Qualified nurses lack adequate knowledge related to oral ...
Upload
independentCategory
view
1download
0
A D U ~ UROLOGY
REFLUXES 1N ORTHOTOPIC NEOBLADDERS: CAN THE ILEOCECAL SPHINCTER BE CONSIDERED AN
ADEQUATE ANTIREFLUX MECHANISM?
EUGENIO ALCINI, M.D. MARCO RACIOPPI, M.D.
ALESSANDRO D'ADDESSI, M.D.
FRANCESCO SASSO, M.D. ANTONIO ALCIN1, M.D.
MARIO G1USTACCHINI, M.D.
From the Surgical Department, Urological Division, Universit~ Cattolica del S. Cuore, Rome, Italy
ABSTRACT--Objectives. To evaluate the usefulness of the ileocecal sphincter in prevent- ing ureteral refluxes in ileocecal orthotopic neobladder, thus avoiding the use of antire- flux technique for ureteroileal anastomosis.
Methods. From 1980 to 1992, 95 patients underwent orthotopic bladder substitution. In SO our detubularized ileal reservoir was used and in 65 first only an integral ileocecal segment was used and subsequently multiple transverse teniamyotomies on the cecal portion to increase the capacity and reduce the pressure. The upper urinary tract was in- directly protected in the ileal reservoir technique by leaving an integral 8 to 10 cm long af- ferent segment folded behind the reservoir and in the ileocecal technique by the ileocecal sphincter, thus keeping the anastomosis between ureters and ileum simple and direct.
Results. The mean follow-up of the 65 patients with ileocecourethrostomy is 37 + 33 months [range, 2 to 141 months); in 13.8% of the patients (9/65! monolateral refluxes appeared, but without any evident clinical consequences. The appearance of monolateral stenosis on the ureterointestinal anastomosis requiring treatment occurred in 4 patients {6%): S underwent an endoscopic treatment and 1 a surgical one. Modifications of renal function with respect to the preoperative status were not verified in any of the patients.
Conclusions. The ileocecal sphincter is an effective antireflux mechanism for an ortho- topic neobladder in which multiple transverse teniamyotomies (S to 7) increase the ca- pacity of the neobladder itself, reduce its internal pressure, and confer a nearly spherical configuration. Moreover, a correct anastomosis between the cecum and membranous urethra decisively reduces the resistance to emptying of the neobladder, thus avoiding too strong pressures against the ileocecal sphincter. The integrity of the circular muscular layer maintains a healthy tonic wall: this fact, combined with the low peripheral resis- tances, ensures good emptying and a stable capacity. The procedure is easy to perform and not time-consuming; these considerations lead us to consider the ileocecal unit an excellent structure for bladder substitution.
Since 1980, we have carried out 95 bladder sub- stitutions with intestinal loops following cystec- tomy: in 30 patients our detubularized ileal reser- voir was used, in the other 65 patients an ileocecal segment was used, at first integral ly and sub- sequent ly with mult iple transverse teniamyot- omies. >4
Submitted: November 23, /993, accepted (with revisions): Feb- ruary 17, 1994
In our opinion, the good results that have been verified by a long follow-up are due to the initia! construction of neobladders of a modest capacity: detubularized reservoirs 100 to 120 mL; cecum with multiple transverse teniamyotomies: 250 t0 280 mL. In fact, with the latter technique, if the circular musculature is kept intact, a satisfactor~ initial capacity is possible since the tone of the neobladder does not allow for later excessive dil- atation; 5 years after the operation the capacity stabilizes at around 450 to 500 mL. 5
38 UROLOGY / JuLY 1994 / VOLUME 44, NUmBeR I

FIGURE 1. (,4) Our bladder re- placement technique using the de- tubularized ileal reservoir. (B) The I0 cm long afferent loop folded behind avoids ureteral refluxes with filled neobladder (from Acta Urologica Italica 4 : 2 77 -28 I, 1989, with permission).
