Gastrin release: Antrum microdialysis reveals a complex neural control
11
Gastrin release: Antrum microdialysis reveals a complex neural control P. Ericsson a, ⁎, R. Håkanson b , J.F. Rehfeld c , P. Norlén a a Experimental and Clinical Pharmacology, Department of Laboratory Medicine, Lund University Hospital, S-221 85 Lund, Sweden b Drug Target Discovery, Department of Experimental Medical Science, University of Lund BMC A 12, S-221 84 Lund, Sweden c Department of Clinical Biochemistry, Rigshospitalet, University of Copenhagen, DK-2100 Copenhagen, Denmark abstract article info Article history: Received 9 May 2009 Received in revised form 6 October 2009 Accepted 11 January 2010 Available online 18 January 2010 Keywords: Endocrine cells Stomach Rat Vagus Tetrodotoxin Acid blockade Omeprazole We used microdialysis to monitor local gastrin release in response to food, acid blockade and acute vagal excitation. For the first time, gastrin release has been monitored continuously in intact conscious rats in a physiologically relevant experimental setting in a fashion that minimizes confounding systemic effects. Microdialysis probes were placed in the submucosa on either side of the antrum, 3 days before the experiments. The concentration of gastrin in the antral submucosal compartment was about 20 times higher than in the microdialysate and estimated to be 5–10 times higher than in serum regardless of the prandial state. The rats were conscious during microdialysis except when subjected to electrical vagal stimulation. Acid blockade (omeprazole treatment of freely fed rats for 4 days), or bilateral sectioning of the abdominal vagal trunks (fasted, 3 days post-op.), raised the gastrin concentration in blood as well as microdialysate. The high gastrin concentration following omeprazole treatment was not affected by vagotomy. Vagal excitation stimulated the G cells: electrical vagal stimulation and pylorus ligation (fasted rats) raised the gastrin concentration transiently in both serum and microdialysate. Food intake induced a 2- to 3-fold increase in serum gastrin, while gastrin in antral microdialysate increased 10- to 15-fold. In unilaterally vagotomized rats (fasted, 3 days post-op.), food evoked a prompt peak gastrin release followed by a gradual decline on the intact side. On the vagotomized side of the antrum, the peak response seemed to be reduced while the microdialysate gastrin concentration remained elevated. Thus, unilateral vagotomy surprisingly raised the integrated gastrin response to food on the denervated side compared to the intact side, indicating that vagotomy suppresses an inhibitory as well as a stimulating effect on the G cells. While local infusion of atropine was without effect, infusion of the neuronal blocker tetrodotoxin (TTX) (which had no effect on basal gastrin) virtually abolished the food-evoked gastrin response and lowered the high microdialysate gastrin concentration in omeprazole-treated rats by 65%. We conclude that activated gastrin release, unlike basal gastrin release, is highly dependent on a neural input: 1) Vagal excitation has a transient stimulating effect on the G cells. The transient nature of the response suggests that the vagus has not only a prompt stimulatory but also a slow inhibitory effect on gastrin release. 2) Although vagal denervation did not affect the gastrin response to anacidity, the TTX experiments revealed that both food-evoked and anacidity-evoked gastrin release depends on neural input. © 2010 Elsevier B.V. All rights reserved. 1. Introduction Gastrin from G cells in the antrum is the main stimulus of gastric acid secretion. Gastrin stimulates the ECL cells in the oxyntic mucosa [1,2] to mobilize histamine [3,4], which in turn stimulates the parietal cells to produce hydrochloric acid [4–8]. Gastrin is released in response to a variety of food-related stimuli, such as elevated luminal pH [9,10], intraluminal peptides, amino acids and amines [11,12], and distension of the stomach [13–15]. In addition to this, agents released from endocrine cells in the vicinity of the G cells (for example, somatostatin released from D cells) [16–18], as well as hormones reaching the antrum via the circulation [19–21], contribute to the control of gastrin release. Further, G-cell secretion is regulated by the enteric nervous system and the autonomic nervous system (via transmitters such as acetylcholine and gastrin-releasing peptide) [19,22–25]. Gastrin release has been the subject of numerous studies in the past using either in vivo or in vitro techniques. The drawback of the in vivo methods is that it is usually difficult to decide whether the G-cell response reflects a direct effect of the experimental intervention or occurs as a consequence of confounding systemic effects. In vitro methods, such as isolated stomachs [4,19,21,22], antral sheets [26] or isolated G cells [12,25,27,28] are generally thought to allow more direct studies of the G cell. However, in vitro methods are inherently “unphysiological” in that nervous and hormonal circuits that may affect the ability of the G cells to respond to stimuli are not operative. Regulatory Peptides 161 (2010) 22–32 ⁎ Corresponding author. Unit of Diabetes & Celiac Diseases, Department of Clinical Sciences, CRC, Entrance 72, Bldg 91, Floor 10, Malmö University Hospital, S-205 02 Malmö, Sweden. Tel.: +46 40 39 19 03; fax: +46 40 39 19 19. E-mail address: [email protected] (P. Ericsson). 0167-0115/$ – see front matter © 2010 Elsevier B.V. All rights reserved. doi:10.1016/j.regpep.2010.01.004 Contents lists available at ScienceDirect Regulatory Peptides journal homepage: www.elsevier.com/locate/regpep
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Gastrin release: Antrum microdialysis reveals a complex neural control

Regulatory Peptides 161 (2010) 22–32
Contents lists available at ScienceDirect
Regulatory Peptides
j ourna l homepage: www.e lsev ie r.com/ locate / regpep
Gastrin release: Antrum microdialysis reveals a complex neural control
P. Ericsson a,⁎, R. Håkanson b, J.F. Rehfeld c, P. Norlén a
a Experimental and Clinical Pharmacology, Department of Laboratory Medicine, Lund University Hospital, S-221 85 Lund, Swedenb Drug Target Discovery, Department of Experimental Medical Science, University of Lund BMC A 12, S-221 84 Lund, Swedenc Department of Clinical Biochemistry, Rigshospitalet, University of Copenhagen, DK-2100 Copenhagen, Denmark
⁎ Corresponding author. Unit of Diabetes & Celiac DiSciences, CRC, Entrance 72, Bldg 91, Floor 10, MalmöMalmö, Sweden. Tel.: +46 40 39 19 03; fax: +46 40 3
E-mail address: [email protected] (P. Ericsso
0167-0115/$ – see front matter © 2010 Elsevier B.V. Adoi:10.1016/j.regpep.2010.01.004
a b s t r a c t
a r t i c l e i n f oArticle history:Received 9 May 2009Received in revised form 6 October 2009Accepted 11 January 2010Available online 18 January 2010
Keywords:Endocrine cellsStomachRatVagusTetrodotoxinAcid blockadeOmeprazole
We used microdialysis to monitor local gastrin release in response to food, acid blockade and acute vagalexcitation. For the first time, gastrin release has been monitored continuously in intact conscious rats in aphysiologically relevant experimental setting in a fashion that minimizes confounding systemic effects.Microdialysis probes were placed in the submucosa on either side of the antrum, 3 days before theexperiments. The concentration of gastrin in the antral submucosal compartment was about 20 times higherthan in the microdialysate and estimated to be 5–10 times higher than in serum regardless of the prandialstate. The rats were conscious during microdialysis except when subjected to electrical vagal stimulation.Acid blockade (omeprazole treatment of freely fed rats for 4 days), or bilateral sectioning of the abdominalvagal trunks (fasted, 3 days post-op.), raised the gastrin concentration in blood as well as microdialysate. Thehigh gastrin concentration following omeprazole treatment was not affected by vagotomy. Vagal excitationstimulated the G cells: electrical vagal stimulation and pylorus ligation (fasted rats) raised the gastrinconcentration transiently in both serum and microdialysate. Food intake induced a 2- to 3-fold increase inserum gastrin, while gastrin in antral microdialysate increased 10- to 15-fold. In unilaterally vagotomizedrats (fasted, 3 days post-op.), food evoked a prompt peak gastrin release followed by a gradual decline on theintact side. On the vagotomized side of the antrum, the peak response seemed to be reduced while themicrodialysate gastrin concentration remained elevated. Thus, unilateral vagotomy surprisingly raised theintegrated gastrin response to food on the denervated side compared to the intact side, indicating thatvagotomy suppresses an inhibitory as well as a stimulating effect on the G cells. While local infusion ofatropine was without effect, infusion of the neuronal blocker tetrodotoxin (TTX) (which had no effect onbasal gastrin) virtually abolished the food-evoked gastrin response and lowered the high microdialysategastrin concentration in omeprazole-treated rats by 65%. We conclude that activated gastrin release, unlikebasal gastrin release, is highly dependent on a neural input: 1) Vagal excitation has a transient stimulatingeffect on the G cells. The transient nature of the response suggests that the vagus has not only a promptstimulatory but also a slow inhibitory effect on gastrin release. 2) Although vagal denervation did not affectthe gastrin response to anacidity, the TTX experiments revealed that both food-evoked and anacidity-evokedgastrin release depends on neural input.
seases, Department of ClinicalUniversity Hospital, S-205 029 19 19.n).
ll rights reserved.
© 2010 Elsevier B.V. All rights reserved.
1. Introduction
Gastrin from G cells in the antrum is the main stimulus of gastricacid secretion. Gastrin stimulates the ECL cells in the oxyntic mucosa[1,2] to mobilize histamine [3,4], which in turn stimulates the parietalcells to produce hydrochloric acid [4–8]. Gastrin is released in responseto a variety of food-related stimuli, such as elevated luminal pH [9,10],intraluminal peptides, amino acids and amines [11,12], and distensionof the stomach [13–15]. In addition to this, agents released fromendocrine cells in the vicinity of the G cells (for example, somatostatin
released from D cells) [16–18], as well as hormones reaching theantrum via the circulation [19–21], contribute to the control of gastrinrelease. Further, G-cell secretion is regulated by the enteric nervoussystem and the autonomic nervous system (via transmitters such asacetylcholine and gastrin-releasing peptide) [19,22–25].
