
Ultra mortem: Metempsychosis aut resurrecctionis possibilitas secundum Platonem et Sanctum Thomam
Upload
independentCategory
view
1download
0
2001;38;2035-2042 J. Am. Coll. Cardiol.Calderón
Fause Attie, Martín Rosas, Nuria Granados, Carlos Zabal, Alfonso Buendía, and Juan randomized clinical trial
Surgical treatment for secundum atrial septal defects in patients >40 years old: A
This information is current as of May 29, 2008
http://content.onlinejacc.org/cgi/content/full/38/7/2035located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by on May 29, 2008 content.onlinejacc.orgDownloaded from

Adult Congenital Heart Disease
Surgical Treatment for SecundumAtrial Septal Defects in Patients �40 Years OldA Randomized Clinical TrialFause Attie, MD, FACC, Martın Rosas, MD, PHD, Nuria Granados, MD, Carlos Zabal, MD,Alfonso Buendıa, MD, Juan Calderon, MDMexico City, Mexico
OBJECTIVES We prospectively examined whether surgical treatment of secundum atrial septal defects(ASDs) in patients �40 years old improves their long-term clinical outcome.
BACKGROUND Surgical treatment of secundum ASDs in adults �40 years old is a subject of controversybecause of the perception of good long-term clinical outcomes in patients with unrepairedASDs and the lack of data from randomized trials.
METHODS We recruited 521 patients �40 years old with secundum ASDs referred for treatment; 48were excluded. Patients were randomly assigned to surgical closure (n � 232) or medicaltreatment (n � 241). The primary and secondary end points were a composite of majorcardiovascular events (death, pulmonary embolism, major arrhythmic event, embolic cere-brovascular event, recurrent pulmonary infection, functional class deterioration or heartfailure) and overall mortality, respectively. We assessed possible prognostic markers. Theanalysis was performed on an intention-to-treat basis.
RESULTS The median follow-up period was 7.3 years (range 2 to 13). The risk of having the primaryend point was significantly higher in the medical group, which had a univariate hazards ratioof 1.99 (95% confidence interval [CI] 1.23 to 3.22) and a multivariate hazards ratio of 1.85(95% CI 1.08 to 3.17). Although the survival analysis did not reveal differences in overallmortality between the surgical and medical treatments (hazards ratio 1.71, 95% CI 0.76 to3.86), the multivariate analysis, adjusted by age at entry, mean pulmonary artery pressure andcardiac index, demonstrated significant differences between the study groups (hazards ratio4.09, 95% CI 1.41 to 11.89).
CONCLUSIONS Surgical closure was superior to medical treatment in improving both the composite of majorcardiovascular events and overall mortality in patients �40 years old with secundum ASDs.This superiority was related to the mean pulmonary artery pressure, age at diagnosis andcardiac index. Because of the higher risk of morbidity and mortality, we believe that anatomicclosure should always be attempted as the initial treatment for ASDs in adults �40 years oldwith pulmonary artery systolic pressure �70 mm Hg and a pulmonary/systemic output ratio�1.7. The operation must be performed as soon as possible, even if the symptoms or thehemodynamic impact seems to be minimal. (J Am Coll Cardiol 2001;38:2035–42) © 2001by the American College of Cardiology
Surgical treatment of atrial septal defects (ASDs) is themost common cardiac surgery performed for congenitalheart disease in adults; however, the long-term survival ofpatients operated on after age 40 years remains controversial(1–7). Comparisons between medical and surgical manage-ment in adults have been based on retrospective data(4,5,8,9). Lamentably, the presence of several biases in theseseries is a common finding. Life expectancy may be short-ened in some patients, but still long in others, regardless ofsurgical treatment. Therefore, the excellent outcome re-ported in some patients included in the surgical groupsmight not necessarily be surgery-related. The identificationof strong predictive risk factors to select adult patients who
may benefit from anatomic closure remains to be demon-strated. The aim of this open, prospective, randomizedclinical trial was to analyze the impact of surgical treatmenton long-term clinical outcome, as well as to identify possiblepredictive factors related to a good long-term prognosiswhen surgical repair is performed.
METHODS
Study group. Between November 1985 and August 1998,the National Institute of Cardiology of Mexico “IgnacioChavez” recruited 521 patients �40 years old, who werereferred for ASD treatment, from major national medicalcenters; 48 patients were excluded. After obtaining writteninformed consent and a medical history and reviewing themost recent echocardiogram, the patients underwent rightheart catheterization. For the purposes of this study, inclu-sion criteria were isolated ASD (only ostium secundum[88.2%] or sinus venosus defect [11.8%]), age �40 years at
From the Departments of Adult Congenital Heart Disease and Pediatric Cardi-ology, National Institute of Cardiology of Mexico “Ignacio Chavez,” Mexico City,Mexico. This study was financially supported by the National Institute of Cardiologyof Mexico “Ignacio Chavez.”
Manuscript received April 2, 2001; revised manuscript received July 26, 2001,accepted August 20, 2001.
