
Support surfaces for treating pressure ulcers
12
Review Support surfaces for treating pressure injury: A Cochrane systematic review Elizabeth McInnes a, *, Asmara Jammali-Blasi a , Nicky Cullum b , Sally Bell-Syer c , Jo Dumville c a Nursing Research Institute – St Vincent’s & Mater Health Sydney & Australian Catholic University, National Centre for Clinical Outcomes Research (NaCCOR), Australia b School of Nursing, Midwifery and Social Work, University of Manchester, United Kingdom c Department of Health Sciences, University of York, United Kingdom What is already known about this topic? Pressure injuries are areas of localised damage to the skin and underlying tissue due to pressure, shear or friction. There are range of low-tech and high-tech devices that may be used in a variety of settings to assist with the treatment of pressure injuries. Currently there is a limited and/or inconclusive evidence base for other pressure injury treatment options includ- ing wound cleansing, electromagnetic therapy, reposi- tioning and therapeutic ultrasound. What this paper adds: There is a paucity of evidence to guide clinicians as to which support surfaces are best for the treatment of pressure injuries. Methodologically sound research is required to enable robust meta-analyses to be performed, and clinically relevant evidence to be produced. International Journal of Nursing Studies 50 (2013) 419–430 A R T I C L E I N F O Article history: Received 1 March 2012 Received in revised form 2 May 2012 Accepted 22 May 2012 Keywords: Support surfaces Pressure ulcer Treatment Pressure injury Systematic review A B S T R A C T Objectives: To examine the effects on healing of pressure relieving support surfaces in the treatment of pressure injury. Design: Systematic review. Data sources: Cochrane Wound Group Specialised Register, The Cochrane Central Register of Controlled Trials, Ovid MEDLINE, Ovid EMBASE and EBSCO CINAHL. The reference sections of included trials were searched for further trials. Review methods: Randomised controlled trials, published or unpublished, assessing the effect of support surfaces in treating all pressure injuries were sought. All included studies had to have reported objective measures of pressure injury healing. Where possible, findings from individual trials were calculated using risk ratio estimates or mean difference with 95% confidence intervals. Results: Eighteen eligible trials involving 1309 participants were identified. There was no statistically significant effect on pressure injury size with low air loss devices compared with foam alternatives. One small trial at high risk of bias found that sheepskin positioned under the legs significantly reduced redness and a very small subgroup analysis favoured a profiling bed when compared with a standard bed in terms of the healing of grade 1 pressure injuries. Conclusions: Overall, there was an absence of good evidence to support the superiority of any pressure relieving device in the treatment of pressure injuries. This review highlights that the current evidence base requires improving by undertaking robust trials to ascertain which support surfaces are most effective for the treatment of pressure injuries. ß 2012 Elsevier Ltd. All rights reserved. * Corresponding author at: Nursing Research Institute – St Vincent’s & Mater Health Sydney & Australian Catholic University, National Centre for Clinical Outcomes Research (NaCCOR), Sydney, NSW 2012, Australia. Tel.: +61 02 8382 3793; fax: +61 02 8382 3792. E-mail address: [email protected] (E. McInnes). Contents lists available at SciVerse ScienceDirect International Journal of Nursing Studies journal homepage: www.elsevier.com/ijns 0020-7489/$ – see front matter ß 2012 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.ijnurstu.2012.05.008
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Support surfaces for treating pressure ulcers

Re
Sure
Elia Nu
Reseb Schc De
� Pa� T
mtr
International Journal of Nursing Studies 50 (2013) 419–430
A R
Artic
Rece
Rece
Acce
Keyw
Sup
Pres
Trea
Pres
Syst
*
Mat
Clin
Tel.:
002
http
view
pport surfaces for treating pressure injury: A Cochrane systematicview
zabeth McInnes a,*, Asmara Jammali-Blasi a, Nicky Cullum b, Sally Bell-Syer c, Jo Dumville c
rsing Research Institute – St Vincent’s & Mater Health Sydney & Australian Catholic University, National Centre for Clinical Outcomes
arch (NaCCOR), Australia
ool of Nursing, Midwifery and Social Work, University of Manchester, United Kingdom
partment of Health Sciences, University of York, United Kingdom
What is already known about this topic?
ressure injuries are areas of localised damage to the skinnd underlying tissue due to pressure, shear or friction.here are range of low-tech and high-tech devices thatay be used in a variety of settings to assist with theeatment of pressure injuries.
� Currently there is a limited and/or inconclusive evidencebase for other pressure injury treatment options includ-ing wound cleansing, electromagnetic therapy, reposi-tioning and therapeutic ultrasound.
What this paper adds:
� There is a paucity of evidence to guide clinicians as towhich support surfaces are best for the treatment ofpressure injuries.� Methodologically sound research is required to enable
robust meta-analyses to be performed, and clinicallyrelevant evidence to be produced.
T I C L E I N F O
le history:
ived 1 March 2012
ived in revised form 2 May 2012
pted 22 May 2012
ords:
port surfaces
sure ulcer
tment
sure injury
ematic review
A B S T R A C T
Objectives: To examine the effects on healing of pressure relieving support surfaces in the
treatment of pressure injury.
Design: Systematic review.
Data sources: Cochrane Wound Group Specialised Register, The Cochrane Central Register
of Controlled Trials, Ovid MEDLINE, Ovid EMBASE and EBSCO CINAHL. The reference
sections of included trials were searched for further trials.
Review methods: Randomised controlled trials, published or unpublished, assessing the
effect of support surfaces in treating all pressure injuries were sought. All included studies
had to have reported objective measures of pressure injury healing. Where possible,
findings from individual trials were calculated using risk ratio estimates or mean
difference with 95% confidence intervals.
Results: Eighteen eligible trials involving 1309 participants were identified. There was no
statistically significant effect on pressure injury size with low air loss devices compared with
foam alternatives. One small trial at high risk of bias found that sheepskin positioned under
the legs significantly reduced redness and a very small subgroup analysis favoured a profiling
bed when compared with a standard bed in terms of the healing of grade 1 pressure injuries.
Conclusions: Overall, there was an absence of good evidence to support the superiority of
any pressure relieving device in the treatment of pressure injuries. This review highlights
that the current evidence base requires improving by undertaking robust trials to ascertain
which support surfaces are most effective for the treatment of pressure injuries.
� 2012 Elsevier Ltd. All rights reserved.
Corresponding author at: Nursing Research Institute – St Vincent’s &
er Health Sydney & Australian Catholic University, National Centre for
ical Outcomes Research (NaCCOR), Sydney, NSW 2012, Australia.
+61 02 8382 3793; fax: +61 02 8382 3792.
E-mail address: [email protected] (E. McInnes).
Contents lists available at SciVerse ScienceDirect
International Journal of Nursing Studies
journal homepage: www.elsevier.com/ijns
0-7489/$ – see front matter � 2012 Elsevier Ltd. All rights reserved.
://dx.doi.org/10.1016/j.ijnurstu.2012.05.008

E. McInnes et al. / International Journal of Nursing Studies 50 (2013) 419–430420
� Further research requires clear evidence of true rando-misation, complete outcome data (allowing for repro-duction of results), validated healing measures and cost–benefit analyses.
1. Introduction
1.1. Rationale
Pressure injury (also known as pressure ulcers, pressuresores, bed sores and decubitus injuries) is an area of localiseddamage to the skin and underlying tissue, believed to becaused by pressure, or caused by both pressure and shear(European Pressure Ulcer Advisory Panel and NationalPressure Ulcer Advisory Panel, 2009). A pressure injury canrange from non-blanching erythema (usually termed agrade 1 pressure injury) to a more serious chronic woundwhich can be debilitating, painful and difficult to heal(Girouard et al., 2008). Grade 2 pressure injuries generallyrefers to partial thickness loss of dermis and grades 3 and 4,respectively, refer to full thickness tissue loss and fullthickness tissue loss with exposed bone, tendon or muscle(EPUAP-NPUAP 2009). Patients at risk of developingpressure injury include those who are seriously ill orneurologically compromised, those with impaired mobility(Allman et al., 1987; Berlowitz et al., 1997; Berlowitz andWilkin, 1990; Bianchetti et al., 1993) or those with impairednutrition (Banks, 1998; Casey, 1997, 1998). Obesity(Gallagher, 1997), poor posture, age, incontinence, impairedcirculation and some medications such as steroids andpregnancy (Hefley and Radcliffe, 1990; Krainski, 1992;Orlando, 1998; Pase and Hoffman, 1998; Prior, 2002; Rondaand Falce, 2002; Spoelhof, 2000; Thomas et al., 1996;Waltman et al., 1991) have also been reported as increasingrisk. Studies conducted in healthcare facilities in Europe,Canada, USA and Australia report pressure injury prevalenceranging from 5% to 26% (Vanderwee et al., 2007; Woodburyand Houghton, 2004; Australian Commission for Safety andQuality in Health Care (ACSQHC), 2005; Posnett et al., 2009).Of these, 57.9% (Europe) and 73% (USA) are classified asgrade/stage two and above (Vanderwee et al., 2007;VanGilder et al., 2009). Annual total costs for treatingpressure injuries in the UK have been estimated as beingbetween 1.4 and 2.1 billion pounds (Phillips and Buttery,2009) and between 2.2 and 3.6 billion dollars in the UnitedStates annually (VanGilder et al., 2009).