Gastrin release has been the subject of numerous studies in thepast using either in vivo or in vitro techniques. The drawback of the invivomethods is that it is usually difficult to decide whether the G-cellresponse reflects a direct effect of the experimental intervention oroccurs as a consequence of confounding systemic effects. In vitromethods, such as isolated stomachs [4,19,21,22], antral sheets [26] orisolated G cells [12,25,27,28] are generally thought to allow moredirect studies of the G cell. However, in vitro methods are inherently“unphysiological” in that nervous and hormonal circuits that mayaffect the ability of the G cells to respond to stimuli are not operative.

23P. Ericsson et al. / Regulatory Peptides 161 (2010) 22–32
The method of microdialysis was first applied to the rat gastricsubmucosa by Bunnett et al. [29]. By using a similar approach, we havedeveloped a protocol for the study of histamine mobilization from theECL cells in the acid-producing part of the rat stomach with the use ofmicrodialysis probes placed in the gastric submucosa [30–32]. Theadvantage of the microdialysis technique, as compared to measuringcirculating concentrations of a substance, lies in the fact that themicrodialysis probe operates as an artificial blood vessel. This allowsthe continuous monitoring of substances in the extracellular fluid intissues of intact conscious animals [33,34]. Also, by reverse micro-dialysis agents can be delivered locally in the gastric submucosa viathe probe, enabling stimulation or inhibition of the target cells withless risk of causing systemic effects [35]. Hence, the microdialysistechnique has the advantage over in vitro methods and over other invivo methods in that specific cell populations can be studied in wholeanimals under physiologically relevant experimental conditions. Theusefulness of the microdialysis technique is limited mainly by thesensitivity of the monitoring assay and the ability of compounds topass the dialysis membrane.
Measurement of gastrin in serum following different kinds ofexperimental manipulations is a conventional approach to monitorgastrin release in vivo. However, these manipulations may interferewith the activity of the G cells. For instance, effects on acid secretion,on the central and peripheral nervous systems or on endocrine cellsother than G cells may influence the G cells in an indirect manner,complicating the interpretation of the results. Another complicatingfactor in the in vivo situation is that following its release, gastrin ispromptly being distributed, and diluted, in the blood stream, makingit difficult to achieve precision in monitoring the process of gastrinrelease by measuring the serum gastrin concentration. The vascularlyperfused rat stomach is an alternative experimental model, whichreduces the impact of confounding systemic factors and makes itpossible to monitor (even control) luminal acidity. However, there areproblems: 1) The stomach is not in continuity with the remainder ofthe digestive tract. 2) Circulation ismaintained artificially by perfusionwith a salt solution. 3) All inputs from extra-gastric neurocrine andendocrine systems have been eliminated.
The present study addresses the control of gastrin release from theG cells in the antrum. The primary purpose was to develop a protocolfor studying gastrin release in intact, conscious rats in physiologicallyrelevant experimental settings by the use of antral submucosalmicrodialysis and to compare measurement of gastrin in blood andmicrodialysate following a series of treatments assumed to influencegastrin release. The secondary purpose of the study was to explore thesignificance of nervous control of the G cells in relation to basal andstimulated gastrin release.
2. Materials and methods
2.1. Ethical approval
The studies were approved by the local AnimalWelfare Committeeof Lund/Malmö.
2.2. Chemicals
The proton pump inhibitor omeprazole was a gift from AstraZe-neca (Mölndal, Sweden). Omeprazole was dissolved in 0.25%Methocel (methyl cellulose) (Dow Corning, Midland, MI, USA) andadministered once daily (400 μmol kg−1 day−1) between 7:00 and9:00 a.m. for 4 days by oral gavage. This treatment is known to blockacid secretion [36]. The last dose was administered in the morning onthe day of the experiment. Saline (0.9% NaCl) was used for perfusionvia the microdialysis probes.
Tetrodotoxin (TTX) (Alomone Labs, Jerusalem, Israel), a drugknown to block nervous conductance [37], and atropine sulphate
(Sigma, St. Louis, MO, USA), a muscarinic receptor blocker, weredissolved in saline for perfusion via the microdialysis probe.
2.3. Animals
130 male and 11 female (as specified) Sprague–Dawley rats (250–300 g)were kept at a 12-h light and12-h dark cycle in plastic cages (2–3 in each cage) with free access to standard rat food pellets (B & KUniversal, Sollentuna, Sweden) and tap water. When the rats were tobe fasted, theywere housed in individualwiremeshbottomcageswithfree access to water overnight for 24 h before the experiments. Inexperiments involving refeeding they were offered standard ratpellets and tap water for 3 h. Microdialysis experiments wereperformed on conscious animals, except those experiments thatinvolved electrical vagal stimulation (see below). During sampling ofmicrodialysate they were kept in Bollman-type restraining cages.Starting 1 week prior to the experiments the rats were familiarizedwith the Bollman cages by daily training for 1–2 h. Food andwaterwasavailable during the training sessions. Blood samples formeasurementof gastrin in serum were drawn from the tip of the tail, usually duringthe equilibration period (just before the start of microdialysatesampling) and at the termination of each experiment (after collectingthe last microdialysate sample). Each rat was killed by exsanguinationfrom the abdominal aorta following an overdose of chloral hydrateintraperitoneally.
2.4. Surgery
2.4.1. AnaesthesiaIf not otherwise stated, surgery, including implantation of the
microdialysis probe (see below), was performed under chloralhydrate anaesthesia (300 mg kg−1 intraperitoneally), 3 days prior tothe microdialysis experiments. Surgery was performed on freely fedrats. Buprenorphine (Temgesic®, Schering-Plough, NJ, USA) wasgiven subcutaneously (0.02 mg kg−1) at the time of surgery toalleviate postoperative pain. No mortality was associated with thesurgery. No antibiotics were used. Experiments involving electricalstimulation of the vagus (see Experimental design) were performedon rats anaesthetized with fluanisone/fentanyl/midazolam (15/0.5/7.5 mg kg−1, intraperitoneally), since this anaesthesia has lessinhibitory effect on gastric endocrine cells than chloral hydrate [31].
2.4.2. Unilateral vagal denervationUnilateral vagotomy was performed by opening the abdominal
cavity by a midline incision and by exposing the ventral vagus nervealong the oesophagus below the diaphragmbefore cutting it as close aspossible to the stomach. The dorsal vagus nervewas left intact. The ratswere fitted with microdialysis probes at the same time (see below).
2.4.3. Bilateral vagal denervationTotal abdominal vagotomy was achieved by cutting both vagal
trunks immediately below the diaphragm. A pyloroplasty wasperformed at the same time to prevent gastric dilation [38], and therats were also fitted withmicrodialysis probes in the dorsal part of theantrum (see below). We have shown previously that pre- and post-prandial serum gastrin concentrations in rats subjected to pylor-oplasty do not differ from unoperated rats [39]. The effectiveness ofthe bilateral vagal denervation was verified by hypergastrinemia inthe fasted state at the time of the experiment, usually 3 days aftersurgery (132±36 pmol l−1, n=5, as compared to 15±2 pmol l−1,n=16, in fasted intact rats).
2.4.4. Pylorus ligationThe surgical procedure of acute pylorus ligation in conscious rats
has been described in detail previously [40]. In short, each rat (freelyfed) was fitted with a microdialysis probe on the dorsal side of the

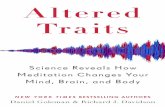
Fig. 1. Histological analysis of antrum with microdialysis probe. Transverse section(12 µm thick) of the antral wall (stained with haematoxylin and erythrosin), showingmucosa (m), microdialysis probe (p) in the submucosa (sm), and muscularis externa(muscle). Bar=200 µm. Implantation of the probe is known to cause tissue damage andan inflammatory response in the stomach wall [32]. Indeed, histological analysisrevealed inflammatory cells around the probe and mild oedema in the submucosa. Themucosa was 360±20 (SEM) µm in thickness (n=10).The distance between theuppermost part of the probe and the basal part of the mucosa, where most of the G cellsare located, was found to be 255±20 µm. The probe (diameter 570 µm) resembles alarge blood vessel. On the basis of themicroanatomy, we suggest that themicrodialysategastrin concentration reflects the gastrin concentration in the extracellular compart-ment of the submucosa (and mucosa) of the antrum.
24 P. Ericsson et al. / Regulatory Peptides 161 (2010) 22–32
stomach (see below). A loose-fitting loop (noose) of silk thread wasplaced around the pylorus. The ends of the thread were passedthrough a plastic catheter that exited in the neck. By pulling the endsof the thread the loop tightens around the pylorus (no anaesthesia),ligating the pylorus without disturbing the rat. Ligation was applied3 days after surgery (fastedmale rats) andmaintained until the animalswere killed 4 h later. Gastric juice was collected at necropsy and itsvolume determined (11±3 ml, n=6), to verify that the ligation wassuccessful.
2.5. Microdialysis
2.5.1. Implantation of the microdialysis probeFlexible microdialysis probes (MAB3.35.4, AgnTho's AB, Stockholm,
length 4 mm, outer diameter 0.57 mm, 35 kDa cut-off) were used. Theabdomen of the anaesthetized rat was opened by a midline incision. Theserosa and the muscle layers of the dorsal or the ventral aspect (at timesboth)of the antrumwere tangentially puncturedbyaneedle (22G)andatunnel (5–8 mmlong)wasmade in the submucosal layer. Theorientationof the tunnel was from the border between corpus and antrum towardsthe pylorus, ending 1–2 mm proximally to the sphincter. In 6 rats,microdialysis probes were also implanted in the ventral aspect of thecorpus. The orientation of the tunnel was from mid corpus towards theborder between the corpus and the antrum, ending 5–10 mmproximallyto the antrum. Themicrodialysis probewas then inserted into the tunneland kept in placewith sutures at the tunnel entrance. The inlet and outlettubes were passed through the abdominal opening and tunnelled underthe skin to a point at the nape of the neck where they were affixed withsutures. The time needed to implant probes was less than 20 min.Immediately upon recovery from the anaesthesia (less than 1 h), the ratswere returned to their cage and given free access to food and water. Thebody weight was not affected by the surgery. In some cases food waswithheld on the third night after surgery in preparation for experimentsthat involved fasted rats.
