Reversal of established rat crescentic glomerulonephritis by blockade of macrophage migration...
12
Molecular Medicine 4: 413-424, 1998 Molecular Medicine © 1998 The Picower Institute Press Reversal of Established Rat Crescentic Glomerulonephritis by Blockade of Macrophage Migration Inhibitory Factor (MIF): Potential Role of MIF in Regulating Glucocorticoid Production Niansheng Yang,' David J. Nikolic-Paterson7 Yee-Yung Ng,4 Wei Mu,2 Christine Metz,5 Michael Bacher,5 Andreas Meinhardt,3 Richard Bucala,5 Robert C. Atkins,2 and Hui Y. Lan2 'The First Hospital, Sun Yat-Sen University of Medical Sciences, Ghongzhou, China 2Department of Nephrology and the 3Institute for Reproduction and Development, Monash Medical Centre, Clayton, Victoria, Australia 4Department of Nephrology, Veterans General Hospital-Taipei, National Yang-Ming University, Taipei, Taiwan 5Picower Institute for Medical Research, Manhasset, New York, U.S.A. Communicated by R. Bucala. Accepted April 28, 1998. Abstract Macrophage migration inhibitory factor (MIF) is a potent pro-inflammatory cytokine that also counter-regulates glucocorticoid action. We investigated whether immu- noneutralization of MIF could reverse established exper- imental crescentic glomerulonephritis and if this treat- ment could modulate endogenous glucocorticoid levels. Accelerated anti-GBM glomerulonephritis was induced in six littermate pairs of rats. Once crescentic disease was established on day 7, one animal in each pair was given a daily injection of neutralizing anti-MIF antibody (Ab) or irrelevant isotype control Ab for 14 days and then killed on day 21. In addition, a group of 6 animals was killed on day 7 of disease without any treatment. Ani- mals receiving the control Ab exhibited a rapidly pro- gressive glomerulonephritis with severe renal injury (proteinuria), loss of renal function (creatinine clear- ance), anemia, and marked histologic damage (including glomerular crescent formation), compared with animals killed on day 7 without treatment. In contrast, anti-MIF Ab treatment partially reversed the disease by restoring normal renal function and reducing histological damage compared with untreated animals killed on day 7 (p < 0.05). Interestingly, anti-MIF Ab treatment also pre- vented severe anemia (p < 0.05). Reversal of disease was associated with a significant reduction in leukocyte infil- tration and activation and renal interleukin- 1 (IL- 1) pro- duction. Importantly, anti-MIF Ab treatment caused a significant increase in endogenous serum corticosterone levels, which correlated with the reversal of disease pa- rameters. In conclusion, this study has demonstrated that blocking MIW activity can partially reverse estab- lished crescentic glomerulonephritis and suggests that MIF operates by both enhancing the cellular immune response and suppressing the endogenous anti-inflam- matory glucocorticoid response. Introduction Macrophage migration inhibitory factor (MIF) was first described over 30 years ago as a product Address correspondence and reprint requests to: Hui Y. Lan, Ph.D., Department of Nephrology, Monash Medical Centre, 246 Clayton Road, Clayton, Victoria 3168, Austra- lia. Phone: 61-3-9550 3534; Fax: 61-3-9550 3530; E-mail: huilan@its-mmccl .cc.monash.edu.au of activated T cells that inhibited the migration of macrophages in vitro and promoted macrophage accumulation in the skin delayed-type hypersen- sitivity reaction (1,2). The recent cloning and characterization of MIF has led to the recognition that this molecule occupies a pivotal position in regulating the inflammatory and immune re- sponses (3). The use of neutralizing antibodies (Ab) has confirmed the central role of MIF in the
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Reversal of established rat crescentic glomerulonephritis by blockade of macrophage migration...

Molecular Medicine 4: 413-424, 1998
Molecular Medicine© 1998 The Picower Institute Press
Reversal of Established Rat CrescenticGlomerulonephritis by Blockade of MacrophageMigration Inhibitory Factor (MIF): Potential Roleof MIF in Regulating Glucocorticoid Production
Niansheng Yang,' David J. Nikolic-Paterson7 Yee-Yung Ng,4Wei Mu,2 Christine Metz,5 Michael Bacher,5 Andreas Meinhardt,3Richard Bucala,5 Robert C. Atkins,2 and Hui Y. Lan2
'The First Hospital, Sun Yat-Sen University of Medical Sciences,Ghongzhou, China2Department of Nephrology and the 3Institute for Reproduction andDevelopment, Monash Medical Centre, Clayton, Victoria, Australia4Department of Nephrology, Veterans General Hospital-Taipei,National Yang-Ming University, Taipei, Taiwan5Picower Institute for Medical Research, Manhasset, New York, U.S.A.Communicated by R. Bucala. Accepted April 28, 1998.
Abstract
Macrophage migration inhibitory factor (MIF) is a potentpro-inflammatory cytokine that also counter-regulatesglucocorticoid action. We investigated whether immu-noneutralization of MIF could reverse established exper-imental crescentic glomerulonephritis and if this treat-ment could modulate endogenous glucocorticoid levels.Accelerated anti-GBM glomerulonephritis was inducedin six littermate pairs of rats. Once crescentic disease wasestablished on day 7, one animal in each pair was givena daily injection of neutralizing anti-MIF antibody (Ab)or irrelevant isotype control Ab for 14 days and thenkilled on day 21. In addition, a group of 6 animals waskilled on day 7 of disease without any treatment. Ani-mals receiving the control Ab exhibited a rapidly pro-gressive glomerulonephritis with severe renal injury(proteinuria), loss of renal function (creatinine clear-ance), anemia, and marked histologic damage (includingglomerular crescent formation), compared with animals
killed on day 7 without treatment. In contrast, anti-MIFAb treatment partially reversed the disease by restoringnormal renal function and reducing histological damagecompared with untreated animals killed on day 7 (p <0.05). Interestingly, anti-MIF Ab treatment also pre-vented severe anemia (p < 0.05). Reversal of disease wasassociated with a significant reduction in leukocyte infil-tration and activation and renal interleukin- 1 (IL- 1) pro-duction. Importantly, anti-MIF Ab treatment caused asignificant increase in endogenous serum corticosteronelevels, which correlated with the reversal of disease pa-rameters. In conclusion, this study has demonstratedthat blocking MIW activity can partially reverse estab-lished crescentic glomerulonephritis and suggests thatMIF operates by both enhancing the cellular immuneresponse and suppressing the endogenous anti-inflam-matory glucocorticoid response.