We wish to concentrate above all in this article on the various ureterointestinal anastomosis an- tire flux techniques and report our results obtained using the ileocecal sphincter as a barrier against neovesicoureteral reflux. Usually the renal func- tion is not modified or altered by the interposi- tioning of an intestinal segment, in the absence of mechanical and/or infectious complications. <r M~nsson et al. 8 reported that in patients with a cecal reservoir, no alteration of glomerular filtra- tion was evident 2 years after the operation. How- ever, with the diffusion and increase in different substitution techniques, there has also been a ten- dency toward the development of a technique that prevents defluxio obstacles, in terms of stenosis or dehiscence of the anastomosis and pathologic re- fluxes. The majority of authors (LeDuc, Carney, Turner-Warwick) use techniques aimed at the ureterointestinal anastomosis; others (Studer) make use of the peristalsis of a relatively long loop.
Modifying our first experiences~ we used the latter concept, 1 integrated with appropriate angulations of the afferent loop, as an antireflux mechanism in our orthotopic substitution with an ileal reservoir (Fig. 1). Others (Kock) make use of the possibility of creating a nipple-type valve mechanism after the anastomosis.
We agree with Gil-Vernet 9 and K/iss et at. lo who, more than 20 years ago, reported their preference for the ileocecal segment, due to the anatomic- physiologic characteristics of the cecum: receptive adaption and near-spherical form that is high- lighted by the multiple transverse teniamyotomies used by us since 1987, and the ileocecal sphincter. The aim of the present article is to summarize the results obtained over 10 years from a clinical point of view, using the usual physiological capacity of the ileocecal junction (ICJ), compared also with the results of the most common antireflux tech- niques reported in literature.
UROLOGY / .JULY 1994 / VoLuta~ 44, NUMBER 1 39

B
FIGURE 2. (,4) Bladder replacement technique by ileocecourethrostomy plus teniamyotomies (ICUS + T): 5 to 6 cm. of the last i leal loop and cecum is used; teniamyotomies are carried out on the ante- r i o r tenia coi l and the tenia omenta l is . (B) ICUS + T at the end of op- erat ion: ureters are di- rectly anastomosed end: to-side to the ileal tract and i leocecal sphincter serves as antireflux mech- anism.
MATERIAL AND METHODS From 1980 to 1992, in 65 patients with vesical
cancer and needing cystoprostatovesiculectomy, an or thotopic recons t ruc t ion of the lower ur inary tract using the ileocecal segment was performed. In the first series of 23 patients the cecal segment was left intact.
From 1987, multiple transverse teniamyotomies have been carried out in 42 patients on the anterior tenia call and tenia omentalis, to obtain release of the cecal wall to allow a similar configuration to the bladder to be formed, to increase the capacity, and to reduce the internal pressure. The techniques have been previously described in detail. 1,2,5 The terminal 5 to 6 cm of i leum and cecum is isolated, the segment is extraperitonealized, and the most inferior part of the cecum is anastomosed to the membranous urethra. In particular, the ureters are end-to-side anastomosed directly to the ileal seg- ment without using antireflux techniques but sim- ply fixed with external seroserous sutures. A num- ber of t e n i a m y o t o m i e s ( f r om five to seven , depending on the morphology, the capacity, and the pressure of the cecum) were carried out on the anterior tenia call and tenia omentalis (Fig. 2).
None of the patients were affected by monolat- eral renal anagenesis or had previously undergone nephrectomy. The mean follow-up of patients was 37 _+ 33 months (range, 2 to 141).
RESULTS
The absence of refluxes following the operation was ensured in 86.2% of the patients. In the re-
maining nine patients monolateral refluxes were present (13.8% of all cases). In patients without teniamyotomies, refluxes were present in 17.4% (4/23) and in patients with teniamyotomies they were present in 11.9% (5/42). It is important !0 emphasize that none of the patients complained Of reflux symptoms. The re fluxes were revealed foil lowing routine cystographic examinations: in two patients the r e fux was grade III, while in the other seven patients it was grades I to II.
