
Speech perception of children using Nucleus, Clarion or Med-El cochlear implants
9
Speech perception of children using Nucleus, Clarion or Med-El cochlear implants Riki Taitelbaum-Swead a,b, * , Liat Kishon-Rabin a , Ricky Kaplan-Neeman a,b , Chava Muchnik a,b , Jona Kronenberg c , Minka Hildesheimer a,b a Department of Communication Disorders, Sackler Faculty of Medicine, Tel-Aviv University, Israel b Speech and Hearing Center, Chaim Sheba Medical Center, Tel-Hashomer, Israel c Department of Otorhinolaryngology and Head and Neck Surgery, Chaim Sheba Medical Center, Tel-Hashomer, Israel Received 30 January 2005; accepted 3 May 2005 International Journal of Pediatric Otorhinolaryngology (2005) 69, 1675—1683 www.elsevier.com/locate/ijporl KEYWORDS Cochlear implants; Performance; Prelingual hearing- impaired children; Speech perception; Age at implantation; Mode of communication Summary Objective: The purpose of this study was to present speech perception achievements of implanted children using commercially available cochlear implant devices: Nucleus, Clarion or Med-El. Study design: A retrospective analysis. Methods: Speech perception data of 96 hearing-impaired children: 27 with Clarion, 49 with Nucleus and 20 with Med-El were collected. Speech tests included the Hebrew Infant Toddlers Meaningful Auditory Integration Scale (HIT-MAIS) for the infants, the Hebrew Early Speech Perception (HESP) closed-set word-identification test and Hebrew Arthur Boothroyd (HAB) open-set one-syllable word recognition test were used for the older children. Results: I HIT-MAIS: (1) Infants showed similar rate of progress, regardless of device. (2) Children implanted under two years of age reached performance within normal development on this test. II HAB: (1) Most children achieved open set results with mean HAB between 40 and 50%, within 1—1.5 years post implantation. (2) Linear regression analyses revealed no statistical differences between the Clarion the Nucleus and the Med-El devices on the mean final measurement of this test. (3) Age of implantation and mode of communication were significant covariate variables: (a) the younger the child is implanted the better the results and (b) oral commu- nication prior to implantation results in better performance than sign language. Conclusions: There are no apparent differences in speech perception performance between implant devices when considering background variables. The data have important implications on the rehabilitation process of hearing impaired children with * Corresponding author. Tel.: +972 3 5352876x105; fax: +972 3 5352868. E-mail address: [email protected] (R. Taitelbaum-Swead). 0165-5876/$ — see front matter # 2005 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijporl.2005.05.002
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Speech perception of children using Nucleus, Clarion or Med-El cochlear implants

International Journal of Pediatric Otorhinolaryngology (2005) 69, 1675—1683
www.elsevier.com/locate/ijporl
Speech perception of children using Nucleus,Clarion or Med-El cochlear implants
Riki Taitelbaum-Swead a,b,*, Liat Kishon-Rabin a,Ricky Kaplan-Neeman a,b, Chava Muchnik a,b,Jona Kronenberg c, Minka Hildesheimer a,b
aDepartment of Communication Disorders, Sackler Faculty of Medicine,Tel-Aviv University, Israelb Speech and Hearing Center, Chaim Sheba Medical Center, Tel-Hashomer, IsraelcDepartment of Otorhinolaryngology and Head and Neck Surgery,Chaim Sheba Medical Center, Tel-Hashomer, Israel
Received 30 January 2005; accepted 3 May 2005
KEYWORDSCochlear implants;Performance;Prelingual hearing-impaired children;Speech perception;Age at implantation;Mode ofcommunication
S
OoNSM4IHHuR(dmrNA(nCbi
* Corresponding author. Tel.: +972 3 5E-mail address: [email protected]
0165-5876/$ — see front matter # 200doi:10.1016/j.ijporl.2005.05.002
ummary
bjective: The purpose of this study was to present speech perception achievementsf implanted children using commercially available cochlear implant devices:ucleus, Clarion or Med-El.tudy design: A retrospective analysis.ethods: Speech perception data of 96 hearing-impaired children: 27 with Clarion,9 with Nucleus and 20 with Med-El were collected. Speech tests included the Hebrewnfant Toddlers Meaningful Auditory Integration Scale (HIT-MAIS) for the infants, theebrew Early Speech Perception (HESP) closed-set word-identification test andebrew Arthur Boothroyd (HAB) open-set one-syllable word recognition test weresed for the older children.esults: I HIT-MAIS: (1) Infants showed similar rate of progress, regardless of device.2) Children implanted under two years of age reached performance within normalevelopment on this test. II HAB: (1) Most children achieved open set results withean HAB between 40 and 50%, within 1—1.5 years post implantation. (2) Linearegression analyses revealed no statistical differences between the Clarion theucleus and the Med-El devices on the mean final measurement of this test. (3)ge of implantation and mode of communication were significant covariate variables:a) the younger the child is implanted the better the results and (b) oral commu-ication prior to implantation results in better performance than sign language.onclusions: There are no apparent differences in speech perception performanceetween implant devices when considering background variables. The data havemportant implications on the rehabilitation process of hearing impaired children with
352876x105; fax: +972 3 5352868.l (R. Taitelbaum-Swead).
