
The conversational skills of school-aged children with cochlear implants
13
The conversational skills of school-aged children with cochlear implants Dianne M Toe, Louise E Paatsch Faculty of Arts and Education, Deakin University, Geelong, Victoria, Australia Children with cochlear implants have been shown to have language skills on a par with children with severe hearing losses who have hearing aids. Earlier implants, bilateral implantation, and focused intervention programmes may result in some children with cochlear implants displaying similar language skills to their hearing peers. The development of pragmatic skills is central to communication competence and underpins the development of friendships. Although some studies of pragmatic skills in children with cochlear implants have been reported, most have used a contrived referential communication task rather than free conversation. Method: This study investigated the conversational skills of 20 children with cochlear implants, aged between 9 and 12 years, in free conversation with their hearing peers. The pragmatic skills of these 20 deaf/hearing pairs or dyads were compared with the pragmatic skills of 20 hearing/hearing dyads. Pragmatic skills were analysed in terms of conversational balance, conversational turn types, and conversational maintenance. The impact of the participants’ level of speech intelligibility was also investigated. Results: Children with cochlear implants tend to dominate conversations with their hearing peers. They initiated more topics, took longer turns, asked more questions, and tended to make more personal comments while their hearing friends tended to use more conversational devices and minimal answers. In contrast, pairs of matched hearing children were very balanced in all of these aspects of conversation. Speech intelligibility did not appear to impact consistently on the pragmatic skills of the children with cochlear implants but all children had a relatively high level of speech intelligibility. Discussion: Rather than being characterized by frequent conversational breakdown as in older studies, children with cochlear implants had a strong grasp of basic conversational rules. They conversed in a similar way to some deaf adults who also have been shown to take control of the conversation. Findings are discussed for their implications for intervention and future research. Keywords: Cochlear Implantation, Children, Conversational skills, Pragmatics, Language development Introduction It is well documented in the literature that hearing impairment impacts on the development of spoken language skills in children (Blamey et al., 2001a, b; Geers et al., 2003; Ibertsson, et al., 2009a). Children with hearing loss produce shorter utterances, fewer different words per minute, and less bound mor- phemes in their overall spoken language compared with their age-matched peers (Geers et al., 2003). Typically, they have smaller lexicons, acquire words at a slower rate compared with children with normal hearing of a similar age, and have delayed receptive and expressive vocabulary development (Blamey et al., 2001b; Boothroyd and Boothroyd-Turner, 2002; Svirsky et al., 2000). Improvements in cochlear implant design and speech processing strategies have provided many children with severe-to-profound, pro- found, and total hearing loss greater access to spoken language. Consequently, many of these children have developed language skills at a faster rate than children with similar degrees of hearing loss who use hearing aids and they perform similarly on language measures to children with severe hearing loss who wear hearing aids (Blamey et al., 2001b; Boothroyd and Boothroyd- Turner, 2002; Geers et al., 2003). For some children, however, despite the increase in language performance after cochlear implantation, scores for syntax, vocabu- lary, reading, and mathematical concepts and problem-solving remain significantly below those of their peers with normal hearing (Fagan et al., 2007; Paatsch et al., 2006). Such outcomes suggest that the enhanced auditory capacity provided by the implant has a positive effect on language development for implanted children, but there is still a need for language-based intervention that would enable more Correspondence to: Dr Dianne M Toe, Faculty of Arts and Education, Deakin University, Geelong, Victoria, Australia. Email: [email protected] © W. S. Maney & Son Ltd 2013 DOI 10.1179/1754762812Y.0000000002 Cochlear Implants International 2013 VOL. 14 NO. 2 67
Transcript of The conversational skills of school-aged children with cochlear implants

The conversational skills of school-agedchildren with cochlear implantsDianne M Toe, Louise E Paatsch
Faculty of Arts and Education, Deakin University, Geelong, Victoria, Australia
Children with cochlear implants have been shown to have language skills on a par with children with severehearing losses who have hearing aids. Earlier implants, bilateral implantation, and focused interventionprogrammes may result in some children with cochlear implants displaying similar language skills to theirhearing peers. The development of pragmatic skills is central to communication competence andunderpins the development of friendships. Although some studies of pragmatic skills in children withcochlear implants have been reported, most have used a contrived referential communication task ratherthan free conversation.Method: This study investigated the conversational skills of 20 children with cochlear implants, aged between9 and 12 years, in free conversation with their hearing peers. The pragmatic skills of these 20 deaf/hearingpairs or dyads were compared with the pragmatic skills of 20 hearing/hearing dyads. Pragmatic skills wereanalysed in terms of conversational balance, conversational turn types, and conversational maintenance.The impact of the participants’ level of speech intelligibility was also investigated.Results: Children with cochlear implants tend to dominate conversations with their hearing peers. Theyinitiated more topics, took longer turns, asked more questions, and tended to make more personalcomments while their hearing friends tended to use more conversational devices and minimal answers. Incontrast, pairs of matched hearing children were very balanced in all of these aspects of conversation.Speech intelligibility did not appear to impact consistently on the pragmatic skills of the children withcochlear implants but all children had a relatively high level of speech intelligibility.Discussion: Rather than being characterized by frequent conversational breakdown as in older studies,children with cochlear implants had a strong grasp of basic conversational rules. They conversed in asimilar way to some deaf adults who also have been shown to take control of the conversation. Findingsare discussed for their implications for intervention and future research.
Keywords: Cochlear Implantation, Children, Conversational skills, Pragmatics, Language development
IntroductionIt is well documented in the literature that hearingimpairment impacts on the development of spokenlanguage skills in children (Blamey et al., 2001a, b;Geers et al., 2003; Ibertsson, et al., 2009a). Childrenwith hearing loss produce shorter utterances, fewerdifferent words per minute, and less bound mor-phemes in their overall spoken language comparedwith their age-matched peers (Geers et al., 2003).Typically, they have smaller lexicons, acquire wordsat a slower rate compared with children with normalhearing of a similar age, and have delayed receptiveand expressive vocabulary development (Blameyet al., 2001b; Boothroyd and Boothroyd-Turner,2002; Svirsky et al., 2000). Improvements in cochlearimplant design and speech processing strategies have
provided many children with severe-to-profound, pro-found, and total hearing loss greater access to spokenlanguage. Consequently, many of these children havedeveloped language skills at a faster rate than childrenwith similar degrees of hearing loss who use hearingaids and they perform similarly on language measuresto children with severe hearing loss who wear hearingaids (Blamey et al., 2001b; Boothroyd and Boothroyd-Turner, 2002; Geers et al., 2003). For some children,however, despite the increase in language performanceafter cochlear implantation, scores for syntax, vocabu-lary, reading, and mathematical concepts andproblem-solving remain significantly below those oftheir peers with normal hearing (Fagan et al., 2007;Paatsch et al., 2006). Such outcomes suggest that theenhanced auditory capacity provided by the implanthas a positive effect on language development forimplanted children, but there is still a need forlanguage-based intervention that would enable more
Correspondence to: Dr Dianne M Toe, Faculty of Arts and Education,Deakin University, Geelong, Victoria, Australia. Email: [email protected]
© W. S. Maney & Son Ltd 2013DOI 10.1179/1754762812Y.0000000002 Cochlear Implants International 2013 VOL. 14 NO. 2 67

of these children to develop age-appropriate spokenlanguage skills, and to access the language of thecurriculum.Despite extensive reports in the literature of delayed
spoken language performance for children withcochlear implants, there is also evidence that somechildren do achieve age-appropriate language skills,and learn expressive and receptive language skills ata similar rate to their age-matched peers (Blameyet al., 2001b; Colletti, 2009; Fagan and Pisoni,2010). The proportion of these children who scorewithin the normal range for spoken language ishigher than that of children with similar hearing losswho use hearing aids (Geers et al., 2003). Many ofthese children use lexical diversity in their spontaneousconversation samples, and develop narrative skills andutterance length that are comparable to their age-matched hearing peers. Research suggests that post-implant spoken language development is influencedby variables such as age of implantation, hearingexperience, and age of onset (Fagan and Pisoni,2010; Geers et al., 2003).
