The structure, metabolism and function of the carcinoembryonic antigen gene family
13
Biochimica et Biophysica Acta, 1032 (1990) 177-189 177 Elsevier BBACAN 87227 The structure, metabolism and function of the carcinoembryonic antigen gene family Peter Thomas, Carol Ann Toth, Kulvinder S. Saini, J. Milburn Jessup and Glenn Steele Jr Laboratory of Cancer Biology, Department of Surgery, New England Deaconess Hospital, Harvard Medical School, Boston, MA (U.S.A.) (Received 13 March, 1990) Contents I. Introduction .............................................................. 177 II. CEA structure and heterogeneity ................................................ 178 A. Structure of the polypeptide backbone ......................................... 178 B. Structure of the oligosaccharide chains ......................................... 180 C. The domain model for carcinoembryonic antigen .................................. 181 D. Relationship to the immunoglobulin supergene family .............................. 181 III. Cloning and expression of CEA gene family members ................................. 181 IV. Regulation of circulating CEA levels ............................................. 183 V. CEA, biological properties and function ........................................... 185 Acknowledgments ............................................................. 186 References ................................................................... 186 I. Introduction Carcinoembryonic antigen (CEA) was first described almost 25 years ago in two papers by Gold and Freed- man [1,2]. They described an antigen which was present in carcinoma of the colon and fetal digestive tract, but was absent from the normal colon. They recognized that the potential measurement of such an antigen could be useful in the detection and monitoring of patients with colorectal cancer. The first clinical studies carried out by this group showed that CEA elevations in the plasma Abbreviations: CEA, carcinoembryonic antigen; GI, gastrointestinal; NCA, non-specific crossreating antigen; BGP, biliary glycoprotein; PSG, pregnancy specific fll-glycoproteins. Correspondence: P. Thomas, Laboratory of Cancer Biology, New England Deaconess Hospital, 50 Binney Street, Boston, MA 02115, U.S.A. of patients with cancer of the colon fell following resec- tion of the tumor [3]. Subsequently, studies using more sensitive procedures demonstrated that CEA was pre- sent in normal tissues and that serum elevations could be associated with benign disease including inflamma- tory disease of the bowel and diseases of the liver such as cirrhosis, hepatitis and bile duct obstruction [4,5]. These observations resulted in some disillusionment with the whole field of tumor markers, but also in renewed efforts amongst some workers to find markers which improved upon CEA and showed the desired tumor specificity [6]. Many potential tumor markers have sub- sequently been evaluated but none have been better than CEA in the monitoring of colorectal cancers. Nev- ertheless, some useful markers such as CA 125 have been developed for ovarian cancer [7] and CA 15-3 for breast cancer [8]. As pointed out by Zamcheck, CEA is the prototype tumor marker and certainly in the colo- rectal area is the standard by which all new tumor markers are judged [9]. In a recent editorial Neville has 0304-419X/90/$03.50 © 1990 Elsevier Science Publishers B.V: (Biomedical Division)
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of The structure, metabolism and function of the carcinoembryonic antigen gene family

Biochimica et Biophysica Acta, 1032 (1990) 177-189 177 Elsevier
BBACAN 87227
The structure, metabolism and function of the carcinoembryonic antigen gene family
Peter Thomas, Carol Ann Toth, Kulvinder S. Saini, J. Milburn Jessup and Glenn Steele Jr
Laboratory of Cancer Biology, Department of Surgery, New England Deaconess Hospital, Harvard Medical School, Boston, MA (U.S.A.)
(Received 13 March, 1990)
Contents
I. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 177
II. CEA structure and heterogeneity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 178 A. Structure of the polypeptide backbone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 178 B. Structure of the oligosaccharide chains . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 180 C. The domain model for carcinoembryonic antigen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181 D. Relationship to the immunoglobulin supergene family . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181
III. Cloning and expression of CEA gene family members . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181
IV. Regulation of circulating CEA levels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183
V. CEA, biological properties and function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 185
Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 186
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 186
I. Introduction
Carcinoembryonic antigen (CEA) was first described almost 25 years ago in two papers by Gold and Freed- man [1,2]. They described an antigen which was present in carcinoma of the colon and fetal digestive tract, but was absent from the normal colon. They recognized that the potential measurement of such an antigen could be useful in the detection and monitoring of patients with colorectal cancer. The first clinical studies carried out by this group showed that CEA elevations in the plasma
Abbreviations: CEA, carcinoembryonic antigen; GI, gastrointestinal; NCA, non-specific crossreating antigen; BGP, biliary glycoprotein; PSG, pregnancy specific fll-glycoproteins.
Correspondence: P. Thomas, Laboratory of Cancer Biology, New England Deaconess Hospital, 50 Binney Street, Boston, MA 02115, U.S.A.
of patients with cancer of the colon fell following resec- tion of the tumor [3]. Subsequently, studies using more sensitive procedures demonstrated that CEA was pre- sent in normal tissues and that serum elevations could be associated with benign disease including inflamma- tory disease of the bowel and diseases of the liver such as cirrhosis, hepatitis and bile duct obstruction [4,5]. These observations resulted in some disillusionment with the whole field of tumor markers, but also in renewed efforts amongst some workers to find markers which improved upon CEA and showed the desired tumor specificity [6]. Many potential tumor markers have sub- sequently been evaluated but none have been better than CEA in the monitoring of colorectal cancers. Nev- ertheless, some useful markers such as CA 125 have been developed for ovarian cancer [7] and CA 15-3 for breast cancer [8]. As pointed out by Zamcheck, CEA is the prototype tumor marker and certainly in the colo- rectal area is the standard by which all new tumor markers are judged [9]. In a recent editorial Neville has
0304-419X/90/$03.50 © 1990 Elsevier Science Publishers B.V: (Biomedical Division)
178
reaffirmed the usefulness of the CEA assay and made the point that many of the advances in tumor marker research lead directly back to the discovery of CEA [6]. In spite of the misgivings that occurred when it was discovered that CEA was not tumor specific, CEA is the most widely used tumor marker, particularly for cancers of the gastrointestinal (GI) tract and increasing num- bers of commercial assays are now available for its measurement. However, its usefulness is not confined solely to GI cancers, for example breast cancer, small cell cancer of the lung, medullary cancer of the thyroid and others can be monitored using the CEA assay [10]. It is possible, however, that in some of the non-gastro- intestinal tumors it is not CEA but other members of its gene family which are being measured. A great deal of effort has been expended on producing antibodies to CEA in the hope that greater specificity for tumors could be achieved. The current CEA assays are very sensitive and can measure CEA levels below 0.5 ng /m l of serum using volumes as low as 0.1 ml. The more modern assay systems employ monoclonal antibody technology usually using multiple monoclonal antibod- ies to different epitopes to both capture and detect CEA. CEA was also one of the first tumor markers to be utilized as a target for the immunolocalization of primary cancers and their metastases [11]. Mouse-hu- man chimeric monoclonal antibodies to CEA have been produced recently in an attempt to overcome the clini- cal problems associated with repeated use of mouse monoclonals in human patients [12,13]. Anti-CEA anti- bodies coupled to cytotoxic agents have been studied as potential therapeutic agents in cell culture and in nude mouse xenografts with human colorectal cancers [14]. Extensive literature on the clinical utility of the CEA assay has accumulated since the first papers of Gold and Freedman and has been reviewed elsewhere [10,15].
It is now recognized that CEA is a member of the immunoglobulin supergene family. The CEA gene family is comprised of at least 17 members, six of these belong to the CEA subgroup and the rest to the pregnancy specific/~l-glycoprotein (PSG) subgroup [16]. The most well studied of these glycoproteins other than CEA is the non-specific crossreacting antigen (NCA) [17]. It is likely that future assays will be developed to detect all members of the CEA gene family individually and as a group.
11. CEA structure and heterogeneity
Studies on the structure of CEA and other members of its gene family began in the early 1970s, but it was not until 1987 that complete structural information on the protein chain of these molecules became available. The earlier structural studies were designed to de- termine if the antibodies which had been raised against
CEA were directed to the carbohydrate structure or the protein chain and were aimed at mapping antigenic sites with a view to producing more specific antibodies that would improve its tumor specificity and hence its clinical use [18]. The majority of antibodies that have been raised against CEA are not directed towards the carbohydrate structures but tend to be directed against specific peptide sequences along the molecule. The reac- tivities and epitope mapping of more than 50 anti-CEA monoclonal antibodies from 11 research groups has been recently described [19]. More detailed information and discussions of the antigenic sites and specificities of monoclonal antibodies raised against CEA and NCA may be found in this and other review articles [19-22].
Most of the studies carried out on CEA used material isolated from liver metastases of colon adenocarcinomas as this has proven to be the best source for CEA purification [23-25]. CEA and CEA-like molecules have also been isolated and at least partially characterized from a variety of other tumors and normal tissues. These include cancers of the breast [26], bladder [27], stomach [28], ovary [29] and intestine. The normal tis- sues and secretions include colon [30], pancreas [31], lung [32], spleen [33], bile [34], saliva [35] and gastric juice [36].
It was evident early that CEA was structurally a very heterogeneous molecule, and that most of this hetero- geneity was due to variations in the structure of the carbohydrate side chains [37]. Many laboratories carried out carbohydrate analyses and considerable variation in carbohydrate content was demonstrated between sam- ples [38]. The general consensus was that CEA was a highly glycosylated molecule consisting of approx. 60% carbohydrate with a molecular weight of 180000- 200000. Heterogeneity as demonstrated by isoelectric focussing was thought largely to be inherent in the carbohydrate chains due in large part to differences in sialic acid content. However, removal of sialic acid, while decreasing heterogeneity does not produce a ho- mogeneous glycoprotein. This residual heterogeneity probably reflects differences in the internal areas of the carbohydrate chains [39]. Amino acid analyses of CEA extracted from various tissues, including hepatic metas- tases from colorectal cancer, and washings of normal colons were always remarkably consistent [40]. These observations gave further weight to the idea that the heterogeneity found in CEA was due to the variable carbohydrate content and led to much speculation as to whether there was a tumor-specific form of CEA [38]. Shively and Todd [41] have defined CEA in terms of many of these physicochemical properties.
H-A. Structure of the polypeptide backbone
The protein portion of the CEA molecule consists of a single polypeptide chain of 668 amino acid residues.