Journal of the American College of Cardiology Vol. 38, No. 7, 2001© 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00Published by Elsevier Science Inc. PII S0735-1097(01)01635-7
by on May 29, 2008 content.onlinejacc.orgDownloaded from

diagnosis, pulmonary/systemic output (Qp/Qs) ratio �1.7and pulmonary artery systolic pressure �70 mm Hg. Ex-clusion criteria were a contraindication for cardiac surgery,severe comorbid disease, previous cardiac surgery, complexcongenital cardiac malformation, rheumatic valve disease,coronary artery disease at diagnosis, mitral or aortic regur-gitation, left ventricular dysfunction and fixed pulmonaryvascular resistance. Patients were randomly assigned on a1:1 basis to surgical treatment of the defect or to continuedmedical surveillance. A randomization procedure was per-formed within six months after the first cardiac catheteriza-tion by an independent researcher who verified the eligibil-ity criteria. For data analysis, we compared the outcomes forboth surgical and medical treatment groups according to theintention-to-treat principle. The cross-over group com-prised patients randomly assigned to receive medical therapywho met any of the following criteria: onset of newsymptoms or worsening of existing symptoms at the discre-tion of the primary physician, refusal of the patient tocontinue in the medical therapy group and a new unsus-pected comorbid disease; these patients were then scheduledfor surgery. To avoid a waiting-time bias, surgically treatedpatients underwent anatomic closure within six monthsafter randomization.Data collection. Because the overall follow-up period be-gan on the date of right heart catheterization (time zero), allclinical, demographic, radiographic, electrocardiographic,echocardiographic and laboratory data were obtained fromthe medical records within three months before cardiaccatheterization; otherwise, the studies were repeated. Datawere collected by two different researchers and comparedafterward. Another researcher performed a third review ifany discordance was detected. Discrepancies were solved byconsensus. Postoperative cardiovascular events were furtherclassified as early (�30 days) or late (�30 days). Theinformation was entered in a computer-designed format tofacilitate analysis by using the Statistical Package for theSocial Sciences (SPSS, version 8.0 for Windows) (10).Follow-up and clinical decisions. All patients were ad-vised to appear for clinical and echocardiographic follow-upevaluations at six- or eight-month intervals, or as soon aseither new symptoms appeared or the previous clinical statedeteriorated. Although the echocardiographic study wasused as one of the main markers to evaluate the hemody-namic impact of ASD during follow-up in the medical
group, the primary physician required complete clinical andhemodynamic evaluations, including right and left catheter-izations before deciding to submit a patient to surgery.End points. The primary end point was a compound indexof major cardiovascular events (assessed as time to firstevent) of cardiac-related death, heart failure, pulmonary orsystemic embolism, recurrent pulmonary infection, sus-tained ventricular tachyarrhythmia and progression of pul-monary hypertension (elevation �20% from baseline). Sec-ondary end points were the median time of survival, overallmortality and incidence of atrial fibrillation or flutter.Statistical analysis. Based on parametric data analysis fromprevious studies in adults (1–9), we estimated a meanfrequency of 37% of the compound index used as a primaryend point in adult patients without surgical interventionafter the age of 40 years at the end of five-year follow-up.For the primary end point, we considered a 15% differencebetween surgical and medical groups as clinically relevant.With 416 patients (208 per group), the study was designedto have a power �80% for a two-tailed test at a 5% level ofsignificance.
Continuous variables are expressed as the mean value �SD. Comparisons between the two groups were conductedby using the Student t test for normally distributed contin-uous variables or the Mann-Whitney U test for thosevariables without normal distribution. For comparisonsamong three or more groups, analysis of variance, or itsequivalent nonparametric test, was used. The chi-square orFisher exact test was used for categorical variables. Theassociation between individual variables and the clinicaloutcome was initially assessed by bivariate analysis. Survivalwas estimated using the Kaplan-Meier method, and differ-ences among groups were assessed by the log-rank test (11).
