Limb Immobilization Induces a Coordinate Down- Regulation ...
Upload
dongnocchiCategory
view
3download
0
IEEE TRANSACTIONS ON NEURAL SYSTEMS AND REHABILITATION ENGINEERING, VOL. 20, NO. 3, MAY 2012 351
Robot Training of Upper Limb in MultipleSclerosis: Comparing Protocols With orWithoutManipulative Task ComponentsIlaria Carpinella, Davide Cattaneo, Rita Bertoni, and Maurizio Ferrarin, Member, IEEE
Abstract—In this pilot study, we compared two protocols forrobot-based rehabilitation of upper limb in multiple sclerosis(MS): a protocol involving reaching tasks (RT) requiring armtransport only and a protocol requiring both objects’ reachingand manipulation (RMT). Twenty-two MS subjects were assignedto RT or RMT group. Both protocols consisted of eight sessions.During RT training, subjects moved the handle of a planar roboticmanipulandum toward circular targets displayed on a screen.RMT protocol required patients to reach and manipulate realobjects, by moving the robotic arm equipped with a handle whichleft the hand free for distal tasks. In both trainings, the robotgenerated resistive and perturbing forces. Subjects were evaluatedwith clinical and instrumental tests. The results confirmed thatMS patients maintained the ability to adapt to the robot-gener-ated forces and that the rate of motor learning increased acrosssessions. Robot-therapy significantly reduced arm tremor andimproved arm kinematics and functional ability. Compared toRT, RMT protocol induced a significantly larger improvementin movements involving grasp (improvement in Grasp ARATsub-score: RMT 77.4%, RT 29.5%, p=0.035) but not precisiongrip. Future studies are needed to evaluate if longer trainings andthe use of robotic handles would significantly improve also finemanipulation.
Index Terms—Motor learning, multiple sclerosis, robot-therapy,upper limb function.
I. INTRODUCTION
A LTHOUGH multiple sclerosis (MS) is the most commoncause of chronic neurological disability in young adults,
current pharmacological therapies are so far not able to sub-stantially improve motor functionality [1]. Although no firmconclusions can be drawn, a recent review suggests that reha-bilitation may be useful to maximize the functional status ofthese subjects [2]. Most studies about motor rehabilitation inMS are focused on walking and mobility [3], but, as the dis-ease progresses, nearly 75% of MS subjects experience alsoupper limb dysfunction [4], mainly related to tremor [5], co-ordination deficit [6] and muscle weakness [7]. Although armimpairment highly contributes to reduce the quality of life of
Manuscript received July 14, 2011; revised October 20, 2011; accepted Jan-uary 29, 2012. Date of current version May 18, 2012. This work was supportedin part by FISM—Fondazione Italiana Sclerosi Multipla.I. Carpinella and M. Ferrarin are with the Biomedical Technology Depart-
ment, DonCarlo Gnocchi FoundationOnlus IRCCS, 20148Milan, Italy (e-mail:[email protected]).D. Cattaneo and R. Bertoni are with the Department of Neurorehabilitation,
Don Carlo Gnocchi Foundation Onlus IRCCS, 20148Milan, Italy (e-mail: [email protected]).Digital Object Identifier 10.1109/TNSRE.2012.2187462
MS subjects [8], only few studies exist about neuromotor reha-bilitation of upper limb inMS [7], [9], [10]. The results emergedfrom these works showed that physical rehabilitation generatedan improvement in arm strength [7], in the execution of the ac-tivities of daily living (ADL) [10] and a tendency to an improvedmanual dexterity, although not significant [9]. Given the paucityof existing studies, more research is needed to explore the ef-fects of neuro-rehabilitation on upper limb dysfunction in MSsubjects.In the last decade, robotic devices for upper limb motor
rehabilitation have been increasingly studied, becoming apromising complement to traditional therapy, as they can pro-vide high-intensity, repetitive and interactive treatment of theimpaired upper limb and, inherently, an objective, quantitativemeasurement of patient’s progress. Although robotic systemsare mostly used in rehabilitation of stroke patients [11], theyappear good candidates also for the treatment of tremor andincoordination due to MS. At present, three studies have ad-dressed the application of robot-based treatment of upper limbin MS [12]–[14]. Gijbels et al. [14] used a gravity-supportingexoskeleton which allowed the subject to execute 3-D taskssimulated in a virtual environment on a computer screen.Carpinella et al. [12] and Vergaro et al. [13] used a planarrobotic system and adaptive training protocols, in which therobot did not assist subjects during the execution of the move-ment, but, rather it provided unfamiliar dynamic environmentsto which subjects were required to adapt, by learning to predictthe effects of perturbing forces [15], [16]. A common findingof these studies was the post-treatment improvement in theexecution of functional tasks implying distal movements notdirectly involved in the training. In particular, robotic trainingconsistently improved manual dexterity, as shown by the NineHole Peg Test score [17] which significantly decreased from157 to 109 s in severe MS subjects [14] and from nearly 60to 48 s in mild/moderate patients [12], [13]. These resultsindicated that, even though the mean improvement was signifi-cant, the post-treatment score was still consistently higher thanthe threshold value typical of healthy adults with comparableage, that is 19 [18]. Starting from these results, onemay wonder if the implementation of a functional-based robottraining, which involves not only the movement of proximaljoints but also the use of distal arm and the manipulation of realobjects should even improve the rehabilitation outcome andfacilitate the skill transfer from the experimental setting to theADL [19]. This approach has been recently applied to strokepatients [20], not yet to MS subjects.
1534-4320/$31.00 © 2012 IEEE

352 IEEE TRANSACTIONS ON NEURAL SYSTEMS AND REHABILITATION ENGINEERING, VOL. 20, NO. 3, MAY 2012
In the present study we designed a robot-based functionaltraining which combines a typical adaptive paradigm, previ-ously applied to stroke [21] and MS subjects [12], [13], [22],with two main principles of motor learning: 1) the use of realobjects during purposeful and challenging functional tasks in-volving whole arm, to enhance motor performance and maxi-mize subjects’ active participation [19] and 2) the execution ofdifferent types of exercises during each session, that has beenshown to promote motor learning [23]. A robot-based protocolincorporating these two concepts was applied to a group of MSsubjects and the results were compared to those obtained bya second group of MS patients treated with a more traditionalrobot-based protocol involving reaching tasks [12], [13]. Goalof this pilot study was to evaluate if a robot therapy approach in-volving both objects’ reaching and manipulation leads to betteroutcomes than training involving only the transport of the arm.
