
Relative deprivation theory: An overview and conceptual critique

ORIGINAL CONTRIBUTION
Survival Following Primary AndrogenDeprivation Therapy Among MenWith Localized Prostate CancerGrace L. Lu-Yao, MPH, PhDPeter C. Albertsen, MDDirk F. Moore, PhDWeichung Shih, PhDYong Lin, PhDRobert S. DiPaola, MDSiu-Long Yao, MD
PROSTATE CANCER IS THE MOST
common nonskin cancer andthe second most commoncause of cancer death among
men.1 For the majority of men with in-cident prostate cancer (approximately85%), disease is diagnosed at local-ized (T1-T2) stages,2 and standard treat-ment options include surgery, radia-tion, or conservative management (ie,deferral of treatment until necessi-tated by disease signs or symptoms).
Although not standard or sanc-tioned by major groups or guidelines,an increasing number of clinicians andpatients have turned to primary andro-gen deprivation therapy (PADT) as analternative to surgery, radiation, or con-servative management, especiallyamong older men.3,4 For example, in a1999-2001 survey, PADT had becomethe second most common treatment ap-proach, after surgery, for localized pros-tate cancer.3
Randomized clinical trials supportthe use of early androgen deprivationtherapy (ADT) as an adjunct to sur-
gery or radiation for patients with high-risk cancer.5-10 In 1 trial,5,8 early ADTreduced mortality by approximately
50% when used with radiation in high-risk disease (poorly differentiated T1-T2or T3-T4); whereas, in another trial,9
See also Patient Page.
Author Affiliations: Department of Environmental andOccupational Medicine, Robert Wood Johnson Medi-cal School (Dr Lu-Yao), and Department of Biostatis-tics, The School of Public Health (Drs Moore, Shih, andLin), University of Medicine and Dentistry of New Jer-sey, Piscataway; Department of Medicine, University ofMedicine and Dentistry of New Jersey, Robert WoodJohnson Medical School, New Brunswick (Drs Lu-Yao,DiPaola, and Yao); Cancer Institute of New Jersey, New
Brunswick (Drs Lu-Yao, Moore, Shih, Lin, DiPaola, andYao); Department of Surgery (Urology), University ofConnecticut, Farmington (Dr Albertsen); and The Deanand Betty Gallo Prostate Cancer Center, New Bruns-wick, New Jersey (Drs Lu-Yao and DiPaola).Corresponding Author: Siu-Long Yao, MD, Cancer In-stitute of New Jersey, Robert Wood Johnson MedicalSchool, 195 Little Albany St, Room 5544, New Bruns-wick, NJ 08901 ([email protected]).
Context Despite a lack of data, increasing numbers of patients are receiving pri-mary androgen deprivation therapy (PADT) as an alternative to surgery, radiation, orconservative management for the treatment of localized prostate cancer.
Objective To evaluate the association between PADT and survival in elderly menwith localized prostate cancer.
Design, Setting, and Patients A population-based cohort study of 19 271 menaged 66 years or older receiving Medicare who did not receive definitive local therapyfor clinical stage T1-T2 prostate cancer. These patients were diagnosed in 1992-2002within predefined US geographical areas, with follow-up through December 31, 2006,for all-cause mortality and through December 31, 2004, for prostate cancer–specificmortality. Instrumental variable analysis was used to address potential biases associ-ated with unmeasured confounding variables.
Main Outcome Measures Prostate cancer–specific survival and overall survival.
Results Among patients with localized prostate cancer (median age, 77 years), 7867(41%) received PADT, and 11 404 were treated with conservative management, notincluding PADT. During the follow-up period, there were 1560 prostate cancer deathsand 11 045 deaths from all causes. Primary androgen deprivation therapy was asso-ciated with lower 10-year prostate cancer–specific survival (80.1% vs 82.6%; hazardratio [HR], 1.17; 95% confidence interval [CI], 1.03-1.33) and no increase in 10-yearoverall survival (30.2% vs 30.3%; HR, 1.00; 95% CI, 0.96-1.05) compared with con-servative management. However, in a prespecified subset analysis, PADT use in menwith poorly differentiated cancer was associated with improved prostate cancer–specific survival (59.8% vs 54.3%; HR, 0.84; 95% CI, 0.70-1.00; P=.049) but notoverall survival (17.3% vs 15.3%; HR, 0.92; 95% CI, 0.84-1.01).
Conclusion Primary androgen deprivation therapy is not associated with improvedsurvival among the majority of elderly men with localized prostate cancer when com-pared with conservative management.JAMA. 2008;300(2):173-181 www.jama.com
©2008 American Medical Association. All rights reserved. (Reprinted) JAMA, July 9, 2008—Vol 300, No. 2 173
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

mortality was reduced by approxi-mately 60% in patients with nodal dis-ease identified at surgery. Conse-quently, many investigators haveconcluded that the early use of ADT isappropriate for patients with higher-risk or intermediate-risk disease in con-junction with local therapy, but stud-ies that assess the use of ADT alone, asprimary therapy, or in lower-risk set-tings are sparse.
The importance of determining theappropriate application of ADT has re-cently increased, because a growingbody of literature now demonstratesthat chronic ADT use has been associ-ated with approximately 10% to 50%increases in the risks of fracture, dia-betes, coronary heart disease, myocar-dial infarction, and sudden cardiacdeath, in addition to adverse effects onfat mass, cholesterol, and quality oflife.11-16 In the Prostate Cancer Out-comes Study (PCOS),17 the risk of gy-necomastia and hot flashes increased500% and a 267% increase in impo-tence was observed after 1 year of treat-ment. In addition, medical ADT iscostly. The costs associated with ADTmedication use in the United Statesreached $1.2 billion in 200318 and ADTdrugs represented the second highestMedicare Part B drug expenditure.
A randomized clinical trial wouldprovide the data needed to determinethe usefulness of PADT vs conserva-tive management in localized disease.However, because of the relatively in-dolent nature of most cases of local-ized prostate cancer, such a trial wouldtake more than a decade to completeand, given current treatment practicesand resources, would probably not befeasible. Observational studies are of-ten used to provide insight under suchcircumstances, although they may bemore subject to biases.
Instrumental variable analysis (IVA)techniques have been applied success-fully to observational medical stud-ies19,20 to help minimize many of thesebiases so that the results of random-ized clinical trials may often be mim-icked with observational data.2 1
Instrumental variable analysis is a
method of capturing the random com-ponent of patient treatment choiceand using it to balance treatmentgroups with respect to measured andunmeasured confounders. We usedthis approach to assess the associationbetween PADT and disease-specificsurvival and overall survival in menwith T1-T2 prostate cancer.
METHODSData Sources
Data were obtained from the popula-tion-based Surveillance, Epidemiol-ogy, and End Results (SEER) programdatabase and linked Medicare files. TheSEER regions encompass approxi-mately 14% of the US population be-fore 2001 and 26% thereafter. TheMedicare database covers approxi-mately 97% of US persons aged 65years or older, and linkage to the SEERdatabase was complete for approxi-mately 93% of the patients.22 Thestudy received institutional reviewboard approval from the University ofMedicine and Dentistry of New Jer-sey, as well as the SEER program, andthe Center for Medicare & MedicaidServices. Informed consent was waivedby the institutional review board be-cause the data did not contain per-sonal identifiers.
Study Participants
The study cohort consisted of 89 877men aged 66 years or older who wereSEER residents and diagnosed withT1-T2 cancer in 1992-2002. Men whodied within 180 days of diagnosis wereexcluded (n = 1761) (inclusion ofpatients dying within 180 days did notsignificantly alter the results). Patientsreceiving definitive local therapy (eg,prostatectomy or radiation) within180 days of diagnosis were alsoexcluded (n=31 485). To ensure thatthe database accurately documentedthe patient’s clinical course, patientswithout both Medicare Part A (hospi-talization) and Part B (physician andoutpatient) as their primary healthcare insurance coverage duringthe study period were excluded(n = 33 987). Patients with missing
data (n = 2995), unknown cancergrade (n=255), or initiation of ADTbefore cancer diagnosis (n=123) werealso excluded. Therefore, a totalcohort of 19 271 men were included inour analysis.
