Treating Crohn's With Diet - The Jewish Press
40
Fighting the Common Cold and Flu By Blanche Reiss INTRODUCTION It is that time of year again when we see “Flu Shots” signs appearing in every pharmacy win- dow and doctor’s office. As the weather turns cooler, we scramble for ways to prevent and fight the common cold and flu. As of now, there is no cure for the common cold or for the flu, but a lit- tle knowledge can go a long way in helping to prevent these nasty infections and fight them off successfully. WHAT CAUSES THE COMMON COLD AND FLU? Colds and flus are both caused by viruses, and may cause some similar symptoms. The common cold is primarily caused by a rhinovirus that invades the upper half of the throat behind the nose. The symptoms, such as excess mucous and watering eyes, are the result of the body’s attempt to fight off the cold virus. The flu is caused by influenza vi- rus A or B. The more common influenza A virus has many types such as H1N1. Some types are more November 2011 A Publication of Medicaid and Home Care: The Next Generation Dealing with the Effects of Medicaid Re-design By: Martin Schwartz CEO of Stay At Home Solutions Assisting families in need of Medicaid and Medicaid services like home care was almost an ex- act science until April 2011. Since April the new regime in Albany, headed by Governor Cuo- mo, has made changes to Medic- aid eligibility criteria and has im- posed restrictions on home care agencies regarding the amount of Medicaid services they can pro- vide to their patients. NY State has the ability to do this because Med- icaid is partially funded by the State, therefore the federal law that established Medicaid gave in- dividual states control over issues that impact their cost. Regarding Medicaid eligibili- ty, many New York State residents over the last decade or more, with the assistance of Elder Care Attor- neys, created life estates. A life estate is when a person in need of Medicaid either transfers the deed to their home to another person(s) or places the home into an irrevocable trust but maintains the right to live in the home for the rest of their life. By doing so, the Medicaid consumer protect- ed the proceeds of any future sale of the home from Medicaid recov- ery. This life estate was honored by Medicaid until mid-Septem- ber. Now, the NYS government has reversed this policy by direct- ing Medicaid to inform consumers that, in its opinion, a person with a life estate is reaping the bene- fits of the home by maintaining Treating Crohn’s With Diet By Yaakov Kornreich We have all been raised in a culture which we are taught to believe in the “miracles of modern medicine.” We trust that when a doctor gives us a pre- scription for a new medicine, or tells us that we need an opera- tion, his advice represents the best that medical science has to offer. But sometimes, when it becomes clear that medical science is up against a health problem that it does not under- stand, and cannot effectively treat, even the most rational pa- tient has no choice but to turn to other approaches to uncon- ventional methods of dealing with that problem. That is clearly the case with Crohn’s disease, a form of in- flammatory bowel disease with a wide variety of debilitating symptoms which can some- times extend beyond the gas- tro-intestinal tract. The disease was named after American gastroenterologist Burril Ber- nard Crohn, who described its symptoms in 1932. Crohn’s dis- ease apparently has a genetic component, because it has be- come disproportionally preva- lent among Ashkenazic Jews, and in the yeshiva communi- ty in Israel. Crohn’s can be difficult to di- agnose and differentiate from other digestive ailments, such as irritable bowel syndrome (IBS). The most common symp- toms are intensive and recur- ring bouts of gastric pain and distress, and an inability of the intestines to properly digest their food, leaving their bod- ies starved for nutrients. Even- tually, the damage done by the disease will cause portions of the intestines to close up, cre- Continued on p.34 Continued on p.20 Continued on p.16 See page 39 A Member of the Beth Abraham Family of Health Services that, in its opinion, a person with Special Special Feature Feature Turning 65 Turning 65
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Treating Crohn's With Diet - The Jewish Press
Fighting the Common Cold and Flu
By Blanche Reiss
INTRODUCTIONIt is that time of year again when we see “Flu
Shots” signs appearing in every pharmacy win-dow and doctor’s offi ce. As the weather turns cooler, we scramble for ways to prevent and fi ght the common cold and fl u. As of now, there is no cure for the common cold or for the fl u, but a lit-tle knowledge can go a long way in helping to prevent these nasty infections and fi ght them off successfully.
WHAT CAUSES THE COMMON COLD AND FLU?
Colds and fl us are both caused by viruses, and may cause some similar symptoms. The common cold is primarily caused by a rhinovirus that invades the upper half of the throat behind the nose. The symptoms, such as excess mucous and watering eyes, are the result of the body’s attempt to fi ght off the cold virus. The fl u is caused by infl uenza vi-rus A or B. The more common infl uenza A virus has many types such as H1N1. Some types are more
November 2011A Publication of
Medicaid and Home Care: The Next Generation Dealing
with the Effects of Medicaid Re-designBy: Martin Schwartz
CEO of Stay At Home Solutions
Assisting families in need of Medicaid and Medicaid services like home care was almost an ex-act science until April 2011.
Since April the new regime in Albany, headed by Governor Cuo-mo, has made changes to Medic-aid eligibility criteria and has im-posed restrictions on home care agencies regarding the amount of Medicaid services they can pro-vide to their patients. NY State has the ability to do this because Med-icaid is partially funded by the State, therefore the federal law that established Medicaid gave in-dividual states control over issues that impact their cost.
Regarding Medicaid eligibili-ty, many New York State residents over the last decade or more, with the assistance of Elder Care Attor-neys, created life estates. A life estate is when a person in need of Medicaid either transfers the deed to their home to another person(s) or places the home into
an irrevocable trust but maintains the right to live in the home for the rest of their life. By doing so, the Medicaid consumer protect-ed the proceeds of any future sale of the home from Medicaid recov-ery. This life estate was honored by Medicaid until mid-Septem-ber. Now, the NYS government has reversed this policy by direct-ing Medicaid to inform consumers
that, in its opinion, a person with a life estate is reaping the bene-fi ts of the home by maintaining
Treating Crohn’s With DietBy Yaakov Kornreich
We have all been raised in a culture which we are taught to believe in the “miracles of modern medicine.” We trust that when a doctor gives us a pre-scription for a new medicine, or tells us that we need an opera-tion, his advice represents the best that medical science has to offer. But sometimes, when it becomes clear that medical science is up against a health problem that it does not under-stand, and cannot effectively treat, even the most rational pa-tient has no choice but to turn
to other approaches to uncon-ventional methods of dealing with that problem.
That is clearly the case with Crohn’s disease, a form of in-flammatory bowel disease with a wide variety of debilitating symptoms which can some-times extend beyond the gas-tro-intestinal tract. The disease was named after American gastroenterologist Burril Ber-nard Crohn, who described its symptoms in 1932. Crohn’s dis-ease apparently has a genetic component, because it has be-come disproportionally preva-lent among Ashkenazic Jews,
and in the yeshiva communi-ty in Israel.
Crohn’s can be difficult to di-agnose and differentiate from other digestive ailments, such as irritable bowel syndrome (IBS). The most common symp-toms are intensive and recur-ring bouts of gastric pain and distress, and an inability of the intestines to properly digest their food, leaving their bod-ies starved for nutrients. Even-tually, the damage done by the disease will cause portions of the intestines to close up, cre-
Continued on p.34
Continued on p.20
Continued on p.16See page 39
A Member of the Beth Abraham Family of Health Services
that, in its opinion, a person with
Special Special FeatureFeatureTurning 65Turning 65
2 | November 2011 HEALTH LIVING

November 2011 | 3HEALTH LIVING
Supplement Publisher Moshe Klass [email protected]
Senior EditorYaakov Kornreich [email protected]
Associate EditorIta Yankovich
Mental Health Consultant Chaim SenderEditorial Staff
Dana Ledereich and Tova RossContributing Writers
Sheryl Mayer, Esther HornsteinSales
David Hoppenwasser at [email protected] Urman at [email protected]
Seasonal Mood Disorder
Whether it is called the ‘Winter Blues,’ ‘Season-al Aff ect Disorder’ or simply SAD -“Seasonal Mood Disorder,’ it is a subtype of depression. It is a seri-ous disorder that aff ects half a million people ev-ery winter. It is due to shorter days and increased darkness, which causes a biochemical imbalance in the brain leading one to feel unhappy.
WHO GETS IT?It is estimated that 6 in every 100 peo-
ple will experience SAD. Women are more susceptible to SAD, especially stay at home mothers with young children who are stuck indoors. People residing in northern coun-tries/states are also more sensitive due to the extended deprivation of natural light. The further one lives from the equator, the high-er the chances of becoming depressed dur-ing winter months. One study reported that people living in New Hampshire were seven times more likely to suffer than people from Florida. People who work the night shift or in building without windows are also more likely to suffer depression. Interestingly, the average age of a SAD patient is 23.
SYMPTOMSThose suff ering from SAD frequently exhibit
symptoms such as over-eating, chronic fatigue and oversleeping, weight gain, social isolation and a general feeling of hopelessness. These symptoms return every year if left untreated.
TREATMENT It is important to get a physical exam to rule
out other medical issues before a diagnosis of SAD can be confi rmed.
Sometimes the solution can be as simple as spending more time outdoors. A brief walk out-side during the sunniest time of day can be as
Table of Contents
Continued on page 38
Medical and Health News 4-5
Issues - Op EdsEthical Issues in Organ Transplants . .6
Taxing Unhealthy Food . . . . . . . . . . .7
Raising Our Childrewn
Melatonin for Sleep Disorders . . . . . .8
Importance of Folic Acid . . . . . . . . . .9
Jews Opting Out of Vaccines? . . . . .10
Preschool ADHD . . . . . . . . . . . . . . .11
Golden YearsMedication Management . . . . . . . . .14
Paying for Healthcare . . . . . . . . . . .17
Helping ‘Uncle Sam’ During Retirement . . . . . . . . . . . . . .18
Understanding Part D Drug Benefits . . . . . . . . . . . . . . . . . .19
L’Chayim to LifeRun For Your Life . . . . . . . . . . . . . . .21
Aneurism Screening . . . . . . . . . . . .22
Blood Thinning . . . . . . . . . . . . . . . .23
Creepy Crawlers . . . . . . . . . . . . . . .24
Skimping on Healthcare . . . . . . . . .25
Mind, Body & SoulTalking to Mourners . . . . . . . . . . . .26
Half Shabbos . . . . . . . . . . . . . . . . . .27
Relationship Boundaries . . . . . . . . .28
Am I Being Abused? . . . . . . . . . . . .29
Teenage Depression . . . . . . . . . . . .30
TMS Alternative Therapy . . . . . . . . .30
Shana Rishona . . . . . . . . . . . . . . . .31
Communicating For Real . . . . . . . . .32
Messages for Yourself . . . . . . . . . . .33
Directory Advertising . . . 35-37
Health Provider Bulletin . . 36-38
At A Glance . . . . . . . . . . . . . . . . 3-38
Health & Living Checklists. . . . . . . . . . . . . . . . 38
From the Doctor’s Desk . 39
At a Glance

4 | November 2011 HEALTH LIVING
Diabetes Affects Astonishing Number of PeopleThe International Diabe-
tes Federation reports that an estimated 366 million peo-ple around the world suffer with diabetes. It is estimated that diabetes causes 4.6 mil-lion deaths each year. Health systems spend $465 billion each year to fi ght the disease, including both Type 1 and Type 2.
Diabetes is a metabol-ic disease in which a person has higher blood sugar than normal, either because the body does not produce enough insulin on its own – Type 1 – or the cells do
not respond to the insulin produced – Type 2. Those high blood sugar levels cause symptoms such as fre-
quent urination, increased thirst, and increased hun-ger. Over an extended peri-od time, uncontrolled diabe-tes can cause a variety of se-rious medical problems, in-cluding blindness and loss of blood circulation in the feet.
Type 1 diabetes, which used to be known as juvenile dia-betes, is, in part, inherited and then triggered by certain in-fections. It is usually diagnosed early in life. Type 2 diabetes,
also known as adult onset diabetes, is due to lifestyle factors, such as diet and obesity, and genetics.
Have Back Pain? Book a Massage at the Nearest Spa
The National Institutes of Health reports that most job-related disabil-ity leaves are relat-ed to low back pain. Back pain is so se-vere that after head-aches, it is the sec-ond biggest culprit behind neurologi-cal complaints.
What can help alleviate chronic low back pain? Ac-cording to a new study by the Annals of Internal Medi-cine, getting regu-lar massages may be the answer. 400 people with chronic low back pain (with the cause unable to be identifi ed) were divided into three groups: one group received medical care for back pain without massage; the second group re-
ceived a relaxation or Swedish massage one hour a week for ten weeks; and the
third group, which received structur-al massage, specif-ically targeting tis-sues and joint struc-tures, also for one a hour a week for ten weeks.
B o t h g r o u p s who received some type of massage, rather than tradi-tional medical treat-ment, reported fee-ing better and the abi l i ty to move around more eas-ily than the group that received the
traditional form of care. The study con-cludes that further research is needed to understand the benefi ts of massage for chronic low back pain conditions.
Lowering Salt Intake Does Not Lead to
Lower Death RatesAn analysis of several studies
found that low-salt diets or reduc-ing overall salt intake does not lead to lower risks for cardiovascular heart attacks and death. The report, pub-lished in the American Journal of Hy -pertension, found that while patients in the studies – those who had high blood pressure and those with nor-mal blood pressure – on reduced-salt diets lowered their blood pressure, there was no signifi cant diff erence in mortality rates.
Doctors said that these results in-dicated that further investigation is needed, since previous studies have linked lower salt intake and lower mortality rates. Some have question whether the total number of patients in these studies, – 6,250 – was not large enough to dispute the results of previous studies that showed health benefi ts from reduced-salt diets.
Medical and Health NewsCOMPILED BY TOVA ROSS, ITA YANKOVICH AND STAFF
Smelly? Might not be Your Fault!The American Journal of Medicine
fi nds that a common genetic disor-der, known as “fi sh-odor syndrome” may be the culprit behind some peo-ple’s unexplained body odor. The dis-order is called trimethylaminuria, and is caused by emitting too much of the compound known as trimethly-amine (TMA).
TMA—which has a strong fi shy odor – is produced when we eat foods rich in
choline, such as some fi sh, eggs, liv-er and soy and kidney beans. When a defect in the gene FMO3 is pres-ent, it causes trimethlyaminuria, and prevents the body’s ability from me-tabolizing TMA properly and turn it into odor-free compounds.
Because the disorder is rare, only a few laboratories in the Unit-ed States conduct the test neces-sary to diagnose suff ers.
Drug-Resistant Forms of TB Spreading Rapidly in Europe
The World Health Organiza-tion (WHO) reports that drug-resis-tant forms of tuberculosis (TB) are spreading rapidly throughout Eu-rope, and unless quick action is tak-en to halt the epi-demic, thousands of people will die.
TB currently kills around 1.7 million people each year. The infection is caused by the bacterium My-cobacterium tuber-culosis and destroys patients’ lung tis-sue. This causes them to cough up the bacteria, which is then spread through the air, leaving others vul-nerable to inhaling it. Once they con-tract the disease and start coughing, they will spread it to others the same way.
15 of the 27 countries with the highest burden of multidrug-resis-tant TB (MDR-TB) are in the WHO’s Eu-ropean region. London has the high-est TB rate of any capital city in West-
ern Europe. It reports about 3,500 cases of TB diagnosed each year, and 2 percent of those are multidrug-re-sistant. Treatment for MDR-TB can cost over $15,000 in drugs alone, and up to over $200,000 in hospital stays, medical care and other related costs.
November 2011 | 5HEALTH LIVING
Medical and Health News continued
Are We Relying Too Much on Cancer Screening?
False positives are a common out-come in many cancer screening tests. In fact, about three of every 10 mam-mograms and about seven of every 10 positive PSA tests result in false alarms. Many people are eager to un-dergo cancer screenings, so that they can rest easy knowing they are being proactive in guarding their health, but the frequency of false positives does raise questions about the idea that screening tests are a surefire weapon against cancer.
We have been taught that early detection of cancer is the best form of prevention. That is why 75% of men over the age of 50 have had a prostate specifi c antigen (PSA) test; 67% of women over the age of 40 have had a mammogram in the past two years; and 55% of women get a Pap smear every year. However, new studies have ignited a debate over whether these tests can sometimes do more harm than good.
Recently, the U.S. Preventive Ser-vices Task Force (USPSTF), a govern-ment-appointed scientific advisory board, recommended against routine PSA tests to screen for prostate cancer. The same panel also suggested that a Pap test every three years is as good as an annual test. Two newly published studies suggest reducing the number of mammograms in women under 50; one went so far as to conclude that “most women with screen-detected breast cancer have not had their life saved by screening. They are instead either diagnosed early (with no eff ect on their mortality) or overdiagnosed.” The reason for this is because studies
have found tests such as PSA, mam-mogram and the Pap smear are less than ideal screeners.
Many patients have been scared literally to death by the outcome of their PSA tests when all along studies have shown that the levels of pros-tate specifi c antigen (the marker for prostate cancer) can be elevated for a variety of other reasons. A mammo-gram can be read as suspicious due to a cyst, a benign fl uid collection; a Pap smear is often reported as abnor-
mal due to abnormal cells caused by a local infection rather than cancer.
The tests are also potentially harmful. They lead to subsequent testing such as a biopsy, which can cause complications such as infec-tion or lead to treatment of a can-cer that would not have otherwise caused any harm.
Researchers are pursuing a variety of improvements for cancer screen-ing tests, including one for prostate cancer that tracks blood calcium lev-els following a PSA test and another that tests urine for a genetic marker, but such tests are years away from being available to the general public.
This does not mean that we should avoid cancer screening tests, but that they should be limited to those who may be at higher risk of certain can-cers because of their age, family histo-ry or presenting symptoms. Similarly, people need to know that a positive outcome from one of these tests is not necessarily a cause for alarm.
Doctors need to address requests for testing for each patient differ-ently.
Red Wine: A Toast to Overall Health
Red wine has been known to off er a bounty of health benefi ts, but now, for the fi rst time, it has been proven and shown to benefi t the body’s metab-olism, reduce blood sugar and pres-sure, triglycerides, cut-ting the accumulation of fat in the liver, and boosting the effi ciency of muscles.
The study involving 11 obese but healthy men found that taking a relatively low dose of resveratrol, (contained in trace amounts in red wine), daily for a month produced a variety of fundamental beneficial effects on their metab-olism.
Resveratrol appeared to protect mice from obe-sity and diabetes, boost the animals’ physical en-durance, reduce their chances of suff ering the ill eff ects of obesity and extend their lives. Such fi ndings prompted some scientists to speculate that the presence of trace amounts of resveratrol in red wine might help explain the “French paradox,” which is that even though the French consume a relatively rich
diet, their life expectancy does not suf-fer because of it.
Some people have even started tak-ing resveratrol, which is sold over-the-counter in health and grocery stores.
But the benefi ts and risks for people taking large doses of reveratrol for long periods of time remain unknown, and some scientists have questioned the validity of some of the early research.
Cocaine Cupcakes?According to recent medical re-
search, cupcakes and other pro-cessed foods and sugary drinks may be just as addictive as cocaine.
Brain scans of obese people and compulsive eaters reveal distur-bances in brain reward circuits sim-ilar to those experienced by drug abusers.
These findings can be detrimen-tal to the $1 trillion food and bever-age industries since if indeed such foods and beverages are found to be addictive then food companies may face the most drawn-out consumer safety battle since the anti-smoking movement took on the tobacco in-dustry a generation ago.
It is natural for our bodies to crave sugars and fats, but what’s changed is modern processing that creates food with concentrated levels of sug-ars, unhealthy fats and refined flour, without redeeming levels of fiber or
nutrients, obesity experts say. Con-sumption of large quantities of those processed foods may be changing the way the brain is wired.
Those changes look a lot like ad-diction to some experts. Addiction “is a loaded term, but there are as-pects of the modern diet that can elicit behavior that resembles addic-tion,” said David Ludwig, a Harvard researcher and director of the New Balance Foundation Obesity Pre-vention Center at Children’s Hospi-tal Boston. Highly processed foods may cause rapid spikes and declines in blood sugar, increasing cravings, his research has found.
The food industry is fighting back by refuting these findings. Swansea University psychologist David Ben-ton recently published a 16-page rebuttal to sugar addiction studies. The paper was partly funded by the World Sugar Research Organization.
6 | November 2011 HEALTH LIVING
Issues - Op Eds
New Organ Transplant Guidelines Raise Ethical Questions
By Joel Berman
One of the most diffi cult moral aspects of organ transplantation is the fact that in many cases, the organ donor must be de-clared clinically dead before the life-saving surgical procedure can begin. For example, surgeons performing a heart transplant operation must wait for a period of time before beginning to make sure that the donor’s heart doesn’t spontaneously start beating again. However, any delay in the re-implantation damages the transplanted heart and reduces the chances of success.
Another moral consideration in the current transplant procedures is the re-quirement to wait until a potential do-nor’s doctors and family members have given up on attempts to save them be-fore beginning any preparations for the procedure.
But the success of cardiac transplant operations in saving patients with failing hearts has put the system under stress be-cause the demand for hearts to transplant now far outstrips the supply. As a result, there are 6,000 Americans who die each year while waiting for an organ transplant.
Family members of patients who are waiting for a lifesaving organ transplant have put pressure on the United Network for Organ Sharing (UNOS), which man-ages the national organ transplant sys-tem for the federal government, to loos-en some of the requirements to qualify as an organ donor.
The issues involved are not simple. Ev-eryone agrees that it would be immoral to take a vital organ from a donor who is not yet dead, but that raises the ques-tion of how we defi ne death. That stan-dard has changed over the years. Histor-ically, the standard was the cessation of the heartbeat, which today is known as “cardiac death.” But that standard was changed in the 1970s, when the medical establishment adopted brain activity as the new determining factor as to whether someone is alive or dead. Since then, the guidelines have called for most organ do-nors to be brain-dead before transplant activities can be started.
But as the demand for life-saving or-gan transplants increased, doctors in the 1990s began advocating a revision of the guidelines to allow transplants to be ini-tiated even before all brain activity has ceased, as long as the heart has stopped beating. This procedure is called “dona-tion after cardiac death,” or DCD, and it has become a growing source of organs used for transplants in recent years.
DCD involves harvesting the organs surgically within minutes after respira-tors and other forms of artifi cial life sup-port have been turned off for patients who no long have a heartbeat, but who are not yet clinically “brain dead.” Candi-dates for DCD are in intensive care after suffering irrecoverable brain damage, due to a car accident or stroke, for ex-ample, but whose brains still show some neurological activity.
The National Academy of Scienc-es concluded in 1997 that DCD was ethical as long as there were suffi-ciently strong protections in place to make sure that the best interests of both the organ donor and their fami-ly members were being respected, and that their wishes were being followed: Guidelines were established to make sure that the decision to withdraw life support must be made independently of the decision to donate organs. The original recommendation also insisted that surgeons must wait at least five minutes after the heart stops before removing any organs, as a precaution against the possibility that the heart could start beating again spontane-ously. But since then, the standard for the minimum amount of time sur-geons must wait has been gradually reduced to two minutes.
Some doctors would like to see the delay shortened even further. At the Children’s Hospital Colorado in Denver, surgeons reduced the waiting period to only 75 seconds before removing hearts from brain-damaged newborn babies to be transplanted into infants. But that touched off such an uproar of objections that the hospital was forced to aban-don the practice and is again requiring
its surgeons to resume waiting at least two minutes.
The additional few minutes of de-lay can mean the difference between the success or failure of the transplant, and the life or death of the organ re-cipient. That is why doctors are seek-ing to find new ways to start perform-ing the transplant as soon as the donor has been declared cardiac dead. One program in Pittsburgh is trying to seek-ing ways to start the transplant proce-dure on patients who have died while they are still in the emergency room. Another program in New York City is exploring the possibility of perform-ing the organ-retrieval procedure in ambulances on potential donors who have been declared dead at the scene of an accident.
The 16-page draft proposal for the new transplant guidelines was published this spring by the UNOS organ procure-ment organization committee. Its 22 members developed the new recom-mendations over the course of a year of deliberations. After waiting for comments from concerned outside parties, the orga-nization is now in the process of fi nalizing the new rules for transplant procedures throughout the United States.
The new guidelines would do away with a specifi c amount of time that trans-plant surgeons must wait to declare car-diac death, leaving that determination to the doctors on a case-by-case basis.
Gail Van Norman, who is a bioethi-cist at the University of Washington, said that according to the new UNOS guide-lines, “every hospital in America can now develop its own defi nition of ‘dead,’ and that is profoundly disturbing. . . . We are, it seems, admitting that we are willing to
take the chance of procuring organs from someone who is not dead yet.”
Those who support the changes in the transplant rules claim that they are simply catching up with the current state of medical knowledge and prac-tice. They also argue that the new guide-lines help to satisfy the wishes of those do who want to donate their organs af-ter their deaths.
“The ultimate goal is to facilitate the dying wishes of patients who wish to be donors and save the lives of the 112,000-plus patients who are in need,” said Charles Alexander, the immediate past president of UNOS. “We are always very aware of our public trust.”
However, opinion within the medical community on the changes in transplant rules is divided. Robert Veatch, a George-town University bioethicist, who serves on the separate, 31-member UNOS eth-ics committee, says that at a recent com-mittee meeting in Chicago, there was an emotional discussion over whether the medical state of DCD patients real-ly should be considered “irreversible.” He called the debate, “a remarkably heat-ed battle.”
Michael A. Grodin, a professor of health law, bioethics and human rights at Boston University suspects the mo-tives of the transplant community say-ing, “The bottom line is that they want to do everything they can to increase or-gan donation.”
They new UNOS guidelines also iden-tify certain types of patients, such as those with severe spinal cord injuries, and terminal diseases such as muscu-lar dystrophy and ALS (Lou Gehrig’s dis-ease), as potential organ donors before they reach the end stage. Critics worry that this will encourage doctors to sub-tly pressure these into voluntarily fore-going the most heroic medical measures in order to gain access to their organs for transplant that much sooner.
Critics of the new UNOS standards say that they increase the risk that potential organ donors will be treated more like liv-ing human tissue banks than critically sick patients who deserving every chance to live, or to have their wishes to die peace-fully respected.
“This change in policy creates the ap-pearance that the patient is always be-ing evaluated as a possible donor, which I think would make the public uneasy, and rightfully so,” said Leslie Whetstine, a Walsh University associate professor of medical ethics.

