
The Zollinger–Ellison Syndrome and Mismeasurement of Gastrin
10
The Zollinger–Ellison Syndrome and Mismeasurement of Gastrin JENS F. REHFELD,* MARIE–HÉLÈNE GINGRAS, ‡ LINDA BARDRAM, § LINDA HILSTED,* JENS P. GOETZE,* and PIERRE POITRAS ‡ Departments of *Clinical Biochemistry and § Surgical Gastroenterology, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark; and ‡ Department of Gastroenterology, CHUM - Hospital Saint-Luc, Université de Montréal, Montréal, Quebec, Canada See editorial on page 1380. BACKGROUND & AIMS: Zollinger–Ellison syndrome (ZES) is characterized by hypersecretion of gastric acid, severe peptic ulcerations in the upper small intestine, and diarrhea. It is usually diagnosed by measuring increased levels of gastrin in plasma. METHODS: We examined the accuracy of commercial kits to measure gastrin (7 radioimmunoassays and 5 enzyme-linked immunosor- bent assays), using plasma from 40 patients suspected or known to have ZES. Each sample was analyzed using the 12 kits and a reference assay that measures bioactive gastrin in plasma, irrespective of size and amino acid derivatization. Known concentrations of peptides with identical sequences to circulating gastrins were also as- sessed by all assays. Molecular patterns in plasma from patients with ZES were examined by chromatography and monitored by kits that measure false-low or false- high concentrations of gastrin. RESULTS: Failure to diagnose gastrinomas has serious consequences. Four kits found false-low concentrations of gastrin in 20% to 80% of the patients. Specificity assessment showed that the antibodies used in these kits bound only gastrin-17. Three kits found false-high concentrations of gastrin, because the reagents had increased reactions to sulfated gastrins or to unspecific factors in plasma. Thus, only 5 of 12 kits tested accurately measure plasma concentra- tions of gastrin. CONCLUSIONS: Seven of 12 tested commercial kits inaccurately measure plasma concen- trations of gastrin; these assays used antibodies with inappropriate specificity that were insufficiently vali- dated. Misdiagnosis of gastrinoma based on lack of specificity of assays for gastrin results in ineffective or inappropriate therapy for patients with ZES. Keywords: Diagnostic Assays; Gastrinoma; Antibody; Gas- trin Quantitation. View this article’s video abstract at www.gastrojournal. org. Z ollinger–Ellison syndrome (ZES) is caused by release of gastrin from endocrine tumors. 1,2 Most gastrino- mas originate in the pancreas or the duodenal mucosa. 3– 6 The syndrome is characterized by hypersecretion of gas- tric acid, severe peptic ulceration in the upper small intestine, and often diarrhea. The diagnosis is usually established by measuring elevated gastrin concentrations in plasma. 4,5,7–13 Clas- sically, 0.3% to 3% of patients with ZES have been reported to have normal or low gastrin concentra- tions. 14 –16 A case of ZES with normal gastrin concen- trations might be explained by unidentified acid stim- ulatory factors that are different from gastrin 17,18 or simply by assays unable to measure gastrin levels cor- rectly. The latter possibility is worth examining be- cause gastrin is not a single molecule but circulates as several peptides of various lengths and amino acid modifications (Figure 1A). 2,19 –21 Moreover, the profile of circulating gastrins in hypergastrinemia deviates from that of healthy subjects (Figure 1B and C). 22–24 The gastrin assays used for diagnosis thus have to be able to measure the pattern present in patients with ZES. Today, diagnostic measurements of gastrin are performed mainly using commercial immunoassay kits. 13,25 We describe here 2 patients suspected to have ZES and the consequences experienced by these patients because gastrin levels in plasma were reported to be normal or only slightly elevated. Motivated by these cases, we com- pared the diagnostic reliability of available gastrin kits with that of an immunoassay that has been fully charac- terized with respect to the pattern of gastrins in patients with gastrinoma. Finally, we characterized the specificity of the kits and are now able to explain “false” low and high concentrations in terms of reactivity with the dif- ferent forms of gastrin. Patients and Methods Patients Two patients from Montreal motivated this study. Their stories are summarized in Results. Abbreviations used in this paper: CT, computed tomography; ELISA, enzyme-linked immunosorbent assay; RIA, radioimmunoassay; ZES, Zollinger-Ellison syndrome. © 2011 by the AGA Institute 0016-5085/$36.00 doi:10.1053/j.gastro.2011.01.051 CLINICAL– ALIMENTARY TRACT GASTROENTEROLOGY 2011;140:1444 –1453
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of The Zollinger–Ellison Syndrome and Mismeasurement of Gastrin

G
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
GASTROENTEROLOGY 2011;140:1444–1453
The Zollinger–Ellison Syndrome and Mismeasurement of Gastrin
JENS F. REHFELD,* MARIE–HÉLÈNE GINGRAS,‡ LINDA BARDRAM,§ LINDA HILSTED,* JENS P. GOETZE,*and PIERRE POITRAS‡
§ ‡
Departments of *Clinical Biochemistry and Surgical Gastroenterology, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark; and Department ofastroenterology, CHUM - Hospital Saint-Luc, Université de Montréal, Montréal, Quebec, Canadasrttusrcsm
See editorial on page 1380.
BACKGROUND & AIMS: Zollinger–Ellison syndrome(ZES) is characterized by hypersecretion of gastric acid,severe peptic ulcerations in the upper small intestine, anddiarrhea. It is usually diagnosed by measuring increasedlevels of gastrin in plasma. METHODS: We examinedthe accuracy of commercial kits to measure gastrin (7radioimmunoassays and 5 enzyme-linked immunosor-bent assays), using plasma from 40 patients suspected orknown to have ZES. Each sample was analyzed using the12 kits and a reference assay that measures bioactivegastrin in plasma, irrespective of size and amino acidderivatization. Known concentrations of peptides withidentical sequences to circulating gastrins were also as-sessed by all assays. Molecular patterns in plasma frompatients with ZES were examined by chromatographyand monitored by kits that measure false-low or false-high concentrations of gastrin. RESULTS: Failure todiagnose gastrinomas has serious consequences. Fourkits found false-low concentrations of gastrin in 20% to80% of the patients. Specificity assessment showed thatthe antibodies used in these kits bound only gastrin-17.Three kits found false-high concentrations of gastrin,because the reagents had increased reactions to sulfatedgastrins or to unspecific factors in plasma. Thus, only 5of 12 kits tested accurately measure plasma concentra-tions of gastrin. CONCLUSIONS: Seven of 12 testedcommercial kits inaccurately measure plasma concen-trations of gastrin; these assays used antibodies withinappropriate specificity that were insufficiently vali-dated. Misdiagnosis of gastrinoma based on lack ofspecificity of assays for gastrin results in ineffectiveor inappropriate therapy for patients with ZES.
Keywords: Diagnostic Assays; Gastrinoma; Antibody; Gas-trin Quantitation.
View this article’s video abstract at www.gastrojournal.org.
Zollinger–Ellison syndrome (ZES) is caused by releaseof gastrin from endocrine tumors.1,2 Most gastrino-
mas originate in the pancreas or the duodenal mucosa.3– 6
The syndrome is characterized by hypersecretion of gas-tric acid, severe peptic ulceration in the upper smallintestine, and often diarrhea.
