The Vitamin D Solution: A 3-Step Strategy to Cure Our Most ...
310
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of The Vitamin D Solution: A 3-Step Strategy to Cure Our Most ...



TableofContents
TitlePageCopyrightPageDedicationAcknowledgementsForewordIntroductionPARTI-THELIGHTOFYOURLIFEANDTHEHEALTHHORMONE
CHAPTER1-WhatIsVitaminD?CHAPTER2-Fish,Phytoplankton,Dinosaurs,Lizards,andYouCHAPTER3-HardBodiesCHAPTER4-AdventuresinGlobe-TrottingCHAPTER5-FindingImmunityCHAPTER6-MindMattersandMixedEmotionsCHAPTER7-AreYouDeficient?PARTII-THREESTEPSTOREBUILDINGYOURVITAMINDLEVELS
CHAPTER8-Step1:LettheSunshineInCHAPTER9-Step2:BoneUponCalciumCHAPTER10-Step3:SupplementSafelyCHAPTER11-SpecialTreatmentCHAPTER12-DethroningtheCover-UpCHAPTER13-Q&ARESOURCEGUIDE
SELECTEDBIBLIOGRAPHYINDEX


HUDSONSTREETPRESSPublishedbythePenguinGroup
PenguinGroup(USA)Inc.,375HudsonStreet,NewYork,NewYork10014,U.S.A.•PenguinGroup(Canada),90EglintonAvenueEast,Suite700,Toronto,Ontario,CanadaM4P2Y3(adivisionofPearsonPenguinCanadaInc.)•PenguinBooksLtd.,80Strand,LondonWC2R0RL,England•PenguinIreland,25St.Stephen’sGreen,Dublin2,Ireland(adivisionofPenguinBooksLtd.)•PenguinGroup(Australia),250CamberwellRoad,Camberwell,Victoria3124,Australia(adivisionofPearsonAustraliaGroupPty.Ltd.)•
PenguinBooksIndiaPvt.Ltd.,11CommunityCentre,PanchsheelPark,NewDelhi-110017,India•PenguinGroup(NZ),67ApolloDrive,Rosedale,NorthShore0632,NewZealand(adivisionofPearson
NewZealandLtd.)•PenguinBooks(SouthAfrica)(Pty.)Ltd.,24SturdeeAvenue,Rosebank,Johannesburg2196,SouthAfricaPenguinBooksLtd.,RegisteredOffices:80Strand,LondonWC2R0RL,
EnglandFirstpublishedbyHudsonStreetPress,amemberofPenguinGroup(USA)Inc.FirstPrinting,April2010
Copyright©MichaelF.Holick,M.D.,2010Allrightsreserved
REGISTEREDTRADEMARK—MARCAREGISTRADA
LIBRARYOFCONGRESSCATALOGING-IN-PUBLICATIONDATA
Holick,M.F.(MichaelF.)
ThevitaminDsolution:a3-stepstrategytocureourmostcommonhealthproblem/MichaelF.Holick;forewordbyAndrewWeil.p.cm.
Includesbibliographicalreferencesandindex.eISBN:978-1-10122293-5
2.VitaminDinhumannutrition.I.Title.QP772.V53H.3’99—dc222009053666Withoutlimitingtherightsundercopyrightreservedabove,nopartofthispublicationmaybereproduced,storedinorintroducedintoaretrievalsystem,ortransmitted,inanyform,orbyanymeans(electronic,mechanical,photocopying,recording,orotherwise),withoutthepriorwrittenpermissionofboththe
copyrightownerandtheabovepublisherofthisbook.PUBLISHER’SNOTE
Everyeffortasbeenmadetoensurethattheinformationcontainedinthisbookiscompleteandaccurate.However,neitherthepublishernortheauthorisengagedinrenderingprofessionaladviceorservicestothe
individualreader.Theideas,procedures,andsuggestionscontainedinthisbookarenotintendedasasubstituteforconsultingwithyourphysician.Allmattersregardingyourhealthrequiremedicalsupervision.Neithertheauthornorthepublishershallbeliableorresponsibleforanylossordamageallegedlyarising
fromanyinformationorsuggestioninthisbook.WhiletheauthorhasmadeeveryefforttoprovideaccuratetelephonenumbersandInternetaddressesatthe
timeofpublication,neitherthepublishernortheauthorassumesanyresponsibilityforerrors,orforchangesthatoccurafterpublication.Further,publisherdoesnothaveanycontroloveranddoesnotassume
anyresponsibilityforauthororthird-partywebsitesortheircontent.Thescanning,uploading,anddistributionofthisbookviatheInternetorviaanyothermeanswithoutthepermissionofthepublisherisillegalandpunishablebylaw.Pleasepurchaseonlyauthorizedelectronic
editions,anddonotparticipateinorencourageelectronicpiracyofcopyrightedmaterials.Yoursupportoftheauthor’srightsisappreciated.
Thisbookisprintedonacid-freepaper.[∞]
http://us.penguingroup.com
Tomybest friendand lovingwife,SallyAnn,whosededication toour familyand unwavering support of all of my activities have been instrumental inmyability to communicate to the world the insidious health consequences of thevitaminD-deficiencypandemic.
ACKNOWLEDGMENTS
This book has been in its making for nearly thirty years. Without theinvolvementofmyfamilymembers,friends,andcolleagues,youwouldnotbereading this; it does takeavillage toput agoodbook together. I ameternallygratefultomywife,Sally,andourchildren,MichaelToddandEmilyAnn,whonotonlyparticipatedinsomeoftheresearchthatIpresentinthisbook,buthavealso been gracious champions of my career and dedication to vitamin Dresearch.WhenBonnieSolowfirstcalledmetoaskaboutdoingabook,Iknewitwas
finallytimetosharetheknowledgethatIandmycolleagueshadbeencollectingthrough years of steadfast researchwith theworld,much ofwhichwas goingunnoticed by the general public but could be used to enhance the health ofmillions.Thankyou,Bonnie, forpaving thewayfor thisbook to finally reachthosemillions;yourleadership,guidance,andenthusiasticsupportofthisprojecthave been invaluable. You are a delight to work with, for your attention todetails,goodhumor,andcommitment tooverseeingeverystep in theproject’sprocessareabonusthatfewauthorsexperiencewiththeiragents.I ammost grateful toKristin Loberg,my ghost writer, who listened tomy
many scientific presentations as well as stories about my experiences withvitaminDimprovingthehealthofKomododragons,iguanas,polarbears,andababygorilla,justtomentionafew.SheskillfullyhelpedmeweavewhatIhopeis a compelling and convincing message about the vitamin D-deficiencypandemic, itsserioushealthconsequences,andhow, in threesimplesteps,youcanimproveyourvitaminDstatusforgoodhealth.Iwillforeverbeindebtedtothenumeroustechnicians,students,fellows,and
colleagueswithwhomIhavecollaboratedovertheyearsinthefieldofvitaminD photobiology, physiology, biochemistry, and clinical application. I ammostgratefultomymentorandfriendformorethanthirtyyears,Dr.JohnT.PottsJr.,forhiswonderfulguidanceandcounsel.IamappreciativeforthesupportfromtheUVFoundationinfundingsomeofmyresearchonvitaminDandcancer.A
big thanksgoesout to JimandKathyShepherd, and JohnOverstreet for yourfriendshipoverthepastdecade.Iamparticularlyappreciativeoftheassistance,counsel, and inspiration given tome byDr. JohnAdams,Mrs.MaryAldrich,R.N.,Dr.MaryAllen,Dr.AndreAraujo,Ms.CaroleBaggerly,Ms.MaraBanks,Dr.HowardBauchner,Dr.ShallyBhasin,Ms.RachaelBiancuzzo,Dr.DouglassBibuld,Dr.HeikeBischoff-Ferrari,Dr.GeorgeBrainard,Dr.JohnCannell,Dr.Laura Carbone, Dr. Tai Chen, Dr. Farhad Chimeh, Dr. Thomas Clemens, Dr.Robert Cousins, Dr. Bess Dawson-Hughes, Mrs. Sheila DeCastro, R.N., Dr.Hector DeLuca, Dr. Emily Demetriou, Dr. Cermina Durakovik, Dr. ChristinaEconomos, Dr. Frank Farraye, Dr. Gary Ferguson, Drs. Cedric and FrankGarland,Dr.WilliamGehrmann,Dr.CatherineGordon,Dr.EdwardGorhan,Dr.WilliamGrant,Dr.SusanGreenspan,Dr.RobertHeaney,Dr.BrettHolmquist,Mr.DanielJamieson,Dr.DavidKenney,Dr.DouglasKiel,Mrs.EllenKlein,Dr.AlbertKligman,Dr.LorenKline,Dr.PolyxeniKoutkia,Dr.RolfdieterKrause,Dr. Joyce Lee, Dr. Linda Linday, Mr. Zhiren Liu, Dr. Cliford Lo, Dr. AlanMalabanan,Dr.TrondMarksted,Mr. JeffreyMathieu,Dr.LoisMatsuoko,Dr.CarlosMautalen,Ms. JuliaMcLaughlin,Ms. JaneenMcNeil,R.N.,Ms.AnneMerewood,Dr.JohanMoan,Dr.CarolynMoore,Dr.HaraikarnNimitphong,Dr.JamesO’Keefe,Dr.JackOmdahl,Dr.JohnParrish,Dr.RalfPaus,Dr.AlbertoPerez, Mr. Kelly Persons, Dr. John Pettifor, Dr. Sara Pietras, Dr. PornpojPramyothin,Dr.KumaravelRajakumar,Dr.RahulRay,Mrs.SwapnaRay,Dr.Jorg Reichrath, Dr. Richard Reitz, Dr. Clifford Rosen, Dr. Irv Rosenberg, Dr.WilliamRosenberg,Dr. JoshSafer,Dr.WaelSalameh,Dr.EdwardSauter,Dr.NevinSchrimshaw,Dr.GarySchwartz,Mr.JimShepherd,Dr.LeonidShinchuk,Dr.AndrzejSlominski,ElizabethSouthworth,Ms.CatherineSt.Clair,Dr.MarkSt.Lezin,Dr.TatsuoSuda,Dr.SusanSullivan,Dr.VinTangpricha,Mr.AndrewTannenbaum,Dr.XiaoTian,Dr.DuaneUlrey,Mr.DemetriusVorgias,Dr.AnnWebb, Mr. LymanWhitlatch, Mr. FredericWolff, Mr. JörgWolff, Dr JacoboWortsman, Dr. Azzie Young, Dr. Vernon Young, Dr.Michael Young, and Dr.SusieZanello.Thank you to the members of the Boston University Medical Center
community, including its executive administrators, clinical research supportstaff, the nurses in thegeneral clinical researchunit, andmy tireless assistant,LorrieButler.Thankyou,Dr.Weil,forpenningmyForewordandbeingsuchapassionateadvocateofmyworkthroughtheyears.TotheteamatHudsonStreetPressandPenguin,whoenduredallofmylast-
minuterequestsandchanges,andwhose insightshavehelpedproduce thebest

book possible for you, the general reader, especiallyCaroline Sutton,MeghanStevenson,ElizabethKeenan,andAlexandraRamstrum.Andfinally,myspecialthanksgotoalltheorganismsoftheworldwhorely
onvitaminDtosustaintheirlife,andwho’vetaughtmeagreatdealaboutthishormone that humans are now beginning to understand, and appreciate, likeneverbefore.

FOREWORD
Dr.AndrewWeil
TheVitaminDSolutionsetsanewstandardinhealthandwell-nessthatIbelievewillchangethefaceofmedicineasweknowit.ThisindispensableguidehelpsyouunderstandwhyvitaminD is socritical toyouroverallhealth, and showshowyou canharness its rewards through a three-part prescription that anyonecan follow. Since identifying the body’s active formof vitaminD some thirtyyears ago, my friend and colleague Dr. Michael F. Holick has stood at theforefront of vitamin D research, pioneering groundbreaking studies that havelinkedawidearrayofdisordersthatafflictupto200millionAmericanswithasinglecommonriskfactor—vitaminDdeficiency.It’sthemostcommonmedicalcondition in the world with sometimes devastating, even fatal, consequences.WhetheryouliveinanorthernregionlikeNewEngland,ornearmeinthesunnysouthwestwherethesunshinesmostdays,youcouldbesufferingfromasilentvitamin D deficiency that undermines all of your efforts to achieve optimalhealth.Contrary to popularwisdom, vitaminD isn’t just about bone health, and it
standsuniquelyapartfromallothervitamins.VitaminDisactuallyahormonethatplaysacentralroleinmetabolismandalsoinmuscle,cardiac,immune,andneurologicalfunctions,aswellas in theregulationof inflammation.Increasingthe amount of vitamin D in the body can prevent or help treat a remarkablenumberofailments,fromobesitytoarthritis,fromhighbloodpressuretobackpain,fromdiabetestomusclecramps,fromupperrespiratorytractinfectionstoinfectious diseases, and from fibromyalgia to cancers of the breast, colon,pancreas,prostate,andovaries.Itcansafeguardpregnancy,supportidealweightmanagement,reduceabnormalcellgrowth,andstaveoffinfectionsandchronicdiseases.Whowouldnotwantthesebenefits?
Themessage ofTheVitaminDSolution is simple yet profound: just aswerequirealittlefatandsaltforsurvival,weneedthesuninmoderation,too—forsunexposure isourbest sourceofvitaminD. It’s awell-documented fact thatsunlight is necessary for human survival, but we’ve been brainwashed intothinking that any exposure to sunlight is bad. This is both unfortunate anduntrue. There is really no substantiated scientific evidence to suggest thatmoderate sun exposure significantly increases risks of benign cancers or, andmore importantly, themost deadly formof skin cancer,melanoma.Dr.HolickshowsyouhowtosafelyandsensiblytakeadvantageofsunlightduringcertaintimesofthedayandyeartobuildandmaintainyournaturallevelsofvitaminDwithoutincreasingyourriskforskincancer.Aspartofhisthree-partstrategy,healsoexplainstheroleandimportanceofcalciumincombinationwithvitaminD,andtellsyouhowmuchyouneedintheformofsupplementstooptimizeyourhealth.Throughout this book, Dr. Holick shares fascinating case studies that have
definedandshapedhisworkoverthepastthirtyyears,someofwhichrevealthedevastating consequences of vitamin D deficiency even in a country like theUnitedStates,wherehealthcare is considered tobe soadvanced. Ihavegreatrespectforhimasaclinician,researcher,andeducator.Weare luckytobelivingduringanexcitingtransformationofmedicineand
health care.We have more knowledge about health than ever before, yet wecontinue to suffer from serious diseases that are largely preventable throughsimple lifestyle changes. I have devoted the past thirty years to developing,practicing, and teaching others about the principles of integrative medicine,which emphasizes prevention through attention to lifestyle. In 1994, Iestablished the Program in IntegrativeMedicine, now the Arizona Center forIntegrative Medicine, a Center of Excellence of the University of ArizonaCollege of Medicine. Its main work is the education of physicians, nursepractitioners, medical students and residents, and other health care providers,andoneof its initiatives is tocreatearobustfieldofnutritionalmedicine.OurcurriculumincludesthesamevaluablelessonsandstrategiesthatDr.Holickhasdevelopedthroughhislife’swork.The Vitamin D Solution is a very practical guide for maintaining optimum
health. Just asDr.Holickprescribes, I take adailyvitaminD supplement andalsogetsomeunprotected,regular,sensiblesunexposurewhileswimminginmypool.Onceyouhavereadthisbook,Iamsureyouwillwanttodothesame.

INTRODUCTION
FromNASAtotheNationalZoo
Bythetimewereachadulthood,mostofushavedevelopedageneralsenseofwhat’s good and bad for our health. Eating fresh fruits and vegetables: good.Drinkingabottleofwhiskeyaday:bad.Exercisinga fewdaysaweek:good.Baskinginthesunwithoutsunscreen:bad.Iagreewiththefirstthreeideasbutemphaticallydisagreewiththenotionthat
sunbathingisalwaysbad.AndI’mgoingtoproveittoyouinthisbook.Infact,I’mgoingtoshowyou—backedbymorethanthirtyyearsofscience,includingsomeastonishingdiscoveriesinjustthelastfewyearsalone—howvaluableandnecessary the sun is in powering up your health, enhancing your well-being,stavingofftypicalcausesofdisease,andextendingyourlife.If I had to give you a single secret ingredient that could apply to the
prevention—and treatment, inmanycases—ofheartdisease, commoncancers,stroke,infectiousdiseasesfrominfluenzatotuberculosis,type1and2diabetes,dementia, depression, insomnia, muscle weakness, joint pain, fibromyalgia,osteoarthritis, rheumatoid arthritis, osteoporosis, psoriasis, multiple sclerosis,andhypertension,itwouldbethis:vitaminD.Surprised? Iactually like tostartwith the fact thatwesuffer fromaserious
shortfallinthisvitaminthatthreatensourlivelihoodandlongevity.IhavebeentravelingaroundtheworldnotonlylecturingaboutvitaminDbutalsohearingfrom physicians how common vitaminD deficiency is. It’s not only themostcommon nutritional deficiency in the world, but it’s also the most commonmedicalcondition,affectingatleastonebillionpeople.
•50percentto100percentofchildrenlivinginEuropeandtheUnitedStatesareathighriskofbeingvitaminDdeficient.
•Arecentstudyrevealedthatthere’sbeena22percentreductioninvitaminDlevelsinthegeneralU.S.populationinthepastdecade.
•In2009researchersfromHarvardandtheUniversityofColoradorevealedthat70percentofwhites,90percentofHispanics,and97percentofblacksintheUnitedStateshaveinsufficientbloodlevelsofvitaminD;theirstudywaspublishedintheArchivesofInternalMedicine.
•Neartheequator—inSouthAfrica,SaudiArabia,India,Australia,Brazil,orMexico,forexample—it’sbeenestimatedthatbetween30percentandupwardsof80percentofchildrenandadultswhohaveminimumsunexposurearevitaminDdeficientorinsufficient.
ThreeoutofeveryfourAmericansaredeficientinvitaminD,upfromoneoutoftwotwentyyearsago.
Youmaywonder:Whyisthishappeningandwhatcanwedoaboutit?Howcanasinglevitaminbeassociatedwithsomanyconditions?That’sexactlywhyIwrotethisbook.Oneofmygoalsistoconveytoyoujust
howcriticalthisvitamin(actuallyahormone)isinourlivesandinspireyoutospringtoactionandwelcometherewardsthatahealthyvitaminDstatushastooffer.Thelistofhealthconditionsassociatedwithadeficiencyisoverwhelming(Ilistedjustachoicefewabove),andtheamountofresearchthathasemergedlatelyonthisvitaminofvitalitybegsforabookthatsharesthislatestknowledgein a way anyone can understand and use to become a healthier, happierindividual.Contrarytopopularwisdom,vitaminDisn’tjustaboutstrongbonesandteeth.Andyoucan’tgetenoughfromfoodsandmultivitaminsalone.Your overall well-being depends in part on developing an appropriate
relationship with the sun. However, it can be a challenge to get the kind ofinformationyouneedtoestablishsucharelationship.Iwillprovideyouwithacomprehensive understanding of the issues at hand. Equipped with thisknowledge, you will be able to make your own decision about what yourrelationshiptothesunshouldbe.You,too,canlearntousesunlightforhealth.(And don’t panic: if the sun truly isn’t for you, there will be alternativessuggested in this book to meet your personal preferences and choices—andsatisfyyourvitaminDrequirement.)IknowthatImayhaveanuphillbattletoclimbforsomereaders,who,upon

the mere thought of sensible sunbathing, immediately think about wrinkles,prematureaging,skincancerssuchasmelanoma,andsoforth,butItrustyou’llbe amazed by the lessons learned in this book. You may also come to thisthinking,IgetplentyofvitaminDbecauseIdrinkalotofmilk,amexposedtocasualsunlightduringthedayjustwalkingaround,andtakeamultivitaminanda calcium supplement with added D. Unfortunately, you are still likely to bewoefullydeficient.You’llsoonunderstandwhyandlearnwhattodoaboutit.
ALifelongFascination
I’vebeen interested in the importanceof vitaminD tohumanhealth formorethan three decades.When Iwas a graduate studentworking onmyPh.D. andM.D.at theUniversityofWisconsinbackin theearly1970s,wedidn’trealizethatvitaminDhadtobeactivatedintheliverandkidneysbeforeitwasavailableforuse in thebody.Whilestudyingunderyoung,up-and-comingprofessorDr.Hector DeLuca, I was responsible for isolating and identifying the majorcirculatingformofvitaminDinhumansaswellastheactiveformproducedbythekidneys.Thesediscoveriesalloweddoctorstoprescribetinyamountsofthisactive hormone substance to people whose bodies could not make their ownactivevitaminDduetokidneyfailureandwhosufferedsevereboneproblemsasa result.When Iwas inmedical school,my roommate and Imade the activeformof vitaminD chemically in a test tube and gave it to patientswhowerewheelchairboundbecausetheyhadkidneydiseaseandassociatedbonedisease.Thosepatientsbeganwalkingagain.Thatwasmy introduction to thepracticalapplicationofvitaminDresearch,andIhaveworkedinthisareaeversince.Call itbeingat therightplaceat theright time,butfromthoseearlyyearsI
was transfixed by my studies of vitamin D—captivated by the fact that wedependonsunlightforvitaminD.Iwantedtoknow:Howdoourbodiesmakeit?Whataffectsthisprocess?Whatfactorsregulateit?Howdosunscreensandskin pigment influence this process? Can our bodies make vitamin D in thewinter?Whathappenswhenweliveinnorthernlatitudes?HowmanypartsandsystemsdoesvitaminDaffect in thebody?What are the consequencesof toolittle vitaminD?Even after all these years and somanydiscoveries about thehealth benefits of vitamin D, I still find this field of science fascinating andneedingfurtherexploration.I have made numerous contributions to the field of the biochemistry,

physiology, metabolism, and photobiology of vitamin D, not only for humannutrition but for animal nutrition aswell. I discovered themechanism for thesynthesisofvitaminDintheskinofhumansaswellasreptiles,birds,fish,andwhales.I’vedemonstratedtheeffectsofaging,obesity,latitude,seasonalchange,sunscreenuse,skinpigmentation,andclothingonthisvitalskin-to-bloodstreamprocess.I’veestablishedglobalrecommendationsadvisingsunlightexposureasan integral source of vitaminD and continue to call for new standards in thegovernment’s recommendationfordailyvitaminDintake. I’vehelped increaseawareness in the pediatric and general medical communities regarding thevitaminDdeficiencypandemicanditsrolenotonlyincausingmetabolicbonediseaseandosteoporosisinadultsbutinincreasingchildren’sandadults’riskofdeveloping common deadly cancers, heart disease, type 2 diabetes, andautoimmune diseases, including type 1 diabetes, multiple sclerosis, Crohn’sdisease, and rheumatoid arthritis. I serve on a number of national committeesand editorial boards and have organized and/or cochaired several internationalsymposia. I continue to perform studies and have published more than threehundred research papers in peer-reviewedmedical journals, including theNewEngland Journal ofMedicine, theLancet, andScience. I’ve alsowrittenmorethan 200 review articles and numerous book chapters, and I’ve edited orcoedited eleven books in academia. My first book to the trade, The UVAdvantage ,crackedopenthedoorforlaypeopletoseesunlightandvitaminDfromanewperspective.In2009IwashonoredwiththeLinusPaulingInstitutePrizeinhealthresearchandtheDSMNutritionAwardformycontributions.
SoWhyVitaminD?
Medicine has long known that there is a clear and undisputed relationshipbetween sun exposure and bone health. Without the vitamin D that humansthroughoutevolutionhavedependedonalmostentirelyfromthesun,ourbonescouldnotobtainthecalciumtheyneedtobestrong.Thechildhoodbonediseasericketsdoesn’t exist inchildrenwhoget enoughsunexposureandcalcium. Infact,oneof themosteffectivewaysof treatingkidswithrickets is toget themintothesunshine.Therelationshipbetweensunexposureandbonehealthissoincontrovertible
thateven theantisun lobby increasinglyhemsandhawsabout this issue in thefaceofnew findings.When its spokespeople areputon the spot, theyusually

mumble something along the lines of “Kids gotta drink more milk.” In fact,vitaminD-fortifiedmilkwasintroducedtocombatrickets,butmuchofthemilksold today that is labeled as rich in vitamin D does not actually contain thevitaminDitissupposedto.Myownstudieshaveprovedthis,andthatresearchhas been backed by other studies, including one by the Food and DrugAdministration(FDA).Evenwhenmilkcontainstheamountstatedonthelabel(100internationalunits,orIU,perserving),aneight-ounceglassprovidesonlyabout5percentto10percentofwhatthebodyrequires.Ricketsisagainontheriseinoursociety—ashockingdevelopmentgiventhe
medicaladvancesduringthepastcentury.ButvitaminDdeficiencygoesmuch,much further than staving off bone-related diseases in children and adults.Recently,scientistshavebecomeinterestedinthefactthatpeoplelivinginsunnyclimates have a lower incidence of organ-and cell-related conditions, such asheart disease, type 1 diabetes, multiple sclerosis, and cancers of the breast,colon, ovaries, and prostate.Unlike the connection between sun exposure andbone health, the link between sun exposure and cellular and organ healthwasmoredifficult toestablish. Inpart this isbecausemuchofwhatwenowknowhasbeenlearnedbyputtingtogetherresearchfindingsfromdifferentpartsoftheworld,whichwasnotpossible inpreviousdecades.Because it took longer forscientiststomaketheconnectionbetweensunexposureandcellularhealth,weonlyrecentlyestablishedwhattheconnectionactuallyis.And it goes even further. Today there is evidence to link sun exposure and
vitaminDtoeveryfacetofmedicineandhealth.AdequatelevelsofvitaminDcan improve fertility, safeguard pregnancy, reduce inflammation, help withweightcontrol,protectagainst infectiousdiseases like thefluand tuberculosis,prevent strokes and dementia, bolster the immune system, boostmemory, andsupportmusclestrength.WhatallofthisreallymeansisthatvitaminDmaybethemost underappreciated andmisunderstood antiaging secret. And unlike somanyotherantiaging“secrets,”thisoneisabsolutelyfree.NodoubtyouwillbesurprisedbysomeofthefindingsIpresent,andyoumay
evenfeeluncomfortableonceIdiveintothefactsaboutsunexposureandwhyit’s so important to let a little sunshine intoyour lifedespitewhatmostof thedermatology community would have you believe. If the noise from thesunphobicdermatologycornerhasyoucuriousaboutmyscientificrationaleforendorsingsensiblesunexposurewithoutsunblock,thenIencourageyoutofliptochapter8andfirstreadthetruthaboutskincancerandtheriskofmelanoma.Otherwise, begin in chapter 1 and take the journey with me through a
comprehensiveexplorationofvitaminD—astory thatbeginsmillionsofyearsbefore humans walked the earth. I’ve chosen to save the skin cancer/sunexposureconversationuntillaterinthebook;bythetimeyoureachit,you’llbebetterpreparedtotaketheknowledgeinanduseitforyourownbenefit.ThoughIwillsaythis:studiessuggestthatthosewhoworkindoorshavehigherratesofthemost deadly skin cancer than those who work outside in the sun all day.That’sbutonefactofmanyyou’ll find in thesepages thatmaygoagainst thegrain of the established “common sense” that you have obtained from thirtyyearsoftheunchallengedmessagetoavoidalldirectsunexposure.Iwillalsopresentasynthesisofcutting-edgeresearchfromaroundtheworld,
offerahistoricalperspectivegoingbackmillionsofevolutionaryyearsthatwillreally put all this into meaningful and, I hope, insightful and enlighteningperspective, and present a practical—“D-lightful”—plan for rebuilding andmaintainingoptimallevelsofvitaminD.Thisplanentailsthreesimplesteps:(1)usingmy formula for sensible sun to determine your daily requiredminimumexposure (with alternative options suggested in lieu of actual sunlight), (2)ensuringadequatecalciumintakealongsidegooddietarysourcesofvitaminD,and(3)supplementing.Specialconsiderationswillbeexplainedforpeoplewithcertain conditions, such as obesity, pregnancy, lactation, advanced age (olderthanseventy),epilepsy,malabsorptionsyndromes,andkidneyandliverdisease.Ireceivetonsofquestionsfrommypatients,friends,andfamily,soI’vealso
devoted a full chapter to frequently asked questions—to ensure that no stonegoesunturnedinsettlingcommonconfusionsandcuriosities.Forexample,doesthewayyoucookfishaffectitsvitaminDcontent?Doesitmatterifthesalmonyoueatiswildcaughtorfarmed?Doyouneedtotakeasupplementevenduringthesummer?What’sthebestsupplementforchildrenwhocannotswallowpills?HowmuchvitaminDshouldpregnantwomentake?Howdoyouinterpretbloodlevels of activevitaminD?Will I increasemy riskof getting a kidney stone?Theanswerstothesequestions,andmanymore,willbecoveredinchapter12.Shouldyouhaveaquestionnotaddressedinthisbook,thenpostitonmyWebsite,www.drholicksdsolution.com.I’llanswerasmanyasIcan.
PartoftheWildKingdom
Thiscrusadeofmineisn’tjustabouthumans.It’sabouteverylivingvertebrateon the planet that relies on the sun to maintain optimal levels of vitamin D,especiallythosethataredeniedadequateexposuretothesun.Take,forexample,Kirmani, the first lowlandgorillabornat theFranklinParkZoo inBoston.Bythetimehercaretakersreachedouttomeforhelpin2005,Kirmaniwasonthebrinkofdeath.Atjustsevenmonthsoldsheshowedsignsofthebone-softeningdiseasericketsandhadseveremuscleweaknessandriskofseizures,makingitdifficult for her to suckle and get enough nutrition fromhermother’smilk. Italso seemed to zookeepers that Kirmani’s illness had put her parents underserious,visiblestress.Herpediatriciansadvisedadministering400IUofvitaminD (twice the recommended daily intake for human infants), but it didn’t domuch.IsuggestedtheyupthevitaminDdosageto5,000IUaday,andloandbehold,Kirmanimade a full recovery. Shewon’t grow to be quite as tall andmightyassheshouldhave,becauseofherbriefboutwithvitaminDdeficiencyandresultingrickets,butshesurvivedandisflourishingtoday.Infact,Iwastheguestofhonoratherfirstbirthday.Thisscenariohasplayedoutacrossthecountryinvariouszooswhereanimals
are caged andoften shaded andprotected from sunlightmost of the time, andI’ve enjoyed a degree of renown for improving the health of four-leggedresidentsofplanetearth.TwinpolarbearsattheDenverZoohavemetothankfor their ability to walk after vitamin D supplementation.When the NationalZoo’sKomododragons showed signsof a die-out because thematedpair hadnonviablehatchlings, Iwas called to the rescue.Thesewere the firstKomododragonsinazoointheUnitedStates,giventothezooasagiftbythepresidentof Indonesia. After I made sure these large lizards got plenty of vitamin D,suddenly a new generation of Komodo dragons was born, and they are nowthrivinginmanyzoosacrosstheUnitedStates.(I liketothinkthepolarbears,gorillas,Komododragons,andiguanashavebeenreadingthetabloids,someofwhich have featured my message; when these animals feel weak and loosetoothed, theymuster thestrength toshout,“CallHolick!”)But it’snot just thetabloids. Other popular publications, such as the New York Times, theWashingtonPost,andtheWallStreetJournalhavepickedupmyinsightsinthepast.IcontinuallyfieldcallsonvitaminDdeficiencyfromrenownedinstitutions
likeNASAand theNationalZoo and advise folks there onhow to safely andassuredly rectify a problem. I’ve even helped develop lighting for reptileenclosuresthatreplicatesnaturalsunshine,andIadvisezoostaffsofhowtokeeptheirvitaminD-dependent animalshealthyand fertile. It’s amatterof life anddeath.Whichmeansitcouldbeamatterof lifeanddeathforyou, too.Soturnthe
page and begin to take charge of your health in a way you never thought ofbefore. Let go of whatever preconceived notions you have about the sun andvitaminD,andopenyourminduptoashiftinperspective.Itcandramaticallychangeyourhealthandyourlife.

PARTI
THELIGHTOFYOURLIFEANDTHEHEALTHHORMONE

CHAPTER1
WhatIsVitaminD?
Isitahormoneoravitamin?Somewhere along the equator a ten-year-old girl is growing up without theluxuriesmost of us enjoy on a daily basis. Shewill never learn how to use acomputer,orderapizzatobedelivered,ordriveacartothemallforclothesandcosmetics.Shespendsmostofherdaysplayingoutsidenearherfarmingparents,and soon shewill join them in tilling the soil. Shewill never learn to readorwrite. She will endure periods of poor nutrition and poverty. And she knowsnothingaboutsunblockandprobablyneverwill.Nowlet’ssailnorthtotheUnitedStatesorEurope,whereanotherten-year-old
girl leads an immensely different life. She is maturing into a savvy user ofelectronics, passes the majority of her days indoors at a rigorous school, hasaccess to the best nutrition and all the benefits that modern medicine canprovide, and will know what SPF means long before graduating from highschoolandpursinghighereducation.Ifbothgirlscontinueontheirseparatepaths,theequatorialgirlwillbeatleast
halfaslikelytogetcancerduringherlifetimeashernortherncounterpart.Shealsowillhavean80percent reduced riskofdeveloping type1diabetes in thefirst thirty years of her life. In fact, barring any freak accident or untreatedmedicalcondition,herlongevityoverallwillbe7percentgreater.The northern girl, on the other hand, faces a host of increased health risks
throughoutherlife,frombreastandovariancancertodepression,obesity,type2diabetes, osteoporosis, arthritis, high blood pressure, heart disease, and stroke.Shewillbemoresusceptibletoupper-respiratory-tractinfections,dentalcavitiesand gum disease, and infectious diseases like the flu and tuberculosis. As agroup,sheandhergirlfriendswillbreaktheirarms56percentmoreoftenthan
theirpeersdid justfortyyearsago.Becauseshewasborninnorthernlatitudesandhaslivedthereforthefirsttenyearsofherlife,fortherestofherlifeshehasa 100 percent increased risk of developingmultiple sclerosis nomatterwhereshechoosestoliveintheworldafterageten.Shewouldlikelyloseinajumpingcontestwithherequatorialsister,whocanjumphigherandwithmoreforce.Ifshecomplainsofmuscleweaknessandwidespreadmuscleand jointpain lateroninadulthood,herdoctorwilllikelydiagnosefibromyalgiaorchronicfatiguesyndromewhentestsdon’t turnupanythingspecific.Theequatorialgirlmightneverexperiencesuchdebilitatingachesorchronicpainandinfactmaydevelopinto amuch stronger, leaner, andmore fertilewoman. If bothwomenbecomepregnant,theequatorialmom-to-bewon’thavetoworryasmuchaboutseriouscomplications like preeclampsia. And shewon’t have trouble giving birth theold-fashionedway.Thenorthernmom-to-be,however,willhaveamuchhigherriskof having anunplannedC-section andof givingbirth to a childwhowillsufferfromschizophrenia.Bythetimethenortherngirlreachesmidlifeandherlateryears,chancesare
goodthatshe’llhavebeentreatedforaninternalcancer(breast,colon,ovarian,pancreatic—takeyourpick)atsomepointandbeenprescribedmultipledrugstocombat chronic ailments like hypertension, osteoporosis, arthritis, depression,obesity, type 2 diabetes, dementia, Alzheimer’s, and perhaps even insomnia.Becauseof a significant lossofbonemass, shewill be terrifiedof fallingandfracturingabone,andthereforewillhave limitedsomeofherfavoriteoutdooractivities,suchastennis,skiing,horsebackriding,andgolf,significantlycuttingbackonphysicalactivity.Andbecauseshewillhavelostaconsiderableamountofmusclestrength,herbiologicalagewillbemucholderthanshereallyis.Theequatorialwomannotonlymayoutlivehernortherncounterpart,butshe’llalsobe less prone to chronic diseases that afflict her northern counterpart. For thisreason,theequatorialwomanmay,overall,enjoyahigherqualityoflife—evenwhenadvancedagesetsin.What’s goingonhere?The answer lies in thedifferencebetween these two
girls’ exposure to natural sunlight, which is our main source of vitamin D.Obviously, I’ve taken some liberty in letting a few assumptions go. Theequatorialgirl’s limitedaccess tohealthcareandpreventativemedicinehas itsown basket of risks, but let’s focus for a moment just on the difference inexposuretosunlightandtheconclusionsthatcanbedrawnfromthatsinglefact.Let’s also assume that these girls growup to exhibit vastly different levels ofvitaminDintheirsystems,whichisnotastretchgiventhedocumentedrecords

ofvitaminDdeficiencypatternsacrosstheglobe.IfIweretotesteachofthesegirls’vitaminDlevels,Iwouldnotbesurprisedtofindthenortherngirl’slevelsterribly low as compared to her equatorial counterpart. And that differencemeanseverything.Thesunisasvital toyourhealthandwell-beingasfood,shelter,water,and
oxygen. I’m going to prove it to you through a comprehensive exploration ofvitaminD.WhatdoesvitaminDhavetodowithaginganddisease?Morethanweeverimagined.
OurMostCommonHealthChallenge
When I tell people that vitamin D deficiency is our most common healthchallenge globally, the response I get is pretty much the same in wealthy,developednations:“Well,thatcan’thappentomeoranyoneelseinmycountry;besides,wehavegreathealthcare.”AndwhenIremindpeoplethatthebestwayto ensure healthy levels of vitaminD is through sensible sun exposure two tothreetimesaweek,acommonthreadisheardintheresponse,whichisalongthelinesof,“Youcan’tbeserious.Thesun is thedemonofcancerandaging.NowayamIgoingtoconsidersunlightasmedicine.It’sjustnotpossible.”The statistics proving otherwise speak volumes, and you’re going to hear
aboutthemthroughoutthisbook.Increasingnumbersofstudiesareconfirmingthe link between vitaminD and optimal health, and attitudes are beginning toshift. Researchers have long known that the “sunshine vitamin” boosts bonestrengthbyencouragingthebodytoabsorbcalcium,butonlyrecentlyhavewebegun to see just how far-reaching vitamin D is in maintaining the health ofevery systemandcell in thebody’s intricatemachinery.VitaminDmaybe asvitaltoyourheartandbrainhealth,forexample,asitistoyourbonehealth.Asnoted in the introduction, increasing the amountofvitaminD in thebodycanpreventorhelptreataremarkablenumberofailments,fromhighbloodpressuretobackpain,fromdiabetestoarthritis,fromupper-respiratory-tractinfectionstoinfectiousdiseases, and from fibromyalgia to cancer. It also seems to improvefertility,weightcontrol,andmemory.Theevidence isclear: justaswerequirea little fatandsalt forsurvival,we
needthesuninmoderation,too.I’lladdtothatthefollowingfact,whichwillbefully explored in chapter 8: there is essentially no substantiated scientificevidence tosuggest thatmoderatesunexposuresignificantly increases risksof

benign skin cancers or, and more importantly, the most deadly form of skincancer,melanoma.Infact,ifyouwereunfortunatelytodevelopmelanoma,youwouldbemorelikelytosurviveit ifyouhadadequatesunexposureasachildandyoungadult.And ifyouhadadequatesunexposureasachild,youwouldhavea40percentreducedriskofdevelopinglymphomaasayoungadult.In the past five years alone there has been a breakthrough in our
understandingofwhysunexposurebenefitshealthinsomanyways,somethingthatwasnotfullycomprehendeduntilnow.Thisbreakthroughhasforcedpeopletotakeacloserlookatthevalueofsunexposure.IamproudtosaythatIhavebeenattheforefrontofthisresearch.
Groundbreaking new research has linked a wide array of disordersthatafflictuptotwohundredmillionAmericanstoasinglecommonfactor—vitamin D deficiency or insufficiency, the most commonmedical condition in the world with sometimes devastating, if notfatal,consequences.
And the research keeps coming from various labs around the worldinvestigating vitamin D. As I write this, doctors at the University ofPennsylvania have revealed that vitamin D can prevent or forestall theirreversibledeclineinrespiratoryfunctionovertimethatleavesmanyasthmaticseven more vulnerable when they suffer an asthma attack. At the same time,scientists at theMoores Cancer Center at the University of California at SanDiegohave raised thepossibility that lowvitaminDmaybe the root causeofcancer.Nodoubtwewillcontinuetoseeremarkablestudiesemerge,andyou’llbe reading about some of the more fascinating and profound studies in theupcomingchapters. It’snowonder that thisvitaminmadeTimemagazine’s listof the top ten medical breakthroughs of 2007. So if you can dramaticallydecreaseyourriskofillnessandage-relateddiseaseandliveahealthier,happierlife—withoutitscostingyouapenny—wouldn’tyouwanttodothat?
CenturiesofProblemSolving
When you put the vitamin D story into the perspective of human history, it
beginswiththeIndustrialRevolution.AstherevolutionbegantosweepacrossnorthernEurope in themid-seventeenthcentury,doctors reportedseeinganewdisease that afflictedyoungchildrenwithaconstellationofphysical signsandsymptoms,notablydeformitiesof theskeleton,suchasbowed legs,misshapenpelvis,enlargedhead,prominentknobbyprojectionsalongtheribs,curvatureofthe spine, poor teeth, and weak and flabby legs. The disease had devastatingconsequences. It not only retarded growth and carried serious risk of upper-respiratory-tract infections including tuberculosisand influenza,but italsohadfar-reaching effects into adulthood and impaired these children’s ability tofunction throughout their lives. Women with a distorted pelvis often haddifficultywith childbirth andwere at high risk of dying or giving birth to anunhealthychild.Several theories about the cause of this debilitating disease called rickets
surfacedintheearly1900s,includinginfection,lackofactivity,poornutrition,andaninheriteddisorder.Althoughcodliveroil(highinvitaminD)appearedtobeeffectiveinpreventingthedisease,itwasprincipallyusedonthecoastlinesoftheScandinavian countries and theUnitedKingdom andwas notwidely usedelsewhere.Thediseasecontinuedtoplaguetheindustrialcentersoftheworld.WhatwashappeningwasthataspeoplebegantocongregateinGreatBritain
andnorthernEurope, they erected citieswhose tightly placedbuildings closedofftosunlightthealleyswherekidswerehangingoutandliving.Compoundingtheproblemwasthegatheringpollutionfromcoalburning,whichthickenedtheair andblocked the sun’s rays.When thesekids started to showsignsofbonedeformities,doctorsbegantotakenote.
“Waterworkswonders,aircandoevenmore,butlightworksbestofall.”
Inthe1820s,aPolishdoctornamedJedrzejSniadeckiobservedthatchildrenwho lived in thecityofWarsawhadamuchhigherprevalenceof rickets thanyoungsters who lived in the Polish countryside. Dr. Sniadecki thought it wasprobably the lack of sunshine in the cramped confines ofWarsaw thatwas toblame for this widespread condition. He was able to successfully treat theafflictedcitykidsbytakingthemintothecountrysideforsunexposure.Buthewasn’t taken seriously. Itwas inconceivable to the scientific communityat thetime that exposure of skin to sunlight could have any impact on the skeleton.Indeed, it would take another seventy years before the British Medical
Associationin1889reportedthatricketswasrarelyseenintheruraldistrictsoftheBritishIslesbutwasprevalentinlargeindustrializedtowns,suggestingthatlackofsunexposurewasresponsibleforthehighincidenceofrickets.Ayearlater,aBritishdoctorcollectedclinicalobservationsfromanumberof
his colleagues throughout the British Empire and the Orient and found thatrickets abounded in the industrialized centers of Great Britain, whereas theimpoverished cities ofChina, Japan, and India,where people lived in squalorandhadpoornutrition,weresparedfromthisbone-deformingdisease.ButlikeDr.Sniadecki, thisearlyvisionary’s findingsweren’t takenseriously.Althoughthe exact relationship between sunlight and bone development was not yetunderstood,ahealthmovementwaspioneeredbyArnoldRikliattheendofthe1800swiththismotto:“Waterworkswonders,aircandoevenmore,but[sun]lightworksbestofall.”Itwasdifficult for thescientificcommunity toembrace theconcept that the
simpleremedyofexposuretosunlightcouldcurethisbone-deformingdisease,and littlewas done to use these insightful observations for the prevention andcure of rickets. When scientists began investigating the connection betweensunlightandhealth,itwasinitiallybelievedthatthewarmthgeneratedbythesunconferred thehealthbenefits. ItwasSirEverardHome,who, in the late1700sandearly1800s,deducedthatitwasn’ttheheatofthesun’sradiationbutrathertheoccurrenceofachemicaleffectonthebodycausedbythesunthatproducedsunburn.Homealsoshowedthatdark-skinnedpeoplehadanaturalresistancetosunburn.By 1900, it was estimated that 80 percent of the children living in the
industrializedcitiesofnorthernEuropeandthenortheasternUnitedStateswereafflictedwithrickets.AlmostonehundredyearsafterDr.Sniadecki’sfirstreport,aGermanphysicianbythenameofKurtHuldschinskyreportedthatexposuretoultravioletradiationfromamercuryarclampwasaneffectivemethodofcuringpatients with severe rickets. He cleverly demonstrated that the effect ofphototherapywasnot a direct effect on the skeleton, inasmuch as exposureofonearmhadan equal anddramatic effecton the cureof rickets inboth arms.People thought hewas nuts for irradiating sick kidswith amercury arc lamp(mindyou, thiswas longbefore skincancerbecamepartof the conversation),butsometookhisideatoheart.Twoyearslater,in1921,twoNewYorkdoctors(Hess andUnger) exposed eight children suffering from rickets to sunlight onthe rooftop of a New York City hospital. They showed through X-rayexamination marked improvement in each child. Finally, the scientific

communitywasreadytolisten.Intheearly1930s,theU.S.governmentsetupanagencythatrecommended
to parents that they put their children outside for a reasonable amount of sunexposure.Severalmanufacturers alsobegan toproduceultraviolet (UV) lampsthatwerethensoldinlocalpharmaciesthroughoutthe1930s,’40s,and’50s.Iknow,difficulttobelievegiventoday’sattitudeonultravioletradiation.
HeliotherapyTakesHold
By the beginning of the twentieth century, scientists had determined that itwastheUVradiationinsunlightthatstimulatedtheproductionofvitaminDinthe humanbody.Theydeduced that thiswas important for a variety of healthreasons.BasedonfindingsthatthevitaminDcreatedbysunexposureimprovedbone health, the dairy industries of Europe and the United States startedfortifying milk with vitamin D. A craze was under way, and vitamin Dfortificationwasbeingtoutedbyfoodandbeveragemanufacturersadnauseam.Products as varied as Bond bread, Richter’s hot dogs, Twang soda, and evenSchlitzbeerweresoldwiththepromiseofdeliveringvitaminD.The first few decades of the twentieth century were the heyday of
photobiology and heliotherapy. Photobiology is the branch of science thatinvestigates the effect of natural and artificial radiation on all life forms;heliotherapyfocuseson thesun’sabilities toheal thesick.Photobiologistsandheliotherapists were credited with developing effective treatments for rickets,tuberculosis, and theskindisorderpsoriasis.HospitalsalloverEuropeand theUnited States built solaria and balconies so they could offer their patients apleasant place to enjoy the sun’s healing rays. In Boston, the then Children’sHospitalputrachiticchildrenonaboatandhadthemexposedtodirectsunlight,whichtheycouldnotgetinthecrowded,polluteddowntownair.ThisgaverisetotheBostonFloatingHospital,whichstillexiststoday(astheFloatingHospitalforChildren)atTuftsMedicalCenter.In1903,photobiologistDr.NielsRybergFinsenwon theNobelPrize formedicineafter successfullydemonstrating thatexposure to sunlight cured many diseases, including lupus vulgaris, ortuberculosisoftheskin.
RicketsontheRise
It’shard to imagineagovernment recommending thedeliberateexposureofchildrentosunlight.Butourgovernmentdidjustthatin1931whenitsetupanagency to encourage parents to expose their children to sunlight to preventrickets. But there’s been a 180-degree turn in just the last forty years. Today,parentsarelikelytobeaccusedofchildendangermentorabuseiftheylettheirkidsroamsunscreen-freeinplaygroundsandatthebeach.Thisallcomeswithaseriousconsequence.Ricketsisnotathingofthepast.It’sbeenontheriselately,andincitieslike
Bostonweseehalfadozencasesayear.Themainreason this ishappening isthat human breast milk today hardly contains any vitamin D, and withoutadequatesunexposureoravitaminDsupplement, infantsareatahighriskofdeveloping rickets. In fact, in one of my studies we looked at forty newbornbabies whose mothers were seemingly doing everything right before givingbirth.Seventypercentofthemtookprenatalvitamins,90percentdrankfortifiedmilk,andallatefish—oneofthebestdietarysourcesforvitaminD—regularlyduringtheirpregnancy.Upongivingbirth,76percentofthemomsandafull81percentofthenewbornswerevitaminDdeficient.
In all, 90 percent to 95 percent of most people’s vitamin Drequirementcomesfromcasualexposuretosunlight.
Anotherreasonricketsiscroppingupagainwithincreasingfrequencyisthatmany kids these days spend toomuch time indoors and out of the sun or areslatheredinsunscreenandmadetowearprotectiveclothingbeforetheygooutto play. Even more alarming is a new epidemic in which bone formation inchildrenappearsnormalbutisactuallymuchsofterthanitshouldbe.Girlstodaybreaktheirarms56percentmoreoftenthantheirpeersdidfortyyearsago.Boysbreaktheirarms32percentmoreoften.Justlastyear,theAmericanAcademyofPediatricsfeltcompelledtodoubleitsrecommendeddailyvitaminDintakefornewborns,children,andadolescents,citingconcernoverrisinglevelsofricketsaswell as theexplosionofnewevidencedemonstrating thathighervitaminDintake may help prevent a wide variety of diseases. Eventually, even theAmericanAcademy ofDermatology, which had been having the hardest timeacceptingrecentstatisticsonricketsandaccompanyingliteratureonvitaminD,chimedin.
In July of 2009, the AmericanAcademy of Dermatology issued a “revisedpositionstatementonvitaminDafteranupdatedreviewoftheincreasingbodyof scientific literature on this vitamin and its importance for optimal health.”Whilestillextremelygun-shyaboutendorsingsensiblesunexposure(infact,thestatementplainly remindedmembers about thedangersofUV radiation in thedevelopment of skin cancer, saying, “VitaminD should not be obtained fromunprotectedexposuretoultravioletradiation”), theacademyurgeditsmembersto remain vigilant about the importance of vitamin D and to pay attention topatientswhoareathighriskofdeficiency.Itsaidthatthosewhoareatriskforadeficiencyshouldbeencouraged toup theirvitaminDintake throughdietandsupplements—not through sun exposure. I am happy to see this baby-stepforward,eventhoughtheacademystillcannotfathomsensiblesunexposureasanoption thatcouldbemoreeffectiveandbeneficialoverall. Iwasamused tolearn that when dermatologists in Australia had their own vitamin D levelschecked, 87 percent of themwere deficient! Indeed, the proof is in their ownpudding. The doctrine of dermatology will take time to rewrite, but in themeantime,eachoneofuscanestablishandfollowourowncanonofhealth.PoorbonehealthandchildhoodricketsisjustthetipofthevitaminDiceberg.
IncreasingnumbersofadultsaredevelopingavitaminDdeficiency-relatedbonecondition known as osteomalacia (pronounced os-tee-oh-muh-LAY-shuh),sometimes called “adult rickets.” Unlike the brittle-bone disease osteoporosis,which doesn’t cause bone pain and is more common in older adults,osteomalaciaischaracterizedbyvaguebutoftenintenseboneandmusclesachesand is frequentlymisdiagnosed as fibromyalgia, chronic fatigue syndrome, orarthritis.The“fibromyalgiaepidemic”thatsomedoctorsrefertomayactuallybeamassive increase invitaminDdeficiency-relatedosteomalacia (seechapter3formoreonthisimportantsubject).I’veestimatedthat40percentto60percentofpatientswhohavebeendiagnosedwithfibromyalgiaorchronicfatiguehaveavitamin D deficiency and suffer from osteomalacia. One such patient whoeventuallyfoundmewaspainfreeafterjustsixmonthsoftreatmenttoraiseherblood levels of vitamin D. Her fibromyalgia simply vanished and her bonedensityimprovedbymorethan25percentafterthefirstyear.AsIchronicledinthecomparisonofthetwofictionalten-year-oldgirlsatthe
startofthischapter,avitaminDdeficiencysetsoneupformyriadhealthrisksacross the board and throughout one’s life. If you are vitamin D deficient inchildhood,youaremorethantwiceaslikelytodeveloptype1diabetes.Ifyoulive above 35 degrees north latitude (roughly the latitude of Atlanta and Los

Angeles),youaretwiceaslikelytodevelopmultiplesclerosis.LivingathigherlatitudesalsomeansahigherriskofCrohn’sdisease,infections,andhighbloodpressure.There’s evidence to suggest that if you raise your level of vitamin D to a
certainamount(andI’llexplainexactlywhatthoselevelsareinchapter2),youcan reduce your risk of colorectal, ovarian, pancreatic, prostate, and breastcancerbyasmuchas30percentto50percent.Youcanalsoreduceyourriskofhypertension, stroke, and heart attack by as much as 50 percent. If you’re awomancontemplatingpregnancy,healthyvitaminDlevelscanimprovefertility,prevent anunplannedC-section, andensure ahealthierbabywhowill enjoyahealthierlife.Womenmaylowertheirriskofrheumatoidarthritisby42percent,anddecreasetheirriskofmultiplesclerosisbymorethan40percent.AndwithadequatelevelsofvitaminDyouwilllivelonger.
AHormone,NotaVitamin
Naturally,we’re disposed to think about vitaminD as a vitamin—a substancethat we get from our diets, like vitamin C or niacin, and that participates inbiological reactions to help the body operate optimally. But despite its name,vitaminDisn’treallyavitamin,andasI’vesaid,youcan’trelyondiettoobtainit;youdo,however,makeitinyourskin.VitaminDisinaclassbyitself;itsfar-reaching effects on the body are alignedwith how hormones act to influencemetabolic pathways, cellular functions, and the expression of myriad genes.VitaminD’sactivemetabolicproduct in thebody, in fact, isamoleculecalled1,25-dihydroxyvitaminD(let’scallit1,25-vitaminDforsimplicity),whichisasecosteroidhormone thatdirectlyor indirectly targetsmore than two thousandgenes,or about6percentof thehumangenome. (I’llbe talkingaboutvitaminD’s twodifferent forms—vitaminD2andvitaminD3.For thepurposesof thebook I’ll be discussing vitaminD2 or vitaminD3 as vitaminD, and I’ll onlyrefertospecificformsofvitaminDwhereappropriate.)Generallyspeaking,vitaminsareorganiccompoundsthatcannotbemadeby
the body but are necessary for proper functioning. (The term vitamin comesfrom“vitalamine”—asubstancethatisessentialforhealthbutcannotbemadebythebody.)Obtainedthroughthedietorsupplementation,vitaminsarevitaltogrowth,development,andmetabolicreactions.Hormones,ontheotherhand,are

synthesizedinthebodyfromsimpleprecursorsandgotodistant tissueswheretheyhaveanintendedeffectandmakemultiplemetabolicimprovements.Inthecase of the manufacture of vitamin D, which requires the help of an outsidesource to trigger a sequence of events, the precursor of a cholesterol-likemoleculefoundintheskincell(7-dehydrocholesterol;provitaminD3)startstheprocessbyabsorbing just theultravioletBportionof sunlight to createwhat’scalledprevitaminD3.PrevitaminD3quickly rearranges itselfwith thehelpofthebody’sheattogivebirthtovitaminD,whichimmediatelyexitstheskincellforthebloodstream.ThefactthatvitaminDismadeinlivingskincellsexplainswhyitisnotpossibletowashoffvitaminDwhenyoubatheafterbeingexposedtothesun.BeforevitaminDcanactasahormone,however,itmustgothroughtwosteps
ofactivation—oneinyourliverandanotherinyourkidneys.I’llbetakingyouthroughthedetailsofhowvitaminDgetsmadeinyourbodyfromsunlighttoitsactive,circulatingforminthenextchapter.Theprocessisyetanotherexampleofhowourbrilliantbodiesoperateandself-regulatetoensureoptimalhealth.IfyouapplyasunscreenwithanSPFof8intoyourskin,itwillabsorbabout
90 percent ofUVB radiation and decrease your ability tomake vitaminD inyourskinbyabout90percent.AnSPFof30reducesyourabilityby99percent.Whileit’struethatmostpeopledon’tputsunscreenonproperly,peoplearenowusingsunscreenwithanSPFof45orabove,soevenifyouputonhalforonethirdoftherecommendedamount,you’restillgettinganSPFof15andreducingyourabilitytomakevitaminDinyourskinbyabout95percent.FarmersintheMidwestwhohadahistoryofnonmelanomaskincancerweretoldtoalwaysusesunprotection,andtheydid.WhenwemeasuredtheirbloodlevelsofvitaminDattheendofthesummer,mostweredeficient.
Mosthumansobtainfromsunexposure theirvitaminDrequirementbetweenthehoursofabout10:00A.M.and3:00P.M.andmainlyinthe late spring, summer, and early fall. Because vitamin D is fatsoluble, it’s stored in body fat and released throughout the wintermonths,allowingyoutobevitaminDsufficientthroughouttheyear.
Hormones are more sophisticated, complex molecules than vitamins. Theycanactintwoways:first,theycansimplyenterthecellandtravelthroughthe

seaofcellularcytoplasmuntiltheyreachthenucleus—thebrainofthecell—andinfluenceitsactivity;second,theycanbindtoareceptoronacellmembraneandtherebytransmitasignaltothecell,tellingittochangewhatitisdoinginanynumber of ways. Activated vitamin D mainly works by interacting with itsreceptorwithinthecell’snucleus.
FromBoneHealthtoBrainHealth
Contrarytowhatwaspreviouslybelieved—thatvitaminDreceptorswereonlyin bones, intestines, and kidneys—wenowknow that vitaminD receptors areeverywhereinthebody.ThereisevenproofthatvitaminDreceptorsexistinthebrainandthattheactiveformofvitaminDstimulatestheproductionofmood-elevatingserotonin.Thisexplainshowitmayhelpreducedepression(orjustachronicallyfoulmood).Fatcells,too,havevitaminDreceptors,andfatcellscanbemoremetabolicallyactive(burnmorecalories)iftheyhavemorevitaminD.People tendto thinkthatfatcellsare like inanimateblobsof lardwheninfacttheyareactiveparticipantsintheprocessbywhichyourbrainlearnsthatyou’refullanddon’tneed to takeanotherbiteof food.Whenyou’vehadenough, fatcells secrete a hormone called leptin that allows you to push away from thetable.AlackofvitaminDwillinterferewiththisappetite-suppressinghormonewhose job it is to regulate your body weight. And we all know what anuncheckedappetitecanleadto:weightgainandahigherriskofdevelopingtype2 diabetes. Speaking of which, vitamin D deficiency has also been shown toexacerbate type 2 diabetes, impair insulin production in the pancreas, andincreaseinsulinresistance.ThefactthateverytissueandcellinyourbodyhasavitaminDreceptorraises
aquestion:whywouldthosereceptorsbethereiftheyweren’tmeanttohaveaneffect? Many of us in the science community think that vitamin D acts as asentinelforyourhealthinthatitcancontrolcellgrowth.Thismeansitcanaffecttheinstigationofcancer.Ifacellbeginstolosecontrolofitsowngrowthandisonapathtobecomingamalignantcancercell,activatedvitaminDcancometothe rescue by either turning on genes to control cell growth or inducingapoptosis—aprocesswhereby the cell kills itself. If the tumor takes hold andbegins to grow, active vitaminDhas onemore trick up its sleeve: it preventsbloodvesselsfromformingtosupplynutritionthatthecancerneedstosurvive.Once the malignant process begins, unfortunately, cancer cleverly develops

systemstobecomeresistanttothebeneficialeffectoftheactiveformofvitaminD.ThisiswhyitissoimportanttobevitaminDsufficientthroughoutyourlife.Just as a gap in your car insurance coverage leaves you vulnerable to costlyaccidents,aperiodoftimewhenyourbodylackssufficientvitaminDtoactonthoseubiquitousreceptorsleavesyouvulnerabletodisease.Infact,itisknownthat ifyouhave lungcancerdetected in thewinter,youare likely todiemorequickly than if you had been diagnosed in the summer. Could that be acoincidence,ordoeslungcancerhavesomethingtodowithvitaminD?Suffice it to say that in some respected medical circles, sunlight is being
described as a “wonder drug.” Dr. William Grant, director of the Sunlight,NutritionandHealthResearchCenter inSanFranciscoandahighly respectedscientist in thefield,hassuggestedthat increasedsunexposurewouldresult in185,000 fewer cases of internal cancers (specifically, cancers of the breast,ovaries,colon,prostate,bladder,uterus,esophagus,rectum,andstomach)everyyearand30,000fewerdeathsintheUnitedStatesalone.Otherresearchershavetakenthisastepfurtherandlookedattheglobalimpact.UniversityofCaliforniaresearchers estimate that 250,000 cases of colon cancer and 350,000 cases ofbreastcancercouldbepreventedworldwidebyincreasingintakeofvitaminD.Sunlight has a similarly dramatic effect on high blood pressure, one of the
leadingcausesofheartattackandstroke.Peoplewhospendtimeinthesunorona tanning bed experience a blood pressure-lowering effect similar to that ofstandardmedicationsthathaveunpleasantsideeffects.Inmystudies,backedbythoseofothers,I’vefoundthatsunlighthasabeneficialeffectonhearthealthonparwiththebenefitsofexercise.Putthosetwothingstogether—physicalfitnessandUVBexposure—andyou’vegotamagicalalchemyofhealthbenefits.

And then, of course, there’s bone health. Sun exposure helps build andmaintainbonedensityandreducesfractures,oneofthemaincausesofdeathanddisability among senior citizens. Humans also need sunlight to control theirbiological clocks, which regulate mood, and appropriate sun exposure isresponsible for keeping down rates of depression associated with seasonalaffectivedisorder(SAD)andpremenstrualsyndrome(PMS).Let’snotforgetthatsunlightplainoldmakesyoufeelbetter—notsomething
tobedismissed in thehigh-stressworld inwhichmanyofus live.Thosewhoheedwarnings to avoid the sunbecause “sunlight is dangerous” are robbedofthe life-sustaining benefits of sun exposure—and the idea that sunlight isdangerousdeniesbasicevolutionaryscience.
TheComplexitiesofaModernEpidemic
Tosay thatour fearof sunlightandourexcessiveuseof sunscreenhaveputa
seriousdamperonourability tomaintain sufficient levelsofvitaminD isonething. But there are other variables that make today’s deficiency epidemic auniquechallenge.Age,gender, race,geographic location,cultural factors,diet,drugs, and even certain health conditions like obesity, liver disease, intestinaldisease, andkidneydisease all factor in.Peoplewhohaveundergonebariatricsurgerytogaincontroloftheirweighthaveaddedchallenges.Forstarters,skincolorhasa tremendous impact,which isevident instudies
donetoidentifypatternsofdeficiency.MyteamdidastudyinBostonattheendofthesummer—atimewhenyouwouldexpectbloodlevelsofvitaminDtobethehighest—andfoundthat40percentofHispanics,34percentofwhites,andabreathtaking84percent ofAfrican-American adults over the ageof fiftywerevitaminDdeficient.Thedarkeryour skin, theharder it is tomakevitaminD,because melanin, your skin’s pigment that gives it color, acts as a naturalsunscreen;AfricanAmericanshavetospendatleasttwotimes(andasmuchastentimes)longerinthesuntomakethesameamountofvitaminDasapersonofIrishorScandinaviandescent(moreonthislater).ThevitaminDdeficiencyin this community may help explain why there’s a health disparity betweenwhites and blacks, with a disproportionate number of African Americanssufferingfromhypertension,heartdisease,type2diabetes,deadlycancers,andstroke,ascomparedtoCaucasians.Another study my colleagues and I published showed that 36 percent of
healthywhitemen andwomen inBoston (medical students and doctors) ageseighteentotwenty-ninewerevitaminDdeficientattheendofwinter.Thiswasdespite thefact that theyoften tookamultivitamin,drankat leastoneglassoffortifiedmilkaday,andatefishatleastonceaweek.Theproblemisworsetheolderyouget—42percentofotherwisehealthyBoston-areaadultsovertheageoffiftywhoparticipatedinthestudywerefoundtobevitaminDdeficient.Theolderyouare,theharderitbecomestosynthesizeenoughvitaminD.Aseventy-year-oldhasonlyaquarterofthevitaminD-makingcapacitythatatwenty-year-oldhas.Thegoodnewsisthatifyouexposeolderpeopletosunlightafewdaysaweek,they—likeanyoneelse—canmaintainadequatelevels.Butalotofourelderlyarenotgettingthebareminimumtimetheyrequireinthesun—sansthesunscreenandfloppyhats—toliterallygettheirvitaminDbloodrunning.That’s not to say, though, that youths are likely to have adequate levels of
vitamin D. Another study in nine-to eleven-year-old girls in Bangor, Maine,revealed that 48 percent were vitamin D deficient at the end of the winter.SeventeenpercentremainedvitaminDdeficientattheendofthesummer.When
theCentersforDiseaseControlandPreventiondidastudyintheUnitedStatesattheendofthewinter,itfoundthat48percentofAfricanAmericanwomen,intheir childbearing years (fifteen to forty-nine years of age) were vitamin Ddeficient. Dr. Catherine Gordon and her colleagues at Boston’s Children’sHospitalreportedthat52percentofadolescentHispanicandAfricanAmericanboys and girls tested were vitamin D deficient throughout the year. The firstnational assessment of this crucial nutrient in young Americans came out inAugustof2009,broadcastingmoremind-bogglingstatistics.About9percentofthoseagesonetotwenty-one,orroughly7.6millionchildren,adolescents,andyoungadults, aredeficient,while an additional 61percent (50.8million) havelevelslowenoughtobeconsideredinsufficient.Thiswasconfirmedbyanotherstudy reporting that 50 percent of children one to five years of age, and 70percentofchildrensixtoelevenyearsofage,wereeithervitaminDinsufficientordeficient.ThiswasnewevidencethatlowvitaminDlevelscouldbeputtingournation’snextgenerationatanincreasedriskforheartdiseaseanddiabetes,two of our biggest health problems worsened by the epidemic of childhoodobesity.Infact,itwasrecentlyreportedthatteenswhowerevitaminDdeficientorinsufficienthadamore-than-200percentincreasedriskofhighbloodpressureand high blood sugar and a 400 percent increased risk of having pre-type 2diabetes (also known as metabolic syndrome), compared to teens who werevitaminDsufficient.ThisthemeisplayedoutwhetheryouliveinFloridaorAlaska.It’spervasive,
in fact, in all parts of the world. It’s natural to assume that Floridians, forinstance, would have no problem keeping their vitamin D levels up. But onestudy demonstrated that their blood levels defy their geography; vitamin DdeficiencyamongFloridianswasstill42percent.After performing a study on themselves, doctors in India reported that 90
percent of Indian physicians—whether they lived inBombay orNewDelhi—weredeficient.Theynowhave reported that50percent to80percentof adultIndiansarevitaminDdeficient.Morethan50percentofchildreninNewDelhiare vitamin D deficient. Even in places like Cape Town, South Africa, andRiyadh,SaudiArabia,vitaminDdeficiencyhasbeenshowntobeaproblem.Ifyoucompareyourskin’svitaminDsyntheticactivityinthesummertowhat
itisinthewinter,you’llseean80percentto100percentreductioninvitaminDsynthesis in thewinter—even in a place likeFlorida. If you live farther norththanAtlanta,Georgia, you essentially can’tmake any vitaminD in your skinfrom aboutNovember throughMarch. In the earlymorning or late afternoon,
even at the equator with the sun shining, you’re still not making vitamin D,becausethezenithangleofthesunissoobliquethatmostoftheUVBphotonsthatmakevitaminDareabsorbedbytheozonelayer.In later chapters I’ll delve more into these as well as other factors that
compound this epidemic, but in brief I want to mention one of the moremisunderstoodfeaturesof thisproblem: the linkbetweenvitaminDdeficiencyandobesity.BecausevitaminDisstoredinfatcells,you’dthinkthatpeoplewithexcess fat would have plenty of extra vitamin D on hand to make up anyshortage.Asitturnsout,thatthinkingiswrong,andaparallelrelationshipexistsbetweenvitaminDdeficiencyandobesity.The fatter youare, thehigheryourriskforadeficiency.Why?ThevitaminDessentiallygetslockedinsidethefatcells,unavailableforuse.Inoneofmystudies,weexposedobeseandnonobeseindividualstothesame
amount of UVB radiation and showed that obese people can only raise theirblood levels of vitamin D by about 45 percent compared to a normal-weightperson.Obesepeople(definedasthosewithabodymassindex,orBMI,above30) oftenneed at least twice asmuchvitaminD to satisfy their body’s needs.WiththemajorityofAmericansoverweightorobesethesedays,it’snotastretchtounderstandwhyasimilarnumberofpeoplearevitaminDdeficient.Thetwoepidemicshaveworsenedinunison.What’s more, obesity and osteomalacia often go hand in hand, tripping a
vicious cycle that worsens the obesity, the osteomalacia, and the vitamin Ddeficiencylikeaperfectstorm.AsIdescribed,osteomalaciaischaracterizedbyextremebone andmuscle pain andweakness.Being overweight predisposes aperson to osteomalacia because the excess fat absorbs and holds on to thevitamin D from the sun and diet so that it cannot be used for properlymineralizing the skeleton or formaintaining cellular health. In addition, obesepeoplearefrequentlyvitaminDdeprivedbecausetheygooutsidemuchless,forpractical and self-esteem-related reasons. This only perpetuates the problem.When an obese person has osteomalacia, the bone and muscle pain andweakness make it virtually impossible to participate in any sort of physicalactivity thatmight help the individual take control of his or herweight.As aresult,theindividualremainsobeseorperhapsgainsmoreweight,whichinturnworsenshisorhervitaminDstatusandexacerbatestheosteomalacia.Treatingaperson’svitaminDdeficiencycancureosteomalaciaandopenthe
worldofexerciseuptoanobeseindividual.AstudyIparticipatedinshowedthatitwaspossibletoincreaseobesepeople’svitaminDlevelsbyexposingthemto
UVBradiation,inthiscasefromatanningbed,orgivingthemmorevitaminDinsupplementform.Thesetreatmentsmayhavebenefitsotherthanenablingthepatients to exercise. Recall that I explained how being vitamin D deficientinterfereswith the secretion of an appetite-suppressing hormone called leptin,which signals thebrainwhenapersonhasconsumedenough fat.Building thevitaminD inaperson’sbloodstreamtonormal levelswill restore thatprocess.Those three elements alone—lessening bone pain, making exercise easier byimprovingmusclestrength,andrebalancingtheappetitehormone—cancombinetohaveadramaticeffectonanindividual’sefforttoputanendtotheobesityandadoptahealthierlife.Muchmoreresearchneedstobedone,butIthinkthereisenormouspotential
forUVBexposure from the sunorartificial sources tobeused to treatpeoplewithobesity.
ButIConsumeLotsofFortifiedMilk,Cereal,andJuice,andITakeaMulti!
When people express doubt over the possibility that they are vitamin Ddeficient because they don’t fall under anyof the usual high-risk categories, Iremind them that it’s nearly impossible tomeet the requirements through dietand a daily multivitamin. As I’ll explain further in chapter 10, the currentrecommendationsareinadequate.Lookatyourmultivitamin’spackaging:Ibetitcontains400IUofvitaminD
and indicates that this is“100%”ofyour recommendeddietaryallowance (theUSDA’s current recommendation,which is twice the200 IU recommendedbytheInstituteofMedicine[IOM]forallchildrenandadultsuptofiftyyearsold).Thisisnotevenhalfofwhatyoushouldbegetting.Andyoucan’tjustdoubleortripleuponyourmultivitamin.ThiscanbedangerousduetothelevelofvitaminAyou’dbeingesting.People assume that if you have a well-balanced diet, you’re getting all the
nutrients you need. There is very little vitamin D from dietary sources. It’sprincipally found in oily fish, mushrooms, or sun-dried mushrooms, and infortifiedfoodslikemilk,orangejuice,yogurt,somecheeses,andsomecereals.Butthereareonly100IUinaglassofmilkorvitaminD-fortifiedjuiceorfoodperserving.(Trivia:MushroomsaretheonlysourceofnaturalvitaminDintheproducesection.Similartothewaythathumansabsorbsunlightandconvertitto

vitamin D, mushrooms contain a plant stool—ergosterol—that converts tovitaminDwhenexposedtolight.Anincreasingnumberofmushroomgrowersaround the world are now exposing their product to ultraviolet light thatproducesevenmorenaturalvitaminD.)What about fish?A serving (3.5 ounces) ofwild salmon can impart 600 to
1,000IU,but fewpeopleeatwildsalmonmostdaysaweek.Aservingofcodliveroilcanprovide400IUperserving,buteventhat’stoolow,andfewpeopleenjoy downingmultiple servings of cod liver oil every day. It’s simply not apracticalwaytogetyourvitaminD,andyoucangettoomuchvitaminA(codliver oil not only contains vitamin D but also vitamin A, similar to amultivitamin).Thesadstateofcommercialfishingcanalsoleadusastray.Afewyearsago
wecomparedfarmedsalmontosalmoncaughtinthewild.BecausewildsalmongetvitaminDfromthefoodchaininnature,wherethereisplentyofvitaminDbecausephytoplanktonandzooplanktonphotosynthesizeit,wildsalmoncontainhigh levels of vitaminD. Farmed salmon, on the other hand, are fed pelletedfoodthathasverylittlebasicnutritionalvalue.ThereisessentiallynovitaminDinit.Whenwecomparedwild-caughttofarmedsalmon,wefoundthatfarmedsalmon had 10 percent to 25 percent of the vitaminD content ofwild-caughtsalmon—notenough toboost levels to anadequate state. (Fora listofdietarysourcesofvitaminDand theirapproximatecontent, refer to thechartonpage227.)
To eat a sufficient amount of vitaminD (1,000 to 2,000 IU), you’dhavetoconsumethreecansofsardines,drinktentotwentyglassesoffortifiedmilk,gulpdowntentotwentybowlsofcereal,snackonfiftytoahundredeggyolks,oreatsevenouncesofwildsalmonfordinnereverynight.
ManyProblems,OneSolution
The inescapable fact is that humans have evolved in such a way as to bedependentonsunshineforlifeandhealth.SunlightisthefuelthatenablesyourbodytomanufacturevitaminD.Whenyourbodyisunable toobtainsufficient