2.5.2. Sampling of microdialysate and bloodMicrodialysate was sampled 3 days after implantation of the
microdialysis probe [32]. At this stage the rats had been fasted overnight(if not otherwise stated). All ratswere consciousduring the experimentsexcept those that were subjected to electrical vagal stimulation. Theinlet tube was connected to a microinfusion pump (Model 361, SageInstrument, ATI Orion, Boston, USA) and the outlet was allowed to draininto 300 μl polyethylene vials. Perfusion of the microdialysis probeswith 0.9% saline (1.2 μl min−1) started at 7 a.m. After a 40 minequilibration period, collection of microdialysate commenced (seebelow). Basal samples were collected for 2 h before start of refeedingor stimulation (if not otherwise stated). Sampling started 3 min (thetime needed for the perfusion medium to travel from the microdialysismembrane to the outlet of the probe) after start of food intake orstimulation. Food and water was made available in the Bollman cage.The amount of food ingested wasmeasured in each case (food availableat the start of the experimentminus the amount of food remainingat theend). In order to compare the gastrin concentration in serumwith thatof the microdialysate, blood was drawn (200 µl) from the tip of the tail,usually once during the equilibration period and once after collectingthe lastmicrodialysate sample, if not otherwise stated. Each rat andeachprobe was used once only. The position of the probe in the submucosawas verified at autopsy. Microdialysate and serum samples were storedat−20 °C until measurement of gastrin.
2.5.3. Determination of microdialysate equilibration periodThe length of the equilibration period was determined in an
experiment in which microdialysate samples were collected every30 min for 3 h after start of perfusion. In the 6 rats that were tested thebaseline concentration of gastrin in the microdialysate was found tobecome stable within 30 min (not shown).
2.5.4. Reverse microdialysisThe microdialysis technique allows local administration of bioac-
tive agents in the gastric submucosa with reduced risk of inducingconfounding systemic effects [35]. In short, by perfusing the probewith a solution containing the agent, the agent will diffuse into thetissue surrounding the microdialysis membrane. Tetrodotoxin (TTX)was administered by reversemicrodialysis at concentrations from 1 to100 µmol l−1 [41,42]. Also, atropine was administered by reversemicrodialysis (0.1 or 1 mmol l−1). The concentration to be used wasdetermined in a separate experiment where 4 rats were consecutivelyperfused with 0.01, 0.1, 1 or 10 mmol l−1 (for 30 min at eachconcentration) of atropine via the microdialysis probes. Systemiceffects of atropine are manifested by pupil dilation [43]. Pupil dilation(1 mm) was seen at 10 mmol l−1 of atropine, but not at 0.01 to1 mmol l−1: Therefore, higher doses than 1 mmol l−1 were not usedin subsequent experiments.
2.6. Histological analysis of probe-carrying antral wall
Specimens of the antral wall (5×5 mm) were collected (3 days afterimplantation of microdialysis probe) from the area surrounding themicrodialysis membrane and fixed by immersion in 4% formaldehyde(1 h). After rinsing in sucrose-enriched buffer (15%, w/v) for 72 h, thespecimens were frozen in Tissue-Tek® O.C.T. (optimal cutting temper-ature) embedding medium and sectioned in a cryostat. Sections (10–12 μm)were cut perpendicularly to the probe and thawed onto gelatine-coated glass slides. The sections were stained with haematoxylin anderythrosine before being mounted in Kaiser´s glycerol gelatine. Theprobe was invariably found to be positioned in the submucosa and thedistancebetween theprobeand thebaseof themucosawas255±20 µm(n=5). A typical picture is shown in Fig. 1. Introduction of themicrodialysis probe in the gastric submucosa is associated with sometissue damage and a reactive inflammatory response. The histological

25P. Ericsson et al. / Regulatory Peptides 161 (2010) 22–32
analysis revealed invasionof inflammatory cells around and into thewallof the probe, and mild oedema in the submucosa.
2.7. Experimental design
2.7.1. RefeedingRats fittedwithmicrodialysis probes in the antrumwere deprived of
food for 24 h and then given free access to food (standard rat pellets)andwater after collection of basalmicrodialysate for 2 h.Microdialysatesamples were collected every 20 min during the first hour of refeedingand then every h. The effect of food intake was assessed: 1) in male ratsfitted with microdialysis probes on both the ventral and the dorsalaspect of the antrum(8 rats), 2) in female ratsfittedwith amicrodialysisprobe on the dorsal aspect of the antrum (7 rats), 3) in male rats thatwere subjected to unilateral vagotomy (ventral side) fitted with probeson both the intact and the vagotomized side of the stomach (18 rats), 4)inmale rats fittedwithmicrodialysis probes on both the ventral and thedorsal aspect of the antrum, receiving TTX (1, 10 or 100 µmol l−1) (17rats) or atropine (0.1 or 1 mmol l−1) (10 rats) via the ventral probe. Inaddition, the contribution of local neurons to gastrin release in responseto elevated luminal pH was assessed in omeprazole-treated (4 daystreatment) female rats fitted with microdialysis probes on both theventral and the dorsal aspect of the antrum, receiving TTX (100 µmol l−1)(5 rats) via the ventral probe. Perfusion with TTX or atropine started 1 hprior to start of refeeding and continued throughout the experiment.Blood sampleswere collected 1.5 h before and 3 h after start of refeeding.At termination of the experiments the stomach contents were collectedand weighed. In order to monitor the serum gastrin response to foodintake, serum was sampled repeatedly from two sets of male rats(equipped with single dummy microdialysis probes) (12 rats) duringfood intake: at 1 h before and 0, 20, 60 min, 2 h and 3 h after start ofrefeeding.
2.7.2. Recovery of gastrinIn vitro recovery: The in vitro recovery of gastrin was calculated
by placing microdialysis probes (n=10) in vials containing serum(37 °C): 1) from omeprazole treated rats with a gastrin concentration of480 pmol l−1, or 2) from normal fasted rats, but with synthetic ratgastrin-17 added up to a final concentration of 35 nmol l−1. The probeswere perfused with 0.9% saline (1.2 μl min−1). The gastrin concentra-tion in theperfusatewasdetermined and the recovery of gastrin (%)wascalculated. The in vitro recovery of gastrin ranged from 4.8±0.9% to5.2±0.7%.
Recovery from corpus and antrum: In 6 omeprazole-treated ratswithintact vagal innervations, microdialysis probes were implanted bothin the antrum and the corpus. Three days later, blood samples(from the tail) and microdialysate samples (1 h) were collected. Thegastrin concentrations in microdialysate from the corpus and antrumwere 10±1 pmol l−1 and 136±30 pmol l−1, respectively. Thecorresponding serum gastrin concentration was 295±30 pmol l−1.Assuming that the microdialysis recovery of gastrin from the corpusand antrum is similar to the in vitro recovery (5%), it can be concludedthat the gastrin concentration in the extracellular space of thesubmucosal compartment of the corpus is in the same range as inserum, while the gastrin concentration in the submucosal compart-ment of the antrum is about 10-fold higher than in serum.
2.7.3. Vagal activation by pylorus ligation and electrical vagal stimulationPylorus ligation is known to cause vagal stimulation [44]. Basal
microdialysate samples were collected for 2 h before the ligation(performed in 6 conscious fastedmale rats as described under Surgery).Microdialysate samples were collected every 20 min during the firsthour of stimulation and then every hour. Blood samples were collected1.5 h before and 3 h after applying the ligature. Electrical vagalstimulation was performed in anaesthetized male rats (see Anaesthe-sia). The rats (fasted for 24 h) had a microdialysis probe implanted on
the ventral side of the antrum andwere kept on a warm surface (37 °C)during the experiment. The abdomenwas opened and the ventral vagusgently exposed. Thirty minutes later collection of basal microdialysatesamples commenced. The ventral vagus was stimulated electrically bymeans of a pair of platinum electrodes (diameter 0.25 mm, distancebetween electrodes 2 mm). A Grass stimulator (S48 stimulator, Astro-Med. Inc., W Warwick, RI, USA) was used to generate 1 ms impulses of5 V at 1 Hz (9 rats), 5 Hz (10 rats) or 20 Hz (7 rats). After 2 h of basalsampling of microdialysate, the electrical stimulation started. Sampleswere collected every 20 min during the electrical stimulation (1 h).Blood samples were collected 30 min before and 15 min afterstimulation. In one experiment, rats were fitted with microdialysisprobes on both sides of the antrum (n=3). Three days later, the rats(fasted state) were anaesthetized and the abdomen was opened. Theanterior vagus was stimulated (5 Hz, 1 h) and microdialysate wascollected from both sides.
2.8. Measurement of gastrin
We applied two different radioimmunoassays (RIAs) to measuregastrin, using two different antisera. The sensitivity of the conven-tional RIA used to measure serum gastrin was not high enough topermit the measurement of gastrin in the microdialysate in a reliableway. This made it necessary to develop an alternative, more sensitiveRIA for this particular purpose. Details are given below.
2.8.1. Microdialysate gastrinGastrin in themicrodialysatewasmeasuredbyaRIAusingantiserum
no. 92132/5 with rat gastrin-17 as standard and monoiodinated 125I-gastrin-17 as tracer [45]. The antiserum was raised in a white Danishrabbit (no. 92132) against a gastrin analog corresponding to O-sulfatedcholecystokinin (CCK)-10 extended at the N-terminus with a diglycinebridge directionally coupled to bovine serum albumin (BSA) [46]. Theantiserum recognizes the bioactive C-terminal pentapeptide amidecommon to gastrin and CCK, but displays an affinity for sulfated gastrin-17which is 8.4 times higher than the affinity for sulfated CCK-8 [46]. Theaffinity (expressed by the “effective” equilibriumconstant, K0
eff [47]) forgastrin-17 (both sulphated and unsulphated) displayed by theantiserum was 32.6×1012 l mol−1 [46]. Since CCK peptides so farhave not been found in the mammalian antrum [48,49], the cross-reactivity with CCK is without significance for the specificity of thegastrin measurements in the antral microdialysate. This premise wasfurther corroborated in the present study by direct control measure-ments in rat antral extracts using an entirely specific CCK assay based onantiserum92128 [46]. Gel chromatographyonSephadexG-50 superfinecolumns of rat antral extracts showed that the present gastrin-assaybased on antiserum no. 92132 measured rat gastrin-34 and gastrin-17with equimolar potency. Antiserum 92132 was diluted 1:700 000,resulting in 35% tracer binding. Barbital buffer (pH 8.5), containing0.025% NaN3, 0.25% BSA and 0.25% EDTA, was used for all dilutions.