November 2011 | 7HEALTH LIVING
Taxing Unhealthy Foods A Jewish Perspective
By Yaakov Kornreich
Chocolate lovers and connoisseurs of rich desserts despaired last month when the new conservative govern-ment of Denmark made headlines around the world by instituting a “sin tax” on fattening foods. The tax kicks in on any food item sold in Denmark whose saturated fat content exceeds 2.3%. In practical terms, it adds about 12 cents to the cost of a bag of potato chips, and about 40 cents to the retail price of a hamburger.
The concept of placing special tax-es on unhealthy foods is not new to Denmark nor is it unique. The Danes were already paying special taxes on sugary items like soda and candy. Denmark may be the fi rst country to specifi cally target saturated fats in the diets of their citizens as a revenue en-hancement opportunity, but it won’t stay unique for very long. Finland and Romania have already started looking into levying similar taxes of their own.
Sin taxes, of course, are not new. In theory, they are meant to create an incentive against bad behavior. Per-haps the most extreme case is the spiraling tax on cigarettes. The tax works, to a certain extent, because most teenagers and low income peo-ple simply can’t aff ord to pay $9 for a pack of cigarettes that cost less than a dollar not that many years ago. But for someone who is chemically ad-dicted to nicotine, the price does not matter. They simply have to have that smoke. It would be another matter if medical science had a safe and reli-able means to help smokers to “kick the habit.” But it doesn’t. They are a captive audience.
The same thing is true when it comes to fighting the obesity epi-demic. The sad truth is that there is no single “magic bullet” that can help us to easily get rid of the excess weight that none of us really want. Diets are too hard to stick with. The pills don’t work, and gastric bypass surgery, aside from being expensive and po-tentially dangerous, also requires a signifi cant change in eating habits in order to succeed in the long run.
Also, since new studies show that some kinds of unhealthy foods can be as addictive as cigarettes or even drugs, it is unlikely that simply by making those foods more expensive by taxing them we will be able to win the war against obesity.
In the end, there is only one reli-able way for any of us to lose weight. It’s the answer that none of us wants to hear – exercising more self control. You don’t really have to read the nutri-tion label on a bag of potato chips to know that its contents aren’t healthy for you, or look at the calorie counts that are now listed by law in New York City on the menu when you walk into an ice cream store. For the most part, we instinctively know what we should or should not be eating, but most of us don’t really care enough to control our impulses. That is the main rea-son why it is never a good idea to go shopping for food when you are feel-ing hungry.
But in this area, religious Jews do have a real advantage. From our ear-liest years, we have been raised to control our impulses when it comes to the kinds of food we are allowed to eat. We have had it drummed into our heads, and ultimately our hearts, that there are certain kinds of foods that we cannot eat at all, and others that we can only eat at certain times. If we want to have a dish of ice cream, we will wait six hours (OK, maybe just fi ve and a half ), after we fi nish our meat meal. And when we go on a road trip, and need to go into the McDonald’s at the turnpike rest area for a cup of coff ee to stay alert behind the wheel, we are not even tempted by the sight and smell of all the treif food that is also on sale there.
An even better example is Pesach, when for 8 days, we adopt a far more restrictive diet than the rest of the year, to avoid chometz.
About 20 years ago, when I be-came really determined to lose a sig-
nifi cant amount of weight, I decided to try the then new Atkins diet, even though I had heard all kinds of hor-ror stories about how hard it was to stay on it. I then hit upon an easy so-lution. I decided to pretend that all of the foods that the Atkins diet forbids were actually “treif,” and for a while, it worked. Over a period of two months, I dropped 20 pounds, and was actual-ly able to go out and buy new clothes a couple of sizes smaller than what I had been wearing before.
But it was too good to last. I
couldn’t help but remember that those foods that Atkins forbade real-ly weren’t “treif,” which caused me to start to cheat... but just a little. Then a Yom Tov came... and you know how my diet ended.
So what is the moral of this story?Most religious Jews, when asked
why they observe kashruth, answer simply because it is a mitzvah. Yes, there have been all kinds of studies over the years showing the health benefi ts from eating only kosher food. But that is not why a religious Jew can walk away from a cheeseburger with-out a second thought.
Our dedication to our faith makes the very idea of eating treif food un-thinkable, and gives us the strength to control our physical impulses.
So let us take that idea one step further. There is another mitzvah in the Torah which should help us to control our impulses to eat unhealthy foods, even the ones that are kosher. It is the mitzvah which instructs us to protect our lives - ushmartem es naf-shosaychem.
That means that maybe I did fi nd the right answer to my own obesity 20 years ago, because, in light of that mitzvah, unhealthy foods really are treif after all.
Issues
SUBMISSION INFORMATION
Health & Living invites readers to submit Letters to the Editor. Letters will be selected for publication at
the sole discretion of the editor, and may be edited for size and content.
Submissions become the proper-ty of The Jewish Press. Please e-mail
your Letter to the Editor to [email protected]

8 | November 2011 HEALTH LIVING
Using Melatonin to Treat Sleep Disorders in Children
By Dana Ledereich
Sleep is essential for the body’s health and growth. It plays a vital role in promoting physical health and emo-tional well-being for both adults and children. It is associated with better attention and mental acuity through-out the day. Sleep promotes healing in the body and so is essential for op-timal health and recovery from a sick-ness or injury.
The amount of sleep required var-ies from child to child. An infant sleeps an average of 14-15 hours; a day; a tod-dler/preschooler sleeps 12-14 hours; a school-age child sleeps 10-12 hours and an adult averages 7-9 hours. These ranges include total sleep throughout a 24-hour period – both nighttime sleep and naptimes.
The best indicator of whether your child is getting enough sleep is to ob-serve his behavior during the day. A
sleep-deprived child will most likely be-come cranky as fatigue sets in. His per-formance in school may suff er and he will have difficulty focusing attention on his school work. A tired child may
also appear clumsier. Oftentimes, sleep deprived children are hyperactive. Their bodies release adrenaline to help keep them going during the day. This makes it harder for them to fall asleep at night and thus perpetuates the cycle. A child who is not getting enough sleep will most like-ly have to be awakened in the morning.
Sleep cycles are regulated by the body’s internal clock. Circadian rhythms control your body’s natural sleep and wakefulness on a 24-hour cycle. Mel-atonin is a hormone produced by the pineal gland that helps to regulate the body’s sleep/wake cycle. Typically, the body produces more melatonin later in the day. Higher levels are maintained throughout the night and drop off in the morning.
Melatonin is also available as a non-prescription food supplement and can be purchased in many health food stores. It is frequently used by adults to help treat insomnia as well as to promote daytime sleep in people who work the night shift, or to minimize the eff ects of jetlag. Studies have shown supplemental melatonin to be safe for adults when taken in low-doses, even for long term usage. It is recommend-ed that one consult with your doctor before taking supplemental melatonin.
Some parents give supplemental melatonin to their children who have diffi culty falling asleep. They report that their children typically fall asleep with-in 20-30 minutes of ingesting the sup-plement, but there is not yet suffi cient research to support the safety of such treatment for young children. Some doctors report Melatonin to be safe for teenagers when used for short periods of time, but there is no research on the
safety of giving Melatonin to toddlers, preschoolers or school-aged children.
Children normally produce a suf-fi cient amount of Melatonin to regu-late their sleep cycles. If a child is hav-ing diffi culty falling asleep, it is more ef-fective to investigate what other prob-lem may be contributing to his diffi cul-ties and address it. Creating a consis-tent bedtime routine is the most wide-ly recommended approach to promote good sleep habits. Putting your child to bed at the same time each day also helps to maintain natural sleep cycles. Refrain from exercise, television, video games, computer and phone usage an hour before bedtime since it can make it more diffi cult for a child to fall asleep. Consider limiting these activities in the later part of the evening. Finally, caff ein-ated drinks can also disrupt sleep. On the other hand, children benefi t from a glass of warm milk and a light, healthy snack before bed as part of their routine.
Because we don’t know the long term eff ects, the use of Melatonin by young children should be closely mon-itored. It’s important to remember that while Melatonin may help your child fall asleep faster, it does not address the un-derlying reason as to why he or she is having diffi culty falling asleep. Even if Melatonin is ultimately recommended and used, it’s important to investigate the underlying causes of the sleep dis-turbances and work on establishing fi rm bedtime routines to promote bet-ter sleep habits.
It’s also important to keep in mind that sufficient amounts of sleep do vary between children. While a par-ticular child may fall asleep later than most children his age, a child who falls asleep on his own and wakes up inde-pendently and refreshed in the morn-ing is most likely getting enough sleep.
Dana Ledereich, MA, OT/L is a pe-diatric occupational therapist who works in Yeshiva of Flatbush and also maintains a private practice. She evaluates and treats children age birth-13 years with sensory pro-cessing issues, poor handwriting, developmental concerns and neuro-logical issues. She has lectured to both parents and professionals on various topics in sensory processing and handwriting development. She is available for lectures as well as to mentor new therapists. She can be reached at 718-252-2939.
Raising Our Children
HUGE SALE GOING ON NOW!

November 2011 | 9HEALTH LIVING
The Importance of Folic Acid in Early PregnancyBy Dana Ledereich
One of the most diffi cult symptoms in the fi rst few months of pregnancy is morning sickness, which for many women, can last all day. Under these circumstances, it can be a challenge to keep anything down, let alone the horse pills that doctors prescribe - oth-erwise known as prenatal vitamins!
The truth is, prenatal vitamins bene-fi t the mother more than the baby – es-pecially at the beginning of a pregnan-cy. The growing baby takes the nutrients that it needs directly from the mother’s body. To the woman who eats a bal-anced diet and supplements it with a regular dose of prenatal vitamins, they are simply replacing the nutrients that her fetus is draining from her. But the woman whose diet is lacking in essential nutrients and who does not take a sup-plemental vitamin is at risk for vitamin defi ciencies as a result of her pregnancy.
Prenatal vitamins contain the recom-mended daily allowance for a multitude of vitamins and nutrients. In the fi rst tri-mester, the most essential of these vita-mins is Folic Acid, otherwise known as Folate. Folic Acid has been found to re-duce the incidence of neural tube de-fects by up to 70%.
An expectant mother’s body needs folic acid by the third week of pregnan-cy, when the embryo begins to form the neural tube which develops into the ner-vous system. If the neural tube does not close completely, the baby is born with a neural tube defect, such as spinal bifi -da, which usually results in some form of paralysis. Other forms of neural tube defects can result in paralysis and/or im-paired cognitive function. Some forms of neural tube defects carry with them a severally shortened life expectancy.
The good news is that folic acid has
been found to severally reduce the in-cidence of neural tube defects. The problem is that the fetus needs the folic acid before the mother is even aware that she is pregnant! Most neural tube birth defects occur in the third and four week of pregnancy. But most women don’t take over-the-counter pregnancy tests until several days after missing a regular menstrual period. By that point they are nearly fi ve weeks pregnant – two weeks after neural tube formation!
Because of this, doctors recommend that women take folic acid supplements even before they become pregnant. Since nearly 50% of pregnancies are unplanned, doctors recommend that ALL women of childbearing age take folic acid supplements on a regular ba-sis. This way, in the event a woman be-comes pregnant, her body is already prepared and fortifi ed with folic acid.
To underline the importance of folic acid, the FDA requires that it be used to fortify all enriched cereals, breads, rice and pastas. Other foods which are nat-urally high in folic acid include:
• Bananas• Oranges and orange juice• Broccoli, spinach and other green
leafy vegetables• Asparagus• Dried beans• Peanuts and other nuts• PeasEven with these natural sources, it
can be diffi cult to consume a diet with enough folic acid to reap the gestation-
al benefi ts. Doctors recommend that all women of childbearing years – wheth-er or not they plan to become pregnant, take at least 400mg of folic acid daily and not to exceed 1000 mg. Pregnant wom-an should continue to take folic acid for at least the fi rst three months of preg-nancy, and some studies have demon-strated added benefi ts from taking folic acid even further into pregnancy.
Despite all the strong and convinc-ing evidence of the extreme impor-tance of folic acid during the begin-ning weeks of pregnancy, it can be a challenge for an expectant mother to convince themselves to swallow those behemoth pills during the “morning sickness months.” Some doctors rec-ommend that their patients reduce the frequency for taking prenatal vita-mins to every other day in order to re-duce the potential nausea side eff ect. If one does not take a prenatal vita-min on a daily basis, it is essential for women in this age category to take a daily folic acid supplement, which, for-tunately, are tiny and typically do not cause nausea. In this way, we can be-gin to provide for our children even be-fore we have them!
Raising Our Children continued
• Short-Term Rehab & Long-Term Care
• Under Frum Ownership & Operation
• Judaic Library for Study and Leisure
• Tehilim Groups
• Weekly Bikur Cholim Visits
• Special Shiurim Delivered by Inspiring Guest Speakers
• Special Monthly and Holiday Events
• NEW! Torah Conferencing Network Shiurim for Residents and the Community
• Shabbos Programming
Dr. Zeitlin, Medical Director
Under the VAAD Horabanim of Queens (VHQ)
78-10 164th Street, Fresh Meadows, New York
For further information please contact Akiva Goldstein 718.591.8300 Ext. 248
FEATURING
The Chai Traditions Program™Created in 2004, our extensive experience servicing the Jewish
resident has allowed us to build an exclusive community resource
MMEADOW PARKREHABILITATION & HEALTH CARE CENTER
den
a.g
rap
hix
718
.701
.112
5
Watch our Video & Virtual Tour at
www.mprcare.com
Drinking Raw Milk Linked to Lower Rates of Asthma in Children
A recent study from Europe fi nds that children who drink raw milk are less like-ly to develop asthma and allergies than those children who drink pasteurized milk.
The study, published in the Journal of Allergy and Clinical Immunology, theorizes that certain milk proteins (whey proteins such as BSA and alpha-lactalbumin) that are destroyed by heat during the pasteur-ization process could be benefi cial to chil-dren’s developing immune systems.
However, researchers are wary to rec-ommend drinking raw milk, as it may also cause serious health risks due to the pos-sible presence of harmful microorgan-isms. In 2008, there was an outbreak of
E. coli in Connecticut that was linked to drinking raw milk. Four people were hos-pitalized with severe illness because of it.
Researchers looked at a large survey in which parents answered questions about their children’s milk consumption, and collected 800 milk samples from those participants’ homes. They found that compared to children who drank only store-bought milk, those who drank raw milk had a 41 percent reduction in their chances of developing asthma. They were also half as likely to develop hay fever.
In the United States, more than seven percent of adults and an even higher per-centage of children have asthma.

10 | November 2011 HEALTH LIVINGRaising Our Children continued
Avoiding The Needle: Can New York Jews Opt Out Of Vaccination?By Esther Hornstein, L.Ac.,
Dipl. Ac.
When Louis Pasture tested the fi rst rabies vaccine for humans in 1885, a major breakthrough in preventative medicine was achieved. Since then, the medical community has endeav-ored to expand the practice of vac-cination to cover every isolatable pathogen.
However, in October, 1915, an ar-ticle published in the British medical journal, Lancet reported on a study of 21 cases of tetanus, in which each patient had received Pasteurian in-oculation against the disease. The conclusion of the article was that in every case, the tetanus had been caused by the inoculation. Its au-thor, Dr. Montais, said that “Pasteur had created a new form of disease.” Other doctors, however, disagreed, and claimed that in those 21 cases, the immunity provided by the vac-cine had diminished so much over time that it could no longer prevent the disease.
The combined measles, mumps and rubella vaccine (MMR) was fi rst licensed for use in the U.S. in 1971.
In 1998, Lancet published a contro-versial article by Andrew Wakefi eld, which claimed that the MMR vacci-nation was the cause of autism spec-trum symptoms in 12 children. Wake-fi eld’s article was retracted from Lan-cet in February 2010 due to the many ethical and clinical errors he made while conducting his study and in-terpreting his results. Even though Wakefi eld’s research has been widely discredited in the mainstream med-ical community, it was influential
enough to shake the faith of some parents in the immunization proce-dure, and to decide not to allow their children to be vaccinated at all with the MMR vaccine.
Under U.S. constitutional law no one has the authority to force one to undergo a medical procedure, such as vaccination. Nevertheless, the conse-quence of U.S. children avoiding im-munizations, aside from possible risk of serious diseases, is being denied acceptance into school.
This policy has been the cause of much debate. On one hand, public health offi cials argue that allowing a child into school without vaccination creates a risk of spreading these dis-eases to or from the other children with whom they will come into con-tact. On the other hand, the act of rejecting an unvaccinated child into school is seen as a method of uneth-ical coercion by the government on the parents to “force” them to have their child vaccinated.
In order to satisfy the rights of those parents who want to avoid the vaccination of their children, each of the states has been given the author-ity to institute specifi c vaccination ex-emptions which allow children to en-ter school without immunizations.
When parents, decide against vac-cinating their child they must justify their choice according to the recog-nized medical, religious or philosoph-ical reasons specifi ed in the exemp-tions allowed in each state.
Most states resist giving parents a blanket vaccination exemption. All states allow medical exemptions to those whose children are immuno-compromised, severely ill or have ana-phylactic allergic reactions to compo-nents of vaccines.
Forty-eight states allow religious exemptions. Mississippi and West Vir-ginia only allow medical exemptions. Eighteen of the fi fty United States al-low vaccination exemptions based on
philosophical beliefs. New York State does not permit exemptions based on any philosophical beliefs.
HOW MANY ARE OPTING OUT?
Only 0.99% of American children obtained non-medical vaccination ex-emptions in 1991. Since then, there has been a huge increase in exemp-tions to 2.54% in 2004. The states that instituted a personal belief exemp-tion have made it simpler to opt out than others, but critics of that poli-cy contend that it makes it too easy for parents to avoid vaccinating their children purely as a matter of conve-nience.
HOLDING CREED IN NEW YORK
There are a number of Christian sects, such as Christian Science, and other schools of belief, such a Scien-tology, which do not permit children to be vaccinated.
However, according to New York State law, a parent does not need to prove that they are a “bona fi de member” of one of these organiza-tions in order to use its objections to vaccination as a reason for exempt-ing their child from the vaccination requirement.
To take advantage of the exemp-tion permitted by the New York State law, the family must describe how their sincere religious beliefs are con-trary to allowing vaccinations.
JEWISH JUSTIFICATION FOR NOT VACCINATING
For religious Jews, the wording of the state law allows one to combine his or her own personal philosophies with psukim that can infer that vacci-nations are against that family’s re-ligious beliefs. “Lo S ertzach, (Do Not Kill)” has been used in a number of ar-guments. One such argument is that some elements of vaccines are known to be carcinogenic, and could theo-retically lead to death. Another is that many vaccines are researched and de-veloped with the use of material ob-tained from aborted fetuses and thus using those vaccines is a substantia-tion of elected fetal death. “Shamor et Nafshecha Meod , (Guard Your Life Greatly),” could also be utilized to show a religious basis for one’s reli-gious belief that vaccines are not for his or her child.
On the other side of this dispute, there are local doctors serving the re-ligious community who are adamant in their insistence that all school age
TRUST US. WE CARE
LOSE 3-7 INCHES IN ONLY 2 WEEKS
ZERONA
4918 Ft. Hamilton Pkwy. Brooklyn, NY 11219 www.inchknocker.com 10 Min. from Belt Pkwy;
5 Min. from Ocean Pkwy
718.972.1500
Clinically proven body slimmingLose stubbon fat off your waist, hips and thighsZERO pain, ZERO downtime,ZERO Surgery
15% OFF TO JUMPSTART YOUR DIET
RESTRICTIONS APPLY
FDA APPROVED
Continued on p.11

November 2011 | 11HEALTH LIVINGRaising Our Children continued
children who do not have specific medical risk factors should be immu-nized for the protection of all. They fear that excessive use of the available legal exemptions by parents could lead to avoidable epidemics in our community, such as the recent mea-sles outbreak, and the unnecessary deaths of children.
I recently made a survey of 15 boys and girls yeshivas in the Brooklyn area as to their policy towards unvaccinat-ed children that have NYS vaccine exemptions. The majority of schools stated that if the child had a NYS ex-emption they would be accepted to school. One school indicated that it had 2 children currently with a mat-ter of exemption on fi le. Some schools had never been approached about the issue and would have to make an
admission decision on a case by case basis. And, of course, some schools didn’t want to speak to “the press.”
As the fi erce dispute over the safe-ty of vaccines continues, we should be aware that the rights of both sides are being protected. Whereas Jewish New Yorkers seeking exemptions from im-munizations for their children may run into hindrances from local schools, they may nonetheless endeavor and succeed in implementing the choices they make for their children.
Esther Hornstein is a New York State licensed acupuncturist and diplomat in acupuncture, practicing in Brooklyn, NY. She is a mother of 2 and a graduate of Pacifi c College of Oriental Medicine. She has par-ticipated in acupuncture research in Lutheran Medical Center, labor and delivery and in hospital projects in NYU Hospital for Joint Diseases. In her practice she addresses pediat-ric ailments, woman’s health, pain management and overall wellness.
52 Madison Ave. Lakewood, NJ 08701 Ph: 732.905.2055 Fax: 732.905.4030
www.lakewoodcourtyard.com
Chanah Daina, CALADirector of Marketing
732.865.8130
R. G
RO
SS
MA
N 7
18.6
77.6
757
We’ve just added the Wii Exercise Program to our already diverse activities calendar!
Music Entertainment, Aerobics Exercise, Shopping Trips, Discussion Groups, Manicures, Baking, Health Lectures, Crafts, Bingo, Jewelery Making, Shiurim, Cultural Outings, Art, Food Decorating, Card Games... & Many More
Keeping both mind and body active
“WiiJuvinating” our recreation department
A GLATT KOSHER
Assisted & Independent
living community
Avoiding The Needle: Can New York Jews Opt Out Of Vaccination?
Continued from p.10
New Treatment Guidelines Approving ADHD Medication for Preschoolers
By Dana Ledereich
The American Academy of Pediat-rics (AAP) recently issued new treat-ment guidelines for 4-5 year old pre-schoolers who are diagnosed with Attention Deficit Hyperactivity Dis-order.
Children with ADHD exhibit a range of symptoms that include rest-lessness, difficulty maintaining at-tention both in the classroom and with independent work, impulsivi-ty, impatience and disorganization. It is one of the most common neu-robehavioral conditions of child-hood, affecting about 8 percent of children. Boys are three times more likely than girls are to be diagnosed with the disorder.
Treatment for ADHD utilizes a combination of behavioral therapy and prescription medication. The stimulant most commonly used to treat ADHD is methylphenidate and sold under brand names like Ritalin and Concerta. Previously, that drug was not approved for use with chil-dren under the age of 6, but the new treatment guidelines from the AAP changes that.
Treatment guidelines for ADHD recommended methylphenidate for children as young as 4 when neces-sary, based on numerous studies that
found the drug to be effective for the preschool sect, though results are better in children over the age of 6. In a study done by the National In-stitutes of Mental Health, preschool-ers were found to require only low doses of the medication, increasing as they grew older. The preschool-ers were also found to be more sen-sitive to side effects from the medi-cation than were older children. The 303 children involved in the 10 week study suffered side effects including slower growth rate, weight loss, in-somnia, loss of appetite, moodiness and skin-picking behavior. 10% of study participants dropped due to the severity of the side effects.
The new AAP guidelines for ADHD treatment in preschoolers empha-size exploring other treatment op-tions before turning to medication, which is only recommended after other interventions, such as behavior management techniques and parent training, have failed. The guidelines recommend that medication should be used in conjunction with behav-ioral intervention, and medication is only recommended for preschoolers with moderate to severe symptoms.
The AAP feels that diagnosing and treating ADHD at a younger age provides the children with great-er chances of succeeding at school.
Critics say that recommending medi-cation gives parents an option to the preferred cure of aggressively pursu-ing behavioral interventions and life-style changes. They also say it can be difficult to distinguish between what may be exuberant but still normal ac-tivity in a 4-5 year old and true ADHD. An incorrect diagnosis can lead to in-tervention that is inappropriate and even harmful when not warranted.
Parents should explore the many other treatment options for ADHD before resorting to medication. One of the best alternatives to medica-tion has been the implementation of Occupational Therapy, which has been found to be an effective form of treatment for children with mild symptoms and can assist in their symptom management. Other ef-fective forms of treatment include changes in diet, specifically to ex-clude sugary sweets and processed foods, frequent exercise for those exhibiting symptoms of hyperactiv-
ity, lifestyle changes, parent training and behavioral therapy. The new AAP guidelines allow for medication, but only as a last resort for children with moderate to severe symptoms who cannot effectively function in a class-room and who don’t respond to oth-er treatments. It is a tool that parents can use to help their child succeed in school, but only when all else fails.
Dana Ledereich, MA, OT/L is a pe-diatric occupational therapist who works in Yeshiva of Flatbush and also maintains a private practice. She evaluates and treats children age birth-13 years with sensory pro-cessing issues, poor handwriting, developmental concerns and neuro-logical issues. She has lectured to both parents and professionals on various topics in sensory processing and handwriting development. She is available for lectures as well as to mentor new therapists. She can be reached at 718-252-2939.

