
The comparison of dual phase Tc99m MIBI and Tc99m MDP scintimammography in the evaluation of breast...
8
ORIGINAL ARTICLE Annals of Nuclear Medicine Vol. 14, No. 1, 39-46, 2000 The comparison of dual phase Tc-99m MIBI and Tc-99m MDP scintimammography in the evaluation of breast masses: Preliminary report Nuri ARSLAN,* Emel OZTURK,* Seyfettin ILGAN,* Yavuz NARIN,* Sabri DUNDAR,* Turgut TUFAN,** Mesut PEKCAN**and Hikmet BAYHAN* Departments of *Nuclear Medicine and **General Surgery, Giilhane Military Medical Academy and Medical FaculO,, Ankara, Turkey The aim of this prospective study was to determine the diagnostic value of Tc-99m MDP scintimammography (SMG) for the detection of breast cancer in patients with breast masses and to compare the results with Tc-99m MIBI scintimammography. Twenty patients, categorized as suspicious, positive or benign for breast cancer according to the mammographic findings were included in the study. Dual phase Tc-99m MIBI and Tc-99m MDP SMG were performed in the prone lateral position within 5 days of each other. Although early and late Tc-99m MIBI SMG showed equal (90.4%) sensitivity, the specificity of late Tc-99m MIBI (87.5%) was found superior to early (62.5%) imaging. The overall sensitivity and specificity of early Tc-99m MDP SMG were 71.4% and 62.5%, respectively. Although late Tc-99m MDP imaging showed 100% specificity, its sensitivity was only 23.8%. In the patients with palpable masses, both early Tc-99m MDP and Tc- 99m MIBI showed equal sensitivity (100%), but the sensitivity of early Tc-99m MIBI (37.5%) was found slightly higher than Tc-99m MDP (25.0%) for nonpalpable breast lesions. The sensitivity of Tc-99m MIBI and Tc-99m MDP SMG in detecting metastatic axillary involvement was 66.6% and 50%, respectively. High sensitivity and specificity together with its low cost, easy availability and the possibility of detecting bone metastases seems to make Tc-99m MDP a contributive agent in the evaluation of breast lesions as an alternative to Tc-99m MIBI. Key words: breast cancer, scintimammography, Tc-99m MIBI, Tc-99m MDP INTRODUCTION BREAST CANCERis the most common visceral neoplasm affecting women. Approximately more than 700,000 breast cancers are diagnosed in the whole world annually and it remains the leading cause of death among women from 40 to 55 years old.l Early detection of breast cancer decreases mortality and facilitates conservative therapy. At present, mammography (MG) remains the only suitable imaging method for screening asymptomatic women. Despite its Received August 16, 1999, revision accepted November 10, 1999. For reprint contact: Nuri Arslan, M.D., G01hane Military Medical Academy, Department of Nuclear Medicine, 06018 Etlik, Ankara, TURKEY. E-mail: [email protected] high sensitivity in the detection of breast abnormalities, the positive predictive value of MG is only between 20 and 30%. 2 Tc-99m hexakis-methoxyisobutyl-isonitrile (MIBI), a cationic iipophilic complex,3 has been proposed and used widely for the differential diagnosis of breast masses. 4-7 The overall sensitivity and specificity of Tc-99m MIBI scintimammography (SMG) is reported to be 94-100% and 88-91% for palpable breast masses and 25-67% and 80-100% for nonpalpable ones, respectively.6-8 The other potential agent for breast imaging is Tc-99m methylene diphosphonate (MDP). Several benign and malignant primary breast tumors have been reported to accumulate Tc-99m-MDP. 9-13 The diagnostic accuracy of late breast imaging was found to be low in the past. 14 On the other hand, early Tc-99m MDP SMG has re- cently gained popularity due to its favorable results. The Vol. 14, No. 1, 2000 Original Article 39
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of The comparison of dual phase Tc99m MIBI and Tc99m MDP scintimammography in the evaluation of breast...

ORIGINAL ARTICLE
Annals of Nuclear Medicine Vol. 14, No. 1, 39-46, 2000
The comparison of dual phase Tc-99m MIBI and Tc-99m MDP scintimammography in the evaluation of breast masses:
Preliminary report
Nuri ARSLAN,* Emel OZTURK,* Seyfettin ILGAN,* Yavuz NARIN,* Sabri DUNDAR,* Turgut TUFAN,** Mesut PEKCAN** and Hikmet BAYHAN*
Departments of *Nuclear Medicine and **General Surgery, Giilhane Military Medical Academy and Medical FaculO,, Ankara, Turkey
The aim of this prospective study was to determine the diagnostic value of Tc-99m MDP scintimammography (SMG) for the detection of breast cancer in patients with breast masses and to compare the results with Tc-99m MIBI scintimammography. Twenty patients, categorized as suspicious, positive or benign for breast cancer according to the mammographic findings were included in the study. Dual phase Tc-99m MIBI and Tc-99m MDP SMG were performed in the prone lateral position within 5 days of each other. Although early and late Tc-99m MIBI SMG showed equal (90.4%) sensitivity, the specificity of late Tc-99m MIBI (87.5%) was found superior to early (62.5%) imaging. The overall sensitivity and specificity of early Tc-99m MDP SMG were 71.4% and 62.5%, respectively. Although late Tc-99m MDP imaging showed 100% specificity, its sensitivity was only 23.8%. In the patients with palpable masses, both early Tc-99m MDP and Tc- 99m MIBI showed equal sensitivity (100%), but the sensitivity of early Tc-99m MIBI (37.5%) was found slightly higher than Tc-99m MDP (25.0%) for nonpalpable breast lesions. The sensitivity of Tc-99m MIBI and Tc-99m MDP SMG in detecting metastatic axillary involvement was 66.6% and 50%, respectively. High sensitivity and specificity together with its low cost, easy availability and the possibility of detecting bone metastases seems to make Tc-99m MDP a contributive agent in the evaluation of breast lesions as an alternative to Tc-99m MIBI.
