
Selective Right Ventricular Unloading and Novel Technical Concepts in Ebstein's Anomaly
7
Selective Right Ventricular Unloading and Novel Technical Concepts in Ebstein’s Anomaly Sunil P. Malhotra, MD, Ed Petrossian, MD, V. Mohan Reddy, MD, Mary Qiu, BS, Katsushide Maeda, MD, Sam Suleman, BS, Malcolm MacDonald, MD, Olaf Reinhartz, MD, and Frank L. Hanley, MD Division of Pediatric Cardiac Surgery, Stanford University School of Medicine, Stanford, California Background. Favorable outcomes in Ebstein’s anom- aly are predicated on tricuspid valve competence and right ventricular function. Successful valve repair should be aggressively pursued to avoid the morbidity of prosthetic tricuspid valve replacement. We report our experience with valve-sparing intracardiac repair, emphasizing novel concepts and techniques of valve repair supplemented by selective bidirectional Glenn (BDG). Methods. Between June 1993 and December 2008, 57 nonneonatal patients underwent Ebstein’s anomaly repairs. The median age at operation was 8.1 years. All were symptomatic in New York Heart Association (NYHA) func- tional class II (n 38), III (n 17), or IV (n 1). Preoperatively, 26 had mild or moderate cyanosis at rest. We used a number of valve reconstructive techniques that differed substantially from those currently described. BDG was per- formed in 31 patients (55%) who met specific criteria. Results. No early or late deaths occurred. At the initial repair, 3 patients received a prosthetic valve. Four patients required reoperation for severe tricuspid regurgitation. Repeat repairs were successful in 2 pa- tients. At follow-up (range, 3 months to 6 years), all patients were acyanotic and in NYHA class I. Tricuspid regurgitation was mild or less in 49 (86%) and moder- ate in 6 (11%). Freedom from a prosthesis was 91% (52 of 57). Conclusions. Following a protocol using BDG for ven- tricular unloading in selected patients with Ebstein’s anomaly can achieve a durable valve-sparing repair us- ing the techniques described. Excellent functional mid- term outcomes can be obtained with a selective one and a half ventricle approach to Ebstein’s anomaly. (Ann Thorac Surg 2009;88:1975– 81) © 2009 by The Society of Thoracic Surgeons E bstein’s anomaly is a complex malformation of both the tricuspid valve and the right ventricle (RV) that exhibits characteristic lesions of variable severity. Tricus- pid valve function is affected by failure of delamination of the valve leaflets, anterior leaflet tethering, annular dila- tation, and apical displacement of the tricuspid valve annulus [1]. This downward displacement of the attach- ments of the septal and posterior leaflets also effectively reduces the functional mass of the RV. RV function is further impaired by the histologically abnormal myocar- dium associated with Ebstein’s anomaly [2]. Clinical manifestations of Ebstein’s anomaly stem from the severity of the component anatomic lesions. Functional limitations typically present as a result of progressive RV dysfunction and ventricular interdependent effects impair- ing left ventricular function. Cyanosis develops as a result of right-to-left shunting through an atrial communication. Massive right atrial dilation contributes to the development of recurrent atrial dysrhythmias. Surgical therapy for Ebstein’s anomaly should restore tricuspid valve competence and address the inadequacy of the inefficient RV. As the surgical experience with Ebstein’s anomaly has accumulated, the approach has evolved from isolated tricuspid valve replacement [3] and repair [4] to tricuspid repair in conjunction with RV reconstructive techniques [5, 6]. The inferior wall of the RV is often thinned and dyskinetic. Suture plication of this segment excludes the nonfunctional portion of the RV, potentially improving efficiency of the right heart. All of the existing major strategies for repair of the Ebstein’s valve described in the literature have in common several similar principles: restoring the functional valve orifice to the anatomic right atrioventricular junction, detachment and reimplantation of the major leaflets, and complete plication of the atrialized portion of the RV [5–7]. The bidirectional Glenn (BDG) has been used to im- prove RV energetics in a variety of lesions that result in borderline RV function [8 –10]. The “one and a half ventricle” strategy uses the superior cavopulmonary con- nection to unload the myopathic RV, reducing RV work during systole. In Ebstein’s anomaly, this approach has been advocated to reduce the preload on a dilated, poorly functioning RV [11, 12]. In patients with significant func- tional limitations, the BDG can relieve the “pancake effect” of a massively dilated RV on the left ventricle, thus Accepted for publication July 2, 2009. Presented at the Forty-fifth Annual Meeting of The Society of Thoracic Surgeons, San Francisco, CA, Jan 26 –28, 2009. Address correspondence to Dr Malhotra, Congenital Heart Center at the University of Florida, PO Box 100296, Gainesville, FL 32610-0296; e-mail: [email protected]fl.edu. © 2009 by The Society of Thoracic Surgeons 0003-4975/09/$36.00 Published by Elsevier Inc doi:10.1016/j.athoracsur.2009.07.019 PEDIATRIC CARDIAC
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Selective Right Ventricular Unloading and Novel Technical Concepts in Ebstein's Anomaly
STSKOD
arsooer(
nTstPusf
Eepttamrfd
tldioMo
A
PS
AUs
©P
elective Right Ventricular Unloading and Novelechnical Concepts in Ebstein’s Anomaly
unil P. Malhotra, MD, Ed Petrossian, MD, V. Mohan Reddy, MD, Mary Qiu, BS,atsushide Maeda, MD, Sam Suleman, BS, Malcolm MacDonald, MD,laf Reinhartz, MD, and Frank L. Hanley, MD
ivision of Pediatric Cardiac Surgery, Stanford University School of Medicine, Stanford, California
iFrtprao
taita
PED
IAT
RIC
CA
RD
IAC
Background. Favorable outcomes in Ebstein’s anom-ly are predicated on tricuspid valve competence andight ventricular function. Successful valve repairhould be aggressively pursued to avoid the morbidityf prosthetic tricuspid valve replacement. We reportur experience with valve-sparing intracardiac repair,mphasizing novel concepts and techniques of valveepair supplemented by selective bidirectional GlennBDG).
