
Spectral-Domain Cirrus Optical Coherence Tomography of Choroidal Striations Seen in the Acute Stage...
8
Spectral-Domain Cirrus Optical Coherence Tomography of Choroidal Striations Seen in the Acute Stage of Vogt- Koyanagi-Harada Disease VISHALI GUPTA, AMOD GUPTA, PAWAN GUPTA, AND AMAN SHARMA ● PURPOSE: To describe changes in the retinal pigment epithelium (RPE) corresponding to the choroidal stria- tions in acute-stage Vogt-Koyanagi-Harada (VKH) dis- ease. ● DESIGN: Prospective, consecutive case series. ● METHODS: Four patients (eight eyes) with acute-stage VKH disease were studied. All underwent fundus fluo- rescein angiography (FFA), ultrasonography, and spec- tral-domain optical coherence tomography (SD OCT). The main outcome measure was the correlation of the findings seen on a 3-dimensional (3D) single-layer RPE map constructed on SD OCT with the serous retinal detachment (RD) and choroidal striations. ● RESULTS: The retina inner to external limiting mem- brane did not show any structural alteration in any of the eyes. The 3D single-layer RPE map showed undu- lations and bumps on the RPE surface in all the eyes. The troughs of the undulations were noted to corre- spond to the choroidal striations seen as hypofluores- cent lines in the early phase of FFA. The bumps over the undulations corresponded to the pinpoint hyper- fluorescent dots on FFA, resulting in the development of serous RDs over the troughs, thus obscuring the hypofluorescent lines in the late phase of fluorescein angiograms. ● CONCLUSIONS: The troughs of the RPE undulations were seen clinically as choroidal striations in the acute uveitic stage of VKH disease. (Am J Ophthalmol 2009;147:148 –153. © 2009 by Elsevier Inc. All rights reserved.) V OGT-KOYANAGI-HARADA (VKH) DISEASE IS A BI- lateral panuveitis that, in the acute uveitic stage, is characterized by the presence of exudative retinal detachment (RD) in the posterior pole. 1 Fluorescein an- giography (FA) shows multiple focal areas of leakage in the early phase with subretinal pooling of dye in the late phase. 1 Conventional time-domain optical coherence to- mography (TD OCT) can detect serous RD as true neurosensory RD, along with intraretinal fluid accumula- tion 2 and the presence of subretinal septae in the multi- lobular serous detachments. 3 Choroidal folds are a recently described sign seen in acute VKH disease. 4 The authors reported that the choroidal folds seen in VKH disease were different from those seen in other diseases because these remained hypofluorescent and were not seen as stripes with alternating hypofluorescent and hyperfluorescent bands on FA-like true choroidal folds. 4 However, the underlying mechanisms of the choroidal folds was not well understood on conventional TD OCT. We believe that these folds are not true and merely represent the undulations of the retinal pigment epithelium (RPE) that are seen clinically as striations. The newer-generation Cirrus high-definition (HD) OCT model 4000 (Carl Zeiss Meditec, Dublin, Califor- nia, USA) uses advanced imaging technology (spectral- domain [SD]), making the data acquisition 70 times faster than the TD Stratus OCT (Carl Zeiss Meditec). This enables the data acquisition in entire cubes that can be viewed in three dimensions and also gives single-layer surface maps of RPE. The HD images with nearly 5 m transverse resolution scans enable better visualization and 3-dimensional (3D) viewing of retinal structures, including the inner segment and outer seg- ment (IS/OS) photoreceptor junction and RPE, contrib- uting to the better understanding of the pathogenetic mechanisms for several retinal diseases. Line scanning laser ophthalmoscope allows the simultaneous capture of OCT fundus, giving a clear image of the retinal area addressed by the scan, and the image display option makes it possible to overlay the internal limiting membrane (ILM) to the RPE thickness map on the OCT fundus for exact localization of the pathologic features. We used SD Cirrus HD OCT to study the structural alterations in the retina and RPE corre- sponding to the choroidal striations seen in the acute uveitic stage of VKH disease. METHODS FOUR CONSECUTIVE PATIENTS WITH VKH DISEASE VISIT- ing our Tertiary Care Institute between October 15, 2007 and January 21, 2008 were enrolled in the study. Accepted for publication Jul 21, 2008. From the Department of Ophthalmology, Advanced Eye Centre (V.G., A.G., P.G.), and the Department of Internal Medicine (A.S.), Post- graduate Institute of Medical Education and Research, Chandigarh, India. Inquiries to Amod Gupta, Advanced Eye Centre, Department of Ophthalmology, Postgraduate Institute of Medical Education and Re- search, Chandigarh 160012, India; e-mail: [email protected] © 2009 BY ELSEVIER INC.ALL RIGHTS RESERVED. 148 0002-9394/09/$36.00 doi:10.1016/j.ajo.2008.07.028
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Spectral-Domain Cirrus Optical Coherence Tomography of Choroidal Striations Seen in the Acute Stage...