IntroductionMacrophage migration inhibitory factor (MIF)was first described over 30 years ago as a product
Address correspondence and reprint requests to: Hui Y.Lan, Ph.D., Department of Nephrology, Monash MedicalCentre, 246 Clayton Road, Clayton, Victoria 3168, Austra-lia. Phone: 61-3-9550 3534; Fax: 61-3-9550 3530; E-mail:huilan@its-mmccl .cc.monash.edu.au
of activated T cells that inhibited the migration ofmacrophages in vitro and promoted macrophageaccumulation in the skin delayed-type hypersen-sitivity reaction (1,2). The recent cloning andcharacterization of MIF has led to the recognitionthat this molecule occupies a pivotal position inregulating the inflammatory and immune re-sponses (3). The use of neutralizing antibodies(Ab) has confirmed the central role of MIF in the

414 Molecular Medicine, Volume 4, Number 6, June 1998
cutaneous response to tuberculin (4). In addi-tion, a requirement for MIF in primary T cellactivation and T cell-dependent immunoglob-ulin production has been demonstrated in vitroand in vivo (5). An unexpected property ofMIF was the discovery that it acts as a counter-regulator for glucocorticoid action. Injection ofdexamethasone into mice causes an increase inserum MIF levels, while the addition of recom-binant MIF overcomes dexamethasone-medi-ated inhibition of lipopolysaccharide-inducedcytokine secretion in vitro (6). In addition,administration of recombinant MIF can over-come dexamethasone inhibition of lethal en-dotoxemia in mice (6). Consistent with its roleas a regulator of glucocorticoids, preformedMIF is present at high levels within secretorygranules of corticotrophic cells of the anteriorpituitary (7). Indeed, MIF is widely expressedin most normal tissues (8,9).
We have recently described constitutiveMIF expression by intrinsic glomerular and tu-bular epithelial cells of the rat kidney. There isa marked increase in both renal and systemicMIF production during the development ofcrescentic glomerulonephritis in the rat, whichis dependent upon tumor necrosis factor-a(TNF-a) activity (10,11). Treatment of ratswith a neutralizing anti-MIF antibody (Ab) sig-nificantly inhibits the induction of this aggres-sive model of kidney disease, providing thefirst evidence that MIF participates in thepathogenesis of immunologically induced dis-ease (12). This inhibition of disease inductionwas associated with a suppression of bloodmonocyte recruitment and subsequent mac-rophage-mediated tissue injury. This findinghas opened up two important questions. First,can anti-MIF Ab treatment reverse establishedcrescentic glomerulonephritis? This is the situ-ation encountered in clinical practice and thesetting in which any new therapy must beeffective. Second, does immunoneutralizationof MIF affect circulating glucocorticoid levels?This may be an important component of thepro-inflammatory actions of MIF in immune-mediated disease. These two questions havebeen addressed in a study in which establishedcrescentic glomerulonephritis in rats wastreated with a neutralizing anti-MIF or irrele-vant isotype control antibody and the effectupon disease progression/resolution and se-rum glucocorticoid levels examined.
Materials and MethodsAntibodies and ProbesThe following mouse antibodies (Ab) were used:IIID9, a mouse anti-murine MIF monoclonal Abraised to purified recombinant mouse MIF,which neutralizes the bioactivity of mouse, rat,and human MIF (13); OX-1; anti-rat CD45, aleukocyte common antigen (14); ED1, an anti-rat CD68 that labels most monocytes and mac-rophages (15,16); R73, which recognizes a non-polymorphic epitope of the af3 T cell receptor(17); NDS 61, an anti-rat CD25, p55 chain of therat interleukin-2 receptor (IL-2R) (18); MCA1397, an anti-rat recombinant IL-1f3 (Serotec,Oxford, UK) (19); and 73.5, a mouse anti-hu-man CD45R mAb that does not react with rattissues; this was used as a negative control. Per-oxidase-conjugated goat anti-mouse IgG andmouse peroxidase anti-peroxidase complexeswere purchased from Dakopatts (Glostrup, Den-mark). Fluorescein isothiocyanate (FITC)-conju-gated goat anti-rat IgG, anti-rat C3, and FITC-conjugated sheep anti-rabbit IgG were purchasedfrom Nordic (Tilburg, The Netherlands).
A 420 bp fragment of mouse MIF cDNAcloned into pBluescript (Stratagene, La Jolla, CA)(20), was used to prepare digoxigenin (DIG)-labeled cRNA sense and anti-sense probes for insitu hybridization according to the manufactur-er's protocol (Boehringer Mannheim, Mann-heim, Germany).
Experimental DesignPassive accelerated anti-GBM disease was in-duced in inbred male Sprague-Dawley rats (150-180 g) (Monash Animal Services, Melbourne) aspreviously described (21). Each experiment con-sisted of a matched pair of inbred littermatesimmunized at the same time by s.c. injection of 5mg normal rabbit IgG in Freund's complete ad-juvant, followed 5 days later (day 0) by i.v. in-jection of 10 ml/kg body weight rabbit anti-ratglomerular basement membrane (GBM) serum(12.5 mg IgG/ml). One animal in each pair wasrandomly assigned to treatment with daily i.p.injections of 2.5 mg/kg anti-MIF Ab or an irrel-evant isotype IgGI (73.5) control Ab from day 7until being killed on day 21. A third group waskilled on day 7 after injection of anti-GBM serumwith no treatment in order to serve as a controlfor the degree of renal injury at the time anti-body treatment commenced. Blood and 24-hrurine collections were taken on days 0, 1, 7, 14,

N. Yang et al.: Reversal of Glomerulonephritis by MIF Blockade 415
and 21. A group of normal rats was also exam-
ined. Animal experiments were approved by theAnimal Experimentation Ethics Committee ofMonash Medical Centre. Urinary protein excre-
tion was determined using the Manual PonceauRed method. Concentrations of serum and urinecreatinine, and serum urea were determined us-
ing the standard Jaffe rate reaction (alkalinepicrate) or NED/OPA assay, respectively. Hepa-rinized blood samples were taken under etheranesthesia at the time of sacrifice and whiteblood cells were analyzed by Coulter Counter(Cell Dyne). All analyses were performed by theDepartments of Biochemistry and Haematology,Monash Medical Centre.
