T cell cytokine patterns in active tuberculosis patients in a northeastern area of Romania
12
T CELL CYTOKINE PATTERNS IN ACTIVE TUBERCULOSIS PATIENTS IN A NORTHEASTERN AREA OF ROMANIA by EUGEN CARASEVICI *1 , CARMEN COZMEI 2 , DANIELA CONSTANTINESCU 3 , ADRIANA SORETE-ARBORE 4 , DOINA GRAMADA 5 , TRAIAN MIHAESCU 6 ( 1 “Gr.T. Popa” University of Medicine and Pharmacy, Department of Immunology, 2 Institute of Public Health, Department of Occupational Medicine, 3 Institute of Public Health, Department of Immunology, 4 Clinical Hospital of Pneumology, Outpatient Service, 5 Clinical Hospital of Pneumology, 6 “Gr.T. Popa” University of Medicine and Pharmacy, Department of Pneumology, Iasi, Romania) ABSTRACT Developing countries like Romania have a high incidence of tuberculosis. Literature data suggest that people in these countries have an important Th2–type immune background which prevents a protective Th1 response of the host against Mycobacterium tuberculosis. Our study is the first attempt in Romania to identify cytokine patterns in active tuberculosis. The study included 15 patients with active pulmonary tuberculosis and 11 healthy volunteers. Peripheral blood mononuclear cells (PBMC), stained with carboxyfluoresceine-diacetate-succinimidylester (CFSE), were incubated for 7 days with purified protein derivate (PPD) or with medium alone. Intracellular synthesis of IFNγ and IL-4 in proliferated (CFSE low ) T cells was detected by flowcytometry. The results showed that both Th1 (IFNγ) and Th2 (IL-4) cytokines are produced in response to in vitro PPD-stimulation of PBMC from pulmonary tuberculosis patients and healthy controls. Moreover, the proportion between IFNγ and IL-4 is tilted in favour of IL-4 in PPD-activated (CD3 + CFSE low ) cells from healthy persons, who did not develop active tuberculosis during the two-year study time interval. This predominance of Th2 effectors points to the need to further investigate the role of IL-4 in the M. tuberculosis infection. Key words: carboxyfluoresceine-diacetate-succinimidylester (CFSE), cytokines, flow-cytometry, tuberculosis. * Correspondence should be addressed to: Prof. Eugen Carasevici, Department of Immunology, „Gr.T. Popa” University of Medicine and Pharmacy, Bd. Independentei 1, Iasi 700111, Romania Phone/Fax: 40 232 213212, e-mail: [email protected] ROM.ARCH.MICROBIOL.IMMUNOL.T.65,Nos.1-2,pp. , Jan.-June, 2006
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of T cell cytokine patterns in active tuberculosis patients in a northeastern area of Romania

T CELL CYTOKINE PATTERNS IN ACTIVE TUBERCULOSIS PATIENTS IN A NORTHEASTERN
AREA OF ROMANIA
by
EUGEN CARASEVICI*1, CARMEN COZMEI
2, DANIELA CONSTANTINESCU3, ADRIANA SORETE-ARBORE
4, DOINA GRAMADA
5, TRAIAN MIHAESCU6
(1 “Gr.T. Popa” University of Medicine and Pharmacy, Department of Immunology, 2Institute of Public Health, Department of Occupational Medicine, 3Institute of Public
Health, Department of Immunology, 4Clinical Hospital of Pneumology, Outpatient Service, 5Clinical Hospital of Pneumology, 6 “Gr.T. Popa” University of Medicine and
Pharmacy, Department of Pneumology, Iasi, Romania)
ABSTRACT
Developing countries like Romania have a high incidence of tuberculosis. Literature data suggest that people in these countries have an important Th2–type immune background which prevents a protective Th1 response of the host against Mycobacterium tuberculosis. Our study is the first attempt in Romania to identify cytokine patterns in active tuberculosis. The study included 15 patients with active pulmonary tuberculosis and 11 healthy volunteers. Peripheral blood mononuclear cells (PBMC), stained with carboxyfluoresceine-diacetate-succinimidylester (CFSE), were incubated for 7 days with purified protein derivate (PPD) or with medium alone. Intracellular synthesis of IFNγ and IL-4 in proliferated (CFSElow) T cells was detected by flowcytometry. The results showed that both Th1 (IFNγ) and Th2 (IL-4) cytokines are produced in response to in vitro PPD-stimulation of PBMC from pulmonary tuberculosis patients and healthy controls. Moreover, the proportion between IFNγ and IL-4 is tilted in favour of IL-4 in PPD-activated (CD3+ CFSElow) cells from healthy persons, who did not develop active tuberculosis during the two-year study time interval. This predominance of Th2 effectors points to the need to further investigate the role of IL-4 in the M. tuberculosis infection.