Studies have shown that having a pressure injury wasassociated with a 2–4-fold increase in risk of death in olderpatients in intensive care units (Bo et al., 2003; Clough,1994; Thomas et al., 1996). The presence of a pressureinjury is also associated with psychological, physical andsocial problems (Franks et al., 2002; Langemo et al., 2000;Fox, 2002) resulting in reduced quality of life (Goreckiet al., 2009). The management of pressure injury ischallenging for clinicians (Franks et al., 2002; Langemoet al., 2000; Fox, 2002) as the evidence base for treatmentssuch as wound cleansing, electromagnetic therapy, repo-sitioning and therapeutic ultrasound is either limited orinconclusive (Moore and Cowman, 2005, 2009; Aziz et al.,2010; Akbari Sari et al., 2009).
The use of pressure relieving (in this review the term‘pressure relieving’ refers to any support surface thatrelieves, redistributes or reduces pressure) support sur-faces for treating pressure injuries has been investigated inseveral trials (Reddy et al., 2008; Russell et al., 2000; Nixonet al., 2006c; Ferrell et al., 1993; Cullum et al., 1995;Allman et al., 1987). Pressure relieving support surfacesaim to reduce the magnitude and/or duration of pressurebetween an individual and the support surface used(‘interface pressure’). In terms of treatment properties,support surfaces work by reducing pressure at the site ofskin damage. The use of pressure-relieving supportsurfaces for healing pressure injuries are generally usedin conjunction with other wound management strategiessuch as positioning and use of dressings. Support surfacesinclude overlays, mattresses, cushions, sheepskins andbeds. These can be classified either as ‘low-tech’ or ‘high-tech’ devices. Low-tech devices are conforming supportsurfaces that mould around the shape of the patient todistribute the body weight over a large area and includeconstant low-pressure devices such as foam mattresses.High-tech devices include alternating support surfaceswhere inflatable cells alternately inflate and deflate(McInnes et al., 2011a) and mechanical support surfacessuch as turning beds/frames which work by motor driventurning and tilting.
There are many pressure relieving support surfacesavailable and treatment should ideally employ initiativeswhich are based on the best available effectivenessevidence. Hence we have undertaken a systematic reviewof randomised controlled trials with the aim of providingclinicians with information on which to base decisionsabout choice of support surfaces for the treatment ofpressure injuries. This review complements a Cochranereview examining support surfaces for the prevention ofpressure injuries which we have recently also published(McInnes et al., 2011b).
1.2. Objectives
To examine (1) whether pressure relieving supportsurfaces are effective in healing existing pressure injuriesand (2) which pressure relieving support surfaces are mosteffective in healing pressure injuries
2. Methods
2.1. Protocol and registration
The Cochrane systematic review on which this article isbased can be accessed from the Cochrane Database ofSystematic Reviews (Art. No: CD009490) (McInnes et al.,2011a). This report adheres to the PRISMA method forreporting on systematic reviews (Moher et al., 2009).
2.2. Eligibility criteria
Randomised controlled trials (RCTs) of support surfaceswhich evaluated pressure injury healing on people withexisting pressure injuries of any grade in any setting. Theprimary outcome of interest was healing of existing
presucareTriasucintestrasup
2.3.
CocDecCon4,
201CitaWeTheCocranmaThecomIntecollseaCon
theanywitscru
2.4.
indrevweof psecsionche
2.5.
revextsioninckeyof
numdesup
meattethe
E. McInnes et al. / International Journal of Nursing Studies 50 (2013) 419–430 421
ssure injuries as measured by some objective methodh as time to complete healing, rate of change in thea/volume of the injuries or number of injuries healed.ls which only measured surrogate outcome measures
h as interface pressure were excluded on the basis thatrface pressure measurements have not been demon-ted to reliably predict the clinical performance ofport surfaces (Cullum et al., 2000).
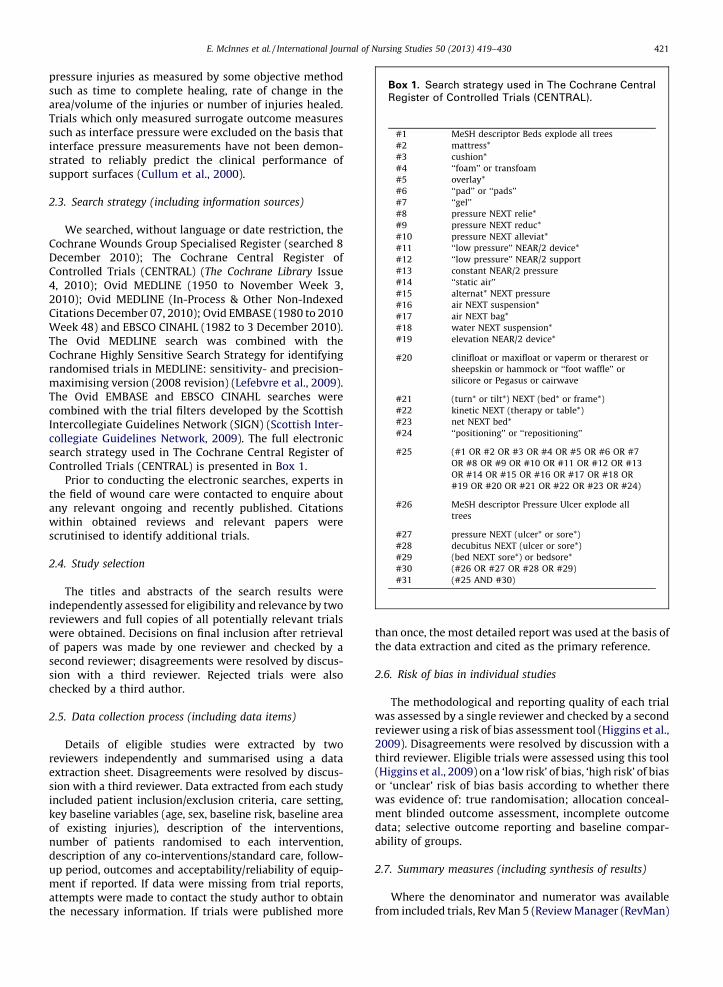
Search strategy (including information sources)
We searched, without language or date restriction, thehrane Wounds Group Specialised Register (searched 8ember 2010); The Cochrane Central Register oftrolled Trials (CENTRAL) (The Cochrane Library Issue
2010); Ovid MEDLINE (1950 to November Week 3,0); Ovid MEDLINE (In-Process & Other Non-Indexedtions December 07, 2010); Ovid EMBASE (1980 to 2010ek 48) and EBSCO CINAHL (1982 to 3 December 2010).
Ovid MEDLINE search was combined with thehrane Highly Sensitive Search Strategy for identifyingdomised trials in MEDLINE: sensitivity- and precision-ximising version (2008 revision) (Lefebvre et al., 2009).
Ovid EMBASE and EBSCO CINAHL searches werebined with the trial filters developed by the Scottishrcollegiate Guidelines Network (SIGN) (Scottish Inter-egiate Guidelines Network, 2009). The full electronicrch strategy used in The Cochrane Central Register oftrolled Trials (CENTRAL) is presented in Box 1.
Prior to conducting the electronic searches, experts in field of wound care were contacted to enquire about
relevant ongoing and recently published. Citationshin obtained reviews and relevant papers weretinised to identify additional trials.
Study selection
The titles and abstracts of the search results wereependently assessed for eligibility and relevance by twoiewers and full copies of all potentially relevant trialsre obtained. Decisions on final inclusion after retrieval
apers was made by one reviewer and checked by aond reviewer; disagreements were resolved by discus-
with a third reviewer. Rejected trials were alsocked by a third author.
Data collection process (including data items)
Details of eligible studies were extracted by twoiewers independently and summarised using a dataraction sheet. Disagreements were resolved by discus-
with a third reviewer. Data extracted from each studyluded patient inclusion/exclusion criteria, care setting,
baseline variables (age, sex, baseline risk, baseline areaexisting injuries), description of the interventions,ber of patients randomised to each intervention,
cription of any co-interventions/standard care, follow-period, outcomes and acceptability/reliability of equip-nt if reported. If data were missing from trial reports,mpts were made to contact the study author to obtain
than once, the most detailed report was used at the basis ofthe data extraction and cited as the primary reference.
2.6. Risk of bias in individual studies
The methodological and reporting quality of each trialwas assessed by a single reviewer and checked by a secondreviewer using a risk of bias assessment tool (Higgins et al.,2009). Disagreements were resolved by discussion with athird reviewer. Eligible trials were assessed using this tool(Higgins et al., 2009) on a ‘low risk’ of bias, ‘high risk’ of biasor ‘unclear’ risk of bias basis according to whether therewas evidence of: true randomisation; allocation conceal-ment blinded outcome assessment, incomplete outcomedata; selective outcome reporting and baseline compar-ability of groups.
2.7. Summary measures (including synthesis of results)
Where the denominator and numerator was available
Box 1. Search strategy used in The Cochrane Central
Register of Controlled Trials (CENTRAL).