Methods. Between June 1993 and December 2008, 57onneonatal patients underwent Ebstein’s anomaly repairs.he median age at operation was 8.1 years. All wereymptomatic in New York Heart Association (NYHA) func-ional class II (n � 38), III (n � 17), or IV (n � 1).reoperatively, 26 had mild or moderate cyanosis at rest. Wesed a number of valve reconstructive techniques that differedubstantially from those currently described. BDG was per-
ormed in 31 patients (55%) who met specific criteria.toEerrRtRovstap
pbvndbfte
niversity of Florida, PO Box 100296, Gainesville, FL 32610-0296; e-mail:[email protected].
2009 by The Society of Thoracic Surgeonsublished by Elsevier Inc
Results. No early or late deaths occurred. At thenitial repair, 3 patients received a prosthetic valve.our patients required reoperation for severe tricuspidegurgitation. Repeat repairs were successful in 2 pa-ients. At follow-up (range, 3 months to 6 years), allatients were acyanotic and in NYHA class I. Tricuspidegurgitation was mild or less in 49 (86%) and moder-te in 6 (11%). Freedom from a prosthesis was 91% (52f 57).Conclusions. Following a protocol using BDG for ven-
ricular unloading in selected patients with Ebstein’snomaly can achieve a durable valve-sparing repair us-ng the techniques described. Excellent functional mid-erm outcomes can be obtained with a selective one andhalf ventricle approach to Ebstein’s anomaly.
(Ann Thorac Surg 2009;88:1975–81)
© 2009 by The Society of Thoracic Surgeonsbstein’s anomaly is a complex malformation of boththe tricuspid valve and the right ventricle (RV) that
xhibits characteristic lesions of variable severity. Tricus-id valve function is affected by failure of delamination of
he valve leaflets, anterior leaflet tethering, annular dila-ation, and apical displacement of the tricuspid valvennulus [1]. This downward displacement of the attach-ents of the septal and posterior leaflets also effectively
educes the functional mass of the RV. RV function isurther impaired by the histologically abnormal myocar-ium associated with Ebstein’s anomaly [2].Clinical manifestations of Ebstein’s anomaly stem from
he severity of the component anatomic lesions. Functionalimitations typically present as a result of progressive RVysfunction and ventricular interdependent effects impair-
ng left ventricular function. Cyanosis develops as a resultf right-to-left shunting through an atrial communication.assive right atrial dilation contributes to the development
f recurrent atrial dysrhythmias.
ccepted for publication July 2, 2009.
resented at the Forty-fifth Annual Meeting of The Society of Thoracicurgeons, San Francisco, CA, Jan 26–28, 2009.
ddress correspondence to Dr Malhotra, Congenital Heart Center at the
Surgical therapy for Ebstein’s anomaly should restorericuspid valve competence and address the inadequacyf the inefficient RV. As the surgical experience withbstein’s anomaly has accumulated, the approach hasvolved from isolated tricuspid valve replacement [3] andepair [4] to tricuspid repair in conjunction with RVeconstructive techniques [5, 6]. The inferior wall of theV is often thinned and dyskinetic. Suture plication of
his segment excludes the nonfunctional portion of theV, potentially improving efficiency of the right heart. Allf the existing major strategies for repair of the Ebstein’salve described in the literature have in common severalimilar principles: restoring the functional valve orifice tohe anatomic right atrioventricular junction, detachmentnd reimplantation of the major leaflets, and completelication of the atrialized portion of the RV [5–7].The bidirectional Glenn (BDG) has been used to im-
rove RV energetics in a variety of lesions that result inorderline RV function [8–10]. The “one and a halfentricle” strategy uses the superior cavopulmonary con-ection to unload the myopathic RV, reducing RV workuring systole. In Ebstein’s anomaly, this approach haseen advocated to reduce the preload on a dilated, poorly
unctioning RV [11, 12]. In patients with significant func-ional limitations, the BDG can relieve the “pancake
ffect” of a massively dilated RV on the left ventricle, thus0003-4975/09/$36.00doi:10.1016/j.athoracsur.2009.07.019
iet
tcltott
mpdd
1
2
3
cr
M
Tctw
PBuoor
cpdto4du
bytwcFsf
F
Fam
1976 MALHOTRA ET AL Ann Thorac SurgNOVEL CONCEPTS IN EBSTEIN’S ANOMALY 2009;88:1975–81
PEDIA
TR
ICC
AR
DIA
C
mproving biventricular function [13]. An additional ben-fit we have realized is that the unloaded RV is amenableo an aggressive tricuspid valve repair strategy.
In patients who require very aggressive valvuloplastyechniques that reduce the functional orifice of the tri-uspid valve, RV unloading permits an otherwise border-ine valve opening to be functionally adequate, avoidinghe need for prosthetic tricuspid valve replacement. Usef the BDG serves to reduce both the risk of postrepairricuspid stenosis and potential progression of residualricuspid regurgitation (TR).
