Results from the Boston Kidney Biopsy Cohort Study - JASN
12
CLINICAL RESEARCH www.jasn.org The Prognostic Value of Histopathologic Lesions in Native Kidney Biopsy Specimens: Results from the Boston Kidney Biopsy Cohort Study Anand Srivastava, 1,2 Ragnar Palsson, 1 Arnaud D. Kaze, 1 Margaret E. Chen, 1 Polly Palacios, 1 Venkata Sabbisetti, 1 Rebecca A. Betensky, 3 Theodore I. Steinman, 4 Ravi I. Thadhani, 5,6,7 Gearoid M. McMahon, 1 Isaac E. Stillman, 8 Helmut G. Rennke, 9 and Sushrut S. Waikar 1 1 Renal Division and 9 Pathology Department, Brigham and Women’s Hospital, Boston, Massachusetts; 2 Division of Nephrology and Hypertension, Center for Translational Metabolism and Health, Institute for Public Health and Medicine, Northwestern University Feinberg School of Medicine, Chicago, Illinois; 3 Department of Biostatistics, Harvard T.H. Chan School of Public Health, Boston, Massachusetts; 4 Renal Division and 8 Department of Pathology, Beth Israel Deaconess Medical Center, Boston, Massachusetts; 5 Division of Nephrology, Massachusetts General Hospital, Boston, Massachusetts; and 6 Departments of Biomedical Sciences and 7 Medicine, Cedars-Sinai Medical Center, Los Angeles, California ABSTRACT Background Few studies have evaluated whether histopathologic lesions on kidney biopsy provide prog- nostic information beyond clinical and laboratory data. Methods We enrolled 676 individuals undergoing native kidney biopsy at three tertiary care hospitals into a prospective, observational cohort study. Biopsy specimens were adjudicated for semiquantitative scores in 13 categories of histopathology by two experienced renal pathologists. Proportional hazards models tested the association between histopathologic lesions and risk of kidney disease progression ($40% eGFR decline or RRT). Results Mean baseline eGFR was 57.5636.0 ml/min per 1.73 m 2 . During follow-up (median, 34.3 months), 199 individuals suffered kidney disease progression. After adjustment for demographics, clinicopatho- logic diagnosis, and laboratory values, the following lesions (hazard ratio; 95% confidence interval) were independently associated with progression: inflammation in nonfibrosed interstitium (0.52; 0.32 to 0.83), moderate and severe versus minimal interstitial fibrosis/tubular atrophy (2.14; 1.24 to 3.69 and 3.42; 1.99 to 5.87, respectively), moderate and severe versus minimal global glomerulosclerosis (2.17; 1.36 to 3.45 and 3.31; 2.04 to 5.38, respectively), moderate and severe versus minimal arterial sclerosis (1.78; 1.15 to 2.74 and 1.64; 1.04 to 2.60, respectively), and moderate and severe versus minimal arteriolar sclerosis (1.63; 1.08 to 2.46 and 2.33; 1.42 to 3.83, respectively). An 11-point chronicity score derived from semi- quantitative assessments of chronic lesions independently associated with higher risk of kidney disease progression (hazard ratio per one-point increase, 1.19; 95% confidence interval, 1.12 to 1.27). Conclusions Across a diverse group of kidney diseases, histopathologic lesions on kidney biopsy provide prognostic information, even after adjustment for proteinuria and eGFR. J Am Soc Nephrol 29: 2213–2224, 2018. doi: https://doi.org/10.1681/ASN.2017121260 Tens of thousands of native kidney biopsies are performed annually across the world for the evalua- tion and management of a variety of forms of kidney disease. 1,2 Information from pathologic examination of biopsy tissue is used for diagnosis as well as prog- nosis. 3–5 Despite the importance of the kidney biopsy in the care of patients with acute kidney diseases and Received December 7, 2017. Accepted April 18, 2018. Published online ahead of print. Publication date available at www.jasn.org. Correspondence: Dr. Sushrut S. Waikar, Renal Division, Brigham and Women’s Hospital, MRB-4, 75 Francis Street, Boston, MA 02115. Email: [email protected] Copyright © 2018 by the American Society of Nephrology J Am Soc Nephrol 29: 2213–2224, 2018 ISSN : 1046-6673/2908-2213 2213 CLINICAL RESEARCH
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Results from the Boston Kidney Biopsy Cohort Study - JASN

CLINICAL RESEARCH www.jasn.org
The Prognostic Value of Histopathologic Lesions inNative Kidney Biopsy Specimens: Results from theBoston Kidney Biopsy Cohort Study
Anand Srivastava,1,2 Ragnar Palsson,1 Arnaud D. Kaze,1 Margaret E. Chen,1 Polly Palacios,1
Venkata Sabbisetti,1 Rebecca A. Betensky,3 Theodore I. Steinman,4 Ravi I. Thadhani,5,6,7
Gearoid M. McMahon,1 Isaac E. Stillman,8 Helmut G. Rennke,9 and Sushrut S. Waikar1
1Renal Division and 9Pathology Department, Brigham and Women’s Hospital, Boston, Massachusetts; 2Division ofNephrology and Hypertension, Center for Translational Metabolism and Health, Institute for Public Health and Medicine,Northwestern University Feinberg School of Medicine, Chicago, Illinois; 3Department of Biostatistics, Harvard T.H. ChanSchool of Public Health, Boston, Massachusetts; 4Renal Division and 8Department of Pathology, Beth Israel DeaconessMedical Center, Boston, Massachusetts; 5Division of Nephrology, Massachusetts General Hospital, Boston, Massachusetts;and 6Departments of Biomedical Sciences and 7Medicine, Cedars-Sinai Medical Center, Los Angeles, California
ABSTRACTBackground Few studies have evaluated whether histopathologic lesions on kidney biopsy provide prog-nostic information beyond clinical and laboratory data.
Methods We enrolled 676 individuals undergoing native kidney biopsy at three tertiary care hospitalsinto a prospective, observational cohort study. Biopsy specimens were adjudicated for semiquantitativescores in 13 categories of histopathology by two experienced renal pathologists. Proportional hazardsmodels tested the association between histopathologic lesions and risk of kidney disease progression($40% eGFR decline or RRT).
ResultsMean baseline eGFR was 57.5636.0 ml/min per 1.73 m2. During follow-up (median, 34.3 months),199 individuals suffered kidney disease progression. After adjustment for demographics, clinicopatho-logic diagnosis, and laboratory values, the following lesions (hazard ratio; 95% confidence interval) wereindependently associated with progression: inflammation in nonfibrosed interstitium (0.52; 0.32 to 0.83),moderate and severe versus minimal interstitial fibrosis/tubular atrophy (2.14; 1.24 to 3.69 and 3.42; 1.99to 5.87, respectively), moderate and severe versus minimal global glomerulosclerosis (2.17; 1.36 to 3.45and 3.31; 2.04 to 5.38, respectively), moderate and severe versus minimal arterial sclerosis (1.78; 1.15 to2.74 and 1.64; 1.04 to 2.60, respectively), and moderate and severe versus minimal arteriolar sclerosis(1.63; 1.08 to 2.46 and 2.33; 1.42 to 3.83, respectively). An 11-point chronicity score derived from semi-quantitative assessments of chronic lesions independently associated with higher risk of kidney diseaseprogression (hazard ratio per one-point increase, 1.19; 95% confidence interval, 1.12 to 1.27).
Conclusions Across a diverse group of kidney diseases, histopathologic lesions on kidney biopsy provideprognostic information, even after adjustment for proteinuria and eGFR.
