Prevention and Management of Pressure Ulcers - Black ...
61
Version 1.4 January 2020 Prevention and Management of Pressure Ulcers Target Audience Who Should Read This Policy All Clinical Staff
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Prevention and Management of Pressure Ulcers - Black ...
Version 1.4 January 2020
Prevention and Management of Pressure Ulcers
Target Audience
Who Should Read This Policy
All Clinical Staff
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020
2
Ref. CONTENTS Page No.
1.0 Introduction 4
2.0 Purpose 4
3.0 Objectives 4
4.0 Process 4-20
5.0 Procedures connected to this policy 20
6.0 Links to relevant Legislation
6.1 Links to relevant National Standards
6.2 Links to other key Policies
6.3 References
20 20 21
21
7.0 Roles and responsibilities for this policy 23
8.0 Training 25
9.0 Equality Impact Assessment 26
10.0 Data Protection and Freedom of Information 26
11.0 Monitoring this Policy is Working in Practice 27
APPENDICES
1 Guidelines for completion of a body map 29
2 Adult Body map chart & skin integrity assessment sheet 30-31
3 Paediatric skin integrity & tissue viability risk assessment tool 32-34
4 Flow chart for prevention & treatment of Pressure Ulcers 35
5 Guide to reporting pressure ulcers - DATIX 36
6 Areas of the body at risk of Pressure Ulcers 37
7 Pressure Ulcer Grading Chart (Categories 1-4 etc.) 38
8 Grade 3 & 4 Pressure Ulcer Review Panel – Terms of Reference 39-40
9 Root Cause Analysis (RCA) for Pressure Ulcer Grades 2, 3 & 4 41-44
10 Wound care and treatment – care plan template 45-46
11 Management & Prevention of Nappy Rash & Moisture Lesions 47
12 Waterlow risk assessment tool 48-49
13 Malnutrtion Universal Screening Tool (MUST) 50-52
14 Pain assessment for people with dementia 53-56
15 Pain assessment for children 57
16 Simple, safe & effective 30° tilt 58
17 Pressure relieving equipment selection flow chart 59
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020
3
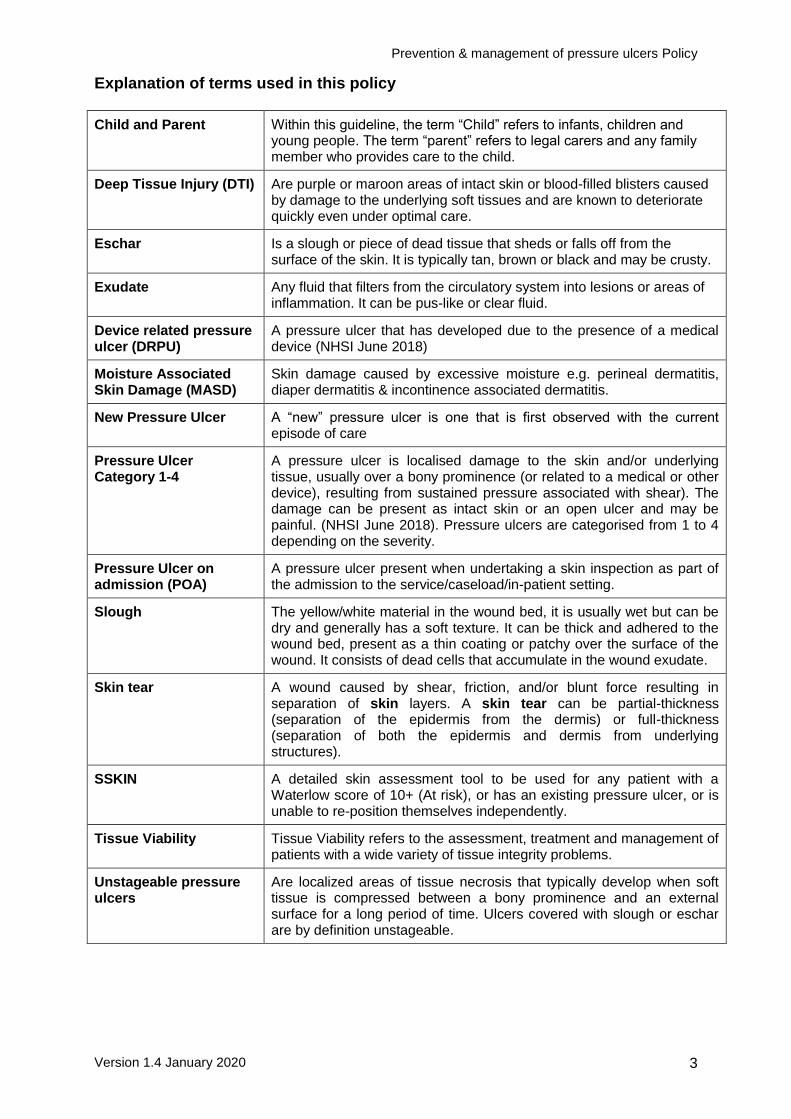
Explanation of terms used in this policy
Child and Parent Within this guideline, the term “Child” refers to infants, children and young people. The term “parent” refers to legal carers and any family member who provides care to the child.
Deep Tissue Injury (DTI) Are purple or maroon areas of intact skin or blood-filled blisters caused by damage to the underlying soft tissues and are known to deteriorate quickly even under optimal care.
Eschar Is a slough or piece of dead tissue that sheds or falls off from the surface of the skin. It is typically tan, brown or black and may be crusty.
Exudate Any fluid that filters from the circulatory system into lesions or areas of inflammation. It can be pus-like or clear fluid.
Device related pressure ulcer (DRPU)
A pressure ulcer that has developed due to the presence of a medical device (NHSI June 2018)
Moisture Associated Skin Damage (MASD)
Skin damage caused by excessive moisture e.g. perineal dermatitis, diaper dermatitis & incontinence associated dermatitis.
New Pressure Ulcer A “new” pressure ulcer is one that is first observed with the current episode of care
Pressure Ulcer Category 1-4
A pressure ulcer is localised damage to the skin and/or underlying tissue, usually over a bony prominence (or related to a medical or other device), resulting from sustained pressure associated with shear). The damage can be present as intact skin or an open ulcer and may be painful. (NHSI June 2018). Pressure ulcers are categorised from 1 to 4 depending on the severity.
Pressure Ulcer on admission (POA)
A pressure ulcer present when undertaking a skin inspection as part of the admission to the service/caseload/in-patient setting.
Slough The yellow/white material in the wound bed, it is usually wet but can be dry and generally has a soft texture. It can be thick and adhered to the wound bed, present as a thin coating or patchy over the surface of the wound. It consists of dead cells that accumulate in the wound exudate.
Skin tear A wound caused by shear, friction, and/or blunt force resulting in separation of skin layers. A skin tear can be partial-thickness (separation of the epidermis from the dermis) or full-thickness (separation of both the epidermis and dermis from underlying structures).
SSKIN A detailed skin assessment tool to be used for any patient with a Waterlow score of 10+ (At risk), or has an existing pressure ulcer, or is unable to re-position themselves independently.
Tissue Viability Tissue Viability refers to the assessment, treatment and management of patients with a wide variety of tissue integrity problems.
Unstageable pressure ulcers
Are localized areas of tissue necrosis that typically develop when soft tissue is compressed between a bony prominence and an external surface for a long period of time. Ulcers covered with slough or eschar are by definition unstageable.
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 4
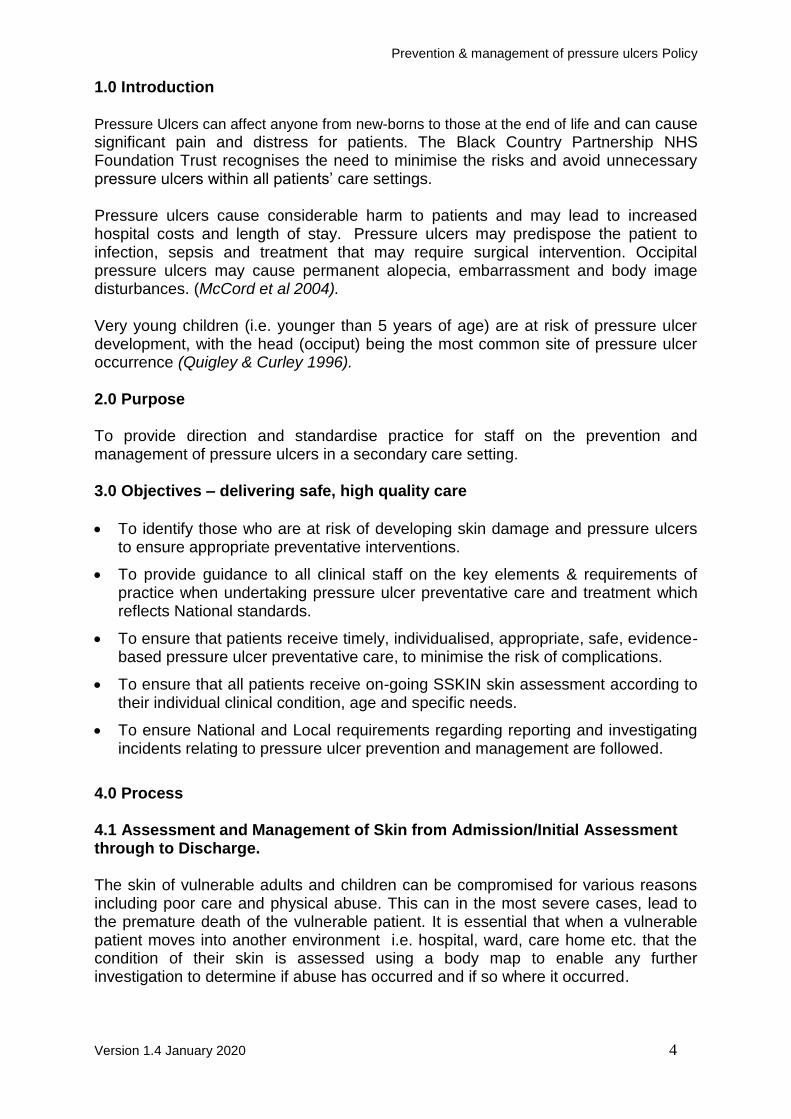
1.0 Introduction Pressure Ulcers can affect anyone from new-borns to those at the end of life and can cause significant pain and distress for patients. The Black Country Partnership NHS Foundation Trust recognises the need to minimise the risks and avoid unnecessary pressure ulcers within all patients’ care settings. Pressure ulcers cause considerable harm to patients and may lead to increased hospital costs and length of stay. Pressure ulcers may predispose the patient to infection, sepsis and treatment that may require surgical intervention. Occipital pressure ulcers may cause permanent alopecia, embarrassment and body image disturbances. (McCord et al 2004). Very young children (i.e. younger than 5 years of age) are at risk of pressure ulcer development, with the head (occiput) being the most common site of pressure ulcer occurrence (Quigley & Curley 1996).
2.0 Purpose To provide direction and standardise practice for staff on the prevention and management of pressure ulcers in a secondary care setting. 3.0 Objectives – delivering safe, high quality care
To identify those who are at risk of developing skin damage and pressure ulcers to ensure appropriate preventative interventions.
To provide guidance to all clinical staff on the key elements & requirements of practice when undertaking pressure ulcer preventative care and treatment which reflects National standards.
To ensure that patients receive timely, individualised, appropriate, safe, evidence-based pressure ulcer preventative care, to minimise the risk of complications.
To ensure that all patients receive on-going SSKIN skin assessment according to their individual clinical condition, age and specific needs.
To ensure National and Local requirements regarding reporting and investigating incidents relating to pressure ulcer prevention and management are followed.
4.0 Process 4.1 Assessment and Management of Skin from Admission/Initial Assessment through to Discharge. The skin of vulnerable adults and children can be compromised for various reasons including poor care and physical abuse. This can in the most severe cases, lead to the premature death of the vulnerable patient. It is essential that when a vulnerable patient moves into another environment i.e. hospital, ward, care home etc. that the condition of their skin is assessed using a body map to enable any further investigation to determine if abuse has occurred and if so where it occurred.
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 5
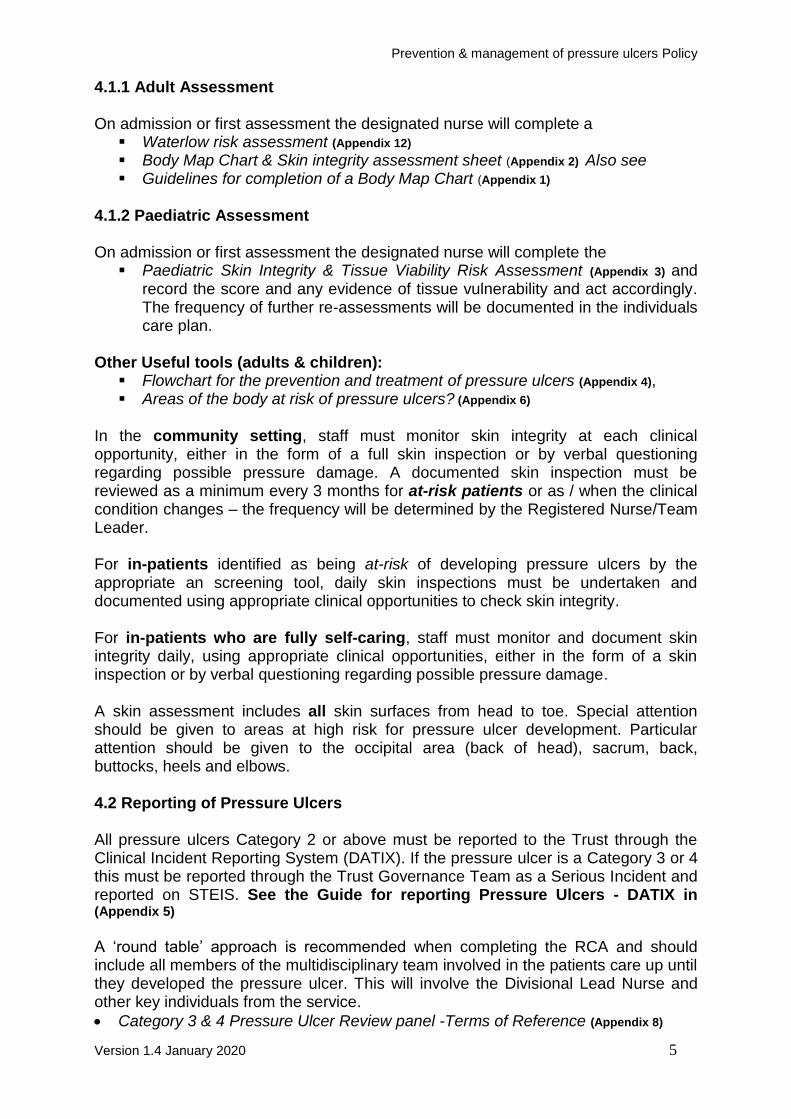
4.1.1 Adult Assessment On admission or first assessment the designated nurse will complete a
Waterlow risk assessment (Appendix 12) Body Map Chart & Skin integrity assessment sheet (Appendix 2) Also see Guidelines for completion of a Body Map Chart (Appendix 1)
4.1.2 Paediatric Assessment On admission or first assessment the designated nurse will complete the
Paediatric Skin Integrity & Tissue Viability Risk Assessment (Appendix 3) and record the score and any evidence of tissue vulnerability and act accordingly. The frequency of further re-assessments will be documented in the individuals care plan.
Other Useful tools (adults & children):
Flowchart for the prevention and treatment of pressure ulcers (Appendix 4), Areas of the body at risk of pressure ulcers? (Appendix 6)
In the community setting, staff must monitor skin integrity at each clinical opportunity, either in the form of a full skin inspection or by verbal questioning regarding possible pressure damage. A documented skin inspection must be reviewed as a minimum every 3 months for at-risk patients or as / when the clinical condition changes – the frequency will be determined by the Registered Nurse/Team Leader. For in-patients identified as being at-risk of developing pressure ulcers by the appropriate an screening tool, daily skin inspections must be undertaken and documented using appropriate clinical opportunities to check skin integrity. For in-patients who are fully self-caring, staff must monitor and document skin integrity daily, using appropriate clinical opportunities, either in the form of a skin inspection or by verbal questioning regarding possible pressure damage. A skin assessment includes all skin surfaces from head to toe. Special attention should be given to areas at high risk for pressure ulcer development. Particular attention should be given to the occipital area (back of head), sacrum, back, buttocks, heels and elbows. 4.2 Reporting of Pressure Ulcers All pressure ulcers Category 2 or above must be reported to the Trust through the Clinical Incident Reporting System (DATIX). If the pressure ulcer is a Category 3 or 4 this must be reported through the Trust Governance Team as a Serious Incident and reported on STEIS. See the Guide for reporting Pressure Ulcers - DATIX in (Appendix 5) A ‘round table’ approach is recommended when completing the RCA and should include all members of the multidisciplinary team involved in the patients care up until they developed the pressure ulcer. This will involve the Divisional Lead Nurse and other key individuals from the service.
Category 3 & 4 Pressure Ulcer Review panel -Terms of Reference (Appendix 8)
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 6
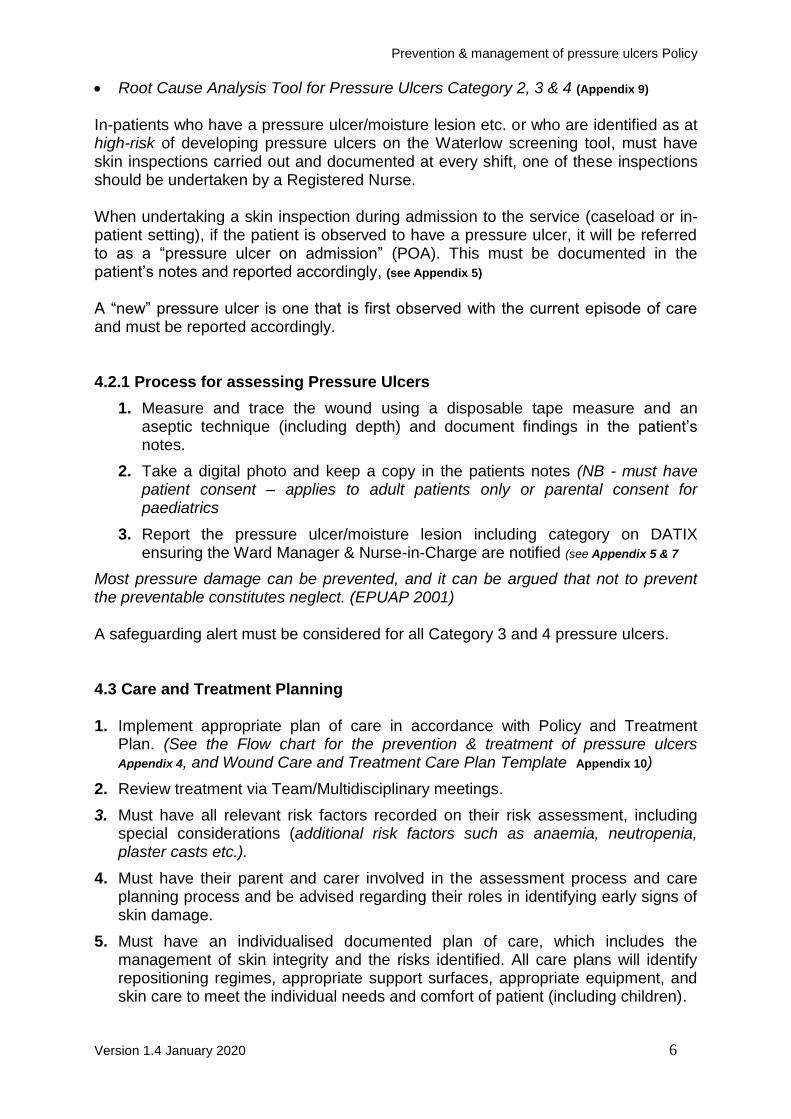
Root Cause Analysis Tool for Pressure Ulcers Category 2, 3 & 4 (Appendix 9) In-patients who have a pressure ulcer/moisture lesion etc. or who are identified as at high-risk of developing pressure ulcers on the Waterlow screening tool, must have skin inspections carried out and documented at every shift, one of these inspections should be undertaken by a Registered Nurse. When undertaking a skin inspection during admission to the service (caseload or in-patient setting), if the patient is observed to have a pressure ulcer, it will be referred to as a “pressure ulcer on admission” (POA). This must be documented in the patient’s notes and reported accordingly, (see Appendix 5)
A “new” pressure ulcer is one that is first observed with the current episode of care and must be reported accordingly. 4.2.1 Process for assessing Pressure Ulcers
1. Measure and trace the wound using a disposable tape measure and an aseptic technique (including depth) and document findings in the patient’s notes.
2. Take a digital photo and keep a copy in the patients notes (NB - must have patient consent – applies to adult patients only or parental consent for paediatrics
3. Report the pressure ulcer/moisture lesion including category on DATIX ensuring the Ward Manager & Nurse-in-Charge are notified (see Appendix 5 & 7
Most pressure damage can be prevented, and it can be argued that not to prevent the preventable constitutes neglect. (EPUAP 2001) A safeguarding alert must be considered for all Category 3 and 4 pressure ulcers. 4.3 Care and Treatment Planning 1. Implement appropriate plan of care in accordance with Policy and Treatment
Plan. (See the Flow chart for the prevention & treatment of pressure ulcers Appendix 4, and Wound Care and Treatment Care Plan Template Appendix 10)
2. Review treatment via Team/Multidisciplinary meetings.
3. Must have all relevant risk factors recorded on their risk assessment, including special considerations (additional risk factors such as anaemia, neutropenia, plaster casts etc.).
4. Must have their parent and carer involved in the assessment process and care planning process and be advised regarding their roles in identifying early signs of skin damage.
5. Must have an individualised documented plan of care, which includes the management of skin integrity and the risks identified. All care plans will identify repositioning regimes, appropriate support surfaces, appropriate equipment, and skin care to meet the individual needs and comfort of patient (including children).

Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 7
6. Patients must be assessed for a high specification pressure-relieving mattress if identified as high-risk, the Tissue Viability Nurse may be able to advice.