For measurement of microdialysate gastrin the procedure was asfollows: Standard samples (15 µl, containing different concentrationsof gastrin) and microdialysate samples (15 µl) were incubated withthe antiserum (200 µl) in polyethylene vials for 4 days (+4 °C). Afteradding tracer (50 µl), the samples were incubated for another 24 h(+4 °C). After the second incubationperiod goat anti rabbitγ-globulin(GAR) was added (250 µl, 2.5% GAR, 5% polyethylene glycol, PEG)together with normal rabbit serum (NRS) (50 µl, 1% NRS, 5% PEG) toseparate bound tracer from free. After 2 h of incubation (+4 °C) withGAR and NRS, barbital buffer (150 µl) was added to each test tube andthe sampleswere centrifuged. After decantation of the supernatant theradioactivity of the sedimented bound tracer was counted in a gammacounter. Gastrin concentrations in themicrodialysate are expressed aspicomole equivalents of rat gastrin-17 per liter.
The gastrin assaywas evaluatedwith respect to detection limit andintra- and interassay precision. The evaluation was performed as

Fig. 2. Correlation between the gastrin concentration in serum andmicrodialysate. Basalgastrin concentration in serum and microdialysate in male rats (fasted for 24 h) withintact vagal innervation (○) (n=8) or subjected to total abdominal vagotomy (VT)(●) (n=5), and in omeprazole-treated male rats with intact vagal innervation(Δ) (n=6) or subjected to VT (▲) (n=5). The microdialysate gastrin concentrationwas well correlated to the serum gastrin concentration (r2=0.71, p<0.001). Assumingthat the in vivo recovery is similar to the in vitro recovery (5%), the gastrin concentrationof the antral submucosal compartment is 5–10 times higher than the serum gastrinconcentration. Blood was drawn from the tail immediately before sampling ofmicrodialysate. Microdialysate was sampled for 1 h. Mean values±SEM (vertical andhorizontal bars). Correlation between serum and microdialysate gastrin concentrationswas determined using Pearson correlation calculations.
26 P. Ericsson et al. / Regulatory Peptides 161 (2010) 22–32
follows: Intraassay precision: The gastrin concentration was measuredten times within the same assay run in three microdialysate samplescontaining low, medium and high gastrin concentration, respectively.The coefficient of variation for the intraassay precision ranged from6.2to 7.7%. Interassay precision: The reproducibility of the estimationswasassessed by five replicate measurements of ten different microdialy-sate samples during a period of two months. The coefficient ofvariation for the interassay precision ranged from 2.7 to 13.2%. De-tection limit: The detection limit was defined as the gastrin concen-tration corresponding to two SD below the mean binding at a gastrinconcentration of zero pmol/l. The calculated minimal detectableamount was 23 amol (i.e. 15 µl microdialysate with a concentrationof 1.5 pmol l−1) in the assay set-up of this study. The sensitivity of thisassay was approximately 5 times higher than the sensitivity of theconventional RIA used to measure serum gastrin (see below).
2.8.2. Serum gastrinThe concentration of gastrin in serumwas measured by a RIA using
antiserum no. 2604 [50] with rat gastrin-17 as standard andmonoiodinated 125I-gastrin-17 as tracer [45]. Antiserum 2604 wasraised against the 2-17 fragment of gastrin-17 and is specific for thebioactive C-terminal octapeptide amide. It binds gastrin-34 and gastrin-17with the same potency, irrespective of the degree of O-sulfation, andit displays no crossreactivity with CCK. The affinity (expressed by the“effective” equilibrium constant, K0
eff [47]) for gastrin-17 (bothsulphated and unsulphated) displayed by the antiserum was1.1×1012 l mol−1 [50]. Interestingly, the affinity for antiserum no.92132 was 30 times higher than for antiserum no. 2604 (see Section2.8.1). The serum gastrin concentrationwasmeasured in 50 µl of serumand expressed as picomole equivalents of rat gastrin-17 per liter. Thereliabilityparameters, including the intraassayand interassayprecisionshave been reported before [51]. In our hands, the minimum detectableamount in the assay tubes was 115 amol.
2.9. Statistics
Results are expressed as mean value±SEM. The integrated gastrinresponses are presented as the rise inmicrodialysate gastrin over basalconcentrations during the period of activation (electrical stimulationand refeeding). Statistical significancewas determined using Student'st test, or by one way analysis of variance (ANOVA) followed byBonferroni's or Dunnett's multiple comparison test. p<0.05 (*) wasconsidered significant. Correlation between serum andmicrodialysategastrin concentrations (Fig. 2) was assessed using Pearson correlationcalculations. Statistics, concentration–response curves and graphswere calculated/constructed using the GraphPad PRISM program(version 3.00, GraphPad Software, San Diego, CA, USA).
3. Results
3.1. Gastrin in serum and microdialysate
Gastrin was measured in serum and microdialysate collected fromthe same fasted or omeprazole-treated male rats with or without intactvagal innervation. The microdialysate gastrin concentration was wellcorrelated to the serum gastrin concentration (Fig. 2) (r2=0.71,p<0.001). The gastrin concentration in fasted rats with intact vagalinnervationwas 14±1.6 pmol l−1 and 5.2±0.9 pmol l−1 in serum andantral microdialysate, respectively (n=8). It should be noted that theactual gastrin concentration in the antral submucosal compartment canbe expected to be 20 times higher than the concentration in themicrodialysate (the recovery of gastrin being 5%), i.e. the gastrin con-centration in the antral submucosal compartment is estimated to bealmost 10 times higher than the concentration of gastrin in serum. Infasted rats subjected to unilateral vagotomy the gastrin concentrationwas 12±1.3 pmol l−1 in serum and 3.5±1.0 pmol l−1 in antral
microdialysate (denervated side) (n=4). The gastrin concentration inboth serum andmicrodialysatewas raised bybilateral vagotomy (3daysbefore) to 132±36 pmol l−1 and 29±2.9 pmol l−1 (n=5), respective-ly, and by omeprazole treatment to 342±75 pmol l−1 and 212±69 pmol l−1 (n=6), respectively. When omeprazole treatment wascombinedwithbilateral vagotomy, the serumandmicrodialysate gastrinconcentrations were 331±65 pmol l−1 and 239±40 pmol l−1, respec-tively (n=5), in fact quite similar to what was seen after omeprazoletreatment alone in intact rats.
3.2. Gastrin release in response to refeeding
The experiment was performed in fasted male and female rats(Fig. 3A) equipped with probes on either side of the antrum (Fig. 3B).All rats started to eat immediately after receiving food, resulting in aprompt increase in the microdialysate gastrin concentration. Theresponse peaked during the first hour with a 15-fold increase in malerats (6.3±2 pmol l−1 versus 96±19 pmol l−1) and 8-fold in femalerats (3±0.9 pmol l−1 versus 26±4.5 pmol l−1) (Fig. 3A, B), whichwas followed by a gradual decline. The gastrin response was similaron either side of the stomach (Fig. 3A). Upon termination of theexperiments (3 h), the concentration of gastrin in the microdialysateremained 2 to 3-fold above the basal concentration in both male andfemale rats. At this time point, the corresponding gastrin concentra-tions in serum were elevated 2-fold in the male rats (17±2 pmol l−1
versus 38±6 pmol l−1) (n=8) and by 50% in the female rats (19±1 pmol l−1 versus 30±3 pmol l−1) (n=7). Male rats consumedmore food than did female rats. At the end of the experiment thestomach content weighed 7.3±0.8 g in male versus 4.7±0.7 g infemale rats (p<0.05). The serum gastrin concentration was increased3-fold 20 and 60 min after food intake in both groups of rats; 3 h afterstart of feeding the serum gastrin concentration was still twice that ofthe basal level (Fig. 3C).
3.3. Gastrin release in response to pylorus ligation
Ligation of the pylorus in conscious fasted male rats raised themicrodialysate gastrin concentration; it peaked within 20–40 min

Fig. 3. Effects of food intake on gastrin mobilization. The gastrin concentration inmicrodialysate in response to food in fastedmale (A) (n=8) and female (B) (n=6) ratsequipped with microdialysis probes on the ventral (○) and dorsal (●) sides of theantrum. Access to food is indicated. Microdialysate samples were collected simulta-neously from both sides of the antrum (male rats). There was no difference between thesides. The peak gastrin response was elevated 15 times over basal (male rats). Male andfemale rats differed in that the microdialysate gastrin concentration was higher in themale rats. The differencemay reflect the fact that male rats eat more than female rats. Atthe end of the experiments the stomach content weighed 7±0.8 g (male rats) and 5±0.7 g (female rats) (p<0.05). The serum gastrin response to food was assessed in fastedmale rats (C) (n=12) (these rats were equipped with dummy microdialysis probes).The blood samples were collected during food intake: at −1 h, and 0, 20, 60 min, 2 hand 3 h after start of refeeding. The peak gastrin response was 3 times over basal. At theend of this experiment the stomach content weighed 8±0.6 g. Mean values±SEM.Statistical significance was assessed by ANOVA, followed by Dunnett's multiplecomparison test (*p<0.05, ***p<0.001). Fig. 4. Gastrin mobilization in response to pylorus ligation. Gastrin was monitored in
microdialysate in response to pylorus ligation (fasted male rats) as indicated.Microdialysis probes were placed on the dorsal side of the antrum 3 days beforeligation (n=6). The pylorus was ligated at time zero and the ligation was maintainedfor 4 h (no anaesthesia). Serum gastrin concentration was determined before (18±2 pmol l-1) and after collection of the microdialysate samples (28±4 pmol l-1). Meanvalues±SEM. The rise in microdialysate gastrin 20 min after ligation (6-fold elevation)was statistically significant. Statistical significance was assessed by ANOVA, followed byDunnett's multiple comparison test (*p<0.05).
