
Th1/Th2 cytokines in patients with systemic lupus erythematosus: is tumor necrosis factor α...
10
Th1/Th2 Cytokines in Patients with Systemic Lupus Erythematosus: Is Tumor Necrosis Factor Protective? Diana Go ´ mez, Paula A. Correa, Luis Miguel Go ´ mez, Jose ´ Cadena, Jose ´ F. Molina, and Juan-Manuel Anaya Objectives: To determine the circulating levels of Th1 and Th2 cytokines in patients with systemic lupus erythematosus (SLE) and to elucidate their association with disease activity and autoimmune response. Methods: We included 52 patients and 25 healthy controls. Serum levels of tumor necrosis factor (TNF) , interferon (IFN) , interleukin (IL)-12p70, IL-10, and IL-4, as well as anti-DNA, -Ro, -La, -RNP, and -Sm antibodies were deter- mined by enzyme-linked immunosorbent assay. Disease activity was recorded according to the Systemic Lupus Erythematosus Disease Activity Index (SLE- DAI) and classified as very active (SLEDAI > 13), moderately active (SLEDAI: 3-12), or inactive (SLEDAI < 2). Results: The mean age of the patients was 34.2 12.6 years, and the mean duration of disease was 4.9 7.6 years. Twelve patients (23%), 20 patients (34.5%), and 20 patients (34.5%) had highly, moderately, and inactive SLE, respectively. Levels of IFN-, TNF-, and IL-12 were significantly higher in patients than in healthy controls (P < .03), as well as the IL-12/IL-10, IL-12/IL-4, IFN/IL-10, IFN/IL-4, TNF/IL-10, and TNF/IL-4 ratios (P < .01), suggesting a major participation of Th1 over Th2 cytokines. Nevertheless, a direct correlation between Th1 (IFN- and TNF-) and Th2 (IL-4 and IL-10) cytokines was ob- served in patients (r > .5, P < .01), indicating a mutual Th1-Th2 participation. TNF- levels and the TNF/IL-10 ratio were higher in patients with inactive disease compared with patients with very active disease and controls (P < .04). IL-12 levels and IL-12/IL-4, as well as IL-12/IL-10, ratios were higher in patients with very active disease than in those with inactive SLE and controls (P < .01). IL-10 levels were associated with anti-DNA, anti-Ro, and anti-La response (P < .01). Conclusion: Our results suggest that TNF- could be a protective factor in SLE patients, whereas IL-12p70 participates in disease activity and IL-10 influ- ences the autoimmune response (autoantibody production). Semin Arthritis Rheum 33:404-413. © 2004 Elsevier Inc. All rights reserved. INDEX WORDS: Systemic lupus erythematosus; cytokines; TNF-; IL-10; IL12; autoantibodies; SLEDAI. From the Cellular Biology and Immunogenetics Unit, Corporacio ´n para Investigaciones Biolo ´gicas, Medellin, Colombia; and Rheuma- tology Unit, Clinica Universitaria Bolivariana, School of Medicine, Universidad Pontificia Bolivariana, Medellin, Colombia. Diana Go ´mez, BSc: Assistant Researcher, Cellular Biology and Immunogenetics Unit, Corporacio ´n para Investigaciones Biolo ´gicas, Medellin, Colombia; Paula A. Correa, MSc: Assis- tant Researcher, Cellular Biology and Immunogenetics Unit, Corporacio ´n para Investigaciones Biolo ´gicas, and Assistant Professor, School of Medicine, Universidad Pontificia Boliva- riana, Medellin, Colombia; Luis Miguel Go ´ mez, MV: Assistant Researcher, Cellular Biology and Immunogenetics Unit, Cor- poracio ´ n para Investigaciones Biolo ´ gicas, Medellin, Colombia; Jose ´ Cadena, MD: Assistant Researcher, Cellular Biology and Immunogenetics Unit, Corporacio ´n para Investigaciones Bio- lo ´gicas, and Rheumatology Unit, Rheumatology Unit, Clı ´nica Universitaria Bolivariana, Medellin, Colombia; Jose ´ F. Molina, MD: Associate Professor, School of Medicine, Universidad Pontificia Bolivariana, Medellin, Colombia Juan-Manuel Anaya, MD: Associate Researcher, Cellular Biology and Im- munogenetics Unit, Corporacio ´n para Investigaciones Biolo ´gi- cas, and Professor of Medicine, School of Medicine, Univer- sidad Pontificia Bolivariana, Medellin, Colombia. Supported by the Asociacio ´n Colombiana de Reumatologı ´a, Bogota ´, and the Corporacio ´n para Investigaciones Biolo ´gicas, Medellı ´n, Colombia. Address reprint requests to: Juan-Manuel Anaya, MD, Cor- poracio ´n para Investigaciones Biolo ´gicas, Cra. 72-A No 78-B- 141, Medellı ´n, Colombia. E-mail: [email protected] © 2003 Elsevier Inc. All rights reserved. 0049-0172/04/3306-0000$30.00/0 doi:10.1016/j.semarthrit.2003.11.002 404 Seminars in Arthritis and Rheumatism, Vol 33, No 6 (June), 2004: pp 404-413
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Th1/Th2 cytokines in patients with systemic lupus erythematosus: is tumor necrosis factor α...

ptU
aBtCPrRpJIl
idad
Im-
iver-
ı
or--
4
Th1/Th2 Cytokines in Patients with Systemic LupusErythematosus: Is Tumor Necrosis Factor � Protective?
Diana Gomez, Paula A. Correa, Luis Miguel Gomez, Jose Cadena,
Jose F. Molina, and Juan-Manuel Anaya
Objectives: To determine the circulating levels of Th1 and Th2 cytokines in
patients with systemic lupus erythematosus (SLE) and to elucidate their
association with disease activity and autoimmune response.
Methods: We included 52 patients and 25 healthy controls. Serum levels of
tumor necrosis factor (TNF) �, interferon (IFN) �, interleukin (IL)-12p70, IL-10,
and IL-4, as well as anti-DNA, -Ro, -La, -RNP, and -Sm antibodies were deter-
mined by enzyme-linked immunosorbent assay. Disease activity was recorded
according to the Systemic Lupus Erythematosus Disease Activity Index (SLE-
DAI) and classified as very active (SLEDAI > 13), moderately active (SLEDAI:
3-12), or inactive (SLEDAI < 2).
