
Resting motor threshold in idiopathic generalized epilepsies: A systematic review with meta-analysis
11
Please cite this article in press as: Brigo, F., et al., Resting motor threshold in idiopathic generalized epilepsies: A systematic review with meta-analysis. Epilepsy Res. (2012), http://dx.doi.org/10.1016/j.eplepsyres.2012.03.020 ARTICLE IN PRESS +Model EPIRES-4745; No. of Pages 11 Epilepsy Research (2012) xxx, xxx—xxx jou rn al h om epa ge: www.elsevier.com/locate/epilepsyres REVIEW Resting motor threshold in idiopathic generalized epilepsies: A systematic review with meta-analysis Francesco Brigo a,b,∗ , Monica Storti c , Maria Donata Benedetti a , Fabio Rossini a , Raffaele Nardone b,d , Frediano Tezzon b , Antonio Fiaschi a , Luigi Giuseppe Bongiovanni a , Paolo Manganotti a a Department of Neurological, Neuropsychological, Morphological and Movement Sciences, Section of Clinical Neurology, University of Verona, Italy b Division of Neurology, Hospital ‘‘Franz Tappeiner’’, Merano, Italy c Department of Medicine, University of Verona, Italy d Department of Neurology, Christian Doppler Clinic, Paracelsus Medical University, Salzburg, Austria Received 30 January 2012; received in revised form 13 March 2012; accepted 28 March 2012 KEYWORDS Idiopathic generalized epilepsy; Juvenile myoclonic epilepsy; Resting motor threshold; Systematic review/meta analysis; Transcranial magnetic stimulation Summary Resting motor threshold (rMT) assessed by means of Transcranial Magnetic Stimula- tion (TMS) is thought to reflect trans-synaptic excitability of cortico-spinal neurons. TMS studies reporting rMT in idiopathic generalized epilepsies (IGEs) yielded discrepant results, so that it is difficult to draw a definitive conclusion on cortico-spinal excitability in IGEs by simple sum- mation of previous results regarding this measure. Our purpose was to carry out a systematic review and a meta-analysis of studies evaluating rMT values obtained during single-pulse TMS in patients with IGEs. Controlled studies measuring rMT by single-pulse TMS in drug-naive patients older than 12 years affected by IGEs were systematically reviewed. rMT values were assessed calculating mean difference and odds ratio with 95% confidence intervals (CI). Fourteen tri- als (265 epileptic patients and 424 controls) were included. Patients with juvenile myoclonic epilepsy (JME) have a statistically significant lower rMT compared with controls (mean differ- ence: −6.78; 95% CI −10.55 to −3.00); when considering all subtypes of IGEs and IGEs other than JME no statistically significant differences were found. Overall considered, the results are indicative of a cortico-spinal hyper-excitability in JME, providing not enough evidence for motor hyper-excitability in other subtypes of IGE. The considerable variability across studies probably reflects the presence of relevant clinical and methodological heterogeneity, and higher tempo- ral variability among rMT measurements over time, related to unstable cortical excitability in these patients. © 2012 Elsevier B.V. All rights reserved. ∗ Corresponding author at: Department of Neurological, Neuropsychological, Morphological and Movement Sciences, Section of Clinical Neurology, University of Verona, Italy, Piazzale L.A. Scuro 10, 37134 Verona, Italy. Tel.: +39 045 8124174; fax: +39 045 8124873. E-mail address: [email protected] (F. Brigo). 0920-1211/$ — see front matter © 2012 Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
Transcript of Resting motor threshold in idiopathic generalized epilepsies: A systematic review with meta-analysis
ARTICLE IN PRESS+ModelEPIRES-4745; No. of Pages 11
Epilepsy Research (2012) xxx, xxx—xxx
jou rn al h om epa ge: www.elsev ier .com/ locate /ep i lepsyres
REVIEW
Resting motor threshold in idiopathic generalizedepilepsies: A systematic review with meta-analysis
Francesco Brigoa,b,∗, Monica Storti c, Maria Donata Benedetti a,Fabio Rossini a, Raffaele Nardoneb,d, Frediano Tezzonb, Antonio Fiaschia,Luigi Giuseppe Bongiovannia, Paolo Manganotti a
a Department of Neurological, Neuropsychological, Morphological and Movement Sciences, Section of Clinical Neurology,University of Verona, Italyb Division of Neurology, Hospital ‘‘Franz Tappeiner’’, Merano, Italyc Department of Medicine, University of Verona, Italyd Department of Neurology, Christian Doppler Clinic, Paracelsus Medical University, Salzburg, Austria
Received 30 January 2012; received in revised form 13 March 2012; accepted 28 March 2012
KEYWORDSIdiopathicgeneralized epilepsy;Juvenile myoclonicepilepsy;Resting motorthreshold;Systematicreview/metaanalysis;Transcranial magneticstimulation
Summary Resting motor threshold (rMT) assessed by means of Transcranial Magnetic Stimula-tion (TMS) is thought to reflect trans-synaptic excitability of cortico-spinal neurons. TMS studiesreporting rMT in idiopathic generalized epilepsies (IGEs) yielded discrepant results, so that itis difficult to draw a definitive conclusion on cortico-spinal excitability in IGEs by simple sum-mation of previous results regarding this measure. Our purpose was to carry out a systematicreview and a meta-analysis of studies evaluating rMT values obtained during single-pulse TMS inpatients with IGEs. Controlled studies measuring rMT by single-pulse TMS in drug-naive patientsolder than 12 years affected by IGEs were systematically reviewed. rMT values were assessedcalculating mean difference and odds ratio with 95% confidence intervals (CI). Fourteen tri-als (265 epileptic patients and 424 controls) were included. Patients with juvenile myoclonicepilepsy (JME) have a statistically significant lower rMT compared with controls (mean differ-ence: −6.78; 95% CI −10.55 to −3.00); when considering all subtypes of IGEs and IGEs otherthan JME no statistically significant differences were found. Overall considered, the results areindicative of a cortico-spinal hyper-excitability in JME, providing not enough evidence for motor
hyper-excitability in other subtypes of IGE. The considerable variability across studies probablyreflects the presence of relevant clinical and methodological heterogeneity, and higher tempo-easu
ral variability among rMT mPlease cite this article in press as: Brigo, F., et al., Restingsystematic review with meta-analysis. Epilepsy Res. (2012), ht
these patients.© 2012 Elsevier B.V. All rights re
∗ Corresponding author at: Department of Neurological, NeuropsycholoNeurology, University of Verona, Italy, Piazzale L.A. Scuro 10, 37134 Vero
E-mail address: [email protected] (F. Brigo).
0920-1211/$ — see front matter © 2012 Elsevier B.V. All rights reserved.http://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
rements over time, related to unstable cortical excitability in
motor threshold in idiopathic generalized epilepsies: Atp://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
served.
gical, Morphological and Movement Sciences, Section of Clinicalna, Italy. Tel.: +39 045 8124174; fax: +39 045 8124873.
