Role of Placental Growth Factor in Mesenteric Neoangiogenesis in a Mouse Model of Portal...
19
Role of Placental Growth Factor in Mesenteric Neoangiogenesis in a Mouse Model of Portal Hypertension CHRISTOPHE VAN STEENKISTE,* ANJA GEERTS,* ELINE VANHEULE,* HANS VAN VLIERBERGHE,* FILIP DE VOS, ‡ KIM OLIEVIER,* CHRISTOPHE CASTELEYN, § DEBBY LAUKENS,* MARTINE DE VOS,* JEAN–MARIE STASSEN, PETER CARMELIET, ¶,# and ISABELLE COLLE* *Faculty of Medicine and Health Sciences, Department of Hepatology and Gastroenterology, Ghent University, Ghent; ‡ Faculty of Pharmaceutical Sciences, Radiopharmacy, Ghent University, Ghent; § Faculty of Veterinary Medicine, Department of Morphology, Ghent University, Merelbeke; ThromboGenics NV, Leuven; ¶ Vesalius Research Center, VIB, Leuven; and # Vesalius Research Center, Leuven, Belgium BACKGROUND & AIMS: Portal hypertension is re- sponsible for the major complications associated with cirrhosis. Angiogenesis has been associated with the pathophysiology of portal hypertension. We investigated the role of placental growth factor (PlGF) and tested the effects of monoclonal antibodies against PlGF (PlGF) in a mouse model of portal hypertension. METHODS: Us- ing a mouse model of prehepatic portal hypertension, we measured PlGF levels in the mesenteric tissue at different time points. We used knockout mice and PlGF to de- termine the role of PlGF in the splanchnic hyperdynamic system and portosystemic collateral formation, examin- ing its effects before and after portal hypertension was induced. RESULTS: PlGF was significantly up-regulated in the mesenteric tissue of mice with portal hypertension. Compared with wild-type animals, the vascular density in the mesentery was reduced in PlGF knockout hyperten- sive mice, preventing collateral formation and attenua- tion of mesenteric artery flow without affecting portal pressure. In the prevention study, PlGF showed similar findings as in the knockout study. In mice with portal hypertension, administration of PlGF resulted in a 32% decrease in portal pressure, compared with mice given immunoglobulin G 1 (control). CONCLUSIONS: Patho- logic angiogenesis in the mesenteric tissues of mice with portal hypertension is mediated by PlGF. Block- ing PlGF could be an effective strategy for reducing collateral formation and lowering portal pressure; further research into the effects in cirrhosis is warranted. P ortal hypertension (PHT) is the most common com- plication of chronic liver disease and develops in the vast majority of patients with cirrhosis. The principal factors leading to PHT are increased resistance to blood flow within the liver and increased blood flow in the splanchnic system. 1 Increased splanchnic blood flow results from well-de- scribed functional 1 and structural vascular alterations 2,3 and is typically observed in more advanced stages of PHT. Several studies have indicated increased angiogenesis— defined as the growth of new blood vessels from a pre- existing vascular tree 4 —as a key structural feature in the splanchnic territory of portal hypertensive rats and cir- rhotic patients. 5–7 Fernandez et al demonstrated that blocking the vascular endothelial growth factor recep- tor-2 (VEGFR-2) signalling pathway reduces vascular density and increases splanchnic arteriolar resistance, re- sulting in decreased splanchnic blood flow. 2,3 Recently, inhibition of angiogenesis and arteriogenesis (the matu- ration of a nascent vascular bed by coverage of smooth muscle cells) by combined VEGF and platelet derived growth factor (PDGF) targeting was shown to decrease portal pressure. 8 Moreover, antagonism of the biologic effects of VEGF with monoclonal antibodies or small molecules can inhibit the development of portosystemic collaterals. 2,3 The present study focuses on the role of placental growth factor (PlGF) in the pathophysiology of portal hypertensive mice. PlGF is a VEGF homologue, originally isolated from the human placenta in 1991. 9 This growth factor is an attractive therapeutic target, with pleiotropic actions in both angiogenesis and arteriogenesis. 9 Further- more, studies in transgenic mice revealed that the angio- genic activity of PlGF is restricted to pathologic condi- tions, without affecting healthy vessels. 10 Importantly, whereas VEGF binds VEGFR-2, PlGF selectively binds VEGFR-1, a receptor that is up-regulated in disease. 9 Treatment with VEGFR-2-inhibitors may cause signifi- cant adverse events such as thrombosis, hypertension, and microvascular changes in healthy organs. 10 In con- trast, preliminary safety studies with a monoclonal anti- PlGF antibody (PlGF) in healthy mice and humans have Abbreviations used in this paper: PlGF, murine anti-PlGF monoclo- nal antibody; SMA, -smooth-muscle actin; MAP, mean arterial pres- sure; PDGF, Platelet-Derived Growth Factor; PHT, portal hypertension; PlGF, Placental Growth Factor; PPVL, partial portal vein ligation; SO, sham-operated; sVEGFR, soluble Vascular Endothelial Growth Factor receptor; VEGF, Vascular Endothelial Growth Factor; VEGFR, Vascular Endothelial Growth Factor Receptor. © 2009 by the AGA Institute 0016-5085/09/$36.00 doi:10.1053/j.gastro.2009.08.068 BASIC–LIVER, PANCREAS, AND BILIARY TRACT GASTROENTEROLOGY 2009;137:2112–2124
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Role of Placental Growth Factor in Mesenteric Neoangiogenesis in a Mouse Model of Portal...

RM
CKP
*R¶
BscpteaimttsiiiCtstpfihdilwicfw
Pvffls
saS
BA
SIC–LIV
ER,
PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
GASTROENTEROLOGY 2009;137:2112–2124
ole of Placental Growth Factor in Mesenteric Neoangiogenesis in aouse Model of Portal Hypertension
HRISTOPHE VAN STEENKISTE,* ANJA GEERTS,* ELINE VANHEULE,* HANS VAN VLIERBERGHE,* FILIP DE VOS,‡
IM OLIEVIER,* CHRISTOPHE CASTELEYN,§ DEBBY LAUKENS,* MARTINE DE VOS,* JEAN–MARIE STASSEN,�
ETER CARMELIET,¶,# and ISABELLE COLLE*
Faculty of Medicine and Health Sciences, Department of Hepatology and Gastroenterology, Ghent University, Ghent; ‡Faculty of Pharmaceutical Sciences,adiopharmacy, Ghent University, Ghent; §Faculty of Veterinary Medicine, Department of Morphology, Ghent University, Merelbeke; �ThromboGenics NV, Leuven;
Vesalius Research Center, VIB, Leuven; and #Vesalius Research Center, Leuven, Belgiumdesrbtdsirmgpemc
ghifamgtwVTcatP
nsPsrE
ACKGROUND & AIMS: Portal hypertension is re-ponsible for the major complications associated withirrhosis. Angiogenesis has been associated with theathophysiology of portal hypertension. We investigatedhe role of placental growth factor (PlGF) and tested theffects of monoclonal antibodies against PlGF (�PlGF) inmouse model of portal hypertension. METHODS: Us-
ng a mouse model of prehepatic portal hypertension, weeasured PlGF levels in the mesenteric tissue at different
ime points. We used knockout mice and �PlGF to de-ermine the role of PlGF in the splanchnic hyperdynamicystem and portosystemic collateral formation, examin-ng its effects before and after portal hypertension wasnduced. RESULTS: PlGF was significantly up-regulatedn the mesenteric tissue of mice with portal hypertension.ompared with wild-type animals, the vascular density in
he mesentery was reduced in PlGF knockout hyperten-ive mice, preventing collateral formation and attenua-ion of mesenteric artery flow without affecting portalressure. In the prevention study, �PlGF showed similarndings as in the knockout study. In mice with portalypertension, administration of �PlGF resulted in a 32%ecrease in portal pressure, compared with mice given
mmunoglobulin G1 (control). CONCLUSIONS: Patho-ogic angiogenesis in the mesenteric tissues of miceith portal hypertension is mediated by PlGF. Block-
ng PlGF could be an effective strategy for reducingollateral formation and lowering portal pressure;urther research into the effects in cirrhosis isarranted.
ortal hypertension (PHT) is the most common com-plication of chronic liver disease and develops in the
ast majority of patients with cirrhosis. The principalactors leading to PHT are increased resistance to bloodow within the liver and increased blood flow in theplanchnic system.1
Increased splanchnic blood flow results from well-de-cribed functional1 and structural vascular alterations2,3
nd is typically observed in more advanced stages of PHT.