This information has been derived from cloning and sequencing of the CEA gene. The use of conventional protein chemistry methodologies to obtain the complete sequence of the CEA molecule proved to be extremely difficult due, in part, to the large amount of carbo- hydrate present on CEA and thus its resistance to degradation with proteinases [42]. It had been known for some time that the glycoprotein contains 12 cysteine residues that hold the conformation of CEA with six disulfide bonds [43]. Four independent laboratories have arrived at the same structure for the polypeptide chain of CEA and published it in 1987 [44-47]. This structure has been further confirmed by comparing the amino acid sequence derived from gene cloning with partial sequences obtained by conventional protein sequencing methods [48]. Similarly, the structure of the related protein NCA-50 has also been determined using gene cloning [49-51] and the structure of this glycoprotein has also been authenticated by comparison with known partial sequences obtained by conventional protein se- quencing [48]. Amino acid sequences deduced from cDNA have shown that CEA is synthesized as a pre- cursor of 702 amino acids [44]. The first 34 amino acids comprise a leader sequence that is not present in the mature form of the glycoprotein. Based on repeated sequences in the molecule, CEA can be divided into three domains of 178 amino acids each containing two disulfide bridges. These domains have approx. 70% ho- mology and the four cysteine residues are at identical positions. In addition, there is a N-terminal domain of 109 amino acids and a small highly hydrophobic do- main at the C-terminus of 26 amino acids [44]. NCA-50 closely resembles CEA with similar N- and C-terminal domains, but with just a single internal loop domain [49-51]. Hinoda et al. isolated and sequenced biliary glycoprotein I (BGPI) another member of the CEA gene family that is found in normal gallbladder and hepatic bile [52]. The BGPI peptide consists of an N-terminal, immunoglo.bulin-like, BGP-specific, trans- membrane and cytoplasmic domains. The nucleotide sequence of the N-terminal and immunoglobulin-like domains exhibit greater than 80% homology with CEA and NCA [52]. More recently, the genes have been cloned and sequences obtained for four other members of the CEA gene family. These are 3.9, 3.7, 2.2 and 1.8 kb cDNAs and a 23 kb genomic transcription unit [53]. These four new gene family members were called trans- membrane CEAs as they have both transmembrane and cytoplasmic domains similar to those of BGP [52]. Two of them BGP b and BGP d (TM2 and TM4) are similar to NCA, while BGP a and BGP c (TM1 and TM3) have homology to CEA, containing sequences similar to the first disulfide bridge domain plus part of the second from CEA. All of the BGP variants, however, are de- rived from an independent gene. They show extensive
179
homology with CEA and NCA, but in addition, these molecules demonstrate a transmembrane and a cyto- plasmic domain at the C-terminus. However, there is no conclusive evidence at present that these cytoplasmic domains survive post-translationally. Indeed in the case of the short cytoplasmic domain there is a possibility that it is cleaved like the short transmembrane domain of CEA to provide for attachment of a glycosyl phos- phoinositol moiety (see below). Nevertheless in the case of the BGP molecules that have the long cytoplasmic domain there is a tyrosine that has the consensus se- quence for phosphorylation although the significance of this is not apparent at present [53]. A further five members of the CEA gene family have been described by Thompson et al. [54], one of which is the human pregnancy specific fll-glycoprotein. The other four des- ignated hsCGM (homo sapiens CEA gene family mem- ber) 1, 2, 3 and 4 have not been identified. These genes have homology to the immunoglobulin supergene family and show conservation of nine out of 13 critical amino acids [54,55]. Recently the nomenclature of the CEA gene family was changed at a workshop held in Frei- berg. The two CEA gene variants, the short and long polyadenylation mRNA variants are CEA a and CEAb, respectively. BGP1 and TM1 are known as BGP a, while TM2, TM3 and TM4 are now known as BGP b, BGP c and BGPo, respectively. A new nomenclature is also suggested for the pregnancy specific fll-glycoproteins (PSG) whose subfamily now numbers at least seven members [56]. The short hydrophobic C-terminal do- mains may be involved in attachment of CEA or BGP to the lipid bilayer of the colon cancer cell surface prior to secretion. Recent studies suggest, however, that some CEAs are attached to the cell surface via an ethanol- amine linked to a glycosyl phosphoinositol [57,58]. Hefta et al. have suggested that this C terminal region of CEA is lost post-translationally from the mature protein and an ethanolamine-glycosylphosphatidylinositol moiety is subsequently added to a residue within the terminal hexapeptide of the third repeating domain [58].
The grouping of the CEA gene family into two subgroups, CEA-like, or PSG-like, is based on the de- gree of sequence homology between the members. Ho- mology between CEA, NCA and BGP is in the region of 70-80%, while homology between the members of the PSG subgroup can be greater than 90%. However, the homology between the two subgroups is much lower, being about 40-50% [42,53-56]. This high degree of intra-subgroup homology but lower inter-subgroup rela- tionship accounts for the nomenclature.
Diagrammatic representations showing the pos- tulated structures of CEA and other sequenced mem- bers of the CEA gene family subgroup are shown in Fig. 1A and B.
180
NH 2 CEA
$ S
TTT TTT
C
NCA CEA
C G
s s
BGPa BGP b BGPc BGPd (TM1) (TM2) (TM3)(TM4)
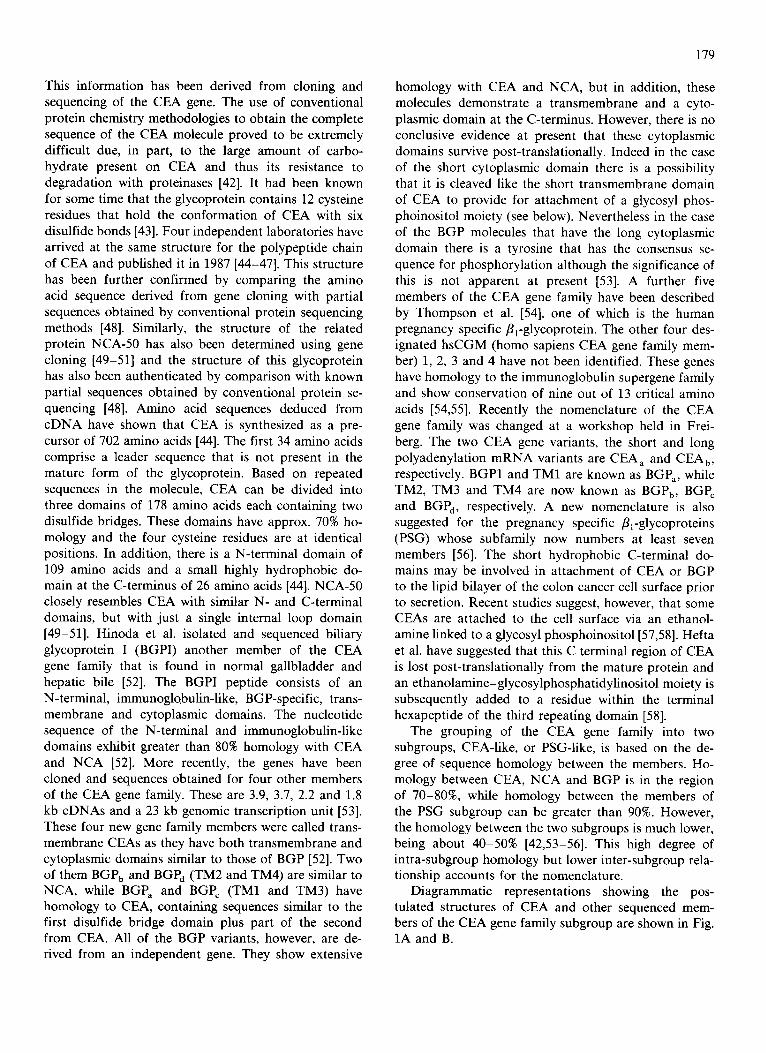
Fig. 1. (A) Structure of CEA. CEA structure is diagrammatically represented based on data from the cDNA sequence. The structure is drawn in the shape expected for a member of the immunoglobul in super gene family [76]. The positions of possible sites of N-linked glycosylation are shown. (B) Relationship of CEA to other members of its gene family. The structure of CEA, NC A and the four trans- membrane forms are shown diagrammatically. The structures are taken from Barnett et al. [53]. It should be noted that BGP b (TM2) and BGP d (TM4) have a free - S H group. Barnett et al. have suggested that dimerization of these molecules may occur by formation of an
intermolecular disulfide bridge [52]. Note new nomenclature [55].