The diagnosis is usually established by measuringelevated gastrin concentrations in plasma.4,5,7–13 Clas-ically, 0.3% to 3% of patients with ZES have beeneported to have normal or low gastrin concentra-ions.14 –16 A case of ZES with normal gastrin concen-rations might be explained by unidentified acid stim-latory factors that are different from gastrin17,18 orimply by assays unable to measure gastrin levels cor-ectly. The latter possibility is worth examining be-ause gastrin is not a single molecule but circulates aseveral peptides of various lengths and amino acid
odifications (Figure 1A).2,19 –21 Moreover, the profileof circulating gastrins in hypergastrinemia deviatesfrom that of healthy subjects (Figure 1B and C).22–24
The gastrin assays used for diagnosis thus have to beable to measure the pattern present in patients withZES. Today, diagnostic measurements of gastrin areperformed mainly using commercial immunoassaykits.13,25
We describe here 2 patients suspected to have ZES andthe consequences experienced by these patients becausegastrin levels in plasma were reported to be normal oronly slightly elevated. Motivated by these cases, we com-pared the diagnostic reliability of available gastrin kitswith that of an immunoassay that has been fully charac-terized with respect to the pattern of gastrins in patientswith gastrinoma. Finally, we characterized the specificityof the kits and are now able to explain “false” low andhigh concentrations in terms of reactivity with the dif-ferent forms of gastrin.
Patients and MethodsPatientsTwo patients from Montreal motivated this study.
Their stories are summarized in Results.
Abbreviations used in this paper: CT, computed tomography; ELISA,enzyme-linked immunosorbent assay; RIA, radioimmunoassay; ZES,Zollinger-Ellison syndrome.
© 2011 by the AGA Institute0016-5085/$36.00
doi:10.1053/j.gastro.2011.01.051
ctdbI
sewhe
asu
ients
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
May 2011 GASTRIN MISMEASUREMENT IN PATIENTS WITH GASTRINOMA 1445
Plasma SamplesSamples from 40 Danish patients with proven or
suspected ZES were examined. They included 21 men and19 women with a median age of 53 years (range, 23–78years). Seven had localized gastrinoma in the pancreas orduodenum, 10 had metastatic gastrinoma, 10 fulfilled theclinical criteria of ZES with no tumor found yet, 7 weremeasured in the follow-up period after removal of one ormore gastrinomas, and 6 were under suspicion but notfinally proven to have a gastrinoma.
The suspicion of a ZES diagnosis was corroborated bymeasurements of gastrin in plasma, using a fully character-ized gastrin radioimmunoassay (RIA),26,27 and subsequentlyonfirmed by the usual diagnostic procedures (computedomography [CT] scan, Octreoscan (Octreoscan, Covi-ien PLC, Dublin, Ireland), surgery, histologic analysis,asal and pentagastrin-stimulated gastric acid secretion).
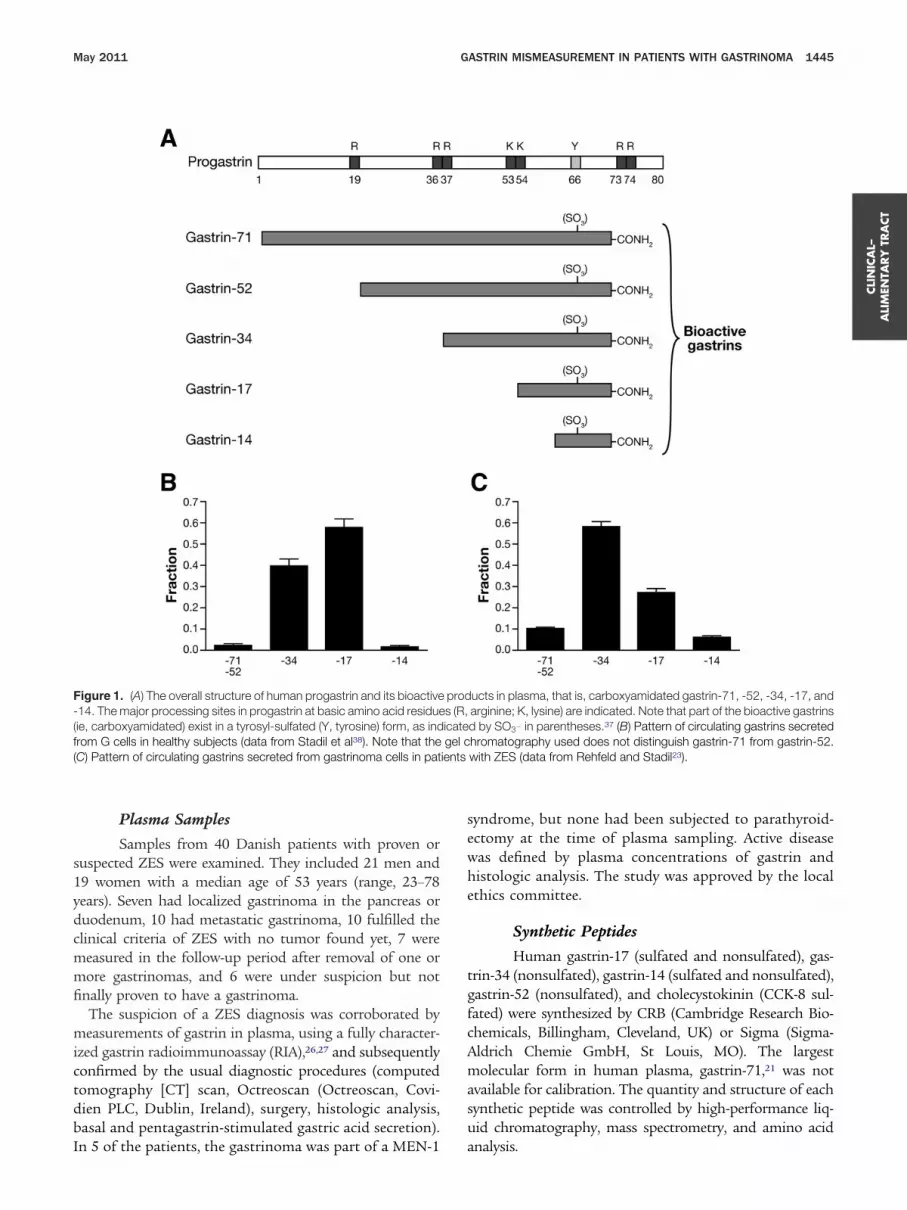
Figure 1. (A) The overall structure of human progastrin and its bioactive-14. The major processing sites in progastrin at basic amino acid residue(ie, carboxyamidated) exist in a tyrosyl-sulfated (Y, tyrosine) form, as indfrom G cells in healthy subjects (data from Stadil et al38). Note that the(C) Pattern of circulating gastrins secreted from gastrinoma cells in pat
n 5 of the patients, the gastrinoma was part of a MEN-1 a
yndrome, but none had been subjected to parathyroid-ctomy at the time of plasma sampling. Active diseaseas defined by plasma concentrations of gastrin andistologic analysis. The study was approved by the localthics committee.