#1 MeSH descriptor Beds explode all trees
#2 mattress*
#3 cushion*
#4 ‘‘foam’’ or transfoam
#5 overlay*
#6 ‘‘pad’’ or ‘‘pads’’
#7 ‘‘gel’’
#8 pressure NEXT relie*
#9 pressure NEXT reduc*
#10 pressure NEXT alleviat*
#11 ‘‘low pressure’’ NEAR/2 device*
#12 ‘‘low pressure’’ NEAR/2 support
#13 constant NEAR/2 pressure
#14 ‘‘static air’’
#15 alternat* NEXT pressure
#16 air NEXT suspension*
#17 air NEXT bag*
#18 water NEXT suspension*
#19 elevation NEAR/2 device*
#20 clinifloat or maxifloat or vaperm or therarest or
sheepskin or hammock or ‘‘foot waffle’’ or
silicore or Pegasus or cairwave
#21 (turn* or tilt*) NEXT (bed* or frame*)
#22 kinetic NEXT (therapy or table*)
#23 net NEXT bed*
#24 ‘‘positioning’’ or ‘‘repositioning’’
#25 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7
OR #8 OR #9 OR #10 OR #11 OR #12 OR #13
OR #14 OR #15 OR #16 OR #17 OR #18 OR
#19 OR #20 OR #21 OR #22 OR #23 OR #24)
#26 MeSH descriptor Pressure Ulcer explode all
trees
#27 pressure NEXT (ulcer* or sore*)
#28 decubitus NEXT (ulcer or sore*)
#29 (bed NEXT sore*) or bedsore*
#30 (#26 OR #27 OR #28 OR #29)
#31 (#25 AND #30)
included trials, Rev Man 5 (Review Manager (RevMan)
necessary information. If trials were published more from
E. McInnes et al. / International Journal of Nursing Studies 50 (2013) 419–430422
Version 5.0, 2008) was used to calculate the risk ratio (RR)for dichotomous variables such as numbers healed or nothealed. Continuous outcome variables such as change inwound volume or mean time of healing were summarisedusing the mean difference (MD) and variance (SD) reportedin the included trials. If data were not available for analysisin Rev Man, the results reported by the trial authors arereported narratively.
We planned to pool trials with similar patients,comparisons, outcomes and low statistical heterogeneity.Heterogeneity was measured by I2, with a value greaterthan 50% indicating substantial heterogeneity which wasconsidered significant when p < 0.10 (Higgins et al., 2011).A random effects model was used if there was significantstatistical heterogeneity, and a fixed effects model wasused in the absence of significant statistical heterogeneity(Higgins et al., 2011). A narrative review was conducted
where meta-analysis was not possible. Included trials weregrouped according to the types of support surfaces andcomparisons evaluated as shown in Box 2.
3. Results
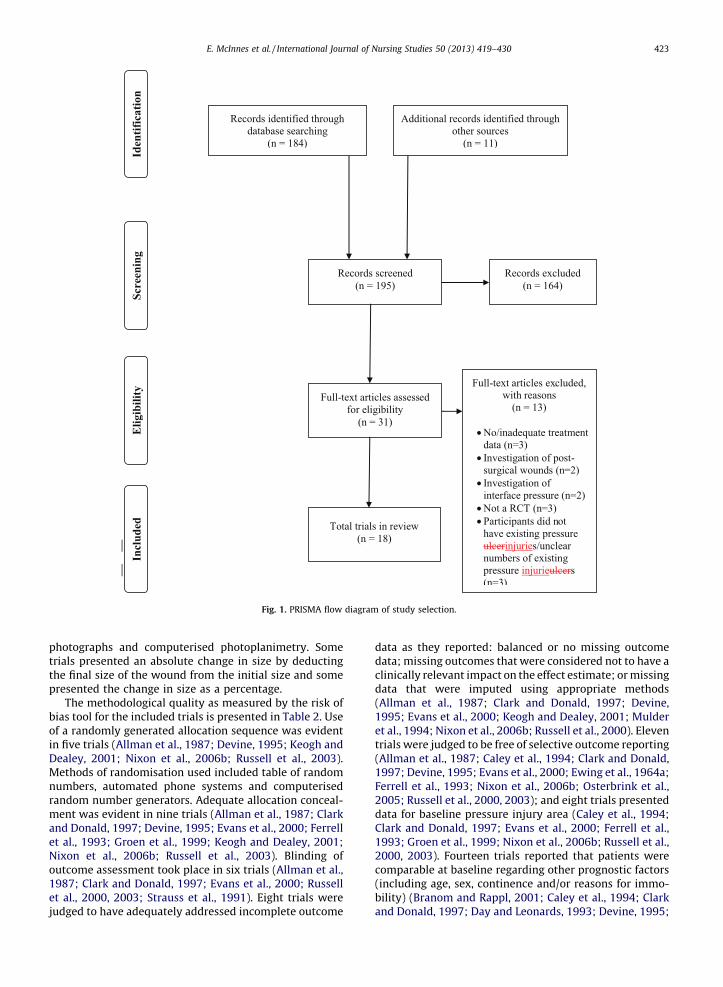
The search identified 31 full text articles which wereassessed for eligibility out of a download of 195 potentiallyrelevant articles (Fig. 1). Eighteen trials met the eligibilitycriteria and 13 were excluded (Fig. 1). Table 1 shows thatmost were rejected on the basis of study design or outcomemeasurement. Fourteen trials involved people withpressure injuries and assessed the treatment effects ofpressure relieving support surfaces. The remaining fourtrials evaluated the effects of support surfaces for bothprevention and treatment of pressure injuries and treat-ment-specific data was extracted from these papers(Ewing et al., 1964b; Keogh and Dealey, 2001; Nixonet al., 2006a; Osterbrink et al., 2005).
The trials were conducted in a variety of settingsincluding nursing homes, care of the elderly hospitalwards, medical and surgical wards. Sample sizes rangedfrom 14 to 160 participants and the reported follow-upperiod for trials ranged from 5 days to 18 months. Therewas evidence of sample size calculation in eight trials(Allman et al., 1987; Clark and Donald, 1997; Ferrell et al.,1993; Groen et al., 1999; Keogh and Dealey, 2001; Nixonet al., 2006b; Russell et al., 2000, 2003). Similar timing ofoutcome assessment between study arms was reported in15 trials and this ranged from 3-day intervals to every2 weeks. In three trials it was unclear whether similartiming of outcome assessment had occurred (Ewing et al.,1964a; Keogh and Dealey, 2001; Strauss et al., 1991).
Healing outcomes were measured in various ways andthere was little standardisation of types of outcomemeasures applied across the trials. Outcomes included:proportion of pressure injuries healed; time to healing;rate of healing; size of wounds healed; number of pressureinjuries healed; number of patients with healed pressureinjuries and the proportion of pressure injuries reported as‘improved’. Wound size measurement techniques includedthe use of mathematical formulae to calculate woundvolume; clinical judgement of ‘improvement’ or ‘healed’with and without a pre-determined scaling instrument;
Box 2. Categories of included trials (n = 18).
‘Low-tech’ constant pressure support surfaces (n = 3)
Air-filled mattress/overlays
Branom et al.
Water-filled supports
Groen et al.
Sheepskins
Ewing et al.
‘High-tech’ constant pressure support surfaces (n = 15)
Low-air-loss supports
Caley et al.
Day et al.
Ferrell et al.
Mulder et al.
Alternating-pressure supports
Allman et al.
Clark et al.
Devine et al.
Evans et al.
Munro et al.
Nixon et al.
Osterbrink et al.
Russell et al. (2000)
Russell et al. (2003)
Strauss et al.
Profiling bed with foam mattress
Keogh et al.
Table 1
Excluded studies (n = 13).
Study Reason for exclusion
Bennett 1998 Authors did not report treatment data: ‘‘too few patients with existing pressure ulcers were treated for
too short a period of time to assess the effect of low air low-air-loss hydrotherapy on pressure sore healing’’
De Roche 2004 Ulcers have been surgically closed and therefore are post-surgical wounds.
Finnegan 2008 Ulcers under investigation had been surgically closed and therefore classified as post-surgical wounds
Gardner 2008 Not looking at pressure injury treatment. Outcome measure of interface pressure
Hardin 2000 Not an RCT, measured interface pressure and included a retrospective chart audit
Lazzara 1991 Participants did not have existing pressure ulcers
Marchand 1993 Retrospective chart audit
Meyers 2008 Study does not investigate the treatment of pressure ulcers
Prebio 2005 Unclear of baseline number of pre-existing pressure ulcers
Rosenthal 1996 Study investigated interface pressures
Rosenthal 2003 Treatment outcomes are inadequately reported. Process of randomisation may have introduced bias
Stoneburg 1986 Participants did not have existing pressure ulcers
Timmons 2008 Not an RCT. Product review
photriathepre
biaof ain fiDeaMenumranmeandet aNixout198et ajud
E. McInnes et al. / International Journal of Nursing Studies 50 (2013) 419–430 423
tographs and computerised photoplanimetry. Somels presented an absolute change in size by deducting
final size of the wound from the initial size and somesented the change in size as a percentage.The methodological quality as measured by the risk ofs tool for the included trials is presented in Table 2. Use
randomly generated allocation sequence was evidentve trials (Allman et al., 1987; Devine, 1995; Keogh andley, 2001; Nixon et al., 2006b; Russell et al., 2003).