Seven demographic, clinical and hemodynamic variableswere assessed by Cox hazards regression to identify predic-tors of death and to examine the adjusted independent effectof the relative hazards associated with factors measurable atclinical presentation, while controlling for possible con-founding variables. The seven variables were age at entry,cardiothoracic ratio (CTR), previous atrial arrhythmia,mean pulmonary artery pressure (mPAP), Qp/Qs ratio,cardiac index and treatment group. Significant continuousvariables were selected for categorical analysis, and cut-offpoints were determined to define subgroups for maximalcomparison with the log-rank statistic. Cox proportionalhazards ratios were estimated for each categorical variable,using the most favorable category as the reference. Formultivariable analysis, first we explored all variables in aforced model, and second, the independent factors associ-ated with reduced time to the end point in stepwise forwardCox proportional hazards modeling (12,13). The validity ofthe proportionality assumption was verified graphically.Checks for possible interactions were explored. Statisticalsignificance was inferred at p � 0.05.
Abbreviations and AcronymsASD � atrial septal defectCI � confidence intervalCTR � cardiothoracic ratiomPAP � mean pulmonary artery pressureNYHA � New York Heart AssociationQp/Qs � pulmonary/systemic output ratio
2036 Attie et al. JACC Vol. 38, No. 7, 2001Atrial Septal Defects in Adults December 2001:2035–42
by on May 29, 2008 content.onlinejacc.orgDownloaded from
RESULTS
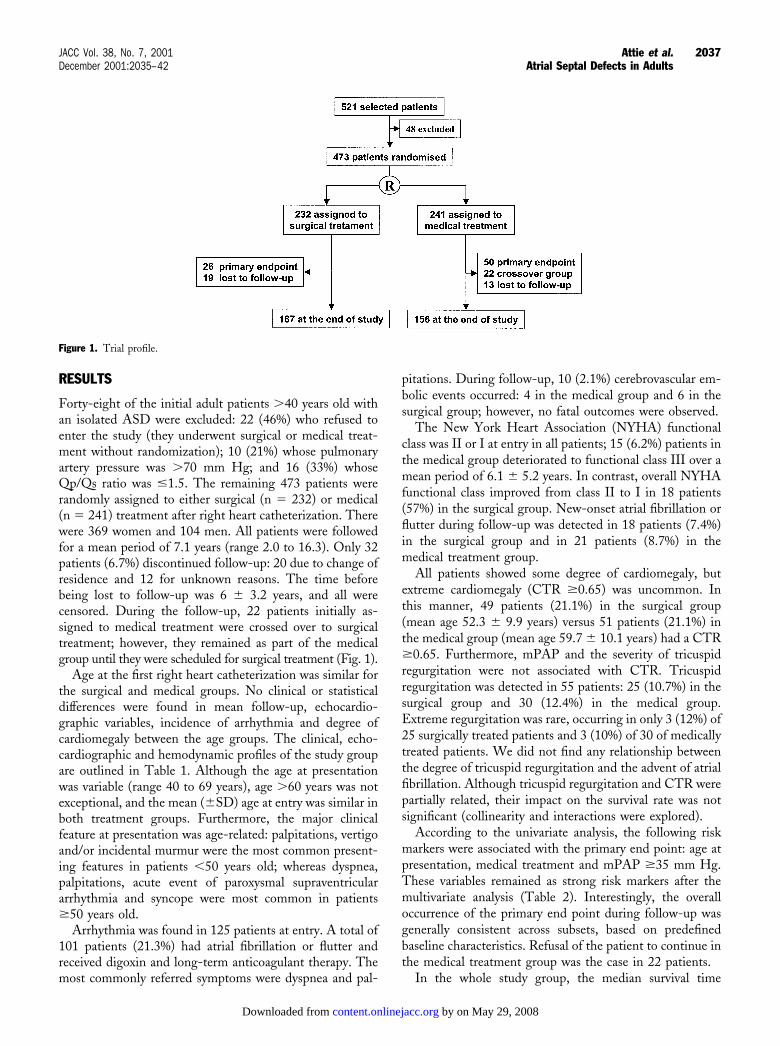
Forty-eight of the initial adult patients �40 years old withan isolated ASD were excluded: 22 (46%) who refused toenter the study (they underwent surgical or medical treat-ment without randomization); 10 (21%) whose pulmonaryartery pressure was �70 mm Hg; and 16 (33%) whoseQp/Qs ratio was �1.5. The remaining 473 patients wererandomly assigned to either surgical (n � 232) or medical(n � 241) treatment after right heart catheterization. Therewere 369 women and 104 men. All patients were followedfor a mean period of 7.1 years (range 2.0 to 16.3). Only 32patients (6.7%) discontinued follow-up: 20 due to change ofresidence and 12 for unknown reasons. The time beforebeing lost to follow-up was 6 � 3.2 years, and all werecensored. During the follow-up, 22 patients initially as-signed to medical treatment were crossed over to surgicaltreatment; however, they remained as part of the medicalgroup until they were scheduled for surgical treatment (Fig. 1).
Age at the first right heart catheterization was similar forthe surgical and medical groups. No clinical or statisticaldifferences were found in mean follow-up, echocardio-graphic variables, incidence of arrhythmia and degree ofcardiomegaly between the age groups. The clinical, echo-cardiographic and hemodynamic profiles of the study groupare outlined in Table 1. Although the age at presentationwas variable (range 40 to 69 years), age �60 years was notexceptional, and the mean (�SD) age at entry was similar inboth treatment groups. Furthermore, the major clinicalfeature at presentation was age-related: palpitations, vertigoand/or incidental murmur were the most common present-ing features in patients �50 years old; whereas dyspnea,palpitations, acute event of paroxysmal supraventriculararrhythmia and syncope were most common in patients�50 years old.
Arrhythmia was found in 125 patients at entry. A total of101 patients (21.3%) had atrial fibrillation or flutter andreceived digoxin and long-term anticoagulant therapy. Themost commonly referred symptoms were dyspnea and pal-
pitations. During follow-up, 10 (2.1%) cerebrovascular em-bolic events occurred: 4 in the medical group and 6 in thesurgical group; however, no fatal outcomes were observed.
The New York Heart Association (NYHA) functionalclass was II or I at entry in all patients; 15 (6.2%) patients inthe medical group deteriorated to functional class III over amean period of 6.1 � 5.2 years. In contrast, overall NYHAfunctional class improved from class II to I in 18 patients(57%) in the surgical group. New-onset atrial fibrillation orflutter during follow-up was detected in 18 patients (7.4%)in the surgical group and in 21 patients (8.7%) in themedical treatment group.
All patients showed some degree of cardiomegaly, butextreme cardiomegaly (CTR �0.65) was uncommon. Inthis manner, 49 patients (21.1%) in the surgical group(mean age 52.3 � 9.9 years) versus 51 patients (21.1%) inthe medical group (mean age 59.7 � 10.1 years) had a CTR�0.65. Furthermore, mPAP and the severity of tricuspidregurgitation were not associated with CTR. Tricuspidregurgitation was detected in 55 patients: 25 (10.7%) in thesurgical group and 30 (12.4%) in the medical group.Extreme regurgitation was rare, occurring in only 3 (12%) of25 surgically treated patients and 3 (10%) of 30 of medicallytreated patients. We did not find any relationship betweenthe degree of tricuspid regurgitation and the advent of atrialfibrillation. Although tricuspid regurgitation and CTR werepartially related, their impact on the survival rate was notsignificant (collinearity and interactions were explored).
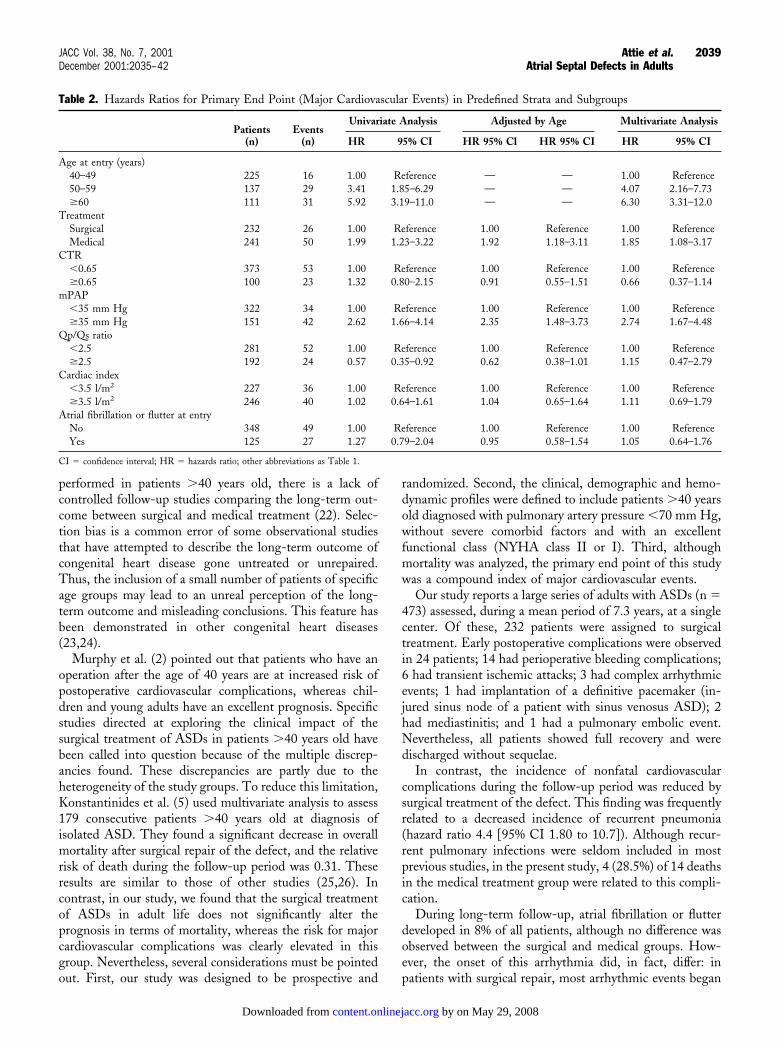
According to the univariate analysis, the following riskmarkers were associated with the primary end point: age atpresentation, medical treatment and mPAP �35 mm Hg.These variables remained as strong risk markers after themultivariate analysis (Table 2). Interestingly, the overalloccurrence of the primary end point during follow-up wasgenerally consistent across subsets, based on predefinedbaseline characteristics. Refusal of the patient to continue inthe medical treatment group was the case in 22 patients.