II-B. Structure of the oligosaccharide chains
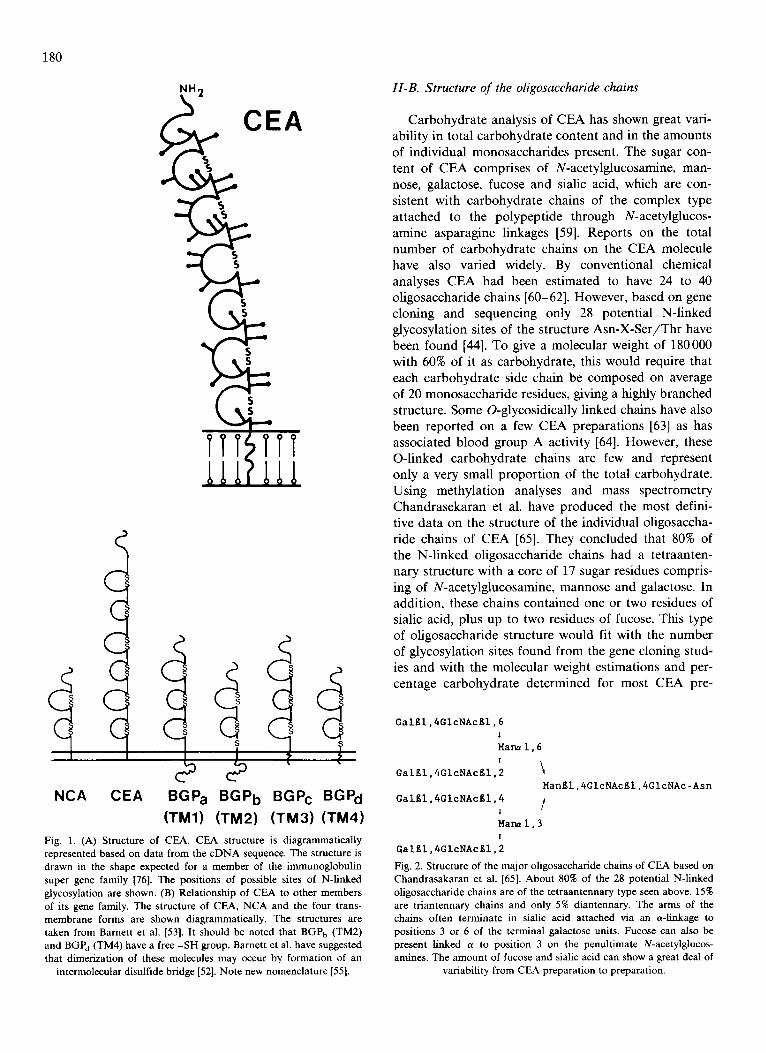
Carbohydrate analysis of CEA has shown great vari- ability in total carbohydrate content and in the amounts of individual monosaccharides present. The sugar con- tent of CEA comprises of N-acetylglucosamine, man- nose, galactose, fucose and sialic acid, which are con- sistent with carbohydrate chains of the complex type attached to the polypeptide through N-acetylglucos- amine asparagine linkages [59]. Reports on the total number of carbohydrate chains on the CEA molecule have also varied widely. By conventional chemical analyses CEA had been estimated to have 24 to 40 oligosaccharide chains [60-62]. However, based on gene cloning and sequencing only 28 potential N-linked glycosylation sites of the structure Asn-X-Ser/Thr have been found [44]. To give a molecular weight of 180 000 with 60% of it as carbohydrate, this would require that each carbohydrate side chain be composed on average of 20 monosaccharide residues, giving a highly branched structure. Some O-glycosidically linked chains have also been reported on a few CEA preparations [63] as has associated blood group A activity [64]. However, these O-linked carbohydrate chains are few and represent only a very small proportion of the total carbohydrate. Using methylation analyses and mass spectrometry Chandrasekaran et al. have produced the most defini- tive data on the structure of the individual oligosaccha- ride chains of CEA [65]. They concluded that 80% of the N-linked oligosaccharide chains had a tetraanten- nary structure with a core of 17 sugar residues compris- ing of N-acetylglucosamine, mannose and galactose. In addition, these chains contained one or two residues of sialic acid, plus up to two residues of fucose. This type of oligosaccharide structure would fit with the number of glycosylation sites found from the gene cloning stud- ies and with the molecular weight estimations and per- centage carbohydrate determined for most CEA pre-
GalKI,4GIcNAcKI, 6
Mana i, 6 !
GalKI,4GIcNAcKI, 2 \ HanEl, 4GIeNAcKI, 4GlcNAc -Asn
GalKl, 4GIcNAcKI, 4 /
Mana i, 3 T
GalEl, 4GIcNAcKI, 2
Fig. 2. Structure of the major oligosaccharide chains of CEA based on Chandrasakaran et al. [65]. About 80% of the 28 potential N-linked oligosaccharide chains are of the tetraantennary type seen above. 15% are tr iantennary chains and only 5% diantennary. The arms of the chains often terminate in sialic acid attached via an a-linkage to positions 3 or 6 of the terminal galactose units. Fucose can also be present linked a to position 3 on the penultimate N-acetylglucos- amines. The amount of fucose and sialic acid can show a great deal of
variability from CEA preparation to preparation.
parations. The remaining 20% of the oligosaccharide chains consist of largely triantennary structures with some diantennary chains. Both arms of the diantennary chains terminate in sialic acid [65]. A carbohydrate structure which may be typical of that found in CEA is shown in Fig. 2. (Based on observations by Chandra- sakaran et al., Ref. 65).
Very little structural work on the carbohydrate side chains has been reported for other members of the CEA gene family aside from simple analyses of NCA and TEX. It is fairly certain that TEX is identical to NCA-50 [66,67]. Other related antigens isolated from meconium or faeces NCA-2 [68], NFA-2 [69], and meconium anti- gen [70] are probably degradation products of CEA [71] though a glycoprotein found in bile (BGP-1) seems to be a distinct member of the family [63].
H-C. The domain model for carcinoembryonic antigen
Based on the structures determined from gene clon- ing described above, CEA contains three major loop domains consisting of 178 amino acids each with two cysteine disulfide bridges (see Fig. 2). It should be noted, however, that the position of the disulfide bridges has not been established and other foldings of the molecule could occur. The electron microscopic studies of Slayter and Colligan [72] determined that CEA was a cruller-shaped particle with dimensions of 9 × 14 nm. Reduction and alkylation of the molecule produced a random configuration in an extended form up to 110 nm in length. They calculated that the length of the fully extended polypeptide backbone would be 220 nm [72]. It is therefore possible that a more compact shape may pertain in CEA where the six disulfide bridges are formed from two cysteines that are not adjacent to each other on the polypeptide chain. Clarification of this awaits the determination of the exact position of the disulfide bridges. Circular dichroism studies by West- wood et al. [73] have shown CEA to be largely in the 13 conformation with over 80% of the molecule being composed of r-sheet and r- turn. The other 20% is random coil and no a-helix can be detected. This would suggest that the loop domains are in the/3 conforma- tion, with the N-terminus probably representing the majority of the random coil regions. Computer analysis of the disulfide bridge domains in CEA have also de- duced that the secondary structure is an antipolar arrangement of /3 strands [74]. Other support for a domain model for CEA has come from studies with a panel of 17 monoclonal antibodies which recognized eight different antigenic sites on the molecule. The specificity of these antibodies to proteolytically cleaved CEA strengthen the idea of the repeating domain model suggested by the cDNA sequence [75].
181
H-D. Relationship to the immunoglobufin supergene family
The proposed structures for CEA and NCA show close similarity to members of the immunoglobulin su- pergene family. Comparison of the CEA gene family members sequence at both the amino acid and nucleo- tide levels show a great deal of homology to other members of the immunoglobulin supergene family [48,76,77]. Members of this gene family that show ho- mology with CEA are: mouse Thy-l.2 antigen [78,79]; mouse r-chain variable region [80]; rabbit polyim- munoglobulin receptor [81]; a- lB glycoprotein [82]; chicken NCAM [83]; and also MAG (myelin associated glycoprotein) [84]. These proteins have greater than 40% homology with CEA at the nucleotide level. In the case of mouse Ig Vk, for example, there is 55.4% homology between the uninterrupted 92 nucleotides in the second disulphide bridge domain of CEA surrounding Cys-311 and the mouse sequence surrounding Cys-88 [74]. The major similarities in protein sequence reside in the three disulfide bridge loop domains. These areas of the mole- cule are composed of an antipolar arrangement of fl strands and this is a typical feature of the immuno- globulin fold [55]. Even though it does not contain a disulfide bond there is sufficient homology in the N- terminal region of CEA and NCA so that it too can be considered as an immunoglobulin-like domain [48].
A recent study by Lin and Guidotti [85,86] has suggested a function for the BGP glycoproteins. They determined the amino acid sequence of the rat hepato- cyte plasma membrane ecto-ATPase and showed a 65% homology to human BGP-1 at the amino acid level. They also showed that the two putative nucleotide binding sequences of the ATPase also occur in the N-terminal and BGP specific domain of BGP and they suggest that BGP is the human form of the ecto-ATPase.
III. Cloning and expression of CEA gene family mem- bers
Like the attempts to determine the amino acid se- quence of CEA, the initial attempts at gene cloning of CEA and related members of its gene family were also found to be extremely difficult. The first experiments to characterize the CEA mRNA used in vitro translation of poly(A) ÷ RNA from a rectal carcinoma [87]. Im- munoprecipitation of the product with anti-CEA anti- bodies identified a polypeptide with a molecular weight of approx. 80 000 and the size of the CEA mRNA was estimated to be 3.1 kb [87]. A major difficulty of isolat- ing a full length cDNA remained however, and was not resolved until additional sequence information was ob- tained by conventional techniques of protein chemistry. cDNA clones for CEA and other members of its gene family were finally isolated and characterized using two
182
different approaches, cDNA libraries were screened using either synthetic oligonucleotides based on known protein sequences [45-47] or were detected in expres- sion vectors using anti-CEA antibodies [44,58]. Using these techniques, cDNAs for CEA, NCA and for the transmembrane forms of CEA have now all been iso- lated and characterized [53], as well as a cDNA coding for BGP [52] and the five new family members de- scribed by Thompson et al. [54]. In addition, CEA-re- lated cDNAs have been cloned from human fetal liver [87] and belong to a further sub-family called the preg- nancy specific fll-glycoprotein/fetal liver non-specific crossreacting antigens. Klemenz et al. [90] have cloned, sequenced and expressed three members of this family. In addition CEA-related genes have been obtained from the stimulation of NIH 3T3 cells with serum growth factors and oncogenes [90]. We can now account for at least fourteen members of the CEA gene family with the possibility of more to be discovered. Studies on the gene expression of members of the CEA gene family have been carried out using both tumor and normal tissue [91]. Probes from both coding and noncoding regions have been used to examine RNAs in Northern blot hybridization analyses. At least six mRNAs have been identified corresponding to CEA, NCA and the four transmembrane members of the gene family [53]. Alter- native splicing was found to be responsible for the existence of multiple mRNAs that code for the four BGP members of the CEA gene family [53]. Expression of CEA and NCA-50 mRNAs have great variability in their absolute and relative amounts. As expected, strong expression for CEA was found in adenocarcinomas of the colon and pancreas [91] and these tumors also tended to express the mRNA for NCA-50 [91,92]. How- ever, carcinomas of the breast were shown to express transcripts for NCA-50 only [92], while squamous cell carcinomas of the lung expressed transcripts for both NCA and BGP. Leukocytes from patients with chronic myelogenous leukemia also express a 2.6 kb mRNA coding for NCA but in addition they also showed an unidentified 2.3 kb transcript which may represent an undefined gene of the CEA family. This transcript is probably the same as the 2.2 kb mRNA reported by Barnett et al. [53]. This transcript has been recently characterized and cloned from human granulocytes and corresponds to a new CEA gene family member hsCGM-6 or NCA-95 [93]. It has also been reported that both normal colon and colon tumors may have a large variability in the amount of CEA message ex- pressed [94]. Recent studies from our laboratory (un- published work) and others [95,96] have indicated that in some cases the normal mucosa adjacent to a colo- rectal carcinoma can express higher levels of CEA mRNA than the tumor itself. This was an unexpected finding as the amounts of CEA found in colon cancer extracts by immunoassay are very much greater (by up
to 100-fold) than that found in the normal colon [94]. These data would strongly suggest that post-transcrip- tional control is important in determining the expres- sion of CEA in colon cancer. In this context Boucher et al. [94] were unable to find a correlation between the level of the CEA mRNA and production of the secreted glycoprotein. They suggested that both transcriptional and post-transcriptional control mechanisms must oper- ate to result in the variable expression of CEA. In addition, the degree of methylation in the 5' region of the CEA gene was inversely correlated to CEA expres- sion [94,95]. This decrease in methylation was even more apparent in cultured colorectal cancer cell lines. In addition to these controls at the RNA level, the differences in CEA content of tumors as opposed to the normal mucosae may also be explained anatomically. In the normal mucosae CEA production is polarized to the luminal face of the cell. This results in secretion of CEA into the lumen of the colon where it is lost. In tumors CEA tends to be associated with all faces of the cell surface and if secretion into a lumen occurs it is often into a blind duct where the CEA may remain trapped, inevitably resulting in higher levels of extractable CEA from tumor tissue. This effect would be independent of transcriptional events.
