
Research proposal final 15
102
Study to investigate factors influencing adoption of mobile devices in the health care environment Abstract In recent years, the potential use of mobile devices has significantly improved the healthcare sector. Despite claims of widespread use of mobile devices in healthcare, its adoption is low. Areas of interest for most researchers have focussed on the planning, implementation, technology and organisational perspectives and individual perspectives. However, adoption of mobile devices form individual perspective concentrating on individual characteristics such as age, gender experience and individual readiness has received less attention. This research aims to assess the extent to which the adopted variables, self-efficacy and relative advantages impact individual readiness to adopt mobile devices in healthcare. This research also aims to elaborate how age, gender and experience operate as mediating factors. The overall aim of the research is to develop a health specific conceptual framework for adoption of mobile devices. For this proposal, an initial conceptual framework is developed from a review of previous literature to understand various factors influencing adoption of mobile devices in healthcare settings. The mixed method approach will be used to arrive at findings of this study. A qualitative approach (focus group technique) will be used to find the determinants that are influencing healthcare professionals and patients for adoption of mobile devices in the healthcare domain. Analysis of qualitative data will be used to refine the initial conceptual framework drawn from the literature. A quantitative approach (web survey) will be used to test the refined conceptual framework. This research hypothesizes that individual readiness, complexity and social influences are mediated by age, gender and experience for individual intention to adopt 1
-
Upload
himlayanstudies -
Category
Documents
-
view
3 -
download
0
Transcript of Research proposal final 15
Study to investigate factors influencing adoption of mobile devices in the health care environment
Abstract
In recent years, the potential use of mobile devices hassignificantly improved the healthcare sector. Despiteclaims of widespread use of mobile devices in healthcare,its adoption is low. Areas of interest for most researchershave focussed on the planning, implementation, technologyand organisational perspectives and individualperspectives. However, adoption of mobile devices formindividual perspective concentrating on individualcharacteristics such as age, gender experience andindividual readiness has received less attention. Thisresearch aims to assess the extent to which the adoptedvariables, self-efficacy and relative advantages impactindividual readiness to adopt mobile devices in healthcare.This research also aims to elaborate how age, gender andexperience operate as mediating factors. The overall aim ofthe research is to develop a health specific conceptualframework for adoption of mobile devices.
For this proposal, an initial conceptual framework isdeveloped from a review of previous literature tounderstand various factors influencing adoption of mobiledevices in healthcare settings. The mixed method approachwill be used to arrive at findings of this study. Aqualitative approach (focus group technique) will be usedto find the determinants that are influencing healthcareprofessionals and patients for adoption of mobile devicesin the healthcare domain. Analysis of qualitative data willbe used to refine the initial conceptual framework drawnfrom the literature. A quantitative approach (web survey)will be used to test the refined conceptual framework.
This research hypothesizes that individual readiness,complexity and social influences are mediated by age,gender and experience for individual intention to adopt
1
mobile devices in healthcare. Furthermore, functionalfeatures of mobile devices and compatibility withhealthcare processes will be mediated by age and gender.
This research will contribute to the body of knowledge onadoption of mobile devices in the healthcare context.Further contribution of this research is in improvement ofhealthcare practices and policies.
1.0 BackgroundModern methods of healthcare are associated with mobility,
flexibility, convenience, real time communication and
connectivity; and mobile devices offer all these features
to modernise healthcare (Ben-Zeev et al. 2013; Morón,
Luque & Casilari 2014; Nah, Siau & Sheng 2005; Sarker,
Urbaczewski & Wells 2002). In recent times iPad and iPhone
are popular mobile devices to access high quality health
care services (Castro, D. 2014). The ability to monitor
patients’ health remotely is making mobile devices’ popular
2
in health (Kang et al. 2010). Moreover, mobile devices have
made health services economical and convenient (The pulse of
telehealth 2014; Deng, Mo & Liu 2013; Hebert, Korabek & Scott
2006; Wu, Wang & Lin 2007). Further, Mobile devices in
collaboration with other technologies (like skype, FaceTime
and internet technology) are now used to provide real time
monitoring (Slaper & Conkol 2014; Zangbar et al. 2014).
Interpretation of images from remote locations have become
easy for physicians due to high resolution mobile devices
such as iPad (Ramey, Fung & Hassell 2011). Hence, mobile
devices have transformed the healthcare delivery process.
Use of mobile devices in healthcare has enhanced the scope
of health care services and in the near future will make
health services more flexible (Wu, Li & Fu 2011) however,
for adopting mobile devices, both healthcare professionals
(HCPs) and patients feel insecure (Fox 2011; Rogers 2003b;
Slaper & Conkol 2014; Wu, Li & Fu 2011; Wu, Wang & Lin
2007). It attracted researcher’s attention to investigate
the factors which influence HCPs’ and patients’ intention
to adopt mobile devices in healthcare.
1.1 Research aim
3
The overall aim of the research is to understand adoption
factors influencing the intention of healthcare
professionals and patients for adoption of mobile devices
in healthcare and build a health specific conceptual
framework for the adoption of mobile devices. The sub aims
of this research are: understanding how self-efficacy and
relative advantages influence individual readiness for
adoption of mobile devices in the healthcare context and
investigate the influence of age, gender and experience as
mediating factors on determinants for adoption of mobile
devices in the healthcare domain.
1.2 Justification of the research
It is evident that adoption of mobile devices in the
healthcare context is low. By understanding adoption of
mobile devices at the individual level may increase the
rate of adoption of mobile devices in healthcare because
the successful use of technology depends upon the
satisfaction and acceptance by the users (Bano & Zowghi
2015; Cellucci, Spil & Wiggins 2014; Zmud 1979). Also,
personal characteristics such as age, gender and experience
are pertinent to adoption of technology in the healthcare
4
because they can ensure the long term profitability and
reduction in organisational cost (Boulos et al. 2011; Lim
et al. 2011; Xue et al. 2012). Moreover, this research
will also provide avenues for future research in the domain
of healthcare for adoption of mobile devices. Also, this
research will contribute to the theoretical knowledge and
practices for the adoption of mobile devices in healthcare.
Therefore, this research is focussed on understanding the
adoption pattern of mobile devices in healthcare and on
developing a rigorous (credible, reliable, valid)
conceptual framework.
1.3 Scope of the research
The scope of the research is limited to Queensland,
Australia with the main activities happening in Brisbane
and Toowoomba however, the findings of the research will be
beneficial for countries also. The healthcare system is
well developed in Australia as people are already using
health services by means of mobile devices. It is
difficult to study the factors in developing countries
where the use of mobile devices for health purposes is not
on a large scale. Further, this research will understand
5
HCPs’ and patient’s intention of for adoption of mobile
devices but intention may differ from actual final
behaviour performance.
2.0 Literature review
In this research the meaning of individual level of
adoption of mobile devices in the healthcare refers to
adoption of mobile devices by HCPs and patients and not by
organisation. Literature indicates that individual level of
adoption of mobile devices is influenced by planning,
implementation, technology and organisational perspectives
(Brown III et al. 2013; Kay 2011; West 2012; Wu, Li & Fu
2011; Wu, Wang & Lin 2007; Yangil & Chen 2007). For
example, Brown III et al. (2013) discusses that individual
adoption of mobile device in the healthcare depend upon
technology aspect. Small size of mobile devices, low
resolution screens, slow operating system, and variable
connectivity may be problematic to use these devices in the
healthcare environment. Further, in a global survey
conducted by world health organisation (WHO) among 114
nations in 2011 resulted that priority, budgetary
restrictions, staff shortage privacy and data security
6
influencing adoption of mobile devices in healthcare which
indicates towards organisational and implementation
perspectives (West 2012). Moreover, Wu, Li and Fu (2011)
explore factors influencing individual intention for
adoption of mobile devices from organizations, ,
technology, system services, and individual psychological
states perspectives. In conclusion, adoption of mobile
devices by individual in the healthcare system is
influenced by many factors.
Theory of planned behaviour (TPB) and diffusion of
innovation theory (DOI) appear to be appropriate for this
research. Various researchers have used TPB to predict
individual behaviour for adoption of technology (Casper
2007; Cheng & Chu 2014; Perkins et al. 2007; Wu, Li & Fu
2011). Casper (2007) has used TPB in the field of health
care to compare mental health professionals intention to
use technology as the assessment tool. Additionally,
Perkins et al. (2007) used TPB to predict clinicians’
behaviour towards clinical practices in mental health
services. Hence, TPB appears acceptable in the domain of
7
healthcare for adoption of mobile devices. All the
variables of TPB are represented in figure 1 below.
Figure 1: TPB Adapted from(Ajzen 1988)
TPB is able to explain fundamental predictors for adoption
of technology from individual perspective however TPB is
unsuccessful to explain adoption of technology from
technology and organisational perspective (Ghodeswar &
Vaidyanathan 2007; Looney, Akbulut & Poston 2008; Moseley
2000) which are important for adoption of mobile devices in
healthcare (Wu, Li & Fu 2011). Diffusion of innovation
(DOI) theory has the potential to cover these aspects.
Figure 2: DOI Adapted from (Rogers 2003a)
8
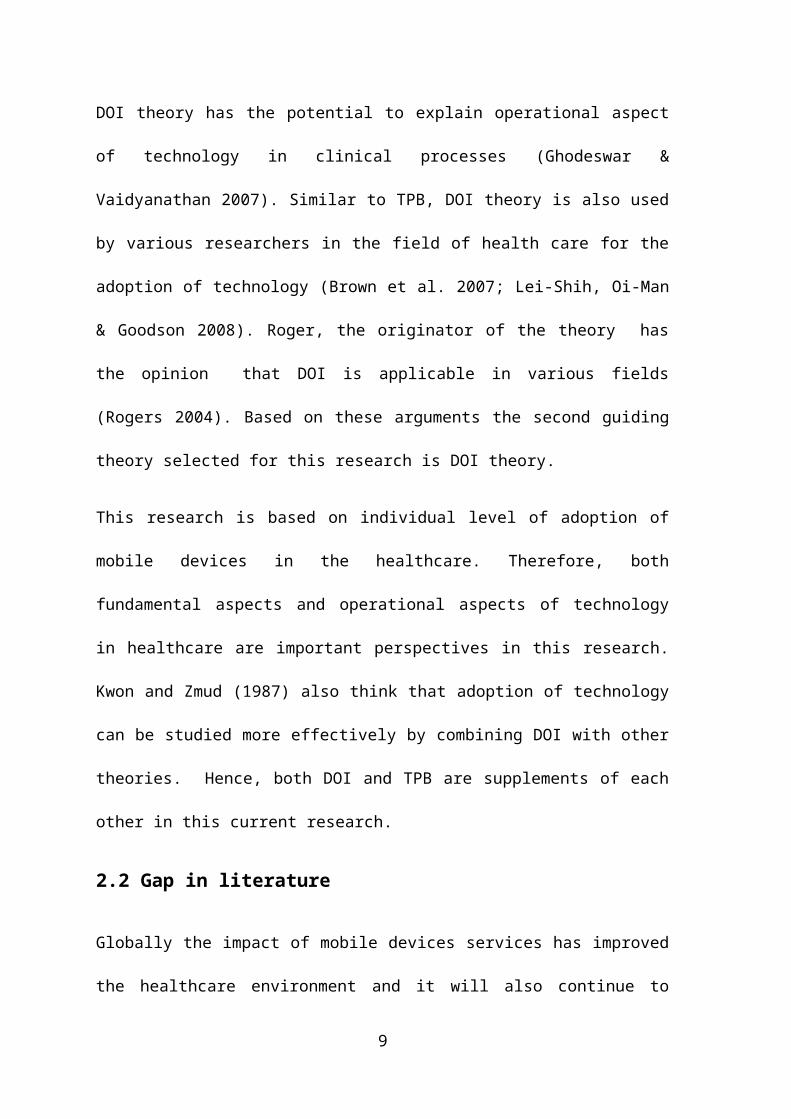
DOI theory has the potential to explain operational aspect
of technology in clinical processes (Ghodeswar &
Vaidyanathan 2007). Similar to TPB, DOI theory is also used
by various researchers in the field of health care for the
adoption of technology (Brown et al. 2007; Lei-Shih, Oi-Man
& Goodson 2008). Roger, the originator of the theory has
the opinion that DOI is applicable in various fields
(Rogers 2004). Based on these arguments the second guiding
theory selected for this research is DOI theory.
This research is based on individual level of adoption of
mobile devices in the healthcare. Therefore, both
fundamental aspects and operational aspects of technology
in healthcare are important perspectives in this research.
Kwon and Zmud (1987) also think that adoption of technology
can be studied more effectively by combining DOI with other
theories. Hence, both DOI and TPB are supplements of each
other in this current research.
2.2 Gap in literature
Globally the impact of mobile devices services has improved
the healthcare environment and it will also continue to
9
take centre stage in the future also (Lim et al. 2011;
Newswire 2014; Slaper & Conkol 2014; Wu, Li & Fu 2011), but
adoption of mobile devices in healthcare is low
(Christensen & Remler 2009; Kay 2011; Wu, Li & Fu 2011).
Previous literature has explored factors influencing
individuals’ adoption of mobile devices from technical,
organisational, implementation and planning, and individual
perspectives (Boulos et al. 2011; Wu, Li & Fu 2011; Yu et
al. 2006). However, the influence of personal factors (age,
gender, experience and individual readiness) on intention
to adopt mobile devices in the healthcare has yet received
less attention. It is evident from literature that age,
gender and experience act as mediating variables for
adoption of technology (Leventhal 2008; Lim et al. 2011;
Venkatesh & Morris 2000; Xue et al. 2012). Wu, Li and Fu
(2011) also agree that personal factors such as gender
differences play a mediating role for adoption of mobile
devices in healthcare. In addition, individual readiness
for adoption is salient in this study because individual
readiness to adopt technology can ensure long term
profitability and reduction in organisational cost being
10
an advantage for an organisation (Caison et al. 2008;
Kuang-Ming, Chung-Feng & Chen-Chung 2013; Thong, Hong & Tam
2006). Previous studies are lacking in the area of the
influences of self-efficacy, relative advantage on
individual readiness for adoption of technology.
Furthermore, research on adoption of mobile devices in
Australian healthcare settings has received less attention
than it has in Asia and America; therefore, this research
is focussing on three main gaps in the literature: 1) how
age, gender and experience as mediating variables influence
the determinants which influence adoption of mobile devices
in healthcare 2) the influence of self-efficacy and
relative advantages on individual readiness 3) different
healthcare contexts (Australia) compared with previous
studies (America and Asia).
2.3 Research questions
This research on adoption of mobile devices at the
individual level in the healthcare domain is focussed on
the following research questions:
RQ1: What factors constitute a conceptual framework for
adoption of mobile devices in healthcare environment?
11
RQ2: How self-efficacy and relative advantages influence
individual readiness for adoption of mobile devices in
healthcare?
RQ3: What is the role of age, gender, and experience as
mediating factors on the determinants of adoption of mobile
devices in healthcare?
2.4 Conceptual framework
In this proposal the initial conceptual framework is
developed from previous literature following six steps.
All these steps and their detailed explanation for the
development of the conceptual framework are attached in
Appendix 4.
Operationalization of constructs and formulation of
hypothesis: Construct operationalization is a practical
step to achieve clear and practical meaning of the
constructs chosen in the hypothetical framework. It
includes an agreed definition of the constructs from
literature, clear meaning of the constructs which is also
suitable for the research and identifying key concepts
properties describing constructs (Ayers & Olander 2013;
Bhattacherjee et al. 2007). These all are helpful to
12
understand constructs and apply them in the existing
research context. Each construct considered for the current
study is operationalized and hypothesised below.
Intention: (Ajzen 1988, p. 42) expresses intention as ‘the
measure of the likelihood to perform the behavior’. In this research
intention is the individual perception towards adoption of
mobile devices in healthcare. User intention is a good
indicator of how a system will be accepted. Intention to
use technology may vary because of many factors (Tiong et
al. 2006). Therefore, intention to adopt mobile devices is
a dependent variable and is included in this research.
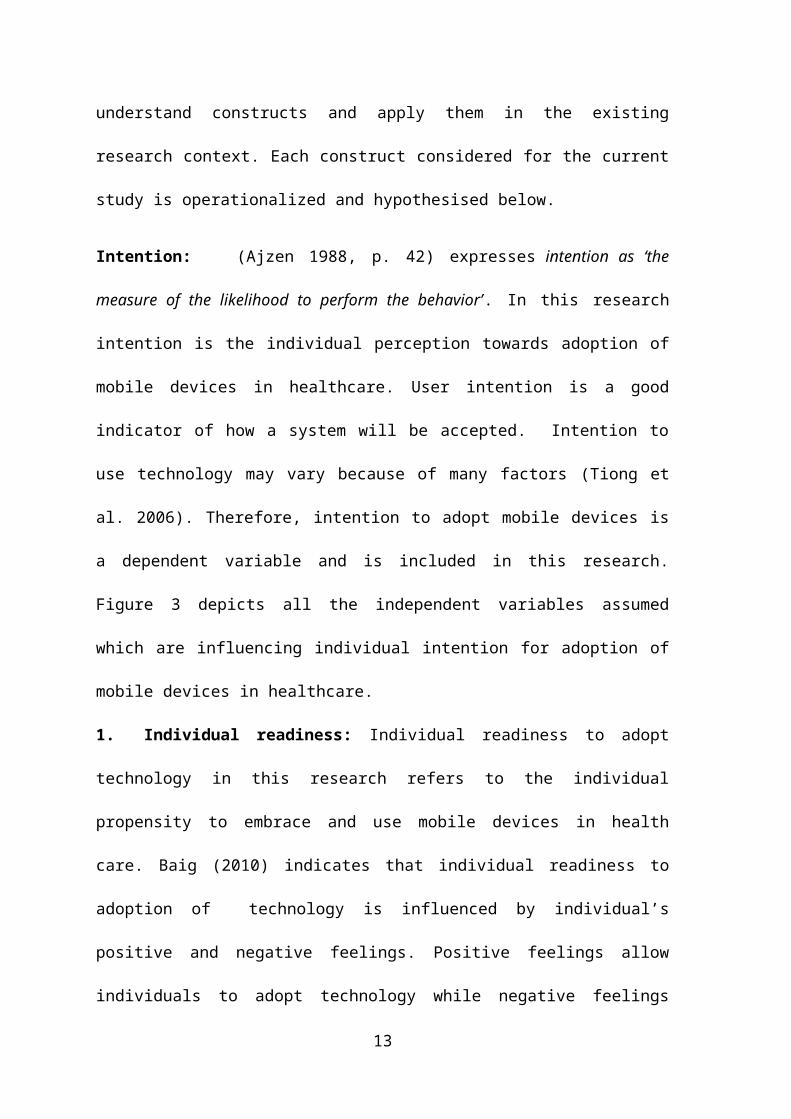
Figure 3 depicts all the independent variables assumed
which are influencing individual intention for adoption of
mobile devices in healthcare.
1. Individual readiness: Individual readiness to adopt
technology in this research refers to the individual
propensity to embrace and use mobile devices in health
care. Baig (2010) indicates that individual readiness to
adoption of technology is influenced by individual’s
positive and negative feelings. Positive feelings allow
individuals to adopt technology while negative feelings
13
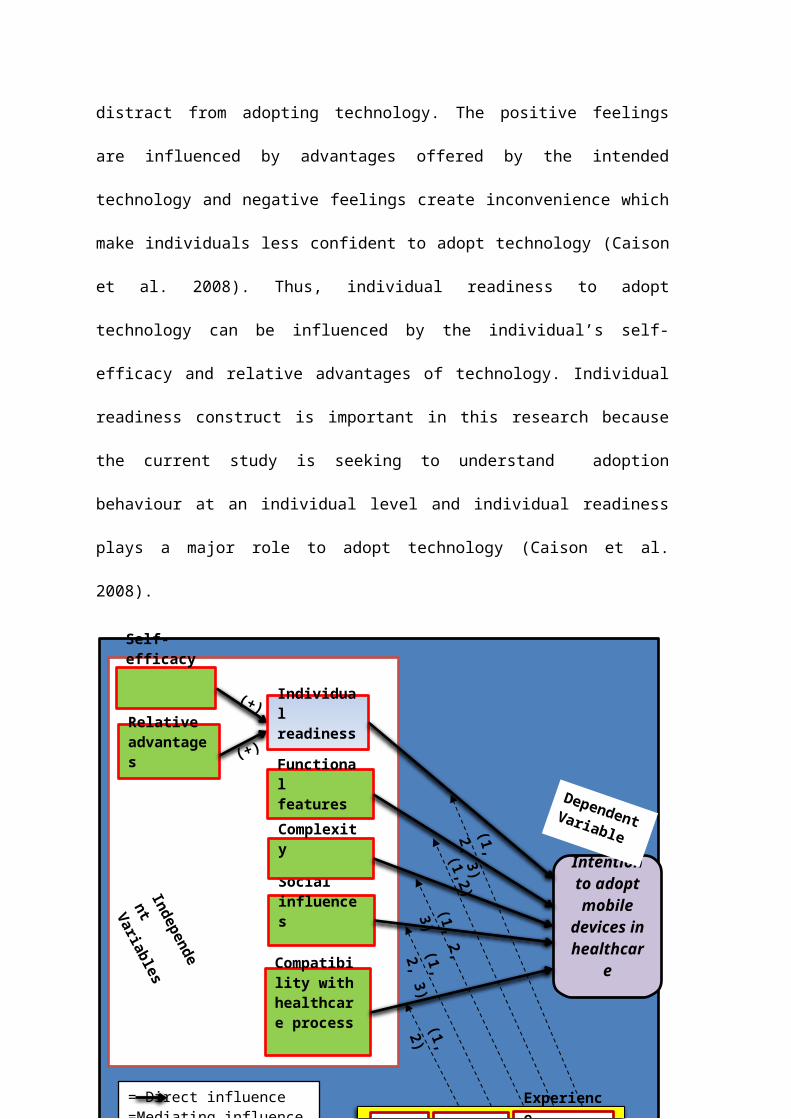
distract from adopting technology. The positive feelings
are influenced by advantages offered by the intended
technology and negative feelings create inconvenience which
make individuals less confident to adopt technology (Caison
et al. 2008). Thus, individual readiness to adopt
technology can be influenced by the individual’s self-
efficacy and relative advantages of technology. Individual
readiness construct is important in this research because
the current study is seeking to understand adoption
behaviour at an individual level and individual readiness
plays a major role to adopt technology (Caison et al.
2008).
14
Intention to adopt mobile
devices in healthcar
e
Dependent Variable
= Direct influence=Mediating influence=Age=Gender=Experience
Social influences
Self-efficacy
Complexity
Relative advantages
Age Gender
Experienceexperienc
e
Compatibility with healthcare process
Functional features
Independe
nt Variables
(1, 2)
(1,2)(1, 2, 3)
(1, 2,
3)(1, 2, 3)
Individual readiness
(+)
(+)
Several studies result relative advantages and self-
efficacy influencing individual intention for adoption of
technology in the healthcare context (Wu, Li & Fu 2011; Wu,
Wang & Lin 2007; Yangil & Chen 2007). However, research is
lacking in the area of influence of relative advantages and
self-efficacy on individual readiness for adoption of
mobile devices in healthcare. Thus, in the conceptual
framework, influence of relative advantages and self-
efficacy on individual readiness is considered for adoption
of mobile devices.
