
New perspectives in electronic fetal surveillance
10
J. Perinat. Med. 41 (2013) 83–92 • Copyright © by Walter de Gruyter • Berlin • Boston. DOI 10.1515/jpm-2012-0024 Review article New perspectives in electronic fetal surveillance* Emily F. Hamilton 1,2, ** and Philip A. Warrick 1 1 PeriGen, Montreal, QC, Canada 2 McGill University, Montreal, QC, Canada Abstract Despite its recognized limitations, fetal heart rate monitoring is a mainstay of intrapartum care. Although the basic technol- ogy in standard electronic fetal monitors has changed little in recent decades, clinical behavior in response to heart rate monitoring has changed considerably. In addition to clearly defined nomenclature and clinical guidelines, there is an increased awareness that environmental and human factors can impair clinical judgment, resulting in delayed intervention and, consequently, birth-related injury. This review examines three essential steps that affect clinical outcome: (1) signal acquisition, (2) associations with physiological outcome, and (3) clinical intervention. Only the third step is directly respon- sible for changing clinical outcome. However, timely initia- tion of interventions is dependent upon the second step, which is dependent upon the first step. Thus, deficiencies at each step tend to accumulate and contribute to the worsening of overall clinical outcome. This review article summarizes advances occurring at each step. The synergy and convergence of inno- vations in engineering, mathematics, and behavioral science shows considerable promise in intrapartum fetal surveillance. Keywords: Electronic fetal monitoring; fetal heart rate; metabolic acidemia. Introduction Controversy is no stranger to electronic fetal monitoring (EFM). Few technologies in medicine can claim associa- tion with such an extensive and debated literature. Despite disagreements, it remains a mainstay of intrapartum care, suggesting that clinicians find its benefits outweigh its dis- advantages. The merits of this clinical behavior are supported by encouraging reports of falling rates of hypoxic-ischemic encephalopathy (HIE). Several large jurisdictions with population-wide statistics have shown steady declines, often reaching reductions in the range of 50% per decade. Preventable intrapartum stillbirths are almost eliminated [4, 7, 17, 32, 54, 67]. A myriad of factors influence outcomes, such as HIE, and it would be incorrect to attribute the improvement to any single one. The basic sensor technology of EFM has changed little over the past few decades. Thus, improvement in outcome is not likely to be related to simply better recording of the fetal heart rate (FHR). In contrast, clinical practices today are very different from those in the mid-1980s, when the larg- est randomized clinical trial (RCT) on EFM was reported. During this randomized study of 12,964 mothers, perina- tal hypoxic death or newborn seizures occurred at a rate of approximately 1 in every 285 births, and primary cesarean rates were around 2.4% [43]. US cesarean rates now exceed 30% [47]. The rise is attributed to a number of factors in addi- tion to an EFM effect. A recent review of over 1.7 million US births in 2004 found no difference in the primary cesarean rate among women with EFM (17.7%) compared with those without EFM (17.8%) [10]. Another change has been a growing recognition that human factors and system failures play a substantial role in adverse outcomes across all of branches of medicine [59]. Human actions, such as delayed recognition of tracing abnor- mality and delayed intervention are reported to have occurred in approximately half of asphyxial injuries or death [11, 23, 35, 57, 63]. The patient safety movement has ascertained many causes of medical error and, drawing from aviation and military experience, provides guidance on how to build less error-prone heath-care systems. Consequently, policies and procedures to redress the reasons underlying human error are now widespread. Some actions are directed at system vulner- abilities, such as legislation to limit working hours, recom- mendations on staff-to-patient ratios, setting standards for the availability of obstetricians and operating room facilities, simulation training for emergency procedures, and formal feedback on performance to clinicians [9, 12, 37, 56]. Other actions are specific to EFM, such as standardizing nomen- clature, defining graded classifications of abnormality, and establishing formal guidelines for clinical management [1, 24, 41, 44, 51, 62]. Finally, improved understanding about the clinical significance between some FHR patterns and out- come helps clinicians respond better. For example, defining the correlation between rates of fetal death, or HIE, and the interval between persistent bradycardia and delivery is cru- cial to establishing desirable response times [39]. *This project received financial support from PeriGen, Princeton, NJ, USA. **Corresponding author: Emily F. Hamilton, MD PeriGen 5252 de Maisonneuve West, Suite 314 Montreal, QC Canada H4A 3S5 Tel.: +1-514-488-3461 Fax: +1-514-488-1880 E-mail: [email protected] Unauthenticated Download Date | 5/15/16 6:49 AM
Transcript of New perspectives in electronic fetal surveillance

J. Perinat. Med. 41 (2013) 83–92 • Copyright © by Walter de Gruyter • Berlin • Boston. DOI 10.1515/jpm-2012-0024
Review article
New perspectives in electronic fetal surveillance *
Emily F. Hamilton 1,2, ** and Philip A. Warrick 1
1 PeriGen , Montreal, QC , Canada 2 McGill University , Montreal, QC , Canada
Abstract
Despite its recognized limitations, fetal heart rate monitoring is a mainstay of intrapartum care. Although the basic technol-ogy in standard electronic fetal monitors has changed little in recent decades, clinical behavior in response to heart rate monitoring has changed considerably. In addition to clearly defi ned nomenclature and clinical guidelines, there is an increased awareness that environmental and human factors can impair clinical judgment, resulting in delayed intervention and, consequently, birth-related injury. This review examines three essential steps that affect clinical outcome: (1) signal acquisition, (2) associations with physiological outcome, and (3) clinical intervention. Only the third step is directly respon-sible for changing clinical outcome. However, timely initia-tion of interventions is dependent upon the second step, which is dependent upon the fi rst step. Thus, defi ciencies at each step tend to accumulate and contribute to the worsening of overall clinical outcome. This review article summarizes advances occurring at each step. The synergy and convergence of inno-vations in engineering, mathematics, and behavioral science shows considerable promise in intrapartum fetal surveillance.
Keywords: Electronic fetal monitoring; fetal heart rate; metabolic acidemia.
Introduction
Controversy is no stranger to electronic fetal monitoring (EFM). Few technologies in medicine can claim associa-tion with such an extensive and debated literature. Despite disagreements, it remains a mainstay of intrapartum care, suggesting that clinicians fi nd its benefi ts outweigh its dis-
advantages. The merits of this clinical behavior are supported by encouraging reports of falling rates of hypoxic-ischemic encephalopathy (HIE). Several large jurisdictions with population-wide statistics have shown steady declines, often reaching reductions in the range of 50 % per decade. Preventable intrapartum stillbirths are almost eliminated [4, 7, 17, 32, 54, 67] .
A myriad of factors infl uence outcomes, such as HIE, and it would be incorrect to attribute the improvement to any single one. The basic sensor technology of EFM has changed little over the past few decades. Thus, improvement in outcome is not likely to be related to simply better recording of the fetal heart rate (FHR). In contrast, clinical practices today are very different from those in the mid-1980s, when the larg-est randomized clinical trial (RCT) on EFM was reported. During this randomized study of 12,964 mothers, perina-tal hypoxic death or newborn seizures occurred at a rate of approximately 1 in every 285 births, and primary cesarean rates were around 2.4 % [43] . US cesarean rates now exceed 30 % [47] . The rise is attributed to a number of factors in addi-tion to an EFM effect. A recent review of over 1.7 million US births in 2004 found no difference in the primary cesarean rate among women with EFM (17.7 % ) compared with those without EFM (17.8 % ) [10] .