Key words: breast cancer, scintimammography, Tc-99m MIBI, Tc-99m MDP
INTRODUCTION
BREAST CANCER is the most common visceral neoplasm affecting women. Approximately more than 700,000 breast cancers are diagnosed in the whole world annually and it remains the leading cause of death among women from 40 to 55 years old.l Early detection of breast cancer decreases mortality and facilitates conservative therapy. At present, mammography (MG) remains the only suitable imaging method for screening asymptomatic women. Despite its
Received August 16, 1999, revision accepted November 10, 1999.
For reprint contact: Nuri Arslan, M.D., G01hane Military Medical Academy, Department of Nuclear Medicine, 06018 Etlik, Ankara, TURKEY.
E-mail: [email protected]
high sensitivity in the detection of breast abnormalities, the positive predictive value of MG is only between 20 and 30%. 2
Tc-99m hexakis-methoxyisobutyl-isonitrile (MIBI), a cationic iipophilic complex, 3 has been proposed and used widely for the differential diagnosis of breast masses. 4-7 The overall sensitivity and specificity of Tc-99m MIBI scintimammography (SMG) is reported to be 94-100% and 88-91% for palpable breast masses and 25-67% and 80-100% for nonpalpable ones, respectively. 6-8
The other potential agent for breast imaging is Tc-99m methylene diphosphonate (MDP). Several benign and malignant primary breast tumors have been reported to accumulate Tc-99m-MDP. 9-13 The diagnostic accuracy of late breast imaging was found to be low in the past. 14 On the other hand, early Tc-99m MDP SMG has re- cently gained popularity due to its favorable results. The
Vol. 14, No. 1, 2000 Original Article 39

sensitivity and specificity of dynamic and early (10-20 minutes) Tc-99m MDP imagings were reported to be 92% and 95%, respectively. J 5
The aim of this prospective study was to determine the diagnostic value of Tc-99m MDP SMG for the detection of breast cancer in patients with breast masses and to compare the results with Tc-99m MIBI SMG and the final histopathological diagnosis.
MATERIALS AND METHODS
Patients Twenty women, aged 26 to 89 years old (mean age = 51 + 14 years) with either suspicious mammographic finding or a mass palpated at physical examination were included in this study. SMG results for 29 lesions (21 palpable, 8 nonpalpable) in 20 consecutive patients were evaluated. Each patient had a comprehensive physical breast exami- nation by an experienced breast surgeon before the study.
Mammography Craniocaudal and mediolateral oblique mammographic projections (Mammomat 3-stereo; Siemens) of all pa- tients were performed with dedicated units. All mam- mograms were interpreted by the attending breast radiolo- gist with full knowledge of available clinical information and previous mammograms. The patients were classified in three categories according to the mammographic findings: suspicion of malignancy, positive (most prob- ably malignant) and negative (most probably benign). The criteria for malignant lesions were poorly defined margins, spicular margins, high density and small, thin, multiple calcifications. The criteria for benign lesions were coarse calcifications or low density lesions with sharp margins. The criteria for the suspicious group were dense breast tissue or parenchymal nodes or mild asym- metry. For statistical analysis, the suspicious group on mammography was considered to be positive for predict- ing malignancy since biopsy and histopathological confirmation were suggested to these patients.
Tc-99m MIBI SMG SMG was performed by using a large field of view gamma camera equipped with a low energy, high-resolution col- limator (GE 400 ACT/STARCAM, GE Medical Systems, Milwaukee, WI). Each patient received intravenous in- jection of 740 MBq of Tc-99m MIBI (Cardiolite, Du Pont Merck Pharmaceutical Co., N.Billerica, MA) in the arm contralateral to the breast lesion. For patients with bilat- eral suspected breast abnormalities, Tc-99m MIBI was given via a pedal vein. Prone lateral imaging of each breast was done for t0 minutes at the 5th minute and one hour after the injection of Tc-99m MIBI, with a 10% window centered at 140 keV, by using a 128 x 128-pixel matrix size and 1.33 zoom factor. Patients were imaged with a specially designed plexiglas table (home-made)
overlay with a lateral cut off which allows the breast to come in close contact with the gamma camera and also allows relaxation of the pectoralis muscle. Anterior chest planar images were also acquired for 10 minutes at the end of each session in the supine position with the arms raised for depiction of the axillary area with a 256 • 256 pixel matrix size. Some obese patients whose chests did not fit completely into the field of view required anterior oblique planar views for each axilla (l,500 kilocounts).
Tc-99m MDP SMG Within 5 days after Tc-99m MIBI SMG, breast imaging was repeated after the injection of 740 MBq Tc-99m MDP. An additional dynamic imaging of the most suspi- cious breast lesion seen on mammography was added to the Tc-99m MDP imaging protocol. Dynamic acquisition was performed for a total of 5.5 minutes (6 frames of 5 sec each, 6 frames of 10 sec each and 16 frames of 15 sec each) by using a low energy, general purpose, parallel-hole collimator. Acquisition parameters of a 64 x 64 matrix with a 20% window centered at 140 keV were used for the dynamic acquisition. Early (5-30 min) and late (2nd hour) static images were performed as described in the Tc-99m MIBI study. Whole body bone scanning was performed for all patients for the detection of possible bone me- tastases after the completion of Tc-99m MDP SMG.