everal studies have indicated increased angiogenesis—efined as the growth of new blood vessels from a pre-xisting vascular tree4—as a key structural feature in theplanchnic territory of portal hypertensive rats and cir-hotic patients.5–7 Fernandez et al demonstrated thatlocking the vascular endothelial growth factor recep-or-2 (VEGFR-2) signalling pathway reduces vascularensity and increases splanchnic arteriolar resistance, re-ulting in decreased splanchnic blood flow.2,3 Recently,nhibition of angiogenesis and arteriogenesis (the matu-ation of a nascent vascular bed by coverage of smooth
uscle cells) by combined VEGF and platelet derivedrowth factor (PDGF) targeting was shown to decreaseortal pressure.8 Moreover, antagonism of the biologicffects of VEGF with monoclonal antibodies or smallolecules can inhibit the development of portosystemic
ollaterals.2,3
The present study focuses on the role of placentalrowth factor (PlGF) in the pathophysiology of portalypertensive mice. PlGF is a VEGF homologue, originally
solated from the human placenta in 1991.9 This growthactor is an attractive therapeutic target, with pleiotropicctions in both angiogenesis and arteriogenesis.9 Further-ore, studies in transgenic mice revealed that the angio-
enic activity of PlGF is restricted to pathologic condi-ions, without affecting healthy vessels.10 Importantly,hereas VEGF binds VEGFR-2, PlGF selectively bindsEGFR-1, a receptor that is up-regulated in disease.9
reatment with VEGFR-2-inhibitors may cause signifi-ant adverse events such as thrombosis, hypertension,nd microvascular changes in healthy organs.10 In con-rast, preliminary safety studies with a monoclonal anti-lGF antibody (�PlGF) in healthy mice and humans have
Abbreviations used in this paper: �PlGF, murine anti-PlGF monoclo-al antibody; �SMA, �-smooth-muscle actin; MAP, mean arterial pres-ure; PDGF, Platelet-Derived Growth Factor; PHT, portal hypertension;lGF, Placental Growth Factor; PPVL, partial portal vein ligation; SO,ham-operated; sVEGFR, soluble Vascular Endothelial Growth Factoreceptor; VEGF, Vascular Endothelial Growth Factor; VEGFR, Vascularndothelial Growth Factor Receptor.
© 2009 by the AGA Institute0016-5085/09/$36.00
doi:10.1053/j.gastro.2009.08.068

sca
PthtvBod
awafBG
lwn
(kitp
S(iniPitwblahaaw
wss
i(
aap
km(fl
bsgaccl
jpfftl
ttq(c
sgbsI
ca
BA
SIC–L
IVER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
December 2009 PlGF IN PORTAL HYPERTENSION 2113
o far not revealed any major adverse effects (personalommunication with ThromboGenics; phase I results fornti-PlGF cancer therapeutic TB-403, 2009).10
The present study describes, for the first time, the role oflGF in the pathophysiology of PHT and supports a poten-ial role for �PlGF in the future treatment of the portalypertensive syndrome. Providing antiangiogenic medica-ion to cirrhosis patients is a feasible approach,11 but ad-erse effects may limit their application in Child–Pugh class
and C patients. In this regard, �PlGF treatment couldffer a new, safe therapeutic perspective for chronic liverisease.
Materials and MethodsAnimals and Surgical ProcedureMale 50% Sv129/50% Swiss mice (aged 5– 8 weeks)
nd PlGF knockout mice of the same genetic backgroundere used as previously described.12 All mice were treatedccording to institutional animal health care guidelines,ollowing study approval by the Institutional Reviewoard at the Faculty of Medicine and Health Sciences ofhent University.Portal hypertension was induced by partial portal vein
igation (PPVL), as previously described.13 Control miceere sham-operated (SO); portal vein was isolated butot ligated.
Knockout Mice Study, Prevention Study, andTherapeutic StudyTo address the role of PlGF in portal hypertension
proof of concept), PlGF signalling was studied in PlGFnockout mice. PPVL and SO (n � 6 in each group) were
nduced in PlGF wild-type and PlGF knockout mice, respec-ively. Animals were killed after 2 weeks, the time at whichortal hypertensive syndrome had fully established.2
For the prevention study, age- and weight-matched 50%v129/50% Swiss mice were treated for 1 week with �PlGFprovided by ThromboGenics, Leuven, Belgium; 50 mg/kgntraperitoneal [IP] injections performed on days 0 and 3;
� 8 in each group), starting immediately after PPVL/SOnduction. To account for passive immunization, matchedPVL and SO groups (n � 6 each) were treated with murine
mmunoglobulin (Ig) G1 (1C8011; ThromboGenics) usinghe same dose and time schedule as for �PlGF. All miceere killed on day 7. The dosing schedule of �PlGF wasased on previous pharmacokinetic studies in mice.10 The
owest effective dose in solid tumors was 25 mg/kg IP twiceweek.10 The half-life for �PlGF was approximately 186
ours. Based on the methods used by Fischer et al10 and inccordance with dosing schedules previously used for otherntiangiogenic antibodies, a dose of 50 mg/kg, IP, twice aeek, was selected.10
For the therapeutic study, �PlGF was administeredhen PHT had already been established. Dose and time
chedule were the same as those used in the prevention
tudy. Here, �PlGF was administered for 2 weeks, start- png from 7 days after induction of PPVL (n � 12) or SOn � 6), respectively. The mice were killed on day 21.
To provide long-term therapeutic data, 4-week �PlGFpplication was also evaluated. Treatment started 1 weekfter induction of PPVL (n � 5), and experiments wereerformed on day 35.
Hemodynamic StudiesThe animals were anesthetized with a mixture of
etamine/xylazine and prepared for measurement of he-odynamic parameters, including arterial blood pressure
MAP), portal pressure, and superior mesenteric arteryow (see Supplementary Materials).
Determination of the Extent of PortosystemicCollateral Vessel FormationThe portosystemic shunt fraction was quantified
y injecting 51Cr microspheres (diameter, 15 � 3 �m;pecific activity, 41 mCi/g; Perkin–Elmer, Zaventem, Bel-ium) into the splenic pulpa.14 Radioactivity in the livernd lungs was measured separately using a �-scintillationounter (Cobra II; Canberra, CT). The shunt fraction wasalculated by the ratio [(lungs counts)/(lungs counts �iver counts)] � 100.2
Western Blot Analysis of CD31 and�-Smooth-Muscle Actin in Mesenteric TissueThe double layer of visceral peritoneum suspending
ejunum and ileum (referred to as “mesenteric tissues”) wasrelevated. Because vascular density may vary between dif-erent parts of the mesentery, the first 6 loops proximalrom the cecum were arbitrarily excised. Samples (each con-aining 100 �g protein) from mesenteric tissues were ana-yzed by Western blotting (see Supplementary Materials).
Enzyme-Linked Immunosorbent AssayProtein lysates from mesenteric tissues were ob-
ained as described in Supplementary Materials. Concen-rations of PlGF, VEGF, sVEGFR-1, and sVEGFR-2 wereuantified by enzyme-linked immunosorbent assay (ELISA)R&D Quantikine; R&D Systems Minneapolis, MN), ac-ording to the manufacturer’s instructions.
To determine the concentration of �PLGF in serumamples, ELISA plates (Sigma–Aldrich, Bochem, Bel-ium) were coated with PlGF (0.5 �g/mL, R&D Systems),locked with BSA and incubated with serial dilutions oferum. Bound �PlGF was detected using goat anti-mousegG1-horseradish peroxidase (HRP; Sigma–Aldrich).
Immunohistochemistry, Measurement of theVascular Area, and Image Analysis ofTissue SectionsSections from paraffin-embedded tissues were in-
ubated with anti-VEGF-R1, anti-VEGFR-2, anti-CD31,nti-�-smooth muscle actin (SMA) antibodies (see Sup-
lementary Materials). Antigen localization was visual-
iC
t-ata
I
CemvLdJT
1
BA
SIC–LIV
ER,
PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
2114 VAN STEENKISTE ET AL GASTROENTEROLOGY Vol. 137, No. 6
zed with 3=-3-diamino benzidene (DAB) as chromogen.ounterstaining was performed with hematoxylin.The vascular density on slides stained for CD31 and
he percentage of cells stained positive for VEGFR-1 and2 were measured quantitatively using light microscopynd computerized image analysis, using an adapted in-ernational consensus method for the quantification ofngiogenesis15 (see Supplementary Materials).
Vascular Corrosion CastingsAfter 24-hour food restriction, mice were killed by
P injection of phenobarbital (150 mg/kg) (Nembutal;
eva Sante Animale, Brussels, Belgium) after proper an-sthesia (ketamine and xylazine, mentioned above). Aidline abdominal incision was made, and the ileocolic
ein was catheterized with a 26-gauge catheter (Terumo,euven, Belgium). Each cast was prepared as previouslyescribed16 and analyzed with a stereomicroscope and a
eol JSM 5600 LV scanning electron microscope (Jeol Ltd,okyo, Japan).