Another change has been a growing recognition that human factors and system failures play a substantial role in adverse outcomes across all of branches of medicine [59] . Human actions, such as delayed recognition of tracing abnor-mality and delayed intervention are reported to have occurred in approximately half of asphyxial injuries or death [11, 23, 35, 57, 63] . The patient safety movement has ascertained many causes of medical error and, drawing from aviation and military experience, provides guidance on how to build less error-prone heath-care systems. Consequently, policies and procedures to redress the reasons underlying human error are now widespread. Some actions are directed at system vulner-abilities, such as legislation to limit working hours, recom-mendations on staff-to-patient ratios, setting standards for the availability of obstetricians and operating room facilities, simulation training for emergency procedures, and formal feedback on performance to clinicians [9, 12, 37, 56] . Other actions are specifi c to EFM, such as standardizing nomen-clature, defi ning graded classifi cations of abnormality, and establishing formal guidelines for clinical management [1, 24, 41, 44, 51, 62] . Finally, improved understanding about the clinical signifi cance between some FHR patterns and out-come helps clinicians respond better. For example, defi ning the correlation between rates of fetal death, or HIE, and the interval between persistent bradycardia and delivery is cru-cial to establishing desirable response times [39] .
* This project received fi nancial support from PeriGen, Princeton, NJ, USA. **Corresponding author:Emily F. Hamilton, MDPeriGen5252 de Maisonneuve West, Suite 314Montreal, QCCanada H4A 3S5Tel.: + 1-514-488-3461Fax: + 1-514-488-1880E-mail: [email protected]
UnauthenticatedDownload Date | 5/15/16 6:49 AM

84 Hamilton and Warrick, New perspectives in electronic fetal surveillance
Three basic steps in clinical monitoring
This brief review of the evolution of fetal monitoring under-scores three essential steps that affect clinical outcome: (1) signal acquisition, (2) associations with physiological out-come, and (3) effective clinical intervention. This article will demonstrate how they interact, discuss evaluation strategies, and present advances that may improve the overall process.
Understanding the hierarchy and dependencies of these steps is essential. Better signal acquisition increases the potential to recognize when intervention is needed. For exam-ple, consistent and reliable detection of the FHR improves its clinical utility. However, failure to intervene when a reli-able test is abnormal would negate any benefi t gained through testing. Thus, each step is dependent upon the preceding step and the ultimate clinical outcome is dependent upon all three. Moreover, each step should be measured separately to iden-tify and rectify weak links in the process.
The most basic step in fetal surveillance is signal acquisition from the monitoring device and subsequent display. Evaluation of this step should include performance measures, such as the frequency of missing signals, accuracy of the readings, and clarity of displays. Practical questions, such as “ how easy is it to use the device ? ” and “ are there complications associated with its application ? ” are also relevant to clinical practice. All fetal surveillance devices are subject to health-care regulatory agencies that scrutinize aspects related to safety and effective-ness carefully in their review process. It is important to note that effectiveness in this context means, “ does the device do what its manufacturer states it does ? ” For example, if the manufac-turer claims that the device can measure the FHR, “ effective-ness ” relates to how well it does exactly that. It does not refer to effectiveness in reducing a particular birth complication. It is up to clinical professional to decide if the device has clinical value. Nevertheless, how often the device actually measures what it is intended to measure is a fundamental determinant of clinical utility. For instance, an imaging device that produces satisfactory images only 50 % of the time is unlikely to ever achieve high diagnostic sensitivity.
The second step in the sequence is the fundamental physio-logical association between the measured parameter mea-sured and the pathology of interest. Exactly what patterns in the FHR recordings are associated with metabolic acidemia ? How often are these patterns found in uncomplicated births and how discriminating are they for adverse outcome ? The task of correctly inferring the state of the baby and its internal environment from its FHR patterns is daunting because the relationships between the FHR and metabolic acidemia are very indirect and non-specifi c. For example, low heart rate variability may indicate a depressed fetal central nervous system in the presence of metabolic acidemia, but it can also be seen in a range of normal conditions from, for example, fetal sleep or with certain medications. Decelerations provide some information about cardiac output, which is related to the development of metabolic acidemia, but decelerations with something relatively innocuous, such as intermittent cord compression may look identical to those with an impending catastrophic event like uterine rupture [29] .
The usual measures of the relationship between a diagnos-tic test and its target disease are sensitivity (rate that the test is positive among diseased individuals) and false-positive rates (rate that the test is positive among healthy individuals). These measures are not entirely appropriate for fetal surveil-lance where the goal is prevention not detection. For example, when a baby is born after an intervention for an abnormal tracing and has a normal outcome, it is not possible to be certain if this was a “ successful prevention ” or an “ unneces-sary intervention ” unless there is a good marker of impend-ing peril. In animal studies, one can create hypoxemia and measure sensitivity and false-positive rates associated with the heart rate patterns without the interference of therapeutic intervention. This is not possible with EFM in humans.
One approach to estimating sensitivity and false-positive rates in humans uses historical cases and measures the incidence of certain patterns in the groups with or without metabolic acidosis at birth. Although this underestimates the properties of the device, because monitoring can instigate intervention that prevents adverse outcome, it does provide some insight on performance.
The third step is clinical intervention: What should be done ? How urgently should it be accomplished ? How effec-tive is the clinical intervention ? Only the third step is directly responsible for changing clinical outcome. However, timely initiation of interventions is dependent upon the second step, which is dependent upon the fi rst step. Thus, defi ciencies at each level tend to accumulate and contribute to worsening the overall clinical outcome. Randomized clinical trials where a clinical outcome is the endpoint measure the combined effect of all three steps.
If we could optimize each of the steps, the task for cli-nicians would be considerably easier than it is today. The next section will focus mostly on exciting developments in engineering and mathematics pertaining to steps 1 and 2. We turn to advances in the social sciences of human behavior and health-care management for the third step.
Step 1: signal acquisition
Standard fetal monitoring devices have changed little in recent decades. FHRs are still calculated based on the identifi cation of cardiac pulsation by either an external Doppler ultrasound sensor or a fetal ECG sensor on the fetal scalp. Uterine pres-sure is measured directly with intrauterine pressure sensors or indirectly using external sensors that measure abdominal wall tension.
There are two broad groups of technologies with respect to innovation in monitoring devices. One group includes external sensors to measure the FHR or uterine contractions non-invasively. With concerns about infection, reliable non-invasive monitoring is highly desirable. Wireless transmis-sion allows the patient to be mobile, provided the sensors can still perform well with ambulation.
External sensors Electrodes placed on the surface of the maternal abdomen can detect changes in the electromagnetic fi eld that arise from uterine contractions and from the fetal
UnauthenticatedDownload Date | 5/15/16 6:49 AM

Hamilton and Warrick, New perspectives in electronic fetal surveillance 85
heart. The changes induced by the beating fetal heart are relatively weak, given its size and are mixed with changes from maternal heart beats and other contracting muscles. It is therefore a challenging engineering problem to isolate the fetal cardiac signal and calculate heart rate and even more challenging to construct the actual ECG complex with suffi cient fi delity to measure fi ne details, such as the R-R interval, ST segment, or other aspects related to altered myocardial function [13, 30] .
