The fetal portal vein: normal blood flow development during the second half of human pregnancy
9
Ultrasound Obstet Gynecol 2007; 30: 52–60 Published online 8 June 2007 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.4054 The fetal portal vein: normal blood flow development during the second half of human pregnancy J. KESSLER*†, S. RASMUSSEN*†‡ and T. KISERUD*† *Department of Clinical Medicine, University of Bergen and †Department of Obstetrics and Gynecology, Haukeland University Hospital, Bergen and ‡Medical Birth Registry of Norway, Locus of Registry Based Epidemiology, University of Bergen and the Norwegian Institute of Public Health, Norway KEYWORDS: blood flow; circulation; Doppler ultrasound; fetus; portal vein ABSTRACT Objectives The umbilical vein is the major source of blood for the fetal liver, but portal blood, which has not been measured directly in human fetuses, probably constitutes a physiologically important contribution. We aimed to establish a method for measuring blood flow in the fetal portal vein and to produce longitudinal reference ranges for diameter, blood flow velocities and volume blood flow during the second half of pregnancy. Methods After a pilot project to develop the measuring technique, 160 low-risk pregnant women were recruited to a longitudinal study that included ultrasound exam- inations at 4–5-week intervals starting at 20–22 weeks of gestation. The inner diameter (D) of the vessel was measured with a perpendicular insonation angle, and the time-averaged maximum blood velocity (TAMXV) and weighted mean velocity (VWMEAN) were recorded with an insonation directed along the long axis of the ves- sel. Portal flow was calculated as: Q = π(D/2) 2 × h × TAMXV (where h is a velocity profile parameter and equals 0.5). Portal flow was normalized for estimated fetal weight based on birth-weight percentiles. Results The portal vein could be visualized and measured in 558/593 (94%) cases. Blood flow was pulsatile. D and TAMXV doubled during the second half of pregnancy (21–39 weeks), from 1.5 to 3.4 mm and from 8.4 to 14.9 cm/s, respectively. Correspondingly, the portal flow increased from 5 to 41 mL/min, and from 10 to 13 mL/min/kg when normalized for fetal weight. Similar results were achieved for VWMEAN. Conclusion Portal flow can be measured with a standardized technique. It increases during the second half of pregnancy, even when normalized for fetal weight, suggesting that it has increasing importance in the fetal liver circulation. Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. INTRODUCTION The fetal liver has a prominent position in the fetal circulation, receiving 70–80% of the venous return from the placenta 1,2 , and its role in the regulation of intrauterine growth is being recognized increasingly 3 . In fetal sheep, umbilical venous liver perfusion seems to drive both the synthesis of insulin-like growth factor 1 in the liver and the proliferation rates of peripheral tissues 4,5 . Data from human pregnancies suggest that the venous flow to the fetal liver is under the influence of maternal factors such as diet and body composition 6 . The venous perfusion of the liver in utero differs substantially from that after delivery. While postnatally all the venous blood is supplied by the portal vein, during prenatal life the liver receives venous blood from both the umbilical and the portal veins (Figure 1). In fetal sheep, the umbilical vein directs the well-oxygenated cord blood mainly to the left liver lobe, while the portal vein blood circulates the right liver lobe 7 , a concept that was also suggested for the human fetus by Lind 8 in 1963. Emery 9 described morphological and functional differences between the left and right fetal liver lobes in humans (from autopsies), and related these differences to the selective perfusion of the liver lobes by the portal and umbilical veins. A recent study supports this concept, showing differences in the gene expression profile between the left and right liver lobes of fetal baboons 10 . While the blood flow in the umbilical vein has been studied extensively both in normal and in compromised pregnancies 2,11–18 , so far flow in the main portal stem has not been measured, although it has been estimated indirectly using Doppler recordings of the intrahepatic branches 19 . The aim of this study was, therefore, first to Correspondence to: Dr J. Kessler, Department of Obstetrics and Gynecology, Haukeland University Hospital, N-5021 Bergen, Norway (e-mail: [email protected]) Accepted: 3 April 2007 Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. ORIGINAL PAPER
Transcript of The fetal portal vein: normal blood flow development during the second half of human pregnancy

Ultrasound Obstet Gynecol 2007; 30: 52–60Published online 8 June 2007 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.4054
The fetal portal vein: normal blood flow development duringthe second half of human pregnancy
J. KESSLER*†, S. RASMUSSEN*†‡ and T. KISERUD*†*Department of Clinical Medicine, University of Bergen and †Department of Obstetrics and Gynecology, Haukeland University Hospital,Bergen and ‡Medical Birth Registry of Norway, Locus of Registry Based Epidemiology, University of Bergen and the Norwegian Instituteof Public Health, Norway
KEYWORDS: blood flow; circulation; Doppler ultrasound; fetus; portal vein
ABSTRACT
Objectives The umbilical vein is the major source ofblood for the fetal liver, but portal blood, which hasnot been measured directly in human fetuses, probablyconstitutes a physiologically important contribution. Weaimed to establish a method for measuring blood flow inthe fetal portal vein and to produce longitudinal referenceranges for diameter, blood flow velocities and volumeblood flow during the second half of pregnancy.
