Understanding the atrial sound - Heart (BMJ)
7
Editorial British Heart Journal, 1973, 35, 229-235. Understanding the atrial sound H. J. N. Bethell 1, 2 and P. G. F. Nixon' Charcelay (I838) first described the presystolic sound which was later termed 'bruit de galop' by Bouillard (Potain, I894). Potain's description (I875) of this presystolic sound has not been bettered: 'This sound is much duller than normal sounds; it is a shock, a distinct pulsation, scarcely a sound. When the ear is applied to the chest it affects the sense of touch more perhaps than the sense of hearing.' Since the I930's this sound has often been called the fourth sound to distinguish it from the protodiastolic third sound. Some clinicians pre- fer to call it the atrial sound because 'fourth' sug- gests that it may be the last rather than the initial sound of a complete cardiac cycle. Others use the terms atrial or presystolic gallop when it is associ- ated with heart disease. We shall use the term 'atrial sound' to refer to the sound associated with atrial systole both in the healthy and the diseased heart; in bradycardia, tachycardia, and normal heart rate; in sinus rhythm and atrioventricular dissociation; and irrespective of whether the vibrations are audible through the stethoscope or require a phono- cardiogram for their detection. We shall use the term 'atrial beat' to refer to the movement of the apex produced by atrial contraction (the 'a' wave of apex displacement). This discussion is only con- cerned with events arising from the left heart. Characteristics of the atrial sound The vibrations of the clinically detectable atrial sound are characteristically of low frequency, be- tween 25 Hz and ioo Hz, and usually near the threshold of human hearing. The sound has a vari- able relation to the P wave of the electrocardiogram, starting not less than 0-07 sec and usually about OI4 sec after the onset of the P wave. The peak vibra- tions of the sound coincide with the peak of the 1 Address: The Cardiac Department, Charing Cross Hospital, London WC2N 4DZ. 2 In receipt of a fellowship from the Board of Governors of the Charing Cross Hospital. atrial beat: the outward movement of the left ven- tricular apex caused by atrial contraction (Fig. I). The relation of the sound to the rounded 'a' wave of the left atrial pressure pulse is variable. The atrial sound is most easily detectable with the patient lying on his left side, semirecumbent. The palpating fingers, placed very lightly on the apex, can feel the presystolic thrust of an enlarged atrial beat. Listening at the same time as feeling enables the atrial beat to be distinguished from the double systolic impulse found in some patients with left ventricular disease. The atrial sound is most easily heard with the bell of the stethoscope placed very lightly over the cardiac apex, but is sometimes easier to hear at the left sternal edge or even at the base of the heart. It may be confused with a split sound or a first sound followed by an ejection click, but the atrial sound usually has vibrations of such small magnitude and low frequency that they can be filtered out by pressing firmly with the bell and so converting the skin into a diaphragm for the stethoscope. Phonocardiograms recorded from microphones in the oesophagus (Orias and Braun-Menendez, I939) or the left atrium (Crevasse et al., I962) show that the atrial sound may be preceded by low fre- quency vibrations, o0o4 sec to o-o6 sec after the onset of the P wave, which are not recorded at the chest wall. In the special case of heart block, instead of a single atrial sound, two components may be recorded at the cardiac apex. The significance of each com- ponent is not known. The first of the two components has all the charac- teristics of the atrial sound of sinus rhythm. It occurs o0o7 to OI4 sec after the onset of the P wave, its peak vibrations usually coincide with the peak of the atrial beat, and it disappears when the atrium contracts against the closed mitral valve during ventricular systole (Fig. 2). The second component occurs o02o to o-28 sec after the onset of the P wave and also disappears when the atrium contracts during ventricular systole. These observa- on January 8, 2022 by guest. Protected by copyright. http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.35.3.229 on 1 March 1973. Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Understanding the atrial sound - Heart (BMJ)

Editorial
British Heart Journal, 1973, 35, 229-235.