II. METHODS
A. Subjects
A consecutive sample of 22 MS subjects were enrolled inthe study within a period of one year and a half. Their demo-graphic and clinical characteristics are shown in Table I. All sub-jects signed an informed consent to the protocol which was con-formed to the standards for human experiments set by the Decla-ration of Helsinki. Subjects fulfilled the following inclusion cri-teria: a definite diagnosis of MS according to McDonald criteria[24], Expanded Disability Status Scale [25] , Nine Hole PegTest [17] score between 30 and 300 s, Mini-Mental State Exam-ination [26] , willing to follow the rehabilitation program.Subjects were excluded if they had reduced and not amendablevisual acuity and/or ocular motility which interfere with the exe-cution of the training tasks. Each subject was allocated to one ofthe following groups: a group receiving a robot-basedrehabilitation program involving the execution of reaching tasks(RT) and a group receiving a robot-based rehabil-itation program involving both objects’ reaching and manipu-lation (RMT). Group allocation was performed following mini-mization method [27], that is a widely acceptable alternative ap-proach to randomization in small trials, as it ensures excellentbalance between groups, even in small samples. In particular,each subject was allocated to one group or the other, dependingon the baseline clinical characteristics of those participants al-ready enrolled, in order to minimize the imbalance between thetwo groups. As shown in Table I, demographic and clinical char-acteristics were similar in both groups.
B. Experimental Equipment
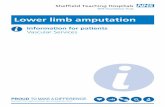
The apparatus consists of a planar robotic manipulandum[Fig. 1(a)] with two back-driveable degrees-of-freedom(Braccio di Ferro, Celin srl, La Spezia, Italy), which has beenfully described elsewhere [28]. It has an 80 40 cm ellipticworkspace and is smoothly impedance-controlled in order togenerate continuous forces up to 25 . Subjects can interactwith the robotic arm through two handles: a “traditional” handlegrasped by the patient [Fig. 1(b)] and a customized “functional”handle [Fig. 1(c)] wrapped around the forearm of the subjectand fastened through velcro stripes leaving the hand free to
TABLE IDEMOGRAPHIC AND CLINICAL CHARACTERISTICS OF TREATED MS SUBJECTS
Fig. 1. (a) Experimental set-up. (b) The “traditional” handle. (c) The “func-tional” handle. (d) Example of a subject executing a functional task, i.e., inserta key in a padlock.
manipulate real objects [Fig. 1(d)]. The “functional” handleis fixed to the robotic arm through a 12-cm-long vertical rodthat supports a cylindrical ball bearing which can rotate aroundthe rod and translate in vertical direction with low friction. Aforearm splint made of thermoplastic material is fixed to theball bearing. The inner surface of the splint is covered withfoam rubber coat to guarantee subject’s comfort.
C. Robot-Based Rehabilitation Protocols
Both RT and RMT protocols were composed of eight ses-sions. The number of sessions was chosen on the basis of theresults obtained by Vergaro et al. [13]. Each session consistedof eight epochs of 20 movements each, for a total of 160 move-ments and a duration of 30–45 min. The most affected arm ofeach subject was treated.In the RT protocol (see also [12], [13], and [22]), subjects sat
on a chair behind a table and grasped the “traditional” handle ofthe robot [Fig. 1(b)]. A 19-in LCD screen, positioned in frontof the subject, was used to display the current position of the

CARPINELLA et al.: ROBOT TRAINING OF UPPER LIMB IN MULTIPLE SCLEROSIS 353
end-effector and the target (circles with a diameter of 1.5 cmand 3 cm, respectively). Subjects performed center-out reachingmovements from the same center position to peripheral targets(directions: 45 and 135 with respect to the horizontal axis)and then they returned to the center (directions: 225 and 315 ).The amplitude of the nominal reaching trajectory was 25 cm. Allsubjects were able to fulfill the task. The movements were ex-ecuted at self-selected speed and the targets were presented ina random order. Each training session consisted of two phases[13], [22]: 1) null field phase (2 epochs, 40 movements) and 2)force field phase (6 epochs, 120 movements). During the nullfield phase, subjects executed the reaching task while the robotdid not generate forces. Null field trials had the purpose to mon-itor the progress of unperturbed reaching movement and the re-tention of the effects of each training session on arm kinematics.During the force field phase, subjects executed the reaching taskwhile the robot generated a velocity-dependent clockwise forcefield [12], [13], [15], [22] to which subjects were requiredto adapt. Perturbing force was perpendicular to the instan-taneous movement direction and had a magnitude proportional
to the handle speed. This force disturbed themovement executed by the subject by deviating hand’s trajec-tory from the nominal straight path. During each epoch, forcewas unexpectedly turned off in 1/5 of the movements (catch
trials, 4 per epoch) to monitor the progress of adaptation. In par-ticular, if adaptation is occurring and the subject is learning theappropriate internal model to predict and cancel the perturba-tions induced by the robot, two effects should be noticed: 1) agradual reduction of the execution errors in the force trials and2) a gradual increase of erroneous movements in directions op-posite to the perturbations in catch trials, when the force is un-expectedly removed (see also [12], [13], [15], [16], [22]). Toincrease the difficulty of the exercise, the robot generated also aspring-like resistive force which opposed hand’s movement.In particular, the force was proportional tothe distance between the current position of the end-effector andthe starting position and was directed along the line which con-nected the starting point and the instantaneous position of thehandle.RMT training sessions also consisted of a null field phase and
a force field phase. During the null field phase (2 epochs, 40movements), subjects executed the reaching task (as in RT pro-tocol), while the robot did not generate forces. At the end of thisphase, the “traditional” handle of the robot was replaced withthe “functional” handle [Fig. 1(c)] and the splint was worn bythe subject. During the force field phase (6 epochs, 120 move-ments), subjects executed a set of 6 functional tasks (one perepoch) involving reaching and manipulation of “real” objects,built using LEGO bricks (LEGO Group, Billund, Denmark)(e.g., small containers, pegs, beads, coin slots) or taken fromtypical activities of daily living (e.g., bottles, jars, padlocks,keys). The set of functional tasks was selected on the basis ofthe specific deficit of each subject, as measured by clinical as-sessment. The tasks included both grasp (e.g., grasp and releaseof water bottles or cylindrical jars) and precision grips, mainlykey grip (e.g., locking of a padlock or insertion of a coin into aslot) and pinch grip (e.g., putting a bead down a needle or inserta rectangular peg into a squared hole). An example is shown in
Fig. 1(d). The objects to be reached and manipulated were fixedon a LEGO supporting base and arranged on the table withinthe elliptic workspace of the manipulandum. The positions ofthe end-effector when each object had been reached were cali-brated for each patient at the beginning of the first training dayand maintained for all sessions. These positions and the instan-taneous position of the handle were represented on the screen bycircles, as in RT protocol. This allowed the operator to check thecorrect execution of the task which was performed by the patientby looking at the objects on the table. Subjects were invited toperform the tasks at self-selected speed, trying to counteract thepull of gravity by maintaining the ball bearing in the middle ofthe handle rod and by avoiding to rest their elbow on the table.During the training, the difficulty of the tasks was increased byvarying the size and the weight of the objects to be manipu-lated. Each functional movement consisted in a transport phase(during which the subject reached the object) and a manipula-tion phase. During the transport phase the robot generated thesame forces and used in the RT protocol. Moreover thesame number of catch trials (4 per epoch) were inserted.To analyze the effect of resistive force , all subjects were
also required to execute the reaching task (1 epoch, 20 move-ments) while only was turned on. This test was performedpre- and post-treatment.
