
Stroke in the Ashanti Region of Ghana: The Politics of Blame and Self-Blame
83
1 1 All pictures are the authors own and permission for the usage was obtained from all informants. Left: Akosi; right: Bubu and Owowusu Social Anthropology Dissertation March 2013 Michaela Hubmann Student Number: 1017555 The Politics of Blame and Self-Blame Stroke in the Ashanti Region of Ghana:
Transcript of Stroke in the Ashanti Region of Ghana: The Politics of Blame and Self-Blame

1
1 All pictures are the authors own and permission
for the usage was obtained from all informants.
Left: Akosi; right: Bubu and Owowusu
Social Anthropology Dissertation March 2013
Michaela Hubmann Student Number: 1017555
The Politics of Blame and Self-Blame
Stroke in the Ashanti Region of Ghana:

` 1
Abstract
This dissertation investigates the lived post-stroke experience in Ghanian Akan
society. It shows that Akan matrilineal values of reciprocity, respect and
deservedness influence both the provision of care and the experience of care.
Investigating the lived experience and illness narratives of afflicted persons and
their care providers is of utmost importance when trying to make sense of
people’s health seeking and care provision behaviour. Only by developing an
emic perspective are the hidden inequalities of care provision within families
highlighted. Such inequalities are influenced by wider structural factors (e.g.
poverty or minimal access to health care) which occur in Akan society and in
Ghana at large.

` 2
Table of Contents
Abstract ......................................................................................................... 1
Acknowledgement ......................................................................................... 4
Chapter 1: Introduction and Background ........................................................ 5
1.1. Introduction ........................................................................................................... 5
1.2. General background: Ghana .................................................................................. 7
1.2.1. The Akan and Asante ...................................................................................... 8
1.2.2. Stroke in Ghana .............................................................................................. 9
Chapter 2: Literature Review ........................................................................ 12
2.1. Studies on stroke in sub-Saharan Africa and Ghana ........................................... 12
2.2. Epidemiological approaches in anthropological perspective .............................. 13
2.3. Anthropological approaches ................................................................................ 15
Chapter 3: Fieldwork, Fieldsites and Methodology ........................................ 20
3.1. Fieldwork in Offinso, Ashanti Region, Ghana ...................................................... 20
3.2. Fieldsite I: Hospital .............................................................................................. 21
3.2.1. Physiotherapy Department .......................................................................... 21
3.3. Methodology ....................................................................................................... 23
3.4. Fieldsite II: Community ........................................................................................ 25
Chapter 4: The syncretisation of different health systems in Ghana ............... 27
4.1 The archaic concept of ‘pluralism’ ........................................................................ 27
4.2. Medical systems in historical context.................................................................. 28
4.3. Preference for choosing herbal treatment .......................................................... 29
4.4. Negative perceptions of herbal treatment .......................................................... 32
4.5. Herbal treatments to ‘go modern’ ...................................................................... 33
4.6. Conclusion ........................................................................................................... 35
Chapter 5: The aetiology of stroke and politics of blame and self-blame ........ 36
5.1. Unhealthy Diets ................................................................................................... 36
5.2. Poor lifestyle practices: Alcoholism ..................................................................... 38
5.3. Witchcraft causation............................................................................................ 40

` 3
5.4. Self-Blame ............................................................................................................ 41
5.5. Conclusion ........................................................................................................... 42
Chapter 6: Experiences of Care and Care Provision ........................................ 44
6.1. The role of the family in care giving .................................................................... 44
6.2. Case study I: Camie .............................................................................................. 45
6.3. Case study II: Akosi .............................................................................................. 48
6.4. Conclusion ........................................................................................................... 55
Chapter 7: Conclusion ................................................................................... 57
Bibliography ................................................................................................. 60
Appendices ................................................................................................... 66
Total Word Count: 14,730

` 4
Acknowledgement
This dissertation would not have been possible without the help of Father Joah,
who was responsible of approving my research in the hospital, and whose natal
family welcomed me into their Offinso home.
In Ghana, my grateful thanks are extended to the members of the
physiotherapy department who provided a warm working and research
environment, and to my research assistant Justice, for liaising with stroke
patients in the community.
I am profoundly grateful to my informants, for their co-operation. For the
purpose of confidentiality, all names have been changed.
I would like to thank Melissa Parker for her invaluable support and guidance
throughout the process of writing this dissertation.
Finally, I wish to thank Nicole for her support and encouragement throughout
my study.
` 5
Chapter 1: Introduction and Background
1.1. Introduction
This dissertation investigates how matrilineal values of reciprocity, respect and
deservedness influences the lived post-stroke experience of the Akan in the
Ashanti region in Ghana. These values determine the level of care provided to
the sick individual whilst at the same time influencing the care giving
experience. The dissertation further analyses my informant’s understandings
and explanations of the aetiology of their affliction, as such views are influenced
by wider socio-political and cultural factors. State-led health education
programmes additionally influence such aetiologies, as primary focus is on the
individual’s lifestyle choices, their health seeking behaviour and the
establishment of risk factors and risk behaviours. This, in turn, fosters a politics
of blame and self-blame, whereby informants either blamed themselves for
becoming sick, or they were accused by others of having led an unhealthy and
‘risky’ lifestyle.
Stroke for my informants was a disruptive event, whereby the sudden
malfunctioning of their body interrupted all aspects of their daily life and those
of their families. Stroke survivors were particularly troubled by the loss of their
personal independence and their role as income generator. This, in turn, caused
familial and emotional consequences. To accelerate recovery a syncretic
approach to health care was employed: The use of contemporary medicine for
treating acute and serious symptoms was coupled with the use of local healers
in order to address the spiritual aspect of their affliction.

` 6
My informants’ illness experience was characterised by inequalities
accessing adequate care and health facilities, as well as by structural factors
such poverty and social inequality. This dissertation therefore highlights the
lived post-stroke experience in order to understand health seeking and care
giving behaviour.
Chapter 1 provides basic demographic information about Ghana, Akan
matrilineal values, and stroke. Chapter 2 places this dissertation in the wider
literature of non-communicable diseases and stroke, focusing on
epidemiological and anthropological approaches. Chapter 3 provides an
introduction to the fieldsites and a discussion of the research methods utilised.
Chapter 4 focuses on the pluralistic health care system found throughout
Ghana, and the treatment preferences of patients and their families. Chapter 5
discusses my informants’ understanding of the aetiology of their stroke, with an
explanation of the most frequently attributed factors. Chapter 6 analyses how
in Akan society matrilineal values such as reciprocity and respect play a
fundamental role in the provision or withdrawal of care.

` 7
Figure 1: Ghana and its neighbouring countries2 Figure 2: Ghana and its
districts
Figure 3: Ashanti Region, with Offinso
1.2. General background: Ghana
Ghana is located on the south-central coast of Africa, sharing boarders with
Togo, Burkina Faso and Cote d’Ivoire (Figure 1 & 2). Before Europeans first set
foot on the shores of Ghana in 1470, its history was derived primarily from oral
2All maps accessed on worldatlas.com:
(http://www.worldatlas.com/webimage/countrys/africa/gh.htm [Accessed on 02/02/2013].
` 8
tradition. The Portuguese arrived in the region in 1472, followed by the Dutch,
Danish, French, and British. The British took over the coastal region in 1821,
followed by the appropriation of the Ashanti region in 1902. In 1957, Ghana
became independent3 (Horton 2001).
1.2.1. The Akan and Asante
Ethnically, Ghana is divided into ethnic groups speaking more than 50 languages
and dialects. English is the official language and the main language used in state
education. The largest ethnic group are the Akan, who consist of many sub-
groups including the Asante (which my informants belonged to), Fanti, and the
Bono. Although the groups are classified as Twi- (which the majority of my
informants spoke) or Fanti- speakers, their matrilineal social system is the same.
That is, every individual belongs to the mother’s clan, successions are
matrilineal, and marriage is exogamous. Sociality is an important aspect for this
dissertation, as these values influence the experiences of sick people and care
providers (Stoeltje 1997; Crentsil 2007). The Asante occupy the Ashanti Region
(Figure 3), which, according to the Population and Housing Census (PHC) (2010),
was the most populous region in Ghana in 20104. The basic economic activity in
the Ashanti region is farming, with yams, cocoyam, oil palm, and plantain as the
main crops.
3Ghana was the first African nation to gain independence.
4For statistical data on Ghana please refer to Appendix A.1.
` 9
1.2.2. Stroke in Ghana
In common with other developing nations, Ghana’s health system is under-
funded and under-resourced. The situation is further intensified by the
increasing burden of infectious (so called ‘communicable’), and chronic (‘non-
communicable’) diseases (de-Graft Aikins et al 2012). Stroke is a non-
communicable disease (NCD) and is the second-leading cause of death amongst
adults worldwide; whereby 87 per cent of stroke deaths occur in middle- and
low-income countries (Agyemang 2012). Furthermore, stroke is reported to be a
major contributor to disability and reduced quality of life (ibid). There are two
known forms of stroke: ischemic and the hemorrhagic stroke5, with the former
accounting for 90 per cent of all stroke cases. The location and the extent of
affected brain tissue determines the physical impairment after the stroke.
However, most stroke patients are left with either paralysis or weakness on one
side of the body, speech-impairment and incontinence (NHS n.d.). The in-
hospital, post-acute care and subsequent rehabilitation management of stroke
are crucial for its treatment. This, however, seems to be a difficult task for
developing countries, as the majority of patients do not have access to life-
saving investigations, which, if they exist, are only available in major cities
(Kengne et al 2006). Furthermore, such investigations are often not covered by
national health systems. Despite the Ghanaian National Health Insurance
(NHIS)6, which aims to provide access to basic health services to the whole
population, many Ghanaians’ cannot afford the annual fee, let alone expensive
5 For more information on the medical definitions of stroke refer to Appendix A.2.
6 For more information on the NHIS refer to Appendix B.

` 10
drugs or treatments. Although rehabilitation management, such as
physiotherapy (PT), is covered by the NHIS, most Ghanaians (including health
professionals) are not aware of this service, (especially in rural areas). This was
also confirmed by one of my informants, Bubu7
When I started here at St Patrick’s hospital, it was difficult, as not
many were aware of the discipline [PT], not even the doctors. Only
hospitals in big cities have PT departments. Even now patients are
suspicious – they rather want to have drugs.
This reflects the findings of the 2010 Ghana’s Health Service Report (GHSR): a
mere 68 physiotherapists were employed throughout Ghana in 2008. The
majority of physiotherapists (30) were employed in the Accra region, in
comparison to only eleven in the Ashanti region. The entire northern region
with a total population of 4,227.665 has only 5 physiotherapists (GHSR 2010,
PHC 2010)8. These findings suggest that the majority of Ghanaians have
inadequate access to post-stroke rehabilitation management. However, it is not
only the Ghanaian health care system that is affected by the social and
economic costs of long-term care for stroke survivors - long-term care also
threatens patients’ households’ livelihoods as care providers are required to
spend substantial periods of time away from work. Lemogoum (2005) suggests
improving the provision of home-based rehabilitation, in order to minimise
disabling conditions and to promote the re-establishment of productivity of an
7 For my informants demographic information’s please refer to Appendix C.
8 For more information on the North-South dichotomy and statistics please refer to Appendix
A.1.

` 11
affected individual. However, considering the scarcity of physiotherapists and
the lack of knowledge about stroke rehabilitation, this is a rather unrealistic
proposal.
The following literature overview contextualises my research into the wider
field of related literature.
` 12
Chapter 2: Literature Review
This chapter provides an overview of the epidemiological and anthropological
literature on stroke and non-communicable diseases (NCDs). A brief outline of
such studies in Ghana and SSA is provided and an anthropological discussion of
the epidemiological approach and its shortfalls is presented. Finally,
anthropological studies in sub-Saharan Africa (SSA) with their focus on the
Explanatory Models (EM) approach of stroke are examined. Taking into account
the reviewed literature, I suggest that when studying the lived experience of
stroke sufferers, more attention should be devoted towards anthropological
approaches of illness narratives, interpretive phenomenology, and biographical
disruption. Furthermore, this literature review revealed the non-existent nature
of anthropological research on stroke in Ghana.
2.1. Studies on stroke in sub-Saharan Africa and Ghana
It is reported that NCDs are an emerging problem in developing countries
including countries in SSA. In their extended literature review on the burden of
stroke in SSA, Kengne & Anderson (2006) argue that current epidemiological
studies are mainly hospital based. The data suggests an increased rate of
stroke, affecting people at much younger ages in SSA than in developed
countries. Lemogoum (2005) further argues that in order to tackle the increased
burden of stroke in SSA, the treatment of high blood pressure (hypertension)
has to be optimised. Cappuccio et al (2004) studied the prevalence of
hypertension in the Ashanti region in Ghana, where 1013 men and 628 women

` 13
were interviewed. The results confirmed the urgent need for preventive
strategies on hypertension control in Ghana. Agyemang et al’s (2012) study
stresses that stroke constitutes a significant cause of morbidity and mortality in
Ghana and an implementation of population-based health education
programmes is suggested. The above mentioned studies are focusing on the
improvement of individuals’ risk factors and risk behaviours without taking the
lived experience of stroke sufferers into account. To my knowledge, no
anthropological research on stroke has been conducted in Ghana.
2.2. Epidemiological approaches in anthropological perspective
Epidemiology studies patterns, causes and effects of health and disease
conditions in defined populations. As such, epidemiology identifies risk factors
and risk behaviours in order to establish preventive medicines and public health
campaigns, thus targeting risk behaviour in a given population (Pool & Geissler
2005). The underlying hypothesis is that there is a rational basis for an
individual’s decision making. Indeed, current epidemiological studies on stroke
and NCDs are promoting an ‘aggressive’ risk factor control-strategy. Such risk
factors include limited health care facilities throughout SSA; poor detection,
treatment and control of high blood pressure9; unhealthy diet; alcohol and
tobacco abuse; and physical inactivity (e.g. Cappuccio et al 2004; Lemogoum
2005; Kegne & Anderson 2006; Agyemand et al 2012).
These studies indicate that NCDs are ‘lifestyle diseases’ that can be
tackled by changing people’s behaviour. This implies, however, that “people can 9 High blood pressure is a major predictor of stoke as nearly 70% of all stroke cases in Ghana are
caused by high blood pressure (Agyemang 2012).