R-R interval measurements or beat-to-beat variability cal-culations are not available with conventional fetal monitors with their standard data exporting methods. Heart rates from the Doppler sensors are averaged over several seconds (i.e., several heart beats) to improve signal-to-noise ratios, thus eliminating the potential to estimate individual R-R intervals. Although scalp electrodes acquire cleaner signals and permit heart rate estimation with each heart beat, the standard pro-tocol for exporting the heart rate does not preserve this level of detail, which is important for characterization of the short-term FHR variability. Thus, both scalp ECG and surface ECG methods could give beat to beat intervals. However, this is not readily available with most current commercial applications [15, 20] .
Surface detection of the fetal ECG complex with suffi cient precision to analyze the P-QRS-T waves would open another dimension of possibilities. Based on the premise that myocar-dial changes induced by hypoxemia are refl ected in changes in the ECG waveform, ECG analysis could provide additional information that helps to determine which fetus is experienc-ing clinically signifi cant hypoxemia [5, 6, 40, 61, 70] .
Uterine contraction detection is also possible with these sensors. Using surface electrodes, Euliano et al. [26] have measured the characteristics of the electrohistogram (EHG) of uterine contractions. In this small study, uterine contrac-tions propagated with less fundal dominance in mothers with active phase arrest of dilation compared with mothers with vaginal delivery. It is not yet clear if the altered contraction characteristics caused non-progressive labor or resulted from it. Lucovnik et al. [42] have used a similar technology with preterm contractions to determine what characteristics of con-tractions discriminate preterm labor from false labor.
Nevertheless, these experimental data indicate the encour-aging potential of wearable sensors to provide clinical advan-tage, particularly if they could provide additional information about the nature or strength of contractions and/or myocardial response to hypoxemia.
Internal sensors A second group of technologies includes specialized internal sensors. Examples include devices that measure fetal oxygen saturation levels or scalp electrodes that can measure fetal oxygen saturation aspects of the ECG waveform, such as the ST segment of the fetal electrocardiogram [5, 6, 21] . Both of these technologies are used in combination with EFM. Logically, we would expect that additional information about the oxygen-carrying capacity of the baby or myocardial reactions that indicate hypoxia would add to our understanding of the fetal cerebral condition. However, fetal O 2 levels in peripheral blood or
fetal ST segment characteristics are still indirectly related to fetal cerebral oxygenation. Compensatory mechanisms can maintain oxygen delivery to the fetal brain cell despite lowered oxygen saturation levels and cerebral perfusion is preserved preferentially over cardiac perfusion. Moreover, some ST segment changes are not specifi c to hypoxemia and can be induced by normal fetal movement. Thus, these measures do not necessarily refl ect actual fetal brain oxygenation [5, 21] . This underscores the critical importance of animal studies to fully understand their associations with metabolic acidemia before launching a clinical trial. A clinical trial using poorly selected thresholds may conclude with negative fi ndings whereas the effect with a different threshold could be positive. A simple analogy might be an RCT based on a subtherapeutic dosage of an anticoagulant.
Step 2: association with metabolic acidemia
Traditional EFM The relationship between EFM and metabolic acidemia has a large literature, which will not be reviewed in detail here, as it is well summarized by several professional societies in the USA, UK, Canada, and Japan [1, 24, 41, 44, 51, 62] . This animal and human literature was the basis for defi ning what combinations of EFM patterns are most closely associated with metabolic acidemia and to describe a graded classifi cation of increasing abnormality, which in turn determines the nature and urgency of clinical management. None of these classifi cations were published with their sensitivity or false-positive measures. This information is critical to understanding their potential clinical effect. High sensitivity of the classifi cation is required to prevent a substantial portion of metabolic acidemia and good specifi city is needed to avoid unnecessary interventions.
We have measured the sensitivity and specifi city of one of the most methodical and detailed classifi cation methods that defi ned fi ve color-coded levels based on baseline variability, baseline level and the severity of recurrent decelerations [25, 51] . Red was the most abnormal, with orange, yellow, and blue defi ning progressively less concerning patterns. Green included only tracings with completely normal features.
We computerized these defi nitions and measured how often the various levels appeared in the last 3-h tracings of babies with metabolic acidemia defi ned by an umbilical artery base defi cit over 8 mM [25, 60] . The digital tracings were ana-lyzed using PeriCALM Patterns ™ version 1.05 (PeriGen, Princeton, NJ, USA), an EFM pattern recognition software that identifi ed and measured baseline, baseline variability, FHR decelerations, and contractions. Table 1 shows the sen-sitivity and specifi city for each of the levels.
This performance is not stellar at fi rst glance and bears dis-cussion. These simple classifi cation defi nitions do not con-sider the duration of tracing abnormality or trends over time. Another key problem is the assessment of baseline variability, which was a defi ning feature for each level of abnormality. Minute variations in baseline variability can change the clas-sifi cation level. A recent review of levels of clinician agree-ment on tracings classifi cation using the ACOG Category defi nitions showed that disagreements were often due to how
UnauthenticatedDownload Date | 5/15/16 6:49 AM

86 Hamilton and Warrick, New perspectives in electronic fetal surveillance
clinician rated the baseline variability [3] . In addition, base-line variability measured electronically can be different from visual estimations. An example of this disparity is provided in Figure 1 .
The tracing in Figure 1 was obtained about 20 min before the birth of a baby with Apgar scores of 0 and 4 and an umbilical artery pH of 7.03 with a base excess of – 10 mM. Severely reduced baseline variability is clearly evident. Most clinicians would describe this as absent variability, but precise automated software measurement of variation around the baseline produces a value of 3.2 beats per minute (bpm).
The stated clinical signifi cance of moderate variability is also problematic. For convenience, the relevant text about baseline variability from the updated NICHD defi nitions is reproduced in Table 2 [44] .