D. Clinical Assessment
All subjects were evaluated pre- and post-treatment by meansof three clinical tests administered by a blinded examiner: NineHole Peg test (9 HPT) [17], Action Research Arm Test (ARAT)[29], and Tremor Severity Scale (TSS) [30].The 9HPT evaluates hand dexterity. The test requires the sub-
ject to place nine pegs in nine holes. Subjects are scored on theamount of time they take to place and remove all nine pegs.The ARAT evaluates proximal and distal function of upper
limb and was used in this study to evaluate the transfer of thetraining effects on functional tasks involving 3-D movementsnot executed during the treatment. The ARAT consists of19 items organized in four sections: Grasp, Grip, Pinch, andGross. Each item is given an ordinal score of 0, 1, 2, or 3, withhigher values indicating better performance. The maximumARAT score is 57. In the present study, total ARAT score andsub-scores related to the four sections were considered. More-over, a variable related to the execution time was analyzed.When a subject was not able to perform some ARAT tasks
, execution time was used to calculateexecution frequency (60/time), that represents the number oftimes an item was executed in a minute. A value of 0 wasassigned when subjects were unable to perform the task. TotalARAT frequency was calculated as the mean frequency of allitems.The TSS measures the severity of tremor in four domains:
1) rest tremor: tremor occurring at rest with the body part sup-ported; 2) postural tremor: tremor occurring while maintaining aposition against gravity; 3) kinetic tremor: tremor during move-ment; and 4) intention tremor: pronounced exacerbation of ki-netic tremor towards the end of a goal directed movement. Eachdomain is rated by a 10-point scale, with higher score indicatingmore severe tremor.

354 IEEE TRANSACTIONS ON NEURAL SYSTEMS AND REHABILITATION ENGINEERING, VOL. 20, NO. 3, MAY 2012
E. Kinematic Analysis
Handle coordinates were sampled at 100 Hz and low-pass fil-tered using a sixth-order Savitzky-Golay filter with a 200 mswindow and a cutoff frequency of 9.4 Hz [12]. The same filterwas used to estimate the subsequent time derivatives of the tra-jectory. Kinematic data were segmented into separated move-ments and, for functional tasks, each movement was dividedinto a reaching phase and a manipulation phase. Then, the fol-lowing parameters were extracted.• Reaching duration: time between reaching onset and ter-mination (first instants in which handle velocity exceededand fell below a threshold of 20% of peak speed, respec-tively [13]).
• Manipulation duration: time elapsed between reaching ter-mination and the end of whole task. This parameter wascalculated only for functional tasks.
• Jerk Index: logarithm of the jerk (norm of the third timederivative of the trajectory), averaged over the movementduration and normalized with respect to the amplitude andduration of the reaching movement [13]. Jerk Index eval-uates the smoothness of the trajectories.
• Mean and maximum lateral deviation: mean andmaximumdistance of the actual trajectory from the nominal trajectory(straight line connecting the start and the end points).
• Normalized path length: length of the actual trajectory nor-malizedwith respect to the length of the nominal trajectory.
• Learning Index : calculated to assess the subjects’ability to adapt to the perturbing force field generated bythe robot. In this study we used the definition of learningindex proposed by Donchin et al. [15] and expressed by
(1)
where and are the maximum lateral deviationsin the field and catch trials, respectively. This index compares asigned measure of execution error (here, maximum lateral devi-ation, positive in the direction of force ) in movements whereforce is turned on (force trials) and where force is turned off(catch trials). Values of equal to 1 indicate a perfect adapta-tion, in which errors in force trials tend to 0, while errors in catchtrials are large and in the opposite direction (negative values)with respect to force [15].
F. Statistical Analysis
Kinematic parameters were analyzed with a two-way mixedANOVA, with session and group (RT versusRMT protocol) as fixed factors. Considering that clinicaldata were not normally distributed (Shapiro-Wilks W test,
), nonparametric procedures were used. In partic-ular, comparisons between pre- and post-treatment data wereevaluated using Wilcoxon matched pairs test (Wt), while dif-ferences between RT and RMT groups were tested by meansof Mann-Whitney U test (MWt). Level of significance was setto 0.05.
III. RESULTS
A. Null Field Trials
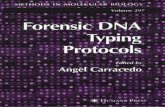
The results related to the unperturbed reaching move-ments performed by the treated MS subjects are shownin Fig. 2. A significant effect of session was found forreaching duration , jerk index
and mean lateral devia-tion , which gradually decreasedduring the training [Fig. 2(a)–(c)], while normalized path lengthremained almost unchanged [seeFig. 2(d)]. The effect of training protocol was not significantfor all parameters. These results indicated that the unperturbedreaching movements of MS subjects became gradually faster,smoother and more linear across sessions, similarly in bothgroups, as shown in the examples reported in Fig. 2(e)–(h).