Synthetic Peptides
Human gastrin-17 (sulfated and nonsulfated), gas-trin-34 (nonsulfated), gastrin-14 (sulfated and nonsulfated),gastrin-52 (nonsulfated), and cholecystokinin (CCK-8 sul-fated) were synthesized by CRB (Cambridge Research Bio-chemicals, Billingham, Cleveland, UK) or Sigma (Sigma-Aldrich Chemie GmbH, St Louis, MO). The largestmolecular form in human plasma, gastrin-71,21 was notvailable for calibration. The quantity and structure of eachynthetic peptide was controlled by high-performance liq-id chromatography, mass spectrometry, and amino acid
ucts in plasma, that is, carboxyamidated gastrin-71, -52, -34, -17, andarginine; K, lysine) are indicated. Note that part of the bioactive gastrinsd by SO3� in parentheses.37 (B) Pattern of circulating gastrins secretedhromatography used does not distinguish gastrin-71 from gastrin-52.with ZES (data from Rehfeld and Stadil23).
prods (R,icategel c
nalysis.
rWmr
tsabbS
B
C
D
D
E
S
M
P
P
P
S
U
n
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
1446 REHFELD ET AL GASTROENTEROLOGY Vol. 140, No. 5
Gastrin KitsSeven RIA and 5 enzyme-linked immunosorbent
assays (ELISA) kits were purchased. They constitutedall the gastrin kits available according to a catalog andInternet search. The kits were used according to themanufacturers’ instructions by a technician with morethan 20 years of experience in measurement of gastrin.Each sample was assayed twice in duplicate. As indi-cated in Table 1, the instructions of 3 kits state “Foresearch only. Not for use in diagnostic procedures.”
e have, nevertheless, included them because correcteasurement is always crucial, both in diagnosis and
esearch.
Reference Assay and Additional Assays Usedfor CharacterizationThe results of plasma measurements obtained
with the kits were compared with those of an in-houseRIA based on antiserum no. 2604, which binds the
Table 1. Assay Information From Manufacturers of Gastrin Im
ManufacturerHuman gastrins used
for specificity testImmunoass
technolog
iohit Gastrin-17 (ns) ELISA
orrelate Gastrin-13 (ns)Gastrin-17 (ns)Gastrin-17 (s)Gastrin-34 (ns)
ELISA
iaSorin Gastrin-17 (ns)Gastrin-17 (s)Gastrin-34 (ns)
RIA
RG Diagnostics Gastrin-17 (ns)Gastrin-17 (s)Gastrin-34 (ns)
RIA
uro-Diagnostica Gastrin-17 (ns)Gastrin 17 (s)Gastrin-34 (ns)
RIA
iemens Immulite 2000 Gastrin-17 (ns)Gastrin-17 (s)Gastrin-34 (ns)Gastrin 34 (s)
ELISA
P Biomed Gastrin-17 (ns)Gastrin-17 (s)Gastrin-34 (ns)
RIA
eninsula Gastrin-17 (ns)Gastrin-34 (ns)
RIA
hoenix EIA Gastrin-17 (ns)Gastrin-34 (ns)
ELISA
hoenix RIA Gastrin-17 (ns)Gastrin-34 (ns)
RIA
iemens RIAa Gastrin-17 (ns)Gastrin-17 (s)Gastrin-34 (ns)
RIA
S Biological Gastrin-17 (ns) ELISA
s, nonsulfated; s, sulfated.a“Mini” gastrin also tested without indication of length or sulfation.
bioactive sequence of all amidated gastrins.26 The anti-
serum binds human gastrin-14, -17, -34, -52, and -71with equimolar potency, irrespective of degree of sul-fation. Moreover, the cross-reactivity with CCK is neg-ligible.26 Under the conditions used, there is no inter-ference from plasma proteins, salt, or other unrelatedsubstances.27 Monoiodinated human nonsulfated gas-rin-17 was used as tracer,28 and the same batch ofynthetic gastrin-17 in its nonsulfated form was useds standard. The assay setup and conditions of incu-ation have been detailed elsewhere.27 The assay haseen used for 4 decades for diagnostic measurement incandinavian countries.9
To corroborate the results obtained with kits thatmeasured only gastrin-17, we repeated the measurementswith another in-house RIA using antiserum no. 90183,which is specific for gastrin-17 without reactivity withlonger or shorter forms of gastrin (but 4 times higheraffinity for sulfated gastrin-17). Moreover, for the chro-matographic examination, we used a gastrin RIA based
oassay Kits
Upper referencelimit Diagnostic use Described limitations
— Hypergastrinemia Human plasmarecommended
— For research use only; not for use indiagnostic procedures
108 pg/mL or52 pmol/L(guideline)
Hypergastrinemia Lipemia
111 pg/mL or53 pmol/L(guideline)
Hypergastrinemia None
60 pmol/L Hypergastrinemia None
115 pg/mL or55 pmol/L(guideline)
Hypergastrinemia None
111 pg/mL or53 pmol/L(guideline)
Hypergastrinemia None
— For research use only; not for use indiagnostic procedures
— Hypergastrinemia None
— Hypergastrinemia Extractionrecommended;intended for invitro use
90 pg/mL or 41pmol/L(guideline)
Hypergastrinemia None
— Not for use in diagnosis of gastrinoma
mun
ayy
antiserum no. 8017 that is specific for N-terminus of

U
NrTl
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
May 2011 GASTRIN MISMEASUREMENT IN PATIENTS WITH GASTRINOMA 1447
human gastrin-17.29 Finally, for the chromatographic exam-ination of the reactivity to sulfation, we used antiserum no.2605, which binds only nonsulfated gastrins.26,30
ChromatographyFor characterization of the gastrins in gastrinoma
plasma, samples were applied to Sephadex (Sephadex, GEHealthcare, Little Chalfont, Buckinghamshire, UK) G50superfine colums.23 The elutions were monitored usingselected immunoassay kits and in-house sequence spe-cific RIA with antibodies as described previously.
StatisticsFor assay comparison, we used Deming regression
analysis, which determines the line of best fit for a 2-di-
Table 2. Gastrin Levels in Plasma From Patients Suspected
Co
Referenceassay Biohit Correlate DiaSorin DRG
Euro-Diagnostica
GroupA7 6 64 17 17 15
13 6 137 20 13 1817 1 94 25 12 2120 5 112 23 15 2235 22 170 32 42 5135 3 151 30 32 3639 31 244 36 45 5445 23 272 41 55 5155 1 64 35 48 5458 59 103 65 83 9071 65 76 94 38 7590 �1 246 59 111 14393 83 250 69 86 11097 26 155 52 74 108
GroupB131 219 124 131 159 169150 272 196 135 226 178158 73 162 75 134 121195 114 350 103 164 208209 157 321 118 226 267255 238 228 189 274 332281 51 293 103 252 279286 70 214 88 173 246293 145 610 230 218 360336 275 585 200 232 380365 660 925 355 479 585387 390 630 260 359 400397 75 640 45 23 545398 0 1850 190 231 230
GroupC495 120 1620 390 345 250500 605 275 380 444 505560 105 810 255 405 510833 600 1540 610 767 1330880 940 505 560 854 1100910 2000 1680 1060 990 1380
1460 1300 1330 1070 1680 25602700 3920 1240 3530 1719 41802830 1990 2020 1240 2412 36705520 6300 15,000 6100 6460 9500
16,000 18,900 44,500 11,300 22,200 800062,340 354,000 1,260,000 456,000 590,000 87,400 3
pper concentration limit for healthy subjects (see also Table 1)50 — — 52 53 60
OTE. Values are expressed as pmol/L. The patients in group A had concentraemoved. The patients in group B had concentrations between 100 and 400 pmhe patients in group C had concentrations �400 pmol/L (reference assay). Thast line of the table for kits providing this information.
aThe upper reference concentration for healthy fasting subjects is approximate
proton pump inhibitors with ensuing moderate hypergastrinemia up to 100 pmol/Lconcentrations �100 pmol/L are false low when the reference assay results are �1mensional data set. Bland–Altman bias plots were alsocalculated; all comparisons were performed using Graph-Pad Prism software (La Jolla, CA).
