The American Journal of Medicine
121
The American Journal of Medicine Volume 120, Issue 12, Pages, 1011-1097(December 2007) Editorial 1. Travel Bugs Page 1011 Marcia R. Silver Review 2. Sepsis Pages 1012-1022 James M. O’Brien Jr, Naeem A. Ali, Scott K. Aberegg and Edward Abraham Diagnostic dilemma 3. Hard to Swallow Pages 1023-1025 Madhusudan Grover, Amit Gupta, Dianne P. Wagner and Mark B. Orringer Images in dermatology 4. A Prickly Pair Pages 1026-1027 Mario Vaccaro, Fabrizio Guarneri, Olga Barbuzza, Giuseppe Galtieri and Serafinella P. Cannavò ECG image of the month 5. Spotting a Zebra by Its Stripes Pages 1028-1030 Deepak Asudani, Martin I. Broder and Sivakumar Natanasabapathy Images in radiology 6. A Cut Above Pages 1031-1033 Elisabeth B. Marsh, Grant V. Chow, Gary X. Gong, Darius A. Rastegar and Emmanuel S. Antonarakis
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of The American Journal of Medicine

The American Journal of Medicine
Volume 120, Issue 12, Pages, 1011-1097(December 2007) Editorial
1. Travel Bugs Page 1011 Marcia R. Silver
Review
2. Sepsis Pages 1012-1022 James M. O’Brien Jr, Naeem A. Ali, Scott K. Aberegg and Edward Abraham
Diagnostic dilemma
3. Hard to Swallow Pages 1023-1025 Madhusudan Grover, Amit Gupta, Dianne P. Wagner and Mark B. Orringer
Images in dermatology
4. A Prickly Pair Pages 1026-1027 Mario Vaccaro, Fabrizio Guarneri, Olga Barbuzza, Giuseppe Galtieri and Serafinella P. Cannavò
ECG image of the month
5. Spotting a Zebra by Its Stripes Pages 1028-1030 Deepak Asudani, Martin I. Broder and Sivakumar Natanasabapathy
Images in radiology
6. A Cut Above Pages 1031-1033 Elisabeth B. Marsh, Grant V. Chow, Gary X. Gong, Darius A. Rastegar and Emmanuel S. Antonarakis
Clinical research studies
7. Viral Elimination Reduces Incidence of Malignant Lymphoma in Patients with Hepatitis C Pages 1034-1041 Yusuke Kawamura, Kenji Ikeda, Yasuji Arase, Hiromi Yatsuji, Hitomi Sezaki, Tetsuya Hosaka, Norio Akuta, Masahiro Kobayashi, Fumitaka Suzuki, Yoshiyuki Suzuki and Hiromitsu Kumada
8. Skin Temperature Monitoring Reduces the Risk for Diabetic Foot Ulceration in High-risk Patients Pages 1042-1046 David G. Armstrong, Katherine Holtz-Neiderer, Christopher Wendel, M. Jane Mohler, Heather R. Kimbriel and Lawrence A. Lavery
9. Hospital Discharge against Advice after Myocardial Infarction: Deaths and Readmissions Pages 1047-1053 Kevin Fiscella, Sean Meldrum and Steve Barnett
10. C-Reactive Protein, Inflammatory Conditions, and Cardiovascular Disease Risk Pages 1054-1062 Ravi Dhingra, Philimon Gona, Byung-Ho Nam, Ralph B. D’Agostino Sr, Peter W.F. Wilson, Emelia J. Benjamin and Christopher J. O’Donnell
11. Outcomes in Patients with Chronic Kidney Disease Referred Late to Nephrologists: A Meta-analysis Pages 1063-1070.e2 Micah R. Chan, Aaron T. Dall, Kathlyn E. Fletcher, Na Lu and Hariprasad Trivedi
12. The Characteristics and Prognostic Importance of NT-ProBNP Concentrations in Critically Ill Patients Pages 1071-1077 Keyur B. Shah, Matthew M. Nolan, Krishnamurti Rao, David J. Wang, Robert H. Christenson, Carl B. Shanholtz, Mandeep R. Mehra and Stephen S. Gottlieb
13. Bloodstream Infections in a Geriatric Cohort: A Population-Based Study Pages 1078-1083 Sarah J. Crane, Daniel Z. Uslan and Larry M. Baddour
14. Oxidative Stress and Severe Walking Disability among Older Women Pages 1084-1089 Richard D. Semba, Luigi Ferrucci, Kai Sun, Jeremy Walston, Ravi Varadhan, Jack M. Guralnik and Linda P. Fried
AJM online Review
15. Combining Neuroendocrine Inhibitors in Heart Failure: Reflections on Safety and Efficacy Pages 1090.e1-1090.e8 Hani Jneid, George V. Moukarbel, Bart Dawson, Roger J. Hajjar and Gary S. Francis
Clinical communications to the editor
16. Noninfective Endocarditis in Rheumatoid Arthritis Pages e1-e2 Christine E. DeLong and Carlos A. Roldan
17. Potential Ipriflavone and Warfarin Interaction Page e3 Douglas C. Anderson Jr and Bernard P. Scoggins
18. Pneumococcal Pyomyositis in a Patient Infected with Human Immunodeficiency Virus Pages e5-e6 Soumya Chatterjee and Maysoon Al-Hihi
19. Incidental Administration of Corticosteroid Can Mask the Diagnosis of Tuberculosis Pages e7-e10 Grace Lui, Nelson Lee, Bonnie Wong, David S. Hui, Clive S. Cockram, Ka-tak Wong, Rebecca K. Lam and Gavin M. Joynt
Letters
20. Individualized Treatment of Foramen Ovale and Stroke Page e11 Richard Alan Rison
21. Patent Foramen Ovale and Cryptogenic Stroke Page e13 Jorge R. Kizer
22. The Reply: Page e15 James E. Dalen
23. Exercise, Vitamins and Respiratory Tract Infections Page e17 Harri Hemilä
24. The Reply Page e19 Cornelia M. Ulrich, Jessica Chubak and Anne McTiernan
25. Anti-TNF Antibodies Associated with Different Risk of Latent Tuberculosis Activation Page e21 Michele Hooper and Eric Chi
26. The Reply Page e23 Gökhan M. Mutlu, Amy Bellmeyer, Ece A. Mutlu and Israel Rubinstein
27. Currently Used Medicines for Alzheimer’s Disease Are Not Very Effective Page e25 Steven Brenner
28. The Reply Page e27 Martin R. Farlow
29. Clinical Perspectives of Statin-induced Rhabdomyolysis Page e29 Amer Alshekhlee and Bashar Katirji
30. Testing for Stain-induced Myopathy Page e31 Mark H. Hyman
31. The Reply Page e33 Paul Sydney Phillips
APM perspectives
32. Predicting, Preparing for, and Creating the Future: What Will Happen to Internal Medicine? Pages 1091-1096 Paul A. Hemmer, Sheila T. Costa, Deborah M. DeMarco, Stuart L. Linas, Don C. Glazier and Barbara L. Schuster
Medical humanities perspectives
33. Cicero and Healthy Aging Page 1097 Dean Gianakos
E
TTotdshcd
ltpscpthnfilmj
flbsnwwoImm
iarntwh
0d
The American Journal of Medicine (2007) 120, 1011
DITORIAL
ravel Bugs
foagb3ittatB
lnedoo
rmslhm
R1
2
3
he SARS (severe acute respiratory syndrome) outbreakf 2006 and fears of avian influenza have sensitized manyo the risks of transmission of especially viral illnessesuring air travel. People worry about recirculated air, andome wear masks during trips. On several recent flights Iave noticed another likely means of viral transmission:areless hygiene practices by flight attendants servingrinks.
Using hands I never see washed or cleaned with water-ess cleaners, and after handling money required for some ofhe drinks, the attendants pull stacks of cups out of theirlastic wrappers and handle the cups by the rims whenerving the drinks. Rims are the business ends of theups—to which we apply our mouths when drinking. Wiserractice would be to place the cups upside down and keephem in their plastic sleeves on the cart, pull them outandling only the bottom outside surfaces of the cups, andever touch the rims from which we drink. The containersrom which the drinks are served should always have open-ngs that don’t require handling the area over which theiquid flows when poured (think about how we handleilk-carton-type containers in which some kinds of orange
uice are packaged).Similar practices should apply in restaurants. Americans
y about 650 million domestic air trips annually. The num-er of meals eaten out annually is about 100 billion. Ob-erve how your waiters handle pitchers and drinking glassesext time you eat in a restaurant. Does your waiter hold theater glass by the rim as he serves it? Does he place theater pitcher on the table and lean against it with his handsn the rim of the pitcher while pleasantly chatting with you?f so, he is putting his customers at risk from germs trans-itted from his hands, from other customers, from handledoney, or from his own nose and skin.The message about the critical importance of hand wash-
ng in health care settings may finally be getting enoughttention to turn heads and decrease nosocomial infectionates. The cleaning products industry has developed manyew, quick, easy methods for sanitizing. But my observa-ions suggest that common sense and thoughtful application ofhat we know about disease transmission—not only in the
ospital setting but also in our everyday lives—are lacking.002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.oi:10.1016/j.amjmed.2007.02.030
We practicing physicians need to carry our greater mind-ulness about sensible hygiene from the hospital and clinicut into the community. It is a matter of social responsibilitynd public health. The costs of the common cold and viralastroenteritis in the US are each estimated at about $40illion annually.1,2 In 10% of acute hepatitis C cases and0% of chronic hepatitis cases, a source of infection can’t bedentified.3 When I was in medical school, we were taughthat hepatitis B could be transmitted only parenterally. Athat time, Medicare funded maintenance dialysis; nursesnd doctors worked without gloves and smoked and ate inhe dialysis units—and lots of them developed hepatitis—without having experienced needle-sticks.
“Doctor” means “teacher.” Our children are inclined toearn more from what we do than what we say. That is, weeed to model good behavior. And we need to speak out toducate the community. Good pedagogy and good parentingepend on repetition. We need to be patient and persistent,bservant and concerned—in our communities as well as inur hospitals. We can make an important difference.
As we enter flu season, and with lots of viral upperespiratory infections already affecting many of our com-unities, more attention to common-sense hygiene could
ignificantly limit the spread of such illnesses. As weearned so unpleasantly in the early history of dialysis,and-to-mouth transmission of viruses like hepatitis B alsoight be prevented.
Marcia R. Silver, MD, FACPAssociate Professor of Medicine
Case Western Reserve University atMetroHealth Medical Center
Division of Nephrology and HypertensionCleveland, Ohio
eferences. Fendrick AM, Monto AS, Nightengale B, Sames M. The economic
burden of non-influenza-related viral respiratory tract infection in theUnited States. Arch Intern Med. 2003;163:487-494.
. Koopmans M. Outbreaks of viral gastroenteritis: what’s new in 2004?Curr Opin Infect Dis. 2005;18:295-299.
. National Digestive Diseases Information Clearinghouse. Chronic hep-atitis C: current disease management. Available at: digestive.niddk.nih.gov/ddiseases/pubs/chronichepc/index.htm. Last accessed Septem-
ber 4, 2007.
R
SJa
o
Dsdincsfc
DBrcifiaote
Mi1
0d
The American Journal of Medicine (2007) 120, 1012-1022
EVIEW
epsisames M. O’Brien, Jr, MD, MSc,a Naeem A. Ali, MD,a Scott K. Aberegg, MD, MPH,a Edward Abraham, MDb
Division of Pulmonary, Allergy, Critical Care and Sleep Medicine, The Ohio State University Medical Center, Columbus; bDepartment
f Medicine, UniSaaidabod
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
versity of Alabama at Birmingham School of Medicine, Birmingham
ABSTRACT
epsis is a clinical syndrome defined by a systemic response to infection. With progression to sepsis-ssociated organ failure (ie, severe sepsis) or hypotension (ie, septic shock) mortality increases. Sepsis is
cause of considerable mortality, morbidity, cost, and health care utilization. Abnormalities in thenflammation, immune, coagulation, oxygen delivery, and utilization pathways play a role in organysfunction and death. Early identification of septic patients allows for evidence-based interventions, suchs prompt antibiotics, goal-directed resuscitation, and activated protein C. Appropriate care for sepsis maye more easily delivered by dividing this clinical entity into various stages and with changes in structuresf delivery that extend across traditional boundaries. Better description of the molecular basis of theisease process also will allow for more targeted therapies. © 2007 Elsevier Inc. All rights reserved.
KEYWORDS: Critical care; Multi-organ failure syndrome; Sepsis; Septic shock; Severe sepsis
eoncwfidnstb
BTahoss2rAo
espite the frequency, mortality, morbidity, and cost ofepsis, explicit patient phenotypes are lacking. Sepsis isefined by nonspecific clinical criteria that do not discrim-nate differences in underlying pathophysiological mecha-isms. With recognition of the major public health impli-ations and resource utilization associated with theyndrome, there is a growing awareness of sepsis and a needor an organized approach to caring for affected patients thatrosses traditional structures of care.
EFINING A SYNDROMEefore 1992, the terminology used to define the systemic
esponse to infection varied widely. To standardize nomen-lature, a consensus conference defined sepsis as a systemicnflammatory response syndrome due to presumed or con-rmed infection (Table 1).1 The description of severe sepsisnd septic shock outlined an increasingly severe spectrumf the response to infection. Subsequent studies validatedhat sepsis-induced organ dysfunction and shock are mark-rs of higher mortality.2,3
Requests for reprints should be addressed to James M. O’Brien, Jr.,D, MSc, Division of Pulmonary, Allergy, Critical Care and Sleep Med-
cine, The Ohio State University Medical Center, 201 Davis HLRI, 4732th Avenue, Columbus, OH 43210.
ront matter © 2007 Elsevier Inc. All rights reserved.ed.2007.01.035
In 2001, the participants of a second consensus confer-nce anticipated that the definition of sepsis would evolve tone based on biological markers.4 However, it was recog-ized that the previous definitions had proven useful forlinicians and researchers. Although existing definitionsere overly sensitive and nonspecific, there were not suf-cient data to provide compelling reasons for alternativeefinitions. A categorization inspired by the TNM (tumor,odes, metastasis) staging of cancer was proposed for con-ideration. While this framework might better classify sep-ic patients by pathophysiology and risk of death, it has noteen validated for clinical use.
URDEN OF SEPSIShere are approximately 750,000 cases of sepsis in the USnnually.5,6 Sepsis is involved in approximately 2% of allospitalizations, and there will be more than 1 million casesf sepsis per year in the US by 2020. Hospital mortality forepsis patients ranges from 18% to 30%, depending on theeries. While the mortality rate has decreased over the past0 years, an increase in the number of sepsis cases hasesulted in a tripling of the number of sepsis-related deaths.n estimated 215,000 deaths (9.3% of all deaths) in the USccurred in patients with sepsis. In the US, care for septic
atients results in hospital costs exceeding $16 billion, re-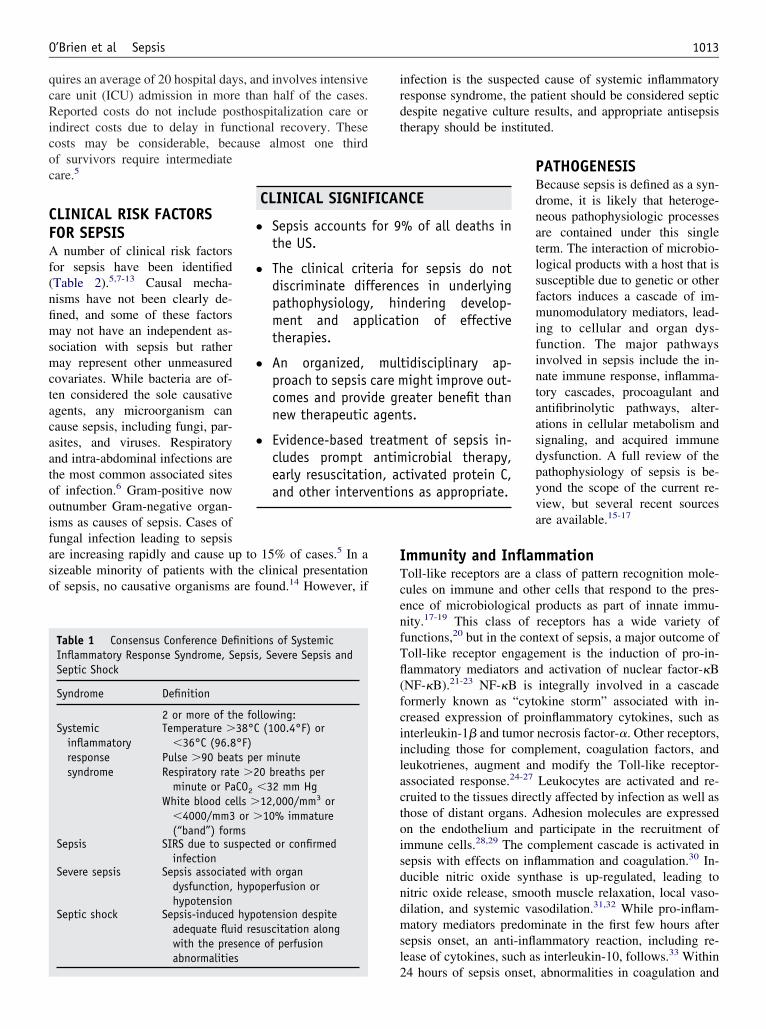
qcRicoc
CFAf(nfimsmctacaatooifaso
irdt
ITcenfTfl(fciilactoisdndmsl
entio
1013O’Brien et al Sepsis
uires an average of 20 hospital days, and involves intensiveare unit (ICU) admission in more than half of the cases.eported costs do not include posthospitalization care or
ndirect costs due to delay in functional recovery. Theseosts may be considerable, because almost one thirdf survivors require intermediateare.5
LINICAL RISK FACTORSOR SEPSIS
number of clinical risk factorsor sepsis have been identifiedTable 2).5,7-13 Causal mecha-isms have not been clearly de-ned, and some of these factorsay not have an independent as-
ociation with sepsis but ratheray represent other unmeasured
ovariates. While bacteria are of-en considered the sole causativegents, any microorganism canause sepsis, including fungi, par-sites, and viruses. Respiratorynd intra-abdominal infections arehe most common associated sitesf infection.6 Gram-positive nowutnumber Gram-negative organ-sms as causes of sepsis. Cases ofungal infection leading to sepsisre increasing rapidly and cause up to 15% of cases.5 In aizeable minority of patients with the clinical presentationf sepsis, no causative organisms are found.14 However, if
Table 1 Consensus Conference Definitions of SystemicInflammatory Response Syndrome, Sepsis, Severe Sepsis andSeptic Shock
Syndrome Definition
2 or more of the following:Systemic
inflammatoryresponsesyndrome
Temperature �38°C (100.4°F) or�36°C (96.8°F)
Pulse �90 beats per minuteRespiratory rate �20 breaths per
minute or PaCO2 �32 mm HgWhite blood cells �12,000/mm3 or
�4000/mm3 or �10% immature(“band”) forms
Sepsis SIRS due to suspected or confirmedinfection
Severe sepsis Sepsis associated with organdysfunction, hypoperfusion orhypotension
Septic shock Sepsis-induced hypotension despiteadequate fluid resuscitation alongwith the presence of perfusionabnormalities
CLINICAL SIGNIF
● Sepsis accountsthe US.
● The clinical critdiscriminate difpathophysiologyment and apptherapies.
● An organized,proach to sepsiscomes and provinew therapeutic
● Evidence-basedcludes promptearly resuscitatioand other interv
2
nfection is the suspected cause of systemic inflammatoryesponse syndrome, the patient should be considered septicespite negative culture results, and appropriate antisepsisherapy should be instituted.
PATHOGENESISBecause sepsis is defined as a syn-drome, it is likely that heteroge-neous pathophysiologic processesare contained under this singleterm. The interaction of microbio-logical products with a host that issusceptible due to genetic or otherfactors induces a cascade of im-munomodulatory mediators, lead-ing to cellular and organ dys-function. The major pathwaysinvolved in sepsis include the in-nate immune response, inflamma-tory cascades, procoagulant andantifibrinolytic pathways, alter-ations in cellular metabolism andsignaling, and acquired immunedysfunction. A full review of thepathophysiology of sepsis is be-yond the scope of the current re-view, but several recent sourcesare available.15-17
mmunity and Inflammationoll-like receptors are a class of pattern recognition mole-ules on immune and other cells that respond to the pres-nce of microbiological products as part of innate immu-ity.17-19 This class of receptors has a wide variety ofunctions,20 but in the context of sepsis, a major outcome ofoll-like receptor engagement is the induction of pro-in-ammatory mediators and activation of nuclear factor-�BNF-�B).21-23 NF-�B is integrally involved in a cascadeormerly known as “cytokine storm” associated with in-reased expression of proinflammatory cytokines, such asnterleukin-1� and tumor necrosis factor-�. Other receptors,ncluding those for complement, coagulation factors, andeukotrienes, augment and modify the Toll-like receptor-ssociated response.24-27 Leukocytes are activated and re-ruited to the tissues directly affected by infection as well ashose of distant organs. Adhesion molecules are expressedn the endothelium and participate in the recruitment ofmmune cells.28,29 The complement cascade is activated inepsis with effects on inflammation and coagulation.30 In-ucible nitric oxide synthase is up-regulated, leading toitric oxide release, smooth muscle relaxation, local vaso-ilation, and systemic vasodilation.31,32 While pro-inflam-atory mediators predominate in the first few hours after
epsis onset, an anti-inflammatory reaction, including re-ease of cytokines, such as interleukin-10, follows.33 Within
CE
% of all deaths in
for sepsis do notces in underlyingndering develop-on of effective
tidisciplinary ap-ight improve out-
eater benefit thants.
ent of sepsis in-icrobial therapy,tivated protein C,
ns as appropriate.
ICAN
for 9
eriaferen, hilicati
mulcare mde gragen
treatmantimn, ac
4 hours of sepsis onset, abnormalities in coagulation and

rm
CPcetttTpScsitchasbeso
CAoddaesu
sottac
ICtccdcacipisiatapn
RStscwb
1014 The American Journal of Medicine, Vol 120, No 12, December 2007
elease of proinflammatory late mediators, such as high-obility group box-1, are found.17,34
oagulation Abnormalitiesro-inflammatory cytokines and complement activate theoagulation cascade in septic patients.35,36 Tissue factor isxpressed on immune and endothelial cells, contributing tohe activation of the extrinsic coagulation system pathwayhat results in conversion of factor VII to an active pro-ease.37 Proinflammatory molecules and the interaction ofoll-like receptors with microbial products up-regulate ex-ression of plasminogen activator inhibitor-1 (PAI-1).38-40
uch events produce an initial activation of endothelialells, coagulation, and fibrinolysis followed by a prolongeduppression of fibrinolysis as PAI-1 levels increase. Anmbalance toward a procoagulant state results, especially inhe micro-circulation.15,41,42 Decreases in endogenous anti-oagulants, including protein C, tissue factor pathway in-ibitor, and antithrombin, coupled with elevated circulatingnd tissue levels of PAI-1, are observed in the majority ofeptic patients.15 Components of the coagulation and fi-rinolytic system, particularly PAI-1 and urokinase, arelevated for prolonged periods in septic patients and haveubstantial proinflammatory effects that may contribute torgan dysfunction.43,44
ellular Metabolismbnormalities in lipid, carbohydrate, and protein metab-lism occur in septic patients.45-48 Inadequate oxygenelivery due to alterations in capillary blood flow andecreased cardiac output may contribute to increasednaerobic metabolism and lactate production.49 However,ven in the presence of adequate tissue oxygen delivery,epsis may cause impaired cellular oxygen extraction and
Table 2 Reported Association of Clinical Risk Factors with Sep
Risk Factor Description
DemographicsAge7 Greater than 65 years vs �6Race5 African American vs Caucasi
Other non-Caucasian race vsSex5 Male vs. female
Co-morbiditiesHIV10 HIV vs no HIVCancer8 Any cancer vs no cancer
Solid tumor vs no cancerHematologic cancer vs no c
Cirrhosis9 Cirrhosis vs no cirrhosisAlcohol dependence13 Ongoing alcoholism or alcoh
Complications of medical careVenous access devices12 Central venous catheter vs pTransfusion11 Packed red cell transfusion
95% CI � 95% confidence interval; HIV � human immunodeficiency*Relative risk.†Odds ratio.
tilization due to mitochondrial dysfunction. Sepsis-as- t
ociated inhibition of cellular oxygen utilization andther metabolic pathways may lead to decreased produc-ion of oxygen radicals by some populations of dysfunc-ional cells.50 This cellular “hibernation” may explain thebsence of cell necrosis when failing organs from fatalases of sepsis are examined.51
mmunosuppression and Depletionirculating monocytes, but not neutrophils, from septic pa-
ients are hyporesponsive to proinflammatory stimuli whenompared with normal cells.52 Additionally, there is in-reased apoptosis of circulating lymphocyte and splenicendritic cells in patients dying of severe sepsis.53 This mayontribute to mortality because inhibition of lymphocytepoptosis through over-expression of anti-apoptotic mole-ules, such as Bcl-2, results in improved survival in exper-mental models.54,55 Enhanced apoptosis of lymphoid cellopulations, as well as diminished monocyte response, mayncrease the risk of nosocomial infections, a cause of con-iderable mortality in critically ill patients who survive theirnitial septic episode. Enhanced sepsis-induced apoptosislso may play a role in the loss of cells in the gastrointes-inal and respiratory tract.56,57 While apoptosis may bedaptive to repair damaged tissues, increased cellular apo-tosis also may contribute to organ dysfunction and immu-osuppression in sepsis.53
ECOGNITION AND TREATMENTeptic patients present with a variety of signs and symp-
oms, and recognition requires consideration of the diagno-is. Sepsis may occur in ambulatory offices, at extendedare facilities, in emergency departments, on the generalard, or in the ICU. Structures and processes of care shoulde considered that extend beyond traditional borders within
d Severe Sepsis
Odds or Risk (95% CI)
s 13.1 (12.6 to 13.6)*1.9 (1.8 to 2.0)*
sian 1.9 (1.8 to 2.0)*1.3 (1.2 to 1.3)*
5.1 (1.2 to 21.2)†2.8 (2.8 to 2.8)*1.8 (1.8 to 18.2)*
15.7 (15.6 to 15.9)*2.6 (1.9 to 3.3)*
hdrawal vs no alcohol dependence 1.5 (1.2 to 1.9)
ral venous catheter 64 (54 to 76)*ransfusion 6.0 (4.0 to 9.2)†
sis an
5 yearanCauca
ancer
ol wit
eriphevs no t
virus.
he health care continuum. As is encouraged in the care of
piEdFbci
RTmpasf
FtwIcRcfcAS recomba t.
1015O’Brien et al Sepsis
atients with myocardial infarction, care may be dividednto different stages based on effectiveness and urgency.arly emphasis in myocardial infarction patients is on hemo-ynamic stabilization and opening of the occluded vessel.ocus then shifts to secondary prevention, recovery, and reha-ilitation. Various studies suggest that an approach to sepsisentered on a similar organized approach to septic patients,
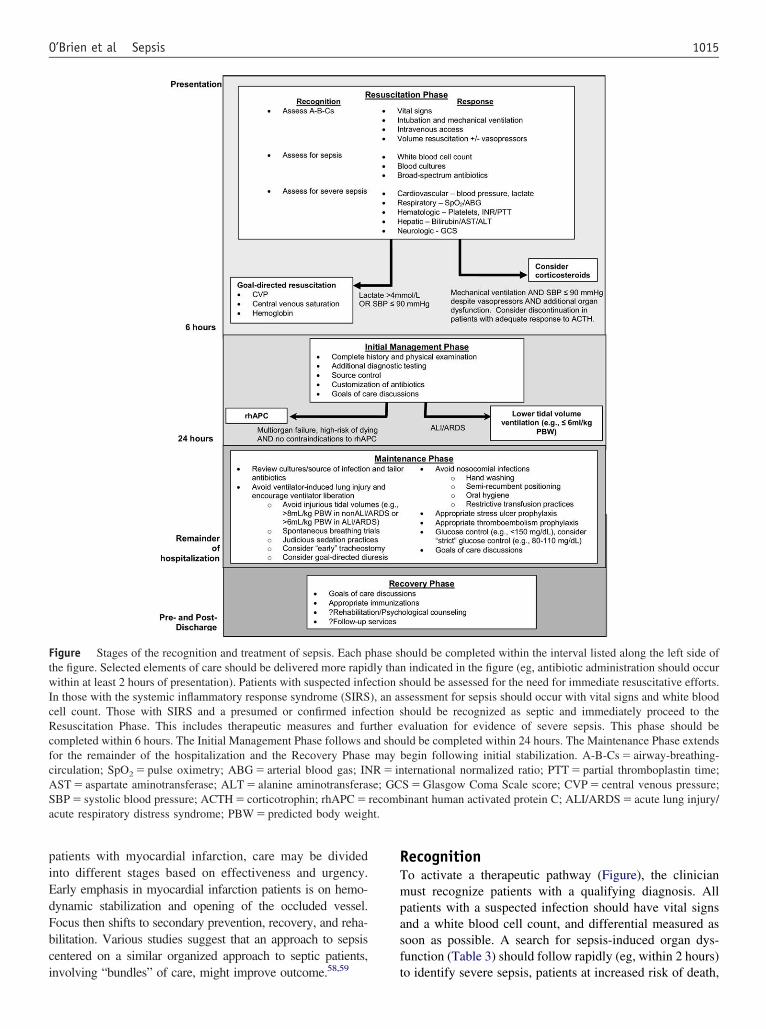
igure Stages of the recognition and treatment of sepsis. Each phe figure. Selected elements of care should be delivered more rapidithin at least 2 hours of presentation). Patients with suspected infe
n those with the systemic inflammatory response syndrome (SIRSell count. Those with SIRS and a presumed or confirmed infeesuscitation Phase. This includes therapeutic measures and fuompleted within 6 hours. The Initial Management Phase follows aor the remainder of the hospitalization and the Recovery Phaseirculation; SpO2 � pulse oximetry; ABG � arterial blood gas; INST � aspartate aminotransferase; ALT � alanine aminotransferaBP � systolic blood pressure; ACTH � corticotrophin; rhAPC �cute respiratory distress syndrome; PBW � predicted body weigh
nvolving “bundles” of care, might improve outcome.58,59 t
ecognitiono activate a therapeutic pathway (Figure), the clinicianust recognize patients with a qualifying diagnosis. All
atients with a suspected infection should have vital signsnd a white blood cell count, and differential measured asoon as possible. A search for sepsis-induced organ dys-unction (Table 3) should follow rapidly (eg, within 2 hours)
ould be completed within the interval listed along the left side ofindicated in the figure (eg, antibiotic administration should occur
hould be assessed for the need for immediate resuscitative efforts.sessment for sepsis should occur with vital signs and white bloodhould be recognized as septic and immediately proceed to thevaluation for evidence of severe sepsis. This phase should be
uld be completed within 24 hours. The Maintenance Phase extendsbegin following initial stabilization. A-B-Cs � airway-breathing-ternational normalized ratio; PTT � partial thromboplastin time;S � Glasgow Coma Scale score; CVP � central venous pressure;inant human activated protein C; ALI/ARDS � acute lung injury/
hase shly thanction s), an asction srther end sho
mayR � in
se; GC
o identify severe sepsis, patients at increased risk of death,

asfao
RTpatacaDsbga
wehomdmttpcsashvrgrc
tlmttrhabpt
cctlpsqalwnmotstaoa
IFtlCi
1016 The American Journal of Medicine, Vol 120, No 12, December 2007
nd candidates for specific therapies. Initial treatmenthould proceed in concert with evaluation for organ dys-unction. Because the incidence of sepsis in patients is highnd specific treatment exists, it is favorable to err on the sidef initial over-diagnosis.
esuscitation Phasehe earliest goals are to assess and secure the airway, torovide adequate volume resuscitation, and to administerppropriate antimicrobial therapy. In patients with respira-ory or hemodynamic compromise, life-sustaining effortsre the first priority. In all patients, obtaining appropriateultures and immediate administration of broad-spectrumntimicrobials should be included in the initial approach.elayed administration of appropriate antimicrobials is as-
ociated with poorer outcomes.60 Choices of agents shoulde guided by suspected site of infection, anticipated patho-ens, penetration of adequate levels into infected tissues,nd local patterns of antibiotic susceptibility (Table 4).
Early intervention is particularly beneficial for patientsith septic shock or evidence of organ hypoperfusion (eg,
levated serum lactate levels, diminished urine output, orypoxemia). Intubation and mechanical ventilation is rec-mmended for patients with respiratory compromise toaintain oxygenation and acid-base status, and to mitigate
iversion of the compromised circulation to the respiratoryuscles. The value of rapid resuscitation directed by objec-
ive measures is illustrated by reduced observed mortality inhe experimental group of a study among septic patientsresenting to an emergency department.61 The protocol in-luded continuous measurement of central venous oxygenaturation as a measure of oxygen delivery-extraction bal-nce, and used fluids, vasopressors, red blood cell transfu-ions, and inotrope therapy for 6 hours after identification ofypotension (systolic blood pressure �90 mm Hg) or ele-ated serum lactate (�4 mmol/L). Other studies of earlyesuscitative interventions support the findings of this sin-le-center study.62,63 The superiority of a particular protocolemains to be established and is being examined in a multi-
Table 3 Measures of Sepsis-induced Organ Dysfunction
Organ System Measures of Dysfunction
Cardiovascular Low systolic arterial blood pressure, low mlow cardiac output, low central or mixed
Respiratory Need for mechanical ventilation, PaO2/FiO2
pressure, low static complianceCoagulation Elevated INR, elevated PTT, elevated D-dimRenal Low urine output, elevated creatinine, neeHepatic Elevated transaminases, elevated bilirubinNeurologic Decreased mental status (eg, low Glasgow
the ICU)Metabolic acidosis Elevated lactate, elevated base deficit, lowGastrointestinal Ilieus
PaO2 � Partial pressure of oxygen in arterial blood; FiO2 � inspirthromboplastin time; ICU � intensive care unit.
entered National Institutes of Health-funded study. s
A central venous catheter is often necessary for diagnos-ic and therapeutic purposes. Subclavian and internal jugu-ar catheters provide advantages over femoral catheters inonitoring capabilities and in reducing infectious and
hrombotic complications.64 There are few data to supporthe superiority of use of crystalloid or colloid solutions foresuscitation.65 Different catecholamine vasopressor agentsave not been compared in large studies, but observationalnd hemodynamic studies suggest that norepinephrine maye preferred.66,67 Vasopressin, a noncatecholamine vaso-ressor, currently lacks compelling data to endorse its rou-ine use.15
Routine corticosteroid replacement in septic shock forritical illness-related corticosteroid insufficiency remainsontroversial. An inadequate response to synthetic cortico-rophin (ACTH; defined as �9 mg/dL increase in cortisolevel 1 hour after administration of 250 �g ACTH) isresent in the majority of patients with septic shock.68 Foreptic patients with hypotension unresponsive to fluids, re-uirement for mechanical ventilation, and the presence of andditional sepsis-associated organ failure, administration ofow doses of corticosteroids improved mortality in patientsith inadequate responses to ACTH but not in those withormal responses.69 In this study, the average time to treat-ent was approximately 7 hours after shock onset. Because
f difficulties in determining ACTH responsiveness withinhis interval, a reasonable course is to perform an ACTHtimulation test and start corticosteroid treatment only inhose with vasopressor-dependent shock, respiratory failure,nd an additional organ failure as soon as possible afternset. Corticosteroids can be discontinued in patients withn adequate response to ACTH.
nitial Management Phaseollowing the resuscitation phase of sepsis, treatment shifts
o consolidation of care. Further diagnostic testing to detectikely pathogens and sites of infection may be appropriate.ontrol of the source of infection, including the removal of
ndwelling catheters, drainage of collections of pus, and
ood pressure, mottled extremities, delayed capillary refill time,s oxygen saturations�300, chest radiograph abnormalities, high plateau airway
platelets, disseminated intravascular coagulationenal replacement therapy
cale), delirium (eg, positive Confusion Assessment Method for
tion of oxygen; INR � International Normalized Ratio; PTT � partial
ean blvenouratio
er, lowd for r
coma s
pH
ed frac
urgical debridement, may be needed. Discussions about
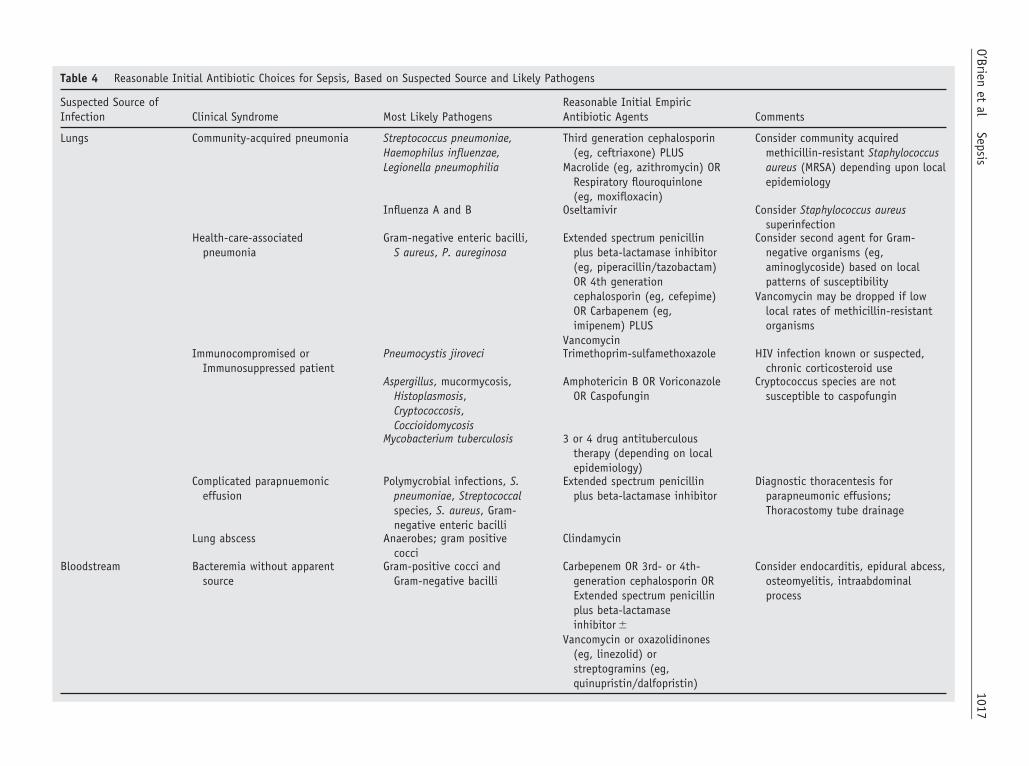
Table 4 Reasonable Initial Antibiotic Choices for Sepsis, Based on Suspected Source and Likely Pathogens
Suspected Source ofInfection Clinical Syndrome Most Likely Pathogens
Reasonable Initial EmpiricAntibiotic Agents Comments
Lungs Community-acquired pneumonia Streptococcus pneumoniae,Haemophilus influenzae,Legionella pneumophilia
Third generation cephalosporin(eg, ceftriaxone) PLUS
Macrolide (eg, azithromycin) ORRespiratory flouroquinlone(eg, moxifloxacin)
Consider community acquiredmethicillin-resistant Staphylococcusaureus (MRSA) depending upon localepidemiology
Influenza A and B Oseltamivir Consider Staphylococcus aureussuperinfection
Health-care-associatedpneumonia
Gram-negative enteric bacilli,S aureus, P. aureginosa
Extended spectrum penicillinplus beta-lactamase inhibitor(eg, piperacillin/tazobactam)OR 4th generationcephalosporin (eg, cefepime)OR Carbapenem (eg,imipenem) PLUS
Vancomycin
Consider second agent for Gram-negative organisms (eg,aminoglycoside) based on localpatterns of susceptibility
Vancomycin may be dropped if lowlocal rates of methicillin-resistantorganisms
Immunocompromised orImmunosuppressed patient
Pneumocystis jiroveci Trimethoprim-sulfamethoxazole HIV infection known or suspected,chronic corticosteroid use
Aspergillus, mucormycosis,Histoplasmosis,Cryptococcosis,Coccioidomycosis
Amphotericin B OR VoriconazoleOR Caspofungin
Cryptococcus species are notsusceptible to caspofungin
Mycobacterium tuberculosis 3 or 4 drug antituberculoustherapy (depending on localepidemiology)
Complicated parapnuemoniceffusion
Polymycrobial infections, S.pneumoniae, Streptococcalspecies, S. aureus, Gram-negative enteric bacilli
Extended spectrum penicillinplus beta-lactamase inhibitor
Diagnostic thoracentesis forparapneumonic effusions;Thoracostomy tube drainage
Lung abscess Anaerobes; gram positivecocci
Clindamycin
Bloodstream Bacteremia without apparentsource
Gram-positive cocci andGram-negative bacilli
Carbepenem OR 3rd- or 4th-generation cephalosporin ORExtended spectrum penicillinplus beta-lactamaseinhibitor �
Vancomycin or oxazolidinones(eg, linezolid) orstreptogramins (eg,quinupristin/dalfopristin)
Consider endocarditis, epidural abcess,osteomyelitis, intraabdominalprocess
1017O’Brien
etal
Sepsis
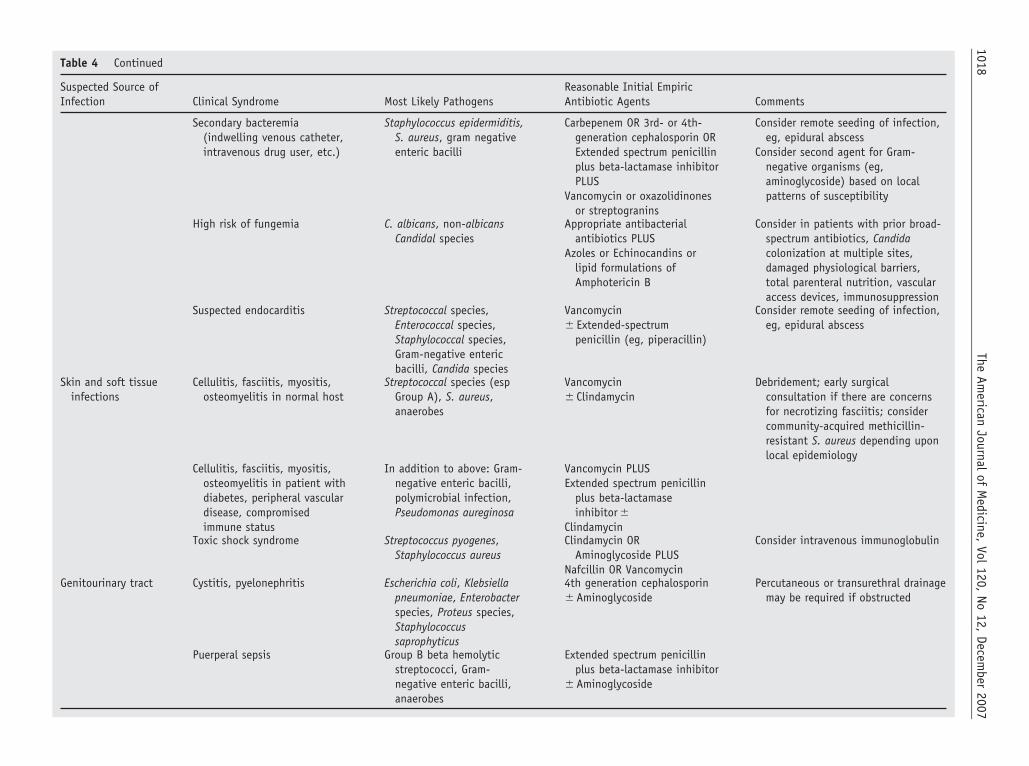
Table 4 Continued
Suspected Source ofInfection Clinical Syndrome Most Likely Pathogens
Reasonable Initial EmpiricAntibiotic Agents Comments
Secondary bacteremia(indwelling venous catheter,intravenous drug user, etc.)
Staphylococcus epidermiditis,S. aureus, gram negativeenteric bacilli
Carbepenem OR 3rd- or 4th-generation cephalosporin ORExtended spectrum penicillinplus beta-lactamase inhibitorPLUS
Vancomycin or oxazolidinonesor streptogranins
Consider remote seeding of infection,eg, epidural abscess
Consider second agent for Gram-negative organisms (eg,aminoglycoside) based on localpatterns of susceptibility
High risk of fungemia C. albicans, non-albicansCandidal species
Appropriate antibacterialantibiotics PLUS
Azoles or Echinocandins orlipid formulations ofAmphotericin B
Consider in patients with prior broad-spectrum antibiotics, Candidacolonization at multiple sites,damaged physiological barriers,total parenteral nutrition, vascularaccess devices, immunosuppression
Suspected endocarditis Streptococcal species,Enterococcal species,Staphylococcal species,Gram-negative entericbacilli, Candida species
Vancomycin� Extended-spectrum
penicillin (eg, piperacillin)
Consider remote seeding of infection,eg, epidural abscess
Skin and soft tissueinfections
Cellulitis, fasciitis, myositis,osteomyelitis in normal host
Streptococcal species (espGroup A), S. aureus,anaerobes
Vancomycin� Clindamycin
Debridement; early surgicalconsultation if there are concernsfor necrotizing fasciitis; considercommunity-acquired methicillin-resistant S. aureus depending uponlocal epidemiology
Cellulitis, fasciitis, myositis,osteomyelitis in patient withdiabetes, peripheral vasculardisease, compromisedimmune status
In addition to above: Gram-negative enteric bacilli,polymicrobial infection,Pseudomonas aureginosa
Vancomycin PLUSExtended spectrum penicillin
plus beta-lactamaseinhibitor �
ClindamycinToxic shock syndrome Streptococcus pyogenes,
Staphylococcus aureusClindamycin OR
Aminoglycoside PLUSNafcillin OR Vancomycin
Consider intravenous immunoglobulin
Genitourinary tract Cystitis, pyelonephritis Escherichia coli, Klebsiellapneumoniae, Enterobacterspecies, Proteus species,Staphylococcussaprophyticus
4th generation cephalosporin� Aminoglycoside
Percutaneous or transurethral drainagemay be required if obstructed
Puerperal sepsis Group B beta hemolyticstreptococci, Gram-negative enteric bacilli,anaerobes
Extended spectrum penicillinplus beta-lactamase inhibitor
� Aminoglycoside
1018The
American
Journalof
Medicine,
Vol120,
No12,
December
2007
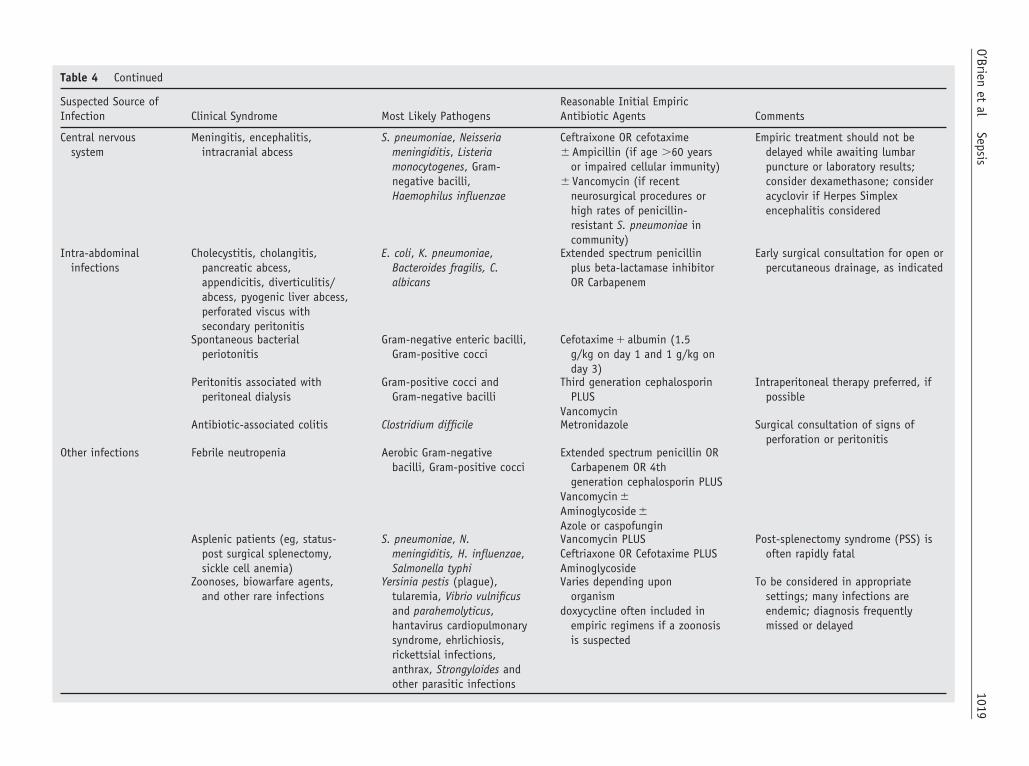
Table 4 Continued
Suspected Source ofInfection Clinical Syndrome Most Likely Pathogens
Reasonable Initial EmpiricAntibiotic Agents Comments
Central nervoussystem
Meningitis, encephalitis,intracranial abcess
S. pneumoniae, Neisseriameningiditis, Listeriamonocytogenes, Gram-negative bacilli,Haemophilus influenzae
Ceftraixone OR cefotaxime� Ampicillin (if age �60 years
or impaired cellular immunity)� Vancomycin (if recent
neurosurgical procedures orhigh rates of penicillin-resistant S. pneumoniae incommunity)
Empiric treatment should not bedelayed while awaiting lumbarpuncture or laboratory results;consider dexamethasone; consideracyclovir if Herpes Simplexencephalitis considered
Intra-abdominalinfections
Cholecystitis, cholangitis,pancreatic abcess,appendicitis, diverticulitis/abcess, pyogenic liver abcess,perforated viscus withsecondary peritonitis
E. coli, K. pneumoniae,Bacteroides fragilis, C.albicans
Extended spectrum penicillinplus beta-lactamase inhibitorOR Carbapenem
Early surgical consultation for open orpercutaneous drainage, as indicated
Spontaneous bacterialperiotonitis
Gram-negative enteric bacilli,Gram-positive cocci
Cefotaxime � albumin (1.5g/kg on day 1 and 1 g/kg onday 3)
Peritonitis associated withperitoneal dialysis
Gram-positive cocci andGram-negative bacilli
Third generation cephalosporinPLUS
Vancomycin
Intraperitoneal therapy preferred, ifpossible
Antibiotic-associated colitis Clostridium difficile Metronidazole Surgical consultation of signs ofperforation or peritonitis
Other infections Febrile neutropenia Aerobic Gram-negativebacilli, Gram-positive cocci
Extended spectrum penicillin ORCarbapenem OR 4thgeneration cephalosporin PLUS
Vancomycin �Aminoglycoside �Azole or caspofungin
Asplenic patients (eg, status-post surgical splenectomy,sickle cell anemia)
S. pneumoniae, N.meningiditis, H. influenzae,Salmonella typhi
Vancomycin PLUSCeftriaxone OR Cefotaxime PLUSAminoglycoside
Post-splenectomy syndrome (PSS) isoften rapidly fatal
Zoonoses, biowarfare agents,and other rare infections
Yersinia pestis (plague),tularemia, Vibrio vulnificusand parahemolyticus,hantavirus cardiopulmonarysyndrome, ehrlichiosis,rickettsial infections,anthrax, Strongyloides andother parasitic infections
Varies depending uponorganism
doxycycline often included inempiric regimens if a zoonosisis suspected
To be considered in appropriatesettings; many infections areendemic; diagnosis frequentlymissed or delayed
1019O’Brien
etal
Sepsis
lfi
t((teblpdadds
dvnptstncdsspp
MFtmciptcntisircbahctpt
ivvivatppei
RMcisSao
CSstbhbodtvb
frribp
R
1020 The American Journal of Medicine, Vol 120, No 12, December 2007
ikely prognosis and goals of care with the patient andamily are appropriate considering the considerable mortal-ty and morbidity attributable to sepsis.
For severe sepsis patients at a high risk of death, such ashose with multiorgan failure or elevated severity of illnesseg, APACHE II score �25), drotrecogin alfa (activated)recombinant activated protein C) should be administered ifhere are no contraindications.70 The most significant sideffect of this agent is bleeding. Patients at greatest risk ofleeding are those with severe thrombocytopenia, coagu-opathy, or an increased risk of intracranial bleeding. Foratients with high risk of death and without such contrain-ications, the risk of bleeding is counterbalanced by anbsolute reduction in mortality. Drotrecogin alfa (activated)oes not appear to be effective in patients at a low risk ofeath and may be harmful in those with recent surgery andingle organ dysfunction.71
A considerable number of severe sepsis patients willevelop acute lung injury. In these patients, lower tidalolumes (eg, 6 mL/kg predicted body weight) and mainte-ance of plateau airway pressure below 30 cmH2O im-roves mortality and organ failure, compared with tradi-ional larger tidal volumes.72 For mechanically ventilatedeptic patients without lung injury, lower tidal volume ven-ilation may prevent its development.73 Recent studies haveot shown benefit from the routine use of pulmonary arteryatheters in patients with acute lung injury,74 but haveemonstrated diminished time on the ventilator with a con-ervative fluid strategy (eg, keeping central venous pres-ures �4 mm Hg).75 Such a strategy was restricted toatients without shock or other signs of inadequate organerfusion.
aintenance Phaseor septic patients surviving 24 hours, attention should turn
o preventing nosocomial complications and restoring pre-orbid functioning. As cultures are available, antimicrobial
hoices, doses, and durations of therapy should be custom-zed. Hyperglycemia is a common occurrence in critically illatients and, in select populations, particularly postopera-ive patients, strict control (eg, maintenance of serum glu-ose at 80-110 mg/dL) may provide benefit by reducingosocomial infections and improving survival.76 The effec-iveness of such therapy in patients with sepsis or in medicalntensive care units is not proven and risks of hypoglycemiahould be carefully considered.77 Anemia occurs frequentlyn critically ill patients, but transfusions (after the initialesuscitation phase) may be harmful, particularly by in-reasing the risk of nosocomial infections.78 Among non-leeding patients, hemoglobin values as low as 7 mg/dL arecceptable, and there is no apparent benefit for maintainingigher levels with transfusion.79 Avoidance of nosocomialomplications also may be reduced in selected patients withhe use of semi-recumbent positioning,80 stress ulcer pro-hylaxis,81 thromboembolism prophylaxis,82 and close at-
ention to hand-washing.83As the patient stabilizes, de-escalation of invasive monitor-ng and life support is indicated. Liberation from mechanicalentilation at the earliest appropriate time reduces the risk ofentilator-associated complications. Judicious sedation, includ-ng daily “holidays” from sedatives, can reduce the number ofentilator and ICU days.84 Assessment of readiness for liber-tion from the ventilator with spontaneous breathing trialsriggered by protocols based on patient recovery, rather thanhysician discretion, reduces mechanical ventilation time.85 Inatients expected to require prolonged mechanical ventilation,arly tracheostomy may reduce mortality, length of stay, andnfectious complications.86
ecovery Phaseortality for sepsis survivors is higher than age-matched
ontrols for at least 5 years.87 The mechanism of this effects unknown. Additionally, survivors of critical illness mayuffer considerable physical and psychological morbidity.88
mall interventional studies utilizing ICU follow-up clinicsnd patient education initiatives following critical care dem-nstrate variable results.89,90
ONCLUSIONepsis is a major cause of mortality and morbidity, and is aource of substantial health care costs. The current defini-ion provides easy identification of affected patients but,ecause of the heterogeneity of patients included, may haveampered the ability to develop effective therapies and toetter classify disease. Other areas of medicine, such asncology, have learned the value in greater description ofisease based on biological mechanisms for prognostic andherapeutic purposes.91-93 It is likely that therapeutic ad-ances in preventing and treating sepsis will be facilitatedy such an approach.94
Sepsis is a condition that involves health care providersrom many disciplines and in a variety of settings. As aesult, organization of therapeutic efforts for these patientsequires coordination across traditional boundaries of med-cine. A concerted, multidisciplinary approach to sepsisased on patient needs, rather than physical location, mayrovide greater benefit than new therapeutic agents.
eferences1. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ
failure and guidelines for the use of innovative therapies in sepsis. TheACCP/SCCM Consensus Conference Committee. American Collegeof Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101(6):1644-1655.
2. Marshall JC, Cook DJ, Christou NV, et al. Multiple organ dysfunctionscore: a reliable descriptor of a complex clinical outcome. Crit CareMed. 1995;23(10):1638-1652.
3. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-relatedOrgan Failure Assessment) score to describe organ dysfunction/fail-ure. On behalf of the Working Group on Sepsis-Related Problems ofthe European Society of Intensive Care Medicine. Intensive Care Med.1996;22(7):707-710.
4. Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med.
2003;31(4):1250-1256.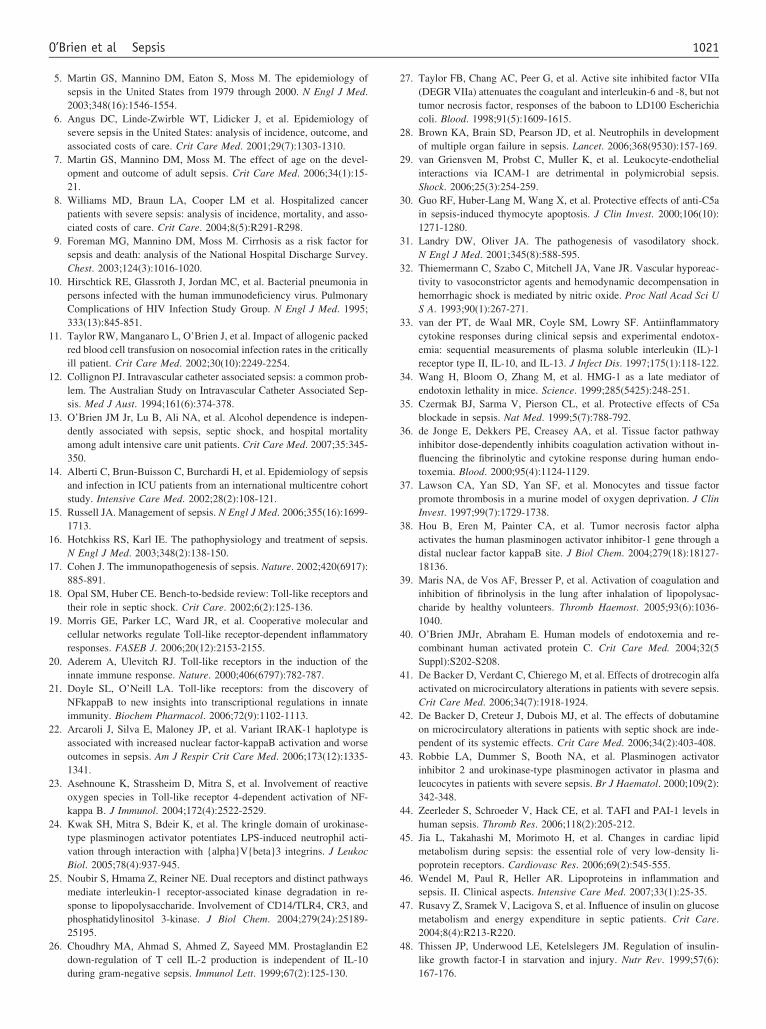
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
1021O’Brien et al Sepsis
5. Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology ofsepsis in the United States from 1979 through 2000. N Engl J Med.2003;348(16):1546-1554.
6. Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology ofsevere sepsis in the United States: analysis of incidence, outcome, andassociated costs of care. Crit Care Med. 2001;29(7):1303-1310.
7. Martin GS, Mannino DM, Moss M. The effect of age on the devel-opment and outcome of adult sepsis. Crit Care Med. 2006;34(1):15-21.
8. Williams MD, Braun LA, Cooper LM et al. Hospitalized cancerpatients with severe sepsis: analysis of incidence, mortality, and asso-ciated costs of care. Crit Care. 2004;8(5):R291-R298.
9. Foreman MG, Mannino DM, Moss M. Cirrhosis as a risk factor forsepsis and death: analysis of the National Hospital Discharge Survey.Chest. 2003;124(3):1016-1020.
0. Hirschtick RE, Glassroth J, Jordan MC, et al. Bacterial pneumonia inpersons infected with the human immunodeficiency virus. PulmonaryComplications of HIV Infection Study Group. N Engl J Med. 1995;333(13):845-851.
1. Taylor RW, Manganaro L, O’Brien J, et al. Impact of allogenic packedred blood cell transfusion on nosocomial infection rates in the criticallyill patient. Crit Care Med. 2002;30(10):2249-2254.
2. Collignon PJ. Intravascular catheter associated sepsis: a common prob-lem. The Australian Study on Intravascular Catheter Associated Sep-sis. Med J Aust. 1994;161(6):374-378.
3. O’Brien JM Jr, Lu B, Ali NA, et al. Alcohol dependence is indepen-dently associated with sepsis, septic shock, and hospital mortalityamong adult intensive care unit patients. Crit Care Med. 2007;35:345-350.
4. Alberti C, Brun-Buisson C, Burchardi H, et al. Epidemiology of sepsisand infection in ICU patients from an international multicentre cohortstudy. Intensive Care Med. 2002;28(2):108-121.
5. Russell JA. Management of sepsis. N Engl J Med. 2006;355(16):1699-1713.
6. Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis.N Engl J Med. 2003;348(2):138-150.
7. Cohen J. The immunopathogenesis of sepsis. Nature. 2002;420(6917):885-891.
8. Opal SM, Huber CE. Bench-to-bedside review: Toll-like receptors andtheir role in septic shock. Crit Care. 2002;6(2):125-136.
9. Morris GE, Parker LC, Ward JR, et al. Cooperative molecular andcellular networks regulate Toll-like receptor-dependent inflammatoryresponses. FASEB J. 2006;20(12):2153-2155.
0. Aderem A, Ulevitch RJ. Toll-like receptors in the induction of theinnate immune response. Nature. 2000;406(6797):782-787.
1. Doyle SL, O’Neill LA. Toll-like receptors: from the discovery ofNFkappaB to new insights into transcriptional regulations in innateimmunity. Biochem Pharmacol. 2006;72(9):1102-1113.
2. Arcaroli J, Silva E, Maloney JP, et al. Variant IRAK-1 haplotype isassociated with increased nuclear factor-kappaB activation and worseoutcomes in sepsis. Am J Respir Crit Care Med. 2006;173(12):1335-1341.
3. Asehnoune K, Strassheim D, Mitra S, et al. Involvement of reactiveoxygen species in Toll-like receptor 4-dependent activation of NF-kappa B. J Immunol. 2004;172(4):2522-2529.
4. Kwak SH, Mitra S, Bdeir K, et al. The kringle domain of urokinase-type plasminogen activator potentiates LPS-induced neutrophil acti-vation through interaction with {alpha}V{beta}3 integrins. J LeukocBiol. 2005;78(4):937-945.
5. Noubir S, Hmama Z, Reiner NE. Dual receptors and distinct pathwaysmediate interleukin-1 receptor-associated kinase degradation in re-sponse to lipopolysaccharide. Involvement of CD14/TLR4, CR3, andphosphatidylinositol 3-kinase. J Biol Chem. 2004;279(24):25189-25195.
6. Choudhry MA, Ahmad S, Ahmed Z, Sayeed MM. Prostaglandin E2down-regulation of T cell IL-2 production is independent of IL-10
during gram-negative sepsis. Immunol Lett. 1999;67(2):125-130.7. Taylor FB, Chang AC, Peer G, et al. Active site inhibited factor VIIa(DEGR VIIa) attenuates the coagulant and interleukin-6 and -8, but nottumor necrosis factor, responses of the baboon to LD100 Escherichiacoli. Blood. 1998;91(5):1609-1615.
8. Brown KA, Brain SD, Pearson JD, et al. Neutrophils in developmentof multiple organ failure in sepsis. Lancet. 2006;368(9530):157-169.
9. van Griensven M, Probst C, Muller K, et al. Leukocyte-endothelialinteractions via ICAM-1 are detrimental in polymicrobial sepsis.Shock. 2006;25(3):254-259.
0. Guo RF, Huber-Lang M, Wang X, et al. Protective effects of anti-C5ain sepsis-induced thymocyte apoptosis. J Clin Invest. 2000;106(10):1271-1280.
1. Landry DW, Oliver JA. The pathogenesis of vasodilatory shock.N Engl J Med. 2001;345(8):588-595.
2. Thiemermann C, Szabo C, Mitchell JA, Vane JR. Vascular hyporeac-tivity to vasoconstrictor agents and hemodynamic decompensation inhemorrhagic shock is mediated by nitric oxide. Proc Natl Acad Sci US A. 1993;90(1):267-271.
3. van der PT, de Waal MR, Coyle SM, Lowry SF. Antiinflammatorycytokine responses during clinical sepsis and experimental endotox-emia: sequential measurements of plasma soluble interleukin (IL)-1receptor type II, IL-10, and IL-13. J Infect Dis. 1997;175(1):118-122.
4. Wang H, Bloom O, Zhang M, et al. HMG-1 as a late mediator ofendotoxin lethality in mice. Science. 1999;285(5425):248-251.
5. Czermak BJ, Sarma V, Pierson CL, et al. Protective effects of C5ablockade in sepsis. Nat Med. 1999;5(7):788-792.
6. de Jonge E, Dekkers PE, Creasey AA, et al. Tissue factor pathwayinhibitor dose-dependently inhibits coagulation activation without in-fluencing the fibrinolytic and cytokine response during human endo-toxemia. Blood. 2000;95(4):1124-1129.
7. Lawson CA, Yan SD, Yan SF, et al. Monocytes and tissue factorpromote thrombosis in a murine model of oxygen deprivation. J ClinInvest. 1997;99(7):1729-1738.
8. Hou B, Eren M, Painter CA, et al. Tumor necrosis factor alphaactivates the human plasminogen activator inhibitor-1 gene through adistal nuclear factor kappaB site. J Biol Chem. 2004;279(18):18127-18136.
9. Maris NA, de Vos AF, Bresser P, et al. Activation of coagulation andinhibition of fibrinolysis in the lung after inhalation of lipopolysac-charide by healthy volunteers. Thromb Haemost. 2005;93(6):1036-1040.
0. O’Brien JMJr, Abraham E. Human models of endotoxemia and re-combinant human activated protein C. Crit Care Med. 2004;32(5Suppl):S202-S208.
1. De Backer D, Verdant C, Chierego M, et al. Effects of drotrecogin alfaactivated on microcirculatory alterations in patients with severe sepsis.Crit Care Med. 2006;34(7):1918-1924.
2. De Backer D, Creteur J, Dubois MJ, et al. The effects of dobutamineon microcirculatory alterations in patients with septic shock are inde-pendent of its systemic effects. Crit Care Med. 2006;34(2):403-408.
3. Robbie LA, Dummer S, Booth NA, et al. Plasminogen activatorinhibitor 2 and urokinase-type plasminogen activator in plasma andleucocytes in patients with severe sepsis. Br J Haematol. 2000;109(2):342-348.
4. Zeerleder S, Schroeder V, Hack CE, et al. TAFI and PAI-1 levels inhuman sepsis. Thromb Res. 2006;118(2):205-212.
5. Jia L, Takahashi M, Morimoto H, et al. Changes in cardiac lipidmetabolism during sepsis: the essential role of very low-density li-poprotein receptors. Cardiovasc Res. 2006;69(2):545-555.
6. Wendel M, Paul R, Heller AR. Lipoproteins in inflammation andsepsis. II. Clinical aspects. Intensive Care Med. 2007;33(1):25-35.
7. Rusavy Z, Sramek V, Lacigova S, et al. Influence of insulin on glucosemetabolism and energy expenditure in septic patients. Crit Care.2004;8(4):R213-R220.
8. Thissen JP, Underwood LE, Ketelslegers JM. Regulation of insulin-like growth factor-I in starvation and injury. Nutr Rev. 1999;57(6):
167-176.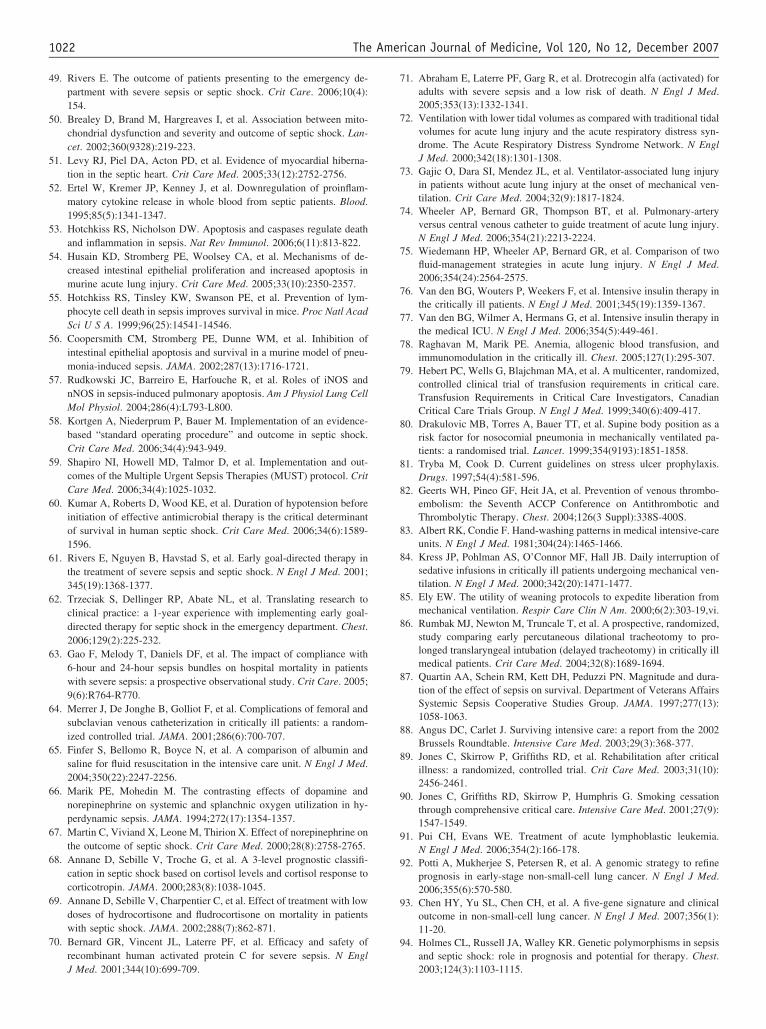
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
7
7
7
7
7
7
7
7
8
8
8
8
8
8
8
8
8
8
9
9
9
9
9
1022 The American Journal of Medicine, Vol 120, No 12, December 2007
9. Rivers E. The outcome of patients presenting to the emergency de-partment with severe sepsis or septic shock. Crit Care. 2006;10(4):154.
0. Brealey D, Brand M, Hargreaves I, et al. Association between mito-chondrial dysfunction and severity and outcome of septic shock. Lan-cet. 2002;360(9328):219-223.
1. Levy RJ, Piel DA, Acton PD, et al. Evidence of myocardial hiberna-tion in the septic heart. Crit Care Med. 2005;33(12):2752-2756.
2. Ertel W, Kremer JP, Kenney J, et al. Downregulation of proinflam-matory cytokine release in whole blood from septic patients. Blood.1995;85(5):1341-1347.
3. Hotchkiss RS, Nicholson DW. Apoptosis and caspases regulate deathand inflammation in sepsis. Nat Rev Immunol. 2006;6(11):813-822.
4. Husain KD, Stromberg PE, Woolsey CA, et al. Mechanisms of de-creased intestinal epithelial proliferation and increased apoptosis inmurine acute lung injury. Crit Care Med. 2005;33(10):2350-2357.
5. Hotchkiss RS, Tinsley KW, Swanson PE, et al. Prevention of lym-phocyte cell death in sepsis improves survival in mice. Proc Natl AcadSci U S A. 1999;96(25):14541-14546.
6. Coopersmith CM, Stromberg PE, Dunne WM, et al. Inhibition ofintestinal epithelial apoptosis and survival in a murine model of pneu-monia-induced sepsis. JAMA. 2002;287(13):1716-1721.
7. Rudkowski JC, Barreiro E, Harfouche R, et al. Roles of iNOS andnNOS in sepsis-induced pulmonary apoptosis. Am J Physiol Lung CellMol Physiol. 2004;286(4):L793-L800.
8. Kortgen A, Niederprum P, Bauer M. Implementation of an evidence-based “standard operating procedure” and outcome in septic shock.Crit Care Med. 2006;34(4):943-949.
9. Shapiro NI, Howell MD, Talmor D, et al. Implementation and out-comes of the Multiple Urgent Sepsis Therapies (MUST) protocol. CritCare Med. 2006;34(4):1025-1032.
0. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension beforeinitiation of effective antimicrobial therapy is the critical determinantof survival in human septic shock. Crit Care Med. 2006;34(6):1589-1596.
1. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy inthe treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368-1377.
2. Trzeciak S, Dellinger RP, Abate NL, et al. Translating research toclinical practice: a 1-year experience with implementing early goal-directed therapy for septic shock in the emergency department. Chest.2006;129(2):225-232.
3. Gao F, Melody T, Daniels DF, et al. The impact of compliance with6-hour and 24-hour sepsis bundles on hospital mortality in patientswith severe sepsis: a prospective observational study. Crit Care. 2005;9(6):R764-R770.
4. Merrer J, De Jonghe B, Golliot F, et al. Complications of femoral andsubclavian venous catheterization in critically ill patients: a random-ized controlled trial. JAMA. 2001;286(6):700-707.
5. Finfer S, Bellomo R, Boyce N, et al. A comparison of albumin andsaline for fluid resuscitation in the intensive care unit. N Engl J Med.2004;350(22):2247-2256.
6. Marik PE, Mohedin M. The contrasting effects of dopamine andnorepinephrine on systemic and splanchnic oxygen utilization in hy-perdynamic sepsis. JAMA. 1994;272(17):1354-1357.
7. Martin C, Viviand X, Leone M, Thirion X. Effect of norepinephrine onthe outcome of septic shock. Crit Care Med. 2000;28(8):2758-2765.
8. Annane D, Sebille V, Troche G, et al. A 3-level prognostic classifi-cation in septic shock based on cortisol levels and cortisol response tocorticotropin. JAMA. 2000;283(8):1038-1045.
9. Annane D, Sebille V, Charpentier C, et al. Effect of treatment with lowdoses of hydrocortisone and fludrocortisone on mortality in patientswith septic shock. JAMA. 2002;288(7):862-871.
0. Bernard GR, Vincent JL, Laterre PF, et al. Efficacy and safety ofrecombinant human activated protein C for severe sepsis. N Engl
J Med. 2001;344(10):699-709.1. Abraham E, Laterre PF, Garg R, et al. Drotrecogin alfa (activated) foradults with severe sepsis and a low risk of death. N Engl J Med.2005;353(13):1332-1341.
2. Ventilation with lower tidal volumes as compared with traditional tidalvolumes for acute lung injury and the acute respiratory distress syn-drome. The Acute Respiratory Distress Syndrome Network. N EnglJ Med. 2000;342(18):1301-1308.
3. Gajic O, Dara SI, Mendez JL, et al. Ventilator-associated lung injuryin patients without acute lung injury at the onset of mechanical ven-tilation. Crit Care Med. 2004;32(9):1817-1824.
4. Wheeler AP, Bernard GR, Thompson BT, et al. Pulmonary-arteryversus central venous catheter to guide treatment of acute lung injury.N Engl J Med. 2006;354(21):2213-2224.
5. Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of twofluid-management strategies in acute lung injury. N Engl J Med.2006;354(24):2564-2575.
6. Van den BG, Wouters P, Weekers F, et al. Intensive insulin therapy inthe critically ill patients. N Engl J Med. 2001;345(19):1359-1367.
7. Van den BG, Wilmer A, Hermans G, et al. Intensive insulin therapy inthe medical ICU. N Engl J Med. 2006;354(5):449-461.
8. Raghavan M, Marik PE. Anemia, allogenic blood transfusion, andimmunomodulation in the critically ill. Chest. 2005;127(1):295-307.
9. Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized,controlled clinical trial of transfusion requirements in critical care.Transfusion Requirements in Critical Care Investigators, CanadianCritical Care Trials Group. N Engl J Med. 1999;340(6):409-417.
0. Drakulovic MB, Torres A, Bauer TT, et al. Supine body position as arisk factor for nosocomial pneumonia in mechanically ventilated pa-tients: a randomised trial. Lancet. 1999;354(9193):1851-1858.
1. Tryba M, Cook D. Current guidelines on stress ulcer prophylaxis.Drugs. 1997;54(4):581-596.
2. Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thrombo-embolism: the Seventh ACCP Conference on Antithrombotic andThrombolytic Therapy. Chest. 2004;126(3 Suppl):338S-400S.
3. Albert RK, Condie F. Hand-washing patterns in medical intensive-careunits. N Engl J Med. 1981;304(24):1465-1466.
4. Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption ofsedative infusions in critically ill patients undergoing mechanical ven-tilation. N Engl J Med. 2000;342(20):1471-1477.
5. Ely EW. The utility of weaning protocols to expedite liberation frommechanical ventilation. Respir Care Clin N Am. 2000;6(2):303-19,vi.
6. Rumbak MJ, Newton M, Truncale T, et al. A prospective, randomized,study comparing early percutaneous dilational tracheotomy to pro-longed translaryngeal intubation (delayed tracheotomy) in critically illmedical patients. Crit Care Med. 2004;32(8):1689-1694.
7. Quartin AA, Schein RM, Kett DH, Peduzzi PN. Magnitude and dura-tion of the effect of sepsis on survival. Department of Veterans AffairsSystemic Sepsis Cooperative Studies Group. JAMA. 1997;277(13):1058-1063.
8. Angus DC, Carlet J. Surviving intensive care: a report from the 2002Brussels Roundtable. Intensive Care Med. 2003;29(3):368-377.
9. Jones C, Skirrow P, Griffiths RD, et al. Rehabilitation after criticalillness: a randomized, controlled trial. Crit Care Med. 2003;31(10):2456-2461.
0. Jones C, Griffiths RD, Skirrow P, Humphris G. Smoking cessationthrough comprehensive critical care. Intensive Care Med. 2001;27(9):1547-1549.
1. Pui CH, Evans WE. Treatment of acute lymphoblastic leukemia.N Engl J Med. 2006;354(2):166-178.
2. Potti A, Mukherjee S, Petersen R, et al. A genomic strategy to refineprognosis in early-stage non-small-cell lung cancer. N Engl J Med.2006;355(6):570-580.
3. Chen HY, Yu SL, Chen CH, et al. A five-gene signature and clinicaloutcome in non-small-cell lung cancer. N Engl J Med. 2007;356(1):11-20.
4. Holmes CL, Russell JA, Walley KR. Genetic polymorphisms in sepsisand septic shock: role in prognosis and potential for therapy. Chest.
2003;124(3):1103-1115.
DC
HMa
M
PDchwaspsbbwsr
ptmiccc
AAbtaouhsmr
DU
0d
The American Journal of Medicine (2007) 120, 1023-1025
IAGNOSTIC DILEMMA: THORACIC MEDICINE
harles M. Wiener, MD, Section Editorard to Swallowadhusudan Grover, MD,a Amit Gupta, MD,a Dianne P. Wagner, MD,a Mark B. Orringer, MD,b
Department of Internal Medicine, Michigan State University, East Lansing, Mich, bSection of Thoracic Surgery, University of
Atgmtsna
DSerswarcmbrecwt
eflsasiiwtc
t
ichigan, Ann Arbor, Mich.
RESENTATIONays after her symptoms began, an 85-year-old woman
oughed up the diagnosis. She was in her usual state ofealth when she presented to her primary care physicianith a 2-day history of dysphagia that began with solid food
nd rapidly progressed to an inability to swallow her ownaliva. She had no nausea, vomiting, chest or abdominalain, or history of reflux. Although her appetite was good,he had lost 7-pounds in the previous 3 months. She recalledeing quite ill with fever and chest discomfort 50 yearsefore, at which time she was told that a “lump” in the chestas seen on an x-ray. At that time, she had opted against
urgery, and the fever and chest discomfort resolved withoutecurrence.
A medical history also was significant for essential hy-ertension, hypothyroidism following partial thyroidec-omy, osteoporosis, and a benign colon polyp. The patient’sother and sister had a history of colon cancer. Medications
ncluded low-dose aspirin, levothyroxine, an angiotensin-onverting enzyme inhibitor, a multivitamin, vitamin D,alcium, and alendronate. The patient had no history ofigarette smoking or alcoholism.
SSESSMENTphysical examination was normal, as were a complete
lood count and serum chemistry panel. An esophagogas-roduodenoscopy revealed dilatation of the proximal esoph-gus and a small amount of retained fluid; narrowing sec-ndary to extrinsic compression in the mid-esophagus;lceration at the gastroesophageal junction; a small hiatalernia; and diffuse erythema in the gastric antrum. Biopsieshowed esophagitis and antral gastritis with no dysplasia oretaplasia. A chest radiograph showed small bilateral pleu-
al effusions and a possible small retrocardiac hiatal hernia.
Requests for reprints should be addressed to Madhusudan Grover, MD,epartment of Internal Medicine, B 301, Clinical Center, Michigan Stateniversity, East Lansing, MI 48842.
cE-mail address: [email protected]
002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.oi:10.1016/j.amjmed.2007.08.022
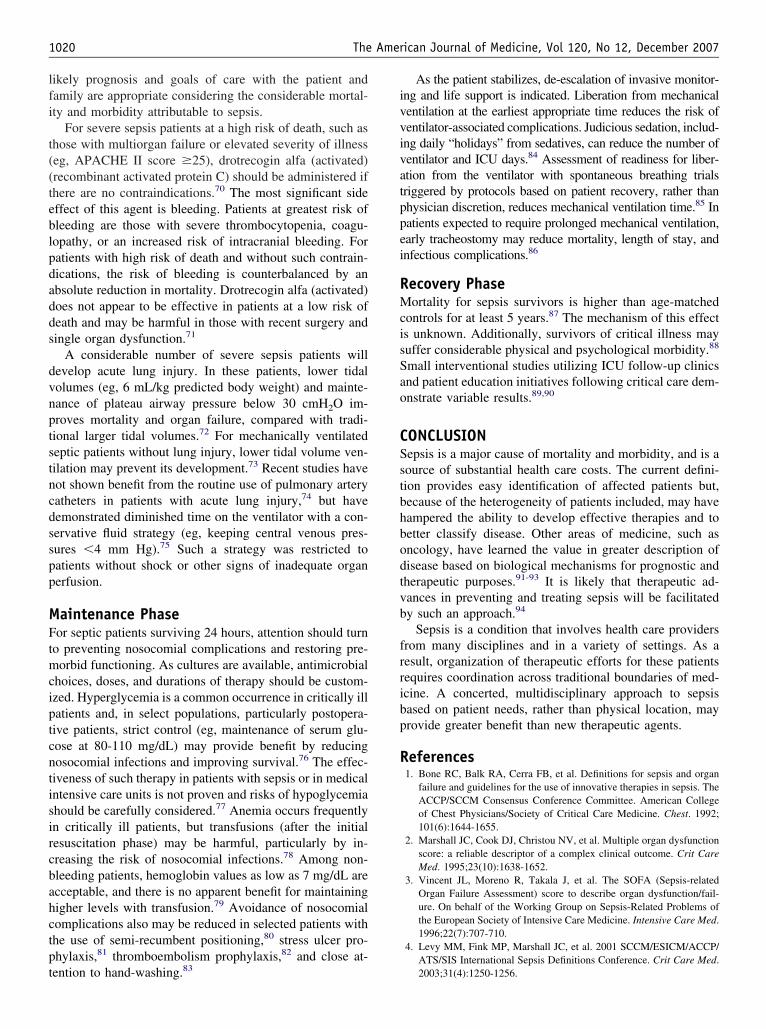
barium esophagogram showed extrinsic compression ofhe mid-esophagus and what was interpreted as an esopha-eal perforation that directly communicated with a posteriorediastinal mass (Figure 1). Contrast enhanced computed
omography of the chest confirmed an 8-cm, fluid-filled,ubcarinal mass in the posterior mediastinum that commu-icated with the esophagus through a fistulous tract in thenterior wall (Figure 2).
IAGNOSIShortly after her hospitalization, the patient had a coughingpisode, felt something “pop” in her high anterior chest, andegurgitated a brownish liquid. After this, she was able towallow her saliva again. The imaging findings combinedith the remote medical history—retrosternal discomfort
ssociated with febrile illness, chest discomfort, and a chestadiographic abnormality—suggested a long-standing bron-hogenic cyst that communicated with the esophageal lu-en. It was assumed that the coughing, regurgitation of
rownish fluid, and recovered ability to swallow salivaepresented sudden decompression of the cyst into thesophagus. Consequently, esophageal compression by theyst was reduced, and swallowing improved. The patientas advised to resume a mechanical soft diet, which she
olerated well.Eight weeks after the patient’s initial presentation, an
lective right posterolateral thoracotomy disclosed an in-amed cystic mass, 7-8 cm in diameter, adhering to theubcarinal soft tissues and communicating with the esoph-geal lumen through a 4-mm fistulous tract. The fistula wastapled closed, and adjacent esophageal muscle was approx-mated over the staple line. Pathology on the resected spec-men indicated ciliated epithelium of respiratory type thatas surrounded with small particles of cartilage and focal
hick lymphoid aggregates consistent with a bronchogenicyst (Figures 3a and 3b).
Mediastinal cysts are rare developmental anomalies ofhe foregut and are usually classified as duplication, bron-
hogenic, or neurenteric cysts, based primarily on histolog-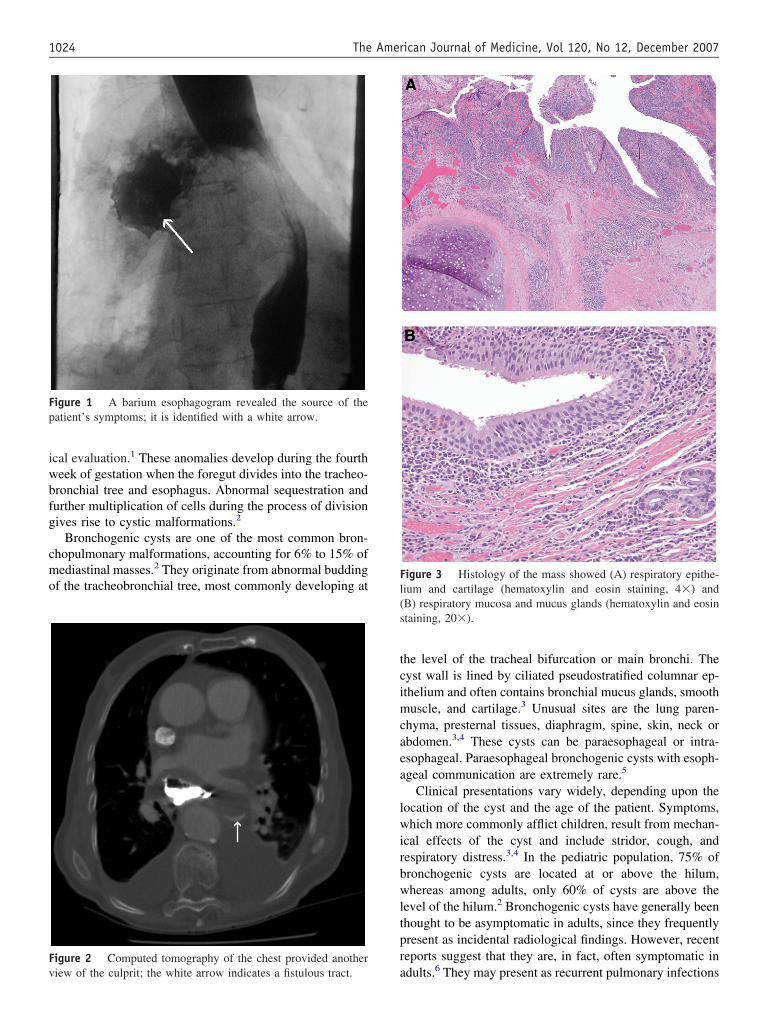
iwbfg
cmo
tcimcaea
lwirbwltpr
Fp
Fv
Fl(s
1024 The American Journal of Medicine, Vol 120, No 12, December 2007
cal evaluation.1 These anomalies develop during the fourtheek of gestation when the foregut divides into the tracheo-ronchial tree and esophagus. Abnormal sequestration andurther multiplication of cells during the process of divisionives rise to cystic malformations.2
Bronchogenic cysts are one of the most common bron-hopulmonary malformations, accounting for 6% to 15% ofediastinal masses.2 They originate from abnormal budding
f the tracheobronchial tree, most commonly developing at
igure 1 A barium esophagogram revealed the source of theatient’s symptoms; it is identified with a white arrow.
igure 2 Computed tomography of the chest provided another
aiew of the culprit; the white arrow indicates a fistulous tract.he level of the tracheal bifurcation or main bronchi. Theyst wall is lined by ciliated pseudostratified columnar ep-thelium and often contains bronchial mucus glands, smoothuscle, and cartilage.3 Unusual sites are the lung paren-
hyma, presternal tissues, diaphragm, spine, skin, neck orbdomen.3,4 These cysts can be paraesophageal or intra-sophageal. Paraesophageal bronchogenic cysts with esoph-geal communication are extremely rare.5
Clinical presentations vary widely, depending upon theocation of the cyst and the age of the patient. Symptoms,hich more commonly afflict children, result from mechan-
cal effects of the cyst and include stridor, cough, andespiratory distress.3,4 In the pediatric population, 75% ofronchogenic cysts are located at or above the hilum,hereas among adults, only 60% of cysts are above the
evel of the hilum.2 Bronchogenic cysts have generally beenhought to be asymptomatic in adults, since they frequentlyresent as incidental radiological findings. However, recenteports suggest that they are, in fact, often symptomatic in
igure 3 Histology of the mass showed (A) respiratory epithe-ium and cartilage (hematoxylin and eosin staining, 4�) andB) respiratory mucosa and mucus glands (hematoxylin and eosintaining, 20�).
dults.6 They may present as recurrent pulmonary infections