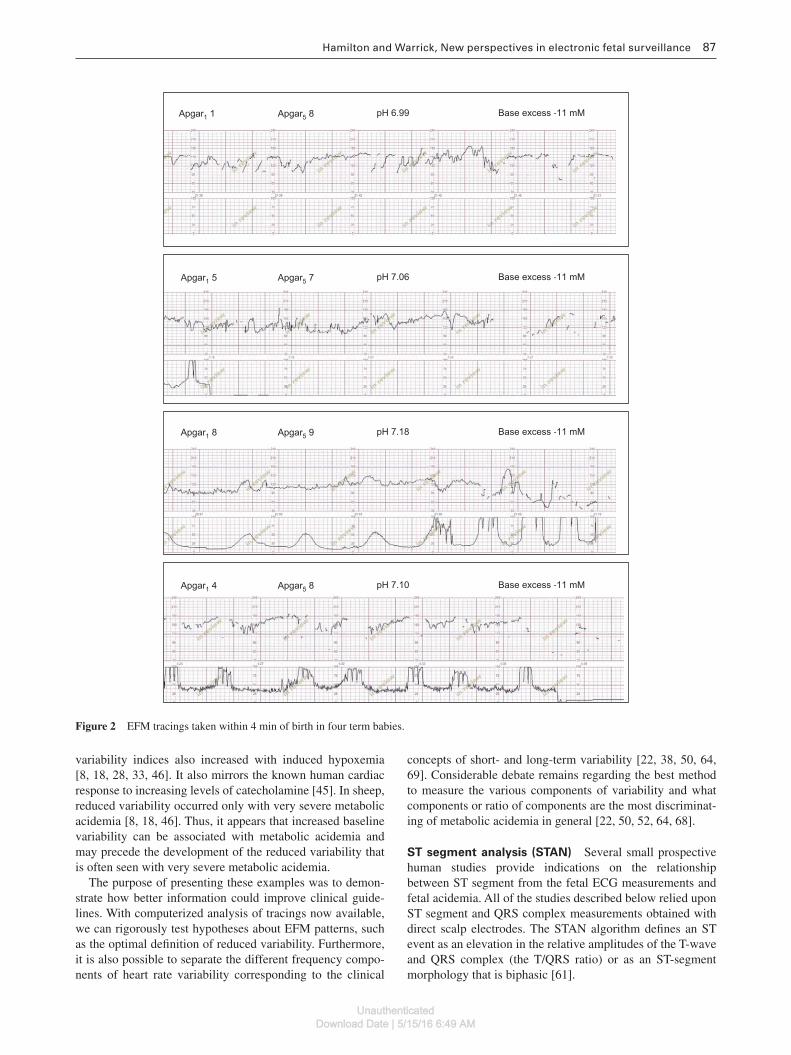
The four tracings in Figure 2 were taken a few minutes before birth. Electronically measured baseline variability exceeds 5 bpm in each panel. All babies showed abnormal base excess levels in the umbilical artery at birth. These cases demonstrate clear exceptions to the statement that “ moder-
ate variability reliably predicts the absence of fetal metabolic acidemia at the time it is observed. ”
To determine if these examples are typical or merely rare exceptions, it is necessary to examine a large number of cases systematically. The following graphs show summarize the analysis of baseline and baseline variability (measured elec-tronically as a single complex) using PeriCALM Patterns ™ from a series of term 3320 babies born with normal umbilical artery gases (base excess over – 8 mM) and a group of 316 with base excess under – 12 mM. We divided each tracing into 10-min segments, with 0 representing the last 10 min before birth. The mean and its 95 % confi dence interval for baseline and baseline variability in each time segment are shown in Figures 3 and 4 .
On average, the baseline heart rate increased slightly and gradually as labor advanced especially in the babies with an elevated base defi cit. Within these groups, some trac-ings developed low variability and others developed exces-sive variability. However, on average, baseline variability increased terminally in both groups, especially those with metabolic acidemia. These observations are consistent with experimental sheep and monkey literature, where heart rate
Table 1 Sensitivity and specifi city of a modern feature- and rule-based classifi cation method.
Percentages of cases that reached
Sensitivity in the group with meta bolic acidemia group (n = 280)
Specifi city in the group with normal umbilical artery gases (n = 2132)
Red 2.9 98.3Orange or above 30.0 81.9Yellow or above 73.2 40.1Blue or above 93.6 13.1
Apgar1 0 Apgar5 4 pH 7.03 Base excess -10 mM
Figure 1 EFM tracing approximately 20 min before birth.
Table 2 Current ACOG defi nition, classifi cation, and clinical signifi cance of baseline variability.
Defi nition Baseline FHR variability is defi ned as fl uctuations in the baseline FHR that are irregular in amplitude and frequency. The fl uctuations are visually quantitated as the amplitude of the peak-to-trough in beats per minute. No distinction is made between short-term variability (or beat-to-beat variability or R-R wave period differences in the electrocardiogram) and long-term variability, because in actual practice, they are visually determined as a unit. Hence, the defi nition of variability is based visually on the amplitude of the complexes, with exclusion of the sinusoidal pattern.
Classifi cation Absent FHR variability: amplitude range undetectable. Minimal FHR variability: amplitude range > undetectable and ≤ 5 bpm. Moderate FHR variability: amplitude range > 6 – 25 bpm. Marked FHR variability: amplitude range > 25 bpm.
Clinical signifi cance
Moderate FHR variability reliably predicts the absence of fetal metabolic acidemia at the time it is observed. Minimal or absent FHR variability alone does not reliably predict the presence of fetal hypoxemia or metabolic acidemia.
UnauthenticatedDownload Date | 5/15/16 6:49 AM
Hamilton and Warrick, New perspectives in electronic fetal surveillance 87
variability indices also increased with induced hypoxemia [8, 18, 28, 33, 46] . It also mirrors the known human cardiac response to increasing levels of catecholamine [45] . In sheep, reduced variability occurred only with very severe metabolic acidemia [8, 18, 46] . Thus, it appears that increased baseline variability can be associated with metabolic acidemia and may precede the development of the reduced variability that is often seen with very severe metabolic acidemia.
The purpose of presenting these examples was to demon-strate how better information could improve clinical guide-lines. With computerized analysis of tracings now available, we can rigorously test hypotheses about EFM patterns, such as the optimal defi nition of reduced variability. Furthermore, it is also possible to separate the different frequency compo-nents of heart rate variability corresponding to the clinical
concepts of short- and long-term variability [22, 38, 50, 64, 69] . Considerable debate remains regarding the best method to measure the various components of variability and what components or ratio of components are the most discriminat-ing of metabolic acidemia in general [22, 50, 52, 64, 68] .
ST segment analysis (STAN) Several small prospective human studies provide indications on the relationship between ST segment from the fetal ECG measurements and fetal acidemia. All of the studies described below relied upon ST segment and QRS complex measurements obtained with direct scalp electrodes. The STAN algorithm defi nes an ST event as an elevation in the relative amplitudes of the T-wave and QRS complex (the T/QRS ratio) or as an ST-segment morphology that is biphasic [61] .
Apgar5 8Apgar1 1 pH 6.99 Base excess -11 mM
Apgar5 7Apgar1 5 pH 7.06 Base excess -11 mM
Apgar5 9Apgar1 8 pH 7.18 Base excess -11 mM
Apgar5 8Apgar1 4 pH 7.10 Base excess -11 mM
Figure 2 EFM tracings taken within 4 min of birth in four term babies.
UnauthenticatedDownload Date | 5/15/16 6:49 AM

88 Hamilton and Warrick, New perspectives in electronic fetal surveillance
Dervaitis et al. [19] examined 143 term patients with umbilical artery blood gases at birth. Metabolic acidemia was defi ned as pH < 7.15 and a base defi cit of ≥ 12 mM. Tracings were classifi ed visually by two authors using the FIGO scor-ing system. Sensitivity for ST segment parameters with the FIGO classifi cation was 43 % (3/7) and specifi city was 75 % (101/136).
A later study by Costa et al. [16] examined the last hour of tracing in 148 term patients. Tracings were analyzed and classifi ed using a computerized EFM pattern recognition program, Omniview Sis Porto 3.5 (Speculum SA, Alfragide, Amadora, Portugal), before applying the STAN algorithm. Metabolic acidemia was defi ned by an umbilical artery pH of ≤ 7.05. Sensitivity was 100 % (7/7) and specifi city was 94 % (133/141) in this study. Vaysserie et al. [72] retrospectively examined 411 term tracings. When the outcome of interest was an umbilical artery pH of < 7.15, sensitivity was 38 % (41/108) and specifi city was 83 % (252/303). When a more stringent outcome (pH < 7.05) was chosen, sensitivity rose to 62.5 % (10/16) and specifi city fell to 79 % (313/395).