7. Patients will be prescribed appropriate dressings as advised by the Tissue Viability Nurse, including alginates, soft silicones, films, hydrogels, and foams.
8. Patients will be given access to an interpreter if English is not the family’s first language, to help with pressure ulcer management.
9. If there is evidence of improvement, continue with current plan of care and review accordingly.
10. If there is no improvement and there is evidence of deterioration the treatment plan must be reviewed with the local Tissue Viability Link Nurse. If the pressure ulcer deteriorates, a new DATIX must be submitted within 24 hours. Appendix
5
4.3.1 Non-compliance with Treatment Plans
Where there is an issue of non-compliance with recommended treatment plans, it is essential to ensure that the choice made is an informed one. Therefore, the patient’s capacity should always be considered and recorded in their records. If necessary, a best interest assessment should be completed and a safeguarding referral should be considered.
Please discuss the case with the relevant Line Manager and a Named Safeguarding Professional, as non-compliance may need to be considered.
In the case of children, the same process should be followed in as much as ensuring that the child is of an age to be deemed Gillick Competent. If the carers are seen as not adhering to any aspect of the care plan then again a safeguarding referral should be considered.
Not all pressure ulcers in an adult or child are the result of neglect or self-neglect but they may be an indication of lack of resources, lack of clinical skill or poor practice. As a result, consideration at each assessment should be given as to whether a Safeguarding Adults or Children’s referral should be made.
4.4 Who is at Risk? Deep tissue damage leading to pressure ulceration often occurs before outward signs are visible. Identifying individuals ‘at risk’ is essential in reducing the incidence of pressure ulceration. See Areas of the body at Risk of pressure ulcer areas diagram (Appendix 6) Although potentially all patients are at risk, some groups have an enhanced risk status these include;
Those with impaired mobility or who are immobile (including a recent fracture/ cast, prosthesis, splints, cardio vascular accident CVA)
Those with physical ill health e.g. chest infection, flu, winter vomiting disease
Those with severe depression leading to lack of motivation to mobilise
Those with anorexia nervosa
Those with impaired/compromised nutrition and/or dehydration
Those with a neurological or sensory deficit; dementia, CVA, MS, diabetes, spinal injuries, epilepsy, motor neurone disease
Those who are obese
Those with poorly controlled pain
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 8
The terminally ill
Those who are incontinent
Wheelchair users
Patients with chronic skin conditions such as eczema/psoriasis etc. should have specialist advice sought from a Dermatology specialist.
Assessment of the persons who have darker skin should have careful attention paid to any purplish/bluish looking areas of skin, localised heat or coolness and oedema
Health professionals also need to be aware that anxiety, a frequent feature of dementia and depression reduces the efficiency of the immune system. This has implications for existing ulceration and increases the risk of wound infection. 4.4.1 General Health When assessing the patient’s risk of pressure ulceration it is imperative that a holistic assessment is performed, as there are many predisposing factors such as:
Age - With increased age there is thinning of the dermis, which leads to decreased elasticity. The collagen in the dermis provides a buffer which helps to prevent disruption of the micro circulation. Also, it takes longer for an ulcer to heal in the older person when compared to a younger person. As age increases so does the likelihood of chronic illness which also predisposes to development of pressure ulcers.
Reduced Mobility - There may be numerous reasons why a patient (including children) has decreased mobility, neurological deficit such as paraplegia, multiple sclerosis, pain, diabetes and spinal injury or degeneration and patients undergoing major surgery. Reduced mobility increases the likelihood of pressure ulcer development.
Decreased Consciousness - There is a strong relationship between reduced movements and the development of pressure ulcers. Therefore, increased risk may be evident in those patients (including children) who are confused or patients on antidepressants or opioids because they may not move of their own accord in order to relieve their pressure areas.
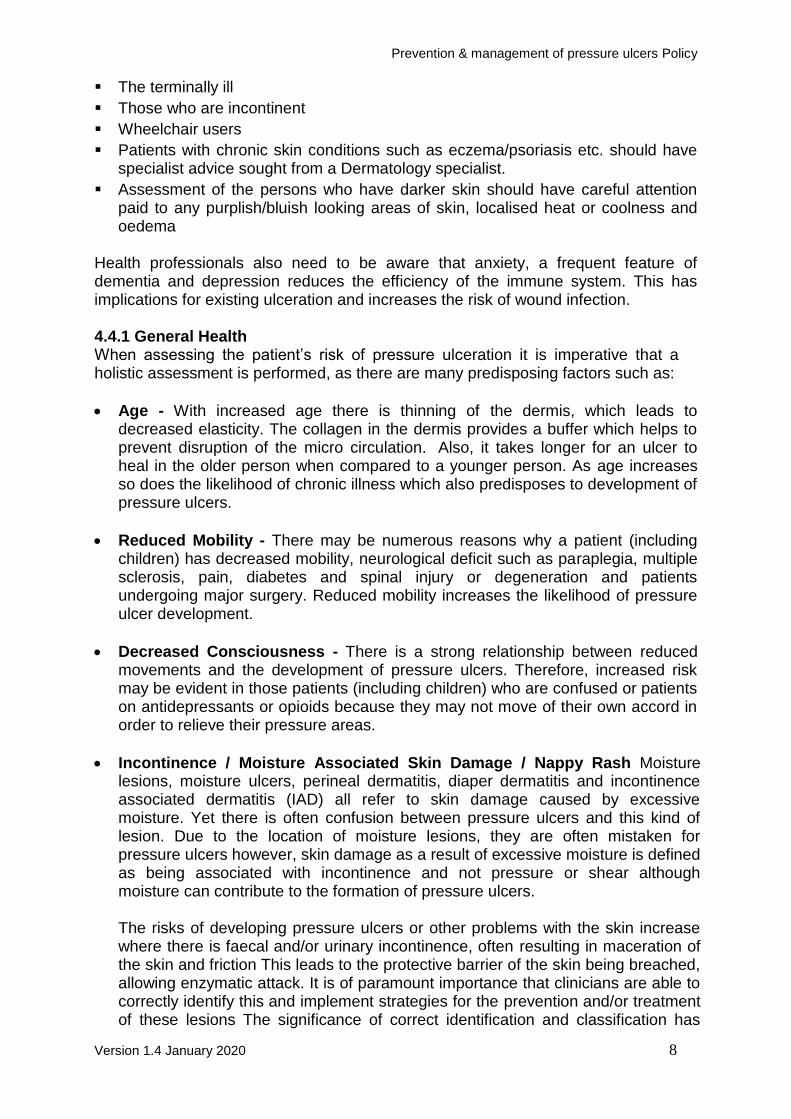
Incontinence / Moisture Associated Skin Damage / Nappy Rash Moisture lesions, moisture ulcers, perineal dermatitis, diaper dermatitis and incontinence associated dermatitis (IAD) all refer to skin damage caused by excessive moisture. Yet there is often confusion between pressure ulcers and this kind of lesion. Due to the location of moisture lesions, they are often mistaken for pressure ulcers however, skin damage as a result of excessive moisture is defined as being associated with incontinence and not pressure or shear although moisture can contribute to the formation of pressure ulcers.
The risks of developing pressure ulcers or other problems with the skin increase where there is faecal and/or urinary incontinence, often resulting in maceration of the skin and friction This leads to the protective barrier of the skin being breached, allowing enzymatic attack. It is of paramount importance that clinicians are able to correctly identify this and implement strategies for the prevention and/or treatment of these lesions The significance of correct identification and classification has
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 9
never been more central, with many trusts identifying that Moisture Associated Skin Damage are often incorrectly categorised as category 2 pressure ulcers. Constant washing removes the body’s natural oils by drying the skin; however, dry skin can also cause problems. (See Management and prevention of nappy rash//Moisture Associated Skin Damage (Appendix 11)
Moisture Associated Skin Damage
Nutrition - Malnutrition is frequently cited as a risk factor for the development and non-healing of pressure ulcers. Malnutrition and specific nutrient deficiencies compromise the body’s ability to heal wounds and make the individual more susceptible to pressure damage. Nutrition plays a vital role in the prevention and treatment of wounds and pressure ulcers. Nutritional status has a direct influence on the health of the body’s tissue and its repair in the event of damage. Wound healing is a complex process which can be further complicated by chronic illness.
The nutrition of the patient (including children) with a pressure ulcer requires a multidisciplinary approach and effective communication between all health care workers. Improving nutrition can improve the quality of life by reducing the risk of infection, increasing the strength of the skin and improving the appearance of the patient’s pressure ulcer.
Many people admitted to hospital have an impaired nutritional intake due to functional or psychological issues, for example, arthritic fingers and self-neglect. Research has shown that nutritional status deteriorates in hospital, particularly in older people.
Malnutrition has direct influence on the development and severity of pressure ulcer (NICE 2005). Skin tolerance is also reduced by dehydration, decreased calorie intake and a fall in serum albumin; this increases the risk of skin breakdown and delays wound healing (NICE 2005). Utilise a dietary intake chart to identify the adequacy of total nutrient intake in in-patient units. The European Pressure Ulcer Advisory Panel (EPUAP) 2009, suggests that every individual with nutritional risk and pressure ulcer risk should be routinely referred to a dietician.
All patients should, be screened on admission/initial assessment for malnutrition using a recognised screening tool. Please see The Waterlow Risk Assessment Tool (Appendix 12), The Malnutrition Universal Screening Tool (MUST) in adults (Appendix 13), and the Paediatric Skin Integrity & Tissue Viability Risk Assessment Tool (Appendix 3).
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 10
Body weight - Emaciated patients have no subcutaneous fat particularly over the bony prominences and so have less protection against pressure ulcers. However, obese patients are also at high risk of pressure damage due to immobility and excess moisture in skin folds causing maceration. Both extremes of patient bodyweight may have poor nutritional status (Dealey 1994(a)). Factors affecting perfusion and oxygenation, diabetes, cardiovascular instability, hypotension, peripheral vascular disease and those with low oxygen saturations have reduced tissue perfusion and risk of pressure ulceration.
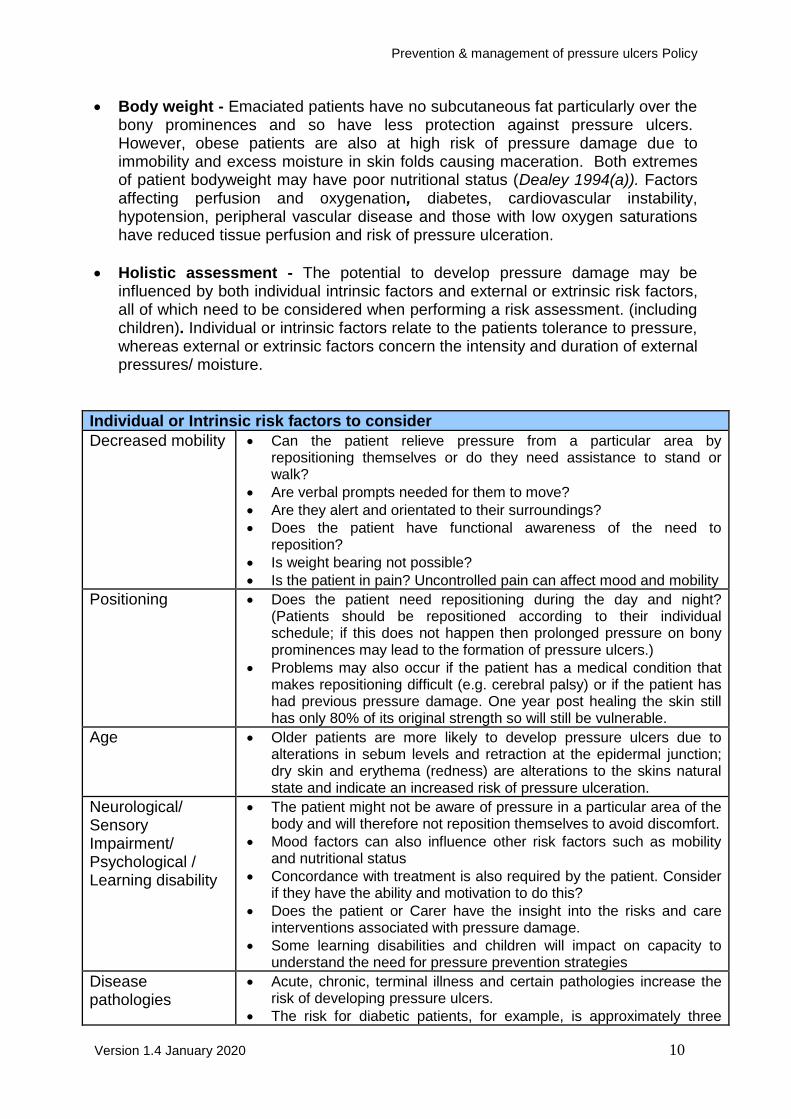
Holistic assessment - The potential to develop pressure damage may be influenced by both individual intrinsic factors and external or extrinsic risk factors, all of which need to be considered when performing a risk assessment. (including children). Individual or intrinsic factors relate to the patients tolerance to pressure, whereas external or extrinsic factors concern the intensity and duration of external pressures/ moisture.
Individual or Intrinsic risk factors to consider
Decreased mobility Can the patient relieve pressure from a particular area by repositioning themselves or do they need assistance to stand or walk?
Are verbal prompts needed for them to move?
Are they alert and orientated to their surroundings?
Does the patient have functional awareness of the need to reposition?
Is weight bearing not possible?
Is the patient in pain? Uncontrolled pain can affect mood and mobility
Positioning Does the patient need repositioning during the day and night? (Patients should be repositioned according to their individual schedule; if this does not happen then prolonged pressure on bony prominences may lead to the formation of pressure ulcers.)
Problems may also occur if the patient has a medical condition that makes repositioning difficult (e.g. cerebral palsy) or if the patient has had previous pressure damage. One year post healing the skin still has only 80% of its original strength so will still be vulnerable.
Age Older patients are more likely to develop pressure ulcers due to alterations in sebum levels and retraction at the epidermal junction; dry skin and erythema (redness) are alterations to the skins natural state and indicate an increased risk of pressure ulceration.
Neurological/ Sensory Impairment/ Psychological / Learning disability
The patient might not be aware of pressure in a particular area of the body and will therefore not reposition themselves to avoid discomfort.
Mood factors can also influence other risk factors such as mobility and nutritional status
Concordance with treatment is also required by the patient. Consider if they have the ability and motivation to do this?
Does the patient or Carer have the insight into the risks and care interventions associated with pressure damage.
Some learning disabilities and children will impact on capacity to understand the need for pressure prevention strategies
Disease pathologies
Acute, chronic, terminal illness and certain pathologies increase the risk of developing pressure ulcers.
The risk for diabetic patients, for example, is approximately three
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 11
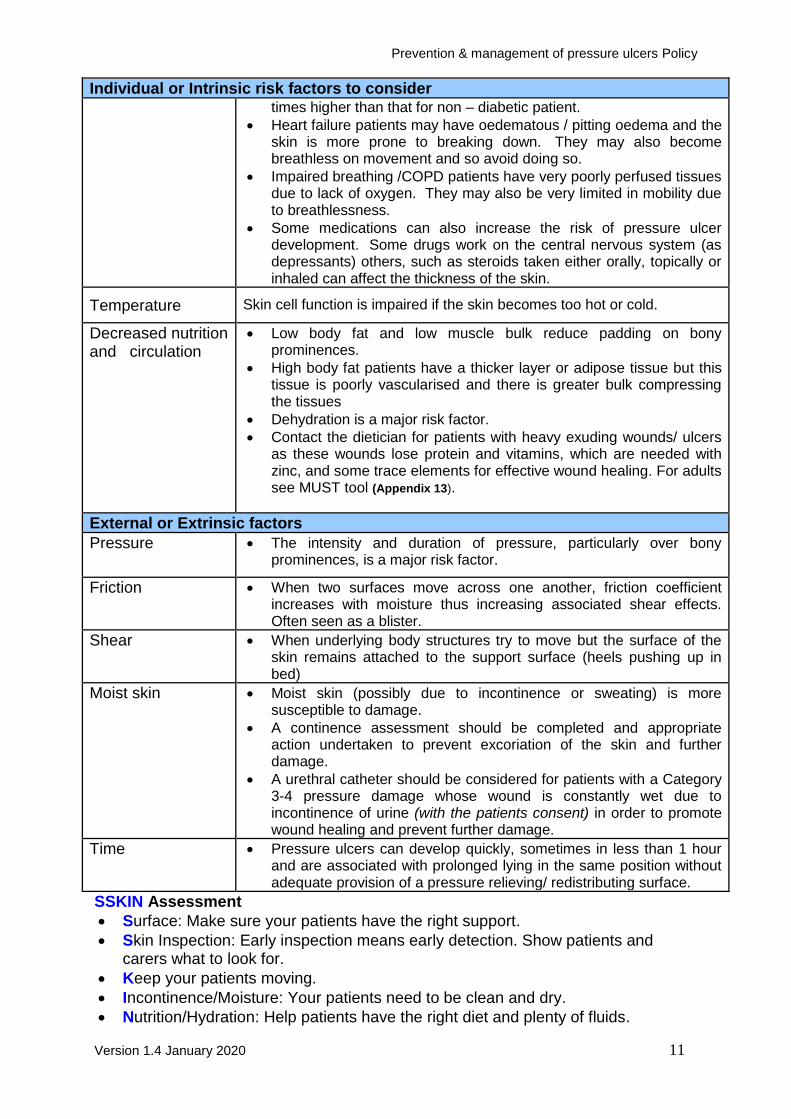
Individual or Intrinsic risk factors to consider times higher than that for non – diabetic patient.
Heart failure patients may have oedematous / pitting oedema and the skin is more prone to breaking down. They may also become breathless on movement and so avoid doing so.
Impaired breathing /COPD patients have very poorly perfused tissues due to lack of oxygen. They may also be very limited in mobility due to breathlessness.
Some medications can also increase the risk of pressure ulcer development. Some drugs work on the central nervous system (as depressants) others, such as steroids taken either orally, topically or inhaled can affect the thickness of the skin.
Temperature Skin cell function is impaired if the skin becomes too hot or cold.
Decreased nutrition and circulation
Low body fat and low muscle bulk reduce padding on bony prominences.
High body fat patients have a thicker layer or adipose tissue but this tissue is poorly vascularised and there is greater bulk compressing the tissues
Dehydration is a major risk factor.
Contact the dietician for patients with heavy exuding wounds/ ulcers as these wounds lose protein and vitamins, which are needed with zinc, and some trace elements for effective wound healing. For adults see MUST tool (Appendix 13).
External or Extrinsic factors
Pressure The intensity and duration of pressure, particularly over bony prominences, is a major risk factor.
Friction When two surfaces move across one another, friction coefficient increases with moisture thus increasing associated shear effects. Often seen as a blister.
Shear
When underlying body structures try to move but the surface of the skin remains attached to the support surface (heels pushing up in bed)
Moist skin Moist skin (possibly due to incontinence or sweating) is more susceptible to damage.
A continence assessment should be completed and appropriate action undertaken to prevent excoriation of the skin and further damage.
A urethral catheter should be considered for patients with a Category 3-4 pressure damage whose wound is constantly wet due to incontinence of urine (with the patients consent) in order to promote wound healing and prevent further damage.
Time Pressure ulcers can develop quickly, sometimes in less than 1 hour and are associated with prolonged lying in the same position without adequate provision of a pressure relieving/ redistributing surface.
SSKIN Assessment
Surface: Make sure your patients have the right support.
Skin Inspection: Early inspection means early detection. Show patients and carers what to look for.
Keep your patients moving.
Incontinence/Moisture: Your patients need to be clean and dry.
Nutrition/Hydration: Help patients have the right diet and plenty of fluids.
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 12
(See Standard Operating Procedure 1 SSKIN Assessment & Appendix 3 for Paeds) Skin inspection Skin inspection provides essential information for pressure ulcer prevention. Regular inspection of vulnerable parts of the body will enable early detection of pressure damage. Skin should be inspected for any ulceration, redness, erythema, non-blanching erythema. It should include inspection of the most vulnerable areas of risk for each patient including children are typically:- occipital areas and ears back of head Temporal regions of the skull Shoulders Spine Scapular Elbows Hips Sacrum Ischial tuberosities Knees Ankles Heels Toes Parts of the body that are affected by the wearing of anti-embolic stockings Parts of the body where pressure, friction or shear is exerted in the course of
an individual’s daily living activities e.g. on the hands of wheelchair users Parts of the body where there are external forces exerted by equipment and
clothing e.g. endotracheal tubes, intravenous lines, catheters, shoes, elastic clothing
Blanch testing of intact skin aids the identification of potential damage. Pressure is applied to the ‘red’ area, healthy microcirculation will cause the skin to turn white, and on removal of pressure, the capillaries will refill and turn the skin back to red. This indicates the skin is healthy and there is no pressure damage. If the skin does not turn white on the application of pressure the microcirculation is already damaged and the patient has a Category 1 pressure ulcer. Sometimes the skin will be slow to turn back to red, this is known as ‘sluggish hyperaemia’ and indicates the need to start or increase repositioning – if this is not done pressure damage will occur.
The assessment of darkly pigmented skin is different. Clinical signs to consider
during skin inspection are; localised heat and purplish/bluish skin hue. If pressure damage has already occurred the area may feel cool, harder, have increased pain and localised oedema. Pressure ulcers are under detected in darkly pigmented skin as early damage is harder to see. (See Appendices for Body maps, guidelines and assessments)
Should patients be using a medical device i.e. callipers, plaster cast or naso-gastric
tube fixers the risk of pressure ulcers should be considered.
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 13
Children with chronic skin conditions such as eczema/psoriasis etc. should have specialist advice sought from a Dermatology specialist if deemed necessary. Pain
Assess for pressure ulcer related pain using a validated pain tool; include non-verbal cues and body language - see Pain Assessment of People with Dementia (Appendix 14) and for Pain Assessment in Children (Appendix 15)
Use appropriate equipment to minimise friction/shear when repositioning, keep sheet smooth and wrinkle free.
Position off the pressure ulcer whenever possible.