` 14
choose how to live and stay healthy through proper self-discipline” (Whyte
2012: 65). For epidemiologists, confronting the context of risk,10 in which stroke
and other NCDs are prevalent, is central to the success of public health
campaigns locally as well as globally. Conversely, anthropological studies
suggest that such risk factors are also an outcome of structural violence and
that ultimately a change of ‘life conditions’ is necessary, as opposed to a change
of ‘lifestyles’ (Pool & Geissler 2005; Whyte 2012). Farmer’s (1992) famous study
on structural violence in Haiti is a good example of how inequalities in Haitian
society are responsible for conditions which foster vulnerability to HIV
infections. Furthermore, such inequalities deprive those infected of necessary
care, appropriate living conditions and drugs that could prevent early death
(ibid)11.
According to my informants, structural violence takes on many forms
in Ghana: e.g. poverty, unequal access to health care and the production of
toxic foods through contemporary agricultural practices. Setel (2003) suggests
that:
A more anthropological or social epidemiological concept of risk, would
encompass structural and social vulnerabilities, as well as biological and
behavioural ones…[A]nthropologists would draw a wide circle around
the notion of ‘risk’ and ‘risk factors.’ In particular, they would explore
10
Lemogoum (2005) summarises risk as follows: “[R]educing the stroke burden will require the increased awareness on the preventable nature of stroke, educate populations and health professionals on the modifiable risk factors, on healthy lifestyles and early warning symptoms… [The implementation of] population-based surveillance [is equally important]” (ibid: 97). 11
The World Health Organisation (WHO) 2010 report has emphasised the importance of such structural factors. However, the same report also stresses the health education on diet and physical activity in order to change people’s life style (WHO 2011).

` 15
how the rise of NCD risk reflects the changing social and economic
position of certain groups and individuals relative to other members of
society. In this model of risk, structural, environmental, and individual
forces would all receive consideration in the design of NCD intervention
and policy (Setel 2003: 151).
In Africa, as elsewhere, confronting the context of risk in which stroke and NCDs
occur, as well as incorporating the emic perspective of the social and cultural
basis of health, healing, and health-seeking behaviour, will be central to the
success of future international public health policies.
2.3. Anthropological approaches
Anthropological research exploring stroke experience in developing countries
has largely focused on Explanatory Model(s) (EM[s]) and health seeking
behaviour (Hundt et al 2004; Mshana et al 2006). The EM of illness was
developed by Arthur Kleinman in order to distinguish between disease and
illness, and to bridge the gap between clinical knowledge and constructions of
clinical reality (Kleinman et al 1978: 251). EMs are used to explain how people
view their illness in terms of causation, personal impact and the effectiveness of
treatment. Such EMs are always embedded within a given culture and social
structure of a particular place and time (Kleinman 1978).
Hundt et al (2004), for example, investigated the lay conceptualisation of
stroke-like symptoms and health-seeking behaviour in South Africa. Individuals
considered stroke-like symptoms as a combination of physical and social
conditions. Mshana et al (2007), furthermore, used EMs to explore the

` 16
causation beliefs of stroke in rural and urban Tanzania, and how Tanzanians
make sense of and respond to their illness. In both studies attention was paid to
treatment decision-making. A recent study (de-Graft Aikins 2012) exploring the
lay representation of chronic diseases in Ghana concluded that individuals draw
on a broad range of sources when forming opinions on the cause of their
illnesses. The most frequently mentioned factors are biomedical and local
medical encounters, mass media, rumours and experiences of people living with
the same condition (de-Graft Aikins 2012).
What these studies have in common is that they focus on the individual
and their understanding of illness. Such studies lose sight of wider social
relations beyond the individual’s perspective. Additionally, the social conditions
of medical knowledge production (e.g. how mass media and health education
programmes influences the individuals EMs) are often perceived as secondary
(Pool & Geissler 2005). Lynch & Medin (2006) further criticise the EM
framework for ignoring the ways social relations shape and distribute illness and
how power relationships between groups (i.e. the family) can shape the
experience of sickness. Indeed, throughout this dissertation it becomes clear
how intra-household relations shaped my informants’ illness experiences, for
instance denying care or access to health care.
Instead of focusing on EMs, I follow Pool & Geissler’s (2005) argument to
focus on Illness Narratives:
Illness narratives are a way of exploring the patients experience of
illness [e.g. how a patient comes to term with disability after stroke;

` 17
the lived experience; blame; self-blame] and the wider cultural
models [e.g. matrilineal decent and cultural understanding of
reciprocity] that underlie or give form to that experience (Pool &
Geissler 62).
Hence, illness narratives are tales of a sick person’s lived experience. In turn, the
lived experience is “influenced by globalisation, urbanisation and local economic
development which alter conditions of day-to-day life of individuals and their
society” (Setel 2003: 151). The ‘lived experience’ or phenomenological approach
is, therefore, of particular interest to this dissertation, as my informants stroke
experience did not end with its onset.
Interpretive phenomenology focuses on human consciousness and on
the sick person’s subjective experience of their surrounding world. Therefore,
through the individuals’ narratives, the meanings behind their experiences can
be uncovered (Desjarlais & Throop 2011). Such narratives, therefore, are always
situated in the social, political and cultural contexts. This phenomenological
framework has subsequently helped anthropologists to better understand
“what it means to be human, to have a body, to suffer and to heal, and to live
amongst others” (Desjarlais & Throop 2011: 87). Thus, the combination of both
ethnography and interpretative phenomenology is an appropriate framework to
understand people’s lived experience. However, two more theoretical
approaches have to be considered when investigating the lived experience of a
sick person: the ‘disruptive life’ and the ‘biographical’ approach.
Stroke as a ‘disruptive’ event is widely discussed in western-based
literature (Becker 1993; Faircloth et al. 2004). That is, an individual’s former

` 18
self-identity is disrupted by the loss of physical and mental ability through
impairment (ibid). Michael Bury’s (1982) concept of biographical disruption is a
useful framework to analyse this loss. According to Bury (1982), stages of
chronic illness are: disruption, a discontinuance of an on-going life, and a critical
situation. The sudden onset of chronic illness throws people’s daily lives into
chaos. Illness begins to dominate their lives, and taken-for-granted assumptions
about the world are thrown into question. Attention is given on bodily states
and how the ill person reconsiders their biography and self-concept, ultimately
resulting in a mobilisation of resources to respond to the disruption (Faircloth et
al 2004).
The disruptive nature of stroke and its subsequent impairments has a
negative impact upon household livelihoods, as income is lost for care providers
staying at home with the afflicted person. This was acknowledged in Crentsil's
(2007) study of HIV-positive individuals and in Van der Geest’s (2002, 2009)
work on care of the elderly Akan in Ghana. In both studies, the focus was on the
lived experience of the carer, the family and the sick person; and how wider
cultural values shape an individual’s illness experience.
All of these studies focus on pluralistic health care systems which are
widely found throughout the developing world. According to Pool & Geissler
(2005), medical pluralism describes “the existence, within one medical system,
or one society, of different medical traditions” (ibid: 39). However, medical
pluralism has been criticised for drawing the line too neatly between different
health systems. In Ghana different medical traditions co-exist next to each
other, and are often intermingled and used together. New modern herbal clinics

` 19
are managed like western hospitals, and herbalists may undergo basic
biomedical training and conversely, scientifically-trained biomedical healers -
called herbatologists - may make use of ‘local’ practices without perceiving it as
a paradox. In such clinics both systems are uniquely combined in what can be
termed a ‘single syncretic health care alternative’ (Tsey 1997). In other words,
medical systems are syncretised, which is “the unifying and merging [of]
different or opposing schools of thought” (Pool & Geissler 2005: 40). It is
therefore important to understand both, the pluralistic health care systems, as
well as the actual (everyday) practice of such systems. Further, it is important to
acknowledge that modernisation, globalisation and other social forces influence
a given health care system.
In summary, the studies on stroke and NCDs have primarily been
informed by either the epidemiological approaches to risk behaviour, or
anthropological investigations of EMs. However, as I have demonstrated, the
focus on illness narratives, the lived experience, interpretive phenomenology,
and biographical disruption of a sick person are of equal importance. The
triangulation of all these theoretical frameworks may contribute to an effective
policy for stroke and NCDs, which constitute an increasing burden both in
Ghana12 and throughout the globe.
12
Stroke is the fourth leading hospital in-patient cause of death in Ghana (Agyemang et al 2012).

` 20
Chapter 3: Fieldwork, Fieldsites and Methodology
3.1. Fieldwork in Offinso, Ashanti Region, Ghana
It was the ‘in-between’ season13 when I arrived in New Offinso14, which is
located 15 miles from Kumasi, the capital of the Ashanti region. Offinso is the
capital of the Offinso South Municipal district15.
During my six-week stay I lived with Father Joah’s natal family. They
were a typical matrilineal family in which the eldest female was the head16.
Twelve family members lived in the house, and during my stay I established
good relationships with each of them, having the closest relationships with the
three granddaughters: Aroha, Abah and Fai. My family and I quickly settled into
a daily routine17, providing me with the stability of a home, in which I could
concentrate on my work (e.g. writing-up of field notes). Staying with a local
family had another key advantage: whilst doing daily chores, such as cooking,
washing clothes, or during and after dinner, I could talk with them in a relaxed
atmosphere. This provided valuable insights into contemporary Ghanaian
affairs, its history, its tradition, together with my host family’s everyday lives. At
dinnertime we often watched TV which displayed many advertisements of new
and modern herbal clinics.
13
For more information on Ghana’s seasons please refer to Appendix A.1. 14
The correct name is New Offinso, but my informants called their city Offinso. I will refer to Offinso throughout this dissertation. 15
For statistical information please refer to Appendix A.1. 16
See Appendix A.3.: lineage of family 17
For more information on the daily routine please refer to Appendix A.4.

` 21
3.2. Fieldsite I: Hospital
The primary fieldsite of this study was St. Patricks Hospital, a Catholic mission
hospital serving a community of approximately 100,000 people in a 60+ km
area. Researchers, especially when not medically trained, often have difficulties
gaining access to hospital settings. They may encounter resistance from
physicians and nurses, who might refuse access to patients’ medical histories
and entrance to operating theatres (Pope 2005). Fortunately, I did not
encounter any of these difficulties, as one of my main gatekeepers in the
hospital was Father Joah - a board member of the hospital. As a key figure in the
hospital he was responsible for approving my research and enabling
unrestricted access to the hospital. Initially I spent three days on the maternity,
outpatient and children’s wards. However these wards did not provide a fruitful
research environment as they were too busy for staff to have sufficient time to
introduce me to patients, translate conversations, or explain patients’ medical
histories.
My restricted time-frame of six weeks, created immense pressure to
collect and produce good and ‘rich’ ethnographic data. Therefore, following
advice from my host family, I decided to observe the Physiotherapy Department
which proved more successful for my research.
3.2.1. Physiotherapy Department (PTD)
The PTD is a small ward at St. Patricks Hospital. It is located along a dark
corridor opposite the men’s ward. The PTD consisted of an exercise room which
was equipped with one therapy bed, one ‘bicycle’, one ‘standing’ machine,

` 22
crutches and other equipment which were stored at the back of the room.
There was also a separate therapy room with one therapy bed, one massage
bed, one infrared machine and a desk and two chairs for patients to be assessed
or treated. Patients needed to register at a desk first, which was located at the
back of the corridor. Two benches were lined along this corridor, where patients
waited for their treatments.
The PTD comprised three permanent members of staff, and one
volunteer18. The department saw patients with a wide range of symptoms: most
commonly people with fractures, lumbago, osteo-arthritis, cervical palsy and
stroke patients. The PTD was generally busy, but this increased during so-called
‘stroke-days’. As discussed in the previous section, stroke is common in Ghana
and due to this demand, the PTD held these ‘stroke-days’ every Tuesday and
Thursday, from 8am until noon. However, patients were not always able to
attend due to a shortage of money. Nevertheless these stroke-days were still
busy, sometimes with more than twenty patients.
Patients were first required to report to Manu at the registration desk.
They then waited until some were called into the therapy room, where hot-
packs and massages were administered. Other patients were taken into the
exercise room where active or passive exercises were performed. In the
exercise room patients could exchange their experiences and thus establish
some sort of support group. It was here where the PTs were most engaged with
the patients, spending time listening to the patients’ worries and providing
personal advice and support. This was unusual in a hospital-setting, in which
18
For further information on the PTD and for pictures please refer to Appendix A.5.