●
ete●
●
VrtTfimd●
btlTsctfloha●
wu2r
Vdgep
A
AgI
Os
1
Spectral-Domain Cirrus Optical Coherence Tomographyof Choroidal Striations Seen in the Acute Stage of Vogt-
Koyanagi-Harada Disease
VISHALI GUPTA, AMOD GUPTA, PAWAN GUPTA, AND AMAN SHARMA
mntldrdraFmonra
OndfTcsnvsmumoftottsss
F
i
PURPOSE: To describe changes in the retinal pigmentpithelium (RPE) corresponding to the choroidal stria-ions in acute-stage Vogt-Koyanagi-Harada (VKH) dis-ase.DESIGN: Prospective, consecutive case series.METHODS: Four patients (eight eyes) with acute-stageKH disease were studied. All underwent fundus fluo-
escein angiography (FFA), ultrasonography, and spec-ral-domain optical coherence tomography (SD OCT).he main outcome measure was the correlation of thendings seen on a 3-dimensional (3D) single-layer RPEap constructed on SD OCT with the serous retinaletachment (RD) and choroidal striations.RESULTS: The retina inner to external limiting mem-
rane did not show any structural alteration in any ofhe eyes. The 3D single-layer RPE map showed undu-ations and bumps on the RPE surface in all the eyes.he troughs of the undulations were noted to corre-
pond to the choroidal striations seen as hypofluores-ent lines in the early phase of FFA. The bumps overhe undulations corresponded to the pinpoint hyper-uorescent dots on FFA, resulting in the developmentf serous RDs over the troughs, thus obscuring theypofluorescent lines in the late phase of fluoresceinngiograms.CONCLUSIONS: The troughs of the RPE undulationsere seen clinically as choroidal striations in the acuteveitic stage of VKH disease. (Am J Ophthalmol009;147:148–153. © 2009 by Elsevier Inc. All rightseserved.)
OGT-KOYANAGI-HARADA (VKH) DISEASE IS A BI-
lateral panuveitis that, in the acute uveitic stage, ischaracterized by the presence of exudative retinal
etachment (RD) in the posterior pole.1 Fluorescein an-iography (FA) shows multiple focal areas of leakage in thearly phase with subretinal pooling of dye in the latehase.1 Conventional time-domain optical coherence to-
ccepted for publication Jul 21, 2008.From the Department of Ophthalmology, Advanced Eye Centre (V.G.,.G., P.G.), and the Department of Internal Medicine (A.S.), Post-
raduate Institute of Medical Education and Research, Chandigarh,ndia.
Inquiries to Amod Gupta, Advanced Eye Centre, Department of
2phthalmology, Postgraduate Institute of Medical Education and Re-
earch, Chandigarh 160012, India; e-mail: [email protected]
© 2009 BY ELSEVIER INC. A48
ography (TD OCT) can detect serous RD as trueeurosensory RD, along with intraretinal fluid accumula-ion2 and the presence of subretinal septae in the multi-obular serous detachments.3 Choroidal folds are a recentlyescribed sign seen in acute VKH disease.4 The authorseported that the choroidal folds seen in VKH disease wereifferent from those seen in other diseases because theseemained hypofluorescent and were not seen as stripes withlternating hypofluorescent and hyperfluorescent bands onA-like true choroidal folds.4 However, the underlyingechanisms of the choroidal folds was not well understood
n conventional TD OCT. We believe that these folds areot true and merely represent the undulations of theetinal pigment epithelium (RPE) that are seen clinicallys striations.
The newer-generation Cirrus high-definition (HD)CT model 4000 (Carl Zeiss Meditec, Dublin, Califor-ia, USA) uses advanced imaging technology (spectral-omain [SD]), making the data acquisition 70 timesaster than the TD Stratus OCT (Carl Zeiss Meditec).his enables the data acquisition in entire cubes thatan be viewed in three dimensions and also givesingle-layer surface maps of RPE. The HD images withearly 5 �m transverse resolution scans enable betterisualization and 3-dimensional (3D) viewing of retinaltructures, including the inner segment and outer seg-ent (IS/OS) photoreceptor junction and RPE, contrib-
ting to the better understanding of the pathogeneticechanisms for several retinal diseases. Line scanning laser
phthalmoscope allows the simultaneous capture of OCTundus, giving a clear image of the retinal area addressed byhe scan, and the image display option makes it possible toverlay the internal limiting membrane (ILM) to the RPEhickness map on the OCT fundus for exact localization ofhe pathologic features. We used SD Cirrus HD OCT totudy the structural alterations in the retina and RPE corre-ponding to the choroidal striations seen in the acute uveitictage of VKH disease.