B. Force Field Trials
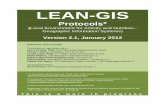
The subjects’ improvement in counteracting the robot-gen-erated disturbing force is shown in Fig. 3. The amplitudeof the perturbing force field [Fig. 3(a)] showed a sig-nificant effect of session .No difference was noticed between RT and RMT groups
but the significant sessiongroup interaction revealed that
amplitude increased mainly in RT group, while remainedalmost stable in RMT group. Despite this difference, therate of force field adaptation was similar in both groups. Asshown in Fig. 3(b), the learning index increased oversessions , similarly in both groups
. The increase of was due to asignificant decrease of the lateral deviation in the force trials
[see Fig. 3(c)] and to a significantincrease (in the opposite direction) of the execution error incatch trials [see Fig. 3(d)]. Exam-ples of the trajectories executed during force field trials by tworepresentative MS subjects from RT and RMT group are shownin Fig. 3(e)–(h), respectively. With respect to the first session[Fig. 3(e) and (g)], in the last training day [Fig. 3(f)–(h)] thedeviation from the straight line decreased during force fieldtrials (continuous lines) and increased in the opposite directionduring catch trials (dashed lines), thus indicating adaptation tothe perturbing force.The results related to the trajectories executed pre and
post-treatment, when only force was turned on revealedthat, after the treatment, MS subjects improved their abilityin counteracting the resistive force which opposed themovement. In particular the trajectories performed againstresistance showed a significant decrease in duration
, jerk index, and lateral deviation, with respect to pre-
treatment evaluation. No statistically significant difference wasnoticed between the two groups. Moreover, similarly in bothgroups, movements executed against were characterized byhigher duration and jerkindex , with respect tounperturbed reaching.

CARPINELLA et al.: ROBOT TRAINING OF UPPER LIMB IN MULTIPLE SCLEROSIS 355
Fig. 2. (a)–(d) Quantitative parameters (mean confidence interval) de-scribing null field trials. Significant differences with respect to session 1 arereported for RT and RMT group . (e)–(h) Unperturbed reaching trajecto-ries executed during the first and the last treatment sessions by two MS subjects(V09 and F03) treated with the RT and the RMT protocols, respectively. -axisrepresents the direction of movement.
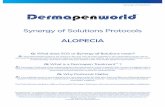
The results related to the duration of the manipulation tasksexecuted by the RMT group are reported in Fig. 4. The timerequired for manipulative tasks involving grasp gradually de-creased across sessions , while thetime of precision grip tasks (i.e., key or pinch grip) remainedalmost unchanged .
C. Clinical Evaluations
At the baseline evaluation (Pre) both groups showedsimilar clinical characteristics (Table II). The MS sub-jects showed moderate to severe upper limb dysfunction(ARAT score: ). All subjects showed cerebellar
Fig. 3. (a)–(d) Quantitative parameters (mean confidence interval) de-scribing force field trials. Significant differences with respect to session 1 arereported for RT and RMT group . (e)–(h) Reaching trajectories executedduring the first and the last treatment sessions by twoMS subjects (V06 and F05)treated with the RT and the RMT protocols, respectively. -axis represents thedirection of movement. Continuous lines: force field trials; dashed lines: catchtrials.
symptoms. In particular, upper limb ataxia (as measured byitems of the Ataxia scale
[31]) was mild/moderate (Ataxia score: 1–3) in 18 subjects andsevere (5–6) in four subjects. Kinetic and intention tremor wasmild/moderate (TSS score: 1–5) in 20 patients and severe (7–8)in two patients.As concerns the effects of training on upper limb function
(see Table II), both groups significantly improved ARAT totalscore and Pinch sub-score, while only RMT group consistentlyincreased Grasp and Grip sub-scores. Gross sub-score did notchange significantly in both groups because of a high ceiling

356 IEEE TRANSACTIONS ON NEURAL SYSTEMS AND REHABILITATION ENGINEERING, VOL. 20, NO. 3, MAY 2012
Fig. 4. Duration (mean confidence interval) of manipulation tasks, in-volving grasp and precision grip, executed by MS subjects during the eight ses-sions of the RMT protocol. ANOVA p-values related to the effect of session andsignificant differences with respect to session are reported.
TABLE IIPRE- AND POST-TREATMENT CLINICAL SCORES FOR RT AND RMT GROUPS
effect. In particular, 16/22 patients (eight per group) showed abaseline Gross score equal to the maximum (nine points) andmaintained the same score after the treatment. The remainingsubjects (three per group) significantly improved their Grosssub-score . A direct comparison of the per-centage change obtained by the two groups after the treatmentconfirmed the above results. As shown in Fig. 5, RMT groupobtained a percentage improvement of Grasp sub-score signifi-cantly higher than that attained by RT group. Analysis of the ex-ecution frequency of ARAT tasks revealed that both groups sig-nificantly increased this parameter after the treatment
. Again, the percentage change in execution frequency ofGrasp items was significantly higher in RMT group [RT: 14.3%
Fig. 5. Post treatment percentage change in ARAT total score and sub-scores.- - . Column: mean; whisker: stan-
dard deviation. P-value from Mann Whitney U test comparing RT and RMTgroups are reported.
(15.8%); RMT: 38.4% (21.3%); ], while a sim-ilar improvement in both groups was noticed for execution fre-quency of Grip [RT: 18.1% (17.8%); RMT: 21.6% (19.8%);
] and Pinch items [RT: 17.2% (20.0%); RMT:17.8% (34.0%); ].As concerns manual dexterity, both groups significantly im-
proved the 9 HPT score after the treatment (Table II). The per-centage change obtained after the training was similar in bothgroups [RT: 14.1% (16.3%); RMT: 12.1% (19.3%);
]. Three subjects in the RT group and five subjects in theRMT group attained an improvement greater than 20% (thethreshold for clinical significance [32]). No subjects showed asignificant worsening.As shown in Table II, both groups significantly reduced in-
tention tremor. A significant reduction of postural tremor wasnoticed in the RMT group.