+ModelE
2
C
I
Entiaeswttcgbcbc‘b(tsnp(t2n
ne
ARTICLE IN PRESSPIRES-4745; No. of Pages 11
F. Brigo et al.
ontents
Introduction............................................................................................................... 00Methods................................................................................................................... 00
Objective............................................................................................................. 00Study selection ....................................................................................................... 00Data sources and search strategy ..................................................................................... 00Data extraction....................................................................................................... 00Statistical analysis.................................................................................................... 00
Results .................................................................................................................... 00Description of studies (Table 1)....................................................................................... 00Risk of bias ........................................................................................................... 00
Quantitative synthesis..................................................................................................... 00rMT values in all types of IGEs (Fig. 2) ................................................................................ 00rMT values in juvenile myoclonic epilepsy (JME) (Fig. 3).............................................................. 00rMT values in IGEs other than JME (Fig. 4) ............................................................................ 00Publication bias ...................................................................................................... 00
Discussion ................................................................................................................. 00Exploration of heterogeneity ......................................................................................... 00Strengths and limitations of the review............................................................................... 00
Conflict of interest statement ............................................................................................. 00Disclosure ................................................................................................................. 00Acknowledgements........................................................................................................ 00Appendix A. Supplementary data........................................................................................ 00Appendix A. Supplementary data........................................................................................ 00References ................................................................................................................ 00
ntroduction
pilepsy is a chronic disorder characterized by heteroge-eous and dynamic pathophysiological processes leadingo an altered balance between excitatory and inhibitorynfluences at cortical level, which may be counteracted byntiepileptic drugs (Tassinari et al., 2003). Idiopathic gen-ralized epilepsies (IGEs) encompass many distinct epilepticyndromes, and are supposed to be the expression of aidespread hyperexcitability involving subcortical and cor-
ical structures in both hemispheres, and especially inhalamo-cortical circuitry. However, each seizure type whichharacterizes IGEs (typical absences, myoclonic jerks andeneralized tonic—clonic seizures, alone or in varying com-inations and severity) involves a distinct hyperexcitableircuitry that in most instances does not comprise the wholerain (Capovilla et al., 2009). As a result of maturation, cir-uits involved may even differ with age. The concept of‘systems,’’ referring to structures and pathways involvedy the ictal event, has been therefore recently introducedWolf, 2006; Avanzini, 2009), based on the assumption thathe neuronal circuits involved in absence seizures, toniceizures, tonic—clonic seizures, and myoclonic seizures areot the same (Capovilla et al., 2009). A paradigmatic exam-le of ‘‘system epilepsy’’ is juvenile myoclonic epilepsyJME), in which an impairment of GABAa-mediated inhibi-
to study pathophysiological mechanisms underlying epilepsyin general, and IGE in particular.
TMS of the motor cortex in epilepsy can assess corti-cal excitability by determining different parameters. Motorthreshold (MT) represents the most easily recorded param-eter. It is defined as the minimum stimulus strengthwhich produces a small motor evoked potential (usually50—100 �V) in the target muscle (conventionally of thehand), in at least 50% of trials (Rossini et al., 1994).MT can be determined at rest (rMT) or during slight iso-metric muscle activation and reflects neuronal membraneexcitability rather than cortical excitability alone (Chen,2000). MT reflects the excitability and the local densityof a central core of excitatory interneurons and corti-cospinal neurons in the muscle representation at the primarymotor cortex level, as well as the excitability of the tar-get spinal motoneurons (Ziemann et al., 1996; Hallett,2000).
rMT represents therefore the physiological and method-ological basis for more complex TMS assessment of corticalexcitability such as the evaluation of intra-cortical inhibition(ICI) or facilitation (ICF) patterns obtained by paired-pulseparadigm (Kujirai et al., 1993). Therefore, in addition tostudies on ICI, ICF and cortical silent period, the determina-tion of rMT in patients with IGEs is essential for an overallassessment of motor excitability in this subgroup of epilepsy.
Please cite this article in press as: Brigo, F., et al., Restingsystematic review with meta-analysis. Epilepsy Res. (2012), ht
ion may lead to motor hyperexcitability (Manganotti et al.,000), without evidence of abnormal processing of cuta-eous afferents (Manganotti et al., 2004).
Trancranial magnetic stimulation (TMS) has been used tooninvasively and directly assess the cortical physiology andxcitability in vivo, thus representing a fascinating method
Fseedw
urthermore, the rMT represents an important safety con-train for therapeutic brain stimulation in epilepsy (Cantello
motor threshold in idiopathic generalized epilepsies: Atp://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
t al., 2007) and in other neurological disorders (Edwardst al., 2008). In the literature there are however importantiscrepancies among different studies reporting rMT in IGEs,ith some studies reporting increased, and others decreased

IN+Model
D
Tas‘bie(
ssrtratieo
D
Wtus
psrcIorap
baob
S
Fcti
acufias
ARTICLEEPIRES-4745; No. of Pages 11
Resting motor threshold in idiopathic generalized epilepsies
interictal values. These discrepancies make it very difficultto draw a definitive conclusion on cortico-spinal excitabil-ity in IGEs by simple summation of previous results. Wetherefore decided to carry out a systematic review and ameta-analysis of studies evaluating rMT values obtained dur-ing single-pulse TMS in drug-naive patients older than 12years affected by IGE.
Some reviews previously assessed the topic of motorcortex hyperexcitability in epilepsy (Ziemann et al., 1998;Macdonell et al., 2002; Tassinari et al., 2003; Chen et al.,2008), but always in a narrative and subjective way, withoutusing systematic and explicit methods to identify, select andcritically appraise studies, to extract data, and to analysethem with statistical methods. To our knowledge the presentreview represents therefore the first attempt to system-atically appraise the available literature on cortico-spinalexcitability in IGEs.
Methods
This review was guided by a written pre-specified proto-col describing research questions, review methods, plan fordata extraction and synthesis.
Objective
Our aim was to critically and systematically evaluate the lit-erature to evaluate rMT obtained during single-pulse TMS indrug-naive patients older than 12 years with IGE, comparedto healthy controls.
Study selection
Inclusion criteria were established a priori. Each controlledstudies reporting data on rMT obtained by single-pulse TMSin drug-naive patients (≥12 years) of either gender with IGE(defined according to International League Against Epilepsycriteria (ILAE, 1989)) and in healthy controls, regardless ofstimulator characteristics (such as coils’ shape, size andmaximum magnetic field strength), were included. rMT wasdefined as the lowest intensity (expressed as a percentage ofmaximal stimulator output) able to produce an electromyo-graphic response in a resting superficial muscle of the handof at least 50 �V peak-to-peak amplitude in at least 50% oftrials (Rossini et al., 1994). Studies indicating patients asaffected by IGE without further specifications on the diag-nostic criteria used were assumed to have adopted the ILAEcriteria (Fig. 1).
Uncontrolled studies, studies conducted in subjectsyounger than 12 years, and studies performing TMS withpaired magnetic stimuli or consecutive TMS were excluded.Also TMS studies using definitions of rMT different fromthat reported above were excluded. To include data in themeta-analysis, the studies must provide mean and standarddeviation (SD) values, or enough data to calculate them; if
Please cite this article in press as: Brigo, F., et al., Restingsystematic review with meta-analysis. Epilepsy Res. (2012), ht
not, principal investigators of provisionally included trialswere contacted and additional information requested. Weexcluded studies from which we did not manage to havedata on rMT mean and SDs.
i
se
PRESS3
ata sources and search strategy
he MEDLINE (accessed by Pubmed; 1966—August 2011)nd EMBASE (1980—August 2011) electronic databases wereearched using the medical subject headings (MeSH):‘Epilepsy, Generalized’’, and following free terms, com-ined in multiple search strategies with Boolean operatorsn order to find relevant articles: ‘‘idiopathic generalizedpilepsy’’, ‘‘generalized epilepsy’’, ‘‘motor threshold’’see appendix).
Two independent reviewers working in pairs (FB and MS)creened the titles and abstracts of the initially identifiedtudies to determine if they satisfied the selection crite-ia. Any disagreement was resolved through consensus. Fullext articles were retrieved for the selected titles, andeference lists of the retrieved articles were searched fordditional publications. We also contacted the authors ofhe retrieved papers for any additional or unpublished stud-es, handsearched conference proceedings and contactedxperts in the field for information about any unpublishedr ongoing study. No language restrictions were applied.
ata extraction
e designed a data collection form before the implemen-ation of the search strategy. Two independent reviewerssed this form to extract the relevant information from theelected studies (FB and MS).
The following data were extracted: number and sex ofarticipants, age, seizure free interval, subtypes of epilepticyndrome/seizures, stimulator characteristics, site of EMGecording. Mean and SD values of rMT were extracted oralculated for inclusion in the meta-analysis (see appendix).n case of missing or incomplete data, principal investigatorsf included trials were contacted and additional informationequested. If requested information was not provided, meannd SD values were obtained from graphs or tables in theapers (if available).