Avoid postures that increase pressure i.e. 90-degree side lying or semi recumbent (30 degree lateral tilt) see Appendix 16.
Handle all wounds gently, irrigate carefully, protect surrounding skin, remove dressings correctly, choose appropriate dressings.
Organise care delivery in co-ordination with pain relief.
Where possible provide pain relief 20-30 minutes prior to intervention.
Encourage the patient/ child to request ‘time out’ if the procedure causes pain.
Re-Positioning Relieving pressure especially over bony prominences is of primary concern. Patients with limited mobility are especially at risk for the development of pressure ulcers. Every effort should be made to redistribute the pressure on the skin, either by repositioning or utilising pressure relieving surfaces. Pressure redistribution can be achieved through repositioning and use of pressure redistribution surfaces & Physiotherapist’s input to the patients care is valued.
Consider mobilising, positioning and repositioning interventions for all patients (including those in beds, chairs and wheelchair users) (NICE, 2005). Frequency of repositioning will be determined by an individual assessment and daily skin inspections. In the community setting the patient’s carer’s may be involved and should have adequate instruction to ensure no further skin damage e.g. due to shearing.
Frequency must be adjusted according to the response of the patients’ skin to pressure/ tissue tolerance, as indicated by changes in skin colour/ texture/ temperature etc. (i.e. if the skin reddens after two hours, reduce the time interval and reassess. If there is no evidence of persistent erythema or any other indication of early tissue damage, then the frequency of repositioning may then be reduced). The acutely at risk patient should still be assessed every two hours (NICE 2005; European Pressure Ulcer Advisory Panel, 1999).
All patients with pressure ulcers should actively mobilize or change their position or be repositioned frequently.
Minimise pressure on bony prominences and avoid positioning on pressure ulcer if present.
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 14
Frequency of repositioning may be restricted by the patients’ medical condition, level of comfort and attached medical devices e.g. IV cannulae, external fixators, urinary catheters. In cases where patients cannot be adequately repositioned suitable support surfaces must be used and regular repositioning introduced as soon as possible.
If unable to turn the patient’s position then a 30° lateral tilt can be achieved to minimise pressure on bony prominences. See Simple Safe Effective 30° Tilt (Appendix 16)
It is important to recognise and prevent the effects on the skin caused by poor
manual handling techniques. A documented care plan to minimise friction, shear, rubbing or dragging on the patients skin should be documented, implemented, and evaluated.
Devices to assist manual handling such as slide sheets and hoists should be used to reduce the potential skin damage to the patient or injury to carers.
Older children/young people at risk of developing pressure ulcers should be discouraged from sitting in chairs for prolonged periods.
Patients who use wheelchairs should be assisted to regularly redistribute their weight. An agreed period of time should be negotiated with the patient and carer and should be recorded in the care plan and should be no longer than two hours. Use of pressure relieving cushions should be based on risk assessment. Specialist advice and expertise on repositioning patients with restricted mobility should be obtained from the Moving & Handling Advisor for the division/Tissue Viability Specialist Nurses and the Physiotherapist.
4.5 Mattresses, Support Surfaces and Equipment
Consideration will need to be given to the utilisation of specialist pressure, redistribution or pressure relieving equipment by the multi-disciplinary team. (See Pressure relieving equipment selection flow chart (Appendix 17)
It is important that the following factors be taken into account: Individual clinical need and general comfort of the patient
Acceptability of the equipment to the patient and carer
Compatibility of the equipment for use with the patient
Ease of use
Impact on care procedures
Cost
All equipment must be used in accordance with the manufacturer’s instructions, and equipment provided must not put the patient at any additional risk to their health and safety.
Staff must not use equipment for which they have not received training; it is their
responsibility to identify and rectify deficits in training needs according to local guidelines.
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 15
The provision of specialist mattresses does not replace the need for repositioning/redistributing the patient’s weight.
Unless there is a clinical contra-indication patients on pressure redistributing/
relieving surfaces still need to be re-positioned as directed by their individual risk assessment.
If additional equipment i.e. pillows, gel pads are used to prevent pressure between knees and ankles, their use must not compromise the pressure redistribution / relief of the support surface the patient is being nursed on.
Patients who have specific moving and handling requirements may also require additional equipment such as:
A hoist
Low friction slide sheets, or handling belts to assist with patient movement that will reduce the risk of problems associated with shear or friction.
N.B. The use of water filled gloves or sheepskins, Doughnut type devices, i.e. ring cushions is no longer acceptable under any circumstances (NICE, 2003). Guidance is given in the selection of the correct pressure relieving equipment on the Pressure relieving Equipment Selection Chart (Appendix 17). Allocation of specialist mattresses should be considered in accordance with an overall assessment and not based solely on the basis of risk assessment scores (EPUAP/NPUAP 2009).
The health professional’s judgement is key here.
Check that the base on which they are placed provides adequate support for the device, as per the manufacturer’s instructions.
Provide information for carers/family/friends, when caring for someone on pressure relieving equipment.
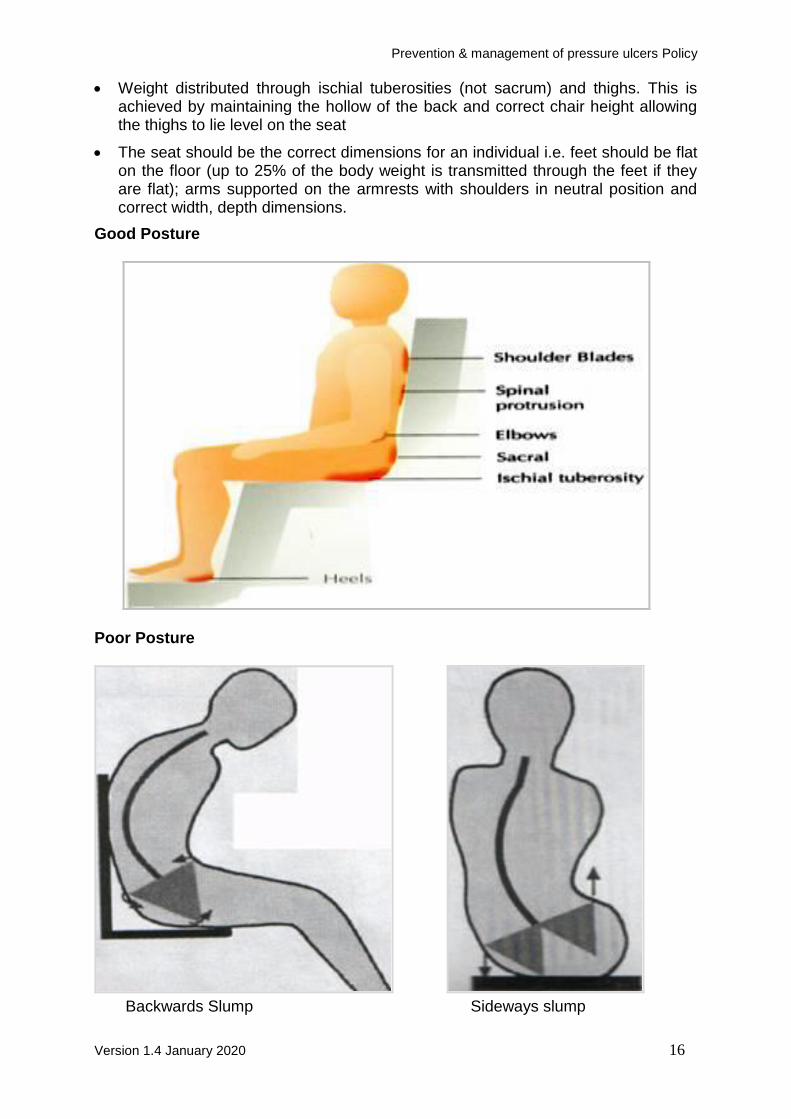
4.5.1 Seated Assessments and Posture A good, stable posture is central to pressure reduction, however poor posture can predispose pressure ulcers and can render ineffective any pressure-reducing cushion. Remember that in any seated position, the body weight is being taken over a much smaller surface area, possibly even smaller if posture is affected, therefore the risk is increased. The physiotherapy & occupational therapist input should be included in the assessment and patient care. A good posture may be described as-
Upright
No gap between pelvis and chair back
Spine supported upright in natural curvature (back supported at a slope will increase shear forces to buttocks)
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 16
Weight distributed through ischial tuberosities (not sacrum) and thighs. This is achieved by maintaining the hollow of the back and correct chair height allowing the thighs to lie level on the seat
The seat should be the correct dimensions for an individual i.e. feet should be flat on the floor (up to 25% of the body weight is transmitted through the feet if they are flat); arms supported on the armrests with shoulders in neutral position and correct width, depth dimensions.
Good Posture
Poor Posture
Backwards Slump Sideways slump

Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 17
4.5.2 Cushions The cushion should provide the optimum postural support and maximum contouring with the patient’s body shape in order to distribute pressure as evenly as possible. Any contouring provided by the cushion will allow the ischial tuberosities to sit lower than the thighs; increasing stability this reduces the slide forward, which reduces both friction and shearing. In children the cushion/contouring is usually built into their seating systems. 4.5.3 Factors to consider for cushions - Cautions:
Placing any cushion on top of a chair will impact on its dimensions/height and in turn its support and stability for the individual. This may affect transfers/posture/functional ability.
User Weight. Please remember all equipment has a user weight.
Alternating Pressure Cushions and Riser-recliners. There are contraindications for use with this type of equipment e.g. alternating cushions that are electric and need to be plugged in can pose a different risk on recliner chairs so risk assessment should be carried out prior to issue. The wires could become trapped in the chair mechanism and the cushion is likely to be less effective, if at all due to changes in position and weight distribution during reclining. These cushions also pose a risk with posture as they can be unstable and increase postural instability and shear. Please seek further advice regarding this option. There are certain types of cushion which require the patient to be positioned correctly on them to be effective e.g. Contoured cushions. If used incorrectly, they may cause further damage. Please seek further advice if unsure.
4.5.4 Reassessment It is important to reassess the patient’s equipment needs regularly, at least weekly or as documented in the individuals care plans. It is important to utilise the equipment as per the patient’s needs this may mean upgrading or down grading equipment. 4.5.5 Continence Management It is generally recognised that incontinence is one of the major causative factors in the development of pressure ulcers/ nappy rash and moisture associated skin damage. It increases the risk of friction and the chemical reaction of urine and faeces on the skin causes further tissue breakdown with ammonia being produced leading to excoriation. This increase in moisture combined with bacterial and enzymatic activity can result in the breakdown of vulnerable skin. Therefore, the treatment of any incontinence needs to be addressed. In incontinence related moisture lesions the skin should be cleansed with cleansing foam and a barrier film is recommended. They must be labelled for individual single patient use.

Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 18
The patients’ skin should be kept clean and dry. The use of soap can destroy the natural oils produced in the sebaceous glands of the skin and it is advisable not to use soap for skin cleansing. Specialist expertise and advice about the care of children with chronic or unusual skin problems should be obtained from the Multidisciplinary Team or via referral to a specialist if deemed necessary. 4.6 Heel Pressure Ulcers Pressure ulcers on the heel can develop as a result of both intrinsic and extrinsic factors, They are the second most common site for the development of pressure ulcers (Cheneworth, 1994). The heel has a relatively low resting blood perfusion level and ulceration can occur if subjected to pressure lower than 32mmHg, friction and shearing forces can reduce the tissue tolerance even further (Cheneworth, 1994). A vascular assessment should be undertaken if ischaemia is suspected. The most effective way of relieving pressure is to totally offload the pressure on the heel. Prevention can be achieved with the following:
Pillows – Carefully placed will relieve pressure but a higher amount of pressure may then be borne by the rest of the limb
The use of the 30° lateral tilt where a pillow is placed to act as a ‘space filler’ (Appendix 16)
Where relevant
The use of a bed cradle to take away the weight of the bedclothes
Foam leg troughs and foam heel suspension boots
Air filled heel protectors i.e. waffle and repose boots.
Gel heel pads
Fibre filled heel pads can be used to protect from friction and shearing but do not offload pressure.
Foam dressing products do not offer any offloading or pressure relief and should not be used for treatment or prevention purposes.
Heel protection devices should elevate the heel completely (offloading) in such a way as to distribute the weight of the leg along the calf without putting pressure on the Achilles tendon. The heel should be in a slight flexion. Pressure reducing mattresses do not appear to be effective in preventing heel ulcers as, mechanisms, which offload pressure. Therefore, their use is questionable for the treatment and prevention of heel ulcers alone (Dinsdale, 1974). Identified patients in inpatient areas who wear compression hosiery or anti-embolism stockings need to be able to have their heels checked daily for any pressure damage (Donnelly, 2001).
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 19
4.7 Infection Prevention High standards of infection prevention must be maintained, using standard precautions, maintaining asepsis and appropriate hand decontamination. Wherever possible the pressure ulcer must be covered. Further advice must be obtained from local Trust guidelines and the Infection Prevention & Control Team. Adults, children /young people who are transferred from other hospitals or community homes should be screened in accordance with the local Infection Prevention & Control Policy. When screening swabs are obtained, they should include swabs of any wounds, lesions or pressure ulcers.
Any patient who has an interruption in the continuity or integrity of their skin is at risk of developing a local or systemic infection and may also pose a risk to other patients. Individual advice should be sought from the Infection Prevention & Control Team. Signs of infection include-
pyrexia
increased pain at the site
cellulitis
malodour
increasing size of ulcer
purulent discharge
tachycardia / tachypnoea Sepsis should be considered as a possibility if the patient becomes unwell. 4.8 Patient / Parent / Carer Information Adults, children, young people referred to BCPFT clinical services (including their parents and carers), will be provided with written peer and patient reviewed information identified on the care plan to include:
A patients risk of pressure ulcers
Pressure ulcer prevention strategies (repositioning, nutrition, equipment, skin inspection, skin care etc.)
Safe use of specialist equipment
Useful contact details see SSKIN patient leaflet found in SOP 1: SSKIN Assessment
The patients and family will be given the opportunity to ask questions and share their views. They will be encouraged to actively participate in care planning and care interventions to maintain or improve their tissue viability. 4.9 Discharge or transfer of patients All patients should be reassessed, including skin assessment, prior to discharge or transfer from BCPFT services. This should be documented accurately and should include a description of the patient’s pressure areas. If any pressure ulcers are present, there should be a wound assessment and details of the treatment plan. When discharging or transferring a patient from hospital it is essential that all the relevant people are informed. This includes District Nurses, Community Paediatric
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 20
Services, General Practitioners, Carers and Nursing Homes. This contact should be timely in order to ensure relevant resources are in place prior to discharge. 4.10 Compliance/Capacity Compliance/capacity refers to patient’s ability to follow a treatment plan that has been agreed between the patient and health care professionals. The nurse should not only assess compliance/capacity but also identify potential reasons for non- compliance. Pressure ulcer treatment and palliative/end of life care
Set treatment goals consistent with the values and goals of the patient whilst considering family input
Set goals to enhance quality of life; healing may not be achievable but reducing pain/odour/exudate
Assess the pressure ulcer at least every two days unless the patient is end of life and document findings
Monitor to ensure the aims of comfort and reduction in wound pain/symptoms are met
Debride the ulcer of devitalised tissue to control infection and odour only if healing can be achieved
Consider charcoal dressings to help control odour
Utilise dressings that do not require frequent changing but manage the wound Symptoms
Utilise a dressing that maintains a moist healing environment and is comfortable for the patient if healing can be achieved. If not and necrosis is dry maintain a desiccated state.
For children who are end of life – liaise with tissue viability and all healthcare professionals involved to plan the appropriate course of action.
5.0 Procedures connected to this Policy Prevention & Management of Pressure Ulcers SOP 1 – SSKIN Assessment.
6.0 Links to Relevant Legislation
Department of Health (2010a) Equity and Excellence Liberating the NHS London:
Department of Health (2010b) The NHS Quality, Innovation, Productivity and Prevention Challenge: An Introduction for Clinicians. London: DH.
Department of Health (2009a) NHS 2010–2015: From Good to Great. Preventative, Peopled-centred, Productive. London: DH.
Department of Health (2009b) The Framework for Quality Accounts: A Consultation on the Proposals. London: DH.
Department of Health (2008) High Quality Care for All: NHS Next Stage Review Final Report.London: DH.
Department of Health 1999. Making a difference: strengthening the nursing
and health visiting contribution to health and healthcare
Department of Health 2001 Essence of care Department of Health London

Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 21
Department of Health 1999 Making a difference: strengthening the nursing and health visiting contribution to health and healthcare
6.1 Links to Relevant National Standards
Care Quality Commission(CQC)
NHS Litigation Authority (NHSLA)
National Institute for Health & Clinical Excellence (NICE)
NICE Clinical Guideline CG179
Pressure Ulcers published April 2014
6.2 Links to other Key Policies
Care Record Keeping
Risk Management Strategy Policy and Process
Infection Prevention and Control Standards and procedures 6.3 References
Bale, S (2005) Chapter 6, Incontinence Care In: Skin Care In Wound Management Assessment Prevention and Treatment, Wounds UK Ltd, Aberdeen.
Cheneworth CC et al. (1994). Portrait of practice: healing heel ulcers. Advances in Wound Care. 7,2, 44-48
Collins, F (2001) How to assess a patient seating needs, some basic principles. Journal of wound care 10(9) 383-386
Cooper P. Gray D. (2001) Comparison of two skin care regimes for incontinence, British Journal of Nursing Tissue Viability Supplement Vol 10 No 6 pS6-S20.
Dealey C. (1994) (a) The Care of Wounds. Blackwell Scientific Publications. Chapter 5 P83.
Department of Health – (1995) Pressure ulcers: A Key Quality indicator. HMSO London.
Defloor, M, (1999). The risk of pressure sores- a conceptual scheme. Journal of clinical nursing, 8 (2) pp63-64
Dinsdale. S.M. (1974). Decubitus ulcers: role of pressure and friction in causation. Arch Phys Med Rehab. 55:4 pp147-152
European Pressure Ulcer Advisory Panel (2001) Pressure Ulcer Prevention Guidelines, EPUAP Business Office. Churchill Hospital Old Road Headington, Oxford
European Pressure Ulcer Advisory Panel (2003) Pressure Ulcer Prevention Guidelines, EPUAP Business Office. Churchill Hospital Old Road Headington, Oxford
European Pressure Ulcer Advisory Panel (1999) Pressure Ulcer Prevention Guidelines, EPUAP Business Office. Wound Healing Unit Department of Dermatology. Churchill Hospital Old Road Headington, Oxford
National Institute for Clinical Excellence (2003), CG29. Pressure ulcers: prevention and pressure relieving devices. NICE. London
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 22
National Statistics online (31st January 2006) Preston K. N. (1988) Position for comfort and pressure relief: the 30 degree alternative. Care Science and Practice 6. 4. 116-9.
Nursing and Midwifery council (2008) The Code: Standards of conduct, performance and ethics for nurses and midwives. NMC. London
Torra I, Bou J, Garcia-fernandez FP, Pancorbo-Hidalgo PL, Furtado K. Risk assessment scales for predicting the risk of developing pressure ulcers. In: Romanelli M, Clark M, Cherry G, et al (eds). Science and practice of pressure Ulcer Management. London: Springer-Verlag, (2006).
Tissue viability society 2009 Seating and Pressure ulcers Clinical Practice Guideline
Waterlow J. (1988) Prevention is cheaper than cure. Nursing Times 84 25 p69-70
Paediatric pressure ulcer guidelines developed by: The West Midlands Paediatric Tissue Viability Regional group (Adapted from Birmingham Children’s Hospital guidelines March 2012)
Buckingham KW and Berg RW. (1986) Etiological factors in diaper dermatitis: The role of faeces. Paediatric Dermatology 3(2) pp.107-12.
Gray M (2004) Which pressure ulcer scales are valid and reliable in the paediatric population? Journal of Wound Ostomy and Continence Nursing 31, pp.157-160.
Bethell E (2005) Wound care for patients with darkly pigmented skin. Nursing Standard 20 (4) pp.41-49.
McGurk V, Holloway B, Crutchley A and Izzard H. (2004) Skin integrity assessment in neonates and children. Paediatric Nursing 16 (3) pp.15-18.
Sims A and McDonald R. (2003) An overview of paediatric pressure care Journal of Tissue Viability 13 (4) pp.144-148.
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 23
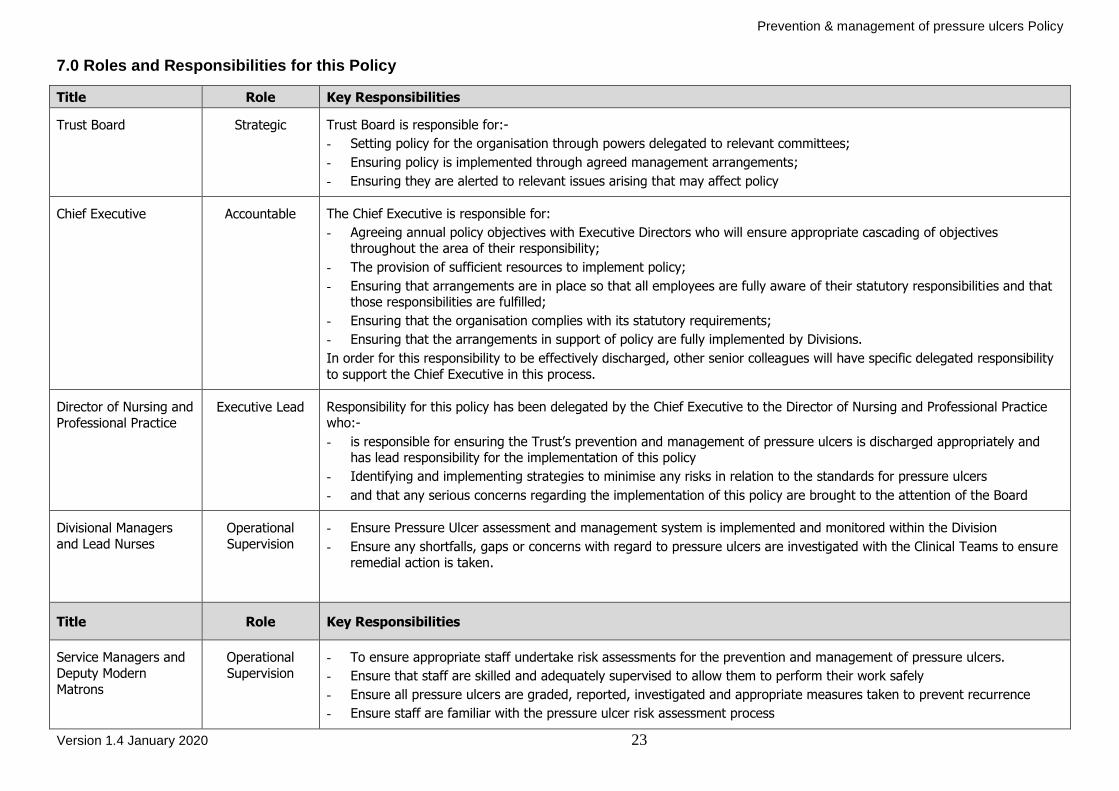
7.0 Roles and Responsibilities for this Policy
Title Role Key Responsibilities
Trust Board Strategic Trust Board is responsible for:-
- Setting policy for the organisation through powers delegated to relevant committees;
- Ensuring policy is implemented through agreed management arrangements;
- Ensuring they are alerted to relevant issues arising that may affect policy
Chief Executive
Accountable The Chief Executive is responsible for:
- Agreeing annual policy objectives with Executive Directors who will ensure appropriate cascading of objectives throughout the area of their responsibility;
- The provision of sufficient resources to implement policy;
- Ensuring that arrangements are in place so that all employees are fully aware of their statutory responsibilities and that those responsibilities are fulfilled;
- Ensuring that the organisation complies with its statutory requirements;
- Ensuring that the arrangements in support of policy are fully implemented by Divisions.