Primary AndrogenDeprivation Therapy
Patients undergoing PADT receivedADT as primary cancer therapy (eg,no surgery or radiation) during thefirst 180 days following diagnosis.Patients in the conservative manage-ment group were those that did notreceive surgery, radiation, or PADTduring this time. A previous studydemonstrated that patients generallystart primary therapy within 6 monthsof diagnosis.23 Using a previouslydescribed algorithm,11 Medicare physi-cian, inpatient and outpatient claimswere used to identify orchiectomy(Healthcare Common Procedure Cod-ing System codes 54520, 54521,54522, 54530, or 54535, or the Inter-national Classification of Diseases,Ninth Revision code 624) and the useof luteinizing hormone-releasing hor-mone agonists (Healthcare CommonProcedure Coding System codesJ1950, J9202, J9217, J9218, or J9219).Luteinizing hormone-releasing hor-mone agonists and orchiectomy werecombined because previous studieshave shown these treatments to beessentially equivalent.24
Study End Points and Covariates
Overall and prostate cancer–specificsurvival was available through Decem-ber 31, 2006, and December 31, 2004,respectively. Underlying cause of deathwas determined from data in the SEERrecords. Studies have shown that causeof death in the SEER data confirm in-formation available in medical rec-ords in 87% to 88% of cases.25,26
Cox proportional hazards regres-sion model covariates included age at di-agnosis, race (self-determined by the pa-tients and included as a variable becauserace can be associated with outcomes inprostate cancer), zip code income, SEERregion, urban area, marital status, can-
HORMONAL THERAPY USE FOR LOCALIZED PROSTATE CANCER
174 JAMA, July 9, 2008—Vol 300, No. 2 (Reprinted) ©2008 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

cer grade, clinical tumor (T) stage,Charlson comorbidity score, and year ofdiagnosis. Charlson score, a powerfulpredictor of longevity in men with lo-calized prostate cancer27-29 was derivedfrom Medicare claims during the year be-fore prostate cancer diagnosis by usinga validated algorithm.30,31 For cancergrade, Gleason score 2 to 4, 5 to 7, and8 to 10 corresponded to well-differen-tiated, moderately differentiated, andpoorly differentiated disease, respec-tively. We used clinical extension infor-mation provided by SEER to determinecancer stage (T1, T2).
Instrumental Variable Analysis
A health service area (HSA) is definedas 1 or more counties that are rela-tively self-contained with respect tothe provision of routine hospitalcare.32 The instrumental variable wasconstructed by first calculating theproportion of patients who receivedPADT in each HSA. Because someHSAs had small numbers of prostatecancer cases, each HSA with less than50 cases was combined with the near-est (in terms of distance between geo-graphic centers) HSA with 50 or morecases. The threshold of 50 or morecases was chosen because lowerthresholds were associated with moreimbalances in patient characteristics inhigh-PADT and low-PADT use areas.The algorithm produced 66 utilizationareas. High-use and low-use areas cor-responded to the top and bottom ter-tiles of PADT utilization and wereused as the (binary) instrumentalvariable for the (binary) treatmentassignment.
Previous studies have demon-strated that PADT use is highly influ-enced by nonmedical factors,33 with tu-mor characteristics accounting for only9.7% of the total variance in use.34 Ourdata confirmed that PADT use variedwidely across HSAs, a key require-ment of an instrumental variable. An in-strumental variable must be associ-ated with outcomes primarily throughits correlation with treatment status andnot through any other independenteffect. We verified this assumption by
comparing baseline characteristics, in-cluding age at diagnosis, cancer stage,and grade at diagnosis, and found thesefactors comparable between low-PADT and high-PADT areas.
Statistical Analyses
Instrumental variable analysis meth-ods based on the Rubin Causal Model21
were used to account for both mea-sured and unmeasured (eg, prostate-specific antigen, family history, diet,weight) confounders. Covariates in theIVA models included age, race, comor-bidity status, cancer stage, cancer grade,income status, urban residence, mari-tal status, and year of diagnosis. All IVAresults were derived from the samemodels. We examined all the requiredassumptions listed above to ensure thevalidity of our IVA. Traditional Coxproportional hazards regression modelresults were also reported for compari-son with the IVA results. Analyses wereconducted by using SAS version 9.1(SAS Institute Inc, Cary, North Caro-lina) and R version 2.7.0 (R Founda-tion for Statistical Computing, Vi-enna, Austria). Cancer grade was apredefined measured covariate. We cal-culated PADT utilization for each can-cer grade so that it was not necessaryto assume that the patterns of PADT uti-lization were the same for all cancergrades within the same area. Results forwell-differentiated cancer (Gleasonscore 2-4) are not shown separately be-cause results were unstable due to thelimited sample size.
Patients who differ in the likeli-hood of receiving PADT are comparedand the treatment effect on the mar-ginal population is estimated. The mar-ginal effect (local average treatmenteffect)21 of PADT was calculated as
where Hi=a geographic area in the up-per tertile of PADT use, Lo=a geo-graphic area in the lower tertile of PADTuse, Pr(PADT | Hi/Lo)=estimated prob-ability of PADT use among men who
had localized prostate cancer and didnot have surgery or radiation as theirprimary cancer therapy in high/low useregion, and Adjusted OutcomesHi/Adjusted OutcomesLo=estimated sur-vival probability at a particular time (eg,5- or 10-year survival) among men whohad localized prostate cancer and didnot have surgery or radiation as theirprimary cancer therapy in high/low useregion.
To compute the populat ion-adjusted survival curves, we substi-tuted the population means (for con-tinuous covariates) into the Coxproportional hazards regression modelfor each combination of the categori-cal covariates to derive an adjusted haz-ard function. Then, a weighted aver-age of these adjusted hazard functionswas computed with weights propor-tional to the numbers of patients in eachclass. In addition, the population-adjusted survival curve was computedfrom the weighted hazard function.35
Estimates of 5- and 10-year overall andcancer-specific survival for men at av-erage risk were derived from these ad-justed curves. Confidence intervals(CIs) were obtained by computing theseadjusted survival curves for each of10 000 bootstrap samples of the origi-nal data. P values and 95% CIs werederived from the bootstrap estimates.Testing was 2-sided, with �=.05. Analy-ses were repeated for different agegroups but results were similar acrossage groups and the interaction be-tween age and PADT use was not sig-nificant; therefore, all age groups werecombined.
Power calculations for determiningthe difference in survival between high-and low-use HSAs were performed byusing simulations. Overall, the studyhad 80% power to detect a 7% differ-ence in overall survival between high-and low-use PADT areas.
RESULTSBaseline CharacteristicsThe total cohort consisted of 19 271men aged 66 years or older with local-ized prostate cancer diagnosed in 1992-2002. By definition, none of these men
Instrumental Variable Estimate = ∆ =
Adjusted OutcomesHi − Adjusted OutcomesLo
Pr(PADT | Hi) − Pr(PADT | Lo),
HORMONAL THERAPY USE FOR LOCALIZED PROSTATE CANCER
©2008 American Medical Association. All rights reserved. (Reprinted) JAMA, July 9, 2008—Vol 300, No. 2 175
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

received definitive local therapies (eg,radiation or surgery) in the first 180days following diagnosis; 41% re-ceived PADT. The median age of thestudy cohort was 77 years and the me-dian follow-up for overall survival was81 months. As expected, patients re-
ceiving PADT and patients receivingconservative management differed inmany characteristics, suggesting thatthere could be differences in unmea-sured characteristics that might not beadjusted for by conventional statisti-cal methods (TABLE 1).
PADT utilization within 180 daysvaried widely across HSAs (31%-53%)(TABLE 2). When we extended the win-dow for defining PADT from 180 daysto 18 months, the high-use and low-use patterns remained the same. Du-ration of PADT use was also longer inhigh-use areas.