Understanding the atrial sound
H. J. N. Bethell 1, 2 and P. G. F. Nixon'
Charcelay (I838) first described the presystolicsound which was later termed 'bruit de galop' byBouillard (Potain, I894). Potain's description (I875)of this presystolic sound has not been bettered:'This sound is much duller than normal sounds; itis a shock, a distinct pulsation, scarcely a sound.When the ear is applied to the chest it affects thesense of touch more perhaps than the sense ofhearing.' Since the I930's this sound has oftenbeen called the fourth sound to distinguish it fromthe protodiastolic third sound. Some clinicians pre-fer to call it the atrial sound because 'fourth' sug-gests that it may be the last rather than the initialsound of a complete cardiac cycle. Others use theterms atrial or presystolic gallop when it is associ-ated with heart disease. We shall use the term 'atrialsound' to refer to the sound associated with atrialsystole both in the healthy and the diseased heart;in bradycardia, tachycardia, and normal heart rate;in sinus rhythm and atrioventricular dissociation;and irrespective of whether the vibrations areaudible through the stethoscope or require a phono-cardiogram for their detection. We shall use theterm 'atrial beat' to refer to the movement of theapex produced by atrial contraction (the 'a' waveof apex displacement). This discussion is only con-cerned with events arising from the left heart.
Characteristics of the atrial soundThe vibrations of the clinically detectable atrialsound are characteristically of low frequency, be-tween 25 Hz and ioo Hz, and usually near thethreshold of human hearing. The sound has a vari-able relation to the P wave of the electrocardiogram,starting not less than 0-07 sec and usually about OI4sec after the onset of the P wave. The peak vibra-tions of the sound coincide with the peak of the
1 Address: The Cardiac Department, Charing Cross Hospital,London WC2N 4DZ.2 In receipt of a fellowship from the Board of Governors ofthe Charing Cross Hospital.
atrial beat: the outward movement of the left ven-tricular apex caused by atrial contraction (Fig. I).The relation of the sound to the rounded 'a' waveof the left atrial pressure pulse is variable.The atrial sound is most easily detectable with
the patient lying on his left side, semirecumbent.The palpating fingers, placed very lightly on theapex, can feel the presystolic thrust of an enlargedatrial beat. Listening at the same time as feelingenables the atrial beat to be distinguished from thedouble systolic impulse found in some patients withleft ventricular disease. The atrial sound is mosteasily heard with the bell of the stethoscope placedvery lightly over the cardiac apex, but is sometimeseasier to hear at the left sternal edge or even at thebase of the heart. It may be confused with a splitsound or a first sound followed by an ejection click,but the atrial sound usually has vibrations of suchsmall magnitude and low frequency that they canbe filtered out by pressing firmly with the bell andso converting the skin into a diaphragm for thestethoscope.
Phonocardiograms recorded from microphonesin the oesophagus (Orias and Braun-Menendez,I939) or the left atrium (Crevasse et al., I962) showthat the atrial sound may be preceded by low fre-quency vibrations, o0o4 sec to o-o6 sec after the onsetof the P wave, which are not recorded at the chestwall. In the special case of heart block, instead of asingle atrial sound, two components may be recordedat the cardiac apex. The significance of each com-ponent is not known.The first ofthe two components has all the charac-
teristics of the atrial sound of sinus rhythm. Itoccurs o0o7 to OI4 sec after the onset of the Pwave, its peak vibrations usually coincide with thepeak of the atrial beat, and it disappears when theatrium contracts against the closed mitral valveduring ventricular systole (Fig. 2). The secondcomponent occurs o02o to o-28 sec after the onset ofthe P wave and also disappears when the atriumcontracts during ventricular systole. These observa-
on January 8, 2022 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.35.3.229 on 1 M
arch 1973. Dow
nloaded from

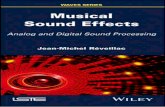
2488A
*..: j
FIG. I (A) The normal diastolic movements and sounds displayed by simultaneous recordingof the apex cardiogram (ADC), the mitral area low frequency phonocardiogram (MALF), andlead II of the electrocardiogram. Diastolic filling of the ventricle occurs in three phases repre-sented by the rapidfilling wave (rfw), the slow filling wave (sfw), and the small 'a' wave causedby atrial systole. (B) The abnormal diastolic movements and sounds in a patient with ischaemicheart disease. The rapid filling wave is attenuated while the 'a' wave is exaggerated and isaccompanied by a loud atrial sound (4).