IV. DISCUSSION
The main goal of the present study was to compare the effectsof two protocols for robot-based rehabilitation of upper limb inMS: a protocol involving reaching tasks (RT) and a protocolrequiring objects’ reaching and manipulation (RMT).The enrolled patients did not report any adverse event in
terms of muscle aches, fatigue or increased muscle stiffness.The results related to the whole sample of treated MS subjects(RT and RMT groups together) confirmed those found inprevious studies and added further evidence that robot-basedtraining significantly improved upper limb coordination, func-tionality and dexterity in people with MS [12]–[14], thusrepresenting a valid complement to traditional rehabilitationapproaches. An important question that arises from these resultsis whether the observed improvements are due to the forcesgenerated by the robot or are just the effect of repeated move-ments. This pilot study did not analyze this aspect, but a recentwork of Vergaro et al. [13] found that, within each session,motor improvements were significant only after robot-assistedtrials, whereas mere exercise alone did not show any effect.This result suggests a specific within-session effect of the robot,

CARPINELLA et al.: ROBOT TRAINING OF UPPER LIMB IN MULTIPLE SCLEROSIS 357
but future studies comparing robot training with unassistedexercise are warranted to explore long term effects.Analysis of instrumental data confirmed that MS subjects
maintained the ability to adapt to novel dynamic environmentsby learning to predict the perturbations induced by the robot. Inparticular the appearance of erroneous movements in oppositedirection of force ,when itwas unexpectedly turned off (catchtrials), suggested that MS subjects reacted to the perturbationby learning a suitable internal model of the disturbing fieldrather than resisting the perturbation by increasing their armstiffness through muscles co-contraction, as found also inhealthy subjects [16]. The time course of learning index
indicated that the capability to adapt was preservednot only within each session, as found by Casadio et al.[22], but also across training days. Similar results were foundby Tomassini et al. [33] who analyzed the learning curvesof MS subjects during the execution of a simple trackingtask. Contrarily to the protocols described by Casadio et al.[22] and Vergaro et al. [13], which forced the subjects tomaintain an approximately constant velocity, in the presentstudy MS patients executed the movements at self-selectedspeed. In particular, MS subjects gradually increased theirreaching velocity across sessions, thus inducing a consequentgradual augmentation of the perturbation generated by therobot. Despite this factor, the parameters describing motorlearning improved along the treatment, thus suggesting thatMS subjects maintain the ability to adapt to the disturbingforce, not only when it remains nearly constant [13], [22]but also when it increases across sessions. Analysis of thelearning curves obtained in the present study revealed thatMS subjects’ adaptation mainly improved in the first part ofthe treatment, with an increase of of approximately 50%during the first four training days, followed by a further butlower increase of about 15% during the last four sessions.This typical asymptotic behavior of motor learning has beenfound also in several studies on healthy subjects and has beendemonstrated to be associated with different mechanisms ofneural plasticity indispensable for the acquisition of new skills(e.g., [34]). This similarity with healthy subjects suggests, inturn, that the mechanisms of force field adaptation and brainplasticity are preserved, at least partly, in MS patients and that,for this reason, these subjects may benefit of adaptive trainingswhich have been shown to promote neural reorganization [35].Interestingly, the rate of adaptation was similar in both groups,thus indicating that subjects treated with the RMT protocoladapted to the perturbing force field similarly to patients whounderwent RT training, even though the exercises proposedin RMT protocol were more complex and the forces weretransmitted to the forearm of the patients and not directlyto the hand as in the RT protocol. The only differencefound in RMT group was the time course of the perturbingforce amplitude, whose increase across sessions was lowerwith respect to RT group. This could be ascribed to thedifficulty of the proposed functional tasks which was graduallyaugmented during the training, thus limiting the increase ofhand velocity and, consequently, of the disturbing force. Despite
this difference, direct comparisons between the two groups,performed separately within each training day, revealed that,during each session, both groups were exposed to forcesof similar amplitude, thus allowing the comparison of theirperformances.Analysis of trials executed when only was turned on, re-
vealed that movements against resistance were slower and lesssmooth than unperturbed reaching. This suggested that addinga spring-like resistive component to the task actually increasedthe difficulty of the exercise. Moreover, after the treatment bothgroups of MS subjects improved their ability in counteractingthe resistive force . This could be ascribed not only to an im-provement in upper limb coordination, but also to an increase inmuscle strength. Future studies should include a direct measureof muscle force to test this hypothesis.Analysis of the reaching trajectories performed by the
subjects during null field trials clearly showed that kinematicsof unperturbed upper limb movements significantly improvedover sessions, independently from the training protocol. Inparticular, arm movements became gradually faster, smootherand more linear, similarly in both groups. According to Fitts’law [36], an increase in movement speed should reducethe accuracy of the trajectory. The fact that the movementsbecame smoother and more linear despite the increased velocitysuggested that the improvements in arm kinematics wereactually due to a beneficial effect of the therapy for bothgroups. Clinical counterpart of this result was the similarimprovement attained by the two groups in Gross sub-scoreof the ARAT, which evaluates the movement of proximalarm only. Taken together, these results suggest that addinga manipulation component to the reaching exercise did notlimit the improvements of proximal arm function in MSsubjects. An opposite result was found by Krebs et al. [20]on chronic stroke patients. In particular, they found that subjectswho underwent a robot-assisted whole-arm training obtaineda significantly larger improvement in wrist/hand movementbut a consistently lower increase in proximal arm function,with respect to stroke patients treated with a robot traininginvolving arm transport only. The authors speculated thatstroke subjects could have focused their attention on thehardest component of the task, that was the manipulation ofthe object, relying on the assistive force generated by therobot for the transport of the arm to the target. This wasnot the case of MS patients treated in the present study, asthey did not receive an assistive force which helped them toextend the elbow, but, rather, resistive and perturbing forceswhich disturbed their movement. This training paradigm, inturn, required the subject to actively participate not only inthe manipulation phase of the task, but also in the reachingphase, thus promoting the active use of whole arm.Importantly, the applied clinical tests showed that both robot-