An obstruction of the ureteroileal anastomosis fob :i I
lowing the operation was present in six patients (9.2%). The m e a n appea rance t ime was 1316; months (range, 2 to 36 months); but in 4 patienis (6.1%) the onse t was p recoc ious , after 2 t o ~ months (mean, 3.5 months); in 2 patients the sten0 ~, sis appeared later (32 and 36 months, respectively) In 4 of 6 patients, treatment was necessary and c o n sisted of reimptanting in 1 case and transnephr011 :: stomic dilatation in the remaining 3 (Table I).
Interestingly, in all patients the renal functi0g was unaltered following the operation. In partic~! lar, one patient experienced a modes t preoperative renal insufficiency that has remained constant ove~, the 13 years following the operation. In all th~ other patients the creatinine and blood urea nitr0": gen (BUN) levels are within a normal range The mean BUN value for patients with a follow-up of 4: months to 13 years is 22,8 +_ 4 mg/dL (range, 17 to 29; normal value [nv], 10 to 23), and that of crea' t inine was 1.15 _ 0.2 mg/dL (range, 0.8 to 16}: nv 0.7 to 1.4). The patients with refluxes havea mean creatinine value of 1.04 + 0.2 mg/dL (mea~
40 UROLOGY / JuLY 1994 / VOLtJME 44, NUMBER
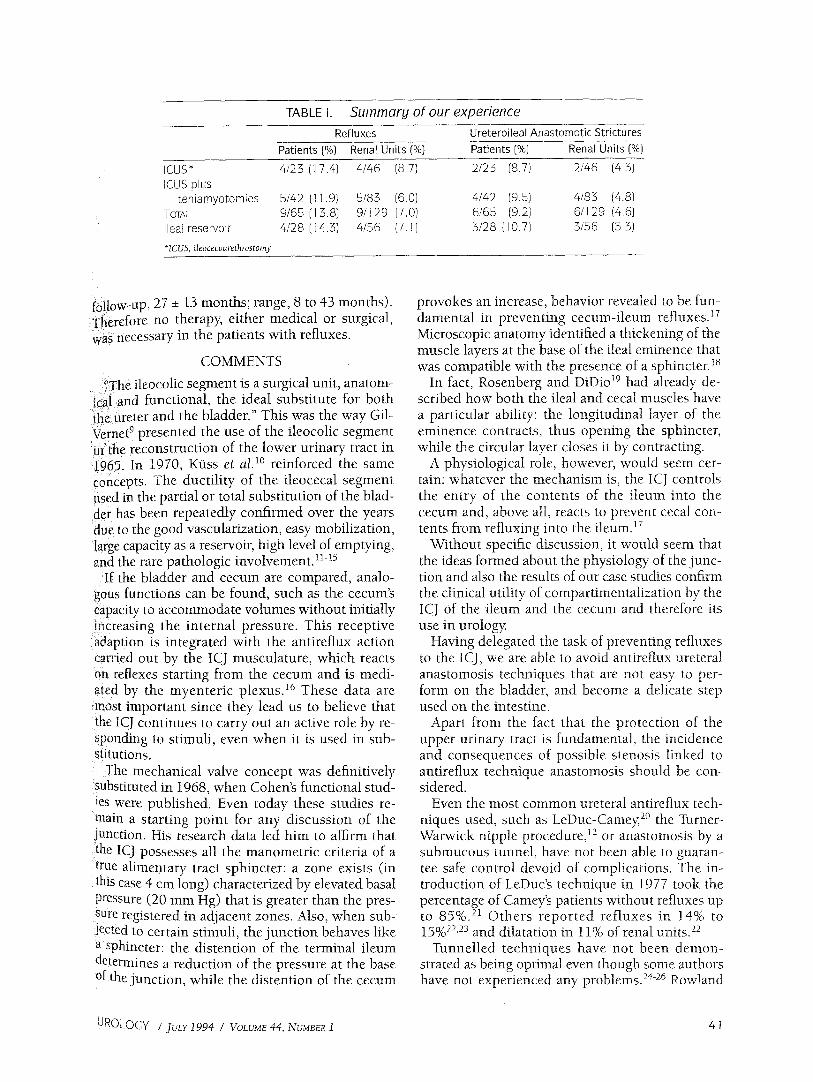
TABLE I. Summary of our experience Refluxes Ureteroileal Anastomotic Strictures
Patients (%) Renal Units (%) Patients (%) Renal Units (%)
ICUS* 4/23 (17.4) 4/46 {8.7) 2/23 (8.7) 2/46 (4.3) IC@S plus
teniamyotomies 5/42 (11.9) 5/83 (6.0) 4/42 {9.5) 4/83 (4.8) TOTAL 9/65 (13.8) 9/129 (7.0) 6/65 (9.2) 6/129 (4.6) Ileal reservoir 4/28 (t 4.3) 4/56 (7.t) 3/28 (10.7) 3/56 (5.3)
* ICU5, ileocecourethrostomy.