sunlight,itcan’tmakeenoughvitaminDonitsown.Whydoesthismatter?TheshortansweristhatthebenefitsofvitaminDtohumanhealtharemany,varied,and profound. As mentioned in the introduction, it’s estimated that anywherefrom30percent to80percentof theU.S.population isvitaminDdeficientorinsufficient.Inmyopinion,thepercentageofvitaminD-deficientor-insufficientcitizensisatleast50andprobablycloserto90percent.The notion that we have to protect ourselves from the sun all the time is
misguided and unhealthy. This sun phobia explains why so many people aresuffering from conditions related to sun deprivation. When the body doesn’thavewhatitneedstooptimizecellularfunctionsandsustainlife,theinevitabledecline that followsoftenmanifests itself in exactly thekindsof illnesses anddiseases that we hear and read about (and fear) daily, such as heart disease,cancer,diabetes,arthritis,osteoporosis,anddementia,tonamejustafew.Theseultimatelyleadtoalossofindependenceandalowerqualityoflife.I’ve touchedupon a lot of issues in this chapter in broad strokes as a swift
preludetothebalanceofthisbook,whichwilltakeyoudeeperintothevitaminDstory.WhatIhaven’tmentioned,however,isthatwecantraceourrelationshiptovitaminDbackmillionsofyearstoatimewhenhumanshadyettomakeanappearance on the planet. Vitamin D’s legacy begins when earth and itsinhabitants looked vastly different fromhow they look today.Casting back tothattimeperiodallowsustoseewhyandhowweevolvedthewaywedidandadmire the ingeniousmakingofnotonly thehumanbody,buteverybody thatsportsaspine.
CHAPTER2
Fish,Phytoplankton,Dinosaurs,Lizards,andYou
TheevolutionofvitaminDandthescienceofsunlight
YouwouldthinkthatIwasverycarefulandthoughtful inmyconsiderationofwhatIwantedtospecializeinasIwasworkingtowardmyPh.D.,butnothingisfurtherfromthetruth.Moststudentswanttoworkinthehottestareaofscientificinvestigation because they believe that willmake them successful. In the late1960s,whenIwasattheUniversityofWisconsin,thebiggesttopicbouncingoffthewalls in laboratories and lecture hallswas how the body uses energy and,morespecifically,howitgeneratesenergyinitspower-producingmitochondria.Atthetime,everybodywantedtostudyenergymetabolismandthegenerationofATP—the energy packer driving all physiological processes. It was mainlypostdoctoral fellows who were lucky enough to be working with the greatestexperts in thatparticular field.When I tried tonudgemyway into the field, Iwas told togo talk toayoung investigatorwhowasworking in thevitaminDarena.AndsoIdid, leaving theprospectofbecominganexperton thehumanbatterytoothers.Icouldn’tthinkofamoreboringsubjectthanvitaminD.Iknewitprevented
rickets in kids, andwe didn’t see rickets anymore, sowhatwas the big deal?WhyshouldIbeinterested?ScientistsinthelabIjoinedalreadyhaddeterminedthatinpigsvitaminDwasconvertedtoamoleculecalled25-hydroxyvitaminD(“25-vitaminD” for short).When Icameonboard, Ineeded togetamaster’sdegree.Myprojectwas to demonstrate thatwhat theyhad found in pig bloodwasfoundinhumanblood.Istartedmyresearchbutsoonrealizedthattherewasa contaminant in humanblood thatwas not found in pig blood. So I couldn’tsimply follow the procedure for pig blood andwas instead compelled to find
anotherwaytoidentify25-vitaminDinhumans.That puzzle forcedme to develop awhole new chromatographic separation
system, which then permitted me to identify 25-vitamin D. After only threemonths, I had completed the research I needed to obtainmymaster’s degree.Then itwas realized that 25-vitaminD took too long toworkon thebody, sotherewasstillabigmissingpiecetothepuzzle.Itwasthoughtthatmaybe25-vitaminDhadtoundergoatransformationtoan“activeform.”Sotheracewason for three different laboratories, each hoping to be the first to identify this“active”formofvitaminD.TheDeLucalaboratory,whereIworked,wasoneofthoselabs.Longstoryshort:formyPh.D.thesis,whichIcompletedaboutayearlater,I
was responsible for the first isolation and identification of the active form ofvitaminD,which is technically called1,25-dihydroxyvitaminD3 (we’ll call iteither “activated vitamin D” or 1,25-vitamin D). In this chapter, we’ll take acloselookathowyourbodymakesandutilizesthisactivatedform,oneof themost vital hormones your body needs for survival, from a ray of ultravioletsunlight.We’llalsoexplorethemagnificentconnectionbetweenvitaminDandcalciumandseewhyallthecalciumintheworldwon’tkeepyourbonesstrongwithoutthehelpofvitaminD.Butbeforewegettothehumanfactor,weneedtoexaminetheevolutionaryfactordatingbackaeons.
FromtheBigBangtoaBigDeal
An understanding of why we all need a little sunlight starts with anunderstanding of how we’ve evolved as humans, or, more specifically, howwe’ve evolved as land-dwelling creatureswith skeletons tomaintain.Humanshavedependedonsunlighttosustainlifeandhealthsinceourancestorsslitheredoutoftheprimordialoceans.VitaminD has existed on this earth formore than 500million years, since
longbeforeorganismscouldcontemplategrowingbackbonesorappendagesorwalking upright on two legs. At the world-famous Woods Hole MarineBiological Laboratory near Martha’s Vineyard, my team and I grew aphytoplanktonthathasexistedunchangedinourAtlanticoceanforthepast500million years. We exposed this ancient life form to simulated sunlight andshowedthatphytoplanktonhavebeenharnessingtheenergyofthesuntomake

vitaminDforatleastthatlong.Photosynthesisofsugarmayhaveitsoriginsinprokaryotes—primitivelifeformsthathadtheirDNAswimmingintheircellularsoup rather than containedwithin a nucleus,which is the case for eukaryotes(wherelifeformsencapsulatedtheirpreciousgeneticmaterialinanenvelope)—some3.5billionyearsago,butitwouldtakeanotherseveralbillionyearsoftheearth’s 4.55 billion-year history for life forms to develop more sophisticatedwaysofusingthesun’senergytoevolveanddiversifyintovariouscreatures.Atsomepointintheearth’sexpansivetimeline,lifeformsgotboredwiththe
oceanandbegantoventureontoland.Butaslifeformsleft thesecalcium-richwaterssome350millionyearsago,theywereconfrontedwithaproblem:therewasessentiallynoaccessiblecalciumonland; itwas lockedup in thesoilandendedupintherootsandleavesofplants.Backinthebubblingsalineoceans,earlylifecouldabsorbcalciumrightintoprimitivevertebrateskeletons.Ortheyate phytoplankton and zooplankton (microscopic animals) rich in vitamin D.Landpresentedmanynewchallenges,especiallyoncelifeformsgotbiggerandhad to find a way to satisfy their vitamin D requirement without relying onplants. This wasmillions of years, by the way, before humans came into thepicture.Land-dwelling organismsmay have started to roam350million yearsago,buttheevolutionarylineleadingtousdidn’tgetgoinguntilabout7millionyears ago in Africa, at which point our apish ancestors finally becamedistinguishedfromtheancestorsofchimpanzeesandgorillas.Eventhen,ittookthe first 5 to 7 million years after our appearance on earth to venture out ofAfricaandevolveintoHomosapiensaroundhalfamillionyearsago.Humansasweknowthemtodaydidn’tinfactemergeuntilabout200,000yearsago.Bythen,vitaminDhadbeenaroundformillionsofyears.Wearerelativelyyoung.VitaminDisancient.Sofor reasonswedon’t fullyunderstand, itwasexposure tosunlighton the
skin—producing vitamin D—that permitted these animals evolving on terrafirmatobeabletoabsorbenoughdietarycalciumfortheirvertebrateskeletons.Themainjobofcalciumistomaintainneuromuscularfunctionaswellasbuildbones, and these ancient relatives of ours developed a system of absorbingcalcium through diet into their bones. This biochemical transport processrequired the presence of vitaminD,whichwasmade in the skinwhen itwasexposedtosunlight.
DidVitaminDDeficiencyWipeOuttheDinosaurs?
It’s longbeen suggested that the dinosaurswere taken out about 65millionyearsagobyagiantasteroidthathittheearthanddisruptedthenaturalbalancebetween the sun and life just long enough to kill sources of food.But there’sanotherideaIthinkisequallyviableandrelatedtothistheoryofwhathappenswhenyoublockthesun’sraysfromfuelingearth’slifeforms.Thecataclysmiccloud of smoke and debris that spread across the land and caused a perpetualwinter after the asteroid hit prevented the penetration of not just sunlight butspecifically theUVB rays that allowed these animals tomake vitaminD andmaintaintheirhugevertebrateskeletons.WhenthedinosaursgrewdeficientinvitaminD,theygrewweaker.Females
beganhavingtroubleproducingeggswithenoughcalciumintheshelltosurviveboth their birth delivery and the environment, and a terminal cycle set in thatculminatedintheseanimals’officialdeparturefromtheplanet.(Asanaside,thepesticide DDT almost caused the extinction of the condors under a similarreasoning; the exposure to the chemical prevented the condors’ eggs fromcalcifying properly. The eggs broke soon after they were laid, killing thedevelopingbabycondors.)Isometimeswonder,didthedinosaursdieofricketsandosteomalacia?Whatiffortifiedfoodshadbeenaround65millionyearsago?Couldtheirextinctionhavebeenthwartedordelayed?Becausenocturnalrodentsatthetimehadminimumexposuretosunlightand
thusproducedlittle,ifany,vitaminD,theyadaptedbymaintainingcalciumandbonemetabolismwithouttheneedforverymuchvitaminDintheirdiet.Eventoday,moleratsinSouthAfricadonotneedvitaminDtosurvive.Wemayoweouroriginstothesenocturnalrodentsinourlongevolutionaryline,butwe,likesomany other animalswith large skeletons, ultimately evolved to require thesun’senergytobuildstrongbonesandhelpcreatebiologicalproductsthatplayrolesinourmetabolismandcellularfunctioning.
VitaminDmadeintheskinlaststwiceaslonginthebloodasvitaminDingestedfromthediet.
When you are exposed to sunlight you make not only vitamin D but alsoseveralotherphotoproductsthatyoucannotobtainfromfood.Wedonotknowifanyofthesephotoproductshaveanyuniquebiologicalactionsthatwouldbeofadditionalbenefitforhealth,butonehastowonder.MyteamandIcontinueto
searchformorecluesinthisarea.But back to the dinosaurs for a moment. When the movie Jurassic Park
became a blockbuster, no doubt due to our fascination with these awesomecreaturesfromonceuponatime,apeakinreptilesalessoonfollowed.Suddenly,kids were asking their parents to buy them iguanas—modern, small-scaleversionsoftheirancestraldinosaurs.Mydaughter,whowasnineyearsoldwhenthemoviecameout,wasequallyintriguedandbeggedmeforthisexoticpet.Isaidyesunderonecondition:theiguanawouldn’tbecomeavictimofvitaminDdeficiencylikesomanyothervertebratesincaptivity.Eachyear,750,000youngiguanasareimportedintheUnitedStatesandEurope,andmanyofthemshowsignsofmuscleweaknessandbonedeformitiesbytheirfirstbirthday.Our family’s iguana is called Raptor, and he and other reptiles provide
dramaticinsightintotheimportanceofUVBradiationonbonehealth.Innature,reptiles continually bathe in the sun to warm their cold-blooded bodies andbecomevitaminD-photosynthesizing factories. In fact,workingwithDr.GaryFergusonatTexasChristianUniversity,myteamandIshowedthatvitaminD-deficientreptilesspentmoretimeinthesunthantheirbrethrenwhoweregivenvitaminD in their diet—proof that even a reptile knowswhat’s good for himwhenhecan’tgetenoughvitaminDfromdietalone.Whenincaptivity,reptileshavedifficultygettinganysuntoensuretheirbonehealthbecausetheyliveinanenclosed environment that’s often encased in glass, camping out in large fishtanksensconcedinbedroomsorlivingrooms.Eveniftheseglassenclosuresaremovednearawindowwherethesunispenetrating,thereptilesstillcan’tmakevitaminDbecausetheUVBcannotgetthroughtheglass.Theymaygetplentyof calcium in their diet, butwithout the accompanying vitaminD they fail tothrive.ImadesureRaptorhadagoodsourceofcalcium(low-fatcreamcheesesandwichedbetweenlettuceleaves)andinstalledalampthatemitsUVBsohecouldmakeplentyofvitaminD.Youngpetreptilesoftenhaverickets,andolderoneshaveosteoporosissobad
thattheybegintotakeontheshapeofanoldhorsewithasway-backasfracturesin their upper spine collapse their backbone (this is the equivalent of an old,osteoporotic woman with the profile of a camel). As a result, even the mostbenign of accidents—such as falling off a perch—can lead to bone fractures,especiallyofthelegsandarms.WhenX-rayed,manycaptivereptilesarefoundto have multiple fractures, which often lead to their death. Responsible andeducatedreptileownersnowunderstand it isessential to installUVBlamps intheir pets’ enclosures. Doing this effectively prevents the kinds of fractures

previously seen in captive reptiles because it results inmuch stronger, denserbones.Thisphenomenonisidenticaltowhathumanbodiesexperiencewhentheydo
notgetenoughsolarUVBexposure—aweakeningof thebones that results inunnecessaryfractures.
HomosapiensHarnesstheSunforHealth
Sowe know that humans have been using sunlight tomake the vitaminDneededtoregulatecalciumnecessaryforbonehealthforlongerthanwe’vebeencalledHomo sapiens. Our hunter-gatherer forefatherswere always exposed tosunlight. Their skin pigment evolved and devolved specifically for theenvironmentinwhichtheylived,inordertoproduceenoughvitaminDandyetprotectthemfromthedamagingeffectsofexcessivesunexposure.Earlyhumanslived near the equator, where sunlight is plentiful, and they developed dark,melanin-rich skin thatprotected themagainst sunburnbut still “let in” enoughsunlighttomakevitaminD.Ashumansstartedtomigrateawayfromtheequatortoregionswheresunlight
is less intense, andwhere for severalmonths of the year the sun isn’t strongenoughforthehumanbodytomakevitaminD,skinbecamelesspigmentedsoitwould more effectively absorb the sun’s rays when they were available. Thefarther north humans migrated, the fairer their skin became to make use ofavailablesunlight.TheNeanderthals,adistincthumanpopulation thatdiedoutbetween thirty thousand and forty thousand years ago and is not related to usotherthanthroughacommonancestoraroundthreehundredthousandyearsago,wereprominentthroughoutEuropeandwesternAsia.TheNeanderthalswerethefirst human species to live outside of the temperate zone of the world andcolonizeareaswhereobtainingamplevitaminDwasachallenge.NeanderthalfossilsrecoveredfromElSidróninnorthernSpainandMontiLessini,Italy,haveafforded us the opportunity to analyze theirDNA.And in 2007 the results ofthose analyses became known, changing the story of Neanderthals inpaleontologicalandanthropologicalcircles.One of the most startling revelations, though not surprising in the grand
schemeofthevitaminDstory,hasbeenashiftinhowwebelieveNeanderthalslooked. Though they are often viewed as embodying the mystique of thecaveman—withdark skin, a small brain, bulging andprimitive facial features,
andalumberingbodymass,wenowhaveadifferentperspectivetoincludeforat least some of these early hominids. What scientists uncovered through acarefulexaminationof theirDNAwasamutation in theso-calledMC1Rgenethatcodesforaproteininvolvedintheproductionoftheskinpigmentmelanin.MelaninalsoprotectstheskinfromUVradiation.Thishasledscientiststothinksome of these early human species struggling to survive in northern climatesprobablyhad redhairand faircomplexions,much likemodern-dayhumansofCelticorigin. In today’shumansofEuropeandescent,mutations in theMC1Rgene are thought to be responsible for red hair and pale skin because themutationhaltstheactivityofthismelanin-producingprotein.ThemutationseeninNeanderthalgenesisnotexactlythesameastheonedocumentedinmodernhumans,buttheeffectappearstobesimilar.Interestinglyenough,it’salsobeensurmisedthatNeanderthalssufferedfrom
vitamin D deficiency, which may explain the popular hunched-over ape-manimageofaNeanderthal.Complexion-wise,theymayhavebeendevolvingawayfromtheirdarker-skinnedAfricanancestorssotheycouldabsorbmoreUVBandthusmakemore vitaminD.Whether their vitaminD deficiencywas partly orsignificantlytoblamefortheirdie-outisanyone’sguess.Debatestillragesastohow this early species of humans left the planet. Many scholars believe theNeanderthalslivedduringaniceage,whichcontributedtopoordietandlackofexposuretothesun.Othersblameaninvadingnewpopulationofhumansbetterequipped tosurvive, forone thing iscertain:when theCro-Magnonsemerged,theNeanderthals’lastdaysonearthwerelooming.Eventually, humans couldn’tmigrate any farther north because therewasn’t
enough sun to make the vitamin D needed to survive. Then somethingfascinating happened—humans developed the means to harvest the seas forvitaminD-richfishandmammalsofthesortstilltraditionallyeatenbyEskimosand Scandinavians, which enable people to live in climates with very littlevitaminD-producingsunlight.Eventoday,peoplewithfairskindon’trequiremuchexposuretosunlightto
makeenoughvitaminD tobehealthy,andpeoplewithdarkskinarenaturallywellprotectedagainstsunburn.Conversely,peoplewithfairskingetsunburnedquiteeasilyandmaybesusceptibletononmelanomaskincancer,whereasdark-complexioned peoplemore easily become vitaminD deficient when living innorthernclimates.Fromthebeginningofrecordedtime,humanshaveworshippedthesunforits
therapeutic and life-saving properties. This can be seen in cave paintings that
show that ancient people believed exposure to sunlightwas necessary for lifeandgoodhealth.Medicalpractitionersreportedthebenefitsofsunexposureonhearthealthsixthousandyearsago,inthetimeoftheancientEgyptianpharaohs,including Akhenaton. In a famous hieroglyphic drawn during this time,Akhenaton,hiswife,Nefertiti,and theirchildrenarepicturedbeingblessedbythemany “hands” of the sun. Sun therapy was also praised by the legendaryHippocrates (creatorof theHippocraticoath)and thedoctorsof ancientRomeandArabia.TheEgyptians,Mesopotamians,andGreeksallhadsundeities,andthe influence of the sun in religious belief also appears in Zoroastrianism,Mithraism,Romanreligion,Hinduism,andBuddhismandamongtheDruidsofEngland, theAztecsofMexico, the IncasofPeru,andmanyNativeAmericangroups.Thatancientpeoplesinstinctivelyunderstoodthatsunshinewasgoodforthemisnotsurprising.The race to understand sun therapy from a scientific standpoint really got
under way more recently, starting in the first few decades of the twentiethcentury. During this heyday of photobiology and heliotherapy, hospitalsthroughoutEuropeandNorthAmericabuiltsolariaandbalconiessotheycouldoffer theirpatientsacomfortableplace toenjoy thesun’shealing radiation fortreatmentofrickets,tuberculosis,andpsoriasis.AsImentionedinthepreviouschapter,theNobelPrizeformedicinewasbestowedonaphotobiologistin1903fordemonstratingthehealthbenefitsofsunlight.But something has happened in the last forty years. For more than two
hundred thousandyearsourspecieshasenjoyedaspecial relationshipwith thesun,evenwhenwehadnoideaexactlywhyitfeltsogoodorwhyweneededalittle bit of sunshine for optimal health.With the revelation that sunlight alsocontributed to skin cancer and prematurely aged skin, attitudes changed. Big-moneyinterestsgotbehindthecampaigntoconvinceusthatallsunisunhealthy,so that people would always wear sunscreens and regularly visit thedermatologist.Thankstothebarrageofinformationthatwas—andcontinuestobe—unleasheduponus,webecamepersuadedofthis“fact.”Forthepastfourdecadesthedermatologycommunityand,morerecently,the
WorldHealthOrganizationhaverecommendedthatpeopleneverbeexposedtodirect sunlight. That has been a major cause of this worldwide pandemic ofvitamin D deficiency. Drug companies can sell fear, but they can’t sell yousunlight, so there’s no promotion of the sun’s health benefits. Since firstidentifyinghowvitaminDgoesfromUVBradiationtoanactivatedhormoneinthebody,I’vewatchedthelobbyforthesunretreat.I’vewatchedtherallyingcry
formoresunscreenandlessexposure(noticehowthatword“exposure”evenhasanegativering to it,as if it relates togerms)growsstrongerandstronger.Butnothingismorepowerfulthaninformation.Andtothatend,let’stakeatourofyourbody’smiraculousmachineryformakingvitaminD.It’sabigdealanywayyoulookatit.
TheScienceofSunlight:FromUVRaystoActivatedVitaminD
Asmentionedearlier, I identified themajorcirculatingformofvitaminD(25-vitamin D) and its subsequent active form (1,25-vitamin D, the only form ofvitamin D that provides humans with direct health benefits) in my graduate-school days more than thirty years ago. Once it was appreciated that theactivationofvitaminDoccurredinthekidneys,itinstantlybecameobviouswhypatients with kidney disease had severe bone disease and had a resistance tovitaminD.AfteractivatedvitaminDwasidentified,wethoughttherewashopeinusingtheactivatedformtotreatpatientswithkidneyfailureandbonedisease,andmaybepostmenopausalosteoporosis.Butwesoondiscoveredthatthiswasjust thebeginningof thevitaminDstory. In1979, theDeLucagroup reportedthatessentiallyeverytissueinthebodyappearedtorecognizetheactiveformofvitaminD.WeandotherswentontoshowthateverytissueandcellinthebodyhasareceptorforvitaminD.AndwebegantounderstandthatmaybevitaminDhad other biological actions than simply regulating calcium and bonemetabolism.OneofthefirstinsightsintovitaminD’spowerwasmadebyaformerpostdoc
whoworkedwithmeintheDeLucagroup,Dr.TatsuoSuda,D.D.S.,Ph.D.Heshowed that if you took leukemic cells that have a vitamin D receptor andincubated themwith the active formof vitaminD in the lab, it inhibited theirgrowth and induced differentiation, thus dampening their cancerous activity.That was the first clue to the potent biological action of vitamin D and itspotentialroleinpreventingcancer.Afterthatobservation,intheearly1980sweshowedthattheactiveformofvitaminDcouldregulateskingrowthandbeusedtotreattheskindisorderpsoriasis.Psoriasisisanonmalignantdiseaseoftheskinwherebyskincellsmultiplyuptotentimesfasterthannormal,causingunsightlyraisedredlesionswithheavy,whitedeadskin.Iwasoneofthefirstscientiststoprove theantiproliferationactivityofactivevitaminD to restorepsoriaticskincells to theirnormalgrowth,and thisquicklybecame the first line therapy for
psoriasis.Allofasudden,itbecameclearthatcellsthathadavitaminDreceptorhada
widevarietyofgenesthatwerebeingturnedonandoffbyactivatedvitaminD.These genes controlled cell growth and induced cells that were malignant toeitherbecomenormalordie.Thus,vitaminDcouldeffectivelycontrolwhetherornotacellbecamecancerous.
SpotTreatment
Untilthemid-1990s,itwasbelievedthatthekidneysmadethebody’sentiresupply of activated vitamin D. The kidneys make this supply from the 25-vitaminDinthebloodstreamthatiscreatedbytheliverfromthevitaminDthatismade in the skin after sun exposure and, to a lesser extent, from foods thatcontain vitamin D (see figure 1). The supply of activated vitamin D that thekidneysactuallymanufactureisverysmall(abouttwotofourmicrogramsaday,whichamountstoaboutonehundredthofagrainofsalt),andthissupplydoesn’tchangenomatterhowmuch25-vitaminDthereisinthebloodstream.Inotherwords, you could dramatically increase the 25-vitamin D content in yourbloodstreamby lyingon thebeach all summer long, drinkinggallonsofmilk,and eating mackerel at every meal, but your kidneys would still produce thesame tiny trickle of activated vitamin D. The main job of this precious littleamountofactivatedvitaminD,itwasthought,wastocontributetobonehealth.As thepersonwhohad actuallydiscovered the activated formofvitaminD, Iwas very closely involvedwithwhatwas happening in the field of vitaminDresearch, and like most researchers who eventually hit the proverbial wall,somethingbegantobotherme.Here’s what I couldn’t figure out. In response to increased exposure to
sunlight, cellular andorganhealthbenefitswereoccurring that appeared tobetheworkofactivatedvitaminD.Thesebenefits included lowerbloodpressureand decreased risk of cancer and autoimmune diseases likemultiple sclerosisandtype1diabetes.However,thiscouldn’tbetheworkofactivatedvitaminDifwhatwebelievedweknewaboutthekidneys’productionofactivatedvitaminDwastrue.Therewasapparentlyaconnectionbetweensunexposureandcellularand organ health. But our naiveté of how activated vitamin D is producedpreventedusfrommakingtheclaimthatonewasresponsiblefortheother.

Figure 1. Once vitamin D is manufactured in your skin from the sun’s UVBradiation,orobtainedfromdietaryorsupplementalsources,yourlivercreatesavitaminDmetabolite called 25-vitaminD (25-hydroxyvitaminD),which thentravelstothekidneystobeturnedintoactivatedvitaminD(1,25-vitaminD;1,25dihydroxyvitaminD).RecentbreakthroughdiscoverieshaveshownthatvitaminDalsocanbeactivatedwithinavarietyofcells,includingthoseoftheimmunesystem, to modulate immune cell activity reducing the development ofautoimmunediseasesandenhancefighting infectiousdiseases,prostate,breast,and colon, where it prevents the unhealthy cell proliferation characteristic ofcancer.All the while, we were teetering on the verge of a breakthrough in our
understandingoftherelationshipbetweensunlightandcellularhealth.Finally,ithappened.Whatmy colleagues and I discovered in studies at the Vitamin D,Skin, and Bone Research Laboratory at BostonUniversityMedical Center, incollaborationwithDr.GarySchwartz andhis teamatWakeForestUniversity,wasthathumanprostatecellscouldactivatevitaminDinawaysimilartowhathadbeenobservedinhumanskinseveralyearsearlierbyDr.DanielBikleandhis team at theUniversity of California at San Francisco. In otherwords,wewere coming to gripswith the fact humans have the ability tomake activated
vitaminDthroughoutthebody.Theprocessisextraordinary.Whereasoncewethoughtthatonlythekidneys
could activate vitaminD,we now understand that a variety of cells have thisability, including thoseof thebreast,prostate,colon, lung,brain,andskin,andprobablymostothertissuesandcells.Whenthe25-vitaminDreachesandentersthesecells,itisconvertedintoactivatedvitaminD.Unlikethekidneys,however,whichmakeactivatedvitaminDfrom25-vitaminDandsenditoutthroughthebloodstream to the intestine and bones, in other cells, such as brain cells, 25-vitaminDisconvertedintoactivatedvitaminDandusedonthespotwithinthecell.Afteritperformsitsimportantfunctionsinthecell,theactivatedvitaminDextinguishesitselfbyinducingitsowndestruction(thatwayitcannotleavethecellandenterthebloodstreamtocreateanoverabundanceofactivevitaminD,which could be toxic). Because this vitamin D activation process begins andendswithinthecell,thereisnoevidenceofincreasedactivatedvitaminDinthebloodstream,not evenwhenmoreactivatedvitaminD isbeingmadeby thesecells. This is why scientists had difficulty making a connection among sunexposure,vitaminD,andreducedriskofmanychronicandoftenfataldiseases.This discovery is significant becausewe nowknow for sure that increasing
25-vitaminDlevelsinourbloodstreamviasunexposure,andtoalesserextentvia diet or supplementation, will help lower the risk of several diseases—especially thosecausedbyabnormalcellgrowth,suchascancer.Wehavealsosince discovered that the immune system has the ability to make activatedvitaminD,meaningthatsunexposuremayhavearoleinpreventingandtreatingautoimmune diseases such as multiple sclerosis, rheumatoid arthritis, Crohn’sdisease,andtype1diabetes.My laboratory studies continued to confirm that activated vitamin D is an
extremely potent substance that is one of the most effective inhibitors ofabnormal cell growth. The discovery bymy laboratory and other laboratoriesthatcellsthroughoutthebodycanactivatevitaminDwasamajorbreakthroughin vitamin D research. It is what’s behind the emerging realization that—contrarytowhatwehearsooften—theadvantagesofsunexposurefaroutweighthepotentialnegativeconsequences(muchmoreonthistopicinchapter8).Add to this the growing body of research showing that sun exposure helps
regulate circadian rhythms, thus preventing mood-related conditions such asseasonal affective disorder, premenstrual syndrome, and depression due todecreased melatonin levels. This expansive body of research has had someinterestingoffshoots, spawning fresh insights intoareasofourphysiology that
weneverwouldhaveexpected.Forexample,werecentlyconfirmedsomethingthatscientistshaddiscoveredinthe1980sbutthathadneverbeenfollowedupon:It’snot just thebrainthatmakesthe“feel-good”substancebetaendorphin.WhenexposedtoUVBradiation,skinalsomakesbetaendorphinsrightthereonthespot.Thismayexplainwhypeopleoftenfeelsogoodafterspendingtimeatthebeachoreveninatanningbed.
TheSun’sTrigger:UVB,NotUVAorUVC
The vitamin D-making miracle starts, of course, with the sun. Sunlightconsistsofamixtureofpackets(technicallycalledphotons)ofelectromagneticradiation energy of variouswavelengths, from the longest and least energetic,calledinfrared,throughred,orange,yellow,green,blue,indigoandviolet,totheshortestandmostenergeticinwavelength,calledultravioletradiation.Ultraviolet,orUV,radiation,consistsofUVA,UVB,andUVC.UVC(200to
280 nanometers) and some of UVB (281 to 289 nanometers) are completelyabsorbedby theozone in the atmosphere, so theynever reach earthor humanskin. UVA (320 to 400 nanometers) andmost UVB (290 to 319 nanometers)reachearth’ssurfacetovaryingdegreesbuthavedifferenteffectsonyourbody.AsmuchasonehundredtimesmoreUVAradiationreachestheearth’ssurfacethanUVB,and thoughUVAcontainsmuch lessenergy thanUVB, it’sable topenetrate deeper into the layers of your skin, where it affects the elasticstructures, increases free radicals, causes wrinkles, and also influences theimmunesystemandmelanocytes,orskin-pigmentcells.Forthisreason,UVAisthoughttobeamajorcauseofmelanomas.UVB,ontheotherhand,isthehigh-energy form of radiation that is absorbed by DNA and proteins and is lesspenetrating.UVBreddensskinandisamajorcontributor,overthelongterm,tononmelanoma skin cancer.When UVB causes sunburns, it may contribute tomelanoma.UVBisalsotheonlyformofUVradiationthatstartsthereactioninskinthat
stimulatestheproductionofvitaminD.Untilrecently,mostsunscreensblockedonlyUVBradiation,whichmayhaveprecipitated the rise inmelanoma in theUnitedStatesandotherWesterncultures.That’sbecausesunscreens thatblockout only the burning UVB radiation enable people to stay out in the sun forunlimitedperiodsoftime,duringwhichtheyarenotprotectedagainstthedeeplypenetratingUVAradiation.Withoutanysunscreenatall,peoplewouldnothave

beenabletostayoutinthesunlongenoughtoreceivethedoseofUVAthatcanincrease the risk of melanoma. Thankfully, researchers have now developed“broadspectrum”sunscreens,whichprotectagainstmostoftheUVAandnearlyalloftheUVBradiation(dependingontheSPF).ThelevelofUVradiationthatreachestheearthvariesdependingonseveral
factors.Oneofthosefactorsisthestratosphericozonelayer,whichabsorbsmostofthesun’sdamagingUVradiation.Buthowmuchitabsorbsdependsonwhattimeofyearitisandothernaturalphenomena.Asawhole,theozonelayerhasthinned due to industrial pollution and now-banned substances previouslyemittedbyrefrigerantsandcertainconsumerproductssuchashairspray.Sevenchief factorsaffecthowmuchUVradiationactually reachesahumanstandingonearth.Timeofday.UVlevelsareattheirmostintenseatmidday,whenthesunisat
itshighestpointinthesky.Whenthesunisatitshighestpoint,theUVradiationhastheshortestdistancetotravelthroughtheatmospheretoearth.Contrarily,thesun’sradiationmustpassthroughtheatmosphereatamoreobliqueangleduringthe early morning and late afternoon, and therefore UV intensity is greatlydiminishedatthosetimes,whichiswhyit’sverydifficulttomakevitaminDinearlymorningorlateafternoonsun.Timeofyear.Theangleofthesunchangeswiththeseasons.Thiscausesthe
intensityoftheUVradiationtovaryaswell.UVintensityisgreatestduringthesummermonths.Latitude.Thesun’sradiationismostintenseattheequator,wherethesunis
directlyoverheadanditsradiationhastotraveltheshortestdistancethroughtheearth’s ozone layer. Therefore, at the equator, more UV radiation reaches theearth’ssurfacefromthesun.AthigherlatitudesthesunislowerintheskyandUV radiationhas to travel a greater distance throughmoreozone to reach theearth’s surface.Thismakes theUV radiation inmiddle andhigh latitudes lessintense. People living in Edmonton, Canada, for example, cannot make anyvitamin D in their skin during seven months of the year (from SeptemberthroughApril).NewYorkerscannotmakevitaminDduringfourmonths(fromNovemberthroughFebruary).Altitude.UVradiationismoreintenseathigheraltitudesbecausethereisless
atmospheretoabsorbit.Whenyouareathigheraltitudes,therefore,youareatgreaterriskofoverexposure.AstudywedidwithDr.EdwardSautercomparingthebody’svitaminD-makingcapacityatEverestBaseCampin theHimalayas(atanaltitudeof17,700feet)provedapersoncanmakevitaminDyear-roundat
suchanelevation,butnotatloweraltitudesnearby.YoucouldstandbytheTajMahalinNovemberandbedeficient.Weather conditions. The more clouds there are, the less UV radiation can
penetrate to the earth’s surface. However, UV radiation can penetrate cloudcover, which explains why you can still get sunburned on a hazy or overcastsummer’sday.Reflection. Certain surfaces reflect UV radiation and increase its intensity
eveninshadedareas.Suchsurfacesincludesnow,sand,orwater.Withincreasedintensitycomesadoubledose.Pollution.An increasingnumberof people livewithpollution in their local
atmosphere,fromthoseinmetropolitansettingslikeLosAngelesandHoustontothoselivinginlessdenselypopulatedareaswherewindpatternsmoveandtrappollutedpocketsofairinotherwisecleanplaces.BecausepollutioncanfilteroutUVradiation,lessreachestheearth’ssurface.ThismayexplainwhyvitaminDdeficiencypersistsinLosAngelesandAtlanta,thetwocitiesjustontheborderoflatitudeswheremakingvitaminDisrelativelyeasymostoftheyear.
ThinkAforAgingandBforBurning
PeoplegetconfusedbetweenUVAandUVB.Ithelps to thinkof theA-typeradiation as contributing to premature wrinkles when exposure is excessive.Wind, pollution, and smoking also can damage the skin, especially if yourexposure to theseelements isextreme. Ironically, likemelanoma, thewrinkledskinyouseeinmanybabyboomersmaybearesultoftheadventofsunscreensinthe1960s.Why?TheseearlysunscreensprotectedpeoplefromUVBradiation—whichcausesburning—enablingthemtospendlengthyperiodsinthesun,butdidn’tshieldthemfromdeeplypenetratingUVA.Atthetime,UVAradiationwasn’tthoughttohaveanyeffect.Wenowknow,
however, that it is mostly the UVA radiation from sunshine that causes thedamage responsible for wrinkles. Thus, early sunscreens contributed toprematurewrinklinginpeoplewhousedthembecausetheycouldspendalongtime in the sun without getting burned. In doing so, they were exposed tounnaturally largedosesofUVAradiation,whichpenetrateddeeplyandhadanaddedimpactontheirimmunesystems.

FromUVBtoActivatedVitaminD
The chain reaction startswhenUVB rays hit the skin’s surface,where, as Iexplained earlier, a precursor to cholesterol called 7-dehydrocholesterol (alsocalledprovitaminD3,or7-DHC)getsconvertedtoprevitaminD3rightthereintheupperlayerofyourskin.ThiscompoundthenrapidlychangestovitaminD3thatcanbereleasedfromtheskincellsandenterthebloodstream.Thisformisalsocalledcholecalciferol,orvitaminD3,andisthesameformsynthesizedfromsheep’s lanolin for vitaminD3supplements. (I’ll distinguish vitaminD3 fromD2shortly.)VitaminD3 isstillbiologically inactiveuntil the liver takes itandcreatesthemajorcirculatingform,25-vitaminD(alternativelycalledcalcidiol).But wait. Before vitamin D even gets to the liver to be changed into 25-
vitaminD,someofitisgoingthroughyoursubcutaneousfat(thelayeroffatjustbeneathyourskin)andbeingstored.VitaminDisfatsoluble,sothat’swhereitcan be stored during winter months and released as needed. Just as a bearhibernatesduringthewinterandrestockshisfatcellsduringthewarmermonthsfromspringtofall,ahumanismeanttostockuponvitaminDduringthesunnymonthsandcashoutthosefatcellsduringthosecoldwinterdays.
The half-life of 25-vitamin D in your circulation is two to threeweeks.Thus,onesensiblesunexposureprobablylastsyouforatleastonetotwoweeks.
I described earlier that before the main circulating form of vitamin D cancarry out its functions, it must go through another gate—the kidneys. This iswhere 25-vitamin D becomes the active form, 1,25-vitamin D. And it is thisactive form that is responsible for regulating calcium metabolism and bonehealth.Ifyoudon’thaveadequatevitaminD,youcan’tusecalcium.Infact,ifyouaredeficient,youabsorbnomorethan10percentto15percentofcalciuminyourdietorsupplements.IfyouarevitaminD insufficient ,youabsorblessthan30percentofdietarycalcium.I’lldefinetheseparametersindetailbelow;in brief, being insufficientmeans you’re technically not deficient but you stillaren’tmeetingyourbody’sfullrequirement.The ability to absorb calcium is significant for everyone, and especially for

peoplewho are taking bone-health drugs like Fosamax (alendronate);Actonel(risedronate); Boniva (ibandronate); Reclast (zoledronic acid); or Forteo(teriparatide). Patients are often instructed to take calcium in addition to theirdrugtreatment,butdoctorsfailtoremindthemaboutadequatevitaminDintake.Without thevitaminDavailable, the calciumyou ingest is less useful.For allintentsandpurposes,thatcalciumisinvisibletothebodyanditshungrybones.Inchapter9I’llgointodetailaboutthecalciumconnectionandbonehealthandexplainhowvitaminDandcalciumworktogetherinsynergy.
TheOnlyTestforVitaminDStatus
Sogivenall thesedifferent formsofvitaminD,you’d think thebestone totestinapersonwouldbetheactiveform,right?Wrong.It turns out that you cannot useyour blood level of activatedvitaminD, or
eventheformthatmovesfromtheskincells totheliver,whichisbiologicallyinert, to arrive at an accurate measurement of vitamin D status. The majorcirculating form—25-vitaminD—is themost important vitaminDmetabolite.It’s the form I and all experts inmy field recommend that doctorsmeasure inpatients to determine their vitamin D status. (On a lab report, you may see“serum 25(OH)D,” which is the correct form.) Doctors are becoming moreawareofthedifferences,butupwardsof20percentofphysiciansstillorderthewrongtest.
VitaminD2versusVitaminD3:What’stheDifference?
I get this question a lot. And I’m not surprised to find that many peoplebelievethatvitaminD2doesnothingandit’sallaboutvitaminD3.Mylabandothershavejustrecentlyputthismythtobed.The vitaminD that ismade in your skin is vitaminD3.VitaminD2,made
fromyeastandusedforfoodfortificationandsupplementsformorethansixtyyears,hasbeenaccusedofbeinglesseffective thanvitaminD3 inmaintaining25-vitaminDlevels.Thelaypresshaspromotedtheideathatpeopleshouldbecareful about their vitamin D supplement and be sure that they are takingvitaminD3andnotvitaminD2.In2008Ireportedthatwhenhealthyyoungand
middle-aged adults ingested 1,000 IU of vitamin D2, they raised their bloodlevelsof25-vitaminDtothesameextentashealthyadultsingesting1,000IUofvitaminD3.TobecertainthatvitaminD2wasn’tenhancingthedestructionofvitaminD3,
Idesignedthestudytoincludeagroupwhoreceived500IUofvitaminD2and500 IU of vitaminD3 in the same capsule.My team and I observed that thebloodlevelsof25-vitaminDincreasedbytennanograms(ng)permilliliterandwascomparabletothelevelachievedbyingestingeither1,000IUofvitaminD2or1,000IUofvitaminD3.Inotherwords,IdemonstratedthatvitaminD2isjustaseffectiveasvitaminD3andputtorestthislong-establishedmyth.Otherlabshavesinceconfirmedthisfindinginchildren.
Because supplemental vitamin D3 comes from an animal source(lanolin), vegans often avoid supplements or think that vitamin D2isn’tgoodenough.Someassays reportbothsetsofvitaminD,as in“25(OH)D2”and“25(OH)D3.”This is fine;you justneed the total25(OH)D.
MostsupplementssoldtodayarevitaminD3,butthere’snoharminobtainingyour supply fromvitaminD2,which is the ideal choice for veganswhodon’twant any animal sources in their supplements. Patients who are treated forseverevitaminDdeficiencywithhighdosesofprescribedvitaminD(tothetuneof50,000IUperdose)receiveD2;it’scurrentlytheonlyFDA-approvedvitaminD available to physicians to treat and prevent vitamin D deficiency at thatdosage,anditworkswell.IhavegivenpatientsthisamountofvitaminDforuptosixyearswithoutanytoxicity(seechapter10formoreaboutthis).
WhatConstitutesaDeficiency?
My extensive studies have helped redefine what it means to be vitamin Ddeficient. Before one of my publications in the Lancet in 1998, vitamin Ddeficiencywasdefinedasahaving25-vitaminDlevelsbelow10nanogramsper

milliliter. I demonstrated, however, that a blood level of twice that—20nanograms per milliliter—is needed to prevent an unhealthy elevation inparathyroidhormonelevel.Iandmycolleagues,includingDr.RobertHeaneyatCreightonUniversity, established that for every100 IUofvitaminD ingested,theblood’s levelof25-vitaminDgoesupby1nanogrampermilliliter.Don’tworryaboutwhat that reallymeans; the importantpoint is thatbasedon theseobservations, it is now recognized the international community now definesvitaminDdeficiencyasahavinga25-vitaminDlevelbelow20nanogramspermilliliter.VitaminDinsufficiencyisbetween21and29nanogramspermilliliter.Ideally,youshouldaimtohavea25-vitaminDlevelofat least30nanogramspermilliliter,and100nanogramspermilliliterissafe.

Clearly,you’renotgoing toseeavitaminDsupplement thatsays“take thispillonceadayanditwillboostyour25-vitaminDlevelsto40nanogramspermilliliter.”Andthesunwon’tstopshiningonceyou’veobtainedenoughtoboostyour vitaminD supplies. So how do you know howmuch you’re getting andhowthatalltranslatestosufficientlevelsinyourbody?

That’swheremythree-stepstrategycomesin,whichI’lltakeyouthroughstepby step in part II. But first, it’s imperative to clear up a few commonmisconceptions about vitamin D that probably still have you scratching yourhead.
Your 25-vitaminD level is the barometer for your vitaminD statusand is a summation of your dietary, supplemental, and sunlightsourcesofvitaminD.Seechapter7formoreabouttesting.
HowMuchIsTooMuch?
Between 1987 and 1991, asmany as forty-four thousand households in theBoston area were at risk of vitamin D “intoxication,” the scientific word foroverdosing.Theculpritwashome-deliveredmilkthathadbeenoverlyfortifiedbyonecarelessemployeeatadairycompany(ratherthan400IUofvitaminDperquart, therewereup to250,000 IUperquart).The index cases included ahealthy seventy-six-year-old woman who died due to vitamin D intoxication,whichcanincreasebloodcalciumandphosphateandcalcifybloodvesselsandkidneys,andayoungchildwhodevelopedkidneyfailure,caseswereportedinthe New England Journal of Medicine. I helped uncover the source of theoutbreak and put a stop to distribution of the tainted milk. The experienceinspired me to conduct a study, published in the New England Journal ofMedicineatthesametime,thatexaminedmilkandinfant-formulapreparations.Milk rarely contains the amount of vitaminD stated on the label, but inmostcases it’s not overfortified—it’s underfortified. Which is why my conclusioncalledforbettermonitoringofthefortificationprocess.(Wedid,however,findthat infant formulas contained at least the amount of vitaminD stated on thelabel.)I’llgiveyouonemoreexampleofanunusualcaseofvitaminDOD.At7:00
onemorning in themid-1990s, I picked up the phone to hear an irate Floridalawyer accuse me of ruining his health by suggesting he take vitamin Dsupplements.“AreyouDr.Holick?”hesaid.“No.”(Iwasn’tinterestedintalkingtoalawyeratthathour.Whois?)
“Well,Iknowyou’reDr.Holickbecauseyou’retheonlyonetherethatearlyinthemorning.AndI’mgonnasueyou.”“Why”?(NowIwasinterested.)“BecauseI’vebeenfollowingyouradviceandIwentontheInternet,bought
somevitaminD, andnow I’ve landed in the emergency roomwithvitaminDintoxication!”Nowonder Iwas at the topof his list of people to call and threatenwith a
lawsuit. Rather than hang up on the poor fellow and call my own lawyer, IkindlyaskedhimtosendhisvitaminDtomesoIcouldtestit.IfoundithardtobelievehecouldbevitaminDintoxicatedfromtheamounthebelievedhewastaking.Sureenough,thecompanyhadforgottentodiluteit.Thetwoteaspoonsaday
hewastakinginpowderformweren’tdeliveringahealthy2,000IUaday.Hewas taking 1,000,000 IU a day—plenty to cause vitamin D intoxication. Hedidn’tsuemein theend,butratherheaskedformyadviceonhowtorecoverfrom his vitamin D intoxication. He then took his complaint up with thesupplementcompany,whichquicklywentoutofbusiness.
SunlightdestroysanyexcessvitaminD thatyourbodymakes, soyou could never become vitaminD intoxicated from sun exposure.Youwouldneedtoingestmorethan10,000IUofvitaminDadayforat least half a year to even begin to worry about potential toxicityfrom supplements. Symptoms of toxicity include nausea, vomiting,loss of appetite, constipation, increased frequency of urination,increasedthirst,disorientation,andweightloss.
Despitethesetwocases,vitaminDintoxicationisextremelyrare.AndwhatIcontinuallytellpeopleisthatthereisabsolutelynowaytooverdoseonvitaminD through exposure to sunlight. The body, not surprisingly, has a way ofregulatingtheamountrequiredsothatthere’sneveranexcessamountofvitaminDcirculatinginthebloodstream.Ifyouexposeyourselftothesuninabathingsuit for longenoughtoseea lightpinkness twenty-fourhoursafterward, that’stheequivalentoftakingbetween15,000and20,000IUofvitaminD.Forawhiteadult,thatwouldbetheequivalentofbeingexposedtosunlightinJuneatnoonfor about ten to fifteenminutes on aCapeCod beach.Your body has a huge
capacitytomakevitaminDatanyage.WhileagingdoesdecreaselevelsoftheprovitaminDmoleculeresponsibleformakingvitaminDintheskin,yourbodystillhasenoughingredientstomakeadequatevitaminDwithadequateamountsofsunshine,evenwhenyouareninetyyearsold.
TheProsBeatthe“Cons”
In 2002, an extraordinary amount of attention was being generated by anannouncement concerning UV radiation and health. The federal government’sNationalToxicologyProgramhad just announced that it had added ultravioletradiation to the list of what it considers “known human carcinogens.” AsunfortunateasthismovewasbyanagencyoftheU.S.DepartmentofHealthandHuman Services, it perfectly encapsulates the misconceptions that prevailconcerningsunlightandhealth.The blanket statement that UV radiation is carcinogenic is confusing. As a
friend of mine put it, saying that UV radiation causes cancer and should beavoidedisakintosayingthatwatercausesdrowning,sodon’tdrinkwater.Itismisleading to place radiation on the list of carcinogens without saying thatoverexposure—not just exposure—is the problem. Too much of just aboutanything can be a problem—too much dietary fat, too much salt, and so on.There’saworldofdifferencebetweenmoderationandexcess.Justasweneedalittlefatandsaltinourdiet,wealsoneedalittlesun.What’sinterestingwhenyoureadsomeofthefinerprintinthegovernment’s
reportoncarcinogensisthatitdoesn’toffernumbersthatdefineparametersforsafetylevels.Itstates,“ListingofsubstancesintheReport...doesnotestablishthat such substances present carcinogenic risks to individuals in their dailylives.”Inmyopinion,excludingthisvitalinformationmakesthelistofcarcinogens
pointless. The situation is similar to one in the 1980s, when the artificialsweetenersaccharinwaslistedintheNationalToxicologyProgram’sReportonCarcinogens. Remember those warnings on soda can labels stating that theproducthadbeenshown tocausecancer in laboratoryanimals?Saccharinwasremovedfromthelistin2002becausetheamountneededtocausecancerevenin lab animals—eight hundred cans of diet soda per rat!—was unrealisticallylarge.It’salsoimportanttokeepinmindthatcarcinogensarepresenteverywherein

nature.Asscaryasitmaysound,thereareknowncarcinogensinmostfoodanddrink, including tap water (chloroform), grain products (ethylene dibromide),baconandotherprocessedmeats(nitrosamines),peanutbutter(aflatoxin),brownmustard (allyl isothiocyanate), basil (estragole),mushrooms (hydrazines), beerandwine(ethylalcohol),and,asIjustpointedout,somedietsodas(saccharin).Here is what the American Council on Science and Health states about yourchancesofbeing freeof all carcinogens: “Nohumandiet canbe free fromallnaturallyoccurringcarcinogensortoxicsubstances.Indeed,itishardtofindanyfoodthatdoesnotcontainsomeharmfulchemicalthateitheroccursnaturallyorisproducedduringcookingorbymicrobialdecomposition.”ThepointI’mmakingisthatcarcinogensareeverywhere,includinginnatural
substances that we need to survive. Just because something is natural doesn’tmeanwecanconsumeor subjectourselves tounlimitedamountsof itwithoutsufferingnegativehealthconsequences.Sugar,salt,andevenwaterandoxygenarealldangerouswhentakeninexcess.DespitetheattentionthetenthReportonCarcinogensreceivedwhenUVradiationwasputonthelist,theinclusionmeansnothingmorethanthatoverexposuretosunlightmayincreaseyourriskofskincancer.Therearefewpeoplearoundwhowoulddenythisfact.Buttherearejustas many people who have a hard time seeing UVB and health in the samecolumn.
TheTruth
Howdidwe reachapoint inourhistorywhensunbecamesomething tobefearedinsteadofrevered?Thesimpleanswerliesinthefactthattherearemanybillionsofdollarstobemadeinemphasizingtheonlymajormedicaldownsideofsunexposure(nonmelanomaskincancer)andnotmuchmoneytobemadeinpromotingthesun’smanybenefits.Thedeclineofsunlightasapopularandsuccessfultreatmentforavarietyof
diseaseswas initiallyhastenedbymajormedicalbreakthroughs. It startedwiththediscoveryofpenicillinin1928.Thesuccessofthisandotherwonderdrugsheralded the beginning of the era of pharmacology and saved the lives ofmillions. However, it also precipitated the eclipse of disciplines such asheliotherapy and photobiology, which appeared quaint and outdated bycomparison. Itwasn’t long before people had been converted enmasse to theidea that synthetic drugs were much more effective in preventing and curing

mostmaladiesthataffecthumankindthananythingMotherNaturehadtooffer—abeliefthatlargelyprevailstoday.Medicine has long known that, despite all the sun’s benefits, a health
downside of sun exposure is nonmelanoma skin cancer. In the 1920s, it wasrecognized that farmers in Europe developed skin cancer on their most sun-exposedareas—theirears,face,nose,andthebacksoftheirhands.By1937theAmericanJournaloftheMedicalSciencespublishedareportbyDr.SigismundPeller ofNewYorkUniversity that theorized howUV radiation could protectagainstthedevelopmentofmoremalignantcancers,albeitinducingbenignandtreatable skin cancer. Dr. Peller’s population study of choice was a group ofpeople famous for its time in the sun by virtue of the job: the U.S. Navy.Comparedtoage-matchedcontrols,therateofskincancerintheU.S.Navywaseighttimeshigher,whilethetotalnumberofdeathsfromothercancerswas60percent less than in the civilianpopulation.And in1941, the first issueof theJournalofCancerputtheissueinperfectperspective,statingthatanincreasedrisk of nonmelanoma skin cancer was one of the prices to be paid for adecreasedriskofcanceroftheprostate,breast,andcolon.Studieslikethiswerelaterrepeated,confirmingthesameconclusion.Alookatnavypersonnelagain,this time over a ten-year period in the 1970s and 1980s, revealed the samepattern.Peoplewhoworkedinjobsthathadthemoutdoorshadthelowestratesofmelanoma.Thosewhotookmostlytotheindoorsforwork,ontheotherhand,hadthehighestincidenceofmelanoma.Unfortunately, in the past quarter century, the relationship between sunlight
and skin cancer has been blown out of proportion. Themajor culprits are thecosmeticwingof the pharmaceutical industry andwhat I consider to be someunenlightened dermatologists. In the 1960s and 1970s, as the leisure cultureexpanded and peoplewere spendingmore time outdoors, the “cosmeceutical”industry developed antisunburn creams that gave the user a false sense ofsecurityandencouragedexcessivesunexposure.Antisunburnproductsbeganmakingextraordinaryamountsofmoneyforthe
companiesthatproducedthem.Althoughtheproductswereinitiallyintroducedto prevent sunburn, they soon were being cannily marketed to prevent skincancer. There is an important role for modern sunscreens in preventing skincancer,andpeopleshouldcontrolsunexposureinthesamewaytheywatchhowmuchsalt, sugar,andfat theyeatandhowmuchalcohol theydrink.However,the sophisticated and aggressive “educational” campaigns funded by thecosmeceuticalindustryhavecreatedanantisunshinehysteriathatisdetrimental

toourhealthbecauseitconvertspeopleintosunphobesbyconvincingthemthatnoamountofunprotectedsunexposureissensibleorimportantforhealth.Sodesperateistheantisunlobbytoconvinceyouofthedangersofthesun(so
that youwill buy its products year-round) that its representativeswill tell youwithastraightfacethatifit’sFebruaryinBostonandyou’replanningtowalktothecornerstore tobuyaquartofmilkorsitoutsideonyour lunchbreak,youshouldwearsunscreen.ThismessagehasrecentlybeentakentotheextremebyaNewYorkCitydermatologistonapopularmorningTVstationsuggesting thatyoushouldwearsunscreenevenindoorsbecausefluorescentlampscandamageyour skin and cause cancer. This is wrongheaded and alarmist. Even on thesunniestFebruaryday,thesunisn’tstrongenoughinNewEngland,NewYork,orSanFranciscotoincreaseyourriskofskincancersignificantly.Thatsaid,itstillhasplentyofUVAradiationthatcandamageyourskin’selasticityandyourimmunesystem.This isbutoneexampleof thekindof inaccurate informationtheantisun lobbyputsout toalarmpeople. Insodoing, itconvincespeopleoftheneedforitsproductsandservicesyear-roundindoorsandout.Thescaretacticsofthecosmeceutical industryhavebeenembracedbymost
of thedermatologyprofession.Thesegroupshaveworked inconcertandhavefrightened the daylights out of people—or,more accurately, frightened peopleoutofthedaylight.Toputthedangersofskincancerincontext,it’sworthwhileto lookatsomestatistics.Nonmelanomaskincancer,whichmaybecausedbylong-termsunexposure,hasanextremelylowdeathrate.Fewerthan0.5percentofpeoplewhodevelopnonmelanomaskincancerdie;nonmelanomaskincancerclaims1,200livesayear in theUnitedStates.Compare thatwithdiseases thatcanbepreventedbyregularsunexposure.Colonandbreastcancers,whicharetwoofthemostcommontypesofcancer
andwhichmaybepreventedbyregularsunexposure,havemortalityratesof20percentto65percentandkillnearly100,000Americansannually.Osteoporosis,a bone disease that can be mitigated by regular sun exposure, is endemic,affecting 25 million Americans. Every year, 1.5 million Americans withosteoporosissufferbonefractures,whichcanbefatalwhenthepersoniselderly;300,000 of those are hip fractures, and 20 percent of patients (or 60,000individuals)willdiewithinthefirstyearaftersuchabreak.WhenIthinkofthemonetarycosts,not tomention theemotionalandpsychological toll, related totreatingthediseasesandinjuriesrelatedtovitaminDdeficiency,thefireinmybellytokeeptalkingaboutallthisdatareignites.
Somefifty thousandtoseventy thousandAmericansdieprematurelyeach year because of insufficient UV exposure, compared with theninethousandtotenthousanddeathsintheUnitedStatesduetoskincancer—skincancerthatcanbepreventedandtreatedwhendetectedearly.
Thoughrare,melanomasarebyfar themostdangerousformofskincancer,and, if left untreated, they are often fatal. Eighty percent of all skin cancerfatalities are attributed to this type of cancer. However—and this is a criticalpoint—thereisnocrediblescientificevidencethatmoderatesunexposurecausesmelanomas. In chapter 8, I will clear up the confusion surrounding therelationship between sun exposure and skin cancer, confusion that the mediadoesn’t seem able to unravel and the antisun lobby has a vested interest inmaintaining.The antisun lobby also plays on people’s fear of developing wrinkles—a
growingconcerninouryouth-obsessedculture.It’struethatsunexposurecausestheskintoageprematurely,butitispossibletotakeadvantageofthebenefitsofsunexposurewhileminimizingwrinkles.So why has no one stood up to the antisun lobby and said, “Hey, wait a
minute, for too long you’ve exaggerated the dangers of sun exposure andignored the fact that human beings need sunlight to live”?Well, I have! Theproblemis,wheneveranyonechallenges theantisun-coalitiondoctrine thatsunexposure does nothing but cause skin cancer and wrinkles—usually bypublishinganewstudy thatdemonstrates apositive linkbetween sunlight anddiseaseprevention—thisnewsisdrownedoutbyanotherwell-fundedroundofdisinformationaboutthehazardsofsunexposure.ThebibliographyattheendofthebooklistsmanyofthepublishedstudiesthatshowthebeneficialassociationbetweenthevitaminDyougetfromsunlightandmanyareasofhealth.It’sdifficulttogetthefactsoutbecausethereisnosunlobby.Sunshineisfree,
after all, so there’s notmuchmoney to bemade extolling its virtues. Clearlythere’salotofworktobedonetopromotetheimportanceofUVradiationforall-around health.This book should help alter public perception of the role ofsunlightinourlives.CertainlyIhopeithelpsyoumakemoreinformeddecisionsaboutyour relationship tosunshineandhumanwell-being. IncreasingnumbersofscholarlyarticlesarebeingpublishedthataddressthebeneficialrelationshipbetweenUVBradiationandhealth—tothepointthatevenmybelovedAmerican
AcademyofDermatology, thevery institution that has criticizedmyadvice inthe past, is showing signs of weakening in the face of so many indisputablepapersfromthemostesteemedcampusesintheworld.TheverydayIwrote thispage,anotherstudyemergeddeclaring thatone in
sevenAmerican teenagers is vitaminDdeficient, including fullyhalf of blackteenagers.Overweightteensaretwiceaslikelytobedeficientasteensofhealthyweight, and girls have twice the risk of boys. These are sobering statistics,especially against the backdrop of our climbing obesity epidemic. The linkbetweenobesityandvitaminDdeficiencyposesanaddedchallengebecauseit’smoredifficultforobeseindividualstopushtheirlevelsofvitaminDup.Dependingonwhatkindofskinyouhave,whereyoulive,andwhattimeof
yearitis,youneedsunexposureinvaryingamountstomaintainadequatelevelsofvitaminD.Itistruethattherearesomedrawbackstoexcessivesunexposure,andIexaminetheseindepthinlaterchaptersofthisbook.However,asyouwillsee,thedrawbacksofsunexposurepaleincomparisonwiththehealthbenefits.Let’s put the pros and cons of sunlight into perspective with an analogy.
Exerciseisanotherexampleofsomethingthathasbothbenefitsanddrawbacksbutthatis,onthewhole,goodforyou.Everyoneknowsthatexercisingisgood.Itpreventsavarietyofchronicillnessesandmakesyoulookandfeelbetter.Butifyouexercise toomuch,or ifyouhavecertainpredisposingriskfactors—flatfeet or a faulty backhand—then youmay develop overuse conditions such asAchilles tendonitisor lateralepicondylitis (“tenniselbow”).Everyyear,peopledie of heart attacks while running or lifting weights. Nevertheless, no self-respecting doctor would take the position that exercise is unhealthy. Mostdoctorswilltellyoutotakecertainprecautionswhenexercising,butnonewouldeveradviseyounottobeactive.The same goes for sun exposure. Sunlight is not unhealthy. Precautions do
needtobetaken,butaregular,moderateamountofunprotectedsunexposureisabsolutelynecessaryforgoodhealth—asyouwillcometodiscoverasyouturnthepagesofthisbook.
CHAPTER3
HardBodies
ThemagicofDonmuscleandbonehealthWhenyou thinkofoldage, thewords frailandweakmaycometomind.Youmightpictureadodderingwomanormanhunchedoveracanewithloose,crepe-likeskin,thinthreadsofhair,andareedyvoice.Whatyoudon’tseeisawell-posturedindividualwithalotoftonedmusclesandsignsofphysicalstrength.Ifthispersononcehadthephysiqueofanathleteorthecarriageofamodel,itisevidentonly inoldphotographs.Fewpeople thinkabout the rolemusclemassplaysintheagingprocess,andhowmuscleworksintandemwithbonetokeepusagile,able-bodied,andaboveall,young.TheaverageAmericangainsonepoundofbodyweighteachyearaftertheage
of twenty-five, yet loses one third to one half a pound ofmuscle.Although afractionofapoundofmusclemassmayseemminuscule,itactuallyaddsuptobe quite remarkable—translating to about a 1 percent to 2 percent loss ofstrength each year. Muscle strength typically peaks between ages twenty andthirty and then gradually decreases, resulting in the majority of peopleexperiencinga30percentlossinoverallstrengthbyageseventy.Ofcourse,thiscanbepartiallyoffsetifoneisdiligentabouttryingtomaintainandcontinuetobuildmusclemassthroughexerciseand,inparticular,strengthtraining.Butformany people, age brings a combination of unique circumstances and physicalconditions thatcan infringeon thequest to retainmusclemass.So thedeclinecontinues, and with this loss of muscle strength we become even less activebecause daily activities become more difficult and exhausting. All of thisexacerbatesthemusclelossandmagnifiesaperson’soverallfrailty.

Thereasonstrengthtraininggetssomuchattentioninfitnesscirclesisthatitsupportsleanmusclemassandcanhelpyoutoincreasemusclemass, strength,andbonehealth.Themusclesyouengagewhenyouliftaweightputpressureonyourbones,forcingthemtogetstronger.Infact,recentstudieshaveshownthatlossofbonedensitymaybeabetter predictor of death from atherosclerosis (hardening of thearteries)thancholesterollevels.Thereareotherbenefits,too.Strengthtraining is an effective antidepressant and can even improve sleepquality.
Wedon’tnormallyhearaboutpeoplelosingoutonlifeordyingfrommuscleloss. But we do hear a lot about bone loss and osteoporosis, especially withregard to women after menopause. Pharmaceutical companies have startedmarketing their osteoporosis drugs directly to consumers, promising to helpwomenmaintainbonedensityandevenreverseboneloss.Twofactstonote:(1)one of these aggressively marketed drugs has no impact on the risk of hipfractures;itonlyreducesspinalfractures,whicharefarlesslifethreateningthanhip breaks; and (2)more than half ofwomen taking these drugs (58 percent)have been shown to be vitaminD deficient or insufficient.One canmarkedlyreducethechanceofhipfracturethroughadequatelevelsofcalciumandvitaminD.Earlier I touched upon bone diseases such as rickets, osteomalacia, and
osteoporosis and their association with vitamin D. Let’s take a closer look atthese conditions and then loop back tomuscle health.You’ll come to see justhowcriticalvitaminDisinyourbody’smusculoskeletalstructureandhowyourown version of “old age” may have everything to do with maintaining yourvitaminDlevels.
GrowingUpandBoningUp
The thought of bones often conjures scenes from archaeological digs or acemetery.Yourbones, though,are livingthingsmadeupofsubstancesthatarecontinually breaking down and being rebuilt. This process is known asremodeling.

Everyyear,20percentto40percentofyourskeletonisrenewed.Children’sbodiesmakenewbonefasterthantheybreakdownexistingbone,whichcausesbone mass to increase. People reach their peak bone mass in their twenties.However, in the late thirties, thebodybegins tobreakdownmorebonethanitmakes.Thisdecreaseisslight;normalbonelossisonlyabout0.3percentto0.5percentperyear.The result of this slow loss is that the skeletonbecomes lessdense and more fragile. The process accelerates the older you get. Aftermenopause,women losebonedensityata rateof2percent to4percenteveryyear.Menlose1percentto2percentaftertheageofsixty.Itgoeswithoutsayingthatifyouaretryingtoensurethehealthofyourbones,
thegoal shouldbe tobuildbonemasswhenyouareyoungand tomaintain itwhenyougetpast theagewhenboneremodelingisat itspeak.Ifyoudothis,chancesareyouwon’thaveproblemswithyourbones later in life.But ifyoudon’t build bonemasswhen you are young, and if you lose bonemass at anexcessiverateafterthepeakbone-buildingage,yourbonescangetmoreporousandbrittle(osteoporosis,apainlessdisease),whichmeanstheycanbreakmoreeasily. If the bone-rebuilding process itself is compromised, you may havesymptomssuchaspersistentpainandbonedeformity(osteomalaciaorrickets).Howcanyoubuildbonemasswhenyouareyoungandmaintainitwhenyou
areolder?Theanswer tobothquestions is thesame:beactiveandgetenoughcalcium in your diet.Whenwe emphasize calcium intake for bone health, theimportanceofvitaminD isoften ignored.ButvitaminD is like theyeast inarecipe forbread.Youcan’tmakebonewithoutvitaminDavailable.And it allstartsinyourparathyroidglandsandintestine.
Theopposingprocessesofboneresorption(thedissolvingofexistingbonetissue)andformation(thefillingof theresultingsmallcavitieswithnewbonetissue)arewellregulatedsothatanadult’stotalmassof bone tissue normally remains nearly constant, but it’s constantlybeingbrokendownandreplacedsuchthat20percentto40percentofanadult’sskeletonisremodeledeveryyear.Inaninfant’sfirstyearoflife,almost100percentofhisorherskeletonisreplaced.
Anumberof factors affect bonedevelopment, growth, and repair, includinghormones,exercise,andvitaminDsynthesis.VitaminDisnecessaryforproper

absorption of calcium in the small intestine, fromwhich it canmove to yourskeletonviayourbloodstreamandbedepositedinthebonestogiventhemtheirstrength—rather like a cement.When vitamin D is absent, calcium is poorlyabsorbed,which compromises the bone-remodeling process—not enoughboneismade to replace thebone that isbrokendown.Theconstantbreakdownandreplacement of bone that occurs throughout your life is spurred largely byparathyroidhormone,whichisreleasedfromyourparathyroidglands,whichsitontheupperandlowerpolesofyourthyroid.WithoutenoughcalciummovingtoyourbonesthankstovitaminD’spresence,thatdelicatedancebetweenbonebreakdownandbonecreationcanbecomeimbalanced.Inotherwords,youcaneatasmuchcalcium-richfood,drinkasmuchmilk,and takeasmanycalciumsupplements as youwant to, but if you don’t have enough vitaminD in yourbody,youwon’tbeabletoeffectivelyabsorbthatcalciumforyourbones.Andyouwon’tbeabletooutpacethebreakdownofbones,leadingtoseriousbone-relatedconditions.Sowhyiscalciumsocritical?Theintercellularcollagenmatrixofbonetissue
needs a considerable amount of calcium hydroxyapatite to have normal bonemineralization. It is estimated that a person who is vitamin D deficient willabsorbonlyaboutonethirdtoonehalfasmuchcalciumasheorshewouldwithahealthyvitaminDstatus.WithoutenoughvitaminDtohelpyourbonesabsorbcalcium—orwithoutenoughcalciumitself—yourbonesdon’tremodelproperly.Thiscanhappenat anyage.And it’snot just aboutbonehealth.Lowcalciumabsorptiontriggersacascadeofphysiologicalproblems,ascalciumisimportantformostmetabolicfunctionsandneuromuscularactivities.
CanOsteoporosisBeAvertedDespiteAdvancedAge?
The most commonly known bone disease is osteoporosis, which ischaracterized by porous, brittle, and weak bones. Vitamin D deficiency cancauseosteoporosis,anditcanmakeitworse.Evenwhenpeopleareconsumingenoughcalcium,numerousstudieshaveshownthattheystillwillnotbuildandmaintainbonemass if theyaredeficient invitaminD.Andevenmore studieshave shown that people who suffer from osteoporosis often have vitamin Ddeficiency.AsI’vebeenreiterating,notgettingenoughvitaminDdoesn’tjustaffectyour
bones in old age. If you don’t get enough vitaminD during those early years

whenit’scrucialtobuildbonemass—upuntilyourthirties—youwon’testablishthe bonemass you need to keep your bones strongwhen you naturally breakdownmoreofthebonestructurethanyoucanmake.Mendogetosteoporosis,butwomenareatmuchgreaterrisk.Becausewomenhavelesstestosterone,theyhave less muscle mass (this also explains why women have a harder timebuildingandmaintainingmusclemass,astestosteronefactorsheavilyintoone’smusclemass).Women,infact,startoutwithlowerbonemassandtendtolivelonger; they also experience a sudden drop in estrogen at menopause thatacceleratesboneloss.Atthebeginningofmenopause,womencanloseasmuchas3percentto4percentofbonemasseveryyear.Slender,small-framedwomenare particularly at risk. Men who have low levels of the male hormonetestosterone are also at increased risk. Doctors can detect early signs ofosteoporosiswithasimple,painlessbonedensitytest(densitometry).YouareatespeciallyhighriskofvitaminDdeficiency-relatedosteoporosisif
you are predisposed to vitamin D deficiency. There is one exception whencomparingtherisksofvitaminDdeficiencyandosteoporosis.Althoughpeopleof African descent living in higher latitudes are at higher risk of vitamin Ddeficiencybecausetheirbodiesdon’tconvertsunlightintovitaminDaseasilyasraceswithfairerskin, theydonotappear tobeatahigherriskofosteoporosisthanthosewithfairerskin.ThereasonforthisisthatpeopleofAfricangeneticlineage tend tostartwith9percent to15percentdenserbones thanCaucasianpeople. However, chronic vitamin D deficiency will overcome this naturalprotectionandcauseAfricanAmericanstosufferincreasedlossofbonedensityandriskoffracture.AnindicationoftheimportanceofvitaminDonthebonedensityofseniors
wasfoundinastudymycolleaguesandIdidofseniorcitizenslivinginMaine,whichshowedthattheylost3percentto4percentoftheirbonemassinthefalland winter and regained it in the spring and summer months. Obviously, themost serious problem associated with osteoporosis is fractures. As notedpreviously,osteoporosisisresponsiblefor1.5millionfractureseachyear,mostnotablyfracturesofthevertebrae(causingthehunchedappearanceoftenseeninelderlywomenandpainfulsciaticaduetonervecompressioninthelowerback),ribs,wrists,andhips.Hipfracturestendtobecripplingandaresometimesfatal.Osteoporosis-related fractures are more common during the winter months,whenmusclestendtobeweakerandthere’sanincreasedriskoffalling.Unlessaperson remainsactiveduring thewintermonths, thuskeepingupmusclemassandbonestrength,there’sagreaterlikelihoodoffallingandbreakingbones.A
vitamin D deficiency could worsen the situation, since UVB-absent wintermonths require adequate storage of vitamin D for use and vitamin Dsupplementation.Becausethereisnopainuntilafractureoccurs,osteoporosisisknownasthe
silent threat. Numerous studies have shown that vitamin D—usually inconjunction with calcium—is an effective treatment for increasing ormaintainingbonedensityandpreventingfracturesassociatedwithosteoporosis.Finnishresearchersfoundthat341elderlypeople(mostlywomenagesseventy-fiveandolder)whoweregivenvitaminDinjectionsexperiencedfewerfracturesthan458peoplewhodidnotreceivethesupplements.AFrenchstudyof3,270elderlywomenshowed43percentfewerhipfracturesinparticipantswhoweregivenan800IUvitaminDsupplementeverydayand800milligramsofcalciumthaninthoseparticipantswhoweregivenaplacebo.Astudyofalesshigh-riskgroupwasdonebyDr.BessDawson-HughesandhercolleaguesintheBostonareawhen391menandwomenagessixty-fiveandolderweregiveneithera700IUvitaminDsupplementoraplacebo.Theresultsshowedthattheparticipantswhoweregiventhesupplementsustainedhalfasmanyfracturesastheplacebogroupandexperiencedsignificantbonedensityincreases.
WhatIsBoneDensitometry?
BonedensitometryisaspecializedkindofX-ray.Bonedensitometrycalculates how much the X-ray beams are absorbed when passingthrough bones. The amount of X-ray beams absorbed reveals todoctorsthedensityofthebonesbeingstudied.(Densityreferstotheamountofcalciuminthebones.Here’sabitoftriviathatfewpeopleknow:thereasonboneslookwhiteonanX-rayorappearmoredenseinbone-mineral-densitytestsisthattheatomicweightofcalciumisatleast two to forty times greater than that of hydrogen, oxygen, andcarbon, which make up the soft tissues and surrounding collagen.Hence, the “heavy” calcium is absorbing more of the X-rays andshowing upmore brightly.)Bone densitometrymay be done on thebonesof the spine,hip,orwrist.VitaminDdeficiencycausesmorebone loss in the wrist and hip than in the spine. The result of adensitometry test is known as a T-score and is calculated based onhowdifferentyourbonesarefromthebonedensityofanormalyoung
personofyourraceandgender.Ascoregreaterthan-2.5putsyouinthe category of having osteoporosis. Sometimes, however, this testisn’t useful. A bone density test done on a person who has acompressionfractureofthespine,forexample,willshowbonesthatappeartobedensebecauseofthecompressionandthepileofcalciuminthatcompression.Inthiscase,youcan’tevaluatethetrueconditionofthebone,muchlessdistinguishgoodbonefrombrittlebone.
HowDrugstoTreatOsteoporosisWork
In 1995, Fosamax became the first medication in a class of drugs calledbisphosphonates to come on the market and be approved for treatingosteoporosis. Since then, other drugs in the same class have followed.Bisphosphonates affect thebone-remodeling cycle,which, again, is thebody’sbalancingactbetweenbreakingbonedownandformingnewbone.Inahealthyindividual, the bone breakdown-formation process is equal, so you form newboneasfastasyoudissolveoldbone.Butwhenthesetwopartsofthecyclearenotinsync,whichcanhappenduetodiseaseormissingingredientslikevitaminDtohelpcompletethecycle,youeventuallyhaveosteoporosis.Bisphosphonates essentially slow or stop the bone-dissolving portion of the
remodeling cycle, thus allowing new bone formation to catch up with boneresorption.Thesedrugshavebeenfoundtoreducespinalfracturesbyasmuchas60percentoverthreeyearsandhipfracturesbyasmuchas50percent.Themostdramaticresultsareseeninthefirstthreetofiveyearsoftakingthemedication,and smaller improvements aremade for up to a total of tenyears. If a patientstops taking thedrug,however,heor shewill begin to lose thebone thatwasinitiallyregained.Thesedrugsare far fromperfect,however.Theycanbecostly,and theyare
not side-effect free for everyone. Some patients experience gastrointestinalproblemsthatcanbetoomuchtobear.Thesesideeffectsexplainwhypatientsare asked to sit in an upright position, which prevents the drug frommovingbackup into the esophagus and causing irritation.Thedrug is not absorbed iffoodisaround,whichiswhypatientsneedtoavoiddrinkingoreatingforthirtyminutes following the drug’s administration, or for sixty minutes after takingBoniva.

Fosamax (alendronate), Actonel (risedronate), and Boniva (ibandronate) areapprovedforboththepreventionandtreatmentofpostmenopausalosteoporosis;however, whereas Fosamax and Actonel have been shown to reduce hip andvertebralfractures,BonivahasonlybeenapprovedbytheFDAtoreducetheriskof spinal fractures.Miacalcin (calcitonin-salmon) andEvista (raloxifene) offerprotectionagainstvertebral fracturesbutnothipfractures.Forteo(teriparatide)actuallystimulatesboneformationandsignificantlyreducesvertebralandnon-vertebral fracture risk.Thismedication is actuallynot a bisphosphonate. It’s amanmadeparathyroidhormoneusedinpostmenopausalwomen,andinmenwhoare at high risk for fracture and who have not responded to bisphosphonatetherapy; long-termuse (greater than twoyears) isnot currently encouraged.AnewerbisphosphonatecalledReclast(zoledronicacidsolution)hassincejoinedthemarket.Thisonce-a-yeartreatmentisgivenintravenouslyinafifteen-minuteprocedure so that it bypasses the gastrointestinal tract.Also a bisphosphonate,Reclast issaid to increasebonestrengthandreducefractures in thehip,spine,wrist,arm,leg,andrib.Despiteouraccesstothesepowerfuldrugstoday, innowaydotheyreplace
theneedtoensureyourcalciumintakeissufficientandyourvitaminDlevelsarestrong.Thesedrugscanonlyworkaswellas their targetbody’s supplyof theraw ingredients that participate in the bone-formation process. Most of thestudies donewith bisphosphonates that reported good results required calciumandvitaminDsupplementation.Thesedrugsaside, ithelps to remember thatvitaminDsupplementationhas
been shown to help reduce the likelihood of falling bymore than 20 percent,which is important for patients with already compromised bone health. In arandomized,double-blindtrial,treatmentwithvitaminDpluscalciumdailyforthreemonths reduced the riskof fallingby49percent comparedwith calciumaloneamongelderlywomeninlong-staygeriatriccare.InmyownstudieswithDr.DouglasKielandhisgroup,we’veshowna72percentdecreaseintheriskoffallingon800IUofvitaminDforfivemonths.AndkeepinmindthatvitaminDhasabroadrangeofactivitiesbeyonditsroleincalciummetabolismandbonehealth.VitaminDhasasayinnumerousillnesses—cancer,rheumatoidarthritis,multiple sclerosis, type 1 diabetes, type 2 diabetes, heart disease, dementia,schizophrenia, and hypertension—many of which come to define a person’squalityoflifeandlifespan.