ResultsCase Report 1A 49-year-old man with diarrhea and profuse
vomiting was hospitalized in the intensive care unit forhypovolemic shock and acute renal failure. A nasogastrictube drained 3 L of liquids daily, and he was treated withintravenous pantoprazole 40 mg twice daily. Computedaxial tomography (CT scan) showed 2 minor hepaticlesions and a large 12-cm lesion with septae and cysts aswell as severe fluid accumulation in intestinal loops.
Control for Gastrinomas
cial gastrin kits
liteMP
Biomed PeninsulaPhoenix
EIAPhoenix
RIASiemens
RIAUS
Biological
14 23 16 30 32 9 910 25 44 21 36 12 713 20 17 18 123 9 2�5 19 20 43 26 9 554 63 40 39 42 33 1936 55 34 37 35 25 364 60 28 33 35 30 2780 79 26 24 31 38 1771 80 28 55 35 47 7
140 104 66 33 45 59 51�5 53 27 125 154 161 43
139 134 74 132 83 117 17140 106 53 52 49 68 70
94 79 46 50 42 68 49
329 147 145 33 86 124 180268 213 182 94 70 202 305176 140 110 266 56 133 68228 210 203 147 89 169 120286 295 219 192 77 216 134430 346 318 282 109 260 181212 268 246 420 92 226 68252 180 191 83 73 175 64515 375 280 330 795 270 195530 330 295 265 98 180 375200 680 575 365 169 405 1370805 625 490 445 86 490 35
15 95 75 195 60 35 0530 430 170 1640 97 230 0
630 570 290 410 222 250 510005 655 540 340 145 505 295710 610 385 905 157 555 80570 1350 660 1850 282 1280 700010 1040 965 1045 223 805 855350 4800 920 1360 264 2710 1280980 1710 1940 5690 283 2050 1150400 2580 2910 1040 978 1440 500080 2170 2450 2720 451 1750 1870400 11,400 4000 17,600 11,800 5500 5400500 10,500 20,500 16,981 1664 8500 12,500000 851,000 510,000 1,129,000 192,100 467,000 240,000
55 53 — — — 41 —
�100 pmol/L (reference assay).a Several in this group had their gastrinomaseference assay). These patients were in treatment with proton pump inhibitors.er concentration limits (pmol/L) for normal fasting subjects are indicated in the
pmol/L, but because patients with dyspeptic symptoms are often treated with
or in
mmer
Immu
1
1
1222
11,4
12,17,
,140,
tionsol/L (re upp
ly 50
, concentrations above this level are in the gastrinoma range. Consequently,00 pmol/L.
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
1448 REHFELD ET AL GASTROENTEROLOGY Vol. 140, No. 5
Gastrointestinal endoscopy revealed mild esophagitisand prominent gastric folds but no ulcers. While stillbeing treated with pantoprazole, the patient’s serumgastrin level was 67 pmol/L (normal, 0 –50 pmol/L;GammaDab Gastrin RIA Kit, DiaSorin, Stillwater,MN). During a secretin test, the gastrin concentrationswere again almost normal (53– 64 pmol/L).
Based on the normal gastrin levels, the diagnosis ofZES was discarded. Attempts to stop pantoprazoletreatment led to profuse acid vomiting and multipleesophageal strictures, prohibiting oral feeding and gas-tric secretory studies. Somatostatin receptor scintigra-phy (Octreoscan) suggested a neuroendocrine tumor inliver segments V, VI, and VII. Considering a diagnosis ofZES, the dosage of intravenous pantoprazole was in-creased to 80 mg every 8 hours before it could be substi-tuted for an oral suspension of esomeprazole 120 mgtwice daily.
Remeasurement with the DiaSorin kit still revealed lowgastrin concentration (64 pmol/L). The same serum sam-ple measured with an Immulite 1000 kit (DiagnosticProducts Corp, Llanberis, Caernafon, Gwynedd, UK)showed an elevated gastrin level (271 pmol/L) suspiciousof gastrinoma.
An exploratory laparotomy revealed bilobar hepaticneuroendocrine tumor metastases, but the primary tu-mor was not identified. Chemoembolization and treat-ment with octreotide stabilized tumor progression. Fouryears later, esomeprazole 80 mg twice daily is still re-quired to maintain basal acid secretion less than 2mmol/h, and esophageal dilatations are performed every2 to 3 months for recurrent strictures.
Case Report 2A 51-year-old man who had a 6-month history of
epigastric pain, diarrhea, and 15-kg weight loss was hos-pitalized for a severe episode of abdominal pain, vomit-ing, diarrhea, and dehydration. He rapidly improved with
Table 3. Gastrin Concentrations in “0” Plasma to Which SynHave Been Added
Added gastrinpeptide
Referenceassay Biohit Correlate DiaSorin
DRGDiagnostics
EDiag
“0” plasma 0 2 96 6 8Gastrin-14 (ns) 13 2 119 9 16Gastrin-14 (s) 55 0 187 33 58Gastrin-17 (ns) 52 45 188 42 69Gastrin-17 (s) 38 220 174 49 64Gastrin-34 (ns) 43 1 193 24 32Gastrin-52 (ns) 12 3 135 8 11CCK-8 (s) (100
pmol/L)2 3 157 5 27
Antral extract 87 310 215 166 158Upper concentration limit for normal subjects (see also Table 1)
50 — — 52 53
NOTE. Values are expressed as pmol/L.ns, nonsulfated; s, sulfated.
intravenous liquids and pantoprazole. Computed tomo-densitometry (CT scan) showed inflammatory changes ofthe third segment of the duodenum and enlarged lymphnodes in the periduodenal area, while liver and pancreaswere normal. Gastrointestinal endoscopy showed severeesophagitis and 3 ulcers in the third segment of theduodenum. Gastrin level in serum was 88 pmol/L (Dia-Sorin kit). The slight increase in gastrin level was attrib-uted to long-term intake of a proton pump inhibitor andacute renal failure due to dehydration.
Two days after stopping treatment with pantoprazole,the severe digestive symptoms relapsed and resolvedwhen pantoprazole was readministered. Endoscopic ul-trasonography suggested enlarged gastric folds andshowed 2-cm lymph nodes where fine needle aspirationindicated neuroendocrine tumor. Octreoscan showed in-creased uptake corresponding to the lymph nodes foundon CT scan and endoscopic ultrasonography. A secondgastrin measurement with the DiaSorin kit was still nor-mal (32 pmol/L). A secretin stimulation test failed toincrease serum gastrin concentrations. Basal gastric acidoutput was 14.5 mEq/h (normal, �5 mEq/h) while treat-ment continued with oral pantoprazole 80 mg twicedaily. Following these results, the diagnosis of ZES wasconfirmed, and the dosage of pantoprazole was increasedto 120 mg twice daily.
At laparotomy, 2 lymph nodes containing metastasisof a neuroendocrine tumor were removed near the pan-creas head, but no primary tumor was identified. Sixyears after surgery, gastric acid hypersecretion is stillcontrolled by esomeprazole 20 mg twice daily.