Other studies using human colorectal cancer cell lines have shown that expression of the CEA gene can be modulated by various agents including sodium butyrate [97], retinoids [98] and recombinant human -/-interferon [99-101]. Unpublished work from our laboratory, using cell lines that produce only low levels of CEA, showed that sodium butyrate causes a > 25- fold increase in CEA mRNA abundance while tran- scription rates are increased only 6-fold, however, CEA mRNA stability is also increased about 10-fold. This suggests that the effect of butyrate on CEA mRNA turnover appears to involve a coordinate response at both transcriptional and post-transcriptional steps. Re- cently it has also been shown that sodium butyrate can effect synthesis of the human pregnancy specific fll- glycoproteins in placental fibroblasts [102]. Using probes that identified the majority of PSGs they showed that butyrate increased the steady state levels of three PSG mRNAs of 2.3, 2.2 and 1.7 kilobases. Because these proteins contain the Arg-Gly-Asp (RGD) sequence, a sequence that is implicated in integrin-mediated cell binding [103], it has been suggested that they may act as recognition molecules that are important in fetal devel- opment [102].
Analysis of cDNAs has revealed major differences in the 3' untranslated regions of NCA-50 mRNA and CEA mRNA, and beyond the first 40 nucleotides di- rectly downstream from the C-terminus. In addition, the NCA-50 mRNA does not have any Alu-like repe- titive sequences [42]. These differences in the 3' un- translated regions may be exploited to distinguish be-

tween the CEA and NCA-50 genes and to investigate their functions. These differences may also serve a regu- latory role in the expression of the two genes.
From an evolutionary point of view much specula- tion has centered around the development of the CEA gene family. For some time CEA was thought to be unique to the higher primates. Using radioimmunoas- says with both the Roche goat anti-CEA and a baboon anti-CEA antibody, circulating CEA could only be de- tected in the human, gorilla and chimpanzee and was absent from the other primates tested including those of the Macaca genus and the common baboon [104,105]. Other workers, however, identified and raised antisera to a CEA-like molecule from 1,2-dimethylhydrazine-in- duced rat colon carcinomas in inbred Fisher rats [106]. These CEA-like molecules were not immunologically crossreactive with antisera made to human CEA. How- ever, antisera made to the rat proteins did crossreact with human CEA [107]. More recently using Southern blot analysis of mouse DNA with probes based on the human cDNA sequence, multiple CEA-like genes have been found. Isolation of a mouse CEA cDNA clone from murine colon showed that both the N-terminal and internal loop domains have been conserved be- tween the two species with particular homology to the N-terminal domain of human NCA-50 [108]. Kodelja et al. [109] have also shown the presence of five discrete genes belonging to the CEA family in the rat. Sequence comparison of these genes, however, showed low simi- larity at the amino acid level with the human proteins. These rat genes are more closely related to the human pregnancy specific protein subgroup than to the CEA subgroup. It is possible that the rat equivalents to members of the CEA subgroup remain to be cloned.
The CEA gene family is also unique in that it has arisen a number of times, in parallel, in different mam- malian orders [42]. Thompson and Zimmerman [42] described in detail a possible evolutionary model for the CEA gene family. In the human, the CEA genes are located on chromosome 19 [109]. In situ hybridization with a cross hybridizing probe from the NCA gene showed that the CEA gene family were localized to the long arm of chromosome 19, with a second locus at the end of the short arm. A CEA cDNA probe was found to hybridize only to the long arm of chromosome 19. These results also agreed with those of Kamarck et al. who probed a panel of mouse /human somatic cell hybrids [45]. Inazawa et al. have also assigned the gene for NCA to chromosome 19 and further localized it to band 19q13.2 [110].
IV. Regulation of circulating CEA levels
The regulation of CEA levels in the circulation is complex and depends on many factors. The input rate of CEA into the circulation is obviously an important
183
consideration, and this will depend on the presence of tumor, its size, localization, degree of invasiveness and its state of differentiation [111]. Access to blood supply is also very important as the secreted forms of CEA have to get into the circulation to be of value as a marker of tumor progression [10]. Tumor differentiation is involved, as the more well differentiated the tumor, the greater the likelihood of it producing large amounts of CEA [111]. Some tumors which are poorly differenti- ated or undifferentiated produce little or no CEA and can account for those patients with a large tumor load but who have serum CEA levels that are normal or only marginally elevated [112]. CEA production by tumor cells in vitro can also be influenced by external factors including biological response modifiers such as polar solvents (DMF and DMSO), retinoids, sodium butyrate or the interferons [97-99]. Under certain circumstances cells that do not normally produce any CEA in culture can be induced to do so using agents such as sodium butyrate [98].
In spite of the clinical and biological importance of CEA little is known about its biosynthesis by colorectal cancer cells or by the normal colonic epithelia. Studies utilizing tunicamycin as an inhibitor of oligosaccharide processing have shown that glycosylation of the mole- cule is not necessary for incorporation into membranes or secretion by colorectal cancer cells [113,114]. Other studies to determine the role of the carbohydrate in CEA processing have not been done, and only recently have serious efforts been made to define a biological role for CEA [115].
A much greater effort has been put into determining the factors responsible for CEA clearance from the circulation and the mechanisms by which this occurs are now quite well understood [109]. In this the liver plays the major role. The first observations that CEA levels may be influenced by the liver were made from the study of plasma CEA levels in patients with benign liver diseases including cirrhosis, hepatitis and extrahepatic biliary obstruction [116,117]. The small or moderate increases seen in plasma CEA levels in these diseases are thought to be due to impaired hepatic clearance of the circulating glycoprotein [108]. The initial laboratory studies on mechanisms of CEA clearance were carried out in rabbits and dogs by Shuster et al. [118]. They showed a biphasic clearance curve for 125I-labeled CEA with over 70% of the glycoprotein being cleared in the rapid phase. The radiolabeled CEA accumulated within the liver. Studies using a rat liver perfusion system also showed that CEA was cleared rapidly by the liver and that removal of sialic acid from CEA by neuraminidase treatment increased this rate [119]. Studies performed in the rat in vivo also confirmed these observations [119]. It has also been shown that the liver is the major organ of clearance in the hamster, and that clearance was retarded in tumor-beating animals [120]. Hepatic
184
clearance of CEA has also been shown in Rhesus monkeys and more recently studies have been made on CEA uptake by isolated human liver cells [121,122]. Measurements of CEA levels in portal and peripheral blood in 87 patients with colorectal tumors showed consistently higher levels in the portal blood [123]. Furthermore studies using fluorescent antibodies have shown that both CEA and NCA are expressed on the surface of Kupffer cells in normal adult liver [124]. All these studies point to the key role of the liver in CEA metabolism.
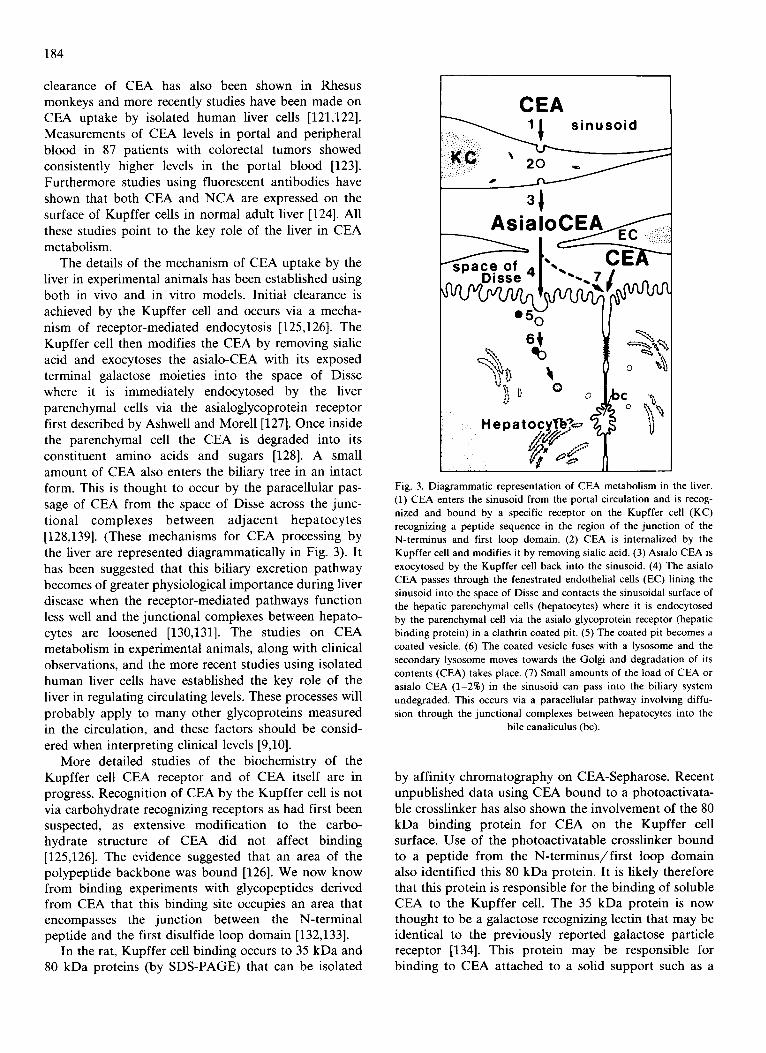
The details of the mechanism of CEA uptake by the liver in experimental animals has been established using both in vivo and in vitro models. Initial clearance is achieved by the Kupffer cell and occurs via a mecha- nism of receptor-mediated endocytosis [125,126]. The Kupffer cell then modifies the CEA by removing sialic acid and exocytoses the asialo-CEA with its exposed terminal galactose moieties into the space of Disse where it is immediately endocytosed by the liver parenchymal cells via the asialoglycoprotein receptor first described by Ashwell and Morell [127]. Once inside the parenchymal cell the CEA is degraded into its constituent amino acids and sugars [128]. A small amount of CEA also enters the biliary tree in an intact form. This is thought to occur by the paracellular pas- sage of CEA from the space of Disse across the junc- tional complexes between adjacent hepa tocytes [128,139]. (These mechanisms for CEA processing by the liver are represented diagrammatically in Fig. 3). It has been suggested that this biliary excretion pathway becomes of greater physiological importance during liver disease when the receptor-mediated pathways function less well and the junctional complexes between hepato- cytes are loosened [130,131]. The studies on CEA metabolism in experimental animals, along with clinical observations, and the more recent studies using isolated human fiver cells have established the key role of the liver in regulating circulating levels. These processes will probably apply to many other glycoproteins measured in the circulation, and these factors should be consid- ered when interpreting clinical levels [9,10].