Data Analysis Tc-99m MIBI and Tc-99m MDP images were evaluated by two experienced nuclear medicine physicians without any clinical information. Images were evaluated both visually and quantitatively. For visual analysis, any focal area of increased uptake either in the early or late imaging session for both agents was considered as positive for malignancy. Bilateral and uniform breast uptake which is equal to soft-tissue uptake and mild to moderate bilateral or unilateral diffuse uptake with no area of focal uptake was considered as negative for malignancy. For semi- quantitative analysis, regions of interests were drawn around the tumor and to an area of 'normal' breast tissue in the same breast, and tumor-to-background (T/Bg) ratios were obtained. Any focal tracer accumulation in the axillary region was interpreted as lymphatic invasion for both studies. Finally, Tc-99m MIBI and Tc-99m MDP SMG results were compared with each other and with the final histopathological diagnosis.
RESULTS
SMG results for 29 lesions (21 palpable, 8 nonpalpable) in 20 consecutive patients were evaluated. 13 patients had a single lesion, five patients had two and two patients had three lesions. Histopathologic diagnoses were obtained by means of excisional biopsy in 14 patients and by fine needle aspiration in 6. According to the final histopatho- logic diagnosis; 21 lesions in 13 patients were diagnosed
40 Nuri Arslan, Emel Ozturk, Seyfettin Ilgan, et al Annals of Nuclear Medicine
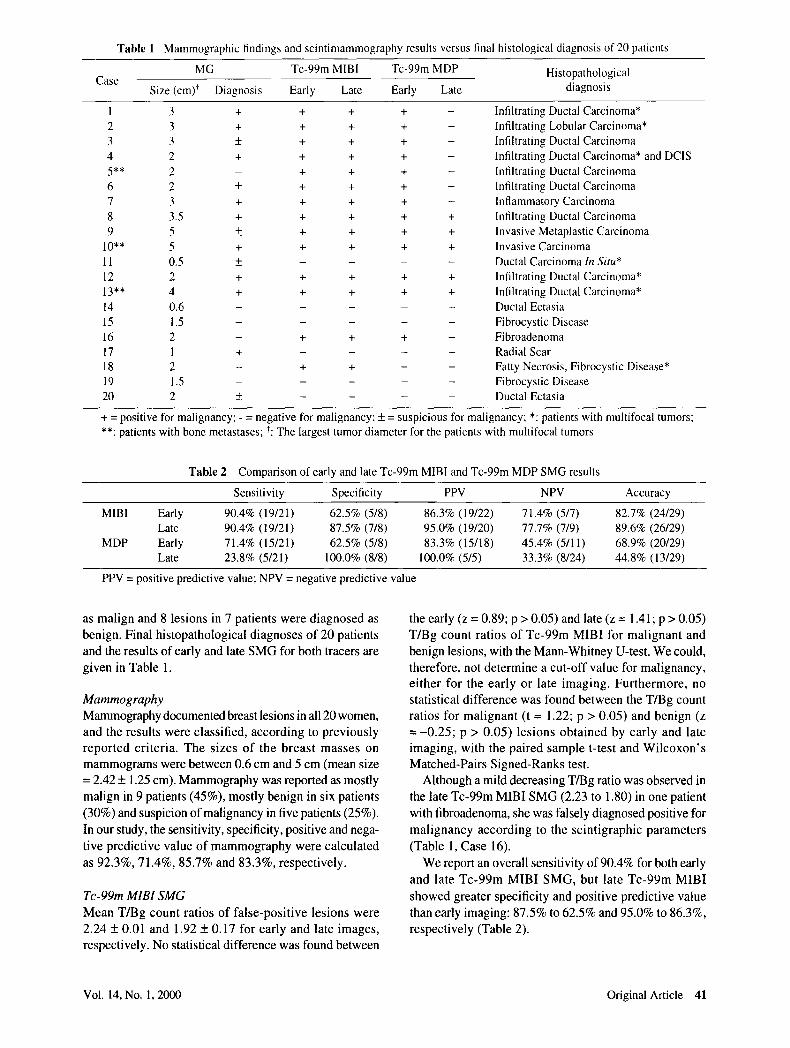
Table 1 Mammographic findings and scintimammography results versus final histological diagnosis of 20 patients
Case MG Tc-99m MIBI Tc-99m MDP Histopathological
Size (cm) t Diagnosis Early Late Early Late diagnosis
1 3 + + + + -
2 3 + + + + - 3 3 • + + + - 4 2 + + + + - 5** 2 - + + + - 6 2 • + + + - 7 3 + + + + -
8 3 . 5 + + + + +
9 5 • + + + + 10"* 5 + + + + + 11 0.5 • . . . . 12 2 + + + + + 13"* 4 + + + + + 14 0.6 . . . . . 15 1.5 . . . . . 16 2 - + + + - 17 1 + . . . . 18 2 - + + - -
1 9 1.5 . . . . . 20 2 • . . . .
Infiltrating Ductal Carcinoma* Infiltrating Lobular Carcinoma* Infiltrating Ductal Carcinoma Infiltrating Ductal Carcinoma* and DCIS Infiltrating Ductal Carcinoma Infiltrating Ductal Carcinoma Inflammatory Carcinoma Infiltrating Ductal Carcinoma Invasive Metaplastic Carcinoma lnvasive Carcinoma Ductal Carcinoma In Situ* Infiltrating Ductal Carcinoma* Infiltrating Ductal Carcinoma* Ductal Ectasia Fibrocystic Disease Fibroadenoma Radial Scar Fatty Necrosis, Fibrocystic Disease* Fibrocystic Disease Ductal Ectasia
+ = positive for malignancy; - = negative for malignancy; + = suspicious for malignancy; *: patients with multifocal tumors; **: patients with bone metastases; *: The largest tumor diameter for the patients with multifocal tumors
Table 2 Comparison of early and late Tc-99m MIBI and Tc-99m MDP SMG results
Sensitivity Specificity PPV NPV Accuracy
MIBI Early 90.4% (19/21) 62.5% (5/8) 86.3% (19/22) 71.4% (5/7) 82.7% (24/29) Late 90.4% (19/21) 87.5% (7/8) 95.0% (19/20) 77.7% (7/9) 89.6% (26/29)
MDP Early 71.4% (15/21) 62.5% (5/8) 83.3% (15/18) 45.4% (5/11) 68.9% (20/29) Late 23.8% (5/21) 100.0% (8/8) 100.0% (5/5) 33.3% (8/24) 44.8% (13/29)
PPV = positive predictive value; NPV = negative predictive value
as malign and 8 lesions in 7 patients were diagnosed as benign. Final histopathological diagnoses of 20 patients and the results of early and late SMG for both tracers are
given in Table 1.