Methods After a pilot project to develop the measuringtechnique, 160 low-risk pregnant women were recruitedto a longitudinal study that included ultrasound exam-inations at 4–5-week intervals starting at 20–22 weeksof gestation. The inner diameter (D) of the vessel wasmeasured with a perpendicular insonation angle, and thetime-averaged maximum blood velocity (TAMXV) andweighted mean velocity (VWMEAN) were recorded withan insonation directed along the long axis of the ves-sel. Portal flow was calculated as: Q = !(D/2)2! h !TAMXV (where h is a velocity profile parameter andequals 0.5). Portal flow was normalized for estimatedfetal weight based on birth-weight percentiles.
Results The portal vein could be visualized and measuredin 558/593 (94%) cases. Blood flow was pulsatile. D andTAMXV doubled during the second half of pregnancy(21–39 weeks), from 1.5 to 3.4 mm and from 8.4to 14.9 cm/s, respectively. Correspondingly, the portalflow increased from 5 to 41 mL/min, and from 10 to13 mL/min/kg when normalized for fetal weight. Similarresults were achieved for VWMEAN.
Conclusion Portal flow can be measured with astandardized technique. It increases during the secondhalf of pregnancy, even when normalized for fetal weight,suggesting that it has increasing importance in the fetal
liver circulation. Copyright ! 2007 ISUOG. Publishedby John Wiley & Sons, Ltd.
INTRODUCTION
The fetal liver has a prominent position in the fetalcirculation, receiving 70–80% of the venous returnfrom the placenta1,2, and its role in the regulation ofintrauterine growth is being recognized increasingly3. Infetal sheep, umbilical venous liver perfusion seems to driveboth the synthesis of insulin-like growth factor 1 in theliver and the proliferation rates of peripheral tissues4,5.Data from human pregnancies suggest that the venousflow to the fetal liver is under the influence of maternalfactors such as diet and body composition6.
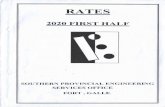
The venous perfusion of the liver in utero differssubstantially from that after delivery. While postnatallyall the venous blood is supplied by the portal vein, duringprenatal life the liver receives venous blood from boththe umbilical and the portal veins (Figure 1). In fetalsheep, the umbilical vein directs the well-oxygenated cordblood mainly to the left liver lobe, while the portal veinblood circulates the right liver lobe7, a concept thatwas also suggested for the human fetus by Lind8 in1963. Emery9 described morphological and functionaldifferences between the left and right fetal liver lobes inhumans (from autopsies), and related these differencesto the selective perfusion of the liver lobes by the portaland umbilical veins. A recent study supports this concept,showing differences in the gene expression profile betweenthe left and right liver lobes of fetal baboons10.
While the blood flow in the umbilical vein has beenstudied extensively both in normal and in compromisedpregnancies2,11–18, so far flow in the main portal stemhas not been measured, although it has been estimatedindirectly using Doppler recordings of the intrahepaticbranches19. The aim of this study was, therefore, first to
Correspondence to: Dr J. Kessler, Department of Obstetrics and Gynecology, Haukeland University Hospital, N-5021 Bergen, Norway(e-mail: [email protected])
Accepted: 3 April 2007
Copyright ! 2007 ISUOG. Published by John Wiley & Sons, Ltd. ORIGINAL PAPER

Fetal portal vein blood flow 53
Figure 1 Venous blood supply of the fetal liver in a transversesuperior view. Red indicates well oxygenated and blue indicatespoorly oxygenated blood; purple represents a mixture of the two.DV, ductus venosus; LPV, left portal branch; PV, main stem of theportal vein; RPV, right portal branch; ST, stomach; SP, spine;UV, umbilical vein.
establish a measurement technique and then to producelongitudinal reference ranges for diameter, blood flowvelocities and volume blood flow in the fetal portal veinduring the second half of pregnancy.
METHODS
Women scheduled for a routine ultrasound examinationbetween 17 and 20 weeks of gestation were invited toparticipate in this study as part of a larger hemodynamicstudy of the umbilical and portal venous circulation(we have published previously on ductus venosus bloodvelocities20). The study protocol was approved by theRegional Committee for Research Ethics (REK-Vest04/3837) and the women were recruited after givinginformed written consent.
First, a pilot study was conducted with 40 participantswho were each examined once. During this study wefocused on the anatomy of the liver vessels to find land-marks for orientation and directions of insonation forthe measurements. Then, 160 healthy pregnant womenconsecutively entered the study during the period ofAugust 2004–July 2005. Gestational age was assessedsonographically in the second trimester21. Reasons forexclusion included: multiple pregnancy, fetal malforma-tion or chromosomal aberration, chronic maternal disease(hypertension, diabetes, rheumatic or autoimmune dis-eases, dyslipidemia) and complicated obstetric history(pre-eclampsia, growth restriction, placental abruption,gestational diabetes, delivery < 37 weeks of gestation).The study protocol aimed to obtain four to five exami-nations per participant at 4–5-week intervals starting at20–22 weeks of gestation. Each session lasted 60 min.After delivery, information on gender, weight, mode ofdelivery and transfer to the neonatal intensive care unit(NICU) were collected from the medical records.