12 | November 2011 HEALTH LIVING
Golden Years
You’re Never Too Old for Exercise
Most people think that exercise is primarily for younger people, and that as you grow older, it is no longer nec-essary or appropriate. Medical experts disagree, and recommend that any-one who is over the age of 50 and does not have a fi tness regimen, had better start one.
According to Tom Prohaska, a pro-fessor of public health and aging at the University of Illinois at Chicago, many older adults “don’t think they are ca-pable of exercising or exercising safe-ly” because of the conditions of old age, such as arthritis, hypertension and heart disease. In fact, he said, studies show that 95 percent of older adults, can work out safely if they do it in the right way.
Another problem is the mistaken conviction of many seniors that they won’t benefit from exercise. “Some people don’t realize... that the things
they attribute to normal aging are re-ally because they aren’t physically fi t,” says Prohaska.
According to the National Institute on Aging (NIA), only 25 percent of peo-ple between the ages of 65 to 74 exer-cise regularly. For those aged 85 and older, the participation rate is just 11 percent. But according to Chhanda Dut-ta, the NIA’s chief of the clinical geron-tology, exercise can help people at that age in many ways. “There’s so much more to life than simply being able to dress yourself,” he added.
The NIA has launched a Go4Life campaign to help all Americans over the age of 50 to start or continue ex-ercising. “I think that a lot of people may not know where to begin,” Dut-ta says. “This campaign shows people that there are ways they can incorpo-rate exercise and physical activity into their busy lives.”
The NIA’s Web site is an integral part of the eff ort. It off ers information on specifi c exercises designed for se-niors, as well as motivational tips, ad-
vice, health and nutrition information. There are also programs designed for the homebound, for the chairbound, and for people recovering from a health setback.
Walking is one of the most popular exercises for seniors. The NIA recom-mends pairing up with a walking part-ner to make the experience more en-joyable.
Another health organization pro-moting the benefi ts of walking is Kai-ser Permanente. It recently launched an Every Body Walk! campaign promot-ing walking’s advantages as the easi-est, most aff ordable and most accessi-ble form of regular exercise. At a Walk-ing Summit held at Kaiser Permanente’s Center for Total Health, in Washington, DC, presenters said that walking can im-prove the quality of life almost instantly, curing depression, strengthening social bonds and reducing health-care costs.
Life-long exercise has many bene-fi ts, in addition to maintaining cardio-vascular fi tness- it preserves a senior’s strength, balance and fl exibility, pre-
vent heart disease, high blood pressure diabetes, and may even help to main-tain mental agility.
There are other things you can do to stave off memory loss, according to clinical psychologist Cynthia Green, the author of “30 Days to Total Brain Health.” Playing computer games can be use-ful, especially those which force you to compete against a clock. Research has also shown that certain cognitive training techniques can help people to absorb information such as names and passwords and to remember them longer. Other memory tools include or-ganizers and to-do lists that can help you keep track of appointments and errands. Maintaining social connec-tions with family and friends on a reg-ular basis can also reduce the risk of memory loss.
Finally, to reduce the risk of develop-ing Alzheimer’s disease and cognitive impairment, researchers at Rush Uni-versity Medical Center in Chicago found that it helps for older people to have a strong sense of purpose in their lives.
used in combination with the
Jaw Rehabilitation ProgramJaw Rehabilitation Programprovides a powerful tool for
developing biting and chewing skills.
For more information callSpeech Pathology Associates, LLC Speech Pathology Associates, LLC
at 207-741-2443207-741-2443
visit us on the web at www.ChewyTubes.comwww.ChewyTubes.com
or
Cen
tral D
esig
n 73
2-94
2-07
46

November 2011 | 13HEALTH LIVINGGolden Years continued
More Evidence Shows Aspirin Effective at Preventing Cancer
Add yet another entry to the long and still growing list of uses for one of the most popular medications in the world- plain, old aspirin. A new study whose results were reported in the British medical journal, The Lan-cet, found that taking two full strength (300 milligram) aspirin tablets a day by people who suff er from Lynch syn-drome cuts their risk of contracting colon cancer by 60 percent.
Lynch syndrome is a genetically in-herited condition which aff ects about one in 1,000 people. About half of them will develop colon, endometrial and ovarian cancers before the age of 45. It was previously known as hered-itary nonpolyposis colorectal cancer (HNPCC), and is believed to be respon-sible for about 3% of all cases of co-lon cancer. The study tracked 861 car-riers of Lynch syndrome for four years.
“Results of this study support as-pirin use for people with Lynch syn-drome, in addition to regular colo-noscopies as recommended by their
health care provider,” said Eric Jacobs, strategic director of pharmacoepide-miology for the American Cancer So-ciety. “However, aspirin use can have side eff ects and should be discussed with a health care provider.” He not-ed that aspirin use is not presently recommended for cancer prevention “because even low-dose aspirin can increase the risk of serious stomach bleeding.” Such bleeding is relatively rare (about 1 in 1000) through mid-
dle age, but the incidence increases sharply after the age of 75.
The fi ndings of the Lynch syndrome study are consistent with a 2010 re-port on a much larger study by Ox-ford University which showed the ef-fectiveness of aspirin in reducing the risk of dying from various forms of can-cer. That study tracked 25,000 patients who took one low dose (75 milligram) aspirin tablet daily for between four and eight years, and found an over-
all reduction in the cancer death risk of more than 20% from some of the most common cancers, for both men and women. That study found a risk re-duction of about 40% for colon cancer, 30% for lung cancer, 10% for prostate cancer and 60% for esophageal cancer.
The results of the Oxford study has prompted other researchers to investi-gate the potential for aspirin to reduce the risk of death from breast cancer.
Aspirin has long been known for a variety of therapeutic eff ects. It acts as an analgesic to relieve minor aches and pains, it reduces fever, cures head-aches and is an anti-infl ammatory. It is also eff ective in preventing the forma-tion of blood clots, which can cause strokes and heart attacks.
Its chemical name is acetylsalicyl-ic acid, and it was fi rst discovered in 1853 by French chemist Charles Fred-eric Gerhardt. Its synthesized form was patented by the German Bayer Com-pany which renamed it aspirin and be-gan silleingit around the world in 1899.
14 | November 2011 HEALTH LIVINGGolden Years continued
Medication ManagementBy Mutty Burstein
Medications can work wonders—they can prevent and control ill-ness, relieve pain and fight infection. However, if they’re taken incorrectly or in the wrong combination, med-icines can also cause serious prob-lems. If you are age 65 or older, you may take more medicines now than ever before. Two-thirds of adults age 65 and older use one or more med-ications each day, and one-quarter (25%) take three medications daily. This is why it is so important to be responsible when it comes to med-ications.
The first thing is to know the names of your medications and why you are taking them. An important point to be aware of is medications can interact with one another and possibly cause sickness or death. Drug interactions can also occur when taking over-the-counter (OTC) medications with prescription drugs. For example, taking two blood thin-ners, or anticoagulants, such as war-
farin (Coumadin) and gink-go (or aspirin, vitamin E, or fish oil) together may cause excess bleeding. Make sure you add OTC drugs to your medication sheet. Before taking a new OTC drug, be sure to ask your doctor or pharmacist to check for po-tential interactions with your usual medications. If possible, have all your prescriptions filled by one pharmacy. This allows your pharmacist to check any new medication for possi-ble interactions with your other medications.
Make sure you read the medicine label and pack-age inserts. I f you have difficulty reading and un-derstanding the label, ask a friend, relative or phar-macist for help. You may need to keep a magnify-ing glass handy to read some of the small warning
labels put on prescription bottles. Make sure you tell your doctor about all the medicines you are present-ly taking, the medication strength, why you are tak-ing it, and who prescribed it. Be sure to include all pre-scription and nonprescrip-tion medicines, as well as dietary supplements, such as vitamins, minerals and herbals. This is especial-ly important if your doctor wants to prescribe a new medication. The more your doctor knows, the more he or she can help you. Be sure you understand all in-structions before leaving the doctor’s office or the pharmacy. Sometimes you might want to write down the instructions for future reference.
Medications are large-ly safe, but like anything else, accidents can happen.
November 2011 | 15HEALTH LIVINGGolden Years continued
Since millions of prescriptions are filled in hos-pitals and pharmacies every year, medication errors, like someone receiving the wrong dose of a medication or the incorrect medication en-tirely, are among the most common medical er-rors. The Institute of Medicine estimates that medication errors hurt at least one million peo-ple each year. Through proper medication man-agement, accidents can be averted. While hos-pitals, nursing homes, and other care facilities often have mechanisms in place to try and pre-vent medication errors, homecare is the setting where a systematic medication review can of-ten be made most efficiently. Clients often get their medications from several different physi-cians and have their prescriptions filled at nu-merous pharmacies so medication reviews at the point of purchase are not always effective. Fur-ther, home health agencies are ideally situated to do reviews as their services are often covered as a Medicare benefit following hospitalization. Contacting a Certified Home Health Agency, al-lows you or your loved one to safely take med-ication while remaining in the comfort of your own home. A licensed nurse will ensure medica-tion safety while coordinating care with you or your loved one’s physician. A nurse can help ed-ucate the patient, family members or care giv-ers about the different medications prescribed and how to set up a safe method of preparing the assorted pills for consumption. People get confused by the similar sounding name, shape and color of medications and could easily con-fuse them. The nurse can help alleviate this prob-
lem by explaining the different medications and what they are taken for.
Over the past 25 years, medication use has been on the rise. More medications have be-come available on the market and address more health problems than ever before. More than 80 percent of adverse drug reactions in the elder-ly are preventable, according to a February 2004 study published in British Journal of Clinical Phar-macology. Working as a team with the physician, pharmacist, and a registered nurse from a Certi-fied Home Health Care Agency, is the best meth-od of prevention.
Mutty Burstein is the Education Outreach Manager of the Patient Relations Department at Americare CSS, a Certifi ed Home Health Agency. The Ameri-care Companies, founded in 1982, provide high quality home care services in the N.Y. metro area, including the 5 boros, Long Island, and Wesches-ter, Rockland, Orange, Dutchess, Putnam, Sulli-van, and Ulster counties, in the Hudson Valley. Americare integrates compassionate patient care with family needs and is ready to serve 24/7 with registered nurses, home health aides, PT’s, OT’s, speech therapists, and social workers. in addition to all the reguler aspects of home care, Americare has a special license to work with patients with mental health issues and patients with dementia, alzheimers, and/or depression, as well as the de-velopmentally disabled. Mutty can be reached at 917-287-1636 or [email protected] for any questions regarding health care or eligibility for medicare, medicaid, and managed care.
Insulin May Help Slow the Progression of
Alzheimer’s DiseaseResearch published in the Archives of Neu-
rology has found that a daily spritz of insu-lin into the nose may halt the progression of Alzheimer’s disease. Researchers split 104 people with mild to moderate memory prob-lems into three groups: thirty-six people in-haled 20 milligrams of insulin twice a day for four months; 38 people inhaled 40 milligrams twice a day for four months; and 30 people were given a saline solution.
After the study period was over, research-ers found that the group treated with 20 mil-ligrams of insulin twice a day for four month improved in memory tests and in their abil-ity to handle day-to—day activities. People who were treated with higher insulin dos-es saw no change in their memory abilities, while those who were treated with the saline solution saw a decline.
Insulin is an essential hormone that is typ-ically associated with diabetes. It is known to help brain function and this study sug-gests that a deficiency of it could potential-ly be a factor in the progression of Alzheim-er’s disease.

16 | November 2011 HEALTH LIVING
The Times, They Are A-changing - Baby Boomers Going On Medicare
By Yaakov Kornreich
I turned 65 a few months ago, and I must admit that it was something of a psychological shock. All my life, I had considered Social Security and Medi-care to be nice programs intended for somebody else, “the old people,” whose ranks I always assumed that I might join some day, but not any time soon. There-fore, you can imagine how I felt when I got a letter from the Social Security ad-ministration this summer notifying me on my upcoming new status.
When the envelope arrived, and I saw where it was from, I quickly fi g-ured out what it probably contained. But instead of opening it immediately, I put it aside, still sealed, where it sat for months before I was fi nally able to work up the courage to face its message.
That was a mistake. When I did open the envelope, I learned that getting set up on Medicare is not so simple as walk-ing into your doctor’s offi ce on the day after your 65th birthday and announc-ing, “Here I am. Take care of me.”
There are many options to consider and decisions to make, and waiting too long to do that can be costly. For exam-ple, when I fi nally decided to register online with the Social Security Admin-istration for my Medicare benefi ts, the week before I turned 65, I learned that the coverage would not become eff ec-tive until the start of the next month. In the interim, my private health insur-ance celebrated my birthday by auto-matically cancelling my policy.
I also had to do some research to de-termine that my wife, who is a few years younger than I am, had to re-register to stay on my old health policy by opting to pay for her own coverage after I was no longer on the plan.
Another thing I learned was that Medicare isn’t free; there are still de-ductibles and co-payments. You also have to pay a separate monthly pre-mium for part B, which covers doctor costs, and part D, which pays for pre-scription medicines. If you don’t want to pay those premiums, you don’t have to sign up for those coverages, but if
you change your mind later, the pre-miums will be higher than if you start-ed as soon as you turned 65.
Then I had to decide whether to buy a Medigap private insurance plan to pay for some of the things that Medi-care doesn’t, or to join a Medicare Ad-vantage plan, which is paid for by Medi-care, but provided by competing pri-vate companies. I quickly learned that each provider off ers somewhat diff er-ent benefi ts.
Then there are the questions about arranging for how to pay for long term care, and whether you can qualify for Medicaid, which is a whole separate government health program with its own set of rules.
In short, turning 65 and going on Medicare has had its ups and downs. The government is now paying for much of my medical costs, but I have had to do a lot of research to deter-mine which of my many options best suits my particular needs.
If you are turning 65 soon, or some-one who you care about is, then you need to learn about these things, too. That is what this special section of Health & Living was designed for.
There is a lot of ground to cover. Consider these articles to be just an in-troduction. As I learned the hard way, sooner or later, we all will have to learn these things, and the sooner, the bet-ter. Let’s get started.
Golden Years continuedTurning 65
residence there. Therefore, the life es-tate will no longer completely protect proceeds of the eventual sale. Medic-aid will have the right to seek a portion of the proceeds of the sale. Whether or not Medicaid decides to seek proceeds from the sale can be dependent on the amount of money it paid out for servic-es for the consumer.
If you created a life estate for your-self, a family member or a loved one, you should contact the attorney (who created the estate) to request a review of your situation and to discuss any op-tions available to you if your attorney hasn’t already done so.
With regard to home care servic-es, the governor’s offi ce has instructed Medicaid to place certifi ed home health agencies (CHHA) under a cap. Before April, if an agency wanted to provide 24-hr home health aide services to a patient, there was no issue. Now, each agency, based on the amount of Medicaid ser-vices they provided in previous years is limited to how many hours of service they can off er to any patient, regardless of how many hours the patient actual-ly needs. The days of CHHAs readily of-fering 24-hr live-in home health aides or split shift services (two 12-hr aides) are gone.
Now, the alternative…the new wave of home care providers are Managed Long-term Care Programs (MLTCP). The MLTCPs are not under any service relat-ed caps. This means, the program can off er home health aide services based on the patient’s actual health care
needs, not based on a government-di-rected service cap. MLTCP is what its name indicates…a managed care pro-gram that receives funding from the government. In most circumstances, even though it is a managed care pro-gram, patients that enroll in one can keep their current physician (the phy-sician doesn’t have to be in the MLTCP network) because the physician is paid by the separate, wholly federally fund-ed Medicare (not Medicaid).
Anybody needing Medicaid today is strongly urged to consult with a Med-icaid planning specialist. There have been too many recent, major changes to the ground rules of the Medicaid pro-gram for anyone to take the risk of ap-plying for eligibility and services with-out expert assistance. Anybody in-need of home care should ask specifi -cally about MLTCPs in the course of ar-ranging for those services.
The growth of New York State’s aging population means that the costs of the Medicaid program will inevitably keep rising, prompting the state government to impose further restrictions on eligibil-ity and the coverage provided the pro-gram. That means that all recipients of Medicaid-provided services or the family members managing their aff airs should keep in close contact with their Medic-aid planning specialist in order to track and evaluate the impact of those chang-es on the recipient’s situation.
Martin Schwartz, founder and CEO of Stay At Home Solutions is certi-fi ed as a Client Representative by NYC Medicaid. He has been assist-ing the community with their Medic-aid planning needs for fi fteen years. You can reach Mr. Schwartz by call-ing 718-758-3910.
Medicaid and Home Care: The Next Generation Dealing with the Effects of Medicaid Re-designContinued from Page 1
November 2011 | 17HEALTH LIVINGGolden Years continued
BY: Eli Stolberg
HOMECARE PLANNING SOLUTIONS
As one approaches retirement, de-cisions need to be made regarding the healthcare options that are available to retired adults. In this article, I will dis-cuss the primary healthcare provider for retired adults - Medicare.
MEDICAREMedicare is the federal govern-
ment’s health insurance for retired adults. All people age 65 or older are eligible to receive Medicare. However, how people receive their Medicare var-ies as we will discuss.
MEDICARE PART AMedicare Part A is hospital insur-
ance and helps to cover the costs of inpatient hospital care, skilled nursing facility, hospice, and home health care. Most people do not pay a Part A premi-um because they or their spouse paid
Medicare taxes while working. If some-one is not eligible to receive Part A free of charge, he may be able to buy it.
MEDICARE PART BMedicare Part B helps to cover
Medical Services such as doctor vis-its, outpatient care, home health ser-vices, and other medical services. In 2011, new enrollees pay a Part B pre-mium of $115.40/month if they earn less than $85,000 a year ($170,000 for
couples). Rates for people with high-er incomes rise substantially. In 2012, the standard Part B premium will be $99.90.
ENROLLMENT IN PART A AND PART B
People who collect Social Security will automatically get Medicare Part A and Part B. If someone is 65 and is not yet getting Social Security or Railroad Retirement Ben-efi ts, he will not get Part A and Part B auto-matically. He will need to contact Social Se-curity or the Railroad Retirement Board to sign up. People who delay signing up for Part B when they are fi rst eligible may have to pay a higher premium; especially if they were not covered under a group employ-er plan at the time of their initial eligibility.
GAPS IN MEDICARE AND MEDIGAP POLICIES
Medicare does not cover every-thing. Some notable gaps that are not covered by Medicare include (2011 levels):
MEDICARE PART A Coinsurance for hospital stays:Yearly Deductible - $1,132.Days 61-90 - $283 per day.
Paying for Healthcare as We AgeMedicare
Continued on p.18
Turning 65