J Am Soc Nephrol 29: 2213–2224, 2018. doi: https://doi.org/10.1681/ASN.2017121260
Tens of thousands of native kidney biopsies areperformed annually across the world for the evalua-tion and management of a variety of forms of kidneydisease.1,2 Information from pathologic examinationof biopsy tissue is used for diagnosis as well as prog-nosis.3–5 Despite the importance of the kidney biopsyin the care of patients with acute kidney diseases and
Received December 7, 2017. Accepted April 18, 2018.
Published online ahead of print. Publication date available atwww.jasn.org.
Correspondence: Dr. Sushrut S. Waikar, Renal Division, Brighamand Women’s Hospital, MRB-4, 75 Francis Street, Boston, MA02115. Email: [email protected]
Copyright © 2018 by the American Society of Nephrology
J Am Soc Nephrol 29: 2213–2224, 2018 ISSN : 1046-6673/2908-2213 2213
CLINICALRESE
ARCH

CKDs,6 there are no widely used standardized guidelines forstructuring and reporting the results of kidney biopsy patho-logic examination. Standardized scoring systems have been de-veloped for specific kidney diseases but not as a global scoringor reporting system.7–15 A recent expert opinion–based pro-posal to score and grade chronic changes on the kidney biopsyspecimen included four lesions and a global chronicity scoreand highlighted the need for studies to examine the prognosticsignificance of each variable.16
It is often claimed that chronic tubulointerstitial lesions are themost important prognostic indicators from kidney biopsies.17–21
Despite this widespread belief, the underlying evidence base isrelatively thin and derives from small numbers of patients withspecific forms of kidney diseases without adequate adjustment forconfounding variables. Few studies have tested the prognosticvalue of histopathologic findings across a diverse set of kidneydiseases with adjustment for clinical variables, such asdemographics, clinicopathologic diagnosis, and laboratoryvariables.22,23 To address this gap in our understanding ofthe prognostic significance of kidney histopathology, weconducted a prospective cohort study, in which biopsieswere re-read by two study pathologists who were unawareof the original clinical or pathologic diagnosis. Each biopsywas reviewed under lightmicroscopy jointly and graded semi-quantitatively for acute and chronic lesions in the glomerular,tubulointerstitial, and vascular compartments. We followedpatients prospectively and tested whether individual histo-pathologic lesions predicted the subsequent development ofkidney disease progression ($40% decline in eGFR or theneed for RRT).
METHODS
Study PopulationThe Boston Kidney Biopsy Cohort (BKBC) is a prospective,observational cohort study of patients undergoing native kid-ney biopsy at three tertiary care hospitals in Boston, Mas-sachusetts. This study includes adult patients ($18 years ofage) who underwent a clinically indicated native kidney biopsybetween September 2006 and June 2016. Patients providedblood and urine samples on the day of kidney biopsy. Exclu-sion criteria included the inability to provide consent, enroll-ment in competing studies, severe anemia, and pregnancy. Allparticipants provided written consent. The study protocol wasapproved by the Partners Human Research Committee (theBrigham and Women’s Hospital Institutional Review Board),and is in accordance with the principles of the Declaration ofHelsinki.
Evaluation of HistopathologyAll biopsies were adjudicated under light microscopy by tworenal pathologists, who provided semiquantitative scores ofkidney inflammation, fibrosis, vascular sclerosis, and tubularinjury. The scoring system for individual histopathologic
lesions was developed by the pathologists for use in this studyon the basis of their review of the literature and clinical expe-rience.12,14,24–30 Formal criteria were not used for individuallesions. In joint pathology review sessions, the pathologistsreviewed the light microscopy slides alongside one anotherand verbally suggested their score for individual histopatho-logic lesion severity in the presence of A.S. and/or S.S.W. Ifthey did not initially agree, the case was discussed in moredetail to obtain consensus on individual histopathologic le-sion severity. Of the 13 categories used, all were scored duringstudy sessions except for the grades of segmental and globalglomerulosclerosis, which were taken from the biopsy report,because they were each calculated as a percentage of the totalnumber of glomeruli. Global glomerulosclerosis was furthergraded as “age related” or “pathologic” on the basis of thenumber of globally sclerosed glomeruli divided by the totalnumber of glomeruli as done by Hommos et al.31 The studypathologists reviewed the slides without knowledge of theoriginal biopsy diagnosis or biopsy report, typically severalmonths after the biopsy procedure and original pathology re-port. Not all lesions were able to be evaluated on all biopsies,but this amounted to ,5% missing data. We reviewed all pa-tients’ charts alongside the final histopathologic diagnosisto identify the primary and any secondary clinicopathologicdiagnoses.
Exposure and OutcomesThe primary exposures were semiquantitative measures of 13separate histopathologic lesions: mesangial expansion, globalglomerulosclerosis, segmental glomerulosclerosis, endocapillaryglomerular inflammation, extracapillary cellular crescents, fi-brinoid necrosis, fibrocellular crescents, interstitial fibrosisand tubular atrophy (IFTA), inflammation in the nonfibrosedinterstitium, inflammation in the fibrosed interstitium, acutetubular injury (ATI), arterial sclerosis, and arteriolar sclerosis.We calculated a kidney biopsy chronicity score on the basis ofthe proposal by Sethi et al.16 for standardized semiquantita-tive grading of chronic changes of glomerulosclerosis (zero tothree), interstitial fibrosis (zero to three), tubular atrophy
Significance Statement
Kidney biopsy remains an important tool in the diagnosis andmanagement of acute kidney disease and CKD. Kidney histopa-thology may provide both diagnostic and prognostic information.Whether histopathologic lesions provide prognostic informationindependent of clinical information has not beenevaluated in detail.In this study of 676 individuals undergoing native kidney biopsy, theauthors found that greater severity of interstitial fibrosis and tubularatrophy, arterial and arteriolar sclerosis, and global glomerulo-sclerosis were independent predictors of future kidney failure, evenafter adjusting for confounders, including eGFR and proteinuria. Achronicity score derived from the sum of semiquantitative assess-ments of chronic histopathologic lesions was also independentlyassociated with kidney failure, and could be incorporated intokidney pathology reports to provide clinicians useful prognosticinformation.
2214 Journal of the American Society of Nephrology J Am Soc Nephrol 29: 2213–2224, 2018
CLINICAL RESEARCH www.jasn.org

(zero to three), and arteriolosclerosis (zero or one). Because thetotal renal chronicity score by Sethi et al.16 adds the score forinterstitial fibrosis and the score for tubular atrophy separately,we weighted our IFTA scores by a factor of two.We also convertedour semiquantitative arterial sclerosis score to a binary score inkeeping with the proposal by Sethi et al.16
The primary outcome was kidney disease progression de-fined as $40% eGFR decline from baseline or the need forRRT (dialysis or kidney transplantation). eGFR during followup was obtained from the electronic medical record (EMR).The secondary outcome was the need for RRT. RRTstatus wasconfirmed by reviewing the EMR and linkage with the USRenal Data System database. Mortality status was confirmedwith the Social Security Death Index. Participants were followedup until the occurrence of death, voluntary study withdrawal,loss to follow-up, or June 30, 2017.