Key words: carboxyfluoresceine-diacetate-succinimidylester (CFSE), cytokines, flow-cytometry, tuberculosis.
* Correspondence should be addressed to:Prof. Eugen Carasevici, Department of Immunology, „Gr.T. Popa” University of Medicine and Pharmacy, Bd. Independentei 1, Iasi 700111, RomaniaPhone/Fax: 40 232 213212, e-mail: [email protected]
ROM.ARCH.MICROBIOL.IMMUNOL.T.65,Nos.1-2,pp. , Jan.-June, 2006

CARASEVICI et al.
INTRODUCTION
Tuberculosis, malaria and HIV infection represent high priority health problems worldwide.
In 2004, according to the World Health Organization, 9 million new cases of tuberculosis and approximately 2 million deaths were recorded (1). While western Europe boasts a declining incidence of tuberculosis, some eastern European countries have difficulties in managing the disease. One of the highest incidences of tuberculosis, 134.6 cases per 100 000 inhabitants in 2004, was registered in Romania (2).
A steady increase of active tuberculosis disease burden including development of resistant strains, or association with HIV infection, prompted recent studies aiming to understand host immunity and to reveal new markers of disease evolution and control.
However, in spite of extensive experimental work and accumulation of new data concerning host–pathogen relationship, there are gaps in our knowledge, which still prevent the development of immune response manipulation for the benefit of the patient. Moreover, the immune background of a certain population group can be largely variable, raising the question of the necessity to carry out an epidemiological immune survey concomitantly with research efforts for developing a new and effective vaccine. Although it became apparent that an efficient immune response to Mycobacterium tuberculosis as an intra-cellular pathogen is associated with Th1 differentiation and IFNγ production (3, 4), the exact mechanism of protection is still unclear (5).
Reduced Th1 activity was associated with active tuberculosis in patients from Gambia and the Republic of Guinea (6). In addition, there are studies reporting failure of peripheral blood mononuclear cells (PBMC) from TB patients to produce IFNγ in response to stimulation with different mycobacterium antigens (7, 8, 9). However, granting that CD4+ cells producing IFNγ is a prominent feature in patients with tuberculosis (10, 11), the amount of the produced cytokine does not seem to be a reliable predictive marker for disease status (12).
Moreover, high levels of anti-inflammatory Th2-like cytokines, especially IL-4, were also reported in human tuberculosis patients (13, 14) and the most spread belief is that IL-4 response to M. tuberculosis would hamper Th1 activity and trigger immunopathology (15). Furthermore, Rook et al. (16) suggest that people from developing countries would have a pre-existing Th2 component, which is exploited by M. tuberculosis to avoid an efficient Th1 response of the host. The present study investigated the Th1/Th2 cytokine profile in patients with active tuberculosis from northeastern Romania, based on T cell response to PPD (purified protein derivate).
We assessed the IFNγ- and IL-4- producing lymphocytes from specifically-activated PBMC of tuberculosis patients at diagnosis and after completion of treatment and of healthy controls.
MATERIALS AND METHODS
Study groups
The study group included 15 patients with active pulmonary tuberculosis aged between 24 and 50, admitted in the Clinical Hospital of Pneumology in Iasi, Romania.
2

Cytokines in active tuberculosis from Romania
Patients were studied before the initiation of antituberculous treatment and 6 months after completion of tuberculosis therapy. Diagnosis of tuberculosis was established after considering the clinical status, chest X-ray and positive sputum culture.
The tuberculin skin test (TST) was performed with 2 units of PPD IC65, produced by N.I.R.D.M.I. „Cantacuzino” in Bucharest, which is bioequivalent to the internationally recognized PPD RT23 produced by the Danish Statens Serum Institute in Copenhagen.
The TST was positive (over 10 mm skin indurations) for five of the fifteen patients before treatment. At the time of the first blood collection, none of the patients received chemotherapy or corticotherapy.