A larger retrospective review of tracings from 787 term tracings underlines the importance of interpreting ST events simultaneously with the EFM tracing [48] . ST events alone were associated with sensitivity for severe acidosis of 79 % (19/24). However, specifi city was only 50 % in the 177 normal
150
Base excess <-12 mM Normal base excess
148
146
Bas
elin
e
142
144
140
138
136240 220 200 180 160 140
min120 100 80 60 40 20 0
Figure 3 Mean baseline during the last 240 min before birth.
17.0
Base excess <-12 mM Normal base excess
Mean (95% CI) baseline variability
16.0
15.0
14.0
Var
iabi
lity
13.0
12.0
11.0
10.0240 220 200 180 160 140 120
min100 80 60 40 20 0
Figure 4 Mean baseline variability during the last 240 min before birth.
controls. Requiring an abnormal EFM tracing in addition to the ST event fi nding reduced sensitivity to 69 % and improved specifi city to 88 % .
Even this small review quickly demonstrates that it is not easy to see the incremental benefi t of a new technology. To draw some reasonable conclusions, the reader needs to see the performance for the same outcome and to be able to match specifi city and then see the changes in specifi city or vice versa .
To date there have been fi ve prospective RCTs using ST segment technology in fi ve different countries and a number of observational studies. Results have not been consistent across the fi ve RCTs with respect to rates of operative delivery and reduction in measures of metabolic acidemia. In some studies (UK and Swedish), the operative interventions decreased in the STAN group but not in others (Finnish, French, and Dutch) [2, 49, 71, 75, 76] . Outcomes related to metabolic acidosis were defi ned differently across the studies. Again, an inconsistent pattern was seen, with reductions in metabolic acidosis related outcomes is reported in some studies (Swedish and Dutch) but unchanged in others (Finnish and French) and borderline in another (UK). Fetal blood sampling is the most defi nitive test of intrapartum acid base status, and its use would strongly affect outcome irrespective of the method of fetal surveillance. The utilization of fetal blood sampling varied greatly from study to study. In addition, focused educational efforts were part of the intervention, and this also affects outcome. Thus, it is not self-evident how STAN would perform in regions where fetal blood sampling is rarely done, such as in North America or where cesarean rates are much higher. Another RCT is under-way in the USA with a projected enrollment of 11,000 women to determine if fetal ECG ST segment and T wave analysis change the rate of cesarean birth, operative vaginal delivery, or fetal compromise defi ned as a composite of several clinical and acid base markers [5] .
Innovative approaches to EFM analysis We have focused on the association between metabolic acidemia and classical EFM parameters and the incremental benefi t of additional parameters, such as measurements of the fetal P-QRS-T complex. We have seen that simple thresholds are inadequate. For example, FHR variability tends to rise before it falls and average baseline variability changes as labor advances. In addition, correct labeling of FHR parameters is essential especially for the correct usage of STAN because certain ST parameters are innocuous with some FHR patterns and hazardous with other FHR patterns. Correct labeling of EFM features can be diffi cult when decelerations are not exactly typical of the “ late ” or “ variable ” type. Inconsistent labeling among clinicians is well-known. Thus, there is need for a method that can address these limitations.
Automated FHR analysis can address labeling inconsis-tency, and many automated FHR analysis techniques have focused on careful detection of contractions and decelera-tions, mimicking visual clinical interpretation. However, even automated labeling of the tracing with classifi cation showed poor discriminating performance as was outlined in Table 1 [25] .
UnauthenticatedDownload Date | 5/15/16 6:49 AM

Hamilton and Warrick, New perspectives in electronic fetal surveillance 89
We have recently proposed a new approach to FHR analy-sis, based on system identifi cation theory, that bypasses the detection phase altogether and focuses directly on the dynamic relationship between uterine pressure (as an input) and the FHR (as an output) [73, 74] .
System identifi cation is a signal analysis method that cor-responds well to recognized fetal physiology. Many years ago, the antepartum contraction stress test (CST) was used to unmask vulnerability for hypoxia by applying a controlled stress via contractions to determine if they induced decel-erations, revealing a potentially compromised fetal-placental unit [14, 55, 58] . In many ways, labor is the ultimate CST. Although the stress of contractions in labor is not controlled, uterine pressure can be measured. With system identifi ca-tion techniques, it is possible to characterize the response of the FHR relative to the uterine contractions it experiences. Rather than delineating individual events, this mathemati-cal method results in a succinct characterization of the over-all response of the FHR to uterine pressure within the time extent of the analysis. This FHR response relative to uter-ine pressure response was very different in babies born with symptomatic metabolic acidosis compared with babies with normal gases at birth.
This novel approach is well suited to current clinical practice. Although the FHR is subject to numerous infl u-ences, uterine pressure is the only input that is accessible by routinely used external monitoring; indeed, clinicians already interpret certain uterine pressure-FHR relationships as indications of pathology. Accounting for measurement noise and artifact, we estimated linear system dynamics in terms of an impulse response function (IRF), a model that represents very-low-frequency FHR energy ( < 0.03 Hz) related to uterine pressure, and is therefore complementary to other FHR components, such as baseline and variabi lity. From this IRF model, we extracted two key parameters, gain and delay, that have direct clinical signifi cance. Gain is an indication of the size of the FHR response, normally manifested as the depth of the deceleration relative to con-traction amplitude. Delay is an indication of the timing of the response, normally observed as a lag between the onset of the deceleration compared with the beginning of the contraction.
We also recognize that there are other associations with metabolic acidosis, such as altered heart rate variability or bradycardia and have developed models to characterize base-line and heart rate variability and how they change over time. Finally, we have applied a machine learning method to con-sider the multiple factors including the IRF parameters, heart rate, and variability parameters as well as trends over time to classify the tracing as normal or pathological. These sta-tistical methods are well suited to biological systems where the relationships between the outcome state and many inter-related time dependent variables are not linear.
In our study, this approach correctly classifi ed more than half of the pathological cases, 1.5 h before delivery with a false-positive rate of 7.5 % . Using the same data set, this method matched the sensitivity of a modern EFM feature- and rule-based approach and bettered its specifi city by 15 % .
Step 3: clinical intervention
As described earlier, clinical intervention, the last step in this hierarchy of dependent steps, is the only one that can directly change outcome. The effectiveness of clinical intervention is not only directly dependent upon the sensitivity and specifi c-ity of the surveillance parameters but also on the lead time it allows making intervention logistically possible.
In practice, the clinician must integrate clinical and moni-toring information as well as project what is likely to happen and how quickly it might happen. This process of recognizing what is going on and what is about to happen is not unique to obstetrics. It has been studied extensively by psychologists and is called situational awareness [53] . Industries, such as aerospace or the military, where processes can degrade rapidly with dire consequences, were among the fi rst to recognize the importance of situational awareness [36, 65, 66] . Situational awareness is now recognized as an essential skill for anesthe-sia and a critical skill throughout health care [27] .
Situational awareness also has three basic and interde-pendent components that bear some similarities to the pre-vious steps discussed with monitoring. However, rather than focusing on the physics of the monitor and the physiology of acidosis, these steps relate to the cognitive processes of the clinicians. Situational awareness depends upon perceiving the relevant information, understanding its meaning, and project-ing what is about to happen.