18 | November 2011 HEALTH LIVING
HELPING “UNCLE SAM” DURING RETIREMENTRita Auerbach
We are constantly being reminded about the fi nancially uncertain times we are living in. High unemployment, the rising cost of living, large stock market swings, and dwindling 401K values have all contribute to making retirement plan-ning increasingly complicated. From the end of 2007 to the fi rst quarter of 2009, the markets lost nearly $2.8 trillion in re-tirement savings.
If you think that Social Security will take care of you during your retirement years -think again! In 2010, the max-imum monthly Social Security retire-
ment benefi t was $2,346, which is not enough for most people to live com-fortably. Also, when our Social Securi-ty system was enacted, life expectan-cy at birth was about 49 years. Today it is about 80 years. This is good news, but it means we have to prepare our-selves fi nancially for many more years of retirement.
Building a systematic withdrawal plan around a sustainable withdrawal rate is a smart way to try to make your money last longer, but this may not be enough. Assume you have $1 million in your retirement portfolio. You make ini-tial annual withdrawals of $50,000 (5%).
Continuing at this rate, your funds will last for 20 years, but in this example, one in ten retired people would outlive their income later in life.
“Asset preservation” must be a top priority for retirees. If only there were guarantees against outliving your in-come. The good news is that there are!
A Lifetime Income Annuity is a fi nan-cial product that does GUARANTEE life-long income.
Another option to supplement re-tirement is a life insurance policy. Life insurance’s primary purpose is to off er guaranteed death benefi t, which pro-vides a generally tax-free legacy to loved
ones. Permanent life insurance also car-ries many living benefi ts. Cash value is money that accumulates within the pol-icy, tax deferred. This means you do not pay taxes on any of the accumulation of cash within the policy. That money can be accessed tax-free through pol-icy loans, and used to supplement So-cial Security.
With proper planning and the use of available vehicles and strategies you can make your retirement years “golden!”
For more information about topics discussed in this article contact Rita Auerbach at (718) 471-8010.
Days 91-150 - $566 per day.Days 151 and above – all costs.Coinsurance for skilled nursing fa-
cility:Days 21-100 - $141.50 per day.Days 101 and above – all costs.
MEDICARE PART B20% of Medicare approved rate for
physician services, outpatient hospital treatment, medical supplies, and dura-ble medical equipment.
Many people purchase supplemen-tal policies that help to cover the gaps in Medicare coverage. These policies are of-ten referred to as Medigap policies. Me-digap policies vary in what they will cov-er and in how much coverage they will provide. Be sure to carefully review what a policy provides before purchasing one.
DO I STILL NEED A MEDIGAP POLICY IF I GET MEDICAID?
In terms of coverage, someone who gets Medicaid will have complete cov-erage for the gaps left by Medicare. They will also be given full Extra Help for Medicare Part D (If they don’t al-ready have a Part D plan, they will be auto-enrolled in one. People who have prescription drug coverage through a pension plan should ask their plan if this will confl ict with their pension coverage, as well as what steps might be taken to avoid any confl ict.). Nev-ertheless, many doctors do not like to take Medicaid and having a Medigap policy can open doors that Medicaid might not.
MEDICARE PART CAnother popular alternative to avoid
the coverage gaps that Medicare leaves is to join a Medicare Part C plan. These plans are also known as Medicare Ad-vantage plans or Managed Medicares
and function much like a traditional HMO or PPO. When someone joins one of these plans, Medicare pays a fi xed amount each month to a private third-party company that provides the plan and that company is in turn responsi-ble for providing his care.
Part C plans must follow rules set forth by Medicare; however, each plan may have diff erent out-of-pocket costs such as yearly deductibles and co-pays, as well as diff erent rules regarding ac-cessing services. Limitations on services may include requiring a referral to see a specialist as well as restricting coverage to in-network and preferred doctors, fa-cilities, or suppliers for non-emergency or non-urgent care. Most Medicare Ad-vantage plans include Medicare pre-scription drug coverage (Part D). Some require a monthly premium in addition to the standard Part B premium, which still must be paid monthly.
Some Medicare Advantage plans of-fer additional perks not covered under traditional Medicare, such as a free gym membership, as a way to attract new members. However, when choosing a plan, remember that none of these perks is worth sacrifi cing elements that are more critical to your healthcare cov-erage. Make sure that your regular doc-tors are included in the plan’s network and try to fi nd out what other people’s experiences have been with the plan. If the Medicare Advantage plan your are considering includes Part D drug cov-erage, check to see if it covers the pre-scription medications which you are currently taking.
Ultimately, having original Medicare Part A and B with a supplemental pol-icy will usually provide more options than a Medicare Advantage plan when it comes to seeing doctors and receiv-ing other services.
PART DMedicare Part D provides prescription
drug coverage. (See the separate article on
“Understanding Part D” in this issue.) Part D is off ered through competing plans by private third-party companies. While the Centers for Medicare and Medicaid Servic-es (CMS) regulates these plans, each plan has its own out of pocket costs, list of cov-ered drugs and participating pharmacies.
PART D COVERAGE GAP THE DONUT HOLE
Part D has a very signifi cant cover-age gap. Under Part D, the consumer is responsible to pay 100% of drug costs above $2,840 until they have spent $4,550 in total out of pocket costs (this includes any deductibles, co-payments, or coinsurance paid while reaching the coverage gap). This gap in coverage is commonly referred to as the donut hole. While this is the rule, it should be noted that there are some Part D plans avail-able that off er varying levels of coverage for someone who is in the donut hole.
EPIC AND EXTRA HELPLow income New Yorkers may be
eligible to receive prescription drug coverage from the Elderly Pharma-ceutical Insurance Coverage program (EPIC) through New York State or “Ex-tra Help” for Medicare Part D from the Social Security Administration. These programs help to cover the cover-age gap left by ordinary Part D plans and can also reduce or eliminate de-ductibles and co-pays. People with full Extra Help will not pay a month-ly premium for their Part D as long as they choose a plan that meets cer-tain requirements that Medicare calls a “benchmark” plan.
ENROLLMENT FOR PART C AND PART D
When initially enrolling in Medi-care you are given the opportunity to enroll in a Medicare Advantage (Part C) and/or Part D plan. Subse-quently, every year you have the op-portunity to make changes in your
Medicare between October 15 and December 7. This period is called open enrollment. Additionally, be-tween January 1 and February 14 you can disenroll from a Medicare Advantage plan and switch to orig-inal Medicare. If you choose to do this, you have until February 14 to enroll in a Part D plan.
CUSTODIAL CAREMedicare does not pay for long-
term care. Medicare views itself only as a provider of medical care. As such, Medicare will not pay for care provid-ed to assist with basic activities of dai-ly living (ADLs) such as dressing, bath-ing, and meal preparation. These ser-vices fall into the category of custodial care, which includes long-term home health care, adult day care, assisted liv-ing, and long-term nursing home care. There are two primary providers that will cover the costs of long-term cus-todial care, Medicaid and private long-term care insurance.
The rules governing payment for healthcare as we age can be very com-plex. Whenever in doubt, those arrang-ing for such care should consult with experts in the fi eld to make sure that they fully understand all the available options.
Disclaimer: Nothing in this ar ticle constitutes legal advic e and should not take the place of seeking compe-tent counsel.
Eli Stolberg is the director of Homec-are Planning Solutions, a division of Edison Home Health Care. Homec-are Planning Solutions provides free assistance with Medicaid applica-tions, pooled-income trusts, long-term care insurance claims, and private pay arrangements for peo-ple who would like to receive homec-are. He is available from 9:00 A.M. – 5:00 P.M and can be reached at 718-838-3838.
Paying for Healthcare as We AgeContinued from Page 17
Golden Years continuedTurning 65
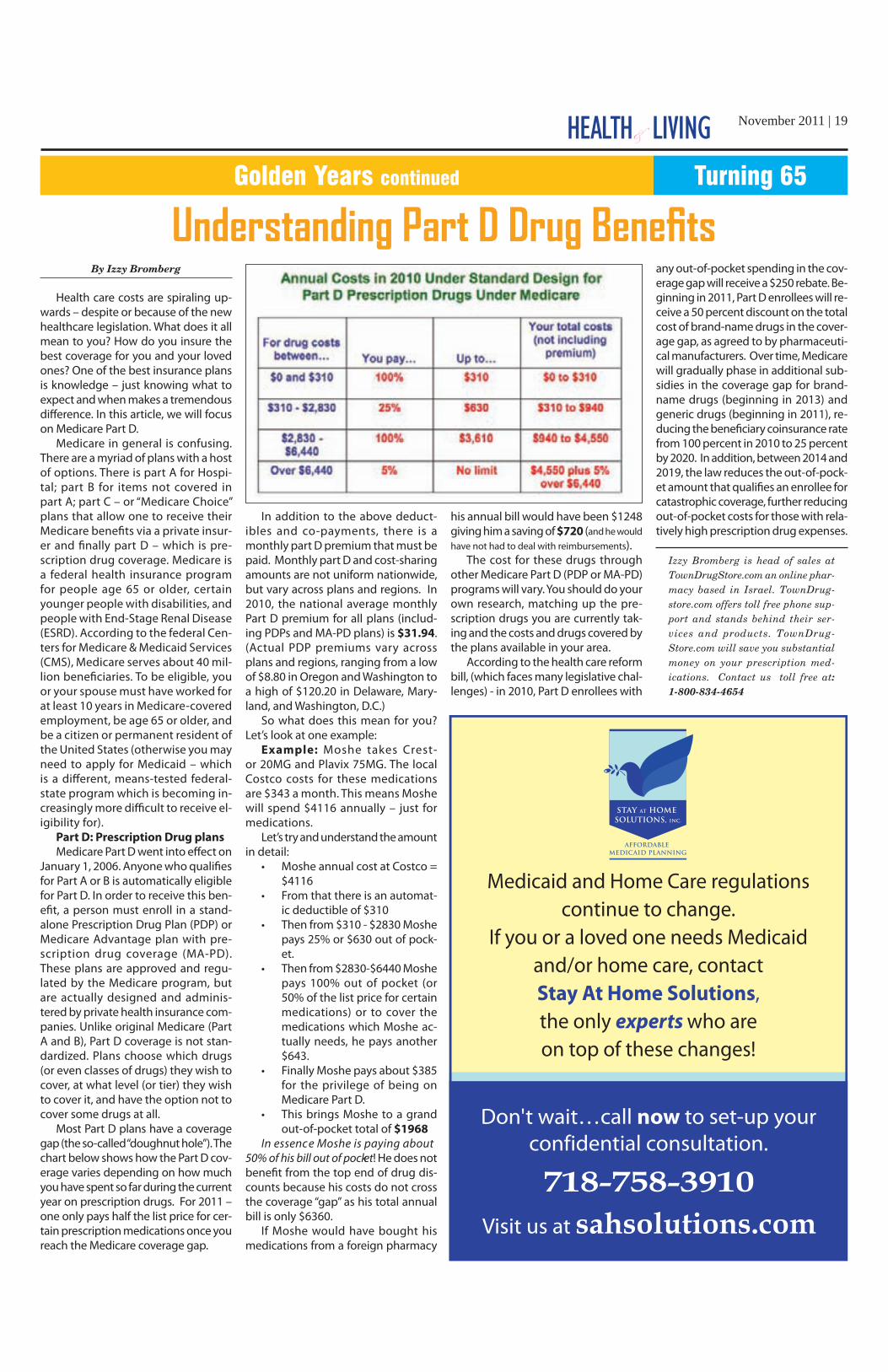
November 2011 | 19HEALTH LIVING
Understanding Part D Drug Benefi tsBy Izzy Bromberg
Health care costs are spiraling up-wards – despite or because of the new healthcare legislation. What does it all mean to you? How do you insure the best coverage for you and your loved ones? One of the best insurance plans is knowledge – just knowing what to expect and when makes a tremendous diff erence. In this article, we will focus on Medicare Part D.
Medicare in general is confusing. There are a myriad of plans with a host of options. There is part A for Hospi-tal; part B for items not covered in part A; part C – or “Medicare Choice” plans that allow one to receive their Medicare benefi ts via a private insur-er and fi nally part D – which is pre-scription drug coverage. Medicare is a federal health insurance program for people age 65 or older, certain younger people with disabilities, and people with End-Stage Renal Disease (ESRD). According to the federal Cen-ters for Medicare & Medicaid Services (CMS), Medicare serves about 40 mil-lion benefi ciaries. To be eligible, you or your spouse must have worked for at least 10 years in Medicare-covered employment, be age 65 or older, and be a citizen or permanent resident of the United States (otherwise you may need to apply for Medicaid – which is a diff erent, means-tested federal-state program which is becoming in-creasingly more diffi cult to receive el-igibility for).
Part D: Prescription Drug plans
Medicare Part D went into eff ect on January 1, 2006. Anyone who qualifi es for Part A or B is automatically eligible for Part D. In order to receive this ben-efi t, a person must enroll in a stand-alone Prescription Drug Plan (PDP) or Medicare Advantage plan with pre-scription drug coverage (MA-PD). These plans are approved and regu-lated by the Medicare program, but are actually designed and adminis-tered by private health insurance com-panies. Unlike original Medicare (Part A and B), Part D coverage is not stan-dardized. Plans choose which drugs (or even classes of drugs) they wish to cover, at what level (or tier) they wish to cover it, and have the option not to cover some drugs at all.
Most Part D plans have a coverage gap (the so-called “doughnut hole”). The chart below shows how the Part D cov-erage varies depending on how much you have spent so far during the current year on prescription drugs. For 2011 – one only pays half the list price for cer-tain prescription medications once you reach the Medicare coverage gap.
In addition to the above deduct-ibles and co-payments, there is a monthly part D premium that must be paid. Monthly part D and cost-sharing amounts are not uniform nationwide, but vary across plans and regions. In 2010, the national average monthly Part D premium for all plans (includ-ing PDPs and MA-PD plans) is $31.94. (Actual PDP premiums vary across plans and regions, ranging from a low of $8.80 in Oregon and Washington to a high of $120.20 in Delaware, Mary-land, and Washington, D.C.)
So what does this mean for you? Let’s look at one example:
Example: Moshe takes Crest-or 20MG and Plavix 75MG. The local Costco costs for these medications are $343 a month. This means Moshe will spend $4116 annually – just for medications.
Let’s try and understand the amount in detail:
• Moshe annual cost at Costco = $4116
• From that there is an automat-ic deductible of $310
• Then from $310 - $2830 Moshe pays 25% or $630 out of pock-et.
• Then from $2830-$6440 Moshe pays 100% out of pocket (or 50% of the list price for certain medications) or to cover the medications which Moshe ac-tually needs, he pays another $643.
• Finally Moshe pays about $385 for the privilege of being on Medicare Part D.
• This brings Moshe to a grand out-of-pocket total of $1968
In essence Moshe is paying about 50% of his bill out of pocket! He does not benefi t from the top end of drug dis-counts because his costs do not cross the coverage “gap” as his total annual bill is only $6360.
If Moshe would have bought his medications from a foreign pharmacy
his annual bi ll would have been $1248 giving him a saving of $720 (and he would have not had to deal with reimbursements).
The cost for these drugs through other Medicare Part D (PDP or MA-PD) programs will vary. You should do your own research, matching up the pre-scription drugs you are currently tak-ing and the costs and drugs covered by the plans available in your area.
According to the health care reform bill, (which faces many legislative chal-lenges) - in 2010, Part D enrollees with
any out-of-pocket spending in the cov-erage gap will receive a $250 rebate. Be-ginning in 2011, Part D enrollees will re-ceive a 50 percent discount on the total cost of brand-name drugs in the cover-age gap, as agreed to by pharmaceuti-cal manufacturers. Over time, Medicare will gradually phase in additional sub-sidies in the coverage gap for brand-name drugs (beginning in 2013) and generic drugs (beginning in 2011), re-ducing the benefi ciary coinsurance rate from 100 percent in 2010 to 25 percent by 2020. In addition, between 2014 and 2019, the law reduces the out-of-pock-et amount that qualifi es an enrollee for catastrophic coverage, further reducing out-of-pocket costs for those with rela-tively high prescription drug expenses.
Izzy Bromberg is head of sales at TownDrugStore.com an online phar-macy based in Israel. TownDrug-store.com offers toll free phone sup-port and stands behind their ser-vices and products. TownDrug-Store.com will save you substantial money on your prescription med-ications. Contact us toll free at: 1-800-834-4654
Golden Years continued Turning 65

20 | November 2011 HEALTH LIVING
dangerous than others. The less dan-gerous infl uenza type A virus invades the nose, throat and mouth.
IS IT A COLD OR THE FLU?How do you know if you have a cold
or the fl u? The symptoms are some-times very similar. In general, fl u symp-toms start suddenly. You can be feel-ing well in the morning and miserable by the evening. Cold symptoms begin more gradually, usually with a scratchy or sore throat, and progress over the course of 7-10 days. Flu symptoms are also more severe than cold symptoms, as are their complications. Use the fol-
lowing chart to help identify wheth-er you have a common cold or the fl u.
PREVENTION IS THE BEST MEDICINE
Although research is underway, to date there is no available cure for the com-mon cold and fl u. At best, cold remedies and herbal supplements can help allevi-ate some of the discomfort, and help pre-vent the common cold and fl u from invad-ing the body. The number one preven-tion for the common cold is eff ective hand washing. Washing hands using soap and running water, can reduce your chance of catching colds and the fl u from others.
Another way to reduce the chances of catching a cold and sometimes the fl u is to be careful about how you use your hands in public areas. The viruses which transmit a cold and even sometimes the fl u are of-ten found lurking on door handles and other surfaces, and are transferred to the hands when they are touched. However, a person is unlikely to contract a cold or the fl u unless their hands carrying the vi-rus then touch their eyes, nose or mouth.
Washing hands with soap and warm water can re-move the virus and pre-vent transmission of the disease.
For the flu, the best means of prevention is getting a fl u vaccine, or nasal mist (not for every-one) each year. The CDC has included protection in its vaccine against in-fl uenza A H1N1, infl uen-za A, H3N2, and infl uenza B virus for the 2011-2012 infl uenza season, and rec-ommends vaccination for anyone over age 6 months. Other means of prevention include eat-ing well and obtaining adequate rest, to help the body fi ght off the infec-tion before a full blown cold and fl u invasion.
There is also some research indicating that Vitamin C may help pre-
vent a cold from attacking, but will not be effective in fighting it off once it strikes. Zinc has shown promise in re-ducing the length and severity of the cold, but can also cause side eff ects such as unpleasant taste, and stomach aches. Beware of nasal sprays contain-ing zinc such as Zicam because they can permanently cause a loss of sense of smell. Echinacea may help as preven-tion in otherwise healthy individuals.
RELIEF FOR THE COMMON COLD AND FLUCOUGH AND COLD PREPARATIONS
Choosing among the many over the counter products available to treat cold and fl u can be daunting.
Here are some guidelines: First, cold, fl u and cough prepara-
tions should not be used by everyone. If you have any condition such as asth-ma, high blood pressure, thyroid dis-ease, or diabetes, or any other health condition listed in the warning section of the Drug Facts label on the box, you
must talk to your doctor or pharmacist before taking an over the counter prod-uct. Experts now agree that giving over the counter cold medication to children under 4 can cause dangerous side ef-fects. Read warning labels carefully.
Second, many combination prod-ucts such as Tylenol Flu, Tylenol, Tri-aminic products as well as other brand name products contain acetamino-phen, which can be dangerous if tak-en in doses exceeding 4000 mg per day for adults (and for some people 2000 mg per day). It is very easy to take too much acetaminophen by combining any of the many over the counter prod-ucts in which it is an active ingredient. You can fi nd out how much acetamin-ophen is contained in each product by checking the active ingredients list on the Drug Facts label which is often found on the back of the box. The same principle is true for other active ingre-dients such as phenylephrine, dextro-methorphan, and antihistamines. Use caution whenever combining over the counter products, and be sure to always
check the active ingredients to guard against an accidental overdose. It is saf-er to use single active ingredient prod-ucts that target your symptoms such as Acetminophen or Ibuprofen for chest pain, throat pain, headache and/or fe-ver, decongestants for nasal stuffi ness and sinus stuffi ness, and dextrometho-rphan to suppress coughing. Again, talk to your doctor before taking any over the counter medication if you have oth-er health conditions.
TRIED AND TESTEDSaline sprays, gels, mists and drops can
provide great relief for nasal stuffi ness, and are generally considered safe in chil-dren, pregnant women, and people with other health conditions (again -- talk to your doctor to make sure). Follow the di-rections on the specifi c saline preparation to make sure you are using it correctly.
Petroleum Jelly is very soothing on sore skin under the nose and lips when suff ering from runny nose and sneez-ing. It helps stop the pain caused by rubbing sore skin.
Fluids are essential for good recov-ery. In fact, water is the best cough ex-pectorant on the market! Drink plenty of hot and cold liquids to loosen mu-cous and prevent dehydration. Chick-en soup (yes, really) has been shown to have anti-infl ammatory properties in addition to mucous thinning properties.
Adequate resting and eating prop-erly will also help the body fi ght off in-fection.
RESEARCHResearch conducted by scientists
at Cambridge University has recently shown that there may be hope to stop the cold virus even after it entered the healthy cell of the infected person. Un-til now, it was believed that once the vi-rus entered the healthy cell, there was no way for the body to fi ght the virus without destroying the whole cell. Re-cently, scientists showed that a protein inside the cell called TRIM21 can recog-nize viruses that have entered the cell with an antibody attached to them, and can destroy the virus without killing the rest of the cell. This discovery may lead to a cure for the common cold as well as other unpleasant viruses.
Wishing everyone and a happy and healthy cold and fl u season!
Dr. Blanche Reiss holds a Pharm.D – a Doctor of Pharmacy degree, and is licensed and registered as a pharma-cist in NY and NJ. She is the found-er of SeniorMed Consulting and pro-vides medication reviews and consul-tations both privately and to long term care facilities. She can be reached at (845) 354-0473 ext 161, or by email at [email protected].
L’Chayim to Life
Fighting the Common Cold and Flu
Continued from Page 1
SYMPTOMS COLD FLU
Fever Rare Characteristic, high(100-103 degrees F); lasts three to four days
Headache Rare Prominent
General Aches, Pains Slight Usual; often severe
Stuff y Nose, sneezing, sore throat Common Sometimes
Chest Discomfort,Cough
Mild to moderate;hacking cough Common; can become severe
Complications Sinus congestionor earache
Bronchitis, pneumonia;can be life-threatening
Prevention Good hygiene Good Hygiene Annual fl u shot or FluMist