In order for this responsibility to be effectively discharged, other senior colleagues will have specific delegated responsibility
to support the Chief Executive in this process.
Director of Nursing and
Professional Practice Executive Lead Responsibility for this policy has been delegated by the Chief Executive to the Director of Nursing and Professional Practice
who:-
- is responsible for ensuring the Trust’s prevention and management of pressure ulcers is discharged appropriately and has lead responsibility for the implementation of this policy
- Identifying and implementing strategies to minimise any risks in relation to the standards for pressure ulcers
- and that any serious concerns regarding the implementation of this policy are brought to the attention of the Board
Divisional Managers
and Lead Nurses
Operational
Supervision
- Ensure Pressure Ulcer assessment and management system is implemented and monitored within the Division
- Ensure any shortfalls, gaps or concerns with regard to pressure ulcers are investigated with the Clinical Teams to ensure
remedial action is taken.
Title Role Key Responsibilities
Service Managers and
Deputy Modern
Matrons
Operational
Supervision
- To ensure appropriate staff undertake risk assessments for the prevention and management of pressure ulcers.
- Ensure that staff are skilled and adequately supervised to allow them to perform their work safely
- Ensure all pressure ulcers are graded, reported, investigated and appropriate measures taken to prevent recurrence
- Ensure staff are familiar with the pressure ulcer risk assessment process

Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 24
- Where pressure ulcers identify a need for additional resources, ensure that the situation is analysed, actions agreed and
implemented.
- Audit of clinical practice as part of documentation audits to ensure this policy is implemented in practice
Ward or Team
Managers
Operational
Supervision
- Ensure staffs understand their responsibilities with regard to the pressure ulcers prevention policy, guidelines and annual audit.
- Ensure staff attend appropriate training and are competent to carry out a Waterlow risk assessment, grading of pressure ulcers where applicable, report accordingly and implement appropriate management plans.
- Ensure staffs talk to service users, carer and family about pressure ulcer prevention and management plans.
- Monitor the implementation of the Pressure Ulcer Prevention policy through line management supervision.
- Support Tissue Viability Link Nurses in their role
- Ensure all pressure ulcers are reported through the Trust incident Reporting system DATIX
- Ensure case note audits undertaken include the compliance monitoring in relation to this policy
Trust Tissue Viability
Nurses/ Link Nurses
(including paediatrics)
Health Care
Professionals
Adherence All Health Care Professionals must:
- Familiarise themselves with this Policy and NICE Prevention and Treatment of Pressure Ulcers Quick Reference Guide. (NICE 2005)
- Ensure the Waterlow Pressure Ulcer risk assessment is completed on all service users admitted to an inpatient setting and a pressure ulcer management plan is formulated where appropriate.
- Assess and manage skin from admission to discharge as per Trust Flowchart for Prevention and Treatment of Pressure Ulcers. (Appendix 1a)
- Ensure any evidence of a pressure area is graded in accordance with the Pressure Ulcer Grading Chart NHS Midlands and East adapted from EPUAP/NPUAP 2009 (Appendix 2a & 2b)
- Ensure continuity of care between shifts via handover
- Ensure service users and carers are involved in treatment and care planning
NB NICE guidance does not override the individual responsibility of health professionals to make decisions appropriate to the
needs of the individual service users.
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 25
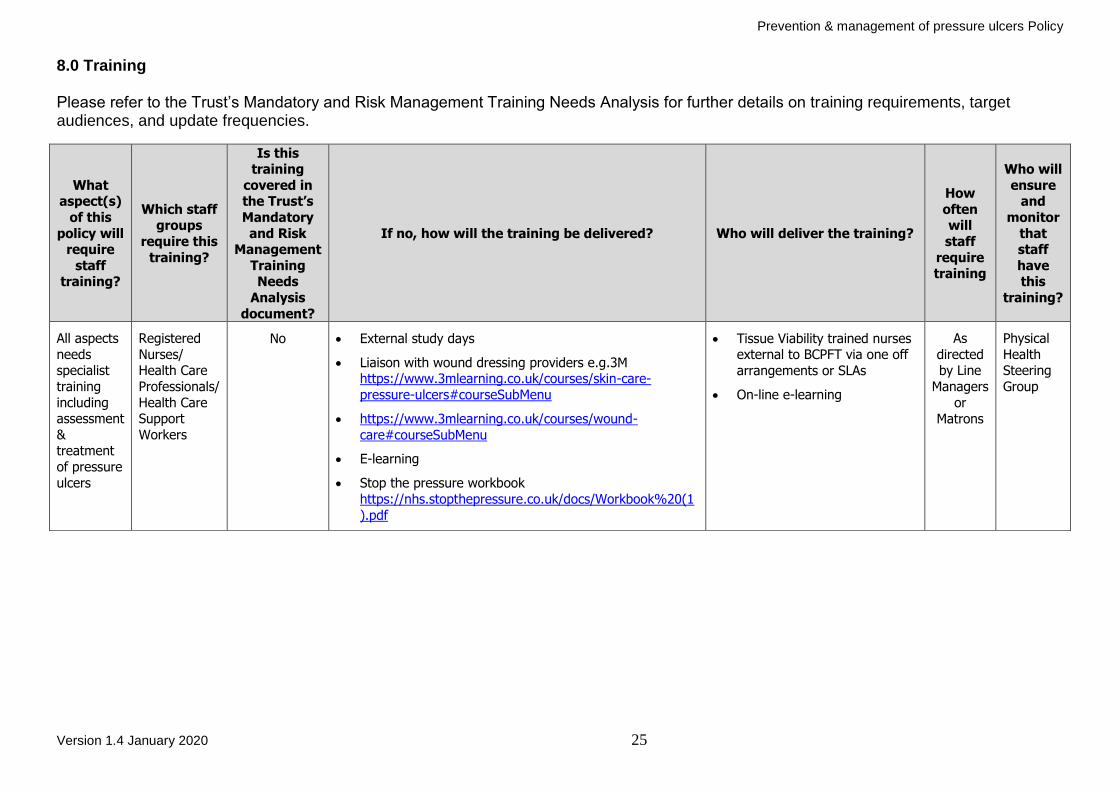
8.0 Training Please refer to the Trust’s Mandatory and Risk Management Training Needs Analysis for further details on training requirements, target audiences, and update frequencies.
What aspect(s)
of this
policy will require
staff training?
Which staff groups
require this
training?
Is this training
covered in the Trust’s
Mandatory
and Risk Management
Training Needs
Analysis
document?
If no, how will the training be delivered? Who will deliver the training?
How
often will
staff
require training
Who will
ensure and
monitor
that staff
have this
training?
All aspects
needs specialist
training
including assessment
& treatment
of pressure
ulcers
Registered
Nurses/ Health Care
Professionals/
Health Care Support
Workers
No External study days
Liaison with wound dressing providers e.g.3M https://www.3mlearning.co.uk/courses/skin-care-
pressure-ulcers#courseSubMenu
https://www.3mlearning.co.uk/courses/wound-
care#courseSubMenu
E-learning
Stop the pressure workbook
https://nhs.stopthepressure.co.uk/docs/Workbook%20(1
Tissue Viability trained nurses external to BCPFT via one off
arrangements or SLAs
On-line e-learning
As
directed by Line
Managers
or
Matrons
Physical
Health Steering
Group
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 26
9.0 Equality Impact Assessment
Black Country Partnership NHS Foundation Trust is committed to ensuring that the way we provide services and the way we recruit and treat staff reflects individual needs, promotes equality and does not discriminate unfairly against any particular individual or group. The Equality Impact Assessment for this policy has been completed and is readily available on the Intranet. If you require this in a different format e.g. larger print, Braille, different languages or audio tape, please contact the Equality & Diversity Team on Ext. 8067 or email [email protected]
10.0 Data Protection and Freedom of Information
Data Protection Act provides controls for the way information is handled and to gives legal rights to individuals in relation to the use of their data. It sets out strict rules for people who use or store data about individuals and gives rights to those people whose data has been collected. The law applies to all personal data held including electronic and manual records. The Information Commissioner’s Office has powers to enforce the Data Protection Act and can do this through the use of compulsory audits, warrants, notices and monetary penalties which can be up to €20million or 4% of the Trusts annual turnover for serious breaches of the Data Protection Act. In addition to this the Information Commissioner can limit or stop data processing activities where there has been a serious breach of the Act and there remains a risk to the data. The Freedom of Information Act provides public access to information held by public authorities. The main principle behind freedom of information legislation is that people have a right to know about the activities of public authorities, unless there is a good reason for them not to. The Freedom of Information Act applies to corporate data and personal data generally cannot be released under this Act. All staffs have a responsibility to ensure that they do not disclose information about the Trust’s activities; this includes information about service users in its care, staff members and corporate documentation to unauthorised individuals. This responsibility applies whether you are currently employed or after your employment ends and in certain aspects of your personal life e.g. use of social networking sites etc. The Trust seeks to ensure a high level of transparency in all its business activities but reserves the right not to disclose information where relevant legislation applies. The Information Governance Team provides a central point for release of information under Data Protection and Freedom of Information following formal requests for information; any queries about the disclosure of information can be forwarded to the Information Governance Team.
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 27
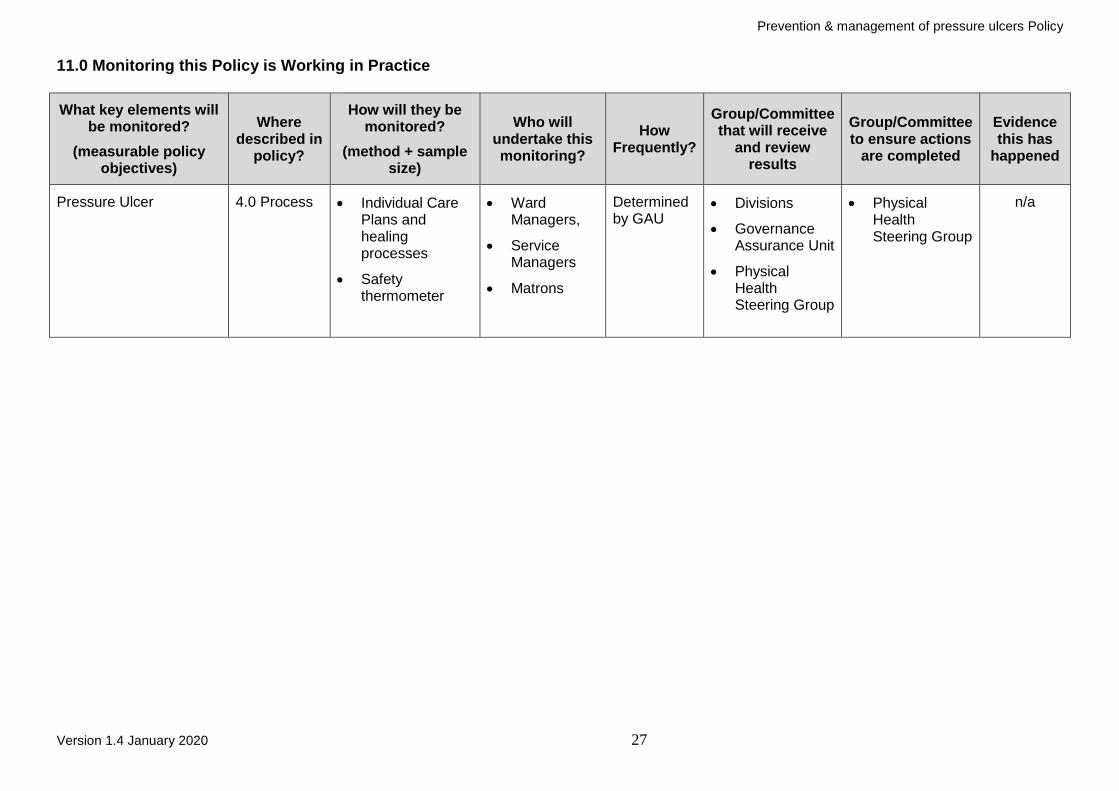
11.0 Monitoring this Policy is Working in Practice
What key elements will be monitored?
(measurable policy objectives)
Where described in
policy?
How will they be monitored?
(method + sample size)
Who will undertake this monitoring?
How Frequently?
Group/Committee that will receive
and review results
Group/Committee to ensure actions
are completed
Evidence this has
happened
Pressure Ulcer 4.0 Process Individual Care Plans and healing processes
Safety thermometer
Ward Managers,
Service Managers
Matrons
Determined by GAU
Divisions
Governance Assurance Unit
Physical Health Steering Group
Physical Health Steering Group
n/a
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 28
APPENDICES TO SUPPORT THIS POLICY

Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 29
GUIDELINES FOR COMPLETION OF BODY CHART
1. Complete body chart on admission or following a significant event.
2. Using the key below, shade onto the body chart the affected area, from the site draw an arrow and put the key next to it. Any characteristics i.e. colour of bruise, length of scar, MUST be added.
3. Sign and date the form.
4. Repeat as advised, remembering to file previous forms in the patients notes.
5. If a DATIX form is used please enter number here:
KEY
1. Bruise 2. Abrasion 3. Skin tear
4. Laceration 5. Haematoma 6. Operation scar
7. Swelling 8. Tattoo 9. Self-harm wound
Please Note See Appendix 4 regarding mandatory reporting of pressure ulcers Different skin shades and types present in different ways. If you are unfamiliar with any discolouration or injuries to a patient, always report it to the nurse in charge, advice can also be sort from the Tissue Viability Lead / link nurses
Appendix 1
DATIX NO:

Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 30
ADULT Body Map Chart & Skin Integrity Assessment Sheet
Patient Name: NHS Number:
Completed by Name: Designation:
DATIX No. (if applicable) Date Completed:
Section 1: Body Map
Appendix 2
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 31
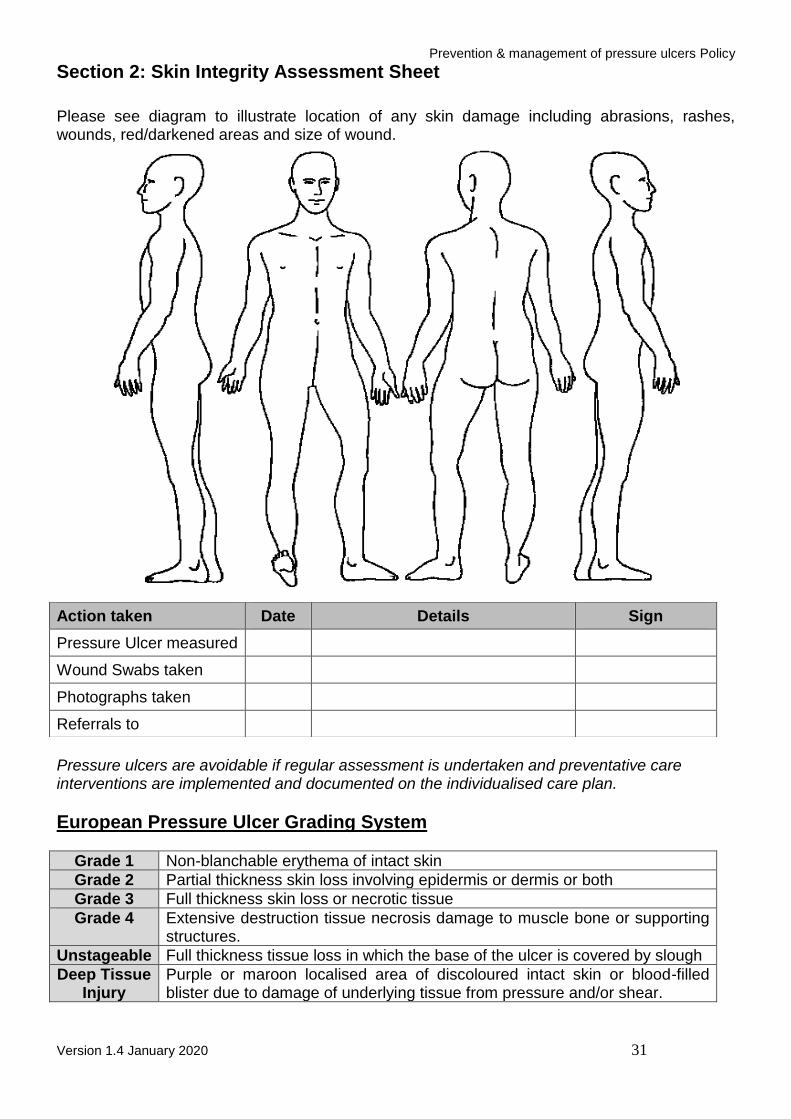
Section 2: Skin Integrity Assessment Sheet
Please see diagram to illustrate location of any skin damage including abrasions, rashes, wounds, red/darkened areas and size of wound.
Pressure ulcers are avoidable if regular assessment is undertaken and preventative care interventions are implemented and documented on the individualised care plan.
European Pressure Ulcer Grading System
Grade 1 Non-blanchable erythema of intact skin
Grade 2 Partial thickness skin loss involving epidermis or dermis or both
Grade 3 Full thickness skin loss or necrotic tissue
Grade 4 Extensive destruction tissue necrosis damage to muscle bone or supporting structures.
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough
Deep Tissue Injury
Purple or maroon localised area of discoloured intact skin or blood-filled blister due to damage of underlying tissue from pressure and/or shear.
Action taken Date Details Sign
Pressure Ulcer measured
Wound Swabs taken
Photographs taken
Referrals to
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 32
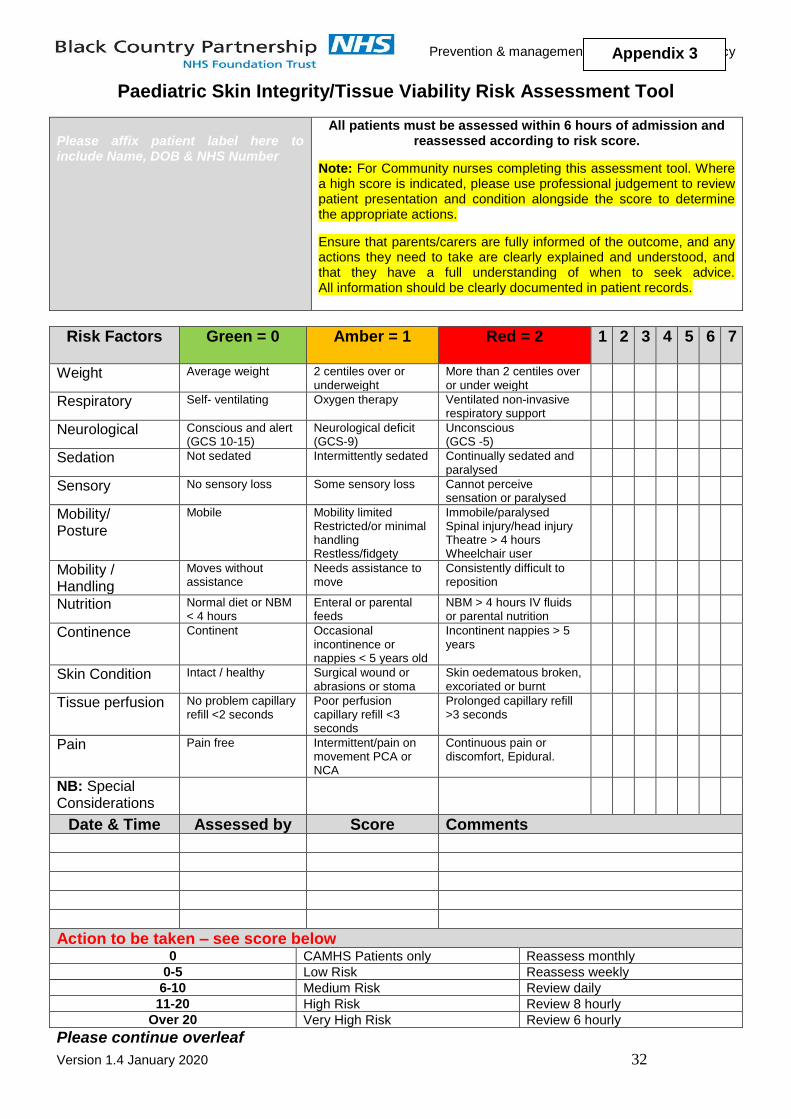
Paediatric Skin Integrity/Tissue Viability Risk Assessment Tool
Please affix patient label here to include Name, DOB & NHS Number
All patients must be assessed within 6 hours of admission and reassessed according to risk score.