Eleven healthy volunteers, aged between 22 and 50, with no clinical history of tuberculosis, were included in the study as controls. Eight of the controls were positive for tuberculin skin test.
All subjects included in this study have been inoculated with BCG vaccine during childhood as confirmed by the skin scar and all of them had a negative human immunodeficiency virus serologic test. Stool samples were collected and tested for the presence of parasites and only individuals uninfected with intestinal parasites were admitted to the study.
Informed consent was obtained from each subject and the Ethical Committee of the Clinical Hospital of Pneumology approved the study.
CFSE staining and cell culture
Twenty-five to forty ml of venous blood were collected in heparinized syringe and processed for mononuclear cells isolation by density gradient sedimentation over Ficoll-Hystopaque. Cell viability was constantly over 95% as tested by trypan blue dye exclusion test.
Before culturing the PBMC, cells were stained with carboxyfluoresceine-diacetate-succinimidylester (CFSE) (Molecular Probes, USA) using a slightly modified technique, originally devised by Lyons et al. (17). Briefly, 1 x 107 cells/ml were incubated with 1.25 μM CFSE for 10 min at 370C. The staining was quenched by adding one volume of cold autologous plasma and the cells were washed twice in cold RPMI 1640.
106 cells/ml were cultured in the presence or absence of PPD in 24-well plates (Nunc, Denmark) at 370C, in humid atmosphere, with 5% CO2 in RPMI 1640 supplemented with antibiotics and 5% autologous plasma. According to previous pilot experiments that showed an optimum of proliferation on the 7th day of culture, the cells were stimulated for up to 7 days with 20 μg/ml PPD free of preservatives. In order to block the cytokine secretion, the cultures were treated with 10 μg/ml Brefeldin A (Sigma, Germany) during the last 6 hours of culture.
Staining and flow-cytometric analysis
At defined time points, the cells were collected, aliquoted and washed in PBS/1%FCS/0.1%NaN3. Next, they were fixed in 2% paraformaldehyde, permeabilized with 2% saponin and incubated for 30 min at room temperature with anti-CD3 PerCP (Becton Dickinson), anti-IFNγ PE or anti-IL-4 PE (Pharmingen). The analysis was
3
CARASEVICI et al.
performed on a FACSCalibur flow cytometer (Becton Dickinson) using the CELL-Quest software. Fifty thousand events per sample were acquired and lymphocytes, the small ones together with the blasts, were gated according to their forward and side scatter characteristics. The CD3+ cells were then selected by gating them on a Fl3/SSC dot-plot and the proportion of the T cells that underwent the blastic transformation (CFSElow) was determined on histograms of CFSE (FL1) fluorescence. This last population was further analyzed to establish the percentage of IFNγ- and IL-4-expressing cells among these antigen-reactive CD3+ cells.
Results are expressed as percentage of proliferated T lymphocytes (CFSElow) from total CD3+ cells and as percentage of IFNγ+CD3+ or IL-4+CD3+ cells from proliferated CD3+CFSElow population of lymphocytes.
Statistical analysis
Data processing was performed using SPSS v12 statistical analysis program. Average values were compared using specific tests for normal distribution series and non-parametrical tests when distribution was not normal.
When Bartlett test confirmed a significant difference between the dispersions of the two data sets, Kruskal-Wallis (or Mann-Whitney/Wilcoxon) tests were used to compare interest variable averages for the studied groups. t test results were considered when no significant difference was noted. A p value of <0.05 was considered significant.
RESULTS
Lymphocytes proliferation
After 7 days of incubation with complete medium alone or in presence of PPD, the cells were stained and analyzed by flow-cytometry. A representative flow-cytometric analysis is depicted in Fig. 1. As the lymphocytes progress through the division process, their CFSE fluorescence intensity diminishes so that we could establish the percentage of activated CD3+ cells (CFSElow) on the CFSE histograms.
