
Grading of cellular rejection after orthotopic liver transplantation
12
Grading of Cellular Rejection After Orthotopic Liver Transplantation SIDDHARTHA DATTA GUPTA,l” MARK HUDSON,~ ANDREW K. BURROUGHS,3 RICHARD MORRIS,4 KEITH ROLLES,3 PETER AM LOT,^ PETER J. SCHEUER,~ AND AMAR P. DHILLON’ All 684 post-orthotopic liver transplantation (OLT) liver biopsies performed at the Royal Free Hospital (RFH) between 1988 and 1993, from 120 patients, were reviewed in order to try to define the relative impor- tance of the histologicalfeatures of immunosuppression- responsive cellular rejection. Twenty histological fea- tures considered to be possible contributors to the diagnosis of cellular rejection were documented in a bi- nary (presenuabsent) fashion. These features in 106 bi- opsy specimens obtained 1 to 8 days after OLT were ana- lyzed using stepwise logistic discriminant analysis. All clinical and treatment records were reviewed, and each biopsy specimen was assigned to a diagnostic category depending on these records and follow-upinformation. Important determinants of the histological diagnosis of cellular rejection (which occurred in 84 of the 106 cases) were moderatdsevere mixed portal inflammation, eosin- ophils, endotheliitis, and bile duct damage. When these all occurred together, the odds of rejection increased 3.6- fold. The original histological diagnosis was recorded, and each biopsy specimen showing cellular rejection was regraded according to the specific criteria of Snover et al., Demetris et al., and a novel RFH scoring system. The latter consists of evaluating portal inflammation, endotheliitis, eosinophils, and bile duct damage, each on a 0 to 3 scale (none, mild, moderate, or severe, respec- tively) and summation. The resulting cellular rejection score thus can range from 0 to 12. The agreement be- tween the different scoring systems was analyzed using K statistics, and there was good concordance (K, 0.64 to Abbreviations: OLT, orthotopic liver transplantation; RFH, Royal Free Hos- pital; PAS, periodic acid-Schiff; CMV, cytomegalovirus; HBs, hepatitis B sur- face antigen; HBc, hepatitis B core antigen; HDV, hepatitis delta virus; HCV, hepatitis C virus; PCR, polymerase chain reaction; ALWATG, antilymphocyte globulidantithymocyttf globulin; TP, true-positives; TN, true-negatives; FP, false-positives; FN, false-negatives; MHC, major histocompatibility complex. From the University Departments of ‘Hisopathology, ‘Medicine, ‘Hepato- biliary and Liver Transplantation Unit (University Departments of Medicine & Surgery), ‘Public Health & Primary Care, and %munology, Royal Free Hospi- tal School of Medicine, Hampstead, London, United Kingdom; and ‘Depart- ment of Pathology, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India. Received October 26, 1993; accepted June 29, 1994. A.P.D. is partly supported by the Frances and Augustus Newman Founda- tion (London, England). Address reprint requests to: Amar P. Dhillon, MA, MD, MRCP, MRCPath, University Department of Histopathology, Royal Free Hospital, School of Medi- cine, Rouland Hill St, Hampstead, London NW3 2PF, United Kingdom. Copyright 0 1995 by the American Association for the Study of Liver Diseases. 0’L70-9139/95/2101-0009$3.00/0 0.78), despite different histological criteria being used to derive each score. Each system showed a similar de- gree of sensitivity (87% to 96%). The specificity ranged from 69% to 77%. We conclude that the histological diag- nosis of cellular rejection relies mainly on the previously described features of mixed portal inflammation, endotheliitis, eosinophils, and duct damage. There is scope for unification and simplification of the existing grading systems, which depend on differing criteria, and we suggest one such scheme. (HEPATOLOGY 1995;21:46- 57.) Serial liver biopsies of the allograft are performed not only to diagnose cellular rejection but also to assess therapeutic response. The criteria for diagnosis of cel- lular rejection after orthotopic liver transplantation (OLT) have been described principally by two group^,(^'^' and grading of such rejection has been pro- posed. Many centers, including ours, routinely use modifications of the published systems. Thus, many different schemes are now in regular use for the histo- logical diagnosis and grading of cellular rejection after OLT. The specific histological criteria of the best estab- lished schemes, those of Snover et all and Demetris et a1,’ are different (Tables 1, 2, and 3). Both systems include histological components now usually regarded as elements of chronic ductopenic rejection and possi- bly related arteriopathy and ischemia in their highest grades. A multicenter study3 reported moderate to excellent intraobserver and interobserver agreement regarding the final diagnosis of cellular rejection, although the agreement was not equally reproducible for individual histological features. Cellular rejection criteria were agreed and defined between the participants in this st~dy,~ but the definitions of each of the histological features used were not stated in that article. The inves- tigators concluded, “Surprisingly, the diagnosis of acute rejection was more reproducible than the individ- ual histopathological findings that were thought to be the basis for the diagn~sis.”