27P. Ericsson et al. / Regulatory Peptides 161 (2010) 22–32
(6-fold increase) but started the return towards basal levels within 1 h(Fig. 4). Four hours after pylorus ligation the serum gastrin concentra-tion was still higher than before ligation (28±4 pmol l−1 versus 18±2 pmol l−1, n=6, p<0.05).
3.4. Gastrin release in response to electrical vagal stimulation
Electrical stimulation (1 Hz, 5 Hz and 20 Hz for 1 h) of the ventralvagus nerve in fasted anaesthetized rats caused a prompt 3- to 10-foldincrease in themicrodialysate gastrin concentration on the stimulatedside (Fig. 5A). At 15 min after start of stimulation, the serum gastrinconcentration had increased 2- to 4-fold (Fig. 5B). In one pilotexperiment of 3 rats, gastrin in the microdialysate was monitored onboth sides following electrical stimulation (5 Hz, 1 h) of the ventralvagus. The gastrin concentration increased on both sides (Fig. 5C).
3.5. Gastrin release in response to refeeding inunilaterally vagotomized rats
The experiments were performed on fasted male rats which hadbeen subjected to unilateral ventral vagotomy 3 days earlier. Unilateralvagotomy per se had no effect on the basal microdialysate gastrinconcentration on either side of the antrum. Intake of food raised themicrodialysate gastrin concentration on the intact side of the antrum(10-fold increase within 20–40 min), after which it declined to reach aplateau at a level 4-fold above the basal concentration (Fig. 6A). Thepeak increase in microdialysate gastrin was similar on the vagotomizedside of the antrum. After the peak (12-fold increase), the gastrinconcentrations stayed at a plateau 10-fold above basal (Fig. 6A). As aconsequence, the integrated gastrin response was more than 2-foldhigher on the vagotomized side than on the intact side (p<0.05)(Fig. 6B). Following food intake in unilaterally vagotomized rats, theserum gastrin concentration increased from 18±2 pmol l−1 (basal) to45±5 pmol l−1 (3 h after start of feeding) (p<0.001), an increasesimilar to that seen in intact rats (Fig. 3C).
3.6. The effect of atropine on food-evoked gastrin release
The experiment was performed in fasted male rats fitted with oneprobe on the ventral and another on the dorsal side of the antrum.Infusion of atropine (0.1 or 1 mmol l−1, starting 1 h prior to foodintake) via the ventral probe did not affect the gastrin response to foodintake, as compared to the dorsal, control side receiving saline (Fig. 7).The serum gastrin concentration (rats treated with 1 mmol l−1)increased from 16±2 pmol l−1 (basal) to 28±4 pmol l−1 (3 h afterstart of feeding) (n=5) (p<0.05).

Fig. 5. Gastrin mobilization in response to electrical vagal stimulation. Gastrin inmicrodialysate (A, C) and serum (B) in response to electrical stimulation of the ventralvagus nerve (as indicated) in anaesthetized, fasted male rats. The vagus nerve wasstimulatedwith 1 ms impulses of 5 V (A, B) at 1 Hz (▲) (n=9), 5 Hz (○) (n=10) or 20 Hz(▼) (n=7), and (C) at 5 Hz (n=3, (○) for ventral and (●) for dorsal sides of the antrum).The serum gastrin concentrations shown in B were determined 30 min before (□) and15 minafter (■) start of theelectrical vagal stimulation (as indicatedby the symbols belowdiagram A). Mean values±SEM. Statistical significance was assessed by Student´s t test orby ANOVA, followed by Dunnett's multiple comparison test (*p<0.05).
Fig. 6. Gastrin mobilization in response to food intake in rats subjected to unilateralvagotomy.Gastrin wasmonitored inmicrodialysate (A) in response to food in fastedmalerats, 3 days after unilateral (ventral) vagotomy; the rats were equippedwithmicrodialysisprobes on the ventral/vagotomized (○) as well as on the dorsal/intact (●) side of theantrum. Access to food is indicated.Microdialysate sampleswere collected fromboth sidesof the antrum (n=18). The serum gastrin concentration was determined once during theequilibration period (just before start of sampling of microdialysate) (18±2 pmol l−1)and at termination of the experiment (after collection of the last microdialysate samples)(45±5 pmol l−1) (n=12). At the end of the experiment the content of the stomachweighed 6±0.8 g. B shows the integrated microdialysate gastrin output on the intact sideand on the vagotomized side during 3 h of refeeding. Mean values±SEM. Statisticalsignificance was assessed by Student's t test (*p<0.05).
28 P. Ericsson et al. / Regulatory Peptides 161 (2010) 22–32
3.7. The effect of TTX on gastrin release
Local infusion of TTX was performed in fasted male rats equippedwith one probe on the ventral and another on the dorsal side (Fig. 8A).Infusion of TTX via the ventral probe started 1 h before food intake.The dorsal probe was used to infuse saline. TTX had no effect on theamount of food ingested (9±1 g at TTX 100 µmol l−1) and no effect on
the basal microdialysate gastrin concentration on either side of theantrum. It did, however, reduce both the peak concentration and theintegrated response to food on the ventral side. Thus, the integratedgastrin response was reduced by 18%, 45% and 83% after infusion of TTXat 1, 10 and 100 µmol l−1, respectively (Fig. 8A, B). The gastrin responseto food was unaffected on the dorsal, untreated side (Fig. 8A, B). Theserumgastrin concentration (rats treatedwith 100 µmol l−1) increasedfrom 14±2 pmol l−1 (basal) to 34±8 pmol l−1 (3 h after start offeeding) (n=5) (p<0.05).
In another experiment, TTX was given by local infusion to rats(female) treated with omeprazole for 4 days and equipped with aprobe on the dorsal side (Fig. 8C). As expected the microdialysategastrin concentration was greatly elevated by omeprazole; localinfusion of TTX (100 µmol l−1) lowered the gastrin concentration inthese rats by 65% (after 1 h) (Fig. 8C).
4. Discussion
Gastrin is released from G cells in response to food-related stimulisuch as elevated luminal pH, distension, and intraluminal amino acidsand amines [9–15,52]. The magnitude of the gastrin response isthought to be affected by signals from paracrine/endocrine as well asneurocrine pathways [15,18,19,22,24,25,52]. The regulation of gastrin

Fig. 7. Gastrin mobilization in response to food intake during local infusion of atropine.Gastrin in microdialysate was monitored in response to food in intact, fasted male ratsequippedwithmicrodialysis probes onboth the ventral (○) and thedorsal (●) sides of theantrum. Access to food is indicated. Local infusion of atropine 1 mmol l−1 (A) (n=5) or0.1 mmol l−1 (B) (n=5)via theventralmicrodialysis probe started1 hbefore start of foodintake and continued throughout the experiment (as indicated). Microdialysate sampleswere collected from both sides of the antrum. In A, the serum gastrin concentration wasdetermined once during the equilibration period (just before start of sampling ofmicrodialysate) (16±2 pmol l−1) and at termination of the experiment (after collectionof the lastmicrodialysate samples) (28±4 pmol l−1) (n=7).At theendof theexperimentthe gastric content weighed 6±1 g. Mean values±SEM Statistical significance wasassessed by ANOVA followed by Bonferroni's multiple comparison test (*p<0.05).
29P. Ericsson et al. / Regulatory Peptides 161 (2010) 22–32
release has been studied extensively in numerous experiments,involving both in vivo and in vitro techniques. However, all thesestudies suffer from the general problems that are associated withconventional in vivo and in vitro methods. Briefly, while conventionalin vivo methods (measuring serum or plasma gastrin) can be used tostudy gastrin release in intact animals, the limitation of this approachlies in the difficulty to monitor changes continuously and todistinguish direct effects on G cells from indirect. The results fromin vivo studies of the effects of injected neurotransmitters on G-cellfunction are difficult to evaluate due to confounding systemic effects.In vitro methods, on the other hand, are compromised by the factthat they are highly artificial and likely to provide a distorted andpotentially misleading view of any physiological process under study.
4.1. Microdialysis in examination of gastrin release
In the present study we have developed a microdialysis proceduretomonitor the concentration of gastrin in the extracellular fluid and to
introduce substances locally into the antral submucosa (reversemicrodialysis) of conscious rats. Implantation of the microdialysisprobe in the gastric submucosa will result in some tissue damage andan inflammatory reaction. However, the histological analysis revealedonly amild inflammatory responsewith invasion of inflammatory cellsaround the probe membrane and mild oedema in the submucosa. Tobe able to translate the gastrin concentration in the microdialysate tothe gastrin concentration in the submucosal compartment, therecovery of gastrin in the microdialysate had to be determined. Therecovery was found to be approximately 5%. The low recovery isthought to reflect the relatively large molecular weight of gastrin:Using a similar setup, the corresponding histamine recovery wasapproximately 50% [30]. Nonetheless, since the in vitro recoverypercentage was independent of the gastrin concentration of themedium, we expect changes observed in microdialysate gastrin toparallel changes in submucosal gastrin.
From the results shown in Fig. 2 it appears that the serum gastrinlevels correlate well to the concentration of gastrin in the micro-dialysate and probably to the gastrin concentration in the extracel-lular compartment of the antral mucosa and submucosa. It has beensuggested that gastrin from the antrum reaches the oxyntic mucosavia a microcirculatory short cut (i.e. a portal system) [53]. Inomeprazole-treated rats with microdialysis probes implanted inboth antrum and corpus, the gastrin concentration in the micro-dialysate was found to be 14 times higher in antral probes than inprobes in the corpus. Based on the recovery of gastrin (5%), thecalculated gastrin concentration in the extracellular compartment ofthe corpus submucosa of omeprazole-treated rats was quite similar tothat observed in serum. This observation is in line with the view thatgastrin is released from G cells to reach the corpus via the systemiccirculation rather than via a direct route from antrum to corpus: Thegastrin concentration in the corpus would presumably have beenmuch higher than in the circulation if gastrin reached the corpus via adirect route from the antrum.