This report summarizes our experience with the surgicalanagement of Ebstein’s anomaly outside of the neonatal
eriod. The study focuses on two major points: First, weescribe the use of valve reconstructive techniques thatiffer substantially from those in the literature:
. A “play it where it lies” approach to the tricuspidvalve in which the reconstruction is performed atthe functional orifice instead of moving the valve tothe anatomic tricuspid annulus;
. Avoidance of detachment and reimplantation ofvalve leaflets; and
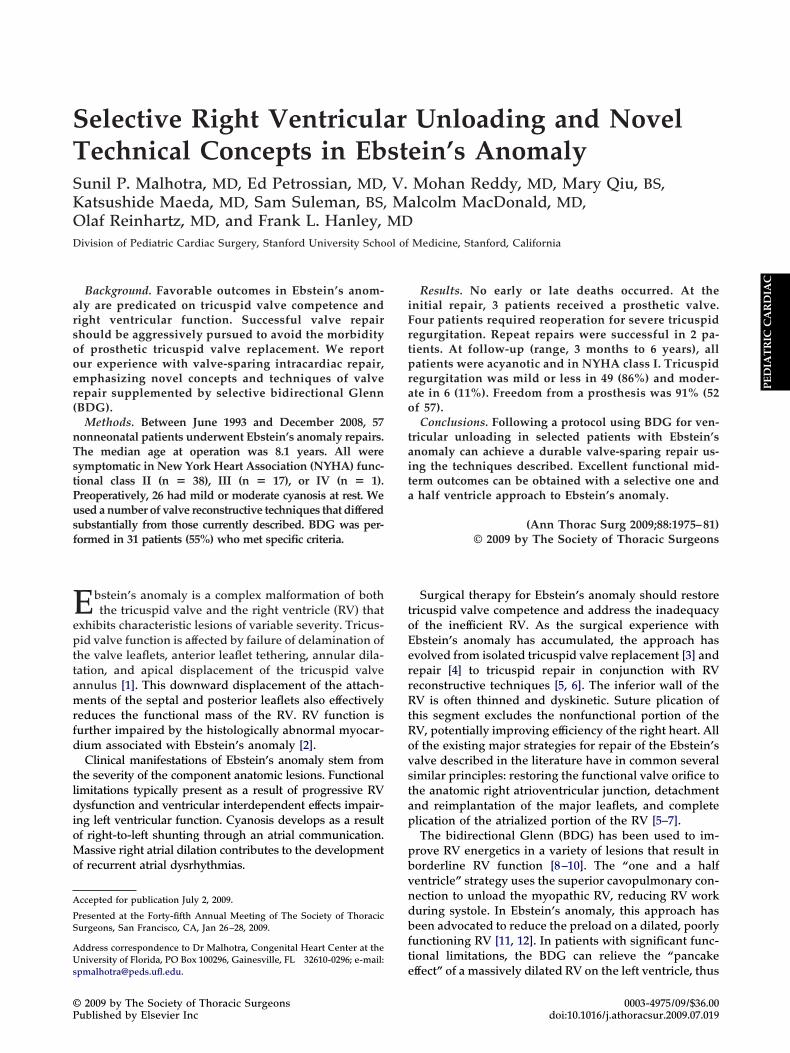
ig 1. Graph shows age distribution of patients at time of operation.
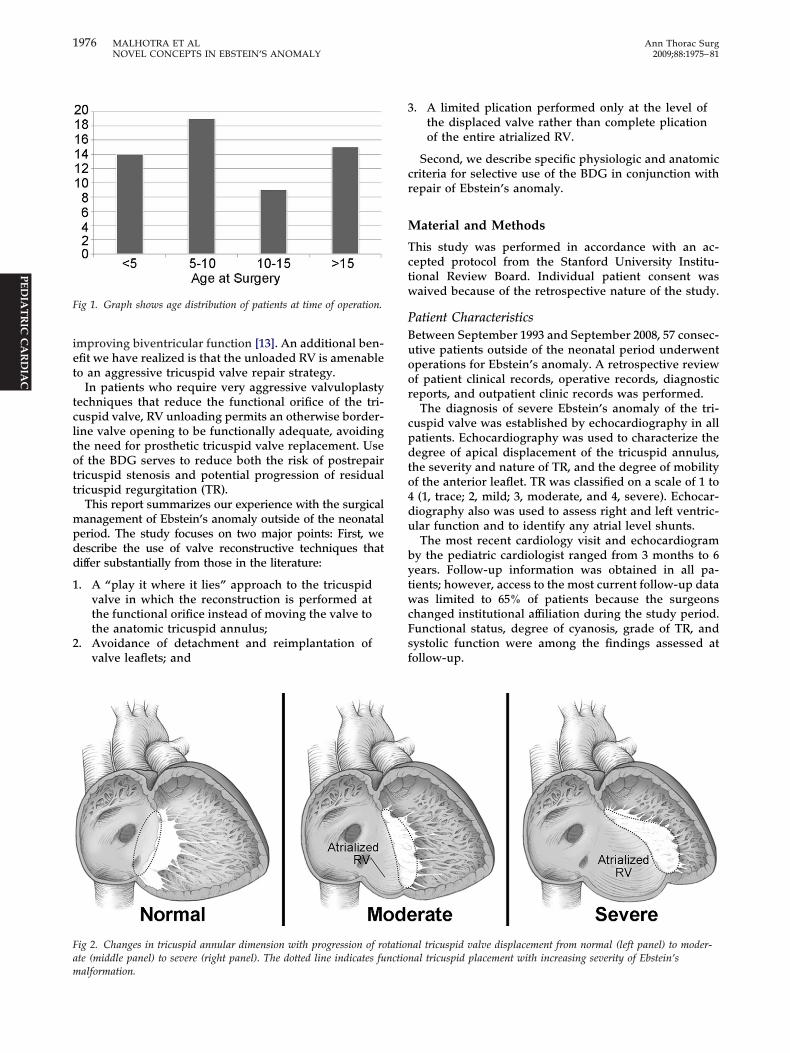
ig 2. Changes in tricuspid annular dimension with progression of rote (middle panel) to severe (right panel). The dotted line indicates fu
alformation.. A limited plication performed only at the level ofthe displaced valve rather than complete plicationof the entire atrialized RV.
Second, we describe specific physiologic and anatomicriteria for selective use of the BDG in conjunction withepair of Ebstein’s anomaly.
aterial and Methods
his study was performed in accordance with an ac-epted protocol from the Stanford University Institu-ional Review Board. Individual patient consent wasaived because of the retrospective nature of the study.
atient Characteristicsetween September 1993 and September 2008, 57 consec-tive patients outside of the neonatal period underwentperations for Ebstein’s anomaly. A retrospective reviewf patient clinical records, operative records, diagnosticeports, and outpatient clinic records was performed.