Skin Delayed-Type Hypersensitivity Response
Twenty-four hours prior to being killed, eachanimal was given three separate intradermal in-jections of 0.1 ml each of I mg/ml rabbit IgG(specific antigen challenge), 1 mg/ml horse IgG(irrelevant antigen control), and phosphate buff-ered saline (PBS) (no antigen control). Skinthickness at the time of killing was measuredusing engineer's callipers.
Histopathology
Tissues were fixed in 4% buffered formalin and4-,um paraffin sections were stained with hema-toxylin and eosin (H&E) or periodic acid-Schiff(PAS) reagent. Glomerular hypercellularity was
graded on the basis of the total glomerular cellcount/glomerular cross section (gcs) scored in100 glomerular cross sections per animal inH&E-stained sections and ranked as previouslydescribed (22): (0), normal (<50 cells/gcs); (1),mild (60-80 cells/gcs); (2), moderate (80-120cells/gcs); (3), severe hypercellularity (>120cells/gcs). The percentage of glomeruli exhibitingsegmental and/or global sclerosis or crescent for-mation was also scored in 100 glomeruli per
animal in PAS-stained sections. A point countingtechnique was used to quantitate tubulointersti-tial damage (tubular atrophy, leukocytic infiltra-tion, and fibrosis) in at least 50 high-power cor-
tical fields in PAS-stained sections (23). Data are
presented as the mean of 6 animals ± SEM.Scoring was performed on blinded slides.
Measurement of the Humoral Immune Response
Circulating levels of rat IgG reactive with rabbitimmunoglobulin were quantitated by a sand-
wich ELISA, as previously described (24). Depo-sition of immune reactants within the kidneywas assessed by direct immunofluorescence. Tis-sues were snap frozen in liquid nitrogen and4-,um cryostat sections were stained with FITC-conjugated polyclonal antibodies to rat IgG, C3,or rabbit IgG. Semi-quantitation of rabbit IgG, ratIgG, and C3 deposition was determined in tissuesections using an antibody titration method(22,24). Sections from each tissue were incu-bated with serial 2-fold dilutions of each anti-body. Slides were blinded and the antibody dilu-tion at which staining became undetectable wasscored.
ImmunohistochemistryThree-layer immunoperoxidase staining wasperformed on cryostat sections of tissues fixed in2% paraformaldehyde-lysine-periodate (PLP) aspreviously described (22). Briefly, sections werepreincubated with 10% fetal calf serum (FCS)and 10% normal goat serum in PBS for 20 min,drained, and labeled with a mouse mAb for 60min, washed (X 3) in PBS, and endogenous per-oxidase inactivated by incubation in 0.3% H202in methanol. Sections were then washed in PBS,incubated with peroxidase-conjugated goat anti-mouse IgG, washed in PBS, and incubated withmouse peroxidase anti-peroxidase complexesand developed with 3,3-diaminobenzidine toproduce a brown color. Sections were counter-stained with PAS minus hematoxylin.
In Situ HybridizationIn situ hybridization was performed on 4-gmparaffin sections of formalin-fixed tissue using amicrowave-based protocol (10,25). After dewax-ing, sections were treated with 2 x 5 min micro-wave oven heating in 0.01 M sodium citrate, pH6.0, at 2450 MHz and 800 W, incubated with 0.2M HCI for 15 min, followed by 1% Triton X-100for 15 min, and then digested for 20 min with 10,g/ml proteinase-K at 37°C (Boehringer Mann-heim). Sections were then washed in 2 X SSC,prehybridized, and then hybridized with 0.3ng/,ul digoxigenin-labeled sense or anti-senseMIF cRNA probe overnight at 42°C in a hybrid-ization buffer containing 50% deionized form-amide, 4 X SSC, 1 mg/ml salmon sperm DNA,and 1 mg/ml yeast tRNA. Sections were washedfinally in 0.1 X SSC at 42°C and the hybridizedprobe detected using alkaline phosphatase-con-jugated sheep anti-digoxigenin F(ab) fragments

416 Molecular Medicine, Volume 4, Number 6, June 1998
and color development with NBT/X-phosphate.Sections were counterstained with PAS minushematoxylin. Hybridization with the MIF cRNAsense probe gave no signal.
Quantitation of Tissue Staining
A standard semi-quantitative method was usedto score the glomerular and tubulointerstitial in-filtrates as previously described (10,22,24). Cellslabeled by each mAb or by the MIF cRNA probewere counted in high-power fields (X40) of 20consecutive glomerular cross sections for eachanimal and expressed as the number of labeledcells per glomerular cross section (gcs). Glomer-ular staining with the anti-IL- 13 Ab was gradedon a scale of (0) no staining; (1) <25% stained;(2) 25-50% stained; (3) >50% of the gcsstained. To assess interstitial staining, corticalareas were selected at random. The number oflabeled interstitial cells was counted in 20 con-secutive high-power fields by means of a 0.02mm2 graticule fitted in the eyepiece of the mi-croscope and expressed as cells per mm2. Thesefields progressed from the outer to inner cortex,avoiding only large vessels and glomerular andimmediate periglomerular areas. For each tissue,the same area was examined in serial sectionslabeled with different Ab. No adjustment of theinterstitial cell count was made for tubules or theluminal space. Tubular expression of MIF andIL- 113 was scored in at least 1000 cortical tubulesin high-power fields as previously described ( 12).Data are expressed as the mean for six animals ±SEM. All counting was performed on blindedslides.
Glomerular MIF ProductionGlomeruli were isolated by differential sieving inwhich a half kidney from each animal was placedin RPMI 1640 medium with 5% FCS, dicedfinely, gently pressed through a 250-,um wiremesh and poured through a 106-,um and then a75-,um wire mesh. Glomeruli remaining on thetop of the 75-,tm mesh were washed extensivelywith RPMI/5% FCS and collected. Isolated glo-meruli were >95% pure as assessed by phase-contrast microscopy. Glomeruli were cultured at3000 glomeruli/ml in RPMI 1640/5% FCS in 5%CO2 at 370C for 24 hr and the supernatant har-vested. The concentration of MIF in the super-natant samples was quantitated by a sandwichELISA (6).