follow, up, 27 - 13 months; range, 8 to 43 months). T~erefore no therapy, either medical or surgical, was necessary in the patients with refluxes.
COMMENTS
', ' " surgical unit, anatom- The lleocollc segment is a icai and functional, the ideal substitute for both the ureter and the bladder." This was the way Gil- Vernet 9 presented the use of the ileocolic segment inthe reconstruction of the lower urinary tract in ,t965. In 1970, K*iss et al. 1° reinforced the same Concepts. The ductility of the ileocecal segment used in the partial or total substitution of the blad- der has been repeatedly confirmed over the years due to the good vascularization, easy mobilization, :large capacity as a reservoir, high level of emptying, and the rare pathologic involvement. 1115
If the bladder and cecum are compared, analo- gous functions can be found, such as the cecum's capacity to accommodate volumes without initially increasing the internal pressure. This receptive ~daption is integrated with the antireflux action Carried out by the ICJ musculature, which reacts 0n. reflexes starting from the cecum and is medi-
:ated by the myenter ic plexus. 16 These data are most important since they lead us to believe that the ICJ continues to carry out an active role by re- Sponding to stimuli, even when it is used in sub- s!itutions.
The mechanical valve concept, was definitively substituted in 1968, when Cohens functional stud- ies were published. Even today these studies re- main a starting point for any discussion of the junction. His research data led him to affirm that the ICJ possesses all the manometric criteria of a true alimentary tract sphincter: a zone exists (in this case 4 Cm long) characterized by elevated basal pressure (20 mm Hg) that is greater than the pres- SUre registered in adjacent zones. Also, when sub- jected to certain stimuli, the junction behaves like a sphincter: the distention of the terminal ileum determines a reduction of the pressure at the base of the junction, while the distention of the cecum
provokes an increase, behavior revealed to be fun- damental in preventing cecum-ileum refluxes. ~7 Microscopic anatomy identified a thickening of the muscle layers at the base of the ileal eminence that was compatible with the presence of a sphincter.18
In fact, Rosenberg and DiDio 19 had already de- scribed how both the ileal and cecal muscles have a particular ability: the longitudinal layer of the eminence contracts, thus opening the sphincter, while the circular layer closes it by contracting.
A physiological role, however, would seem cer- tain: whatever the mechanism is, the ICJ controls the entry of the contents of the i leum into the cecum and, above all, reacts to prevent cecal con- tents from refiuxing into the ileum. ~r
Without specific discussion, it would seem that the ideas formed about the physiology of the junc- tion and also the results of our case studies confirm the clinical utility of compartimentalization by the ICJ of the ileum and the cecum and therefore its use in urology.
Having delegated the task of preventing refluxes to the ICJ, we are able to avoid antireflux ureteral anastomosis techniques that are not easy to per- form on the bladder, and become a delicate step used on the intestine.