All measurements were carried out by one observer(J.K.) using a Sonos 7500 ultrasound machine (Philips,Seattle, WA, USA) with a 3.5-MHz (2–6-MHz) curvedlinear transducer including color Doppler (2.5 MHz) andpulsed Doppler (3 MHz) facilities. The high-pass filter wasset at 50 Hz. The mechanical index (MI) and the thermalindex for soft tissue (TIS) were usually 1.1 or less; in a fewobese participants, higher energy output was occasionallyneeded and the TIS and MI were increased to 1.4.
The main stem of the portal vein was identified usingcolor Doppler. Starting with a transverse left or rightlateral insonation similar to the transection used for themeasurement of the fetal abdominal circumference, themain portal stem was identified at the point at whichit divides into the left and right branches. The arteriahepatica propria usually crossed the main portal stembefore it branched and helped to identify the site formeasurement of diameter.
The inner diameter of the portal vein was measured ina longitudinal insonation perpendicular to the vessel wall.For this purpose the transducer was tilted to a slightlymore oblique insonation, thus visualizing the vessel wallimmediately upstream of the branching point (Figure 2).After the site was identified, the color Doppler mode wasswitched off, the image of the vessel zoomed in, andboth gain and compression were reduced to sharpen theinterface between vessel wall and blood. The diameterbetween the inner edges of the vessel wall was measuredseveral (median, 4; range, 1–6) times and the mean foreach individual session was used for further analysis andflow calculation.
At the same location, but with an insonation along thelong axis of the vessel with an angle as low as possible andalways < 30", the blood flow velocities (time-averagedmaximum velocity, TAMXV; time averaged weightedmean velocity, VWMEAN) were measured in the absenceof fetal movements (Figure 3).
The volume blood flow (Q) was calculated as Q =!(D/2)2 ! h ! TAMXV, where D is the inner diameterof the portal vein and h is the velocity profile (h = 0.5)and assuming a parabolic velocity profile in the mainportal stem. In order to test this assumption, flow wasalso calculated as Q = !(D/2)2 ! VWMEAN. A plot ofdifference from the mean was used to compare VWMEANand 0.5 TAMXV for the calculation of volume flow22.Blood flow was normalized for estimated fetal weightbased on birth-weight percentiles23,24.
Statistical analysis
Our power calculation followed that of Royston andAltman25, who, anticipating that a cross-sectional studyneeds a certain number of participants (Nc), calculatedthe corresponding number in a longitudinal study (Nl)for the same purpose as Nl = Nc/2.3. Approximately15 observations per gestational week are necessaryfor the calculation of reliable percentiles accordingto previous experience in cross-sectional studies1,26,27.Thus, an observation period of 20 weeks corresponds to
Copyright ! 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 30: 52–60.

54 Kessler et al.
Figure 2 Color Doppler image with perpendicular insonation of theportal vein (PV) for the measurement of its inner diameter (arrow)at 22 + 1 weeks of gestation, showing color signals in the left portalbranch (LPV) and the ductus venosus (DV). Due to the insonationangle and filter setting no color signals are visible in the PV, rightportal branch (RPV) or umbilical vein (UV). The diametermeasurement was made without simultaneous color Dopplertracing.
Figure 3 Pulsed Doppler recording at the main stem of the portalvein with the typical monophasic pulsatile velocity pattern at27 + 6 weeks of gestation. The crossing arteria hepatica propria(HA, thick arrows) and the ductus venosus (DV, thin arrow) serveas anatomical landmarks. RPV, right portal branch; UV, umbilicalvein.
Nc = 300 and Nl = 130; an anticipated success rate of80% increased the study population to 160 participants.
Statistical analysis was carried out using SPSS (Statisti-cal Package for the Social Sciences, SPSS Inc. Chicago,IL, USA) and MlWin (MlWin, Centre for MultilevelModelling, University of Bristol, Bristol, UK). Multilevelmodeling using the MlWin program was used to construct
mean and percentile curves for each variable accordingto gestational age. The assumption of normal distributionwas checked for the outcome variables and the power intowhich the dependent variables was transformed was deter-mined using Box-Cox transformation. Fractional polyno-mials were specified as two components, a fixed one anda random one. Goodness-of-fit was assessed by deviancestatistics. Formulae for the gestational age-specific meansand SDs are presented online in Appendix S1.
The 2.5th, 5th, 10th and 25th percentiles were calculatedby subtracting 1.96, 1.645, 1.282 and 0.674 SD,respectively, from the mean and the 97.5th, 95th, 90th
and 75th percentiles were estimated by adding theserespective multiples of the SD to the mean. The confidenceinterval of the mean was obtained from the standarderror (SE) of the mean as provided by the MlWinprogram. To obtain the SE of the 5th and 95th percentiles,transformed observations ± 1.645 were regressed againstgestational age. The SEs around the regression lines, whichequalled the 5th and 95th percentiles, were used to obtainapproximate 95% CIs around the percentiles. The 95%CI around the mean can be used to assess the significanceof changes. If the 95% CIs at specific gestational ages donot overlap, the change of the dependent variable duringthis period is considered as being significant.
The intraobserver variation for the measurement of theportal stem diameter and flow velocities was calculatedusing limits of agreement22.