Results: The mean age of the patients was 34.2 � 12.6 years, and the mean
duration of disease was 4.9 � 7.6 years. Twelve patients (23%), 20 patients
(34.5%), and 20 patients (34.5%) had highly, moderately, and inactive SLE,
respectively. Levels of IFN-�, TNF-�, and IL-12 were significantly higher in
patients than in healthy controls (P < .03), as well as the IL-12/IL-10, IL-12/IL-4,
IFN/IL-10, IFN/IL-4, TNF/IL-10, and TNF/IL-4 ratios (P < .01), suggesting a major
participation of Th1 over Th2 cytokines. Nevertheless, a direct correlation
between Th1 (IFN-� and TNF-�) and Th2 (IL-4 and IL-10) cytokines was ob-
served in patients (r > .5, P < .01), indicating a mutual Th1-Th2 participation.
TNF-� levels and the TNF/IL-10 ratio were higher in patients with inactive disease
compared with patients with very active disease and controls (P < .04). IL-12 levels
and IL-12/IL-4, as well as IL-12/IL-10, ratios were higher in patients with very active
disease than in those with inactive SLE and controls (P < .01). IL-10 levels were
associated with anti-DNA, anti-Ro, and anti-La response (P < .01).
Conclusion: Our results suggest that TNF-� could be a protective factor in
SLE patients, whereas IL-12p70 participates in disease activity and IL-10 influ-
ences the autoimmune response (autoantibody production).
Semin Arthritis Rheum 33:404-413. © 2004 Elsevier Inc. All rights reserved.
INDEX WORDS: Systemic lupus erythematosus; cytokines; TNF-�; IL-10; IL12;
autoantibodies; SLEDAI.
From the Cellular Biology and Immunogenetics Unit, Corporacio´nara Investigaciones Biolo´gicas, Medellin, Colombia; and Rheuma-
ology Unit, Clinica Universitaria Bolivariana, School of Medicine,niversidad Pontificia Bolivariana, Medellin, Colombia.Diana Gomez, BSc: Assistant Researcher, Cellular Biology
nd Immunogenetics Unit, Corporacio´n para Investigacionesiologicas, Medellin, Colombia;Paula A. Correa, MSc: Assis-
ant Researcher, Cellular Biology and Immunogenetics Unit,orporacion para Investigaciones Biolo´gicas, and Assistantrofessor, School of Medicine, Universidad Pontificia Boliva-
iana, Medellin, Colombia;Luis Miguel Gomez, MV: Assistantesearcher, Cellular Biology and Immunogenetics Unit, Cor-oracion para Investigaciones Biolo´gicas, Medellin, Colombia;ose Cadena, MD: Assistant Researcher, Cellular Biology andmmunogenetics Unit, Corporacio´n para Investigaciones Bio-
Universitaria Bolivariana, Medellin, Colombia;Jose F. Molina,MD: Associate Professor, School of Medicine, UniversPontificia Bolivariana, Medellin, ColombiaJuan-ManuelAnaya, MD: Associate Researcher, Cellular Biology andmunogenetics Unit, Corporacio´n para Investigaciones Biolo´gi-cas, and Professor of Medicine, School of Medicine, Unsidad Pontificia Bolivariana, Medellin, Colombia.
Supported by the Asociacio´n Colombiana de Reumatolog´a,Bogota, and the Corporacio´n para Investigaciones Biolo´gicas,Medellın, Colombia.
Address reprint requests to: Juan-Manuel Anaya, MD, Cporacion para Investigaciones Biolo´gicas, Cra. 72-A No 78-B141, Medellı´n, Colombia. E-mail: [email protected]
© 2003 Elsevier Inc. All rights reserved.0049-0172/04/3306-0000$30.00/0
ogicas, and Rheumatology Unit, Rheumatology Unit, Clı´nica doi:10.1016/j.semarthrit.2003.11.002
04 Seminars in Arthritis and Rheumatism, Vol 33, No 6 (June), 2004: pp 404-413

Sciwlmrm
mDtnwmciI(mIhBpt(pcnrdci
swt
S
wCbCtpeaw
C
tddacvea
wAwnjeaebtuNplaoaopcdcaupacppnc
pslcsl
405TNF-� IN SLE
YSTEMIC LUPUS erythematosus (SLE) is aheterogeneous, chronic autoimmune disease
haracterized by the deposit of immune complexesn different organs. The disease primarily affectsomen between the third and fourth decades of
ife. Even though the etiology of SLE is unknown,any predisposing factors playing an important
ole have been found, including genetic, environ-ental, infectious, and hormonal factors (1).In SLE, B-cell hyperactivity and the presence ofultiple autoantibodies are observed (2,3). Anti-IgGNA antibodies are present in nearly 70% of pa-
ients, and some studies have suggested that they areephrotoxic (3,4). Another characteristic of patientsith SLE is the abnormality in the T-cell response,anifested by an imbalance in the production of
ytokines. Cytokines have been functionally dividednto 2 subgroups: Th1, mainly interleukin (IL)-2,L-12, interferon (IFN) �, and tumor necrosis factorTNF) � and �, which mainly activate the cellularachinery of the immune system; and Th2 (IL-4,
L-5, IL-10, and IL-13) cytokines, which activate theumoral machinery (5–8). In patients with SLE,-cell hyperactivity has been associated with a highroduction of Th2 cytokines. However, the participa-ion of Th1 cytokines has been equally demonstrated9). Both Th1 and Th2 cytokines can participate inromoting or inhibiting autoimmune diseases; thus, alear-cut distinction between Th1 and Th2 patterns isot without complexity (10). In SLE, the differentesults concerning cytokines should be consideredepending on the studied model, because discrepan-ies exist between murine and human (patients) stud-es (10–22).
In the present study, the simultaneous relation-hips between the levels of Th1-Th2 cytokinesith the production of autoantibodies and the ac-
ivity of SLE in a group of patients was evaluated.
METHODS
tudy Population
This was a cross-sectional study. SLE patientsere enrolled in the Rheumatology Unit at thelinica Universitaria Bolivariana, Medellin, Colom-ia. All patients fulfilled 4 or more of the Americanollege of Rheumatology criteria for the classifica-
ion of SLE (23). Healthy people unrelated to theatients, without inflammatory or autoimmune dis-ase, matched to patients by age (�5 years), gender,nd geography were included as controls. This study
as approved by the local ethics committee. alinical Variables
Information on patient demographics and cumula-ive clinical and laboratory manifestations over theisease course were obtained either by verificationuring discussion with the patient or by chart review,nd were recorded in a standard data-collection formreated for that purpose. Each clinical and laboratoryariable was registered as “present” or “absent” forvery specific patient during the course of the diseasend at the time of blood sample collection.