tions do not support the widely held view (Kincaid-Smith and Barlow, I959a) that the first componentis an audible vibration which is retained when theatrium contracts against a closed mitral valve andthat the second component corresponds with theatrial sound of sinus rhythm.
Methods of recording left atrial activityA variety of techniques has been used to take
graphic records of the chest wall vibrations causedby atrial and ventricular activity. The patterns ob-tained depend upon the aspects of motion to whichthe transducer is sensitive, its frequency response,time constant, and sensitivity, as well as any modifi-cations created by its electronic circuitry. The tech-niques include apex cardiography (Marey, i88i),impulse cardiography (Beilin and Mounsey, I962),kinetocardiography (Eddleman et al., 1953), vibro-cardiography (Agress et al., I96I), and accelero-cardiography (Rosa et al., I96I). Apex cardiographyis the oldest and most widely used of these tech-niques. By recording the displacement of the apex
beat, it most closely represents the physical signsfelt by the fingers, and is well suited to the detec-tion and measurement of the atrial impulse ('a'wave). A commonly used device is a cup connectedto a piezoelectric device. The disadvantages of thissystem include the relatively large area covered bythe cup, the unsuitability of most crystals to recordvery low frequency movements, a relatively shorttime constant, and dependence upon an air-filledconducting system. We have preferred an apparatuswith a moving probe which is sensitive, specific fordisplacement, allows a single point to be selectedfor recording, and incorporates a microphone topick up sound vibrations from an area around thepoint (Nixon, Hepburn, and Ikram, I964). It iseasy to use at the bedside and the records obtainedare reproducible.To assess whether a given 'a' wave is normal or
abnormal, it is customary to compare its amplitudewith the total apical movement, the upper limit ofnormal being taken as 15 to 20 per cent. There are
obvious disadvantages to the comparison of one
diastolic filling wave with the sum of three diastolic
230 Bethell and Nixon
on January 8, 2022 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.35.3.229 on 1 M
arch 1973. Dow
nloaded from

Understanding the atrial sound 231
FIG. 2 The apex cardiogram (ADC), mitral area low frequency phonocardiogram (MALF),and lead II of the electrocardiogram in a case of complete heart block. The P waves are labelled.The firstP wave is followed by an apical 'a' wave and atrial sound (4) with two components. Thefirst component starts 0*14 sec after the onset of the P wave and its peak vibrations coincide withthe peak of the apical 'a' wave. The second component starts o23 sec after the onset of the P wave.The second P wave is followed by an 'a' wave which coincides with the rapid filling wave toproduce a 'summation' sound (S). The third P wave occurs during ventricular systole and isnot followed by either component of the atrial sound.
filling waves and a systolic movement. It is simplerand more logical to compare the 'a' wave amplitudewith the total diastolic excursion since early and latediastolic filling are interdependent, one waning as
the other waxes. Using this technique the upperlimit of normal for the 'a' wave is 40 per cent.Pathologically enlarged 'a' waves are usually pal-pable.
It is less easy to assess the normality or abnor-mality of presystolic sound vibrations. The phono-cardiographic appearance of atrial sound vibrationsis not a reliable guide either to whether the soundis audible or whether it represents a physiologicalor pathological event. There is great need for stan-dardization of methods for recording heart soundsand pulsations, so that comparable records can beproduced from different centres and the problemof normal limits resolved, as has been done for theelectrocardiogram.