5 Elsevier Ireland Ltd. All rights reserved.

1676 R. Taitelbaum-Swead et al.
cochlear implants in relation to device selection, age at implantation and mode ofcommunication prior to implantation.# 2005 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
The communicative benefit of cochlear implantationin profoundly deaf children has been documentedextensively. The amount of benefit, however, variesacross individuals and appears to depend on severalfactors. These factors include demographic andhearing characteristics of the child, as well as fea-tures of the implant device. Most studies to date,have primarily investigated the contribution of thechild’s demographic and hearing characteristics toperformance. These characteristics include age ofimplantation, amount of residual hearing, mode ofcommunication and family support [1—3]. Of thefeatures related to the device, the majority of theresearch focused on the effect of speech codingstrategy within the implanted device, usually inpostlingually deafened adults and only a few focusedon prelingually hearing-impaired children [4,5].
The availability of a variety of Food and DrugAdministration (FDA) approved cochlear implantdevices, introduced an additional source of variabil-ity in performance of cochlear implantees, namelythe type of implant device. The decision as to theselectionof implantdevice for implantation is usuallybasedonmanyconsiderations suchasmedical, esthe-tical, financial, and performance. Of these factors,the difference in performance between the differenttypes of implant devices received little attention.Furthermore, the studies that addressed this issuefound inconclusive results. In postlingual deafenedadults, higher speech perception scores and greaterrate of progress were found in those using the Clariondevice compared to those using an earlier generationofNucleus speech coding strategies [6]. This Clarion’sadvantage was maintained in a recent study usingmore advanced systems with ear level processors ofboth devices [7]. Better speech perception scoreswith the Clarion device were also found compared tothe Ineraid device [8]. In contrast, Battmer et al. [9]showed no difference between the Nucleus 22 andthe Clarion device in either quiet or noise. Similarly,no difference in speech perception performance wasfound between the Med-El and the Nucleus 24implant devices [10].
Considering children are not ‘‘small adults’’ [11],and that today most cochlear implant candidatesare young toddlers, implant device comparison stu-
dies need to focus on this population. To date, onlyfew studies compared speech perception betweendevices in prelingually hearing impaired children.Meyer and Svirsky [12] found no significant differ-ences between the Clarion and the Nucleus 22devices. Young et al. [13] found better auditoryperception skills in children with the Clarion deviceduring the first year post implantation compared tochildren implanted with the Nucleus 22. Theyargued that processing strategy of CIS that wasimplemented in the Clarion device used high rateof stimulation (800 pulses/s) compared to the SPEAKstrategy in the Nucleus 22 device that used lowerrate of stimulation (180—300 pulses/s). These dif-ferences might explain the higher scores of theClarion’s implanted children.
Currently, the three FDA approved cochlearimplant devices (Calrion, Med-El and Nucleus)encode the speech signal in different ways. WhileNucleus uses a channel picking strategy, whichselects typically 8—12 channels for each cycle ofstimulation, in strategies used by Clarion and Med-El, all channels are stimulated in each cycle ofstimulation. There is therefore a need to compareperformance between the advanced versions ofthese three implant devices in children and findout if the different strategies are equally capableof providing high levels of speech recognition. Ide-ally, such a comparison should be conducted bymatching children in each device group by back-ground information and audiologic characteristics.An alternative approach is to treat statisticallyfactors that may influence performance. The pur-poses of the present study were: (1) to presentspeech perception performance of implanted chil-dren using different commercial devices and (2) tocompare the results between the devices taking intoaccount audiologic and demographic variables.