In the whole study group, the median survival time
Figure 1. Trial profile.
2037JACC Vol. 38, No. 7, 2001 Attie et al.December 2001:2035–42 Atrial Septal Defects in Adults
by on May 29, 2008 content.onlinejacc.orgDownloaded from

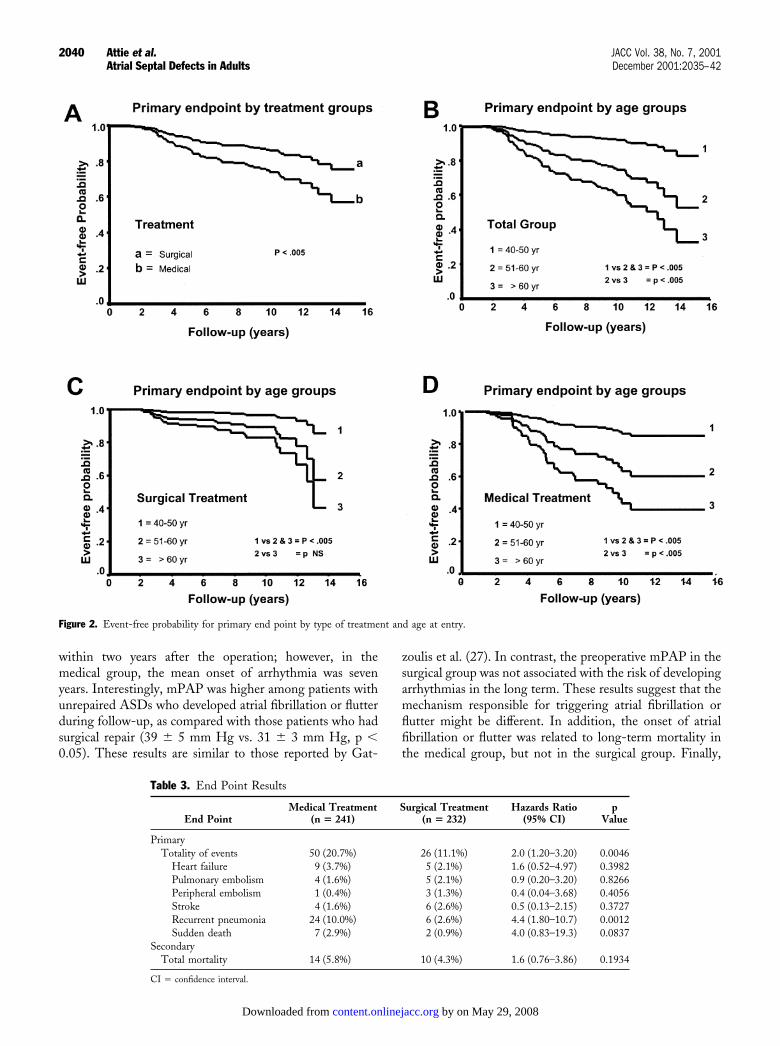
without a major cardiovascular event (primary end point)was 13.7 � 0.2 years (95% confidence interval [CI] 12.9 to14.9 years). Of the 473 patients included, 76 had a majorcardiovascular event at 15 years, with an estimated cumu-lative overall event-free survival rate of 99% at 1 year, 89%at 5 years, 79% at 10 years and 58% at 15 years of follow-up.Significant differences for the primary end point were foundwhen the analysis was performed according to the type oftreatment and age at entry (Figs. 2A and 2B). The log-rankstatistic showed differences between the three groups of ageat entry in both the medical and surgical groups (Figs. 2Cand 2D).
There were 50 events (20.7%) in the medically treatedversus 26 events (11.1%) in the surgically treated patients(hazard ratio 2.0 [95% CI 1.20 to 3.2], p � 0.004). Thetotal number of heart failures, strokes and embolic eventsdid not differ significantly (Table 3). Using a forwardmultivariate Cox regression model to identify the bestassociated variables with the primary end point duringfollow-up, we found that age at diagnosis, mPAP �35 mmHg and medical treatment were the main risk markers.
