Spectral processing technique based on feature selection and artificial neural networks for...
8
http://www.jclinpharm.org Pharmacology The Journal of Clinical 1999; 39; 366 J. Clin. Pharmacol. A el-Yazigi, S Shabib, S al-Rawithi, A Yusuf, ES Legayada and A al-Humidan with hepatocellular diseases Salivary clearance and urinary metabolic pattern of caffeine in healthy children and in pediatric patients http://www.jclinpharm.org/cgi/content/abstract/39/4/366 The online version of this article can be found at: Published by: http://www.sagepublications.com On behalf of: American College of Clinical Pharmacology can be found at: The Journal of Clinical Pharmacology Additional services and information for http://www.jclinpharm.org/cgi/alerts Email Alerts: http://www.jclinpharm.org/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: © 1999 American College of Clinical Pharmacology. All rights reserved. Not for commercial use or unauthorized distribution. at King Abdulaziz City for on April 11, 2008 http://www.jclinpharm.org Downloaded from
Transcript of Spectral processing technique based on feature selection and artificial neural networks for...
http://www.jclinpharm.orgPharmacology
The Journal of Clinical
1999; 39; 366 J. Clin. Pharmacol.A el-Yazigi, S Shabib, S al-Rawithi, A Yusuf, ES Legayada and A al-Humidan
with hepatocellular diseasesSalivary clearance and urinary metabolic pattern of caffeine in healthy children and in pediatric patients
http://www.jclinpharm.org/cgi/content/abstract/39/4/366 The online version of this article can be found at:
Published by:
http://www.sagepublications.com
On behalf of: American College of Clinical Pharmacology
can be found at:The Journal of Clinical Pharmacology Additional services and information for
http://www.jclinpharm.org/cgi/alerts Email Alerts:
http://www.jclinpharm.org/subscriptions Subscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
© 1999 American College of Clinical Pharmacology. All rights reserved. Not for commercial use or unauthorized distribution. at King Abdulaziz City for on April 11, 2008 http://www.jclinpharm.orgDownloaded from

EL- YAZIGI ET ALSALI VARY CLEAR ANCE AND META BOLIC PAT TERN OF CAF FEINEPE DI AT RICS
Sali vary Clear ance and Uri nary Meta bolic Pat tern of Caf feine in Healthy Chil dren and inPe di at ric Pa tients with He pa to cel lu lar Dis eases
Ad nan El- Yazigi, Souheil Shabib, Sa meer Al- Rawithi, PhD, Ah med Yusuf,Er linda S. Le gay ada, and Ab dul karim Al- Humidan
Con ven tional hepatic func tion tests such as themeas ure ment of serum lev els of endoge nous trac -
ers such as albu min, clot ting fac tors, bile acids, andvari ous enzymes are of lim ited value for assess inghepatic dys func tion since they reflect increased hepa -to cel lu lar per me abil ity rather than func tional capac -ity. Efforts have been inten si fied in recent years for thedevel op ment of tests that quan tify hepatic func tion byinves ti gat ing the metabo lism of model drugs. Caf feineis exten sively con sumed in bev er ages and food and is,reput edly, the world’s most widely con sumed drug.1,2
Owing to desir able phar ma coki netic and meta bolicchar ac ter is tics,3-8 caf feine has recently found a role asa probe for hepatic func tion assess ment. It pro vides anesti mate of the func tional reserve capac ity of the liver.Caf feine is com pletely and rap idly absorbed fol low ingoral inges tion9 and is con sid ered an “ideal com pound”for this inves ti ga tion since its admini stra tion as a sin -gle oral dose dur ing a clear ance test is asso ci ated withno tox ic ity in humans.6
As depicted in Fig ure 1, caf feine (1,3,7-tri-methylxanthine, 137X) under goes oxi da tive demeth y -la tion and hydroxy la tion to form a number of uri narymetabo lites, includ ing 1,3,7-trimethyluric acid(137U), 1,3-dimethylxanthine (theo phyl line or 13X),3,7-dimethylxanthine (theo bro mine or 37X),1,7-dimethylxanthine (par ax an thine or 17X),1,3-dimethyluric acid (13U), 1,7-dimethyluric acid(17U), 3,7-dimethyluric acid (37U), 1-methylxanthine(1X), 3-methylxanthine (3X), 7-methylxanthine (7X),
366 • J Clin Phar ma col 1999;39:366-372
From the Phar ma coki net ics Labo ra tory, Depart ment of Bio logi cal andMedi cal Research (El- Yazigi, Al- Rawithi, Yusuf, Legay ada, Al- Humidan)and Pedi at ric Gas tro en ter ol ogy (Shabib), Depart ment of Pedi at rics, KingFaisal Spe cial ist Hos pi tal and Research Cen tre, Riyadh, Saudi Ara bia. Sub -mit ted for pub li ca tion June 5, 1998; revised ver sion accepted Novem ber22, 1998. Address for reprints: Dr. Adnan El- Yazigi, FCP, Phar ma coki net icsLabo ra tory, King Faisal Spe cial ist Hos pi tal and Research Cen tre, P.O. Box3354, Riyadh 11211, Saudi Ara bia.
Meas ure ment of sali vary clear ance and uri nary metabo litesof caf feine is an excel lent non in va sive tool for assess ing liverfunc tion, par ticu larly the activ ity of cyto chrome P4501A2(CYP1A2), N-acetyltransferase (NAT), and xan thine oxi dase(XO). This study was under taken to meas ure the clear ance ofcaf feine using saliva as a bio logi cal fluid and to assess theactivi ties of the above- mentioned enzymes in healthy chil dren and pedi at ric patients with liver dis eases using uri nary molarratios of dif fer ent caf feine metabo lites. The well- establishedtwo- sample saliva approach was used to meas ure the clear -ance of caf feine in nine pedi at ric patients with liver dis eases(LD) and in nine healthy chil dren. The caf feine metabo liteswere also meas ured in the urine of these sub jects by high- performance liq uid chro ma tog ra phy, and uri nary molarratios of 5-acetylamino- 6- formylamino- 3- methyluracil(AFMU), 1-methylxanthine (1X), 1-methyluric acid (1U), and
1,7-dimethyluric acid (17U) were employed to esti mate theactivi ties of CYP1A2, NAT, and XO. The caf feine sali vary clear -ance and the per cent age of the dose excreted in the form ofvari ous metabo lites were sig nifi cantly (p < 0.035) smaller inthe LD patients than those in healthy chil dren. The uri narymolar ratio of [AFMU + 1U + 1X]/17U, which reflects theactiv ity of CYP1A2, was also sig nifi cantly (p < 0.0005)reduced in these patients. How ever, there were no sig nifi cantdif fer ences between the two groups in the ratios of AFMU/1Xand 1U/1X, which esti mate the activi ties of NAT and XO,respec tively. In con clu sion, the data obtained sug gest thatliver dis ease in pedi at ric sub jects sig nifi cantly reduces thesali vary clear ance of caf feine and the activ ity of cyto chromeP4501A2, but it has no impact on the activi ties of NAT and XO.