CovariatesWe collected patient information at the biopsy visit, includingdemographics, detailed medical history, medication lists, andpertinent laboratory data. Study data were collected and man-aged using REDCap electronic data capture tools hosted atPartners HealthCare.32 We obtained serum creatinine (SCr)from the EMR on the day of biopsy. In participants for whomthis was unavailable (n=117), we measured SCr in individualswith available blood samples collected on the day of biopsy(n=82). If no samples were available (n=35), we used the mostrecent SCr values available in the EMR from the date of kidneybiopsy up to 3 months before biopsy. We obtained spot urineprotein-to-creatinine ratio or urine albumin-to-creatinine ra-tio from the date of kidney biopsy to 3 months before biopsyfrom the EMR. If a participant did not have any of these values,we measured urine albumin-to-creatinine ratio from urinecollected on the day of the kidney biopsy (n=54). SCr andurinary creatinine were measured using a Jaffe-based method,and urine albumin was measured by an immunoturbidometricmethod. We used the creatinine-based Chronic Kidney DiseaseEpidemiology Collaboration equation to calculate the eGFR.33
Statistical AnalysesDescriptive statistics were summarized as mean6SD ormedian (interquartile range) for continuous variables, andfrequency distribution is presented with percentages for cate-gorical variables. For skewed data distributions, we performednatural logarithmic transformation as appropriate. Weassessed for associations between categorical variables andtwo-group comparisons using chi-squared tests. For evalua-tions between continuous variables and multiple group com-parisons, we used ANOVA (for normally distributed variables)and Kruskal–Wallis tests (for non-normally distributed vari-ables). We used Spearman correlation coefficients to deter-mine the associations between continuous variables andhistopathologic lesion scores. We calculated the weightedk-statistic to evaluate the reproducibility of histopathologicscores.
For the primary outcome (time to either $40% decline ineGFR or starting RRT), we treated the data as interval censored,because the exact date of the event may not be known (e.g., theexact time to $40% decline in eGFR could have occurred anytime in the interval between two successive laboratory mea-surements). We evaluated the association between individualhistopathologic lesions and subsequent kidney disease
Table 1. Baseline characteristics of the Boston KidneyBiopsy Cohort
Characteristics n=676
Age, yr 52.2616.5Women, % 52.5Race, %White 63.8Black 20.6Other 15.7
eGFR, ml/min per 1.73 m2 57.5636.0Serum creatinine, mg/dl 1.41 [0.94–2.24]Proteinuria, g/g creatinine 1.74 [0.43–4.38]No. of glomeruli on biopsy 31 [20–43]Reason for biopsy,a %Proteinuria 59.2Hematuria 27.4Nephrotic syndrome 14.5Nephritic syndrome 2.5Abnormal eGFR 53.5
Primary clinicopathologic diagnosis, %Proliferative GN 30.2Nonproliferative glomerulopathies 18.2Advanced glomerulosclerosis 11.5Diabetic nephropathy 11.1Vascular 8.0Tubulointerstitial 7.3Paraprotein 7.3Other 6.5
Comorbid conditions, %Diabetes mellitus 22.6Hypertension 49.3SLE 14.8Hepatitis C 2.5Malignancy 13.0
Medications, %ACEi/ARB 45.9Mineralocorticoid receptor antagonists 1.9Calcium channel blockers 23.4b-Blockers 29.4Immunosuppression 17.8Corticosteroids 17.6
Clinical site, %Site 1 57.8Site 2 32.0Site 3 10.2
Data presented as percentages,mean6SD, andmedian [interquartile range].ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptorblocker.aPercentages do not add to 100, because there may have been multiplereasons for biopsy.
J Am Soc Nephrol 29: 2213–2224, 2018 Prognostic Value of Histopathology 2215
www.jasn.org CLINICAL RESEARCH

progression using a nonparametric survival function for inter-val-censored datawith differences assessed by the generalized logrank test.34,35Wemodeled the data using Cox proportional haz-ards (PH) regression models that accommodated interval-censored times to event.36,37 Cox PH models were used for thesecondary outcome of time to RRT. All PH models were fit firstwithout adjustment and then stratified by site withmultivariableadjustment for covariates, including age, sex, race, baselineeGFR, natural log-transformed proteinuria, angiotensin-converting enzyme inhibitor or angiotensin receptor blockeruse, and primary clinicopathologic diagnostic category of kidneydisease.
To test the predictive models, we calculated c statistics forthe outcome of RRT using a base model (including age, sex,log-transformed proteinuria, and baseline eGFR) and themodel further including the chronicity score.38,39 Resultsfrom subdistribution hazards models that acknowledged thecompeting risk of death were performed as a sensitivity anal-ysis for the outcome of RRT, but they were qualitatively
unchanged; therefore, they are not reported.40 We confirmedno violations of the PH assumption using the Kolmogorov-type supremum test, and the functional forms of the covariateswere assessed by checking martingale residuals. All statisticaltests were two sided, and P values ,0.05 were consideredsignificant. Statistical analyses were performed using SAS soft-ware version 9.4 (SAS Institute Inc., Cary, NC).
RESULTS
Study Population CharacteristicsPatient characteristics in the BKBC at the time of kidney biopsyare presented in Table 1. The mean age was 52.2616.5 yearsold, 52.5% were women, and 63.8% were white. The meaneGFR was 57.5636.0 ml/min per 1.73 m2, and median pro-teinuria was 1.74 g/g creatinine [interquartile range, 0.43–4.38 g/g creatinine]. The most common reasons for kidneybiopsy were proteinuria, abnormal eGFR, and hematuria.
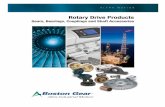
Figure 1. Distribution of semiquantitative severity scores for each of the adjudicated 13 histopathological lesions in the BostonKidney Biopsy Cohort. The histopathologic categories were graded by percentage of renal cortical volume or affected glomeruli:none, #10%; mild, 11%–25%; moderate, 26%–50%; and severe, .50%. ATI, acute tubular injury; IFTA, interstitial fibrosis andtubular atrophy.
2216 Journal of the American Society of Nephrology J Am Soc Nephrol 29: 2213–2224, 2018
CLINICAL RESEARCH www.jasn.org

Table
2.Prim
aryclinicop
atho
logic
diagno
ses
ProliferativeGN,
n=20
4
Nonp
roliferative
Glomerulopathies
,n=12
3
Parap
rotein,
n=49
DN,
n=75
Vascu
lar,
n=54
Tubulointerstitial,
n=49
Adva
nced
,n=78
Other,
n=44
IgAne
phrop
athy
(73)
Mem
brano
usne
phrop
athy
(47)
ALam
yloid(21)
DN
(75)
Vascu
lar
sclerosis(37)
AIN
(14)
Seco
ndary
TBM
(15)
Lupus
nephritis
Minim
alch
ange
disea
se(24)
MIDD
(15)
TMA(12)
ATN
(14)
FSGS(40)
Normal
(15)
Class
2(8)
IdiopathicFS
GS(15)
AAam
yloid(5)
APL
S(2)
Chron
ic/active
IN(6)
Adva
nced
chronic
chan
ges
(37)
Lympho
ma
infiltration(7)
Class
3(A
orA/C
)(14
)Lu
pus
nephritis
Cast
nephrop
athy
(4)
Scleroderma
(1)
Oxalate
nephrop
athy
(6)
Aden
oviru
s(1)
Mild
IFTA
(7)
Class
3+5
(Aor
A/C
)(11
)Class
2+5(1)
Immun
otac
toid
GN
(1)
CNItox
icity
(1)
CIN
(3)
Class
4(A
orA/C
)(23
)Class
3(C)(1)
Light-cha
incrystal
tubulop
athy
(1)
Cho
lesterol
emboli(1)
Granu
lomatou
sIN
(3)
Class
4+5
(Aor
A/C
)(9)
Class
4(C)(5)
Light-cha
inproteinuria
(1)
Phos
pha
tene
phrop
athy
(2)
Class
4+6
(Aor
A/C
)(1)
Class
3(C)+
5(1)
Multip
lemye
loma(1)
Teno
fovir
nephrotoxicity
(1)
ANCA(27)
Class
4(C)+
5(1)
Immun
eco
mplex
GN
(14)
Class
5(23)
Postinfectious
GN
(3)
Class
6(1)
Cryog
lobulinem
ia(4)
Collapsing
glomerulop
athy
(3)
PGNMID
(2)
C1q
nephrop
athy
(1)
C3GN
(4)
Idiopathicno
dular
glomerulosclerosis(1)
HIV
immun
eco
mplex
GN
(1)
Fibrillary
GN
(3)
Hered
itary
nephritis(1)
Mem
brano
proliferative
GN
(2)
Crescen
ticGN
(3)
Actua
lnum
ber
ofpatients(n)inea
chcategory.D
N,d
iabeticne
phrop
athy
;AL,am
yloidlig
htch
ain;
AIN
,acu
teinterstitialn
ephritis;TB
M,thinbasem
entm
embrane
;MID
D,m
ono
clon
alim
mun
oglobulindep
osition
disea
se;T
MA,throm
boticmicroan
giopathy
;ATN
,acu
tetubular
necros
is;A
A,serum
amyloidAprotein;A
PLS,
antip
hosp
holip
idsynd
rome;
IN,interstitialne
phritis;IFTA
,interstitialfibrosisa
ndtubular
atrophy
;CNI,
calcineu
rininhibito
rtox
icity
;CIN
,chron
icinterstitialn
ephritis;PG
NMID
,proliferativeGN
with
mon
oclona
limmun
oglobulin
dep
osits
.