dc
tvumabp
igtoaggdn
aroacfdrhsgTca
MOrachascupw
mib
rfltatdsm
R
1
1
1
1
1
1025Grover et al Hard To Swallow
ue to partial bronchial obstruction or as dysphagia due toompression of the esophagus.
Complications, such as infection or hemorrhage withinhe cyst, can occur.3 Pulmonary artery stenosis, superiorena caval obstruction, pericardial tamponade, arrhythmias,nilateral pulmonary edema, bronchial atresia, and carcino-atous or sarcomatous changes have been reported in
dults.4 It is likely that in our patient, pressure necrosisetween the cyst and esophageal wall occurred, and the cystartially decompressed as it contents were regurgitated.
The diagnosis is usually made with a combination ofmaging and endoscopic modalities. A barium esophago-ram can detect a nonspecific, often smooth, rounded, in-ramural or paraesophageal process that narrows the lumenf the esophagus. A fistulous connection between the cystnd the esophagus might be discovered as well. Esophago-astroduodenoscopy usually reveals a bulge in the esopha-us with overlying normal mucosa. The procedure helps toistinguish between submucosal, intramural, and intralumi-al tumors.
Computed tomography and endoscopic ultrasonographyre the imaging tests of choice. Although computed tomog-aphy is helpful in evaluating the topographical relationshipf the mass in order to plan the most appropriate surgicalpproach, it cannot definitely exclude a malignancy, as theomputed tomography density of a bronchogenic cyst variesrom typical water (0-20 Hounsfield units) to soft tissueensity (80-90 Hounsfield units).7 Endoscopic ultrasonog-aphy accurately differentiates solid and cystic lesions, andelps in determining their relationship with the adjacenttructures.8 Nonetheless, definitive diagnosis of a broncho-enic cyst requires excision and pathological evaluation.he differential diagnosis includes esophageal duplicationyst, esophageal leiomyoma, pleural fibroma, granuloma,nd lymphadenopathy.9
ANAGEMENTur patient’s postoperative course was uneventful, and she
esumed normal oral intake. Resection, even in asymptom-tic patients, has been recommended as the treatment ofhoice for bronchogenic cysts.10 This eliminates the likeli-ood of future complications—as occurred in our patient—nd rules out malignancy.11 In elderly patients with highurgical risk or asymptomatic patients who refuse surgery,lose follow-up with computed tomography or endoscopicltrasonography might be appropriate, but the risk of com-lications continues to exist.4,12 Minimally invasive surgery
ith videothoracosopic technique is less traumatic andight be as effective as open thoracotomy, but intensenflammatory reaction surrounding a chronically infectedronchogenic cyst might preclude thoracoscopic removal.13
Postoperative outcome is generally favorable, and recur-ence after complete resection is exceedingly unusual. Re-ux symptoms might occur after resection of distal cysts if
heir mobilization results in disruption of the lower esoph-geal sphincter mechanism. When extensive dissection ofhe musculature is required for cyst removal, esophagealysmotility might follow, but this is seldom of clinicalignificance.14 Long-term follow-up is recommended toonitor for these complications.
eferences1. Foker EJ, Boyle EMJ. Pediatric disorders: congenital anomalies. In:
Pearson FG, Cooper JD, Deslauriers J, et al, eds. Esophageal Surgery.2nd ed. New York: Churchill Livingstone; 1995:184-199.
2. Ribet ME, Copin MC, Gosselin B. Bronchogenic cysts of the medi-astinum. J ThoracCardiovasc Surg. 1995;109:1003-1010.
3. Fraser RB, Pare JAP, Pare PD, et al. Pulmonary abnormalities ofdevelopmental origin. In: Diagnosis of diseases of the chest. Vol 2.Philadelphia: WB Saunders; 1989:675-773.
4. Patel SR, Meeker DP, Biscotti CV, et al. Presentation and managementof bronchogenic cysts in the adult. Chest. 1994;106:79-85.
5. Knezevic J, Radovanovic N, Simic A, et al. A paraesophageal bron-chogenic cyst with esophageal communication. Dis Esophagus. 1999;12:321-323.
6. St. Georges R, Deslauriers J, Duranceau A, et al. Clinical spectrum ofbronchogenic cysts of the mediastinum and lung in the adult. AnnThorac Surg. 1991;52:6-13.
7. Haddon MJ, Bowen A. Bronchopulmonary and neuroenteric forms offoregut anomalies. Imaging for diagnosis and management. RadiolClin North Am. 1991;29:241-254.
8. Geller A, Wang KK, DiMagno EP. Diagnosis of foregut duplicationcysts by endoscopic ultrasonography. Gastroenterology. 1995;109:838-842.
9. Cartmill JA, Hughes CF. Bronchogenic cysts: a persistent dilemma.Aust N Z J Surg. 1989;59:253-256.
0. Postlethwait RW, Lowe JE. Benign tumors and cysts of the esophagus.In Zuidema GD, Yeo CJ, Orringer MB, et al, eds. Shackelford’ssurgery of the Alimentary Tract. Vol 1.4th ed. Philadelphia: WBSaunders; 1996:369-386.
1. Miralles Lozano F, Gonzalez-Martínez B, Luna More S, ValenciaRodríguez A. Carcinoma arising in a calcified bronchogenic cyst.Respiration. 1981;42:135-137.
2. Kuhlman JE, Fishman EK, Wang KP, et al. Mediastinal cysts: diag-nosis by CT and needle aspiration. AJR Am J Roentgenol. 1988;150:75-78.
3. Watson DI, Britten-Jones R. Thoracoscopic excision of bronchogeniccyst of the esophagus. Surg Endosc. 1995;9:824-825.
4. Van Dam J, Rice TW, Sivak MV Jr. Endoscopic ultrasonography andendoscopically guided needle aspiration for the diagnosis of uppergastrointestinal tract foregut cysts. Am J Gastroenterol. 1992;87(6);
762-765.
IP
AMSa
PCgesb
shbwaghld
ghpaotc
AOatdfsh
I9
0d
The American Journal of Medicine (2007) 120, 1026-1027
MAGES IN DERMATOLOGY
arwathi “Uma” Paniker, MD, Section EditorPrickly Pairario Vaccaro, MD, PhD,a Fabrizio Guarneri, MD, PhD,a Olga Barbuzza, MD, PhD,b Giuseppe Galtieri, MD,b
erafinella P. Cannavò, MDa
b Univer
ttwsIt
DIcoefstobebflpbp
uoTcoaddnsfipo
Institute of Dermatology and Institute of Occupational Health,
RESENTATIONertain occupational hazards are more than obvious – dogroomers are at high risk of dog bites, for example. How-ver, some hazards are more unexpected. The 2 cases de-cribed here illustrate an unusual occupational hazard commonoth to dog groomers and hairdressers.
In the first case, a 60-year-old male hairdresser haduffered recurrent erythema, papulae, and pustules on bothands for 2 years. He reported that the lesions had initiallyurned and itched, and that the symptoms had progressivelyorsened to the point of intense pain and bleeding associ-
ted with purulent drainage from sinuses between his fin-ers. His general practitioner had removed multiple foreignairs from the lesions on previous occasions, had treated theesions with several courses of antibiotics, and also hadrained abscesses from the sinuses.
In the second case, a 52-year-old male professional dogroomer complained of repeated infections of his hands,air fragments trapped under his fingernails (subungually),apulae and pustules in the web spaces between his fingers,nd separation of his fingernails from the nail bed (onych-lysis). As he was able to remove the embedded hairs withweezers, he had not previously seen a physician for theseomplaints.
SSESSMENTn examination, the hairdresser was found to have multiple
reas of chronic inflammation, nodules, and sinuses in allhe interdigital web spaces (Figure 1). These lesions hin-ered extension of his fingers. Palpation of the interdigitalolds revealed the presence of a cyst in the second webpace of the right hand, in the first web space of the leftand, and provoked discharge of purulent fluid.
Requests for reprints should be addressed to Mario Vaccaro, MD, PhD,nstitute of Dermatology, Policlinico Universitario, Via Consolare Valeria,8125 Messina, Italy.
pE-mail address: [email protected]
002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.oi:10.1016/j.amjmed.2007.08.029
sity of Messina, Italy.
Examination of the dog groomer revealed a small sinusract with no visible hairs and an area of chronic inflamma-ion in the third web space of his right hand, onycholysisith hairs embedded under the right thumbnail, and oblique
plit with hairs embedded under the left index fingernail.nflammatory papules were present at some sites of pene-ration of hair fragments (Figure 2).
IAGNOSISn both cases, the observed symptoms indicated tri-hogranuloma (also known as pilonidal sinus), an uncommonccupational dermatosis that afflicts hairdressers, sheep shear-rs, dog groomers, and cow milkers.1-3 This disease resultsrom an inflammatory response to penetration of short,harp fragments of hairs into the epidermis, particularly intohe interdigital spaces of the hand. It only rarely occurs inther locations, such as the finger pulp, periungual area,reast, back, feet, and popliteal fossa. Subungual hair pen-tration appears to be much less common,4-5 but if the hairsecome embedded and are not promptly removed, an in-ammatory reaction, formation of sinus tracts, and chronic,urulent drainage can result. Possible complications includeacterial or fungal infections, abscesses, cellulitis, lym-hangitis, and, rarely, osteomyelitis.6
The first clinical symptoms of trichogranuloma are pap-les and cysts. These lesions can develop into sinuses, withr without protruding hairs of various lengths and colors.hese hairs readily distinguish trichogranuloma from otheronditions of the differential diagnosis, which includesther traumatic implantations, bite reactions, deep fungal ortypical mycobacterial infections, orf virus infection, pyo-erma, erosio-interdigitalis blastomycetica (interdigital can-idiasis), onychodystrophy, onychomycosis, and psoriaticail disease.4-8 Subsequently, connections among severalinuses can form within the skin, leading to development ofstulas in one or several interdigital spaces. Inflammatoryapules, subungually embedded hairs, onycholysis, andblique split in the distal pulp tissue with discharge of
urulent fluid are characteristic features of the subungual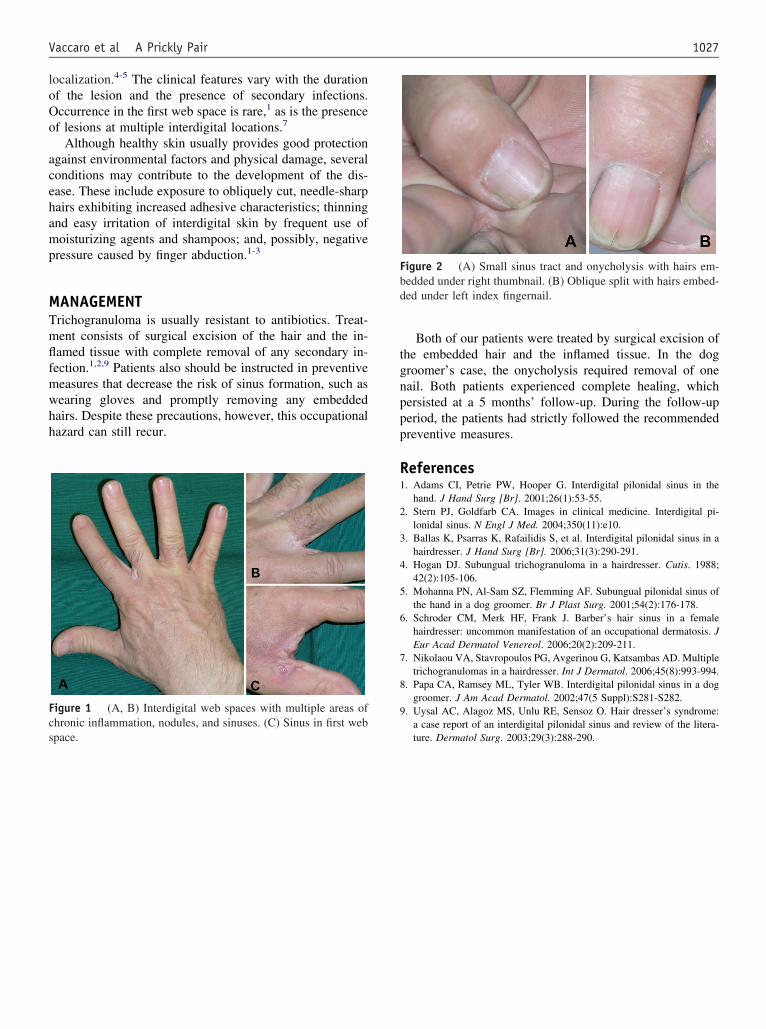
loOo
acehamp
MTmflfmwhh
tgnppp
R1
2
3
4
5
6
7
8
9Fcs
Fbd
1027Vaccaro et al A Prickly Pair
ocalization.4-5 The clinical features vary with the durationf the lesion and the presence of secondary infections.ccurrence in the first web space is rare,1 as is the presencef lesions at multiple interdigital locations.7
Although healthy skin usually provides good protectiongainst environmental factors and physical damage, severalonditions may contribute to the development of the dis-ase. These include exposure to obliquely cut, needle-sharpairs exhibiting increased adhesive characteristics; thinningnd easy irritation of interdigital skin by frequent use ofoisturizing agents and shampoos; and, possibly, negative
ressure caused by finger abduction.1-3
ANAGEMENTrichogranuloma is usually resistant to antibiotics. Treat-ent consists of surgical excision of the hair and the in-amed tissue with complete removal of any secondary in-ection.1,2,9 Patients also should be instructed in preventiveeasures that decrease the risk of sinus formation, such asearing gloves and promptly removing any embeddedairs. Despite these precautions, however, this occupationalazard can still recur.
igure 1 (A, B) Interdigital web spaces with multiple areas ofhronic inflammation, nodules, and sinuses. (C) Sinus in first web
pace.Both of our patients were treated by surgical excision ofhe embedded hair and the inflamed tissue. In the dogroomer’s case, the onycholysis required removal of oneail. Both patients experienced complete healing, whichersisted at a 5 months’ follow-up. During the follow-uperiod, the patients had strictly followed the recommendedreventive measures.
eferences. Adams CI, Petrie PW, Hooper G. Interdigital pilonidal sinus in the
hand. J Hand Surg [Br]. 2001;26(1):53-55.. Stern PJ, Goldfarb CA. Images in clinical medicine. Interdigital pi-
lonidal sinus. N Engl J Med. 2004;350(11):e10.. Ballas K, Psarras K, Rafailidis S, et al. Interdigital pilonidal sinus in a
hairdresser. J Hand Surg [Br]. 2006;31(3):290-291.. Hogan DJ. Subungual trichogranuloma in a hairdresser. Cutis. 1988;
42(2):105-106.. Mohanna PN, Al-Sam SZ, Flemming AF. Subungual pilonidal sinus of
the hand in a dog groomer. Br J Plast Surg. 2001;54(2):176-178.. Schroder CM, Merk HF, Frank J. Barber’s hair sinus in a female
hairdresser: uncommon manifestation of an occupational dermatosis. JEur Acad Dermatol Venereol. 2006;20(2):209-211.
. Nikolaou VA, Stavropoulos PG, Avgerinou G, Katsambas AD. Multipletrichogranulomas in a hairdresser. Int J Dermatol. 2006;45(8):993-994.
. Papa CA, Ramsey ML, Tyler WB. Interdigital pilonidal sinus in a doggroomer. J Am Acad Dermatol. 2002;47(5 Suppl):S281-S282.
. Uysal AC, Alagoz MS, Unlu RE, Sensoz O. Hair dresser’s syndrome:a case report of an interdigital pilonidal sinus and review of the litera-
igure 2 (A) Small sinus tract and onycholysis with hairs em-edded under right thumbnail. (B) Oblique split with hairs embed-ed under left index fingernail.
ture. Dermatol Surg. 2003;29(3):288-290.
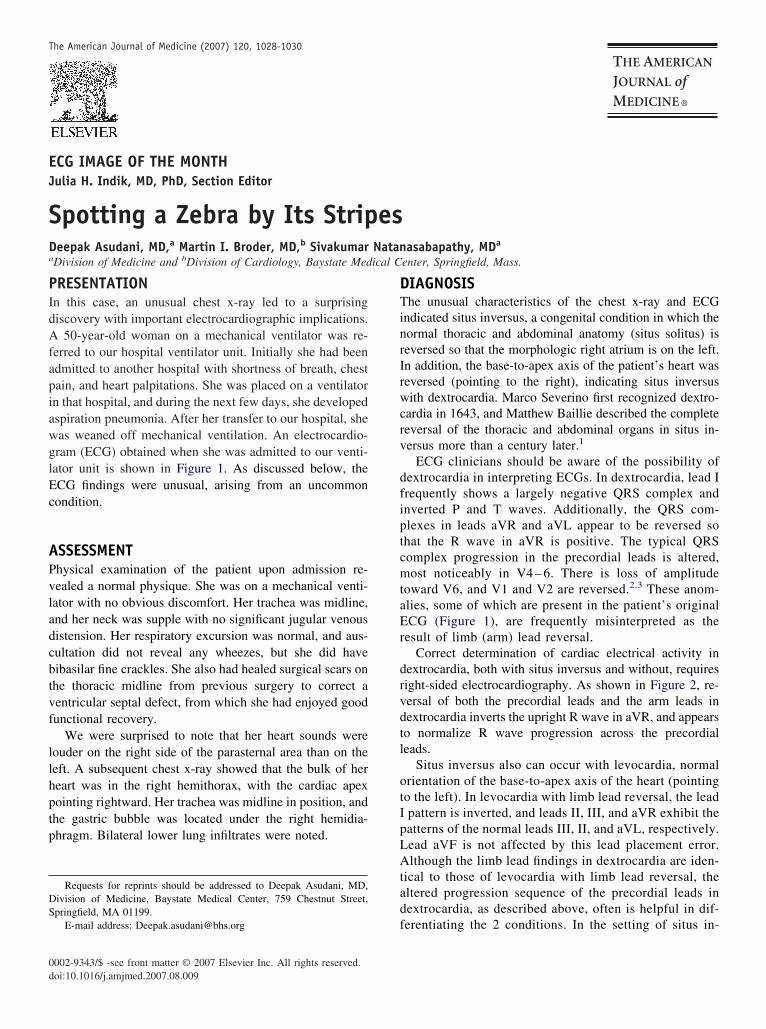
EJ
SDa
PIdAfapiawglEc
APvladcbtvf
llhptp
DS
0d
The American Journal of Medicine (2007) 120, 1028-1030
CG IMAGE OF THE MONTH
ulia H. Indik, MD, PhD, Section Editorpotting a Zebra by Its Stripeseepak Asudani, MD,a Martin I. Broder, MD,b Sivakumar Natanasabapathy, MDa
b ical C
DTinrIrwcrv
dfiptcmtaEr
drvdtl
otIpLAtad
Division of Medicine and Division of Cardiology, Baystate Med
RESENTATIONn this case, an unusual chest x-ray led to a surprisingiscovery with important electrocardiographic implications.
50-year-old woman on a mechanical ventilator was re-erred to our hospital ventilator unit. Initially she had beendmitted to another hospital with shortness of breath, chestain, and heart palpitations. She was placed on a ventilatorn that hospital, and during the next few days, she developedspiration pneumonia. After her transfer to our hospital, sheas weaned off mechanical ventilation. An electrocardio-ram (ECG) obtained when she was admitted to our venti-ator unit is shown in Figure 1. As discussed below, theCG findings were unusual, arising from an uncommonondition.
SSESSMENThysical examination of the patient upon admission re-ealed a normal physique. She was on a mechanical venti-ator with no obvious discomfort. Her trachea was midline,nd her neck was supple with no significant jugular venousistension. Her respiratory excursion was normal, and aus-ultation did not reveal any wheezes, but she did haveibasilar fine crackles. She also had healed surgical scars onhe thoracic midline from previous surgery to correct aentricular septal defect, from which she had enjoyed goodunctional recovery.
We were surprised to note that her heart sounds wereouder on the right side of the parasternal area than on theeft. A subsequent chest x-ray showed that the bulk of hereart was in the right hemithorax, with the cardiac apexointing rightward. Her trachea was midline in position, andhe gastric bubble was located under the right hemidia-hragm. Bilateral lower lung infiltrates were noted.
Requests for reprints should be addressed to Deepak Asudani, MD,ivision of Medicine, Baystate Medical Center, 759 Chestnut Street,pringfield, MA 01199.
fE-mail address: [email protected]
002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.oi:10.1016/j.amjmed.2007.08.009
enter, Springfield, Mass.
IAGNOSIShe unusual characteristics of the chest x-ray and ECG
ndicated situs inversus, a congenital condition in which theormal thoracic and abdominal anatomy (situs solitus) iseversed so that the morphologic right atrium is on the left.n addition, the base-to-apex axis of the patient’s heart waseversed (pointing to the right), indicating situs inversusith dextrocardia. Marco Severino first recognized dextro-
ardia in 1643, and Matthew Baillie described the completeeversal of the thoracic and abdominal organs in situs in-ersus more than a century later.1
ECG clinicians should be aware of the possibility ofextrocardia in interpreting ECGs. In dextrocardia, lead Irequently shows a largely negative QRS complex andnverted P and T waves. Additionally, the QRS com-lexes in leads aVR and aVL appear to be reversed sohat the R wave in aVR is positive. The typical QRSomplex progression in the precordial leads is altered,ost noticeably in V4 – 6. There is loss of amplitude
oward V6, and V1 and V2 are reversed.2,3 These anom-lies, some of which are present in the patient’s originalCG (Figure 1), are frequently misinterpreted as the
esult of limb (arm) lead reversal.Correct determination of cardiac electrical activity in
extrocardia, both with situs inversus and without, requiresight-sided electrocardiography. As shown in Figure 2, re-ersal of both the precordial leads and the arm leads inextrocardia inverts the upright R wave in aVR, and appearso normalize R wave progression across the precordialeads.
Situs inversus also can occur with levocardia, normalrientation of the base-to-apex axis of the heart (pointingo the left). In levocardia with limb lead reversal, the leadpattern is inverted, and leads II, III, and aVR exhibit theatterns of the normal leads III, II, and aVL, respectively.ead aVF is not affected by this lead placement error.lthough the limb lead findings in dextrocardia are iden-
ical to those of levocardia with limb lead reversal, theltered progression sequence of the precordial leads inextrocardia, as described above, often is helpful in dif-
erentiating the 2 conditions. In the setting of situs in-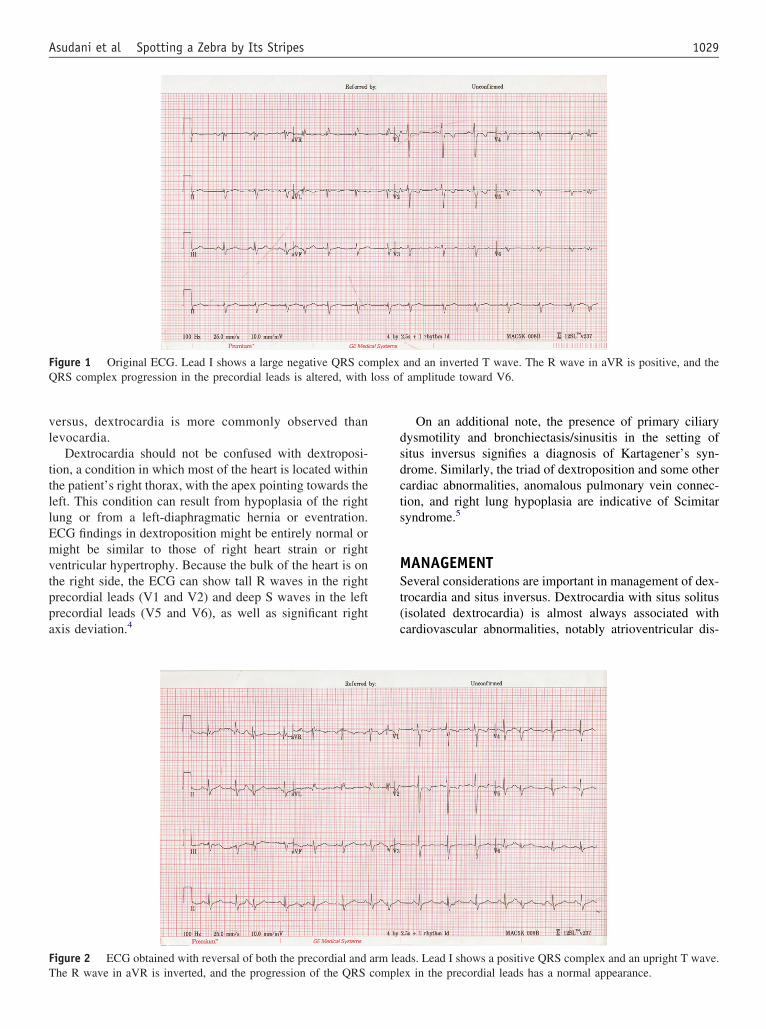
vl
ttllEmvtppa
dsdcts
MSt(c
FQ loss of
FT
1029Asudani et al Spotting a Zebra by Its Stripes
ersus, dextrocardia is more commonly observed thanevocardia.
Dextrocardia should not be confused with dextroposi-ion, a condition in which most of the heart is located withinhe patient’s right thorax, with the apex pointing towards theeft. This condition can result from hypoplasia of the rightung or from a left-diaphragmatic hernia or eventration.CG findings in dextroposition might be entirely normal oright be similar to those of right heart strain or right
entricular hypertrophy. Because the bulk of the heart is onhe right side, the ECG can show tall R waves in the rightrecordial leads (V1 and V2) and deep S waves in the leftrecordial leads (V5 and V6), as well as significant rightxis deviation.4
igure 1 Original ECG. Lead I shows a large negative QRS coRS complex progression in the precordial leads is altered, with
igure 2 ECG obtained with reversal of both the precordial and
he R wave in aVR is inverted, and the progression of the QRS compleOn an additional note, the presence of primary ciliaryysmotility and bronchiectasis/sinusitis in the setting ofitus inversus signifies a diagnosis of Kartagener’s syn-rome. Similarly, the triad of dextroposition and some otherardiac abnormalities, anomalous pulmonary vein connec-ion, and right lung hypoplasia are indicative of Scimitaryndrome.5
ANAGEMENTeveral considerations are important in management of dex-
rocardia and situs inversus. Dextrocardia with situs solitusisolated dextrocardia) is almost always associated withardiovascular abnormalities, notably atrioventricular dis-
and an inverted T wave. The R wave in aVR is positive, and theamplitude toward V6.
ds. Lead I shows a positive QRS complex and an upright T wave.
mplex
arm lea
x in the precordial leads has a normal appearance.
ctolcihplld
dtpt
fr
R1
2
3
4
5
1030 The American Journal of Medicine, Vol 120, No 12, December 2007
ordance, anomalous pulmonary venous return, transposi-ion of the great arteries, atrial or ventricular septal defect,r single ventricular defect. Normal life expectancy in iso-ated dextrocardia is severely limited. In contrast, dextro-ardia with situs inversus is seldom associated with congen-tal heart disease. Our patient was unusual in this respect,aving been born with a ventricular septal defect. Typically,atients with dextrocardia and situs inversus have a normalife expectancy. In the rare instances of cardiac anomalies,ife expectancy is reduced, depending on the severity of theefect.
Finally, dextrocardia is an important consideration inetermining the placement of electrodes during defibrilla-ion, as the position of the apex is significantly altered, andrecaution is necessary when placing anterior apex or an-
erior posterior schemes. In the setting of situs inversus,ailure to recognize an atypical history in the setting ofeversed anatomy might result in surgical mishaps.
eferences. Wilhelm A. Situs inversus. Available at: http://www.emedicine.com/
radio/topic639.htm. Accessed Feb. 14, 2007.. Marelli AJ. Congenital heart disease in adults. In: Goldman L, Bennett
JC, eds. Cecil Textbook of Medicine, 21st ed. Philadelphia: WB Saun-ders Co; 2000; pp. 2779-2911.
. Demangone D. ECG manifestations: noncoronary heart disease. EmergMed Clin North Am. 2006;24:113-131.
. Surawicz B, Knilans T. Diseases of the heart and lungs. Chou’s Elec-trocardiography in Clinical Practice. Philadelphia: WB Saunders Co;2001; pp. 256-309.
. Desai PR, Babu M. Scimitar syndrome as a differential diagnosis in achild with recurrent wheeze. Arch Dis Child. 2002;87:357 No abstract
available. Erratum in: Arch Dis Child. 2003;88:93.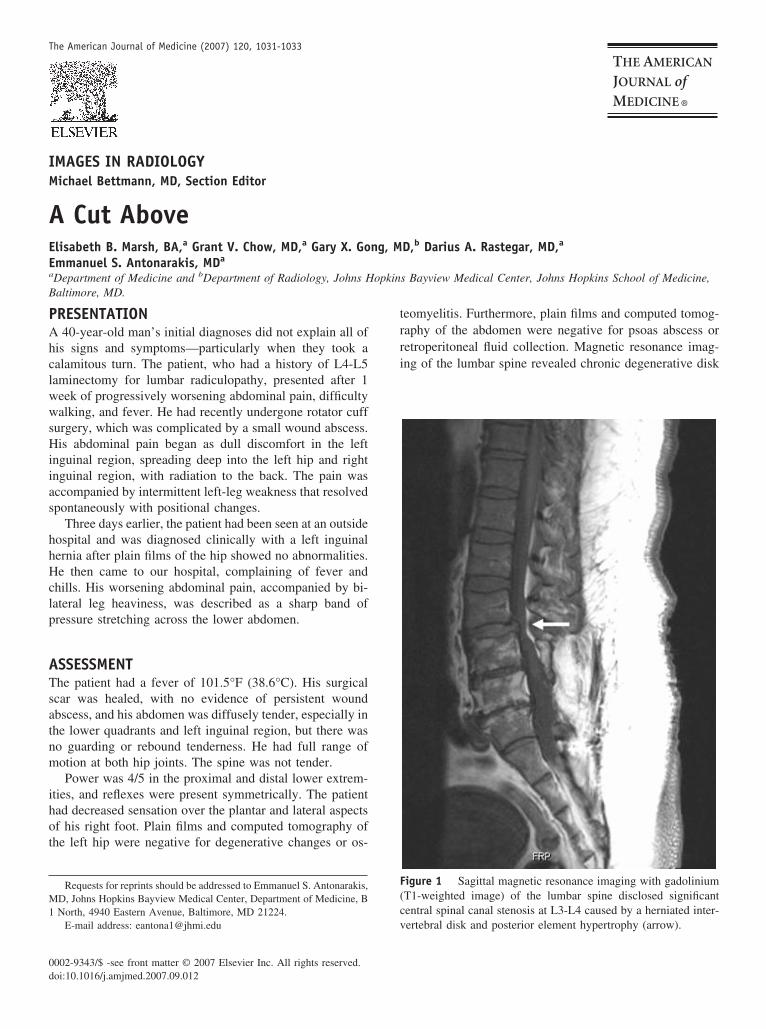
IM
AEEa
B
PAhclwwsHiias
hhHclp
ATsatnm
ihot
M1
0d
The American Journal of Medicine (2007) 120, 1031-1033
MAGES IN RADIOLOGY
ichael Bettmann, MD, Section EditorCut Abovelisabeth B. Marsh, BA,a Grant V. Chow, MD,a Gary X. Gong, MD,b Darius A. Rastegar, MD,a
mmanuel S. Antonarakis, MDa
Department of Medicine and bDepartment of Radiology, Johns Hopkins Bayview Medical Center, Johns Hopkins School of Medicine,
trri
F(c
altimore, MD.
RESENTATION40-year-old man’s initial diagnoses did not explain all of
is signs and symptoms—particularly when they took aalamitous turn. The patient, who had a history of L4-L5aminectomy for lumbar radiculopathy, presented after 1eek of progressively worsening abdominal pain, difficultyalking, and fever. He had recently undergone rotator cuff
urgery, which was complicated by a small wound abscess.is abdominal pain began as dull discomfort in the left
nguinal region, spreading deep into the left hip and rightnguinal region, with radiation to the back. The pain wasccompanied by intermittent left-leg weakness that resolvedpontaneously with positional changes.
Three days earlier, the patient had been seen at an outsideospital and was diagnosed clinically with a left inguinalernia after plain films of the hip showed no abnormalities.e then came to our hospital, complaining of fever and
hills. His worsening abdominal pain, accompanied by bi-ateral leg heaviness, was described as a sharp band ofressure stretching across the lower abdomen.
SSESSMENThe patient had a fever of 101.5°F (38.6°C). His surgicalcar was healed, with no evidence of persistent woundbscess, and his abdomen was diffusely tender, especially inhe lower quadrants and left inguinal region, but there waso guarding or rebound tenderness. He had full range ofotion at both hip joints. The spine was not tender.Power was 4/5 in the proximal and distal lower extrem-
ties, and reflexes were present symmetrically. The patientad decreased sensation over the plantar and lateral aspectsf his right foot. Plain films and computed tomography ofhe left hip were negative for degenerative changes or os-
Requests for reprints should be addressed to Emmanuel S. Antonarakis,D, Johns Hopkins Bayview Medical Center, Department of Medicine, BNorth, 4940 Eastern Avenue, Baltimore, MD 21224.
E-mail address: [email protected] v
002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.oi:10.1016/j.amjmed.2007.09.012
eomyelitis. Furthermore, plain films and computed tomog-aphy of the abdomen were negative for psoas abscess oretroperitoneal fluid collection. Magnetic resonance imag-ng of the lumbar spine revealed chronic degenerative disk
igure 1 Sagittal magnetic resonance imaging with gadoliniumT1-weighted image) of the lumbar spine disclosed significantentral spinal canal stenosis at L3-L4 caused by a herniated inter-
ertebral disk and posterior element hypertrophy (arrow).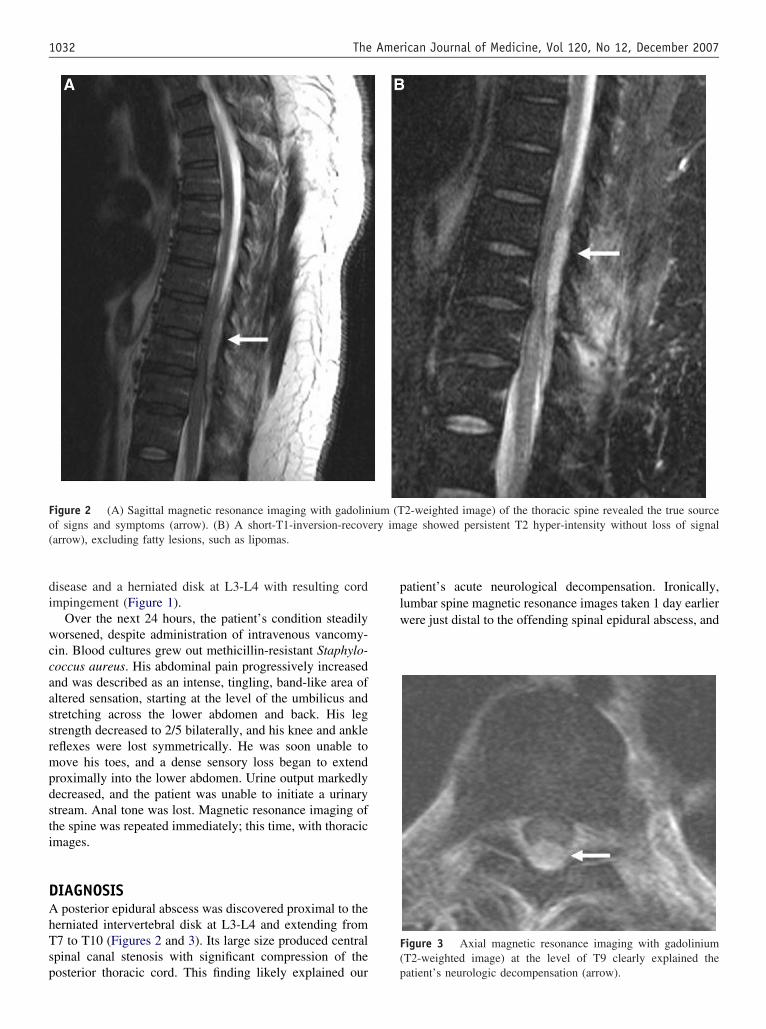
di
wccaassrmpdsti
DAhTsp
plw
F(
Fo(
1032 The American Journal of Medicine, Vol 120, No 12, December 2007
isease and a herniated disk at L3-L4 with resulting cordmpingement (Figure 1).
Over the next 24 hours, the patient’s condition steadilyorsened, despite administration of intravenous vancomy-
in. Blood cultures grew out methicillin-resistant Staphylo-occus aureus. His abdominal pain progressively increasednd was described as an intense, tingling, band-like area ofltered sensation, starting at the level of the umbilicus andtretching across the lower abdomen and back. His legtrength decreased to 2/5 bilaterally, and his knee and ankleeflexes were lost symmetrically. He was soon unable toove his toes, and a dense sensory loss began to extend
roximally into the lower abdomen. Urine output markedlyecreased, and the patient was unable to initiate a urinarytream. Anal tone was lost. Magnetic resonance imaging ofhe spine was repeated immediately; this time, with thoracicmages.
IAGNOSISposterior epidural abscess was discovered proximal to the
erniated intervertebral disk at L3-L4 and extending from7 to T10 (Figures 2 and 3). Its large size produced centralpinal canal stenosis with significant compression of the
igure 2 (A) Sagittal magnetic resonance imaging with gadolinf signs and symptoms (arrow). (B) A short-T1-inversion-recovearrow), excluding fatty lesions, such as lipomas.
osterior thoracic cord. This finding likely explained our p
atient’s acute neurological decompensation. Ironically,umbar spine magnetic resonance images taken 1 day earlierere just distal to the offending spinal epidural abscess, and
igure 3 Axial magnetic resonance imaging with gadoliniumT2-weighted image) at the level of T9 clearly explained the
2-weighted image) of the thoracic spine revealed the true sourceage showed persistent T2 hyper-intensity without loss of signal
ium (Try im
atient’s neurologic decompensation (arrow).

tp
1cbpsmPtaar
witnhepc
mnnmcacsl
iotaaidees
MPitatcrt
ol
pacotacc
pwhfepc3Ps
R
1
1
1
1
1
1
1033Marsh et al A Cut Above
he diagnosis was missed. Rapid progression of symptomsrompted imaging of the thoracic spine.
Spinal epidural abscesses are rare, affecting only 1 in0,000 hospitalized patients.1 The classic presentation in-ludes a triad of fever, back pain, and neurologic deficits,ut few patients have all 3 components. Often, the initialresentation is nonspecific. A review of 63 patients withpinal epidural abscess found that a correct diagnosis wasade after 1 to 8 visits to the emergency department.2
atients have even undergone exploratory laparotomy prioro receiving a correct diagnosis.3 Our patient’s abdominalnd hip pain were misleading, although abdominal pain,ttributed to thoracic nerve root involvement, has beeneported as an early sign of epidural abscess.3-6
Our patient lacked many of the risk factors associatedith epidural abscess, including diabetes, alcoholism, HIV
nfection, foreign travel, or trauma.1 He had a remote his-ory of intravenous drug use, and a recent HIV test wasegative. It is most likely that the infection associated withis recent surgery entered the bloodstream and seeded thepidural space, leading to epidural abscess. Like 60% ofatients with epidural abscess, he did have a positive bloodulture.7
Untreated spinal epidural abscess can progress quickly touscle weakness, bowel and bladder dysfunction, and fi-
ally paralysis.8,9 Magnetic resonance imaging, the diag-ostic imaging modality of choice, should be obtained im-ediately upon the first clinical suspicion of spinal cord
ompromise. Anatomically, the adult spinal cord terminatest the L1-L2 vertebral body level. Therefore, if spinal cordompression is suspected, imaging of the thoracic spinehould always be included, even if symptoms initially seemocalized to lower spinal levels.
Epidural abscesses are more common in the thoracic thann the lumbar region because of the relatively large amountsf fat within the epidural space of the thoracic spine.10 Forhis same reason, they are almost always found posteriorly,s the dura is attached directly to the vertebral bodiesnteriorly. Ideally, short-T1-inversion-recovery sequencemages should be applied, because they suppress the epi-ural fat signal and greatly increase the efficacy of thexamination (Figure 2B). Finally, it is not uncommon for anpidural abscess to extend longitudinally over 3-5 spinalegments, as was seen with our patient.8
ANAGEMENTaralysis from a spinal epidural abscess can quickly become
rreversible.11,12 The immediate treatment goals are reduc-ion of the inflammatory mass impinging on the spinal cordnd eradication of the causative organism with antibioticherapy. Surgical decompression within the first 24 hours isrucial to improving long-term prognosis, and neurologicecovery after surgery is indirectly related to the duration of
he untreated neurologic deficit.12 Irreversible paraplegiaccurs in up to 25% of patients, and substantially more areeft with residual motor weakness.10,13
Long-term antibiotic therapy alone might allow someatients to achieve full recovery, as shown in a retrospectivenalysis of 57 patients.14 However, medical management isurrently reserved only for selected patients with a knownrganism and no neurologic impairment.15 Almost two-hirds of all cases of epidural abscess are caused by S.ureus, with skin and soft tissue infections being the mostommon sites of bacterial origin.7 The incidence of methi-illin-resistant S. aureus is steadily increasing.1
Our patient underwent emergency spinal cord decom-ression and epidural abscess drainage. Two days later, heas able to move his toes and had regained some strength inis legs. Bilateral reflexes returned, and bowel and bladderunction were restored. A bacterial culture from the drainedpidural abscess grew methicillin-resistant S. aureus. Theatient, who was transferred to a rehabilitation facility,ontinued intravenous vancomycin for 6 weeks. At a-month follow-up visit, he was ambulating with a cane.ower was 4/5 in the right leg and 5/5 in the left. Hisensory paresthesias were gone.
eferences1. Darouiche RO. Spinal epidural abscess. N Engl J Med. 2006;355:
2012-2020.2. Davis DP, Wold RM, Patel RJ, et al. The clinical presentation and
impact of diagnostic delays on emergency department patients withspinal epidural abscess. J Emerg Med. 2004;26:285-291.
3. Hagan G, Adjogatse J. Spinal epidural abscess presenting as acuteabdomen. Ann R Coll Surg Engl. 2004;86:W15-W17.
4. Lim EC, Seet RC. Abdominal pain from a thoracic epidural abscess.J Gen Intern Med. 2006;21:C8-C10.
5. Bremer AA, Darouiche RO. Spinal epidural abscess presenting asintra-abdominal pathology: a case report and literature review.J Emerg Med. 2004;26:51-56.
6. Flikweert ER, Postema RR, Briel JW, et al. Spinal epidural abscesspresenting with abdominal pain. Eur J Pediatr Surg. 2002;12:141-143.
7. Gellin BG, Weingarten K, Gamache FW Jr, et al. Epidural abscess. In:Scheld WM, Whitley RJ, Durack DT, eds. Infections of the CentralNervous System. 2nd Ed. Philadelphia, PA: Lippincott-Raven Publish-ers; 1997:507.
8. Darouiche RO, Hamill RJ, Greenberg SB, et al. Bacterial spinal epi-dural abscess. Review of 43 cases and literature survey. Medicine(Baltimore). 1992;71:369-385.
9. Rigamonti D, Liem L, Wolf AL, et al. Epidural abscess in the cervicalspine. Mt Sinai J Med. 1994;61:357-362.
0. Danner RL, Hartman BJ. Update on spinal epidural abscess: 35 casesand review of the literature. Rev Infect Dis. 1987;9:265-274.
1. Mooney RP, Hockberger RS. Spinal epidural abscess: a rapidly pro-gressive disease. Ann Emerg Med. 1987;16:1168-1170.
2. Liem LK, Rigamonti D, Wolf AL, et al. Thoracic epidural abscess.J Spinal Disord. 1994;7:449-454.
3. Khanna RK, Malik GM, Rock JP, Rosenblum ML. Spinal epiduralabscess: evaluation of factors influencing outcome. Neurosurgery.1996;39:958-964.
4. Wheeler D, Keiser P, Rigamonti D, Keay S. Medical management ofspinal epidural abscesses: case report and review. Clin Infect Dis.1992;15:22-27.
5. Siddiq F, Chowfin A, Tight R, et al. Medical vs. surgical management
of spinal epidural abscess. Arch Intern Med. 2004;164:2409-2412.
C
VLYTHD
Hcp1eb
MH
Dn
0d
The American Journal of Medicine (2007) 120, 1034-1041
LINICAL RESEARCH STUDY
iral Elimination Reduces Incidence of Malignantymphoma in Patients with Hepatitis C
usuke Kawamura, MD, Kenji Ikeda, MD, Yasuji Arase, MD, Hiromi Yatsuji, MD, Hitomi Sezaki, MD,etsuya Hosaka, MD, Norio Akuta, MD, Masahiro Kobayashi, MD, Fumitaka Suzuki, MD, Yoshiyuki Suzuki, MD,iromitsu Kumada, MD
epartment of HPimwMaR0lyd1ip(Clic
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
epatology, Toranomon Hospital, Tokyo, Japan.
ABSTRACT
URPOSE: A high prevalence of malignant lymphoma among patients with hepatitis C virus (HCV)nfection has been reported. The aim of this retrospective study was to determine the incidence ofalignant lymphoma and the relationship between malignant lymphoma and viral elimination in patientsith HCV.ETHOD: We studied 501 consecutive HCV-infected patients who had never received interferon therapy
nd 2708 consecutive HCV-infected patients who received interferon therapy.ESULTS: In the non-interferon group, the cumulative rates of malignant lymphoma development were.6% at the 5th year, 2.3% at the 10th year, and 2.6% at the 15th year. The cumulative rates of malignantymphoma development in interferon-treated patients with sustained virologic response were 0% at the 5thear, 0% at the 10th year, and 0% at the 15th year. The cumulative rates of malignant lymphomaevelopment with persistent infection were 0.4% at the 5th year, 1.5% at the 10th year, and 2.6% at the5th year. The malignant lymphoma development rate was higher in patients with persistent infection thann patients with sustained virologic response (P � .0159). The hazard ratio of lymphomagenesis in 1048atients with sustained virologic response was significantly lower than in patients with persistent infectionhazard ratio: 0.13; P � .049).ONCLUSION: Our retrospective study is the first to determine the annual incidence of malignantymphoma among patients with HCV at 0.23%. Our results indicate that sustained virologic responsenduced by interferon therapy protects against the development of malignant lymphoma in patients withhronic HCV. © 2007 Elsevier Inc. All rights reserved.
KEYWORDS: Cohort study; Hepatitis C virus; Hepatocellular carcinoma; Interferon; Malignant lymphoma; Sus-tained virologic response; Viral elimination\
icsftapitw
t
epatitis C virus (HCV) is a major risk for hepatocellulararcinoma.1-10 The incidence of hepatocellular carcinoma inatients with HCV-related cirrhosis is estimated at 5% to0% per year, and it is one of the major causes of death,specially in Asian countries.10 On the other hand, HCV haseen detected not only within infected hepatocytes but also
The present work was supported in part by Grants-in-Aid from Okinakaemorial Institute for Medical Research and the Japanese Ministry ofealth, Labour and Welfare.
Requests for reprints should be addressed to Yusuke Kawamura, MD,epartment of Hepatology, Toranomon Hospital 2-2-2, Toranomon, Mi-ato-ku, Tokyo 105-8470, Japan.
ront matter © 2007 Elsevier Inc. All rights reserved.ed.2007.06.022
n blood cells, such as lymphocytes,11 and has been impli-ated as a putative agent of cryoglobulinemia.12 The virusustains clonal expansion of B lymphocytes in HCV-in-ected patients.13 Moreover, the prevalence of HCV infec-ion in B-cell non-Hodgkin’s lymphoma also is high,14 andnti-HCV seropositivity is a risk factor of malignant lym-homa.15 Zuckerman et al16 suggested that HCV mightnduce clonal proliferation of B-cell and t(14;18) transloca-ion. However, the mechanism of lymphomagenesis is notell known in patients with HCV.There are many reports on the prevalence of HCV infec-
ion in malignant lymphoma,14 but there is little or no
nformation on the cumulative incidence and influence of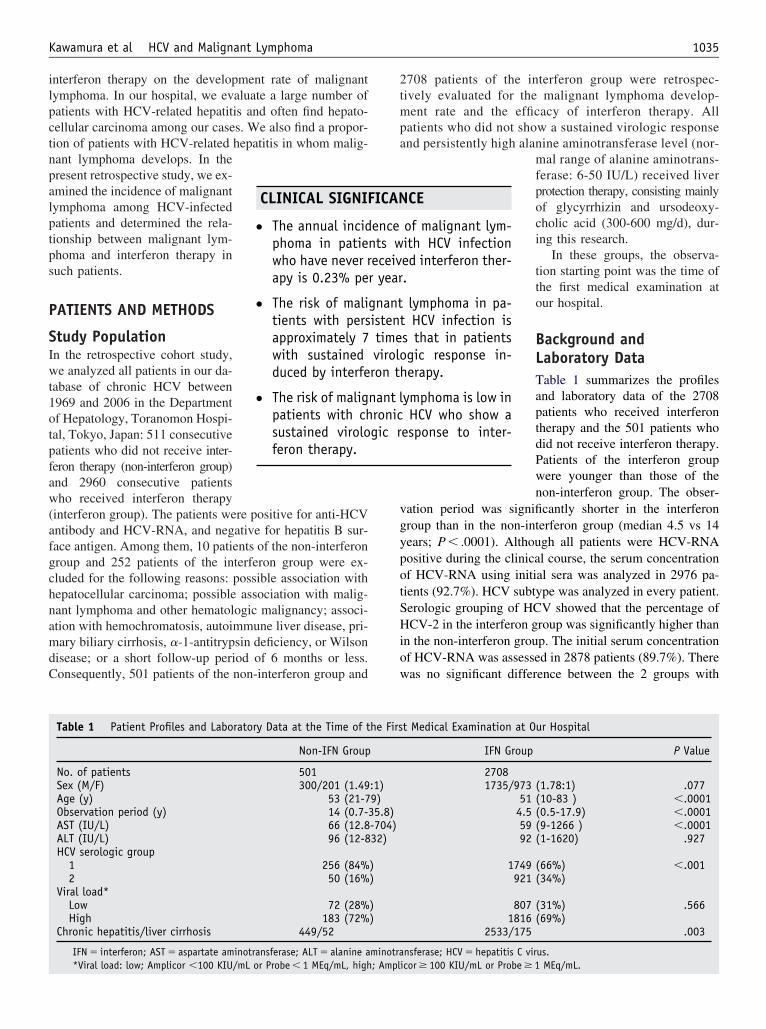
ilpctnpalptps
P
SIwt1otpfaw(afgchnamdC
2tmpa
vgypotSHiow
1035Kawamura et al HCV and Malignant Lymphoma
nterferon therapy on the development rate of malignantymphoma. In our hospital, we evaluate a large number ofatients with HCV-related hepatitis and often find hepato-ellular carcinoma among our cases. We also find a propor-ion of patients with HCV-related hepatitis in whom malig-ant lymphoma develops. In theresent retrospective study, we ex-mined the incidence of malignantymphoma among HCV-infectedatients and determined the rela-ionship between malignant lym-homa and interferon therapy inuch patients.
ATIENTS AND METHODS
tudy Populationn the retrospective cohort study,e analyzed all patients in our da-
abase of chronic HCV between969 and 2006 in the Departmentf Hepatology, Toranomon Hospi-al, Tokyo, Japan: 511 consecutiveatients who did not receive inter-eron therapy (non-interferon group)nd 2960 consecutive patientsho received interferon therapy
interferon group). The patients were positive for anti-HCVntibody and HCV-RNA, and negative for hepatitis B sur-ace antigen. Among them, 10 patients of the non-interferonroup and 252 patients of the interferon group were ex-luded for the following reasons: possible association withepatocellular carcinoma; possible association with malig-ant lymphoma and other hematologic malignancy; associ-tion with hemochromatosis, autoimmune liver disease, pri-ary biliary cirrhosis, �-1-antitrypsin deficiency, or Wilson
isease; or a short follow-up period of 6 months or less.onsequently, 501 patients of the non-interferon group and
CLINICAL SIGNIF
● The annual incidphoma in patienwho have never rapy is 0.23% pe
● The risk of malitients with persapproximately 7with sustainedduced by interfe
● The risk of maligpatients with chsustained viroloferon therapy.
Table 1 Patient Profiles and Laboratory Data at the Time of t
Non-IFN Group
No. of patients 501Sex (M/F) 300/201 (1.49Age (y) 53 (21-7Observation period (y) 14 (0.7-3AST (IU/L) 66 (12.8ALT (IU/L) 96 (12-8HCV serologic group
1 256 (84%2 50 (16%
Viral load*Low 72 (28%High 183 (72%
Chronic hepatitis/liver cirrhosis 449/52
IFN � interferon; AST � aspartate aminotransferase; ALT � alanine a
*Viral load: low; Amplicor �100 KIU/mL or Probe � 1 MEq/mL, high; Ampl708 patients of the interferon group were retrospec-ively evaluated for the malignant lymphoma develop-ent rate and the efficacy of interferon therapy. All
atients who did not show a sustained virologic responsend persistently high alanine aminotransferase level (nor-
mal range of alanine aminotrans-ferase: 6-50 IU/L) received liverprotection therapy, consisting mainlyof glycyrrhizin and ursodeoxy-cholic acid (300-600 mg/d), dur-ing this research.
In these groups, the observa-tion starting point was the time ofthe first medical examination atour hospital.
Background andLaboratory DataTable 1 summarizes the profilesand laboratory data of the 2708patients who received interferontherapy and the 501 patients whodid not receive interferon therapy.Patients of the interferon groupwere younger than those of thenon-interferon group. The obser-
ation period was significantly shorter in the interferonroup than in the non-interferon group (median 4.5 vs 14ears; P � .0001). Although all patients were HCV-RNAositive during the clinical course, the serum concentrationf HCV-RNA using initial sera was analyzed in 2976 pa-ients (92.7%). HCV subtype was analyzed in every patient.erologic grouping of HCV showed that the percentage ofCV-2 in the interferon group was significantly higher than
n the non-interferon group. The initial serum concentrationf HCV-RNA was assessed in 2878 patients (89.7%). Thereas no significant difference between the 2 groups with
CE
of malignant lym-ith HCV infectioned interferon ther-.
lymphoma in pa-HCV infection is
s that in patientsgic response in-erapy.
ymphoma is low inHCV who show a
esponse to inter-
t Medical Examination at Our Hospital
IFN Group P Value
27081735/973 (1.78:1) .077
51 (10-83 ) �.00014.5 (0.5-17.9) �.000159 (9-1266 ) �.000192 (1-1620) .927
1749 (66%) �.001921 (34%)
807 (31%) .5661816 (69%)
2533/175 .003
nsferase; HCV � hepatitis C virus.
ICAN
encets w
eceivr year
gnantistenttimeviroloron th
nant lronicgic r
he Firs
:1)9)5.8)
-704)32)
))
))
minotra
icor � 100 KIU/mL or Probe � 1 MEq/mL.
rcvPaAssi
TIArbfbisopAgat
VDsdnHbSaDgos
HLpwawawhpp
FMPfi
nisswpwtfizeAbcnf
SNbWafhtcfptwlfmdvcaPspptci
R
IWI1ylts
1036 The American Journal of Medicine, Vol 120, No 12, December 2007
egard to the initial viral load (low viral load; Ampli-or � 100 KIU/mL [Cobas Amplicor HCV Monitor Test,2.0, Roche Molecular Systems, Inc, Belleville, NJ] orrobe � 1 MEq/mL, high viral load [branched DNA probessay; version 2.0; Chiron, Dai-ichi Kagaku, Tokyo, Japan];mplicor � 100 KIU/mL or probe � 1 MEq/mL). In this
tudy, the percentage of patients with chronic hepatitis wasignificantly higher in the interferon group than in the non-nterferon group.
ype of Interferon and Judgment ofnterferon Effectmong 2708 patients with interferon therapy, 1675 patients
eceived interferon-alpha, 415 patients received interferon-eta, 33 patients received both interferon-alpha and inter-eron-beta, and the remaining 585 patients received a com-ination therapy of interferon and ribavirin. The response tonterferon therapy was based on a sustained virologic re-ponse (elimination of HCV-RNA at 6 months after the endf treatment). Among patients treated with interferon, 1048atients (38.7%) acquired a sustained virologic response.mong 1660 patients in the nonsustained virologic responseroup, there were 1012 patients with a relapse of HCV RNAfter temporal viral clearance, and the remaining 648 pa-ients had nonviral clearance during treatment.
iral Markers of Hepatitis B and C Virusesiagnosis of HCV infection was based on the detection of
erum HCV antibody and positive RNA. Anti-HCV wasetected using a second-generation enzyme-linked immu-osorbent assay (Abbott Laboratories, North Chicago, Ill).CV-RNA was determined by the Amplicor method (Co-as Amplicor HCV Monitor Test, v2.0, Roche Molecularystems, Inc, Belleville, NJ) or the branched DNA probessay (branched DNA probe assay; version 2.0; Chiron,ai-ichi Kagaku, Tokyo, Japan). Hepatitis B surface anti-en was tested by radioimmunoassay (Austria, Abbott Lab-ratories, Detroit, Mich). The used serum samples weretored �80°C at the first consultation.
istopathologic Examination of Liveriver biopsy specimens were obtained percutaneously or ateritoneoscopy using a modified Vim-Silverman needleith an internal diameter of 2 mm. All specimens for ex-
mination contained at least 6 portal areas. Chronic hepatitisas diagnosed on the basis of histopathologic assessment
ccording to the scoring system of Desmet et al.17 Patientsho did not undergo liver biopsy were diagnosed with chronicepatitis on the basis of the presence of irregular liver surface,ortal-hypertension, and/or ascites by ultrasonography, com-uted tomography (CT), and/or endoscopy.
ollow-up, Diagnosis, and Classification ofalignant Lymphoma
atients were followed up monthly to trimonthly after the
rst medical examination at our hospital. Physical exami- mation and biochemical tests were conducted at each exam-nation together with a regular checkup with CT or ultra-onography imaging in each patient. When a patient had anyymptoms in relation to malignant lymphoma (unexplainedeight loss, fever, and lymphadenopathy), we further ex-lored possible malignant lymphoma. Malignant lymphomaas diagnosed by histopathologic examination. Classifica-
ion was based on the Revised European-American Classi-cation of lymphoid neoplasms/new World Health Organi-ation classification18 revised by Harris.19 Staging andxtranodal involvement were determined according to thenn Arbor classification by physical examination, totalody CT scan, and bone marrow biopsy. The number ofases lost to follow-up included 78 patients (15.6%) in theon-interferon group and 184 patients (6.8%) in the inter-eron group.
tatistical Analysisonparametric procedures were used for the analysis ofackground features of the patients, including the Mann-hitney U test and chi-square method. The cumulative
ppearance rate of malignant lymphoma was calculatedrom the period between the first medical examination at ourospital to the appearance of malignant lymphoma, usinghe Kaplan-Meier method. Differences in lymphomagenesisurves were tested using the log-rank test. Independentactors associated with the incidence rate of malignant lym-homa were analyzed by a time-dependent Cox propor-ional hazard model, using the term of interferon therapyith “waiting time” as a time-dependent variable. The fol-
owing 9 variables were analyzed for potential covariatesor incidence of malignant lymphoma at the time of firstedical examination at our hospital: age, sex, state of liver
isease (chronic hepatitis or liver cirrhosis), viral serotype,iral load, history of interferon therapy, efficacy of virallearance by interferon therapy, serum concentrations ofspartate aminotransferase, and alanine aminotransferase. A
value of less than .05 in a 2-tailed test was consideredignificant. Data analysis was performed using the computerrogram SPSS version 11.0 (SPSS Inc, Chicago, Ill). Thehysicians in charge explained the purpose and method ofhis clinical trial to each patient, who gave their informedonsent for participation. This study was approved by thenstitutional review board of our hospital.
ESULTS
ncidence of Malignant Lymphoma in Patientsithout Interferon Therapy
n the interferon group, malignant lymphoma developed in2 patients (2.4%) during a median observation period of 14ears. The cumulative rate of newly diagnosed malignantymphoma was 0.62% at the end of the 5th year, 2.26% athe 10th year, and 2.62% at the 15th year (Figure 1). Table 2ummarizes the characteristics of patients who developed
alignant lymphoma. The period between the first medical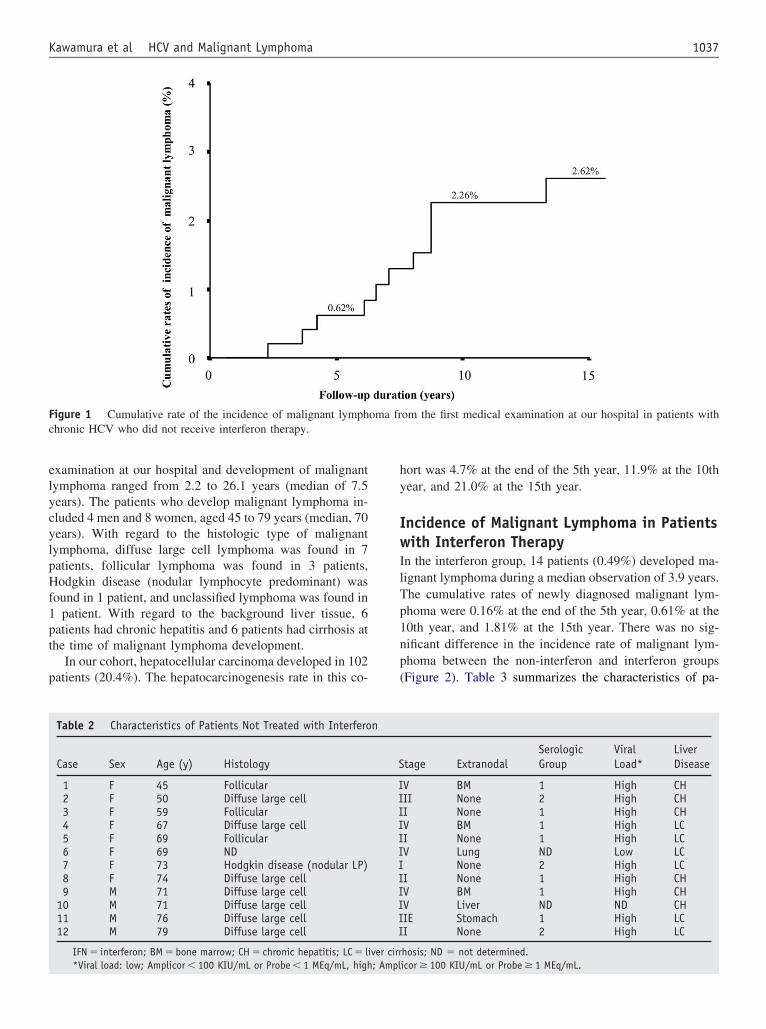
elycylpHf1pt
p
hy
IwIlTp1np(
Fc
1037Kawamura et al HCV and Malignant Lymphoma
xamination at our hospital and development of malignantymphoma ranged from 2.2 to 26.1 years (median of 7.5ears). The patients who develop malignant lymphoma in-luded 4 men and 8 women, aged 45 to 79 years (median, 70ears). With regard to the histologic type of malignantymphoma, diffuse large cell lymphoma was found in 7atients, follicular lymphoma was found in 3 patients,odgkin disease (nodular lymphocyte predominant) was
ound in 1 patient, and unclassified lymphoma was found inpatient. With regard to the background liver tissue, 6
atients had chronic hepatitis and 6 patients had cirrhosis athe time of malignant lymphoma development.
In our cohort, hepatocellular carcinoma developed in 102atients (20.4%). The hepatocarcinogenesis rate in this co-
igure 1 Cumulative rate of the incidence of malignant lymphhronic HCV who did not receive interferon therapy.
Table 2 Characteristics of Patients Not Treated with Interfero
Case Sex Age (y) Histology
1 F 45 Follicular2 F 50 Diffuse large cell3 F 59 Follicular4 F 67 Diffuse large cell5 F 69 Follicular6 F 69 ND7 F 73 Hodgkin disease (nodular LP)8 F 74 Diffuse large cell9 M 71 Diffuse large cell
10 M 71 Diffuse large cell11 M 76 Diffuse large cell12 M 79 Diffuse large cell
IFN � interferon; BM � bone marrow; CH � chronic hepatitis; LC � li
*Viral load: low; Amplicor � 100 KIU/mL or Probe � 1 MEq/mL, high; Amplort was 4.7% at the end of the 5th year, 11.9% at the 10thear, and 21.0% at the 15th year.
ncidence of Malignant Lymphoma in Patientsith Interferon Therapy
n the interferon group, 14 patients (0.49%) developed ma-ignant lymphoma during a median observation of 3.9 years.he cumulative rates of newly diagnosed malignant lym-homa were 0.16% at the end of the 5th year, 0.61% at the0th year, and 1.81% at the 15th year. There was no sig-ificant difference in the incidence rate of malignant lym-homa between the non-interferon and interferon groupsFigure 2). Table 3 summarizes the characteristics of pa-
om the first medical examination at our hospital in patients with
tage ExtranodalSerologicGroup
ViralLoad*
LiverDisease
V BM 1 High CHII None 2 High CHI None 1 High CHV BM 1 High LCI None 1 High LCV Lung ND Low LC
None 2 High LCI None 1 High CHV BM 1 High CHV Liver ND ND CHIE Stomach 1 High LCI None 2 High LC
hosis; ND � not determined.
oma fr
n
S
IIIIIIIIIIII
ver cirr
icor � 100 KIU/mL or Probe � 1 MEq/mL.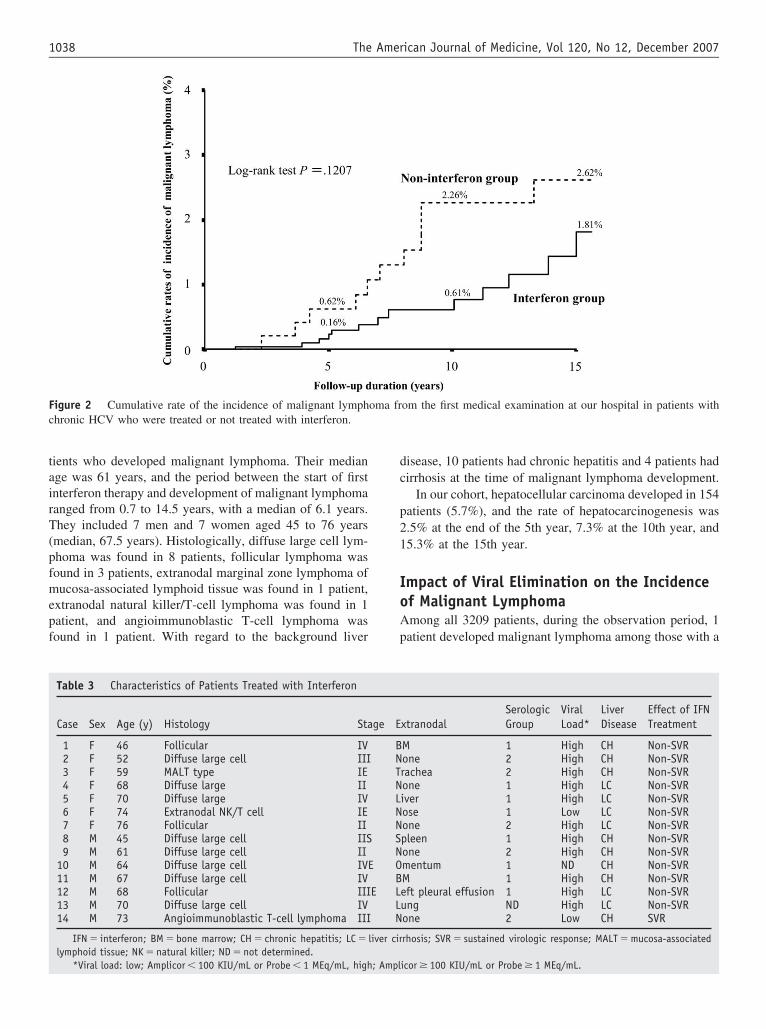
tairT(pfmepf
dc
p21
IoAp
Fc
1038 The American Journal of Medicine, Vol 120, No 12, December 2007
ients who developed malignant lymphoma. Their mediange was 61 years, and the period between the start of firstnterferon therapy and development of malignant lymphomaanged from 0.7 to 14.5 years, with a median of 6.1 years.hey included 7 men and 7 women aged 45 to 76 years
median, 67.5 years). Histologically, diffuse large cell lym-homa was found in 8 patients, follicular lymphoma wasound in 3 patients, extranodal marginal zone lymphoma ofucosa-associated lymphoid tissue was found in 1 patient,
xtranodal natural killer/T-cell lymphoma was found in 1atient, and angioimmunoblastic T-cell lymphoma wasound in 1 patient. With regard to the background liver
igure 2 Cumulative rate of the incidence of malignant lymphhronic HCV who were treated or not treated with interferon.
Table 3 Characteristics of Patients Treated with Interferon
Case Sex Age (y) Histology Sta
1 F 46 Follicular IV2 F 52 Diffuse large cell III3 F 59 MALT type IE4 F 68 Diffuse large II5 F 70 Diffuse large IV6 F 74 Extranodal NK/T cell IE7 F 76 Follicular II8 M 45 Diffuse large cell IIS9 M 61 Diffuse large cell II
10 M 64 Diffuse large cell IVE11 M 67 Diffuse large cell IV12 M 68 Follicular III13 M 70 Diffuse large cell IV14 M 73 Angioimmunoblastic T-cell lymphoma III
IFN � interferon; BM � bone marrow; CH � chronic hepatitis; LC �lymphoid tissue; NK � natural killer; ND � not determined.
*Viral load: low; Amplicor � 100 KIU/mL or Probe � 1 MEq/mL, high; Ampl
isease, 10 patients had chronic hepatitis and 4 patients hadirrhosis at the time of malignant lymphoma development.
In our cohort, hepatocellular carcinoma developed in 154atients (5.7%), and the rate of hepatocarcinogenesis was.5% at the end of the 5th year, 7.3% at the 10th year, and5.3% at the 15th year.
mpact of Viral Elimination on the Incidencef Malignant Lymphomamong all 3209 patients, during the observation period, 1atient developed malignant lymphoma among those with a
om the first medical examination at our hospital in patients with
xtranodalSerologicGroup
ViralLoad*
LiverDisease
Effect of IFNTreatment
M 1 High CH Non-SVRone 2 High CH Non-SVRrachea 2 High CH Non-SVRone 1 High LC Non-SVRiver 1 High LC Non-SVRose 1 Low LC Non-SVRone 2 High LC Non-SVRpleen 1 High CH Non-SVRone 2 High CH Non-SVRmentum 1 ND CH Non-SVRM 1 High CH Non-SVReft pleural effusion 1 High LC Non-SVRung ND High LC Non-SVRone 2 Low CH SVR
rhosis; SVR � sustained virologic response; MALT � mucosa-associated
oma fr
ge E
BNTNLNNSNOB
E LLN
liver cir
icor � 100 KIU/mL or Probe � 1 MEq/mL.
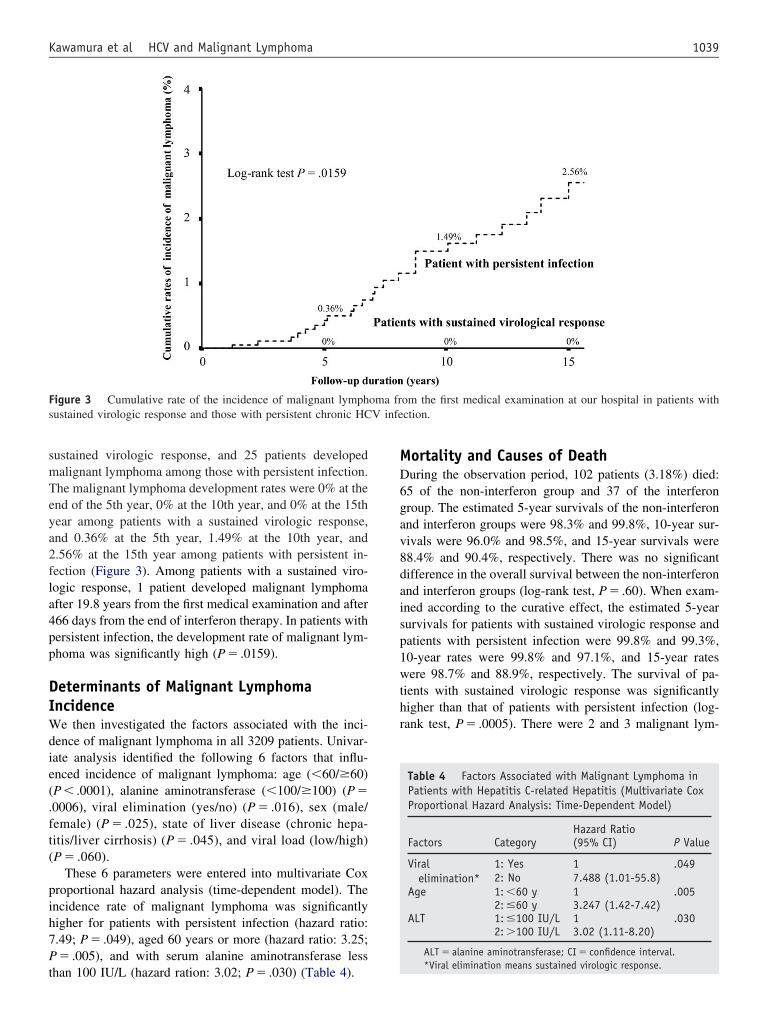
smTeya2fla4pp
DIWdie(.ft(
pih7Pt
MD6gav8daisp1wthr
Fs V infe
1039Kawamura et al HCV and Malignant Lymphoma
ustained virologic response, and 25 patients developedalignant lymphoma among those with persistent infection.he malignant lymphoma development rates were 0% at thend of the 5th year, 0% at the 10th year, and 0% at the 15thear among patients with a sustained virologic response,nd 0.36% at the 5th year, 1.49% at the 10th year, and.56% at the 15th year among patients with persistent in-ection (Figure 3). Among patients with a sustained viro-ogic response, 1 patient developed malignant lymphomafter 19.8 years from the first medical examination and after66 days from the end of interferon therapy. In patients withersistent infection, the development rate of malignant lym-homa was significantly high (P � .0159).
eterminants of Malignant Lymphomancidencee then investigated the factors associated with the inci-
ence of malignant lymphoma in all 3209 patients. Univar-ate analysis identified the following 6 factors that influ-nced incidence of malignant lymphoma: age (�60/�60)P � .0001), alanine aminotransferase (�100/�100) (P �0006), viral elimination (yes/no) (P � .016), sex (male/emale) (P � .025), state of liver disease (chronic hepa-itis/liver cirrhosis) (P � .045), and viral load (low/high)P � .060).
These 6 parameters were entered into multivariate Coxroportional hazard analysis (time-dependent model). Thencidence rate of malignant lymphoma was significantlyigher for patients with persistent infection (hazard ratio:.49; P � .049), aged 60 years or more (hazard ratio: 3.25;� .005), and with serum alanine aminotransferase less
igure 3 Cumulative rate of the incidence of malignant lymphustained virologic response and those with persistent chronic HC
han 100 IU/L (hazard ration: 3.02; P � .030) (Table 4).
ortality and Causes of Deathuring the observation period, 102 patients (3.18%) died:5 of the non-interferon group and 37 of the interferonroup. The estimated 5-year survivals of the non-interferonnd interferon groups were 98.3% and 99.8%, 10-year sur-ivals were 96.0% and 98.5%, and 15-year survivals were8.4% and 90.4%, respectively. There was no significantifference in the overall survival between the non-interferonnd interferon groups (log-rank test, P � .60). When exam-ned according to the curative effect, the estimated 5-yearurvivals for patients with sustained virologic response andatients with persistent infection were 99.8% and 99.3%,0-year rates were 99.8% and 97.1%, and 15-year ratesere 98.7% and 88.9%, respectively. The survival of pa-
ients with sustained virologic response was significantlyigher than that of patients with persistent infection (log-ank test, P � .0005). There were 2 and 3 malignant lym-
om the first medical examination at our hospital in patients withction.
Table 4 Factors Associated with Malignant Lymphoma inPatients with Hepatitis C-related Hepatitis (Multivariate CoxProportional Hazard Analysis: Time-Dependent Model)
Factors CategoryHazard Ratio
P Value(95% CI)
Viralelimination*
1: Yes 1 .0492: No 7.488 (1.01-55.8)
Age 1: �60 y 1 .0052: �60 y 3.247 (1.42-7.42)
ALT 1: �100 IU/L 1 .0302: �100 IU/L 3.02 (1.11-8.20)
ALT � alanine aminotransferase; CI � confidence interval.
oma fr
*Viral elimination means sustained virologic response.