The diagnosis of severe Ebstein’s anomaly of the tri-uspid valve was established by echocardiography in allatients. Echocardiography was used to characterize theegree of apical displacement of the tricuspid annulus,
he severity and nature of TR, and the degree of mobilityf the anterior leaflet. TR was classified on a scale of 1 to(1, trace; 2, mild; 3, moderate, and 4, severe). Echocar-iography also was used to assess right and left ventric-lar function and to identify any atrial level shunts.The most recent cardiology visit and echocardiogram
y the pediatric cardiologist ranged from 3 months to 6ears. Follow-up information was obtained in all pa-ients; however, access to the most current follow-up dataas limited to 65% of patients because the surgeons
hanged institutional affiliation during the study period.unctional status, degree of cyanosis, grade of TR, andystolic function were among the findings assessed atollow-up.
al tricuspid valve displacement from normal (left panel) to moder-al tricuspid placement with increasing severity of Ebstein’s
tationnction

(cdacapo
OAdmdtwccgtarr
AAEnipo
1
2
Ftoocb
1977Ann Thorac Surg MALHOTRA ET AL2009;88:1975–81 NOVEL CONCEPTS IN EBSTEIN’S ANOMALY
PED
IAT
RIC
CA
RD
IAC
The median patient age at operation was 8.1 yearsrange, 7 months to 40.4 years). Patients requiring surgi-al intervention as a neonate were excluded. The ageistribution is displayed in Figure 1. There were 28 malesnd 29 females. Clinical status at presentation was exer-ise intolerance in 40, cyanosis in 26, RV failure in 18, andtrial dysrhythmias in 8. TR was moderate or severe in 50atients (87.7%). An atrial septal defect or patent foramenvale was present in 46 (80.7%).
perative Techniquestandardized approach using median sternotomy, car-
iopulmonary bypass with mild or moderate hypother-ia, bicaval cannulation, aortic cross-clamping, and in-
uction of cardioplegia-induced arrest is followed. Thericuspid valve is exposed through a right atriotomy,hich extends from the appendage to the inferior vena
aval junction. If present, intraatrial communications arelosed by primary suture closure or with a patch oflutaraldehyde-treated autologous pericardium. Rou-inely, at the end of the procedure, wide strips of righttrial free wall on each side of the right atrial incision areemoved before atrial closure, achieving a significantight atrial reduction plasty.
pproaches to the Tricuspid Valvenumber of well-known technical approaches to the
bstein’s tricuspid valve have been reported. We haveot followed any of these. We believe there are several
mportant concepts that have not been emphasized in theublished reports that have an important influence onur method of tricuspid valve repair:
. The detrimental effects of a very large tricuspid annu-lus—The functional opening of the tricuspid valveis markedly enlarged in Ebstein’s anomaly due tothe leaflet displacement. As the displacement be-comes more severe, the annular dimension pro-gressively enlarges (Fig 2). As a result, significantcomponents of the valve cross-sectional area can beobliterated, as necessary, to achieve valve compe-tence. The tricuspid valve cross-sectional diametermay be as large as 6 cm in severely displacedvalves. A 70-kg adult requires a valve diameter ofonly 2.5 cm or less. We believe that “excess” valvediameter after repair increases the chances of bothearly and late valve instability and has no counter-balancing benefits. Thus, our approach is to reducethe valve opening to approximately 2.5 cm in the70-kg patient (or indexed appropriately for smallerpatients). This is achieved by using a number oftechnical maneuvers in various combinations asneeded. One of these maneuvers, the limited plica-tion of the atrialized RV, is described in point 2. Theother maneuvers are listed in point 4.
. The goal of plication of the atrialized RV—Varioustechnical approaches and general philosophiesrelating to the atrialized portion of the RV havebeen described. Our approach and philosophy
differs from these. We believe that the plicationmaneuver is useful only as a component of thevalve repair; thus, we do not plicate the entireatrialized portion all the way to the anatomictricuspid annulus. Complete plication runs therisk of distorting major coronary arteries, or atthe very least creates myocardial ischemia simplyfrom tissue compression. Rather, we focus onlyon the portion of the atrialized RV closest to theRV apex, at the point of maximal displacement,essentially where the displaced posterior leaflet,if present, would be positioned (Fig 3). We ag-gressively perform plication in this region usingone, or at most, 2 separate heavy (2-0) polypro-pylene pledgetted mattress sutures placed inter-nally within the RV. Particular care is taken toavoid occlusion or distortion of all coronary ar-teries running on the surface of the RV with thesesutures. We specifically avoid extending the pli-cation towards the anatomic tricuspid annulus(atrioventricular groove) out of concerns for dis-torting the main right coronary artery or its majorbranches; thus, we perform neither a classic ra-dial plication (Danielson) nor a complete verticalplication (Carpentier). The 1 or 2 plication su-tures we do place are oriented similarly to thevertical plication technique. The resulting plica-tion essentially coapts the most apical aspect ofthe anterior leaflet with the apical aspect of theseptal leaflet, in essence achieving a functionalbicuspid valve. This plication maneuver as de-scribed may reduce the orifice size by as much
ig 3. The “play it where it lies” approach involves limited plica-ion of the tricuspid valve. Points A and B are approximated with 1r 2 mattress sutures at the level of the native valve, not to the levelf the true tricuspid annulus. This results in approximating the api-al aspects of the septal and anterior leaflets, effectively creating aicuspid valve.
as 50%.