Afifty-year-oldwhitefemalehasa40percentriskofexperiencinganosteoporotic fracture inher lifetime. If sheminimizesherbone loss,however, and can postpone bone loss by ten years, her risk offracturingabonegoesdownbyasmuchas50percentlaterinlife.
WhyOsteomalaciaIsSoPainful
Boneproblemsdon’t justcropup late in lifeafter they’vehad time tobrewover the years unnoticed. There’s somewhat of an expectation that an elderlypersonwill haveweaker bones than a younger counterpart.Age does, in fact,decreaseboneresilience.Afifty-year-oldandaseventy-year-oldwiththesamebonedensitywillhaveverydifferentriskforfractures.Theseventy-year-oldwillhaveatwotofourtimesgreaterriskoffracture.Age-related bone issues aside, few people think about serious bone-related
disorders in younger people,which canmake formore challenging diagnoseswhendoctorscan’tput their fingeronadiagnosisforapatientcomplainingofgeneralachesandpains.Ifyouhavebonepainandyourmusclesacheandfeelweak,youmayhaveavitaminDdeficiency-relatedconditionIdescribedearliercalled osteomalacia.Osteomalacia is frequently described as “softening of thebones.” This is slightly misleading. Osteomalacia is a condition in which thebonesdon’thardenproperlyduring thebuildingphase.A lackofvitaminD isthemostcommoncauseofosteomalacia.Unlike osteoporosis, which is often referred to as a silent disease because
there are no symptoms until a fracture occurs, the chief characteristic ofosteomalaciaissevere,unrelenting,deepbonepain.Thispainisfeltinthebonesof thearms, legs,chest,spine,and/orpelvis.Usually there is tendernessof theboneswhen the doctor pushes down even lightly on the area, and this can bemisinterpretedasatriggerpointforfibromyalgia.Thepainfromosteomalaciaisaresultoftheunhardened,Jell-O-likebonematterpressingoutwardagainsttheperiosteum,whichisthenerve-filledfibroussheaththatcoversthebones.Peoplewith osteomalacia often complain of throbbing, aching bone pain andmuscleachesandweakness.Osteomalaciamostseverelyaffectssufferersduringthewintermonths,when
lackofvitaminDproductionismostpronounced.Oftenthepainassociatedwith
osteomalaciaisconstant,pounding,andsevere.Asaresult,itcaninterferewithdaily activities and sleep. Muscle aches and weakness are also common andcome and go unexpectedly. This pain can increase the risk of injuries fromfalling. If youhaveosteomalacia that continues unabated, itwillweakenyourbones and predispose you to fractures, especially of the lower spine, hip, andwrist.How do we test for osteomalacia? X-rays and bone density tests aren’t
effectivediagnostictoolsbecausetheycannotdistinguishbetweenosteomalaciaandosteoporosis.Ifmypatientcomplainsofthecharacteristicsymptomsofthiscondition and a physical examination reveals bone pain when I press downlightlyonthebreastbone(sternum),theoutsideoftheshinofthelowerleg,andthe forearms, then I diagnose that person with vitamin D deficiency-relatedosteomalacia and initiate intensive vitaminD therapy, includingmoderate sunexposureinspring,summer,andfall.Toconfirmthediagnosis,Iorderabloodtest tomeasure the serum levelof25-vitaminD, themostaccurategaugeofaperson’svitaminDstatus.Iprescribe50,000IUofvitaminD2onceaweekforeightweeks.Aftertwomonths,Itestthepatient’sbloodagaintomakesurethevitamin D deficiency shows signs of improvement. If it does not, I prescribeanothereight-weekcourseof50,000IUdosesofvitaminD2onceaweek;obesepatients may need twice as much to raise levels of vitamin D. Usually thetherapyIprescribe resolves thecondition, though it’snotanovernightsuccessstory. It can take up to a full year before the patient feels better and levels ofvitaminDareconsistentlysufficient.Yourdoctorcangetmore informationonhow to treat and prevent vitamin D deficiency on my Web site,www.drholicksdsolution.com.Countless studies have reported great results from treating osteomalacia
patientswithaprotocoltoupvitaminDlevels.Restoring25-vitaminDlevelstonormalinpatientswiththisconditionhasresultedincompleteresolutionofpain,though I’ll admit that the healing process takes time and patience. It can takemonths or years to develop osteomalacia, and it may take just as long toovercomeit.
CanFibromyalgiaBeDisguisedOsteomalacia?
Muscle pain, bone aches, feelings of weakness, and fatigue that just won’tquit.These are thehallmarksof fibromyalgia.Andosteomalacia.Are they the

samething?Therehasbeenadramaticincreaseinvariousconditionswithvaguesymptoms and no proven way to diagnose them. Among these conditions isfibromyalgia (sometimes known by the names fibrositis, chronic muscle painsyndrome, psychogenic rheumatism, or tension myalgias). Fibromyalgia wasunknown until twenty years ago. There is no specific test to confirm that apersonhasfibromyalgia.Itisadiagnosisofexclusion.Thatis,wheneverythingelsehasbeenruledout,thismustbewhat’swrong.Manypeoplewhoaretoldtheyhavefibromyalgiaactuallyhaveosteomalacia.
When someone shows up at a doctor’s officewith fuzzy symptoms of achingbonepainandmuscleweakness,thephysicianisusuallynotawarethatthesearesymptomsof vitaminDdeficiency.Thus, the patient’s vitaminD status is nottested. If it were, doctors would discover that many of the people with thesesymptoms are vitaminD deficient. Between 40 percent and 60 percent of thepeople who come to my clinic having been diagnosed with fibromyalgia orchronic fatigue or written off as having depression actually have vitamin Ddeficiency-relatedosteomalacia.ThesepatientscanbesuccessfullytreatedwithvitaminDsupplementationandexposuretosunlight.
Between 40 percent and 60 percent of the peoplewho come tomyclinic having been diagnosed with fibromyalgia or chronic fatigueactuallyhavevitaminDdeficiency-relatedosteomalacia.Manyhavealsobeenwrittenoffasvictimsofdepression.
A study of Muslim women living in Denmark who had muscle pain andsymptoms consistent with the symptoms of fibromyalgia revealed that 88percentofthemwerevitaminDdeficient.Womeninthisculturetendtogetlittlesunlight because they spend a lot of time at home andwhen they go out areobliged to cover themselves entirely. Similar observations have beenmade inSaudiArabia,Qatar,andtheUnitedArabEmirates.Other studies have also demonstrated how a misdiagnosis as simple as
missingavitaminDdeficiencycanleadtoanexhaustiveprocessofeliminationthatkeepspatientsinpainandprolongstheircorrectivetreatment.Dr.GregoryA.Plotnikoffof theUniversityofMinnesotaMedicalSchool reported in2003that among 150 children and adults aged ten to sixty-five years old whopresented to an emergency department complaining of nonspecific muscular
skeletal aches and pains, 93 percent were vitaminD deficient. These patientswere initially given a wide variety of diagnoses, including degenerative jointdisease, chronic depression (technically called dysthymia), chronic fatiguesyndrome,arthritis,and,ofcourse, fibromyalgia.Theywerealsogivenawiderangeoftreatments;youngwomenweresenthomeonover-the-counterNSAIDs(nonsteroidal anti-inflammatory drugs, e.g., Aleve) whereas an older AfricanAmericangentleman(fifty-eightyearsold)wassenthomeonanarcotic,amongmanyotherpowerfuldrugs.Dr.Plotnikoffwasstunnedtofindno25-vitaminDatallinfivepatientswhohadbeentoldtheirpainwas“allintheirhead.”In a remarkable case solved by doctors at the University of Connecticut, a
seventy-eight-year-oldmanwith severemuscleweakness andmuscle twitcheswassuspectedtohaveamyotrophiclateralsclerosis(ALS,commonlyknownasLou Gehrig’s disease). This was a misdiagnosis. All of the elderly man’ssymptomsdisappearedafterhisunderlyingvitaminDdeficiencywasidentifiedandcorrected.
APainintheBack
Back pain is the most common neurological complaint in North America,secondonlytoheadache.InAmerica,morethan$50billionisspenteachyearontreatment,muchofittonoavailifaspecificcauseisnotfound.Chronicbackpainisoftenprogressive,andmanysufferersnevergetdiagnosedwithanythingspecifictotargetincuringthebackpainforever.IstherealinkbetweensomeofthesecasesandvitaminDdeficiency?AnarticlepublishedintheJournaloftheAmericanBoardofFamilyMedicine
in2008lookedatsixcaseswherepatientshadexperiencedeitherchronicbackpainorfailedbacksurgery.Afterraisingtheir25-vitaminDlevelsfromastateof insufficiency or deficiency to sufficiency, they showed significantimprovement. Some were actually cured of their back ailments entirely,prompting the author of the article,Dr.GerrySchwalfenberg, to call formoreattention to possible vitaminD deficiencies in patientswho complain of backpain.
RicketsRevisited
Let me add a few more facts about rickets, also known as pediatricosteomalacia, that I left out earlier. The sad fact about bone-developmentproblemsinchildrenisthattheyusuallyaren’tdetectedearlyenoughtothwartsomeofthelifelongsideeffects.Inadults,nomatterhowbadthepain,therearenovisiblesymptomsofosteomalacia.Inchildrenwhosebonesarestillgrowing,however, bones that don’t harden properlymay bend under theweight of thechild’s body due to gravity as the child begins to stand and walk. The mostprominent signs of rickets are legs that bend inward or outward and a sunkenchestwithrivetlikeboneprotrusionsupanddownbothsidesofthebreast.Theendsofthebonesofthearmsandlegsmaybewiderthannormal.Inadditiontothesevisibledeformities,childrenwithricketsexperiencebone
painandmuscleweaknessbutmaynotbeabletosuccessfullyconveytheirpain.Ricketswas first identified inEurope in themid-1600s, and, as you knowbynow,itbecameamajorproblemduringtheIndustrialRevolution.Doctorsoftheeraweredismayedtofindwidespreadbonedeformationinurbanyoungstersthatwasunknown inEuropean farmkidsor even thepoorest childrenofAsiaandAfrica.Dr. JedrzejSniadecki ofPolanddetermined that ricketswas causedbylackofsunlight.Europeancitieswereamazeofdarkalleywayswherethesundid not penetrate, and overhead the skies were clouded with heavy pollution.Furthermore, many children of this period were forced to work all day infactories.Itwasn’t until the 1920s thatDrs.AlfredHess andLesterUnger—working
fromthe researchofDr.SniadeckiandDr.Huldschinsky—finallygotpeople’sattention when they demonstrated in New York that sunlight was the magicbullet to cure rickets. Even though a handful of scientists and doctors hadrealizeddecadesearlierthatUVradiationfromthesunwasimportantforhealthandcouldcurerickets,ittookalongtimefortheevidencetocatchoningeneralcirclesandbeaccepted.Soon after sunlight became the standard treatment for rickets (artificial
sunlight frommercury arc lamps was also used), scientists discovered it waspossible to fortifymilkwithvitaminD,andgovernments inEuropeandNorthAmericasanctioned thefortificationofmilkandother foods. (Asanaside,Dr.HarrySteenbochattheUniversityofWisconsin-Madisondemonstratedthatyoucouldirradiatefoodstoimpartanti-rachiticactivity.ThisisthesamelabthatDr.DeLucatookoverafterDr.Steenbochretired.)Rickets,forthetimebeing,waseffectivelyeradicated.However,inthe1950s,therewasanoutbreakofelevatedcalciumininfantsintheUnitedKingdomthatcausedpermanentbraindamage.
Governmentofficialsunjustlyattributedit totheoverfortificationofmilksincevitaminDfortificationwasunregulated.Althoughoverfortifiedmilkwasneverproven to be the reason, European governments moved quickly to pass lawsprohibitingthefortificationofmilkoranyotherfoodproductswiththisvitamin.Andricketshasagainbecomeasignificanthealthprobleminchildrenlivingincramped European urban communities such as London, Glasgow, and Paris.Sweden and Finland, however, do now fortify milk, margarine, and cereals,whileotherEuropeancountriesonlyfortifymargarineandcereals.TheUnitedStateshasseenaresurgenceofricketsinthelastfewyears.This
has motivated the American Academy of Pediatrics to voice its concern andreconsideritsrecommendeddailyvitaminDintakeforchildrenandadolescents.Because the disease had become so rare, doctors are not required by law toreport it, so no national statistics are available. Doctors trained in an era thathasn’tseenricketsarealsonotuptospeedonspottingandtreatingit.Thatmaychangeinthenearfuture.Themain reasons for the reemergence of this condition are the increase in
breast-feeding of infants (humanmilk contains almost no vitamin D) and thedecline in young children’s exposure to natural sunlight. Breast-feeding isimportantforachild’shealth,butitisimportantthatbothinfantandmothertakeavitaminDsupplement,whichI’llcoverinchapter10.AlthoughtheincidenceofricketsamongAmericanchildrenisstillextremely
low, it isagrowingproblem.Parentsneed tobevigilantabout theirchildren’sdietandlifestyle.Thefoundationoftreatmentforricketsisrestoringthechild’svitaminD status.Bracing and sometimes surgerymaybe necessary to correctskeletal deformities that have occurred. Once a child has been affected byrickets,there’snoturningbackfrommanyofitsravages.Heorshemaynevergrowtobecomeastallorasstrongasprogrammedbygenetics.Andthechild’srisk of other diseases, such as certain cancers, type 1 diabetes, and multiplesclerosis,isalsomarkedlyincreased.Notagreatwaytostartalong,healthylife—especiallygiventhefactthisdiseaseiscompletelypreventablewithadequatevitaminD and calcium. Even a childwho suffers from less severe vitaminDdeficiencywillbeheldbackfromreachinghisorherfulldevelopmentandpeakbone mass. If the child continues on through adulthood with below-adequatelevelsofvitaminD,heorshewilllikelyexperienceahormonalimbalancecalledsecondary hyperparathyroidism, which then accelerates bone turnover andprogressiveboneloss—allof this leadingtoanincreasedriskforosteomalaciaandosteoporosis.Osteoporosis,bytheway,canstartdecadesbefore“oldage”;
peopleasyoungastwentysomethinghavebeendiagnosedwiththisdebilitatingcondition. (In 2002, aUniversity ofArkansas study revealed that 2 percent ofcollege-age women already have osteoporosis, and a further 15 percent havesustainedsignificantlossesinbonedensity.)Along-termbone-healthstudyofU.S.childrenisnowbeingdoneinresponse
to this resurgence in rickets, and researchers are concerned that widespreadosteoporosismaybewaitingforthisyoungergenerationinadulthood.Butsomeresearchers are just as concerned about the less well-known effects that lowvitaminD levelsmayhaveon these children later in life.Dr.CedricGarland,who has been researching vitaminD for over twenty years, estimates thatwecouldprevent75percentofcancersbygettingeveryone’svitaminDbloodlevelintoanoptimalrange.(Moreonthiscancerconnectioniscomingupinthenextchapter.)
LeapsandBounds
Ifyouhadtoletonethinggoinlife,whichwoulditbe:muscleorbone?Hardchoicetomake,isn’tit?Thesetwotissuesworkinsyncthroughoutthebodyandarewhatallowustokeepourformandfunction.Musclesinparticularprovidetheforceformovementofbodyparts,andyourmuscularsystemisconnectedtoeveryothersystemofthebody,includingyourskeletalsystem(hencethetermmusculoskeletalsystem).Musclesplayacrucialroleinthedevelopmentofbonesandthemaintenanceoftheirintegrity,andthecalciumyouabsorbwiththehelpofvitaminDinyourintestinesisalsoessentialfornerve-impulseandmuscularfunctions. Bones are not freewheeling parts. If they weren’t attached to yourskeletalmuscles,witha shared interest inhavingample suppliesofvitaminDandcalciumavailable, youwouldn’t be able towalk,dance, talk, or eat.Yourmusculoskeletalsystemisasmuchpartofyoursurvivalasistheairyoubreathe.Soit’snosurprisethat theintertwiningofthesetwotissuesmeansthatwhat
can damage one may also damage the other. Several cross-sectional studiesdating years back byDr.HeikeBischoff-Ferrari and others have shown that alow25-vitaminDlevelisrelatedtolowermusclestrength,increasedbodysway,falls,anddisabilityinoldermenandwomen.InAprilof2000Dr.AnuPrabhalaandhis colleaguesatSUNYBuffalo reportedon the treatmentof fivepatientsconfinedtowheelchairswithsevereweaknessandfatigue.BloodtestsrevealedthatallsufferedfromseverevitaminDdeficiency.Thepatientsreceived50,000

IUofvitaminDperweek,andallbecamemobilewithinsixweeks.TheirresultswerepublishedinArchivesofInternalMedicine.NewerevidencefurtherconfirmsthatlowlevelsofvitaminDmaybeafactor
in lossofmusclemassandmusclestrength,whichwesawat thebeginningofthis chapter is among the more defining consequences to growing older andweaker.Onepopulation-based study from theNetherlands reported thathigherlevelsofcirculating25-vitaminDinbothactiveandsedentaryadultssixtyyearsor older were associated with better musculoskeletal function in the legs andloweroddsofdeclineinphysicalperformanceascomparedtocounterpartswithlowerlevelsof25-vitaminD.Beingabletohavefullfunctionofyourlegs—nottomentionotherbodyparts
—laterinlifecanmakeasignificantdifferenceintheabilitytostayactiveandmaintainacertainqualityoflife—which,inturn,affectsaperson’scapacitytocontinuetomaintainandbuildtheseleantissues.Bothmuscleandbonerequirethegoodkindofphysicalstress thatcomeswithexerciseandstrength training(weight-bearingexercise)thatsupportsthehealthofthesespecialtissues.I’llgointomoredetailaboutthatonpage211.Recall our two ten-year-old girls from chapter 1 and how, hypothetically
speaking,eachmayfaceadifferentfatebasedonherenvironmentandlevelofvitaminD.Imentionedthattheequatorialgirlmaybeabletojumphigherandwithmoreforcethanhernortherncounterpart.Why?Becausestudieshavealsoshownthat levelsof25-vitaminDcorrelatewithmusclepowerandforce.Onestudy in particular that was reported in 2009 looked at adolescent girls andrevealedthatvitaminDispositivelyrelatedtomusclepower,force,velocity,andjumpheight.Thisfindingalertedresearcherstocontinueinvestigatingthisarea,becauseamaturingadolescentwithsuboptimalmuscularforcemayhavelong-termconsequencesinfullbonedevelopment.Laterinthisbook,whenwegettothehow-to’sofmaintainingoptimallevels
ofvitaminD,I’llelaborateonwhyphysicalexerciseissoessentialtothehealthandmaintenanceofyourbonesandmuscles.AdequatevitaminDandcalciumintake,alongwithexercises that stressyourmusculoskeletal system,constitutethe dynamic trio.This is true for both older adults andprepubescent children,whose bone development can be positively influenced by physical activity.StudiescontinuetocomeoutaddressingtheperfectstormofnotenoughvitaminD,notenoughcalcium,andnotenoughexercise.Notonlydoesbeing indoorsattached to the computer and television keep children out of the vitamin D-makingraysofthesun,butitalsokeepsthemfromdoingtheessentialweight-

bearingexercises,suchasrunningandjumping,thatencourageyoungbonestogrowdenserandstronger.What’smore,somestudiessuggestthatchildrenandteens today get 20 percent less calcium than isminimally recommended. Theculprit?Toomuchprocessedfoodandsoda.Unfortunately,withtherecommendeddailyintakeofvitaminDunchangedfor
over fifty years for children and adults up to fifty years of age, andwith ourproblem of childhood obesity deepening, our youngest generationmay be thefirst generation in the history of humankind to suffer the most healthconsequencesasaresultofbeingdeprivedofadequatevitaminD.There isnoexcusefornotgettingenoughvitaminDwhenit’sfreelyavailablefromthesun,butweallknowthatthereareplentyofexcusestouseinstayingoutofthesunandforgettingwhatwe’remissing.Untilit’stoolate.
CHAPTER4
AdventuresinGlobe-Trotting
Docommonkillerslikecancerandheartdiseasesharecommongeography?
One of the most exciting breakthroughs in my field has been the undeniableconnectionsmadebetweenvitaminDdeficiencyandahigherriskofavarietyofcellularhealthconditions, suchas internalcancers, cardiovasculardisease, andcertainmetabolicconditions.Doctorshavelongunderstoodthatsundeprivationcausesboneproblems,butonlyrelativelyrecentlyhavetheseotherassociationsbetween sunlight and health been made. When epidemiologists (doctors whostudythecauseandtransmissionofdiseaseswithinpopulations)ruledoutotherfactorsthatmightexplainthebettercellularandorganhealthofpeoplewholivein sunnier climates—such as diet, exercise, and alcohol and tobacco use—thesearchwasontodiscovertheconnectionbetweensunshineanddecreasedriskofcertaincommondiseases.Those of us in the vitamin D community felt sure there was a connection
betweenthisimportantvitaminandgoodhealth.Asitturnedout,wewereright.Increasingly, epidemiologists are discovering that people who live in sunnierclimateshavealowerincidenceofthesekillerdiseasesthanpeoplewholiveinclimates with are limited amounts of sunlight. Indeed, this is where locationmeanseverything.
Location,Location,Location!
Takea lookat thefollowinggraphicsshowingcancer ratesandbloodpressure

readingsonamap.Findthepattern.Inthenextchapter,you’llseeasimilarpatternwhenexaminingtheincidence
ofmultiplesclerosisacrossthemap.AsearlyasthedaysofWorldWarIitwasappreciatedthatifyoulivedata
higherlatitude,youwereatgreaterriskofdyingofcancer—eventhoughitwasalso appreciated that, yes, if you lived down south andwere exposed tomoresunlight,youcould increaseyour riskofnonmelanomaskincancer.FollowingDr. Peller’s analysis of navy personnel, who showed higher rates ofnonmelanomaskincancerbutmuchlowerratesofother,moredeadlytypesofcancer than the general public, scientists hunted for further clues to thismysterious connection between howmuch sun people get throughout the yearand their riskofdisease. In1941Dr.FrankApperly analyzed cancer statisticsthroughout North America and Canada. Compared with cities at a latitudebetween10and30degrees,citiesbetween30and40degreeslatitudeaveraged85percenthigheroverall cancerdeath rates, citiesbetween40and50degreeslatitude averaged118percent higher cancerdeath rates, and cities between50and60degreeslatitudeaveraged150percenthighercancerdeathrates.
Figure3.ThismapshowstheratesofprostatecancerindifferentregionsoftheUnitedStates.Asyoucantell,thesunniertheregion,thefewerprostatedeathsthere are. The same trend has been identified in analyses of breast and coloncancerrates.

Figure4.Thefartheryoulivefromtheequator,thehigheryourbloodpressureislikely to be. Why? Because the farther you live from the equator, the lessavailable sun there is tomake adequate vitaminD.ANewYorker is likely tohave higher blood pressure than someone who lives in Austin, Texas, forexample.Numerous studies have since confirmed these findings. In the 1980s and
1990s,brothersCedricandFrankGarlandoftheUniversityofCaliforniaatSanDiego and Dr. Ed Gorham, among other researchers, picked up where Dr.Apperly had left off and began looking at geography and relating it to cancerincidence. They first looked at colorectal cancer incidence and showed thatpeople living in the northeast had a 10 percent increased risk of developingcolorectal cancer. Then they did further studies showing that the higher thelatitude at which a person lived, the higher his risk of colorectal, breast, andseveralothercancers.Scores of other investigators have found similar associations and further
cracked this code of cancer. In 2007, Dr. Joan Lappe and her colleagues atCreightonUniversity reported that postmenopausalwomenwho took 1,400 to1,500 milligrams of calcium and 1,100 IU of vitamin D daily for four yearsreducedtheirriskofdevelopingallcancersbymorethan60percentcomparedtoaplacebogroup.Inmyownrecentresearch,aftergivingmicecoloncancerandfollowing them for twenty days, we observed a marked reduction in tumorgrowthaftersimplyensuringtheygotamplevitaminDintheirdiet.Therewasa40percentreductionintumorsize.Thisgatheringphalanxofresearchprovidesstrong new evidence that vitaminD could in fact be the singlemost effectivemedicine in preventing cancer, perhaps even outpacing the benefits of otherpreventivemeasuresknowntomodernscience,suchaseatingahealthydiet.
The bold but unequivocal argument that started with Dr. Peller’s and Dr.Apperly’s findingscontinues togather force today:nonmelanomaskincancersare relatively easy to detect and treat, unlike lethal colon, prostate, and breastcancer,whichwenowknowareassociatedwithlackofsunexposure.Wealsoknowthatthesun’sprotectionagainstcancerisduetovitaminD.You’llhavetoforgiveme for sounding a little repetitivewith all this research and publishedworks confirming the same or similar conclusions; the statistics can becomedizzying, but they are astonishing. All these insights have truly reshaped ourviewonsunlightaswellasgivenusareasontoviewthelastdecadeasagreatleapforwardinscientificcircles.
CrackingOneofCancer’sCodes
A1990studypublishedinPreventiveMedicineshowedthatwomenlivinginthesunniersouthwestoftheUnitedStateswereonlyabouthalfaslikelytodiefrombreastcanceraswerewomenintheleastsunnynortheastregionofthecountry.A 1992 article in the same journal analyzing fifty years of epidemiologicalcancerdatasuggestedthatincreasingsunexposurewouldreducethenumberofbreastandcoloncancerdeathsbythirtythousand,oronethird.In2001, theLancetpublishedanarticle thatdirectly linkedsunexposure to
decreased prostate cancer rates. This study showed that Britishmenwho hadgottensunburnedaschildren,whovacationedinsunnycountries,andwhomadeahabitofsunbathingweremuchlesslikelytodevelopprostatecancer.Theyalsofound thatpeoplewhospent lotsof time in thesun tended todevelopprostatecancer later than thosewho spent little time in the sun (at an average of 67.7years old as compared to 72.1 years). Because prostate cancer grows veryslowly,thisfive-yeardelayintheageatdiagnosisishighlysignificant.Twomajorstudiespublishedin2002reinforcedthelinkbetweensunlightand
cancer prevention. Doctors from the National Cancer Institute reported thatpeoplewhoeitherworkedoutdoorsorlivedinsunnyclimateswerelesslikelytodie from breast or colon cancer. They also found that the risk of dying fromcancersof theovariesandprostatewere loweramongpeople livingnearer theequator. In the journal Cancer a month earlier, a researcher described howsunlightwas responsible for preventing a rangeof cancersof the reproductiveand digestive systems. The study’s author, Dr. William Grant, revealed that,comparedwithresidentsoftheSouthwest,peopleinNewEnglandweretwiceas
likelytodevelopcancersofthebreast,ovaries,colon,prostate,bladder,uterus,esophagus,rectum,andstomach.Based on the statistics available, Grant calculated that in 2002 alone,
insufficient sun exposure amongAmericans caused eighty-five thousandmorecases of cancer and thirty thousandmore deaths thanwould have occurred ifeveryone in theUnited States had gotten asmuch sun as people living in theSouthwest.SimilarobservationshavebeenmadeinEurope.Youmayask,Whatabouttheincreasedratesofmelanomaandnonmelanoma
skincancerthatwould,hypothetically,resultfromthisadditionalsunexposure?Grant calculated the additional number of deaths from skin cancer would bethreethousand—atragicallyhighnumber,butonefarsmallerthanthenumberofdeathscausedbyunderexposuretosunlight.Recallthatmostmelanomasoccurin the leastsun-exposedareas,andworkingoutside in thesunallday(what issometimesreferredtoasoccupationalexposure)lowersone’sriskformelanoma.Certain types of cancer have strong gender associations. Breast cancer affectsmostly women, and only men get prostate cancer. Both breast and prostatecancerarestronglyinfluenced—inapreventivemanner—bysunexposure.
TheGarlandbrothersandtheircolleaguesandDr.WilliamGranthaveshown that if you start out with a 25-vitamin D of at least 20nanograms per milliliter, you reduce your risk of developingcolorectal,breast,andawidevarietyofothercancersby30percentto50percent.It’sestimatedthat ifyoutake1,000IUofvitaminDperday, you reduce your risk of developing colorectal, breast, prostate,andovariancancerbyapproximately50percent.
Canceralsohasstrongracialassociations.It’swelldocumentedthatthere’sahigher incidenceof cancer amongAfricanAmericans than amongCaucasians.Theyalsohavelowersurvivalratesoncediagnosedwithcancer.ScientistshavelonghypothesizedthatthisdisparitycouldbedueinparttovitaminDstatus,asvitamin D deficiency is more prevalent and pronounced among AfricanAmericans,whosemelanin-richskinabsorbssolarUVBradiationandcompeteswith7-DHCforthesevitamin-Dproducingrays,thusdecreasingtheamountofvitamin D that can be manufactured in the skin. When Dr. William Grantreportedon this in2006 for theJournalof theNationalMedicalAssociation ,
statingthatlowercancersurvivalratescouldbeattributedtolower25-vitaminDlevels in the black community, he even took factors like smoking, alcoholconsumption,accesstohealthcare,andpovertyintoconsideration.Large-scale studies performed by researchers at Harvard found that, after
adjusting for multiple dietary, lifestyle, and medical risk factors, AfricanAmericanmenwereat32percentgreaterriskof totalcancer incidenceand89percentgreaterriskoftotalcancermortalitythanwhitemen.AfricanAmericanmen also have been shown to be at an especially high risk of cancer in thedigestive tract (colon, rectum,mouth, esophagus, stomach, andpancreas)—theverygroupofcancersstronglyassociatedwithlow25-vitaminDlevels.In2005,atameetingof theAmericanAssociationforCancerResearch,Harvard’s leadresearcheron these studies,Dr. EdwardGiovannucci, a professor ofmedicineandnutrition,laidouthiscaseinakeynotelecturethathadvirtuallyeveryone’searsprickedup.HisresearchsuggeststhatvitaminDmighthelppreventthirtydeathsforeachonecausedbyskincancer.
BreastCancer
Here’s a staggering statistic:Womenwho are deficient in vitaminD at thetimetheyarediagnosedwithbreastcancerarenearly75percentmorelikelytodiefromthediseasethanwomenwithsufficientvitaminDlevels.What’smore,theircanceristwiceaslikelytometastasizetootherpartsofthebody.IntheUnitedStates,morethanfortythousandwomendiefrombreastcancer
every year—making it the deadliest killer of women after heart disease. Onewoman ineighteitherhasorwilldevelopbreastcancer inher lifetime.To themore than two hundred thousandwomenwho are diagnosedwith this diseaseeachyear,therearenotonlyphysicalconsequencesbutemotionalonestoo.Self-esteemissuesassociatedwithbreastcancercanbeprofound.
There are 214,000 new cases and 41,000 deaths from breast cancereachyearintheUnitedStates.A2008studyfoundthatwomenwhohad a vitamin D deficiency at the time they were diagnosed withbreastcancerwere94percentmorelikelytohavetheircancerspreadthanwomenwithadequate25-vitaminDlevelsintheirbodies.

InMay1999,alandmarkstudybyDr.EstherJohn,basedonthemeticulousanalysis of breast cancer statistics from the National Health and NutritionExamination Survey, was published. The results provide extraordinary insightinto the relationship between sun exposure and breast cancer. The authorsconcludedefinitively that sun exposure andavitaminD-richdiet significantlylowertheriskofbreastcancer.The John study demonstrates that increased sun exposure alone could
potentially reduce the incidence and death rate of breast cancer in theUnitedStatesby35percentto75percent.Thiswouldmeanthattheincidenceofnewcases might be reduced by 70,000 to 150,000 each year and that 17,500 to37,500deathscouldbeprevented.Aconservativeestimateisthatincreasedsunexposure couldprevent100,000newcasesofbreast cancer and27,500deathsfromthisdisease.CombiningincreasedsunexposurewithavitaminD-richdietorsupplementscouldmakethediseasepreventionanddeathratefigures150,000and38,000,respectively.In2007,researcherspooledtheresultsfromtwostudies—theHarvardNurses’
HealthStudyandtheSt.George’sHospitalStudyinLondon—andpublishedareport that saidpatientswith thehighestblood levelsof25-vitaminDhad thelowestriskofbreastcancer.Raising25-vitaminDlevelsmaypreventuptohalfofbreastandtwothirdsofcolorectalcancercasesintheUnitedStatesalone.In2008,Dr.Garlandandhiscolleaguesagaindocumentedanassociationamongalackofsunlightexposure,low25-vitaminD,andbreastcancer.Thesestatisticslikely replicate inothercountriesat similar latitudes.Basedonhisstudies,Dr.William Grant estimates that lack of sun exposure is responsible forapproximately25percentofthedeathsfrombreastcancerinEurope.Recently,Dr.JuliaKnightoftheUniversityofTorontoreportedthatwomenwhohadthemost sun exposure as teenagers and young adults had amore than 60 percentreducedriskofdevelopingbreastcancercomparedtowomenwhohadtheleastsunexposure.Onecanonlyimaginetheexcitement thatwouldresult ifadrugwereinventedthatyieldedsuchpreventiveresults!Again,youmightaskaboutskincancerrates.Wouldn’ttheyriseinresponse
to increased sun exposure? Approximately 500 women a year die fromnonmelanoma skin cancer. Given that the above statistics show that 27,500women die prematurely because of underexposure to sunlight, it becomesevidentthat55womendieprematurelybecauseofunderexposuretosunlightforevery1whodiesprematurelyfromoverexposuretosunlight.Hangtight:I’llbeansweringallyourquestionsaboutsunlightandskincancer

inchapter8.Fornow,let’skeepthefocusonthetypesofcancerthatkillmorepeopleanddon’tcrymercytoooftenwhendiagnosedandtreated.
ProstateCancer
Onlyheartattacksandlungcancerkillmorementhancanceroftheprostate,which every year claims more than fifty thousand lives in the United Statesalone.Prostatecancerkillsoneinfourmenwhogetthisdisease,makingitoneof themost deadly forms of cancer. About forty thousandAmericanmen dieeveryyearfromprostatecancer—morethantentimesasmanyasarekilledbymelanomas.Canceroftheprostateisespeciallyfearedbymenbecausesurgicaltreatment
for this formof cancer frequently results in impotence.A study in theAugust2001 issue of theLancet proves that the risk of developing prostate cancer isdirectlyrelatedtosunlightexposure.Thestudydividedpeopleintofourgroupsaccordingtohowmuchsunlighttheyhadbeenexposedto.Thelowestquarter,or quartile, of the study participants were three times more likely to developprostate cancer than those in the highest quartile of sun exposure. The resultsshowthatthoseinthehighestquartilereducedtheirriskofdevelopingprostatecancer by 66 percent. Those in the second and third quartiles also had asignificantlylowerchanceofgettingprostatecancercomparedwiththoseinthelowestquartile,whoreceivedtheleastsunexposure.Anotherstudytookalonglook,overalmosttwoyears,atmenwithprostatecancerwhoreceived2,000IUofvitaminDadayandfoundthatoverallthemenhada50percentreductionintheriseoftheirlevelsofprostate-specificantigen(PSA),whichisanindicatorofprostatecanceractivity.Only about six hundredmen die prematurely each year from nonmelanoma
skin cancer, but thirty-seven thousand men die prematurely each year fromprostatecancer.It’spossibletoconcludethatfifty-fivemendieprematurelyfromunderexposure to sunlight for every one who dies prematurely due tooverexposure.Evenwhenyouincludemelanoma—forwhichexcessivesunshineisonlyoneofseveralriskfactors—thenumbersarestill lopsided:about tentoone.
ColonCancer

Cancerofthecolonanditsneighboringarea,knownsometimesascolorectalcancer, affects both men and women. Like breast cancer and prostate cancer,colorectal cancer is seenmuchmore frequently than skincancers and ismuchmoredeadly.About150,000Americansaretoldeachyearthattheyhavecoloncancer,andabout35percentofthesewilldieofit.Therearemanycontributingfactors in why someone gets colon cancer, but the most commonlyacknowledged one is diet. Diets high in fat and nonorganic non-grass-fed redmeat are especially dangerous. Other diets, such as diets high in fruits,vegetables,andothernaturalrawandorganicfoods,helppreventcoloncancer.AstudypublishedintheJournalofClinicalOncologyin2008,conductedby
lead researcherDr.KimmieNgof theDana-FarberCancer Institute inBostonfound that high blood levels of 25-vitaminD increased colon cancer patients’survivalrateby48percent.Inthisstudy,Dr.Ngandherteamcollecteddataon304patientswhohadbeendiagnosedwithcoloncancerbetween1991and2002.Everyone in the study had had their 25-vitamin D blood levels measured aminimum of two years before being diagnosedwith the disease. The patientsweretrackeduntiltheydiedoruntilthestudyendedin2005;123patientsdied,96ofthemfromcolonorrectalcancerduringthefollow-upperiod.Dr.Ngandher team found that thepatientswith thehighest 25-vitaminD levelswere39percent less likely todie fromcolorectal cancer than thepatientswhohad thelowestlevels.These findings are consistentwith dozens and dozens of other observations
thathavebeenmadeinthepastdecade,includingthosebyDr.CedricGarland.Hislabreportsthatyouarethreetimeslesslikelytodiefromcoloncancerifyouhavehealthylevelsof25-vitaminDinyourbloodstream.
HowVitaminDTakestheLifeoutofCancer
The link between vitaminD and cancermay have gained a strong footholdjustrecentlywithinthemedicalcommunityatlarge,buttheresearchstartedlongago.Towardtheendofthe1980s,Iwaspartofasmallbutgrowingmovementofmedicalscientistswhobelievedthat theactiveformofvitaminDthatIhaddiscoveredadecadeearlierhadbenefitswellbeyondbonehealth.Wetheorizedthat peoplewho lived in sunnier climates had lower rates of cancer and heartdisease because the vitamin D produced by their exposure to the sun wassomehowbenefitingcells throughoutthebody.Afewstudiesbackedthisupat
thetime,butwhatexactlywascausingthis?My fellow researchers had successfully proved the relationship between
sunlight andcellularhealth,but Ibelieved their conclusionas towhy sunlightandincreasedvitaminDproductionbenefitedcellularhealthwasincorrect.TheythoughtthatvitaminDbenefitedcellsthroughoutthebodyinthesamewayweunderstooditbenefitedbonehealth.Thatis,themoresunshineyouget,themore25-vitaminDthere iscirculatinginyourbloodstreamthatcanbeconvertedbythe kidneys into activated vitamin D. According to this theory, this activatedvitaminDwouldthenbesentbythekidneystodifferentpartsofthebody,whereitwouldbenefitdifferentcellgroupsbyregulatingtheirgrowthandpreventingthem frombecomingmalignant.This theory assumes that themore vitaminDyougetfromthesunandyourdiet,themoreactivatedvitaminDyourkidneyswillmake.Ibelievedsomethingquitedifferent.At the time,my theorywasconsidered
heretical,anditprobablystillwouldbeifmycolleaguesandIhadn’tprovedit.Weunderstood thatactivatedvitaminDisoneof themostpotent inhibitorsofabnormalcellgrowth,butweknewthatnomatterhowmuchyouincreasedthesupply of 25-vitamin D in a person’s body through sunlight and diet, youcouldn’t get the kidneys tomake any additional activated vitaminD. I didn’tthink the very limited amount of activated vitamin D the kidneys are able toproducecouldberesponsibleforallthecellularbenefitsthatwehadidentified.Inotherwords,thekidneyscouldnotbethesolerulerinthevitaminDland.IbelievedthattherehadtobeanothersourceofactivatedvitaminD.WhatmycolleaguesandIproposedwasthatcellsthroughoutthebodydon’t
have to rely on the meager supply of activated vitamin D from the kidneysbecause each group of cells has its own enzymatic machinery to convert 25-vitaminD into activated vitaminD. In otherwords, cells canmake their ownactivatedvitaminDon the spotwithouthaving to relyonactivatedvitaminDsentfromthedistantkidneys.(Ifthisstorysoundsfamiliar,that’sbecauseItolditearlierfromaslightlydifferentangleandinbroaderstrokes.)Weprovedthistheoryinastudypublishedin1998thatinvolvedcollaboration
withDr.GarySchwartzandmycolleagueDr.TaiChen.OurfindingscompletelychangedthewaymedicalscienceperceivestherelationshipbetweenvitaminDandcellularandorganhealth.Inthisstudyweexposednormalprostatecellsto25-vitaminD to seewhatwouldhappen.The cells converted25-vitaminD toactivatedvitaminD(1,25-vitaminD).Wethenexposedprostatecancercellsto25-vitaminD.Incancerousfashion,thesecellswerereproducingoutofcontrol.
Whenwe exposed these prostate cancer cells to 25-vitaminD, they convertedthatsubstance intoactivatedvitaminDandstopped theirchaotic reproduction.Whatwehadactuallyprovedwasthat,justlikethekidney,normalprostatecellsand prostate cancer cells could make activated vitamin D. But unlike theactivatedvitaminDmadebythekidneys,whichregulatescalciummetabolismand promotes bone health, the activated vitaminD createdwithin the prostatehas the job of ensuring healthy cell growth. Not only was this confirmed insubsequent studies, but similar studies by my research group and otherresearchersfoundthatthesameenzymaticmachinerytoactivatevitaminDalsoexistsinthecellsofthecolon,breast,lung,andbrain.Thisfindinghelpedmakemoresenseoutofothermysteriesaboutthebody’s
useofvitaminD.ThevitaminDactivatedinthekidneysspecificallytravelstotheintestineandbonetoregulatecalciummetabolism.Soifyourkidneyswereto make a lot more active vitamin D, there would be negative healthconsequences, such as hypercalcemia (high blood calcium) and hypercalciuria(highurinecalcium).Whatthebodycleverlydoesinsteadisallowothertissuesandcells inyourbodytoactivatevitaminD.Ifyouhaveapatientwhohasnokidneys,hehasnocirculatingbloodlevelsofactivatedvitaminD.Therefore,itusedtobeassumedthatonlythekidneysmadeactivatedvitaminD.Whatwasshownbymylabandotherswas that thebodywassmarterandcouldactivatevitaminDlocallyintheprostate,colon,andbreast.Activated vitamin D, locally produced, can regulate up to two thousand
different genes that control cell growth and other cellular functions, produceinsulin in the pancreas, and regulate production of the hormone renin in thekidneys. Once it carries out these functions, activated vitamin D triggers theexpression of 25-vitamin D-24-hydroxylase, which is an enzyme that rapidlydestroys activated vitamin D. Activated vitamin D never leaves the cell, andthereforeitssignatureisneverpickedupinthebloodstream.It’sasilentsoldierthatessentiallycommitssuicideonceitstaskisfinishedonsite.Anotherbrilliantexampleofhowthebodyself-regulates.Theconsequencesofthisdiscoveryaremind-boggling.Wehaddiscoveredthe
likely reason why sun exposure has such a profound effect on cancer rates.When you are exposed tomore sunlight andmakemore vitaminD, it can beconvertedbytheliverinto25-vitaminD,whichcanbeactivatedbytheprostate,colon,ovaries,breast,pancreas,brain,andprobablymostothertissuestopreventunhealthy cell growth. Themore 25-vitamin D youmake, the healthier thesedisease-prone tissues will be. Because we don’t have to rely on a supply of

activatedvitaminDfromourkidneys,thereisanenormouscapacitytopreventcancer just by having ample supplies of 25-vitamin D around that originateeitherfromthesunlight’sactionintheskinorfromsupplementationofvitaminD2orD3.PowerfulnewsyntheticformsofactivatedvitaminDalsoarebeingstudiedtoseehowtheycouldhindercancergrowth.While the potential for activated vitamin D to be used as a treatment for
cancerseemslogicalgivenvitaminD’spreventiveactionsoncells,there’smoreto the cancer story that bears understanding. For one thing, cancer cells areclever.Onceamalignancytakeshold,thosecancerouscellsbegintomakemoreof aprotein that controls theexpressionofgenes, calleda transcription factor.And one of those transcription factors, called Snail, binds to the vitamin Dreceptor and renders it dysfunctional. Once that happens, activated vitaminDcannolongerregulategeneexpressionandthuscannolongerworkoncellstoprotect them. It’s like a switch that’s been flipped off. The cancerous cellsessentiallybecomeclosedforbusinesswithactivatedvitaminDand,lefttotheirowndevices,continuetogrowandinflictharmonnearbytissues.
ANewModelforCancer?
Though it’s a stretch to say vitaminD can totally prevent and cure cancer,some scientists have been bold enough to suggest a whole new theory aboutcancer.Just lastyear, theGarlandbrothers raised thepossibility that there’sanother
storybehindcancer’sgenesisinthebody.Thecurrentscientificmodelassumesthatageneticmutationiscancer’spointoforigin.Butwhatifthatassumptioniswrong?Whatifthereisanotherwaytoexplainhowcancerdevelops?Thosearethe questions the Garlands put forth, which were published in the Annals ofEpidemiologyandimmediatelypickedupbythemedia.First, Dr. Cedric Garland and his team pointed to a host of research that
suggestscancerdevelopswhencellslosetheabilitytosticktogetherinahealthy,normalway.Hewentontoarguethatthekeyfactorinthisinitialtriggeringofamalignancy could well be a lack of vitamin D. According to Dr. Garland,researchershavedocumentedthatwithenoughactivatedvitaminDpresent,cellsadheretooneanotherintissueandactasnormal,maturecells.ButifthereisadeficiencyofactivatedvitaminD,cellscanlosethisstick-to-each-otherquality,aswellastheiridentityasdifferentiatedcells.Theresult?Theymayreverttoa

dangerous,immaturestateandbecomecancerous.What can stop this process from occurring, says Dr. Garland, is ample
suppliesofvitaminDinthebody.WhenenoughactivatedvitaminDispresent,itmay halt the first stage of the cancer process by reestablishing connectionsamong cells that have an intact vitamin D receptor. No activated vitamin Daround,noactiononthecelltohelpchangeitscourse.Thisnewmodelofcancer’scausehasbeendubbedDINOMITbyDr.Garland
and his colleagues. Each letter stands for a different phase of cancerdevelopment:Dreferstodisjunction,orlossofcommunicationbetweencells;Iisforinitiation,whengeneticmutationsbegintoplayarole;Nreferstonaturalselectionofthefastest-reproducingcancercells;Oisforovergrowthofcells;Mstands for metastasis, the spread of a malignancy to other tissues; I refers toinvolutionandTfortransition,bothdormantstatesthatmayoccurincancerandcanpotentiallybealteredbyincreasingvitaminD.Whetherornot this theorycanbeproven truewillbe toldby future studies
andresearch.Cluesaboutapossiblecause-and-effectassociationbetweenalackofvitaminDandcancer’sdevelopmenthaverapidlyaccumulatedoverthepastfew years.No doubtmore clueswill continue tomount and slowly crush theincessantchatterthatsunlightisalwaysbadandthatskincancershouldbefirstandforemostoneveryone’sworrylist.Icouldgoonandonlistingstudies;theoriesassociatingvitaminDwithmany
cancers have been tested and confirmed in over two hundred epidemiologicalstudies.Inaddition,morethan2,500laboratorystudieshavebeenconductedthatprovide an understanding of the physiological basis of vitamin D’s link tocancer.Seeforyourself:GooglevitaminDandcancerandyou’llfindthousandsof links to papers and articles pouring out of themost prestigious universitiesand research centers around the world. The flip side of this optimistic coin,though, is the fact thatmost cancer patients are vitaminD deficient.My ownstudies,inadditiontoothers,havedocumentedthis,anditisnotasurprisegiventhatthegeneralpopulation’slevelof25-vitaminDis,forthemostpart,woefullydeficient. Add to that the fact that cancer patients usually don’t feel well, sothey’renotoutsideandarenotactive,andoftenhaveupsetstomachs,sotheyarenot eating very well and as a result are not fully absorbing whatever littlevitaminDmaybe in theirdiet.My teamhas found thatwhenwegivecancerpatients vitaminD, they report feeling better.Theirmuscle strength improves,andtheiroverallfeelingofwell-beingclimbs.
BeatingDownHeartDisease
Whenyou lookback at the graphonpage 76 that showsbloodpressure ratesacrossdifferent latitudes,you’llseethat thefartherawayfromtheequatoryoulive,thehigheryourbloodpressuregets.Whatgives?Isitintheair?Thewater?Thefood?No,it’sinthesky—thesun,orlackthereof.BecauseofvitaminD’sactionsinthebody,sunexposurehasadramaticeffect
on heart and circulatory disease. High blood pressure, also known ashypertension, is a very serious condition that is themain cause of stroke andheartattack.Ifyouliveinasunnyclimate,youarelesslikelytohavehighbloodpressure than if you live somewherewith less sunlight at certain times of theyear. People tend to have healthier blood pressure during the summer thanduring the winter because there’s more sunlight available—and thus morevitaminD in thebody.When exposed to the sameamountof sunlight, peoplewithfairerskinhavehealthierbloodpressurethanthosewithdarkskin,thankstohigherlevelsofvitaminD(thedarkeryourskin,themoremelaninthereisinit,andconsequently themoredifficult it is foryou toproducevitaminDfromthesun).There’snowspecificevidencethatpeoplewholiveinsunnierclimateshave fewer heart attacks. Heart failure is also associated with vitamin Ddeficiency.
TheHeartoftheMatter
Scientists nowbelieve that theworkwedid on themechanismof action ofactivatedvitaminDoncellgrowthalsohasabearingonthosecellsimportanttoheartandcirculatoryhealth,especiallythebloodvessels.Bloodvesselsarethetubular channels—the arteries and veins—through which blood circulatesthroughout your body.High blood pressure can occur if the blood vessels getstiffandnarrow,whichincreasesthepressureinsidethem.The work showing that there are vitamin D receptors in various cells
throughout the body and that these cells activate vitaminD ledme and otherscientiststoconcludethattherearealsovitaminDreceptorsinthecellsofourbloodvessels.TheeffectofvitaminDonthebloodvesselsistomakethemrelaxandbemoreflexible.Itdoesthisintwoways.Itlessenstheeffectsonthebloodvesselsoftherenin-angiotensinsystem,whichisacomplexhormonesystemthatregulatesbloodpressureandwaterbalanceinthebody,anditworksdirectlyon
vesselsandsmoothmuscletorelaxthem.Thus,thebloodflowsmoreefficientlythrough them, because there is less pressure against the blood vessel walls.What’s more, when 25-vitamin D levels are low, calcium can accumulate inartery walls and promote formation of dangerous fatty plaques. And it’s thebreakupoftheseplaquesthatleadstotheocclusionsandclotsthatarethedirectcausesofheartattacks,heartfailure,andstrokes.Atthesametime,bonescanbedeprivedofcalciumasvitaminDdeficiency
prevents proper absorption of calcium from the intestines. This constitutes adoublewhammy:weakerbonesandsickarteries,ascalciumaccumulatesinthewrongarea.Thishardeningofthearteriesisalsoknownasatherosclerosis.
Womenwithosteoporosis tendtohavemorecalciuminthewallsoftheirarteries,andtheyrunagreaterriskofcardiacdeaththanwomenwithstrong,densebones.
Researchinto the linkbetweenlow25-vitaminDandcardiovascular troubledatesbacktwentyyears.In1990,ProfessorRobertScraggoftheUniversityofAucklandpublishedthediscoverythatheartattackvictimshadlower25-vitaminD levels than theirhealthycounterparts.His teamexamined two setsofbloodsamples, one taken from 179 heart-attack patients within twelve hours of theonsetofsymptoms,andanothertakenfromhealthypeopleonthesameday.Thiscontrolgroupmatchedtheheartpatientsintermsofageandgenderdistribution.Dr.Scragg’sgroupfoundthattheheart-attackpatientshadasignificantlyloweraverage25-vitaminDlevelthanthehealthycontrols.Theriskofaheartattackwas calculated as being 57 percent lower among the people with higher 25-vitaminDlevelsthanamongthosewithlowerlevels.In2002,moreevidenceemergedwhenateamofresearchersledbyDr.Paul
Varosy at the University of California at San Francisco looked at nearly tenthousandwomenoveragesixty-fivewhohadparticipatedinanearlierstudyofosteoporotic fractures. Some of these women either had taken supplementalvitaminDinthepastorwerecontinuingtodoso.Dr.Varosywashopingtofindout how taking a supplementwould impact thewomen’s risk for heart-relatedproblems.Afterfollowingthewomenforanaverageofaboutelevenyears,hedetermined that thosewho used vitaminD supplements enjoyed a 31 percentreduction in the riskofheartdisease-relateddeathcomparedwithwomenwho
did not. The researchers were quick to point out that the use of calciumsupplements didnot affect their results.They alsomanaged toweedout otherfactorsthatpotentiallycouldhaveskewedtheirresults,includingdiet,genetics,lifestyle,healthconditions,andeducation.Ihaveparticipatedinseveralstudiesoverthelasttwodecadestoinvestigate
the effects of UVB irradiation on heart health. Dr. Rolfdeiter Krause andmycolleagues and I have found that regularly exposing patients with high bloodpressure to UVB radiation in a tanning bed caused their blood pressure tobecome normal—in other words, they got healthier. The best known of thesestudieswaspublishedintheLancetbackin1998.Inthisstudy,weshowedthatexposing hypertensive patients to brief periods ofUVB radiation in a tanningbedthreetimesaweekforthreemonthselevatedbloodstream25-vitaminDby180 percent and reduced diastolic blood pressure by 6millimeters ofmercury(mmHg)andsystolicbloodpressureby6mmHg,bringingthemintothenormalrange.(That’saboutasmuchasmostblood-pressuremedicationsdo,butwithouttheunpleasantsideeffects!)HowdidweknowthattheUVBradiationwasatworkratherthanthewarmth
and relaxing environment effecting this change? We provided the sametreatments toa separate setofhypertensivepatientsusingaUVA tanningbed,and thismadenodifference to25-vitaminD levels or bloodpressure.For theentire nine months we followed them, those patients who continued with thetanning-bedtreatmentsmaintainedahealthier,lowerbloodpressure.RememberthathighbloodpressureisoneoftheleadingcausesofdeathintheUnitedStatesandtherestoftheindustrializedworldbecauseitisamaincauseofheartattackandstrokeandamajorcauseofkidneyfailure.MycolleaguesandIalsostudiedareasofhearthealthotherthanhypertension.
Iwaspartofateamofresearcherswho,toconfirmthepioneeringworkofDrs.MalteBühringandRolfdeiterKrause,exposedagroupofheart-diseasepatientstoUVBradiationthreetimesaweekforamonth.Increasing25-vitaminDlevelsin the body in this way improved heart health in a variety of ways—heartstrength(asmeasuredbyblood-pumpingability)wasincreasedandheartstrain(asmeasuredbyrestingandnonrestingheartrateandtheaccumulationoflacticacid)wasdecreased.Ourstudiesandotherresearchteams’effortsshowthatthebenefitsofUVBtohearthealtharesimilartothoseofanexerciseprogram.And,asImentionedearlier,whencombinedwithphysicalfitness,UVBexposurehasbeenshowntohaveextremelybeneficialresults.
Ifyou takepeoplewithhypertensionandput them ina tanningbedforbriefperiods thatsimulatessunlight three timesaweekfor threemonths, you can increase their blood level of 25-vitamin D by asmuchas180percentandlowertheirbloodpressuretonormallevels—nodrugsrequired.
In2006,anItalianteamofresearchersmeasuredtheamountofatheroscleroticplaqueinthearteriesof390diabeticpatients,aswellasthepatients’25-vitaminD levels.Whatdid they find?Low25-vitaminDblood levelswereassociatedstronglywithagreaterdegreeofatherosclerosis.Laterthatyear,thesameteamfoundvitaminDdeficiencies in threeoutoffivepeoplediagnosedwith type2diabetes.TherateofvitaminDdeficiencywas61percentinthediabeticsversusonly 43 percent in the nondiabetic controls. This was in line with the team’spreviousfinding,as the31percentof thediabeticswithcardiovasculardiseasewereverylikelytoalsohavelowbloodlevelsof25-vitaminD.Most recently, a study ledbyDr.ThomasWangatHarvardMedicalSchool
andpublishedintheAmericanHeartAssociation’sjournal,Circulation,unveiledastoundingstatisticsregardingtherelationshipofvitaminDdeficiencytoone’srisk of heart attacks, strokes, and other cardiovascular events. Researchersfollowed 1,739 people for five years, assessing their 25-vitamin D levels bymeansofregularbloodtests.Theaverageageofparticipantswasfifty-nine.Allparticipantswerewhite,hadnopriorhistoryofcardiovasculardisease,andwerethechildrenoftheoriginalparticipantsinalandmark,edtheFraminghamHeartStudy.Participantswithlowlevelsof25-vitaminDhada60percenthigherchance
of experiencing a cardiovascular event, includingheart attack,heart failure, orstroke,duringthestudyperiodthanparticipantswithhighbloodlevels.AnotherstudyhasfurthershowedthatpeoplewhoinfactdosufferheartattacksaremorelikelytosurviveitiftheyarevitaminDsufficientasopposedtoinsufficientordeficient.(NotethatthisprettymuchconfirmsexactlywhatDr.Scraggobservedtwentyyearsago.)Thecorrelationremainedevenafterresearchersadjustedforother risk factors such as diabetes, high blood pressure, and high cholesterol.ThosewhohadbothvitaminDdeficiencyandhighbloodpressurehadtwicetheriskofcardiovasculareventsasthosewhohadvitaminDdeficiencyalone.Theresults of the studies treating heart and circulatory healthwithUVB radiationdemonstratewhypeoplewhospendtimeinthesuntendtohavehealthierblood
pressureandbetterall-aroundhearthealth.AttheAmericanHeadacheSociety’sfiftiethannualmeetingin2008,vitamin
D got a round of applause when Dr. SteveWheeler from the RyanWheelerHeadacheTreatmentCenterinMiamipresentedhisstory.Turnsouthehadbeenreading up on vitamin D deficiency in the medical literature, coming acrossseveral ofmy studies, and this prompted him to take a look at the vitaminDstatus of his patients suffering from chronic migraine. Migraines are uniquetypesofheadachesthattypicallyentailthrobbing,pulsatingpainononesideofthe head, accompanied by nausea and sensitivity to light. To a large extent,migraines remain a mystery, but we know they are related to blood-vesselcontractionsandotherchangesinthebrain.Dr.Wheelernoticedthatnoonehadever looked at the vitamin D status of the forty-fivemillionmigraineurs, yetpatientswithmigraineoftenhaveother health concerns such as increased riskfor cardiovascular disease, cerebrovascular disease, and fibromyalgia—allconditionsthathavealsobeenlinkedtovitaminDdeficiency.Butfirst,Dr.Wheelerstartedwithhimself.Amigrainesufferer,hediscovered
that his 25-vitaminD levelswere drastically low, a scanty 8.2 nanograms permilliliter. Dr. Wheeler was inspired to immediately start testing his patients,finding that 41.8 percent of the fifty-five patients he assessed at a singleoutpatientlaboratoryoverasix-monthperiodhadsub-optimallevelsofvitaminD. Specifically, 27.3 percent of these 41.8 percent of people had insufficientlevels (between 20 and 30 nanograms per milliliter) and 14.5 percent haddeficientlevels(20nanogramspermilliliterorbelow).Dr. Wheeler’s examination confirmed what other studies had previously
found.Therewasatrendtowardhypertensionandtype2diabetesinhisvitaminD-deficient patients. His team also uncovered a trend toward earlier onset ofheadache(14.3yearsofageversus18)andmigraine(16.7yearsoldversus22.2)in his vitamin D-deficient patients. Those with vitamin D insufficiency weremore likely to have osteopenia (the precursor to osteoporosis), and thosedeficientweremorelikelytohaveosteoporosis.ThispromptedDr.Wheeler toconclude that vitamin D deficiency is an unrecognized yet treatable cause ofcardiovasculardiseaseandcouldaggravateproblemswithmigraine.
TheBeatGoesOn
Finally, there’s one more study I want to point out related to the
cardiovascularsystemthat justcameout in2009, thisonefromSweden.Fortythousand women had been followed for about eleven years, one thousandwomenperyearofagefromtwenty-fivetosixty-four.Thegoalofthestudywasto see if sun-exposure habits were related to the risk of so-called venousthromboembolism(VTE)events,which, insimpleterms,arebloodclots in theveins. These can be deadly. About six hundred thousand Americans developVTEeachyear,andonehundredthousandofthosedie.VTEincludesdeepveinthrombosis(DVT),inwhichclotsforminthedeepveins,ofteninthelegs,andwhenletloosetraveltothelungs,causingapulmonaryembolism.Swedishwomenwho sunbathedduring the summer, onwintervacations, or
whenabroadoruseda tanningbedwereat30percent lowerriskofVTEthanthosewhodidnot.Thispercentagedidnotchangeevenafterthescientistsmadeadjustmentsfordemographicvariables.TheriskofVTEincreasedby50percentinwinterascomparedtotheotherseasons.And,nottoosurprisingly,thelowestrisk was found in the summer. The researchers speculated that greater UVBradiationexposurewasthereason.ItimproveslevelsofvitaminD,whichinturnenhances the body’s anticoagulant (declotting) properties and improvesconditionsinthebodythathelppreventsuchcatastrophicclots.
Hypertension:TheSilentKiller
One in four adult Americans—fifty million in all—suffers fromhypertension, themain sign of which is high blood pressure.Morethan half of Americans (67 percent) older than sixty havehypertension.It’sexpected toaffect1.6billionpeopleworldwidebythe year 2025. Despite its prevalence, high blood pressure is oftenignored or undiagnosed because it has no symptoms. However,hypertension is a prime risk factor for heart disease and stroke, thefirst and third leading causes of death in this country. It’s a chieffactor in our nation’s struggle with chronic disease, disability, andeven death. Because it is an insidious and deadly disease,hypertensionissometimescalledthesilentkiller.WeknowthatbloodvesselshavevitaminDreceptors.Theactive
formofvitaminDwill enhancecontractionof theheartmuscleandimprovevascularsmooth-musclefunction,asDr.RobertU.SimpsonfromtheUniversityofMichiganshowedmanyyearsago.Weknow

thatactivatedvitaminDaltersinflammatoryactivity,whichisamajorfactor in the development of atherosclerosis. And there is evidencethattheactiveformofvitaminDregulatesthemajorblood-pressure-regulatinghormonerenininyourkidneys.Thegatheringevidenceonvitamin D’s active role in regulating blood pressure has promptednumerous studies lately, as researchers continue to look for clues toconqueringthissilentkiller.
BloodSugarandMetabolicSyndrome
Highbloodpressure.Highblood sugar.Unhealthy cholesterol and triglyceridelevels. Excess abdominal (belly) fat. If you were to look into a crowd ofAmericans,say,atafootballgameorlargeconcert,andstartcountinghowmanyof them could check off all of these conditions as relating to them, you’d betagging one of every six people. That’s forty-seven million Americans.Collectively,thissetofconditionshasastrangename:metabolicsyndrome,or,strangerstill,syndromeX.Youmaynotintuitivelyputhighbloodpressure,forexample,inthesamecategoryasmetabolism,butalloftheseconditionsshareauniquerelationship.Andwhentheycombineinthebody,theycanhaveanepicimpact. These risk factors double your risk of blood-vessel and heart disease,whichcanleadtoheartattacksandstrokes.Theyincreaseyourriskofdiabetesbyfivetimes.Whenyouheartheworddiabetes,mostlikelyit’srelatedtotype2,so-called
adultonsetdiabetes.It’sthemostcommonformofdiabetes;ofthe23.6millionpeoplewithdiabetes,90percentto95percenthavetype2.Liketype1,thisformdisrupts the body’s ability to metabolize sugar for fuel, but type 2 is not anautoimmunedisease.Intype2diabetes,thebetacellsofthepancreascontinuetomakeinsulin,butwhenthereistoomuchfat,thereisaresistancetoinsulin,sothe body cannot use it effectively.When that happens, a person is said to beinsulin resistant and prediabetic.As the disease progresses, insulin productionslowsdownafterseveralyears,andtheresultissimilartowhatoccursintype1diabetes:glucose,thebody’spreferredformofenergy,buildsupinthebloodandthebodycannotmakeefficientuseofitsmainsourceoffuel.Unlike type 1,which I’ll describe in the next chapter as being autoimmune
related, this form of diabetes is associated with older age, obesity, a family
historyofdiabetes,physicalinactivity,andethnicity.About80percentofpeoplewithtype2diabetesareoverweight,whichiswhythistypegetssomuchmediaexposurenowthatobesityrateshavesoared.Forsome,reversingthisdiseaseispossiblethroughchangesindietandexercisehabits.Butforothers,theravagesofthisdiseasecanmakeforalongstrugglethatdestroysthequalityoflifeandbringsacomplicatedmorassofmedicalchallenges.BecauseactivatedvitaminDcanincreaseinsulinproduction, it’snosurprise
that researchhas indicated thatUVB radiation—andhence, adequate levels of25-vitamin D in the body—may have an indirect role in preventing type 2diabetes.WehaveyettolearntheexacteffectvitaminDhasontheriskfortype2 diabetes, but the evidence continues to collect showing a clear associationbetween sufficient vitamin D and efficient cellular metabolism. Numerouslongitudinalstudieshaveconsistentlydemonstratedthatpeoplewhosufferfromtype2diabetestypicallyhavelow25-vitaminDlevels.Justlastyearateamofscientists from Harvard and Tufts reported in the Journal of Nutrition thatvitaminDstatusmaybeanimportantdeterminantfortype2diabetes,basedontheir findingswhenstudying the relationshipbetween25-vitaminD levelsandinsulinresistance.What we do know is that a lack of vitamin D is related to both insulin
resistanceandimpairedpancreaticbetacells,whicharethesourcesofinsulinforthe body’s metabolism and which do possess vitamin D receptors. In studiesdone with mice, beta cells lose their capacity to secrete insulin when theirvitaminDreceptorisn’tfunctioningasitshouldbecauseoflow25-vitaminD.In 2004, researchers at UCLA unveiled their findings after trying to make
better sense of the CARDIA (Coronary Artery Risk Development in YoungAdults) Study, a population-based look at vitamin D’s role in metabolicsyndrome.TheCARDIAStudyexaminedasamplingof3,157blackandwhiteadultsagedeighteen to thirtyyears fromfourmetropolitanareas in theUnitedStates.What it foundwasthatamongoverweightadults, themoremilkpeopledrank,thelesslikelytheyweretobeinsulinresistant.Thenumbers,infact,arequite staggering—peoplewith thehighestdairy consumptionhada72percentlower incidence of metabolic syndrome. The study concluded that dairyconsumptioncouldreducetheriskoftype2diabetesandcardiovasculardisease.The UCLA team confirmed this conclusion in its own study and reportedspecificallyonhowhigherlevelsof25-vitaminDcorrelatedtothisloweredrisk.EvenmorerevealinghavebeenthestudiesdoneontheeffectbothvitaminD
and calcium—the high-powered couplewe’ll explore again in chapter 9—can
haveonreducingone’sriskfordiabetes.Onelargestudypublishedin2006byDiabetesCare that looked atmiddle-agedwomen concluded that a high dailyintake of vitamin D (greater than 800 IU) and calcium (greater than 1,200milligrams)wasassociatedwitha33percentlowerriskoftype2diabetes.Type2diabeticstendtobestuckinaviciouscyclewherebytheybattleweight
problems and lack the energy or motivation to exercise, precipitating otherhealthchallenges—fromtheiroverworkedorganstotheirinabilitytogetagoodnight’ssleep.Thenumberofpotentialhazardsthatflowfromtheirconditionandresulting secondaryconditions ispractically limitless.Add to that avitaminDdeficiency,knowingalltheareasinwhichvitaminDcanhaveapositiveimpact,and you can quickly grasp the magnitude and intricacy of this problem.Achievingabreakinthecycletypicallyrequiresacompletelifestyleanddietarychange,aswellasafocusonreducingstresslevelsthatcanthwartweight-losseffortsandperpetuatehormonalimbalances.Inthelastfewyears,thespotlighthasbeenturnedonteens,whoarecurrently
changingtheactuarialtables.Soaringobesityratesamongouradolescentsmayactually shift their longevity, snipping two to five years off their life spans ascomparedtotheirparents’.Andnewresearchhasalsolinkedlowlevelsof25-vitaminD tohighbloodpressureandhighbloodsugar in thisagegroup—thevery risk factors for heart disease and conditions associated with this elusivemetabolicsyndrome.AteamofresearchersledbyJaredReisofJohnsHopkins’sBloombergSchoolofPublicHealthfoundthatteens(3,600boysandgirlsagestwelvetonineteen)withthelowest25-vitaminDlevelsweremorethantwiceaslikelytohavehighbloodpressureandhighbloodsugarthanthosewithhigher25-vitaminD levels.Theywerealso four timesmore likely tohavemetabolicsyndrome than their counterparts with optimal levels of 25-vitamin D. ThevitaminD-deficiencypatternwasconsistentwithearlier findings in thatblackshad the lowest levels, followed by the Mexican Americans; whites had thehighest levels, but all of the teens showed a deficiency. Further research willdeterminetheextenttowhichvitaminDliesbehindthesehealthproblemsandhowmuchofanimpact itcanhaveinpreventing, treating,andreversingtheseproblems.
Do you have a teenagerwho is vitaminD deficient?New researchproves teenswith low levels of vitaminD have a high risk of highbloodpressureandbloodsugar,whichcancontributetoheartdisease
andotherseriousconditions.
CHAPTER5
FindingImmunity
CanvitaminDbethebody’ssecretweaponagainstgermsandautoimmunedisease?
InadditiontorespondingtotheNewYorkTimesorCNN,someofmyproudestmoments have been responding to feedback after landing in such esteemedpublications asPeople, theNational Enquirer, and theGlobe (not the BostonGlobe,butratherthetabloidyoufindatsupermarketcheckouts).Inthelate1980sIwenttoadermatologymeetingandgaveatalkonaFriday
afternoonaboutmyclinicalresearchusingactivatedvitaminDtotreatpsoriasis.This was just after I had tried to publish a study on activated vitamin D’sprofound effects on this painful skin disorder when applied topically in anointment. The New England Journal of Medicine had flatly rejected mysubmission.But thatdidn’tmeanIcouldn’tgoandreportmyfindings to localdermatologists,hopingafewinquisitivesoulswouldlisten.Asyoucanimagine,thereweren’tmanypeoplepresentatthattimeofdayon
theeveofaweekend.Halfaroomfulofpeopleshowedup,lookingeagertoendtheworkweek.Iwastold,though,thattheBostonGlobewastherefishingforahuman-interest story. I presented my results and recommended this newtreatmentforpsoriasis.IhadshowninclinicaltrialsthataddingactivevitaminDtoVaselineandapplyingittopicallycoulddramaticallyreducetheexcessivecellproliferation that causes psoriasis. Well, suffice it to say my talk ultimatelywoundupbeingpickedup in theother “Globe”publication (the second-most-readtabloidintheworld)severalmonthslaterundertheheadline“BreakthroughforPsoriasis:CallHolick” (strategicallyplaced right next tonews about then-popularprimetimesoapDynasty).My phonewas ringing off the hook the followingweek.More than twenty
thousandpeoplesufferingfrompsoriasiswrotetomeaskingtoparticipateinmystudy.Today,mymethodhasbecomeoneofthefirst-linetreatmentsforpsoriasis.I
hadoneof the largestpsoriasispatientpopulationsofanydermatologist in thecountryandcontinuetotreatpsoriasispatientswithactivatedformsofvitaminD.
TheBetrayal
Itmayseenunfathomablethatthebodycouldturnagainstitselfandinflictharmby ordering the immune system to attack its own tissues and cells. But that’sexactly what happens in the case of autoimmune diseases such as multiplesclerosis,type1diabetes,andrheumatoidarthritis.Thesecanbeamongthemostperplexing illnessesorconditions tostudyand try tounderstandfromapurelyscientificandevolutionarystandpoint.HowcanMotherNatureletthishappen?Howmany triggers of autoimmune diseases are there?Will we ever find thesilverbullettoresetanimmunesystemgoneawry?Psoriasis,while typicallyplacedunder the“autoimmunediseases”umbrella,
isnotactuallyanautoimmunedisease.I’llexplainwhyIdon’tlikecallingitanautoimmune disease a bit later in this chapter. Psoriasis deserves attentionalongsidethemoreofficialautoimmuneillnesses,though,becauseitinvolvestheimmunesystematsomepointinitsprogression.Controversycontinuestoswirlaround psoriasis’s story, but you’ll find that to be the case for most of themysterious autoimmune diseases that have yet to be fully decoded andcategorized as bona fide autoimmunediseases or something else entirely.Onething is certain: psoriasis is probably one of the longest-known illnesses ofhumansandsimultaneouslyoneofthemostmisunderstood.Similarly,vitaminDmaybe the oldest hormone on the planet and one of themostmisunderstood.Theoddcoupleindeed.
YourAutomaticWeapon
Surely you have some memory from high-school biology about the immunesystem—the intricate system of special cells that defend the body against

invadingmicroorganisms,suchasvirusesandbacteria.Theimmunesystemdoesthis by producing antibodies or particular kinds of white blood cells, calledsensitizedlymphocytes,toattacktheseunwelcomeinvaders.Ifyourimmunesystemisworkingasitshould,itwon’tattackfellowcells;it
willonlyrespondtothreatsfromrealtrespassers.Butifsomethinggoeswrong,your immune system can malfunction and signal antibodies and sensitizedlymphocytestoattackyourowncells.Thisusuallyoccursbecauseofanexternaldisturbance of your immune system by a medication, bacteria, or virus,combinedwithageneticpredispositiontoautoimmunedisease.Whileitmaybeironicthatthebodycanbecomeavictimofitsowndesign,astheverysystemsetuptodealwithinvaderscanbetrickedbythem,agatheringbodyofevidenceimplicatesoutsidersastheinstigatorsofawidevarietyofautoimmunediseases.Theimmunesystem,itturnsout,maynotbeasinfallibleaswe’dlike.ButthatmakesthecaseforitsconnectiontovitaminDallthestronger.Aswasrecentlydiscovered,oneofthemainreasonsforthisdisproportionate
incidence of autoimmune diseases across the globe may be the vitamin Dreceptors of the immune system. Because immune cells have vitamin Dreceptors(VDRs),theymaybenefitfromthevitaminDthebodygeneratesfromsunexposure.Afterall,whywould thesecellshave receptors forvitaminD ifthereweren’tapurposeforthemandaconcomitantneedforvitaminDtoactonthem?And, as we explored previously, vitamin D also promotes other areas of
cellular health, which makes it less likely that an undesirable autoimmuneresponsewilloccur.Inotherwords,whenthebodyisfunctioningoptimallyandhas all the ingredients it needs to fulfill its cellular obligations, conditions areideal and there’s less likely to be a mishap somewhere in the millions ofreactions that take place every day without your even thinking about them.Becauseof themountingevidence that sunexposure isaneffectivepreventivemeasureagainstautoimmunediseases, activatedvitaminDandartificial formsofthissubstance(knownasactivatedvitaminDanalogs)areincreasinglybeingtestedasatherapyfordiseasesthathaveanautoimmunecomponent.
SicknessWheretheSunDoesn’tShineSoBright
Forsometime,epidemiologistshaveknownthatautoimmunediseasesarelesscommon in regions close to the equator, where there is more sunshine
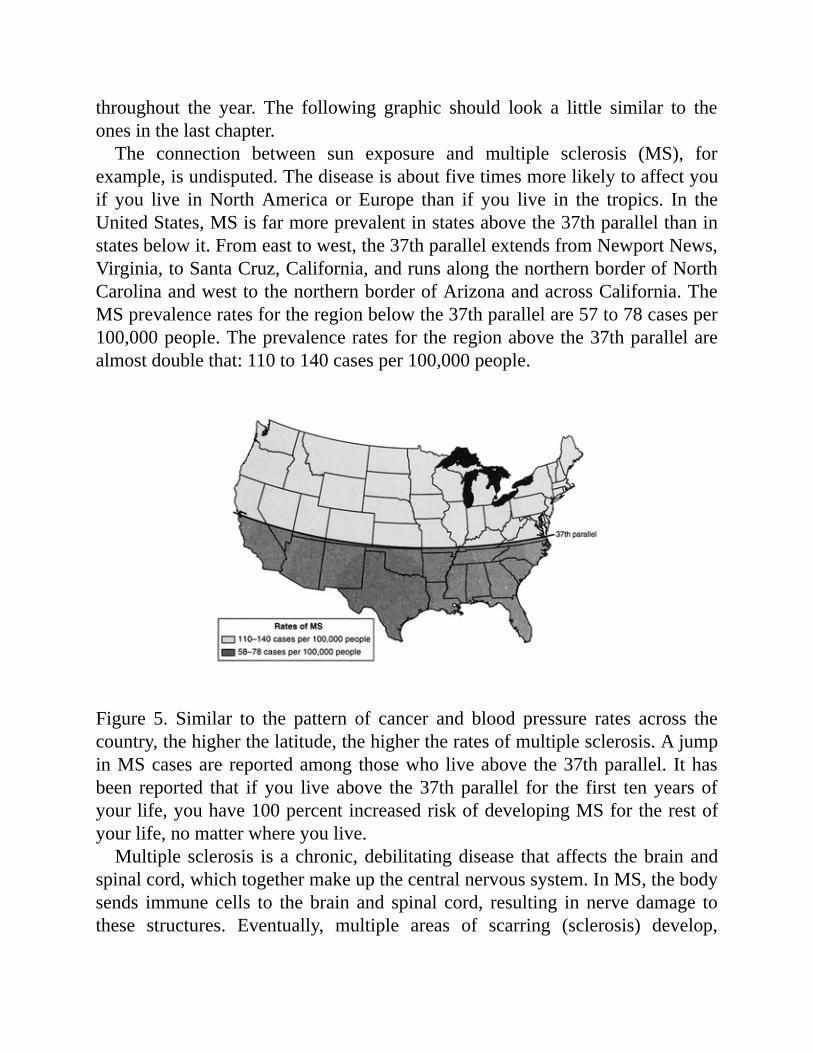
throughout the year. The following graphic should look a little similar to theonesinthelastchapter.The connection between sun exposure and multiple sclerosis (MS), for
example,isundisputed.Thediseaseisaboutfivetimesmorelikelytoaffectyouif you live inNorthAmerica or Europe than if you live in the tropics. In theUnitedStates,MSisfarmoreprevalentinstatesabovethe37thparallelthaninstatesbelowit.Fromeasttowest,the37thparallelextendsfromNewportNews,Virginia,toSantaCruz,California,andrunsalongthenorthernborderofNorthCarolinaandwesttothenorthernborderofArizonaandacrossCalifornia.TheMSprevalenceratesfortheregionbelowthe37thparallelare57to78casesper100,000people.Theprevalenceratesfortheregionabovethe37thparallelarealmostdoublethat:110to140casesper100,000people.
Figure 5. Similar to the pattern of cancer and blood pressure rates across thecountry,thehigherthelatitude,thehighertheratesofmultiplesclerosis.AjumpinMScasesare reportedamong thosewho liveabove the37thparallel. Ithasbeen reported that if you live above the37thparallel for the first tenyears ofyourlife,youhave100percentincreasedriskofdevelopingMSfortherestofyourlife,nomatterwhereyoulive.Multiple sclerosis isachronic,debilitatingdisease thataffects thebrainand
spinalcord,whichtogethermakeupthecentralnervoussystem.InMS,thebodysends immune cells to thebrain and spinal cord, resulting innervedamage tothese structures. Eventually, multiple areas of scarring (sclerosis) develop,