pi
DTBwotpaftgpl
dattf2vdH0r(tpo
ano(tpfoHotwiislmti
iro
tltSi
aslislsolac
nfi
COcidH
R
1
1
1040 The American Journal of Medicine, Vol 120, No 12, December 2007
homa-related deaths in the non-interferon group and thenterferon group, respectively.
ISCUSSIONhe reported significant incidence of HCV infection in-cell non-Hodgkin’s lymphoma in several areas of theorld indicates a link between viral infection and this subsetf lymphoproliferative disorder. The controversial results ofhe different research groups may be explained by the lowrobability of HCV carriers who develop lymphoma; thus,n accurate assessment of the exact risk could only comerom a large cohort study.20 Recent reports attesting tohe efficacy of interferon therapy for HCV-related, low-rade B-cell non-Hodgkin’s lymphoma21 support the hy-othesis of a link between HCV infection and B-cellymphoma.
Little is known about the relationship between the inci-ence of malignant lymphoma and interferon therapy. Theim of this research was to clarify the relationship in pa-ients with HCV. Our retrospective cohort study showedhat 12 of 501 cases without interferon therapy (non-inter-eron group) developed malignant lymphoma and 14 of708 cases with interferon treatment (interferon group) de-eloped malignant lymphoma. This epidemiologic studyemonstrates the malignant lymphoma occurrence rate inCV-positive patients: The annual appearance rate was.23% in the non-interferon group. The annual appearanceate was higher than that in the general Japanese population�0.008%). Furthermore, our results clearly indicate thathe hazard ratio for malignant lymphoma development inatients with HCV elimination is 0.133 compared with thatf patients with persistent infection (Table 4).
Multivariate analysis identified age, HCV elimination,nd alanine aminotransferase level as significant determi-ants of malignant lymphoma development. Interpretationf this finding requires further examination and analysisTable 4). Zuckerman et al16 reported that chromosomeranslocation of B-cell improved after interferon therapy inatients with malignant lymphoma complicating HCV in-ection. Our results are in agreement with those of a previ-us study that showed interferon-induced improvement ofCV-related lymphoma.21 In our study, the incidence ratef malignant lymphoma was significantly lower among pa-ients with a sustained virologic response than in patientsith persistent infection for both the non-interferon and
nterferon groups (Figure 3). Thus, our results indicate thatnterferon therapy coupled with sustained virologic re-ponse reduces the likelihood of development of malignantymphoma. We again emphasize the high prevalence ofalignant lymphoma in HCV-positive patients without in-
erferon therapy and the significance of viral elimination bynterferon in regard to the suppression of lymphomagenesis.
Although it is safe to conclude that malignant lymphomas not a risk in patients who achieve a sustained virologicesponse by interferon therapy, malignant lymphoma devel-
ped in 1 patient after achieving an interferon-induced sus-ained virologic response. However, the cause of malignantymphoma is not clear, that is, whether it is de novo, mu-ation of genome by infection of HCV, or other factors.tudies are under way in our laboratories to investigate this
ssue.We also analyzed the incidence of malignant lymphoma
ccording to the subtype of malignant lymphoma. The re-ults showed a significant prevalence of diffuse large-cellymphoma (P � .029) and follicular lymphoma (P � .005)n our cohort compared with the distribution of the sameubtypes of malignant lymphoma in Japan.22 Malignantymphoma cases with HCV-related hepatitis may develop apecific subtype of non-Hodgkin’s lymphoma. However,ur cohort included only a small number of malignantymphoma cases, and this finding should be confirmed innother study with a large number of malignant lymphomaases with HCV-related hepatitis.
Although the design of our study was retrospective inature, multicenter prospective studies are needed to con-rm the results described in this report.
ONCLUSIONur retrospective cohort study reported for the first time the
umulative incidence rate of malignant lymphoma in HCV-nfected patients and indicated that interferon therapy re-uces the incidence of malignant lymphoma in patients withCV-related hepatitis.
eferences1. Bruix J, Barrera JM, Calvet X, et al. Prevalence of antibodies to
hepatitis C virus in Spanish patients with hepatocellular carcinoma andhepatic cirrhosis. Lancet. 1989;ii:1004-1006.
2. Colombo M, Kuo G, Choo QL, et al. Prevalence of antibodies tohepatitis C virus in Italian patients with hepatocellular carcinoma.Lancet. 1989;ii:1006-1008.
3. Hasan F, Jeffers LJ, De Medina M, et al. Hepatitis C-associatedhepatocellular carcinoma. Hepatology. 1990;12:589-591.
4. Kew MC, Houghton M, Choo QL, et al. Hepatitis C virus antibodiesin southern African blacks with hepatocellular carcinoma. Lancet.1990;335:873-874.
5. Ohkoshi S, Kojima H, Tawaraya H, et al. Prevalence of antibodyagainst non-A, non-B hepatitis virus in Japanese patients with hepa-tocellular carcinoma. Jpn J Cancer Res. 1990;81:550-553.
6. Saito I, Miyamura T, Ohbayashi A, et al. Hepatitis C virus infection isassociated with the development of hepatocellular carcinoma. ProcNatl Acad Sci U S A. 1990;87:6547-6549.
7. Kiyosawa K, Furuta S. Review of hepatitis C in Japan. J GastroenterolHepatol. 1991;6:383-391.
8. Alter MJ, Margolis HS, Krawczynski K, et al. The natural history ofcommunity acquired hepatitis C in the United States. N Engl J Med.1992;327:1899-1905.
9. Tsukuma H, Hiyama T, Tanaka S, et al. Risk factors for hepatocellularcarcinoma among patients with chronic liver disease. N Engl J Med.1993;328:1797-1801.
0. Ikeda K, Saitoh S, Koida I, et al. A multivariate analysis of risk factorsfor hepatocellular carcinogenesis: a prospective observation of 795patients with viral and alcoholic cirrhosis. Hepatology. 1993;18:47-53.
1. Ferri C, Monti M, La Civita L, et al. Infection of peripheral bloodmononuclear cells by hepatitis C virus in mixed cryoglobulinemia.
Blood. 1993;82:3701-3704.
1
1
1
1
1
1
1
1
2
2
2
1041Kawamura et al HCV and Malignant Lymphoma
2. Agnello V, Chung RT, Kaplan LM. A role for hepatitis C virusinfection in type II cryoglobulinemia. N Engl J Med. 1992;327:1490-1495.
3. Franzin F, Efremov DG, Pozzato G, et al. Clonal B-cell expansions inperipheral blood of HCV-infected patients. Br J Haematol. 1995;90:548-552.
4. Gisbert JP, Garcia-Buey L, Pajares JM, et al. Prevalence of hepatitis Cvirus infection in B-cell non-Hodgkin’s lymphoma: systematic reviewand meta-analysis. Gastroenterology. 2003;125:1723-1732.
5. Matsuo K, Kusano A, Sugumar A, et al. Effect of hepatitis C virusinfection on the risk of non-Hodgkin’s lymphoma: a meta-analysis ofepidemiological studies. Cancer Sci. 2004;95:745-752.
6. Zuckerman E, Zuckerman T, Sahar D, et al. The effect of antiviraltherapy on t(14;18) translocation and immunoglobulin gene rearrange-ment in patients with chronic hepatitis C virus infection. Blood. 2001;
97:1555-1559.7. Desmet VJ, Gerber M, Hoofnagle JH, et al. Classification of chronichepatitis: diagnosis, grading and staging. Hepatology. 1994;19:1513-1520.
8. Harris NL, Jaffe ES, Stein H, et al. A revised European-Americanclassification of lymphoid neoplasms: a proposal from the Interna-tional Lymphoma Study Group. Blood. 1994;84:1361-1392.
9. Harris NL. Principles of the revised European-American LymphomaClassification (from the International Lymphoma Study Group). AnnOncol. 1997;8(Suppl 2):11-16.
0. Turner NC, Dusheiko G, Jones A. Hepatitis C and B-cell lymphoma.Ann Oncol. 2003;14:1341-1345.
1. Vallisa D, Bernuzzi P, Arcaini L, et al. Role of anti-hepatitis C virus(HCV) treatment in HCV-related, low-grade, B-cell, non-Hodgkin’slymphoma: a multicenter Italian. J Clin Oncol. 2005;23:468-473.
2. Lymphoma Study Group of Japanese Pathologists. The World HealthOrganization classification of malignant lymphomas in Japan: inci-
dence of recently recognized entities. Pathol Int. 2000;50:696-702.
C
SDDHa
CPH
vnAtd(
CG
0d
The American Journal of Medicine (2007) 120, 1042-1046
LINICAL RESEARCH STUDY
kin Temperature Monitoring Reduces the Risk foriabetic Foot Ulceration in High-risk Patients
avid G. Armstrong, DPM, PhD,a Katherine Holtz-Neiderer, DPM,b Christopher Wendel, MS,b M. Jane Mohler, PhD,b,c
eather R. Kimbriel,b Lawrence A. Lavery, DPM, MPHd
Scholl’s Center for Lower Extremity Ambulatory Research (CLEAR), Rosalind Franklin University of Medicine and Science, Northhicago, Ill; bSouthern Arizona Veterans Affairs Medical Center, Tucson; cDepartment of Epidemiology and Biostatistics, College ofublic Health, University of Arizona, Tucson; dDepartment of Surgery, Texas A&M College of Medicine at Scott & White Memorial
ospital, TemplePuMatfGTsRlvauFgoCur
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
.
ABSTRACT
URPOSE: To evaluate the effectiveness of home temperature monitoring to reduce the incidence of footlcers in high-risk patients with diabetes.ETHODS: In this physician-blinded, 18-month randomized controlled trial, 225 subjects with diabetes
t high risk for ulceration were assigned to standard therapy (Standard Therapy Group) or dermalhermometry (Dermal Thermometry Group) groups. Both groups received therapeutic footwear, diabeticoot education, regular foot care, and performed a structured foot inspection daily. Dermal Thermometryroup subjects used an infrared skin thermometer to measure temperatures on 6 foot sites twice daily.emperature differences �4°F between left and right corresponding sites triggered patients to contact thetudy nurse and reduce activity until temperatures normalized.ESULTS: A total of 8.4% (n � 19) subjects ulcerated over the study period. Subjects were one third as
ikely to ulcerate in the Dermal Thermometry Group compared with the Standard Therapy Group (12.2%s 4.7%, odds ratio 3.0, 95% confidence interval, 1.0 to 8.5, P � .038). Proportional hazards regressionnalysis suggested that thermometry intervention was associated with a significantly longer time tolceration (P � .04), adjusted for elevated foot ulcer classification (International Working Group Riskactor 3), age, and minority status. Patients that ulcerated had a temperature difference that was 4.8 timesreater at the site of ulceration in the week before ulceration than did a random 7 consecutive-day samplef 50 other subjects that did not ulcerate (3.50 � 1.0 vs 0.74 � 0.05, P � .001).ONCLUSIONS: High temperature gradients between feet may predict the onset of neuropathiclceration and self-monitoring may reduce the risk of ulceration. © 2007 Elsevier Inc. All rightseserved.
KEYWORDS: Diabetes; Foot; Thermometry; Ulcer; Wound
IeMsbatpa
This study was supported by VA HSR&D Merit Award 20-059. Theiews expressed in this article are those of the authors and do notecessarily reflect the position or policy of the Department of Veteransffairs. All authors had full access to all of the data in the study and all
ake responsibility for the integrity of the data and the accuracy of theata analysis. This protocol has been registered with Clintrials.govNCT00105755).
Requests for reprints should be addressed to David G. Armstrong,LEAR, Rosalind Franklin University of Medicine and Science, 3333reen Bay Road, North Chicago, IL 60064.
ront matter © 2007 Elsevier Inc. All rights reserved.ed.2007.06.028
n diabetes, as in other chronic diseases, self-care is anssential element of disease management and prevention.ost diabetic lower extremity complications involve sen-
ory neuropathy; patients do not recognize that their feet areeing injured until a wound develops.1,2 Wounds are invari-bly preceded by inflammation.3-6 Therefore, it would stando reason that identifying preulcerative inflammation mightredict foot ulceration. Temperature assessment seems to belikely surrogate to measure inflammation.Studies of dermal thermometry have suggested that vari-
tions in temperature �4°F (2.2°C) could be helpful in skin
spmptslisawstppthsoau
MImtwcutwstTtDtTdataepttmticr
PASy
FchRt
ltw
ITwwpdtadgo
OWhitequipc
heir
1043Armstrong et al Diabetic Foot Ulceration
urveillance.7-12 More recently, 2 randomized trials ap-eared to confirm that dispensing simple “personal ther-ometers” to neuropathic patients might serve as useful
revention tools.13,14 The second of these studies appearedo suggest that this preventative effect is independent ofimply increasing visual surveil-ance of the foot.14 Previous stud-es using temperature as a self-as-essment and monitoring toolppear promising; however, theyere either conducted over rather
hort time frames (6 months)13 orhey studied very specific patientopulations.14 Therefore, the pur-ose of this study was to evaluatehe effectiveness of an infraredome temperature monitoring in-trument to reduce the incidencef foot complications in patientst high risk for diabetic footlceration.
ETHODSn this physician-blinded, 18-onth randomized controlled
rial, 225 United States veteransith diabetes at high risk for ul-
eration (neuropathy and deformity or previous history oflceration) were assigned to standard therapy or dermalhermometry groups. Both groups received therapeutic foot-ear, diabetic foot education, and regular foot care. All
ubjects were instructed to perform a structured foot inspec-ion daily and record their findings in a logbook. If Standardherapy Group subjects identified any foot abnormalities,
hey were to contact the study coordinator immediately.ermal Thermometry Group subjects used an infrared skin
hermometer (TempTouch, Xilas Medical, San Antonio,ex) to measure temperatures on 6 sites on the foot twice aay. Temperature differences �4°F (�2.2°C) between leftnd right corresponding sites triggered patients to contacthe study coordinator and reduce activity until their temper-tures normalized. As a practical measure, the oppositextremity was used as a control because both feet are ex-osed to the same repetitive stresses during walking andherefore represented a built-in comparison source. Becausehe disease processes of neuropathic ulceration involvesultiple factors that affect lower extremity perfusion and
emperature regulation, we felt that it would be difficult todentify an absolute skin temperature level that could beonsidered normal or one that could be used as a universaleference.
articipantsll patients with type 2 diabetes receiving foot care at theouthern Arizona VA Health Care System, aged 18-80
CLINICAL SIGNIF
● Diabetic footcomplex and cquently causedthe foot, causskin breakdown.
● The results of thsimple device uidentify potentiation and allowactivity before u
● In this mannertheir activity byperatures muchlin by checking t
ears, who fit category 2 or 3 of the International Diabetic T
oot Risk Classification System,15 were candidates for in-lusion in the study. Risk Group 3 included patients with aistory of either a foot ulcer or of a partial foot amputation.isk Group 2 included patients with neuropathy and struc-
ural foot deformity or limited joint mobility.15 There wereapproximately 4800 patients withtype 2 diabetes receiving care atthe Southern Arizona VA HealthCare System. Of these, 1942 wereidentified as high risk for develop-ment of foot ulcers (neuropathyand deformity), and at least 300had been treated for a foot ulcer ora partial foot amputation in 1999.
Candidates were not admittedto the study if any of the followingcriteria were present: active openulcers, amputation sites, or footinfections; active Charcot arthrop-athy; severe peripheral vasculardisease, as evidenced by nonpal-pable foot pulses or an ankle-bra-chial index �0.8 on either extrem-ity; dementia or impaired cognitivefunction; active drug abuse or his-tory of drug or alcohol abusewithin 1 year of the study; sightimpaired (ie, unable to read the
arge (2.5 cm) digital display characters on the dermalhermometer); or unable to walk without the assistance of aheelchair or crutches.
nterventionshe TempTouch thermometer (Xilas Medical) is equippedith a “touch sensor” that detects tip contact with skin,hich allows the user to just simply touch the end of therobe to the skin to take a measurement. To operate theevice, the user would place the tip of the device onhe skin, which would then automatically trigger a temper-ture measurement and display it on an LCD (liquid crystalisplay) screen. The thermometer utilized incorporates aooseneck design, which allows the user to reach any pointn the bottom or sides of the foot.
bjectivese evaluated the effectiveness of self-administered in-
ome infrared temperature probe monitoring to reduce thencidence of diabetic foot ulcers in high-risk veterans withype 2 diabetes. Secondary objectives were to measure theffect of the intervention on type of ulcer, health-relateduality of life, self-efficacy, satisfaction with care, and mod-lation of activity. We tested the hypothesis that self-mon-tored temperatures would: reduce the rate of foot ulcers andositively influence health-related quality of life, self-effi-acy and satisfaction with care, and modulation of activity.
CE
ds are common,. They are fre-petitive stress tonflammation and
dy suggest that ay the patient canmaging inflamma-atient to modifyion.
ients may modifying their skin tem-y dose their insu-glucose.
ICAN
wounostlyby reing i
is stused blly dathe plcerat
, patcheckas the
his article addresses the primary outcome of foot ulcer
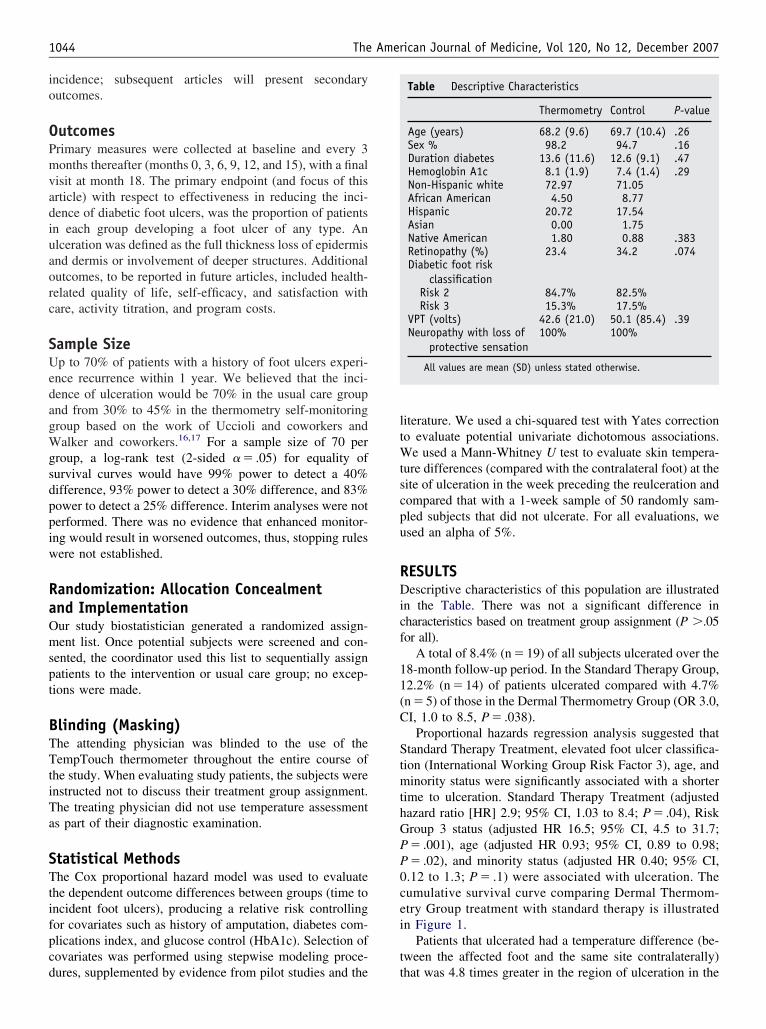
io
OPmvadiuaorc
SUedagWgsdppiw
RaOmspt
BTTtiTa
STtifpcd
ltWtscpu
RDicf
11(C
StmthGPP0cei
t
1044 The American Journal of Medicine, Vol 120, No 12, December 2007
ncidence; subsequent articles will present secondaryutcomes.
utcomesrimary measures were collected at baseline and every 3onths thereafter (months 0, 3, 6, 9, 12, and 15), with a final
isit at month 18. The primary endpoint (and focus of thisrticle) with respect to effectiveness in reducing the inci-ence of diabetic foot ulcers, was the proportion of patientsn each group developing a foot ulcer of any type. Anlceration was defined as the full thickness loss of epidermisnd dermis or involvement of deeper structures. Additionalutcomes, to be reported in future articles, included health-elated quality of life, self-efficacy, and satisfaction withare, activity titration, and program costs.
ample Sizep to 70% of patients with a history of foot ulcers experi-
nce recurrence within 1 year. We believed that the inci-ence of ulceration would be 70% in the usual care groupnd from 30% to 45% in the thermometry self-monitoringroup based on the work of Uccioli and coworkers andalker and coworkers.16,17 For a sample size of 70 per
roup, a log-rank test (2-sided � � .05) for equality ofurvival curves would have 99% power to detect a 40%ifference, 93% power to detect a 30% difference, and 83%ower to detect a 25% difference. Interim analyses were noterformed. There was no evidence that enhanced monitor-ng would result in worsened outcomes, thus, stopping rulesere not established.
andomization: Allocation Concealmentnd Implementationur study biostatistician generated a randomized assign-ent list. Once potential subjects were screened and con-
ented, the coordinator used this list to sequentially assignatients to the intervention or usual care group; no excep-ions were made.
linding (Masking)he attending physician was blinded to the use of theempTouch thermometer throughout the entire course of
he study. When evaluating study patients, the subjects werenstructed not to discuss their treatment group assignment.he treating physician did not use temperature assessments part of their diagnostic examination.
tatistical Methodshe Cox proportional hazard model was used to evaluate
he dependent outcome differences between groups (time toncident foot ulcers), producing a relative risk controllingor covariates such as history of amputation, diabetes com-lications index, and glucose control (HbA1c). Selection ofovariates was performed using stepwise modeling proce-
ures, supplemented by evidence from pilot studies and the titerature. We used a chi-squared test with Yates correctiono evaluate potential univariate dichotomous associations.
e used a Mann-Whitney U test to evaluate skin tempera-ure differences (compared with the contralateral foot) at theite of ulceration in the week preceding the reulceration andompared that with a 1-week sample of 50 randomly sam-led subjects that did not ulcerate. For all evaluations, wesed an alpha of 5%.
ESULTSescriptive characteristics of this population are illustrated
n the Table. There was not a significant difference inharacteristics based on treatment group assignment (P �.05or all).
A total of 8.4% (n � 19) of all subjects ulcerated over the8-month follow-up period. In the Standard Therapy Group,2.2% (n � 14) of patients ulcerated compared with 4.7%n � 5) of those in the Dermal Thermometry Group (OR 3.0,I, 1.0 to 8.5, P � .038).
Proportional hazards regression analysis suggested thattandard Therapy Treatment, elevated foot ulcer classifica-
ion (International Working Group Risk Factor 3), age, andinority status were significantly associated with a shorter
ime to ulceration. Standard Therapy Treatment (adjustedazard ratio [HR] 2.9; 95% CI, 1.03 to 8.4; P � .04), Riskroup 3 status (adjusted HR 16.5; 95% CI, 4.5 to 31.7;� .001), age (adjusted HR 0.93; 95% CI, 0.89 to 0.98;� .02), and minority status (adjusted HR 0.40; 95% CI,.12 to 1.3; P � .1) were associated with ulceration. Theumulative survival curve comparing Dermal Thermom-try Group treatment with standard therapy is illustratedn Figure 1.
Patients that ulcerated had a temperature difference (be-ween the affected foot and the same site contralaterally)
Table Descriptive Characteristics
Thermometry Control P-value
Age (years) 68.2 (9.6) 69.7 (10.4) .26Sex % 98.2 94.7 .16Duration diabetes 13.6 (11.6) 12.6 (9.1) .47Hemoglobin A1c 8.1 (1.9) 7.4 (1.4) .29Non-Hispanic white 72.97 71.05African American 4.50 8.77Hispanic 20.72 17.54Asian 0.00 1.75Native American 1.80 0.88 .383Retinopathy (%) 23.4 34.2 .074Diabetic foot risk
classificationRisk 2 84.7% 82.5%Risk 3 15.3% 17.5%
VPT (volts) 42.6 (21.0) 50.1 (85.4) .39Neuropathy with loss of
protective sensation100% 100%
All values are mean (SD) unless stated otherwise.
hat was 4.8 times greater in the region of ulceration in the
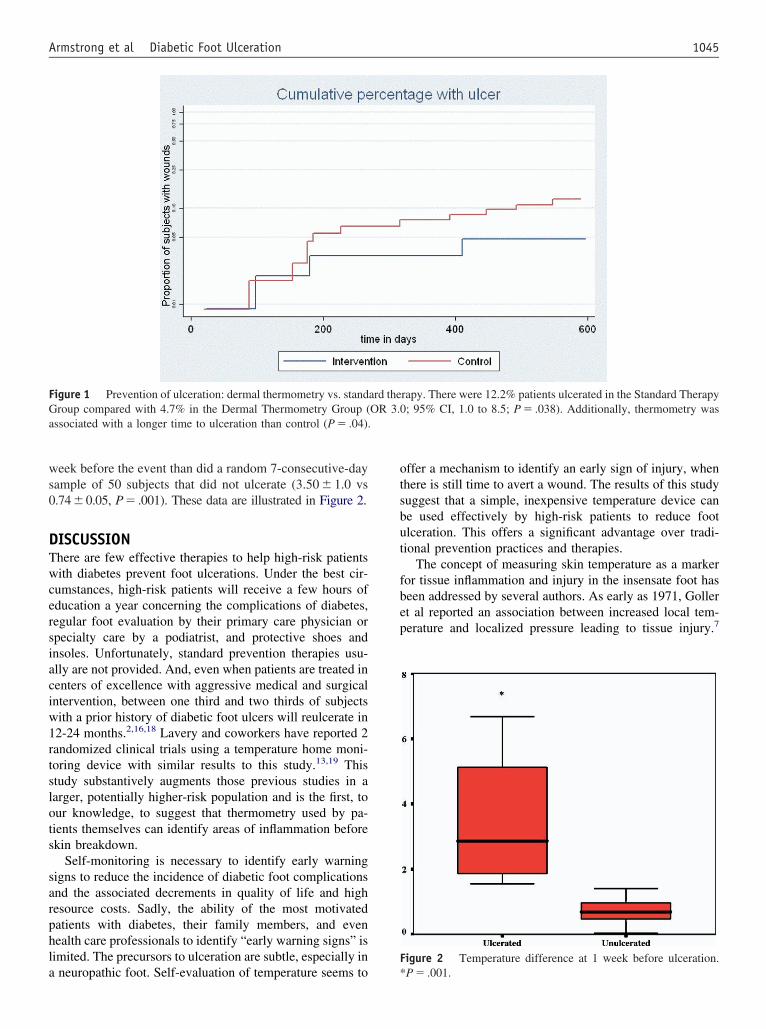
ws0
DTwcersiaciw1rtslots
sarphla
otsbut
fbep
F
FGa
1045Armstrong et al Diabetic Foot Ulceration
eek before the event than did a random 7-consecutive-dayample of 50 subjects that did not ulcerate (3.50 � 1.0 vs.74�0.05, P� .001). These data are illustrated in Figure 2.
ISCUSSIONhere are few effective therapies to help high-risk patientsith diabetes prevent foot ulcerations. Under the best cir-
umstances, high-risk patients will receive a few hours ofducation a year concerning the complications of diabetes,egular foot evaluation by their primary care physician orpecialty care by a podiatrist, and protective shoes andnsoles. Unfortunately, standard prevention therapies usu-lly are not provided. And, even when patients are treated inenters of excellence with aggressive medical and surgicalntervention, between one third and two thirds of subjectsith a prior history of diabetic foot ulcers will reulcerate in2-24 months.2,16,18 Lavery and coworkers have reported 2andomized clinical trials using a temperature home moni-oring device with similar results to this study.13,19 Thistudy substantively augments those previous studies in aarger, potentially higher-risk population and is the first, tour knowledge, to suggest that thermometry used by pa-ients themselves can identify areas of inflammation beforekin breakdown.
Self-monitoring is necessary to identify early warningigns to reduce the incidence of diabetic foot complicationsnd the associated decrements in quality of life and highesource costs. Sadly, the ability of the most motivatedatients with diabetes, their family members, and evenealth care professionals to identify “early warning signs” isimited. The precursors to ulceration are subtle, especially in
igure 1 Prevention of ulceration: dermal thermometry vs. standroup compared with 4.7% in the Dermal Thermometry Group (
ssociated with a longer time to ulceration than control (P � .04).
neuropathic foot. Self-evaluation of temperature seems to *
ffer a mechanism to identify an early sign of injury, whenhere is still time to avert a wound. The results of this studyuggest that a simple, inexpensive temperature device cane used effectively by high-risk patients to reduce footlceration. This offers a significant advantage over tradi-ional prevention practices and therapies.
The concept of measuring skin temperature as a markeror tissue inflammation and injury in the insensate foot haseen addressed by several authors. As early as 1971, Gollert al reported an association between increased local tem-erature and localized pressure leading to tissue injury.7
igure 2 Temperature difference at 1 week before ulceration.
rapy. There were 12.2% patients ulcerated in the Standard Therapy; 95% CI, 1.0 to 8.5; P � .038). Additionally, thermometry was
ard theOR 3.0
P � .001.

Sawuppwfrapimea
acdncaIp
h(oGlapiwaaDcm
taatmat
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
1046 The American Journal of Medicine, Vol 120, No 12, December 2007
androw and coworkers subsequently used thermometry astool to diagnosis occult neuropathic fractures in patientsith diabetes in 1972.20 Stess and colleagues described these of infrared thermography to assess skin temperatures inatients with diabetes, patients with diabetes with neuro-athic fractures, patients with diabetes with ulcers, patientsith leprosy, and controls.21 They found that neuropathic
oot ulcers frequently had increased skin temperatures sur-ounding a central necrotic area, and suggested that temper-ture assessment may be a useful technique to identifyatients at risk for ulceration. Similar findings were revealedn a larger study by Armstrong et al using standard ther-ometers.22 The concept is elegant in its simplicity, and
ven challenging patient populations appear to have beenble to successfully use the device.
Veterans treated in the Department of Veterans Affairsre older, poorer, and have more comorbidities than generalommunity dwellers. However, they are not appreciablyifferent from the disproportionately low income and mi-ority population with diabetes in regards to ulcer out-omes.23,24 Therefore, the results of this study should bepplicable to both veteran and nonveteran populations alike.n fact, a less challenged population might realize betterreventative outcomes.
In this study we evaluated 2 risk groups: patients with aistory of previous diabetic foot ulceration or amputationRisk Group 3) and those with sensory neuropathy and lossf protective sensation with structural foot deformities (Riskroup 2). The majority of subjects enrolled were in the
atter group, and this group had a lower incidence of ulcer-tion than expected. Our sample size estimate was based onublished outcomes using “standard prevention” in diabet-cs with a history of pathology (Risk Group 3). Therefore,e underestimated the sample size needed to evaluate Di-
betic Foot Risk Group 2 subjects, and we disproportion-bly enrolled fewer Diabetic Foot Risk Group 3 subjects.espite these errors, the smaller patient sample was suffi-
ient to show a significant impact when home temperatureonitoring was used.Quality of life, functional status, self-efficacy, satisfac-
ion with care, and cost outcomes from this study will beddressed in future articles. While smaller studies in thisrea have mirrored the current project,13,19 it is unknown ifhe same outcomes and compliance would be observed in aulticenter clinical trial over an extended period of evalu-
tion. We look forward to work that might continue to refinehis method’s usefulness in a variety of settings.
eferences1. Pecoraro RE, Reiber GE, Burgess EM. Pathways to diabetic limb
amputation: basis for prevention. Diabetes Care. 1990;13:513-521.2. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients
with diabetes. JAMA. 2005;293(2):217-228.3. Armstrong DG, Abu-Rumman PL, Nixon BP, Boulton AJ. Continuous
activity monitoring in persons at high risk for diabetes-related lower-
extremity amputation. J Am Podiatr Med Assoc. 2001;91(9):451-455.4. Armstrong DG, Lavery LA, Holtz-Neiderer K, et al. Variability inactivity may precede diabetic foot ulceration. Diabetes Care. 2004;27(8):1980-1984.
5. Maluf KS, Morley RE, Richter EJ, et al. Foot pressures during levelwalking are strongly associated with pressures during other ambula-tory activities in subjects with diabetic neuropathy. Arch Phys MedRehabil. 2004;85(2):253-260.
6. Maluf KS, Mueller MJ. Novel Award 2002. Comparison of physicalactivity and cumulative plantar tissue stress among subjects with andwithout diabetes mellitus and a history of recurrent plantar ulcers. ClinBiomech (Bristol, Avon). 2003;18(7):567-575.
7. Goller H, Lewis DW, McLaughlin RE. Thermographic studies ofhuman skin subjected to localized pressure. Am J Roentgenol RadiumTher Nucl Med. 1971;113(4):749-754.
8. Stess RM, Sisney PC, Moss KM, et al. Use of liquid crystal thermog-raphy in the evaluation of the diabetic foot. Diabetes Care. 1986;9(3):267-272.
9. Armstrong DG, Lavery LA, Liswood PJ, et al. Infrared dermal ther-mometry for the high-risk diabetic foot. Phys Ther. 1997;77(2):169-175.
0. Benbow SJ, Chan AW, Bowsher DR, et al. The prediction of diabeticneuropathic plantar foot ulceration by liquid-crystal contact thermog-raphy. Diabetes Care. 1994;17(8):835-839.
1. Bergtholdt HT, Brand PW. Thermography: an aid in the managementof insensitive feet and stumps. Arch Phys Med Rehabil. 1975;56(5):205-209.
2. Clark RP, Goff MR, Hughes J, Klenerman L. Thermography andpedobarography in the assessment of tissue damage in neuropathic andatherosclerotic feet. Thermology. 1988;3:15-20.
3. Lavery LA, Higgins KR, Lanctot DR, et al. Home monitoring of footskin temperatures to prevent ulceration. Diabetes Care. 2004;27(11):2642-2647.
4. Lavery LA, Higgins KR, Lanctot D, et al. Preventing diabetic footulcer recurrence in high-risk patients: the use of temperature monitor-ing as a self-assessment tool. Diabetes Care. 2007;30(1):14-20.
5. Peters EJ, Lavery LA. International Working Group on the DiabeticFoot. Effectiveness of the diabetic foot risk classification system of theInternational Working Group on the Diabetic Foot. Diabetes Care.2001;24(8):1442-1447.
6. Uccioli L, Faglia E, Monticone G, et al. Manufactured shoes in theprevention of diabetic foot ulcers. Diabetes Care. 1995;18(10):1376-1378.
7. Walker SC, Helm PA, Pulliam G. Total contact casting and chronicdiabetic neuropathic foot ulcerations: healing rates by wound location.Arch Phys Med Rehabil. 1987;68:217-221.
8. Mueller MJ, Sinacore DR, Hastings MK, et al. Effect of achillestendon lengthening on neuropathic plantar ulcers. A randomized clin-ical trial. J Bone Joint Surg Am. 2003;85-A(8):1436-1445.
9. Lavery LA, Higgins KR, Armstrong DG, et al. Randomized clinicaltrial to evaluate a novel home temperature monitoring device to reducethe incidence of diabetic foot complications (Abstract). Diabetologia.2002;45(Suppl 2):A342.
0. Sandrow RE, Torg JS, Lapayowker MS, Resnick EJ. The use ofthermography in the early diagnosis of neuropathic arthropathy in thefeet of diabetics. Clin Orthop. 1972;88:31-33.
1. Stess RM, Sisney PC, Koss KM, et al. Use of liquid crystal thermog-raphy in the evaluation of the diabetic foot. Diabetes Care. 1986;9:267-272.
2. Armstrong DG, Lavery LA, Liswood PJ, et al. Infrared dermal ther-mometry for the high-risk diabetic foot. Phys Ther. 1997;77(2):169-175; discussion 176-177.
3. Reiber GE, Koepsell TD, Maynard C, et al. Diabetes in nonveterans,veterans, and veterans receiving Department of Veterans Affairs healthcare. Diabetes Care. 2004;27(Suppl 2):B3-B9.
4. Reiber GE, Boyko EJ. Diabetes research in the Department of Veter-
ans Affairs. Diabetes Care. 2004;27(Suppl 2):B95-B98.
C
HIKDR
Aptdb
Q
DOn
0d
The American Journal of Medicine (2007) 120, 1047-1053
LINICAL RESEARCH STUDY
ospital Discharge against Advice after Myocardialnfarction: Deaths and Readmissionsevin Fiscella, MD, MPH,a,b,c Sean Meldrum, MS,a Steve Barnett, MDa
epartments of aFamily Medicine, bCommunity & Preventive Medicine, and cOncology, University of Rochester School of Medicine,
ochester, NY.BsiMmwWoRmyp(pfsl1CaE
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
ABSTRACT
ACKGROUND: Approximately 1% of patients leave hospitals against medical advice, but the clinicalignificance of premature hospital discharge is unknown, particularly after admission for acute myocardialnfarction (AMI).ETHODS: We used California hospital discharge data (1998-2000) to compare readmissions andortality among patients admitted for AMI who were discharged against medical advice with those whoeren’t. Effects were adjusted for age, race, income, comorbidity, insurance, and hospital characteristics.e also examined whether the effects of premature hospital discharge were partly explained by lower rates
f coronary revascularization.ESULTS: There were 1079 patients (1.1% of the sample) with AMI on admission who left againstedical advice. Compared with those who didn’t leave against medical advice, these patients were
ounger, more often male, low income, black, insured through Medicaid or uninsured, and had lesshysical comorbidity, but greater mental health comorbidity. Their mean length of stay was shorter4 vs 8 days) than those who stayed. They were transferred less often. They received fewer cardiacrocedures, including coronary revascularization. In multivariate analyses, they had 60% higher riskor death or re-admission for AMI or unstable angina up to 2 years postdischarge than patients withtandard discharge (hazard ratio 1.59; 95% confidence interval, 1.43-1.77). Adjustment for revascu-arization attenuated, but did not eliminate, this risk (hazard ratio 1.39; 95% confidence interval,.25-1.55).ONCLUSIONS: Discharge against medical advice after AMI is associated with appreciable morbiditynd mortality. These results should be used to manage AMI patients contemplating such discharge. © 2007lsevier Inc. All rights reserved.
KEYWORDS: Hospitalization; Mortality; Myocardial infarction; Patient compliance; Patient discharge
sm
apwsgpact
pproximately 1 in 100 medical inpatients leave the hos-ital against their physician’s advice.1,2 For selected condi-ions such as alcohol abuse, asthma, and human-immuno-eficiency-virus-related complications, such discharge haseen associated with increased risk of hospital readmis-
This study was supported by the Agency for Healthcare Research anduality R01 HS10910-02.
Requests for reprints should be addressed to Kevin Fiscella, MD, MPH,epartments of Family Medicine, Community & Preventive Medicine, andncology, University of Rochester School of Medicine, 1381 South Ave-ue, Rochester, NY 14620.
ront matter © 2007 Elsevier Inc. All rights reserved.ed.2007.08.024
ion,3-6 but the association with inpatient procedures andortality is not known.In this study, we assessed the association of discharge
gainst medical advice among patients admitted with arimary diagnosis of acute myocardial infarction (AMI)ith either death or hospital readmission for acute coronary
yndrome, defined as myocardial infarction or unstable an-ina. We chose to examine premature discharges amongatients admitted for AMI because hospitalization for it isssociated with appreciable postdischarge mortality and be-ause many hospital-based interventions have been showno reduce AMI-associated mortality.7,8 We also examined
hether any observed effect from premature discharge
mc
M
SWhcsIthfotdwpo2slhnfittthpptc
d1bas1wsfTItS
RWovcst
dhcla
peevo
dwoa(c
OTflcamwm2
SWhd
ients
1048 The American Journal of Medicine, Vol 120, No 12, December 2007
ight be explained in part by lower rates of coronary revas-ularization.
ETHODS
tudy Populatione conducted a retrospective co-
ort study using hospital dis-harge data for 1998-2000 ab-tracted from California Statenpatient Data. We identified pa-ients 30 years and older whoad not been admitted to a Cali-ornia hospital with a diagnosisf AMI (International Classifica-ion of Diseases [ICD]-9 proce-ure code 410) during 1998, butere subsequently admitted with arimary diagnosis of AMI presentn admission between 1999 and000.9 We used encrypted socialecurity numbers, age, and sex toink patient discharge data acrossospitalizations and to the Califor-ia Mortality file. The mortalityle contained the encrypted iden-
ifiers and dates of death of pa-ients that died during the 2-year follow-up period. Charac-eristics of the hospitals were obtained by matching theospital discharge data to an abstract of the American Hos-itals Association (AHA) database from 1998. We excludedatients with missing encrypted social security numbers,hose that died while hospitalized, and those with missingovariates.
We excluded those patients who were admitted for AMIuring 1998 to increase the probability that the admission in999-2000 represented the patient’s first event rather thaneing one among a series of closely occurring events. Whenpatient experienced multiple admissions for AMI, we
elected the first admission that occurred beginning January, 1999. When patients were transferred to another hospital,e combined the information from each admission into a
ingle patient event. The length of follow-up time availableor each subject ranged from 1 day to 2 years (mean 1 year.)his study was approved by the University of Rochester
nstitutional Review Board and the Committee for the Pro-ection of Human Subjects, California Health and Humanervices Agency.
isk Factorse assessed discharge against medical advice based on type
f discharge specified in billing data using a dichotomousariable (discharge against medical advice or other). Patientharacteristics included age, sex, race/ethnicity, insurancetatus, zip code-derived median household income by quar-
CLINICAL SIGNIF
● One in 100 patieagainst medicalmyocardial infar3 days.
● Premature dischreceipt of fewercluding revasculastantially higherity and mortality
● These findings inpatients considereinforce the neelow-up when pat
ile (obtained by matching patient zip code to 2000 census c
ata), and patient morbidity categories developed by Elix-auser et al (series of 30 diagnostic categories such asongestive heart failure, arrhythmias, pulmonary disease,iver disease, renal disease, hypertension, and diabetes,mong others).10,11 Use of conditions present on hospital
admission has been shown to pro-duce mortality prediction modelsfor AMI that are similar to modelsthat include clinical data.9,12 Be-cause substance abuse and mentalhealth diagnoses have been previ-ously shown to predict dischargeagainst medical advice among med-ical inpatients,2,3,5,13,14 we exam-ined the effect of inclusion of diag-noses for drug abuse, alcoholdependence, depression, and psy-chosis in the models although thereliability of these hospital codesis not known. All comorbidity waslimited to those present upon hos-pital admission.
Hospital characteristics derivedfrom the AHA file included hos-pital ownership and hospital loca-tion. Hospital characteristics de-rived from the data included the
ercentage of total discharges in the Major Diagnostic Cat-gory grouping of Diagnosis-Related Group codes, “Dis-ases and disorders of the circulatory system.” Hospitalolume, a proxy for size, was derived from the total numberf annual discharges for any diagnosis.
To examine use of commonly performed inpatient car-iac procedures, we used the Clinical Classification Soft-are groupings of ICD-9 procedure codes for implantationf a pacemaker (48), angiography (47), thrombolytic ther-py (46), percutaneous transluminal coronary angioplasty45), coronary artery bypass graft (44), or the ICD-9 pro-edure codes for insertion of a coronary artery stent (3606).
utcomeshe primary outcome was subsequent hospital admission
or acute coronary syndrome or all-cause death during fol-ow-up. Acute coronary syndrome was defined as a dis-harge diagnosis of AMI (ICD-9 code 410) or unstablengina (ICD-9 code 411). Death was based on Californiaortality data. Hospital re-admissions for “other diagnoses”ere based on any ICD-9 codes other than 410 or 411. Theaximal follow-up period for assessment of outcomes wasyears. We examined outcomes at 30, 60, 90, and 365 days.
tatistical Analysise compared type of discharge across various patient and
ospital characteristics. We examined the association ofischarge against medical advice with receipt of selected
CE
eaves the hospitalce after an acutehalf do so within
is associated withary procedures in-ion, and with sub-discharge morbid-
efforts to counseluch discharge andcontinuity in fol-
leave prematurely.
ICAN
nts ladvi
ction;
argecoronrizatpost.
formring sd for
ardiac procedures and also with admission for acute coro-
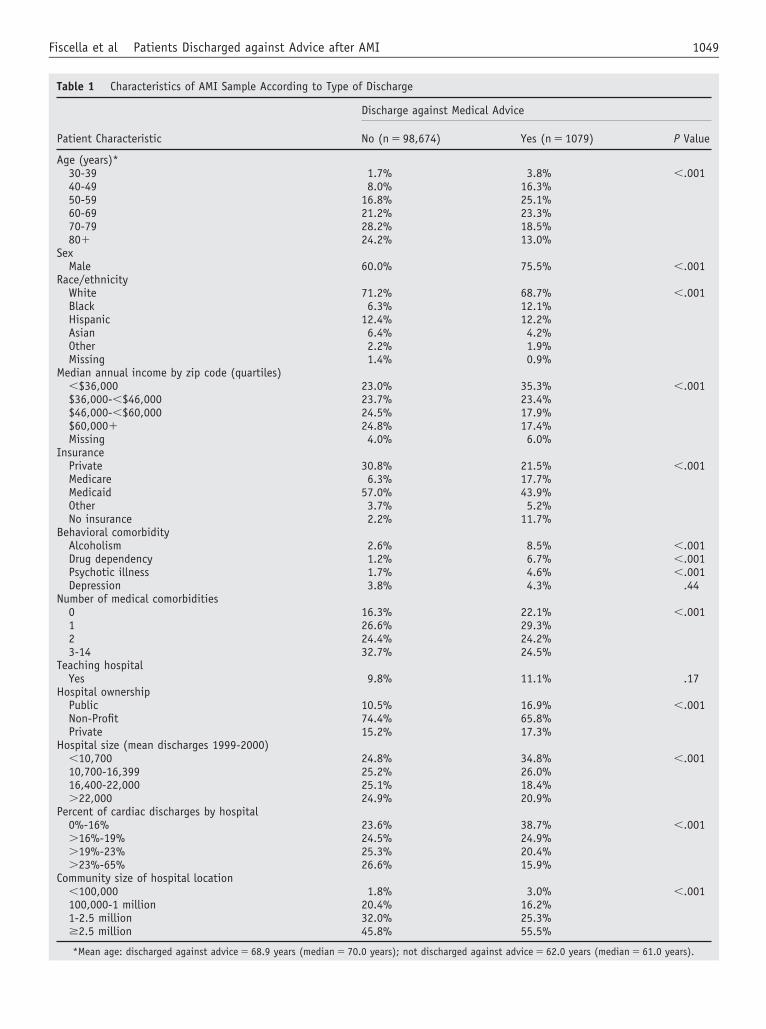
1049Fiscella et al Patients Discharged against Advice after AMI
Table 1 Characteristics of AMI Sample According to Type of Discharge
Patient Characteristic
Discharge against Medical Advice
No (n � 98,674) Yes (n � 1079) P Value
Age (years)*30-39 1.7% 3.8% �.00140-49 8.0% 16.3%50-59 16.8% 25.1%60-69 21.2% 23.3%70-79 28.2% 18.5%80� 24.2% 13.0%
SexMale 60.0% 75.5% �.001
Race/ethnicityWhite 71.2% 68.7% �.001Black 6.3% 12.1%Hispanic 12.4% 12.2%Asian 6.4% 4.2%Other 2.2% 1.9%Missing 1.4% 0.9%
Median annual income by zip code (quartiles)�$36,000 23.0% 35.3% �.001$36,000-�$46,000 23.7% 23.4%$46,000-�$60,000 24.5% 17.9%$60,000� 24.8% 17.4%Missing 4.0% 6.0%
InsurancePrivate 30.8% 21.5% �.001Medicare 6.3% 17.7%Medicaid 57.0% 43.9%Other 3.7% 5.2%No insurance 2.2% 11.7%
Behavioral comorbidityAlcoholism 2.6% 8.5% �.001Drug dependency 1.2% 6.7% �.001Psychotic illness 1.7% 4.6% �.001Depression 3.8% 4.3% .44
Number of medical comorbidities0 16.3% 22.1% �.0011 26.6% 29.3%2 24.4% 24.2%3-14 32.7% 24.5%
Teaching hospitalYes 9.8% 11.1% .17
Hospital ownershipPublic 10.5% 16.9% �.001Non-Profit 74.4% 65.8%Private 15.2% 17.3%
Hospital size (mean discharges 1999-2000)�10,700 24.8% 34.8% �.00110,700-16,399 25.2% 26.0%16,400-22,000 25.1% 18.4%�22,000 24.9% 20.9%
Percent of cardiac discharges by hospital0%-16% 23.6% 38.7% �.001�16%-19% 24.5% 24.9%�19%-23% 25.3% 20.4%�23%-65% 26.6% 15.9%
Community size of hospital location�100,000 1.8% 3.0% �.001100,000-1 million 20.4% 16.2%1-2.5 million 32.0% 25.3%�2.5 million 45.8% 55.5%
*Mean age: discharged against advice � 68.9 years (median � 70.0 years); not discharged against advice � 62.0 years (median � 61.0 years).
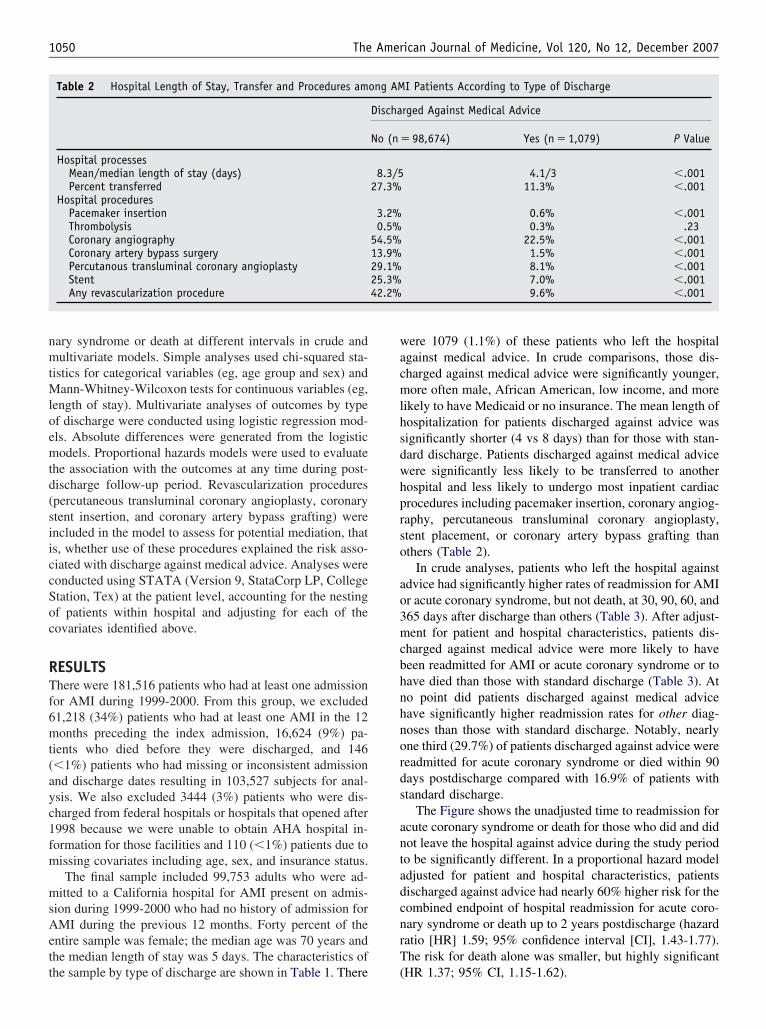
nmtMloemtd(siiccSoc
RTf6mt(ayc1fm
msAett
wacmlhsdwhprso
ao3mcbhnhnords
antadcnrT
1050 The American Journal of Medicine, Vol 120, No 12, December 2007
ary syndrome or death at different intervals in crude andultivariate models. Simple analyses used chi-squared sta-
istics for categorical variables (eg, age group and sex) andann-Whitney-Wilcoxon tests for continuous variables (eg,
ength of stay). Multivariate analyses of outcomes by typef discharge were conducted using logistic regression mod-ls. Absolute differences were generated from the logisticodels. Proportional hazards models were used to evaluate
he association with the outcomes at any time during post-ischarge follow-up period. Revascularization procedurespercutaneous transluminal coronary angioplasty, coronarytent insertion, and coronary artery bypass grafting) werencluded in the model to assess for potential mediation, thats, whether use of these procedures explained the risk asso-iated with discharge against medical advice. Analyses wereonducted using STATA (Version 9, StataCorp LP, Collegetation, Tex) at the patient level, accounting for the nestingf patients within hospital and adjusting for each of theovariates identified above.
ESULTShere were 181,516 patients who had at least one admission
or AMI during 1999-2000. From this group, we excluded1,218 (34%) patients who had at least one AMI in the 12onths preceding the index admission, 16,624 (9%) pa-
ients who died before they were discharged, and 146�1%) patients who had missing or inconsistent admissionnd discharge dates resulting in 103,527 subjects for anal-sis. We also excluded 3444 (3%) patients who were dis-harged from federal hospitals or hospitals that opened after998 because we were unable to obtain AHA hospital in-ormation for those facilities and 110 (�1%) patients due toissing covariates including age, sex, and insurance status.The final sample included 99,753 adults who were ad-
itted to a California hospital for AMI present on admis-ion during 1999-2000 who had no history of admission forMI during the previous 12 months. Forty percent of the
ntire sample was female; the median age was 70 years andhe median length of stay was 5 days. The characteristics of
Table 2 Hospital Length of Stay, Transfer and Procedures am
Hospital processesMean/median length of stay (days)Percent transferred
Hospital proceduresPacemaker insertionThrombolysisCoronary angiographyCoronary artery bypass surgeryPercutanous transluminal coronary angioplastyStentAny revascularization procedure
he sample by type of discharge are shown in Table 1. There (
ere 1079 (1.1%) of these patients who left the hospitalgainst medical advice. In crude comparisons, those dis-harged against medical advice were significantly younger,ore often male, African American, low income, and more
ikely to have Medicaid or no insurance. The mean length ofospitalization for patients discharged against advice wasignificantly shorter (4 vs 8 days) than for those with stan-ard discharge. Patients discharged against medical adviceere significantly less likely to be transferred to anotherospital and less likely to undergo most inpatient cardiacrocedures including pacemaker insertion, coronary angiog-aphy, percutaneous transluminal coronary angioplasty,tent placement, or coronary artery bypass grafting thanthers (Table 2).
In crude analyses, patients who left the hospital againstdvice had significantly higher rates of readmission for AMIr acute coronary syndrome, but not death, at 30, 90, 60, and65 days after discharge than others (Table 3). After adjust-ent for patient and hospital characteristics, patients dis-
harged against medical advice were more likely to haveeen readmitted for AMI or acute coronary syndrome or toave died than those with standard discharge (Table 3). Ato point did patients discharged against medical adviceave significantly higher readmission rates for other diag-oses than those with standard discharge. Notably, nearlyne third (29.7%) of patients discharged against advice wereeadmitted for acute coronary syndrome or died within 90ays postdischarge compared with 16.9% of patients withtandard discharge.
The Figure shows the unadjusted time to readmission forcute coronary syndrome or death for those who did and didot leave the hospital against advice during the study periodo be significantly different. In a proportional hazard modeldjusted for patient and hospital characteristics, patientsischarged against advice had nearly 60% higher risk for theombined endpoint of hospital readmission for acute coro-ary syndrome or death up to 2 years postdischarge (hazardatio [HR] 1.59; 95% confidence interval [CI], 1.43-1.77).he risk for death alone was smaller, but highly significant
I Patients According to Type of Discharge
rged Against Medical Advice
� 98,674) Yes (n � 1,079) P Value
4.1/3 �.00111.3% �.001
0.6% �.0010.3% .23
22.5% �.0011.5% �.0018.1% �.0017.0% �.0019.6% �.001
ong AM
Discha
No (n
8.3/527.3%
3.2%0.5%
54.5%13.9%29.1%25.3%42.2%
HR 1.37; 95% CI, 1.15-1.62).
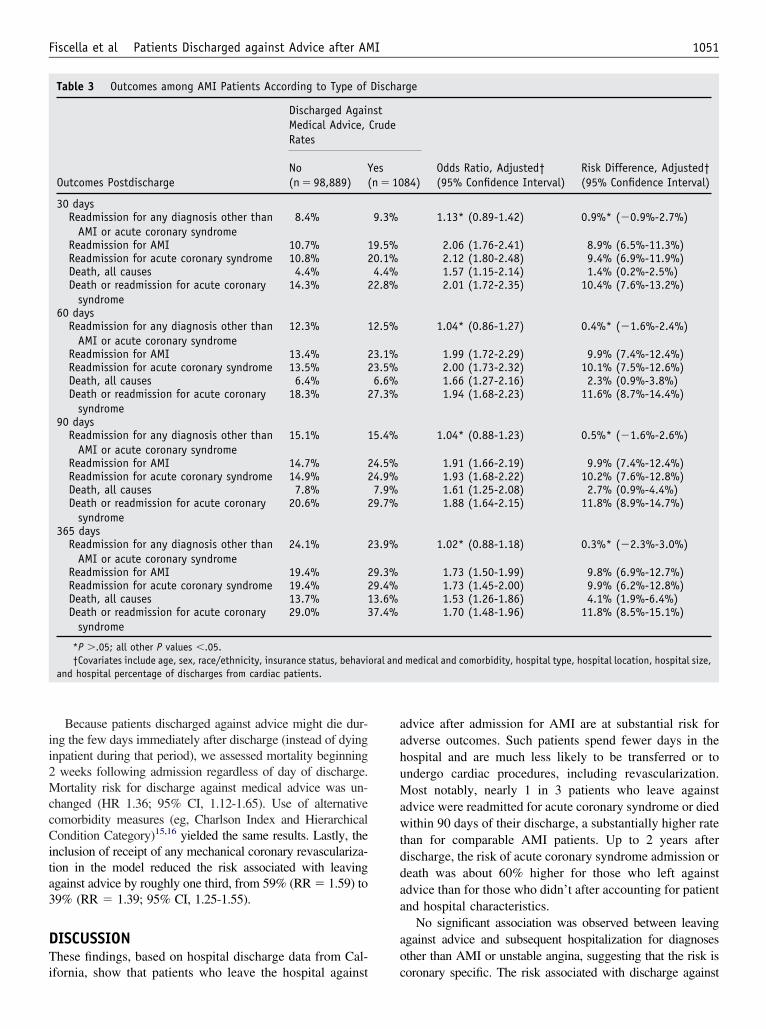
ii2MccCita3
DTi
aahuMawtddaa
ao
1051Fiscella et al Patients Discharged against Advice after AMI
Because patients discharged against advice might die dur-ng the few days immediately after discharge (instead of dyingnpatient during that period), we assessed mortality beginning
weeks following admission regardless of day of discharge.ortality risk for discharge against medical advice was un-
hanged (HR 1.36; 95% CI, 1.12-1.65). Use of alternativeomorbidity measures (eg, Charlson Index and Hierarchicalondition Category)15,16 yielded the same results. Lastly, the
nclusion of receipt of any mechanical coronary revasculariza-ion in the model reduced the risk associated with leavinggainst advice by roughly one third, from 59% (RR � 1.59) to9% (RR � 1.39; 95% CI, 1.25-1.55).
ISCUSSIONhese findings, based on hospital discharge data from Cal-
Table 3 Outcomes among AMI Patients According to Type of
Outcomes Postdischarge
Discharged AgainMedical Advice,Rates
No(n � 98,889)
Y(
30 daysReadmission for any diagnosis other than
AMI or acute coronary syndrome8.4%
Readmission for AMI 10.7% 1Readmission for acute coronary syndrome 10.8% 2Death, all causes 4.4%Death or readmission for acute coronary
syndrome14.3% 2
60 daysReadmission for any diagnosis other than
AMI or acute coronary syndrome12.3% 1
Readmission for AMI 13.4% 2Readmission for acute coronary syndrome 13.5% 2Death, all causes 6.4%Death or readmission for acute coronary
syndrome18.3% 2
90 daysReadmission for any diagnosis other than
AMI or acute coronary syndrome15.1% 1
Readmission for AMI 14.7% 2Readmission for acute coronary syndrome 14.9% 2Death, all causes 7.8%Death or readmission for acute coronary
syndrome20.6% 2
365 daysReadmission for any diagnosis other than
AMI or acute coronary syndrome24.1% 2
Readmission for AMI 19.4% 2Readmission for acute coronary syndrome 19.4% 2Death, all causes 13.7% 1Death or readmission for acute coronary
syndrome29.0% 3
*P �.05; all other P values �.05.†Covariates include age, sex, race/ethnicity, insurance status, behavio
and hospital percentage of discharges from cardiac patients.
fornia, show that patients who leave the hospital against c
dvice after admission for AMI are at substantial risk fordverse outcomes. Such patients spend fewer days in theospital and are much less likely to be transferred or tondergo cardiac procedures, including revascularization.ost notably, nearly 1 in 3 patients who leave against
dvice were readmitted for acute coronary syndrome or diedithin 90 days of their discharge, a substantially higher rate
han for comparable AMI patients. Up to 2 years afterischarge, the risk of acute coronary syndrome admission oreath was about 60% higher for those who left againstdvice than for those who didn’t after accounting for patientnd hospital characteristics.
No significant association was observed between leavinggainst advice and subsequent hospitalization for diagnosesther than AMI or unstable angina, suggesting that the risk is
rge
84)Odds Ratio, Adjusted†(95% Confidence Interval)
Risk Difference, Adjusted†(95% Confidence Interval)
1.13* (0.89-1.42) 0.9%* (�0.9%-2.7%)
2.06 (1.76-2.41) 8.9% (6.5%-11.3%)2.12 (1.80-2.48) 9.4% (6.9%-11.9%)1.57 (1.15-2.14) 1.4% (0.2%-2.5%)2.01 (1.72-2.35) 10.4% (7.6%-13.2%)
1.04* (0.86-1.27) 0.4%* (�1.6%-2.4%)
1.99 (1.72-2.29) 9.9% (7.4%-12.4%)2.00 (1.73-2.32) 10.1% (7.5%-12.6%)1.66 (1.27-2.16) 2.3% (0.9%-3.8%)1.94 (1.68-2.23) 11.6% (8.7%-14.4%)
1.04* (0.88-1.23) 0.5%* (�1.6%-2.6%)
1.91 (1.66-2.19) 9.9% (7.4%-12.4%)1.93 (1.68-2.22) 10.2% (7.6%-12.8%)1.61 (1.25-2.08) 2.7% (0.9%-4.4%)1.88 (1.64-2.15) 11.8% (8.9%-14.7%)
1.02* (0.88-1.18) 0.3%* (�2.3%-3.0%)
1.73 (1.50-1.99) 9.8% (6.9%-12.7%)1.73 (1.45-2.00) 9.9% (6.2%-12.8%)1.53 (1.26-1.86) 4.1% (1.9%-6.4%)1.70 (1.48-1.96) 11.8% (8.5%-15.1%)
medical and comorbidity, hospital type, hospital location, hospital size,
Discha
stCrude
esn � 10
9.3%
9.5%0.1%4.4%2.8%
2.5%
3.1%3.5%6.6%7.3%
5.4%
4.5%4.9%7.9%9.7%
3.9%
9.3%9.4%3.6%7.4%
ral and
oronary specific. The risk associated with discharge against
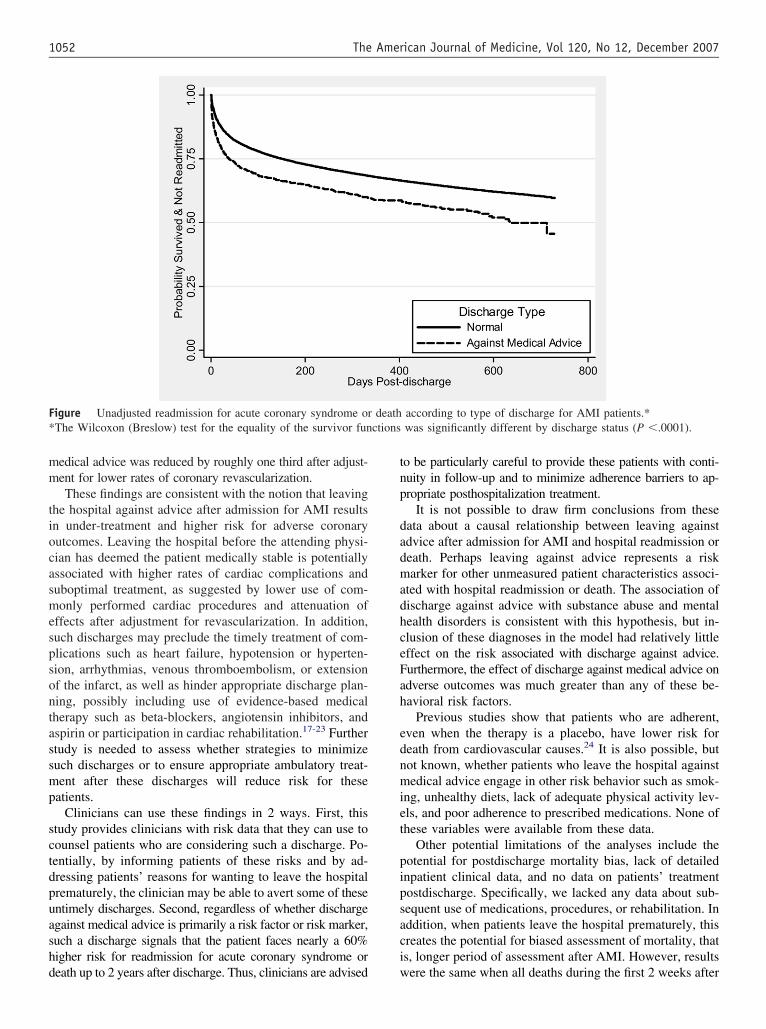
mm
tiocasmespsontassmp
sctdpuashd
tnp
dadmadhceFah
ednmiet
pipsaci
F* ctions
1052 The American Journal of Medicine, Vol 120, No 12, December 2007
edical advice was reduced by roughly one third after adjust-ent for lower rates of coronary revascularization.These findings are consistent with the notion that leaving
he hospital against advice after admission for AMI resultsn under-treatment and higher risk for adverse coronaryutcomes. Leaving the hospital before the attending physi-ian has deemed the patient medically stable is potentiallyssociated with higher rates of cardiac complications anduboptimal treatment, as suggested by lower use of com-only performed cardiac procedures and attenuation of
ffects after adjustment for revascularization. In addition,uch discharges may preclude the timely treatment of com-lications such as heart failure, hypotension or hyperten-ion, arrhythmias, venous thromboembolism, or extensionf the infarct, as well as hinder appropriate discharge plan-ing, possibly including use of evidence-based medicalherapy such as beta-blockers, angiotensin inhibitors, andspirin or participation in cardiac rehabilitation.17-23 Furthertudy is needed to assess whether strategies to minimizeuch discharges or to ensure appropriate ambulatory treat-ent after these discharges will reduce risk for these
atients.Clinicians can use these findings in 2 ways. First, this
tudy provides clinicians with risk data that they can use toounsel patients who are considering such a discharge. Po-entially, by informing patients of these risks and by ad-ressing patients’ reasons for wanting to leave the hospitalrematurely, the clinician may be able to avert some of thesentimely discharges. Second, regardless of whether dischargegainst medical advice is primarily a risk factor or risk marker,uch a discharge signals that the patient faces nearly a 60%igher risk for readmission for acute coronary syndrome or
igure Unadjusted readmission for acute coronary syndrome orThe Wilcoxon (Breslow) test for the equality of the survivor fun
eath up to 2 years after discharge. Thus, clinicians are advised w
o be particularly careful to provide these patients with conti-uity in follow-up and to minimize adherence barriers to ap-ropriate posthospitalization treatment.
It is not possible to draw firm conclusions from theseata about a causal relationship between leaving againstdvice after admission for AMI and hospital readmission oreath. Perhaps leaving against advice represents a riskarker for other unmeasured patient characteristics associ-
ted with hospital readmission or death. The association ofischarge against advice with substance abuse and mentalealth disorders is consistent with this hypothesis, but in-lusion of these diagnoses in the model had relatively littleffect on the risk associated with discharge against advice.urthermore, the effect of discharge against medical advice ondverse outcomes was much greater than any of these be-avioral risk factors.
Previous studies show that patients who are adherent,ven when the therapy is a placebo, have lower risk foreath from cardiovascular causes.24 It is also possible, butot known, whether patients who leave the hospital againstedical advice engage in other risk behavior such as smok-
ng, unhealthy diets, lack of adequate physical activity lev-ls, and poor adherence to prescribed medications. None ofhese variables were available from these data.
Other potential limitations of the analyses include theotential for postdischarge mortality bias, lack of detailednpatient clinical data, and no data on patients’ treatmentostdischarge. Specifically, we lacked any data about sub-equent use of medications, procedures, or rehabilitation. Inddition, when patients leave the hospital prematurely, thisreates the potential for biased assessment of mortality, thats, longer period of assessment after AMI. However, results
according to type of discharge for AMI patients.*was significantly different by discharge status (P �.0001).
death
ere the same when all deaths during the first 2 weeks after