4
Cytokines in active tuberculosis from Romania
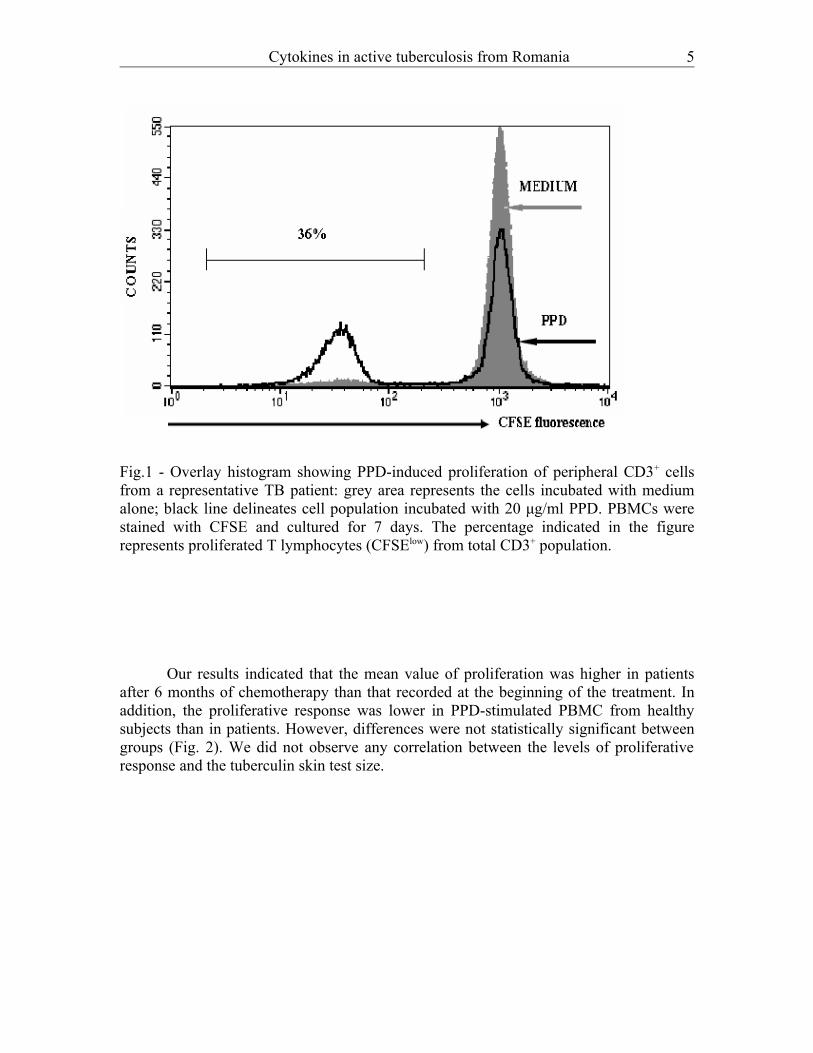
Fig.1 - Overlay histogram showing PPD-induced proliferation of peripheral CD3+ cells from a representative TB patient: grey area represents the cells incubated with medium alone; black line delineates cell population incubated with 20 μg/ml PPD. PBMCs were stained with CFSE and cultured for 7 days. The percentage indicated in the figure represents proliferated T lymphocytes (CFSElow) from total CD3+ population.
Our results indicated that the mean value of proliferation was higher in patients after 6 months of chemotherapy than that recorded at the beginning of the treatment. In addition, the proliferative response was lower in PPD-stimulated PBMC from healthy subjects than in patients. However, differences were not statistically significant between groups (Fig. 2). We did not observe any correlation between the levels of proliferative response and the tuberculin skin test size.
5

CARASEVICI et al.