causing slowed or blockedmuscle coordination,weakness, double vision, andeventually loss of sight and other nerve signals. Most people develop MSbetween the ages of twenty and forty. An estimated 400,000Americans haveMS,andtherearethoughttobe2.5millionsufferersworldwide.Thediseaseisatleasttwiceascommoninwomenasinmen.There is a well-established genetic component inMS—if someone in your
familyhadthedisease,youaremuchmorelikelytogetit.About20percentofpeople with MS have at least one affected relative. If you’re a first-degreerelative, such as a child or a sibling, of someone with MS, your chance ofeventuallydevelopingMSistwentytofortytimesgreaterthanifyouweren’t.Interestingly,earlysunexposurehasproventobekey,andwhereyougrowup
determinesthelikelihoodthatyouwilldevelopMS.Fifteenyearsoldseemstobe thecutoffage. Inotherwords, ifyougrowup in the tropicsandmove toacountry in thenorthern latitudes after age fifteen, your riskof developingMSstayslow,andconversely,ifyougrowupinthenorthernlatitudesandmovetothetropicsafteragefifteen,youcontinuetohaveahigherriskofdevelopingMSfor the rest of your life. While the exact causes of MS remain unknown,researchers believe a lack of vitamin D in early life may prevent the thymusfromkillingcellsthateventuallyattackthenervesandeliminatetheprotective,insulatingmyelin sheath that iswrapped around the nerves that controlmotorfunction.
Studieshaveshownthatwomenwhohavehighlevelsof25-vitaminDreducetheirriskofdevelopingMSbyabout42percent.
ScandinaviansandCelticpeopleofnorthernEuropeappeartobepredisposedto MS, especially those who don’t eat a vitamin D-rich diet. As a result ofgenerationsofsundeprivation,thesepopulationsmayhaveahigherriskofMS.Basedonepidemiologicalstudies,scientistshypothesizethatalackofvitaminDfrom sunlight caused the immune systems of some people living in thesenorthernlatitudestogoawryandattacktheirnervoussystems.ConfirmationofthistheoryisfoundinstudiesshowingthatNorwegianswholivenearthecoastandeatadiethighinvitaminD-richfoodshaveamuchlowerriskofMSthanthosewholiveinland.Becausetheyliveathighlatitudes,bothgroupsareatriskof not getting enough natural sunlight. On the other hand, there is almost no

incidenceofMSamongEskimoswholiveatveryhighlatitudes.Thisisthoughtto be because of their traditional vitamin D-rich diet of polar bear liver, sealblubber,andoilyfish.Whenimmunecells,which,again,havevitaminDreceptors,areexposedto
appropriate amounts of activated vitamin D, some of which is made by theimmunecellsthemselves,theyrespondbydoingthejobtheyshoulddoandnotlaunching attacks against the body they are supposed to protect. Recently,researchersat theUniversityofOxfordandtheUniversityofBritishColumbiahavelinkedvitaminDwithageneticvariantthatinfluencesthedevelopmentofmultiplesclerosis.A group led by Dr. Hector DeLuca used lab studies to demonstrate that
pretreating mice with activated vitamin D and then trying to trigger theautoimmune response that causesMS resulted in noMS symptoms. ThiswasduetotheprotectiveeffectoftheactivatedvitaminD.Unfortunately,despitethetantalizing possibility that vitamin D may be the key to treating MS, so fardoctors haven’t been able to develop an activated vitamin D therapy thateffectively slowsorhalts theprogressionof thedisease inhumans (although IhaveusedvitaminDsuccessfullytotreatsomeofthemuscleweaknessandbonepaincausedbyvitaminDdeficiencyinpeoplewithMS).Partoftheproblemisthat by the time a person is diagnosed with MS, it’s too late to reverse theautoimmune process that causes the nerve damage. Researchers are testingdifferentwaysofadministeringlargedosesofactivatedvitaminDtopeoplewithMS,buttheresultshavebeendisappointing.Ihavefound,inafewofmyfriendsandpatientswiththefirstsymptomsofMS,thattheyhavenothadanyfurtherepisodesofthediseasesincetheybegantaking50,000IUofvitaminD2or itsequivalenteverytwoweeks,whichispositive.We’restillholdingouthopethatonedaywewilldevelopamethodoftreating
MSwithactivatedvitaminDthatcanhelpthemillionsofpeopleworldwidewhohavethisdevastatingdisease.Untilthen,itisreasonabletosuggestthatyoucanlessenyourownandyourchildren’s riskofdevelopingMSbygettingenoughsunexposuretobuildappropriatelevelsof25-vitaminDand,failingthat,takinga supplementwith enoughvitaminD in it tomeet yourminimumdaily needs(refertopartIIforguidelines).ThisisespeciallyimportantifyougrewupinthenorthernlatitudesorareofScandinavianorCelticheritage.Type 1 diabetes (also called juvenile diabetes or insulin-dependent diabetes
mellitus)isachronicdiseasethatoccurswhenthespecialpancreaticcellscalledbeta islet cells, which are responsible for making the hormone insulin, are
attacked and eventually destroyed by the immune system. This condition isdifferentfromtype2,or“adultonset,”diabetes,whichoccursinadulthoodandis not a disease of the immune system. In type 1 diabetes, the pancreas can’tproduce enough insulin to regulate blood sugar levels and eventually can’tproduce any insulin at all because all the beta islet cells havebeendestroyed.Thisdiseasealmostalwaysoccursinchildhood.Althoughitisacknowledgedtobeanautoimmunedisease,thecausesoftype1diabetesarestillconsideredtobeunknown.Without enough insulin, glucose builds up in the bloodstream instead of
enteringthecells.Thebodycan’tusetheglucoseforenergy,despitehighlevelsinthebloodstream.Thiscausessymptomssuchasexcessivethirst,frequentneedtourinate,andhunger.Fivetotenyearsaftertheonsetofdiabetes,thebetaisletcellsaredestroyedandthepancreasisunabletomakeanyinsulinatall.Severeconditions, includingblindness,kidneyfailure,hypertension,andheartdisease,are among the regrettable complications of type 1 diabetes. Circulation maydeterioratetotheextentthatulcersonthelegsdon’theal,andamputationsofthefootorlegsmaybenecessary.
About fifteen thousand new cases of type 1 diabetes mellitus arediagnosedeachyearintheUnitedStates,makingitthesecond-most-common chronic disease in children after asthma. It has beenestimated that1.5millionpeoplehave type1diabetes in theUnitedStates.
Although epidemiological studies have long suggested that vitaminD fromsunexposureprovidesimmunitytodiabetes,astudydoneinFinlandrockedthemedical establishment and confirmed what many of us believed about therelationshipbetweenvitaminDandthisdisease.NorthernFinnsexperienceonlytwohours of sunlight onDecember days, andFinland has theworld’s highestreported incidence of type 1 diabetes. The study followed more than twelvethousandbabiesbornin1966.ThosewhoweregivenavitaminDsupplementof2,000IUadayduringthefirstyearoflifehadanearly80percentreducedriskofdevelopingdiabetescomparedwithbabieswhodidnotreceiveasupplement.Thestudy’s leadresearcher,Dr.ElinaHyppönen,followedthemedical recordsofthesechildrenforthirty-oneyears.ThosewhowerevitaminDdeficientand

had rickets had a 2.4-fold risk of developing type 1 diabetes. In 2008, theGarlandbrotherswerepartofateamofresearcherswhoanalyzedthepatternofdiabetesintheworldaccordingtolatitudeandstrengthofsolarUVBradiation.Theirresults furtherconfirmedthisgeographical trendindiabetes.Peoplewholiveinsunnyclimatestendtohavealowerriskoftype1diabetes.Conversely,regionswith limited amounts of sunlight have a higher incidence of diabetes.Thisdiseaseisveryrareinequatorialregions.TheyalsoconfirmedthatchildrenwhosemothershadpoorvitaminDstatusorwhothemselveslackedvitaminDhadahigherriskoftype1diabetes.We know that activated vitamin D may help prevent type 1 diabetes by
makingthebetaisletcellsmoreresistanttoattackfromtheimmunesystemandbyenhancinginsulinoutputbythesecells.Itcanalsoimprovethehealthoftheimmune system as awhole,making it less likely that it willmalfunction andattack the beta islet cells in the first place. What we don’t know, though, iswhetherafuturecurefortype1diabeteswillentailactivatedvitaminDorthisvitamin in a cocktail with other substances. As with MS, the challenge isreversingthecourseoftheimmunesystemonceithasalreadygoneoffcourse.Inotherwords,preventingdiseasefromhappeninginthefirstplaceisideal,andadequatevitaminDmayhelpinthepreventionofcertainconditions.
TamingtheFlamesofRheumatoidArthritis
ScientistsbegantestingtheeffectsofvitaminDonrheumatoidarthritis(RA)inthe1940s,butinitialoverdosescausedtestingtobesuspendeduntilrenewedinterestarose in the1990s.Whywas there renewed interest?Becausewenowbetter understood the role of activated vitamin D on cellular health and hadmuch more efficient and safer ways of administering vitamin D treatment, itbecamereasonabletorevisittheprospectofusingvitaminDtotreatRA.Rheumatoidarthritis isachronic inflammatorydisease thatprimarilyaffects
thejointsbutcanalsoaffectotherorgansystems.Althoughthediseasecanstrikea person at any age, it usually comes on between the ages of twenty-five andfifty-five. The disease is more common in older people.Women are affectedalmost three times as often as men. Between 1 percent and 2 percent ofAmericans have RA. The rate of advance and severity of the illness varies agreatdealfrompersontoperson.Theareasofthebodymostcommonlyaffectedbyrheumatoidarthritisarethe
wrists, knees, elbows, fingers, toes, ankles, and neck. Individuals with RAexperiencebilateral jointpain, joint stiffness, jointwarmth, and joint swelling.Othercommonsymptomsincludethefollowing:
•fatigue•discomfort•appetiteloss•mildfever•morningstiffnessformorethanonehour•jointdeformitiesinthehandsandfeet•round,painlessnodulesundertheskin•skinrednessorinflammation•eyeirritationanddischarge•numbnessand/ortingling
WhenapersongetsRA,theimmunesystemattackstheliningofthejoints,asubstance known as synovium, which then becomes inflamed. The process isusually bilateral, which means it affects both knees, both wrists, and so on.Symptomsincludepain,swelling,andstiffnessofthejointsthatcanleadtojointdeformity.Thesesymptomsdistinguishrheumatoidarthritisfromosteoarthritis,whichisamorecommonanddegenerative“wear-and-tear”arthritis.Complications ofRA can be very severe andmay include joint destruction,
heart failure, lung disease, anemia, lowor high platelets, eye disease, cervical(neck) spine instability, neuropathy, and vasculitis (inflammation of bloodvessels).Therearenoknownways topreventRA,althoughthedisease’sprogression
canbeslowedwithearlydetectionandaggressivetreatment.Currenttreatmentfocuses on reducing inflammation of the joints with anti-inflammatory orimmunosuppressivemedicationssuchasprednisone,methotrexate,andEnbrel.Unfortunately,most of the successful pharmacological treatments have seriousside effects, from life-threatening gastrointestinal bleeding to osteoporosis.Infections also may occur because of the suppression of the immune system.MillionsuponmillionsofdollarsarebeingspenttodevelopeffectivetreatmentsforRAthatdonothaveserioussideeffects.StudiesarecurrentlyunderwayexamininghowvitaminDmayalleviateRA.
Preliminary studies suggest that activated vitamin D may be an effectivetreatment for RA. Mice with RA that were given activated vitamin Dexperiencedadiminishmentofthecellularactivityresponsibleforthisimmune

disease,givingrisetotheexpectationthat theremaycomeadaywhenwecansuccessfully treat RAwith injections of activated vitamin D or oral activatedvitaminDpills.
PuttingPsoriasisinItsProperPlace
Back topsoriasis, the semiautoimmunedisease thatmaybegettingwronglybilledasafull-fledgedautoimmunedisease.Here’smythinking.Plaquepsoriasisisachronicskindiseasethathumankindhasknownaboutfor
millennia (the word psoriasis is the ancient Greek word for itch). Today thisdisease affects 5.5 million people in the United States and 50 million peopleworldwide. The condition mostly affects adults, and the symptoms can beextremelydistressing,bothphysicallyandpsychologically.Thecharacteristicsymptomsofpsoriasisareraisedpatchesofthick,redskin
coveredwithsilveryscales.Theseunsightlypatches,sometimescalledplaques,generally itch and may burn. Psoriasis usually occurs on the elbows, knees,scalp, lower back, face, palms, and soles of the feet, but it can affect skinanywhere on the body. In areas such as the knees and elbows, the skin maycrack.Thediseasesometimesaffects thefingernails, thetoenails,andthefleshinside the mouth. About 15 percent of people with psoriasis have jointinflammation, which produces a crippling form of arthritis called psoriaticarthritis.Undernormalcircumstances,skincellsgrow,divide,andreplacethemselves
inanorderly fashion,butwithpsoriasis,cells start reproducingoutofcontrol.Psoriaticskinmay“turnover”(bereplaced)inaslittleasfourdays,comparedwith normal skin,which turns over in twenty-eight days. This rapid turnover,combined with altered maturation of skin cells, results in the characteristicsymptomsofpsoriasis.Long before doctors established that psoriasis would respond to directed
vitaminDtherapy,peoplewithpsoriasisknewthattheirconditionimprovedinresponse to sun exposure. Folk remedies for psoriasis invariably includedsunbaths. One of the first modernmedical breakthroughs in treating psoriasiswith UV radiation was made in the 1920s by the German doctor WilliamGoeckerman. Goeckerman theorized that, because sunlight helped lessen thesymptomsofpsoriasis,increasingtheintensityofthesun’sradiationontheskinofapersonwhohadpsoriasiscouldincreasethehealthyeffectsofthesun.He
applied a solution of coal tar to the affected areas of skin and then subjectedthoseareas to theradiationofasunlamp.Thecoal tardid indeed intensify theeffectof the sun’s radiationand reduced the symptomsofpsoriasis evenmorethan didUV radiation alone.Versions ofGoeckerman’s treatment of psoriasisarestillusedtodaybymanydermatologists,whobelievethatcoaltarisstillthemosteffectivesensitizingagentforthesun’sradiation.UVBirradiationalsohasbeeneffectivelyusedtotreatpsoriasis.Morecommonforseverepsoriasis,though,areoralmedicationsthatmakea
patient’s skin highly sensitive to sunlight and carefully controlled exposure toUVA radiation at a dermatology clinic (a treatment called psoralen UVAphotochemotherapy, or PUVA).Over the years,more than thirty skin diseaseshave been shown to respond positively to PUVA treatment. This treatment isveryeffective,butPUVAtherapyisquiteinconvenientforthepatient,whohastovisit theclinictwoor threetimesaweek.Also,whendonetoomanytimes,PUVA causes nonmelanoma skin cancer, melanomas, and cataracts. For thatreasonPUVAisnowconsideredoutdatedbysome.Until recently, treatment for psoriasis was based on the premise that the
diseaseofpsoriasisstartswithadefectiveimmunesystem.Idon’tbelievethistobe the case and stated my claim in an editorial in the journal ExperimentalDermatology.Myresearchshowsthatalthoughtheimmunesystemiscertainlyinvolved, the problem begins with a defect in the skin cells themselves. Thisdefectcausestheskincellstoreproduceoutofcontrol.Onlyaftertheskincellsstartoverproducingdoestheautoimmunesystemsensethere’ssomethingwrongandgetinvolved,whichonlycausestheproblemtogetworse.In other words, in psoriasis the autoimmune response is secondary to the
initialproblemintheskincells.Mosttreatmentsforpsoriasisweredesignedtosuppresstheautoimmunesystem.Notonlydoesthisnotaddresstherootcauseoftheproblem—adefectintheskincellsthatcausesthemtoreproduceoutofcontrol—but it can also have serious side effects.Medications to suppress theautoimmune system, such as cyclosporine, prednisone, and methotrexate, canraisebloodpressure,damagethekidneysandliver,andcauseosteoporosis,andtopical steroids thin the skin (sometimespermanently).Suppressing thebody’sautoimmunesystemmayalsoopenthedoortoinfectionandskincancer.Afirst-line therapyfor treatingpsoriasis isa treatment Ihelpeddevelop.As
detailed at the beginning of this chapter, I discovered that by applying to theaffected skin an ointment containing activated vitamin D it was possible todramaticallyreducethesymptomsofpsoriasis.GaldermaLaboratories’Vectical
(whosegenericname is calcitriol)ointment is the formofactivatedvitaminDcurrently available on the market. Another topical drug that developed as anatural progression of my research is Dovonex (calcipotriene), which is ananalogofactivatedvitaminD.ThisapproachofusingactivatedvitaminDandits analogs differs from previous treatments: instead of suppressing theautoimmune response to skin-cell defects, it corrects the skin-cell defectsthemselves.Unlike other forms of treatment for psoriasis, activated vitamin D and
calcipotriene have no serious side effects (mild skin irritation may occur insensitiveareas).Patientsapplytheointmentorcreamtwiceadayforsixtoeightweeks,andthevastmajorityexperiencemoderatetogoodresultswithinamatterofweeks.Sometimesthesetreatmentsareusedinconjunctionwithavarietyofotheroraland topicalmedications,aswellasexposure toUVBradiation fromthe sun or a sunlamp. Another more recent option is Vectical, from the drugcompany Galderma, which specifically serves the dermatology community.Vectical delivers threemicrograms of calcitriol (activated vitamin D) per onegramofointmentandisavailablebyprescription.Can sunlight alone be used to treat psoriasis? Sunlight is, after all, a main
source of vitaminD, and peoplewith psoriasis seem to fare better during thesummermonths, when it’s sunnier. If I see someone who has amild case ofpsoriasis and never gets any natural sunlight, I advise the individual to spendmore time in the sun to find out whether this alone is enough to treat thesymptoms. If this measure is successful, then I advise the person to use anindoor-tanning facilityduring thenonsunnymonths (under specific guidelines,though, thatyou’ll readabout inchapter8). If theconditiondoesnot improve,theindividualshouldseektheservicesofadermatologistexperiencedintreatingpsoriasis.Alongwithotherresearchers,mycolleaguesandIfoundthattheskinhasthe
enzymaticmachinery toactivatevitaminD, thesubstance thatmosteffectivelypreventsunhealthycellreproductionofthesortcharacteristicofpsoriasis.Thismay be the explanation for why sun exposure and UVB irradiation are soeffectiveintreatingpsoriasis.
EverythingbuttheKitchenSink
The fact that your immune cells possess vitamin D receptors explains why

vitamin D has been shown to influence a spectrum of illnesses blamed onspecific infections. Take, for example, tuberculosis. At the turn of the lastcentury,solariaweresetupspecificallyforTBpatients.Wehavealwaysknownthatmacrophages—germ-killing cells of the immune system—activatevitaminD. Butwe never understoodwhy they did so until recently, whenDr. RobertModlin’s and Dr. John Adams’s teams at UCLA revealed that the reasonmacrophagesactivatevitaminDisthatactivatedvitaminDtellsthemacrophagetomakecathelicidin,aproteinthatspecificallykillsinfectiveagentssuchasTB.TheirworkwaspublishedinSciencein2006,sheddinglightonwhatwehad
knownformorethanacentury:sunlightcantreat tuberculosis.Sowenowarebeginning to realize why vitamin D is so important to innate immunity,especiallyagainstinfectiousagentswecancontractinourenvironment.Astudyofpostmenopausalwomenwhotook2,000IUofvitaminDadayshowedthattheyhada90percentreductioninupper-respiratory-tractinfectionscomparedtowomenwho took just 400 IU of vitaminD a day.This study is supported byother observations that risk of upper-respiratory-tract infection is reduced inadultswhohavethehighestcirculatingbloodlevelsof25-vitaminD.Extendingthisobservationtootherrelatedinfections,wecansurmisethatvitaminDmayhave an impact on whether you become infected with influenza, which, as Iwrite this, iscircling theglobe inanewstraincalledH1N1,orswineflu. Is itpossible that just correcting vitaminD deficiency could decrease your risk ofcontractingtheflutobeginwith?IthinkitbehoovesallofustobeawareofourvitaminDstatus.
Duringthe1916fluepidemic,ifyouwereexposedtoinfluenza,youwere less likely todie ifyou lived inTexas than ifyou lived in theNortheast.
In2009,Dr.WilliamGrantpresentedahypothesisinanarticleforDermato-EndocrinologystatingthatlowlevelsofvitaminDareariskfactorforsepsis,aseriousbloodconditionusuallybroughtonbyinvadingbacteria.Thatsameyear,agroupattheUniversityofPittsburghpublishedastudystatingthatvitaminDdeficiency is associated with bacterial vaginosis, a highly prevalent vaginalinfection that plagues many women and can lead to complications duringpregnancy.
Youmightrecallaseeminglyweirdconnectionmadeafewyearsagobetweengumdiseaseandheartattacks.On thesurface, it’sanoddpairing:howcananoral infection or inflammation (periodontitis) cause a heart attack?When youconnectthedotsfromthemouthtothecardiovascularsystem,youcanseehowthis can happen.One theory is that bacteria in themouth can affect the heartwhen they enter the bloodstream. From there, the bacteria can attach to fattyplaques in the heart’s blood vessels and contribute to the formation of a clot.Once thosebloodclotsgetbigenough toobstruct the flowofblood,nutrientsand oxygen get restricted and the heart begins to decline in performance.Eventually,aheartattackcanoccur.Anothertheoryisthattheinflammationthataccompanies the periodontal disease increases the plaque buildup, which thencauses arteries to swell. People with periodontal disease are almost twice aslikely to suffer from coronary artery disease as those without periodontaldisease.SohowdoesvitaminDfitinhere?BecausevitaminDhasthepowertoassist
the body’s natural defense against bad bacteria and inflammation, keepinghealthy levels of 25-vitamin D (so that the immune cells can activate it)ultimatelyreducestheriskofthischainofeventshappening.Themechanismisthesameastheonefortuberculosis:1,25-vitaminDpromotestheproductionofaprotein(cathelicidin)thatfightsbacterialinfectionsinthemouth.
Toothdecay (cavities)andperiodontaldiseaseare linked to low25-vitaminDlevels.
Thisalsoexplainswhydentalcavities(toothdecay)havebeenassociatedwithvitaminDdeficiency.Asmostpeopleknow,dentalcavitiesaremorecommonamongyoungerpeople(belowtheageoffifty)andperiodontaldiseaseismorecommon in older people. We were aware of a connection between sunlightexposure and the prevalence of cavities as far back as the 1930s, when anecologicalstudyreportedaninverserelationshipbetweenmeanhoursofsunlightandthepresenceoftoothdecayinboysagedtwelvetofourteenyearslivinginrural or semirural regions of theUnited States. In otherwords,more sunlightexposurecorrelatedwithfewercavities.Therewasageneralincreaseincavities,going from 2.9 cavities per boy for those living where there weremore than3,000 hours of sunshine a year to 4.9 cavities per boy for those livingwhere

therewerelessthan2,200hoursofsunshineayear.Theanti-inflammatoryqualityofvitaminDexplainswhyit’sbeenassociated
with theprevention and treatment of asthma and allergic reactions. It has alsobeen touted as a great addition to steroid-based treatments for asthmaticswhotypically don’t respond well to traditional steroid inhalers or tablets. WhenvitaminD is added to a steroid regimen in these patients, the immune systemresponds as T cells synthesize amolecule called IL-10. Thismolecule,whichacts as a signal, can inhibit the immune responses that cause the symptomsofallergicandasthmaticdisease.Lateron,whenIcovera fewpregnancy issues,you’llsee thatvitaminD’s immunologicalpowercanplayasignificant role inpreventing a lifetime of allergic diseases in unborn children. The power ofvitaminDtosupporttheimmunesystemisproofagainthatitservesaprofoundfunctioninourlivesfromstarttofinish.I believe we’re just beginning to understand the power of vitamin D in
preserving and enhancing the immune system. Just before this book went topress,morestudiesemergedshowingthatvitaminDcanboosttheproductionofproactive compounds in the skin itself and may ultimately help prevent skininfections, particularly those caused by microbial invasions. But that’s justscratchingthesurface,sotospeak.VitaminD,asyouknowbynow,respondstoreceptorsalloverthebodyandinitsdeepestcellsandtissues.TosayvitaminDhas anti-inflammatory, antimicrobial, antiviral, anti-anything properties is anunderstatement.VitaminDmaybeoneofourmostreliableproactiveingredientsin bolstering comprehensive immunity and reinforcing the body’s naturaldefenses.Inthenextchapter,we’llmakeadeparturefromtheimmunesystembutsee
that vitamin D serves an equally comprehensive role in aidingmatters of themind,includingemotions.
CHAPTER6
MindMattersandMixedEmotions
Thefactsoflightonmood,mentalstates,andsenseofwell-being
Avoidingthesuncansometimesfeellikeyou’retryingtoavoideatingafreshlybakedchocolate-chipcookiewhenyou’rewatchingyourdiet.Somethinginyourbrainstartstalkingtoyou,triggeringyouto(quitesubconsciously)takeasmallbiteofthecookie,or,inthiscase,letyourbodybeexposedtoalittlesunshine(justafewsecondswon’thurt!).Ittastes—andfeels—delicious.Youcan’tstopeatingthecookie.Youcan’tstopsoakingupsomerays.Bitesbecomethewholething.Secondsturnintominutes.Isthereareasonwhythesuncanfeelsogood?Thatsenseofwell-beingafterexposuretoUVradiationisveryphysicaland
probablyhasbeeningrainedinourDNAforlongerthanwe’vebeenhuman.Sunexposure provides a natural high by stimulating the release of “feel-good”substancesinyourbody,suchasserotonin,dopamine,andbetaendorphins,thebody’snaturalopiate.(Anequivalentresponsecanbeobtainedfromeatingthecookie,assomeofthosesamehormonesgetreleased—contributingtothatall-too-familiar rush of euphoria.) Sunshine also suppresses hormones likemelatonin,whichmakeyoufeelsluggishand“down.”Weusedtothinkthatthisrelease of hormones had to begin in the hypothalamus, our brain’s commandcenterforemotionsandtheoriginofcountlesshormonalreactions.Butrecentlyscientistshaveunlockedthesecretmessagingservicethattakesplacerightthereinyourskincells.Itturnsoutourskinandnervoussystemsharealanguageweare just beginning to understand. We now know, for example, that thosehormoneskeytomoodmaynotoriginateonlyinthebrain.TheycanbecreatedbyskincellsuponexposuretoUVradiationandthenenterthebloodstreamandtraveltothebrain.Nowthat’satwo-waystreet.
Sunshine hasmore than a short-term impact on your psychological state. Italmostcompletelycontrolsthebiologicaltempoofyourlife—yourdailypatternof body temperature highs and lows, levels of alertness, sleeping patterns,hormonalsecretions,andotherbasicbiologicalfunctions,suchaswhenyoueat.Itmayeven factor intoyour riskofdementia later in life.Let’s takea lookatthese connections.Along theway I’ll call out further connections that involvevitaminD.
YourBiologicalClock
Biological clocks, while sometimes pigeonholed as referring mainly to awoman’sreproductivetimeframe,tickinallhumansanddon’thaveanythingtodo with procreation. Everyone has what’s called a circadian rhythm,characterized by a cycle of changes your body undergoes every day.Much ofthisrhythmiscarefullycontrolledbytheebbandflowofhormonesthroughoutyourday,which factor into things likeyour sleep, appetite, and energy levels.Until theearly1980s,scientistsbelievedhumanshadevolvedtoapointwherewecontrolledourowncircadianrhythms.Butwe’veuncoveredalotmoreaboutour bodies since then, andonly in the past fewyears have scientists begun tounderstandhowourcircadianrhythmaffectsourabilitytothinkandact.Andit’snotarhythmthatbeatstothedrumofourwillfulwantsanddesires.While it could be nice to have a biological clock fully under our own
conscious control and subject to our personal commands, circadian rhythmsanswertosunshine.Ourbiologicalclockiskeptonatwenty-four-hourscheduleby the rise and fall of light. Without sunshine and darkness signals, yoursleep/wakeschedulewouldshiftforwardbyanhoureveryday—or“freerun”—asitdoesinsubmariners,astronauts,andanyoneelsewholiveswithoutregularexposure tonatural sunlight.Howdoes thismechanismwork? It’s reallyquiteintriguing.Your biological clock is made up of a small cluster of cells called the
suprachiasmatic nucleus (SCN),which is located near the center of the brain.Sunlighthitsthephotoreceptorsintheretinaofyoureye,andthissignaltravelsvia the optic nerve to the hypothalamus, your brain’s emotional headquarters,wheretheSCNislocated.InadditiontohousingtheSCN,thehypothalamusisresponsibleforavarietyofinvoluntaryfunctionsthatcontrolyourmood.Oneofthemostimportantjobsofthehypothalamusistosendsignalstothe

pinealgland,apea-sizedstructureknownasthethirdeyelocateddeepbetweenthehemispheresofyourbrain (it looks likea tinypinecone—hence itsname).Whenitisdarkoutside,theglandreleasesasubstancecalledmelatonin,whichmakesyoursystemslowdownandpreparesyouforsleep.Conversely,whentheSCNreceivessignalsthatlightisaround,itsendsmessagestothepinealglandto shut down production of melatonin and increase production of serotonin,whichmakesyoufeelhappyandalert.How canwe be so biologically influenced by the sun?When our ancestors
werefirstevolving,humanslivedbytheriseandfallofthesun.Inotherwords,withoutelectricityandaway toworkpastnightfall,peoplesloweddownaftersunsetandrestedforthenextday.Thus,ourphysiologyevolvedinsuchawayastoshutdownwhendarknessbeganandstartupinresponsetosunlight.Itisn’tjustthesleep-wakecyclethatisaffectedbyyourcircadianrhythms;avarietyofother psychological and physical functions are profoundly influenced as well.Many peoplewho suffer from sleep problems have an internal clock that hasbecomeoutofsyncormismatchedwiththeday-nightcycle.Thatistosay,theirbodies’physiologiesdon’tmeshwithsociety’stwenty-four-hourclock.Everyone’s circadian clockor “pacemaker” ticks at a different rate.And, in
fact,a teamofGermanscientists in2008discoveredthatyoucanlookatyourskincellgenestodeterminewhetheryouarealark(wholikestogetupearly)oranowl (who likes to stayup late).Ourpreferences for rising earlyor late areencoded in our genes, including those found in skin cells. These scientistsengineered a way to observe and measure individual “clocks” in human skincells.After taking skin samples fromvolunteers, they inserted intoeachcell agenethatlightsupinultravioletlightwhenthecellismetabolicallymostactive.The gene allowed the scientists to follow the circadian rhythm of the cells asthey changed over a twenty-four-hour period. In essence, they were able toidentify and track skin cells’ built-in timing mechanism set by the centralbiological clock of the body. This is possible becausemost cell types have ageneticimprintofaperson’suniquecircadianphysiology.Youmaynotgivemuchthoughttoyourcircadianrhythm.Youprobablytake
forgrantedthatyouwillbesleepyatnightandthenfeelawakeandalertduringtheday.Yourmoodmayvary,butyoumanagetonavigatelife’ssemipavedroad.Somedaysyoumaywakeuponthewrongsideofthebed,butforthemostpartyouarereasonablygood-humored.Science is still trying to understand completely how our body clockswork,
andevenhowmanybodyclockswehave.Inadditiontotheclocksetbycuesof

dayandnight,wealsohaveaneurologicalclockthathasaninternalschedulesetin the brain. When these two clocks don’t agree on the same schedule andcompetewithoneanother,wefeel“off,”whichiswhathappenswithclassicjetlag.Ifyourcircadianrhythmissynchronizedwithyourdailylife,thenchancesare yourmood state will be a vibrant one. However,millions of people havecircadianrhythmdysfunction,andtheyexperiencemood-relatedproblemssuchas seasonal affective disorder and other forms of depression, premenstrualsyndrome, and sleeping disorders characterized by not being able to sleepenough, sleeping toomuch,ornotbeingable tosleepat the right time. Ifyouhavewhat’scalleddelayedsleepphasesyndrome,forexample,yourclockissetlater.Youmayfinditdifficulttofallasleepuntiltheearlyhoursofthemorning—sometimestwoorthreeo’clock—andmaynotbealertuntilnoontimeorlater.Peoplewithadvancedsleepphasesyndromehaveabiologicalclock that issetearlierthantheirnaturalenvironment.Theytendtofeelgroggyandtiredintheafternoon, fallasleep in theveryearlyevening, thenwakeup in themiddleofthenightwithoutbeingabletofallbacktosleep.Sometimes the cure for simple circadian rhythm imbalances is to hit your
“reset” button by exposure to light (preferably bright morning light) and byactivity.Thiswillhelpsynchronizeyourbiologicalclockthatbeatstothetuneofdaylightversusnighttimeandyourneurologicalclock.Forexample,whenyouwant to be alert and awake but your body doesn’t want to follow, you canstimulateyourbodytoresetitselfjustbygoingoutsideintothesunlightfortenorfifteenminutesorengaginginsomephysicalactivity,preferablyoutsideinthebrightlight.Circadian rhythm disorders are also thought to be associated with physical
illnesses, including heart disease and gastrointestinal disorders. Based on ourgrowingunderstandingoftheimportanceofsunshineonthefunctioningofthebiological clock, scientists are now able to successfully treat most circadianrhythm-relatedconditionsusingartificialbrightlight.
MoodTherapyThroughSunlight
Spendingmore time in the sun to improve your circadian rhythm healthmayalsoimproveyourvitaminDstatus,butthebright-lighttreatmentsthatareattheheart ofmodern treatment of circadian rhythm disorderswill not increase thevitaminD in your bloodstream.Not only is your biological clock set by light

hitting your eyes—not your skin—but the kind of light your body prefers forcalibrating its clock is early-morning light.At this timeofday, too littleUVBradiationispenetratingtheatmospheretoalsogetagooddoseofvitaminD.In addition to scheduling morning exposure to sunlight to help keep the
biologicalclocktickingintimewiththetwenty-four-hourday,oneofthemostcommonmethodsused today toaddresscircadianrhythmdisorders is the lightbox.Lightboxesemitup to10,000 lux (ameasurementof light intensity)andmimicnaturalsunshineataroundnoontime.Thelightemittedbythesedevicesistwenty times the intensity of average indoor light (500 to 1,000 lux), which,mostpeoplearesurprisedtofindout,isonlyasstrongasthenaturaltwilight.Thelightboxesthemselvesconsistofasetoffluorescentbulbsinstalledina
boxwithadiffusingscreenthatspreadsthelightevenlyandfiltersoutallUVBandmostUVAradiation.Usingalightboxiseasy.Yousimplypositiontheboxonanearby tableordesktopandsitcomfortably for the treatmentsession. It’simperativetositorstandclosetothelightbox,withorwithouttheroomlightson,andyoureyesmustbeopen.Lookingdirectlyat the lights isunnecessary;instead,light-boxuserspassthetimereading,writing,watchingTV,oreatingameal. The only reported side effects are occasional slight headaches. Theduration of bright-light treatment sessions varies from fifteenminutes to threehoursaday,dependingonyourindividualneedsandtheequipmentyouuse.Themorepowerfultheunit,thelesstimeyouhavetospendinfrontofittogetthesameeffect.Also,theneareryouaretothelightsource,thehighertheintensityof light shining through your eyes and the quicker and more effective thetreatment.The timing of light treatments is extremely important and varies with each
person, depending on the type of circadian rhythm disorder being addressed.Peoplewhohavelate-nightinsomnia,forexample,andthushavetroublegettingupinthemorningaftergoingtobedtoolate,mayonlyneedonebrieftreatmenta day in the morning to speed the body clock up; those with early-morninginsomniahave the reverseproblem—theywakeup tooearlyand fall asleep inthe early evening.Thesepeopleneed to slowdown theirbodyclocks andcantypicallydosowithearlyeveningsessionsofbright-lighttherapytoaverttheirsuperearly bedtimes and align their bodies with the twenty-four-hour day.Knowing exactly what kind of rhythm disorder you may have and thenscheduling the right kind of light therapy is important, and this reinforces theneed to use bright-light treatment under the supervision of a qualified sleeptherapist.

You don’t need a prescription for a light box, but anyone suffering from aseriousmood-relateddisordershouldcertainlyseekadoctor’srecommendationbeforeobtainingaunit anduse itunder thedoctor’s supervision.Chooseyourdoctorwisely,andquestiononewhoonlyprescribesdrugssuchassedativesorantidepressantsforyourcondition.Somedoctorsareunawareofthesuccessfulresultsofbrightlighttherapy.Severalreputablecompaniesselllightboxes(seetheResourceGuideonpage
269). The key to successful bright-light treatment is using a product thatprovides strong light at a reasonable unit-to-user distance. It is important thatyoupurchaseyourlightboxfromatrustedcompany,becausethere’snowayyoucan measure the lux output of a bright-light unit. If your symptoms don’timprove,youwon’tknowifitisbecausetheinexpensivelightboxyouboughtisnotemittingstrongenoughlightorbecauseyourconditionisresistanttobright-light treatment. Tests of products sold by disreputable companies demonstratethatcertainlightboxesdon’tputouttheamountoflighttheyareadvertisedasemitting. Also, poor-quality screens may not filter out enough UV radiation,whichmaydamageyoureyes.Aportableunitmightsuityouifyoutravelalot,oronewithastandmayfityourneedsifyouplantogetbright-lighttreatmentwhileworkingoutonatreadmillorstairclimber.Numerousaccessoriesarealsoavailable,includingpaddedcarryingcasesandstandsthatletyouplacethelightboxindifferentpositions.Theseunitscancostbetweentwohundredandsevenhundreddollars,dependingonavarietyoffactors,themostimportantbeingtheunit’s lux output and the distance it can project that light intensity. Manyinsurancecompanieswill reimburse thepurchasepriceof light fixtures for thetreatmentofseasonalaffectivedisorder,PMS,andsleepdisorders.
SeasonalAffectiveDisorder(SAD)
Ifyouliveatahigherlatitude,youareprobablyawareofsomeminorchangesinyourselfthataccompanythelengtheningdaysoflatefallandwinter.Becausethere’s less light—in terms of both intensity and duration—your hibernationimpulsemakesyouwanttoeatmoreandbelessenergetic.Mostofuscopequitewellwiththesechanges,andindeed,somebecomeenergizedbytheprospectofbriskJanuarydaysandwintersports.However,asignificantnumberofpeopleareextremelysensitivetochangesin
thelengthoftheday,somuchsothatforthemlivinganormallifeinthemodern

age is difficult. In winter, their biological clocks tell them to hibernate, eventhough life tells them they have work to do, meetings to attend, prime-timetelevisionshowstowatch,andkidstofeed.Mostofthesepeoplefinditdifficulttofulfilltheeverydaydemandsoflifeduringthewintermonths.Thissyndromehasbeenknownformillennia.Hippocratesidentifieditinthe
time of the ancient Greeks. On May 16, 1898, Arctic voyager Dr. FrederickCook wrote poignantly of psychological changes his fellow explorers wereexperiencinginresponsetothelackofsunlight:
Thewinterandthedarknesshaveslowlybutsteadilysettledoverus....It isnotdifficult to readon the facesofmycompanions their thoughtsandmoodydispositions. . . .Thecurtainofblacknesswhichhas fallenovertheouterworldoficydesolationhasalsodescendedupontheinnerworldofoursouls.Aroundthetables.. .menaresittingaboutsadanddejected, lost indreamsofmelancholy fromwhich, nowand then, onearouseswith an empty attempt at enthusiasm.For briefmoments sometrytobreakthespellbyjokes, toldperhapsfor thefiftieth time.Othersgrindoutacheerfulphilosophy,butalleffortstoinfusebrighthopesfail.
Thisconditionwas formally identified in1984byDr.NormanRosenthalofthe National Institute of Mental Health and was given the name seasonalaffectivedisorder,orSAD(ahighlyappropriateacronym).Rosenthalestablishedthat this was a bona fide disorder by taking a group of people who reportedserioussymptomsof“winterdepression”andtrackingthemthroughthevariousseasons.Withstartlingaccuracy,heshowedthattheirsymptomsworsenedwiththe shortening days and improved as the days got longer. Since Rosenthal’slandmarkstudy,manyotherresearchershaveconfirmedhisfindings.
HowDoYouKnowIfYouHaveSAD?
ThecharacteristicsymptomofSADistheonsetofmajordepressivefeelingsatcertaintimesoftheyear.Physicalactivitydecreases.Youfeelverylethargicandevensluggish.Almostanyphysicalactivityseemstobetoomucheffort.Onthe other hand, your appetite increases and you have a particular craving forcarbohydrates and sugars, such as starches, pastries, and other sweets, andalcohol.ThisexplainswhypeoplewithSADusuallyputonweightduring thewinter.MostpeoplewithSADsleepforlonghours—orwishtheycould!They

may lose interest in sex, become irritable andbad tempered, and have troublethinkingclearlyandquickly,whichmayleadtomistakes.
SymptomsofSAD
The“blahs”or“cabinfever”arenotthesameasSAD.Symptomsoffull-blownSADincludethefollowing:
•depressionthatbeginsinfallorwinter•lackofenergy•decreasedinterestinworkorimportantactivities•increasedappetitewithweightgain•carbohydrateandsugarcravings•increasedneedforsleepandexcessivedaytimesleepiness•socialwithdrawal• extreme afternoon slumps with decreased energy andconcentration
•decreasedsexdrive
Epidemiologists estimate that 2 percent to 3 percent of Americans developfull-blown SAD,with another 7 percent suffering a less extreme form of thiscondition.Womenare four timesas likely togetSAD,and theaverageageofonset is twenty-three. Because winter days are shorter at higher latitudes, thefarther you live from the equator the greater the chance you’ll develop SAD.About1.5percentofpeoplewholive inFloridagetSAD,while thisconditionafflictsalmost10percentofpeopleinNewHampshire.ThetermholidayblueshasbeenusedtodescribeSAD.That’sbecauseinthe
Northern Hemisphere, the onset of SAD symptoms begins when people aregearingupforThanksgiving,Christmas,andtheNewYear,andtheomnipresentgood cheer contrasts with many people’s “blue mood.” Until Dr. Rosenthalpublished his study, many people thought the holiday season itself wasresponsibleforarousingdepressivefeelingsinthosewhocouldn’tbewiththeirlovedonesorwhofeltstressinanticipationoffamilyget-togethers.What exactly is happening topeoplewhodevelopSAD? I described earlier
howdarknesscausesthepinealglandtoreleasemelatonintomakeusslowdown
andgotosleep.Winterwreakshavocwithsomepeople’sphysiology,andunlikethe rest of us, individualswith SAD aren’t able to suppress the production ofmelatoninintheirsystemcausedbythedimwinterlight.SADisamajordepressivesyndromewithclinicalmanifestations.Thanksto
the pioneeringwork of doctors likeNormanRosenthal, it is now listed in theAmericanPsychiatricAssociation’sstandardtext,theDiagnosticandStatisticalManual ofMental Disorders. In the past, SAD has been treated using strongantidepressantdrugsandevenelectricshocktherapy.However,byfarthemosteffective treatment forSAD is sunlight, or artificial bright light that replicatesthe effect of sunshine in the summer. InNormanRosenthal’s study, he told alargegroupofpatientsthathewasgoingtoexposethemtobrightlight,whichmightormightnothelptheircondition.Heexposedhalfthepatientstothekindofhigh-intensity light that simulatesmidday summer sunshine (between5,000and10,000 lux)and the rest to theequivalent tobright indoorhousehold light(brightofficelightingemitsbetween500and700lux,whichisequalonlytothelight at duskordawn).Thepatients didnotknowwhich typeof light therapytheyweregetting.Almostall theSADpatientswhowereexposedto thehigh-intensitylightsexperiencedadramaticreductioninsymptoms,whereasthoseintheyellow-lightgroupsawnoimprovement.Numerousstudieshaveduplicatedthese results. Bright-light treatment administered by a light box is now thetreatment of choice if you haveSAD. 80 percent of peoplewith SADbenefitfrom it.Remember, it’s important to have a qualifieddoctor provideyouwithguidelinesforusingyourlightbox,althoughyouwillfindthroughtrialanderrorwhatworksbestforyou.Therapistsusuallyhave theirSADpatients startwitha single ten-to fifteen-
minutesessioneveryday,graduallyincreasingtheirexposuretothirtytoforty-fiveminutes.Ifsymptomspersistorworsenasthedaysshorten,twosessionsadaymaybetheprotocol—oneinthemorning,uponwaking,andanotherintheevening. As with any bright-light treatment, however, figuring out the idealtimingtotreataspecificconditionshouldbedoneunderthecareofadoctorortherapisttrainedinthisarena.Totaldailyexposureisusuallylimitedtobetweenninetyminutes and twohours.Keep inmind that the light boxesused to treatSADarenotsunlamps,soyouwillnotgetatanfromthem—noranyvitaminDbenefits. Studies have shown thatmorning bright-light sessionswork better totreatthesymptomsofSAD.TheClinicalPracticeGuidelinesissuedbytheU.S.DepartmentofHealthand
Human Services recognize bright light as a generally accepted treatment for
SAD. However, on the rare occasion that bright-light treatments don’t work,antidepressantmedicationsmay be prescribed for use in conjunctionwith thiskindoftherapy.SADsymptomsusuallyimproveafterjustafewdaysofbright-lighttherapy.
Thebestresultsareseeninpeoplewhosticktoaconsistentschedulebeginningin the fall orwinter and continuing until the spring.A commonmistake is todiscontinue treatmentsas soonasyou feelbetter. In suchcases, the symptomsreturn. This reinforces the need to keep up treatments throughout the wintermonths.
GuidelinesforMinimizingthe“WinterBlahs”
Ifyourspiritsinevitablysinkalittleduringthewintermonths,youmayhavenotseasonalaffectivedisorderbuta lessserious,orsubclinical,versionof thisconditioncolloquiallyreferredtoasthewinterblahs.Beattunedtoyourmoodsand energy levels. If you start feeling “low” toward the end of summer, takepreventiveaction,includingsomeofthefollowingmeasures:
•Getasmuchnaturalsunlightaspossible.Whenit’ssunny,spendasmuchtime as you can outdoors. Early-morning sunlight is ideal, as this canhelpcalibrateacircadianrhythmgonehaywire.
• If you are at home during the day, keep the curtains open as much aspossible.
•Ifyouworkinanoffice,trytogetaworkspacethat’snearawindow.• Be physically active, and begin your physical activity before thesymptomsstart.Physicalactivityoutsideinthebrightmorninglightisawin-win.
•Try toestablishamind-set thatwillenableyou toenjoy thewintertime.Planactiveeventsforyourselfinadvanceofthefall.Schedulethingstolookforwardto.
Ifyoufeelyourselfsuccumbing,don’tfeelashamedortrytohideit.Youareby no means alone. Seek competent professional help. What you learn thiswinteryoucanapplyinwinterstocome.
NonseasonalDepression

Therearedifferentdegreesofnonseasonaldepression.Mild depression, or the “blues,” may be brought on by an unhappy event,
suchasadivorceor thedeathofarelative,and ischaracterizedbyfeelingsofsadness,gloominess,oremptiness,whichmaybeaccompaniedbylethargy.Chronic low-grade depression, also known as dysthymia, exists when a
personfeelsdepressedmostofthetimeforaperiodoftwoyears.Thesefeelingsare accompaniedby changes in energy, appetite, or sleep, aswell as low self-esteemandfeelingsofhopelessness.Major depression involves severe, persistent mood depression and loss of
interest and pleasure in daily activities, accompanied by decreased energy,changes in sleep and appetite, and feelings of guilt or hopelessness. Thesesymptomsmustbepresentforatleasttwoweeks,causesignificantdistress,andbesevereenoughtointerferewithfunctioning.Ifthedepressionisverysevere,itmay be accompanied by psychotic symptoms or by suicidal thoughts orbehaviors.Until recently, few studies had measured the effect of bright light on
nonseasonal depression. The success of bright-light treatment on seasonalaffective disorder, however, has prompted numerous researchers to studywhether this therapy would be effective for the treatment of nonseasonaldepression.Theresultshavebeenextremelyencouraging.Several studies have shown that bright-light therapy alone is as effective as
antidepressantmedicationsinreducingthesymptomsofnonseasonaldepression.One study showed that just a single hour of bright-light treatment was aseffectiveasseveralweeksonastandardmedicationfordepression.SomeofthemostsignificantworkinthisareaisbeingdoneattheUniversityofCaliforniaatSanDiegoandattheUniversityofVienna.Researchersattheseinstitutionshavefound thatcombiningbright-light therapyandantidepressantmedications isanextremelysuccessfulwaytoalleviatethesymptomsofdepression.Bright-light therapy is a fundamental component of the latest and most
successfultreatmentfornonseasonaldepression.Thisformoftherapyinvolvesathree-pronged approach: bright-light exposure, antidepressant medication, and“waketherapy.”Inwaketherapy,patientswakethemselveshalfwaythroughthenightonthefirstnighttheirprogrambeginsandstayawakeuntiltheyhavetheirbright-lighttreatmentataroundbreakfasttime(thesepatientshadalreadybegunantidepressantmedications,sotheeffectsofthedrughadbegun).Waketherapyseemstointensifytheeffectivenessofthebright-lighttherapy,perhapsbecauseit jump-starts the suppression ofmelatonin production and increases serotonin

production. Patients who have undergone this “triple-whammy” depressiontherapyhaveexperienceda27percentdecreaseinsymptomsinoneweek.The success of bright light in treating depressive disorders has inspired
doctors to use this therapy to treat conditions such as bulimia, chronic fatiguesyndrome, post-and antepartum depression, alcohol withdrawal syndrome,adolescentdepression,jetlag,andcertainformsofmentalillness.
TheVitaminDLinktoDepression
Whileseveralfactorsmayplayintotheonsetandprogressionofdepression,whethermildor severe,vitaminDdeficiencyhasbeen shown tocontribute todepressionandevenchronicfatigue.ThisisduetothefactthatactivatedvitaminD in the adrenal glandshelps regulate an enzymecalled tyrosinehydroxylase,which is necessary for the production of dopamine, epinephrine, andnorepinephrine—those hormones critical to mood, stress management, andenergy. The adrenal glands pump these hormones to help us cope with dailystress.WithoutamplevitaminDtokeeptheadrenalsincheck,theycancontinueto pump these powerful hormones out and the body can begin to experienceconstantexhaustionthatmaythenleadtochronicfatigue.Andthere’snodoubtthatbeinginachronicfatiguedstatecanperpetuatefeelingsofdepression.One insightful study performed in Minneapolis tested for vitamin D
deficiency among 150 children and adults at an inner-city primary-care clinic.Manyofthesepeoplewereimmigrantsfromvariouscornersoftheglobe,andallof them had come into the clinic between February 2000 and June 2002complainingofvague,nonspecificpain.Amongthemyriadsymptomsrecordedby doctors were achy lower-back pain, insomnia, fatigue, weakness, and adepressedmood.Manyofthemwerediagnosedwithdepressionandsenthomewithnonsteroidalanti-inflammatorydrugs(NSAIDs,suchasAleveandMotrin)tohelptaketheedgeofftheirelusivepains,andinsomecases,antidepressantswereprescribed.Imentionedthisstudybackinchapter3,buthereIwanttogiveyouacloserlookattheindividualprofilesofthesepatients,whichturnupsomeinterestingfindingswithregardtotheirvitaminDstatus,theirspecificethnicity,andhowtheyweretreated.Noneof thepatientshadanyknowndisorder thatwouldprevent themfrom
manufacturing vitamin D in the body, and none had ever been tested for 25-vitaminD.Lessthan10percentweretakingavitaminsupplementatthetimeof
the study, andmore than 90 percent had been evaluated by a doctor for theirpersistentmusculoskeletal pain one year ormore before the screening for 25-vitaminD.A full 93percentof all thesepeoplewere shown tohavedeficientlevels of 25-vitamin D. Every single one of the East Africans and Hispanicstested low for 25-vitaminD (specifically, they had 25-vitaminD levels of 20nanogramspermilliliterorless);89percentoftheSoutheastAsiansalsoscoredthislow.Andtotheresearchers’surprise,alloftheAfricanAmericans,alloftheAmerican Indians, and 83 percent of the white patients were proved to bevitaminDdeficient.Perhaps the most alarming finding of all was what the screening revealed
when looked at by age group.Thedegree of severity of vitaminDdeficiencywas inversely proportionate by age group. The youngest patients showed thelowest 25-vitamin D levels, and of the five who had undetectable serum 25-vitamin D levels, four were thirty-five years of age or younger.Many of thepatientswere given vastly different diagnoses and treatments.A twenty-three-yearoldwhitefemalediagnosedwithdepression,nondegenerativejointdisease,and low-back pain was given over-the-counter and prescription nonsteroidalanti-inflammatories.Afifty-eight-yearoldAfricanAmericanmale,ontheotherhand,diagnosedwithapanoplyofhealthconditions,wasgivenacorrespondingpanoplyofdrugs,includingnarcoticsandanantidepressant.Could any or all of these serious health challenges have been averted had
thesepatientsmaintainedsufficientlevelsof25-vitaminD?Onethingiscertain:peoplewho suffer frompersistent, nonspecific pain andwho are subsequentlydiagnosedasshowingsignsofdepressionalongsideelusiveothersymptomslikefatigueandinsomniawoulddowelltohavetheir25-vitaminDlevelscheckedorsimplytakevitaminDasIprescribeinchapter10.
TakingDepressionSymptomsSeriously
Justbecauseyourdepressionsymptomsoccuronlyatcertaintimesoftheyeardoesn’tmeantheyareallinyourhead.Thesymptomsofdepression—seasonalor nonseasonal—must be taken very seriously. Proper diagnosis and treatmentare essential. If youexperiencepersistent sadness that lasts formore than twoweeks, accompanied by problems with sleep, appetite, concentration, andenergy, seek professional help. This is especially important if you areexperiencingthoughtsofsuicideorofhurtingyourself.
There’snomechanicaldevicetomeasuredepression,sohowdodoctorstellifantidepression treatments suchasbright lightareworking?Scientists ratehowdepressedpatientsarebeforeandaftertreatmentwith“depressionratingscales.”Theyinterviewpatientsandaskthemtoscorehowsad,guilty,withoutappetite,suicidal,andsoforth theyare,andthentheyaddupthepoints toreacha totaldepression score.After therapy, the researchers ask the same questions. If thescoreisthesameorhigher,theyconcludethatthetreatmentmadenodifferenceor perhaps made the patient’s condition worse. But if the score is lower, thetreatmenthasworked.
PremenstrualSyndrome(PMS)
Premenstrual syndrome (PMS) refers to a cluster of symptoms that occurregularly in conjunction with a woman’s monthly menstrual period. Thesymptoms tend to occur five to eleven days before her period starts and stopwhenherperiodbegins.Most women are affected by PMS at some point during their childbearing
years. Between 30 percent and 40 percent of women have PMS symptomssevereenoughtointerferewithdailyliving,and10percentsuffersymptomssosevere they are debilitating. PMS can cause extremedifficulties in awoman’srelationshipswithfriends,family,andcolleagues.TheincidenceofPMSishigherinthosebetweentheirlatetwentiesandearly
forties, those with at least one child, those with a family history of a majordepressiondisorder,andthosewithapastmedicalhistoryofeitherpostpartumdepressionor someother affectivemooddisorder, such asSAD. It used to bethoughtthatPMSsymptomswerecausedbyahormonalimbalancethatoccurredduring the menstrual cycle. Now it’s understood that PMS is a result ofinsufficient serotonin—the chemical that carriesmessages between the nervesandmakesusfeelcalm,happy,andalert.Justbeforeawomangetsherperiod,herlevelsofserotoninnaturallydropandthengobackupagainwhenherperiodstarts.Ifshehasnaturallylowbaselevelsofserotonin,symptomsofPMSwillprobablyoccurasserotoninlevelsdropbelowthepointatwhichtheyareneededtomaintaingoodpsychologicalhealth.SeveralresearchershavedemonstratedthatPMSrespondswelltobright-light
treatment.ThereasonbrightlightworkstoreducethesymptomsofPMSisquitestraightforward:serotoninlevelsinthebodyincreaseinresponsetobrightlight;
remember, too, that vitaminD helps regulate the production of dopamine, theothermood-friendlyhormone,inthebrain.OneofthemostimportantstudiesinthelastdecadeofhowbrightlightcanbeusedtotreatPMSwasledbyDr.D.J.Anderson and published in the Journal of Obstetrics and Gynecology. Dr.Anderson’s six-month study involved a group of twenty women who hadunsuccessfully tried in a variety of ways to reduce their serious, ongoingproblemswithPMS.Thewomenweregiven fifteen to twenty-nineminutesofbright-lighttherapyeverydayforfourconsecutivemenstrualperiods.Attheendof the study, Dr. Anderson and his colleagues found that the bright-lighttreatments had reduced by 76 percent the severity of PMS symptoms such asdepression, anxiety, irritability, poor concentration, fatigue, food cravings,bloating,andbreastpain.TheremaybeavitaminDlinkaswell.Becauseovarianhormonesinfluence
calcium,magnesium, andvitaminDmetabolism, scientists have longbelievedthatPMScanbepartlyblamedonlowlevelsofthesemicronutrients.Dr.SusanThys-JacobsofColumbiaUniversitypublishedastudyin2000makingastrongcase for calcium, highlighting that the addition of not just calcium but alsomagnesium and vitamin D can completely reverse PMS. A year before thatstudy, Dr. Thys-Jacobs’s investigations revealed that polycystic ovariansyndromealsocouldbecorrectedbysupplementationofvitaminDandcalcium.Polycystic ovarian syndrome is a condition in which a woman’s hormonesbecome imbalanced, often causing a disruption in her menstrual cycle andinfertility. Dr. Thys-Jacobs examined thirteen premenopausal women with ahistoryofabnormalovulationand relatedmenstrualproblems.Theirmean25-vitaminD levelswere11.2 (yes, that’sdeficient).After theywere treatedwithcalciumtherapyandtheirvitaminDbroughtuptosufficientlevels,sevenofthewomenhadnormalmenstrualcycleswithintwomonths,includingtwowhohadresolved previously dysfunctional bleeding. Two of the women becamepregnant,andtheotherfourpatientsmaintainednormalmenstrualcycles.Anothersideeffectof somewomen’smonthlycycle—menstrualmigraine—
hasalsobeenassociatedwithlowlevelsofvitaminDandcalcium.Recall thatwe saw earlier how vitamin D deficiency is common in chronic migrainesufferers;thisisasidefromthemenstrualfactorandincludesmen,too.
SymptomsofPremenstrualSyndrome
YouhavePMSiffiveormoreofthesesymptomsareassociatedwithyourmenstrualperiod:
•feelingofsadnessorhopelessness,possiblesuicidalthoughts•feelingsoftensionoranxiety•moodswingsmarkedbyperiodsofcrying•persistentirritabilityorangerthataffectsotherpeople•disinterestindailyactivitiesandrelationships•troubleconcentrating•fatigueorlowenergy•foodcravingsorbinging•sleepdisturbances•feelingsofbeingoutofcontrol• Physical symptoms, such as bloating, breast tenderness,headaches,andjointormusclepain
ShiftWorkerSyndrome
Tens of millions of Americans work the night shift. Night-shift workersexperienceavarietyofproblems,suchasahigherriskofpsychologicalailmentsandanincreasedlikelihoodoffatigue-relatedaccidents.Nightworkersalsohavehigherratesofheartdisease,cancer,diabetes,andgastrointestinaldisorders.Despite the additional expenseofpayingpeople towork thenight shift and
the problems it causes for the workers, in this modern age we need peopleworkingunfavorablehours.Certainindustries,suchasoilrefining,shipping,andtransportation, need to operate around the clock; others find it economicallydesirable to keep the assembly line moving; emergency response and lawenforcementneedpersonneloperatingtheirstationstwenty-fourhoursaday;andconveniencestoresneedtokeeptheirdoorsopenincasesomeoneneedsagallonofmilkattwoo’clockinthemorning.Night-shift workers experience problems because their lives operate in
opposition to their circadian rhythms.Nomatterhow longapersonworks thenightshift,whenheleavesworkandwalksintothedaylighttogohometobed,hisbodyclocktellshimitistimetowakeup.Thatmakesithardforthatpersontogetafullnight’ssleepduringtheday.

Studiesofnight-shiftworkershaveshownthat,onaverage,theysleeponetotwohourslessthandayworkers.Thatsleeplossiscumulativeandisprimarilyresponsiblefortheproblemsnightshiftworkerstendtohavestayingalertduringtheirshiftsandexperiencingafulfillinglifeoutsidework.Shiftworkersalsopaya huge toll in their relationships with others and ability to maintain a stablehousehold.A largenumberof studieshaveshown thatbright-light therapy isextremely
helpfulinhelpingnight-shiftworkersadapttotheirworkschedules.Companiesthat have employees working the night shift should fully utilize bright-lighttechnology to improveworkermorale and reduce errors and accidents on thejob.Thekeystothisarehavingtheappropriatebright-lightequipmentinstalledand timing its use to synchronize workers’ body clocks to their working andsleepinghours.
GuidelinesforDecreasingCircadianRhythmDisruptionsCausedbyShiftWork
•Reducethenumberofconsecutivenightshiftsyouwork.Night-shiftworkersgetlesssleepthandayworkers.Overseveraldays,theybecomeprogressivelymoresleepdeprived.Ifyoulimitthenumberofnightshiftsyouworktofiveorfewer,withdaysoffinbetween,youaremorelikelytorecoverfromsleepdeprivation.Ifyouworkatwelve-hourshiftinsteadoftheusualeighthours,limitthistofourconsecutiveshifts.Afterseveralconsecutivenightshifts,youshouldideallyreceiveaforty-eight-hourbreak.
•Avoidworkingprolongedshifts,workingexcessiveovertime,andtakingonlyshortbreaks.
•Avoidlongcommutes,becausetheywastetimeyoucouldspendsleeping.•Avoidrotatingshiftsmorethanonceaweek.Itismoredifficulttocopewithsuchalterationthanitistoworkthesameshiftforextendedperiods.Thesequenceofshiftrotationcanbeimportantaswell.Workingthefirstshift,thenthesecondshift,andthenthethirdshiftiseasierthanworkingthefirst,thethird,andthenthesecond.
•Getenoughsleeponyourdaysoff.Practicegood“sleephygiene”byplanningandarrangingasleepscheduleandbyavoidingcaffeine,alcohol,andnicotinetohelpyousleeporstayawake.
•Avoidrelianceonstimulants,over-the-counterandotherwise.Caffeineandstay-awakepillsonlytemporarilytrickthebodyintothinkingitisfunctioningproperly,whichwillonlyfurtherdisruptyourcircadianrhythms.
SleepDisturbancesandElderCare
Bright light is being used with increasing frequency and success to treat avariety of disorders that affect our older citizens, especially sleep-patterndisturbancesandformsofdementiasuchasAlzheimer’sdisease.As people get older, their circadian rhythms “flatten out” and they become
predisposedtosleepdisturbances.Thisusuallymanifestsitselfingoingtosleeptoo early and then waking before the sun comes up—often at three or fouro’clockinthemorning.Inthemostextremecases,elderlynursinghomepatientsmaysleepatanyhourofthedayornight,sometimesevensleepingforpartofeveryhourintheday.Bright-lighttherapyfirstthinginthemorning,followingthe same guidelines used for seasonal affective disorder, has been effective inresettingelderlypeople’sbiologicalclocksandrestoringtheircircadianrhythms.Increasingly, attention is being paid to the kinds of lighting that should beprovidedforseniors,notjustintheformofdirectedtherapybutalsoasitshouldbe incorporated into the design and architecture of homes and group livingfacilities.
SleepTips
Wantabetternight’ssleep?Trythefollowing:
• Cut down on caffeine (including caffeinated soda) after 2:00P.M.andavoidalcohol.
• Drink fewer fluids before going to sleep so you won’t beawakenedbybladderdiscomfort.
•Avoidheavymealsclosetobedtime.•Avoidnicotine,whichactsasastimulant—notarelaxant.•Exerciseregularly,butdosointheearlyafternoon,notinthelateafternoonorevening.

•Relaxinahottuborbathbeforebedtime.•Establish a regular bedtimeandwake-time schedule.Keep tothatscheduleontheweekends.
If your sleep problems become chronic, consider bright-lighttherapy. Even peoplewithmild sleeping disorders can benefit frombright-lighttreatment.Forexample,apersonwhowantstogotosleepatelevenintheeveningbutcan’tnodoffuntiloneinthemorningcanreset the body’s clock by having a leisurely breakfast in front of alightbox.
TheFutureofTreatmentforCircadianRhythmDisorders
Bright-light treatment isanexcitingbreakthrough in the treatmentofmood-relatedconditionscausedbycircadianrhythmdysfunction.Treatmentsaresafeand economical, and light boxes have no side effects.Light boxes represent aone-timecostofafewhundreddollars,versusseventydollarspermonthforanantidepressant that has side effects and other risks. However, bright-lighttreatments can be extremely effective when used in conjunction withantidepressantmedicationsinsomecases.Recent breakthroughs have demonstrated that bright “blue light” treatments
may have even more applications than we fully understand. Rather than thetraditional 10,000-lux full-spectrum light therapy devices, blue-light devicesemit exactlywhat they say: blue light,which is a very specific range of lightwithinthevisiblespectrumthathasawavelengthof526nanometers.Forsometime, blue light treatments have been usedwith great success for babieswithjaundice.Morerecently,bluelighttreatmentshavebeenusedtostimulateweightgaininprematurebabies.TheDepartmentofArchitectureattheMassachusettsInstitute of Technology is studying how to maximize natural daylight andminimize artificial light in buildings. It is developing tools to measure howilluminationcanbemanipulatedtomeethumancircadianneedsinordertohelparchitectsmakelight-relateddesigndecisions.Acolleagueofminehasbeenatthe forefront of creating headlamps that a person can simply put on to beexposedtobluelight.Blue-light therapy can have multiple benefits. One recent study found that
usingblue light helpedofficeworkers staymore alert during theday, reduced

evening fatigue, and improved night sleep. Some research suggests this isbecause blue light targets a recently discoveredphotoreceptor in the eye.Thismayhelpthosewhodon’trespondwelltotraditionalwhite-lighttherapy.Studiesareunderwaytoseeifothertypesoflighttreatment,includingsynchronizationto individualmelatoninrhythmsorsimulateddawns,might improve individualhealthandperformance.Newevidencefrommylaboratory—thatit’snotjustourbrainsthatmakethe
powerful mood-enhancing beta endorphins in response to UVB exposure butalsoourskin—isanothermajorstepforward.Mostrecently,mycolleaguesandIidentified two genes in the skin that are responsible for regulating the body’scircadianrhythms.Thediscoverythatwehavebiologicalclocksalloverourbodies,not just in
the hypothalamus, has also been a major breakthrough. These advances wereinitiallymade in research involving fruit flies andmice.Then, in a study thatrocked the circadian rhythm research community, a group successfully resetpeople’s body clocks byblindfolding themand exposing the area behind theirknees to light. Although other researchers have had difficulty replicating theresults,thisdiscoveryhassignificantimplications.Itincreasesthelikelihoodthatwemay soon have the ability to treat a variety of other conditions associatedwith circadian rhythm disruption, including heart disease, diabetes, and evencancer.
TheDangersofNightLight
Theprofound impact that light canhaveonourbodiesmayalso includeanunwantedoutcome, asnew research links exposure to lightatnight to cancer.The associationwas first observed byEvaSchernhammer,M.D.,who noticedthat twoofhercolleagues—healthywomen in their thirties—developedcancerwith no risk factors or a history of the disease. Dr. Schernhammer workedrotatingnightshifts inaVienna,Austria,cancerward from1992 to1999.Shehadtopull tenall-nightersamonthinadditiontoherregularhours.Whenshelanded atHarvardMedical School three years later, she curiously tapped intomedical,work,andlifestylerecordsofnearlyseventy-ninethousandnursesanddiscoveredthatnurseswho’dworkedthirtyormoreyearsonnightshiftshada36percenthigherrateofbreastcancerthanthosewho’dworkedonlydayshifts.She continued to uncover unsettling news, and by late 2005 she published

reports that her fellow female night owls exhibited a 48 percent rise in breastcancer.Blindwomen,ontheotherhand,hada50percentreducedriskofbreastcancer,comparedtotheirseeingcounterparts.Thesefindingssuggestthatexposuretolightatnightmayraisetheriskofnot
onlybreastcancerbutalsoseveralothertypesofcancer.Futurestudieswillbearthis out. It also confirms the far-reaching influence that light can have on ourbodies,notablyourabilitytofightdiseaseslikecancer.It’snotsomuchthelightitself that is harmful, but ratherwhat the light does to the body’s physiology.Melatonin,itturnsout,haspowerfulanticancercapabilities.Allcells—includingcancerouscells—havereceptorsthatbindtomelatonin,thehormoneresponsiblefor lulling us to sleep at night after the sun sets.When amelatoninmoleculebinds toabreastcancercell, it counteractsestrogen’s tendency toactivatecellgrowth.Melatoninalsoaffectsreproductivehormones,whichmightexplainwhyitappearstoprotectagainstcancersrelatedtothereproductivecycle—ovarian,endometrial, breast, and testicular. Another feature of melatonin’s cancer-fightingstrengthisitsabilitytoboostthebody’sproductionofimmunecellsthatspecificallytargetcancercells.Dr.Schernhammer’sstudies,publishedintheJournaloftheNationalCancer
Institutein2001,providethefirstevidencethatthere’sabiologicalrelationshipbetweencancerandadisturbedcircadianrhythm.Thissurelyputsanewspinonthe“graveyard”shift.
Sun,BrainHealth,andVitaminD
There’sareasonI tookadetour tocovercircadianrhythmdisorders thatdon’trevolve primarily around vitamin D levels. The role sunlight plays in ourbiologicalclocks,whicharedirectlytiedtoourphysiologicalrhythmsandthus,ultimately,tohowwefeel—sleepyoralert,hungryorfull,hotorcold,andsoon—reinforces the importanceofsunlight inour lives.Butnowlet’s turn tohowvitaminDplays directly into ourmental health, startingwith some interestingrecentfindingsaboutvitaminDanddementia.Dementia is among themost feared conditionsof old age.Noonewants to
endup in a catatonic state characterized by the inability to communicatewithothers,recallmemories,dosimplemath,recognizefamilymembers,andhaveagrasponthegoings-onintheworld.Recently,twostudieslookedattheroleofvitaminDinmaintainingbrainfunction.Oneexaminedevidencelinkingvitamin
Ddeficiencytobraindysfunction,andtheotherexploredtheroleofvitaminDinpreventingthecollapseofmentalperformance.Takentogether,manyofthesereportslaythegroundworkforthehypothesisthatvitaminDcanreducetheriskofdementia.The termdementia is a bit misleading because it’s not necessarily a single
disease. Rather, dementia encompasses a spectrum of brain-related diseases,including Alzheimer’s disease, vascular dementia, Lewy body disease, andwhat’sknownasfrontotemporaldementia.ThedistinctionbetweenAlzheimer’s,a progressive, degenerative disease of the brain that causes impairedmemory,thinking, and behavior and is probably the most commonly thought-of braindiseaseofoldage,andvasculardementiaissomewhatblurred.Asmanyas45percentofthosewithdementiamayhavemixeddementia,oracombinationofAlzheimer’sandvasculardementia.Vasculardementiaistypicallycharacterizedbypreviousstrokes,heartdisease,hypertension,anddiabetes.Themultifaceted nature of dementia means that there is no single, defined
path to dementia—there are many, from inflammation and oxidative stress(otherwise known as free-radical damage) to small strokes and the death ofneurons in thebrain.Andthereare justasmanyriskfactorsorconditions thatoftenprecededementia,includingcardiovasculardiseases,diabetes,depression,osteoporosis,andevendentalcavitiesandperiodontaldisease.Notonlydoallofthese increase the risk of dementia later in life, but notice that they are allassociatedwith low levels of 25-vitaminD. The laboratory evidence includesseveral findings on the role of vitaminD in protecting the brain and reducinginflammation.PeoplewithParkinson’sandAlzheimer’s,forexample,havebeenfoundtohavelowerlevelsof25-vitaminD.It’s not that boosting levels of 25-vitamin D will reverse or cure dementia
(thoughIwouldstronglysuggestthatpatientsalreadydiagnosedwithdementiakeeptheir25-vitaminDlevelsinthehealthyrange);thegoalhereistomaintainadequate 25-vitamin D levels to reduce the risk of the pathways that lead todementia—namely,theonesIjustmentioned.A study done by University of Manchester scientists in collaboration with
colleaguesfromotherEuropeaninstitutionscomparedthecognitiveperformanceofmore than three thousandmen between the ages of forty and seventy-nineyears at eight test centers. This study, published in the Journal of Neurology,Neurosurgery,andPsychiatry,woundupbeingquiteremarkablebecauseitwasthefirsttolookspecificallyattherelationshipbetweenvitaminDandcognitiveperformance (for example, how fast you can multiply two times two). In

studyingthislargepopulationsample,theresearcherstookintoaccountpotentialinterferinghealthandlifestylefactors,suchasdepression,education,andlevelofphysicalactivity—allofwhichcanaffectmentalabilityinolderadults.Theyfoundthatthemiddle-agedandoldermenwiththehigherlevelsof25-vitaminDshowedthebestmentalagility.Infact,themenwithhigherlevelsof25-vitaminDperformedconsistentlybetterinasimpleandsensitiveneuropsychologicaltestthatdocumentsanindividual’sattentionandspeedofinformationprocessing.Themostunexpected findingof thestudywas that increasedvitaminDand
fasterinformationprocessingweremorestronglyassociatedinmenovertheageof sixty, although thebiological reasons for this remainunclear.The scientistsconcludedthatvitaminDappearstohaveextraordinarilypositiveeffectsonthebrain.ThestudyalsoraisesthepossibilitythatvitaminDcouldminimizeaging-relateddeclinesincognition.Wedon’tknowexactlyhowvitaminDandmentalagility may be connected, but it wouldn’t surprise me to see future studiesdemonstrate vitamin D’s role in increasing certain hormonal activity or otherbiological reactions that ultimately protect neurons and that confer healthierbrains.It’s common for people with dementia to suffer disturbances in circadian
rhythm, too, because of the damage occurring to their brains.A vicious cycleoften begins, with the dementia-induced circadian rhythm disturbancesexacerbated by indoor confinement and lack of exercise, both of whichcontribute tocircadian rhythmdisorders.Apersonwithdementia typicallyhasproblems sleeping through the night and may wander out of bed and beconfused. Sedatives have traditionally been used to treat circadian rhythmsymptomsassociatedwithdementia,but theyarenotparticularlyeffectiveandhavesignificantsideeffects.Anumberofstudieshaveproventhatbright-lighttreatmentscanbeextremelyhelpful.Asyoucandeduceonyourownbynow,bright-light therapy helps people with various forms of dementia by resettingtheirbiologicalclocks,helpingthembecomemorealertduringthedaysotheygo on fewer night wanderings. In addition, recent research has shown thatreducing circadian rhythm disturbances using bright-light treatments canimprovethementalfunctionofpeoplewithearlystagesofdementia.
FromWombtoOlderAge
Thisbrainprotectionactuallybeingsinutero—inthewomb.Livingathigher
latitudeshasbeenshowntoincreasetheriskofschizophrenia,therootsofwhichmay take hold in a developing baby’s brain long before symptoms emerge inyoungadulthood.Infact,oneof thecausal links thathavebeenmadebetweenschizophreniaandvitaminDisbasedonthetheorythatvitaminDdeficiencyinutero alters brain development. This helps explain schizophrenia’s oddcharacteristic of occurring more frequently in those born in winter or earlyspring.Dr. JohnMcGrath,professorofpediatrics,biochemistry,andmolecularbiologyattheMedicalUniversityofSouthCarolina,stateditperfectlywhenhesaidthatvitaminDdeficiencyduringpregnancynotonlyislinkedtoamother’sskeletal preservation and her baby’s skeletal formation, but also is vital to thefetal “imprinting” thatmay affect chronic disease susceptibility later in life aswellassoonafterbirth.Thatistosay,thevitaminDstatusofapregnantwomandirectlyimpactswhetherornotherchilddevelopscertainillnessesanddiseases,fromdiabetesasanadolescenttoosteoporosisanddementiaasanelder.TothinkthatprebirthvitaminDdeterminesourbonehealthforlifeandeven
ourriskforcancerandautoimmunediseases,amongalitanyofotherillnesses,isamazing.Theconnectionwouldn’tnormally leapoutatyou,but themountingevidenceisclearandpersuasive.Evenachild’slungsareaffectedbyamother’svitamin D levels. Asthma, a common childhood problem, has been linked tovitaminDdeficiency inmothers.When the journalClinical andExperimentalAllergyin2009publishedanarticleentitled“ChildhoodAsthmaIsaFat-SolubleVitaminDeficiencyDisease,”laypeopleanddoctorsaliketooknotice.Thepaperoutlineda strong linkbetweenvitaminDandchildhoodasthma. (I’llbegoingintomuchmoredetailaboutpregnancyandvitaminDinchapter10.)Giventhisdelugeofnewinformation,it’snosurprisethatpeopleoftenhave
more than one vitamin D-sensitive disease during their lives. The questionyou’relikelyaskingyourselfnowis,howbadisyourdeficiency?
CHAPTER7
AreYouDeficient?
Aquickself-testtodetermineyourlevelofdeficiency
When thebody aches for something it needs, it oftenhas awayof tellingus.Whenwe’redehydrated,thirstsignalsfromthebrainencourageustodrink.Thesame goes for being fuel-deficient (hunger), sleep-deprived (drowsiness), andeven faced with serious danger. The famous fight-or-flight stress responseexemplifieshowthebodymaintainsitsownbrilliantsurvivalsystemforlife.Allanimals,infact,survivebysimilarmechanismsthatdon’trequireahighIQoraPh.D., much less a complex brain that can ruminate over the past and worryabout thefuture.ButwhataboutsensingavitaminDdeficiency?Howdoyouknow?It’sfunnytothinkthat,withtheexceptionofhumans,animalsthatrelyonthe
sunforenergyandvitaminDknowinstinctivelytosoakinthoserays.Theymaynot pass a driver’s test or read health books, but at least they “know”what’sgood enough for their survival needs. It’swell documented, for example, thatlizardswhoarevitaminDdeficientseekoutUVBradiationjustastheywouldwaterwhenthirsty.Humans,ontheotherhand,havethisextraordinarycapacity—thankstotheadvancedbrainsthataffordustheabilitytocriticallyanalyzeandjudgetoourhearts’content,whetherthatjudgmentturnsouttoberightorwrong—totalkourselvesintoandoutofanything,includingtheverythingsthatcouldbehealthyorunhealthy.Sometimes,though,itpaystoactlikealizard.By now, if you’ve been digesting the previous chapters and thinking about
your geography and habits in the sun, you probably have a feeling you’revitaminDdeficienttosomedegree.YoumayevenhavetheurgetorunoutandbuyabottleofvitaminDsupplementsandcallitaday.Unfortunately,youcan’t
satisfyabody’sneedformorevitaminDwithaquicktriptothemarketlikeyoucansatisfyhungerand thirstwithquickaccess to foodandwater.Abody thathasbeendeprivedofadequatesuppliesofvitaminDforawhilerequiresalong-term commitment to restocking the system day by day andmonth bymonth,slowlybuildingitbackupovertime.That’swhatpartIIwillbeabout,asItakeyou through on a fail-proof plan to elevate your vitamin D levels back intohealthfulterritory—andkeepthemthere.
If you are vitamin D deficient or insufficient, then your vitamin Dtank is empty and needs to be filled as quickly as possible. Sunexposureforonlyafewdaysandover-the-countersupplementsinpillformusuallyaren’tenough.
Agood(andquick)preludetopartII,however,isgettingsomegeneralsenseofapotentialdeficiencyandwhatyoucandotogettestedunderadoctor’scareforarealdiagnosis.Andthat’sexactlywhatthischapterisabout.
PopQuiz
Howmanyofthefollowingstatementsapplytoyou?
❑Irarelygooutinthesun.❑IwearsunblockandcoverupmyskinwhenIgooutinthesun,especiallyduringthesummermonthsorwhenI’moutsideinthemiddleoftheday.
❑Mywardrobetypicallycoversmostofmyskin,includingarmsandlegs.❑Iliveabove35degreeslatitudeintheNorthernHemisphere(northofAtlantaandLosAngeles).
❑Ilivebelow35degreeslatitudeintheSouthernHemisphere(southofSydney,Australia,Santiago,Chile,orBuenosAires,Argentina).
❑IdonottakeamultivitaminalongwithavitaminDsupplementeveryday.
❑IdonottakeaseparatevitaminDsupplementeveryday.❑Idonoteatwild,oilyfish(salmon,mackerel,herring,sardines,etc.)twotothreedaysaweek.