thods of randomisation used included table of randombers, automated phone systems and computerised
dom number generators. Adequate allocation conceal-nt was evident in nine trials (Allman et al., 1987; Clark
Donald, 1997; Devine, 1995; Evans et al., 2000; Ferrelll., 1993; Groen et al., 1999; Keogh and Dealey, 2001;on et al., 2006b; Russell et al., 2003). Blinding ofcome assessment took place in six trials (Allman et al.,7; Clark and Donald, 1997; Evans et al., 2000; Russelll., 2000, 2003; Strauss et al., 1991). Eight trials were
ged to have adequately addressed incomplete outcome
data as they reported: balanced or no missing outcomedata; missing outcomes that were considered not to have aclinically relevant impact on the effect estimate; or missingdata that were imputed using appropriate methods(Allman et al., 1987; Clark and Donald, 1997; Devine,1995; Evans et al., 2000; Keogh and Dealey, 2001; Mulderet al., 1994; Nixon et al., 2006b; Russell et al., 2000). Eleventrials were judged to be free of selective outcome reporting(Allman et al., 1987; Caley et al., 1994; Clark and Donald,1997; Devine, 1995; Evans et al., 2000; Ewing et al., 1964a;Ferrell et al., 1993; Nixon et al., 2006b; Osterbrink et al.,2005; Russell et al., 2000, 2003); and eight trials presenteddata for baseline pressure injury area (Caley et al., 1994;Clark and Donald, 1997; Evans et al., 2000; Ferrell et al.,1993; Groen et al., 1999; Nixon et al., 2006b; Russell et al.,2000, 2003). Fourteen trials reported that patients werecomparable at baseline regarding other prognostic factors(including age, sex, continence and/or reasons for immo-bility) (Branom and Rappl, 2001; Caley et al., 1994; Clarkand Donald, 1997; Day and Leonards, 1993; Devine, 1995;
Fig. 1. PRISMA flow diagram of study selection.

E. McInnes et al. / International Journal of Nursing Studies 50 (2013) 419–430424
Evans et al., 2000; Ferrell et al., 1993; Groen et al., 1999;Keogh and Dealey, 2001; Nixon et al., 2006a,b,c; Osterbrinket al., 2005; Russell et al., 2000, 2003; Strauss et al., 1991).Fifteen trials reported having similar timing of outcomesfor each study arm; for three trials this was unclear (Ewinget al., 1964a; Keogh and Dealey, 2001; Strauss et al., 1991).Fifteen trials indicated the grade of injury of the studyparticipants (in this paper, we use the term ‘grade’ forconsistency). Of these, seven analysed pressure injuriesgrade 2 and above (Clark and Donald, 1997; Day andLeonards, 1993; Devine, 1995; Ferrell et al., 1993; Nixonet al., 2006b; Osterbrink et al., 2005; Russell et al., 2000);two investigated injuries grade 2–3 (Evans et al., 2000;Munro et al., 1989); four investigated those grade 3–4(Branom and Rappl, 2001; Groen et al., 1999; Mulder et al.,1994; Strauss et al., 1991); and two investigated allpressure grades (Allman et al., 1987; Russell et al., 2000). Arange of classification systems was used in grading theinjuries in the included trials including the TorrenceClassification (Russell et al., 2000), European PressureAdvisory Panel (EPUAP) grading (Keogh and Dealey, 2001;
Osterbrink et al., 2005; Russell et al., 2003) and the Sheascale (Allman et al., 1987; Ferrell et al., 1993).
Following the classification system used in a previoussystematic review (McInnes et al., 2011b), trials wereclassified into those that evaluated high-tech and low-techsupport surfaces. Four trials evaluated low-tech constantpressure relief supports (air-filled mattress/overlay, waterfilled supports and sheepskin overlay) (Table 3). Fourteentrials evaluated high-tech pressure relief supports (alter-nating-pressure mattresses, alternating-pressure mattressoverlays, alternating-pressure cushion, air-fluidised ther-apy and profiling beds) (Table 4).
3.1. Comparisons including low-tech constant pressure
support surfaces
Three trials investigated the use of low-tech constantpressure support surfaces compared with standard hospi-tal equipment, foam mattresses and/or overlays (Table 3)(Branom and Rappl, 2001; Ewing et al., 1964a; Groen et al.,1999). There was insufficient information to enable us to
Table 2
Risk of bias of included trials (n = 18).
Study Adequate
sequence
generation
Allocation
concealment
Blinding Incomplete
outcome data
addressed
Free of
selective
reporting
ITT analysis Groups
similar at
baseline
Timing of outcome
assessment similar
in all groups
Allman Low risk Low risk Low risk Low risk Low risk Low risk High risk Low risk
Branom High risk Unclear Unclear Unclear Unclear High risk Low risk Low risk
Caley Unclear Unclear High risk Unclear Low risk Unclear Low risk Low risk
Clark Unclear Low risk Low risk Low risk Low risk High risk Low risk Low risk
Day Unclear Unclear Unclear Unclear High risk High risk Low risk Low risk
Devine Low risk Low risk High risk Low risk Low risk High risk Low risk Low risk
Evans Unclear Low risk Low risk Low risk Low risk Unclear Low risk Low risk
Ewing Unclear High risk High risk Unclear Low risk High risk Unclear Unclear
Ferrell Unclear Low risk Unclear Unclear Low risk Low risk Low risk Low risk
Groen Unclear Low risk High risk Unclear High risk High risk Low risk Low risk
Keogh Low risk Low risk Unclear Low risk High risk Low risk Low risk Unclear
Mulder Unclear Unclear Unclear Low risk High risk Low risk Unclear Low risk
Munro Unclear Unclear High risk Unclear High risk Unclear Unclear Low risk
Nixon Low risk Low risk High risk Low risk Low risk Low risk Low risk Low risk
Osterbrink Unclear Unclear Unclear Unclear Low risk Low risk Low risk Low risk
Russell 2000 Unclear Unclear Low risk Low risk Low risk High risk Low risk Low risk
Russell 2003 Low risk Low risk Low risk Unclear Low risk High risk Low risk Low risk
Strauss Unclear Unclear Low risk Unclear Unclear Low risk Low risk Unclear
Table 3
Characteristics of included trials – low-tech constant pressure support surfaces (n = 3).
Study, Date (Country) Participants Design (intervention) Outcomes assessed Reported follow-up
Branom, 2001 (USA) Long-term and sub-acute
inpatients
RCT, non-powered mattress
(Pressure Guard CFT) (n = 10)
vs. Low-air-loss mattress
(n = 10)
Meeting treatment goals
(including wound closure,
maintenance of condition and
preparation for flap), rate of
wound healing
8 weeks
Ewing, 1964 (Australia) Elderly patients, confined to
bed, with reduced mobility in
lower limbs secondary to
neurological
disorder or fixed joints,
peripheral vascular disease
RCT, sheepskin (18) vs. No
sheepskin (n = 18)
Relief of redness, pressure
injury healing, comfort
6 months
Groen, 1999 (Holland) Nursing home patients, aged
greater than 59 years, grade
3 or 4 pressure injury on trunk
RCT, Foam replacement
mattress (n = 60) vs.
Water mattress
on top of standard mattress
Proportion of ulcers healed at
4 weeks, mean pressure injury
severity score at 4 weeks
4 weeks
(Secutex) (n = 60)

Table 4
Characteristics of included trials – High-tech pressure support surfaces (n = 15).
Study, Date
(country)
Participants Design (Intervention) Outcomes Assessed Reported
follow-up
Allman, 1987 (USA) Surgical patients, aged over
18 years, patients expected to be
limited to bed/chair, in hospital for
at least 1 week
RCT; Air fluidised therapy
(CLINITRON) (n = 31) vs.
Conventional treatment (n = 34)
Median change in injury total
surface area, improvement in
condition of pressure injury,
pain response
Mean = 13 days
(range: 4–77)
Caley, 1994 (USA) Acute patients with existing
pressure ulcers with low-air loss
therapy recommendations
RCT, Low-air-loss bed (Monarch)
(n = 23) vs. Low-air-loss overlay
(SPR Plus) (n = 32)
Median change in injury area,
healing progress over time
Mean = 24 days
Clark and Donald,
1997 (UK)
Elderly patients in acute care and
nursing home settings,
established pressure ulcers
RCT, Cushion (ProActive 2) (n = 14)
vs. Cushion (ROHO) (n = 11)
Number of ulcers healed
completely, rate of healing
Mean = 58.6
(Proactive)
Mean = 43.7
(ROHO)
Day, 1993 (USA) Hospitalised, adult patients with
existing grade 2–4 ulcers
RCT, Air suspension bed
(Therapulse) (n = 44) vs. Foam
mattress overlay (Geomatt) (n = 39)
Mean injury size,
mean comfort score
Minimum
7 days
Devine, 1995 (UK) Elderly patients with ulcers
grade 2 or above
RCT, Alternating pressure mattress
(Nimbus I) (n = 22) vs. Alternating
pressure mattress (Pegasus
Airwave) (n = 19)
Complete healing, comfort,
reduction in area, withdrawal
rates
4 weeks
Evans, 2000 (UK) Hospital and nursing home
patients, aged greater than
65 years, minimum grade
2 injury, one of the following;
difficult to reposition in bed,
unable to tolerate 30 degree
tilt, unable to move in bed,
in bed for greater that 20 h,
greater than 108 kg and bed
bound, undergone spinal
anaesthesia
RCT, Alternating pressure mattress
(Nimbus III) (n = 17) vs. Alternating
pressure mattress overlay (nursing
home patients)/Alternating
pressure mattress replacement
system (hospital patients) (n = 15)
Absolute and relative reduction
in wound surface area, comfort
2 weeks
Ferrell, 1993 (USA) Elderly nursing home residents,
trunk or trochanter pressure
ulcers (grade 2 or greater)
RCT, Low-air-loss bed (KINAIR)
(n = 43) vs. Foam overlay on top
of standard mattress (n = 41)
Rate of healing, ulcers
completely healed
33–40 days
Keogh, 2001 (UK) Patients from surgical and medical
wards, aged greater than 18 years,
Waterlow score of 15–25, tissue
damage no greater than grade 1
RCT, Profiling bed (n = 50) vs.