Jour nal of Clini cal Phar ma col ogy, 1999;39:366-372©1999 the Ameri can Col lege of Clini cal Phar ma col ogy
© 1999 American College of Clinical Pharmacology. All rights reserved. Not for commercial use or unauthorized distribution. at King Abdulaziz City for on April 11, 2008 http://www.jclinpharm.orgDownloaded from
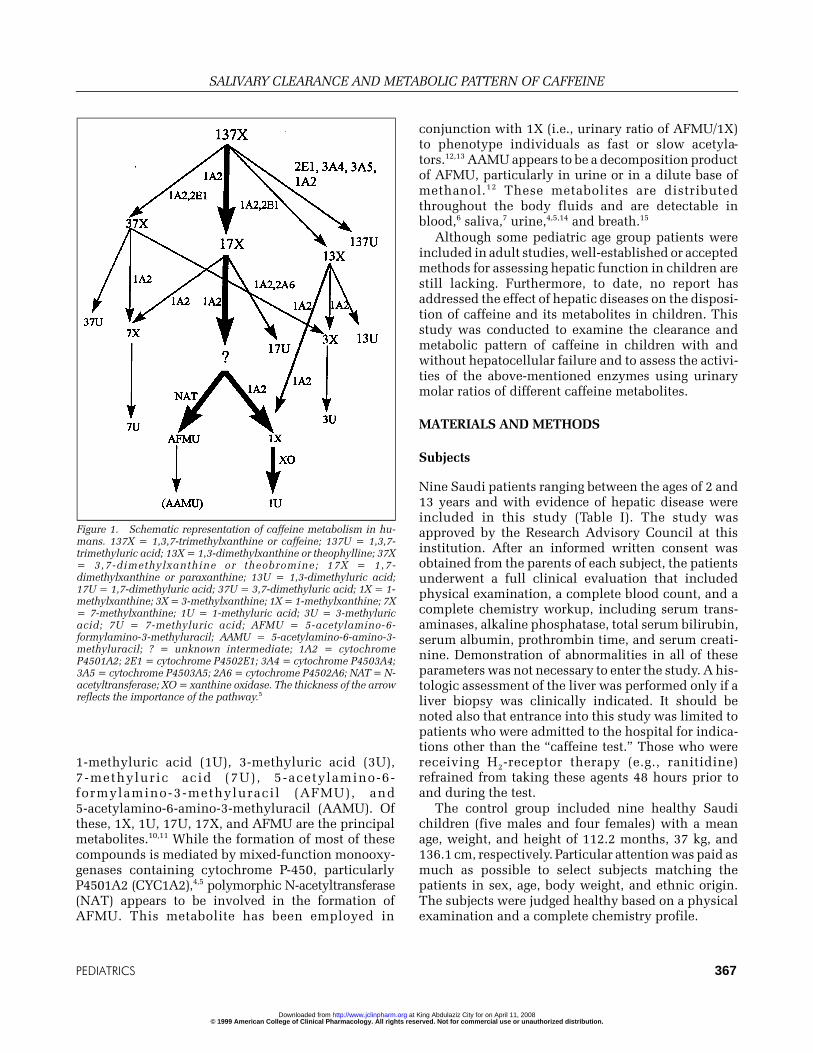
1-methyluric acid (1U), 3-methyluric acid (3U),7-methyluric acid (7U), 5-acetylamino- 6- formylamino- 3- methyluracil (AFMU), and5-acetylamino- 6- amino- 3- methyluracil (AAMU). Ofthese, 1X, 1U, 17U, 17X, and AFMU are the prin ci palmetabo lites.10,11 While the for ma tion of most of thesecom pounds is medi ated by mixed- function mono oxy -ge nases con tain ing cyto chrome P-450, par ticu larlyP4501A2 (CYC1A2),4,5 poly mor phic N-acetyltransferase(NAT) appears to be involved in the for ma tion ofAFMU. This metabo lite has been employed in
con junc tion with 1X (i.e., uri nary ratio of AFMU/1X)to phe no type indi vidu als as fast or slow ace ty la -tors.12,13 AAMU appears to be a decom po si tion prod uct of AFMU, par ticu larly in urine or in a dilute base ofmetha nol.12 These metabo lites are dis trib utedthrough out the body flu ids and are detect able inblood,6 saliva,7 urine,4,5,14 and breath.15
Although some pedi at ric age group patients wereincluded in adult stud ies, well- established or accepted meth ods for assess ing hepatic func tion in chil dren arestill lack ing. Fur ther more, to date, no report hasaddressed the effect of hepatic dis eases on the dis po si -tion of caf feine and its metabo lites in chil dren. Thisstudy was con ducted to exam ine the clear ance andmeta bolic pat tern of caf feine in chil dren with andwith out hepa to cel lu lar fail ure and to assess the activi -ties of the above- mentioned enzymes using uri narymolar ratios of dif fer ent caf feine metabo lites.
MA TE RI ALS AND METH ODS
Sub jects
Nine Saudi patients rang ing between the ages of 2 and13 years and with evi dence of hepatic dis ease wereincluded in this study (Table I). The study wasapproved by the Research Advi sory Coun cil at thisinsti tu tion. After an informed writ ten con sent wasobtained from the par ents of each sub ject, the patientsunder went a full clini cal evalua tion that includedphysi cal exami na tion, a com plete blood count, and acom plete chem is try workup, includ ing serum trans -ami nases, alka line phos phatase, total serum bili ru bin,serum albu min, prothrom bin time, and serum creati -nine. Dem on stra tion of abnor mali ties in all of theseparame ters was not nec es sary to enter the study. A his -to logic assess ment of the liver was per formed only if aliver biopsy was clini cally indi cated. It should benoted also that entrance into this study was lim ited topatients who were admit ted to the hos pi tal for indi ca -tions other than the “caf feine test.” Those who werereceiv ing H2-rece ptor ther apy (e.g., rani ti dine)refrained from tak ing these agents 48 hours prior toand dur ing the test.