Survival Outcomes
There were 1560 prostate cancerdeaths and 11 045 deaths from allcauses in the study cohort. Unadjustedand adjusted prostate cancer–specificsurvival and overall survival wereworse for patients treated with PADTwhen analyses were conducted using atraditional Cox multivariate model(TABLE 3). The Cox proportional haz-ards regression model approach, how-ever, is unable to adjust for unmea-sured confounders and selectionbiases (eg, higher-risk patients may bepreferentially selected for PADT, thusyielding apparently adverse outcomesfor this group). When IVA was used(Table 3, TABLE 4, TABLE 5, andFIGURE), PADT was still associatedwith increased unadjusted andadjusted prostate cancer–specificmortality (hazard ratio [HR], 1.17;95% CI, 1.03-1.33), but there was nosignificant associated effect on unad-justed, and adjusted median overallsurvival (82 months vs 82 months;HR, 1.00; 95% CI, 0.96-1.05) .Results were similar when analyses
Table 1. Characteristics of the Study Cohorta
CharacteristicsPADT
(n = 7867)Conservative Management
(n = 11 404)
Age, median (IQR), y 79 (74-83) 77 (72-81)
Black race 758 (9.6) 1307 (11.5)
Married at diagnosis 4911 (62.4) 7302 (64.0)
Urban residence 6299 (80.1) 9411 (82.5)
Income, median (IQR), US $ 42 890 (33 861-57468) 44 022 (34 214-57983)
SEER regionsNortheast 840 (10.7) 964 (8.5)
North central 1984 (25.2) 3134 (27.5)
West 4816 (61.2) 6903 (60.5)
South 227 (2.9) 403 (3.5)
Cancer gradeWell differentiated 64 (0.8) 244 (2.1)
Moderately differentiated 5115 (65.0) 9545 (83.7)
Poorly differentiated 2688 (34.2) 1615 (14.2)
Clinical stage at diagnosisT1 3915 (49.8) 7325 (64.2)
T2 3952 (50.2) 4079 (35.8)
Comorbidity statusCharlson comorbidity score 0-1 7446 (94.7) 10 664 (93.5)
Charlson comorbidity score �2 421 (5.3) 740 (6.5)
Year of cancer diagnosis1992-1997 2876 (36.6) 5348 (46.9)
1998-2002 4991 (63.4) 6056 (53.1)Abbreviations: IQR, interquartile range; PADT, primary androgen deprivation therapy; SEER, Surveillance, Epidemiol-
ogy, and End Results.aData are presented as No. (%) unless otherwise specified. Race was self-determined by the patients. For cancer grade,
a Gleason score of 2 to 4, 5 to 7, and 8 to 10 corresponded to well-differentiated, moderately differentiated, andpoorly differentiated disease, respectively. Clinical extension information provided by SEER was used to determinecancer stage (T1, T2). Charlson comorbidity score was derived from Medicare claims during the year before pros-tate cancer diagnosis by using a validated algorithm.30,31
Table 2. Characteristics of Men With Localized Prostate Cancer in High-Use and Low-Use PADT Health Service Areas
Characteristics
Moderately Differentiated Poorly Differentiated All Localized Cancers
High(n = 4278)
Low(n = 5898)
High(n = 1433)
Low(n = 1478)
High(n = 6302)
Low(n = 6673)
PADT within 180 d, No. (%) 2058 (48.1) 1502 (25.5) 1058 (73.8) 757 (51.2) 3321 (52.5) 2041 (30.6)
PADT within 18 mo, No. (%) 2067 (48.3) 1652 (28.0) 1081 (75.6) 815 (55.1) 3396 (53.9) 2247 (33.7)
Duration of PADT use,mean (SD), mo
21 (30) 16 (29) 34 (34) 26 (33) 24 (31) 19 (31)
Age at diagnosis,median (IQR), y
78 (73-82) 77 (72-81) 79 (75-83) 79 (74-83) 78 (74-82) 77 (73-81)
Zip code–levelincome, median(IQR), US $
41 284(33 816-56 958)
44 939(34 490-56 912)
42 545(35 091-59 722)
41 580(31 166-52 645)
42 408(34 382-60 669)
44 107(33 176-56 041)
Charlson score, mean(SD)a
0.22 (0.63) 0.22 (0.64) 0.19 (0.58) 0.22 (0.64) 0.21 (0.61) 0.22 (0.64)
Clinical stage T1, No. (%)a 2619 (61.2) 3742 (63.5) 698 (48.7) 739 (50.0) 3651 (57.9) 3901 (58.5)Abbreviations: IQR, interquartile range; PADT, primary androgen deprivation therapy.aSee Table 1 for explanations of Charlson score and clinical stage tumor (T1).
HORMONAL THERAPY USE FOR LOCALIZED PROSTATE CANCER
176 JAMA, July 9, 2008—Vol 300, No. 2 (Reprinted) ©2008 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013
were restricted to men with comor-bidity scores of 0 or without othercancers, suggesting that the resultswere independent of comorbidity.
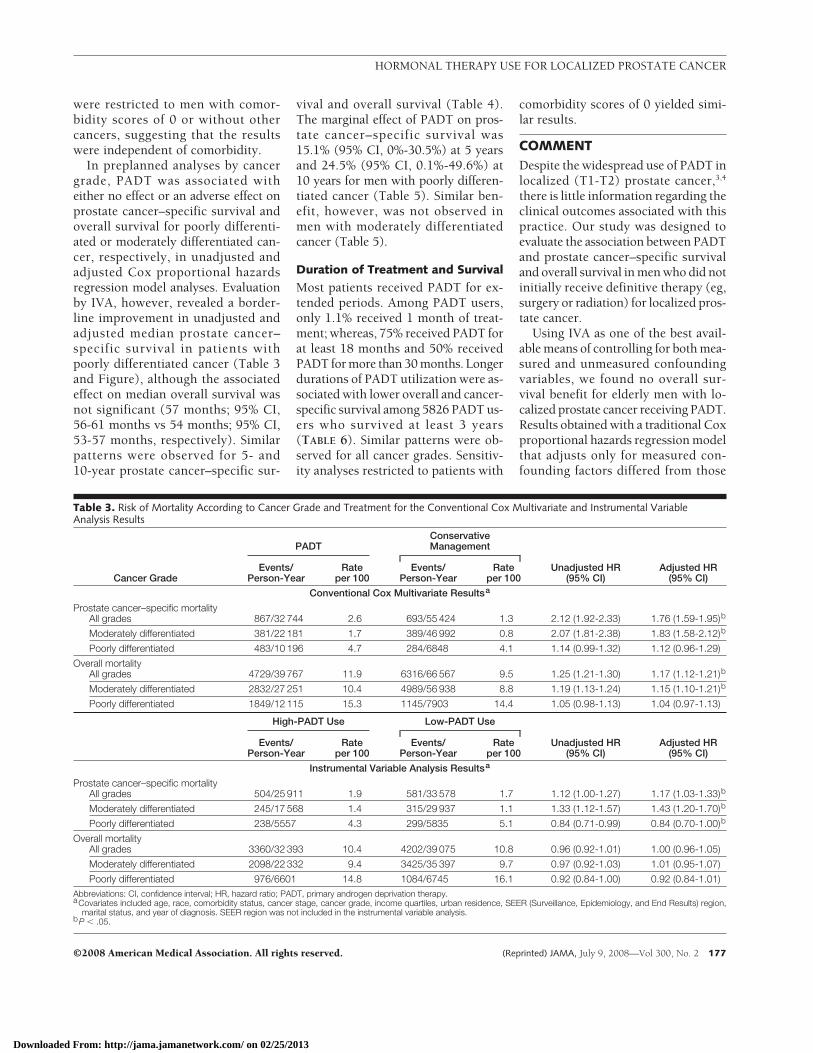
In preplanned analyses by cancergrade, PADT was associated witheither no effect or an adverse effect onprostate cancer–specific survival andoverall survival for poorly differenti-ated or moderately differentiated can-cer, respectively, in unadjusted andadjusted Cox proportional hazardsregression model analyses. Evaluationby IVA, however, revealed a border-line improvement in unadjusted andadjusted median prostate cancer–specific survival in patients withpoorly differentiated cancer (Table 3and Figure), although the associatedeffect on median overall survival wasnot significant (57 months; 95% CI,56-61 months vs 54 months; 95% CI,53-57 months, respectively). Similarpatterns were observed for 5- and10-year prostate cancer–specific sur-
vival and overall survival (Table 4).The marginal effect of PADT on pros-tate cancer–specific survival was15.1% (95% CI, 0%-30.5%) at 5 yearsand 24.5% (95% CI, 0.1%-49.6%) at10 years for men with poorly differen-tiated cancer (Table 5). Similar ben-efit, however, was not observed inmen with moderately differentiatedcancer (Table 5).
Duration of Treatment and Survival
Most patients received PADT for ex-tended periods. Among PADT users,only 1.1% received 1 month of treat-ment; whereas, 75% received PADT forat least 18 months and 50% receivedPADT for more than 30 months. Longerdurations of PADT utilization were as-sociated with lower overall and cancer-specific survival among 5826 PADT us-ers who survived at least 3 years(TABLE 6). Similar patterns were ob-served for all cancer grades. Sensitiv-ity analyses restricted to patients with
comorbidity scores of 0 yielded simi-lar results.