Statistical AnalysesData analysis was performed with SPSS version
5.0 (SPSS Inc, Chicago, IL). In case of normally dis-
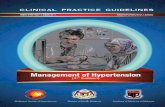
Figure 1. Vascular castingimages of mice by injectingBatson solution in the ileocolicvein. (A) General overview of avenous vascular cast. (B) Pres-ence of increased angiogene-sis in PPVL mice comparedwith SO. View on a newlyformed vascular network withirregular, tortuous, and imma-ture vessels (star) betweenbranches of the portal vein(white arrow) and the inferiorcaval vein (in the depth, notshown on this image). (C) Rep-resentative stereomicroscopicand (D) scanning electron mi-croscopy photographs of themesentery show an increasedsplanchnic neoangiogenesis inPPVL mice as compared with
SO mice.
tttp(tn
vfis
riPe
ptatc�tsbh
FknsPdpot1ntbaP.tlSdsWP.
BA
SIC–L
IVER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
December 2009 PlGF IN PORTAL HYPERTENSION 2115
ributed data, groups were compared with the Studenttest for independent samples. For other types of data,he Mann–Whitney U test was performed. Data areresented as the mean � standard error of the mean
SEM) or median � range when indicated. P values lesshan .05 (2-tailed probability) were considered as sig-ificant.
ResultsIncreased Neoangiogenesis in PortalHypertensive MiceVascular proliferation in PPVL/SO mice was in-
estigated via vascular casting (Figure 1A). A newlyormed vascular network with irregular, tortuous, andmmature vessels could be detected as an extrahepatic
igure 2. Effects of PlGFnockout (KO) on mesentericeovascularization and porto-ystemic collateral formation inPVL mice on day 14 after in-uction (proof-of-principle ex-eriment). (A) Histologic imagesf CD31 staining of mesen-eries (original magnification,0�) and quantification. (a) Sig-ificant differences in mesen-eric vascularization were seenetween PPVL wild-type micend PlGF KO mice, P � .02. (b)PVL WT vs sham WT, P �
016. Arrows represent endo-helia of blood vessels. (B) Col-ateral formation in PPVL andO mice with or without PlGFeficiency. (a) PPVL WT vsham WT, P � .001; (b) PPVLT vs PPVL KO, P � .01; (c)PVL KO vs sham KO, P �
001.
hunt between branches of the portal vein and the infe- t
ior caval vein (Figure 1B). Consistent with previous stud-es, increased splanchnic angiogenesis was present only inPVL mice (stereomicroscopic examination and scanninglectron microscopy; Figure 1C and D).
In addition, increased splanchnic neovascularization inortal hypertensive mice was confirmed by immunohis-ochemistry for CD31 (Figure 2A; n � 5, P � .016 vs SO),
marker of endothelial cells (ie, angiogenesis).8 The ex-ent of portosystemic collateral formation was signifi-antly increased on day 14 after PPVL induction (94% vs1% for SO, respectively, P � .001) (Figure 2B). In addi-
ion, PPVL mice showed significantly higher portal pres-ure and spleen enlargement compared with SO (Table 1,oth P � .01). Beyond 14 days postligation, splanchnicyperemia disappeared, and a significant decrease in por-
al pressure and collateral formation was noted, reflect-
iS
(wiTotata
rStaVv1scw(utoasi
sm
twddcm
nka(smoai
59.l(rrvt
apstMps
T
MPSHM
NBa
b
c
d
BA
SIC–LIV
ER,
PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
2116 VAN STEENKISTE ET AL GASTROENTEROLOGY Vol. 137, No. 6
ng the natural course of PPVL in this murine model (seeupplementary Materials).
Overexpression and Kinetics of AngiogenicMediators in the Splanchnic Microvasculatureof Portal Hypertensive MiceThe time frame in which PlGF and soluble
s)VEGFR-1 are expressed in the mesentery of PHT miceas assessed by ELISA at different time points after PPVL
nduction (days 1, 2, 5, 7, and 14; n � 5 in each group).he results were compared with the corresponding databtained for VEGF and sVEGFR-2. With sVEGFR-1 an-agonizing VEGF and PlGF in pathologic conditions9
nd because sVEGFR-2 can also inhibit angiogenesis,17
he ratio of pro- and antiangiogenic factors can be useds an index of angiogenic activity.18
Significant up-regulation of VEGF and PlGF was al-eady observed 1 day after PPVL induction (P � .05 vsO) and was followed by a time-dependent increase, withhe highest levels detected on day 14 and day 5 for VEGFnd PlGF, respectively (Figure 3A and B). SolubleEGFR-1 was significantly decreased on day 5 (P � .05s SO), following a decreasing trend observed from day
(Figure 3C). There was no significant change inVEGFR-2 expression (Figure 3D). Finally, immunohisto-hemistry demonstrated that VEGFR-1 and VEGFR-2ere up-regulated in PPVL mice compared with SO mice
Figure 4). The decreased ratio of sVEGFR-1/PlGF (Fig-re 3E) and sVEGFR-2/VEGF (Figure 3F) contributed tohe increased angiogenesis noticed within the mesenteryf the portal hypertensive mice. The present results showtime-dependent increase in VEGF, PlGF, and their re-
pective receptors during splanchnic neovascularizationn portal hypertensive mice, indicating neoangiogenesis.
PlGF Deficiency Decreases PortosystemicCollateral Vessel Formation in PortalHypertensive Mice and Attenuates SplanchnicHyperdynamic CirculationTo address the role of PlGF in portal hyperten-
ion, PlGF signalling was first studied in PlGF knockout
able 1. Splanchnic and Hemodynamic Changes in PPVL/SOMice
Parameters Sham WT
ean arterial pressure (mm Hg) 110 � 9ortal pressure (mm Hg) 4.7 � 0.3pleen weight (g/10 g BW) 0.033 � 0.003eart rate (beats/min) 438 � 26esenteric artery flow (mL/min) 0.87 � 0.02
OTE. Results are shown as mean � SEM.W, body weight.PPVL WT vs Sham WT, P � .01.PPVL KO vs PPVL WT, P � .07.PPVL KO vs PPVL WT, P � .01.PPVL KO vs PPVL WT, P � .05.
ice as a proof-of-concept experiment. Inactivation of m
he PlGF gene in PlGF knockout mice was associatedith a 47% reduction in splanchnic neovascularization 14ays after PPVL induction, as indicated by a significantecrease in CD31 expression observed by immunohisto-hemical staining, to a level comparable with that of SOice (Figure 2A).PlGF deficiency also affected the splanchnic hyperdy-
amic circulation (Table 1). Portal hypertensive PlGFnockout mice exhibited a 32% reduction in mesentericrtery blood flow compared with wild-type PPVL mice0.95 mL/min vs 1.41 mL/min, respectively, P � .04), andhowed a tendency for lower portal pressure (10 � 0.7
m Hg vs 11.2 � 0.8 mm Hg, respectively, P � .07). Lackf PlGF in portal hypertensive mice did not affect MAPnd heart rate, and there were no significant differencesn hemodynamic parameters in both SO groups.
The extent of portosystemic collaterals was reduced by2% in portal hypertensive PlGF knockout mice (42% vs4% shunting in wild-type PPVL mice, respectively; P �
01) (Figure 2B). Spleen weights were also significantlyower in PlGF knockout mice than in the wild-type group0.045 g/10 g body weight vs 0.068 g/10 g body weight,espectively, P � .003) (Table 1). In conclusion, theseesults indicate that PlGF contributes to splanchnic neo-ascularization, hyperdynamic circulation, and portosys-emic collateral formation in portal hypertensive mice.
Prevention Study: �PlGF Partially Preventsthe Formation of Portosystemic Collateralsand the Development of SplanchnicHemodynamic Changes in PHT
Continuing on the results in PlGF knockout mice,subsequent experiment assessed the effect of �PlGF ap-
lication on PHT development. Treatment with �PlGF,tarting immediately after induction of PPVL and con-inuing for 1 week, resulted in no detectable toxicity.
ortality and average body weights on day 7 were com-arable in both groups of portal hypertensive mice. Theerum concentration of �PlGF (trough level) in PPVL
Wild-Type Mice, Compared With PPVL/SO PlGF Knockout
PPVL WT Sham KO PPVL KO
99 � 8 105 � 9 101 � 10.2 � 0.8a 4.8 � 0.4 10 � 0.7b
68 � 0.005a 0.032 � 0.004 0.045 � 0.004c
59 � 47 448 � 57 483 � 5941 � 0.26 0.98 � 0.002 0.95 � 0.08d
PlGF
110.0
41.
ice was in the therapeutic range (991 � 280 �g/mL).10

5lmsacwi(
cp�mm
(dstS
(lr.iimtk
Fevi 5 vs B
ASI
C–L
IVER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
December 2009 PlGF IN PORTAL HYPERTENSION 2117
Confirming an immunohistochemical trend (FigureB), Western blot showed a significant decrease in CD31
evels (Figure 5A), indicating that treatment of PPVLice with �PlGF was highly effective in suppressing
planchnic neovascularization. Treatment with �PlGFlso reduced arteriogenesis, as demonstrated by signifi-antly reduced �-SMA expression (a marker of pericytes,hich cover the newly formed vessels, ie, arteriogenesis)
n Western blot (Figure 5C) and immunohistochemistryFigure 5D).