~ It seems as though experienced observers are able to reliably and reproducibly diagnose and grade cellular rejection, using different sets of histological criteria, despite differing in the precise assessment of individual histological features. The observer variability in as- sessing cellular rejection and the histological features 46
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Grading of cellular rejection after orthotopic liver transplantation

Grading of Cellular Rejection After Orthotopic Liver Transplantation
SIDDHARTHA DATTA GUPTA,l” MARK HUDSON,~ ANDREW K. BURROUGHS,3 RICHARD MORRIS,4 KEITH ROLLES,3 PETER AM LOT,^ PETER J. SCHEUER,~ AND AMAR P. DHILLON’
All 684 post-orthotopic liver transplantation (OLT) liver biopsies performed at the Royal Free Hospital (RFH) between 1988 and 1993, from 120 patients, were reviewed in order to try to define the relative impor- tance of the histological features of immunosuppression- responsive cellular rejection. Twenty histological fea- tures considered to be possible contributors to the diagnosis of cellular rejection were documented in a bi- nary (presenuabsent) fashion. These features in 106 bi- opsy specimens obtained 1 to 8 days after OLT were ana- lyzed using stepwise logistic discriminant analysis. All clinical and treatment records were reviewed, and each biopsy specimen was assigned to a diagnostic category depending on these records and follow-up information. Important determinants of the histological diagnosis of cellular rejection (which occurred in 84 of the 106 cases) were moderatdsevere mixed portal inflammation, eosin- ophils, endotheliitis, and bile duct damage. When these all occurred together, the odds of rejection increased 3.6- fold. The original histological diagnosis was recorded, and each biopsy specimen showing cellular rejection was regraded according to the specific criteria of Snover et al., Demetris et al., and a novel RFH scoring system. The latter consists of evaluating portal inflammation, endotheliitis, eosinophils, and bile duct damage, each on a 0 to 3 scale (none, mild, moderate, or severe, respec- tively) and summation. The resulting cellular rejection score thus can range from 0 to 12. The agreement be- tween the different scoring systems was analyzed using K statistics, and there was good concordance (K, 0.64 to
Abbreviations: OLT, orthotopic liver transplantation; RFH, Royal Free Hos- pital; PAS, periodic acid-Schiff; CMV, cytomegalovirus; HBs, hepatitis B sur- face antigen; HBc, hepatitis B core antigen; HDV, hepatitis delta virus; HCV, hepatitis C virus; PCR, polymerase chain reaction; ALWATG, antilymphocyte globulidantithymocyttf globulin; TP, true-positives; TN, true-negatives; FP, false-positives; FN, false-negatives; MHC, major histocompatibility complex.
From the University Departments of ‘Hisopathology, ‘Medicine, ‘Hepato- biliary and Liver Transplantation Unit (University Departments of Medicine & Surgery), ‘Public Health & Primary Care, and %munology, Royal Free Hospi- tal School of Medicine, Hampstead, London, United Kingdom; and ‘Depart- ment of Pathology, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India.
Received October 26, 1993; accepted June 29, 1994. A.P.D. is partly supported by the Frances and Augustus Newman Founda-
tion (London, England). Address reprint requests to: Amar P. Dhillon, MA, MD, MRCP, MRCPath,
University Department of Histopathology, Royal Free Hospital, School of Medi- cine, Rouland Hill St, Hampstead, London NW3 2PF, United Kingdom.
Copyright 0 1995 by the American Association for the Study of Liver Diseases.
0’L70-9139/95/2101-0009$3.00/0
0.78), despite different histological criteria being used to derive each score. Each system showed a similar de- gree of sensitivity (87% to 96%). The specificity ranged from 69% to 77%. We conclude that the histological diag- nosis of cellular rejection relies mainly on the previously described features of mixed portal inflammation, endotheliitis, eosinophils, and duct damage. There is scope for unification and simplification of the existing grading systems, which depend on differing criteria, and we suggest one such scheme. (HEPATOLOGY 1995;21:46- 57.)
