The extended clinical phenotype of dome-shaped macula
10
MEDICAL OPHTHALMOLOGY The extended clinical phenotype of dome-shaped macula Marie-Hélène Errera & Michel Michaelides & Pearse A. Keane & Marie Restori & Michel Paques & Anthony T. Moore & Jonathan Yeoh & Derek Chan & Catherine A. Egan & Praveen J. Patel & Adnan Tufail Received: 16 September 2013 /Revised: 16 December 2013 /Accepted: 31 December 2013 /Published online: 25 January 2014 # Springer-Verlag Berlin Heidelberg 2014 Abstract Purpose To describe the phenotype, associations, and com- plications of dome-shaped macula (DSM) through the com- bination of spectral-domain optical coherence tomography (OCT) imaging and B-scan ultrasonography, when available. This retroprospective cohort study aims to gain further path- ophysiological understanding in eyes with DSM. Methods Fifty-eight eyes of 36 patients were identified as having OCT features of DSM. Retinal and choroidal thick- nesses were determined from enhanced depth imaging (EDI)- OCT image sets, with scleral thickness subsequently calculat- ed by subtraction from the B-scan ultrasound-derived mea- surements of posterior coat thickness. Results DSM was associated with myopia in 81 % of eyes. The underlying clinical diagnosis was variable: central serous chorioretinopathy (CSCR)-like entity, choroidal neovascular- ization, and inherited retinal disorders. The subfoveal choroi- dal thickness of the nine highly myopic eyes with a CSCR- like phenotype was thicker than the 25 eyes without CSCR (p =0.169). The mean subfoveal scleral thickness of the highly myopic eyes was 585±196 μm, which was significantly dif- ferent from those with a refractive error less than 6 diopters (1133 ± 290 μm) (P<0.0001). Conclusions This study highlights the novel observation of a thickened choroid when CSCR is present. In addition, we ex- pand the associations of DSM to eyes with hypermetropia and acquired disease, and to those with inherited retinal dystrophies. Keywords Optical coherence tomography . Ultrasonography . Dome-shaped macula . Enhanced depth imaging . Myopia Abbreviations DSM dome-shaped macula OCT optical coherence tomography EDI enhanced depth imaging VA visual acuity CSCR central serous chorioretinopathy CNV choroidal neovascularization RPE retinal pigment epithelium FA fluorescein angiography ICGA indocyanine green angiography D diopters SD standard deviation Introduction Dome-shaped macula (DSM) is a morphologic feature recent- ly described using optical coherence tomography (OCT), and characterized by an inward or anterior deviation of the macula with respect to the chorioretinal concavity. This feature was first reported exclusively in myopic patients with posterior staphyloma [1], but more recently has also been described in those patients without staphyloma [2]. Furthermore, using enhanced depth imaging (EDI)-OCT, Spaide and co-workers have demonstrated normal choroidal thickness, with a local- ized increase in scleral thickness in the area of the DSM [2]. The cause of DSM is not known; however, authors have postulated a range of theories, ranging from localized choroi- dal thickening, to scleral in-folding, to vitreomacular traction. The work of Spaide and co-workers suggests that scleral rather than choroidal thickening may underlie the changes seen in DSM, and that this may relate to the process of ocular expansion seen in myopia [1]. The aim of this study is to describe the clinical phenotype of a series of patients with DSM, reporting refractive error, Presented as a poster at the Association for Research in Vision and Ophthalmology Meeting Seattle, May 2013 M.<H. Errera : M. Michaelides : P. A. Keane : M. Restori : A. T. Moore : J. Yeoh : D. Chan : C. A. Egan : P. J. Patel : A. Tufail NIHR Biomedical Research Centre for Ophthalmology, Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology, London, UK M.<H. Errera (*) : M. Paques Ophthalmology Department IV, Centre Hospitalier National des Quinze-Vingts, UPMC Univ Paris 06, 28 rue de Charenton, 75012 Paris, France e-mail: [email protected] Graefes Arch Clin Exp Ophthalmol (2014) 252:499–508 DOI 10.1007/s00417-013-2561-7
Transcript of The extended clinical phenotype of dome-shaped macula

MEDICAL OPHTHALMOLOGY
The extended clinical phenotype of dome-shaped macula
Marie-Hélène Errera & Michel Michaelides & Pearse A. Keane & Marie Restori &Michel Paques & Anthony T. Moore & Jonathan Yeoh & Derek Chan &
Catherine A. Egan & Praveen J. Patel & Adnan Tufail
Received: 16 September 2013 /Revised: 16 December 2013 /Accepted: 31 December 2013 /Published online: 25 January 2014# Springer-Verlag Berlin Heidelberg 2014
AbstractPurpose To describe the phenotype, associations, and com-plications of dome-shaped macula (DSM) through the com-bination of spectral-domain optical coherence tomography(OCT) imaging and B-scan ultrasonography, when available.This retroprospective cohort study aims to gain further path-ophysiological understanding in eyes with DSM.Methods Fifty-eight eyes of 36 patients were identified ashaving OCT features of DSM. Retinal and choroidal thick-nesses were determined from enhanced depth imaging (EDI)-OCT image sets, with scleral thickness subsequently calculat-ed by subtraction from the B-scan ultrasound-derived mea-surements of posterior coat thickness.Results DSM was associated with myopia in 81 % of eyes.The underlying clinical diagnosis was variable: central serouschorioretinopathy (CSCR)-like entity, choroidal neovascular-ization, and inherited retinal disorders. The subfoveal choroi-dal thickness of the nine highly myopic eyes with a CSCR-like phenotype was thicker than the 25 eyes without CSCR (p=0.169). The mean subfoveal scleral thickness of the highlymyopic eyes was 585±196 μm, which was significantly dif-ferent from those with a refractive error less than 6 diopters(1133 ± 290 μm) (P<0.0001).Conclusions This study highlights the novel observation of athickened choroid when CSCR is present. In addition, we ex-pand the associations of DSM to eyes with hypermetropia andacquired disease, and to those with inherited retinal dystrophies.