Genesis of the atrial soundThe atrial sound coincides with the peak of outwardmovement of the left ventricular apex which iscaused by atrial systole-it marks the end of a rapidfilling phase when the apex and the mitral annulusare carried furthest apart. It is reasonable to suggestthat sudden tension of the mitral cusps and chordaetendineae at this time causes vibrations heard as theatrial sound. This hypothesis is supported by thefact that the sound is amplified by manoeuvreswhich enhance atrial transport such as hypervol-aemia and exercise; and myocardial diseases whichreduce early diastolic filling of the ventricle.The involvement of the mitral apparatus in the
genesis of diastolic sound has been studied morefully in the case of the third heart sound (Dock,Grandell, and Taubman, i955), and it seems likelythat the third sound and atrial sound have a com-mon origin. They have similar frequency character-
on January 8, 2022 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.35.3.229 on 1 M
arch 1973. Dow
nloaded from

232 Bethell and Nixon
istics, both are related to rapid filling periods of theventricle, and both have maximum vibrations at thepeak of an outward movement of the ventricularapex. When they occur in disease they appear torepresent exaggerations of normal physiologicalevents. An illustration of the involvement of themitral valve apparatus in the production of diastolicmovement and sound is provided by mitral incom-petence. In rheumatic cases, where the cusps andchordae are present, the rapid filling peak andthird sound are prominent (Nixon, I96I), whereasin severe regurgitation round a prosthetic mitralvalve, the filling peak and third sound are absent orrudimentary.
Factors influencing timing and audibilityof the atrial sound
A variety of factors determines whether the atrialsound can be heard by the trained observer. Perhapsthe most important of these is the time interval be-tween the atrial sound and the first sound (Spodicket al., I97I). This depends upon the PR interval,the interval between the P wave and the atrialsound, and the interval between the Q wave and thefirst sound.
In first-degree heart block the atrial sound isoften audible and at certain heart rates it will sum-mate with the protodiastolic third sound to create a'summation gallop'.The interval between the P wave and the atrial
sound shortens with deteriorating heart function(Duchosal, I931-I932). It lengthens with recoveryfrom myocardial infarction (Hill et al., I969; Ben-nett, Smithen, and Sowton, 1972), with treatment ofhypertension, and with manoeuvres which reducecardiac filling, such as the application of venoustourniquets and the use of glyceryl trinitrate (Kin-caid-Smith and Barlow, 1959b). These types ofchange tend to make the atrial sound merge withthe first sound, to make it inaudible, and to make itappear as an 'atrial component' of the first soundon the phonocardiogram.The interval between the Q wave and the first
sound is lengthened by left ventricular hypertrophy,and so the atrial sound is often well separated fromthe first sound in hypertension. It is shortened bysympathetic stimulation of the heart as may be seenimmediately after myocardial infarction (Jain andLindahl, 1971).
Other factors which influence the audibility of theatrial sound include its amplitude and its frequencycharacteristics. Those manoeuvres and changes thatshorten the interval between the P wave and theatrial sound also tend to amplify the atrial sound.
FIG. 3 The apex cardiogram (ADC), mitral arealow frequency phonocardiogram (MALF), and lead IIof the electrocardiogram in a patient with severe heartdisease. The 'a' wave is prominent but rounded and anatrial sound is not discernible.
In some cases of long-standing left ventriculardisease, the peak of the atrial beat tends to becomesharp and the atrial sound may develop high fre-quency components, particularly in the physicallyactive subject. In some cases with severe heartdisease, the atrial beat is early and easily palpable,but rounded: vibrations of the corresponding atrialsound may be of low amplitude and frequency andbe inaudible (Fig. 3).