based protocols significantly reduced intention tremor and im-proved upper limb functionality and dexterity. A hypothesisabout tremor reduction arises from the indication that cerebellarsymptoms typical of MS (including coordination deficit andtremor), may partly depend on the alteration of the anticipatory

358 IEEE TRANSACTIONS ON NEURAL SYSTEMS AND REHABILITATION ENGINEERING, VOL. 20, NO. 3, MAY 2012
(feed-forward) component of motor control and, thus, on thereduced, although present, capability to predict the motor com-mands required to perform a complex task [37]. The fact thatforce field adaptation exercises specifically train these feed-for-ward control mechanisms could thus explain tremor reduction.As concerns the improvements of upper limb function, the re-
sults related to the RT group confirmed those previously foundin [12]–[14] and suggested that the effect of robot-therapy maypartly transfer to tasks more related to ADL. This could be as-cribed to two factors. Firstly, the reduction of tremor and theimprovement of coordination between shoulder and elbow mayhave improved the control of proximal arm, thus allowing abetter orientation of the hand in space, that is a fundamentalprerequisite for a correct grip. Secondly, the beneficial effect ofthe adaptive training on the feed-forward control mechanisms,strongly involved in manipulative tasks [38], could explain theimprovement observed also in distal functions not directly in-volved in the treatment.Interestingly, the comparison between the two groups re-
vealed that MS subjects treated with the RMT protocol obtaineda significantly higher improvement in 3-D tasks involving graspbut not precision grip (i.e., key and pinch grip). This findingwas confirmed by instrumental results, which revealed a signif-icant decrease in the execution time of grasp tasks only. Thiscould be due to different factors. First of all, precision gripis more complex than grasp, as it requires independent fingermovements that involve fine control of the directions and mag-nitudes of fingertip forces [38]. This aspect has been confirmedby fMRI studies which showed that precision grip engagesdifferent and more complex neural circuits with respect to thoseinvolved during grasp [39]. Moreover, it has been demonstratedthat MS subjects reported more difficulties in pinch than grasp[40]. This could be ascribed not only to motor problems, butalso to altered and/or reduced tactile sensibility [41] which canimpair the feedback control of fingertip actions mainly duringmanipulation of small and light objects. On the basis of theseconsiderations, it could be possible that more training sessionsare necessary to obtain a further improvement in precision grip.A second hypothetical explanation could be ascribed to thesplint of the “functional” handle, which highly reduced forearmprono-supination movements. Possibly, this characteristic mayhave facilitated the subjects during the training by reducingthe degrees of freedom to be controlled and, consequently, bysimplifying the whole motor problem to be solved. This, in turn,may have limited the transfer of the acquired skill to the morecomplex 3-D tasks measured by ARAT. A third hypothesis canalso be formulated. In particular, in the investigated protocolthe haptic device generated forces only during the reachingphase of the tasks while the patient-robot interaction was indeednull during the manipulation phase. Moreover such forces wereapplied to the forearm/wrist and not to the fingers. This leavesopen the possibility that assistive/resistive/perturbing forcesoperating directly on the hand and/or fingers (as describedfor example in [42], [43]) might be a significant factor for afurther improvement in manipulation tasks and, in particular,in precision skills.
There are some limitations that need to be addressed re-garding the present study. Considering that no correlation wasfound between the baseline clinical characteristics and the levelof post-treatment improvement, studies on a greater numberof patients are warranted to identify the MS subjects whowould mostly benefit of robot therapy and to make the resultsgeneralizable to the entire population with MS. A secondlimitation concerns the design of the “functional” handle. Inparticular, future studies should include the use of wearablesensorized robotic handles which can generate forces operatingon the distal part of the upper limb (i.e., hand and fingers) andwhich can provide an objective, quantitative measurement ofhand’s movement. The third limitation concerns the parametersand related to the forces generated by the robot, that
were maintained fixed for all subjects and during all trainingsessions. Given the high variability of the symptoms typicalof MS, these parameters should be tuned on the basis of theindividual capabilities and gradually adjusted to account forthe change of performance across the training sessions. Futurestudies should include automatic procedures for the fine tuningof the exercises.In conclusion the present pilot study confirmed that adaptive
robot training may be a useful approach to improve upper limbkinematics and functional ability in subjects with MS. Eventhough caution must be taken given the small sample size, thepresent results suggested that the inclusion of a manipulationcomponent to the typical reaching exercise can significantly im-prove the execution of functional tasks involving grasp. Fur-ther larger studies including follow-up evaluations are needed toevaluate if longer treatments, which involve the use of a wear-able robotic handle, could induced also significant ameliorationof precision grip and if the beneficial effects of robot therapyare maintained long-term.
REFERENCES
[1] S. J. Pittock and C. F. Lucchinetti, “The pathology ofMS: New insightsand potential clinical applications,” Neurologist, vol. 13, pp. 45–56,Mar. 2007.
[2] F. Khan, L. Turner-Stokes, L. Ng, and T. Kilpatrick, “Multidisciplinaryrehabilitation for adults with multiple sclerosis,” Cochrane. DatabaseSyst. Rev., pp. CD006036–CD006036, 2007.
[3] E. M. Snook and R. W. Motl, “Effect of exercise training on walkingmobility in multiple sclerosis: A meta-analysis,” Neurorehabil. NeuralRepair, vol. 23, pp. 108–116, Feb. 2009.
[4] S. Johansson, C. Ytterberg, I. M. Claesson, J. Lindberg, J. Hillert, M.Andersson, H. L. Widen, and L. von Koch, “High concurrent presenceof disability in multiple sclerosis. Associations with perceived health,”J. Neurol., vol. 254, pp. 767–773, Jun. 2007.
[5] P. Feys, F. Maes, B. Nuttin, W. Helsen, V. Malfait, G. Nagels, A.Lavrysen, and X. Liu, “Relationship between multiple sclerosis inten-tion tremor severity and lesion load in the brainstem,” Neurorep., vol.16, pp. 1379–1382, Aug. 2005.
[6] A. J. Bastian, T. A.Martin, J. G. Keating, andW. T. Thach, “Cerebellarataxia: Abnormal control of interaction torques across multiple joints,”J. Neurophysiol., vol. 76, pp. 492–509, Jul. 1996.