J Am Soc Nephrol 29: 2213–2224, 2018 Prognostic Value of Histopathology 2217
www.jasn.org CLINICAL RESEARCH

Supplemental Figure 1 shows a flow diagram for individualsenrolled in the BKBC.
Histopathologic and Clinicopathologic ClassificationAll biopsies were reviewed under light microscopy duringstudy sessions with two experienced renal pathologists whojointly adjudicated each biopsy semiquantitatively for acuteand chronic lesions as shown in Supplemental Table 1. Figure1 shows the breakdown of the semiquantitative scores for his-topathologic lesions. To test the reproducibility of the adjudi-cated scores, we had study pathologists rescore 26 selectedkidney biopsies several months after their initial review.Weighted k-statistics (95% CI) were 0.92 (0.77–1.00) forendocapillary glomerular inflammation, 1.00 (1.00–1.00) forcellular crescents, 0.72 (0.56–0.89) for fibrinoid necrosis, 0.65(0.02–1.00) for fibrocellular crescents, 0.54 (0.12–0.69) formesangial expansion, 0.67 (0.45–0.89) for ATI, 0.46 (0.16–0.76) for inflammation in the nonfibrosed interstitium, 0.52(0.27–0.78) for inflammation in the fibrosed interstitium, 0.72
(0.52–0.93) for IFTA, 0.64 (0.41–0.87) for arterial sclerosis,and 0.66 (0.44–0.87) for arteriolar sclerosis. Weightedk-statistics for global and segmental glomerulosclerosis werenot performed, because these lesions were not readjudicatedbut rather, were abstracted from the biopsy report.
Patients were classified into eight primary clinicopatho-logic diagnostic categories using histopathologic informationand review of the medical record. All primary clinicopatho-logic diagnoses included within each category are presented inTable 2.
Correlations with HistopathologySupplemental Figure 2 shows the distribution of eGFR andproteinuria categories in all patients with biopsies. The histo-pathologic lesions that most strongly correlated with eGFRwere IFTA (Rs=20.62, P,0.001), arteriolar sclerosis(Rs=20.48, P,0.001), inflammation in the fibrosed interstitium(Rs=20.47, P,0.001), global glomerulosclerosis (Rs=20.46,P,0.001), arterial sclerosis (Rs=20.44, P,0.001), and ATI
Figure 2. Histopathologic lesions are significantly associated with eGFR and proteinuria. Boxplots show significant differences be-tween grades of adjudicated histopathologic lesions and (A) eGFR or (B) proteinuria.
2218 Journal of the American Society of Nephrology J Am Soc Nephrol 29: 2213–2224, 2018
CLINICAL RESEARCH www.jasn.org

Table 3. Individual histopathologic lesions and the risk of kidney disease progression
Histopathologic Lesion N Events per 100 person-yra Model 1 HR [95% CI] Model 2 HR [95% CI] Model 3 HR [95% CI]
Glomerular compartmentEndocapillary glomerular
inflammationAbsent 569 13.0 — — —
Present 101 10.6 0.91 [0.61 to 1.35] 1.22 [0.74 to 2.02] 1.33 [0.81 to 2.20]Cellular crescentsAbsent 586 13.1 — — —
Present 85 9.0 0.72 [0.45 to 1.15] 0.99 [0.56 to 1.78] 1.02 [0.54 to 1.95]Fibrinoid necrosisAbsent 611 13.3 — — —
Present 60 5.9 0.47 [0.24 to 0.92] 0.57 [0.28 to 1.16] 0.61 [0.29 to 1.27]Fibrocellular crescentsAbsent 602 12.9 — — —
Present 68 9.8 0.84 [0.52 to 1.36] 1.18 [0.68 to 2.06] 1.08 [0.59 to 1.96]Mesangial expansionNone or mild 438 8.9 — — —
Moderate 155 15.1 1.59 [1.13 to 2.23] 1.35 [0.92 to 1.98] 1.25 [0.85 to 1.83]Severe 69 38.1 3.64 [2.52 to 5.25] 1.56 [0.92 to 2.64] 1.21 [0.71 to 2.07]
Segmental sclerosisAbsent 532 12.0 — — —
Present 138 14.8 1.19 [0.85 to 1.66] 1.17 [0.82 to 1.67] 1.09 [0.71 to 1.69]Global glomerulosclerosisMinimal (#10%) 255 5.1 — — —
Mild (11%–25%) 164 9.8 1.76 [1.11 to 2.79] 1.62 [1.00 to 2.61] 1.54 [0.95 to 2.48]Moderate (26%–50%) 149 18.1 3.31 [2.18 to 5.02] 2.63 [1.66 to 4.14] 2.17 [1.36 to 3.45]Severe (.50%) 104 39.1 6.30 [4.18 to 9.48] 4.61 [2.91 to 7.32] 3.31 [2.04 to 5.38]
Tubulointerstitial compartmentAcute tubular injuryAbsent 412 10.4 — — —
Present 254 16.8 1.47 [1.11 to 1.95] 1.25 [0.92 to 1.70] 0.95 [0.68 to 1.33]Inflammation, nonfibrosedinterstitiumAbsent 560 13.1 — — —
Present 104 10.0 0.79 [0.53 to 1.20] 0.68 [0.43 to 1.08] 0.52 [0.32 to 0.83]Inflammation, fibrosed interstitiumNone or mild 436 9.5 — — —
Moderate 187 18.7 1.84 [1.36 to 2.48] 1.47 [1.07 to 2.02] 1.09 [0.79 to 1.50]Severe 45 28.3 2.51 [1.53 to 4.10] 2.52 [1.48 to 4.27] 1.74 [0.99 to 3.06]
Interstitial fibrosis/tubular atrophyMinimal (#10%) 249 4.3 — — —
Mild (11%–25%) 142 8.6 1.85 [1.13 to 3.05] 1.63 [0.96 to 2.75] 1.34 [0.78 to 2.31]Moderate (26%–50%) 118 18.2 3.71 [2.34 to 5.88] 2.99 [1.83 to 4.90] 2.14 [1.24 to 3.69]Severe (.50%) 158 38.3 7.15 [4.73 to 10.8] 5.07 [3.17 to 8.09] 3.42 [1.99 to 5.87]
Vascular compartmentArterial sclerosisNone or mild 287 6.3 — — —
Moderate 204 14.2 2.18 [1.49 to 3.19] 1.97 [1.18 to 3.28] 1.78 [1.15 to 2.74]Severe 194 22.8 3.18 [2.20 to 4.61] 2.13 [1.25 to 3.64] 1.64 [1.04 to 2.60]
Arteriolar sclerosisNone or mild 331 6.0 — — —
Moderate 204 15.5 2.31 [1.62 to 3.29] 2.08 [1.41 to 3.08] 1.63 [1.08 to 2.46]Severe 131 36.7 4.90 [3.44 to 7.00] 3.06 [1.93 to 4.84] 2.33 [1.42 to 3.83]
Model 1 is unadjusted. Model 2 is stratified by site and adjusted for age, sex, race, log-transformed proteinuria, primary clinicopathologic diagnosis, andangiotensin-converting enzyme inhibitor or angiotensin receptor blocker medication use. Model 3 includes Model 2 and further adjusts for eGFR. HR, hazardratio; 95% CI, 95% confidence interval; —, reference group.aApproximate events per 100 person-years. If an event occurred, the time used is one half of the interval width plus all of the time before the interval as theapproximate exposure time (the exact time an event occurred is not known if a $40% decline in eGFR occurred).