Diagnostic Sensitivity of the Gastrin KitsTable 2 shows the results of the measurements in
plasma from 40 fasting patients with ZES using thecommercial immunoassay kits. Defined by the referenceassay, the first group of 14 patients had concentrationsless than 100 pmol/L (Table 2, group A). The patients
c Human Peptides and an Extract of Human Antral Mucosa
Commercial gastrin kits
a ImmuliteMP
Biomed PeninsulaPhoenix
EIAPhoenix
RIA SiemensUS
Biological
0 8 8 91 1 0 00 19 16 0 0 15 00 78 54 29 3 54 0
79 79 77 116 18 47 77233 80 28 0 22 28 250
48 48 9 33 4 44 09 14 7 0 4 6 00 34 28 0 5 9 0
290 175 136 28 27 91 250
55 53 — — — 41 —
theti
uro-nostic
57
1215654512113
109
60
nat
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
May 2011 GASTRIN MISMEASUREMENT IN PATIENTS WITH GASTRINOMA 1449
with the lowest concentrations were those with con-trolled disease after surgical removal of gastrinomas (nos.1–5, 8, and 11 in Table 2 [group A]). Five of the patients(nos. 6, 7, 12, 13, and 14 [Table 2, group A]) still hadactive disease and 2 (nos. 10 and 14 [Table 2, group A])were strongly suspected of having ZES yet without his-tochemical verification of gastrinoma. In group A, theBiohit and US Biological kits measured false-low concen-trations in 5 and 4 patients, respectively.
The second group of 14 patients with gastrinoma werenot surgically treated but on long-term medication withproton pump inhibitors. The medication was stopped for5 days before blood was drawn for measurement of gas-trin until the diagnosis was established. According to thereference assay, they had concentrations ranging between100 and 400 pmol/L (Table 2, group B). The results showthat the Biohit ELISA, US Biological ELISA, and PhoenixRIA failed to provide adequate diagnostic measurementsin 35%, 43%, and 77% of patients, respectively. In addi-tion, the DiaSorin and the Phoenix ELISA kits measuredtoo low concentrations in 2 and 3 cases, respectively.
The last 12 patients had concentrations greater than400 pmol/L (Table 2, group C). Despite a considerableinterkit variation, the concentrations in this group are sohigh that they support a diagnosis of gastrinoma anyway.The only exception was a patient in whose plasma the USBiological kit measured a concentration of 80 pmol/L.
In all groups of patients, the Siemens Immulite kitmeasured false-high concentrations due to overreactivityagainst sulfated gastrins (Table 3 and Figure 2C). Toohigh concentrations were also measured by the Correlatekit, both in the low and the intermediate ranges (Table2), apparently due to unspecific interference from plasmaproteins (Table 3).
Considering patients at risk for an erroneous diagnosiswhen basal gastrin level is between 50 and 400 pmol/L(20 patients in our series), the kits provided the correctdiagnosis in the following percentages of patients: Euro-Diagnostica 100%, MP Biomed and Siemens RIA 95%,DRG and Siemens Immulite 90%, Peninsula and PhoenixEIA 75%, DiaSorin and Biohit 60%, US Biological 55%,and Phoenix RIA 40%. The kit from Correlate measuredelevated gastrin concentrations in 100% of patients with
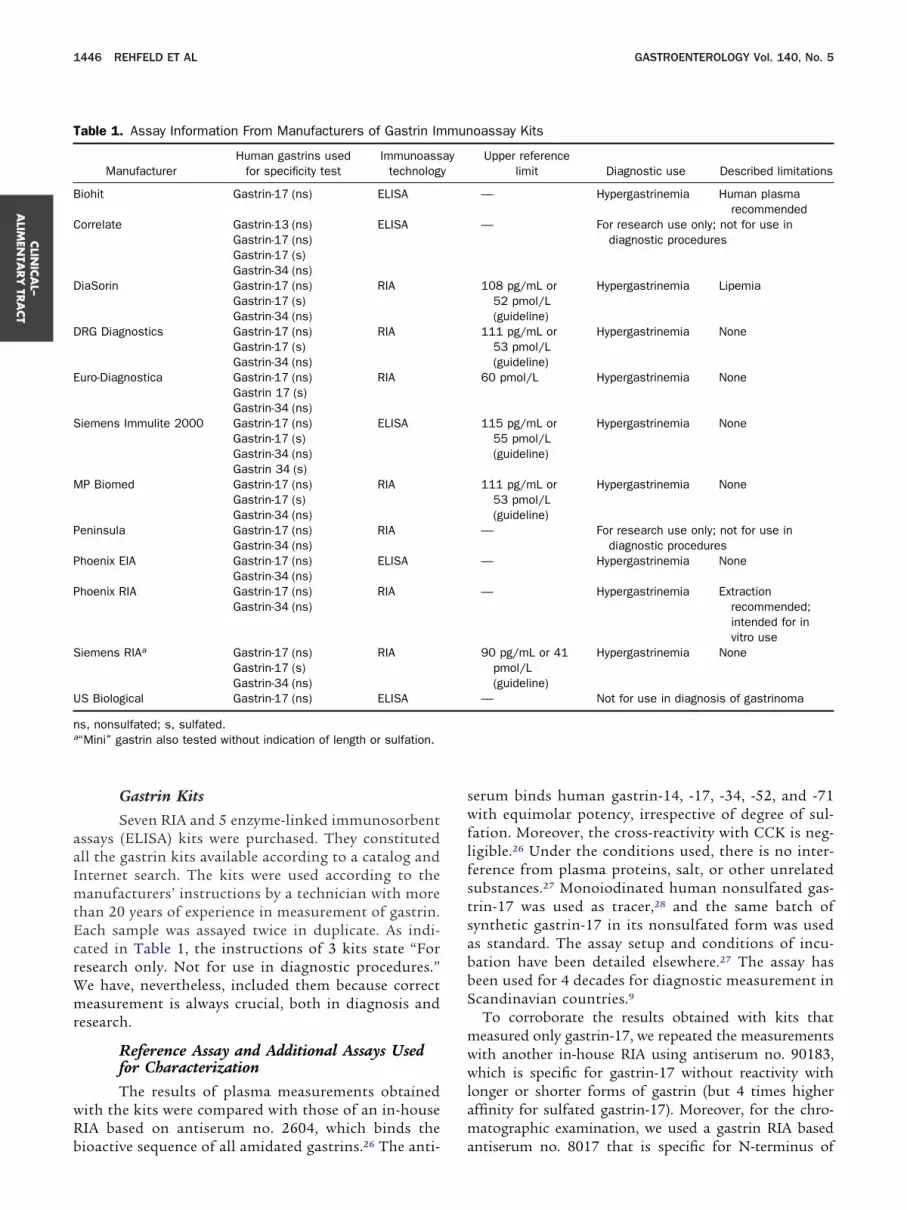
4™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™Figure 2. Gel chromatography (Sephadex G50 superfine column) ofplasma from a patient with ZES. The elution was monitored using 5 gastrinimmunoassays that all use synthetic human nonsulfated gastrin-17 asassay calibrator and tracer. (A) The elution monitored by the Biohit ELISAkit. (B) The elution monitored by an RIA specific for the N-terminus (Nt) ofhuman gastrin-17.29 (C) The elution monitored by the Siemens Immulite kit.(D) The elution monitored by an RIA that uses antibody 2605, whichbinds the amidated C-terminus of bioactive gastrins in nonsulfated formonly.30 (E) The elution monitored by the reference RIA that uses antibodyo. 2604, which binds the carboxyamidated C-terminus of all the bio-ctive gastrins and binds these gastrins with equimolar affinity, irrespec-
ive of the degree of tyrosyl sulfation.26,27
vtw
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
1450 REHFELD ET AL GASTROENTEROLOGY Vol. 140, No. 5
hypergastrinemia, but it also provided false-positive re-sults in 8 of 8 patients with normal gastrin levels.