METHODS
OUR CONSECUTIVE PATIENTS WITH VKH DISEASE VISIT-
ng our Tertiary Care Institute between October 15,
007 and January 21, 2008 were enrolled in the study.LL RIGHTS RESERVED. 0002-9394/09/$36.00doi:10.1016/j.ajo.2008.07.028
TreeeaiwatFCMc
s(fsrwR
wsubIflwtgocccipgsals
FlVosdio
V
he diagnosis of VKH disease was made based on theevised diagnostic criteria.5 The inclusion criteria atnrollment included VKH disease with presence ofxudative RD and choroidal striations seen on fundusxamination and fundus fluorescein angiography (FFA)nd diffuse choroidal thickening of more than 1.75 mmn the posterior pole on ultrasound B-scan. The patientsho already were receiving systemic corticosteroid ther-py before enrollment were excluded from the study. Allhe enrolled patients underwent Cirrus HD OCT andFA at presentation. The acquisition protocols forirrus HD OCT included five lines raster scans and theacular cube 200 � 200 and Macular cube 512 � 128
ombination.High-difinition image analysis of the five lines raster
can was carried out. The external limiting membraneELM) was identified in all eight eyes, and the outeroveal thickness was measured between the line repre-enting ELM and the inner border of RPE fit, a lineepresenting normal parabolic RPE. The IS/OS junctionas identified as the third highly reflective band (the
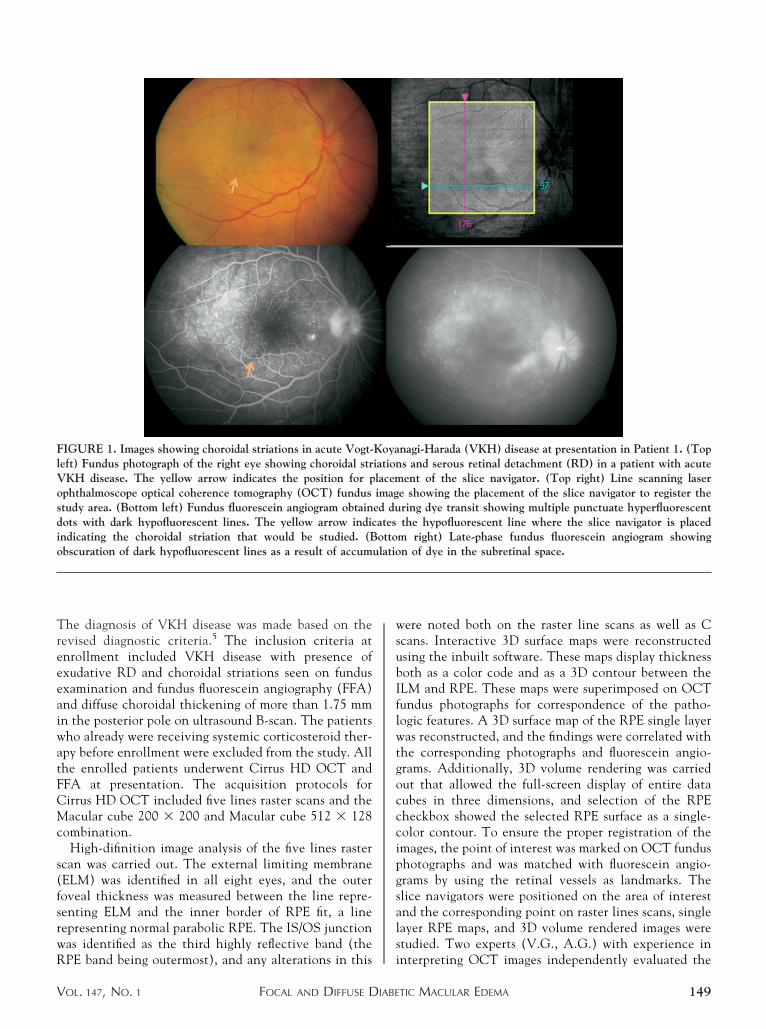
IGURE 1. Images showing choroidal striations in acute Vogt-eft) Fundus photograph of the right eye showing choroidal strKH disease. The yellow arrow indicates the position for pphthalmoscope optical coherence tomography (OCT) fundustudy area. (Bottom left) Fundus fluorescein angiogram obtainots with dark hypofluorescent lines. The yellow arrow indicndicating the choroidal striation that would be studied. (Bbscuration of dark hypofluorescent lines as a result of accum
PE band being outermost), and any alterations in this i
FOCAL AND DIFFUSE DIABEOL. 147, NO. 1
ere noted both on the raster line scans as well as Ccans. Interactive 3D surface maps were reconstructedsing the inbuilt software. These maps display thicknessoth as a color code and as a 3D contour between theLM and RPE. These maps were superimposed on OCTundus photographs for correspondence of the patho-ogic features. A 3D surface map of the RPE single layeras reconstructed, and the findings were correlated with
he corresponding photographs and fluorescein angio-rams. Additionally, 3D volume rendering was carriedut that allowed the full-screen display of entire dataubes in three dimensions, and selection of the RPEheckbox showed the selected RPE surface as a single-olor contour. To ensure the proper registration of themages, the point of interest was marked on OCT fundushotographs and was matched with fluorescein angio-rams by using the retinal vessels as landmarks. Thelice navigators were positioned on the area of interestnd the corresponding point on raster lines scans, singleayer RPE maps, and 3D volume rendered images weretudied. Two experts (V.G., A.G.) with experience in
nagi-Harada (VKH) disease at presentation in Patient 1. (Tops and serous retinal detachment (RD) in a patient with acuteent of the slice navigator. (Top right) Line scanning laser
e showing the placement of the slice navigator to register thering dye transit showing multiple punctuate hyperfluorescentthe hypofluorescent line where the slice navigator is placed
m right) Late-phase fundus fluorescein angiogram showingn of dye in the subretinal space.