Note: For Community nurses completing this assessment tool. Where a high score is indicated, please use professional judgement to review patient presentation and condition alongside the score to determine the appropriate actions.
Ensure that parents/carers are fully informed of the outcome, and any actions they need to take are clearly explained and understood, and that they have a full understanding of when to seek advice. All information should be clearly documented in patient records.
Please continue overleaf
Risk Factors
Green = 0 Amber = 1 Red = 2 1 2 3 4 5 6 7
Weight Average weight 2 centiles over or underweight
More than 2 centiles over or under weight
Respiratory Self- ventilating Oxygen therapy Ventilated non-invasive respiratory support
Neurological Conscious and alert (GCS 10-15)
Neurological deficit (GCS-9)
Unconscious (GCS -5)
Sedation Not sedated Intermittently sedated Continually sedated and paralysed
Sensory No sensory loss Some sensory loss Cannot perceive sensation or paralysed
Mobility/ Posture
Mobile Mobility limited Restricted/or minimal handling Restless/fidgety
Immobile/paralysed Spinal injury/head injury Theatre > 4 hours Wheelchair user
Mobility / Handling
Moves without assistance
Needs assistance to move
Consistently difficult to reposition
Nutrition Normal diet or NBM < 4 hours
Enteral or parental feeds
NBM > 4 hours IV fluids or parental nutrition
Continence Continent Occasional incontinence or nappies < 5 years old
Incontinent nappies > 5 years
Skin Condition Intact / healthy Surgical wound or abrasions or stoma
Skin oedematous broken, excoriated or burnt
Tissue perfusion No problem capillary refill <2 seconds
Poor perfusion capillary refill <3 seconds
Prolonged capillary refill >3 seconds
Pain Pain free Intermittent/pain on movement PCA or NCA
Continuous pain or discomfort, Epidural.
NB: Special Considerations
Date & Time Assessed by Score Comments
Action to be taken – see score below 0 CAMHS Patients only Reassess monthly
0-5 Low Risk Reassess weekly
6-10 Medium Risk Review daily
11-20 High Risk Review 8 hourly
Over 20 Very High Risk Review 6 hourly
Appendix 3
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 33
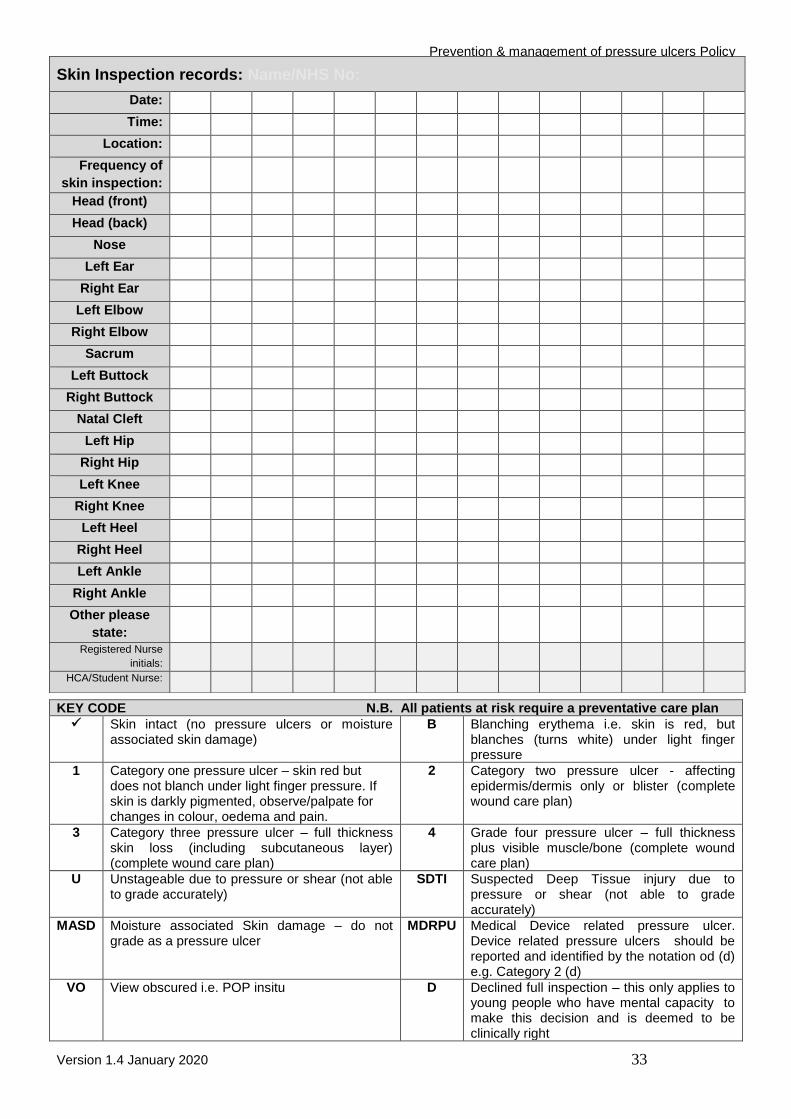
KEY CODE N.B. All patients at risk require a preventative care plan Skin intact (no pressure ulcers or moisture
associated skin damage) B Blanching erythema i.e. skin is red, but
blanches (turns white) under light finger pressure
1 Category one pressure ulcer – skin red but does not blanch under light finger pressure. If skin is darkly pigmented, observe/palpate for changes in colour, oedema and pain.
2 Category two pressure ulcer - affecting epidermis/dermis only or blister (complete wound care plan)
3 Category three pressure ulcer – full thickness skin loss (including subcutaneous layer) (complete wound care plan)
4 Grade four pressure ulcer – full thickness plus visible muscle/bone (complete wound care plan)
U Unstageable due to pressure or shear (not able to grade accurately)
SDTI Suspected Deep Tissue injury due to pressure or shear (not able to grade accurately)
MASD Moisture associated Skin damage – do not grade as a pressure ulcer
MDRPU Medical Device related pressure ulcer. Device related pressure ulcers should be reported and identified by the notation od (d) e.g. Category 2 (d)
VO View obscured i.e. POP insitu D Declined full inspection – this only applies to young people who have mental capacity to make this decision and is deemed to be clinically right
Skin Inspection records: Name/NHS No:
Date:
Time:
Location:
Frequency of
skin inspection:
Head (front)
Head (back)
Nose
Left Ear
Right Ear
Left Elbow
Right Elbow
Sacrum
Left Buttock
Right Buttock
Natal Cleft
Left Hip
Right Hip
Left Knee
Right Knee
Left Heel
Right Heel
Left Ankle
Right Ankle
Other please
state:
Registered Nurse
initials:
HCA/Student Nurse:
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 34
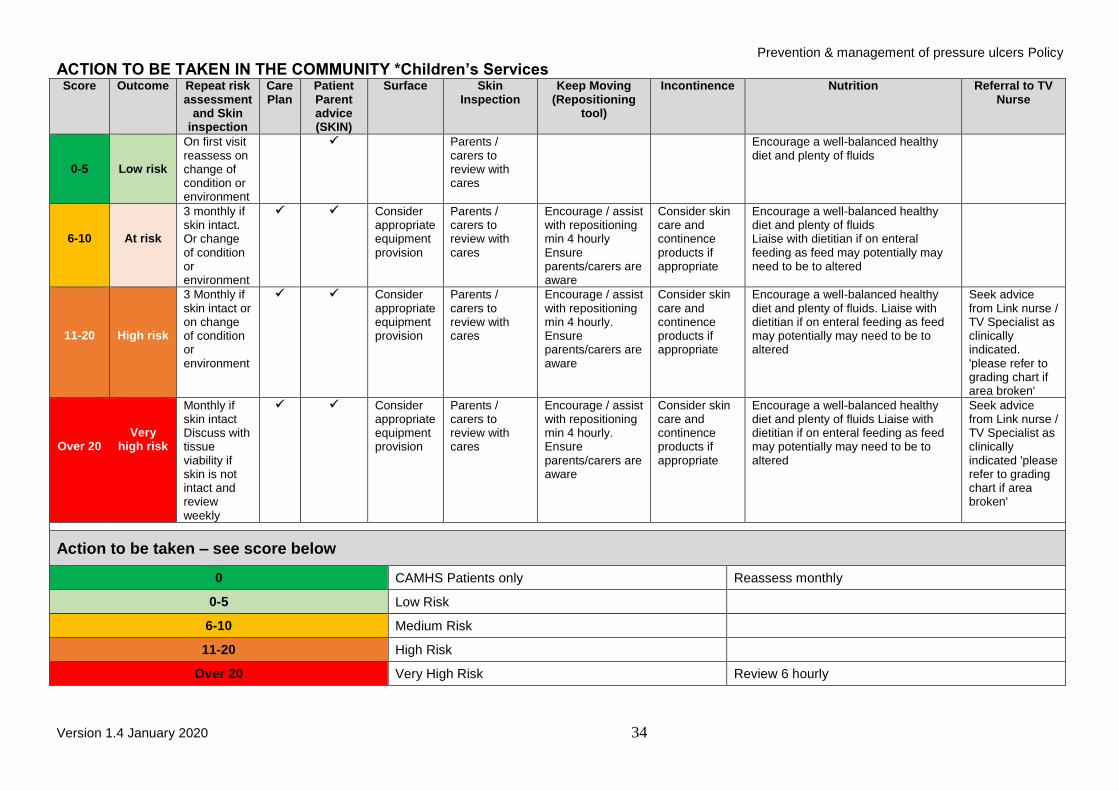
ACTION TO BE TAKEN IN THE COMMUNITY *Children’s Services Score Outcome Repeat risk
assessment and Skin
inspection
Care Plan
Patient Parent advice (SKIN)
Surface Skin Inspection
Keep Moving (Repositioning
tool)
Incontinence Nutrition Referral to TV Nurse
0-5
Low risk
On first visit reassess on change of condition or environment
Parents / carers to review with cares
Encourage a well-balanced healthy diet and plenty of fluids
6-10
At risk
3 monthly if skin intact. Or change of condition or environment
Consider appropriate equipment provision
Parents / carers to review with cares
Encourage / assist with repositioning min 4 hourly Ensure parents/carers are aware
Consider skin care and continence products if appropriate
Encourage a well-balanced healthy diet and plenty of fluids Liaise with dietitian if on enteral feeding as feed may potentially may need to be to altered
11-20
High risk
3 Monthly if skin intact or on change of condition or environment
Consider appropriate equipment provision
Parents / carers to review with cares
Encourage / assist with repositioning min 4 hourly. Ensure parents/carers are aware
Consider skin care and continence products if appropriate
Encourage a well-balanced healthy diet and plenty of fluids. Liaise with dietitian if on enteral feeding as feed may potentially may need to be to altered
Seek advice from Link nurse / TV Specialist as clinically indicated. 'please refer to grading chart if area broken'
Over 20
Very high risk
Monthly if skin intact Discuss with tissue viability if skin is not intact and review weekly
Consider appropriate equipment provision
Parents / carers to review with cares
Encourage / assist with repositioning min 4 hourly. Ensure parents/carers are aware
Consider skin care and continence products if appropriate
Encourage a well-balanced healthy diet and plenty of fluids Liaise with dietitian if on enteral feeding as feed may potentially may need to be to altered
Seek advice from Link nurse / TV Specialist as clinically indicated 'please refer to grading chart if area broken'
Action to be taken – see score below
0 CAMHS Patients only Reassess monthly
0-5 Low Risk
6-10 Medium Risk
11-20 High Risk
Over 20 Very High Risk Review 6 hourly
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 35
Community and Day Care Flow Chart
Appendix 4
Appendix 5
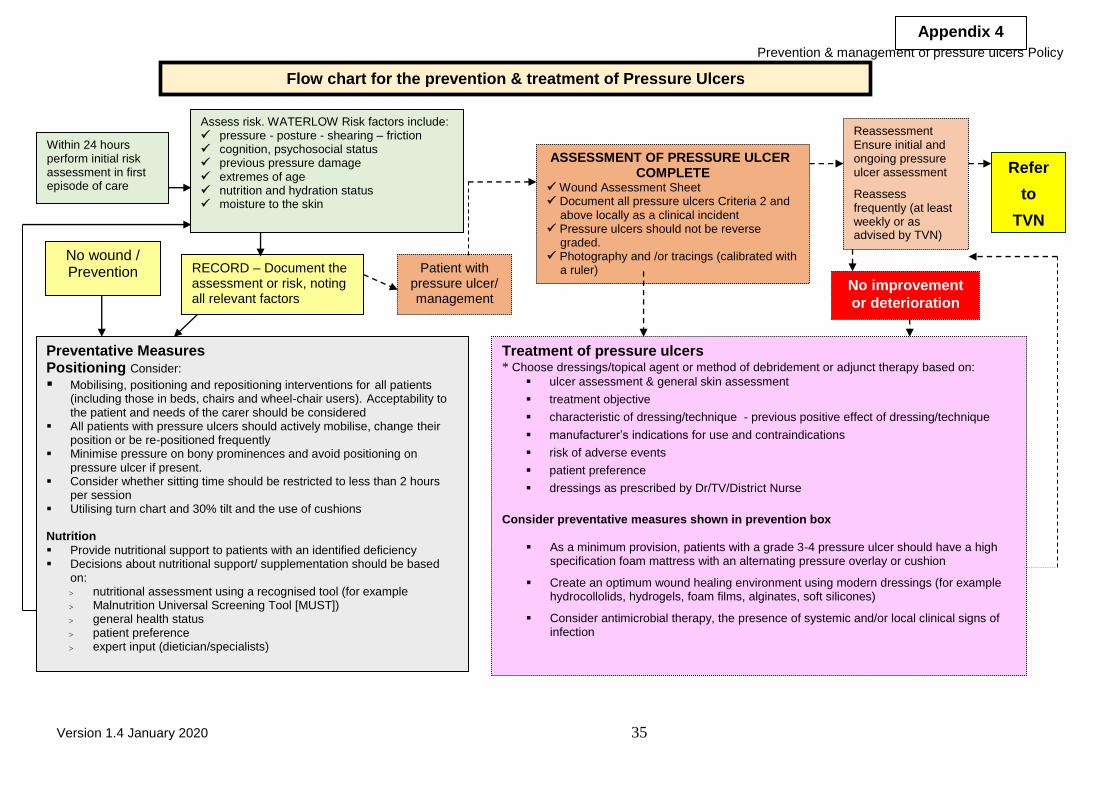
Flow chart for the prevention & treatment of Pressure Ulcers
Within 24 hours perform initial risk assessment in first episode of care
Assess risk. WATERLOW Risk factors include: pressure - posture - shearing – friction cognition, psychosocial status previous pressure damage extremes of age nutrition and hydration status moisture to the skin
RECORD – Document the assessment or risk, noting all relevant factors
Patient with pressure ulcer/ management
No wound / Prevention
Preventative Measures Positioning Consider:
Mobilising, positioning and repositioning interventions for all patients (including those in beds, chairs and wheel-chair users). Acceptability to the patient and needs of the carer should be considered
All patients with pressure ulcers should actively mobilise, change their position or be re-positioned frequently
Minimise pressure on bony prominences and avoid positioning on pressure ulcer if present.
Consider whether sitting time should be restricted to less than 2 hours per session
Utilising turn chart and 30% tilt and the use of cushions Nutrition
Provide nutritional support to patients with an identified deficiency Decisions about nutritional support/ supplementation should be based
on: nutritional assessment using a recognised tool (for example Malnutrition Universal Screening Tool [MUST]) general health status patient preference expert input (dietician/specialists)
ASSESSMENT OF PRESSURE ULCER COMPLETE
Wound Assessment Sheet Document all pressure ulcers Criteria 2 and above locally as a clinical incident Pressure ulcers should not be reverse graded. Photography and /or tracings (calibrated with a ruler)
Reassessment Ensure initial and ongoing pressure ulcer assessment
Reassess frequently (at least weekly or as advised by TVN)
No improvement
or deterioration
Refer
to
TVN
Treatment of pressure ulcers * Choose dressings/topical agent or method of debridement or adjunct therapy based on:
ulcer assessment & general skin assessment
treatment objective
characteristic of dressing/technique - previous positive effect of dressing/technique
manufacturer’s indications for use and contraindications
risk of adverse events
patient preference
dressings as prescribed by Dr/TV/District Nurse
Consider preventative measures shown in prevention box
As a minimum provision, patients with a grade 3-4 pressure ulcer should have a high
specification foam mattress with an alternating pressure overlay or cushion
Create an optimum wound healing environment using modern dressings (for example hydrocollolids, hydrogels, foam films, alginates, soft silicones)
Consider antimicrobial therapy, the presence of systemic and/or local clinical signs of infection
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 36
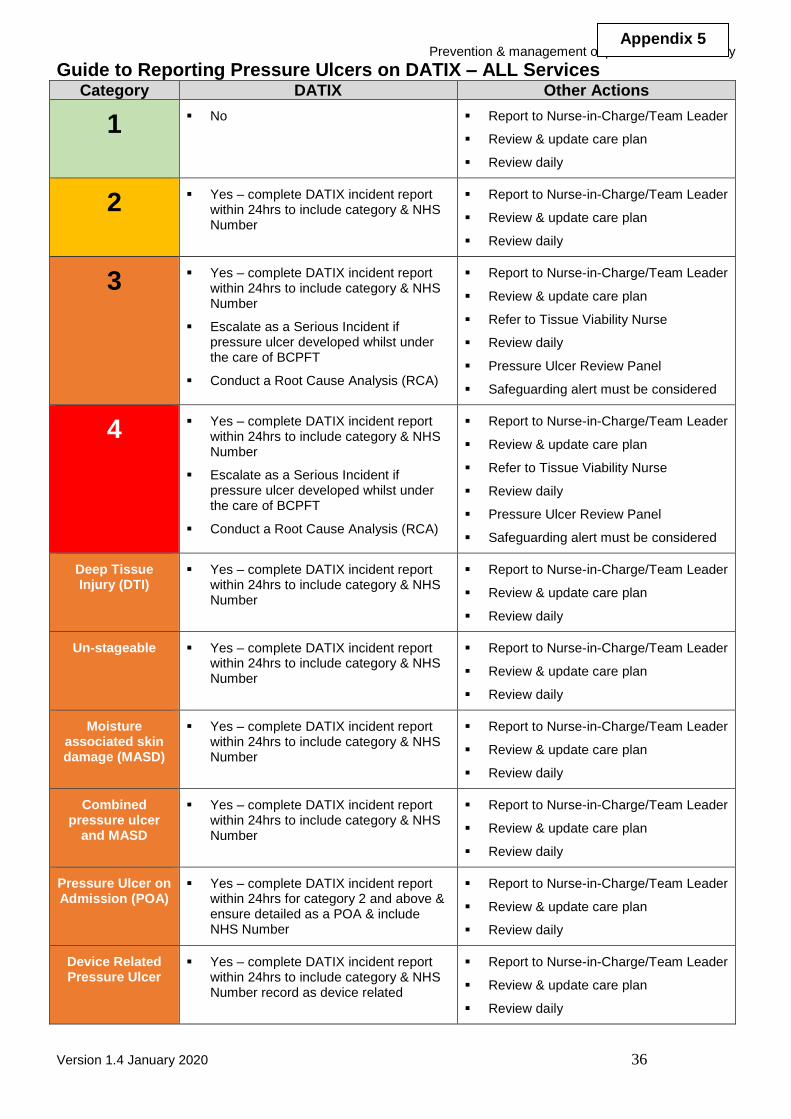
Guide to Reporting Pressure Ulcers on DATIX – ALL Services Category DATIX Other Actions
1 No Report to Nurse-in-Charge/Team Leader
Review & update care plan
Review daily
2 Yes – complete DATIX incident report within 24hrs to include category & NHS Number
Report to Nurse-in-Charge/Team Leader
Review & update care plan
Review daily
3 Yes – complete DATIX incident report within 24hrs to include category & NHS Number
Escalate as a Serious Incident if pressure ulcer developed whilst under the care of BCPFT
Conduct a Root Cause Analysis (RCA)
Report to Nurse-in-Charge/Team Leader
Review & update care plan
Refer to Tissue Viability Nurse
Review daily
Pressure Ulcer Review Panel
Safeguarding alert must be considered
4 Yes – complete DATIX incident report within 24hrs to include category & NHS Number
Escalate as a Serious Incident if pressure ulcer developed whilst under the care of BCPFT
Conduct a Root Cause Analysis (RCA)
Report to Nurse-in-Charge/Team Leader
Review & update care plan
Refer to Tissue Viability Nurse
Review daily
Pressure Ulcer Review Panel
Safeguarding alert must be considered
Deep Tissue Injury (DTI)
Yes – complete DATIX incident report within 24hrs to include category & NHS Number
Report to Nurse-in-Charge/Team Leader
Review & update care plan
Review daily
Un-stageable Yes – complete DATIX incident report within 24hrs to include category & NHS Number
Report to Nurse-in-Charge/Team Leader
Review & update care plan
Review daily
Moisture associated skin damage (MASD)
Yes – complete DATIX incident report within 24hrs to include category & NHS Number
Report to Nurse-in-Charge/Team Leader
Review & update care plan
Review daily
Combined pressure ulcer
and MASD
Yes – complete DATIX incident report within 24hrs to include category & NHS Number
Report to Nurse-in-Charge/Team Leader
Review & update care plan
Review daily
Pressure Ulcer on Admission (POA)
Yes – complete DATIX incident report within 24hrs for category 2 and above & ensure detailed as a POA & include NHS Number
Report to Nurse-in-Charge/Team Leader
Review & update care plan
Review daily
Device Related Pressure Ulcer
Yes – complete DATIX incident report within 24hrs to include category & NHS Number record as device related
Report to Nurse-in-Charge/Team Leader
Review & update care plan
Review daily
Appendix 5
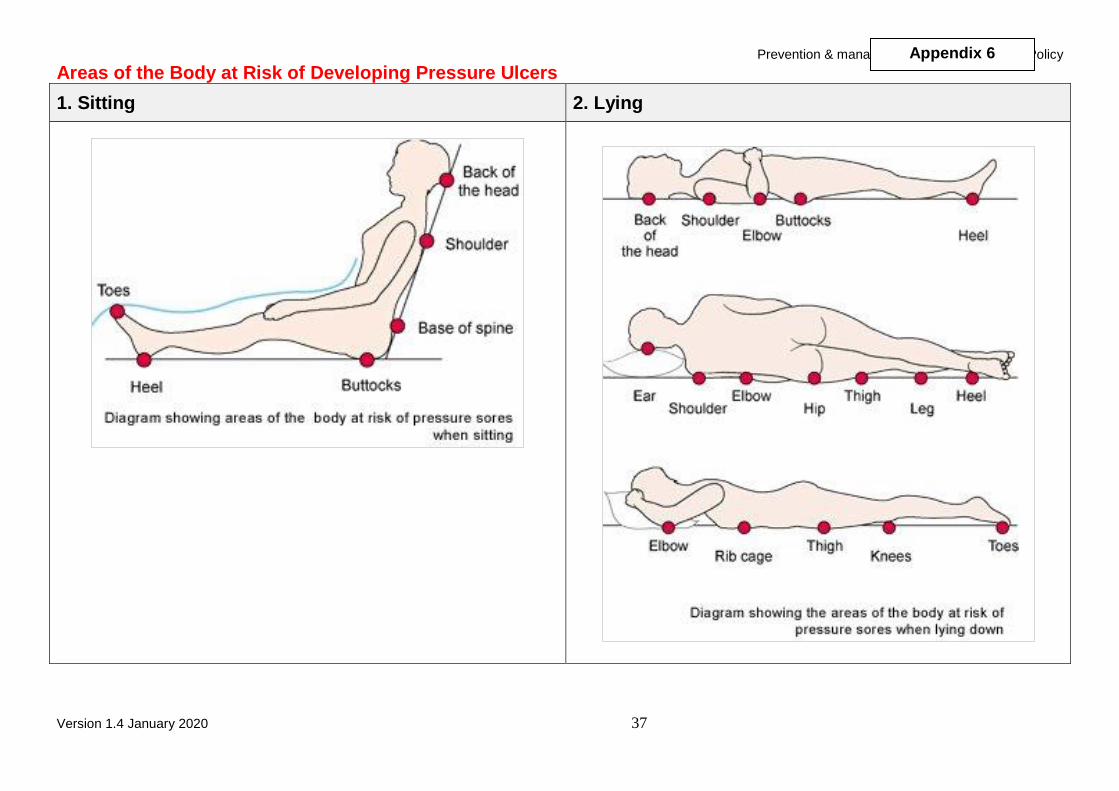
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 37
Areas of the Body at Risk of Developing Pressure Ulcers
1. Sitting 2. Lying
Appendix 6
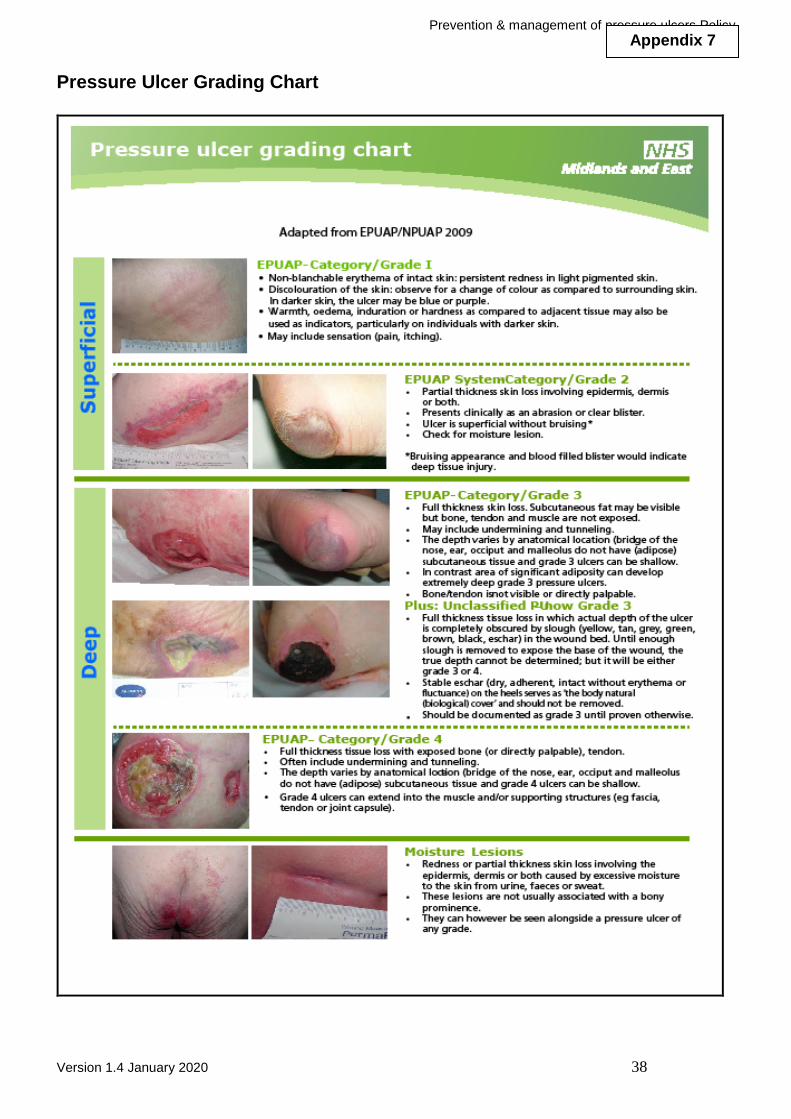
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 38
Pressure Ulcer Grading Chart
Appendix 7
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 39
Category 3 and 4 Pressure Ulcer Review Panel TERMS OF REFERENCE & MEMBERSHIP
1. Objectives 1.1 The Category 3 & 4 Pressure Ulcer Review Panel’s purpose is to review the Determination
of Causative Factors in the development of Category 3 and 4 Pressure Ulcers for those ulcers acquired in Black Country Partnership NHS Trust care.