Keywords Opticalcoherence tomography .Ultrasonography .
Dome-shapedmacula . Enhanced depth imaging .Myopia
AbbreviationsDSM dome-shaped maculaOCT optical coherence tomographyEDI enhanced depth imagingVA visual acuityCSCR central serous chorioretinopathyCNV choroidal neovascularizationRPE retinal pigment epitheliumFA fluorescein angiographyICGA indocyanine green angiographyD dioptersSD standard deviation
Introduction
Dome-shaped macula (DSM) is a morphologic feature recent-ly described using optical coherence tomography (OCT), andcharacterized by an inward or anterior deviation of the maculawith respect to the chorioretinal concavity. This feature wasfirst reported exclusively in myopic patients with posteriorstaphyloma [1], but more recently has also been described inthose patients without staphyloma [2]. Furthermore, usingenhanced depth imaging (EDI)-OCT, Spaide and co-workershave demonstrated normal choroidal thickness, with a local-ized increase in scleral thickness in the area of the DSM [2].
The cause of DSM is not known; however, authors havepostulated a range of theories, ranging from localized choroi-dal thickening, to scleral in-folding, to vitreomacular traction.The work of Spaide and co-workers suggests that scleralrather than choroidal thickening may underlie the changesseen in DSM, and that this may relate to the process of ocularexpansion seen in myopia [1].
The aim of this study is to describe the clinical phenotypeof a series of patients with DSM, reporting refractive error,
Presented as a poster at the Association for Research in Vision andOphthalmology Meeting Seattle, May 2013
M.<H. Errera :M. Michaelides : P. A. Keane :M. Restori :A. T. Moore : J. Yeoh :D. Chan :C. A. Egan : P. J. Patel :A. TufailNIHR Biomedical Research Centre for Ophthalmology, MoorfieldsEye Hospital NHS Foundation Trust and UCL Institute ofOphthalmology, London, UK
M.<H. Errera (*) :M. PaquesOphthalmology Department IV, Centre Hospitalier National desQuinze-Vingts, UPMC Univ Paris 06, 28 rue de Charenton,75012 Paris, Francee-mail: [email protected]
Graefes Arch Clin Exp Ophthalmol (2014) 252:499–508DOI 10.1007/s00417-013-2561-7

relative symmetry of findings between eyes in individuals,and other ocular associations. Furthermore, we report thechoroidal and scleral thickness in these eyes, and de-scribe possible associations of DSM including choroidalneovascularization (CNV) and subretinal fluid (serousmacular detachment).
Materials and methods
Data collection
All Spectralis-OCTs performed during a 4-year period atMoorfields Eye Hospital were reviewed in search for DSMprofile, and these are the only cases. Data from those patientswith DSM on OCTwere retrospectively collected.
Eyes with a previous history of photodynamic therapy, orof intravitreal anti-angiogenic therapy, were excluded from thestudy. Approval for the study was obtained from theresearch governance committee at Moorfields Eye Hos-pital. The research adhered to the tenets set forth in theDeclaration of Helsinki.
Information about age, gender, refractive error, and dura-tion of follow-up were gathered before clinical ophthalmicexamination and OCT image acquisition. Best-corrected visu-al acuity (VA) was measured using Snellen VA charts.
Optical coherence tomography imaging
For each subject, OCT image sets were obtained using a singleSpectralis OCT device (Heidelberg Engineering, Germany).All image sets were obtained using the EDI-OCT protocols[3], with horizontal line scans through the fovea. Seven hor-izontal line scans were performed in the macula.
For measurement of subfoveal retinal thickness, automatedsegmentation of the inner and outer retinal boundaries wasperformed by the proprietary software of the Spectralis OCTsystem (HEYEX, Heidelberg Eye Explorer). In each case, theresults of this process were inspected to ensure the absence ofsegmentation error. Measurement of subfoveal choroidalthickness was made with the manual calipers provided bythe HEYEX software. The choroid was measured from theouter portion of the reflective line corresponding to the retinalpigment epithelium (RPE) to the inner surface of the sclera.Two examiners performed the measurements of subfovealchoroidal thickness independently. The repeatability of thisapproach has previously been described [5].
Ultrasonography and other imaging
Additional imaging, including color fundus photography, fluo-rescein angiography (FA), and indocyanine green angiography(ICGA) were performed when clinically indicated. B-scan
ultrasonography (Siemens Acuson 512 with a 14 MHz lineararray probe) was performed by one single experienced opera-tor (MR) when clinically indicated (e.g., to rule out posteriorscleritis), and allowed determination of axial length manuallyand posterior coat thickness in a subset of patients. Retinal andchoroidal thicknesses were determined from OCT image sets,with scleral thickness subsequently calculated by subtractionfrom the ultrasound-derived measurements of posterior coatthickness. The presence or absence of a staphyloma was alsonoted. When a posterior staphyloma was present, the positionof the apex of the dome in relation to it was determinedbased on a combination of biomicroscopic and imagingexamination.
A previous study showed that the measurement precisionreached±0.1 mm under optimal conditions [4].
Data analysis and statistical methods
For the purpose of analysis, the patient cohort was subdividedinto two pre-defined groups based on spherical equivalentrefractive error and report of “myopia” versus “high myopia”in the patients’ notes. “Group 1” included eyes with≤-−6diopters (D) refractive error, while “group 2” includedeyes with≥-−6 D refractive error. A cut-off of −6 Drefractive error was chosen to allow for comparisonwith previously published normative data on scleralthickness [6].
