The sinus tarsi syndrome
14
International Orthopaedics (SICOT) (1981) 5 : 117-130 International Orthopaedics © Springer-Verlag 1981 The Sinus Tarsi Syndrome Willy Taillard 1, Jean-Marc Meyer 2, Jean Garcia 3, and Yves Blanc 4 1, 2 H6pital Cantonal universitaire, Department of Surgery, Orthopaedic Clinic, 1211 Geneva 4, Switzerland 3 H6pital Cantonal universitaire, Department of Radiology, Geneva, Switzerland 4 H6pital Cantonal universitaire, Laboratory of Electromyocinesigraphy of the Orthopaedic Clinic, Geneva, Switzerland Summary. The sinus tarsi syndrome is now a well- defned entity of foot pathology. Usually post-trau- matic, it is eharacterised by pain over the lateral opening of the sinus tarsi and a feeling of instability of the ankle. We were able to define two objective criteria for the syndrome: arthrography of the subtalar joint shows specific abnormalities and recording of the electromyographic function of the peronei demon- strates abnormalities during walking. Conservative treatment is successful in about two-thirds of the cases. In other cases a simple sur- gical procedure can cure or improve 90% of the pa- tients. R~sum& Le syndrome du sinus du tarse est une en- tit~ bien d~finie de la pathologie du pied. Le plus souvent post-traumatique, il se caract~rise par une douleur d l'orifice externe du sinus du tarse et une instabilitk de l'arrikre-pied. Nous avons pu dbfinir deux symptrmes objectifs de ce syndrome parfois difficile d diagnostiquer: l'arthrographie de l'articulation sous-astragalienne rkvkle des anomalies spbcifiques clans tousles cas et l'enregistrement de la fonction automatique des pk- roniers durant la marche montre kgalement des mo- difications claires de cette activitk. Le traitement conservateur est suffisant dans environ 2/3 des cas. Chez les autres, une interven- tion chirurgicale simple gukrit ou amkliore notable- ment 90% des patients. Key words: Foot pain, Arthrography, Subtalar joint, Sinus tarsL Cinesiology, Foot surgery Address offprint requests to: W. Taillard Clinical research supported by Hoffmann La Roche, Switzer- land In 1958, O'Connor [23] read a paper at the 25th meeting of the American Orthopaedic Academy entitled "Sinus Tarsi Syndrome". Since then, nearly 220 cases of this syndrome have been re- ported in numerous papers describing the clinical features and methods of treatment [5, 7, 8, 11, 15, 21, 22]: Diagnosis of the syndrome has usually been based on subjective features, principally pain on the lateral side of the foot that is increased by pressure over the lateral opening of the sinus tarsi together with a feeling of instability in the hind- foot. The pain is usually abolished by injection of a few ml of local anaesthetic into the sinus tarsi. O'Connor [23] reported 45 cases, 14 of them hav- ing been cured by surgical excision of the fatty tis- sue and ligaments of the sinus tarsi. During the last five years, a team of orthopae- dic surgeons, histopathologists, radiologists and electrophysiologists have attempted to establish more objective criteria for the syndrome and this paper reports the results of their investigations. Normal Anatomy We can compare the sinus tarsi to the intercondy- lar fossa of the knee. The talo-calcaneal sulcus constitutes a funnel-shaped tunnel with a large opening on the lateral side of the foot and a very narrow opening on the medial side, just behind the sustentaculum tali below the medial malleo- lus. The walls of the sinus are irregular and show many vascular foraminae. The sinus is almost completely filled with the interosseous talo-calcaneal ligament which is broad and very strong. At its medial end it forms a single fibrous band but in its lateral half it is split into two bands separated by fatty pads con- 0341-2695/81/0005/0117/$ 02.80
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The sinus tarsi syndrome
International Orthopaedics (SICOT) (1981) 5 : 117-130 International Orthopaedics
© Springer-Verlag 1981
The Sinus Tarsi Syndrome
Willy Taillard 1, Jean-Marc Meyer 2, Jean Garcia 3, and Yves Blanc 4
1, 2 H6pital Cantonal universitaire, Department of Surgery, Orthopaedic Clinic, 1211 Geneva 4, Switzerland 3 H6pital Cantonal universitaire, Department of Radiology, Geneva, Switzerland 4 H6pital Cantonal universitaire, Laboratory of Electromyocinesigraphy of the Orthopaedic Clinic, Geneva, Switzerland
Summary. The sinus tarsi syndrome is now a well- defned entity o f foot pathology. Usually post-trau- matic, it is eharacterised by pain over the lateral opening of the sinus tarsi and a feeling of instability o f the ankle.
We were able to define two objective criteria for the syndrome: arthrography o f the subtalar joint shows specific abnormalities and recording of the electromyographic function o f the peronei demon- strates abnormalities during walking.