November 2011 | 21HEALTH LIVING
“Run For Your Life!”By Shaindy Urman
For some people, the word “run-ning” conjures up images of pain, sweat, and a tedious workout that they will avoid at all costs. For others, it is an idealistic dream that seems unattain-able. Yet for actual runners – running is a way of life.
There are plenty of workouts out there, each of which has its own unique advantages and health benefi ts. Yet one of the most accessible, simple, and benefi cial forms of exercise is run-ning. Technically, all you need to run is a good pair of sneakers and a healthy dose of determination.
Among its numerous health ben-efits, running has been proven to strengthen the heart, prevent heart disease, stroke, and diabetes, lower blood pressure, raise good cholester-ol, and boost immunity to colds and other viruses. It slows down the aging process, and could reduce both dis-ability and risk of death by increasing cardio fi tness and bone mass, lower-ing infl ammation, improving response to vaccination, and improving think-ing, learning, and memory functions. Like regular exercise in general, it re-duces the risk of many kinds of can-cers, including colon, breast, endome-trial, and lung. Running has also been recognized as an extremely eff ective method of treating psychological dis-orders, such as clinical depression, and drug and alcohol addiction.
The reason it is so eff ective is be-cause running, a rigorous cardiovas-cular exercise, makes the heart work faster, which in turn makes it stronger. Running bolsters your cartilage by in-creasing oxygen fl ow and fl ushing out toxins, and by strengthening the liga-ments around your joints. It also gives your bones a boost, helping to prevent osteoporosis.
Many people believe that they can work out all their problems “on the road,” and the fact is that when exer-cising, the body releases endorphins, the brain’s natural opiates, for an un-matched feeling of euphoria, or to-tal relaxation. Running is a wonderful and healthy way to relieve stress and reduce anxiety.
One organization that is no strang-er to running is Yachad, the National Jewish Council for Disabilities. Yachad is dedicated to addressing the needs of people with disabilities, and in-cluding them in the Jewish communi-ty. This year, for the third consecutive year, Yachad has put together a team of runners from all over the country, to
compete in the ING Mi-ami Marathon and Half Marathon in January 2012. The goal of Team Yachad is to raise funds for this very worthwhile organization, with each team member com-mitting to raise a set amount of money in exchange for running in the race. It is a fun, healthy, and exciting way to get people in-volved, and many of Yachad’s past runners have continued to in-corporate running into their lives long after the race has ended.
C o a c h J a s m i n e “Jaz” Graham, an RRCA (Road Runner’s Club of America) certified training coach who is the coach for Team Yachad, says that, “Running is the best stress relief as it releases endorphins that improves your mood, dissipates negative emo-tions and decreases stress. It’s as easy as going home and lacing up your sneakers and hitting the pavement. With every step, you leave the pres-sures of the day behind. Running can also be a spiritual experience. Some people pray as they run or refl ect on life and what changes need to be made to make it better, or they med-itate. Coming up with a positive man-tra to repeat as you run can really as-sist in improving your mood, as well.”
Chaim Backman, a physical ther-apist and triathlon instructor from Crown Heights, Brooklyn, also talks about the amazing mental benefits from running. “Running is a great time to take a break from all the craziness of the day and just allow you to relax and get in touch with yourself,” he says. “That’s why it’s a good idea to run with-out music, so as to keep distractions to a minimum. Running is also the best quality time you can spend with your kids. It’s personal one-on-one time in a non-confrontational setting, and it can be a very bonding experience. You’re moving around, you’re seeing beau-tiful sights, breathing in fresh air, and it’s an overall great activity to engage in with family.”
Running takes commitment, ded-ication, and perseverance. It can also change your life. Once you begin on a regularly scheduled regimen, you will find that running will improve all ar-eas of your life, not just your health. Yet
with all the many benefi ts to exercise, it’s important to keep in mind that, like all things, exercise must be performed
in moderation. It is possible to become addicted to working out and this can result in serious damage. Addiction to anything is harmful and destructive, and running is no exception. So take it slow and don’t overwork yourself. Your body will know when you’re pushing it too hard, and it will fi ght back. Remem-ber, slow and steady wins the race. So what are you waiting for? Lace up those sneakers, grab a bottle of water, and let’s get running!
Shaindy Urman is a freelance writer living in Brooklyn. She will be run-ning with Team Yachad this year in the ING Miami Marathon. To spon-sor Shaindy and donate to a great cause, visit her page, www.teamy-achad.com/shaindy. All proceeds, no matter the sum, go to benefit Yachad, the Natinal Jewish Coun-cil for Disabilities. Shaindy can be reached at [email protected]. Chaim Backman is a physical ther-apist and certifi ed USA triathlon coach. See ad on page 36 for web-site information.
L’Chayim to Life continued
Want to be part of something ?
Sunday, January 29, 2012
Yachad is an agency of the
Orthodox Union
www.teamyachad.com212.613.8301
COMMIT TO RAISE $3,000 FOR YACHAD AND THE REST IS ON US!
WE WILL PROVIDE:
ING MIAMI MARATHON AND HALF MARATHON
• Roundtrip airfare to Miami
• Hotel accommodations
• Unforgettable Yachad Shabbaton at the beautiful Newport Beach Resort and Spa
• Guaranteed race admission and registration
• Pre-Race Pasta Party and Post-Race BBQ
• Personalized training regimen
• Awesome Team Yachad gear
FOR MORE INFORMATION ABOUT TEAM YACHAD OR TO SIGN UP,please join us at our First Training Event on October 30th
Finish Line Physical Therapy • 119 W. 23rd St., Ste. 304, NYC • 12:00 pm
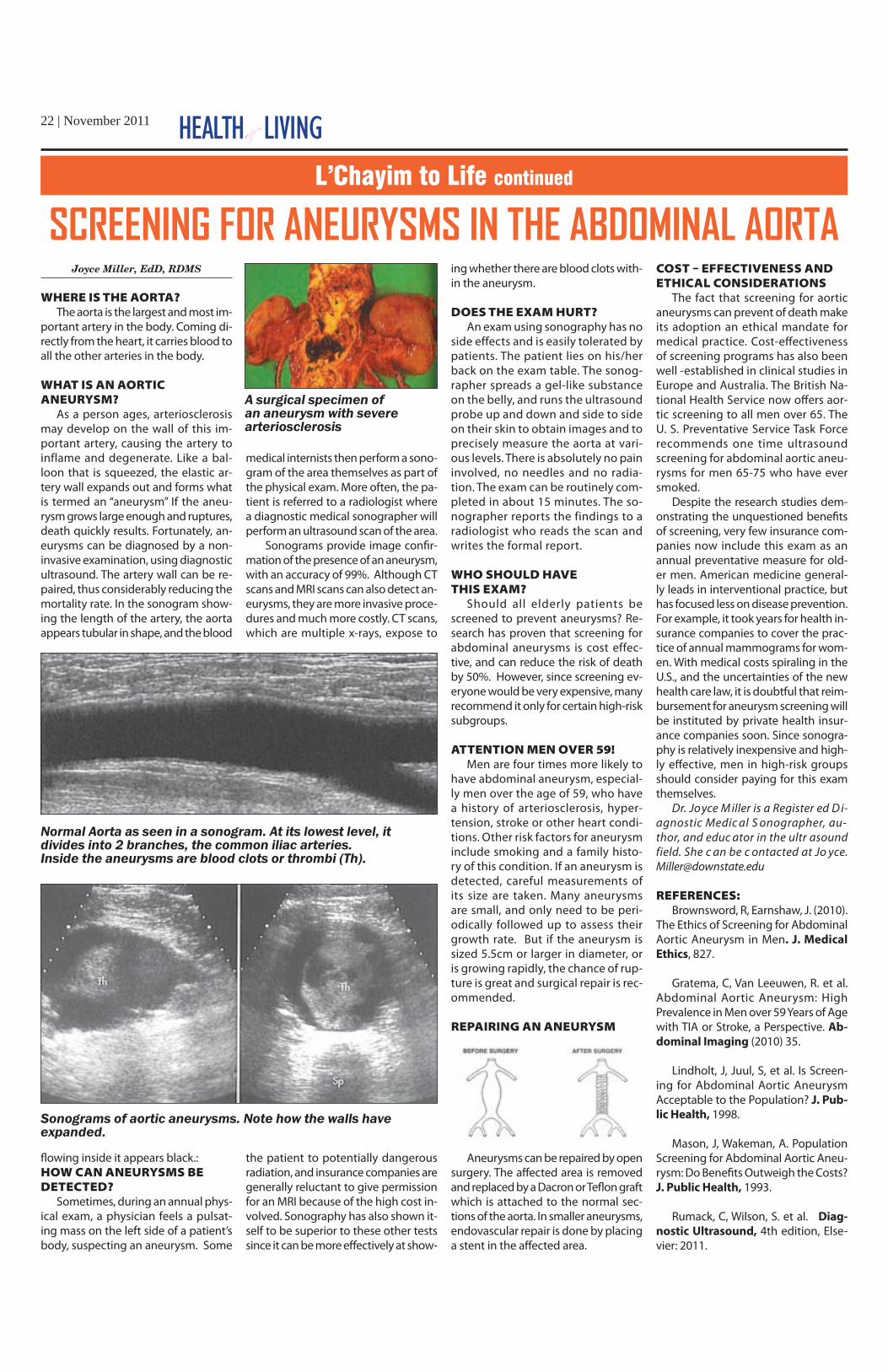
22 | November 2011 HEALTH LIVINGL’Chayim to Life continued
SCREENING FOR ANEURYSMS IN THE ABDOMINAL AORTAJoyce Miller, EdD, RDMS
WHERE IS THE AORTA? The aorta is the largest and most im-
portant artery in the body. Coming di-rectly from the heart, it carries blood to all the other arteries in the body.
WHAT IS AN AORTIC ANEURYSM?
As a person ages, arteriosclerosis may develop on the wall of this im-portant artery, causing the artery to inflame and degenerate. Like a bal-loon that is squeezed, the elastic ar-tery wall expands out and forms what is termed an “aneurysm” If the aneu-rysm grows large enough and ruptures, death quickly results. Fortunately, an-eurysms can be diagnosed by a non-invasive examination, using diagnostic ultrasound. The artery wall can be re-paired, thus considerably reducing the mortality rate. In the sonogram show-ing the length of the artery, the aorta appears tubular in shape, and the blood
fl owing inside it appears black.: HOW CAN ANEURYSMS BE DETECTED?
Sometimes, during an annual phys-ical exam, a physician feels a pulsat-ing mass on the left side of a patient’s body, suspecting an aneurysm. Some
medical internists then perform a sono-gram of the area themselves as part of the physical exam. More often, the pa-tient is referred to a radiologist where a diagnostic medical sonographer will perform an ultrasound scan of the area.
Sonograms provide image confi r-mation of the presence of an aneurysm, with an accuracy of 99%. Although CT scans and MRI scans can also detect an-eurysms, they are more invasive proce-dures and much more costly. CT scans, which are multiple x-rays, expose to
the patient to potentially dangerous radiation, and insurance companies are generally reluctant to give permission for an MRI because of the high cost in-volved. Sonography has also shown it-self to be superior to these other tests since it can be more eff ectively at show-
ing whether there are blood clots with-in the aneurysm.
DOES THE EXAM HURT?An exam using sonography has no
side effects and is easily tolerated by patients. The patient lies on his/her back on the exam table. The sonog-rapher spreads a gel-like substance on the belly, and runs the ultrasound probe up and down and side to side on their skin to obtain images and to precisely measure the aorta at vari-ous levels. There is absolutely no pain involved, no needles and no radia-tion. The exam can be routinely com-pleted in about 15 minutes. The so-nographer reports the findings to a radiologist who reads the scan and writes the formal report.
WHO SHOULD HAVE THIS EXAM?
Should all elderly patients be screened to prevent aneurysms? Re-search has proven that screening for abdominal aneurysms is cost effec-tive, and can reduce the risk of death by 50%. However, since screening ev-eryone would be very expensive, many recommend it only for certain high-risk subgroups.
ATTENTION MEN OVER 59! Men are four times more likely to
have abdominal aneurysm, especial-ly men over the age of 59, who have a history of arteriosclerosis, hyper-tension, stroke or other heart condi-tions. Other risk factors for aneurysm include smoking and a family histo-ry of this condition. If an aneurysm is detected, careful measurements of its size are taken. Many aneurysms are small, and only need to be peri-odically followed up to assess their growth rate. But if the aneurysm is sized 5.5cm or larger in diameter, or is growing rapidly, the chance of rup-ture is great and surgical repair is rec-ommended.
REPAIRING AN ANEURYSM
Aneurysms can be repaired by open surgery. The aff ected area is removed and replaced by a Dacron or Tefl on graft which is attached to the normal sec-tions of the aorta. In smaller aneurysms, endovascular repair is done by placing a stent in the aff ected area.
COST EFFECTIVENESS AND ETHICAL CONSIDERATIONS
The fact that screening for aortic aneurysms can prevent of death make its adoption an ethical mandate for medical practice. Cost-eff ectiveness of screening programs has also been well -established in clinical studies in Europe and Australia. The British Na-tional Health Service now off ers aor-tic screening to all men over 65. The U. S. Preventative Service Task Force recommends one time ultrasound screening for abdominal aortic aneu-rysms for men 65-75 who have ever smoked.
Despite the research studies dem-onstrating the unquestioned benefi ts of screening, very few insurance com-panies now include this exam as an annual preventative measure for old-er men. American medicine general-ly leads in interventional practice, but has focused less on disease prevention. For example, it took years for health in-surance companies to cover the prac-tice of annual mammograms for wom-en. With medical costs spiraling in the U.S., and the uncertainties of the new health care law, it is doubtful that reim-bursement for aneurysm screening will be instituted by private health insur-ance companies soon. Since sonogra-phy is relatively inexpensive and high-ly eff ective, men in high-risk groups should consider paying for this exam themselves.
Dr. Joyce M iller is a Register ed D i-agnostic Medic al S onographer, au-thor, and educ ator in the ultr asound field. She c an be c ontacted at Jo yce. [email protected]
REFERENCES:Brownsword, R, Earnshaw, J. (2010).
The Ethics of Screening for Abdominal Aortic Aneurysm in Men. J. Medical
Ethics, 827.
Gratema, C, Van Leeuwen, R. et al. Abdominal Aortic Aneurysm: High Prevalence in Men over 59 Years of Age with TIA or Stroke, a Perspective. Ab-
dominal Imaging (2010) 35.
Lindholt, J, Juul, S, et al. Is Screen-ing for Abdominal Aortic Aneurysm Acceptable to the Population? J. Pub-
lic Health, 1998.
Mason, J, Wakeman, A. Population Screening for Abdominal Aortic Aneu-rysm: Do Benefi ts Outweigh the Costs? J. Public Health, 1993.
Rumack, C, Wilson, S. et al. Diag-
nostic Ultrasound, 4th edition, Else-vier: 2011.
Normal Aorta as seen in a sonogram. At its lowest level, it divides into 2 branches, the common iliac arteries.Inside the aneurysms are blood clots or thrombi (Th).
A surgical specimen of an aneurysm with severe arteriosclerosis
Sonograms of aortic aneurysms. Note how the walls have expanded.

November 2011 | 23HEALTH LIVINGL’Chayim to Life continuedL’Chayim to Life continued
The Art of Medicine: Advances in “Blood Thinning”By Jason Esses
If you are reading the health sec-tion regularly, you have probably heard of the commonly prescribed medication warfarin, better known by its trade name, Coumadin.
Warfarin is in a class of medica-tions known as anticoagulants or “blood thinners”, which is a misno-mer, as the drug prevents clotting (i.e. coagulation) and doesn’t actual-ly thin the blood. It has been used medically for over half a century, and is the most prescribed oral anticoag-ulant in the country. Common indica-tions for prescribing warfarin include stroke prevention in patients with atri-al fi brillation, the most common car-diac arrhythmia, which aff ects almost 10% of eighty year olds, and venous blood clots, potentially a life threat-ening illness.
It has prevented many medical problems, but physicians have been looking for other alternatives for sev-eral decades now. Why? Although war-farin is very eff ective, its eff ects can be unpredictable. It is aff ected by many external factors such as other medica-
tions, and food items, and can harm a person’s “quality of life”.
Because every patient reacts diff er-ently to the drug, people taking it must have their blood checked frequently, usually bimonthly, but sometimes as often as biweekly. Unfortunately, war-farin has what physicians refer to as a “narrow therapeutic window”. If you give too much, and the blood is “too thin”, it could lead to uncontrolled bleeding. If you don’t give enough, it may not work. The only way to know for sure is to test the blood, checking the “INR” (International Normalized Ra-tio) to determine if you are in the cor-rect range (an INR of 2-3). The goal is to keep the patient in the therapeutic range at least 60% of the time to pro-vide the necessary protection against clotting.
Many common foods and medi-cations interact with the drug. Foods such as green leafy vegetables that contain signifi cant amounts of vitamin K, can inhibit its ability to prevent clot-ting. Alcohol or cranberry juice can in-crease its anti-clotting eff ect. Similarly, many common antibiotics and heart medications can cause either problem.
This is why researchers have been looking for decades for a substitute for warfarin that can be given in pill and is more predictable, because it doesn’t interact with many common foods or medications, eliminating the need for frequent blood tests. Dabi-gatran (“Pradaxa”) is the fi rst of sev-eral new drugs that fulfi ll these cri-teria. It was introduced last year. Ex-pected shortly on the market is an-other such medication called Rivar-oxaban (“Xarelto”). These warfarin re-placement medications have the po-tential to revolutionize treatment by eliminating the frequent blood tests, preventing strokes caused when the blood is “not thin enough”, and avoid-ing potentially life- threatening bleed-ing when the blood becomes “too thin” due to the eff ects of warfarin.
Of course, most new drugs are cost-ly, and Dabigatran is no diff erent. Its cost can be prohibitive for some pa-tients, especially when the insurance company refuses to pay for it because warfarin is a much cheaper, but not al-ways a better option.
There are other drawbacks to the new medications. Contrary to war-
farin, if someone does develop life-threatening bleeding because of the new drugs, it can be much harder to control. (The ability to easily reverse the eff ect of warfarin is one of the ad-vantages to the drug).
Which patients are aff ected most by these new drugs? Ask any one of the millions of patients who take war-farin already. If someone is already tak-ing warfarin, should they switch? Not necessarily. Many patients are well controlled with warfarin, and have mastered the skill of getting the INR in the therapeutic range. However, pa-tients who have never been on war-farin, or who are poorly controlled on warfarin, are potential candidates for these new medications.
So who should get it? Whenever a new drug comes out I remember my father-in-law’s voice whispering to me a quote from Alexander Pope, “Be not the irst by whom the new are tried, nor yet the last to lay the old aside”. Knowing when is the art of medicine.
Jason Esses is a practicing cardiol-ogist in Brooklyn, and is affi liated with Maimonides Medical Center.
HYPERBAL Herbal Tea Remedy
COLESTEL Herbal Tea Remedy
√ Naturally stabilizes blood pressure levels
√ Has a calming effect on the circulatory system
√ Relaxes and slackens the blood vessel system
√ Aids in the relief of Hypertension symptoms such as:
Insomnia, stress, anxiety, headaches, etc.
√ Lowers LDL and total cholesterol levels
√ Promotes healthy liver and kidney function
√ Removes poisons out of the body
√ Helps the liver to break down fats
√ Clinically tested
√ Contains 100 tea bags
√ 100% Natural
√ Kosher √ Tasteful
√ No side effects
Or Call: (713) 936-2248
A Natural Israeli Remedy Balances Blood Pressure
Now Also Available at Your Nearest Health Food Store
www.GalileeTisanes.comFor a List of Stores Visit:

24 | November 2011 HEALTH LIVING
Creepy Facts About “Crawly” ThingsBy Rochelle Rothman
I really don’t want to “gross” you out with this article, but the subject is too important to ignore! In my over 40 years of selling Tupperware, help-ing homemakers organize their small to large kitchen space, this problem has always existed, yet no one has ever asked me to stop “bugging” them about it! The information I am about to provide you was given to me at one of our national conventions by an ex-perienced exterminator from the Or-kin company.
Bugs in your home are the last thing you want. The fact is though, unless we take precautions, they will fi nd a way to get in. The following information will acquaint you with some common pests found in food and food storage areas, and the pre-cautions you can take to avoid them.
The greatest damage caused by roaches is not the food they eat, but from their habit of feeding and liv-ing in damp, unsanitary places. You may not see them crawling around on your surfaces, but they are and when they do, they pick up organisms and
dirt, spreading them to food supplies, preparation surfaces, dishes, and utensils, which are then transmitted to humans. Besides for being unsani-tary and disgusting, the bigger threat is the potential for stomach problems like food poisoning, dysentery, diar-rhea and even asthma.
A few interesting facts about cock-roaches:
There are over 3500 species worldwide (55 live in the U.S.)
They’ve been around since time began.
They live in small cracks and crevices.
They’re not social insects, as ants and wasps.
They’re found in all 50 states.
Has this ever happened to you? You are ready to make dinner and you have all the ingredients lined up on your counter; you open one of the containers, and are horrifi ed to see little critters crawling around, or evi-dence of insect feces.
Did you know that even if roaches can’t get to your food, they can live a
long and happy life eating the glue used in cardboard? Help keep your home pest-free by storing your food in Modular Mates products and trash-ing cardboard boxes and bags!
The most important thing you need to know about the common house roach:
They can live up to one year. Females produces 4-8 egg
capsules (30-48 eggs in each) in their lifetime. Hatching time takes 28 days.
Roaches are most active at night (avoiding humans).
They prefer to live near food and moisture (kitchens).
They’re especially fond of : starches, sweets, grease, and meat products; but will also eat cheese, beer, leather, bak-ery products, starch in book bindings, glue and the glue that seals our food packages and boxes. They eat hair, fl akes of dried skin, dead animal, and some plants.
If there’s water, roaches can live about a month without food!
When food is scarce, roach-es will feed on crumbs, soiled clothing, and some cosmetics.
Roaches come into the home through very small openings, or by “hitchhiking” in grocery bags, food packages, and box-es.
Some pests are found in the food you bring home. There’s not much you can do if you see them except dis-pose of the infested food This is why, we always recommend you transfer all dry staples into Tupperware Modular containers as soon as you bring home food from the store. Once your food is safely in the containers, your food is is airtight, leak proof and bug-proof! In case you did unknowingly “transport” some moths, bus etc. with a specifi c food, it will be “trapped” in that con-tainer and NOT spread throughout your cabinet and infest other food. You will see the problem when you open it, and attempt to use it, there-by disposing of it properly.
I cannot tell you how many hun-dreds of times, during my long career, I received phone calls with “cries for help” with this issue.
Recently, there was a moth prob-lem in a particular barley brand. Sev-eral women from a local area called me to order Modulars for their food to avoid further bug problems in their cabinets. It was not their fault because it was brought in with their food packages from the store. One
woman used a half of a bag of barley, closed it with a tie band before put-ting it on her shelf. The next morn-ing, when she opened her pantry door, moths came flying out! Need-less to say, she lost at least a hun-dred dollars worth of food that day, as moths were in all her dry semi-opened boxes. If infested, dry food is left in the carton or bag it comes in, and stored in your or pantry, there’s a chance food will be infested. If it’s stored in an airtight container, pests will be contained.
Weevils like to infest whole grains (oats, wheat rye), beans, and nuts while beetles infest fl our, breakfast cereals, dried fruit, dried peas and beans, spices, macaroni, dried meats, dried plants, and chocolate, and grain mites are often found in grain, fl our, and macaroni.
In order to prevent pests from en-tering your home, you should dis-pose of paper shopping bags, box-es, and trash immediately. Always check packaged food at the store, for any cracks or breaks in seals and/or wrapping. Look at the packaging for freshness (date) and look for insects in foods packaged in clear plastic or waxed paper.
Transfer dry foods to airtight con-tainers. Ordinary metal canisters are generally not tight enough. Card-board, paper, or plastic wrapping will not prevent infestation. Use old packages before newer ones; opened packages before unopened ones.
Keep the drip pan under your re-frigerator dry. Store garbage contain-ers in dry areas and empty them daily.
Once you implement these mea-sures, you and your family can en-joy meals together knowing with full confidence that all your food stor-age areas are organized, dry, clean and bug-free.
Over 550 recipes and tips are fea-tured in Rochelle ’s humorous and entertaining cookbook, NOT JUST A COOKBOOK. It also fea-tures many “multi-ethnic” recipes that were adapted for the kosher cook. Rochelle’s book examines food around the year by month. Her new DVD recipe organizer includes the book. Check out www.facebook.com/greatrecipeorganizer for FREE recipes and to order your copy on-line, or call 718-258-0415 for store information. Rochelle is available for cooking demo events for fund-raisers as well as Tupperware dem-onstrations. Call to fi nd out about the MODULAR sales going on un-til JAN. 28th!!
L’Chayim to Life continued
Family Forum and Sibs Speak Can Be Sent To:Email: [email protected] - Fax: 347-342-3152
All submissions become property of the Jewish Press and cannot bereturned. All submissions will be responded to in a timely manner.
Ruchi Eisenbach, the Author of Hidden Gems - Our Special Children, will once again compile and edit the “Family Forum and Sibs Speaks.” All submissions that are printed will receive a copy of Hidden Gems.
SIBS SPEAKIf you are a sibling of a child with special needs, we want to hear
from you! Send us a short essay (1-3 paragraphs) about your sibling. Can be a story, advice, complaint, suggestion or anything.
FAMILY FORUMParents & Adult Family Members
Do you have questions that you would like answered by specialists in the field? Helpful hints or tips that made life easier? Suggestions to improve the system? Write an inspiring story about how you or a family member with special needs that over-came great obstacles & succeeded?
SHARE IT WITH US! WE WANT TO KNOW!Please include your full name, address, and/or e-mail address & age. (We will only print your first name or an alias & age.)
A SPECIAL NEEDS MAGAZINEA SPECIAL NEEDS MAGAZINE

November 2011 | 25HEALTH LIVINGL’Chayim to Life continued
Many Skimping on Medical Care to Save MoneyBy Ita Yankovich
Pessie Klein* of Boro Park doesn’t tell her doctor that she has been splitting her blood pressure pills in half to make them last longer. Med-ication is expensive and she is one of the tens of millions of Americans without prescription drug insurance coverage. Tzvi Silverman* of Marine Park admitted that he no longer goes for yearly checkups if he feels fine since his company’s insurance plan recently increased his co-payment for an office visit to $25.
These are not isolated cases; many Americans today are go-ing without needed medical at-tention to save money. Ameri-cans are cutting back on doc-tor’s visits and delaying filling their prescriptions because they simply can’t afford them. A recent Consumer Reports survey revealed that almost half of the 1,226 consumers taking at least one medi-cation said they didn’t fill prescriptions, took less medicine than a pre-scribed dose or failed to undergo a medical test advised by their physician.
Others simply live with the pain and avoid treatments or surgery be-cause they are fearful of taking too much time off from work. “I have been having severe neck pain for years,” complains Bill Shannon, a re-cently employed graphic designer. “My doctor recommends surgery, but there is no way I am going to ask for weeks off now after being unem-ployed for 2 years.” As the economy continues to struggle, sales of med-ical devices, artificial hips and knee joints are on the decline.
Patients should tell their phy-sicians when they are having eco-nomical difficulty because the doc-tor will then be more inclined to prescribe less expensive gener-ic forms of the drugs that may be needed, or to give the patient free samples provided to doctors by the drug companies.
One of the more recent phenom-enons due to the high cost of health care in American today is so-called medical tourism. Many Americans are now traveling overseas to un-dergo plastic surgery or costly in-fertility treatments, which are not covered by health insurance. Today there are many doctors in countries like Brazil, India and China who are well qualified to carry out these pro-
cedures at a small fraction of their cost
in the USA. D o c t o r s w a r n t h a t
avoiding medical attention is not a wise way to save money.
In fact, it can be very expensive. If a diabetic, for example, decides to cut his expenses by reducing his insulin dosage, he can potentially wind up in a hospital getting a limb amputat-ed, or worse. The money that can be saved by playing such games simply isn’t worth the risk.
So what can Americans do to save money on their healthcare?
Shop Around - Even if you get in-surance from your employer, you may still have a choice of providers and the level of coverage. Before the open en-rollment period, talk to whoever deals with the insurance plan at work and re-view the available plans. Health care providers and hospitals are required to post their fees online (in 33 states). Make sure that the plans you are con-sidering cover the specific medical procedures that you are most likely to need. Check out different pharmacies. Wal-Mart, for example, charges $4 for a 30 day supply of many common ge-neric prescriptions. Partnership for Prescription is an organization that can help with costs too. Certain pre-scription drugs may be significantly cheaper if ordered by mail, or from a reputable foreign pharmacy.
Speak Up - The insurance com-panies want to keep you as their consumer, so if you’re unhappy, call the members’ help line or log onto
the patient website for infor-mation about a multitude of cost and quality mea-sures for com-mon diagnos-tic exams, visits, and medical pro-cedures.
Facilitate Fa-
cilities - Special-ized medical cen-
ters are generally less expensive than
hospitals. Don’t be so committed to a specific
hospital. Most communities have a subsidized clinic or hos-
pital that serves the entire popula-tion regardless of income or ability to pay. Visiting one of these local clinics for short term care or vaccinations, or medications can help you save. If your employer doesn’t off er dental insur-ance, go to a university dental clinic, which are staff ed by dental interns and off er dental care for less money.
HSA-Compatible Health Insur-
ance- If you are generally in good health and do not need to see doc-
tors often, consider joining an HSA-compatible insurance plan. The plan has a high deductible that works with a Health Savings Ac-count, which allows one to set aside pre-taxed dollars from your regular paycheck to pay for health expenses.
Kids - If your family doesn’t qual-ify for Medicaid, but you cannot af-ford private health coverage, by law the government must provide your kids with the Children’s Health Insur-ance Program (CHIP). Eligibility is de-pendent on your income, and if you qualify, kids will be insured at low or no cost. Generally, the income cut-off is $23,000 for a family of 2 and $35,000 for a family of 4. Some states offer low-cost family plans if the in-come doesn’t exceed $55,000. For more information call (877) 543-7669 or visit www.insurekidsnow.gov.
*names have been changed to pro-tect the identities
Ita Yankovich is a freelance writer and reporter. She also teaches Eng-lish and Literature at Kingsbor-ough and Touro College. She can be reached at [email protected]
Feeling lost in a sea of services for your child?
TAFKID assists families
whose children have been diagnosed
with a variety of disabilities and
special needs.
TAFKID is a not-for-profit organization services
are free of charge to all families.For more information call TAFKID at
(718) 252-2236 or e-mail: [email protected]
TAFKID can help!Services provided by TAFKID include:
Family Support Services & Information Educational Advocacy Individual Case Consultation Referrals to Doctors, Therapists,
Schools and Government Programs Parent Matching Family Recreation Programs Parent Training and Meetings Guest Lecturers Community Sensitivity and Training Informational Publications Pediatric Equipment Lending Program Tape/Video Lending
Ce
ntr
al
De
sig
n 7
32
-94
2-0
74
6
TAFKID

26 | November 2011 HEALTH LIVING
Mind, Body & Soul
What To Say (And Not Say) To The Bereaved
By: Bernie Kastner, PhD, MPH
While a good formal education can provide us with the basic knowledge that we need in the areas of math, language, science, history, and the like, there are other areas of life in which we do not get enough basic training in school are: an-ger management, boundary issues, ne-gotiating skills, and what to say or not to say when someone is grieving.
There are books that have been writ-ten on the proper conduct upon enter-ing a house of mourning. These books do contain some good tips, but most of these guidelines are rather technical in na-ture, so I would like to address the more spiritual side.
Saying the wrong thing to someone who just lost a loved one can be very hurt-ful, to say the least. Many mourners have told me that they have become down-right angry and bewildered with visitors who may have had good intentions, but
nevertheless did more harm than good by their visit.
Some examples of well-meaning but inappropriate and hurtful comments in-
clude: “Hashem wanted it to work out that way,” “Be strong - that’s how your fa-ther would want you to be,” “Don’t wor-ry - everything will be alright,” “Come on, get a hold of yourself,” “Don’t cry in front of
the children,” “He’s in a better place now, “It was his time to go,” “So did you hear about the incredibly large sale I made a few days ago?”
Sometimes even common sense won’t help us fi gure out how to behave when sit-ting in front of someone bereaving. There are those who will initiate and steer a con-versation away from the subject of the de-ceased in order to “take one’s mind away from” the grieving. But distraction really fl ies in the face of the whole point of sit-ting shiva. Sometime, our own inability to face the bare facts ourselves causes us to fail in our responsibility to bring comfort to those in their ultimate moment of need.
So what can we do? What can we say that will make a diff erence?
First of all, we need to recognize that there are two processes going on here si-multaneously - the fi rst is the person who is grieving and the pain he/she is feeling. The second is the pain of the soul who just departed. On some level, we need to be prepared to deal with and address both.
Many of the books recommend wait-ing until the griever turns to you and ad-dresses you fi rst. Then take the lead from him and respond accordingly. This is gen-erally good advice, but what if the mourn-er is not the talkative type? Is it better to just sit in silence thereby giving the mourn-er the feeling of “being there” for him, or is it better to come armed with something inspirational to say?
Sitting in silence can be awkward, in-deed. Some will impulsively say anything just to break the silence. That can turn out to be the opposite of what the mourner wants to hear. So acknowledging the si-lence would be a better approach. Con-sider saying: “I am embarrassed to say that I didn’t come prepared with any particular words of wisdom for you, so instead, if it is OK with you, I’ll just sit here next to you in silence while letting you know that I share your hurt and pain.” Brutal honesty works.
I can guarantee you that no mourner will respond by saying “in that case, what good are you to me?”
There are those who come armed with funny jokes. While that could indeed be entertaining, we don’t want to turn the house of mourning into a house of frivoli-ty. If the jokes are ones that the deceased used to tell, that would shed a diff erent light on them. Humor can certainly be in-jected into a discussion, as long as it can be tied in a positive way to the deceased.
The main focus should be on the soul of the departed. After all, death is about the deceased - not about those who are left behind. Many times we get this basic fact backwards, and it turns the mourning environment into an emotional fest that is very diffi cult to alter or tolerate.
I believe that it is safer to talk about the departed than it is to speak to the emotional state of the grieving family. Of course it is perfectly acceptable to off er help by asking questions like: “Can I do any shopping for you today?” Would you like me to pick up your child from school?” “I would like to prepare supper for your fami-ly - would you prefer a meat or dairy meal?”
But beyond those “to do” things, an-other good approach would be to fi nd a way to comfortably direct the discussion towards the departed soul for the grieving family. Relating a heartwarming personal story which is not well known about the deceased, or recapping the acts of kind-ness he used to do, are good places to start. Or ask the mourner to tell you what particular personal quality about the de-ceased stands out in their minds. What specifi c quality in the deceased can we strengthen in ourselves in order to make us into better people?
Those of us who have grieved in similar circumstances also may be in a position to contribute to the comfort of the mourners if it is done with humility. Ever since I lost a 19-year old son to an illness, when paying a shiva call to parents who lost a child, I fi nd myself less intimidated by the atmosphere in the house. Of course I would never say “I know what you’re going through”. Never is the pain exactly the same for people in simi-lar circumstances of loss. But I do feel an ob-ligation to say something like “time will do its part. Look at me - I am capable of smiling again - hopefully one day, you too, will be able to do the same”. Coming from some-one who is a member of the same “club” (in this case, the bereaved parents club) has a better chance of being heard. Those of
Continued on p.27
SF
De
sign
s917-416-6952
Coming from someone who is a member of the same “club” (in this case, the bereaved parents club) has a better chance of being heard. Those of you who fi nd themselves in similar circumstances as the bereaved one ought not be shy; take the initiative and lead by example. You would be doing a tremendous chesed by giving someone just the right amount of chizzuk in their hour of need.