The clinical and laboratory variables associatedith SLE, including each feature of the revisedmerican College of Rheumatology criteria (23),ere evaluated and defined as follows: 1) arthritis:onerosive arthritis involving 2 or more peripheraloints, characterized by tenderness, swelling, orffusion; 2) malar rash; 3) photosensitivity; 4)lopecia; 5) discoid lupus; 6) Raynaud’s phenom-non; 7) renal involvement, as evidenced by a renaliopsy result showing the World Health Organiza-ion’s (WHO) class II-V histopathology, activerinary sediment, or proteinuria �500 mg/24 h.ephrotic syndrome was defined as �3.5 g/d ofroteinuria, hypoalbuminemia (�2.8 g/dL), hyper-ipidemia, and edema. Lupus nephritis was defineds present or absent according to the abnormalitiesf the previous tests. 8) Neurologic involvement,s evidenced by seizures or psychosis without anyther definable cause, or other conditions such aseripheral neuropathy, stroke, transverse myelitis,horea, or other central nervous system lesionsirectly attributable to SLE in the absence of otherauses; 9) pleuritis: pleural rub and/or effusionnd/or typical pleuritic pain; 10) pericarditis: doc-mented by electrocardiogram, rub, or evidence ofericardial effusion; 11) autoimmune hemolyticnemia, with a hematocrit �35%, reticulocyteount �4%, and positive Coombs test; 12) leuko-enia, white cells �4000/mm3; 13) thrombocyto-enia, platelets �100,000/mm3; 14) arterial or ve-ous thrombosis diagnosed on clinical grounds andonfirmed by appropriate tests.
Comorbility was also recorded, and included theresence or absence of infection, arterial hyperten-ion (blood pressure levels � 140/90), diabetes mel-itus (fasting glycemia � 126 mg/dl in 2 occasions),oronary disease (history of myocardial infarction,table or unstable angina), hyperlipidemia (LDL cho-esterol � 130 mg/dl and triglycerides � 150 mg/dl),
nd hypothyroidism (TSH � 5 mU/L).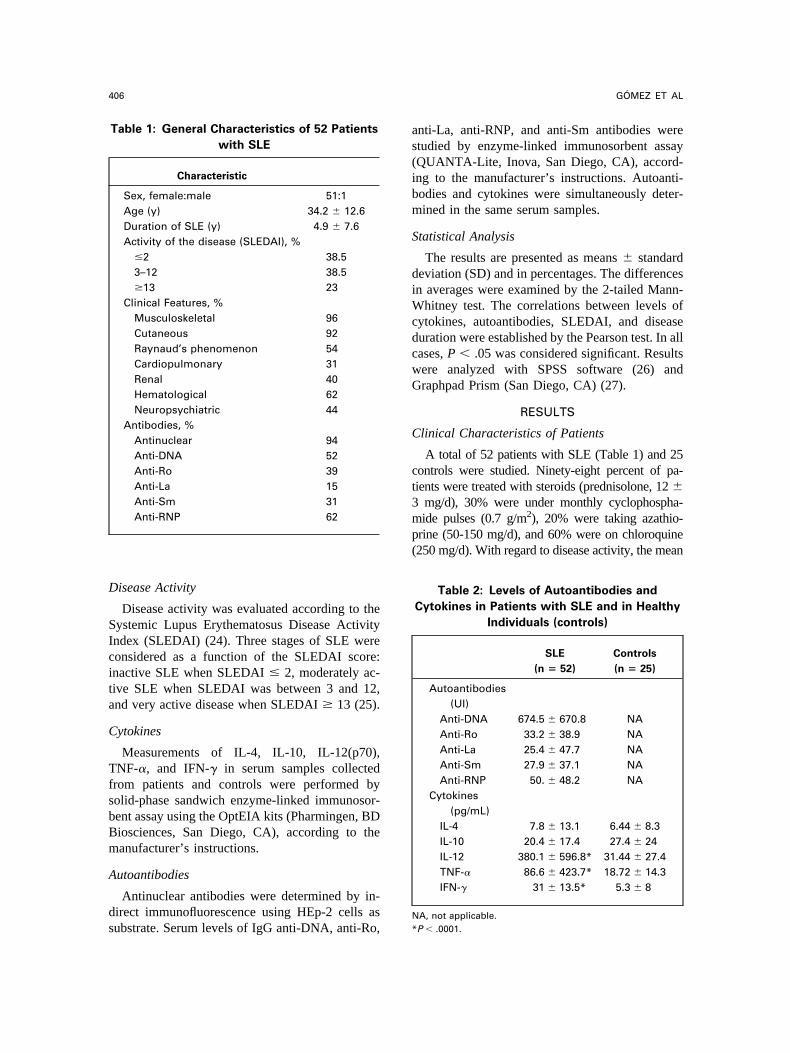
D
SIcita
C
TfsbBm
A
ds
as(ibm
S
diWcdcwG
C
ct3mp(
N
406 GOMEZ ET AL
isease Activity
Disease activity was evaluated according to theystemic Lupus Erythematosus Disease Activityndex (SLEDAI) (24). Three stages of SLE wereonsidered as a function of the SLEDAI score:nactive SLE when SLEDAI � 2, moderately ac-ive SLE when SLEDAI was between 3 and 12,nd very active disease when SLEDAI � 13 (25).
ytokines
Measurements of IL-4, IL-10, IL-12(p70),NF-�, and IFN-� in serum samples collected
rom patients and controls were performed byolid-phase sandwich enzyme-linked immunosor-ent assay using the OptEIA kits (Pharmingen, BDiosciences, San Diego, CA), according to theanufacturer’s instructions.
utoantibodies
Antinuclear antibodies were determined by in-irect immunofluorescence using HEp-2 cells as
Table 1: General Characteristics of 52 Patients
with SLE
Characteristic
Sex, female:male 51:1Age (y) 34.2 � 12.6Duration of SLE (y) 4.9 � 7.6Activity of the disease (SLEDAI), %
�2 38.53–12 38.5�13 23
Clinical Features, %Musculoskeletal 96Cutaneous 92Raynaud’s phenomenon 54Cardiopulmonary 31Renal 40Hematological 62Neuropsychiatric 44
Antibodies, %Antinuclear 94Anti-DNA 52Anti-Ro 39Anti-La 15Anti-Sm 31Anti-RNP 62
ubstrate. Serum levels of IgG anti-DNA, anti-Ro, *
nti-La, anti-RNP, and anti-Sm antibodies weretudied by enzyme-linked immunosorbent assayQUANTA-Lite, Inova, San Diego, CA), accord-ng to the manufacturer’s instructions. Autoanti-odies and cytokines were simultaneously deter-ined in the same serum samples.
tatistical Analysis
The results are presented as means � standardeviation (SD) and in percentages. The differencesn averages were examined by the 2-tailed Mann-
hitney test. The correlations between levels ofytokines, autoantibodies, SLEDAI, and diseaseuration were established by the Pearson test. In allases, P � .05 was considered significant. Resultsere analyzed with SPSS software (26) andraphpad Prism (San Diego, CA) (27).