Conservative treatment is successful in about two-thirds o f the cases. In other cases a simple sur- gical procedure can cure or improve 90% of the pa- tients.
R~sum& Le syndrome du sinus du tarse est une en- tit~ bien d~finie de la pathologie du pied. Le plus souvent post-traumatique, il se caract~rise par une douleur d l'orifice externe du sinus du tarse et une instabilitk de l'arrikre-pied.
Nous avons pu dbfinir deux symptrmes objectifs de ce syndrome parfois difficile d diagnostiquer: l'arthrographie de l'articulation sous-astragalienne rkvkle des anomalies spbcifiques clans tousles cas et l'enregistrement de la fonction automatique des pk- roniers durant la marche montre kgalement des mo- difications claires de cette activitk.
Le traitement conservateur est suffisant dans environ 2/3 des cas. Chez les autres, une interven- tion chirurgicale simple gukrit ou amkliore notable- ment 90% des patients.
Key words: Foot pain, Arthrography, Subtalar joint, Sinus tarsL Cinesiology, Foot surgery
Address offprint requests to: W. Taillard Clinical research supported by Hoffmann La Roche, Switzer- land
In 1958, O'Connor [23] read a paper at the 25th meeting of the American Orthopaedic Academy entitled "Sinus Tarsi Syndrome". Since then, nearly 220 cases of this syndrome have been re- ported in numerous papers describing the clinical features and methods of treatment [5, 7, 8, 11, 15, 21, 22]:
Diagnosis of the syndrome has usually been based on subjective features, principally pain on the lateral side of the foot that is increased by pressure over the lateral opening of the sinus tarsi together with a feeling of instability in the hind- foot. The pain is usually abolished by injection of a few ml of local anaesthetic into the sinus tarsi. O'Connor [23] reported 45 cases, 14 of them hav- ing been cured by surgical excision of the fatty tis- sue and ligaments of the sinus tarsi.
During the last five years, a team of orthopae- dic surgeons, histopathologists, radiologists and electrophysiologists have attempted to establish more objective criteria for the syndrome and this paper reports the results of their investigations.
Normal Anatomy
We can compare the sinus tarsi to the intercondy- lar fossa of the knee. The talo-calcaneal sulcus constitutes a funnel-shaped tunnel with a large opening on the lateral side of the foot and a very narrow opening on the medial side, just behind the sustentaculum tali below the medial malleo- lus. The walls of the sinus are irregular and show many vascular foraminae.
The sinus is almost completely filled with the interosseous talo-calcaneal ligament which is broad and very strong. At its medial end it forms a single fibrous band but in its lateral half it is split into two bands separated by fatty pads con-
0341-2695/81/0005/0117/$ 02.80

118
taining vessels and nerves [17] and sometimes a small bursa has been observed both anatomically and at surgery [8, 11, 14, 16]. The interosseous lig- ament separates the two halves of the subtalar joint and both sides of the interosseous ligament are lined with synovial membrane [21].
On the posterior surface the synovium forms small superior and inferior recesses and occasio- nally papillary folds due to simple hyperplasia of the lining cells. On the anterior surface similar small recesses have been observed. These features, as we shall see later, are of great importance in
W. Taillard et al.: The Sinus Tarsi Syndrome
the interpretation of artfirograms of the subtalar joint (Fig. 1).
Some authors have demonstrated the presence of nerve endings in the ligaments and consider the calcaneo-tibial ligament as a "carrier" of proprio- ceptive nerve fibres which play an important role in the biomechanics of the hindfoot [9, 17, 25, 27].
The interosseous ligament within the sinus tar- si lies in a fairly central position on the prolonga- tion of the weight-bearing axis of the leg, sur- rounded by the talo-tarsal joints. It takes part in every movement of the subtalar joint around the
Fig. 1. a and b Topography of the sinus tarsi and the interosseous ligament. 1. Subtalar joint; 2. The two main bands of the ligament separated by fatty pads and vessels; 3. Recessus synovialis adjacent to the ligamentum talo-calcaneum. c The recessus synovialis with its multiple papil- lary folds creating the micro-recesses observed on arthrography. Lower right: The origin of the interosseous ligament

W. Taillard et al.: The Sinus Tarsi Syndrome 119
6
5
Fig. 2 a -d . a Drawing of the ligaments of the postero-lateral side of the foot: 1. Lateral malleolus; 2. Ligamentum talo-fibulare anterius; 3. Ligamentum calcaneo-fibulare; 4. Ligamentum talo-calcaneum laterale; 5. Ligamentum talo-calcaneum interos- seum; 6. Subtalar joint. b Sequence of ligament-tearing in progressive varus of the heel and in neutral position of the ankle. 3. Rupture of the lig. calcaneo-fibulare; 4. The second to give way is the lig. talocalcaneum laterale; 5. The last to be torn is the lig. interosseum. c and d Surgical exploration of a freshly sprained ankle with an isolated rupture of the ligamentum calcaneo fibulare. 1. Lateral malleolus; 2. Torn lig. calcaneo-fibulare; 3. Ankle joint; 4. Subtalar joint; 5. Sinus tarsi filled with blood clots and tearing of some fibres of the ligament interosseum (see arthrography Fig. No. 5); 6. Lig. talo-fibulare anterius intact
axis of Henke and is subjected to traction as well as to torsional stresses [12, 14, 16, 18, 29]. The li- gament is taut in supination of the foot and rela- xed in pronation.