Data were independently extracted and cross-checkedy two review authors (FB, MS), who also independentlyssessed the methodological quality of each study and riskf bias, focusing on blinding and other potential sources ofias.
tatistical analysis
or each included study the differences in demographicharacteristics (age, sex) among patients and healthy con-rols were evaluated using chi-square (categorical data) andndependent t tests (continuous data).
We planned to summarize the results in a meta-nalysis. rMT values (continuous data) were analyzed byalculating the mean difference for each trial, with thencertainty in each study being expressed using 95% con-dence intervals (CI). A weighted effect across studies waslso calculated. In studies performing TMS over both hemi-pheres, only data from left (or dominant) hemisphere were
motor threshold in idiopathic generalized epilepsies: Atp://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
ncluded.In case of sufficient data, we planned to undertake
ubgroup analyses by assessing the effect of the type ofpileptic syndrome, age, time to the diagnosis, number
ARTICLE IN PRESS+ModelEPIRES-4745; No. of Pages 11
4 F. Brigo et al.
Records iden�fied throughdatabase se arching
(n = 24 1 )
Screen
ing
Includ
edEligibility
Iden
�fica�
on Addi�onal records iden�fiedthrough other sources
(n = 2 )
Records a� er dup licates remov ed(n = 77 )
Records screened(n = 77 )
Records excluded(n = 38 )
Full-text ar�cles assesse dfor eligibil ity(n = 39)
Full-text ar�cles exclud ed,with reasons(n = 16 )
Stud ies includ ed inqualita�ve synthesis
(n =23 )
Stud ies includ ed in quan�ta�ve synth esi s(meta-analysis)
(n = 14 )(5 studies inc luded in subg roup anal ysis on JME
pa�ents; 4 studies in clud ed in subgroup anal ysis onpa�ents with IGE s other than JME)
study
agsi
atttwiami(mrmiw
wo
ssgput
iiitwpwcgtet
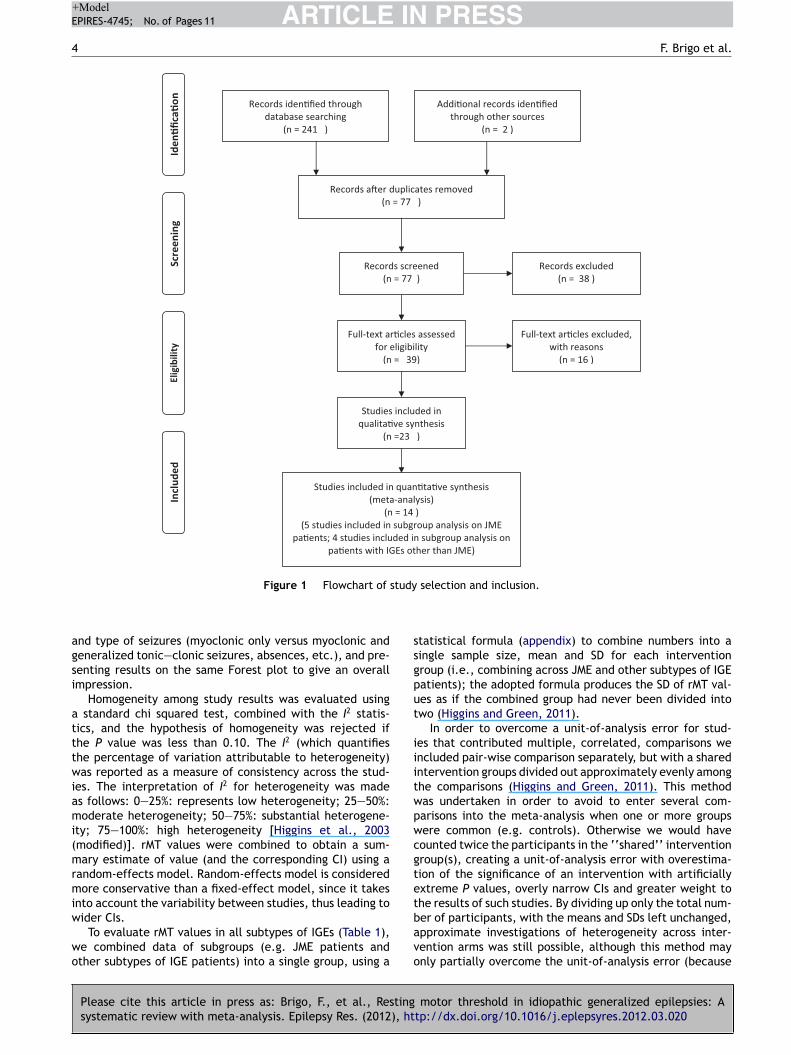
Figure 1 Flowchart of
nd type of seizures (myoclonic only versus myoclonic andeneralized tonic—clonic seizures, absences, etc.), and pre-enting results on the same Forest plot to give an overallmpression.
Homogeneity among study results was evaluated using standard chi squared test, combined with the I2 statis-ics, and the hypothesis of homogeneity was rejected ifhe P value was less than 0.10. The I2 (which quantifieshe percentage of variation attributable to heterogeneity)as reported as a measure of consistency across the stud-
es. The interpretation of I2 for heterogeneity was mades follows: 0—25%: represents low heterogeneity; 25—50%:oderate heterogeneity; 50—75%: substantial heterogene-
ty; 75—100%: high heterogeneity [Higgins et al., 2003modified)]. rMT values were combined to obtain a sum-ary estimate of value (and the corresponding CI) using a
andom-effects model. Random-effects model is consideredore conservative than a fixed-effect model, since it takes
nto account the variability between studies, thus leading to
Please cite this article in press as: Brigo, F., et al., Restingsystematic review with meta-analysis. Epilepsy Res. (2012), ht
ider CIs.To evaluate rMT values in all subtypes of IGEs (Table 1),
e combined data of subgroups (e.g. JME patients andther subtypes of IGE patients) into a single group, using a
bavo
selection and inclusion.
tatistical formula (appendix) to combine numbers into aingle sample size, mean and SD for each interventionroup (i.e., combining across JME and other subtypes of IGEatients); the adopted formula produces the SD of rMT val-es as if the combined group had never been divided intowo (Higgins and Green, 2011).
In order to overcome a unit-of-analysis error for stud-es that contributed multiple, correlated, comparisons wencluded pair-wise comparison separately, but with a sharedntervention groups divided out approximately evenly amonghe comparisons (Higgins and Green, 2011). This methodas undertaken in order to avoid to enter several com-arisons into the meta-analysis when one or more groupsere common (e.g. controls). Otherwise we would haveounted twice the participants in the ‘‘shared’’ interventionroup(s), creating a unit-of-analysis error with overestima-ion of the significance of an intervention with artificiallyxtreme P values, overly narrow CIs and greater weight tohe results of such studies. By dividing up only the total num-
motor threshold in idiopathic generalized epilepsies: Atp://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
er of participants, with the means and SDs left unchanged,pproximate investigations of heterogeneity across inter-ention arms was still possible, although this method maynly partially overcome the unit-of-analysis error (because

Please cite
this article
in press
as: Brigo,
F., et
al., Resting
motor
threshold in
idiopathic generalized
epilepsies: A
systematic
review w
ith m
eta-analysis. Epilepsy
Res. (2012),
http://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
AR
TIC
LE
IN P
RE
SS
+Model
EPIRES-4745;
No.
of Pages
11
Resting m
otor threshold
in idiopathic
generalized epilepsies
5
Table 1 Included studies (only data from subjects included in the meta-analysis comparisons are reported).