More detailed studies of the biochemistry of the Kupffer cell CEA receptor and of CEA itself are in progress. Recognition of CEA by the Kupffer cell is not via carbohydrate recognizing receptors as had first been suspected, as extensive modification to the carbo- hydrate structure of CEA did not affect binding [125,126]. The evidence suggested that an area of the polypeptide backbone was bound [126]. We now know from binding experiments with glycopeptides derived from CEA that this binding site occupies an area that encompasses the junction between the N-terminal peptide and the first disulfide loop domain [132,133].
In the rat, Kupffer cell binding occurs to 35 kDa and 80 kDa proteins (by SDS-PAGE) that can be isolated
CEA
AsialoCEA
CEA v Disse 4/ " ' - , 7 1 ^ _l
I( _ I
Hepatocy. .~ ,~ ~_~ o ~,
Fig. 3. Diagrammatic representation of CEA metabolism in the liver. (1) CEA enters the sinusoid from the portal circulation and is recog- nized and bound by a specific receptor on the Kupffer cell (KC) recognizing a peptide sequence in the region of the junction of the N-terminus and first loop domain. (2) CEA is internalized by the Kupffer cell and modifies it by removing sialic acid. (3) Asialo CEA is exocytosed by the Kupffer cell back into the sinusoid. (4) The asialo CEA passes through the fenestrated endothelial ceils (EC) lining the sinusoid into the space of Disse and contacts the sinusoidal surface of the hepatic parenchymal cells (hepatocytes) where it is endocytosed by the parenchymal cell via the asialo glycoprotein receptor (hepatic binding protein) in a clathrin coated pit. (5) The coated pit becomes a coated vesicle. (6) The coated vesicle fuses with a lysosome and the secondary lysosome moves towards the Golgi and degradation of its contents (CEA) takes place. (7) Small amounts of the load of CEA or asialo CEA (1-2%) in the sinusoid can pass into the biliary system undegraded. This occurs via a paracellular pathway involving diffu- sion through the junctional complexes between hepatocytes into the
bile canaliculus (bc).
by affinity chromatography on CEA-Sepharose. Recent unpublished data using CEA bound to a photoactivata- ble crosslinker has also shown the involvement of the 80 kDa binding protein for CEA on the Kupffer cell surface. Use of the photoactivatable crosslinker bound to a peptide from the N- te rminus / f i r s t loop domain also identified this 80 kDa protein. It is likely therefore that this protein is responsible for the binding of soluble CEA to the Kupffer cell. The 35 kDa protein is now thought to be a galactose recognizing lectin that may be identical to the previously reported galactose particle receptor [134]. This protein may be responsible for binding to CEA attached to a solid support such as a
cell [135]. Similar to many other protein recognizing receptors, binding requires Ca 2÷ [136]. The lung al- veolar macrophage also carries this receptor and in the rat it has a similar binding constant (1 • 10-8 M) and a similar number of receptors (16000) to those of the Kupffer cell [137]. The resting peritoneal macrophage, however, has no detectable receptor activity, nor do a number of macrophage-like cell lines [137]. We have shown that peritoneal macrophages elicited with thio- glycolate, however, are capable of endocytosing CEA, suggesting an up-regulation of the receptor on partial activation. This is unlike the macrophage surface man- nose receptor where activation causes loss of receptor function [138]. It may be that Kupffer cells because of their contact with gut derived endotoxins, and alveolar macrophages because of their contact with airborne materials, may all be at least partially activated and this may account for the presence of the CEA binding protein on these cells. There is a major difference be- tween CEA uptake and processing by the lung macro- phage and by the Kupffer cell. This difference is in the rate at which internalized CEA is exocytosed. The rat Kupffer cell exocytoses CEA at approx. 4-times the rate of the lung macrophage [137]. The reason for this dif- ference between these cells is not known, but it may be significant that in the liver two cells are involved in CEA processing. For processing by the hepatocyte mod- ified CEA must be released from the Kupffer cell. In the lung only one cell appears to be involved and is capable of degrading CEA without the involvement of other cell types.
CEA clearance is a heterogeneous process and rates of removal from the circulation are often multiphasic [139]. Different CEA preparations will show different kinetics of clearance, some tend to have largely rapid- phase clearance while others have higher proportions of the more slowly clearing forms. These more slowly clearing CEAs have been isolated from ascitic fluid from patients with colorectal cancer [140]. These pa- tients all had extraordinary high CEA levels and this probably reflected the preponderance of the slow clear- ing forms. Analysis of both forms of CEA showed a higher content of sialic acid in the slower clearing samples. This was found to be due to the presence of an acidic glycoprotein related to al-acid glycoprotein, that associates with CEA and presumably binds in the re- gion of the Kupffer cell binding site. Because of its structural relationship to al-acid glycoprotein (orosomucoid), including sequence homology around one of the methionines (unpublished results), we have called this glycoprotein carcinoma orosomucoid related antigen (CORA) [141].
The highest plasma CEA levels are seen in patients with colorectal cancer liver metastases especially when they are associated with cholestasis (bile stasis produced by mechanical obstruction of the major bile ducts) [142]
185
and the highest plasma CEA levels seen in benign liver disease are also associated with inter- or extrahepatic biliary obstruction [143]. Thus, the effect of biliary obstruction on CEA circulatory clearance rates and uptake by the liver has been examined. In the rat, ligation of the bile duct for 3 days will cause impaired circulatory clearance of CEA [130]. As membrane bound receptors can be affected by the action of detergents, a likely cause of CEA elevations in cholestasis would be the detergent effects of bile salts refluxed into the circulation. These can damage Kupffer cell membranes and impair CEA receptor binding. Injection of mice with the non-ionic detergent Triton WR-1339 increases the half life of CEA in the circulation [144], this agent is known to cause membrane damage to the Kupffer cells [1451.
More recently the effects of individual bile salts on Kupffer cell endocytosis have been studied and it has been shown that CEA endocytosis is impaired in treated cells and that bile acids of greatest polarity had the greatest effect [146]. This correlates with the ability of bile acids to act as detergents and also with their membrane damaging properties [147]. The evidence for the effects of liver damage on CEA metabolism seen in experimental animal systems reflects that seen in the patient with liver disease and adds further support that the mechanisms for clearance are similar in the human.
V. CEA, biological properties and function
Twenty-five years after its discovery [1,2] the func- tion of CEA is beginning to be unravelled. Because CEA is now known to be conserved in mammals at least as far down the evolutionary chain as the rat and mouse [108,109], it seems likely that its function is important. Its structural similarity to members of the immuno- globulin supergene family, in particular to molecules such as N-CAM [81], T cell [148] and growth factor receptors [149], would suggest a potential adhesion function for CEA. Recently Benchimol et al. [115] have shown that CEA can function as an intracellular ad- hesion molecule, by mediating homotypic aggregation of cultured human colon cancer cells. Unlike the bind- ing of CEA to macrophages this aggregation does not require Ca 2÷. Oikawa et al. [150] also showed a similar effect using CHO cells transfected with the CEA or NCA genes CHO cells expressing CEA aggregated rapidly, although aggregation was not as strong with the NCA expressing cells. They also showed that the CEA- induced aggregation could be blocked using the Fab' fragment of an anti-CEA antibody. Benchimol et al. also showed that CEA would promote aggregation of rodent cells (LR-73) transfected with a full length func- tional CEA cDNA using the construct in the antisense orientation as the control [115]. More recently Zhou et al. [151] showed that rodent cells transfected with the

186
NCA gene would also homotypically aggregate in a Ca 2÷ independent manner. Unlike CEA which contains three immunoglobulin-like domains, NCA contains only one, thus these experiments demonstrate the require- ment for only a single domain for homotypic binding. In this study they also showed that mixtures of CEA- and NCA-transfected cells could also form heterotypic aggregates. However, these cells would not form hetero- typic aggregates with cells transfected with the genes for neural cell adhesion molecule (NCAM) or the long form of myelin-associated glycoprotein (MAG). These authors suggest, therefore, that only closely related members of the immunoglobulin gene family can induce both homo- typic and heterotypic cell aggregates, while less closely related family members will only participate in homo- typic interactions [151]. Both Benchimol et al. [115] and Nap et al. [152] demonstrated, using immunohistoche- mistry, that while CEA is located on the luminal side of the cell in adult large bowel, in the embryo and in colonic tumors it is located on adjacent cell membranes and Shi et al. [153] showed that 80-95% of the CEA in colorectal tumors is associated with the cell membrane. This configuration will allow the epithelium to assume a multilayered arrangement. It has been suggested [115] that because of this effect, overproduction of CEA could result in disruption of the normal orderly pattern of differentiation [154], and represent an early event in tumorigenesis. The pattern of CEA staining in colo- rectal cancers has been used to indicate prognosis [155]. Patients whose tumors have a pattern of staining in which CEA is contained in the apical cytoplasm, similar to that seen in the normal adult colon [156,157] had a better outcome than those where CEA was distributed over the entire membrane, a pattern similar to that seen in the 8-9 week fetal colon [115,151].