Mammography Mammography documented breast lesions in all 20 women, and the results were classified, according to previously repor ted cri teria. The sizes of the breas t masses on mammograms were between 0.6 cm and 5 cm (mean size = 2.42 + 1.25 cm). Mammography was reported as mostly
malign in 9 patients (45%), mostly benign in six patients
(30%) and suspicion of malignancy in five patients (25%). In our study, the sensitivity, specificity, positive and nega-
tive predictive value of mammography were calculated
as 92.3%, 71.4%, 85.7% and 83.3%, respectively.
Tc-99m MIBI SMG Mean T/Bg count ratios of false-posi t ive lesions were 2.24 + 0.01 and 1.92 + 0.17 for early and late images, respectively. No statistical difference was found between
the early (z = 0.89; p > 0.05) and late (z = 1.41; p > 0.05) T/Bg count ratios of Tc-99m MIBI for mal ignant and benign lesions, with the Mann-Whitney U-test. We could, therefore, not determine a cut-off value for malignancy, ei ther for the ear ly or late imaging. Fur thermore , no statistical difference was found between the T/Bg count ratios for mal ignant (t = 1.22; p > 0.05) and benign (z = - 0 . 2 5 ; p > 0.05) lesions obtained by early and late imaging, with the paired sample t-test and Wi lcoxon ' s Matched-Pairs Signed-Ranks test.
Although a mild decreasing T/Bg ratio was observed in the late Tc-99m MIBI SMG (2.23 to 1.80) in one patient
with fibroadenoma, she was falsely diagnosed positive for
mal ignancy according to the scintigraphic parameters
(Table 1, Case 16).
We report an overall sensitivity of 90.4% for both early
and late Tc-99m MIBI SMG, but late Tc-99m MIBI
showed greater specificity and positive predictive value than early imaging: 87.5% to 62.5% and 95.0% to 86.3%, respectively (Table 2).
Vol. 14, No. 1, 2000 Original Article 41
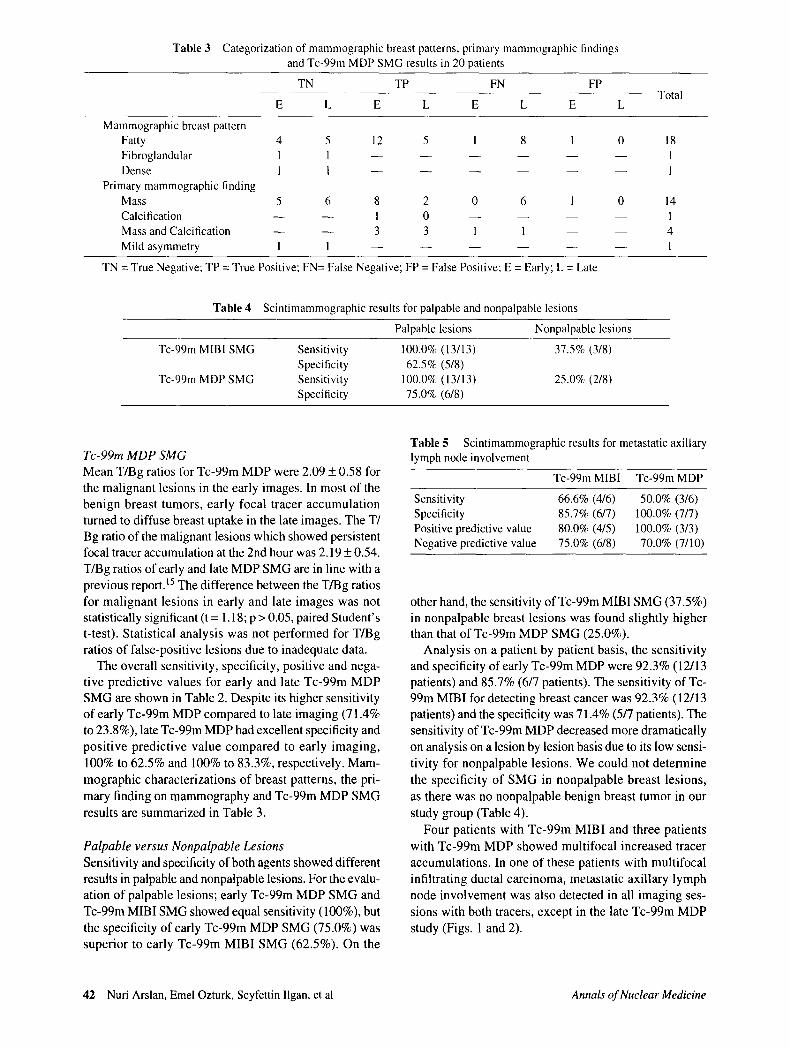
Table 3 Categorization of mammographic breast patterns, primary mammographic findings and Tc-99m MDP SMG results in 20 patients
TN TP FN FP
E L E L E L E L Total
Mammographic breast pattern Fatty 4 5 12 5 1 8 1 0 18 Fibroglandular 1 1 . . . . . . 1 Dense 1 1 . . . . . . 1
Primary mammographic finding Mass 5 6 8 2 0 6 1 0 14 Calcification - - - - 1 0 . . . . 1 Mass and Calcification - - - - 3 3 1 1 - - - - 4 Mild asymmetry 1 1 . . . . . . 1
TN = True Negative; TP --- True Positive; FN= False Negative; FP = False Positive; E = Early; L = Late
Table 4 Scintimammographic results for palpable and nonpalpable lesions
Palpable lesions Nonpalpable lesions
Tc-99m MIBI SMG Sensitivity 100.0% (13/13) 37.5% (3/8) Specificity 62.5% (5/8)
Tc-99m MDP SMG Sensitivity 100.0% (13/13) 25.0% (2/8) Specificity 75.0% (6/8)
Tc-99m MDP SMG Mean T/Bg ratios for Tc-99m MDP were 2.09 + 0.58 for the malignant lesions in the early images. In most of the benign breast tumors, early focal tracer accumulation turned to diffuse breast uptake in the late images. The T/ Bg ratio of the malignant lesions which showed persistent focal tracer accumulation at the 2nd hour was 2.19 + 0.54. T/Bg ratios of early and late MDP SMG are in line with a previous report.t5 The difference between the T/Bg ratios for malignant lesions in early and late images was not statistically significant (t = 1.18; p > 0.05, paired Student' s t-test). Statistical analysis was not performed for T/Bg ratios of false-positive lesions due to inadequate data.