2. Materials and methods
2.1. Subjects
A total of 250 children were implanted at the ShebaMedical Center, Tel-Hashomer, Israel between 1993and 2004. Of these, 96 children with advancedcoding strategies, monolingual Hebrew speakers

Speech perception of implanted children 1677
Table 1 Background information of the implanted children
Nucleus Clarion Med-El
Number of subjects 49 27 20
Age at implantationMean (years) (S.D.) 3.8 (2.9) 3.5 (1.9) 7.6 (5.6)Range 11 m—13 y 12 m—7.6 y 14 m—16.7 yMedian (years) 2.75 3.4 6.5
Etiology (n)Unknown 25 16 13Genetic 22 7 4CMV 2 1 2Meningitis 2Wardenburg 1Mondini 1
Mode of communication preimplant (n)Oral 14 6 10Gestures 24 13 7Total 3 4 2Sign 8 4 1Unaided PTA (dBHL) 106.1 106.8 107.6
Speech perception preimplant (n) *
HESP categories 1 and 2 9 15 3HESP categories 3 and 4 7 1 3HAB 0—20% 3 4HAB 21—40% 3 1 3
* Not included 44 infants who were evaluated prior to implantation by the Hebrew Infant Toddler Meaningful Auditory IntegrationScale (HIT-MAIS). m: months, y: years, PTA: pure tone average, dBHL: decibel hearing level, HESP: Hebrew Early Speech Perceptionand HAB: Hebrew Arthur Bootroyd.
(Arabic and Yiddish speakers were excluded), noadditional problems (such as autism, mental retar-dation and cerebral palsy), and congenital hearingloss, were selected for the present study. Forty-ninechildren were implanted with the Nucleus 24 device(Cochlear Corporation, Lane Cove, NSW, Australia),twenty-seven children were implanted with theClarion device (Advance Bionics Corporation, Syl-mar, California, USA) and 20 children wereimplanted with the Med-El device (Med-EL Corpora-tion, Innsbruck, Austria). The background informa-tion of the subjects is summarized in Table 1.
2.2. Implant devices and strategy ofstimulation
Three types of implants were used in the presentstudy: the Nucleus, the Clarion and the Med-Eldevices. Forty-nine children were implanted withthe Nucleus device and were using the AdvancedCombination Encoder (ACE) strategy. In ACE, thefrequency spectrum of the incoming sound is dividedto 22 channels, and typically 8—12 channels with thehighest amplitudes, ‘‘maxima’’, are selected foreach cycle of stimulation, in stimulation rates thatvary between 500 and 2400 Hz.
Of the children implanted with the Clariondevice, 11 children used the Continuous Inter-leaved Sampler (CIS), 13 used the SimultaneousAnalog Stimulation (SAS) and three used the PairedPulsatile Sampler (PPS). All strategies used in theClarion device extract the signal’s envelope afterseparation of the signal to different frequencybands. In CIS, the processed signals are deliveredsequentially across all eight channels at the rate of813 Hz per channel. In PPS, signals are deliveredto pairs of electrodes, sequentially. Conseque-ntly, the rate of stimulation is 1445 Hz per channel.In SAS, all channels are stimulated simultaneo-usly, with overall stimulation rate of more than90,000 Hz.
Twenty children were implanted with the Med-Eldevice and were using the CIS strategy. The CISstrategy implemented in the Med-EL device istermed ‘‘CIS+’’. It differs from the Clarion’s CISmainly in the envelope extraction process per-formed in Med-El using the Hilbert Transformation.The rate of stimulation is 1515 Hz. Childrenimplanted with the Clarion device were initiallyprogrammed with the SAS strategy, followingAdvanced Bionics recommendations. Children weretransferred to the CIS and PPS strategies for two

1678 R. Taitelbaum-Swead et al.
reasons: unsatisfactory speech perception perfor-mance and/or high levels of most comfortable levels(M levels) in the presence of compliance limits.
The Nucleus group used one of three types ofelectrodes: CI24M (30 children), CI24K (7 children)and CI24R (CS) (12 children). The Clarion group alsoused one of three types of electrodes EnhancedBipolar 1.2 (15 children), Highfocus (8 children) orCII (4 children). The Med-El group used the Combi40+.