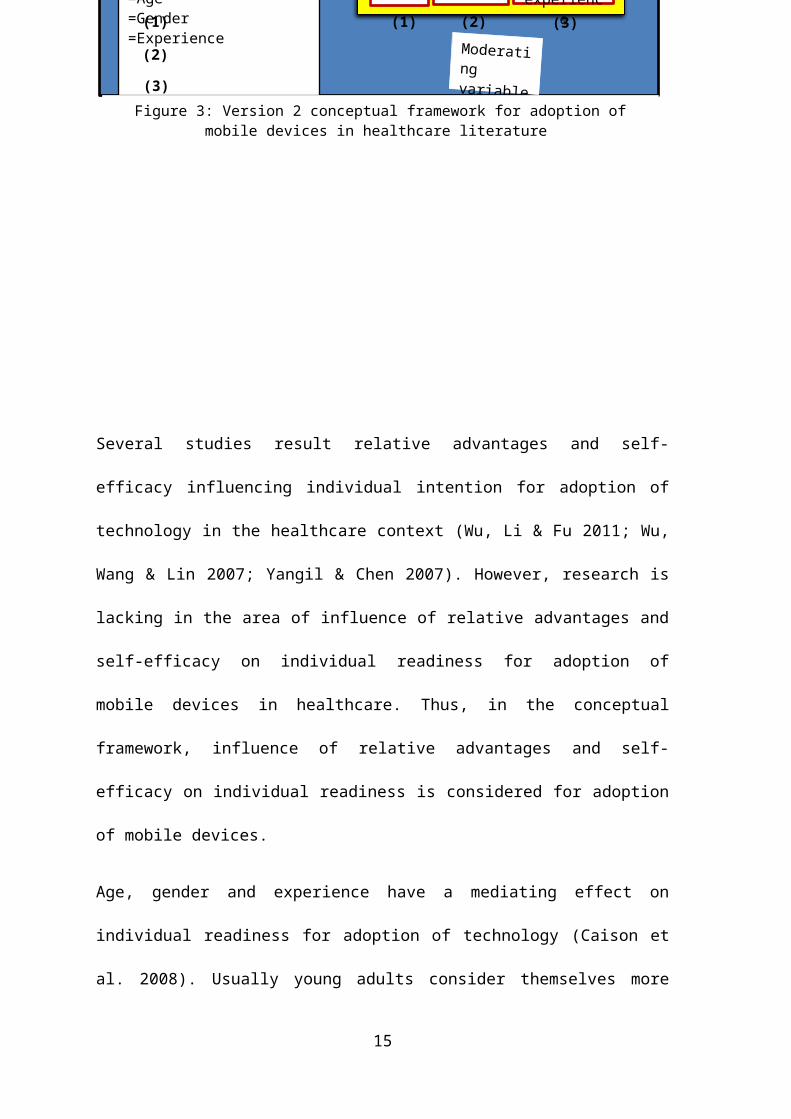
Age, gender and experience have a mediating effect on
individual readiness for adoption of technology (Caison et
al. 2008). Usually young adults consider themselves more
15
= Direct influence=Mediating influence=Age=Gender=Experience
Age Gender
Experienceexperienc
e(1)
(2)
(3)(1) (2)
(3)
Moderating variablesFigure 3: Version 2 conceptual framework for adoption of
mobile devices in healthcare literature
tech- savvy (Lim et al. 2011; Xue et al. 2012) and this
affect is more obvious in men as compared to women.
Durndell and Haag (2002) suggest that men have more
internet experience then women which can make them more
self-efficacious. Lim et al. (2011) studies in this area
explore how women have less confidence in their ability to
adopt technology as compared to men (Lim et al. 2011). Men
are more task oriented and they want to see the benefits
which technology can provide to do their office work is
more (as it can be useful for them to achieve their goal)
(Taylor & Todd 1995; Xue et al. 2012). Overall, young
experienced men are more self-efficacious as compared to
women so their individual readiness for the adoption of
mobile devices in healthcare will be greater than women.
Moreover, Caison et al. (2008) results shows that young
male medical students have more curiosity for adoption of
technology. Therefore, the mediating effect of age, gender
and experience on individual readiness can be studied and
hypothesized for this research.
H1: The influences of individual readiness on intention to
adopt mobile devices in healthcare will be moderated by
16
age, gender and experience, such that the effect will be
stronger for young, and particularly experienced males.
a. Self- efficacy: Self- efficacy in current research
is defined as the individual’s confidence in his own
capabilities and strength to use mobile devices in the
healthcare environment. Self-efficacy is the individual’s
confidence on his skills to perform the behaviour. In TPB
self-efficacy is termed as perceived behaviour control.
Self-efficacy is defined by Bandura as ‘people’s perception
about their capability to execute a task’ (Bandura 1986).
Thus, the meaning of self- efficacy remains the same
whether it is denoted by some researcher in terms of
perceived behaviour control. Many researchers have
demonstrated self- efficacy as an important construct for
adoption of technology especially in mobile computing and
wireless technology in healthcare (Lim et al. 2011; Wu,
Wang & Lin 2007; Yangil & Chen 2007). Hence, self-efficacy
is considered as an important construct in this research.
Previous studies have investigated the direct positive
influence of self-efficacy on individual intention for
adoption of technology (Ajzen 2005; Wu, Wang & Lin 2007;
17
Yangil & Chen 2007). This research will investigate the
positive impact of self-efficacy on individual readiness
for adoption of mobile devices in healthcare.
H1a: Individual readiness for adoption of mobile devices in
healthcare will be positively influenced by self-efficacy
of the individual to use these devices in healthcare.
b. Relative advantages: Relative advantages in this
research refer to benefits of mobile devices in the
healthcare processes. Rogers (2003b, p. 239)outlines
relative advantage as ‘the degree to which an innovation is perceived as
better than the idea it supersedes’. It can be measured using various
parameters such as cost, features and compatibility. This
means benefits offered by innovation positively impact the
individual to adopt technology (Wang et al. 2010; Wu, Li &
Fu 2011). In the technology acceptance model (TAM) the
term ‘perceived usefulness’ is used in place of relative
advantages (Davis 1985). Many researchers have studied the
direct influence of relative advantage on individual
intention for adoption of technology (Daim, Basoglu &
Topacan 2013; Gagnon et al. 2012; Kim 2009) This research
18
is investigating the influence of relative advantages on
individual readiness as is hypothesised below.
H1b: Individual readiness for adoption of mobile devices
in healthcare will be positively influenced by relative
advantages offered by mobile devices in the healthcare
process.
2. Functional features: In this research functional
features refer to the general features of mobile devices
which can influence individual intention for adoption of
mobile devices in healthcare. In the healthcare environment
the most important concern is a person’s health and adopted
technology should have good supporting features with
healthcare process (Wu, Li & Fu 2011). Ghodeswar and
Vaidyanathan (2007) think technology features are
responsible for performance of technology. Therefore,
whatever technology is used it should have good supporting
features within healthcare settings. Mobile devices
features such as size of the screen, image quality, battery
life and layout effect (Kargin & Basoglu 2006; Lu et al.
2005) may influence HCP and patient intention for adoption
of technology because individuals use health services on19
mobile device screen and both the sensory and functional
needs of the individual should be satisfied (Massey, Khatri
& Montoya-Weiss 2007). Therefore, it important to study the
impact of functional features of mobile devices and hence
is included in this research.
It is assumed that functional features of mobile devices
are mediated by age and gender. For older people negative
attribution dominantly affect mind and body which makes
them disinterested in technology use (Thimm, Rademacher &
Kruse 1998). For example, poor eyesight in old age affects
viewing ability (Leventhal 2008). Elderly people may prefer
mobile devices with bigger screen size, good image quality
and touch screen (Boulos et al. 2011). Further, new mobile
devices have many features which may be difficult for old
people to handle (Boulos et al. 2011). Besides age, gender
differences may also affect reaction to mobile device
features. Generally, women have more health complications
than men (Lim et al. 2011) which can increase their
difficulty to operate the mobile device functional
featuring. Thus, it can be inferred that the mediating
effect of age and gender on mobile devices functional
20
features will impact more on older women as compare to
older men.
H2: The influence of mobile device feature’s on intention
to adopt mobile devices in healthcare will be moderated by
age and gender such that the effect will be stronger for
older women.
3. Complexity: Complexity in this research refers to the
degree to which HCPs and patients experiences difficulty in
using mobile devices for health care services. Rogers
(2003b, p. 257) states complexity as ‘the degree to which an
innovation is perceived as relatively difficult to understand and use.’ In the
context of adoption of mobile devices in healthcare, if an
individual has to struggle with use of technology in health
process, then individual’s intention for adoption of mobile
devices will be weak. Many researchers proposed complexity
as one of the major factors for adoption of technology in
healthcare, with antonyms like simple/ easy to
use/perceived easiness, perceived ease of use (Daim,
Basoglu & Topacan 2013). Complexity can be an important
factor for adoption of mobile devices in healthcare
environments as if HCPs and patients find it difficult to21
operate these devices in healthcare process; their
intention for adoption will be low. Thus, complexity
negatively affects adoption of mobile devices and is
included in this research.
Age, gender and experience have a mediating effect on
complexity. In the healthcare domain various other
technologies are also used (Baig 2010) and users
experience, age and gender with the use of those
technologies can influence individual intention for
adoption of technology (Venkatesh et al. 2003). Lim et al.
(2011) recognises that gender has a moderating effect for
adoption of technology and this effect is more prevalent in
females (Taylor & Todd 1995).Venkatesh and Morris (2000)
describes that complexity to use technology is mediated by
gender differences and prior experience with technology.
Women who do not have prior experience with technology may
feel more uncomfortable in using technology (Lim et al.
2011). Therefore, it can be hypothesised that complexity of
operation of mobile devices in the healthcare process is
moderated by age, gender and experience and this influence
is more predominant in women.
22
H3: The influence of complexity on intention to adopt
mobile devices in healthcare will be moderated by age,
gender and experience such that the effect will be greater
for older inexperienced women.
4. Social influences: Social influences in this research
are defined as the influences of people on individuals for
adoption of mobile devices in healthcare services. Goswami
and Chandra (2013, p. 68) define social influences as the
‘influence of the people associated with the individual’. In the theory of
reasoned action (TRA), TAM2, TPB, C-TAM-TPB the term social
norm is used and has the same meaning as social influences.
according to Ajzen (1991, p. 188) subjective norm refers
to ‘the perceived social pressure to perform behaviour’.
Social influences are the influences of peers on the
individual (Morris, Venkatesh & Ackerman 2005). Social
influences have a great influence on individual adoption of
innovation (Rogers 2003b) and is considered one of the
essential constructs in the present research setting.
Social influences are moderately affected by age, gender
and experience. It is observed that women are easily
influenced by the people with whom they interact (Morris,23
Venkatesh & Ackerman 2005). Further, women prefer more
social interactions and are more socially active as
compared to men and as a result they are more involved in
the socialization process and more likely to listen and
follow the opinions of their friends and co-workers
(Hodgson & Watson 1987). It has been observed that elderly
people who have little experience in technology usage, rely
more on their friends (Lim et al. 2011; Morris & Venkatesh
2000; Venkatesh et al. 2003). Thus, it is concluded that
social influences are moderated by age, gender and
experiences and this leads to the following hypothesis.
H4: The influence of social influence on intention to adopt
mobile devices in healthcare will be moderated by age,
gender and experience such that the effect will be stronger
for women, particularly older women who have less
experience with technology.
5. Compatibility with healthcare processes: Compatibility
of clinical practices in this research refers to the
consistency of mobile devices with clinical processes.
defines compatibility as ‘the degree to which an innovation
is perceived as consistent with the existing values, past24
experiences, and needs of potential adopters’. Both HCPs
and patients show less interest for adoption of new
technology (Rogers 2003b; Wu, Li & Fu 2011). However, if
the technology is compatible with HCP’s work process,
they like to adopt it (Xue et al. 2012). Additionally, in
the health care environment new technology is adopted if it
supports the existing system and adds newness to the system
and mobile devices have that potential (Daniel Castro, Ben
miller & Nager 2014). Therefore, compatibility construct is
added in the conceptual framework.
Age and gender have a mediating effect on compatibility.
Generally elderly people are resistant to technology change
but if technology is suitable with their work process it
changes their mindset to adopt technology (Xue et al.
2012). Further, men’s ability to perform mental rotation
tasks is better compared to women. Rotation tasks are the
asks of reposition of 2D or 3D objects (Roberts & Bell
2000). For the use of health services in mobile devices,
individuals have to interact with various 2D and 3D
objects on the screen with which older females may feel
more difficulty than men because they are considered to be
25
less tech-savvy (Xue et al. 2012). Therefore, it is
considered that age and gender have a mediating effect on
compatibility with clinical process for adoption of mobile
devices.
H5: The influence of compatibility on intention to adopt
mobile devices in healthcare will be moderated by age and
gender such that the effect will be stronger for older
women.
2.0 Research methodology
This research is using a mixed method which provides
strength to research by overcoming the drawbacks of both
qualitative and quantitative approaches (Klassen et al.
2012; Onwuegbuzie & Johnson 2006); and heighten the
validity of research (Greene, Caracelli & Graham 1989).
Venkatesh, Brown and Bala (2013) suggest that selection of
mix method depends upon the research questions, purpose and
context. The aim of the research is to develop a conceptual
framework; and the nature of the research questions is
exploratory and confirmatory which gives support for a
mixed methodology in this research. Further, mixed method
is a vital method for research whose aims are either of26
these: developmental, completeness, complementarity,
expansion, confirmation, compensation and diversity; and
having research questions that are exploratory and
confirmatory (Onwuegbuzie & Collins 2007; Venkatesh, Brown
& Bala 2013). Moreover, Creswell et al. (2011) have a
notion that mixed method is suitable for problems which are
influenced by a number of levels such as individual,
organisation and policies. Based on above discussion, this
research will use a sequential mix method approach with the
qualitative method followed by quantitative method.
3.1 Research philosophy
Research philosophy is a belief about the nature of reality
(ontology), values (axiology) and how knowledge is obtained
by the researcher (epistemology) (Saunders, Lewis &
Thornhill 2012). Saunders, Lewis and Thornhill (2012, p.
127) define ‘Research philosophy is an over-arching term relating to the
development of knowledge and the nature of that knowledge’. This
statement shows that research philosophy can be selected
considering three aspects: epistemology, ontology and
axiology. Epistemology is concerned with the question: ‘how
we know? What we know? ‘, ontology refers to the ‘nature of
27
reality’ and axiology refers to belief about values of
research (what is good? what is right? what is important?).
Saunders, Lewis and Thornhill (2012) claim that selection
of research philosophy is based upon the research
question(s), research methodology and how a researcher
understands the research process. Depending upon these
arguments, pragmatism is the underlying research philosophy
in this research (Ethridge 2004; Fisher 2004; Saunders,
Lewis & Thornhill 2012). Pragmatists can use either or both
subjective or objective epistemology and ontology (Feilzer
2010; Saunders, Lewis & Thornhill 2012). Also, pragmatism
is applicable for mixed method and multilevel research
(Denscombe 2008). Morgan (2007) thinks that pragmatism is
suitable for research which supports transferability of
results. This research will use mixed methodology and work
with the holistic view of qualitative and quantitative
research. Therefore, pragmatic research philosophy is a
suitable philosophy. A comparison of pragmatism with
interpretivism, positivism and realism is given in Appendix
12.
3.2 Research approaches
28
This research will use both qualitative and quantitative
approaches sequentially to achieve research objectives.
Qualitative approach is preferable when research has to
determine motivation, perception or beliefs (Milena,
Dainora & Alin 2008). Creswell et al. (2011) signify that
qualitative research helps to obtain information for those
processes which evolve over time and the use of mobile
devices such as iPad in healthcare is an emerging idea
which is progressing with the passage of time. Thus, in
this research context a qualitative approach is useful to
determine constructs and hypotheses and formulate a
conceptual framework. On the other hand, quantitative
research aims at testing of hypotheses (Yilmaz 2013) and
hence, in this research it will provide validation for the
conceptual framework developed in qualitative research.
In qualitative and quantitative research design focus group
and web survey techniques will be used respectively. The
objective of qualitative research is to determine
constructs, develop hypotheses and develop a conceptual
framework. Focus groups can provide valuable information to
29
achieve that aim because in focus groups the responses come
after a relaxed, comfortable and enjoyable discussion (Baig
2010; Kai-Wen 2014) . As a result, more and more
information can be collected (Hussey & Hussey 1997;
Kitzinger 1994). In contrast, quantitative research aims at
testing hypotheses and validating conceptual framework
which can be achieved if researcher is able to collect
large number of responses. Cavana, Delahaye and Sekeran
(2001) have the idea that web survey is an effective
techniques to get more responses in less time and cost in
the new area of research. To increase the response rate in
this study respondents will be contacted through email and
personally prior to being sent the survey questionnaire
(Kaplowitz, Hadlock & Levine 2004). In conclusion, in this
research focus groups and web survey are the appropriate
research techniques in qualitative and quantitative
research design correspondingly.
3.3 Population, sampling and sample size
In this research purposive (convenience) sampling is
considered most appropriate techniques. It is the suitable
techniques for the researchers who have to select
30

participants deliberately based on a certain criteria and
who can provide good information (Cavana, Delahaye &
Sekeran 2001; Guarte & Barrios 2006; Teddlie & Yu 2007). In
the healthcare domain not all the HCPs can participate in
this research due to their workload (Wu, Li & Fu 2011).
Also, it is difficult to receive responses from all the
patients. Therefore, purposive (convenience) sampling is
the best technique to choose participants who are
available conveniently and are willing to participate
(Onwuegbuzie & Collins 2007).
Selecting sample size for both qualitative and quantitative
research is a critical task (Onwuegbuzie & Collins 2007).
Kotrlik and Higgins (2001) think that sample size selection
depends upon target population. Further, Onwuegbuzie and
Collins (2007) suggest that sample size depends upon
research design. In qualitative research design, a small
sample is sufficient to collect information (Johnson &
Christensen 2010). Various researchers suggest different
sample sizes (such as 6- 9, 6-10, 6-12, 8-10) for focus
groups data collection, (Christensen & Remler 2009;
Johnson & Christensen 2010). In this study 6-8 respondents
31
will be selected per focus group and 6-9 sessions of focus
groups will be held depending upon when researcher reach at
saturation point. Hence, in total 36-81 participants will
be needed in this research to conduct the focus groups
discussions.
In quantitative research design a large sample is needed to
generalise the results. Roscope (1975) cited in (Baig
2010) clarifies that in the quantitative research
paradigm, if data is divided into different themes then a
sample of 30 responses is enough for each theme. Currently
the conceptual framework drawn from the literature uses 4
themes, therefore 120 participants are required, but in
this research respondents will be selected based on number
of constructs and 25 responses are considered enough for
each construct. Therefore, in total 200 participants are
required for 8 constructs. However, the final sample size
will be decided after qualitative data analysis.
3.4 Data collection and analysis techniques
This research is using both primary as well as secondary
data. The main aim of secondary data collection is to
become familiar with the factors which influence adoption
32
of technology in healthcare and create an initial
conceptual framework. Alternatively, the main goal of
primary data collection is to answer research questions on
which this research is based. Thus both primary and
secondary data is important to achieve the overall aim of
the research. For Secondary data, (already collected for
this research) information is retrieved from articles
published in peer reviewed journals, books, reports and
magazines. Primary data will be collected and analysed in
two phases: 1) focus group 2) web survey.
Phase1: Focus group data collection and analysis
The first phase of primary data collection will be
completed in two steps: 1) pre-focus group, pilot focus
group and 2) focus group data collection. The first step
will provide experience for conducting actual focus group
interviews (Baig 2010). Pre-focus group and pilot focus
group are similar to focus groups, but the number of
participants remains less compared to the actual focus
group (Baig 2010). For the pre-focus and pilot study 4-5
participants will be selected. Each session will be held
for approximately 90 minutes. For focus group data
33
collection a semi-structured approach will be used which
encourages participants to contribute as much as possible
(Saunders, Lewis & Thornhill 2012). The objective and
description of the appropriate participants will be clearly
stated so that the findings of the research will be
reliable and on track.
Focus groups discussions will be recorded (both audio and
video) and transcribed. This transcribed file will be
converted into Microsoft word version 10. Further it will
be edited by the researcher to eliminate the information
identifying participants and will be uploaded into Nvivo to
analyse the data for repeated items, themes and categories.
Data analysis is a process of converting raw data into
intelligent information (Zikmund 2010).
Data obtained from focus group discussions will be analysed
to improve constructs, hypothesises and the version 2 of
the conceptual framework developed from literature. For
analysing qualitative data, content analysis techniques
will be used. It is a technique of analysing written,
verbal or visual communication messages (Cole 1988). The
34
benefit of content analysis is that words can be
categorised into smaller categories (Elo & Kyngäs 2008).
Hence, this phase will provide refinement to the conceptual
framework developed from literature and help to design a
survey questionnaire.
Phase2: Web survey data collection and analysis
In the second phase of primary data collection, cross-
sectional, web survey technique will be used. The aim of
this phase is to test the hypothesis generalise the
conceptual framework drawn from phase1 data collection. Web
survey is a cost effective method to collect information in
short duration of time (Fan & Yan 2010). The survey
questionnaire will be uploaded to the USQ website and
responses will be collected in the USQ database. The survey
questionnaire will require approximately one hour. Data
will be collected using a five point Likert scale.
In the survey questionnaire descriptive and inferential
analysis will be conducted using SPSS (AMOS) software.
Descriptive analysis of data will be helpful for
summarizing and simplifying data which will provide
descriptive validity. Inferential analysis will be used to
35
understand meanings and implications which can be attained
using statistical techniques (such as t- test, Chi Square
test, regression and structural equation modelling) to get integrative
validity (Baig 2010). A rough draft of the sample of the
survey questionnaire is attached in Appendix7: this will be
modified after phase 1 data collection and analysis.
3.5 Reliability and validity
Reliability means that the measured outcome should remain
consistent while repeating the same experiment many times.
(Cavana, Delahaye & Sekeran 2001; Neuman 2003). The
qualitative phase is a subjective phase and it is difficult
to get the same response each time the test is repeated
with the same individual (Bashir, Afzal & Azeem 2008)
however, the responses will be analysed to sift out the
same central ideas or themes. Reliability of quantitative
data will be ensured by using a standard reliability test
(Cronbach’s alpha test).
Validity of research ensures the quality of research. Poor
sampling and inaccurate and misleading responses may
challenge the validity of research (Hussey & Hussey 1997).
In qualitative approach four types of validity will be
36
ensured in this research: 1) descriptive validity: refers
to validity of factual accuracy of the data collected which
will be ensured by providing actual transcribed data. 2)
Interpretive validity: refers to respondents own word
validity which will be achieved by providing direct quote
supported by researcher’s interpretation. 3) Internal
validity: refers to uniformity of procedure which will be
confirmed by same set of questions and audio-video
recording of discussions. 4) External/ theme: refers to
theme and construct validity which will be achieved by
reviewing the items by researcher, discussing with
supervisors and consulting literature (Baig 2010;
Onwuegbuzie & Collins 2007; Onwuegbuzie & Johnson 2006).
In the quantitative approach the validation process is
followed to check the validity of the survey instrument and
will be conducted in three stages (Cavana, Delahaye &
Sekeran 2001). First stage: initial validation will be
conducted to check completeness, wording, and
appropriateness of the instrument which is called face
validity (Zikmund 2010). Face validity will be conducted
using pre-testing among PhD students and staff members.
37
Second stage: item validity which is the degree that a
measure covers the domain of interest, will be tested
through a pilot study (Zikmund 2010). Third stage: two
types of construct validity, namely convergent and
discriminant validity will be conducted. A correlation
coefficient helps to measure both types of validity. Both
will ensure that the items are measured with a higher
degree of correlation. However, the value of convergent
validity should not be too high as compared to discriminant
validity. As a rule of thumb when the value of convergent
validity is higher than 0.75 its discriminant validity is
interrogated (Zikmund 2010) which shows that two related
constructs are separate identities.
4.0 Outcomes and contributions of research
It is anticipated that individual readiness, complexity and
social influences are mediated by age, gender and
experience for individual intention for adoption of
technology; and general features of mobile devices and
compatibility with healthcare processes will be mediated by
age and gender.
38
This research will provide significant contributions in
theory, practice and policies. The conceptual model
developed in this research will be the first of its type
for adoption of mobile devices in healthcare at the
individual level. This model will serve as a pathway for
the healthcare and information technology domain to design
information communication tools for healthcare. Moreover,
this study will contribute to policy makers in healthcare.
They can redesign policies for the use of technology which
can fit in the healthcare environment (with users and
technology context). Also, the results from this research
can be transferable to the other part of Australian
healthcare settings.
4.1 Limitations and future research
This study is based more on intention rather than actual
behaviour as actual behaviour may change prior to intention
performance. This drawback can be overcome by studying the
actual use of mobile devices in healthcare. Further, policy
makers and management people are not included in this study
which can provide additional information about adoption of
mobile devices in the healthcare system. It is therefore
39

important to include those people in future research. In
addition to it, future research can be conducted for
adoption of mobile devices in a particular application such
as tele radiology and tele dermatology.
40
4.0 References
Agarwal, R & Prasad, J 1999, 'Are individual differences germane to the acceptance of new information technologies?', Decision Sciences, vol. 30, no. 2, pp. 361-91.