Haemodynamic correlations of the atrialsound
In the normal heart, the pressure-volume relationsof the left ventricle are such that relatively largeincreases in volume are accomplished with littlerise in pressure. Most of the filling of the left ven-tricle is achieved in early diastole and the contribu-tion from left atrial systole is small (Stott et al.,1970). The apex cardiogram reflects this in a largerapid filling wave and a small 'a' wave. In myocar-dial disease the pressure-volume relation of the leftventricle alters: the ventricle fills less well in earlydiastole and increases in volume cause greater pres-
on January 8, 2022 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.35.3.229 on 1 M
arch 1973. Dow
nloaded from

Understanding the atrial sound 233
sure rises. The reduction in early diastolic fillingleaves a larger volume of blood to be moved intothe left ventricle by left atrial systole at a time whenleft ventricular pressure rises steeply with eachincrement of diastolic volume. The result is a risein the left ventricular end-diastolic pressure, thoughthe mean left atrial pressure and the left ventriculardiastolic pressure before atrial systole remain nor-mal (Cohn et al., 197I). The apex cardiogram reflectsthis situation with a reduction in the size of therapid filling wave and enlargement of the 'a' wave,which is usually accompanied by the atrial sound.
Deterioration in heart function tends to exagger-ate these changes, but when the heart goes intoclinical failure with abnormally high mean left atrialand left ventricular diastolic pressures, the patternreverses. There is a return of early diastolic rapidfilling, frequently accompanied by a pathologicalthird sound ('ventricular gallop'), while the 'a'waves of the left ventricular pressure curve and ofthe apex cardiogram become less prominent. Whenthe mean left atrial pressure exceeds 20 mmHg, the'a' wave of the apex cardiogram usually becomesquite small and the atrial sound is lost (Taylor andNixon, I972). If the heart rate is fast enough tocause early diastolic rapid filling to coincide withatrial contraction, a summation gallop results, andthis rate is often adopted tenaciously by the failingheart.
It is interesting to note that cardiac deteriorationcauses the interval between the onset of the P waveand the peak of the 'a' wave of left atrial and leftventricular pressure to lengthen, whereas it causesthe time from the onset of the P wave to the atrialsound and the peak of the atrial beat to shorten(O'Rourke, I970). This is because maximum move-ment of the apex away from the mitral annulus isachieved progressively earlier in left atrial systole asthe heart function deteriorates.
Significance of the atrial soundThe significance given to a diastolic sound usuallydepends upon the diagnosis of the heart conditionmade by other methods. A third sound in a youngathlete is called physiological while a similar soundin a patient with heart failure is called a gallop. Inthe past many clinicians have regarded any audibleatrial sound as pathological. However, the earlierfindings of Potain (I875) who believed that thediastolic sounds were exaggerations of normalevents and that the atrial sound could be heard inhealth, are now being confirmed (Spodick et al.,1971; Benchimol and Desser, 1971). We have,therefore, to distinguish between the physiologicaland the pathological atrial sound.
In the absence of overt heart disease, the atrialsound may be heard in the following circumstances.i) In childhood Here the circulation is brisk andthe chest wall thin. All the detectable diastolic eventsappear amplified and the pattern of left ventricularfilling movement is normal. The atrial sound, whenpresent, is much less prominent than the thirdsound, and the apex cardiogram shows a normalrelation between the rapid filling wave and the 'a'wave.2) In hyperdynamic and hypervolaemic states Theoveractive circulation of certain emotional states,fever, anaemia, exercise, and pregnancy may soexaggerate the normal diastolic events as to makethe atrial sound audible, but if the heart is normalthe atrial sound and beat are overshadowed by thethird sound and rapid filling wave. If a hyper-dynamic state unmasks myocardial disease, an ab-normal left ventricular filling pattern with a large'a' wave and an atrial sound may be found.3) In middle age As middle age advances, the inci-dence of the atrial sound in apparently normal sub-jects appears to increase. The increasing incidencemay be due to increasing stiffness in the mitral val-var apparatus which causes it to become more pro-ductive of noise (Dock, I959) or to changes in theleft ventricular filling pattern. Unlike the sound, the'a' wave of the apex cardiogram does not increasein amplitude with increasing age in normal subjects(Ginn et al., I967). The atrial sound, then, is encoun-tered in two different clinical circumstances, eitherwith or without enlargement of the 'a' wave. Insome cases where the 'a' wave is normal in size andimpalpable, the atrial sound may be a physiologicalevent (Spodick et al., I971). In others, however, itmay owe its presence to a healed myocardial infarc-tion, to the cardiac effect of hypertension, or tocovert heart disease. More investigation is neededto clarify the significance of the lone atrial sound,when it is the only questionable sign to be detectedin a middle-aged heart.We believe that an atrial sound associated with
an enlarged 'a' wave and a palpable atrial beat isnearly always abnormal, and most frequentlycaused by hypertensive and/or ischaemic heartdisease. Where this is found in subjects withoutother evidence of heart disease, it can be the conse-quence of a small healed myocardial infarction afterwhich the electrocardiogram has returned to normal.In others it may be the first evidence of underlyingischaemic heart disease or cardiomyopathy. Morestudy will be needed to determine the significanceof the 'lone atrial gallop', and it would be usefulto include apex recordings in long-term populationstudies.