heow2
bfvdila
dnsndFhra
AfCpm
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
1053Fiscella et al Patients Discharged against Advice after AMI
ospital admission were excluded. We could not assess thextent of patients lost to follow-up, that is, those who movedut-of-state whose hospital admissions (but not deaths)ould be missed, but this number is likely to be small overyears.We lacked detailed clinical data on patients, such as
lood pressure or serum creatinine levels, left ventricularunction, oxygenation, and other clinical variables, but pre-ious studies show similar performance between AMI pre-iction models derived from discharge data and those thatncluded detailed clinical data.12 Thus, we think it is un-ikely that more detailed clinical data would significantlylter our findings.
It is possible, if not probable, that patient behavior afterischarge contributed to higher death rates. As previouslyoted, discharge against medical advice was associated withubstance abuse and mental health disorders. These diag-oses are almost certainly under-coded in hospital dischargeata, so control for these factors was likely incomplete.urthermore, it is plausible that patients who leave theospital against advice are less adherent to medications,ecommendations for lifestyle changes, and follow-upppointments.
In conclusion, discharge against medical advice afterMI is associated with a 60% higher risk for readmission
or acute coronary syndrome or death for up to 2 years.linicians should use these findings when caring for AMIatients who are considering leaving the hospital againstedical advice.
eferences1. Franks P, Meldrum S, Fiscella K. Discharges against medical advice:
are race/ethnicity predictors? J Gen Intern Med. 2006;21:55-60.2. Moy E, Bartman BA. Race and hospital discharge against medical
advice. J Natl Med Assoc. 1996;88:658-660.3. Hwang SW, Li J, Gupta R, et al. What happens to patients who leave
hospital against medical advice? Can Med Assoc J. 2003;168:417-420.4. Baptist AP, Warrier I, Arora R, et al. Hospitalized patients with asthma
who leave against medical advice: characteristics, reasons, and out-comes. J Allergy Clin Immunol. 2007;119:924-929.
5. Anis AH, Sun H, Guh DP, et al. Leaving hospital against medicaladvice among HIV-positive patients. Can Med Assoc J. 2002;167:633-637.
6. Palepu A, Sun H, Kuyper L, et al. Predictors of early hospital read-mission in HIV-infected patients with pneumonia. J Gen Intern Med.2003;18:242-247.
7. Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelinesfor the management of patients with ST-elevation myocardial infarc-
tion: a report of the American College of Cardiology/American HeartAssociation Task Force on Practice Guidelines. Circulation. 2004;110:e82-292.
8. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA 2002 guide-line update for the management of patients with unstable angina andnon-ST-segment elevation myocardial infarction--summary article: areport of the American College of Cardiology/American Heart Asso-ciation task force on practice guidelines (Committee on the Manage-ment of Patients With Unstable Angina). J Am Coll Cardiol. 2002;40:1366-1374.
9. Stukenborg GJ, Wagner DP, Harrell FE Jr, et al. Present-at-admissiondiagnoses improved mortality risk adjustment among acute myocardialinfarction patients. J Clin Epidemiol. 2007;60:142-154.
0. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity mea-sures for use with administrative data. Med Care. 1998;36:8-27.
1. Southern DA, Quan H, Ghali WA. Comparison of the Elixhauser andCharlson/Deyo methods of comorbidity measurement in administra-tive data. Med Care. 2004;42:355-360.
2. Pine M, Jordan HS, Elixhauser A, et al. Enhancement of claims data toimprove risk adjustment of hospital mortality. JAMA. 2007;297:71-76.
3. Corley MC, Link K. Men patients who leave a general hospital againstmedical advice: mortality rate within six months. J Stud Alcohol.1981;42:1058-1061.
4. Smith DB, Telles JL. Discharges against medical advice at regionalacute care hospitals. Am J Public Health. 1991;81:212-215.
5. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method forclassifying prognostic comorbidity in longitudinal studies: develop-ment and validation. J Chronic Dis. 1987;40:373-383.
6. Pope GC, Kautter J, Ellis RP, et al. Risk adjustment of Medicarecapitation payments using the CMS-HCC model. Health Care FinancRev. 2004;25:119-141.
7. Menon V, Harrington RA, Hochman JS, et al. Thrombolysis andadjunctive therapy in acute myocardial infarction: the Seventh ACCPConference on Antithrombotic and Thrombolytic Therapy. Chest.2004;126:549S-575S.
8. Yusuf S, Wittes J, Friedman L. Overview of results of randomizedclinical trials in heart disease. II. Unstable angina, heart failure, pri-mary prevention with aspirin, and risk factor modification. JAMA.1988;260:2259-2263.
9. Yusuf S, Wittes J, Friedman L. Overview of results of randomizedclinical trials in heart disease. I. Treatments following myocardialinfarction. JAMA. 1988;260:2088-2093.
0. Olsson G, Wikstrand J, Warnold I, et al. Metoprolol-induced reductionin postinfarction mortality: pooled results from five double-blind ran-domized trials. Eur Heart J. 1992;13:28-32.
1. Domanski MJ, Exner DV, Borkowf CB, et al. Effect of angiotensinconverting enzyme inhibition on sudden cardiac death in patientsfollowing acute myocardial infarction. A meta-analysis of randomizedclinical trials. J Am Coll Cardiol. 1999;33:598-604.
2. Freemantle N, Cleland J, Young P, et al. beta Blockade after myocar-dial infarction: systematic review and meta regression analysis. BMJ.1999;318:1730-1737.
3. Taylor RS, Brown A, Ebrahim S, et al. Exercise-based rehabilitationfor patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trial. Am J Med. 2004;116:682-692.
4. Simpson SH, Eurich DT, Majumdar SR, et al. A meta-analysis of theassociation between adherence to drug therapy and mortality. BMJ.
2006;333:15.
C
CCRPa
LBDH
NtR
Av
MF
0d
The American Journal of Medicine (2007) 120, 1054-1062
LINICAL RESEARCH STUDY
-Reactive Protein, Inflammatory Conditions, andardiovascular Disease Risk
avi Dhingra, MD,a,b,c Philimon Gona, PhD,a,d Byung-Ho Nam, PhD,a,d Ralph B. D’Agostino, Sr, PhD,a,d
eter W. F. Wilson, MD,a,e Emelia J. Benjamin, MD, MS,a,f Christopher J. O’Donnell, MD, MPHa,g,h
National Heart Lung and Blood Institute’s (NHBLI) Framingham Heart Study, Framingham, Mass; bAlice Peck Day Memorial Hospital,ebanon, NH; cDivision of Aging, Brigham and Women’s Hospital, Harvard Medical School, Boston, Mass; dDepartment of Mathematics,oston University, Boston, Mass; eGeneral Clinical Research Center, Medical University of South Carolina, Charleston; fCardiologyivision, Boston University School of Medicine, Boston, Mass; gCardiology Division, Massachusetts General Hospital, Boston; hNational
eart, Lung andBpMfipiRvmCr(accmCwd
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
Blood Institute, Bethesda, Md.
ABSTRACT
ACKGROUND: It is uncertain to what extent high C-reactive protein (CRP) concentrations reflect theresence of inflammatory conditions in the community.ETHODS: We evaluated 3782 Framingham Offspring Study participants (mean age 55 years; 52% women)
ree of baseline cardiovascular disease. Logistic regression models examined the prevalence of commonnflammatory conditions by CRP categories, while a separate matched case-referent analysis evaluated therevalence of uncommon inflammatory conditions. Cox models were used to assess the influence of commonnflammatory conditions on relations between CRP and incident cardiovascular disease.ESULTS: Common inflammatory conditions were reported by nearly half of the participants; these indi-iduals were more likely to have markedly high CRP concentrations (�10 mg/L, P for trend � .001). Inultivariable models, there were increased odds of having at least one common inflammatory condition withRP concentrations of 1-3.0, 3.01-10, and �10 mg/L, compared with the referent category (�1 mg/L); the
espective odds ratios with 95% confidence intervals were 1.41 (1.07-1.86), 1.45 (1.07-1.98), and 1.641.09-2.47) in men, and 1.08 (0.82-1.43), 1.07 (0.80-1.44), and 1.38 (0.97-1.96) in women. In case-referentnalyses, uncommon inflammatory conditions were more common in individuals with CRP �10 mg/Lompared with those with CRP �1 mg/L (12.1% vs 6.6%; P � .0001). In multivariable models, higher CRPategories were not associated with incident cardiovascular disease, and with additional adjustment for inflam-atory conditions, results remained unchanged.ONCLUSION: There is high prevalence of common and uncommon inflammatory conditions in individualsith high CRP concentrations. Higher CRP concentrations should be interpreted with caution in cardiovascularisease risk assessment. © 2007 Elsevier Inc. All rights reserved.
KEYWORDS: Arthritis; C-reactive protein; Cardiovascular disease; Cohort study; Inflammation
Cmedhrtouh
Supported by the NHLBI’s Framingham Heart Study contract NHLBI01 HC 25195; R01 HL 073272 01, R01 HL 64753, and R01 HL 076784; and
he Donald W. Reynolds Foundation Program in Clinical Cardiovascularesearch.
Part of this article was presented as a poster at the American Heartssociation annual scientific sessions, New Orleans, Louisiana, on No-ember 9, 2004.
Requests for reprints should be addressed to Christopher J. O’Donnell,D, MPH, NHLBI’s Framingham Heart Study, 73 Mount Wayte Avenue #2,
ramingham, MA 01702-5827.
s: [email protected], [email protected]ront matter © 2007 Elsevier Inc. All rights reserved.ed.2007.08.037
-reactive protein (CRP) is a nonspecific marker of inflam-ation and a predictor of incident coronary heart dis-
ase,1 cardiovascular disease,2 and subclinical vascularisease.3,4 Available evidence suggests that moderatelyigh CRP concentrations (3-10 mg/L) predict increasedisk of myocardial infarction5 and stroke,6 even thoughhe optimal way to assess the prognostic utility of CRPver and above other traditional risk factors remainsncertain.7,8 Nevertheless, in some studies, markedlyigh CRP concentrations (�10 mg/L) also have been
hown to predict cardiovascular risk.9
ttcCcaamcflrlvaaadtacc
pssdciraspt
M
STsmtceepucatflcpaw
pR
M
ARAhtIi
eeocc(cpet
AIItact
1055Dhingra et al CRP and Inflammatory Conditions
Several factors are known to influence the CRP concentra-ions, including body mass index (BMI),10 diabetes,10 hyper-ension,11 cigarette smoking,12 estrogen replacement therapy,13
holesterol concentrations,2 and genetic polymorphisms in theRP gene.14,15 There are large intra-individual variations inirculating CRP concentrations,16
s well as differences by ethnicitynd sex.17 Prior studies have docu-ented associations of high CRP
oncentrations with numerous in-ammatory conditions, such asheumatoid arthritis18,19 or chronicung conditions,20 as recently re-iewed.21 CRP, an acute phase re-ctant, is also known to increase incute inflammatory states such ascute viral infections.22-24 However,ata are sparse regarding the extento which inflammatory conditionsre associated with circulating con-entrations of CRP in theommunity.
High-sensitivity CRP has beenroposed for use in cardiac risktratification and preventive deci-ion-making.5,25 Therefore, to ad-ress the influence of inflammatoryonditions on CRP concentrationsn the community, we examined theelations between higher concentrations of CRP with commonnd uncommon inflammatory diseases in the Framingham Off-pring Study participants. Additionally, we examined the im-act of common inflammatory conditions on the relation be-ween CRP concentrations and incident cardiovascular disease.
ETHODS
tudy Samplehe design and selection criteria for Framingham Off-pring Study have been described previously.26 For pri-ary analyses, we selected all participants who attended
he fifth examination cycle (1991-1995) and had CRPoncentrations measured (n � 3782; 1973 women). Wexcluded participants with prevalent cardiovascular dis-ase at baseline (n � 365), resulting in an available sam-le of 3417 (1842 women) participants. This sample wassed to assess the prevalence of common inflammatoryonditions (as described below) cross-sectionally and tonalyze the incidence of cardiovascular disease prospec-ively. For assessing the prevalence of uncommon in-ammatory conditions (from the same examination cy-le), we conducted a case-referent analysis matching 463articipants with CRP concentrations �10 mg/L by agend smoking status to a referent group of 463 participants
CLINICAL SIGNIF
● We evaluated 378women free of cainflammatory conreactive protein(referent), 1-3.mg/L.
● There was a higmon and uncomditions in thosetration (�10 mgmg/L).
● High CRP levelsevidence of an ucondition and ctesting.
ith CRP concentrations �1 mg/L. fl
All participants signed the informed consent and therotocol for the study was approved by the Institutionaleview Board of the Boston Medical Center.
easurements of CRPBlood samples for CRP weredrawn from the antecubital veinof individuals after an overnightfast. For examination cycle 5,CRP concentrations were mea-sured by an enzymatic immuno-assay (Hemagen Diagnostics, Inc.,Columbia, Md) as described previ-ously.6 The coefficient of variationfor replicate CRP measurements on36 subjects was 0.86. CRP was usedas a categorical predictor in ouranalyses, and the kappa statistic was0.75 for CRP values in the fourthcompared with the first throughthird quartiles, as previously de-scribed.6 For examination 7 cycleparticipants, CRP was measured byDade Behring BN100 nephelometer(Deerfield, Ill), and the mean coef-ficient of variation on 139 phantomreplicates was 3.2%.
scertainment of Cardiovascular Disease andisk Factorst each examination visit, participants underwent a medicalistory, physical examination, anthropometry, and labora-ory assessment of risk factors, as previously described.26
ndividuals who reported smoking 1 or more cigarettes/dayn the year of examination were considered current smokers.
Surveillance for cardiovascular events occurred duringach examination cycle and adjudication occurred by anndpoint committee consisting of 3 investigators, as previ-usly described.27 A cardiovascular event was defined asoronary heart disease (stable angina, coronary insuffi-iency, and myocardial infarction), cerebrovascular diseasestroke and transient ischemic attack), intermittent claudi-ation, or congestive heart failure. A family history ofremature cardiovascular disease was present if a validatedvent occurred in the father before the age of 55 years or inhe mother before age 65 years, as previously described.28
scertainment of Common and Uncommonnflammatory Conditionsnformation on common inflammatory conditions was ob-ained from the database collected during the clinic visit onstructured questionnaire administered at each examination
ycle by physician-examiners blinded to CRP concentra-ions. Participants were classified as having a common in-
CE
dle-aged men andascular disease forns according to C-) categories: �101-10, and �10
revalence of com-inflammatory con-high CRP concen-
ersus low CRP (�1
nt evaluation forying inflammatoryeration of repeat
ICAN
2 midrdiovditio(CRP
0, 3.
her pmonwith a/L) v
warranderlonsid
ammatory condition if they answered “yes” during the