The con trol group included nine healthy Saudichil dren (five males and four females) with a meanage, weight, and height of 112.2 months, 37 kg, and136.1 cm, respec tively. Par ticu lar atten tion was paid as much as pos si ble to select sub jects match ing thepatients in sex, age, body weight, and eth nic ori gin.The sub jects were judged healthy based on a physi calexami na tion and a com plete chem is try pro file.
PE DI AT RICS 367
SALI VARY CLEAR ANCE AND META BOLIC PAT TERN OF CAF FEINE
Fig ure 1. Sche matic rep re sen ta tion of caf feine me tabo lism in hu -mans. 137X = 1,3,7- trimethylxanthine or caf feine; 137U = 1,3,7- trimethyluric acid; 13X = 1,3- dimethylxanthine or theo phyl line; 37X= 3,7- dimethylxanthine or theo bro mine; 17X = 1,7- dimethylxanthine or par ax an thine; 13U = 1,3- dimethyluric acid;17U = 1,7- dimethyluric acid; 37U = 3,7- dimethyluric acid; 1X = 1- methylxanthine; 3X = 3- methylxanthine; 1X = 1- methylxanthine; 7X= 7- methylxanthine; 1U = 1- methyluric acid; 3U = 3- methyluricacid; 7U = 7- methyluric acid; AFMU = 5- acetylamino- 6- formylamino- 3- methyluracil; AAMU = 5- acetylamino- 6- amino- 3- methyluracil; ? = un known in ter me di ate; 1A2 = cy to chromeP4501A2; 2E1 = cy to chrome P4502E1; 3A4 = cy to chrome P4503A4;3A5 = cy to chrome P4503A5; 2A6 = cy to chrome P4502A6; NAT = N- acetyltransferase; XO = xan thine oxi dase. The thick ness of the ar rowre flects the im por tance of the path way.5
© 1999 American College of Clinical Pharmacology. All rights reserved. Not for commercial use or unauthorized distribution. at King Abdulaziz City for on April 11, 2008 http://www.jclinpharm.orgDownloaded from
Drug Ad min istra tion
Sub jects refrained from caf feine intake for a 72- hourperiod prior to admini stra tion orally of a 2 mg/kg doseof caf feine in the form of a caf fein ated cola bev er agepro vided at least 3 hours after inges tion of the lastmeal. After chew ing on parafilm for 5 to 10 min utes,saliva sam ples (1-2 mL) were col lected from each sub -ject at 4 to 5 hours (i.e., even ing sam ple) and 16 to 17hours (i.e., morn ing sam ple) (time of sam pling wasexactly recorded) after drug admini stra tion and storedin a speci men con tainer at –80ºC until analy sis.
Urine was col lected for 48 hours after caf feineinges tion in a 2-liter con tainer con tain ing 2 g ofsodium meta bi sul fite as an anti oxi dant sta bi lizer andwas kept refrig er ated through out the col lec tion period. At the end of this period, the urine vol ume was mea-s ured, and an ade quate ali quot (10 mL) was taken andstored fro zen at –80ºC until analy sis.
Sam ple Analy sis
Con cen tra tions of caf feine and its metabo lites weredeter mined in saliva and urine by high- performanceliq uid chro ma tog ra phy accord ing to a modi fi ca tion ofthe method by El- Yazigi, Chaleby, and Mar tin.13 Toensure a full sepa ra tion of the metabo lites in urine andsaliva, chro ma tog ra phy was per formed at 35ºC, andthe mobile phase con sisted of two buff ers deliv ered bya lin ear gra di ent. Buffer A (A) was ace tic acid (0.05%
v/v, adjusted to pH 4.5 with a con cen trated solu tion ofammo nium hydrox ide), and buffer B (B) was a mix ture of A and metha nol (50:50 v/v, adjusted to pH 4.5 withcon cen trated ace tic acid). Ini tially, A was pumped iso -crati cally for 8 min utes, after which the mobile phasewas changed line arly to a mix ture of A and B at 93:7(v/v) attained after 15 min utes. The change in themobile phase com po si tion con tin ued line arly, and theA:B ratio was 84:16, 62:38, 100:0 (all v/v) at 35, 45, and56 min utes from the begin ning of each run, respec -tively. The flow rate was 1.2 ml/min, and the pres surewas < 1200 psi; 4-acetaminophenol was used as theinter nal stan dard (IS). The extrac tion pro ce dure wasiden ti cal to that described ear lier,13 but the resi due ofthe chlo ro form/iso pro pa nol (50:50 v/v) extract ofsaliva and that of the chlo ro form/iso pro pa nol (95:5v/v) extract of urine were recon sti tuted in 125 µl of amix ture of sodium ace tate solu tion (0.01 M, pH = 4.74) and metha nol (90:10 v/v). After vor tex mix ing for 30sec onds, a 125 µl ali quot of sodium ace tate solu tion(0.01 M, pH = 4.74) con tain ing tetra bu tyl ammo niumphos phate (0.05 M) was added and vor tex mixed for 30 sec onds. A 50 µl ali quot was injected into thechro ma tograph.