J Am Soc Nephrol 29: 2213–2224, 2018 Prognostic Value of Histopathology 2219
www.jasn.org CLINICAL RESEARCH

(Rs=20.40, P,0.001) (Supplemental Table 2). The histo-pathologic lesions that most strongly correlated with protein-uria were mesangial expansion (Rs=0.29, P,0.001), IFTA(Rs=0.13, P,0.001), endocapillary glomerular inflamma-tion (Rs=0.11, P=0.004), segmental sclerosis (Rs=0.11,P,0.01), arteriolar sclerosis (Rs=0.09, P=0.02), inflamma-tion in the fibrosed interstitium (Rs=0.09, P=0.03), andATI (Rs=0.08, P=0.03) (Supplemental Table 2). Figure 2shows boxplots between grades of histopathologic lesionsthat were most significantly associated with eGFR and pro-teinuria.
We found a number of significant correlations among his-topathologic lesions of glomerular, tubulointerstitial, andvascular injury (Supplemental Table 3). IFTA moderatelycorrelated with global glomerulosclerosis (Rs=0.64,P,0.001), inflammation in the fibrosed interstitium(Rs=0.61, P,0.001), arteriolar sclerosis (Rs=0.59,P,0.001), and arterial sclerosis (Rs=0.52, P,0.001). Crescentscorrelated with necrosis (Rs=0.69, P,0.001) and fibrocellularcrescents (Rs=0.60, P,0.001).
Prognostic Significance of Histopathologic LesionsDuring a median follow-up time of 34.3 months, 199 individualsexperienced subsequent kidney disease progression, and 111 in-dividuals were started on RRT. Table 3 shows the unadjusted andmultivariable-adjusted associations between each individual his-topathologic lesion and kidney disease progression. Results forprogression to RRTwere similar (Supplemental Table 4).
Glomerular LesionsHigherdegrees of global glomerulosclerosiswere associated with an increased risk ofkidney disease progression (Figure 3A)(generalized log rank P,0.001). The asso-ciation between global glomerulosclerosisand kidney disease progression was con-founded by eGFR. In a fully multivari-able-adjusted clinical model includinglog-transformed proteinuria and eGFR,26%–50% and .50% versus #10% globalglomerulosclerosis were associated withmore than two- and more than threefoldincreased risks of kidney function loss, re-spectively (Table 3). After accounting forage-related or no global glomerulosclerosisas previously described,31,41 global glomer-ulosclerosis deemed pathologic (abnormalfor age) was associated with a higher risk ofkidney disease progression after multivari-able adjustment (hazard ratio, 1.87; 95%confidence interval, 1.29 to 2.73). Age-related global glomerulosclerosis was notassociated with an increased risk of kidneydisease progression compared with noglobal glomerulosclerosis after multivari-able adjustment (hazard ratio, 0.97; 95%
confidence interval, 0.51 to 1.81). In multivariable-adjustedmodels, pathologic global glomerulosclerosis with involve-ment of 26%–50% and .50% glomeruli, compared with noor age-related global glomerulosclerosis, remained associatedwith an increased risk of kidney disease progression (Supple-mental Table 5).
Tubulointerstitial LesionsIncreasing severity of IFTAwas associatedwith subsequent lossof kidney function (Figure 3B) (generalized log rankP,0.001). The association was strongly confounded byeGFR. In a fully multivariable-adjusted model including log-transformed proteinuria and eGFR, 26%–50% and .50%IFTAversus#10% IFTAwere associated with a 2.1- and nearly3.5-fold increased risks of kidney disease progression, respec-tively (Table 3). Severe inflammation in the fibrosed intersti-tium was associated with 1.7-fold increased risk of kidneydisease progression that did not reach statistical significanceafter multivariable adjustment, but it was significant for theoutcome of RRT (Supplemental Table 4). Inflammation in thenonfibrosed interstitium (present versus absent) was associ-ated with a lower rather than a higher risk of kidney diseaseprogression in the fully adjusted model (Table 3).
Vascular LesionsBecause of the low number of scores of “none” for both arterialand arteriolar lesions, “none” and “mild”were collapsed into asingle category for analyses. The severity of arterial sclerosis
Figure 3. Chronic histopathologic lesions are associated with kidney disease progression.(A) Global glomerulosclerosis. (B) Interstitial fibrosis/tubular atrophy. (C) Arterial sclerosis. (D)Arteriolar sclerosis. Generalized log rank P,0.001 for all lesions.
2220 Journal of the American Society of Nephrology J Am Soc Nephrol 29: 2213–2224, 2018
CLINICAL RESEARCH www.jasn.org

and arteriolar sclerosis were both associated with future kidneydisease progression (Figure 3, C and D) (generalized log rankP,0.001). The association of arterial and arteriolar sclerosiswith subsequent kidney disease progression was confounded byeGFR.Moderate arterial sclerosis and severe arterial sclerosis (ver-sus none/mild) remained associated with nearly 1.8- and 1.7-foldincreased risks of kidney disease progression after multivariableadjustment, respectively (Table 3). Moderate arteriolar sclerosisand severe arteriolar sclerosis (versus none/mild) were associatedwith 1.6- and 2.3-fold increased risks of kidney disease progres-sion after multivariable adjustment, respectively (Table 3).
Kidney Biopsy Chronicity ScoreSethi et al.16 proposed a standardized grading of chronic changes innative kidney biopsy specimens on the basis of the following fourvariables: interstitial fibrosis, tubular atrophy, arteriosclerosis(without mention of arterioles), and glomerulosclerosis—all ofwhich were found in our study to be independently associatedwith kidneydisease progression. Results on the associationbetweenthe chronicity score and kidney disease progression are shown inTable 4.Results for the outcomeofRRTwere similar and are shownin Supplemental Table 6.We calculated total renal chronicity scoresfor each individual in this studyon thebasis of theproposal by Sethiet al.16 and tested the performance of the score for predicting 5-yearrisk of RRT; we compared the score with the Kidney Failure RiskEquation (KFRE), which includes age, race, sex, proteinuria, andeGFR.42,43The c statistic of themodelwithonly the chronicity scorewas 0.84 (95% confidence interval, 0.80 to 0.88). The c statistic ofthemodel with KFRE variables was 0.85 (95% confidence interval,0.81 to 0.89). The c statistic of the model with both the chronicityscore and the KFRE variables increased to 0.87 (95% confidenceinterval, 0.83 to 0.90; P=0.13 for comparison with the c statistic ofthe KFRE model).
DISCUSSION
In this prospective studyof adjudicated histopathologic lesionsacross a diverse set of kidney diseases, we found that severalhistopathologic lesions were independent predictors of kidneydisease progression. Themain findings were that IFTA, arterial
and arteriolar sclerosis, and global glomerulosclerosis were eachassociated with kidney disease progression even after adjustingfor a number of clinical predictors, including eGFR, proteinuria,and clinicopathologic diagnosis. Apreviously proposed chronicityscore from the sum of semiquantitative grading of chronic lesionswas also independently associatedwith kidneydisease progressionbut did not change risk prediction appreciably as judged by thechange in c statistic. The final findings were that the presence ofinflammation in the fibrosed interstitium and the presence ofinflammation in nonfibrosed interstitium were associated withhigher and lower risk of subsequent kidney disease progression,respectively; the latter was presumably due to the treatable natureof such lesions.