RESULTS
All 160 participants were Caucasian, with a meanmaternal age of 29 (range, 20–43) years at inclusion,94 (59%) being para 0. There were 16 smokers in thestudy population. The mean gestational age at birth was40 + 3 weeks (range, 33 + 3 to 42 + 4). Eighty-two malesand 78 females were delivered, and the neonates hada mean birth weight of 3550 (range, 2100–4700) g.There were 15 (9.4%) Cesarean sections and seven (4.4%)newborns were admitted to the NICU.
A total of 593 examinations was carried out (mean, 3.7;range, 1–5 per participant). Measurement of the vesseldiameter was successful in 573 (97%) of these and theblood flow velocities were measured in 576 (97%). Forthe estimation of the volume blood flow, data from 558(94%) examinations were eligible for statistical analysis.
With color Doppler we were able to visualize the mainstem of the portal vein regularly as a vessel going in acranial, anterior and right lateral direction, connectingto the right and left portal veins, to the right side ofthe origin of the ductus venosus (Figure 3). The distancebetween the division of the main stem of the portal veinand the inlet of the ductus venosus was approximately4 mm at midgestation, increasing to 9 mm near term.There was considerable variation with respect to both theangle between the main stem of the portal vein and the leftportal vein and the distance between the ductus venosusand the branching of the portal vein. We also observeddifferent connection types of the main portal stem to the
Copyright ! 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 30: 52–60.

Fetal portal vein blood flow 55
left and right branches. In most cases, the left and rightportal branch formed a straight sinus and the junctionwith the main stem was at a right angle (Figure 4a).However, in some cases the main stem continued furtherto the right with a direct communication with the rightposterior branch and a less developed junction with theleft portal branch which seemed to continue into the rightanterior branch (Figure 4b). At 21 weeks of gestation,the portal stem had a diameter of 1.5 mm, increasing to3.4 mm at 39 weeks (Figure 5, Table 1).
In all measurements, the blood flow in the main portalstem was directed towards the liver. The blood flowwas found to be pulsatile in all but six measurements.Typically, we observed a waveform shape with onevelocity peak and one nadir during the heart cycle(Figure 3). When recording the arteria hepatica propriaand the portal vein simultaneously, we found identicalpulse rates for the two pulsations, but with a shiftbetween the peaks corresponding to half of the durationof the pulse (Figure 6). The presence of fetal respiratorymovements modified the blood flow pattern as shown inFigure 7, and any measurements thus affected were notincluded in the statistics. The angle correction for thevelocity recordings was 0"for 137 of 576 measurements,with the median angle correction being 10 (range, 0–30)"
for the total of 576 measurements.The TAMXV in the portal vein increased throughout
the second half of gestation, from 8.4 cm/s at 21 weeksto 14.9 cm/s at 39 weeks (Figure 8 and Table S1 online).Similarly, VWMEAN increased from 4.1 cm/s at 21 weeksto 7.6 cm/s at 39 weeks (Figure S1 online). In parabolicflow, VWMEAN equals 0.5 TAMXV, and they couldbe used interchangeably for the calculation of volumeflow. When comparing 0.5 TAMXV with VWMEAN in aBland-Altman plot22, we found good agreement but there
0.5
0.4
0.3
0.2
0.1
0.020 24 28 32 36 40
Dia
met
er (c
m)
Gestational age (weeks)
Figure 5 Longitudinal reference ranges for the growth of thediameter of the main stem of the fetal portal vein, based on 573observations in 160 low-risk pregnancies. The 5th, 50th and 95th
percentiles are presented (solid lines) with 95% CIs (dashed lines).
was slight skewing towards a blunted flow profile whenthe mean velocity reached 8-10 cm/s (Figure 9). However,the effect was mild and velocities observed at this levelwere rare and did not impact the calculated referenceranges, which were almost identical. The mean volumeflow based on 0.5 TAMXV was 4.6 mL/min at 21 weeksof gestation, rising exponentially to 41.4 mL/min at39 weeks (Figures 10 and 11 and Table S2 online),much the same as the flow calculation based on
Figure 4 Power Doppler images of the fetal portal system showing anatomical variations. (a) Conventional anatomy, with the right portalbranch (RPV) starting at the junction with the left portal branch (LPV) and main stem (PV) and then branching into the right anterior (RA)and right posterior (RP) branches (30 + 2 weeks). (b) The conventional RPV is replaced by the LPV and the PV running approximatelyparallel, joined through a small communicating window and feeding the RA and RP, respectively (36 + 2 weeks). In both cases, the arteriahepatica propria (arrow) runs close to the PV.
Copyright ! 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 30: 52–60.