The intra- (within- day) and inter as say (between-day) coef fi cient of varia tion (CV) of the con cen tra tionat 2.5 and 10 µg/mL of caf feine in saliva was ≤ 10.6%,and that of most metabo lites in urine was ≤ 15.03%.The detec tion limit and con cen tra tion range of caf -feine in saliva were 0.2 µg/mL and 0.25 to 20 µg/mL,
EL- YAZIGI ET AL
368 • J Clin Phar ma col 1999;39:366-372
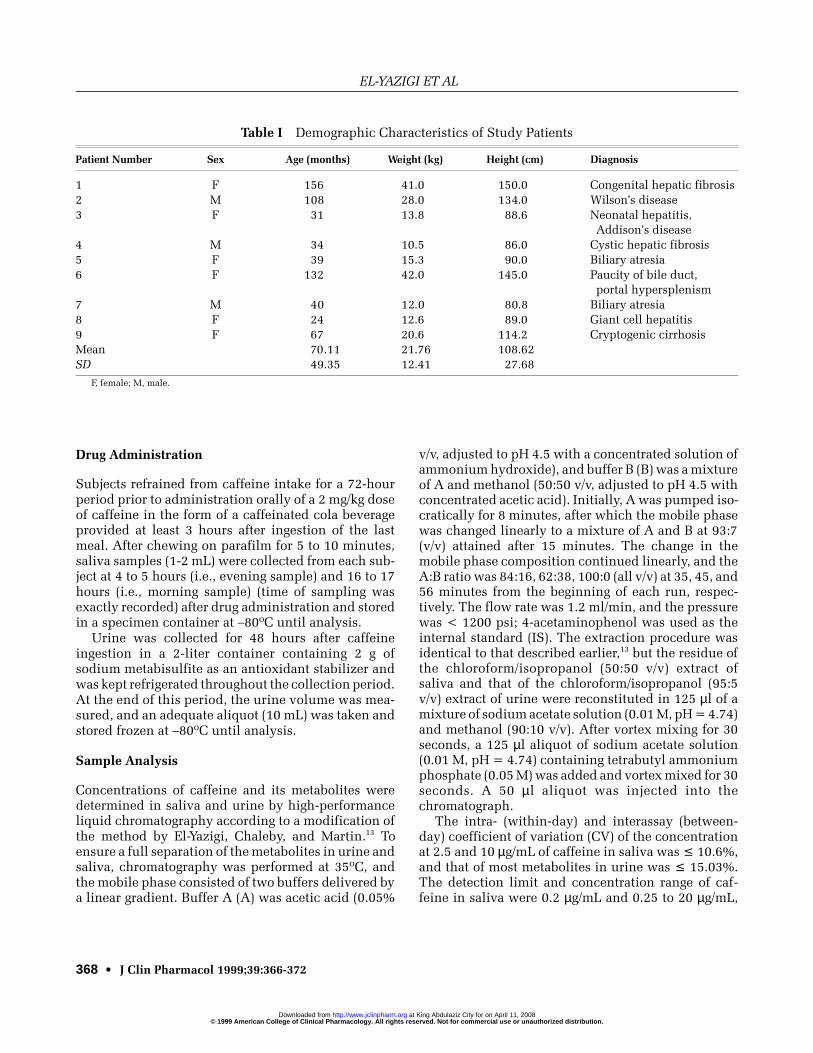
Ta ble I Demo graphic Char ac ter is tics of Study Pa tients
Pa tient Num ber Sex Age (months) Weight (kg) Height (cm) Di ag no sis
1 F 156 41.0 150.0 Con geni tal he patic fi bro sis2 M 108 28.0 134.0 Wil son’s dis ease3 F 31 13.8 88.6 Neo na tal hepa ti tis,
Ad di son’s dis ease4 M 34 10.5 86.0 Cys tic he patic fi bro sis5 F 39 15.3 90.0 Bili ary atresia6 F 132 42.0 145.0 Pau city of bile duct,
por tal hy per splen ism7 M 40 12.0 80.8 Bili ary atresia8 F 24 12.6 89.0 Gi ant cell hepa ti tis9 F 67 20.6 114.2 Cryp to genic cir rho sisMean 70.11 21.76 108.62SD 49.35 12.41 27.68
F, fe male; M, male.
© 1999 American College of Clinical Pharmacology. All rights reserved. Not for commercial use or unauthorized distribution. at King Abdulaziz City for on April 11, 2008 http://www.jclinpharm.orgDownloaded from
respec tively, and those of the caf feine metabo lites inurine were 0.25 µg/mL and 0.25 to 10 µg/mL,respec tively.
Cal cu la tion
Caf feine clear ance (Clcaf) was cal cu lated using thewell- established two- sample approach accord ing tothe fol low ing equa tion:16,17
Clcaf = Vd [ln Ct1/Ct2]/T,
where Vd is the vol ume of dis tri bu tion (Vd) that isassumed to be equiva lent to 0.6 liters per kg bodyweight,7,16-19 Ct1 is the con cen tra tion of caf feine insaliva in the first (i.e., even ing) sam ple, Ct2 is the con -cen tra tion of caf feine in saliva in the sec ond (i.e.,
morn ing) sam ple, and T is the time inter val sepa rat ingthe two col lec tions, assum ing first- order kinet ics forcaf feine.
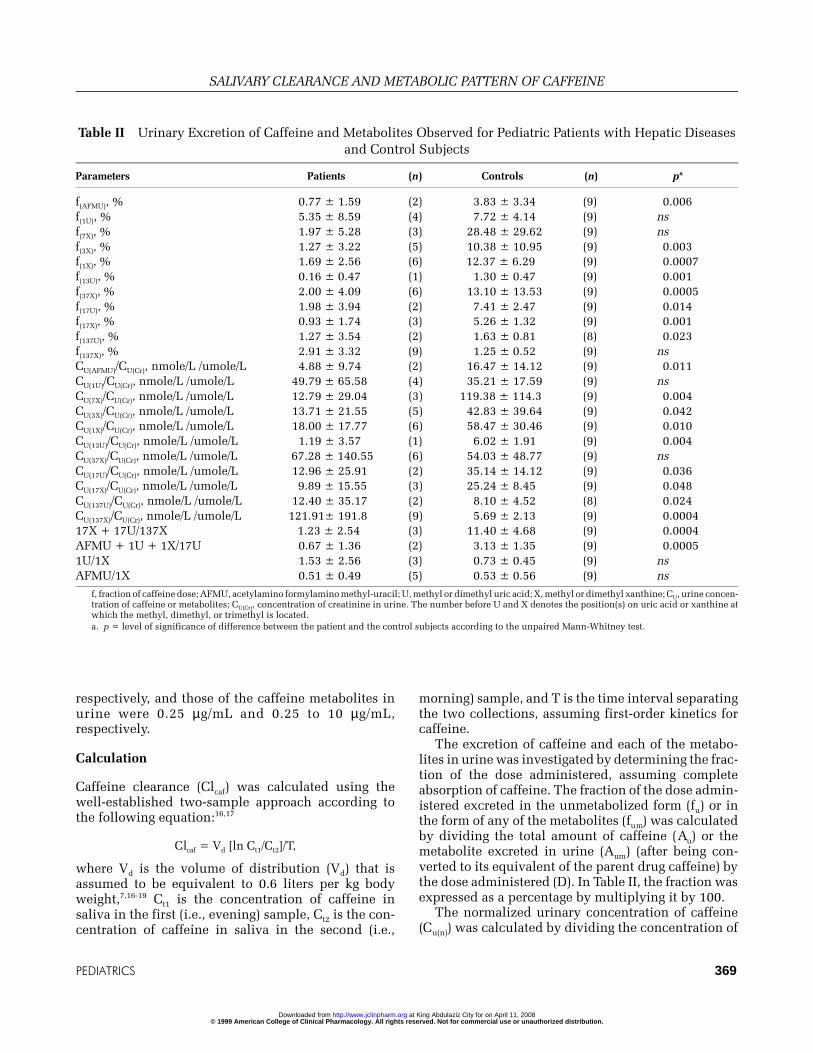
The excre tion of caf feine and each of the metabo -lites in urine was inves ti gated by deter min ing the frac -tion of the dose admin is tered, assum ing com pleteabsorp tion of caf feine. The frac tion of the dose admin -is tered excreted in the unme tabo lized form (fu) or inthe form of any of the metabo lites (fum) was cal cu latedby divid ing the total amount of caf feine (Au) or themetabo lite excreted in urine (Aum) (after being con -verted to its equiva lent of the par ent drug caf feine) bythe dose admin is tered (D). In Table II, the frac tion wasexpressed as a per cent age by mul ti ply ing it by 100.