Food intake induced a great and prompt increase in microdialysategastrin (Fig. 3A, B). In fact, the microdialysate gastrin concentrationpeaked within the first hour with an almost 20-fold increase overbasal, after which it declined to a level about 2- to 3-fold above basal.This corresponds to a 3-fold increase (p<0.001) in circulating gastrinduring the first hour (Fig. 3C). After 3 h, the serum gastrin level wasstill elevated 2-fold over basal (p<0.001) (Fig. 3C). Thus, the food-evoked rise in gastrinwasmuchmore prominent in themicrodialysatethan in the circulation. It seems that rapid changes, including quitesmall changes, can be monitored locally, while they are likely to beblunted in the circulation due to the impact of distribution or dilution.
In female rats the increase in microdialysate gastrin after foodintakewas lower than inmale rats (Fig. 3B). Likewise, the basal gastrinlevels in omeprazole-treated ratswere 3-fold lower in female rats thanin male rats (Fig. 2 versus Fig. 8C). Conceivably, this is a long-termconsequence of the difference in pattern of food consumption in maleversus female rats [54] (see also Results). This difference is manifestedin a smaller number of G cells and in a smaller gastrin response to ameal in females than in males. As can be expected, the difference infeeding pattern is associated with a greater and more rapid weightincrease in male rats.
4.2. Vagal control of gastrin release
The role of the vagus in the regulation of G-cell gastrin release isnot fully understood. Gastrin release has been reported to be eitherstimulated or inhibited by vagal excitation (for reviews see [55,56]).Indeed, there is evidence that central vagal stimulation increasescirculating gastrin [57]; whether this is a direct or an indirect effect onthe G-cells is not known. The G cells are probably not directlyinnervated by vagal fibers [58,59]. Instead, the vagus is thought toexercise indirect control of cells in the mucosa (including endocrine

30 P. Ericsson et al. / Regulatory Peptides 161 (2010) 22–32
cells) through the enteric nervous system [59]. Electrical vagalstimulation is known to stimulate gastrin release [24,40,60,61]. Inthe present study, electrical vagal activation (anaesthetized rats) for1 h raised the microdialysate as well as the circulating gastrinconcentrations at all frequencies tested (1, 5 and 20 Hz). The increasewas 3- to 10-fold in the microdialysate and 2- to 4-fold in serum. Theinterpretation of the results is complicated by the fact that electricalvagal stimulation can be expected to activate both afferent andefferent fibers. Hence, it cannot be excluded that sensory afferentsmay impact on the results as suggested by Nojima et al. [62]. Pylorusligation is said to induce vagal excitation [44,63]. In our experiments,pylorus ligation (conscious rats) resulted in a prompt but transientincrease in themicrodialysate gastrin concentration. In contrast, it haspreviously been reported that pylorus ligation does not affect theserum gastrin concentration [64,65], perhaps simply because it ismore difficult to monitor gastrin release in blood than in micro-dialysate. It is also possible that the discrepancy can be explained by
differences in the experimental setup: In the present study, pylorusligation was applied in rats that were conscious throughout theexperiment, whereas previous studies used rats that were anaesthe-tized during the actual ligation [64,65].
The ventral vagal trunk innervates the ventral side of the acid-producing part of the stomach (corpus), while the dorsal trunkinnervates the dorsal side,with little overlap fromone side to the other[38,66,67]. Bilateral vagal denervation suppresses acid secretion and asexpected causes secondary hypergastrinemia [68,69]. Unilateral vagaldenervation, on the other hand, suppresses acid secretion on thedenervated but not on the intact side [38] and does not affect thecirculating gastrin concentration. These observations were confirmedin the present study as bilateral vagotomy resulted in a 5- to 10-foldincrease in the serum gastrin concentration, which unilateralvagotomy failed to do.
In the antrum, the vagal innervation of the two sides (i.e. theventral and the dorsal side) seems to overlap more than in the acid-producing part of the stomach. Berthoud et al. [70] reported thatelectrical stimulation of the ventral vagal trunk in anaesthetized ratsactivated not only the enteric neurons on the ventral side of theantrum but also one third of the neurons on the dorsal side. This wassupported by our finding that gastrin was released also from the non-stimulated dorsal side of the antrum in response to selective electricalstimulation of the ventral vagus.
Food-evoked gastrin release on the denervated side differedgreatly from that on the innervated side in unilaterally vagotomizedrats. While food intake resulted in an immediate gastrin responsefollowed by a gradual decline on the intact side of the antrum, thegastrin concentration increased and stayed elevated for the durationof the experiment on the vagotomized side. Considering the fact thatacute vagal excitation stimulated gastrin release (as e.g. shown by thegastrin response to pylorus ligation and electrical vagal stimulation),it was quite surprising that the integrated gastrin response to foodwas higher on the vagotomized side. The seemingly paradoxical effectof unilateral vagotomy, illustrated in Fig. 6, can be interpreted tomeanthat a vagally dependent inhibition of the G cells is eliminated by thevagotomy (desinhibition).
Omeprazole is a powerful inhibitor of acid secretion [71], and vagaldenervation suppresses acid secretion [68]. Blockade or suppressionof acid secretion, regardless of cause leads to hypergastrinemia[68,72]. In the present study, the concentration of gastrin in blood aswell as in the antral microdialysate was increased in both omepra-zole-treated rats and bilaterally vagotomized rats. The combination ofbilateral vagal denervation and omeprazole treatmentwas as effectiveas omeprazole treatment alone when it comes to raising themicrodialysate (or serum) gastrin concentration. These observations
Fig. 8. Gastrinmobilization in response to food intake during local infusion of TTX. Gastrinin microdialysate (A) was monitored in response to food intake in intact, fasted male ratsequippedwithmicrodialysis probes on both the ventral (○, Δ) and the dorsal (●) sides ofthe antrum. Access to food is indicated. Local infusion of TTX 0.01 mmol l−1 (○) (n=7)orTTX0.1 mmol l−1 (Δ) (n=6)via the ventralmicrodialysis probe started 1 h before start offood intake and continued throughout the experiment (as indicated). Microdialysatesamples were collected from both sides of the antrum. The serum gastrin concentrationwas determined once during the equilibration period (just before start of sampling ofmicrodialysate) (14±2 pmol l−1 in both groups of rats) and at termination of theexperiment (after collectionof the lastmicrodialysate samples) (37±6 pmol l−1 and34±8 pmol l−1 after 0.01 and 0.1 mmol l−1 of TTX, respectively). At the end of the experimentthe gastric content weighed 9±1 g in rats treated with 0.1 mmol l−1 of TTX. B shows theintegrated microdialysate gastrin response on the TTX-treated, ventral side (at 0, 0.001,0.01 and0.1 mmol l−1 of TTX)andon thenon-treated, dorsal side during3 hof food intake(n=4–8). Gastrin inmicrodialysate (C)wasmonitored in response to local infusionof TTX0.1 mmol l−1 in omeprazole treated female rats (n=5) equipped with microdialysisprobes on the dorsal side of the antrum. Infusion of TTX started at time zero and continuedthroughout the experiment (as indicated).Meanvalues±S.E.M. The statistical significanceof the difference between untreated and TTX-treated sides was assessed by ANOVAfollowedbyBonferroni's (A)multiple comparison test, or by Student's t test (B) (*p<0.05).The statistical significance of the decrease in microdialysate gastrin concentrationfollowing local infusion of TTX in omeprazole-treated rats was assessed by ANOVAfollowed by Dunnett's (C) multiple comparison test (*p<0.05).

31P. Ericsson et al. / Regulatory Peptides 161 (2010) 22–32
are in line with the view that 1) lack of acid in the lumen representsthe main stimulus of gastrin release, 2) that vagotomy does not add tothe omeprazole-induced anacidity, and 3) that the G cells do notdepend on an intact vagal innervation to be able to respond to aprolonged period of achlorhydria.
All in all, the results of our studies of vagal stimulation and vagaldenervation are in line with the following conclusions: 1) there is apartial vagal overlap from one side of the antrum to the other, 2) vagalexcitation causes a prompt stimulation of gastrin release followed byinhibition and 3) the antrum is dependent on an intact vagalinnervation for a normal gastrin response to food intake (but not forthe gastrin response to acid blockade).
4.3. Local neuronal control of gastrin release
Acetylcholine has been put forward as one of the neurotransmit-ters most likely to control G-cell activity [15,73,74]. Interestingly,however, one-sided microinfusion of the muscarinic receptor antag-onist atropine (0.1 or 1 mmol l−1) failed to impair the gastrinresponse to food intake as compared to the non-atropinized side.This observation seems to suggest that local acetylcholine, acting viamuscarinic receptors, is not essential for food-evoked gastrin release.
To further investigate the influence of local neurons (entericneurons) on the G cells, the neuronal conductance blocker TTX wasadministered via the microdialysis probe in order to inactivate localneurons [41,42]. Infusion of TTX had no effect on basal gastrin (and noeffect on basal acid secretion, see Refs. 75,76) but reduced the gastrinresponse to anacidity (omeprazole) and to food in a dose-dependentmanner. The amount of food ingested was not affected by TTX. At thehighest concentration of TTX (100 µmol l−1) the food-evoked gastrinresponse was virtually abolished on the TTX-treated side, while anormal (15-fold) increase was seen on the control side of the antrum.G cells are known to respond, directly or indirectly, to alterations ingastric acidity [9,10,63,71,72] and to food-derived luminal stimulantssuch as amino acids and amines [12,77]. The G cells are of the opentype, and it has been suggested that the stimulatory effect of e.g.dietary constituents is mediated directly on the G cells [28]. However,the failure of food to release gastrin after local administration of TTXsuggests that the gastrin response is mediated by local neurons, or atleast dependent on the permissive action of such neurons. This view isin line with the report that omeprazole-induced gastrin release ismediated by the neuropeptide gastrin-releasing peptide [78]. Indeed,subsequent studies have revealed that also capsaicin-sensitive afferentneurons participate in the control of gastrin release [62]. We concludethat in the basal state, gastrin release is unaffected by neuronal input,while such mechanisms are important for activated gastrin release.