Corticosterone Assay
Animals were bled under ether anesthesia be-tween 9 and 10 a.m. and serum samples pre-pared. Serum corticosterone levels were mea-sured by radioimmunoassay using an antiserumprepared by immunizing rabbits with 4-pregnen-111,21 -diol-3,20-dione 3-CMO: BSA conjugate(Steraloids Inc., Wilton, NH). A known amountof unlabeled corticosterone, or the test serumsample, was adjusted to a 0.2 ml volume in gel-atin buffer (0.1% gelatin in PBS, pH 7.5) andincubated with 0.1 ml (-8000 cpm) of [1,2,6,7-3H] corticosterone (TRK 406, Amersham Inter-national, Buckinghamshire, UK) and 0.1 ml of a1:16,000 dilution of corticosterone antiserum,both in gelatin buffer. After overnight incubationat 40C, 0.2 ml of 0.25% dextran-coated charcoalwas added, incubated for 15 min in an ice bath,and tubes centrifuged at 1000 X g for 15 min.The supernatant was removed and mixed with 3ml of liquid scintillation fluid (Ready Safe, Beck-man, CA) and radioactivity counted on a Wallace1409 automated 13-counter (Pharmacia, Stock-holm, Sweden). Duplicate samples covering arange of 2.5 to 1200 pg of corticosterone wereassayed to form the standard curve. The level ofdetection of the assay was 5 pg corticosterone pertube. Inhibition curves produced by extractedrat serum were parallel to that of unlabeledcorticosterone. The intra-assay and interassaycoefficients of variation were 3.3% and 9.2%,respectively.
Statistical AnalysisData were analyzed by one-way analysis of vari-ance (ANOVA) using the Complete StatisticalSystems program (Statsoft, Tulsa, OK).
ResultsRenal Function and Histological DamageAll animals on day 7 of anti-GBM disease exhib-ited significant proteinuria (p < 0.001 vs. nor-mal), a significant increase in serum creatininelevels (p < 0.01 versus normal), and a decreasein creatinine clearance (not significant) (Fig. 1).Animals killed on day 7 of disease with no treat-ment exhibited significant glomerular and tubu-lar lesions, including glomerular crescent forma-tion (Fig. 2). There was rapid progression ofcrescentic glomerulonephritis in those animalstreated with the irrelevant control Ab over days7 to 21, with ascites evident in 3 of 6 animals.

N. Yang et al.: Reversal of Glomerulonephritis by MIF Blockade
(a) Proteinuria
]P<0.05
//, Treatment with anti-M F mAb,
Fig. 1. Anti-MIF Ab treatment improves renalfunction in rat anti-GBM disease. The effect ofanti-MIF Ab (open circles, dotted line) and irrele-vant control Ab treatment (closed circles, solid line)was assessed in terms of (a) urinary protein excre-tion, (b) serum urea levels, (c) serum creatinine lev-els, and (d) the rate of creatinine clearance. Data areshown as the mean ± SEM for six animals. *p <0.05, **p < 0.01, ***p < 0.001 versus time-matchedcontrol Ab-treated animals; #p < 0.05, ##p < 0.01,###p < 0.001 versus day 7 by ANOVA. The group ofsix animals killed on day 7 of disease without anytreatment had 291 ± 42 mg protein/24 hr, 17.3 +3.5 nmol urea/L, 63 ± 6.8 ,umol creatinine/L, and0.48 ± 0.03 ml/min creatinine clearance..d(b) Serum Urea
Treatment with anti.MIF mAbL-----------------------------__ -_--_--_--_ ___ __J,
(c) Serum creatinine
Treatment with anti.MIF mAb,.-
This is consistent with previous studies in whichanimals treated with saline or an irrelevant con-trol antibody developed a very similar, rapid pro-gressive disease (8,12,26). In contrast, those an-imals treated with the anti-MIF Ab showed apartial reversal of established crescentic glomer-ulonephritis. In particular, serum levels of ureaand creatinine returned to the normal range andanimals exhibited hyperfiltration (increased cre-atinine clearance) (Fig. 1). Furthermore, therewas a significant reduction in glomerular hyper-cellularity, segmental lesions, and crescent for-mation in animals treatment with anti-MIF Abcompared with animals killed on day 7 withoutany treatment (Fig. 2).
75-
c" 60-
a).0045
i' 30-a2 3-1L
15-
(d) Creatinine clearance
j
Treatment with anti-MIF mAb
7 14 21
Days after induction of disease
0-
***NS *** *****NS
T T Tr _
Fig. 2. Anti-MIF Ab treatment partially re-verses renal histological damage in rat anti-GBM disease. The percent of glomeruli exhibitinghypercellularity (GHYP), focal and segmental lesions(FSL), and crescents (CRES) and the percent corticalinterstitial lesions (TL) were scored in animals killedon day 7 of disease without any treatment (openbars), and after treatment with an irrelevant controlAb (closed bars) or an anti-MIF Ab (hatched bars)over days 7 to 21. Note that none of these glomeru-lar or interstitial lesions are seen in normal animals.Data are shown as the mean ± SEM for six animals.*p < 0.05, **p < 0.01, ***p < 0.001, and not signifi-cant (NS), by ANOVA.
500-U)= 400-
AI 300-i
2 200-
¾100-0-
30-
24--j
L- 18-
E 12-
6-
10L -
-j
Cc.E
I
E
75-
50-
25-
2.0-
1.5-
1.0-
0.5-
0.0-
L~~
FSL CRES TL
0
IyI I I
u- . . .
{J-uII~~~~~~~~~~~~~~~~~~~~~~~~
417
k
4 fv%
.. R....