Apart from the fact that the protection of the upper urinary tract is fundamental, the incidence and consequences of possible stenosis linked to antireflux technique anastomosis should be con- sidered.
Even the most common ureteral antireflux tech- niques used, such as LeDuc-Camey, 2° the Turner- Warwick nipple procedure, ~2 or anastomosis by a submucous tunnel, have not been able to guaran- tee safe control devoid of complications. The in- troduction of LeDuc's technique in 1977 took the percentage of Camey's patients without refluxes up to 85%. 21 Others repor ted refluxes in 14% to 15% 22,23 and dilatation in 11% of renal units . 22
Tunnelled techniques have not been demon- strated as being optimal even though some authors have not experienced any problems. 24-26 Rowland
UROLOGY / JULY 1994 / VOLUME 44, NUMBER 1 4 1

et al. 27 reported refluxes in 7% of subjects with continent reservoirs. Ahlering et al. 28 reported ob- struct ions in 4.2% of patients wi th the Indiana pouch; using the Mainz pouch, Narayan et al. 29 re- ported dilated renal units in 18% of their patients. In turn, the indirect protection of the anastomosis by the intussusception of the intestinal loop, which creates a valve mechanism, is not wi thout prob- lems: Rock et al. 3° report sliding or eversion of the in tussuscepted valve in the cons t ruc t ion of the Rock orthotopic reservoir in 42% of patients. In our technique of constructing a neobladder with an ileal reservoi r as an a l t e rna t ive to i teoce- coureterostomy, partially modifying our first expe- riences, we actually use an integral segment of af- ferent loop (8 to 10 cm long) to which we directly inosculate the ureters in the orad extremity. The loop is then folded back to the reservoir, impeding refluxes in 85.7% of cases due to the acute angle formed when the neobladder is full. An efferent loop only 1 to 2 cm long is entirely used for the anastomosis to the urethra TM (Figs. 3,4).
Another possibility is provided using the natural function of the ICJ. Gil-Vernet and others have af- firmed their preference for the ileocecal segment using the junct ion as an antireflux system. 1°,12,32-36 Some of these authors have further increased its ef- ficacy following Gittes' example. 32 He was the first to reinforce the ICJ using a plication; however, in 1983 he reported refluxes in 18% of cases. 3r Zin- man and Libertino, n using their modified fundo- plication technique, reported no refluxes in 80% of cases. Robertson and King, 34 in creating bladder enlargement, reinforced the ICJ making it compe- tent up to pressures of 80 to 90 cm water, but ne-
F I G U R E 3. Voiding cystograrn o f i leal reservoir::~ years after the operation: no reflux is shown.
cessltatmg in some cases nephrostomlc denvat vg,
procedures. In general, the results obtained w t~ cecoplication and intussusception techniques sho~{{' that these techniques are not capable of preventi~i refluxes 33 and can easily determine ureteral o1~! structions (Table II). When dealing with bladd~il enlargements and conserving the prostatic urethr~{il which are systems of high resistance, the ileocec.~
T A B L E II. S u m m a r y o f rev iewed ar t ic les
Upper Ur inary Tract Author(s) Year No. Pat ients Refluxes (%) D i la ta t ions (%)
Carney > 1 9 8 5 4 0 2 1 5 . . Roeh rbo rn et al. 22 1 9 8 7 1 4 1 4 11
of renal uni ts of renal uni ts
Gotdwasser eta/. 2~ 1 9 8 7 10 1 5 . . of renal uni ts
Marsha l l et ot. 24 1 991 25 . . . . Lockha r t 2s 1 9 8 7 11 . . . . L ight and Marks 26 1 9 9 0 11 . . . . Rowland eta/. 27 t 9 8 7 22 7 . . Ah le r ing eta/. 28 1 991 70 . . 4 Na rayan etal. 29 ] 991 22 . . 1 8
K o c k e t af. 3° 1 9 8 9 4 3 4 2 . . W h i t m o r e and Gi t tes s7 1 9 8 3 33 1 8 . . Z inman and L iber t ino H 1 9 8 6 14 2 0 . . Rober tson and King 34 1 9 8 6 21 33 1 4
4 2 U R O L O G Y / JuLY 1994 / VOLUME 44, NUMBE~!