Speech intelligibilitySpeech intelligibility is a joint product of a speaker andlistener and is often used as a way of measuring howwell an individual with hearing loss can be understoodby others (Peng et al., 2004). Wide variation in speechintelligibility ratings in children who use cochlearimplants and those who use hearing aids is well docu-mented in the literature (Ching et al., 2001; Gantzet al., 2000). For children who use cochlear implants,variables such as age of implantation, communicationmode, and years of experience with a cochlear implantcontribute to differences in speech intelligibility ratings(Blamey et al., 2001a; Uchanski and Geers, 2003).Typically, children who receive implants early, havebetter speech intelligibility (Colletti, 2009; Penget al., 2004) and levels of speech intelligibility appearto improve after 2–3 years of implant experience(Chin et al., 2003; Tobey et al., 2003). Colletti (2009)reported that children implanted between the ages of6 and 11 months had better levels of speech intelligibil-ity than those children who were implanted later, andsuggested that early implantation provides long-termcommunication benefits. In more recent years, withthe establishment of universal newborn screening pro-grammes, and advancement in technology andimproved speech-coding strategies, children withcochlear implants are developing higher levels ofspeech intelligibility than previously reported(Flipsen, 2008). For example, Peng et al. (2004) inves-tigated the speech intelligibility levels of 24 prelin-gually deaf cochlear implant users with seven yearsof implant use. Results showed that children usingcochlear implants with more advanced speech-coding
strategies had better speech intelligibility scores.Similarly, in a review of 10 studies investigating thespeech intelligibility levels of children with cochlearimplants during spontaneous conversation, Flipsen(2008) reported that the speech intelligibility is con-siderably better than has been seen historically inthese children. Some studies suggest that childrenwith cochlear implants may exhibit highly intelligiblespeech that is on par with hearing peers. Efrat et al.(2008) found that school-aged children with cochlearimplants were similar to their hearing peers in termsof speech intelligibility and general languagemeasures, but still observed significant delays in theareas of syntax, morphology, and more sophisticatedmetalinguistic skills such as knowledge of idioms.Research has also shown that there is a strong relation-ship between speech intelligibility levels and the effec-tiveness of communication during conversation.Ibertsson et al. (2009a) investigated the relationshipbetween speech recognition abilities and conversa-tional skills, as measured during a referential com-munication task, in a group of 13 children/adolescents aged between 11 and 19 years withcochlear implants. Findings showed a significantassociation between the listener’s speech recognitionabilities and the time it took for the hearing peer tocomplete the referential task (i.e. the ability of a lis-tener to select the correct picture from descriptionsgiven by the speaker). However, speech intelligibilityis only one way of measuring the effectiveness of com-munication in children with cochlear implants. Inorder to be considered a competent interpersonal com-municator, a speaker must develop a range of prag-matic skills to ensure effective communication inconversation (Jeanes et al., 2000).
Conversational skills of students with hearinglossPragmatics is often referred to as the social use oflanguage and requires the development of particularbehaviours and rules needed to use language effec-tively (Most et al., 2010). It is the aspect of languagethat incorporates syntax, semantics, morphology,and phonology within a particular social context.Typically, pragmatic skills develop within the first 8years of life through everyday conversations whereparticipants develop the role of both speaker and lis-tener (Ibertsson et al., 2009a, b; Most, 2002; Toeet al., 2007). Pragmatic skills include the ability to:take turns; select, introduce, maintain, and changetopics; seek clarification; maintain eye contact; andrespond to the partner’s utterances (Prutting andKirchner, 1987; Toe et al., 2007). Conversation is ajoint activity, which is co-constructed by both part-ners, whereby contributions rely on the ability to con-sider prior contributions and prepare contributions
Toe and Paatsch The conversational skills of school-aged children with cochlear implants
Cochlear Implants International 2013 VOL. 14 NO. 268

which follow (Ibertsson et al., 2009b). Spontaneousand informal conversation is the foundation for inter-actions and the development of peer relationships.True friendships are more likely to develop whenthere are ample opportunities for informal conversa-tions (Stinson and Foster, 2000).Much of the research which has investigated the
pragmatic skills of children and teenagers withhearing loss has measured these skills either in conver-sation with an adult or during referential communi-cation tasks (Lloyd et al., 2001, 2005; Most et al.,2010; Tye-Murray, 2003). A referential communi-cation task involves a speaker describing someone orsomething so that the listener can identify what isbeing described. This task is more structured than aspontaneous conversation but provides opportunitiesto investigate the communication skills used duringinteraction.Students with hearing loss appear to show an ability
to use some pragmatic behaviour similar to theirhearing peers (Most et al., 2010; Toe et al., 2007).However, other studies have shown that there are sig-nificant differences in the appropriate use of pragmaticskills between students with hearing loss and their age-matched peers (Ibertsson et al., 2009a). For example,Most et al. (2010) investigated the pragmatic skills of24 children aged 6–9 years who used cochlear implantsor hearing aids and found that these children used awide variety of communication functions. Somebehaviour, such as topic selection and introduction,and conversation initiation, were rated similarly totheir hearing peers. However, none of these childrenwere able to demonstrate contingency (i.e. the abilityto continue sharing the same topic as introduced bytheir partner in prior utterances) and showed moreincidents of inappropriate use of pragmatic beha-viours. Results also showed that the cochlear implantgroup had similar pragmatic skills to the childrenwith severe hearing loss who used hearing aids.Jeanes et al. (2000) reported that students aged 8, 11,14, and 17 years using spoken language and signedcommunication were able to seek general clarificationand respond to their partner’s requests. These childrenwere all hearing aid users. However, differences werereported in their use of specific requests and the appro-priateness of responses to their partner’s requests forclarification. More recently, Lloyd et al. (2005)found that a group of 20 children with hearing loss(aged 10 years) performed similarly to that of ayounger group of hearing children during a referentialcommunication task, suggesting a developmental lagin pragmatic skills.In a UK study by Lloyd et al., (2001), the pragmatic
skills of 12 children with hearing loss (mean age of 8years, 8 months) were assessed as they constructedtwo Lego models; one with a hearing peer and the
other with their specialist teacher of the deaf.Measures of the deaf children’s pragmatic skills werecompared between child-peer and child-teacherdyads. Communication skills of both the teachersand peers were analysed as communication partnersof the deaf children. Quantitative analysis includedmean length of utterance in morphemes and words,mean length of turn (MLT), number of non-verbalturns, number of unintelligible utterances, and turnendings. Conversational categories for coding turnendings included questions, personal contributions,conversational devices, minimal answers, extendedanswers, directives, and tagged contributions. Resultsshowed that the frequency of spoken utterances andturns for the deaf children was higher with the teacherscompared with their peers, suggesting that the teacherswere more successful at eliciting communication thanwere their hearing peers. However, when communicat-ing with their hearing peers, the deaf children’s turnsand utterances tended to be longer in relation to wordsand morphemes. In terms of types of turn endings,results showed that the child–teacher conversations con-tained a much higher proportion of question–answersequences compared with child–peer conversations. Incontrast, child–peer conversations contained a higherproportion of conversational devices and personal con-tributions than did the child-teacher conversations.Further results showed that the deaf children askedmore questions when in conversation with their peersthan when conversing with their teachers.
Pragmatic and conversational skills of studentswith cochlear implantsThere is paucity of research which has investigatedpragmatic skills in students with cochlear implantswhile in conversation. Moreover, there appears to beeven fewer studies which have investigated the prag-matic skills of children with cochlear implants inconversation with their hearing peers. Typically, prag-matic skills have been measured during interactionswith adults or using referential communication tasks.Research into the pragmatic skills of students with
cochlear implants shows that many of these childrenare active communicators and are able to use effectivepragmatic skills during structured and informal com-munication tasks with adults and peers. Ibertssonet al. (2009a) investigated the conversational skills of13 children/teenagers aged 11–19 years who usedcochlear implants. Conversational skills were assessedin a referential communication task with a hearingpeer. The interactions during this task were codedaccording to the number of requests for clarificationand the proportion of different types of requests forclarification asked by the participants with cochlearimplants. Speech recognition skills were also assessedto explore the relationship between speech recognition
Toe and Paatsch The conversational skills of school-aged children with cochlear implants
Cochlear Implants International 2013 VOL. 14 NO. 2 69

and requests for clarification. Results showed thatthere was a significant correlation between thenumber of requests for clarification and speech recog-nition scores, suggesting that children with cochlearimplants with better speech recognition make fewerrequests for clarification. Further findings from thisstudy revealed that only 3% of the requests for clarifi-cation were requests for elaboration, while 70% of therequests were requests for confirmation of new infor-mation, and 16% of the requests were requests foralready given information. The improved speech per-ception afforded by cochlear implants appears toimpact these pragmatic skills, resulting in a reducedneed to request clarification and improved conversa-tional fluency. Ibertsson and colleagues suggest thatthe group of cochlear implant users in their studyappeared to be active and competent communicatorswith little evidence of communication breakdown,with a comparable number of words and utterancesas their hearing peers, and few non-specific requestsfor clarification. However, one of the limitations high-lighted in this study is related to the structure of thetask. A referential communication task is more struc-tured and does not replicate conditions in which spon-taneous communication occurs, such as in freeconversation. Further research is warranted whichinvestigates the communication skills of childrenusing cochlear implants during spontaneous conversa-tion, to ascertain whether improved speech perceptionskills and language skills result in more fluent spon-taneous conversations.Research investigating pragmatic skills of children
with cochlear implants during conversation withadults has found that many children demonstrate awide variety of skills. Tye-Murray (2003) investigatedthe conversational fluency of 181 children aged 8 or9 years old during a semi-structured interview withan unfamiliar adult. Results showed that the childrenwith cochlear implants spent more time in communi-cation breakdown and more time in silence thantheir hearing peers. However, those children withcochlear implants who had better speech intelligibilityand better receptive and expressive language skills alsohad better conversational fluency. Toe et al. (2007)found that the group of students in their study (18 chil-dren aged 6–16 years) demonstrated very little conver-sational breakdown in conversation with their familiarteacher of the deaf. Differences in findings betweenthese studies may be attributed to factors such aslevels of: familiarity of the conversational partner;speech intelligibility; spoken language skills; and ageof participants.Given the importance of effective communication
with peers and the development of true friendships,clearly further research is warranted which investi-gates the pragmatic skills of children with cochlear
implants and their hearing peers. The purpose ofthis present study was to investigate the pragmaticskills of a group of primary-school aged childrenduring a less-structured communication task; a taskwhich more closely represents the type of conversa-tion which occurs between friends. Specifically, thisstudy will investigate the pragmatic skills of childrenwith cochlear implants in conversation with theirhearing peers in terms of conversational balance,conversational turn types, and conversational main-tenance. In addition, pragmatic skills occurring inthese deaf/hearing (D/H) dyads will be comparedwith the pragmatic skills of the same hearing peersin conversation with another hearing peer (hearing/hearing (H/H) dyads). This experimental designallowed for the investigation of the following researchquestions:1. What are the similarities and differences in conversa-
tional skills between children who are deaf or hearingimpaired who use cochlear implants and childrenwith normal hearing?