Analytical Specificity of the Gastrin KitsAccording to the manufacturers, all the immuno-
assay kits were examined against nonsulfated gastrin-17;10 kits were also examined against nonsulfated gas-trin-34 and 6 kits against sulfated gastrins (Table 1). Toextend the specificity examination, we spiked humanplasma that had first been charcoal stripped of endoge-nous gastrins (“0” plasma) with different synthetic hu-man gastrins. As shown in Table 3, gastrin-14 (sulfated aswell as nonsulfated) was not measured by the Biohit,Siemens Immulite, Phoenix ELISA, Phoenix RIA, and USBiological kits. Gastrin-17 (sulfated and nonsulfated) wasmeasured by all kits, but the Biohit, Immulite, and USBiological kits overestimated the sulfated form of gas-trin-17 6- to 7-fold, whereas the Phoenix ELISA kit didnot measure sulfated gastrin-17 at all. Human gastrin-34(nonsulfated) was not measured by the Biohit, PhoenixRIA, and US Biological kits but measured fully by theremaining kits. The same pattern of reactivity was foundwith synthetic gastrin-52 (nonsulfated).
Gel chromatography confirmed that kits that did notbind gastrin-14, gastrin-34, and gastrin-52 in the speci-ficity test recognized only gastrin-17 in plasma frompatients with ZES (Figure 2A). The result was confirmedboth by our in-house gastrin-17 specific RIA, using anti-body no. 90183 (data not shown), and the RIA specific forthe N-terminus of gastrin-17 (Figure 2B). Gel chroma-tography also confirmed that kits that overestimatedsulfated forms of synthetic gastrins also did so in plasmafrom patients with gastrinoma (Figure 2C).
Unspecific plasma interference was assessed using thepreviously mentioned human “0” plasma stripped free ofendogenous gastrins. Significant interference was found
Table 4. Deming Regression Analysis Comparing the ResultsGastrin Immunoassays From Diagnostic Companies
Manufacturer Slope95% confidence
intervalY-i
Biohit 1.16 0.59–1.72Correlate 3.61 2.23–5.00DiaSorin 0.66 0.50–0.82DRG Diagnostics 0.82 0.61–1.04Euro-Diagnostica 1.17 1.03–1.31Siemens Immulite 2.34 1.59–3.09MP Biomed 1.35 1.05–1.64Peninsula 1.04 0.75–1.32Phoenix EIA 2.67 1.35–4.00Phoenix RIA 0.73 0.00–1.50Siemens RIA 0.86 0.61–1.10US Biological 2.75 0.75–4.76
NOTE. Thirty samples were included, defined from a cutoff from the goTable 2).
in the Correlate and the Phoenix ELISA kits (Table 3).
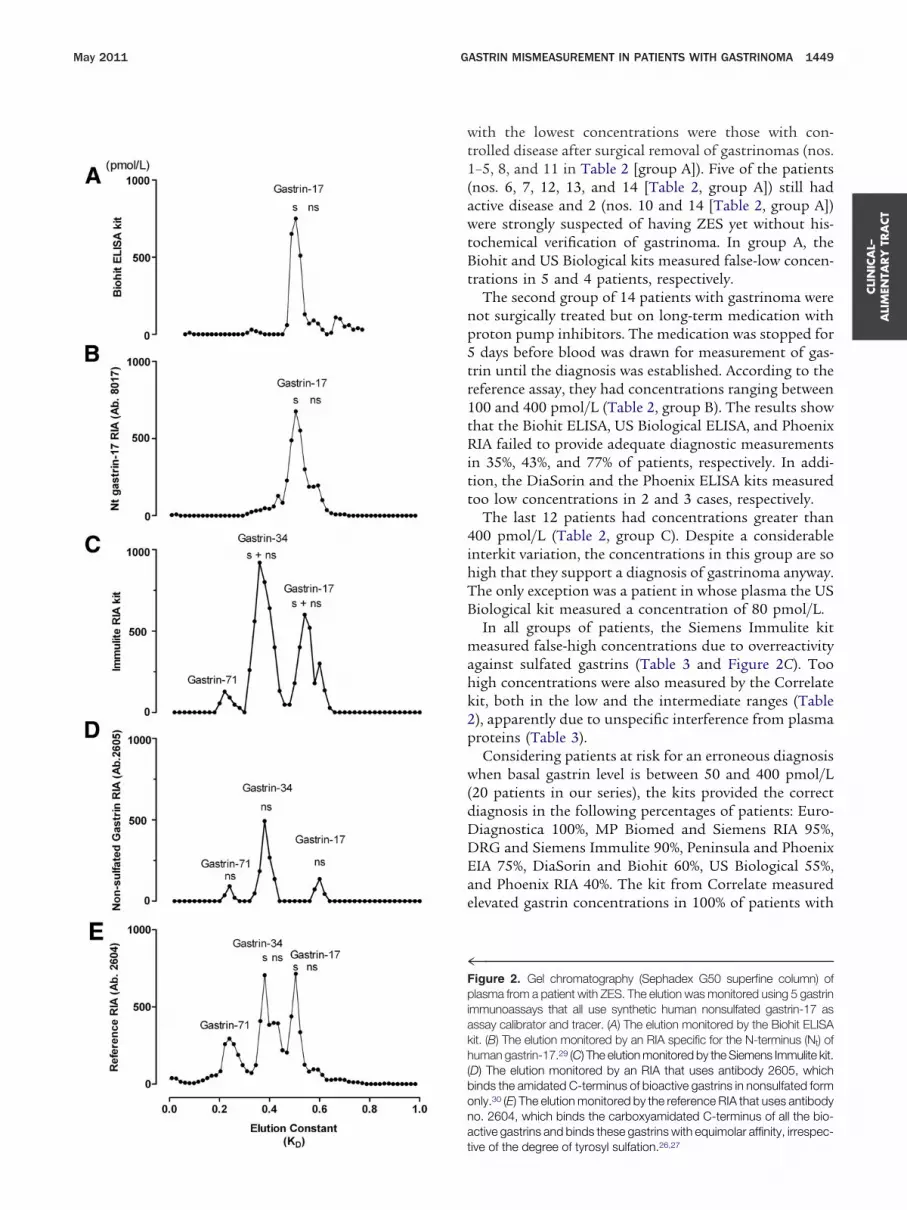
In Deming regression analysis, the correlation betweenthe reference assay and each commercial gastrin kit wasfound to vary considerably. Thus, the r value (Pearson)aried from 0.34 to 0.96 (Table 4). The variation is fur-her illustrated for 3 kits: one that is gastrin-17 specificith frequent false-low measurement (Biohit, Figure 3A
and B); one that overreacts with sulfated gastrin, whichcauses false-positive measurements (Siemens Immulite,Figure 3C and D), and one with acceptable correlation(Siemens RIA, Figure 3E and F).