❑Idonoteatalotofmushrooms.❑Idrinkfewerthantenglassesoffortifiedmilkororangejuiceaday.❑IamnaturallydarkskinnedoramofAfricanorHispanicdescent.❑Iamolderthansixty.❑Iamyoungerthantwenty.❑Iamoverweightandcarryaconsiderableamountofextrafat.❑WhenIpressfirmlyonmysternum(breastbone)withmythumborforefinger,ithurts.
❑WhenIpressfirmlyonmyshins,Ifeelpain.❑IfeellikeIhavelessenergyandmusclestrengththanIshould.❑ItakeantiseizureorAIDSmedication.❑Itakeglucocorticoids(e.g.,prednisone).❑Ihaveceliacdisease.❑Ihaveintestinaldisease.❑Ihavehadgastricbypasssurgery.
Ifyoucheckedanyoftheaboveboxes,thenthere’sahighchancethatyousufferfromavitaminDdeficiency.Ifyoucheckedseveralboxes,thenIencourageyoutotakepartII’sprotocolseriouslyand,ifyou’recurious,askyourdoctortotestyourvitaminDstatus.It’simportant,though,tomakesureyourequestaspecifictest.
Testing,Testing,1-2-3
The only surefire way to know for certain the extent of your vitamin Ddeficiencyistoaskfora25-hydroxyvitaminDtest,alsocalleda25(OH)Dtest.Again,thisisthecirculatingformofvitaminDthatthelivergeneratesandthatthenbecomesactivatedbythekidneys.Whileit’sintuitivetothinkyou’dwantto test for thebody’s“active form” rather than just aprecursor, testing for theactivated vitamin D (1,25-vitamin D) actually does not give an accurateportrayalofyourvitaminDstatus.Andhere’s therub:manydoctorsorder thewrongtest,andwhentheresultscomebackshowinganormallevelofactivatedvitaminD, they think everything isD-okay.You could, however, be sufferingfromaseriousdeficiencyeventhoughyouractivatedlevelsappearnormal—orevenelevated.Thismaysoundincomprehensible,butnotonceyouunderstandafewfactsaboutvitaminD’sbiology.
Anydoctor canorder the 25(OH)D test for you, but if theyuse thewrongcodingwhen submitting the claim to the insurance company,theywon’tgetreimbursedandyouwillwinduphavingtopayforthetest. (The actual cost of vitamin D testing can vary significantlydependingonthelabusedandwhetheralargenumberofassaysarebeing performed by an individual doctor’s office or hospital. Theassaycostcanrangefromapproximately$40to$225pertest,soaskyour health care provider. Medicare currently reimburses you for$40.)ThecodeforvitaminDdeficiencyis268.9,orifthedoctorhasa code for osteoporosis or for other related diseases for vitamin Ddeficiency,heorshemaybeabletousethat.But268.9isforvitaminDdeficiency, andusing that canhelpminimize costs andmaximizereimbursements. (Other codes of interest: osteomalacia = 268.2;osteoporosis=733.00;osteopenia=733.90.)
The active form of vitamin D circulates at one thousand times lowerconcentration than 25-vitamin D, which, when created by your body from asupplement, has a half-life in your circulation of two to threeweeks.The 25-vitaminDmadebyyourbody in response to sunlight, however, lasts twiceaslonginthebody.Half-lifesimplyreferstotheamountoftimeittakesthebodytoeliminateonehalfofthetotalamountof25-vitaminDand1,25-vitaminDinyourblood.On theotherhand, theactive formofvitaminDhasahalf-lifeofonly two to four hours, meaning that the concentration of active D in yourbloodstreamisreducedbyhalfeverytwotofourhours.AsyoubecomevitaminD deficient, the body immediately responds by increasing the production ofparathyroidhormone,which tellsyourkidneys toactivatevitaminD,which iswhy your activated vitamin D (1,25-vitamin D) levels are either normal orelevatedwhenyouarevitaminDdeficientorinsufficient.Howisthatpossible?AndhowcanyoubevitaminDdeficientifthekidneys
thencrankoutmoreactivatedD?Myguess is thatyour target tissues,namelyyourintestinesandbones,stillcan’tgetenough,eventhoughyourbloodlevelsare normal. Serum calcium is usually normal in the vitaminD-deficient state.Mostphysiciansalso tripuponcalcium levels.That is to say, if theymeasurecalcium levels in the blood and see nothing off the mark, they automaticallyassume this translates to a correspondingnormal vitaminD status.But in fact
thisisn’tnecessarilytrue.NeithercalciumlevelsnoractivatedvitaminDlevelsinthebloodcantellyouwhetherornotyouarevitaminDdeficient.Youmustmeasure 25-vitamin D; do not accept any other marker no matter what yourdoctortellsyou.So,whereshouldyour25-vitaminDlevelsbe?Theunitofmeasurementused
forvitaminDisnanogramspermilliliter,andmostexperts—myselfincluded—agree that vitamin D deficiency is defined as 25-vitamin D of less than 20nanograms per milliliter. Vitamin D insufficiency is between 21 and 29nanogramspermilliliter.AndvitaminDsufficiencybeginsat30nanogramspermilliliter. To obtain the full benefits of vitamin D for health, many expertsrecommendthatbloodlevelsbecloserto40nanogramspermilliliter.Thereasonfor this is that higher levels have been associated with a decreased risk forcancer,heartdisease,autoimmunedisease,andsoon.VitaminDintoxicationistypically not seen until blood levels are above 150 to 200 nanograms permilliliter;lifeguards,forexample,arefamousfortoutinglevelsof25-vitaminDinthe100-nanograms-per-milliliterrange,andyoudon’thearaboutthemfallingvictimtovitaminDtoxicity—principallybecausethey’regettingmostoftheirDfrom the sun and it’s impossible to get toomuch from this source. Similarly,tannerswhousetanningbedsonceaweektypicallymaintainlevelsinthe40-to60-nanograms-per-milliliter range throughout the winter. If you rely onsupplements for your vitamin D, it takes about a month to fall below 20nanogramspermilliliterifyourregularsupplementationgoesonhiatus.
The assay for 25-vitamin D is now the most ordered assay in theUnitedStates.
Here’s anotherway to look at it: for every100 IUof vitaminDyou ingestthrough, say, a supplement, your blood level of 25-vitamin D increases by 1nanogrampermilliliter.This iswhybothchildrenandadultsneed tobeonatleast1,000IUofvitaminDadaywhen theyhave inadequatesunexposure tosatisfytheirbody’svitaminDrequirement.Ipersonallytakeabout2,700IUofvitaminDdailyfromsupplementsandmilk(thisisinadditiontoanyvitaminDI get from sensible sun exposure), and my blood level is 50 nanograms permilliliterthroughouttheyear.

ReadingDifferentAssays
Therearetwomainassaysthattestaperson’svitaminDstatus,oneofwhichisbetterthantheother.Liquid chromatography tandemmass spectrometry (I know, it’s amouthful
usually abbreviated as just LCMSMS) is, in my opinion, the state-of-the-art,gold-standardassaythatdeterminesyourbloodlevelsofboth25-vitaminD2and25-vitaminD3.Whatyoucareaboutisthetotal25-vitaminD,soyou’dsimplyadduptheresultsofthisassaytoarriveatyourgrandtotal.Forexample,ifyourresults show20nanogramspermilliliterofvitaminD2 and15nanogramspermilliliterofvitaminD3,thenyourtotalvitaminDis35nanogramspermilliliter.WhatmakesthisassaybestisthatitcandifferentiatebetweenthetwotypesofvitaminD.Remember,vitaminD2 isavailableonlyasapharmaceutical.So ifyou’re being treated for a deficiency using pharmaceutical-gradeD2 but yourbloodlevelofD2doesnotgoup,thatindicatesthatyourbodyisnotabsorbingvitaminD2.Theotherassayoutthereisaradioimmunoassay.Itmeasuresonlyyourtotal
25-vitaminDandcannotdistinguishbetweenD2 andD3. If youdon’t have achoiceinwhichassayisusedandarestuckwiththeradioimmunoassay,it’sstilla reliable source that can suffice. If possible, however, request the LCMSMSassayforamorein-depthanalysis.
WhyAge,Place,andRaceMatter
I’ve already covered how these circumstances factor into the vitamin D-deficiencyequation,butletmeremindyoubriefly.Age.Theolderyouare,theharderitisforyourbodytomakevitaminDfrom
sunlight,becausetheprecursorofvitaminDinthebodydeclineswithage.Thatsaid,theskinhasalargecapacitytomakeamplevitaminDdespitethisphysicaldecline in the “assembly line.” Assuming there’s a 50 percent to 70 percentreduction in the body’s ability tomakevitaminDby the ageof seventy, all aseventy-year old would need to do to be able to make plenty of necessaryvitaminD is exposemore areas of skin (say, the arms and legs) three to four

timesaweek.Theseventy-year-oldwon’tmakewhatatwenty-toforty-year-oldwillinthesun(theequivalentofa20,000IUsupplement),butthe3,000to5,000IUhemakeswillsuffice.Unfortunately,olderpeopleareespeciallyreceptivetothealarmistwarningsaboutexcessivesunexposure.Theelderlyoftendecreasetheirsunexposureatatimewhentheyneedmoreofit tobehealthy.StudiesIhaveparticipatedinhaveshownthatwelloverhalfofAmericansagesixty-fiveand older are vitaminD deficient. If you are a senior citizen, you need to bemuchmoreconcernedabouttheriskoffracturingahipbecauseyouarevitaminDdeficientthanabouttheriskofgettingwrinklesorskincancer.Considerthisalarmingstatistic:approximatelythreehundredthousandhipfractureswilloccurinelderlymenandwomenthisyear;20percentofthosepeoplewilldiewithinayear, and 50 percent will never regain mobility and will have to move to anursinghome.Althoughyoumayhaveheardthatbefore,itbearsrepeating.Lifestyle. Themore time you spend indoors during daylight hours, the less
opportunity you have to make vitamin D. The lifestyles of most Americans,Europeans,andothers inwealthynationsfarabove theequator typicallyentaillongindoordaysandafixationonavoidingthesun’sUVraysduringanytimespent outside. This explains why nearly sixty million American children andteens—that’s 70 percent of the entire youth population—may have less thansufficient 25-vitamin D in their bloodstreams. One in seven teenagers is nowwalkingaroundinatotallydeficientstate.Geographicallocation.Ifyouliveinaplacewithrelativelylongwinters,you
getlesssunoverthecourseoftheyearbecauseUVBrayscannothitthesurfaceof the earth at the ideal angle formaking vitaminD in the skin during thosewintermonths.Theozone layerabsorbsmostof theUBVtrying toreachyourskin.Also,ifyouliveinacitywithlotsofD-defyingozonepollution,yourriskincreases.Race.Peoplewithverydarkskin,especiallythoseofAfricandescent,findit
difficulttomakevitaminDfromlimitedsunlight,astheirancestorsevolvedinapartoftheworldwheresunshinewasavailableyear-round.Thatthiskindofskinisnotefficientatconvertingthesun’sradiationintovitaminDisn’tanissueinAfrica because there are unlimited amounts of sunshine on that continent.However,whenpeopleofAfricandescent liveatnorthern latitudes, theyoftenbecomevitaminDdeficientbecausetheirsuperprotectiveskinmightnotconvertenough of the less UVB-containing sunlight into vitamin D. Studies I haveparticipatedinshowthatupto80percentofelderlyAfricanAmericans(overtheageofsixty-five)arevitaminDdeficient.TheCentersforDiseaseControland
Prevention recently reported that 42 percent of African American women ofchildbearing age (fifteen to forty-nine years old) throughout the entireUnitedStatesarevitaminDdeficientby theendofwinter—aremarkablenumber.Onaverage, 40 percent to 60 percent of African American adults are vitamin Ddeficient. African Americans are at increased risk of a variety of conditionsassociated with vitamin D deficiency, including type 2 diabetes and moreaggressive forms of cancer in the breast and prostate. Americans of Africandescentarealsomorelikelytohaveformsofhighbloodpressure(hypertension)andheart disease that aremore resistant to drug treatment. It tookmillions ofyears for equatorial inhabitants to develop their skin type in response to theirgeography, and itwill takemillionsmore for evolution to catchupwith thosewho have migrated elsewhere and who no longer need such a skin type tosurviveinUVB-deprivedterritories.Culture.Certaincultures require that theirwomencover themselvesentirely
inheavyclothingthatblocksoutthesun.Thismayexplainwhystudiesdoneonpeople in sunny spots across the Middle East and India and have foundwidespreadvitaminDdeficiency.Menarenotexcludedfromthisfatebecauseanother factor is atwork here: bothmen andwomen in these regions tend toavoidthesuningeneralbecausetheydon’twanttheirnaturallydarkskintogetanydarker.
WhoShouldOrdertheTest?
IfyouhavesymptomsthatareconsistentwithvitaminDdeficiencyandyouhavebeentakingavitaminDsupplementoverthelastsixmonthsintherangeofat least 1,000or2,000 IUperday, then it’s inyourbest interest toget tested.People who have or are at higher risk for the following health concerns alsoshouldconsidergettingtheir25-vitaminDlevelstestediftheyarenottakinganadequateamountofvitaminDasIprescribeinchapter10:
•familyhistoryorpersonalhistoryofcancer•highbloodpressure(hypertension)•osteoporosis/osteopenia•osteoarthritis• autoimmune conditions (such as lupus, ankylosing spondylitis,multiplesclerosis,rheumatoidarthritis,Crohn’sdisease,type1diabetes)
•PCOS(polycysticovariansyndrome)•schizophrenia•depression•migraines•epilepsy•diabetes(eithertype1ortype2)•fibromyalgia• general aches andmusculoskeletal pain in the body that have not beendiagnosed
•low-backpain•jointpain•muscleweakness•chronicfatiguesyndrome•poornerveconduction•poorbalance
Ifyou’reonMedicare,thetestshouldbetotallycovered.Withhealth-carecostscontinually scrutinized, physicians are quick to cut back on expensive andunnecessary tests. The 25-vitamin D assay can be costly at some labs, anddoctors who are not knowledgeable about the vitamin D-deficiency epidemicmay view such a test as gratuitous and unnecessary. Some doctors still don’tbelievevitaminDdeficiencycanhappenintheirpatients.Thatsaid,oftentimeswhendoctorsfindthatjustoneoftheirpatientsis(surprisingly)deficient, theybegin ordering 25-vitaminD tests on all of their patients. First, find out howmuchyour25-vitaminD testwill cost, and if it seemsunreasonable, askyourdoctor where you can go and get tested. If you reach a dead end, call yourhealth-careproviderorfindanotherdoctor.WordaboutvitaminDdeficiencyisfinally getting around, which is why the test for 25-vitamin D is the mostorderedtestintheUnitedStatestoday.
PARTII
THREESTEPSTOREBUILDINGYOURVITAMINDLEVELS

CHAPTER8
Step1:LettheSunshineIn
Practicingsensiblesunexposureforoptimalhealth
Wehave just seenwhyweall need enoughvitaminD inourbloodstreams toensurethehealthofourbonesandtohelppreventavarietyofdeadlydiseases,including cancer, diabetes, multiple sclerosis, and hypertension. I have alsohintedthroughoutthediscussionthatthere’snobetterwaytoobtainyoursupplyofvitaminDthantoliterallyletthesunshineintoyourlife.Ofallthelessonslearnedinthisbook,thisonemaybethehardestmedicineto
swallow:givingyourselfpermissiontoexposeyourskinforaspecificamountoftimeinthesun—withoutsunprotection.Howmuchshouldyouallow?When?And,mostrelevanttothedebate,whybotherifyoucanjustpopapill?
Why:SunandSupplementsAren’ttheSame
LetmestartmydiscussionofwhyIcallforsensiblesunexposureinadditiontosupplementationwith this: it’snoteasy toboostyourvitaminDstatus into thehealthy range of at least 30 nanograms permilliliter through supplementationalone.Thereissomuchpublishedliteraturenowtodemonstratethateven1,000IU a day will not raise your blood level above 30 nanograms per milliliter.RachaelBiancuzzo,mystudent,andmygroupjustpublishedastudyofmostlyhealthy adults living in Boston during the wintertime showing that 1,000 IUvitamin D2 or vitamin D3 a day did not raise their blood level above 30nanogramspermilliliter.

IlikenthisphenomenontotheconceptofTheRealThing.Whichwouldyouprefer:acubiczirconiaoradiamond,therealthing?AgenericcanofsodaoraCoke,therealthing?AvirtualtriptoHawaiiatanIMAXtheatertoseethelavaoozingfromthevolcanoesoranactual trip toviewtheminpersonon theBigIsland, the real thing? I assume you’d choose the latter in all these decisions.Well, if the body could say which method it prefers to get its daily dose ofvitaminD, itwouldhandsdowngiveastandingovationtosunlightsourcesofvitamin D rather than a bottle. After all, why else would it spend so manymillions of years perfecting this clever and self-regulating process? There’ssomething to be said for the fact that the body can in no way overdose onvitaminDcreated through sunlight, as it can through supplementation. I thinkthatfactalonespeaksvolumesaboutwhatweshouldbedoing.Anotherwaytolookatit:ifyouwereMotherNatureandwantedtoguaranteethatallvertebratesand humans got an essential vitamin hormone,what betterway than from thesun?Here’s somethingelse toconsider:vitaminDmade in the skin lasts at least
twiceas long in thebloodasvitaminD ingested from thediet.Whenyouareexposedtosunlight,youmakenotonlyvitaminDbutalsoatleastfiveanduptotenadditionalphotoproducts thatyouwouldneverget fromdietary sourcesorfrom a supplement. So the obvious question is,whywouldMotherNature bemakingallofthesevitaminDphotoproductsiftheyweren’thavingabiologicaleffect?MycolleaguesandIareintheprocessofidentifyingthephotoproductstosee if theyhaveaspecialbiological function. In themeantime,we’regoing toexposemenwithprostatecancertosimulatedsunlightusingaspecificsunlampcalledtheSpertilamp(www.sperti.com)toraisetheirbloodlevelof25-vitaminDtothesamelevelasthatofpatientswhoaretakingoralvitaminD3(fromVitalNutrientsofMiddletown,Connecticut)andseewhetherthereissomeadditionalbenefit.And then there’s thestraightforwardfact thatsunlight is freelyaccessible. It
doesn’taskformoneyinexchangeforitsdoseofhealth,anditcanimpartmorethanjusttherawingredientstomakevitaminDinthebody.Sunlight,aswe’veseen, boosts mood, keeps the circadian rhythm in check, and helps us sleepsoundlyatnightsowecanrejuvenateandrehabilitate thebodybeforeanotherday.
OurrichestsourceofvitaminDisthesun.Mostofusneedonlyafew

minutesadayofsunexposureduringthesummermonthstomaintainhealthyvitaminDlevelsthroughouttheyear.
HowMuch?
Iwant to be clear right from the get-go that I do not advocate tanning, and Irecommendyougetonlyenoughsunexposuretoestablishandmaintainhealthy25-vitaminDlevelsandtoimproveyourpsychologicalhealthasMotherNatureintended.At the same time, if youhavedecided that the feelingofwell-beingyougetfromUVBexposurefaroutweighsthedangers,IwouldnotdiscourageyoufromUVBexposure inexcessof thatwhich isneededforgoodhealth,aslongasyouknowandaccepttherisksandneverburn.Clearly, just because “some is good” doesn’t mean that “a lot is better.”
Undesirableconsequencescanresultifyougettoomuchsun,justasifyoueator exercise too much. Those consequences include nonmelanoma skin cancerandwrinkles.(I’llbeaddressingtheskin-cancersun-melanomaissuehead-oninthischapter,sohangtight.)Ifsunisessentialforgoodhealth,buttoomuchcanbeunhealthy, this raisesanobviousquestion:what is therightamount?Ihavebeen at the forefront of developing a scientific answer to this question andprovidingeasy-to-useguidelinesforthepublic.If I diagnose osteopenia, osteoporosis, or osteomalicia in someone whose
blood test reveals she isvitaminDdeficient (the25-vitaminD inherblood isless than30nanogramspermilliliter;1/33,000ofagramin1gramofblood),then I will prescribe an intensive program to restore her 25-vitamin D level,generallyconsistingof50,000 IUofvitaminD2weekly for eightweeks.Thishigh-doseprotocolcanonlybeprescribedbyadoctor.Thealternativeistotake3,000to4,000IUofvitaminD2orvitaminD3adayforeightweeks(youcanbuy a 1,000 or 2,000 IU supplement from your pharmacy). Although thepatient’s25-vitaminDlevelwillgoupquickly,thesymptomsrelatedtovitaminDdeficiencymaytakeseveralweeksormonths to lessenandmanymonths toresolvecompletely.Sunexposureisjustaseffectiveawaytobuildaperson’s25-vitaminDlevel.
Ifyousunbatheinabathingsuitonthebeachorinyourbackyard,youwillhavereceivedadoseofbetween10,000and25,000IUofvitaminDwhenyouhave

sunbathed longenough tobe slightlypink twenty-fourhours later (technically,this is called a minimal erythemal dose, or “1 MED”). I always discourageanyone from getting a burn and always encourage protection of their face.Spendingonequartertoonehalftheamountoftimeinthesunthatittakesyoutogetpink is thesafestway tobuildyour25-vitaminD levels,anddoing thisthreetimesaweekwillprovideyouwithaweeklydoseofvitaminDequivalenttoingestingabout20,000to30,000IU.ThisamountofsunexposureisusuallyenoughtocorrectavitaminDdeficiency.Ifyouworkduringtheday,anindoor-tanning facility canprovide the samebenefits (andyes, I’ll be addressing thishotlydebatedtopicinthischapter).Ihavecalculatedthattomakeapproximately2,000to4,000IUofvitaminD
you need to expose your arms and legs (about 25 percent of your body) forbetweenonefourthandonehalfthetimeittakesyourskintobepinkfromthesun twenty-four hours later. This calculation is based on my finding thatexposingmostofyourskininabathingsuitto1MEDwillcauseanincreaseinvitaminDinyourbodyequivalent to takingbetween10,000and25,000IUofvitamin D orally. But actually it is equal to taking 20,000 to 50,000 IU ofvitaminD in a supplement, because the vitaminD you get from the sun laststwiceaslonginyourbody.Again,IwanttostressthatIamnotadvocatingthatyouactuallyget1MED.However, it is important tofigureout,basedonyourskintypeand1MEDtime,howlongyoursensibleandhealthfulsunexposuretimeis.
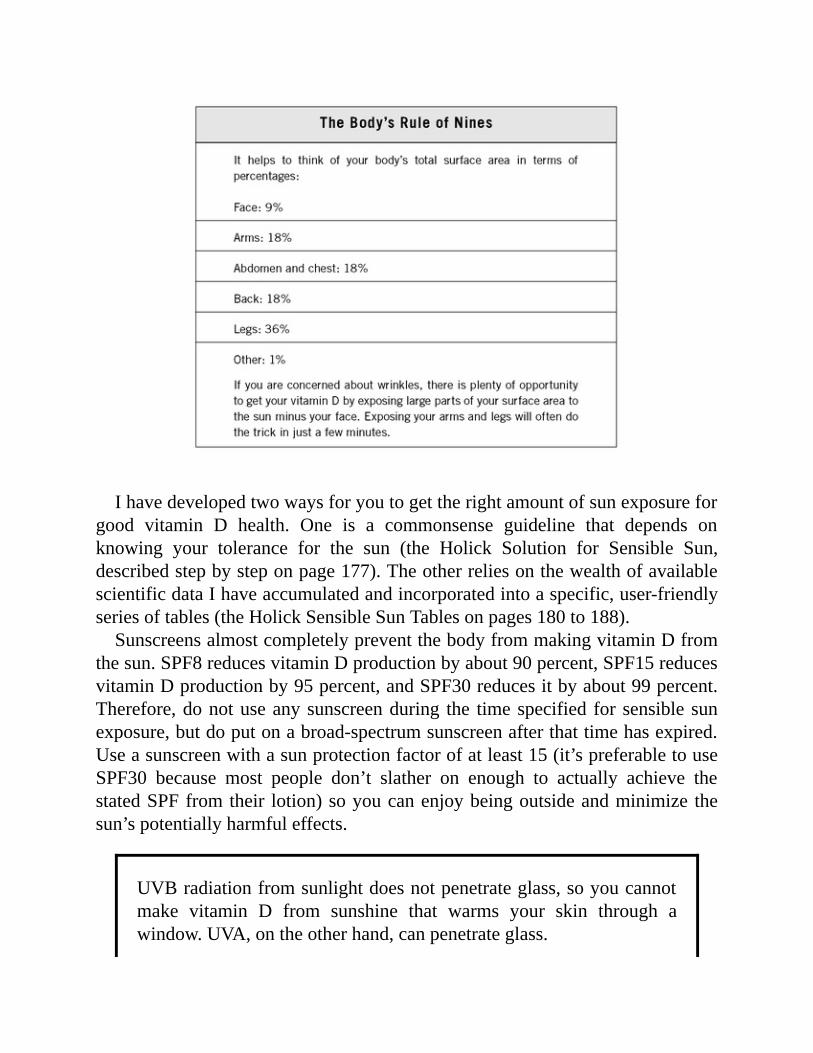
Ihavedevelopedtwowaysforyoutogettherightamountofsunexposureforgood vitamin D health. One is a commonsense guideline that depends onknowing your tolerance for the sun (the Holick Solution for Sensible Sun,describedstepbysteponpage177).TheotherreliesonthewealthofavailablescientificdataIhaveaccumulatedandincorporatedintoaspecific,user-friendlyseriesoftables(theHolickSensibleSunTablesonpages180to188).SunscreensalmostcompletelypreventthebodyfrommakingvitaminDfrom
thesun.SPF8reducesvitaminDproductionbyabout90percent,SPF15reducesvitaminDproductionby95percent,andSPF30reducesitbyabout99percent.Therefore,donotuseanysunscreenduring the timespecified for sensible sunexposure,butdoputonabroad-spectrumsunscreenafterthattimehasexpired.Useasunscreenwithasunprotectionfactorofatleast15(it’spreferabletouseSPF30 because most people don’t slather on enough to actually achieve thestatedSPFfromtheir lotion)soyoucanenjoybeingoutsideandminimize thesun’spotentiallyharmfuleffects.
UVBradiationfromsunlightdoesnotpenetrateglass,soyoucannotmake vitamin D from sunshine that warms your skin through awindow.UVA,ontheotherhand,canpenetrateglass.

Butbeforegettingtoofarintothedetailsofsensiblesunning,let’stackletheissueofskincancerandprematureagingcausedbythesun.
SkinographyandMythology
Thateveryonecanseeyourskinisjustoneindicationofhowimportantitis.Itisyour body’s largest organ and weighs about six pounds. Skin provides aprotectivecoveringforyourentirebodyandprotectsyoufromsunlight,heatandcold,infections,toxins,andinjury.Otherimportantfunctionsoftheskinarethatitregulatesbodytemperatureandretainswater.And,ofcourse,yourskinhelpsyouconvertsunshineintovitaminD.Yourskinhastwolayers,theouterepidermisandtheinnerdermis.Thesetwo
layersarequitedifferent.Theinnerdermislayercontainsbloodvessels,lymphducts,nerve fibersandnerveendings,andhair follicles. It alsocontains sweatand sebaceous glands, which produce sweat to keep you cool and an oilysubstancecalledsebumthathelpsprevent theskinfromdryingout.Sweatandsebumgettotheskin’ssurfacethroughtinyholescalledpores.Theouterepidermis is thinner than thedermisand ismadeupof squamous
cells (also known as keratinocytes). Beneath these squamous cells are fuller-shapedcellscalledbasalcells.Basalcellsareconstantlydividingtorejuvenatetheskin.Theyrisetothetopoftheepidermis,wheretheyareprogrammedtodieand become the dead outer layer of our skin, known as the stratum corneum.ThisouterlayeractslikeamirrortoreflectUVAandUVBawayfromtheskin.Underneath and interspersed between the basal cells are melanocytes.Melanocytesproducemelanin,apigmentthatgivesskinandhairtheircolor.Themoremelanin you have in your skin, the darker it is. For example, people ofAfrican descent have more melanin in their skin than people of Norwegiandescent.Theimportanceofmelaninisthatitabsorbstheultravioletradiationofthe sun, thus protecting the skin cells against sunburn. Because dark-skinnedpeople have evolved to live in sunny regions, thosewith darker skin producemelaninallthetime,whereaslight-skinnedpeoplemainlyproducemelaninonlyinresponsetosunexposure.Asyou’reabouttofindout,however,everyonewhoproducesmelanin in their skin—which iseveryoneexceptvery fair-skinnedorfreckled,red-hairedpersons—hasanaturaldefenseagainstthesun’sradiation.

SunburnversusSuntan
Oneofthemostimportantjobsoftheepidermis—especiallyinlight-skinnedpeople—is to adapt quickly to protect skin cells from the sun’s radiation.Thedefensemechanismtheskinusesagainstsunburniswhatwecalltanning,whichisan ingeniousprocess. In response to sunexposure, themelanocytesproducemelaninthatmakestheskindarker.Theproductionofmoremelaninistriggeredthrough an increase in the activity of an enzyme called tyrosinase. MelaninprotectstheskinbyabsorbingUVradiation.Evenshortburstsofsunexposurewilltriggerthemelanocytestoproducemoremelanin.Dark-skinnedpeopledonothavemoremelanocytes,buttheirmelanocytesare
moreactive,whichexplainswhytheirskinisalwayspigmented.Italsoexplainswhy theriskofall formsofskincancer is lower fordark-skinnedpeople—thecellsoftheirskinarealwaysmoreprotectedfromdamagingUVBandUVAbythe presence of melanin, which acts like an umbrella, shielding the cell’svulnerableDNAand proteins fromUVdamage due to sun exposure.Melaninactuallymigrates upward and, like anumbrella, shades thenucleusof the cellfromdamagingUVradiation.Sunburnisquitedifferentfromasuntan.Whenyougetasunburn,yourskin
turnsredandcansometimesblisterandpeel.Thisredness,knowninscientifictermsaserythema,isactuallycausedbyincreasedbloodflowtotheskin.Thisbegins approximately four hours after the sun exposure and reaches its peakbetweeneightand twenty-fourhoursafterexposure.Bloodisbeingsent to theskin to attend to cells that have been damaged by the sun. When severelydamaged squamous and basal cells cannot repair themselves, they “commitsuicide”sotheywon’treplicateinamutatedstateandcausecancer(thisresultsinpeeling).Thisformofcellsuicideisknownasapoptosis,orprogrammedcelldeath.Fear of skin cancer is one of the main reasons for the hysteria over sun
exposure.As is thecasewithsomanyhealthaxioms, therelationshipbetweensunshine and cancer isn’t as straightforward asmostpeople think.There are anumberofmythsassociatedwithwhatcausesskincancer.
MythsExposed
Manymythsareassociatedwithskincancer, thanks to thebarrageofpublic

misinformationonthistopic.Herearesomeofthem.(I’vetoucheduponmanyofthesealready,buttheybearrepeating.)Anyandallsunexposurecausesskincancer.BecauseUVBexposureisthe
easiestwaytoincreaselevelsof25-vitaminD,whichhumanscan’tlivewithout,this statementneeds tobequestioned.While it’s true thatUVBradiation fromsunlight—especiallychronicoverexposure tosunlight—is thought tobeoneofthecausesofnonmelanomaskincancer,virtuallyallnonmelanomaskincancersare treatable and curable when detected early, and sunlight is proven to haveprotectivebenefitsoverthemoredeadlyinternalcancers.Thetrade-offbetweenthe risk of basal-cell carcinoma, for example, and the risk of stage 4 breastcancer cannot be understated. And you’ll hear me state this more than once:there is no data to suggest that sensible sun exposure increases the risk ofnonmelanomaskincancer.Sunexposureisthemaincauseofmelanoma.Thereisnoscientificevidence
that regular, moderate sun exposure causes melanoma. As the FDA observedaftera1995conferenceonmelanoma, the relationshipbetweenmelanomaandsunlightisbaffling.Melanomaisseenmoreofteninpeoplewhodonotreceiveregular,moderate sun exposure than in thosewho regularly spend time in thesun.Mostmelanomasalsooccuronpartsofthebodythatreceivelittleornosunexposure.This suggests thatgeneticsplays amuchmore important role in thedevelopmentofskincancerthandoesregular,moderatesunexposure.Thereisalso evidence thatUVB-protection-only sunscreensmaydistort theUVB/UVAratio thatpenetrates into theskin, thuscontributing tomelanomadevelopment.Remember, UVA penetrates much more deeply than UVB, bombardingmelanocytes and immune cells. Sunburns as a child or young adult increase aperson’s risk of melanoma, especially in areas least exposed to sunlight. Apossible explanation for this is that sunburnsmay damage somemelanocytes.Normally, thiswould trigger the immune system to jump into action to attackandkillthedefectivemelanocytes.(Thisisknownasimmuno-surveillanceandisaverygood thing forkeepingdefectivecells incheck so theydon’t lead tocancer.)However, if the immunesystem isalsoaffectedbyexcessiveUVBorUVA exposure, this immuno-surveillance system can become compromised. Itthenmaynolongeridentifydamagedmelanocytes,andamajormechanismforpreventingout-of-controlmelanocytesfromgrowingintoadeadlycancer isallbutlost.Weareinthemidstofaskincancer“epidemic.”It isinaccuratetocallthe
increasing incidence of skin cancer an epidemic. Skin cancer rates have been
risingsteadilysincetheearlytwentiethcentury.Skincancerratesaregoingupsolely becausemore people are excessively sunbathing. Although skin cancerrateshavebeenrisingsteadilysince theearly twentiethcentury, itwasn’tuntilthe 1960s that a tanned skin was considered desirable. Present-day peopleactuallyspendlesstimeoutdoorsthandidourforebears,mostofwhomworkedthelandbeforetheIndustrialRevolution.Workingoutdoorsthroughouttheyearprobablyhelpedpreviousgenerationsbuildaresistancetosunburnintheformoftannedskin.More recently—especially in the 1970s and 1980s, when a severe sunburn
wasconsideredaprerequisiteforaneventualsummertan—peoplehavebecomemore likely to get sunburned. Adding insult to injury, the use of UVB-protection-onlysunscreensprobablycontributedtotheriseofmelanomabecausethey promoted massive exposure to deeply-penetrating UVA. There’s onehundredtoonethousandtimesmoreUVAthanUVBinsunlight.What’smore,ithelpstobearinmindthatnonmelanomaskincancerhasanextremelylowdeathrate.IntheUnitedStates,itclaimsabout1,200livesayear.
If you get regular,moderate sun exposure, you have less chance ofdevelopingmalignantmelanoma.NewresearchshowsthatmelanomaismoreprevalentinEuropeandNorthAmericathanintheequatoriallatitudes,whichagainsuggeststhatregularsunexposuremaypreventmelanoma.Attheveryleast,moderatesunexposurewillnotincreasetheriskofmelanoma.
There’s no such thing as a safe tan. Tanned skin protects you againstsunburn,thoughttobethemaincauseofmelanoma.Also,it’smoredangeroustoavoidsunexposurecompletelythanitistogetregular,moderatesunexposure.Ifyouavoidgettingsunburned, thebenefitsof sunexposurewill faroutweighthepossibledangers.Independentscientificresearchhasshownthatifyouliveinasunnyclimate,orifyouliveinanot-so-sunnyclimatebutexposeyourselftosun,thenyourincreasedproductionofvitaminDduetoUVBradiationwillhelplowerriskofahostofdebilitatingandfataldiseases.Colon,prostate,andbreastcancer—whichtogetherclaimmorethan115,000liveseachyear—caninsomecasesbepreventedbyregular,moderatesunexposure.Peoplewhogetregular,moderate sunexposureare less likely toget amalignantmelanoma than those
whodon’t.Anddon’tforgetaboutalltheresearchbackingsunlight’seffectonamultitudeofcommonillnessesanddiseases,includinginternalcancers.Tanning is like smoking toyourskin.Wrong.Tanning isnatural. It isyour
body’snaturaldefenseagainstsunburn.Smokingisanunnaturalhabitthatyourbodyrejectsbybecomingill.
SoWhatIsSkinCancer?
Ourbodiesfunctionnormallywhenthecellsthatmakeupthedifferenttissues—suchastheprostate,breast,andcolon—grow,divide,andreplacethemselvesinanorderlyfashion.Occasionally,cellsdividetoorapidlyandmultiplyoutofcontrol;thiscanleadtocancer.Skincancerresultswhenthisprocessoccursinthecellsof theskin.Thereareseveralformsofskincancer,butallof themfitintotwobroadcategories:nonmelanomaskincancerandmelanoma.NonmelanomaSkinCancer.Byfarthemostcommonformsofnonmelanoma
skincancerarebasal-cellcarcinomaandsquamouscellcarcinoma(carcinomaisthemedicaltermforcancer).Basal-cellcarcinoma(BCC)affectsthebasalcellsin the epidermis and is themost common form of nonmelanoma skin cancer.BCCusuallyoccursonareasofyourskinthataremostexposedtothesunandthataremostlikelytohavebeensunburned,suchasthenose,face,topsoftheears,andbacksofthehands.OftenBCCappearsasasmall,raisedbumpthathasasmooth,“pearly”appearance.SometimesBCClookslikeascarandfeelsfirmwhenyoupressonit.BCCmayexpandinsizeandspreadtotissuesaroundit,butthesecellsrarelyspreadtootherpartsofthebody.Squamouscellcarcinoma(SCC)alsooccursonareasoftheepidermisthatare
mostoftenexposedtoexcessiveamountsofsun.OftenSCCappearsasafirm,redbump.Thetumormayfeeldry,itchy,andscaly,maybleed,ormaydevelopacrust. SCC very occasionally spreads to nearby lymph nodes (lymph nodesproduce and store infection-and cancer-fighting immune cells). SCCmay alsoappearonpartsofyourskinthathavebeenburned,exposedtochemicals,orhadX-raytherapy.Bothtypesofnonmelanomaskincancerarethoughttobecausedbylong-term
exposuretosunshine.Suchexposureovermanyyearsmaycausedamagetotheskincellsthemselvessothattheyeventuallystartreplicatingoutofcontrol.Sunexposure over many years may also desensitize the skin’s immune system insuchawaythatitwillnotrecognizeandactagainstcancerousskincells.

Finally, researchers have been looking at the p53 gene, a “quality-control”gene that is responsible for fixing a damaged cell or causing it to kill itself(apoptosis). There is mounting evidence that the p53 gene system may bedamagedbyexcessive,long-termsunexposure.Eachpersonhastwop53genes—onefromeachparent.Whenonep53geneisdamaged,theskincellbecomessickandmultipliesabnormallytoformaprecancerous,scalylesionknownasanactinickeratosis.Whenbothp53genesaredamagedandcannolongerfunctionproperly, the skin cell may start replicating out of control and become anonmelanomaskincancer.Thep53geneissoimportantthatitwasdeclaredthemoleculeof theyearby theeditorsof the journalScienceandappearedon thecoverofNewsweek.The likelihood that youwill developnonmelanoma skin cancer is greater if
yourexposure tosunshinebeganwhenyouwereachild,adolescent,oryoungadult.Duringtheseearlyyears, theskinisespeciallyvulnerabletosunburning.Thereisalsothesimplefact that theearlierinlifethatskincellsaredamaged,thelongerthechancetheyhavetoreplicateinamutatedstate.There’salsomoretimetodamagethatsecondp53gene.Remember,noteveryonewhoisexposedtostrongsunshinefromayoungage
is going to develop nonmelanoma skin cancer. Some people are geneticallypredisposedtothisdisease.Thisexplainswhycertainpeoplegetnonmelanomaskincancerwhileothersdon’t—evenwhentheyhavethesameskintypeandareexposedtojustaboutthesameamountofsun.It’salsobelievedthatafattydietmaypredisposeyoutoavarietyofcancers,includingnonmelanomaskincancer.People who suffer from DNA-repair-enzyme diseases such as a xerodermapigmentosum(XP)alsoexperienceamuchhigherriskofskincancer.XPisanextremely rare skin disorder whose sufferers are highly sensitive to sunexposure.ThecauseofXPishypersensitivityoftheskincells toUVradiationdue to a defect in the gene’s DNA repair system. PeoplewithXP experiencepremature aging of the skin andmultiple skin cancers. The disease is usuallydiagnosed in infancy when the child with XP exhibits severe skin problems,includingskinreddening,scaling,andfreckling.Skincancersusuallyappearinearlychildhood,asdochroniceyeproblems.There isnocure for thisdisease,andtheonlycourseofactionistostayoutofthesun.Melanoma.Melanomaisadifferentstory.Althoughrare,melanomaismuch
moredeadlythannonmelanomaskincancer.Comprisinglessthan5percentofall skin cancers, melanomas are responsible for the majority of skin-cancerdeaths, killing about 8,600 Americans annually. The number of new cases of

melanoma in theUnited States has not changedmuch in the last eight years.Overall, the lifetime riskofgettingmelanoma is aboutone in fifty forwhites,oneinonethousandforblacks,andoneintwohundredforHispanics.Melanomasoccurinthedeeperpigment-producingcellslocatedbetweenthe
dermis and epidermis, known as themelanocytes.Whenmelanocytes becomecancerous,ormalignant,thesecellsgrowuncontrollablyandaggressivelyinvadesurroundinghealthy tissues.Melanomamaystay in theskin,butmoreoften itspreads, ormetastasizes, through the blood or lymph system to the bones andorgans,includingthebrain,lungs,andliver.Melanomasometimesoccursinanexistingmoleorotherskinblemishsuchasadysplasticnevus(pronounceddis-PLAS-tikNEE-vus),butitoftendevelopsinotherwiseunmarkedskin.Inmen,melanomadevelopsmost oftenon theupperback, and inwomen it is usuallyseenonthelegs,althoughitmayoccuranywhere.Melanoma ismost common in peoplewith fair skin and thosewho have a
largenumberofmoles,althoughitaffectspeopleofallraces.Melanomausuallyresemblesaflatbrownorblackmolewithanirregular,unevenborder.Usuallytheblemishisnotsymmetrical.Melanomalesionsareoften6millimeters(0.24inches)ormore indiameter.Anychange in theshape,size,orcolorofamolemayindicatemelanoma.Amelanomamaybelumpyorrounded,changecolor,becomecrusty,ooze,orbleed.Therearenumerousriskfactorsformelanoma.Excessiveexposuretothesun
is but one. But as you already know, melanomas occur in people who don’tspendtimeinthesunandareoftenseenonpartsof thebodythataren’tmuchexposedtothesun.Someofthenonradiationriskfactorsincludethefollowing:
•Heredity.Iftwoormoreofyourfamilymembershavehadamelanoma,youaremuchmorelikelytogetone.
•Dysplasticnevi.Thesekindsofmolesaremorelikelythannormalmolestobecomemelanomas.
•Manynormalmoles.Ifyouhavemorethanfiftymolesonyourbody,thisincreases your chance of developing a melanoma because melanomausuallybeginsinthemelanocytesofanormalmole.
•Weakenedimmunesystem.Peoplewhoseimmunesystemisweakenedbycertain other forms of cancer, certain drugs (such as cyclosporine)prescribed after organ transplants, or AIDS have a greater risk ofdevelopingmelanoma.
•Previousmelanoma.Peoplewhohave alreadyhad amelanomaare at ahighriskofdevelopinganother.
• Defective DNA repair system. People with the extremely rare skindisorderxerodermapigmentosum(XP),describedabove,tendtohaveadefectiveDNArepairsystemandareatahigherriskofmelanoma.
This brings us to the relationship between sun exposure and melanoma.Normalsunexposureofthetypethatbuildsatandoesn’tseemtoberesponsibleformelanoma.NumerousstudiespioneeredbyDrs.CedricandFrankGarland,andDr.EdGorhamshowthatpeoplewhoworkoutsidehavealowerincidenceofmelanomathandopeoplewhoworkinside.Despite thefact that theUnitedStateswasforseveralcenturiesarural,agriculture-basednationwhosecitizenswere outdoors much of the time, melanoma was so rare then that separatestatisticsweren’tkeptonthediseaseuntilthe1950s.So what’s going on?Why are melanoma rates increasing rapidly and have
been doing so at a rate of 2 percent per year formore than thirty years? Theanswer is surprising—it may be because people are exposed to sunshine lessduring theirworkinghours.Sunburns are a risk factor formelanoma.Becausepeople these days—young and old alike—work outside less and therefore getless regular sun exposure than did previous generations, they are at increasedriskofgettingsunburnedratherthansuntannedwhentheydogooutinthesun.Another explanation for the rise inmelanomamay surprise you evenmore:
the use of sunscreens starting in the 1950s. Before any of you heave yoursunscreen into the trash, letmemake thepoint that the typeof sunscreen thatprobably contributed to the rise of melanoma is the kind that protected onlyagainst UVB radiation. As I detailed earlier, until the late 1990s, UVB-protection-onlysunscreenwasallthatwasavailable,andthishadbeenthecasesincethe1940s.Inthepastfewyears,thistypeofsunscreenhasbeenphasedoutinfavorofsunscreensthatprotectagainstbothUVBandUVAradiation.RecallwhenIexplainedthatsunscreenwasfirstdevelopedtoenablepeopleto
avoid sunburn and thereby spend more time in the sun, either tanning orparticipating in outdoor recreation. Although these early sunscreens protectedagainst the burning radiation of UVB, they did not protect against UVAradiation.Atthetime,UVAradiationwasnot thoughttobeharmfulbecauseitdidn’tcausetheobvioussymptomsofsunburn.Theincreaseinmelanomamaybe partially due to the fact that by protecting people againstUVB,UVB-onlysunscreen use enabled people to receive massive doses of UVA, whichpenetratesdeep into the epidermis anddermis todamage themelanocytes andcause immune tolerance.We now know that UVA is partially responsible formelanoma,andthecosmeceuticalindustryhasintroducedsunscreensthatprotect
against both UVB and UVA radiation—so-called broad-spectrum sunscreens.You should always use broad-spectrum sunscreen when trying to preventsunburn.Look for sunscreens that clearly state they protect against bothUVAandUVB,becausediscrepanciesstillexistinthemarket.Beaware,too,thatnosunscreencanfullyprotectyou.Withallthisinmind,itisimportanttorepeatthatmelanomausuallyoccursin
partsofthebodythatarenotexposedtothesunandisseeninpeoplewhodonotspendmuchtimeinthesun,twofactorsthatindicatethatsunexposuremaynotbeariskfactorforthisseriousdisease.
GoingHome
Researchinthelastfewyearsalonehasfinallybeguntounravelthemysteryofwhymelanoma can be so invasive, radically efficient in spreading quickly,andremarkablypotent.Unlikeothercancercells,whichtaketimetospreadandcanbeclumsyindoingso,melanomadoesnothavetolearnhowtoreachdistanttissuesandorganstoinflictharm.Usually,themovementofcancerouscellsfromoneplacetoanother,aprocess
knownasmetastasis, isahighly inefficientandmultistepprocess that requirescancer cells to leapmanyhurdles.First, cellsmust invadeanearby tissueandfindtheirwaytothebloodstreamorlymphaticsystemtohitcharidetoadistantsite,wheretheythendisembarktoestablishnewcolonies.Melanomaseemstohavethisjourneydownpat,liketheflipofaswitch,andnowweknowhow.Itturns out that asmelanocytesmorph into cancer cells, they immediately stir adormantcellularprocessthatletsthemtravelswiftlythroughthebody.KeytothisawakeningprocessisagenecalledSlug.(Ifyou’rehearingechoes
ofthe“Snail”geneItalkedaboutearlier,you’reright;thisisjustanothergeneticingredientthatcontrolscellularfunctionsandhasanironicname.)Slugplaysanimportant role inallowingmelanocytes to travelaround thedevelopinghumanembryointhewomb.Thesemelanocytesbegininthemidbrainofadevelopingembryo and migrate to distant sites, including the skin, during the embryo’sdevelopment.ButtheSluggeneispermanentlyturnedoffoncethemelanocytesarriveattheirdestination.In2005researchersdiscoveredthatwhenmelanocytesbecomemalignant, they reactivateSlug—turning thegenebackon.Thisgivesthe cell an immediate ability to spread, especially to the brain. It aims to “gohome”—back from whence it came. The gene literally commands the cell to
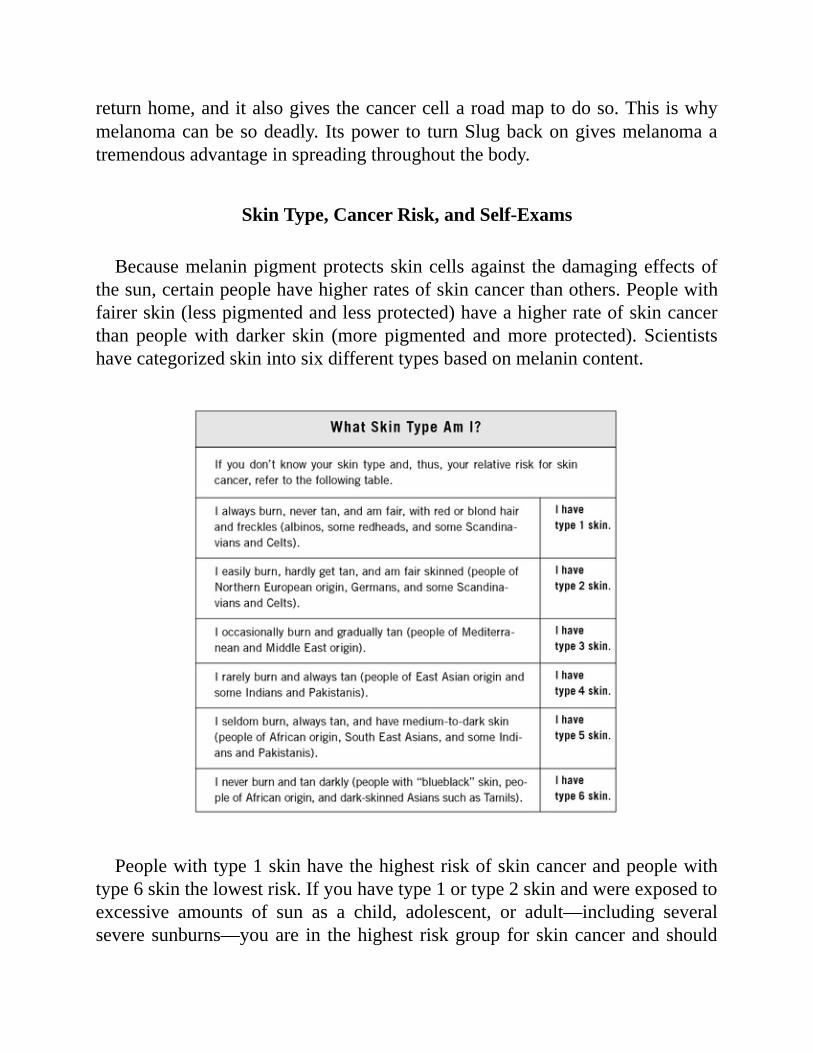
returnhome,anditalsogivesthecancercellaroadmaptodoso.Thisiswhymelanomacanbesodeadly. Itspower to turnSlugbackongivesmelanomaatremendousadvantageinspreadingthroughoutthebody.
SkinType,CancerRisk,andSelf-Exams
Becausemelaninpigmentprotectsskincellsagainst thedamagingeffectsofthesun,certainpeoplehavehigherratesofskincancerthanothers.Peoplewithfairerskin(lesspigmentedandlessprotected)haveahigherrateofskincancerthan peoplewith darker skin (more pigmented andmore protected). Scientistshavecategorizedskinintosixdifferenttypesbasedonmelanincontent.
Peoplewithtype1skinhavethehighestriskofskincancerandpeoplewithtype6skinthelowestrisk.Ifyouhavetype1ortype2skinandwereexposedtoexcessive amounts of sun as a child, adolescent, or adult—including severalseveresunburns—youare in thehighest riskgroup for skincancerandshould

get screened. Some people never get tan, principally those who are very fairskinned or red haired and freckled; they have type 1 skin. The reason peoplewith type 1 skin don’t tan is that themelanocytes in their skin are unable toproduceprotectivemelanin pigment.Because their skin is unprotected againstthesun’sradiation,thesepeoplearehighlysusceptibletosundamage,includingsunburn,andarethereforeatthehighestriskforskincancer.Oneofthecharacteristicsofskincanceristhat,unlikeallothercancers,itis
visible.Ifeveryonewerevigilantaboutdetectingskincancerinitsearlystagesthrough self-exams, themortality rate for nonmelanoma skin cancerwould godown to virtually zero.Weknowhow to catch skin cancer in its early stages,which is the key to reducing its severity. So the key to early detection andtreatmentofskincancerisverymuchinyourhands.There’snoneedforpanicoroverreaction,butyouneedtobeonthelookoutandknowwhattolookfor.Just as women should do regular breast self-exams, each person should
periodicallycheckhisorherskinforearlysignsofskincancer.Howoftenyoudo thisdependsonyour riskfactors. Ifyouoracloserelativehasahistoryofskincancer,orifotherriskfactorsapplytoyou—suchasifyouhavefairskin,burneasily,andhadalotofsunexposureasachild—examineyourskinonceamonth. Otherwise, once every six months is probably sufficient. Checkingyourself every day is counterproductive because you may not notice subtlechangesthatcouldbesignsofskincancer.Aredflagforskincancerisachangeinyourskin’sappearance,suchasanew
growthorasorethatdoesn’theal.Lookforthesewarningsignsthatyoumighthaveanonmelanomaskincancer:
•alumpthatissmall,smooth,shiny,and“waxy”looking•alumpthatisfirmandred•alumpthatbleedsordevelopsacrustysurface•aflat,redareathatisrough,dry,itchy,orscaly•ascarlikegrowththatgraduallygetslarger
Ifyou see anyof these changesonyour skin, consult yourpersonalphysicianimmediatelytodeterminetheircause.What about signs ofmelanoma?This very rare but dangerous form of skin
cancer generally begins as an irregular-shaped, flat blemish colored amottledlightbrowntoblack.Melanomasareusuallyatleastonequarterinchacross.Theblemishmaycruston thesurfaceandbleed.Melanomasusuallyappearon theupperback,torso,bellybutton,backsofthelegs,lowerlegs,head,orneck.They

alsocanbedetectedinthegenitalareas.Seekmedicalattentionforamolethatchangessize,shape,orcolor;anewmole;oramolethatlooksoddorunsightlyorbeginstogrow.Rememberthatpainisnotanindicatorofaskincancer.Untilitprogressestoquiteanadvancedstage,askincancerwon’thurtorsting.Thisfact reinforces the need to see a doctor as soon as you have any legitimatesuspicion.
If you examine your skin regularly, youwill become familiarwithwhat onyourbodyisnormal.Ifyoufindanythingsuspiciousduringthecourseofyourexamination, see your doctor right away.Remember, the earlier skin cancer isfound, the more straightforward the treatment program is and the greater thechanceforsuccessfulresolution.Ifadoctorthinksagrowthlookssuspicious,heorshewillorderabiopsy.Inthissimpleofficeprocedure,thepatientisgivenalocalanestheticandallorsomeofthesuspect tissueisremovedandexaminedunderamicroscope.If skin cancer is diagnosed, there are various options for treatment. The
doctor’s goalwill be to totally remove or destroy the cancerwhile leaving assmall a scar as possible. Types of surgery include cryosurgery (destruction byfreezingwithliquidnitrogen), lasersurgery(usingalaserbeamtocutawayorvaporizegrowths),andcurettageandelectrodesiccation(usingaspoonlikebladeto scoop out the growth, then destroying surrounding tissue with an electricneedle). Occasionally, other treatments, such as radiation therapy orchemotherapy,maybeusedaloneorincombination.Precise treatment and follow-up for both nonmelanoma skin cancer and
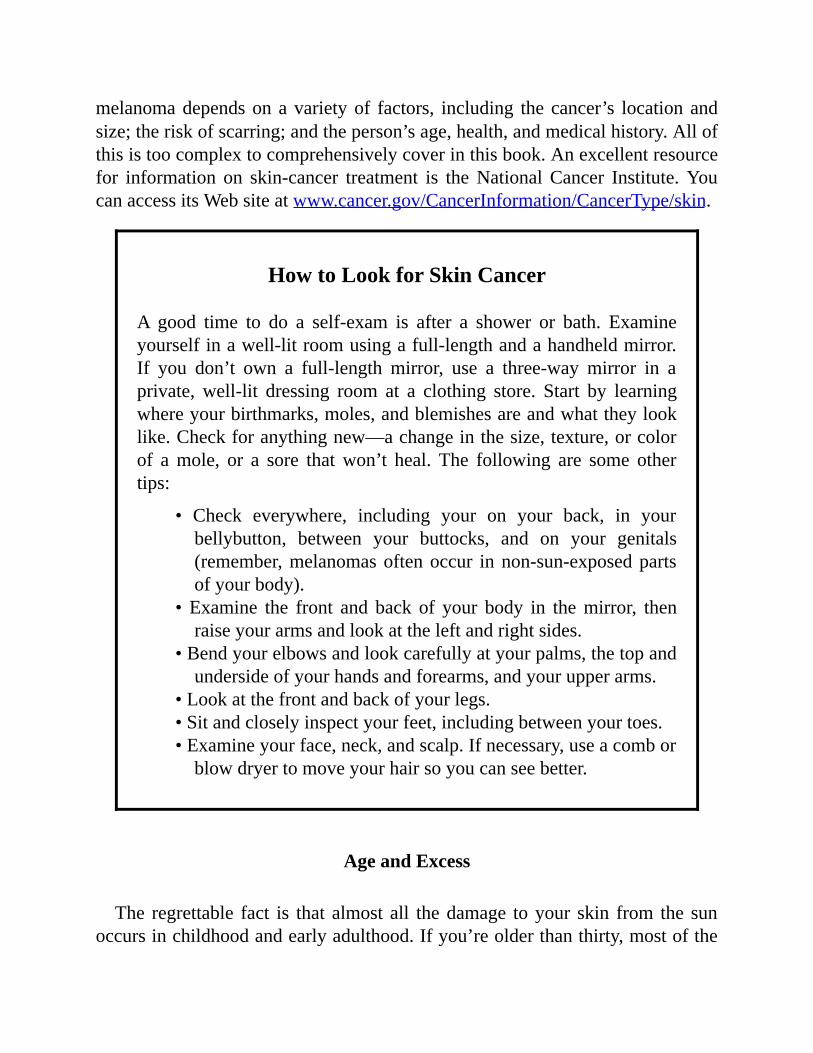
melanomadependsonavarietyof factors, including the cancer’s locationandsize;theriskofscarring;andtheperson’sage,health,andmedicalhistory.Allofthisistoocomplextocomprehensivelycoverinthisbook.Anexcellentresourcefor information on skin-cancer treatment is theNationalCancer Institute.YoucanaccessitsWebsiteatwww.cancer.gov/CancerInformation/CancerType/skin.
HowtoLookforSkinCancer
A good time to do a self-exam is after a shower or bath. Examineyourselfinawell-litroomusingafull-lengthandahandheldmirror.If you don’t own a full-length mirror, use a three-way mirror in aprivate, well-lit dressing room at a clothing store. Start by learningwhereyourbirthmarks,moles,andblemishesareandwhattheylooklike.Checkforanythingnew—achangeinthesize,texture,orcolorof amole, or a sore thatwon’t heal. The following are some othertips:
• Check everywhere, including your on your back, in yourbellybutton, between your buttocks, and on your genitals(remember,melanomasoftenoccur innon-sun-exposedpartsofyourbody).
• Examine the front and back of your body in themirror, thenraiseyourarmsandlookattheleftandrightsides.
•Bendyourelbowsandlookcarefullyatyourpalms,thetopandundersideofyourhandsandforearms,andyourupperarms.
•Lookatthefrontandbackofyourlegs.•Sitandcloselyinspectyourfeet,includingbetweenyourtoes.•Examineyourface,neck,andscalp.Ifnecessary,useacomborblowdryertomoveyourhairsoyoucanseebetter.
AgeandExcess
The regrettable fact is that almost all thedamage toyour skin from the sunoccursinchildhoodandearlyadulthood.Ifyou’reolderthanthirty,mostofthe

sundamagethatmayhavecontributedtoyourriskofnonmelanomaskincancerandmelanomahasalready takenplace.Still, youcan reduceyour riskof skincancertosomeextentbybeingjudiciousabouthowmuchsunexposureyougetin thefuture.Althoughsunexposureandsunburnearly in lifedon’tmeanyouwillnecessarilygetskincancer,yourchancesarehigher.Therefore,fromtheageofthirtyonwardyoushouldfocusonearlydetection.
It’s also important to educate younger familymembers about the risks of skindamagefromlong-termsunexposureandintermittentsunburn.Explaintothemhowtheycansafelygetthebenefitsofsunexposure,aneasyformulaexplainedbelow. Folks over age seventy need not worry about trying to prevent skincancerbystayingoutof thesun.Inpeopleof thisagewhohavespenta lotoftime in the sun, the damage has almost certainly been done. In addition tovigilance in regard to skin-cancer detection, the concern among older peopleshouldbewhethertheyaregettingenoughsuntoachieveandmaintainahealthy25-vitaminDlevel.OlderpeoplearemuchmorelikelytodiefromavitaminDdeficiency-relatedhipfractureduetoosteoporosisthanfromskincancer.Ifyouareyounger than thirtyandhavehadagreatdealofunprotected sun
exposureinyourlife,youshouldavoidanymoreUVexposurethanisnecessaryto maintain good health. It is especially important that you protect againstsunburnandstaywithinthelimitsofmyformulaforsensiblesun.
TheHolickSolutionforSensibleSun:Estimate,Expose,Protect
It’s themillion-dollarquestion:howdoyoumanage this finebalancebetweenrisk and reward—the risk of skin cancer and the rewards of UVB exposure?Here’showtousetheHolickSolutiontogetsensibleamountsofsunexposureandmakeenoughvitaminDforgoodhealth:
1.Estimatehowlongittakesintheparticularconditionsinwhichyouwillbe sunning yourself for you to get a mild pinkness (known as oneminimalerythemaldose,or1MED).
2.Then,withoutapplyingsunscreen,exposeyourarmsandlegsforabout25percentto50percentofthatlengthoftime.Ihavecalculatedthatthatamount of sun exposure two to three days aweek enables the body tomakeenoughvitaminDtostayhealthy.
3.Aftergettingthisamountofsunexposure,protectyourskinbyputtingonabroad-spectrumsunscreenwithanSPFofatleast15,andpreferably
use SPF30. Thiswill prevent overexposure and lessen the risk of skincancer and wrinkles. The more skin you expose to the sun, the morevitaminDyouwillmake.Ifyouarewearingaswimsuit,itwilltakeyoulesstimepersessionthan25percentto50percentof1MEDtomaketheminimumamountofvitaminDyouneedforgoodhealth.Remember,itdoesn’tmatterwhichareaofyourbodyisexposedtothesun,solongasat least 25 percent is. I don’t recommend exposing your face, whichcomprises only 9 percent of your body’s total surface area anyhow.Follow the directions on the sunscreen label tomake sure you use thecorrect amount. SPF refers to the length of time a particular productprotects against skin reddening fromUVB exposure compared to skinwithout protection. For example, if your skin takes twenty minutes tobeginreddeningwithoutprotection,applyinganSPF15sunscreenshouldpreventreddeningfifteentimeslonger—aboutfivehours(thoughitmaytake up to twenty-four hours after sun exposure for redness to becomevisible). To maintain the SPF protection, it is important to reapplysunscreeneveryfourhoursandalwaysafterswimming.Toget theSPFadvertisedontheproductlabel,anadultinabathingsuittypicallyneedstousefullyonequarterofafour-ouncebottleofsunscreentocoverhisorher body. Studies have consistently shown that people do not applyenoughsunscreen,whichmeanstheyarenotgettingtheprotectiontheythinktheyare.
Here’sanexampleoftheHolickSolutioninaction.SayyouliveinNewYorkandfrequentthebeachesofLongIsland.Ifyouhavequitefairskin(type2skin)and estimate it would take you half an hour of sun exposure on the beach atmidday in July to be pink twenty-four hours later (because you haven’t spentmuchtimeinthesunlately),thenyoushouldspendfivetotenminutes—anduptofifteenminutes—inthesunbeforeputtingonsunscreen.Thisshouldnotcauseyou toburn. If you arewearing abathing suit and are exposing75percent ofyourbodytosunlight,thenyourtimewithoutsunscreencanbereducedtwotothreefoldandthenjusttwoorfiveminutesanduptotenminutes.Whynotmakemore vitamin D in less time and fewer exposures? If you are a dark-skinnedAfricanAmericanandcanspendhoursandhoursoutinthesunonthebeachesofLongIslandbeforegettingburned—ifyougetburnedatall—thenspendhalfanhourinthesunbeforeputtingonanysunscreen.Forthoseinbetweenthesetwo skin types who get pink in one hour, fifteen to thirty minutes of sunexposurewillsuffice.