Kidney biopsies provide diagnostic and also prognostic in-formation.3–6 A key strength of our study is the inclusion ofdiverse forms of kidney disease and multivariable adjustmentfor clinicopathologic diagnosis as well as demographics andlaboratory values. Our findings extend and validate findingsfrom the published literature dating back to the 1960s.17,44,45
It is commonly stated that interstitial fibrosis is the histo-pathologic lesionmost strongly associated with a higher risk ofkidney failure.18,19,22,46 The evidence base for this assertion,however, derives from a number of studies restricted to spe-cific etiologies47–50 and studies that did not adjust compre-hensively for known confounders, such as clinicopathologicdiagnosis, eGFR, and proteinuria.20,51,52 Our findings confirmthe importance of IFTA and expand on the importance ofinterstitial inflammation,53 global glomerulosclerosis, arterialsclerosis, and arteriolar sclerosis. Our finding that kidneydisease progression is more common in those with global glo-merulosclerosis exceeding the expected degree on the basis ofage is consistent with the findings of Hommos et al.31 andsupport the need to take into account age-related pathologicchanges.
A number of studies have developed scoring systems forrenal pathology. Examples include activity and chronicity in-dices in lupus nephritis,50 the Oxford classification in IgAnephropathy,13,14 the Nephrotic Syndrome Study Networkdigital pathology scoring system,54 and prior suggestions forglobal chronicity scores.20,49,55 More recently, Sethi et al.16
suggested that biopsies should include semiquantitative scores
Table 4. Risk of kidney disease progression using the kidney biopsy chronicity score
Chronicity Scorea N Events per 100 person-yr Model 1 HR [95% CI] Model 2 HR [95% CI] Model 3 HR [95% CI]
Per one-point change 654 12.1 1.28 [1.22 to 1.33] 1.23 [1.17 to 1.30] 1.19 [1.12 to 1.27]Minimal chronic changes (0–1) 199 3.6 — — —
Mild chronic changes (2–4) 168 8.1 2.02 [1.17 to 3.48] 1.72 [0.97 to 3.06] 1.53 [0.85 to 2.75]Moderate chronic changes (5–7) 146 17.3 4.24 [2.55 to 7.04] 3.81 [2.20 to 6.59] 2.92 [1.61 to 5.31]Severe chronic changes ($8) 141 39.6 8.67 [5.35 to 14.1] 6.09 [3.51 to 10.6] 4.42 [2.37 to 8.22]
Shown are HRs (95% CIs) per one-point increase in the score (range from zero to ten) or compared to the reference group of minimal chronic changes. Model 1 isunadjusted.Model 2 isModel 1 stratified by site and adjusted for age, sex, race, log-transformed proteinuria, primary clinicopathologic diagnosis, and angiotensin-converting enzyme inhibitor or angiotensin receptor blocker medication use. Model 3 includes Model 2 and adjusts for eGFR. HR, hazard ratio; 95% CI, 95%confidence interval; —, reference group.aChronicity score is calculated by adding scores of global glomerulosclerosis (zero to three), interstitial fibrosis and tubular atrophy (zero to three), and arterialsclerosis (zero to one). Interstitial fibrosis and tubular atrophy are counted twice, because interstitial fibrosis and tubular atrophy are scored separately in theproposal by Sethi et al.16 Arterial sclerosis is given a score of zero for none/mild and one for moderate/severe lesions.
J Am Soc Nephrol 29: 2213–2224, 2018 Prognostic Value of Histopathology 2221
www.jasn.org CLINICAL RESEARCH

for the degree of glomerulosclerosis, interstitial fibrosis, tubularatrophy, and arteriosclerosis alongwith an overall chronicity scoreequal to the sum of the individual scores. Our findings provideempirical evidence in support of such a scoring system. The pro-posed scoring system by Sethi et al.16 did not include arteriolarsclerosis, but our study provides evidence for the prognostic im-portance of arteriolar sclerosis for kidney disease progression. Thedegrees of arterial and arteriolar lesions, although correlated, candiverge from one another on the basis of our finding of a modestcorrelation between the two scores (R=0.68). These findings sug-gest that nephropathologists should score arterial and arteriolarlesions separately because they both associate with kidney diseaseprogression and may represent different pathologic processes.Given the importance of arterial and arteriolar lesions, greaterstandardization by pathologists—in both terminology and grad-ing criteria—would be desirable.
eGFR and proteinuria are used by clinicians for prognosticassessment, but they do not capture the full extent of kidneypathology. Our results of independent associations betweenhistopathology and kidney disease progression reflect the in-adequacy of SCr and proteinuria as risk markers and pointtoward well described hypotheses on the causal associationsbetween histopathologic lesions and progression of kidneydisease. Global glomerulosclerosis and IFTA, for example,may denote focal nephron loss and adaptive responses of sur-viving nephrons that ultimately prove to be detrimental tokidney function.56,57 Arterial and arteriolar lesions couldbe a reflection (or cause) of systemic hypertension and failureof glomerular autoregulation.58–60 Whether chronic lesionsfrom kidney biopsy findings can direct specific treatments tomodify disease progression (for example, antifibrotic agentsfor those with excessive IFTA) is an area in need of more re-search and clinical trials. It is tempting to speculate that kidneybiopsies could provide value in patients who do not currentlyundergo kidney biopsy, such as individuals with presumedhypertension-associated CKD and presumed diabetic ne-phropathy. Indeed, the Kidney Precision Medicine Projectlaunched by the National Institute of Diabetes, Digestive andKidney Diseases is conducting multicenter studies to expandthe role for kidney biopsies and their molecular interrogationin individuals with common forms of CKD and AKI.
Several limitations should be noted in our study.We did notinclude readjudication of electron microscopy or immunoflu-orescence results primarily due to logistic constraints. We alsodid not perform quantitative morphometry or quantify fea-tures, such as podocyte number or peritubular capillary den-sity, which are important in the pathogenesis and progressionof variouskidneydiseases.Wedidnot take into account therapyadministered after the biopsy, which could alter an individual’strajectory to the outcome, particularly in individuals requiringimmunosuppressive therapy. The two renal pathologists didnot use formalized definitions and criteria for each gradingcategory; this is not a source of bias for our findings, however,because they were completely blinded to clinical variables,reason for biopsy, and original diagnosis. The relatively low
k-statistics for certain lesions could have biased results towardthe null hypothesis of no association between a given lesionand the outcomes tested. Although our cohort was diverse(from three separate academic medical centers) and large rel-ative to other biopsy cohorts with adjudicated histopathologicscores, it includes only individuals who underwent biopsiesfor specific clinical indications with diseases that are not nec-essarily reflective of the majority of patients with CKD andpatients with AKI. The number of biopsies from individualdisease categories was also small, particularly for rare forms ofkidney disease. Our readjudication process provided inter-nally consistent scoring for biopsies; however, it is not neces-sarily generalizable, because we relied on two expert renalpathologists who convened to score biopsies together in studysessions. Further development of standardized criteria forscoring lesions, as has been done by the Banff group for trans-plant biopsies, would be important to allow adoption by othercenters and enhance generalizability. The development of im-age analysis algorithms using digital pathology could also befocused on lesions that provide prognostic information, suchas we have described.