2.3. Speech perception tests
The tests administered to each child were deter-mined based on his/her age, cognitive and languageabilities. We used a questionnaire as well as closedand open-set tests.
1. T
he questionnaire included the IT-MAIS–—InfantToddler Meaningful Auditory Integration Scalewhich was adapted to Hebrew. This question-naire includes 10 questions that are posed tothe parents in an interview schedule regardingtheir child’s spontaneous listening behaviors ineveryday situations. The questions reflect threedifferent areas of auditory skills development:changes in vocalization associated with deviceuse; alertness to sounds in everyday environ-ments and derivation of meaning from sound.Scores for each question range from 0 (‘‘neverdemonstrates the behavior’’) to 4 (‘‘alwaysdemonstrates the behavior’’). The total possiblepoints on the IT-MAIS are 40 (10 ques-tions � maximum score of 4). This questionnairewas administrated to the parents of 109 normalhearing infants [1] for establishing validity andreliability.2. T
Fig. 1 HIT-MAIS scores (in %) of Nucleus (n = 24), Clarion(n = 10) and the Med-El device (n = 5), as a function of
he closed set test included the Early SpeechPerception Test, adapted to Hebrew. In this testthe child is asked to point to one of the picturesfollowing an audio presentation of each word. Inorder to ensure that the child is familiar with thevocabulary presented in the pictures, the audio-visual condition was administrated prior to test-ing in the auditory only condition. The childperformance is categorized to one of four cate-gories according his scores. These include: cate-gory 1–—no pattern perception, category 2–—pattern perception, category 3–—two syllableword identification and category 4–—one syllableword identification.
chronological age. The rate of progress of each implanted
3. Tinfant is demonstrated by the connecting lines betweendata points. The solid curve represents the best-fittingcurve to data of 109 normal-hearing infants [1]. Dottedlines show �2S.D. of the mean of normative data.
he open set word test included the Arthur Boot-hroyd (AB) adapted to Hebrew (HAB). This testincludes one-syllable CVC isophonemic meaning-ful word lists, testing in open set. Each listincludes, 10 words represent of each consonant
of the Hebrew language once and each voweltwice. The child is asked to repeat the words.
All tests were adapted to Hebrew based on theunderling criteria upon which they were developedin English.
Speech perception of implanted children 1679
2.4. Procedure
Speech perception abilities were measured atapproximately 3, 6, 12, 24, 36 and 44 months postimplantation. Note that not all the subjects wereavailable at all times. As stated before, the testsadministered to the child were determined basedon his/her age, cognitive and language abilities:Infants younger than 2.5 years old were usually eval-uatedwithHIT-MAIS.Childrenabove2.5yearsoldwhowere not able to perceive speech in open set, wereadministered the HESP test. Children above 2.5 yearsold, whowere able to repeat words in open set, weretested with the open-set word stimuli (HAB). All spe-echperception testswerepresentedat70—75 dBSPL.
2.5. Statistical analysis
The factors that may affect the performance usingimplant devices were addressed statistically. Linearregression analyses were therefore, performed onthe HIT-MAIS and HAB data while adjusting for con-founding factors, such as, age of implantation,mode of communication, duration of implant useand speech perception results pre implantation. Inthe regression model, categorical variables with ncategories were represented by n � 1 dummy vari-ables and the last category is regarded as a refer-ence category. Therefore, each category wascompared to the reference category. To enable allpossible pair-wise comparisons between categoriesof the categorical variables, an analysis of variancewith covariates (ANCOVA) was also conducted.