Fig.2 - Comparison of peripheral lymphocytes proliferation in response to PPD stimulation in TB patients before treatment, patients after 6 months of treatment and subjects in the control group. PBMCs were stained with CFSE and cultured with 20 μg/ml PPD for 7 days. Results are presented as mean percentage of proliferated T lymphocytes (CD3+CFSElow) from total CD3+ population
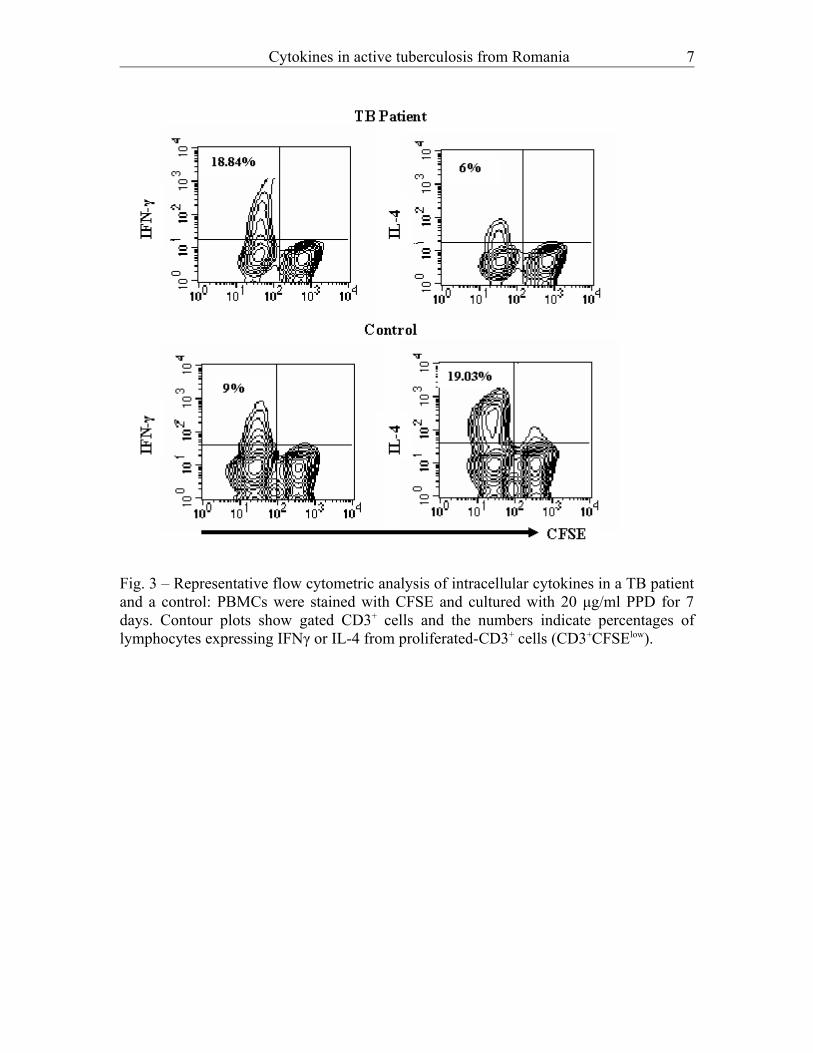
PPD-activated CD3+ cells expressing cytokinesThe CFSE dye dilution technique allowed us to measure the frequencies of cytokine-secreting lymphocytes among the specifically-activated CD3+ cells (Fig. 3). The frequency of PPD-activated lymphocytes (CD3+CFSElow) expressing IFNγ was higher in TB patients as compared to the healthy controls and showed a tendency to decrease from the beginning to the end of treatment. High percentages of IL-4-producing CD3+CFSElow
cells were recorded in controls so that the analysis of the IFN/IL-4 ratio of percentages showed a significant difference between patients at diagnosis and healthy individuals (p=0.046) (Fig. 4).
6
Cytokines in active tuberculosis from Romania
Fig. 3 – Representative flow cytometric analysis of intracellular cytokines in a TB patient and a control: PBMCs were stained with CFSE and cultured with 20 μg/ml PPD for 7 days. Contour plots show gated CD3+ cells and the numbers indicate percentages of lymphocytes expressing IFNγ or IL-4 from proliferated-CD3+ cells (CD3+CFSElow).
7
CARASEVICI et al.