Furthermore, �PlGF was associated with markedhanges in hemodynamic parameters (Table 2). Com-ared with IgG1-treated PPVL mice, administration ofPlGF to portal hypertensive mice significantly decreasedesenteric artery flow by 35% (1.29 � 0.03 vs 0.84 � 0.14
igure 3. Expression of angiogenic mediators (ELISA) in mesentericxpression. (a) P � .05 vs SO; (b) P � .05 vs D1. (B) PlGF expression.s SO; (b) P � .05 vs D2 and D7. (D) sVEGFR-2 expression. (E) sVEGFRn favor of increased mesenteric angiogenesis in PPVL mice. (a) P � .0
L/min, respectively, P � .02) and increased MAP by 26% T
93 � 3 vs 118 � 10 mm Hg, respectively, P � .04). Noifferences were shown in spleen weight and portal pres-ure. There were no significant changes in MAP, mesen-eric artery flow, portal pressure, and heart rate in bothO mouse groups (Table 2).
Importantly, PPVL mice demonstrated a significant48%) reduction in the formation of portosystemic col-aterals after 7 days of �PlGF treatment (43% vs 91%,espectively, shunting in IgG1-treated PPVL mice, P �015) (Figure 5E). To evaluate whether �PlGF therapynduced a compensatory angiogenic program that couldn turn trigger resistance to antiangiogenic medication,10
esenteric expression of VEGF was assessed. Impor-antly, �PlGF treatment did not induce expression of thisey angiogenesis regulator (Supplementary Figure 2A).
es at different time points during the development of PHT. (A) VEGF� .05 vs SO; (b) P � .05 vs D1. (C) sVEGFR-1 expression. (a) P � .05GF ratio. (F) sVEGFR-2/VEGF ratio. The lower ratios in PPVL vs SO areSO.
tissu(a) P-1/Pl
aken together, these data confirm the previous results

orpdt
assm
m(a
WttaMivnira
nmp.(
FVi and
BA
SIC–LIV
ER,
PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
2118 VAN STEENKISTE ET AL GASTROENTEROLOGY Vol. 137, No. 6
f the knockout study and indicate that �PlGF therapyeduced splanchnic neovascularization, resulting in therevention of portosystemic collateral formation and re-uction in arterial mesenteric blood flow in portal hyper-ensive mice.
Therapeutic Study: Beneficial Effects of�PlGF on Splanchnic and Portal CollateralCirculation Resulting in a Reduction inPortal PressureIn the therapeutic setting, �PlGF therapy was
gain well tolerated, and no drug-induced mortality orignificant effects on body weight were observed. Theerum concentration of �PlGF (trough level) in PPVL
ice was in the therapeutic range (1114 � 110 �g/mL).Compared with IgG1-treated PPVL animals, 2-week ad-inistration of �PlGF significantly reduced the CD31
Figure 6A and B) and �-SMA overexpression (Figure 6C
igure 4. Immunohistochemical staining for VEGFR-1 and VEGFR-2EGFR-2 in PPVL and SO (original magnification, 20�). (C) Computerize
n mesenteric VEGFR-1 and -2 were seen on day 14 between SO mice
nd D) in portal hypertensive mice, demonstrated by .
estern blotting and immunohistochemistry. In addi-ion, stereomicroscopy and electron microscopic evalua-ion of vascular casts revealed increased splanchnicngiogenesis in IgG1-treated PPVL (see Supplementaryaterials and Supplementary Figures 3, 4, and 5), reflect-
ng different mechanisms of angiogenesis. Interestingly,ascular pruning and decreased vascular density wereoticed after treatment with �PlGF. Together, these find-
ngs indicate that preventing PlGF from binding to itseceptor can reverse mesenteric neovascularization andrteriogenesis in portal hypertensive mice.
In addition, �PlGF had a significant effect on splanch-ic hemodynamics (Table 2). Compared with IgG1 treat-ent, 2-week �PlGF treatment caused a 32% decrease in
ortal pressure (10.4 � 0.4 vs 7.1 � 0.3, respectively; P �001) and a 43% reduction in mesenteric artery flow1.36 � 0.35 vs 0.78 � 0.12 mL/min, respectively; P �
Histologic images of mesenteric tissue stained for VEGFR-1 and (B)antification of VEGFR-1 and -2 in the mesentery. Significant differencesPPVL, both for VEGFR-1 and VEGFR-2, (a) P � .05 vs SO.
. (A)d qu
002). Moreover, �PlGF did not modify MAP, spleen

Fm(tmt
BA
SIC–L
IVER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
December 2009 PlGF IN PORTAL HYPERTENSION 2119
igure 5. Effects of �PlGF on mesenteric neovascularization and arteriogenesis in prophylactic setting. (A) Western blot analysis of CD31 inesenteric tissues of �PlGF or IgG1-treated PPVL/SO. (a) PPVL IgG1 vs PPVL �PlGF, P � .05. (B) Histologic images of CD31 staining of mesenteries
original magnification, 10�) and quantification. Arrows represent endothelial cells of blood vessels. (C) Western blot analysis of �-SMA in mesentericissues of �PlGF or IgG1-treated PPVL/SO. (a) PPVL IgG1 vs PPVL �PlGF, P � .05. (D) Histologic images of �-SMA staining of mesenteries (originalagnification, 10�) and quantification. (a) P � .05. Arrows represent smooth muscle cells in blood vessels. (E) Collateral formation in PPVL/SO mice
reated with �PlGF or IgG1. (a) PPVL IgG1 vs sham IgG1, P � .001; (b) PPVL IgG1 vs PPVL �PlGF, P � .05; (c) PPVL �PlGF vs sham �PlGF, P � .001.

wd�msc2
�30ptTwmrim
apnc
iVaisce
tdaficcbkrTCttpp
f
™FoCo.P�
T
MPSHM
MPSHM
NBa
b
c
d
BA
SIC–LIV
ER,
PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
2120 VAN STEENKISTE ET AL GASTROENTEROLOGY Vol. 137, No. 6
eights, or heart rate (Table 2). A significant (52%) re-uction in collateral formation was noticed after 2-weekPlGF treatment (46% vs 98% shunting for IgG1 treat-ent, respectively; P � .01) (Figure 6E), and no compen-
atory up-regulation of VEGF in the mesenteric tissueould be demonstrated after �PlGF treatment (FigureB).
Again compared with IgG1-treated PPVL mice, 4-weekPlGF treatment of portal hypertensive mice induced a8% and 29% reduction in mesenteric artery flow (1.18 �.03 vs 0.73 � 0.09 mL/min, respectively; P � .05) andortal pressure (9.2 � 0.2 vs 6.5 � 0.4 mm Hg, respec-ively; P � .001, respectively) (Supplementary Table 2).reatment with �PlGF did not affect MAP, spleeneights, or heart rate. In addition, 4-week �PlGF treat-ent was accompanied by a modest but significant (20%)
eduction in collateral formation (45.8% vs 65.8% shunt-ng for IgG1 treatment, respectively; P � .042; Supple-
entary Figure 6).
DiscussionThe present study highlights the importance of
ngiogenesis and the involvement of PlGF in the patho-hysiology of PHT. Previous studies have shown thatumerous growth factors are up-regulated in PHT andontribute to the development and/or maintenance of
™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™igure 6. Effects of �PlGF on mesenteric neovascularization and arterif CD31 in mesenteric tissues of �PlGF- or IgG1-treated PPVL/SO. (a) PD31 staining of mesenteries (original magnification, 10�) and quantificf �PlGF- or IgG1-treated PPVL/SO. Blots are displayed as negative im05. (D) Histologic images of �-SMA staining of mesenteries (original mPVL/SO mice treated with �PlGF or IgG1. (a) PPVL IgG1 vs sham IgG1
able 2. Splanchnic and Hemodynamic Changes in PPVL/ShSetting
Prevention Sham IgG1
ean arterial pressure (mm Hg) 99 � 7ortal pressure (mm Hg) 4.7 � 0.7pleen weight (g/10 g BW) 0.037 � 0.002eart rate (beats/min) 458 � 31esenteric artery flow (mL/min) 1.04 � 0.07
Therapeutic (2-wk treatment) Sham IgG1
ean arterial pressure (mm Hg) 122 � 3ortal pressure (mm Hg) 4.1 � 0.8pleen weight (g/10 g BW) 0.033 � 0.005eart rate (beats/min) 501 � 18esenteric artery flow (mL/min) 0.84 � 0.06
OTE. Results are shown as mean � SEM.W, body weight.PPVL �PlGF vs PPVL IgG1, P � .05.PPVL �PlGF vs PPVL IgG1, P � .001.PPVL �PlGF vs sham IgG1, P � .001.PPVL �PlGF vs PPVL IgG1, P � .01.
PlGF, P � .001.
ncreased splanchnic blood flow.2,3,8,19 In particular, theEGF-A/VEGFR-2 interaction has recently received widettention and was reported to be one of the main factorsnvolved in normal and pathologic angiogenesis.2,3 Con-istent with these reports, we also demonstrated in-reased angiogenesis in association with high VEGF lev-ls in the mesenteric tissue of portal hypertensive mice.