Flat-based bed (n = 50)
Proportion with healed
grade 1 ulcers
5–10 days
Mulder, 1994 (USA) Nursing home patients with
grade 3–4 ulcers
RCT, Air suspension bed
(Therapulse) (n = 31) vs.
Convoluted foam mattress
overlay (Geomatt) (n = 18)
Wound closer, pressure injury
improvement, wound surface
area, injury volume
Maximum
12 weeks
Munro, 1989 (USA) Male patients, grade 2–3 pressure
injury, expected hospital stay of at
least 15 days
RCT, Air fluidised bed
(Clinitron) (n = 20) vs.
Standard care (n = 20)
Change in mean injury area,
final injury area, pain levels,
patient satisfaction
15 days
Nixon, 2006 (UK) Patients aged at least 55 years,
expected hospital stay of least
1 week, Braden score = 1–2 or
existing grade 2 injury
RCT, Alternating pressure
overlay (n = 989) vs.
Alternating pressure
mattress (n = 982)
Proportion of patients with
new grade 2 + pressure injury,
time to development of new
pressure injury, proportion of new
ulcers developed within 30 days,
healing of existing pressure ulcers,
patient acceptability
30 days
Osterbrink,
2005 (Germany)
Patients from aged care facility,
acute care hospitals and home
care settings, aged greater than
18 years, at least one grade 2
pressure injury at a bony
prominence
RCT, Repose device (n = 28) vs.
Small cell alternating pressure
mattress (n = 12) vs. Large cell
alternating pressure mattress
(n = 10)
Wound healing success, weekly
changes in wound
Maximum
6 weeks
Russell, 2000 (UK) Patients from care of the elderly
units, existing grade 2 or greater
pressure injury
RCT, Alternating cell mattress
(Nimbus III) & cushion (Aura)
(n = 70) vs. Alternating cell mattress
(Cairwave) & cushion (Proactive 2)
Injury healing 18 month
follow-up
Russell, 2003 (UK) Hospital patients with
grade 1–2 ulcers
RCT, Alternating pressure mattress
(Nimbus III) (n = 83) vs. Fluid
overlay mattress (RIK static)
(n = 75)
Improved injury response,
length of hospital stay
Mean = 22 days
Strauss, 1991 (USA) Participants with at least one
grade 3–4, likely to require future
hospitalisations for pressure
ulcers, severely limited mobility,
aged over 16 years
RCT, Home air fluidised therapy
(CLINITRON) (n = 47) vs.
Conventional or standard
therapy (n = 50)
Pressure injury improvement,
pressure injury related
hospitalisations and costs,
pressure injury related
hospital days
36 weeks
E. McInnes et al. / International Journal of Nursing Studies 50 (2013) 419–430 425

E. McInnes et al. / International Journal of Nursing Studies 50 (2013) 419–430426
calculate the risk ratio or MD. Pooling of these studies wasnot appropriate due to heterogeneity regarding type ofsupport surfaces, comparators, patient characteristics,outcome measures and follow-up time of patients, there-fore we have reported results narratively.
A small trial involving 36 participants comparedsheepskin overlays with standard hospital mattresses ina geriatric care setting (grade of pressure injury notspecified) (Ewing et al., 1964a). Results favoured the use ofa sheepskin overlay in reducing redness and healingpressure injuries, however, no formal analyses wereperformed (Ewing et al., 1964a). Our analysis of ‘resolutionof redness’ favoured the sheepskin (RR 29; 95% CI 1.86–425.00). However, the confidence interval is very wide andthe trial was assessed as having a high risk of bias (Table 2).
A trial of 120 nursing home patients aged over 60 yearswith grade 3–4 pressure injuries (grading system notspecified), found no statistically significant difference ineffectiveness between a foam replacement mattress (45%healed) compared with a water mattress overlay (48%healed) (Groen et al., 1999). A total of 30 patients were lostto follow up (n = 19 foam replacement mattress, n = 11water mattress overlay), mainly as a result of severe illnessor discharge from the nursing home (Groen et al., 1999).We did not find a statistically significant difference in theproportion of pressure injuries completely healed betweenthe two groups (RR 0.93, 95% CI 0.63–1.37).
Twenty patients from long-term and subacute carecentres who were on bed rest and had grade 3 or greaterpressure injuries were randomised to a non-poweredmattress or a low-air-loss mattress (Branom and Rappl,2001). Study participants were followed-up for 8 weeksbut no data were provided by the study authors regardingnumbers lost to follow-up. The study authors reported thatthe rate of wound closure at the end of the study forpatients on the non-powered mattress was 9% (�4.8%)compared with 5% (�3.7%) for patients on the low-air-lossmattress (Branom and Rappl, 2001). The study did not reportwhether these results were statistically significant and thelack of data reported meant that we could not calculate themean difference in pressure injury healing.
3.2. Comparisons including high-tech constant pressure
support surfaces
Fifteen trials evaluated the effectiveness of high-techpressure support surfaces against other high-tech alter-nating-pressure mattresses and overlays, low-air loss beds,air-filled devices, dry flotation cushion, profiling beds andstandard therapies (Table 4) (Allman et al., 1987; Caleyet al., 1994; Clark and Donald, 1997; Day and Leonards,1993; Devine, 1995; Evans et al., 2000; Ferrell et al., 1993;Mulder et al., 1994; Munro et al., 1989; Nixon et al., 2006b;Osterbrink et al., 2005; Russell et al., 2000, 2003; Strausset al., 1991; Keogh and Dealey, 2001).
No statistically significant difference was foundbetween two different alternating mattresses in 41hospital patients with grade 2 or above pressure injuries(RR 0.57, 95% CI 0.26–1.27), or the number of pressureinjuries that decreased in size (RR 0.58, 95% CI 0.21–1.65)(Devine, 1995). A larger trial of 141 elderly patients with
pressure injuries grade 2 and above, also reported nosignificant differences in pressure injury healing andimprovement between two newer alternating-pressuredevices (see Table 2), one combined with four hourlyturning and use of a cushion and the other combined witheight hourly turning and use of a seating cushion (RR 0.99,95% CI 0.90–1.09). Participants were followed up for18 months. A total of 71 participants were lost to follow-up(n = 26 died and n = 45 did not complete the study). Co-interventions varied between the two groups (Russellet al., 2000).
In another study, participants from either a hospital ornursing homes with at least grade 2 pressure injuries, wererandomised to either an air-filled device or an alternating-pressure mattress (either small cell or large cell). The air-filled devices consisted of a range of air-filled productsincluding a mattress overlay, foot protectors and a wedgepillow. There were significant differences when examiningthe proportion of patients with completely healed pressureinjuries (Osterbrink et al., 2005) (RR 5.35, 95% CI 0.70–40.84).
No statistically significant differences were found inthree RCTs that evaluated various alternative pressuremattresses compared with different types of overlays(Evans et al., 2000; Nixon et al., 2006b; Russell et al., 2003).Pooled analysis was not possible due to differences in thedevices evaluated; the different outcomes and lack of datapresented. In one trial it was difficult to discern if the lackof treatment effect was due to either the non-effect of theexperimental device and/or because the co-intervention ofre-positioning frequency was not standardised, andpatients could request additional turning (Russell et al.,2003).
A small study of 25 patients with grade 2 and abovepressure injuries, compared a dry flotation with analternating pressure cushion. Three pressure injuries inthe alternating pressure cushion group and five pressureinjuries in the dry flotation group healed completely (Clarkand Donald, 1997); this difference was not statisticallysignificant (RR 0.47, 95% CI 0.14–1.56).
Four of the fifteen trials in this category compared theuse of a low air loss (LAL) bed with a foam overlay (Caleyet al., 1994; Day and Leonards, 1993; Ferrell et al., 1993;Mulder et al., 1994). These studies could not be pooled asthe pressure injuries under investigation were of differentgrades and healing rates were measured in different ways.Nursing home residents (n = 84) with a grade 2 or greaterpressure injury were randomised to a low-air-loss bed or afoam overlay with a foam mattress. No data were providedregarding numbers lost to follow-up. Statistically signifi-cant results favouring low-air-loss beds was reported inthe trial report for decreased time to healing (p = 0.0002),and a decrease in surface area (as measured by tracing thewound border) (p = 0.004) (Ferrell et al., 1993). However,our analysis found the result for proportion of woundscompletely healed was non-significant (RR 1.30, 95% CI0.87–1.96).