Youdon’tneedtospendtimeonthebeachtomakevitaminD.Youcandoitsittingoutsideorwalkingwhileonyour lunchbreak.Butyoudoneedtohaveyourskinexposedtodirectsunlightbetweenthehoursof10:00A.M.and3:00P.M.You cannotmake vitaminD in high latitudes during thewintermonths.However,ifyouliveinthenortheasternUnitedStatesandfollowthisguidelinebetweenMayandOctober,youwillmakeenoughvitaminDtolastyouthroughthewinter.VitaminDisstoredinyourbodyfatandreleasedinthewinterwhenyouneedit.(However,ifyouareobese,thisprocessismuchlessefficient,asthebody tenaciously holds onto the vitamin D.) If you don’t get this amount ofsunlight between May and October, then during the winter months consideralternate forms of vitamin D, such as pill supplements and indoor-tanningfacilities(forguidelinesonthis,refertopage193).Always adjust your calculationsdependingon the situation.For example, if
youareatthebeachatteninthemorningorfourintheafternoon,thesunislessstrong,soyoucanspendlonger in thesunwithoutprotection. (Ifyouestimatethatatthattime,basedonyourexperience,itwouldtakeanhourforyoutogeta1MED,thenyoucanspendaboutfifteentothirtyminutesinthesunwithoutanysunscreenon.)Remember, Idonotadvocate thatyouevergetamildsunburn,butsimply thatyouestimatehow long itwould takeyou toget a1MEDandmakeyourcalculationsofsensiblesuntimeaccordingly.What if you live in a climate such asFloridawhere the sun shines all year
round?Thesameprincipleapplies.Youshouldtrytogetafewminutesofsunexposure two to three times aweek for a lengthof time thatdependsonyourskintype(seebox)andthetimeofyear.Makesureyoutakeadvantageofprimetime:between10:00A.M.and3:00P.M.Eventhoughat7:00A.M.thesuninFlorida appears to be strong enough during certain times of the year tomakevitaminD,itsraysarenotUVB-richenoughatthishourtomakeamplevitaminD.
TheHolickSensibleSunTables
Thesecondaccurateandconvenientmethodyoucanusetodeterminehowmuchsunyouneed iswith tables Ihavecreatedbasedonmyresearch.These tablesprovidesensiblesuntimefordifferentclimaticlocationsanddifferentskintypes.Themostimportantthingsyouneedtoknowbeforeyoustartiswhatskintype
youhaveandwhatlatitudecategoryyouarein.Usethedescriptionsinthebox
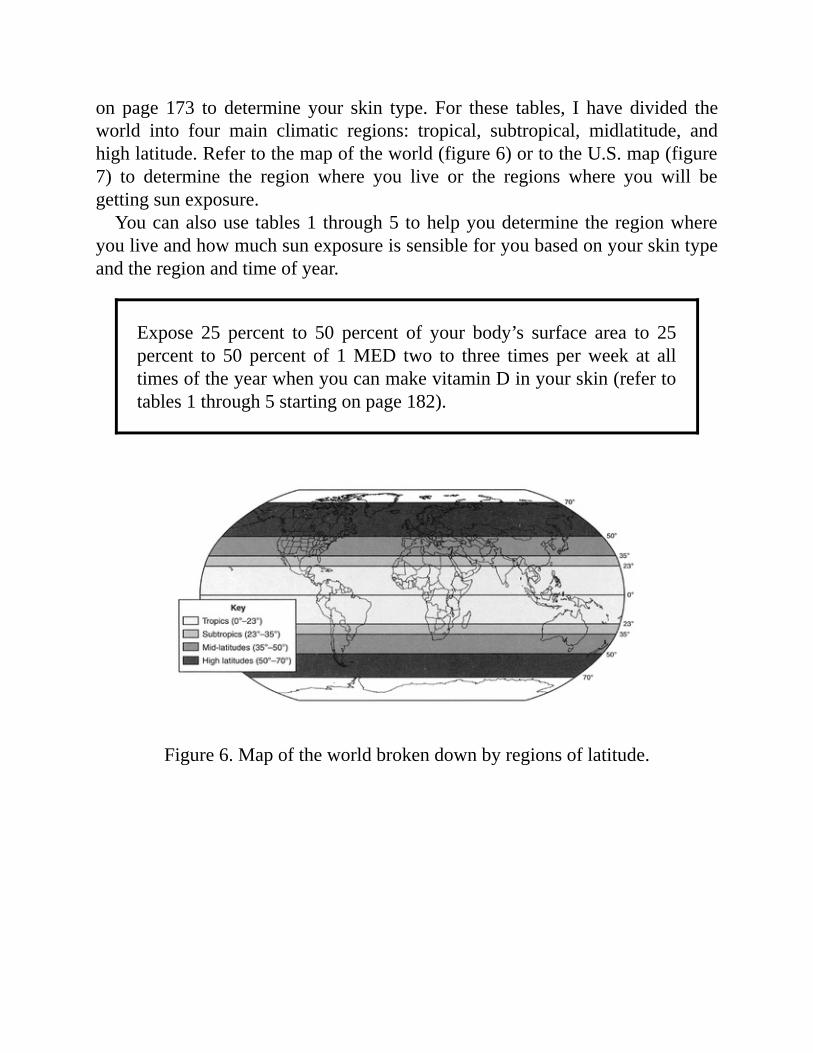
on page 173 to determine your skin type. For these tables, I have divided theworld into four main climatic regions: tropical, subtropical, midlatitude, andhighlatitude.Refertothemapoftheworld(figure6)ortotheU.S.map(figure7) to determine the region where you live or the regions where you will begettingsunexposure.Youcanalsouse tables1 through5 tohelpyoudetermine theregionwhere
youliveandhowmuchsunexposureissensibleforyoubasedonyourskintypeandtheregionandtimeofyear.
Expose 25 percent to 50 percent of your body’s surface area to 25percent to 50 percent of 1MED two to three times perweek at alltimesoftheyearwhenyoucanmakevitaminDinyourskin(refertotables1through5startingonpage182).
Figure6.Mapoftheworldbrokendownbyregionsoflatitude.
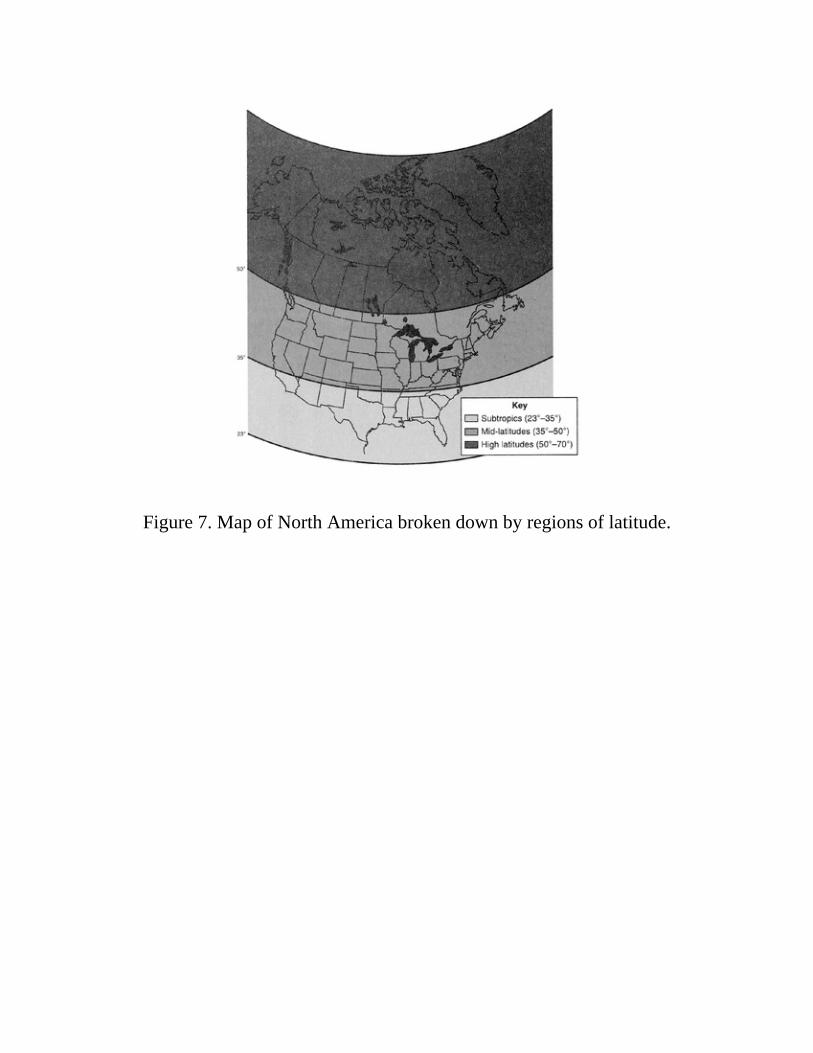
Figure7.MapofNorthAmericabrokendownbyregionsoflatitude.
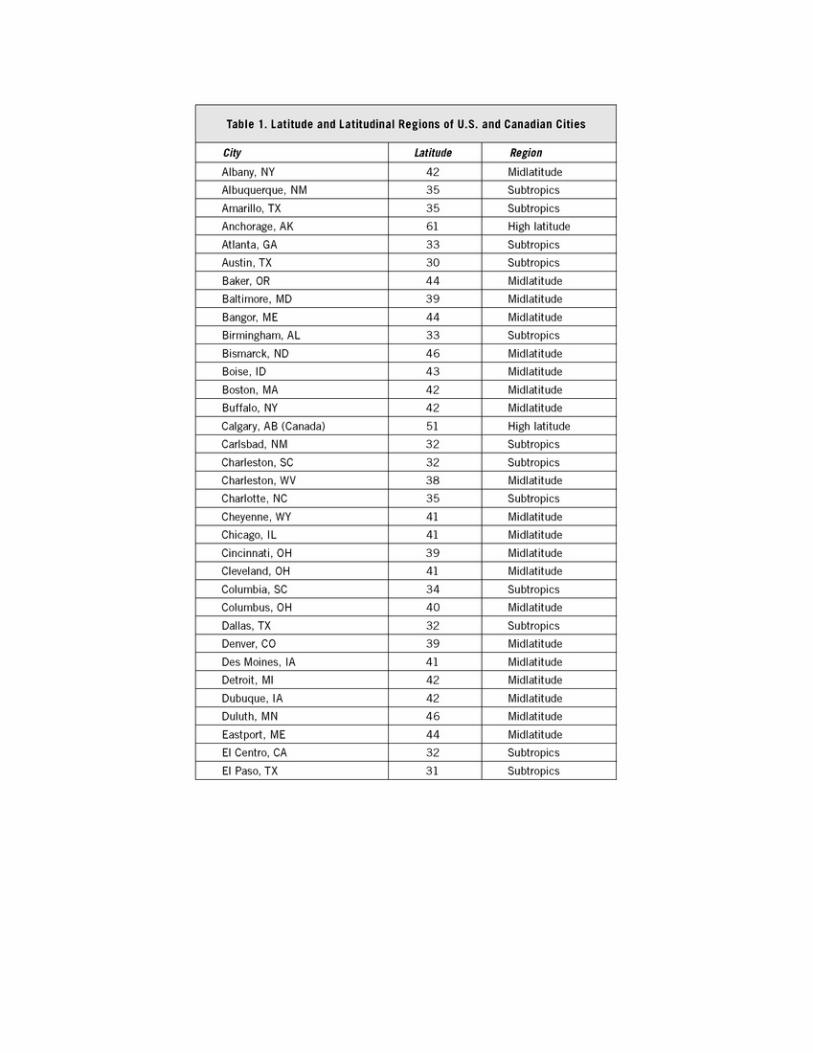

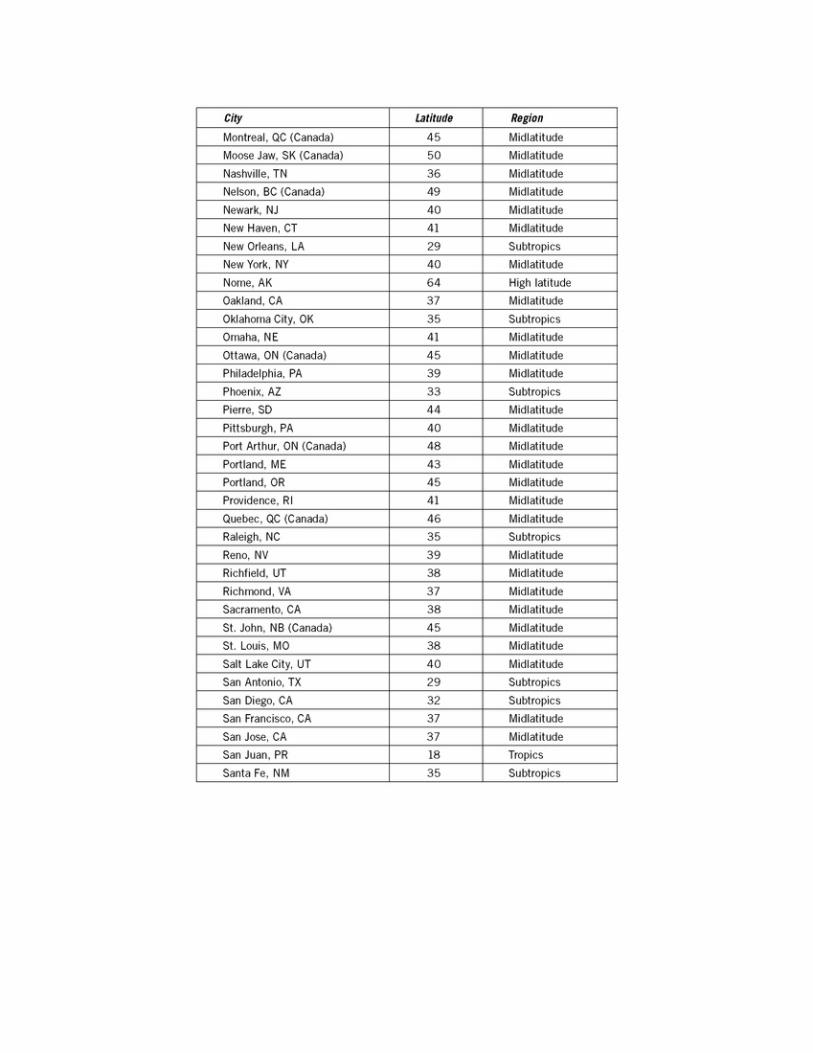

Table2.SafeandEffectiveSunExposure(inMinutes)forVitaminDProduction:TropicalLatitudes(approx.0-25degrees,e.g.,Honolulu,
Jamaica,U.S.VirginIslands)
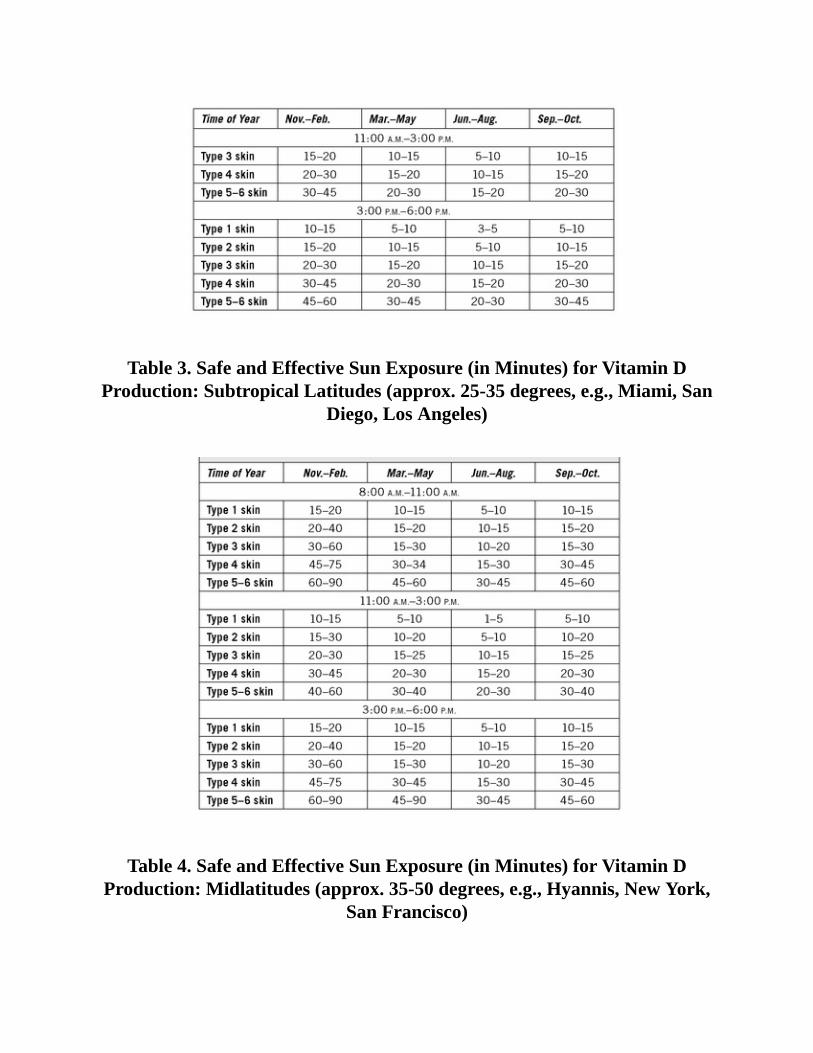
Table3.SafeandEffectiveSunExposure(inMinutes)forVitaminDProduction:SubtropicalLatitudes(approx.25-35degrees,e.g.,Miami,San
Diego,LosAngeles)
Table4.SafeandEffectiveSunExposure(inMinutes)forVitaminDProduction:Midlatitudes(approx.35-50degrees,e.g.,Hyannis,NewYork,
SanFrancisco)

Table5.SafeandEffectiveSunExposure(inMinutes)forVitaminDProduction:HighLatitudes(approx.50-75degrees.e.g.,Anchorage,
Stockholm)

AreTanningBedsRightforYou?
Inaperfectworld,allofuswouldhavethetimeandopportunitytostripoffourclothesandstepoutsideforseveralminutesadayfortheamountofsunweneedto make enough vitamin D to be healthy, especially between spring and fall,whenwecanstockupforthewinter.Regrettably,that’snotthecase,andreallife(nottomentionofficedresscodes)tendstointerferewiththisgoal.Everyday,approximatelyonemillionAmericans frequentan indoor-tanning
facilitytolookandfeelbetter.AlthoughIamnotanadvocateoftanningperse,Idobelieve in the importance ofUVBexposure formaking the vitaminDyouneedtobehealthyandfeelinvigorated.Ifyoudon’thavetheopportunitytogoout in the sun or prefer a more private and controlled environment, indoor-tanningfacilitiesareaviablealternativetonaturalsunshine.Am I crazy? Don’t I know that tanning beds were officially listed as a
carcinogen last year by the World Health Organization? And that theInternationalAgency for Research on Cancer elevated sun beds to its highestcancerriskcategory?WhatkindofadoctoramItobetoutingthebenefitsofsunbedswhenthepowersthatbehavepracticallydeclaredwarontanningsalons?I am a realist. I know that many of you will continue to frequent indoor-
tanning facilities because of the way you look and feel afterward. I dounderstandtheconcern,though;tanningbedscanbeabusedbypeoplewhodon’tknow how to use them safely, especially the young, who are at high risk ofdamaging their skin fora lifetime. I alsobelieve that ifyouhaveall the facts,

youhavetherighttomakethechoicetoenjoyUVBexposureindoorsoroutside.It’s ludicrous and, frankly, irresponsible for the these institutions to say thattanningbedsareonparwitharsenicandmustardgas.Could thesamebesaidaboutsaturatedfatandsodium?Certainlynot.Weneedthoseforsurvival,justasweneedUVBinmoderation.Andthat’sthemessage:moderation—apointI’vebeendrivinghomesincethefirstpageofthisbook.Sowithallthisinmind,ifyouchoosetotanindoors,makesureyouusethistechnologyresponsibly.Thankfully, the indoor-tanning industry, through the efforts of the Indoor
TanningAssociation, is doing its part by introducing quality-controlmeasuresand offering education and certification for its personnel. Keep in mind thatthere’s no such thing as artificial UV radiation. A UVB photon (packet ofenergy)isaphotonwhetheritisproducedbythesunorbyatanningbedwithfluorescent lamps. The fact that the radiation you are exposed to in indoor-tanning facilities is thesameaswhatyouget from thesunmeansyouneed totakethesameprecautionsyouwouldifyouwereinthenaturalsunlight.Aswithnaturalsunlight,whenusingindoortanningequipmentthereisthepotentialforthekindofoverexposure that isassociatedwithnonmelanomaskincancerandprematurelyagedskin.Aboveall,makesuretheindoor-tanningfacilityyouusefeaturesappropriate
equipment. At one time, indoor-tanning facilities used equipment that emittedhigh-intensityUVBradiation.WhenUVBradiationwaslinkedtobasal-cellandsquamouscell skincancer, the industry switched toUVA-only“high-pressure”lamps,whichwere considered safebecause theydidn’t causeburning.Then itwasdiscoveredthatUVAradiationmaycontributetomelanomaandwrinkles,aswell as increase the risk of nonmelanoma skin cancer. Therefore, the trend inrecenttimeshasbeentowardlow-pressureandmedium-pressurelampsthatemitabalanceofUVAandUVBradiation(94percentto97.5percentUVAand2.5percent to 6 percent UVB) that replicates natural sunshine. Before using anindoor-tanning facility, make sure it features low-pressure lamps (look forfluorescent tubes, not round lamps). Facilities that use high-pressure lampsshouldbe avoidednot onlybecauseof those lamps’ potential for causing skindamageandcertain typesofcancersbutalsobecause theydonotprovideanysortofvitaminDbenefit.Ifyourequireassistance,findafacilitywherethestaffhasbeencertifiedby
anindustryassociationsuchastheInternationalSmartTanNetwork.Aqualifiedstaffmembershoulddothefollowing:
•Discussyour skin typeandexposure-timechartscarefullywithyouand

ensurethatyouhaveaccesstothisinformationatalltimes.•Recommendanexposureschedulethatwilltanyoumoderatelyandavoidanypinknessandespeciallysunburn.
•Discusswithyouanything thatmaycauseyou to reactadversely toUVexposure(certainmedicines,birthcontrolpills,cosmetics,orsoapsmayincreaseyourriskofasun-sensitivereaction).
•ProvideyouwithFDA-approvedeyewearwithusageinstructions.•Guideyouthroughyourfirsttanningexperience.
Followstaffguidelinesand thoseof theequipmentmanufacturers.Wearsunprotection on your face. Do not exceed the recommended exposure time. Beaware that areas not usually exposed to sunlight can still get pink—anotherreasontoconsiderspendinglesstimethanisrecommended,whichissupposedtobe0.75MED.IndoortanningexposuretimesarebasedonFDAandFederalTrade Commission guidelines, which allow a per-session UV exposureequivalentto75percentof1MED.Thisisquiteliberalbecauseyourequireonly25 percent to 50 percent of 1MED (again, the time itwould take you to getpink)togetenoughvitaminD(equivalenttotakingabout4,000to10,000IUofvitaminDorally).Ifyouareconcernedabout thepotentialharmofUVBradiationandarenot
interestedinatan,youcangetall themedicalbenefitsofUVBexposurefromjust 25 percent of 1 MED (about 4,000 IU of vitamin D). One of the mostpopular reasons for using indoor-tanning facilities is to build a “base tan” inanticipation of awinter visit to a tropical destination such as theCaribbean. Ithinkthat’ssmart,andI’llexplainwhy.As I’vemade clear, I’mnot a proponent of tanning, but I dobelieve in the
importance of skin health and of protecting skin against strong sunshine.Increasing the melanin content in your skin by going to an indoor-tanningfacilitywill provide youwith a certain amount of natural protection against aburn. Start increasing themelanin content in your skin by visiting an indoor-tanning facilityat leastonemonthbeforeyou leave,andhave threesessionsaweek. When you arrive at your tropical or subtropical destination, take theappropriatemeasurestoprotectyourselfagainstaburn.Dependingonyourskintype, the protection you get from prevacation tanning salon exposure isequivalent to using a sunscreen with a sun protection factor of two or three(SPF2orSPF3),whichmeans you can stay outside twoor three times longerthanyoucouldifyoudidn’thavethe“basetan.”Somepeoplechoosetopurchasetanningequipmentforuseintheirhomes.I

aminfavorofdoingthisifyourprimarygoalistomakevitaminDandimproveyour psychological health. Follow the same guidelines and precautions youwould observe in commercial facilities or in natural sunshine. It is especiallyimportant to avoid overexposure, which can be a temptation because of youreasy access to the equipment. Again, be sure your equipment uses low-ormedium-pressurelamps—thosethatemitabalanceofUVAandUVBradiationthatmostcloselyreplicatesnaturalsunlight.
Remember: Tanning beds that only emit UVA radiation will notproduce any vitamin D in the skin. There’s only one lamp on themarketthathasbeenapprovedtoclaimithelpsboostvitaminD;youcan learn more about the Sperti Sunlamp at www.sperti.com. MycolleaguesandIhaveshownthatthislampisveryefficientinmakingvitaminDintheskin.Onlythreetofiveminutesofexposingthelegsorabdomenthreetimesaweekcanbeeffective.Dr.VinTangpricha,whospenttimeatBostonUniversityandisnowatEmoryUniversityrunninghisownlaboratory,andourgroupreportedin2007thatafteronlyeightweeksofexposure,patientswithcysticfibrosiswhowereunable to absorb vitaminDwere able to significantly increase their25-vitaminDlevels.
Most people use tanning facilities for cosmetic reasons—in otherwords, tolookandfeelbetter.IusethiskindofequipmentextensivelytotesttheeffectsofUV radiationonhealth. Inoneof themostdramatic examplesofhow indoor-tanningequipmentcanbeusedtherapeutically,ImanagedtorelieveexcruciatingbonepaininawomanwithsevereCrohn’sdiseasewhowasvitaminDdeficientbecause90percentofherintestineshadbeenremovedinsurgeryandnoamountoforalvitaminDcouldenableherintestinestoabsorbenoughvitaminDtokeepher bones healthy. Her bone pain, caused by the condition known asosteomalacia (see chapter 3), was relieved in a month thanks to three-times-weekly sessions on a tanning bed, observing the manufacturer’s exposureguidelines.IfyouhavetroubleabsorbingvitaminDfromyourdiet,speaktoyourdoctor
about whether indoor tanning sessions would help correct your vitamin Ddeficiency. Three of the most common conditions associated with difficulty
absorbing vitamin D through the small intestine are Crohn’s disease,inflammatoryboweldisease,andcysticfibrosis.Lamps that emit UVB radiation were originally invented to treat medical
conditionsinthe1930s.Tanningbedsasweknowthemtoday,however,didn’tgainafootholduntilmuchlater.Themancreditedwithbeingthe“fatherofthetanning industry” is the Swiss engineer Friedrich Wolff. While studying thebeneficialeffectsofultravioletlightonathletesdecadesago,Wolfftooknoteofthe tanned-skin side effect and went on to found the indoor tanning industry.Mimicking German and Eastern European spas, Wolff brought his Europeantechnology to the United States in 1978, and an industry was born to takeadvantage of people’s desire to look as if they had just returned from anexpensivevacationinthetropics.WiththenewinformationthatvitaminDissoimportantforgoodhealth,Ihopeyouwillstarttoregardindoor-tanningfacilitiesasplacesnottobronzeyourselfbutrathertoundergotherapytostimulateyourproduction of vitaminD.Whenmy colleagues and I compared two groups ofBostonians—oneagroupoftannersandanotherwhodidn’ttan,matchedupintermsofageandsex,weshowedthatthetannersboastedabloodlevelofabout45nanogramspermilliliter,which,again,isthoughttomarkedlyreducetheriskof myriad health problems. Their counterparts who never visited a tanningfacility, however, had 25-vitamin D levels in the 18-nanogram-per-milliliterrange,farbelowthelevelrequiredformaximumhealthprotection.
GuidelinesforIndoorTanning
•Educateyourself.KnowtheprosandconsofUVexposureandhowtouseitandprotectyourself.
•Uselow-pressureormedium-pressurelamps.Lookforbedsthathavefluorescenttubes,asopposedtoroundlamps.Asktheattendantworkingatthefacilitywhetherheorsheknowsforsurethatthelampsatthatfacilityarelowpressure(thosethatemitabalanceofUVAandUVB).High-pressurelampsemitonlyUVA,whichpenetratesdeepintotheskinandmaycauseskincancerandwrinklesandalteryourimmunesystem.Bydefinition,fluorescenttubesemitUVB,whereasround,high-pressurelampsemitUVA.
•Usecommonsenseandpracticemoderation.Refertothe
guidelinesinthischapterforhowmuchUVexposureyouneed.Keepinmindthatindoor-tanningfacilitiesemitUVradiationequivalenttothesunshineattropicallatitudes.Restrictyourexposureto50percentofthemanufacturer’srecommendedtimeofexposure,orthetimedefinedbymyguidelines—whicheverisless.Protectyourfaceandwearlipsunscreen.
•Knowtheconsequencesofusingoil.Rubbingoilintoyourskinflattenstheverytoplayerofskin(thestratumcorneum,whichactslikeafieldoflittlemirrorsreflectingtheUVAandUVB)andincreasesthepenetrationofmuchoftheUVAandUVBradiationthatwouldotherwisebereflectedofftheskin.Ifyouusesuchproducts,cutyourUVexposuretimebyatleast30percent.
•Weargogglesorpeepers.Makesurethefacilityprovideseyewearthatfitssnugly.Ifthefacilityoffersgoggles,makesurethegogglesaresterilizedaftereachusetopreventthespreadofeyeinfections.Iftheyarenot,purchaseyourownpairofgoggles.
•Consideryourmedicalhistory.Ifyouarebeingtreatedforlupusortendtogetcoldsores,theseconditionscanbeactivatedthroughexposuretoUVradiationfromindoor-tanninglamps,justastheyarebynaturalsunlight.Forexample,ifyoucarrytheherpesvirus,UVexposuretotheareasaffected,suchaslipsandthegenitalregion,caninduceactivityofthevirusandthuscoldsores.YourskinmayalsobemoresensitivetoUVradiationifyoutakecertainmedications,suchasantibiotics,antihistamines,tranquilizers,waterpills,diuretics,orbirthcontrolpills.Awell-runindoortanningfacilitywillkeepafilewithinformationaboutyourmedicalhistory,medications,andtreatments.Makesureyouhelpthestaffkeepthefileuptodate.
EvolutionandAdaptationatWork

Weshouldgivethehumanbodymorecreditthanitsometimesgets.Peopledon’tshrivel,shatter,orshutdownatthefirstsignofstress.Instead,thehumanbodyoperatesonthe“overloadprinciple”—whensubjectedtooutsideforces,itadaptsbygettingstronger.Examplesofthisphenomenonaboundinthehumanbody.Your muscles don’t pop and your bones don’t break if you regularly lift
weights—theygetbiggerandmorepowerfulsotheycanhandleaheavierload.Yourheartandlungsdon’texplodeorcollapseifyougorunningeverymorning—theybecomemoreefficientandyour lungcapacityexpands.Your ligamentsandtendonsdon’tsnapifyoudostretchingexercises—theygetmoreflexible.The same goes for your skin’s exposure to sunshine. If your skin receives
regular,moderateexposuretosunshine,itadaptsbyproducingmelanintoabsorbthesun’sradiation,therebyprotectingitselfagainstafutureburn.ItalsoinducesDNA repair enzymes to spring into action. This is the human body’s naturaladaptation tooutsidestress.Ofcourse, suddenandextremeexposure tostrongsunshineafter anextendedperiodofnonexposurewill result in sunburn in thesameway that exposure to sudden and extreme physical activity can result indamagetothemuscle-bonesystemortheheart.Remember, too, that skin did not evolve solely to resist the power of the
sunshine—yourskinisalsotheconduitthroughwhichyourbodyusesthesun’sradiationtocreatethevitaminDyouneedforyourverysurvival.Plus,youhavean entire DNA-repair system made up of enzymes whose job is to repairdamagedDNAandreplaceitwithhealthynewmaterial.MycolleaguesandIaredoingresearchtodetermineiftheskin’sDNArepairprogramisenhancedwhenitisexposedtomoderatesunlight,andIsuspectthatitis.Allthisistosaythatyourbodyisdesignedtoaccommodate theeffectsofsunshine.Tosuggest thatsunshine is necessarily harmful to your skin is to underestimate the humanspecies’abilitytoadapttoitsenvironment.Antisun activists argue that to differentiate between the causes of
nonmelanomaskincancerandthecausesofmelanomaistoconfusetheissue—theymaintainthatyouneedtoavoidallsunshineandbecomeasunphobe.Thisignoresthefact thatsomesunexposureisnecessarytosurviveandbehealthy.Theamountof sun exposure that causes thepotentiallydeadlymelanoma—anamount that results in a sunburn—should be stringently avoided, but themoderate, regular sun exposure, which is yourmain source of vitaminD andwhichisassociatedwiththerarelydeadlyandeasilytreatednonmelanomaskincancer, shouldnotbe forsaken. If it is,you increaseyour riskofdevelopingavarietyofmoreseriousanddeadlydiseases.

Some people enjoy being in the sun and using indoor-tanning facilities somuch that theywill risknonmelanomaskincancer in favorofall thepotentialbenefitsofsunexposure.OthersmaychoosetogetonlytheminimumamountofUVB exposure necessary to build and maintain vitamin D levels. These arechoices only you can make. However, we know a couple of things for sure.Subjecting yourself to unlimited amounts of UVB is potentially harmful. ButdenyingyourselfanyandallUVBcanleadtoserioushealthproblemsifyouarenot taking enoughvitaminD fromdietary and supplemental sources to satisfyyourbody’srequirementforvitaminD.
TheHolick Solution for Sensible Sun is a guide to howmuch sunexposure youneed tomaintain appropriate vitaminD levels.Here’showitworks.Youestimatehowlong itwould take foryou togetamildsunburn(whenyourskingetspink—thisamountofexposureisknown as 1MED), then two to three times aweek, you expose 25percentofyourbody(e.g.,armsandlegs)for25percentto50percentof that time. Inotherwords, if itwould take thirtyminutes foryourskintogetpinkinthesunshine(asitwouldformeatnoononaCapeCodbeachinthesummertime),thentwotothreetimesaweek,spendeighttofifteenminutesinthesunbeforeputtingonSPF30sunscreen.Usetheseguidelinesifyouchoosetovisitatanningsalon,too,butdonotexceed50percentofthemanufacturer’smaximumrecommendedtimeofexposure.

CHAPTER9
Step2:BoneUponCalcium
ThedynamicduoofcalciumandvitaminDcansustainyourlife
Virtually everyone can recite the milk industry’s campaign slogan: It does abodygood.Muchof this goodness no doubt hinges on the calciumcontent ofmilk.Calcium is themost abundantmineral in the human body,with over 99percentoftheamountpresentbeingfoundinthebonesandteeth.Forthegrowthandmaintenanceofhealthybonesitisessentialthatwehavesufficientcalciumintake;we are at risk of developing bone diseases such as osteoporosiswhencalcium leaching isnotbalancedbydietary ingestion.But calcium isnotonlyimportant for the skeleton; it also has a role to play in nerve function, bloodclotting,musclehealth,andotherareas.And,likeanorphanchildwithoutaparenttoguideitproperly,calciumcannot
workproperlyinthebodywithoutthehelpofvitaminD.CalciumandvitaminDshare a special relationship that plays into everything about you, from yourabilitytobuildandmaintainbonestrengthtoyourneuromuscularfacultiesandbrainpower.I’vealreadytouchedupontheseideasinearlierchapters,buthereI’llexploremoreaboutthiscalcium-vitaminDconnectionandencourageyoutopayattentiontoyourcalciumintakeasmuchasyourvitaminDintake.
It is also well recognized that vitamin D aids in the absorption ofcalciumaswellasphosphate.

TheMissingLinkBetweenVitaminDandBoneHealth
Todiscoverthatsunlightheldasecretingredienttopreventingandtreatingbonediseases like rickets was one thing, but understanding why and how this allworked, from a single ray of UVB to health in the human body, was clearlyanother. It took scientists severaldecades touncover themechanismbywhichvitaminDproducedintheskincouldeffectsomanypositivehealthbenefits.OneofthereasonsittooksolongtoteaseoutvitaminD’scomplexbiological
pathwayandinfluenceonotherphysiologicalprocessesisthatwesimplydidn’thavethetoolstotrackvitaminDdown.Itwasn’tuntil themid1960sthatnewlaboratory techniques emerged to afford researchers the opportunity to followvitamin D’s intricate actions using radioactively labeled substances. Between1969and1971,asIwasmakinganameformyselfinarenownedlabheadedbyHectorF.DeLucaattheUniversityofWisconsin,researchers,myselfincluded,weremakinggreatstridesinunderstandingthemetabolicprocessingofvitaminD.By1971itwasclearthatvitaminDwentthroughsequentialtransformationsin the body that entailed inactivemetabolites along theway until the kidneysconverted the major circulating form (25-vitamin D) to activated vitamin D(1,25-vitaminD).Thesefindingswereconfirmedbyotherteamsofresearchers,includingAnthonyW.NormanandhiscolleaguesattheUniversityofCaliforniaatRiverside andEgonKodicekandhis coworkers atCambridgeUniversity inEngland.Isolating and determining the molecular structure of all these vitamin D
metaboliteshelpedput to rest thebiggestmystery thathad troubledvitaminDscientists for decades: just howdid vitaminD influence calciumdeposition tobuildstrongbones? In theearly1950s, theSwedish researcherArvidCarlssondiscovered, much to everyone’s surprise, that vitamin D can actually removecalciumfromboneswhenitisneededbythebody.Ataboutthesametime,theNorwegianbiochemistRagnarNicolaysen,whohadbeentestingdifferentdietsonanimalsforyears,concludedthattheuptakeofcalciumfromfoodisguidedbysomeunknown“endogenousfactor.”Hebelievedthisendogenousfactorsentamessage to the intestines that thebodyneededcalcium.Thatmessage turnedouttobeactivatedvitaminD.WithvitaminD’sidentitysolved,answersbegantoemergeintheexperimentstracingtheactivationofvitaminD.Oncewehadour fingeronactivatedvitaminD,andhowitcame tobe ina
complex series of conversions through organs and the bloodstream, it was
apparentthatweweren’tdealingwithjustanothervitamin.Weweredecipheringapreviouslyvagueandconvolutedpictureofhow“vitaminD”workedon thebody. And because of its profound effects, which we were just beginning tounravel and interpret, we quickly realized that it belonged in the hormonecategory. No sooner had we singled out 1,25-vitamin D, the active form ofvitamin D, than we reclassified it as a hormone that controlled calciummetabolism,whichreferstohowthebodymaintainsadequatelevelsofcalcium(more on this below). Thismarked the genesis of understanding not only therelationshipofvitaminDtothebody’sendocrinesystemandcalciumregulationbut also how vitamin D could effect positive change of myriad biologicalprocesses,frommodulatingtheimmunesystemtoinhibitingtheskincellgrowththatleadstoskindisorderslikepsoriasis.As detailed in chapter 1, hormones are unique substances produced in the
body.TheworditselfisderivedfromtheGreekverbhorman,meaning“tostirthings up.” Acting as internal signals, hormones control not only differentaspects of metabolism but also many other functions—from cell and tissuegrowth to blood sugar, heart rate, blood pressure, and even the activity of thereproductive system. By definition, hormones are produced by one organ andthen transported in the bloodstream to a target organ,where they can cause aspecificbiologicalaction.EvidenceforreclassifyingtheactiveformofvitaminDcamewiththerealizationthat1,25-vitaminDisproducedbythekidneysandthatitssecretionbythekidneysintothebloodstream,whereitcanthentraveltothe small intestine, leads to its buildup in cell nuclei of the intestine,where itregulatestheefficiencyoftheabsorptionofdietarycalcium.By1975,MarkR.Haussler at the University of Arizona confirmed the discovery of a proteinreceptor thatbinds theactivevitaminDmetabolite in thenucleiofcells in theintestine.WithvitaminDnowassociatedwith the intestine, scientistswerezeroing in
onthemechanismofcalciumcontrol.Itwasnotedthatasthelevelofcalciuminthedietrises,theamountofactivevitaminDhormoneinthebodyfalls,andviceversa.Thisfeedback-looppatternfurtherconfirmedtheideathatactivevitaminDwasahormone,specificallyacalcium-regulatingone.Thehuntwasthenontofind out how this exceptional hormone was linked to the rest of the body’sendocrinesystem.MyresearchcolleaguesandIfoundthatahormoneproducedby the parathyroid gland (hence called parathyroid hormone) is critical tomaintaining adequate levels of active vitaminD hormone in the blood.Whencalcium isneeded, theparathyroidgland sends thishormone to thekidneys to

trigger production of vitaminD hormone. That hormone, in turn, prompts theintestinestotransfercalciumfromfoodtotheblood.Whencalciumintakeistoolow to supportnormal functions,bothvitaminDand theparathyroidhormonetriggeraprocessinwhichstoredcalciumismobilizedfromthebones(asArvidCarlssondiscoveredfiftyyearsago).Itdoesthisbysignalingbone-formingcellscalled osteoblasts to express on their surface a protein known as RANKL(receptor activator ofNF-kappaB ligand),which acts as amagnet to attach tomonocyticcells (a typeofwhitebloodcell) in thebonemarrow.This intimateconnection results in the birth of giant cells with multiple nuclei that releaseacids and enzymes to dissolve bone and unleash its stored calcium into thebloodstream.Toooftenpeoplediscredit,orsimplydon’tknow,theroleofcalciumintheir
everyday functions. Calcium is required for skeletal and cardiac musclecontraction,blood-vesselexpansionandcontraction,secretionofhormonesandenzymes,andtransmissionofimpulsesthroughoutthenervoussystem.Thebodystrivestomaintainconstantconcentrationsofcalciuminblood,muscle,tissues,and intercellular fluids, though less than 1 percent of total body calcium isneeded to support these functions. The rest of your calcium—99 percent—isstored in your bones and teeth, where it supports their structure. And, as Iexplained earlier, bone itself undergoes continuous remodeling, with constantresorption (breakdown of old bone) and deposition of calcium into a newlyformed bone collagen matrix. The balance between bone resorption anddeposition changes with age. Bone formation exceeds resorption in growingchildren,whereasinearlyandmiddleadulthoodthetwoprocessesarerelativelyequal.Inagingadults,particularlyamongpostmenopausalwomenandmenoversixtyyearsold,bonebreakdownexceeds formation, resulting inbone loss thatincreasestheriskofosteoporosisovertime.Weallneedcalciumtosurvive, justasweneedwater.But there isacertain
balance to be struck, a so-called homeostasis. In fact, you can think of thehomeostasisofcalciumionsinthebodyasacenterofgravityforanumberofphysiologicalprocesses.Ifthereistoolittlecalciuminyourblood(aconditioncalled hypocalcemia), soft-tissue cells—especially nerves and muscle, whichrely on calcium to operate—becomedysfunctional.Your entire neuromuscularsystem will become abnormally excitable, and impulses may be triggeredspontaneously. This, in effect, sends your body into convulsions as muscles,including those of the respiratory system, contract uncontrollably. In thissituation,apersoncandiefromfailuretobreathe.Theheart,whichalsodepends

on calcium to beat properly, can lose its rhythm, with fatal consequences.Conversely, if there is too much calcium in the blood (a condition calledhypercalcemia),organscalcifyandeventuallyceasetowork.This isespeciallytrue for thekidneys.Bloodvesselswill calcify, rendering them lesspliant andthus increasing the risk of stroke and myocardial infarction. Those excesscalcium ions have an opposite effect on the nervous system, abnormallydepressing it and causing depression, constipation, and confusion. Having toomuchcalciumcanbejustashazardousashavingtoolittle.Soyoucanseehow important it is tomaintain steadyandhealthy levelsof
calciuminthebody.YoucanalsoseehowvitaminDpromoteshealthybonesbyindirectly maintaining adequate serum calcium and phosphorus for bonemineralizationtooccur.VitaminDcontrolsthelevelofcalciumintheblood.Ifthereisnotenoughcalciuminthediet,thenitwillbedrawnfromthebone.HighlevelsofvitaminD (from thedietor fromsunlight)will actuallydemineralizeboneifsufficientcalciumisnotpresent.We know that if you are vitaminD deficient, asmostAmericans are, your
bodywillstealthecalciumoutofyourbones.Thatiswhatwouldcauseyoutohaveosteopeniaorosteoporosis,severelowbonedensitywithincreasedriskoffracture.ButbeingvitaminDdeficientalsopreventscalciumfromcomingintothe bones. And as a result, there’s nothing more than a Jell-O-like collagenmatrixleftbehind,anditwillgethydratedjustlikeJell-Oandwater.Womenwhocomplainofthrobbing,achingbonepainaresometimesmetwith
doctorswhocan’t understand it.When thedoctorpresseson apatient’sbonesalmostanywhere,shewilloftenwinceinpain,andthat’sbecausethedoctorispressingdownwhere there’snomineralizedboneon the surface. It’s simplyaJell-O-like substance, triggering significant discomfort. The covering on theboneisfullofnerveendings,andif thereisnomineralizedboneunderneathitbut instead a rubbery “Jell-O,” then when the doctor presses on it, thatcompressesthecoveringandexcitesthosenerveendings,resultinginpain.LikeJell-O,thecollagenmatrixexpandsundertheperiostealbonecovering,causingthrobbing,achingbonepain.Whenpeoplearesittingwithachesintheirhipsorlying in bed with throbbing aches in their bones, it can be very hard forphysicianstoimmediatelythinkofvitaminDdeficiency.Butoftenthat’sexactlywhat’scausingtheproblem.Makingsenseofthisremarkablerelationshipbetweencalciumregulationand
vitaminDhasopenedmanynewdoorsinscienceandmedicine.Inadditiontoshifting thecourseof treatment forpeoplesuffering frombonediseases, ithas

pavedanewpathforpeoplesufferingfromcalcium-regulationdisordersduetounderlying medical conditions. It suddenly became possible, for example, totreat patientswho had lost their parathyroid glands or their kidneys and, as aresult,couldnolongerregulatethelevelofcalciumintheirblood.Nowthatwehad the ability to synthesize activated vitamin D hormone commercially, wecouldtreatthesepatientswithactivatedvitaminDandcalcium.Theeffectsweredramatic, putting an end to their painful muscle spasms, convulsions, andchronicbonedisease.
YourBonesSavingsAccount
Whilecalciumisakeymineralforbothsexes, it isespecially important to thehealthofwomen.Aftertheageofthirty-five,mostmenandwomenstartlosingcalcium from their bones due to poor calcium and vitamin D intake. Duringmenopause,however,therateoflossincreasesrapidlyforwomen.Itisthereforevitalthatcalciumneedsbesatisfiedthroughdietsothatcalciumisnotleachedfrom the bones. Maintaining sufficient levels during this period is critical ifwomenaretoavoidmajorskeletalproblems.Notaswellknownisthefactthatthe degree of osteoporosis suffered in later life is largely dependent on theamountofbonemassachievedbyearlyadulthood.Forthisreason,thebuildingof strong bones—requiring regular calcium intake—should be a priority forwomen from childhood onward.By the age of eighty, 25 percent ofmenwillhavesufferedahipfracture.Thisiswhymenshouldbeequallyconcernedabouttheirbonehealth.Menhavehigherbonedensitythanwomenbecauseofhighermusclemass,butthey,too,willlosebonemass.Infact,12percentofmenwillhaveanosteoporoticfractureintheirlifetime.Whenyouareborn,youaregivena“bonessavingsaccount.”This iswhere
yourbodystorescalcium.Youareabletomakedepositsintothisaccountforthefirst thirty to thirty-five years of your life.After that point, that account is inretirement,andwheneveryourbodyrequirescalcium,especiallywhenitcomesto remodelingbones, it can take fromyourdietarysourcesor it can take fromyourbones.Obviously,youwantyourbankaccounttobefullandyouwantyourbodytouseitssavingsaslittleaspossible.You’dreallyliketohavethataccountas an emergency fund and rely on your diet and supplementation to get thecalcium you need. But if you end upwith ameasly account inmidlife, yourboneswillpaytheprice.

Without an adequate, constant supply of calcium the bones becomeweakerandthinneranddeveloptinyholesorpores(aconditioncalledporosity).Theseporousbonesarewhatleadstoosteoporosis.CurrentlytenmillionAmericans—80 percent of whom are women—have osteoporosis. Moreover, thirty-fourmillionAmericansareconsideredtohaveboneloss that’saprematureformofosteoporosis called osteopenia, which can progress to osteoporosis. Havingeitherdiseaseincreasestheriskoffracturesinthehip,spine,wrist,pelvis,andribs. Osteoporosis was once considered an older women’s issue. However, asI’vealreadypointedout,itcanstrikebothsexesatanyageandhasbeenreportedinchildrenasyoungastwelveyearsold.
It is estimated that nearly60percent of dietary calcium is absorbedduringchildhoodandadolescence,whenbonesaregrowingandneedas much calcium as they can get. This is why teenagers areencouragedtoingest1,300milligramsofcalciumaday.Inadultstheabsorptionratedecreasesto30percentto40percent.
Luckily, calcium, unlike vitaminD, is easy to obtain from diet alone. Richsources of calcium include dairy products (milk, yogurt, cheese), leafy greenvegetables(includingkale,escarole,collardgreens,andbokchoy),soyproducts(including tofu), nuts (especially almonds andpistachios), legumes, seeds, andcalcium-fortifiedjuices.Sidenote:althoughspinachishighincalcium,it’shardtoget thecalciumfromitbecause itcontainsa lotofoxalate,asubstance thattightly binds calcium so that it cannot be absorbed into the body (not thatspinachdoesn’tofferothernutritionalbenefits,however). Ifyoueatwell, thenyoumaynotneedtotakeacalciumsupplement.Butifyoufeelthatyou’renotgettingenough(seebox), thenbyallmeansaddacalciumsupplement toyourdailyregimen.
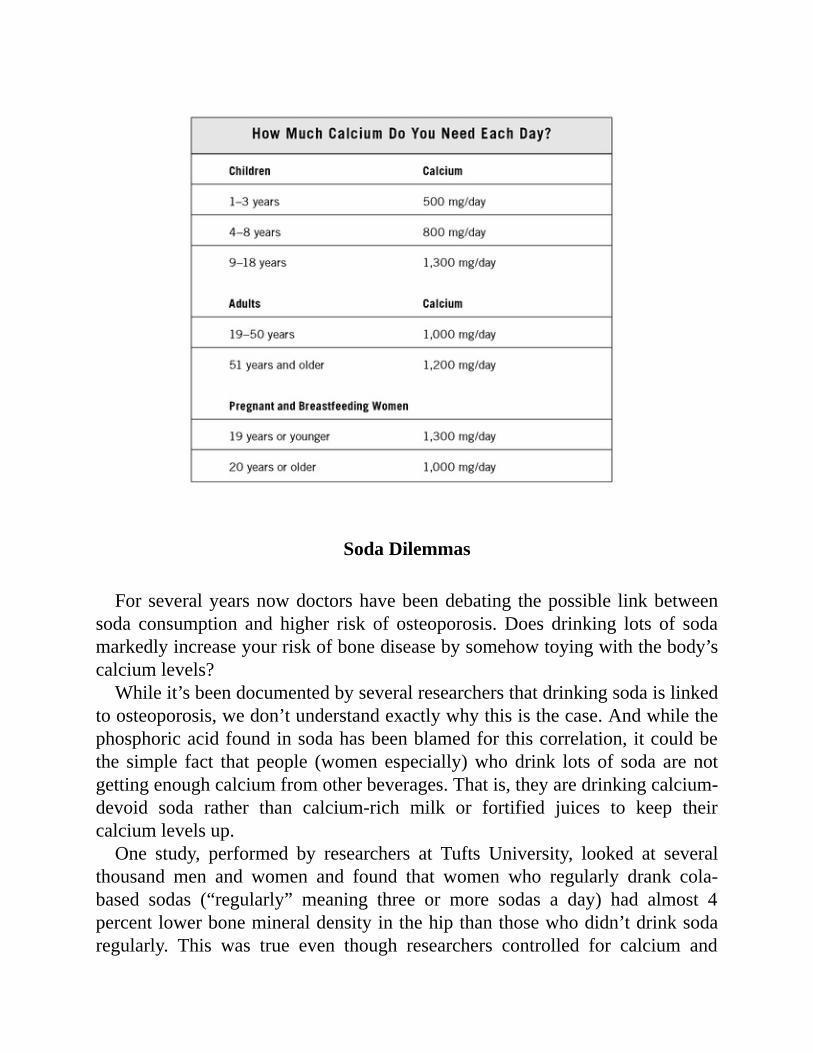
SodaDilemmas
Forseveralyearsnowdoctorshavebeendebating thepossible linkbetweensoda consumption and higher risk of osteoporosis.Does drinking lots of sodamarkedlyincreaseyourriskofbonediseasebysomehowtoyingwiththebody’scalciumlevels?Whileit’sbeendocumentedbyseveralresearchersthatdrinkingsodaislinked
toosteoporosis,wedon’tunderstandexactlywhythisisthecase.Andwhilethephosphoricacidfoundinsodahasbeenblamedforthiscorrelation,itcouldbethe simple fact that people (women especially)whodrink lots of soda are notgettingenoughcalciumfromotherbeverages.Thatis,theyaredrinkingcalcium-devoid soda rather than calcium-rich milk or fortified juices to keep theircalciumlevelsup.One study, performed by researchers at Tufts University, looked at several
thousand men and women and found that women who regularly drank cola-based sodas (“regularly” meaning three or more sodas a day) had almost 4percentlowerbonemineraldensityinthehipthanthosewhodidn’tdrinksodaregularly. This was true even though researchers controlled for calcium and
vitamin D intake. But women who drank noncola soft drinks, like Sprite orMountainDew,didn’tappeartohavelowerbonedensity.Cloudingthisstudy,however,andtheissueathand,arethepotentialeffectsof
caffeine.We’velongknownthatcaffeinecaninterferewithcalciumreabsorptionin the kidneys, increasing calciumexcretion into the urine. In theTufts study,both caffeinated and noncaffeinated colas were associated with lower bonedensity. And the caffeinated drinks appeared to do more damage than thecaffeine-freedrinks.Thebrouhahaoverthisdebatewillcontinue,butregardless,the“moderation”
messageshouldbeobvious.Mostpeoplewoulddowelltomoderatetheirintakeof these ingredients that, forwhatever reason,seemto interferewithachievingideal calcium levels in the body. When you limit soda and caffeine, youautomatically move toward healthier ingredients overall that pack a morepowerfulpunchofnutritionanyhow.
CalciumSupplements
Calcium supplements are an excellent alternative for people who fear theirdietpreferencesarenotgivingthemenoughcalcium.Thisisespeciallytrueforpeoplewho avoid dairy orwho are lactose intolerant.The twomain forms ofcalcium in supplements are carbonate and citrate. Calcium carbonate is morecommonlyavailableandisbothinexpensiveandconvenient.Thecarbonateandcitrateformsaresimilarlywellabsorbed,andbothcanbetakenwithorwithoutfood. One caveat, however, relates to people who don’t make much stomachacid,asisthecaseforthosetakingaproton-pumpinhibitororhydrogenblocker(moreonthiscomingrightup).Inthisscenario,takingthecalciumsupplementwith a meal is best. Other calcium forms in supplements or fortified foodsinclude gluconate, lactate, and phosphate. Calcium citrate malate is a well-absorbedformofcalciumfoundinsomefortifiedjuices.Howwellyourbodyabsorbscalciumfromasupplementdepends,inpart,on
howconcentratedelementalcalciumisinthatsupplement.Absorptionishighestindosesequaltoorlessthan500milligrams.So,forexample,ifyouliketotake1,000milligramsofcalciumperdayfromsupplements,it’sidealtosplitthedoseandtake500milligramsatatime,twoseparatetimesduringtheday.Thosewhotakeaproton-pumpinhibitorlikePrilosecorNexiumtocontrolacidrefluxandgastroesophageal refluxdisease (GERD),orTagametorZantac (whichworka

differentwaybuthavethesameeffectofinhibitingtheproductionofacidinthestomach), need to be extra careful about getting enough calcium. Becausestomachacidhelpsthebodyabsorbcalciumbydissolvingthecalciumpill,thusfreeing the calcium so it can be absorbed by the small intestine, loweringstomachacidlevelsmaystopitsproperabsorption.In2006,theJournaloftheAmerican Medical Association published a study suggesting that long-term(morethanayear)useofproton-pumpinhibitorsinhighdosesincreasedtheriskofhipfractureby245percent.Thesubjectsinthestudywereallovertheageoffifty,andtheresearcherssaidtheeffectswereparticularlyexaggeratedinpeoplealreadyatriskofosteoporosis.However, if you take your calcium pill with ameal, as yourmeal is being
ground up in the stomach so, too, is the calcium pill—without the need forstomachacid.ThisiswhyItellmypatientstotaketheircalciumpillwiththeirmeals.Some people who take calcium supplements experience gas, bloating,
constipation,oracombinationofthesesymptoms.Thesesymptomscanoftenberesolved by spreading out the calcium dose throughout the day, taking thesupplementwithmeals, or changing the brand of supplement used. The olderyou get, the harder it becomes to produce adequate stomach acid, as you didwhen you were younger (and able to down just about anything withoutgastrointestinalproblems).For thisreason, takingacalciumsupplementwithamealisbest.SupplementsthatcombinecalciumandvitaminDareanevenbetteroption,
asthevitamin,onceitgetsactivatedintheliverandkidneys,increasescalciumabsorption and provides other health benefits. Vitamin D is essential to theuptake of calcium fromyour diet, helping the calcium to becomemore easilyabsorbedinthebloodstreamandbones.
Becauseofitsabilitytoneutralizestomachacid,calciumcarbonateisfoundinseveralover-the-counterantacidproducts,suchasTumsandRolaids.Thusthesedrugsservetwopurposes—calmingstomachacidandprovidingbioavailablecalcium.Thefactthatyou’rechewingthecalciummakesiteasilyabsorbed.

TheDietFactor
Given the general state of our dietary habits,whereby processed foods takecenterstageinthelivesofmillions,Ithinkaplausibleargumenttoexplainwhymany Americans fail to meet their calcium needs is the mere lack of goodnutrition.What’smore,eatingahealthydiet isa little-knownbutextremely important
waytopreventskincancer.A1995studypublishedintheInternationalJournalofCancerreportedthatpeoplewhoatealow-fatdiethad90percentlesschanceofgettingskincancerthanthosewhoateahigh-fatdiet.Conversely,adiethighinfatshortensthetimebetweenUVexposureandtheonsetofskincancerandincreasesthenumberoftumorsthatdevelop.Accordingtothissamearticle,themagnitudeofthedietaryeffectisalmostdirectlyrelatedtotheamountandkindoffatconsumed(saturatedfatappearstobemostcloselyrelatedtoskincancer).Unfortunately,foracenturynow,theAmericandiethasbeengettinghigherin
fat—especially in the extra-unhealthy saturated fats. This may partly explainwhyskincancerrateshavegoneup,aswellasdiabetesandheartdisease.TheaverageAmericandietisabout16percentsaturatedfat,whereasmostqualifieddieticians will tell you it should be nomore than one third of that. Tomakematters worse, there has been a trend toward fad weight-loss programsadvocatinghighfatcontent(theAtkinsdietisprobablythebestknownofthese).Leaving aside whether these diets actually work in the long term to help
peoplekeepweightoff,dietshigh in saturated fatmaycauseavarietyof life-
threatening health problems and probably contribute to skin cancer, not tomention all other types of cancer. But you don’t necessarily have to go on atraditional“diet”toachievetheresultsyou’relookingfor.Youjustneedtostartmovingtowardfoodslowerinsaturatedfatandtrytolimitorevictthosefoodsthat contain excessive amounts of fat—which is typically found in processedproducts(whichalsousuallycontainlotsofsaltandsugar)andmarbledmeats.Thereareseveralexcellenteatingplansouttherethatadvocateeatingthisway.It’sbeyondthescopeofthisbooktoofferspecificsontheperfectdiet,butI’ll
saythatahealthyeatingregimencallsforplentyoffreshfruitsandvegetables,high-qualityproteins (“high-quality”meaning theyare low in saturated fatbutcanbehigh inhealthymonounsaturated fats,as is thecasewithwildsalmon),andwholegrains.
TheBenefitsofBoostingCalcium:AlltheWaytoWeightLoss
Anestimated44percentto87percentofAmericansdon’tgetenoughcalcium,including children, who are falling severely short on this mineral critical forproper growth and development. Unfortunately, there are not usually anyobvious symptoms of a calcium deficiency, and people can go for years in acalcium-deficient state before any noticeable problems occur. Most of thesymptoms thatmightoccurdue toacalciumdeficiencywouldbe seenonly ifcalciumlevelsare lowin theblood.Because thebodyisverygoodatkeepingthe blood calcium levels steady (often at the expense of bone strength),mostpeoplewillneverexperienceanysymptomsofadeficiencyuntiltheirbonesaresignificantlyweakenedandfracture.Thebenefitsofboostingcalciumgofarbeyondtheobviousreasonsofhelping
tonormalizecalciumlevelsandensurehealthyphysiologicalprocessing.Severalrecentstudieshaveshown linksbetween increasedcalcium intakeandspecifichealthbenefitsinanarrayofconditions.Premenstrual syndrome. As noted earlier, Dr. Susan Thys-Jacobs of St.
Luke’s-RooseveltHospitalCenter inNewYorkfounda50percentdecrease inPMS symptoms forwomen given calcium supplementation, compared to a 30percent decrease for the placebo group. Thys-Jacobs concluded that “no otherdrugaddressesall thesesymptomsaseffectively.”Anotherreport,basedonanepidemiological studyofmore than two thousandwomen, found a strong linkbetween calcium and vitamin D intake and the risk of PMS. The authors

concludedthat“ahighintakeofcalciumandvitaminDmayreducetheriskofPMS.”Weight loss. Other studies at Creighton University, the University of
Tennessee, and Purdue University have demonstrated links between increasedcalcium intake and weight loss. One of the researchers, Dr. Michael Zemel,reported thatcalciumplaysakeyrole inmetabolicdisorders linked toobesity,andalsothathighcalciumdietsleadtothereleaseofahormonethatleadstothebody’s fat cells losing weight. This is the basis on which the milk industryclaimsitsproducthelpscinchawaistline,bolsteringthe“itdoesabodygood”mantra.Highbloodpressure.Clinicaltrialshavealsolinkedlowcalciumlevelswith
highbloodpressure.Argentineanresearchshowedthatwomenwhotakecalciumduring pregnancy may lower their children’s future risk of blood-pressureproblems. Studies done at Rockefeller University showed that calciumsupplementswereofgeneralbenefittobothmotherandbabyduringpregnancy.Coloncancer. Researchers at theUniversity ofNorthCarolina andCornell
Universityhavelinkedcalciumwiththepreventionofcoloncancer.Stroke.Harvardscientists reportedona linkbetween increasedcalciumand
thepreventionofstroke.Cholesterol. Researchers at the University of Texas Southwestern Medical
CenterhaveshownthatincreasedcalciumcanlowerLDL(bad)cholesterol.
TheExFactor
Youknowyou can’t get through a health bookwithout amention of the “ex”factor, or exercise. I won’t go into exhaustive detail about the benefits ofexercise that you already know, if even subconsciously, by now. Iwon’t evenbroachthesubjectofexercise’sbenefitsinweightcontrol,mood,cardiovascularhealth,andmetabolism.ButIwillsaythatphysicalactivitydirectlytiesintotheconversation about bone and muscle health. Physical exercise, especially theweight-bearingkind,putshealthystressonyourbonestokeepthemstrongandforcethemtobeevenstronger.Italsoworksthemusclesthatkeepyounimbleandquickonyourfeet.Youngwomenandmenwhoexerciseregularlygenerallyachievegreaterpeak
bone mass than those who do not. Exercising allows us to maintain musclestrength, coordination, and balance, which in turn helps to prevent falls and
related fractures. This is especially important for older adults and peoplewhohave been diagnosed with osteoporosis. The exercise you choose needn’t becomplicated,boring,oroverlychallengingordemanding.Thebestexerciseforyourbonesisthekindthatforcesyoutoworkagainstgravity,evenifit’ssimplybyworkingagainstyourownbodyweight,as is thecase formodern formsofyoga, mat Pilates, and the use of a resistance band. Other examples includeweighttraining,hiking,jogging,climbingstairs,tennis,dancing,and,ofcourse,walking.It’stheconstantpoundingonthegroundthattranslatestobettermusclestrength in the hips and lower back, maintaining or increasing bone density.Thesearethetwoplacesthatareathighestriskforfracture.Sopicksomethingyoulikeandjustgodoitmoreoften.

CHAPTER10
Step3:SupplementSafely
HowtosupplementasabackupplanWheneverIgiveapresentation,oneofthefirstthingsthathappensisthatalltheattendees rush to their local pharmacy and buy a big bottle of vitamin Dsupplements.Whentheyhearthestoryandappreciatewhat’sgoingon,theygetreligion. (You can hear one of my presentations if you go to my Web site,www.drholicksdsolution.com.)Iwas in SouthAfrica, for example, giving some talks for a pharmaceutical
company,andthepresidentandCEOofthecompanywassittingintheaudience.Immediatelyaftermytalk,hewentoutandgot1,000-IUtabletsofvitaminDforhimselfandhisfamilymembers.Oncepeoplehearthestoryandappreciatethatthere is no downside to increasing your vitamin D intake and there is asignificant upside, everybody complies. But it’s incomprehensible to manyphysiciansthatthissimplevitaminthateverybodyhasalwaystakenforgrantedcanhaveallofthesehealthbenefits.Thereisstillgreatskepticism.The driving force in convincing the medical community of the insidious
consequencesofthevitaminDdeficiencyepidemichasbeenmainstreammediaoutlets, which promote the health benefits of vitamin D. This has includedcoverageinpopularmagazinesandnewspaperssuchasFitness,VogueandTeenVogue, theWall Street Journal, and even theEnquirer—both in print and ontelevision in appearances by representatives of these publications. This hascreatedawaveofawarenessfromthelaypublictodoctors,asmediacoverageofthis information inspires viewers and readers to ask their doctors for a 25-vitaminDtest.Somearemetwithhesitant, incredulousdoctors. It’sonlyafterpatients’ insistingon the test thatdoctors reluctantlyorder it and likely find—much to their surprise—that theirpatientsarevitaminDdeficient.And testing

frombydoctors’officesofalloftheirpatientscommences.MycolleaguesandIalsofindthatifwecanconvincephysicianstoorder25-
vitamin D assay on a couple of their patients, all the results come back asdeficient.This oftenwill convince the doctors.They’ve got religion, and nowtheyorderthetestonalltheirpatients.TheyrealizethatvitaminDdeficiencyisamajorhealthissue.We’vestillgotalongwaytogoinspreadingthismessageaboutvitaminD,butthosewhoaregettingitreallyappreciateit.AlthoughIstaunchlyadvocatethatsunlightbemostpeople’smainsourceof
vitaminD,vitaminDsupplementationgetsmysealofapprovaltomakeupforanyshortfallinthevitaminDobtainedfromsensiblesunexposure.BecauseyoucannotoverdoseonvitaminDfromsunlight,there’snothingwrongwithtakingasupplementtosatisfythat“just-in-case”factor.Moreover,Iknowthattherewillbe some people who just won’t expose themselves to sunlight withoutprotection.Thischoicemaybebasedonpersonalfears,oritmaybemadeinauniquecaseinwhichapersoncannotgointosunlightforhealth-relatedreasons.Peoplewho take certain antibiotics or antihypertensionmedications thatmakethemexceptionallysunsensitive,forinstance,mayopttoavoidthesunentirelyand choose supplementation. Supplementsmay also be useful for peoplewithtype 1 skin, who have trouble going out into the sun without getting burnedrelativelyquickly,andthosewiththerarediseasexerodermapigmentosum,whocannotexposetheirskinatalltothesun.Alwaysrememberthatsupplementsareno remedy for poor nutritional habits, so it’s important to eat awell-balanceddiet.Otherwise,anutritionalsupplementwillbeineffective.If you live at a high latitude but spend plenty of time outside during the
summermonths,thentakingavitaminDsupplementduringthewintermaynotbe necessary, but itwillmake absolutely sure you have healthy 25-vitaminDlevels year-round. To find out if you have enough 25-vitaminD, you can getyourstatuscheckedwithabloodtest;atyourrequest,yourdoctorwilldrawasmall amount of your blood and send it off to a lab for testing (as explainedearlier,makesurethedoctortestsforyour25-vitaminDlevels,notyourlevelsof activated vitamin D, also known as 1,25-vitamin D). You want your 25-vitamin D levels to be in the range of 30 to 100 nanograms per milliliter ofblood.Anythingbelow20nanogramspermilliliter isconsidereddeficient,andanythingbetween21and29nanogramspermilliliterisinsufficient.
OutdatedScience,InadequateRecommendations
In1995,whentheInstituteofMedicine(IOM)formedaninternalcommitteeofwhichIbecameamember,wewereaskedbytheNationalAcademyofSciencesand the Food and Nutrition Board of the Institute of Medicine to make arecommendation on vitamin D intake based on published literature. Wedeliberated for two years. Dr. Robert Heaney, Dr. Bess Dawson-Hughes, Dr.Connie Weaver, Dr. Bonny Specker, and I were the experts in the field ofcalciumandvitaminD.Werealizedevenbackthen,basedonourownworkthathadyetnotbeenpublished,thatourrecommendationswereprobablygoingtobeinadequate; that is,althoughweknewfromourunpublishedinvestigationsthatthe recommendations should be higher than what we suggested, we wereobligatedtomakerecommendationsbasedonlyonpublishedstudies.Therewas essentially none thatwas very relevant at that time.Most of the
literature in the1940sand1950sshowedthatgiving100IUofvitaminDtoachildwouldprevent rickets,sodoubling thedose to200IUwas thought tobeboth effective and safe for preventing rickets in children. But rickets is thegrossest manifestation of vitamin D deficiency; we now have a much moreadvancedknowledgeabouttheeffectsofvitaminDdeficiencyfarbeyondricketsalone. Before 1997, when the IOM issued the new recommendations, therecommendationwas 200 IU for everybody. In fact, itwas determined by theInstitute ofMedicine in 1997 that therewas insufficient evidence to establishany recommendeddailyallowanceforvitaminD.Instead,aso-calledadequateintake(AI)—alevelofintakesufficienttomaintainwhatwasthenperceivedasahealthy blood level of 25-vitamin D—was established. The recommendationsremainunchangedat thiswriting.Thegoodnewsis thatanewpanelhasbeenformedandplanstoissuenewrecommendationsthisyear.Wefeltthatwehadmadeatleastsomecontributionbecausewecould,based
ontheliteraturepublishedbefore1995,showthatatleast400IUwasneededtobenefitadultsages fifty tosixty-nine,and600IUforpeopleagedseventyandolder. But now many experts agree that both children and adults need aminimumof 1,000 IUof vitaminD a day (and preferably 2,000 IU a day) tomaintainabloodlevelof25-vitaminDthatweconsidertobehealthful,whichisabove30nanogramspermilliliter.It’sabitofashamethateventhoughallthisfascinatingandalarmingresearch
hasemergedsince1997tochangeourperspectiveonvitaminD,thegovernmentcontinues to advocate subadequate daily allowances. It takes time for suchrecommendations toformallychange, though.I think that thisyear,withalloftheemergingscientificstudiesbeingpublishedinwell-respectedpeer-reviewed

journals, the newly formed IOM panel will suggest significant increases invitaminDintakeforchildrenandadults.We’vealreadywatchedgroupswithinthe medical industry, such as the American Academy of Pediatrics, publiclyannouncechangestotheirownrecommendationsinlightofrecentfindingsthatcall attention to the vitamin D deficiency pandemic and its consequences forinfantsandyoungchildren.These scanty government recommendations are also holding back the food
and multivitamin industry, as they continue to base fortification andsupplementationlevelsontheInstituteofMedicine’soutdatedrecommendationsregardingthesafeupperlimit,whichis1,000IUforchildrenuptooneyearand2,000 IU for children older than one year and all adults. Most Europeancountries still forbid the fortification of most foods with vitamin D. That’sbecauseof anobservation in the1950s,which turned out to be incorrect, thatvitaminDintoxicationinyoungchildrenwasduetotheoverfortificationofmilkwith vitaminD.As a result of public outrage, European governments bannedfortification of dairy products with vitamin D. They even went so far as tooutlawvitaminDinskincreams.Inmyopinion,youcouldeasily take5,000IUofvitaminDaday,probably
forever. I typicallyrecommendtaking1,000to2,000IUofvitaminDaday—that should be adequate along with a multivitamin that contains 400 IU ofvitamin D. I personally take 2,700 IU of vitamin D a day (400 in mymultivitamin,another2,000fromastand-alonevitaminDsupplement,and300fromthreeglassesofmilk).Inthespring,summer,andfall,Icyclewithoutsunprotectionforaperiodoftimeandthenputsunprotectionon.Weknowfrommyown study, in collaboration with Dr. Robert Heaney, that you can take up to10,000IUofvitaminDadayforatleastfivemonthswithouttoxicity.Youwouldhavetotakeprobably30,000to50,000IUofvitaminDadayfor
long periods of time,months or years, to become vitaminD intoxicated. Thetypical vitamin D intoxication incident is inadvertent, and usually, more thanseveral hundred thousand IU tomillions of IU have been ingested daily for aprolongedperiodoftime.VitaminDintoxicationisoneofthemostraremedicalconditionsworldwide.Youonlyneedtobecarefulifyouhaveagranulomatousdisordersuchassarcoidosis,a rareautoimmuneconditioncharacterizedby theformation of small lumps of cells (“granulomas”), usually in the lungs,wherethey can interfere with breathing, but sometimes in the skin, brain, and otherorgans.
HowMuchtoTakeandWhen
Ofcourse,themajorissuewithobtainingvitaminDfromapillisthatyouhavetoremembertotakethepill.Nowadays,it’seasytofindsupplementswith1,000IUoreven2,000IUpertabletorcapsule.Thiswasn’tthecasejustafewyearsago. You can readily find supplements where you find other vitamins. Anynationalbrandwilldo.ThereisevenaliquidsupplementfromWellessethathas500 IUper teaspoon,which is ideal forchildrenandadultswhodon’twant totakeapillorhavetroubleswallowingpills.Everyonefromtheageofoneonwardshouldbetakinga1,000IUsupplement
dailyinadditiontoamultivitaminthathas400IU.Inall,youwillbeingestingbetween 1,500 and 2,000 IU of vitamin D daily among the supplements,multivitamin, and dietary sources. That’s perfectly fine and right on target.(Don’t forget to include calcium by drinking milk or orange juice containingcalcium and vitaminD.) If your doctor tests you and determines that you aredeficient,thenyoucancertainlyupthedosageto5,000to6,000IUadayunderyourdoctor’scare(again,thiswillbeinadditiontoyourmultivitamin,soyou’llbeingestingupto6,400IUadayfortwotothreemonthsinsupplementform).Depending on your level of deficiency, your doctor may prescribe a moreaggressive treatment,withhighdosesofvitaminDforacertain timeperiod. Itreatwith50,000IUofvitaminD2onceaweekforeightweeks(which is theequivalentoftaking6,000IUaday)tofillanemptyvitaminDtank.Tomaintaina full tank, I then administer 50,000 IU once every two weeks, which is theequivalentof3,000IUaday.Remember, too, that it doesn’tmatter whether you take vitaminD2 orD3,
thoughD3appearstobethemostavailableformnowonthemarket.(D2istheonlyformavailableasapharmaceutical.)Youalsoneedn’tworryaboutwhenorhowtotakeit.VitaminDsupplementscanbetakenwithfood,withmilk,oronanemptystomach.Youdonotneedtoingestthemwithfattyfood,contrarytoapopular belief. I do suggest takingyour vitaminD supplementwhenyou takeyourmultivitaminandanyothersupplementsyoumightalreadybe taking;getinto the routineof taking thispill everyday.Agingdoesnot affect thebody’sabilitytoabsorbvitaminDeitherfromthedietorfromsupplements.Andthereis no advantage to taking smaller dosesmore frequently rather than one largedoseof1,000to2,000IUaday.Thisalsomeansthatyoucouldtakeeither1,000IUofvitaminDonceadayorseven1,000IUofvitaminDsupplementsoncea

week.Itwillworkthesameway,thoughIthinkthisisanimpracticalwaytogo,asyouaremorelikelytoforget.Ifyouforgetjustoneday,youcantaketwopillsthenextday.
Irecommendthateveryonetakeatleast1,000IUofvitaminDaday(andpreferably2,000 IU) alongwith amultivitamin containing400IU of vitaminD, all year long. This will not cause any buildup ofvitamin D in the body, and by following this routine, you are lesslikelytoforgetitinthewinter.Fornewbornsintheirfirstyearoflife,I recommend at least 400 IU a day and up to 1,000 IU. This isperfectly safe and may be more beneficial than just 400 IU(remember, Finnish children who took 2,000 IU a day for the firstyear of life had a 78 percent reduced risk of developing type 1diabetes31years later).Irecommendthatchildrenbetweenoneandtwelve years old take at least 1,000 IU of vitamin D a day. For abreakdownofallmyrecommendationsbyageandcondition,seethetableonthefollowingpage.
RectifyingavitaminDdeficiencytakestime.Youwon’tseebloodlevelsriseovernight.Frommyexperience,healthyadults taking1,000IUofvitaminDadaycanreachtheirpeakbloodlevelinfivetosixweeks.WhenItreatseverelydeficient patientswith50,000 IUofvitaminD2once aweek for eightweeks,theirbloodlevelbeginstoincreasebythefirstweekandlevelsoffbythefourththroughsixthweeksoftreatment.
Forevery100IUofvitaminD2orvitaminD3youingest,youraiseyourbloodlevelof25-vitaminDby1nanogrampermilliliter.
“WhyDon’tIJustTakeaSupplement?”
That’s the attitudeofmanypeoplewhen theyhear thenew findings about thebenefitsofvitaminD.TheirrationaleisthatbytakingavitaminDsupplement,

theycanavoidthehealthrisksofsunexposurewhilestillavailingthemselvesofallthehealthbenefitsofthisvitamin.Unfortunately,it’snotthatstraightforward.For one thing, vitamin D taken orally—whether in whole foods or pill
supplements—maynotprovideasmuchbenefitas thevitaminDyougetfromthe sun. The vitamin D you get from sunlight stays in your body longer andthereforeprovideslonger-lastingbenefits.Inaddition,sunlightcausesyourbodytomake not just vitaminD itself but also vitaminD-related substances calledphotoisomers.Wearecurrentlydoingresearchonthesephotoisomers,whicharemade in the skin and could offer health benefits, butwhich are not present insupplements.
Keep inmind that neither vitaminD-rich foods nor supplementswill causeyour body to produce feel-good substances such as beta endorphins, whichcreatethesenseofwell-beingyoufeelafterbeinginthesunorusinganindoor-tanningfacility.Andnothingbutthesuncanregulateyourcircadianrhythmandmaintainahealthysleep-wakecycle.Finally,unlikevitaminDsupplements,neithersunexposurenoratanningbed

can cause vitamin D toxicity. Though difficult to do unless you’re takingsupplements thatmistakenly contain toxic levels of vitaminD, if you overusevitamin D supplements you are at risk of vitamin D toxicity. You cannotoverdosebyspendingtoomuchtimeinthesunoronatanningbed.VitaminDtoxicitycausesanumberofserioussymptoms,includingnausea,vomiting,lossof appetite, constipation, increased thirst, increased frequency of urination,depression, and weight loss. Elevated calcium levels brought on by thisconditioncancauseavarietyofphysicalconditions,suchascalcificationofthekidneys,causingkidneyfailure,calcificationofthemajorarteries,andconfusionandbizarrebehavior.
VitaminDtoxicityisdefinedashavinglevelsof25-vitaminDabove150nanogramspermilliliterwithhighbloodcalcium.
Idon’tmeanthistoalarmyou,however.VitaminDtoxicityisextremelyrareand happens only in unusual circumstances. My chief message here is theimportanceofbothlettingsomesunshineintoyourlife,asnatureintended,andsafeguardingyourvitaminDlevelsbytakingasupplementdailythroughouttheyear.Thereisnoharmin“doublingup”yourvitaminDintakethroughsensiblesunexposureandsupplementation.
Double trouble:Do not double or triple up on yourmultivitamin togetmorevitaminD.Thiscanbedangerousbecauseofothervitaminsthat you’d subsequently also be doubling or tripling up on and thatcan be toxic at high levels. Excessive amounts of vitamin A, forexample,havebeenassociatedwithbirthdefectsandosteoporosis.
SupplementationDuringandAfterPregnancy
Therulesforpregnantwomenmightsurpriseyou.TheIOMrecommendationatthiswriting (200 IU of vitaminD a day) is inadequate for both pregnant andlactating women. My colleagues and I reported that 76 percent of pregnant

womenwhotookaprenatalvitamin(containing400IUofvitaminD)anddranktwoglassesofmilkdaily,thusgetting600IUofvitaminDaday,werevitaminDdeficientwhentheygavebirth.Andfully81percentoftheirnewbornswerevitaminDdeficient.Inmyopinion,pregnantwomenneedtobeonatleast1,400and up to 2,000 IU of vitamin D a day to maintain their blood level of 25-vitamin D above 30 nanograms per milliliter. A study currently under waysuggests that a lactating woman can take as much as 4,000 to 6,000 IU ofvitaminDperdaywithoutcausinganytoxicityeithertoherselfortoherinfant,and,more importantly, that it takes thisamountofvitaminD tobe transferredintohermilktosatisfytheinfant’srequirement.
Human breast milk today contains little vitamin D today becauselactating women take only 400 IU in a multivitamin and may getanother400IUfromacalcium+vitaminDsupplement.Thisisafarcry fromourhunter-gatherer foremothers,whoweremakingseveralthousand IUofvitaminDaday that found itsway into themilk tosatisfytheirinfants’needs.
Thisisanongoingstudy,andwedonotknowwhetherthereareanylong-termconsequences for either themother or the infantwhen themother is ingesting4,000to6,000IUofvitaminDdaily.Frommyexperience,Iwouldsuspectthatthestudywillshownotoxicityandthatitisperfectlysafetotakethisamountofvitamin D. Until the results come out, I will refrain from advocating thatbreastfeedingmotherstakesuchahighdoseofvitaminD,butI’dtellanynewmothertoatleastincreaseherintaketo2,000IUaday.Becausemostpregnantwomen take a prenatal vitamin, which will have 400 IU of vitamin D in it,addinganother1,000IUto2,000IUinsupplementformshouldbeconsideredthebareminimum.Thisisn’taboutjustthemother’shealth,butalsothatofherunbornchild.Morethan50percentofinfantsbornintheUnitedStatesareborninavitamin
D-deficient or insufficient state. As a consequence, they will not reach theirfullestpotential inheightandbonedensity.Theirconditioncan thenworsen iftheyarenotgivenenoughvitaminDduringinfancyandchildhood.OneofthechiefculpritshereisthelackofvitaminDinhumanbreastmilktoday,causedbylactating mothers’ own vitamin D deficiency. It contains very little. Humans
evolved to livemuch of their lives outdoors. For centuries people in agrariansocieties spent hours outdoors,making thousandsof units of vitaminDaday.Thus,thisvitaminDcouldbestoredinthemilkfortheinfant’sneeds.SincetheIndustrialRevolution, our bodies haven’t evolved to accommodate the shift tolivingmostlyindoors,essentiallyevictingthesunfromourlives.As I outlined earlier, studies have linked vitamin D deficiency during
pregnancytoanincreasedriskofthechild’sdevelopingschizophreniaduringhisorheradultlife.ThisgoestoshowhowcriticalvitaminDisinthedevelopingbrain and psychological faculties of a fetus, even though we may not fullyunderstandalltheintricatemechanismsbywhichvitaminDhelpssafeguardthehealthydevelopmentofahumanveryearlyinlife.Onethingiscertain:vitaminDreceptorsarepresentinhumanembryos.Andit’sbeenshownthatvitaminDdeficiencyduringpregnancyisariskfactorforproblemsnotonlyinfetalgrowthandcalciummetabolismbutalsointhedevelopmentofthefetalimmunesystem.Don’tforgetthatvitaminDalsoreducestheriskofpregnantwomendevelopingthe serious complication preeclampsia. It alsomaymake childbirth easier andreducetheneedforaC-section.
Head sweating at night is one of the hallmark signs of vitamin Ddeficiencyinanewborn.
Several studies have proved that women who take vitamin D duringpregnancy also protect their young children from upper-respiratory-tractinfectionsandwheezingdiseases.Low levelsof25-vitaminD, inbothmotherand child, are also associatedwith a high risk of low birthweight and of thechild’sdevelopingautoimmunediseasessuchastype1diabetesandasthma.Justrecently, in the summer of 2009, a Finnish report published in the journalClinicalandExperimentalAllergystatedthattakingvitaminDduringpregnancywas inverselyassociatedwithasthmaandallergic rhinitis (inflammationof thenasal passages) in five-year-old children. That is to say, thewomenwho tookvitamin D during pregnancy were less likely to have children suffering fromallergiesandasthmabythetimetheywerefiveyearsold.Someexpertshavegoneas farasmakinganassociationbetweenvitaminD
deficiencyandautism,butthereisnocurrentproofthatthetwoarerelated.Weneedmoreclinicaltrialstoexplorethatconnectionfurtherundertherigorsofthe

scientific method. (However, there are vitamin D receptors in the brain, andvitaminDdeficiencyhasbeenassociatedwithpoormuscle function; thus, it’simportant to ensure that children with autism have an adequate amount ofvitaminD.Autisticchildrenareoftenindoors,andvitaminDdeficiencycauseslethargy,muscleweakness,andadepressedmood.)Inchapter2IretoldthedinosaurextinctionstorywithafocusonvitaminD
deficiency. I posited that pregnant femaleswith a severevitaminDdeficiencywouldhavehadadifficulttimeproducingviableegghatchlings.Overtime,thedwindling numbers of healthy dinosaurs able to procreate could havecompounded other challenges they faced in a harsh environment that was nolongerconducivetotheirsurvival.Unlikethedinosaurs,humans—byvirtueofouradvancedbrainsandabilityto
develop technology—have managed to circumvent challenges posed by ourcircumstances,conditions,andinsomecasesourenvironment.(Thoughthislastis increasingly the subject of debate over how our impact has altered theenvironment and whether we may someday face a fate similar to thedinosaurs’—nomatterwhattechnologiesorbrainystrategiesweemploy.)We’velearned, forexample,howto transport largeamountsofcleanwater todistant,dry locations to sustainpopulations;we’vemastered the art of agriculture andcan fortify foods to boost nutrition. And we’ve developed ways to prolonghuman life and intervenewithmedicinewhen life-threatening situations arise,suchaswhenawomancannotgivebirthnaturallyforwhateverreason.Caesarean sections have been around since the Roman Empire, though the
namemistakenlylinksthemtoJuliusCaesar,whowasnotbornbythissurgicalmethodofdelivery.Itusedtobethedeliverymethodoflastresortwhennaturalchildbirth was not possible because of the health of or risks to the baby, themother,orboth.ButinthelastdecadeC-sectionshavegainedpopularityamongwomen who prefer to schedule their deliveries (and not endure the pain ofnaturalchildbirth)ratherthanwaitfortheirchildtoarrivevaginallyaftergoingintolabor.AlthoughtheWorldHealthOrganizationrecommendsthattherateofcaesareansectionsnotexceed15percentinanycountry,theU.S.rateofbirthsbyC-sectionwas31.1percentin2006,thelastyearwithavailabledata.This trend may reverse itself, however, as new studies point to other risks
relatedtoC-sections.BecauseC-sectionsaremajorsurgery,theyentailtheusualadditionalrelatedrisks,fromtheuseofanesthesiatorespiratorydifficultiesandtheneed tostay longer in thehospital,whereboth themotherandchildareatriskofdevelopingahospital-borneinfection.
Forwomenwhoplanonvaginalbirth,thenewsthattheyneedaC-sectionisnotalwayswelcome.TheyarenotlikelytobetoldthatavitaminDdeficiencycouldbetoblame,butitmayjustbe.In2008,AnneMerewoodandDr.HowardBauchnerandmyteamreporteda
landmark study indicating thatwomenwhohad low25-vitaminD levelsweremore likely to have aC-section.The findingswere part of a larger study thatlooked at the 25-vitamin D levels of women within seventy-two hours afterdelivery.NoneofthewomeninthestudyhadpreviousC-sections,andtherateofC-sectionsinthestudywas17percent.Wefound36percentofthesewomentobevitaminDdeficientand23percenttobeseverelydeficient.Weconcludedthatawomanwithlow25-vitaminDlevelsisfourtimesmorelikelytodeliverbyC-sectionthanawomanwithahigherlevel.What’s the connection?Howcan this be?VitaminDdoesn’t have anything
directlytodowithgivingbirth,doesit?The reason behind this is actually quite straightforward, and you can think
back to thosedinosaurs foramoment toseewhy.Childbirth requiresacertainlevelofstrengthtoendure.Afemaletryingtogivelivebirthmustundergolabor,whichcanlastforhoursordays.Thistraumatoafemale’sreproductiveorgansdemandsmuscle strength and abdominal power.Granted, if females had to beathletestogivebirththehumanracewouldn’texistasweknowit.Millionsofwomengivebirtheverydaywhocanhardlydoasit-up.ButI’mnotreferringtojusttheobviousmusclesemployedduringchildbirth.Theuterusitselfismadeofmuscle, and as such, it can becomeweak and lose some of its strength if theperson(oranyvertebrateanimal,forthatmatter,includingadinosaur)isoverallvitaminDdeficient.And if awoman’s birthingmuscles, including her uterus,areweak,thismayhinderherabilitytodeliverthebabyvaginally.
ClampingDownonPreeclampsia
One of the reasons a woman may find herself going in for an unplanned C-section is that she’s been diagnosed with preeclampsia. It’s among the mostcommon yet more severe complications during pregnancy, a disordercharacterized by suddenweight gain, fluid retention, high blood pressure, andswellinginthesecondandthirdtrimesters.Itcanevenlastforawhileafterthewoman has given birth. Other symptoms, including vision changes andheadaches, may not always appear in rapidly advancing cases. Preeclampsia
affects5percentto8percentofallpregnanciesandisthecauseof15percentofpremature births. Preeclampsia is one of the most perplexing enigmas ofpregnancyandhasnocure;patientswhosuffer from it aremonitoredby theirdoctorstopreventfurthercomplicationsthatthreatenthelifeandhealthofbothmother and child. Sometimes the condition can worsen to the point where adoctorwillinducelabor.IncollaborationwithDr.LisaBodnarattheUniversityofPittsburghSchoolof
the Health Sciences, my colleagues and I reported that the occurrence ofpreeclampsiawasfivetimeshigherinwomenwhose25-vitaminDmeasuredlowduring early pregnancy.We also stressed that even slightly low 25-vitaminDmeasurements in pregnant women may double the likelihood of having thedisorder. Even those who took prenatal vitamins showed a high risk for thedeficiency. This isn’t surprising given that prenatal vitamins don’t containenoughvitaminDforpropersupplementation.
MakingSureYourBabyGetsEnough
TheAmericanAcademyofPediatricsnowrecommends thatall children, frombirth through childhood, receive at least 400 IU of vitaminD each day.MostchildrencangetthisamountfromdrinkingthreetofourservingsofavitaminD-fortified infant formula, milk, or orange juice, but infants who are breastfedexclusively will need an additional supplement of at least 400 IU. As Imentionedearlier,WellessemakesaflavoredliquidvitaminDsupplementthatcanbemixedwithinfantformula,milk,ororangejuice.Itdelivers500IUperteaspoon.YoucanalsooptforamultivitaminthatcontainsvitaminDinitsmix.Speakwith your pediatrician aboutwhich one to choose. Bear inmind that Ibelieve400IUisthebareminimumandatotalof1,000IUshouldbeadvocated.Infantscanbeexposedtodirectsunlight,butyoushouldalwaysprotecttheir
faces,asyouwouldyourown.Atoneyearold,it’sfinetograduateachildupto1,500 IU vitamin D a day in supplement form. This can be in addition tofortifiedmilk, infant formula,multivitamins, and sensibleexposure to the sun.Troublegettingachildtoswallowatabletorcapsule?Grindoneupandmixitintoacupofmilkorjuice,orgetyourselfsomeliquidvitaminDfromWellesseoranothermanufacturer.