3. Results
3.1. HIT-MAIS questionnaire scores
HIT-MAIS scores with the Nucleus (n = 24), Clarion(n = 10) and the Med-El device (n = 5), as a function
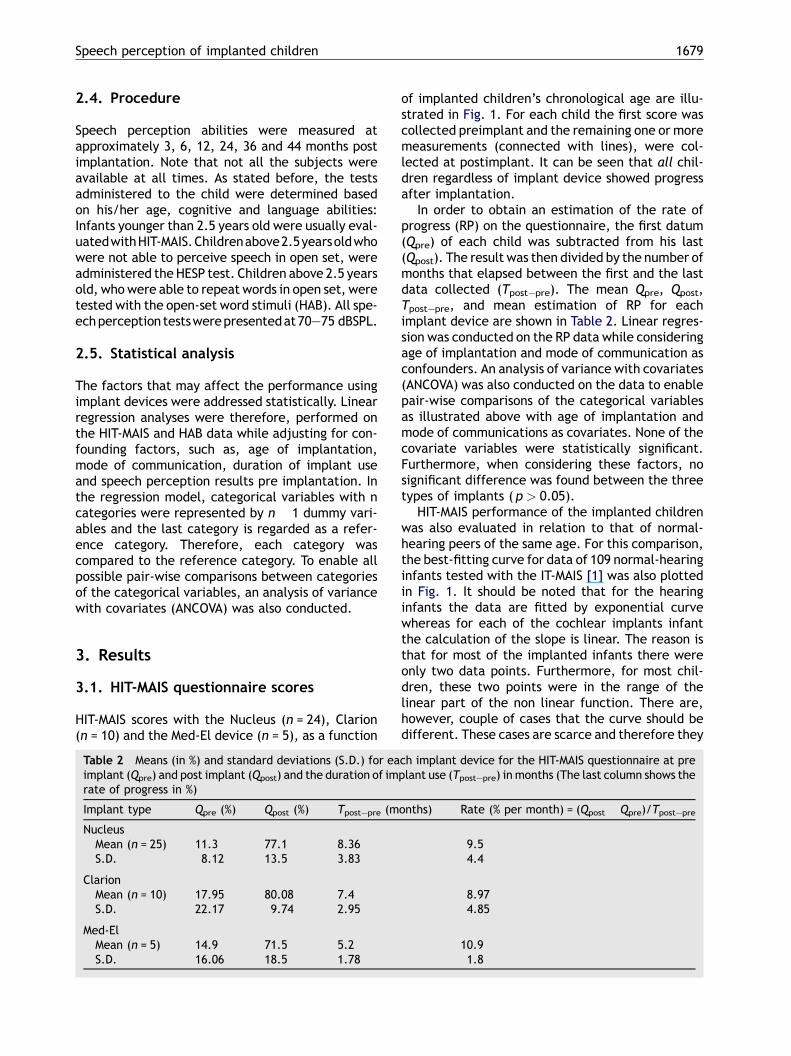
Table 2 Means (in %) and standard deviations (S.D.) for eaimplant (Qpre) and post implant (Qpost) and the duration of imrate of progress in %)
Implant type Qpre (%) Qpost (%) Tpost—pre (m
NucleusMean (n = 25) 11.3 77.1 8.36S.D. 8.12 13.5 3.83
ClarionMean (n = 10) 17.95 80.08 7.4S.D. 22.17 9.74 2.95
Med-ElMean (n = 5) 14.9 71.5 5.2S.D. 16.06 18.5 1.78
of implanted children’s chronological age are illu-strated in Fig. 1. For each child the first score wascollected preimplant and the remaining one or moremeasurements (connected with lines), were col-lected at postimplant. It can be seen that all chil-dren regardless of implant device showed progressafter implantation.
In order to obtain an estimation of the rate ofprogress (RP) on the questionnaire, the first datum(Qpre) of each child was subtracted from his last(Qpost). The result was then divided by the number ofmonths that elapsed between the first and the lastdata collected (Tpost—pre). The mean Qpre, Qpost,Tpost—pre, and mean estimation of RP for eachimplant device are shown in Table 2. Linear regres-sion was conducted on the RP data while consideringage of implantation and mode of communication asconfounders. An analysis of variance with covariates(ANCOVA) was also conducted on the data to enablepair-wise comparisons of the categorical variablesas illustrated above with age of implantation andmode of communications as covariates. None of thecovariate variables were statistically significant.Furthermore, when considering these factors, nosignificant difference was found between the threetypes of implants ( p > 0.05).