RESULTS
linical Characteristics of Patients
A total of 52 patients with SLE (Table 1) and 25ontrols were studied. Ninety-eight percent of pa-ients were treated with steroids (prednisolone, 12 �
mg/d), 30% were under monthly cyclophospha-ide pulses (0.7 g/m2), 20% were taking azathio-
rine (50-150 mg/d), and 60% were on chloroquine250 mg/d). With regard to disease activity, the mean
Table 2: Levels of Autoantibodies and
Cytokines in Patients with SLE and in Healthy
Individuals (controls)
SLE
(n � 52)
Controls
(n � 25)
Autoantibodies(UI)
Anti-DNA 674.5 � 670.8 NAAnti-Ro 33.2 � 38.9 NAAnti-La 25.4 � 47.7 NAAnti-Sm 27.9 � 37.1 NAAnti-RNP 50. � 48.2 NA
Cytokines(pg/mL)
IL-4 7.8 � 13.1 6.44 � 8.3IL-10 20.4 � 17.4 27.4 � 24IL-12 380.1 � 596.8* 31.44 � 27.4TNF-� 86.6 � 423.7* 18.72 � 14.3IFN-� 31 � 13.5* 5.3 � 8
A, not applicable.
P � .0001.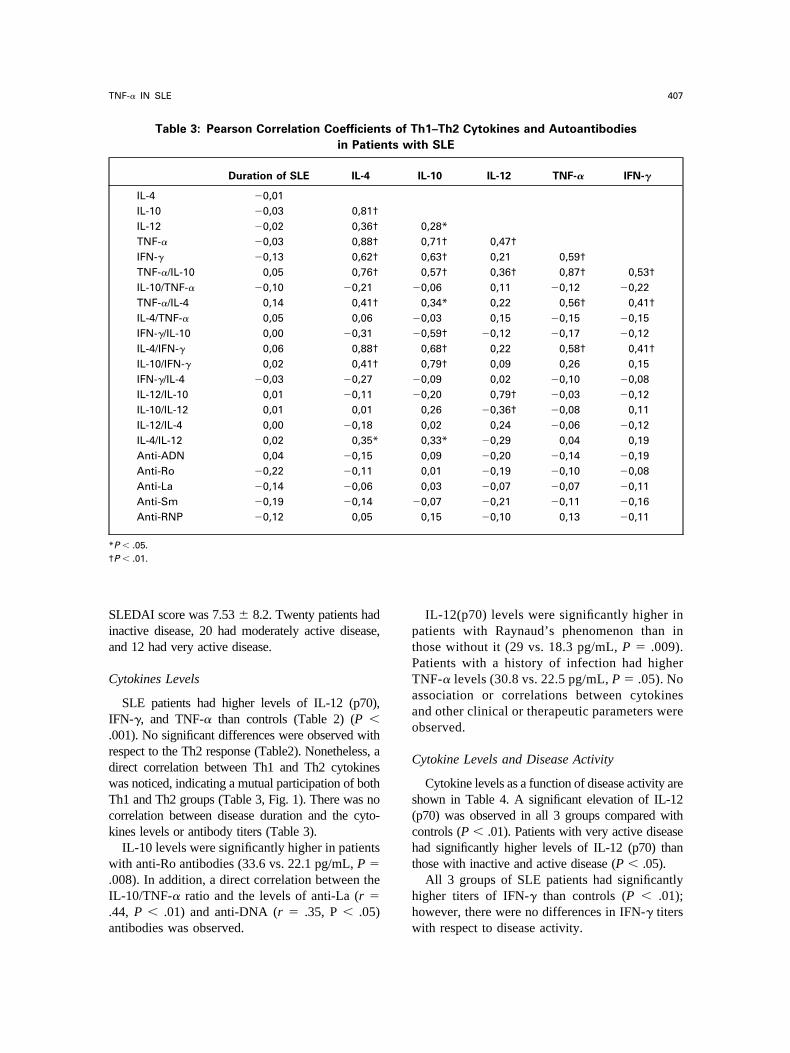
Sia
C
I.rdwTck
w.I.a
ptPTaao
C
s(cht
hh
*†
407TNF-� IN SLE
LEDAI score was 7.53 � 8.2. Twenty patients hadnactive disease, 20 had moderately active disease,nd 12 had very active disease.
ytokines Levels
SLE patients had higher levels of IL-12 (p70),FN-�, and TNF-� than controls (Table 2) (P �001). No significant differences were observed withespect to the Th2 response (Table2). Nonetheless, airect correlation between Th1 and Th2 cytokinesas noticed, indicating a mutual participation of bothh1 and Th2 groups (Table 3, Fig. 1). There was noorrelation between disease duration and the cyto-ines levels or antibody titers (Table 3).
IL-10 levels were significantly higher in patientsith anti-Ro antibodies (33.6 vs. 22.1 pg/mL, P �
008). In addition, a direct correlation between theL-10/TNF-� ratio and the levels of anti-La (r �44, P � .01) and anti-DNA (r � .35, P � .05)
Table 3: Pearson Correlation Coefficien
in Patie
Duration of SLE IL-4
IL-4 �0,01IL-10 �0,03 0,81†IL-12 �0,02 0,36†TNF-� �0,03 0,88†IFN-� �0,13 0,62†TNF-�/IL-10 0,05 0,76†IL-10/TNF-� �0,10 �0,21TNF-�/IL-4 0,14 0,41†IL-4/TNF-� 0,05 0,06IFN-�/IL-10 0,00 �0,31IL-4/IFN-� 0,06 0,88†IL-10/IFN-� 0,02 0,41†IFN-�/IL-4 �0,03 �0,27IL-12/IL-10 0,01 �0,11IL-10/IL-12 0,01 0,01IL-12/IL-4 0,00 �0,18IL-4/IL-12 0,02 0,35*Anti-ADN 0,04 �0,15Anti-Ro �0,22 �0,11Anti-La �0,14 �0,06Anti-Sm �0,19 �0,14Anti-RNP �0,12 0,05
P � .05.P � .01.
ntibodies was observed. w
IL-12(p70) levels were significantly higher inatients with Raynaud’s phenomenon than inhose without it (29 vs. 18.3 pg/mL, P � .009).atients with a history of infection had higherNF-� levels (30.8 vs. 22.5 pg/mL, P � .05). Nossociation or correlations between cytokinesnd other clinical or therapeutic parameters werebserved.
ytokine Levels and Disease Activity
Cytokine levels as a function of disease activity arehown in Table 4. A significant elevation of IL-12p70) was observed in all 3 groups compared withontrols (P � .01). Patients with very active diseasead significantly higher levels of IL-12 (p70) thanhose with inactive and active disease (P � .05).