Pignatelli et al. [158] have suggested that CEA may also function as an accessory adhesion molecule mediat- ing the binding of some colorectal cancer cells to a type 1 collagen matrix. While CEA will not bind to collagen itself monoclonal antibodies to CEA inhibit binding of SW1222 cells to collagen [158]. It has also been sug- gested [159,160] that CEA may be a possible marker for tumor progression along the adenoma-carcinoma se- quence.
The suggestion also has been made that CEA pro- duction may be a factor in the development of metast- ases from colorectal cancers, in particular those to the liver [161]. It has been known for some time that the highest plasma levels of CEA are associated with pa- tients with liver metastases [9,10,142]. It was assumed that this was due to tumor load, good access to the circulation and to impaired circulatory clearance [111]. Recent studies have suggested an additional factor, that CEA production by tumor cells is associated with a proclivity to form liver metastases [162,163]. There is now data to suggest that the adhesion properties of
CEA may be involved in the ability of tumor cells to arrest in the hepatic sinusoids [164,165]. This process is a prerequisite to the extravasion of the tumor ceils into the parenchyma, and may involve binding between tumor cells and Kupffer cells via the receptor system described above. Using a splenic injection model in nude mice [166] to assess the ability of human tumor cells to grow in the liver, Hostetter et al. [165] have shown that pre-injection of the mice with CEA caused a moderately metastatic tumor, where only 2% of the animals produced hepatic tumors, to become more ag- gressive with 48% of the CEA-treated animals now forming liver metastases. They also showed that these tumor cells were capable of binding to CEA coated onto plastic, while cell lines in which CEA had no effect on metastases formation did not bind to the CEA-coated plastic [164,165]. A study using a poorly differentiated colorectal cancer cell line with a low rate of metastases from intrasplenic injection showed an increase in metastases to both liver and lung on prior injection with CEA. Prior injection of asialo-CEA, however did not show this effect [167]. A recent review [168] discusses these data and the possible role of CEA in metastases formation more fully.
While evidence is mounting for CEAs role as an adhesion molecule in the fetal colon and in colorectal cancers its role in the adult colon is still a mystery. The normal colon produces large amounts of CEA [169,170] but exports it into the lumen. What could its function be? Does it have an adhesive function in the adult lumen possibly sticking bacteria together? Recent evi- dence suggests that this may be so. Leusch et al. [171] have shown that both CEA and NCA can bind to Escherichia coli of human origin. They also showed that binding was mannose-dependant and suggested that CEA may be involved in bacterial recognition by the colonic epithelial cells. This also raises the possibility that CEA serves a protective function in conjunction with the colonic mucus. Other questions to be answered are, how does CEA promote metastases of some colo- rectal cancers? Is this due to its properties as an ad- hesion molecule? In the liver, is the Kupffer cell and its CEA-binding protein involved in this process? These questions all require further investigation but should be resolved in the next few years.
Acknowledgements
Supported by grants R01CA42589, R01CA44586 and P01CA44704 from the U.S. Department of Health and Human Services. Ms Arleen Frasca is thanked for the drawings.
References
1 Gold, P. and Freedman, S.O. (1965) J. Exp. Med. 121,439-462. 2 Gold, P. and Freedman, S.O. (1965) J. Exp. Med. 122, 467-481.

3 Thompson, D.M.P., Krupey, J., Freedman, S.O. and Gold, P. (1969) Proc. Natl. Acad. Sci. USA 64, 161-167.
4 Loewenstein, M.S. and Zamcheck, N. (1977) Gastroenterology 72, 161-164.
5 Khoo, S.K. and Mackay, I.R. (1973) J. Chn. Pathol. 26, 470-475. 6 Neville, A.M. (1988) Tumor Biol. 9, 61-62. 7 Bast, R.C., Klug, T.L., St. John, E., Jenison, E., Niloff, J.M.,
Lazarus, H., Berkowitz, R.S., Leavitt, T., Griffiths, C.T., Parker, L., Zurawski, V.R. and Knapp, R.C. (1983) N. Engl. J. Med. 309, 883-887.
8 Hayes, D.F., Zurawski, V.R. and Kufe, D.W. (1986) J. Clin. Oncol. 4, 1542-1550.
9 Zamcheck, N. (1981) Cancer Bull. 4, 141-151. 10 Zamcheck, N., Steele, G., Thomas, P. and Mayer, R. (1986) in
Manual of Clinical Laboratory Immunology. (Rose, N.R., Freid- man, H. and Fahey, J.L., eds.), pp. 802-809, American Society for Microbiology, Washington, DC.
11 Goldenberg, D.M., Deland, F.H., Kim, E., Bennett, S., Primus, F.J., Van Nagell, J.R., Estes, N., DeSimone, P. and Rayburn, P. (1978) N. Engl. J. Med. 298, 1394-1398.
12 Beidler, C.B., Ludwig, J.R., Cardenas, J., Phelps, J, Papworth, C.G., Melcher, E., Sierzega, M., Myers, L.M., Unger, B.W., Fisher, M., David, G. and Johnson, N.J. (1988) J. Immunol. 141, 4053-4060.
13 Hardman, N., Gill, L.L., De Winter, F.J., Wagner, K., Hollis, M., Buchegger, F., Ammaturo, D., Buchegger, F., Mach, J.-P. and Heusser, C. (1989) Int. J. Cancer 44, 424-433.
14 Levin, L.V., Griffin, T.W., Haynes, L.R. and Sedor, C.J. (1982) J. Biol. Response Mod. 1, 149-162.
15 Go, V.L.W. (1976) Cancer 37, 562-566. 16 Zoubir, F., Khan, W.N. and Hammerstrom, S. (1990) Biochem.
Biophys. Res. Commun. 169, 203-216. 17 Von Kleist, S., Chavanel, G. and Burtin, P. (1972) Proc. Natl.
Acad. Sci. USA 60, 2492-2494. 18 Rogers, G.T. (1983) Biochim. Biophys. Acta 695, 227-249. 19 Hammerstrom, S., Shively, J.E., Paxton, R.J., Beatty, B.G., Lars-
son, A., Ghosh, R., Bormer, O., Buchegger, F., Mach, J.-P., Burtin, P., Seguin, P., Darbouret, B., Degorce, F., Sertour, J., Jolu, J.P., Fuks, A., Kalthoff, H., Schmiegel, W., Arndt, R., Kloppel, G., Von Kleist, S., Grunert, F., Schwarz, K., Matsuoka, Y., Masahide, K., Wagener, C., Weber, T., Yachi, A., Imai, K., Hishikawa, N. and Tsujisaki, M. (1989) Cancer Res. 49, 4852- 4858.
20 Reynoso, G., Keane, M. and Reynoso, M.A. (1985) in Cancer, (Sell, S. and Reisfeld, R., eds), pp. 19-40, Humana Press, Clifton, NJ.
21 Muraro, R., Wunderlich, D., Thor, A., Lundy, J., Noguchi, P., Cunningham, R. and Schlom J. (1985) Cancer Res. 45, 5769-5780.
22 Schwarz, K., Mehnert-Solzer, C., Von Kleist, S. and Grunert, F. (1988) Mol. Immunol. 25, 889-898.
23 Krupey, J., Wilson, T., Freedman, S.O. and Gold, P. (1972) Immunochemistry 9, 617-622.
24 Laurence, D.J.R., Turberville, C., Anderson, S.G. and Neville, A.M. (1975) Br. J. Cancer. 32, 295-299.
25 Coligan, J.E., Pritchard, D.G., Schnute, W.C. and Todd, C.W. (1976) Cancer Res. 36, 1915-1917.
26 Denk, H., Tappeiner, G., Ekerstorfer, R. and Holzner, J.H. (1972) Int. J. Cancer. 10, 262-272.
27 Martin, E.W., Kibbey, W.E., DiVecchia, L., Anderson, G., Catalano, P. and Minton, J.P. (1976) Cancer Res. 37, 62-81.
28 Denk, H., Tappeiner, G., Davidovits, A., Ekerstorfer, R. and Holzner, J.H. (1974) J. Natl. Cancer Inst. 53, 933-942.
29 Hill, R., Daunter, B., Khoo, S.K. and Mackay, E.V. (1981) Mol. Immunol. 18, 647-653.
30 Goldenberg, D.M., Pant, K.D. and Dahlman, H.L. (1976) Cancer Res. 36, 3455-3463.
187
31 Khoo, S.K., Warner, N.L., Lie, J.T. and Mackay, I.R. (1973) Int. J. Cancer. 11,681-688.
32 Pusztaszeri, G. and Mach, J.-P. (1973) Immunochemistry 10, 197. 33 Burtin, P., Chavanel, G. and Hirsch-Marie, H. (1973) J. Im-
munol. 111, 1926-1928. 34 Svenberg, T. (1976) Int. J. Cancer. 17, 588-596. 35 Martin, F. and Devant, J. (1973) J. Natl. Cancer Inst. 50,
1375-1379. 36 Vuento, M., Engvall, E., Seppala, M. and Ruoslahti, E. (1976)
Int. J. Cancer 18, 156-162. 37 Rogers, G.T. (1976) Biochim. Biophys. Acta 458, 355-373. 38 Westwood, J.H., Bessell, E.M., Bukhari, M.A., Thomas, P. and
Walker, J.M. (1974) Immunochemistry 11, 811-818. 39 Coligan, J.E., Henkart, P.A., Todd, C.W. and Terry, W.D. (1973)
Immunochemistry 10, 591-597. 40 Coligan, J.E., Egan, M.L., Guyer, R.L., Schnute, W.C. and Todd,
C.W. (1975) Ann. NY Acad. Sci. 259, 355-365. 41 Shively, J.E. and Todd, C.W. (1978) Scand. J. Immunol. 7, 19-31. 42 Thompson, J. and Zimmermann, W. (1988) Tumor Biol. 9, 63-83. 43 Westwood, J.H. and Thomas, P. (1975) Br. J. Cancer 32, 708-719. 44 Oikawa, S., Nakazato, H. and Kosaki, G. (1987) Biochem. Bio-
phys. Res. Commun. 142, 511-518. 45 Kamarck, M., Elting, J., Hart, J., Goebel, S., Rae, P.M.M.,
Northdurft, M.A., Nedwin, J. and Barnett, T. (1987) Proc. Natl. Acad. Sci. USA 84, 5350-5354.