PlGF is a member of the VEGF subfamily and par-icipates in the angiogenic process by stimulating en-othelial cell growth, migration, and survival, as wells the subsequent stabilization and maturation of newlyormed vessels.9,20 This pleiotropic action is particularlymportant because previous studies have shown that theombined inhibition of angiogenesis and smooth muscleell vessel coverage can have synergistic action.8 PlGF haseen described in a variety of pathologies,19,21 but, to ournowledge, there have been only 3 reports that indicate aole for PlGF in the field of PHT and cirrhosis.19,22,23
ugues et al reported marked abundance of PlGF inCL4 cirrhotic livers.19 Interestingly, Salcedo et al showed
hat serum levels of PlGF were elevated in chronic hepa-itis C patients, correlating to the stage of fibrosis.23 Theresent study is the first to describe a role for PlGF in theathophysiology of portal hypertension.Unlike VEGF, PlGF selectively binds to VEGFR-1. Dif-
erent direct and indirect effects can lead to increased an-
™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™3esis in therapeutic setting (2-week treatment). (A) Western blot analysisIgG1 vs PPVL �PlGF and SO groups, P � .05. (B) Histologic images of. (a) P � .05. (C) Western blot analysis of �-SMA in mesenteric tissuesto optimize contrasts. (a) PPVL IgG1 vs PPVL �PlGF and SO IgG1, P �cation, 10�) and quantification, (a) P � .05. (E) Collateral formation in.001; (b) PPVL IgG1 vs PPVL �PlGF, P � .01; (c) PPVL �PlGF vs sham
Treated With �PlGF or IgG1 in Prevention and Therapeutic
PPVL IgG1 Sham �PlGF PPVL �PlGF
93 � 3 97 � 9 118 � 10a
10.1 � 0.3 5.4 � 0.7 11.7 � 1.0.072 � 0.008 0.044 � 0.008 0.067 � 0.013529 � 22 526 � 29 476 � 381.29 � 0.03 0.97 � 0.16 0.84 � 0.14a
PPVL IgG1 Sham �PlGF PPVL �PlGF
94 � 4 120 � 12 84 � 410.4 � 0.4 4.5 � 0.7 7.1 � 0.3b,c
.056 � 0.004 0.032 � 0.003 0.065 � 0.005469 � 32 484 � 22 467 � 471.36 � 0.11 0.77 � 0.13 0.78 � 0.05d
™™™ogenPVLation
agesagnifi, P �
am,
0
0

BA
SIC–L
IVER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
December 2009 PlGF IN PORTAL HYPERTENSION 2121

gutvgiutsiisP
umPadatshwcrbi
tasesatvataapasS
mat((twpat
tfltltebhn
gaats(ptrapocpdtssmosd
CosiaTtnicpwgpa
bPanmc
BA
SIC–LIV
ER,
PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
2122 VAN STEENKISTE ET AL GASTROENTEROLOGY Vol. 137, No. 6
iogenesis. Among these, PlGF has been proposed to stim-late angiogenesis by displacing VEGF from VEGFR-1,hereby increasing the fraction of VEGF available to acti-ate VEGFR-2. Alternatively, PlGF might stimulate an-iogenesis by direct signalling via VEGFR-1 or by form-ng heterodimers with VEGF.6 In contrast to VEGF,24 thenderlying mechanisms that initiate PlGF release in por-al hypertension remain unclear. A number of provokingtimuli with potential relevance in portal hypertension,ncluding shear stress and hypoxia, have been proposedn other pathologic circumstances.9 However, detailedtudies specifically addressing these molecular signals inHT are not available.The present results show for the first time that PlGF is
p-regulated in mesenteric tissues of portal hypertensiveice. As soon as 1 day after PPVL induction, mesenteric
lGF levels were significantly increased, peaking on day 5nd remaining significantly elevated until 14 days postin-uction. Because PlGF is also involved in subsequentrteriogenesis, this prolonged increase may have facili-ated stabilization and maturation of the vessel wall withmooth muscle cells. Furthermore, VEGFR-1 levels wereigher in the mesenteric tissue of PPVL mice comparedith SO mice, whereas sVEGFR-1 levels tended to de-
rease. The potent proangiogenic action of PlGF and theelative deficiency in the antiangiogenic effect modulatedy sVEGFR-1 likely created a suitable environment for
ncreased blood vessel formation.However, the main novelty reported in this study was
he capacity of �PlGF to prevent and reverse mesentericngiogenesis, portosystemic collaterals, and portal pres-ure in a pure portal hypertensive model. The observedffects of �PlGF were most likely caused by inhibition ofplanchnic neoangiogenesis and arteriogenesis, althoughn additional indirect vasoconstricting effect of �PlGF inhe long-term cannot be ruled out. According to recent initro data,25 PlGF is known to have some vasodilatorctivity mediated in part by endothelial nitric oxide syn-hase activation, although increased levels of PlGF in vivore not associated with clinical detectable vasodilatoryctivities.26 In an additional experiment, we examined aotential in vivo “direct” vasoactive effect of �PlGF aftercute administration to portal hypertensive mice, but noignificant hemodynamic effects could be observed (seeupplementary Materials and Supplementary Table 3).
In the first part of our study examining PlGF knockoutice, we provided evidence that PlGF was involved in the
ctive development of portal hypertensive syndrome andhat PlGF deficiency prevented collateral formation�52%) and markedly reduced splanchnic hyperemia�32%), without significant effect on portal pressure. Inhe prevention study in which mice received �PlGF for 1eek immediately after induction of PHT, the extent ofortosystemic collateralization (�48%) and mesentericrtery blood flow (�31%) was also significantly reduced,
o a similar extent as in the knockout study. The finding that PlGF deficiency decreased mesenteric arterial bloodow in both the knockout mouse study and the preven-ion strategy, without affecting portal pressure, is mostikely due to concomitant inhibition of collateral forma-ion and the subsequent increase in portosystemic collat-ral resistance. The observed decrease in splanchniclood flow and significant increase in MAP are bothallmark hemodynamic features of diminished hyperdy-amic circulation.The most interesting clinical application of antiangio-
enic drugs was investigated in experiments in whichnimals are treated when PHT and complications arelready established. In this therapeutic setting, 2-weekreatment with �PlGF resulted in significant attenuatedplanchnic hyperemia (�43%) and collateral formation�52%) but also caused a significant reduction (�32%) inortal pressure. It should be emphasized that, accordingo Ohm’s law (P � Q � R), a decrease in portal pressureesults from simultaneous changes in portal inflownd/or portal vascular resistance.1 In this regard, a moreronounced decrease in mesenteric blood flow couldvercome a less explicit reduction in collateralization,onsequently tipping the scale in favor of a lower portalressure. This mechanism is likely to be the basis of theiminished portal pressure detected in therapeutic set-ing. Because portosystemic collaterals are large-sized ves-els with a high degree of maturation compared withplanchnic neovessels, the splanchnic vascular network
ight be more susceptible to the antiangiogenic effectsf �PlGF,27 resulting in a more pronounced effect onplanchnic neovascularization and a less accentuated re-uction in collaterals.Other cirrhotic portal hypertensive models, such as the
CL4 model,19 may be of interest for studying the impactf �PlGF on intrahepatic vascular resistance and its sub-equent net effect on portal pressure. Preliminary, pos-tive safety data for �PlGF have been established innimals10 and humans (personal communication withhromboGenics; phase I results for anti-PlGF cancer
herapeutic TB-403, 2009). In choosing among the manyewly tested antiangiogenic molecules, the safety profile
s a pivotal factor, especially considering potential appli-ation in critically ill portal hypertensive patients. Theresent data confirm that short-term �PlGF therapy isell tolerated in mice. Most importantly, the antiangio-enic effects of �PlGF were specific for the diseasedortal hypertensive mice and were not observed in the SOnimals.
Until recently, most studies examining �PlGF haveeen published in the field of oncology.10 Unlike VEGF,lGF plays a negligible role in physiologic angiogenesisnd is not required as a survival signal for the mainte-ance of quiescent vessels in healthy tissues. However, itarkedly amplifies the activity of VEGF in pathologic
onditions.12 Fischer et al demonstrated that administra-
ion of �PlGF in mice was not associated with vascular
pafiyfi(awcwim
trgwtwTso
tnPitlWcaci
mpTap�tcit
aG1
1
1
1
1
1
1
1
1
1
1
2
BA
SIC–L
IVER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
December 2009 PlGF IN PORTAL HYPERTENSION 2123
runing (regression) in different healthy organs, did notlter the clinical chemistry or hematological blood pro-le, resulted in normal embryonic development, andielded healthy litters.10 Consistent with this report, arst phase I study for a monoclonal anti-PlGF antibody
TB-403) in healthy individuals met all primary safetynd tolerability end points (personal communicationith ThromboGenics; phase I results for anti-PlGF can-
er therapeutic TB-403, 2009). In contrast, treatmentith �VEGFR-2 is associated with teratogenicity, prun-
ng of healthy vessels, thrombosis, hypertension, andany other adverse effects.Another important issue in clinical application of an-
iangiogenic medication is the potential development ofesistance through induction of compensatory angio-enic stimuli (eg, up-regulation of VEGF). In accordanceith previous studies10 and in contrast to �VEGFR-2
reatment, this effect was not observed after treatmentith �PlGF, at least for VEGF in the mesenteric tissues.aken together, these data suggest that �PlGF can be
afely administered and is effective without “switchingn” an angiogenic rescue program.