In conclusion, greater severity of lesions on native kidneybiopsies—independent of clinical factors, including clinico-pathologic diagnosis, eGFR, and proteinuria—associateswith a greater risk of kidney disease progression across a va-riety of kidney disease etiologies. A kidney biopsy chronicityscore also provides additional prognostic value above routineclinical variables. Our findings highlight the prognostic valueof careful review and semiquantitative scoring of the kidneybiopsy specimen.
ACKNOWLEDGMENTS
We thank themembers of the laboratory of S.S.W. for their invaluable
assistance in the Boston Kidney Biopsy Cohort.
This study is supported by National Institutes of Health (NIH)
grant R01DK093574 (to S.S.W.). A.S. was supported by NIH grant
F32DK11106. S.S.W. is also supported by NIH grants U01DK085660,
U01DK104308, and UG3DK114915.
This work was conducted with support from Harvard Catalyst. The
Harvard Clinical and Translational Science Center (National Center for
Advancing Translational Sciences, National Institutes of Health Award
UL1 TR001102) and financial contributions from Harvard University
and its affiliated academic healthcare centers. The content is solely the
responsibility of the authors and does not necessarily represent the of-
ficial views of Harvard Catalyst, Harvard University and its affiliated
academic healthcare centers, or the National Institutes of Health.
Part of this work was presented as a poster at the 2016 American
Society of Nephrology Scientific Session on November 19 in Chicago,
Illinois.
DISCLOSURESNone.
2222 Journal of the American Society of Nephrology J Am Soc Nephrol 29: 2213–2224, 2018
CLINICAL RESEARCH www.jasn.org

REFERENCES
1. Fiorentino M, Bolignano D, Tesar V, Pisano A, Van Biesen W, D’ArrigoG, et al.; ERA-EDTA Immunonephrology Working Group: Renal biopsyin 2015–from epidemiology to evidence-based indications. Am
J Nephrol 43: 1–19, 20162. O’Shaughnessy MM, Hogan SL, Thompson BD, Coppo R, Fogo AB,
Jennette JC: Glomerular disease frequencies by race, sex and region:Results from the International Kidney Biopsy Survey [published onlineahead of print July 2, 2017].Nephrol Dial Transplant doi: 10.1093/ndt/gfx189
3. Richards NT, Greaves I, Lee SJ, Howie AJ, Adu D, Michael J: In-creased prevalence of renal biopsy findings other than diabeticglomerulopathy in type II diabetes mellitus.Nephrol Dial Transplant
7: 397–399, 19924. Gambara V, Mecca G, Remuzzi G, Bertani T: Heterogeneous nature of
renal lesions in type II diabetes. J Am Soc Nephrol 3: 1458–1466, 19935. Mazzucco G, Bertani T, Fortunato M, Bernardi M, Leutner M, Boldorini
R, et al.: Different patterns of renal damage in type 2 diabetes mellitus:A multicentric study on 393 biopsies. Am J Kidney Dis 39: 713–720,2002
6. Richards NT, Darby S, Howie AJ, Adu D, Michael J: Knowledge of renalhistology alters patientmanagement in over 40%of cases.Nephrol Dial
Transplant 9: 1255–1259, 19947. Zweiman B, Kornblum J, Cornog J, Hildreth EA: The prognosis of lupus
nephritis. Role of clinical-pathologic correlations. Ann Intern Med 69:441–462, 1968
8. Baldwin DS, Lowenstein J, Rothfield NF, Gallo G, McCluskey RT: Theclinical course of the proliferative and membranous forms of lupusnephritis. Ann Intern Med 73: 929–942, 1970
9. Cheatum DE, Hurd ER, Strunk SW, Ziff M: Renal histology and clinicalcourse of systemic lupus erythematosus. A prospective study. ArthritisRheum 16: 670–676, 1973
10. Baldwin DS, Gluck MC, Lowenstein J, Gallo GR: Lupus nephritis. Clin-ical course as related to morphologic forms and their transitions. AmJ Med 62: 12–30, 1977
11. Appel GB, Silva FG, Pirani CL, Meltzer JI, Estes D: Renal involvement insystemic lupud erythematosus (SLE): A study of 56 patients emphasiz-ing histologic classification. Medicine (Baltimore) 57: 371–410, 1978
12. Weening JJ, D’Agati VD, Schwartz MM, Seshan SV, Alpers CE, AppelGB, et al.: The classification of glomerulonephritis in systemic lupuserythematosus revisited. J Am Soc Nephrol 15: 241–250, 2004
13. Cattran DC, Coppo R, Cook HT, Feehally J, Roberts IS, Troyanov S,et al.; Working Group of the International IgA Nephropathy Networkand the Renal Pathology Society: The Oxford classification of IgA ne-phropathy: Rationale, clinicopathological correlations, and classifica-tion. Kidney Int 76: 534–545, 2009
14. Roberts IS, Cook HT, Troyanov S, Alpers CE, Amore A, Barratt J, et al.;Working Group of the International IgA Nephropathy Network and theRenal Pathology Society: TheOxford classification of IgA nephropathy:Pathology definitions, correlations, and reproducibility. Kidney Int 76:546–556, 2009
15. Sethi S, Haas M, Markowitz GS, D’Agati VD, Rennke HG, Jennette JC,et al.: Mayo clinic/renal pathology society consensus report on path-ologic classification, diagnosis, and reporting of GN. J AmSocNephrol
27: 1278–1287, 201616. Sethi S, D’Agati VD, Nast CC, Fogo AB, De Vriese AS, Markowitz GS,
et al.: A proposal for standardized grading of chronic changes in nativekidney biopsy specimens. Kidney Int 91: 787–789, 2017
17. Risdon RA, Sloper JC, De Wardener HE: Relationship between renalfunction and histological changes found in renal-biopsy specimensfrom patients with persistent glomerular nephritis. Lancet 2: 363–366,1968
18. Nath KA: Tubulointerstitial changes as a major determinant in theprogression of renal damage. Am J Kidney Dis 20: 1–17, 1992
19. Nath KA: The tubulointerstitium in progressive renal disease.Kidney Int54: 992–994, 1998
20. Howie AJ, Ferreira MA, Adu D: Prognostic value of simple measure-ment of chronic damage in renal biopsy specimens. Nephrol Dial
Transplant 16: 1163–1169, 200121. Rodríguez-Iturbe B, Johnson RJ, Herrera-Acosta J: Tubulointerstitial
damage and progression of renal failure.Kidney Int Suppl 99: S82–S86,2005
22. Mariani LH, Martini S, Barisoni L, Canetta PA, Troost JP, Hodgin JB,et al.: Interstitial fibrosis scored onwhole-slide digital imaging of kidneybiopsies is a predictor of outcome in proteinuric glomerulopathies.Nephrol Dial Transplant 33: 310–318, 2018
23. Menn-Josephy H, Lee CS, Nolin A, Christov M, Rybin DV, WeinbergJM, et al.: Renal interstitial fibrosis: An imperfect predictor of kidneydisease progression in some patient cohorts. Am J Nephrol 44:289–299, 2016
24. Tervaert TW, Mooyaart AL, Amann K, Cohen AH, Cook HT,DrachenbergCB, et al.; Renal PathologySociety: Pathologic classificationofdiabetic nephropathy. J Am Soc Nephrol 21: 556–563, 2010
25. Mauer SM, Steffes MW, Ellis EN, Sutherland DE, Brown DM, Goetz FC:Structural-functional relationships in diabetic nephropathy. J Clin In-
vest 74: 1143–1155, 198426. D’Agati VD, Fogo AB, Bruijn JA, Jennette JC: Pathologic classification
of focal segmental glomerulosclerosis: A working proposal. Am J Kid-