The nor mal ized uri nary con cen tra tion of caf feine(Cu(n)) was cal cu lated by divid ing the con cen tra tion of
PE DI AT RICS 369
SALI VARY CLEAR ANCE AND META BOLIC PAT TERN OF CAF FEINE
Ta ble II Uri nary Ex cre tion of Caf feine and Me tabo lites Ob served for Pe di at ric Pa tients with He patic Dis easesand Con trol Sub jects
Pa rame ters Pa tients (n) Con trols (n) pa
f(AFMU), % 0.77 ± 1.59 (2) 3.83 ± 3.34 (9) 0.006f(1U), % 5.35 ± 8.59 (4) 7.72 ± 4.14 (9) nsf(7X), % 1.97 ± 5.28 (3) 28.48 ± 29.62 (9) nsf(3X), % 1.27 ± 3.22 (5) 10.38 ± 10.95 (9) 0.003f(1X), % 1.69 ± 2.56 (6) 12.37 ± 6.29 (9) 0.0007f(13U), % 0.16 ± 0.47 (1) 1.30 ± 0.47 (9) 0.001f(37X), % 2.00 ± 4.09 (6) 13.10 ± 13.53 (9) 0.0005f(17U), % 1.98 ± 3.94 (2) 7.41 ± 2.47 (9) 0.014f(17X), % 0.93 ± 1.74 (3) 5.26 ± 1.32 (9) 0.001f(137U), % 1.27 ± 3.54 (2) 1.63 ± 0.81 (8) 0.023f(137X), % 2.91 ± 3.32 (9) 1.25 ± 0.52 (9) nsCU(AFMU)/CU(Cr), nmole/L /umole/L 4.88 ± 9.74 (2) 16.47 ± 14.12 (9) 0.011CU(1U)/CU(Cr), nmole/L /umole/L 49.79 ± 65.58 (4) 35.21 ± 17.59 (9) nsCU(7X)/CU(Cr), nmole/L /umole/L 12.79 ± 29.04 (3) 119.38 ± 114.3 (9) 0.004CU(3X)/CU(Cr), nmole/L /umole/L 13.71 ± 21.55 (5) 42.83 ± 39.64 (9) 0.042CU(1X)/CU(Cr), nmole/L /umole/L 18.00 ± 17.77 (6) 58.47 ± 30.46 (9) 0.010CU(13U)/CU(Cr), nmole/L /umole/L 1.19 ± 3.57 (1) 6.02 ± 1.91 (9) 0.004CU(37X)/CU(Cr), nmole/L /umole/L 67.28 ± 140.55 (6) 54.03 ± 48.77 (9) nsCU(17U)/CU(Cr), nmole/L /umole/L 12.96 ± 25.91 (2) 35.14 ± 14.12 (9) 0.036CU(17X)/CU(Cr), nmole/L /umole/L 9.89 ± 15.55 (3) 25.24 ± 8.45 (9) 0.048CU(137U)/CU(Cr), nmole/L /umole/L 12.40 ± 35.17 (2) 8.10 ± 4.52 (8) 0.024CU(137X)/CU(Cr), nmole/L /umole/L 121.91± 191.8 (9) 5.69 ± 2.13 (9) 0.000417X + 17U/137X 1.23 ± 2.54 (3) 11.40 ± 4.68 (9) 0.0004AFMU + 1U + 1X/17U 0.67 ± 1.36 (2) 3.13 ± 1.35 (9) 0.00051U/1X 1.53 ± 2.56 (3) 0.73 ± 0.45 (9) nsAFMU/1X 0.51 ± 0.49 (5) 0.53 ± 0.56 (9) ns
f, frac tion of caf feine dose; AFMU, ace tylamino formylamino methyl- uracil; U, methyl or di methyl uric acid; X, methyl or di methyl xan thine; CU, urine con cen -tra tion of caf feine or me tabo lites; CU(Cr), con cen tra tion of cre ati nine in urine. The number be fore U and X de notes the po si tion(s) on uric acid or xan thine atwhich the methyl, di methyl, or tri methyl is lo cated.a. p = level of sig nifi cance of dif fer ence be tween the pa tient and the con trol sub jects ac cord ing to the un paired Mann- Whitney test.
© 1999 American College of Clinical Pharmacology. All rights reserved. Not for commercial use or unauthorized distribution. at King Abdulaziz City for on April 11, 2008 http://www.jclinpharm.orgDownloaded from
caf feine in urine (Cu) by the con cen tra tion of creati -nine (Cr) in the same sam ple (Cu(Cr)). Creati nine con -cen tra tion in urine was deter mined using a Jaffe- basedreac tion (Boe hrin ger Mann heim Auto mated Analy sisfor BM Hitachi Sys tems 747/737) on a Hitachi 737ana lyzer.
Sta tis ti cal Analy sis
Data were ana lyzed using a non para met ric sta tis ti caltest (unpaired Mann- Whitney test) using theSTATGRAPHICS Sta tis ti cal Graphic Sys tem pack age(Sta tis ti cal Graph ics Co., Rockville, MD). The dif fer -ence was con sid ered sig nifi cant when p was ≤ 0.05.