In summary, the present study shows, for the firstime, that the development, progression, and mainte-ance of PHT in mice are at least in part regulated by thelGF-signalling pathway. From a therapeutic perspective,
nhibition of PlGF-dependent angiogenesis can diminishhe extent of collaterals and simultaneously render themess prone to bleeding by lowering the portal pressure.
hereas nonselective �-blockers constrict the collateralirculation, leading to decreased portal pressure, thisntiangiogenic approach targets structural splanchnichanges and diminishes or prevents collateral formationn a pure portal hypertensive model.
In addition, blocking the PlGF pathway, either byonoclonal antibodies or by using PlGF-deficient mice,
revented angiogenesis in the mesentery of PHT mice.his translated into an attenuation of the mesentericrterial blood flow, as well as in a significant decrease inortosystemic shunting. Furthermore, treatment withPlGF reduced portal pressure in mice with PHT. Impor-
antly, because of the excellent safety profile of �PlGF, itsombined action on angiogenesis and arteriogenesis andts negligible induction of VEGF, �PlGF is an attractivearget for new therapeutic strategies in portal hypertension.
Supplementary Data
Note: To access the supplementary materialccompanying this article, visit the online version ofastroenterology at www.gastrojournal.org, and at doi:0.1053/j.gastro.2009.08.068.
References
1. Colle I, Geerts AM, Van Steenkiste C, et al. Hemodynamicchanges in splanchnic blood vessels in portal hypertension. Anat
Rec (Hoboken) 2008;291:699–713.2. Fernandez M, Vizzutti F, Garcia-Pagan JC, et al. Anti-VEGF recep-tor-2 monoclonal antibody prevents portal-systemic collateral ves-sel formation in portal hypertensive mice. Gastroenterology2004;126:886–894.
3. Fernandez M, Mejias M, Angermayr B, et al. Inhibition of VEGFreceptor-2 decreases the development of hyperdynamic splanch-nic circulation and portal-systemic collateral vessels in portalhypertensive rats. J Hepatol 2005;43:98–103.
4. Carmeliet P. Angiogenesis in health and disease. Nat Med 2003;9:653–660.
5. Cejudo-Martin P, Ros J, Navasa M, et al. Increased production ofvascular endothelial growth factor in peritoneal macrophages ofcirrhotic patients with spontaneous bacterial peritonitis. Hepatol-ogy 2001;34:487–493.
6. Geerts AM, Colle I. Angiogenesis in portal hypertension: involve-ment in increased splanchnic blood flow and collaterals? ActaClin Belg 2007;62:271–275.
7. Perez-Ruiz M, Ros J, Morales-Ruiz M, et al. Vascular endothelialgrowth factor production in peritoneal macrophages of cirrhoticpatients: regulation by cytokines and bacterial lipopolysaccha-ride. Hepatology 1999;29:1057–1063.
8. Fernandez M, Mejias M, Garcia-Pras E, et al. Reversal of portalhypertension and hyperdynamic splanchnic circulation by com-bined vascular endothelial growth factor and platelet-derivedgrowth factor blockade in rats. Hepatology 2007;46:1208–1217.
9. Autiero M, Luttun A, Tjwa M, et al. Placental growth factor and itsreceptor, vascular endothelial growth factor receptor-1: noveltargets for stimulation of ischemic tissue revascularization andinhibition of angiogenic and inflammatory disorders. J ThrombHaemost 2003;1:1356–1370.
0. Fischer C, Jonckx B, Mazzone M, et al. Anti-PlGF inhibits growth ofVEGF(R)-inhibitor-resistant tumors without affecting healthy ves-sels. Cell 2007;131:463–475.
1. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advancedhepatocellular carcinoma. N Engl J Med 2008;359:378–390.
2. Carmeliet P, Moons L, Luttun A, et al. Synergism between vas-cular endothelial growth factor and placental growth factor con-tributes to angiogenesis and plasma extravasation in pathologi-cal conditions. Nat Med 2001;7:575–583.
3. Geerts AM, Vanheule E, Praet M, et al. Comparison of threeresearch models of portal hypertension in mice: macroscopic,histological and portal pressure evaluation. Int J Exp Pathol2008;89:251–263.
4. Chojkier M, Groszmann RJ. Measurement of portal-systemicshunting in the rat by using �-labeled microspheres. Am J Physiol1981;240:G371–G375.
5. Danese S, Sans M, Spencer DM, et al. Angiogenesis blockade asa new therapeutic approach to experimental colitis. Gut 2007;56:855–862.
6. Callewaert BL, Loeys BL, Casteleyn C, et al. Absence of arterialphenotype in mice with homozygous slc2A10 missense substi-tutions. Genesis 2008;46:385–389.
7. Robak E, Sysa-Jedrzejewska A, Robak T. Vascular endothelialgrowth factor and its soluble receptors VEGFR-1 and VEGFR-2 inthe serum of patients with systemic lupus erythematosus. Medi-ators Inflamm 2003;12:293–298.
8. Levine RJ, Lam C, Qian C, et al. Soluble endoglin and othercirculating antiangiogenic factors in preeclampsia. N Engl J Med2006;355:992–1005.
9. Tugues S, Fernandez-Varo G, Munoz-Luque J, et al. Antiangio-genic treatment with sunitinib ameliorates inflammatory infiltrate,fibrosis, and portal pressure in cirrhotic rats. Hepatology 2007;46:1919–1926.
0. Fischer C, Mazzone M, Jonckx B, et al. FLT1 and its ligandsVEGFB and PlGF: drug targets for anti-angiogenic therapy? Nat
Rev Cancer 2008;8:942–956.
2
2
2
2
2
2
2
R
DHB
A
Mc
C
dCpdwr
F
(
BA
SIC–LIV
ER,
PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
2124 VAN STEENKISTE ET AL GASTROENTEROLOGY Vol. 137, No. 6
1. Roncal C, Buysschaert I, Chorianopoulos E, et al. Beneficialeffects of prolonged systemic administration of PlGF on lateoutcome of post-ischaemic myocardial performance. J Pathol2008;216:236–244.
2. Huang XX, McCaughan GW, Shackel NA, et al. Up-regulation ofproproliferative genes and the ligand/receptor pair placentalgrowth factor and vascular endothelial growth factor receptor 1 inhepatitis C cirrhosis. Liver Int 2007;27:960–968.
3. Salcedo MX, Sanz-Cameno P, Medina J, et al. Association be-tween angiogenesis soluble factors and disease progressionmarkers in chronic hepatitis C patients. Rev Esp Enferm Dig2005;97:699–706.
4. Abraldes JG, Iwakiri Y, Loureiro-Silva M, et al. Mild increases inportal pressure up-regulate vascular endothelial growth factorand endothelial nitric oxide synthase in the intestinal microcircu-latory bed, leading to a hyperdynamic state. Am J Physiol Gas-trointest Liver Physiol 2006;290:G980–G987.
5. Osol G, Celia G, Gokina N, et al. Placental growth factor is apotent vasodilator of rat and human resistance arteries. Am JPhysiol Heart Circ Physiol 2008;294:H1381–H1387.
6. Julian CG, Galan HL, Wilson M, et al. Lower uterine artery blood flowand higher endothelin relative to nitric oxide metabolite levels areassociated with reductions in birth weight at high altitude. Am JPhysiol Regul Integr Comp Physiol 2008;295:R906–R915.
7. Escorsell A, Bosch J. Pathophysiology of variceal bleeding. In:Groszmann RJ, Bosch J, eds. Portal hypertension in the 21stcentury. Dordrecht, The Netherlands: Kluwer Academic Publish-
ers, 2004:155–166. bReceived January 17, 2009. Accepted September 8, 2009.
eprint requestsAddress requests for reprints to: Isabelle Colle, MD, PhD,
epartment of Hepatology and Gastroenterology, Ghent Universityospital, building K12 first floor IE, De Pintelaan 185, 9000 Ghent,elgium. e-mail: [email protected]; fax: (32) 9-3324984.
cknowledgmentsThe authors thank Julien Dupont, Maria De Mol, and Huberteoreau for their technical assistance and Koen Boussery for his
ritical discussions.C.V.S. and A.G. contributed equally to this work.
onflicts of interestThe authors disclose the following: Jean-Marie Stassen: senior
irector of research and development, Thrombogenics. Peterarmeliet: Peter Carmeliet declares to be named as inventor on aatent, claiming subject matter that is partially based on the resultsescribed in this paper. The aforementioned patent is licensed,hich may result in a royalty payment to Peter Carmeliet. The
emaining authors disclose no conflicts.
undingSupported by a grant from the Fund for Scientific Research
Aspirant mandaat-FWO Vlaanderen, 1.1.466.09.N.0; to C.V.S.) and
y a Methusalem grant (to P.C.).