COMMENTDespite the widespread use of PADT inlocalized (T1-T2) prostate cancer,3,4
there is little information regarding theclinical outcomes associated with thispractice. Our study was designed toevaluate the association between PADTand prostate cancer–specific survivaland overall survival in men who did notinitially receive definitive therapy (eg,surgery or radiation) for localized pros-tate cancer.
Using IVA as one of the best avail-able means of controlling for both mea-sured and unmeasured confoundingvariables, we found no overall sur-vival benefit for elderly men with lo-calized prostate cancer receiving PADT.Results obtained with a traditional Coxproportional hazards regression modelthat adjusts only for measured con-founding factors differed from those
Table 3. Risk of Mortality According to Cancer Grade and Treatment for the Conventional Cox Multivariate and Instrumental VariableAnalysis Results
Cancer Grade
PADTConservativeManagement
Unadjusted HR(95% CI)
Adjusted HR(95% CI)
Events/Person-Year
Rateper 100
Events/Person-Year
Rateper 100
Conventional Cox Multivariate Resultsa
Prostate cancer–specific mortalityAll grades 867/32 744 2.6 693/55 424 1.3 2.12 (1.92-2.33) 1.76 (1.59-1.95)b
Moderately differentiated 381/22 181 1.7 389/46 992 0.8 2.07 (1.81-2.38) 1.83 (1.58-2.12)b
Poorly differentiated 483/10 196 4.7 284/6848 4.1 1.14 (0.99-1.32) 1.12 (0.96-1.29)
Overall mortalityAll grades 4729/39 767 11.9 6316/66 567 9.5 1.25 (1.21-1.30) 1.17 (1.12-1.21)b
Moderately differentiated 2832/27 251 10.4 4989/56 938 8.8 1.19 (1.13-1.24) 1.15 (1.10-1.21)b
Poorly differentiated 1849/12 115 15.3 1145/7903 14.4 1.05 (0.98-1.13) 1.04 (0.97-1.13)
High-PADT Use Low-PADT Use
Unadjusted HR(95% CI)
Adjusted HR(95% CI)
Events/Person-Year
Rateper 100
Events/Person-Year
Rateper 100
Instrumental Variable Analysis Resultsa
Prostate cancer–specific mortalityAll grades 504/25 911 1.9 581/33 578 1.7 1.12 (1.00-1.27) 1.17 (1.03-1.33)b
Moderately differentiated 245/17 568 1.4 315/29 937 1.1 1.33 (1.12-1.57) 1.43 (1.20-1.70)b
Poorly differentiated 238/5557 4.3 299/5835 5.1 0.84 (0.71-0.99) 0.84 (0.70-1.00)b
Overall mortalityAll grades 3360/32 393 10.4 4202/39 075 10.8 0.96 (0.92-1.01) 1.00 (0.96-1.05)
Moderately differentiated 2098/22 332 9.4 3425/35 397 9.7 0.97 (0.92-1.03) 1.01 (0.95-1.07)
Poorly differentiated 976/6601 14.8 1084/6745 16.1 0.92 (0.84-1.00) 0.92 (0.84-1.01)Abbreviations: CI, confidence interval; HR, hazard ratio; PADT, primary androgen deprivation therapy.aCovariates included age, race, comorbidity status, cancer stage, cancer grade, income quartiles, urban residence, SEER (Surveillance, Epidemiology, and End Results) region,
marital status, and year of diagnosis. SEER region was not included in the instrumental variable analysis.bP � .05.
HORMONAL THERAPY USE FOR LOCALIZED PROSTATE CANCER
©2008 American Medical Association. All rights reserved. (Reprinted) JAMA, July 9, 2008—Vol 300, No. 2 177
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

with the NA approach. These observa-tions suggest that there is significant un-accounted residual bias associated withtraditional analytical methods in thissetting and that the NA approach may
be particularly advantageous. In addi-tion, 1 potential advantage of this studyover clinical trials is that it includes real-world patients that would often be ex-cluded from clinical trials, even though
these patients would receive the treat-ment in practice.
In our study, cancer-specific sur-vival but not overall survival appearedworse for men with lower risk cancertreated with PADT. This observationhas been previously documented in arandomized controlled study of PADTin men with T0-T4 disease.36 Theauthors suggested several possibleexplanations for this finding, includ-ing competing causes of death, mis-classification, and statistical varia-tion.36 Another possibility could bethat suppression of moderately orwell-differentiated cells not destinedto harm a patient’s overall survivalmay allow for the establishment orovergrowth of more rapidly growingmalignant clones (as observed in pre-clinical models)37-39 that increase theprobability of death due to prostatecancer instead of a competing cause ofdeath. As shown in the Figure, thelikelihood of death from competingcauses normally exceeds the risk ofdeath from prostate cancer in thispopulation; this balance may bealtered if PADT preferentially allowsfor the establishment or overgrowth ofa more malignant fraction of a tumor.
Our study had some limitations.The study was limited to men aged66 years or older; therefore, the re-sults could differ for younger men. TheSEER-Medicare database does not cap-ture information on antiandrogen use.
Table 4. Adjusted Percentage Overall and Prostate Cancer–Specific Survival in High-Use andLow-Use Areasa
Cancer Grade
High-PADT Use Low-PADT UseHigh vs LowDifference(95% CI)
Deaths/Person-Year
AdjustedSurvival, %
Deaths/Person-Year
AdjustedSurvival, %
Prostate cancer–specificsurvival
5-y all grades 378/21 757 91.6 408/25 386 92.7 −1.1(−2.1 to −0.1)
5-y moderately 180/14 759 93.8 196/22 689 95.7 −1.9(−2.8 to −0.9)
5-y poorly 190/4782 79.2 248/4863 75.8 3.4(0.01 to 11.1)
10-y all grades 500/25 709 80.1 570/33 022 82.6 −2.5(−4.7 to −0.3)
10-y moderately 242/17 430 83.1 308/29 456 88.0 −4.9(−7.4 to −2.4)
10-y poorly 237/5529 59.8 298/5783 54.3 5.5(0.01 to 11.1)
Overall survival5-y all grades 2349/25 444 62.0 2632/26 987 62.1 −0.1
(−1.5 to 1.3)
5-y moderately 1456/17 558 65.5 2085/24 459 65.9 −0.3(−1.9 to 1.3)
5-y poorly 717/5376 47.3 823/5281 44.9 2.4(−0.7 to 5.6)
10-y all grades 3238/31 770 30.2 3949/37 499 30.3 −0.1(−1.8 to 1.6)
10-y moderately 2012/21 914 33.9 3211/33 971 34.4 −0.4(−2.5 to 1.7)
10-y poorly 953/6518 17.3 1054/6598 15.3 2.0(−0.6 to 4.6)
Abbreviations: CI, confidence interval; PADT, primary androgen deprivation therapy.aCovariates included age, race, comorbidity status, cancer stage, cancer grade, income quartiles, urban residence, mari-
tal status, and year of diagnosis. 95% CIs are bootstrapped. Because date of last follow-up differed for overall (Decem-ber 31, 2006) and cancer-specific survival (December 31, 2004), the number of person-years of follow-up differs foreach end point.
Table 5. Marginal Effect of PADT on Overall and Prostate Cancer–Specific Survival in High-Use and Low-Use Areasa
Cancer Grade
5-Year Survival 10-Year Survival
Risk Difference,%
Difference inPADT Use, %
Marginal Effect(95% CI)
Risk Difference,%
Difference inPADT Use, %
Marginal Effect(95% CI)
Prostate cancer–specificsurvival
All localized −1.1 21.9 −5.0 (−9.4 to −0.6) −2.5 21.9 −11.2 (−21.2 to −1.3)
Moderatelydifferentiated
−1.9 22.6 −8.3 (−12.5 to −4.1) −4.9 22.6 −21.7 (−32.8 to −10.8)
Poorlydifferentiated
3.4 22.6 15.1 (0 to 30.5) 5.5 22.6 24.5 (0.1 to 49.6)
Overall survivalAll localized −0.1 21.9 −0.4 (−6.7 to 6.0) −0.1 21.9 −0.5 (−8.1 to 7.3)
Moderatelydifferentiated
−0.3 22.6 −1.5 (−8.5 to 5.6) −0.4 22.6 −2.0 (−11.2 to 7.4)
Poorly differentiated 2.4 22.6 10.7 (−3.1 to 24.8) 2.0 22.6 8.8 (−2.5 to 20.4)Abbreviations: CI, confidence interval; PADT, primary androgen deprivation therapy.aAnalyses used 95% bootstrapped CIs. Marginal effect is the risk difference (obtained from Table 4) divided by the difference in PADT use (obtained from Table 2).