Study Diagnosis (no.of subjects,female/male)
Age(mean ± SD)
Subtypes ofepilepsy/seizures
Seizure freeinterval
Equipment,stimulator,Co/MF/CD
Migraine/menstrualphase
Site of EMG recording
Reutens andBerkovic(1992)
Ep (11,nr)C (71,nr)
Ep 26 ± 7C 28 ± 8NS
7 Absences,5 myoclonicseizures, 10GTCS
Not reported Magstim 200C/2.0/90
nr Abductor digitiminimi of thedominant hand
Reutenset al. (1993)
Ep (20,13/7)C (89,62/27)NS
Ep 20 ± nrC28 ± nr
6 JME, 8CAE-JAE, 6not clearlydefined/17GTCS alone,10myoclonicseizures, 12absence
Not reported Magstim 200C/2.0/90
nr Abductor digitiminimi of thedominant hand
Michelucciet al. (1997)
Ep (19, nr)C (50, nr)
Ep nrC nr
Notexplicitlyreported
Not reported Cadwellnr/nr/nr
nr Contralateral tenarmuscles (bilateralTMS)
Brodtmannet al. (1999)
Ep (7,2/5)C (16,9/7)NS
Ep 25 ± nrC 29 ± nr
3 JME, 1JAE, 3 GTCSalone
All patients hadexperienced aseizure within 2weeks of TMS.
Magstim 200C/-/140
nr Abductor pollicisbrevis of thedominant hand
Manganottiet al. (2000)
Ep (3,2/1)C (12,7/5)NS
Ep24.3 ± 0.6C (24-39)
3 JME Not reported Magstim 200E/-/70
nr Right thenareminence muscles
Macdonellet al. (2001)
Ep (21,nr)C (19,nr)
Ep 17.4 ± nrC 25.7 ± nr
9 JME, 1JAE, 11unspecified(CGTS only)
All patients hadexperienced aseizure within 2weeks of TMS.
Magstim 200C/-/140
nr Abductor digitiminimi of thedominant hand
Groppaet al. (2008)
Ep (17,12/5)C (13,10/3)NS
Ep14.9 ± 2.6C 36.8 ± 7S, P < 0.01
3 GTCSalone, 14JAE
At least 6months ofseizurefreedom beforeTMS
Magstim 200E/-/-
nr Right abductorpollicis brevis
Badawyet al. (2006)
Ep (15,8/7)C (13,6/7)NS
Ep 32.3 ± nrC 39.2 ± nr
5 JME, 10unspecified
All patients hadexperienced aseizurebetween 2 and4 weeks beforeTMS
Magstim 200C/-/140
nr Right abductorpollicis brevis

Please cite
this article
in press
as: Brigo,
F., et
al., Resting
motor
threshold in
idiopathic generalized
epilepsies: A
systematic
review w
ith m
eta-analysis. Epilepsy
Res. (2012),
http://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
AR
TIC
LE
IN P
RE
SS
+Model
EPIRES-4745;
No.
of Pages
11
6
F. Brigo
et al.
Table 1 (Continued)
Study Diagnosis (no.of subjects,female/male)
Age(mean ± SD)
Subtypes ofepilepsy/seizures
Seizure freeinterval
Equipment,stimulator,Co/MF/CD
Migraine/menstrualphase
Site of EMG recording
Cantelloet al. (2006)
Ep (8, 3/5)C (18,8/10)NS
Ep19.4 ± 7.5C 25.3 ± 8.7NS
2 JME, 4absenceepilepsy, 2GTCS onawakening
At least 3weeks ofseizurefreedom beforeTMS
Magstim 200C/-/90
nr Contralateral firstdorsal interosseus(bilateral TMS)
Badawyet al. (2007)
Ep (35,18/17)C (29,12/17)NS
Ep 25 ± nrC33 ± nr
11 JME, 2JAE, 22unspecified
All patients hadexperienced aseizurebetween 2 and4, weeksbefore TMS
Magstim 200C/-/140
nr Contralateralabductor pollicisbrevis (bilateral TMS)
Badawyet al.(2009a,b)
Ep (20, 12/8)C (10,6/4)NS
Ep 31 ± nrC 29 ± nr
10 JME, 1JAE, 9,GTCS alone
At least 2weeks ofseizurefreedom beforeTMS
Magstim 200C/-/140
nr Abductor pollicisbrevis of thedominant hand
Klimpeet al. (2009)
Ep (15,10/5)C (20,12/8)NS
Ep30 ± 16.34C27.45 ± 8.32NS
9 JME, 6GTCS alone
At least 24 h ofseizurefreedom beforeTMS
Magstim 200E/2.2/90
nr First dorsalinterosseus of thedominant hand
Badawyet al.(2010a)
Ep (19,10/9)C (32,20/12)NS
Ep16.5 ± 6.5C 31 ± nr
19 JME At least 2weeks oftonic—clonicseizurefreedom beforeTMS
Magstim 200C/-/140
nr Abductor pollicisbrevis of thedominant hand
Badawyet al.(2010b)
Ep (55,nr)C (32,20/12)
Ep 28 ± 23C 31 ± nr
Notexplicitlyreported
Not reported Magstim 200C/-/140
TMS performedduring the samephase of themenstrual cycle
Abductor pollicisbrevis of thedominant hand
-: not reported; C: controls; CD: outer coil diameter (mm); Ci: circular; CNS: central nervous system; Co: Shape of coil; E: figure-of-eight; EMG: electromyography; Ep: epileptic patients;GTCS: generalized tonic—clonic seizures; JAE: juvenile absence epilepsy; JME: juvenile myoclonic epilepsy; MF: peak magnetic flux (Tesla); NS: difference not statistically significant; S:difference statistically significant; SD: standard deviation; TMS: transcranial magnetic stimulation.

IN+Model
irbl
weocl
Q
r
Tpisaf
r(
Fcsswad
r
FctsweC
P
Fn
D
ImaAf
ARTICLEEPIRES-4745; No. of Pages 11
Resting motor threshold in idiopathic generalized epilepsies
the resulting comparisons remain correlated) (Higgins andGreen, 2011).
Statistical analyses were undertaken with the ReviewManager software developed by the Cochrane Collaboration(5.1).
Results
Description of studies (Table 1)
The search strategy described above yielded 243 results (25MEDLINE, 216 EMBASE, 2 conference abstracts found throughhandsearching). Of the 243 references, 166 duplicates(identified using reference manager and manual checks)were excluded. After the initial screening of the title andabstract, a further 38 citations were excluded, leaving 39articles for retrieval. Full text assessment of these arti-cles resulted in 23 eligible studies that were provisionallyincluded in our review. Of these 23 studies provisionally con-sidered for inclusion, 9 were later excluded: one (Delvauxet al., 2001) performed TMS in untreated patients havingexperienced only a first ‘‘grand mal’’ seizure, thus lackingthe minimum criteria for a diagnosis of epilepsy (definedaccording to ILAE, 1997); one study (Kazis et al., 2006)adopted a rMT definition different from that adopted inthe present review; one study was conducted on epilep-tic patients under antiepileptic treatment (Aguglia et al.,2000); one study performed consecutive TMS (Badawy et al.,2009a); from five studies it was impossible to obtain meanand SD values of rMT even after contacting principal inves-tigators (Michelucci et al., 1990; Tataroglu et al., 2004; Jooet al., 2008; Hwang et al., 2010; Badawy et al., 2011).
One study using TMS early in the morning and late in theafternoon to investigate the effect of diurnal variability oncortical excitability was included, since in pooled analysisdata regarding such a variable would be balanced (Badawyet al., 2009b). The same was made with another study eval-uating cortical excitability after sleep deprivation (Badawyet al., 2006). These studies performing multiple comparisons(morning/late afternoon; sleep deprivation/no sleep depri-vation) with one or more groups in common were assessed asdescribed above (statistical analysis and appendix) to avoidunit-of-analysis errors.