56 Kessler et al.
Table 1 Longitudinal reference ranges for the diameter (in cm) ofthe main portal stem, based on 573 observations in 160 low-riskpregnancies
PercentileGestation(weeks) 50th 2.5th 5th 10th 25th 75th 90th 95th 97.5th
22 0.16 0.14 0.14 0.14 0.15 0.17 0.18 0.18 0.1923 0.17 0.14 0.15 0.15 0.16 0.18 0.19 0.19 0.2024 0.18 0.15 0.16 0.16 0.17 0.19 0.20 0.21 0.2125 0.19 0.16 0.17 0.17 0.18 0.20 0.21 0.22 0.2226 0.20 0.17 0.18 0.18 0.19 0.21 0.22 0.23 0.2427 0.21 0.18 0.19 0.19 0.20 0.23 0.24 0.24 0.2528 0.23 0.19 0.20 0.20 0.21 0.24 0.25 0.26 0.2629 0.24 0.20 0.21 0.21 0.22 0.25 0.26 0.27 0.2830 0.25 0.21 0.22 0.22 0.24 0.26 0.28 0.29 0.2931 0.26 0.22 0.23 0.23 0.25 0.28 0.29 0.30 0.3132 0.27 0.23 0.24 0.25 0.26 0.29 0.31 0.32 0.3233 0.29 0.24 0.25 0.25 0.27 0.30 0.32 0.33 0.3434 0.30 0.25 0.26 0.26 0.28 0.32 0.33 0.35 0.3635 0.31 0.25 0.26 0.27 0.29 0.33 0.35 0.36 0.3736 0.32 0.26 0.27 0.28 0.30 0.34 0.36 0.37 0.3937 0.33 0.27 0.28 0.29 0.31 0.35 0.37 0.39 0.4038 0.34 0.27 0.28 0.29 0.31 0.36 0.38 0.40 0.41
Figure 6 Simultaneous pulsed Doppler recording of the main stemof the portal vein (thick arrow) and the arteria hepatica propria(thin arrow) at 21 + 3 weeks of gestation, showing identical pulserates but a shift in peak velocities corresponding to half of theduration of the pulse.
VWMEAN (Figure S2 online). The mean portal bloodflow normalized for estimated fetal weight remained at10–11 mL/min/kg until 28 weeks, and increased steadily(and significantly, with non-overlapping 95% CIs ofthe mean) thereafter, to 13 mL/min/kg at 39 weeks ofgestation (Figure 12, Table S3 online).
The intraobserver variation for the velocity anddiameter measurements was low, with lower and upperlimits of agreement for measurements being #2.03 and2.43 for TAMXV, #1.26 and 1.49 for VWMEAN, and#0.04 and 0.03 for diameter of the portal main stem.The calculation was based on 211 repeat velocity and 554diameter measurements.
DISCUSSION
We have established a reliable technique for examining themain portal stem in the human fetus and have investigatedsystematically the development of diameter, blood flow
Figure 7 Pulsed Doppler recording at the main stem of the portalvein in the presence of fetal respiratory movements (31 + 1 weeksof gestation).
20
16
12
8
4
020 24 28 32 36 40
TA
MX
V (c
m/s
)
Gestational age (weeks)
Figure 8 Longitudinal reference ranges showing the development ofthe time-averaged maximum velocity (TAMXV) in the main stemof the fetal portal vein during the second half of pregnancy, basedon 576 observations in 160 low-risk pregnancies. The 5th, 50th and95th percentiles are presented (solid lines) with 95% CIs (dashedlines).
velocities and volume flow of this vessel during the secondhalf of pregnancy.
In contrast to normalized combined cardiac output,which remains at 400 mL/min/kg for the second half ofpregnancy28, the normalized blood flow in the main portalstem increased during gestational weeks 26–39. This isin line with the higher fraction of umbilical blood beingdirected to the liver during the same period1,2, indicatinga high circulatory priority of the fetal liver during thethird trimester. In addition to regulating growth in fetaltissues4,5, during this period the fetal liver also seemsto be involved in metabolic adaptation reflecting the
Copyright ! 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 30: 52–60.

Fetal portal vein blood flow 57
2.5
2.0
1.5
1.0
0.5
0.0
!0.5
!1.0
!1.5
!2.0
!2.5
0.5
TA
MX
V !
VW
MEA
N (c
m/s
)
0 2 4 6 8 10Portal vein mean velocity (cm/s)(0.5 TAMXV + VWMEAN)/2
Figure 9 Bland–Altman plot22 showing the agreement betweentime-averaged weighted mean velocity (VWMEAN) and 0.5 !time-averaged maximum velocity (TAMXV). Dashed linesrepresent 95% limits of agreement. Solid line represents the meandifference between 0.5 ! TAMXV and VWMEAN.
70
60
50
40
30
20
10
20 24 28 32 36 400
Vol
ume
bloo
d flo
w (m
L/m
in)
Gestational age (weeks)
Figure 10 Longitudinal reference ranges showing the developmentof the volume flow in the main stem of the fetal portal vein, basedon 0.5 ! time-averaged maximum velocity from 558 observationsin 160 low-risk pregnancies. The 5th, 50th and 95th percentiles arepresented (solid lines) with 95% CIs (dashed lines).
maternal nutritional state and diet6. We believe that thetechniques and results presented here provide a goodbasis for studying the role of the liver in prenatal life,both its role in growth and more specifically its role in theincreasing splanchnic circulation. Increase in portal bloodflow is known to occur after meals in adults29. Similarly,a substantial velocity increase in the superior mesentericartery has been described in newborns after breast-milk
80
70
60
50
40
30
20
20 24 28 32 36 40
10
0
Vol
ume
bloo
d flo
w (m
L/m
in)
Gestational age (weeks)
Figure 11 Individual variation and development of the volumeblood flow in the main portal stem; flow calculation based on 558longitudinal observations in 160 low-risk pregnancies.