HORMONAL THERAPY USE FOR LOCALIZED PROSTATE CANCER
178 JAMA, July 9, 2008—Vol 300, No. 2 (Reprinted) ©2008 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

Therefore, patients using antiandro-gens only might be misclassified intothe conservative management cohortand, because a previous study40 sug-gested that antiandrogens may result inadverse outcomes in these patients, itis possible that the conservative man-agement group performed unusuallypoorly. However, previous data fromanother large database (CaPSURE)41
showed that the use of antiandrogensas sole treatment for localized pros-tate cancer is relatively uncommon (ap-proximately 2%) and it is unlikely thatthis small subset could alter the out-comes of the conservative manage-ment group overall.
Just like the success of a random-ized study is dependent on factors suchas the attainment of a sufficient sample
size to balance both measured and un-measured characteristics in differenttreatment groups, the use of IVA to bal-ance treatment group characteristics(eg, prostate-specific antigen levels,family history, diet, body mass) de-pends on finding a suitable, partlyrandom, varying factor (instrumentalvariable) that can be used to balancetreatment groups. Our instrumental
Figure. Adjusted Prostate Cancer–Specific Survival and Overall Survival in High-Use and Low-Use Health Service Areas by Cancer Grade
Poorly differentiated prostate cancer
Poorly differentiated prostate cancer
Moderately differentiated prostate cancer
Moderately differentiated prostate cancer
Moderately differentiated prostate cancer
Low-PADT useHigh-PADT use
5898 5210 3379 2002 1105 4354278 3779 1699 828 420 133
Poorly differentiated prostate cancer
Low-PADT useHigh-PADT use
1478 1159 581 290 134 451433 1184 561 236 116 29
Prostate Cancer–Specific Survival
5898 5210 4233 2719 1575 8394278 3779 3084 1364 626 287
1478 1159 789 399 188 971433 1184 840 388 144 66
Overall Survival
1.0
0.4
0.2
0.6
0.8
0 2 4 6 8 10Time, y
Sur
viva
l Pro
babi
lity
Health Service AreaPADT Use
LowHigh
1.0
0.4
0.2
0.6
0.8
0 2 4 6 8 10Time, y
Sur
viva
l Pro
babi
lity
PADT indicates primary androgen deprivation therapy. Error bars represent 95% confidence intervals (CIs) at 5 and 10 years. For cancer-specific survival, results wereadjusted for age, race, income, marital status, urban residence, comorbidity status, year of diagnosis, and cancer stage. Prostate cancer–specific survival was lower inhigh- vs low-PADT use areas among men with moderately differentiated cancer (bootstrap P� .001). Prostate cancer–specific survival was borderline statistically dif-ferent between high- and low-PADT use areas among men with poorly differentiated cancer (bootstrap P=.049). Overall survival was similar in high- and low-PADTuse areas among men with moderately differentiated cancer; median overall survival was 89 and 90 months for high- and low-use areas, respectively (bootstrap P=.67).Difference in overall survival between high- and low-PADT use areas among men with poorly differentiated cancer did not reach statistical significance (bootstrapP=.13). Median overall survival was 57 and 54 months for high- and low-PADT use areas, respectively. The difference in median overall survival between high- andlow-PADT use areas was 3 months (95% CI, −1 to 7 months).
Table 6. Adjusted HRs for Overall and Cancer-Specific Mortality Among 5826 Patients With PADT Surviving at Least 3 Years
Cancer Grade
Cancer-Specific Mortality Rate per 100(Deaths/Person-Year)
Overall Mortality Rate per 100(Deaths/Person-Year)
Duration of PADTAdjusted HR
(95% CI)a
Duration of PADTAdjusted HR
(95% CI)a�12 mo 13-36 mo �12 mo 13-36 mo
Moderatelydifferentiated
0.39 (16/4056) 1.24 (199/16 031) 2.22 (1.32-3.74) 4.40 (242/5498) 7.43 (1457/19 613) 1.32 (1.14-1.52)
Poorly differentiated 0.72 (7/969) 2.32 (179/7700) 2.44 (1.14-5.23) 5.42 (73/1347) 9.70 (895/9227) 1.46 (1.14-1.86)
All localized 0.45 (23/5103) 1.58 (379/23 988) 2.42 (1.58-3.72) 4.61 (320/6934) 8.18 (2381/29 119) 1.36 (1.20-1.53)Abbreviations: CI, confidence interval; HR, hazard ratio; PADT, primary androgen deprivation therapy.aCovariates included age, race, comorbidity status, cancer stage, cancer grade, income quartiles, urban residence, SEER (Surveillance, Epidemiology, and End Results) region,
marital status, and year of diagnosis.
HORMONAL THERAPY USE FOR LOCALIZED PROSTATE CANCER
©2008 American Medical Association. All rights reserved. (Reprinted) JAMA, July 9, 2008—Vol 300, No. 2 179
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

variable (high- and low-PADT useHSAs) had excellent properties. How-ever, as in randomized studies, it is pos-sible that some unmeasured factors stillmay have been imbalanced betweengroups. Nonetheless, sensitivity analy-ses, using various geographic-based in-struments and removing patients withother cancers or comorbidity scores ofmore than 0, yielded similar results andsuggested that the analyses were ro-bust. However, it is still possible thatthe use of an NA approach in this set-ting does not adequately control for un-known confounding variables; there-fore, if possible, a randomized trialshould be considered.
There are few data comparing PADTwith conservative management, or anyother established treatment option (eg,surgery or radiation), in men with lo-calized (T1-T2, NO, M0) prostate can-cer, even though the popularity ofPADT has increased in this pop-ulation by 2- to 3-fold in recent years.3
Published studies have generally notprovided data specific for localized (T1-T2) disease and have had limitedsample sizes.42,43 The largest publishedstudy describing PADT use amongpatients with T1-T2 disease was de-scriptive, noncomparative, and had lim-ited follow-up.41 The randomized EarlyProstate Cancer trial44 had a largesubset of patients with T1-T2 diseasebut a nontraditional form of PADT(bicalutamide) was used. Results fromthis trial revealed a trend toward de-creased overall survival in patientstreated with PADT.40 The VeteransAdministration Co-operative UrologicalResearch Group study45 also used anonconventional form of PADT (dieth-ylstilbestrol). Results were inconsis-tent, with benefit in T2 disease but harmin T1 disease. In a related randomizedstudy, European Organization for Re-search and Treatment of Cancer trial30891,36 which included patients withboth localized and advanced disease (eg,T0-4, N0-2), a modest overall survivalbenefit was found in favor of PADT butfurther analyses suggested that this ben-efit was associated with a group of pa-tients with high-risk disease.46 Studies
by the Medical Research Council,47 theEuropean Organization for Researchand Treatment of Cancer trial 30846,10
and the Swiss Group for Clinical Can-cer Research48 focused on patients withmore advanced disease. In general, al-though the designs, therapies, and set-tings vary significantly from our study,the findings of these previous studiesare inferentially consistent with ourdocumentation of a lack of overall ben-efit, and some suggestion of potentialbenefit in high-risk or advanced-disease subgroups.
In conclusion, our analyses suggestthat PADT is not associated with im-proved survival among the majority ofelderly men with T1-T2 prostate can-cer. The significant adverse effects andcosts associated with PADT, along withour finding of a lack of overall sur-vival benefit, suggest that cliniciansshould carefully consider the ratio-nale for initiating PADT in elderly pa-tients with T1-T2 prostate cancer.