Patients of one study (Reutens et al., 1993) were classi-fied as affected by JME (6 patients) or other IGEs (8 patientswith absence seizures only) on the basis of clinical data pro-vided in the research paper; the other 6 patients were notincluded in meta-analysis B and C (rMT in JME patients/ rMTin IGEs other than JME) because it was not clear whetheralso these subjects may have a definite diagnosis of JME.
Thus 14 trials, including 265 epileptic patients and 424control subjects, contributed to this review: the earliest waspublished in 1992 and the most recent in 2010.
Risk of bias
Several studies had at least one author in common (Reutens,
Please cite this article in press as: Brigo, F., et al., Restingsystematic review with meta-analysis. Epilepsy Res. (2012), ht
Badawy) and were published within a few years apart, sothat the probability of overlapping cases and/or controlscould not be ruled out, also because, when contacted,Authors did not clarify such an aspect. Thus, it was
stsc
PRESS7
mpossible to determine whether some included papers rep-esent duplicate publications (risk of multiple publicationias). The inclusion of duplicated data may therefore haveead to overestimation of results from these studies.
Only in one study the neurophysiologist performing TMSas blinded to the different groups of participants (Groppat al., 2008). However, unlike occipital TMS with evaluationf phosphene threshold, measuring rMT is an objective pro-edure, so that its results are not likely to be influenced byack of blinding.
uantitative synthesis
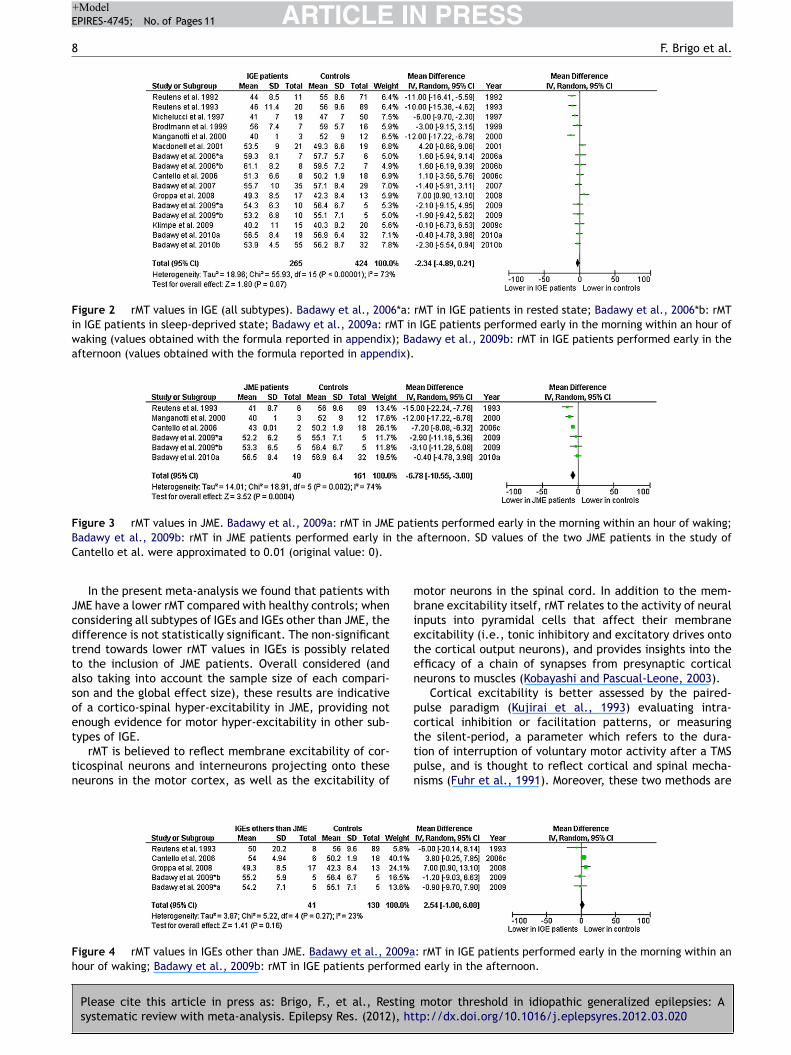
MT values in all types of IGEs (Fig. 2)
here were 14 studies with 689 participants (265 epilepsyatients, 424 controls). Statistically significant heterogene-ty among trials was detected. There was no statisticallyignificant difference in rMT between IGE and control group,lthough a trend towards lower values in IGE patients wasound (mean difference: −2.34; 95% CI −4.89 to 0.21).
MT values in juvenile myoclonic epilepsy (JME)Fig. 3)
ive studies with 201 participants (40 epilepsy patients, 161ontrols) reported rMT values of JME patients to allowing aubgroup analysis relative of this subset of IGEs. Statisticallyignificant heterogeneity among trials was detected. Thereas a statistically significant difference in rMT between JMEnd control group, with lower values in JME patients (meanifference: −6.78; 95% CI −10.55 to −3.00).
MT values in IGEs other than JME (Fig. 4)
our studies with 171 participants (41 epilepsy patients, 130ontrols) reported rMT values of patients with IGEs otherhan JME to allowing a subgroup analysis. No statisticallyignificant heterogeneity among trials was detected. Thereas no statistically significant difference in rMT betweenpilepsy patients and controls (mean difference: 2.54; 95%I −1.00 to 6.08).
ublication bias
unnel plot qualitative analysis showed no evidence of sig-ificant publication bias (Egger et al., 1997).
iscussion
n this systematic review we used systematic and explicitethods to identify, select and critically appraise studies,
nd to extract data, analysing them with a meta-analysis. meta-analysis is the statistical combination of resultsrom two or more separate studies, allowing an increase in
motor threshold in idiopathic generalized epilepsies: Atp://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
tatistical power, and an improvement in precision, some-imes permitting to answer questions not posed by individualtudies and to settle controversies arising from conflictinglaims.
ARTICLE IN PRESS+ModelEPIRES-4745; No. of Pages 11
8 F. Brigo et al.
Figure 2 rMT values in IGE (all subtypes). Badawy et al., 2006*a: rMT in IGE patients in rested state; Badawy et al., 2006*b: rMTin IGE patients in sleep-deprived state; Badawy et al., 2009a: rMT in IGE patients performed early in the morning within an hour ofwaking (values obtained with the formula reported in appendix); Badawy et al., 2009b: rMT in IGE patients performed early in theafternoon (values obtained with the formula reported in appendix).
Figure 3 rMT values in JME. Badawy et al., 2009a: rMT in JME patients performed early in the morning within an hour of waking;B the
C
Jcdttasoet
tn
mbieten
pct
Fh
adawy et al., 2009b: rMT in JME patients performed early inantello et al. were approximated to 0.01 (original value: 0).
In the present meta-analysis we found that patients withME have a lower rMT compared with healthy controls; whenonsidering all subtypes of IGEs and IGEs other than JME, theifference is not statistically significant. The non-significantrend towards lower rMT values in IGEs is possibly relatedo the inclusion of JME patients. Overall considered (andlso taking into account the sample size of each compari-on and the global effect size), these results are indicativef a cortico-spinal hyper-excitability in JME, providing notnough evidence for motor hyper-excitability in other sub-ypes of IGE.
Please cite this article in press as: Brigo, F., et al., Restingsystematic review with meta-analysis. Epilepsy Res. (2012), ht
rMT is believed to reflect membrane excitability of cor-icospinal neurons and interneurons projecting onto theseeurons in the motor cortex, as well as the excitability of
tpn
igure 4 rMT values in IGEs other than JME. Badawy et al., 2009aour of waking; Badawy et al., 2009b: rMT in IGE patients performe
afternoon. SD values of the two JME patients in the study of
otor neurons in the spinal cord. In addition to the mem-rane excitability itself, rMT relates to the activity of neuralnputs into pyramidal cells that affect their membranexcitability (i.e., tonic inhibitory and excitatory drives ontohe cortical output neurons), and provides insights into thefficacy of a chain of synapses from presynaptic corticaleurons to muscles (Kobayashi and Pascual-Leone, 2003).