ijunction alone can encounter problems. With a :{io@~pressure system and overall negligible periph- ierial resistance, as occurs with orthotopic substi-
maf ter cystoprostatovesiculectomy, any even- ref lux is o f t en of l i t t le i m p o r t a n c e . 3s,39
i!heMore, in this case, the ever-present risk of pro- iduCing an obstruction in the upper tract is evalu- {atedl The damage that can be caused is certainly }i~ore severe when compared to the damage pro- iduced by low-pressure reflux. The ICJ is capable of }cti~ely resisti-ng counterpressures of up to 60 cm >ater: in a low-pressure system where higher pres- }urn will not be reached, the ICJ alone can be an ef- fective bar r ie r against refluxes. The sph inc te r Nechanism can be rendered more efficacious using ten!amyotomies, as we did in our orthotopic sub- Stitution, since the in ternal pressures and the :!notflity of the cecal reservoir are reduced.
Since we are concerned with a sphincter mecha- h ism, we do not believe that it is appropriate to in-
FIGURE 4. T h r e e - s t e p intra-
v e n o u s urogram (IVU) of the ileal reservoir 8 years after the operation. (A) Upper urinary tract is normal. (B) The afferent loop folded behind is first filled by contrast medium and (C) the reservoir reaches o goocl ca- pacity.
terfere with its action, distorting its physiology and installing reinforcement techniques.
CONCLUSION
The data tha t emerge f rom our expe r i ence demonstrate the functional validity of the ICJ. The reflux observed was discovered during routine cys- tographic examinations: however, the obstacle the sphincter displays is demonstrated by the fact that the reflux is asymptomatic and associated with a modest dilatation of the upper urinary tract. Spe- cific symptoms were not present in any of the sub- jects. A long-term study of our patients (a follow- up of up to 13 years) has not ev idenced any alterations of preoperative renal function in any subjects. It does not seem possible to expect opti- mal continence in every patient. Also a preopera- uve enema evaluation can give an unreal picture due to the fact that, when carrying out the exami- nation, pressures 4° inside the colon can be over 90
[JRQLOGY / JuLY 1994 / VOLVM~ 44, NU~4BeR 1 43

FIGURE 5. Intravenous urogram of ICUS + T 6 years after the operation: upper urinary tract has a normal morphology and the neobladder capacity is 450 mL.
FIGURE 6. Voiding cystogram of ICUS + T 6 years after the operation (same patient as in Fig. 5): due the teniamyotomies the neobladder morphology is nearly spherical and ileocecal sphincter avoids refluxes.
cm water, thus dis tor t ing the physiology. Using the an t i r e f lux m e c h a n i s m of the ICJ in the i leoce- cou re th ro s tom y plus t en i amyo tomies , wh ich was successful in 88.1% of cases, the ureteroi leal anas-
tomos i s was m a i n t a i n e d direct, quick, and easy to p e r f o r m (Figs. 5,6).
The usefulness of t e n i a m y o t o m i e s in increasing .capacity, r e d u c i n g i n t e rna l p re s su re , mod i fy ing m o r p h o l o g y whi le ma in t a in ing a tonic wall to en- sure good empty ing , and avoid ing late decompen- sa t ion due to the in tegr i ty of the circular muscular layer leads us, c o m b i n e d wi th the val idi ty of ileo: cecal sphincter , as our exper ience has shown, to cons ider the i leocolic uni t an excel lent structure for b l adder rep lacement .
Marco Racioppi, M.D. Via Bartolomeo Capasso, 19:
00179 Rome, Italy
REFERENCES 1. Alcini E, Pescatori M, D'Addessi A, Destito A, and Cas-
tiglioni GC: Bladder reconstruction after cystectomy for can- cer: use of the ileal reservoir. BrJ Urol 57: 245-247, 1985.