Two groups of ligaments are especially impor-
tant for the stability of the subtalar joint: the cal- caneo-fibular ligament and ' the interosseous talo- calcaneal ligament together with the smaller late- ral talo-calcaneal ligament.
If we test the resistance of the ligaments on the

120 w. Taillard et al.: The Sinus Tarsi Syndrome
Fig. 3 a-e. The anatomopatholo- gy of the sinus tarsi syndrome, a (Case 3883/74). Synovial hyper- plasia without inflammatory cells. On the lower half of the specimen: ligament tissue (Van Gieson x 20). b (Case 3883/74). Synovial hyperplasia with some remnants of ligament (~) (Von Gieson x 270). c (Case 14840/ 80). Synovial hyperplasia with haemosiderin deposits appearing like a blue line in the synovial membrane (Prussian Blue x 80). d and e (Case 8163/80). Fibrous scar tissue in the interosseous li- gament, d Normal light, e Polari- zed light showing differences in structure between ligament bun- dles (white area) and fibrous scar tissue (black area) (Hematoxylin- eosin x 50) (Prof. R. Lagier, In- stitute of Pathology, Osteoarticu- lar Unit, Geneva)

W. Taillard et al.: The Sinus Tarsi Syndrome 121
lateral side of the hindfoot whilst maintaining it in a neutral position (i. e. without any dorsiflexion or extension), we find that progressive inversion of the heel provokes rupture of the ligaments in the following sequence: a) The calcaneo-fibular ligament. b) The lateral talo-calcaneal ligament. c) The interosseous talo-calcaneal ligament (Fig.
2b). Thus the ligament of the sinus tarsi is the last
ligament to be ruptured and we find that the inter- osseous ligament is never damaged unless the la- teral talo-calcaneal ligament and the calcaneo-fi- bular ligament have already been divided. It
seems therefore that an isolated lesion of the inter- osseous ligament is very rare and it is almost al- ways associated with lesions of the other compo- nents of the lateral ligament complex of the ankle.
Surgical exploration of fresh traumatic lesions has confirmed the anatomical study and has shown tears of the ligament or bleeding within the sinus tarsi. It is certainly advisable to check the state of the sinus tarsi at every operation for a se- vere ankle sprain, especially when there is instabi- lity of the hindfoot (Fig. 2 c-d) .
Most of the patients suffering from the sinus tarsi syndrome have sustained either single or re- peated ankle sprains. In these patients it is rare to
122 W. Taillard et aI.: The Sinus Tarsi Syndrome
find any macroscopic abnormality when explor- ing the sinus but histological examination often reveals remodelling of the soft tissues [21]. We have usually found synovial hyperplasia obliterat- ing the synovial recesses of the subtalar joint and healing of the ligaments with scar tissue (Fig. 3). There are also deposits of haemosiderin indicat- ing old haemorrhage.
Pathological changes in the sinus have been observed in other conditions also, such as chronic inflammation, gout, rheumatoid arthritis and osteoarthritis [l, 5, 8, 1 l].
Clinical Signs and Symptoms
Most of the cases reported in the literature have suffered at least once from a severely sprained an- kle which has generally been neglected or poorly treated. We may speak therefore of a "post-trau- matic syndrome". Our experience is based on 21 patients, each of them with a diagnosis confirmed by arthrography. Fifteen of these patients have been treated surgically so that we have available complete documentation of their syndrome with the findings at radiology, arthrography, electro- myography and histology.
Among the 220 cases reported in the literature, 70% are considered as post-traumatic. The remain- ing 30% have been attributed to various causes, mainly inflammatory conditions like rheumatoid arthritis, ankylosing spondylitis or gout and oth- ers to deformity of the foot such as pes cavus or pes planus with chronic instability of the hind- foot.
Pain localised in the sinus tarsi may also ac- company tenosynovitis of the peronei, sciatica, calcaneal spur syndrome or the tarsal tunnel syn- drome. We have never observed a case in infants, children or adolescents and most of the patients are within their twenties or thirties.