Koyaiationlacemimaged duatesotto
ulatio
nterpreting OCT images independently evaluated the
TIC MACULAR EDEMA 149
Oflfacd
fmplr
B
pfrc
ewytidrtcsspt(
lsct(
FfpwipTrc
1
CT scans and compared them with OCT fundus anduorescein angiograms. All the OCT scans were per-ormed twice for each patient. All the scans were viewednd also evaluated thrice by each expert to assess theonsistency of analysis, including analysis on differentays. Both the experts agreed on all scans.All patients received intravenous methylprednisolone
ollowed by oral corticosteroids at the dosage of 1 to 1.5g/kg daily. The tapering of oral corticosteroids was
erformed only when no residual fluid was seen on rasterine scans. All patients had follow-up scans at intervalsanging between four and 12 weeks (median, 5.5 weeks).
RESULTS
ETWEEN OCTOBER 15, 2007 AND JANUARY 21, 2008, SEVEN
atients with acute VKH disease were seen. Of these,our fulfilled the study criteria and were enrolled. Theemaining three patients already were receiving oral
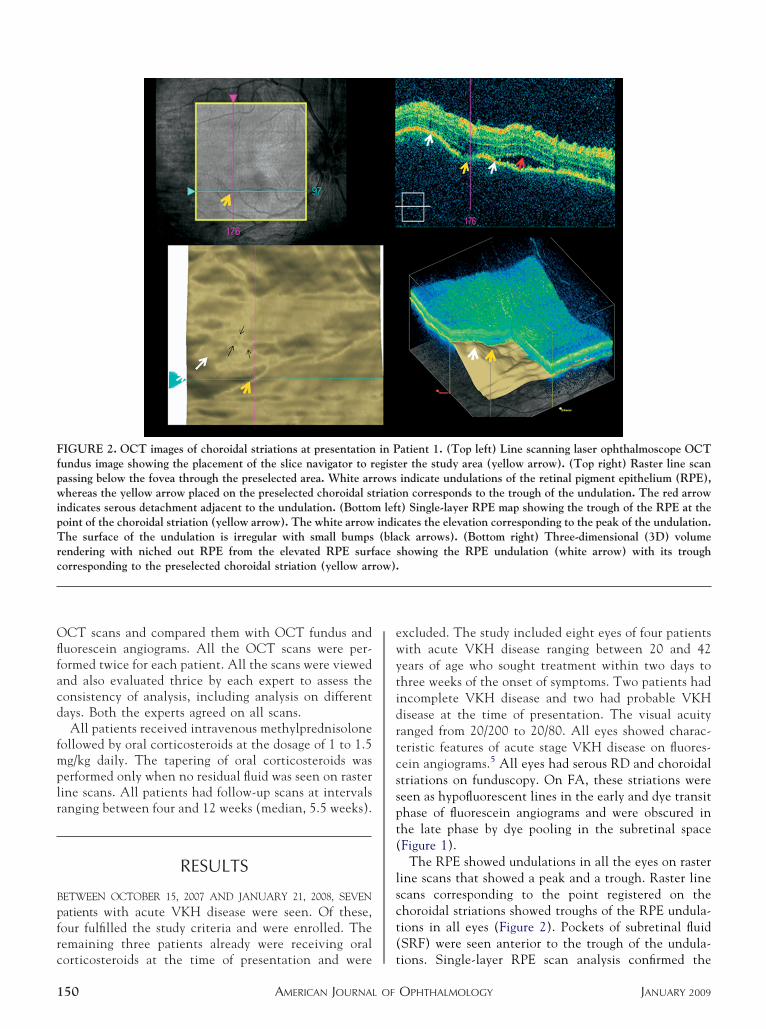
IGURE 2. OCT images of choroidal striations at presentationundus image showing the placement of the slice navigator to rassing below the fovea through the preselected area. White arhereas the yellow arrow placed on the preselected choroidal st
ndicates serous detachment adjacent to the undulation. (Bottomoint of the choroidal striation (yellow arrow). The white arrowhe surface of the undulation is irregular with small bumps
endering with niched out RPE from the elevated RPE surforresponding to the preselected choroidal striation (yellow arr
orticosteroids at the time of presentation and were t
AMERICAN JOURNAL OF50
xcluded. The study included eight eyes of four patientsith acute VKH disease ranging between 20 and 42ears of age who sought treatment within two days tohree weeks of the onset of symptoms. Two patients hadncomplete VKH disease and two had probable VKHisease at the time of presentation. The visual acuityanged from 20/200 to 20/80. All eyes showed charac-eristic features of acute stage VKH disease on fluores-ein angiograms.5 All eyes had serous RD and choroidaltriations on funduscopy. On FA, these striations wereeen as hypofluorescent lines in the early and dye transithase of fluorescein angiograms and were obscured inhe late phase by dye pooling in the subretinal spaceFigure 1).