Ajzen, I 1988, Attitudes, personality, and behavior, Open University Press, Milton Keynes, England.
Ajzen, I 1991, 'The theory of planned behavior', OrganizationalBehavior and Human Decision Processes, vol. 50, no. 2, pp. 179-211.
Ajzen, I 2005, Attitudes, personality, and behavior, 2nd, Open University Press, New York, <http://ezproxy.usq.edu.au/login?url=http://www.USQ.eblib.com.au/EBLWeb/patron?target=patron&extendedid=P_287791_0&>.
Ayers, S & Olander, EK 2013, 'What are we measuring and why? Using theory to guide perinatal research and measurement', Journal of Reproductive and Infant Psychology, vol. 31, no. 5, pp. 439-48.
Baig, AH 2010, 'Study to investigate the adoption of wireless technology in the Australian healthcare system', Doctor of Philosophy thesis, University of Southern Queensland, Toowoomba.
Bandura, A 1986, Social foundations of thought and action, Prentice Hall, Englewood Cliffs, USA.
Bano, M & Zowghi, D 2015, 'A systematic review on the relationship between user involvement and system success', Information and Software Technology, vol. 58, pp. 148-69.
41
Bashir, M, Afzal, MT & Azeem, M 2008, 'Reliability and validity of qualitative and operational research paradigm', Pakistan Journal of Statistics and Operation Research, vol. 4, no. 1, pp.35-45.
Ben-Zeev, D, Kaiser, SM, Brenner, CJ, Begale, M, Duffecy, J& Mohr, DC 2013, 'Development and usability testing of FOCUS: a smartphone system for self-management of schizophrenia', Psychiatric Rehabilitation Journal, vol. 36, no. 4, pp. 289-96.
Bhattacherjee, A, Hikmet, N, Menachemi, N, Kayhan, VO & Brooks, RG 2007, 'The differential performance effects of healthcare information technology adoption', Information SystemsManagement, vol. 24, no. 1, pp. 5-14.
Boulos, MN, Wheeler, S, Tavares, C & Jones, R 2011, 'How smartphones are changing the face of mobile and participatory healthcare: an overview, with example from eCAALYX', Biomedical Engineering Online, vol. 10, no. 1, pp. 1-14.
Bradford, NK, Young, J, Armfield, NR, Herbert, A & Smith, AC 2014, 'Home telehealth and paediatric palliative care: clinician perceptions of what is stopping us?', BMC Palliative Care, vol. 13, no. 1, pp. 1-19.
Brewster, L, Mountain, G, Wessels, B, Kelly, C & Hawley, M 2014, 'Factors affecting front line staff acceptance of telehealth technologies: a mixed-method systematic review', Journal of Advanced Nursing, vol. 70, no. 1, pp. 21-3.
Brown, I, Stride, C, Psarou, A, Brewins, L & Thompson, J 2007, 'Management of obesity in primary care: nurses' practices, beliefs and attitudes', Journal of Advanced Nursing, vol. 59, no. 4, pp. 329-41.
Brown III, W, Yen, P-Y, Rojas, M & Schnall, R 2013, 'Assessment of the health IT usability evaluation model
42
(health-ITUEM) for evaluating mobile health (mhealth) technology', Journal of Biomedical Informatics, vol. 46, no. 6, pp. 1080-7.
Caison, AL, Bulman, D, Pai, S & Neville, D 2008, 'Exploringthe technology readiness of nursing and medical students ata Canadian university', Journal of Interprofessional Care, vol. 22, no. 3, pp. 283-94.
Casper, E 2007, 'The theory of planned behavior applied to continuing education for mental health professionals', Psychiatric Services, vol. 58, no. 10, pp. 1324-9.
Cavana, R, Delahaye, BL & Sekeran, U 2001, Applied business research: qualitative and quantitative methods, John Wiley & Sons Queensland.
Cellucci, L, Spil, CLT & Wiggins, C 2014, 'Introduction to IT adoption, diffusion, and evaluation in healthcare', Proceedings of the 47th Hawaii international conference on system sciences(HICSS), IEEE Computer Society, Hawaii, p. 2685.
Cheng, P-Y & Chu, M-C 2014, 'Behavioral factors affecting students' intentions to enroll in business ethics courses: a comparison of the theory of planned behavior and social cognitive theory using self-identity as a moderator', Journal of Business Ethics, vol. 124, no. 1, pp. 35-46.
Christensen, MC & Remler, D 2009, 'Information and communications technology in U.S. health care: why is adoption so slow and is slower better?', Journal of Health Politics, Policy & Law, vol. 34, no. 6, pp. 1011-34.
Cimperman, M, Brenčič, MM, Trkman, P & Stanonik, MdL 2013, 'Older adults' perceptions of home telehealth services', Telemedicine & e-Health, vol. 19, no. 10, pp. 786-90.
43
Cole, FL 1988, 'Content analysis: process and application', Clinical Nurse Specialist, vol. 2, no. 1, pp. 53-7.
Creswell, JW, Klassen, AC, Plano Clark, VL & Smith, KC 2011, 'Best practices for mixed methods research in the health sciences', Bethesda (Maryland): National Institutes of Health, pp.1-36.
Daim, TU, Basoglu, N & Topacan, U 2013, 'Adoption of healthinformation technologies: the case of a wireless monitor for diabetes and obesity patients', Technology Analysis & Strategic Management, vol. 25, no. 8, pp. 923-38.
Daniel Castro, Ben miller & Nager, A 2014, 'Unlocking the potential of physician-to-patient telehealth services', The Information Technology and Innovation Foundation, pp. 1-21.
Davis, FD 1985, 'A technology acceptance model for empirically testing new end-user information systems: theory and results', Doctor of philosphy thesis, Massachusetts Institute of Technology.
Deng, Z, Mo, X & Liu, S 2013, 'Comparison of the middle-aged and older users’ adoption of mobile health services inChina', International Journal of Medical Informatics, vol. 83, no. 3, pp. 210-24.
Denscombe, M 2008, 'Communities of practice a research paradigm for the mixed methods approach', Journal of Mixed Methods Research, vol. 2, no. 3, pp. 270-83.
Durndell, A & Haag, Z 2002, 'Computer self efficacy, computer anxiety, attitudes towards the Internet and reported experience with the Internet, by gender, in an East European sample', Computers in Human Behavior, vol. 18, no.5, pp. 521-35.
44
Elo, S & Kyngäs, H 2008, 'The qualitative content analysis process', Journal of Advanced Nursing, vol. 62, no. 1, pp. 107-15.
Ethridge, DE 2004, Research methodology in applied economics: organizing, planning, and conducting economic research, Blackwell Publishing, Ames, Iowa.
Fan, W & Yan, Z 2010, 'Factors affecting response rates of the web survey: a systematic review', Computers in Human Behavior, vol. 26, no. 2, pp. 132-9.
Feilzer, MY 2010, 'Doing mixed methods research pragmatically: implications for the rediscovery of pragmatism as a research paradigm', Journal of Mixed Methods Research, vol. 4, no. 1, pp. 6-16.
Fichman, RG 1992, 'Information technology diffusion: a review of empirical research', Proceedings of the international conference on information system, pp. 195-206.
Fisher, CM 2004, Researching and writing a dissertation for business students, Pearson/Prentice Hall Financial Times, Harlow.
Fox, S 2011, The social life of health information, 2011, Pew Internet and American Life Project, Washington, DC, <http://pewinternet. org/~/media/Files/Reports/2011/PIP_Social_Life_of_Health_Info. pdf >.
Furukawa, MF, Raghu, TS, Spaulding, TJ & Vinze, A 2008, 'Adoption of health information technology for medication safety in U.S. Hospitals, 2006', Health Affairs, vol. 27, no. 3,pp. 865-75.
Gagnon, M-P, Godin, G, Gagné, C, Fortin, J-P, Lamothe, L, Reinharz, D & Cloutier, A 2003, 'An adaptation of the theory of interpersonal behaviour to the study of
45
telemedicine adoption by physicians', International Journal of Medical Informatics, vol. 71, no. 2-3, pp. 103-15.
Gagnon, M-P, Lamothe, L, Fortin, J-P, Cloutier, A, Godin, G, Gagné, C & Reinharz, D 2005, 'Telehealth adoption in hospitals:an organisational perspective', Journal of Health Organization and Management, vol. 19, no. 1, pp. 32-56.
Gagnon, MP, Desmartis, M, Labrecque, M, Car, J, Pagliari, C, Pluye, P, Fremont, P, Gagnon, J, Tremblay, N & Legare, F2012, 'Systematic review of factors influencing the adoption of information and communication technologies by healthcare professionals', Journal of Medical System, vol. 36, no. 1, pp. 241-77.
Ghodeswar, BM & Vaidyanathan, J 2007, 'Organisational adoption of medical technology in healthcare sector', Journal of Services Research, vol. 7, no. 2, pp. 57-81.
Goodhue, DL & Thompson, RL 1995, 'Task-technology fit and individual performance', MIS Quarterly, pp. 213-36.
Goswami, S & Chandra, B 2013, 'Convergence dynamics of consume innovativeness vis-à-vis technology acceptance propensity: an empirical study on adoption of mobile devices', The IUP Journal of Marketing Management, vol. 12, no. 3, pp. 63-87.
Greene, JC, Caracelli, VJ & Graham, WF 1989, 'Toward a conceptual framework for mixed-method evaluation designs', Educational Evaluation and Policy Analysis, vol. 11, no. 3, pp. 255-74.
Guarte, JM & Barrios, EB 2006, 'Estimation under purposive sampling', Communications in Statistics—Simulation and Computation, vol. 35, no. 2, pp. 277-84.
46
Hafeez-Baig Abdul & Raj, G 2010, 'Adoption phenomena for wireless handheld devices in the healthcare environment', Journal of Communication in Healthcare, vol. 3, no. 3/4, pp. 228-39.
Hebert, MA, Korabek, B & Scott, RE 2006, 'Moving research into practice: a decision framework for integrating home telehealth into chronic illness care', International Journal of Medical Informatics, vol. 75, no. 12, pp. 786-94.
Heidarian, A & Mason, D 2013, 'Health information technology adoption in New Zealand optometric practices', Clinical & Experimental Optometry, vol. 96, no. 6, pp. 557-65.
Hodgson, R & Watson, E 1987, 'Gender-integrated management teams', Business Quarterly, vol. 52, pp. 68-72.
Honka, A, Kaipainen, K, Hietala, H & Saranummi, N 2011, 'Rethinking health: ICT-enabled services to empower people to manage their health', IEEE Reviews in Biomedical Engineering vol. 4, pp. 119-39.
Howe, KR 1988, 'Against the quantitative-qualitative incompatibility thesis or dogmas die hard', Educational Researcher, vol. 17, no. 8, pp. 10-6.
Hussey, J & Hussey, R 1997, Business research: a practical guide for undergraduate and postgraduate students, Macmillan, London.
Johnson, B & Christensen, L 2010, Educational research: quantitative,qualitative, and mixed approaches, 3 edn, Sage, Thousands Oaks.
Kai-Wen, C 2014, 'A study on applying focus group interviewon education', Reading Improvement, vol. 51, no. 4, pp. 381-4.
Kang, HG, Mahoney, DF, Hoenig, H, Hirth, VA, Bonato, P, Hajjar, I & Lipsitz, LA 2010, 'In situ monitoring of health
47
in older adults: technologies and issues', Journal of the American Geriatrics Society, vol. 58, no. 8, pp. 1579-86.
Kaplowitz, MD, Hadlock, TD & Levine, R 2004, 'A comparison of web and mail survey response rates', Public Opinion Quarterly, vol. 68, no. 1, pp. 94-101.
Karahanna, E, Straub, DW & Chervany, NL 1999, 'Information technology adoption across time: a cross-sectional comparison of pre-adoption and post-adoption beliefs', MIS Quarterly, vol. 23, no. 2, pp. 183-213.
Kargin, B & Basoglu, N 2006, 'Adoption factors of mobile services', Proceedings of the international conference on mobile business (ICMB'06), IEEE, Copenhagen, pp. 1-41.
Kay, M 2011, 'mHealth: new horizons for health through mobile technologies', World Health Organization, pp. 66-71.
Kim, D 2009, 'Adoption of personal information system: innovation diffusion theory and task technology fit', Academy of Information and Management Sciences, vol. 13, no. 2, pp.50-73.
Kim, S & Garrison, G 2008, 'Investigating mobile wireless technology adoption: an extension of the technology acceptance model', Information Systems Frontiers, vol. 11, no. 3, pp. 323-33.
Kitzinger, J 1994, 'The methodology of focus groups: the importance of interaction between research participants', Sociology of Health & Illness, vol. 16, no. 1, pp. 103-21.
Klassen, AC, Creswell, J, Plano Clark, VL, Smith, KC & Meissner, HI 2012, 'Best practices in mixed methods for quality of life research', Quality of Life Research, vol. 21, no. 3, pp. 377-80.
48
Kluge, EH 2011, 'Ethical and legal challenges for health telematics in a global world: telehealth and the technological imperative', International Journal of Medical Informatics, vol. 80, no. 2, pp. 1-5.
Kotrlik, JWKJW & Higgins, C 2001, 'Organizational research:determining appropriate sample size in survey research appropriate sample size in survey research', Information Technology, Learning, and Performance Journal, vol. 19, no. 1, p. 43.
Kuang-Ming, K, Chung-Feng, L & Chen-Chung, M 2013, 'An investigation of the effect of nurses' technology readinesson the acceptance of mobile electronic medical record systems', BMC Medical Informatics & Decision Making, vol. 13, no. 1,pp. 1-14.
Kwon, TH & Zmud, RW 1987, 'Unifying the fragmented models of information systems implementation', Proceedings of the criticalissues in information systems research, John Wiley & Sons, New York, pp. 227-51.
Lei-Shih, C, Oi-Man, K & Goodson, P 2008, 'US health educators' likelihood of adopting genomic competencies intohealth promotion', American Journal of Public Health, vol. 98, no. 9, pp. 1651-7.
Leventhal, J 2008, 'News & features', Journal of Visual Impairment & Blindness, vol. 102, no. 6, pp. 365-8.
Lim, S, Xue, L, Yen, CC, Chang, L, Chan, HC, Tai, BC, Duh, HBL & Choolani, M 2011, 'A study on Singaporean women's acceptance of using mobile phones to seek health information', International Journal of Medical Informatics, vol. 80, no. 12, pp. 189-202.
Looney, CA, Akbulut, AY & Poston, RS 2008, 'Understanding the determinants of service channel preference in the early
49
stages of adoption: a social cognitive perspective on online brokerage services', Decision Sciences, vol. 39, no. 4, pp. 821-57.
Lu, Y-C, Xiao, Y, Sears, A & Jacko, JA 2005, 'A review and a framework of handheld computer adoption in healthcare', International Journal of Medical Informatics, vol. 74, no. 5, pp. 409-22.
Massey, AP, Khatri, V & Montoya-Weiss, MM 2007, 'Usability of online services: the role of technology readiness and context', Decision Sciences, vol. 38, no. 2, pp. 277-308.
Michael J. Ackerman, Rosemarie Filart, Lawrence P. Burgess,Insup Lee & Poropatich, RK 2010, 'Developing next-generation telehealth tools and technologies: patients, systems, and data perspectives', Telemedicine and E-Health, vol. 16, no. 1, pp. 93-5.
Milena, ZR, Dainora, G & Alin, S 2008, 'Qualitative research methods: a comparison between focus-group and in-depth interview', Annals of the University of Oradea, Economic Science Series, vol. 17, no. 4, pp. 1279-83.
Morgan, DL 1997, Focus groups as qualitative research, Sage, ThousandOaks.
Morgan, DL 2007, 'Paradigms lost and pragmatism regained methodological implications of combining qualitative and quantitative methods', Journal of Mixed Methods Research, vol. 1, no. 1, pp. 48-76.
Morón, MJ, Luque, R & Casilari, E 2014, 'On the capability of smartphones to perform as communication gateways in medical wireless personal area networks', Sensors vol. 14, no.1, pp. 575-94.
50
Morris, MG & Venkatesh, V 2000, 'Age differences in technology adoption decisions: implications for a changing work force', Personnel Psychology, vol. 53, no. 2, pp. 375-403.
Morris, MG, Venkatesh, V & Ackerman, PL 2005, 'Gender and age differences in employee decisions about new technology:an extension to the theory of planned behavior', IEEE Transactions on Engineering Management, vol. 52, no. 1, pp. 69-84.
Moseley, MJ 2000, 'Innovation and rural development: some lessons from Britain and Western Europe', Planning Practice & Research, vol. 15, no. 1/2, pp. 95-115.
Nah, FF-H, Siau, K & Sheng, H 2005, 'The value of mobile applications', Communications of the ACM, vol. 48, no. 2, pp. 85-90.
Neuman, WL 2003, Dimensions of research, 5th edn, Allyn and Bacon, Boston, Massachusetts.
Newswire, P 2014, 'War Memorial Hospital - Michigan to deploy JEMS telehealth system across all divisions, specialists,' viewed 20/092014 <http://ezproxy.usq.edu.au/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=bwh&AN=201407290929PR.NEWS.USPR.DE78966&site=ehost-live>.
Ngwenyama, OK & Lee, AS 1997, 'Communication richness in electronic mail: critical social theory and the contextuality of meaning', MIS Quarterly, vol. 21, no. 2, pp. 145-67.
Onwuegbuzie, AJ & Leech, NL 2005, 'On becoming a pragmatic researcher: the importance of combining quantitative and qualitative research methodologies', International Journal of Social Research Methodology, vol. 8, no. 5, pp. 375-87.
51
Onwuegbuzie, AJ & Johnson, RB 2006, 'The validity issue in mixed research', Research in the Schools, vol. 13, no. 1, pp. 48-63.
Onwuegbuzie, AJ & Collins, KM 2007, 'A typology of mixed methods sampling designs in social science research', Qualitative Report, vol. 12, no. 2, pp. 281-316.
Peddle, K 2007, 'Telehealth in context: socio-technical barriers to telehealth use in labrador, Canada', Computer Supported Cooperative Work (CSCW), vol. 16, no. 6, pp. 595-614.
Perkins, M, Jensen, P, Jaccard, J, Gollwitzer, P, Oettingen, G, Pappadopulos, E & Hoagwood, K 2007, 'Applyingtheory-driven approaches to understanding and modifying clinicians' behavior: what do we know?', Psychiatric Services, vol. 58, no. 3, pp. 342-8.
The pulse of telehealth 2014, Research and Markets <http://ezproxy.usq.edu.au/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=n5h&AN=16PU3412843375&site=ehost-live>.
Ramey, J, Fung, KM & Hassell, LA 2011, 'Use of mobile high-resolution device for remote frozen section evaluation of whole slide images', Journal of Pathology Informatics, vol. 2, no. 1, pp. 235-8.
Randle, M, Mackay, H & Dudley, D 2014, 'A comparison of group-based research methods', Market & Social Research, vol. 22,no. 1, pp. 22-38.
Roberts, JE & Bell, MA 2000, 'Sex differences on a mental rotation task: variations in electroencephalogram hemispheric', Developmental Neuropsychology, vol. 17, no. 2, p. 199.
52
Rogers, EM 2003a, Diffusion of innovations, Free Press, New York.
Rogers, EM 2003b, Diffusion of innovations, 5th edn, Free Press, New York.
Rogers, EM 2004, 'A prospective and retrospective look at the diffusion model', Journal of Health Communication, vol. 9, no.1, pp. 13-9.
Saad, NM, Alias, RA & Ismail, Z 2013, 'Initial framework onidentifying factors influencing individuals' usage of telehealth', Proceedings of the 3rd international conference on research and innovation in information systems – 2013 (ICRIIS’13), IEEE, Malaysia, 2013, pp. 174-9.
Sanders, C, Rogers, A, Bowen, R, Bower, P, Hirani, S, Cartwright, M, Fitzpatrick, R, Knapp, M, Barlow, J & Hendy,J 2012, 'Exploring barriers to participation and adoption of telehealth and telecare within the whole system demonstrator trial: a qualitative study', BMC Health Services Research, vol. 12, no. 1, p. 220.
Sarker, S, Urbaczewski, A & Wells, JD 2002, 'Understanding hybrid wireless device use and adoption: an integrative framework based on an exploratory study', Proceedings of the 36thHawaii international conference on system sciences (HICSS’03), IEEE Computer Society, Hawaii.
Saunders, M, Lewis, P & Thornhill, A 2012, Research methods for business students, 6th edn, Pearson, New York.
Singh, R, Mathiassen, L, Stachura, ME & Astapova, EV 2010, 'Sustainable rural telehealth innovation: a public health case study', Health Services Research, vol. 45, no. 4, pp. 985-1004.
53
Singh, R, Lichter, MI, Danzo, A, Taylor, J & Rosenthal, T 2012, 'The adoption and use of health information technology in rural areas: results of a national survey', Journal of Rural Health, vol. 28, no. 1, pp. 16-27.
Slaper, MR & Conkol, K 2014, 'mHealth tools for the pediatric patient-centered medical home', Pediatric Annals, vol.43, no. 2, pp. 39-43.
Sun, H & Zhang, P 2006, 'The role of moderating factors in user technology acceptance', International Journal of Human-ComputerStudies, vol. 64, no. 2, pp. 53-78.
Taylor, S & Todd, P 1995, 'Assessing IT usage: the role of prior experience', MIS Quarterly, vol. 19, no. 4, pp. 561-70.
Teddlie, C & Yu, F 2007, 'Mixed methods sampling a typologywith examples', Journal of Mixed Methods Research, vol. 1, no. 1, pp. 77-100.
Thimm, C, Rademacher, U & Kruse, L 1998, 'Age stereotypes and patronizing messages: features of age-adapted speech intechnical instructions to the elderly', Journal of Applied Communication Research, vol. 26, no. 1, pp. 66-82.
Thomas, D, Yao, Y & Guo, X 2014, 'Environment versus partnering experience: an exploration of Chinese healthcareIT manager attitudes toward innovation of services', Proceedings of the 47th Hawaii international conference on system sciences (HICSS), IEEE Computer Society, Hawaii, pp. 2741-50.
Thong, JY, Hong, S-J & Tam, KY 2006, 'The effects of post-adoption beliefs on the expectation-confirmation model for information technology continuance', International Journal of Human-Computer Studies, vol. 64, no. 9, pp. 799-810.
54
Tiong, I, Hafeez-Baig, A, Gururajan, R & Soar, J 2006, 'Preliminary investigation to explore perceptions of security issues associated with wireless technology in healthcare in Australia', Proceedings of bridging the digital divide: clinician, consumer and computer, Health Informatics Society of Australia, Sydney, 20-22 August 2006.
Venkatesh, V & Morris, MG 2000, 'Why don't men ever stop toask for directions? Gender, social influence, and their role in technology acceptance and usage behavior', MIS Quarterly, vol. 24, no. 1, pp. 115-39.
Venkatesh, V, Brown, SA & Bala, H 2013, 'Bridging the qualitative-quantitative divide: guidelines for conducting mixed methods research in information systems', MIS Quarterly, vol. 37, no. 1, pp. 21-54.
Venkatesh, V, Morris, MG, Davis, GB & Davis, FD 2003, 'Useracceptance of information technology: toward a unified view', MIS Quarterly, vol. 27, no. 3, pp. 425-78.
Wang, A, Redington, L, Steinmetz, V & Lindeman, D 2010, 'The ADOPT model: accelerating diffusion of proven technologies for older adults', Ageing International, vol. 36, no. 1, pp. 29-45.
West, D 2012, 'How mobile devices are transforming healthcare', Issues in Technology Innovation, vol. 18, no. 1, pp. 1-14.
Wu, I-L, Li, J-Y & Fu, C-Y 2011, 'The adoption of mobile healthcare by hospital's professionals: an integrative perspective', Decision Support Systems, vol. 51, no. 3, pp. 587-96.
Wu, J-H, Wang, S-C & Lin, L-M 2007, 'Mobile computing acceptance factors in the healthcare industry: a structural
55
equation model', International Journal of Medical Informatics, vol. 76,no. 1, pp. 66-77.
Xue, L, Yen, CC, Chang, L, Chan, HC, Tai, BC, Tan, SB, Duh,HBL & Choolani, M 2012, 'An exploratory study of ageing women's perception on access to health informatics via a mobile phone-based intervention', International Journal of Medical Informatics, vol. 81, no. 9, pp. 637-48.