25
20
20 24 28 32 36 40
15
10
5
0
Vol
ume
bloo
d flo
w (m
L/m
in/k
g)
Gestational age (weeks)
Figure 12 Longitudinal reference ranges showing the developmentof the volume flow in the main stem of the fetal portal veinnormalized for fetal weight and based on 558 observations in 160low-risk pregnancies; flow calculation based on 0.5 !time-averaged maximum velocity. The 5th, 50th and 95th
percentiles are presented (solid lines) with 95% CIs (dashed lines).
feeding30. Whether these responses exist prenatally hasnot been investigated. However, both the developmentof fetal gall bladder activity31 and our results supportthe assumption that intestinal activity and splanchniccirculation increase during gestation.
Although the fetal portal vein is only half the diameterof the umbilical vein, we achieved a 97% success rate
Copyright ! 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 30: 52–60.

58 Kessler et al.
for the diameter and velocity measurements, indicatingthat this technique is robust. We used an insonation tech-nique similar to that first published by Jeanty et al.32,but with some modifications to optimize diameter andvelocity measurements. These authors also described a‘cross’ formed by the left portal branch, the ductus veno-sus, and the right anterior and posterior portal branch.Scrutinizing the corresponding figure in their publication,the vessel that they identify as the ductus venosus mayrather represent the main stem of the portal vein, as seenin our Figure 4.
The investigation of anatomical variations was not theprimary aim of our study. However, we noted that in somecases we could not identify a right portal branch in theusual sense. The main stem continued directly as the (right)posterior branch and parallel to the left portal branch,which continued as the (right) anterior branch (Figure 4).This observation fits well with the three types of con-nection defined previously based on studies of resin castsof 27 aborted fetuses33. The most common (Type I) was‘endolateral’, which corresponds to our Figure 4a, whilethe laterolateral types (Types II and III) were character-ized by two separate veins running parallel and connectedthrough the lateral wall (Type II) or by a short anastomo-sis (Type III), corresponding to our Figure 4b. There wereno cases of absence of the portal vein in our study, whichseems to be a rare malformation and is often associatedwith caval, umbilical or cardiac abnormalities34,35.
A previous study on the blood velocity pattern of theportal system found pulsatile flow in 7/48 (15%) of thefetuses36. This is at variance with our results (570/576;99%) and may be due to differences in the recordingsite. We believe that the neighboring hepatic artery is thesource of pulsation when recordings are made at the mainportal stem, while recording more distally, at the rightportal branch, detects pulsation less commonly, whichmight have been the case in the previous study.
The TAMXV in the portal vein was initially approx-imately one third that observed in the umbilical vein atthe same gestational age14 and increased throughout theobservation period to become half the velocity in theumbilical vein near term. The TAMXV of the fetal portalvein at term was about half that observed in adults29,suggesting a further substantial increase in blood flowvelocities after birth.
For the estimation of volume blood flow, we usedtwo concepts of velocity measurement: the VWMEAN1
and the TAMXV, corrected by a factor according tothe velocity profile in the vessel17. Both concepts havepotential sources of error37,38. We used 0.5 TAMXV tocalculate the volume flow, assuming a parabolic velocityprofile in the main portal stem, and had an internal controlby using VWMEAN for the flow calculation; we foundvirtually no difference between them, indicating that bothmethods can be used interchangeably.
Estimation of volume flow has potential sources oferror, measurement of the vessel diameter being themost prominent. To reduce random error, we performedrepeated diameter measurements (median, 4)39. The low
intraobserver variation for the diameter measurementis reassuring for this measurement technique. As theintraobserver variation for the velocity measurementswas also low, we believe that our results provide areliable reflection of the general development of theportal circulation in the second half of pregnancy. Itshould be mentioned at this point that the calculationof normalized blood flow was based not on direct fetalbiometry but on estimated fetal weight at the time ofexamination, according to birth-weight percentile andassuming stable growth rate throughout gestation; thishas been shown to be valid both for low-risk populationsand for growth-restricted fetuses23,40,41. Inevitably, thecalculated weight is encumbered with potential error;however, fetal weight based on biometry has also beenshown to differ from actual weight, by 7.5–18%42.Although not aimed at clinical management, we believeour normalized flow results represent useful physiologicalinformation, particularly with regards to the developmentseen with increasing gestational age, since all techniqueswere used consistently throughout this longitudinal study.
There has been no previous direct assessment of fetalportal volume flow, though Haugen et al.19 made anindirect estimate based on a cross-sectional study of 91low-risk pregnant women at 36 weeks of gestation. Theyestimated the portal flow to be 37 mL/min by subtractingthe flow in the left portal branch from that in the right. Ourdirect measurements showed a mean value of 32 mL/minat the corresponding gestational age, confirming that theirestimation was reasonable. The notable increase in portalvolume flow during gestation is attributed mainly to fetalweight gain. However, there is still a significant flowincrease after correction for fetal weight, signifying anincreased importance of the splanchnic circulation duringthe last weeks of pregnancy.
In short, we have established a method for Dopplersonographic assessment of the main stem of the portalvein in the human fetus. The blood flow was pulsatileand increased with gestation due to both vessel growthand increase in velocity. The presented techniques andreference ranges make it possible to study global venousblood supply to the fetal liver under various physiologicalconditions, as well as the alterations imposed bymaldevelopment and pregnancy complications.
ACKNOWLEDGMENTS
This study received financial support from the NationalHealth Council, Norway and Haukeland UniversityHospital, Bergen.