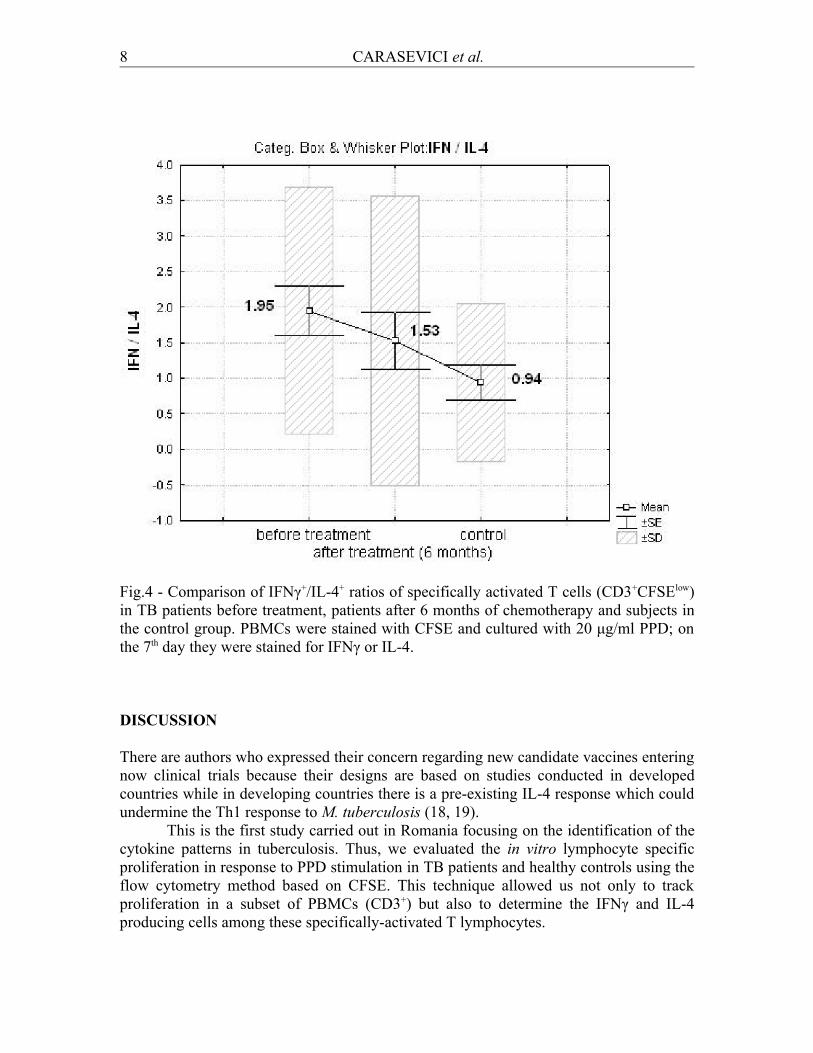
Fig.4 - Comparison of IFNγ+/IL-4+ ratios of specifically activated T cells (CD3+CFSElow) in TB patients before treatment, patients after 6 months of chemotherapy and subjects in the control group. PBMCs were stained with CFSE and cultured with 20 μg/ml PPD; on the 7th day they were stained for IFNγ or IL-4.
DISCUSSION
There are authors who expressed their concern regarding new candidate vaccines entering now clinical trials because their designs are based on studies conducted in developed countries while in developing countries there is a pre-existing IL-4 response which could undermine the Th1 response to M. tuberculosis (18, 19).
This is the first study carried out in Romania focusing on the identification of the cytokine patterns in tuberculosis. Thus, we evaluated the in vitro lymphocyte specific proliferation in response to PPD stimulation in TB patients and healthy controls using the flow cytometry method based on CFSE. This technique allowed us not only to track proliferation in a subset of PBMCs (CD3+) but also to determine the IFNγ and IL-4 producing cells among these specifically-activated T lymphocytes.
8

Cytokines in active tuberculosis from Romania
Similarly to other reports (20) we did not find significant differences between groups under the scrutiny (patients and controls) concerning the T cells responsiveness to in vitro PPD stimulation. Our results showed that peripheral T-lymphocytes in TB patients react to PPD in vitro stimulation by proliferating at a slightly higher level as compared to healthy subjects, and by increasing the proliferation process after treatment. This higher percentage of CD3+ specific proliferating cells in culture recorded after 6 months of treatment could be an indicator for recirculation of a highly activated effector/memory lymphocyte pool trafficking from and to the site of inflammation.
These specific antigen-activated T lymphocytes were further evaluated for cytokine production and we recorded the predominance of Th1 effectors in patients before the administration of treatment. This type of response was modified by treatment, i.e., the Th1-response diminished as healing took place. It is well known that IFNγ is a key mediator of the inflammation process by sustaining the macrophage activation and infection control. But the excess of inflammatory response and TNFα macrophage overproduction induce local tissue damage (21, 22).
Our results showed that the Th1/Th2 balance was significantly tilted in favor of a Th2 type of response in healthy controls compared to patients before treatment. Taken collectively, these data, together with the fact that healthy controls under observation did not develop active disease during the two-year study time interval, suggest a possible interpretation of IL-4 as having a protective role rather than a clearly defined pathogenic one, at least in the population studied by us and relying on our system of investigation for specific T lymphocytes.