Another trial (Mulder et al., 1994) compared the effectsof a convoluted foam mattress overlay with a low-air-lossbed on a sample of 49 residents in 25 nursing homes whohad a grade 3 or 4 pressure injury (defined by the authors

as
imminfewegrostatparwagrasurbedweana
alloma(DainjuUlcPanlimfoll(n =a rInteperianinjusignthe
ovepreup
signof cTheor wins
westua spreexpinithadinjumeDeaanasigncom(RR
Stracom(n =(n =and(All
E. McInnes et al. / International Journal of Nursing Studies 50 (2013) 419–430 427
sized from 1.5 cm2 to 10 cm � 20 cm). Those withune deficiencies, inadequate nutritional status and
cted pressure injuries were excluded. Ten participantsre lost to follow-up (reasons not given, nor whichups to which these participants were allocated). Aistically significant reduction in pressure injury size inticipants randomised to the low-air-loss bed (p < 0.04)s reported. When adjusting for differences in the initialde of the injuries, it was reported that the percentageface area change was 77% higher for the low-air-loss
group; however, no p-values were reported and therere insufficient data reported for us to conduct anlysis (Mulder et al., 1994).The change in mean injury size in 77 patients who werecated to either an air suspension bed or a foamttress overlay was examined in a hospital based studyy and Leonards, 1993) Participants had pressureries grade 2–4 (NPUAP grading) (European Pressure
er Advisory Panel and National Pressure Ulcer Advisoryel, 2009) and activity during hospitalisation wasited to a chair or bed. There was a minimum 7-dayow-up with 35 participants being lost to follow-up
16 foam overlay group, n = 19 air-suspension group) asesult of death or being discharged from hospital.ntion-to-treat analysis does not appear to have been
formed. The authors reported that analysis of covar-ce (to remove possible bias from the difference in meanry size between the two groups) found no statisticallyificant difference in the healing of pressure injuries in
two groups (Day and Leonards, 1993).A comparison of a low-air-loss bed with a low-air-lossrlay in 93 hospital patients (hospital ward or includedssure injury grades not specified) who were followedfor 1 month or until discharged, reported no statistically
ificant difference between the two therapies in termshanges in surface area (p = 0.06) (Caley et al., 1994).re was no information regarding loss to follow-up rateshether intention-to-treat analysis was performed, and
ufficient data available for us to conduct analyses.The healing rates of existing grade 1 pressure injuriesre evaluated in a small convenience subgroup of largerdy comparing a profiling bed and a foam mattress withtandard hospital bed used in combination with assure relieving mattress. Study participants wereected to stay in bed for at least 12 h a day and onial assessment had a Waterlow score of 15–25 (that is,
a high to very high risk of developing a pressurery). Healing occurred in 4/4 patients in the experi-
ntal group and 2/10 of the control group (Keogh andley, 2001). The study authors did not report a statisticallysis of the healing data. Our analysis found thatificantly more grade 1 pressure injuries healedpletely in the patients receiving the profiling bed
5.00, 95% CI 1.45–17.27).Three trials (Allman et al., 1987; Munro et al., 1989;uss et al., 1991) evaluated air-fluidised devicespared with other devices. Air-fluidised therapy
31) was compared to conventional treatment 34) (two hourly turns, heel and elbow protectors alternating-pressure mattress) in surgical patientsman et al., 1987) Inclusion criteria included presence of
a pressure injury (all grades as measured using the Sheascale) on the sacrum, buttocks, trochanters or back, withmobilisation limited to a bed or chair for at least 1 weekand life expectancy of at least 1 week, and no skin graft orflap planned for the pressure injury within 1 week. Astatistically significant reduction in the median surfacearea of people in the air-fluidised group was reported;�1.2 cm3 (range: �38.0 to 15.5) compared with +0.5 cm3
(range: �55.1 to 94.7) in the conventional therapy group(p = 0.01). In addition, it was reported that there was astatistically significant decrease in the median surface areaof the pressure injuries that were greater than or equal to7.8 cm2 in size for patients randomised to the air-fluidisedtherapy (p = 0.01) (Allman et al., 1987). However, the lackof published variance data meant that we could notconduct an analysis. There was no evidence of intention-to-treat analyses.
A second trial investigated standard patient care(positioning or massage and sheepskins or gel pads underthe pressure injuries) compared with an air-fluidisedmattress by randomising 40 male hospital patients withgrade 2 and 3 pressure injuries, who weighed less than250 pounds and were expected to remain in hospital for atleast 15 days (Munro et al., 1989). No data regardingnumbers lost to follow-up were reported nor was thereinformation regarding whether an intention-to-treatanalysis was performed. A statistically significant decreasein pressure injury size in the intervention group at the 15-day follow-up was reported (p = 0.05) (Munro et al., 1989).There were insufficient variance data available from thestudy for us to calculate the mean difference between thetwo interventions.
The third trial was a home-based study whichcompared air-fluidised therapy with conventional therapy(which included alternating-pressure pads, air mattresses,water mattresses and foam pads and mattresses) inparticipants with at least one grade 3 or 4 pressure injury(Strauss et al., 1991). The trial authors reported that ahigher proportion of patients randomised to the air-fluidised therapy had pressure injuries classified as‘improved’ (Strauss et al., 1991), however, we found thatthis finding was not statistically significant (RR 1.23; 95%CI 0.84–1.86).
4. Discussion
A systematic review of trials examining the effects of avariety of support surfaces for treating existing pressureinjuries was undertaken. A major strength of this review isthat it is rigorous, having followed the methods outlined bythe Cochrane Collaboration (Higgins et al., 2011; Higginsand Green, 2009). Although systematic searches wereconducted to identify all relevant trials it is accepted thatno search strategy is infallible and, in common with allsystematic reviews, eligible unpublished trials may nothave been identified. Therefore the possible effect ofpublication bias on this review should not be discounted.Other strengths are the standardised and comprehensiveassessment of risk of bias, and that the sifting, selection,quality assessment and data extraction processes involvedtwo reviewers at each stage. Many of the trials in this

E. McInnes et al. / International Journal of Nursing Studies 50 (2013) 419–430428
review were conducted over 10 years ago and may haveevaluated technologies now no longer used or which havebeen modified. However, it is important for systematicreviews to report such results as older technologies maystill be used in some settings and countries.
The evidence base regarding the effectiveness of anypressure relieving device for the treatment of existingpressure injuries is limited and characterised by metho-dologically weak and under-powered studies. There is anabsence of evidence to support the superiority of anypressure relieving device in the treatment of pressureinjuries. Overall the trials were characterised by lowquality and small sample sizes. There was considerableclinical and methodological heterogeneity which meantthat we could not undertake pooled analysis. Theinconclusive findings of this review are congruent withfindings of another systematic review published in 2008which evaluated support surfaces for treating pressureinjuries (Reddy et al., 2008).
Two studies showed significant improvements inpressure injury healing following use of sheepskins (Ewinget al., 1964a) and profiling beds (Keogh and Dealey, 2001)but both trials were very small, not clearly reported, orwere appraised as being at high risk of bias. The studycomparing a non-powered mattress versus a low air lossmattress (Branom and Rappl, 2001) reported differencesfavouring the LAL mattress in treating pressure injuries butdid not report if these results were significant. In commonwith some other trials in this review, we could notreplicate the analysis because raw data were not reported.
Trials evaluating high-tech, air-fluidised therapy withstandard or conventional therapies (Allman et al., 1987)reported statistically significant reductions in mediansurface area and overall size of pressure injury, however,we regard this evidence as being unclear. While the Allmantrial3 was evaluated as being at low risk of bias (as a resultof having seven of the eight risk of bias categories classifiedas low risk), the results should be viewed with caution asthere was a high drop-out rate in the group allocated airfluidised therapy. The Munro trial was at high risk of bias,did not report baseline comparability for initial pressureinjury size nor wholly accounted for attritions and drop-out rates (Munro et al., 1989). In both of the studies,variance data was not reported so we could not replicatethe reported analyses. Our analysis of the third trial of air-fluidised therapy did not find the results to be statisticallysignificant (Strauss et al., 1991).
Differences in the reporting and measurement ofpressure injury healing outcomes also prevented poolingto allow estimation of effect size. Specifically, a range ofsubjective and objective methods were used to measurechange in injury size or volume, time to healing, rate ofhealing and number of patients with healed pressureinjuries. Subjective outcome assessments of wound healingby clinicians were used in six trials which relied onretrospective methods and judgements such as ‘better,worse or unsure’, to assess changes in size, severity or overallimprovement. Important variables such as the number ofinjuries healed or mean change in size of injuries were ofteninadequately reported. For example, not reporting thenumerator and denominator, only reporting the surface
area of the wounds as opposed to a more clinically significantvolume measure, omitting to report standard deviationalongside the mean, or selectively reporting statisticalanalysis for some outcomes such as comfort, healthcareresource utilisation but failing to report statistical analysis ofhealing outcomes was also a problem and suggestive ofpossible outcome reporting bias (Williamson et al., 2010).
It should also be noted that when assessing woundhealing outcomes, a criteria or definition of healing isnecessary (Cullum et al., 1999), and the lack of such adefinition was a common shortcoming of the included trials.In addition, the number of pressure injuries healed wasincluded in some trials as the outcome while in others thenumber of patients with healed pressure injuries was theoutcome and unit of analysis. This further complicatedcomparison of results across trials. We were unable toreplicate most comparisons because of the lack of differ-entiation of pressure injury grade or simply that there wasunclear data. Eight trials (44%) did not provide sufficientdata (numerator and denominator) to allow us to undertakeour own analyses. For one trial that reported significance,our analysis did not confirm this finding (Ferrell et al., 1993).