The RPE showed undulations in all the eyes on rasterine scans that showed a peak and a trough. Raster linecans corresponding to the point registered on thehoroidal striations showed troughs of the RPE undula-ions in all eyes (Figure 2). Pockets of subretinal fluidSRF) were seen anterior to the trough of the undula-
atient 1. (Top left) Line scanning laser ophthalmoscope OCTer the study area (yellow arrow). (Top right) Raster line scanindicate undulations of the retinal pigment epithelium (RPE),n corresponds to the trough of the undulation. The red arrow
t) Single-layer RPE map showing the trough of the RPE at thecates the elevation corresponding to the peak of the undulation.ck arrows). (Bottom right) Three-dimensional (3D) volumeshowing the RPE undulation (white arrow) with its trough
in Pegistrowsriatio
lefindi(bla
aceow).
ions. Single-layer RPE scan analysis confirmed the
OPHTHALMOLOGY JANUARY 2009
pbmlfltortttob
sttc
sdd(tbr
aslrcdt
O
oimOwfsRw
tpa
Fpss
V
resence of undulations and also showed multiple smallumps on the RPE surface in all the eight eyes. Theseultiple small bumps seen on the peak of these undu-
ations corresponded to the areas of punctuate hyper-uorescence on fluorescein angiograms. The trough ofhese undulations corresponded to the points registeredn the choroidal striations (Figure 2). 3D volumeendering and selection of the RPE checkbox showedhat the elevation of the RPE surface corresponded tohe peak and that the depression corresponded to therough of the undulation (Figure 2). The informationbtained by analyzing all the scans at least three timesy each expert was consistent.With corticosteroid therapy, the single-layer RPE
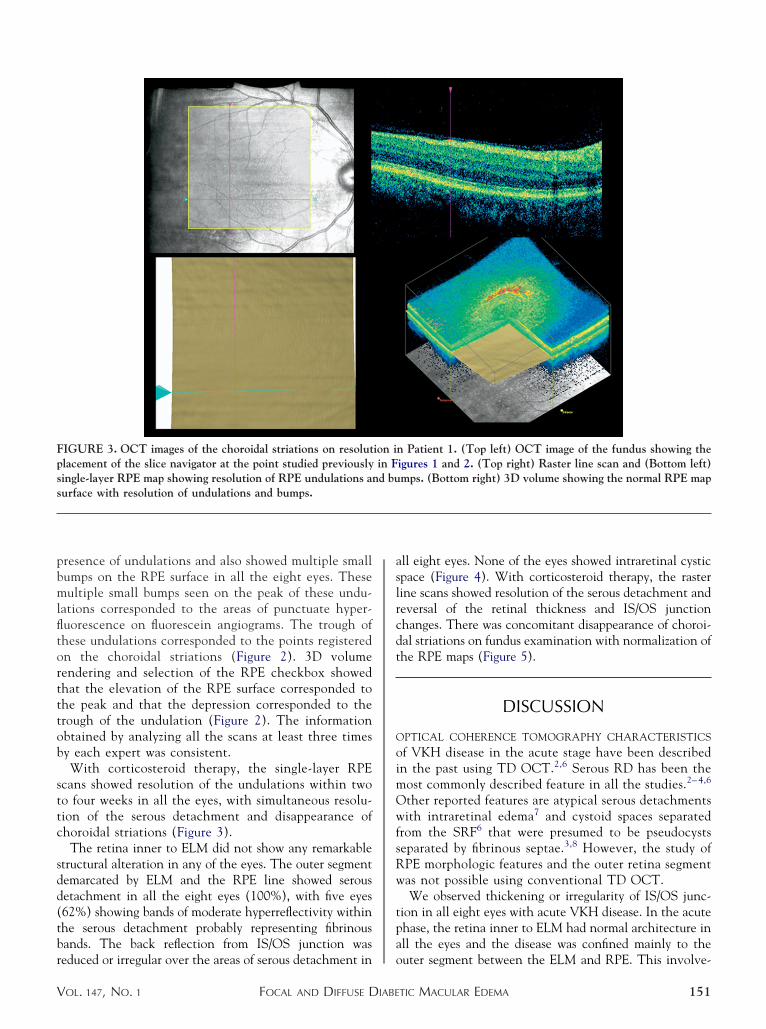
cans showed resolution of the undulations within twoo four weeks in all the eyes, with simultaneous resolu-ion of the serous detachment and disappearance ofhoroidal striations (Figure 3).