The Panel’s core functions:
To ensure that all Category 3 & 4 pressure ulcers are investigated appropriately.
To monitor the quality and content of the notes and reviews submitted.
To ensure that lessons learnt are acted upon following review.
To ensure that all pressure injuries (Category 3+) that are identified as being acquired in BCPFT are recorded as a Serious Incident (SI) as per the Trust’s Risk Policy.
To ensure that any pressure injury acquired while under the care of BCPFT will be escalated and a Root Cause Analysis report delivered to SI panel in the required format and within agreed timescales.
2. Authority The Category 3 & 4 Pressure Ulcer Review Panel is authorised to carry out the activities specified within these Terms of Reference.
3. Review Panel Membership
The membership of the Category 3 & 4 Pressure Ulcer Review Panel includes: Core Panel Members
Chair -
Director/Deputy Director of Nursing
Service Director representation
Older Person’s Mental Health representation
Tissue Viability Specialist Nurse
Infection Prevention & Control Specialist
Clinical Risk Manager
Safeguard Lead
Community Nursing/Paediatric representation/designate as appropriate (if community paediatric involvement in patient care)
Associate Panel Members
Physiotherapy /Occupational Therapy Lead
Safeguarding Adults Lead / Designate
Safeguarding children’s lead / Designate other specialist co-opted as necessary 4. Terms of Reference Specific duties for the Category 3 & 4 Pressure Ulcer Review Panel include:
Appendix 8

Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 40
Review of the 72-hour report and chronological notes review and Waterlow tool assessment of pressure ulcers acquired in BCPFT care at Category at 3 & 4 in a timely manner.
Monitoring compliance with BCPFT policies at locality level, consistent with efficient and economic use of resources throughout the Trust.
Review clinical activity related to Category 3 & 4 pressure injuries on an ongoing basis.
Discussion of any identified issues specifically related Category 3 & 4 pressure ulcers acquired in BCPFT.
The 72 hour report and notes review will be submitted to the Risk Management Team by the service completing the Determination of Causative Factors in the development of Category 3 & 4 Root Cause Analysis Pressure Ulcers Risk Assessment Tool (Appendix 9)
5. Frequency of panel meetings
The Panel will ‘meet’ in response to the submission of a Datix Report and 72 hours Report Review to the Risk Management Team, identifying a pressure ulcer acquired in Black Country Partnership NHS Foundation Trust. 6. Timescale All requests for review will be circulated within 2 working days of receipt to the Risk Management Team. 7. Decision Making
Panel members will discuss the Route Cause Analysis findings and any associated evidence that has been collated, as a result of the review of the Pressure Ulcer.
The Risk Management Team will collate responses and action appropriately given the panel decision.
8. Quorum No business shall be transacted at the panel unless the following are present:
Chairperson or Chair’s Designate
With a minimum of five of the membership three of whom will be core panel members.
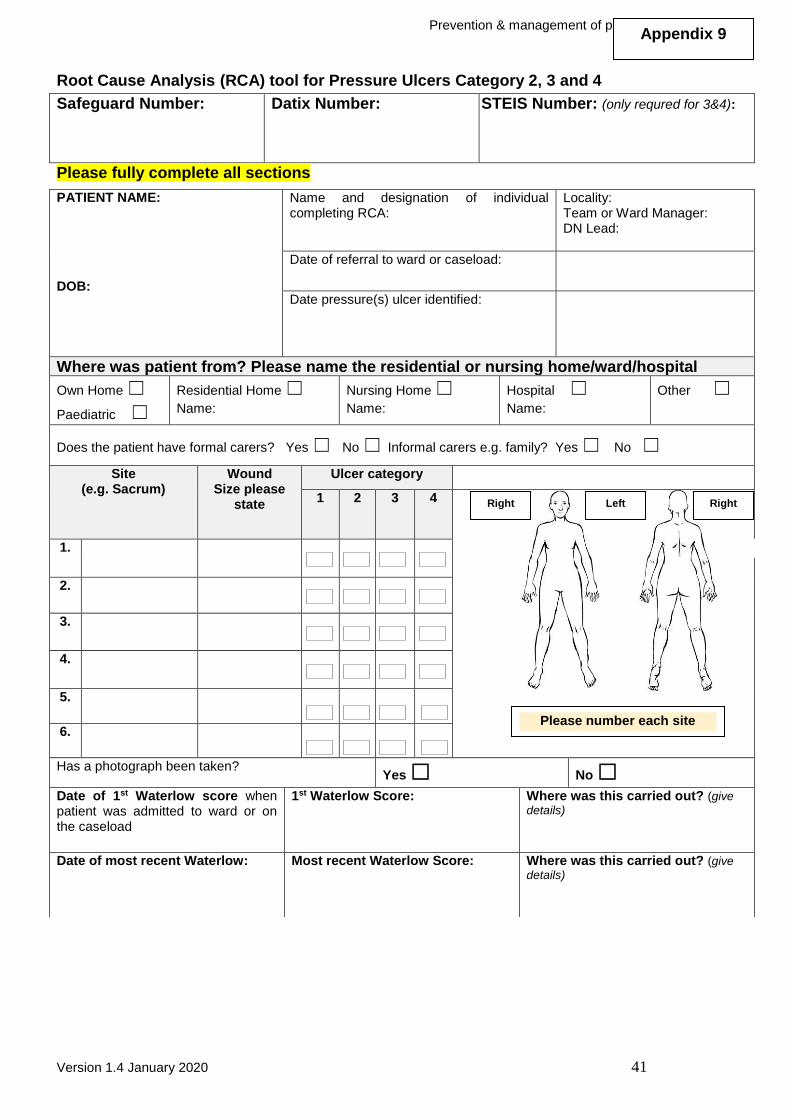
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 41
Root Cause Analysis (RCA) tool for Pressure Ulcers Category 2, 3 and 4
Safeguard Number:
Datix Number:
STEIS Number: (only requred for 3&4):
Please fully complete all sections
PATIENT NAME:
DOB:
Name and designation of individual completing RCA:
Locality: Team or Ward Manager: DN Lead:
Date of referral to ward or caseload:
Date pressure(s) ulcer identified:
Where was patient from? Please name the residential or nursing home/ward/hospital
Own Home ☐
Paediatric ☐
Residential Home ☐
Name:
Nursing Home ☐
Name:
Hospital ☐
Name:
Other ☐
Does the patient have formal carers? Yes ☐ No ☐ Informal carers e.g. family? Yes ☐ No ☐
Site (e.g. Sacrum)
Wound Size please
state
Ulcer category
1 2 3 4
1.
2.
3.
4.
5.
6.
Has a photograph been taken? Yes ☐ No ☐
Date of 1st Waterlow score when patient was admitted to ward or on the caseload
1st Waterlow Score:
Where was this carried out? (give
details)
Date of most recent Waterlow:
Most recent Waterlow Score:
Where was this carried out? (give
details)
Right Left Right
Appendix 9
Please number each site
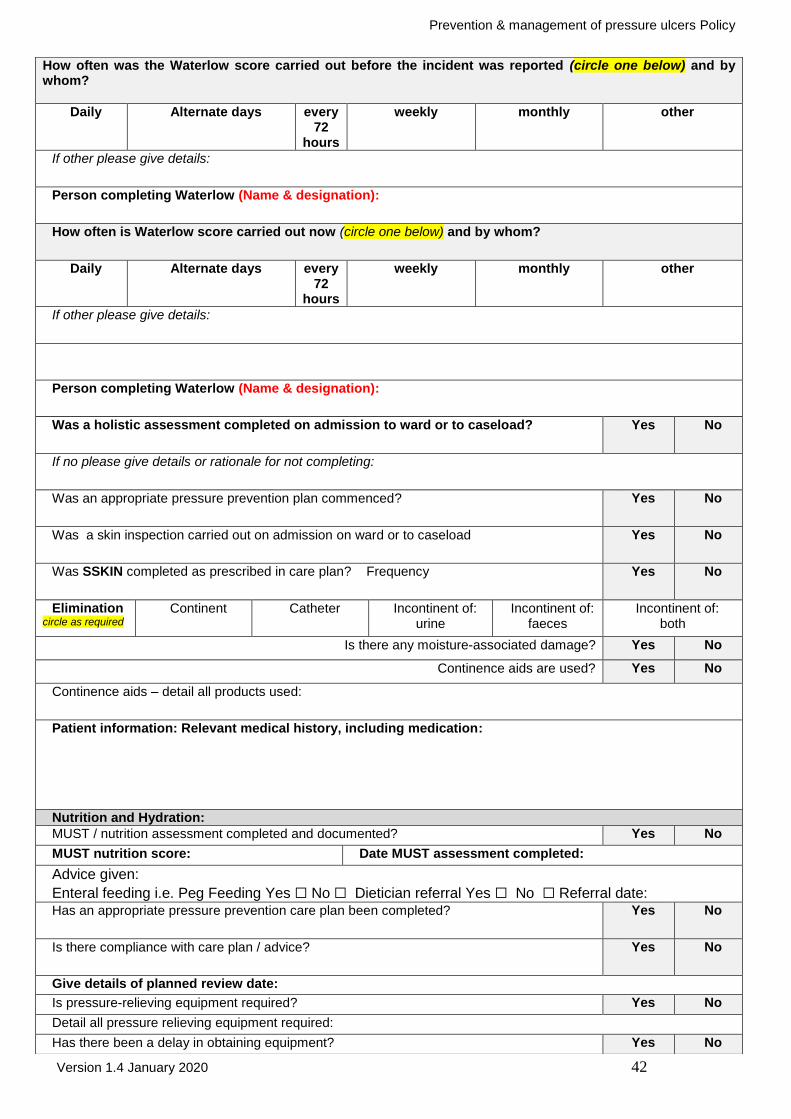
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 42
How often was the Waterlow score carried out before the incident was reported (circle one below) and by whom?
Daily Alternate days every 72
hours
weekly monthly other
If other please give details:
Person completing Waterlow (Name & designation):
How often is Waterlow score carried out now (circle one below) and by whom?
Daily Alternate days every 72
hours
weekly monthly other
If other please give details:
Person completing Waterlow (Name & designation):
Was a holistic assessment completed on admission to ward or to caseload?
Yes No
If no please give details or rationale for not completing:
Was an appropriate pressure prevention plan commenced? Yes No
Was a skin inspection carried out on admission on ward or to caseload Yes No
Was SSKIN completed as prescribed in care plan? Frequency Yes No
Elimination circle as required
Continent Catheter Incontinent of: urine
Incontinent of: faeces
Incontinent of: both
Is there any moisture-associated damage? Yes No
Continence aids are used? Yes No
Continence aids – detail all products used:
Patient information: Relevant medical history, including medication:
Nutrition and Hydration:
MUST / nutrition assessment completed and documented? Yes No
MUST nutrition score: Date MUST assessment completed:
Advice given:
Enteral feeding i.e. Peg Feeding Yes ☐ No ☐ Dietician referral Yes ☐ No ☐ Referral date: Has an appropriate pressure prevention care plan been completed? Yes No
Is there compliance with care plan / advice?
Yes No
Give details of planned review date:
Is pressure-relieving equipment required? Yes No
Detail all pressure relieving equipment required:
Has there been a delay in obtaining equipment? Yes No
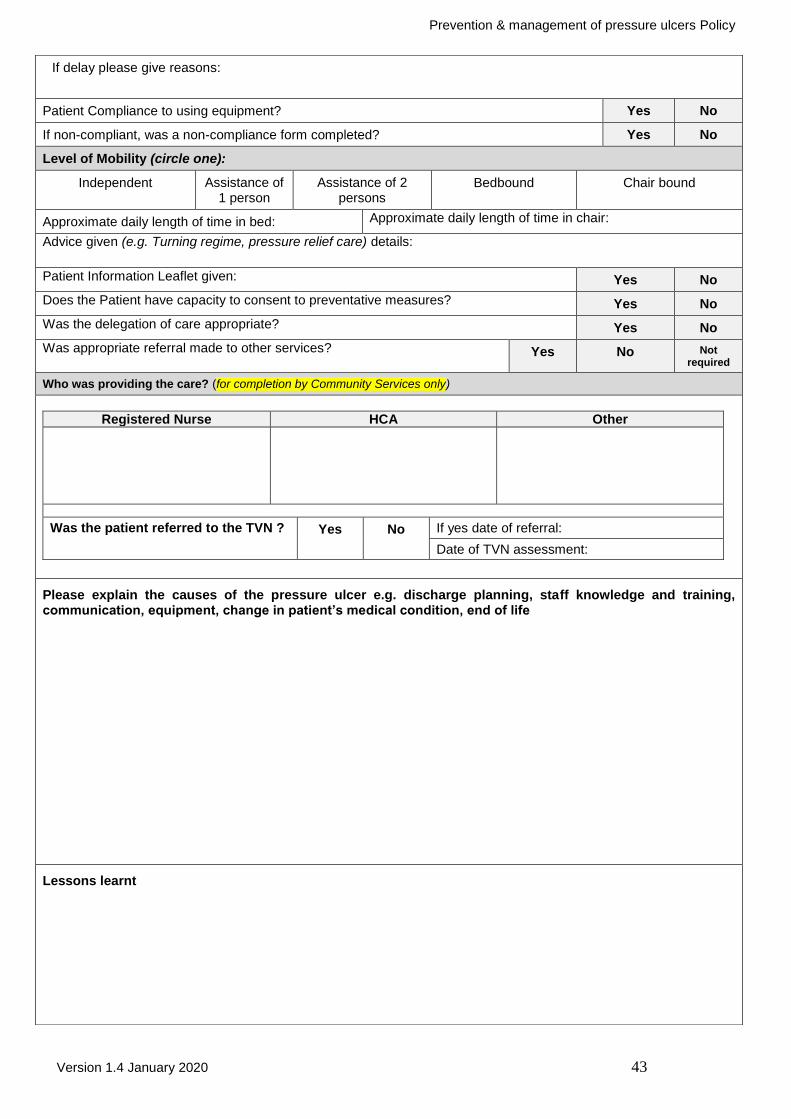
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 43
If delay please give reasons:
Patient Compliance to using equipment? Yes No
If non-compliant, was a non-compliance form completed? Yes No
Level of Mobility (circle one):
Independent Assistance of 1 person
Assistance of 2 persons
Bedbound Chair bound
Approximate daily length of time in bed: Approximate daily length of time in chair:
Advice given (e.g. Turning regime, pressure relief care) details:
Patient Information Leaflet given: Yes No
Does the Patient have capacity to consent to preventative measures? Yes No
Was the delegation of care appropriate? Yes No
Was appropriate referral made to other services? Yes No Not required
Who was providing the care? (for completion by Community Services only)
Registered Nurse HCA Other
Was the patient referred to the TVN ? Yes No If yes date of referral:
Date of TVN assessment:
Please explain the causes of the pressure ulcer e.g. discharge planning, staff knowledge and training, communication, equipment, change in patient’s medical condition, end of life
Lessons learnt
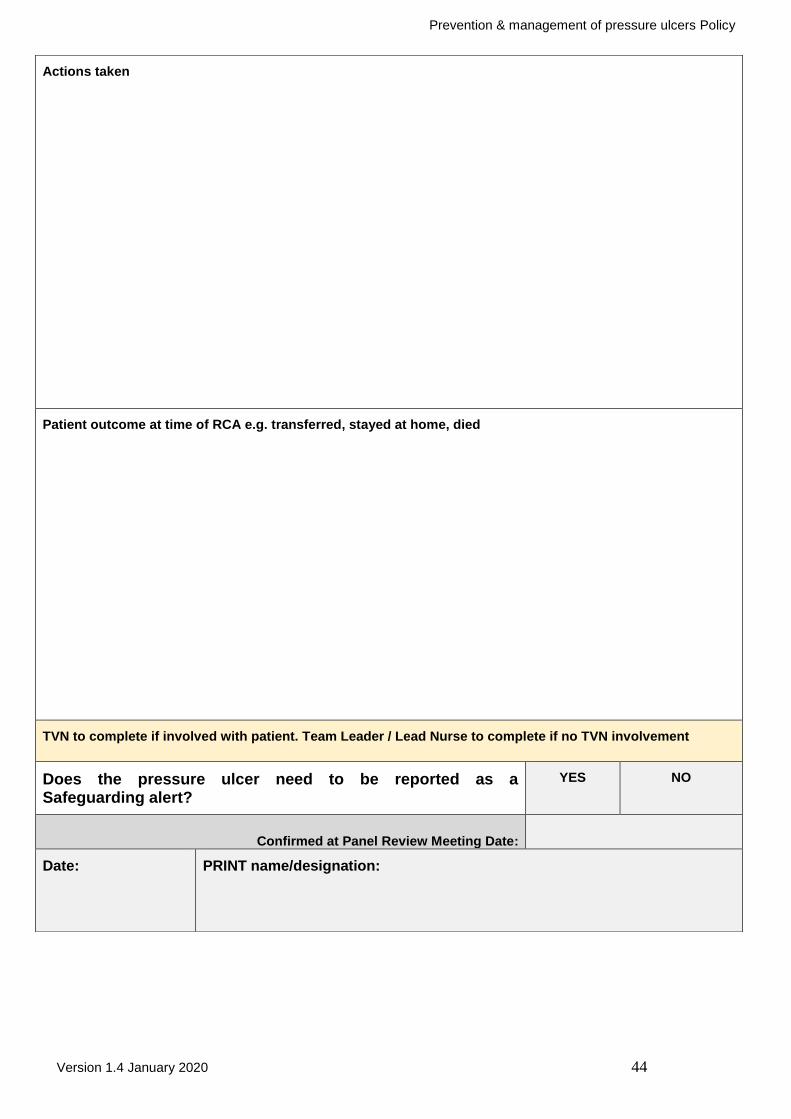
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 44
Actions taken
Patient outcome at time of RCA e.g. transferred, stayed at home, died
TVN to complete if involved with patient. Team Leader / Lead Nurse to complete if no TVN involvement
Does the pressure ulcer need to be reported as a Safeguarding alert?