2. Alcini E, Vincenzoni M, Destito A, D'Addessi A, and: Castiglioni GC: lteocaeco-urethroplasty after total cystec, tomy for bladder cancer. BrJ Urol 57: 160-163, 1985.
3. Alcini E, Pescatori M, D'Addessi A, Grassetti F, Anasta- sia G, Giustacchini M, and Grasso G: Multiple taeniamy~ atomy of the replaced caecum after restorative cystoprosta- tovesiculectomy for bladder cancer. Br J Urol 66: 441-442, 1990.
4. Alcini E, D'Addessi A, Giustacchini M, Sasso F, Grass0 G, and Castiglioni GC: Bladder reconstruction after cystec- tomy: use of ileocecal segment and three-loop ileal reservoir. Urology 31: 10-13, 1988.
5. Alcini E, D'Addessi A, Racioppi M, Menchinelli E Anas- tasia G, Grassetti E Destito A, and Giustacchini M: Four years' experience with bladder replacement using an ileoceca[ segment with multiple transverse teniamyotomies. J Ur01: 149: 735-738, 1993.
6. Lilien OM, and Carney M: 25 year experience with re~ placement of the human bladder (Camey procedure). J Urd 132: 886-891, 1984.
7. Label B, and SoretJY: Intestine et chirurgie urologique, J Urol (Paris) 93: 379-394, 1987.
8. M~nsson W, Colleen S, Forsberg L, Larsson I, Sundin~ and White T: Renal function after urinary diversion. A study of continent caecal reservoir, ileal conduit and colonic cofi~ duit. ScandJ Urol Nephrot 18: 307-315, 1984.
9. Gil-Vernet JM Jr: The ileocolic segment in urologiCa! surgery. J Urol 94: 418-426, 1965.
10. Ktiss R, Bitker M, Camey M, Chatelain C, and LasSa~ JP: Indications and early and late results of intestino-cyst0¢ plasty: a review of 185 cases. J Urol 103: 53-63, 1970.
11. Zinman L, and Libertino JA: Right colocystoplasty f0! bladder replacement. Urol Clin North Am 13: 321-33L 1986.
12. Turner-Warwick R, and Ashken MH: The function}! results of partial subtotal cystoplasty with special reference to ureterocystoplasty, selective sphincterotomy and cyst0" cystoplasty. BrJ Urol 39: 3-12, 1967.
13. Rampal M, Ivaldi A, Coulange C, Lacoste J, and Ga ~ vin C: La caecocystoplastie. Apropos de quatorze obser va' tions. Ann Urol 19: 184-189, 1985.
i4. Merricks JW: A continent substitute bladder and ure thra, in King LR, Stone AR, and Webster GD (Eds): BladM
44 URQLQGY / JvLY 1994 / VOLUME 44, NUmBeR1

;Reconstruction and Continent Urinary Diversion, Chicago, ;Lol~don, Year Book Medical Publishers, 1987, pp 179-203.
15. Libertino JA, and Zinman L: Ileocecal segment for temporary and permanent urinary diversion. Urol Clin North Am !3: 241-250, 1986. i !6. Guyton AC: Textbook on Medical Physiology, Philadel- ! ,~hia, W.B. Saunders Co, 1971, pp 863-864.
17. Cohen S Harris LD and Levitan B: Manometric char- ~;acteristie of the human ileocecal junctional zone. Gastroen- ter01ogy 54: 72-75, 1968. ! 1 8 . Quigley EM, and Phillips SF: The ileocecal (ileo-
i colonic) sphincter. Z Gastroenterol 21: 47-55, 1983. 19. Rosenberg JC, and DiDio LJ: Anatomic and clinical
i!as,pects of the junction of the ileum with the large intestine. Dis Colon Rectum 13: 220-224, 1970.