All 3 groups of SLE patients had significantlyigher titers of IFN-� than controls (P � .01);owever, there were no differences in IFN-� titers
h1–Th2 Cytokines and Autoantibodies
ith SLE
IL-10 IL-12 TNF-� IFN-�
0,28*0,71† 0,47†0,63† 0,21 0,59†0,57† 0,36† 0,87† 0,53†0,06 0,11 �0,12 �0,220,34* 0,22 0,56† 0,41†0,03 0,15 �0,15 �0,150,59† �0,12 �0,17 �0,120,68† 0,22 0,58† 0,41†0,79† 0,09 0,26 0,150,09 0,02 �0,10 �0,080,20 0,79† �0,03 �0,120,26 �0,36† �0,08 0,110,02 0,24 �0,06 �0,120,33* �0,29 0,04 0,190,09 �0,20 �0,14 �0,190,01 �0,19 �0,10 �0,080,03 �0,07 �0,07 �0,110,07 �0,21 �0,11 �0,160,15 �0,10 0,13 �0,11
ts of T
nts w
�
�
�
�
�
�
ith respect to disease activity.

scw
tFTe
F
N*†‡§�
408 GOMEZ ET AL
Significantly higher levels of TNF-� were ob-erved in the inactive and active groups whenompared with the controls (P � .01). Patientsith inactive disease had statistically higher levels
ig 1. Mutual participation of representative cyto
Table 4: Th1/Th2 Cytokines and Autoant
of Dise
Characteristics
A
SLEDAI <2
(n � 20)
S
Age (y) 36.3 � 16.4Duration of SLE (y) 5.3 � 9IL-4 (pg/mL) 11.8 � 25IL-10 (pg/mL) 22.9 � 25 1IL-12 (pg/mL) 303 � 546† 3TNF-� (pg/mL) 196 � 675.5† 2IFN-� (pg/mL) 32.5 � 14.8†TNF-�/IL-4 ratio 6.8 � 13.6TNF-�/IL-10 ratio 2.8 � 7�
IFN-�/IL-10 ratio 2.5 � 1.6†IL-12/IL-4 ratio 149 � 521† 6IL-12/IL-10 ratio 14.5 � 13.7† 3Anti-DNA (UI/mL) 578 � 589 5Anti-Ro (Units) 34 � 35 3Anti-La (Units) 12.3 � 15.1 3Anti-Sm (Units) 27.4 � 38.5 3Anti-RNP (Units) 48 � 52 5
A, not applicable.P � .05 compared with the SLEDAI �2 group.P � .01 compared with the control group.P � .05 compared with the SLEDAI 3–12 group.P � .05 compared with SLEDAI �13.
P � .05 compared with the control group.han those in the very active group (P � .01).inally, no significant differences were found inh2 (IL-4, IL-10) cytokines as a function of dis-ase activity (Table 4).
of the Th1 and Th2 response in patients with SLE.
Levels in Patients with SLE in Function
ctivity
of SLE Control
Group
(n � 25)
3–12
20)
SLEDAI >13
(n � 12)
8.1 34.8 � 12.3 33 � 9.24 7.2 � 7.6 NA7.4 4.1 � 4.8 6.4 � 8.39.6 19.6 � 10 27.4 � 24579† 629 � 726*‡† 31.4 � 2469.8† 8.1 � 17.4 19 � 14.3§
15.4† 26.45 � 5.2† 5.3 � 87.8 4.6 � 10 6.5 � 8.24† 1 � 3� 0.9 � 0.61.6† 1.7 � 0.8† 0.13 � 0.186.4† 574.5 � 1126† 6.8 � 6.865.3† 43.2 � 51.1† 1.4 � 1.6672.6 996.3 � 787.7 NA48.4 26 � 30.4 NA63.2 10.8 � 4.3 NA45 17 � 11 NA53 43 � 34.4 NA
kines
ibody
ase A
ctivity
LEDAI
(n �
32 �
3.2 �
5.3 �
7.6 �
24 �
5.1 �
32 �
3.3 �
1.3 �
2.3 �
1.4 �
0.6 �
81 �
6.3 �
8.4 �
5.1 �
6.3 �

TtscmsIu
aTpcsTailloesafwtTdrrrdeotaTostlcsdppflt
deaapiotrst7fpt1sssd(otf(pwtcm
eclsunmcItsItiw
1a
409TNF-� IN SLE
DISCUSSION
We evaluated the relationship between Th1-h2 cytokine levels with the production of au-
oantibodies and the activity of SLE. Our resultshow a mutual participation of Th1 and Th2ytokines in the disease, and suggest that TNF-�ay play a protective role. The importance of
erum IL-12p70 in the activity of disease and ofL-10 in the synthesis of autoantibodies is doc-mented.TNF-� is a 17-kd protein containing 157
mino acids (28,29). The major sources ofNF-� are the cells of the monocyte/macro-hage lineage. T lymphocytes, neutrophils, mastells, and endothelium also contribute to itsynthesis under different circumstances (29).he induction by TNF-� of multiple chemokinesnd adhesion molecules is of major importancen rapidly attracting immune and inflammatoryeukocytes to the site of injury and TNF-� re-ease. TNF-� acutely up regulates the functionf the immune system, but following prolongedxposure, excessive TNF-� is immunosuppres-ive (28,29). High levels of this cytokine gener-te systemic effects that include the induction ofever, the synthesis of acute-phase proteins, asell as cachexia. It also causes intravascular
hrombosis and shock (28,29). We found thatNF-� levels were diminished as a function ofisease activity, suggesting a possible protectiveole in SLE (Table 4), as has been previouslyeported (17,30,31). Nearly 10% of patients withheumatoid arthritis treated with TNF-� blockersevelop anti-DNA antibodies (31,32), and sev-ral patients treated with such blockers devel-ped SLE (33). On the other hand, in popula-ions with a high exposure to infectious diseases,nd therefore with a continuous synthesis ofNF-�, the prevalence of SLE is low (31,34). Inur patients, higher levels of TNF-� were ob-erved in those with a history of infection (al-hough not statistically significant). Neverthe-ess, it is possible that TNF-� acts as a 2-faceytokine in SLE. First, it could be an immuno-uppressive mediator, chronically produced as aefense mechanism (28,29) or acting as a sup-ressor of autoantibody synthesis at the T-lym-hocyte level (35). Second, it might be a proin-ammatory factor acutely released in the local
issues (35). d