“ Sizing up ” a situation is challenging in the presence of an overwhelming amount of information. The medical mind must focus on what is important and disregard the irrelevant. However, in doing so, the brain is vulnerable to well-described biases. The psychological phenomenon of “ tunnel vision ” refers to the tendency to perceive and confi rm information that aligns with a particular viewpoint and discard contradict-ing information. Variations of this include “ framing bias, ” which refers to a tendency to create a coherent interpretation without examining all the available information, and “ con-fi rmation bias, ” which refers to seeking only the information that supports a particular opinion. EFM assessments are also prone to these biases. The rarity of adverse outcome coupled with frequent “ false alarms ” further exacerbates the potential for bias.
Table 3 lists some of the impediments to situational aware-ness with some specifi c examples from labor and delivery. This list provides clues about how we can optimize the envi-ronment in labor and delivery to facilitate situational aware-ness among clinicians.
There is an important role here for intelligent electronic medical records or automated tracing analysis because they are not vulnerable to the subjectivity biases and impediments described above. Electronic medical records hold informa-tion on the evolution of the patient ’ s status and can display this in formats that help clinicians quickly grasp the situation. In addition, they can apply virtual checklists, perform trend analysis and escalate its alerts and reminders as the clinical condition warrants. The desirable characteristics of an intel-ligent medical record are well described by Hasely [31] and examples are in use today. Psychological testing has also
UnauthenticatedDownload Date | 5/15/16 6:49 AM

90 Hamilton and Warrick, New perspectives in electronic fetal surveillance
contributed greatly to our understanding of the importance of simplicity and clarity of information display on computer screens. Overcrowded or confusing displays may themselves lead to medical error. High rates of false alarms lead to frus-tration and disregard of the device.
The future of fetal surveillance
The search for better physiological sensors and pathogno-monic features will continue. There are exciting prospects on the horizon with new sensors and better ways of character-izing fetal condition. A large prospective RCT is underway in the USA to examine the impact of adding ST segment infor-mation to traditional EFM. Non-invasive detection of fetal ECG and contractions via surface electrodes on the mother ’ s abdomen are now available for clinical use. The largest ever perinatal trial examining the effects of computer-assisted trac-ing interpretation and management reminders at the bedside is underway in the UK [34] .
Perhaps with greater understanding that clinical outcomes are related to the cumulative effects at each of the three hier-archical steps outlined in this review, we will pay more atten-tion to performance at each level. Correcting defi ciencies at each level will maximize the potential to improve outcome, which is the ultimate clinical goal.
In addition, there are important lessons to be learned from past experiences. We must use reliable tools, not merely visual inspection, to measure parameters of interest. We must take the time to fully understand the relationship between the parameters in question and fetal metabolic acidemia. Relationships are complex and the evolution of patterns over time may not proceed in simple linear fashions. Until these data are obtained, it is premature to defi ne clinical manage-ment guidelines or launch a clinical trial using a threshold that is potentially suboptimal.
Finally, any clinical trial on fetal surveillance measures both the capacity of the device and the effect of clinician behavior. As the intention of the new monitoring device is to change clinician behavior to improve the state of the baby,
the preferable clinical trial design would use randomization of clinician groups. For example, a clinician who uses a new adjunctive technique, such as computerized analysis and management suggestions, will gradually alter his interpreta-tion of EFM. The computerized tool is providing constant and immediate feedback, which are powerful teaching tools for adult learners. Newly learned behavior will not completely disappear when caring for his next patient who has a similar tracing but does not have the computer analysis component. Unconsciously, the clinician will use these acquired skills with tracings that do not have computerized analysis. This behavior tends to bring benefi t to the control group, causing “ contamination ” and diminishing the capacity of the study to ascertain differences between the groups. Contamination is less likely to occur when the randomized clinical groups are geographically separate.
The early 20 th century mathematician David Hilbert, who laid some of the mathematical foundations underlying mod-ern digital signal processing, said, “ every real advance goes hand in hand with the invention of sharper tools and simpler methods. ” In the case of fetal surveillance, the future is bright because many “ sharper tools ” are emerging with the conver-gence of innovations in engineering, mathematics, and behav-ioral science.
References
[1] American College of Obstetricians and Gynecologists. Intrapartum fetal heart rate monitoring: nomenclature, inter-pretation, and general management principles. ACOG Practice Bulletin 106, 2009.
[2] Amer-W å hlin I, Hellsten C, Nor é n H, Hagberg H, Herbst A, Kjellmer I, et al. Cardiotocography only versus cardiotocogra-phy plus ST analysis of fetal electrocardiogram for intrapartum fetal monitoring: a Swedish randomised controlled trial. Lancet. 2001;358:534 – 8.
[3] Bannerman CG, Grobman WA, Antoniewicz L, Hutchinson M, Blackwell S. Assessment of the concordance among 2-tier, 3-tier, and 5-tier fetal heart rate classifi cation systems. Am J Obstet Gynecol. 2011;205:288.e1 – 4.
Table 3 Impediments to situational awareness.
Perceiving information • Unreliable information – fetal monitor posts “ maternal ” heart rate as the “ fetal ” heart rate • Incomplete information or delayed communication – handover snapshots of selected portions
of tracing rather than full review • Cluttered overcrowded spaces that impede visibility or access to critical information • Interruptions/multitasking • Limited time • Alert fatigue • Stress • Inexperience
Understanding its meaning • Knowledge gaps regarding basic physiology related to EFM • Knowledge gaps regarding the progression of coexisting/underlying diseases • Erroneous assumptions • Deference to authority fi gures despite a contrary personal opinion
Projection • Disregard of impending problem because it has a low incidence and false alarms are common • Time to actual delivery exceeds expectation • Fixation on achieving vaginal birth
UnauthenticatedDownload Date | 5/15/16 6:49 AM
Hamilton and Warrick, New perspectives in electronic fetal surveillance 91
[4] Becher JC, Stenson BJ, Lyon AJ. Is intrapartum asphyxia pre-ventable ? Br J Obstet Gynaecol. 2007;114:1442 – 4.
[5] Belfort MA, Saade GR. ST segment analysis as an adjunct to electronic fetal monitoring, Part I: background, physiology, and interpretation. Clin Perinatol. 2011;38:143 – 57.
[6] Belfort MA, Saade GR. ST segment analysis (STAN) as an adjunct to electronic fetal monitoring, Part II: clinical studies and future directions. Clin Perinatol. 2011;38:159 – 67.
[7] Bell R, Glinianaia SV, Rankin J, Wright C, Pearce MS, Parker L. Changing patterns of perinatal death, 1982 – 2000: a ret-rospective cohort study. Arch Dis Child Fetal Neonatal Ed. 2004;89:F531 – 6.
[8] Bocking AD. The relationship between heart rate and asphyxia in the animal fetus. Clin Invest Med. 1993;16:166 – 75.
[9] Bohmer RM. The four habits of high-value health care organi-zations. N Engl J Med. 2011;365:2045 – 7.
[10] Chen HY, Chauhan SP, Ananth CV, Vintzileos AM, Abuhamad AZ. Electronic fetal heart rate monitoring and its relationship to neonatal and infant mortality in the United States. Am J Obstet Gynecol. 2011;204:491.e1 – 10.
[11] Clark SL, Belfort MA, Dildy GA, Meyers JA. Reducing obstet-ric litigation through alterations in practice patterns. Obstet Gynecol. 2008;112:1279 – 83.