ifdnptctts
wefmptciiCsccflaCtpsflfleoa
SSafl
Pscmmc
CtmccTcB
dl(Cii
PRevttm(o
CmMto�piad
RMwcspc
PCTcma(wicttcmdm
1056 The American Journal of Medicine, Vol 120, No 12, December 2007
nterview by a physician-examiner about any one of theollowing conditions: chronic urinary tract diseases (urinaryiseases), chronic gastro-duodenal ulcer (ie, gastro-duode-al diseases), chronic cough, chronic bronchitis, asthma (ie,ulmonary diseases), rheumatoid arthritis, gout, degenera-ive joint disease (ie, musculoskeletal diseases), or any can-er (excluding nonmelanoma skin cancers). These condi-ions were further categorized according to body system/ype—urinary, gastro-duodenal, pulmonary, musculo-keletal, and cancers.
Information about uncommon inflammatory conditionsas elicited during the participant’s interview and physical
xamination by the physician-examiner and noted in textorm on the questionnaire. Information about these uncom-on inflammatory conditions was not recorded in the com-
uterized database and could be obtained only by retrospec-ive review of the participants’ medical charts (heart studyharts). Therefore, to assess the prevalence of uncommonnflammatory conditions, we selected a total of 926 partic-pants by matching all participants in the markedly highRP category (�10 mg/L; n � 463) for age and smoking
tatus to equal number of referent participants with lowoncentrations of CRP (�1 mg/L). Before conducting thehart review, a separate prespecified list of uncommon in-ammatory conditions was made after reviewing the liter-ture for conditions associated with high concentrations ofRP29 and by consensus of 2 cardiologists and a rheuma-
ologist (Appendix 1). All charts were reviewed by a singlehysician blinded to CRP concentration and case-referenttatus. Charts were then screened for the prespecified in-ammatory conditions (eg, connective tissue disorders, in-ammatory bowel disease) for the fifth, sixth, or the seventhxamination cycle visits. For intra-observer reproducibilityf chart review, we re-reviewed 20 randomly selected chartsnd found high concordance (�95%) of results.
tatistical Analysesex-specific baseline characteristics of participants weressessed according to presence or absence of common in-ammatory conditions.
revalence of Common Inflammatory Conditions. Inex-specific analyses, prevalence of common inflammatoryonditions was calculated according to the clinically recom-ended CRP categories: low (�1 mg/L), borderline (1-3g/L), moderately high (3.01-10 mg/L), and markedly high
oncentrations (�10 mg/L).5,9
ross-sectional Analyses of CRP to Common Inflamma-ory Conditions. Sex-specific multiple logistic regressionodels30 were constructed to examine the relations of CRP
oncentrations in categories to the presence or absence ofommon inflammatory conditions (dichotomous variable).he following sex-specific models were constructed hierar-hically: (a) age-adjusted models; (b) adjusting for age,
MI, systolic blood pressure, antihypertensive medications, ciabetes mellitus, total/high-density lipoprotein (HDL) cho-esterol, smoking status, and estrogen replacement therapyin women). Additionally, we repeated these analyses usingRP concentrations in quartiles. We also investigated for
nteractions of the relations of CRP categories with commonnflammatory conditions by age or by smoking status.
rospective Analyses of CRP to Cardiovascular Diseaseisk. Sex-specific Cox proportional hazard regression mod-
ls were constructed to analyze the risk of incident cardio-ascular disease on follow-up, according to CRP concen-rations in continuous models (log transformed to normalizehe distribution) and by CRP categories (as above). Allodels were adjusted for covariates as described above
models a and b) with and without adjustment for presencef common inflammatory condition.
ase-referent Analyses of CRP to Uncommon Inflam-atory Conditions. In the case-referent analysis, Cochranantel-Haenszel31 test and chi-squared test accounting for
he matched design (age and smoking status) compared thedds of uncommon inflammatory conditions in cases (CRP10 mg/L) with referents (CRP �1 mg/L). Further, sex-
ooled multivariable conditional-logistic regression adjust-ng for all the covariates (model b, as above) was used tossess the odds of having an uncommon inflammatory con-ition in cases compared with referents.
ESULTSean age of the participants was 55 � 10 years (52%omen; Table 1). Participants with prevalent inflammatory
onditions were more likely to report current cigarettemoking. Blood pressure, total/HDL cholesterol ratio, andrevalence of diabetes were slightly higher among menompared with women.
revalence of Common Inflammatoryonditionshe prevalence of inflammatory conditions in participants ac-ording to CRP concentrations is presented in Table 2. Com-on inflammatory conditions were reported by 30.9% of men
nd 30.8% of women. Markedly high CRP concentrations�10 mg/L) were present in 9.4% of men and 14.0% ofomen overall. Chronic inflammatory conditions were signif-
cantly less likely to be present in men and women with CRPoncentrations �1 mg/L (P� .001; Table 2). A test for linearrend showed increasing prevalence of inflammatory condi-ions from the lowest CRP concentration to the highest CRPoncentration (P for both sex �.001). The prevalence of com-on inflammatory conditions according to body system/type is
isplayed in Table 3. Pulmonary conditions and cancer wereost common, followed by gastro-duodenal, urinary, and mus-
uloskeletal conditions.
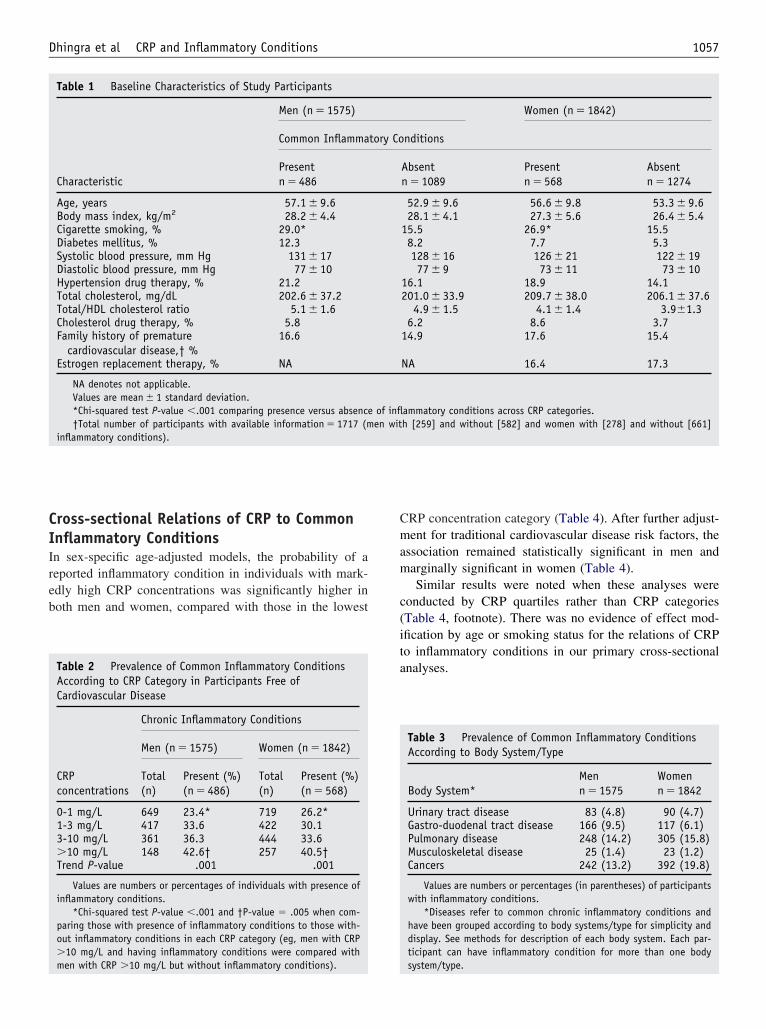
CIIreb
Cmam
c(ita
1057Dhingra et al CRP and Inflammatory Conditions
ross-sectional Relations of CRP to Commonnflammatory Conditionsn sex-specific age-adjusted models, the probability of aeported inflammatory condition in individuals with mark-dly high CRP concentrations was significantly higher inoth men and women, compared with those in the lowest
Table 1 Baseline Characteristics of Study Participants
Characteristic
Men (n � 1575)
Common Inflamma
Presentn � 486
Age, years 57.1 � 9.6Body mass index, kg/m2 28.2 � 4.4Cigarette smoking, % 29.0*Diabetes mellitus, % 12.3Systolic blood pressure, mm Hg 131 � 17Diastolic blood pressure, mm Hg 77 � 10Hypertension drug therapy, % 21.2Total cholesterol, mg/dL 202.6 � 37.2Total/HDL cholesterol ratio 5.1 � 1.6Cholesterol drug therapy, % 5.8Family history of premature
cardiovascular disease,† %16.6
Estrogen replacement therapy, % NA
NA denotes not applicable.Values are mean � 1 standard deviation.*Chi-squared test P-value �.001 comparing presence versus absence†Total number of participants with available information � 1717 (m
inflammatory conditions).
Table 2 Prevalence of Common Inflammatory ConditionsAccording to CRP Category in Participants Free ofCardiovascular Disease
CRPconcentrations
Chronic Inflammatory Conditions
Men (n � 1575) Women (n � 1842)
Total(n)
Present (%)(n � 486)
Total(n)
Present (%)(n � 568)
0-1 mg/L 649 23.4* 719 26.2*1-3 mg/L 417 33.6 422 30.13-10 mg/L 361 36.3 444 33.6�10 mg/L 148 42.6† 257 40.5†Trend P-value .001 .001
Values are numbers or percentages of individuals with presence ofinflammatory conditions.
*Chi-squared test P-value �.001 and †P-value � .005 when com-paring those with presence of inflammatory conditions to those with-out inflammatory conditions in each CRP category (eg, men with CRP�10 mg/L and having inflammatory conditions were compared with
men with CRP �10 mg/L but without inflammatory conditions).RP concentration category (Table 4). After further adjust-ent for traditional cardiovascular disease risk factors, the
ssociation remained statistically significant in men andarginally significant in women (Table 4).Similar results were noted when these analyses were
onducted by CRP quartiles rather than CRP categoriesTable 4, footnote). There was no evidence of effect mod-fication by age or smoking status for the relations of CRPo inflammatory conditions in our primary cross-sectionalnalyses.
Women (n � 1842)
nditions
Absentn � 1089
Presentn � 568
Absentn � 1274
52.9 � 9.6 56.6 � 9.8 53.3 � 9.628.1 � 4.1 27.3 � 5.6 26.4 � 5.4
15.5 26.9* 15.58.2 7.7 5.3128 � 16 126 � 21 122 � 1977 � 9 73 � 11 73 � 10
16.1 18.9 14.1201.0 � 33.9 209.7 � 38.0 206.1 � 37.6
4.9 � 1.5 4.1 � 1.4 3.9�1.36.2 8.6 3.7
14.9 17.6 15.4
NA 16.4 17.3
ammatory conditions across CRP categories.h [259] and without [582] and women with [278] and without [661]
Table 3 Prevalence of Common Inflammatory ConditionsAccording to Body System/Type
Body System*Menn � 1575
Womenn � 1842
Urinary tract disease 83 (4.8) 90 (4.7)Gastro-duodenal tract disease 166 (9.5) 117 (6.1)Pulmonary disease 248 (14.2) 305 (15.8)Musculoskeletal disease 25 (1.4) 23 (1.2)Cancers 242 (13.2) 392 (19.8)
Values are numbers or percentages (in parentheses) of participantswith inflammatory conditions.
*Diseases refer to common chronic inflammatory conditions andhave been grouped according to body systems/type for simplicity anddisplay. See methods for description of each body system. Each par-ticipant can have inflammatory condition for more than one body
tory Co
of inflen wit
system/type.
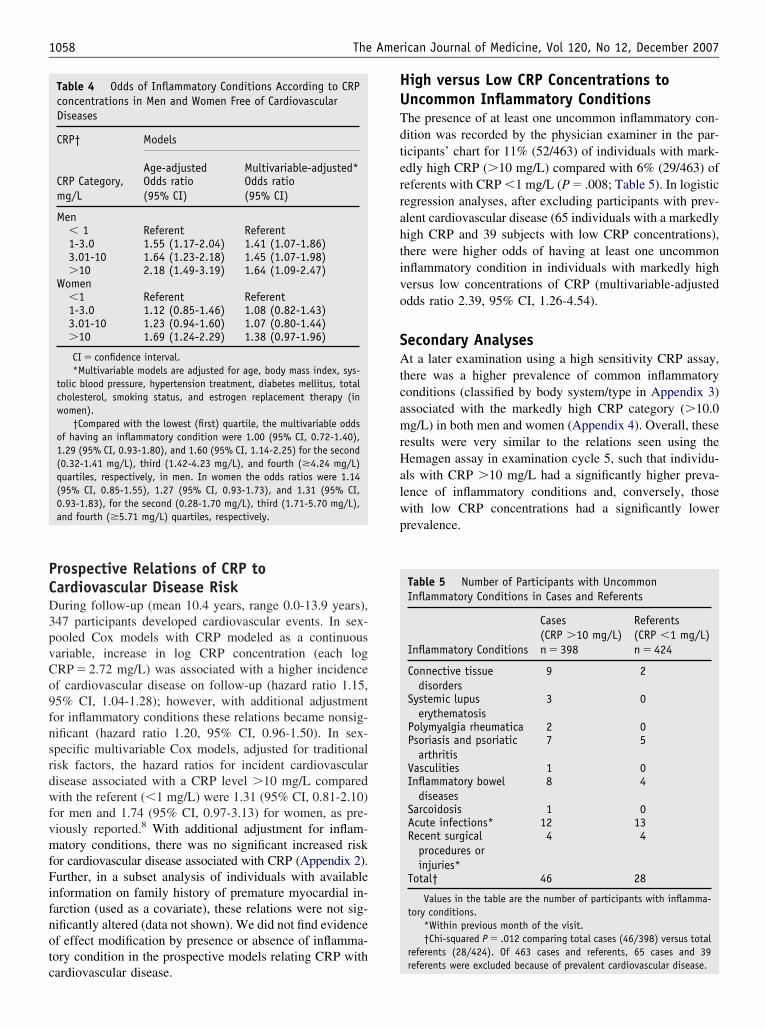
PCD3pvCo9fnsrdwfvmfFifnotc
HUTdterrahtivo
SAtcamrHalwp
1058 The American Journal of Medicine, Vol 120, No 12, December 2007
rospective Relations of CRP toardiovascular Disease Riskuring follow-up (mean 10.4 years, range 0.0-13.9 years),47 participants developed cardiovascular events. In sex-ooled Cox models with CRP modeled as a continuousariable, increase in log CRP concentration (each logRP � 2.72 mg/L) was associated with a higher incidencef cardiovascular disease on follow-up (hazard ratio 1.15,5% CI, 1.04-1.28); however, with additional adjustmentor inflammatory conditions these relations became nonsig-ificant (hazard ratio 1.20, 95% CI, 0.96-1.50). In sex-pecific multivariable Cox models, adjusted for traditionalisk factors, the hazard ratios for incident cardiovascularisease associated with a CRP level �10 mg/L comparedith the referent (�1 mg/L) were 1.31 (95% CI, 0.81-2.10)
or men and 1.74 (95% CI, 0.97-3.13) for women, as pre-iously reported.8 With additional adjustment for inflam-atory conditions, there was no significant increased risk
or cardiovascular disease associated with CRP (Appendix 2).urther, in a subset analysis of individuals with available
nformation on family history of premature myocardial in-arction (used as a covariate), these relations were not sig-ificantly altered (data not shown). We did not find evidencef effect modification by presence or absence of inflamma-ory condition in the prospective models relating CRP with
Table 4 Odds of Inflammatory Conditions According to CRPconcentrations in Men and Women Free of CardiovascularDiseases
CRP† Models
Age-adjusted Multivariable-adjusted*CRP Category,mg/L
Odds ratio(95% CI)
Odds ratio(95% CI)
Men� 1 Referent Referent1-3.0 1.55 (1.17-2.04) 1.41 (1.07-1.86)3.01-10 1.64 (1.23-2.18) 1.45 (1.07-1.98)�10 2.18 (1.49-3.19) 1.64 (1.09-2.47)
Women�1 Referent Referent1-3.0 1.12 (0.85-1.46) 1.08 (0.82-1.43)3.01-10 1.23 (0.94-1.60) 1.07 (0.80-1.44)�10 1.69 (1.24-2.29) 1.38 (0.97-1.96)
CI � confidence interval.*Multivariable models are adjusted for age, body mass index, sys-
tolic blood pressure, hypertension treatment, diabetes mellitus, totalcholesterol, smoking status, and estrogen replacement therapy (inwomen).
†Compared with the lowest (first) quartile, the multivariable oddsof having an inflammatory condition were 1.00 (95% CI, 0.72-1.40),1.29 (95% CI, 0.93-1.80), and 1.60 (95% CI, 1.14-2.25) for the second(0.32-1.41 mg/L), third (1.42-4.23 mg/L), and fourth (�4.24 mg/L)quartiles, respectively, in men. In women the odds ratios were 1.14(95% CI, 0.85-1.55), 1.27 (95% CI, 0.93-1.73), and 1.31 (95% CI,0.93-1.83), for the second (0.28-1.70 mg/L), third (1.71-5.70 mg/L),and fourth (�5.71 mg/L) quartiles, respectively.
ardiovascular disease.
igh versus Low CRP Concentrations toncommon Inflammatory Conditionshe presence of at least one uncommon inflammatory con-ition was recorded by the physician examiner in the par-icipants’ chart for 11% (52/463) of individuals with mark-dly high CRP (�10 mg/L) compared with 6% (29/463) ofeferents with CRP �1 mg/L (P � .008; Table 5). In logisticegression analyses, after excluding participants with prev-lent cardiovascular disease (65 individuals with a markedlyigh CRP and 39 subjects with low CRP concentrations),here were higher odds of having at least one uncommonnflammatory condition in individuals with markedly highersus low concentrations of CRP (multivariable-adjusteddds ratio 2.39, 95% CI, 1.26-4.54).
econdary Analysest a later examination using a high sensitivity CRP assay,
here was a higher prevalence of common inflammatoryonditions (classified by body system/type in Appendix 3)ssociated with the markedly high CRP category (�10.0g/L) in both men and women (Appendix 4). Overall, these
esults were very similar to the relations seen using theemagen assay in examination cycle 5, such that individu-
ls with CRP �10 mg/L had a significantly higher preva-ence of inflammatory conditions and, conversely, thoseith low CRP concentrations had a significantly lowerrevalence.
Table 5 Number of Participants with UncommonInflammatory Conditions in Cases and Referents
Inflammatory Conditions
Cases(CRP �10 mg/L)n � 398
Referents(CRP �1 mg/L)n � 424
Connective tissuedisorders
9 2
Systemic lupuserythematosis
3 0
Polymyalgia rheumatica 2 0Psoriasis and psoriatic
arthritis7 5
Vasculities 1 0Inflammatory bowel
diseases8 4
Sarcoidosis 1 0Acute infections* 12 13Recent surgical
procedures orinjuries*
4 4
Total† 46 28
Values in the table are the number of participants with inflamma-tory conditions.
*Within previous month of the visit.†Chi-squared P � .012 comparing total cases (46/398) versus total
referents (28/424). Of 463 cases and referents, 65 cases and 39
referents were excluded because of prevalent cardiovascular disease.
DImucoccCmmammccfltCch
emgtltdaicfiti(sfdmgwtpdi
mrdtnmwo
scwtcvtdt
hipH(hbwRwactawnpHiifiu
CImsartCcfiaau
R
1059Dhingra et al CRP and Inflammatory Conditions
ISCUSSIONn our sample of middle-aged to elderly men and women,arkedly high CRP concentrations (�10 mg/L) were not
ncommon (9.4% of men and 14.0% women). At least onehronic inflammatory condition was reported by nearly halff men and women who were free of prevalent cardiovas-ular disease. The prevalence of common inflammatoryonditions increased with increasing concentrations of CRP.onversely, participants with low CRP concentrations (�1g/L) were less likely to report a common chronic inflam-atory condition. In prospective multivariable-adjusted
nalyses for incident cardiovascular disease, further adjust-ent for common inflammatory conditions did not alter theagnitude or direction of the relations between CRP con-
entrations and incident cardiovascular disease. Finally, inase-referent analyses, we documented that uncommon in-ammatory conditions occur infrequently, as expected, but
end to occur more commonly in those with markedly highRP concentrations. To our knowledge, this is the firstomprehensive study of inflammatory conditions related toigh CRP concentrations in a community-based sample.
An American Heart Association (AHA)/Centers for Dis-ase Control and Prevention (CDC) statement (2002)5 and aore recent CDC/AHA workshop statement (2004) sug-
ested clinically relevant CRP categories and emphasizedhe existence of considerable biological variability in circu-ating CRP concentrations.25 Intermediate to high concen-rations of CRP clearly confer increased risks for myocar-ial infarction, stroke, and other cardiovascular disease,2,6,9
lthough it is unclear whether and how to implement screen-ng.32,33 Considering large intra-individual variability in theoncentrations of CRP,16,22 and apparently important dif-erences by race,17 our data support repeat testing for CRPn subjects with high CRP concentrations. In addition, cau-ion should be exercised if a chronic inflammatory conditions present or suspected. Indeed, the AHA/CDC statement2002) recommended that patients with active infection orystemic inflammatory conditions should not be tested.5 Aew studies have shown that CRP concentrations also pre-ict the risk of death from cardiovascular disease in inflam-atory arthritis patients.34,35 In this respect, some investi-
ators even believe that CRP can be proinflammatory,36,37
hereas others disagree.38,39 An important objective of fur-her research is to assess whether there is any utility, andarticularly what is the risk/benefit ratio, of initiation ofrug therapy in the setting of markedly high values of CRPn patients with documented inflammatory conditions.
Our study has some potential limitations. First, inflam-atory conditions were collected retrospectively from the
esearch charts, and we were not able to validate eachiagnosis of inflammatory conditions reported by the par-icipants, and some common inflammatory conditions mayot have been ascertained. Thus, our data may underesti-ate the prevalence and acuity of inflammatory conditions,hich would likely lead to a bias towards the null. We hope
ur study findings will motivate accurate, validated pro-pective collection of information about common and un-ommon inflammatory conditions and the inter-relationsith CRP in cardiovascular cohort studies. Second, due to
he cross-sectional design of our study, we cannot infer aausal relation between inflammatory conditions and ele-ated CRP concentrations. Third, the majority of our par-icipants are middle-aged to elderly Whites of Europeanescent, which may limit the generalizability of our findingso other ethnic/racial and age groups.
A final, important potential limitation is that variousigh-sensitivity CRP assays may differ in their reproduc-bility characteristics even if they might not differ in theirredictive value.40 The coefficient of variation for theemagen assay is somewhat higher at low concentrations
CRP �1.00 mg/L), but it is within an acceptable range atigher (CRP �1.00 mg/L) concentrations.6 Moreover, theetween-assay agreement as assessed by the kappa statisticas excellent for CRP categories used in our analyses.6
eductions in reproducibility at low CRP concentrationsould be expected to bias associations toward the null. To
ddress potential limitations of the Hemagen CRP assay, weonducted a similar cross-sectional analysis of the associa-ion of CRP categories with inflammatory conditions during
later Offspring examination cycle 7 (1999-2002) using aidely used high-sensitivity CRP assay (Dade-Behring,ephelometric assay) and found very similar results (Ap-endices 3, 4). Although our prospective analyses using theemagen assay do not suggest any significant impact of
nflammatory conditions on associations between CRP andncident cardiovascular disease, these findings warrant con-rmation in other prospective cohorts using the more widelysed high-sensitivity CRP assay.
ONCLUSIONn our community-based sample, elevated and, in particular,arkedly high concentrations of CRP (�10 mg/L) are as-
ociated with a significantly higher prevalence of common,s well as uncommon, inflammatory conditions. Furtheresearch is warranted using comprehensive, validated ascer-ainment of inflammatory conditions and high-sensitivityRP assays to assess the impact of common inflammatoryonditions on cardiovascular disease risk prediction. Ourndings reinforce previous statements that the presence ofctive inflammatory conditions should be excluded beforessessing an individual’s risk of cardiovascular disease bysing CRP concentrations.
eferences1. Koenig W, Sund M, Frohlich M, et al. C-Reactive protein, a sensitive
marker of inflammation, predicts future risk of coronary heart diseasein initially healthy middle-aged men: results from the MONICA (Mon-itoring Trends and Determinants in Cardiovascular Disease) AugsburgCohort Study, 1984 to 1992. Circulation. 1999;99:237-242.
2. Ridker PM, Rifai N, Rose L, et al. Comparison of C-reactive proteinand low-density lipoprotein cholesterol levels in the prediction of first
cardiovascular events. N Engl J Med. 2002;347:1557-1565.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
1060 The American Journal of Medicine, Vol 120, No 12, December 2007
3. Wang TJ, Nam BH, Wilson PW, et al. Association of C-reactiveprotein with carotid atherosclerosis in men and women: the Framing-ham Heart Study. Arterioscler Thromb Vasc Biol. 2002;22:1662-1667.
4. Wang TJ, Larson MG, Levy D, et al. C-reactive protein is associatedwith subclinical epicardial coronary calcification in men and women:the Framingham Heart Study. Circulation. 2002;106:1189-1191.
5. Pearson TA, Mensah GA, Alexander RW, et al. Markers of inflam-mation and cardiovascular disease: application to clinical and publichealth practice: a statement for healthcare professionals from theCenters for Disease Control and Prevention and the American HeartAssociation. Circulation. 2003;107:499-511.
6. Rost NS, Wolf PA, Kase CS, et al. Plasma concentration of C-reactiveprotein and risk of ischemic stroke and transient ischemic attack: theFramingham study. Stroke. 2001;32:2575-2579.
7. Danesh J, Wheeler JG, Hirschfield GM, et al. C-reactive protein andother circulating markers of inflammation in the prediction of coronaryheart disease. N Engl J Med. 2004;350:1387-1397.
8. Wilson PW, Nam BH, Pencina M, et al. C-reactive protein and risk ofcardiovascular disease in men and women from the Framingham HeartStudy. Arch Intern Med. 2005;165:2473-2478.
9. Ridker PM, Cook N. Clinical usefulness of very high and very lowlevels of C-reactive protein across the full range of Framingham RiskScores. Circulation. 2004;109:1955-1959.
0. Ford ES. Body mass index, diabetes, and C-reactive protein amongU.S. adults. Diabetes Care. 1999;22:1971-1977.
1. Sesso HD, Buring JE, Rifai N, et al. C-reactive protein and the risk ofdeveloping hypertension. JAMA. 2003;290:2945-2951.
2. Bazzano LA, He J, Muntner P, et al. Relationship between cigarettesmoking and novel risk factors for cardiovascular disease in the UnitedStates. Ann Intern Med. 2003;138:891-897.
3. Ridker PM, Hennekens CH, Rifai N, et al. Hormone replacementtherapy and increased plasma concentration of C-reactive protein.Circulation. 1999;100:713-716.
4. Carlson CS, Aldred SF, Lee PK, et al. Polymorphisms within theC-reactive protein (CRP) promoter region are associated with plasmaCRP levels. Am J Hum Genet. 2005;77:64-77.
5. Kathiresan S, Larson MG, Vasan RS, et al. Contribution of clinicalcorrelates and 13 C-reactive protein gene polymorphisms to interindi-vidual variability in serum C-reactive protein level. Circulation. 2006;113:1415-1423.
6. Macy EM, Hayes TE, Tracy RP. Variability in the measurement ofC-reactive protein in healthy subjects: implications for reference in-tervals and epidemiological applications. Clin Chem. 1997;43:52-58.
7. Khera A, McGuire DK, Murphy SA, et al. Race and gender differencesin C-reactive protein levels. J Am Coll Cardiol. 2005;46:464-469.
8. Guidelines for the management of rheumatoid arthritis: 2002 update.Arthritis Rheum. 2002;46:328-346.
9. Nielen MM, van Schaardenburg D, Reesink HW, et al. Increasedlevels of C-reactive protein in serum from blood donors before theonset of rheumatoid arthritis. Arthritis Rheum. 2004;50:2423-2427.
0. Mannino DM, Ford ES, Redd SC. Obstructive and restrictive lungdisease and markers of inflammation: data from the Third NationalHealth and Nutrition Examination. Am J Med. 2003;114:758-762.
1. Kushner I, Rzewnicki D, Samols D. What does minor elevation ofC-reactive protein signify? Am J Med. 2006;119:166.e17-166.e28.
2. Anderson NL, Anderson NG. The human plasma proteome: history,character, and diagnostic prospects. Mol Cell Proteomics. 2002;1:845-
867.3. Pepys MB, Baltz ML. Acute phase proteins with special reference toC-reactive protein and related proteins (pentaxins) and serum amyloidA protein. Adv Immunol. 1983;34:141-212.
4. Zimmerman MA, Selzman CH, Cothren C, et al. Diagnostic implica-tions of C-reactive protein. Arch Surg. 2003;138:220-224.
5. Myers GL, Rifai N, Tracy RP, et al. CDC/AHA Workshop on Markersof Inflammation and Cardiovascular Disease: Application to Clinicaland Public Health Practice: report from the laboratory science discus-sion group. Circulation. 2004;110:e545-e549.
6. Kannel WB, Feinleib M, McNamara PM, et al. An investigation ofcoronary heart disease in families. The Framingham offspring study.Am J Epidemiol. 1979;110:281-290.
7. Kannel WB, Wolf PA, Garrison RJ, eds. The Framingham Study: AnEpidemiological Investigation of Cardiovascular Disease. Section 34.Some risk factors related to the annual incidence of cardiovasculardisease and death in pooled repeated biennial measurements: Framing-ham Heart Study, 30-year follow up (NIH publication no. 87-2703).Bethesda, MD: National Heart, Lung and Blood Institute; 1987.
8. Lloyd-Jones DM, Nam BH, D’Agostino RB Sr, et al. Parental cardio-vascular disease as a risk factor for cardiovascular disease in middle-aged adults: a prospective study of parents and offspring. JAMA.2004;291:2204-2211.
9. Pepys MB, Hirschfield GM. C-reactive protein: a critical update.J Clin Invest. 2003;111:1805-1812.
0. Hosmer DW, Lemeshow S. Applied Logistic Regression. New York,NY: John Wiley and Sons, Inc.; 1989.
1. Cochran WG. The comparison of percentages in matched samples.Biometrika. 1950;37:256-266.
2. Koenig W. C-reactive protein and cardiovascular risk: has the timecome for screening the general population? Clin Chem. 2001;47:9-10.
3. Mosca L. C-reactive protein—to screen or not to screen? N EnglJ Med. 2002;347:1615-1617.
4. Goodson NJ, Symmons DP, Scott DG, et al. Baseline levels of C-re-active protein and prediction of death from cardiovascular disease inpatients with inflammatory polyarthritis: a ten-year followup study ofa primary care-based inception cohort. Arthritis Rheum. 2005;52:2293-2299.
5. Pasceri V, Yeh ET. A tale of two diseases: atherosclerosis and rheu-matoid arthritis. Circulation. 1999;100:2124-2126.
6. Cermak J, Key NS, Bach RR, et al. C-reactive protein induces humanperipheral blood monocytes to synthesize tissue factor. Blood. 1993;82:513-520.
7. Nakagomi A, Freedman SB, Geczy CL. Interferon-{gamma} and li-popolysaccharide potentiate monocyte tissue factor induction by C-re-active protein: relationship with age, sex, and hormone replacementtreatment. Circulation. 2000;101:1785-1791.
8. Hirschfield GM, Gallimore JR, Kahan MC, et al. Transgenic humanC-reactive protein is not proatherogenic in apolipoprotein E-deficientmice. Proc Natl Acad Sci U S A. 2005;102:8309-8314.
9. Pepys MB, Hawkins PN, Kahan MC, et al. Proinflammatory effects ofbacterial recombinant human C-reactive protein are caused by con-tamination with bacterial products, not by C-reactive protein itself.Circ Res. 2005;97:e97-e103.
0. Clarke JL, Anderson JL, Carlquist JF, et al. Comparison of differingC-reactive protein assay methods and their impact on cardiovascular
risk assessment. Am J Cardiol. 2005;95:155-158.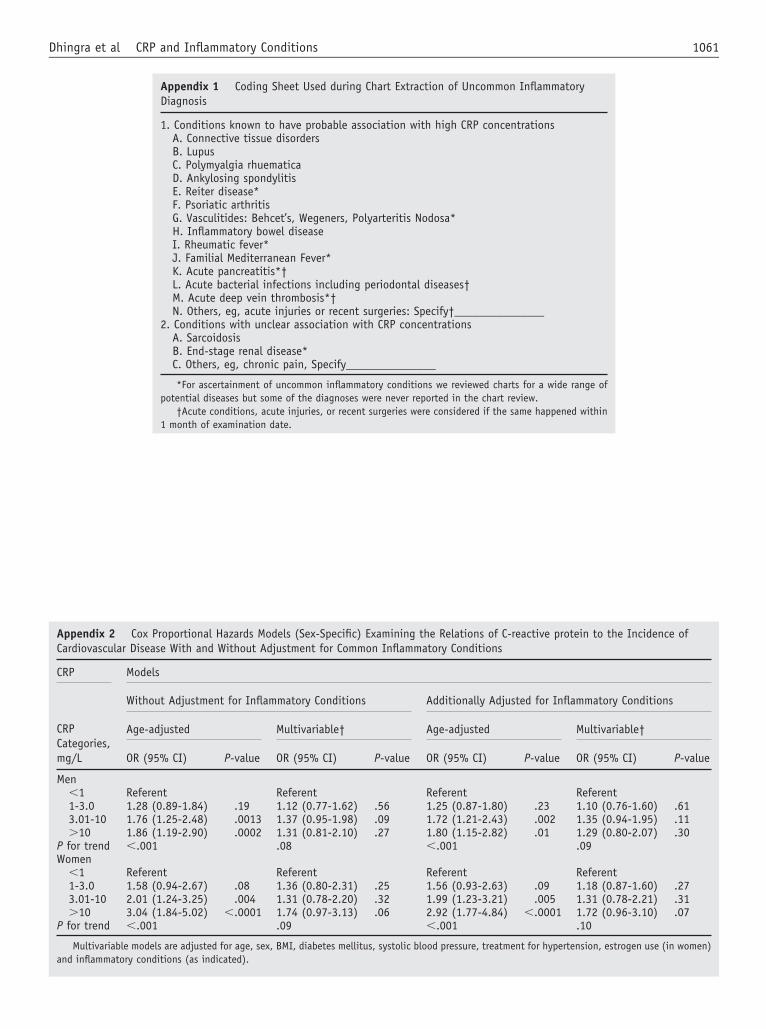
1061Dhingra et al CRP and Inflammatory Conditions
Appendix 1 Coding Sheet Used during CDiagnosis
1. Conditions known to have probable assoA. Connective tissue disordersB. LupusC. Polymyalgia rhuematicaD. Ankylosing spondylitisE. Reiter disease*F. Psoriatic arthritisG. Vasculitides: Behcet’s, Wegeners, PolyH. Inflammatory bowel diseaseI. Rheumatic fever*J. Familial Mediterranean Fever*K. Acute pancreatitis*†L. Acute bacterial infections including pM. Acute deep vein thrombosis*†N. Others, eg, acute injuries or recent su
2. Conditions with unclear association withA. SarcoidosisB. End-stage renal disease*C. Others, eg, chronic pain, Specify____
*For ascertainment of uncommon inflammatpotential diseases but some of the diagnoses w
†Acute conditions, acute injuries, or recent1 month of examination date.
Appendix 2 Cox Proportional Hazards Models (Sex-Specific) ECardiovascular Disease With and Without Adjustment for Commo
CRP Models
Without Adjustment for Inflammatory Conditions
CRPCategories,mg/L
Age-adjusted Multivariable†
OR (95% CI) P-value OR (95% CI)
Men�1 Referent Referent1-3.0 1.28 (0.89-1.84) .19 1.12 (0.77-1.62)3.01-10 1.76 (1.25-2.48) .0013 1.37 (0.95-1.98)�10 1.86 (1.19-2.90) .0002 1.31 (0.81-2.10)
P for trend �.001 .08Women
�1 Referent Referent1-3.0 1.58 (0.94-2.67) .08 1.36 (0.80-2.31)3.01-10 2.01 (1.24-3.25) .004 1.31 (0.78-2.20)�10 3.04 (1.84-5.02) �.0001 1.74 (0.97-3.13)
P for trend �.001 .09
Multivariable models are adjusted for age, sex, BMI, diabetes mellitusand inflammatory conditions (as indicated).
hart Extraction of Uncommon Inflammatory
ciation with high CRP concentrations
arteritis Nodosa*
eriodontal diseases†
rgeries: Specify†_______________CRP concentrations
___________
ory conditions we reviewed charts for a wide range ofere never reported in the chart review.surgeries were considered if the same happened within
xamining the Relations of C-reactive protein to the Incidence ofn Inflammatory Conditions
Additionally Adjusted for Inflammatory Conditions
Age-adjusted Multivariable†
P-value OR (95% CI) P-value OR (95% CI) P-value
Referent Referent.56 1.25 (0.87-1.80) .23 1.10 (0.76-1.60) .61.09 1.72 (1.21-2.43) .002 1.35 (0.94-1.95) .11.27 1.80 (1.15-2.82) .01 1.29 (0.80-2.07) .30
�.001 .09
Referent Referent.25 1.56 (0.93-2.63) .09 1.18 (0.87-1.60) .27.32 1.99 (1.23-3.21) .005 1.31 (0.78-2.21) .31.06 2.92 (1.77-4.84) �.0001 1.72 (0.96-3.10) .07
�.001 .10
, systolic blood pressure, treatment for hypertension, estrogen use (in women)
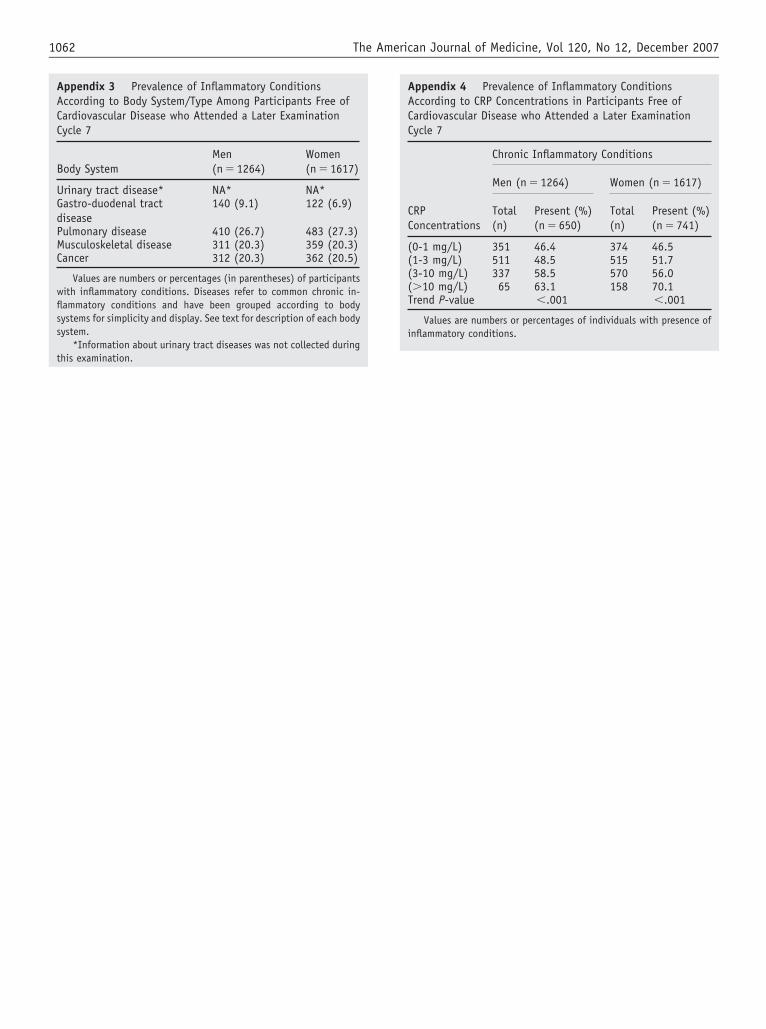
this examination.
1062 The American Journal of Medicine, Vol 120, No 12, December 2007
Appendix 4 Prevalence of Inflammatory ConditionsAccording to CRP Concentrations in Participants Free ofCardiovascular Disease who Attended a Later ExaminationCycle 7
CRPConcentrations
Chronic Inflammatory Conditions
Men (n � 1264) Women (n � 1617)
Total(n)
Present (%)(n � 650)
Total(n)
Present (%)(n � 741)
(0-1 mg/L) 351 46.4 374 46.5(1-3 mg/L) 511 48.5 515 51.7(3-10 mg/L) 337 58.5 570 56.0(�10 mg/L) 65 63.1 158 70.1Trend P-value �.001 �.001
Values are numbers or percentages of individuals with presence ofinflammatory conditions.
Appendix 3 Prevalence of Inflammatory ConditionsAccording to Body System/Type Among Participants Free ofCardiovascular Disease who Attended a Later ExaminationCycle 7
Body SystemMen(n � 1264)
Women(n � 1617)
Urinary tract disease* NA* NA*Gastro-duodenal tractdisease
140 (9.1) 122 (6.9)
Pulmonary disease 410 (26.7) 483 (27.3)Musculoskeletal disease 311 (20.3) 359 (20.3)Cancer 312 (20.3) 362 (20.5)
Values are numbers or percentages (in parentheses) of participantswith inflammatory conditions. Diseases refer to common chronic in-flammatory conditions and have been grouped according to bodysystems for simplicity and display. See text for description of each bodysystem.
*Information about urinary tract diseases was not collected during
C
ORMa
c
o
CwU(ciptdcrr
a
MWM
0d
The American Journal of Medicine (2007) 120, 1063-1070
LINICAL RESEARCH STUDY
utcomes in Patients with Chronic Kidney Diseaseeferred Late to Nephrologists: A Meta-analysis
icah R. Chan, MD, MPH,a Aaron T. Dall, MD,a Kathlyn E. Fletcher, MD, MA,b Na Lu, PhD,c Hariprasad Trivedi, MDd
Department of Medicine, Division of General Internal Medicine, bDivision of General Internal Medicine, Zablocki VA Medical Center,Health Policy Institute, Graduate School of Biomedical Sciences, Division of Biostatistics, dDivision of Nephrology, Medical College
f Wisconsin andPtMnsRehaCmc2
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
Affiliated Hospitals, Milwaukee.
ABSTRACT
URPOSE: The study purpose was to compare differences in mortality and the duration of hospitaliza-ion in patients with chronic kidney disease who are referred early versus late to nephrologists.ETHODS: We searched English-language literature from 1980 through December 2005, along withational conference proceedings, the Web of Science Citation Index, and reference lists of all includedtudies. Twenty-two studies with a total sample size of 12,749 met inclusion criteria.ESULTS: There was significantly increased overall mortality in the late referral group as compared with thearly referral group (relative risk 1.99; 95% confidence interval [CI], 1.66 to 2.39, P �.0001). The duration ofospital stay, at the time of initiation of renal replacement therapy, was greater in the late referred group by anverage of 12 days (95% CI, 8.0 to 16.1, P � .0007). Significant heterogeneity was detected for both outcomes.ONCLUSION: Timing of referral emerged to be a significant factor impacting homogeneity in theortality outcome. Our results suggest significantly higher mortality and increased early hospitalization of
hronic kidney disease subjects referred late to nephrologists as compared with earlier referred subjects. ©007 Elsevier Inc. All rights reserved.
KEYWORDS: Chronic kidney disease; Dialysis; Hospitalization; Mortality; Referral; Timing
tfbHaptuidtt
usrec
hronic kidney disease is a continually growing problemorldwide. It has been estimated that 8 million people in thenited States have a calculated glomerular filtration rate
GFR) �60 mL/min/1.73m2 and another 12 million have mi-roalbuminuria.1 The prevalence of end-stage renal disease hasncreased over the past decade and continues to grow. Therevalence in the US was �450,000 in 2003 and is estimatedo exceed 650,000 by 2010.1,2 Subjects with end-stage renalisease have an exceedingly high morbidity and mortality asompared with the general population. The annual mortalityate has consistently exceeded 170 per 1000 patient-years-atisk.1
Along with the increase in end-stage renal disease prev-lence, the costs of care have increased. In the year 2010,
Requests for reprints should be addressed to Micah R. Chan, MD,PH, Department of Medicine, Division of Nephrology, University ofisconsin Hospitals and Clinics, 3034 Fish Hatchery Road, Suite B,adison, WI 53713-3125.
ront matter © 2007 Elsevier Inc. All rights reserved.ed.2007.04.024
he projected direct health care costs borne by the Centersor Medicare and Medicaid is projected to increase to $28.3illion, more than double the Medicare cost in 1998.2,3
ospitalization is a significant component, constitutingbout 39.6% of direct costs in 2003. Hospital days peratient-year have consistently exceeded 13.6 from 1994hrough 2004.1 Probably prompted by these alarming fig-res, Healthy People 2010 includes among its goals improv-ng the mortality of chronic kidney disease subjects andecreasing the economic costs. Defining contributing fac-ors related to patient outcomes is paramount to improvinghese dismal statistics.
Over the past several years, interest has evolved in eval-ating the timing of nephrology referral in the predialytictage of chronic kidney disease as an important variableelated to prognosis. Specifically, it is of interest whetherarly versus late referral of these subjects improves out-ome. The definition of the time factor “late” is somewhat
rbitrary and varies in the literature, ranging from �1 month
tpar
mrTptophaimmotsssctitm
M
SWrrWtsrfrrm
LWcrbWr(sdafd
t1aa
aaitwt
DOttanis
afasarf
ST
n est
1064 The American Journal of Medicine, Vol 120, No 12, December 2007
o 1 year before renal replacement therapy. In general, aatient is considered to have been referred late “when man-gement could have been improved by earlier contact withenal services.”4
Potential benefits of early referral include aggressiveanagement of several dialysis-
elated and nondialysis issues.5
hese include control of bloodressure, treatment of anemia, at-ention to nutrition, and correctionf metabolic abnormalities in theredialysis period. The underlyingypotheses are that these issuesre better managed in the special-sts’ realm as opposed to the pri-ary care setting, and that betteranagement leads to improved
utcome. Prior individual studieshat have explored this issue con-ist of relatively small sampleizes and are predominantly retro-pective. Further, results may beonfounded by case-mix charac-eristics and regional differencesn practice patterns. Therefore, therue benefit of early referral re-ains uncertain.
ETHODS
tudy Questionse intended to answer the following questions: What is the
isk of mortality in end-stage renal disease patients who areeferred to nephrologists late versus those referred early?
hat is the difference in the duration of hospitalization, athe initiation of renal replacement therapy, between end-tage renal disease patients who are referred late and thoseeferred early? In addition, we analyzed differences in theollowing laboratory parameters at the initiation of renaleplacement therapy in subjects referred late versus thoseeferred early: serum creatinine; creatinine clearance; albu-in; hemoglobin; and hematocrit.
iterature Sources and Search Termse conducted a computerized search of the literature for
linical studies that addressed the issue of referral to neph-ologists published during the period 1980 through Decem-er 2005 using MEDLINE, PREMEDLINE, and CINAHL.e used combinations of terms related to referral (referral,
eferral and consultation, timing, time factors), nephrologychronic kidney disease, CKD, chronic kidney failure, end-tage renal disease, and ESRD), and dialysis (dialysis, renalialysis, renal replacement therapy, and RRT). This strategylso combined 5 exploded Medical Subject Headings (re-erral and consultation, time factors, chronic kidney failure,
CLINICAL SIGNIF
● Early nephrologylytic stage of chrproves outcomedisease.
● In dialysis patieshortened hospimortality by hareferral.
● Primary care phincreased traininuation of chronicvalue of comareferral.
● Specific guidelinhave not yet bee
ialysis, and renal replacement therapy). t
Further, we hand searched journals that were indexed inhe Web of Science-Science Citation Index from the years998 through 2005. We also examined the reference lists ofll articles identified in the search as well as those of reviewrticles. We reviewed the abstracts of the American Society
of Nephrology, European RenalAssociation/European DialysisTransplant Association, and Na-tional Kidney Foundation annualscientific meetings from 1995through 2005. Whenever possible,we corresponded with the authorsof the abstracts to clarify ques-tions or obtain data.
Study SelectionInclusion criteria were a measureof timing of referral to nephrol-ogy, defined as early or late, andan assessment of outcomes relatedto mortality or duration of hospi-talization. It was decided, a priori,to exclude any of the followingcategories of articles: wrong top-ics, editorials, reviews, practiceguidelines, patient education ma-terial, or pediatric studies.
From among 325 identified ci-tations, we reviewed all relevant
rticles (Figure 1). Of those, 111 were abstracts or articlesppropriate for detailed review. Two authors (MRC, ATD)ndependently reviewed each article from the initial searcho determine if inclusion criteria were met. Disagreementas resolved by consensus and, when necessary, with arbi-
ration from a third author (HT).
ata Abstractionf the 111 studies reviewed in detail, 36 were eliminated due
o non-English studies, duplicate reports, case reports, simula-ion-based data, or reviews. Of the remaining 75 studies thatssessed the timing of referral to nephrology, 53 were elimi-ated due to undefined or inestimable time factors, outcome ofnterest not available, or insufficient relevant data. Finally, 22tudies were retained for further analysis.
The data from each included article were abstracted by 2uthors (MRC, ATD). We used a standardized abstractionorm that included patient number, demographics, controlnd study group information, study design, primary andecondary outcomes, and methodological concerns. Dis-greements were resolved through consensus or by a thirdeviewer (HT). We were able to correspond with authorsrom 2 of the 4 studies for which we needed clarification.
tatistical Analysishe primary outcomes of interest were mortality and dura-
CE
rral in the predia-kidney disease im-
end-stage renal
prior early referralays and decreasedmpared with late
ns should receiveiagnosis and eval-ey disease and theent and timely
r “early referral”ablished.
ICAN
refeonics in
nts,tal stlf, co
ysiciag in dkidn
nagem
es fo
ion of hospitalization in the late versus early referred
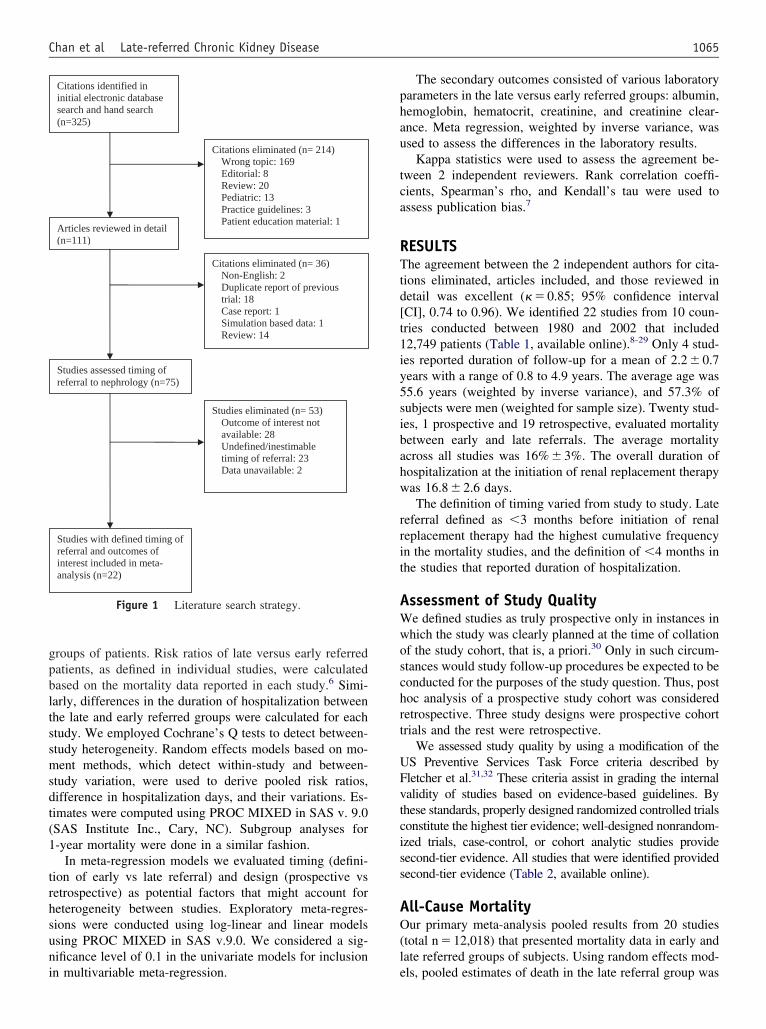
gpbltssmsdt(1
trhsuni
phau
tca
RTtd[t1iy5sibahw
rrit
AWwoschrt
UFvtciss
AO(l
1065Chan et al Late-referred Chronic Kidney Disease
roups of patients. Risk ratios of late versus early referredatients, as defined in individual studies, were calculatedased on the mortality data reported in each study.6 Simi-arly, differences in the duration of hospitalization betweenhe late and early referred groups were calculated for eachtudy. We employed Cochrane’s Q tests to detect between-tudy heterogeneity. Random effects models based on mo-ent methods, which detect within-study and between-
tudy variation, were used to derive pooled risk ratios,ifference in hospitalization days, and their variations. Es-imates were computed using PROC MIXED in SAS v. 9.0SAS Institute Inc., Cary, NC). Subgroup analyses for-year mortality were done in a similar fashion.
In meta-regression models we evaluated timing (defini-ion of early vs late referral) and design (prospective vsetrospective) as potential factors that might account foreterogeneity between studies. Exploratory meta-regres-ions were conducted using log-linear and linear modelssing PROC MIXED in SAS v.9.0. We considered a sig-ificance level of 0.1 in the univariate models for inclusion
Citations identified ininitial electronic databasesearch and hand search(n=325)
Citations eliminated (n= 214)Wrong topic: 169
Editorial: 8 Review: 20 Pediatric: 13
Practice guidelines: 3 Patient education material: 1
Articles reviewed in detail(n=111)
Citations eliminated (n= 36) Non-English: 2
Duplicate report of previoustrial: 18Case report: 1 Simulation based data: 1
Review: 14
Studies assessed timing ofreferral to nephrology (n=75)
Studies eliminated (n= 53)Outcome of interest notavailable: 28
Undefined/inestimabletiming of referral: 23Data unavailable: 2
Studies with defined timing ofreferral and outcomes of interest included in meta-analysis (n=22)
Figure 1 Literature search strategy.
n multivariable meta-regression. e
The secondary outcomes consisted of various laboratoryarameters in the late versus early referred groups: albumin,emoglobin, hematocrit, creatinine, and creatinine clear-nce. Meta regression, weighted by inverse variance, wassed to assess the differences in the laboratory results.
Kappa statistics were used to assess the agreement be-ween 2 independent reviewers. Rank correlation coeffi-ients, Spearman’s rho, and Kendall’s tau were used tossess publication bias.7
ESULTShe agreement between the 2 independent authors for cita-
ions eliminated, articles included, and those reviewed inetail was excellent (� � 0.85; 95% confidence intervalCI], 0.74 to 0.96). We identified 22 studies from 10 coun-ries conducted between 1980 and 2002 that included2,749 patients (Table 1, available online).8-29 Only 4 stud-es reported duration of follow-up for a mean of 2.2 � 0.7ears with a range of 0.8 to 4.9 years. The average age was5.6 years (weighted by inverse variance), and 57.3% ofubjects were men (weighted for sample size). Twenty stud-es, 1 prospective and 19 retrospective, evaluated mortalityetween early and late referrals. The average mortalitycross all studies was 16% � 3%. The overall duration ofospitalization at the initiation of renal replacement therapyas 16.8 � 2.6 days.The definition of timing varied from study to study. Late
eferral defined as �3 months before initiation of renaleplacement therapy had the highest cumulative frequencyn the mortality studies, and the definition of �4 months inhe studies that reported duration of hospitalization.
ssessment of Study Qualitye defined studies as truly prospective only in instances inhich the study was clearly planned at the time of collationf the study cohort, that is, a priori.30 Only in such circum-tances would study follow-up procedures be expected to beonducted for the purposes of the study question. Thus, postoc analysis of a prospective study cohort was consideredetrospective. Three study designs were prospective cohortrials and the rest were retrospective.
We assessed study quality by using a modification of theS Preventive Services Task Force criteria described byletcher et al.31,32 These criteria assist in grading the internalalidity of studies based on evidence-based guidelines. Byhese standards, properly designed randomized controlled trialsonstitute the highest tier evidence; well-designed nonrandom-zed trials, case-control, or cohort analytic studies provideecond-tier evidence. All studies that were identified providedecond-tier evidence (Table 2, available online).
ll-Cause Mortalityur primary meta-analysis pooled results from 20 studies
total n � 12,018) that presented mortality data in early andate referred groups of subjects. Using random effects mod-
ls, pooled estimates of death in the late referral group was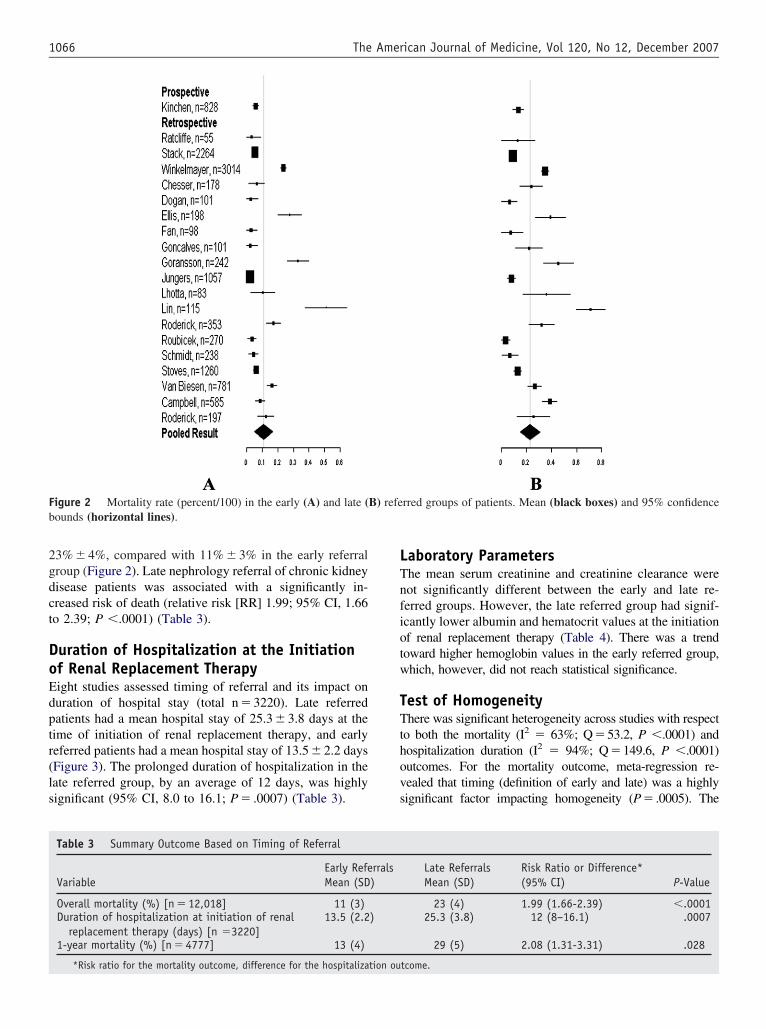
2gdct
DoEdptr(ls
LTnfiotw
TTthovs
Fb
1066 The American Journal of Medicine, Vol 120, No 12, December 2007
3% � 4%, compared with 11% � 3% in the early referralroup (Figure 2). Late nephrology referral of chronic kidneyisease patients was associated with a significantly in-reased risk of death (relative risk [RR] 1.99; 95% CI, 1.66o 2.39; P �.0001) (Table 3).
uration of Hospitalization at the Initiationf Renal Replacement Therapyight studies assessed timing of referral and its impact onuration of hospital stay (total n � 3220). Late referredatients had a mean hospital stay of 25.3 � 3.8 days at theime of initiation of renal replacement therapy, and earlyeferred patients had a mean hospital stay of 13.5 � 2.2 daysFigure 3). The prolonged duration of hospitalization in theate referred group, by an average of 12 days, was highlyignificant (95% CI, 8.0 to 16.1; P � .0007) (Table 3).
igure 2 Mortality rate (percent/100) in the early (A) and late (ounds (horizontal lines).
Table 3 Summary Outcome Based on Timing of Referral
VariableEarly RefeMean (SD
Overall mortality (%) [n � 12,018] 11 (3)Duration of hospitalization at initiation of renal
replacement therapy (days) [n �3220]13.5 (2.2
1-year mortality (%) [n � 4777] 13 (4)
*Risk ratio for the mortality outcome, difference for the hospitalization ou
aboratory Parametershe mean serum creatinine and creatinine clearance wereot significantly different between the early and late re-erred groups. However, the late referred group had signif-cantly lower albumin and hematocrit values at the initiationf renal replacement therapy (Table 4). There was a trendoward higher hemoglobin values in the early referred group,hich, however, did not reach statistical significance.
est of Homogeneityhere was significant heterogeneity across studies with respect
o both the mortality (I2 � 63%; Q�53.2, P �.0001) andospitalization duration (I2 � 94%; Q�149.6, P �.0001)utcomes. For the mortality outcome, meta-regression re-ealed that timing (definition of early and late) was a highlyignificant factor impacting homogeneity (P� .0005). The
rred groups of patients. Mean (black boxes) and 95% confidence
Late ReferralsMean (SD)
Risk Ratio or Difference*(95% CI) P-Value
23 (4) 1.99 (1.66-2.39) �.000125.3 (3.8) 12 (8–16.1) .0007
29 (5) 2.08 (1.31-3.31) .028
B) refe
rrals)
)
tcome.
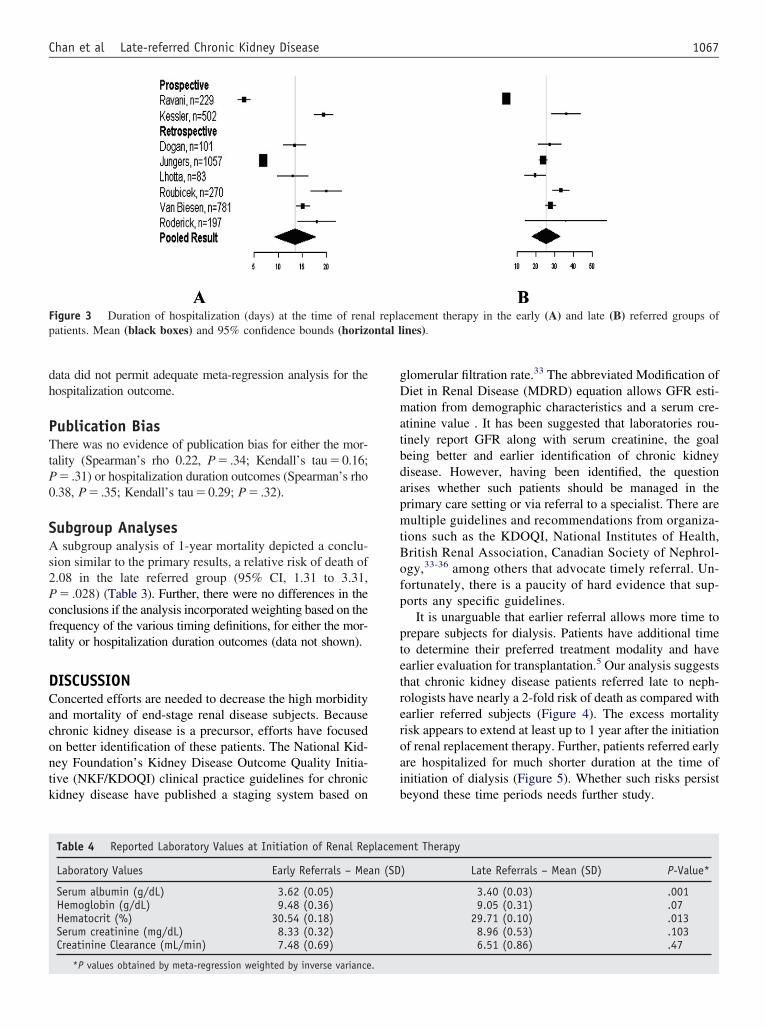
dh
PTtP0
SAs2Pcft
DCacontk
gDmatbdapmtBofp
ptetreroaib
Fp ontal l
1067Chan et al Late-referred Chronic Kidney Disease
ata did not permit adequate meta-regression analysis for theospitalization outcome.
ublication Biashere was no evidence of publication bias for either the mor-
ality (Spearman’s rho 0.22, P� .34; Kendall’s tau�0.16;� .31) or hospitalization duration outcomes (Spearman’s rho
.38, P� .35; Kendall’s tau�0.29; P� .32).
ubgroup Analysessubgroup analysis of 1-year mortality depicted a conclu-
ion similar to the primary results, a relative risk of death of.08 in the late referred group (95% CI, 1.31 to 3.31,� .028) (Table 3). Further, there were no differences in the
onclusions if the analysis incorporated weighting based on therequency of the various timing definitions, for either the mor-ality or hospitalization duration outcomes (data not shown).
ISCUSSIONoncerted efforts are needed to decrease the high morbiditynd mortality of end-stage renal disease subjects. Becausehronic kidney disease is a precursor, efforts have focusedn better identification of these patients. The National Kid-ey Foundation’s Kidney Disease Outcome Quality Initia-ive (NKF/KDOQI) clinical practice guidelines for chronicidney disease have published a staging system based on
igure 3 Duration of hospitalization (days) at the time of renaatients. Mean (black boxes) and 95% confidence bounds (horiz
Table 4 Reported Laboratory Values at Initiation of Renal Rep
Laboratory Values Early Referrals – Me
Serum albumin (g/dL) 3.62 (0.05)Hemoglobin (g/dL) 9.48 (0.36)Hematocrit (%) 30.54 (0.18)Serum creatinine (mg/dL) 8.33 (0.32)Creatinine Clearance (mL/min) 7.48 (0.69)
*P values obtained by meta-regression weighted by inverse variance.
lomerular filtration rate.33 The abbreviated Modification ofiet in Renal Disease (MDRD) equation allows GFR esti-ation from demographic characteristics and a serum cre-
tinine value . It has been suggested that laboratories rou-inely report GFR along with serum creatinine, the goaleing better and earlier identification of chronic kidneyisease. However, having been identified, the questionrises whether such patients should be managed in therimary care setting or via referral to a specialist. There areultiple guidelines and recommendations from organiza-
ions such as the KDOQI, National Institutes of Health,ritish Renal Association, Canadian Society of Nephrol-gy,33-36 among others that advocate timely referral. Un-ortunately, there is a paucity of hard evidence that sup-orts any specific guidelines.
It is unarguable that earlier referral allows more time torepare subjects for dialysis. Patients have additional timeo determine their preferred treatment modality and havearlier evaluation for transplantation.5 Our analysis suggestshat chronic kidney disease patients referred late to neph-ologists have nearly a 2-fold risk of death as compared witharlier referred subjects (Figure 4). The excess mortalityisk appears to extend at least up to 1 year after the initiationf renal replacement therapy. Further, patients referred earlyre hospitalized for much shorter duration at the time ofnitiation of dialysis (Figure 5). Whether such risks persisteyond these time periods needs further study.
cement therapy in the early (A) and late (B) referred groups ofines).
ent Therapy
) Late Referrals – Mean (SD) P-Value*
3.40 (0.03) .0019.05 (0.31) .07
29.71 (0.10) .0138.96 (0.53) .1036.51 (0.86) .47
l repla
lacem
an (SD
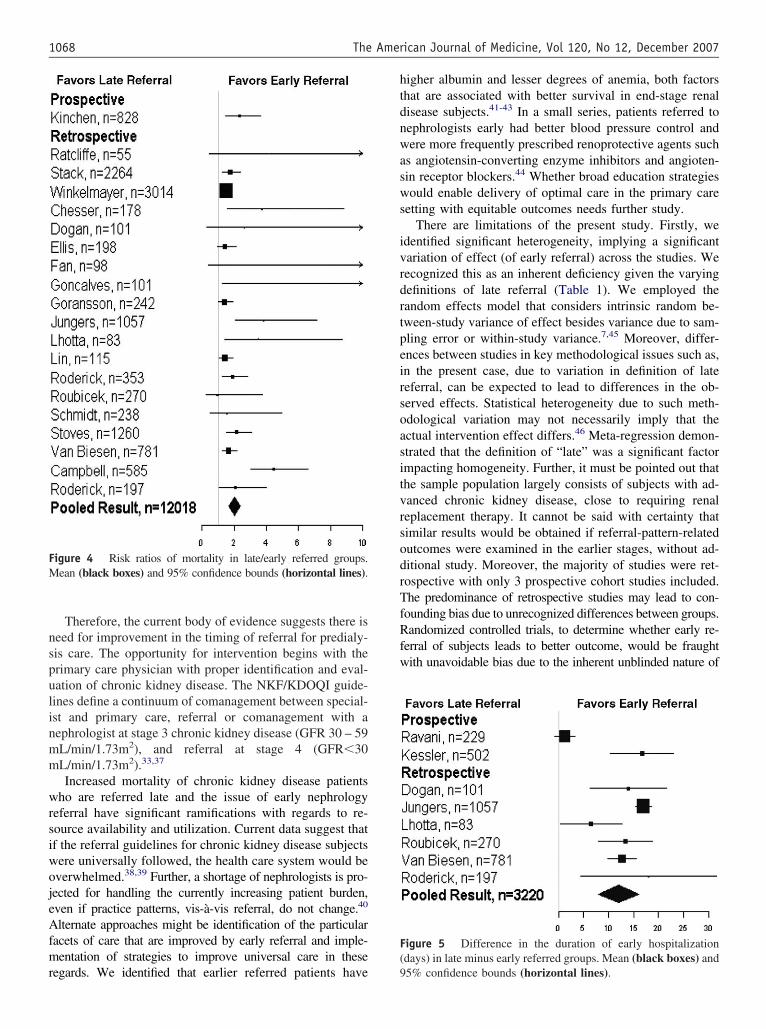
nspulinmm
wrsiwojeAfmr
htdnwasws
ivrdrtpeirsoasitvrsodrTfRfw
F(
FM
1068 The American Journal of Medicine, Vol 120, No 12, December 2007
Therefore, the current body of evidence suggests there iseed for improvement in the timing of referral for predialy-is care. The opportunity for intervention begins with therimary care physician with proper identification and eval-ation of chronic kidney disease. The NKF/KDOQI guide-ines define a continuum of comanagement between special-st and primary care, referral or comanagement with aephrologist at stage 3 chronic kidney disease (GFR 30 – 59L/min/1.73m2), and referral at stage 4 (GFR�30L/min/1.73m2).33,37
Increased mortality of chronic kidney disease patientsho are referred late and the issue of early nephrology
eferral have significant ramifications with regards to re-ource availability and utilization. Current data suggest thatf the referral guidelines for chronic kidney disease subjectsere universally followed, the health care system would beverwhelmed.38,39 Further, a shortage of nephrologists is pro-ected for handling the currently increasing patient burden,ven if practice patterns, vis-à-vis referral, do not change.40
lternate approaches might be identification of the particularacets of care that are improved by early referral and imple-entation of strategies to improve universal care in these
igure 4 Risk ratios of mortality in late/early referred groups.ean (black boxes) and 95% confidence bounds (horizontal lines).
egards. We identified that earlier referred patients have 9
igher albumin and lesser degrees of anemia, both factorshat are associated with better survival in end-stage renalisease subjects.41-43 In a small series, patients referred toephrologists early had better blood pressure control andere more frequently prescribed renoprotective agents such
s angiotensin-converting enzyme inhibitors and angioten-in receptor blockers.44 Whether broad education strategiesould enable delivery of optimal care in the primary care
etting with equitable outcomes needs further study.There are limitations of the present study. Firstly, we
dentified significant heterogeneity, implying a significantariation of effect (of early referral) across the studies. Weecognized this as an inherent deficiency given the varyingefinitions of late referral (Table 1). We employed theandom effects model that considers intrinsic random be-ween-study variance of effect besides variance due to sam-ling error or within-study variance.7,45 Moreover, differ-nces between studies in key methodological issues such as,n the present case, due to variation in definition of lateeferral, can be expected to lead to differences in the ob-erved effects. Statistical heterogeneity due to such meth-dological variation may not necessarily imply that thectual intervention effect differs.46 Meta-regression demon-trated that the definition of “late” was a significant factormpacting homogeneity. Further, it must be pointed out thathe sample population largely consists of subjects with ad-anced chronic kidney disease, close to requiring renaleplacement therapy. It cannot be said with certainty thatimilar results would be obtained if referral-pattern-relatedutcomes were examined in the earlier stages, without ad-itional study. Moreover, the majority of studies were ret-ospective with only 3 prospective cohort studies included.he predominance of retrospective studies may lead to con-
ounding bias due to unrecognized differences between groups.andomized controlled trials, to determine whether early re-
erral of subjects leads to better outcome, would be fraughtith unavoidable bias due to the inherent unblinded nature of
igure 5 Difference in the duration of early hospitalizationdays) in late minus early referred groups. Mean (black boxes) and
5% confidence bounds (horizontal lines).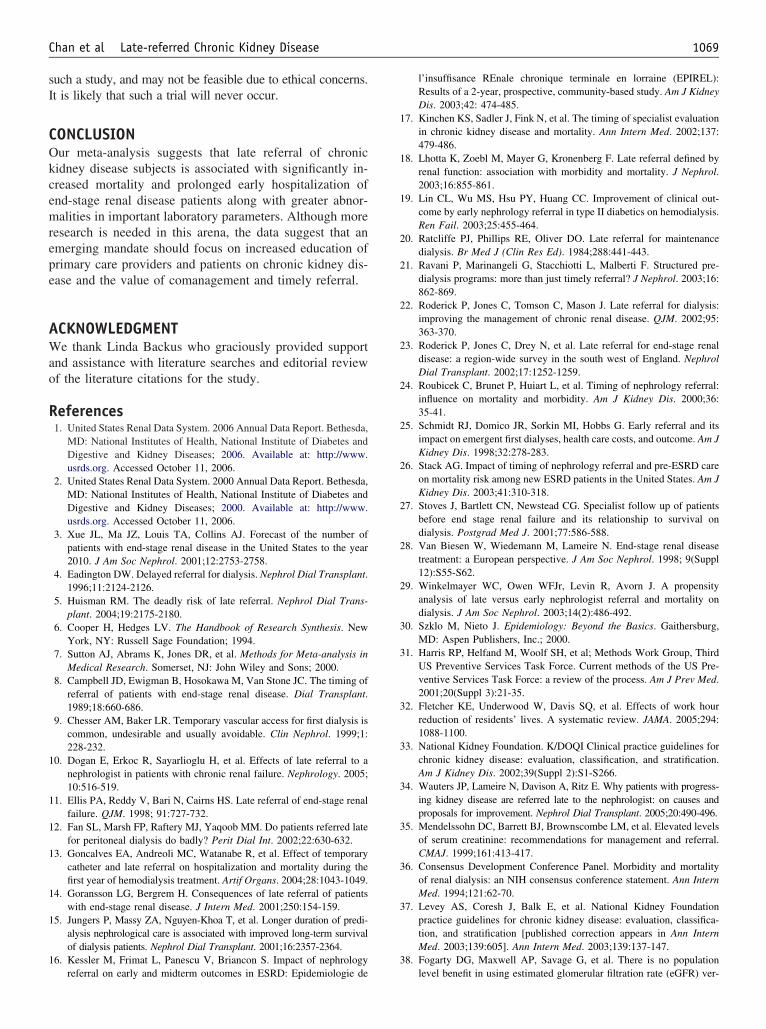
sI
COkcemrepe
AWao
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
1069Chan et al Late-referred Chronic Kidney Disease
uch a study, and may not be feasible due to ethical concerns.t is likely that such a trial will never occur.
ONCLUSIONur meta-analysis suggests that late referral of chronicidney disease subjects is associated with significantly in-reased mortality and prolonged early hospitalization ofnd-stage renal disease patients along with greater abnor-alities in important laboratory parameters. Although more
esearch is needed in this arena, the data suggest that anmerging mandate should focus on increased education ofrimary care providers and patients on chronic kidney dis-ase and the value of comanagement and timely referral.
CKNOWLEDGMENTe thank Linda Backus who graciously provided support
nd assistance with literature searches and editorial reviewf the literature citations for the study.
eferences1. United States Renal Data System. 2006 Annual Data Report. Bethesda,
MD: National Institutes of Health, National Institute of Diabetes andDigestive and Kidney Diseases; 2006. Available at: http://www.usrds.org. Accessed October 11, 2006.
2. United States Renal Data System. 2000 Annual Data Report. Bethesda,MD: National Institutes of Health, National Institute of Diabetes andDigestive and Kidney Diseases; 2000. Available at: http://www.usrds.org. Accessed October 11, 2006.
3. Xue JL, Ma JZ, Louis TA, Collins AJ. Forecast of the number ofpatients with end-stage renal disease in the United States to the year2010. J Am Soc Nephrol. 2001;12:2753-2758.
4. Eadington DW. Delayed referral for dialysis. Nephrol Dial Transplant.1996;11:2124-2126.
5. Huisman RM. The deadly risk of late referral. Nephrol Dial Trans-plant. 2004;19:2175-2180.
6. Cooper H, Hedges LV. The Handbook of Research Synthesis. NewYork, NY: Russell Sage Foundation; 1994.
7. Sutton AJ, Abrams K, Jones DR, et al. Methods for Meta-analysis inMedical Research. Somerset, NJ: John Wiley and Sons; 2000.
8. Campbell JD, Ewigman B, Hosokawa M, Van Stone JC. The timing ofreferral of patients with end-stage renal disease. Dial Transplant.1989;18:660-686.
9. Chesser AM, Baker LR. Temporary vascular access for first dialysis iscommon, undesirable and usually avoidable. Clin Nephrol. 1999;1:228-232.
0. Dogan E, Erkoc R, Sayarlioglu H, et al. Effects of late referral to anephrologist in patients with chronic renal failure. Nephrology. 2005;10:516-519.
1. Ellis PA, Reddy V, Bari N, Cairns HS. Late referral of end-stage renalfailure. QJM. 1998; 91:727-732.
2. Fan SL, Marsh FP, Raftery MJ, Yaqoob MM. Do patients referred latefor peritoneal dialysis do badly? Perit Dial Int. 2002;22:630-632.
3. Goncalves EA, Andreoli MC, Watanabe R, et al. Effect of temporarycatheter and late referral on hospitalization and mortality during thefirst year of hemodialysis treatment. Artif Organs. 2004;28:1043-1049.
4. Goransson LG, Bergrem H. Consequences of late referral of patientswith end-stage renal disease. J Intern Med. 2001;250:154-159.
5. Jungers P, Massy ZA, Nguyen-Khoa T, et al. Longer duration of predi-alysis nephrological care is associated with improved long-term survivalof dialysis patients. Nephrol Dial Transplant. 2001;16:2357-2364.
6. Kessler M, Frimat L, Panescu V, Briancon S. Impact of nephrology
referral on early and midterm outcomes in ESRD: Epidemiologie del’insuffisance REnale chronique terminale en lorraine (EPIREL):Results of a 2-year, prospective, community-based study. Am J KidneyDis. 2003;42: 474-485.
7. Kinchen KS, Sadler J, Fink N, et al. The timing of specialist evaluationin chronic kidney disease and mortality. Ann Intern Med. 2002;137:479-486.
8. Lhotta K, Zoebl M, Mayer G, Kronenberg F. Late referral defined byrenal function: association with morbidity and mortality. J Nephrol.2003;16:855-861.
9. Lin CL, Wu MS, Hsu PY, Huang CC. Improvement of clinical out-come by early nephrology referral in type II diabetics on hemodialysis.Ren Fail. 2003;25:455-464.
0. Ratcliffe PJ, Phillips RE, Oliver DO. Late referral for maintenancedialysis. Br Med J (Clin Res Ed). 1984;288:441-443.
1. Ravani P, Marinangeli G, Stacchiotti L, Malberti F. Structured pre-dialysis programs: more than just timely referral? J Nephrol. 2003;16:862-869.
2. Roderick P, Jones C, Tomson C, Mason J. Late referral for dialysis:improving the management of chronic renal disease. QJM. 2002;95:363-370.
3. Roderick P, Jones C, Drey N, et al. Late referral for end-stage renaldisease: a region-wide survey in the south west of England. NephrolDial Transplant. 2002;17:1252-1259.
4. Roubicek C, Brunet P, Huiart L, et al. Timing of nephrology referral:influence on mortality and morbidity. Am J Kidney Dis. 2000;36:35-41.
5. Schmidt RJ, Domico JR, Sorkin MI, Hobbs G. Early referral and itsimpact on emergent first dialyses, health care costs, and outcome. Am JKidney Dis. 1998;32:278-283.
6. Stack AG. Impact of timing of nephrology referral and pre-ESRD careon mortality risk among new ESRD patients in the United States. Am JKidney Dis. 2003;41:310-318.
7. Stoves J, Bartlett CN, Newstead CG. Specialist follow up of patientsbefore end stage renal failure and its relationship to survival ondialysis. Postgrad Med J. 2001;77:586-588.
8. Van Biesen W, Wiedemann M, Lameire N. End-stage renal diseasetreatment: a European perspective. J Am Soc Nephrol. 1998; 9(Suppl12):S55-S62.
9. Winkelmayer WC, Owen WFJr, Levin R, Avorn J. A propensityanalysis of late versus early nephrologist referral and mortality ondialysis. J Am Soc Nephrol. 2003;14(2):486-492.
0. Szklo M, Nieto J. Epidemiology: Beyond the Basics. Gaithersburg,MD: Aspen Publishers, Inc.; 2000.
1. Harris RP, Helfand M, Woolf SH, et al; Methods Work Group, ThirdUS Preventive Services Task Force. Current methods of the US Pre-ventive Services Task Force: a review of the process. Am J Prev Med.2001;20(Suppl 3):21-35.
2. Fletcher KE, Underwood W, Davis SQ, et al. Effects of work hourreduction of residents’ lives. A systematic review. JAMA. 2005;294:1088-1100.
3. National Kidney Foundation. K/DOQI Clinical practice guidelines forchronic kidney disease: evaluation, classification, and stratification.Am J Kidney Dis. 2002;39(Suppl 2):S1-S266.
4. Wauters JP, Lameire N, Davison A, Ritz E. Why patients with progress-ing kidney disease are referred late to the nephrologist: on causes andproposals for improvement. Nephrol Dial Transplant. 2005;20:490-496.
5. Mendelssohn DC, Barrett BJ, Brownscombe LM, et al. Elevated levelsof serum creatinine: recommendations for management and referral.CMAJ. 1999;161:413-417.
6. Consensus Development Conference Panel. Morbidity and mortalityof renal dialysis: an NIH consensus conference statement. Ann InternMed. 1994;121:62-70.
7. Levey AS, Coresh J, Balk E, et al. National Kidney Foundationpractice guidelines for chronic kidney disease: evaluation, classifica-tion, and stratification [published correction appears in Ann InternMed. 2003;139:605]. Ann Intern Med. 2003;139:137-147.
8. Fogarty DG, Maxwell AP, Savage G, et al. There is no population
level benefit in using estimated glomerular filtration rate (eGFR) ver-
3
4
4
4
4
4
4
4
1070 The American Journal of Medicine, Vol 120, No 12, December 2007
sus serum creatinine for identifying and referring patients with CKD[Abstract]. J Am Soc Nephrol. 2005;61:319A.
9. Van Biesen W, Vanholder R, Veys N, et al. The importance ofstandardization of creatinine in the implementation of guidelines andrecommendations for CKD: implications for CKD management pro-grammes. Nephrol Dial Transplant. 2006;21:77-83.
0. Suki WN. Are physician assistants the answer to a shortage of neph-rologists? Am J Kidney Dis. 1999;33:796-797.
1. Dwyer JT, Larive B, Leung J, et al. Are nutritional status indicatorsassociated with mortality in the Hemodialysis (HEMO) Study? KidneyInt. 2005;68:1766-1776.
2. Revicki DA, Brown RE, Feeny DH, et al. Health-related quality of lifeassociated with recombinant human erythropoietin therapy for predialysis
chronic renal disease patients. Am J Kidney Dis. 1995;25:548-554.3. Xue JL, St. Peter WL, Ebben JP, et al. Anemia treatment in thepre-ESRD period and associated mortality in elderly patients. Am JKidney Dis. 2002;40:1153-1161.
4. Martinez-Ramirez HR, Jalomo-Martinez B, Cortes-Sanabria L, et al.Renal function preservation in type 2 diabetes mellitus patients withearly nephropathy: a comparative prospective cohort study betweenprimary health care doctors and a nephrologist. Am J Kidney Dis.2006;47(1):78-87.
5. Egger M, Smith GD, Phillips AN. Meta-analysis: principles and pro-cedures. BMJ. 1997;315:1533-1537.
6. Higgins JPT, Green S. Analysing and presenting results. CochraneHandbook for Systematic Reviews of Interventions. 4.2.5 [updatedMay 2005]. Available at: http://www.cochrane.org/resources/hand-
book/hbook.htm. Accessed December 8, 2006.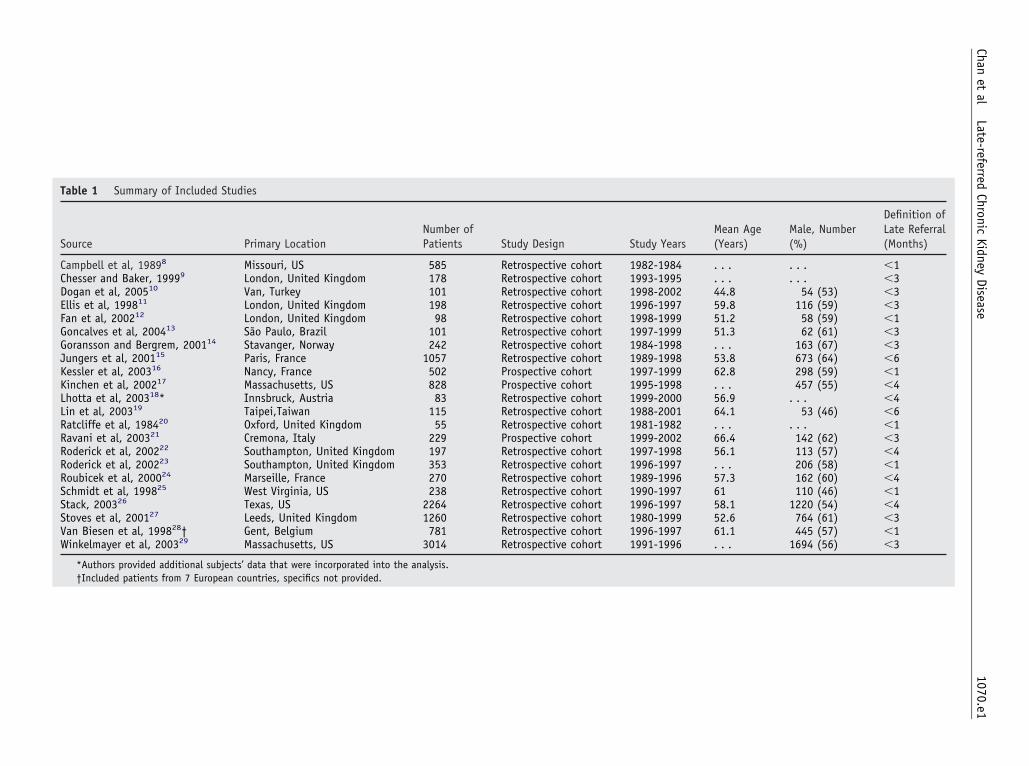
Number ofPatients Study Design Study Years
Mean Age(Years)
Male, Number(%)
Definition ofLate Referral(Months)
585 Retrospective cohort 1982-1984 . . . . . . �1178 Retrospective cohort 1993-1995 . . . . . . �3101 Retrospective cohort 1998-2002 44.8 54 (53) �3198 Retrospective cohort 1996-1997 59.8 116 (59) �398 Retrospective cohort 1998-1999 51.2 58 (59) �1
101 Retrospective cohort 1997-1999 51.3 62 (61) �3242 Retrospective cohort 1984-1998 . . . 163 (67) �3
1057 Retrospective cohort 1989-1998 53.8 673 (64) �6502 Prospective cohort 1997-1999 62.8 298 (59) �1828 Prospective cohort 1995-1998 . . . 457 (55) �483 Retrospective cohort 1999-2000 56.9 . . . �4
115 Retrospective cohort 1988-2001 64.1 53 (46) �655 Retrospective cohort 1981-1982 . . . . . . �1
229 Prospective cohort 1999-2002 66.4 142 (62) �3dom 197 Retrospective cohort 1997-1998 56.1 113 (57) �4dom 353 Retrospective cohort 1996-1997 . . . 206 (58) �1
270 Retrospective cohort 1989-1996 57.3 162 (60) �4238 Retrospective cohort 1990-1997 61 110 (46) �1
2264 Retrospective cohort 1996-1997 58.1 1220 (54) �41260 Retrospective cohort 1980-1999 52.6 764 (61) �3781 Retrospective cohort 1996-1997 61.1 445 (57) �1
3014 Retrospective cohort 1991-1996 . . . 1694 (56) �3
into the analysis.d.
1070.e1Chan
etal
Late-referredChronic
KidneyDisease
Table 1 Summary of Included Studies
Source Primary Location
Campbell et al, 19898 Missouri, USChesser and Baker, 19999 London, United KingdomDogan et al, 200510 Van, TurkeyEllis et al, 199811 London, United KingdomFan et al, 200212 London, United KingdomGoncalves et al, 200413 São Paulo, BrazilGoransson and Bergrem, 200114 Stavanger, NorwayJungers et al, 200115 Paris, FranceKessler et al, 200316 Nancy, FranceKinchen et al, 200217 Massachusetts, USLhotta et al, 200318* Innsbruck, AustriaLin et al, 200319 Taipei,TaiwanRatcliffe et al, 198420 Oxford, United KingdomRavani et al, 200321 Cremona, ItalyRoderick et al, 200222 Southampton, United KingRoderick et al, 200223 Southampton, United KingRoubicek et al, 200024 Marseille, FranceSchmidt et al, 199825 West Virginia, USStack, 200326 Texas, USStoves et al, 200127 Leeds, United KingdomVan Biesen et al, 199828† Gent, BelgiumWinkelmayer et al, 200329 Massachusetts, US
*Authors provided additional subjects’ data that were incorporated†Included patients from 7 European countries, specifics not provide
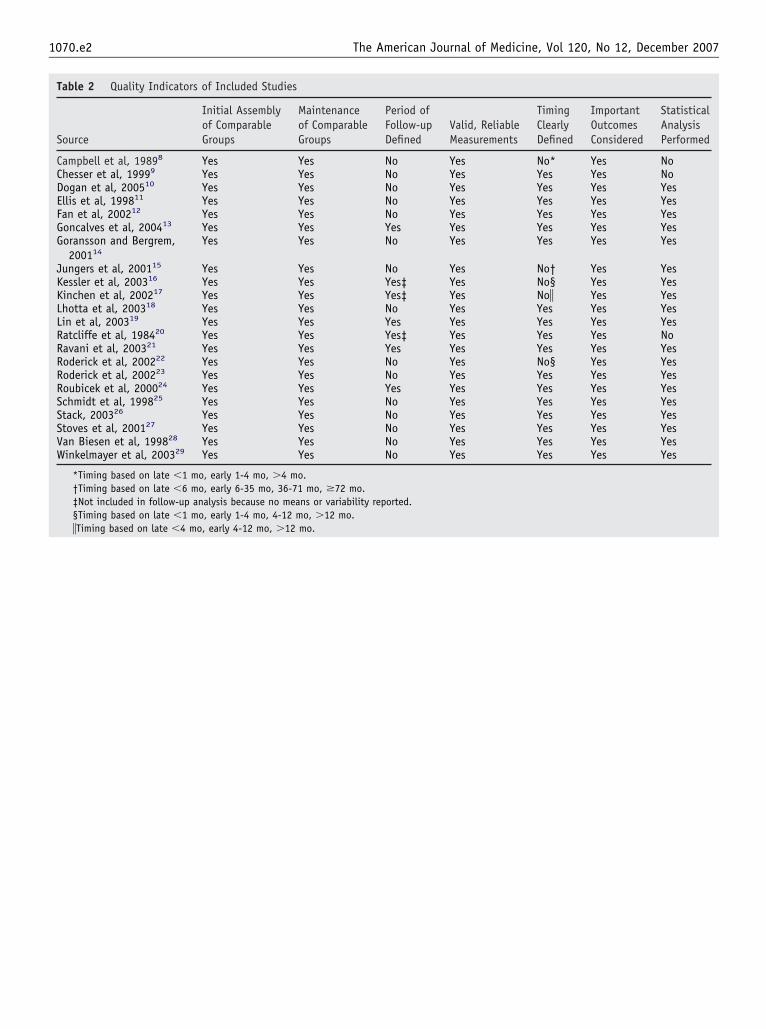
1070.e2 The American Journal of Medicine, Vol 120, No 12, December 2007
Table 2 Quality Indicators of Included Studies
Source
Initial Assemblyof ComparableGroups
Maintenanceof ComparableGroups
Period ofFollow-upDefined
Valid, ReliableMeasurements
TimingClearlyDefined
ImportantOutcomesConsidered
StatisticalAnalysisPerformed
Campbell et al, 19898 Yes Yes No Yes No* Yes NoChesser et al, 19999 Yes Yes No Yes Yes Yes NoDogan et al, 200510 Yes Yes No Yes Yes Yes YesEllis et al, 199811 Yes Yes No Yes Yes Yes YesFan et al, 200212 Yes Yes No Yes Yes Yes YesGoncalves et al, 200413 Yes Yes Yes Yes Yes Yes YesGoransson and Bergrem,
200114Yes Yes No Yes Yes Yes Yes
Jungers et al, 200115 Yes Yes No Yes No† Yes YesKessler et al, 200316 Yes Yes Yes‡ Yes No§ Yes YesKinchen et al, 200217 Yes Yes Yes‡ Yes No� Yes YesLhotta et al, 200318 Yes Yes No Yes Yes Yes YesLin et al, 200319 Yes Yes Yes Yes Yes Yes YesRatcliffe et al, 198420 Yes Yes Yes‡ Yes Yes Yes NoRavani et al, 200321 Yes Yes Yes Yes Yes Yes YesRoderick et al, 200222 Yes Yes No Yes No§ Yes YesRoderick et al, 200223 Yes Yes No Yes Yes Yes YesRoubicek et al, 200024 Yes Yes Yes Yes Yes Yes YesSchmidt et al, 199825 Yes Yes No Yes Yes Yes YesStack, 200326 Yes Yes No Yes Yes Yes YesStoves et al, 200127 Yes Yes No Yes Yes Yes YesVan Biesen et al, 199828 Yes Yes No Yes Yes Yes YesWinkelmayer et al, 200329 Yes Yes No Yes Yes Yes Yes
*Timing based on late �1 mo, early 1-4 mo, �4 mo.†Timing based on late �6 mo, early 6-35 mo, 36-71 mo, �72 mo.‡Not included in follow-up analysis because no means or variability reported.§Timing based on late �1 mo, early 1-4 mo, 4-12 mo, �12 mo.
�Timing based on late �4 mo, early 4-12 mo, �12 mo.
C
TNKRa
Btmstf
DB
0d
The American Journal of Medicine (2007) 120, 1071-1077
LINICAL RESEARCH STUDY
he Characteristics and Prognostic Importance ofT-ProBNP Concentrations in Critically Ill Patients
eyur B. Shah, MD,a,b Matthew M. Nolan, MD,a,b Krishnamurti Rao, BS,a,b David J. Wang, MD,a,b
obert H. Christenson, PhD,a Carl B. Shanholtz, MD,a Mandeep R. Mehra, MD,a Stephen S. Gottlieb, MDa,b
University of M b
BitcMfdwoPbRpsseA(Cspv
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
aryland School of Medicine, Baltimore and Baltimore Veteran’s Affairs Medical Center.
ABSTRACT
ACKGROUND: There are limited data for prognostic and diagnostic use of natriuretic peptides inntensive care unit (ICU) patients. We evaluate amino-terminal brain natriuretic peptide (NT-proBNP) inhe medical ICU, specifically its correlation with noncardiac admission diagnosis and prognosis ofritically ill patients.ETHODS: NT-proBNP (pg/mL) was measured in 179 ICU patients without acute decompensated heart
ailure or acute coronary syndrome. Death during hospitalization (mortality), APACHE II score, laboratoryata, echocardiograms, medical history, and demographics were assessed. NT-proBNP concentrationsere compared with established cutoffs for congestive heart failure (�450 pg/mL for patients �50 yearsf age, �900 pg/mL for patients 50-70 years of age, and �1800 pg/mL for patients �70 years of age).redictors of mortality and of NT-proBNP were analyzed by regression analysis. Tertiles were comparedy analysis of variance and chi-squared test.ESULTS: NT-proBNP was elevated in these ICU patients (median 2139 pg/mL, 25th percentile 540g/mL, 75% percentile 7389 pg/mL ). Severity of illness and renal dysfunction (APACHE II score anderum creatinine) increased with rising NT-proBNP. The incidence of acute respiratory distress syndrome,epsis, death, history of coronary artery disease (CAD) or congestive heart failure (all P �.05) increased withach tertile. Independent predictors of increased NT-proBNP were creatinine (P �.001), CAD (P �.001),PACHE II score (P �.05), and sepsis (P �.001). Overall hospital mortality was 26%, and log NT-proBNP
P �.05), APACHE II (P �.001), and CAD (P �.05) were independent predictors of mortality.ONCLUSIONS: For patients admitted to the ICU without decompensated heart failure or acute coronaryyndrome, NT-proBNP concentrations are markedly elevated, especially in patients with sepsis. NT-roBNP strongly and independently predicts mortality. However, NT-proBNP should not be used to directolume management in critically ill patients. © 2007 Elsevier Inc. All rights reserved.
KEYWORDS: Amino-terminal probrain natriuretic peptide; Congestive heart failure; Intensive care unit; Natriureticpeptide; Sepsis
lddr
Ntvat
rain natriuretic peptide (BNP) is synthesized primarily inhe cardiac ventricles. Gene expression of the BNP prohor-one is rapidly increased during periods of ventricular wall
tretch. The prohormone is enzymatically cleaved to formhe active BNP molecule and an inactive amino-terminalragment (NT-proBNP), which are secreted into the circu-
Requests for reprints should be addressed to Stephen Gottlieb, MD,ivision of Cardiology, University of Maryland Hospital, 22 S. Greene St.,altimore, MD 21201.
ront matter © 2007 Elsevier Inc. All rights reserved.ed.2007.07.032
ation. The BNP molecules activate surface receptors toecrease intracardiac pressure by diuresis, peripheral vaso-ilatation, and suppression of the renin-angiotensin-aldoste-one-axis.1
Measuring circulating serum concentrations of BNP orT-proBNP has proven useful for identifying cardiac pa-
hology. In the emergency room or outpatient setting, ele-ated levels help distinguish cardiac causes of dyspnea.2,3 Insymptomatic individuals, elevated serum concentrations ofhese cardiac markers maintain prognostic value for identi-
ying risk of cardiovascular events and mortality.4
(cItupOtrarp
emtAahpWtdotscctt
M
STU2b
poroawpewjcwimds
tc
BW
rtswiaucumvfPsE
d
STvaftocM
atient
1072 The American Journal of Medicine, Vol 120, No 12, December 2007
In critically ill patients admitted to the intensive care unitICU), the specificity of natriuretic peptides for identifyingardiac pathology and congestive heart failure is unclear.nitial studies with BNP were dominated by surgical pa-ients, and peptide concentrations identified the presence ofnderlying heart disease withoutroviding prognostic information.5,6
ther studies focusing on only pa-ients with severe sepsis or shockeported diffusely elevated valuesnd differing conclusions about theole of BNP and NT-proBNP as arognostic tool.7-12
A heterogeneous array of dis-ase processes, complications, andedical interventions affect pa-
ients admitted to the medical ICU.n inclusive survey of patients
dmitted to the ICU is needed toelp characterize the role of NT-roBNP in the intensive care unit.hether NT-proBNP concentra-
ions are elevated because of car-iac dysfunction, volume overload,r other reasons is not known. Weherefore conducted a large pro-pective study characterizing criti-ally ill patients without a primaryardiac reason for admission andhe relationship of these characteristics to NT-proBNP concen-rations and prognosis.
ETHODS
tudy Designhis was a prospective observational study conducted at theniversity of Maryland Medical Center, July 2004 to July005. The protocol was approved by the institutional reviewoard of the University of Maryland Medical Center.
Adult patients admitted to the ICU were eligible if theatient did not have an acute cardiac condition (acute cor-nary syndrome, acute decompensated heart failure, or ar-hythmia) as determined by the primary team. The presencef an acute coronary syndrome was based on the presence ofmyocardial infarction or unstable angina. Unstable anginaas defined as the presence of angina at rest, increase inreviously stable angina, or ST segment depression on thelectrocardiogram. The diagnosis of myocardial infarctionas based on serum troponin concentrations and clinical
udgment of the ICU physician. Patients with preexistingoronary artery disease or history of congestive heart failureere included in the study. Patients transferred from other
ntensive care units were excluded. If a patient requiredultiple admissions to the ICU, data were collected only
uring the initial admission. One hundred seventy-nine con-
CLINICAL SIGNIF
● In intensive carprimary cardiac paterminal brain nproBNP) are mar
● Myocardial diseanant cause ofthese patients.
● Elevated NT-proBfection, organ faease severity, andent predictor o
● NT-proBNP is novolume status orin critically ill p
ecutive patients were enrolled in the study. The institu- d
ional review board waived the requirement for patientonsent.
lood Samplese obtained blood samples in additive-free tubes to mea-
sure serum NT-proBNP concen-trations within 24 hours of admis-sion to the ICU. The blood wasimmediately transported to the hos-pital’s central laboratory where itwas centrifuged and stored at�70°C. The NT-proBNP concen-tration was determined with an elec-trochemiluminescent immunoassayElecSys 2010 (Roche Diagnostics,Mannheim, Germany). The interas-say coefficient of variance (total im-precision) is �3.0%. The analyticrange is from 20 to 35,000 pg/mL.The age-based cutoffs for diagnos-ing congestive heart failure havebeen established elsewhere (�450pg/mL for patients �50 years ofage, �900 pg/mL for patients 50-70years of age, and �1800 pg/nL forpatients �70 year of age).13
Data CollectionAn investigator blinded to the se-
um natriuretic peptide concentration collected data fromhe patient chart, nursing notes, and the computerized dataystem. The demographic and clinical data included: age,eight, height, sex, race, reason for admission, acute med-
cal issues, medical history, outpatient medications, temper-ture, blood pressure, pulse, respiratory rate, oxygen sat-ration, serum creatinine concentration, serum bilirubinoncentration, and chest radiographic findings. We doc-mented acute therapies and interventions includingechanical ventilation, intravenous antibiotics, steroids,
asoactive agents, volume resuscitation, and blood trans-usion. Disease severity was scored according to the Acutehysiology and Chronic Health Evaluation (APACHE II)ystem, with higher values indicating more severe illness.14
chocardiography was obtained in 98 patients.A second investigator reviewed the chart after hospital
ischarge or death to ensure complete and accurate records.
tatistical Analysishe continuous data are expressed as mean � standard de-iation. Dichotomous variables are presented as percent-ges. For the data analysis, NT-proBNP was log trans-ormed to promote normality, and the data are compared byertiles. For the univariate analysis among tertiles, analysisf variance was used to compare continuous variables andhi-squared analysis was used to compare discrete variables.ultivariate stepwise regression analysis was performed to
CE
t patients withoutgy, levels of amino-retic peptide (NT-elevated.
not the predomi-ted NT-proBNP in
orrelates with in-and increased dis-strong, indepen-
tality.
good indicator ofestive heart failures.
ICAN
e unitholoatriukedly
se iseleva
NP cilure,d is af mor
t acong
etermine the relationship of NT-proBNP and in-hospital
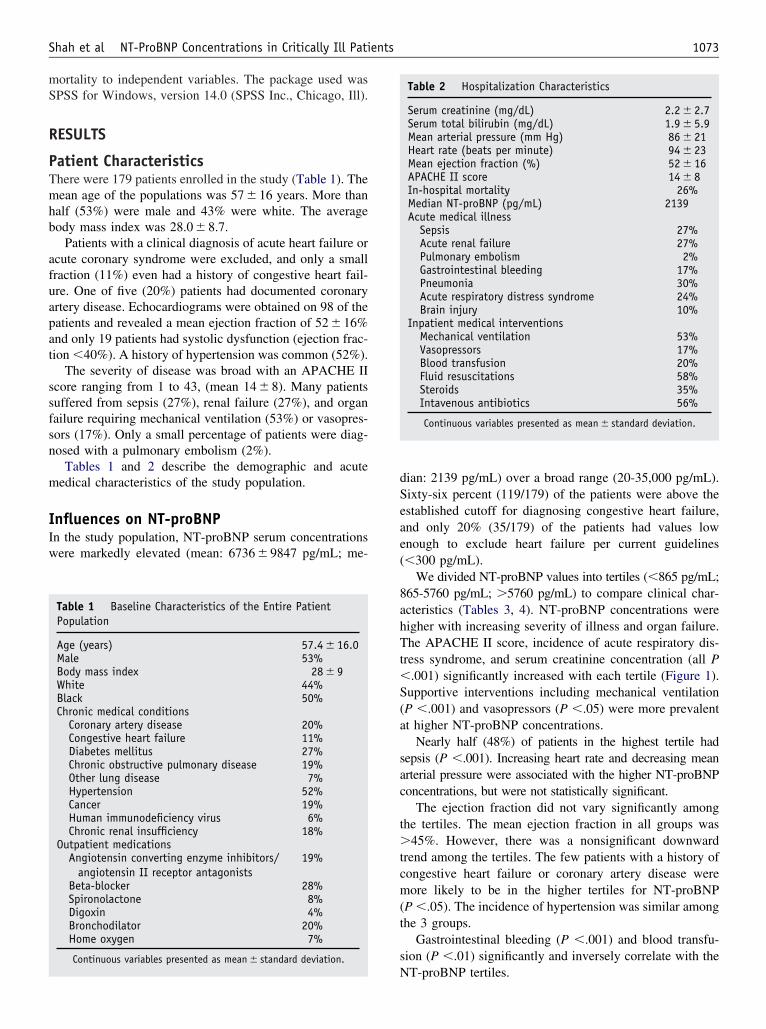
mS
R
PTmhb
afuapat
ssfsn
m
IIw
dSeae(
8ahTt�S(a
sac
t�tcm(t
s
1073Shah et al NT-ProBNP Concentrations in Critically Ill Patients
ortality to independent variables. The package used wasPSS for Windows, version 14.0 (SPSS Inc., Chicago, Ill).
ESULTS
atient Characteristicshere were 179 patients enrolled in the study (Table 1). Theean age of the populations was 57 � 16 years. More than
alf (53%) were male and 43% were white. The averageody mass index was 28.0 � 8.7.
Patients with a clinical diagnosis of acute heart failure orcute coronary syndrome were excluded, and only a smallraction (11%) even had a history of congestive heart fail-re. One of five (20%) patients had documented coronaryrtery disease. Echocardiograms were obtained on 98 of theatients and revealed a mean ejection fraction of 52 � 16%nd only 19 patients had systolic dysfunction (ejection frac-ion �40%). A history of hypertension was common (52%).
The severity of disease was broad with an APACHE IIcore ranging from 1 to 43, (mean 14 � 8). Many patientsuffered from sepsis (27%), renal failure (27%), and organailure requiring mechanical ventilation (53%) or vasopres-ors (17%). Only a small percentage of patients were diag-osed with a pulmonary embolism (2%).
Tables 1 and 2 describe the demographic and acuteedical characteristics of the study population.
nfluences on NT-proBNPn the study population, NT-proBNP serum concentrationsere markedly elevated (mean: 6736 � 9847 pg/mL; me-
Table 1 Baseline Characteristics of the Entire PatientPopulation
Age (years) 57.4 � 16.0Male 53%Body mass index 28 � 9White 44%Black 50%Chronic medical conditions
Coronary artery disease 20%Congestive heart failure 11%Diabetes mellitus 27%Chronic obstructive pulmonary disease 19%Other lung disease 7%Hypertension 52%Cancer 19%Human immunodeficiency virus 6%Chronic renal insufficiency 18%
Outpatient medicationsAngiotensin converting enzyme inhibitors/
angiotensin II receptor antagonists19%
Beta-blocker 28%Spironolactone 8%Digoxin 4%Bronchodilator 20%Home oxygen 7%
Continuous variables presented as mean � standard deviation.
Nian: 2139 pg/mL) over a broad range (20-35,000 pg/mL).ixty-six percent (119/179) of the patients were above thestablished cutoff for diagnosing congestive heart failure,nd only 20% (35/179) of the patients had values lownough to exclude heart failure per current guidelines�300 pg/mL).
We divided NT-proBNP values into tertiles (�865 pg/mL;65-5760 pg/mL; �5760 pg/mL) to compare clinical char-cteristics (Tables 3, 4). NT-proBNP concentrations wereigher with increasing severity of illness and organ failure.he APACHE II score, incidence of acute respiratory dis-
ress syndrome, and serum creatinine concentration (all P.001) significantly increased with each tertile (Figure 1).
upportive interventions including mechanical ventilationP �.001) and vasopressors (P �.05) were more prevalentt higher NT-proBNP concentrations.
Nearly half (48%) of patients in the highest tertile hadepsis (P �.001). Increasing heart rate and decreasing meanrterial pressure were associated with the higher NT-proBNPoncentrations, but were not statistically significant.
The ejection fraction did not vary significantly amonghe tertiles. The mean ejection fraction in all groups was
45%. However, there was a nonsignificant downwardrend among the tertiles. The few patients with a history ofongestive heart failure or coronary artery disease wereore likely to be in the higher tertiles for NT-proBNP
P �.05). The incidence of hypertension was similar amonghe 3 groups.
Gastrointestinal bleeding (P �.001) and blood transfu-ion (P �.01) significantly and inversely correlate with the
Table 2 Hospitalization Characteristics
Serum creatinine (mg/dL) 2.2 � 2.7Serum total bilirubin (mg/dL) 1.9 � 5.9Mean arterial pressure (mm Hg) 86 � 21Heart rate (beats per minute) 94 � 23Mean ejection fraction (%) 52 � 16APACHE II score 14 � 8In-hospital mortality 26%Median NT-proBNP (pg/mL) 2139Acute medical illness
Sepsis 27%Acute renal failure 27%Pulmonary embolism 2%Gastrointestinal bleeding 17%Pneumonia 30%Acute respiratory distress syndrome 24%Brain injury 10%
Inpatient medical interventionsMechanical ventilation 53%Vasopressors 17%Blood transfusion 20%Fluid resuscitations 58%Steroids 35%Intavenous antibiotics 56%
Continuous variables presented as mean � standard deviation.
T-proBNP tertiles.
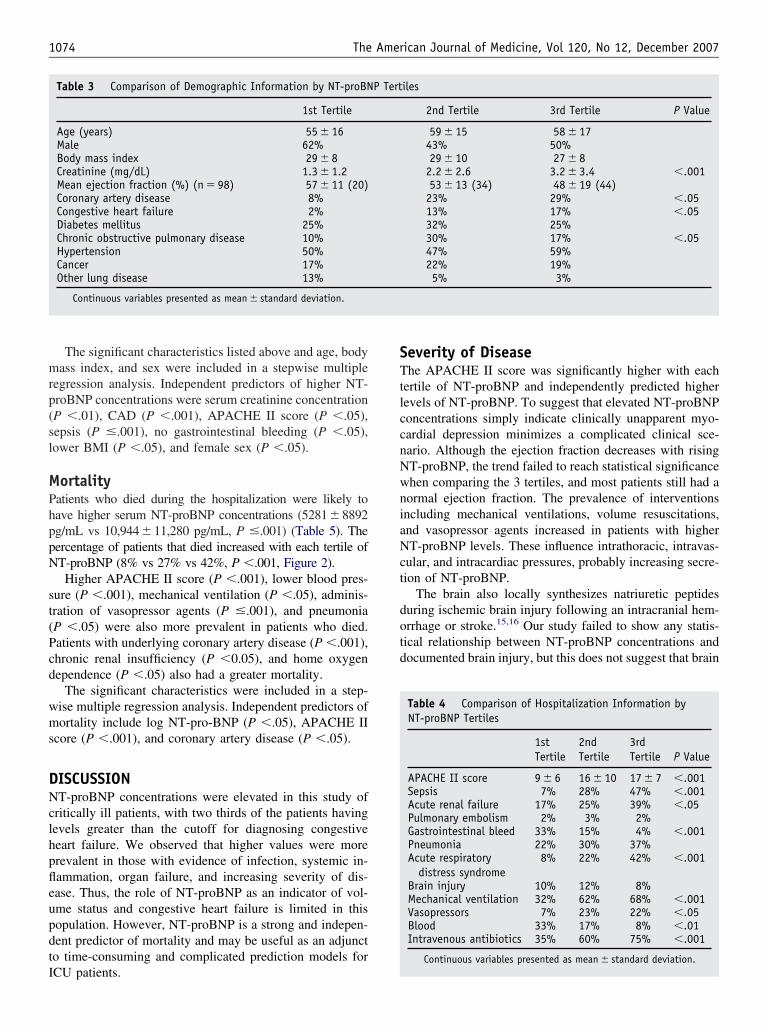
mrp(sl
MPhppN
st(Pcd
wms
DNclhpfleupdtI
STtlccnNwniaNct
dotd
1074 The American Journal of Medicine, Vol 120, No 12, December 2007
The significant characteristics listed above and age, bodyass index, and sex were included in a stepwise multiple
egression analysis. Independent predictors of higher NT-roBNP concentrations were serum creatinine concentrationP �.01), CAD (P �.001), APACHE II score (P �.05),epsis (P �.001), no gastrointestinal bleeding (P �.05),ower BMI (P �.05), and female sex (P �.05).
ortalityatients who died during the hospitalization were likely toave higher serum NT-proBNP concentrations (5281�8892g/mL vs 10,944�11,280 pg/mL, P �.001) (Table 5). Theercentage of patients that died increased with each tertile ofT-proBNP (8% vs 27% vs 42%, P �.001, Figure 2).Higher APACHE II score (P �.001), lower blood pres-
ure (P �.001), mechanical ventilation (P �.05), adminis-ration of vasopressor agents (P �.001), and pneumoniaP �.05) were also more prevalent in patients who died.atients with underlying coronary artery disease (P �.001),hronic renal insufficiency (P �0.05), and home oxygenependence (P �.05) also had a greater mortality.
The significant characteristics were included in a step-ise multiple regression analysis. Independent predictors ofortality include log NT-pro-BNP (P �.05), APACHE II
core (P �.001), and coronary artery disease (P �.05).
ISCUSSIONT-proBNP concentrations were elevated in this study of
ritically ill patients, with two thirds of the patients havingevels greater than the cutoff for diagnosing congestiveeart failure. We observed that higher values were morerevalent in those with evidence of infection, systemic in-ammation, organ failure, and increasing severity of dis-ase. Thus, the role of NT-proBNP as an indicator of vol-me status and congestive heart failure is limited in thisopulation. However, NT-proBNP is a strong and indepen-ent predictor of mortality and may be useful as an adjuncto time-consuming and complicated prediction models for
Table 3 Comparison of Demographic Information by NT-proBN
1st Tertile
Age (years) 55 � 16Male 62%Body mass index 29 � 8Creatinine (mg/dL) 1.3 � 1.2Mean ejection fraction (%) (n � 98) 57 � 11 (20)Coronary artery disease 8%Congestive heart failure 2%Diabetes mellitus 25%Chronic obstructive pulmonary disease 10%Hypertension 50%Cancer 17%Other lung disease 13%
Continuous variables presented as mean � standard deviation.
CU patients.
everity of Diseasehe APACHE II score was significantly higher with each
ertile of NT-proBNP and independently predicted higherevels of NT-proBNP. To suggest that elevated NT-proBNPoncentrations simply indicate clinically unapparent myo-ardial depression minimizes a complicated clinical sce-ario. Although the ejection fraction decreases with risingT-proBNP, the trend failed to reach statistical significancehen comparing the 3 tertiles, and most patients still had aormal ejection fraction. The prevalence of interventionsncluding mechanical ventilations, volume resuscitations,nd vasopressor agents increased in patients with higherT-proBNP levels. These influence intrathoracic, intravas-
ular, and intracardiac pressures, probably increasing secre-ion of NT-proBNP.
The brain also locally synthesizes natriuretic peptidesuring ischemic brain injury following an intracranial hem-rrhage or stroke.15,16 Our study failed to show any statis-ical relationship between NT-proBNP concentrations andocumented brain injury, but this does not suggest that brain
Table 4 Comparison of Hospitalization Information byNT-proBNP Tertiles
1stTertile
2ndTertile
3rdTertile P Value
APACHE II score 9 � 6 16 � 10 17 � 7 �.001Sepsis 7% 28% 47% �.001Acute renal failure 17% 25% 39% �.05Pulmonary embolism 2% 3% 2%Gastrointestinal bleed 33% 15% 4% �.001Pneumonia 22% 30% 37%Acute respiratory
distress syndrome8% 22% 42% �.001
Brain injury 10% 12% 8%Mechanical ventilation 32% 62% 68% �.001Vasopressors 7% 23% 22% �.05Blood 33% 17% 8% �.01Intravenous antibiotics 35% 60% 75% �.001
Continuous variables presented as mean � standard deviation.
iles
2nd Tertile 3rd Tertile P Value
59 � 15 58 � 1743% 50%29 � 10 27 � 82.2 � 2.6 3.2 � 3.4 �.00153 � 13 (34) 48 � 19 (44)23% 29% �.0513% 17% �.0532% 25%30% 17% �.0547% 59%22% 19%5% 3%
P Tert
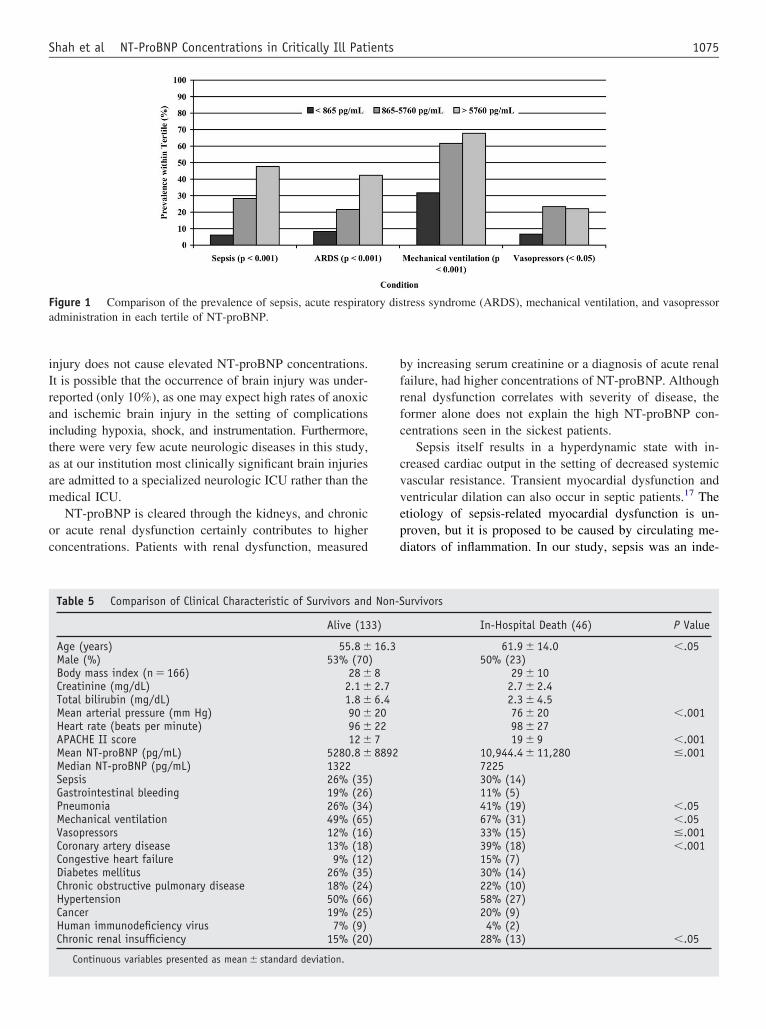
iIraitaam
oc
bfrfc
cvvepd
Fa
1075Shah et al NT-ProBNP Concentrations in Critically Ill Patients
njury does not cause elevated NT-proBNP concentrations.t is possible that the occurrence of brain injury was under-eported (only 10%), as one may expect high rates of anoxicnd ischemic brain injury in the setting of complicationsncluding hypoxia, shock, and instrumentation. Furthermore,here were very few acute neurologic diseases in this study,s at our institution most clinically significant brain injuriesre admitted to a specialized neurologic ICU rather than theedical ICU.NT-proBNP is cleared through the kidneys, and chronic
r acute renal dysfunction certainly contributes to higheroncentrations. Patients with renal dysfunction, measured
igure 1 Comparison of the prevalence of sepsis, acute respiratdministration in each tertile of NT-proBNP.
Table 5 Comparison of Clinical Characteristic of Survivors and
Alive (13
Age (years) 55.8 �Male (%) 53% (70Body mass index (n � 166) 28 �Creatinine (mg/dL) 2.1 �Total bilirubin (mg/dL) 1.8 �Mean arterial pressure (mm Hg) 90 �Heart rate (beats per minute) 96 �APACHE II score 12 �Mean NT-proBNP (pg/mL) 5280.8 �Median NT-proBNP (pg/mL) 1322Sepsis 26% (35Gastrointestinal bleeding 19% (26Pneumonia 26% (34Mechanical ventilation 49% (65Vasopressors 12% (16Coronary artery disease 13% (18Congestive heart failure 9% (12Diabetes mellitus 26% (35Chronic obstructive pulmonary disease 18% (24Hypertension 50% (66Cancer 19% (25Human immunodeficiency virus 7% (9)Chronic renal insufficiency 15% (20
Continuous variables presented as mean � standard deviation.
y increasing serum creatinine or a diagnosis of acute renalailure, had higher concentrations of NT-proBNP. Althoughenal dysfunction correlates with severity of disease, theormer alone does not explain the high NT-proBNP con-entrations seen in the sickest patients.
Sepsis itself results in a hyperdynamic state with in-reased cardiac output in the setting of decreased systemicascular resistance. Transient myocardial dysfunction andentricular dilation can also occur in septic patients.17 Thetiology of sepsis-related myocardial dysfunction is un-roven, but it is proposed to be caused by circulating me-iators of inflammation. In our study, sepsis was an inde-
tress syndrome (ARDS), mechanical ventilation, and vasopressor
urvivors
In-Hospital Death (46) P Value
61.9 � 14.0 �.0550% (23)
29 � 102.7 � 2.42.3 � 4.576 � 20 �.00198 � 2719 � 9 �.001
10,944.4 � 11,280 �.001722530% (14)11% (5)41% (19) �.0567% (31) �.0533% (15) �.00139% (18) �.00115% (7)30% (14)22% (10)58% (27)20% (9)4% (2)
28% (13) �.05
ory dis
Non-S
3)
16.3)82.76.4202278892
)))))))))))
)
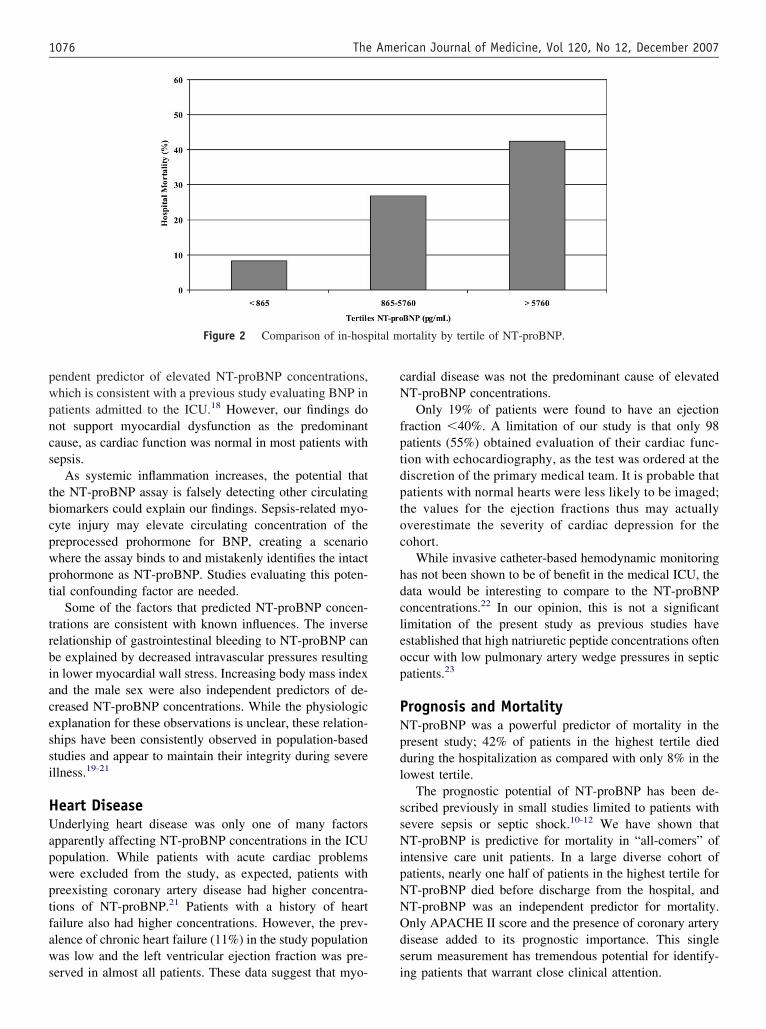
pwpncs
tbcpwpt
trbiacessi
HUapwptfaws
cN
fptdptoc
hdcleop
PNpdl
ssNipNNOds
ital m
1076 The American Journal of Medicine, Vol 120, No 12, December 2007
endent predictor of elevated NT-proBNP concentrations,hich is consistent with a previous study evaluating BNP inatients admitted to the ICU.18 However, our findings doot support myocardial dysfunction as the predominantause, as cardiac function was normal in most patients withepsis.
As systemic inflammation increases, the potential thathe NT-proBNP assay is falsely detecting other circulatingiomarkers could explain our findings. Sepsis-related myo-yte injury may elevate circulating concentration of thereprocessed prohormone for BNP, creating a scenariohere the assay binds to and mistakenly identifies the intactrohormone as NT-proBNP. Studies evaluating this poten-ial confounding factor are needed.
Some of the factors that predicted NT-proBNP concen-rations are consistent with known influences. The inverseelationship of gastrointestinal bleeding to NT-proBNP cane explained by decreased intravascular pressures resultingn lower myocardial wall stress. Increasing body mass indexnd the male sex were also independent predictors of de-reased NT-proBNP concentrations. While the physiologicxplanation for these observations is unclear, these relation-hips have been consistently observed in population-basedtudies and appear to maintain their integrity during severellness.19-21
eart Diseasenderlying heart disease was only one of many factors
pparently affecting NT-proBNP concentrations in the ICUopulation. While patients with acute cardiac problemsere excluded from the study, as expected, patients withreexisting coronary artery disease had higher concentra-ions of NT-proBNP.21 Patients with a history of heartailure also had higher concentrations. However, the prev-lence of chronic heart failure (11%) in the study populationas low and the left ventricular ejection fraction was pre-
Figure 2 Comparison of in-hosp
erved in almost all patients. These data suggest that myo- i
ardial disease was not the predominant cause of elevatedT-proBNP concentrations.Only 19% of patients were found to have an ejection
raction �40%. A limitation of our study is that only 98atients (55%) obtained evaluation of their cardiac func-ion with echocardiography, as the test was ordered at theiscretion of the primary medical team. It is probable thatatients with normal hearts were less likely to be imaged;he values for the ejection fractions thus may actuallyverestimate the severity of cardiac depression for theohort.
While invasive catheter-based hemodynamic monitoringas not been shown to be of benefit in the medical ICU, theata would be interesting to compare to the NT-proBNPoncentrations.22 In our opinion, this is not a significantimitation of the present study as previous studies havestablished that high natriuretic peptide concentrations oftenccur with low pulmonary artery wedge pressures in septicatients.23
rognosis and MortalityT-proBNP was a powerful predictor of mortality in theresent study; 42% of patients in the highest tertile dieduring the hospitalization as compared with only 8% in theowest tertile.
The prognostic potential of NT-proBNP has been de-cribed previously in small studies limited to patients withevere sepsis or septic shock.10-12 We have shown thatT-proBNP is predictive for mortality in “all-comers” of
ntensive care unit patients. In a large diverse cohort ofatients, nearly one half of patients in the highest tertile forT-proBNP died before discharge from the hospital, andT-proBNP was an independent predictor for mortality.nly APACHE II score and the presence of coronary arteryisease added to its prognostic importance. This singleerum measurement has tremendous potential for identify-
ortality by tertile of NT-proBNP.
ng patients that warrant close clinical attention.