Yangil, P & Chen, JV 2007, 'Acceptance and adoption of the innovative use of smartphone', Industrial Management & Data Systems, vol. 107, no. 9, pp. 1349-65.
Yilmaz, K 2013, 'Comparison of quantitative and qualitativeresearch traditions: epistemological, theoretical, and methodological differences', European Journal of Education, vol. 48, no. 2, pp. 311-25.
Yu, P, Wu, MX, Yu, H & Xiao, GQ 2006, 'The challenges for the adoption of M-health', Proceedings of the IEEE international conference on service operations and logistics, and informatics (SOLI'06), IEEE, Shanghai, 21-23 June 2006, pp. 181-6.
Zangbar, B, Pandit, V, Rhee, P, Aziz, H, Hashmi, A, Friese,RS, Weinstein, R & Joseph, B 2014, 'Smartphone surgery: howtechnology can transform practice', Telemedicine & e-Health, vol.20, no. 6, pp. 590-2.
Zigurs, I & Buckland, BK 1998, 'A theory of task/technologyfit and group support systems effectiveness', MIS Quarterly, vol. 22, no. 3, pp. 313-34.
Zikmund, WG 2010, Business research methods, 8th edn, South-Western, Mason, OH.
Zinszer, K, Tamblyn, R, Bates, DW & Buckeridge, DL 2013, 'Aqualitative study of health information technology in the
56
Canadian public health system', BMC Public Health, vol. 13, no.1, p. 509.
Zmud, RW 1979, 'Individual differences and MIS success: a review of the empirical literature', Management Science, vol. 25, no. 10, pp. 966-79.
57
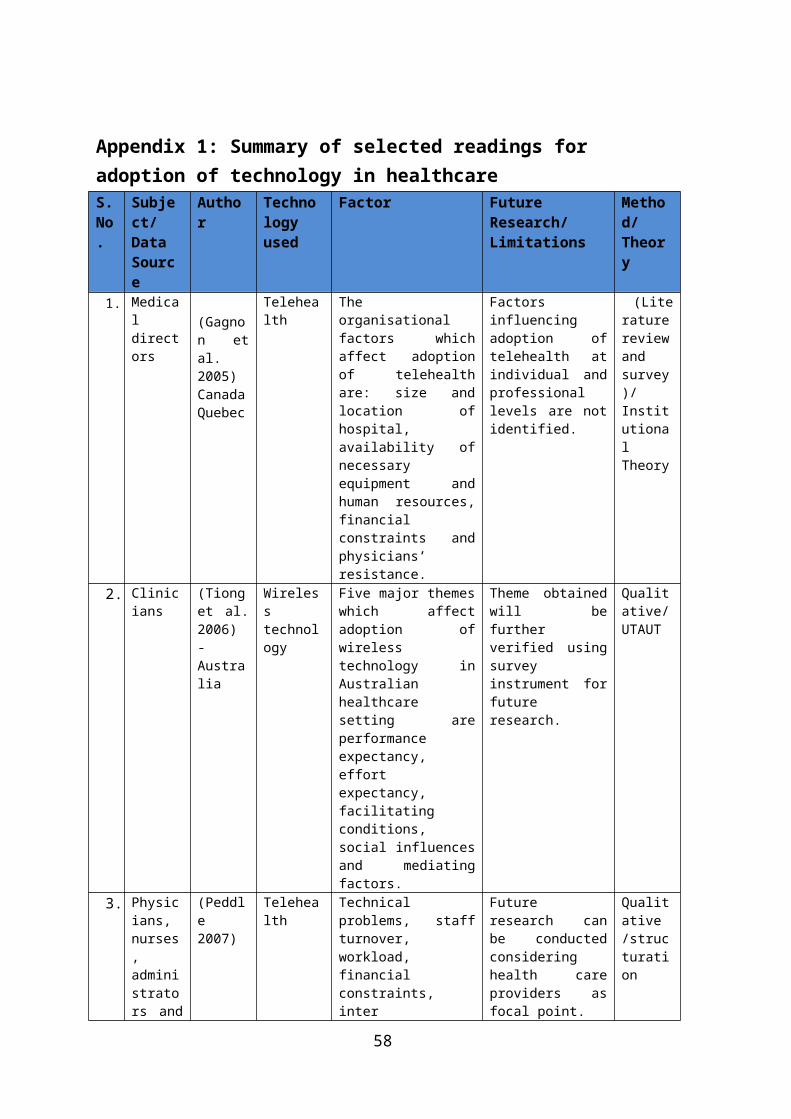
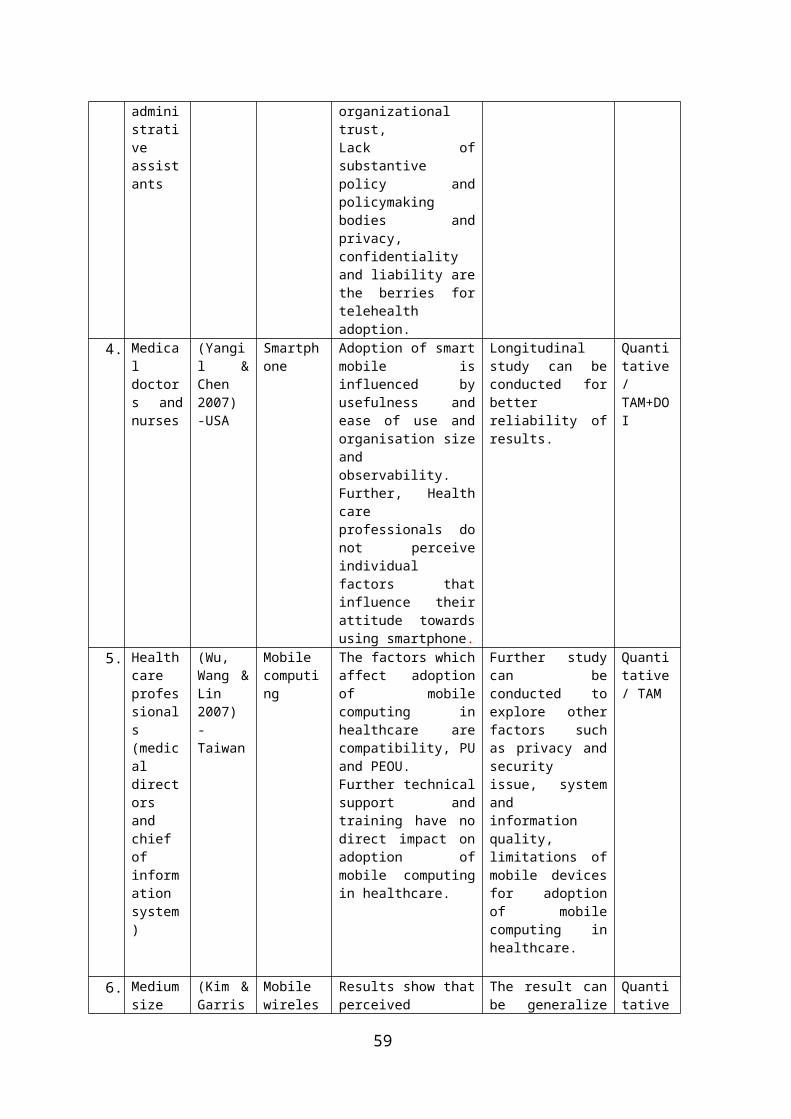
Appendix 1: Summary of selected readings for adoption of technology in healthcareS.No.
Subject/ Data Source
Author
Technology used
Factor Future Research/ Limitations
Method/Theory
1. Medicaldirectors
(Gagnon etal.2005)CanadaQuebec
Telehealth
Theorganisationalfactors whichaffect adoptionof telehealthare: size andlocation ofhospital,availability ofnecessaryequipment andhuman resources,financialconstraints andphysicians’resistance.
Factorsinfluencingadoption oftelehealth atindividual andprofessionallevels are notidentified.
(Literaturereviewandsurvey)/InstitutionalTheory
2. Clinicians
(Tionget al.2006)-Australia
Wirelesstechnology
Five major themeswhich affectadoption ofwirelesstechnology inAustralianhealthcaresetting areperformanceexpectancy,effortexpectancy,facilitatingconditions,social influencesand mediatingfactors.
Theme obtainedwill befurtherverified usingsurveyinstrument forfutureresearch.
Qualitative/UTAUT
3. Physicians,nurses,administrators and
(Peddle2007)
Telehealth
Technicalproblems, staffturnover,workload,financialconstraints,inter
Futureresearch canbe conductedconsideringhealth careproviders asfocal point.
Qualitative /structuration
58
administrativeassistants
organizationaltrust,Lack ofsubstantivepolicy andpolicymakingbodies andprivacy,confidentialityand liability arethe berries fortelehealthadoption.
4. Medicaldoctors andnurses
(Yangil &Chen2007)-USA
Smartphone
Adoption of smartmobile isinfluenced byusefulness andease of use andorganisation sizeandobservability.Further, Healthcareprofessionals donot perceiveindividualfactors thatinfluence theirattitude towardsusing smartphone.
Longitudinalstudy can beconducted forbetterreliability ofresults.
Quantitative/TAM+DOI
5. Healthcareprofessionals(medicaldirectorsandchiefofinformationsystem)
(Wu,Wang &Lin2007)-Taiwan
Mobilecomputing
The factors whichaffect adoptionof mobilecomputing inhealthcare arecompatibility, PUand PEOU.Further technicalsupport andtraining have nodirect impact onadoption ofmobile computingin healthcare.
Further studycan beconducted toexplore otherfactors suchas privacy andsecurityissue, systemandinformationquality,limitations ofmobile devicesfor adoptionof mobilecomputing inhealthcare.
Quantitative/ TAM
6. Mediumsize
(Kim &Garris
Mobilewireles
Results show thatperceived
The result canbe generalize
Quantitative
59
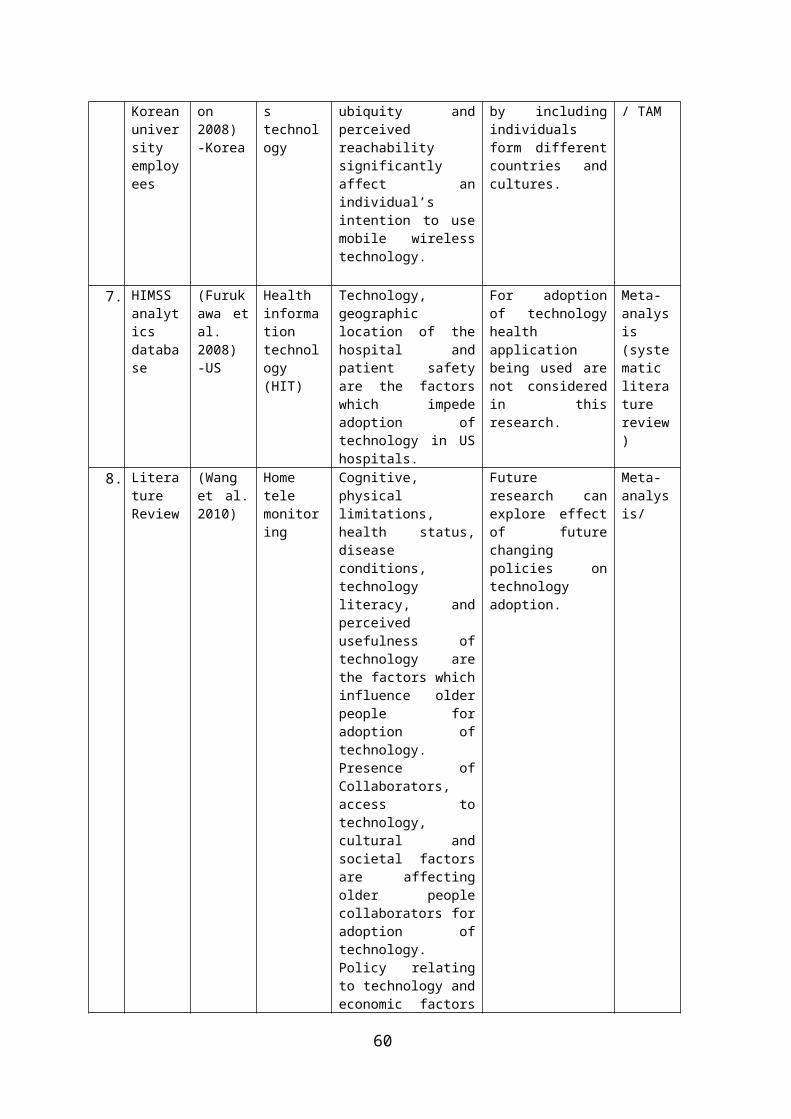
Koreanuniversityemployees
on2008)-Korea
stechnology
ubiquity andperceivedreachabilitysignificantlyaffect anindividual’sintention to usemobile wirelesstechnology.
by includingindividualsform differentcountries andcultures.
/ TAM
7. HIMSSanalyticsdatabase
(Furukawa etal.2008)-US
Healthinformationtechnology(HIT)
Technology,geographiclocation of thehospital andpatient safetyare the factorswhich impedeadoption oftechnology in UShospitals.
For adoptionof technologyhealthapplicationbeing used arenot consideredin thisresearch.
Meta-analysis(systematicliteraturereview)
8. LiteratureReview
(Wanget al.2010)
Hometelemonitoring
Cognitive,physicallimitations,health status,diseaseconditions,technologyliteracy, andperceivedusefulness oftechnology arethe factors whichinfluence olderpeople foradoption oftechnology.Presence ofCollaborators,access totechnology,cultural andsocietal factorsare affectingolder peoplecollaborators foradoption oftechnology.Policy relatingto technology andeconomic factors
Futureresearch canexplore effectof futurechangingpolicies ontechnologyadoption.
Meta-analysis/
60
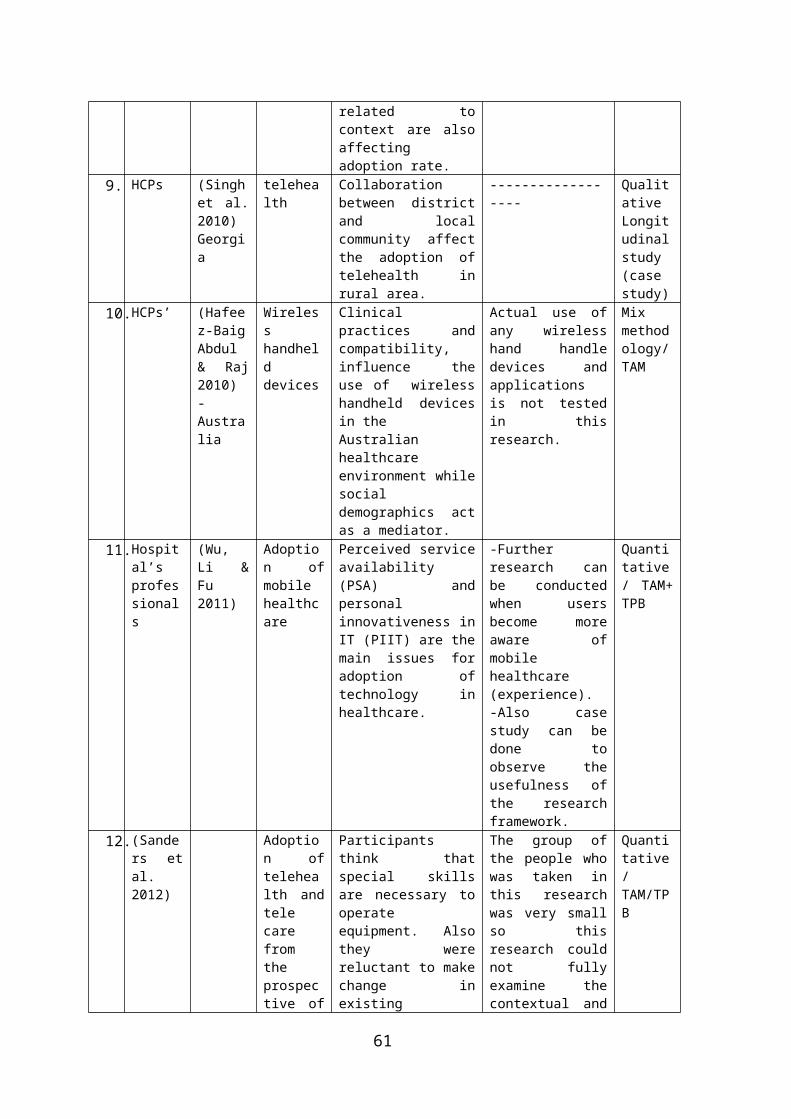
related tocontext are alsoaffectingadoption rate.
9. HCPs (Singhet al.2010)Georgia
telehealth
Collaborationbetween districtand localcommunity affectthe adoption oftelehealth inrural area.
------------------
QualitativeLongitudinalstudy(casestudy)
10.HCPs’ (Hafeez-BaigAbdul& Raj2010)-Australia
Wirelesshandhelddevices
Clinicalpractices andcompatibility,influence theuse of wirelesshandheld devicesin theAustralianhealthcareenvironment whilesocialdemographics actas a mediator.
Actual use ofany wirelesshand handledevices andapplicationsis not testedin thisresearch.
Mixmethodology/TAM
11.Hospital’sprofessionals
(Wu,Li &Fu2011)
Adoption ofmobilehealthcare
Perceived serviceavailability(PSA) andpersonalinnovativeness inIT (PIIT) are themain issues foradoption oftechnology inhealthcare.
-Furtherresearch canbe conductedwhen usersbecome moreaware ofmobilehealthcare(experience).-Also casestudy can bedone toobserve theusefulness ofthe researchframework.
Quantitative/ TAM+TPB
12.(Sanders etal.2012)
Adoption oftelehealth andtelecarefromtheprospective of
Participantsthink thatspecial skillsare necessary tooperateequipment. Alsothey werereluctant to makechange inexisting
The group ofthe people whowas taken inthis researchwas very smallso thisresearch couldnot fullyexamine thecontextual and
Quantitative/TAM/TPB
61
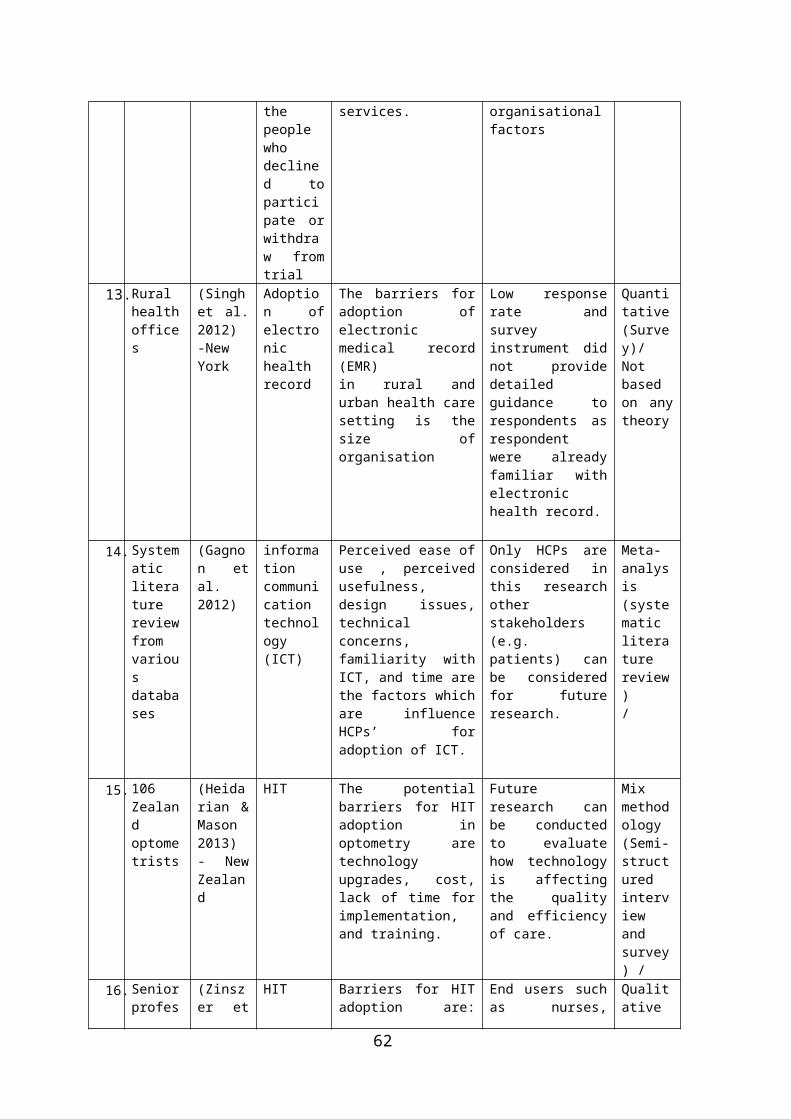
thepeoplewhodeclined toparticipate orwithdraw fromtrial
services. organisationalfactors
13.Ruralhealthoffices
(Singhet al.2012)-NewYork
Adoption ofelectronichealthrecord
The barriers foradoption ofelectronicmedical record(EMR)in rural andurban health caresetting is thesize oforganisation
Low responserate andsurveyinstrument didnot providedetailedguidance torespondents asrespondentwere alreadyfamiliar withelectronichealth record.
Quantitative(Survey)/Notbasedon anytheory
14.Systematicliteraturereviewfromvariousdatabases
(Gagnon etal.2012)
informationcommunicationtechnology(ICT)
Perceived ease ofuse , perceivedusefulness,design issues,technicalconcerns,familiarity withICT, and time arethe factors whichare influenceHCPs’ foradoption of ICT.
Only HCPs areconsidered inthis researchotherstakeholders(e.g.patients) canbe consideredfor futureresearch.
Meta-analysis(systematicliteraturereview)/
15.106Zealandoptometrists
(Heidarian &Mason2013)- NewZealand
HIT The potentialbarriers for HITadoption inoptometry aretechnologyupgrades, cost,lack of time forimplementation,and training.
Futureresearch canbe conductedto evaluatehow technologyis affectingthe qualityand efficiencyof care.
Mixmethodology(Semi-structuredinterviewandsurvey) /
16.Seniorprofes
(Zinszer et
HIT Barriers for HITadoption are:
End users suchas nurses,
Qualitative
62
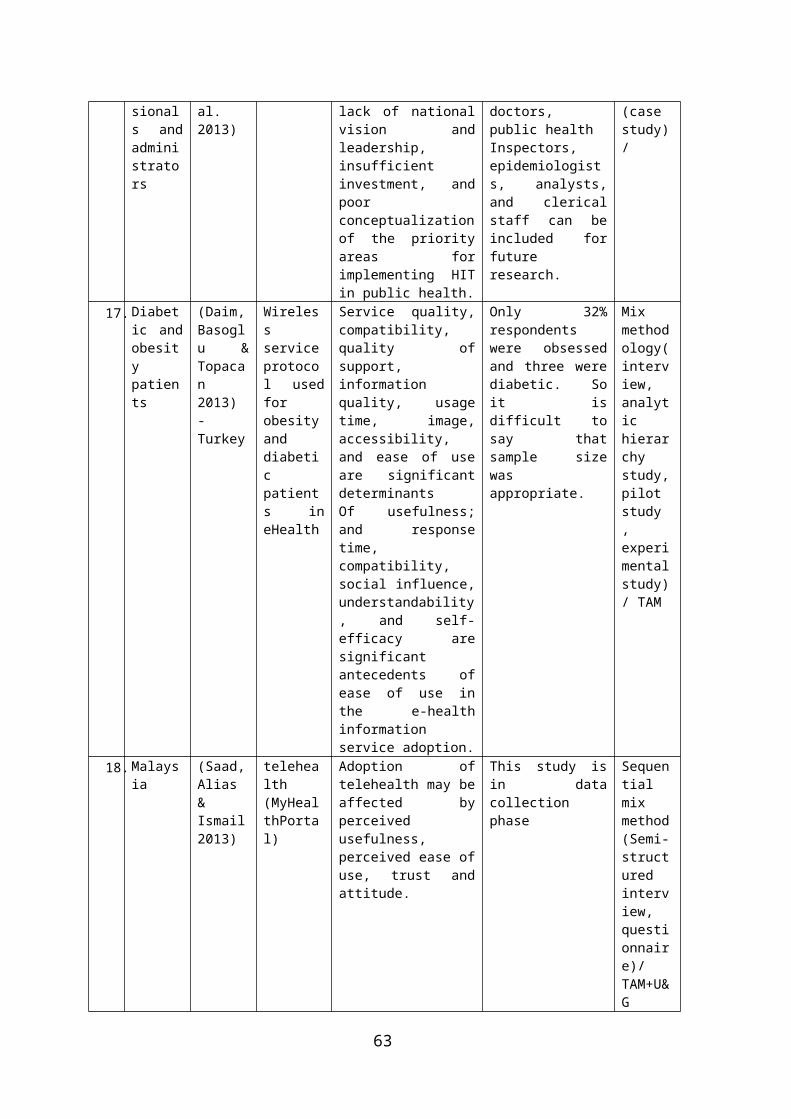
sionals andadministrators
al.2013)
lack of nationalvision andleadership,insufficientinvestment, andpoorconceptualizationof the priorityareas forimplementing HITin public health.
doctors,public healthInspectors,epidemiologists, analysts,and clericalstaff can beincluded forfutureresearch.