PuttingtheDinDiet
Though I’ve made it clear by now that it’s virtually impossible to obtain anadequate amount of vitaminD fromyour diet, Imust note thatmore fortifiedfoodsandbeveragesarelikelytoemergeonthemarkettohelpfillthegap.Thetop sources of vitaminD from diet are salmon (preferablywild),mushrooms,fortified orange juice and milk, fortified cereals, fortified bread, and fortifiedyogurt.Mushroomsmay seem like an unlikely source for vitamin D, but notonly do mushrooms naturally contain some vitamin D, growers are nowexposingtheirproducttoultravioletlighttoenhancethatvitaminDcontent.IncollaborationwithCoca-Cola,which ownsMinuteMaid, I did a study on thevitaminDcontentintheirpopularorangejuicebrand,showingthatitwasableto raise blood levels of 25-vitaminD in both children and adults. Below is achartshowingsourcesofvitaminD.
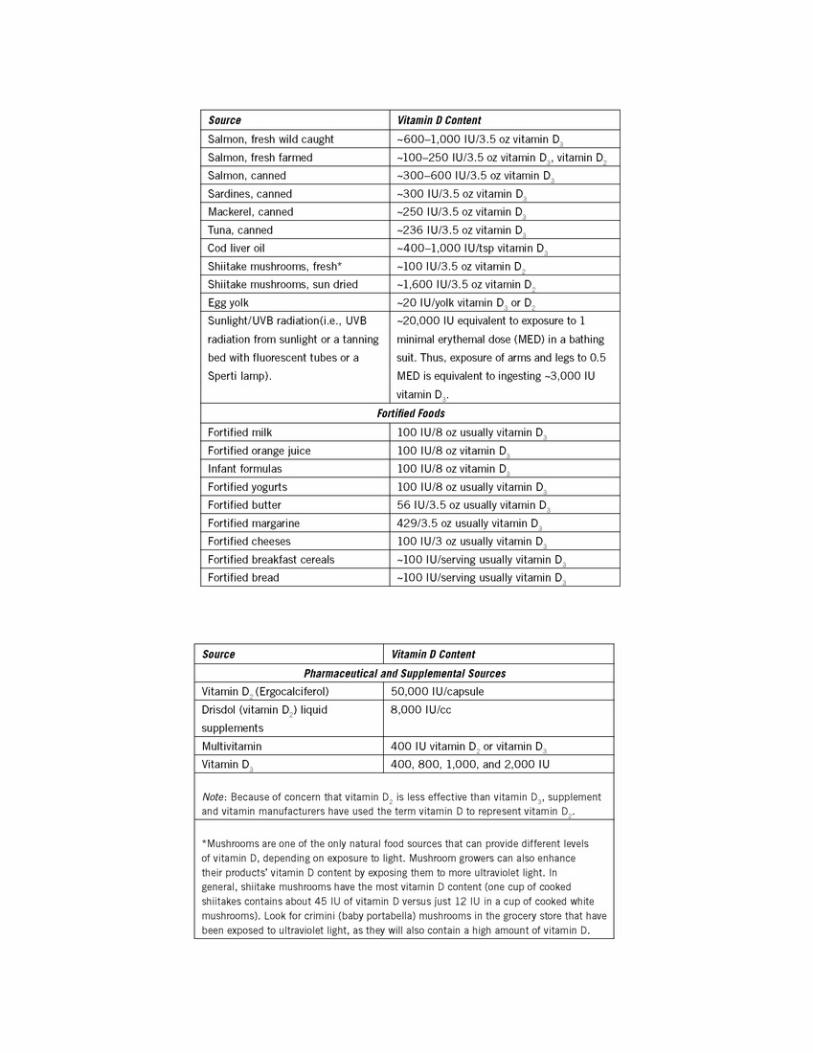

CHAPTER11
SpecialTreatment
OthercausesofvitaminDdeficiencyNodaypasseswithouthearingaboutanotherreportontheobesityepidemic.Noweek goes by without a magazine rack displaying countless publications thatshout out another trick to losingweight. Fast! Effortless! Fun! If it were thateasy,wewouldn’tseetheobesitynumberscontinuetogrowwithourwaistlines.Obesity-related conditions now account for nearly 10 percent of all medicalspending,havingdoubledinthelastdecade.It’shardtobelievethattheobesityrate could rise 37 percent in just eight years alone, but that’s exactly whathappened between 1998 and 2006—bringing a breathtaking one third of theadultAmericanpopulationinto theobesecamp.Whythespikeinsuchashorttimeframe?What reallywentonduring thoseyears thatmade it so incrediblyeasy(frankly,effortless)formillions—millions—ofindividualstosuddenlygainenoughweighttoqualifyforthisnewanddangerouslabel?Ourbodiescertainlydidn’tchange,fromanevolutionarystandpoint. It’snot
likewewokeupinthelateninetieswithbodiesthatcouldnolongermetabolizefoodproperly,butclearlyweweredoingsomethingtotipthescales.Now,thatwholediscussionastowhyandhowthisalloccurredisatopicforanotherbook.Mypointisthatwenowhaveaprobleminoursocietysomassivethatitcannolonger be considered uncommon. That is to say, obesity is a common healthchallenge today that gives rise topilesofotherhealth challenges.AndamongtheseisvitaminDdeficiency.Inthischapter,I’llshareinsights intounderlyingconditionsthataggravatea
vitamin D deficiency. Exposure to sunlight, diet, and supplementation aside,there are certain caseswhere keepingoptimal levels of vitaminD is a seriousuphillbattle.

ABig,FatProblem
Startingwiththeobesityissueislogical.It’scolossal,affectingsomanypeopleastobeuniversal.Itdoesn’tsingleoutadults;rather,it’sbeenreportedthatthecurrentgenerationofAmericanchildrenmayhaveshorterlifeexpectanciesthantheir parents because of the rapid rise in childhoodobesity.The report,whichwaspublishedina2005NewEnglandJournalofMedicinepiece,wentasfarasto say that childhood obesity could cut life spans by as much as five years.Clearly, it’snot theobesityper se that’s thekiller—it’s theassociateddiseasesand complications: type 2 diabetes, heart disease, stroke, kidney failure, andcancer.Thereportalsostatedthattheaveragelifeexpectancyofadults,roughlyseventy-sevenyears,hasalreadybeenadjustedfor theobesityepidemic.It’satleast four to nine months shorter than it would be if there were no obesity.Obesity, it turns out, is already shortening average life spans by a greater ratethan accidents, homicides, and suicides combined. We are, in effect, killingourselves.Idescribedearlierhowwe’veevolvedtostorevitaminDinfat.Thisallowsus
to have ample supplies on hand during the long winter months, when it’svirtuallyimpossibletomakevitaminD—whentheactivesynthesisofvitaminDfrom the sun is in hibernation until the spring. But humans did not evolve tocarrysuchcopiousamountsofexcessivefatthatthisfatbeginstohavenegativeeffectson thebody’smetabolismandhormonalbalance.Contrary towhatyoumightthink,overweightpeopledon’thavehigherlevelsof25-vitaminDduetotheirhigherfatcontent.Theyhavelowerlevels,becausetheexcessfatabsorbsand holds onto the vitaminD so that it cannot be used for bone building andcellular health.Unlike a normal-weight person,whose fat is continually beingrecycled so the vitaminD can be released, thosewith relatively immobile fatstorescannotaccesstheirvitaminD,whichisliterallylockedupintheiradiposetissue.Makingmattersworse,obesepeoplearefrequentlyvitaminDdeficienttostartwithbecausetheygooutsidemuchless,trippingaviciouscycle.
The price tag on obesity-related medical care is nearly 60 percenthigherthanexpensesforalltypesofcancercombined.
It’sbeenwelldocumentedbyDr.NormanBell andbyothers, includingmy

team,thatobesepeopletendtohavedeplorable25-vitaminDlevels.Mostobesepeoplehavemuscleweakness and aches andpains in their bones andmusclesandarelethargic.VitaminDdeficiencyisassociatedwithallofthosesymptoms.Myteamdidastudytoprovethepoint.Wetookobeseandnonobesepeopleandputthemintanningbeds.ObesesubjectsraisedtheirbloodlevelsofvitaminDonly50percentasmuchasnormal-weightindividuals.Tobesurethatthishadnothing to do with body surface, we also gave an oral dose of 50,000 IU ofvitamin D2 to obese and to nonobese individuals and saw exactly the samephenomenon—vitaminD levels roseabout50percent in theobese individualscomparedtothenonobeseindividuals.Clearly, themosteffective treatment for these individuals isweight lossand
higherdosesofvitaminDtocompensatefortheirimpairedabilitytokeepupthe25-vitaminD level in theirblood.Obesepeopleneed two to three timesmorevitaminDaday than thoseofnormalweight,soIadvisesuchpatients to takebetween3,000and6,000IUofvitaminDaday.Thisdoesnotentailanyriskoftoxicityandmayevenultimatelyhelpapersontoloseweight,givenvitaminD’spositive impact on insulin metabolism. It can also improve muscle strength,lessenachesandpainsinbones,muscles,andjoints,andinspirepeopletoboosttheiractivitylevel.Theweightlossalonewilllikelyhaveanimpactonmultiplemedical levels, decreasing all the risk factors for vitamin D deficiency. Asdiscussed earlier, the so-called metabolic syndrome typically seen in obeseindividuals is a collectionof symptoms, includingbelly fat,whichputsone athighriskofheartdisease,stroke,anddiabetes.Theheartbreakingtruthaboutbeingobese,asanyonesufferingfromthiscan
attest,isthatlosingweightisdifficult.Geneticsandenvironmentaside,themerecondition adds another formidable obstacle to surmount. And some of thatobstacle is linked to vitamin D and calcium. Studies have determined thatsunlight, UVB, and vitamin D help normalize food intake and blood sugar.Therefore,weight normalization is associatedwith higher levels of vitaminDandadequatecalcium.When the diet lacks calcium, there is an increase in fatty acid synthase, an
enzyme that converts calories into fat.Higher levels of calciumwith adequatevitaminDinhibitthisenzyme,whiledietslowincalciumincreasethisenzymebyasmuchas fivefold.Moreof thisenzyme’sactivitymeansmore fatgettingstored from calories coming in. In one study, genetically obese rats lost 60percent of their body fat in six weeks on a diet that had moderate caloriereductionbutwashighincalcium.Allratssupplementedwithcalciumshowed

increased body temperature, indicating a shift from calorie storage to calorieburning(aprocessknownasthermogenesis).What thismeans is that in thepresenceofcalciumandvitaminD, thebody
turns down the volume on this fat-storing enzyme.Without adequate calciumand vitamin D available, the body turns up the volume on this fat-storingenzyme,andwhatyouendupwithisjustthat—ahighervolumeoffatworkingagainst everything an individualwould like to see happen in his or her body.This is yet another reason to focus on upping calcium and vitamin D intakewhilereducingcaloricconsumptiontoforcethebodytoconvertfatintofuelandreduce theweight load.Asmuchasweightgaincan feel likeaspiral, so, too,cantheweight-lossexperience;asthepoundsfallaway,thedominoeffectofthebenefitsaddsupandhelpscatapulttheweight-losseffortsfurther.I’vewitnessedinnumerable transformations among peoplewho commit to losingweight andwho consequently change their vitamin D status along the way. One of mypatientswhocorrectedavitaminDdeficiencylostthirteenpoundsinsixmonths,whichforherwas“thoselasttenpounds.”
ObesitySurgery:ACruelParadox
In thesummerof2009,a surprisingstudyemerged from theMayoClinic thatthe Associated Press posted with the headline “Obesity Surgery May ThinBones, Causing Breaks. Bariatric Patients May Be More Likely to FractureHandsorFeet.”Itseemslikeacrueljoke.Whywouldobesitysurgeryleadtothinnerbones?
Wouldn’t losing all that fat reverse the obesity-related problems, includingvitaminDdeficiency?The irony in all this is that it turns out that obesity protects bones.Why?
Becausethebodyisn’tstupid;obesepeoplewouldcrushthemselvesundertheirownweightifthebodydidn’tincreaseitsbonemineraldensity.Whatwedon’tknowyet, though, iswhetherbariatricpatientsdoendupwithworsebonesorsimply go through a transition period as their bones adjust to their new bodysize. About fifteen million Americans are classified as extremely (morbidly)obese, defined as being one hundred pounds or more overweight. Diet andexercise alone don’t help these people enough to stave off diabetes and otherhealthproblems,whichiswhysurgeryisfastbecomingapopularoption.Therearecurrentlytwoformsofthesurgery,onethatinvolvesstomachstapling,called

gastricbypass,andanotherthat’slessinvasive,calledstomachbanding.Patientstend to lose between 15 percent and 25 percent of their original weight, anddiabetes dramatically improves. More than 1.2 million U.S. patients haveundergone the surgery in the past decade, 220,000 in the last year alone,accordingtotheAmericanSocietyforMetabolicandBariatricSurgery.Wein themedicalcommunityhave longknownthat radicalweight losscan
speed bone turnover, causing the breakdown of old bone to outpace theformation of new bone. Recent studies have shown that a year after gastricbypass, hip density among adult patients drops by as much as 10 percent.Stomachbandingcauses less thinningbecause it doesn’t changeasmuchhownutrientsareabsorbedintothebody.Wealsoknowthatgastricbypassmakesithardertoabsorbcalcium,promptingdoctorstoadvisetheirpatientstoincreasetheirintakeofcalciumandvitaminD.Whetherornottheycomplyisanyone’sguess. You would think that losing one hundred pounds of fat, with all thevitamin D in it, would boost 25-vitamin D levels, but my colleagues and Ishowed that it does not. The change in the transit time of food through thedigestivetractaddsanotherhurdletothebody’sabilitytoabsorbvitaminDfromthediet.Likewise,othernutrientsinthedietcanbedifficulttoabsorb.Teams of researchers are currently trying to get to the bottom of this
phenomenonandfindoutwhetherittranslatesintomorefracturesamonggastricbypasspatients.Inonealarmingobservation,sixyearsaftersurgerypatientshadmore hand and foot fractures than a control group and had a nearly fourfoldincrease over their rate of such fractures before the surgery. Adding to themysteryis that thebreakagewasto thehandsandfeet, rather thanotherareas.Arethesepeoplegettingmoreactiveintheirlighterbodiesandfallingmoreasaresult?Because somany teenagers resort to this surgery—at a timewhen they are
buildingtheirbonemass—there’sapressingneedtoexaminetheimpactamongadolescentsandhowtheyfarefurtherdowntheroadasaresultofthissurgery.Onequestionyettobeanswered:doesgastricbypasssurgerychangethebody’shormonalchemistrysuchthatitcannolongersupportoptimalbonestrength?Until now, bariatric surgery has called for annual screening of calcium,
phosphorus,magnesium,andalbumin(abloodprotein).Thisnewstudy,whichunderscores the increased risk of vitamin D deficiency among gastric bypasspatients,callsforaddingtothislistboth25-vitaminDandparathyroidhormone,thechiefhormonesincalciummetabolism.As with obese patients, I recommend that patients who have had gastric

bypasssurgerytaketwotofivetimesasmuchvitaminDasanormalperson—3,000to10,000IUdaily.Tocorrectadeficiency,Ihavegivenpatientsasmuchas50,000IUofvitaminD2threetimesaweekforeighttosixteenweekstogettheir blood level of 25-vitamin D up to between 30 and 100 nanograms permilliliter.ThenIputthemon50,000IUofvitaminD2onceortwiceaweekandmonitor their serum 25-vitamin D level every one to two months until itstabilizes. One caveat: often these patients are unable to digest the gelatincapsule that thepharmaceuticalvitaminDcomes in, so Ioftenadvise them tocutthecapsuleopen,putitintoaglassofskimmilk,swirlitaround,anddrinkthemilkwithout the capsule. Iwould implore all suchpatients to discuss thiswiththeirdoctor.Maintaininghealthylevelsof25-vitaminDpostsurgerycannodoubt assist in recovery, speed weight loss, and prevent this potentiallydevastatingboneweaknessanddensityloss.
ChronicKidneyDisease
Thisisnotasuncommonasyoumightthink.Chronickidneydiseaseaffectsonethird of the population, about the same number of peoplewho are obese. It’smainly seen in African Americans and is mostly due to hypertension, which,again,isariskfactorforvitaminDdeficiency.Thesadpartaboutkidneydiseaseis that it runs silently through the first three of five stages, so by the time apersonisdiagnosed,theprognosiscanbebleak.All patients with chronic kidney disease should be receiving vitamin D
supplementation so theymaintainablood levelof25-vitaminDof at least30nanogramspermilliliter;abloodlevelofupto100nanogramspermilliliter issafe.Theexactformoftreatmentwillvarydependingonthepatient’sbaselinevitamin D status. When I treat vitamin D deficiency in patients who are ondialysis,forexample,Itypicallyadminister50,000IUofvitaminDonceaweekforeightweeksasanoralcapsule,andonce theirblood levelof25-vitaminDpasses30nanogramspermilliliter,ImaintaintheirvitaminDstatusbyplacingthem on 50,000 IU of vitamin D2 once every two weeks. (This is what theNationalKidneyFoundation,initsso-calledKDOQIguidelines,recommends.)If you are diagnosed with chronic kidney disease, your doctor will likely
performa25-vitaminDtest.Haveadiscussionabouthowtosafelybringyourlevels up, which you will certainly benefit from. Formore information about
chronic kidney disease as it relates to vitamin D, go towww.drholicksdsolution.com and the National Kidney Foundation’s Web site(www.kidney.org).Forpatientswithstage3,4,or5kidneydisease,theirkidneysmaynotbeabletoproduceenoughactivatedvitaminD,andthustheymayneedtobetreatedwithactivatedvitaminD(calcitriol)oroneoftheactivevitaminDanalogs that include paracalcitriol and 1-hydroxyvitamin D2. But even thesepatientsneedvitaminD,aswell,tokeeptheirbloodlevelof25-vitaminDabove30nanogramspermilliliter.
Over-the-CounterandPrescriptionDrugAlerts
While there are no negative interactions with vitamin D supplements andmedications, certain medications and even some over-the-counter herbalremedies can interferewith the body’s ability tomaintain robust levels of 25-vitaminD.Here’stherundown.Antiseizuremedications.Drugsused to treatepilepsyultimatelydestroy25-
vitaminD,makingpatientswhoareonantiseizuremedicationsathigherriskfordevelopingvitaminDdeficiencyandosteomalaciaorrickets.OftentwotothreetimesasmuchvitaminDisrequiredtomaintainabloodlevelof25-vitaminDabove 30 nanograms per milliliter; 2,000 to 6,000 IU of vitamin D a day isusually needed.An alternative, under a doctor’s care, is to take 50,000 IU ofvitaminD2eitheronceeveryweekoronceeverytwoweeks,dependingontheserum 25-vitamin D level. You want this level to be between 30 and 100nanogramspermilliliter.Prednisone. Similarly, prednisone, an anti-inflammatory and steroid used to
treat a variety of conditions, will increase the destruction of 25-vitamin D,requiringpatientstoincreasetheirvitaminDintakeaswellastheircalcium,asprednisonealsodecreasescalciumabsorptioninthegut.Immunotherapy.TherehavebeenafewstudieslookingatvitaminDstatusin
immunocompromised patients, including those who have had organtransplantation(heart, lung,andkidney)andthosewhosufferfromAIDS.Themedications that these patients are on increase the destruction of vitamin D,giving them a higher risk of vitamin D deficiency. These patients often havesignificant bone loss, causing osteoporosis. Thus, patients who are onimmunotherapyorareimmunocompromisedshouldhavetheirvitaminDstatusevaluated and appropriately treated. Often these patients need twice as much
vitaminDtocorrect theirvitaminDdeficiency,andI therefore typicallyplacethemon50,000IUofvitaminD2onceaweekforsixteenweeks, followedby50,000IUofvitaminD2onceaweekoronceeverytwoweekstomaintaintheirblood level of 25-vitamin D above 30 nanograms per milliliter. (For moreinformation,gotomyWebsite,www.drholicksdsolution.com.)St. John’s wort. This popular herbal supplement, touted as a brain booster,
willenhancethedestructionof25-vitaminDin thebody.Ifyoutakethisherbconsistently, at aminimum Iwould recommend being on at least 2,000 IU ofvitaminDadayandhavingyourbloodlevelof25-vitaminDmonitored.Thisgoestoshowthatthesimplestthingsyoucouldbetaking,includingseeminglyharmless over-the-counter herbal remedies, can affect your ability to absorbvitaminD.Obesity-relateddrugs.Patientsonorlistat,adrugmarketedasXenicalorAlli,
are at increased risk of vitamin D deficiency because the drug decreasesabsorptionofvitaminD(andofdietaryfats—thepurposeofthedrug).Forthesepatients,IrecommendthattheyincreasetheirvitaminDintakefrom2,000IUofvitaminDperdayto3,000to4,000IUofvitaminDperday.Discussthiswithyourdoctorifyoutakethismedication.Cholestyramine(brandnameQuestran).Usedtolowercholesterol,thisdrug
canalso interferewith theabsorptionofvitaminD.Peoplewho take thisdrugoverthelongtermtolowercholesterolshoulddiscusswiththeirdoctoruppingtheirvitaminDintake,andattheveryleastshouldrequesta25-vitaminDtest.TheyshouldtaketheirvitaminDsupplementatleasttwo—andpreferablyuptofour—hoursaftertakingcholestyramine.
EtCetera:StillOtherCausesofVitaminDDeficiency
Somepeoplehavegeneticproblemsormalfunctionsintheirkidneysorliverthatprevent their bodies from making the active form of vitamin D that benefitshealth. Remember, these are the key organs to the production of activatedvitaminD in the body. Here aremore reasons why some peoplemay have avitaminD deficiency that requiresmore aggressive treatment than the normalprotocol.Fatmalabsorptionsyndromes. Peoplewhose ability to absorbdietary fat is
compromised(fatmalabsorption)mayneedtogettheirextravitaminDfromsun

ortanning-bedexposureorfromtheFDASANCTIONEDvitaminD-producingSpertilamp.Somecausesoffatmalabsorptionarepancreaticenzymedeficiency,Crohn’s disease, cystic fibrosis, celiac disease (sprue), liver disease, surgicalremoval of part or all of the stomach, and small-bowel disease. MultiplesurgeriesforCrohn’s,forexample,canleaveamuchsmallerbowel;Ioncehadapatient whose resected bowel (reduced to just two feet) required the use of atanning bed to get his vitamin D levels up andmaintained. Symptoms of fatmalabsorptionincludediarrheaandgreasyandsmellystools.PatientswithcysticfibrosisoftenhaveadifficulttimeabsorbingvitaminD,andmycolleaguesandIshowed that exposure to the Sperti lamp was effective in raising their bloodlevelsof25-vitaminD.Crohn’s disease. Patients with Crohn’s disease, especially of the proximal
small intestine, often have difficulty absorbing vitamin D. I take threeapproachesintreatingandpreventingvitaminDdeficiencyinCrohn’spatients.The firstapproach is togive50,000IUofvitaminD2onceaweekor twiceaweekforatleasteightweekstoseeifthevitaminDdeficiencycanbecorrected.Here,too,Iusethetrickofhavingthepatientcutthecapsuleinhalfandplaceitinmilk,orangejuice,orsomeotherdrinkandthendrinkthecontentbutnotthecapsule. The second approach is to give much higher doses of vitamin D—startingwith asmuch as 50,000 IU once a day until the serum 25-vitaminDreachesalevelbetween30to100nanogramspermilliliterandthentailoringthedose to maintain this blood level. The third alternative is to have the patienteither go to a tanning salon or buy a vitamin D-producing lamp such as theSperti lamp, which can be purchased at www.sperti.com. We showed that apatientwith only two feet of small intestine left respondedverywell to beingexposed three times a week to our tanning bed for 50 percent of the timerecommendedfortanning(wearingsunprotectiononherface).Alloftheachesand pains in her bones and muscles associated with vitamin D deficiencyvanished,andherqualityoflifemarkedlyimprovedafterthreemonths.Wewereable to maintain her at a normal 25-vitamin D level by exposing her to thetanningbedonceortwiceaweekthereafter.Kidneyfailure.Severekidneydiseasecaninterferewiththeconversionof25-
vitamin D to activated vitamin D. But someone with compromised kidneyswouldstillneedadequatevitaminDtobenefitfromallitsotherhealthbenefitsandsupportthelocalproductionofactivatedvitaminDinparathyroidglandstohelpcontrol theparathyroidhormonelevels,whichusually increase inpatientswithstages4and5kidneydisease.

VitaminD-dependent rickets (types 1, 2, and 3). Type 1 rickets affects thebody’s ability to convert 25-vitaminD to its active form, 1,25-vitaminD, andtype 2 interferes with the body’s ability to recognize 1,25-vitamin D. Type 3makestoomuchofaproteinthatpreventsvitaminDfromworking.AllofthesepatientsneedtotakevitaminDandmayalsobenefitfromtaking1,25-vitaminD(calcitriol);thisisespeciallytruefortype1.Seizuredisorders (epilepsy).As I explained just above, long-term treatment
with anticonvulsant medications, such as phenytoin and phenobarbital, canincreasedestructionof25-vitaminD.Celiacdisease.It’sestimatedthatupto10percentofthepopulationhassilent
celiac disease (sprue).The first timemanyof these people notice they have aproblemiswhentheyfindouttheyarevitaminDdeficientbutdonotrespondtotherapy,especiallyfromsupplementation.Patientswithceliacdiseaseoftenhavetrouble absorbing fat-soluble vitamins, including vitaminD.And unless thesepatientsaregettingenoughUVBtomaintainhealthy levelsofvitaminD, theywill become vitamin D deficient—even when taking vitamin D supplements.Vitamin D deficiency is very common in patients with celiac disease. I havefound that patients with celiac disease who are appropriately treated with agluten-free diet and who are treated for their vitamin D deficiency havesignificant improvement in their feelingofwell-being, improvement inmusclestrength,andadecreaseinachesanddiscomfortintheirbones.TheinitialdoseofvitaminDthatIrecommendformypatientsis50,000IUofvitaminD2onceaweek for eightweeks to fill the empty vitaminD tank and achieve a bloodlevelof25-vitaminDabove30nanogramspermilliliter.Ithenmaintainthetankonfullbygivingthemeither50,000IUofvitaminD2onceeverytwoweeksor2,000IUofvitaminD2orvitaminD3daily.Eating disorders. People with anorexia or bulimia routinely score low on
bone density, can show signs of osteopenia (the prelude to the more severeosteoporosis), andmayhave lowvitaminD levels. I advise that thesepatientsreceive 50,000 IU of vitamin D2 once every two weeks from their doctor tomaintainvitaminDsufficiency.Monitoringtheirbloodlevelsof25-vitaminDisalso a must to ensure that it remains above 30 nanograms per milliliter.Obviously,puttinganendtotheeatingdisordershouldalsobeontheagenda.Liver failure.Liver failuredecreasesproductionof25-vitaminD,especially
whenmorethan80percentoftheliverisdestroyed.Liverdiseasealsomakesitdifficult for the intestine to absorb fat aswell as vitaminD, calling formore

aggressiveadministrationofvitaminD.TheassociatedfatmalabsorptioninmildtomoderateliverpatientsisamajorcauseofvitaminDdeficiency.Primarybiliary cirrhosis. This disease causes destruction of the bile ducts,
preventingbilefromreachingtheintestines,whereit’s importantforabsorbingvitaminD. I treat these patientswith 50,000 IUof vitaminDonceor twice aweekifnecessary.Cysticfibrosis.Alsoadisease that leads to fatmalabsorptionandvitaminD
deficiency, cystic fibrosis calls for aggressive vitamin D2 treatment and/orexposure to UVB radiation such as that found in a Sperti lamp. The CysticFibrosis Foundation’s practice guidelines now call for this protocol, givenstudies thatdemonstrate itsbeneficialeffectson improvingpatients’vitaminDstatus.Anyonewho suffers from any of the above conditions should discuss their
vitaminD statuswith their doctor and take action to rectify the problemwithhighdosesofvitaminDunderadoctor’scare.Othercauses.Patientswithhyperparathyroidismandelevatedserumcalcium
are often advised not to take any vitamin D because of worseninghypercalcemia. This, however, is incorrect. Two studies have shown thatcorrecting vitamin D deficiency does not increase serum calcium levels butinsteadcanhelptodecreasecalciumandparathyroidlevels.Thus,it’simportanttocorrectvitaminDdeficiencyinthesepatients.Other causes of vitamin D deficiency due to hypersensitivity to vitamin D
include patients with chronic granulomatous disorders, such as sarcoidosis,tuberculosis, and fungal infections. These patients are at an increased risk ofdeveloping vitaminD deficiency because their immune systems are activatingvitaminD.They need to be treated for their vitaminDdeficiency but receivemuchlessvitaminDthanpatientswhoareotherwisenormalandbeingtreatedforadeficiency;otherwise,theycansufferfromhighcalciumintheirurineandblood. I typically treat these patientswith enough vitaminD tomaintain theirbloodlevelof25-vitaminDbetween20and30nanogramspermilliliter.
CHAPTER12
DethroningtheCover-Up
AnothergiantleapformedicineandmankindMytaskisonlybeginning.WhenIfirststartedworkingwithvitaminD,IneverdreamedofwhatIandfellowscientistswoulddiscoveroverthecourseofthreedecades.MyfirstexperimentstoisolatetheactiveformofvitaminDinthebodywereakin tocomingacrossapartiallyburiedweathervanestickingoutof theground.AndsoIstartedtodig...anddigsomemore,eventuallyunearthinganentire castle underneath filledwith treasures. In the 1980s I grew increasinglyconcerned about themessage of abstinence from the sun and its potential forcausing a vitaminD deficiency epidemic.But I never imagined thatwe’d seesuchgreatdepthsofvitaminDdeficiencyworldwideorthatpushingbackwithour findings against the ever-powerful antisun campaigns would be soproblematic, divisive, and contentious—very much contrary to the spirit ofresearchanddevelopmentinhumanmedicine.Forme,theevidencehasalwaysbeencrystalclear.Nowit’sjustoverwhelmingandcompelling.DespitealltherecognitionthatI’vebeenhonoredtoreceive,Ihavetoadmit
thatsomeofmyworkandresultingadviceisasourceofcontroversyandfieryrhetoricamongcolleagues in thefieldofdermatology.In2004Iwasforced togiveupmypositionasprofessorofdermatologyatBostonUniversityMedicalCenter,apositionIhadheldfornearlytenyears.Mystalwartsupportofsensiblesunexposurejustdidn’tjibewiththeviewsofthechairofthedepartment.Istilldon’t see eye to eye with many of my fellow members of the AmericanAcademyofDermatology.Shameonmeforchallengingoneof thedogmasofdermatology, but think about it: what if we had never experimented withinoculating a healthy individual with a weakened or dead form of a virus toimpart immunity?What if we couldn’t shift our focus from spicy foods to acommon bacterium in the search to understand the cause of most stomach
ulcers?WhatifAlexanderFlemminghadn’tthoughttwiceabouttheplatewheremoldwaskillingthebacteriathathadbeengrowingonitoveralongweekend?Wemightnothavethevaccinesandantibioticswedotodaytotreatanarrayofillnessesanddiseases. Iamalso remindedof thestoryabouthandwashingbydoctors, which was pioneered by the Hungarian-born physician IgnazSemmelweisinthemid-nineteenthcentury.Whileworkingatanobstetricsclinicin Vienna, Dr. Semmelweis noticed that fatal childbed (or “puerperal”) feveroccurredsignificantlymorefrequentlyinwomenwhowereassistedbymedicalstudents than in thosewere assisted bymidwives.After realizing the studentsoftenassisted in childbirth afterperformingautopsiesonpeoplewhohaddiedfrom infections—and not washing their hands between procedures—heinstigatedastricthand-washingpolicy.Butitdidn’tcatchonrightaway.Ittookdecades for Semmelweis’s “theory” to earnwidespread acceptance. Followinganallegednervousbreakdown,Semmelweislandedinanasylum,wherehediedattheageofforty-seven.Yearsafterhisdeath,LouisPasteurconfirmedthegermtheoryandhandwashingbecamethenormamongdoctors.The point of all this? Perceptions mean everything. And the dermatology
communityhashadalongtimetoinoculateuswithmisperceptions.The last time I promoted a book for the lay public,TheUVAdvantage , I
found myself frequently on the defensive, perpetually shoved in the “guilty”cornerwithout a fair trial.But itwas only amatter of time. I knew the proofwouldeventually stackup likeapileofneglectedmail tobeopenedandpaidattention to. And unless that proof is wholeheartedly acknowledged, theconsequencesofavoidingitonlycontinuetostackup...justlikethoseignoredbillsanddismissedcorrespondence.Thesunhasbeenavitalpartnerinourhealth,butit’sbeendemonizedunfairly
(and toourdetriment) in the last fortyyears,especially since the1970s,whenthe dermatology community gained momentum. Ironically, there’s been aparallel relationship between the rise of the unrelenting message of thiscommunity(andtheenormouslyprofitablesunscreenindustry) thatyoushouldnever be exposed to direct sunlight because it’s going to cause serious skincanceranddeathandtheriseinvitaminDdeficiency.Sadly,asaresult,wenowhaveapopulationlargelyvitaminDdeficientandludicrouslyfearfulofthesun.Maythisbookhelpchangethat.Thegoodnewsisthatafteralmosttwenty-fiveyearsofmytryingtoalertthe
world to thevitaminDdeficiencyproblem,people—andphysicianswhooncepooh-poohedmyadvice—arefinallystartingtogetthemessage.ThevitaminD
deficiency and insufficiency that afflict at least half of theworld’s population,andremainoneofthemostundiagnosedmedicalconditions,arereal—andveryserious. They have grave health consequences for unborn children and adultsalike.And they could lie at the root of ourmost enigmatic and vexing healthchallenges. Last year, when a panel of vitamin D researchers, including Dr.Grant, the Garland brothers, and Dr. Gorham—all of whom have beenmentionedinthisbook—publishedapaperthatattemptedtoputapricetagonvitamin D deficiency in Western Europe, they concluded that raising thepopulation’s25-vitaminDlevelsto40nanogramspermillilitercouldresultsinasavings of 187,000 million euros a year. That translates to more than $260billion.That’s a lot of health savings, and I’d expect the numbers to be similar in
America, where health-care costs continue to climb commensurate with thepopulation’s increasing need for care.Dr.Grant projected that, ifmean serum25-vitaminDlevelswereraisedinthegeneralpopulationto45nanogramspermilliliter by solar UVB radiation, the rate of premature deaths in the UnitedStates couldbe reducedby about fourhundred thousandperyear.Thatwouldtranslatetoasignificantsavingsinhealth-carecosts.Dr.Grantalsorecentlyleda study to estimate the economic burden and premature death rate in Canadaattributable to low 25-vitamin D. (Canadians have mean serum 25-vitamin Dlevelsaveragingonly27nanogramspermilliliter.)Thestudyconcludedthat ifCanadianscouldincreasetheir25-vitaminDto40nanogramspermilliliter,thedeathratecouldfallby40,600ayear,or18percent,andtheeconomicburdencoulddropby$18.3billionayear,or8.7percent.Long considered calcium’s comrade in supporting strong bones and teeth,
vitaminD has been radically redefined in history and themedical books, andwillcontinuetoearnnewcreditthatplacesitinitsownuniquecategoryandfarfromeveryother“vitamin.” In the first sixmonthsof2009alone—justbeforethis bookwent to press—more than 2,270 studieswere published referencingthisvitaminofhealth.Nodoubtbythetimeyoureadthis,thatnumberwillhavesoaredtogreaterheights.Twentyyearsago,onlyasmallhandfulofstudieshadeverbeenpublishedon the subject, andwhen Iwrotemy first book,wewerestandingonthevergeofthisincredibleexplosionintheresearch.“Greatleaps”areoftentalkedaboutinscientificcircles,referringtothegiant
leaps that propel an industry to a new paradigm—as well as launch societyforward.Thediscoveryofantibiotics,forexample,couldbeconsideredagreatleap in medicine. The steam engine and the invention of the lightbulb led to

otherkindsofleaps.Leapscanalsobemadewithinthehumangenepool,suchaswhenwebrokeawayfromourapeancestorsandlearnedtowalkupright,andlater when we constructed complex languages to communicate with far moresophistication,meaning,andprecision.Ibelieveournewfoundappreciationforvitamin D constitutes a great leap forward in medicine, and I applaud thenumerous investigators worldwide who today are robustly investigating thisarea. But to the dismay of the dermatology community, a leap we haven’texperiencedyetisoneinourbodies’abilitytothrivewithoutalittlehelpfromthe sun. We just haven’t yet evolved to a point where we can make amplesuppliesofvitaminDwithoutUVB.Takeawayaccesstothosesupplementsandyou’dbehard-pressedtosurvive.For some, evenphysicians, it’s incomprehensible that vitaminDcan reduce
the risk of heart attack by asmuch as 50 percent; reduce the risk of commoncancersofthecolon,prostate,andbreastbyasmuchas50percent;reducetheriskofinfectionsdiseases,includinginfluenza,byasmuchas90percent;reducetheriskoftype1diabetesby78percentinachildwhogets2,000IUofvitaminDadayinthefirstyearoflife;decreasetheriskoftype2diabetes;decreasetheriskofdementiaanddepression;wipeoutcasesoffibromyalgiathathavebeenmisdiagnosed;anddramaticallydecreasetheriskofmultiplesclerosisandotherautoimmunediseases.Whenindoubt,Ialwaysgobacktothissimplefact:everytissueandcellinthebodyhasavitaminDreceptor.Whywouldtheybethereiftheyweren’thavinganeffect?WearegraduallycomingtoanunderstandingthatperhapsallcellsinourbodiesrespondpositivelytoactivatedvitaminD,raisingtheprospect of anuntoldnumberof benefit associatedwith exposure toUVBradiationfromnaturalorartificialsources.I amnot suggesting that vitaminD is a cure-all, but I think thatwe canno
longerkeepourblindersontothespecialbondourbodieshavehadwiththesunin ensuring our health for millennia. The dermatology community mightcontinuetoplaywithitseyeshalfopentoalltheresearch,butnowthatyouhavetheknowledge,yougettodecidehowtoliveyourlife.Iexpectlotsofcriticismfrommyfellowdermatologists,andthat’sfine.I’mprepared.Alwayshavebeen.Thosewhohaveavestedinterestinpromotingsunphobiadon’tmuchcarethatpeer-reviewed studies are being published with increasing frequency thatcontradicttheirclaims.Theirattitudeisthatmostpeopledon’treadthesestudiesand any news of them in themainstreammedia can be quashedwith another“Stay out of the sun!” and “Cover up!” campaign accompanied by vaguerecommendationstojusteatanddrinkmorefortifiedfoodsandmilk(which,of

course,can’tprovidenearlyenoughvitaminDtobenefithealth).Thinkaboutit:our bodies evolved during a time when we spent most of our days outside,making in our skin an amount of vitaminD equivalent to ingesting 10,000 to20,000 IU a day.Today, asmost of us hunker down indoors,we getmaybe ameasly few hundred IU from diet sources. That cannot even make a dent infilling our empty tanks—a trickle in a well run dry. Don’t be fooled bygeography. Recall that 87 percent of dermatologists in a place as sunny asAustralia—the skin cancer capital of the world—have been shown to bedeficient in the summer, prompting the Australian College of Dermatologists,AustralianandNewZealandBoneandMineralSociety,OsteoporosisAustralia,andtheCancerCouncilAustraliatopublishpublichealthalertsandoffercleardirectionsonhowtousesensiblesunexposureforoptimalhealth.Itwillbehardforanyonetodismisstheclaimsandresearchcontainedinthis
book as “unscientific.”They all arise frompeer-reviewed studies published inprestigious medical journals. This means that when they were submitted forpublication,thestudieswerescrutinizedbyarelentlessandconscientiouspanelofdoctors and scientistswhocarefully judged thembasedonhowsound theirmethodology was, the importance of their results to the particular area ofscience, and how well they were executed. Only a very small percentage ofstudies submitted tomedical journals are accepted forpublication.The fact somany have been published on vitamin D in the last five years alone sayssomethingsignificant.Extremelysignificant.Which brings me to why I’ve included such an extensive bibliography
(comingup at thebackof this book). Iwant you tohave all the facts at yourdisposal.Youcanreadmoreabout thesestudiesbysearchingthenamesof thepaperson theNationalLibraryofMedicine’sWebsite (keyword:pubmed)orsimply going to www.pubmed.com. As more studies are published, I will befeaturingthemonmyWebsite,www.drholicksdsolution.com,sopleasefeelfreetovisitandseewhat’snewinthisexcitingfield.I believe Charles Schulz said it the best in hisPeanuts comic strip, in the
cartoonwhereLinus issitting in theschoolyardandopenshis lunch tofindanote fromhismother inwhichsheencourageshim to“makegoodfriends,getgoodgrades”andnotes,“Ihopethatyouaresittinginthesun,foralittlesunisgoodaslongaswedon’toverdoit.Perhaps10minutesadaythistimeoftheyearisaboutright.”SchulzwasrightontargetforsomeonelivinginSanDiego.Hopefullythismessagewillbeheardandthisrecommendationwillbeadoptedworldwide.
Figure 8. This wittyClassic Peanuts comic strip first appeared in 1974, andremains as relevant as ever. Charles Schultz lived in San Diego and therecommendationthatLinusreceivesfromhismothertositinthesunforafewminutes at that latitude is right on target. (Peanuts:United Feature Syndicate,Inc.)
CHAPTER13
Q&A
OddsandendsandafewmoreremindersintheclassicFAQstyle
FollowingareanswerstosomefrequentlyaskedquestionsIgetfromthelayandacademic communities alike. In many of these answers you’ll find echoes ofinformationfromprevioussectionsofthebook,andattimesIwillreferbacktothosepages.Ifyouhaveaquestionnotansweredbelow,justlogontomyWebsite,www.drholicksdsolution.comandaskmethere.You’llfindotherQ&Asonthesite,too.
General
Q.WhathappenswhenyoucookfoodsrichinVitaminD,likewildsalmon?Dotheylosetheirpotency?A.VitaminDisrelativelystableinfoods.Storage,processing,andcookinghavelittle effect on its activity. Vitamin D is stable when heated to boilingtemperatureof212°F.Q.Ifyoufryfishinoil,doesthatremovethevitaminD?A.Yes,morethan50percentof thevitaminDis lostwhenyoufryfishinoil.Youwoulddowelltobake,broil,orgrillthefish.Q.DoesvitaminDinteractwithanymedications?A. Vitamin D does not interact with any medications. However, some

medications,suchasantiseizuredrugs,AIDSmedications,andprednisone,willincreasethedestructionof25-vitaminD,thusrequiringpatientstoincreasetheirvitaminDintake(seechapter11).Q.Doesgeneticsplayaroleintheabilitytomaintain25-vitaminDlevels?A.ThereissomeevidencethatgeneticsdoesplayasmallroleintheabilitytomaintainvitaminDstatus.However,frommyexperience,ifyouingestbetween1,500and2,000 IUofvitaminDaday, andyouarenotobese, thisoftenwillsatisfyyourvitaminDrequirement.Q. Can you receive vitamin D from sunlight through windows? Whatimpactdoescloudcoverhave?A.SunlightcomingthroughwindowglasswillnotproduceanyvitaminDintheskin because the glass absorbs the vitaminD-producingUVB radiation. YourskinmustbeexposedtodirectsunlightinordertomakevitaminD.Cloudcoverwill decrease the amount of UVB radiation penetrating to the earth and canreducevitaminD3synthesisbyasmuchas50percentto75percent.Q.IsthereanageatwhichvitaminDsupplementationdoesn’twork?A.Absolutelynot.VitaminDsupplementationiseffectiveinchildrenandadultsofallages.Agingdoesnotaffect thebody’sability toabsorbvitaminDeitherfrom the diet or from supplements. At least 1,000 IU of vitamin D day isappropriate for all ages, from children one year old to geriatric patients.Newbornsduringthefirstyearoflifeshouldtakeatleast400IUaday,andupto1,000IUisreasonable.Q.DoesagingaffectmyabilitytomakevitaminDinmyskin?A. Yes, but the skin has such a large capacity that even with a 70 percentreductionbythetimeyou’reseventyyearsold,youcanstillmakeenoughjustbyexposingmoreskin.Q.IhaveheardthatitisimportanttotakemagnesiumalongwithvitaminD.Isthereanyreasonforthis?A. There is no need to take magnesium along with vitamin D. Vitamin D isefficientlyabsorbedwithorwithoutmagnesium.
Q.Howmuchcalciumshouldyouhavewith1,000IUofvitaminDaday?A.The InstituteofMedicine recommends that all adultsup to the ageof fiftyingest1,000milligramsofcalciumadayandadultsovertheageoffifty1,200milligrams of calcium a day. Teenagers require 1,300 milligrams a day tomaximizetheirbonehealth.Q.IsitokaytotakevitaminDwithouttakingcalciumsupplements?A.Yes.However,tomaximizevitaminD’seffectonskeletalhealth,youneedtoingest, either from supplements or from diet, 1,000 to 1,200 milligrams ofcalciumadaydependingonyourage(seechapter9).Teensneedevenmore—1,300milligramsaday.Q.DocarbonatedbeveragesaffectvitaminDorcalciumlevels?A.No.CarbonatedbeveragesdonotaffectvitaminDorcalciumlevels.Q.ShouldyoustoptakingvitaminDsupplements justbeforehavingyourvitaminDstatuschecked?A. There is no need to stop your vitaminD to have your 25-vitaminD levelchecked.Q.HowdoyouinterpretdifferentvitaminDlabnumbers(i.e.,doyoulookat25-vitaminD2,25-vitaminD3,ortotal25-vitaminD)?A.When you check the blood level of 25-vitaminD, the only number that isimportant is the total 25-vitaminD,which shouldbe above30nanogramspermilliliter. The 25-vitaminD2 level reflects vitaminD2 intake (usually from avitaminD2prescription), and the25-vitaminD3 level reflects the vitaminD3ingested from diet, supplements, and sun exposure. Adding together the 25-vitaminD2 and 25-vitaminD3 numbers gives the total 25-vitaminD number.For example, if your results show a vitaminD2number of 15 nanogramspermilliliterandavitaminD3countof20nanogramspermilliliter,thenyourtotalvitaminDwouldbe35nanogramspermilliliter.Q. Is itpossible togetvitaminD toxicitywithvitaminDsupplementationandadiethighinvitaminD-fortifiedfoodsalongwithsunexposure?A.Inmyopinion,becauseveryfewfoodscontainvitaminDandtheamountof

vitamin D is relatively small in comparison to what the body requires, it isdoubtful that you could become vitamin D toxic by taking a vitamin Dsupplementof1,000to2,000IUofvitaminDaday.Youcannotgettoomuchfrom the sun, either.Most of the literature suggests that adults have to ingestmorethan10,000IUofvitaminDadayforatleastfivemonthsbeforetheyhaveto begin to be concerned about vitaminD toxicity. If you have sarcoidosis oranothergranulomatousdisorderliketuberculosis,youcouldbemoresensitivetovitaminDandneedtocheckwithyourdoctor.Q.IsfarmedsalmonagoodsourceofvitaminD?A.MycolleaguesandIfoundthatfarmedsalmonhasonlyabout10percentto25 percent of the vitaminD found inwild-caught salmon.Wehave tested theVital Choicewild-caught salmon available atwww.vitalchoice.com and foundthatithasbetween800and1,000IUofvitaminDin3.5ounces.Q.WhydosometextbooksstillcallvitaminDthemosttoxicvitamin?A. Indeed, most textbooks still call vitamin D the most toxic vitamin. Itdefinitely isnot.VitaminAismuchmoretoxicandcanrapidlycausedeathinveryhighconcentrations.(ThiswasdiscoveredbyearlyexplorersinAlaskawhobeganeatingpolarbearliverandbecameseverelyvitaminAintoxicated,leadingto death.) Given the plethora of data emerging on the safety of vitamin D, Iexpectthetextbooksmayberewritten.Q.Shouldchildrenwhodonotdrinkmuchmilkandwhowearsunscreengettheirbloodlevelsof25-vitaminDchecked?A.It’snotunreasonabletohaveyourchildrentestedifyouareconcernedabouttheirbeingvitaminDdeficientbecausetheydon’tdrinkmilkorwearsunscreenall the time.Thiswill help convince you and the pediatrician that the child isvitaminDdeficientandrequiresvitaminDtreatment.However,becausethistestisrathercostly,Ioftenrecommendthatchildrensimplytake1,000IUofvitaminDadayalongwithamultivitamincontaining400IUofvitaminDaday.Q.Doestimeofdaymatterforrecommendedsunexposure?A.The timeof day doesmatter, because the angle of the sun is different. It’sverydifficulttomakevitaminDintheearlymorningorlateafternoon,eveninthe summer, and youwillmakemore vitaminDbetween noon and 2:00P.M.thanyouwilleithermakeat10:00A.M.or3:00P.M.(seetablesstartingonpage
182).Q.ArethereanyvitaminD-stimulatinglightbulbsforhumans?A.VitaminDwillnotbeproducedbyexposuretoincandescentlightbulbs.Youneed to be exposed to a vitaminD-producing lamp that emitsUVB radiation.The Sperti lamp is the only FDASANCTIONED vitamin D-producing lamp.TanningbedsthathavefluorescentlampsalsoemitUVBradiation.Q.Does itmatterwhether Iwear sunglasseswhen I exposemyself to thesun?A. I always recommend some face protection and sunglasses or other eyeprotectiontoreducetheriskofcataracts.Q.Doesboilingcow’smilkdestroyvitaminD?A.Boiling cow’smilkwill not destroyvitaminD.VitaminD is heat stable atleastuptoatemperatureofabout300°F.Q.IsvitaminDbetterabsorbedfromfortifieddairyorfromfortifiedjuice?A. My colleagues and I have recently completed a study with Minute Maidfortified orange juice finding that vitamin D is equally bioavailable fromfortifiedjuice,fortifiedmilk,andvitaminDsupplementcapsules.Q.I’veheardthatvitaminDinskimornonfatmilkisn’tasbioavailable.Isthistrue?A.VitaminD is just as bioavailable from skim and nonfatmilk as it is fromwholemilk.FatisnotneededtoefficientlyabsorbvitaminD.Q.Isn’tvitaminDfat soluble?Is thereawater-soluble formofvitaminDthatisusedtofortifyorangejuiceandskimmilk?A.ThevitaminDthatisusedinorangejuiceisinamicronizedformthatmakesitwater soluble.ThevitaminD in skimmilk is the samevitaminD that is inwholemilkandisperfectlybioavailable.Q.Will Iwashoff thevitaminDIproduce inmyskin if I takeabathorshowerwithinthirtyminutesofbeingexposedtosunlight?A.No.VitaminDismadeinlivingcellsintheskin.Youcannotwashitoff!
Dosage
Q. How long does it take to increase 25-vitamin D levels after startingsupplementation?A.Frommyexperience,healthyadultstaking1,000IUofvitaminDadayreachtheirpeakbloodlevelwithinfivetosixweeks.WhenItreatpatientswith50,000IUofvitaminD2onceaweekforeightweekstotreatadeficiency,theirbloodlevelbegins to increaseby the firstweekand levelsoffby theeighthweekoftreatment.Q. Is there any advantage to taking smallerdosesmore frequently ratherthanonelargedoseperday?A.Thereisnoadvantagetotakingsmallerdosesmorefrequentlyratherthanalargedoseof1,000or2,000IUofvitaminDaday.Indeed,youcantake2,000IUofvitaminDadayor14,000IUofvitaminDonceaweekor60,000IUofvitaminDonceamonth;theyallworkthesameway.Iliketogivemypatients50,000 IU of vitamin D2 once every two weeks, but if they forget, taking100,000IUonceamonthissafe.Q.Doyouneedtotakeasupplementevenduringthesummer?A.Ifyou’regoodaboutgettingplentyofsensiblesunexposurethroughoutthesummermonths, or you live in a sunny place like Florida, then youmay notnecessarilyneedtosupplement.However,it’smucheasiertogetintotheroutineoftakingasupplementyear-round.AndevenFloridianshavebeenshowntobelargelydeficient,becausetheyavoidthesunorwearsunprotection.YoucannotoverdoseonsunlightexposureandbecomevitaminDintoxicated,sonomatterhowmuchsunyougetduringthesummer, takinganadditional1,000to2,000IUsupplementcannothurtyou.Irecommendthateveryonetake1,000to2,000IUofvitaminDadayalongwithamultivitamincontaining400IUofvitaminD.ThiswillnotcauseanybuildupofvitaminDinthebody,andbyusingthisroutine,youarelesslikelytoforgetitinthewinter.Ipersonallytake2,000IUadayplusamultivitaminandthreeglassesofmilk.Ifyouareobeseorhavefatmalabsorptionsyndromeduetoanunderlyingmedicalcondition,youmayneedtwotothreetimesasmuch(seechapter10).Q.Howmanyunits of vitaminDwould a personhave to take to become

toxic?A. Vitamin D intoxication will not occur until a person is taking more than10,000 IUofvitaminDaday formore than sixmonths.Adultswho received10,000IUofvitaminDadayforfivemonthsshowednosignsoftoxicity.YoucannotoverdoseonvitaminDfromexposure tosunlightora tanningbedoraUVB-producinglamp,nomatterhowmuchUVByouget.Q.Whatisthebestsupplementforchildrenwhocannotswallowpills?A. InfantscanbeadministeredvitaminD throughpediatricvitamindrops (seetheResourceGuide).Ifyouhavechildrenwhocannotorwillnotswallowpills,youcancrushavitaminDtabletorsqueezethecontentsofagelcapsuleintoaglassofmilkorjuice.AgoodproductthathasemergedonthemarketandthatIhave used for my young patients is a liquid form of vitamin D. Made byWellesse,itcontains500IUofvitaminDperteaspoon.Q.DoestherecommendeddoseofvitaminDsupplementneedtobetakenwithfat(notinatabletform)?A.TherecommendeddoseofvitaminDsupplementdoesnotneedtobetakenwith fat.My labhas shown that vitaminD is equallybioavailable in cornoil,milk,andorangejuice.Q. How should a vegan or vegetarian make sure he or she gets enoughvitaminD?A.Vegans should supplementswith at least 1,000 IUofvitaminDaday, andpreferably 2,000 IU. This would be in addition to a multivitamin. Vegansconcerned about animal sources of supplemental vitamin D3 can opt forsupplementscontainingvitaminD2,whichcomesfromyeast.Q.Whatisyouradviceforveganorvegetarianchildren?A.Irecommendthatallchildren,includingveganchildren,ingestatleast400IUofvitaminDaday, andpreferably1,000 IUofvitaminDaday, alongwithamultivitamin,especiallyiftheyarenotgettingadequateexposuretosunlight.Q.IfapersonisnotvitaminDdeficient,whatisthebestover-the-counterformanddosetotake?WhatifthepersonisvitaminDdeficient?A. If a person is not vitaminD deficient, tomaintain vitaminD sufficiency I
recommendthatthepersontakeatleast1,000IUofvitaminD2or1,000IUofvitaminD3aday inaddition toamultivitaminwith400IUofvitaminD. Ifaperson isvitaminDdeficient, then Idoubleor triple thedoseand recommendthat he or she take 2,000 to 3,000 IU of vitamin D a day along with amultivitamin. A person who is severely vitamin D deficient should consult adoctor to inquire about prescription-level treatment (see chapter 10 for moredetails).Q.Whatformofsupplementationdoyourecommend—D2orD3?A. In my experience, 1,000 IU of vitamin D2 is as effective as 1,000 IU ofvitaminD3inraisingbloodlevelsof25-vitaminD.Eitherformcanbeused.Butnote:toraisebloodlevelsof25-vitaminDtoabove30nanogramspermilliliter,youneedtotakemorethan1,000IU.Q. Is the prescription form of vitamin D different from what’s availableoverthecounter?A. In the United States, the only vitaminD form available by prescription isvitamin D2, also known as ergocalciferol. It comes either in a capsule with50,000IUofvitaminD2or ina liquidform(forpediatricpatients)with8,000IUofvitaminD2per1milliliter.VitaminD2canalsobefound insomeover-the-countersupplements,andit’sjustaseffectiveasD3.Q.Whatisthebestsupplementbrand?A.Anynationalbrandwilldo.Foralistofideas,seetheResourceGuide.Q.Canaprescriptiondoseof50,000IUofvitaminD2(tocorrectdeficiency)causefatigue?A. I do find that someofmypatientswho take50,000 IUofvitaminD2 feelfatigued.Ibelievethatthismaybeduetothegelatincapsuleratherthantothe50,000IUofvitaminD2.Trycuttingthecapsule,dumpingitintomilkororangejuice,anddrinkingthecontentwithoutthecapsule.Q.Aretheresideeffectsfromtaking50,000IUatonetime?A.Inmyexperience,therearenosideeffectsfromtaking50,000IUofvitamin

D2atonetime.However,somepatientsarenotabletotolerateitorhavesomeGIissues.Ibelievethatthisisduetothegelatincapsule,notthevitaminD.Forthesepatients,Irecommendthattheycutthecapsuleopen,dumpitintoaglassofmilkororangejuice,anddrinkthecontentswithoutthecapsule.Q.WhatdoesvitaminDtoxicitylooklike?A.VitaminDtoxicityisoftendifficulttodiagnose.Thediagnosisismadebasedonthebloodbiochemistriesthatincludeelevatedbloodcalcium(usuallyabove10.4milligramsperdeciliter)alongwithamarkedlyelevatedlevelof25-vitaminD, usually above 200 nanograms per milliliter. The hypercalcemia and oftenhyperphosphatemiaassociatedwithvitaminDintoxicationcancausethekidneystocalcify,increasetheriskofdevelopingkidneystones,andincreasetheriskofcalcifyingbloodvessels(whichultimatelycanleadtodeath).Theelevatedbloodcalcium also causes constipation, confusion, depression, increased thirst,increasedurination,andchangesintheelectrocardiogram.Q.WhatisthesafestwayfortoddlerstoingestvitaminDpills?Shouldaninfant’sortoddler’sbloodlevelof25-vitaminDbethesameasanadult’s?A. For infants and toddlers, Poly Vi-Sol is a liquid vitamin supplement thatcontains 400 IUof vitaminDpermilliliter.Alternatively, I have suggested toparentsthat theycanbuythe1,000IUvitaminDtablet,grinditup,putit intothetoddler’sorangejuiceormilk,andthenhavehimorherdrinkit.Oryoucanpurchase the liquid form of vitamin D from Wellesse (available at Costco’sdrugstoreoronlineatwww.wellesse.com)andaddtwoteaspoons(foratotalof1,000 IU) to the child’s beverage of choice. All children and adults shouldmaintainabloodlevelof25-vitaminDofatleast30nanogramspermilliliterallthetime.SeeResourceGuideformore.Q.Atwhat agedo you recommend children start taking 1,000 IUaday?HowmuchvitaminDdoyourecommendforinfants?A.Ibelievethatallchildrenovertheageofoneyearshouldbeon1,000IUofvitaminD a day plus amultivitamin. Infants should be on at least 400 IU ofvitaminDaday,and,asIhavepointedout,1,000IUofvitaminDadayshouldnotcauseanyharmandmayprovideadditionalbenefits.Q.Doveryleanpeoplerequirealower-dosesupplement?
A.Normalweightpeopleandvery leanpeopledonot requirea lowerdoseofvitamin D. However, anorexic patients have been found to have marginallyhigherbloodlevelsof25-vitaminDfromtakingthesameamountofvitaminDthat a normal weight person would take. However, this is of little clinicalsignificance.Q.Do you recommend higher amounts of vitaminD supplementation forthosewhoareobese?A.IdorecommendthatobesepeopledoubleortripletheirintakeofvitaminD,so instead of taking 1,000 to 2,000 IU of vitamin D a day they should takebetween4,000and6,000IUofvitaminDaday.Q.Itakefishoilcapsuleseveryday.Don’tthosecontainvitaminD?A.No. Fish oil capsules do not contain any vitaminD. Soldmostly for theiromega-3fattyacids,fishoilcapsulesarenotnecessarilymadefromvitaminD-rich fish like cod or salmon. The refining process isolates the omega-3 fattyacids,andanyvitaminDpresentisleftbehind,whichiswhyyoudon’tseeanyvitaminD(orvitaminA,forthatmatter)listedonthelabel.Q.Idon’tmindcodliveroil.Whycan’tIjustrelyonthat?A.BecauseofthehighvitaminAcontentofcodliveroil,it’snotagoodideatodownlotsofitandriskvitaminAtoxicity.Ifyouenjoycodliveroil,sticktoasingle servingand seekadditionalvitaminD throughsensible sunexposureorsupplements.
PregnancyandNewborns
Q.WhatareyourrecommendationsforvitaminDduringpregnancy?A. I recommend thatallpregnantwomen takeaprenatalvitamin thatcontains400IUofvitaminDadayalongwithavitaminDsupplementof1,000IUaday.Their calcium supplements may also contain 400 IU of vitamin D. At aminimum,allpregnantwomenshouldbetakingatleast1,400IUofvitaminDaday,and2,000IUofvitaminDday is fine,especially forobesewomen.Theyshouldhaveabloodlevelof25-vitaminDbetween30and100nanogramspermilliliter.

Q.WhatisyourrecommendationfordispensingvitaminDtobreastfeedinginfants?A. The American Academy of Pediatrics recently came out with therecommendationthatallinfants,includingbreastfedinfants,shouldreceive400IUofvitaminDaday.AlthoughIagreewith this recommendation, this is thebare minimum. Remember, 2,000 IU a day during the first year of life candecrease a child’s risk of diabetes by nearly 80 percent. Thus, giving infants1,000IUadaymaybemorebeneficialtotheirhealth.Q.Ifawomanisalreadytaking400IUofvitaminDinaprenatalvitamin,howmuchmoreisneededduringpregnancyandbreastfeeding?A. I encourage all pregnant and lactatingwomen to take the prenatal vitamincontaining400IUofvitaminDadayalongwithanadditional1,000IUvitaminDsupplement,foratotalofat least1,400IUofvitaminDaday.Theyshouldalsotakecalciumsupplements(1,000milligramsaday,whichcanbesplit intotwo servings of 500 milligrams each). Or they can obtain their calcium bydrinking three to four glasses of skimmilk or calcium-fortified orange juice,whichwill likely be fortifiedwith vitaminD, too. I believe that pregnant andlactatingwomencaneasily take2,000 IUofvitaminDadaywithout causingany toxicity. They shouldmaintain a blood level of 25-vitaminD between 30and100nanogramspermilliliter.Q.Weusedto thinktoomuchvitaminD inpregnantwomenwouldcausethefetus’sheadgrowthtobestunted.Isthatamyth?A.Yes,itisamyth.I’mnotsurewhatyoumeanby“toomuchvitaminD,”butcertainlytakingtherecommended1,400to2,000IUofvitaminDadaywillnotstuntthefetus’sheadgrowth.VitaminDdeficiencyinutero,however,can.Q.Whyareinfantsonlytoreceive400IU?Howaboutprematureinfants?A.InfantsappeartosatisfymostoftheirvitaminDrequirementforbonehealthbyreceiving400IUofvitaminDaday.ThisistherecommendationmadebytheAmericanAcademyofPediatrics and theCanadianPediatricSociety.There issomeevidencethatprematureinfantsmaynotbeabletometabolizevitaminDasefficiently,buttherearenodatatosuggestthatgivingaprematureinfantmorethan 400 IU of vitamin D a day has any additional benefit. Thus, I wouldrecommendthatinfants,includingprematureinfants,receiveatleast400IUof

vitaminDaday,andIbelievethatupto1,000IUofvitaminDadayissafeforthem.Q.Iaminmythirdtrimesterandhavebeensupplementingwith1,400IUofvitaminD3aday.Mydoctorwantsmetostopsupplementingbecausemylevels of activated vitamin D are twice normal and my 25-vitamin D isnormal.She’sworriedabouttoxicity.ShouldIbe?A. Absolutely not. Activated vitamin D (1,25-vitamin D) goes up during thesecond and third trimester; this is in response to your body’s making morevitamin D-binding protein and your need to increase your efficiency ofabsorbing dietary supplemental calcium for fetal mineralization. You areperfectly fineandshouldcontinue to takeyourvitaminD.Youandyourbabywillbenefit.
Disease,Disorders,andSpecialConditions
Q. Once you are diagnosed with cancer, does it help to take vitamin Dsupplements?A.Wedon’tknowwhether increasingvitaminDonceadiagnosisofcancer ismadeprovidesanybenefitinreducingthegrowthofthecancerorthecancer’soutcome.However,thereisnoreasonnottohaveallcancerpatientstakeenoughvitaminD tomaintain their blood level of 25-vitaminD between 30 and 100nanogramspermilliliter. Itmay improvemuscle strengthandbonestrengthaswell as possibly enhancing the therapeutic benefit of any cancer treatment.Patients with cancer often have aches and pains in their bones, muscles, andjoints,aswellasgastrointestinalupset.Curing themofavitaminDdeficiencycanhelp.Mystudieshaveshownthatcancerpatientsaretypicallydeficient.WehavealsodemonstratedinmicethatcolonandprostatecancercellgrowthislessinmicereceivingadequatevitaminD.Q. Are vitamin D supplements safe during chemotherapy, or could theyinteractwiththeactionoftheseagents?A. There is no evidence that vitamin D supplements will interact withchemotherapy. Therefore, vitamin D supplementation is safe duringchemotherapy. My lab has found that more than 50 percent of patients with
variouscancerswhowereonchemotherapywereseverelyvitaminDsufficient.Q.Isitnecessarytohave25-vitaminDlevelsbetween60and80nanogramspermillilitertopreventcancer?A.Itdoesappearthatabloodlevelof25-vitaminDisatleast30nanogramspermillilitermaydecreasetheriskofmanydeadlycancers.Itisunknown,however,the blood level needs to be 60 nanograms per milliliter. There is no harm inkeepingthebloodlevelatbetween60and80nanogramspermilliliter.IhaveallofmypatientsonenoughvitaminDtomaintain theirbloodlevelsbetween40and 100 nanograms per milliliter, which I believe to be both therapeutic andpreventativeofchronicdiseasesincludingcommoncancers.Q.IsvitaminDdeficiencylinkedtothyroiddisease?A. Vitamin D deficiency does not cause thyroid disease, but patients withhyperthyroidism(anoveractivethyroidthatleadstoanimbalanceofthebody’smetabolic hormones, tripping a cascade of health problems) have increaseddestructionof25-vitaminDandareathigherriskofvitaminDdeficiency(seechapter11).Q. Is there any correlation between vitamin D deficiency andhypothyroidism(anunderactivethyroid)?A.There is no correlation between vitaminD deficiency and hypothyroidism.VitaminDdeficiencyissocommonthatoftenpatientswithhypothyroidismarealsovitaminDdeficient.Allpatients,includinghypothyroidpatients,shouldbetreated for their vitamin D deficiency and prevent vitamin D deficiency bystayingonanadequateamountofvitaminD.Q.WhenchildrenraisedinequatorialareasmovetotheUnitedStatesanddevelophighratesofautism,couldthisberelatedtoVitaminDdeficiency?A.Thereislittleinformationregardingthecauseofautism,andtherehasbeenasuggestion thatvitaminDdeficiencymay increase riskof it.However, todatethere have not been any clinical trials demonstrating that vitaminD improvesautism.However, it is important thateveryone, includingchildrenwithautism,have an adequate amount of vitamin D to maintain their blood level of 25-vitaminDofbetween30and100nanogramspermilliliter.