` 23
power-relations and inequalities between doctors/nurses and patients were
regularly played out within the different wards. Bubu explained:
I know about the way nurses and doctors treat patients on the
ward, this is partly due to the unwillingness to become too
emotionally attached to the patient. Here [PTD] we think that we
need to treat the patient as equal. Only then they will cooperate
with us, which is very important for a successful therapy.
All PTs were very engaged, encouraging and, most importantly, they gave the
patient a positive environment. Bubu and Manu, especially, joked with patients;
hence there was constant laughter and a light-hearted mood.
3.3. Methodology
I travelled to Ghana with the aim of recording every interview on my voice
recorder, but I discovered that this interrupted the interactions with my
informants. Therefore, I collected most data by taking fieldnotes with pen and
paper.
After two weeks of observing the daily routines in the PTD and talking to
PTs and patients I decided to focus on stroke patients. I observed treatments,
and at the same time interviewed patients and their accompanying
family/friends. My colleagues functioned as both a valuable source of
information and as interpreters. The PTD seemed to be a somewhat ‘natural’
setting for my informants, due to the longevity of their rehabilitation. Such
long-term treatment allowed my informants to get to know other patients and
` 24
their PTs, as they met and talked during the stroke-days. This also contributed
to the establishment of a natural setting, which in turn was favourable for me
as a researcher: individual patients did not feel exposed by my presence, which
created a sense of ease for the informants under observation (O’Reilly 2009).
Interviews with PTs and patients were informal and unstructured at
first; whilst I used semi-structured interviews at a later stage, to build upon the
previous ones. According to Fetterman (2009), informal interviews are casual
conversations with specific but implicit research agendas. They provide an
opportunity to discover what people think and how one person’s perceptions
differ from others. Such comparisons help to identify shared values in the
community - that is, values that inform behaviour.
The above mentioned establishment of a natural setting was further
fostered by the participatory aspect of my research. Van der Geest et al (2004)
have suggested three possibilities for the researcher to become a ‘native’
within a hospital environment: joining the staff, being a patient, or a visitor. As
a former professional massage therapist, I actively participated in the day to
day running of the PTD (e.g. administering massage to patients). This helped to
establish a good rapport with my informants, and also to define my role within
the team.
Despite the above mentioned positive aspects of my research, I also
encountered problems and limitations. The language barrier was the most
difficult one to overcome. My inability to communicate in Twi (the local
language in Offinso) meant that I was dependent on translators, such as my

` 25
colleagues and English-speaking relatives of the patients. However, given the
fact that English is the official language of Ghana, many of my informants were
sufficiently fluent. Nevertheless, as the PT was a busy department, it was
sometimes not possible to rely upon my colleagues for translating. At such
times I was restricted to the role of an observer, which according to Lawson
(2001) can also be an advantage. Non-verbal communication - e.g. how people
move through space and how they occupy it; facial expressions; body language
- can give the observer vital information of patients physical and mental states
(Lawson 2001).
After three weeks of working in the PTD, a pattern of pro-biomedical
and anti-herbal healers came to the fore: my colleagues were in favour of the
former, whereas many of my informants reported to make use of herbal
treatments. Therefore, the urge to acquire an understanding of how stroke is
affecting people and their social environment in the neighbouring community
emerged.
3.4. Fieldsite II: Community
One day when I was observing the treatment of PT-patients, Justice - who later
became my research assistant - came in with two young children and their
parents. Whilst the children were assessed and treated by Fedu and Bubu, I
talked with Justice. He runs a charity in the neighbouring community, serving
mentally and physically impaired children. As he lived in the community his
entire life, he knew stroke patients and agreed to help me gain access to them.
From that day onwards Justice and I met up regularly in order to interview

` 26
‘community’ informants. As time passed, we expanded our terrain by visiting
my ‘hospital’ informants in their villages, and thus in the natural settings of
their family homes19.
In the community, I made use of informal and unstructured interviews,
followed by semi-structured interviews, with handwritten fieldnotes as the
primary mode of note-taking. In this setting the language barrier was an even
greater limitation, as I solely relied on Justice as an interpreter. Although Justice
had previous research assistant experience20 and good knowledge of English,
during the first interviews he tended to summarise informants’ answers rather
than translating word-by-word. According to O’Reilly (2009), even the best
translation runs the risk of losing subtle nuances and context. After addressing
my concerns, Justice’s interpretation style improved, yet I started to re-read my
notes to him in order to verify, and if necessary, to amend the information.
Using an interpreter might have contributed to loss of data, but at the same
time it opened unique opportunities for me, e.g. the access to sick people in
their family homes.
Conducting ethnographic research in the PTD and in the community has given
me valuable insights in the post-stroke lived experience of my informants.
These lived-experiences are the focus in the chapters to come. The next chapter
deals with the diverse health systems which were available to my informants.
19
For these visits Justice’s uncle lend his car to us. I paid for the petrol and our food. In turn, Justice invested his time, and also showed me the surrounding area. It was not long before Justice and I became good friends, and I partly owe my research-success to him and his support. 20
Physiotherapy students from Europe were studying disability in Offinso.

` 27
Chapter 4: The syncretisation of different health systems in Ghana
This chapter discusses the different treatment options available to the Akan and
to Ghanaians in general. It begins by discussing concepts of medical pluralism,
and by situating Ghana’s medical systems in historical context. Next, attention is
drawn towards the co-existence of the diverse medical systems present in
contemporary Ghana. Consideration is given to herbal treatment options and its
syncretisation with biomedicine and how some of my informants prefer herbal
treatment whilst others have a negative perception of it. Attention is paid
towards the modernisation of the herbal sector, how modern herbal clinics
operate and how stroke patients are excluded or discriminated against in the
health care system.
4.1. The archaic concept of ‘pluralism’
Medical systems are described by anthropologists as cultural entities, in which a
community’s ideas and practices related to illness and health come to the fore
(Pool & Geissler 2005). In Ghana different medical systems co-exist and
anthropologists use the concept of ‘pluralism’ to analyse such sectors (Tsey
1997). Pluralism however, has been criticised for being too static, and ignoring
the fact that such medical systems - including the biomedical one - are
constantly shaped, reconstructed and renewed by socio-political, economic and
historical forces (Pool & Geissler 2005). For instance, biomedicine in non-
Western societies undergoes an indigenisation process, whereby biomedical
` 28
knowledge and practices are adapted to local environments and influenced by
local culture21. Furthermore, medical traditions are often intermingled and used
together. In other words, medical systems are syncretised, which is “the
unifying and merging [of] different or opposing schools of thought” (ibid: 40).
Therefore, I use the concept of syncretisation to explain the health seeking
behaviour of my informants. Furthermore, instead of using the term
‘traditional’ (which is often used to refer to static, closed systems) I employ the
term ‘local’ in order to describe non-biomedical health systems.
4.2. Medical systems in historical context
In the past, the Akan and Ghanaians in general have sought health advice from,
amongst others, herbalists, cult healers, fetish priests and church leaders. It has
been reported that the use of herbalists was the most sought after treatment
option until colonial rule (Tsey 1997; Darko 2009). Herbalists were understood
to have contact with the spiritual world, where the ancestors of the ill were
contacted and if necessary calmed. Illness was therefore regarded to be both
physical and spiritual, and could only be cured by being treated holistically
(Darko 2009). Throughout colonial rule in Ghana western-led medical services
were established, equipped with the newest technologies and medicines of the
time. In order to promote colonial ‘modernity’ local health systems were often
suppressed, local healers accused of being ‘witchdoctors’, depicted as
‘backward’ and portrayed to be the ‘enemy of colonial modernity’ (Pool &
Geissler 2005: 103). After Ghanaian independence importance was given to the
21
The case study of Edjala, an herbalist, illustrates this point further (Appendix D).
` 29
rediscovery of ‘heritage’, including the revival of local medicine. This revival,
however, was greatly influenced by the biomedical model, and professional
bodies of local healers and western-style herbal clinics were established (ibid).
In 1975 the government established the Scientific Research into Plant
Medicine (CSRPM), in order to “regulate, investigate, and coordinate the
activities of herbal practitioners so as to avoid the dangerous and wasteful use
of plants” (Darko 2009: 42). Only in 2003, however, did the Ghanaian
government legally recognise herbal practitioners as a body that offered
healthcare to its population (ibid). The Ghanaian administration, like many
other African and Asian governments, aims to incorporate local herbal medicine
into the formal healthcare sector. Another consequence of modernisation is the
rise of the so-called herbatologists who are scientifically trained medical
practitioners, who work in ‘hygienic’ and ‘sterile’ western-style clinics, and who
use herbal medicine to treat illnesses.
4.3. Preference for choosing herbal treatment
Most of my informants exhibited a distrust of being treated in hospital.
Nevertheless, the hospital was often the first starting point for treatment of
serious and life-threatening conditions. Because of my informants wariness of
hospitals and biomedicine at large, herbal treatment options were a recurring
theme. Thus, herbal healers22 are an important alternative to biomedicine and
may possibly be the preferred method of treatment for many Ghanaians today.
In addition to general distrust, other factors determining whether my 22
For more information on spiritual and non-spiritual herbal healers please refer to Appendix D.1.
` 30
informants chose the biomedical route were accessibility to a hospital, the
seriousness of the symptoms and financial matters.
This preference for herbal treatment is partly due to the local understanding
of illness, which is based on spirituality (i.e. the relationship between a supreme
being, ancestors, lesser gods, deities and man) (Speck, cited in Darko 2009).
Whilst contemporary medicine denies spiritual causes of illness, most local
healers employ spiritual treatment. Many of my informants combined both
systems: the former to treat serious symptoms, and the latter to employ
spiritual healing in order to accelerate recovery. They frequently reported that
friends, family members, neighbours and church members advised them to go
to the herbalist. Alibama, for instance, was considering going to the herbalist
following his release from the hospital based on such advice.
Some herbalists, especially older ones, are inexpensive or may just ask for
appreciation if the patient gets better. Bubu and Manu agreed:
In the past the herbalist had only one herbal medicine for a specific
illness and they did not charge much, if anything. There are new
herbalists who produce one medicine very cheaply which they then sell
very expensive for all illnesses. This also happens in those modern
herbal clinics. People normally do not go back to those healers and
clinics.
Financial concerns were an additional factor for the preference of herbal
medicine. Despite the NHIS, many of my informants were so poor that they

` 31
could not afford the annual fee23 and therefore could not pay for expensive
drugs or treatments. When people are faced with expensive healthcare they
have to be resourceful. Alfred, for instance, took advice from relatives who
argued: “if you have that [herbal] medicine, why do you need to go to the
hospital?” Margaret confirmed that patients improvise to gain access to
expensive biomedical drugs:
People who work or are very poor do not have time to go to the
hospital as that would mean loss of income for them. People with
‘same symptoms’ give them their drugs.
Faith and confidence in the abilities, methods and tools of local herbal healers
were for many of my informant’s reason enough to choose this treatment.
Herbalists are “accepted without question and his or her success [is] greatly
appreciated and applauded and his and her failures [is] understood and
condoned as acts of God” (Anfom, 1986, cited in Darko 2009: 23).
Comfort’s brother had unlimited faith in the herbalist and took her to one
after she was discharged from hospital. At that time she could not talk and
could not raise her concerns about the herbalist. The herbalist treated her with
herbal ointments and knife-cuts into the skin, in which he rubbed the herbs.
Fedu once told me that knife-cuts cause the muscles to contract and blood
circulation to slow down, which may worsen the condition. However, the
herbalist, and consequently Comfort’s brother, interpreted the contraction to
23
The annual insurance fee starts from four cedis (GBP 1,37) for the very poor and young children, whereas the highest fee accumulates at seventy cedis (GBP 24,00) for the very rich. For more information on the NHIS please refer to Appendix B.