HIT-MAIS performance of the implanted childrenwas also evaluated in relation to that of normal-hearing peers of the same age. For this comparison,the best-fitting curve for data of 109 normal-hearinginfants tested with the IT-MAIS [1] was also plottedin Fig. 1. It should be noted that for the hearinginfants the data are fitted by exponential curvewhereas for each of the cochlear implants infantthe calculation of the slope is linear. The reason isthat for most of the implanted infants there wereonly two data points. Furthermore, for most chil-dren, these two points were in the range of thelinear part of the non linear function. There are,however, couple of cases that the curve should bedifferent. These cases are scarce and therefore they
ch implant device for the HIT-MAIS questionnaire at preplant use (Tpost—pre) in months (The last column shows the
onths) Rate (% per month) = (Qpost � Qpre)/Tpost—pre
9.54.4
8.974.85
10.91.8

1680 R. Taitelbaum-Swead et al.
Fig. 2 Each symbol type represents data of one child using the Nucleus (n = 32) device (in the upper graph), Clarion(n = 22) device (in the middle graph) and Med-El (n = 18) device (in the lowest graph), as a function of his/herschronological age. The first data point for each child shows performance before implantation. HESP categories are shownin the lower part of each graph and HAB scores (in %) above the solid line.

Speech perception of implanted children 1681
Table 3 Linear regression on the HAB data
Variable Coefficient t-value p
Age at implantation �2.1 �2.06 0.04 *
Perception pre implant (vs. open-set)HESP 1—2 �14.6 �1.32 0.19HESP 3—4 �10.9 �1.31 0.19Duration of implant use 0.45 1.3 0.2
Mode of communication (vs. oral)Gesture �17.18 �1.68 0.1Total �13.56 �1.43 0.15Sign �27.02 �2.65 0.01 *
Type of implant (vs. Med-El)Nucleus 2.88 0.33 0.74Clarion �3.37 �0.33 0.73
* p < 0.05.
do not have significant effect on the results. It canbe seen that 44% (11/25) of the children with theNucleus, 60% (6/10) of the children with the Clarionand two of five children with the Med-El were withinthe �2S.D. of the mean normative values. Theseresults are difficult to compare because of the smallnumbers of infants in the Clarion and Med-Eldevices. Nonetheless, one outcome common to alldevices is that most of these children who reachednormative values were implanted before 2 years ofage: 18 infants using the Nucleus device, 8 using theClarion device and 2 using the Med-El device. This isillustrated in Fig. 1.
3.2. Speech perception scores
Speech perception scores of the HESP and the HABtests of 32 children with the Nucleus, 22 childrenwith the Clarion and 18 with the Med-El cochlearimplant devices are shown in Fig. 2. These graphsdemonstrate the progress of the children from thecategories of the closed-set test ESP to the open-word identification test of the HAB. Again, for eachchild the first score was collected pre implant andthe remaining scores (connected with lines) werecollected postimplant. It can be seen that mostchildren achieved open set results within 1—1.5years post implantation, regardless of device type.In order to compare open-set performance betweenthe Nucleus the Clarion and the Med-El devices, onlythe final measurement for each subject wasincluded in the statistical analyses. The distributionof these data is shown in the box and whiskers plot inFig. 3. The mean final measurement for childrenusing the Nucleus device was 47.5 (S.D. = 18.7), for
Fig. 3 Distribution of the final measurement of the HABtest for each child with the Nucleus, Clarion or Med-Eldevices. The box represents the inter-quartile range,which contains 50% of the values. The line within thebox marks the median, the whiskers above and below thebox extend to the 90th and 10th percentiles, and theoutlying data are graphed as filled circles.
children using the Clarion device 40.6 (S.D. = 19.8),and for children using the Med-El device 39.7(S.D. = 26.4). Linear regression was conducted onthe HAB data while adjusted for age of implanta-tion, mode of communication, perception preim-plantation and duration post implantation asconfounders. Summary of the statistical analysis isshown in Table 3. An analysis of variance withcovariates (ANCOVA) was also conducted with ageat implantation, duration of implant use, mode ofcommunication and perception pre implant as cov-ariates. The summary of this statistical analysis isshown in Table 4. It can be seen that of the covariatevariables, age at implantation was statistically sig-nificant (p < 0.05) and mode of communicationapproached significance (p = 0.08). These findingssuggest that age of implantation is inversely relatedto speech perception performance–—the youngerthe age of implantation the better the results.Ryan—Einot—Gabriel—Welsch method used for mul-tiple comparisons between the various modes ofcommunication (oral, gesture, total and sign)revealed that children who used oral communica-tion preimplantation performed better than thosewho communicated by sign language. When consid-ering the confounding factors mentioned above, no
Table 4 Analysis of variance with covariates(ANCOVA) results to the HAB scores
Variable d.f. p F
Implant type (2,40) 0.68 0.38Age at implantation (1,40) 0.04 * 4.24Duration of implant use (1,40) 0.2 1.68Mode of communication (3,40) 0.08 2.4Speech perception
preimplant(2,40) 0.3 1.15
* p < 0.05.