IL-12 is a proinflammatory cytokine that in-uces the production of IFN-�, favors the differ-ntiation of Th1 cells, and links innate resistancend adaptive immunity (36,37). Dendritic cellsnd phagocytes produce IL-12 in response toathogens during infection. Production of IL-12s dependent on different regulation mechanismsf expression of the genes encoding IL-12, pat-erns of Toll-like receptor expression, and cross-egulation between the different dendritic cellsubsets, involving cytokines such as IL-10 andype I IFN (36,37). Biologically active IL-12 is a0-kd heterodimeric cytokine (IL-12p70) maderom disulfide-linked p35 (a) and p40 (b) chains.35 is constitutively produced by almost all cellypes, whereas p40 expression (and thereby IL-2p70 production) is restricted to antigen-pre-enting cells, neutrophils, keratinocytes and Ep-tein-Barr Virus–transformed B cells. In ourtudy, we observed that an increase in the pro-uction of IL-12p70 was associated with SLETables 2 and 4). Previous studies, similar to ourwn, have shown diverse results as a function ofhe studied subunit (Table 5). Our results differrom those of Liu et al (19) and Lauwerys et al20), who observed the absence of IL-12p70 inatients with SLE. Our study of this cytokineas replicated and the results confirmed in pa-
ients as well as in controls. Differences in theapturing antibody and the patients studiedight explain these discrepancies.IL-10 is a multifunctional cytokine with diverse
ffects on most hemopoietic cell types. The prin-ipal routine function of IL-10 appears to be toimit, and ultimately terminate, inflammatory re-ponses. In addition to these activities, IL-10 reg-lates growth and/or differentiation of B cells,atural killer cells, cytotoxic and helper T cells,ast cells, granulocytes, dendritic cells, keratino-
ytes, and endothelial cells (38). We observed thatL-10 was associated with the synthesis of autoan-ibodies, as previously reported (Table 6). Othertudies have demonstrated a relationship betweenL-10 levels and activity of the disease (22). Ver-helyi et al (39) did not find a significant differencen IL-10–secreting cells in SLE patients comparedith healthy controls.IFN-� is a dimeric glycoprotein with subunits of
46 amino acids. The 2 forms of the active proteinre 20 and 25 kd, respectively (28,40). It is pro-
�
uced principally by T cells, CD4 as well as
CtqeitwIsga
kltToammBocu
P
P
410 GOMEZ ET AL
D8�, and natural killer cells. Its main function ishe activation of macrophages in innate and ac-uired response. Its activity increases in the pres-nce of TNF-� and TNF-� (28). We observed anncrease of IFN-� in patients with respect to con-rols, although no association to disease activityas found. Previous studies showed an increase in
FN-� in SLE, and an association with the synthe-is of IL-18. Nevertheless, results differ with re-ard to the association of its levels and diseasectivity (Table 7).
IL-4 is a glycoprotein of 129 amino acids (20
Table 5: IL-12 i
Type N
Type of
Study/Sample
IL-12 (total) 49 In vitro (PBMC) Decreased20 In vitro (PBMC) Increased p24 In vitro (PBMC) Negative co
of IL-10, t39 Serum Increased le20 Serum Increased le36 Serum Increased le60 Serum Increased le34 Serum Decreased40 Serum Decreased20 In vitro (PBMC) Decreased
p40 20 In vitro (PBMC) Gene expre28 Serum Increased le
BMC, peripheral blood mononuclear cells.
Table 6: IL-10 i
N
Type of Study/
Sample
49 In vitro (PBMC) Increased producti24 In vitro (PBMC) Increased producti20 In vitro (PBMC) Increased producti
but diminished w20 In vitro (PBMC) Inhibited expressio34 In vitro (PBMC) Increased producti20 Serum Increased levels20 Serum, and in vitro
(PBMC)Increased levels
52 Serum Correlation with th79 In vitro (PBMC) Similar IL-10 secre
BMC, peripheral blood mononuclear cells.
d) produced by a subpopulation of activated Tymphocytes (Th2). It contains 6 residues of cys-ein involved in the formation of disulfide bridges.hese bonds are essential to the biological activityf the molecule. IL-4 promotes the proliferationnd differentiation of activated B cells and aug-ents the expression of class II molecules of theajor histocompatibility complex. The latter helpslymphocytes respond to stimuli proceeding from
ther B cells and aids in presenting antigens to Tells. This cytokine inhibits the activation of nat-ral killer cells and stimulates the proliferation of
ents with SLE
Results Reference
tion 11tion 15on between its production and thatf anti-DNA and disease activity
12
13101416
nction of activity 17in nephritis 18tion 19diminished 19nd correlation with disease activity 20
ents with SLE
Results Reference
inhibitory effect on IL-12 1112
patients with anti-DNA antibodies,spect to the controls
15
L-12 and IFN-� 19171021
ity of SLE 22lls in patients and controls 39
n Pati
producroducrrelatiiters ovelsvelsvelsvels
as a fulevelsproducssionvels a
n Pati
on andonon inith ren by Ion
e activting ce

tfcttasls
imiGflIaa
bvk
(Sp(wstltmeS
Sstaph
P
P
411TNF-� IN SLE
hymocytes (28). We did not find significant dif-erences in IL-4 levels between SLE patients andontrols, nor was there a statistical difference be-ween the levels of this cytokine and disease ac-ivity. However, a direct correlation between IL-4nd the levels of Th1 cytokines was noticed. Othertudies have shown similar results or diminishedevels (Table 8), suggesting that IL-4 does not haveuch a preponderant role in SLE.
Despite the fact that we did not observe signif-cant differences in cytokine levels related to treat-ent, it remains possible that that level may be
nfluenced by immunosuppressive therapy (3).lucocorticoids inhibit the production of proin-ammatory cytokines, such as IL-12, TNF-�, andFN-�, whereas they stimulate the production ofnti-inflammatory cytokines, such as IL-10, IL-4,nd transforming growth factor � (41).