` 32
be a ‘good’ reaction to the therapy. Yet, once Comfort regained speech she
stated her preference for physiotherapy.
Those informants who employed a syncretised approach sought out
herbal treatment in order to treat ‘small’ or ‘normal’ symptoms and sicknesses,
e.g. fever, stomach pain and headache. Manu confirmed this:
I am not against herbal treatment per se. ‘Small’ symptoms are
successfully treated with herbs. When a sickness goes ‘deeper into the
body’ one needs to go to the hospital.
Both health systems - herbal and biomedical - are used successively, as most of
my informants employed a syncretised form of treatment following hospital
discharge in hope of a quick recovery. This hope was fuelled by the belief that
western medicine may be effective in dealing with naturally caused illnesses,
but only local herbal healers can treat illnesses involving spiritual agents.
4.4. Negative perceptions of herbal treatment
Not all of my informants had a positive attitude towards local herbalists. Some
had seen their relatives die or had never seen someone recover when being
treated solely by an herbalist. The most common argument, however, was that
only ‘uneducated’, rural people go to the herbalist. Bubu explained:
This is due to the influence of [our] old traditions: the herbalists were
there before doctors came, hence rural and uneducated people believe
more in it. Educated as well as illiterate prefer herbal treatment, but when

` 33
an educated person chose herbal treatment he/she is looked down by
his/her peers, as one should only make use of biomedical treatment and
not being backward and go to the herbalist.
This illustrates the way in which the state was successful in producing
‘biomedical citizens’, but does not explain why herbal treatment is still popular
amongst the educated middle class. The analysis of the ‘go modern’ approach
from herbalists, especially the large herbal clinics, might offer an explanation.
4.5. Herbal treatments to ‘go modern’
In contemporary Ghana large, modern herbal clinics are built nationwide and
promoted through aggressive advertisement via mass media. TV adverts depict
such clinics as mirror-images of biomedical ones. These herbal clinics have the
same advanced laboratory equipment, the newest tools for analysing and taking
blood, x-ray machines, computed tomography equipment, and fully equipped
physiotherapy units. The Centre of Scientific Research into Herbal Medicine is
one such clinic, where patients can choose between herbal and biomedical
treatment. The centre is located next door to the Tetteh Quarshie Memorial
Hospital24 and patients are referred back and forth, depending on their financial
capabilities (Tsey 1998).
Some of my informants had similar experiences of syncretised
treatment. For example, Rose went to an herbalist clinic where on arrival she
was given an attendance card. After waiting for some time she was called into
the consulting room where the doctor examined Rose by touching her hand. He
24
Both institutions are located less than an hour’s drive east of Accra, the capital of Ghana.

` 34
then wrote out a prescription and Rose collected the pre-packed medication
from the clinic’s pharmacy. In Rose’s case, there was no consultation fee as the
charge is included in the medicine, for which she paid an inexpensive six25 cedis.
She explained the cheap price as follows:
I think they do not charge a consultation fee as the clinic needs to
advertise their business. This clinic is fairly new. They earn money
when a patient needs more medicine. This will then pay for the
herbalist and the clinic.
What becomes apparent from Rose’s statement is that the structure of the
clinic was much like a western hospital. According to Stoner (1986), herbalists
might have had a basic biomedical training and conversely, scientifically-trained
biomedical healers may make use of local practices without experiencing a
paradox. In such clinics both systems are uniquely combined in what can be
termed a ‘single syncretic health care alternative’ (ibid).
Much of the symbolic content of the biomedical treatment system, i.e.
attendance card or pre-packed medicines, has been exported directly to the
herbal clinic. These herbal clinics are thus a ‘modern’ health-care resource,
exhibiting elements of both local and biomedical systems of illness diagnosis
and treatment (Tsey 1997). Plants are tested in laboratories and later
industrially produced and exchanged within capitalist markets. Hence modern
herbal medicines become commodities, detached from the producers of the
medicines and lose what was once so important for herbal treatment - the
25
Six cedis are GBP 1,95; conversion rate of 13/01/2013.
` 35
interpersonal, social relationship between the healer and the patient. As with all
commodities, mass produced herbal remedies are becoming increasingly more
expensive (due to the high cost of testing). This, in turn, will undermine the ease
of access which is often associated with local medicine (ibid). Consequently, this
could reinforce a two-tier society with problems of access to herbal health
systems similar to those experienced with Western-style treatments (Pool &
Geissler 2005; Tsey 1998).
4.6. Conclusion
There is a pluralistic health care system in Ghana, and fieldwork among the
Akan revealed that it is used in a syncretised way. For my informants, the
interpersonal relationship between healer and patient was regarded as playing
a part in the healing process, as only through the healer can the ‘spirits’ heal.
Yet, with new forms of herbal clinics - which are on the increase especially in
urban areas in Ghana - the interpersonal relationship between healer and
patient is lost. Such clinics resemble their western counterpart in
administration, mass-treatment and mass-production of herbal medicines. The
cost of herbal products rises, due to investment in modern laboratories and
equipment for mass production. This may undermine access to local medicine,
and reinforce a two-tier society and access to health systems. Moreover, the
spiritual aspect of local healing is lost in such clinics, as herbatologists are
scientifically-trained, medical practitioners. In the following chapter, another
element of my informants’ lived experience of stroke is discussed: questions of
blame and deservedness, which plays an important role in the provision of care.

` 36
Chapter 5: The aetiology of stroke and politics of blame and self-blame
This chapter analysis my informants understanding of the aetiology of their
illness, whereby unhealthy diet, poor lifestyle practices (e.g. alcoholism), and
witchcraft were the factors frequently cited to have caused their affliction. This
understanding was fostered by Ghana’s health education programme. As a
result, some informants either blamed themselves for becoming sick, or were
accused by others to have led an unhealthy or ‘risky’ lifestyle, and thus
‘deserved’ to be ill. Others made sense of their illness by attributing their
‘undeserved’ illness to the malice of another person. In all cases, however,
stroke and its disabling symptoms invoked self-blame, as none of my informants
were able to contribute to the household livelihood.
5.1. Unhealthy Diets
My informants reported that there were two aspects to their diet and food
practices which impacted on their stroke. The first aspect related to self-
practice: e.g. what my informants ate in their everyday life, in particular the
consumption of high fat and starchy foods. The second aspect related to
practises by others, for instance the production of toxic foods through
contemporary agricultural practices. Rose’s husband illustrates this point26:
26
All interviews were conducted in Twi. Justice translated what was said into English.

` 37
[Rose] got it [the stroke] from the food (aduane). The food we eat
now is no good because of the chemicals. We are using the
chemical to make tomatoes grow better.
In Ghana health education is publicised via TV and radio, and such programmes
are focused on promoting a healthy lifestyle through healthy food intake (Tsey
1997). This was also confirmed by Mr Opoua:
I once listened to a programme on the radio, where they talked
about veins and blood flow and that the body is not used to fat and
fatty food. The fat can cause blockage of blood and this is the reason
why stroke (ndwodwoe3)27 occurs. At another time there was a
programme on blood groups. For blood group ‘A’ yam is supposed to
be not good. Also we should use palm oil, as it is good oil. No fatty
meat should one eat, and the chicken should be left on the fire to
reduce the fat. Okra28 is also not good for stroke patients; I am not
eating Okra anymore.
Radio programmes in Ghana argue that fatty and oily foods are the cause of all
sorts of problems, from stomach pain to cardiovascular diseases, and a low-fat,
more nutritious and varied diet is promoted. However, the reality is that the
local food in Ghana, called Fufu29, is still widely eaten by the poor, elderly and
rural population. Fufu is considered unhealthy by health officials, as it is rich in
carbohydrates, and therefore ‘too fat’ and ‘heavy’. The older generation, as
well as the poor and rural population, are reluctant to change their diet, partly
27
According to Justice the Twi word for stroke, ndwodwoe3, can be translated as paralysis. For more information on the local aetiology please refer to Appendix E. 28
For an explanation of Twi terms please refer to the Glossary in Appendix C.2. 29
(ibid).

` 38
because they are not used to anything but Fufu. This was affirmed by my host
family’s father: “I would miss it, even when I just have one other meal, it would
not feel right. Fufu is the food we [elderly] are used to, and we love our Fufu”.
Poverty is another factor why Ghanaians are holding on to this local meal as
they cannot afford a more nutritious, more varied or healthier diet.
Through the media, therefore, the sick person is made responsible for
their condition due to failure to adhere to a healthy diet. Moreover, Mr Opua’s
statement indicates that he is now actively attempting to improve or rectify his
situation by adhering to a healthier diet, thus becoming a ‘biological citizen’
(Rose and Novas 2005). However, such a model fails to address the fact that
there are much broader socio-political (e.g. the production of toxic foods
through contemporary agricultural practices) and structural factors (e.g.
poverty) involved in an individual’s health behaviour. These practices may play
a central role in influencing and constraining health behaviour and creating
vulnerability (Pool & Geissler 2005).
5.2. Poor lifestyle practices: Alcoholism
My informants attributed unhealthy lifestyle practices, such as unhealthy diet,
drinking and smoking, to be the cause of their affliction30. Two of my
informants31 were decade-long alcohol abusers and through their and others’
accounts, I could experience how Akosi and Oseja Yaw not only blamed
themselves, but were stigmatised and disadvantaged within the intra-
30
In Ghana there is a general culture of social drinking which is promoted by a powerful alcohol production industry with aggressive advertising campaigns (Luginaah 2008). 31
Akosi and Oseja Yaw.
` 39
household care provision. Furthermore, the access to essential medical
treatment was often denied to them (see next chapter).
Akpeteshie is the cheap, preferred alcoholic drink of poor Ghanaians.
Akpeteshie is distilled from fermented palm wine or sugar cane juice and the
alcohol strength is estimated between 40% and 50% volume. Drinks are called
‘kill me quick’, ‘take me and fly’ and ‘let me kill the bastard’ (Luginaah 2008).
Those names are an indication of a wider societal problem: it takes the drinker
away from the problems of their daily lives, but may also lead to violent
behaviour.
In Akosi’s case, alcoholism forced him to be separated from his wife and
children. Their former landlord evicted him and his family from their compound
due to the ongoing violence which occurred between Akosi and his wife. Since
then they were living separately: Akosi with his family, while his wife Roberta
and their children live in a small compound in another part of Offinso. Justice
knows the family well:
In the past Akosi hit and abused his wife and he didn’t treat his
family well either. Now that Akosi is sick, the family does not treat
him well too. Same, same…. If stroke patient has a good relationship
with family, this pays back as they will be good caretakers. Stroke is
a punishment for drinking.
It becomes apparent that Akosi’s stroke was perceived to be a consequence of
his excessive drinking, interpreted by his family to be risky and unsafe health
behaviour and as an intentional ‘wrong-doing’ (Finerman & Bennett 1995).

` 40
Furthermore, this accountability for his abusive drinking behaviour limited his
deservedness for appropriate care, since his “sickness and sick role status serve
as indices that patients [were] irresponsible [in the past]” (Finerman & Bennett
1995: 2). I discuss care, respect, reciprocity and deservedness in more depth in
the next chapter.
5.3. Witchcraft causation
Many of my informants made sense of their illness with reference to witchcraft.
As Evans-Pritchard (1937) points out in his famous monograph on collapsing
granaries in Zandeland, witchcraft can provide explanations of seemingly
random coincidences which afflict people at different times and places.
Additionally, witchcraft can provide a framework for moral agency (ibid). For
my informants, witchcraft was a synonym for their undeserved misfortune
(stroke), where the malice of another person was deemed to be the source of
their suffering. My informant, Owowusu, articulated this in the following way:
I think that my village people believed that I am suffering from a
‘different disease’. I also think that my extended family members
tried to kill me by using Muju [witchcraft]. They wanted to gain
access to my land. Everyone could do it when ‘bad motives’ are
there.
Through Owowusu’s statement it becomes apparent that the origin of his
misfortune is social: another person is blamed to have caused the stroke. This
was confirmed in a recent study on lay causation of chronic diseases in Ghana.