(casestudy)/
17.Diabetic andobesitypatients
(Daim,Basoglu &Topacan2013)-Turkey
Wirelessserviceprotocol usedforobesityanddiabeticpatients ineHealth
Service quality,compatibility,quality ofsupport,informationquality, usagetime, image,accessibility,and ease of useare significantdeterminantsOf usefulness;and responsetime,compatibility,social influence,understandability, and self-efficacy aresignificantantecedents ofease of use inthe e-healthinformationservice adoption.
Only 32%respondentswere obsessedand three werediabetic. Soit isdifficult tosay thatsample sizewasappropriate.
Mixmethodology(interview,analytichierarchystudy,pilotstudy ,experimentalstudy)/ TAM
18.Malaysia
(Saad,Alias&Ismail2013)
telehealth(MyHealthPortal)
Adoption oftelehealth may beaffected byperceivedusefulness,perceived ease ofuse, trust andattitude.
This study isin datacollectionphase
Sequentialmixmethod(Semi-structuredinterview,questionnaire)/TAM+U&G
63
19.Middleagedandolderpeople
(Deng,Mo &Liu2013)-china
mHealth Behaviorintention to usemobile healthservices for theolder users’depend uponperceived value,attitude,perceivedbehavior control,technologyanxiety, andself-actualizationneeds positivelyaffect adoptionof m healthservices.
Furtherresearch caninclude seniorcitizens whohavedisabilitiesand are lesssociallyactive.
Quantitative/ValueAttitudeBehaviourModel+TPB
20. ITmanager
(Thomas, Yao& Guo2014)China
mobileandInternettechnologies
Experience andSecurityare the factorsthat motivatehealthcare ITmanagers toinnovate servicesusing mobile andInternettechnologies
Furtherresearch canbe conductedto find outadditionalfactors whichaffect ITmanagerattitudestowardsupportinginnovation.
Quantitative(Survey)/
21.Report (DanielCastro, Benmiller&Nager2014)-US
Telehealth
Right policiesare essential fortelehealthimplementation
------------------
TAM
22.Palliativecareclinicians
(Bradford etal.2014)-RoyalChildren’sHospitalBrisba
Telehealth
According toclinician’sperspectives themajor factors forhome telehealthadoption programare: Technology,Individual andService.
A small sampleis used inthis studyandinterviewer ispreviouslyknown tointerviewees.
Qualitative/
64
neQueenslandAustralia
65
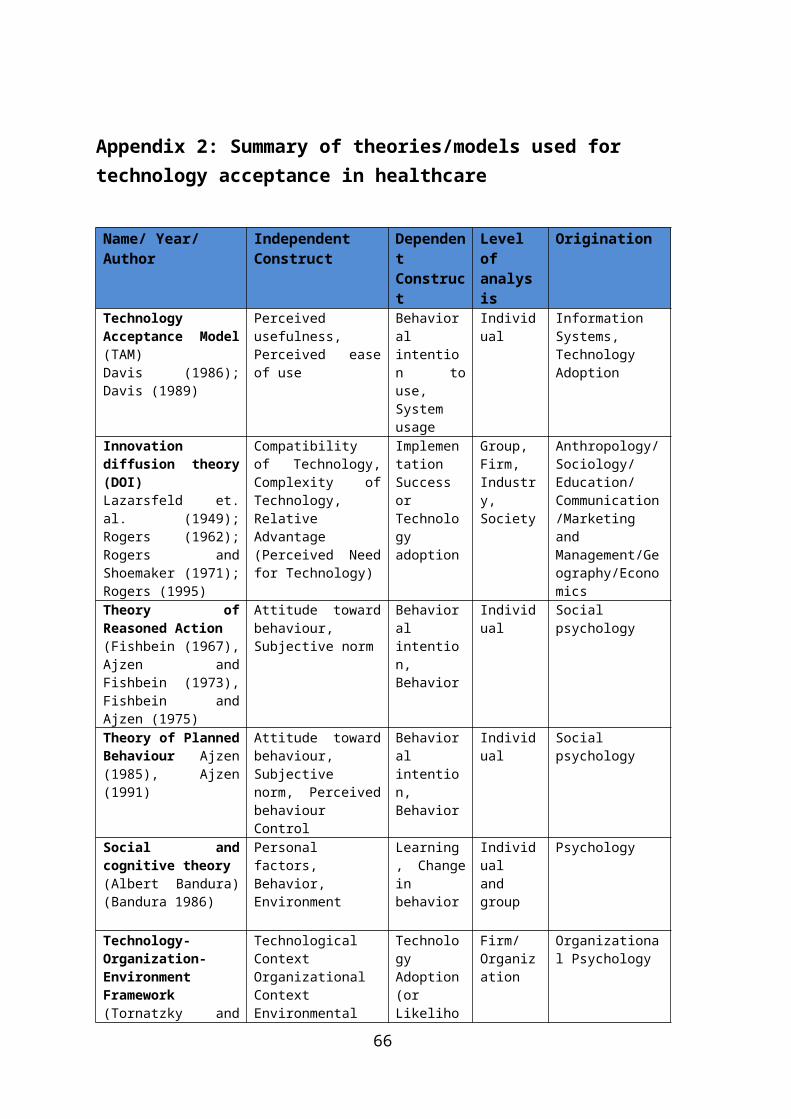
Appendix 2: Summary of theories/models used for technology acceptance in healthcare
Name/ Year/ Author
Independent Construct
Dependent Construct
Level of analysis
Origination
TechnologyAcceptance Model(TAM)Davis (1986);Davis (1989)
Perceivedusefulness,Perceived easeof use
Behavioralintention touse,Systemusage
Individual
InformationSystems,TechnologyAdoption
Innovationdiffusion theory(DOI)Lazarsfeld et.al. (1949);Rogers (1962);Rogers andShoemaker (1971);Rogers (1995)
Compatibilityof Technology,Complexity ofTechnology,RelativeAdvantage(Perceived Needfor Technology)
ImplementationSuccessorTechnologyadoption
Group,Firm,Industry,Society
Anthropology/Sociology/Education/Communication/MarketingandManagement/Geography/Economics
Theory ofReasoned Action(Fishbein (1967),Ajzen andFishbein (1973),Fishbein andAjzen (1975)
Attitude towardbehaviour,Subjective norm
Behavioralintention,Behavior
Individual
Socialpsychology
Theory of PlannedBehaviour Ajzen(1985), Ajzen(1991)
Attitude towardbehaviour,Subjectivenorm, PerceivedbehaviourControl
Behavioralintention,Behavior
Individual
Socialpsychology
Social andcognitive theory(Albert Bandura)(Bandura 1986)
Personalfactors,Behavior,Environment
Learning, Changeinbehavior
Individualandgroup
Psychology
Technology-Organization-EnvironmentFramework(Tornatzky and
TechnologicalContextOrganizationalContextEnvironmental
TechnologyAdoption(orLikeliho
Firm/Organization
Organizational Psychology
66
Fleisher1990ework)
Context od ofAdoption,Intention toAdopt,ExtentofAdoption)
Task technologyFit (TTF)(Goodhue &Thompson 1995;Zigurs & Buckland1998)
Taskcharacteristics, Technologycharacteristics
Individualperformance,Systemutilization
Individual
InformationSystems
Unified theory ofacceptance anduse of technology(UTAUT)(Venkatesh et al.2003)
Performanceexpectancy,Effortexpectancy,Socialinfluence,Facilitatingconditions,Gender, Age,Experience,Voluntarinessof use
Behavioralintention, Usagebehavior
Individual
InformationSystems,TechnologyAdoption
67
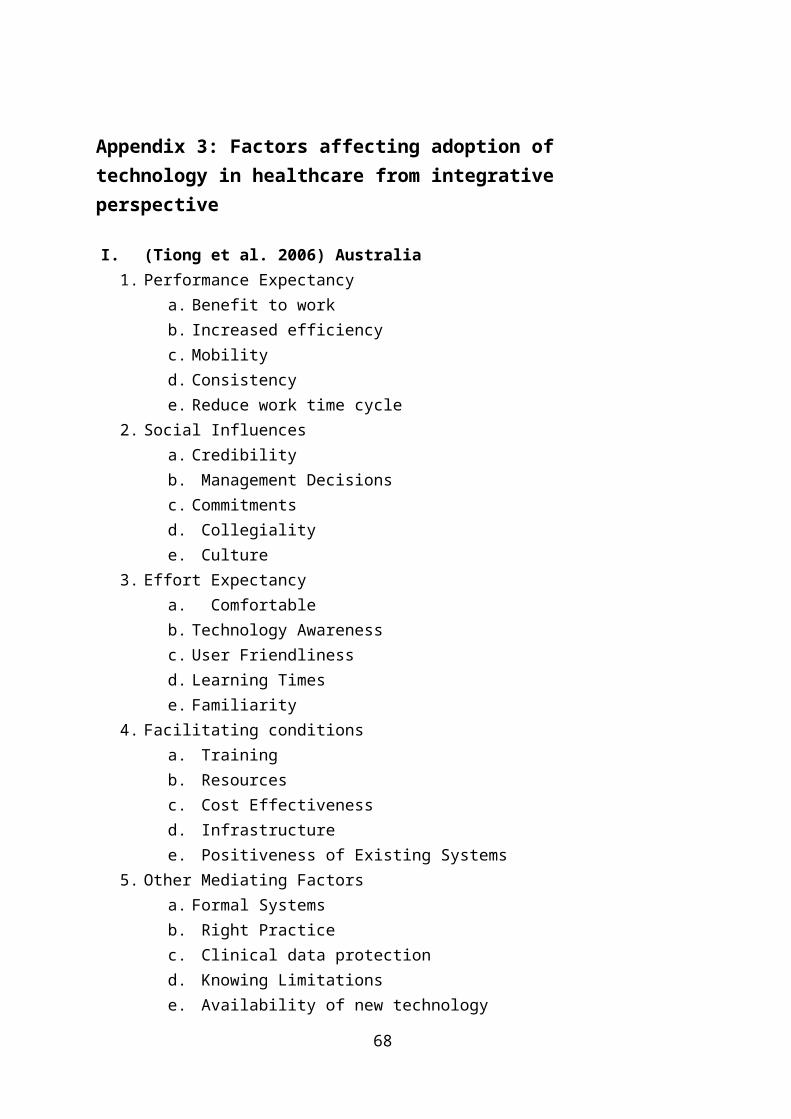
Appendix 3: Factors affecting adoption of technology in healthcare from integrative perspective
I. (Tiong et al. 2006) Australia1. Performance Expectancy
a. Benefit to work b. Increased efficiency c. Mobility d. Consistency e. Reduce work time cycle
2. Social Influencesa. Credibilityb. Management Decisions c. Commitmentsd. Collegiality e. Culture
3. Effort Expectancya. Comfortable b. Technology Awareness c. User Friendliness d. Learning Times e. Familiarity
4. Facilitating conditionsa. Trainingb. Resources c. Cost Effectiveness d. Infrastructure e. Positiveness of Existing Systems
5. Other Mediating Factorsa. Formal Systems b. Right Practice c. Clinical data protection d. Knowing Limitations e. Availability of new technology
68
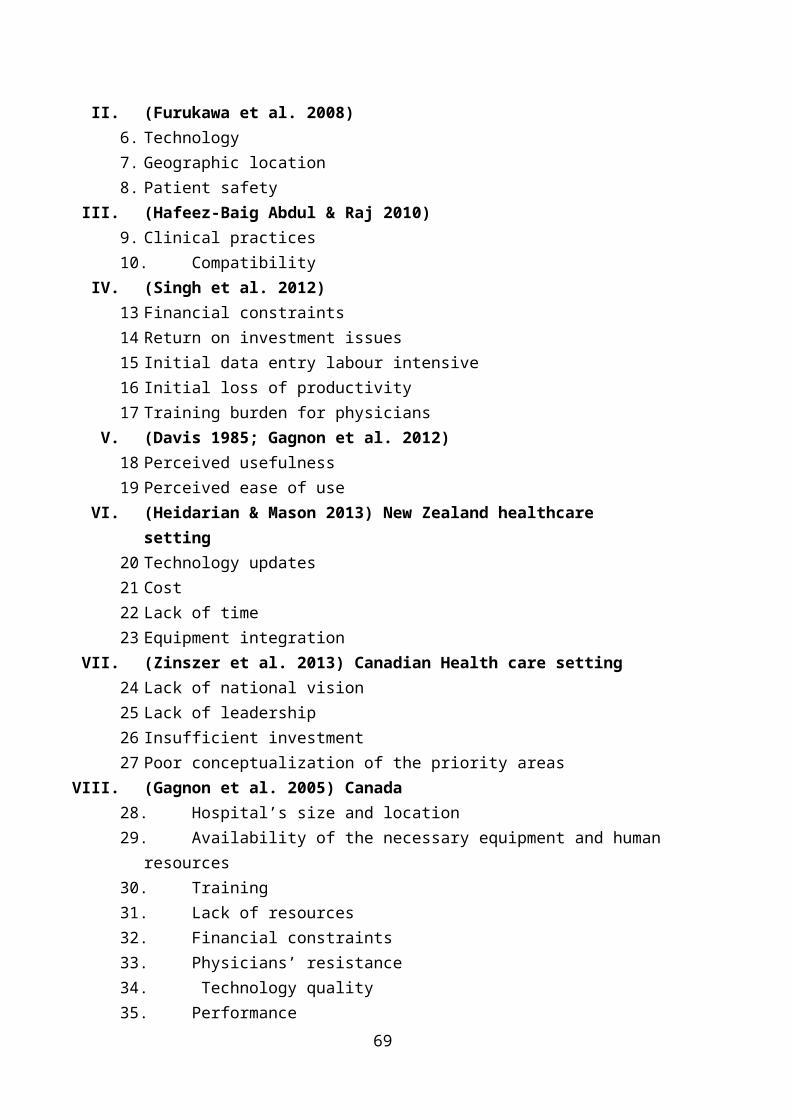
II. (Furukawa et al. 2008)6. Technology7. Geographic location8. Patient safety
III. (Hafeez-Baig Abdul & Raj 2010)9. Clinical practices10. Compatibility
IV. (Singh et al. 2012)13 Financial constraints14 Return on investment issues15 Initial data entry labour intensive16 Initial loss of productivity17 Training burden for physicians
V. (Davis 1985; Gagnon et al. 2012)18 Perceived usefulness 19 Perceived ease of use
VI. (Heidarian & Mason 2013) New Zealand healthcare setting
20 Technology updates21 Cost 22 Lack of time 23 Equipment integration
VII. (Zinszer et al. 2013) Canadian Health care setting24 Lack of national vision 25 Lack of leadership26 Insufficient investment27 Poor conceptualization of the priority areas
VIII. (Gagnon et al. 2005) Canada28. Hospital’s size and location29. Availability of the necessary equipment and human
resources30. Training31. Lack of resources32. Financial constraints 33. Physicians’ resistance34. Technology quality35. Performance
69
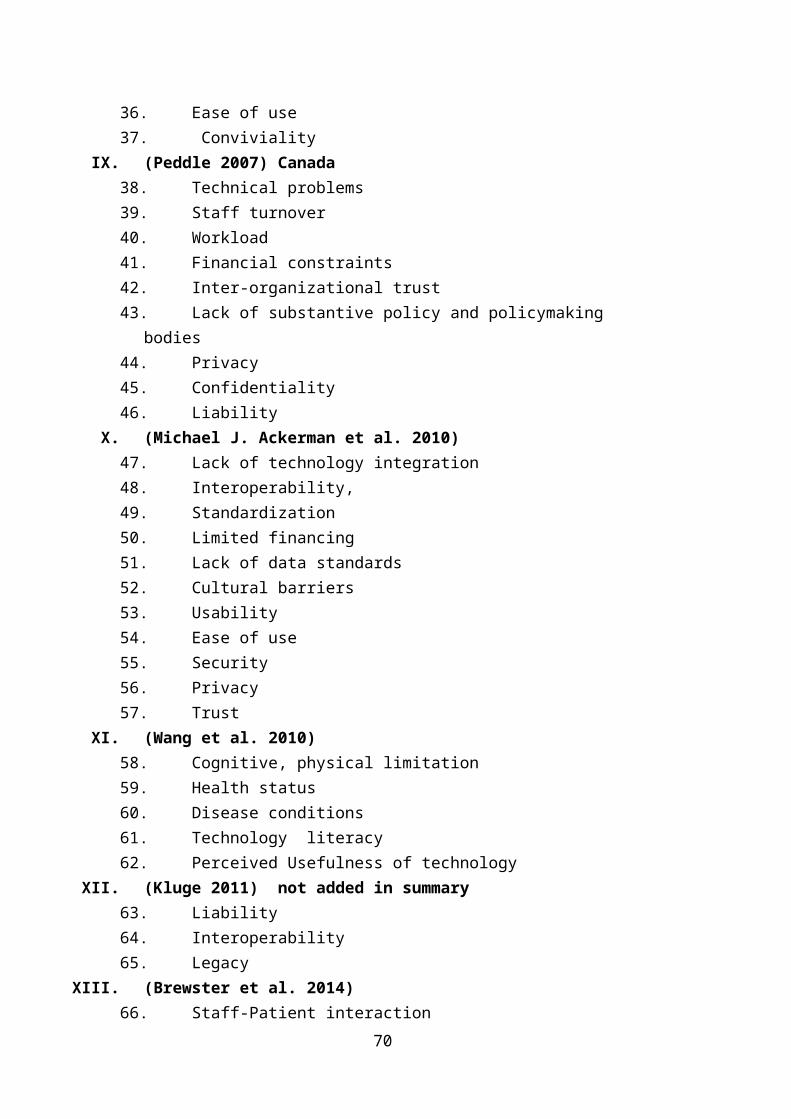
36. Ease of use37. Conviviality
IX. (Peddle 2007) Canada38. Technical problems39. Staff turnover40. Workload41. Financial constraints42. Inter-organizational trust43. Lack of substantive policy and policymaking
bodies44. Privacy45. Confidentiality 46. Liability
X. (Michael J. Ackerman et al. 2010)47. Lack of technology integration48. Interoperability,49. Standardization50. Limited financing 51. Lack of data standards52. Cultural barriers53. Usability54. Ease of use55. Security56. Privacy57. Trust
XI. (Wang et al. 2010)58. Cognitive, physical limitation59. Health status60. Disease conditions61. Technology literacy62. Perceived Usefulness of technology
XII. (Kluge 2011) not added in summary63. Liability64. Interoperability65. Legacy
XIII. (Brewster et al. 2014)66. Staff-Patient interaction
70
67. Credibility68. Negative impact of service change69. Autonomy70. Technical issues
XIV. (Daim, Basoglu & Topacan 2013)71 Usefulness72 Quality of Services73 Compatibility With User’s Life Style74 Quality of Support75 Quality of Information76 Image of Technology77 Usages Time78 Accessibility79 Easy to Use
XV. (Cimperman et al. 2013) 80. Security 81. Usability
XVI. (Daniel Castro, Ben miller & Nager 2014)82. Standard of care83. State licensing policies84. Compatibility 85. Interoperabiliy
XVII. (Bradford et al. 2014) Australia86. Technical ( setting up equipment, username and
password )87. Individual (culture, linguistic and social
variations)88. Service factors (Lack of staff)
XVIII. (Wu, Wang & Lin 2007)89. Device Size90. Access Procedure91. Ease of use92. Attitude93. Self- efficacy94. Compatibility95. Technical Support and Training
XIX. (Yangil & Chen 2007)71
96 Attitude of individual (healthcare professional) 97 Perceived usefulness98 Perceived ease of use99 Self-efficacy100 Organisation size101 Observability
XX. (Kim & Garrison 2008)102 Cognitive Influence Process
a. Job relevanceb. Perceived ease of usec. Perceived usefulness
103 Technological Influence Processa. Ubiquityb. Reachabilityc.
XXI. (Wu, Li & Fu 2011)104 Personal innovativeness105 Availability
XXII. (Goswami & Chandra 2013)106 Interface clarity107 User friendliness108 Social influences109 Support of product and services provided110 Learning predisposition
XXIII. (Deng, Mo & Liu 2013)111 Physical condition112 Resistance to change113 Technology anxiety114 Self-actualization needs
72
Appendix 4: Steps followed for development of conceptual frameworkStep1: Thorough study of literature for adoption of technology in healthcare
In step 1 thorough study of literature is conducted tobecome familiar with the topic of the research. Severalkeywords are used to search the literature. Some of themare: adoption of technology, factors for adoption oftechnology, technology and healthcare, mobile devices inhealthcare, user intention for technology use, telehealth,mHealth and eHealth. Databases used to search literatureare: EBSCOhost MegaFILE Complete which covers topic onvarious fields such as arts, biological and physicalsciences, business, education, engineering and spatialsciences, maths computing, and nursing. Other secondarysources used for this research are web of sciences, Medlinelibrary and Wily online library, USQ library, googlescholar etc. A list of all the research articles read forthis research is attached in Appendix 1.
Step2: Identification of factors influencing adoption of technology in healthcare.
In this phase various factors influencing adoption oftechnology are identified. This step provides a broad viewof all the factors which can influence adoption oftechnology in healthcare environment. Factors identified inthis step are related to adoption of various technologiessuch as EHR, wireless technology, HIT, telehealth, hometele monitoring, eHealth mobile computing and mobile health(Daim, Basoglu & Topacan 2013; Deng, Mo & Liu 2013;Heidarian & Mason 2013; Singh et al. 2012; Wang et al.2010; Zinszer et al. 2013). After completing step2 it isidentified that some studies are conducted for adoption oftechnology in the healthcare from an individual andorganisational level. (Appendix 3 attached in research
73
proposal shows a list factors found from various researcharticles.) So, step3 is followed to separate out factors atindividual level and organisational level of adoption oftechnology.
Step3: Identification of factors influencing adoption of technology in healthcare at individual level
This step is followed to understand factors influencingindividual level of adoption of technology in thehealthcare. Therefore, factors are put into two categories.The scrutiny of factors is accomplished based on whetherthe study is conducted from organisational perspective orindividual perspective. For example, the studies which areconducted for adoption of technology from management peopleperspective, implementation of an application in healthcareand policies are put in the category of organisation levelof adoption of technology (Gagnon et al. 2005; Peddle 2007;Zinszer et al. 2013). Further the studies which areconducted for adoption of technology in the healthcare byHCPs, patients are considered at individual level ofadoption (Bradford et al. 2014; Deng, Mo & Liu 2013; Gagnonet al. 2003; Wang et al. 2010). In this step main focus isto select the factors which influence HCPs and patients foradoption of technology. There are, numerous factorsaffecting adoption of technology in healthcare atindividual level but it is not necessary that all thefactors found in literature at this stage may influenceadoption of mobile devices in healthcare. So there isfurther need to choose factors appropriate for adoption ofmobile devices in the healthcare which is explained in nextstep.