November 2011 | 27HEALTH LIVINGMind, Body & Soul continued
The “Half Shabbos” PhenomenonMichael J. Salamon, Ph.D.
We have recently been bombarded with a spate of articles on what is be-ing called the “Half Shabbos” situation, where people, mostly teens and people in their early 20’s, are said to keep all the laws of Shabbos and kashrus but can-not seem to go without their iPhones or Blackberries or hand held comput-ers for the 25 hours of Shabbos. So on Shabbos they surreptitiously text and Tweet and read and write Facebook posts to their friends while rationaliz-ing that it is not really wrong because it is not the same as actual writing.
One journalist says this situation is most likely to occur among those the writer labels as modern orthodox be-cause, according to this individual, they tend not to be as careful with their ob-servance of certain mitzvoth. Anoth-er essayist suggests that this new phe-nomenon happens more often among Yeshivish people because of the forbid-den fruit theory. Not only is it wrong to communicate digitally on Shabbos but they are told that it is even wrong to have a Smartphone. For some of these young Yeshivish people two negatives make a positive. Each writer approach-es the phenomenon from their own perspective and experience. Each also tends to assign responsibility for the problem to either parents who are not teaching their children about the im-portance of the laws Shabbos or to Rab-beim who are not eff ective in commu-nicating the special warmth of a truly meaningful day of rest.
From my experience, I can state that this situation is not limited to any partic-ular group, nor can we place the blame squarely on any specifi c segment of the community. All groups bear equal re-sponsibility for this condition. Half Shab-bos is also not as pervasive as some of these reports would lead us to believe. While it is next to impossible to get any hard data on how many young people participate in Half Shabbos, it is not yet widespread. That is not an attempt to ex-cuse or minimize it, but rather to keep it in proper context. Most importantly, half Shabbos is really not a new phenomenon.
When small, portable battery driv-en televisions became available in the
late 1970’s, there were people in shuls who could not only update us on sports scores but might also report the latest news on Shabbos afternoons. This is not to mention the practice of some who leave their televisions on for all of Shab-bos and who have done so for years. Back in the days when battery-powered
transistor radios were still new, people somehow knew just the right person to ask for the baseball scores on Shab-bos. Only later did I learn that some en-terprising teenage baseball afi ciona-dos concocted secret ways to keep their transistor radios on all of Shabbos, lis-tening surreptitiously through an ear-piece, while the radio was hidden from plain sight. When no one was looking at them, they would listen through the earpiece to track their favorite sports team, and they could always be count-ed upon for timely updates of the box scores. Some of those same individuals are now among the most upstanding members of the community.
There are several important points that are too easily discounted when the topic of Half Shabbos is discussed. First, and what I think is most impor-tant, is the fact that the teen years are a time of experimentation and rebellious-ness. For many teens, laws are made to be broken. The vast majority of teens rebel, but the large majority of them do so in very minor ways. A moderate re-sponse to these small rebellions is thus indicated. For many young people who experiment with it, Half Shabbos is not a statement that they are breaking with religion; rather, it is a way to get through this stage of testing. A too strong reac-tion by a parent or a Rebbe might actu-ally push the teen farther away from re-ligious observance.
As I indicated, this form of experi-mentation has always occurred in one form or another and most of those in-
volved have become completely in-volved in religious observance over time. Pointing fi ngers at any particular group also causes more problems than it solves. There is a delusional idea that somehow divisiveness strengthens a group by separating it. On the contrary, we have much more in common with
other segments of Orthodoxy than not. By continuing to make such distinctions, we are only adding to the confusion that our children experience and we are in-advertently giving them license to be-come even more rebellious.
Cell phones, Smart phones, tablet computers – they are all here to stay. Pretending that they do not exist, confi s-cating them or legislating against them will not work. Many of these devices are available very inexpensively, and teens
will quickly learn just how to use them from their peers. What is truly lacking, and not just among young people or in the Jewish world, is the proper social eti-quette for these technological advances, and simple, clear rules for when and how to use them. As with all technological ad-vances, we will eventually learn how to adapt to these changes. Until we do, try-ing to force compliance is missing the point. We can only show young people the correct ways of adherence to Jew-ish life by providing healthy role mod-els and proper discipline, not by trying to enforce rules against reality.
Dr. Michael Salamon, a fellow of the American Psychological Asso-ciation, is the founder and direc-tor of ADC Psychological Services in Hewlett, New York and a board member of P’TACH. He is the au-thor of numerous articles and sev-eral psychological tests and books including his newest book Abuse in the Jewish Community, The Shid-duch Crisis: Causes and Cures” (both fromUrim Publications) and “Every Pot Has a Cover” (Universi-ty Press of America).
Not only is it wrong to communicate digitally on Shabbos but they are told that it is even wrong to have a Smartphone. For some of these young Yeshivish people two negatives make a positive.
you who fi nd themselves in similar circum-stances as the bereaved one ought not be shy; take the initiative and lead by example. You would be doing a tremendous chesed by giving someone just the right amount of chizzuk in their hour of need.
What To Say (And Not Say) To The BereavedContinued from Page 26
Dr. Bernie Kastner is a Psychother-
apist in private practice with offi c-
es in Jerusalem and Ramat Beit
Shemesh. He is also the author
of Understanding the Afterlife in
This Life and Masa El Haor. Feel
free to visit his website at www.
drbkastner.com. He can be reached

28 | November 2011 HEALTH LIVINGMind, Body & Soul continued
Roles and Boundaries(Unshackle Them)
Chana Mark, L.C.S.W.
Somehow, we are failing in our roles as parents. How? What went wrong? The chil-dren are unmannered and undisciplined. They are unhappy and discontent despite our endless eff orts to please them. The happier we try to make them, the more rude and demanding they become. They are miserable and we are miserable. We are the adults; it is up to us to fi x it.
Many believe that it is the role of a par-ent to make his child happy. Let us exam-ine this idea.
The word happy comes from an old-er English word hap which means luck or good fortune. The origin of this word is an indicator that the notion of happiness (based on this defi nition) may not be a To-rah concept. We certainly would like to see our children accomplished and feel fulfi lled. We would like to see them get on well with people. We would certainly like them to feel confi dent and comfort-able with themselves. How shall we help them achieve these goals?
What we are really asking is, “What is
my role as a parent?” This question is not a simple one. During the era of World War II and its aftermath the role of the parents was clear- family survival. Do everything possible to put bread on the table, get To-rah education for the kids and try to keep
the family together. Today, baruch Hash-em most of us are not fi ghting for survival; our nisayon is in a way more diffi cult due to our many choices.
THE ROLE OF THE PARENTThe role of a parent is to take respon-
sibility for building our child’s character. Because we were blessed with a Torah to guide us, we have it easier than others. We do not have to struggle with what to im-part. Our struggle revolves around how to impart it. The fi rst step for us is to remem-ber that we are the adults. The judgment
and authority belong to us, not to the chil-dren. Many adults fi nd parental authori-ty too – well – authoritative. Democracy is a good model for government, but it is not a good model for parenting. Our hes-itation about our parental authority is not
helpful to our children, who need to feel relaxed in trusting that we will set bound-aries and provide them with guidance they can rely on.
Authority does not mean harshness. It means that we are confi dent in ourselves and in the value of what we are convey-ing. It also means that we accept the fact that we are the adults and that they are the children. When we are confi dent in our authority we are then free to be the parents we want to be: be gentle in our re-buke, generous in our understanding, fi rm without resorting to harshness.
Children do not take well to having their behavior curtailed or corrected. No one does. They will protest and complain. We do not have to deny his feelings. He may be feeling wronged or slighted. How-ever a child’s feelings are not always an indicator that his perception of reality is correct.
If a child has a complaint that persists over time, this is an indication that some-thing may really be wrong. We must ex-plore the situation, refl ect upon it and cor-rect it without surrendering our dignity.
Children are not yet emotionally or in-tellectually developed enough to see reali-ty clearly. Of course we should consult with others in order to inform our judgment: our spouse, a wise friend and our Rav. In the end though, our judgment must pre-vail over the judgment of children. This is not rigi d or mean. It is being the adult. We do not need our children to constant-ly like us. There may be times when they don’t. Sometimes it takes time before a child comes to understand the wisdom of our judgment. Of course this makes us sad, but that does not mean that we are wrong.
It may happen that a child comes home from school feeling that he has been wronged by his teacher. Children who feel wronged by adults express themselves in a very intense way. These strong feelings in our children may cause us to get angry at the person who wronged our own fl esh and blood. When we behave like angry
children ourselves and lose our adult judg-ment we do our child no favors. Here too, we do not have to deny our child’s feel-ings. We must let him know that, before we can come to a judgment, we must fi rst talk to the teacher. The child may not like this. He may even feel angry or betrayed, and ask, “Don’t you trust me?” It is better to remain separate and calm. We really will not know what happened until we speak to the teacher, the other adult.
A WORD ABOUT CHUTZPAHWhat exactly is chutzpah/ disrespect?
It is a challenge or attack on our parental authority, usually delivered in an angry or hurtful way. It makes us feel enraged and humiliated.
Enraged and humiliated people are not capable of careful and considered thought, no matter how adult they are. Therefore: If we strike back in a hurtful or self-righteous (read self-preserving) rage we are certain to fail. And we will proba-bly make things worse.
What to do?First and foremost, we must take care
of ourselves in a way that preserves our dignity. We may tell the child something like, “What you just said was out of line and very hurtful. Right now I want to be alone for a while. We’ll talk later.” Of course, this is easier said than done, especially in that ter-rible moment of pain and rage. We need to prepare ourselves for the possibility of that moment. (Who said this was going to be easy?) By separating and preserv-ing our dignity, we create enough space for the child to realize that he went too far. And when we respect ourselves, we earn the respect of our children.
Next, we should wait for the right mo-ment to revisit the subject. It doesn’t mat-ter who initiates the next conversation, as long as two conditions are met.
1) Both sides have had enough time to cool off . This may take a while.
2) “Who starts the conversation” should not become a power strug-gle.
If we will give this matter thought and refl ection, we will realize just how perva-sive it is. Truly dealing eff ectively with the problem means looking at the specifi cs of each situation, which is beyond the scope of this article. But in general, cultivating a better understanding of our roles and boundaries will help us to deal more ef-fectively with our children.
Chana Mark is a psychotherapist
with a private practice in Suffern,
N.Y. If you have questions or com-
ments about this article or about
matters of psychological concern
you can e-mail her at chanaspcyh@
optonline.net
Find a Therapist
a free service provided by
Nefesh International the organization for Orthodox Mental Health Professionals
PO Box 3027 Teaneck NJ 07666 T:201-384-0084 F:201-384-0018E:[email protected] www.nefesh.org
sfrank
el.design@
gmai
l.com
917.416.69
52
Authority does not mean harshness. It means that we are confi dent in ourselves and in the value of what we are conveying.

November 2011 | 29HEALTH LIVINGMind, Body & Soul continued
I’m So Confused, Am I Being Abused?By Lisa Twerski, LCSW
DIFFERENTIATING BETWEEN DYSFUNCTION, DISORDERS AND DOMESTIC ABUSE
It can be very confusing to peo-ple who feel abused in their mar-riage, to try and determine if the cause is a dysfunctional relationship that may have some abusive fea-tures, a spouse with a mental illness or domestic abuse. In fact, some of the abusive ways one may be treat-ed by their spouse, may be similar in each of these situations. What deter-mines which type of situation one is actually faced with is the underly-ing dynamic.
Why is it important to make the distinction between whether the emotional abuse (for example) is due to mental illness, dysfunction or is domestic abuse? Because the most appropriate intervention will vary depending on what the underlying issue is, in a given situation.
In the case of domestic abuse, the abuser employs a pattern of sys-tematic, coercive tactics, to instill fear in order to gain and maintain power and control in the marriage. The most common tactics used by the abuser are: economic abuse, emotional abuse, threats, intimi-dation, isolation, and sometimes physical or sexual abuse. The abus-er does this because he (or she) be-lieves it is his absolute entitlement to have power and control, of his wife, in his marriage. For the abus-er, it ’s all about this entitlement. It is his (or her) conviction that he has the right to everything revolve around him without having to con-sider the needs, wants or concerns of his spouse.
FEELING ABUSED DOES NOT ALWAYS MEAN DOMESTIC ABUSE
There are times, when a spouse might have been subjected to one or more abusive tactics by their spouse, but it is actually not a case of do-mestic abuse. To understand what else might be going wrong, it’s best to begin by describing what a mar-riage looks like when things are go-ing right.
A healthy relationship is one in which each spouse feels responsi-ble, and sees it as his or her tafkid, to enjoy, consider and take care of the other – emotionally, spiritually, physically and psychologically. When this dynamic is present, we can refer to this as a functional marriage, be-
cause both partners are function-ing in their intended roles, and the marriage works in the way it was in-tended.
In general terms, a dysfunction-al marriage can be defined as one in which one or both spouses is not abiding by the principle that de-fines a healthy, functional marriage. The times when that breakdown in functioning can be so bad as to feel abusive, usually fall into one of two categories: 1) certain mental illness-es 2) where one or both spouses has a profound inability to function in a healthy way as a spouse: manage conflict, negotiate, communicate effectively or appropriately, think of marriage in terms of giving instead of getting, which leads to the spo-radic use of an abusive tactic.
MENTAL ILLNESSES THAT CAN FEEL LIKE DOMESTIC ABUSE:
There are a variety of disorders which can cause someone to react to their inner turmoil in ways that then
feels abusive to his/her spouse. The following are a couple of examples:
Borderline Personality Disorder (BPD): One of the hallmarks of BPD is the person’s intense fear of aban-donment. This fear often causes the person to be controlling as well as exacting with his or her spouse. Any attempt on the part of his or her spouse to have independence in be-lief or action that is contrary to theirs, provokes the fear of abandonment which, in turn, becomes rage. In that rage someone with BPD can become very abusive, but again, the etiology (root cause), as well as intention, is very different.
Another example can occur when married to someone with intense anxiety, or obsessive compulsive dis-order (OCD). In the case of OCD, peo-ple use rituals of various types in an attempt to calm their anxiety. If the person with the disorder is prone to ‘include’ their spouse in their attempt
to alleviate anxiety, it can feel very abusive. Take for example, someone who uses obsessive orderliness in an attempt to alleviate anxiety. Upon coming home to things being ‘out of place’ they might launch a vicious verbal attack that would sound sim-ilar to an abuser’s use of emotional or psychological abuse.
The key to differentiating be-tween mental illness and domestic abuse, would lie in looking at the bigger picture surrounding the abu-sive behavior.
A PROFOUND INABILITY TO FUNCTION IN A HEALTHY WAY AS A SPOUSE:
When a spouse can only think in terms of what s/he should be getting out of marriage, in the ex-treme, this can look very much like domestic abuse. If this spouse also does not know how to manage con-flicts or communicate appropriate-ly, disagreements can, at times, dis-solve into name calling or even a fit of rage. There may be a demand for
things to revolve around him/her; or, an expectation that is more focused on self rather than giving. The abil-ity or interest in compromise, or re-solving conflict, rather than having thing’s all one’s own way, may seem to be non-existent.
What differentiates a case of do-mestic abuse from one of dysfunc-tion is twofold. First, while there may be abusive behavior, there is not a systematic pattern of coercive con-trol. Again, looking at the bigger context will give some clues. When the dysfunctional spouse’s behavior is examined carefully, one can see that the abusive treatment is sporad-ic and often only comes at times of conflict or potential conflict.
Second, while the spouse who is trying to be giving and caring may get overwhelmed by the demand-ing, self centered behavior of the dysfunctional spouse, s/he actually could step out of that role and say
“no” to the excessive demands. Not that it would be easy. The healthy spouse in a marriage has always wanted and expected to fulfill that role in an appropriate way. Also, this intentional role change may be frightening, because the anger, or perhaps the fragility, that the un-healthy spouse displays seems diffi-cult to challenge.
In fact, a challenge to the dys-functional spouse’s self-centered-ness may at first make the marriage seem even more dysfunctional, be-cause it increases discord, as both spouses are now “fighting” for their own needs. However, in a dysfunc-tional marriage it is possible to stop assuming the caretaking role and as-sert one’s own needs. In this situa-tion the absolute belief in the right to power and control does not exist. Consequently, there is a limit to how far the dysfunctional spouse will ac-tually go, leaving the other spouse with more options.
In true domestic abuse cases, the abused spouse doesn’t have the op-tion of fighting to get her needs or her opinions considered, because if she did try to stand up for herself, she would have to contend with much more than just discord or unpleas-antness. In an abusive relationship, the abuser will continue to escalate the consequences, making things in-creasingly unbearable or frightening for his spouse, until she feels that she must either comply with his expec-tations or leave. If she is not willing to leave, she then feels that her one option is to capitulate to the abus-er’s demands.
It is impossible to overstate the importance of making the distinc-tion between these categories of ‘marital problems.’ What is an ap-propriate intervention for one situ-ation is a waste of time for another. What would be helpful in that situa-tion would be unsafe in still anoth-er. If you are struggling with feeling abused, but don’t quite know what to do, getting a proper assessment of the situation will be the best first step towards help and health.
Lisa Twerski, LCSW, has been work-ing with victims of domestic violence for over twenty years, maintains a private practice in Brooklyn and lec-tures locally and nationally on many subjects including domestic abuse, marriage, and dating. Parts of this article have been excerpted from her book, I’m So Confused, Am I Being Abused? due out at the end of 2011.
A healthy relationship is one in which each
spouse feels responsible, and sees it as his or
her tafkid, to enjoy, consider and take care of
the other –emotionally, spiritually, physically
and psychologically

30 | November 2011 HEALTH LIVINGMind, Body & Soul continued
More than Moody -Understanding Adolescent Depression
By Evan Kroll, Ph.D.
The teenage years are no picnic for both the teenager and the parents. Par-ents of young children yearn for these days, which they assume will be care-free childrearing, but are rudely intro-duced to a challenging parental time. Teenagers assume they are halfway onto adulthood and expect adoles-cents to be time of freedom but soon fi nd it instead to be a time fi lled with of a lot of demands and responsibility. Teenagers are bombarded with pres-sures from many diff erent sources. Be-tween school, family, friends, and even from within, the pressure is constant-ly building up in a teenager. Wanting to look one’s best, refl ect well on one’s family, get good grades, and be a loy-al friend are but a few of the pressures that teenagers face. Sometimes such pressures can be too much for a teen-ager to handle. When this happens, it can lead to depression.
About 20 percent of teens will ex-perience teen depression before they reach adulthood. Depression can af-fect a teen regardless of gender, so-cial background, income level, race, or school. While teenage girls report suf-fering from depression more often than boys, boys are less likely to seek help or recognize that they are suff ering from depression.
When a teenager is depressed, common symptoms like anger, irrita-bility, and moodiness are often down-played. Parents are in denial that some-thing is actually wrong, and may attri-bute long lasting unhappiness to be-ing a “typical teenager.” It can be very hard for a parent to believe that their child is depressed. If you begin to no-tice a pattern about your teen’s behav-ior, don’t be quick to dismiss it. If some-thing “doesn’t feel right,” go with your
instincts and deal with it. Try to fi gure out how long it’s been going on, how extreme it is, and admit the possibility that your teen is depressed.
WARNING SIGNS• Trouble with school and concentra-
tion. Depressed teens often fi nd it diffi cult to concentrate on school-work or stay interested in hobbies they once enjoyed. Depressed teens don’t “care” anymore; therefore, it is not uncommon for a depressed, for-merly good student to get into trou-ble, skip classes, or let grades slip.
• Isolation or changes in relationships. Making friends and keeping them takes eff ort. In an attempt to reduce the demands and pressures upon them, depressed teens will begin to spend more time alone, keep few-er relationships, and pull away from their families.
• Unexplained illnesses. Emotional pain can wreak havoc on the body, especially when it is unexpressed. Depressed teens complain of head-aches, stomachaches, and menstru-al pain. When a physical exam from your child’s doctor doesn’t reveal a medical problem, don’t overlook the possibility that their unexplained symptoms may be a cry for help with their depression.
• Extreme habit changes. Depression may lead to dramatic changes in ev-eryday activities. A depressed teen might sleep all day or not at all, eat excessively or stop eating entirely, or spend endless hours watching TV or playing games on the internet. Life-style changes are not unusual in an adolescent, but when they are dras-tic, they can also signal something much larger.
• Substance Use – The use of drugs and alcohol is often the result of ad-
olescent experimentation, but sub-stance abuse can also be a sign that your child is depressed or unhappy and using substances as means of self-medicating. When the depres-sion is left untreated, the substance abuse can escalate into an addic-tion and become a problem in its own right. Just because teenagers spend most
of their day at school and with friends, that doesn’t mean that parents can’t have a major impact on their psyche. Those few hours with the people who love them most can make all the dif-ference.• Treat the problem – not the symp-
tom. For a depressed teen, being dis-respectful and acting out are symp-toms of feeling out of balance and unhappy inside. These teens are ex-tra sensitive to parental reactions. When parents react with harsh lec-tures, yelling, expressions of dis-appointment, and aggravation, it makes depressed teenagers feel like a failure and often even more de-pressed. While a parent should nev-er condone negative behavior, it is important to keep in mind that the behavior itself is only half the story.
• Communicate without judgment. Your teen needs someone she trusts more than ever. Most depressed teens feel completely alone and are embarrassed by what they are feel-ing, so build them up and let them know you are there for them. Often-times, teens don’t try to communi-cate and connect because they are afraid they will have trouble explain-ing what they are feeling and get fl ustered. Encourage your child to talk to you. If he’s willing to talk, try your best to listen in a non-judgmen-tal manner that conveys understand-ing and empathy. You can also en-
courage your teen to write in a jour-nal. Writing can be extremely ther-apeutic. It is an opportunity to sort out feelings without the worry of be-ing judged.
• Encourage the positive – studies have shown that exercise and health-ful eating are useful tools in manag-ing stress and combatting depres-sion. Persuade your teen to social-ize with good friends, play sports, and participate in extracurricular activities – anything that will keep your teen busy and provide a posi-tive sense of identity.
• Seek professional treatment. Most teens fi nd the idea of seeing a ther-apist embarrassing and frightening. Find a therapist that has extensive experience working with teens, who knows how to relate to them and make teenagers feel comfortable. No teen should ever have to feel de-
pressed or unhappy, but sometimes it happens. When it does, your teenager needs you. Talk to them. They may not be verbalizing “please help me” but I as-sure you, that is what they want. When a teenager with depression is handled properly and immedialty, the benefi ts for everyone involved are long lasting.
Evan Kroll, Ph.D. is a licensed psy-chologist in Teaneck, New Jer-sey. He specializes in therapy for teens, young adults, and families. Dr. Kroll is a certifi ed Marijuana and Alcohol Treatment Specialist. He consults to yeshivas, schools, and camps about teen’s at-risk, substance use and behavior disor-ders. He lectures in a wide range of settings about psychology in the schools, parenting, and social de-velopment. To contact Dr. Kroll, please call 201-357-2825 or visit www.evankroll.com.
TMS – An Alternative Therapy for DepressionBy Yael Genack, MA (Rockland
TMS and Wellness Center, Administrative Coordinator)
Depression affects over 14 mil-lion American adults every year. De-pression can be a debilitating disor-der that interferes with an individ-ual’s thoughts, mood, behavior and physical health. The effects of this illness can ruin relationships, cause problems at work, make it diffi cult to
overcome serious illnesses, and even result in suicide.
While the exact cause of depression is unknown, the leading scientifi c theory is that it is caused by an imbalance in the brain’s neurotransmitters. Neurotrans-mitters are chemical messengers that send signals between brain cells. The symptoms of depression are most often treated with medications which increase the levels of these neurotransmitters, but antidepressants don’t always work.
Many patients do not achieve symptom relief and often suff er debilitating side eff ects from the treatment. The reported side eff ects including, but are not limit-ed to, nausea, insomnia, anxiety, restless-ness and weight gain. Despite advances in treatment, four million depressed pa-tients each year have poor responses to, or cannot tolerate their antidepressant medication.
Now there is another option! A new FDA-approved device is now being
used in Transcranial Magnetic Stimu-lation (TMS) to treat major depressive disorders without the use of medica-tion and its side eff ects. This innovative treatment was approved by the FDA in 2009, and treats depression by using an electromagnetic fi eld, similar those used by MRI machines. The magnetic fi eld produces electric pulses, stimulat-ing the brain to heal itself through neu-
Continued on Next Page