3
4
SAEmrptri(twT
SSwaSFm
T
Ar
TE
R
1978 MALHOTRA ET AL Ann Thorac SurgNOVEL CONCEPTS IN EBSTEIN’S ANOMALY 2009;88:1975–81
PEDIA
TR
ICC
AR
DIA
C
An important point is that the resulting functionalvalve orifice, although markedly reduced in size, isnot moved from its displaced position. Moreover,leaflet detachment and reimplantation is never per-formed. A number of additional valve reconstruc-tive maneuvers are almost always used, in variouscombinations, to achieve the best result with re-spect to valve competence. These are described inpoint 4. Most of these maneuvers further reduce theopening of the valve (see subsequent discussion ofBDG).
. Selective use of the BDG—We use the BDG in twoseparate and independent circumstances. The firstis physiologic. Cyanosis at rest is a marker for aninadequate RV pump. We typically perform a BDGin these patients as part of the overall operation. Ifthe patient is fully saturated at rest but becomescyanotic with exercise, this is a relative marker of aninadequate RV pump, and we will have a lowthreshold for placing a BDG. Typically, we willseparate the patient from cardiopulmonary bypassafter valve repair and monitor right and left atrialpressure. If the right atrial pressure exceeds 1.5times the left atrial pressure under these relativelyunstressed conditions of an open chest in an anes-thetized patient, we will perform a BDG. If thepatient presents with an intact atrial septum or anatrial septal defect with left-to-right shunting, aBDG is not performed.The second circumstance for placing a BDG isanatomic and relates to the ultimate size of thefunctional tricuspid annulus after repair. If it isnecessary to make the functional tricuspid orificesubstantially less than 2.5 cm (in a 70-kg patient) toachieve a competent valve, we will assess inflowvelocity across the tricuspid after separation fromcardiopulmonary bypass using transesophagealechocardiography. If obstruction is demonstrated, aBDG is placed. We acknowledge that many of themaneuvers used to make a regurgitant valve com-petent involve reducing the valve opening. Thisoption for BDG use frees us to aggressively reducethe functional valve orifice as much as necessary toachieve a stable, competent valve repair.
. Other maneuvers on the tricuspid valve—In additionto the modified plication of the atrialized RV,other maneuvers may be used in varying combi-
able 1. Surgical Procedures for Ebstein’s Anomaly Repair
Procedure No.
Valvuloplasty 51Valve replacement 3Plication of atrialized RV 55Right atrial reduction plasty 52ASD/PFO closure 46Bidirectional Glenn 31
0SD � atrial septal defect; PFO � patent foramen ovale; RV �
ight ventricle.
nations as needed to further reduce the valve sizeand address the regurgitation. These include clo-sure of primary commissures, closure of “second-ary commissures” (those within an individualvalve leaflet, usually the large anterior leaflet),true anatomic annuloplasty for that component ofthe valve (anterior leaflet) that is not displaced,primary or patch closure of leaflet fenestrations,and placement of a polytetrafluoroethylene dia-phragm in the position of the displaced septalleaflet (acting as a nonmoving buttress for theanterior leaflet to close against) in those caseswhere the coaptation surface is limited by thecombination of insufficient anterior leaflet andabsent septal leaflet tissue.
urgical Proceduresll 57 patients underwent an initial operation forbstein’s anomaly. Component procedures are sum-arized in Table 1. A valve-sparing Ebstein’s anomaly
epair was performed in 54 patients; of these, valvulo-lasty was performed in conjunction with plication of
he atrialized RV in 50. Prosthetic tricuspid valveeplacement was performed in 3 patients (5.4%) at thenitial operation, and a BDG was performed in 3155%). Atrial septal defects were closed in all 46 pa-ients. Concomitant procedures at time of initial repairere performed in 13 patients and are reported inable 2.
tatistical Analysistatistical analysis was performed with Prism 5.0 soft-are (GraphPad Inc, San Diego, CA). Data are described
s median with ranges or mean with standard deviation.erial data are compared between groups using the t test.reedom from tricuspid valve replacement was deter-ined by actuarial Kaplan-Meier analysis. Values of p �
able 2. Concomitant Procedures Performed at Initialbstein’s Anomaly Repair
Procedures No.
Electrophysiologic procedures 8Ablation of accessory pathway 2Maze procedures
Bilateral 2With pacemaker 1
Right-sided 3With pacemaker 1
Pacemaker alone 1Partial anomalous pulmonary vein repair 1Pulmonary valve replacement 1Relief of RV outflow tract obstruction 2Supravalvar pulmonary stenosis repair 1
V � right ventricular.
.05 were considered statistically significant.
R
NrprdAna
OAw(pmbpt
pmop
f9
FAf(eaPocc9
OAwB9cdtup
ccpuv(r
gut5sF
4
Fr
Ff0
1979Ann Thorac Surg MALHOTRA ET AL2009;88:1975–81 NOVEL CONCEPTS IN EBSTEIN’S ANOMALY
PED
IAT
RIC
CA
RD
IAC
esults
o early or late deaths occurred. Early reoperation wasequired in 2 patients. One patient required pacemakerlacement for atrioventricular nodal block and 1 patientequired placement of an implantable cardioverter-efibrillator device for recurrent ventricular arrhythmias.t follow-up echocardiography, RV systolic function wasormal in 52 patients, mildly reduced in 3, and moder-tely reduced in 2 patients.