DiscussionThe patient reports show that failure to measure
gastrin levels in plasma correctly can have deleteriousconsequences. The ensuing assay examination showedthat the failures are due to antibodies that do not appro-priately recognize the molecular forms of gastrin secretedby gastrinomas.
Gastrinomas are well known for their short-term andlong-term complications. Short-term complications arerelated to gastric acid hypersecretion and aggressive pep-tic disease, often with ulcer perforation. Fortunately, pep-tic complications can now be treated effectively withproton pump inhibitors. Modern management of pa-tients with ZES can therefore focus on long-term com-plications of tumor growth.
The consequences of missing a diagnosis of ZES areserious. Our first patient developed esophagitis and pep-tic stenosis that prohibited oral alimentation for weeksand forced serial dilatations of the esophagus for years.The second patient had repeated episodes of dehydrationand severe ulcerations with microperforation of the distalduodenum. In these situations, the clinician disregardedthe diagnosis of ZES because of low gastrin concentra-tions and therefore failed to prescribe the antisecretory
he Reference Gastrin Assay With Those of Commercial
ept when0
95% confidenceinterval P value
r(Pearson)
86 �221 to 49 �.0001 0.6292 �622 to 38 �.0001 0.71�2 �40 to 37 �.0001 0.85
2 �50 to 54 �.0001 0.83�4 �38 to 29 �.0001 0.9657 �342 to 28 �.0001 0.7832 �103 to 38 �.0001 0.8729 �97 to 40 �.0001 0.8184 �597 to 29 �.0001 0.6231 �213 to 151 �.0001 0.34�6 �66 to 54 �.0001 0.8064 �842 to 114 �.0001 0.47
ndard analysis with plasma gastrin concentration �500 pmol/L (see
of t
ntercX �
��2
�1��
�2�
�3
ld sta
regimen that would have been appropriate.
Cw( igh c
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
May 2011 GASTRIN MISMEASUREMENT IN PATIENTS WITH GASTRINOMA 1451
Accurate measurement of gastrin in plasma togetherwith assessment of gastric acid secretion are decisive for
Figure 3. Deming regression analyses (left panels) and the corresponand D, and E and F, respectively) with the reference assay. Only sampere included (n � 30). The dashed lines indicate the 95% confidence
bias, �67%; SD, 78%) and the Siemens Immulite kit measures false-h
diagnosis of ZES. Gastrin, however, circulates in multiple c
forms, both in healthy subjects and in patients with ZES(Figure 1).22–24 Moreover, the peptide pattern and the
ias plots (right panels) comparing 3 commercial gastrin kits (A and B,ith a gastrin concentration �500 pmol/L defined by the reference assayal. Note that the Biohit kit measures false-negative low concentrationsoncentrations (bias, 28%; SD, 54%).
ding bles winterv
oncentration vary considerably, not only between

ppl
kdwipgatmrkFichTsn1cfp
rsnrgiT1
pwb
1
1
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
1452 REHFELD ET AL GASTROENTEROLOGY Vol. 140, No. 5
healthy subjects and patients with ZES as such (Figure 1Band C), but also among the individual patients withgastrinoma.23,24,30 To ensure a high diagnostic sensitivity,the first-line assays should therefore measure all the bio-active (ie, amidated) gastrin peptides, irrespective of sizeand modification such as tyrosyl sulfation.23,24 A fewpatients with gastrinoma can have truly normal concen-trations of amidated gastrin in plasma.14 –16 For these
atients, assays that measure progastrin or “the totalrogastrin product”31–35 may be necessary in a second
ine of measurement.During the past decades, commercial immunoassay
its have, to a large extent, been implemented in routineiagnostic measurements.13,25 An open question is tohat extent these kits meet the pathognomonic specific-
ty. Prompted by missed diagnoses of ZES, we have in theresent study compared the measurements of availableastrin kits with those of a fully characterized referencessay (Tables 2– 4). The study shows considerable varia-ion of the gastrin concentration in the same sample as
easured by different kits. The 40 plasma samples wereandomly collected among patients known to have,nown to have had, or strongly suspected to have ZES.alse-low concentrations were frequently encountered us-
ng 4 of the kits. The diagnostic significance of false-lowoncentrations is minor for the group of patients whoave plasma concentrations greater than 400 pmol/L.he major problem is the false-low concentrations mea-
ured in patients with moderately but diagnostically sig-ificant increased plasma gastrin concentrations (50 or00 – 400 pmol/L [Table 2, groups A and B]). In thisategory, false-low measurements may be responsible forailure to establish the correct diagnosis, putting theatients at risk for severe, even lethal complications.Our study also uncovers the causes of the deviating
esults in precise molecular terms. Hence, false-low re-ults are due to antibodies that bind only gastrin-17, buteither shorter nor longer forms (Figures 1 and 2A). Theesults, however, depend not only on the length of theastrin peptide. The antibody binding is also heavilynfluenced by modifications such as tyrosine sulfation.hus, a study of different gastrin antisera showed a00-fold variation in reactivity with sulfated gastrins.36
Moreover, while approximately half of each gastrin formis sulfated in normal human tissue and plasma,24,30 the
attern changes in a highly individual manner in patientsith gastrinoma, where sulfation has been found to varyetween 11% and 82%.24 The variation is further compli-
cated by the observation that some antibodies of thegastrin-17 specific kits also underreact or overreact withsulfated gastrins. Hence, if plasma contains a large frac-tion of sulfated gastrin-17, the gastrin-17 specific assaysmeasure false-high gastrin concentrations, as seen for theBiohit and US Biological kits. Accordingly, the gastrin-17specific Phoenix RIA kit measures more consistently
false-low concentrations (Table 2) because the antibodyreacts poorly with sulfated gastrin. These results empha-size the necessity of evaluating not only peptide lengthbut also amino acid derivatizations.
The study also reveals examples of false-high gastrinconcentrations. The explanation seems 2-fold. Two kitsare sensitive to unspecific plasma effects (Table 3). Theother factor is tyrosine sulfation, as discussed previously.This seems true also for a kit that is not gastrin-17specific such as the Siemens Immulite kit, where thefalse-high results (Table 2) are caused by overreactionwith sulfated gastrins (Figure 2C). The implications offalse-high concentrations may be less severe than false-low concentrations because the tumor diagnosis is notmissed. On the other hand, false-high concentrations area cause of anxiety, and patients have to undergo unnec-essary and costly investigations. At its extreme, they canlead to unnecessary surgery and inappropriate, lifelongtreatment.
A broader perspective of the present study is thatneuroendocrine tumors in general release peptide hor-mones and chromogranins that, like gastrin, circulate indifferent molecular forms. An obvious question is, there-fore, whether the immunoassay kits used for the otherneuroendocrine tumors have the necessary diagnosticsensitivity and specificity. The perspective becomes evenwider when diagnostic use of immunoassays as such ischallenged. Do antibodies in diagnostic assays today thuscover the complexity of substances unveiled by modernbiochemistry in normal and diseased tissue and plasma?
References
1. Gregory RA, Grossman MI, Tracy HJ, et al. Nature of the gastricsecretagogue in Zollinger-Ellison tumours. Lancet 1967;2:543–544.
2. Gregory RA, Tracy HJ, Agarwal KL, et al. Aminoacid constitution oftwo gastrins isolated from Zollinger-Ellison tumour tissue. Gut1969;10:603–608.