In contrast to the inhibitory effect of TTX, vagotomy failed to lowerfood-evoked gastrin release; the integrated gastrin response actuallybeing increased on the vagotomized side (Fig. 6). Further, TTX andvagotomy differed in their effects on omeprazole-induced gastrinrelease. Local infusion of TTX (100 µmol l−1) promptly lowered themicrodialysate gastrin concentration in omeprazole-treated hyper-gastrinemic rats (by 65%), whereas vagotomy was without effect.Thus, blockade of local neurons seems to inhibit the G cells whereasvagotomy does not. TTX is known to selectively block neuronalconduction [37]. However, it cannot be excluded that TTX impairedthe function of the G cells. In a parallel study we could show that theeffect of gastrin-releasing peptide was unimpaired by local infusionof TTX (100 µmol l−1) (Ericsson et al., unpublished observation),confirming that TTX per se does not impair the function of the G cells.
4.4. Concluding remarks
Themicrodialysis techniquewas found to be useful for the study oflocal gastrin release in conscious rats and to offer advantages overmeasurements of gastrin in serum in that 1) changes in gastrin
concentrations were more prominent in antral microdialysate than inserum, that 2) the technique allows each side of the antrum to serve asa convenient control for the other when studying effects of localstimulation or inhibition, and that 3) the technique allows thecontinuous monitoring of gastrin in intact conscious rats. In fact,antral submucosal microdialysis revealed a complex neural control ofgastrin release. From the results it seems that vagal excitation bringsabout an acute stimulating effect on G cells in the antrum, as indicatedby the gastrin response to electrical vagal stimulation and pylorusligation. This response is followed by a slow and sustained inhibitoryeffect on gastrin release, as illustrated by the surprising finding thatunilateral vagotomy augmented the gastrin response to food on thevagotomized side. Thus, it seems that a vagally dependent inhibition ofthe G cells is eliminated by the vagotomy. However, local administra-tion of TTX abolished the gastrin response to food and lowered themicrodialysate gastrin concentration in omeprazole-treated rats. Wetherefore suggest that the magnitude of the gastrin response to foodand acid blockade depends on a complex interplay between localneurons and the vagus. To some extent, our results confirm, andextend, earlier observations summarized by e.g. Schubert andMakhlouf [52]. However, it is important to note that while our studieswere performed on intact and (in most cases) conscious rats, previousdata are based on either whole body studies that are compromised byconfounding systemic effects, or on in vitro models, which are lesslikely to provide physiologically relevant information.
Acknowledgements
This study was supported by grants from the Påhlsson Foundation,the Åke Wiberg Foundation, the Magnus Bergvall Foundation, theNovo-Nordisk Foundation, Nio Meter Liv, the Swedish Society ofMedical Science, the Crafoord Foundation, Svenska Läkaresällskapet,the Royal Physiographic Society of Lund, and the Medical Faculty ofLund University (ALF), as well as by the Danish Research Council andthe Danish Biotechnology Program for Peptide Research.
References
[1] Håkanson R, Kroesen JH, Liedberg G, Oscarsson J, Rehfeld JF, Stadil F. Correlationbetween serum gastrin concentration and rat stomach histidine decarboxylaseactivity. J Physiol 1974;243:483–98.
[2] Håkanson R, Chen D, Sundler F. The ECL cells. In: Johnson LR, editor. Physiology ofthe gastrointestinal tract. New York: Raven Press; 1994. p. 1171–84.
[3] Kahlson G, Rosengren E, Svahn D, Thunberg R. Mobilization and formation ofhistamine in the gastric mucosa as related to acid secretion. J Physiol 1964;17:400–16.
[4] Sandvik AK, Waldum HL, Kleveland PM, Schulze Søgnen B. Gastrin produces animmediate and dose-dependent histamine release preceding acid secretion in thetotally isolated, vascularly perfused rat stomach. Scand J Gastroenterol 1987;22:803–8.
[5] Håkanson R, Sundler F. Histamine-producing cells in the stomach and their role inthe regulation of acid secretion. Scand J Gastroenterol 1991;26:88–94.
[6] Waldum HL, Sandvik AK, Brenna E, Petersen H. Gastrin–histamine sequence in theregulation of gastric acid secretion. Gut 1991;32:698–701.
[7] Andersson K, Cabero JL, Mattsson H, Håkanson R. Gastric acid secretion afterdepletion of enterochromaffin-like cell histamine. A study with α-fluoromethyl-histidine in rats. Scand J Gastroenterol 1996;31:24–30.
[8] Lindström E, Chen D, Norlén P, Andersson K, Håkanson R. Control of gastric acidsecretion: the gastrin-ECL cell-parietal cell axis. Comp Biochem Physiol A MolIntegr Physiol 2001;128:505–14.
[9] Walsh JH, Richardson CT, Fordtran JS. pH dependence of acid secretion and gastrinrelease in normal and ulcer subjects. J Clin Invest 1975;55:462–8.
[10] Schusdziarra V, Harris V, Conlon JM, Arimura A, Unger R. Pancreatic and gastricsomatostatin release in response to intragastric and intraduodenal nutrients andHCl in the dog. J Clin Invest 1978;62:509–18.
[11] Strunz UT, Walsh JH, Grossman JM. Stimulation of gastrin release in dogs byindividual amino acids. Proc Soc Exp Biol Med 1978;157:440–1.
[12] Lichtenberger LM, Delansorne R, Graziani LA. Importance of amino acid uptakeand decarboxylation in gastrin release from isolated G cells. Nature 1982;295:698–700.
[13] Lloyd KC, Raybould HE, Taché Y, Walsh JH. Role of gastrin, histamine, andacetylcholine in the gastric phase of acid secretion in anaesthetized rats. Am JPhysiol 1992;262:747–55.
[14] Mailliard ME, Wolfe MM. Effect of antibodies to the neuropeptide GRP ondistention-induced gastric acid secretion in the rat. Regul Pept 1989;26:287–96.

32 P. Ericsson et al. / Regulatory Peptides 161 (2010) 22–32
[15] SchubertML,Makhlouf GM.Gastrin secretion induced by distension ismediated bygastric cholinergic and vasoactive intestinal peptide neurons in rats. Gastroenter-ology 1993;104:834–9.
[16] Alumets J, Ekelund M, El Munshid HA, Håkanson R, Lorén I, Sundler F. Topographyof somatostatin cells in the stomach of the rat: possible functional significance.Cell Tissue Res 1979;202:177–88.
[17] Larsson LI, Goltermann N, DeMagistris L, Rehfeld JF. Somatostatin cell processes aspathway for paracrine secretion. Science 1979;205:1393–5.
[18] Saffouri B, Weir GC, Bitar KN, Makhlouf GM. Gastrin and somatostatin secretion byperfused rat stomach: functional linkage of antral peptides. Am J Physiol1980;238:495–501.
[19] Chiba T, Taminato T, Kadowaki S, Able H, Chihara K, Seino Y, Matsukura S, Fujita T.Effects of glucagon, secretin, and vasoactive intestinal polypeptide on gastricsomatostatin and gastrin release from isolated perfused rat stomach. Gastroen-terology 1980;79:67–71.
[20] Wolfe MM, Reel GM, McGuigan JE. Inhibition of gastrin release by secretin ismediated by somatostatin in cultured rat antral mucosa. J Clin Invest 1983;72:1586–93.
[21] Sandvik AK, Kleveland PM, Waldum HL. The effect of secretin on acid and pepsinsecretion and gastrin release in the totally isolated vascularly perfused ratstomach. Regul Pept 1987;17:143–9.
[22] DuVal JW, Saffouri B, Weir GC, Walsh JH, Arimura A, Makhlouf GM. Stimulation ofgastrin and somatostatin secretion from the isolated rat stomach by bombesin. AmJ Physiol 1981;241:242–7.
[23] Schubert ML, Saffouri B, Walsh JH, Makhlouf GM. Inhibition of neurally mediatedgastrin secretion by bombesin antiserum. Am J Physiol 1985;248:456–62.
[24] Madaus S, Bender H, Schusdziarra V, Kehe K, Munzert G, Weber G, Classen M.Vagally induced release of gastrin, somatostatin and bombesin-like immunoreac-tivity from perfused rat stomach. Effect of stimulation frequency and cholinergicmechanisms. Regul Pept 1990;30:179–92.
[25] Schepp W, Prinz C, Håkanson R, Schusdziarra V, Classen M. Bombesin-likepeptides stimulate gastrin release from isolated rat G-cells. Regul Pept 1990;28:241–53.
[26] Hayes JR, Williams RH. The effect on gastrin secretion of agents which increase theintracellular concentration of 3´, 5´-adenosine monophosphate. Endocrinology1975;97:1210–4.
[27] Dial EJ, Huang J, Delansorne R, Lichtenberger LM. Monoamine oxidase: animportant intracellular regulator of gastrin release in the rat. Gastroenterology1986;90:1018–23.
[28] Kidd M, Hauso Ø, Drozdov I, Gustafsson BI, Modlin IM. Delineation of thechemomechanosensory regulation of gastrin secretion using pure rodent G cells.Gastroenterology 2009;137:231–41.
[29] Bunnett NW, Mogard M, Orloff MS, Corbet HJ, Reeve Jr JR, Walsh JH. Catabolism ofneurotensin in interstitial fluid of the rat stomach. Am J Physiol 1984;246:675–82.
[30] Kitano M, Norlén P, Håkanson R. Gastric submucosal microdialysis: a method tostudy gastrin- and food-evoked mobilization of ECL-cell histamine in consciousrats. Regul Pept 2000;86:113–23.