Cortical excitability is better assessed by the paired-ulse paradigm (Kujirai et al., 1993) evaluating intra-ortical inhibition or facilitation patterns, or measuringhe silent-period, a parameter which refers to the dura-
motor threshold in idiopathic generalized epilepsies: Atp://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
ion of interruption of voluntary motor activity after a TMSulse, and is thought to reflect cortical and spinal mecha-isms (Fuhr et al., 1991). Moreover, these two methods are
: rMT in IGE patients performed early in the morning within and early in the afternoon.

IN+Model
epfbs(
saasscc
eea2do2tesieaippte
eaopeio(l
S
Pe2stMcrse
ARTICLEEPIRES-4745; No. of Pages 11
Resting motor threshold in idiopathic generalized epilepsies
performed with different procedures, so that a direct com-parison of pooled results from studies using these techniqueswould be extremely difficult because of an excessive amountof methodological heterogeneity. A methodological hetero-geneity is intrinsic to paired-pulse TMS procedure since theamount of intra-cortical inhibitory and facilitatory eventscan vary depending on the size of test MEPs, so that it iscritical to maintain the patients relaxed and adjust the sizeof test MEPs across trials and subjects.
In IGE, myoclonic jerks are thought to depend on theinvolvement of thalamocortical structures, that recruit mus-cles via fast-conducting corticospinal pathways (Tassinariet al., 1998). In JME, generalized myoclonus is the main clin-ical feature, whereas in other IGE subtypes myoclonic jerksare an accessory finding. Interestingly, our meta-analysissuggests that the excitability of corticospinal pathways isgreater when considering JME alone than when consider-ing all subtypes of IGE. Lower rMT values in patients withJME compared with healthy controls are therefore indica-tive of an imbalance of excitatory and inhibitory influencesin the primary motor cortex, eventually resulting in hyper-excitability. This result is consistent with other findingsobtained by different neurophysiological methods of assess-ing motor excitability (ICI, ICF, and cortical silent period),that, overall, suggest that a GABAa-mediated inhibitionmay lead to motor hyperexcitability (Manganotti et al.,2000), without abnormal processing of cutaneous afferents(Manganotti et al., 2004). Such a rather selective involve-ment of distinct hyperexcitable circuitry might thereforejustify the concept of ‘‘system epilepsy’’ with regards toJME.
Although the results of meta-analytic comparison C (rMTvalues in IGEs other than JME) were not statistically signifi-cant and based on only 41 patients, the trend towards higherrMT values in IGE might represent an interictal protectivemechanism against the spread or recurrence of seizures, andis consistent with the findings of previous reports (Delvauxet al., 2001; Badawy et al., 2009a).
Exploration of heterogeneity
In the meta-analysis a considerable statistical heterogeneitybetween comparisons A (rMT values in all types of IGEs) and B(rMT values in JME), indicative of inconsistency in the resultsof included studies, was found. The term ‘‘statistical het-erogeneity’’ describes the degree of variation in the effectestimates from a set of studies, and indicates the presenceof variability among studies beyond the amount expecteddue chance alone.
The heterogeneity found in the meta-analysis is relatedto the presence of some outlying studies with results con-flicting with the rest of the studies. However, the limitednumber of included studies prevents us from performing asensitivity analysis to better investigate heterogeneity.
Such a statistical heterogeneity may be howeverexplained both by differences in clinical characteristics ofstudy participants (clinical heterogeneity) and by different
Please cite this article in press as: Brigo, F., et al., Restingsystematic review with meta-analysis. Epilepsy Res. (2012), ht
stimulation procedures (methodological heterogeneity).The main aspect to be considered is the homogene-
ity of included patients. IGEs should not be consideredas a homogeneous entity, but rather as a spectrum of
svtn
PRESS9
pileptic syndromes, each of them with potentially differentathophysiological mechanisms. TMS studies should there-ore adopt strict inclusion criteria (e.g. grouping patientsy epileptic syndrome, etiology, severity, treatment, andeizure-free interval) in order to increase data consistencyTassinari et al., 2003).
Due to lack of data it was not possible to evaluate thetatistical differences in demographic features (age, sex) forll included studies. A statistically significant difference inge of epilepsy patients and controls was found in only onetudy (Groppa et al., 2008). However, because of the limitedtatistical power of this study (5.9%) it is unlikely that thislinical heterogeneity has affected the overall result of theomparison between rMT in IGEs and healthy controls.
Other clinical factors which might influence corticalxcitability are the ovarian cycle (Smith et al., 1999; Smitht al., 2002; Hattemer et al., 2006; Badawy et al., 2010c)nd the presence of migraine (Aurora et al., 1998, 1999,003). All included studies but one (Badawy et al., 2010b)id not explicitly assess these two variables, whose effectn cortical excitability is still matter of debate (Young et al.,001; Boros et al., 2009). Another relevant aspect to beaken into account, especially when evaluating JME, is theffect of sleep deprivation on rMT, as some studies haveuggested an increase in overall higher cortical excitabil-ty after sleep deprivation in this IGE subtype (Manganottit al., 2006; Del Felice et al., 2011). The inconsistencymong meta-analysis results might be explained also by anntrinsic high variability of results in MT values among IGEatients. Such a high variability might be due to higher tem-oral variability among MT measurements over time, relatedo unstable excitability levels in these patients (Delvauxt al., 2001; Badawy et al., 2009a).
Regarding methodological heterogeneity, potentially rel-vant aspects to be considered are the coils’ shape, sizend maximum magnetic field strength, and the directionf the current through the stimulating coil (mono- or bi-hasic); these stimulator characteristics are sometimes notxplicitly reported in the studies, although they may deeplynfluence the results. For example, compared with a figure-f-eight coil, a circular coil stimulates a larger cortical areaCohen et al., 1990; Hallett, 2000), and may generate, ateast theoretically, a stronger electric current.
trengths and limitations of the review
revious narrative reviews have evaluated the motor hyper-xcitability in IGE (Ziemann et al., 1998; Macdonell et al.,002; Tassinari et al., 2003; Chen et al., 2008), but ourystematic review is the first attempt to pool togetherhe different existing studies that evaluated rMT in IGE.oreover, results of this review contributed to settle theontroversies arising from discrepant data among studieseporting rMT in JME patients, providing further data toupport the presence of a cortical hyperexcitability in thispileptic syndrome.
Due to lack of enough data, the only subgroup analy-
motor threshold in idiopathic generalized epilepsies: Atp://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
es which we managed to undertake were on JME patientsersus IGEs other than JME. Despite our intentions, we couldherefore not assess the effect of age, time to the diagnosis,umber and type of seizures presenting results on the same
IN+ModelE
1
Flsscart
ivo
Cfreewp
C
N
D
Wic
A
WkttwF
A
Sfj
R
A
A
A
A
A
B
B
B
B
B
B
B
B
B
B
C
C
C
C
C
C
ARTICLEPIRES-4745; No. of Pages 11
0
orest plot to give an overall impression. Considering theimited data available, which prevented us from performingubgroup analyses on each subgroup of IGE, and the con-iderable statistical heterogeneity found in meta-analyticomparisons, any definite conclusions should be cautious,nd further studies should be done to confirm or refute theesults of our analyses, especially with regards to IGEs otherhan JME.