Serial liver biopsies of the allograft are performed not only to diagnose cellular rejection but also to assess therapeutic response. The criteria for diagnosis of cel- lular rejection after orthotopic liver transplantation (OLT) have been described principally by two group^,(^'^' and grading of such rejection has been pro- posed. Many centers, including ours, routinely use modifications of the published systems. Thus, many different schemes are now in regular use for the histo- logical diagnosis and grading of cellular rejection after OLT. The specific histological criteria of the best estab- lished schemes, those of Snover et all and Demetris et a1,’ are different (Tables 1, 2, and 3). Both systems include histological components now usually regarded as elements of chronic ductopenic rejection and possi- bly related arteriopathy and ischemia in their highest grades.
A multicenter study3 reported moderate to excellent intraobserver and interobserver agreement regarding the final diagnosis of cellular rejection, although the agreement was not equally reproducible for individual histological features. Cellular rejection criteria were agreed and defined between the participants in this s t ~ d y , ~ but the definitions of each of the histological features used were not stated in that article. The inves- tigators concluded, “Surprisingly, the diagnosis of acute rejection was more reproducible than the individ- ual histopathological findings that were thought to be the basis for the diagn~sis.”~
It seems as though experienced observers are able to reliably and reproducibly diagnose and grade cellular rejection, using different sets of histological criteria, despite differing in the precise assessment of individual histological features. The observer variability in as- sessing cellular rejection and the histological features
46
HEPATOLOGY Vol. 21, NO. 1, 1995 GUPTA E T A L 47
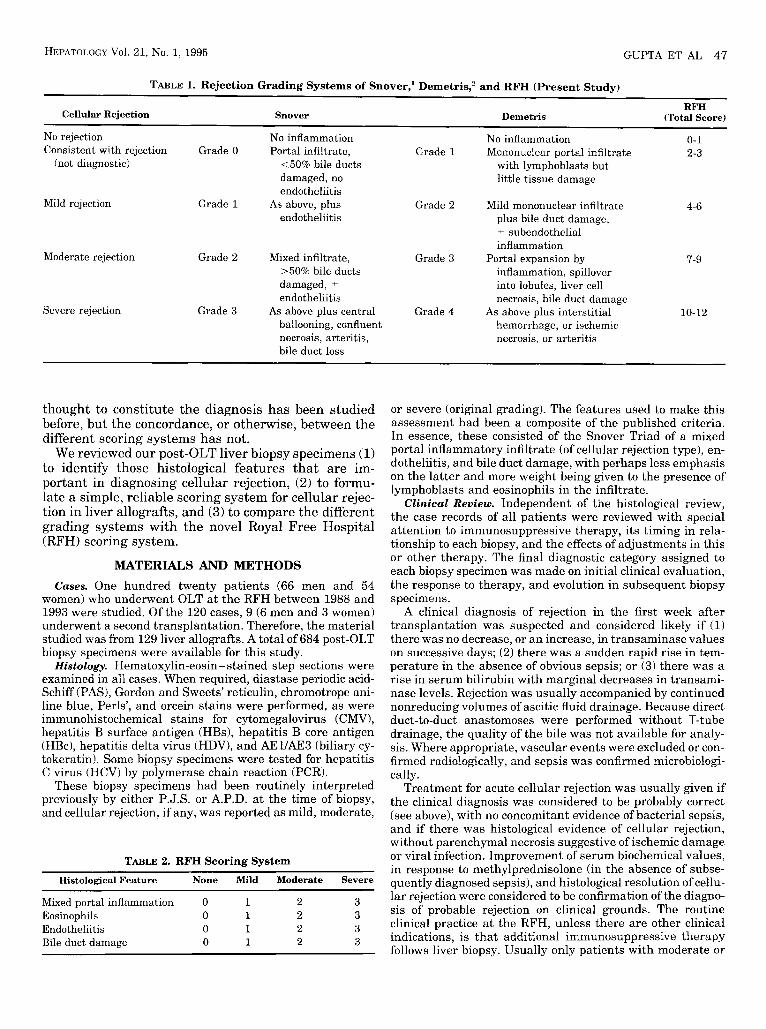
TABLE 1. Rejection Grading Systems of Snover,' Demetris,' and RFH (Present Study)
RFH Cellular Rejection Snover Demetris (Total Score)
No rejection No inflammation No inflammation 0-1 Consistent with rejection Grade 0 Portal infiltrate, Grade 1 Mononuclear portal infiltrate 2-3
(not diagnostic) <50% bile ducts with lymphoblasts but damaged, no little tissue damage endotheliitis
endotheliitis plus bile duct damage, Mild rejection Grade 1 As above, plus Grade 2 Mild mononuclear infiltrate
-t subendothelial inflammation
Moderate rejection Grade 2 Mixed infiltrate, Grade 3 Portal expansion by 7-9 >50% bile ducts inflammation, spillover damaged, -C
endotheliitis necrosis, bile duct damage
ballooning, confluent hemorrhage, or ischemic
into lobules, liver cell
Severe rejection Grade 3 As above plus central Grade 4 As above plus interstitial 10-12
4-6
necrosis, arteritis, bile duct loss
necrosis, or arteritis
thought to constitute the diagnosis has been studied before, but the concordance, or otherwise, between the different scoring systems has not.