November 2011 | 31HEALTH LIVINGMind, Body & Soul continued
rogenesis—the creation of new neu-rons that grow and form new internal brain connections.
TMS Therapy uses a highly focused, pulsed magnetic field to stimulate nerve cells in the area of the brain that controls mood. The treatment is done as an outpatient procedure. The pa-tient undergoes an initial evaluation, and if they are deemed a good can-didate, treatment begins. The typical treatment course consists of fi ve treat-ments a week for six weeks, for a total of thirty treatments, and then six ta-pering-off sessions. Each treatment session lasts about 37 minutes. Dur-ing that time, the device delivers rap-id “pulses” of the magnetic fi eld which last for four seconds at thirty second in-terval. The pulse is said to feel like tap-
ping on the scalp. Because the fi eld is narrowly focused, the magnetic energy used in a full course of TMS Therapy is a small fraction of that used in just one brain scan with an MRI.
During the procedure the patient re-mains fully awake and alert, so that it is possible to use the thirty-seven min-utes of the procedure to conduct a psy-chotherapy session at the same time. This is entirely optional, but it can help the patient enormously, since during the treatment process the brain has more plasticity and is more open than usual to suggestions.
The most exciting part of the treat-ment is the near total lack of side ef-fects. Unlike the case when using an-tidepressant medications, there are no systemic side effects; no weight gain, no sedation, no nausea, no dry mouth, no adverse eff ects on concen-tration or memory, no hospitalization, and no anesthesia. Since TMS is ad-
ministered directly to the spot on the brain requiring the pulse, and does not reach further into the body, the system is considered safe even for expectant or nursing mothers and can be used to treat postpartum depression. This is a major advantage over antidepres-sant drugs, which circulate through-out the body and can have numerous side eff ects.
In clinical studies, more than half of the patients treated for symptoms of depression with TMS experienced significant improvement. About a third had complete relief of their symptoms at the end of six weeks. Patients undergoing TMS treatment also experienced a significant de-crease in anxiety and physical symp-toms like the appetite changes, aches and pains, and lack of energy associ-ated with depression.
The benefi ts of TMS can last any-where from six months to two years
or more. The patient can remain en-tirely drug free during that period and beyond. If symptoms return, a short booster session can be initiat-ed to bring the depression back un-der control.
Though not yet FDA approved for these conditions, TMS Therapy may ul-timately be used to help those suff ering from, ADHD, migraines, stroke symp-toms, Post Traumatic Stress Disorder, bipolar disorder and Schizophrenia.Re-search on the use of TMS for all of these conditions is now ongoing.
Rockland TMS & Wellness Cen-ter is directed by Dr. Isaac Schech-ter, PSyD., and medical opera-tions are directed by Dr. Richard L. Price, M.D. For more informa-tion please call 845-678-6070 or email us at [email protected]. You can also visit our website at www.rocklandtms.org.
Shana Rishona CounselingBy Moishe Herskowitz, M.S.,
LCSW
Disillusionment is a common fac-tor for most married couples. Soon af-ter the wedding, people often come to the conclusion that the person they married is not the same person they thought they were while they were dating. The unconscious mind will al-ways mistake our partners by compar-ing them to our parents. By understand-ing this, we can get beneath the surface and heal childhood wounds.
WHAT IS THIS DISILLUSIONMENT?
Psycho-Pharmacologist have learned that couples ‘in love’ have high levels of natural hormones fl ow-ing through their systems, with high levels of the neurotransmitter sero-tonin within the brain. These chemi-cals in the brain will produce a natural positive reaction, so if something up-setting happens to one spouse in the relationship, it will cause that spouse to respond with positive and correc-tive feedback.
When I was an academic advisor at Touro College, an interesting case was brought to my attention. A student walked into my offi ce very upset be-cause after six months of marriage, his brother was getting divorced. When I questioned him as to why, he re-sponded that his sister-in law had lied. She had not told this student’s broth-er that she was bi-polar. To make mat-ters worse, she claims that when she was dating this student’s brother, she no longer showed signs of depression, and as a result, she felt she no longer
needed medications, and subsequent-ly stopped taking them. How can that be possible?
I then asked the student “how did your brother fi nd out that she “was bi-polar”?
He responded that after sheva bra-chos, she told his brother that before they had dated, she was diagnosed as bi-polar, but once their relationship began, she no longer suff ered from any symptoms.
When the chosson’s family heard about her diagnosis, and conceal-ment, they were outraged. They won-dered how it could be possible that symptoms of this type of manic de-pression can be gone without med-ication!
I responded that it is my belief that this is defi nitely possible for this de-pression to be suspended in a buff er state, for a very long time. When the couple was dating she was in love, and for all intensive purposes she still is. Because of the infl ux of hormones , the levels of serotonin in her brain rose, and compensated for the missing neu-rotransmitters- leaving her in a symp -tom-free state without the need for
chemical altering medications. She did not mean to lie, she honestly felt that her bi-polar was gone, and for her it must have felt like a true miracle.
It is important to understand that for some people this anesthesia or “smoke screen” may wear off right af-ter sheva brachos, and for other cou-ples it can last, far beyond Shana Re-shona (the fi rst year of marriage).
New research using brain scans with various couples in diff erent stag-
es of their marriage, shows that these chemicals produced in the brain dur-ing the beginning of the relationship do not completely leave the brain over time, but rather are stored in the brain; in a temporary state of what neuro-scientist Dr. Dan Siegel calls implicit memory. Interestingly, these chemi-cals in the brain can be retrieved, re-vitalized, and can be re -programmed to be utilized upon request.
The beginning story has a happy ending. The student who confi ded in me was able to convince his brother to come in to see me, and with some coaching, explanations, and accep-tance, B”H he was able to avoid di-vorce.
As a general note, I have shifted my view on premarital counseling. I still believe that it would be benefi-cial for a couple to attend sessions prior to their wedding in order to learn about marriage, and how to live with another person. In fact, I feel it should be mandatory for any individual or couple that is enter-ing a second marriage, or is marring someone who is divorced, to come in before they were married. Now, I also assert that most other couples can best be also served by counsel-ing after Sheva Br achos. I feel that counseling can help at the point where many marriages may take a turn for the worse, and eventual-ly lead to divorce, after the Honey-moon phase ends and the anesthe-sia starts to fade.
Moshe Herskowitz, MS., LCSW, de-veloped the T.E.A.M. (Torah Educa-tion & Awareness for a better Mar-riage) approach based on 20 suc-cessful years of counseling couples. As a licensed clinical social worker and family therapist, he developed this seminar to guide new couples through easy-to-accomplish steps towards a happy, healthy marriage. Moishe Herskowitz is a Graduate School Professor at the Touro Col-lege Mental Health Program. To discuss topics from an article, or ask questions, he can be contact-ed at [email protected] or 718-435-7388. If you would like to read Moishe Herskowitz’s archived arti-cles, log onto www.jewishpress.com and, in the search box on the page, type in Moishe Herskowitz.
TMS
Continued from Previous Page
It is important to understand that for some
people this anesthesia or “smoke screen” may
wear off right after sheva brachos, and for
other couples it can last, far beyond Shana
Resho (the fi rst year of marriage)

32 | November 2011 HEALTH LIVINGMind, Body & Soul continued
Communicating For Real In Relationships That Count
By Dvora Levy
Every person is a unique world unto themselves, and communication is the bridge we lay down that connects our world to that of another person. Posi-tive communication leads to secure and close con-nections. Communication requires a sender, a mes-sage and an intended recipient. When the message I am attempting to convey is received the way I in-tended it to be, that is positive communication. Most people with experience being in relationships con-sider this to be very hard. Communication often does not go smoothly. Let’s look at why that is.
Communication happens on three levels: ver-bal, nonverbal and paraverbal. Verbal communi-cation is the words we use, the content that de-scribes what we are trying to convey. We often take our verbal communications for granted. We’ve taken cues from our environment growing up re-garding how to share certain things and what to share. Before we talk, we seldom think of the im-pact our words will have on the listener. We often take it for granted that our words will be received as we intended them to be, without fully appreci-ating that our listener will hear what we are saying through his or her fi lter. This creates a challenge to positive communication.
Nonverbal communication, also known as body and facial language and tone, is another way we com-municate that is very strongly picked up by our lis-tener – if not consciously, then certainly unconscious-ly. Our face is an important conveyor of emotional information. Our face can express a smile, laughter, empathy, eye contact or, on the other hand, a frown, sneer, cry, smirk, anger or disgust. We show positive body language with touch, open arms, attention, relaxation and leaning forward. We show negative body expression with neck and hand tension, rude gestures, a point, jab and inattention.
The tone we use provides another avenue of com-munication. With our tone, we can express caring, warmth, tenderness, empathy, aff ection and cheer-fulness, or we can have a tone that expresses cold-ness, tension, fear, impatience, anger and more. Our tone makes a diff erence in how our words are un-derstood.
There are times when our communication is in-consistent. We say “Of course I’m listening to you!,” while reading the paper. When communication is inconsistent, nonverbal communication is believed over what’s verbally said. “You have my full atten-tion,” says the wife while preparing dinner. “I’m just closing my eyes for a spell, tell me what happened,” says the husband after his full day of work. “Of course I love you,” he/she tells his or her spouse impatient-ly. These partners’ nonverbal communication leaves the speaker feeling very much unheard and doesn’t establish a positive connection.
Paraverbal communication is how we say some-thing; the tone, pitch and pacing of our voice. How to understand the husband returning from work and asking his wife, “You cleaned the family room?” Is it “YOU cleaned the family room?” thereby expressing
surprise that his wife did something, “You CLEANED the family room?” questioning whether the family room is cleaned or “You cleaned the FAMILY ROOM?” questioning something about the room that was cleaned. Same words, but it is impossible to under-stand the intent without listening to the paraverbal communication. How we say something is not lost on the listener, but is often something speakers pay little attention to.
If we are more conscious of how we deliver our message, paying close attention to the diff erent ways we communicate, then we will be clearer, thereby maximizing our chances of having our message be received the way it is intended.
The second part to positive communication, and the key to receiving messages eff ectively, is listen-ing. Listening is conveyed two ways, nonverbally and verbally.
The “art” of listening involves giving full, physi-cal attention to another person. This is conveyed by leaning forward toward the speaker, facing the other person squarely, maintaining an open posture with arms and legs uncrossed, and appropriate head nod-ding and facial expression. Paying attention to the speaker’s nonverbal communications gives us insight and understanding into the feeling and content of the message. In order to understand the total mes-sage of the speaker, we need to gain an understand-ing of the feeling and content, which adds depth of experience to the communication.
Verbal listening skills involve responding to the speaker by restating, in our words, the feeling and/or content of what is being expressed. This gives the speaker the experience of being heard and ac-knowledged and also provides the speaker with the opportunity to give us feedback about the ac-curacy of our perceptions. Tools we can use for ef-fective verbal listening are paraphrasing, refl ecting and summarizing.
A magical key in the art of listening is validation. An example of validation is the story of a wise Rab-bi who was approached by a couple experiencing marital distress. The Rabbi fi rst called the wife into his study and, with his assistant nearby, heard her recount all the complaints she had about her hus-band. When she was fi nished, he compassionate-ly said “You’re right.” She left feeling lighter in her heart. Next to come in was the husband who re-counted all his grievances against his wife. The Rab-bi sagely stroked his beard and said “You’re right.” The man left feeling better. The assistant turned to the Rabbi and, feeling extremely puzzled, asked “Rabbi, how could they both be right?” “You’re right, too,” answered the Rabbi.
The power of validation in making someone feel heard and strengthening a relationship cannot be overstated. We need to come to our partners, chil-dren, siblings and friends with a mindset that even if we don’t agree with them or we don’t understand where they are coming from, we know there is a rea-son why they feel and react the way they do.
Don't Suffer Alone!
Are you struggling witha medical or mental issue?
Meet other frum peoplewho are suffering
from similar conditions
Free & Anonymousonline support group
www.FrumSupport.com
Continued on p.33

November 2011 | 33HEALTH LIVINGMind, Body & Soul continued
WHAT MESSAGES DO YOU TELL YOURSELF?
By Elisheva Rabinowitz
When you woke up this morning, did you tell yourself?
1. “I want to have a good day” or “I want to have a bad day”
2. “I want to have a day fi lled with peace and tran-quility”; or “I want to fi ght with my children, family members, coworkers and/or friends?”
Throughout the day, we give ourselves messag-es. These messages usually refl ect a desire to have a serene day. On the other hand, if we feel stressed and have negative thoughts, they pull us away from having a close relationship to Hashem and a sense of peacefulness. I would recommend that you im-plement one of the following three suggestions to increase your tranquility:
1. Hakaras Hatov (gratitude)- We need to train ourselves to focus on the positive aspects of our life and observe how Hashem has provided for us in countless ways. When we see Hashem’s hand in our life and all around us, we strengthen our Emunah and our lives are more pleasurable and tranquil.
I recommend you make a list of fi ve (or more) bra-chos (blessings) that Hashem has given you and how Hashem has aided you.
2. Our Thoughts. What is your fi rst thought when: a. You receive a gift?b. Your friend does not return your call?c. Your neighbor refuses to lend you something?d. Your boss calls you into his/her offi ce?e. You do not receive an aliyah in shul?We make split second judgments based on our
view and perspective of ourselves, the people around us and the world. If our view of ourselves, others or situations are negative, then positive self-statements can help us restore our emotional and mental health. When we use positive self-statements we are more cognizant of our thoughts and focus on the positive; however, if an issue needs to be addressed, it should not be denied or ignored.
I recommend that on a daily basis, you repeat one of the following positive self-statements:
Ein O d M ilvado - There is no other than Him Hashem loves me. I can remain calm. I am loveable. In the beginning, if you do not believe what you are telling yourself, just keep practicing the self-state-ments and you will become more positive.
After you pick one of the positive statements above or any other positive statement, you should repeat it to yourself throughout the day.
3. Breathing/Relaxation Exercises. Breath-ing and relaxing are important tools to learn because as soon as we think something nega-tive or our mind perceives something negative or stressful our muscles become tense and our breathing changes. Some simple forms of relax-ation are listening to soft music, taking a bath, visualizing yourself somewhere peaceful (i.e. Kosel, garden, field) and listening to relaxation CDs. Recently, I started making relaxation CDs for my clients to help them learn how to relax. After listening to them, my clients report feel-ing calmer and more peaceful. These exercis-es can help you notice the tension, lower your stress level and handle the situation in a more effective manner.
I recommend that on a daily basis, you prac-tice one form of relaxation and/or breathing ex-ercise.
After choosing and implementing the tools of hav-ing hakaras hatov, saying positive self-statements, or performing relaxation/breathing exercises, you will feel more relaxed and peaceful.
Elisheva Rabinowitz is a counselor in private prac-tice, specializing in anger and stress reduction, eat-ing disorders and loss and grief issues. In addi-tion, she is the moderator of workshops and tele-conferences on methods to decrease anger, stress and negativity and increase shalom in your life and develop a healthier life through movement and nutrition. For more information about her work-shops, CDs or counseling issues, she can be reached at 410-736-8118 and/or her e-mail address is [email protected].
A ten-year-old boy came home from school one day. His mother was making eggs for him and his sister. She put cheese on the eggs. The boy saw the cheese and burst into tears. “You know I don’t like cheese!” he shouted. How should the mom respond? The boy appears to be overreact-ing. Think for yourself how you would respond and then read on.
The mom asked him what had made him so up-set. He said that he feels no one considers what he wants. Mom understood that there was more at is-sue here than just dinner. There were other factors going on in the family that were beyond the boy’s
control and in that context, it made sense that he would be easily upset.
Communication is an important art in creating meaningful relationships. Be a speaker who is aware of his/her verbal, nonverbal and paraverbal messages. Be a listener who conveys understanding and validation. If we don’t understand the other’s message, inquire a bit more into what the other is really saying. Sometimes, good communication requires that we pull out an-other frying pan and start making eggs all over again.
Dvorah Levy, LCSW is a psychotherapist in pri-vate practice working with individuals and cou-ples. She maintains offi ces in Hewlett and Flat-bush and specializes in marriage, parenting and dating issues. Dvorah can be reached at (516) 660-7157.
CommunicatingContinued from Page 32
Making that first therapy appointment is tough. When you cal l, I wil l help lead you on a journey that is ful l of acceptance, empathy, growth,
and insight.
Women-centeredtherapy focused
on life’s turbulenceand transitions
Dodi Lee Lamm, 516-255-2009
Dodi Lee Lamm, Licensed Clinical Social Worker, 100 North Village Avenue, Suite 20
Rockville Centre, NY 11570

34 | November 2011 HEALTH LIVING
Feature Story
ating a blockage, requiring surgery to removed. But surgery does not stop the course of the disease. While powerful medications, including an-ti-inflammatories, immunosuppres-sives and corticosterouids, are used to treat its symptoms, they, too, are not a cure, and have serious side ef-fects, limiting their long-term useful-ness. After years of treatments with the best doctors and medications available, many Crohn’s patients see little or no improvement in their con-dition, and are willing to try anything that offers any hope for a cure.
That was the situation which faced Elaine Gottschall in the 1950’s when her four-year-old daughter was diagnosed with ulcerative colitis which refused to respond to standard medical thera-py. Desperate, she chanced to meet Dr. Sidney V. Haas, then 92 years old, who, years before, had written a widely used text book presenting his nutritional ap-proach to intestinal healing.
But by that time, modern med-icine had passed Haas by, and the doctors treating Gottschall’s daugh-
ter were recommending surgery. Gottschall was already frustrated with the inability of the doctors to help her daughter, and decided she had nothing to lose by letting old Dr. Haas examine her. The first ques-tion Haas asked Gottschall after ex-amining the girl was “What has this child been eating?” Gottschall then followed Haas’ simple nutritional ap-proach in feeding her daughter, and within ten days, she started show-ing marked improvement. Within a
few months, the girl’s symp-toms had subsided, and after two years on the diet, she was totally symptom free.
By that time, Haas had died, and Gottschall was the only one who appreciated the val-ue of his work. She became determined to prove that his approach to treating Crohn’s was medically valid. Through her research into the medi-cal literature, she was able to verify the scientific basis for Haas’ approach, and eventual-ly wrote a self-published book, called “Breaking the Vicious Cy-cle” to make Haas’ nutritional treatment theories accessible
to Crohn’s patients looking for a dif-ferent answer.
For many years, the medical com-munity remained skeptical, but it also failed to come up with any new approaches that offered hope for a real cure. Meanwhile, more desper-ate Crohn’s patients read Gottschall’s book, and tried the nutritional ap-proach it recommended, known as the Specific Carbohydrate Diet (SCD). It is an extremely difficult diet to fol-low, because it calls for the elimina-
tion of all sugars and starches. But for a surprisingly large number of those Crohn’s patients who were able to stick with it, the results justified the effort. Many say that they have been symptom-free without medication, and a smaller but significant number claim that they are completely cured .
The theory behind it, as explained by Yitzy Gruen, of Brooklyn, who has been totally symptom free for 7 years after a year on the diet, is that the disease is caused by harmful micro-organisms in the intestines which feed off sugar and starch. The only way to cure Crohn’s is to slowly kill off the micro-organisms by shutting off their food supply. But these or-ganisms are hardy, and any cheating at all on the diet, even something as innocuous as chewing a sweetened gum, can provide food for the germs, and perpetuate the disease. To work, the Specific Carbohydrate Diet must be followed strictly, at all times, with no cheating at all. This requires a lot of determination on the part of the patient, and support and planning by their family members and friends to help keep them going.
Treating Crohn’s With Diet
Continued from Page 1
Continued on p.35

November 2011 | 35HEALTH LIVING
Feature Story Directory Advertising
Treating Crohn’s With Diet
Continued from Page 34
Gruen admitted that the fi rst time he tried the diet, he couldn’t stick with it. The body’s adjust-ment to the diet during the fi rst two weeks is ex-tremely painful, and many patients, like him, can’t
get through it. But Gruen said that his Crohn’s symptoms were so serious that he was forced to try the diet a second time, and now knowing what to expect, he succeeded.
Gruen’s doctor was skeptical, but he didn’t try to stop him. However, he urged Yitzy to stay on his medications while on the diet. One key to Yitzy’s success the second time was careful preparation. His wife learned how to cook a variety of foods which meet the strict requirements of the diet. It felt strange giving up eating challah on Shabbos, but defeating Crohn’s was worth it. It also helps when other members of the family are eating the same things, so the patient doesn’t feel deprived. Yitzy learned to take his SCD foods with him wher-ever he went, and to eat an SCD meal immediate-ly before going to a party or a dinner, so that he wouldn’t be tempted to cheat. It also helps to have another Crohn’s suff erer as a partner on the diet, a sponsor to help support one another at times of weakness.
He emphasized that with the SCD diet there is no margin for error, no tolerance at all for cheating. But the benefi ts were worth it. After getting over the initial period of extreme pain and discomfort, Yitzy started to feel stronger and healthier. After six months on the diet, he felt confi dent enough to stop taking his medication, and doing so caused no ill eff ects. The next time he was examined by his doctor, who pronounced himself satisfi ed with Yitzy’s progress, he told him that he had stopped taking the medication. The doctor shrugged, unim-pressed. Yitzy continued to improve. After another few months on the diet, Yitzy started to cautiously work his way back onto regular foods, one at a time.
When his doctor examined his intestines with a colonoscopy, he could fi nd no signs of active dis-ease. The blockages had cleared up. Long painful-ly thin because his body could not properly absorb nutrients, Yitzy started to put on weight. Eventu-ally, he came to believe that he was fully cured of the disease. He was able to start eating dairy foods, with no ill eff ects, even though he had suf-
fered from lactose intolerance since he was a child.Now, seven years later, promoting the Gottschall
diet to other Crohn’s suff erers has become one of Yitzy’s missions in life. He and his wife meet with Crohn’s couples to give them advice and encour-agement. There are more like Yitzy, throughout the US and in Israel, who credit the SCD diet with curing of Crohn’s. Today they provide support and
resources for those who have tried the traditional medical treatments, and are still look-ing for something that will work better.
One resource which pro-vides all kinds of raw and pre-pared foods and ingredients for people the SCD diet is an on-line site: www.diges-tivewellness.com, It was start-ed by a Crohn’s suff erer named Rochel Weiss, whose personal experience and success with the Gottschall diet parallel’s Gruen’s, and she, too, feels like she is on a mission. Operated with the assistance of mem-bers of her family, the on-line
store off ers a full range of SCD compliant-products, including baking and cooking ingredients, snacks and beverages, condiments and sauces, as well as lots of advice and encouragement for those trying to stay on the diet for the 2 years it typically takes to cure them, if it works.
The SCD diet doesn’t work for everyone. Some Crohn’s suff erers try it, and stick to it, but see no improvement. According to Dr. Stuart Ditchek, who is one of the few doctors in Brooklyn who actually recommends the SCD diet, it seems to work with about 80% of his Crohn’s patients who can stick with it long enough. Apparently there are signif-icant individual variations among those who suf-fer from the disease, and factors which determine whether the diet will or will not work for them.
There are other types of diets and unconven-tional treatments that are available for Crohn’s suf-ferers, but they do not have the successful track re-cord of the SCD diet, nor, in Dr. Ditchek’s opinion, an equally sound nutritional and scientifi c basis.
Ditchek notes that it is very hard to do a tradi-tional double-blind scientifi c study of how a diet works, because no two people follow a diet ex-actly the same way. That is why many doctors are still skeptical of the SCD diet’s eff ectiveness. But it is hard to argue with the successful results that many patients have had with it, avoiding surgery, and being able to stay symptom free with medi-cation. Even though the results are still considered anecdotal, they are impressive.
Today, Ditchek says, even the most treatment-oriented physician is more open to a nutritional ap-proach, as long it is used in combination with, rath-er than as a substitute for, traditional medications.
The bottom line, according to Ditchek, is that those with Crohn’s who are able to control their symptoms with medication do have a choice. Stay-ing on the diet is diffi cult, and it doesn’t work for everyone. However, those for whom medication is not working to control their symptoms appar-ently have little to lose and everything to gain by trying it.