2. What are the similarities and differences in conversa-tional balance, conversational turn types, and con-versational maintenance between deaf–hearingdyads and hearing–hearing dyads?
MethodParticipantsSixty children (42 girls and 18 boys), aged between 9years 0 months and 12 years 4 months, participated inthis study. Twenty children had profound hearing lossand used a cochlear implant. Forty children hadnormal hearing. Participants were organized intosets of pairs, with 20 dyads comprising one childwith a cochlear implant and profound hearing lossand one child with normal hearing (D/H dyad).Twenty dyads comprised two children with normalhearing (H/H dyad). One child with normal hearingparticipated in both D/H dyad and the H/H dyad.All dyads were matched by gender and year level atschool.
Hearing levels were calculated using pure tonethresholds averaged across the three frequencies 500,1000, and 2000 Hz in the better ear. Pure-Tone-Average (PTA) figures were taken from the mostrecent pre-operative audiogram. Pre-operative audio-grams were not available for two of the children(Child 2 and Child 12) because they had beenimplanted in countries other than Australia. It wasassumed, considering their year of implantation, thatthese children would have had hearing levels of90 dB+HL. Seventeen students wore unilateralimplants. Three participants (Participants 13, 19, and20) had received a second cochlear implant withinthe last year and were participating in an auditoryhabilitation programme at their schools.
Toe and Paatsch The conversational skills of school-aged children with cochlear implants
Cochlear Implants International 2013 VOL. 14 NO. 270
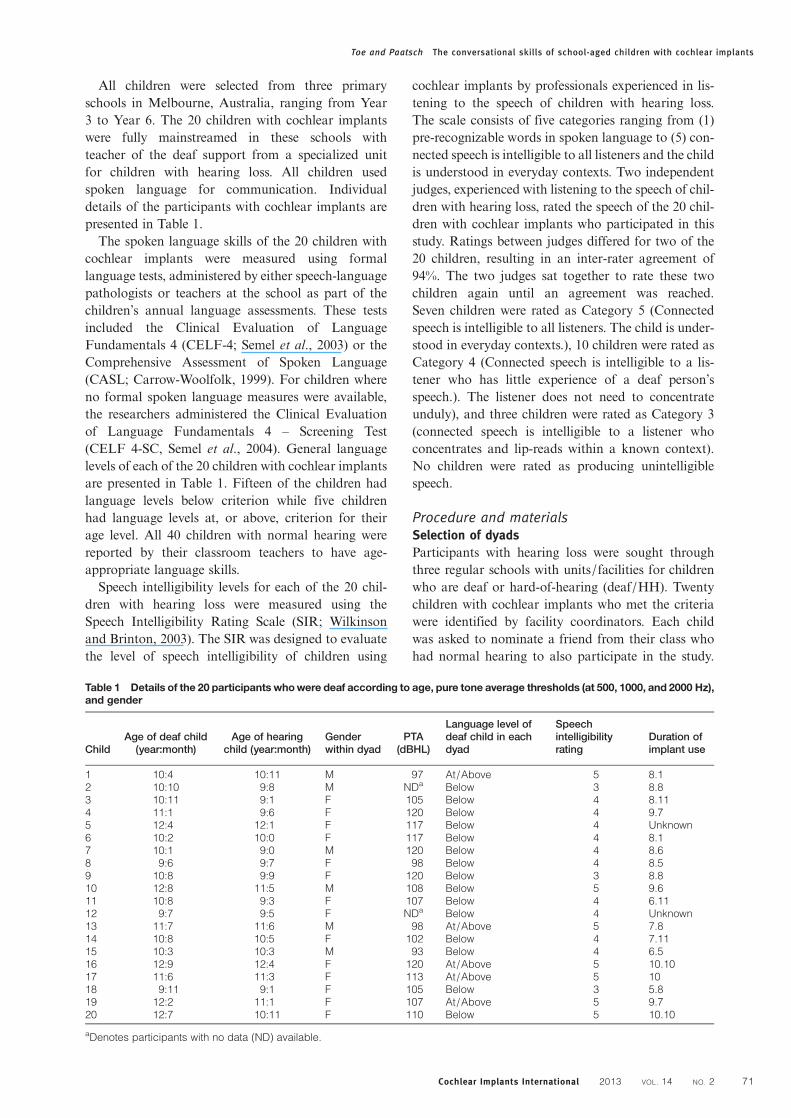
All children were selected from three primaryschools in Melbourne, Australia, ranging from Year3 to Year 6. The 20 children with cochlear implantswere fully mainstreamed in these schools withteacher of the deaf support from a specialized unitfor children with hearing loss. All children usedspoken language for communication. Individualdetails of the participants with cochlear implants arepresented in Table 1.The spoken language skills of the 20 children with
cochlear implants were measured using formallanguage tests, administered by either speech-languagepathologists or teachers at the school as part of thechildren’s annual language assessments. These testsincluded the Clinical Evaluation of LanguageFundamentals 4 (CELF-4; Semel et al., 2003) or theComprehensive Assessment of Spoken Language(CASL; Carrow-Woolfolk, 1999). For children whereno formal spoken language measures were available,the researchers administered the Clinical Evaluationof Language Fundamentals 4 – Screening Test(CELF 4-SC, Semel et al., 2004). General languagelevels of each of the 20 children with cochlear implantsare presented in Table 1. Fifteen of the children hadlanguage levels below criterion while five childrenhad language levels at, or above, criterion for theirage level. All 40 children with normal hearing werereported by their classroom teachers to have age-appropriate language skills.Speech intelligibility levels for each of the 20 chil-
dren with hearing loss were measured using theSpeech Intelligibility Rating Scale (SIR; Wilkinsonand Brinton, 2003). The SIR was designed to evaluatethe level of speech intelligibility of children using
cochlear implants by professionals experienced in lis-tening to the speech of children with hearing loss.The scale consists of five categories ranging from (1)pre-recognizable words in spoken language to (5) con-nected speech is intelligible to all listeners and the childis understood in everyday contexts. Two independentjudges, experienced with listening to the speech of chil-dren with hearing loss, rated the speech of the 20 chil-dren with cochlear implants who participated in thisstudy. Ratings between judges differed for two of the20 children, resulting in an inter-rater agreement of94%. The two judges sat together to rate these twochildren again until an agreement was reached.Seven children were rated as Category 5 (Connectedspeech is intelligible to all listeners. The child is under-stood in everyday contexts.), 10 children were rated asCategory 4 (Connected speech is intelligible to a lis-tener who has little experience of a deaf person’sspeech.). The listener does not need to concentrateunduly), and three children were rated as Category 3(connected speech is intelligible to a listener whoconcentrates and lip-reads within a known context).No children were rated as producing unintelligiblespeech.
Procedure and materialsSelection of dyadsParticipants with hearing loss were sought throughthree regular schools with units/facilities for childrenwho are deaf or hard-of-hearing (deaf/HH). Twentychildren with cochlear implants who met the criteriawere identified by facility coordinators. Each childwas asked to nominate a friend from their class whohad normal hearing to also participate in the study.
Table 1 Details of the 20 participants whowere deaf according to age, pure tone average thresholds (at 500, 1000, and 2000 Hz),and gender
ChildAge of deaf child
(year:month)Age of hearing
child (year:month)Genderwithin dyad
PTA(dBHL)
Language level ofdeaf child in eachdyad
Speechintelligibilityrating
Duration ofimplant use
1 10:4 10:11 M 97 At/Above 5 8.12 10:10 9:8 M NDa Below 3 8.83 10:11 9:1 F 105 Below 4 8.114 11:1 9:6 F 120 Below 4 9.75 12:4 12:1 F 117 Below 4 Unknown6 10:2 10:0 F 117 Below 4 8.17 10:1 9:0 M 120 Below 4 8.68 9:6 9:7 F 98 Below 4 8.59 10:8 9:9 F 120 Below 3 8.810 12:8 11:5 M 108 Below 5 9.611 10:8 9:3 F 107 Below 4 6.1112 9:7 9:5 F NDa Below 4 Unknown13 11:7 11:6 M 98 At/Above 5 7.814 10:8 10:5 F 102 Below 4 7.1115 10:3 10:3 M 93 Below 4 6.516 12:9 12:4 F 120 At/Above 5 10.1017 11:6 11:3 F 113 At/Above 5 1018 9:11 9:1 F 105 Below 3 5.819 12:2 11:1 F 107 At/Above 5 9.720 12:7 10:11 F 110 Below 5 10.10
aDenotes participants with no data (ND) available.