The clinical signs are: (a) Pain at the lateral side of the foot increased by
firm pressure over the lateral opening of the si- nus tarsi. The pain is most severe when stand- ing, walking on uneven ground or during the movements of supination and adduction of the foot. It usually disappears at rest and is eased by a firm bandage or a support holding the heel in pronation or a valgus position.
(b) A feeling of instability of the hindfoot on un- even ground.
(c) An injection of a few ml of Novocaine into
the sinus tarsi reduces the pain and often the feeling of instability for a few hours. All our patients demonstrated these three fea- tures.
(d) Routine clinical and radiological examination did not reveal any sign of instability of the an- kle joint. Our attempts to obtain objective signs of instability of the subtalar joint have all been unsuccessful and we could not find any convincing increase in the talo-calcaneal angle on forced supination of the heel as re- ported by Vidal [28], except in those cases pre- senting instability of the ankle joint [4]. Standard X-ray pictures of the foot do not
show any abnormalities. The only two procedures that have proved to
be reliable in providing objective confirmation of the diagnosis are arthrography of the posterior subtalar joint and a study of the automatic func- tion of the peronei in walking.
Arthrography of the Subtalar Joint
During the last ten years we have attempted to in- vestigate the subtalar joint by arthrography. Our experience now extends to 150 cases with diffe- rent lesions of the hindfoot [20]. In 33 patients with clinical signs of a sinus tarsi syndrome, we found an abnormal arthrogram of the subtalar joint in 21 of them. In others we were able to de- monstrate instability of the ankle joint only. We have also tried to demonstrate fresh lesions of the ligaments of the sinus tarsi in 36 cases with recent ankle sprains.
The technique is simple but it does require some experience [20]. Under local anaesthesia a fine needle is introduced at a point 1.5 cm cranial from the tip of the lateral malleolus and 1.5 cm behind the posterior ridge of the fibula (Fig. 4a). With the aid of an image intensifier, the needle is directed to the posterior joint space passing through its fibrous capsule. When the tip of the needle touches the bone it is likely to have reach- ed the posterior joint recess (Fig. 4b).
Watersoluble contrast medium is injected slowly and filling of the joint cavity observed un- der X-ray control in order t o detect any leakage of the contrast and observe any communication between the posterior part of the subtalar joint and the anterior part of the subtalar joint or the tibiotalar joint. Communication with a tendon sheath of the peronei or the flexor hallucis longus is also possible. Usually an injection of 2-3 ml of contrast medium is sufficient.
W. Taillard et al.: The Sinus Tarsi Syndrome 123
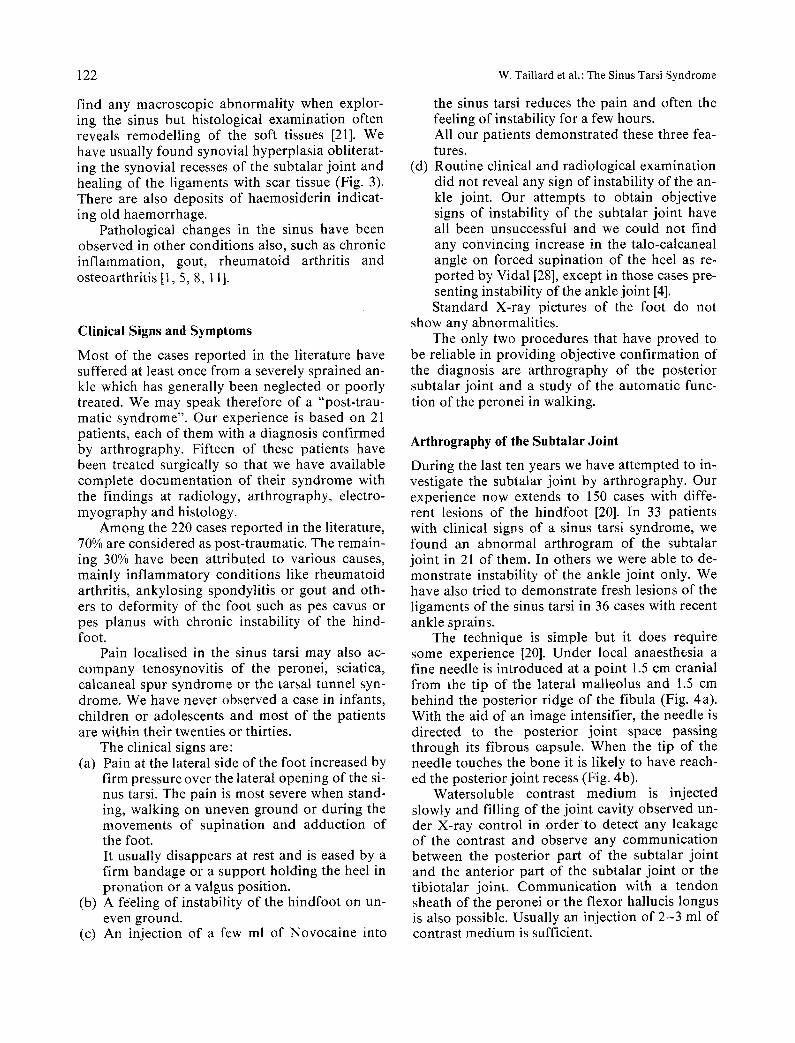
Fig. 4 a -g . Arthrography of the subtalar joint, a Landmarks for in- troduction of the needle, b X-ray control of the position of the tip of the needle in the posterior recess before injection of the contrast medium, e and d Position of the foot for the oblique X-ray which best demonstrates the sinus tarsi, e Normal arthrogram with the typi- cal micro-recesses along the inter- osseous ligament, f and g Arthro- gram of a normal foot in maximal dorsal flexion and in maximal plantar flexion. Note the different appearance of the recesses in the sinus tarsi which demonstrate the normal mobility of the synovial membrane