[7] N. F. Taylor, K. J. Dodd, D. Prasad, and S. Denisenko, “Progressive re-sistance exercise for people with multiple sclerosis,”Disabil. Rehabil.,vol. 28, pp. 1119–1126, Sep. 2006.
[8] N. Yozbatiran, F. Baskurt, Z. Baskurt, S. Ozakbas, and E. Idiman,“Motor assessment of upper extremity function and its relation withfatigue, cognitive function and quality of life in multiple sclerosis pa-tients,” J. Neurol. Sci., vol. 246, pp. 117–122, Jul. 2006.

CARPINELLA et al.: ROBOT TRAINING OF UPPER LIMB IN MULTIPLE SCLEROSIS 359
[9] L. K. Storr, P. S. Sorensen, and M. Ravnborg, “The efficacy of multi-disciplinary rehabilitation in stable multiple sclerosis patients,” Mult.Scler., vol. 12, pp. 235–242, Apr. 2006.
[10] V. W. Mark, E. Taub, K. Bashir, G. Uswatte, A. Delgado, M. H.Bowman, C. C. Bryson, S. McKay, and G. R. Cutter, “Constraint-In-duced Movement therapy can improve hemiparetic progressivemultiple sclerosis. Preliminary findings,” Mult. Scler., vol. 14, pp.992–994, Aug. 2008.
[11] G. Kwakkel, B. J. Kollen, and H. I. Krebs, “Effects of robot-assistedtherapy on upper limb recovery after stroke: A systematic review,”Neurorehabil. Neural Repair, vol. 22, pp. 111–121, Mar. 2008.
[12] I. Carpinella, D. Cattaneo, S. Abuarqub, andM. Ferrarin, “Robot-basedrehabilitation of the upper limbs in multiple sclerosis: Feasibilityand preliminary results,” J. Rehabil. Med., vol. 41, pp. 966–970,Nov. 2010.
[13] E. Vergaro, V. Squeri, G. Brichetto, M. Casadio, P. Morasso, C. So-laro, and V. Sanguineti, “Adaptive robot training for the treatment ofincoordination inMultiple Sclerosis,” J. Neuroeng. Rehabil., vol. 7, pp.37–37, 2010.
[14] D. Gijbels, I. Lamers, L. Kerkhofs, G. Alders, E. Knippenberg, and P.Feys, “The Armeo Spring as training tool to improve upper limb func-tionality in multiple sclerosis: A pilot study,” J. Neuroeng. Rehabil.,vol. 8, pp. 5–5, 2011.
[15] O. Donchin, L. Sawaki, G. Madupu, L. G. Cohen, and R. Shadmehr,“Mechanisms influencing acquisition and recall of motor memories,”J. Neurophysiol., vol. 88, pp. 2114–2123, Oct. 2002.
[16] J. L. Patton and F. A. Mussa-Ivaldi, “Robot-assisted adaptive training:Custom force fields for teaching movement patterns,” IEEE TransBiomed. Eng., vol. 51, no. 4, pp. 636–646, Apr. 2004.
[17] D. E. Goodkin, D. Hertsgaard, and J. Seminary, “Upper extremity func-tion in multiple sclerosis: Improving assessment sensitivity with box-and-block and nine-hole peg tests,” Arch. Phys. Med Rehabil., vol. 69,pp. 850–854, Oct. 1988.
[18] G. K. Oxford, K. A. Vogel, V. Le, A. Mitchell, S. Muniz, and M. A.Vollmer, “Adult norms for a commercially available Nine Hole PegTest for finger dexterity,” Am. J. Occup. Ther., vol. 57, pp. 570–573,Sep. 2003.
[19] J. Carr and R. Shepherd, A Motor Relearning Programme for Stroke, 2ed. Rockville, MD: Aspen, 1987.
[20] H. I. Krebs, S.Mernoff, S. E. Fasoli, R. Hughes, J. Stein, and N. Hogan,“A comparison of functional and impairment-based robotic training insevere to moderate chronic stroke: A pilot study,” NeuroRehabil., vol.23, pp. 81–87, 2008.
[21] J. L. Patton, M. Kovic, and F. A. Mussa-Ivaldi, “Custom-designedhaptic training for restoring reaching ability to individuals with post-stroke hemiparesis,” J. Rehabil. Res. Develop., vol. 43, pp. 643–656,Aug. 2006.
[22] M. Casadio, V. Sanguineti, P. Morasso, and C. Solaro, “Abnormal sen-sorimotor control, but intact force field adaptation, in multiple sclerosissubjects with no clinical disability,”Mult. Scler., vol. 14, pp. 330–342,Apr. 2008.
[23] V. S. Huang and J. W. Krakauer, “Robotic neurorehabilitation: A com-putational motor learning perspective,” J. Neuroeng. Rehabil., vol. 6,pp. 5–5, 2009.
[24] W. I. McDonald, A. Compston, G. Edan, D. Goodkin, H. P. Hartung, F.D. Lublin, H. F. McFarland, D. W. Paty, C. H. Polman, S. C. Reingold,M. Sandberg-Wollheim, W. Sibley, A. Thompson, N. S. van den, B. Y.Weinshenker, and J. S. Wolinsky, “Recommended diagnostic criteriafor multiple sclerosis: Guidelines from the International Panel on thediagnosis of multiple sclerosis,” Ann. Neurol., vol. 50, pp. 121–127,Jul. 2001.
[25] J. F. Kurtzke, “Rating neurologic impairment in multiple sclerosis:An expanded disability status scale (EDSS),” Neurology, vol. 33, pp.1444–1452, Nov. 1983.
[26] E. Pfeiffer, “A short portable mental status questionnaire for the assess-ment of organic brain deficit in elderly patients,” J. Am. Geriatr. Soc.,vol. 23, pp. 433–441, Oct. 1975.
[27] D. G. Altman and J.M. Bland, “Treatment allocation byminimisation,”BMJ, vol. 330, pp. 843–843, Apr. 2005.
[28] M. Casadio, V. Sanguineti, P. G.Morasso, and V. Arrichiello, “Bracciodi Ferro: A new haptic workstation for neuromotor rehabilitation,”Technol. Health Care, vol. 14, pp. 123–142, 2006.
[29] R. C. Lyle, “A performance test for assessment of upper limb functionin physical rehabilitation treatment and research,” Int. J. Rehabil. Res.,vol. 4, pp. 483–492, 1981.