CNideTpenbflc
dipmr
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
1077Shah et al NT-ProBNP Concentrations in Critically Ill Patients
ONCLUSIONT-proBNP serum concentrations are elevated in critically
ll patients. Even without clinically apparent acute heartisease, 66% of the patients had levels greater than thestablished cutoff, suggesting a diagnosis of heart failure.he likely explanation is multifactorial, including a hy-er-sympathetic state, administration of exogenous cat-cholamines, mechanical ventilation, aggressive intrave-ous resuscitation, secretion of natriuretic peptides from therain, unmasking of clinically quiescent heart disease, in-ammation-related cardiac depression, and decreased renallearance of NT-proBNP.
NT-proBNP increases with severity of disease and pre-icts mortality. The prognostic utility of NT-proBNP makest a useful, minimally invasive test for identifying ICUatients with a poor prognosis at higher risk for in-hospitalortality. However, NT-proBNP measures should not di-
ect volume management in these complicated patients.
eferences1. Levin ER, Gardner DG, Samson WK. Natriuretic peptides. N Engl
J Med. 1998;339:321-328.2. Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid measurement of
B-type natriuretic peptide in the emergency diagnosis of heart failure.N Engl J Med. 2002;347:161-167.
3. Lainchbury JG, Campbell E, Frampton CM, et al. Brain natriureticpeptide and n-terminal brain natriuretic peptide in the diagnosis ofheart failure in patients with acute shortness of breath. J Am CollCardiol. 2003;42:728-735.
4. Wang TJ, Larson MG, Levy D, et al. Plasma natriuretic peptide levelsand the risk of cardiovascular events and death. N Engl J Med.2004;350:655-663.
5. Berendes E, Van Aken H, Raufhake C, et al. Differential secretion ofatrial and brain natriuretic peptide in critically ill patients. AnesthAnalg. 2001;93:676-682.
6. McLean AS, Tang B, Nalos M, et al. Increased B-type natriureticpeptide (BNP) level is a strong predictor for cardiac dysfunction inintensive care unit patients. Anaesth Intensive Care. 2003;31:21-27.
7. Tung RH, Garcia C, Morss AM, et al. Utility of B-type natriureticpeptide for the evaluation of intensive care unit shock. Crit Care Med.2004;32:1643-1647.
8. Witthaut R, Busch C, Fraunberger P, et al. Plasma atrial natriureticpeptide and brain natriuretic peptide are increased in septic shock:Impact of interleukin-6 and sepsis-associated left ventricular dysfunc-
tion. Intensive Care Med. 2003;29:1696-1702.9. Jefic D, Lee JW, Jefic D, et al. Utility of B-type natriuretic peptide andN-terminal pro B-type natriuretic peptide in evaluation of respiratoryfailure in critically ill patients. Chest. 2005;128:288-295.
0. Brueckmann M, Huhle G, Lang S, et al. Prognostic value of plasmaN-terminal pro-brain natriuretic peptide in patients with severe sepsis.Circulation. 2005;112:527-534.
1. Roch A, Allardet-Servent J, Michelet P, et al. NH2 terminal pro-brainnatriuretic peptide plasma level as an early marker of prognosis andcardiac dysfunction in septic shock patients. Crit Care Med. 2005;33:1001-1007.
2. Januzzi JL, Morss A, Tung R, et al. Natriuretic peptide testing for theevaluation of critically ill patients with shock in the intensive care unit:a prospective cohort study. Crit Care. 2006;10:R37.
3. Januzzi JL Jr, van Kimmenade R, Lainchbury J, et al. NT-proBNPtesting for diagnosis and short-term prognosis in acute destabilizedheart failure: an international pooled analysis of 1256 patients: theInternational Collaborative of NT-proBNP Study. Eur Heart J. 2006;27:330-337.
4. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II:a severity of disease classification system. Crit Care Med. 1985;13:818-829.
5. Makikallio AM, Makikallio TH, Korpelainen JT, et al. Natriureticpeptides and mortality after stroke. Stroke. 2005;36:1016-1020.
6. Berendes E, Walter M, Cullen P, et al. Secretion of brain natriureticpeptide in patients with aneurysmal subarachnoid haemorrhage. Lancet.1997;349:245-249.
7. Parker MM, Shelhamer JH, Bacharach SL, et al. Profound but revers-ible myocardial depression in patients with septic shock. Ann InternMed. 1984;100:483-490.
8. Cuthbertson BH, Patel RR, Croal BL, et al. B-type natriuretic peptideand the prediction of outcome in patients admitted to intensive care.Anaesthesia. 2005;60:16-21.
9. Costello-Boerrigter LC, Boerrigter G, Redfield MM, et al. Amino-terminal pro-B-type natriuretic peptide and B-type natriuretic peptidein the general community: determinants and detection of left ventric-ular dysfunction. J Am Coll Cardiol. 2006;47:345-353.
0. Das SR, Drazner MH, Dries DL, et al. Impact of body mass and bodycomposition on circulating levels of natriuretic peptides: results fromthe Dallas Heart Study. Circulation. 2005;112:2163-2168.
1. Goetze JP, Christoffersen C, Perko M, et al. Increased cardiac BNPexpression associated with myocardial ischemia. FASEB J. 2003;17:1105-1107.
2. The National Heart, Lung, and Blood Institute Acute RespiratoryDistress Syndrome (ARDS) Clinical Trials Network. Pulmonary-ar-tery versus central venous catheter to guide treatment of acute lunginjury. N Engl J Med. 2006;354:2213-2224.
3. Forfia PR, Watkins SP, Rame JE, et al. Relationship between B-typenatriuretic peptides and pulmonary capillary wedge pressure in the
intensive care unit. J Am Coll Cardiol. 2005;45:1667-1671.
C
BASa
M
Imnobgdsw
DF
0d
The American Journal of Medicine (2007) 120, 1078-1083
LINICAL RESEARCH STUDY
loodstream Infections in a Geriatric Cohort:Population-Based Study
arah J. Crane, MD,a,b Daniel Z. Uslan, MD,a,c Larry M. Baddour, MDa,c
Department of Medicine, bDivision of Primary Care Internal Medicine, and cDivision of Infectious Diseases, Mayo Clinic College of
edicine, RocheParscMbMtiafRamcciCpm
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
ster, Minn.
ABSTRACT
URPOSE: Health care-associated infections are those that do not meet the definition of nosocomial butre acquired by patients with extensive exposure to the health care system placing them at higher risk foresistant organisms. This category is particularly common among elderly patients. The objective of thistudy was to describe and compare the epidemiologic characteristics of community-acquired, healthare-associated and nosocomial bloodstream infections in a geriatric population.ETHODS: A population-based, retrospective study of all patients aged 65 years or greater with positivelood cultures (n � 636) identified between January 1, 2003 and December 31, 2005 in Olmsted County,innesota. Exposures and clinical information were ascertained through complete chart review, utilizing
he resources of the Rochester Epidemiology Project. A total of 347 incident patients with bloodstreamnfection were identified. Bloodstream infections were described as community-acquired, health care-ssociated or nosocomial using standardized definitions. Variables analyzed included source, isolate, riskactors, and mortality.ESULTS: The distribution of bloodstream infection cases that were community-acquired, health care-ssociated, and nosocomial was 159 (46%), 151 (44%), and 37 (10%), respectively. The prevalence ofethicillin-resistant Staphylococcus aureus among S. aureus isolates was 54% and 44% for health
are-associated and nosocomial cases, respectively. Fourteen-day mortality among bloodstream infectionases was the same in health care-associated and nosocomial infections (15% vs 14%), and was lessn community-acquired (6%) cases (P � .04).ONCLUSIONS: The category of health care-associated infection identified a unique group of geriatricatients at increased risk of methicillin-resistant Staphylococcus aureus infection and with increasedortality. © 2007 Elsevier Inc. All rights reserved.
KEYWORDS: Aged; Bacteremia; Bloodstream infection; Geriatric; Population-based
feAptismaich
ndividuals who are 65 years of age and older comprise theajority of patients who are admitted to hospitals, live in
ursing homes, and likely are exposed to antibiotics. Notnly is this cohort at increased risk of bloodstream infection,ut they are also at increased risk of infection due to patho-ens exhibiting antimicrobial resistance.1 An appropriateesignation into specific risk categories is critical whenelection of an empiric antibiotic regimen is desired, orhen considering isolation precaution procedures. Hereto-
Requests for reprints should be addressed to Sarah J. Crane, MD,epartment of Internal Medicine, Mayo Clinic College of Medicine, 200irst St. SW, Rochester, MN 55905.
ront matter © 2007 Elsevier Inc. All rights reserved.ed.2007.08.028
ore, the primary interest in bloodstream infections in thelderly has focused on nursing home-acquired infections.2-5
lthough nursing home exposure is important in the elderlyopulation, it does not account for the many other exposureso the health care system that older patients experience,ncluding recurrent hospitalization, home care, hemodialy-is, infusion center exposure, and chronic wound manage-ent. Thus, the relatively new category of “health care-
ssociated” infection has gained favor in the investigation ofnfectious diseases. We hypothesized that patients with healthare-related exposures, not limited to nursing homes, wouldave a higher risk of infection due to antimicrobial resistant
rganisms than patients without health care exposures.
cfutdtptpdtppo
siPspMircorf
M
STMoT1iotsc
lCandus
CAumw
lai
e
cBm
EPmbicaksa
p
●
●
●
●
●
e of t
1079Crane et al Bloodstream Infection in a Geriatric Cohort
When describing the epidemiology of a new exposurelassification, it is important to consider a whole population,ree of referral bias. Administrative database searches areseful, but do not allow for an adequately accurate descrip-ion of patient characteristics to investigate epidemiologicetails. Studies performed at ter-iary care centers have significantotential for referral bias due tohe increased complexity of theatient population, and studies thato not include outpatient popula-ions may miss specific high-riskopulations, such as hematologyatients, who are often treated asutpatients.
We therefore undertook a retro-pective, population-based study us-ng the Rochester Epidemiologyroject (REP) to characterize blood-tream infection in the geriatricopulation of Olmsted County,innesota and to determine the
mpact of the 3 exposure catego-ies (nosocomial, health care-asso-iated, and community-acquired)n the distribution of antimicrobial-esistant pathogens, sources of in-ection, and 14-day mortality.
ETHODS
tudy Settinghe study was conducted in Olmsted County, Minnesota, aidwestern county in the United States. The county has
nly one mid-sized metropolitan area and is otherwise rural.he population size, according to the 2000 census, was24,277 and was predominately non-Hispanic white. Med-cal care in the area is provided primarily by a small numberf institutions, the Mayo Clinic and Olmsted Medical Cen-er. These institutions’ microbiology laboratories provideervice to all local providers, including hospitals, outpatientlinics, and nursing homes.6
The Rochester Epidemiology Project is a medical recordinkage system that indexes medical records for Olmstedounty residents, regardless of care provider. This linkagellows for complete review of records, including all physicianotes, hospital notes, laboratory results, pathology results, ra-iology records, and procedures notes.6 The system has beensed in previous studies to study specific infectious diseaseyndromes using a population-based approach.7
ase Identificationlist of all positive blood cultures obtained between Jan-
ary 1, 2003 and December 31, 2005 was obtained from theicrobiology laboratories of both institutions. The records
CLINICAL SIGNIF
● Methicillin-resistfection is as coassociated infectmial infections.
● Fourteen-day mpatients infectedtant staphylococcin health-care anosocomial infecspectively) but lquired cases (6%
● Hospitalized gericreased risk forThis study reveaincreased risk foinfection, outsid
ere initially screened for Olmsted County residency of at
east 1 year before the culture date, age of 65 years or older,nd patient authorization for medical record review. Bothnpatient and outpatient cultures were included.
To avoid ascertainment bias in determining clinical rel-vance of bloodstream isolates, a standardized definition of
contamination was used. A bloodculture was designated as contam-inated if one or more of the fol-lowing organisms were identifiedin only one of a series of bloodcultures: coagulase-negative staph-ylococci, Propionibacterium acnes,Micrococcus species, viridans groupstreptococci, Corynebacterium spe-cies, or Bacillus species.8 The caseswere individually abstracted, andcultures that were deemed “con-taminants” were excluded.
Only initial episodes of blood-stream infection were included asincident cases. If a patient hadmore than one positive blood cul-ture during the study period, thelatter cultures were documentedbut were not included in the sta-tistical analysis. Patients with re-current or relapsing cultures mayrepresent a unique population thatcould bias the current question ofexposure categories. All positive
ultures that grew either bacteria or fungi were included.lood cultures were labeled as polymicrobial if multipleicroorganisms grew within a 48-hour period.
xposure Definitionatient exposures were divided into 3 categories—nosoco-ial, health care-associated, and community-acquired—
ased on medical and environmental history. Nosocomialnfection was defined as that which did not become clini-ally evident until 48 hours or later following hospitaldmission.9 “Clinically evident” was defined as fever, leu-ocytosis, mental status changes suggestive of delirium, orite-specific complaints such as urinary tract symptoms,bdominal pain, or respiratory complaints.
Health care-associated infection was designated if theatient had experienced any of the following exposures10:
received IV therapy at home in the previous 30 daysreceived any wound care or other specialized nursing careat home in the previous 30 daysattended a hemodialysis clinic or received IV chemother-apy in the 30 days before infection onsetwas hospitalized in an acute care hospital for 2 or moredays in the past 90 days before infection onsetresided in a nursing home or long-term care facility at the
CE
taphylococcal in-n in health care-as it is in nosoco-
ty among elderlymethicillin-resis-
reus was the sameted infection and15% and 14%, re-in community-ac-
patients are at in-stream infection.t they are also atth care-associatedhe hospital.
ICAN
ant smmoions
ortaliwith
us aussociation (ower).
atricbloodls thar heal
time of infection diagnosis.
wa
SStobasrpiaPw
OSTbptro
DDccgva
pa2Fp2fyCC
RBpfasr
mwwca
DDacitcda
1080 The American Journal of Medicine, Vol 120, No 12, December 2007
Community-acquired infections were infections thatere not included in the nosocomial or health care-associ-
ted categories.
ource Identificationecondary bacteremia sources were identified when a cul-
ure was obtained from a specific site, such as urine, sputumr wound, which grew the same microorganism as theloodstream infection isolate based on species designationnd in vitro susceptibility results. For pulmonary infections,ources were defined as a new infiltrate described on chestadiograph, symptoms consistent with pneumonia, and alausible bloodstream organism identified on culture. Fornfections with a gastrointestinal source, clinical symptomsnd appropriate positive radiologic studies were required.rimary bacteremia was defined as those in which no sourceas identified.
utcomesurvival was evaluated as all-cause mortality at 14 days.his definition was selected instead of inpatient mortalityecause outpatients were included in the study, and someatients elected hospice and died outside the hospital. Four-een days was chosen because a longer time period mightisk including deaths caused by unrelated complications orther comorbid conditions independent of the infection.
ata Analysisescriptive statistics were reported as means (with SD) for
ontinuous variables and frequencies and percentages forategorical variables. Differences in the means among the 3roups were initially evaluated using one-way analysis ofariance technique. If a significant difference was foundmong the 3 categories, pairwise, 2-sample t tests were then
Table 1 Patient Demographics Compared for Community-acquOlmsted County, Minnesota, 2003-2005
Community-Acquired(n � 159)
Health Care-Associated(n � 151)
Age (SD) 80 (8) 81 (8)Male no. (%) 74 (47) 86 (57)Living environment no. (%)
Nursing home 0 66 (48)Assisted living 20 (13) 9 (6)
Comorbidities no. (%)Dementia 15 (9) 46 (30)Chronic renal failure 13 (8) 33 (22)Dialysis 0 22 (15)Vascular 9 (6) 19 (13)Diabetes 38 (24) 43 (29)Cancer 22 (14) 36 (24)Immunocompromised 10 (6) 32 (21)Stroke 14 (9) 32 (22)
ANOVA � analysis of variation between groups; CA � community-a
erformed between groups. Differences in proportionsmong groups were analyzed using a chi-squared test for the� 3 contingency table or, if numbers were small, theisher’s exact test was used instead. Where the global test ofroportions among the 3 groups was significant, individual� 2 tables were then analyzed. The level of significance
or all statistical tests was 2-sided, with � � 0.05. All anal-ses were conducted in JMP (Version 6, SAS Institute Inc.,arey, NC) The Institutional Review Boards of both Mayolinic and Olmsted Medical Center approved the study.
ESULTSetween January 1, 2003 and December 31, 2005, 636ositive blood cultures were identified. Two hundred forty-our (39%) met the standardized definition of contaminationnd 45 cultures represented sustained or relapsing blood-tream infection and were excluded from analysis. Theemaining 347 patients were included in the analysis.
Thirty-seven (10%) bloodstream infections were nosoco-ial, 151 (44%) were health care-associated, and 159 (46%)ere community acquired. Eleven (3%) of 347 patientsere never admitted to the hospital, of which 8 represented
ommunity-acquired infections, 2 were dialysis patients,nd 1 was receiving chemotherapy.
emographics and Comorbiditiesemographic features are described in Table 1. The average
ge of patients in the 3 groups was similar, although noso-omial patients were slightly younger. There was a signif-cantly larger proportion (48%) of nursing home patients inhe health care-associated category than were in the noso-omial (19%) group. Dementia, chronic renal failure, andialysis patients were most common in the health care-ssociated group, but the other comorbidities were evenly
ealth Care-associated and Nosocomial Bloodstream Infections,
ocomial� 37)
ANOVAP Value
CA vs HCAP Value
HCA vs NP Value
CA vs NP Value
(8) .01 .11 .005 .07(62) .11
(9) �.0001 �.0001 .008 �.0001(3) .05 .05 .69 .14
(14) �.0001 �.0001 .04 .54(16) .004 .001 .51 .21(5) �.0001 �.0001 .17 .03(5) .07(32) .47(24) .06(16) .0007 .0001 .65 .09(22) .006 .002 1.0 .04
; HCA � health care-associated; N � nosocomial.
ired, H
Nos(n
7723
71
5622
12968
cquired
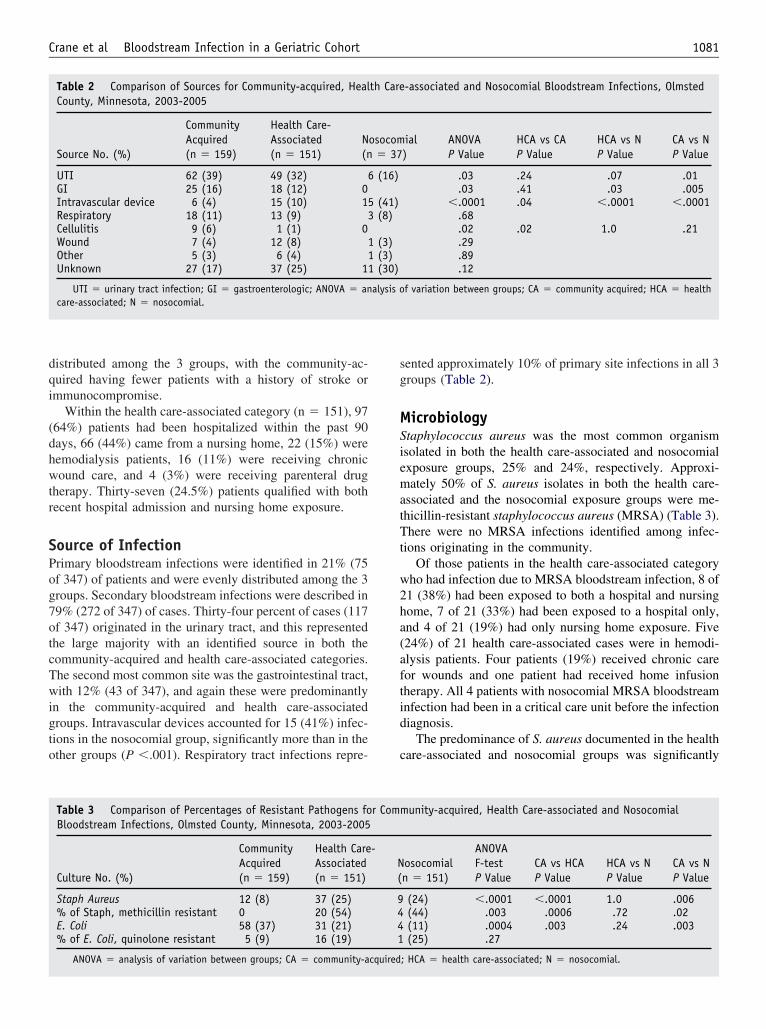
dqi
(dhwtr
SPog7otcTwigto
sg
MSiematTt
w2ha(aftid
c
1081Crane et al Bloodstream Infection in a Geriatric Cohort
istributed among the 3 groups, with the community-ac-uired having fewer patients with a history of stroke ormmunocompromise.
Within the health care-associated category (n � 151), 9764%) patients had been hospitalized within the past 90ays, 66 (44%) came from a nursing home, 22 (15%) wereemodialysis patients, 16 (11%) were receiving chronicound care, and 4 (3%) were receiving parenteral drug
herapy. Thirty-seven (24.5%) patients qualified with bothecent hospital admission and nursing home exposure.
ource of Infectionrimary bloodstream infections were identified in 21% (75f 347) of patients and were evenly distributed among the 3roups. Secondary bloodstream infections were described in9% (272 of 347) of cases. Thirty-four percent of cases (117f 347) originated in the urinary tract, and this representedhe large majority with an identified source in both theommunity-acquired and health care-associated categories.he second most common site was the gastrointestinal tract,ith 12% (43 of 347), and again these were predominantly
n the community-acquired and health care-associatedroups. Intravascular devices accounted for 15 (41%) infec-ions in the nosocomial group, significantly more than in thether groups (P �.001). Respiratory tract infections repre-
Table 2 Comparison of Sources for Community-acquired, HealCounty, Minnesota, 2003-2005
Source No. (%)
CommunityAcquired(n � 159)
Health Care-Associated(n � 151)
N(n
UTI 62 (39) 49 (32) 6GI 25 (16) 18 (12) 0Intravascular device 6 (4) 15 (10) 15Respiratory 18 (11) 13 (9) 3Cellulitis 9 (6) 1 (1) 0Wound 7 (4) 12 (8) 1Other 5 (3) 6 (4) 1Unknown 27 (17) 37 (25) 11
UTI � urinary tract infection; GI � gastroenterologic; ANOVA � ancare-associated; N � nosocomial.
Table 3 Comparison of Percentages of Resistant Pathogens foBloodstream Infections, Olmsted County, Minnesota, 2003-2005
Culture No. (%)
CommunityAcquired(n � 159)
Health CareAssociated(n � 151)
Staph Aureus 12 (8) 37 (25)% of Staph, methicillin resistant 0 20 (54)E. Coli 58 (37) 31 (21)% of E. Coli, quinolone resistant 5 (9) 16 (19)
ANOVA � analysis of variation between groups; CA � community-a
ented approximately 10% of primary site infections in all 3roups (Table 2).
icrobiologytaphylococcus aureus was the most common organismsolated in both the health care-associated and nosocomialxposure groups, 25% and 24%, respectively. Approxi-ately 50% of S. aureus isolates in both the health care-
ssociated and the nosocomial exposure groups were me-hicillin-resistant staphylococcus aureus (MRSA) (Table 3).here were no MRSA infections identified among infec-
ions originating in the community.Of those patients in the health care-associated category
ho had infection due to MRSA bloodstream infection, 8 of1 (38%) had been exposed to both a hospital and nursingome, 7 of 21 (33%) had been exposed to a hospital only,nd 4 of 21 (19%) had only nursing home exposure. Five24%) of 21 health care-associated cases were in hemodi-lysis patients. Four patients (19%) received chronic careor wounds and one patient had received home infusionherapy. All 4 patients with nosocomial MRSA bloodstreamnfection had been in a critical care unit before the infectioniagnosis.
The predominance of S. aureus documented in the healthare-associated and nosocomial groups was significantly
-associated and Nosocomial Bloodstream Infections, Olmsted
ial)
ANOVAP Value
HCA vs CAP Value
HCA vs NP Value
CA vs NP Value
.03 .24 .07 .01
.03 .41 .03 .005�.0001 .04 �.0001 �.0001
.68
.02 .02 1.0 .21
.29
.89
.12
f variation between groups; CA � community acquired; HCA � health
unity-acquired, Health Care-associated and Nosocomial
osocomialn � 151)
ANOVAF-testP Value
CA vs HCAP Value
HCA vs NP Value
CA vs NP Value
(24) �.0001 �.0001 1.0 .006(44) .003 .0006 .72 .02(11) .0004 .003 .24 .003(25) .27
; HCA � health care-associated; N � nosocomial.
th Care
osocom� 37
(16)
(41)(8)
(3)(3)(30)
alysis o
r Comm
-N(
9441
cquired

dwTi
MOMhl(
DTcuauhwhc
tipoetaUe(ibacsctsbwMascpw
dTbiab
hht
iwgtgatpa
rnalwatmattwragOmu
iOdSdhepaartgcsio
spdu
1082 The American Journal of Medicine, Vol 120, No 12, December 2007
ifferent from the community-acquired infection group,here the most common pathogen was Escherichia Coli.he prevalence of fluoroquinolone resistance among E. coli
solates was similar in all 3 exposure groups (Table 3).
ortalityverall, all-cause 14-day mortality was 11% (38 of 347).ortality rates were similar (15% and 14%, respectively) in
ealth care-associated and nosocomial exposure groups andess in the community-acquired bloodstream infection group6%, P � .04).
ISCUSSIONhis study of bloodstream infection was significant whenompared with previous studies in that it employed a pop-lation-based approach that included medical records fromll inpatient and outpatient clinics in the county, making itnique in its completeness. It also selected for a moreomogenous subgroup of patients, age 65 years and older,ho have a high level of exposure to hospitals, nursingomes, wound care clinics, infusion centers, and dialysisenters.
The most striking finding of the current investigation washat patients in the health care-associated category had andentical risk of bloodstream infection due to MRSA as didatients included in the nosocomial group. The findings inur geriatric population are reflective of those described inarlier studies10,11 that were not limited to older adult pa-ients. In a prior investigation,10 patients admitted to onecademic medical center and 2 community hospitals in theS had identical rates of MRSA bloodstream infection with
ither health care-associated (52%) or nosocomial infection61%). In a more recent report from western Europe involv-ng 3 tertiary care hospitals in Ireland and France,11 rates ofloodstream infection due to MRSA were also similar (33%nd 41%, respectively) among patients with either healthare-associated or nosocomial infection. These observationshould prompt serious consideration for providing antibioticoverage for MRSA in the empiric treatment of patients inhe “health care-associated” exposure category who may beeriously ill or at risk for developing serious illness due toloodstream infection. It is noteworthy that 8 of 21 patientsith health care-associated bloodstream infection due toRSA did not receive empiric coverage for this organism
s part of their initial antibiotic treatment regimen. Thetudy’s findings also require a broader look at infectionontrol procedures that empirically isolate defined high-riskatient groups. The isolation of nursing home patients aloneould greatly underestimate the group at risk for MRSA.Community-associated MRSA has emerged as the pre-
ominate cause of skin and soft tissue infection in the US.12
o date, bloodstream infection due to this organism haseen less commonly seen.13 There were no cases of MRSAdentified in our community population. The health care-ssociated and nosocomial MRSA infections had antimicro-
ial susceptibility patterns most consistent with strains that fave historically been associated with hospital or nursingome exposure, but no genotyping was performed to verifyhat assignment.
Urinary and gastrointestinal tract sources predominatedn the community-acquired bloodstream infection group,hich was in marked contrast to the other 2 exposureroups. The similar distribution of fluoroquinolone resis-ance among E. coli bloodstream isolates among the 3roups is noteworthy. Although complete data for priorntibiotic exposure was not collected in our work, it is likelyhat the widespread use of fluoroquinolones in the localopulation in both ambulatory and hospital settings couldccount for this observation.
The all-cause, 14-day mortality rates (15% and 14%,espectively) for both the health care-associated and theosocomial groups were low. For patients with community-cquired bloodstream infection, the mortality rate was eveness (6%). A previous community hospital-based studyhich did not stratify by exposure risk group, demonstrated
n overall case-fatality rate of 11.9%,14 which was similaro that (11%) described in our work. Patients in our com-unity-acquired group had fewer co-morbidities and likelyhigher functional status than did the other 2 groups and
his likely accounted for the low mortality rate. The mor-ality rate (23%; 17 of 56) of our nursing home populationas consistent with that identified in a previously published
eview of 7 nursing home bloodstream infection studies,3
nd suggests that the population locally is similar to otherroups and that our findings are more broadly generalizable.ther factors that could be responsible for the relatively lowortality rates seen in our population-based cohort remain
ndefined.One of the primary concerns with population-based stud-
es is their generalizability to larger or different populations.ne of the most significant differences between infectiousiseases in Olmsted County, Minnesota and other Unitedtates locations is the low prevalence of human immuno-eficiency virus infection. This is an uncommon infection,owever, in the geriatric population and we would thereforexpect our results to be generalizable to other geriatricopulations with similar characteristics. Olmsted County islso unique in that a large, tertiary referral center providessubstantial amount of the primary care. This could bias
esults if there were exposure of the primary care populationo referral patient populations. At the time of this investi-ation, however, within the Mayo Clinic system, primaryare medicine for local residents was provided by differenttaff and the 2 populations were predominantly hospitalizedn separate locations, minimizing their exposure to eachther.
The blood culture contamination rate identified in thistudy was somewhat higher than anticipated or identified inrevious studies. The reason for this was unclear as a stan-ardized definition identified by previous investigators wastilized.8 The rate was consistent, however, with findings
rom this population and institution previously published.1
pTeptcctgpamrir
AWCem
R
1
1
1
1
1
1083Crane et al Bloodstream Infection in a Geriatric Cohort
When studying new definitions of disease, the validityrovided by using a population-based approach is essential.his study provides a unique opportunity to define newxposure categories without the bias introduced by an in-atient, referral center practice. Finally, to our knowledge,his is the first study of health care-associated infections tooncentrate on the geriatric patient population, which has aharacteristically high risk of these exposures. A popula-ion-based investigation of infectious diseases in this sub-roup has not been performed, and this approach shouldermit the examination of many important questions, suchs defining the optimal management of infection due toultidrug-resistant organisms. If we can better identify at-
isk populations, it may also be feasible to more effectivelymplement isolation measures that will diminish infectionisk.
CKNOWLEDGMENTSe thank the statisticians and epidemiologists from the
enter for Patient Oriented Research, Mayo Clinic, Roch-ster for their assistance with data analysis and review of theanuscript.
eferences1. Uslan D, Crane S, St. Sauver J, et al. Age-associated Trends in Blood-
stream Infections: A Population-based Study in Olmsted County, Minne-sota. Arlington, VA: Infectious Diseases Society of America; 2006.
2. Mylotte J, Tayara A, Goodnough S. Epidemiology of bloodstreaminfection in nursing home residents: evaluation in a large cohort from
multiple homes. Clin Infect Dis. 2002;35:1484-1490.3. Mylotte J. Nursing home-acquired bloodstream infection. Infect Con-trol Hosp Epidemiol. 2005;26:833-837.
4. Nicolle L. Bacteremia in a long term care facility. Can J Infect Dis.1994;5:130-132.
5. Sinclair D, Svendsen A, Marrie T. Bacteremia in nursing home pa-tients: prevalence among patients presenting to an emergency depart-ment. Can Fam Physician. 1998;44:317-322.
6. Melton L. History of the Rochester Epidemiology Project. Mayo ClinProc. 1996;71:266-274.
7. Tleyjeh I, Steckelberg J, Murad H, et al. Temporal trends in infectiveendocarditis: a population-based study in Olmsted County, Minnesota.JAMA. 2005;293:3061-3062.
8. Bekeris L, Tworek J, Walsh M, Valenstein P. Trends in blood culturecontamination: a College of American Pathologists Q-Tracks study of356 institutions. Arch Pathol Lab Med. 2005;129:1222-1225.
9. Garner J, Jarvis W, Emori T, et al. CDC Definitions for NosocomialInfections. St. Louis, MO: Mosby; 1996.
0. Friedman N, Kaye K, Stout J, et al. Health care-associated blood-stream infections in adults: a reason to change the accepted defi-nition of community-acquired infections. Ann Intern Med. 2002;137:791-798.
1. Lesens O, Hansmann Y, Brannigan E, et al. Healthcare-associatedStaphylococcus Aureus bacteremia and the risk for methicillin resis-tance: is the Centers for Disease Control and Prevention definition forcommunity-acquired bacteremia still appropriate? Infect Control HospEpidemiol. 2005;26:204-209.
2. Moran G, Krishnadasan A, Gorwitz R, et al. Methicillin-resistant S.aureus infections among patients in the emergency department. N EnglJ Med. 2006;355:666-674.
3. Naimi T, LeDell K, Como-Sabetti K, et al. Comparison of community-and health care-associated methicillin-resistant Staphylococcus aureusinfection. JAMA. 2003;290:2976-2984.
4. Scheckler W, Bobula J, Beamsley M, Hadden S. Bloodstream infec-tions in a community hospital: a 25-year follow-up. Infect Control
Hosp Epidemiol. 2003;24:936-941.
C
OORa
o
Sasodsi
ANtN
DB
0d
The American Journal of Medicine (2007) 120, 1084-1089
LINICAL RESEARCH STUDY
xidative Stress and Severe Walking Disability amonglder Women
ichard D. Semba,a Luigi Ferrucci,b Kai Sun,a Jeremy Walston,a Ravi Varadhan,a Jack M. Guralnik,c Linda P. Frieda
Johns Hopkins University School of Medicine, Baltimore, Md; bLongitudinal Studies Section, Clinical Research Branch, National Institute
n Aging, Baltimo c d.BampMwmiRcfc1Cpl
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
re, Md; Laboratory of Epidemiology, Demography, and Biometry, National Institute on Aging, Bethesda, M
ABSTRACT
ACKGROUND: Oxidative stress has been implicated in sarcopenia and the loss of muscle strength withging, but the relationship between oxidative stress and decrease in muscle strength and physical perfor-ance has not been well characterized. Serum protein carbonyls are markers of oxidative damage to
roteins and are caused by oxidative stress.ETHODS: Serum protein carbonyls were measured at baseline and compared with a decrease inalking speed and development of severe walking disability (inability to walk or walking speed �0.4/sec) over 36 months of follow-up in 545 moderately to severely disabled women, aged �65 years, living
n the community in Baltimore, Maryland (the Women’s Health and Aging Study I).ESULTS: After adjusting for age, body mass index, smoking, and chronic diseases, loge proteinarbonyls (nmol/mg) were associated with a decrease in walking speed over 36 months (P � .002). Duringollow-up, 154 women (28.2%) developed severe walking disability. After adjusting for the same potentialonfounders, loge protein carbonyls were associated with incident severe walking disability (hazards ratio.42, 95% confidence interval, 1.02-1.98, P � .037).ONCLUSION: High oxidative stress, as indicated by oxidative damage to proteins, is an independentredictor of decrease in walking speed and progression to severe walking disability among older womeniving in the community. © 2007 Elsevier Inc. All rights reserved.
KEYWORDS: Aging; Disability; Oxidative stress; Protein carbonyls; Walking
iRzasv
batsmtPo
arcopenia, or loss of muscle strength and muscle mass, isn important factor underlying mobility difficulties such asevere walking disability and a decrease in walking speed inlder adults.1 There is initial evidence that excessive oxi-ative stress is involved in the pathogenesis of age-relatedarcopenia and subsequent decrease of strength and mobil-ty.2,3 Reactive oxygen species are formed as intermediates
This work was supported by National Institute on Aging Grant R01G027012, NIH-NCRR, OPD-GCRC Grant RR00722, and NIA Contract01-AG12112, the Johns Hopkins Older Americans’ Independence Cen-
er, and the Intramural Research Program, National Institute on Aging,ational Institutes of Health.
Requests for reprints should be addressed to Richard Semba, MD,epartment of Ophthalmology, Johns Hopkins School of Medicine, 550 N.roadway, Suite 700, Baltimore, MD 21205.
ront matter © 2007 Elsevier Inc. All rights reserved.ed.2007.07.028
n reduction-oxidation (redox), mostly within mitochondria.eactive oxygen species are balanced by antioxidant en-ymes such as superoxide dismutase, catalase, thioredoxin,nd glutathione peroxidase, and exogenous antioxidantsuch as carotenoids, tocopherols, ascorbate, selenium, fla-onoids, and other plant polyphenols.
Oxidative stress refers to the condition in which thealance between oxidants and antioxidant defenses is upset,nd excess reactive oxygen species cause oxidative damageo nucleic acids, proteins, and lipids.4 Reactive oxygenpecies have an extremely short half-life and are difficult toeasure in humans, but it is possible to measure the damage
hat oxidative stress causes to protein, lipids, and DNA.rotein carbonyls are the most studied marker of proteinxidation.5-7 Protein carbonyls represent several pathways
f oxidative protein damage and are useful in epidemiologic
ss
aaibasoahtbst
MSwwHIsapsMipmtt
●
●
●
●
adcTra
pSss
PsmtbfirhuwuawcipswtCbc
Hiadsfdd
mun
1085Semba et al Oxidative Stress and Severe Walking Disability
tudies because they are stable and can be measured inerum or plasma.7
The relationship between oxidative damage to proteinsnd functional status has not been characterized in olderdults. We hypothesized that higher oxidative stress, asndicated by serum protein car-onyl levels, was associated withn accelerated decline of walkingpeed and excessive risk of devel-ping severe walking disabilitymong older adults. To address thisypothesis, we examined the rela-ionship between serum protein car-onyl concentrations and walkingpeed among older women living inhe community.
ETHODSubjects in this study wereomen, aged 65 years and older,ho participated in the Women’sealth and Aging Study I (WHAS
), a population-based study de-igned to evaluate the causes and course of physical dis-bility in older women living in the community. WHAS Iarticipants were recruited from an age-stratified randomample of women aged 65 years and older selected fromedicare enrollees residing in 12 contiguous zip code areas
n Baltimore.8 Women were screened to identify self-re-orted physical disability that was categorized into 4 do-ains. The domains of disability were ascertained in a 20-
o 30-minute home interview that included questions relatedo:
Mobility and exercise tolerance, that is, walking for aquarter of a mile, walking up 10 steps without resting,getting in and out of bed or chairs;Upper extremity function, that is, raising your arms upover your head, using your fingers to grasp or handle,lifting or carrying something as heavy as 10 pounds;Higher functioning tasks (a subset of instrumental activ-ities of daily living, not including heavy housework, forexample, using the telephone, doing light housework,preparing your own meals, shopping for personal items);andBasic self-care tasks (a subset of non-mobility-dependentactivities of daily living, for example, bathing or show-ering, dressing, eating, using the toilet).
WHAS I enrolled the one third most disabled womenged 65 years and older, those with disability in 2 or moreomains. Of the 1409 women who met study eligibilityriteria, 1002 agreed to participate in the study in 1992.here were no major differences in sociodemographic or
eported health characteristics between eligible participants
CLINICAL SIGNIF
● Although oxidatplicated in the pnia, the relationstress and physicbeen well charac
● Oxidative damagciated with an inin walking speedsevere walking dliving in the com
nd those who declined to participate.8 w
Standardized questionnaires were administered in thearticipants’ homes by trained interviewers. Mini-Mentaltatus Examination (MMSE) was recorded.8 Race was as-essed in a questionnaire as black, white, or other; currentmoking as yes or no; and education as 0-8 years, 9-11
years, 12 years, or more than 12years as the highest level of for-mal education achieved. Twoweeks later, a trained registeredfull-time study nurse conducted anexamination of each study partic-ipant in her home, using a stan-dardized protocol that includedphysical performance measuresand a standardized physical exami-nation. Approximately 75% ofwomen also consented to phlebot-omy performed during a separatevisit by a trained phlebotomist whofollowed a standardized protocol.Further details on the methods andsampling design of the WHAS stud-ies are published elsewhere.8
Participants were asked to walk over a 4-meter course.articipants were instructed to stand with both feet at thetarting line and to start walking after a specific verbal com-and. Timing began when the command was given. In this
est, subjects could use canes, walkers, or other walking aids,ut not the aid of another person. The times to complete therst meter and the entire path were recorded. The test wasepeated 3 times, twice at the woman’s usual pace, and once ater fastest possible pace. The speed of the faster of the 2sual-pace walks was used in the analyses. The length of thealk expressed in meters divided by the time in seconds wassed to calculate the walking speed.8 Women were categorizeds having severe walking disability based upon being unable toalk or having a walking speed �0.4 m/sec.9 The 0.4 m/sec
utoff point was approximately at the top of the lowest quartilen the WHAS population at baseline10 and has been shown toredict functional dependence.11 Demographic characteristics,elf-rated health, and information about appetite and eatingere measured in the WHAS questionnaires. An interim his-
ory of hospitalizations was obtained at each study visit.hronic diseases were adjudicated by WHAS co-investigatorsased on the questionnaire, physical examination, and physi-ian contact.8
There were 1002 women enrolled in the Women’sealth and Aging Study I, of whom 753 women participated
n the blood drawing and had serum nutrient measurementst baseline. Of the 753 women, 150 had severe walkingisability at baseline, 554 of the 753 women did not haveevere walking disability at baseline and had at least oneollow-up visit, and 49 women did not have severe walkingisability at baseline but did not have a follow-up visit (17ropped out and 32 died). Of the 554 women without severe
CE
ress has been im-enesis of sarcope-between oxidativerformance has notd.
proteins was asso-ed risk of a declinehe development ofity in older womenity.
ICAN
ive stathogshipal peterize
e tocreasand tisabil
alking disability at baseline, there were 545 women who
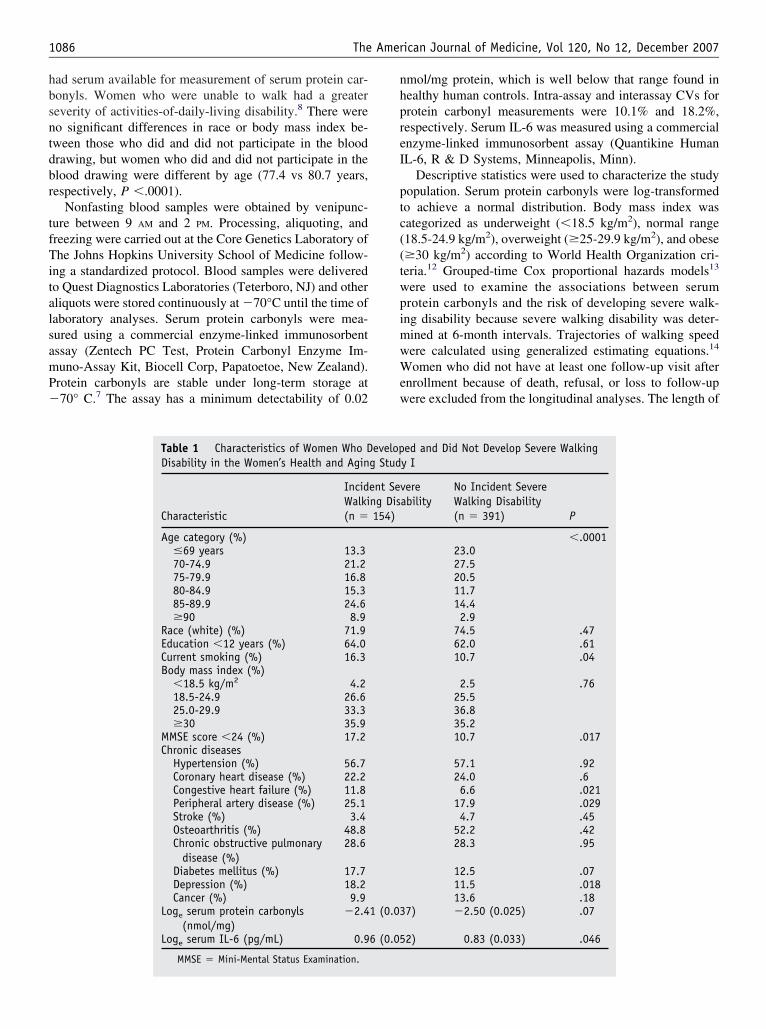
hbsntdbr
tfTitalsamP�
nhpreI
ptc((twpimwWew
1086 The American Journal of Medicine, Vol 120, No 12, December 2007
ad serum available for measurement of serum protein car-onyls. Women who were unable to walk had a greatereverity of activities-of-daily-living disability.8 There wereo significant differences in race or body mass index be-ween those who did and did not participate in the bloodrawing, but women who did and did not participate in thelood drawing were different by age (77.4 vs 80.7 years,espectively, P �.0001).
Nonfasting blood samples were obtained by venipunc-ure between 9 AM and 2 PM. Processing, aliquoting, andreezing were carried out at the Core Genetics Laboratory ofhe Johns Hopkins University School of Medicine follow-
ng a standardized protocol. Blood samples were deliveredo Quest Diagnostics Laboratories (Teterboro, NJ) and otherliquots were stored continuously at �70°C until the time ofaboratory analyses. Serum protein carbonyls were mea-ured using a commercial enzyme-linked immunosorbentssay (Zentech PC Test, Protein Carbonyl Enzyme Im-uno-Assay Kit, Biocell Corp, Papatoetoe, New Zealand).rotein carbonyls are stable under long-term storage at70° C.7 The assay has a minimum detectability of 0.02
Table 1 Characteristics of Women Who DDisability in the Women’s Health and Agin
Characteristic
IncidWalki(n �
Age category (%)�69 years 13.370-74.9 21.275-79.9 16.880-84.9 15.385-89.9 24.6�90 8.9
Race (white) (%) 71.9Education �12 years (%) 64.0Current smoking (%) 16.3Body mass index (%)
�18.5 kg/m2 4.218.5-24.9 26.625.0-29.9 33.3�30 35.9
MMSE score �24 (%) 17.2Chronic diseases
Hypertension (%) 56.7Coronary heart disease (%) 22.2Congestive heart failure (%) 11.8Peripheral artery disease (%) 25.1Stroke (%) 3.4Osteoarthritis (%) 48.8Chronic obstructive pulmonary
disease (%)28.6
Diabetes mellitus (%) 17.7Depression (%) 18.2Cancer (%) 9.9
Loge serum protein carbonyls(nmol/mg)
�2.4
Loge serum IL-6 (pg/mL) 0.9
MMSE � Mini-Mental Status Examination.
mol/mg protein, which is well below that range found inealthy human controls. Intra-assay and interassay CVs forrotein carbonyl measurements were 10.1% and 18.2%,espectively. Serum IL-6 was measured using a commercialnzyme-linked immunosorbent assay (Quantikine HumanL-6, R & D Systems, Minneapolis, Minn).
Descriptive statistics were used to characterize the studyopulation. Serum protein carbonyls were log-transformedo achieve a normal distribution. Body mass index wasategorized as underweight (�18.5 kg/m2), normal range18.5-24.9 kg/m2), overweight (�25-29.9 kg/m2), and obese�30 kg/m2) according to World Health Organization cri-eria.12 Grouped-time Cox proportional hazards models13
ere used to examine the associations between serumrotein carbonyls and the risk of developing severe walk-ng disability because severe walking disability was deter-ined at 6-month intervals. Trajectories of walking speedere calculated using generalized estimating equations.14
omen who did not have at least one follow-up visit afternrollment because of death, refusal, or loss to follow-upere excluded from the longitudinal analyses. The length of
ed and Did Not Develop Severe Walkingy I
ereability
No Incident SevereWalking Disability(n � 391) P
�.000123.027.520.511.714.42.9
74.5 .4762.0 .6110.7 .04
2.5 .7625.536.835.210.7 .017
57.1 .9224.0 .66.6 .021
17.9 .0294.7 .45
52.2 .4228.3 .95
12.5 .0711.5 .01813.6 .18
7) �2.50 (0.025) .07
2) 0.83 (0.033) .046
evelopg Stud
ent Sevng Dis154)
1 (0.03
6 (0.05
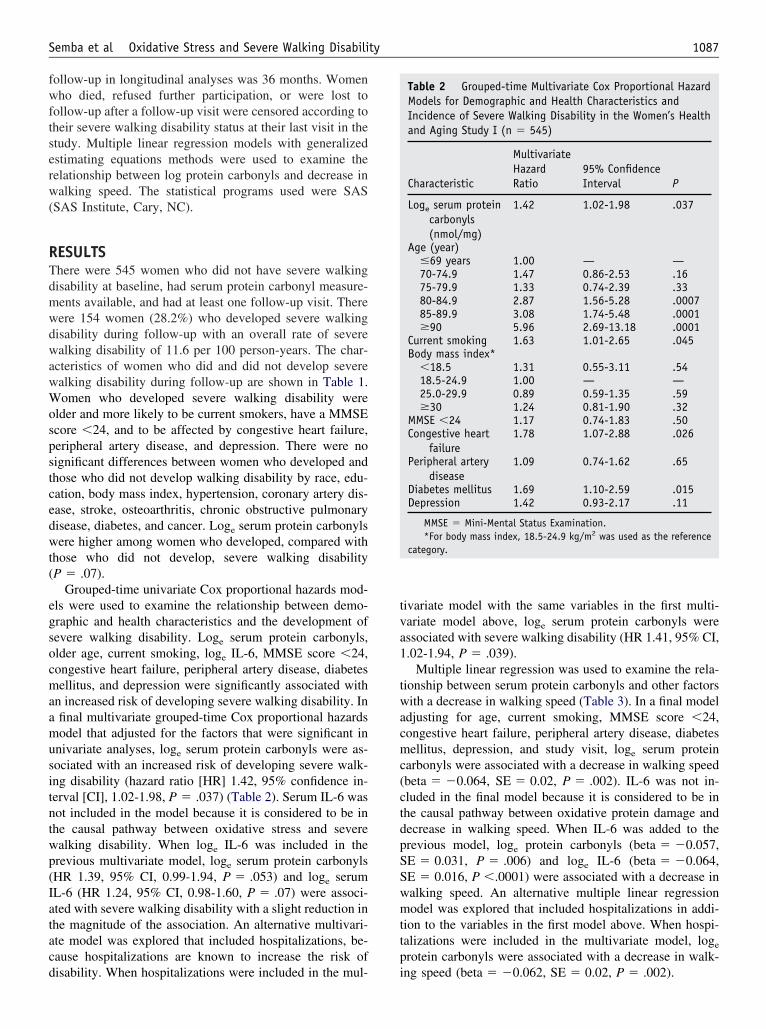
fwftserw(
RTdmwdwawWospstcedwt(
egsocmaamusitntwp(Iatacd
tva1
twacmc(ctdpSSwmttp
1087Semba et al Oxidative Stress and Severe Walking Disability
ollow-up in longitudinal analyses was 36 months. Womenho died, refused further participation, or were lost to
ollow-up after a follow-up visit were censored according toheir severe walking disability status at their last visit in thetudy. Multiple linear regression models with generalizedstimating equations methods were used to examine theelationship between log protein carbonyls and decrease inalking speed. The statistical programs used were SAS
SAS Institute, Cary, NC).
ESULTShere were 545 women who did not have severe walkingisability at baseline, had serum protein carbonyl measure-ents available, and had at least one follow-up visit. Thereere 154 women (28.2%) who developed severe walkingisability during follow-up with an overall rate of severealking disability of 11.6 per 100 person-years. The char-
cteristics of women who did and did not develop severealking disability during follow-up are shown in Table 1.omen who developed severe walking disability were
lder and more likely to be current smokers, have a MMSEcore �24, and to be affected by congestive heart failure,eripheral artery disease, and depression. There were noignificant differences between women who developed andhose who did not develop walking disability by race, edu-ation, body mass index, hypertension, coronary artery dis-ase, stroke, osteoarthritis, chronic obstructive pulmonaryisease, diabetes, and cancer. Loge serum protein carbonylsere higher among women who developed, compared with
hose who did not develop, severe walking disabilityP � .07).
Grouped-time univariate Cox proportional hazards mod-ls were used to examine the relationship between demo-raphic and health characteristics and the development ofevere walking disability. Loge serum protein carbonyls,lder age, current smoking, loge IL-6, MMSE score �24,ongestive heart failure, peripheral artery disease, diabetesellitus, and depression were significantly associated with
n increased risk of developing severe walking disability. Infinal multivariate grouped-time Cox proportional hazardsodel that adjusted for the factors that were significant in
nivariate analyses, loge serum protein carbonyls were as-ociated with an increased risk of developing severe walk-ng disability (hazard ratio [HR] 1.42, 95% confidence in-erval [CI], 1.02-1.98, P � .037) (Table 2). Serum IL-6 wasot included in the model because it is considered to be inhe causal pathway between oxidative stress and severealking disability. When loge IL-6 was included in therevious multivariate model, loge serum protein carbonylsHR 1.39, 95% CI, 0.99-1.94, P � .053) and loge serumL-6 (HR 1.24, 95% CI, 0.98-1.60, P � .07) were associ-ted with severe walking disability with a slight reduction inhe magnitude of the association. An alternative multivari-te model was explored that included hospitalizations, be-ause hospitalizations are known to increase the risk of
isability. When hospitalizations were included in the mul- iivariate model with the same variables in the first multi-ariate model above, loge serum protein carbonyls weressociated with severe walking disability (HR 1.41, 95% CI,.02-1.94, P � .039).
Multiple linear regression was used to examine the rela-ionship between serum protein carbonyls and other factorsith a decrease in walking speed (Table 3). In a final model
djusting for age, current smoking, MMSE score �24,ongestive heart failure, peripheral artery disease, diabetesellitus, depression, and study visit, loge serum protein
arbonyls were associated with a decrease in walking speedbeta � �0.064, SE � 0.02, P � .002). IL-6 was not in-luded in the final model because it is considered to be inhe causal pathway between oxidative protein damage andecrease in walking speed. When IL-6 was added to therevious model, loge protein carbonyls (beta � �0.057,E � 0.031, P � .006) and loge IL-6 (beta � �0.064,E � 0.016, P �.0001) were associated with a decrease inalking speed. An alternative multiple linear regressionodel was explored that included hospitalizations in addi-
ion to the variables in the first model above. When hospi-alizations were included in the multivariate model, loge
rotein carbonyls were associated with a decrease in walk-
Table 2 Grouped-time Multivariate Cox Proportional HazardModels for Demographic and Health Characteristics andIncidence of Severe Walking Disability in the Women’s Healthand Aging Study I (n � 545)
Characteristic
MultivariateHazardRatio
95% ConfidenceInterval P
Loge serum proteincarbonyls(nmol/mg)
1.42 1.02-1.98 .037
Age (year)�69 years 1.00 — —70-74.9 1.47 0.86-2.53 .1675-79.9 1.33 0.74-2.39 .3380-84.9 2.87 1.56-5.28 .000785-89.9 3.08 1.74-5.48 .0001�90 5.96 2.69-13.18 .0001
Current smoking 1.63 1.01-2.65 .045Body mass index*
�18.5 1.31 0.55-3.11 .5418.5-24.9 1.00 — —25.0-29.9 0.89 0.59-1.35 .59�30 1.24 0.81-1.90 .32
MMSE �24 1.17 0.74-1.83 .50Congestive heart
failure1.78 1.07-2.88 .026
Peripheral arterydisease
1.09 0.74-1.62 .65
Diabetes mellitus 1.69 1.10-2.59 .015Depression 1.42 0.93-2.17 .11
MMSE � Mini-Mental Status Examination.*For body mass index, 18.5-24.9 kg/m2 was used as the reference
category.
ng speed (beta � �0.062, SE � 0.02, P � .002).
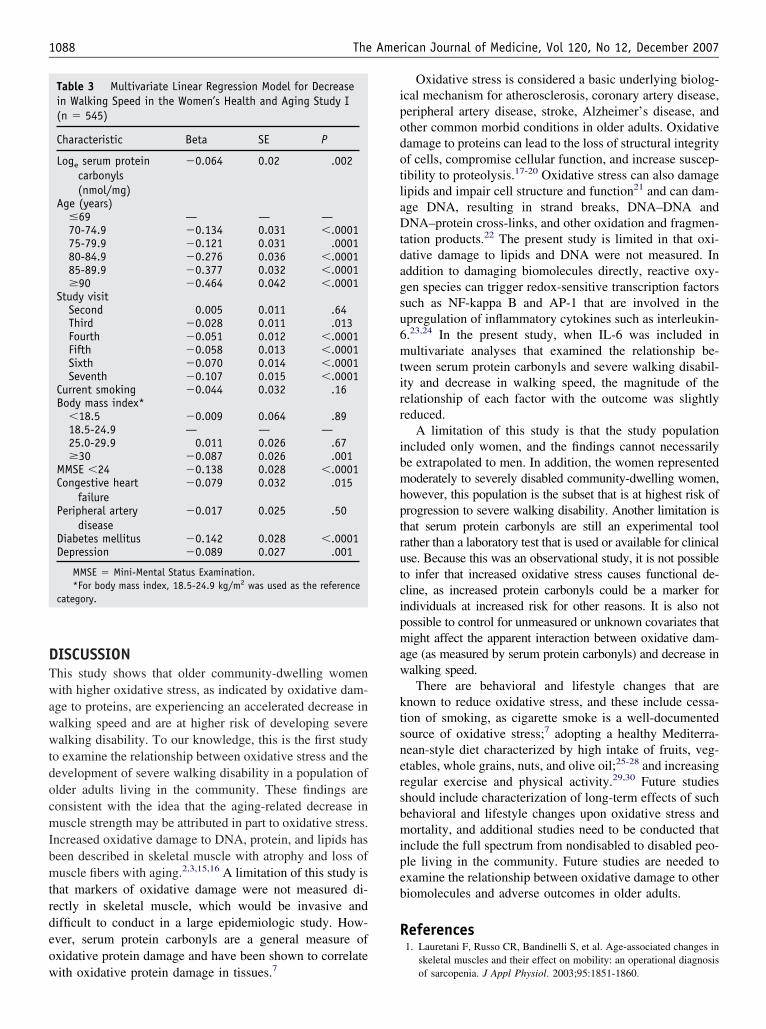
DTwawwtdocmIbmtrdeow
ipodotlaDtdagsu6mtirr
ibmhptrutcipmaw
ktsnersbmipeb
R
1088 The American Journal of Medicine, Vol 120, No 12, December 2007
ISCUSSIONhis study shows that older community-dwelling womenith higher oxidative stress, as indicated by oxidative dam-
ge to proteins, are experiencing an accelerated decrease inalking speed and are at higher risk of developing severealking disability. To our knowledge, this is the first study
o examine the relationship between oxidative stress and theevelopment of severe walking disability in a population oflder adults living in the community. These findings areonsistent with the idea that the aging-related decrease inuscle strength may be attributed in part to oxidative stress.
ncreased oxidative damage to DNA, protein, and lipids haseen described in skeletal muscle with atrophy and loss ofuscle fibers with aging.2,3,15,16 A limitation of this study is
hat markers of oxidative damage were not measured di-ectly in skeletal muscle, which would be invasive andifficult to conduct in a large epidemiologic study. How-ver, serum protein carbonyls are a general measure ofxidative protein damage and have been shown to correlate
Table 3 Multivariate Linear Regression Model for Decreasein Walking Speed in the Women’s Health and Aging Study I(n � 545)
Characteristic Beta SE P
Loge serum proteincarbonyls(nmol/mg)
�0.064 0.02 .002
Age (years)�69 — — —70-74.9 �0.134 0.031 �.000175-79.9 �0.121 0.031 .000180-84.9 �0.276 0.036 �.000185-89.9 �0.377 0.032 �.0001�90 �0.464 0.042 �.0001
Study visitSecond 0.005 0.011 .64Third �0.028 0.011 .013Fourth �0.051 0.012 �.0001Fifth �0.058 0.013 �.0001Sixth �0.070 0.014 �.0001Seventh �0.107 0.015 �.0001
Current smoking �0.044 0.032 .16Body mass index*
�18.5 �0.009 0.064 .8918.5-24.9 — — —25.0-29.9 0.011 0.026 .67�30 �0.087 0.026 .001
MMSE �24 �0.138 0.028 �.0001Congestive heart
failure�0.079 0.032 .015
Peripheral arterydisease
�0.017 0.025 .50
Diabetes mellitus �0.142 0.028 �.0001Depression �0.089 0.027 .001
MMSE � Mini-Mental Status Examination.*For body mass index, 18.5-24.9 kg/m2 was used as the reference
category.
ith oxidative protein damage in tissues.7
Oxidative stress is considered a basic underlying biolog-cal mechanism for atherosclerosis, coronary artery disease,eripheral artery disease, stroke, Alzheimer’s disease, andther common morbid conditions in older adults. Oxidativeamage to proteins can lead to the loss of structural integrityf cells, compromise cellular function, and increase suscep-ibility to proteolysis.17-20 Oxidative stress can also damageipids and impair cell structure and function21 and can dam-ge DNA, resulting in strand breaks, DNA–DNA andNA–protein cross-links, and other oxidation and fragmen-
ation products.22 The present study is limited in that oxi-ative damage to lipids and DNA were not measured. Inddition to damaging biomolecules directly, reactive oxy-en species can trigger redox-sensitive transcription factorsuch as NF-kappa B and AP-1 that are involved in thepregulation of inflammatory cytokines such as interleukin-.23,24 In the present study, when IL-6 was included inultivariate analyses that examined the relationship be-
ween serum protein carbonyls and severe walking disabil-ty and decrease in walking speed, the magnitude of theelationship of each factor with the outcome was slightlyeduced.
A limitation of this study is that the study populationncluded only women, and the findings cannot necessarilye extrapolated to men. In addition, the women representedoderately to severely disabled community-dwelling women,
owever, this population is the subset that is at highest risk ofrogression to severe walking disability. Another limitation ishat serum protein carbonyls are still an experimental toolather than a laboratory test that is used or available for clinicalse. Because this was an observational study, it is not possibleo infer that increased oxidative stress causes functional de-line, as increased protein carbonyls could be a marker forndividuals at increased risk for other reasons. It is also notossible to control for unmeasured or unknown covariates thatight affect the apparent interaction between oxidative dam-
ge (as measured by serum protein carbonyls) and decrease inalking speed.There are behavioral and lifestyle changes that are
nown to reduce oxidative stress, and these include cessa-ion of smoking, as cigarette smoke is a well-documentedource of oxidative stress;7 adopting a healthy Mediterra-ean-style diet characterized by high intake of fruits, veg-tables, whole grains, nuts, and olive oil;25-28 and increasingegular exercise and physical activity.29,30 Future studieshould include characterization of long-term effects of suchehavioral and lifestyle changes upon oxidative stress andortality, and additional studies need to be conducted that
nclude the full spectrum from nondisabled to disabled peo-le living in the community. Future studies are needed toxamine the relationship between oxidative damage to otheriomolecules and adverse outcomes in older adults.
eferences1. Lauretani F, Russo CR, Bandinelli S, et al. Age-associated changes in
skeletal muscles and their effect on mobility: an operational diagnosis
of sarcopenia. J Appl Physiol. 2003;95:1851-1860.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
1089Semba et al Oxidative Stress and Severe Walking Disability
2. Mecocci P, Fanó G, Fulle S, et al. Age-dependent increases in oxida-tive damage to DNA, lipids, and proteins in human skeletal muscle.Free Radic Biol Med. 1999;26:303-308.
3. Pansarasa O, Bertorelli L, Vecchiet J, et al. Age-dependent changes ofantioxidant activities and markers of free radical damage in humanskeletal muscle. Free Radic Biol Med. 1999;27:617-622.
4. Sies H. Oxidative stress. Introductory remarks. In: Sies H, ed. Oxida-tive Stress. London: Academic Press; 1985:1-8.
5. Chevion M, Berenshtein E, Stadtman ER. Human studies related toprotein oxidation: protein carbonyl content as a marker of damage.Free Radic Res. 2000;33:S99-S108.
6. Beal MF. Oxidatively modified proteins in aging and disease. FreeRadic Biol Med. 2002;32:797-803.
7. Dalle-Donne I, Rossi R, Giustarini D, et al. Protein carbonyl groups asbiomarkers of oxidative stress. Clin Chim Acta. 2003;329:23-38.
8. Guralnik JM, Fried LP, Simonsick EM, et al. The Women’s Health andAging Study: Health and Social Characteristics of Older Women withDisability (NIH Publication No. 95-4009). Bethesda, MD: NationalInstitute on Aging; 1995.
9. Ferrucci L, Harris TB, Guralnik JM, et al. Serum IL-6 level and thedevelopment of disability in older persons. J Am Geriatr Soc. 1999;47:639-646.
0. Rantanen T, Guralnik JM, Ferrucci L, et al. Coimpairments as predic-tors of severe walking disability in older women. J Am Geriatr Soc.2001;49:21-27.
1. Tinetti ME, Inouye SK, Gill TM, Doucette JT. Shared risk factors forfalls, incontinence, and functional dependence. JAMA. 1995;273:1348-1353.
2. James PT, Leach R, Kalamara E, Shayeghi M. The worldwide obesityepidemic. Obes Res. 2001;9(suppl 4):228S-233S.
3. Prentice RL, Gloeckler LA. Regression analysis of grouped survivaldata with application to breast cancer data. Biometrics. 1978;34:57-67.
4. Diggle PJ, Liang KY, Zeger SL. Analysis of Longitudinal Data. Ox-ford, UK: Clarendon Press; 1994.
5. Gianni P, Jan KJ, Douglas MJ, et al. Oxidative stress and the mito-chondrial theory of aging in human skeletal muscle. Exp Gerontol.2004;39:1391-1400.
6. Bua EA, McKiernan SH, Wanagat J, et al. Mitochondrial abnormali-ties are more frequent in muscles undergoing sarcopenia. J Appl
Physiol. 2002;92:2617-2624.7. Stadtman ER. Protein oxidation and aging. Free Radic Res. 2006;40:1250-1258.
8. Davies KJA, Lin SW, Pacifici RE. Protein damage and degradation byoxygen radicals. IV. Degradation of denatured protein. J Biol Chem.1987;262:9914-9920.
9. Agarawal S, Sohal RS. Differential oxidative damage to mitochondrialproteins during aging. Mech Ageing Dev. 1995;85:59-63.
0. Grune T, Shringarpure R, Sitte N, Davies K. Age-related changes inprotein oxidation and proteolysis in mammalian cells. J Gerontol ABiol Sci Med Sci. 2001;56:B459-B467.
1. Stark G. Functional consequences of oxidative membrane damage.J Membr Biol. 2005;205:1-16.
2. Evans MD, Cooke MS. Factors contributing to the outcome of oxida-tive damage to nucleic acids. Bioessays. 2004;26:533-542.
3. Kabe Y, Ando K, Hirao S, et al. Redox regulation of NF-�B activation:distinct redox regulation between the cytoplasm and the nucleus.Antioxid Redox Signal. 2005;7:395-403.
4. Karin M, Takahashi T, Kapahi P, et al. Oxidative stress and geneexpression: the AP-1 and NF-�B connections. Biofactors. 2001;15:87-89.
5. Lopes HF, Martin KL, Nashar K, et al. DASH diet lowers bloodpressure and lipid-induced oxidative stress in obesity. Hypertension.2003;41:422-430.
6. Sanchez-Moreno C, Cano MP, de Ancos B, et al. Consumption ofhigh-pressurized vegetable soup increases plasma vitamin C and de-creases oxidative stress and inflammatory biomarkers in healthy hu-mans. J Nutr. 2004;134:3021-3025.
7. Rao LG, Mackinnon ES, Josse RG, et al. Lycopene consumptiondecreases oxidative stress and bone resorption markers in postmeno-pausal women. Osteoporos Int. 2007;18:109-115.
8. Machowetz A, Poulsen HE, Gruendel S, et al. Effect of olive oils onbiomarkers of oxidative DNA stress in Northern and Southern Euro-peans. FASEB J. 2007;21:45-52.
9. Lazarevic G, Antic S, Cvetkovic T, et al. A physical activity pro-gramme and its effects on insulin resistance and oxidative defense inobese male patients with type 2 diabetes mellitus. Diabetes Metab.2006;32:583-590.
0. Rector RS, Warner SO, Liu Y, et al. Exercise and diet induced weightloss improves measures of oxidative stress and insulin sensitivity inadults with characteristics of the metabolic syndrome. Am J Physiol
Endocrinol Metab. 2007;293:E500-E506.
R
CRHa
K
Ntdtts(gbrtai
o
0d
The American Journal of Medicine (2007) 120, 1090.e1-1090.e8
EVIEW
ombining Neuroendocrine Inhibitors in Heart Failure:eflections on Safety and Efficacy
ani Jneid, MD,a George V. Moukarbel, MD,a Bart Dawson, MD,b Roger J. Hajjar, MD,a Gary S. Francis, MDc
Division of Cardiology, Massachusetts General Hospital, Harvard Medical School, Boston; bDivision of Cardiology, University of
entucky, Lexing cNghihpowvbicfiE
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
ton; Department of Cardiovascular Medicine, Cleveland Clinic Foundation, Cleveland, Ohio.
ABSTRACT
euroendocrine activation in heart failure has become the major target of pharmacotherapy for thisrowing epidemic. Agents targeting the renin-angiotensin-aldosterone and sympathetic nervous systemsave shown cardiovascular and survival benefits in clinical trials. Beta-blockers and angiotensin-convert-ng enzyme (ACE) inhibitors remain the mainstream initial therapy. The benefits of aldosterone antagonistsave been demonstrated in advanced heart failure (spironolactone) and after myocardial infarction com-licated by left ventricular dysfunction and heart failure (eplerenone). Emerging clinical evidence dem-nstrated that angiotensin receptor blockers may be a reasonable alternative to ACE inhibitors in patientsith heart failure (candesartan) and following myocardial infarction complicated by heart failure or leftentricular dysfunction (valsartan). Angiotensin receptor blockers (candesartan) also provided incrementalenefits when added to ACE inhibitors in chronic heart failure. Thus, combining neuroendocrine inhibitorsn heart failure appears both biologically plausible and evidence-based. However, this approach raisedoncerns about side effects, such as hypotension, renal insufficiency, hyperkalemia, and others. Closeollow-up and implementation of evidence-based medicine (ie, using agents and doses proven beneficialn clinical trials) should therefore be undertaken when combining neuroendocrine inhibitors. © 2007lsevier Inc. All rights reserved.
KEYWORDS: Aldosterone; Angiotensin; Beta-blocker; Heart failure; Neuroendocrine; Systolic dysfunction
drcbtp
TIHnamehtc
euroendocrine activation in heart failure has become thearget of modern pharmacotherapy for this growing epi-emic. Over the past 2 decades, beta-blockers and angio-ensin-converting enzyme (ACE) inhibitors have becomehe standard of care in the treatment of heart failure.1-6 Theubsequent advent of angiotensin-II receptor blockersARBs) and aldosterone antagonists in recent years hasenerated debates over how and when these agents shoulde added to block the neuroendocrine axis. The results ofecent clinical trials offer insights into the use of “tripleherapy” (beta-blocker, ACE inhibitor, plus an ARB orldosterone antagonist) in heart failure and after myocardialnfarction.7-15
The current report reviews the effects of triple neuroen-
Requests for reprints should be addressed to Hani Jneid, MD, Divisionf Cardiology, Massachusetts General Hospital, Boston, MA 02114.
ront matter © 2007 Elsevier Inc. All rights reserved.ed.2007.02.029
ocrine inhibition in patients with heart failure based onecent evidence from the medical literature. We try to spe-ifically answer the following questions: Does triple com-ination therapy decrease morbidity and mortality? Is itolerable and safe for a wide range of patients? What is theroper time and sequence for adding these agents?
HE ROLE OF NEUROENDOCRINE ACTIVATIONN HEART FAILUREeart failure results in the activation of the sympatheticervous and the renin-angiotensin-aldosterone systems byrterial underfilling and by hemodynamic and hormonallyediated effects on the kidney.16 Elevated plasma cat-
cholamines levels and direct sympathetic activity on theeart result in tachycardia, vasoconstriction, increased con-ractility, and ventricular hypertrophy.17 Beta-blockersounteract these deleterious effects and improve survival in
eart failure.1-3 On the other hand, direct adrenergic and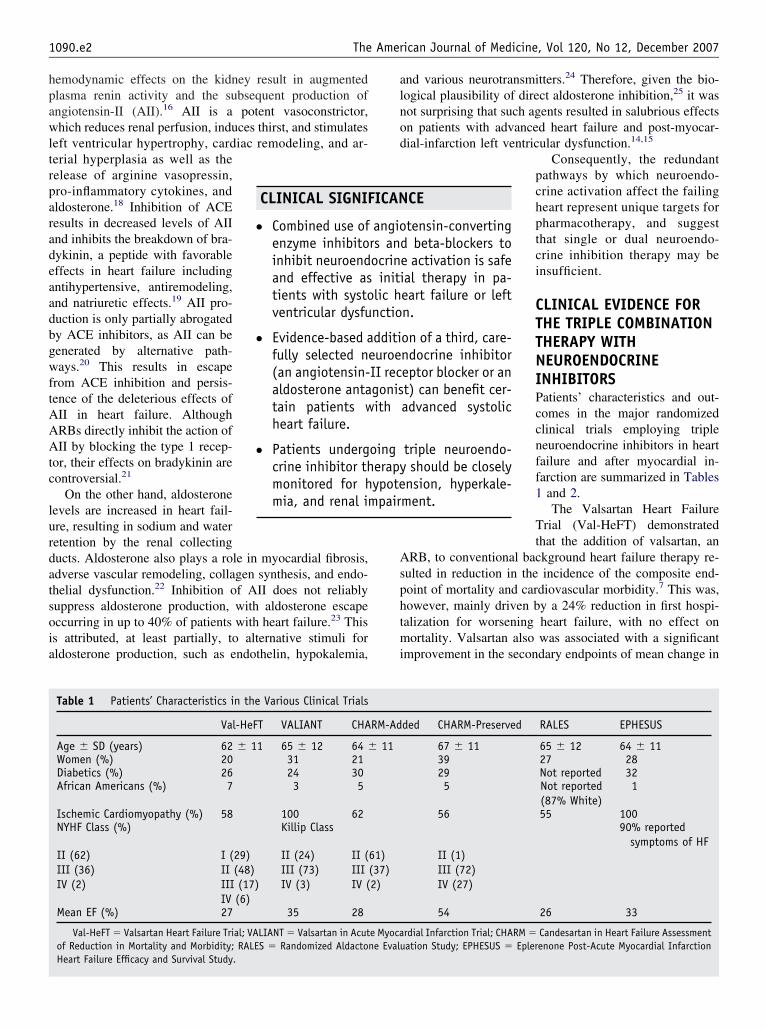
hpawltrparadeaadbgwftAAAtc
lurdatsoia
alnod
Asphtmi
pair
1090.e2 The American Journal of Medicine, Vol 120, No 12, December 2007
emodynamic effects on the kidney result in augmentedlasma renin activity and the subsequent production ofngiotensin-II (AII).16 AII is a potent vasoconstrictor,hich reduces renal perfusion, induces thirst, and stimulates
eft ventricular hypertrophy, cardiac remodeling, and ar-erial hyperplasia as well as theelease of arginine vasopressin,ro-inflammatory cytokines, andldosterone.18 Inhibition of ACEesults in decreased levels of AIInd inhibits the breakdown of bra-ykinin, a peptide with favorableffects in heart failure includingntihypertensive, antiremodeling,nd natriuretic effects.19 AII pro-uction is only partially abrogatedy ACE inhibitors, as AII can beenerated by alternative path-ays.20 This results in escape
rom ACE inhibition and persis-ence of the deleterious effects ofII in heart failure. AlthoughRBs directly inhibit the action ofII by blocking the type 1 recep-
or, their effects on bradykinin areontroversial.21
On the other hand, aldosteroneevels are increased in heart fail-re, resulting in sodium and wateretention by the renal collectingucts. Aldosterone also plays a role in myocardial fibrosis,dverse vascular remodeling, collagen synthesis, and endo-helial dysfunction.22 Inhibition of AII does not reliablyuppress aldosterone production, with aldosterone escapeccurring in up to 40% of patients with heart failure.23 Thiss attributed, at least partially, to alternative stimuli forldosterone production, such as endothelin, hypokalemia,
CLINICAL SIGNIF
● Combined use ofenzyme inhibitoinhibit neuroendand effective astients with systoventricular dysfu
● Evidence-based afully selected n(an angiotensin-aldosterone antatain patients wheart failure.
● Patients undergcrine inhibitor thmonitored for hmia, and renal im
Table 1 Patients’ Characteristics in the Various Clinical Trials
Val-HeFT VALIANT CHA
Age � SD (years) 62 � 11 65 � 12 64 �Women (%) 20 31 21Diabetics (%) 26 24 30African Americans (%) 7 3 5
Ischemic Cardiomyopathy (%) 58 100 62NYHF Class (%) Killip Class
II (62)III (36)IV (2)
I (29)II (48)III (17)IV (6)
II (24)III (73)IV (3)
II (IIIIV (
Mean EF (%) 27 35 28
Val-HeFT � Valsartan Heart Failure Trial; VALIANT � Valsartan in Acutof Reduction in Mortality and Morbidity; RALES � Randomized AldactoHeart Failure Efficacy and Survival Study.
nd various neurotransmitters.24 Therefore, given the bio-ogical plausibility of direct aldosterone inhibition,25 it wasot surprising that such agents resulted in salubrious effectsn patients with advanced heart failure and post-myocar-ial-infarction left ventricular dysfunction.14,15
Consequently, the redundantpathways by which neuroendo-crine activation affect the failingheart represent unique targets forpharmacotherapy, and suggestthat single or dual neuroendo-crine inhibition therapy may beinsufficient.
CLINICAL EVIDENCE FORTHE TRIPLE COMBINATIONTHERAPY WITHNEUROENDOCRINEINHIBITORSPatients’ characteristics and out-comes in the major randomizedclinical trials employing tripleneuroendocrine inhibitors in heartfailure and after myocardial in-farction are summarized in Tables1 and 2.
The Valsartan Heart FailureTrial (Val-HeFT) demonstratedthat the addition of valsartan, an
RB, to conventional background heart failure therapy re-ulted in reduction in the incidence of the composite end-oint of mortality and cardiovascular morbidity.7 This was,owever, mainly driven by a 24% reduction in first hospi-alization for worsening heart failure, with no effect onortality. Valsartan also was associated with a significant
mprovement in the secondary endpoints of mean change in
CE
tensin-convertingd beta-blockers toe activation is safeal therapy in pa-eart failure or leftn.
on of a third, care-ndocrine inhibitoreptor blocker or ant) can benefit cer-advanced systolic
triple neuroendo-should be closely
nsion, hyperkale-ment.
ded CHARM-Preserved RALES EPHESUS
67 � 11 65 � 12 64 � 1139 27 2829 Not reported 325 Not reported
(87% White)1
56 55 10090% reported
symptoms of HFII (1)III (72)IV (27)
54 26 33
rdial Infarction Trial; CHARM � Candesartan in Heart Failure Assessmentation Study; EPHESUS � Eplerenone Post-Acute Myocardial Infarction
ICAN
angiors anocrininiti
lic hnctio
dditieuroeII recgonisith
oingerapyypote
RM-Ad
11
61)(37)2)
e Myocane Evalu
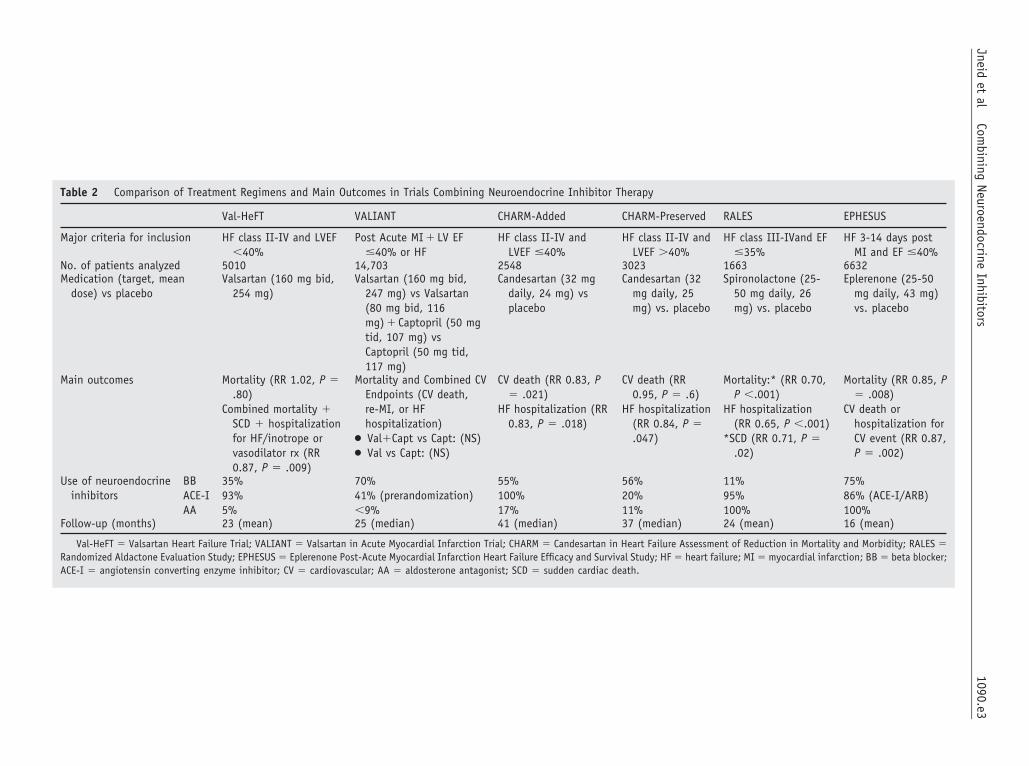
Table 2 Comparison of Treatment Regimens and Main Outcomes in Trials Combining Neuroendocrine Inhibitor Therapy
Val-HeFT VALIANT CHARM-Added CHARM-Preserved RALES EPHESUS
Major criteria for inclusion HF class II-IV and LVEF�40%
Post Acute MI � LV EF�40% or HF
HF class II-IV andLVEF �40%
HF class II-IV andLVEF �40%
HF class III-IVand EF�35%
HF 3-14 days postMI and EF �40%
No. of patients analyzed 5010 14,703 2548 3023 1663 6632Medication (target, mean
dose) vs placeboValsartan (160 mg bid,
254 mg)Valsartan (160 mg bid,
247 mg) vs Valsartan(80 mg bid, 116mg) � Captopril (50 mgtid, 107 mg) vsCaptopril (50 mg tid,117 mg)
Candesartan (32 mgdaily, 24 mg) vsplacebo
Candesartan (32mg daily, 25mg) vs. placebo
Spironolactone (25-50 mg daily, 26mg) vs. placebo
Eplerenone (25-50mg daily, 43 mg)vs. placebo
Main outcomes Mortality (RR 1.02, P �.80)
Combined mortality �SCD � hospitalizationfor HF/inotrope orvasodilator rx (RR0.87, P � .009)
Mortality and Combined CVEndpoints (CV death,re-MI, or HFhospitalization)
● Val�Capt vs Capt: (NS)● Val vs Capt: (NS)
CV death (RR 0.83, P� .021)
HF hospitalization (RR0.83, P � .018)
CV death (RR0.95, P � .6)
HF hospitalization(RR 0.84, P �.047)
Mortality:* (RR 0.70,P �.001)
HF hospitalization(RR 0.65, P �.001)
*SCD (RR 0.71, P �.02)
Mortality (RR 0.85, P� .008)
CV death orhospitalization forCV event (RR 0.87,P � .002)
Use of neuroendocrineinhibitors
BBACE-IAA
35%93%5%
70%41% (prerandomization)�9%
55%100%17%
56%20%11%
11%95%100%
75%86% (ACE-I/ARB)100%
Follow-up (months) 23 (mean) 25 (median) 41 (median) 37 (median) 24 (mean) 16 (mean)
Val-HeFT � Valsartan Heart Failure Trial; VALIANT � Valsartan in Acute Myocardial Infarction Trial; CHARM � Candesartan in Heart Failure Assessment of Reduction in Mortality and Morbidity; RALES �Randomized Aldactone Evaluation Study; EPHESUS � Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study; HF � heart failure; MI � myocardial infarction; BB � beta blocker;ACE-I � angiotensin converting enzyme inhibitor; CV � cardiovascular; AA � aldosterone antagonist; SCD � sudden cardiac death.
1090.e3Jneid
etal
Combining
NeuroendocrineInhibitors