Although the overall mortality rate did not differ signif-
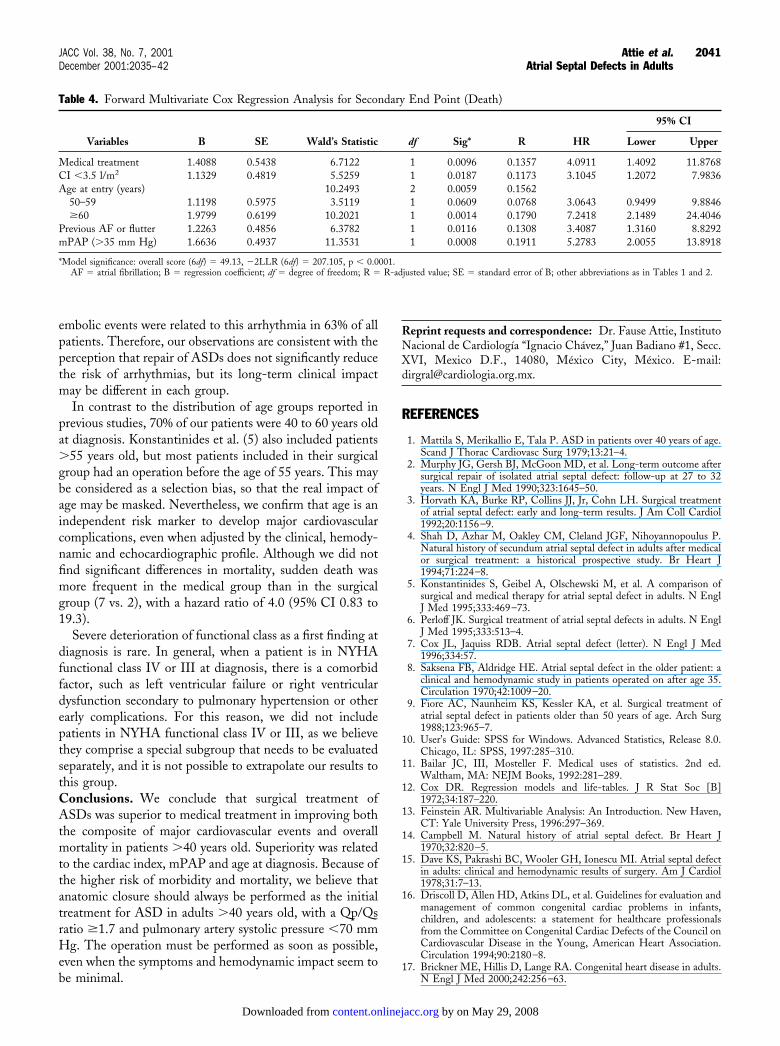
icantly in the surgical (5.8%) and medical (4.3%) groups(hazard ratio 1.6 [95% CI 0.76 to 3.86]), sudden death wasmore frequent in the medical than in the surgical group(2.9% vs. 0.9%, respectively), with a hazard ratio of 4.0 (95%CI 0.83 to 19.3; p � 0.08). Interestingly, when multivariateCox regression analysis was adjusted by age at entry, mPAP�35 mm Hg, previous atrial fibrillation or flutter andcardiac index �3.5 l/m2, a significant difference in mortalitywas found between the surgical and medical groups (Table 4).
DISCUSSION
Surgical repair is still the main therapy for ASDs. Thus, thelife expectancy of patients with unrepaired ASDs is gener-ally thought to be shortened (2,4,14–17). However, thisconclusion is supported by the results of several retrospectivestudies that have mainly included young adult patients(16,18,19). The previous belief that only 50% of patientswith unrepaired ASDs survive beyond the age of 40 yearsand �10% reach the age of 60 years, has not been confirmedin many other observational studies (5,8,20,21). Further-more, although the surgical closure of ASDs is frequently
Table 1. Characteristics at Trial Entry in Predefined Strata and Subgroups
Treatment Groups
VariableTotal Group
(n �473)Surgical
(n � 232)Medical
(n � 241) p Value
Females 369 (78.0%) 183 (78.9%) 186 (77.1%) 0.680Age at entry (yrs) 50.8 � 10.4 50.1 � 9.3 51.9 � 10.8 0.059
40–50 225 (47.6%) 118 (50.1%) 107 (44.4%) 0.11451–60 137 (28.9%) 69 (29.7%) 68 (28.2%)�60 111 (23.5%) 45 (19.3%) 66 (27.4%)
Age at last examination (yr) 58.3 � 13.3 57.6 � 10.0 59.1 � 10.6 0.116Follow-up (yrs) 7.1 � 3.7 7.5 � 3.5 6.7 � 3.7 0.023Cardiomegaly
CTR 0.50–0.59 129 (27.3%) 60 (25.9%) 69 (28.6%) 0.991CTR 0.60–0.69 244 (51.6%) 123 (53.0%) 121 (50.2%)CTR 0.70–0.80 100 (21.1%) 49 (21.1%) 51 (21.2%)
Previous arrhythmias 125 (26.4%) 58 (25.0%) 67 (27.8%) 0.532Atrial fibrillation or flutter 101 (21.3%) 45 (19.4%) 56 (23.2%)SVT 24 (05.0%) 13 (05.6%) 11 (04.6%)
Echocardiographic profileEF (%) 65.0 � 11.0 63.1 � 11.0 66.1 � 11.3 0.849
�55 115 (24.3%) 73 (31.5%) 42 (17.4%) 0.016�55 358 (75.7%) 159 (68.5%) 199 (82.6%)
RVDD (mm) 40.6 � 6.4 40.8 � 6.2 40.4 � 6.7 0.480LVDD (mm) 41.0 � 6.3 40.0 � 6.4 41.9 � 6.1 0.310LVSD (mm) 28.7 � 5.4 28.5 � 5.7 28.9 � 5.2 0.410
Hemodynamic profilemRAP (mm Hg) 5.3 � 3.4 5.3 � 3.4 5.3 � 3.3 0.981mPAP (mm Hg) 30.5 � 12.6 28.7 � 11.9 32.2 � 13.0 0.171Qp/Qs ratio 2.3 � 0.7 2.5 � 0.8 2.1 � 0.5 0.061Sao2 (%) 89.1 � 6.1 89.9 � 5.0 88.3 � 6.8 0.156CO (L/min) 5.7 � 2.2 5.9 � 2.4 5.5 � 2.0 0.186RVEDP (mm Hg) 5.6 � 3.4 5.5 � 3.4 5.8 � 3.5 0.113PVR (Wood’s unit) 3.4 � 1.8 3.3 � 1.8 3.5 � 1.8 0.176
Data are expressed as the mean value � SD or number of patients (%).CO � cardiac output; CTR � cardiothoracic ratio; EF � ejection fraction; LVDD � left ventricular diastolic diameter;
LVSD � left ventricular diastolic diameter; mRAP � mean right atrial pressure; mPAP � mean pulmonary artery pressure;PVR � pulmonary vascular resistance; Qp/Qs � systemic/pulmonary output ratio; RVDD � right ventricular diastolic diameter;RVEDP � right ventricular end-diastolic pressure; Sao2 � arterial oxygen saturation; SVT � supraventricular tachyarrhythmia.