Three X-rays are then taken (Fig. 4 c -d ) : a) An A. P. exposure of the ankle. b) A lateral view of the hindfoot. c) An oblique view with the leg in 45 ° internal ro-
tation and the foot in neutral position. Ninety arthrograms of subjects of different
ages without any history of ankle trauma have
established the criteria defining a normal appear- ance of the subtalar joint. These are (Fig. 4 e-g) : a) The contrast medium must appear to move
freely in different positions of the foot (forced flexion, extension and pronation and supina- tion).
b) The medial and lateral recesses of the talo-cal-

124 w. Taillard et al. : The Sinus Tarsi Syndrome
Fig. 5 a-d . Arthrography of the subtalar joint in a fresh lesion of the ankle with a tear of the lig. calcaneo-fibular and partial lesion of the lig. interosseous (see Fig. 2 c-d) . a X-ray in forced varus showing a slight tilt of the talus, b X-ray in forced forward traction of the foot showing the absence of anterior shift, c Lea- kage of the contrast medium around the fibula and in the sinus tarsi (--+). d Pe- netrat ion of the contrast medium in the sinus tarsi ( ~ )
caneal joint should be free and well-defined and the synovial membrane must lie closely against the interosseous ligament.
c) In oblique X-ray projections, numerous micro- recesses binding the talo-calcaneal interosse- ous ligament should be apparent (Fig. 4e). We have demonstrated in a series of post-mortem
a n d post-amputation specimens that these re- cesses are present along the entire length of the talo-calcaneal ligament. They correspond to imprints on the synovial membrane by peri and intraligamentous adipose tissue and to synovial papillary folds.
d) In many patients there are communications linking the subtalar joint with the ankle or with Chopart 's joint or with the tendon sheaths of the peronei or flexor hallucis longus. These communications appear as small, well-defined canals usually situated at the lateral side of the posterior joint of the foot, just in front of the fibula. These communications are normal but
any other leakage of the contrast medium into the soft tissues around the joint is a definite sign of a tear in the capsule. A normal interarticular communication can
often mask the sinus tarsi so that it is no longer visible on the X-ray films (Fig. 6a).
In 36 fresh lesions we observed (Fig. 5 c -d ) : 1. Frequently blood mixed with synovial fluid ran
out of the needle as soon as it reached the joint space.
2. Dispersal of the contrast medium which then no longer outlined the anatomical structure of the joint recesses, thus signifying a rupture of the capsule.
3. In some cases we also saw the disappearance of the small synovial recesses which were proba- bly filled with blood clot or fibrinous material.
In 21 cases with old lesions, two radiological features were usually observed (Fig. 6 b - c ) : 1. During the injection, the contrast medium nor-
mally filled the posterior recess of the joint at

W. Taillard et al.: The Sinus Tarsi Syndrome 125
Fig. 6 a -c . Arthrography of the subtalar joint in chronic sinus tarsi syndrome, a Normal communication between the subtalar, the talo-navicular and the ankle joint. Moulding of the sinus tarsi is no longer visible (~) . b and c Two cases of sinus tarsi syndrome demonstrating the absence of recesses along the interosseous ligament which appears completely smooth ( ~ )
the tip of the needle. It ran freely into the joint space and was then abruptly stopped when it reached the sinus tarsi. The lateral recess was blocked and could not be filled by the contrast medium (Fig. 6 c).