Author Contributions: Dr Lu-Yao had full access toall of the data in the study and takes responsibility forthe integrity of the data and the accuracy of the dataanalysis.Study concept and design: Lu-Yao, Albertson, Yao.Acquisition of data: Lu-Yao.Analysis and interpretation of data: Lu-Yao, Albertson,Moore, Shih, Lin, DiPaola, Yao.Drafting of the manuscript: Lu-Yao, Lin, Yao.Critical revision of the manuscript for important in-tellectual content: Lu-Yao, Albertson, Moore, Shih,Lin, DiPaola, Yao.Statistical analysis: Lu-Yao, Moore, Shih, Lin, Yao.Obtained funding: Lu-Yao.Administrative, technical, or material support: Lu-Yao,Albertson.Study supervision: Lu-Yao, Shih, DiPaola.Financial Disclosures: None reported.Funding/Support: This study was supported in part byaward DAMD17-01-1-0755 from the US Army Medi-cal Research Acquisition Activity, Fort Detrick, Mary-land, and by the Cancer Institute of New Jersey; awardW81XWG-05-1-0235 from the Department of De-fense, Ohl Foundation; and by grants R01 CA116399from the National Cancer Institute and NCI CA-72720-10 from the Cancer Institute of New Jersey.Role of Sponsors: The Department of Defense did notplay any role in the design and conduct of the study,in the collection, management, analysis, and inter-pretation of the data, or in the preparation, review,or approval of the manuscript. The National CancerInstitute (NCI) sponsored the collection and manage-ment of the data, and reviewed and approved the studyprotocol and manuscript. However, NCI did not playany role in the analysis and interpretation of the data.Disclaimers: This study used the Linked SEER-Medicare Database. The interpretation and report-ing of these data are the sole responsibility of the au-thors. The content of the information does notnecessarily reflect the position or the policy of the USGovernment, and no official endorsement should beinferred.
Additional Contributions: We thank the Applied Re-search Branch, Division of Cancer Prevention and Popu-lation Science, National Cancer Institute; Office of In-formation Services and Office of Strategic Planning,Centers for Medicare & Medicaid Services; Informa-tion Management Services Inc; and the SEER pro-gram tumor registries in the creation of the SEER-Medicare database. Thanusha Puvananayagam, MPH(Cancer Institute of New Jersey assistant staff ) pro-vided outstanding administrative and technical assis-tance. Ms Puvananayagam did not receive any com-pensation.
REFERENCES
1. Jemal A, Siegel R, Ward E, Murray T, Xu J, ThunMJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57(1):43-66.2. Cooperberg MR, Broering JM, Litwin MS, et al. Thecontemporary management of prostate cancer in theUnited States: lessons from the Cancer of the Pros-tate Strategic Urologic Research Endeavor (Cap-SURE), a national disease registry. J Urol. 2004;171(4):1393-1401.3. Cooperberg MR, Grossfeld GD, Lubeck DP, CarrollPR. National practice patterns and time trends in an-drogen ablation for localized prostate cancer. J NatlCancer Inst. 2003;95(13):981-989.4. Akaza H. Trends in primary androgen depletiontherapy for patients with localized and locally ad-vanced prostate cancer: Japanese perspective. Can-cer Sci. 2006;97(4):243-247.5. Bolla M, Collette L, Blank L, et al. Long-term re-sults with immediate androgen suppression and ex-ternal irradiation in patients with locally advanced pros-tate cancer (an EORTC study): a phase III randomisedtrial. Lancet. 2002;360(9327):103-106.6. D’Amico AV, Manola J, Loffredo M, et al. 6-Monthandrogen suppression plus radiation therapy vs ra-diation therapy alone for patients with clinically lo-calized prostate cancer: a randomized controlled trial.JAMA. 2004;292(7):821-827.7. D’Amico AV, Loffredo M, Renshaw AA, LoffredoB, Chen MH. Six-month androgen suppression plusradiation therapy compared with radiation therapyalone for men with prostate cancer and a rapidly in-creasing pretreatment prostate-specific antigen level.J Clin Oncol. 2006;24(25):4190-4195.8. Bolla M, Gonzalez D, Warde P, et al. Improved sur-vival in patients with locally advanced prostate can-cer treated with radiotherapy and goserelin. N Engl JMed. 1997;337(5):295-300.9. Messing EM, Manola J, Sarosdy M, Wilding G,Crawford ED, Trump D. Immediate hormonal therapycompared with observation after radical prostatec-tomy and pelvic lymphadenectomy in men with node-positive prostate cancer. N Engl J Med. 1999;341(24):1781-1788.10. Schröder FH, Kurth KH, Fossa SD, et al. Early ver-sus delayed endocrine treatment of pN1-3 M0 pros-tate cancer without local treatment of the primary tu-mor: results of European Organisation for the Researchand Treatment of Cancer 30846: a phase III study.J Urol. 2004;172(3):923-927.11. Shahinian VB, Kuo YF, Freeman JL, Goodwin JS.Risk of fracture after androgen deprivation for pros-tate cancer. N Engl J Med. 2005;352(2):154-164.12. Kapoor D, Malkin CJ, Channer KS, Jones TH. An-drogens, insulin resistance and vascular disease in men.Clin Endocrinol (Oxf ). 2005;63(3):239-250.13. Makhsida N, Shah J, Yan G, Fisch H, Shabsigh R.Hypogonadism and metabolic syndrome: implica-tions for testosterone therapy. J Urol. 2005;174(3):827-834.14. Smith MR, Finkelstein JS, McGovern FJ, et al.Changes in body composition during androgen dep-rivation therapy for prostate cancer. J Clin Endocri-nol Metab. 2002;87(2):599-603.
HORMONAL THERAPY USE FOR LOCALIZED PROSTATE CANCER
180 JAMA, July 9, 2008—Vol 300, No. 2 (Reprinted) ©2008 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

15. D’Amico AV, Denham JW, Crook J, et al. Influ-ence of androgen suppression therapy for prostatecancer on the frequency and timing of fatal myocar-dial infarctions. J Clin Oncol. 2007;25(17):2420-2425.16. Keating NL, O’Malley AJ, Smith MR. Diabetes andcardiovascular disease during androgen deprivationtherapy for prostate cancer. J Clin Oncol. 2006;24(27):4448-4456.17. Potosky AL, Reeve BB, Clegg LX, et al. Qualityof life following localized prostate cancer treatedinitially with androgen deprivation therapy orno therapy. J Natl Cancer Inst. 2002;94(6):430-437.18. Weight CJ, Klein EA, Jones JS. Androgen depri-vation falls as orchiectomy rates rise after changes inreimbursement in the U.S. Medicare population.Cancer. 2008;112(10):2195-2201.19. Earle CC, Tsai JS, Gelber RD, Weinstein MC,Neumann PJ, Weeks JC. Effectiveness of chemo-therapy for advanced lung cancer in the elderly: in-strumental variable and propensity analysis. J ClinOncol. 2001;19(4):1064-1070.20. Stukel TA, Fisher ES, Wennberg DE, Alter DA,Gottlieb DJ, Vermeulen MJ. Analysis of observa-tional studies in the presence of treatment selectionbias: effects of invasive cardiac management onAMI survival using propensity score and instrumen-tal variable methods. JAMA. 2007;297(3):278-285.21. Angrist JD, Imbens GW, Rubin DB. Identifica-tion of causal effects using instrumental variables.J Am Stat Assoc. 1996;91(434):444-455.22. Warren JL, Klabunde CN, Schrag D, Bach PB, RileyGF. Overview of the SEER-Medicare data: content, re-search applications, and generalizability to the UnitedStates elderly population. Med Care. 2002;40(8)(suppl):IV-3-IV-18.23. Potosky AL, Davis WW, Hoffman RM, et al. Five-year outcomes after prostatectomy or radiotherapyfor prostate cancer: the Prostate Cancer OutcomesStudy. J Natl Cancer Inst. 2004;96(18):1358-1367.24. Seidenfeld J, Samson DJ, Hasselblad V, et al. Single-therapy androgen suppression in men with ad-vanced prostate cancer: a systematic review andmeta-analysis. Ann Intern Med. 2000;132(7):566-577.25. Albertsen PC, Walters S, Hanley JA. A compari-son of cause of death determination in men previ-ously diagnosed with prostate cancer who died in 1985or 1995. J Urol. 2000;163(2):519-523.