Articles published in the last decade underline the importance of IL4-δ2, a splice variant and antagonist of IL-4 (23) in TB. Thus, high levels of IL4δ2 were identified in active tuberculosis (24) and in HIV-positive patients co-infected with M. tuberculosis after completion of chemotherapy (25). Also, high levels of IL-4δ2 mRNA were described in ESAT-6 responders of TB contacts (26) and in healthy individuals with latent TB infection in a TB-endemic area (27) suggesting a possible association between this high expression and protection against M. tuberculosis.
In this context, it would not be surprising that further research could prove a less prominent role of IFNγ in host defense against M. tuberculosis (28) and a more important one for the IL-4/IL4δ2 ratio (15).
The detection of intracellular cytokines by flow-cytometry did not allow us to discriminate between IL-4 and IL-42, yet this does not rule out the existence of the latter so it was possible that both were included in our measurements. Therefore, the Th2 response which was shown to be dominant in healthy individuals could be determined by the presence of IL-4δ2. This is an aspect that has to be clarified in subsequent studies we are already planning for.
CONCLUSIONS
The present study indicates that in our study groups, TB patients and controls from a Northeastern Area of Romania, both Th1 and Th2 effectors are produced in response to PPD stimulation with a predominance of IL-4 response in healthy persons.
9
CARASEVICI et al.
These findings stress the need for further immunoepidemiological studies aimed to assist in the design and evaluation of tuberculosis vaccine candidates to be used in different populations.
ACKNOWLEDGEMENTS
This research was partly supported by a grant (33353/2004) from the CNCSIS (National Council for Academic Research, Romanian Ministry of Education, Research and Youth). We express our gratitude to Dr. Henriette Stavri from the Cantacuzino Institute of Bucharest who kindly provided us with the PPD.
REFERENCES
1. World Health Organization. Global tuberculosis control: surveillance, planning, financing. WHO report 2006. Geneva, (WHO/HTM/TB/2006.362)2. xxx Principalele boli infectioase si parazitare in Romania. I: Anuar de Statistica Sanitara 2004, Ministerul Sanatatii – Centrul de Calcul si Statistica Sanitara Bucuresti. (2005) 62-713. Kaufmann SH. Immunity to intracellular bacteria. Annu Rev Immunol. 11 (1993) 129-1634. Kahnert A, Seiler P, Stein M, Bandermann S, Hahnke K, Mollenkopf H and Kaufmann SHE. Alternative activation deprives macrophages of a coordinated defense program to Mycobacterium tuberculosis. Eur J Immunol. 36 (2006) 631-6475. Boom WH, Canaday DH, Fulton SA, Gehring AJ, Rojas RE, Torres M. Human immunity to M. tuberculosis: T cells subsets and antigen processing. Tuberculosis, 88 (2003) 98-1066. Leinhardt C, Azzuri A, Amedei A, Fielding K, Sillah J, Sow OY, Bah B, Benagiano M, Diallo A, Manetti R, Manneh K, Gustafson P, Bennett S, D’Elios MM, McAdam K, Del Prete G. Active tuberculosis in Africa is associated with reduced Th1 and increased Th2 activity in vivo. Eur J Immunol 32 (2002) 1605-16137. Torres M, Herrera T, Villareal H, Rich ER, Sada E. Cytokine profiles for peripheral blood lymphocytes from patients with active pulmonary tuberculosis and healthy household contacts in response to the 30-kilodalton antigen of Mycobacterium tuberculosis. Infect Immun 66 (1998) 176-1808. Garcia M, Vargas JA, Castejon R, Navas E, Durantes A. Flow-cytometric assessment of lymphocyte cytokine production in tuberculosis. Tuberculosis 82 (2002) 37-419. Smith SM, Klein MR, Malin AS, Sillah J, McAdam KPWJ, Dockrell HM. Decreased IFN and increased IL-4 production by human CD8 T cells in response to Mycobacterium tuberculosis in tuberculosis patients. Tuberculosis 82 (2002) 7-1310. Tesfa L, Koch FW, Pankow W, Volk HD, Kern F. Confirmation of Mycobacterium tuberculosis infection by flow cytometry after ex vivo incubation of peripheral blood T cells with an ESAT-6 derived peptide pool. Cytometry 60B (2004) 47-53