418 Molecular Medicine, Volume 4, Number 6, June 1998
(a)NS
NS NSI
UC)
C,)
NSNS
(b) NS1000- '** *
750- NSE INS
-u) 500-
250- NS
OX-1+ ED1+ R73+ NDS61 +leukocytes macrophages T cells IL-2R+cells
Fig. 3. Anti-MIF Ab treatment prevents ane-
mia in rat anti-GBM disease. White blood cellcounts (a), red blood cell counts (b), and blood he-mioglobin levels (c) were mcasured before diseaseinduction (day 0, open bars), and after treatmentwith an irrelevant control Ab (closed bars) or an an-
ti-MIF Ab (hatched bars) over days 7 to 21. Data are
shown as the mean ± SEM for six animals. *p <0.05, and NS, not significant by ANOVA.
Blood Cell Counlts
Immunization of rats with rabbit IgG caused a
significant increase in the white blood cell (wbc)count (15.2 + 3.8 vs. 7.8 + 2.3 X 106 wbc/ml innormal rats, p < 0.05). White blood cell countsremained elevated in both the anti-MIF- andcontrol Ab-treated rats over the 21-day study(Fig. 3a). Severe anemia was evident in controlAb-treated animals on day 21, with a significantreduction in red blood cell counts and bloodhemoglobin levels. In contrast, animals treatedwith the anti-MIF Ab prevented the develop-ment of anemia (Fig. 3b, c).
Renial Leutkocytic In?filtrationl
Compared with normal rats, there was a 10-foldincrease in glomerular leukocytes and a 5-fold
Fig. 4. Anti-MIF Ab treatment halts renal leu-kocyte infiltration in rat anti-GBM disease. Thenumber of leukocytes per glomcrular cross section(gcs) (a) or per mm2 of the cortical interstitium (b)was scored in animals killed oIn day 7 of diseasewithout treatmnent (open bars) and after treatnwentwith an irrelevant control Ab (closed bars) or ani an-ti-MIF Ab (hatched bars) over days 7 to 21. Data areshown as the mcan + SEM for six animals. *p <0.05, **p < 0.01, and NS, not significant by ANOVA.
increase in interstitial leukocytes oIn day 7 ofanti-GBM disease (p < 0.01). Macrophages werethe main infiltrating cell type in the glomerulus,while a mixed macrophage and T cell infiltratewas seen in the interstitium (Fig. 4). A furtherincrease in macrophage and T cell infiltration,including T cell activation (interleukin-2 recep-tor expression ), was seen in those animalstreated with the control Ab over days 7 to 21.This increase inl leukocyte infiltratioIn and activa-tion was abrogated by anti-MIF Ab treatmlent(Fig. 4).
Renal Produ ctioni of MIF and IL-]
Constitutive MIF mRNA and protein expressionis evident in some glomerular and tubular epi-thelial cells in normal rat kidney (Figs. 5A and 6).Both the number of MIF positive cells and theintensity of staining was increased in glomeruliand tubules on day 7 of untreated disease(Figs. 5B and 6). A further increase in renal MIFexpression was evident in those animals treatedwith the control Ab over days 7 to 21 (Figs. 5C
(a)25-
:1 20-22-EO 15-xC. io-
5-
0-
(b)10.0-
-J 7.5-E0
X 5.0-
25m2.5 -
O .0 -
Day 0 Day 21 Day 21Control Ab Anti-MIF Ab
NSr
'I
I-T
I

N. Yang et al.: Reversal of Glomerulonephritis by MIF Blockade 419
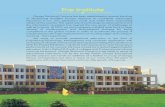
Fig. 5. In situ hybridization of MIF mRNA ex- tubular MIF mRNA expression is seen on day 21 ofpression in tissue sections of normal and dis- anti-GBM disease treated with the control Ab. Noteeased kidney. (A) Normal rat kidney showing con- the expression of MIF mRNA in a glomerular cres-stitutive MIF mRNA expression by a few podocytes cent (asterix). (D) Reduction in glomerular and tu-in the glomerulus and some tubular epithelial cells. bular MIF mRNA expression on day 21 of anti-GBM(B) Up-regulation of MIF mRNA on day 7 of un- disease following treatment with the anti-MIF Abtreated rat anti-GBM disease. Note the increase in compared with control Ab shown in (C). Sectionsthe number of glomerular MIF mRNA+ cells and in were counterstained with PAS minus hematoxylin.the focal pattern of increased tubular MIF expres- Magnification, X250.sion. (C) Further up-regulation of glomerular and
Mif-f
,~w. z:si....zf
.ito, ...
. ..
*f:: ,:,....
or
Ain,s

420 Molecular Medicine, Volume 4, Number 6, June 1998
Glomerulus Tubules
(C) NS
(b)30 ** **
II25-
cn
0) 2Con 20-
o 15-
2 10-
n,
Day 7 LDay 21 Day 21Untreated Control Ab AtIVIIF Ab
(d) NS
100]1I *:: 80-
a} 60-
+ 40-
20 -
O-n_, v-
AA 11
Day 7Untreated
Fig. 6. Anti-MIF Ab treatment suppressesrenal MIF production in rat anti-GBM dis-ease. Quantitation of in situ hybridization andimmunohistochemistry staining of tissue sectionswas used to determine the number of glomerularcells (a, b) and tubules (c, d) expressing MIFmRNA (a, c) and MIF protein (b, d) in animalskilled on dav 7 of disease without treatment(open bars), and after treatment with an irrele-vant control Ab (closed bars) or an anti-MIF Ab(hatched bars) over days 7 to 21. Data are shownas the mean + SEM for six animals. *p < 0.05,**p < 0.01, ***p < 0.001, and NS, not significantby ANOVA. Values for normal rats are 6.5 + 1MIF mRNA+ cells/gcs; 0.8 + 0.2 MIF protein+cells/gcs; 29 + 2.5% MIF mRNA+ tubules, and23 + 2.5 MIF protein+ tubules (all p < 0.01 ver-sus day 7 untreated).
and 6). In contrast, no further increase in renalMIF expression was seen in anti-MIF Ab-treatedanimals (Figs. 5D and 6). As a second method toevaluate MIF production, secretion of MIF byisolated glomeruli cultured for 24 hr was quan-titated. There was no increase in the level of MIFsecretion by glomeruli at day 7 of disease com-pared with glomeruli from normal animals(1894 + 150 versus 1955 + 169 pg/ml, respec-tively, p = N.S.). However, animals receiving theirrelevanit control Ab over days 7 to 21 showed asignificant increase in glomerular MIF secretion(4249 + 977 pg/ml, p < 0.05 versus untreatedday 7 disease), which was suppressed by anti-MIF Ab treatment (1571 + 177 pg/ml, p < 0.05versus control Ab treated).