26. Penson DF, Albertsen PC, Nelson PS, Barry M,Stanford JL. Determining cause of death in prostatecancer: are death certificates valid? J Natl Cancer Inst.2001;93(23):1822-1823.27. Albertsen PC, Fryback DG, Storer BE, Kolon TF,Find J. Long-term survival among men with conser-vatively treated localized prostate cancer. JAMA. 1995;274(8):626-631.28. Fowler JE Jr, Terrell FL, Renfroe DL. Co-morbidities and survival of men with localized pros-tate cancer treated with surgery or radiation therapy.J Urol. 1996;156(5):1714-1718.29. D’Hoore W, Sicotte C, Tilquin C. Risk adjust-ment in outcome assessment: the Charlson comor-bidity index. Methods Inf Med. 1993;32(5):382-387.30. Deyo RA, Cherkin DC, Ciol MA. Adapting a clini-cal comorbidity index for use with ICD-9-CM admin-istrative databases. J Clin Epidemiol. 1992;45(6):613-619.31. Klabunde CN, Potosky AL, Legler JM, Warren JL.Development of a comorbidity index using physicianclaims data. J Clin Epidemiol. 2000;53(12):1258-1267.32. Makuc DM, Haglund B, Ingram DD, KleinmanJC, Feldman JJ. Health service areas for the UnitedStates. Vital Health Stat 2. 1991;(112):1-102.33. Shahinian VB, Kuo YF, Freeman JL, Orihuela E,Goodwin JS. Increasing use of gonadotropin-releasing hormone agonists for the treatment of lo-calized prostate carcinoma. Cancer. 2005;103(8):1615-1624.34. Shahinian VB, Kuo Y-F, Freeman JL, Goodwin JS.Determinants of androgen deprivation therapy use forprostate cancer: role of the urologist. J Natl CancerInst. 2006;98(12):839-845.35. Therneau TM, Grambsch PM. Modeling Sur-vival Data: Extending the Cox Model. New York, NY:Springer; 2000.36. Studer UE, Whelan P, Albrecht W, et al. Imme-diate or deferred androgen deprivation for patients withprostate cancer not suitable for local treatment withcurative intent: European Organisation for Researchand Treatment of Cancer (EORTC) Trial 30891. J ClinOncol. 2006;24(12):1868-1876.37. Isaacs JT, Coffey DS. Adaptation versus selec-tion as the mechanism responsible for the relapse ofprostatic cancer to androgen ablation therapy as stud-ied in the Dunning R-3327-H adenocarcinoma. Can-cer Res. 1981;41(12 pt 1):5070-5075.38. Han G, Buchanan G, Ittmann M, et al. Mutationof the androgen receptor causes oncogenic transfor-
mation of the prostate. Proc Natl Acad Sci U S A. 2005;102(4):1151-1156.39. Banach-Petrosky W, Jessen WJ, Ouyang X, et al.Prolonged exposure to reduced levels of androgenaccelerates prostate cancer progression in Nkx3.1;Pten mutant mice. Cancer Res. 2007;67(19):9089-9096.40. Iversen P, Johansson JE, Lodding P, et al. Bicalu-tamide (150 mg) versus placebo as immediate therapyalone or as adjuvant to therapy with curative intentfor early nonmetastatic prostate cancer: 5.3-year me-dian follow-up from the Scandinavian Prostate Can-cer Group Study Number 6. J Urol. 2004;172(5 pt 1):1871-1876.41. Kawakami J, Cowan JE, Elkin EP, Latini DM,Duchane J, Carroll PR. Androgen-deprivation therapyas primary treatment for localized prostate cancer: datafrom Cancer of the Prostate Strategic Urologic Re-search Endeavor (CaPSURE). Cancer. 2006;106(8):1708-1714.42. Akaza H, Homma Y, Usami M, et al. Efficacy ofprimary hormone therapy for localized or locally ad-vanced prostate cancer: results of a 10-year follow-up.BJU Int. 2006;98(3):573-579.43. Labrie F, Candas B, Gomez JL, Cusan L. Can com-bined androgen blockade provide long-term controlor possible cure of localized prostate cancer? Urology.2002;60(1):115-119.44. McLeod DG, Iversen P, See WA, Morris T,Armstrong JON, Wirth MP. Bicalutamide 150 mgplus standard care vs standard care alone for earlyprostate cancer. BJU Int. 2006;97(2):247-254.45. Treatment and survival of patients with cancer ofthe prostate: the Veterans Administration Co-operative Urological Research Group. Surg GynecolObstet. 1967;124(5):1011-1017.46. Studer UE, Collette L, Whelan P, et al. Using PSAto guide timing of androgen deprivation in patientswith T0-4 N0-2 M0 prostate cancer not suitable forlocal curative treatment (EORTC 30891). Eur Urol.2008;53(5):941-949.47. Immediate versus deferred treatment for ad-vanced prostatic cancer: initial results of the MedicalResearch Council Trial: the Medical Research CouncilProstate Cancer Working Party Investigators Group.Br J Urol. 1997;79(2):235-246.48. Studer UE, Hauri D, Hanselmann S, et al. Imme-diate versus deferred hormonal treatment for pa-tients with prostate cancer who are not suitable forcurative local treatment: results of the randomized trialSAKK 08/88. J Clin Oncol. 2004;22(20):4109-4118.
HORMONAL THERAPY USE FOR LOCALIZED PROSTATE CANCER
©2008 American Medical Association. All rights reserved. (Reprinted) JAMA, July 9, 2008—Vol 300, No. 2 181
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

Primary Androgen Deprivation Therapyin Men With Prostate Cancer
To the Editor: The analysis of prostate cancer–specific andoverall survival by Dr Lu-Yao and colleagues1 concluded thatprimary androgen deprivation therapy (PADT) offered nobenefit compared with conservative management in el-derly men with localized prostate cancer. Since their com-parison was based on epidemiologic data rather than thoseobtained in a prospective randomized trial, there is a pos-sibility that confounding variables may have influenced pa-tient outcomes.
Serum prostate-specific antigen (PSA) has been shown tobe an independent predictor of outcome in newly diag-nosed patients2 and may often be used by clinicians to chooserecommended therapy. It seems likely that men with higherPSA levels (and thus worse prognoses) were those who weregiven PADT. However, the study by Lu-Yao et al does notinclude an analysis of PSA data and their possible influ-ence on treatment recommendations. In the absence of thisinformation, it is not possible to conclude that PADT con-fers no benefit, especially to a high–PSA-level subpopula-tion of patients.
Leslie Laufman, [email protected], Ohio
Financial Disclosures: None reported.
1. Lu-Yao GL, Albertsen PC, Moore DF, et al. Survival following primary andro-gen deprivation therapy among men with localized prostate cancer. JAMA. 2008;300(2):173-181.2. O’Dowd G, Veltri R, Orozco R, Miller M, Oesterling J. Update on the appro-priate staging evaluation for newly diagnosed prostate cancer. J Urol. 1997;158(3 pt 1):687-698.
In Reply: As noted in our article, an important limitationof nonrandomized studies is the potential for biases asso-ciated with unmeasured confounding variables. Tradi-tional statistical methods have been limited in the abilityto adjust for unmeasured or unknown biases.
Instrumental variable analytic (IVA) methods, like the onewe used, have been used to better overcome these chal-lenges and limitations. Previous studies have shown that IVAmethods can very effectively adjust for unmeasured or un-known imbalances,1,2 such as might have occurred with PSAvalues. Although we could not unequivocally document bal-ance in PSA values, examination of other factors, such asage, comorbidity, stage, and grade, demonstrated balancein the comparison groups, suggesting that the IVA methodaccomplished its goal. In addition, the results of our studywere consistent with other similar studies,3-6 further sug-gesting that the results are likely valid.
Nonetheless, it is still possible that there could have beensome residual imbalance, much like that which sporadi-cally occurs when many baseline variables are examined atthe completion of a randomized study. As we recom-mended in our discussion, it would thus be best to conducta large randomized trial, although there could be consid-
erable difficulty in doing so because of existing patient andclinician beliefs, as well as the resources and length of fol-low-up required for such a study. Absent such a trial, wehope our study provides some reasonable data for physi-cians and their patients as they make important personalclinical decisions.
Grace L. Lu-Yao, PhDWeichung Shih, PhDSiu-Long Yao, [email protected] Institute of New JerseyNew Brunswick
Financial Disclosures: Dr Siu-Long Yao reported that during the last 5 years hehas been employed by Sanofi-Aventis and Schering-Plough in the area of clinicalcancer research. Dr Grace Lu-Yao reported having received clinical research fund-ing from the New Jersey Commission on Cancer Research and the Agency for Health-care Research and Quality and employment with HealthStat. Dr Shih reported hav-ing received clinical research funding from Myriad.