RE SULTS
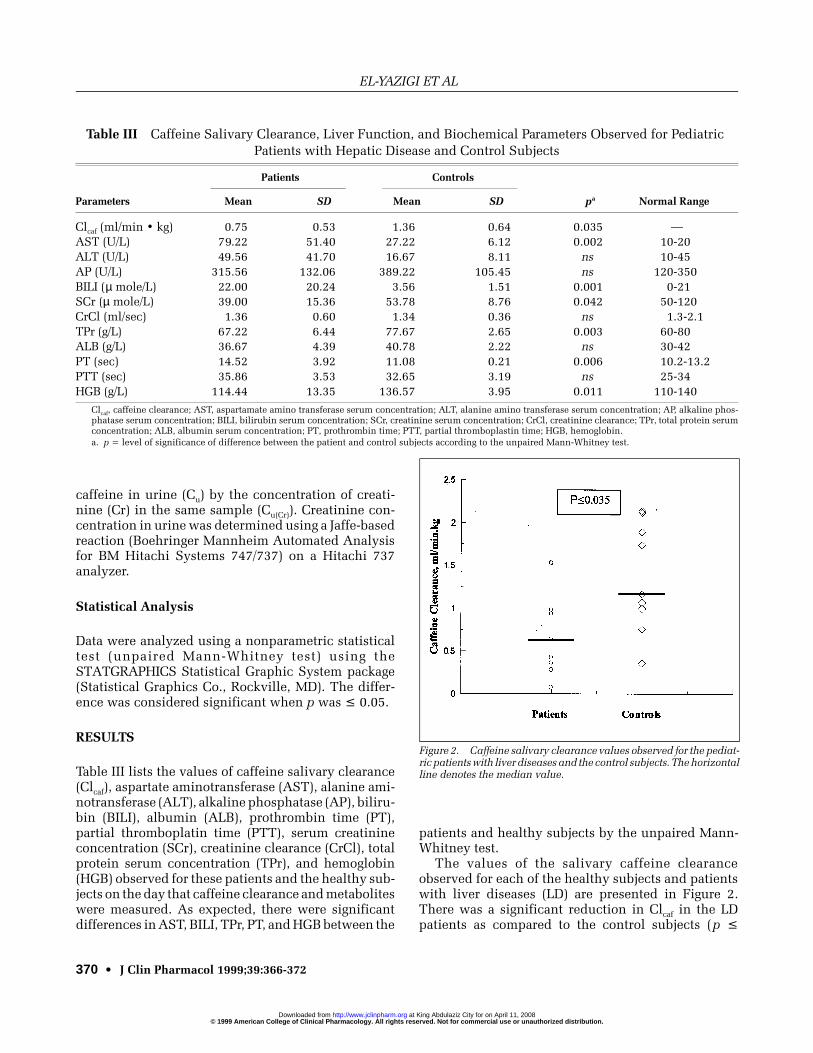
Table III lists the val ues of caf feine sali vary clear ance(Clcaf), aspar tate ami no trans fe rase (AST), alanine ami -no trans fe rase (ALT), alka line phos phatase (AP), bili ru -bin (BILI), albu min (ALB), prothrom bin time (PT),par tial throm bo platin time (PTT), serum creati ninecon cen tra tion (SCr), creati nine clear ance (CrCl), totalpro tein serum con cen tra tion (TPr), and hemo glo bin(HGB) observed for these patients and the healthy sub -jects on the day that caf feine clear ance and metabo lites were meas ured. As expected, there were sig nifi cantdif fer ences in AST, BILI, TPr, PT, and HGB between the
patients and healthy sub jects by the unpaired Mann- Whitney test.
The val ues of the sali vary caf feine clear anceobserved for each of the healthy sub jects and patientswith liver dis eases (LD) are pre sented in Fig ure 2.There was a sig nifi cant reduc tion in Clcaf in the LDpatients as com pared to the con trol sub jects (p ≤
EL- YAZIGI ET AL
370 • J Clin Phar ma col 1999;39:366-372
Ta ble III Caf feine Sali vary Clear ance, Liver Func tion, and Bio chemi cal Pa rame ters Ob served for Pe di at ric Pa tients with He patic Dis ease and Con trol Sub jects
Pa tients Con trols
Pa rame ters Mean SD Mean SD pa Nor mal Range
Clcaf (ml/min • kg) 0.75 0.53 1.36 0.64 0.035 —AST (U/L) 79.22 51.40 27.22 6.12 0.002 10- 20ALT (U/L) 49.56 41.70 16.67 8.11 ns 10- 45AP (U/L) 315.56 132.06 389.22 105.45 ns 120- 350BILI (µ mole/L) 22.00 20.24 3.56 1.51 0.001 0-21SCr (µ mole/L) 39.00 15.36 53.78 8.76 0.042 50- 120CrCl (ml/sec) 1.36 0.60 1.34 0.36 ns 1.3-2.1TPr (g/L) 67.22 6.44 77.67 2.65 0.003 60- 80ALB (g/L) 36.67 4.39 40.78 2.22 ns 30- 42PT (sec) 14.52 3.92 11.08 0.21 0.006 10.2-13.2PTT (sec) 35.86 3.53 32.65 3.19 ns 25- 34HGB (g/L) 114.44 13.35 136.57 3.95 0.011 110- 140
Clcaf, caf feine clear ance; AST, as par ta mate amino trans fe rase se rum con cen tra tion; ALT, al anine amino trans fe rase se rum con cen tra tion; AP, al ka line phos -phatase se rum con cen tra tion; BILI, bili ru bin se rum con cen tra tion; SCr, cre ati nine se rum con cen tra tion; CrCl, cre ati nine clear ance; TPr, to tal pro tein se rumcon cen tra tion; ALB, al bu min se rum con cen tra tion; PT, prothrom bin time; PTT, par tial throm bo plas tin time; HGB, he mo glo bin.a. p = level of sig nifi cance of dif fer ence be tween the pa tient and con trol sub jects ac cord ing to the un paired Mann- Whitney test.
Fig ure 2. Caf feine sali vary clear ance val ues ob served for the pe di at -ric pa tients with liver dis eases and the con trol sub jects. The hori zon tal line de notes the me dian value.
© 1999 American College of Clinical Pharmacology. All rights reserved. Not for commercial use or unauthorized distribution. at King Abdulaziz City for on April 11, 2008 http://www.jclinpharm.orgDownloaded from

0.035); the median (range) of this parame ter was 1.16(0.35-2.14) and 0.64 (0.07-1.53) ml/min ≤ kg,respec tively.
0.035); the median (range) of this parame ter was 1.16(0.35-2.14) and 0.64 (0.07-1.53) ml/min ≤ kg,respec tively.