3. Zollinger RM, Ellison EH. Primary peptic ulcerations of the jeju-num associated with islet cell tumors of the pancreas. Ann Surg1955;142:709–723.
4. Creutzfeldt W, Arnold R, Creutzfeldt C, et al. Pathomorphologic,biochemical, and diagnostic aspects of gastrinomas (Zollinger-Ellison syndrome). Hum Pathol 1975;6:47–76.
5. Wolfe MM, Jensen RT. Zollinger-Ellison syndrome. Current con-cepts in diagnosis and management. N Engl J Med 1987;317:1200–1209.
6. Metz DC, Jensen RT. Gastrointestinal neuroendocrine tumors:pancreatic endocrine tumors. Gastroenterology 2008;135:1469–1492.
7. Walsh JH, Grossman MI. Gastrin. N Engl J Med 1975;292:1377–1384.
8. Malagelada JR, Davis CS, O’Fallon WM, et al. Laboratory diagno-sis of gastrinoma. I. A prospective evaluation of gastric analysisand fasting serum gastrin levels. Mayo Clin Proc 1982;57:211–218.
9. Jacobsen O, Bardram L, Rehfeld JF. The requirement for gastrinmeasurements. Scand J Clin Lab Invest 1986;46:423–426.
0. Rehfeld JF, van Solinge WW. The tumor biology of gastrin andcholecystokinin. Adv Cancer Res 1994;63:295–347.
1. Varro A, Ardill JE. Gastrin: an analytical review. Ann Clin Biochem
2003;40:472–480.
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
May 2011 GASTRIN MISMEASUREMENT IN PATIENTS WITH GASTRINOMA 1453
12. Berna MJ, Hoffmann KM, Serrano J, et al. Serum gastrin inZollinger-Ellison syndrome: I. Prospective study of fasting serumgastrin in 309 patients from the National Institutes of Health andcomparison with 2229 cases from the literature. Medicine (Bal-timore) 2006;85:295–330.
3. Rehfeld JF. The art of measuring gastrin in plasma: a dwindlingdiagnostic discipline? Scand J Clin Lab Invest 2008;68:353–361.
4. Wolfe MM, Jain DK, Edgerton JR. Zollinger-Ellison syndrome as-sociated with persistently normal fasting serum gastrin concen-trations. Ann Intern Med 1985;103:215–217.
5. Zimmer T, Stolzel U, Bader M, et al. Brief report: a duodenalgastrinoma in a patient with diarrhea and normal serum gastrinconcentrations. N Engl J Med 1995;333:634–636.
6. Jais P, Mignon M. Normal serum gastrin concentration in gastri-noma. Lancet 1995;2:1421–1422.
7. Dubois A, Eerdewegh PV, Gardner JD. Gastric emptying andsecretion in Zollinger-Ellison syndrome. J Clin Invest 1977;59:255–263.
8. Song Y, Chey WY, Chang TM, et al. Mechanism of gastric acidhypersecretion in patients with islet cell tumor without hypergas-trinemia: studies in rats. Gastroenterology 1997;113:1129–1135.
9. Gregory RA, Tracy HJ. Isolation of two “big gastrins” fromZollinger-Ellison tumour tissue. Lancet 1972;2:797–799.
0. Gregory RA, Tracy HJ, Harris JI, et al. Minigastrin; correctedstructure and synthesis. Hoppe Seylers Z Physiol Chem 1979;360:73–80.
1. Rehfeld JF, Johnsen AH. Identification of gastrin component I asgastrin-71. The largest possible bioactive progastrin product. EurJ Biochem 1994;223:765–773.
2. Rehfeld JF, Stadil F, Vikelsoe J. Immunoreactive gastrin compo-nents in human serum. Gut 1974;15:102–111.
3. Rehfeld JF, Stadil F. Gel filtration studies on immunoreactivegastrin in serum from Zollinger-Ellison patients. Gut 1973;14:369–373.
4. Andersen BN, Petersen B, Borch K, et al. Variations in thesulfation of circulating gastrins in gastrointestinal diseases.Scand J Gastroenterol 1983;18:565–569.
5. Wolfe MM, Paquet RJ, Reel GM. Specificity of commercially avail-able antibodies used for gastrin measurement. J Lab Clin Med1985;105:417–421.
6. Rehfeld JF, Stadil F, Rubin B. Production and evaluation of anti-bodies for the radioimmunoassay of gastrin. Scand J Clin LabInvest 1972;30:221–232.
7. Stadil F, Rehfeld JF. Determination of gastrin in serum. An eval-uation of the reliability of a radioimmunoassay. Scand J Gastro-enterol 1973;8:101–112.
8. Stadil F, Rehfeld JF. Preparation of 125 I-labelled synthetic hu-man gastrin I for radioimmunoanalysis. Scand J Clin Lab Invest
1972;30:361–368.29. Bardram L, Rehfeld JF. Production and evaluation of monospe-cific antibodies for a processing-independent sequence of humanprogastrin. Scand J Clin Lab Invest 1989;49:173–182.
30. Andersen BN, De Magistris L, Rehfeld JF. Radioimmunochemicalquantitation of sulfated and non-sulfated gastrins in serum. ClinChim Acta 1983;127:29–39.
31. Bardram L, Rehfeld JF. Processing-independent radioimmuno-analysis: a general analytical principle applied to progastrin andits products. Anal Biochem 1988;175:537–543.
32. Bardram L. Progastrin in serum from Zollinger-Ellison patients. Anindicator of malignancy? Gastroenterology 1990;98:1420–1426.
33. Jais P, Mignon M, Rehfeld JF. Processing-independent assay ofserum gastrin for diagnosis of liver metastases in the Zollinger-Ellison syndrome. Int J Cancer 1997;71:308–309.
34. Jorgensen NR, Rehfeld JF, Bardram L, et al. Processing-indepen-dent analysis in the diagnosis of gastrinomas. Scand J Gastro-enterol 1998;33:379–385.
35. Rehfeld JF. Processing of precursors of gastroenteropancreatichormones: diagnostic significance. J Mol Med 1998;76:338–345.
36. Rehfeld JF, De Magistris L, Andersen BN. Sulfation of gastrin:effect on immunoreactivity. Regul Peptides 1981;2:333–342.
37. Rehfeld JF, Zhu X, Norrbom C, et al. Prohormone convertases1/3 and 2 together orchestrate the site-specific cleavages ofprogastrin to release gastrin-34 and gastrin-17. Biochem J 2008;415:35–43.
38. Stadil F, Rehfeld JF, Christiansen L, et al. Patterns of gastrincomponents in serum during feeding in normal subjects andduodenal ulcer patients. Scand J Gastroenterol 1975;10:863–868.
Received November 11, 2010. Accepted January 24, 2011.
Reprint requestsAddress requests for reprints to: Professor Jens F. Rehfeld, MD,
DSc, Department of Clinical Biochemistry, Rigshospitalet, DK-2100Copenhagen, Denmark. e-mail: [email protected]; fax: (45)3545 2880.
AcknowledgmentsThe authors thank Alice von der Lieth for skillful technical
assistance and Diana Skovgaard for skillful secretarial assistance.
Conflicts of interestThe authors disclose no conflicts.
FundingThe earlier gastrin assay studies upon which the present study is
based have been supported by grants from the Danish MedicalResearch Council, the Danish Cancer Union, and the Lundbeck and
the Novo Nordisk Foundations.



