The study on cytokines in SLE patients could beetter assessed, if the genetic background of indi-iduals were taken into account. For instance, it isnown that carriers of the 8.1 ancestral haplotype
Table 7: IFN-� i
N
Type of Study/
Sample
24 In vitro (PBMC) Positive correlation with34 In vitro (PBMC) Tendency to diminish w20 In vitro (PBMC) IFN-� diminishes the exp39 Serum Increased levels20 Serum Correlation with IL-18 le79 In vitro (PBMC) Lower number of IFN-�
than in controls
BMC, peripheral blood mononuclear cells.
Table 8: IL-4 in
N
Type of Study/
Sample
20 Serum Increased levels and34 In vitro (PBMC) Decreased productio20 Peripheral blood
T cellsIntracellular expressi
lack of correlation79 In vitro (PBMC) Lower number of IL-
patients than in co
BMC, peripheral blood mononuclear cells.
autoimmune haplotype), which is associated withLE but is also common in the general population,roduce more TNF-� and IL-10 than noncarriers42,43). Thus, to extend the findings of the presentork, it would be necessary to design longitudinal
tudies to establish a cause-effect relationship, ando develop methods that not only evaluate cytokineevels, but also determine the function and regula-ion of their expression, including their gene poly-orphism (44–47). The results obtained should
nhance our understanding of the immunology ofLE and other autoimmune diseases.
ACKNOWLEDGMENT
The authors thank Drs. Seema S. Ahuja andunil Ahuja, Health Science Center at the Univer-ity of Texas, San Antonio, TX, for their contribu-ions in the development of the present work. Theylso express their gratitude to the patients whoarticipated in this study and to Monica Stone forer help with the manuscript.
ients with SLE
esults Reference
levels 12ease activity 17n of IL-10 19
1310
ng cells in premenopausal patients 39
nts with SLE
esults Reference
ve correlation with IL-18 levels. 1417
L-4 similar to that of controls andisease activity.
15
ting cells in premenopausal 39
n Pat
R
IL-12ith disressio
velssecreti
Patie
R
negatinon of Iwith d4 secrentrols

lm
e1
P
an
ce
pp
1
Dget1
BAt
CltaC
ss1
scIt
Ksd
pke
ie
Jg
412 GOMEZ ET AL
REFERENCESie
timWA
ege
pfiI8
ibL
NpbpA
Rcl
Rc2
GLRe
aWW
C
u
kA
Sp5
P
1. McAlindon T. Update on the epidemiology of systemicupus erythematosus: New spins on old ideas. Curr Opin Rheu-atol 2000;12:104-12.2. Klinman DM, Steinberg AD. Systemic autoimmune dis-
ase arises from polyclonal B cell activation. J Exp Med987;165:1755-60.3. Wallace DJ, Hahn BH. Dubois’ lupus erythematosus.
hiladelphia:Lippincott Williams and Wilkins, 2002.4. Williams RC, Malone C, Blood B, Silvestris F. Anti-DNA
nd anti-nucleosome antibody affinity—a mirror image of lupusephritis? J Rheumatol 1999;26:331-46.5. Funauchi M, Ikoma S, Enomoto H, Horiuchi A. De-
reased Th1-like and increased Th2-like cells in systemic lupusrythematosus. Scand J Rheumatol 1998;27:219-24.
6. Mosmann TR, Coffman RL. TH1 and TH2 cells: Differentatterns of lymphokine secretion lead to different functionalroperties. Annu Rev Immunol 1989;7:145-73.7. Romagnani S. The Th1/Th2 paradigm. Immunol Today
997;18:263-6.8. Viallard JF, Pellegrin JL, Ranchin V, Schaeverbeke T,
ehais J, Longy-Boursier MTh1 [IL-2, interferon-gamma (IFN-amma)] and Th2 (IL-10, IL-4) cytokine production by periph-ral blood mononuclear cells (PBMC) from patients with sys-emic lupus erythematosus (SLE). Clin Exp Immunol 1999;115:89-95.9. Theofilopoulos AN, Koundouris S, Kono DH, Lawson
R. The role of IFN-gamma in systemic lupus erythematosus:challenge to the Th1/Th2 paradigm in autoimmunity. Arthri-
is Res 2001;3:136-41.10. Amerio P, Frezzolini A, Abeni D, Teofoli P, Girardelli
R, De Pita O, et al. Increased IL-18 in patients with systemicupus erythematosus: Relations with Th-1, Th-2, pro-inflamma-ory cytokines and disease activity. IL-18 is a marker of diseasectivity but does not correlate with pro-inflammatory cytokines.lin Exp Rheumatol 2002;20:535-8.11. Liu TF, Jones BM. Impaired production of IL-12 in
ystemic lupus erythematosus. I. Excessive production of IL-10uppresses production of IL-12 by monocytes. Cytokine 1998;0:140-7.12. Liu TF, Jones BM. Impaired production of IL-12 in
ystemic lupus erythematosus. II: IL-12 production in vitro isorrelated negatively with serum IL-10, positively with serumFN-gamma and negatively with disease activity in SLE. Cy-okine 1998;10:148-53.
13. Tokano Y, Morimoto S, Kaneko H, Amano H, Nozawa, Takasaki Y, et al. Levels of IL-12 in the sera of patients with
ystemic lupus erythematosus (SLE)-relation to Th1- and Th2-erived cytokines. Clin Exp Immunol 1999;116:169-73.14. Wong CK, Ho CY, Li EK, Lam CW. Elevation of
roinflammatory cytokine (IL-18, IL-17, IL-12) and Th2 cyto-ine (IL-4) concentrations in patients with systemic lupusrythematosus. Lupus 2000;9:589-93.
15. Chang DM, Su WL, Chu SJ. The expression and signif-cance of intracellular T helper cytokines in systemic lupusrythematosus. Immunol Invest 2002;31:1-12.
16. Robak E, Robak T, Wozniacka A, Zak-Prelich M, Sysa-edrzejowska A, Stephen H. Proinflammatory interferon-
amma–inducing monokines (interleukine-12, interleukine-18,nterleukine-15)—serum profile in patients with systemic lupusrythematosus. Eur Cytokine Netw 2002;13:364-8.
17. Jones BM, Liu T, Wong RW. Reduced in vitro produc-ion of interferon-gamma, interleukin-4 and interleukin-12 andncreased production of interleukin-6, interleukin-10 and tu-our necrosis factor-alpha in systemic lupus erythematosus.eak correlations of cytokine production with disease activity.utoimmunity 1999;31:117-24.18. Min DJ, Cho ML, Cho CS, Min SY, Kim WU, Yang SY,
t al. Decreased production of interleukin-12 and interferon-amma is associated with renal involvement in systemic lupusrythematosus. Scand J Rheumatol 2001;30:159-63.