Toe and Paatsch The conversational skills of school-aged children with cochlear implants
Cochlear Implants International 2013 VOL. 14 NO. 2 71

This hearing friend was then also asked to nominateanother hearing friend to participate in the study.Consent was obtained from all children and theirparents.A quiet room in the school was provided for data
collection. The deaf/hearing dyad was invited tocome to the room for a spontaneous chat with eachother. Students were seated at the corner of the tableso that they could easily hear and see each other andso that they could be videotaped. A single digitalvideo camcorder on a tripod was used to video eachconversation. Each dyad was invited to converseabout any topic of interest. The following instructionswere provided by the researchers. ‘Thanks for beingpart of our study. What we’d like you to do is tohave a talk with each other about anything you like.You might want to talk about the weekend, the holi-days, things you like to do, or anything that’s happen-ing at school. There will be a video recorder switchedon so that we can have a look at your conversationslater. We will be busy doing our own work while youtalk with each other, so just ignore us. We may evenwork in the next room. If you don’t know what totalk about then there are some pictures here thatmay help you. These pictures include favouritemovies, favourite sports, pets etc’.Conversations were videotaped for 10 minutes. If
conversations continued for longer than 10 minutes,participants were interrupted by the researchers. Ifstudents became stuck, and could not think of any-thing to talk about, then some visual topic sugges-tions were available in the form of a page withwords and pictures relating to sport, favourite TVshows, and pets. These visual prompts were veryrarely required. In order to create as comfortableand naturalistic environment as possible, the research-ers ‘appeared’ to be busy with paperwork and satsome distance from the dyad. All videotaped conver-sations were later transcribed into the SALT(Systematic Analysis of Language Transcripts)program. This process was facilitated by the intelligi-ble speech of the participants.
Coding conversationsConversation turnsThe definition of conversational turn used in this studycomes from Caissie and Rockwell (1993). They definea turn as one or more utterances or non-verbal com-municative acts preceded, and followed by a changeof speaker or a pause of two or more seconds.
Conversational balanceBalanced conversations provide both conversationalpartners with the opportunity to share in the inter-action and feel equally valued. One-sided conversationmay be reported as dissatisfying and discourage
further interaction (Erber, 1996). In this study severalmeasures of conversational balance were used suchas number of turns per partner and the number ofinitiations per conversational partner. A topicinitiation was defined as any introduction of a newtopic that was unrelated to the topic of the previousturn or turns (Caissie, 2000). MLT in words per con-versational partner was calculated as the totalnumber of words in each turn divided by the numberof turns. MLT has been used in previous studies(Lloyd et al., 2001). It was calculated using theSystematic Analysis of Language Transcriptsprogram. Revisions and self-repetitions (Mazes) wereexcluded from the analysis, as were unintelligible utter-ances, singing, random vocalizations with no apparentpurpose, and speech addressed to the investigators.
Conversational turn typeA system for coding conversational turn types wasdeveloped from work by Wood and his colleagues(Wood et al., 1982; Wood and Wood, 1984) and alsoused by Lloyd et al. (2001). This system uses the turnas the unit of analysis. Each turn is coded accordingto turn type. When a turn includes more than oneturn type or ‘move’, only the turn ending or finalmove is coded. For example,
‘I really love strawberry ice-cream. What is yourfavourite ice-cream flavour?’
This example is one turn because there is no change ofspeaker and no pause of greater than two secondsbetween utterances. There are two ‘moves’. The firstis a personal contribution followed by a question. Inthis coding system, only the final move (i.e. the ques-tion) is coded as the turn type for this turn. Table 2contains the five turn types with descriptions used inthe analysis in this study.
Conversational maintenanceSeveral broad measures of conversational mainten-ance were used. These included:1. The number of topics per conversation2. The number of turns per topic3. The number of pauses between turns4. The average pause time between turns
It was hypothesized that conversations that involve asmaller number of topics suggest that conversationpartners are able to sustain a topic for longer than con-versations that involve many new topics.Consequently, the number of new topics for each con-versation was coded. In addition, the number of dyadturns for each topic was calculated. Long pausesbetween turns suggest that conversational fluency islow and conversational partners may be struggling tomaintain the flow of conversation and having diffi-culty thinking of what to say. To measure this
Toe and Paatsch The conversational skills of school-aged children with cochlear implants
Cochlear Implants International 2013 VOL. 14 NO. 272

phenomena the number of pauses of greater than 2seconds that occurred between turns were calculatedfor each dyad. Any pauses of 2 seconds or morewere tallied and an average pause time between turnswas also calculated for each dyad conversation.
ResultsConversational balanceEach conversation transcript was analysed accordingto the mean number of turns per partner, the meannumber of topic initiations, and the MLT. A compari-son of means was undertaken using T-tests for inde-pendent samples. Results are shown in Table 3.There were no significant differences found between
the two hearing children in the hearing/hearing (H/H) dyads in terms of the three measures of
conversational balance, turns, topic initiations, orMLT. This finding suggests that a very even balancewas maintained between these two conversationalpartners. In contrast, in the deaf/hearing (D/H)dyads the children with cochlear implants werefound to initiate a significantly higher percentage ofconversation topics than their hearing partners. Thechildren with cochlear implants also took significantlylonger turns as measured by the mean number ofwords per turn. There was no difference between thedeaf and hearing conversational partners in terms ofthe percentage of conversational turns. These wereevenly balanced in a similar way to the hearing/hearing dyads. These data suggest that children withcochlear implants took longer turns and initiatedmore topics, thus permitting them to take greatercontrol of these conversations.
Conversational turn typeThe transcripts of each dyad’s conversation werecoded according to turn type. Results for eachmember of the deaf/hearing dyad and hearing/hearing dyad are presented in Fig. 1. T-tests for inde-pendent samples were undertaken to compare turntypes between hearing and deaf conversational part-ners and to compare the two hearing partners.Inspection of Fig. 1 suggests that when the childrenwho were deaf/HH were conversing with a hearingpeer they asked more questions than did theirhearing partner. This finding was confirmed with aT-test for independent samples (t= 3.46, p= 0.01,df= 38). There was no significant difference betweendeaf and hearing partners for personal contributionsor extended answers, although personal contributionsapproached significance (t= 1.88, P= 0.07, d.f.= 38).When conversing with a partner who is deaf, hearingchildren used significantly more conversationaldevices (e.g. ahh, really, cool) and respond withmore minimal answers (conversational devices,t=−2.03, P= 0.05, d.f.= 38 and minimal answers,t=−2.98, P= 0.005, d.f.= 38). In contrast, the
Table 2 Conversational turn types with descriptions forcoding of conversational turns (final move)
Turn type Description with example
Question Including closed (two choice) andopen questions (Wh-type)
Example: ‘What did you do on theweekend?’
Personal contribution Comments and statementsExamples: ‘I love mango smoothies’‘I went to Dotti to buy my graduation
dress’Conversational devices Phatics
‘Yeah’, ‘OK’, ‘Oh’Filled Pauses‘Um’, ‘Like’
Minimal answers Provides an answer to a question butadds no further information
In response to the question what didyou do on the weekend
Examples: ‘Played basketball’‘Yes’, ‘No’, ‘Not much’
Extended answers Answers a question and thenprovides additional information ormakes a further contribution
Examples: ‘Was there a ride there?’‘Yes there was a rollercoaster. I goon many rollercoasters’
Other Singing, speech directed to theresearchers, incomplete utterances
Completely unintelligible utterances
Table 3 Conversational balance: means, standard deviations, and T-tests for independent samples for deaf/hearing andhearing/hearing dyads
Conversational balance
Deaf/hearing dyad Hearing/hearing dyad
Measure ofconversationalbalance
Deaf mean(SD)
Hearing 1mean (SD)
Tvalue
Pvalue d.f.
Hearing 1mean (SD)
Hearing 2mean (SD)
Tvalue
Pvalue d.f.
Mean percentage oftotal turns
49.7 (4.0) 48.9 (3.93) .647 0.52 38 50.61 (1.9) 49.45 (2.02) 1.87 0.08 38
Mean percentage oftopic initiations
59.25 (24.6) 41.25 (24.6) 2.32 0.03* 38 50.10 (23.6) 49.90 (23.6) 0.27 0.98 38
Mean length of turnin words
9.99 (3.9) 7.47 (4.13) 1.99 0.05* 38 8.56 (4.6) 9.76 (5.19) −0.772 0.46 38
*P< 0.05, **P< 0.01.