In some studies, it was not possible to separate outresults that included grade 1 pressure injuries (which arenot open wounds) from all other grades because the studyauthors had not differentiated the different grades.According to EPUAP guidelines, a grade one pressureinjury is defined as ‘non-blanching erythema’ (p. 9)(European Pressure Ulcer Advisory Panel and NationalPressure Ulcer Advisory Panel, 2009). This grade helps inidentifying those at risk of a more clinically significantpressure injury of a higher grade. Trials have demonstratedthat grade 1 pressure injuries may be reversible andtherefore while they may be recorded as a researchoutcome, they may disappear within a few hours (Halfinset al., 2001). However, a number of trials have identifiedmodels that would label a grade 1 injury irreversible andcould therefore progress to further skin breakdown(Maklebust and Sieggreen, 1996; Allman et al., 1995).Further research is therefore required to determine theextent to which resolution of grade 1 injuries is a valid andreliable outcome for treatment trials. Other shortcomingsof the included trials were related to the variability of thedifferent staging systems used to classify pressure injuriesacross trials and the fact that most of the trials undertakenwere under-powered. It should also be noted that the useof support surfaces is usually one strategy that is part of awound protocol consisting of a number of strategies forhealing pressure injury. However, there were importantvariables that were not considered and discussed by thestudy authors or which were not clearly reported in thestudies. These included patient turning schedules imple-mented concurrently with pressure reduction surfaces,thickness of foam mattress alternatives, type(s) of woundcare treatments being used for wound healing (i.e. thewound healing protocol used in addition to the supportsurface).
The evidence base in this field requires improving byundertaking robust trials to ascertain which supportsurfaces are most effective for the treatment of pressureinjuries. This should include clear descriptions of any

confor
arepreranclinpreinjusettgicadesshotriaimpshoadediffthaof theacomagepreabidurThethecosnat
5. C
be dof
injurepuse(dubasstatoveandpro
Con
Ack
in tcoc
Ref
Akb
Allm
E. McInnes et al. / International Journal of Nursing Studies 50 (2013) 419–430 429
current wound healing strategies and wound protocolsthe study groups as it is unlikely that support surfaces
used as the sole treatment modality in the event ofssure injury. Independent, well-designed, multi-centre,domised controlled trials are needed to compare theical and cost-effectiveness of different types ofssure relieving devices used to treat existing pressureries for patients at different level of risk, in a variety ofings. Future research should address the methodolo-l deficiencies associated with much of the research
cribed in this review and shown in Table 1. Patientsuld be truly randomised (with concealed allocation),ls should be of sufficient size to detect clinicallyortant differences as statistically significant and trialsuld have clear criteria for assessing outcomes and havequate follow-up. Pressure injuries of grade 1 should beerentiated from all other included pressure injuries sot analysis of the trials can investigate the true effect sizehe intervention. Validated measures of pressure injuryling are required to assist with standardisation andparability of results. Researchers should be encour-
d to develop measures to assess patient experiences ofssure relieving equipment, e.g. comfort and accept-lity and these outcomes along with reliability andability of the device should be measured in these trials.
trials should also have adequate follow-up and stratifyir results by pressure injury size. Evaluations of thet–benefit trade-off of pressure injury treatment alter-ives should also be undertaken.
onclusion
In summary, the firmness with which conclusions canrawn and guidance given to clinicians about the choice
support surface for the purpose of treating pressureries was hampered by the variable quality and poor
orting of many of the trials and the small sample sizesd, resulting in increased risk of false positive resultse to chance imbalances between treatment groups ateline) and false negative results (due to lack ofistical power). Nonetheless, we have provided anrview of the state of the evidence relating to this topic
have identified areas for further research to helpgress this field of research.
flict of interest
None declared.
nowledgement
This paper is based on a Cochrane review first publishedhe Cochrane library (McInnes et al., 2011a) (www.the-hranelibrary.com for information).
erences
ari Sari, A., Flemming, K., Cullum, N., Wollina, U., 2009. Therapeuticultrasound for pressure ulcers. Cochrane Database of SystematicReviews (3), http://dx.doi.org/10.1002/14651858.CD001275.pub2.
limitation. Journal of the American Medical Association 273, 865–870.
Allman, R.M., Walker, J.M., Hart, M.K., Laprade, C.A., Noel, L.B., Smith, C.R.,1987. Air-fluidized beds or conventional therapy for pressure sores. Arandomized trial. Annals of Internal Medicine 107, 641–648.
Australian Commission for Safety and Quality in Health Care (ACSQHC),2005. Adverse Event Rates Fact Sheet. Commonwealth of Australia.
Aziz, Z., Flemming, K., Cullum, N., Olyaee Manesh, A., 2010. Electromag-netic Therapy for Treating Pressure Ulcers. .
Banks, V., 1998. Nutrition and pressure area management. Journal ofWound Care 7, 318–319.
Berlowitz, D.R., Brandeis, G.H., Anderson, J., Brand, H.K., 1997. Predictorsof pressure ulcer healing among long-term care residents. Journal ofthe American Geriatrics Society 45, 30–34.
Berlowitz, D.R., Wilkin, S.V.B., 1990. Risk factors for pressure sores:acomparison of cross-sectional and cohort derived data. Journal ofthe American Geriatrics Society 37, 1043–1050.
Bianchetti, A., Zanetti, O., Rozzini, R., Trabucchi, M., 1993. Risk factors forthe development of pressure sores in hospitalized elderly patients:results of a prospective study. Archives of Gerontology and Geriatrics16, 225–232.
Bo, M., Massaia, M., Raspo, S., et al., 2003. Predictive factors of in-hospitalmortality in older patients admitted to a medical intensive care unit.Journal of American Geriatric Society 51, 529–533.
Branom, R., Rappl, L.M., 2001. ‘Constant force therapy’ versus low-air-losstherapy in the treatment of pressure ulcers. Ostomy Wound Manage-ment 46, 38–46.
Caley, L., Jones, S., Freer, J., Muller, J.S., 1994. Randomised prospective trialof two types of low air loss therapy. In: Proceedings of the 9th AnnualClinical Symposium on Pressure Ulcer and Wound Management,Nashville, TN, October.
Casey, G., 1997. Nutrition helps wound healing. Nursing New Zealand 3,19.
Casey, G., 1998. The importance of nutrition in wound healing. NursingStandard 13, 51–52.
Clark, M., Donald, I.P., 1997. A randomised controlled trial comparing thehealing of pressure sores upon two pressure-redistributing seatcushions. In: Proceedings of the 7th European European Conferenceon Advances in Wound Management, Harrogate, UK, 18–20November, pp. 122–125.
Clough, N.P., 1994. The cost of pressure area management in an intensivecare unit. Journal of Wound Care 3, 33–35.
Cullum, N., Deeks, J., Sheldon, T., Song, F., Fletcher, A., 2000. Beds,Mattresses and Cushions for Preventing and Treating PressureSores.
Cullum, N., Nelson, E.A., Nixon, J.E., 1999. Pressure Sores. Clinical Evi-dence. BMJ Publishing Group and American College of Physicians-American Society of Internal Medicine, London, pp. 785–791.
Cullum, N.A., Deeks, J.J., Fletcher, A.W., Sheldon, T.A., Song, F., 1995.Preventing and treating pressure sores. Quality in Health Care 4,289–297.
Day, A., Leonards, F., 1993. Seeking quality care for patients with pressureulcers. Decubitus 6, 32–43.
Devine, B., 1995. Alternating pressure air mattresses in the managementof established pressure sores. Journal of Tissue Viability 5, 94–98.
European Pressure Ulcer Advisory Panel & National Pressure Ulcer Advi-sory Panel, 2009. Prevention and Treatment of Pressure Ulcers: QuickReference Guide. National Pressure Ulcer Advisory Panel, Washing-ton, DC.
Evans, D., Land, L., Geary, A., 2000. A clinical evaluation of the Nimbus 3alternating pressure mattress replacement system. Journal of WoundCare 9, 181–186.
Ewing, M., Garrow, C., Presley, T., Ashley, C., Kinsella, N., 1964a. Furtherexperiences in the use of sheep skins as an aid in nursing. TheAustralian Nurses’ Journal (September), 215–219.
Ewing, M.R., Garrow, C., Presley, T.A., Ashley, C., Kinsella, N.M., 1964b.Further experiences in the use of sheep skins as an aid in nursing. TheAustralian Nurses’ Journal (September), 215–219.
Ferrell, B.A., Osterweil, D., Christenson, P., 1993. A randomised trial of lowair loss beds for treatment of pressure ulcers. Journal of the AmericanMedical Association 269, 494–497.
Fox, C., 2002. Living with a pressure ulcer: a descriptive study of patients’experiences. British Journal of Community Nursing 7, 10, 12, 14, 16,20, 22.
Franks, P.J., Winterburg, J.H., Moffatt, C.J., 2002. Health-related quality oflife and pressure ulceration assessment in patients treated in thecommunity. Wound Repair and Regeneration 10, 133–140.