YES NO
Confirmed at Panel Review Meeting Date:
Date: PRINT name/designation:
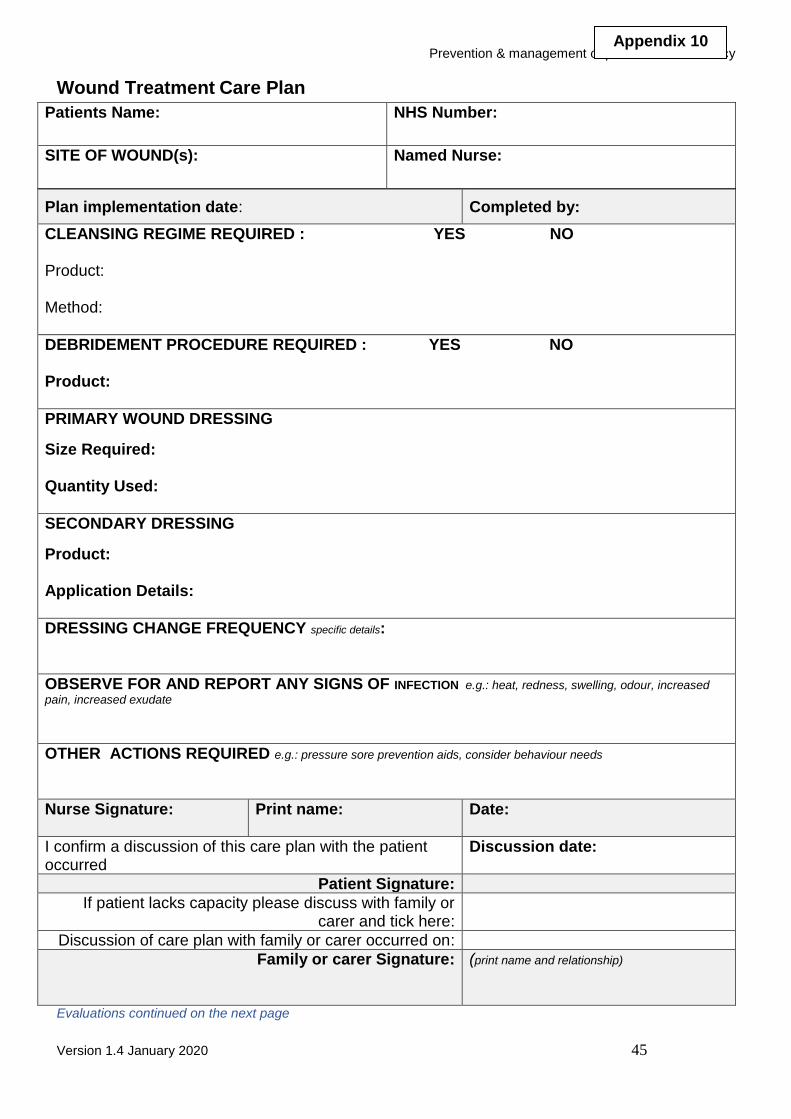
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 45
Wound Treatment Care Plan
Patients Name: NHS Number:
SITE OF WOUND(s): Named Nurse:
Plan implementation date: Completed by:
CLEANSING REGIME REQUIRED : YES NO Product: Method:
DEBRIDEMENT PROCEDURE REQUIRED : YES NO Product:
PRIMARY WOUND DRESSING
Size Required: Quantity Used:
SECONDARY DRESSING
Product: Application Details:
DRESSING CHANGE FREQUENCY specific details:
OBSERVE FOR AND REPORT ANY SIGNS OF INFECTION e.g.: heat, redness, swelling, odour, increased
pain, increased exudate
OTHER ACTIONS REQUIRED e.g.: pressure sore prevention aids, consider behaviour needs
Nurse Signature:
Print name: Date:
I confirm a discussion of this care plan with the patient occurred
Discussion date:
Patient Signature:
If patient lacks capacity please discuss with family or carer and tick here:
Discussion of care plan with family or carer occurred on:
Family or carer Signature:
(print name and relationship)
Evaluations continued on the next page
Appendix 10
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 46
DATE & TIME
Insert Patients Name & DOB
WOUND CARE EVALUATION
SIGNATURE

Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 47
Management and Prevention of Nappy Rash & Moisture Lesions
Atypical presentation Normal bowel
habit
Prophylaxis
For intact skin prior to therapy that may
alter bowel habit
Excoriation
Superficial epidermal
erosion and surrounding erythema
Ulceration
Damage extending to the
dermis
Bright red rash, satellite lesions,
pustules at margins. Rash
extends to areas not in contact with faeces e.g. groin
Other skin conditions such as eczema, psoriasis or ringworm can also be present in the perineal area. If you are unsure about the appearance of a presenting lesion then please contact your medical team, tissue viability or dermatology
3MTMCavilon TM No Sting Barrier
(NSBF) Every 48 -72 hrs
Continue with Cavilon while bowel
habit persists. (Cavilon NSBF not
to be used on babies less than 4
weeks old use Cavilon DBC)
3MTMCavilonT
M
No Sting Barrier (NSBF)
Every 48-72 hours. (Cavilon NSBF not to be used on babies
less than 4 weeks old, use Cavilon DBC)
Classic nappy rash
Mild to moderate
perineal erythema
Follow good nappy
care Clotrimazole 1%
TDS. Continue until rash clears plus 2 weeks Do not use any other
preparations at the same time e.g. Cavilon. This will reduce the effect of the Clotrimazole cream.
Altered bowel habit (or expectation of altered bowel habit due to intervention
e.g. antibiotic therapy
Candidiasis
3MTM Cavilon TM
Durable Barrier Cream (DBC) Re-apply every 3rd nappy change until bowel altering therapy stopped. (Highly concentrated. Only small amount req’d)
Healed No improvement/not healed after 7 days refer to Tissue Viability
Barrier
Prevention
GOOD NAPPY CARE
Frequent changing of gel core nappy
Nappy changes MUST take place as soon as possible after soiling
Use an emollient to clean the skin such as Dermol 500 (Named patient use only – remember to label the container) DO NOT USE SOAP
Apply barrier agents sparingly
Expose skin where possible N.B. ALL treatments MUST be prescribed
Appendix 11
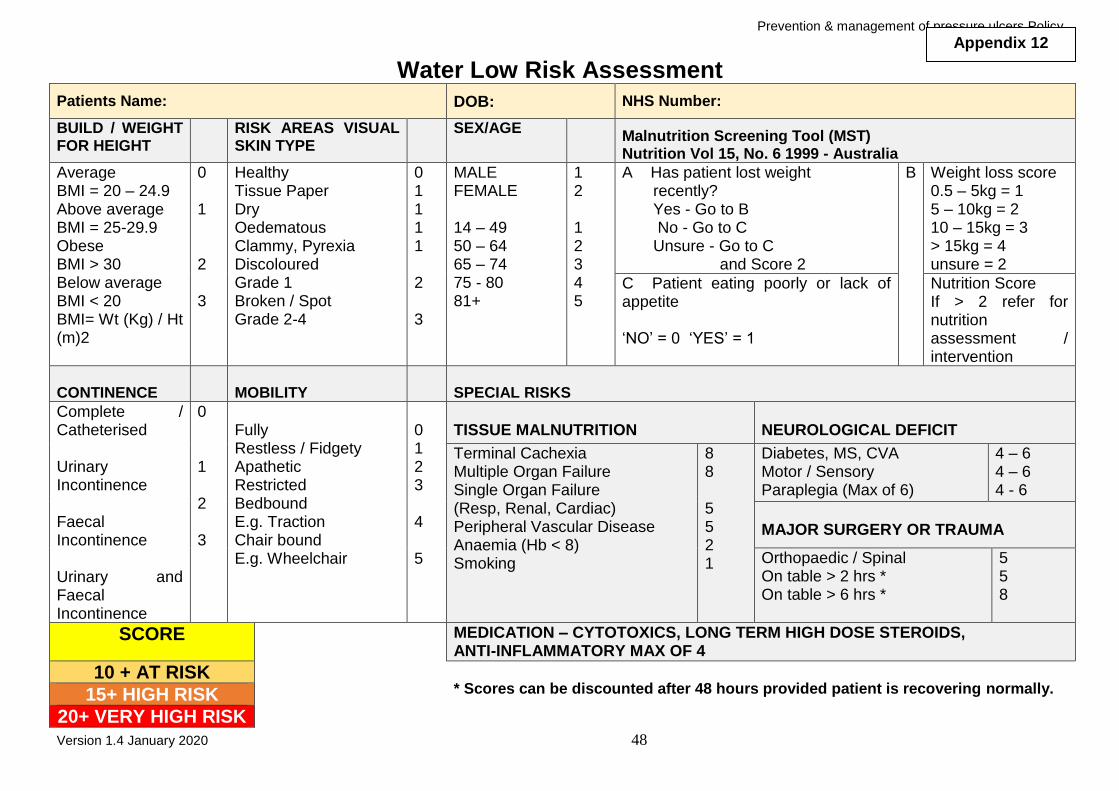
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 48
Water Low Risk Assessment
Patients Name: DOB: NHS Number:
BUILD / WEIGHT FOR HEIGHT
RISK AREAS VISUAL SKIN TYPE
SEX/AGE Malnutrition Screening Tool (MST) Nutrition Vol 15, No. 6 1999 - Australia
Average BMI = 20 – 24.9 Above average BMI = 25-29.9 Obese BMI > 30 Below average BMI < 20 BMI= Wt (Kg) / Ht (m)2
0 1 2 3
Healthy Tissue Paper Dry Oedematous Clammy, Pyrexia Discoloured Grade 1 Broken / Spot Grade 2-4
0 1 1 1 1 2 3
MALE FEMALE 14 – 49 50 – 64 65 – 74 75 - 80 81+
1 2 1 2 3 4 5
A Has patient lost weight recently? Yes - Go to B No - Go to C Unsure - Go to C and Score 2
B Weight loss score 0.5 – 5kg = 1 5 – 10kg = 2 10 – 15kg = 3 > 15kg = 4 unsure = 2
C Patient eating poorly or lack of appetite ‘NO’ = 0 ‘YES’ = 1
Nutrition Score If > 2 refer for nutrition assessment / intervention
CONTINENCE
MOBILITY
SPECIAL RISKS
Complete / Catheterised Urinary Incontinence Faecal Incontinence Urinary and Faecal Incontinence
0 1 2 3
Fully Restless / Fidgety Apathetic Restricted Bedbound E.g. Traction Chair bound E.g. Wheelchair
0 1 2 3 4 5
TISSUE MALNUTRITION
NEUROLOGICAL DEFICIT
Terminal Cachexia Multiple Organ Failure Single Organ Failure (Resp, Renal, Cardiac) Peripheral Vascular Disease Anaemia (Hb < 8) Smoking
8 8 5 5 2 1
Diabetes, MS, CVA Motor / Sensory Paraplegia (Max of 6)
4 – 6 4 – 6 4 - 6
MAJOR SURGERY OR TRAUMA
Orthopaedic / Spinal On table > 2 hrs * On table > 6 hrs *
5 5 8
SCORE
MEDICATION – CYTOTOXICS, LONG TERM HIGH DOSE STEROIDS, ANTI-INFLAMMATORY MAX OF 4
10 + AT RISK * Scores can be discounted after 48 hours provided patient is recovering normally. 15+ HIGH RISK
20+ VERY HIGH RISK
Appendix 12

Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 49
WATER LOW RISK ASSESSMENT cont.
Patients Name: Date of Birth: NHS No:
DATE BUILD/
WEIGHT
SKIN
TYPE
SEX/
AGE
MST CONTINENCE MOBILITY SPECIAL
RISK
TOTAL
SCORE
ASSESSMENT
RATING
ASSESSOR SIGNATURE
NEXT REVIEW
DATE

Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 50
Malnutrition Universal Screening Tool - ADULTS
SCORE 2
NO CARE PLAN REQUIRED
REFER
TO
DIETICIAN
CARE PLAN AS PER DIETICIAN
RECOMMENDATION
SCORE 0
WEEKLY
RE-SCREEN
NO CARE PLAN REQUIRED
SCORE 1
MONITOR DIET AND FLUIDS
DISCUSS WITH MEDICAL TEAM ABOUT NUTRITIONAL SUPPORT
ENCOURAGE HIGH CALORIE INTAKE AND SNACKS BETWEEN MEALS
RESCORE WEEKLY AND REVIEW IN
MDM MEETING
Appendix 13
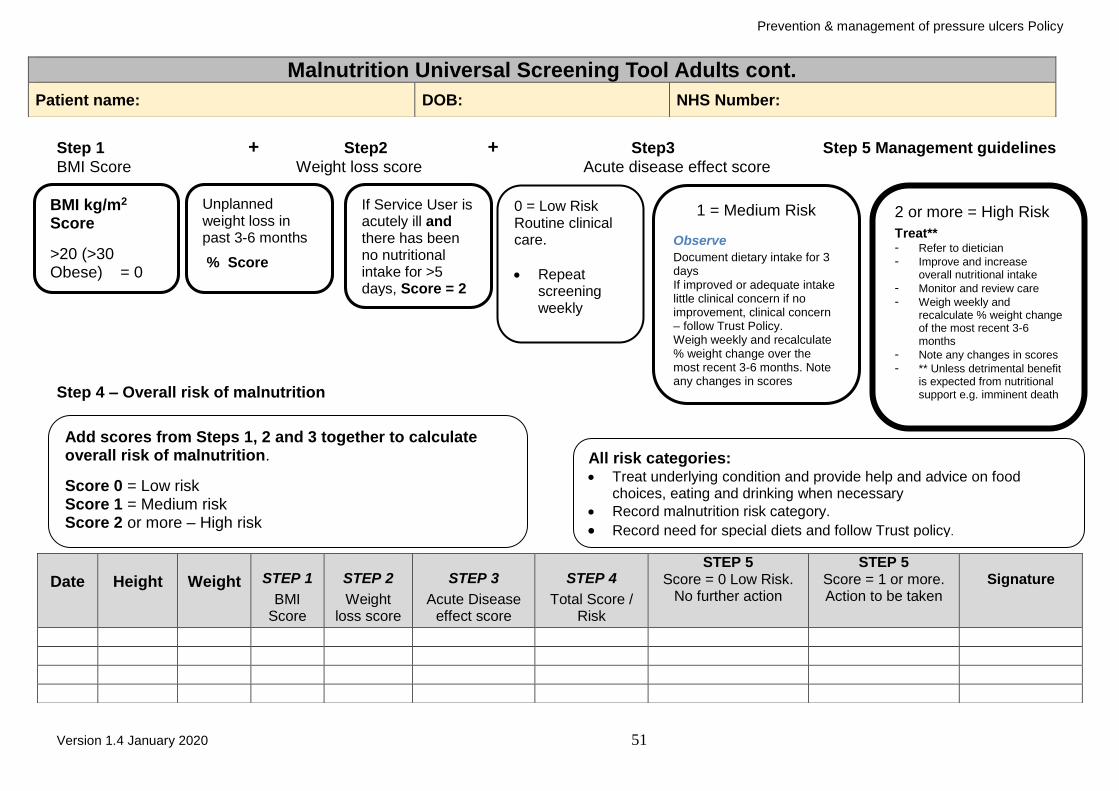
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 51
Step 1 + Step2 + Step3 Step 5 Management guidelines
BMI Score Weight loss score Acute disease effect score
Step 4 – Overall risk of malnutrition
Malnutrition Universal Screening Tool Adults cont.
Patient name: DOB: NHS Number:
Date
Height
Weight STEP 1
BMI Score
STEP 2
Weight loss score
STEP 3
Acute Disease effect score
STEP 4
Total Score / Risk
STEP 5 Score = 0 Low Risk.
No further action
STEP 5 Score = 1 or more. Action to be taken
Signature
BMI kg/m2 Score
>20 (>30 Obese) = 0
If Service User is acutely ill and there has been no nutritional intake for >5 days, Score = 2
Unplanned weight loss in past 3-6 months
% Score
0 = Low Risk Routine clinical care.
Repeat screening weekly
1 = Medium Risk
Observe
Document dietary intake for 3 days If improved or adequate intake little clinical concern if no improvement, clinical concern – follow Trust Policy. Weigh weekly and recalculate % weight change over the most recent 3-6 months. Note any changes in scores
2 or more = High Risk
Treat** - Refer to dietician
- Improve and increase overall nutritional intake
- Monitor and review care
- Weigh weekly and recalculate % weight change of the most recent 3-6 months
- Note any changes in scores
- ** Unless detrimental benefit is expected from nutritional support e.g. imminent death
Add scores from Steps 1, 2 and 3 together to calculate overall risk of malnutrition.
Score 0 = Low risk Score 1 = Medium risk Score 2 or more – High risk
All risk categories: Treat underlying condition and provide help and advice on food
choices, eating and drinking when necessary
Record malnutrition risk category.
Record need for special diets and follow Trust policy.
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 52
Patient name: DOB: Hospital number:
Date
Height
Weight
STEP 1 BMI
Score
STEP 2 Weight
loss score
STEP 3 Acute Disease
effect score
STEP 4 Total Score /
Risk
STEP 5 Score = 0 Low Risk.
No further action
STEP 5 Score = 1 or more.
Action to be taken
Signature
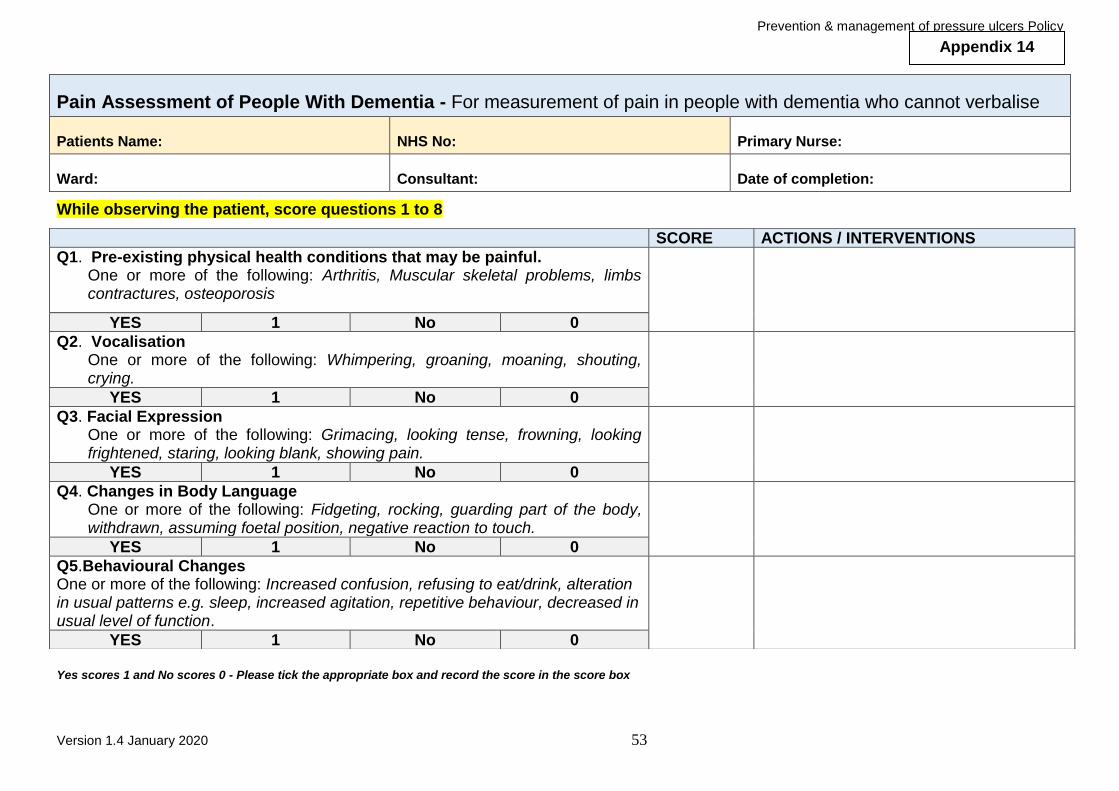
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 53
Pain Assessment of People With Dementia - For measurement of pain in people with dementia who cannot verbalise
Patients Name: NHS No: Primary Nurse:
Ward: Consultant: Date of completion:
While observing the patient, score questions 1 to 8
Yes scores 1 and No scores 0 - Please tick the appropriate box and record the score in the score box
SCORE ACTIONS / INTERVENTIONS
Q1. Pre-existing physical health conditions that may be painful. One or more of the following: Arthritis, Muscular skeletal problems, limbs contractures, osteoporosis
YES 1 No 0
Q2. Vocalisation One or more of the following: Whimpering, groaning, moaning, shouting, crying.