10
Cytokines in active tuberculosis from Romania
11. Hughes AJ, Hutchinson P, Gooding T, Freezer NJ, Holdsworth SR, Johnson PDR. Diagnosis of Mycobacterium tuberculosis infection using ESAT-6 and intracellular cytokine cytometry. Clin Exp Immunol 142 (2005) 132-13912. Flynn JA. Immunology of tuberculosis and implications in vaccine development. Tuberculosis 84 (2004) 93-10113. Surcel HM, Troye-Blomberg M, Paulie S, Andersson G, Moreno C, Pasvol G, Ivanyi J. Th1/Th2 profiles in tuberculosis, based on the proliferation and cytokine response of blood lymphocytes to mycobacterial antigens. Immunology 81 (1994) 171-17614. Seah GT, Rook GA. High levels of mRNA encoding IL-4 in unstimulated peripheral blood mononuclear cells from tuberculosis patients revealed by quantitative nested reverse transcriptase-polymerase chain reaction; correlations with serum IgE levels. Scand J Infect Dis 33 (2001) 106-10915. Rook GAW, Hernandez-Pando R, Dheda K, Seah GT. IL-4 in tuberculosis: implications for vaccine design. Trends Immunol 25 (2004) 483-48916. Rook GAW, Dheda K, Zumla A. Do successful tuberculosis vaccines need to be immunoregulatory rather than merely Th1-boosting?. Vaccine 23 (2005) 2115-2120.17. Lyons AB, Hasbold J, Hodgkin PD. Flow cytometric analysis of cell division history using dilution of carboxyfluorescein diacetate succinimidyl ester, a stably integrated fluorescent probe. Methods Cell Biol 63 (2001) 375-39718. Rook GAW, Dheda K, Zumla A. Immune systems in developed and developing countries; implications for the design of vaccines that will work where BCG does not. Tuberculosis 86 (2006) 152-16219. Rook GAW, Dheda K, Zumla A. Immune responses to tuberculosis in developing countries: implications for new vaccines. Nat Rev Immunol 5 (2005) 661-66720. Wilkinson RJ, Vordermeier HM, Wilkinson KA, Sjölund A, Moreno C, Pasvol G, Ivanyi J. Peptide-specific T Cell Response to Mycobacterium tuberculosis: clinical spectrum, compartmentalization, and effect of chemotherapy. J Infect Dis 178 (1998) 760-76821. Collins HL, Kaufmann SHE. The many faces of host responses to tuberculosis. Immunology 103 (2001) 1-922. Kaplan G, Freedman VH. The role of cytokines in the immune response to tuberculosis. Res Immunol 147 (1996) 565-57223. Atamas SP, Choi J, Yurovsky VV, White B. An alternative splice variant of human IL-4, IL-4δ2, inhibits IL-4-stimulated T cell proliferation. J Immunol 156 (1996) 435-44124. Dheda K, Chang JS, Breen RAM, Kim LU, Haddock JA, Huggett JF, Johnson MA, Rook GAW, Zumla A. In vivo and in vitro studies of a novel cytokine, interleukin 4δ2, in pulmonary tuberculosis. Am J Respir Crit Care Med 172 (2005) 501-50825. Dheda K, Chang JS, Breen RAM, Haddock JA, Lipman MC, Kim LU, Kim LU, Huggett JF, Johnson MA, Rook GA, Zumla A. Expression of a novel cytokine, IL-4delta2, in HIV and HIV-tuberculosis co-infection. AIDS 19 (2005) 1601-1606
11

CARASEVICI et al.
26. Fletcher HA, Owiafe P, Feffries D, Hill P., Rook GAW, Zumla A, Doherty TM, Brookes RH, and VACSEL Study Group. Increased expression of mRNA encoding interleukin (IL)-4 and its splice variant IL-4δ2 in cells from contacts of Mycobacterium tuberculosis, in the absence of in vitro stimulation. Immunology 112 (2004) 669-67327. Demissie A, Abebe M, Aseffa A, Rook G, Fletcher H, Zumla A., Weldingh K, Brock I, Andersen P, Doherty TM, and VACSEL Study Group. Healthy individuals that control a latent infection with Mycobacterium tuberculosis express high levels of Th1 cytokines and the IL-4 antagonist IL-4δ2. J Immunol 172 (2004) 6938-694328. Van de Vosse E., Hoeve MA, Ottenhoff THM. Genetics of intracellular infectious diseases: molecular and cellular immunity against mycobacteria and salmonellae. Lancet Infect Dis 4 (2004) 739-749
12