1. Earle CC, Neumann PJ, Gelber RD, Weinstein MC, Weeks JC. Impact of refer-ral patterns on the use of chemotherapy for lung cancer. J Clin Oncol. 2002;20(7):1786-1792.2. Stukel TA, Fisher ES, Wennberg DE, Alter DA, Gottlieb DJ, Vermeulen MJ. Analy-sis of observational studies in the presence of treatment selection bias: effects ofinvasive cardiac management on AMI survival using propensity score and instru-mental variable methods. JAMA. 2007;297(3):278-285.3. Studer UE, Whelan P, Albrecht W, et al. Immediate or deferred androgen dep-rivation for patients with prostate cancer not suitable for local treatment with cura-tive intent: European Organisation for Research and Treatment of Cancer (EORTC)Trial 30891. J Clin Oncol. 2006;24(12):1868-1876.4. Iversen P, Johansson JE, Lodding P, et al; Scandinavian Prostatic Cancer Group.Bicalutamide (150 mg) versus placebo as immediate therapy alone or as adjuvantto therapy with curative intent for early nonmetastatic prostate cancer: 5.3-yearmedian followup from the Scandinavian Prostate Cancer Group Study Number 6.J Urol. 2004;172(5 pt 1):1871-1876.5. Kawakami J, Cowan JE, Elkin EP, Latini DM, Duchane J, Carroll PR; CaPSUREInvestigators. Androgen-deprivation therapy as primary treatment for localized pros-tate cancer: data from Cancer of the Prostate Strategic Urologic Research En-deavor (CaPSURE). Cancer. 2006;106(8):1708-1714.6. The Veterans Administration Co-operative Urological Research Group. Treat-ment and survival of patients with cancer of the prostate. Surg Gynecol Obstet.1967;124(5):1011-1017.
Failure to Report Financial Disclosure Information
To the Editor: We would like to apologize to the readersand editors of JAMA for a difference in understanding of theJAMA policy for reporting financial disclosures and resul-tant failure to report our disclosure information in our ar-ticle.1 The basis of our omission of financial information wasthat we did not foresee a reasonable likelihood of financialgain or bias as a consequence of our activities or employ-ment in other areas of the fields of prostate cancer or can-cer research that were separate from our study in early stageprostate cancer and, therefore, did not believe that there wereadditional relevant disclosures.
In the interest of full transparency and to avoid any po-tential misunderstanding, we hereby report that duringthe past 5 years, including during the time the study wasconducted and the manuscript was submitted to JAMA, DrSiu-Long Yao has been employed by Sanofi-Aventis andSchering-Plough in the area of clinical cancer research. Sanofi-Aventis and Schering-Plough contributed no funding andplayed no role whatsoever in the design, interpretation, or
LETTERS
©2009 American Medical Association. All rights reserved. (Reprinted) JAMA, January 7, 2009—Vol 301, No. 1 35
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

drafting of our study or manuscript. In addition, during thepast 5 years, the following authors have received financialsupport and maintained affiliations as follows: Dr Lu-Yaohas received clinical research funding from the New JerseyCommission on Cancer Research and the Agency for Health-care Research and Quality and employment with Health-Stat; Dr Peter Albertson has received clinical research fund-ing from Sanofi-Aventis and consultation fees from BlueCross/Blue Shield; and Dr Weichung Shih has received clini-cal research funding from Myriad. None of these entities con-tributed funding or played any role whatsoever in the de-sign, interpretation, or drafting of our study or manuscript.We regret any misunderstanding that resulted from the omis-sion of these disclosures.
Grace Lu-Yao, MPH, PhDRobert Wood Johnson Medical SchoolNew Brunswick, New JerseyPeter Albertsen, MDUniversity of ConnecticutFarmingtonWeichung Shih, PhDUniversity of Medicine and Dentistry of New JerseyPiscatawaySiu-Long Yao, [email protected] Wood Johnson Medical SchoolNew Brunswick
Financial Disclosures: Dr Siu-Long Yao reported that during the last 5 years hehas been employed by Sanofi-Aventis and Schering-Plough in the area of clinicalcancer research. Dr Grace Lu-Yao reported having received clinical research fund-ing from the New Jersey Commission on Cancer Research and the Agency for Health-care Research and Quality and employment with HealthStat. Dr Albertson re-ported having received clinical research funding from Sanofi-Aventis and consultationfees from Blue Cross/Blue Shield. Dr Shih reported having received clinical re-search funding from Myriad.
1. Lu-Yao GL, Albertsen PC, Moore DF, et al. Survival following primary andro-gen deprivation therapy among men with localized prostate cancer. JAMA. 2008;300(2):173-181.
RESEARCH LETTER
Respirator Tolerance in Health Care Workers
To the Editor: Anticipated respirator intolerance and sup-ply shortages during future influenza pandemics promptedthe Institute of Medicine to review respirator use in healthcare workers1 and consider whether disposable models couldbe reused or modified for reuse.2 One option involves plac-ing a medical mask over a disposable respirator to dimin-ish contamination and attrition.1 However, little is knownabout the workplace tolerability of respirators commonlyworn by health care workers, who may be called on to wearrespiratory protection for the duration of their work shiftsfor several consecutive weeks during a pandemic.3,4 We es-timated the length of time health care workers would tol-erate wearing commonly used respirators while perform-ing their typical occupational duties.
Methods. Participants were 27 volunteers (mean [SD] age,48 [11] years; range, 25-65 years; 15 women) among approxi-mately 225 health care workers employed by the local Veter-ans Health System who were approached. The inclusion cri-terion was having worn a respirator in the context of dutiesat least once; all participants were accustomed to wearing N95respirators (filters �95% of particles approximately 0.3 µmin size) for brief periods. Exclusion criteria included sys-temic disease or pregnancy. The sample comprised 16 nurses,2 nurse practitioners, 4 nurse technicians, 2 telemetry tech-nicians, 2 respiratory therapists, and 1 clerical assistant fromthe intensive care unit (n=15), emergency department (n=6),and medical/surgical ward (n=6). Each provided written in-formed consent, underwent a prestudy examination, and wasfit-tested for each respirator. The study was approved by thelocal institutional review board.
In this unblinded multiple crossover study, before eachwork shift (intersession interval, �1 day) each participantwas randomly assigned a respirator ensemble (TABLE 1) towear as long as he or she was “willing to tolerate” the ef-fects while performing typical occupational duties, not in-cluding interposed break periods (15 minutes at 2 and 6hours; 30 minutes at 4 hours). Those who experienced in-tolerance before 8 hours reported up to 3 reasons for pre-mature discontinuation.
Sample size was chosen to achieve power of 0.8 orgreater to detect a difference of 2 hours in median toler-ance times. Kaplan-Meier estimates of survival were usedfor descriptive purposes. Tolerance time for the cup-shaped N95 was compared with a medical mask and withthe N95 with an exhalation valve. The 2 respirators thathad a medical mask placed over the respirator surface toprotect against contamination were compared with thesame respirators without a mask. An extended Coxmodel,5 which accounted for correlation between repeatedmeasures within participant, was used to compare the timeto doff among respirators by controlling for the effects ofsex and age. SAS 9.1 (SAS Institute, Cary, North Carolina)was used for the analyses. The Bonferroni step-downmethod6 was used to adjust the P values for 2-sided tests toaccount for multiple tests.
Results. Each participant wore all 8 respirators except 1 whofailed the duckbill N95 fit test. No sequence or period effectswere found.Tolerance timevariedbyrespiratormodel (Table1).Women were significantly more likely than men to experi-ence intolerance before 8 hours (hazard ratio, 1.97; 95% con-fidence interval, 1.02-3.75; P=.04). Participants discontin-ued wearing the respirator ensembles before 8 hours in 126of 215 total sessions (59%), reporting a variety of reasons forintolerance, including communication interference (TABLE 2).
Comment. A large percentage of participants wereunwilling to wear the respirator ensembles for the entire8-hour work shift, even with interposed break periods.No respirator was ideal: users of disposable models fre-quently experienced facial heat and pressure, and users of
LETTERS
36 JAMA, January 7, 2009—Vol 301, No. 1 (Reprinted) ©2009 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013
Copyright © 2022 FDOKUMEN




