2038 Attie et al. JACC Vol. 38, No. 7, 2001Atrial Septal Defects in Adults December 2001:2035–42
by on May 29, 2008 content.onlinejacc.orgDownloaded from
performed in patients �40 years old, there is a lack ofcontrolled follow-up studies comparing the long-term out-come between surgical and medical treatment (22). Selec-tion bias is a common error of some observational studiesthat have attempted to describe the long-term outcome ofcongenital heart disease gone untreated or unrepaired.Thus, the inclusion of a small number of patients of specificage groups may lead to an unreal perception of the long-term outcome and misleading conclusions. This feature hasbeen demonstrated in other congenital heart diseases(23,24).
Murphy et al. (2) pointed out that patients who have anoperation after the age of 40 years are at increased risk ofpostoperative cardiovascular complications, whereas chil-dren and young adults have an excellent prognosis. Specificstudies directed at exploring the clinical impact of thesurgical treatment of ASDs in patients �40 years old havebeen called into question because of the multiple discrep-ancies found. These discrepancies are partly due to theheterogeneity of the study groups. To reduce this limitation,Konstantinides et al. (5) used multivariate analysis to assess179 consecutive patients �40 years old at diagnosis ofisolated ASD. They found a significant decrease in overallmortality after surgical repair of the defect, and the relativerisk of death during the follow-up period was 0.31. Theseresults are similar to those of other studies (25,26). Incontrast, in our study, we found that the surgical treatmentof ASDs in adult life does not significantly alter theprognosis in terms of mortality, whereas the risk for majorcardiovascular complications was clearly elevated in thisgroup. Nevertheless, several considerations must be pointedout. First, our study was designed to be prospective and
randomized. Second, the clinical, demographic and hemo-dynamic profiles were defined to include patients �40 yearsold diagnosed with pulmonary artery pressure �70 mm Hg,without severe comorbid factors and with an excellentfunctional class (NYHA class II or I). Third, althoughmortality was analyzed, the primary end point of this studywas a compound index of major cardiovascular events.
Our study reports a large series of adults with ASDs (n �473) assessed, during a mean period of 7.3 years, at a singlecenter. Of these, 232 patients were assigned to surgicaltreatment. Early postoperative complications were observedin 24 patients; 14 had perioperative bleeding complications;6 had transient ischemic attacks; 3 had complex arrhythmicevents; 1 had implantation of a definitive pacemaker (in-jured sinus node of a patient with sinus venosus ASD); 2had mediastinitis; and 1 had a pulmonary embolic event.Nevertheless, all patients showed full recovery and weredischarged without sequelae.
In contrast, the incidence of nonfatal cardiovascularcomplications during the follow-up period was reduced bysurgical treatment of the defect. This finding was frequentlyrelated to a decreased incidence of recurrent pneumonia(hazard ratio 4.4 [95% CI 1.80 to 10.7]). Although recur-rent pulmonary infections were seldom included in mostprevious studies, in the present study, 4 (28.5%) of 14 deathsin the medical treatment group were related to this compli-cation.
During long-term follow-up, atrial fibrillation or flutterdeveloped in 8% of all patients, although no difference wasobserved between the surgical and medical groups. How-ever, the onset of this arrhythmia did, in fact, differ: inpatients with surgical repair, most arrhythmic events began
Table 2. Hazards Ratios for Primary End Point (Major Cardiovascular Events) in Predefined Strata and Subgroups
Patients(n)
Events(n)
Univariate Analysis Adjusted by Age Multivariate Analysis
HR 95% CI HR 95% Cl HR 95% CI HR 95% CI
Age at entry (years)40–49 225 16 1.00 Reference — — 1.00 Reference50–59 137 29 3.41 1.85–6.29 — — 4.07 2.16–7.73�60 111 31 5.92 3.19–11.0 — — 6.30 3.31–12.0
TreatmentSurgical 232 26 1.00 Reference 1.00 Reference 1.00 ReferenceMedical 241 50 1.99 1.23–3.22 1.92 1.18–3.11 1.85 1.08–3.17
CTR�0.65 373 53 1.00 Reference 1.00 Reference 1.00 Reference�0.65 100 23 1.32 0.80–2.15 0.91 0.55–1.51 0.66 0.37–1.14
mPAP�35 mm Hg 322 34 1.00 Reference 1.00 Reference 1.00 Reference�35 mm Hg 151 42 2.62 1.66–4.14 2.35 1.48–3.73 2.74 1.67–4.48
Qp/Qs ratio�2.5 281 52 1.00 Reference 1.00 Reference 1.00 Reference�2.5 192 24 0.57 0.35–0.92 0.62 0.38–1.01 1.15 0.47–2.79
Cardiac index�3.5 l/m2 227 36 1.00 Reference 1.00 Reference 1.00 Reference�3.5 l/m2 246 40 1.02 0.64–1.61 1.04 0.65–1.64 1.11 0.69–1.79
Atrial fibrillation or flutter at entryNo 348 49 1.00 Reference 1.00 Reference 1.00 ReferenceYes 125 27 1.27 0.79–2.04 0.95 0.58–1.54 1.05 0.64–1.76
CI � confidence interval; HR � hazards ratio; other abbreviations as Table 1.