In conclusion, the results of this systematic review arendicative of a cortico-spinal hyper-excitability in JME, pro-iding not enough evidence for motor hyper-excitability inther subtypes of IGE.
rMT showed considerable variability between studies.linical and methodological heterogeneity may accountor these discrepancies. A high temporal variability amongMT measurements over time, related to unstable corticalxcitability levels in these patients, should also be consid-red. Further studies adopting a unique, shared protocolith stricter inclusion criteria to study more homogeneousopulations are required to confirm our results.
onflict of interest statement
one of the authors has any conflict of interest to disclose.
isclosure
e confirm that we have read the Journal’s position on issuesnvolved in ethical publication and affirm that this report isonsistent with those guidelines.
cknowledgements
e are in debt with Dr. S. Groppa and Prof. R. Cantello, whoindly provided us additional information, thus allowing uso include also their studies in the meta-analysis. We alsohank Dr. G. Rubboli, Dr. A. Brodtmann and Dr. R. Badawyho kindly gave us information on their studies. We thankrancesco Passarella for graphical support.
ppendix A. Supplementary data
upplementary data associated with this article can beound, in the online version, at http://dx.doi.org/10.1016/.eplepsyres.2012.03.020.
eferences
guglia, U., Gambardella, A., Quartarone, A., Girlanda, P., Le Piane,E., Messina, D., Oliveri, R.L., Zappia, M., Quattrone, A., 2000.Interhemispheric threshold differences in idiopathic generalizedepilepsies with versive or circling seizures determined with focalmagnetic transcranial stimulation. Epilepsy Res. 40, 1—6.
urora, S.K., Ahmad, B.K., Welch, K.M., Bhardhwaj, P., Ramadan,N.M., 1998. Transcranial magnetic stimulation confirms hyper-excitability of occipital cortex in migraine. Neurology 50,
Please cite this article in press as: Brigo, F., et al., Restingsystematic review with meta-analysis. Epilepsy Res. (2012), ht
1111—1114.urora, S.K., Cao, Y., Bowyer, S.M., Welch, K.M., 1999. The occipi-
tal cortex is hyperexcitable in migraine: experimental evidence.Headache 39, 469—476.
D
PRESSF. Brigo et al.
urora, S.K., Welch, K.M., Al-Sayed, F., 2003. The threshold forphosphenes is lower in migraine. Cephalalgia 23, 258—263.
vanzini, G., 2009. System epilepsy: reply to Lüders et al. Epilepsia50, 2326.
adawy, R.A.B., Curatolo, J.M., Newton, M., Berkovic, S.F.,Macdonell, R.A.L., 2006. Sleep deprivation increases corticalexcitability in epilepsy: syndrome-specific effects. Neurology67, 1018—1022.
adawy, R.A.B., Curatolo, J.M., Newton, M., Berkovic, S.F.,Macdonell, R.A.L., 2007. Changes in cortical excitability dif-ferentiate generalized and focal epilepsy. Ann. Neurol. 61,324—331.
adawy, R., MacDonell, R., Jackson, G., Berkovic, S., 2009a. Theperi-ictal state: cortical excitability changes within 24 h of aseizure. Brain 132, 1013—1021.
adawy, R.A.B., Macdonell, R.A.L., Jackson, G.D., Berkovic, S.F.,2009b. Why do seizures in generalized epilepsy often occur inthe morning? Neurology 73, 218—222.
adawy, R.A., Macdonell, R.A., Jackson, G.D., Berkovic, S.F., 2010a.Can changes in cortical excitability distinguish progressive fromjuvenile myoclonic epilepsy? Epilepsia 51, 2084—2088.
adawy, R.A.B., Macdonell, R.A.L., Berkovic, S.F., Newton, M.R.,Jackson, G.D., 2010b. Predicting seizure control: corticalexcitability and antiepileptic medication. Ann. Neurol. 67,64—73.
adawy, R.A., MacDonell, R.A., Berkovic, S.F., Jackson, G.D., 2010c.Cortical excitability and the menstrual cycle: reversal of normalpatterns in new onset epilepsy. Clin. Neurophysiol. 121 (Suppl.1), S197.
adawy, R., Macdonell, R., Berkovic, S., Jackson, G., 2011.Epilepsy: an ever changing state of cortical hyper-excitability.Clin. Neurophysiol. 122 (Suppl. 1), S61.
oros, K., Poreisz, C., Paulus, W., Antal, A., 2009. Does the men-strual cycle influence the motor and phosphene thresholds inmigraine? Eur. J. Neurol. 16, 367—374.
rodtmann, A., Macdonell, R.A.L., Gilligan, A.K., Curatolo,J., Berkovic, S.F., 1999. Cortical excitability and recov-ery curve analysis in generalized epilepsy. Neurology 53,1347—1349.
antello, R., Civardi, C., Varrasi, C., Vicentini, R., Cecchin, M.,Boccagni, C., Monaco, F., 2006. Excitability of the human epilep-tic cortex after chronic valproate: a reappraisal. Brain Res. 1099,160—166.
antello, R., Rossi, S., Varrasi, C., Ulivelli, M., Civardi, C., Bartalini,S., Vatti, G., Cincotta, M., Borgheresi, A., Zaccara, G., Quar-tarone, A., Crupi, D., Laganà, A., Inghilleri, M., Giallonardo,A.T., Berardelli, A., Pacifici, L., Ferreri, F., Tombini, M., Gilio,F., Quarato, P., Conte, A., Manganotti, P., Bongiovanni, L.G.,Monaco, F., Ferrante, D., Rossini, P.M., 2007. Slow repetitiveTMS for drug-resistant epilepsy: clinical and EEG findings of aplacebo-controlled trial. Epilepsia 48, 366—374.
apovilla, G., Berg, A.T., Cross, J.H., Moshe, S.L., Vigevano, F.,Wolf, P., Avanzini, G., 2009. Conceptual dichotomies in classify-ing epilepsies: partial versus generalized and idiopathic versussymptomatic April 18—20, 2008, Monreale, Italy. Epilepsia (May).
hen, R., 2000. Studies of human motor physiology with transcranialmagnetic stimulation. Muscle Nerve Suppl. 9, S26—S32.
hen, R., Cros, D., Curra, A., Di Lazzaro, V., Lefaucheur, J.P.,Magistris, M.R., Mills, K., Rösler, K.M., Triggs, W.J., Ugawa, Y.,Ziemann, U., 2008. The clinical diagnostic utility of transcra-nial magnetic stimulation: report of an IFCN committee. Clin.Neurophysiol. 119, 504—532.
ohen, L.G., Roth, B.J., Nilsson, J., Dang, N., Panizza, M.,Bandinelli, S., Friauf, W., Hallett, M., 1990. Effects of coil design
motor threshold in idiopathic generalized epilepsies: Atp://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
on delivery of focal magnetic stimulation. Technical considera-tions. Electroencephalogr. Clin. Neurophysiol. 75, 350—357.
el Felice, A., Fiaschi, A., Bongiovanni, G.L., Savazzi, S., Mangan-otti, P., 2011. The sleep-deprived brain in normals and patients

IN+Model
M
M
M
M
M
R
R
R
S
S
T
T
T
W
Y
Z
ARTICLEEPIRES-4745; No. of Pages 11
Resting motor threshold in idiopathic generalized epilepsies
with juvenile myoclonic epilepsy: a perturbational approach tomeasuring cortical reactivity. Epilepsy Res. 96, 123—131.
Delvaux, V., Alagona, G., Gérard, P., De Pasqua, V., Delwaide,P.J., Maertens de Noordhout, A., 2001. Reduced excitabilityof the motor cortex in untreated patients with de novo idio-pathic ‘‘grand mal’’ seizures. J. Neurol. Neurosurg. Psychiatry71, 772—776.
Edwards, M.J., Talelli, P., Rothwell, J.C., 2008. Clinical applicationsof transcranial magnetic stimulation in patients with movementdisorders. Lancet Neurol. 7, 827—840.
Egger, M., Davey Smith, G., Schneider, M., Minder, C., 1997. Biasin meta-analysis detected by a simple, graphical test. BMJ 315,629—634.
Fuhr, P., Agostino, R., Hallett, M., 1991. Spinal motor neuronexcitability during the silent period after cortical stimulation.Electroencephalogr. Clin. Neurophysiol. 81, 257—262.
Groppa, S., Siebner, H.R., Kurth, C., Stephani, U., Siniatchkin, M.,2008. Abnormal response of motor cortex to photic stimulationin idiopathic generalized epilepsy. Epilepsia 49, 2022—2029.