The overall sensitivity, specificity, positive and nega- tive predictive values for early and late Tc-99m MDP SMG are shown in Table 2. Despite its higher sensitivity of early Tc-99m MDP compared to late imaging (71.4% to 23.8%), late Tc-99m MDP had excellent specificity and positive predictive value compared to early imaging, 100% to 62.5% and 100% to 83.3%, respectively. Mam- mographic characterizations of breast patterns, the pri- mary finding on mammography and Tc-99m MDP SMG results are summarized in Table 3.
Palpable versus Nonpalpable Lesions Sensitivity and specificity of both agents showed different results in palpable and nonpalpable lesions. For the evalu- ation of palpable lesions; early Tc-99m MDP SMG and Tc-99m MIBI SMG showed equal sensitivity (100%), but the specificity of early Tc-99m MDP SMG (75.0%) was superior to early Tc-99m MIBI SMG (62.5%). On the
Table 5 Scintimammographic results for metastatic axillary lymph node involvement
Tc-99m MIBI Tc-99m MDP
Sensitivity 66.6% (4/6) 50.0% (3/6) Specificity 85.7% (6/7) 100.0% (7/7) Positive predictive value 80.0% (4/5) 100.0% (3/3) Negative predictive value 75.0% (6/8) 70.0% (7/10)
other hand, the sensitivity of Tc-99m MIBI SMG (37.5%) in nonpalpable breast lesions was found slightly higher than that of Tc-99m MDP SMG (25.0%).
Analysis on a patient by patient basis, the sensitivity and specificity of early Tc-99m MDP were 92.3% (12/13 patients) and 85.7% (6/7 patients). The sensitivity of Tc- 99m MIBI for detecting breast cancer was 92.3% (12/13 patients) and the specificity was 71.4% (5/7 patients). The sensitivity of Tc-99m MDP decreased more dramatically on analysis on a lesion by lesion basis due to its low sensi- tivity for nonpalpable lesions. We could not determine the specificity of SMG in nonpalpable breast lesions, as there was no nonpalpable benign breast tumor in our study group (Table 4).
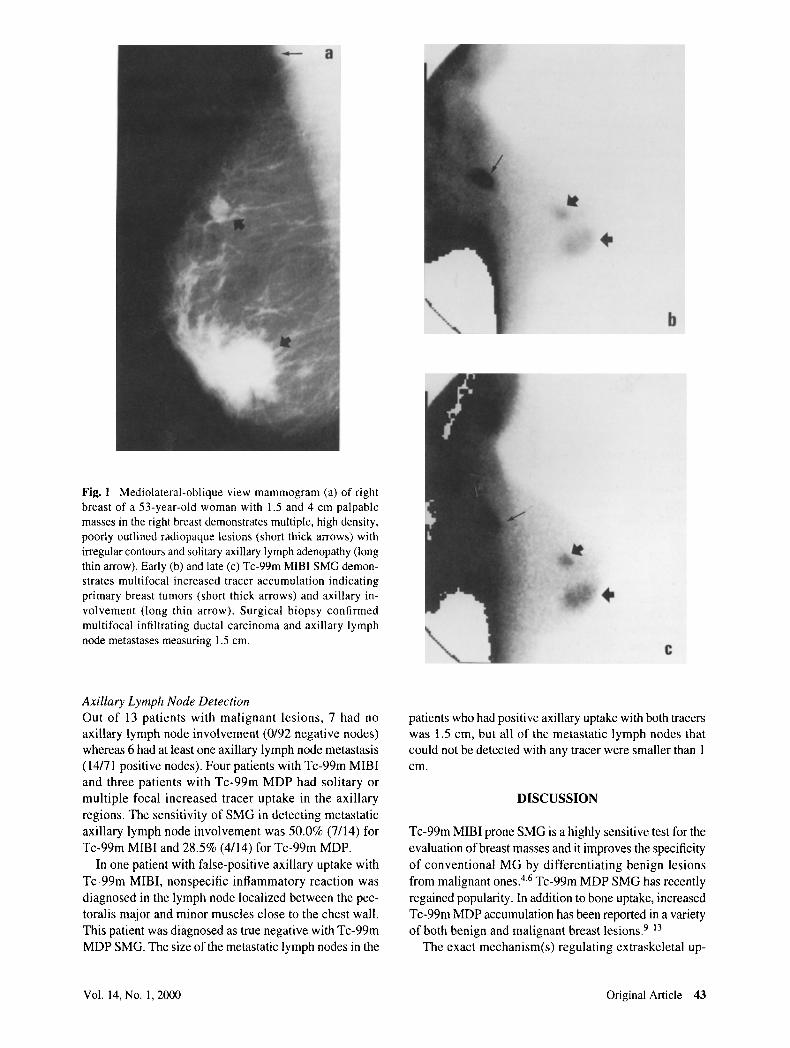
Four patients with Tc-99m MIBI and three patients with Tc-99m MDP showed multifocal increased tracer accumulations. In one of these patients with multifocal infiltrating ductal carcinoma, metastatic axillary lymph node involvement was also detected in all imaging ses- sions with both tracers, except in the late Tc-99m MDP study (Figs. 1 and 2).