2. The most distinctive feature and the most im- portant one was the complete disappearance of the micro-recesses along the interosseus liga- ment. The anterior margin of the posterior sub- talar joint bordering on the sinus tarsi is com- pletely flat and smooth.
In a series of 15 arthrograms demonstrating the above changes surgery was performed and the contents of the sinus tarsi submitted to histologi- cal study. In 13 cases the pathologist was able to demonstrate evidence of old lesions of the liga- ments and of the adjacent tissue such as hyperpla- sia of the synovium, proliferation of the fibrous tissue and obliteration of all the synovial recesses together with slight deposition of haemosiderin indicative of old haemorrhage. In several cases remnants of ligaments embedded in the scar tissue were found (Fig. 3).
It is important to point out that these histolo- gical changes which we consider to be confirma- tory signs of a ligamentous lesion were only ob- served in those cases where the arthrogram was clearly abnormal. In two patients suffering with painful symptoms of the hindfoot in which the ar- throgram showed some abnormality, the patholo- gist was unable to discover convincing evidence of a lesion of the ligamentous structures of the si- nus tarsi.
Electromyography
a) Technical Data
We recorded the automatic function of the extrin- sic foot muscles, the gastrocnemius, tibialis ante- rior and especially both of the peronei in normal subjects and in patients both standing in different postures and walking [2]. We used mini-Beckman surface electrodes, placed at the sites determined by Basmajian and Blumenstein [3] for minimum "cross-talk" between the peroneus longus and so- leus (Fig. 7). In particular we attempted to separa- te the recordings of the electrical activity between peroneus longus and brevis (Fig. 7b). We found that it was quite possible to separate the voluntary contraction of peroneus longus and brevis; the foot of the patient is held by the examiner in a neutral position without any flexion or extension. Then the patient is asked to tilt his hindfoot into valgus without making any attempt at flexion or dorsiflexion of the toes or foot. The examiner ca- refully checks that the other muscles and tendons are relaxed. The EMG recording shows isolated activity of the peroneus brevis very well during this movement (Fig. 7c). When strong resistance to this movement is exerted, or when the patient flexes his foot or toes, the peroneus longus also contracts to assist the brevis. In extension, it is the tibialis anterior which becomes active with the pe- roneus brevis.
The results with the surface electrodes were carefully compared with implanted fine wire elec- trodes in order to confirm that the electrical acti-

126 W. Taillard et al. : The Sinus Tarsi Syndrome
Fig. 7 a -d . Electromyocinesigraphy of foot muscles in a normal subject. a and b The position of the surface electrodes for good separation of the electrical activity of both pero- nei. The patient can walk quite free- ly with the telemetric system of re- cording, c Selective activity of pero- neus longus and brevis muscles when the patient tilts his hindfoot in pure valgus against increasing resi- stance. The peroneus longus begins its contraction when the peroneus brevis is already at its maximal level of activity. The signals on tibialis anterior and soleus may be cross- talk from the peronei muscles, d Usual recording of foot muscle acti- vity using surface electrodes from a normal subject walking at his com- fortable speed, on level ground
vity we were recording came from each separate muscle. It is particularly important to avoid "cross-talk" between both the peronei as well as the extensors of the toes.
We then analysed the pattern of automatic ac- tivity of the muscles during standing and walking in t2 adults (24 to 68 years) and in 16 children (4 to 16 years). In walking, the peronei usually con- tract during the second half of the stance phase [13], but we did not observe a constant phasic acti- vity of the peroneus brevis during the swing phase as has been described by Scherb [24] (Fig. 7 d).
We next examined 18 patients with a "sinus tarsi syndrome", six of these were examined both pre-operatively and post-operatively. In this en- tire group of patients we observed definite abnor- malities in the automatic function of the peronei, the other muscles remaining normal (Fig. 8 a). The features observed in this group were as follows: 1. Reduction in electrical activity or complete
electrical silence of either the peroneus brevis or the peroneus longus or both muscles.
Abnormal activity of the peroneus brevis
.
.
was detected in 75% of the walking cycles. Of the 18 patients examined, 14 showed abnormal activity of the peroneus brevis in 75% of the walking cycles; 13 showed abnormal activity of the peroneus longus in 70% of the walking cyc- les, and 15 showed an abnormality of both pe- ronei in 81% of the walking cycles. Only 3 pa- tients showed normal activity of peroneus lon- gus and brevis when compared with the control group.
We never observed a change in the phasic activity of the peronei in patients walking on le- vel ground. On uneven ground, or grass, we oc- casionally observed a short contraction of the peroneus brevis in the middle of the swing pha- se.
A temporary diminution or disappearance of the activity of the peronei during one or several walking cycles, especially when walking on un- even ground.
Less frequently we noted a "block contraction" of both peronei during the entire stance phase.