The difference in choroidal thickness and scleral thicknessmeasurements between groups of patients was comparedusing a Mann–Whitney U test. To examine the relationshipbetween the subfoveal choroidal/scleral thickness and degreeof myopia, 24 eyes were analyzed, and non-parametric Spear-man correlation tests were performed. P values<0.05 wereconsidered statistically significant.
Results
Baseline characteristics
We identified 58 eyes of 36 patients with DSM. Mean patientage was 53 years (standard deviation (SD): ± 17 years; range:11–80 years). Twenty patients were male (54 %), while 16were female (44 %). In Group 1 (n=24 eyes), the meanrefractive error was −1.47 D (range: +4.50 D to −5.00 D),while the mean axial length was 23.7 mm (for axial length,n=7 as this measurement was not available in all eyes). InGroup 2 (n=34 eyes), mean refractive error was −12.00 D(range: −6.00D to −22.00 D), while the mean axial length was30.6 mm (n=8 eyes). The mean duration of follow-up was 21months (range: 3–48 months).
500 Graefes Arch Clin Exp Ophthalmol (2014) 252:499–508

Tab
le1
Summaryof
choroidaland
thickness,clinicalfeatures,and
diagnosesin
patientsscanned.Group
1(refractiveerror<
−6D)
Patient
number
Eye
Age
(years)/gender
Refractive
error
AL
(mm)
Clinicaldiagnosis(genotypeifknow
n)Presence
ofCSC
.(durationin
monthsM)
Presence
ofCNV
Other
phenotypes
EDIOCT
choroid
thickness
Bscan
ultrasound
scleral
thickness
VA
Snellen
VA
logM
AR
R/L
1L
45/M
N/A
N/A
Choroiderem
ia(deletionof
exons9-15
intheRef-1
gene)
––
–72
N/A
20/30
0.3
2R
44/M
-2.50
N/A
–CSC
(26M).Sp
ontaneous
resolutio
n.–
–354
1335
20/30
0.3
3R
61/M
+2
N/A
–CSC
(12M)
––
284
1349
20/60
0.5
L+1.50
N/A
–CSC
(4M)
––
320
1139
20/18
0
4R
44/F
−2N/A
–CSC
(16M)
––
366
N/A
20/30
0.2
L−3
N/A
––
––
366
N/A
20/20
0
5R
74/M
−3N/A
––
CNV (ranibizum
abIV
T)
–144
N/A
20/40
0.3
6R
51/M
−2.75
25.94
–CSC
(36M)
norm
alpattern
ERG,E
RG
flashandEOGin
2002:
norm
almacular
functio
non
electrophysiology.
––
251
799
20/20
0
L−3
.25
25.79
–CSC
(9M)
––
271
1118
20/18
0
7R
59/F
−4.50
N/A
––
PICin
fello
weye
246
N/A
20/40
0.3
8L
64/M
0N/A
––
–retin
alschisis
192
N/A
20/20
0
9R
34/M
0N/A
Xlin
kedretin
oschisis(RS1
gene
specifically
p.R200C
)–
––
371
N/A
20/40
0.3
L0
N/A
––
–391
N/A
20/60
0.5
10R
75/M
N/A
N/A
Bilateralretinaldysfunctionaffecting
rodandcone,sym
metrical:
late-onsetretin
aldystrophy
(orCARless
likely)
––
–114
1406
20/40
0.3
11R
61/F
+4.5
21.90
––
–224
1281
20/20
0
L+4.5
22.08
CSC
(24M)
––
172
982
20/30
0.2
12R
73/F
+0.50
N/A
––
–194
N/A
20/30
0.2
L+0.50
N/A
––
–222
N/A
20/30
0.2
13R
52/M
−5N/A
CSC
(recent)
––
123
N/A
20/20
0
L−5
N/A
CSC
––
130
N/A
20/20
0
14R
66/M
−5N/A
––
CNV (×10
ranibizumab
IVT)
–136
528
20/40
0.3
23R
76/F
−2.25
23.22
––
CNV(×6ranibizumab
IVT)
–150
N/A
20/50
0.4
Graefes Arch Clin Exp Ophthalmol (2014) 252:499–508 501

Choroidal and scleral morphology
A summary of the choroidal and scleral changes, clinicalfeatures, and patient diagnoses is provided in Tables 1 and 2.A posterior staphyloma was seen in 42 eyes (72 % of eyes). In19 eyes (45 % of eyes with staphyloma), the DSM was foundat the edge of the staphyloma, while in the remaining 23 eyes(55 % of eyes with staphyloma) the DSM was found withinthe area of staphyloma. In 16 eyes (28 %), posteriorstaphyloma was not detected on clinical examination.
Central serous chorioretinopathy and choroidalneovascularization
Nineteen eyes with DSM had subretinal fluid and/or focalhyperfluorescent areas on FA, with no leakage beyond thelesion borders, in keeping with a central serouschorioretinopathy (CSCR)-like phenotype (32.7 %). In eyeswith a CSCR-like phenotype, no evidence of CNV was de-tected on clinical examination or imaging (FA, ICGA, OCT).In patients with both OCTand fundus autofluorescence (FAF)imaging, there were four eyes with subretinal deposits onOCT, corresponding to hyperautofluorescent areas on FAF(patients 2, 11, 15, 35). Twelve eyes (21 %) had evidence ofCNV confirmed by FA and/or ICG imaging (Fig. 1).