` 41
It is argued that witchcraft and sorcery can occur in four ways: due to
unprovoked envy or jealousy; as a result of past and on-going family conflicts;
as form of disciplinary action and as revenge for moral misbehaviour (de-Graft
Aikins et al 2012; see also Tsey 1997). The sick person can therefore be seen as
victim (Owowusu), or as culprit (i.e. through alcohol abuse in Akosi’s case), and
thus, to be deserving or undeserving of care and affection.
5.4. Self-Blame
My informants reacted to their diagnosis with feelings of shock, self-blame,
anger or depression. The feeling of becoming emotionally, economically and
socially dependent on relatives put pressure upon my informants, and often
contributed to intra-household tensions. This situation was aggravated if the
sick person had been a contributor or the sole income provider for the family
(Dilger 2008). Individuals in Akan society are expected to contribute to the
families’ household in various ways: financially, with their labour, and by
looking after one another in times of hardship (Crentsil 2007). Due to the
disabling symptoms of stroke most of my informants perceived themselves to
be a burden for the family. Owowusu, for instance, was proud of his past
achievements in launching a large and successful cocoa, palm tree and orange
plantation, and was especially troubled by the fact that he needed to “beg for
money” from his sons after his stroke.
A growing body of literature suggests that people who suffer from a
disabling or chronic illness have experienced loss of income with its
accompanied hardship through poverty. This literature implies that under such

` 42
constrained circumstances self-blame becomes most prevalent as it is often not
possible to maintain the living standards of the family (Crentsil 2007; Dilger
2008). Rose’s case study demonstrates this in a dramatic way.
Rose was thirty-five when she suffered a stroke. Before the onset of her
affliction she was tilling her family’s field and was the main care provider for her
eight children. Her husband was away for long periods of time as he worked as a
seasonal carpenter. The family lived fairly well on the husband’s income and the
harvests from their farm. However, since Rose suffered the stroke she was not
able to work on the fields, and her husband was unable to pursue his
profession. He obtained local work only occasionally, which put the family
under immense financial and emotional pressure. Due to the loss of income,
their elder children had to drop out of school and work on the fields in order to
meet their basic food requirements. Rose and her husband were hoping for a
quick recovery, so that they were able to take out a micro-loan to establish a
small business for Rose (a small market store to sell clothes and sandals). This
would then enable her husband to take up his seasonal work again, which in
turn would enable the children to continue with their education. This example
demonstrates how loss of income, poverty, and the accompanied dependency
on others, are all contributors to invoke self-blame in a sick person.
5.5. Conclusion
This chapter has drawn upon my informants’ understandings of the aetiology of
their affliction. Many attributed unhealthy diet (e.g. fatty food) to their illness

` 43
and blamed themselves for being responsible for their affliction. Conversely, my
informants also employed ‘the politics of blame’ where they either blamed
someone (i.e. a jealous family member), or something (i.e. witchcraft) to have
caused their affliction. Peoples’ explanations of the cause of their illness form
an important aspect of their illness narratives and such narratives have to be
analysed within the context of a whole set of socio-cultural and individual
idiosyncrasies.
My informants understanding of their affliction was further fostered by
Ghana’s health education programmes. Such programmes often rely on
assumptions similar to those employed in the Health Belief Model (HBM) of risk
behaviour, which according to Pool & Geissler (2005) focuses on the individual.
The underlying hypothesis is that there is a rational basis for an individual’s
decision making, thus health is “knowable, mutable, improvable, eminently
manipulable” (Rose and Novas 2005: 442), by, for instance, leading a healthy
lifestyle.
Lastly, I introduced the reader to the fact that if a sick person displayed
abusive behaviour towards his family before the onset of his/her stroke, this
behaviour was reciprocated in times of their sickness by limiting ones
deservedness for appropriate care. This will be discussed in more detail in the
following chapter.

` 44
Chapter 6: The Experience of Care and Care Provision
Due to the lack of a comprehensive social security system, the family continues
to be the dominant source of care for the elderly and chronically sick in Ghana.
This chapter draws upon two case studies: Camie, a fifty-eight year old female
whose husband and female relatives were amongst the most engaged in caring,
and Akosi, a sixty-six year old male whose family provided the minimum of care.
These two case studies illustrate the way in which reciprocity and respect
influence both, the provision and withdrawal of care for the sick in Akan society.
The level of care delivered by the family is often a consequence of the patient’s
behaviour towards the family and children before the onset of the affliction. If
the sick did not respect the family it will be evident in phases of illness and
dependence. To quote a Ghanaian proverb: Panyin fεre ne mma a, na ne mma
suro no, it means: If the elder respects his children, the children will fear
(respect) the elder (van der Geest 2002: 26).
6.1. The role of the family in care giving
Akan families are traditionally organised in extended family clans of three or
four generations, descended in a direct line of female members. This includes
parents, grandparents, brothers, sisters, children, cousins, and in-laws (Apt
1993). The extended family also functions as a social security system, as
members are required to assist each other in times of crisis. During periods of
sickness, the all-encompassing nature of Akan matrilineage becomes most
visible, as caring for the sick means trying to ‘restore’ them to health (Crentsil

` 45
2007). Furthermore, providing care contributes to the way people make sense
of health and illness in general. The role of relatives as carers extends to the
hospital setting, where they provide informal care for the sick on the ward
(Crentsil 2007). I have often seen patients being accompanied by their relatives
when attending the ‘stroke-days’ on the physiotherapy ward. Relatives either
waited patiently on a bench in the hospital corridor, or they actively
participated in the therapy process. Conversely, van der Geest (2002) argues
that the social and cultural bases of care are undergoing profound changes32 in
Ghana and through these changes, care providers are under immense pressure
to provide for the sick and the family. Through the care process, care providers
are required to spend time away from work and this may lead to intra-
household tensions, often resulting in the denial of the patients’ illness (Crentsil
2007).
During my fieldwork I encountered both sides of care: the positive,
where family members were eager to care for the sick and took pride in it; and
the negative, where the sick family member was neglected and left to their own
devices.
6.2. Case study I: Camie
Camie, aged fifty-eight and obese, was brought into the PTD in a wheelchair by
her brother and several female members of her family. Her brother, an
orthopaedic surgeon, came from Germany in order to assist his sister during the
32
For more information please refer to Appendix F.

` 46
first weeks after her acute stroke33. He managed to organise the best possible
treatment, including CT scans34 of the brain, which was provided in Komfo
Anokye Teaching Hospital35, located in Kumasi. Furthermore he organised post-
rehabilitation, where it was agreed that Bubu would attend her at home for the
first two weeks. Camie did not show any improvement during this time, hence
Fedu, the head of department, decided to pay her a visit in order to get an idea
of the situation.
I accompanied Fedu and noticed six female family members in the room
with Camie. One of her sisters (68) was sleeping in the same room, and was the
primary carer. Camie was lying on a mattress on the floor and appeared
withdrawn. During the day most of the family members were at work or on the
fields, and in the evening the family was busy feeding and bathing her. There
was no time to perform exercises with the patient. This, however, was a vicious
circle: due to the lack of mobilisation, Camie was in constant pain which
prevented her from having restful sleep during the night. It was thus agreed
that the family should bring Camie to at least one stroke-day per week. In
addition to the lack of exercises, the family also made use of herbal treatments
in the hope of a faster recovery. This might also be the reason why the family
was initially reluctant to perform exercises with Camie.
The next day, which was a stroke-day in the PTD, Camie arrived in a
wheelchair pushed by her husband, accompanied by three female family
33
The first weeks after a stroke are the most important (because most effective) ones in terms of providing rehabilitation. 34
For explanation of medical diagnostic tools please refer to Appendix G. 35
Komfo Anokye Teaching Hospital is the main referral hospital in the Ashanti, Brong Ahafo, Northern, Upper East and Upper West Regions.

` 47
members. This was remarkable, as other patients were normally escorted by
only one or two family members, if any. Bubu and Fedu actively including
Camie’s family members in the therapy process and all of them were
participating enthusiastically.
In the following two weeks Camie’s family regularly brought her to the
stroke-days, resulting in Camie going from being depressed and withdrawn to
being an alert, happy, responsive and actively participating patient. This was
partly due to regular attendance at the stroke-days in the PTD, but mainly made
possible through the excellent care the family provided. After three weeks, the
physiotherapists decided that Camie was well enough to start with active
exercise, i.e. standing and walking with the walker.
This case study demonstrates the all-encompassing nature of Camie’s
matrilineage, as caring became an indirect self-fulfilment for the family members
(van der Geest 2002). Care for Camie had an emotional meaning, as it expressed
concern, dedication and attachment, and brought the family closer together
(ibid). This dedication and concern was displayed in the appearance of Camie.
Cleanliness is an important value in Akan culture and to be dressed in clean and
neat clothes is a sign of respect towards the sick (ibid). Furthermore, good care
can impact positively upon the well-being of the sick person, as it provides them
with a sense of self-worth, dignity and belonging (Crentsil 2007). By following
the instructions and explanations of the physiotherapists, resulting in small but
visible improvements, Camie’s family was able to make sense of her illness
(Darko 2009). Moreover, the caring nature of the family members and Camie’s
husband indicates that her family considered her as a valuable family member

` 48
and wife before the stroke occurred, and therefore was deserving the good care
provided.
6.3. Case study II: Akosi
My research included stroke patients from the community. The first stroke
sufferer we visited was Akosi, a 66 year-old former revenue collector. It was
widely acknowledged amongst his community that Akosi suffered from alcohol
addiction, resulting in abusive behaviour towards his wife and children and
refusal to support his extended family.
Akosi’s family lived in an impoverished neighbourhood, with no running
water and only one public toilet facility for hundreds of families. The compound
was small and Akosi’s room was separated on the outer part of the main house.
This was the first sign of neglect: traditionally the architecture of the houses
(i.e. a compound surrounded by rooms) allows communal living which takes
place outside the rooms of the compound (van der Geest 2002). When we
stood outside Akosi’s room, Justice pointed to the door bolted with a lock: “this
is what I meant that such [chronically ill/disabled] people are locked away”.
When we entered the room the first I noticed was the smell. One of the
accompanying symptoms of stroke is incontinence of faeces and urine, and
patients are required to wear diapers (Lemogoum et al. 2005). The smelly, dark
and stuffy room indicated that Akosi’s diapers had not been changed since the
previous evening, and that the room was not aired often. The interior consisted
of Akosi’s decrepit bed; a rug opposite the bed, which belonged to James (the
older brother), and a wheelchair, folded neatly on the other wall. Additionally

` 49
there were several household items and suitcases stored in the room, making it
more akin to a storage room rather than a bedroom.
On our first visit, Akosi was lying on one side and turned away from the
door. It was obvious that he was stationary in the same position throughout the
night. Due to this immobility, it seemed as if Akosi was in constant agony. He
looked malnourished and much older for his sixty-six years. When I first saw
Akosi, my first impression was that the family provided only minimal care.
However, with every visit36 it became apparent that this case was far more
complicated than I had first anticipated. In order to make sense of and analyse
Akosi’s suffering and neglect, it is important to acknowledge the different views
of the people involved in this case: the patient himself, his estranged wife and
the different family members. In doing so, I employ the explanatory model37
approach, which reveals how people make sense of illness, as well as their
experiences of living with it and caring for a sick person. Rather than using this
model to understand different explanations of Akosi’s illness, I aim to
demonstrate how intra-household power relationships were played out and
how they affected Akosi’s care.
Akosi and Roberta
When Justice and I first visited Akosi, he complained of being neglected by his
family and expressed his wish for more attention from the family. The reason
for the neglect was, in Akosi’s opinion, his lack of financial resources: “No
36
I visited Akosi three times in total. I also had the chance to interview Akosi’s wife away from the family, in her workplace. In addition I conducted interviews with various family members, his brother James for instance, during Akosi’s physiotherapy treatment. 37
For further information on the EM please refer to Appendix H.
` 50
money means no food, no care and no time for me. This is the reason why I am
left alone”. This was also confirmed by Roberta, Akosi’s wife:
They [the family] rather let him lie in his own excrements and wait for
me to come. I am the only one who is cleaning him up, who changes his
diapers and who turns him.
Both blamed Edward (the senior brother) for the situation, as “he only cares
about money”. Two of Akosi’s sisters live abroad, one in the US and the other in
Europe. Both have sent money for Akosi’s care, however, neither Roberta nor
Akosi have received any of that money. To my question on whether Akosi feels
that herbal treatment has helped him, he answered:
At first yes, but ever since I come for exercises [to the PTD] I do not
like herbal treatment anymore. I can feel immediate improvement
through exercises, which the family also acknowledges.
Because of her low status as a ‘married in’, Roberta is not included in decision-
making processes (e.g. the choice of treatment). According to Roberta it was
Edward’s sole decision to employ an herbalist. Roberta also believes that the
senior brother is possessed by witchcraft:
How else could he [Edward] develop such a negative attitude towards
my husband? A friend of mine asked Edward about Akosi’s health: ‘We
want him to die’ was Edward’s answer. When I confront other family

` 51
members they are rather annoyed with Edward, and they disagree on
how he treats Akosi.
The EM’s of Akosi and Roberta demonstrate that both perceive themselves as
victims of Edward’s dominance and decision-making. Edward is further criticised
and blamed for destroying the harmony of the family as he is divorced and his
children do not want contact with him.
James
James, Akosi’s brother, aged sixty-nine, accompanied Akosi to every
physiotherapy session. This offered me the chance to interview James by
himself. He disagreed with Edward's handling of the situation with Akosi:
I am not happy with Edward’s decisions. In the last three months,
Akosi was just lying in bed. No exercises. I am not happy with the
herbal treatment, but what can I do? I have to agree.
James attributed the worsening of Akosi’s condition to the herbal treatment,
which in James’s eyes is/was ineffective. James also blamed Akosi directly for
not co-operating with the family: “He does not do anything, not even wash
himself”. It seems that James did not know, or refused to acknowledge that
Akosi’s ‘disobedience’ was due to his ill health and not due to his unwillingness
to help. In James’ EM it is clear that Edward’s decisions were culpable for the
worsening of Akosi’s condition.