2039JACC Vol. 38, No. 7, 2001 Attie et al.December 2001:2035–42 Atrial Septal Defects in Adults
by on May 29, 2008 content.onlinejacc.orgDownloaded from
within two years after the operation; however, in themedical group, the mean onset of arrhythmia was sevenyears. Interestingly, mPAP was higher among patients withunrepaired ASDs who developed atrial fibrillation or flutterduring follow-up, as compared with those patients who hadsurgical repair (39 � 5 mm Hg vs. 31 � 3 mm Hg, p �0.05). These results are similar to those reported by Gat-
zoulis et al. (27). In contrast, the preoperative mPAP in thesurgical group was not associated with the risk of developingarrhythmias in the long term. These results suggest that themechanism responsible for triggering atrial fibrillation orflutter might be different. In addition, the onset of atrialfibrillation or flutter was related to long-term mortality inthe medical group, but not in the surgical group. Finally,
Figure 2. Event-free probability for primary end point by type of treatment and age at entry.
Table 3. End Point Results
End PointMedical Treatment
(n � 241)Surgical Treatment
(n � 232)Hazards Ratio
(95% CI)p
Value
PrimaryTotality of events 50 (20.7%) 26 (11.1%) 2.0 (1.20–3.20) 0.0046
Heart failure 9 (3.7%) 5 (2.1%) 1.6 (0.52–4.97) 0.3982Pulmonary embolism 4 (1.6%) 5 (2.1%) 0.9 (0.20–3.20) 0.8266Peripheral embolism 1 (0.4%) 3 (1.3%) 0.4 (0.04–3.68) 0.4056Stroke 4 (1.6%) 6 (2.6%) 0.5 (0.13–2.15) 0.3727Recurrent pneumonia 24 (10.0%) 6 (2.6%) 4.4 (1.80–10.7) 0.0012Sudden death 7 (2.9%) 2 (0.9%) 4.0 (0.83–19.3) 0.0837
SecondaryTotal mortality 14 (5.8%) 10 (4.3%) 1.6 (0.76–3.86) 0.1934
CI � confidence interval.
2040 Attie et al. JACC Vol. 38, No. 7, 2001Atrial Septal Defects in Adults December 2001:2035–42
by on May 29, 2008 content.onlinejacc.orgDownloaded from
embolic events were related to this arrhythmia in 63% of allpatients. Therefore, our observations are consistent with theperception that repair of ASDs does not significantly reducethe risk of arrhythmias, but its long-term clinical impactmay be different in each group.
In contrast to the distribution of age groups reported inprevious studies, 70% of our patients were 40 to 60 years oldat diagnosis. Konstantinides et al. (5) also included patients�55 years old, but most patients included in their surgicalgroup had an operation before the age of 55 years. This maybe considered as a selection bias, so that the real impact ofage may be masked. Nevertheless, we confirm that age is anindependent risk marker to develop major cardiovascularcomplications, even when adjusted by the clinical, hemody-namic and echocardiographic profile. Although we did notfind significant differences in mortality, sudden death wasmore frequent in the medical group than in the surgicalgroup (7 vs. 2), with a hazard ratio of 4.0 (95% CI 0.83 to19.3).
Severe deterioration of functional class as a first finding atdiagnosis is rare. In general, when a patient is in NYHAfunctional class IV or III at diagnosis, there is a comorbidfactor, such as left ventricular failure or right ventriculardysfunction secondary to pulmonary hypertension or otherearly complications. For this reason, we did not includepatients in NYHA functional class IV or III, as we believethey comprise a special subgroup that needs to be evaluatedseparately, and it is not possible to extrapolate our results tothis group.Conclusions. We conclude that surgical treatment ofASDs was superior to medical treatment in improving boththe composite of major cardiovascular events and overallmortality in patients �40 years old. Superiority was relatedto the cardiac index, mPAP and age at diagnosis. Because ofthe higher risk of morbidity and mortality, we believe thatanatomic closure should always be performed as the initialtreatment for ASD in adults �40 years old, with a Qp/Qsratio �1.7 and pulmonary artery systolic pressure �70 mmHg. The operation must be performed as soon as possible,even when the symptoms and hemodynamic impact seem tobe minimal.
Reprint requests and correspondence: Dr. Fause Attie, InstitutoNacional de Cardiologıa “Ignacio Chavez,” Juan Badiano #1, Secc.XVI, Mexico D.F., 14080, Mexico City, Mexico. E-mail:[email protected].
REFERENCES
1. Mattila S, Merikallio E, Tala P. ASD in patients over 40 years of age.Scand J Thorac Cardiovasc Surg 1979;13:21–4.
2. Murphy JG, Gersh BJ, McGoon MD, et al. Long-term outcome aftersurgical repair of isolated atrial septal defect: follow-up at 27 to 32years. N Engl J Med 1990;323:1645–50.
3. Horvath KA, Burke RP, Collins JJ, Jr, Cohn LH. Surgical treatmentof atrial septal defect: early and long-term results. J Am Coll Cardiol1992;20:1156–9.
4. Shah D, Azhar M, Oakley CM, Cleland JGF, Nihoyannopoulus P.Natural history of secundum atrial septal defect in adults after medicalor surgical treatment: a historical prospective study. Br Heart J1994;71:224–8.
5. Konstantinides S, Geibel A, Olschewski M, et al. A comparison ofsurgical and medical therapy for atrial septal defect in adults. N EnglJ Med 1995;333:469–73.
6. Perloff JK. Surgical treatment of atrial septal defects in adults. N EnglJ Med 1995;333:513–4.
7. Cox JL, Jaquiss RDB. Atrial septal defect (letter). N Engl J Med1996;334:57.
8. Saksena FB, Aldridge HE. Atrial septal defect in the older patient: aclinical and hemodynamic study in patients operated on after age 35.Circulation 1970;42:1009–20.
9. Fiore AC, Naunheim KS, Kessler KA, et al. Surgical treatment ofatrial septal defect in patients older than 50 years of age. Arch Surg1988;123:965–7.