on January 8, 2022 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.35.3.229 on 1 M
arch 1973. Dow
nloaded from

234 Bethell and Nixon
Clinical applications of the atrial soundIschaemic heart diseaseAcute myocardial infarction The atrial sound,usually accompanied by an enlarged atrial beat, isso consistently present after acute myocardial in-farction (Hill et al., I969; Jain and Lindahl, I97I)that the diagnosis is unlikely in its absence. Duringthe first day or two, when the first and secondsounds may be quiet, the atrial sound can be verydifficult to detect, presumably because the cardiacoutput is reduced and the atrium is transportingsmaller volumes of blood. As the patient recovers,the first and second sounds become louder, and theatrial sound becomes easier to detect: it may bewidely separated from the first sound, particularlywhen cardiac damage is severe (Krohn and Davis,I964). As the patient continues to improve, theatrial beat wanes, the interval between the P waveand the atrial sound lengthens, and the atrial soundtends to become incorporated in the first sound (Hillet al., I969; Bennett et al., I972). Thus, serial ob-servations of the state of the diastolic heart soundsand movements provide valuable information aboutheart function after infarction and can be a usefulguide to the speed with which the patient should bemobilized. The persistence of an atrial sound afterinfarction carries a worse prognosis than its dis-appearance (Kincaid-Smith and Barlow, I959b) andis more often associated with continuing symptoms(Benchimol and Dimond, I963). The persistenceof the atrial sound in association with a prominentthird sound usually indicates a ventricular aneurysm(McGinn, Gould, and Lyon, I968).
Diagnosis of early ischaemic heart diseaseThe atrial gallop is a common finding in anginapectoris (Banks and Shugoll, I967). In cases withoutprevious myocardial infarction it is commoner thanan abnormal resting electrocardiogram (Nixon andBethell, I972). In some cases the atrial sound andenlarged atrial beat may become apparent onlyduring attacks of angina, or may appear in responseto exercise in patients with ischaemic heart disease(Benchimol and Dimond, I963). The presence ofan atrial sound and palpable atrial beat in subjectswith 'atypical chest pain', or symptoms consistentwith reducing left ventricular function, is a valuableindication of underlying heart disease and shouldlead to further investigation (Nixon and Bethell,1971).
Management of chronic ischaemic heartdisease In any patient with established ischaemicheart disease, increasing amplitude of the atrial
sound and atrial beat is an indication of deterioratingheart function which often appears before the elec-trocardiogram worsens, and calls for appropriatetreatment.
HypertensionPotain first postulated that the atrial gallop wasassociated with arterial hypertension in some cases,though he was unable to measure the blood pressure.It has now been shown that in hypertensive disease,the atrial sound and beat correlate with the levelof blood pressure (Kincaid-Smith and Barlow,1959b) and electrocardiographic evidence of leftventricular hypertrophy (Beilin and Mounsey,I962). Treatment of the hypertension tends tolengthen the interval between the P wave and theatrial sound which merges with the first sound andis lost (Kincaid-Smith and Barlow, I959b), thoughan atrial sound persists in some patients, despiteadequate blood pressure control (Grayzel, I960). Itis reasonable to use the presence of an atrial soundand palpable atrial beat as one indication for startingtreatment of the hypertensive patient.