Interleukin- 1 (IL- 1) is another pro-inflam-matory cytokine known to participate in leuko-cyte recruitment in this disease model (22,27).Therefore, we examined the effect of anti-MIFAb treatment on renal IL-1X3 production. Therewas a significant increase in the glomerular IL- 1 3staining score on day 7 of the disease comparedwith normal rat kidney (p < 0.05). There was afurther increase in the glomerular IL- 1(3 scoreand a significant increase in the percentage ofcortical tubules expressing IL-1,3 over days 7 to21 with control Ab treatment, but this was sup-pressed by anti-MIF Ab treatment (Fig. 7).
Cellular auid Hunioral Antigen ResponisesSince MIF has previously been shown to play animportant role in both the skin delayed-type hy-persensitivity (DTH) response and the primary
antibody response in vivo (4,5), we examinedthe effect of anti-MIF Ab treatment on theseaspects of the immune response in this disease
nsI
***-- I**(a)
J
-j
co
(b)
a)n3+0
u-
Day 7 Dy 21 Dy 21LUneated Control Ab ArtiMF Ab
Fig. 7. Anti-MIF Ab treatment suppresses re-nal IL-113 production in rat anti-GBM disease.Immunohistochemistry staining of IL-103 protein wasassessed in (a) glomeruli and (b) cortical tubules.Data arc shown as the mean + SEM for six animalskilled on day 7 of disease without treatment (openbars), and after treatment with an irrelevant controlAb (closed bars) or an anti-MIF Ab (hatched bars)over days 7 to 21. *p < 0.05, **p < 0.01, ***p <0.001, and NS, not significant by ANOVA. Values fornormal rats are 0.8 + 0.1 glomerular IL-1(3+ score(p < 0.001 versus day 7 untreated) and 53 + 7%IL-1,B3 tubules (p = N.S. versus day 7 uLntreated).
i NS

N. Yang et al.: Reversal of Glomerulonephritis by MIF Blockade 421
E
cz00
1.0-
0.8-
0.6-
0.4-
0.2-
0.0-
0 2500 5000 7500Serum dilution (inverse xl)
10000
Fig. 8. Anti-MIF Ab treatment does not affectthe humoral immune response in rat anti-GBMdisease. Serum levels of rat antibodies against theimmunizing antigen (rabbit IgG) were determinedby ELISA in diseased animals treated with the con-trol Ab (closed circles, solid line) or anti-MIF Ab(open circles, dotted line). Serum from normal, non-immunized rats (open squares, dashed line), showsthe assay background. Data are shown as themean ± SEM for six animals.
Table 1. Serum corticosterone levels correlatewith disease parameters in rat anti-GBMdisease
Day 21 SerumDisease Parameter CorticosteroneMeasured on Day 21a Levela
Glomerular MIF mRNA+ cells r = -0.77, p = 0.005Tubular MIF mRNA+ cells r = -0.87, p < 0.001Glomerular ED1 + macrophage r = -0.57, p = N.S.Interstitial ED1+ macrophages r = -0.57, p < 0.001Interstitial IL-2R+ cells r = -0.82, p = 0.002Proteinuria r = -0.61, p = 0.046Serum creatinine r = -0.82, p = 0.002Creatinine clearance r = 0.72, p = 0.013Serum urea r = -0.72, p = 0.013
a Data are pooled from both control and anti-MIF Ab-treated animals on day 21 (n = 12) and analyzed using thePearson single correlation coefficient.
model. Animals treated with the control Abmounted a vigorous skin response to the immu-nizing antigen (rabbit IgG), but not to an irrele-vant antigen (horse IgG) (3.25 ± 0.23 versus2.13 ± 0.17 mm, respectively; p < 0.001) or toPBS. There was a lesser degree of skin swelling inresponse to challenge with rabbit IgG comparedwith the irrelevant antigen in animals treatedwith the anti-MIF Ab (2.68 ± 0.08 versus 2.23 ±0.1, respectively; p < 0.001), which represents a60% reduction in the antigen-specific skin re-sponse compared with control Ab-treated ani-mals (p < 0.001). In contrast, there was no dif-
E 1001
2 75-10
0 50-0
0
E 25-20
0-
0 7 14 21Days after disease inducton
Fig. 9. Anti-MIF Ab treatment increases serumcorticosterone levels in rat anti-GBM disease.Serum corticosterone levels were measured using aradioimmunoassay in rats receiving control Ab(closed circles, solid line) or anti-MIF Ab (open cir-cles, dotted line) treatment over days 7 to 21. Nor-mal rat serum corticosterone levels (day 0) areshown. Data are shown as the mean + SEM for sixanimals. "p < 0.05 versus day 7 by ANOVA.
ference in the titer of circulating rat antibodiesagainst the immunizing antigen between the twotreatment groups (Fig. 8). Similarly, no differ-ences between the two Ab treatment groupswere evident in glomerular deposition of rabbitIgG, rat IgG, or C3 as assessed by semi-quantita-tive immunofluorescence staining (data notshown).
Endogenous Corticosterone LevelsSerum samples were taken between 9 and10 a.m. from anesthetised animals to minimizevariation in corticosterone levels. Comparedwith serum corticosterone levels in normal rats(35.6 ± 5.8 pg/ml), there was a significant fall incorticosterone levels on day 7 of rat anti-GBMdisease (p < 0.01 vs. normal) (Fig. 9). Animalsreceiving control Ab treatment showed a re-bound with serum corticosterone returning tonormal levels by day 21 of the disease. However,animals treated with anti-MIF Ab showed a morerapid and significantly greater rebound in endog-enous serum corticosterone levels comparedwith control Ab-treated animals (Fig. 9). Indeed,corticosterone levels in animals treated with theanti-MIF Ab were significantly elevated abovenormal levels by day 21 (p < 0.05).