W. Taillard et al. : The Sinus Tarsi Syndrome 127
NORf4AI. SlOE d
4. The EMG abnormalities disappeared 10 to 20 minutes after local anaesthesia of the sinus tarsi and reappeared a few hours later (Fig. 8 b).
5. The phasic activity improves or returns to nor- mal after successful surgery but disappearance of pain is the main measure of the success of the operation.
6. It is interesting to point out that local anaesthe- sia of the sinus tarsi does not modify the electri- cal pattern of the peronei in cases of instability of the ankle joint. In these cases we rarely find a permanent abnormality in the automatic function of the peronei, abnormalities being de- tected usually only in a few walking cycles. This observation may be a useful diagnostic aid for differentiating the type of instability occurring in the foot.
Treatment
a) Conservative Treatment
In many patients the pain can be lessened or com- pletely relieved by repeated injections of local anaesthetic and steroids into the sinus tarsi. Five to six injections at weekly intervals are usually sufficient. Komprda [15] treated 116 patients in this way with complete cure in 73 and a marked improvement in 25 patients.
Local infiltration should be supplemented by re-education of the peronei and proprioceptive re- sponses in the manner described by Freeman [10] and Castaing [6, 8]. Such a re-education program- me is especially effective in young patients or in sportsmen.
In some instances immobilisation in a walking


W. Taillard et al.: The Sinus Tarsi Syndrome 129
C
6UP.. ~ - 1 9 5 5 ~ ,-Is I ~ 7 100 ,~ F1 ~ ~ t 5, '90 i
R.Ttb. ant. 7
! t i t ! ,~ ,
L ~ . I~ev. .,~ ~,~ ,
7i *
R.Solous
Right foot lifalk~.g barefoot ~ the l~,el 4 aontlm after
1 s t a . c o " 'i .st e i ~j %
Left foot : ~aoce
i i i
I, ' , s t a n c e ,
S t _ M l ~ . : . ; . . . . 7
Fig. 8 a -e . Electromyocinesigraphy in a patient with sinus tarsi syndrome (DUP. M. 1955). a Hypoactivity of both peronei as well as the soleus. The activity of tibialis anterior is normal, h Definite improvement of the electrical pattern of both peronei and soleus after local anesthesia of the sinus tarsi, e Normal activity 4 months after successful surgery
plaster for three to four weeks followed by a re- education programme proves effective.
b) Surgical Treatment If conservative measures remain unsuccessful, ex- cision of the tissue filling the lateral half of the si- nus tarsi is a simple procedure that yields good re- sults [23]. It is important not to extend the exci- sion of the fibroligamentous tissue for more than 1 to 1.5 cm into the sinus because the blood sup- ply to the talus is in part provided by the many vessels that penetrate the bone in the medial half of the sinus [26]. Post-operatively the patient wears a walking caliper for four weeks followed by a muscle re-education programme.
The results of this simple procedure are usual- ly excellent with complete disappearance of the pain in the majority. A review of the literature [5,
8, 11, 15, 19, 22, 23] produced 73 cases treated sur- gically with results graded as excellent 55, good 13, failure 5.
In our series of 15 patients treated operatively the results were excellent 11, good 3 and one case poor because the pain was only slightly reduced.
Recently Claustre [7], Marrera [19], and Vidal [28] have proposed combining curettage of the si- nus tarsi with a ligamentoplasty using part of the tendon of peroneus brevis; the tendon is freed proximally and then passed through holes bored through the calcaneum, the sinus tarsi and the neck of the talus to reconstruct a substitute for the interosseus ligament. This technique may be use- ful in severe instability of the subtalar joint but we have had no experience with it.
In resistant cases triple arthrodesis may be the only possible surgical solution.

130
Conclusion
The sinus tarsi syndrome can now be considered as a well-defined entity with a history of predispo- sing relatively severe trauma to the hindfoot in about 70% of the cases. The syndrome is character- ised by pain that is increased by pressure over the lateral opening of the sinus tarsi and reduced by local anaesthesia at the site together with a feeling of instability of the ankle.
We were able to define two types of objective abnormality: firstly, arthrography of the subtalar joint showed in all cases specific abnormalities in the synovial recesses of the sinus tarsi. Secondly, recording the electromyographic function of the peronei when standing and walking (electromyo- cinesigraphy) also demonstrated characteristic ab- normalities which in many cases allowed us to di- stinguish between the sinus tarsi syndrome and chronic instability of the ankle joint.
Conservative treatment in successful in about 50-60% of cases and in others a simple surgical procedure can cure or considerably improve 90% of the patients.
The objective methods of examination describ- ed in this paper may be helpful in deciding whe- ther surgical treatment is indicated and also in re- solving medico-legal problems.