20. LeDuc A, and Camey M: Un proc4d4 d'implantation ~lrfitero2il4al4 anti-reflux dans l'ent4rocystoplastie. J Urol iNephrol (Paris) 85: 449-454, 1979. ! 211 Carney M: Bladder replacement by ileocystoplasty fol- lowing r adical cystectomy. World J Urol 3: 161-166, !985. ~e 2 Z Roehrborn CG, Teigland CM, and Sagalowsky AI: };unCtional characteristics of the Carney ileal bladder. J Urol ~38: 739-742, 1987. :231 Goldwasser B, Rife CC, Benson RCJr, Furlow WL, and
j3a}:ret DM: Urodynamic evaluation of patients after the ~alngy operation. J Urol 138: 832-835, 1987. 1:241 Marshall FF, Mostwin JL, Radebaugh LC, Walsh PC, ~nd Brendter CB: Ileocolic neobladder post-cystectomy: con- Iiffence and potency. J Urol 145: 502-504, 1991. i ~51 Lockhart JL: Remodeled right colon: an alternative mnary reservoir. J Urol 138: 730-734, 1987. ' : 2 6 Light JK, and Marks JL: Total bladder replacement in ii~ male and female using the ileocol0nic segment (Le Bag). ~r.J Urol 65: 467-472, 1990. 271 Rowland RG, Mitchell ME, and Bihrle R: Alternative
e&niques for a continent urinary reservoir Urol Clin North iifi' 14: 797-804, 1987. ~81 Ahlering TE, Weinberg AC, and Razor B: Modified In-
diana pouch. J Urol 145: 1156-1158, 199t. 29. Narayan E Broderick GA, and Tanagho EA: Bladder
substitution with ileocaecal (Mainz) pouch. Clinical perfor- mance over 2 years. BrJ Urol 68: 588-595, 1991.
30. Kock NG, Ghoneim MA, Lycke KG, and Mahran MR: Replacement of the bladder by the urethral Kock pouch: functional results, urodynamics and radiological features. J Urol 141: l l l l - i i 1 6 , 1989.
31. Cukier J, Dubernard JM, and Grasset D: Atlas de chirurgie urologique (enterocistoplastie ileale detubulee selon Alcini), Paris, Masson, vol 2, 1991, pp 77-78.
32. Gittes RF: Ileocecocystoplasty for contracted bladder with reinforcement of the ileocecal valve. Technica! exhibit, American Urological Association, Philadelphia, 1970.
33. Kay R, and Straffon R: Augmentation cystoplasty. Urol Clin North Am 13: 295-305, 1986.
34. Robertson CN, and King LR: Bladder substition in children. Urol Clin North Am 13: 333-344, 1986.
35. Khafagy M, E1-Bolkainy MN, Barsoum RS, and E1- Tatawy S: The ileocecal bladder: a new method for urinary diversion after radical cystectomy (a preliminary report). J Urol 113: 314-316, 1975.
36. Skinner DG: Secondary urinary reconstruction: use of the ileocecal segment. J Urol 112: 48-51, 1974.
37. Whitmore WF 3d, and Gittes RF: Reconstruction of the urinary tract by cecal and ileocecal cystoplasty: review of a 15 year experience. J Urol 129: 494-498, 1983.
38. Bejany D, Suarez G, Penalver M, and Politano V: Non- tunneled ureteroeolonic anastomosis: an alternative to the tunneled implantation. J Urol 142: 961-963, 1989.
39. Kirby RS, and Turner-Warwick R: Substitution cysto- plasty, in King LR, Stone AR, and Webster GD (Eds): Bladder Reconstruction and Continent Urinary Diversion, Chicago, London, Year Book Medical Publishers, 1987, pp 41-63.
40. Rendleman DE Anthony JE, Davis C Jr, Buenger RE, Brooks AJ, and Beattie EJ Jr: Reflux pressure studies on the ileocecal valve of dogs and humans. Surgery 44: 640-643, 1958.
~ R O L Q G y / JvLr 1994 / VOLUME 44, NUMBER 1 45
Copyright © 2022 FDOKUMEN