Toe and Paatsch The conversational skills of school-aged children with cochlear implants
Cochlear Implants International 2013 VOL. 14 NO. 2 73
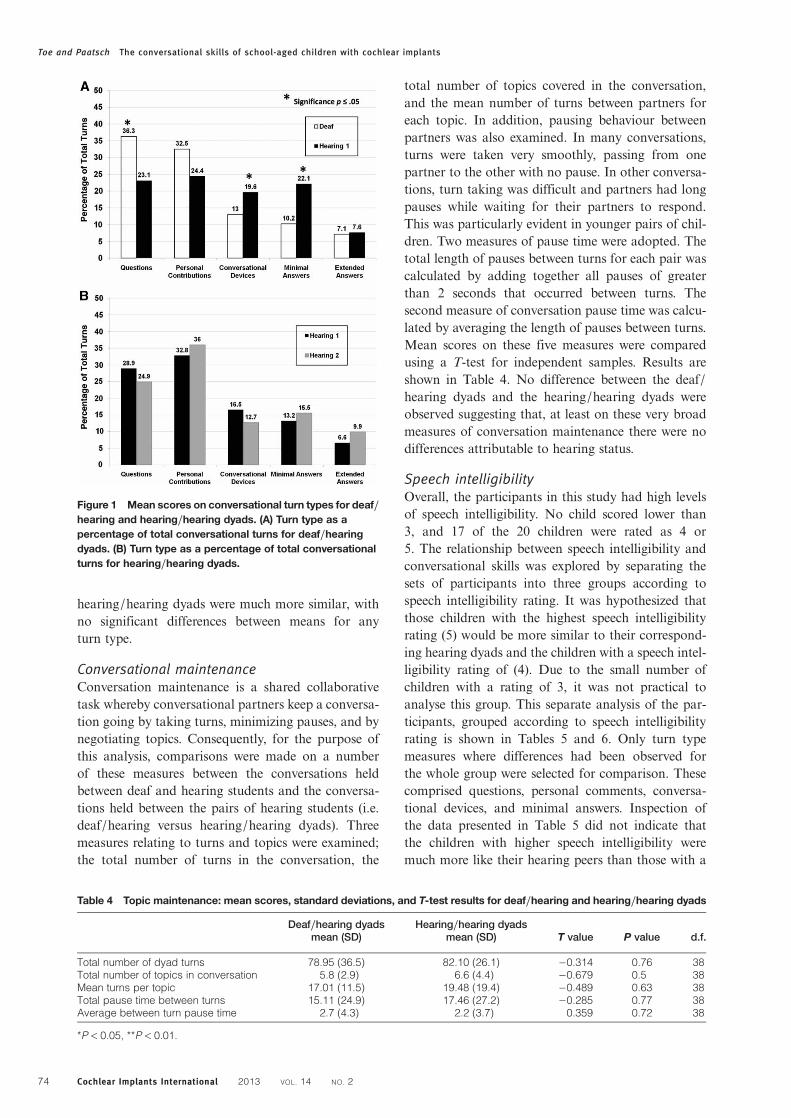
hearing/hearing dyads were much more similar, withno significant differences between means for anyturn type.
Conversational maintenanceConversation maintenance is a shared collaborativetask whereby conversational partners keep a conversa-tion going by taking turns, minimizing pauses, and bynegotiating topics. Consequently, for the purpose ofthis analysis, comparisons were made on a numberof these measures between the conversations heldbetween deaf and hearing students and the conversa-tions held between the pairs of hearing students (i.e.deaf/hearing versus hearing/hearing dyads). Threemeasures relating to turns and topics were examined;the total number of turns in the conversation, the
total number of topics covered in the conversation,and the mean number of turns between partners foreach topic. In addition, pausing behaviour betweenpartners was also examined. In many conversations,turns were taken very smoothly, passing from onepartner to the other with no pause. In other conversa-tions, turn taking was difficult and partners had longpauses while waiting for their partners to respond.This was particularly evident in younger pairs of chil-dren. Two measures of pause time were adopted. Thetotal length of pauses between turns for each pair wascalculated by adding together all pauses of greaterthan 2 seconds that occurred between turns. Thesecond measure of conversation pause time was calcu-lated by averaging the length of pauses between turns.Mean scores on these five measures were comparedusing a T-test for independent samples. Results areshown in Table 4. No difference between the deaf/hearing dyads and the hearing/hearing dyads wereobserved suggesting that, at least on these very broadmeasures of conversation maintenance there were nodifferences attributable to hearing status.
Speech intelligibilityOverall, the participants in this study had high levelsof speech intelligibility. No child scored lower than3, and 17 of the 20 children were rated as 4 or5. The relationship between speech intelligibility andconversational skills was explored by separating thesets of participants into three groups according tospeech intelligibility rating. It was hypothesized thatthose children with the highest speech intelligibilityrating (5) would be more similar to their correspond-ing hearing dyads and the children with a speech intel-ligibility rating of (4). Due to the small number ofchildren with a rating of 3, it was not practical toanalyse this group. This separate analysis of the par-ticipants, grouped according to speech intelligibilityrating is shown in Tables 5 and 6. Only turn typemeasures where differences had been observed forthe whole group were selected for comparison. Thesecomprised questions, personal comments, conversa-tional devices, and minimal answers. Inspection ofthe data presented in Table 5 did not indicate thatthe children with higher speech intelligibility weremuch more like their hearing peers than those with a
Figure 1 Mean scores on conversational turn types for deaf/hearing and hearing/hearing dyads. (A) Turn type as apercentage of total conversational turns for deaf/hearingdyads. (B) Turn type as a percentage of total conversationalturns for hearing/hearing dyads.
Table 4 Topic maintenance: mean scores, standard deviations, and T-test results for deaf/hearing and hearing/hearing dyads
Deaf/hearing dyadsmean (SD)
Hearing/hearing dyadsmean (SD) T value P value d.f.
Total number of dyad turns 78.95 (36.5) 82.10 (26.1) −0.314 0.76 38Total number of topics in conversation 5.8 (2.9) 6.6 (4.4) −0.679 0.5 38Mean turns per topic 17.01 (11.5) 19.48 (19.4) −0.489 0.63 38Total pause time between turns 15.11 (24.9) 17.46 (27.2) −0.285 0.77 38Average between turn pause time 2.7 (4.3) 2.2 (3.7) 0.359 0.72 38
*P< 0.05, **P< 0.01.
Toe and Paatsch The conversational skills of school-aged children with cochlear implants
Cochlear Implants International 2013 VOL. 14 NO. 274
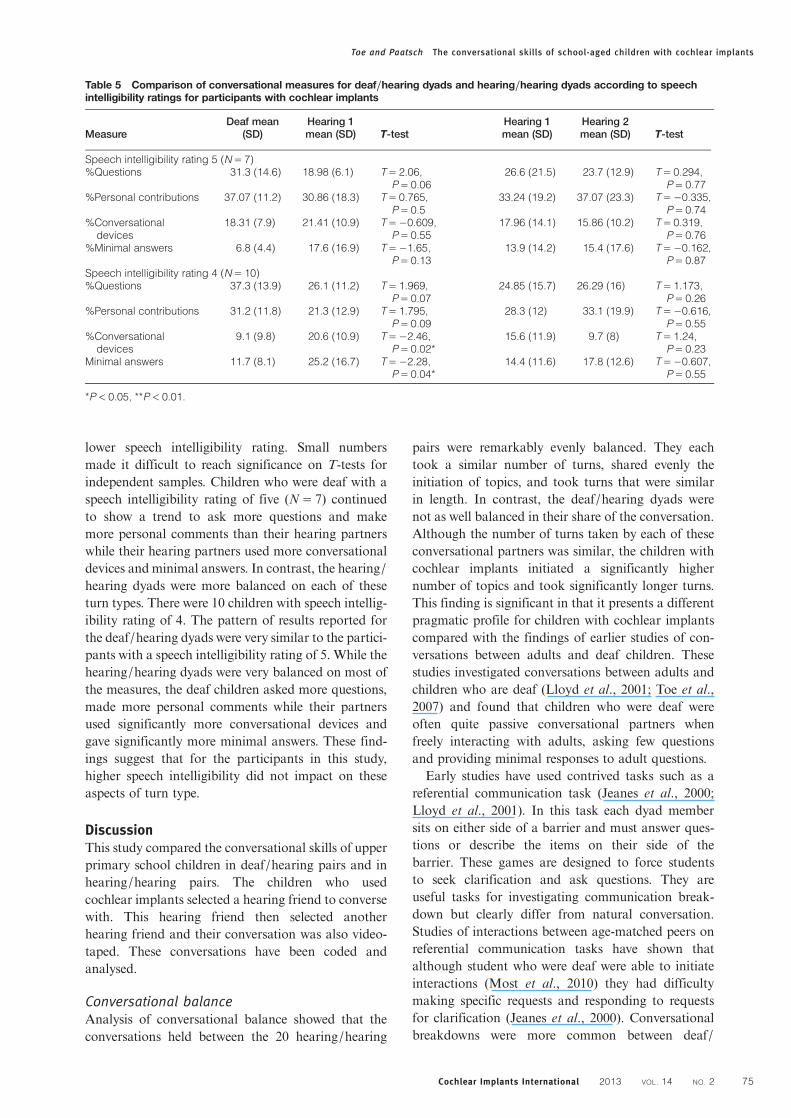
lower speech intelligibility rating. Small numbersmade it difficult to reach significance on T-tests forindependent samples. Children who were deaf with aspeech intelligibility rating of five (N= 7) continuedto show a trend to ask more questions and makemore personal comments than their hearing partnerswhile their hearing partners used more conversationaldevices and minimal answers. In contrast, the hearing/hearing dyads were more balanced on each of theseturn types. There were 10 children with speech intellig-ibility rating of 4. The pattern of results reported forthe deaf/hearing dyads were very similar to the partici-pants with a speech intelligibility rating of 5. While thehearing/hearing dyads were very balanced on most ofthe measures, the deaf children asked more questions,made more personal comments while their partnersused significantly more conversational devices andgave significantly more minimal answers. These find-ings suggest that for the participants in this study,higher speech intelligibility did not impact on theseaspects of turn type.