36 | November 2011 HEALTH LIVING
Health Provider BulletinDirectory Advertising
Edison Home Health Care Event Draws Overfl ow Crowd In Boro Park
On November 9th at Bais Yaa-kov of Boro Park Elementary School, Edison Home Health Care sponsored an evening titled “Are You Concerned About Caring For a Loved One At Home?”
The importance and rele-vance of the subject was dem-onstrated by the many partici-pants who turned out to listen to the experts, who discussed the complex regula-tions governing eligibility regarding home care ser-vices and Medicaid. Most of the participants were members of the so called “sandwich generation” who are confronted with the problem of dealing with elderly parents and felt the need to be prop-erly informed about the options available to them, as they face the need to make the right decision.
The highlight of the evening was Rabbi Paysach Krohn who spoke on the topic “Caring for our Par-ents as they Cared for Us.”
The panel included Mr. Isaac Soskin, CEO of Re-vival Home Care. He explained to the audience that it is very diffi cult to reverse bad decisions once they are in place. “We are here to urge you to get the right
information, we are here to help you make the right decision.”
Mr. Eli Stolberg, who is a Med-icaid Consultant from Edison Home Care, gave a most detailed and professional presentation as to the steps that need to be tak-en in order to secure eligibility for Medicaid.
The importance of selecting the right home care agency was also emphasized at the seminar. When a patient or family member is hospitalized and home care will be needed after discharge, the patient or family have the right to choose the agency most appropriate for their spe-cial needs. Unless they make their choice known to the social worker or case manager before discharge, total strangers will make the right choice for them. So if you or a loved one are in need of home care, make the right choice and choose Edison Home Health Care. Edison understands the needs of the Orthodox Jewish community and will help you nav-igate the road to recovery.
For more information on Edison Home Care, please call 718-705-5800.
Dicon: A Breakthrough in the Treatment of Irritable
Bowel Symptoms IBS, or Irritable Bowel Syndrome is a devastating
condition characterized by lower abdominal pain or discomfort, diarrhea, constipation (or alternating di-arrhea & constipation), gas, bloating, and nausea. IBS affl icts up to 20% of the world’s population and is the most common chronic health disorder in the United States, aff ect-ing more people than asthma, dia-betes, and depression combined.
There is no cure for IBS and cur-rent treatments focus on attempt-ing to manage the symptoms. There are several drugs that are used to treat IBS, though many have nega-tive side eff ects. In 2007 Zelnorm, a drug used to treat IBS Con-stipation, was removed from the market due to FDA con-cerns about possible adverse cardiovascular eff ects.
RAM Biotech LTD, an Israeli biotech start-up, de-veloped Dicon after years of research. Dicon is an all natural supplement and contains CHT (Combination Herbal Therapy), a patent pending combination of herbs that recalibrates and regulates the body’s di-gestive system. It can be purchased without a pre-scription.
To determine the eff ectiveness of Dicon in treat-ing IBS, RAM Biotech conducted a double blind pla-cebo controlled clinical trial under the auspices of Hadassah Hospital in Jerusalem, Israel. The partici-
pating patients were suff ering from a range of typi-cal IBS complaints such as constipation, diarrhea and pain-predominant IBS. Each of the test subjects was given a daily dose of either Dicon or a placebo for a
four-week period and the eff ects were monitored. The clinical trial showed that Dicon eliminates the symptoms of Irritable Bowel Syndrome charac-
terized by constipation with positive trends towards treat-ing IBS characterized by diar-rhea. The clinical trial also indi-cated that patients taking Di-con enjoyed prolonged ben-efi ts even after discontinuing use of the medicine.
Subsequent to the results from the clinical trial, RAM Bio-
tech received seed money from the Offi ce of the Chief Scientist [OCS], the Is-
raeli agency tasked with supporting and incubating Israeli hi tech and biotech startups. Backed by the Is-raeli agency and encouraged by the overwhelming success of the clinical studies, RAM Biotech began production of Dicon.
Dicon has just been introduced to the US market and is currently being sold in GNC & Vitamin World. Dicon is also available online at www.diconDS.com as well as in health stores and pharmacies.
For more information or to contact us, please go to our website, www.diconDS.com
PESACH TIKVAH/DOOR OF HOPEFAMILY AND CHILDREN SERVICES
$ $ $$
Pesach TikvahDoor Of HopeFamily & Children Services• Services for Children with Special Needs• Recovery Based Residences• Respite Program • Family Counseling Center• Psychiatric Assessment and Treatment• Continuing Day Treatment Program• Holocaust Survivors Program• Summer Program for Children with Developmental Disabilities
PESACH TIKVAHHOPE DEVELOPMENT, INC.18 Middleton StreetBrooklyn, NY 11206Tel: 718-875-6900Fax: 718-875-6999Web: www.pesachtikvah.orgE-Mail: [email protected]
ACHIEVE INNER BALANCE
AND OUTWARD HARMONY WITH ACUPUNCTURE
www.2ndNatureAcu.com /[email protected]
Dbmm!gps!bo!Bqqpjounfou!ps!Dpotvmubujpo!Upebz"
ma
Upebz"z
AcupunctureFacial Rejuvenation
CuppingPediactric Acupunctre
Placenta EncapsulationAuricular Acupuncture
Ftuifs!Ipsotufjo!M/Bd/!!:28.525.4942
Parents Educating and Advocating for our Children’s Health
(PEACH)Call # 212 -200- 5010
Pin#61370
Will be hosting conference calls every Tuesday evening from
9pm- 10pm est.
Moderated by Mrs. Chany Silber on the subject of on the recent
concerns regarding vaccination.

November 2011 | 37HEALTH LIVING
Health Provider Bulletin Directory Advertising
NYM is The Only Hospital in Brooklyn to Offer Navigational Bronchoscopy
New York Methodist Hospital’s Comprehensive Lung Cancer Center (CLCC) now off ers navigational bronchoscopy, a minimally invasive diagnostic pro-cedure that provides new options for the diagnosis and treatment of lung disease.
Lung cancer is the number one cause of cancer-related deaths in the United States, among both men and women. The disease claims more lives than colon, prostate and breast cancer combined. Smoking ac-counts for about 85 to 90 percent of lung cancer cas-es, with other causes relating to secondhand smoke, air pollution, and exposure to asbestos.
Lung screenings are recommended for individu-als between the ages of 50 and 80 who have a family history of lung cancer, have a smoking history of at least one pack of cigarettes per day for 10 years, have a past history of smoking less than ten years ago, or have had repeated exposure to secondhand smoke or other cancer-causing agents such as asbestos or radon. Lung cancer screenings may be performed using standard chest x-rays, sputum cytology, or CT (computed tomography) scans, a procedure which involves a rotating, low-dose x-ray beam.
Previously, if a tumor or unknown mass was de-tected during the screening, a needle or surgical bi-
opsy was performed. Both of these procedures could cause complications and discomfort.
Traditionally, bronchoscopy is a procedure used to examine the major air passages of the lungs through a thin lighted tube called a bronchoscope. This allows a physician to evaluate the lungs and collect small tis-sue samples to diagnose lung disease and lung can-cer. However, traditional bronchoscopy cannot reach the distant regions of the lung, where more than two-thirds of all lung lesions are found.
Unlike traditional bronchoscopy, navigational bronchoscopy uses GPS-like technology to posi-tion small, flexible catheters deep into the lungs, using natural airway access. This allows physi-cians to take remote tissue samples that can lead to earlier diagnosis and staging of lung abnormal-ities. “With navigational bronchoscopy, recovery from biopsy is faster than for patients who have had more invasive biopsy procedures,” said Suhail Raoof, M.D., chief of pulmonary and critical care medicine at NYM.
Navigational bronchoscopy can also be used to place markers in the lungs that guide radiation on-cologists to a specifi c area that is targeted for treat-ment with radiation.
Robotic-Assisted RehabilitationNew York Methodist Hospital recently acquired a
robotic-assisted rehabilitation system, known as the Lokomat, and it is already helping many patients re-cover from diseases and disorders like spinal cord in-jury, stroke, traumatic brain injury, multiple sclerosis, cerebral palsy, and Parkinson’s disease. While there is currently no cure, certain treatments have been shown to greatly improve quality of life.
One of these treatments places the patient in a harness suspended slightly above a moving platform while a therapist physically moves the patient’s legs. In advanced versions of treadmill training, the orthosis mechanically moves the pa-tient’s legs, training the gait more naturally and accurately. The Lokomat, in conjunction with oth-er kinds of physical therapy, helps patients re-
gain mobility. The computerized robot, which is manned by one of the trained physical therapists at NYM, not only controls the speed and level of difficulty, but monitors how much effort the pa-tient is making, providing constant feedback and personalized assessment.
The premise of this robotic-assisted rehabilitation is that new movement or an improvement to an ex-isting movement in a patient with a neurological dis-order can be achieved only through a very high num-ber of repetitions of that movement. The new tech-nology allows patients to repeat movements at a high level of accuracy.
“I have witnessed notable improvements with pa-tients who have been rehabilitated on our machine, in less than three weeks,” said Mr. Manuel Wilfred, P.T., chief of physical therapy.
In addition to the Lokomat, used for rehabilita-tion involving walking and gait, New York Method-ist Hospital has also acquired the Armeo, a machine for the upper body, which aims to increase mobil-ity in the arms and fi ngers for patients who have experienced neurological illness. The occupation-al therapy exercises made possible by this machine are designed to provide patients with the specifi c skills needed to reach the highest level of indepen-dence in daily activities. The Armeo provides com-puterized games and activities to improve coordi-nation and functional ability. An “assisted spring” in the device gives patients the boost they need to complete the tasks set for them by occupation-al therapists.
For more information, please call the Depart-ment of Neurosciences’ Rehabilitation Division at 718.780.3248.
Manuel Wilfred, P.T., chief of physical therapy monitors output on the newly acquired robotic orthosis machine.
38 | November 2011 HEALTH LIVING
Health & Living Checklists
helpful as two hours under artifi cial light. If one cannot go outdoors or is homebound, other so-lutions can include opening the curtains to al-low more sunlight to penetrate rooms, sitting near a lamp or under a skylight.
If these tips do not work then the next pre-scribed method is light or phototherapy. This entails 30 minutes of sitting in front of special fl orescent lights, which are 25 times stronger than regular lights. This is thought to be a safer alternative to medication since no major side ef-fects were reported; however, for pregnant pa-tients, light therapy has not yet been systemat-ically evaluated. Common side eff ects from this therapy include headaches, eyestrains and irri-tability. Medicaid does not cover this treatment, but some insurance companies will reimburse for it. One can purchase a wide variety of SAD lights online without a prescription, but it is rec-ommended to seek a professional for treatment.
If all else fails, then the next step is taking a prescription anti depressant such as Prozac, Zoloft, Paxil, and Celexa which increase sero-tonin levels in the brain. Wellbutrin XL (bupro-pion hydrochloride) became the fi rst drug ap-proved specifi cally for SAD in the U.S.
The Center for Environmental Therapeutics (CET), a non-profi t organization which provides educational materials about SAD, off ers free self-assessment questionnaires that you can download from their site, http://www.cet.org/ as well as interpretation guides, to help you de-termine if you should seek professional advice.
Psychotherapy is also highly recommend-ed and should work in conjunction with med-ication.
Continued from page 3
Checklist:Winterizing Your Home
CLEAN GUTTERS
After Fall, chances are your gutters are clogged with leaves and debris. Before the snow and heavy rain come, it would be wise to remove (by hand or with a water hose) all the dirt that collected in your gutters. If you don’t do this then winter’s rain and melting snow cannot properly drain. Clogged drains can form ice dams, in which water backs up, freezes and causes water to seep into the house. You should also examine the roof for missing or cracked shingles. You may need to re-place a broken tile to avoid ice and snow build-up, which can be a costly problem to fix later, and make your house cold.
PROTECT YOUR PIPES Winter’s bitter chill can freeze your pipes mak-
ing them susceptible to bursting, and causing a major flood. This is particularly true to pipes that are exposed to the outside air in winter. Shut off the main water supply to outdoor hose bibs and sprinkler systems. In addition, the water in the ex-terior part of the pipes should be drained to pre-vent it from freezing and cracking the pipe. Make sure to examine your home’s pipes in unheated areas (look at attics, uninsulated basements, ga-rages and crawl spaces) to make sure they are properly insulated. Wrap them with pre-mold-ed foam rubber sleeves or fiberglass insulation, which can be purchased at your local hardware store. To keep pipes from freezing, you can wrap them with heating tape, which contains an elec-trical cord that emits heat.
PLAN FOR YOUR PLANTSPlant evergreens close to your home; they
are good at blocking strong winds and add ex-tra privacy to your windows. Trim tree limbs and branches that overhang the house—they can cause major damage when snow accumulates and can bring down power lines. You may also want to fertilize and reseed your lawn.
SEAL AIR DRAFTSCheck all windows and doors for air pockets.
A little escaped air here and there can lead to bigger monthly heating bills. Inspect the weath-er stripping and caulking around doors and win-dows. Install door sweeps to the bottom of out-side doors to prevent air leakage. There are var-ious door sweeps on the market today, but until you get to the store to buy one, a simple rolled up bath towel will do the trick just fine. Install storm windows or inexpensive window film to add ad-ditional window insulation. Use insulated win-dow curtains to prevent heat loss. If possible, re-move window air conditioner units for the win-ter. If you can’t, install a plastic cover on each unit to keep the cold wind outside from blowing into your house through the vents.
TAKE THE HEAT You don’t want to be surprised to learn on
the first cold day of the winter that you have a broken heating system. Before winter sets in, do a test run by turning the thermostat to heat mode and setting it to 80 degrees. If everything is running smoothly, you will hear the furnace turn on and feel the heat come up within a few minutes. A good way to save money is by hav-ing a programmable thermostat installed. You can then set it to turn the heat down at those times when people are sleeping snug under the covers, or when the house is usually empty, and bring the heat back up just before people wake up or return home.
ALARM SOUND OFFMake sure your fire alarm and carbon mon-
oxide detectors are functioning and have work-ing batteries.
SAFETYIf you are going away at any time, have a neigh-
bor pick up your mail and any circulars left on your property. If possible have someone park in the driveway and place the garbage cans out to make the house look lived-in.
Make sure your street address is visible from the street to allow emergency personnel to find it quickly, if they are needed. You should also re-place outdoor lights as soon as they burnt out, so people don’t trip or fall on your property. Proper lighting also deters burglars.
Stock up on your favorite over-the-counter medications, as well as flashlights, batteries and non-perishable foods in case of blackout or pow-er outage.
CARCheck your car battery. Put snow tires in your
trunk together with other emergency items such as shovels, scraper, and jumper cables. Also, make sure you have enough windshield washer fluid.
UNCLE SAM TO THE RESCUEThe federal Energy Tax Credit was part of the
American Recovery and Reinvestment Act set up to boost the economy by helping homeown-ers make energy-saving home upgrades to get the credits. The tax credits are not as high as last year but are still worth exploring. There are also state tax credit programs and rebates available from local utility companies to help pay for the purchase and installation of the most energy ef-ficient appliances or insulated windows. To quali-fy, you made need to buy specific models or have them installed by a participating contractor, so do your homework. Check out the web sites of your local utilities or on line resources which special-ize in this information such as www.DSIRE.org.
At a Glance
Staphylococcus aureus) which used to only be seen in hospital patients, but is now showing up in the com-munity. Fortunately, we do have a few drugs that can treat MRSA, but the situation bears watching close-ly. In addition, we now have a broad variety of vac-cines which we can use to safely protect virtually all adults and children against the most common forms of the fl u, and senior citizens against pneumonia in-fections, which are a special threat to that age group. Ask your primary care doctor about which vaccines are recommended to keep you healthy during the current fl u season.
In conclusion, when asked to give an answer “on one leg” to the age old question of “what should I do to stay healthy?” I would answer that you need to do the simple, basic things that keep our bodies healthy and our immune systems strong, including drinking plenty of fl uids, getting enough rest, and davening for siyata d’shamaya to keep us well.
Shira Burnstein MD is a Board Certifi ed Internist and mother of eight children who has been in prac-tice for twenty-six years. She has a Primary Care private practice at 2044 Ocean Avenue in Brooklyn New York. Her offi ce screens for diabetes, high blood pressure, high cholesterol, and heart disease in ad-dition to many other diseases. Flu vaccines, blood tests and EKGs done on premises. Dr. Burnstein can be contacted at 718-998-1700 for further questions.
Dr.’s Desk Continued from Page 39

November 2011 | 39HEALTH LIVING
Prevention is the Best CureWhile doctors are known for healing
the sick, the best thing that they can do for their patients is to keep them healthy, and help them to avoid getting sick in the fi rst place.
In addition to developing powerful new medications that provide hope for the cure of diseases which have been the scourge of mankind through history, med-ical science has given us a much more so-phisticated understanding of how bodies work, and some of its latest fi ndings fl y in the face of what many of us have long considered to be “common sense” about healthy living.
For example, it is widely known that obesity has reached epidemic propor-tions in our country. Obesity is a major risk factor for developing diabetes and cardiovascular disease, and poses a seri-ous threat to the health of young and old alike. It is also well known that the exces-sive amount of sugar and other high cal-orie sweeteners contained in the foods that we eat are major factors driving the obesity epidemic. This leads many to con-clude that foods which substitute low cal-orie artificial sweeteners are better for our health. However, new research indi-cates that consuming low calorie artifi cial sweeteners may also lead to obesity, lead-ing to many of the same kinds of health problems caused by excess sugar.
I have conducted an informal survey among my own patients regarding artifi -cial sweeteners and obesity that supports this same conclusion. In the end, my pa-tients who drink diet sodas loaded with artifi cial sweeteners were not much better off than those who drank the higher calo-rie versions in terms of the impact on their bodies. The healthier alternative turns out to be consuming drinks which have fewer added sweeteners of any kind, such as wa-ter, unfl avored seltzer, or low fat milk (if you are not lactose intolerant). If you must have something that tastes sweet, you are much better off drinking something natural, like orange juice (if you don’t have acid refl ux or diabetes), which has real nutritional value.
Although eating a healthy diet is very important, it is also necessary to consult with your doctor to make sure that the “healthy food” that you are eating does not interfere with your medications. For example, grapefruit juice, which contains many important daily vitamins, may inter-fere with the eff ectiveness of some pre-scription medications. Leafy green veg-etables, which contain folic acid and oth-er vitamins may interfere with the eff ec-tiveness of certain blood thinning med-ications. People who drink a lot of cran-berry juice in an eff ort to safeguard them-selves against urinary tract infections can bring on an infl ammation of the bladder wall known as interstitial cystitis.
Thanks to the advances of modern medicine, we and our children can look forward to a much longer life, on average, than our parents and grandparents could. But if we want to remain active and pro-ductive during those extra years, we need to apply the lessons of recent medical re-search to the way we lead our daily lives.
One of the other fastest growing health problems we face today is memory loss, which is increasing among our senior cit-izens as they are living longer. The most important thing to do if you notice mem-ory loss in yourself or your loved one is to make an appointment with your prima-ry care doctor. There are several reversible causes of memory loss such as hypothy-roidism (where your thyroid does not func-tion as well as it should) and vitamin B12 defi ciency that your doctor can test for and treat. Although we have no cure for other types of memory loss, such as that which is associated with Alzheimer’s disease, there are certain medications that can slow its progression. Ask your primary care doctor about what can be done to slow the pro-gression of Alzheimer’s disease if you or your loved one has this diagnosis. Studies have shown that one of the best ways to keep our minds sharp as we grow older is to keep mentally active. A crossword puz-zle a day is probably the best way that we know to “keep dementia away.”
Another way that seniors can maintain their health is to remain physically active. Even something as easy as taking a brisk walk for 45 minutes 4 times a week, along with certain vitamins and supplements, can help prevent worsening of osteopo-rosis. Seniors should ask their primary care doctor to test them for the fi rst signs of the diseases of old age which we can treat to-day before they impact their quality of life.
In order to protect the health of their children, parents of infants and young chil-dren need to maintain proper hygiene. They need to be careful about the trans-mission of germs, keep their hands clean through frequent washing, and use dis-posable towels and food utensils only once. Hand washing is the most eff ective way of preventing the spread of disease. Proper hand washing consists of lathering soap on your hands for a total of fi fteen seconds (approximately the amount of time required to sing the ABCs at a mod-erate speed) before rinsing. This is espe-cially important in today’s multi-genera-tional households in which young chil-dren and their grandparents are living in close proximity to each other.
Finally, there are new threats that we need to protect ourselves against. One of them is a new strain of drug-resistant bac-teria known as MRSA (Methicillin-Resistant
From the Doctor’s Desk: Shira Burnstein MD
Board Certifi ed Internist
™
164-11 Chapin Parkway, Jamaica Hills, NY 11432718-298-7800 • www.margarettietz.org
A Member of the Beth Abraham Family of Health Services
Centrally located near the Queens communities of Kew Gardens Hills, Hillcrest & Jamaica Estates. Only 20 minutes from Brooklyn, Manhattan & the Five Towns.
adlib
unlim
ited.
com
Our newly renovated roomsare reflective of our
upscale ambiance.
Our impressively expansive dedicated rehab gymis well-stocked with the latestcutting edge equipment.
We are proud to unveil the transformed Margaret Tietz Center –featuring state-of-the-artsubacute and long-term care in a brand new luxurious setting.
State of the Art Rehab: Physical, Occupational & Speech Therapies• Specializing in quick recovery for
orthopedic conditions such as Hip/Knee replacements & fractures
• Holistic Team approach focused onachieving independence and speedyreturn to the community
Continued on p.38

OR RECOMMEND ZAHLER HeightFactor™.
YOU CAN TIPTOE AROUND THE ISSUE...
NOW THERE’S A NATURAL SUPPLEMENT THAT HELPS CHILDREN REACH THEIR FULL GROWTH POTENTIAL.
Zahler’s HeightFactorTM is an advanced, proprietary blend of vitamins, minerals and nutrients that help stimulate the pituitary system in its production of growth hormones, and provide the proper nutrition to sustain necessary growth.
These statements have not been evaluated by the food & drug administration. These products are not intended to diagnose, treat, cure, or prevent any disease. HeightFactor™ is a trademark of Advanced Nutrition by Zahler.
Every vitamin developed by Zahler goes through rigorous testing and is manufactured and bottled in a state-of-the-art GMP, NNFA & NSF® certified facility.
Ask ZahlerHave Questions? Call 1-877-ASK-ZAHLER and identify yourself as a health supplements retailer or distributor.
Online at: www.Zahlers.com or www.AskZahler.com
If your aren’t carrying Zahler yet, Call us. And find out why we’re one of the fastest growing brands in the industry.
Contact Nathan at: 1-212-444-9936 x 202 or Email: [email protected]
New!
THE ONLY AUTHENTIC HEIGHT & GROWTH FORMULA
KOSHER PAREVE UNDER STRICT SUPERVISION OF RABBI S. STERN AND THE ORTHODOX UNION