ney Dis 43: 368–382, 200427. Berden AE, Ferrario F, Hagen EC, Jayne DR, Jennette JC, Joh K, et al.:
Histopathologic classification of ANCA-associated glomerulonephritis.J Am Soc Nephrol 21: 1628–1636, 2010
28. Farris AB, Adams CD, Brousaides N, Della Pelle PA, Collins AB, MoradiE, et al.: Morphometric and visual evaluation of fibrosis in renal bi-opsies. J Am Soc Nephrol 22: 176–186, 2011
29. Racusen LC, Solez K, Colvin RB, Bonsib SM, CastroMC, Cavallo T, et al.:The Banff 97 working classification of renal allograft pathology. KidneyInt 55: 713–723, 1999
30. Bajema IM, Hagen EC, Hansen BE, Hermans J, Noël LH, Waldherr R,et al.: The renal histopathology in systemic vasculitis: An internationalsurvey study of inter- and intra-observer agreement. Nephrol Dial
Transplant 11: 1989–1995, 199631. Hommos MS, Zeng C, Liu Z, Troost JP, Rosenberg AZ, Palmer M, et al.:
Global glomerulosclerosis with nephrotic syndrome; the clinical im-portance of age adjustment. Kidney Int 93: 1175–1182, 2018
32. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG: Re-search electronic data capture (REDCap)–a metadata-driven method-ology and workflow process for providing translational researchinformatics support. J Biomed Inform 42: 377–381, 2009
33. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, FeldmanHI, et al.; CKD-EPI (Chronic Kidney Disease Epidemiology Collabora-tion): A new equation to estimate glomerular filtration rate. Ann Intern
Med 150: 604–612, 200934. Wellner JA, Zhan Y: A hybrid algorithm for computation of the non-
parametric maximum likelihood estimator from censored data. J Am
Stat Assoc 92: 945–959, 199735. Zhao Q, Sun J: Generalized log-rank test for mixed interval-censored
failure time data. Stat Med 23: 1621–1629, 200436. Sun J: A non-parametric test for interval-censored failure time data with
application to AIDS studies. Stat Med 15: 1387–1395, 199637. Zhang Z, Sun J: Interval censoring. Stat Methods Med Res 19: 53–70, 201038. PencinaMJ, D’Agostino RB: Overall C as a measure of discrimination in
survival analysis: Model specific population value and confidence in-terval estimation. Stat Med 23: 2109–2123, 2004
39. PencinaMJ, D’Agostino RB Sr., D’Agostino RB Jr., Vasan RS: Evaluatingthe added predictive ability of a newmarker: From area under the ROCcurve to reclassification and beyond. Stat Med 27: 157–172, 2008
40. Fine J, Gray R: A proportional hazardsmodel for the subdistribution of acompeting risk. J Am Stat Assoc 94: 496–509, 1999
J Am Soc Nephrol 29: 2213–2224, 2018 Prognostic Value of Histopathology 2223
www.jasn.org CLINICAL RESEARCH

41. Kremers WK, Denic A, Lieske JC, Alexander MP, Kaushik V, ElsherbinyHE, et al.: Distinguishing age-related from disease-related glomer-ulosclerosis on kidney biopsy: The Aging Kidney Anatomy study.Nephrol Dial Transplant 30: 2034–2039, 2015
42. Tangri N, Stevens LA, Griffith J, Tighiouart H, Djurdjev O, Naimark D,et al.: A predictive model for progression of chronic kidney disease tokidney failure. JAMA 305: 1553–1559, 2011
43. Tangri N, Grams ME, Levey AS, Coresh J, Appel LJ, Astor BC, et al.;CKD Prognosis Consortium: Multinational assessment of accuracy ofequations for predicting risk of kidney failure: A meta-analysis. JAMA315: 164–174, 2016
44. Striker GE, Schainuck LI, Cutler RE, Benditt EP: Structural-functionalcorrelations in renal disease. I. A method for assaying and classifying his-topathologic changes in renal disease. Hum Pathol 1: 615–630, 1970
45. Schainuck LI, Striker GE, Cutler RE, Benditt EP: Structural-functional corre-lations in renal disease. II. The correlations. Hum Pathol 1: 631–641, 1970
46. SerónD, Alexopoulos E, RafteryMJ, Hartley B, Cameron JS: Number ofinterstitial capillary cross-sections assessed by monoclonal antibodies: Re-lation to interstitial damage. Nephrol Dial Transplant 5: 889–893, 1990
47. Walsh M, Sar A, Lee D, Yilmaz S, Benediktsson H, Manns B, et al.:Histopathologic features aid in predicting risk for progression of IgAnephropathy. Clin J Am Soc Nephrol 5: 425–430, 2010
48. Ford SL, Polkinghorne KR, Longano A, Dowling J, Dayan S, Kerr PG,et al.: Histopathologic and clinical predictors of kidney outcomes inANCA-associated vasculitis. Am J Kidney Dis 63: 227–235, 2014
49. An Y, Xu F, LeW,Ge Y, ZhouM, ChenH, et al.: Renal histologic changesand the outcome in patients with diabetic nephropathy. Nephrol DialTransplant 30: 257–266, 2015
50. Yu F, Wu LH, Tan Y, Li LH, Wang CL, WangWK, et al.: Tubulointerstitiallesions of patients with lupus nephritis classified by the 2003 In-ternational Society of Nephrology and Renal Pathology Society system.Kidney Int 77: 820–829, 2010
51. Bohle A,Mackensen-Haen S, vonGiseH,GrundKE,WehrmannM, BatzC, et al.: The consequences of tubulo-interstitial changes for renal
function in glomerulopathies. Amorphometric and cytological analysis.Pathol Res Pract 186: 135–144, 1990
52. Bohle A, Wehrmann M, Bogenschütz O, Batz C, Müller CA, Müller GA:The pathogenesis of chronic renal failure in diabetic nephropathy. In-vestigation of 488 cases of diabetic glomerulosclerosis. Pathol ResPract 187: 251–259, 1991
53. Mannon RB, Matas AJ, Grande J, Leduc R, Connett J, Kasiske B, et al.;DeKAF Investigators: Inflammation in areas of tubular atrophy in kidneyallograft biopsies: A potent predictor of allograft failure. Am J Trans-plant 10: 2066–2073, 2010
54. Barisoni L, Troost JP, Nast C, Bagnasco S, Avila-Casado C, Hodgin J,et al.: Reproducibility of the NEPTUNE descriptor-based scoring sys-tem on whole-slide images and histologic and ultrastructural digitalimages. Mod Pathol 29: 671–684, 2016
55. To KF, Choi PC, Szeto CC, Li PK, TangNL, LeungCB, et al.: Outcome ofIgA nephropathy in adults graded by chronic histological lesions. AmJ Kidney Dis 35: 392–400, 2000
56. Hostetter TH, Olson JL, Rennke HG, Venkatachalam MA, Brenner BM:Hyperfiltration in remnant nephrons: A potentially adverse response torenal ablation. Am J Physiol 241: F85–F93, 1981
57. Fogo AB: Mechanisms of progression of chronic kidney disease. Pe-diatr Nephrol 22: 2011–2022, 2007
58. Bidani AK, Griffin KA: Pathophysiology of hypertensive renal damage:Implications for therapy. Hypertension 44: 595–601, 2004
59. Hill GS, Heudes D, Jacquot C, Gauthier E, Bariéty J: Morphometricevidence for impairment of renal autoregulation in advanced essentialhypertension. Kidney Int 69: 823–831, 2006
60. Tracy RE: Renal vasculature in essential hypertension: A review of somecontrarian evidence. Contrib Nephrol 169: 327–336, 2011
This article contains supplemental material online at http://jasn.asnjournals.org/lookup/suppl/doi:10.1681/ASN.2017121260/-/DCSupplemental.
2224 Journal of the American Society of Nephrology J Am Soc Nephrol 29: 2213–2224, 2018
CLINICAL RESEARCH www.jasn.org