DiscussionThis study compared the conversational skills of upperprimary school children in deaf/hearing pairs and inhearing/hearing pairs. The children who usedcochlear implants selected a hearing friend to conversewith. This hearing friend then selected anotherhearing friend and their conversation was also video-taped. These conversations have been coded andanalysed.
Conversational balanceAnalysis of conversational balance showed that theconversations held between the 20 hearing/hearing
pairs were remarkably evenly balanced. They eachtook a similar number of turns, shared evenly theinitiation of topics, and took turns that were similarin length. In contrast, the deaf/hearing dyads werenot as well balanced in their share of the conversation.Although the number of turns taken by each of theseconversational partners was similar, the children withcochlear implants initiated a significantly highernumber of topics and took significantly longer turns.This finding is significant in that it presents a differentpragmatic profile for children with cochlear implantscompared with the findings of earlier studies of con-versations between adults and deaf children. Thesestudies investigated conversations between adults andchildren who are deaf (Lloyd et al., 2001; Toe et al.,2007) and found that children who were deaf wereoften quite passive conversational partners whenfreely interacting with adults, asking few questionsand providing minimal responses to adult questions.Early studies have used contrived tasks such as a
referential communication task (Jeanes et al., 2000;Lloyd et al., 2001). In this task each dyad membersits on either side of a barrier and must answer ques-tions or describe the items on their side of thebarrier. These games are designed to force studentsto seek clarification and ask questions. They areuseful tasks for investigating communication break-down but clearly differ from natural conversation.Studies of interactions between age-matched peers onreferential communication tasks have shown thatalthough student who were deaf were able to initiateinteractions (Most et al., 2010) they had difficultymaking specific requests and responding to requestsfor clarification (Jeanes et al., 2000). Conversationalbreakdowns were more common between deaf/
Table 5 Comparison of conversational measures for deaf/hearing dyads and hearing/hearing dyads according to speechintelligibility ratings for participants with cochlear implants
MeasureDeaf mean
(SD)Hearing 1mean (SD) T-test
Hearing 1mean (SD)
Hearing 2mean (SD) T-test
Speech intelligibility rating 5 (N= 7)%Questions 31.3 (14.6) 18.98 (6.1) T= 2.06,
P= 0.0626.6 (21.5) 23.7 (12.9) T= 0.294,
P= 0.77%Personal contributions 37.07 (11.2) 30.86 (18.3) T= 0.765,
P= 0.533.24 (19.2) 37.07 (23.3) T=−0.335,
P= 0.74%Conversational
devices18.31 (7.9) 21.41 (10.9) T=−0.609,
P= 0.5517.96 (14.1) 15.86 (10.2) T= 0.319,
P= 0.76%Minimal answers 6.8 (4.4) 17.6 (16.9) T=−1.65,
P= 0.1313.9 (14.2) 15.4 (17.6) T=−0.162,
P= 0.87Speech intelligibility rating 4 (N= 10)%Questions 37.3 (13.9) 26.1 (11.2) T= 1.969,
P= 0.0724.85 (15.7) 26.29 (16) T= 1.173,
P= 0.26%Personal contributions 31.2 (11.8) 21.3 (12.9) T= 1.795,
P= 0.0928.3 (12) 33.1 (19.9) T=−0.616,
P= 0.55%Conversational
devices9.1 (9.8) 20.6 (10.9) T=−2.46,
P= 0.02*15.6 (11.9) 9.7 (8) T= 1.24,
P= 0.23Minimal answers 11.7 (8.1) 25.2 (16.7) T=−2.28,
P= 0.04*14.4 (11.6) 17.8 (12.6) T=−0.607,
P= 0.55
*P< 0.05, **P< 0.01.
Toe and Paatsch The conversational skills of school-aged children with cochlear implants
Cochlear Implants International 2013 VOL. 14 NO. 2 75
hearing than hearing/hearing dyads (Tye-Murray,2003). In contrast, recent studies using referential com-munications tasks with children with cochlearimplants have shown that these children are activeand competent communicators with few communi-cation breakdowns, a wide repertoire of language,and few non-specific requests for clarification(Ibertsson et al., 2009a). There have been no studiesreported that have compared spontaneous conversa-tion between a deaf and hearing peer with conversa-tions between two hearing peers. However, the
findings of the present study have some similaritiesto research conducted with deaf adults and theirhearing conversational partners (Tye-Murray andWitt, 1996). Caissie et al. (1998) compared videotapedconversations between adults with hearing loss and ahearing partner with conversations held between twohearing adults. They found that in the deaf/hearingdyads the deaf adults tended to dominate the conversa-tion by taking longer turns and initiating more topics.Deaf adults with cochlear implants use a similar strat-egy, thus ensuring, presumably, that they were less at
Table 6 Conversational transcripts between hearing/deaf dyad and hearing/hearing dyad
Conversational transcripts
Transcript of conversation between a deaf child with a cochlear implant (d) and a hearing child (1)Girls in Year 6 (Context: lead up to Year 6 graduation)(<> indicates overlap between speakers)1 I’m going to get new ones to go with my dressd have you bought it yet?1 nupd what colour are you going to get?1 a dress?d yeah, what colour?1 I don’t know1 I haven’t found anything nice yetd no because I saw this really cool dress in this pattern book that might be at my mum’s work, and it’s (um) it’s like (um) it goes it’s
poofy, out the back, (it’s like poofy,) and then it’s got a bow there {indicates side}>1 does it have like (that) that material that goes on the tutu/s?d (yeah, no no, what, yeah,) yeah1 yeah, <what colour is it>?d <(it) and it poofs out>d in the book it was orange1 <orange>?d <except> no it looked really coold except (um) I’m going to get a different colourd I don’t like the orange1 are you allowed to get black?d {nods} no, wait, my mum just like oh if you really want to get black then get black but I’m like, I’m getting black1 that’s good1 are you going to get your hair done by a hairdresser, person?d I might get it curled except I don’t know if I should1 you would look okay with curls
Girls in Year 6 (Context just before graduation)NB: Hearing (1) is the same child in both conversations(<> indicates overlap between speakers)1 we have school2 yeah (um) I forgot1 at five, at about four_thirty or something, th.2 yeah I know1 we’re not going to have much time to get ourself ready2 oh yeah, that’s like really weird but we just bring our dress over and stuff, and <get changed>1 <what about our> hair, are you going to get yours done at a hairdresser?2 yeah2 (I want) my mum says to get them done a few day/s earlier, so yeah1 yeah but I’m going to get mine styled on the day and then I’m going to put make up and then I’ll bring my dress to Jess’s or
something2 what you should do is, that you should like go in the middle of the day of the school and then come back with your hair done, on
the day1 oh yeah maybe2 like could you leave it early and then <come back>1 <but the> thing is we have half an hour for a disco2 (oh I wonder was that half), oh no we have an hour and a half for (the not) the school disco but only (a) half an hour for this1 are you going to the school disco?2 (um) I might be, I don’t know what to wear though1 yeah, me neither2 because normally it depends what you wear because (you) you always like wear Roxy stuff so I don’t know what to wear {laughs}1 I might wear, I don’t know what I’ll wear because I have really bad clothes
Toe and Paatsch The conversational skills of school-aged children with cochlear implants
Cochlear Implants International 2013 VOL. 14 NO. 276

risk for misunderstandings and for communicationbreakdown (Tye-Murray and Witt, 1996). Similarly,in the present study, children with cochlear implantstended to take control of the conversation by initiatingmore topics and taking longer turns. This findingsuggests that rather than being passive conversational-ists, as reported in early studies, children with cochlearimplants are actively using their pragmatic skills totheir advantage.