46 Beauchemin, N., Benchimol, S., Cournoyer, D., Fuks, A. and Stanners, C.P. (1987) Mol. Cell Biol. 7, 3221-3230.
47 Zimmermann, W., Ortlieb, B., Friederich, R. and Von Kleist, S. (1987) Proc. Natl. Acad. Sci. USA 84, 2960-2964.
48 Paxton, R., Mooser, G., Pande, H., Lee, T.D. and Shively, J.E. (1987) Proc. Natl. Acad. Sci. USA 84, 920-924.
49 Thompson, J.A., Pande, H., Paxton, R., Shively, L., Padma, A., Simmer, R., Todd, C.W., Riggs, A.D. and Shively, J.E. (1987) Proc. Natl. Acad. Sci. USA 84, 2965-2969.
50 Neumaier, M., Zimmerman, W., Shively, L., Hinoda, Y., Riggs, A. and Shively, J. (1988) J. Biol. Chem. 263(7), 3202-3207.
51 Barnett, T., Goebel, S.J., Nothdurf, M.A. and Etling, J.J. (1988) Genomics 3, 59-66.
52 Hinoda, Y., Neumaier, M., Hefta, S., Drzeniek, Z., Wagener, C., Shively, L., Hefta, L.J.F., Shively, J.E. and Paxton, R.J. (1988) Proc. Natl. Acad. Sci. USA 85, 6959-6963.
53 Barnett, T.R., Kretschmer, A., Austen, D.A., Goebel, S.J., Hart, J.T., Elting, J.J. and Kamarck, M.E. (1989) J. Cell Biol. 108, 267-276.
54 Thompson, J.A., Mauch, E.-M., Chen, F.-S., Hinoda, Y., Schrewe, H., Berling, B., Barnert, S., Von Kleist, S., Shively, J.E. and Zimmermann, W. (1989) Biochem. Biophys. Res. Commun. 158, 996-1004.
55 Williams, A.F. (1987) Immunol. Today 8, 298-303. 56 Barnett, T. and Zimmermann, W. (1990) Tumor Biol. 11, 59-63. 57 Sack, T., Gum, J., Low, M. and Kim, Y. (1988) J. Clin. Invest. 82,
586-593. 58 Hefta, S., Hefta, L., Lee, T., Paxton, R. and Shively, J. (1988)
Proc. Natl. Acad. Sci. USA 85, 4648-4652. 59 Todd, C.W. and Shively, J.E. (1978) Glycoproteins Glycolipids
Dis. Process. 19, 342-356. 60 Hammarstrom, S., Engvall, E., Johansson, B.G., Svensson, S.,
Sundblad, G. and Goldstein, l.J. (1975) Proc. Natl. Acad. Sci. USA 72, 1528-1532.
61 Coligan, J.E., Pritchard, D.G., Schnute, W.C. and Todd, C.W. (1976) Cancer Res. 36, 1915-1917.
62 Bessell, E.M., Thomas, P. and Westwood, J.H. (1975) Carbohydr. Res. 45, 257-268.
63 Shively, J.E. and Beatty, J.D. (1985) CRC Crit. Rev. Oncol. Hematol. 2, 355-399.
188
64 Magous, R., Lecou, C. and Bali, J.-P. (1978) Biochem. Biophys. Res. Commun. 85, 1453-1459.
65 Chandrasekaran, E.V., Davila, M. Nixon, D.W., Goldfarb, M. and Mendicino, J. (1983) J. Biol. Chem. 258, 7213-7222.
66 Kessler, M.J., Shively, J.E., Prichard, D.G. and Todd, C.W. (1978) Cancer Res. 38, 1041-1048.
67 Westwood, J.H., Thomas, P., Edwards, R.G. and Neville, A.M. (1975) Protides Biol. Fluids Proc. Colloq. 24, 413-418.
68 Burtin, P., Chavanel, G. and Hirch-Marie, H. (1973) J. Immunol. 111, 1926-1928.
69 Kuroki, M., Koga, Y. and Matsuoka, Y. (1981) Cancer Res. 41, 713-720.
70 Primus, F.J., Freeman J.W. and Goldenberg, D.M. (1983) Cancer Res. 43, 679-685.
71 Kuroki, M., Shinoda, T., Takayasu, T., Koga, Y. and Matsuoka, Y. (1982) Mol. Immunol. 19, 399-406.
72 Slayter, H. and Coligan, J. (1975) Biochemistry 14(11), 2323-2330. 73 Westwood, J.H., Thomas, P., Edwards, R.G., Scopes, P.M. and
Barrett, M. W. (1978) Br. J. Cancer. 37, 183-189. 74 Oikawa, S., Imajo, S., Noguchi, T., Kosaki, G. and Nakazato, H.
(1987) Biochem. Biophys. Res. Commun. 144, 634-642. 75 Schwarz, K., Mehnert-Solzer, C., Von Kleist, S. and Grunert, F.
(1988) Mol. Immunol. 25, 889-898. 76 Williams, A.F. and Gagnon, J. (1982) Science 216, 696-703. 77 Wilfiams, A.F. and Barclay, A.N. (1988) Annu. Rev. Immunol. 6,
381-405. 78 Tse, A.G.D., Barkley, A.N., Watts, A. and Williamson, A.F.
(1985) Science 230, 1003-1008. 79 Cunningham, B., Hemperly, J., Murray, B., Prediger, E., Bracken-
bury, R. and Edelman, B. (1987) Science 236, 766-806. 80 Kabat, E.A., Wu, T.T., Bilofsky, H., Reid-Miller, M. and Perry,
H. (1983) Sequences of Proteins of Immunological Interest, Na- tional Institutes of Health, Bethesda, MD.
81 Mostov, K.E., Friedlander, M. and Blobel, G. (1984) Nature 308, 37-43.
82 Ishioka, N., Takahashi, N. and Putnam, F.W. (1986) Proc. Natl. Acad. Sci. USA 83, 2363-2367.
83 Hemperly, J.J., Murray, B.A., Edelman, G.M. and Cunningham, B.A. (1986) Proc. Natl. Acad. Sci. USA 83, 3037-3041.
84 Salzer, J., Holmes, W. and Coleman, D. (1987) J. Cell Biol. 104, 957-965.
85 Lin, S.-H. (1989) J. Biol. Chem. 264, 14403-14407. 86 Lin, S.-H. and Guidotti, G. (1989) J. Biol. Chem. 264, 14408-
14414. 87 Zimmermann, W., Friedrich, R., Grunert, F., Luckenbach, G.A.,
Thompson, J.A. and Von Kleist, S. (1983) Ann. NY Acad. Sci. 417, 21-30.
88 Khan, W.N., Osterman, A. and Hammarstrom, S. (1989) Proc. Natl. Acad. Sci. USA 86, 3332-3336.
89 Khan, W.N. and Hammarstrom, S. (1989) Biochem. Biophys. Res. Commun. 161,525-535.
90 Klemenz, R., Hoffmann, S. and Werenskiold, A.K. (1989) Proc. Natl. Acad. Sci. USA 86, 5708-5712.
91 Zimmermann, W., Thompson, J., and Grunert, F. (1984) Contrib. Oncol. 19, 64-74.
92 Cournoyer, D., Beauchemin, N., Boucher, D., Benchimol, S., Fuks, A. and Stanners, C.P. (1988) Cancer Res. 48, 3153-3157.
93 Arakawa, F., Kuroki, M., Misumi, Y., Oikawa, S., Nakazato, H. and Matsuoka, K. (1990) Biochem. Biophys. Res. Commun. 166, 1063-1071.
94 Boucher, D., Cournoyer, D., Stanners, C.P. and Fuks, A. (1989) Cancer Res. 48, 847-852.
95 Toribara, N.W., Sacks, T.C., Gum, J.R., Ho, S.B., Shively, J.E., Wilson, J.K. and Kim, Y.S. (1989) Cancer Res. 49, 3321-3327.
96 Sato, C., Miyaki, M., Oikawa, S., Nakazato, H. and Kosaki, G. (1988) Jpn. J. Cancer Res. 79, 433-437.
97 Tsao, D., Morita, A., Bella, A., Shi, Z., Wong, A. and Kim, Y.S. (1982) Cancer Res. 42, 1052-1058.
98 Niles, R., Wilhelm, S.A., Thomas, P. and Zamcheck, N. (1988) Cancer Invest. 6, 39-45.
99 Toth, C.A., Kowal, A. and Thomas, P. (1988) Biochem. Soc. Trans. 16, 1027-1028.
100 Zimmerman, W., Weber, B., Ortlieb, B., Rudert, F., Schempp, W., Fielig, H., Shively, J., Von Kleist, S. and Thompson, J. (1988) Cancer Res 48, 2550-2554.
101 Kantor, J., Tran, R., Greiner, J., Pestka, S., Fisher, P.B., Shively, J.E. and Schlom, J. (1989) Cancer Res. 49, 2651-2655.
102 Chou, J.Y., Sartwell, A.D., Lei, K.-J. and Plouzek, C.A. (1990) J. Biol. Chem. 265, 8788-9794.
103 Ruoslahti, E. and Pierschbacher, M.D. (1987) Science 238, 491- 497.
104 Haagensen, D.E., Metzgar, R.S., Swensen, B., Dilley, B., Cox, C.E., Davis, S., Murdoch, J., Zamcheck, N. and Wells, S.A. (1982) J. Natl. Cancer Inst. 69, 1073-1076.
105 Haagensen, D.E., Metzgar, R.S., Sawlivich, W., Swenson, B., Davis, D., Newman, E., Zamcheck, N., Wells, S.A. and Hansen, H.J. (1987) Cancer Res. 47, 5606-5611.