42 Nuri Arslan, Emel Ozturk, Seyfettin Ilgan, et al Annals of Nuclear Medicine
4.
b
Fig. 1 Mediolateral-oblique view mammogram (a) of right breast of a 53-year-old woman with 1.5 and 4 cm palpable masses in the right breast demonstrates multiple, high density, poorly outlined radiopaque lesions (short thick arrows) with irregular contours and solitary axillary lymph adenopathy (long thin arrow). Early (b) and late (c) Tc-99m MIBI SMG demon- strates multifocal increased tracer accumulation indicating primary breast tumors (short thick arrows) and axillary in- volvement (long thin arrow). Surgical biopsy confirmed multifocal infiltrating ductal carcinoma and axillary lymph node metastases measuring 1.5 cm.
C
Axillary Lymph Node Detection Out of 13 patients with malignant lesions, 7 had no axillary lymph node involvement (0/92 negative nodes) whereas 6 had at least one axillary lymph node metastasis (14/71 positive nodes). Four patients with Tc-99m MIBI and three patients with Tc-99m MDP had solitary or multiple focal increased tracer uptake in the axillary regions. The sensitivity of SMG in detecting metastatic axillary lymph node involvement was 50.0% (7/14) for Tc-99m MIBI and 28.5% (4/14) for Tc-99m MDP.
In one patient with false-positive axillary uptake with Tc-99m MIBI, nonspecific inflammatory reaction was diagnosed in the lymph node localized between the pec- toralis major and minor muscles close to the chest wall. This patient was diagnosed as true negative with Tc-99m MDP SMG. The size of the metastatic lymph nodes in the
patients who had positive axillary uptake with both tracers was 1.5 cm, but all of the metastatic lymph nodes that could not be detected with any tracer were smaller than 1 c m .
DISCUSSION
Tc-99m MIBI prone SMG is a highly sensitive test for the evaluation of breast masses and it improves the specificity of conventional MG by differentiating benign lesions from malignant ones. 4,6 Tc-99m MDP SMG has recently regained popularity. In addition to bone uptake, increased Tc-99m MDP accumulation has been reported in a variety of both benign and malignant breast lesions. 9-13
The exact mechanism(s) regulating extraskeletal up-
Vol. 14, No. 1, 2000 Original Article 43
0 I!
b
take of Tc-99m MDP is unclear. The selective skeletal uptake of Tc-99m MDP in bone is described as "chemi- sorption" of the agent on the surface of hydroxyapatite crystals of bone. Since microscopic calcification was not found by light microscopy in every biopsied breast tissue (Table 3), it could appear that a mechanism other than chemisorption must be involved in extraskeletal uptake. A wide spectrum of reliable mechanisms has been formu- lated including increased blood flow, inflammatory changes, modification of local metabolism (Ca +2 content, pH) and collagen deposits. 12 Other possible factors that affect uptake of MDP are thought to be changes in cell metabolism, enlargement of the interstitial space, cell wall damage, microcalcification in necrotic degenerative tissues and hormonal effects (estradiol, etc.). 9,15,16 An-
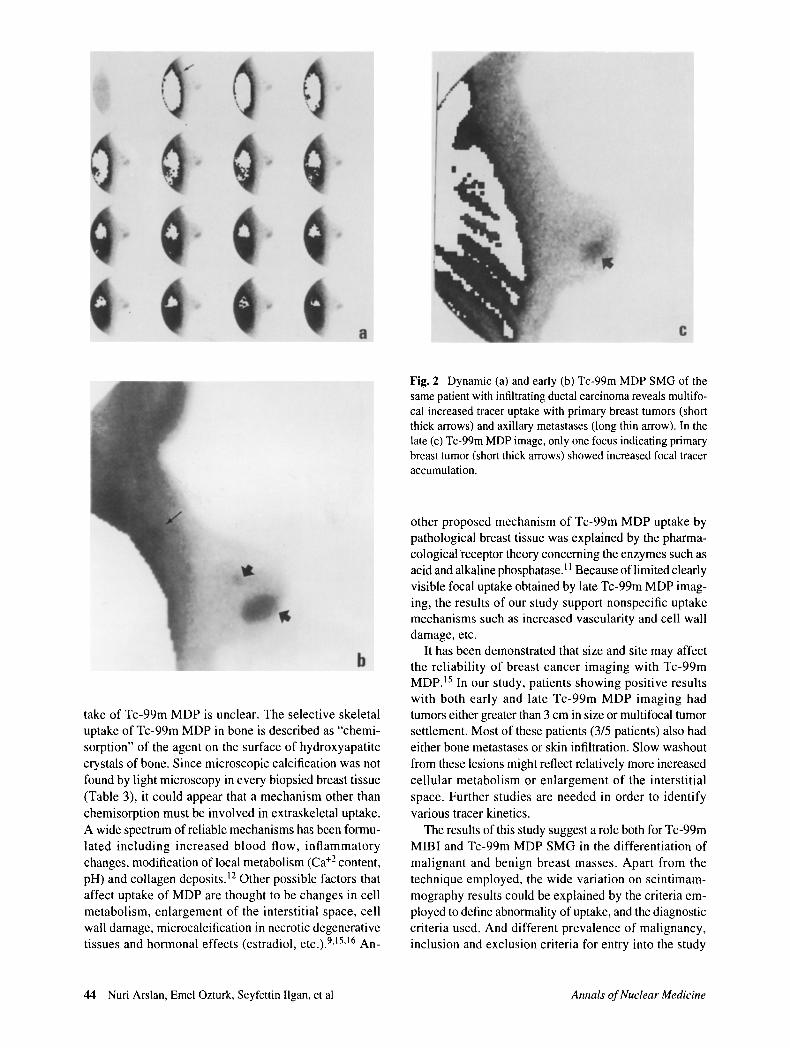
Fig. 2 Dynamic (a) and early (b) Tc-99m MDP SMG of the same patient with infiltrating ductal carcinoma reveals multifo- cal increased tracer uptake with primary breast tumors (short thick arrows) and axillary metastases (long thin arrow). In the late (c) Tc-99m MDP image, only one focus indicating primary breast tumor (short thick arrows) showed increased focal tracer accumulation.