eMhiVttapercs
Mto4svacot
lRgasCwCiweCcwrc.cbcshgmTpscsra
tthbCtpc
(acc7brwat
hoases(tv1hPaaAbo
ANDiub
HIhctcttpt
1090.e4 The American Journal of Medicine, Vol 120, No 12, December 2007
jection fraction, New York Heart Association class, theinnesota Living with Heart Failure questionnaire, and
eart failure symptoms. However, the enthusiasm for utiliz-ng valsartan was dampened by a post hoc analysis inal-HeFT showing a 42% increased mortality (P �.009) in
he 30% of patients (n � 1610) who received all 3 agentsogether (ARB, ACE inhibitor, and beta-blocker), but notmong those treated with any combination of 2 agents. Theossibility that excessive neuroendocrine inhibition is del-terious or that these findings represented a chance occur-ence could not be sorted out initially. However, this in-reased mortality in Val-HeFT7 has not been confirmed inubsequent studies.
Others attempted to address this controversial subject.cKelvie et al8 examined the effects of various combina-
ions of candesartan, enalapril, and metoprolol on surrogatesf ventricular remodeling following 43 weeks of therapy in26 patients with heart failure. This small, mechanistictudy demonstrated a decrease in end-diastolic and systolicolumes and the largest improvement in ejection fractionmong patients utilizing the triple combination therapyompared with the others. This lent support to the improvedutcomes subsequently demonstrated in larger trials usingriple combination therapy.
The largest trial of ARBs in various heart failure popu-ations was the Candesartan in Heart Failure Assessment ofeduction in Mortality and Morbidity (CHARM) pro-ram.10 The investigators utilized a novel design enrollingbout 7600 patients in the research program into any of 3tudies: the CHARM-Added, CHARM-Preserved, andHARM-Alternative trials.11-13 Pooled data on all patientsere reported in the CHARM-Overall study.10 TheHARM-Added11 and CHARM-Preserved12 trials exam-
ned the use of triple combination therapy in heart failure,ith the latter enrolling patients with heart failure and
jection fraction �40% (ie, diastolic heart failure). TheHARM-Added trial demonstrated the benefits of addingandesartan to ACE inhibitors and beta-blockers (whichere administered in 100% and 55% of study patients,
espectively): a 15% reduction in the combined endpoint ofardiovascular death and heart failure hospitalization (P �011) compared with placebo was observed.11 Patients re-eiving all 3 agents (n � 702) demonstrated significantenefits with �20% reduction in the combined cardiovas-ular endpoint vs. placebo (P �.05).11 The CHARM-pre-erved trial addressed the use of candesartan in patients witheart failure and preserved ejection fraction on top of back-round therapy with ACE inhibitors and beta-blockers (ad-inistered to 20% and 56% of patients, respectively).12
his trial, with a relatively higher enrollment of femaleatients (40%) (Table 1), demonstrated a 16% borderline-ignificant reduction in heart failure hospitalization withandesartan (P � .047) but no impact on mortality. Amaller number of patients in the CHARM-Preserved trialeceived triple therapy and the addition of an ARB was not
ssociated with adverse cardiovascular outcomes.12 Taken wogether, the CHARM-Added and -Preserved trials refutedhe previous post hoc findings of Val-HeFT of potentialarm from combining ACE inhibitor, ARB, and beta-locker therapy in heart failure. In CHARM-Added andHARM-Preserved, 17.4% and 11.3% of patients in the
reatment arms received spironolactone, respectively. Theroportions of patients who received all 4 classes of medi-ations together were not reported.
The Valsartan in Acute Myocardial Infarction TrialVALIANT) evaluated the effects of valsartan, captopril,nd their combination in 14,703 patients with recent myo-ardial infarction and systolic dysfunction.9 Although theombination of both medications (with a background of0% beta-blocker therapy) did not confer an incrementalenefit to either alone, valsartan was shown to be noninfe-ior to captopril after a median follow-up of 25 months andas well tolerated.9 VALIANT demonstrated augmented
dverse effects when the combination of valsartan and cap-opril was employed.9
Another issue facing clinicians caring for patients witheart failure and recent myocardial infarction is the choicef agent to be added to an ACE inhibitor and a beta-blocker:n ARB or an aldosterone antagonist? Two trials demon-trated robust cardiovascular effects (on top of beta-block-rs and ACE inhibitors) of aldosterone antagonists in bothettings.14,15 The Randomized Aldactone Evaluation StudyRALES) demonstrated a 30% reduction in mortality withhe use of spironolactone in over 1600 patients with ad-anced heart failure.14 In that study, initially reported in999, 95% of the patients were treated with ACE inhibitors;owever, only 11% received beta-blockers. The Eplerenoneost-Acute Myocardial Infarction Heart Failure Efficacynd Survival Study (EPHESUS) demonstrated benefits ofdding eplerenone, a selective aldosterone antagonist, toCE inhibitors or ARBs (in 87% of patients) and beta-lockers (75%), including a 15% and 17% reduction inverall and cardiovascular mortality, respectively.15
DVERSE EFFECTS OF COMBININGEUROENDOCRINE INHIBITORSespite the benefits of combining neuroendocrine inhibitors
n heart failure, a multitude of side effects might limit theirse (Table 3). Clinicians should therefore balance theirenefits against their side effects.
YPOTENSIONn addition to the renin-angiotensin-aldosterone system in-ibitors, diuretics, nitrates, and other vasodilators mayause hypotension. In the CHARM-Added and -Preservedreatment arms,11,12 the blood pressure decreased signifi-antly more than with placebo, causing discontinuation ofhe study medication in 4.5% and 2.4% of patients, respec-ively. In VALIANT,9 more patients in the valsartan/capto-ril arm discontinued treatment due to hypotension than inhe captopril arm (1.9% vs 0.8%, P � .05). However, there
as no differential increase in hypotension in the Val-HeFT
tb(ba
HWtlumitVCotwEicwnsmwiilmaamlC(AnpEa
RAtnsoocCc(oab
le3
Com
pari
son
ofSi
deEf
fect
sin
Vari
ous
Tria
lsCo
mbi
ning
Neur
oend
ocri
neIn
hibi
tor
Ther
apy
Val-
HeF
TVA
LIAN
TCH
ARM
-Add
edCH
ARM
-Pre
serv
edRA
LES
EPH
ESU
S
ypot
ensi
on1.
3%vs
0.8%
(P�
.124
)1.
9%vs
0.8%
(P�
.05)
4.5%
vs3.
1%(P
�.0
79)
2.4%
vs1.
1%(P
�.0
09)
Nosi
gnifi
cant
chan
ges
betw
een
grou
psBP
incr
ease
dm
ore
inth
etr
eatm
ent
grou
p(P
�0.
01)
yper
kale
mia
K�le
vels
:1
0.12
vs2
0.07
mm
ol/L
(P�
.001
)
0.2%
vs0.
1%(N
S)34
%vs
0.7%
(P�
.000
1)1.
5%vs
0.6%
(P�
.029
)K�
leve
l:1
0.30
mm
ol/L
inac
tive
trea
tmen
tar
m(P
�.0
01)
K��
6m
mol
/L:
2%vs
1%(N
S)
K�le
vels
:1
0.30
vs1
0.2
mm
ol/
L(P
�.0
01)
K��
6m
mol
/L:
5.5%
vs3.
9%(P
�.0
02)
enal
impa
irm
ent
1.1%
vs0.
2%(P
�.0
01)
1.3%
vs0.
8%(P
�.0
5)7.
8%vs
4.1%
P�
.000
14.
8%vs
2.4%
P�
.000
5Cr
leve
l:1
0.05
-0.1
0in
acti
vetr
eatm
ent
arm
(P�
.001
)
Crle
vel:
10.
06vs1
0.02
mg/
dL(P
�.0
01)
otal
drop
out
rate
10%
vs7%
(P�
.001
)23
%vs
22%
*(P
�.0
5)*9
%vs
8%du
eto
adve
rse
drug
even
t(P
�.0
5)
24.2
vs18
.3(P
�.0
003)
17.8
vs13
.5(P
�.0
01)
8%vs
5%(P
�NS
)15
.9%
vs14
.9%
(P�
NS)
Val-
HeF
T�
Vals
arta
nH
eart
Failu
reTr
ial;
VALI
ANT
�Va
lsar
tan
inAc
ute
Myo
card
ialI
nfar
rtio
nTr
ial;
CHAR
M�
Cand
esar
tan
inH
eart
Failu
reAs
sess
men
tof
Redu
ctio
nin
Mor
talit
yan
dM
orbi
dity
;RA
LES
�an
dom
ized
Alda
cton
eEv
alua
tion
Stud
y;EP
HES
US
�Ep
lere
none
Post
-Acu
teM
yoca
rdia
lIn
farr
tion
Hea
rtFa
ilure
Effic
acy
and
Surv
ival
Stud
y;BP
�bl
ood
pres
sure
;Cr
�cr
eati
nine
;K�
�po
tass
ium
.Ra
tes
fdi
scon
tinu
atio
nof
stud
ydr
ugdu
eto
side
effe
cts.
Allco
mpa
riso
nsar
eac
tive
trea
tmen
tvs
.pl
aceb
o.
1090.e5Jneid et al Combining Neuroendocrine Inhibitors
rial,7 possibly because of lesser (35%) utilization of beta-lockers compared with the CHARM (55%) and VALIANT70%) trials. Conversely, the addition of an aldosteronelocker did not adversely affect blood pressure in RALES14
nd EPHESUS.15
YPERKALEMIAhen multiple neuroendocrine inhibitors are combined,
hey have increased propensity to raise serum potassiumevels. This may be detrimental in patients with heart fail-re, who possess higher predilection for serious arrhyth-ias.26 Minor elevations of potassium levels were observed
n Val-HeFT;7 however, RESOLVD (Randomized Evalua-ion of Strategies for Left Ventricular Dysfunction)8 andALIANT9 demonstrated only nonsignificant trends. InHARM-Added11 and Charm-Preserved,12 discontinuationf the study drug due to hyperkalemia was more frequent inhe treatment groups. Hyperkalemia also is a major concernhen adding aldosterone antagonists. In RALES andPHESUS, the average increase in serum potassium levels
n the treatment groups was 0.3 mmol/L;14,15 and the in-reased incidence of serious hyperkalemia (�6.0 mmol/L)ith the aldosterone blocker, although not statistically sig-ificant in RALES,14 was significant in the EPHESUStudy,15 where patients with creatinine clearance �70 mL/in or potassium level �5.5 mmol/L at 1-week follow-upere at higher risk. Juurlink et al27 showed a significant
ncrease in hyperkalemia-associated morbidity and mortal-ty, attributed to increased spironolactone prescription fol-owing the publication of RALES. To minimize hyperkale-ia, guidelines recommend checking serum potassium 3
nd 7 days following initiation of an aldosterone antagonist,t least monthly for the first 3 months, and then every 3onths. Similar monitoring schedule is recommended fol-
owing dose adjustment of an ACE inhibitor or ARB.28
linicians should screen patients for predisposing factorsrenal insufficiency, diabetes, use of ACE inhibitor orRB), and use appropriate doses of aldosterone antago-ists.29-31 Patients with serum creatinine �2.5 mg/dL orotassium �5.0 mmol/L were excluded from RALES andPHESUS.14,15 Thus, aldosterone antagonists should bevoided in these patients.
ENAL IMPAIRMENTnearly 20% increase in serum creatinine is expected with
he use of ACE inhibitors, ARBs, and aldosterone antago-ists. In RALES, EPHESUS, and Val-HeFT, an increase inerum creatinine ranging from 0.05 to 0.18 mg/dL wasbserved.7,14,15 There was a significantly higher incidencef discontinuation of the study medication due to risingreatinine in the treatment arms of the VALIANT9 andHARM-Added trials.11 Patients with preexisting signifi-ant renal impairment were excluded from the clinical trialscreatinine �3.0 mg/dL in CHARM and �2.5 mg/dL in thethers).7-10,14,15 Given that renal insufficiency is an inde-
pendent risk factor for cardiovascular disease32 and is as-
T H H R T R o
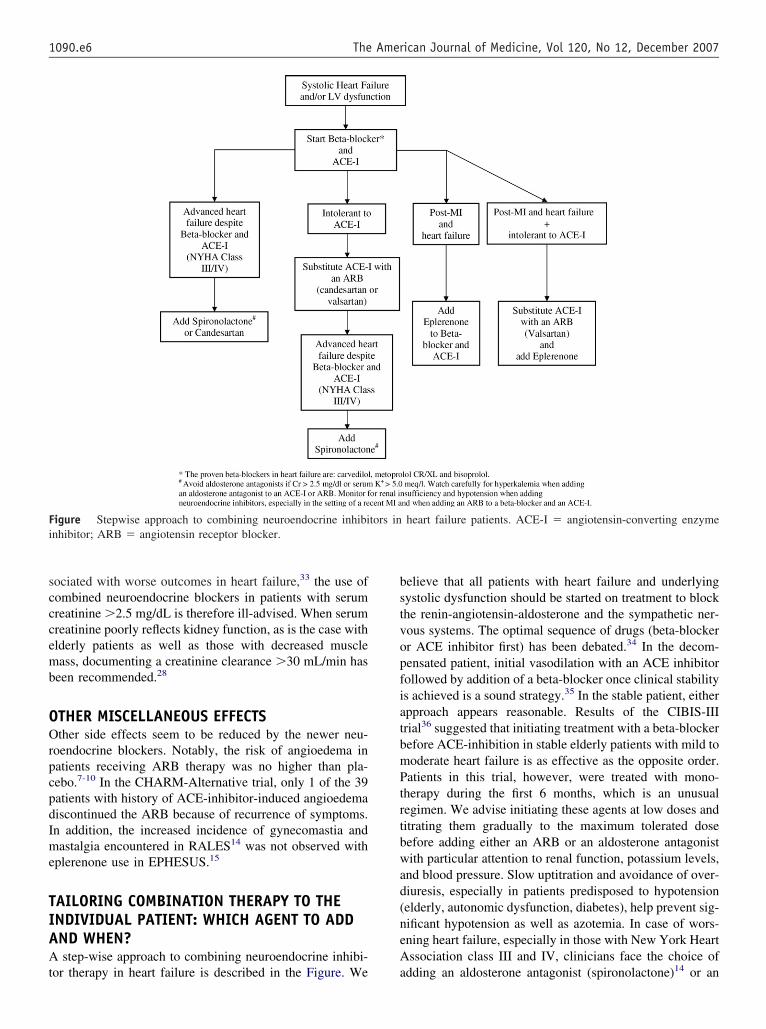
scccemb
OOrpcpdIme
TIAAt
bstvopfiatbmPtrtbwad(neA
Fi
1090.e6 The American Journal of Medicine, Vol 120, No 12, December 2007
ociated with worse outcomes in heart failure,33 the use ofombined neuroendocrine blockers in patients with serumreatinine �2.5 mg/dL is therefore ill-advised. When serumreatinine poorly reflects kidney function, as is the case withlderly patients as well as those with decreased muscleass, documenting a creatinine clearance �30 mL/min has
een recommended.28
THER MISCELLANEOUS EFFECTSther side effects seem to be reduced by the newer neu-
oendocrine blockers. Notably, the risk of angioedema inatients receiving ARB therapy was no higher than pla-ebo.7-10 In the CHARM-Alternative trial, only 1 of the 39atients with history of ACE-inhibitor-induced angioedemaiscontinued the ARB because of recurrence of symptoms.n addition, the increased incidence of gynecomastia andastalgia encountered in RALES14 was not observed with
plerenone use in EPHESUS.15
AILORING COMBINATION THERAPY TO THENDIVIDUAL PATIENT: WHICH AGENT TO ADDND WHEN?step-wise approach to combining neuroendocrine inhibi-
igure Stepwise approach to combining neuroendocrine inhibinhibitor; ARB � angiotensin receptor blocker.
or therapy in heart failure is described in the Figure. We a
elieve that all patients with heart failure and underlyingystolic dysfunction should be started on treatment to blockhe renin-angiotensin-aldosterone and the sympathetic ner-ous systems. The optimal sequence of drugs (beta-blockerr ACE inhibitor first) has been debated.34 In the decom-ensated patient, initial vasodilation with an ACE inhibitorollowed by addition of a beta-blocker once clinical stabilitys achieved is a sound strategy.35 In the stable patient, eitherpproach appears reasonable. Results of the CIBIS-IIIrial36 suggested that initiating treatment with a beta-blockerefore ACE-inhibition in stable elderly patients with mild tooderate heart failure is as effective as the opposite order.atients in this trial, however, were treated with mono-
herapy during the first 6 months, which is an unusualegimen. We advise initiating these agents at low doses anditrating them gradually to the maximum tolerated doseefore adding either an ARB or an aldosterone antagonistith particular attention to renal function, potassium levels,
nd blood pressure. Slow uptitration and avoidance of over-iuresis, especially in patients predisposed to hypotensionelderly, autonomic dysfunction, diabetes), help prevent sig-ificant hypotension as well as azotemia. In case of wors-ning heart failure, especially in those with New York Heartssociation class III and IV, clinicians face the choice of
heart failure patients. ACE-I � angiotensin-converting enzyme
tors indding an aldosterone antagonist (spironolactone)14 or an

Ahtasr(acs
tbmatcii
aAacecis
ahst
cdtpwpluw(ncawadnrrtep
tsss
CFbnsimwcAiibatems
R
1
1
1090.e7Jneid et al Combining Neuroendocrine Inhibitors
RB (candesartan)11 to their dual therapy. If patients witheart failure are intolerant to ACE inhibitors, the substitu-ion with an ARB (valsartan or candesartan) is appropri-te.9,13 When started on an ACE inhibitor, ARB, or aldo-terone antagonists, close monitoring of electrolytes andenal function should be undertaken. Nephrotoxic agentssuch as nonsteroidal anti-inflammatory drugs) should bevoided and potassium supplements discontinued or de-reased substantially, depending on the follow-up potas-ium levels.
If a patient’s symptoms deteriorate while on chronicherapy, it is recommended to continue treatment with beta-locker at the same dose or reduce the current dose mo-entarily while undergoing therapy for congestion and ex-
cerbating factors. Abrupt withdrawal of beta-blockerherapy should be avoided.37 If the patient is symptomati-ally hypotensive, then one should ascertain that the patients not hypovolemic from overdiuresis. If not, then the ACEnhibitor dose could be reduced.
In the post-myocardial-infarction patients, eplerenonend not an ARB9 should be added to a beta-blocker and anCE-inhibitor within the first few days (3 to 14 days after
cute myocardial infarction) if the patient is stable andontinued for at least 16 months.15 Probably, the soonerplerenone is added, the better. If patients with postmyo-ardial infarction heart failure are intolerant to ACE inhib-tor, an ARB (valsartan) appears to be an appropriateubstitute.9
In patients with diastolic heart failure, candesartan isssociated with moderately lower incidence of heart failureospitalization.12 There is otherwise a paucity of evidenceupporting the preferential use of one drug over the other inhis setting.
The vast majority of data on ARBs include valsartan andandesartan, so that one should strive to use these 2 in theoses prescribed in the clinical trials.7,9-12 The ARB losar-an, given at a dose of 50 mg once daily, did not showromising results when compared with captopril in patientsith heart failure (ELITE II)38 and systolic dysfunctionostmyocardial infarction (OPTIMAAL),39 probably re-ated to the low dose of losartan utilized in these trials. It isnknown whether better results may have been achievedith higher doses. The other members of the ARB class
irbesartan, telmesartan, olmesartan, and eprosartan) haveot been extensively studied in heart failure. It also seemslear that ACE inhibitors and ARBs are reasonably equiv-lent with regard to efficacy, but they are not equivalentith regard to the mechanism of action and patient toler-
nce. In addition, there are few data using all 4 classes ofrugs together, which could be unsafe. It also is important toote that certain patient subpopulations are always under-epresented in clinical trials. For example, women and Af-ican-Americans constitute less than 30% and 5%, respec-ively, of patients enrolled in various trials. The safety andfficacy of neuroendocrine inhibitors in these patient sub-
opulations are still unclear.7-15 In blacks with heart failure,he benefit of adding isosorbide dinitrate and hydralazine totandard treatment with beta-blockers and ACE inhibitors isupported by evidence from the A-HeFT trial, showing atriking 43% relative risk reduction in mortality.40
ONCLUSIONor most patients with heart failure, the principal goal is tolock the renin-angiotensin-aldosterone and the sympatheticervous systems. The current literature clearly supports theafety and efficacy of therapy with beta-blockers and ACEnhibitors in systolic heart failure. The ARB candesartanay provide incremental benefit when added to therapyith a beta-blocker and an ACE inhibitor. Spironolactone
an be added to a beta-blocker and an ACE inhibitor orRB for patients with severe heart failure. Post-myocardial-
nfarction patients with heart failure may benefit from add-ng eplerenone to an ACE inhibitor or ARB, and a beta-locker. Valsartan and candesartan appear to be reasonablelternatives to an ACE inhibitor for postmyocardial infarc-ion and chronic heart failure, respectively. Renal function,lectrolytes, and blood pressure of patients started andaintained on triple neuroendocrine inhibitor therapy
hould be closely monitored.
eferences1. Packer M, Bristow MR, Cohn JN, et al. The effect of carvedilol on
morbidity and mortality in patients with chronic heart failure. U.S.Carvedilol Heart Failure Study Group. N Engl J Med. 1996;334(21):1349-1355.
2. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a random-ised trial. Lancet. 1999;353(9146):9-13.
3. Effect of metoprolol CR/XL in chronic heart failure: MetoprololCR/XL Randomised Intervention Trial in Congestive Heart Failure(MERIT-HF). Lancet. 1999;353(9169):2001-2007.
4. Effect of enalapril on survival in patients with reduced left ventricularejection fractions and congestive heart failure. The SOLVD Investi-gators. N Engl J Med. 1991;325(5):293-302.
5. Pfeffer MA, Braunwald E, Moye LA, et al. Effect of captopril onmortality and morbidity in patients with left ventricular dysfunctionafter myocardial infarction. Results of the survival and ventricularenlargement trial. The SAVE Investigators. N Engl J Med. 1992;327(10):669-677.
6. Effect of ramipril on mortality and morbidity of survivors of acutemyocardial infarction with clinical evidence of heart failure. TheAcute Infarction Ramipril Efficacy (AIRE) Study Investigators. Lan-cet. 1993;342(8875):821-828.
7. Cohn JN, Tognoni G. A randomized trial of the angiotensin-receptorblocker valsartan in chronic heart failure. N Engl J Med. 2001;345(23):1667-1675.
8. McKelvie RS, Rouleau JL, White M, et al. Comparative impact ofenalapril, candesartan or metoprolol alone or in combination on ven-tricular remodelling in patients with congestive heart failure. EurHeart J. 2003;24(19):1727-1734.
9. Pfeffer MA, McMurray JJ, Velazquez EJ, et al. Valsartan, captopril, orboth in myocardial infarction complicated by heart failure, left ven-tricular dysfunction, or both. N Engl J Med. 2003;349(20):1893-1906.
0. Pfeffer MA, Swedberg K, Granger CB, et al. Effects of candesartan onmortality and morbidity in patients with chronic heart failure: theCHARM-Overall programme. Lancet. 2003;362(9386):759-766.
1. McMurray JJ, Ostergren J, Swedberg K, et al. Effects of candesartanin patients with chronic heart failure and reduced left-ventricularsystolic function taking angiotensin-converting-enzyme inhibitors: the
CHARM-Added trial. Lancet. 2003;362(9386):767-771.
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
1090.e8 The American Journal of Medicine, Vol 120, No 12, December 2007
2. Yusuf S, Pfeffer MA, Swedberg K, et al. Effects of candesartan inpatients with chronic heart failure and preserved left-ventricular ejec-tion fraction: the CHARM-Preserved Trial. Lancet. 2003;362(9386):777-781.
3. Granger CB, McMurray JJ, Yusuf S, et al. Effects of candesartan inpatients with chronic heart failure and reduced left-ventricular systolicfunction intolerant to angiotensin-converting-enzyme inhibitors: theCHARM-Alternative trial. Lancet. 2003;362(9386):772-776.
4. Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone onmorbidity and mortality in patients with severe heart failure. Random-ized Aldactone Evaluation Study Investigators. N Engl J Med. 1999;341(10):709-717.
5. Pitt B, Remme W, Zannad F, et al. Eplerenone, a selective aldosteroneblocker, in patients with left ventricular dysfunction after myocardialinfarction. N Engl J Med. 2003;348(14):1309-1321.
6. Francis GS, Tang WH. Pathophysiology of congestive heart failure.Rev Cardiovasc Med. 2003;4(Suppl 2):S14-S20.
7. Mann DL, Kent RL, Parsons B, Cooper G. Adrenergic effects on thebiology of the adult mammalian cardiocyte. Circulation. 1992;85(2):790-804.
8. Weber KT. Aldosterone in congestive heart failure. N Engl J Med.2001;345(23):1689-1697.
9. Sharma JN. Does the kinin system mediate in cardiovascular abnor-malities? An overview. J Clin Pharmacol. 2003;43(11):1187-1195.
0. Matsusaka T, Ichikawa I. Biological functions of angiotensin and itsreceptors. Annu Rev Physiol. 1997;59:395-412.
1. Cruden NL, Witherow FN, Webb DJ, et al. Bradykinin contributes tothe systemic hemodynamic effects of chronic angiotensin-convertingenzyme inhibition in patients with heart failure. Arterioscler ThrombVasc Biol. 2004;24(6):1043-1048.
2. Falkenstein E, Christ M, Feuring M, Wehling M. Specific nongenomicactions of aldosterone. Kidney Int. 2000;57(4):1390-1394.
3. Struthers AD. The clinical implications of aldosterone escape in con-gestive heart failure. Eur J Heart Fail. 2004;6(5):539-545.
4. Lee AF, MacFadyen RJ, Struthers AD. Neurohormonal reactivation inheart failure patients on chronic ACE inhibitor therapy: a longitudinalstudy. Eur J Heart Fail. 1999;1(4):401-406.
5. Schrier RW, Abraham WT. Hormones and hemodynamics in heartfailure. N Engl J Med. 1999;341(8):577-585.
6. Zipes DP, Wellens HJ. Sudden cardiac death. Circulation. 1998;98(21):2334-2351.
7. Juurlink DN, Mamdani MM, Lee DS, et al. Rates of hyperkalemiaafter publication of the Randomized Aldactone Evaluation Study.N Engl J Med. 2004;351(6):543-551.
8. Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 GuidelineUpdate for the Diagnosis and Management of Chronic Heart Failure in
the Adult: a report of the American College of Cardiology/AmericanHeart Association Task Force on Practice Guidelines (WritingCommittee to Update the 2001 Guidelines for the Evaluation andManagement of Heart Failure): developed in collaboration with theAmerican College of Chest Physicians and the International Societyfor Heart and Lung Transplantation: endorsed by the Heart RhythmSociety. Circulation. 2005;112(12):e154-e235.
9. Svensson M, Gustafsson F, Galatius S, et al. Hyperkalaemia andimpaired renal function in patients taking spironolactone for conges-tive heart failure: retrospective study. BMJ. 2003;327(7424):1141-1142.
0. Wrenger E, Muller R, Moesenthin M, et al. Interaction of spironolac-tone with ACE inhibitors or angiotensin receptor blockers: analysis of44 cases. BMJ. 2003;327(7407):147-149.
1. Jarman PR, Kehely AM, Mather HM. Hyperkalaemia in diabetes:prevalence and associations. Postgrad Med J. 1995;71(839):551-552.
2. Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and therisks of death, cardiovascular events, and hospitalization. N EnglJ Med. 2004;351(13):1296-1305.
3. McAlister FA, Ezekowitz J, Tonelli M, Armstrong PW. Renal insuf-ficiency and heart failure: prognostic and therapeutic implications froma prospective cohort study. Circulation. 2004;109(8):1004-1009.
4. Fang JC. Angiotensin-converting enzyme inhibitors or beta-blockersin heart failure: does it matter who goes first? Circulation. 2005;112(16):2380-2382.
5. Johnson W, Omland T, Hall C, et al. Neurohormonal activation rapidlydecreases after intravenous therapy with diuretics and vasodilators forclass IV heart failure. J Am Coll Cardiol. 2002;39(10):1623-1629.
6. Willenheimer R, van Veldhuisen DJ, Silke B, et al. Effect on survivaland hospitalization of initiating treatment for chronic heart failure withbisoprolol followed by enalapril, as compared with the opposite se-quence: results of the randomized Cardiac Insufficiency BisoprololStudy (CIBIS) III. Circulation. 2005;112(16):2426-2435.
7. Heart Failure Society of America 2006 Comprehensive Heart FailurePractice Guideline. J Card Fail. 2006;12(1):e1-e122.
8. Pitt B, Poole-Wilson PA, Segal R, et al. Effect of losartan comparedwith captopril on mortality in patients with symptomatic heart failure:randomised trial—the Losartan Heart Failure Survival Study ELITE II.Lancet. 2000;355(9215):1582-1587.
9. Dickstein K, Kjekshus J. Effects of losartan and captopril on mortalityand morbidity in high-risk patients after acute myocardial infarction:the OPTIMAAL randomised trial. Optimal Trial in Myocardial Infarc-tion with Angiotensin II Antagonist Losartan. Lancet. 2002;360(9335):752-760.
0. Taylor AL, Ziesche S, Yancy C, et al. Combination of isosorbidedinitrate and hydralazine in blacks with heart failure. N Engl J Med.
2004;351(20):2049-2057.
ATsAm
F
PFPDa
Bc
DAo
Imtmrobipirgachst
wgf
DdW
APMPerspectives
0d
PM Perspectiveshe Association of Professors of Medicine (APM) is the national organization of departments of internal medicine at the US medicalchools and numerous affiliated teaching hospitals as represented by chairs and appointed leaders. As the official sponsor of Themerican Journal of Medicine, the association invites authors to publish commentaries on issues concerning academic internaledicine.
or the latest information about departments of internal medicine, please visit APM’s website at www.im.org/APM.
redicting, Preparing for, and Creating theuture: What Will Happen to Internal Medicine?
aul A. Hemmer, MD,a Sheila T. Costa, MA,b Deborah M. DeMarco, MD,c Stuart L. Linas, MD,d
on C. Glazier, MPH,e Barbara L. Schuster, MDf
Department of Medicine, Uniformed Services University of the Health Sciences F. Edward Hébert School of Medicine,ethesda, Md; bDepartment of Meetings and Communications, Alliance for Academic Internal Medicine, Washington, DC;
Department of Graduate Medical Education, University of Massachusetts Medical School, Worcester; dDivision of Renaliseases and Hypertension, Department of Medicine, University of Colorado School of Medicine, Denver; eFinance anddministration, Department of Medicine, Oregon Health and Science University School of Medicine, Portland; fDepartment
f Internal Medicine, Wright State University Boonshoft School of Medicine, Dayton, Ohio.pttcpcTmbtii
Iadtbsle
tcc
t is the year 2025. During the past 20 years, internaledicine as a discipline continued to become less pres-
igious, less respected, and more fragmented. As feweredical students chose internal medicine as a career,
esidency programs began to close. Those that remainedpen filled with fewer graduates of US medical schoolsut filled with more US citizens who graduated fromnternational medical schools, more graduates of osteo-athic medical schools, and more foreign graduates ofnternational medical schools. Due to lack of adequateemuneration and a shift of primary care provision fromeneralist physicians to nurse practitioners and physicianssistants, training in general internal medicine as a patientare specialty ceased. Generalist internal medicine careersave been replaced by tracks designed to foster healthervices research or academic careers; internal medicineraining graduates subspecialty physicians.
Although the projected collapse of Medicare in 2019as avoided, severe cuts in federal funding for under-raduate and graduate medical education programsorced medical schools and residency programs to com-
Requests for reprints should be addressed to Sheila T. Costa, MA,epartment of Meetings and Communications, Alliance for Aca-emic Internal Medicine (AAIM), 2501 M Street, NW, Suite 550,ashington, DC 20037-1325.
tE-mail address: [email protected].
002-9343/$ -see front matter © 2007 The Association of Professors of Meoi:10.1016/j.amjmed.2007.09.013
ete for federal funds. As a result, medical schooluition became prohibitive, for-profit health care sys-ems viewed medical education as a significant costenter and chose to limit the size of their residencyrograms, and community-based training programsould not withstand the financial pressures and closed.he result was a reduced supply of internists. Further-ore, compliance with the regulatory burden imposed
y accrediting organizations—such as the Accredita-ion Council for Graduate Medical Education—drovendividuals from sustained careers in education, furthermpacting the viability of training programs.
At the same time, federal funding for the Nationalnstitutes of Health (NIH) has been severely restricted,nd the US research enterprise has become increasinglyependent on the pharmaceutical industry, the private sec-or (including foundations), or specific projects endorsedy federal research supporters. Few internists opt for re-earch careers because the risk is high while the fundingevels are low. More research is performed by basic sci-ntists and PhDs in departments of internal medicine.
In 2025, it appears that the quality and safety of inpa-ient care may have improved as more residents havehosen hospital medicine as a career; however, patientsomplain about the lack of continuity in their care in both
he ambulatory and inpatient setting. More than one halfdicine. All rights reserved.

oiran
tiUsmUwibnpBpmwd
fitpmoirbscfs
AositmiPclooeAp
tte
fiui“
pic
EAsiPpa(ivpst
tabcvp
gib
1092 The American Journal of Medicine, Vol 120, No 12, December 2007
f the nation’s citizens have insufficient or no healthnsurance; the failure to address the obesity epidemic hasesulted in an enormous burden of complex illness inmbulatory and inpatient settings. The cost of health careow exceeds 20% of the gross national product.
This bleak scenario ishe current trajectory ofnternal medicine in thenited States and repre-
ents a logical outcome ofaintaining the status quo.nless the discipline as ahole is willing to change,
nternal medicine will likelyecome increasingly insig-ificant in the practice androvision of medical care.ut what might the otherossible futures of internaledicine look like and inhich direction should theiscipline head?
In fall 2005, the Allianceor Academic Internal Med-cine (AAIM) charged aask force to consider theossible futures of internaledicine. As the largest academically focused specialty
rganization, AAIM is uniquely positioned to influencenternal medicine and the health care system through itsoles in education, research, and patient care. Representedy AAIM, departments of internal medicine at medicalchools and teaching hospitals represent 27% of full-timelinical faculty,1 teach nearly 30% of all residents andellows,2 and conduct the most industry and NIH-spon-ored research (28% of all extramural awards).3
Inspired by the International Campaign to Revitalisecademic Medicine,4 the task force used the techniquef scenario planning to develop and reflect on the pos-ible changes for internal medicine. Scenario plannings “a disciplined method for imagining possible futures”hat examines multiple aspects of an issue, considersultiple, simultaneous changes, and applies subjective
nterpretations of objective analyses.5 According toaul J.H. Schoemaker, “scenario planning attempts toapture the richness and range of possibilities, stimu-ating decision makers to consider changes they wouldtherwise ignore. At the same time, scenario planningrganizes those possibilities into narratives that areasier to grasp and use than great volumes of data.bove all, the scenarios are aimed at challenging therevailing mind-set.”5
In beginning its work, the task force found it usefulo describe 2 extremes. In the “Doomsday” scenario,errorism and the federal debt have reduced the gov-
PERSPECTIVES VIEW
● Using the basic tplanning, several pfor the future of intpresented.
● The scenarios coverbilities, from the comedicine to the“superinternist.”
● The common themefuture of academic inexamined as well ainternists to considefuture.
rnment to focusing on only what is essential, with all s
unding eliminated for education and research, limitednterventions to sustain life (eg, no dialysis and limitedse of intensive care units), the end of health carensurance for Americans, and virtually no internists. InUtopia,” medical education and research are fully
funded, all Americans have full andequal access to care, and internalmedicine is the model for educa-tion, research, and patient care,leading to resurgence in respect andinterest in the discipline.
Envisioning these unlikely ex-tremes led to the development of 6scenarios for the future of internalmedicine: Status Quo, Evolution,Revolution, Science Fiction, TheGeneralist Returns, and Global. Ineach scenario, the task force tried toaddress the effects of the envisionedfuture on education, research, pa-tient care, academic internal medi-cine, and the discipline of internalmedicine itself. Neither the taskforce nor AAIM endorses any ofthese scenarios but simply providesthe scenarios as a stimulus for con-tinued discussion. If even one as-
ect of a single scenario becomes reality, internal med-cine as whole will be better prepared for havingonsidered the myriad possibilities.
VOLUTIONn enlightenment on the part of legislators and con-
umers about the importance and role of internal med-cine results in a more specialized hierarchy of care.rimary care is provided by midlevel providers, such ashysician assistants and nurse practitioners, working onteam with an ambulatory internist. Secondary care
which involves the care of patients with complex med-cal problems and includes geriatric medicine) is pro-ided by internists outside the hospital. Tertiary care isrovided by internists (including hospitalists and sub-pecialists) in the hospital. Quarternary care, such asransplant medicine, occurs only in regional centers.
Redistribution of public and private funding ensureshat all internists—general internists and subspecialistslike—are paid more equitably. Performance-based payecomes the standard. Procedural subspecialties be-ome more cognitive because of technological ad-ances that allow midlevel providers to do many of therocedures.
Undergraduate and graduate medical education pro-rams develop innovative ways to improve accessibil-ty to teachers, provide better role models, train office-ased professionals for their roles, and ensure that
TS
of scenariotial outcomesmedicine are
nge of possi-e of academicnology-driven
arent for thel medicine arenecessity forto shape the
POIN
enetsotenernal
a rallapstech
s appterna
s ther how
tudents and residents have equal access to training in

tcla
psqrTotb
ectpslpf
RPbsccfmc
pcfsbscmsbr
esmsrttlg
e
ptspaacmca
sdtlIhEMet
sia(e
dtoefsdmSpr
SG22cwdirssci
m
1093Hemmer et al The Future of Internal Medicine
he hospital and the ambulatory setting. Residents re-eive explicit training in principles of effective ambu-atory team leadership and management practices, withn emphasis on health services delivery.
Research is directed toward outcomes-based care,atient safety, and quality. Few internists perform basiccience or clinical research because of increasing re-uirements for patient care. However, translationalesearch, especially from bench to patient, increases.o meet the demands of ensuring and measuringutcomes and performance, combined medical doc-or-masters of public health (MD-MPH) programsecome more prevalent.
Patient safety and quality of care increase as doesfficiency, access, and patient satisfaction. As physi-ian outcome data become more readily available, pa-ients use this information to choose providers andractices. Ambulatory internists will have greater over-ight responsibilities as more care is conducted by mid-evel providers. Advances in technology will improveatient information portability, make telemedicine moreeasible, and advance rural health care.
EVOLUTIONublic demand for more internists and the crushingurden of student debt combine to call for shorter, morepecialized training. In response, the internal medicineommunity elects to focus almost entirely on inpatientare; as a direct result, internal medicine educationragments. Hospital medicine and subspecialty internaledicine create their own residencies, to which medi-
al students match directly out of medical school.Meanwhile, the internal medicine clerkship disap-
ears and is replaced by 2 months of inpatient adultare; a requirement to follow x number of patients oramilies during the course of a year; rotations in sub-pecialty disciplines for x number of weeks, or a com-ination of these models. For example, a standard set ofubspecialty experiences embedded in a longitudinallinical experience becomes the standard. The last 6onths of medical school become a “real” subintern-
hip as students matched to a subspecialty residencyegin to fulfill core requirements and competencies foresidency in the final months of medical school.
During residency training, no continuity outpatientxposure occurs beyond the context of the selectedubspecialty training. Ambulatory competencies com-on to the care of all adults would be expanded in
ubspecialty-specific education. The current model ofeimbursing residents and fellows would likely extendo subspecialty residents. As a result of these changes,he overall length of training decreases, which requiresess graduate medical education funding and allowsraduates to begin to repay their loans more quickly.
General internal medicine as a unique outpatient
xpertise ceases to exist. In the inpatient setting, hos- aitalists—with subspecialty consultation—care for pa-ients with complex, multisystem disease. Family phy-icians, physician assistants, and nurse practitionersrovide routine ambulatory care as well as preventivend primary care for noncomplex problems, includingcute illnesses (such as urinary tract infections) andhronic diseases (such as stable asthma and dyslipide-ia). With assistance from midlevel providers, subspe-
ialists care for more complex and unstable illnesses indisease management model.Departments of internal medicine disappear as
ubspecialties have their own departments and resi-ency programs. Interdisciplinary, disease-specific cen-
ers proliferate, as do departments of hospital medicineed by the “general internist.” The American Board ofnternal Medicine evolves to certify subspecialties andospital medicine. The Liaison Committee on Medicalducation and Accreditation Council for Graduateedical Education work collaboratively to ensure that
nd-of-medical school experiences fulfill residency en-rance requirements.
In conjunction with interdisciplinary and disease-pecific centers, a new emphasis on translational med-cine appears. New methods and technologies are testedcross subspecialties. The current structure of NIHspecialty-directed institutes) transitions into more dis-ase-specific institutes.
The change in training increases competency butecreases scope of practice. Patients have direct accesso subspecialists, but this access, combined with a lackf knowledge among the patient population, increasesmergency department utilization or use of urgent careacilities managed by family physicians, physician as-istants, and nurse practitioners. Providers seeking aifferent practice environment will promote “boutiqueedicine,” but such practices are in the minority.6
ubspecialists often provide principal care to adultatients known to them through earlier subspecialty-elated care.
CIENCE FICTIONiven the drastic changes witnessed between 1985 and005, subsequent advances in technology by the year025 will completely alter the face of internal medi-ine. The proliferation of technology will decrease theorkforce needs of subspecialties, especially proce-ure-based subspecialists. The prevalence of geneticnformation, proteomics, imaging, pharmacogenetics,obotics, nanotechnology, laser surgery, and noninva-ive surgery make telemedicine and distance care main-tream. Testing and procedures are executed by techni-ians; the internist becomes “Dr. McCoy”: diagnostician,nterpreter, and manager for the patient.
Despite access to software and databases to helpanage the proliferation of science, internists require
dvanced understanding of modern scientific princi-

pspIiserboptsp
gpirtt
tatciPht(pppl
rsnct
TTitsatmaafsao
ctaipotnrTgapsilpgpltfl
tcomcHfc
tedwi
GThidigcdccls
s
1094 The American Journal of Medicine, Vol 120, No 12, December 2007
les, medical technology, and emerging as well as clas-ic disease entities. The specific internal medicine com-etency remains “finely honed diagnostic reasoning.”nternal medicine attracts “the best of the best,” restor-ng the respect and prestige of the discipline. Medicalchool curricula meld basic science with clinical sci-nce throughout all years of medical school, effectivelyeversing the trend of the late 20th century decrease inasic science education. Collaboration among collegesf medicine, nursing, pharmacy, and allied medicalrofessions becomes commonplace. Scientific educa-ion is central to postgraduate and continuing profes-ional education; clinical experience reverts to an ap-renticeship model.
Translational research increases significantly; inte-rative departments grow at the expense of traditionalhysiology, cell biology, and molecular biology. Clin-cal internists take an active role in developing theesearch agenda, establishing quality outcome parame-ers, and changing guidelines. Basic science is executedhrough collaborative, cross-institution teams.
Employers and federal government provide accesso health care through wellness centers. Results of di-gnostic investigations executed in the wellness centerriggers necessary physician visits. Costs are kept ac-eptable by incorporating only evidence-based testingn cost-effective centers. No personal physicians exist.atients accept the bulk of responsibility for their ownealth; technology provides in-home monitoring andhe ability to “plug in” for testing and diagnosticsblood draw, heart rate monitors). Preventive care andrimary care are provided by wellness centers. Afterreliminary diagnostics to address problems are com-leted in the local wellness center, patient data is up-inked to an internal medicine physician.
The internist is responsible for diagnosis, clinicaleasoning, and decision-making. Other medical andurgical interventions are assigned to procedural tech-icians. Specialist care is available only at regional careenters, which may be accessed through distanceechnology.
HE GENERALIST RETURNShe “medical home” for the adult patient is the general
nternist and a practice team.7 Internal medicine returnso the pre-NIH funding, pre-Medicare funding, pre-pecialty boards model of the 1960s and early 1970s:ll nonsurgical physicians who care for adults are in-ernists. In a 4-year paradigm for residency training, 24onths are dedicated to core training and 24 months are
n individualized track in an area of special interest;dditional training beyond 4 years would be requiredor “invasive” aspects of a subspecialty or for a re-earch track. Generalist reimbursement is more equiv-lent to specialty reimbursement, with incentives based
n outcomes and efficiency. uIn undergraduate medical education, internal medi-ine returns to power within the medical school struc-ure, teaching preclinical and clinical students. Studentsre increasingly interested in internal medicine becausenternists truly manage patient problems, are paid ap-ropriately for their expertise, and work in true collab-ration with subspecialists. Medical school is struc-ured like law school: the goal is only to teach students,ot worry about other academic issues (such as NIHankings). Faculty members are full-time educators.he medical school becomes smaller and more inte-rated into the university. Private practitioners teachnd supervise students and residents in communityractices and community hospitals. Faculty precept andupervise in the medical centers. Internal medicine res-dents spend their final (fourth) year of residency tai-oring their education to future practice (for example,ursuing masters’ degrees in business or public health);eneral internal medicine “fellowships” are common-lace. Current federal funding for residency and fel-owship would be redistributed to fund the 4 years ofraining. The model could also allow for full tuitionunding by the government; students would “pay back”oans with money or service.
Generalists increase their participation in transla-ional research, both inpatient and outpatient. Subspe-ialists routinely include a generalist expert on everyutcomes research collaborative. The removal of for-al research as an essential component of training
hanges the expectation of the “triple threat” internist.owever, the training model—which offers additional
unded training for individuals interested in researchareers—increases the number of physician-scientists.
Well-coordinated adult care becomes the norm. Pa-ient access to care increases, care delivery is morefficient, and costs of health care decrease as referralsecrease. This model provides better “holistic” care asell as offers a broader span of care by an individual
nternist.
LOBALhe United Nations agrees to manage and deliver basicealth care to all people in the world. All nations,ncluding the United States, agree to fund the effort asisease and terrorism pose threats to all. Each countrys assessed according to its resources. Additionally,lobal foundations contribute funds to pay for healthare. Cost-efficiency and effectiveness are the basis ofecisions about what services are delivered. Wealthierountries and affluent individuals are able to buy healthare above and beyond the basic provisions. Care de-ivery systems require a significant increase in nonphy-ician providers.
The United Nations implements worldwide medicalchool standards, competencies, and core curricula. Ed-
cation incorporates increased use of technology, in-
ciao“stwlP
stwpGs
fldaic
DIsSgoslwaatti
owAtDc
●
●
●
●
●
●
●
tssirpac
ssdwsimcpsssgo
acaotiCmw
1095Hemmer et al The Future of Internal Medicine
luding the “virtual medical school.”8 Worldwide med-cal school accreditation, certification, and licensinglso exist. Admission to medical school is availablenly through regional competition, effectively endingbuying” admission. A single-language medium andtandardized entrance examination and training are es-ablished. Greater emphasis is placed on public health,hich becomes a core medical student competency and
eads to a proliferation of MD-MPH and MD-Doctor ofublic Health programs.
Technology allows for worldwide collaborative re-earch efforts. Through global collaboration, transla-ional research studies incorporate patient populationsith greater genetic and cultural diversity. Funds forublic health and epidemiological research increase.rants from foundations and individuals play a sub-
tantial role in funding disease eradication efforts.Worldwide patient care improves but individuals in
ormer first world countries become disgruntled, be-ieving care has regressed to the mean. “VIP care”isappears although boutique medicine becomes avail-ble for alternative health care delivery. Internal med-cine is the core coordinator of adult health care, in-luding care of the elderly.
ISCUSSIONnternal medicine is the largest specialty, includingome 200,000 of 800,000 physicians in the Unitedtates. The pressures being exerted on medicine ineneral, and internal medicine specifically, are numer-us and will force change. Given the decline in medicaltudent and resident interest in internal medicine,9 theack of career satisfaction among practicing internistsho are leaving internal medicine at an alarming rate,10
n aging and retiring cohort of internists,10 the rapidlyging population,11 the rising cost of health care, andhe increased concerns about future funding for educa-ion and research, internal medicine must be proactiven shaping the health care system of the future.
By using scenario planning, the AAIM Task Forcen the Future of Internal Medicine sought to anticipatehat might be true in the future, given today’s trends.lthough no single scenario is likely to come to frui-
ion, aspects of several different ones might occur.espite the differences among the scenarios, several
ommon themes emerge.
An overall decrease in federal funding for medicaleducation at the undergraduate and graduate levels aswell as for basic and clinical science research willoccur. The loss of Title VII funding, the reductions inNIH funding, the growing rate of “earmarked” re-search endeavors, and the looming bankruptcy inMedicare (the single largest source of governmentfunding for education) are all clear harbingers ofsignificant reductions in governmental support of
medical education. hThe lack of funds for research and education alsowill alter the practice of primary care and access tohealth care.Technology will alter subspecialty care and the roleof subspecialists.Internists will practice more subspecialty care andless primary care, which will be turned over to otherswho are likely to be nonphysicians. As a result, thedelivery of primary/preventive principal care for pa-tients will change substantially in the future.Successes in basic science research necessitate clini-cians trained to possess competence in translationalresearch.The processes for and requirements by government,licensing, regulatory, accreditation, and certifyingbodies are strong forces that will continue to shapemedical education and the practice of medicine inunanticipated ways.Generational changes in the workforce and medicalstudents will have a profound influence on careerchoice.
From support of medical education and residencyraining to physician payment and support of the re-earch enterprise, whether from the federal or privateector, financing plays an enormous role in the future ofnternal medicine. Societal needs and demands willemain a powerful factor on wide-ranging issues ofatient safety, quality of care, measures of performancend success in patient care and education, access toare, and continuity of care.
The task force believes that some aspects of thecenarios should guide current efforts, such as rede-igning internal medicine education and increasing stu-ent interest in internal medicine. For example, howould undergraduate medical education look with a
hift from subspecialty fellowships to subspecialty res-dencies? Would this change raise the appeal of internaledicine for medical students? If the internal medicine
ommunity truly values the role that general internistslay in patient care, education, and research, then suchtatements should be made public and accompanied bytrategies to enhance that career choice; internists them-elves must refrain from portraying and referring toeneral internal medicine as a “fall back” or an inferiorption to a subspecialty career.
It is in the best interest of internal medicine to directnd lead the change, rather than be forced to react tohange driven by the federal government, regulatorygencies, and finances. The five member organizationsf AAIM—the Association of Professors of Medicine,he Association of Program Directors in Internal Med-cine, the Association of Specialty Professors, thelerkship Directors in Internal Medicine, and the Ad-inistrators of Internal Medicine—have different rolesithin the internal medicine community. Within AAIM,
owever, the associations share common goals of pre-
swe
cacCsftiaecldfbi
mtpancslarb
ATa
tasDo
R
1
1
1096 The American Journal of Medicine, Vol 120, No 12, December 2007
erving financing of medical education and research asell as ensuring high-quality care for patients and ad-
quate reimbursement for internists.AAIM represents the interests and concerns of the
ontinuum of academic internal medicine. The alliancend its constituent organizations have developed criti-al relationships and collaborations with the Americanollege of Physicians, the nearly 40 internal medicine
pecialty societies, and the organizations responsibleor evaluating the quality of internal medicine and in-ernists (such as the American Board of Internal Med-cine), as well as federal legislative and regulatorygencies, to change accreditation, increase funding forducation and research, and redesign the educationalontinuum (with an initial focus on residency and fel-owship training). These relationships provide the foun-ation for addressing future challenges and shaping theuture of health care. Admittedly, initial efforts haveeen aimed at “evolutionary” changes, which may bensufficient to address future challenges.
But how will the scenarios described guide internaledicine efforts for the future? The task force hopes
hat these scenarios do not become a typical “strategiclan” that sits idly on a shelf, but rather generate debatend discussion within the internal medicine commu-ity. The task force does not seek to engage in endlessircular conversations about nuances of the individualcenarios; such discussions only promote limited evo-ution of internal medicine. But debate and discussionre necessary to understand the limits of the scenarios,ecognize major oversights, force people to thinkroadly about issues, and generate innovative solutions.
CKNOWLEDGMENTShe authors thank Tod Ibrahim, Steven M. Humphrey,
nd Tayloe H. Loftus, MD, for their contributions tohis article. The statements and opinions detailed in thisrticle belong solely to the authors and are not repre-entative of AAIM, its constituent organizations, theepartment of Defense or any other federal agencies,r the authors’ affiliated institutions.
eferences1. Clayton CP, Grover A, O’Connell M. By the numbers: data on
medical school-based departments of internal medicine. Am JMed. 2004;116:213-216.
2. Accreditation Council for Graduate Medical Education. Listof ACGME Accredited Programs and Sponsoring Institutions.Available at: http://www.acgme.org/adspublic. Accessed Febru-ary 20, 2006.
3. National Institutes of Health. Medical Schools Ranking Tables2005 Department Listing: Internal Medicine, Medicine. Avail-able at: http://grants1.nih.gov/grants/award/rank/MedSchool_Departments.cfm?Department � INTERNAL%20MEDICINE,%20MEDICINE. Accessed March 9, 2007.
4. Clark J. Five futures for academic medicine: the ICRAM sce-narios. Br Med J. 2005;331:101-104.
5. Schoemaker PJH. Scenario planning: a tool for strategic think-ing. MIT Sloan Manage Rev. 1995;36(2):25-40.
6. Hoffman F. Fed up, some doctors turn to “boutique medicine.”ACP-ASIM Observer. October 2001. Available at: http://www.acponline.org/journals/news/oct01/new_model.htm. Accessed Feb-ruary 20, 2007.
7. American College of Physicians. The Advanced Medical Home:A Patient-Centered, Physician-Guided Model of Health Care.Philadelphia, PA: American College of Physicians; 2006.
8. Harden RM. International medical education and future directions:a global perspective. Acad Med. 2006;81(12 Suppl):S22-S29.
9. Association of American Medical Colleges. Electronic Resi-dency Application Service Database Information. Washington,DC: Association of American Medical Colleges; 2004.
0. Leigh JP, Kravitz RL, Schembri M, et al. Physician career satisfac-tion across specialties. Arch Intern Med. 2002;162:1577-1584.
1. Hazzard WR, Woolard N, Regenstrief DI. Internal medicine: atthe nexus of the health care system in responding to the demo-graphic imperative of an aging population. Am J Med. 2001;
110(6):507-513.
MH
CDL
Ipob
fCSyh
aofasfhanmsfiootmw
tt
Lb
0d
The American Journal of Medicine (2007) 120, 1097
EDICAL HUMANITIES PERSPECTIVES
elle Mathiasen, Cand Mag., PhD, Section Editoricero and Healthy Agingean Gianakos, MD
tltcado
aomyrtmswi
pticag
aoaym
p
R1
ynchburg Family Medicine Residency, Lynchburg, VA
have never assented to that ancient and much quotedroverb, which advises: Become old early if you would beld long. For my part I would rather not be old so long thane old before my time.
From De Senectute1 On Old Age, Cicero, 106-43 BC.
Advice on how to cope with old age has universal appealor one reason: few of us escape its burdens. Marcus Tulliusicero, the great Roman politician and orator, dedicated Deenectute to his friend, Atticus, in order “to lighten both forou and for me our common burden of old age.”1 I believeis advice has relevance for today’s patients and physicians.
Cicero gives philosophy the most credit for easing thefflictions of old age, “since she enables the man who isbedient to her precepts to pass every season of life freerom worry.”1 What are these precepts? For Cicero, there is
natural progression of aging. Youth enjoy physicaltrength and sensual pleasures. The old enjoy influence,riendship, and memories of a life well lived. He believesumanity should give up the pleasures of one stage tossume the joys and challenges of the next stage. Humanseed to accept the stages of life–infancy, youth, adulthood,iddle age, old age–as the inevitable course of Nature. Each
tage bears fruit for the individual: “Life’s race-course isxed; Nature has only a single path and that path is run butnce, and to each stage of existence has been allotted itswn appropriate quality; so that the weakness of childhood,he impetuosity of youth, the seriousness of middle life, theaturity of old age–each bears some of Nature’s fruit,hich must be garnered in its own season.”1
Second, Cicero believes every age is burdensome tohose ill equipped for virtue and happiness. Old age is nothe problem, though humans blame old age for the loss of
Requests for reprints should be addressed to Dean Gianakos, MD,ynchburg Family Medicine Residency, 2097 Langhorne Road, Lynch-urg, VA 24501.
E-mail address: [email protected]
002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.oi:10.1016/j.amjmed.2007.10.001
heir sensual life and physical strength. Work early in yourife, says Cicero, to develop a character that is wise, just,emperate, and courageous–one that understands that de-line is natural and inevitable: “Therefore as the pleasuresnd pursuits of the earlier periods of life fall away, so alsoo those of old age; and when that happens man has his fillf life and the time is ripe for him to go.”1
How does a 21st century person move gracefully into oldge from middle age (or old age to old-old age!) in an erabsessed with youth and beauty, and the technologicaleans to prolong life and remodel bodies to resemble
outh? How does one learn to accept aging? Cicero wouldespond: accept the fact that aging is natural and inevi-able; study philosophy; understand that the soul is im-ortal, and work to develop a virtuous character at every
tage of one’s life: “For to those who have not the meansithin themselves of a virtuous and happy life every age
s burdensome.”1
His regimen would also include many things today’shysicians prescribe: exercise, particularly intellectual ac-ivity (writing itself provided solace to Cicero); moderationn food and alcohol intake; nurturance of friendships andonversation; mentoring youth; and public service. Cicerolso believes in the healing qualities of soil; cultivatingardens, vineyards, and orchards.
Perhaps the best, general advice Cicero offers patientsnd physicians today are these words: “For just as I approvef the young man in whom there is a touch of age, so Ipprove of the old man in whom there is some flavour ofouth. He who strives thus to mingle youthfulness and ageay grow old in body, but old in spirit he will never be.”1
To adopt that attitude requires wisdom, something worthursuing at any age.
eference. Cicero. De Senectute, Falconer, WA, translator. Cambridge, MA: Har-
vard University Press; 1923.
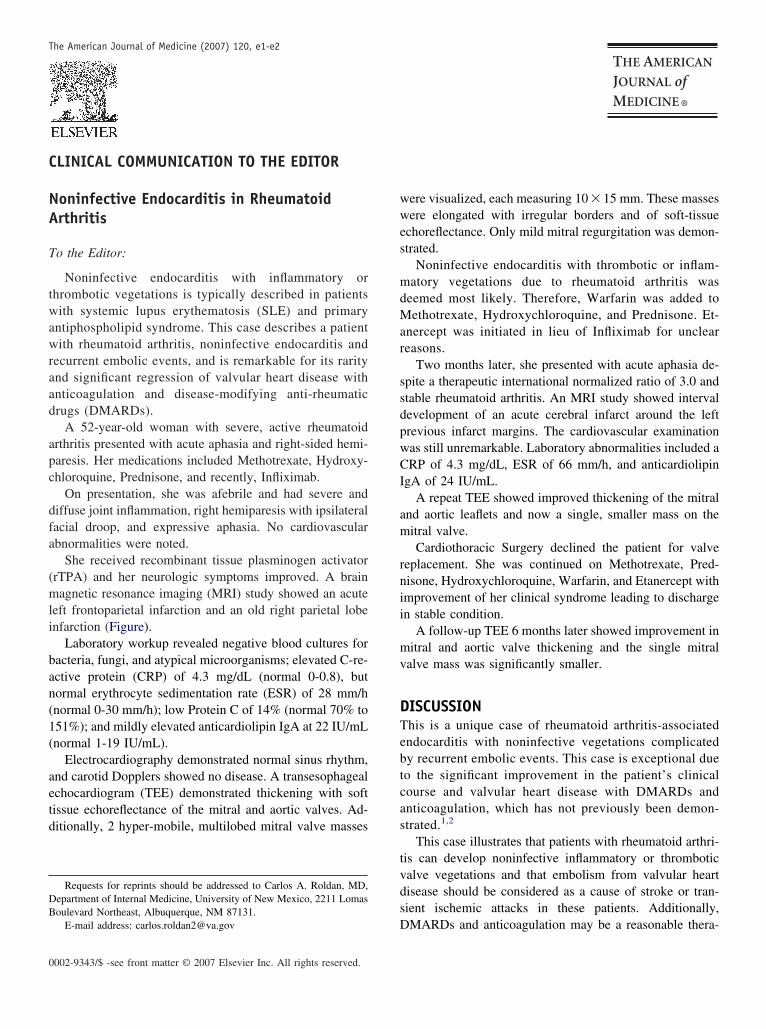
C
NA
T
twawraad
apc
dfa
(mli
ban(1(
aetd
DB
0
The American Journal of Medicine (2007) 120, e1-e2
LINICAL COMMUNICATION TO THE EDITOR
wwes
mdMar
ssdpwCI
am
rnii
mv
DTebtcas
tvds
oninfective Endocarditis in Rheumatoidrthritis
o the Editor:
Noninfective endocarditis with inflammatory orhrombotic vegetations is typically described in patientsith systemic lupus erythematosis (SLE) and primary
ntiphospholipid syndrome. This case describes a patientith rheumatoid arthritis, noninfective endocarditis and
ecurrent embolic events, and is remarkable for its raritynd significant regression of valvular heart disease withnticoagulation and disease-modifying anti-rheumaticrugs (DMARDs).
A 52-year-old woman with severe, active rheumatoidrthritis presented with acute aphasia and right-sided hemi-aresis. Her medications included Methotrexate, Hydroxy-hloroquine, Prednisone, and recently, Infliximab.
On presentation, she was afebrile and had severe andiffuse joint inflammation, right hemiparesis with ipsilateralacial droop, and expressive aphasia. No cardiovascularbnormalities were noted.
She received recombinant tissue plasminogen activatorrTPA) and her neurologic symptoms improved. A brainagnetic resonance imaging (MRI) study showed an acute
eft frontoparietal infarction and an old right parietal lobenfarction (Figure).
Laboratory workup revealed negative blood cultures foracteria, fungi, and atypical microorganisms; elevated C-re-ctive protein (CRP) of 4.3 mg/dL (normal 0-0.8), butormal erythrocyte sedimentation rate (ESR) of 28 mm/hnormal 0-30 mm/h); low Protein C of 14% (normal 70% to51%); and mildly elevated anticardiolipin IgA at 22 IU/mLnormal 1-19 IU/mL).
Electrocardiography demonstrated normal sinus rhythm,nd carotid Dopplers showed no disease. A transesophagealchocardiogram (TEE) demonstrated thickening with softissue echoreflectance of the mitral and aortic valves. Ad-itionally, 2 hyper-mobile, multilobed mitral valve masses
Requests for reprints should be addressed to Carlos A. Roldan, MD,epartment of Internal Medicine, University of New Mexico, 2211 Lomasoulevard Northeast, Albuquerque, NM 87131.
DE-mail address: [email protected]
002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
ere visualized, each measuring 10 � 15 mm. These massesere elongated with irregular borders and of soft-tissue
choreflectance. Only mild mitral regurgitation was demon-trated.
Noninfective endocarditis with thrombotic or inflam-atory vegetations due to rheumatoid arthritis was
eemed most likely. Therefore, Warfarin was added toethotrexate, Hydroxychloroquine, and Prednisone. Et-
nercept was initiated in lieu of Infliximab for uncleareasons.
Two months later, she presented with acute aphasia de-pite a therapeutic international normalized ratio of 3.0 andtable rheumatoid arthritis. An MRI study showed intervalevelopment of an acute cerebral infarct around the leftrevious infarct margins. The cardiovascular examinationas still unremarkable. Laboratory abnormalities included aRP of 4.3 mg/dL, ESR of 66 mm/h, and anticardiolipin
gA of 24 IU/mL.A repeat TEE showed improved thickening of the mitral
nd aortic leaflets and now a single, smaller mass on theitral valve.Cardiothoracic Surgery declined the patient for valve
eplacement. She was continued on Methotrexate, Pred-isone, Hydroxychloroquine, Warfarin, and Etanercept withmprovement of her clinical syndrome leading to dischargen stable condition.
A follow-up TEE 6 months later showed improvement initral and aortic valve thickening and the single mitral
alve mass was significantly smaller.
ISCUSSIONhis is a unique case of rheumatoid arthritis-associatedndocarditis with noninfective vegetations complicatedy recurrent embolic events. This case is exceptional dueo the significant improvement in the patient’s clinicalourse and valvular heart disease with DMARDs andnticoagulation, which has not previously been demon-trated.1,2
This case illustrates that patients with rheumatoid arthri-is can develop noninfective inflammatory or thromboticalve vegetations and that embolism from valvular heartisease should be considered as a cause of stroke or tran-ient ischemic attacks in these patients. Additionally,
MARDs and anticoagulation may be a reasonable thera-
pp
R1
2
Fm(L .
e2 The American Journal of Medicine, Vol 120, No 12, December 2007
eutic alternative for noninfective endocarditis in patientsosing a high surgical risk.
Christine E. DeLong, MDCarlos A. Roldan, MD
Department of Internal MedicineUniversity of New Mexico
Veteran’s Administration Medical Center
igure A. MRI (coronal view) showing left frontoparietal acuteasses (arrows). C. TEE at 2 months showing improvement in
arrow). D. TEE at 6 months showing marked improvement of vA � left atrium; LV � left ventricle; aml � anterior mitral leaflet
Albuquerque, New Mexico
doi:10.1016/j.amjmed.2006.07.023
eferences. Gonzalez-Juanatey C, Garcia-Porrua C, Testa A, Gonzalez-Gay MA.
Potential role of mitral valve strands on stroke recurrence in rheumatoidarthritis. Arthritis Rheum. 2003;49:866-868.
. Kang H, Baron M. Embolic complications of a mitral valve rheumatoid
tion (arrow). B. Initial TEE showing multiple large mitral valvehickening and a single large posterior mitral valve leaflet massickening and a very small remaining mitral valve mass (arrow).
infarcMV t
alve th
nodule. J Rheumatol. 2004;31:1001-1003.