Inherited retinal dystrophies
The spectrum ofmyopic and emmetropic patients in this studyincluded those with inherited retinal dystrophies (11 eyes ofseven patients). These dystrophies included: X-linked retinos-chisis (two eyes, one patient), late onset retinal dystrophy (oneeye, one patient), congenital stationary night blindness (twoeyes, one patient), X-linked retinal dystrophy (gene RS1;oneeye, one patient), cone dystrophy with super normal rodelectroretinogram (gene KCNV2; two eyes, one patient),choroideremia (one eye, one patient) and rod–cone dystrophy(two eyes, one patient) (Fig. 2). Of these, myopia coexistedwith inherited retinal dystrophies in 17 % of eyes identifiedwith DSM (8/47 myopic eyes). Four of these seven patientshad symmetrical disease.
Visual acuity
Thirty-five eyes (21 patients) had VA of 20/40 or better. Of the21 eyes (15 patients) with VA<20/40, five eyes (three pa-tients) had an inherited retinal dystrophy, seven eyes (sixpatients) had age-related macular degeneration with CNV,three eyes (two patients) had CSCR-like features withsubretinal fluid, three eyes (two patients) had myopic retinaldegeneration with myopic retinoschisis, one eye (one patient)had a full-thickness macular hole and one eye (one patient)had a lamellar hole.T
able1
(contin
ued)
Patient
number
Eye
Age
(years)/gender
Refractive
error
AL
(mm)
Clinicaldiagnosis(genotypeifknow
n)Presence
ofCSC
.(durationin
monthsM)
Presence
ofCNV
Other
phenotypes
EDIOCT
choroid
thickness
Bscan
ultrasound
scleral
thickness
VA
Snellen
VA
logM
AR
R/L
L−3
.25
23.12
––
––
159
N/A
20/40
0.3
35R
56/F
−4.50
24Right
supero-nasalorbitalcavernous
haem
angiom
a5yearspriorCSC
.Choroidalfoldsatpresentatio
n.Po
st-operativ
esteroidusefollo
wing
anterior
orbitotomy.
CSC
spontaneousregression
ofSR
Fin
4monthstim
e.–
–288
1,400
20/40
0.3
CSC
centralserouschorioretin
opathy,SRFsubretinalfluid,CNVchorioretin
alneovascularizatio
n,IVTintravitrealtreatment,PEDposteriorepith
eliald
etachm
ent,PIC
Punctuateinnerchoroidopathy,N/A
resultnotavailable.CARcarcinom
a-associated
retin
opathy.M
(months)
502 Graefes Arch Clin Exp Ophthalmol (2014) 252:499–508
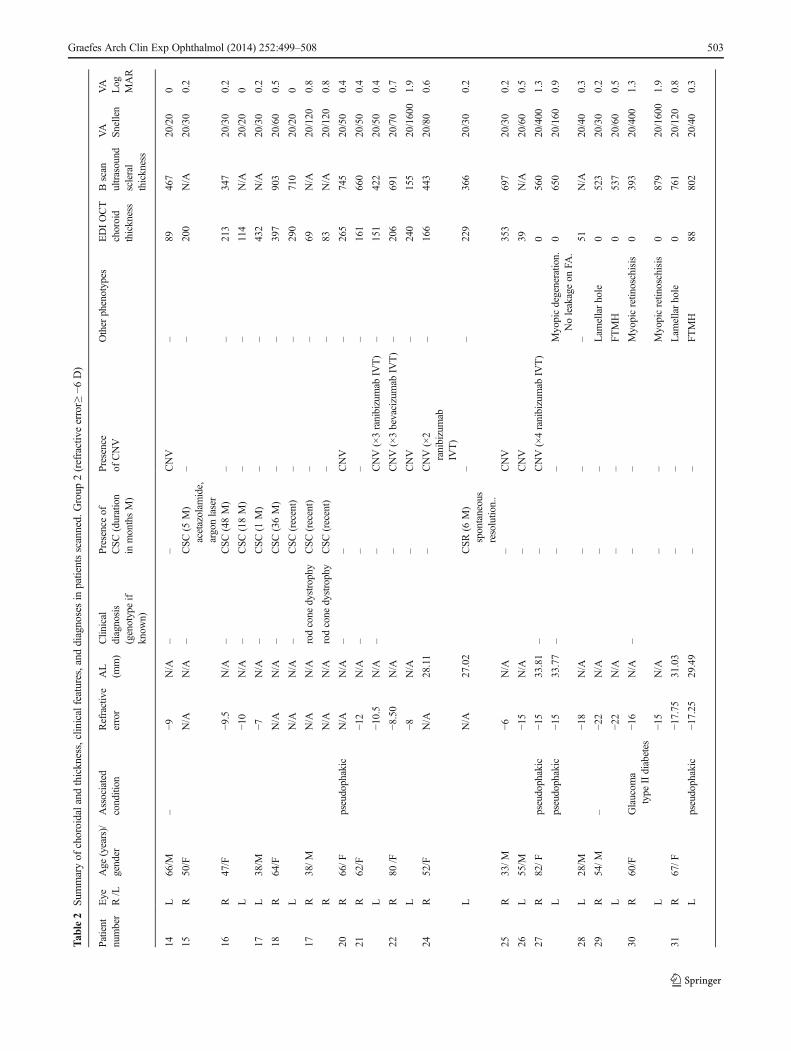
Tab
le2
Summaryof
choroidaland
thickness,clinicalfeatures,and
diagnosesin
patientsscanned.Group
2(refractiveerror≥
−6D)
Patient
number
Eye
Age
(years)/
gender
Associated
condition
Refractive
error
AL
(mm)
Clin
ical
diagnosis
(genotypeif
know
n)
Presenceof
CSC
(duration
inmonthsM)
Presence
ofCNV
Other
phenotypes
EDIOCT
choroid
thickness
Bscan
ultrasound
scleral
thickness
VA
Snellen
VA
Log
MAR
R/L
14L
66/M
–−9
N/A
––
CNV
–89
467
20/20
0
15R
50/F
N/A
N/A
–CSC
(5M)
acetazolam
ide,
argonlaser
––
200
N/A
20/30
0.2
16R
47/F
−9.5
N/A
–CSC
(48M)
––
213
347
20/30
0.2
L−1
0N/A
–CSC
(18M)
––
114
N/A
20/20
0
17L
38/M
−7N/A
–CSC
(1M)
––
432
N/A
20/30
0.2
18R
64/F
N/A
N/A
–CSC
(36M)
––
397
903
20/60
0.5
LN/A
N/A
–CSC
(recent)
––
290
710
20/20
0
17R
38/M
N/A
N/A
rodcone
dystrophy
CSC
(recent)
––
69N/A
20/120
0.8
RN/A
N/A
rodcone
dystrophy