To analyze the relationship between cortico-sterone levels and disease, we compared the
r ~ ~ ~ ~ I-

422 Molecular Medicine, Volume 4, Number 6, June 1998
plasma corticosterone levels in all animals on day21 (n = 12) with various disease parametersusing the Pearson single correlation coefficient(Table 1). The number of glomerular and tubularcells expressing MIF mRNA gave a highly signif-icant negative correlation with corticosteronelevels. The number of interstitial macrophagesand immune-activated cells (IL-2R+), but notglomerular macrophage infiltration, gave a neg-ative correlation with corticosterone levels. Inaddition, parameters of renal injury and renalfunction gave a significant negative correlationwith corticosterone levels (Table 1).
DiscussionWhile a variety of intervention strategies havebeen shown to be successful in preventing theinduction of the immune response that leads tothe development of immune-mediated diseases,it has proven far more difficult to halt or evenpartially reverse progressive tissue injury once itis established. Indeed, this is the crucial test ofany new therapeutic strategy, as patients invari-ably present to the clinician after their disease isalready established. The present study has, there-fore, extended previous results by demonstratingthat antibody-based neutralization of MIF activ-ity can halt and even partially reverse establishedcrescentic glomerulonephritis in the rat.
The ability of anti-MIF Ab treatment to in-hibit established disease can be attributed to twodistinct mechanisms. First, MIF is known to par-ticipate directly in the cellular immune response(4,5). Consistent with a previous study (12), thecellular immune response in this disease wassuppressed by anti-MIF Ab treatment as demon-strated by inhibition of the skin DTH response, areduced macrophage and T cell infiltrate withinthe kidney, and a reduction in immune activa-tion (IL-2R expression) of the mononuclear cellinfiltrate. The inhibition of leukocyte infiltrationmay be due in part to inhibition of local IL-i 3production since this cytokine is known to pro-mote renal leukocyte accumulation through in-duction of molecules such as intercellular adhe-sion molecule- 1 and monocyte chemoattractantprotein-i (27-29). In contrast to the cellular im-mune response, anti-MIF Ab treatment had noeffect upon the secondary antibody response.
The second mechanism by which neutraliza-tion of MIF activity suppressed this disease isthrough counter-regulation of glucocorticoidproduction. Whereas administration of recombi-
nant MIF has been shown to inhibit dexameth-asone mediated suppression of lethal endotoxae-mia in mice (6), the relationship betweenendogenous production of MIF and glucocorti-coids in immune-mediated disease is unknown.There is an increase in both circulating MIF lev-els and local renal MIF production during thedevelopment of rat anti-GBM disease (10,11).The current study showed that increased MIFproduction during the early phase of disease de-velopment was associated with a suppression ofserum corticosterone levels. In addition, neutral-ization of MIF activity caused an increase in cor-ticosterone levels to above that seen in normalanimals. These findings suggest that endogenousMIF may act to regulate glucocorticoid levels inimmune-mediated glomerulonephritis. Further-more, the increase in corticosterone levels seenwith anti-MIF Ab treatment may have contrib-uted to the suppression of the cellular immuneresponse. Indeed, a sharp rise in endogenousglucocorticoid levels has been shown to play acrucial role in the resolution of acute paralyzinginjury in rat experimental allergic encephalomy-elitis (EAE) (30). Also, the basal level of endog-enous serum corticosterone has been shown tobe an important factor in the susceptibility ofLewis, but not PVG.RTIC, rats to the induction ofEAE (31). The finding that serum corticosteronedid not rise above normal levels in control Ab-treated anti-GBM disease probably reflects thevery aggressive nature of this disease model,which progresses rapidly towards end-stage renalfailure.
Erythropoietin is produced by interstitialcells within the kidney (32,33). Anemia is a com-mon complication of renal failure caused by areduction in erythropoietin production in theinjured renal interstitium (34). In the currentstudy, anti-MIF Ab treatment of established anti-GBM disease prevented the development of se-vere anemia, demonstrating that neutralizingMIF activity provides substantial protectionagainst interstitial injury during disease progres-sion.
In summary, this study has demonstratedthat blocking MIF activity can partially reverseestablished crescentic glomerulonephritis. WhileMIF has been identified previously to act as acounter-regulator of glucocorticoid action (6),the present data suggest that in vivo MIF mayalso influence glucocorticoid levels, providing anadditional level of regulation on the ensuing in-flammatory and immune responses.

N. Yang et al.: Reversal of Glomerulonephritis by MIF Blockade 423
AcknowledgmentsThis study was supported by grants from theNational Health and Medical Research Council ofAustralia (no. 9960106) and the National Insti-tutes of Health (no. 13591). We are grateful toMs. M. Lo for corticosterone assay.
References1. David JR. (1966) Delayed hypersensitivity in
vitro: its mediation by cell-free substances formedby lymphoid cell-antigen interaction. Proc. Natl.Acad. Sci. U.S.A. 56: 72-77.
2. Bloom BR, Bennett B. (1966) Mechanism of areaction in vitro associated with delayed-type hy-persensitivity. Science 153: 80-82.
3. Calandra T, Bucala R. (1997) Macrophage migra-tion inhibitory factor (MIF): a glucocorticoidcounter-regulator within the immune system.Crit. Rev. Immunol. 17: 77-88.
4. Bernhagen J, Bacher M, Calandra T, et al. (1996)An essential role for macrophage migration inhib-itory factor in the tuberculin delayed-type hyper-sensitivity reaction. J. Exp. Med. 183: 277-282.
5. Bacher M, Metz CN, Calandra T, et al. (1996) Anessential regulatory role for macrophage migra-tion inhibitory factor in T-cell activation. Proc.Natl. Acad. Sci. U.S.A. 93: 7849-7854.
6. Calandra T, Bernhagen J, Metz CN, et al. (1995)MIF as a glucocorticoid-induced modulator of cy-tokine production. Nature 376: 68-71.
7. Nishno T, Bernhagen J, Shijki H, Calandra T, DohlK, Bucala R. (1995) Localization of macrophagemigration inhibitory factor (MIF) to secretorygranules within the corticotrophic and thyrotro-phic cells of the pituitary gland. Mol. Med. 1: 781-788.
8. Bacher M, Meinhardt A, Lan HY, et al. (1997)Migration inhibitory factor expression in experi-mentally induced endotoxemia. Am. J. Pathol. 150:235-246.
9. Calandra T, Bernhagen J, Mitchell RA, Bucala R.(1994) The macrophage is an important and pre-viously unrecognized source of macrophage mi-gration inhibitory factor. J. Exp. Med. 179: 1895-1902.