YES 1 No 0
Q3. Facial Expression One or more of the following: Grimacing, looking tense, frowning, looking frightened, staring, looking blank, showing pain.
YES 1 No 0
Q4. Changes in Body Language One or more of the following: Fidgeting, rocking, guarding part of the body, withdrawn, assuming foetal position, negative reaction to touch.
YES 1 No 0
Q5.Behavioural Changes One or more of the following: Increased confusion, refusing to eat/drink, alteration in usual patterns e.g. sleep, increased agitation, repetitive behaviour, decreased in usual level of function.
YES 1 No 0
Appendix 14

Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 54
Pain assessment for people with Dementia continued SCORE
ACTIONS / INTERVENTIONS
Q6. Physiological Changes One or more of the following: Change in temperature, pulse, BP, respirations, perspiration, flushing, pale.
YES 1 No 0
Q7. Physical Changes One or more of the following: Skin tears, pressure areas, arthritis, contractures, previous injuries, immobility, unable to weight bear, deterioration in mobility.
YES 1 No 0
Q8. Changes in Communication One or more of the following: Changes in level of communication, patient demands attention in an unusual manner, absence or refusal of any form of communication.
YES 1 No 0
Q9. Changes in Social Life One or more of the following: Refuses to participate in any activity, only participates when asked.
YES 1 No 0
TOTAL
Signature:
Print name: Carers Notified (if required) :
Date seen by Doctor(if required): Pain relief commenced (if required)::
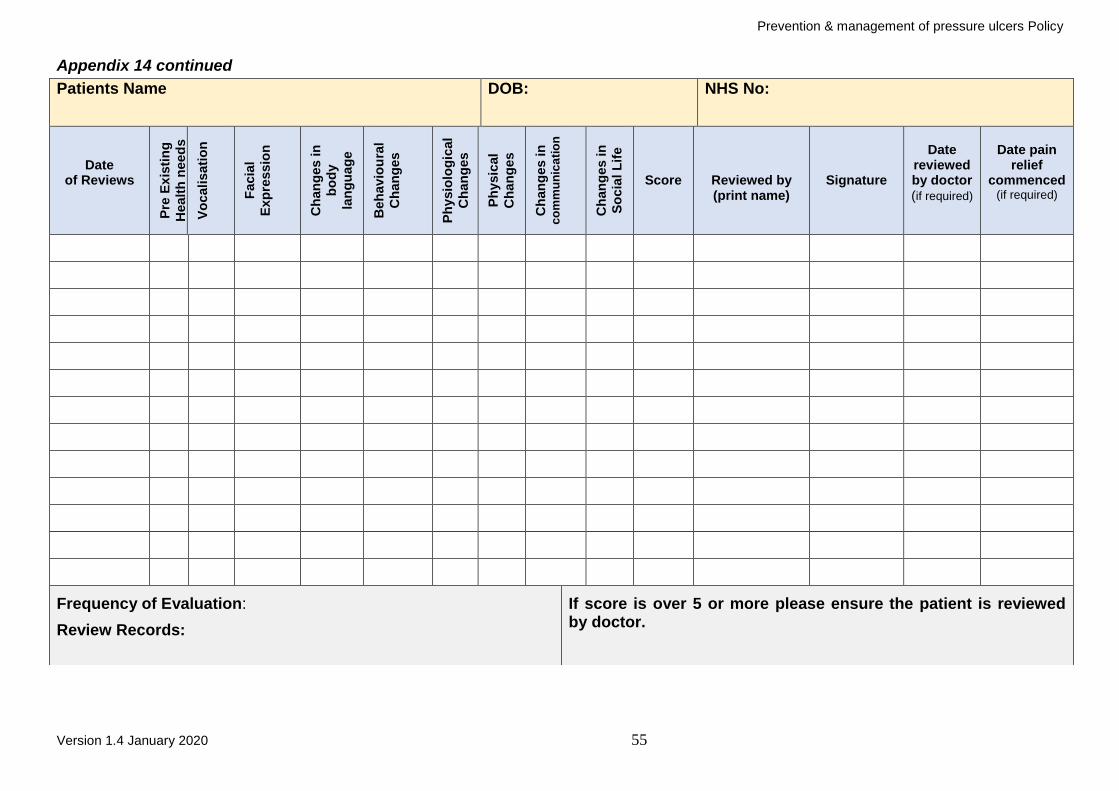
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 55
Appendix 14 continued
Patients Name DOB: NHS No:
Date of Reviews
Pre
Ex
isti
ng
Healt
h n
eed
s
Vo
cali
sati
on
Facia
l
Exp
ressio
n
Ch
an
ges in
bo
dy
lan
gu
ag
e
Beh
avio
ura
l
Ch
an
ges
Ph
ysio
log
ical
Ch
an
ges
Ph
ysic
al
Ch
an
ges
Ch
an
ges in
c
om
mu
nic
ati
on
Ch
an
ges in
So
cia
l L
ife
Score
Reviewed by (print name)
Signature
Date
reviewed by doctor (if required)
Date pain
relief commenced
(if required)
Frequency of Evaluation:
Review Records:
If score is over 5 or more please ensure the patient is reviewed by doctor.
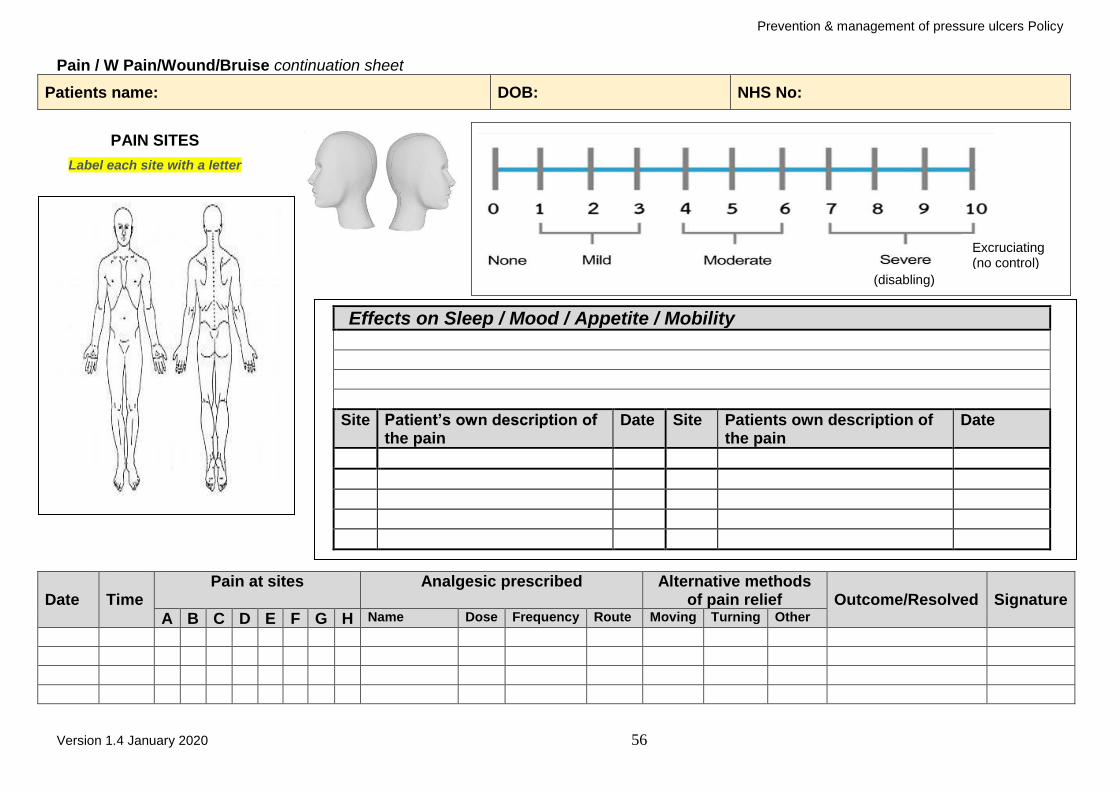
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 56
Pain / W Pain/Wound/Bruise continuation sheet
Patients name: DOB: NHS No:
PAIN SITES
Label each site with a letter
(disabling)
Date
Time
Pain at sites Analgesic prescribed Alternative methods of pain relief
Outcome/Resolved
Signature
A B C D E F G H Name Dose Frequency Route Moving Turning Other
Excruciating (no control)
Effects on Sleep / Mood / Appetite / Mobility
Site Patient’s own description of the pain
Date Site Patients own description of the pain
Date
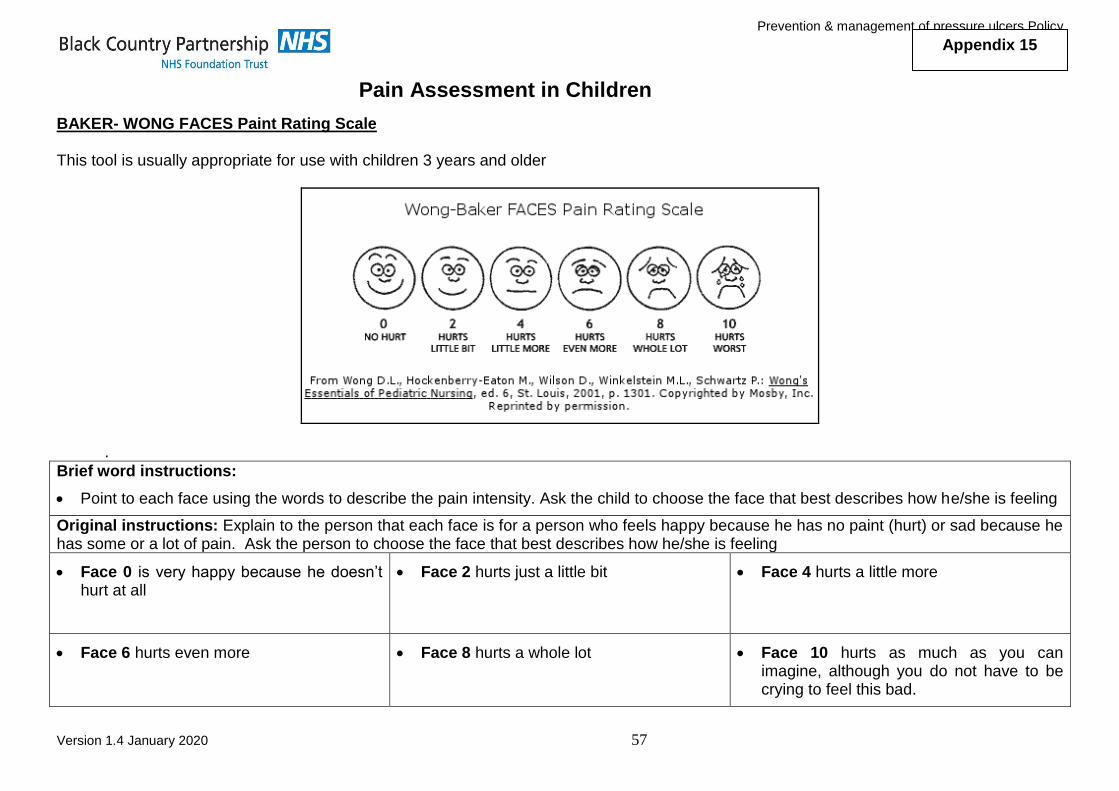
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 57
Pain Assessment in Children
BAKER- WONG FACES Paint Rating Scale This tool is usually appropriate for use with children 3 years and older
.
Brief word instructions:
Point to each face using the words to describe the pain intensity. Ask the child to choose the face that best describes how he/she is feeling
Original instructions: Explain to the person that each face is for a person who feels happy because he has no paint (hurt) or sad because he has some or a lot of pain. Ask the person to choose the face that best describes how he/she is feeling
Face 0 is very happy because he doesn’t hurt at all
Face 2 hurts just a little bit
Face 4 hurts a little more
Face 6 hurts even more
Face 8 hurts a whole lot
Face 10 hurts as much as you can imagine, although you do not have to be crying to feel this bad.
Appendix 15
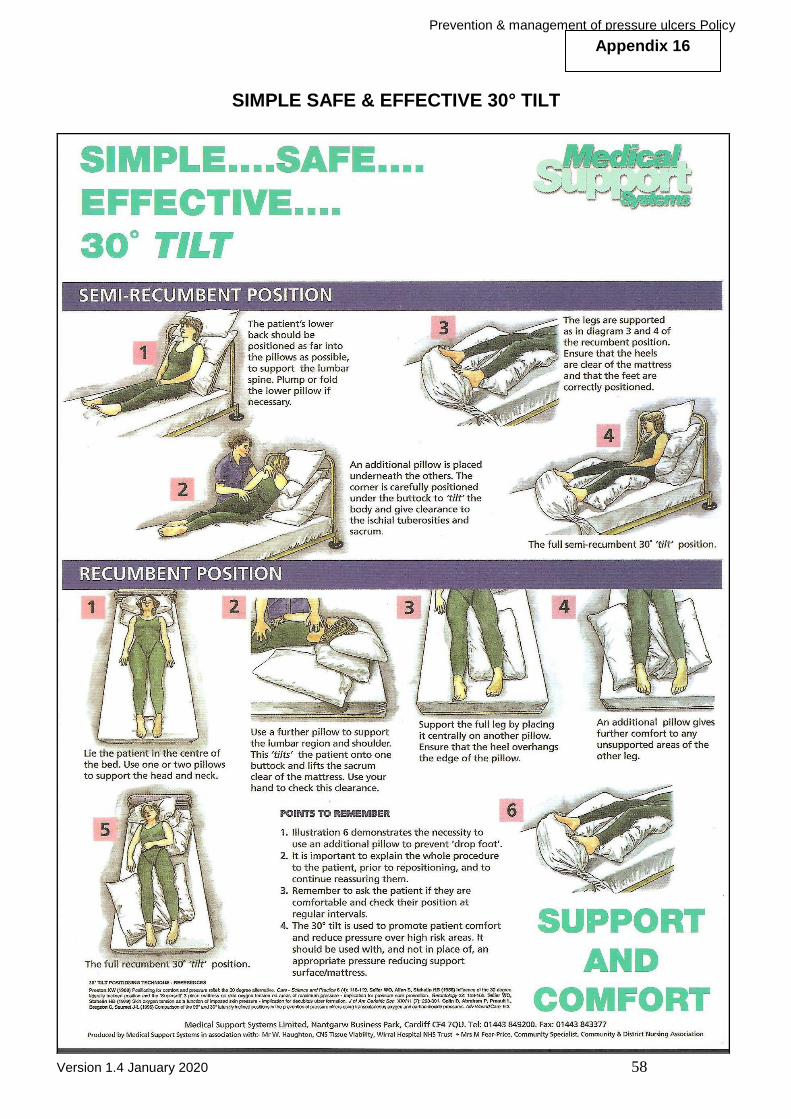
Prevention & management of pressure ulcers Policy
Version 1.4 January 2020 58
SIMPLE SAFE & EFFECTIVE 30° TILT
Appendix 16
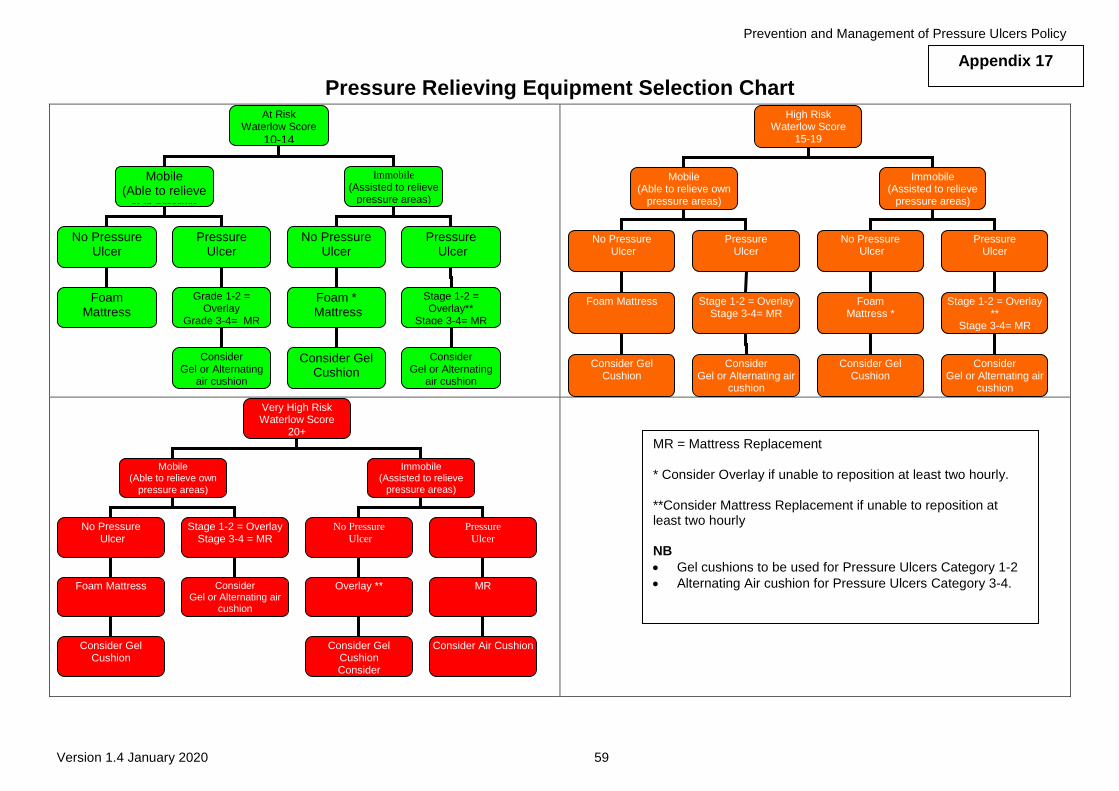
Prevention and Management of Pressure Ulcers Policy
Version 1.4 January 2020 59
Pressure Relieving Equipment Selection Chart
Very High Risk Waterlow Score
20+
Mobile (Able to relieve own
pressure areas)
Immobile (Assisted to relieve
pressure areas)
No Pressure Ulcer
No Pressure
Ulcer
Pressure
Ulcer
Foam Mattress
Stage 1-2 = Overlay Stage 3-4 = MR
Overlay ** MR
Consider Gel Cushion
Consider Gel or Alternating air
cushion
Consider Gel Cushion Consider
Gel or Alternating air
cushion
Consider Air Cushion
High Risk Waterlow Score
15-19
Mobile (Able to relieve own
pressure areas)
Immobile (Assisted to relieve
pressure areas)
No Pressure Ulcer
Pressure Ulcer
No Pressure Ulcer
Pressure Ulcer
Foam Mattress
Stage 1-2 = Overlay Stage 3-4= MR
Foam Mattress *
Stage 1-2 = Overlay **
Stage 3-4= MR
Consider Gel Cushion
Consider Gel or Alternating air
cushion
Consider Gel Cushion
Consider Gel or Alternating air
cushion
At Risk Waterlow Score
10-14
Mobile (Able to relieve
own pressure
areas)
Immobile
(Assisted to relieve pressure areas)
No Pressure Ulcer
Pressure Ulcer
No Pressure Ulcer
Pressure Ulcer
Foam Mattress
Grade 1-2 = Overlay
Grade 3-4= MR
Foam * Mattress
Stage 1-2 =
Overlay** Stage 3-4= MR
Consider Gel or Alternating
air cushion
Consider Gel Cushion
Consider Gel or Alternating
air cushion
MR = Mattress Replacement * Consider Overlay if unable to reposition at least two hourly. **Consider Mattress Replacement if unable to reposition at least two hourly NB
Gel cushions to be used for Pressure Ulcers Category 1-2
Alternating Air cushion for Pressure Ulcers Category 3-4.
Appendix 17

Prevention and Management of Pressure Ulcers Policy
Version 1.4 January 2020 60
Policy Details
* For more information on the consultation process, implementation plan, equality impact assessment, or archiving
arrangements, please contact Corporate Governance
Review and Amendment History
Version Date Details of Change
1.4 Jan 2020
Reviewed to ensure this policy complies with National guidelines following a gap analysis comparison against existing policy.
Explanation of terms expanded as per revised guidelines (June 2018)
Objectives reviewed & updated
Update includes more detail on moisture lesions
Appendices re-ordered & re-formatted
Appendix 3 (Paediatric tool) updated
Appendix 4 added – Reporting pressure ulcers
Appendix 6 updated to mirror the one in the Trust’s SSKIN standard procedure
Title of Policy Prevention and Management of Pressure Ulcers Policy
Unique Identifier for this policy BCPFT-PH-POL-01
State if policy is New or Revised Revised
Previous Policy Title where applicable n/a
Policy Category Clinical, HR, H&S, Infection Control etc.
Physical Health
Executive Director whose portfolio this policy comes under
Director of Nursing
Policy Lead/Author Job titles only
Matron of OA supported by Head of Nursing (Physical Health)
Committee/Group responsible for the approval of this policy
Nursing Board
Month/year consultation process completed *
January 2020
Month/year policy approved February 2020
Month/year policy ratified and issued March 2020
Next review date January 2023
Implementation Plan completed * Yes
Equality Impact Assessment completed * Yes
Previous version(s) archived * Yes
Disclosure status ‘B’ can be disclosed to patients and the public
Key Words for this policy Policy, Pressure Ulcer, Tissue Viability, Tissue Injury, Treatment of Ulcers, Assessment of Ulcers, Management of patients with Ulcers, Moisture lesions
Prevention and Management of Pressure Ulcers Policy
Version 1.4 January 2020 61
1.3 Nov 2019 Appendix 9 amended to include Community Nurses Processes
Version Date Details of Change continued
1.2 May 2018 Reviewed in new Trust Policy template with updates made to section 5.0, 7.0, 8.0 and 11.0.
1.1 Nov 2014 Policy reviewed following publication of NICE Clinical Guideline CG179 April 2014
1.0 Mar 2013 New policy for BCPFT- Policy for BCPFT newly established organisation.