10. User’s Guide: SPSS for Windows. Advanced Statistics, Release 8.0.Chicago, IL: SPSS, 1997:285–310.
11. Bailar JC, III, Mosteller F. Medical uses of statistics. 2nd ed.Waltham, MA: NEJM Books, 1992:281–289.
12. Cox DR. Regression models and life-tables. J R Stat Soc [B]1972;34:187–220.
13. Feinstein AR. Multivariable Analysis: An Introduction. New Haven,CT: Yale University Press, 1996:297–369.
14. Campbell M. Natural history of atrial septal defect. Br Heart J1970;32:820–5.
15. Dave KS, Pakrashi BC, Wooler GH, Ionescu MI. Atrial septal defectin adults: clinical and hemodynamic results of surgery. Am J Cardiol1978;31:7–13.
16. Driscoll D, Allen HD, Atkins DL, et al. Guidelines for evaluation andmanagement of common congenital cardiac problems in infants,children, and adolescents: a statement for healthcare professionalsfrom the Committee on Congenital Cardiac Defects of the Council onCardiovascular Disease in the Young, American Heart Association.Circulation 1994;90:2180–8.
17. Brickner ME, Hillis D, Lange RA. Congenital heart disease in adults.N Engl J Med 2000;242:256–63.
Table 4. Forward Multivariate Cox Regression Analysis for Secondary End Point (Death)
Variables B SE Wald’s Statistic df Sig* R HR
95% CI
Lower Upper
Medical treatment 1.4088 0.5438 6.7122 1 0.0096 0.1357 4.0911 1.4092 11.8768CI �3.5 l/m2 1.1329 0.4819 5.5259 1 0.0187 0.1173 3.1045 1.2072 7.9836Age at entry (years) 10.2493 2 0.0059 0.1562
50–59 1.1198 0.5975 3.5119 1 0.0609 0.0768 3.0643 0.9499 9.8846�60 1.9799 0.6199 10.2021 1 0.0014 0.1790 7.2418 2.1489 24.4046
Previous AF or flutter 1.2263 0.4856 6.3782 1 0.0116 0.1308 3.4087 1.3160 8.8292mPAP (�35 mm Hg) 1.6636 0.4937 11.3531 1 0.0008 0.1911 5.2783 2.0055 13.8918
*Model significance: overall score (6df) � 49.13, �2LLR (6df) � 207.105, p � 0.0001.AF � atrial fibrillation; B � regression coefficient; df � degree of freedom; R � R-adjusted value; SE � standard error of B; other abbreviations as in Tables 1 and 2.
2041JACC Vol. 38, No. 7, 2001 Attie et al.December 2001:2035–42 Atrial Septal Defects in Adults
by on May 29, 2008 content.onlinejacc.orgDownloaded from

18. Edward RK, Evangelista JK, Nigrin DJ, Erickson LC. Impact ofanatomic treatment on somatic growth among small, asymptomaticchildren. Am J Cardiol 2000;85:1472–5.
19. Gatzoulis MA, Redington AN, Somerville J, Shore DF. Shouldatrial septal defects in adults be closed? Ann Thorac Surg 1996;61:657–9.
20. Nasrallah AT, Hall RJ, Garcia E, Leachman RD, Cooley DA.Surgical repair of atrial septal defect in patients over 60 years of age:long-term results. Circulation 1976;53:329–31.
21. St John Sutton MG, Tajik AJ, McGoon DC. Atrial septal defect inpatients ages 60 years or older: operative results and long-termpostoperative follow-up. Circulation 1981;64:402–9.
22. Ward C. Secundum atrial septal defect: routine surgical treatment isnot of proven benefit. Br Heart J 1994;71:219–23.
23. Celermajer DS, Cullen S, Sullivan ID, Spiegelhalter DJ, Wyse RKH,Deanfield JE. Outcome in neonates with Ebstein’s anomaly. J Am CollCardiol 1992;19:1041–6.
24. Attie F, Rosas M, Rirlaarsdam M, et al. The adult patient withEbstein anomaly: outcome in 72 unoperated patients. Medicine(Baltimore) 2000;79:27–36.
25. Hopkins WE. Atrial septal defect. Curr Treat Options CardiovascMed 1999;1:301–10.
26. Thilen U, Berlin S, Varnauskas E. Atrial septal defect in adults:38-year follow-up of a surgically and a conservatively managed group.Scand Cardiovasc J 2000;34:79–83.
27. Gatzoulis MA, Freeman MA, Samuel CS, Webb GD, Harris L.Atrial arrhythmia after surgical treatment of atrial septal defects inadults. N Engl J Med 1999;340:839–46.
2042 Attie et al. JACC Vol. 38, No. 7, 2001Atrial Septal Defects in Adults December 2001:2035–42
by on May 29, 2008 content.onlinejacc.orgDownloaded from
2001;38;2035-2042 J. Am. Coll. Cardiol.Calderón
Fause Attie, Martín Rosas, Nuria Granados, Carlos Zabal, Alfonso Buendía, and Juan randomized clinical trial
Surgical treatment for secundum atrial septal defects in patients >40 years old: A
This information is current as of May 29, 2008
& ServicesUpdated Information
http://content.onlinejacc.org/cgi/content/full/38/7/2035including high-resolution figures, can be found at:
References
http://content.onlinejacc.org/cgi/content/full/38/7/2035#BIBLat: This article cites 21 articles, 12 of which you can access for free
Citations
cleshttp://content.onlinejacc.org/cgi/content/full/38/7/2035#otherartiThis article has been cited by 17 HighWire-hosted articles:
Rights & Permissions
http://content.onlinejacc.org/misc/permissions.dtltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://content.onlinejacc.org/misc/reprints.dtl
Information about ordering reprints can be found online:
by on May 29, 2008 content.onlinejacc.orgDownloaded from
Copyright © 2022 FDOKUMEN




