Step 4: Selection of factors appropriate for adoption for mobile devices in healthcare at individual level
The motive of this step is to select most appropriatefactors influencing adoption of mobile devices inhealthcare. Research articles selected for this criterion
74
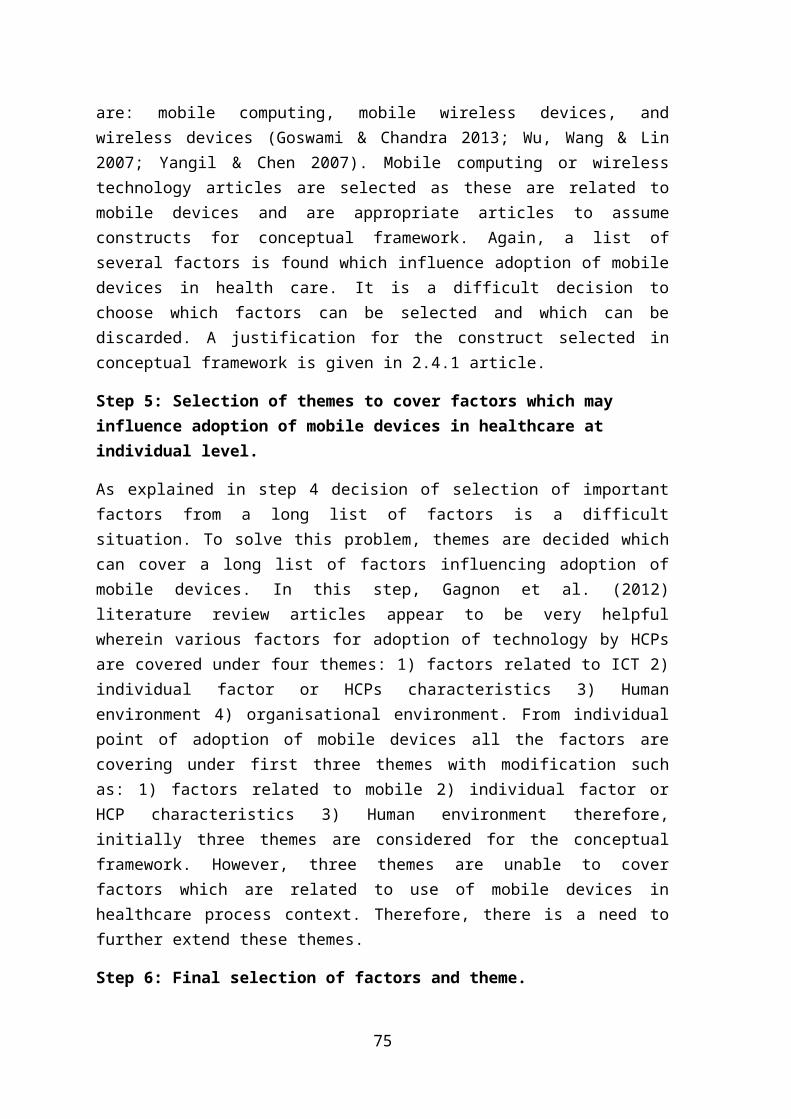
are: mobile computing, mobile wireless devices, andwireless devices (Goswami & Chandra 2013; Wu, Wang & Lin2007; Yangil & Chen 2007). Mobile computing or wirelesstechnology articles are selected as these are related tomobile devices and are appropriate articles to assumeconstructs for conceptual framework. Again, a list ofseveral factors is found which influence adoption of mobiledevices in health care. It is a difficult decision tochoose which factors can be selected and which can bediscarded. A justification for the construct selected inconceptual framework is given in 2.4.1 article.
Step 5: Selection of themes to cover factors which may influence adoption of mobile devices in healthcare at individual level.
As explained in step 4 decision of selection of importantfactors from a long list of factors is a difficultsituation. To solve this problem, themes are decided whichcan cover a long list of factors influencing adoption ofmobile devices. In this step, Gagnon et al. (2012)literature review articles appear to be very helpfulwherein various factors for adoption of technology by HCPsare covered under four themes: 1) factors related to ICT 2)individual factor or HCPs characteristics 3) Humanenvironment 4) organisational environment. From individualpoint of adoption of mobile devices all the factors arecovering under first three themes with modification suchas: 1) factors related to mobile 2) individual factor orHCP characteristics 3) Human environment therefore,initially three themes are considered for the conceptualframework. However, three themes are unable to coverfactors which are related to use of mobile devices inhealthcare process context. Therefore, there is a need tofurther extend these themes.
Step 6: Final selection of factors and theme.
75
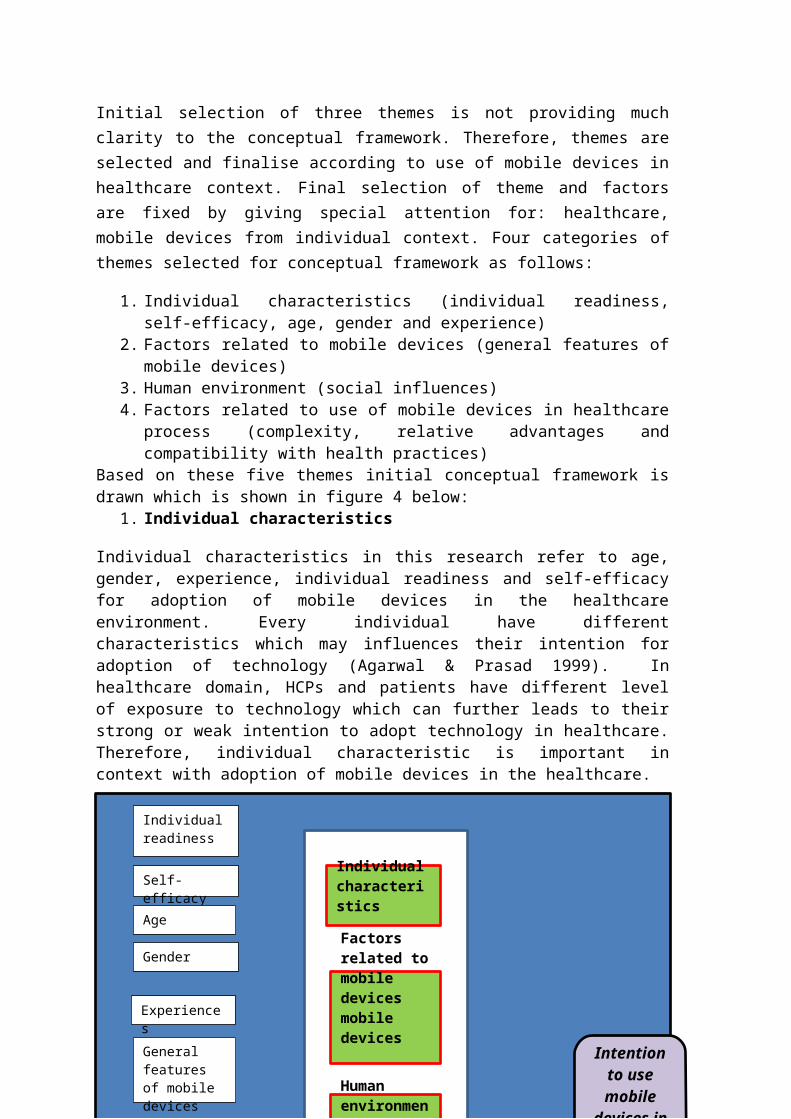
Initial selection of three themes is not providing muchclarity to the conceptual framework. Therefore, themes areselected and finalise according to use of mobile devices inhealthcare context. Final selection of theme and factorsare fixed by giving special attention for: healthcare,mobile devices from individual context. Four categories ofthemes selected for conceptual framework as follows:
1. Individual characteristics (individual readiness,self-efficacy, age, gender and experience)
2. Factors related to mobile devices (general features ofmobile devices)
3. Human environment (social influences)4. Factors related to use of mobile devices in healthcare
process (complexity, relative advantages andcompatibility with health practices)
Based on these five themes initial conceptual framework isdrawn which is shown in figure 4 below:
1. Individual characteristics
Individual characteristics in this research refer to age,gender, experience, individual readiness and self-efficacyfor adoption of mobile devices in the healthcareenvironment. Every individual have differentcharacteristics which may influences their intention foradoption of technology (Agarwal & Prasad 1999). Inhealthcare domain, HCPs and patients have different levelof exposure to technology which can further leads to theirstrong or weak intention to adopt technology in healthcare.Therefore, individual characteristic is important incontext with adoption of mobile devices in the healthcare.
76Intention
to use mobile
devices in telehealth
Human environment
Factors related to mobile devices mobile devices
Individual characteristics
Individual readiness
Self-efficacy
General features of mobile devices
Age
Gender
Experiences
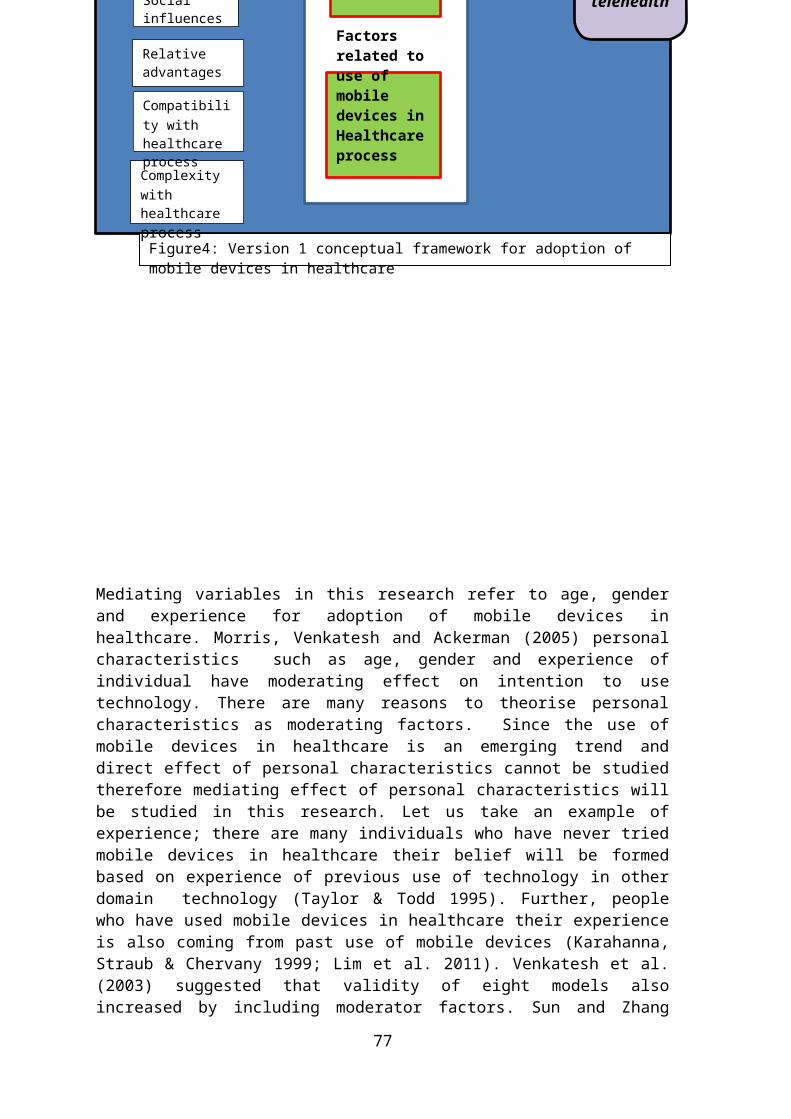
Mediating variables in this research refer to age, genderand experience for adoption of mobile devices inhealthcare. Morris, Venkatesh and Ackerman (2005) personalcharacteristics such as age, gender and experience ofindividual have moderating effect on intention to usetechnology. There are many reasons to theorise personalcharacteristics as moderating factors. Since the use ofmobile devices in healthcare is an emerging trend anddirect effect of personal characteristics cannot be studiedtherefore mediating effect of personal characteristics willbe studied in this research. Let us take an example ofexperience; there are many individuals who have never triedmobile devices in healthcare their belief will be formedbased on experience of previous use of technology in otherdomain technology (Taylor & Todd 1995). Further, peoplewho have used mobile devices in healthcare their experienceis also coming from past use of mobile devices (Karahanna,Straub & Chervany 1999; Lim et al. 2011). Venkatesh et al.(2003) suggested that validity of eight models alsoincreased by including moderator factors. Sun and Zhang
77
Intention to use mobile
devices in telehealth
Figure4: Version 1 conceptual framework for adoption of mobile devices in healthcare
Human environment
Factors related to use of mobile devices in Healthcare process
Complexity with healthcare process
Compatibility with healthcare process
Relative advantages
Social influences
(2006) also identified age, gender and experience asmoderator variables and their importance in his meta-analysis research. Therefore, age, gender and experienceare studied as moderator factors in current research.
2. Factors related to mobile devicesRefers to those features of mobile devices which caninfluence their use in the health care setting. The factorsconsidered under this theme are the general factors ofmobile devices such as image quality, battery life andscreen size.
3. Factors related to use of mobile devices in healthcareprocess
Refer to those factors of mobile devices which caninfluence use of mobile devices in the healthcareprocesses. This theme is understood from Fichman (1992)which states : characteristics of innovation are thecharacteristics posed by innovation and considered byadopters to adopt innovation. Every innovation has its ownspecific characteristics. For example, people usually wantto see the benefits of innovation. In this research,mobile devices are considered innovation and theiradvantages; complexity to operate, compatibility withhealthcare environment can influence individual intentionfor adoption of these devices in healthcare. Therefore,factors proposed in this theme are: complexity level tooperate mobile devices in healthcare practices, relativeadvantages and compatibility with health care practices.
4. Human environment
Human environment in this research is defined as people whoinfluence an individual for adoption of mobile devices inthe healthcare. They may by peer group, colleagues andrelatives. Human environment play a major role for adoptionof technology. In human environment one factor that is‘social influences’ is considered which affect individualfor adoption of mobile device in healthcare.
78
79
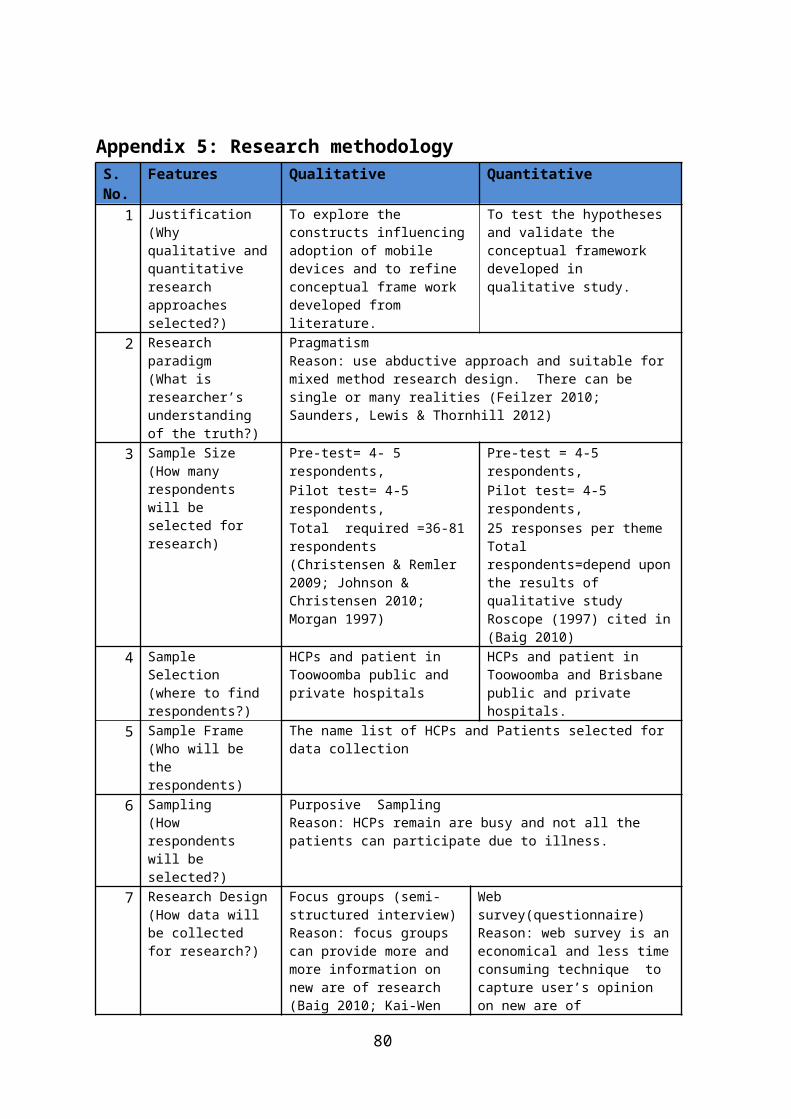
Appendix 5: Research methodologyS. No.
Features Qualitative Quantitative
1 Justification(Why qualitative andquantitative research approaches selected?)
To explore the constructs influencing adoption of mobile devices and to refine conceptual frame work developed from literature.
To test the hypotheses and validate the conceptual framework developed in qualitative study.
2 Research paradigm(What is researcher’s understanding of the truth?)
PragmatismReason: use abductive approach and suitable for mixed method research design. There can be single or many realities (Feilzer 2010; Saunders, Lewis & Thornhill 2012)
3 Sample Size (How many respondents will be selected for research)
Pre-test= 4- 5 respondents,
Pre-test = 4-5 respondents,
Pilot test= 4-5 respondents,
Pilot test= 4-5 respondents,
Total required =36-81 respondents (Christensen & Remler 2009; Johnson & Christensen 2010; Morgan 1997)
25 responses per themeTotal respondents=depend uponthe results of qualitative study Roscope (1997) cited in(Baig 2010)
4 Sample Selection (where to find respondents?)
HCPs and patient in Toowoomba public and private hospitals
HCPs and patient in Toowoomba and Brisbane public and private hospitals.
5 Sample Frame(Who will be the respondents)
The name list of HCPs and Patients selected for data collection
6 Sampling(How respondents will be selected?)
Purposive SamplingReason: HCPs remain are busy and not all the patients can participate due to illness.
7 Research Design(How data will be collected for research?)
Focus groups (semi- structured interview)Reason: focus groups can provide more and more information on new are of research(Baig 2010; Kai-Wen
Web survey(questionnaire)Reason: web survey is aneconomical and less timeconsuming technique to capture user’s opinion on new are of
80
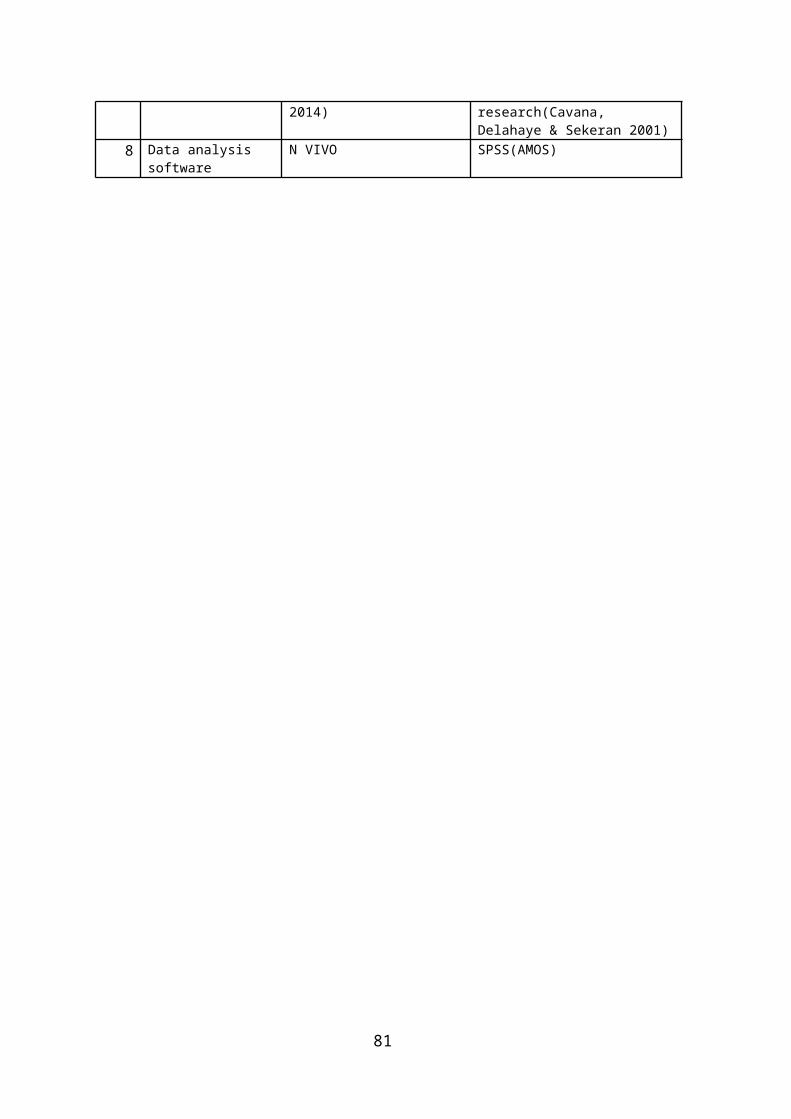
2014) research(Cavana, Delahaye & Sekeran 2001)
8 Data analysis software
N VIVO SPSS(AMOS)
81
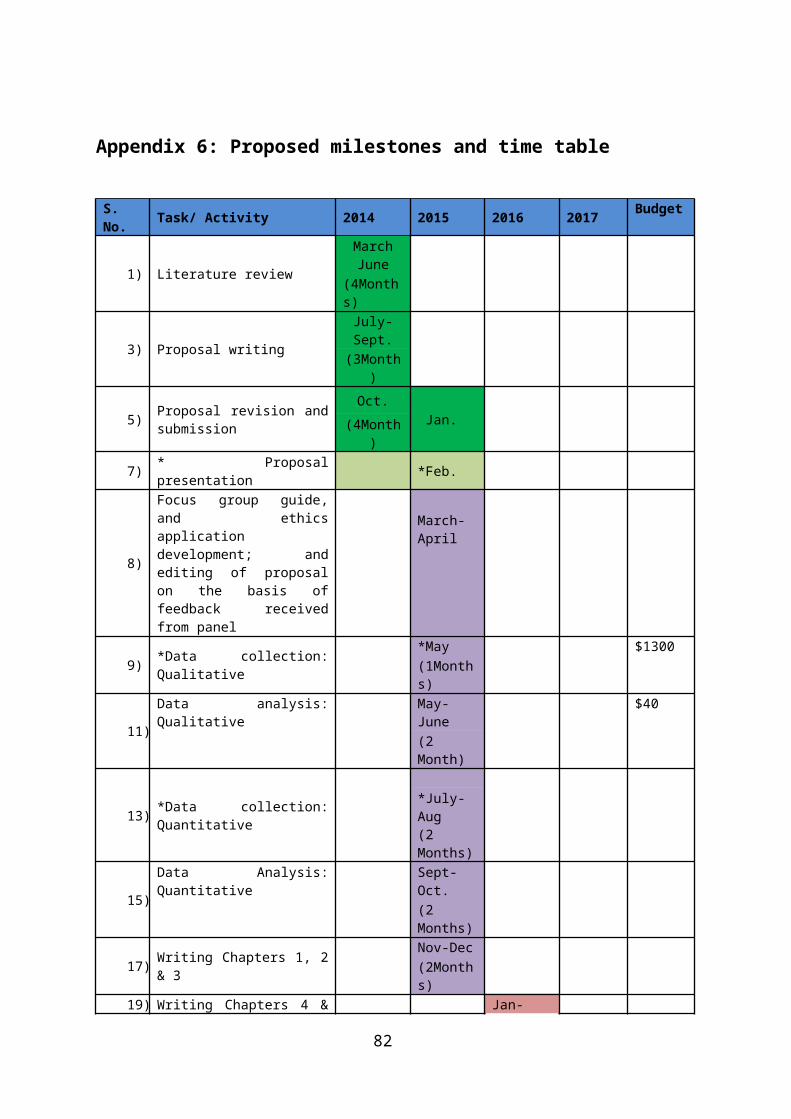
Appendix 6: Proposed milestones and time table
S. No. Task/ Activity 2014 2015 2016 2017 Budget
1) Literature review
MarchJune
(4Months)
3) Proposal writing
July-Sept.(3Month
)
5) Proposal revision andsubmission
Oct. Jan.(4Month
)
7) * Proposalpresentation *Feb.