Q. Is there any evidence that treating patients with autoimmune diseaseswithvitaminDcanlessentheirsymptoms?A.Therearenoprospectivestudiesthathavetreatedpatientswithautoimmunediseases with high doses of vitamin D, so we do not know whether suchtreatment would lessen their symptoms. However, vitamin D deficiency isassociated with many nonspecific symptoms, including muscle weakness,muscleachesandpains,boneachesandpains,andjointachesandpains,whichcan be associated with autoimmune diseases including multiple sclerosis andrheumatoid arthritis. In my experience, not only does treating patients withmultiplesclerosiswithvitaminDimprovetheiroverallfeelingofwell-beingandmusclestrength,butsomeofmypatientsalsohavehadanextendedhoneymoonfromtheirdisease.PatientswithrheumatoidarthritiswhoarevitaminDdeficientalso have improvement in muscle function and decreased aches and pains intheirbonesandjointswhenthedeficiencyistreated.Q.CanvitaminDhelpwiththesymptomsofmultiplesclerosis(MS)?WillvitaminDsupplementationdelaytheprogressionofMSinsomeonewhohasMS?A. I have found that my patients with multiple sclerosis are often vitamin Ddeficient.SincevitaminDdeficiencycausesmuscleweakness,Ihavefoundthatcorrecting their vitamin D deficiency significantly improves overall musclefunction. A few of my patients who had their first symptoms of multiplesclerosis and thenwere treatedwith 50,000 IU of vitaminD once aweek foreightweeksandeveryotherweekthereafter,haveremainedintheirhoneymoonperiod.Thus,ifyouhavemultiplesclerosis,thereisnoreasonnottohaveyourvitaminDstatuschecked,betreatedforyourvitaminDdeficiency,andpreventtherecurrenceofvitaminDdeficiency.Q. Inmild tomoderate cases of osteopenia (the prelude to osteoporosis),would taking adequate vitamin D and calcium be enough to preventosteoporosis,thuseliminatingneedforosteoporosismedications?A.Inmyexperience,manymenandwomenwhopresentwithmildormoderateosteopeniaarevitaminDdeficientandcalciumdeficient.I typicallytreat themfortheirvitaminDdeficiencyandthenmaintainthemon50,000IUofvitaminD2everytwoweeks.Inaddition,foradultsundertheageoffifty,Iplacethemona total of 1,000milligramsof calcium, either fromdietary sourcesor fromsupplements, and for adults over the age of fifty, I increase this by 200

milligrams, so that they ingest approximately 1,200 to 1,500 milligrams ofcalciumadayfromdietandsupplements.Irecommendthatthecalciumbetakenin twoor three divided doses, rather than all at once, because itwill bemorebioavailable.ThevitaminDcanbetakenanytime.Ifollowthesepatients,andoftenafterone to twoyears, I reevaluate theirbonemineraldensity.Often thepatients either have a small increase in their bone mineral density or nosignificantchange.Butsomecanhaveadramatic increaseof10percent to15percentiftheyhaveosteomalaciaduetovitaminDdeficiency.OnlywhenIseethat the bone density is reduced by more than 5 percent within a year do Ibecomeaggressiveinconsideringgivingmedicationtopreventosteoporosis.Q.Does vitaminDhave any associationwith scoliosis in adolescent girls?CanvitaminDsupplementationhelpcorrectspinalcurvature?A.IamnotawareofanyassociationbetweenscoliosisandvitaminDdeficiencyinadolescentgirls.However,manyadolescentgirlsarevitaminDdeficient,andtomaximizetheirbonehealth,theyshouldbereceivinganadequateamountofvitaminDandcalcium(seeboxonpage204).ButvitaminDsupplementationwillnot correct spinal curvature.Unfortunately, this is a permanent deformity.But if thevitaminDdeficiency isexacerbating thespinalcurvature,correctingvitaminDdeficiencymayhelppreventfurthercurvaturefromoccurring.Keepin mind that vitamin D will also improve muscle strength; a study out ofLebanonshowedthat2,000IUadaytogirlstentoseventeenyearsolddidjustthat.Another recent study,whichexamined the influenceof low25-vitaminDlevelsonbonemass,boneturnover,andmusclestrengthin301healthyChineseadolescent girls, also confirmed the importance of adequate vitamin D inreachingpeakbonemassandmusclestrength.Q.Would your recommendations be the same for Down’s syndrome andintellectualdisabilitypatients?A.Irecommendthatchildrenoveroneyearandadultsreceiveatleast1,400to2,000 IU of vitamin D a day if they are not getting adequate exposure tosunlight. This also applies to patients with Down’s syndrome and withintellectual disabilities. (Again, newborns should receive at least 400 IU ofvitaminD,andupto1,000IUadayissafeandmaybemorebeneficial.)Q.DoanyofthestudiesciteddemonstrateanincreasedincidenceofkidneystonesinpatientstakingthelevelsofvitaminDyousuggest?

A. In my opinion, there is no increased risk of developing kidney stones inpatients who are treated for vitamin D deficiency and maintain vitamin Dsufficiency as I have recommended.Most of the studies that have reported anassociation were poorly designed or poorly controlled. I have not found anyincreased riskofkidney stones inmypatientswhomIhave treatedvitaminDdeficiencyandmaintainedatanormalvitaminDstatus. Ibelieve that this isamyth.Q.Ihaveprimaryhyperparathyroidismandmycalcium iselevatedandIamvitaminDdeficient.MydoctorsaystakingvitaminDwill increasemycalciumlevelandthereforeIshouldavoidvitaminD.True?A.Thisisnottrue.Twostudieshaveprovedthat,ifanything,yourparathyroidhormone and calcium levels will be improved by correcting the vitamin Ddeficiency.Q. I have sarcoidosis and my doctor says I should not take vitamin Dbecauseitcouldcausemycalciumtoelevateabovenormal.True?A.ItistruethatexcessiveexposuretosunlightortakingtoomuchvitaminDcancausethemacrophagesinthesarcoidtissuetomaketoomuchactivatedvitaminD.However, patients should not remain vitaminD deficient, because that cancausemuscleweaknessandsymptomsofosteomalacia(achesandpainsinbonesand muscles). I treat my sarcoidosis patients with just enough vitamin D tomaintain their25-vitaminD levelbetween20and30nanogramspermilliliter,and Imonitor their serum calcium to be certain it does not elevate above thenormalrange.Q.Ihavekidneydiseaseandamondialysis.Mydoctorsaidthatsincemykidneys cannotmake activated vitaminD from 25-vitaminD, there is noneedformetotakevitaminDtomaintainmybloodlevelsof25-vitaminDabove30nanogramspermilliliter.Isthiscorrect?A.No.TheNationalKidneyFoundationandIrecommendthatallpatientswithkidney failure—evenpatientswithnokidneys—shouldmaintain25-vitaminDlevelsof30to100nanogramspermilliliter.Q.What about people who have a vitamin D receptor (VDR) defect andneedmorevitaminD?A.PatientswhohaveaVDRdefect can sometimesbenefitby increasing their

vitaminDintake.ItdependsupontheseverityofthealterationintheVDRgene.Patientswith theVDRgenemutation known as vitaminD-resistant rickets orvitaminD-dependent rickets type IIwill sometimesbenefit frombeing treatednotonlywithvitaminDbutalsowiththeactiveformofvitaminD,1,25-vitaminD.Q.Itakemedicationsthatmakemeextrasensitivetothesun.WhatshouldIdo?A. If you cannot expose yourself to the sun for any amount of time, thensupplementation is key.Aim to take 2,000 IUof vitaminD a day year-round.This can be in addition to anymultivitamin containing vitaminD, vitaminD-fortifiedfoodsandbeverages,andD-richfishyouconsume.Q. A lot of women are being given gabapentin for hot flashes instead ofestrogen.Canitlower25-vitaminDlevels?A.Wedo not knowwhether gabapentin (brand nameNeurontin orGabarone)used for treating hot flasheswill lower 25-vitaminD levels.However,we doknowthatmanydrugsandevenSt.John’swortwillenhancethedestructionofvitaminDinthebody.Thus,ataminimumIwouldrecommendbeingonatleast2,000 IU of vitamin D a day and having your blood level of 25-vitamin Dmonitored.

RESOURCEGUIDE
Thefollowinglistofresourcesisintendedasaguidetohelpyoumaximizetheprogramoutlinedinthisbook.SomeoftheseproductsIhavedoneresearchonorhaveused.Itisbynomeansexhaustivebecauseit’simpossibletolisteverytrustedresourceavailabletoyou.Exploreoptionsinyourlocalarea,andIinviteyoutoalsogotowww.drholicksdsolution.comforupdatedinformationandhelpinfindingthebestproductstosupportyourhealth.VitaminD-ProducingLightSpertiLampmfg.byKBD,[email protected]
WildSeafood
VitalChoicePOBox4121Bellingham,WA98227www.vitalchoice.comSalesLine:800-608-4825CustomerService:866-482-5887
SupplementBrands
Wellessewww.wellesse.com1-800-232-4005VitalNutrientswww.vitalnutrients.com1-888-328-9992LaneLabswww.lanelabs.com1-800-526-3005VitalChoicePOBox4121Bellingham,WA98227www.vitalchoice.comSalesLine:800-608-4825CustomerService:866-482-5887Perque*Perque’s“D3CellGuard”issoldthroughdoctorsandhealth-careprofessionals1-800-525-7352www.perque.cominfo@perque.comNatureMadewww.naturemade.com1-800-276-2878Metagenicswww.metagenics.comNewChapterNewChapterBoneHealthvitaminDandcalciumsupplementwww.newchapter.com
PediatricVitaminDrops
Enfamilwww.enfamil.com1-800-BABY-123(1-800-2229-123)JustDInfantVitaminDropswww.sunlightvitamins.comD-FriendlySunscreen(asunscreenthatpermitsyoutomakevitaminD)DSunSolutionSunscreenwww.dsunsolution.cominfo@dsunsolution.comVitaminD-FortifiedProductsBrands and general products to seek out at your local grocery store (youwilloftenfindthatbrandsadvertiserightonthelabelthattheirproductisfortified):
MinuteMaidorangejuicefortifiedwithcalciumandvitaminDVitaminD-fortifiedmilk,yogurt,cheese,andcottagecheeseVitaminD-fortifiedcerealsVitaminD-fortifiedbreadsMushroomsandmushroomsexposedtosunlightorsimulatedsunlightVitaminDyeastBodavitaminenergydrinkwithvitaminD(checkoutwww.urstuff.com)
LightBoxesforSeasonalAffectiveDisorderThe following list of suppliers’Web sites is only a sampling of the availablesources:
www.sunalux.com/s_lightboxes.cfmwww.verilux.comwww.consumer.philips.comhttp://sunbox.com/www.bio-light.com
SELECTEDBIBLIOGRAPHY
Atthetimethisbookwenttopress,newstudiescontinuedtoemergebackingupthe claims of researchers that maintaining healthy levels of vitamin D isfundamental to optimal health. A book that showcases every single publishedstudyonvitaminDwouldspanthousandsofpages,for it’sevenimpossible tolistall therecentstudies thathaveemergedin just the last twentyyears in thisbook.Whatfollowsisabibliographythathighlightssomeofthemoreprominentstudies published, including the ones that are featured in the book. Thebibliography isdivided intosections thatcovervarioushealth issuesaddressedthroughout thisvolume.Toaccessmore researchand find relatedstudies,visitmyWebsiteatwww.drholicksdsolution.comandcheckouttheNationalInstituteofHealth’sonlinepublicationlibraryatwww.pubmed.com.
AutoimmuneDiseases(multiplesclerosis,rheumatoidarthritis,type1diabetes,etc.)
Cantorna MT, Hayes CE, DeLuca HF. “1,25-Dihydroxyholecalciferol inhibitsthe progression of arthritis in murine models of human arthritis.” Journal ofNutrition1998;128:68-72.CantornaMT, Hayes CE, DeLuca HF. “1,25-Dihydroxyvitamin D3 reversiblyblocks the progression of relapsing encephalomyelitis, a model of multiplesclerosis.”ProceedingsoftheNationalAcademyofSciencesoftheUnitedStatesofAmerica1996;93:7861-64.Embry AF, Snowdon LR, Vieth R. “Vitamin D and seasonal fluctuations ofgadolinium-enhancing magnetic resonance imaging lesions in multiplesclerosis.”AnnalsofNeurology2000;48:271-72.EURODIAB Substudy 2 Study Group. “Vitamin D supplement in earlychildhood and risk for Type I (insulin-dependent) diabetes mellitus.”

Diabetologia1999;42:51-54.Harris SS. “Vitamin D and type 1 diabetes.” American Journal of ClinicalNutrition2004;79;889-90.HernánMA,OlekMJ,AscherioA. “GeographicvariationofMS incidence intwoprospectivestudiesofUSwomen.”Neurology1999;51:1711-18.HyppönenE,LääräE,JärvelinM-R,VirtanenSM.“IntakeofvitaminDandriskoftype1diabetes:Abirth-cohortstudy.”Lancet2001;358:1500-1503.MathieuC,BadenhoopK.“VitaminDandtype1diabetesmellitus:Stateoftheart.TrendsinEndocrinologyandMetabolism2005;16:261-66.Merlino LA, Curtis J, Mikuls TR, Cerhan JR, Criswell LA, Saag KG. Iowa“Women’s health study. Vitamin D intake is inversely associated withrheumatoidarthritis.”ArthritisandRheumatism2004;50(1):72-77.Mohr SB, Garland CF, Gorham ED, Garland FC. “The association betweenultravioletBirradiance,vitaminDstatusandincidenceratesoftype1diabetesin51regionsworldwide.”Diabetologia2008Aug;51(8):1391-98.Munger KL, Zhang SM, O’Reilly E, Hernán MA, Olek MJ, Willett WC,AscherioA.“VitaminDintakeandincidenceofmultiplesclerosis.”Neurology2004;62(1):60-65.Munger KL, Levin LI, Hollis BW, Howard NS, Ascheino A. “Serum 25-hydroxyvitaminDlevelsandriskofmultiplesclerosis.”JournaloftheAmericanMedicalAssociation2006;296:2832-38.Ponsonby AL, Lucas RM, van der Mei IA. “UVR, vitamin D and threeautoimmune diseases-multiple sclerosis, type 1 diabetes, rheumatoid arthritis.”PhotochemistryandPhotobiology2005;81:1267-75.VanAmerongenBM,DijkstraCD,LipsP,andPolmanCH.“Multiple sclerosisand vitamin D: An update.” European Journal of Clinical Nutrition 2004;58(8):1095-109.
BrainHealth(Alzheimer’s,dementia,depression,seasonalaffectivedisorder,schizophrenia,etc.)
Ancoli-IsraelS,MartinJL,KripkeDF,MarlerM,andKlauberMR.“Effectoflight treatment on sleep and circadian rhythms in demented nursing homepatients.”JournaloftheAmericanGeriatricsSociety2002;50(2):282-89.Brainard GC, Hanifin JP, Rollag MD, Greeson, J, et al. “Human melatoninregulationisnotmediatedbythethreeconephotopicvisualsystem.”Journalof
ClinicalEndocrinologyandMetabolism2001;86(1):433-36.Colenda CC, et al. “Phototherapy for patients with Alzheimer disease withdisturbedsleeppatterns:Resultsofacommunity-basedpilot study.”AlzheimerDiseaseandAssociatedDisorders1997;11(3):175-78.CzeislerCA,etal.“Useofbrightlighttotreatmaladaptationtonightshiftworkandcircadianrhythmsleepdisorders.”JournalofSleepResearch1995;4(S2):70-73.DaviesG,WelhamJ,ChantD,TorreyEF,McGrathJ.“Asystematicreviewandmeta-analysisofNorthernHemisphereseasonofbirthstudiesinschizophrenia.”SchizophreniaBulletin2003;29(3):587-93.Eastman CI, et al. “Bright light treatment of winter depression.” Archives ofGeneralPsychiatry1998;55:883-89.EylesDW, Smith S,KinobeR,HewisonM,McGrath JJ. “Distribution of theVitaminD receptorand1α-hydroxylase inhumanbrain.”JournalofChemicalNeuroanatomy2005;29:21-30.GlothFM,AlamW,andHollisB.“VitaminDvsbroadspectrumphototherapyinthetreatmentofseasonalaffectivedisorder.”JournalofNutrition,HealthandAging1999;3:5-7.KendellRE,AdamsW. “Exposure to sunlight, vitaminD and schizophrenia.”SchizophreniaResearch2002;54(3):193-98.Kripke DF. “Light treatment for nonseasonal depression: Speed, efficacy, andcombinedtreatment.JournalofAffectiveDisorders1998;49(2):109-17.LamRW,LevittAJ(eds.).“Canadianconsensusguidelinesforthetreatmentofseasonalaffectivedisorder:AsummaryofthereportoftheCanadianconsensusgrouponSAD.”CanadianJournalofDiagnosis2000.Levins PC, Carr DB, Fisher JE, Momtaz K, Parrish JA. “Plasma [beta]-endorphin and [beta]-lipotropin response to ultraviolet radiation.” Lancet1983;2(8342):166.LewyAJ, et al. “Morning vs. evening light treatment of patients with winterdepression.”ArchivesofGeneralPsychiatry1998;55:890-96.McGrathJ,EylesD,MowryB,YolkenR,BukaS.“LowmaternalvitaminDasariskfactorforschizophrenia:Apilotstudyusingbankedsera.”SchizophreniaResearch2003;63:73-78.MishimaK,etal.“Morningbrightlighttherapyforsleepandbehaviordisordersinelderlypatientswithdementia.”ActaPsychiatricaScandinavica1994;89(1):1-7.RosenthalNE.“Diagnosisandtreatmentofseasonalaffectivedisorder.”Journal
oftheAmericanMedicalAssociation1993;270(22):2717-20.Sato Y, Iwamoto J, Kanoko T, Satoh K. “Amelioration of osteoporosis andhypovitaminosis D by sunlight exposure in hospitalized, elderly women withAlzheimer’s Disease: A randomized controlled trial.” Journal of Bone andMineralResearch2005;20:1327-33.Terman M, Lewy AJ, Dijk DJ, Boulos Z, et al. “Light treatment for sleepdisorders:Consensusreport.IV.Sleepphaseanddurationdisturbances.”JournalofBiologicalRhythms1995;10:135-47.Zanello SB, JacksonD,HolickMF. “Expression of the circadian clock genesclock and period 1 in human skin.” Journal of Investigative Dermatology2000;115(4):757-60.
Cancer(oftheinternalorgans,e.g.,breast,colon,prostate,ovarian,pancreatic,etc.)
AhonenMH,TenkanenL,TeppoL,HakamaM,TuohimaaP.“Prostatecancerrisk and prediagnostic serum 25-hydroxyvitamin D levels (Finland).”CancerCausesControl2000;11:847-52.Apperly FL. “The relation of solar radiation to cancer mortality in NorthAmerica.”CancerResearch1941;1:191-95.Bertone-JohnsonER,ChenWY,HolickMF,etal.“Plasma25-hydroxyvitaminD and 1,25-Dihydroxyvitamin D and risk of breast cancer.” CancerEpidemiology,BiomarkersandPrevention2005;14:1991-97.Bischoff-FerrariHA,GiovannucciE,WillettWC,DietrichT,Dawson-HughesB. “Estimation of optimal serum concentrations of 25-hydroxyvitamin D formultiplehealthoutcomes.”AmericanJournalofClinicalNutrition2006;84:18-28.BodiwalaD, Luscombe CJ, Liu S, SaxbyM, FrenchM, Jones PW. “Prostatecancer risk and exposure to ultraviolet radiation: Further support for theprotectiveeffectofsunlight.”CancerLetters2003;192(2):145-49.Chen TC, Holick MF. “Vitamin D and prostate cancer prevention andtreatment.”TrendsinEndocrinologyandMetabolism2003;14:423-30.Cross HS, Kallay E, Lechner D, Gerdenitsch W, et al. “Phytoestrogens andvitamin D metabolism: A new concept for the prevention and therapy ofcolorectal, prostate and mammary carcinoma.” Journal of Nutrition 2004May;134(5):1207S-1212S.
Feldman D, Zhao XY, Krishnan AV. Editorial/Mini-review: “Vitamin D andprostatecancer.”Endocrinology2000;141:5-9.FeskanichJM,FuchsCS,KirknerGJ,HankinsonSE,etal.“PlasmavitaminDmetabolites and risk of colorectal cancer in women.” Cancer Epidemiology,BiomarkersandPrevention2004;13(9):1502-8.FreedmanDM,DosemeciM,McGlynnK.“Sunlightandmortalityfrombreast,ovarian, colon, prostate, and nonmelanoma skin cancer: A composite deathcertificatebasedcase-controlstudy.”OccupationalandEnvironmentalMedicine2002;59:257-62.Garland CF, Garland FC, Shaw EK, Comstock GW, et al. “Serum 25-hydroxyvitamin D and colon cancer: Eight-year prospective study.” Lancet1989;18:1176-78.GarlandFC,GarlandCF,GorhamED,YoungJF.“GeographicvariationinbreastcancermortalityintheUnitedStates:Ahypothesisinvolvingexposuretosolarradiation.”PreventiveMedicine1990;19:614-22.GarlandCF,GarlandFC,GorhamED,etal. “The roleofvitaminD incancerprevention.”AmericanJournalofPublicHealth2006;96(2):252-61.Garland CF, Gorham ED, Mohr SB, Garland FC. “Vitamin D for cancerprevention:Globalperspective.”AnnalsofEpidemiology2009Jul;19(7):468-83.GarlandCF,GorhamED,MohrSB,GrantWB,etal.“VitaminDandpreventionof breast cancer: Pooled analysis.” Journal of Steroid Biochemistry andMolecularBiology2006;103(3-5):708-11.Giovannucci E, Liu Y, Rimm EB, Hollis BW, et al. “Prospective study ofpredictors of vitamin D status and cancer incidence and mortality in men.”JournaloftheNationalCancerInstitute2006;98(7):451-59.GiovannucciE,LiuY,WillettWC.“CancerincidenceandmortalityandvitaminD in black ad white male health professionals.” Cancer Epidemiology,BiomarkersandPrevention2006;15(12):2467-72.Gorham ED, Garland CF, Garland FC, et al. “Optimal vitamin D status forcolorectalcancerprevention:Aquantitativemetaanalysis.”AmericanJournalofPreventiveMedicine2007;32(3):210-16.Grant WB. “An estimate of premature cancer mortality in the U.S. due toinadequatedosesofsolarultraviolet-Bradiation.”Cancer2002;70:2861-69.GrantWB.“Howstrong is theevidence that solarultravioletBandvitaminDreducetheriskofcancer?”Dermato-Endocrinology2009;1:17-24.Grant WB. “Lower vitamin-D production from solar ultraviolet-B irradiancemayexplainsomedifferencesincancersurvivalrates.”JournaloftheNational

MedicalAssociation2006;98(3):357-64.HanchetteCL,SchwartzGG.“Geographicpatternsofprostatecancermortality.”Cancer1992;70:2861-69.HolickMF. “Calcium plus vitaminD and the risk of colorectal cancer.”NewEnglandJournalofMedicine2006;354(21):2287.HolickMF.“VitaminDandsunlight:Strategiesforcancerpreventionandotherhealthbenefits.”Clinical Journalof theAmericanSocietyofNephrology2008Sep;3(5):1548-55.JohnEM,SchwartzGG,DreonDM,KooJ.“VitaminDandbreastcancerrisk:TheNHANES I epidemiologic follow-up study,1971-1975 to1992.”NationalHealth and Nutrition Examination Survey. Cancer Epidemiology, BiomarkersandPrevention1999;8:399-406.KnightJA,LesoskyM,BarnettH,RaboudJM,ViethR.“VitaminDandreducedrisk of breast cancer: A population-based case-control study.” CancerEpidemiology,BiomarkersandPrevention2007;16(3):422-99.LappeJM,Travers-GustafsonD,DaviesKM,ReckerRR,HeaneyRP.“VitaminD and calcium supplementation reduces cancer risk: Results of a randomizedtrial.”AmericanJournalofClinicalNutrition2007;85(6):1586-91.LefkowitzES,GarlandCF.“Sunlight,vitaminD,andovariancancermortalityratesinUSwomen.”InternationalJournalofEpidemiology1994;23:1133-36.PalmerHG,LarribaMJ,GarciaJM,Ordonez-MoranP,etal.“Thetranscriptionfactor SNAIL represses vitamin D receptor expression and responsiveness inhumancoloncancer.”NatureMedicine2004;10:917-19.PellerS,StephensonCS.“SkinirritationandcancerintheUnitedStatesNavy.”AmericanJournaloftheMedicalSciences1937;194:326-33.Schwartz GG,Whitlatch LW, Chen TC, Lokeshwar BL, HolickMF. “Humanprostate cells synthesize 1,25-dihydroxyvitamin D3 from 25-hydroxyvitaminD3.”CancerEpidemiology,BiomarkersandPrevention1998;7:391-95.Spina CS, Tangpricha V, Uskokovic M, Adorinic L, et al. “Vitamin D andcancer.”AnticancerResearch2006;26(4a):2515-24.Wactawski-WendeJ,KotchenJM,AndersonGL,etal.“CalciumplusvitaminDsupplementation and the risk of colorectal cancer.” New England Journal ofMedicine2006;354:684-96.
CardiovascularHealth

BostickR,KushiLH,WuY,MeyerKA,etal.“Relationofcalcium,vitaminDand dietary food intake to ischemic heart disease mortality among postmenopausalwomen.”AmericanJournalofEpidemiology1999;149:151-61.CarboneLD,RosenbergEW,TolleyEA,HolickMF,etal.“25-HydroxyvitaminD, cholesterol, and ultraviolet irradiation.” Metabolism Clinical andExperimental2008;57:741-48.DobnigH,PilzS,ScharnaglH,RennerW,etal.“Independentassociationoflowserum25-hydroxyvitaminDand1,25-dihyroxyvitaminD levelswith all-causeand cardiovascular mortality.” Archives of Internal Medicine 2008;168(12):1340-49.Fahrleitner A,Dobnig H, Obernosterer A,et al. “Vitamin D deficiency andsecondary hyperparathyroidism are common complications in patients withperipheralarterialdisease.”JournalofGeneralInternalMedicine2002;17:663-69.GiovannucciE,LiuY,HollisBW,RimmEB.“25-HydroxyvitaminDandriskofmyocardial infarction in men.” Archives of Internal Medicine 2008;168(11):1174-80.Holick MF. “Sunlight and vitamin D: Both good for cardiovascular health.”JournalofGeneralInternalMedicine2002;17(9):733-35.JordeR,BønaaK.“Calciumfromdairyproducts,vitaminDintake,andbloodpressure: The Tromsø study.” American Journal of Clinical Nutrition2000;71:1530-35.KrauseR,BühringM,HopfenmüllerW,HolickMF,SharmaAM.“UltravioletBandbloodpressure.”Lancet1998;352(9129):709-10.KumarJ,MuntnerP,KaskelFJ,HailpernSM,MelamedML.“Prevalenceandassociations of 25-hydroxyvitamin D deficiency in US children: NHANES2001-2004.”Pediatrics2009;124;e362-e370.LeeJH,O’KeefeJH,BellD,HensrudDD,HolickMF.“VitaminDdeficiency:Animportant,common,andeasilytreatablecardiovascularriskfactor?”JournaloftheAmericanCollegeofCardiology2008Dec9;52(24):1949-56.LindL,HanniA,LithellH,HvarfnerA,etal. “VitaminD is related to bloodpressure and other cardiovascular risk factors inmiddle-agedmen.”AmericanJournalofHypertension1995;8:894-901.MartinsD,WolfM,PanD,ZadshirA,etal.“Prevalenceofcardiovascularriskfactorsandtheserumlevelsof25-hydroxyvitaminDintheUnitedStates:DatafromtheThirdNationalHealthandNutritionExaminationSurvey.”ArchivesofInternalMedicine2007;167-(11):1159-65.

Melamed ML, Muntner P, Michos ED, Uribarri J, et al. “Serum 25-hydroxyvitaminDlevelsandtheprevalenceofperipheralarerialdisease:Resultsfrom NHANES 2001 to 2004.” Arteriosclerosis, Thrombosis, and VascularBiology2008;28(6):1179-85.PfeiferM,BegerowB,MinneHW,NachtigallD,HansenC.“Effectsofashort-termvitaminD3andcalciumsupplementationonbloodpressureandparathyroidhormone levels in elderly women.” Journal of Clinical Endocrinology andMetabolism2001;86:1633-37.PooleKE, LoveridgeN, Barker PJ,HalsallDJ, et al. “Reduced vitaminD inacutestroke.”Stroke2006;37(1):243-45.ReisJP,vonMühlenD,MillerER3rd,MichosED,AppelLJ.“VitaminDstatusand cardiometabolic risk factors in the United States adolescent population.”Pediatrics.2009;Aug3.Rostand SG. “Ultraviolet light may contribute to geographic and racial bloodpressuredifferences.”Hypertension1997;30(2pt1):150-56.WangTJ,PencinaMJ,BoothSL,JacquesPF,etal.“VitaminDdeficiencyandriskofcardiovasculardisease.”Circulation2008;117(4):503-11.ZittermannA,SchleithoffSS,TenderichG,BertholdHK,etal.“LowvitaminDstatus:A contributing factor in the pathogenesis of congestive heart failure? ”JournaloftheAmericanCollegeofCardiology2003;41:105-12.
Immunity
Aloia JR, Li-NgM. “Epidemic influenza and vitamin D.” Epidemiology andInfection2007;12:1-4.CannellJJ,ViethR,UmhauJC,HolickMF,GrantWB,MadronichS,GarlandCF, Giovannucci E. “Epidemic influenza and vitamin D.” Epidemiology andInfection2006;134(6):1129-40.Cantorna MT, Zhu Y, Froicu M, Wittke A. “Vitamin D status, 1,25-dihydroxyvitaminD3, and the immune system.”American Journal of ClinicalNutrition2004;80(suppl):1717S-1720S.ChanTYK.“VitaminDdeficiencyandsusceptibilitytotuberculosis.”CalcifiedTissueInternational2000;66(6):476-78.Ginde AA, Mansbach JM, Camargo CA Jr. “Association between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the ThirdNational Health and Nutrition Examination Survey.” Archives of Internal
Medicine2009Feb23;169(4):384-90.Krause R, Kuhn G, Pose M, Dobberke, et al. “Suberythemal UV-irradiationincreases immunologicalcapacity inchildrenwith frequentcolds.” InBiologiceffectsoflight1998.ProceedingsofasymposiumBasel,SwitzerlandNovember1-3, 1998. M. F. Holick and E. G. Jung, editors. Boston: Kluwer AcademicPublishers,1999:49-51.Liu PT, Stenger S, Li H,Wenzel L, et al. “Toll-like receptor triggering of avitaminD-mediatedhumanantimicrobialresponse.”Science2006;311:1770-73.
KidneyDisease
Dusso AS, Brown AJ, Slatopolsky. “Vitamin D.” American Journal ofPhysiology—RenalPhysiology2005;289:F8-F28.JonesG.“ExpandingroleforvitaminDinchronickidneydisease: Importanceof blood 25-OH-D levels and extra-renal 1α-hydroxylase in the classical andnonclassical actions of 1α,25-dihydroxyvitamin D3.” Seminars in Dialysis2007;20(4):316-24.
MuscleStrength
Bischoff-Ferrari HA, Dietrich T, Orav EJ, Hu FB, Zhang Y, Karlson EW,Dawson-HughesB.“Higher25-hydroxyvitaminDconcentrationsareassociatedwith better lower-extremity function in both active and inactive persons aged≥60y.”AmericanJournalofClinicalNutrition2004;80(3):752-58.Bischoff-FerrariHA,Dawson-HughesB,WillettWC,etal.“EffectofvitaminDon falls: A meta-analysis.” Journal of the American Medical Association2004;291:1999-2006.Bischoff-Ferrari HA, Orav EJ, Dawson-Hughes B. “Effects of cholecalciferolplus calcium on falling in ambulatory older men and women.” Archives ofInternalMedicine2006;166:424-30.BolandR.“RoleofvitaminDinskeletalmusclefunction.”EndocrineReviews1986;7:434-38.BroeKE,ChenTC,WeinbergJ,Bischoff-FerrariHA,etal. “AhigherdoseofvitaminD reduces the risk of falls in nursing home residents: A randomized,multiple-dose study.” Journal of the American Geriatrics Society

2007;55(2):234-39.Holick MF. “Sunlight ‘D’ilemma: Risk of skin cancer or bone disease andmuscleweakness.”Lancet2001;357(9249):4-6.Pfeifer M, Begerow B, Minne HW, et al. “Vitamin D status, trunk musclestrength, body sway, falls, and fractures among 237 postmenopausal womenwith osteoporosis.” Experimental and Clinical Endocrinology and Diabetes2001;109:87-92.Pfeifer M, Begerow B, Minne H, Abrams C, et al. “Effects of a short-termvitamin D and calcium supplementation on body sway and secondaryhyperparathyroidisminelderlywomen.”JournalofBoneandMineralResearch2000;15:1113-15.Visser M, Deeg DJ, Lips P, Longitudinal Aging Study Amsterdam. “Lowvitamin D and high parathyroid hormone levels as determinants of loss ofmuscle strength and muscle mass (sarcopenia): Longitudinal Aging StudyAmsterdam.”JournalofClinicalEndocrinologyandMetabolism2003;88:5766-72.
ObesityandMetabolicSyndrome
ArunabhS,PollackS,YehJ,AloiaJF.“Bodyfatcontentand25-hydroxyvitaminDlevelsinhealthywomen.”JournalofClinicalEndocrinologyandMetabolism2003;88:157-61.BellNH,EpsteinS,GreeneA,Shary J,OexmannMJ,ShawS.“Evidence foralteration of the vitamin D-endocrine system in obese subjects.” Journal ofClinicalInvestigation1985;76:370-73.FordES,AjaniUA,McGurieLC,LiuS:“Concentrationsof serumvitaminDandthemetabolicsyndromeamongU.S.adults.”DiabetesCare2005;28:1228-30.Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF. “DecreasedbioavailabilityofvitaminDinobesity.”AmericanJournalofClinicalNutrition2000;72:690-93.Wortsman J, Matsuoka LY, Chen TC, Zhiren L, Holick MF. “DecreasedbioavailabilityofvitaminDinobesity.”AmericanJournalofClinicalNutrition2000;72:690-93. Erratum in: American Journal of Clinical Nutrition2003;77:1342.
OralHealth
Dietrich T, Nunn M. Dawson-Hughes B, Bischoff-Ferrari HA. “Associationbetween serum concentrations of 25-hydroxyvitamin D and gingivalinflammation.”AmericanJournalofClinicalNutrition2005;82:575-80.DietrichT,JoshipuraKJ,Dawson-HughesB,Bischoff-FerrariHA.“Associationbetweenserumconcentrationsof25-hydroxyvitaminD3andperiodontaldiseaseintheUSpopulation.”AmericanJournalofClinicalNutrition2004;80:108-13.Krall EA,Wehler C,Garcia RI, Harris SS,Dawson-Hughes B. “Calcium andvitaminD supplements reduce tooth loss in the elderly.”American Journal ofMedicine2001;111:452-56.
OsteomalaciaandFibromyalgia
Glerup H, Mikkelsen K, Poulsen L, Hass E, et al. “Hypovitaminosis Dmyopathy without biochemical signs of osteomalacic bone involvement.”CalcifiedTissueInternational2000Jun;66(6):419-24.Plotnikoff GA, and Quigley JM. “Prevalence of severe hypovitaminosis D inpatients with persistent, nonspecific musculoskeletal pain.” Mayo ClinicProceedings2003;78:1463-70.Malabanan AO, Turner AK, Holick MF. “Severe generalized bone pain andosteoporosis in a premenopausal black female: Effect of vitamin Dreplacement.”JournalofClinicalDensitometry1998(1):201-4.HolickMF.“VitaminDdeficiency:Whatapainitis.”MayoClinicProceedings2003;78(12):1457-59.
Osteoporosis,BoneDensity,andCalciumAbsorption
AbramsSA,GriffinIJ,HawthorneKM,GunnSK,etal.“RelationshipsamongVitamin D levels, parathyroid hormone, and calcium absorption in youngadolescents.”JournalofEndocrinologyandMetabolism2005;90(10):5576-81.Araujo AB, Travison TG, Esche GR, Holick MF, et al. “Serum 25-hydroxyvitamin D and bone mineral density among Hispanic men.”OsteoporosisInternational2009Feb;20(2):245-55.ArisRM,MerkelPA,BachrachLK,BorowitzDS,etal.“Consensusstatement:

Guide to bone health and disease in cystic fibrosis.” Journal of ClinicalEndocrinologyandMetabolism2005;90(3):1888-96.BakhtiyarovaS,LesnyakO,KyznesovaN,BlankensteinMA,LipsP.“VitaminD status among patients with hip fracture and elderly control subjects inYekaterinburg,Russia.”OsteoporosisInternational2006;17(3):441-46.BeardMK,LipsP,HolickMF,etal.“VitaminDinadequacyisprevalentamongpostmenopausalosteoporoticwomen.”Climateric2005;8(Suppl2):199-200.Bischoff-Ferrari HA, Willet WC, Wong JB, Giovannucci E, et al. “Fractureprevention with vitamin D supplementation: A meta-analysis of randomizedcontrolledtrials.”JournaloftheAmericanMedicalAssociation2005;293:2257-64.Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T, and Dawson-HughesB.“Estimationofoptimalserumconcentrationsof25-hydroxyvitaminDfor multiple health outcomes.” American Journal of Clinical Nutrition2006;84:18-28.Bischoff-Ferrari HA, Dietrich T, Orav J, Dawson-Hughes B. “Positiveassociation between 25-hydroxyvitaminD levels and bonemineral density:Apopulation-based studyofyounger andolder adults.”Journal of theAmericanMedicalAssociation2004;116:634-39.ChapuyMC,ArlotME,DuboeufF,BrunJ,etal.“VitaminD3andcalciumtoprevent hip fractures in elderly women.” New England Journal of Medicine1992;327(23):1637-42.Cooper C, Javaid K, Westlake S, Harvey N, Dennison E. “Developmentaloriginsofosteoporotic fracture:TheroleofmaternalvitaminDinsufficiency.”JournalofNutrition2005;135:2728S-2734S.Dawson-Hughes B, Harris SS, Krall EA, Dallal GE. “Effect of calcium andvitaminDsupplementationonbonedensityinmenandwomen65yearsofageorolder.”NewEnglandJournalofMedicine.1997;337:670-76.Di Daniele N, Carbonelli MG, Candeloro N, Iacopino L, et al. “Effect ofsupplementation of calcium and vitaminD on bonemineral density and bonemineral content in peri-and post-menopause women; a double-blind,randomized,controlledtrial.”PharmacologicalResearch2004;50:637-41.FeskanichD,WillettWC,ColditzGA.“Calcium,vitaminD,milkconsumption,and hip fractures: A prospective study among postmenopausal women.”AmericanJournalofClinicalNutrition2003;77:504-11.GlowackiJ,HurwitzS,ThornhillTS,KellyM,LeBoffMS.“Osteoporosisandvitamin D deficiency among postmenopausal women with osteoarthritis
undergoing total hip arthroplasty.” Journal of Bone and Joint Surgery2003;85A:2371-77.Heaney RP, Dowell MS, Hale CA, Bendich A. “Calcium absorption varieswithin the reference range for serum 25-hydroxyvitamin D.” Journal of theAmericanCollegeofNutrition2003;22(2),142-46.HeaneyRP,DaviesKM,ChenTC,HolickMF,Barger-LuxMJ.“Humanserum25-hydroxycholecalciferol response to extended oral dosing withcholecalciferol.”AmericanJournalofClinicalNutrition2003;77:204-10.Terris S. “Calcium plus vitamin D and the risk of fractures.” New EnglandJournalofMedicine2006;354(21):2285.
PregnancyandLactation
Bodnar LM, Catov JM, Simhan HN, HolickMF, et al. “Maternal vitamin Ddeficiency increases the risk of preeclampsia.” Journal of ClinicalEndocrinologyandMetabolism2007;92(9):3517-22.Bodnar LM, Krohn MA, Simhan HN. “Maternal vitamin D deficiency isassociatedwithbacterialvaginosis in thefirst trimesterofpregnancy.”JournalofNutrition2009Jun;139(6):1157-61.Camargo Jr CA, Rifas-Shiman SL, Litonjua AA, Rich-Edwards JW, et al.“ProspectivestudyofmaternalintakeofvitaminDduringpregnancyandriskofwheezing illnesses inchildrenatage2years.”JournalofAllergyandClinicalImmunology2006;117:721-22.Camargo Jr CA, Rifas-Shiman SL, Litonjua AA, et al. “Maternal intake ofvitaminDduringpregnancyandriskof recurrentwheeze inchildrenat3yofage.”AmericanJournalofClinicalNutrition2007;85(3)788-95.Merewood A, Mehta SD, Chen TC, Bauchner H, Holick MF. “Associationbetween vitamin D deficiency and primary caesarean section.” Journal ofClinicalEndocrinologyandMetabolism2009Mar;94(3):940-45.HollisBW,WagnerCL.“AssessmentofdietaryvitaminDrequirementsduringpregnancyandlactation.”AmericanJournalofClinicalNutrition2004;79:717-26.HollisBW,WagnerCL. “VitaminD requirements during lactation:High-dosematernalsupplementationastherapytopreventhypovitaminosisDforboththemother and the nursing infant.” American Journal of Clinical Nutrition2004;80:1752S-1758s.

Lee JM, Smith JR, Philipp BL, Chen TC, et al. “Vitamin D deficiency in ahealthygroupofmothersandnewborninfants.”ClinicalPediatrics2007;46:42-44.McGrathJ.“Does‘imprinting’withlowprenatalvitaminDcontributetotheriskof various adult disorders?”Medical Hypothesis 2001;56:367-71. Pawley N,Bishop NJ. “Prenatal and infant predictors of bone health: The influence ofvitamin D.” American Journal of Clinical Nutrition 2004; 80(suppl):1748S-1751S.
PremenstrualSyndrome
AndersonDJ,LeggNJ,RidoutDA.“Preliminarytrialofphoticstimulationforpremenstrualsyndrome.”JournalofObstetricsandGynecology1997;17(1):76-79.LamRW,etal. “Acontrolled studyof light therapy inwomenwith late lutealphasedysphoricdisorder.”PsychiatryResearch1999;86(3):185-92.Parry BL, et al. “Blunted phase-shift responses to morning bright light inpremenstrual dysphoric disorder.” Journal of Biological Rhythms 1997;12(5):443-56.Thys-Jacobs S. “Micronutrients and the premenstrual syndrome: The case forcalcium.”JournaloftheAmericanCollegeofNutrition2000Apr;19(2):220-27.
Psoriasis
Bourke JF, Berth-Jones J, Iqbal SJ, Hutchinson PE. “High-dose topicalcalcipotriol in the treatmentofextensivepsoriasisvulgaris.”BritishJournalofDermatology1993;129:74-76.HolickMF.“Clinicalefficacyof1,25-dihydroxyvitaminD3anditsanaloguesinthetreatmentofpsoriasis.”Retinoids1998;14:7-12.NickoloffB,SchroderJ,vondenDrieschP,RaychaudhuriS,etal.“IspsoriasisaT-celldisease?”ExperimentalDermatology2000;9:359-75.Perez A, Chen TC, Turner A, Raab R, et al. “Efficacy and safety of topicalcalcitriol (1,25-dihydroxyvitamin D3) for the treatment of psoriasis.” BritishJournalofDermatology1996;134:238-46.PerezA,RaabR,ChenTC,TurnerA,HolickMF.“Safetyandefficacyoforal
calcitriol (1,25-dihydroxyvitamin D3) for the treatment of psoriasis.” BritishJournalofDermatology1996;134:1070-78.
Rickets
DeLucia MC, Mitnick ME, Carpenter TO. 2003. “Nutritional rickets withnormal circulating 25-hydroxyvitamin D: A call for reexamining the role ofdietary calcium intake in North American infants.” Journal of ClinicalEndocrinologyandMetabolism2003;88:3539-45.HessAF,UngerLJ. “Thecureof infantile ricketsby sunlight.”Journalof theAmericanMedicalAssociation1921;77:39-41.HessAF,UngerLJ.“Useof thecarbonarc light in thepreventionandcureofrickets.”JournaloftheAmericanMedicalAssociation1922;78:1596-98.Holick MF. “Resurrection of vitamin D deficiency and rickets.” Journal ofClinicalInvestigation2006;116(8):2062-72.HolickMF,LimR,DigheAS.“Case3-2009:A9-month-oldboywithseizures.”NewEnglandJournalofMedicine2009;360:398-407.Huldschinsky K. “Heilung von Rachitis durch Kunstliche Hohensonne.”DeutscheMedWochenschr1919;45:712-13.Huldschinsky,K.“Theultravioletlighttreatmentofrickets.”NewJersey:AlpinePress,1928,3-19.KreiterSR,SchwartzRP,KirkmanHN,CharltonPA,etal.“Nutritional ricketsinAfricanAmericanbreast-fedinfants.”JournalofPediatrics2000;137:2-6.PettiforJM.“VitaminDdeficiencyandnutritionalricketsinchildreninvitaminD.” InVitaminD, second edition.David Feldman, J.Wesley Pike, FrancisH.Glorieux,eds.Boston:ElsevierAcademicPress,2005,1065-84.SniadeckiJ.JerdrzejSniadecki(1768-1838)onthecureofrickets.(1840)CitedbyW.Mozolowski.Nature1939;143:121-24.Wagner CL, Greer FR; American Academy of Pediatrics Section onBreastfeeding; American Academy of Pediatrics Committee on Nutrition.“Prevention of rickets and vitamin D deficiency in infants, children, andadolescents.”Pediatrics2008Nov;122(5):1142-52.
SkinCancer

Berwick M, Armstrong BK, Ben-Porat L et al. “Sun exposure and mortalityfrommelanoma.”JournaloftheNationalCancerInstitute2005;97,195-99.Bikle D. “Vitamin D receptor, UVR, and skin cancer: A potential protectivemechanism.”JournalofInvestigativeDermatology2008;128:2357-61.Black H, et al. “Evidence that a low-fat diet reduces the occurrence ofnonmelanomaskincancer.”InternationalJournalofCancer1995;62(2):165-69.GarlandFC,GarlandCF.“OccupationalsunlightexposureandmelanomaintheU.S.Navy.”ArchivesofEnvironmentalHealth1990;45,261-67.KennedyC,BajdikCD,WillemzeR,deGruijlFR,BavinckJN.“Theinfluenceofpainfulsunburnsandlifetimeofsunexposureontheriskofactinickeratoses,seborrheicwarts,melanocytic nevi, atypical nevi and skin cancer.” Journal ofInvestigativeDermatology2003;120(6):1087-93.Newton-Bishop JA,BeswickS,Randerson-Moor J,ChangYM,etal. “Serum25-hydroxyvitamin D3 levels are associated with breslow thickness atpresentationandsurvival frommelanoma.”JournalofClinicalOncology2009Nov10;27(32):5439-44.ZieglerA, JonasonAS,LeffellDJ, Simon JA,etal. “Sunburn and p53 in theonsetofskincancer.”Nature1994;372:773-76.
TanningBedTherapy
KoutkiaP,LuZ,ChenTC,HolickMF.“TreatmentofvitaminDdeficiencyduetoCrohn’s diseasewith tanning bed ultravioletB radiation.”Gastroenterology2001;121:1485-88.TangprichaV,TurnerA,SpinaC,DecastroS,etal.“TanningisassociatedwithoptimalvitaminDstatus(serum25-hydroxyvitaminDconcentration)andhigherbonemineral density.”American Journal of Clinical Nutrition. 2004;80:1645-49.PetersonCA,HeffernanME, SiskKA, andRing SM. “The effects of regulartanning bed use and increased vitamin D status on serum markers of boneturnoverinhealthyadultwomen.”ClinicalMedicine:Women’sHealth2009:21-7.
Type-2Diabetes

BorissovaAM,TankovaT,KirilovG,DakovskaL,KovachevasR.“Theeffectof vitaminD3 on insulin secretion and peripheral insulin sensitivity in type 2diabeticpatients.”InternationalJournalofClinicalPractice2003;57:258-61.BoucherBJ. “Inadequate vitaminD status:Does it contribute to the disorderscomprisingsyndromeX?”BritishJournalofNutrition1998;80:585.ChiuKC,ChuA,GoVLW,SaadMF. “HypovitaminosisD is associatedwithinsulin resistance and β cell dysfunction.” American Journal of ClinicalNutrition2004;79:820-25.Isai G,Giorgino R, andAdami S. “High prevalence of hypovitaminosisD infemaletype2diabeticpopulation.”DiabetesCare2001;24:1496-98.KumarS,DaviesM,ZakariaY,etal. “Improvement in glucose tolerance andbeta-cell function inapatientwithvitaminDdeficiencyduring treatmentwithvitaminD.”PostgraduateMedicalJournal1994;70:440-43.Oh J,Weng S, Felton SK, Bhandare S, et al. “1,25(OH)2 vitamin D inhibitsfoam cell formation and suppressesmacrophage cholesterol uptake in patientswithtype2diabetesmellitus.”Circulation2009Aug25;120(8):687-98.PittasAG,Dawson-HughesB,LiT,VanDamRM,WillettWC,etal.“VitaminDandcalcium intake in relation to type2diabetes inwomen.”DiabetesCare2006;29(3):650-56.PittasAG,LauJ,HuFB,Dawson-HughesB.Review:TheroleofvitaminDandcalciumintype2diabetes.Asystematicreviewandmeta-analysis.”JournalofClinicalEndocrinologyandMetabolism2007;92:2017-29.SchwalfenbergG. “VitaminD and diabetes: Improvement of glycemic controlwithvitaminD3repletion.”CanadianFamilyPhysician2008;54:864-66.Scragg R, Holdaway I, Singh V, et al. “Serum 25-hydroxyvitamin D3 levelsdecreased in impaired glucose tolerance and diabetes mellitus.” DiabetesResearchandClinicalPractice1995;27:181-88.
VitaminD2vs.D3
Holick MF, Biancuzzo RM, Chen TC, Klein EK, et al. “Vitamin D2 is aseffective as vitamin D3 in maintaining circulating concentrations of 25-hydroxyvitamin D.” Journal of Clinical Endocrinology and Metabolism2008;93(3):677-81.Armas LAG, Hollis B, Heaney RP. “Vitamin D2 is much less effective than
vitamin D3 in humans.” Journal of Clinical Endocrinology and Metabolism2004;89:5387-91.
VitaminDDeficiencyandIntoxication
Bodnar LM, Simhan HN, Powers RW, FrankMP, et al. “High prevalence ofvitamin D insufficiency in black and white pregnant women residing in thenorthernUnitedStatesandtheirneonates.”JournalofNutrition2007;137:447-52.CalvoMS,WhitingSJ,BartonCN.“VitaminDintake:Aglobalperspectiveofcurrentstatus.”JournalofNutrition2005;135:310-16.Dawson-HughesB,HeaneyRP,HolickMF,LipsP,etal.“EstimatesofoptimalvitaminDstatus.”OsteoporosisInternational(Editorial)2005;16:713-16.El-Hajj Fuleihan G, Nabulsi M, Choucair M, et al. “Hypovitaminosis D inhealthyschoolchildren.”Pediatrics2001;107:E53.GindeAA,LiuMC,CamargoJr.CA.“Demographicdifferencesand trendsofvitaminDinsufficiencyintheUSpopulation,1988-2004.”ArchivesofInternalMedicine2009Mar23;169(6):626-32.GordonCM,DePeterKC, EstherannG, Emans SJ. “Prevalence of vitaminDdeficiency among healthy adolescents.”Archives of Pediatrics andAdolescentMedicine2004;158:531-37.Gordon CM, Feldman HA, Sinclair L, Williams AL, et al. “Prevalence ofvitamin D deficiency among healthy infants and toddlers.” Archives ofPediatricsandAdolescentMedicine2008;162(6):505-12.GrantWE,GarlandCF andHolickMF. “Comparisons of estimated economicburdensduetoinsufficientsolarultravioletirradianceandvitaminDandexcesssolar UV irradiance for the Untied States.”Photochemistry and Photobiology2005;81(6):1276-86.HanleyDA,DavisonKS.“VitaminDinsufficiencyinNorthAmerica.”JournalofNutrition2005;135:332-37.HarrisSS,Dawson-HughesB.“Seasonalchangesinplasma25-hydroxyvitaminDconcentrationsyoungAmericanblackandwhitewomen.”AmericanJournalofClinicalNutrition1998;67(6):1232-36.HolickMF. “Too little vitamin D in premenopausal women:Why should wecare?”AmericanJournalofClinicalNutrition2002;76:3-4.HolickMF,JenkinsM.TheUVAdvantage.NewYork:iBooks;2003.
Holick MF. “Sunlight and vitamin D for bone health and prevention ofautoimmunediseases,cancers,andcardiovasculardisease.”AmericanJournalofClinicalNutrition2004;80:1678S-1688S.HolickMF, Siris ES, BinkleyN, BeardMK, et al. “Prevalence of vitamin Dinadequacy among postmenopausal North American women receivingosteoporosis therapy.” Journal of Clinical Endocrinology and Metabolism2005;90:3215-24.Holick MF. “High prevalence of vitamin D inadequacy and implications forhealth.”MayoClinicProceedings2006;81(3):353-73.Holick MF. “Vitamin D deficiency.” New England Journal of Medicine2007;357:266-81.HolickMF,ChenTC.“VitaminDdeficiency:Aworldwideproblemwithhealthconsequences.”AmericanJournalofClinicalNutrition2008;87(4):1080S-6S.Jacobus CH, Holick MF, Shao Q, Chen TC, et al. “Hypervitaminosis Dassociated with drinking milk.” New England Journal of Medicine 1992;326:1173-77.Koutkia P, Chen TC, HolickMF. “Vitamin D intoxication associated with anover-the-counter supplement.” New England Journal of Medicine2001;345(1):66-67.MalabananA,Veronikis IE,HolickMF.“RedefiningvitaminD insufficiency.”Lancet1998;351:805-6.MansbachJM,GindeAA,andCarmargoJr.CA.“Serum25-hydroxyvitaminDlevelsamongUSchildrenaged1to11Years:DochildrenneedmorevitaminD?”PediatricsNov.2009;124:1404-10.ParkS,JohnsonMA.“Livingin low-latituderegionsin theUnitedStatesdoesnotpreventpoorvitaminDstatus.”NutritionReviews2005;63:203-9.SullivanSS,RosenCJ,HaltemanWA,ChenTC,HolickMF.“AdolescentgirlsinMaineatriskforvitaminDinsufficiency.”Journalof theAmericanDieteticAssociation2005;105:971-74.Tangpricha V, Pearce EN, Chen TC, Holick MF. “Vitamin D insufficiencyamong free-living healthy young adults.” American Journal of Medicine2002;112(8):659-62.
VitaminDNutrition
ChandraP,WolfendenLL,ZieglerTR,Tian J,etal. “Treatment of vitaminD

deficiency with UV light in patients with malabsorption syndromes: A caseseries.” Photodermatology, Photoimmunology, and Photomedicine 2007;23(5):179-85.Chen TC, Chimeh F, Lu Z, Mathiew J, et al. “Factors that influence thecutaneoussynthesisanddietarysourcesofvitaminD.”ArchivesofBiochemistryandBiophysics2007;460(2):213-17.HolickMF, ShaoQ, LiuWW,Chen TC. “The vitaminD content of fortifiedmilkandinfantformula.”NewEnglandJournalofMedicine1992;326:1178-81.TangprichaV,Koutkia P, Rieke SM,Chen TC, et al. “Fortification of orangejuicewithvitaminD:AnovelapproachtoenhancevitaminDnutritionalhealth.”AmericanJournalofClinicalNutrition2003;77:1478-83.Vieth R, Garland C, Heaney R, et al. “The urgent need to reconsiderrecommendationsforvitaminDnutritionintake.”AmericanJournalofClinicalNutrition2007;85:649-50.
VitaminDSkinSynthesis
Clemens TL, Henderson SL, Adams JS, HolickMF. “Increased skin pigmentreducesthecapacityofskintosynthesisvitaminD3.”Lancet1982;1(8263):74-76.HolickMF,MacLaughlin JA,ClarkMB,HolickSA,etal. “Photosynthesis ofprevitamin D3 in human skin and the physiologic consequences.” Science1980;210:203-5.MacLaughlin J, Holick MF. “Aging decreases the capacity of human skin toproducevitaminD3.”JournalofClinicalInvestigation1985;76:1536-38.Matsuoka LY, Ide L, Wortsman J, MacLaughlin J, Holick MF. “Sunscreenssuppress cutaneous vitamin D3 synthesis.” Journal of Clinical EndocrinologyandMetabolism1987;64:1165-68.Webb AR, Kline L, Holick MF. “Influence of season and latitude on thecutaneous synthesisofvitaminD3:Exposure towinter sunlight inBoston andEdmontonwill not promote vitaminD3 synthesis in human skin.” Journal ofClinicalEndocrinologyandMetabolism1988;67:373-78.
INDEX
ActivatedvitaminD,autoimmunediseasesandcalciummetabolismanddestructionofdiabetes(type2)andhalf-lifeofashormonehypertensionandinflammationreductionandinstigationofcancerandlowercancerratesandproductionofpsoriasisandrheumatoidarthritisandtestingforActivatedvitaminDanalogsActonel(risedronate)Adams,JohnAdequateintake(AI)Adrenalglands“Adultrickets,”AfricanAmericansAge,skindamageandAge-relatedvitaminDdeficiencyAgingAkhenatonAllergicreactionsAllergicrhinitisAlzheimer’sdiseaseAmericanAcademyofDermatologyAmericanAcademyofPediatricsAmericanAssociationforCancerResearch

AmericanCouncilonScienceandHealthAmericanJournaloftheMedicalSciencesAmericanPsychiatricAssociationAmericanSocietyforMetabolicandBariatricSurgeryAncientpeoples,sunworshipbyAnderson.J.AnnalsofEpidemiologyAnti-seizuremedicationsAntisunlobbyApoptosisApperly,FrankAppetite-suppressinghormoneArchivesofInternalMedicineArthritisosteoarthritispsoriaticrheumatoidAssociatedPressAsthmaAtherosclerosisAutismAutoimmunediseases
BackpainBacterialinfectionsBasal-cellcarcinomaBasalcellsBauchner,HowardBell,NormanBetaendorphinsBetaisletcellsBiancuzzo,RachaelBikle,DanielBiologicalclockBiphosphonates

Bischoff-Ferrari,HeikeBladdercancerBloodpressurehigh,seeHypertensionregulationofBloodvesselsBloombergSchoolofPublicHealth,JohnsHopkinsUniversityBlue-lighttherapyBodnar,LisaBodyfat,storageinBonedensitometryBonedensityBoneformationBonehealthcalciummetabolismandexerciseandfibromyalgiaandobesityandosteomalaciaandosteoporosisand,seeOsteoporosisremodelingandricketsand,seeRicketsBonepainBoneresorptionBonestrengthBoniva(ibandronate)BostonFloatingHospitalBostonGlobeBostonUniversityMedicalCenterBrain,activatedvitaminDproductioninBrainhealthBreast,activatedvitaminDproductioninBreastcancerBreastfeedingBreastmilkBright-lighttherapydementiaanddepressionand
premenstrualsyndrome(PMS)andseasonalaffectivedisorder(SAD)andshiftworkersyndromeandsleepdisturbancesinelderlyandBritishMedicalAssociationBühring,Malte
Caesareansections(C-sections)CaffeineCalcidiol,see25-vitaminDCalciumamountneededatomicweightofbalancebetweenboneresorptionanddepositionandbonemassand“bonessavingsaccount”anddiabetes(type2)andfromdietdinosaurextinctionandevolutionoflandanimalsandhealthbenefitsfromboostingintakeofhomeostasisofmenstrualmigraineandmetabolismofmuscularfunctionandobesityandosteoporosisandpremenstrualsyndrome(PMS)androleineverydayfunctionsvitaminDdeficiencyandbloodlevelsofwomenandCalciumcarbonateCalciumdeficiencyCalciumsupplementsCanadianPediatricSociety

Cancerapoptosisandbladderbreastcolon(colorectal)DINOMITmodelofesophagealgeographicaldifferencesinsunexposureandlungnightlightexposureand,ovarianpancreaticpreventionofprostateraceandskin,seeSkincancerstomachsunexposureanddecreasedriskoftheoryofvitaminDdeficiencyascauseof,uterinevitaminDsupplementationand,Carcinogens,misconceptionsabout,CARDIAStudyCarlsson,ArvidCathelicidinCeliacdiseaseCellularhealthandsunexposure,CentersforDiseaseControlandPreventionChemotherapyChen,Tai“ChildhoodAsthmaIsaFat-SolubleVitaminDeficiencyDisease,”Childrenremodelinginricketsin,seeRicketsveganorvegetarianvitaminDdeficiencyin,vitaminDsupplementationfor,Children’sHospital,Boston
Cholecalciferol,seeVitaminD3CholesterolChronicdiseasesChronicfatiguesyndromeChroniclow-gradedepression,CircadianrhythmdisordersCirculationClinicalandExperimentalAllergy,CloudcoverCoca-ColaCompanyCodliveroilColon,activatedvitaminDproductioninColon(colorectal)cancerCook,FrederickCooking,effectsofCornellUniversityCosmeticwingofpharmaceuticalindustryCreightonUniversityCrohn’sdiseaseCryosurgeryCulture,vitaminDdeficiencyandCurettageCyclosporineCysticfibrosisCysticFibrosisFoundation
Dailyintake,seeRecommendedintakeDana-FarberCancerInstituteDawson-Hughes,BessDeficiencycalciumvitaminD,seeVitaminDdeficiency7-dehydrocholesterolDelayedsleepphasesyndromeDeLuca,HectorF.DeLucalaboratory
DementiaDentalcavitiesDepressionDepressionratingscalesDermatologycommunityDiabetestypetypeDiagnosticandStatisticalManualofMentalDisordersDietarysourcesofcalciumDietarysourcesofvitaminDfortifiedsourcesinadequacyof1-dihydroxyvitaminD,seeActivatedvitaminDDINOMITmodelDNA-repair-enzymediseasesDopamineDovonex(calciptriene)Down’ssyndromedrholicksdsolution.comDrugcompanies,seePharmaceuticalcompaniesDrugsforosteoporosisvitaminDdeficiencyandDysplasticnevusEatingdisordersElderlyosteoporosisandskincancerandsleepdisturbancesandvitaminDdeficiencyinElectrodessicationEnquirerEpidemiologistsEpidermisEpinephrine

Ergocalciferol,seeVitaminD2EskimosEsophagealcancerEvista(raloxifene)EvolutionExerciseExperimentalDermatology
FAQsFatcellsFatigueFatmalabsorptionsyndromesFattyacidsynthaseFattydiet,cancerandFederalTradeCommission(FTC)FibromyalgiaFinsen,NielsRybergFishFishoilcapsulesFitnessFlemming,AlexanderFluForteo(teriparatide)Fosamax(alendronate)Frontotemporaldementia
GabapentinGaldermaLaboratoriesGarland,CedricGarland,FrankGastricbypassGeographicaldifferencesinsunexposureautoimmunediseasesandcancerand

ricketsandultravioletradiation(UV)andvitaminDdeficiencyandGiovannucci,EdwardGlobe,theGoeckerman,WilliamGordon,CatherineGorham,EdGrant,WilliamGumdisease
H1N1(swineflu)HarvardNurses’HealthStudyHaussler,MarkR.Health,optimalHeaney,RobertHeartattackHeartdiseaseHeartfailureHeliotherapyHeredityHess,AlfredHighbloodpressure,seeHypertensionHigh-latitudesHippocratesHispanicsHolickSensibleSunTablesHolickSolutionforSensibleSunHolidaybluesHome,SirEverardHormonalactionHuldschinsky,KurtHumans,early25-hydroxyvitaminDtestHyperparathyroidism

HypertensionHyperthyroidismHypocalcemiaHypothalamusHyppönen,Elina
IguanasIL-10ImmunefunctionImmuno-surveillanceImmunotherapyIndianphysicians,vitaminDdeficiencyinIndoorTanningAssociationIndustrialrevolutionInfectiousdiseasesInflammationInfluenzaInnerdermisInsomniaInstituteofMedicine(IOM)Insufficiency,vitaminD,InsulinInternationalAgencyforResearchonCancerInternationalSmartTanNetworkIntoxication
John,EstherJointpainJournalofCancerJournalofClinicalOncologyJournalofNeurology,Neurosurgery,andPsychiatryJournalofNutritionJournalofObstetricsandGynecologyJournaloftheAmericanBoardofFamilyMedicine
JournaloftheAmericanMedicalAssociationJournaloftheNationalCancerInstituteJournaloftheNationalMedicalAssociationJuice,fortified
Kidneydisease,chronicKidneyfailureKidneysKidneystonesKiel,DouglasKodicek,EgonKrause,Rolfdeiter
LancetLanolinLappe,JoanLasersurgeryLatitudinalregionsLeptinLewybodydiseaseLifestyle,vitaminDdeficiencyandLightboxesLiquidchromatographytandemmassspectometry(LCMSMS)LiverLiverfailureLongevityLungcancerLungs,activatedvitaminDproductioninLupusvulgarisLymphoma
MacrophagesMagnesium
MajordepressionMayoClinicMcGrath,JohnMCIRgene1MED(minimalerythemaldose)Mediaoutlets,mainstreamMedicareMelaninMelanocytesMelanomaappearanceofincreasingratesofinvasivenessofmoderatesunexposureandriskofmortalityratesofmythofsunexposureasmaincauseofnonradiationriskfactorsforsunexposureandlowerincidenceofUVBradiationandUVradiationasprotectionagainstwarningsignsofMelatoninMenstrualmigraineMerewood,AnneMestasisMetabolicsyndromeMethotrexateMiacalcin(calcitonin-salmon)Mid-latitudesMigraineschronicmenstrualMilddepressionMilkbreastcow’s,fortified

MinuteMaidorangejuiceMixeddementiaModlin,RobertMoleratsMolesMood-relatedhealthMooresCancerCenter,UniversityofCaliforniaatSanDiegoMultiplesclerosisMusclehealthMusclelossMusclepainMuscleweaknessMushroomsMuslimwomen
NationalCancerInstituteNationalHealthandNutritionExaminationSurveyNationalKidneyFoundationNationalLibraryofMedicineNationalToxicologyProgramNeanderthalsNefertitiNewEnglandJournalofMedicineNg,KimmieNicolaysen,RagnarNightlight,dangersofNight-shiftworkersNonmelanomaskincancergeneticpredispositionforincreasedincidenceduetosunoverexposurelowmortalityrateoftrade-offbetweenriskofinternalcancersandriskofUVBandwarningsignsofNorepinephrine
Norman,AnthonyW.
ObesityObesity-relateddrugsObesitysurgeryOrangejuice,fortifiedOrganhealthOsteoarthritisOsteoblastsOsteomalaciaOsteopeniaOsteoporosiscalciumanddrugsforgenderdifferencesinmortalityratefromfracturesduetoinreptilesriskoffracturesandsodaconsumptionandvitaminDdeficiencyandOvariancancerOvarianhormonesOvaries,activatedvitaminDproductioninOverexposure
p53genePancreasPancreas,activatedvitaminDproductioninPancreaticcancerParathyroidglandsParathyroidhormonePasteur,LouisPeanutsPeer-reviewedstudies
Peller,SigismundPeriodontaldiseasePharmaceuticalcompaniesosteoporosisdrugsandsunscreensandPhotobiologyPhotoisomersPhotoproductsPhytoplanktonPinealglandPlotnikoff,GregoryA.PolycysticovariansyndromePolyVi-SolPorosityPrabhala,AnuPrebirthvitaminD,PrednisonePreeclampsiaPregnancyPrematureinfantsPremenstrualsyndrome(PMS)PreventiveMedicinePrevitaminD3,PrilosecPrimarybiliarycirrhosisProductionProstate,activatedvitaminDproductioninProstatecancerProto-pumpinhibitorsProvitaminD3,PsoralenUVAphotochemotherapy(PUVA)PsoriasisPsoriaticarthritis
RacecancerandvitaminDdeficiencyandRadioimmunoassayRANKLReclast(zoledronicacid)Recommendedintakeinadequate,oftheInstituteofMedicineReis,JaredRemodelingReptilesResearchResourceguideRespiratoryfunctionRheumatoidarthritisRicketsfortifiedmilkandravagesofrecommendedsupplementationforinreptilesresurgenceofsunexposureandvitaminDdeficiencyandRikli,ArnoldRockefellerUniversityRosenthal,NormanRuleofninesofbody
St.Luke’s-RooseveltHospitalCenterSt.George’sHospitalStudySt.John’swortSalmonSarcoidosisSchernhammer,EvaSchizophrenia

Schulz,CharlesSchwalfenberg,GerrySchwartz,GaryScienceScoliosisScragg,RobertSeasonalaffectivedisorder(SAD)SeasonalfactorsinvitaminDdeficiencySeizuredisordersSemmelweis,IgnazSerotoninShiftworkersyndromeSimpson,RobertSkinactivatedvitaminDproductioninadaptationtosunexposurebycircadianrhythmandmoodhormonereleaseandphysiologyofSkincancerageandchangingattitudestowardsunexposureandmelanoma,seeMelanomamoderatesunexposureandmythsaboutnonmelanoma,seeNonmelanomaskincancerscaretacticsofantisunlobbyandself-examsforskintypeandsunexposureandriskoftreatmentofwarningsignsofSkincolorSkintypeSleepdisordersSluggene

SnailgeneSniadecki,JedrzejSodaconsumption,osteoporosisandSpecker,BonnySpertilampSpottreatmentSquamous-cellcarcinomaSquamouscellsSteenboch,HarryStomachbandingStomachcancerStratumcorneumStrengthtrainingStrokeSubtropicallatitudesSuda,TatsuoSufficiencySunburnmelanomaandpreventionofsunscreensand,seeSunscreensvs.suntanSunexposureadaptationbyskintoantisunlobbyandautoimmunediseasesandbonedevelopmentandbonehealthandbreastcancerandcellularhealthandcircadianrhythmdisordersanddeclineof,aspopulartreatmentdecreasedriskofinternalcancersanddentalcavitiesanddermatologycommunityanddinosaurextinctionand
earlyhumansandearlyresearchonbenefitsofexaggerationofdangersofgeographicaldifferencesin,seeGeographicaldifferencesinsunexposurehearthealthandHolickSensibleSunTablesHolickSolutionforSensibleSunhypertensionandimportanceoflowerincidenceofmelanomasandmisconceptionsaboutnonmelanomaskincancerandobesityandolderpeopleandpsoriasisandreptilesandricketsandseasonalaffectivedisorder(SAD)andsensible,foroptimalhealthskincolorandskintypeandsunburnvs.suntanastherapytimeofdayandvitaminDintoxicationandvs.vitaminDsupplementationwinterblahsandSeealsoBright-lighttherapySeealsoUltravioletradiation(UV)SunglassesSunscreensantisunlobbyandbroadspectrummelanomaandSPFnumberUVBand
SuntablesSunworshipSUNYBuffaloSupplementationcalciumvitaminD,seeVitaminDsupplementationSuprachiasmaticnucleus(SCN)
TagametTanningmythsaboutvs.sunburnTanningfacilitiesTeenagers,vitaminDdeficiencyinTeenVogueTestsTherapyThermogenesisThyroiddiseaseThys-Jacobs,SusanToxicity,vitaminD,TranscriptionfactorTropicallatitudesTryosinehydroxylaseTuberculosisTuftsUniversity
UltravioletBradiation(UVB)activatevitaminDproductionandamountofexposuretobetaendorphinproductionandcloudcoverandhearthealthandindoortanningand

melanomaandmythsaboutobesityandozonelayerandpsoriasisandsunscreensandvs.ultravioletAradiation(UVA)windowglassandUltraviolet(UV)lampsUltravioletradiation(UV)factorsinfluencingintensityofmisconceptionsaboutobesityandprotectionagainstmalignantcancerswithpsoriasisandreptilesandsunburnvs.suntanandUVAUVB,seeUltravioletBradiation(UVB)UVCSeealsoSunexposureUnger,LesterU.S.cities,latitudeandlatitudinalregionsofU.S.DepartmentofHealthandHumanServicesClinicalPracticeGuidelinesofU.S.NavyUniversityofArizonaUniversityofArkansasUniversityofBritishColumbiaUniversityofCaliforniaUniversityofCaliforniaatLosAngelesUniversityofCaliforniaatRiversideUniversityofCaliforniaatSanDiegoUniversityofCaliforniaatSanFranciscoUniversityofManchesterUniversityofNorthCarolina
UniversityofOxfordUniversityofPennsylvaniaUniversityofPittsburghSchooloftheHealthSciencesUniversityofTexasSouthwesternMedicalCenterUniversityofViennaUniversityofWisconsinUpper-respiratory-tractinfectionsU.S.DepartmentofAgriculture(USDA)requirements,inadequacyofUterinecancerUVAdvantage(Holick)
Varosy,PaulVasculardementiaVectical(calcitriol)VegansorvegetariansVenousthromboembolism(VTE)VirusesVitaminD24-hydroxylase25-vitaminD(25-hydroxyvitaminD)bloodlevelofcolorectalcancerandconversiontoactivatedvitaminD,deficiencydefinitionanddiabetes(type2)andhalf-lifeofhearthealthandmusclehealthandover-the-counter/prescriptiondrugsandlevelsofsunexposureandtestingforupper-respiratory-tractinfectionsandVitaminDdeficiencyageandautismandbackpainand
breastcancerandcalciummetabolismandascauseofcancer,theoryofceliacdiseaseandinchildrenchronickidneydiseaseandCrohn’sdiseaseandcultureandcysticfibrosisanddefineddentalcavitiesanddepressionanddiabetes(type1)anddiabetes(type2)andDINOMITmodelofcancerandVitaminDdeficiency(cont.)dinosaursandeatingdisordersandepidemicofextentof,inU.S.populationfatmalabsorptionsyndromesandgastricbypasssurgeryandgeographicaldifferencesinsunexposureandhearthealthandinfluenzaandkidneyfailureandliverfailureandmainstreammediaandawarenessofmigrainesandmortalityratesduetomultiplesclerosisandmusclehealthandinNeanderthalsnonspecificmuscularskeletalachesandobesityandosteomalaciaand

osteoporosisandpregnancyandpremenstrualsyndrome(PMS)andprescriptiondrugsandpricetagofprimarybiliarycirrhosisandraceandresearchonricketsandrisksassociatedwithSt.John’swortandseizuredisordersandself-testforskincolorandsunexposureandsupplementationand,seeVitaminDsupplementationtestsforVitamin D, Skin, and Bone Research Laboratory, Boston University MedicalCenterVitaminDinsufficiencyVitaminDreceptor(VDR)defectVitaminDreceptors(VDRs)VitaminDsufficiencyVitaminDsupplementationageandauthor’sdailyintakeofbodyweightandcancerandforchildrenchoosingfordeficientpeopledosagesizegastricbypasssurgeryandhigh-doseprotocolinadequaterecommendationoftheInstituteofMedicineingesting

“justincase”factorandobesityandpregnancyandprescriptiondrugsandrecommendedintakeriskoffallingandSt.John’swortandvs.sunexposuretimingofbloodlevelincreasetoxicityandvitaminD2andVitaminD2,SeealsoVitaminDsupplementationVitaminD3,SeealsoVitaminDsupplementationVitaminDtoxicityVitaminsVogue
WakeForestUniversityWaketherapyWallStreetJournalWang,ThomasWarsaw,PolandWeaver,ConnieWeight-bearingexerciseWeightlossWellesseliquidsupplementWheeler,SteveWindowglassWinterblahsWolff,FriedrichWoodsHoleMarineBiologicalLaboratoryWorldHealthOrganization(WHO)Wrinkles

Xerodermapigmentosum(XP)
ZantacZemel,Michael