TmPwliphve
scasNab
fa0pmbRa
maI7TtBbaonmtmaC(lImb
cIg
fi(wpc1((fitoV3eifboirafiDPv
(itaciMscTkmtmer
spn
December 2009 PlGF IN PORTAL HYPERTENSION 2124.e1
Materials and Methods
Hemodynamic StudiesAll studies were performed in overnight-fasted mice.
he animals were anesthetized with an intraperitoneal (IP)ixture of ketamine (100 mg/kg body weight, Ketalar;
fizer, Brussels, Belgium) and xylazine (10 mg/kg bodyeight, Rompun; Bayer, Brussels, Belgium). Both the jugu-
ar vein and the carotid artery were cannulated for admin-stration of fluid and monitoring of the mean arterial bloodressure (mm Hg) (MAP), respectively. To evaluate portalypertension, the portal pressure (mm Hg) was measuredia cannulation of the ileocolic vein with a 24-gauge cath-ter (Becton Dickinson, Erembodegem-Aalst, Belgium).
All catheters were connected to highly sensitive pres-ure transducers of a multichannel computer-based re-order (Powerlab; AD Instruments, Spechbach, Germany)nd analyzed with Chart 5 (AD Instruments). An ultra-onic blood flow probe (Transonic Systems Inc, Ithaca,Y) was placed around the superior mesenteric artery,
llowing measurements of the superior mesenteric arterylood flow (milliliters/minute).
Western Blot Analysis of CD31 and �-SmoothMuscle Actin in Mesenteric TissueSnap-frozen mesenteric tissues (3 loops proximal
rom the caecum) were lysed in radioimmunoprecipitationssay buffer (25 mmol/L Tris, 50 mmol/L NaCl, 0.5% NP40..5% deoxycholate, 0.1% SDS, 0.555 g/mL �-glycerophos-hate, 1 mmol/L DTT, phosphatase inhibitor cocktail, andini-EDTA-free protease inhibitor) by sonication in an ice
ath. Total protein content was determined with the Bio-ad DC protein assay kit (Bio–Rad, Hercules, CA), andbsorbance was measured on a plate reader at 590 nm.
One hundred micrograms of protein per lane wasixed with LDS sample buffer (Nupage; Invitrogen, Se-
ttle, WA) and a sample reducing agent (dithiothreitol,nvitrogen). The proteins were denatured by heating at0°C for 10 minutes, subsequently loaded into 10% Bis-ris gel (Invitrogen), separated, and transferred to a ni-
rocellulose membrane (GE Healthcare, Little Chalfont,uckinghamshire, United Kingdom). Membranes werelocked in Tris-buffered saline containing 0.05% Tweennd 5% non-fat milk (TBST/5% milk). Blots were probedvernight at 4°C with anti-CD31 (Santa Cruz Biotech-ology, Santa Cruz, CA; dilution 1:200) or anti-�-smoothuscle actin (SMA) (Sigma–Aldrich, St. Louis, MO; dilu-
ion 1:400) antibodies. After 3 washes with TBST, theembranes were incubated for 1 hour with secondary
ntibodies (CD31: Santa Cruz Biotechnology; �-SMA:ell Signaling, Beverly, MA). Horseradish peroxidase
HRP) detection was carried out with an enhanced chemi-uminescence substrate (Roche Diagnostics, Indianapolis,N). Blots were subsequently stripped and reprobed with
onoclonal antibodies against �-tubulin (Abcam, Cam-
ridge, United Kingdom; dilution 1:5000) as an internal sontrol for protein loading. ImageJ software (Nationalnstitutes of Health, Bethesda, MD; http://rsb.info.nih.ov/ij/) was used to quantify Western blot signals.
Immunohistochemistry, Measurement of theVascular Area, and Image Analysis of TissueSectionTissue samples of the mesentery were immediately
xed in 4% phosphate-buffered formaldehyde solutionSigma–Aldrich) and embedded in paraffin. Serial sectionsere cut at a thickness of 3 �m. Immunostaining waserformed using the following primary antibodies and con-entrations: VEGF-R1 (dilution 1:50), VEGFR-2 (dilution:50) (all Santa Cruz Biotechnology), CD31 (dilution 1:500)BD Pharmingen, San Jose, CA), and �-SMA (no dilution)Biogenex, San Ramon, CA). Tissue sections were deparaf-nized, rehydrated, and incubated with ethylenediamine-etraacetic acid (EDTA) buffer (Invitrogen; in a microwaveven [10 minutes, 750 W, 20-minute cool down]) forEGFR-1 and -2 stainings or Trypsin (Sigma–Aldrich;7°C) for CD31 to retrieve the respective antigens. Endog-nous peroxidase and nonspecific binding were blocked byncubating sections with 0.3% hydrogen peroxide-methanolor 15 minutes at room temperature. Sections were incu-ated with primary antibodies for 1 hour (VEGFR-1 and -2)r overnight (CD31) at room temperature. For CD31 stain-
ng, a secondary antibody (rabbit anti-rat; Dako, Carpinte-ia, CA; 1:300) was applied for 45 minutes. Detection waschieved using a commercialized streptavidin-biotin ampli-cation system (VEGFR-1 and -2: LSAB�system-HRP;ako; CD31: Tyramide Signal Amplification biotin system;erkin Elmer, Waltham, MA) and antigen localization wasisualized with 3=-3-diamino benzidene (DAB kit; Dako).
An immunostained section was screened at low power10�) to detect the 3 most vascularized areas (“hot spots”)n the mesentery. Three pictures were taken of those areas athe appropriate magnification (20�) in which the vascularrea was calculated. A camera (Optronics Colour digitalamera; Olympus Corporation, Tokyo, Japan) and special-zed software (Cell D; Olympus Soft Imaging Solutions,
ünster, Germany) were used to generate a value corre-ponding to the area (�m2) encompassed by the DABolor component within a predefined region of interest.he color component and region of interest settings wereept constant throughout the analysis. The means of alleasurements per section (1 section per mouse) were de-
ermined and averaged with the mean vascular area of 3–5ice per group in each experimental group. Results are
xpressed as the mean area (in �m2 � SEM) stained (rep-esenting blood vessels or cells positive for VEGFR-1 or -2).
Because arteriogenesis is of interest only in medium-ized and large vessels, manual counting of the �-SMAositive vessels was easier and more convenient. Theumber of �-SMA-positive cells was determined in 3
uccessive fields (20�) by 2 blinded observers.
taos(hsonhadtsicTs(
Ettwnttmat
biflcmisTepcalciSa
tt
ahmw
spiCnvmpiipd
vacPwiat
1
2124.e2 VAN STEENKISTE ET AL GASTROENTEROLOGY Vol. 137, No. 6
Results
Natural Course of Murine PPVL ModelBeyond 14 Days PostligationThe natural course of the partial portal vein liga-
ion model has been extensively studied in numerousnimal studies in the past, particularly in rats.1– 6 In mostf these studies, portal hypertensive rats developedplanchnic hyperdynamic circulation, with a high degree�90%) of portosystemic shunting associated with portalypertension, 2 weeks after ligation. However, differentcenarios have been described in the long-term evolutionf PPVL rats, suggesting that the sequence of hemody-amic events is far from uniform. In these chronic portalypertensive models, the hyperdynamic circulation dis-ppears,7 and, although a variable (often decreasing5–7)egree of portosystemic shunting persists in the long-erm, this is not always associated with portal hyperten-ion.1 It has been proposed that long-term vasculopathyn portal hypertensive rats constitutes a remodeling pro-ess, with or without persisting portal hypertension.3
herefore, this experimental model is studied mostly inhort-term (14 –28 days) rather than in chronic stages6 –14 months).
We have studied the natural course of PPVL in mice.xperiments were performed in 3 groups of portal hyper-
ensive mice (n � 5 in each group), divided according toime from the portal vein ligation, respectively 2 weeks, 4eeks, and 7 weeks after ligation. We measured hemody-amic parameters such as portal pressure (PP), mesen-eric artery flow, mean arterial pressure (MAP), and por-osystemic shunt fraction (PSS; using the 51Cr radioactive
icrosphere technique) as well as spleen weight. All datare displayed in Supplementary Table 4 and Supplemen-ary Figure 4.
The natural course of the PPVL model was characterizedy disappearance of the splanchnic hyperemia over time, as
ndicated by the significant decrease in mesenteric arteryow (�55% on week 7 vs week 2), to a level that wasomparable with that of sham-operated (SO) mice. Becauseaintenance of portal hypertension is highly dependent on
ncreased blood flow in the splanchnic system, portal pres-ure was significantly reduced over time (Supplementaryable 1). Furthermore, the extent of portosystemic collat-ral formation was significantly reduced as the postligationeriod increased (�40% on week 7 vs week 2), which alsoontributed to the ultimate decrease observed in mesentericrtery flow (Supplementary Figure 1). According to Ohm’saw, a more pronounced reduction in mesenteric flow couldounteract a less marked decrease in portosystemic shunt-ng, resulting in a significant decrease in portal pressure.pleen weights and MAP were not significantly differentmong the 3 different time points.