Hallett, M., 2000. Transcranial magnetic stimulation and the humanbrain. Nature 406, 147—150.
Hattemer, K., Knake, S., Reis, J., Oertel, W.H., Rosenow, F., Hamer,H.M., 2006. Cyclical excitability of the motor cortex in patientswith catamenial epilepsy: a transcranial magnetic stimulationstudy. Seizure 15, 653—657.
Higgins, J.P.T., Thompson, S.G., Deeks, J.J., Altman, D.G., 2003.Measuring inconsistency in meta-analyses. BMJ 327, 557—560.
Higgins, J.P.T., Green, S. (Eds.), 2011. Cochrane Handbook forSystematic Reviews of Interventions Version 5.1.0 [updatedMarch 2011]. The Cochrane Collaboration. , Available fromwww.cochrane-handbook.org.
Hwang, W.S., Lee, J.Y., Kim, H.-J., Kim, S.-W., Hong, S.B., Joo,E.Y., 2010. Prolonged cortical silent period (CSP) in patients withgeneralized or partial epilepsy. Epilepsia 51 (Suppl. 4), 158.
International League Against Epilepsy (ILAE), 1989. Proposal forrevised classification of epilepsies and epileptic syndromes.Commission on Classification and Terminology of the Interna-tional League Against Epilepsy. Epilepsia 30, 389—399.
International League Against Epilepsy (ILAE). Commission Report,1997. The epidemiology of the epilepsies: future directions.International League Against Epilepsy. Epilepsia 38, 614—618.
Joo, E.Y., Kim, S.H., Seo, D.W., Hong, S.B., 2008. Zonisamidedecreases cortical excitability in patients with idiopathic gen-eralized epilepsy. Clin. Neurophysiol. 119, 1385—1392.
Kazis, D.A., Kimiskidis, V.K., Papagiannopoulos, S., Sotirakoglou, K.,Divanoglou, D., Vlaikidis, N., Mills, K.R., Kazis, A., 2006. Theeffect of valproate on silent period and corticomotor excitabil-ity. Epileptic Disord. 8, 136—142.
Klimpe, S., Behrang-Nia, M., Bott, M.C., Werhahn, K.J., 2009.Recruitment of motor cortex inhibition differentiates betweengeneralized and focal epilepsy. Epilepsy Res. 84, 210—216.
Kobayashi, M., Pascual-Leone, A., 2003. Transcranial magnetic stim-ulation in neurology. Lancet Neurol. 2, 145—156.
Kujirai, T., Caramia, M.D., Rothwell, J.C., Day, B.L., Thompson,P.D., Ferbert, A., Wroe, S., Asselman, P., Marsden, C.D., 1993.Corticocortical inhibition in human motor cortex. J. Physiol. 471,501—519.
Macdonell, R.A.L., King, M.A., Newton, M.R., Curatolo, J.M.,Reutens, D.C., Berkovic, S.F., 2001. Prolonged cortical silentperiod after transcranial magnetic stimulation in generalized
Please cite this article in press as: Brigo, F., et al., Restingsystematic review with meta-analysis. Epilepsy Res. (2012), ht
epilepsy. Neurology 57, 706—708.Macdonell, R.A., Curatolo, J.M., Berkovic, S.F., 2002. Transcranial
magnetic stimulation and epilepsy. J. Clin. Neurophysiol. 19,294—306.
Z
PRESS11
anganotti, P., Bongiovanni, L.G., Zanette, G., Fiaschi, A., 2000.Early and late intracortical inhibition in juvenile myoclonicepilepsy. Epilepsia 41, 1129—1138.
anganotti, P., Tamburin, S., Bongiovanni, L.G., Zanette, G.,Fiaschi, A., 2004. Motor responses to afferent stimulation injuvenile myoclonic epilepsy. Epilepsia 45, 77—80.
anganotti, P., Bongiovanni, L.G., Fuggetta, G., Zanette, G.,Fiaschi, A., 2006. Effects of sleep deprivation on corticalexcitability in patients affected by juvenile myoclonic epilepsy:a combined transcranial magnetic stimulation and EEG study. J.Neurol. Neurosurg. Psychiatry 77, 56—60.
ichelucci, R., Rubboli, G., Forti, A., Plasmati, R., Salvi, F., Parmeg-giani, L., Passarelli, D., Plazzi, G., Riguzzi, P., Buzzi, A.M.,Tassinari, C.A., 1990. Increased threshold intensity to tran-scranial magnetic stimulation in drug-treated with epilepsypatients. Bollettino — Lega Italiana contro l’Epilessia 70—71,191—192.
ichelucci, R., Passarelli, D., Pastorelli, F., Zaniboni, A., Tassinari,C.A., 1997. Decrease of threshold intensity to transcranial mag-netic stimulation in idiopathic generalized epilepsy. Bollettino— Lega Italiana contro l’Epilessia 99, 263—264.
eutens, D.C., Berkovic, S.F., 1992. Increased cortical excitabilityin generalised epilepsy demonstrated with transcranial magneticstimulation. Lancet 339, 362—363.
eutens, D.C., Berkovic, S.F., Macdonell, R.A., Bladin, P.F., 1993.Magnetic stimulation of the brain in generalized epilepsy: rever-sal of cortical hyperexcitability by anticonvulsants. Ann. Neurol.34, 351—355.
ossini, P.M., Barker, A.T., Berardelli, A., Caramia, M.D., Caruso,G., Cracco, R.Q., Dimitrijevic, M.R., Hallett, M., Katayama,Y., Lücking, C.H., Maertens de Noordhout, A.L., Marsden, C.D.,Murray, N.M.F., Rothwell, J.C., Swash, M., Tomberg, C., 1994.Non-invasive electrical and magnetic stimulation of the brain,spinal cord and roots: basic principles and procedures for routineclinical application. Report of an IFCN committee. Electroen-cephalogr. Clin. Neurophysiol. 91, 79—92.
mith, M.J., Adams, L.F., Schmidt, P.J., Rubinow, D.R., Wasser-mann, E.M., 2002. Effects of ovarian hormones on human corticalexcitability. Ann. Neurol. 51, 599—603.
mith, M.J., Keel, J.C., Greenberg, B.D., Adams, L.F., Schmidt, P.J.,Rubinow, D.A., Wassermann, E.M., 1999. Menstrual cycle effectson cortical excitability. Neurology 53, 2069—2072.
assinari, C.A., Rubboli, G., Shibasaki, H., 1998. Neurophysiologyof positive and negative myoclonus. Electroencephalogr. Clin.Neurophysiol. 107, 181—195.
assinari, C.A., Cincotta, M., Zaccara, G., Michelucci, R., 2003.Transcranial magnetic stimulation and epilepsy. Clin. Neurophys-iol. 114, 777—798.
ataroglu, C., Ozkiziltan, S., Baklan, B., 2004. Motor corticalthresholds and cortical silent periods in epilepsy. Seizure 13,474—478.
olf, P., 2006. Basic principles of the ILAE syndrome classification.Epilepsy Res. 70 (Suppl. 1), S20—S26.
oung, W.B., Oshinsky, M.L., Shechter, A.L., Wassermann, E.M.,2001. Consecutive transcranial magnetic stimulation inducedphosphene thresholds in migraineurs and controls. Neurology 56,A142.
iemann, U., Lönnecker, S., Steinhoff, B.J., Paulus, W., 1996.Effects of antiepileptic drugs on motor cortex excitability inhumans: a transcranial magnetic stimulation study. Ann. Neurol.
motor threshold in idiopathic generalized epilepsies: Atp://dx.doi.org/10.1016/j.eplepsyres.2012.03.020
40, 367—378.iemann, U., Steinhoff, B.J., Tergau, F., Paulus, W., 1998. Transcra-
nial magnetic stimulation: its current role in epilepsy research.Epilepsy Res. 30, 11—30.




