Aortic stenosisIn aortic stenosis, an enlarged apical 'a' wave andatrial sound usually signify a peak systolic gradientacross the valve of at least 70 mmHg and a leftventricular end-diastolic pressure of more thanii mmHg (Braunwald et al., I963; Tavel et al.,I965). The development of these signs of augmentedleft atrial activity indicates that the left ventricle hasbecome dependent upon atrial contraction for ade-quate filling. An arrhythmia which removes thisatrial transport function may cause sudden death.Thus, the development of a palpable atrial beat andan atrial sound may be useful signs that the timehas arrived for surgical treatment to be offered.
ReferencesAgress, C. M., Fields, L. G., Wegner, S., Wilburne, M.,
Shickman, M. D., and Muller, R. M. (I96I). The normalvibrocardiogram. American Journal of Cardiology, 8, 22.
Banks, T., and Shugoll, G. I. (I967). Confirmatory physicalfindings in angina pectoris. Journal of the American Medi-cal Association, 200, I031.
Beilin, L., and Mounsey, P. (I962). The left ventricular im-pulse in hypertensive heart disease. British Heart Journal,24, 409.
Benchimol, A., and Desser, K. B. (I97i). The fourth heartsound in patients with proven normal hearts (abstract).Circulation, 44, Suppl. 2, I40.
Benchimol, A., and Dimond, E. G. (I963). The apexcardio-gram in normal older subjects and in patients with arterio-sclerotic heart disease. Effect of exercise on the 'a' wave.American Heart3Journal, 65, 789.
on January 8, 2022 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.35.3.229 on 1 M
arch 1973. Dow
nloaded from

Understanding the atrial sound 235
Bennett, E. D., Smithen, C. R., and Sowton, E. (1972). Sig-nificance of atrial sound in acute myocardial infarction(abstract). British HIeart Journal, 34, 202.
Braunwald, E., Goldblatt, A., Aygen, M. M., Rockoff, S. D.,and Morrow, A. G. (I963). Congenital aortic stenosis:clinical and haemodynamic findings in ioo patients.Circulation, 27, 426.
Charcelay, A. (I838). Memoire sur plusieurs cas remarquablesde defaut de synchronisme des battements et des bruits desventricules du coeur. Archives Generales de Medecine, 3rdnew series, Vol. 3, 393.
Cohn, P. F., Vokonas, P. S., Williams, R. A., Herman, M. V.,and Gorlin, R. (I97i). Diastolic heart sounds and fillingwaves in coronary artery disease. Circulation, 44, I96.
Crevasse, L., Wheat, M. W., Wilson, J. R., Leeds, R. F., andTaylor, W. J., (I962). The mechanism of the generationof the third and fourth heart sounds. Circulation, 25, 635.
Dock, W. (I959). The forces needed to evoke sounds fromcardiac tissues, and the attenuation of heart sounds. Cir-culation, 19, 376.
Dock, W., Grandell, F., and Taubman, F. (I955). The physio-logic third heart sound: its mechanism and relation toprotodiastolic gallop. American Heart Journal, So, 449.
Duchosal, P. (I93I-I932). A study of gallop rhythm by a com-bination of phonocardiographic and electrocardiographicmethods. American Heart_Journal, 7, 6I3.
Eddleman, E. E., Willis, K., Reeves, T. J., and Harrison, T. R.(1953). The kinetocardiogram. I. Method of recordingprecordial movements. Circulation, 8, 269.
Ginn, W. M., Sherwin, R. W., Harrison, W. K., and Baker,B. M. (I967). Apex-cardiography: use in coronary heartdisease and reproducibility. American Heart J'ournal, 73,I68.