REFERENCES
1. Kiserud T, Rasmussen S, Skulstad S. Blood flow and the degreeof shunting through the ductus venosus in the human fetus. AmJ Obstet Gynecol 2000; 182: 147–153.
2. Bellotti M, Pennati G, De Gasperi C, Battaglia FC, Ferrazzi E.Role of ductus venosus in distribution of umbilical blood flowin human fetuses during second half of pregnancy. Am J PhysiolHeart Circ Physiol 2000; 279: H1256–H1263.
Copyright ! 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 30: 52–60.

Fetal portal vein blood flow 59
3. Straus DS, Ooi GT, Orlowski CC, Rechler MM. Expression ofthe genes for insulin-like growth factor-I (IGF-I), IGF-II, andIGF-binding proteins-1 and -2 in fetal rat under conditionsof intrauterine growth retardation caused by maternal fasting.Endocrinology 1991; 128: 518–525.
4. Tchirikov M, Kertschanska S, Sturenberg HJ, Schroder HJ.Liver blood perfusion as a possible instrument for fetal growthregulation. Placenta 2002; 23 (Suppl A): S153–S158.
5. Tchirikov M, Kertschanska S, Schroder HJ. Obstruction ofductus venosus stimulates cell proliferation in organs of fetalsheep. Placenta 2001; 22: 24–31.
6. Haugen G, Hanson M, Kiserud T, Crozier S, Inskip H, God-frey KM. Fetal liver-sparing cardiovascular adaptations linkedto mother’s slimness and diet. Circ Res 2005; 96: 12–14.
7. Barclay AE, Franklin KJ, Prichard MML. The Foetal Circula-tion and Cardiovascular System, and the Changes they Undergoat Birth. CC Thomas: Springfield, 1945.
8. Lind J. Changes in the liver circulation at birth. Ann N Y AcadSci 1963; 111: 110–120.
9. Emery JL. Functional asymmetry of the liver. Ann N Y Acad Sci1963; 111: 37–44.
10. Cox LA, Schlabritz-Loutsevitch N, Hubbard GB, Nijland MJ,McDonald TJ, Nathanielsz PW. Gene expression profile dif-ferences in left and right liver lobes from mid-gestation fetalbaboons: a cautionary tale. J Physiol 2006; 572: 59–66.
11. Kiserud T, Kessler J, Ebbing C, Rasmussen S. Ductus venosusshunting in growth-restricted fetuses and the effect of umbilicalcirculatory compromise. Ultrasound Obstet Gynecol 2006; 28:143–149.
12. Jouppila P, Kirkinen P. Umbilical vein blood flow as anindicator of fetal hypoxia. Br J Obstet Gynaecol 1984; 91:107–110.
13. Gill R, Kossoff G, Warren P, Garrett W. Umbilical venous flowin normal and complicated pregnancy. Ultrasound Med Biol1984; 10: 349–363.
14. Acharya G, Wilsgaard T, Rosvold Berntsen GK, Maltau JM,Kiserud T. Reference ranges for umbilical vein blood flow inthe second half of pregnancy based on longitudinal data. PrenatDiagn 2005; 25: 99–111.
15. Boito S, Struijk PC, Ursem NT, Stijnen T, Wladimiroff JW.Umbilical venous volume flow in the normally developingand growth-restricted human fetus. Ultrasound Obstet Gynecol2002; 19: 344–349.
16. Barbera A, Galan HL, Ferrazzi E, Rigano S, Jozwik M,Battaglia FC, Pardi G. Relationship of umbilical vein bloodflow to growth parameters in the human fetus. Am J ObstetGynecol 1999; 181: 174–179.
17. Kiserud T, Eik-Nes SH, Blaas HG, Hellevik LR, Simensen B.Ductus venosus blood velocity and the umbilical circulation inthe seriously growth-retarded fetus. Ultrasound Obstet Gynecol1994; 4: 109–114.
18. Laurin J, Lingman G, Marsal K, Persson PH. Fetal blood flowin pregnancies complicated by intrauterine growth retardation.Obstet Gynecol 1987; 69: 895–902.
19. Haugen G, Kiserud T, Godfrey K, Crozier S, Hanson M. Portaland umbilical venous blood supply to the liver in the human fetusnear term. Ultrasound Obstet Gynecol 2004; 24: 599–605.
20. Kessler J, Rasmussen S, Hanson M, Kiserud T. Longitudinalreference ranges for ductus venosus flow velocities andwaveform indices. Ultrasound Obstet Gynecol 2006; 28:890–898.
21. Johnsen SL, Rasmussen S, Sollien R, Kiserud T. Fetal ageassessment based on ultrasound head biometry and the effect ofmaternal and fetal factors. Acta Obstet Gynecol Scand 2004;83: 716–723.
22. Bland J, Altman D. Measuring agreement in method compari-son studies. Stat Methods Med Res 1999; 8: 135–160.
23. Johnsen SL, Rasmussen S, Wilsgaard T, Sollien R, Kiserud T.Longitudinal reference ranges for estimated fetal weight. ActaObstet Gynecol Scand 2006; 85: 286–297.
24. Skjaerven R, Gjessing HK, Bakketeig LS. Birthweight by gesta-tional age in Norway. Acta Obstet Gynecol Scand 2000; 79:440–449.