CSC
(recent)
––
83N/A
20/120
0.8
20R
66/F
pseudophakic
N/A
N/A
––
CNV
–265
745
20/50
0.4
21R
62/F
−12
N/A
––
––
161
660
20/50
0.4
L−1
0.5
N/A
––
CNV(×3ranibizumab
IVT)
–151
422
20/50
0.4
22R
80/F
−8.50
N/A
–CNV(×3bevacizumab
IVT)
–206
691
20/70
0.7
L−8
N/A
–CNV
–240
155
20/1600
1.9
24R
52/F
N/A
28.11
–CNV(×2
ranibizumab
IVT)
–166
443
20/80
0.6
LN/A
27.02
CSR
(6M)
spontaneous
resolutio
n..
––
229
366
20/30
0.2
25R
33/M
−6N/A
–CNV
353
697
20/30
0.2
26L
55/M
−15
N/A
–CNV
39N/A
20/60
0.5
27R
82/F
pseudophakic
−15
33.81
––
CNV(×4ranibizumab
IVT)
0560
20/400
1.3
Lpseudophakic
−15
33.77
––
–Myopicdegeneratio
n.Noleakageon
FA.
0650
20/160
0.9
28L
28/M
−18
N/A
––
–51
N/A
20/40
0.3
29R
54/M
–−2
2N/A
––
Lam
ellarhole
0523
20/30
0.2
L−2
2N/A
––
FTMH
0537
20/60
0.5
30R
60/F
Glaucom
atype
IIdiabetes
−16
N/A
––
–Myopicretin
oschisis
0393
20/400
1.3
L−1
5N/A
––
Myopicretin
oschisis
0879
20/1600
1.9
31R
67/F
−17.75
31.03
––
Lam
ellarhole
0761
20/120
0.8
Lpseudophakic
−17.25
29.49
––
FTMH
88802
20/40
0.3
Graefes Arch Clin Exp Ophthalmol (2014) 252:499–508 503

Choroidal thickness
Results from choroidal thickness measurement are summa-rized in Table 3.
In group 1 eyes (n=24 eyes; refractive error<−6 D), themean subfoveal choroidal thickness was 259±87 μm (range172–417 μm).
No difference was noted between mean subfoveal choroi-dal thickness in this group and that measured recently in acohort of “normal” (< −6 D) eyes (287±76 μm) [3]. In group1, eyes with subretinal fluid (or a CSCR-like phenotype; n=10eyes) had a mean subfoveal choroidal thickness of 256±87 μm. This was similar to that of other eligible eyes withno subretinal fluid in the same group 1 (254±101 μm) (n=14eyes) (p=0.1868).
The mean choroidal thickness in group 2 eyes (≥ −6 D) was176±159 μm (n=34 eyes). The subfoveal choroidal thicknessin these highly myopic patients with DSM was thicker thanthe normal range established in a recent study which found themean choroidal thickness in highly myopic eyes to be 93.2±62.5 μm [6]. Among the eyes in group 2, eyes with subretinalfluid or leaks on FA (CSCR-like phenotype) had evidence ofincreased choroidal thickness compared with eyes withoutsubretinal fluid: 239±144 μm, (n=9) versus 153±361 μm (n=25), (p=0.4883).
Scleral thickness
Results from scleral thickness measurement are summarizedin Table 3.
The mean subfoveal scleral thickness of the highlymyopic eyes was 585±196 μm ,which was significantlydifferent from those with a refractive error less than 6diopters (1133 ±290 μm) (P<0.0001).
In group 1 eyes, the mean subfoveal scleral thicknesswas 1133±290 μm (n=10 eyes with ultrasonographyperformed), and was in keeping with the mean scleralthickness in normal subjects as described by Normanet al. (996±181 μm) [7].
In group 2, the mean subfoveal scleral thickness was 585±196 μm (n=20 eyes with ultrasonography performed), a resultsignificantly higher than that of highly myopic eyes withoutDSM (281±85 μm; scleral thickness measured with EDIOCT) reported by Imamura et al. [2].