8)
Focus group guide,and ethicsapplicationdevelopment; andediting of proposalon the basis offeedback receivedfrom panel
March-April
9) *Data collection:Qualitative
*May $1300(1Months)
11)
Data analysis:Qualitative
May-June
$40
(2 Month)
13) *Data collection:Quantitative
*July-Aug(2 Months)
15)
Data Analysis:Quantitative
Sept-Oct.(2 Months)
17) Writing Chapters 1, 2& 3
Nov-Dec(2Months)
19) Writing Chapters 4 & Jan-
82
5March(3Months)
21) Dissertation review
April- July(4Months)
23) *Conferenceattendance
*Aug $3000(1 month)
25) Thesis proof reading,printing and binding Aug $600
26) *Dissertationsubmission
*1st Sept.(1 Month)
28) External examination
Oct.-Dec(3Months)
30) Dissertation revision Jan-Feb (2month)
31) Completion date /total
1 March
4940
Appendix 7: Thesis layout
Chapter Title of the ChapterChapter 1 Introduction
Chapter 2 Literature review
Chapter 3 Research methodology
Chapter 4 Focus group data collection
Chapter 5 Focus group data analysis, results discussion and improved conceptual framework
Chapter 6 Quantitative data collection
83
Chapter 7 Quantitative data analysis and results discussion, final conceptual framework
Chapter 9 Conclusions, limitations, contributions and future research
84
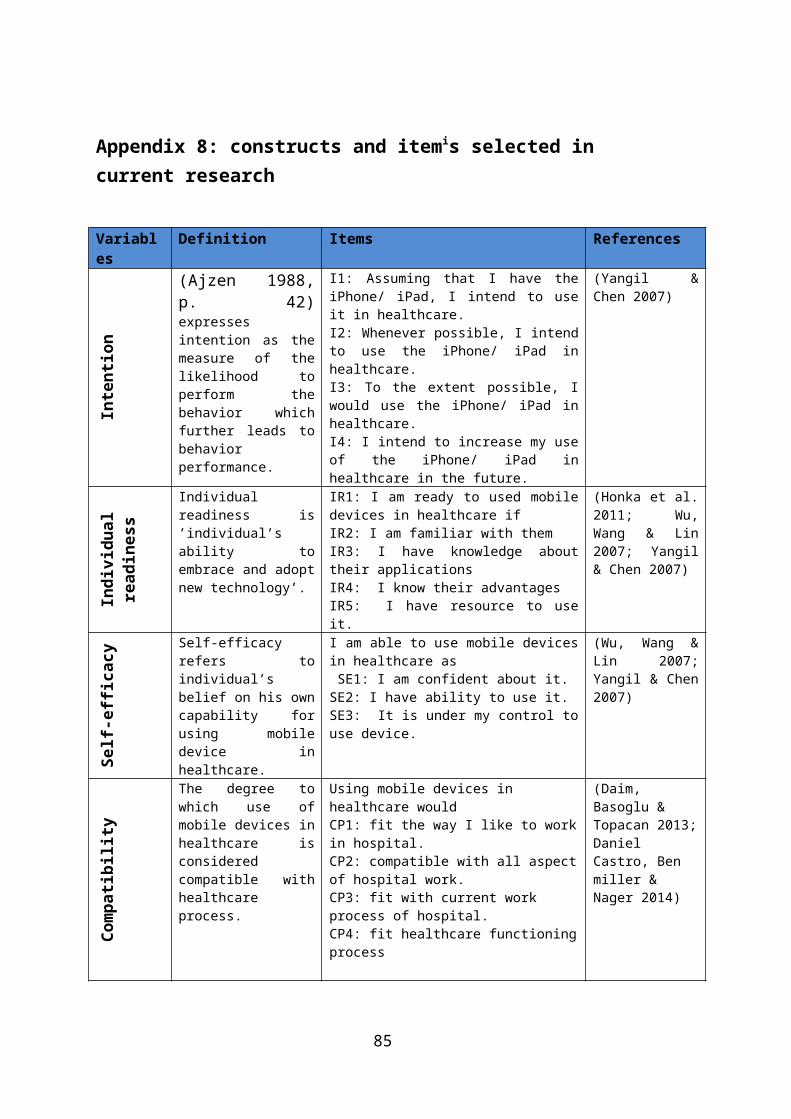
Appendix 8: constructs and itemis selected in current research
Variables
Definition Items References
Inte
ntio
n
(Ajzen 1988,p. 42)expressesintention as themeasure of thelikelihood toperform thebehavior whichfurther leads tobehaviorperformance.
I1: Assuming that I have theiPhone/ iPad, I intend to useit in healthcare.I2: Whenever possible, I intendto use the iPhone/ iPad inhealthcare.I3: To the extent possible, Iwould use the iPhone/ iPad inhealthcare.I4: I intend to increase my useof the iPhone/ iPad inhealthcare in the future.
(Yangil &Chen 2007)
Indivi
dual
readines
s
Individualreadiness is’individual’sability toembrace and adoptnew technology’.
IR1: I am ready to used mobiledevices in healthcare ifIR2: I am familiar with themIR3: I have knowledge abouttheir applicationsIR4: I know their advantagesIR5: I have resource to useit.
(Honka et al.2011; Wu,Wang & Lin2007; Yangil& Chen 2007)
Self-e
fficacy Self-efficacy
refers toindividual’sbelief on his owncapability forusing mobiledevice inhealthcare.
I am able to use mobile devicesin healthcare as SE1: I am confident about it.SE2: I have ability to use it.SE3: It is under my control touse device.
(Wu, Wang &Lin 2007;Yangil & Chen2007)
Compat
ibil
ity
The degree towhich use ofmobile devices inhealthcare isconsideredcompatible withhealthcareprocess.
Using mobile devices in healthcare wouldCP1: fit the way I like to workin hospital.CP2: compatible with all aspectof hospital work.CP3: fit with current work process of hospital.CP4: fit healthcare functioningprocess
(Daim, Basoglu & Topacan 2013;Daniel Castro, Ben miller & Nager 2014)
85
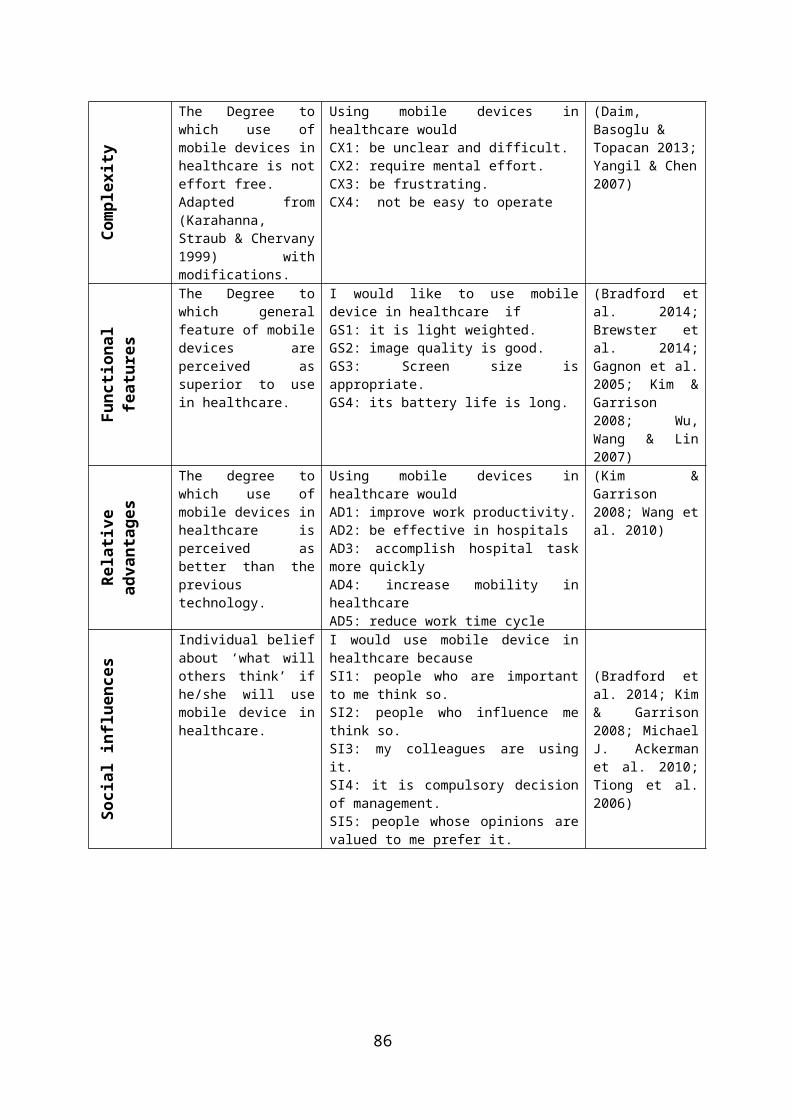
Comp
lexity
The Degree towhich use ofmobile devices inhealthcare is noteffort free.Adapted from(Karahanna,Straub & Chervany1999) withmodifications.
Using mobile devices inhealthcare wouldCX1: be unclear and difficult.CX2: require mental effort.CX3: be frustrating.CX4: not be easy to operate
(Daim, Basoglu & Topacan 2013;Yangil & Chen2007)
Func
tional
feat
ures
The Degree towhich generalfeature of mobiledevices areperceived assuperior to usein healthcare.
I would like to use mobiledevice in healthcare ifGS1: it is light weighted.GS2: image quality is good.GS3: Screen size isappropriate.GS4: its battery life is long.
(Bradford etal. 2014;Brewster etal. 2014;Gagnon et al.2005; Kim &Garrison2008; Wu,Wang & Lin2007)
Relative
advant
ages
The degree towhich use ofmobile devices inhealthcare isperceived asbetter than theprevioustechnology.
Using mobile devices inhealthcare wouldAD1: improve work productivity.AD2: be effective in hospitalsAD3: accomplish hospital taskmore quicklyAD4: increase mobility inhealthcareAD5: reduce work time cycle
(Kim &Garrison2008; Wang etal. 2010)
Soci
al influence
s
Individual beliefabout ‘what willothers think’ ifhe/she will usemobile device inhealthcare.
I would use mobile device inhealthcare becauseSI1: people who are importantto me think so.SI2: people who influence methink so.SI3: my colleagues are usingit.SI4: it is compulsory decisionof management.SI5: people whose opinions arevalued to me prefer it.
(Bradford etal. 2014; Kim& Garrison2008; MichaelJ. Ackermanet al. 2010;Tiong et al.2006)
86
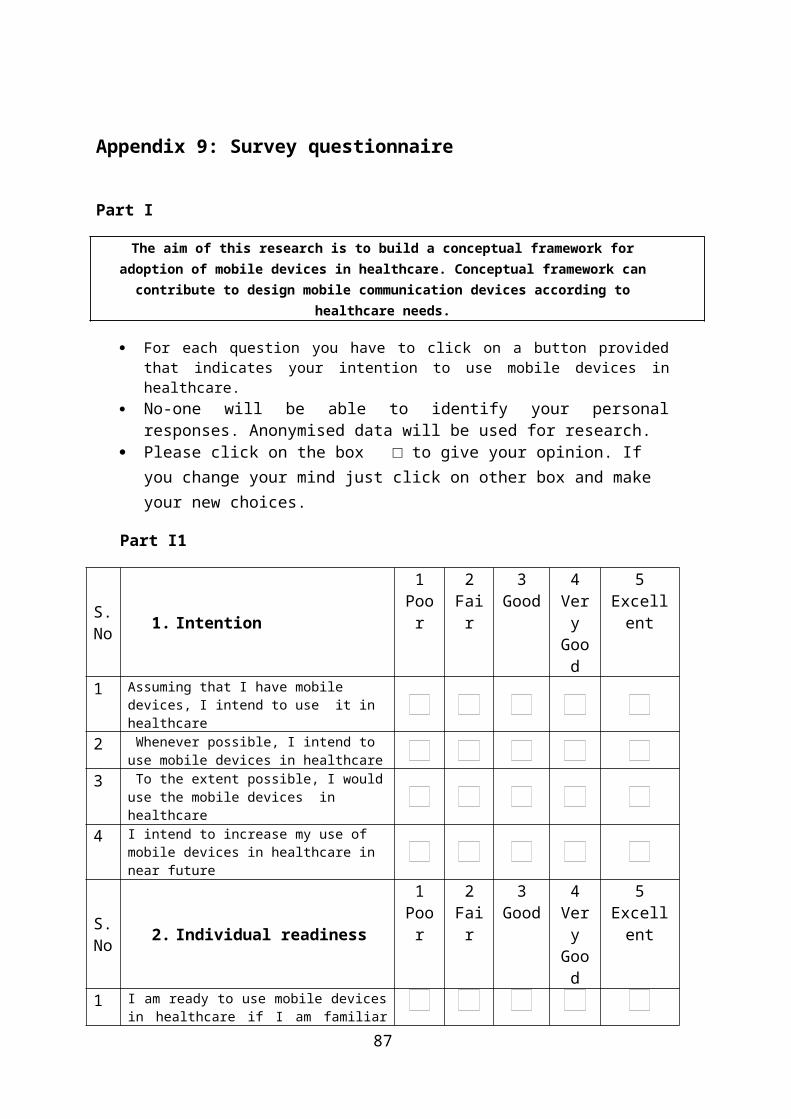
Appendix 9: Survey questionnaire
Part I
The aim of this research is to build a conceptual framework foradoption of mobile devices in healthcare. Conceptual framework cancontribute to design mobile communication devices according to
healthcare needs.
For each question you have to click on a button providedthat indicates your intention to use mobile devices inhealthcare.
No-one will be able to identify your personalresponses. Anonymised data will be used for research.
Please click on the box □ to give your opinion. If you change your mind just click on other box and make your new choices.
Part I1
S.No 1. Intention
1Poor
2Fair
3Good
4VeryGood
5Excellent
1 Assuming that I have mobile devices, I intend to use it in healthcare
2 Whenever possible, I intend to use mobile devices in healthcare
3 To the extent possible, I woulduse the mobile devices in healthcare
4 I intend to increase my use of mobile devices in healthcare in near future
S.No 2. Individual readiness
1Poor
2Fair
3Good
4VeryGood
5Excellent
1 I am ready to use mobile devicesin healthcare if I am familiar
87
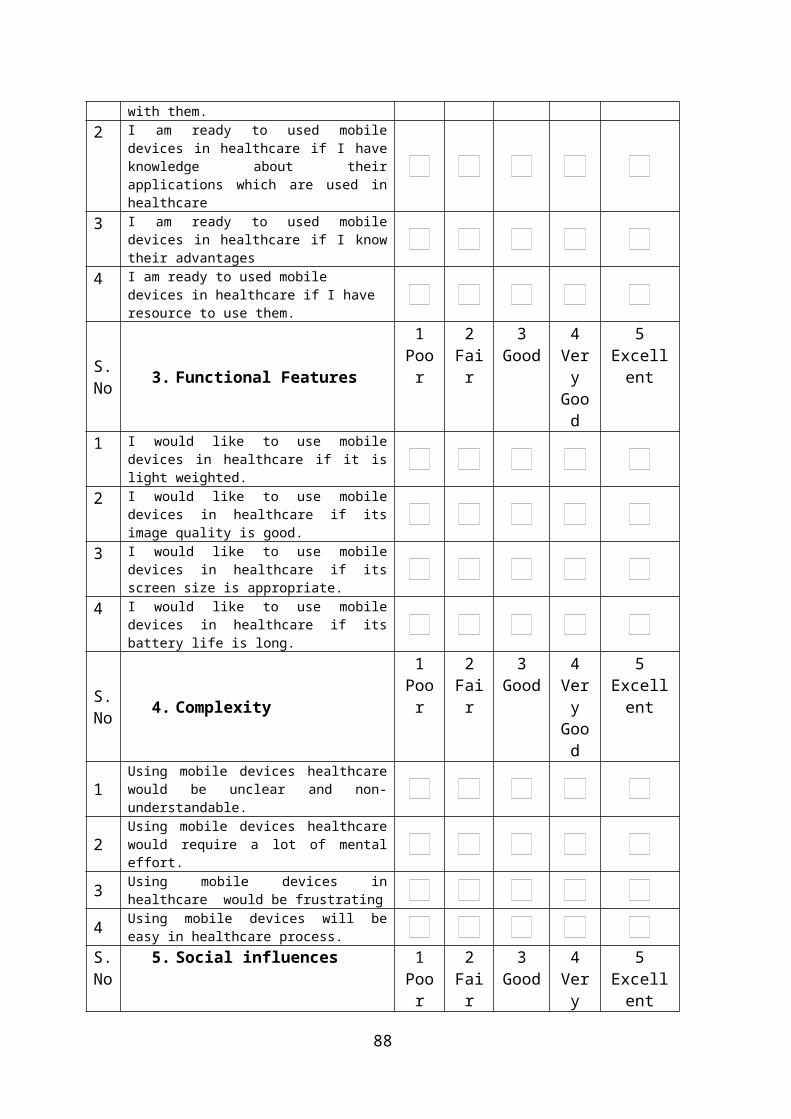
with them.2 I am ready to used mobile
devices in healthcare if I haveknowledge about theirapplications which are used inhealthcare
3 I am ready to used mobiledevices in healthcare if I knowtheir advantages
4 I am ready to used mobile devices in healthcare if I have resource to use them.
S.No 3. Functional Features
1Poor
2Fair
3Good
4VeryGood
5Excellent
1 I would like to use mobiledevices in healthcare if it islight weighted.
2 I would like to use mobiledevices in healthcare if itsimage quality is good.
3 I would like to use mobiledevices in healthcare if itsscreen size is appropriate.
4 I would like to use mobiledevices in healthcare if itsbattery life is long.
S.No 4. Complexity
1Poor
2Fair
3Good
4VeryGood
5Excellent
1Using mobile devices healthcarewould be unclear and non-understandable.
2Using mobile devices healthcarewould require a lot of mentaleffort.
3 Using mobile devices inhealthcare would be frustrating
4 Using mobile devices will beeasy in healthcare process.
S.No
5. Social influences 1Poor
2Fair
3Good
4Very
5Excellent
88
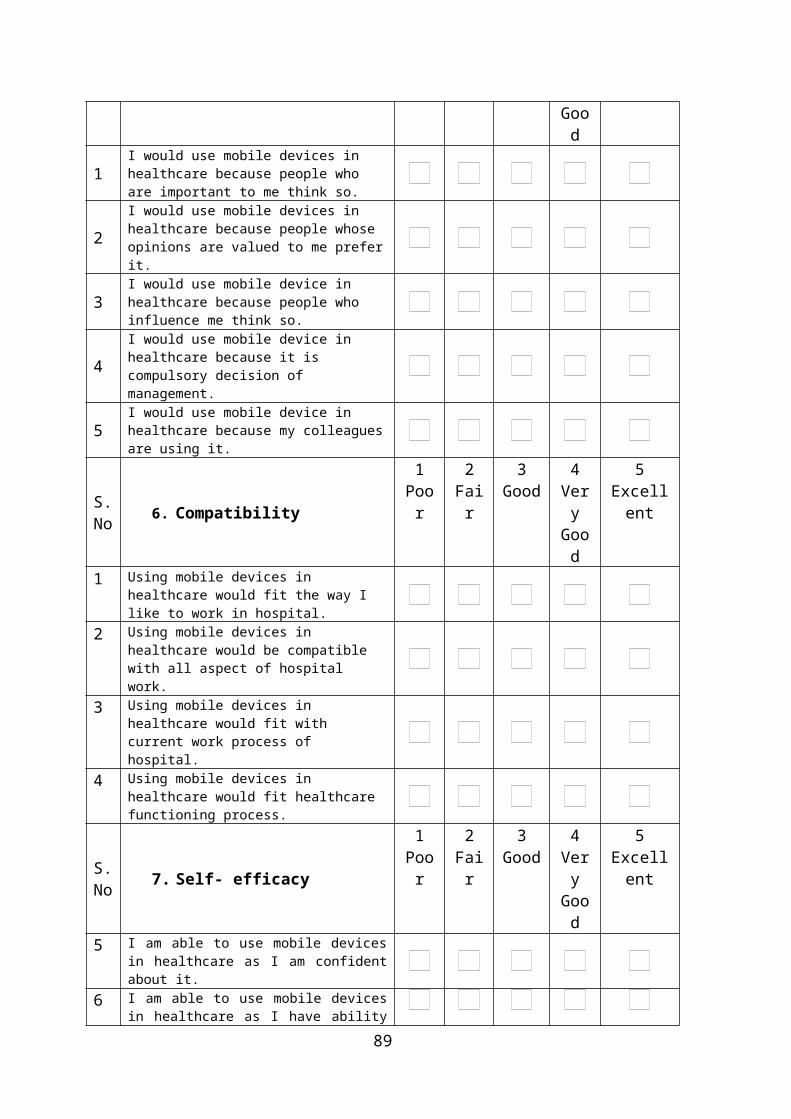
Good
1I would use mobile devices in healthcare because people who are important to me think so.
2I would use mobile devices in healthcare because people whose opinions are valued to me preferit.
3I would use mobile device in healthcare because people who influence me think so.
4I would use mobile device in healthcare because it is compulsory decision of management.
5I would use mobile device in healthcare because my colleaguesare using it.
S.No 6. Compatibility
1Poor
2Fair
3Good
4VeryGood
5Excellent
1 Using mobile devices in healthcare would fit the way I like to work in hospital.
2 Using mobile devices in healthcare would be compatible with all aspect of hospital work.
3 Using mobile devices in healthcare would fit with current work process of hospital.
4 Using mobile devices in healthcare would fit healthcare functioning process.
S.No 7. Self- efficacy
1Poor
2Fair
3Good
4VeryGood
5Excellent
5 I am able to use mobile devicesin healthcare as I am confidentabout it.
6 I am able to use mobile devicesin healthcare as I have ability
89
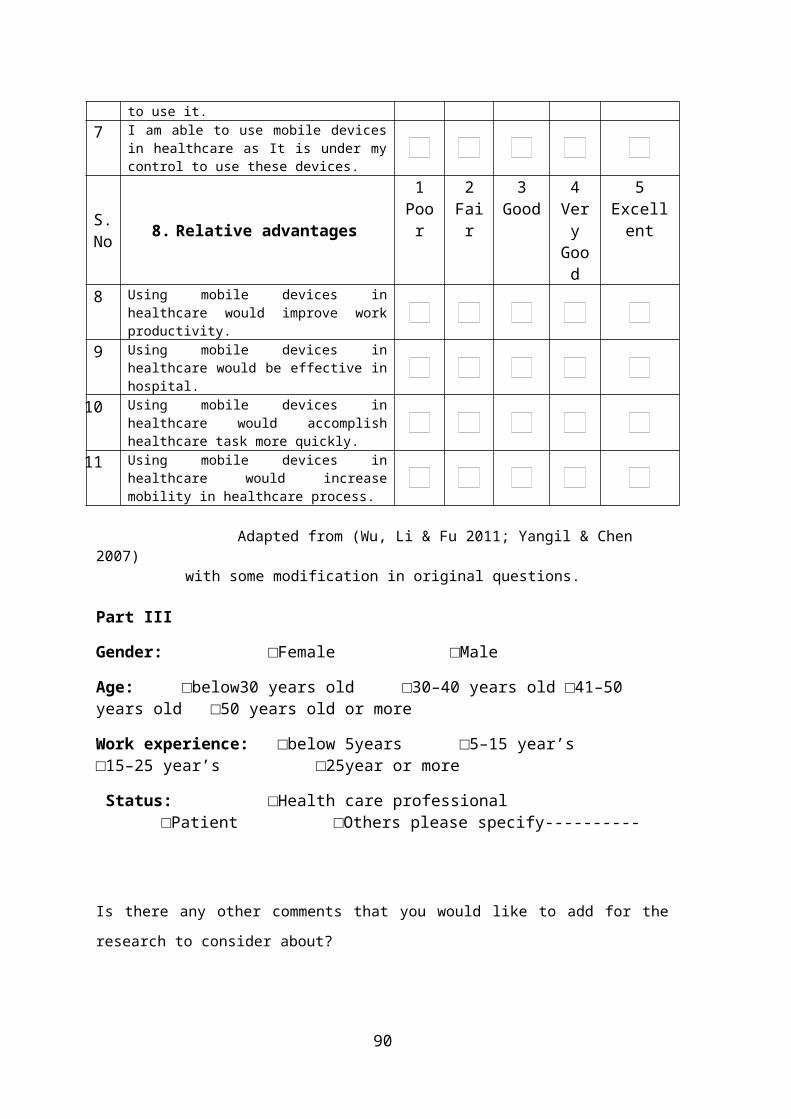
to use it.7 I am able to use mobile devices
in healthcare as It is under mycontrol to use these devices.