The retina inner to ELM did not show any remarkabletructural alteration in any of the eyes. The outer segmentemarcated by ELM and the RPE line showed serousetachment in all the eight eyes (100%), with five eyes62%) showing bands of moderate hyperreflectivity withinhe serous detachment probably representing fibrinousands. The back reflection from IS/OS junction was
IGURE 3. OCT images of the choroidal striations on resolutlacement of the slice navigator at the point studied previouslyingle-layer RPE map showing resolution of RPE undulations anurface with resolution of undulations and bumps.
educed or irregular over the areas of serous detachment in o
FOCAL AND DIFFUSE DIABEOL. 147, NO. 1
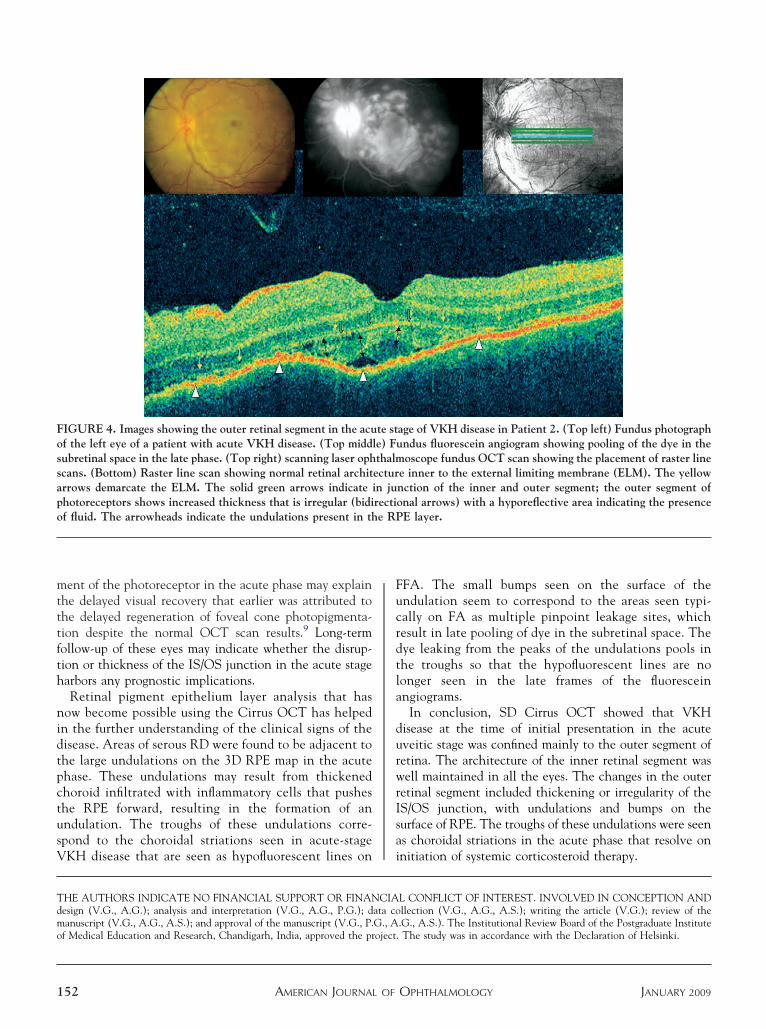
ll eight eyes. None of the eyes showed intraretinal cysticpace (Figure 4). With corticosteroid therapy, the rasterine scans showed resolution of the serous detachment andeversal of the retinal thickness and IS/OS junctionhanges. There was concomitant disappearance of choroi-al striations on fundus examination with normalization ofhe RPE maps (Figure 5).