Relationships between choroidal/scleral thickness and myopia
Subfoveal scleral thickness showed a positive correlation withrefractive error, (r=0.646, p<0.01) (Fig. 3, top). Subfovealchoroidal thickness was also positively correlated with theaxial length (r=0.694, p<0.01) (Fig. 3, bottom).T
able2
(contin
ued)
Patient
number
Eye
Age
(years)/
gender
Associated
condition
Refractive
error
AL
(mm)
Clin
ical
diagnosis
(genotypeif
know
n)
Presenceof
CSC
(duration
inmonthsM)
Presence
ofCNV
Other
phenotypes
EDIOCT
choroid
thickness
Bscan
ultrasound
scleral
thickness
VA
Snellen
VA
Log
MAR
R/L
32R
34/M
−10
N/A
KCNV2
––
–104
N/A
20/120
0.8
L−1
0N/A
KCNV2
––
–35
N/A
20/120
0.8
33R
37/M
N/A
N/A
Xlinkedretinal
dystrophy
––
223
N/A
20/60
0.5
34R
12/M
N/A
N/A
Congenital
stationary
nightb
lindness
––
569
N/A
20/30
0.3
LN/A
N/A
Congenital
stationary
nightb
lindness
––
–527
N/A
20/40
0.
36R
56/F
–N/A
N/A
–CSR
(recent)
––
278
N/A
N/A
N/A
LN/A
N/A
–CSR
(recent)
––
420
N/A
N/A
N/A
CSC
centralserouschorioretin
opathy,SRFsubretinalfluid,
CNVchorioretin
alneovascularizatio
n,PEDposteriorepith
eliald
etachm
ent,N/A
resultnotavailable,IVTintravitrealinjectio
n.M
months
FAfluoresceinangiography
504 Graefes Arch Clin Exp Ophthalmol (2014) 252:499–508

Discussion
The initial descriptions of DSM were in myopic eyes eitherwith or without an associated staphyloma [1]. In this caseseries, we extend the associations of DSM, describing thisabnormality in both emmetropic and hypermetropic eyes. Wealso report the occurrence of DSM in the presence of othermacular and retinal disease. Using the technique of EDI-OCT,Imamura and co-workers imaged the choroid and sclera in aseries of 15 patients (23 eyes) with DSM. Surprisingly, they
reported that choroidal thickness was only slightly increasedover eyes without DSM, but that eyes with DSM had alocalized area of scleral thickening in the macular region [2].The development of DSM in myopic eyes could represent anadaptive phenomenon in a proportion of myopic patients toreduce defocus in the macula [8]. Recently, Ellaban and co-workers showed that a 3-dimensional reconstruction of theirswept-source OCT image sets in highly myopic eyes (≥ −6 D),allowed visualization of a horizontal ridge formed within theposterior staphyloma, consistent with the dome shaped con-vexity appearance on OCT sections [9].
In the present study, we report the largest series of patientsto date with DSM, and report the novel finding of DSM innon-myopic eyes with average, or shorter than average, axiallengths. We also observed a higher proportion of patients withbilateral DSM (78 % of cases) compared to the publishedliterature (50-53%) [1, 2]. Moreover, the association of retinaldystrophy with dome-shaped macula eyes has not previouslybeen described. We suggest the high prevalence of inheriteddiseases (19.6 %) was probably related to the high rate ofmyopia in genetic ocular diseases and the tertiary referralnature of our institution. Given our observation of DSM innon-myopic eyes, prospective studies may be needed to assessthe true incidence and prevalence of DSM in both myopic andnon-myopic eyes.
The cause of subfoveal fluid in association with DSMwithout CNV is unknown. It has been suggested in previousstudies that the presence of subretinal fluid in these eyes maybe due to RPE dysfunction, rather than true CSCR [1].Asdiscussed in the work by Imamura and co-workers, potentialcauses include obstruction of outflow of choroidal fluid by a
Fig. 1 Patient with dome-shapedmacula (DSM) within a posteriorstaphyloma (patient 24). Fifty-one-year-old woman presentingwith idiopathic choroidalneovascular membrane in theright eye. Color fundusphotograph (a) and fluoresceinangiography (FA) (c) showshemorrhage and leakage in theperifoveal area. She wasasymptomatic in the left eye;however, there is some slightsubretinal fluid on OCT scan (f)and no active leakage on FA (d).Note the normal fundusphotograph (b). DSM is seen inboth eyes on Spectralis-OCT(Heidelberg Engineering,Germany). In the left eye, B-scanultrasonography demonstratesmacular elevation (g)
Fig. 2 Patient with dome-shaped macula (DSM) with inherited disease.(patient 12): 19-year-old high myope male diagnosed with rod-conedystrophy. Fundus autofluorescence shows a slight increase in back-ground autofluorescence in the parafoveal area, surrounding an area ofrelative hypoautofluorescence at the fovea in both eyes. Spectralis opticalcoherence tomography (OCT) examination reveals bilateral DSM withsubfoveal fluid (b, d)
Graefes Arch Clin Exp Ophthalmol (2014) 252:499–508 505

thick sclera as in nanophthalmos [2]. Another pathophysio-logical association may be choroidal thickening, as seen incases of more typical CSCR [10]. Imamura and co-workerssuggest that the modest increases in choroidal thickness seenin DSM and high myopia are unlikely to account for thesubfoveal fluid in cases of DSM [2]. In the present study,however, we report a higher proportion of eyes with DSM andsubfoveal fluid in the absence of CNV (28.5 %) compared tothe report by Imamura et al. (9 %) [2]. Moreover, we haveshown increased choroidal thickness in highly myopic eyeswith DSM with subfoveal fluid compared to highly myopiceyes and DSM without subfoveal fluid. We therefore suggest
that choroidal thickening relative to normal thicknesses inhighly myopic eyes may contribute to the pathophysiologyeven though, in absolute terms, the choroidal thicknesses aremuch thinner than those seen in emmetropic eyes with CSCR.
The finding of localized macular scleral thickening inhighly myopic patients with DSM supports findings in theprevious report by Imamura et al., though in the current studywe used ultrasound assessment of macular scleral thicknessrather than EDI-OCT [2]. However, in eyes with DSM notassociated with high myopia, we found no evidence of in-creased macular scleral thickness.