[30] P. G. Bain, L. J. Findley, P. Atchison, M. Behari, M. Vidailhet, M.Gresty, J. C. Rothwell, P. D. Thompson, and C. D. Marsden, “As-sessing tremor severity,” J Neurol. Neurosurg. Psychiatry, vol. 56, pp.868–873, Aug. 1993.
[31] S. H. Alusi, J. Worthington, S. Glickman, and P. G. Bain, “A study oftremor in multiple sclerosis,” Brain, vol. 124, pp. 720–730, Apr. 2001.
[32] S. R. Schwid, A. D. Goodman, M. P. McDermott, C. F. Bever, and S.D. Cook, “Quantitative functional measures in MS: What is a reliablechange?,” Neurology, vol. 58, pp. 1294–1296, Apr. 2002.
[33] V. Tomassini, H. Johansen-Berg, L. Leonardi, L. Paixao, S. Jbabdi, J.Palace, C. Pozzilli, and P. M. Matthews, “Preservation of motor skilllearning in patients with multiple sclerosis,” Mult. Scler., vol. 17, pp.103–115, Jan. 2011.
[34] L.Ma, B.Wang, S. Narayana, E. Hazeltine, X. Chen, D. A. Robin, P. T.Fox, and J. Xiong, “Changes in regional activity are accompanied withchanges in inter-regional connectivity during 4 weeks motor learning,”Brain Res., vol. 1318, pp. 64–76, Mar. 2010.
[35] R. J. Nudo, “Adaptive plasticity in motor cortex: Implications for re-habilitation after brain injury,” J. Rehabil. Med., pp. 7–10, May 2003.
[36] P. M. Fitts, “The information capacity of the human motor system incontrolling the amplitude of movement. 1954,” J. Exp. Psychol. Gen.,vol. 121, pp. 262–269, Sep. 1992.
[37] V. Sanguineti, P. G.Morasso, L. Baratto, G. Brichetto,M. G. Luigi, andC. Solaro, “Cerebellar ataxia: Quantitative assessment and cyberneticinterpretation,” Hum. Mov Sci., vol. 22, pp. 189–205, Apr. 2003.
[38] J. R. Flanagan, M. C. Bowman, and R. S. Johansson, “Control strate-gies in object manipulation tasks,” Curr. Opin. Neurobiol., vol. 16, pp.650–659, Dec. 2006.
[39] H. H. Ehrsson, A. Fagergren, T. Jonsson, G. Westling, R. S. Johansson,and H. Forssberg, “Cortical activity in precision- versus power-griptasks: An fMRI study,” J. Neurophysiol., vol. 83, pp. 528–536, Jan.2000.
[40] C. C. Chen, N. Kasven, H. I. Karpatkin, and A. Sylvester, “Handstrength and perceived manual ability among patients with multiplesclerosis,” Arch. Phys. Med Rehabil., vol. 88, pp. 794–797, Jun. 2007.
[41] V. Iyengar, M. J. Santos, M. Ko, and A. S. Aruin, “Grip force controlin individuals with multiple sclerosis,” Neurorehabil. Neural Repair,vol. 23, pp. 855–861, Oct. 2009.
[42] A. E. Fiorilla, F. Nori, L. Masia, and G. Sandini, “Finger impedanceevaluation by means of hand exoskeleton,” Ann. Biomed. Eng., Aug.2011.
[43] L. Masia, H. I. Krebs, P. Cappa, and N. Hogan, “Design and character-ization of hand module for whole-arm rehabilitation following stroke,”IEEE/ASME Trans. Mechatron., vol. 12, pp. 399–407, Aug. 2007.
Ilaria Carpinella was born in Vigevano, Italy, in1977. She received the M.Sc. degree in biomedicalengineering from thr Polytechnic of Milan, Milan,Italy, in 2002, with a thesis developed at the Univer-sity of Glasgow, Glasgow, U.K.Since 2003, she has been a Researcher with
the Biomedical Technology Department, Don C.Gnocchi Foundation Research Hospital, Milan, andfrom 2005 to 2007 she was a Professor of electricand electronic measures at the University of Milan.Her main research interests include rehabilitation
engineering and robotics, motor control, and movement analysis.
Davide Cattaneo was born in Milan, Italy, in 1970.He received the M.Sc. degree in rehabilitation sci-ence in 2007 and the Ph.D. degree in biomedical en-gineering in 2010.He is Research Coordinator at the Larice Lab, Don
C. Gnocchi Foundation Research Hospital,Milan. Hehas published papers on the assessment and treatmentof functional disorders in subjects with neurologicaldiseases using traditional and innovative instruments.He is a reviewer for several peer-reviewed interna-tional journals and international research institutions.
Dr. Cattaneo is a member of the European Group for Rehabilitation in Mul-tiple Sclerosis.

360 IEEE TRANSACTIONS ON NEURAL SYSTEMS AND REHABILITATION ENGINEERING, VOL. 20, NO. 3, MAY 2012
Rita Bertoni was born in Milan, Italy, in 1982. Shegraduated as a Sport Scientist from the UniversitàCattolica del Sacro Cuore in 2005 and received theB.S. degree in physical therapy, in 2008, from theUniversity of Milan with a thesis on the robotic re-habilitation in people with multiple sclerosis.Since 2010, she has worked as a Physical Thera-
pist and researcher at Don Carlo Gnocchi FoundationOnlus IRCCS, Milan.
Maurizio Ferrarin (M’97) received the M.Sc. andPh.D. degrees in biomedical engineering.He is Research Coordinator with the Biomed-
ical Technology Department, Don C. GnocchiFoundation Research Hospital, Milan, Italy. Hewas Professor of rehabilitation engineering at thePolytechnic of Milan (1997–2003) and, since 2003,has been a Professor of electronic bioengineeringat the University of Milan. His research interestsinclude movement analysis, FES, motor control,rehabilitation robotics. He authored 60 full papers in
peer-reviewed journals and two books.He is member of IFESS and a Founding Member of the Italian Society of
Clinical Movement Analysis. He served in the board of directors of IFESS(2003–2006) and SIAMOC (2009–present).
Copyright © 2022 FDOKUMEN