Simi larly, as shown in Table II, with the excep tion of 1U and 7X, the frac tions of caf feine dose excreted inurine in the forms of vari ous metabo lites (fu(m)) frompatients were smaller than those exhib ited by the con -trol sub jects, but the frac tion of caf feine dose excretedunchanged (fu(137X)) was higher. Simi lar results wereobserved with the ratio of uri nary con cen tra tion of caf -feine (Cu(137X)/Cu(Cr)) or metabo lites (Cu(m)/Cu(Cr)) and thatof creati nine (Cr) (Table II). This nor mali za tion wascon sid ered use ful for elimi nat ing the impact of miss -ing (i.e., unin tended, if any) a frac tion when the urinewas col lected and to negate the effect of the hydra tionstate of the patient on the uri nary con cen tra tion. Itshould be noted that out of nine patient urine sam plesana lyzed, theo phyl line and 13U were meas ur able inone sam ple only; AFMU, 3U, 17U, and 137U weremeas ur able in two sam ples; 7X and par ax an thine were meas ur able in three sam ples; IU was meas ur able infour sam ples; 3X was meas ur able in five sam ples; 1Xand theo bro mine were meas ur able in six sam ples; caf -feine was meas ur able in all nine sam ples; and 7U wasdetected in no sam ple. This undoubt edly explains thelarge stan dard devia tions observed with the data gen -er ated for the patients (Table II). On the other hand,while no 3U, 7U, or theo phyl line was detected in anyof the nine con trol sam ples, all other metabo litesexam ined were meas ur able in each sam ple.
DIS CUS SION
The excel lent cor re la tion found between plasma andsaliva caf feine clear ance3,7,17,20 and the innocu ousnature of saliva sam pling have made the meas ure mentof over night sali vary clear ance of caf feine meas uredafter a sin gle oral dose highly suit able for the assess -ment of hepatic func tion, par ticu larly in pedi at ricpopu la tions. More recently, the deter mi na tion of themolar ratio of vari ous uri nary metabo lites of caf feinefor the evalua tion of cyto chrome P4501A2 (CYP1A2),xan thine oxi dase (XO), and NAT activi ties has becomevery popu lar.4,5,14,21-23 Undoubt edly, com bin ing thesetwo non in va sive approaches makes it easy to exam inevari ous enzy matic sys tems in healthy sub jects who are or are not receiv ing enzyme- inducing or enzyme- inhibiting drugs and in patients with hepatic dis eases,such as the case in this study.
As clearly dem on strated in Fig ure 2, caf feine sali -vary clear ance in the LD patients in com pari son to thecon trol sub jects was sig nifi cantly reduced, indi cat ingthat hepatic func tion, par ticu larly the activ ity of
CYP1A2, was mark edly depressed since caf feine clear -ance has been employed as a marker for the activ ity ofthis enzyme.24 It should be noted that there was anover lap in caf feine clear ance val ues of some patientswith those of some healthy con trols, mak ing this testless than sen si tive and opti mal for clini cal use. It hasbeen shown that CYP1A2 cata lyzes theN-demethylation of caf feine to form par ax an thine(17X), theo phyl line (13X), and theo bro mine (37X),which rep re sent the bulk (> 84%) of pri mary caf feinemetabo lism.23,25 The depres sion of the CYP1A2 activ -ity in the LD patients is also evi dent from the smalleruri nary molar ratios of [17X + 17U]/137X and [AFMU+ 1U + 1X]/17U (Table II) observed in these patients as com pared to the con trols. It should be noted that theseratios have recently been employed for assess ing theactiv ity of CYP1A2.5,20,22,26,27
On the other hand, the lack of sig nifi cant dif fer encein the ratio AFMU/1X (Table II), which has beenwidely used to evalu ate the activ ity of NAT12,13
between LD patients and con trols, indi cates that theactiv ity of this enzyme sys tem is not affected byhepatic dis eases in pedi at ric patients. This comes asno sur prise since this enzyme has been employed todeter mine the ace ty la tion phe no type of the indi vid ual(i.e., fast or slow ace ty la tor), which is known to beinflu enced by the genetic con sti tu tion of the indi vid -ual and by vari ous dis eases other than those of theliver (i.e., dia be tes mel li tus, blad der can cer, etc.).28,29
Although there was no sig nifi cant dif fer ence in theuri nary molar ratio of 1U/1X that reflects the activ ity of XO4,21,22,30 between LD patients and con trols, themean value observed in the patients was twice that inthe con trol sub ject (Table II). This sug gests no or aslight link between XO and LD. It is note wor thy thatwhile the infor ma tion on the role of XO in physio logi -cal sys tems remains lim ited, it has been reported thatXO is the best source of oxygen- generated free radi -cals,31 which are known to induce tis sue dam age.32
How ever, due to the small number of patients and con -trols included in this study, this find ing, as well as thatwith the other enzyme sys tems exam ined, should becon sid ered pre limi nary and need not be over em pha sized.
In con clu sion, the data pre sented here—par ticu -larly those on the activi ties of CYP1A2, NAT, andXO—are the first to be reported in pedi at ric patientswith hepatic dis eases. While the activ ity of CYP1A2was sig nifi cantly sup pressed in these patients as com -pared to the healthy sub jects, the activi ties of NAT andXO appeared to be unaf fected, although XO tended tobe more active in the patients. Fur ther stud ies involv -ing more patients, pref era bly with dif fer ent degrees of LD sever ity, and con trol sub jects are needed to expand on
PE DI AT RICS 371
SALI VARY CLEAR ANCE AND META BOLIC PAT TERN OF CAF FEINE
© 1999 American College of Clinical Pharmacology. All rights reserved. Not for commercial use or unauthorized distribution. at King Abdulaziz City for on April 11, 2008 http://www.jclinpharm.orgDownloaded from

these find ings and pos si bly explore the impact of LDsever ity on the activi ties of these enzymes.
The authors wish to thank the Admin istra tion of the King FaisalSpe cial ist Hos pi tal and Research Cen tre for its sup port of the phar -ma coki net ics and clini cal phar ma col ogy pro gram in this insti tu tion.
REF ER ENCES
1. Weid ner G, Ist van J: Die tary sources of caf feine. NEJM1985;313:1421.
2. Bun ker ML, McWil liams M: Caf feine con tent of com mon bev er -ages. J Am Diet As soc 1979;74:28- 32.
3. Lewis FW, Rec tor WG: Caf feine clear ance in cir rho sis: the value ofsim pli fied de ter mi na tions of liver meta bolic ca pac ity. J He pa tol1992;14:157- 162.
4. Hamelin BA, Xu K, Valle F, Man seau L, Richer M, Le Bel M: Caf -feine me tabo lism in cys tic fi bro sis: en hanced xan thine oxi dase ac -tiv ity. Clin Phar ma col Ther 1994;56:521- 529.
5. Rost KL, Roots I: Ac cel er ated caf feine me tabo lism af ter ome pra -zole treat ment is in di cated by uri nary me tabo lite ra tios: co in ci dence with plasma clear ance and breath test. Clin Phar ma col Ther1994;55:402- 411.
6. Varag nolo M, Ple bani M, Mus sap M, Ne metz L, Pa leari CD, Bur lina A: Caf feine as an in di ca tor of meta bolic func tions of mi cro so malliver en zymes. Clinica Chemica Acta 1989;183:91- 94.