10. Lan HY, Mu W, Yang N, et al. (1996) De novorenal expression of macrophage migration inhib-itory factor (MIF) during the development of ratcrescentic glomerulonephritis. Am. J. Pathol. 149:1119-1127.
11. Lan HY, Yang N, Metz C, et al. (1997) TNF-alphaup-regulates renal MIF expression in rat crescen-tic glomerulonephritis. Mol. Med. 3: 136-144.
12. Lan HY, Bacher M, Yang N, et al. (1997) Thepathogenic role of macrophage migration inhibi-tory factor in immunologically induced kidneydisease in the rat. J. Exp. Med. 185: 1455-1465.
13. Bernhagen J, Calandra T, Mitchell RA, et al.(1993) MIF is a pituitary-derived cytokine thatpotentiates lethal endotoxaemia. Nature 365:756-759.
14. Sunderland CA, McMaster WR, Williams AF.(1979) Purification with monoclonal antibody of apredominant leukocyte-common antigen and gly-coprotein from rat thymocytes. Eur. J. Immunol. 9:155-159.
15. Dijkstra CD, Dopp EA, Joling P, Kraal G. (1985)The heterogeneity of mononuclear phagocytes inlymphoid organs: distinct macrophage subpopula-tions in the rat recognized by monoclonal antibod-ies EDI, ED2 and ED3. Immunology 54: 589-599.
16. Damoiseaux JG, Dopp EA, Calame W, Chao D,MacPherson GG, Dijkstra CD. (1994) Rat macro-phage lysosomal membrane antigen recognizedby monoclonal antibody ED 1. Immunology 83:140-147.
17. Hunig T, Wallny HJ, Hartley JK, Lawetzky A, Tie-fenthaler G. (1989) A monoclonal antibody to aconstant determinant of the rat T cell antigenreceptor that induces T cell activation. Differentialreactivity with subsets of immature and mature Tlymphocytes. J. Exp. Med. 169: 73-86.
18. Tellides G, Dallman MJ, Morris PJ. (1989) Mech-anism of action of interleukin-2 receptor (IL-2R)monoclonal antibody (MAb) therapy: target celldepletion or inhibition of function?. Transplant.Proc. 21: 997-998.
19. Schotanus K, Holtkamp GM, Meloen RH, et al.(1995) Domains of rat interleukin 1 beta involvedin type I receptor binding. Endocrinology 136: 332-339.
20. Mitchell R, Bacher M, Bernhagen J, PushkarskayaT, Seldin MF, Bucala R. (1995) Cloning and char-acterization of the gene for mouse macrophagemigration inhibitory factor (MIF). J. Immunol. 154:3863-3870.
21. Lan HY, Paterson DJ, Atkins RC. (1991) Initiationand evolution of interstitial leukocytic infiltrationin experimental glomerulonephritis. Kidney Int.40: 425-433.
22. Lan HY, Nikolic-Paterson DJ, Zarama M, VanniceJL, Atkins RC. (1993) Suppression of experimen-tal crescentic glomerulonephritis by the interleu-kin-I receptor antagonist. Kidney Int. 43: 479-485.
23. Lan HY, Nikolic-Paterson DJ, Mu W, Atkins RC.(1995) Local macrophage proliferation in the pro-gression of glomerular and tubulointerstitial in-jury in rat anti-GBM glomerulonephritis. KidneyInt. 48: 753-760.
24. Lan HY, Zarama M, Nikolic-Paterson DJ, Kerr PG,Atkins RC. (1993) Suppression of experimentalcrescentic glomerulonephritis by deoxyspergua-lin. J. Am. Soc. Nephrol. 3: 1765-1774.
25. Lan HY, Mu W, Ng Y-Y, Nikolic-Paterson DJ, At-kins RC. (1996) A simple, reliable, and sensitivemethod of nonradioactive in situ hybridization:use of microwave heating to improve hybridiza-

424 Molecular Medicine, Volume 4, Number 6, June 1998
tion efficiency and preserve tissue morphology.J. Histochem. Cytochem. 44: 281-287.
26. Yu XQ, Nikolic-Paterson DJ, W. Mu, et al. (1998)A functional role for osteopontin in experimentalcrescentic glomerulonephritis in the rat. Proc. As-soc. Am. Physicians 110: 50-64.
27. Nikolic-Paterson DJ, Lan HY, Hill PA, Vannice JL,Atkins RC. (1994) Suppression of experimentalglomerulonephritis by the interleukin-1 receptorantagonist: inhibition of intercellular adhesionmolecule-1 expression. J. Am. Soc. Nephrol. 4:1695-1700.
28. Tang WW, Feng L, Vannice JL, Wilson CB. (1994)Interleukin- 1 receptor antagonist ameliorates ex-perimental anti-glomerular basement membraneantibody-associated glomerulonephritis. J. Clin.Invest. 93: 273-279.
29. Tang WW, Qi M, Warren JS. (1996) Monocytechemoattractant protein 1 mediates glomerularmacrophage infiltration in anti-GBM Ab GN. Kid-ney Int. 50: 665-671.
30. MacPhee IA, Antoni FA, Mason DW. (1989)Spontaneous recovery of rats from experimental
allergic encephalomyelitis is dependent on reg-ulation of the immune system by endogenousadrenal corticosteroids. J. Exp. Med. 169: 431-445.
31. Mason DW, MacPhee IA, Antoni FA. (1990) Therole of the neuroendocrine system in determin-ing genetic susceptibility to experimental aller-gic encephalomyelitis in the rat. Immunology 70:1-5.
32. Lacombe C, Da SJ, Bruneval P, et al. (1988) Peri-tubular cells are the site of erythropoietin synthe-sis in the murine hypoxic kidney. J. Clin. Invest. 81:620-623.
33. Maxwell PH, Ferguson DP, Nicholls LG, JohnsonMH, Ratcliffe PJ. (1997) The interstitial responseto renal injury-fibroblast-like cells show pheno-typic changes and have reduced potential forerythropoietin gene expression. Kidney Int. 52:715-724.
34. Eschbach JW. (1989) The anemia of chronic renalfailure: pathophysiology and the effects of recom-binant erythropoietin. Kidney Int. 35: 134-148.