other proposed mechanism of Tc-99m MDP uptake by pathological breast tissue was explained by the pharma- cological receptor theory concerning the enzymes such as acid and alkaline phosphatase. ]l Because of limited clearly visible focal uptake obtained by late Tc-99m MDP imag- ing, the results of our study support nonspecific uptake mechanisms such as increased vascularity and cell wall damage, etc.
It has been demonstrated that size and site may affect the reliability of breast cancer imaging with Tc-99m MDP. 15 In our study, patients showing positive results with both early and late Tc-99m MDP imaging had tumors either greater than 3 cm in size or multifocal tumor settlement. Most of these patients (3/5 patients) also had either bone metastases or skin infiltration. Slow washout from these lesions might reflect relatively more increased cellular metabolism or enlargement of the interstitial space. Further studies are needed in order to identify various tracer kinetics.
The results of this study suggest a role both for Tc-99m MIBI and Tc-99m MDP SMG in the differentiation of malignant and benign breast masses. Apart from the technique employed, the wide variation on scintimam- mography results could be explained by the criteria em- ployed to define abnormality of uptake, and the diagnostic criteria used. And different prevalence of malignancy, inclusion and exclusion criteria for entry into the study
44 Nuri Arslan, Emel Ozturk, Seyfettin llgan, et al Annals of Nuclear Medicine

could influence both mammography and SMG results. In the evaluation of Tc-99m MDP SMG results on a patient by patient basis, the sensitivities obtained by early (92.3%) and late (38.4%) images were similar to the study reported by Piccolo and co-workers. ~5 Demonstration of multi- focality with Tc-99m MDP similar to Tc-99m MIBI indicates that Tc-99m MDP SMG may be useful in patients who are candidates for lumpectomy. In one patient who was diagnosed as having fatty necrosis (1.5 cm) and fibrocystic disease (2 cm) with severe epithelial hyperplasia on histopathological examination (Table 1, Case 18), increased focal tracer accumulation of Tc-99m MIBI was observed in the fibrocystic lesions. On the other hand, none of these lesions showed increased uptake of Tc-99m MDP. Similar to our finding of a false positive fibrocystic lesion, accumulation of Tc-99m MIBI was reported in proliferative and hyper cellular benign breast tumors. 4.s Conversely, a true negative result with Tc-99m MDP in this common benign tumor may be an advantage for Tc-99m MDP SMG. This issue needs further evalua- tion.
Although our patient population is small, we found that early static images with Tc-99m MDP demonstrated equal sensitivity and higher specificity in palpable breast lesions than with early Tc-99m MIBI imaging for the detection of breast malignancy. On the other hand, we obtained superior sensitivity with Tc-99m MIBI than Tc- 99m MDP in nonpalpable malignant tumors. Therefore it is likely that Tc-99m MDP is not as useful as Tc-99m MIBI for the nonpalpable malignant lesions.
In the majority of malignant cases only early Tc-99m MDP images showed focal tracer uptake. Because of limited image quality and a low uptake ratio in soft tissue, late Tc-99m MDP SMG is not diagnostic and reliable alone, and therefore cannot be used to differentiate be- tween benign and malignant breast lesions precisely. Dynamic and early static imaging with Tc-99m MDP were found to be more sensitive than late imaging, and it seems that the best imaging time for Tc-99m MDP is within 30 minutes after the injection. Despite the low sensitivity (23.8%), the excellent overall specificity (100%) of late Tc-99m MDP SMG for lesions was extremely interesting. According to the PPV of each tracer, late imaging with either Tc-99m MIBI (95.0%) or Tc-99m MDP (100%) gave more favorable results than early imaging. Our impression is that late imaging in addition to an early study could be useful in reducing the number of false positive results and may increase the positive predictive value of SMG, but it is obvious that the diag- nostic criteria used for SMG could influence the predic- tive values of the test, especially for Tc-99m MDP. In our study, we accept only focal increased tracer accumulation as a positive study for each tracer.
We report a false positive study for axillary lymph node imaging with Tc-99m MIBI in one patient with reactive lymphoid tissue, but Tc-99m MIBI was found superior to
Tc-99m MDP for the detection of axillary lymphatic involvement, which is consistent with a previous report. 17 Low soft tissue uptake and high lung background activity restrict the use of Tc-99m MDP in axillary lymph node detection, particularly in the early images. Although Piccolo, et al. 15 could not detect an axillary lymph node smaller than 3 cm in size, the smallest lymph node detected in our study was 1.5 cm. According to our study, the poor detection rate for metastatic lymph nodes still remains a major disadvantage with Tc-99m MDP for SMG. On the other hand, the ability to perform whole body bone scan with Tc-99m MDP is an important advan- tage over Tc-99m MIBI SMG.