25. Royston P, Altman DG. Design and analysis of longitudinalstudies of fetal size. Ultrasound Obstet Gynecol 1995; 6:307–312.
26. Altman DG, Chitty LS. New charts for ultrasound dating ofpregnancy. Ultrasound Obstet Gynecol 1997; 10: 174–191.
27. Skulstad SM, Kiserud T, Rasmussen S. Degree of fetal umbilicalvenous constriction at the abdominal wall in a low-riskpopulation at 20–40 weeks of gestation. Prenat Diagn 2002;22: 1022–1027.
28. Kiserud T, Ebbing C, Kessler J, Rasmussen S. Fetal cardiacoutput, distribution to the placenta and impact of placentalcompromise. Ultrasound Obstet Gynecol 2006; 28: 126–136.
29. Barbaro B, Palazzoni G, Prudenzano R, Cina A, Manfredi R,Marano P. Doppler sonographic assessment of functionalresponse of the right and left portal venous branches to ameal. J Clin Ultrasound 1999; 27: 75–80.
30. Martinussen M, Brubakk AM, Linker DT, Vik T, Yao AC.Mesenteric blood flow velocity and its relation to circulatoryadaptation during the first week of life in healthy term infants.Pediatr Res 1994; 36: 334–339.
31. Tanaka Y, Senoh D, Hata T. Is there a human fetal gallbladdercontractility during pregnancy? Hum Reprod 2000; 15:1400–1402.
32. Jeanty P, Romero R, Hobbins JC. Vascular anatomy of thefetus. J Ultrasound Med 1984; 3: 113–122.
33. Czubalski A, Aleksandrowicz R. Connection types between por-tal vein and portal sinus during foetal life. Folia Morphologica(Warsz) 2000; 59: 97–98.
34. Venkat-Raman N, Murphy KW, Ghaus K, Teoh TG,Higham JM, Carvalho JS. Congenital absence of portal veinin the fetus: a case report. Ultrasound Obstet Gynecol 2001;17: 71–75.
35. Hofstaetter C, Plath H, Hansmann M. Prenatal diagnosis ofabnormalities of the fetal venous system. Ultrasound ObstetGynecol 2000; 15: 231–241.
36. Mari G, Uerpairojkit B, Copel J. Abdominal venous system inthe normal fetus. Obstet Gynecol 1995; 86: 729–733.
37. Fei D. A theory to correct the systematic error caused by theimperfectly matched beam width to vessel diameter ratio onvolumetric flow measurements using ultrasound techniques.Ultrasound Med Biol 1995; 21: 1047–1057.
38. Pennati G, Bellotti M, De Gasperi C, Rognoni G. Spatialvelocity profile changes along the cord in normal human fetuses:can these affect Doppler measurements of venous umbilicalblood flow? Ultrasound Obstet Gynecol 2004; 23: 131–137.
39. Kiserud T, Rasmussen S. How repeat measurements affect themean diameter of the umbilical vein and the ductus venosus.Ultrasound Obstet Gynecol 1998; 11: 419–425.
40. Rasmussen S, Kiserud T, Albrechtsen S. Foetal size and bodyproportion at 17–19 weeks of gestation and neonatal size,proportion, and outcome. Early Hum Dev 2006; 82: 683–690.
41. Vik T, Vatten L, Jacobsen G, Bakketeig L. Prenatal growth insymmetric and asymmetric small-for-gestational-age infants.Early Hum Dev 1997; 48: 167–176.
42. Nahum GG, Stanislaw H. Ultrasonographic prediction of termbirth weight: how accurate is it? Am J Obstet Gynecol 2003;188: 566–574.
Copyright ! 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 30: 52–60.

60 Kessler et al.
SUPPLEMENTARY MATERIAL ON THE INTERNET
The following material is available from the Journal homepage:
http://www.interscience.wiley.com/jpages/0960-7692/suppmat (restricted access)
Figure S1 Longitudinal reference ranges showing the development of the time-averaged weighted mean velocity(VWMEAN) in the main stem of the fetal portal vein based on 576 longitudinal observations in 160 low-riskpregnancies. The 5th, 50th and 95th percentiles are presented (solid lines) with 95% CIs (dashed lines).
Figure S2 Longitudinal reference ranges showing the development of the volume flow in the main stem of the fetalportal vein based on time-averaged weighted mean velocity (VWMEAN) from 558 observations in 160 low-riskpregnancies. The 5th, 50th and 95th percentiles are presented (solid lines) with 95% CIs (dashed lines).
Table S1 Longitudinal reference ranges for time-averaged maximum velocity (in cm/s) of the main portal stembased on 576 observations in 160 low-risk pregnancies.
Table S2 Longitudinal reference ranges for volume blood flow (in mL/min) of the main portal stem based on 558observations in 160 low-risk pregnancies and the use of 0.5 ! time-averaged maximum blood velocity.
Table S3 Longitudinal reference ranges for volume blood flow (in mL/min/kg) of the main portal stem based on558 observations in 160 low-risk pregnancies and the use of 0.5 ! time-averaged maximum blood velocity.
Appendix S1 Formulae for the gestational age-specific means and SDs.
Copyright ! 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 30: 52–60.