19. Liu TF, Jones BM, Wong RW, Srivastava G. Impairedroduction of IL-12 in systemic lupus erythematosus. III: De-cient IL-12 p40 gene expression and cross-regulation of IL-12,L- 10 and IFN-gamma gene expression. Cytokine 1999;11:05-11.20. Lauwerys BR, Van Snick J, Houssiau FA. Serum IL-12
n systemic lupus erythematosus: Absence of p70 heterodimersut presence of p40 monomers correlating with disease activity.upus 2002;11:384-7.21. Ronnelid J, Tejde A, Mathsson L, Nilsson-Ekdahl K,
ilsson B. Immune complexes from SLE sera induce IL10roduction from normal peripherical blood mononuclear cellsy an FcgammaRII dependent mechanism: Implications for aossible vicious cycle maintaining B cell hyperactivity in SLE.nn Rheum Dis 2003;62:37-42.22. Miret C, Font J, Molina R, Garcıa-Carrasco M, Filella X,
amos M, et al. Relationship of oncogenes (sFas, Bcl-2) andytokines (IL-10, alpha-TNF) with the activity of systemicupus erythematosus. Anticancer Res 2001;21:3053-9.
23. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ,othfield NF, et al. The 1982 revised criteria for the classifi-ation of systemic lupus erythematosus. Arthritis Rheum 1982;5:1271-7.24. Gladman DD, Urowitz MB, Goldsmith CH, Fortin P,
inzler E, Gordon C, et al. The reliability of the Systemicupus International Collaborating Clinics/American College ofheumatology Damage Index in patients with systemic lupusrythematosus. Arthritis Rheum 1997;40:809-13.
25. Grossman JM, Kalunian KC. Definition, classification,ctivity, and damage indices: Dubois’ lupus erythematosus. Inallace DJ, Hahn BH Philadelphia, Lippincott Williams andilkins, 19-31, 200226. SPSS, Inc. SPSS 9.05 for Windows Reference Guide.
hicago, IL, SPSS Inc., 1999.27. GraphPad Prism version 3.00 for Windows User Man-
al. San Diego, CA, GraphPad Inc., 2001.28. Oppenheim JJ, Francis W, Ruscetti, Faltynek C. Cyto-
ines. In Immunology. Basic & clinical, ed 8. Stites DP, TerrI, Parslow TG, eds. Appleton & Lance 1994:105-23.29. Aggarwal BB, Kohr WJ, Hass PE, Moffat B, Spencer
A, Henzel WJ, et al. Human tumor necrosis factor. Production,urification, and characterization. J Biol Chem 1985;260:2345-4.30. Jacob CO. Tumor necrosis factor � in autoimmunity:
retty girl or old witch? Immunol Today 1992;13:122-5.
31. Mageed RA, Isenberg DA. Tumour necrosis factor alpha
ip
RiiFa
Om
sa
ct
J
Il
AI
sp
i1
mA
Cal
GsHH
ms
Ttm
GeHG
lI1
413TNF-� IN SLE
n systemic lupus erythematosus and anti-DNA autoantibodyroduction. Lupus 2002;11:850-5.32. Charles PJ, Smeenk RJ, De Jong J, Feldmann M, Maini
N. Assessment of antibodies to double-stranded DNA inducedn rheumatoid arthritis patients following treatment with Inflix-mab, a monoclonal antibody to tumor necrosis factor alpha:indings in open-label and randomized placebo-controlled tri-ls. Arthritis Rheum 2000;43:2383-90.
33. Debant M, Vittecoq O, Descamps V, Le Loet X, Meyer. Anti–TNF-�–induced systemic lupus syndrome. Clin Rheu-atol 2003;22:56-61.34. Ballou SP, Khan MA, Kushner I. Clinical features of
ystemic lupus erythematosus: Differences related to race andge of onset. Arthritis Rheum 1982;25:55-60.
35. Aringer M, Smolen JS. Complex cytokine effects in aomplex autoimmune disease: Tumor necrosis factor in sys-emic lupus erythematosus. Arthritis Res Ther 2003;5:172-7.
36. Abdi K. IL-12: The role of p40 versus p75. ScandImmunol 2002;56:1-11.37. Bertagnolli MM, Lin BY, Young D, Herrmann SH.
L-12 augments antigen-dependent proliferation of activated Tymphocytes. J Immunol 1992;149:3778-83.
38. Moore KW, de Waal Malefyt R, Coffman RL, O’Garra. Interleukin-10 and the interleukin-10 receptor. Annu Rev
mmunol 2001;19:683-765.39. Verthelyi D, Petri M, Ylamus M, Klinmann DM. Disas-
ociation of sex hormone levels and cytokine production in SLEatients. Lupus 2001;10:352-358.40. Farrar MA, Schreiber RD. The molecular cell biology of
nterferon-gamma and its receptor. Annu Rev Immunol 1993;1:571-611.41. Elenkov IJ, Chrousos GP. Stress hormones, proinflam-atory and antiinflammatory cytokines, and autoimmunity.nn N Y Acad Sci 2002;966:290-303.42. Price P, Witt C, Allcock R, Sayer D, Garlepp M, Kok
C, et al. The genetic basis for the association of the 8.1ncestral haplotype (A1, B8, DR3) with multiple immunopatho-ogical diseases. Immunol Rev 1999;167:257-274.
43. Lio D, Candore G, Colombo A, Colonna Romano G,ervasi F, Marino V, et al. A genetically determined high
etting of TNF-alpha influences immunologic parameters ofLA-B8,DR3 positive subjects: Implications for autoimmunity.um Immunol 2001;62:705-713.44. Wu MC, Huang CM, Tsai JJ, Chen HY, Tsai FJ. Poly-orphisms of the interleukin-4 gene in chinese patients with
ystemic lupus erythematosus in Taiwan. Lupus 2003;12:21-5.45. Miyake K, Nakashima H, Akahoshi M, Inoue Y, Nagano S,
anaka Y, et al. Genetically determined interferon-gamma produc-ion influences the histological phenotype of lupus nephritis. Rheu-
atol 2002;41:518-24.46. Van der Linden MW, van der Slik AR, Zanelli E,
iphart MJ, Pieterman E, Schreuder GM, et al. Six microsat-llite markers on the short arm of chromosome 6 in relation toLA-DR3 and TNF-308A in systemic lupus erythematosus.enes Immun 2001;2:373-80.47. Eskdale J, Wordsworth P, Bowman S, Field M, Gal-
agher G. Association between polymorphisms at the humanL-10 locus and systemic lupus erythematosus. Tissue Antigens997;49:635-9.




