` 52
Edward
Edward is the eldest son in Akosi’s natal family and hence the head of the
family. He is also the main decision-maker when it comes to Akosi’s treatment.
When Justice and I visited Akosi for a second time, Edward was also present.
Akosi was made ‘presentable’, i.e. he was bathed and wore fresh diapers. After
introducing ourselves, I wanted to know why Akosi was so thin. Edward gave a
curious answer:
Because he is always lying in bed and cannot move, his muscles are
atrophied. Akosi is eating plenty of food. In the morning we feed him
porridge, in the afternoon rice with stew or beans, and evening fufu or
banku [a cooked maize meal] with soup.
When we inquired about the money that the sisters had sent from abroad,
Edward argued that the money was used for paying the herbalist’s bills. For a
three-month treatment the herbalist apparently charges 300 cedis38 - where
170 cedis have to be paid up front.
Edward told us that he did not know that exercise would be good for
Akosi. Later, however, he mentioned that the Komfo Anokye Teaching
Hospital39 had referred Akosi for rehabilitation treatment back at St. Patrick’s
Hospital. Hence, Edward knew about the available PTD, and according to
Edward, the family was planning to bring him to the PTD, if after three months
of herbal treatment, Akosi’s condition had not improved. Here we can see that
38
300 cedis are GBP 98, and 170 cedis are GBP 56; conversion rate from 14/01/13. 39
Akosi was first admitted to St Patricks Hospital, but as his condition was severe, he was referred to Komfo Anokye Teaching Hospital.

` 53
Edward has a completely different explanation of Akosi’s deteriorating
condition, which is Akosi’s physical immobility.
Situating Akosi’s case study into a theoretical framework
Akosi’s case study demonstrates how the willingness to care for a sick person is
dependent on that person’s behaviour towards their family prior to the onset of
the sickness (van der Geest 2002). As Akosi was an alcohol addict in the past, he
could not contribute productively towards his natal family, nor was he able to
support his wife and children. This was reciprocated by his family by way of
withdrawing basic care and denying food in his time of need. Akosi rightly
identified his lack of financial resources to be one of the reasons why his family
is neglecting him. Individuals in Akan society are expected to contribute to the
family’s household and look after one another in times of hardship (Crentsil
2007). Akosi’s stroke was a cause of economic hardship (e.g. cost of medicines
and therapy) for his family, and his disease produced constant conflict in the
family. Dilger’s study suggest that:
Acts of care and support are situated in the specific relations
between social persons that define themselves not primarily as
‘caregiver’ and ‘patient’, but first and foremost through their
relationships as siblings, parent, child and so forth (2008: 108).
In Akosi’s case, the family treated him the same way he had treated them
before he suffered the stroke and, according to Roberta, the responsibility of

` 54
care was shifted to her. Akosi’s case also demonstrates how power relations are
played out within the family. Pool and Geissler (2005) argue that:
Power, according to Foucault, is no commodity or attribute of status,
but a strategic relationship. Power is inherent within a relationship,
but dominance - manifested and felt imbalances and inequalities in
that strategic relationship – varies (2005: 68).
The dominance of the senior brother, Edward, was perceived differently by the
various family members. For instance, Roberta felt his dominance was due to
her low status of being “only married in”.
It has been reported that caring for a chronic sick person over a longer
period of time can lead to the discrediting of the ill person and frustration and
hostility towards them. Furthermore, through the fatigue of caring duties, the
‘sick-role’ might be denied to the chronic sick (Crentsil 2007). This was reflected
in James’s complaint about Akosi’s disobedience of washing himself.
Lastly, Akosi’s case study might also demonstrate that caring for the sick is a
private domain, and it also draws upon the unwillingness to spend money on a
sick person. Van der Geest (2009) points out that:
Funerals are public events but sickbed and death occur in the seclusion
of the house. Medical care is expensive and the outcome is uncertain, so
the willingness to spend money on a sick person who is going to die
anyway is limited” (2009:268).
This was also confirmed by Bubu:
` 55
[The] family is rather interested in a funeral then in treatment. If a
family member suffers a stroke, the family thinks that the illness cannot
be cured. The patient should die as soon as possible so that they can
‘earn’ money at the funeral, as the mourners need to ‘pay’ their respect.
Sometimes family members give patient a poisoned drink so that he/she
dies faster.
Bubu’s statement in turn corresponds with van der Geest (2009), who further
argues that:
Money spent on a funeral, however, is much more certain to be
effective and bear fruit. Death, indeed, is eclipsed by the funeral, in
many ways (2009:268).
6.4. Conclusion
Care in Akan society is a complex endeavour and matrilineage emerges as the
central unit in the care process of a sick person. Ideally, the family should
function as a social security system, as its members are required to assist each
other in times of crisis. The all-encompassing nature of matrilineage comes to
the fore in times of crises, as through care-giving people make sense of illness.
Reciprocity and respect are important values in Akan society and even more so
in times of sickness and hardship. Yet, the social and cultural basis of care is
undergoing profound changes particularly in Akan society but generally across
Ghana. The shift from the extended to a more nuclear family, and the migration
of the younger generation into cities are two major changes of note.

` 56
The two case studies also demonstrate how illness is constructed in
Akan society. Stroke, which renders someone immobile and dependent,
disrupts the coherence of the meaning of everyday life. Good health is
associated with an individual’s ability to perform duties and roles. Illness is
therefore perceived as a disturbance in the health balance, as it reduces the
productivity of an individual. As both informants were completely dependent
upon the family, they could not participate in the reciprocal character of the
support networks, e.g. contributing to the family’s income. In turn, this led to
considerable intra-household tensions with a resulting breakdown of the key
social support networks of the matrilineal kin. Some people even regard a dead
person as better than a chronically sick person, as funerals generate income.
In summary, how a sick person is cared for depends on how that sick
person behaved towards the family before the onset of his/her sickness. Being
cared for is not an automatic right, but a notion that requires considerable
investment.

` 57
Chapter 7: Conclusion
This dissertation has demonstrated that stroke, with its accompanying physical
impairment, disrupted the lives of my informants and their families. Stroke
often had a negative impact upon the livelihood of my informants’ households,
since the care process prevented care providers from pursuing income
generating activities. Unique manifestations of Akan matrilineal values of
reciprocity, respect and sense of deservedness influence the provision of care,
and thus impact the individual’s experience of illness. Illness experiences and
narratives, therefore, are never produced within a socio-cultural vacuum, but
are always situated in the wider social, political and cultural contexts of a given
society.
For my informants, these matrilineal values not only determined the
type and amount of care they received, but these values were also influential on
other aspects of their lives. For instance, decisions concerning possible
treatment, if any, were often made without the patient’s consent. This can be
related back to the reciprocal character of Akan society - whether a patient
‘deserves’ treatment or not was dependent on how they behaved towards the
family before the onset of the affliction. Moreover, the choice of treatment was
influenced by accessibility, costs and other factors, which may or may not
exclude certain groups from a particular form of treatment.
The experience of care and care giving, however, is always influenced by
much wider political, economic and structural factors and restrictions. State-run
health education programmes, for instance, with their focus on the individual’s

` 58
life style choices, are blame-oriented as “the disease [and the] onset and
outcome [of that disease] are directly ascribed to the afflicted themselves”
(Finerman & Bennett 1995:1). Such programmes, therefore, instil anxiety and
fear: in the case of my informants, fear about a future living with the disabilities
of stroke, the fear of not being able to pay for their children’s education, and
the fear of becoming dependent on their family in a society where individuals
are expected to contribute to the family’s household.
Risk factors as advertised by health education programmes might be an
outcome of structural factors. Due to poverty, for instance, my informants’
often had no other choice than to consume unhealthy, fatty and nutritionally
deficient diets. Poverty and poverty-related stress (e.g. depression and anxiety)
often had physical and psychological implications for my informants, including
the adoption of addictive behaviours. Considerable alcohol consumption as a
‘risk factor’ in Ghana, therefore, might be rooted in poverty.
Furthermore, my informants’ illness experience was characterised by
inequalities accessing adequate care and health facilities. As Ghana’s health
system is underfunded and underdeveloped it lacks basic and sophisticated
medical equipment and technologies, necessary for stroke diagnosis or
treatment and rehabilitation (especially in rural areas). As demonstrated earlier,
the in-hospital, post-acute care and subsequent rehabilitation management of
stroke are crucial for the treatment of stroke. However, such medical care is
often not covered by the NHIS and the majority of Ghanaians do not have
adequate access to post-stroke rehabilitation management. Structural factors
such as poverty and social inequality, therefore, greatly impacted on my
` 59
informants’ illness experience. Ultimately a change of ‘life conditions’ is
necessary, as opposed to a change of ‘styles’ in order to tackle the increasing
burden of stroke not only in Ghana but elsewhere in developing and developed
countries (Finerman & Bennett 1995).
The attempt to analyse this research in relation to the wider literature
on stroke in Ghana has proven difficult: though epidemiological literature is
available, the opposite is true for anthropological studies and publications. This
might be due to the fact that non-communicable diseases in Ghana, including
stroke, have not gained prominence in anthropological research as the primary
focus has been on infectious and parasitic diseases, such as HIV/AIDS, malaria
and neglected tropical diseases. Thus, the need for future anthropological
research on stroke in Ghana is prevalent, and a triangulation of diverse
disciplines would help the establishment of a well-formed body of knowledge
on morbidity and mortality rates, the individuals’ aetiology of their affliction,
their health care seeking behaviour, and the lived-experience of stroke sufferers
and their care givers. This triangulation might provide useful information for
the implementation of future health care programmes on stroke and other
NCDs, not only in Ghana and SSA but also throughout the globe.
In summary, this dissertation has highlighted the importance of
investigating the lived experience of stroke sufferers in the Ashanti region of
Ghana in order to understand health seeking and care giving behaviour.

` 60
Bibliography
Agyemang, C, Attah-Adjepong, G., Owusu-Dabo, E., de-Graft Aikins, A., Addo, J.,
Edusei, AK., Nkum, B.C., Ogedegbe, G. (2012). Stroke in the Ashanti Region
of Ghana. Ghana Medical Journal. 46(2): 12–17.
Apt, N. A. (1993). Care of the elderly in Ghana: An emerging issue. Journal of
Cross-Cultural Gerontology. 8(4): 301–312.
Becker, G. (1993). Continuity after a stroke: implications of life course disruption
in old age. The Gerontologist. 31(2): 631–9.
Bury, M. (1982). Chronic illness as biographical disruption. Sociology of Health
and Illness. 4(2): 167–82.
Cappuccio F.P., Micah F.B., Emmett, L., Kerry S.M., Antwi, S., Martin-Peprah, R.,
(2004). Prevalence, detection, management, and control of hypertension in
Ashanti, West Africa. Hypertension. 43(5): 1017–22.
Crentsil, P. (2007). Death, Ancestors, and HIV / AIDS among the Akan of Ghana.
PhD Thesis. University of Helsinki.
Darko, I. N. (2009). Ghanaian Indigenous Health Practices: The use of herbs.
Master Thesis. University of Toronto.
de-Graft Aikins, A., Anum, A., Agyemang, C., Addo, J. and Ogedegbe, O et al.
(2012). Lay Representations of Chronic Diseases in Ghana. Ghana Medical
Journal. 46(2): 59–68.

` 61
Desjarlais, R. & Throop, J. C. (2011). Phenomenological Approaches in
Anthropology. Annual Review of Anthropology. 40(1): 87–102.
Dilger, H. (2008). “We Are All to Die” Kinship, Belonging, and the Morality of
HIV/AIDS-Related Illnesses and Deaths in Rural Tanzania. Anthropological
Quarterly. 81(1): 207–232.
Evans-Pritchard, E. E. (1937). Witchcraft, Oracles and Magic amongst the
Azande. Oxford: Oxford University Press.
Faircloth, C., Boylstein, C., Rittman, M., Young, M. E., Gubrium, J. (2004). Sudden
illness and biographical flow in narratives of stroke recovery. Sociology of
Health & Illness. 26(2): 242–261.
Farmer, P. (1992). AIDS and Accusation: Haiti and the Geography of Blame.
Berkeley: University of California Press.
Fettermann, D. M. (1998). (eds.). Ethnography: Step by Step. SAGE Publications,
Inc.: California.
Finerman, R. and Bennett, L. A. (1995). Guilt Blame and Shame: Responsibility in
Health and Sickness. Soc. Sci. Med. 40(1): 1–3.
Ghana Statistical Service. (2012). 2010 Population and Housing Census:
Summary Report of Final Results. Accra: Sakoa Press Limited.
Ghana Health Service. (2010). The Health Sector in Ghana: Facts and Figures.