S.No 8. Relative advantages
1Poor
2Fair
3Good
4VeryGood
5Excellent
8 Using mobile devices inhealthcare would improve workproductivity.
9 Using mobile devices inhealthcare would be effective inhospital.
10 Using mobile devices inhealthcare would accomplishhealthcare task more quickly.
11 Using mobile devices inhealthcare would increasemobility in healthcare process.
Adapted from (Wu, Li & Fu 2011; Yangil & Chen 2007)
with some modification in original questions.
Part III
Gender: □Female □Male
Age: □below30 years old □30–40 years old □41–50 years old □50 years old or more
Work experience: □below 5years □5–15 year’s □15–25 year’s □25year or more
Status: □Health care professional □Patient □Others please specify----------
Is there any other comments that you would like to add for the
research to consider about?
90

Thank you for your time and effort to complete this survey.Your cooperation is valued and very much appreciated!
91
Appendix 10: Focus group questions
Part I
The aim of this research is to build a conceptual framework foradoption of mobile devices in healthcare. Conceptual framework cancontribute to design mobile communication devices according to
healthcare needs.
Time for this session is approximately 1hour. This session will be recorded (both audio and video) because all
the information provided by you is important to the researcher. No-one will be able to identify your personal responses.
Anonymised data will be used for research. This session is about to know your experiences or perception with
adoption/ use of mobile devices in healthcare. Participation to this session is voluntary; you are free to end
this session at any time.
Part II
1. Can you tell me your intention for adoption of mobile devices in healthcare?
Probe: if I have, to some extent, in coming future.
2. What do you think about your readiness for adoption of mobile devices in healthcare?
Probe: if I am familiar, if I have knowledge, if I have resources.
3. Do you think features of mobile devices can affect their adoptionin healthcare?
Probe: weight, image quality, screen size and battery life.
4. What is your perception about complexity level for the use of mobile devices in healthcare?
Probe: unclear, no understandable, need lot of mental effort,frustrating.
5. Do you think you will be influenced by your social circle for adoption of mobile devices in healthcare?
Probe: friends, relatives or colleagues.
92
6. Do you think use of mobile devices in healthcare will be compatible with healthcare process?
Probe: current work process, all work process, my style of working
7. Do you think you are able to use mobile devices in healthcare?
Probe: I am confident, I am able, it is under my control.
8. Can you tell me the advantages of using mobile devices in healthcare?
Probe: productivity, effective, fast.
9. Do you think other there are some other factors which can influence you for adoption of mobile devices in healthcare?
Part III
Gender: □Female □Male
Age: □below30 years old □30–40 years old □41–50 years old □50years old or more
Work experience: □below 5years □5–15 year’s □15–25 year’s □25year or more
Status: □Health care professional □Patient □Others please specify----------
Appendix 11: Topic introduction for unfocused groupMy name is Vasundhara and I am a PhD research student in USQ Toowoomba. I am trying to find out health care professionals and patients intention for adoption of mobiledevices, especially iPad and iPhone.
This discussion is very relaxed and open-ended. Instead of knocking on your door or ringing up and asking questions, it is simply to chat about the subject we’re interested in.So that’s what’s going to happen: I will explain what we’retrying to find out and then I will leave it to you to say whatever you would like to say about that subject.
It is going to be very informal. There are no rules. I am not in charge – I am just going to sit here and listen and
93
take a few notes. I will record the discussion as well – just so I don’t miss any of the things you’re saying. Is that OK with everybody?
The comments you make will be combined with comments made by other people in groups like this that I am conducting invarious public and private hospitals in Toowoomba, and those comments will form the basis of my research. Of course, your comments will be completely anonymous – I willnot use people’s names in any part of my research, and I don’t even need to know what your names are.
Thank you for giving up your time this evening/ morning – obviously, this kind of research depends on people like youbeing prepared to give us your time and your opinions. So thank you.
Okay then let’s get started. I simply want to know you perception about adoption of mobile devices in healthcare. In other words, what do you think if you have to adopt mobile devices like iPad /iPhone? It’s entirely up to you what you’d like to say … how you’d like to tackle the subject. There are no right or wrong answers.
Okay … over to you … leave me right out of it. I’m just here to listen. So … if one of you would like to start, let’s just see how the conversation goes from there …
Adapted from (Randle, Mackay & Dudley 2014) with some minorchanges
94
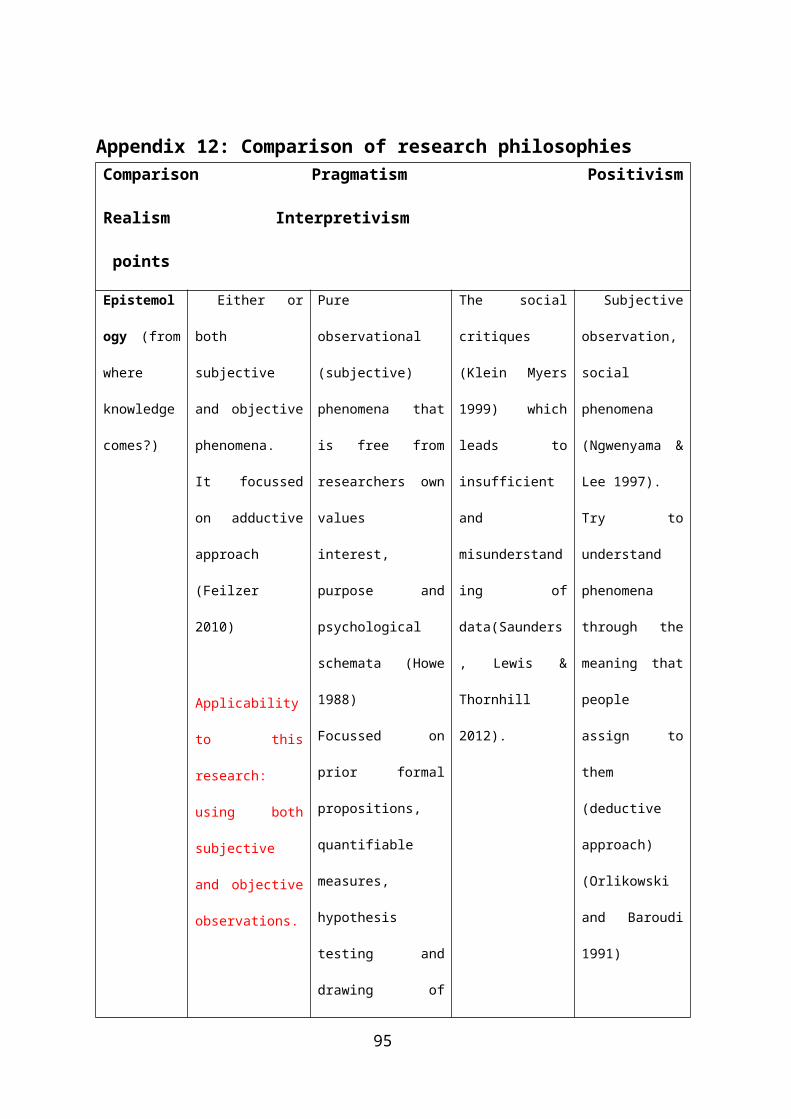
Appendix 12: Comparison of research philosophiesComparison Pragmatism Positivism
Realism Interpretivism
points
Epistemol
ogy (from
where
knowledge
comes?)
Either or
both
subjective
and objective
phenomena.
It focussed
on adductive
approach
(Feilzer
2010)
Applicability
to this
research:
using both
subjective
and objective
observations.
Pure
observational
(subjective)
phenomena that
is free from
researchers own
values
interest,
purpose and
psychological
schemata (Howe
1988)
Focussed on
prior formal
propositions,
quantifiable
measures,
hypothesis
testing and
drawing of
The social
critiques
(Klein Myers
1999) which
leads to
insufficient
and
misunderstand
ing of
data(Saunders
, Lewis &
Thornhill
2012).
Subjective
observation,
social
phenomena
(Ngwenyama &
Lee 1997).
Try to
understand
phenomena
through the
meaning that
people
assign to
them
(deductive
approach)
(Orlikowski
and Baroudi
1991)
95
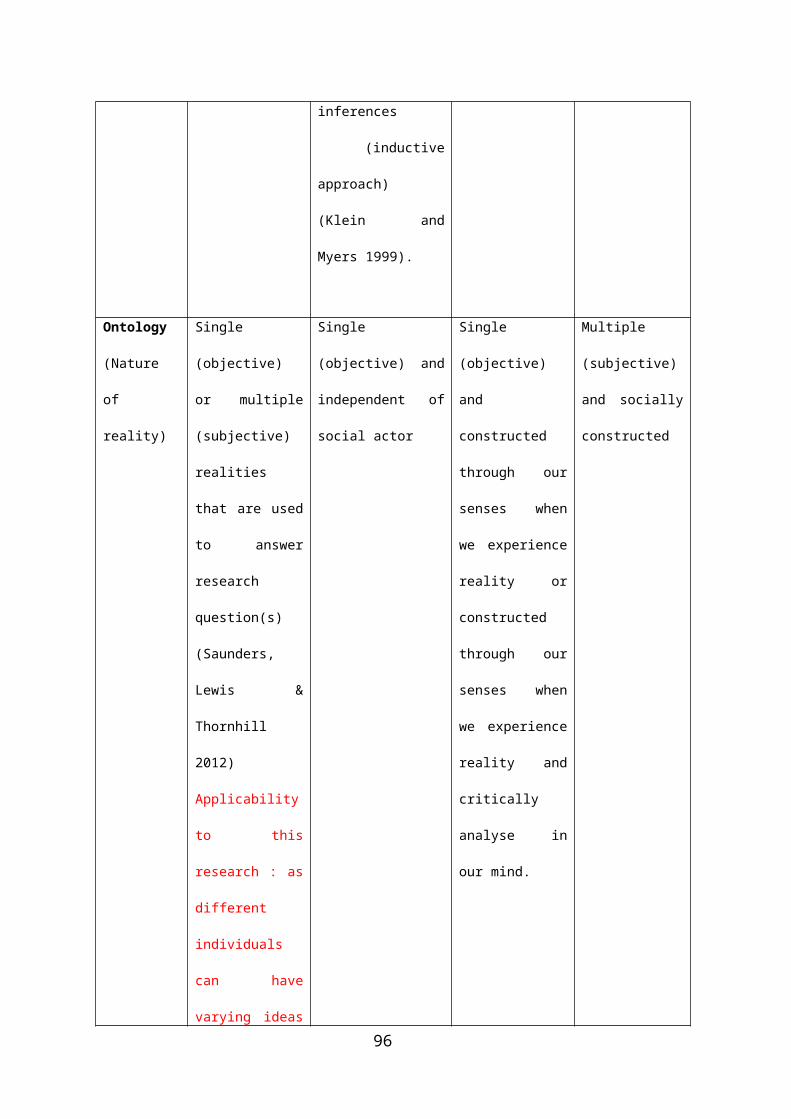
inferences
(inductive
approach)
(Klein and
Myers 1999).
Ontology
(Nature
of
reality)
Single
(objective)
or multiple
(subjective)
realities
that are used
to answer
research
question(s)
(Saunders,
Lewis &
Thornhill
2012)
Applicability
to this
research : as
different
individuals
can have
varying ideas
Single
(objective) and
independent of
social actor
Single
(objective)
and
constructed
through our
senses when
we experience
reality or
constructed
through our
senses when
we experience
reality and
critically
analyse in
our mind.
Multiple
(subjective)
and socially
constructed
96
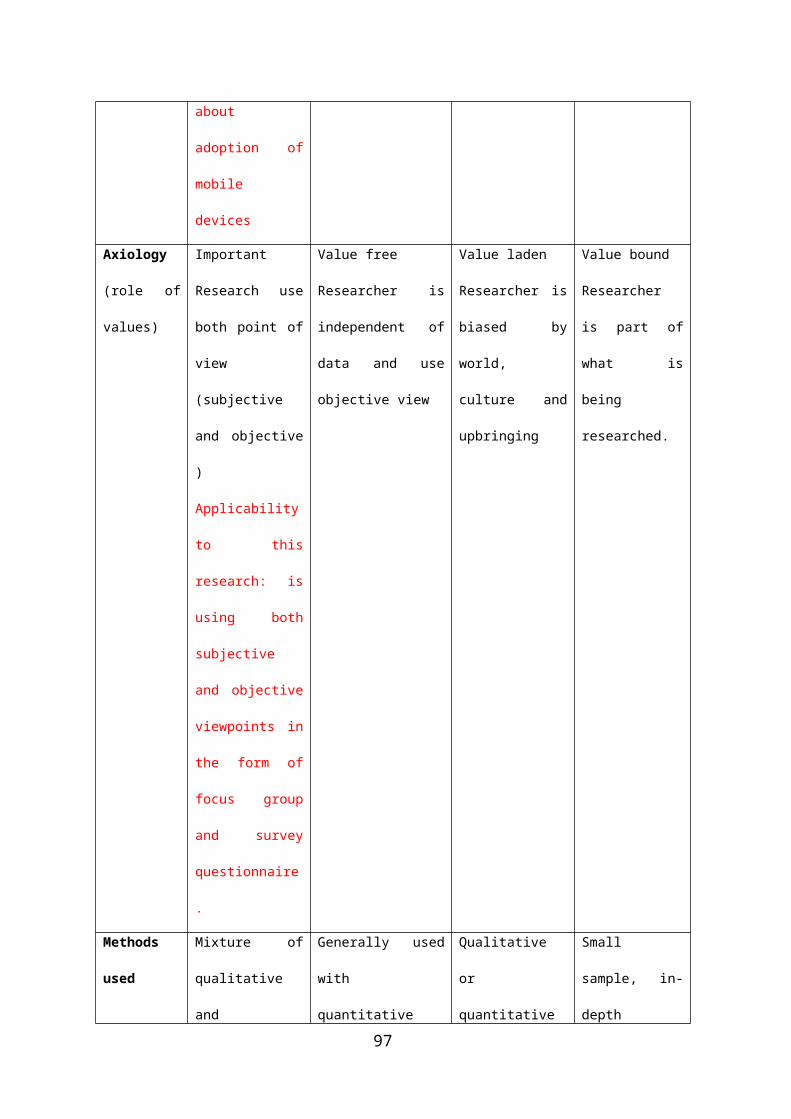
about
adoption of
mobile
devices
Axiology
(role of
values)
Important
Research use
both point of
view
(subjective
and objective
)
Applicability
to this
research: is
using both
subjective
and objective
viewpoints in
the form of
focus group
and survey
questionnaire
.
Value free
Researcher is
independent of
data and use
objective view
Value laden
Researcher is
biased by
world,
culture and
upbringing
Value bound
Researcher
is part of
what is
being
researched.
Methods
used
Mixture of
qualitative
and
Generally used
with
quantitative
Qualitative
or
quantitative
Small
sample, in-
depth
97
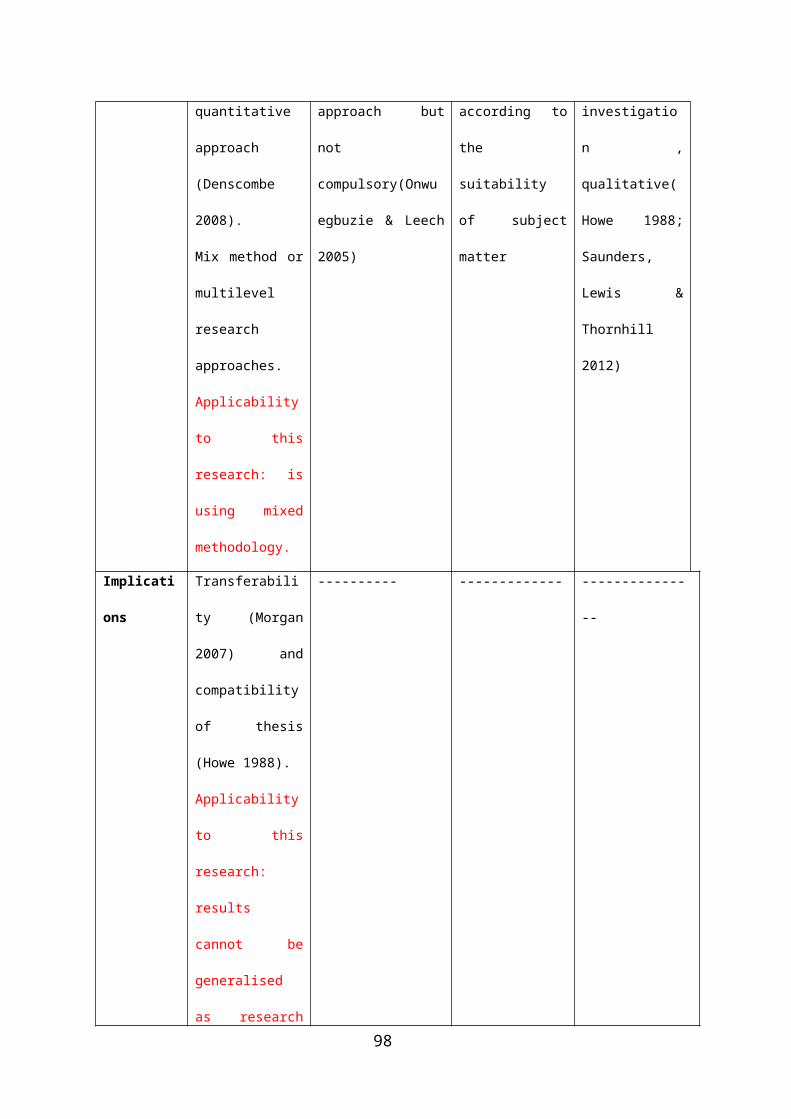
quantitative
approach
(Denscombe
2008).
Mix method or
multilevel
research
approaches.
Applicability
to this
research: is
using mixed
methodology.
approach but
not
compulsory(Onwu
egbuzie & Leech
2005)
according to
the
suitability
of subject
matter
investigatio
n ,
qualitative(
Howe 1988;
Saunders,
Lewis &
Thornhill
2012)
Implicati
ons
Transferabili
ty (Morgan
2007) and
compatibility
of thesis
(Howe 1988).
Applicability
to this
research:
results
cannot be
generalised
as research
---------- ------------- -------------
--
98
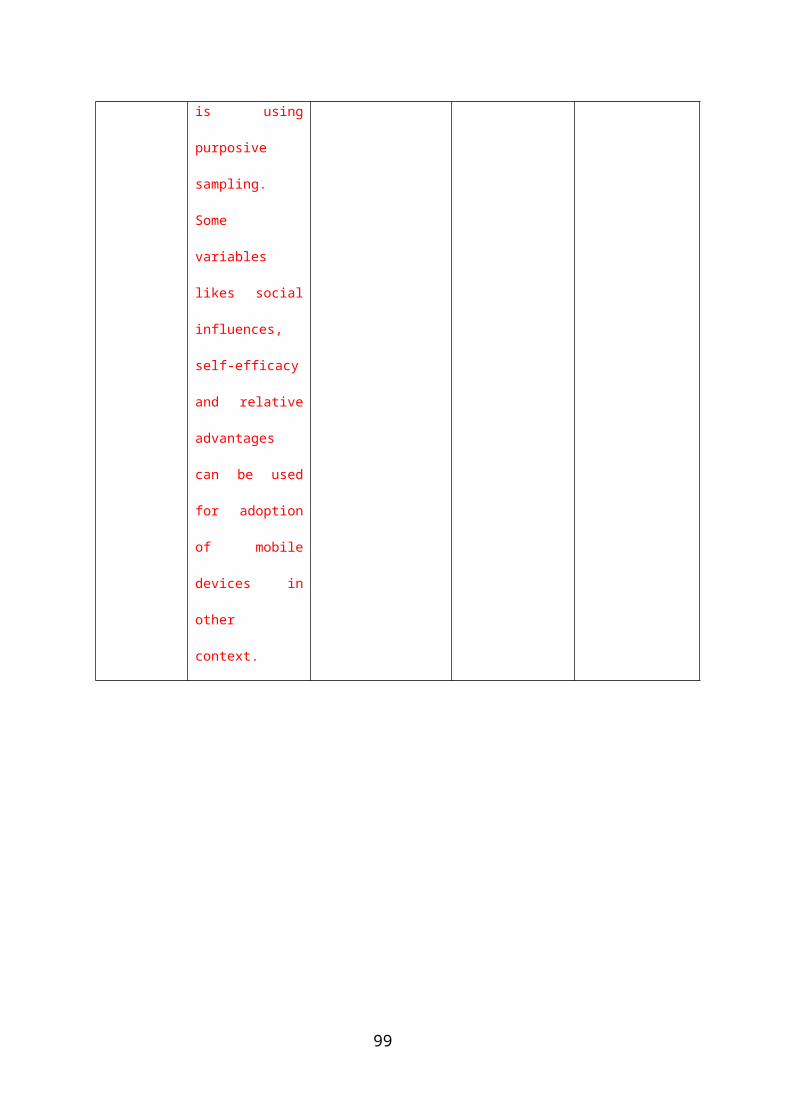
is using
purposive
sampling.
Some
variables
likes social
influences,
self-efficacy
and relative
advantages
can be used
for adoption
of mobile
devices in
other
context.
99
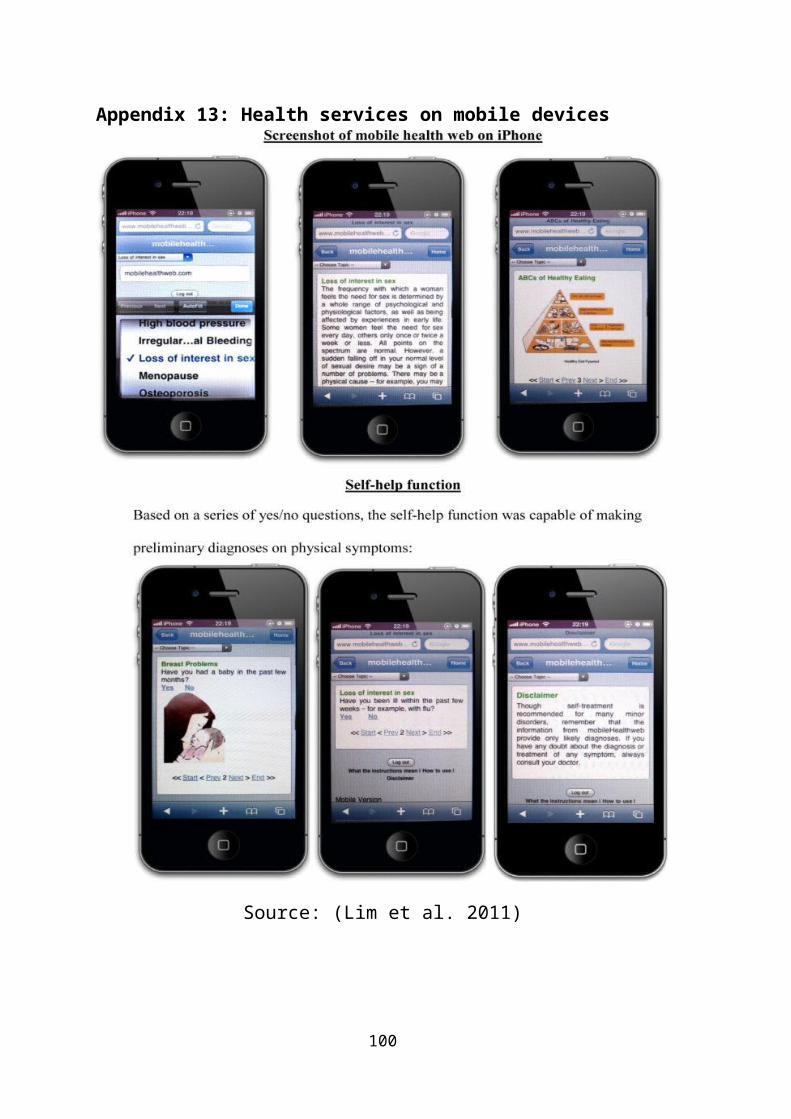
Appendix 13: Health services on mobile devices
Source: (Lim et al. 2011)
100
Adapted from Boulos et al. (2011)
101

i




