DISCUSSION
PTICAL COHERENCE TOMOGRAPHY CHARACTERISTICS
f VKH disease in the acute stage have been describedn the past using TD OCT.2,6 Serous RD has been theost commonly described feature in all the studies.2– 4,6
ther reported features are atypical serous detachmentsith intraretinal edema7 and cystoid spaces separated
rom the SRF6 that were presumed to be pseudocystseparated by fibrinous septae.3,8 However, the study ofPE morphologic features and the outer retina segmentas not possible using conventional TD OCT.We observed thickening or irregularity of IS/OS junc-
ion in all eight eyes with acute VKH disease. In the acutehase, the retina inner to ELM had normal architecture inll the eyes and the disease was confined mainly to the
n Patient 1. (Top left) OCT image of the fundus showing theigures 1 and 2. (Top right) Raster line scan and (Bottom left)mps. (Bottom right) 3D volume showing the normal RPE map
ion iin Fd bu
uter segment between the ELM and RPE. This involve-
TIC MACULAR EDEMA 151
mtttfth
nidtpctusV
Fucrdtla
durwrIsa
Tdmo
Fossapo
1
ent of the photoreceptor in the acute phase may explainhe delayed visual recovery that earlier was attributed tohe delayed regeneration of foveal cone photopigmenta-ion despite the normal OCT scan results.9 Long-termollow-up of these eyes may indicate whether the disrup-ion or thickness of the IS/OS junction in the acute stagearbors any prognostic implications.Retinal pigment epithelium layer analysis that has
ow become possible using the Cirrus OCT has helpedn the further understanding of the clinical signs of theisease. Areas of serous RD were found to be adjacent tohe large undulations on the 3D RPE map in the acutehase. These undulations may result from thickenedhoroid infiltrated with inflammatory cells that pusheshe RPE forward, resulting in the formation of anndulation. The troughs of these undulations corre-pond to the choroidal striations seen in acute-stage
IGURE 4. Images showing the outer retinal segment in the acuf the left eye of a patient with acute VKH disease. (Top middubretinal space in the late phase. (Top right) scanning laser ophcans. (Bottom) Raster line scan showing normal retinal architrrows demarcate the ELM. The solid green arrows indicatehotoreceptors shows increased thickness that is irregular (bidif fluid. The arrowheads indicate the undulations present in th
KH disease that are seen as hypofluorescent lines on i
AMERICAN JOURNAL OF52
FA. The small bumps seen on the surface of thendulation seem to correspond to the areas seen typi-ally on FA as multiple pinpoint leakage sites, whichesult in late pooling of dye in the subretinal space. Theye leaking from the peaks of the undulations pools inhe troughs so that the hypofluorescent lines are noonger seen in the late frames of the fluoresceinngiograms.
In conclusion, SD Cirrus OCT showed that VKHisease at the time of initial presentation in the acuteveitic stage was confined mainly to the outer segment ofetina. The architecture of the inner retinal segment wasell maintained in all the eyes. The changes in the outer
etinal segment included thickening or irregularity of theS/OS junction, with undulations and bumps on theurface of RPE. The troughs of these undulations were seens choroidal striations in the acute phase that resolve on
age of VKH disease in Patient 2. (Top left) Fundus photographndus fluorescein angiogram showing pooling of the dye in theoscope fundus OCT scan showing the placement of raster line
e inner to the external limiting membrane (ELM). The yellownction of the inner and outer segment; the outer segment ofonal arrows) with a hyporeflective area indicating the presenceE layer.
nitiation of systemic corticosteroid therapy.
HE AUTHORS INDICATE NO FINANCIAL SUPPORT OR FINANCIAL CONFLICT OF INTEREST. INVOLVED IN CONCEPTION ANDesign (V.G., A.G.); analysis and interpretation (V.G., A.G., P.G.); data collection (V.G., A.G., A.S.); writing the article (V.G.); review of theanuscript (V.G., A.G., A.S.); and approval of the manuscript (V.G., P.G., A.G., A.S.). The Institutional Review Board of the Postgraduate Institute
f Medical Education and Research, Chandigarh, India, approved the project. The study was in accordance with the Declaration of Helsinki.
te stle) Futhalmecturin jurectie RP
OPHTHALMOLOGY JANUARY 2009
1
2
3
4
5
6
7
8
9
FOrsfslr(c
V
REFERENCES
. Moorthy RS, Inomata H, Rao NA. Vogt-Koyanagi-Haradasyndrome. Surv Ophthalmol 1995;39:265–292.
. Maruyama Y, Kishi S. Tomographic features of serous retinaldetachment in Vogt-Koyanagi-Harada syndrome. OphthalmicSurg Lasers Imaging 2004;35:239–42.
. Yamaguchi Y, Otani T, Kishi S. Tomographic features ofserous retinal detachment with multilobular dye pooling inacute Vogt-Koyanagi-Harada disease. Am J Ophthalmol 2007;144:260–265.
. Wu W, Wen F, Huang S, Luo G, Wu D. Choroidal folds inVogt-Koyanagi-Harada disease. Am J Ophthalmol 2007;143:900–901.