[12] Clark SL, Meyers JA, Frye DK, Perlin JA. Patient safety in obstetrics – the Hospital Corporation of America experience. Am J Obstet Gynecol. 2011;204:283 – 7.
[13] Clifford G, Sameni R, Ward J, Robinson J, Wolfberg AJ. Clinically accurate fetal ECG parameters acquired from mater-nal abdominal sensors. Am J Obstet Gynecol. 2011;205:47.e1 – 5.
[14] Cooper JM, Soffronoff EC, Bolognese RJ. Oxytocin chal-lenge test in monitoring high-risk pregnancies. Obstet Gynecol. 1975;45:27 – 33.
[15] Corometrics 120 series V3.5 operators manual P/N 2015589-001 Rev. C. Barrington, IL, USA: GE Medical Systems Information Technologies.
[16] Costa A, Ayres-de-Campos D, Costa F, Santos C, Bernardes J. Prediction of neonatal acidemia by computer analysis of fetal heart rate and ST event signals. Am J Obstet Gynecol. 2009;201:464.e1 – 6.
[17] Cyr RM, Usher RH, McLean FH. Changing patterns of birth asphyxia and trauma over 20 years. Am J Obstet Gynecol. 1984;148:490 – 8.
[18] Dalton KJ, Dawes GS, Patrick JE. Diurnal, respiratory, and other rhythms of fetal heart rate in lambs. Am J Obstet Gynecol. 1977;127:414 – 24.
[19] Dervaitis KL, Poole M, Schmidt G, Penava D, Natale R, Gagnon R. ST segment analysis of the fetal electrocardiogram plus elec-tronic fetal heart rate monitoring in labor and its relationship to umbilical cord arterial blood gases. Am J Obstet Gynecol. 2004;191:879 – 84.
[20] Digital interface protocol specifi cations. Programmer ’ s guide. Series 50 fetal monitors part number M1350-9074S. Germany: Philips; 2002.
[21] Dildy GA. Fetal pulse oximetry. Clin Obstet Gynecol. 2011;54:66 – 73.
[22] Doret M, Helgason H, Abry P, Goncalves P, Gharib C, Gaucherand P. Multifractal analysis of fetal heart rate variability in fetuses with and without severe acidosis during labor. Am J Perinatol. 2011;28:259 – 66.
[23] Draper ES, Kurinczuk JJ, Lamming CR, Clarke M, James D, Field D. A confi dential enquiry into cases of neona-tal encephalopathy. Arch Dis Child Fetal Neonatal Ed. 2002;87:F176 – 80.
[24] Electronic fetal heart rate monitoring: research guidelines for interpretation. National Institute of Child Health and Human Development research planning workshop. Am J Obstet Gynecol. 1997;177:1385 – 90.
[25] Elliott C, Warrick PA, Graham E, Hamilton EF. Graded clas-sifi cation of fetal heart rate tracings: association with neona-tal metabolic acidosis and neurologic morbidity. Am J Obstet Gynecol. 2010;202:258.e1 – 8.
[26] Euliano NR, Principe J, Edwards RK. Spatiotemporal elec-trohysterography patterns in normal and arrested labor. Am J Obstet Gynecol. 2009;200:54.e1 – 7.
[27] Fioratou E, Flin R, Glavin R, Patey R. Beyond monitoring: distributed situation awareness in anaesthesia. Br J Anaesth. 2010;105:83 – 90.
[28] Frasch MG, M ü ller T, Weiss C, Schwab K, Schubert H, Schwab M. Heart rate variability analysis allows early asphyxia detec-tion in ovine fetus. Reprod Sci. 2009;16:509 – 17.
[29] Freeman R, Garite T, Nageotte M. Fetal heart monitoring. Philadelphia, PA: Lippincott, Williams & Wilkins; 2003.
[30] Graatsma EM, Jacod BC, van Egmond LA, Mulder EJ, Visser GH. Fetal electrocardiography: feasibility of long-term fetal heart rate recordings. Br J Obstet Gynaecol. 2009;116:334 – 7.
[31] Hasley SK. Decision support and patient safety: the time has come. Am J Obstet Gynecol. 2011;204:461 – 5.
[32] Hull J, Dodd KL. Falling incidence of hypoxic-ischaemic encephalopathy in term infants. Br J Obstet Gynaecol. 1992;99:386 – 91.
[33] Ikenoue T, Martin CB Jr, Murata Y, Ettinger BB, Lu PS. Effect of acute hypoxemia and respiratory acidosis on the fetal heart rate in monkeys. Am J Obstet Gynecol. 1981;141:797 – 806.
[34] INFANT clinical trial. Available at https://www.npeu.ox.ac.uk/infant. Accessed 21 May 2012.
[35] Joint Commission on Accreditation of Healthcare Organizations, USA. Preventing infant death and injury during delivery. Sentinel Event Alert. 2004;30:1 – 3.
[36] Jones DG, Endsley MR. Sources of situation awareness errors in aviation. Aviat Space Environ Med. 1996;67:507 – 12.
[37] Knox GE, Simpson KR. Perinatal high reliability. Am J Obstet Gynecol. 2011;204:373 – 7.
[38] Kwon JY, Park IY, Shin JC, Song J, Tafreshi R, Lim J. Specifi c change in spectral power of fetal heart rate variability related to fetal acidemia during labor: comparison between preterm and term fetuses. Early Hum Dev. 2012;88:203 – 7.
[39] Leung TY, Chung PW, Rogers MS, Sahota DS, Lao TT, Hung Chung TK. Urgent cesarean delivery for fetal bradycardia. Obstet Gynecol. 2009;114:1023 – 8.
[40] Lewinsky RM. Cardiac systolic time intervals and other para-meters of myocardial contractility as indices of fetal acid-base status. Baillieres Clin Obstet Gynaecol. 1994;8:663 – 81.
[41] Liston R, Sawchuck D, Young D. Society of Obstetrics and Gynaecologists of Canada, British Columbia Perinatal Health Program. Fetal health surveillance: antepartum and intrapartum consensus guideline. J Obstet Gynaecol Can. 2007;29(Suppl):S3 – 56 [erratum in: J Obstet Gynaecol Can. 2007;29:909].
[42] Lucovnik M, Maner WL, Chambliss LR, Blumrick R, Balducci J, Novak-Antolic Z, et al. Noninvasive uterine electromyogra-phy for prediction of preterm delivery. Am J Obstet Gynecol. 2011;204:228.e1 – 10.
[43] MacDonald D, Grant A, Sheridan-Pereira M, Boylan P, Chalmers I. The Dublin randomized controlled trial of intra-partum fetal heart rate monitoring. Am J Obstet Gynecol. 1985;152:524 – 39.
UnauthenticatedDownload Date | 5/15/16 6:49 AM

92 Hamilton and Warrick, New perspectives in electronic fetal surveillance
[44] Macones GA, Hankins GDV, Spong CY, Hauth J, Moore T. The 2008 National Institute of Child Health and Human Development workshop report on electronic fetal monitoring. Update on defi nitions, interpretation, and research guidelines. Obstet Gynecol. 2008;112:661 – 6.
[45] Martin CB Jr. Physiology and clinical use of fetal heart rate variability. Clin Perinatol. 1982;9:339 – 52.