utcomes of Tricuspid Valve Repairt initial operation, 54 of 57 patients (94.7%) under-ent a valve-sparing Ebstein’s anomaly repair, and 4
7.4%) required reoperation for recurrent TR. Twoatients underwent successful repeat repair at 7onths and 4.1 years after the initial operation, and
oth had mild TR at follow-up. Two patients requiredrosthetic valve replacement at 1.5 and 5.6 years after
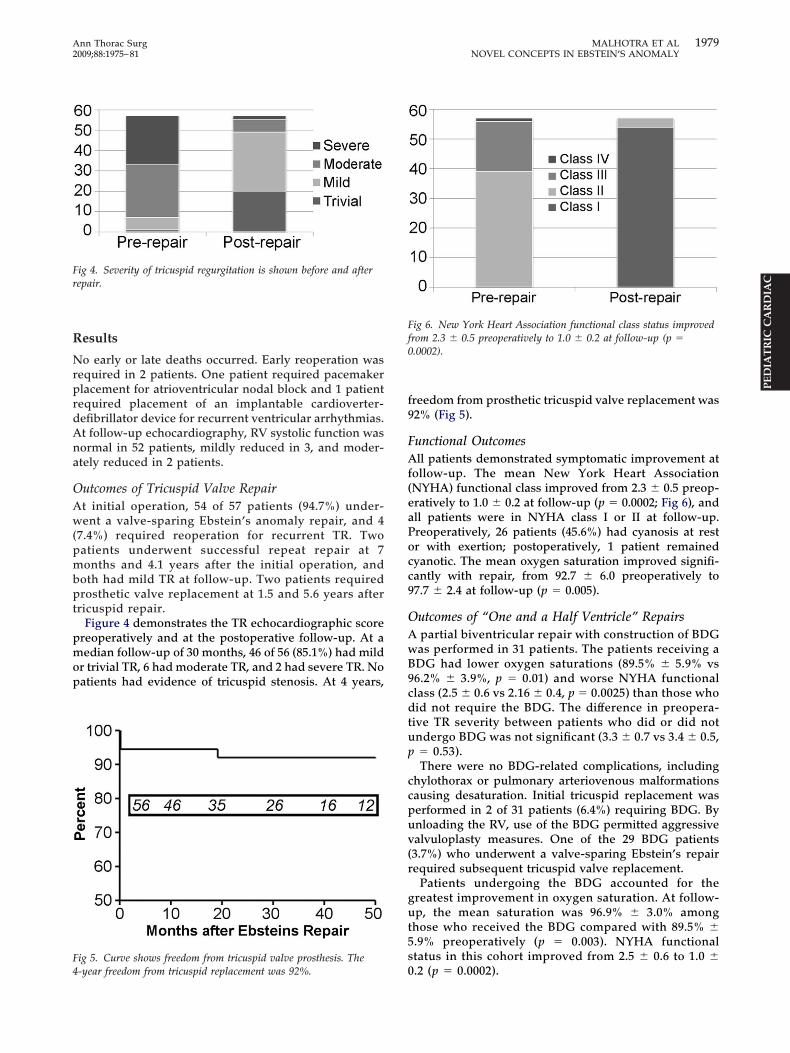
ricuspid repair.Figure 4 demonstrates the TR echocardiographic score
reoperatively and at the postoperative follow-up. At aedian follow-up of 30 months, 46 of 56 (85.1%) had mild
r trivial TR, 6 had moderate TR, and 2 had severe TR. Noatients had evidence of tricuspid stenosis. At 4 years,
ig 5. Curve shows freedom from tricuspid valve prosthesis. The
ig 4. Severity of tricuspid regurgitation is shown before and afterepair.
0-year freedom from tricuspid replacement was 92%.
reedom from prosthetic tricuspid valve replacement was2% (Fig 5).
unctional Outcomesll patients demonstrated symptomatic improvement at
ollow-up. The mean New York Heart AssociationNYHA) functional class improved from 2.3 � 0.5 preop-ratively to 1.0 � 0.2 at follow-up (p � 0.0002; Fig 6), andll patients were in NYHA class I or II at follow-up.reoperatively, 26 patients (45.6%) had cyanosis at restr with exertion; postoperatively, 1 patient remainedyanotic. The mean oxygen saturation improved signifi-antly with repair, from 92.7 � 6.0 preoperatively to7.7 � 2.4 at follow-up (p � 0.005).
utcomes of “One and a Half Ventricle” Repairspartial biventricular repair with construction of BDGas performed in 31 patients. The patients receiving aDG had lower oxygen saturations (89.5% � 5.9% vs6.2% � 3.9%, p � 0.01) and worse NYHA functionallass (2.5 � 0.6 vs 2.16 � 0.4, p � 0.0025) than those whoid not require the BDG. The difference in preopera-
ive TR severity between patients who did or did notndergo BDG was not significant (3.3 � 0.7 vs 3.4 � 0.5,� 0.53).There were no BDG-related complications, including
hylothorax or pulmonary arteriovenous malformationsausing desaturation. Initial tricuspid replacement waserformed in 2 of 31 patients (6.4%) requiring BDG. Bynloading the RV, use of the BDG permitted aggressivealvuloplasty measures. One of the 29 BDG patients3.7%) who underwent a valve-sparing Ebstein’s repairequired subsequent tricuspid valve replacement.
Patients undergoing the BDG accounted for thereatest improvement in oxygen saturation. At follow-p, the mean saturation was 96.9% � 3.0% among
hose who received the BDG compared with 89.5% �.9% preoperatively (p � 0.003). NYHA functionaltatus in this cohort improved from 2.5 � 0.6 to 1.0 �
ig 6. New York Heart Association functional class status improvedrom 2.3 � 0.5 preoperatively to 1.0 � 0.2 at follow-up (p �.0002).
.2 (p � 0.0002).

C
Lobtnmvogs
mmvpqtfwTm
brsqeptetrfadaal
tappomdpn1dui
mspws
sBvt
dBcwbTo
ites
rEssvsaetp
ngeriiMacsbtp
touivfr
R
1980 MALHOTRA ET AL Ann Thorac SurgNOVEL CONCEPTS IN EBSTEIN’S ANOMALY 2009;88:1975–81
PEDIA
TR
ICC
AR
DIA
C
omment
ong-term prognosis for Ebstein’s anomaly is predicatedn tricuspid valve competence and RV function. Weelieve our approach to this complex lesion is applicable
o the entire spectrum of anatomy and physiology ofon-neonatal Ebstein’s anomaly. Our surgical manage-ent has focused on preserving the native tricuspid
alve and maximizing RV function. The outcomes fromur 15-year experience with Ebstein’s anomaly reflect theoals of improving functional status, eliminating cyano-is, and minimizing the need for reoperations.