7. Bi an chetti MG, Krae mer R, Passweg J, Jost J, Prei sig R: Use of sali -vary lev els to pre dict clear ance of caf feine in pa tients with cys tic fi -bro sis. J Pe di atr Gas tro and Nutr 1988;7:688- 693.
8. Soto J, Sac ris tan JA, Al sar MJ: Use of sali vary caf feine tests to as -sess the in ducer ef fect of a drug on he patic me tabo lism. Ann Phar -ma co ther 1996;30:736- 739.
9. Blan cha rad J, Saw ers SJA: The ab so lute bioa vail abil ity of caf feinein man. Eur J Clin Phar ma col 1983;24:93- 98.
10. Grant DM, Tang BK, Ka low W: Poly mor phic N- acetylation of acaf feine me tabo lite. Clin Phar ma col Ther 1983;33:355- 359.
11. Grant DM, Tang BK, Ka low W: Vari abil ity in caf feine me tabo lism. Clin Phar ma col Ther 1983;33:591- 602.12. Grant DM, Tang BK, Ka low W: A sim ple test for ace ty la tor phe no -type us ing caf feine. Br J Clin Phar ma col 1984;17:459- 464.
13. El- Yazigi A, Chaleby K, Mar tin CR: Sim pli fied and rapid test forace ty la tor phe no typ ing by use of the peak height ra tio of two uri narycaf feine me tabo lites. Clin Chem 1989;35:848- 851.
14. Ull rich D, Com pag none D, Munch B, Brandes A, Hille H, BircherJ: Uri nary caf feine me tabo lites in man: age- dependent changes andpat tern in vari ous clini cal situa tions. Eur J Clin Phar ma col1992;43:167- 172.
15. Ko take AN, Schoel ler DA, Lam bert GH, Baker AL, Schaf fer DD,Jo sephs H: The caf feine CO2 breath test: dose re sponse and route ofN- demethylation in smok ers and non- smokers. Clin Phar ma col Ther1982;32:261- 269.
16. Bircher J: Quan ti ta tive as sess ment of de ranged he patic func tion:a missed op por tu nity? Sem Liver Dis ease 1983;3:275- 284.
17. Wahl lander A, Mohr S, Paum gart ner G: As sess ment of he paticfunc tion: com pari son of caf feine clear ance in se rum and sa liva dur -ing the day and at night. J He pa tol 1990;10:129- 137.
18. Ren ner E, Wi etholtz H, Hu guenin P, Ar naud MJ, Prei sig R: Caf -feine: a model com pound for meas ur ing liver func tion. He pa tol1984;4:38- 46.
19. Des mond PV, Pat ward han RV, John son RF, Schen ker S: Im pairedelimi na tion of caf feine in cir rho sis. Dig Dis Sci 1980;25:193- 197.
20. Camp bell ME, Spiel berg SP, Ka low W: A uri nary me tabo lite ra tiothat re flects sys temic caf feine clear ance. Clin Phar ma col Ther1987;42:157- 165.
21. Bosso JA, Liu Q, Evans WE, Rel ling MV: CYP2D6, N- acetylation,and xan thine oxi dase ac tiv ity in cys tic fi bro sis. Phar ma co ther1996;16:749- 753.
22. Ras mussen BB, Bro sen K: De ter mi na tion of uri nary me tabo litesof caf feine for the as sess ment of cy to chrome P4501A2, xan thine oxi -dase, and N- acetyltransferase ac tiv ity in hu mans. Ther Drug Mo nit1996;18:254- 262.
23. No tari anni LJ, Ol iver SE, Do brocky P, Ben nett PN, Sil ver man BW: Caf feine as a meta bolic probe: a com pari son of the meta bolic ra tiosused to as sess CYP1A2 ac tiv ity. Br J Clin Phar ma col 1995;39:65- 69.
24. Wi etholtz H, Zys set T, Mar schall H-U, Ge neret K, Ma tern S: Thein flu ence of ri fampin treat ment on caf feine clear ance in healthyman. J He pa tol 1995;22:78- 81.
25. But ler MA, Iwa saki M, Guen gerich FP, Kad lu bar FF: Hu man cy to -chrome P- 450PA (P4501A2), the phena cetin O- deethylase, is pri -mar ily re spon si ble for the he patic 3- demethylation of caf feine andN- oxidation of car cino genic arylamines. Proc Natl Acad Sci USA1989;86:7696- 7700.26. Fuhr U, Rost KL: Sim ple and re li able CYP1A2 phe no typ ing bythe par ax an thine/caf feine ra tio in plasma and in sa liva. Phar ma co -ge net 1994;4:109- 116.
27. But ler MA, Lang NP, Young JF, Ca po raso NE, Vi neis P, Hayes RB,Teitel CH, Mas sen gill JP, Law sen MF, Kad lu bar FF: De ter mi na tion ofCYP1A2 and NAT2 phe no types in hu man popu la tions by analy sis of caf feine uri nary me tabo lites. Phar ma co ge net 1992;2:116- 127.28. Clark DWJ: Ge neti cally de ter mined vari abil ity in ace ty la tion and oxi da tion: thera peu tic im pli ca tion. Drugs 1985;29:342- 375.
29. El- Yazigi A, Jo han sen K, Raines DA, Dos ing M: N- acetylationpoly mor phism and dia be tes mel li tus among Saudi Ara bi ans. J ClinPhar ma col 1992;32:905- 910.
30. Boda D, Ne meth I: Meas ure ment of uri nary caf feine me tabo litesre flect ing the “in vivo” xan thine oxi dase ac tiv ity in pre ma ture in -fants with RDS and in hy poxic states of chil dren. Bio med Bio chemActa 1989;48:S31- S35.
31. Parks DA, Granger DN: Xan thine oxi dase: bio chem is try, dis tri bu -tion and physi ol ogy. Acta Physiol Scand 1986;S548:87- 99.
32. Kato M, Mo ri kawa A, Kimura H, Shimizu T, Nakano M, KuroumeT: Ef fects of an tiasthma drugs on su per ox ide an ion gen era tion fromhu man poly mor pho nu clear leu ko cytes or hypoxanthine- xanthineoxi dase sys tems. Int Arch Al lergy Appl Im mu nol 1991;96:128- 133.
EL- YAZIGI ET AL
372 • J Clin Phar ma col 1999;39:366-372
© 1999 American College of Clinical Pharmacology. All rights reserved. Not for commercial use or unauthorized distribution. at King Abdulaziz City for on April 11, 2008 http://www.jclinpharm.orgDownloaded from