[46] Martin CB Jr, de Haan J, van der Wildt B, Jongsma HW, Dieleman A, Arts TH. Mechanisms of late decelerations in the fetal heart rate. A study with autonomic blocking agents in fetal lambs. Eur J Obstet Gynecol Reprod Biol. 1979;9:361 – 73.
[47] Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Mathews TJ, Kirmeyer S, et al. Births: fi nal data for 2007. Natl Vital Stat Rep. 2010;58:1 – 85.
[48] Melin M, Bonnevier A, Cardell M, Hogan L, Herbst A. Changes in the ST-interval segment of the fetal electrocardiogram in relation to acid-base status at birth. Br J Obstet Gynaecol. 2008;115:1669 – 75.
[49] Ojala K, V ä ä r ä sm ä ki M, M ä kikallio K, Valkama M, Tekay A. A comparison of intrapartum automated fetal electrocardiography and conventional cardiotocography – a randomised controlled study. Br J Obstet Gynaecol. 2006;113:419 – 23.
[50] Oppenheimer LW, Lewinsky RM. Power spectral analysis of fetal heart rate. Baillieres Clin Obstet Gynaecol. 1994;8:643 – 61.
[51] Parer JT, Ikeda T. A framework for standardized management of intrapartum fetal heart rate patterns. Am J Obstet Gynecol. 2007;197:26.e1 – 6.
[52] Parer WJ, Parer JT, Holbrook RH, Block BS. Validity of math-ematical methods of quantitating fetal heart rate variability. Am J Obstet Gynecol. 1985;153:402 – 9.
[53] Parush A, Campbell C, Hunter A, Ma C, Calder L, Worthington J, et al. Situational awareness. Ottawa, ON: Royal College of Physicians and Surgeons of Canada; 2011. Available at http://rcpsc.medical.org/canmeds/resources/primer_situational_awareness_patient_safety_e.pdf. Accessed 10 January 2011.
[54] Pasupathy D, Wood AM, Pell JP, Fleming M, Smith GC. Rates of and factors associated with delivery-related perinatal death among term infants in Scotland. JAMA. 2009;302:660 – 8.
[55] Peck T. Electronic monitoring evidence of fetal distress in high-risk pregnancies. J Reprod Med. 1980;24:103 – 8.
[56] Pettker CM, Thung SF, Raab CA, Donohue KP, Copel JA, Lockwood CJ, et al. A comprehensive obstetrics patient safety program improves safety climate and culture. Am J Obstet Gynecol. 2011;204:216.e1 – 6.
[57] Ransom SB, Studdert DM, Dombrowski MP, Mello MM, Brennan TA. Reduced medicolegal risk by compliance with obstetric clinical pathways: a case-control study. Obstet Gynecol. 2003;101:751 – 5.
[58] Ray M, Freeman R, Pine S, Hesselgesser R. Clinical experi-ence with the oxytocin challenge test. Am J Obstet Gynecol. 1972;114:1 – 9.
[59] Reason JT. Understanding adverse events: the Hyman factor. In: Vincent C, editor. Clinical risk management. London, UK: BMJ Books; 2001.
[60] Riley RJ, Johnson JW. Collecting and analyzing cord blood gases. Clin Obstet Gynecol. 1993;36:13 – 23.
[61] Rosen KG, Amer-Wahlin I, Luzietti R, Noren H. Fetal ECG waveform analysis. Best Pract Res Clin Obstet Gynaecol. 2004;18:485 – 514.
[62] Royal College of Obstetricians and Gynecologists Clinical Effectiveness Support Unit. The use of electronic fetal
monitoring. Evidence-based clinical guideline no. 8. London: RCOG Press; 2001.
[63] Saphier CJ, Thomas EJ, Studdert D, Brennan TA, Acker D. Applying no-fault compensation criteria to obstetric malprac-tice claims. Prim Care Update Ob Gyns. 1998;5:208 – 9.
[64] Siira SM, Ojala TH, Vahlberg TJ, Jalonen JO, V ä lim ä ki IA, Ros é n KG, et al. Marked fetal acidosis and specifi c changes in power spectrum analysis of fetal heart rate variability recorded during the last hour of labour. Br J Obstet Gynaecol. 2005;112:418 – 23.
[65] Singh H, Davis Giardina T, Petersen LA, Smith MW, Paul LW, Dismukes K, et al. Exploring situational awareness in diagnos-tic errors in primary care. BMJ Qual Saf. 2011;21:30 – 8.
[66] Singh H, Petersen LA, Thomas EJ. Understanding diagnostic errors in medicine: a lesson from aviation. Qual Saf Health Care. 2006;15:159 – 64.
[67] Smith J, Wells L, Dodd K. The continuing fall in incidence of hypoxic-ischaemic encephalopathy in term infants. Br J Obstet Gynaecol. 2000;107:461 – 6.
[68] Street P, Dawes GS, Moulden M, Redman CW. Short-term vari-ation in abnormal antenatal fetal heart rate records. Am J Obstet Gynecol. 1991;165:515 – 23.
[69] van Laar JO, Peters CH, Vullings R, Houterman S, Bergmans JW, Oei SG. Fetal autonomic response to severe acidaemia dur-ing labour. Br J Obstet Gynaecol. 2010;117:429 – 37.
[70] van Wijngaarden WJ, James DK, Symonds EM. The fetal electrocardiogram. Baillieres Clin Obstet Gynaecol. 1996;10:273 – 94.
[71] Vayssi è re C, David E, Meyer N, Haberstich R, Sebahoun V, Roth E, et al. A French randomized controlled trial of ST-segment analysis in a population with abnormal cardiotocograms during labor. Am J Obstet Gynecol. 2007;197:299.e1 – 6.
[72] Vayssiere C, Haberstich R, Sebahoun V, David E, Roth E, Langer B. Fetal electrocardiogram ST-segment analysis and prediction of neonatal acidosis. Int J Gynaecol Obstet. 2007;97:110 – 4.
[73] Warrick PA, Hamilton EF, Precup D, Kearney RE. Identifi cation of the dynamic relationship between intrapartum uterine pres-sure and fetal heart rate for normal and hypoxic fetuses. IEEE Trans Biomed Eng. 2009;56:1587 – 97.
[74] Warrick PA, Hamilton EF, Precup D, Kearney RE. Classifi cation of normal and hypoxic fetuses from systems modeling of intrapartum cardiotocography. IEEE Trans Biomed Eng. 2010;57:771 – 9.
[75] Westerhuis ME, Visser GH, Moons KG, van Beek E, Benders MJ, Bijvoet SM, et al. Cardiotocography plus ST analysis of fetal electrocardiogram compared with cardiotocography only for intrapartum monitoring: a randomized controlled trial. Obstet Gynecol. 2010;115:1173 – 80 [erratum in: Obstet Gynecol. 2011;117(Pt 1):412].
[76] Westgate J, Harris M, Curnow JS, Greene KR. Plymouth ran-domized trial of cardiotocogram only versus ST waveform plus cardiotocogram for intrapartum monitoring in 2400 cases. Am J Obstet Gynecol. 1993;169:1151 – 60.
The authors stated that there are no confl icts of interest regarding the publication of this article.
Received February 2, 2012. Revised April 23, 2012. Accepted April 30, 2012. Previously published online June 12, 2012.
UnauthenticatedDownload Date | 5/15/16 6:49 AM




