Grayzel, J. (I960). Gallop rhythm of the heart. American Jour-nal of Medicine, 28, 578.
Hill, J. C., O'Rourke, R. A., Lewis, R. P., and McGranahan,G. M. (I969). The diagnostic value of the atrial gallop inacute myocardial infarction. American Heart Journal, 78,194.
Jain, S. R., and Lindahl, J. (197I). Apex cardiogram and sys-tolic time intervals in acute myocardial infarction. BritishHeart Journal, 33, 578.
Kincaid-Smith, P., and Barlow, J. (1959a). The atrial soundand the atrial component of the first heart sound. BritishHeart Journal, 21, 470.
Kincaid-Smith, P., and Barlow, J. (1959b). Atrial sound inhypertension and ischaemic heart disease. British HeartJ7ournal, 21, 479.
Krohn, B. G., and Davis, W. H. (I964). The apex cardiogramas a prognostic tool in acute ischaemic heart disease. 4thEuropean Congress of Cardiology, Abstracts, p. i88.
McGinn, F. X., Gould, L., and Lyon, A. F. (I968). Thephonocardiogram and apexcardiogram in patients withventricular aneurysm. American Journal of Cardiology, 2I,467.
Marey, E. J. (i88i). La Circulation du Sang a l'Etat Physio-logique et dans les Maladies. Masson, Paris.
Nixon, P. G. F. (I96I). The third heart sound in mitral re-gurgitation. British Heart Journal, 23, 677.
Nixon, P. G. F., and Bethell, H. J. N. (I97I). Coronary deaths- how unexpected? British MedicalJournal, 4, 486.
Nixon, P. G. F., and Bethell, H. J. N. (I972). Atrial gallop indiagnosis of early coronary heart disease (abstract). BritishHeart3Journal, 34, 202.
Nixon, P. G. F., Hepburn, F., and Ikram, H. (1964). Simul-taneous recording of heart pulses and sounds. BritishMedical Journal, I, II69.
Orias, O., and Braun-Menendez, E. (I939). The Heart Sounds inNormal and Pathological Conditions. Oxford UniversityPress, London.
O'Rourke, R. A. (I970). The atrial sound. Factors regulatingits occurrence and timing. American Heart3Journal, 80, 715.
Potain, P. C. E. (I875). Du rhythme cardiaque appele bruitde galop, de son mecanisme et de sa valeur s6meiologique.Bulletin et Metmoires de la Societe Midicale des Hopitaux deParis, 12, I37. (Quoted by V. A. McKusick in Cardiovas-cular Sound in Health and Disease (I958). Williams andWilkins, Baltimore.)
Potain, P. C. E. (I894). Clinique Medicale de la Charite. Mas-son, Paris.
Rosa, L. M., Constantino, J. P., Reich, R., Karsak, N., andZezmer, B. (I96I). The precordial accelerogram in normalsubjects and noncardiac patients. Experimental Medicineand Surgery, 19, 207.
Spodick, D. H., Rectra, E., Khan, A., and Pigott, V. (I97I).Audibility of the fourth heart sound: a prospective,blinded investigation (abstract). Circulation, 44, Suppl. 2,33.
Stott, D. K., Marpole, D. G. F., Bristow, J. D., Kloster, F. E.,and Griswold, H. E. (1970). The role of left atrial transportin aortic and mitral stenosis. Circulation, 41, I031.
Tavel, M. E., Campbell, R. W., Feigenbaum, H., and Stein-metz, E. F. (1965). The apex cardiogram and its relation-ship to haemodynamic events within the left heart. BritishHeart Journal, 27, 829.
Taylor, D. J. E., and Nixon, P. G. F. (1972). Assessment ofleft ventricular function after myocardial infarction. BritishHeart Journal, 34, 905.
Requests for Reprints to Dr. P. G. F. Nixon, CardiacDepartment, Charing Cross Hospital, London WC2N4DZ.
on January 8, 2022 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.35.3.229 on 1 M
arch 1973. Dow
nloaded from