Imamura’s paper also hypothesized that, rather than local-ized macular thickening, relative preservation of the fovea,with thinning of the surrounding sclera may account for thecharacteristic dome-shape. It would be helpful to know ifDSM is an adaptive and protective mechanism to maintainvisual acuity/refraction for a certain axial length/keratometryor a pathologic process.
There have been several theories postulated for the mech-anism and pathophysiological processes leading to the forma-tion of DSM in myopic eyes. These theories include: 1/hypotonia in the area of staphyloma, with the consequentlower wall tension responsible for the inward collapse of thesclera shell [11], 2/ the tangential vitreomacular traction al-ready involved in retinal abnormalities in highly myopic eyes[11], 3/ the resistance of the sclera to the staphylomatousdeformation [1], 4/ a localized thickening of the choroid [1],or 5/ an adaptive mechanism to minimize defocus in highlymyopic eyes undergoing axial length increases [2]. Our find-ings in the subgroup of eyes with high myopia support thislatter theory. Indeed, DSM may develop as a result of ana-tomical changes in the morphology of layers of the posteriorcoat of the globe, similarly to that reported in chicks afterform-deprivation and optical defocus [12, 13]. In chicks,choroidal thickening at the posterior pole is seen in recoveryof prior deprivation induced myopia [14]. In humans, thisanatomical change could be a response that acts to minimizerefractive error in high myopic eyes and trying to maintain
Fig. 3 Scatter-plot of Spectralis optical coherence tomography (OCT)measurements of choroidal thickness and scleral thickness in 24 eyes.Subfoveal choroidal thickness is (top left) positively correlated withrefractive error (r=0.646, p<0.01. Population standard deviation:366.91; sample standard deviation: 374.47); subfoveal scleral thicknessis also (top left) positively correlated with the refractive error (r=0.694,p<0.01. population standard deviation: 123.73; sample standard devia-tion: 126.28),D: diopters
Table 3 Summary of comparisons among eyes with refractive errors (< −6 D), highly myopic eyes (≥ −6 D) and reports of the literature
Mean subfoveal choroidalthickness (μm)
P Mean subfoveal scleralthickness (μm)
P
Group 1 eyes (< −6 D) n=24 259±87 0.9497*** 1,133 ±290* 0.20Normal eyes (< −6 D) (Margolis, 2009) [3] 287 ±76 996±181
Group 2 eyes (≥ −6 D) n=34 176±159 NP 585±196** NPHighly myopic eyes (−5.0 to −26.0 D) (Fujiwara, 2009)[6] 93.2 um ± 62.5um 281±85
n number of eyes* n=10 eyes with ultrasonography performed, ** n=20 eyes with ultrasonography performed. *** With regard to choroidal thickness, because of anegative correlation to age, statistical comparison may not be fair; NB: Please note that reference 6 was derived from MRI scans on enucleated humanglobes. Considering that the method for scleral thickness measurement in this study was completely different from the reference [6], no statisticalcomparison was done
506 Graefes Arch Clin Exp Ophthalmol (2014) 252:499–508

emmetropization [7]. In addition to choroidal thickness chang-es in the macula, increases in scleral thickness have beenreported in chicks after form deprivation and occurring pri-marily at the posterior pole [15]. In chicks, development ofmyopia is associated with increased scleral growth at theposterior pole of the eye [16–19] following transient increasesin choroidal thickening. Mechanisms involved in the devel-opment of increased scleral thickness may be related to mo-lecular signals that originate in the choroid and pass through itin controlling ocular elongation [20, 21].
The finding of DSM in a proportion of eyes with highmyopia may represent a similar process, given the findingsof increased macular scleral thickness and increased macularchoroidal thickness in highly myopic eyes with DSM com-pared to highly myopic eyes without DSM. More studies arenecessary to determine whether the equator and ora serratademonstrate abnormalities in scleral and choroidal thickness,though the work by Imamura and co-workers suggests thatthese potentially adaptive changes in choroidal and scleralthickness are localized to the macular. Experimental work inchick models of myopia has also previously shown that re-sponses in the extreme periphery are different from changesseen at the macula [2].
It is unclear what pathophysiological mechanisms underliethe development of DSM in non-myopic eyes, and furtherwork is needed to further explore the prevalence and incidenceof DSM in these eyes.
To our knowledge, the current study is the first to show,in vivo, that the scleral thickness is correlated positively withthe refractive error, and further supports existing data showingthe choroidal thickness was correlated positively with therefractive error [22].
However, our report has several limitations. This is aretrospective study, and we were unable to obtain axiallength measurements in all patients. Moreover, the use ofultrasound to measure sclera is probably a weakness andmore studies are needed using the recent technology ofswept-source OCT. Because DSM was diagnosed on hori-zontal section only, we did not document the “vertical oval-shaped dome” pattern as described recently by Caillauxet al. [23]. Finally, the primary diagnosis and associationsappear very heterogeneous (e.g., association with inheriteddiseases, CNV or CSC), and can be regarded as a result ofthe selection process.
Conflicts of interest The authors have no proprietary interests in thematerial presented.
Drs. Keane, Egan, Tufail, and Patel have received a proportion of theirfunding from the Department of Health’s NIHR Biomedical ResearchCentre for Ophthalmology at Moorfields Eye Hospital, and UCL Instituteof Ophthalmology. The views expressed in the publication are those ofthe author and not necessarily those of the Department of Health.
Dr. Tufail has been on advisory boards for Novartis, Pfizer, GSK,Thrombogenics, Bayer and Allergan. Drs. Keane and Patel have receivedtravel grants from the Allergan European Retina Panel. Dr. Patel has beenon advisory boards for Novartis UK. Dr. Michaelides is supported by aFoundation Fighting Blindness Career Development Award.