Tc-99m MIBI is a transport substrate recognized by the multidrug-resistant (MDR) P-glycoprotein (Pgp), and the tumor cell accumulation of the tracer is enhanced by inhibition of the efflux transport function. 18 High levels of Pgp or MDR1 mRNA have been found in both treated and untreated human malignant tumors, including renal, co- lonic, adrenal and breast. 19,2~ Scintimammography with Tc-99m MIBI offers a potential advantage over various other imaging methods in non-invasive functional imag- ing for the presence of Pgp and in the prediction of the re- sponse to chemotherapy, when diminished accumulation of Tc-99m MIBI implies the presence of Pgp-enriched tissue. Tc-99m MIBI also has a potential application in monitoring acquired drug resistance during chemo- therapy.19 Because all positive cases detected with early Tc-99m MIBI imaging showed signs of persistent tracer accumulation on late images, it is highly probable that all of the Tc-99m MIBI positive cases in our study were chemosensitive. Unfortunately, Pgp expressions could not be determined and we do not have enough clinical follow-up data to determine whether or not all of these patients were chemosensitive. Furthermore, quantifica- tion of uptake levels in early and late images and drawing a time-activity curve until two or three hours later after the injection of Tc-99m MIBI could have provided more favorable results on the drug resistance status.
Insufficient sensitivity for the detection of axillary lymph node involvement, and not allowing to predict the presence of MDR gene expression and the response to chemotherapy are the main drawbacks in using Tc-99m MDP for scintimammographic studies, but obtaining high sensitivity and specificity with a combination of early and late images, low cost, easy availability and the possibility of detection of bone metastases seem to make Tc-99m MDP a contributive agent in the evaluation of breast lesions as an alternative to Tc-99m MIBI.
REFERENCES
1. Robert AS. The epidemiology of breast cancer. In Daniel BK, Ellen BM (eds.): Syllabus: A.categorical course in breast imaging. 81 st scientific assembly and annual meeting of the Radiological Society of North America, pp. 7-20,
Vol. 14, No. 1, 2000 Original Article 45

November 26--December 1, 1995. 2. Kopans DB. The positive predictive value of mammogra-
phy. AJR 158: 521, 1992. 3. Savi A, Gemndini P, Zoli P. et al. Biodistribution of Tc-99m
Methoxy-lsobutyl-lsonitrile (MIBI) in Humans. Eur J Nucl Med 15: 597, 1989.
4. Khalkhali I, Cutrone JA, Mena IG, et aI. Scintimam- mography: The complementary role of Tc-99m sestamibi prone breast imaging for the diagnosis of breast carcinoma. Radiology 196: 421, 1995.
5. Taillefer R, Robidoux A, Lambert R, et al. Technetium- 99m-Sestamibi prone scintimammography to detect pri- mary breast cancer and axillary lymph node involvement. J NuclMed36: 1758, 1995.
6. Villanueva-Meyer JV, Leonard MH Jr, Briscoe E, et al. Mammoscintigraphy with Technetium-99m-Sestamibi in Suspected Breast Cancer. J Nucl Med 37: 926, 1996.
7. Palmedo H, Schomburg A, Grunwald F, et al. Technetium- 99m-MIBI scintimammography for suspicious breast le- sions. J Nucl Med 37: 626, 1996.
8. Khalkhali I, Cutrone J, Mena I, et al. Technetium-99m- sestamibi scintimammography of breast lesions: clinical and pathologic follow-up. J Nucl Med 36:1784, 1995.
9. Berg GR, Kalisher L, Osmond JD, et al. 99m-Tc- diphosphonate concentration in primary breast carcinoma. Radiology 109: 393, 1973.
10. Mc Dougall IR, Pistenma DA. Concentration of 99m-Tc- diphosphonate in breast tissue. Radiology 112: 655, 1974.
11. Schmitt GH, Holmes RA, Isitman AT, et al. A proposed mechanism for Tc-99m-labeled polyphosphate and diphosphonate uptake by human breast tissue. Radiology
112: 733, 1974. 12. Bumett KR, Lyons KP, Brown WT. Uptake of osteotropic
radionuclides in the breast. Semin Nucl Med 14: 48, 1984. 13. Hobbs S, Neumann RD, Merino MJ. Gunzenhauser J,
Carrasquillo JA. Localization of Tc-99m-MDP in cysto- sarcoma phyllodes. Clin Nuct Med 17: 58, 1992.
I4. Serafini AN, Raskin MM, Zand LC, et ai. Radionuclide breast scanning in carcinoma of the breast. J Nucl Med 15: 1149, 1974.
15. Piccolo S, Lastoria S, Mainolfi C, et al. Technetium-99m- methylene diphosphonate scintimammography to image primary breast cancer. J Nucl Med 36: 718, 1995.
16. Worsley DF, Lentle BC. Uptake of technetium-99m MDP in primary amyloidosis with a review of the mechanisms of soft-tissue localization of bone seeking radiopharma- ceuticals. J Nucl Med 34: 1612, 1993.
17. Lastoria S, Piccolo S, Varrella P, et al. Comparative results of Tc-99m MIBI and Tc-99m MDP scintimammography in patients with breast abnormalities. J Nucl Med 36 (suppl): 51, 1995. (abstract)
18. Piwnica-Worms D, Chiu ML, Budding M, et al. Functional imaging of multidrug-resistant P-glycoprotein with an organo-technetium complex. Cancer Res 53: 977, 1993.
19. Moretti JL, Caglar M, Duran-Cordobes M, Morere JF, et al. Can nuclear medicine predict response to chemotherapy? Eur J Nucl Med 22: 97, 1995.
20. Vecchio SD, Ciarmiello A, Potena MI, et al. In vivo detec- tion of multidrug-resistant (MDR1) phenotype by tech- netium-99m sestamibi scan in untreated breast cancer patients. Eur J Nucl Med 24: 150, 1997.
46 Nuri Arslan, Emel Ozturk, Seyfettin Ilgan, et al Annals of Nuclear Medicine




