As previously reported,8 a 10% mortality was noticed inhe PPVL group, mostly because of technical failure of too
ight ligation of the portal vein with subsequent ischemiand bowel necrosis. These deaths were observed within 24ours after partial portal vein ligation. Afterwards, the PPVLice had a normal activity level, and no excessive mortalityas observed during 12 weeks after induction.Taken together, sequential long-term hemodynamic
tudies in the murine PPVL model indicate that theortal hypertensive syndrome decreases over time, mak-
ng this model less appropriate for long-term experiments.onsistent with these findings, Sikuler et al described aormal splanchnic blood flow and 24% (nonsignificant, Palue not reported) reduction in portosystemic shunting 6onths after PPVL in rats, although portal hypertension
ersisted.7 Stauber et al reported a significant 20% decreasen PSS after 3 months in PPVL rats.6 Therefore, the exper-mental model of PPVL is mostly used in a short-termeriod (day 7–day 28) when the portal hypertensive syn-rome is fully developed.
Discussion
Direct In Vivo Vasoactive Effect of �PlGFBriefly, �PlGF was acutely administered to portal
ein ligated mice (n � 3) 14 days after PPVL induction, asn intravenous bolus injection through a jugular veinatheter at the same dose used previously (50 mg/kg).ortal pressure (PVP), mesenteric artery flow, and MAPere continuously measured for 10 minutes after �PlGF
njection. No significant differences in PVP, mesentericrtery flow, and MAP were observed after acute adminis-ration of �PlGF (Supplementary Table 3).
References
1. Aller MA, Arias JL, Cruz A, et al. Inflammation: a way to under-standing the evolution of portal hypertension. Theor Biol MedModel 2007;4:44.
2. Benoit JN, Womack WA, Korthuis RJ, et al. Chronic portal hyper-tension: effects on gastrointestinal blood flow distribution. Am JPhysiol 1986;250:G535–G539.
3. Chojkier M, Groszmann RJ. Measurement of portal-systemicshunting in the rat by using �-labeled microspheres. Am J Physiol1981;240:G371–G375.
4. Dieguez B, Aller MA, Nava MP, et al. Chronic portal hypertensionin the rat by triple-portal stenosing ligation. J Invest Surg 2002;15:329–336.
5. Geraghty JG, Angerson WJ, Carter DC. Portal venous pressure andportasystemic shunting in experimental portal hypertension. Am JPhysiol 1989;257:G52–G57.
6. Stauber RE, Ruthardt FW, Tauxe WN, et al. Evaluation of portal-systemic shunting in rats from mesenteric and splenic beds. DigDis Sci 1991;36:209–215.
7. Sikuler E, Groszmann RJ. Hemodynamic studies in long- andshort-term portal hypertensive rats: the relation to systemic glu-cagon levels. Hepatology 1986;6:414–418.
8. Geerts AM, Vanheule E, Praet M, et al. Comparison of threeresearch models of portal hypertension in mice: macroscopic,histological and portal pressure evaluation. Int J Exp Pathol2008;89:251–263.
9. Clauss M, Breier G. Mechanisms of angiogenesis. BirkhäuserVerlag, 2005.
0. De SL, Simoens P, Lauwers H, et al. The hyaloid vascular systemof the pig. A light and scanning electron microscopic study. Anat
Embryol (Berl) 1989;180:549–554.
SPP
St 1
apeutic setting (2-week treatment).
December 2009 PlGF IN PORTAL HYPERTENSION 2124.e3
0
10
20
30
40
50
60
70
80
90
100
2 weeks 4 weeks 7 weeks Sham
Colla
tera
ls (m
ean
+/-s
em)
94%
67%
54%
<1%
a
- 27%
upplementary Figure 1. Collateral formation at different weeks afterPVL, compared with SO. (a) PPVL 2 weeks vs PPVL 4 weeks andPVL 7 weeks, P � .001.
upplementary Figure 2. Expression of VEGF (ELISA) in mesentericissues in �PlGF- or IgG -treated PPVL. (A) Prevention setting. (B) Ther-

St
2124.e4 VAN STEENKISTE ET AL GASTROENTEROLOGY Vol. 137, No. 6
upplementary Figure 3. (A) Vascular casting by injecting Batson solution in the ileocolic vein. Representative stereomicroscopic photographs of
he mesentery showed an increased splanchnic neoangiogenesis in IgG1-treated PPVL mice (A) as compared with �PlGF treatment (B).
Smt(sfat
Sp
December 2009 PlGF IN PORTAL HYPERTENSION 2124.e5
upplementary Figure 4. Vascular casting by injecting Batson solution in the ileocolic vein: scanning electron microscopy photographs of theesentery of PPVL mice, treated with IgG1 or �PlGF. (A and B) Illustration of intussusceptive angiogenesis in IgG1-treated mice. Incipient
ranscapillary pillars appear as small depressions on the surface of the blood vessel cast (arrowhead) indicating the initial stages of pillar formationA). As the 2 opposite components of the pillar approximate, there is fusion and subsequent perforation (arrow) of the vascular lumen (B), ultimatelyplitting into 2 new vessels.9 Also see Supplementary Figure 5. (C and D) Casts from IgG1-treated animals showed an increased vascular arborization,orming honeycomb-like vascular networks (D). In addition, sprouting angiogenesis was observed more frequently in IgG1-treated animals (blackrrows) (C). (E and F) Treatment with �PlGF-induced vascular pruning (regression), appearing as thread-like appendices.10 Also, the continuous and
ortuous network disappeared, characterized by a decrease in ramification, involution of complexity, and a more straight course of the vessels.upplementary Figure 5. Different steps in the generation of new vascular segments by intussusceptive angiogenesis. Protrusion of a capillary
illar from opposite sides into the vascular lumen is followed by perforation of the vessel. After Claus et al.9 Reprinted with permission from the author.
S�P
S
MPSM
NBa
b
c
d
S
MPSM
NB
S
MPMP
Nshown as mean � SEM.
2124.e6 VAN STEENKISTE ET AL GASTROENTEROLOGY Vol. 137, No. 6
0
10
20
30
40
50
60
70
80
PPVL IgG1 PPVL αPlGF
Colla
tera
ls (m
ean
+/-s
em)
66%
46%
a
- 20%
upplementary Figure 6. Collateral formation in PPVL treated withPlGF or IgG1 during 4 weeks in therapeutic setting. (a) PPVL IgG1 vs
PVL �PlGF, P � .05.upplementary Table 1. Natural Course of PPVL Mice: Splanchnic and Hemodynamic Changes at Different Weeks AfterPartial Portal Vein Ligation Compared With SO
Parameters Sham 2 Wk 4 Wk 7 Wk
ean arterial pressure (mm Hg) 110 � 9 99 � 8 93 � 4 103 � 9ortal pressure (mm Hg) 4.7 � 0.3 11.2 � 0.8 10.2 � 0.8 7.8 � 0.3a,b
pleen weight (g/10 g BW) 0.033 � 0.003 0.068 � 0.005 0.054 � 0.009 0.066 � 0.009esenteric artery flow (mL/min) 0.87 � 0.02 1.41 � 0.26 1.16 � 0.07 0.63 � 0.1c,d
OTE. Results are shown as mean � SEM.W, body weight.PPVL 7 weeks vs PPVL 4 weeks, P � .05.PPVL 7 weeks vs PPVL 2 weeks, P � .05.PPVL 7 weeks vs PPVL 2 weeks, P � .05.
PPVL 7 weeks vs PPVL 4 weeks, P � .05.upplementary Table 2. Splanchnic and Hemodynamic Changes in PPVL Mice Treated With �PlGF or IgG1 During 4 Weeks inTherapeutic Setting
Parameters PPVL IgG1 PPVL �PlGF P value IgG1 vs �PlGF
ean arterial pressure (mm Hg) 96 � 3 104 � 4 NSortal pressure (mm Hg) 9.2 � 0.2 6.5 � 0.4a P � .001pleen weight (g/10 g BW) 0.076 � 0.013 0.063 � 0.008 NSesenteric artery flow (mL/min) 1.18 � 0.03 0.73 � 0.09b P � .05
OTE. Results are shown as mean � SEM.
W, body weight.upplementary Table 3. Mean Change in HemodynamicParameters After Acute �PlGFInjection
Parameter Mean change (%) P value
ean arterial pressure (mm Hg) 0.02 � 0.00079 P � .05ortal pressure (mm Hg) 0.8 � 0.021 P � .05esenteric artery flow (mL/min) 0.2 � 0.037 P � .05ulse (beats/min) 0.0015 P � .05
OTE. Mean change is in reference to preinjection value. Results are