Dr Marie-Hélène Errera has received a travel grant from NovartisFrance.
DrMarie-Hélène Errera wants to thank Dr Pablo Goldschmidt, CentreHospitalier des Quinze-Vingts, for helpful discussion in statistics.
Clinical trial registration number ERRM1003 (Moorfields Eye Hos-pital, London, UK)
References
1. Gaucher D, Erginay A, Lecleire-Collet A, Haouchine B, Puech M,Cohen SY, Massin P, Gaudric A (2008) Dome-shaped macula in eyeswith myopic posterior staphyloma. Am J Ophthalmol 145:909–914
2. Imamura Y, Iida T, Maruko I, Zweifel SA, Zweifel SA, Spaide RF(2011) Enhanced depth imaging optical coherence tomography of thesclera in dome-shaped macula. Am J Ophthalmol 151:297–302
3. Margolis R, Spaide RF (2009) A pilot study of enhanced depthimaging optical coherence tomography of the choroid in normal eyes.Am J Ophthalmol 147:811–815
4. Guthoff R, Berger RW, Dreager J (1987) Ultrasonographic measure-ment of the posterior coats of the eye and their relation to axial length.Graefes Arch Clin Exp Ophthalmol 225:374–376
5. Rahman W, Chen FK, Yeoh J, Patel P, Tufail A, Da Cruz L (2011)Repeatability of manual subfoveal choroidal thickness measurementsin healthy subjects using the technique of enhanced depth imagingoptical coherence tomography. Invest Ophthalmol Vis Sci 8(52):2267–2271
6. Fujiwara T, Imamura Y, Margolis R, Slakter JS, Spaide RF (2009)Enhanced depth imaging optical coherence tomography of the cho-roid in highly myopic eyes. Am J Ophthalmol 148:445–450
7. Norman RE, Flanagan JG, Rausch SM, Sigal IA, Tertinegg I, EilaghiA, Portnoy S, Sled JG, Ethier CR (2010) Dimensions of the humansclera: thickness measurement and regional changes with axiallength. Exp Eye Res 90:277–284
8. Keane PA,Mitra A, Khan IJ, Quhill F, Elsherbiny SM (2012). Dome-shaped macula: a compensatory mechanism in myopic anisometro-pia? Ophthalmic Surg Lasers Imaging 43 Online:e52–e54
9. Ellabban AA, Tsujikawa A, Matsumoto A, Yamashiro K, Oishi A,Ooto S, Nakata I, Akagi-Kurashige Y, Miyake M, Elnahas HS,Radwan TM, Zaky KA, Yoshimura N (2013) Three-dimensionaltomographic features of dome-shaped macula by swept-sourceoptical coherence tomography. Am J Ophthalmol 155:320–328
10. Imamura Y, Fujiwara T, Margolis R, Spaide RF (2009) Enhanceddepth imaging optical coherence tomography of the choroid in centralserous chorioretinopathy. Retina 29:1469–1473
11. Mehdizadeh M, Nowroozzadeh MH (2008) Dome-shaped macula ineyes with myopic posterior staphyloma. Am J Ophthalmol 146:478
12. Ehrlich D, Sattayasai J, Zappia J, Barrington M (1990) Effects ofselective neurotoxins on eye growth in the young chick. CIBA FoundSymp 155:63–84
13. Beresford JA, Crewther SG, Crewther DP (1998) Anatomical corre-lated of experimentally inducedmyopia. Aust N ZOphthalmol 26(1):S84–S87
14. Wallman J, Wildsoet C, Xu A, Gottlieb MD, Nickla DL, Marran L,Krebs W, Christensen AM (1995) Moving the retina: choroidalmodulation of refractive state. Vision Res 35:37–50
15. Gottlieb MD, Joshi HB, Nickla DL (1990) Scleral changes in chickswith form-deprivation myopia. Curr Eye Res 9:1157–1165
Graefes Arch Clin Exp Ophthalmol (2014) 252:499–508 507

16. Rada JA, Thoft RA, Hassell JR (1991) Increased aggrecan (cartilageproteoglycan) production in the sclera of myopic chicks. Dev Biol147:303–312
17. Rada JA, McFarland AL, Cornuet PK, Hassell JR (1992)Proteoglycan synthesis by scleral chondrocytes is modulated by avision dependent mechanism. Curr Eye Res 11:767–782
18. Rada JA, Matthews AL, Brenza H (1994) Regional proteoglycansynthesis in the sclera of experimentally myopic chicks. Exp Eye Res59:747–760
19. Christensen AM, Wallman J (1991) Evidence that increased scleralgrowth underlies visual deprivation myopia in chicks. InvestOphthalmol Vis Sci 32:2143–2150
20. Wallman J, Winawer J (2004) Homeostasis of eye growth and thequestion of myopia. Neuron 43:447–468
21. Nickla DL, Wallman J (2010) The multifunctional choroid. ProgRetin Eye Res 29:144–16
22. Sogawa K, Nagaoka T, Takahashi A, Tanano I, Tani T, Ishibazawa A,Yoshida A (2012) Relationship between choroidal thickness andchoroidal circulation in healthy young subjects. Am J Ophthalmol153:1129–1132
23. Caillaux V, Gaucher D, Gualino V, Massin P, Tadayoni R, Gaudric A(2013). Morphologic characterization of dome-shaped macula inmyopic eyes with serous macular detachment. Am J Ophthalmol156(5):958.e1–967.e1
508 Graefes Arch Clin Exp Ophthalmol (2014) 252:499–508