` 62
Horton, R. (2001). Ghana: defining the African challenge. Lancet. 358(9299):
2141–2149.
Hundt, G., Stuttaford, M., Ngoma, B. (2004). The Social Diagnostics of Stroke-
Like Symptoms: Healers, Doctors and Prophets in Agincourt, Limpopo
Province, South Africa. Journal of Biosocial Science. 36(4): 433–443.
Kengne, A. P. and Anderson, C. (2006). The neglected burden of stroke in Sub-
Saharan Africa. International Journal of Stroke. 1(4): 180–190.
Kleinman, A. M., Eisenberg, L., Good, B. (1978). Culture, Illness, and Care. Annals
of International Medicine. 88(2): 251–258.
Lawson, B. (2001). The Language of Space. Oxford: Reed Educational and
Professional Publishing Ltd.
Lemogoum, D., Degaute, J-P., Pascal Bovet, P. (2005). Stroke prevention,
treatment, and rehabilitation in sub-saharan Africa. American Journal of
Preventive Medicine. 29(5 Suppl 1): 95–101.
Luginaah, I. (2008). Local gin (Akpeteshie) and HIV/AIDS in the Upper West
Region of Ghana: the need for preventive health policy. Health & Place.
14(4): 806–816.
Lynch, E. & Medin, D. (2006). Explanatory models of illness: a study of within-
culture variation. Cognitive psychology. 53(4): 285–309.

` 63
Mshana, G., Plummer, M.L., Wamoyi, J., Shigongo, Z.S., Ross, D.A., Wight, D.
(2006). “She was bewitched and caught an illness similar to AIDS”: AIDS
and sexually transmitted infection causation beliefs in rural northern
Tanzania. Culture, health & sexuality. 8(1): 45–58.
National Health Insurance Scheme. (2010). Annual Report. Accra: National
Health Insurance Authority.
O’Reilly, K. (2009). Key concepts in Ethnography. SAGE Publications Ltd.:
London.
Pool, R. & Geissler, W. (2005). Medical Anthropology: Understanding Public
Health. London: London School of Hygiene and Tropical Medicine.
Pope, C. (2005). Conducting ethnography in medical settings. Medical Education
39(12): 1180-1187.
Rose, N & Novas, C. (2005). 'Biological citizenship', in Stephen J. Collier & Aihwa
Ong (eds.) Global assemblages: Technology, politics, and ethics as
anthropological problems. Malden, Mass. ; Oxford: Blackwell Publishing.
Setel, P. W. (2003). Non-Communicable Diseeases, Political Economy, and
Culture in Africa: Anthropological Applications of an Emerging Pandemic.
Ethnicity & Disease. 13(2): 2–167.
Stoeltje, B. J. (1997). Asante Queen Mothers: A Study in Female Authority.
Annals of the New York Academy of Sciences. 810(1): 41–71.

` 64
Stoner, B. P. (1986). Understanding Medical Systems: Traditional, Modern and
Syncretic Health Care Alternatives. Medical Anthropology Quarterly. 17(2):
44–48.
Tsey, K. (1997). Traditional Medicine in Contemporary Ghana: A Public Policy
Analysis. Social Science & Medicine. 45(7): 1065–1074.
Tsikata, D. and Seini, W. (2004). Identities, Inequalities and Conflicts in Ghana.
Working Paper. CRISE: Centre of Research and Inequality, Human Security
and Ethnicity. Oxford University: 3–50.
Van der Geest, S. (2002). ‘I want to go!’ How Older People in Ghana look
forward to death. Ageing and Society. 22(1): 7-28.
Van der Geest, S. and Finkler, K. (2004). Hospital ethnography: Introduction.
Social Science and Medicine 59(10): 1995-2001.
Van der Geest, S. (2009). 'End of Life Care in Ghana and the Netherlands: Good
Death, Bad Death and Euthanasia', in Christine Oppong et al. (eds.) Care of
the seriously sick and dying: perspectives of Ghana. Bergen, Norway: BRIC.
Ventevogel, P. (1996). Whiteman’s Things. Amsterdam: Het Spinhuis.
World Health Organisation (WHO). (2011). Global Status Report on non-
communicable diseases 2010. Geneva: World Health Organization
Whyte, S. R. (2012). Chronicity and control: framing “noncommunicable
diseases ” in Africa. Anthropology & Medicine. 19(1): 37–41.

` 65
Websites:
Government of Ghana. (2013). Ashanti: Introduction. Available at:
http://www.ghana.gov.gh/index.php/about-ghana/regions/ashanti
[24/01/2013].
NHS UK. (n.d.). CT scans: Introduction. Available at:
http://www.nhs.uk/conditions/ct-scan/pages/introduction.aspx [22/01/2013].
NHS UK. (n.d.). Stroke. Available at:
http://www.nhs.uk/Conditions/Stroke/Pages/Intro-duction.aspx [22/01/2013]
World-map. (n.d.). Ghana. Available at:
http://www.worldatlas.com/webimage/countrys/africa/gh.htm [02/02/2013].
` 66
Appendices
Appendix A A.1. General information and statistics on Ghana The Offinso muncipal is one of 2740 districts in the Ashanti region and according
to the 2010 household census, the population in this district comprised of 76,
89541 inhabitants. Offinso , the district capital has a population of approximately
30,000.
In 2010 the estimated population of Ghana was 24,658,823. The Ashanti region
as the most populated region accounted for a total population of 4,780,380,
compared to 4,010,054 in the Greater Accra region (Accra is the capital of
Ghana) (Population and Housing Census Report 2010). Greater Accra is the
smallest but most developed region (especially in terms of health care facilities)
in Ghana. For example: 466 Health facilities (including hospitals and health
centres) are found in Greater Accra, compared to 548 in the Ashanti region.
In West Africa, widening inequalities between a more developed south coastal
area and an underdeveloped periphery in the Sahelian north has been reported.
In Ghana the root of the North-South dichotomy can be traced back to colonial
dependency. The internal production of goods and services had a dual
structure: a dynamic modern export sector (Southern Ghana) and a backward
and underdeveloped subsistence sector (Northern Ghana, including Upper East,
40
For further information refer to the official governmental website of Ghana: (http://www.ghana.gov.gh/index.php/about-ghana/regions/ashanti [accessed on 24/01/2013]). 41
Population and Housing Census 2010.

` 67
Upper West and Northern region) that also served as a labour reserve for the
modern sector. Northern underdevelopment therefore stood, and still stands, in
stark contrast to the relative development of the South. Recent studies in
Ghana revealed that most of the poor (70 percent, with earnings of less than
GBP 298) and the extreme poor (59 percent, with earnings of less than GBP 231)
were to be found in the rural savannah (North), while less poverty was found in
the rural forest (South) – where 38 percent were poor and 21 percent extremely
poor (Tsikata & Seini 2004).
The ‘in-between’ season occurs between the two rainy seasons. The Ashanti
region experiences its first and major rainy season in March until July, the
second and minor one starting from September to November. December to
February is dry, hot, and dusty.
A.2. Medical definitions of stroke
Ischemic stroke occurs when a blood clot occurs as a result of an obstruction
within a blood vessel supplying blood to the brain. Hemorrhagic stroke is more
aggressive: it occurs when a blood vessel on the brain’s surface ruptures and
blood streams in either the space between brain and skull, or the brain’s
surrounding tissue. This then causes pressure on the brain. In most cases, this
form of stroke is fatal and people die within minutes. Hypertension is the most
common cause for hemorrhagic stroke (NHS n.d.).

` 68
A.3. Lineage of family
A.4. Daily routine in Offinso
I was getting up in the morning at around 7am; having breakfast (usually
porridge) in Aroha’s kitchen; going to work (between 8-9am) by taxi for 1 Cedi
(GBP 0,33) per person each way; having lunch around 1pm with Fai, who at that
time, completed a two-month internship for the administration at the hospital. I
usually finished the working-day between 5 and 6pm. On Saturdays my family
either just relaxed at home, or travelled to Kumasi for shopping. On Sundays it
was time to go to church, followed by a visit of the Sunday market in town, and
later to wash our cloths by hand. However, we did not adhere to this routine
(especially for the church services) too strictly: it dependent very much on the
weather and on our mood.

` 69
A.5. Further information on the Physiotherapy Department Permanent staff members included: Physiotherapist Fedu42,, physiotherapy
assistants Bubu and Manu, and the volunteer Alian. Fedu was the head of the
department, as he held a degree in physiotherapy, and thus was regarded to be
the best trained personnel in this department. Bubu obtained a diploma from
the physiotherapy assistant college. He gained experience in other PTDs, before
joining St. Patricks Hospital two years prior. Manu was the newest member of
staff, joining the department recently. As he came fresh out of college, this was
his first work experience. Alian was a trained physician assistant, but planned to
retrain as a physiotherapist assistant.
After the first week in the PTD I started to realise that there was a power-
struggle going on between Fedu and Bubu. I had the impression that Fedu tried
to embarrass Bubu in front of the patients. Furthermore it was Bubu who did
the majority of treatments. Fedu was mainly in the therapy room, sitting behind
his desk and doing work on his computer. At first I thought that it was because
of me, as he might have felt obliged to explain as much as possible. As time
progressed I began to feel the tension within the PTD and at times I was very
uncomfortable with Fedu’s treatment of Bubu. But when I spent the majority of
my time with patients and hence with Bubu, Fedu’s behaviour towards Bubu
deteriorated. After three weeks in the PTD, Fedu needed to attend an advanced
training in Accra which would last three weeks. This allowed me to discuss my
42
Informed consent was obtained from all informants. However, due to the size of the department, it was clear that even though I change the names, the characters will be still recognisable. I informed my respondents of this, but none raised any concerns about the identification problems.
` 70
impressions with Bubu, who told me that he felt bullied and treated badly by
Fedu. It was Bubu who established the PTD at St Patricks and not Fedu, and
Bubu, Manu and Alian confirmed that Fedu is not very helpful for the
department. In Fedu’s absence, the mood of the department changed
drastically: the three remaining staff members clearly relaxed and thus opened
up to me. This was also the time in which I was allowed to become an active
member of the team, and helped with administering therapies to patients. As a
former professional massage therapist, I greatly enjoyed this time.

` 71
Pictures of the Physiotherapy Department
Corridor and waiting area for patients
Treatment Room
` 72
Exercise Room

` 73
Appendix B: National Health Insurance Scheme (NHIS)
Since independence in 1957, the Ghanaian government has committed itself to
a welfare system that includes a ‘free health care for all’ policy. Between 1957
and 1966, Ghanaians could seek medical attention for free. In 1982, user fees
were introduced in government run facilities to supplement limited health
financing resources. This led to a dramatic decline in health care utilisation. In
1997, with the help of donor funding, voluntary Mutual Health Organisations
(MHOs) were introduced to certain districts throughout the country, which in
2002 consisted of around 159 MHOs, with 67 Ghanian districts involved. In
2003, Ghana introduced the National Health Insurance Scheme (NHIS), which
aimed to cover the entire population with affordable access to basic health
services within five years. The membership of NHIS is open to all persons
resident in Ghana by subscription. Exempt from the fees are: children under
eighteen years; the elderly aged seventy and above; the poor and, since 2008,
free ante-natal and post-natal care to all pregnant women. At present the NHIS
benefits package covers 95% of the most common disease conditions in Ghana,
and includes outpatient and inpatient care, delivery care, diagnostic tests,
generic (cheap) medicine, emergency care and rehabilitations care. The insured
has to go to his/her district hospital to receive treatment (NHIS Report 2010).
In comparison to other African countries, Ghana is certainly a role model
in terms of public health system. However, as with all great policy intentions,
the NHIS has major flaws, which on the ground affect the poor the most.
According to my informants the annual insurance fee starts from four cedis
(GBP 1,37) for the very poor and young children, and goes up to forty cedis (GBP
` 74
13,74). According to the NHIS Report the highest fee accumulated at seventy
cedis (GBP 24,00) for the very rich. I was somewhat surprised to read in the
same report that children under the age of eighteen and the poor should be
exempt from the insurance. My informants had to pay for their young children,
no matter how old they were. Justice pays the insurance for every child in his
charity. There are of course advantages with this system, such as the out and
inpatient care and the free ante- and post-natal care. However only basic
treatment is covered, e.g. a cast for a broken bone is not covered by the NHIS.
Conversely, rehabilitation after the removal of the cast is covered. The current
NHIS policy, therefore, is creating the same inequality as in the year 1982. Many
of the poor cannot afford the annual fees for themselves and their family, hence
they turn to local healers.
When I first heard about the NHIS it reminded me of the NHS here in the
UK and this was confirmed by Fedu:
The policy makers wanted to install the same medical system as in
UK, where every patient is treated in his/her own district and is
seldom referred to another hospital. In Ghana this does not work as
people attend hospitals in districts where their relatives live. These
hospitals then refer them back to their original district hospital. But
by then it is often too late.
In Fedu’s opinion, more applied medical personnel need to get into policy
making and politics in order to improve healthcare.
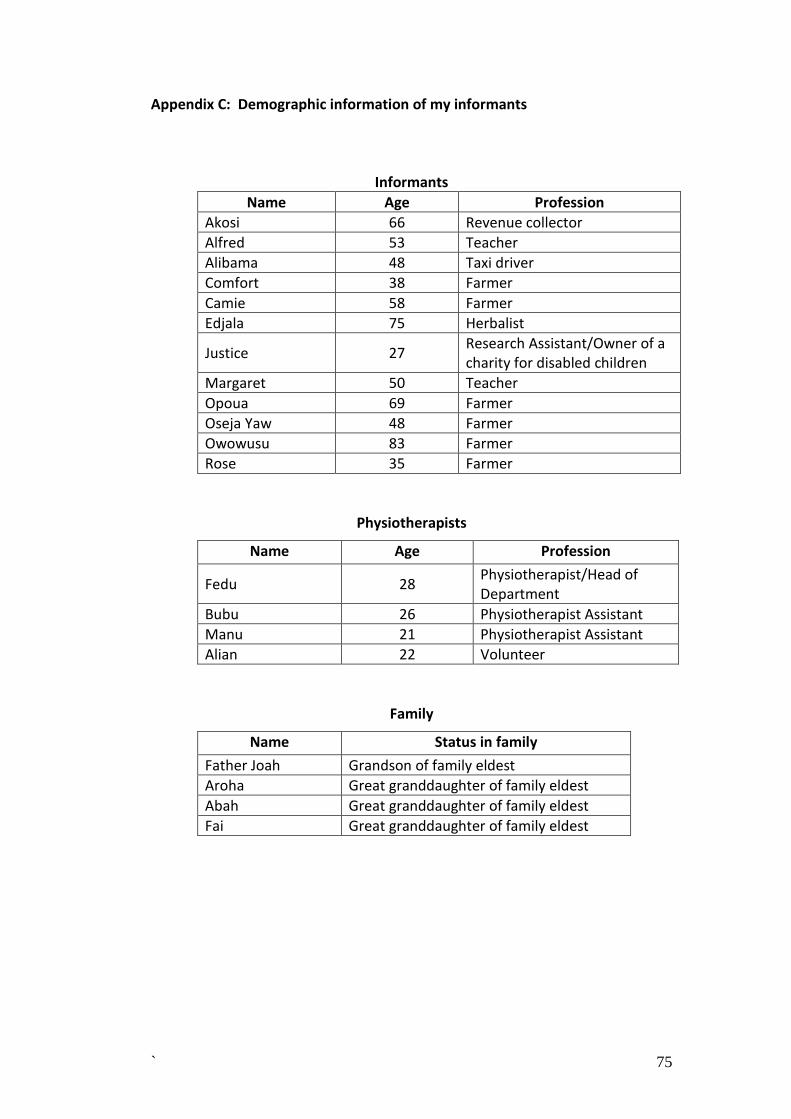
` 75
Appendix C: Demographic information of my informants
Informants
Name Age Profession
Akosi 66 Revenue collector
Alfred 53 Teacher
Alibama 48 Taxi driver
Comfort 38 Farmer
Camie 58 Farmer
Edjala 75 Herbalist
Justice 27 Research Assistant/Owner of a charity for disabled children
Margaret 50 Teacher
Opoua 69 Farmer
Oseja Yaw 48 Farmer
Owowusu 83 Farmer
Rose 35 Farmer
Physiotherapists
Name Age Profession
Fedu 28 Physiotherapist/Head of Department
Bubu 26 Physiotherapist Assistant
Manu 21 Physiotherapist Assistant
Alian 22 Volunteer
Family
Name Status in family
Father Joah Grandson of family eldest
Aroha Great granddaughter of family eldest
Abah Great granddaughter of family eldest
Fai Great granddaughter of family eldest