Gallagher, S.M., 1997. Morbid obesity: a chronic disease with an impact
on wounds and related problems. Ostomy Wound Management 4318–24, 26–27.an, R., Goode, P., Patrick, M., Burst, N., Barolucci, A., 1995. Pressureulcer risk factors among acute care hospitalized patients with activity

E. McInnes et al. / International Journal of Nursing Studies 50 (2013) 419–430430
Girouard, K., Harrison, M., VanDenKerkof, E., 2008. The symptom of painwith pressure ulcers: a review of the literature. Ostomy WoundManagement 54 30–40, 42.
Gorecki, C., Brown, J., Nelson, E., et al., 2009. European Quality of LifePressure Ulcer Project group. Impact of pressure ulcers on quality oflife in older patients: a systematic review. Journal of AmericanGeriatric Society 57, 1175–1183.
Groen, H.W., Groenier, K.H., Schuling, J., 1999. Comparative study of afoam mattress and a water mattress. Journal of Wound Care 8, 333–335.
Halfins, R., Bours, G., Van Ast, W., 2001. Relevance of the diagnosis ‘stage 1pressure ulcer’: an empirical study of the clinical course of stage 1ulcers in acute care and long-term care hospital populations. Journalof Clinical Nursing 10, 748–757.
Hefley, M.L., Radcliffe, J., 1990. The 1988–1989 decubitus study. Can astandardization of treatment be set for the elderly patient withdecubiti ulcers stage III? Hawaii Medical Journal 49 346, 346–349, 350.
Higgins, J., Altman, D., On behalf of the Cochrane Statistical Methods Groupthe Cochrane Bias Methods Group, 2009. Chapter 8: Assessing risk ofbias in included studies. In: Higgins, J.P.T., Green, S. (Eds.), CochraneHandbook for Systematic Reviews of Interventions Version 5.0.2[updated September 2009]The Cochrane Collaboration (Available fromwww.cochrane-handbook.org).
Higgins, J., Altman, D., Sterne, J., 2011. Chapter 8. Assessing risk of bias inincluded studies. In: Higgins, J.P.T., Green, S. (Eds.), Cochrane Hand-book for Systematic Reviews of Interventions Version 5.0.1 [updatedMarch 2011]The Cochrane Collaboration (Available from www.co-chrane-handbook.org).
Higgins, J., Green, S., 2009. Cochrane Handbook for Systematic Reviews ofInterventions Version 5.0.2 [updated September 2009] The CochraneCollaboration.
Keogh, A., Dealey, C., 2001. Profiling beds versus standard hospital beds:effects on pressure ulcer incidence outcomes. Journal of Wound Care10, 15–19.
Krainski, M.M., 1992. Pressure ulcers and the elderly. Ostomy WoundManagement 38, 22.
Langemo, D., Melland, H., Hanson, D., Olson, B., Hunter, S., 2000. The livedexperience of having a pressure ulcer: a qualitative analysis.Advances in Skin and Wound Care 13, 225–235.
Lefebvre, C., Manheimer, E., Glanville, J., On behalf of the CochraneInformation Retrieval Methods Group, 2009. Chapter 6. Searchingfor studies. In: Higgins, J.P.T., Green, S. (Eds.), Cochrane Handbook forSystematic Reviews of Interventions Version 5.0.2 [updated Septem-ber 2009]The Cochrane Collaboration (Available from www.co-chrane-handbook.org).
Maklebust, J., Sieggreen, M., 1996. Pressure Ulcers: Guidelines for Pre-vention and Nursing Management. Springhouse Corporation, Spring-house.
McInnes, E., Dumville, J.C., Jammali-Blasi, A., Bell-Syer, S.E.M., 2011a. Sup-port surfaces for treating pressure ulcers. Cochrane Database of Sys-tematic Reviews (12), http://dx.doi.org/10.1002/14651858. CD009490.
McInnes, E., Jammali-Blasi, A., Bell-Syer, S., Dumville, J., Cullum, N., 2011b.Support surfaces for pressure ulcer prevention. Cochrane Database ofSystematic Reviews (4), http://dx.doi.org/10.1002/14651858.CD001735.pub4.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D., The PRISMA Group, 2009.Preferred reporting items for systematic reviews and meta-analyses:the PRISMA statement. British Medical Journal 339.
Moore, Z., Cowman, S., 2005. Wound Cleansing for Pressure Ulcers. .Moore, Z., Cowman, S., 2009. Repositioning for Treating Pressure Ulcers. .Mulder, G.D., Taro, N., Seeley, J., Andrews, K., 1994. A study of pressure
ulcer response to low air loss beds vs. conventional treatment. Journalof Geriatric Dermatology 2, 87–91.
Munro, B.H., Brown, L., Heitman, B.B., 1989. Pressure ulcers: one bed oranother? Geriatric Nursing 10, 190–192.
Nixon, J., Cranny, G., Iglesias, C., et al., 2006a. Randomised, controlled trialof alternating pressure mattresses compared with alternating pressureoverlays for the prevention of pressure ulcers: PRESSURE (pressurerelieving support surfaces) trial. British Medical Journal 332, 1416.
Nixon, J., Cranny, G., Iglesias, C., et al., 2006b. Randomised, controlled trialof alternating pressure mattresses compared with alternating pres-sure overlays for the prevention of pressure ulcers: PRESSURE (pres-sure relieving support surfaces) trial. British Medical Journal 332,1413–1415.
Nixon, J., Nelson, E.A., Cranny, G., Iglesias, C.P., Hawkins, K., Cullum, Na,et al., 2006c. Pressure relieving support surfaces: a randomisedevaluation. Health Technology Assessment 10 iii–iv, ix–x, 1–163.
Orlando, P.L., 1998. Pressure ulcer management in the geriatric patient.Annals of Pharmacotherapy 32, 1221–1227.
Osterbrink, J., Mayer, H., Schroder, G., 2005. Clinical evaluation of theeffectiveness of a multimodal statis pressure relieving device. In:Journal of Wound Healing European Wound Conference ‘‘From theLaboratory to the Patient: Future Organisation and Care of ProblemWounds’’, September, pp. 15–17.
Pase, M.N., Hoffman, R.G., 1998. Selection and use of risk assessment toolsand treatment protocol in extended care facilities in the southwest.Journal of Wound Ostomy and Continence Nursing 25, 44–50.
Phillips, L., Buttery, J., 2009. Exploring pressure ulcer prevalence andpreventative care. Nursing Times 105, 34–36.
Posnett, J., Gottrup, F., Lundgren, H., Saal, G., 2009. The resource impact ofwounds on health-care providers in Europe. Journal of Wound Care18, 154–161.
Prior, J., 2002. The pressure is on: midwives and decubitus ulcers. RCMMidwives Journal 5, 196–200.
Reddy, M., Gill, S., Kalkar, S., Wu, W., Anderson, P., Rochon, P., 2008.Treatment of pressure ulcers: a systematic review. Journal of theAmerican Medical Association 300, 2647–2662.
The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen.Ronda, L., Falce, R.L., 2002. Skin care in older people. Primary Health Care
12, 51–57.Russell, L., Reynolds, T.M., Carr, J., Evans, A., Holmes, M., 2000. Rando-
mised controlled trial of two pressure-relieving systems. Journal ofWound Care 9, 52–55.
Russell, L., Reynolds, T.M., Towns, A., Worth, W., Greenman, A., Turner, R.,2003. Randomized comparison trial of the RIK and the Nimbus 3mattresses. British Journal of Nursing 12, 254–259.
Scottish Intercollegiate Guidelines Network, 2009. Search filters. http://www.sign.ac.uk/methodology/filters.html#random.
Spoelhof, G.D., 2000. Management of pressure ulcers in the nursing home.Annals of Long Term Care 8, 69–77.
Strauss, M.J., Gong, J., Gary, Bd., Kalsbeek, W.D., Spear, S., 1991. The cost ofhome air-fluidized therapy for pressure sores. A randomized con-trolled trial. Journal of Family Practice 33, 52–59.
Thomas, D.R., Goode, P.S., Tarquine, P.H., Allman, R.M., 1996. Hospitalaquired pressure ulcers and risk of death. Journal of the AmericanGeriatric Society 44, 1435–1440.
Vanderwee, K., Clark, M., Dealey, C., Gunningberg, L., Defloor, T., 2007.Pressure ulcer prevalence in Europe: a pilot study. Journal of Evalua-tion in Clinical Practice 13, 227–235.
VanGilder, C., Amlung, S., Harrison, P., Meyer, S., 2009. Results of the2008–2009 international pressure ulcer prevalence survey and a 3-year, acute care, unit-specific analysis. Ostomy Wound Management55, 39–45.
Waltman, N.L., Bergstrom, N., Armstrong, N., Norvell, K., Braden, B., 1991.Nutritional status, pressure sores, and mortality in elderly patientswith cancer. Oncology Nursing Forum 18, 867–873.
Williamson, P., Blazeby, J., Altman, D., Clarke, M., 2010. Core reporting ofoutcomes in effectiveness trials. Cochrane Methods (Suppl. 1).
Woodbury, M., Houghton, P., 2004. Prevalence of pressure ulcers inCanadian healthcare settings. Ostomy Wound Management 50, 22–24, 26, 28, 30, 32, 34, 36–38.




