Conversational turn typeThe present study adapted the turn type codingscheme used by Lloyd et al. (2001) to explore therange of turn types used in spontaneous conversationsbetween deaf and hearing pairs, and hearing/hearingpairs. Results showed that the children with cochlearimplants used the range of turn types including ques-tions, personal contributions, conversational devices,extend answers, and minimal answers. Comparisonsbetween the dyads showed some interesting and stat-istically significant patterns. Children with cochlearimplants asked significantly more questions andmade more personal contributions than did theirhearing partners. These hearing partners used signifi-cantly more conversational devices (e.g. phatics, suchas Oh, really, cool, etc.) and tended to respond witha higher proportion of minimal answers. Both partnersused a very similar number of extended responseswhich made up less than 10% of the total number ofturn types. In contrast, the hearing pairs were verybalanced. Each partner used a similar number of ques-tions, personal contributions, conversational devicesand minimal answers. Although these findings showthat children with cochlear implants were competentcommunicators with the range of turn types withintheir repertoire, they also demonstrate that childrenwith cochlear implants tended to take control of theconversations by asking questions and offering morestatements or personal contributions. These resultssuggest these children were doing more of the workin their conversation while their hearing partnersresponded with minimal answers and supporting con-versational devices. This suggests that their hearingpartners might have adopted a more passive rolewhen conversing with their deaf friends. A similarobservation has been made by Caissie et al. (1998) intheir work with adults who are deaf. Hearing adultsin their studies tended to alter their conversationalapproach when conversing with a deaf partner. Thisfinding also raises some questions about the qualityof friendship between the pairs. Although they wereself-selected it was not possible to test the level ordepth of friendship. It is possible that the hearingpairs were more closely aligned and hence the conver-sational space more evenly shared.
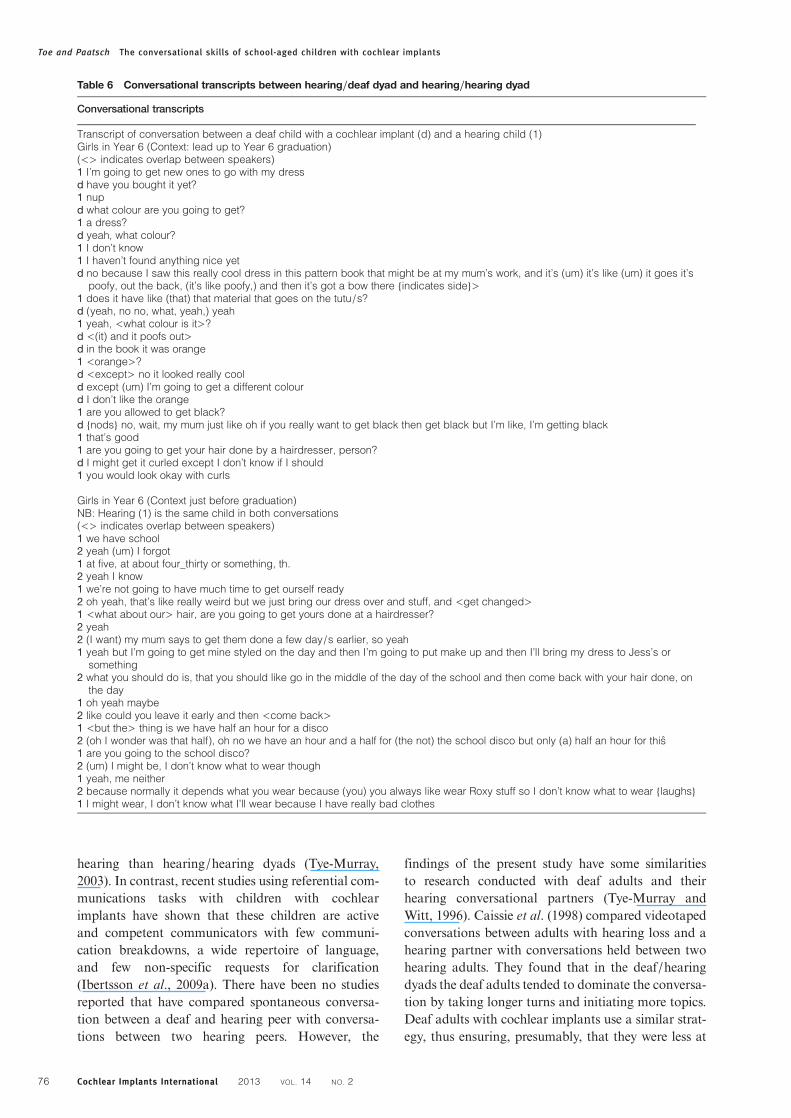
These data may also indicate some more subtleaspects of conversational skills that were not asevident in the pairs of deaf/hearing children. Askingmore questions and receiving more minimal responsessuggest that these conversations may have been a littleone sided. Contingency is a key factor in conversa-tional fluency and satisfaction (Erber, 1996). This isoften seen in the third turn whereby a conversationalpartner follows up on a question or response byexpanding or returning to the topic previouslyinitiated. Contingent conversations flow well andprovide even exchanges of shared information. Thetwo conversations, taken from the present study andshown in Table 6, suggest that there were manysubtle differences in contingency between the deaf/hearing and hearing/hearing pairs.A comparison of these two transcripts provides
some clues into some of the subtle differencesbetween the deaf/hearing dyad and the same hearingchild conversing with another hearing friend. In thedeaf/hearing dyad, the transcript reads more like aninterview, with the child with the cochlear implanttaking longer turns and keeping the topic focusedupon her choice of dress. In the second transcript thetwo hearing girls move freely back and forth on thetopic of where and when to get dressed for graduation.The topic is shared and continually renegotiated,picking up threads from previous turns as it developsthe ideas, almost as one stream of consciousness. Forexample, girl (1) commences with ‘we have school’ fol-lowed by 2 ‘Yeah I forgot’ Girl 1 then contributes ‘atfive, at about four -thirty or something’, appearingto finish her previous sentence. Further analysis isrequired to explore the issue of contingency andwhere and why it appears to be missing from the con-versations held between the children with cochlearimplants and their partners. This finding is consistentwith the work of Most et al. (2010) who found littlecontingency in the conversations between childrenwho were deaf compared to hearing children.
Conversational maintenanceConversational partners use their pragmatic skills tomaintain a conversation by taking turns, initiating ormaintaining topics, and minimizing pausing betweenturns. In this study, three broad measures of conversa-tional maintenance were investigated. The deaf/hearing dyads were compared to the hearing/hearingdyads on three measures, the total number of turnsin the conversation, the total number of topicscovered, and the mean number and length of pausesbetween turns. There was no significant differenceobserved on any of these measures for the deaf/hearing and hearing/hearing dyads. Observation ofthe data suggests that younger children (Grade 3 and4) did tend to take longer pauses between turns,
Toe and Paatsch The conversational skills of school-aged children with cochlear implants
Cochlear Implants International 2013 VOL. 14 NO. 2 77

presumably because they were less sophisticated con-versationalists, but this was evident in both deaf/hearing and hearing/hearing pairs and hence wasnot analysed for the purpose of this paper.
Speech intelligibilitySeveral recent studies have found a link between speechintelligibility and conversational skills in children withcochlear implants.Tye-Murray (2003) showed that chil-dren with cochlear implants with better speech intellig-ibility conversed more fluently than those with poorerspeech intelligibility. Similarly, Ibertsson et al. (2009a)linked more intelligible speech with better pragmaticskills in children with cochlear implants. Childrenrated as having speech intelligible to all listeners werecompared to the students rated as having speech thatwas intelligible to listeners who have had little experi-ence with deaf people’s speech on the measures ofTurn Type that had emerged as differentiating thedeaf/hearing and hearing/hearing dyads such as,number of questions, conversational devices, andminimal answers. Most of the children in the presentstudy had highly intelligible speech. It was hypoth-esized that the dyads with participants with more intel-ligible speech would be more similar to the hearing/hearing dyads than those with less intelligible speech.No such differences were observed. It is likely that, inthe present study, the overall high level of speech intel-ligibility and the small number of participants made itdifficult to observe any differences between groups.This study has found some interesting patterns in the
pragmatic skills of childrenwith cochlear implants con-versingwith hearing partners. These upper primary stu-dents displayed a wide range of turn types and wereequally skilful in maintaining a conversation whencompared to their hearing pairs. Rather than passiveconversationalists, the children with cochlear implantsin this study operated more like adults with hearingloss by taking control of conversations through themechanisms of longer turns and more topic initiations.Their hearing partner appeared to become morepassive, using more conversational devices and moreminimal turns as compared to when they conversedwith a hearing partner. It is unclear whether thisresponse is adaptive or avoidant, and requires furtherinvestigation. In addition, further analysis is requiredto explore the complex issue of contingency.Anecdotal differences between dyads require newapproaches to analysis to reveal subtle differences inpragmatic skills. This study has confirmed that childrenwith cochlear implants are able to make significantdevelopments in a wide range of language skills.
ConclusionThis study has shown that school-aged children withcochlear implants have a range of pragmatic skills
that enabled them to conduct fluent conversationswith hearing friends. In contrast to older studies,these interactions were not characterized by frequentbreakdowns but flowed smoothly with similarnumbers of turns, topics, and pauses to pairs ofhearing children. Pairs of hearing children werefound to engage in very even or balanced conversa-tional exchanges; however, the children with cochlearimplants appeared to take a more dominant role,asking more questions, initiating more topics, andtaking longer turns than their self-selected hearingfriend. Their hearing partners appeared to take amore passive role in the conversation, using more con-versational devices and minimal answers. This patternwas quite similar to those seen in previous researchwith hearing impaired adults. It suggests that theseupper primary school children have a range of effectivepragmatic skills but have also developed some survivalstrategies to make sure that they can maintain a con-versation. These strategies may not be productivelong-term strategies for developing strong friendships.Inspection of a sample transcript highlighted reducedcontingency in the conversations between childrenwith cochlear implants and their hearing peers.Further analysis of these data is required, in order toexplore the issue of contingency and to find ways tosupport children with cochlear implants to developmore contingent conversation behaviours. Hearingchildren may also need support from teachers to takea more active role in conversation with their deafpeers. Teachers of the deaf and regular classroom tea-chers can support further development of pragmaticskills by encouraging students with cochlear implantsto share the conversational space more evenly withtheir peers. These students require specific supportstrategies to help them fine tune their pragmaticskills and to develop greater sensitivity towards theirconversational partners.