Avoiding prosthetic tricuspid valve replacement is aajor guiding force in our philosophy of the surgicalanagement of Ebstein’s anomaly. Prosthetic tricuspid
alve replacement in the pediatric population is certainlyroblematic, with issues of somatic growth and subse-uent need for reoperation, thromboembolic complica-
ions, risk of endocarditis, and the effect on long-term RVunction. In a 15-year experience, a valve-sparing repairas achieved in 54 of 57 patients at the initial operation.he overall rate of prosthetic replacement at either pri-ary or subsequent operation was 8.8%.The valvuloplasty techniques are reproducible and
ased on the basic principles of valve repair and RVemodeling. As illustrated in Figure 2, the true annulus ismaller than the displaced functional annulus. Conse-uently, plication using the technique described hereffectively reduces the tricuspid annulus and also accom-lishes valvuloplasty. Concerns exist about more tradi-
ional plication, and we agree with these concerns. In anxtensive experience of 539 patients undergoing opera-ions for Ebstein’s anomaly, Brown and colleagues [14]eported that RV plication is no longer routinely per-ormed due to the development of intractable ventricularrrhythmias. Using the modified plication techniquesescribed here, we have not encountered any cases ofcute coronary insufficiency and one case of ventricularrrhythmias requiring placement of an internal defibril-ator after ventriculoplasty.
Our approach to the Ebstein’s tricuspid repair relies onhe redundant nature of the anterior leaflet to createlmost all of the coaptation surface area, the use oflication as a form of “annuloplasty” and “valvulo-lasty,” and aggressive reduction in the functional valverifice using the various techniques described. Detach-ent of the anterior leaflet from the tricuspid annulus,
escribed in several Ebstein repairs, including the Car-entier technique and, more recently, the “cone” tech-ique, has never been necessary in our experience [6, 7,5]. In instances where the annulus required significantownsizing, the cavopulmonary connection has beensed successfully to prevent tricuspid stenosis by reduc-
ng tricuspid valve inflow.The BDG has been a valuable adjunct for the surgicalanagement of Ebstein’s anomaly. We have followed a
elective protocol in which the BDG is added in allatients with resting cyanosis and in selected patientsith effort-induced cyanosis. In these patients, the BDG
erves to off-load a marginal RV that has required con-
iderable right-to-left shunting. Intraoperatively, theDG may be used if it is judged that the extensivealvuloplasty measures required would create functionalricuspid stenosis.
In addition to facilitating significant annular reductionuring tricuspid repair, the volume load reduction fromDG alone can lead to reduction in severity of TR. Threeyanotic patients in our early experience underwent BDGithout valvuloplasty and had mild TR that was found toe trivial at follow-up. This observation of a reduction inR with a cavopulmonary connection alone was previ-usly reported by Marianeschi and colleagues [16].In cyanotic patients with significant right-to-left shunt-
ng, the BDG reduces the volume load on the dysfunc-ional RV. The reduced volume along with improved RVfficiency resulting from RV plication permits safe clo-ure of the intraatrial communication in these patients.
Our approach contrasts with other groups who haveeserved the BDG for only the most severe forms ofbstein’s anomaly. Quinonez and colleagues [17] de-cribed using the BDG in 14 critically ill patients withevere RV dysfunction or dilation in which 11 requiredalve replacements. Chauvaud and colleagues [11] de-cribed improved survival when BDG was performed in
cohort of high-risk Ebstein’s anomaly patients. Ourxperience demonstrates the value of the selective use ofhe BDG for both durable valve repair and improved RVerformance, leading to the resolution of cyanosis.This study had several limitations. Its retrospective
ature prevents a uniform approach to echocardio-raphic interpretation. This is especially noted in thevaluation of RV function, which is challenging to accu-ately gauge by echocardiography. Future studies shoulddeally incorporate magnetic resonance imaging, whichs a more reliable tool in the evaluation of RV function.
oreover, the follow-up was limited to the short-termnd medium-term. Although no trends have emerged toause concern for long-term outcomes, longer cross-ectional follow-up will be necessary to assess the dura-ility of this approach in the long-term. Finally, exercise
esting is necessary to gain an accurate assessment ofostrepair improvements in functional status.In conclusion, we have described a surgical approach
o Ebstein’s anomaly that incorporates unique methodsf valvuloplasty, ventricular remodeling, and ventricularnloading. Our management strategy for these challeng-
ng patients has yielded a high rate of native tricuspidalve preservation, a low incidence of recurrent TR,avorable functional status and RV function, and markedesolution of cyanosis.
eferences
1. Zuberbuhler JR, Allwork SP, Anderson RH. The spectrum ofEbstein’s anomaly of the tricuspid valve. J Thorac Cardio-vasc Surg 1979;77:202–11.
2. Anderson KR, Lie JT. The right ventricular myocardium inEbstein’s anomaly: a morphometric histopathologic study.
Mayo Clinic Proc 1979;54:181–4.
1
1
1
1
1
1
1
1
D
DdMlGptbsflgG
pvopaptod
fnmitvwpr
1981Ann Thorac Surg MALHOTRA ET AL2009;88:1975–81 NOVEL CONCEPTS IN EBSTEIN’S ANOMALY
PED
IAT
RIC
CA
RD
IAC
3. Barnard CN, Schirire V. Surgical correction of Ebstein’smalformation with prosthetic tricuspid valve. Surgery 1963;54:302–8.
4. Hardy KL, May IA, Webster CA, Kimball KG. Ebstein’sanomaly: a functional concept and successful definitiverepair. J Thorac Cardiovasc Surg 1964;48:927–40.
5. Danielson GK, Driscoll DJ, Mair DD, Warnes CA, OliverWC. Operative treatment of Ebstein’s anomaly. J ThoracCardiovasc Surg 1992;104:1195–200.