` 76
C.1. Glossary of Twi terms
Twi term English word / explanation
Aduane Food
Akpeteshie Cheap alcoholic drink
Banku A cooked maize meal
Fufu
Fufu is made by boiling starchy vegetables like cassava, yams or plantains, which are then pounded into a dough-like consistency. It is eaten with an accompanying soup, e.g. peanut, palm nut or groundnut soup, which is often made with different kinds of meat or fish.
Mogya Blood
Muju Witchcraft
Ndwodwoe3 Paralysis (in connection to stroke)
Okra Okra is a plant that produces an edible pod that is eaten as a vegetable
Yafunu Belly
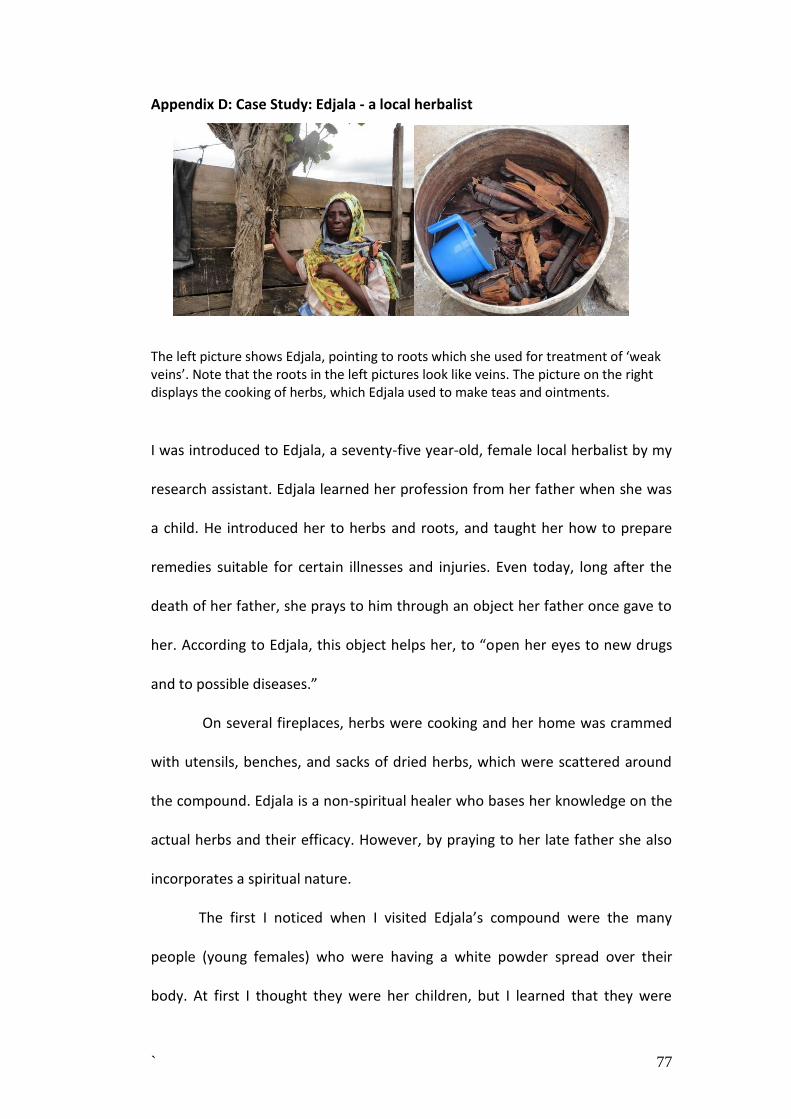
` 77
Appendix D: Case Study: Edjala - a local herbalist
The left picture shows Edjala, pointing to roots which she used for treatment of ‘weak veins’. Note that the roots in the left pictures look like veins. The picture on the right displays the cooking of herbs, which Edjala used to make teas and ointments.
I was introduced to Edjala, a seventy-five year-old, female local herbalist by my
research assistant. Edjala learned her profession from her father when she was
a child. He introduced her to herbs and roots, and taught her how to prepare
remedies suitable for certain illnesses and injuries. Even today, long after the
death of her father, she prays to him through an object her father once gave to
her. According to Edjala, this object helps her, to “open her eyes to new drugs
and to possible diseases.”
On several fireplaces, herbs were cooking and her home was crammed
with utensils, benches, and sacks of dried herbs, which were scattered around
the compound. Edjala is a non-spiritual healer who bases her knowledge on the
actual herbs and their efficacy. However, by praying to her late father she also
incorporates a spiritual nature.
The first I noticed when I visited Edjala’s compound were the many
people (young females) who were having a white powder spread over their
body. At first I thought they were her children, but I learned that they were
` 78
patients, staying with her in her compound or in her ‘hospital’ not far from the
compound. Accommodation in this hospital is free - however, food and care
have to be provided by the patients’ relatives. In the past, Edjala did not charge
anything for the treatment. Her patients simply showed their appreciation after
they recovered. Nowadays, with increased living expenses to cover, she is
forced to charge one-hundred cedis.
Cause of stroke
Edjala’s believes that stroke is a vein disease. If the vein is not strong enough,
the blood flow is blocked, hence a stroke occurs. The lesser the blood flow, the
thinner the vein will become. If a person is thin and has no blood, Edjala advises
the patient to go to the hospital in order to “make blood and veins stronger”
(through blood transfusions). If the patient has no “hospital disease”, the doctor
will send him/her back to her. Different diseases are transmitted by air and they
enter the person’s body through the skin. If a person wakes up paralysed in the
morning it is caused by the air.
According to Edjala, diet is another factor for causing stroke, as today’s
food does not contain enough energy due to the added chemicals. The food is
also too fatty and oily. This notion was also repeated by many of my informants.
She further argued that “white people are stronger then black people. White
people can take better care of themselves and they have a better diet”. People
also believe in witchcraft, although they cannot see witches. Edjala explained:
“A person’s jealousy can also cause stroke, as when someone thinks about
someone in a jealous way the other person will be possessed by witchcraft.”

` 79
Witchcraft can be interpreted to have not only a spiritual but also a social origin
(Evans-Pritchard 1937; Tsey 1997; de-Graft Aikins et al 2012).
Edjala has ‘indigenised’ biomedical knowledge and is using it for her
advantage (Pool & Geissler 2005). Equally, contaminated and fatty food,
witchcraft and her claim that white people are stronger then black people,
points to structural violence which occurs in the daily lives of the Ghanaians,
especially the poor. Such structural violence incorporates unequal access to
healthcare, education, employment and, due to poverty, lack of access to
nutritious food (Darko 2009, Pool & Geissler 2005, Tsey 1998, Stoner 1986).
Another interesting fact which we can see through Edjalas case study is
that she refers patients who have ‘no blood’ to the hospital. In turn, hospital
doctors refer them back to her when they cannot help the patient with
conventional treatments. A syncretised form of health care takes place as both
systems co-exist and complement each other.
D.1. Explanations of the profession of herbal healers
In Ghana, there are spiritual and non-spiritual herbal healers, and several routes
of training can lead to this trade. The first is through informal learning from a
close family member. A second method is through a three-year apprenticeship,
and the third route is through ‘spiritual calling’. The former two base their
knowledge on herbs and their efficacy. Spirituality (for explanations of
spirituality please refer to the next section) is a very important, though
secondary component. These herbalists usually also provide some sort of
accommodation for their patients. The last group of herbalists have a strong link

` 80
to the spiritual world, and herbal treatment serves as a mere means of driving
away evil spirits, destroying the supernatural powers responsible for any illness,
or involving the help of good spirits. Local priests/priestesses, cult healers, fetish
priests and pastors are part of this group (Tsey 1997; Darko 2009).

` 81
Appendix E: Further information on the local aetiology of stroke
The blockage of blood therefore might suggest either an upcoming paralysis,
which is an actual symptom of stroke or a weakening of the veins, which Edjala
the herbalist also suggested. Another important fact to note is that in the Akan
conceptualisation of disease, the belly (yafunu) is often regarded to be the
center from where diseases originate. The belly in turn is connected with the
blood (mogya). Often, therefore, disease aetiology is explained in terms of
‘blood that has changed’ or ‘something is in the belly’ (Ventevogel 1996: 16).
Appendix F: Changes in the socio and cultural foundations of care
Van der Geest (2002) writes about the care of the elderly, which is also
important for this dissertation as many of my informants were elderly. Van der
Geest (2002) identifies four major developments in care giving: The first, he
argues, comes from the shift from lineage and extended family to the nuclear
family. Families began to exclude non-nuclear relatives, so that extended family
members were denied access to their income, possessions and heritage. At the
same time however, the new established nuclear-families were keen to
maintain some sort of ties to their matrilineage. For example, at funerals, it is
considered prestigious to summon as many family members as possible. The
second development affecting care-giving is the continuous migration of the
younger generation into cities and therefore they are not able to provide
immediate care. What they can provide, however, is care from the distance by
sending money and food contribution back home, which is the third
development. The fourth development is the shift from the appreciation of the

` 82
knowledge and wisdom of the elderly, which is based on long life experience, to
a knowledge based on school education and general changes in society (van der
Geest 2002).
Appendix G
A CT scan is a computerised tomography scan. It uses X-rays and a computer to
create detailed images of the inside of your body. The images produced by a CT
scan are called tomograms and are more detailed than standard X-rays. A CT
scan can produce images of structures inside the body including the internal
organs, blood vessels, bones and tumours (NHS n.d.).
Appendix H
The explanatory model of illness was developed by Arthur Kleinman in 1978. He
developed these models and related questionnaires in an attempt to distinguish
between disease and illness, and to bridge the gap between clinical knowledge
and constructions of clinical reality. Questions for informants included: What do
you think has caused your problems? Why do you think it started when it did?
(Kleinman 1978: 251). Explanatory models (EM[s]) are often used to explain
how people view their illness in terms of how it happens, what causes it, how it
affects them, and what will make them feel better. It is a method used in both
clinical settings and qualitative research as a way to obtain individual
explanations about a particular phenomenon




