AcknowledgementThe authors would like to acknowledge DeafnessFoundation (Victoria) for their generous financialsupport for this study. They are also very grateful tothe children who participated in this study with suchenthusiasm.
ReferencesBlamey P.J., Barry J.G., Bow C.P., Sarant J.Z., Paatsch L.E., Wales
R.J. 2001a. The development of speech production followingcochlear implantation. Clinical Linguistics and Phonetics,15(5): 363–382.
Blamey P.J., Sarant J.Z., Paatsch L.E., Barry J.G., Bow C.P., WalesR.J., et al. 2001b. Relationships among speech perception, pro-duction, language, hearing loss, and age in children withimpaired hearing. Journal of Speech, Language, and HearingResearch, 44: 264–285.
Boothroyd A., Boothroyd-Turner D. 2002. Postimplantation audi-tion and educational attainment in children with prelinguallyacquired profound deafness. Annals of Otology, Rhinology,and Laryngology, 111(5): 79–84.
Toe and Paatsch The conversational skills of school-aged children with cochlear implants
Cochlear Implants International 2013 VOL. 14 NO. 278
Caissie R. 2000. Conversational topic shifting and its effect on com-munication breakdown for individuals with hearing loss. VoltaReview, 102: 45–56.
Caissie R., Rockwell E. 1993. A videotape analysis procedure forassessing conversational fluency in hearing-impaired adults.Ear and Hearing, 14: 202–209.
Caissie R., Dawe A.L., Donovan C., Brooks H., MacDonald S.M.1998. Conversational performance of adults with a hearingloss. Journal of the Academy of Rehabilitative Audiology, 31:45–46.
Carrow-Woolfolk E. 1999. Comprehensive Assessment of SpokenLanguage (CASL). MN: American Guidance Service, CirclePines.
Chin S.B., Tsai P.L., Gao S. 2003. Connected speech intelligibility ofchildren with cochlear implants and children with normalhearing. American Journal of Speech-Language Pathology, 12:440–451.
Ching T.Y.C., Psarros C., Incerti P., Hill M. 2001. Management ofchildren using cochlear implants and hearing aids. VoltaReview, 103(1): 39–57.
Colletti L. 2009. Long-term follow-up of infants (4–11months)fitted with cochlear implants. Acta Oto-Laryngologica, 129:361–366.
Efrat A., Schorr F., Roth N.A., Fox A. 2008. Comparison of speechand language skills of children with cochlear implants and chil-dren with normal hearing. Communication Disorders Quarterly,29: 195–210.
Erber N. 1996. Communication Therapy for Adults with SensoryLoss. 2nd edn. Victoria, Australia: Clavis Publishing.
Fagan M.K., Pisoni D.B. 2010. Hearing experience and receptivevocabulary development in deaf children with cochlearimplants. Journal of Deaf Studies and Deaf Education, 15(2):149–161.
Fagan M.K., Pisoni D.B., Horn D.L., Dillon C.M. 2007.Neuropsychological correlates of vocabulary, reading, andworking memory in deaf children with cochlear implants.Journal of Deaf Studies and Deaf Education, 12: 461–471.
Flipsen P. 2008. Intelligibility of spontaneous conversational speechproduced by children with cochlear implants: a review.International Journal of Pediatric Otorhinolaryngology, 72:559–564.
Gantz B.J., Rubinstein J.T., Tyler R.S., Teagle H.F.B., Cohen N.L.,Waltzman S.B., et al. 2000. Long-term results of cochlearimplants in children with residual hearing. Annals ofOtology, Rhinology and Laryngology, 109(12 Part 2 Suppl.185): 33–36.
Geers A.E., Nicholas J.G., Sedey A.L. 2003. Language skills of chil-dren with early cochlear implantation. Ear and Hearing, 24(1Suppl.): 46S–58S.
Ibertsson T., Hansson K., Asker-Arnason L., Sahlen B. 2009a.Speech recognition, working memory and conversation in chil-dren with cochlear implants. Deafness and EducationInternational, 11(3): 132–151.
Ibertsson T., Hansson K., Maki-Torkko E., Willstedt-Svensson U.,Sahlen B. 2009b. Deaf teenagers with cochlear implants in con-versation with hearing peers. International Journal of Languageand Communication Disorders, 44(3): 319–337.
Jeanes R.C., Nienhuys T.G., Rickards F.W. 2000. The pragmaticskills of profoundly deaf children. Journal of Deaf Studies andDeaf Education, 5: 3, 237–247.
Lloyd J., Lieven E., Arnold P. 2001. Oral conversations betweenhearing-impaired children and their normally hearing peersand teachers. First Language, 21: 83–107.
Lloyd J., Lieven E., Arnold P. 2005. The oral referential communi-cation skills of hearing-impaired children. Deafness andEducation International, 7(1): 22–42.
Most T. 2002. The use of repair strategies by children with andwithout hearing impairment. Language, Speech, and HearingServices in Schools, 33: 112–123.
Most T., Shinga-August E., Meilijson S. 2010. Pragmatic abilities ofchildren with hearing loss using cochlear implants and hearingaids compared to hearing children. Journal of Deaf Studies andDeaf Education, 15(4): 422–437.
Paatsch L.E., Blamey P.J., Sarant J.Z., Bow C.P. 2006. The effects ofspeech production and vocabulary training on different com-ponents of spoken language performance. Journal of DeafStudies & Deaf Education, 11(1): 39–55.
Peng S., Spencer L., Tomblin J.B. 2004. Speech intelligibility of pedi-atric cochlear implant recipients with 7 years of device experi-ence. Journal of Speech, Language, and Hearing Research, 47:1227–1236.
Prutting C.A., Kirchner D.M. 1987. A clinical appraisal of the prag-matic aspects of language. Journal of Speech and HearingDisorders, 52: 105–119.
Semel E., Wiig E.H., Secord W.A. 2003. Clinical Evaluation ofLanguage Fundamentals (CELF-4). 4th edn. Toronto,Canada: The Psychological Corporation/A HarcourtAssessment Company.
Semel E., Wiig E.H., Secord W.A. 2004. Clinical Evaluation ofLanguage Fundamentals Screening Test (CELF-4 ScreeningTest). 4th edn. Toronto, Canada: The PsychologicalCorporation/A Harcourt Assessment Company.
Stinson M.S., Foster S. 2000. Socialization of deaf children andyouths in school. In: Spencer P.E., Erting C.J., Marschark M.(eds) The Deaf Child in the Family and at School,pp. 191–209. Mahwah, NJ: Lawrence Erlbaum.
Svirsky M., Robbins A.M., Kirk K.I., Pisoni D.B., Miyamoto R.T.2000. Language development in profoundly deaf children withcochlear implants. Psychological Science, 11(2): 153–158.
Tobey E.A., Geers A.E., Brenner C., Altuna D., Gabbert G. 2003.Factors associated with development of speech productionskills in children implanted by age five. Ear and Hearing, 24(1Suppl.): 36S–45S.
Toe D., Beattie R., Barr M. 2007. The development of pragmaticskills in children who are severely and profoundly deaf.Deafness and Educational International, 9(2): 101–117.
Tye-Murray N. 2003. Conversational fluency of children who usecochlear implants. Ear and Hearing, 24(1S): 82S–89S.
Tye-Murray N., Witt S. 1996. Conversational moves and conversa-tional styles of adults cochlear implant users. Journal of theAcademy of Rehabilitative Audiology, 29: 11–25.
Uchanski R.M., Geers A.E. 2003. Acoustic characteristics of thespeech of young cochlear implant users: a comparison withnormal-hearing age-mates. Ear and Hearing, 24(1S):p90S–105S.
Wilkinson A., Brinton J. 2003. Speech intelligibility rating ofcochlear implant children: inter-rater reliability. CochlearImplant International, 4(1): 22–30.
Wood H.A., Wood D.J. 1984. An experimental evaluation of theeffects of five styles of teacher conversation on the languageof hearing-impaired children. Journal of Child Psychology,Psychiatry, and Allied Disciplines, 25: 45–62.
Wood D.J., Wood H.A., Griffiths A.J., Howarth S.P., Howarth C.I.1982. The structure of conversations with 6- to 10-year-old deafchildren. Journal of Child Psychology, Psychiatry, and AlliedDisciplines, 23: 295–308.
Toe and Paatsch The conversational skills of school-aged children with cochlear implants
Cochlear Implants International 2013 VOL. 14 NO. 2 79




