C
P
T
ofltdettocbsicwh
vwfveCmrGfceo
PwmA
0
The American Journal of Medicine (2007) 120, e3
LINICAL COMMUNICATION TO THE EDITOR
cthhmnhhntspctrw
R1
2
3
4
5
otential Ipriflavone and Warfarin Interaction
o the Editor:
The patient is a 68-year-old white woman with a historyf atrial fibrillation, osteoporosis, and gastroesophageal re-ux disease who is anticoagulated with warfarin. Her os-
eoporosis had been treated with risedronate sodium, but sheiscontinued this medication when she learned that gastro-sophageal reflux was a common adverse effect. She wento a local pharmacy that specializes in herbal and nontradi-ional medications to seek an over-the-counter treatment forsteoporosis. The pharmacist recommended a supplementontaining ipriflavone, calcium, and vitamin D. The patientrought this with her to her next primary care visit becausehe wanted her primary care physician to review the med-cation before she started taking it. She was particularlyoncerned about the possibility of an interaction with herarfarin therapy even though the pharmacist had reassureder that there would be no interaction.
Ipriflavone is a synthetic isoflavone derivative. Isofla-one belongs to a group of compounds called flavonoids,hich are widely found in many fruits and vegetables, and
ound in particularly high concentrations in grapefruit.1 Fla-onoids are well known to be inhibitors of cytochrome P450nzymes.1 Ipriflavone has been shown to inhibit bothYP2C9 and 3A4, both of which are involved in warfarinetabolism.2,3 However, a MEDLINE search revealed no
eports of interactions between ipriflavone and warfarin. Aoogle search revealed many websites selling ipriflavone
or the treatment of osteoporosis. One well-designed clini-al trial found that ipriflavone and calcium were no moreffective than placebo and calcium at preventing bone lossr improving markers of bone metabolism.4
Requests for reprints should be addressed to Douglas C. Anderson, Jr,harmD, DPh, CACP, Clinical Associate Professor and Director, South-est Georgia Pharmacy Program, University of Georgia College of Phar-acy, c/o Albany State University, 504 College Drive, ACAD-161,lbany, GA 31705.
E-mail address: [email protected]
002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
Health care providers receive little training in herbal oromplementary medicines. With the many herbal medica-ions that are currently being marketed, it is essential thatealth care providers develop a working knowledge oferbal medications and identify useful databases to supple-ent their knowledge. Moreover, health care professionals
eed to act responsibly when counseling patients abouterbals. The current case demonstrates the potential forarm that could be done when health care professionals doot counsel patients in a responsible manner. Fortunately, inhis case the patient did not settle with the initial counselinghe received and sought other advice, thus averting theotential drug interaction. This is not usually the case be-ause patients often do not disclose herbal medication use toheir providers.5 Finally, we urge all health care providers tooutinely screen for and discuss use of herbal medicationsith their patients.
Douglas C. Anderson, Jr, PharmD, DPhSouthwest Georgia Pharmacy Program
University of Georgia College of PharmacyAlbany
Bernard P. Scoggins, MDAlbany Area Primary Health Care, Inc.
Albany
doi:10.1016/j.amjmed.2006.08.028
eferences. Fuhr U. Drug interactions with grapefruit juice. Extent, probable mech-
anism and clinical relevance. Drug Saf. 1998;18:251-272.. Monostory K, Vereczkey L, Levai F, Szatmari I. Ipriflavone as an
inhibitor of human cytochrome P450 enzymes. Br J Pharmacol. 1998;123:605-610.
. Monostory K, Vereczkey L. Interaction of theophylline and ipriflavoneat the cytochrome P450 level. Eur J Drug Metab Pharmacokinet.1920;(1):43-47.
. Alexandersen P, Toussaint A, Christiansen C, et al. Ipriflavone in thetreatment of postmenopausal osteoporosis: a randomized controlledtrial. JAMA. 2001;285:1482-1488.
. Stout CW, Weinstock J, Homoud MK, Wang PJ, Estes NA III, LinkMS. Herbal medicine: beneficial effects, side effects, and promisingnew research in the treatment of arrhythmias. Curr Cardiol Rep. 2003;
5:395-401.
C
PI
T
c3stbdle
CTh(0geTitnBcwr(m
DMsemd
MoRA
0
The American Journal of Medicine (2007) 120, e5-e6
LINICAL COMMUNICATION TO THE EDITOR
icr
MPpiwtri
DPrgmSgwa7pcbccGbaamnapmea
neumococcal Pyomyositis in a Patientnfected with Human Immunodeficiency Virus
o the Editor:
A 41-year-old man infected with human immunodefi-iency virus, who had not received antiretroviral therapy for
years, was admitted with severe pain and progressivewelling of the right shoulder and right upper extremity forhe previous 10 days. He denied any fever, shortness ofreath, or cough. He also denied current or past intravenousrug abuse. The right upper extremity was profusely swol-en and exquisitely tender, with overlying hot, shiny skinxtending from the shoulder down to the hand.
ASE REPORThe patient’s initial laboratory study results were as follows:emoglobin, 9.5 g/dL; white blood cell count, 6.4�109/Lneutrophils, 5.2 � 109/L; bands, 0.3 � 109/L; lymphocytes,.6 � 109/L), platelet count, 136 � 109/L; blood urea nitro-en, 100 mg/dL; creatinine, 5.0 mg/dL; liver function andlectrolytes, normal; and creatine phosphokinase, 77 U/L.he patient’s CD4 count was 702 cells/�L, and his human
mmunodeficiency virus-1 RNA by polymerase chain reac-ion was 75,000 copies/mL. Doppler ultrasound scan wasegative for a right upper-extremity deep vein thrombosis.lood culture was positive for penicillin-sensitive Strepto-occus pneumoniae. A course of intravenous penicillin Gas started. Purulent fluid (60 mL) was aspirated from the
ight shoulder, which had a nucleated cell count of 175,000/�L88% neutrophils, 5% lymphocytes). Gram stain, bacterial,ycobacterial, and fungal cultures were negative.
IAGNOSISagnetic resonance images revealed extensive generalized
oft tissue and intramuscular edema of the entire right upperxtremity and shoulder. Prominent abscess collections (pyo-yositis) demonstrating rim enhancements were seen, pre-
ominantly within the deltoid muscle and also involving the
Requests for reprints should be addressed to Soumya Chatterjee, MD,S, MRCP, FACP, Assistant Professor, Cleveland Clinic Lerner College
f Medicine of Case Western Reserve University, Staff, Department ofheumatic and Immunologic Diseases, Cleveland Clinic, 9500 Euclidvenue/Desk A50, Cleveland, OH 44195.
E-mail address: [email protected] or [email protected]
002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
nfraspinatus, supraspinatus, biceps, and coracobrachialis mus-les (Figure 1). The magnetic resonance image also showedight lower lobe consolidation (Figure 1B).
ANAGEMENTenicillin G was continued. Under contrast-enhanced com-uted tomography guidance, a pigtail catheter was insertednto the fluid collection, and 75 mL of dark purulent fluidas drained. After 7 days there was significant reduction in
he size of the multiloculated fluid collections. The patientecovered with a prolonged course of intravenously admin-stered antibiotic.
ISCUSSIONyomyositis is a bacterial infection of the skeletal musclesesulting in single or multiple intramuscular abscesses. It isenerally a tropical disease.1 However, nontropical pyo-yositis is being increasingly recognized in the Unitedtates.2 The infection most often selects the larger muscleroups, such as the quadriceps, glutei, and so forth.1 World-ide, Staphylococcus aureus is the most common infectious
gent1; it is seen in up to 90% of cases in tropical areas and5% of cases in temperate countries.3 In temperate regions,yomyositis usually occurs in people with immune defi-iency states. Pneumococcal pyomyositis is less commonut has been reported in patients with human immunodefi-iency virus infection4 or diabetes.5 Abscess fluid culturesan be sterile in 15% to 30% cases.6 In our case, too, theram stain and bacterial cultures were negative, perhapsecause the patient was already receiving an appropriatentibiotic when rheumatology service was consulted and thebscess was aspirated. The diagnosis is suggested when theagnetic resonance image demonstrates fluid collection sig-
als with peripheral enhancement on post-gadolinium im-ges.7 Appropriate antibiotic therapy and drainage of theus are important components of management. Pyomyositisust be considered in the differential diagnosis of a swollen
xtremity, because mortality is high2 and early recognitionnd treatment are essential to prevent a fatal outcome.
Soumya Chatterjee, MDa
Maysoon Al-Hihi, MDb
aCleveland Clinic Lerner College of Medicine ofCase Western Reserve University
Department of Rheumatic and Immunologic Diseases
Cleveland Clinic, Cleveland, Ohio
R1
2
3
4
5
6
7
Fdman
e6 The American Journal of Medicine, Vol 120, No 12, December 2007
bHarper University HospitalWayne State University
Detroit, Mich
doi:10.1016/j.amjmed.2007.05.007
eferences. Chauhan S, Jain S, Varma S, Chauhan SS. Tropical pyomyositis (my-
ositis tropicans): current perspective. Postgrad Med J. 2004;80:267-270.
. Gomez-Reino JJ, Aznar JJ, Pablos JL, et al. Nontropical pyomyositis in
igure 1 Fat-saturated post-gadolinium magnetic resonance imaemonstrating intramuscular abscesses in the deltoid and infraspinauscles (arrows) consistent with myositis; right lower lobe cons
bscess collections (arrows) extending from the acromioclavicularot included).
adults. Semin Arthritis Rheum. 1994;23:396-405.
. Christin L, Sarosi GA. Pyomyositis in North America: case reports andreview. Clin Infect Dis. 1992;15:668-677.
. Pallangyo K, Hakanson A, Lema L, et al. High HIV seroprevalence andincreased HIV-associated mortality among hospitalized patients withdeep bacterial infections in Dar es Salaam, Tanzania. AIDS. 1992;6:971-976.
. Watanabe Y, Ohashi H, Asahina T, et al. Pneumococcal paraspinalpyomyositis in a diabetic man: a case report. Diabetes Obes Metab.2000;2:385-386.
. Shepherd JJ. Tropical myositis: is it an entity and what is its cause?Lancet. 1983;2:1240-1242.
. Soler R, Rodriguez E, Aguilera C, Fernandez R. Magnetic resonance
: Axial images of the right shoulder and proximal right humerusscles (arrows). B: Enhancement in the biceps and coracobrachialison (black arrow). C: Sagittal image demonstrates intramuscularto approximately 10 cm above the elbow joint (the elbow joint is
ges. Atus muolidatijoint
imaging of pyomyositis in 43 cases. Eur J Radiol. 2000;35:59-64.
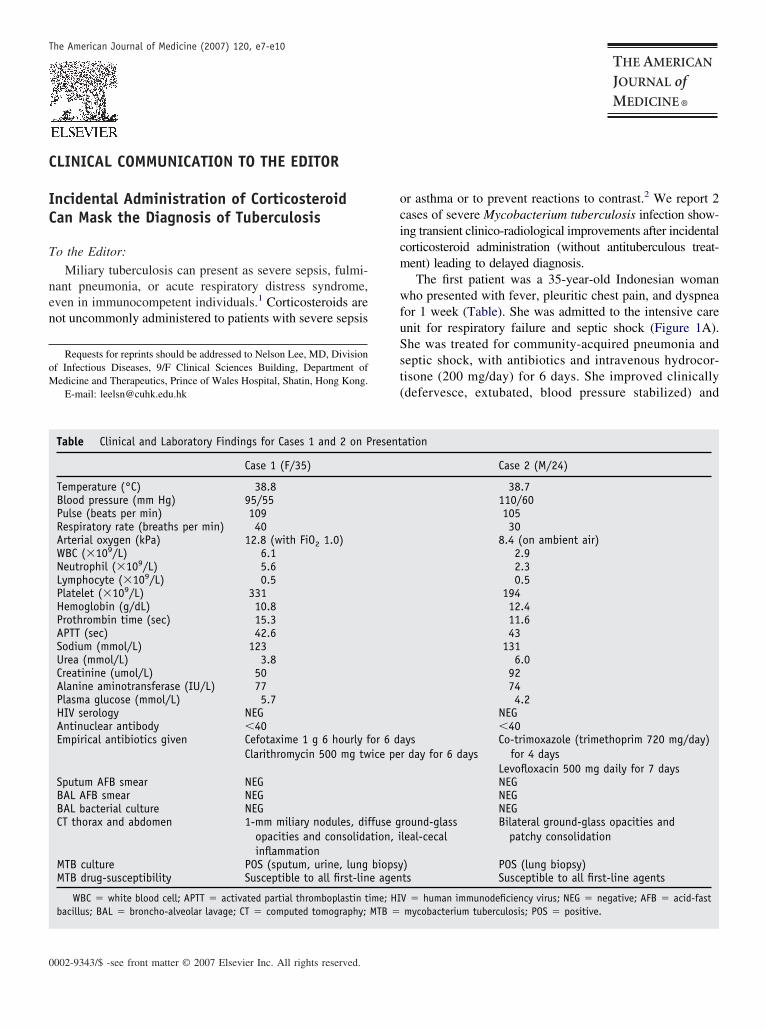
C
IC
T
nen
oM
0
The American Journal of Medicine (2007) 120, e7-e10
LINICAL COMMUNICATION TO THE EDITOR
ocicm
wfuSst(
ncidental Administration of Corticosteroidan Mask the Diagnosis of Tuberculosis
o the Editor:
Miliary tuberculosis can present as severe sepsis, fulmi-ant pneumonia, or acute respiratory distress syndrome,ven in immunocompetent individuals.1 Corticosteroids areot uncommonly administered to patients with severe sepsis
Requests for reprints should be addressed to Nelson Lee, MD, Divisionf Infectious Diseases, 9/F Clinical Sciences Building, Department ofedicine and Therapeutics, Prince of Wales Hospital, Shatin, Hong Kong.
E-mail: [email protected]
Table Clinical and Laboratory Findings for Cases 1 and 2 on P
Case 1 (F/35)
Temperature (°C) 38.8Blood pressure (mm Hg) 95/55Pulse (beats per min) 109Respiratory rate (breaths per min) 40Arterial oxygen (kPa) 12.8 (with FiO2 1.0)WBC (�109/L) 6.1Neutrophil (�109/L) 5.6Lymphocyte (�109/L) 0.5Platelet (�109/L) 331Hemoglobin (g/dL) 10.8Prothrombin time (sec) 15.3APTT (sec) 42.6Sodium (mmol/L) 123Urea (mmol/L) 3.8Creatinine (umol/L) 50Alanine aminotransferase (IU/L) 77Plasma glucose (mmol/L) 5.7HIV serology NEGAntinuclear antibody �40Empirical antibiotics given Cefotaxime 1 g 6 hourly f
Clarithromycin 500 mg tw
Sputum AFB smear NEGBAL AFB smear NEGBAL bacterial culture NEGCT thorax and abdomen 1-mm miliary nodules, dif
opacities and consolidainflammation
MTB culture POS (sputum, urine, lungMTB drug-susceptibility Susceptible to all first-lin
WBC � white blood cell; APTT � activated partial thromboplastin tbacillus; BAL � broncho-alveolar lavage; CT � computed tomography;
002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
r asthma or to prevent reactions to contrast.2 We report 2ases of severe Mycobacterium tuberculosis infection show-ng transient clinico-radiological improvements after incidentalorticosteroid administration (without antituberculous treat-ent) leading to delayed diagnosis.The first patient was a 35-year-old Indonesian woman
ho presented with fever, pleuritic chest pain, and dyspneaor 1 week (Table). She was admitted to the intensive carenit for respiratory failure and septic shock (Figure 1A).he was treated for community-acquired pneumonia andeptic shock, with antibiotics and intravenous hydrocor-isone (200 mg/day) for 6 days. She improved clinicallydefervesce, extubated, blood pressure stabilized) and
ation
Case 2 (M/24)
38.7110/6010530
8.4 (on ambient air)2.92.30.5
19412.411.643
1316.0
92744.2
NEG�40
ysr day for 6 days
Co-trimoxazole (trimethoprim 720 mg/day)for 4 days
Levofloxacin 500 mg daily for 7 daysNEGNEGNEG
round-glassleal-cecal
Bilateral ground-glass opacities andpatchy consolidation
) POS (lung biopsy)ts Susceptible to all first-line agents
V � human immunodeficiency virus; NEG � negative; AFB � acid-fastmycobacterium tuberculosis; POS � positive.
resent
or 6 daice pe
fuse gtion, i
biopsye agen
ime; HIMTB �
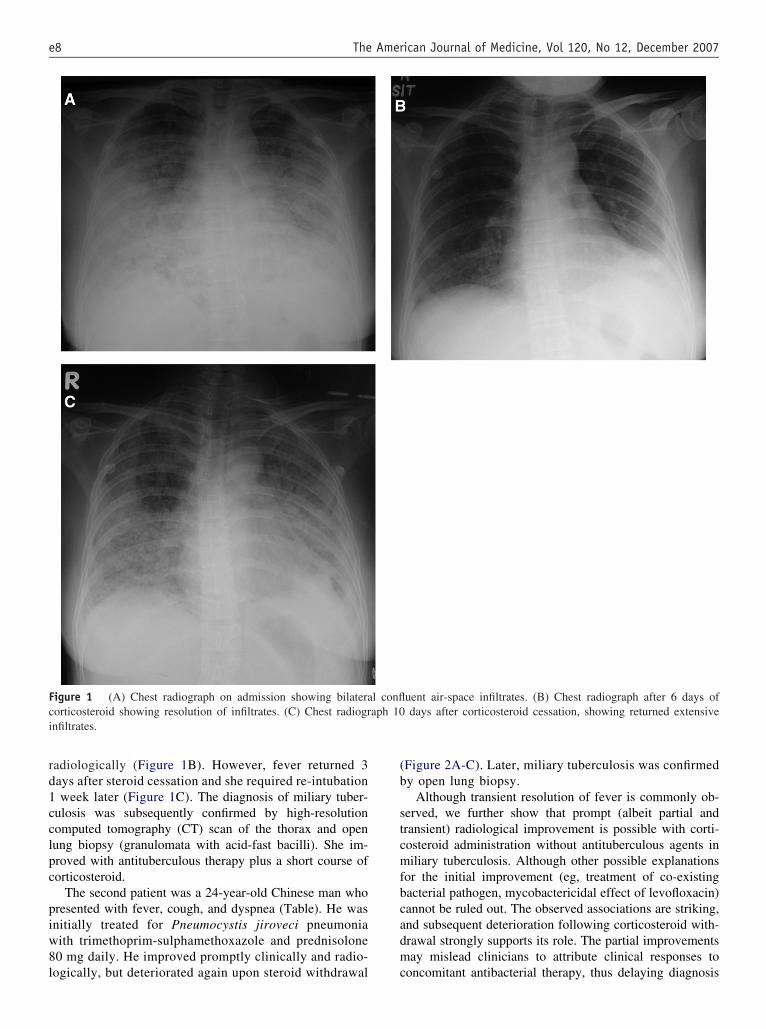
rd1cclpc
piw8l
(b
stcmfbcadm
Fci
e8 The American Journal of Medicine, Vol 120, No 12, December 2007
adiologically (Figure 1B). However, fever returned 3ays after steroid cessation and she required re-intubationweek later (Figure 1C). The diagnosis of miliary tuber-
ulosis was subsequently confirmed by high-resolutionomputed tomography (CT) scan of the thorax and openung biopsy (granulomata with acid-fast bacilli). She im-roved with antituberculous therapy plus a short course oforticosteroid.
The second patient was a 24-year-old Chinese man whoresented with fever, cough, and dyspnea (Table). He wasnitially treated for Pneumocystis jiroveci pneumoniaith trimethoprim-sulphamethoxazole and prednisolone0 mg daily. He improved promptly clinically and radio-
igure 1 (A) Chest radiograph on admission showing bilateraorticosteroid showing resolution of infiltrates. (C) Chest radiogrnfiltrates.
ogically, but deteriorated again upon steroid withdrawal c
Figure 2A-C). Later, miliary tuberculosis was confirmedy open lung biopsy.
Although transient resolution of fever is commonly ob-erved, we further show that prompt (albeit partial andransient) radiological improvement is possible with corti-osteroid administration without antituberculous agents iniliary tuberculosis. Although other possible explanations
or the initial improvement (eg, treatment of co-existingacterial pathogen, mycobactericidal effect of levofloxacin)annot be ruled out. The observed associations are striking,nd subsequent deterioration following corticosteroid with-rawal strongly supports its role. The partial improvementsay mislead clinicians to attribute clinical responses to
uent air-space infiltrates. (B) Chest radiograph after 6 days ofdays after corticosteroid cessation, showing returned extensive
l conflaph 10
oncomitant antibacterial therapy, thus delaying diagnosis
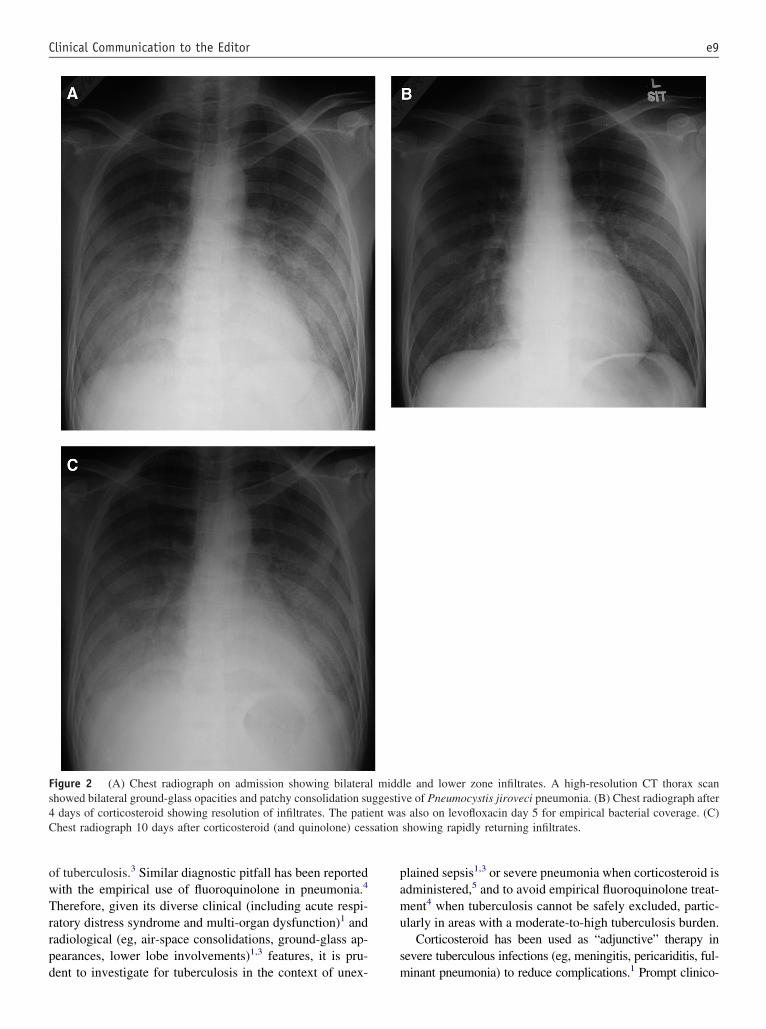
owTrrpd
pamu
s
Fs4C sation
e9Clinical Communication to the Editor
f tuberculosis.3 Similar diagnostic pitfall has been reportedith the empirical use of fluoroquinolone in pneumonia.4
herefore, given its diverse clinical (including acute respi-atory distress syndrome and multi-organ dysfunction)1 andadiological (eg, air-space consolidations, ground-glass ap-earances, lower lobe involvements)1,3 features, it is pru-
igure 2 (A) Chest radiograph on admission showing bilaterahowed bilateral ground-glass opacities and patchy consolidation sudays of corticosteroid showing resolution of infiltrates. The patihest radiograph 10 days after corticosteroid (and quinolone) ces
ent to investigate for tuberculosis in the context of unex- m
lained sepsis1,3 or severe pneumonia when corticosteroid isdministered,5 and to avoid empirical fluoroquinolone treat-ent4 when tuberculosis cannot be safely excluded, partic-
larly in areas with a moderate-to-high tuberculosis burden.Corticosteroid has been used as “adjunctive” therapy in
evere tuberculous infections (eg, meningitis, pericariditis, ful-
le and lower zone infiltrates. A high-resolution CT thorax scanve of Pneumocystis jiroveci pneumonia. (B) Chest radiograph afters also on levofloxacin day 5 for empirical bacterial coverage. (C)showing rapidly returning infiltrates.
l middggesti
ent wa
inant pneumonia) to reduce complications.1 Prompt clinico-

rjvtkepsjsaD
R1
2
3
4
5
6
e10 The American Journal of Medicine, Vol 120, No 12, December 2007
adiological responses also are observed for Pneumocystisiroveci pneumonia, severe acute respiratory syndrome, andaricella pneumonia, where immunopathogenesis is impor-ant. Skewed Th2 cytokine responses (eg, elevated interleu-in-4, interleukin-10, and interleukin-13) are demonstrated inxtensive/cavitatory pulmonary and miliary tuberculosis.1 Hy-er-production of tumor necrosis factor-� and interleukin-1�,timulated by lipoarabinomannan, also triggers acute lung in-ury. Corticosteroids can inhibit expression of these cytokines,uppressing symptoms.6 It is important for clinicians to beware that corticosteroid may mask the diagnosis of tuberculosis.elay in antituberculous treatment may lead to higher mortality.1
Grace Lui, MRCP (UK)Nelson Lee, MRCP (UK)
Bonnie Wong, MRCP (UK)David S. Hui, MD
Clive S. Cockram, FRCPDepartment of Medicine and Therapeutics
Prince of Wales HospitalThe Chinese University of Hong Kong
Shatin, Hong Kong
Ka-tak Wong, FRCPDepartment of Diagnostic Radiology and Organ Imaging
Prince of Wales HospitalThe Chinese University of Hong Kong
Shatin, Hong Kong
Rebecca K. Lam, MRCPathDepartment of Microbiology
Prince of Wales HospitalThe Chinese University of Hong Kong
Shatin, Hong Kong
Gavin M. Joynt, MBChBDepartment of Anesthesia and Intensive Care
Prince of Wales HospitalThe Chinese University of Hong Kong
Shatin, Hong Kong
doi:10.1016/j.amjmed.2007.01.034
eferences. Sharma SK, Mohan A, Sharma A, Mitra DK. Miliary tuberculosis: new
insights into an old disease. Lancet Infect Dis. 2005;5(7):415-430.. Keh D, Sprung CL. Use of corticosteroid therapy in patients with sepsis
and septic shock: an evidence-based review. Crit Care Med. 2004;32(Suppl):S527-S533.
. Kunimoto D, Long R. Tuberculosis: still overlooked as a cause ofcommunity-acquired pneumonia—how not to miss it. Respir Care ClinN Am. 2005;11:25-34.
. Wang JY, Hsueh PR, Jan IS, et al. Empirical treatment with a fluoro-quinolone delays the treatment for tuberculosis and is associated with apoor prognosis in endemic areas. Thorax. 2006;61(10):903-908.
. Confalonieri M, Urbino R, Potena A, et al. Hydrocortisone infusion forsevere community-acquired pneumonia: a preliminary randomizedstudy. Am J Respir Crit Care Med. 2005;171(3):242-248.
. Rock RB, Hu S, Gekker G, et al. Mycobacterium tuberculosis-inducedcytokine and chemokine expression by human microglia and astrocytes:
effects of dexamethasone. J Infect Dis. 2005;192(12):2054-2058.
L
Ia
T
wr
vtt5o
Taiatrr
Pooe
lwcyonp
0
The American Journal of Medicine (2007) 120, e11
ETTER
oovc
R1
2
3
4
5
6
ndividualized Treatment of Foramen Ovalend Stroke
o the Editor:
I read with interest Dalen’s editorial1 on whether patientsho harbor a patent foramen ovale (PFO) are at increased
isk of strokes or not, and contend the following:In regard to the increased risk of recurrent stroke and
enous thromboembolism, 41% of patients with stroke orransient ischemic attack (TIA) were found to have a PFO inhe Lausanne study.2 Venous thrombosis was detected in.5%, and other studies show annual stroke recurrence ratesf up to 12% in patients with cryptogenic stroke.2-4
The French Study Group3 found that the risk of stroke orIA was not increased in patients with cryptogenic strokend a PFO alone treated with aspirin, but the risk wasncreased from 4.7% to 8.0% in patients with a PFO and antrial septal aneurysm (ASA). Therefore, many of us thinkhat the combination of an ASA and a PFO is a significantisk factor for cerebral embolic ischemia in patients withecurrent cryptogenic stroke.
There are conflicting reports on transvenous closure ofFOs and the risk of recurrent stroke. Ruchat et al.5 dem-nstrated that patients with PFOs and cryptogenic strokes,r TIA who underwent closure had no recurrent vascularvents. Similar results have been reported elsewhere.6
There are situations in which a right-to-left shunt with aarge PFO and ASA are found in the workup of a patientith cryptogenic TIA or ischemic stroke in whom one
onsiders anticoagulation or PFO closure. What about aoung diver with no other risk factors? What about therthopedic surgery patient who has a TIA from fat emboli ineed of more surgery? What about the patient with a hy-
ercoagulable state? Although we would all like the results002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
f properly designed randomized clinical trials before rec-mmendations regarding PFO closure can be made, indi-idual patient presentations and characteristics must guidelinical decision making.
Richard Alan Rison, MDWhittier Presbyterian Intercommunity Hospital Stroke Center
Whittier, CalifUniversity of Southern California
Keck School of MedicineLos Angeles County Medical Center
Los Angeles, CalifNeurology Consultants Medical Group
Whittier, Calif
doi:10.1016/j.amjmed.2007.06.027
eferences. Dalen JE. Are patients with a patent foramen ovale at increased risk of
stroke? A billion dollar question Am J Med. 2007;120:472-474.. Bogousslavsky J, Garazi S, Jeanrenaud X, et al. Stroke recurrence in
patients with patent foramen ovale: the Lausanne Study: LausanneStroke with Paradoxical Embolism Study Group. Neurology. 1996;46:1301-1305.
. Mas JL, Zuber M. Recurrent cerebrovascular events in patients withpatent foramen ovale, atrial septal aneurysm, or both and cryptogenicstroke or transient ischemic attack: French Study Group on PatentForamen Ovale and Atrial Septal Aneurysm. Am Heart J. 1995;130:1083-1088.
. Cujec B, Mainra R, Johnson DH. Prevention of recurrent cerebralischemic events in patients with patent foramen ovale and cryptogenicstrokes or transient ischemic attacks. Can J Cardiol. 1999;15:57-64.
. Ruchat P, Bogousslavsky J, Hurni M, et al. Systematic surgical closureof patent foramen ovale in selected patients with cerebrovascular eventsdue to paradoxical embolism: early results of a preliminary study. EurJ Cardiothorac Surg. 1997;11:824-827.
. Devuyst G, Bogousslavsky J, Ruchat P, et al. Prognosis after strokefollowed by surgical closure of patent foramen ovale: a prospectivefollow-up study with brain MRI and simultaneous transesophageal and
transcranial Doppler ultrasound. Neurology. 1996;47:1162-1166.
L
P
T
r(to
etiicdcpfc
atndli
ipadiyTl
0
The American Journal of Medicine (2007) 120, e13
ETTER
ogawsytftwb
iwp
R1
2
3
4
5
atent Foramen Ovale and Cryptogenic Stroke
o the Editor:
In his recent commentary,1 Dalen details uncertaintiesegarding the pathogenic role of patent foramen ovalePFO) in ischemic stroke and the appropriateness of percu-aneous closure. Dalen’s piece raises valid points, but somef its assertions warrant additional comment.
Dalen’s contention that cryptogenic strokes may not bembolic overlooks existing data showing otherwise. Cryp-ogenic strokes are, by definition, nonlacunar infarcts lack-ng a demonstrable arterial or cardiac cause. Necropsy stud-es document that many large-artery strokes are embolic,haracterized by thrombi lacking mural attachment or un-erlying atheroma.2 Angiographic studies show that intra-ranial occlusions frequently undergo early recanalization, ahenomenon typical for thromboembolism.3 Such emboliceatures predominate in cryptogenic infarcts, supporting theoncept that these often represent unexplained embolism.4
Still, the frequent absence of a right-to-left gradientcross the foramen and failure to detect concurrent venoushrombosis do cast doubt on a paradoxical embolic mecha-ism.1 Transient reversal of the left-to-right transeptal gra-ient does occur normally in early systole, however, andack of detectable venous thrombosis may reflect challengesn identification rather than genuine absence.5
Longitudinal studies of PFO have failed to demonstratencreased cerebrovascular risk,1 but apart from being under-owered, such studies have not focused on the appropriatege group. Given that clinical or subclinical atheroscleroticisease may dwarf the risk of PFO for cerebral infarction,ncreased prevalence of such disease in cohorts over 45ears of age might bias findings toward the null hypothesis.o maximize the chance of detecting the PFO signal, large
ongitudinal studies in younger cohorts are necessary.
002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
In recognizing the shortfalls in available data, what thenf following the American College of Chest Physiciansuidelines of aspirin therapy endorsed by Dalen? Althoughstudy found no difference in stroke recurrence or death forarfarin versus aspirin in the subset with cryptogenic
troke, warfarin nonsignificantly halved the risk.5 In aounger cohort with cryptogenic stroke receiving aspirin,he combination of PFO and atrial septal aneurysm con-erred a 4% yearly risk of recurrence.5 These data suggesthat aspirin may well be insufficient for younger patientsith high-risk PFO features, and that such patients might beetter served by anticoagulation or closure.
Only randomized trials can definitively answer outstand-ng treatment questions. Until then, one cannot but agreeith Dalen that the prevailing zeal in closing every PFO isremature and unjustified.
Jorge R. Kizer, MD, MScDepartments of Medicine and Public HealthWeill Medical College of Cornell University
New York
doi:10.1016/j.amjmed.2007.07.024
eferences. Dalen JE. Are patients with a patent foramen ovale at increased risk of
stroke? A billion dollar question. Am J Med. 2007;120:472-474.. Jorgensen L, Torvik A. Ischaemic cerebrovascular diseases in an au-
topsy series. I. Prevalence, location and predisposing factors in verifiedthrombo-embolic occlusions, and their significance in the pathogenesisof cerebral infarction. J Neurol Sci. 1966;3:490-509.
. Fieschi C, Argentino C, Lenzi GL, et al. Clinical and instrumentalevaluation of patients with ischemic stroke within the first six hours.J Neurol Sci. 1989;91:311-321.
. Sacco RL, Ellenberg JH, Mohr JP, et al. Infarcts of undetermined cause:the NINCDS Stroke Data Bank. Ann Neurol. 1989;25:382-390.
. Kizer JR, Devereux RB. Clinical practice. Patent foramen ovalein young adults with unexplained stroke. N Engl J Med. 2005;353:
2361-2372.
L
T
tndeihtptt
srHcTs
ci
t
oos
0
The American Journal of Medicine (2007) 120, e15
ETTER
ldflct
dc
R1
2
3
4
he Reply:
I agree with Rison that there are many inconsistencies inhe reports of stroke and patent foramen ovale (PFO). Heotes that in the Lausanne study,1 venous thrombosis wasetected in 5.5% of patients with stroke or transient isch-mic attack (TIA). If the stroke/TIAs were due to paradox-cal embolism, the incidence of venous thrombosis wouldave been much higher. The French study group2 reportedhat the risk of recurrent stroke/TIA was not increased inatients with cryptogenic stroke and a PFO who werereated with aspirin. However, aspirin is relatively ineffec-ive in preventing venous thrombosis.3
He notes that many feel that the combination of an atrialeptal aneurysm and PFO is a significant risk factor forecurrent stroke/TIA in patients with cryptogenic stroke.owever, Homma et al,4 in a study of 265 patients with
ryptogenic stroke, found that the recurrence rate of stroke/IA was the same in PFO patients with or without an atrialeptal aneurysm.
I agree that, until randomized clinical trials are reported,linical judgment should determine the appropriate therapyn patients with cryptogenic stroke who have a PFO.
Kizer cites compelling evidence that cryptogenic strokeshat are not lacunar are likely to be embolic in origin.
In patients in whom right-to-left shunting can be dem-nstrated only in early systole, paradoxical embolism couldccur only if a venous thrombus of the appropriate small
ize reaches the PFO at the brief interval in which right-to-002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
eft shunting occurs. I agree with his point that the lack ofetectable venous thrombosis in nearly all cases could re-ect challenges in identification of venous thrombosis. Itould also reflect the absence of venous thrombosis andherefore the absence of paradoxical embolism.
We all agree that randomized clinical trials are needed toetermine if it is appropriate to close PFOs in patients withryptogenic strokes.
James E. Dalen, MD, MPHProfessor Emeritus
University of ArizonaTucson
doi:10.1016/j.amjmed.2007.08.026
eferences. Bogousslavsky J, Garazi S, Jeanrenaud X, et al. Stroke recurrence in
patients with patent foramen ovale: the Lausanne Study. Neurology.1996;46:1301-1305.
. Mas JL, Zuber M. Recurrent cerebrovascular events in patients withpatent foramen ovale, atrial septal aneurysm, or both and cryptogenicstroke or transient ischemic attack: French Study Group on PatentForamen Ovale and Atrial Septal Aneurysm. Am Heart J. 1995;130:1083-1088.
. Patrano C, Coller B, FitzGerald GA, et al. Platelet-active drugs: therelationships among dose, effectiveness and side effects. Chest. 2004;126:234S-264S.
. Homma S, Sacco RL, DiTullio MR, et al. Effect of medical treatmentin stroke patients with patent foramen ovale. Circulation. 2002;105:
2625-2631.
L
ET
T
ent3sis
amAai
irmaieirio6gCmgm
0
The American Journal of Medicine (2007) 120, e17
ETTER
vrAcwt(bos
R1
2
3
4
5
6
xercise, Vitamins and Respiratoryract Infections
o the Editor:
Chubak and colleagues1 reported that moderate-intensityxercise training reduced common cold incidence but hado effect on the total incidence of upper respiratory infec-ions. As a motivation for the trial, they cited 2 randomized- to 4-month trials2,3; however, these trials did not find atatistically significant effect on upper respiratory infectionncidence from moderate exercise, but the studies weremall (N � 36).
In their article, Chubak et al1 failed to refer to our studynalyzing the relation between physical activity and com-on cold incidence in middle-aged Finnish men of theTBC Study cohort (N � 14,401). Physical activity at work
nd at leisure had no association with common coldncidence.4
In Chubak et al’s trial,1 less severe upper respiratorynfections were classified as “the common cold,” and theemaining episodes included “flu” and were, on average,ore severe. The causes of the illnesses in these 2 groups
re largely overlapping, but the difference in severity ismportant. There was no significant difference in the sum ofpisodes between the 2 treatment groups. However, accord-ng to Table 2 in Chubak et al’s article, the severity of upperespiratory infections was considerably dissimilar in the 2ntervention groups. In the exercising group, the proportionf episodes classified as “the common cold” was 35% (23/5), whereas it was significantly higher in the stretchingroup: 67% (47/70) (P [2-t] � .0004, Fisher exact test).onsequently, the more severe episodes were substantiallyore frequent in the exercising group (65% vs 33%), sug-
esting that exercise might, in fact, have caused harm by
aking upper respiratory infections more severe.002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
Finally, Chubak et al1 mentioned the possibility thatitamins might affect the immune system, but they did notefer to controlled trials with physically active people. In theTBC Study cohort, vitamin E had no effect on common
old incidence in those who had heavy physical activity atork or at leisure.4,5 Nevertheless, in 6 placebo-controlled
rials with participants under heavy acute physical stresscombined N � 642), vitamin C reduced common cold risky 50% (95% confidence interval: �34% to �62%).5,6 Fourf the trials studied marathon runners; thus, the latter findinghould be generalized cautiously.
Harri Hemilä, PhD, MDDepartment of Public Health
University of HelsinkiHelsinki, Finland
doi:10.1016/j.amjmed.2006.11.025
eferences. Chubak J, McTiernan A, Sorensen B, et al. Moderate-intensity exercise
reduces the incidence of colds among postmenopausal women. Am JMed. 2006;119:937-942.
. Nieman DC, Nehlsen-Cannarella SL, Markoff PA, et al. The effects ofmoderate exercise training on natural killer cells and acute upper respi-ratory tract infections. Int J Sports Med. 1990;11:467-473.
. Nieman DC, Henson DA, Gusewitch G, et al. Physical activity andimmune function in elderly women. Med Sci Sports Exerc. 1993;25:823-831.
. Hemilä H, Virtamo J, Albanes D, Kaprio J. Physical activity and thecommon cold in men administered vitamin E and �-carotene. Med SciSports Exerc. 2003;35:1815-1820.
. Hemilä H. Do vitamins C and E affect respiratory infections? [Disser-tation]. Helsinki, Finland: University of Helsinki; 2006:48-50, 66-67.Available at: http://ethesis.helsinki.fi/julkaisut/laa/kansa/vk/hemila/. Lastaccessed April 11, 2007.
. Douglas RM, Hemilä H. Vitamin C for preventing and treating the
common cold. PLoS Med. 2005;2:e168.
L
T
prssv
tsisftoieascidwhtn
htvicseiu
0
The American Journal of Medicine (2007) 120, e19
ETTER
eHWcgo
twiigmi
R1
2
he Reply:
We appreciate the interest in our work by Hemilä. As heoints out, the motivation for our study came from previousandomized trials with promising results but limitations intudy size and relatively short intervention periods. Ourtudy was the first to test the effects of an exercise inter-ention on the incidence of colds in a larger trial.1
Hemilä refers to a larger epidemiologic study (ATBCrial, limited to male smokers) in which no association waseen between physical activity and upper respiratory tractnfections.2 There are several possible reasons that thistudy may not have detected an association if one does, inact, exist. For example, smoking can affect immune func-ion and also is likely to affect the reporting and occurrencef upper respiratory tract infections. Our study did notnclude smokers. The ATBC trial and other large-scalepidemiologic studies have a limited assessment of physicalctivity, which may result in misclassification, biasing re-ults to the null. The central advantage of a randomizedontrolled trial, such as ours, is that the exposure of interests randomly assigned—thus it provides the most rigorousesign for testing hypotheses. Another feature of our trialas that participants were given explicit instructions aboutow to classify their upper respiratory tract infections,hereby reducing the likelihood of misclassification. This isot always possible in large epidemiologic studies.
Hemilä suggests that the exercisers in our study mayave experienced more severe infections. We do not believehat this conclusion is appropriate. As discussed, the inter-ention and control groups had different proportions ofnfluenza vaccination at baseline (Table 1) and during theourse of the intervention, which may have affected thetudy results and contributed to our null findings for influ-nza or upper respiratory tract infections overall. It also ismportant to note that a comparison of the proportion of
pper respiratory tract infections that were not colds in002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
xercisers compared with stretchers, as suggested byemilä, is not appropriate if the overall rates are not similar.e hope that our findings of a reduction in the incidence of
olds with exercise will spur similar research that investi-ates exercise effects on the incidence of influenza andther infections.
We agree with Hemilä that the potential interaction be-ween vitamin use and exercise on the risk of colds is notell defined. Our ability to examine this question was lim-
ted, in part, by the size of our study. Future large random-zed controlled trials should be undertaken to verify oureneral findings and to investigate whether the use of vita-in supplements modifies the apparent benefits of exercise
n preventing colds.
Cornelia M. Ulrich, PhDJessica Chubak, MBHL
Anne McTiernan, MD, PhDFred Hutchinson Cancer Research Center
Cancer Prevention ProgramSeattle, Wash
Department of EpidemiologyUniversity of Washington
Seattle, Wash
Anne McTiernan, MD, PhDDepartment of Medicine
University of WashingtonSeattle, Wash
doi:10.1016/j.amjmed.2006.12.012
eferences. Chubak J, McTiernan A, Sorensen B, et al. Moderate-intensity exercise
reduces the incidence of colds among postmenopausal women. Am JMed. 2006;119:937-942.
. Hemilä H, Virtamo J, Albanes D, Kaprio J. Physical activity and thecommon cold in men administered vitamin E and �-carotene. Med Sci
Sports Exerc. 2003;35:1815-1820.
L
ADA
T
ATcapipafa
oaeeas
icpfwprrr
ab
0
The American Journal of Medicine (2007) 120, e21
ETTER
R1
2
3
4
5
nti-TNF Antibodies Associated withifferent Risk of Latent Tuberculosisctivation
o the Editor:
We read with interest the article entitled “Pulmonarydverse Events of Anti-Tumor Necrosis Factor-� Antibodyherapy,” by Mutlu and colleagues.1 In this article, etaner-ept is classified as an anti-tumor necrosis factor (TNF)-�ntibody. In fact, etanercept is a soluble dimeric fusionrotein including 2 covalently linked proteins each consist-ng of the extracellular ligand-binding portion of the human75 receptor (receptor 2) fused to the Fc region of anntibody. As such, etanercept has a different structure andunction than the anti-TNF-� antibodies infliximab anddalimumab.
Higher incidence rates of tuberculosis and shorter time tonset of tuberculosis have been seen in patients treated withnti-TNF-� antibodies compared with patients treated withtanercept.2-4 This finding may be attributable to the differ-ntial effects of the therapies in terms of cytokine responsend granuloma formation and maintenance, as well as thehorter clearance time of etanercept.2-5
Although the authors correctly state in the text that theres a significantly lower incidence of tuberculosis in etaner-ept-treated patients, the incidence rate of tuberculosis inatients with rheumatoid arthritis treated with etanerceptrom Keane et al4 was reported as 20.7 per 100,000 patients,hen, in fact, it is 8.8 per 100,000 patients (9/102,000atients). Also, the reported crude worldwide tuberculosisate of 47.6 per 100,000 patients is specific for patientseceiving infliximab.4 The table shows the correct incidenceates and labels.
In closing, it is important for physicians to have the mostccurate information to appropriately assess the risks and
enefits of therapy.002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
Michele Hooper, MD, MSEric Chi, PhD
Amgen, IncThousand Oaks, Calif
doi:10.1016/j.amjmed.2006.11.023
eferences. Mutlu GM, Mutlu EA, Bellameyer A, Rubinstein I. Pulmonary adverse
events of anti-tumor necrosis factor-� antibody therapy. Am J Med.2006;119:639-646.
. Rychly DJ, DiPiro JT. Infections associated with tumor necrosis fac-tor-� antagonists. Pharmacotherapy. 2005;25:1181-1192.
. Gardam MA, Keystone EC, Menzies R, et al. Anti-tumor necrosis factoragents and tuberculosis risk: mechanisms of action and clinical man-agement. Lancet Infect Dis. 2003;3:148-155.
. Keane J, Gershon S, Wise RP, et al. Tuberculosis associated withinfliximab, a tumor necrosis factor alpha-neutralizing agent. N EnglJ Med. 2001;345:1098-1104.
. Saliu OY, Sofer C, Stein DS, et al. Tumor-necrosis-factor blockers:differential effects on mycobacterial immunity. J Infect Dis. 2006;194:
Table Incidence of Tuberculosis Associated with DifferentAnti-Tumor Necrosis Factor Therapies
LocationIncidence per100,000
United StatesPatients who have rheumatoid arthritisWithout anti-TNF therapy 6.2With infliximab 24.4-54With etanercept 8.8-28
EuropeRheumatoid arthritis without anti-TNF
therapy6.2
Rheumatoid arthritis with infliximab 173Worldwide (calculated crude rate)Rheumatoid arthritis with infliximab
therapy47.6
TNF � tumor necrosis factor.
486-492.

L
T
e7ret
metee
risTtU1Sfppair
0
The American Journal of Medicine (2007) 120, e23
ETTER
apmtca
sinott
R1
2
3
4
5
6
he Reply:
We thank Hooper and Chi for their comments. To this end,tanercept is composed of 2 naturally occurring soluble human5-kDa TNF-R2 receptors ligated to the crytallizable (Fc)egion of human immunoglobulin G1.
1 Accordingly, it is anngineered soluble antibody that competitively binds TNF,hereby hindering its binding to its receptors.
We recognize that “TNF� inhibitor” would have beenore appropriate words to describe the biologic effects of
tanercept. However, our intention in choosing “TNF� an-ibody” instead was to describe the ability of this class ofngineered proteins, unlike receptor antagonists and block-rs, to bind human TNF�.
We inadvertently misplaced the etanercept-associated crudeate of tuberculosis worldwide (20.7 per 100,000)2 with thencidence of tuberculosis due to etanercept in the US,3 whichhould have been 8.8 per 100,000, and have now revised theable accordingly. Although the majority (94%) of patients
reated with etanercept were from the US, patients outside theS also were included in the analysis, so a rate of 8.8 per00,000 may not be representative of the US population.3
ubsequent to the report of Keane et al,3 reanalysis of datarom the Food and Drug Administration’s Adverse Event Re-orting System revealed 16 additional patients (total of 25atients including the initial 9) who developed tuberculosisfter etanercept administration. This figure corresponds to anncidence of 15 per 100,000 (17 of 113,238 patients whoeceived etanercept in the US).4
Table Incidence of Tuberculosis Associated with Anti-TNF�Therapy
LocationIncidence/Rate(per 100,000)
United States (incidence)Patients who have rheumatoid arthritisWithout TNF� therapy 6.2With infliximab 24.4-54With etanercept 8.8,3 15,4 285
Worldwide (calculated crude rate)With infliximab 47.62
With etanercept 20.72
002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
Available evidence suggests that the lower incidence ofctive tuberculosis in patients treated with etanercept com-ared with infliximab may be attributed to differences inechanism(s) of action and pharmacokinetics. However,
his difference also may be related, in part, to differences inase reporting and inconsistencies in voluntary reporting ofdverse events to both drugs.4-6
The above notwithstanding, the risk of active tuberculo-is associated with etanercept, although lower than that withnfliximab, is still significantly higher than that of patientsot being treated with etanercept. Accordingly, we stand byur key take-home message that clinicians should screenheir patients for latent tuberculosis infection regardless ofheir anti-TNF� drug of choice.
Gökhan M. Mutlu, MDAmy Bellmeyer, MS
Pulmonary and Critical Care MedicineNorthwestern University Feinberg School of Medicine
Chicago, Ill
Ece A. Mutlu, MDGastroenterology and Nutrition
Rush University Medical CollegeChicago, Ill
Israel Rubinstein, MDPulmonary, Critical Care and Sleep Medicine
University of Illinois at ChicagoJesse Brown VA Medical Center
Chicago, Ill
doi:10.1016/j.amjmed.2006.12.017
eferences. Mutlu GM, Mutlu EA, Bellmeyer A, Rubinstein I. Pulmonary adverse
events of anti-tumor necrosis factor-alpha antibody therapy. Am J Med.2006;119:639-646.
. Gardam MA, Keystone EC, Menzies R, et al. Anti-tumour necrosisfactor agents and tuberculosis risk: mechanisms of action and clinicalmanagement. Lancet Infect Dis. 2003;3:148-155.
. Keane J, Gershon S, Wise RP, et al. Tuberculosis associated withinfliximab, a tumor necrosis factor alpha-neutralizing agent. N EnglJ Med. 2001;345:1098-1104.
. Mohan AK, Cote TR, Block JA, Manadan AM, Siegel JN, Braun MM.Tuberculosis following the use of etanercept, a tumor necrosis factorinhibitor. Clin Infect Dis. 2004;39:295-299.
. Wallis RS, Broder MS, Wong JY, et al. Granulomatous infectiousdiseases associated with tumor necrosis factor antagonists. Clin InfectDis. 2004;38:1261-1265.
. Schaible TF. Inconsistencies in reporting of granulomatous infectiousdiseases associated with infliximab and etanercept. Clin Infect Dis.
2004;39:1255-1256; reply 1256.
L
CD
T
pi
aAdmff
ttptl
em
0
The American Journal of Medicine (2007) 120, e25
ETTER
rw
sep
R1
2
3
urrently Used Medicines for Alzheimer’sisease Are Not Very Effective
o the Editor:
I read the article by Farlow and Cummings on effectiveharmacologic management of Alzheimer’s disease withnterest.1
My concern with the point of the article is that thereren’t really any effective pharmacologic treatments forlzheimer’s disease. An article by Courtney2 indicatedonepezil is not cost effective, with benefits below mini-ally relevant thresholds. The article concluded more ef-
ective treatments than cholinesterase inhibitors are neededor Alzheimer’s disease.2
The medications are accepted as “symptomatic” treatmentshat help delay functional decline but don’t alter the course ofhe disease. Advocates maintain it is unethical not to treatatients with these compounds to prolong any remaining func-ional abilities while critics note modest efficacy, high cost andack of any detectable improvement in most patients.3
There is probably little improvement in quality of life,specially in patients with advanced dementia, from the
edications.002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
There is not one patient I am aware of who has actuallyecovered from moderate to advanced Alzheimer’s disease,ith treatment, enough to resume a normal life.Although the cholinesterase inhibitors are widely pre-
cribed for patients with Alzheimer’s disease, beneficialffects might not be discernable in many, if not most,atients.
Steven Brenner, MDDepartment of Neurology
St. Louis VA Medical CenterSt. Louis
Neurology DepartmentSt. Louis University
doi:10.1016/j.amjmed.2007.05.008
eferences. Farlow M, Cummings J. Effective pharmacologic management of Alz-
heimer’s disease. Am J Med. 2007;120:388-397.. Courtney C, Farrell D, Gray R, et al. Long term donepezil treatment in
565 patients with Alzheimer’s disease (AD2000): randomized double-blind trial. Lancet. 2004;363:2105-2115.
. Nair A, Green R. A century of Alzheimer’s: progress and pitfalls.
Practical Neurology. 2006;5:22-29.
L
T
pifddtCicavmatc
tosrt
ste
0
The American Journal of Medicine (2007) 120, e27
ETTER
pp
tAdar
R1
2
3
4
5
he Reply:
Contrary to the opinion and personal experience ex-ressed by Brenner, the evidence base for cholinesterasenhibitors being effective and clinically significant therapiesor Alzheimer disease is strong. The measure in previousouble-blind, placebo-controlled trials that most directlyemonstrates appreciable significant clinical effects forhese drugs is the Clinician Interview Based Impression ofhange with Caregiver Input.1 This assessment is by an
ndependent clinician who evaluates the patient and theiraregiver separately and makes a judgment on whether theyre mildly, moderately, or strongly improved, or worseersus their own baseline. This instrument clearly is a globaleasure and does assess overall quality of life. All of the
vailable cholinesterase inhibitors have been demonstratedo have appreciable clinically significant effects versus pla-ebo treatments by this measure.2-4
However, progressive deterioration naturally occurs inhe course of Alzheimer disease, and the beneficial effectsf cholinesterase inhibitors in the individual patient may betabilization of clinical symptoms or less rapid deteriorationather than improvement, a benefit that may be difficult forhe caregiver to appreciate.
It also is important to understand that modest benefitseen in cholinesterase inhibitor studies are group means andhat some patients are better responders, whereas other ben-
fit hardly at all. Moderate stage of disease and rapidly002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
rogressive disease are factors that seem to predict betteratient responses to cholinesterase inhibitor therapy.5
In summary, cholinesterase inhibitors do improve symp-oms for substantial periods of time in many patients withlzheimer disease. Even after disease progression-delayingrugs are developed, they are likely to remain a usefulnd necessary component of future Alzheimer therapyegimens.
Martin R. Farlow, MDIndiana University School of Medicine
Indianapolis, Ind
doi:10.1016/j.amjmed.2007.07.031
eferences. Schneider LS, Olin JT, Doody RS, et al. Validity and reliability of the
Alzheimer’s disease Cooperative Study-Clinical Global Impression ofChange. Alzheimer Dis Assoc Disord. 1997;11(Suppl 2):S22-S32.
. Schneider LS, Anand R, Farlow MR. Systematic review of the efficacyof rivastigmine for patients with Alzheimer’s disease. Int J GeriatrPsychopharmacol. 1998;1(Suppl 1):S26-S34.
. Rogers SL, Farlow MR, Doody RS, Mohs R, Friedhoff LT and theDonepezil Study Group. A 24-week, double-blind, placebo-controlledtrial of donepezil in patients with Alzheimer’s disease. Neurology.1998;50:136-145.
. Tariot PN, Solomon PR, Morris JC, et al. A 5-month, randomized,placebo-controlled trial of galantamine in AD. The Galantamine USA-10Study Group. Neurology. 2000;54:2269-2276.
. Gauthier S, Vellas B, Farlow M, Burn D. Aggressive course of disease
in dementia. Alzheimers Dement. 2006;2:210-217.
L
CR
T
l
sfaadpcocfwnrctiiwpmhpmmdsf
0
The American Journal of Medicine (2007) 120, e29
ETTER
rmdtdcseTmfsdtn
R1
2
3
4
linical Perspectives of Statin-inducedhabdomyolysis
o the Editor:
We read with interest the article by Antons and col-eagues.1 Two points in their article attracted our attention.
We are in agreement that statins pose a burden to phy-icians because of myotoxicity. Neurologic evaluation isrequently sought for myalgia, cramps, muscle tenderness,nd sometimes rhabdomyolysis with proximal weaknessfter therapy with statin. As mentioned, a major differentialiagnosis is acute inflammatory muscle disease, such asolymyositis and dermatomyositis. However, we do notount inclusion body myositis in the differential diagnosisf rhabdomyolysis because this disorder is unique in itshronicity and phenotype. Electromyography (EMG) is arequently used diagnostic test during the acute phase ofeakness to differentiate acute necrotizing myopathies fromoninflammatory myonecrosis “rhabdomyolysis.” Severaleports showed a good correlation among muscle weakness,reatine kinase elevation, and EMG findings in polymyosi-is.2 We recently reported a low utility of EMG in evaluat-ng rhabdomyolysis in 15 cases, one of which was precip-tated by statin.3 Needle EMG of 117 muscles in patientsith rhabdomyolysis who had a median creatine kinaseeak of 48,000 �/L showed variable proximal myopathicotor unit action potentials in 16%. None of those patients
ad persistent active denervation. The study concluded thatatients with rhabdomyolysis are less likely to show abnor-al EMG results when compared with patients with poly-yositis. We believe that EMG has a good negative pre-
ictive value in diagnosing rhabdomyolysis and in a correctetting, such as statin myonecrosis, would obviate the need
or a muscle biopsy.002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
The authors referred to heavy exercise as an exogenousisk factor for statin myotoxicity. Indeed, heavy exerciseay cause myonecrosis in patients with enzymatic muscle
isorders (eg, myophosphorylase and carnitine palmitoyl-ransferase deficiency), even without statin use, suggesting aisorder of the mitochondrial respiratory chain. A low mus-le coenzyme Q10 concentration and altered skeletal muscleterol metabolism in those with statin myopathy are furthervidence of statin-induced mitochondrial dysfunction.4
herefore, a family history of inherited enzymatic oretabolic muscle disorder or statin myotoxicity is help-
ul to indicate a potential harmful effect of statin. Phy-icians should be aware of statin myotoxicity, but not toeter patients from pursuing physical fitness, especiallyhose who have a high risk for vascular disease and doot manifest exercise intolerance.
Amer Alshekhlee, MD, MScBashar Katirji, MDNeurological Institute
University Hospital Case Medical CenterCleveland, Ohio
doi:10.1016/j.amjmed.2006.08.034
eferences. Antons KA, Williams CD, Baker SK, Phillips PS. Clinical perspectives
of statin-induced rhabdomyolysis. Am J Med. 2006;119:400-409.. Tymms KE, Beller EM, Webb J, et al. Correlation between tests of
muscle involvement and clinical muscle weakness in polymyositis anddermatomyositis. Clin Rheumatol. 1990;9:523-529.
. Al-Shekhlee A, Hachwi R, Jaberi MM, Katirji B. The electromyo-graphic features of acute rhabdomyolysis. J Clin Neuromusc Dis. 2005;6:114-118.
. Lamperti C, Naini AB, Lucchini V, et al. Muscle coenzyme Q10 level
in statin-related myopathy. Arch Neurol. 2005;62:1709-1712.
L
T
T
gratl
0
The American Journal of Medicine (2007) 120, e31
ETTER
R1
2
esting for Stain-induced Myopathy
o the Editor:
The clinically important article by Antons et al.1 placesreat weight on use of the creatinine kinase test in their algo-ithm (Figure 2). I have been interested in whether there is anylternative testing that might be more clinically reliable.2 Havehe authors any experience with alternative blood testing in
ight of their described limits in creatinine kinase testing?002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
Mark H. Hyman, MDAssociate Clinical Professor Medicine, UCLA
Los Angeles, Calif
doi:10.1016/j.amjmed.2006.05.065
eferences. Antons KA, Williams CD, Baker SK, et al. Clinical perspectives of
statin-induced rhabdomyolysis. Am J Med. 2006;119:400-409.. Hyman MH. Statin-associated myopathy with normal creatinine kinase
levels. Ann Intern Med. 2003;138:12:1007.

L
T
GatAteaeciwaa
twsniwtctymnnb
0
The American Journal of Medicine (2007) 120, e33
ETTER
ma
itcmntlf
R1
2
3
4
5
he Reply:
We appreciate the observations of Hyman and Al-shekhlee.iven the limits of creatine kinase in detecting statin-ssociated muscle disorders, Hyman correctly points outhe need for alternative screening tests for this disorder.s yet, no biomarker is sufficiently sensitive or specific
o be used routinely to diagnose statin myotoxicity. Skel-tal troponins,1 lipidomics analyses,2 and urinary organiccid profiles3 each hold some promise and remain undervaluation. In the meanwhile we must depend on aombination of clinical criteria described in the article,ncluding typical symptoms, dynamometer-measuredeakness, abnormalities on cardiopulmonary exercise,
nd a constellation of tests excluding other disorders torrive at this diagnosis.
The patient evaluation plan we recommended includedhe approach to patients with less serious muscle symptomshile receiving statins, as well as to patients with muscle
ymptoms after statin-induced rhabdomyolysis.4 Although aegative electromyogram has not been useful in distinguish-ng patients with purported statin-induced muscle pain andeakness, it is certainly useful in distinguishing inflamma-
ory from other causes of acute rhabdomyolysis. The mostommon reason for muscle biopsy in patients with persis-ent symptoms after suspected statin-induced rhabdomyol-sis is to exclude polymyositis or an underlying metabolicyopathy. We agree with Al-shekhlee and Katirji that a
egative electromyogram will exclude the former. We doot agree that a negative electromyogram obviates a muscle
iopsy in patients with persistent symptoms after rhabdo-002-9343/$ -see front matter © 2007 Elsevier Inc. All rights reserved.
yolysis. A significant number of these patients have met-bolic muscle disease, as we recently observed.5
Both correspondents point to the complexity in evaluat-ng and treating statin-induced muscle disorders that con-inues to make work in this area both challenging andontroversial. Fear of serious muscle toxicity remains theost common reason that our patients and colleagues are
ot compliant with aggressive lipid-lowering recommenda-ions. Further work to clarify the mechanism by whichipid-lowering therapies cause muscle toxicity is essentialor the appropriate application of lipid-lowering therapies.
Paul Sydney Phillips, MDScripps-Mercy Hospital
San Diego, Calif
doi:10.1016/j.amjmed.2007.08.005
eferences. Simpson JA, Labugger R, Hesketh GG, et al. Differential detection of
skeletal troponin I isoforms in serum of a patient with rhabdomyolysis:markers of muscle injury? Clin Chem. 2002;48:1112-1114.
. Laaksonen R, Katajamaa M, Paiva H, et al. A systems biology strategyreveals biological pathways and plasma biomarker candidates for po-tentially toxic statin-induced changes in muscle. PLoS ONE. 2006;1:e97.
. Phillips PS, Haas RH, Barshop B, et al. Utility of abnormal 3-methyl-glutaconic aciduria (3MGA) in diagnosing statin associated myopathy.Arterioscler Thromb Vasc Biol. 2002;22:878.
. Antons K, Williams C, Baker SK, Phillips PS. Clinical perspectives ofstatin-induced rhabdomyolysis. Am J Med. 2006;119:400-409.
. Vladutiu GD, Simmons Z, Isackson PJ, et al. Genetic risk factors andmetabolic myopathies associated with lipid-lowering drugs. Muscle
Nerve. 2006;34:153-162.