References
1. Andr6, J.: Etude histopathologique des 16sions de d~g~n6- rescence au niveau de Farticulation sous-astragalienne. Po- dologie 1, 18-23 (19,62) '
2. Basmajian, J. W., Benzon, J: W.: An electromyographic study of certain muscles of the leg and foot in the standing position. Surg. Gynecol. Obstet. 98, 662-666 (1954)
3. Basmajian, J. W., Blumenstein, R.: Electrode placement in EMG biofeedback, p. 84, p. 87. Baltimore: Williams and Wilkins 1980
4. Brantigan, J. W., Pedegana, L. R., Lippert, F. G.: Instabili- ty of the subtalar joint. J. Bone Joint Surg. (Am.) 59, 321- 324 (1977)
5. Brown, J. E.: The sinus tarsi syndrome. Clin. Orthop. 18, 231-233 (1960)
6. Castaing, J.: Les entorses de la cheville. Conf. Enseigne- ment SOFCOT, Paris. Expansion Scientifique Frangaise, pp. 23-41 (1968)
W. Taillard et al.: The Sinus Tarsi Syndrome
7. Claustre, J., Simon, L., Allieu, Y.: Le syndrome du sinus du tarse existe-t-il? Rhumatologie 31, 19-23 (1979)
8. Debrunner, H. V.: Das Sinus Tarsi Syndrom. Schw. Med. Wschr. 93, 1660-1664 (1963)
9. Delplace, J., Castaing, J.: Place de la r~6ducation proprio- ceptive dans les instabilit6s musculo-ligamentaires externes de la cbeville. Ann. M~d. Phys. 18, 605-617 (1975)
10. Freeman, M. A. R., Dean, M. R., Hanham, I. W. F.: The etiology and prevention of functionnal instability of the foot. J. Bone Joint Surg. (Br.) 47, 678-685 (1965) Hauser, E. D. W.: The sinus tarsi syndrome. Ann. Pod. l, 11-14(1962) Inman, V. T., Mann, R. A.: Biomechanics of the foot and ankle. In: Surgery of the foot, de Vries, ed., pp. 3-22. Phi- ladelphia: Saunders 1973
13. Jonsson, B., Rundgren, A.: The peroneus longus and bre- vis muscles. Electromyography 11, 93-103 (1971)
14. Kapandji, I. A.: Physiologic articulaire. Membre inf~rieur. Paris: Maloine 1971
15. Komprda, J.: Le syndrome du sinus du tarse. Ann. Podol. 5, 11-17 (1966)
16. Lanz, J., Wachsmuth, W.: Praktische Anatomic. Bein und Statik. Berlin: Springer 1972
17. Lopez, A. R., Marrero, R. M.: Inervacion y sindrome del seno tarsiano. Actualit~s M6d. Chir. Pied XI, 181-184. Pa- ris: Masson 1978
18. Manter, J. T.: Movements of the subtalar and transverse tarsal joints. Anat. Rec. 80, 397-410 (1941)
19. Marrero, R. M., Lopez, A. R.: Tratamiento quirurgico de la lesion cronica del seno del tarso. Nota previa. Actnalitbs M6d. Chir. Pied XI, pp. 173-179. Paris: Masson 1978
20. Meyer, J. M., Taillard, W.: L'arthrographie de l'articula- tion sous-astragalienne dans les syndromes douloureux post-trauma'tiques du tarse post6rieur. Rev. Chir. Orthop. 60, 321-330 (1974)
21. Meyer, J. M., Lagier, R.: Post-traumatic sinus tarsi syndro- me. Acta Orthop. Scand. 48, 122-128 (1977)
22. Navarre, M.: Apropos du syndrome du sinus du tarse. Acta Orthop. Belg. 32, 743-754 (1966)
23. O'Connor, D.: Sinus tarsi syndrome. A clinical entity. J. Bone Joint Surg. (Am.) 40, 720 (1958)
24. Scherb, R.: Kinetisch-diagnostische Analyse von Gehst6- rungen. Stuttgart: Enke 1952
25. Stilwell, D. L.: The innervation of deep structures of the foot. Am. J. Anat. 101, 59-73 (1957)
26 Trueta, J.: Studies of the development and decay of the hu- man frame. London: Heinemann 1968
27. Valenti, V. : Personal communication 28. Vidal, J., Fassio, B., Buscayret, Ch., Escare, Ph., Allieu, Y.:
Instabilit6 externe de la cheville. Rev. Chir. Orthop. 60, 635-642 (1974)
29. Wright, D. G., Desai, S. M., Henderson, W. H.: Action of the subtalar and ankle-joint complex during the stance phase of walking. J. Bone Joint Surg. (Am.) 46, 361-382 (1964)
11.
12.