6. Da Silva JP, Baumgratz JF da Fonseca L, et al. The conereconstruction of the tricuspid valve in Ebstein’s anomaly.The operation: early and midterm results. J Thorac Cardio-vasc Surg 2007;133:215–23.
7. Carpentier AC, Chavaud S, Mace L. A new reconstructiveoperation for Ebstein’s anomaly of the tricuspid valve. J Tho-rac Cardiovasc Surg 1988;96:92–101.
8. Mavroudis C, Backer CL, Kohr LM, et al. Bidirectional Glennshunt in association with congenital heart repairs: the 1-1/2ventricle repair. Ann Thorac Surg 1999;68:976–82.
9. Chowdhury UK, Airan B, Sharma R, et al. One and a halfventricle repair with pulsatile bi-directional Glenn: resultsand guidelines for patient selection. Ann Thorac Surg 2001;71:1995–2002.
0. Reddy VM, McElhinney DB, Silverman NH, et al. Partialbiventricular repair for complex congenital heart defects: an
intermediate option for complicated anatomy or functionallyesonance imaging] would be a better method to assess RV
fh
cya
a
DDggtapcGtcu
stto
tfbEs
borderline right complex heart. J Thorac Cardiovasc Surg1998;116:21–7.
1. Chauvaud S, Fuzellier JF, Berrebi A, et al. Bi-directionalcavopulmonary shunt associated with ventriculo and valvu-loplasty in Ebstein’s anomaly: benefits in high risk patients.Eur J Cardiothorac Surg 1998;13:514–9.
2. Corno A, Chassot P, Payot M, Sekarski N, Tozzi P, vonSegesser LK. Ebstein’s anomaly: one and a half repair. SwissMed Wkly 2002;132:485–8.
3. Dearani JA, O’Leary PW, Danielson GK. Surgical treatmentof Ebstein’s malformation: state of the art in 2006. CardiolYoung 2006;16(suppl 3):12–20.
4. Brown ML, Dearani JA, Danielson GK, et al. The outcomes ofoperations for 539 patients with Ebstein anomaly. J ThoracCardiovasc Surg 2008;135:1120–36.
5. Quaegabeur JM, Sreeram N, Fraser AG, et al. Surgery forEbstein’s anomaly: the clinical and echocardiographic eval-uation of a new technique. J Am Coll Cardiol 1991;17:722–8.
6. Marianeschi SM, McElhinney DB, Reddy VM, et al. Alterna-tive approach to the repair of Ebstein’s malformation: intra-cardiac repair with ventricular unloading. Ann Thorac Surg1998;66:1546–50.
7. Quinonez LG, Dearani JA, Puga FJ, et al. Results of the 1.5ventricle repair for Ebstein anomaly for the failing right
ventricle. J Thorac Cardiovasc Surg 2007;133:1303–10.ISCUSSION
R JOSEPH A. DEARANI (Rochester, MN): Thank you, Presi-ent Chitwood, Secretary Wood. I have no disclosures. Dralhotra and colleagues, your findings are consistent with the
iterature and with my own experience that the bidirectionallenn is a helpful adjunct when treating Ebstein’s anomaly,articularly when the right ventricle is dilated and dysfunc-
ional. In contrast to many others who have employed theidirectional Glenn routinely in Ebstein’s, you have utilized aelective strategy and have applied it in typical Frank Hanleyashion—thoughtful, rational, and protocolized. Your physio-ogic and anatomic indications will be helpful in guiding sur-eons to know when it is important to use the bidirectionallenn.My first comment and question has to do with the adult
atient. There is concern about the earlier development ofenous collaterals and pulmonary AV [arteriovenous] fistula inlder patients with a bidirectional Glenn. How many olderatients with Ebstein’s anomaly received a bidirectional Glennnd what are your indications for using the Glenn outside of theediatric population? This is a practical issue since many pa-
ients with Ebstein’s anomaly undergo their first or repeatperation in adulthood when RV function is often significantlyepressed.My second question has to do with RV [right ventricular]
unction. Echocardiography is a poor method at accurate determi-ation of RV function. I would challenge your findings in theanuscript that postoperative RV systolic function was “normal”
n more than 90% of your patients. This would be uncommon inhis patient population, whose primary problem is a rightentricular myopathy to begin with. What would be helpfulould be a comparative analysis of postoperative RV function inatients with and without the Glenn. Obviously, MRI [magnetic
unction, but could you comment on the differences you mayave noted between these two groups?Finally, it has been shown that New York Heart functional
lass correlates poorly with exercise capacity, particularly inoung patients. Do you have any exercise data, and, if so, is thereperformance benefit in one group over the other?Congratulations to the authors for an important contribution,
nd thank you to the Society for the privilege of discussing it.
R MALHOTRA: Thank you for your kind comments, Drearani. Your contributions to this field are tremendous andreatly appreciated by all of us that deal with this challengingroup of patients. Regarding the adult population, in reviewinghe data, approximately half of the adults underwent a Glennnd the conditions or criteria were unchanged regardless ofatient age. We have not seen development of pulmonary AVollaterals. This is likely due to the fact that this is a pulsatilelenn with antegrade flow through the pulmonary artery from
he right ventricle. But we do not change the criteria for adults tohildren, it is the same criteria, and we have not seen anyntoward events following that.Regarding RV function, I agree wholeheartedly with your
tatement about RV function assessed by echo as being subop-imal. It would be a very valuable adjunct to use MRI to look athe function, because I think, as I stated, echo is a poor indicatorf RV function.Regarding New York Class Association vs exercise testing,
hat is a very salient point. Exercise testing is the gold standardor performance status in these patients, and we are currentlyeginning to look at exercise improvement in patients after anbstein’s repair, but no conclusions can be made until after thattudy is completed.
Thank you again.




