106 Abeyounis, C.J. and Milgrom, F. (1976) J. Immunol. 116, 30-34. 107 Abeyounis, C.J., Kim, J.G., Wilhelm, S.A., Diakun, K.R. and
Milgrom, F. (1989) Immunol. Invest. 18, 143-157. 108 Beauchemin, N., Turbide, C., Afar, D., Raymond, M., Stanners,
C.P. and Fuks, A. (1989) Cancer Res. 49, 2017-2021. 109 Kodelja, V., Lucas, K., Barnert, S., Von Kleist, S., Thompson, J.
and Zimmerman, W. (1989) J. Biol. Chem. 264, 6906-6912. 110 Inazawa, J., Abe, T., Inoue, K., Misawa, S., Oikawa, S., Nakazato,
H. and Yoshida, M.C. (1989) Cytogenet. Cell Genet. 52, 28-31. 111 Thomas, P. and Zamcheck, N. (1983) Dig. Dis. Sci. 28, 216-224. 112 Niles, R.M., Wilhelm, S.A., Steele, G.D., Burke, B., Christensen,
T., Dexter, D., O'Brien, N.J., Thomas, P. and Zamcheck, N. (1987) Cancer Invest. 5, 545-552.
113 Hartshorn-Mottola, C., Lorenzoni, P. and Ceccarini, C. (1988) Biochem. J. 255, 943-948.
114 Miura, S. and Kim, Y.S. (1986) Int. J. Cancer. 38, 197-205. 115 Benchimol, S., Fuks, A., Jothy, S., Beauchemin, N., Shirota, K.
and Stanners, C. (1989) Cell 57, 327-334. 116 Moore, J.L., Dhar, P., Zamcheck, N., Keeley, A., Gottlieb, L. and
Kupchik H. (1979) Gastroenterology 63, 88-94. 117 Lurie, B.B., Loewenstein, M. and Zamcheck, N. (1975) J. Am.
Med. Assoc. 233, 326-330. 118 Shuster, J., Silverman, M. and Gold, P. (1973) Cancer Res. 33,
65-68. 119 Thomas, P. and Hems, D. (1975) Biochem. Biophys. Res. Com-
mun. 67, 1205-1209. 120 Primus, F.J., Hansen, H. and Goldenberg, D.M. (1974) 249,
837-838. 121 Thomas, P., Zamcheck, N., Rogers, A. and Fox, J.G. (1982) Clin.
Lab. Med. 2, 459-467. 122 Toth, C.A., Rapoza, A., Kowal, A., Steele, G. and Thomas, P.
(1988) Biochem. Soc. Trans. 16, 1027-1028. 123 Shimoyama, T., Fukuda, Y., Takahira, R., Kawaguchi, A.,
Tohchika, H., Nakao, H., Kusano, H., Shimizu, T., Nakagoe, T., Hirano, T., Sakai, T., Miura, T. and Tomita, M. (1988) Acta Med. Nagasaki 33, 221-227.
124 Kodama, T., Fugino, N., Endo, Y., Fukayama, N., Sugiura, N., Oda, T., Wada, T. and Burtin, P. (1979) in Carcinoembryonic Proteins, Vol. 2. (Lehmann, F., ed.), pp. 93-97, Elsevier Biomedi- cal Press, New York.
125 Toth, C.A., Thomas, P., Broitman, S. and Zamcheck, N. (1982) Biochem. J. 204, 377-381.
126 Toth, C.A., Thomas, P., Broitman, S. and Zamcheck, N. (1985) Cancer Res. 45, 392-397.
127 Ashwell, G. and Morell, A.G. (1974) Adv. Enzymol. 41, 99-128.
128 Thomas, P. (1980) Biochem. J. 192, 837-843. 129 Thomas, P., Toth, C.A. and Zamcheck, N. (1982) Hepatology 2,
800-803. 130 Thomas, P., O'Neil, P.F. and Zamcheck, N. (1982) Biochem. Soc.
Trans. 10, 459-460. 131 Thomas, P., O'Neil, P.F. and Zamcheck, N. (1985) Hepatology 5,
207-210. 132 Thomas, P. and Toth, C.A. (1989) Biochem. Soc. Trans. 17,
1121-1122. 133 Thomas, P. and Toth, C.A. (1990) Biochem. Biophys. Res. Com-
mun. 170, 391-396. 134 Roos, P.H., Hartmann, H.-J., Schlepper-Schafer, J., Kolb, H. and
Kolb-Bachofen, V. (1985) Biochim. Biophys. Acta 847, 115-121. 135 Schlepper-Schafer, J., Raffelsiefer, A. and Kolb-Bachofen, V.
(1989) in Cells of the Hepatic Sinusoid, Vol. 2 (Wisse, E., Knook, D.L. and Decker, K., eds.) pp. 115-119, The Kupffer Cell Foundation, Rij swijk.
136 Thomas, P., Byrn, R.A. and Toth, C.A. (1988) FASEB J. 2, 623A. 137 Toth, C.A., Rapoza, A., Zamcheck, N. Steele, G. and Thomas, P.
(1989) J. Leukocyte Biol. 45, 370-376. 138 Stahl, P. and Gordon, S. (1982) J. Cell. Biol. 93, 48-55. 139 Byrn, R.A., Medrek, P., Thomas, P., Jeanloz, R. and Zamcheck,
N. (1985) Cancer Res. 45, 3137-3142. 140 Saravis, C.A., Thomas, P. and Zamcheck, N. (1986) Proc. Am.
Assoc. Cancer Res. 27, 1. 141 Toth, C.A., Thomas, P., Rapoza, A., Sherman, M. and Steele, G.
(1988) FASEB J. 2, A851. 142 O'Brien, M.J., Bronstein, B., Zamcheck, N., Saravis, C., Burke, B.
and Gottlieb, L.S. (1980) J. Natl. Cancer Inst. 64, 1291-1294. 143 Scapa, E., Thomas, P., Loewenstein, M.S. and Zamcheck, N.
(1985) Eur. J. Cancer Clin. Oncol. 21, 1037-1042. 144 Thomas, P. and Jones, M. (1978) Biochem. J. 178, 981-983. 145 Cotmore, S.F. and Carter, R.L. (1973) Int. J. Cancer. 11,725-738. 146 Thomas, P. and Toth, C.A. (1989) in Cells of the Hepatic
Sinusoid, Vol. 2 (Wisse, E., Knook, D.L. and Decker, K., eds.), pp. 302-304, The Kupffer Cell Foundation, Rijswijk.
147 Scholmerich, J., Becher, M.-S., Schmidt, K., Schubert, R., Kremer, B., Feldhaus, S. and Gerok, W. (1984) Hepatology 4, 661-666.
148 Huang, H.-J., Jones, S., Strominger, J.L. and Herzenberg, L.A. (1987) Proc. Natl. Acad. Sci. USA 84, 204-208.
149 Yarden, Y., Escobedo, J.A., Kuang, W.-J., Yang-Feng, T.L., Daniel, T.O., Tremble, P.M., Chen, E.Y., Ando, N., Harkins, R.N., Franke, U., Fried, V.A., Ullrich, A. and Williams, L.T. (1986) Nature 323, 226-232.
150 Oikawa, S., Inuzuka, C., Kuroki, N., Matsuoka, Y., Kosaki, G. and Nakazato, H. (1989) Biochem. Biophys. Res. Commun. 164, 39-45.
189
151 Zhou, H., Fuks, A. and Stanners, C.P. (1990) Cell Growth Differ. 1,209-215.
152 Nap, M., Mollgard, K., Burtin, P. and Fleuren, G. (1988) Tumor Biol. 9, 145-153.
153 Shi, Z.R., Tsao, D. and Kim, Y.S. (1983) Cancer Res. 43, 4045- 4049.
154 Chang, W.W.L. and Leblond, C.P. (1971) Am. J. Anat. 131, 73-100.
155 Wiggers, T., Arends, J.W., Verstijnen, C., Noerkerk, P.M. and Bosman, F.T. (1986) Br. J. Cancer. 54, 409-414.
156 Huitric, E., Laumonier, R., Burtin, P. and Von Kleist, S. (1976) Lab. Invest. 34, 97-105.
157 Ahnen, D.J., Nakane, P.K. and Brown, W.R. (1982) Cancer. 49, 2077-2090.
158 Pignatelli, N., Durbin, H. and Bodmer, W.F. (1990) Proc. Natl. Acad. Sci. USA 87, 1541-1545.
159 Zamcheck, N., Liu, P., Thomas, P. and Steele, G.D. (1988) in Basic and Clinical Perspectives of Colorectal Polyps and Cancer (Steele, G., Burt, R., Winawer, S.J. and Karr, J.P., eds.), pp. 251-275 Alan R. Liss, New York.
160 Berry, R.D. and Paraskeva, C. (1988) Carcinogenesis 9, 447-450. 161 Steele, G.D. and Thomas, P. (1988) in Gastrointestinal Cancer:
Current approaches to diagnosis and treatment (Levin, B. ed.), pp. 211-224, University of Texas Press, Austin.
162 Giavazzi, R., Jessup, J.M., Campbell, D.E., Walker, S.M. and Fidler, I.J. (1986) Cancer Res. 46, 1928-1933.
163 Jessup, J.M., Giavazzi, R., Campbell, D.E., Cleary, K. Morikowa, K. and Fidler, I.J. (1988) Cancer Res. 48, 1689-1692.
164 Hostetter, R., Augustus, L.B., Mankarious, R., Chi, K., Fan, D., Toth, C.A., Thomas, P. and Jessup, J.M. (1990) J. Natl. Cancer Inst. 82, 380-385.
165 Hostetter, R., Campbell, D.E., Kerkhoff, S., Cleary, K., Ullrich, S. Thomas, P. and Jessup, J.M. (1990) Arch. Surg. 125, 300-304.
166 Giavazzi, R., Jessup, J.M., Campbell, D.E., Walker, S.M. and Fidler, I.J. (1986) J. Natl. Cancer Inst. 77, 1303-1308.
167 Wagner, H.E., Thomas, P., Wolf, B.C., Zamcheck, N., Jessup, J.M. and Steele, G.D. (1990) Invasion Metastasis, in press.
168 Jessup, J.M. and Thomas, P. (1989) Cancer and Metastasis Rev. 8, 263-280.
169 Egan, M.L., Pritchard, D.G., Todd, C.W. and Go, V.L.W. (1977) Cancer Res. 37, 2638-2643.
170 Shively, J.E., Todd, C.W., Go, V.L.W. and Egan, M.L. (1978) Cancer Res. 38, 503-505.
171 Leusch, H.-G., Hefta, S.A., Drzeniek, Z., Hummel, K., Markos- Pusztai, Z. and Wagner, C. (1990) FEBS Lett. 261,405-409.