1682 R. Taitelbaum-Swead et al.
significant difference was found between the threetypes of implants ( p > 0.05).
4. Discussion
The present study was designed to evaluate retro-spectively speech perception results of childrenusing the Nucleus, the Clarion or the Med-El devices.Our results suggest that implanted children showconsiderable progress in speech perception abilitiesregardless of their implant device. This was foundfor the rate of progress when using the HIT-MAISquestionnaire in the very young implanted children,as well as for the final speech perception score in theolder children who were administrated with theopen-set HAB test. These results are in keeping withthe scarce published data on comparison betweendevices in young implanted children [12].
The present data also reveal the variability in theamount of benefit that hearing-impaired young chil-dren receive from their cochlear implants. None-theless, it appears that most infants who receivedtheir implant before 2 years of age reached norma-tive values in the HIT-MAIS questionnaire regardlessof device. In fact, most of these infants reached anaverage of 80—100% on the HIT-MAIS before 1 yearpostimplant. Our results are in keeping with thepublished data regarding age of implantation sug-gesting that for congenitally deaf children, earlierimplantation leads to better auditory performance[1,14]. McConkey Robbins et al. [1] for example,found using the IT-MAIS questionnaire that childrenimplanted before the age of 2 years showed highscores, which fell within normative values comparedto children implanted between 2 and 3 years of age.Govaerts et al. [14] also found, that childrenimplanted before the age of 2 years showed norma-tive values at three months post implantation on theCategories of Auditory Performance (CAP).
Data with the open-set HAB speech perceptionmeasure showed that implanted children using anyof the devices reached mean word identificationscore of 40—50% on the HAB word lists. The rangeof scores is large possibly due to factors such as ageof implantation, anatomical malformation, and typeof hearing loss. The data suggests that childrenimplanted at very young ages tended to performbetter than children implanted at older ages.Further comparison of the HAB word scores of theyoungest implanted children with those of normal-hearing children (aged 2.5—4 years) matched bychronological age [15] suggests that within thisage group, implanted children did not reach norma-tive performance. Noteworthy is the fact that therewere six older implanted children (four Nucleus and
two Med-El) who had either progressive hearing lossor significant open-set recognition prior to implan-tation. These children showed high HAB word scores(up to 80%) 2—3 years after implantation. This is inkeeping with Gray et al. [16] who showed high word-in-sentences scores (63—94%) in seven olderimplanted children with progressive hearing loss.
Mode of communication was also found to be asignificant contributor to performance with theimplant. Children who used oral communicationprior to implantation performed better with theirimplant than those who communicated via signlanguage. These finding are in keeping with otherpublished data that found better performance inchildren who used oral communication [3].
The present study suggests that when adjustingfor confounding factors such as age of implantation,mode of communication and duration of implantuse, there are no apparent differences in speechperception scores when comparing data of im-planted children using different cochlear implantsdevices. These results, however, are limited to themeasures used in this study. It is possible that onaverage, implanted children’s outcome perfor-mance is not device dependent or alternatively,auditory, speech, language and psycho-social fac-tors override any differences between devices.Nonetheless, it is clear that when using a retro-spective analysis design of existing data, the differ-ent factors that possibly influence the scores aredifficult to control for. We attempted to addressthese issues using a statistical approach.
The present data contributes to the knowledgeregarding the question commonly asked by bothprofessional and parents whether there are differ-ences in speech perception performance betweendevices. Because of obvious reasons, we cannotcompare, implant devices using a with-in subjectdesign. We are therefore required to continue to usebetween-subject comparisons while attempting toconsider the different influencing factors on audi-tory behavior and speech performance.
4.1. Conclusions
Speech perception outcomes of implanted childrenwho use new generations of the three cochlearimplants devices are similar, and depend on factorssuch as age at implantation and mode of commu-nication. These results have important implicationswhen counseling parents regarding type of implantdevice. The three devices may be different in var-ious characteristics (esthetic, battery supply, devicefailure and telemetry options) however the out-comes in terms of open set abilities and rate ofprogress are similar.