. Read RW, Holland GN, Rao NA, et al. Revised diagnostic
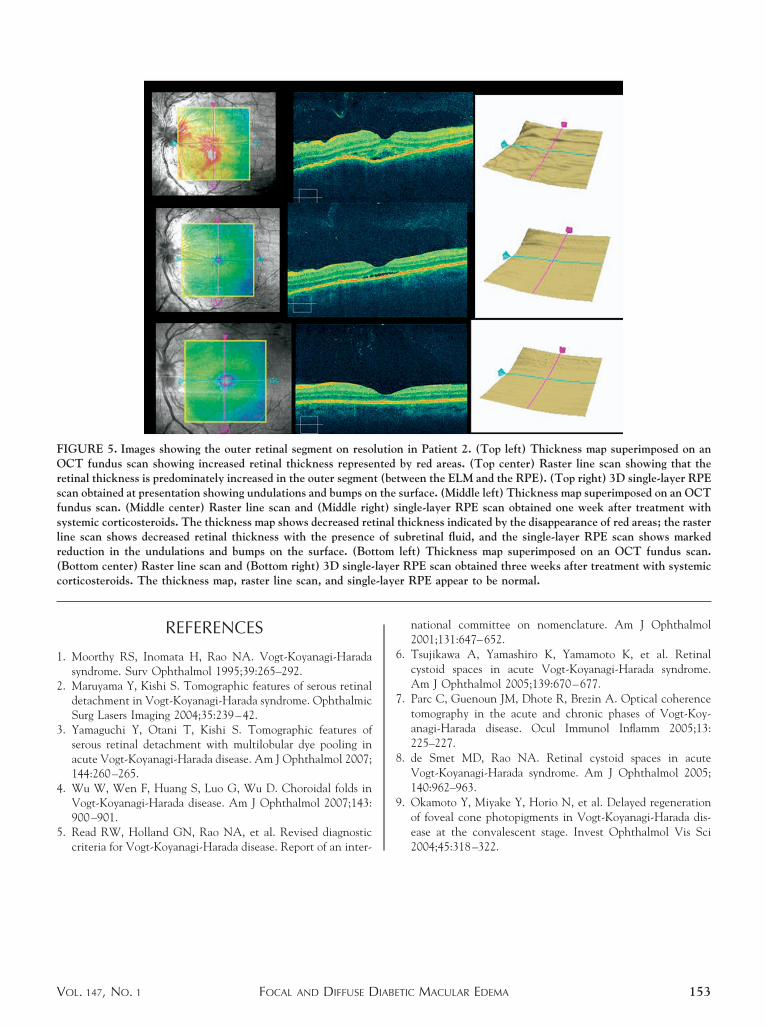
IGURE 5. Images showing the outer retinal segment on resoCT fundus scan showing increased retinal thickness represe
etinal thickness is predominately increased in the outer segmencan obtained at presentation showing undulations and bumps onundus scan. (Middle center) Raster line scan and (Middle rigystemic corticosteroids. The thickness map shows decreased retine scan shows decreased retinal thickness with the presenceeduction in the undulations and bumps on the surface. (BotBottom center) Raster line scan and (Bottom right) 3D single-orticosteroids. The thickness map, raster line scan, and single
criteria for Vogt-Koyanagi-Harada disease. Report of an inter-
FOCAL AND DIFFUSE DIABEOL. 147, NO. 1
national committee on nomenclature. Am J Ophthalmol2001;131:647–652.
. Tsujikawa A, Yamashiro K, Yamamoto K, et al. Retinalcystoid spaces in acute Vogt-Koyanagi-Harada syndrome.Am J Ophthalmol 2005;139:670–677.
. Parc C, Guenoun JM, Dhote R, Brezin A. Optical coherencetomography in the acute and chronic phases of Vogt-Koy-anagi-Harada disease. Ocul Immunol Inflamm 2005;13:225–227.
. de Smet MD, Rao NA. Retinal cystoid spaces in acuteVogt-Koyanagi-Harada syndrome. Am J Ophthalmol 2005;140:962–963.
. Okamoto Y, Miyake Y, Horio N, et al. Delayed regenerationof foveal cone photopigments in Vogt-Koyanagi-Harada dis-ease at the convalescent stage. Invest Ophthalmol Vis Sci
n in Patient 2. (Top left) Thickness map superimposed on anby red areas. (Top center) Raster line scan showing that the
tween the ELM and the RPE). (Top right) 3D single-layer RPEsurface. (Middle left) Thickness map superimposed on an OCTingle-layer RPE scan obtained one week after treatment withthickness indicated by the disappearance of red areas; the rasterubretinal fluid, and the single-layer RPE scan shows markedleft) Thickness map superimposed on an OCT fundus scan.RPE scan obtained three weeks after treatment with systemicr RPE appear to be normal.
lutiontedt (bethe
ht) sinalof s
tomlayer-laye
2004;45:318–322.
TIC MACULAR EDEMA 153
VVCt
1
Biosketch
ishali Gupta is currently working as an Associate Professor in the Department of Ophthalmology (in the subspecialty ofitreo-retina and Uvea) at the Advanced Eye Centre at the Postgraduate Institute of Medical Education and Research,handigarh, India. Dr Gupta’s major areas of interest are the intraocular infections, diabetes, and imaging modalities for
he retinal diseases.
AMERICAN JOURNAL OF OPHTHALMOLOGY53.e1 JANUARY 2009
AId
V
Biosketch
mod Gupta is a Professor and Heads the Department of Ophthalmology at the Advanced Eye Centre at the Postgraduatenstitute of Medical Education and Research, Chandigarh, India. Dr Gupta has extensively published original work iniseases of Retina and Uvea.
FOCAL AND DIFFUSE DIABETIC MACULAR EDEMAOL. 147, NO. 1 153.e2




