[31] Norlén P, Kitano M, Lindström E, Håkanson R. Anaesthetic agents inhibit gastrin-stimulated but not basal histamine release from rat stomach ECL cells. Br JPharmacol 2000;130:725–30.
[32] Ericsson P, Norlén P, Bernsand M, Alm P, Höglund P, Håkanson R. ECL-cellhistamine mobilization studied by gastric submucosal microdialysis in awake rats.Methodological considerations. Pharmacol Toxocol 2003;93:57–65.
[33] Benveniste H, Huttemeier PC. Microdialysis—theory and application. ProgNeurobiol 1990;35:195–215.
[34] Ungerstedt U. Microdialysis—principles and applications for studies in animalsand man. J Intern Med 1991;230:365–73.
[35] Norlén P, BernsandM, Konagaya T, Håkanson R. ECL-cell histaminemobilization inconscious rats: effects of locally applied regulatory peptides, candidate neuro-transmitters and inflammatory mediators. Br J Pharmacol 2001;134:1767–77.
[36] Ryberg B, Mattsson H, Larsson H, Carlsson E. Correlation between inhibition ofgastric acid secretion, plasma gastrin, and oxyntic mucosal histidine decarbox-ylase activity in the rat. Scand J Gastroenterol 1989;24:287–92.
[37] Kao CY. Tetrodotoxin, saxitoxin and their significance in the study of excitationphenomena. Pharmacol Rev 1966;18:997–1049.
[38] Håkanson R, Liedberg G. Mechanism of activation of rat stomach histidinedecarboxylase after vagal denervation. Eur J Pharmacol 1971;16:78–89.
[39] Alumets J, El Munshid HA, Håkanson R, Hedenbro J, Liedberg G, Oscarson J, RehfeldJF, Sundler F, Vallgren S. Gastrin cell proliferation after chronic stimulation. Effectof vagal denervation or gastric surgery in the rat. J Physiol 1980;298:557–69.
[40] Norlén P, Ericsson P, Kitano M, Ekelund M, Håkanson R. The vagus regulateshistamine mobilization from rat stomach ECL cells by controlling their sensitivityto gastrin. J Physiol 2005;564:895–905.
[41] Boehnke SE, Rasmusson DD. Time course and effective spread of lidocaine andtetrodotoxin delivered via microdialysis: an electrophysiological study in cerebralcortex. J Neurosci Methods 2001;105:133–41.
[42] van Duuren E, van der Plasse G, van der Blom R, Joosten RNJMA, Mulder AB,Pennartz CMA, Feenstra MGP. Pharmacological manipulation of neuronalensemble activity by reverse microdialysis in freely moving rats: a comparativestudy of the effects of tetrodotoxin, lidocaine, andmuscimol. J Pharmacol Exp Ther2007;323:61–9.
[43] EkelundM, Håkanson R, Vallgren S. Effects of cimetidine, atropine, and pirenzepineon basal and stimulated gastric acid secretion in the rat. Eur J Pharmacol 1987;138:225–32.
[44] Brodie DA. The mechanism of gastric hyperacidity produced by pylorus ligation inthe rat. Am J Dig Dis 1966;11:231–41.
[45] Stadil F, Rehfeld JF. Preparation of 125I-labelled synthetic human gastrin forradioimmunoanalysis. Scand J Clin Lab Invest 1972;30:361–9.
[46] Rehfeld JF. Accurate measurement of cholecystokinin in plasma. Clin Chem1998;44:991–1001.
[47] Ekins R, Newman B. Theoretical aspects of saturation analysis. Acta Endocrinol1970;147:11–36.
[48] Larsson LI, Rehfeld JF. Distribution of gastrin and CCK cells in the ratgastrointestinal tract. Histochemistry 1978;58:23–31.
[49] Rehfeld JF, Bardram L, Hilsted L. Ontogeny of procholecystokinin maturation in ratduodenum, jejunum and ileum. Gastroenterology 1992;103:424–30.
[50] Rehfeld JF, Stadil F, Rubin B. Production and evaluation of antibodies for theradioimmunoassay of gastrin. Scand J Clin Lab Invest 1972;30:221–32.
[51] Stadil F, Rehfeld JF. Determination of gastrin in serum: an evaluation of thereliability of a radioimmunoassay. Scand J Gastroent 1973;8:101–13.
[52] Schubert ML, Makhlouf GM. Neural, hormonal, and paracrine regulation of gastrinand acid secretion. Yale J Biol Med 1992;65:553–60.
[53] Taylor TV, Torrance B. Is there an antral-body portal system in the stomach? Gut1975;16:781–4.
[54] Lichtenberger LM, Nance DM, Gorski RA, Grossman MI. Sex-related difference inantral and serum gastrin levels in the rat. Proc Soc Exp Biol Med 1976;151:785–8.
[55] Grossman M. Vagal stimulation and inhibition of acid secretion and gastrinrelease: which aspects are cholinergic? In: Rehfeld JF, Amdrup E, editors. Gastrinand the vagus. London–New York: Academic Press, 1979:105–14.
[56] Soll AH,Walsh JH. Regulation of gastric acid secretion.AnnRevPhysiol 1979;41:35–53.[57] Song M, Yang H, Walsh JH, Wong H, Taché Y. Intracisternal TRH analog increases
gastrin release and corpus histidine decarboxylase activity in rats. Am J Physiol1999;276:901–8.
[58] BerthoudHR, JedrzejewskaA, PowleyTL. Simultaneous labelingof vagal innervationsof the gut and afferent projections from the visceral forebrain with dil injected intothe dorsal vagal complex in the rat. J Comp Neurol 1990;301:65–79.
[59] Holst MC, Kelly JB, Powley TL. Vagal preganglionic projections to the entericnervous system characterized with Phaseolus vulgaris-leucoagglutinin. J CompNeurol 1997;381:81–100.
[60] Uvnäs B, Uvnäs-Wallensten K, Nilsson G. Release of gastrin on vagal stimulation inthe cat. Acta Physiol Scand 1975;94:167–76.
[61] Nishi S, Seino Y, Takemura J, Ishida H, Seno M, Chiba T, Yanaihara C, Yanaihara N,Imura H. Vagal regulation of GRP, gastric somatostatin, and gastrin secretion invitro. Am J Physiol 1985;248:425–31.
[62] Nojima K, Sumii K, Sumii M, Okahara S, Haruma K, Yoshihara M, Kajiyama G. Acid-sensitive and alkaline-sensitive sensory neurons regulate pH dependent gastrinsecretion in rat. Dig Dis Sci 2000;45:1217–26.
[63] Brodie DA, Knapp PG. The mechanism of the inhibition of gastric secretionproduced by esophageal ligation in the pylorus-ligated rat. Gastroenterology1966;50:787–95.
[64] Alumets J, Ekelund M, Håkanson R, Hedenbro J, Rehfeld JF, Sundler F, Vallgren S.Gastric acid response to pylorus ligation in rats: is gastrin or histamine involved?J Physiol 1982;323:145–56.
[65] Zhao C-M, Chen D, Monstein H-J, Ding X-Q, Sundler F, Håkanson R. Rat stomachenterochromaffin-like cells are not stimulated by pylorus ligation. A biochemicaland ultrastructural study. Scand J Gastroenterol 1996;31:31–7.
[66] Legros G, Griffith CA. The abdominal vagal system in rats. An anatomical studywith emphasis upon the distribution of the gastric vagi to the stomach. J Surg Res1969;9:183–6.
[67] Håkanson R, Vallgren S, Ekelund M, Rehfeld JF, Sundler F. The vagus exerts trophiccontrol of the stomach in the rat. Gastroenterology 1984;86:28–32.
[68] Håkanson R, Hedenbro J, Liedberg G, Vallgren S. Effect of vagotomy on gastric acidsecretion in the rat. Acta Physiol Scand 1982;115:135–9.
[69] Vallgren S, Ekelund M, Håkanson R. Mechanism of inhibition of gastric acidsecretion by vagal denervation in the rat. Acta Physiol Scand 1983;119:77–80.
[70] Berthoud HR, Patterson LM, Zheng H. Vagal-enteric interface: vagal activation-induced expression of c-Fos and p-CREB in neurons of the upper gastrointestinaltract and pancreas. Anat Rec 2001;262:29–40.
[71] Larsson H, Carlsson E, Junggren U, Olbe L, Sjöstrand SE, Skånberg I, Sundell G.Inhibition of gastric acid secretion by omeprazole in the dog and rat. Gastroen-terology 1983;85:900–7.
[72] Ryberg B, Mattsson H, Carlsson E. Effects of omeprazole and ranitidine on gastricacid secretion, blood gastrin levels and [3H]-thymidine incorporation in theoxyntic mucosa from dogs and rats. Digestion 1988;39:91–9.
[73] Harty RF, McGuigan JE. Effects of carbachol and atropine on gastrin secretion andsynthesis in rat antral organ culture. Gastroenterology 1980;78:925–30.
[74] Schubert ML, Coy DH,Makhlouf GM. Peptone stimulates gastrin secretion from thestomach by activating bombesin/GRP and cholinergic neurons. Am J Physiol1992;262:685–9.
[75] Angus JA, Black JW. The interaction of choline esters, vagal stimulation and H2-receptor blockade on acid secretion in vitro. Eur J Pharmacol 1982;80:217–24.
[76] Black JW, Shankley NP. The isolated stomach preparation of the mouse: aphysiological unit for pharmacological analysis. Br J Pharmacol 1985;86:571–9.
[77] Dial EJ, Cooper LC, Lichtenberger LM. Amino acid- and amine-induced gastrinrelease from isolated rat endocrine granules. Am J Physiol 1991;260:175–81.
[78] Takehara Y, Sumii K, Tari A, Yoshihara M, Sumii M, Haruma K, Kajiyama G, Wu SV,Walsh JH. Evidence that endogenous GRP in rat stomach mediates omeprazole-induced hypergastrinemia. Am Physiol Soc 1996;271:799–804.