Speech perception of implanted children 1683
Acknowledgments
The authors would like to thank the clinicians OrnaSegal, Shira Cohen and Yifaat Yaar-Sofer of thecochlear-implant team at the Sheba Medical Centerfor their contribution in the collection of the data.We would also like to thank Mrs. Eti Shabtai for thestatistical analyses.
References
[1] A. McConkey Robbins, D.B. Koch, M.J. Osberger, S. Zimmer-man-Phillips, L. Kishon-Rabin, Effect of age at cochlearimplantation on auditory skill development in infants andtoddlers, Arch. Otol. Head Neck Surg. 130 (2004) 570—574.
[2] R.C. Dowell, P.J. Blamey, G.M. Clark, Factor affecting out-come in children with cochlear implants, in: G. Clark (Ed.),Proceeding of the XVI World Congress on Cochlear Implants,Moduzzi Editore, Sydney, 1997.
[3] T.A. Meyer, M.A. Svirsky, I.K. Kirk, R.T. Miyamoto, Improve-ments in speech perception by children with profound pre-lingual hearing loss: effect of device, communication modeand chronological age, J. Speech Hear Res. 41 (1998) 846—858.
[4] M.J. Osberger, L. Fisher, SAS-CIS preference study in post-lingually deafened adults implanted with the Clarioncochlear implant, Ann. Otol. Rhinol. Laryngol. Suppl. 177(1999) 74—79.
[5] C.E. Psarros, K.L. Plant, K. Lee, J.A. Decker, L.A. Whitford,R.S. Cowan, Conversion from the SPEAK to the ACE strategyin children using the Nucleus 24 cochlear implant system:speech perception and speech production outcomes, EarHear Suppl. 23 (2002) 18—27.
[6] R.D. Battmer, D. Gnadeberg, D.J. Allum-Mecklenburg, T.Lenarz, Matched-pair comparison for adults using the Clar-ion or Nucleus Devices, Ann. Otol. Rhinol. Laryngol. Suppl.166 (1995) 251—254.
[7] A.J. Spahr, M.F. Dorman, Performance of subjects fit with theAdvanced Bionics CII and Nucleus 3G cochlear implantdevices, Arch. Otol. Head Neck Surg. 130 (2004) 624—628.
[8] R.S. Tyler, B.J. Gantz, A.J. Parkinson, G.G. Woodworth,M.W. Lowder, W.S. Parkinson, Initial comparison betweenthe Clarion, Nucleus and Ineraid Cochlear Implants, Adv.Otorhinolaryngol. 52 (1997) 274—278.
[9] R.D. Battmer, J.M. Reid, T. Lenarz, Performance in quiet andin noise with the Nucleus Spectra 22 and the Clarion CIS/CAcochlear implant devices, Scand. Audiol. 26 (1997) 240—246.
[10] M. Kompis, M. Jenk, M.W. Vischer, E. Seifert, R. Hausler,Intra-and intersubject comparison of cochlear implant sys-tems using the Esprit and the Tempo+ behind the ear speechprocessor, Int. J. Audiol. 41 (2002) 555—562.
[11] G.E. Loeb, Speech processing strategies designed for chil-dren, Otolaryngol. Head Neck Surg. 117 (1997) 170—173.
[12] T.A. Meyer, M.A. Svirsky, Speech perception by children withthe Clarion (CIS) or nucleus 22 (SPEAK) cochlear implant orhearing aids, Ann. Otol. Rhinol. Laryngol. Suppl. 185 (2000)49—51.
[13] N.M. Young, K.M. Grohne, V.N. Carrasco, C.J. Brown, Speechperception in young children using nucleus or Clarioncochlear implants: effect of communication mode, Ann.Otol. Rhinol. Suppl. 185 (2000) 77—79.
[14] P.J. Govaerts, C. De Beukelaer, K. Daemers, G. De Ceulaer,M. Yperman, T. Somers, et al. Outcome of cochlear implan-tation at different ages from 0 to 6 years, Otol. Neurotol. 23(2002) 885—890.
[15] L. Kishon-Rabin, Assessing benefit in infants with cochlearimplants, Presented at the 4th European Investigators Meet-ing, London, UK, November 20—21, 2003.
[16] R.F. Gray, S.E.M. Jones, I. Court, Cochlear implantation forprogressive hearing loss, Arch. Dis. Child 88 (2003) 708—711.




