We reviewed our post-OLT liver biopsy specimens (1) to identify those histological features that are im- portant in diagnosing cellular rejection, (2) to formu- late a simple, reliable scoring system for cellular rejec- tion in liver allografts, and (3) to compare the different grading systems with the novel Royal Free Hospital (RFH) scoring system.
MATERIALS AND METHODS Cases. One hundred twenty patients (66 men and 54
women) who underwent OLT a t the RFH between 1988 and 1993 were studied. Of the 120 cases, 9 (6 men and 3 women) underwent a second transplantation. Therefore, the material studied was from 129 liver allografts. A total of 684 post-OLT biopsy specimens were available for this study.
Histology. Hematoxylin-eosin-stained step sections were examined in all cases. When required, diastase periodic acid- Schiff (PAS), Gordon and Sweets' reticulin, chromotrope ani- line blue, Perls', and orcein stains were performed, as were immunohistochemical stains for cytomegalovirus (CMV), hepatitis B surface antigen (HBs), hepatitis B core antigen (HBc), hepatitis delta virus (HDV), and AEUAE3 (biliary cy- tokeratin). Some biopsy specimens were tested for hepatitis C virus (HCV) by polymerase chain reaction (PCR).
These biopsy specimens had been routinely interpreted previously by either P.J.S. or A.P.D. a t the time of biopsy, and cellular rejection, if any, was reported as mild, moderate,
TABLE 2. RFH Scoring System
Histological Feature None Mild Moderate Severe
Mixed portal inflammation 0 1 2 3 Eosinophils 0 1 2 3 Endotheliitis 0 1 2 3 Bile duct damage 0 1 2 3
or severe (original grading). The features used to make this assessment had been a composite of the published criteria. In essence, these consisted of the Snover Triad of a mixed portal inflammatory infiltrate (of cellular rejection type), en- dotheliitis, and bile duct damage, with perhaps less emphasis on the latter and more weight being given to the presence of lymphoblasts and eosinophils in the infiltrate.
Clinical Review. Independent of the histological review, the case records of all patients were reviewed with special attention to immunosuppressive therapy, its timing in rela- tionship to each biopsy, and the effects of adjustments in this or other therapy. The final diagnostic category assigned to each biopsy specimen was made on initial clinical evaluation, the response to therapy, and evolution in subsequent biopsy specimens.
A clinical diagnosis of rejection in the first week after transplantation was suspected and considered likely if (1) there was no decrease, or an increase, in transaminase values on successive days; (2) there was a sudden rapid rise in tem- perature in the absence of obvious sepsis; or (3) there was a rise in serum bilirubin with marginal decreases in transami- nase levels. Rejection was usually accompanied by continued nonreducing volumes of ascitic fluid drainage. Because direct duct-to-duct anastomoses were performed without T-tube drainage, the quality of the bile was not available for analy- sis. Where appropriate, vascular events were excluded or con- firmed radiologically, and sepsis was confirmed microbiologi- cally.
Treatment for acute cellular rejection was usually given if the clinical diagnosis was considered to be probably correct (see above), with no concomitant evidence of bacterial sepsis, and if there was histological evidence of cellular rejection, without parenchymal necrosis suggestive of ischemic damage or viral infection. Improvement of serum biochemical values, in response to methylprednisolone (in the absence of subse- quently diagnosed sepsis), and histological resolution of cellu- lar rejection were considered to be confirmation of the diagno- sis of probable rejection on clinical grounds. The routine clinical practice a t the RFH, unless there are other clinical indications, is that additional immunosuppressive therapy follows liver biopsy. Usually only patients with moderate or
48 GUPTA ET AL HEPATOLOGY January 1995
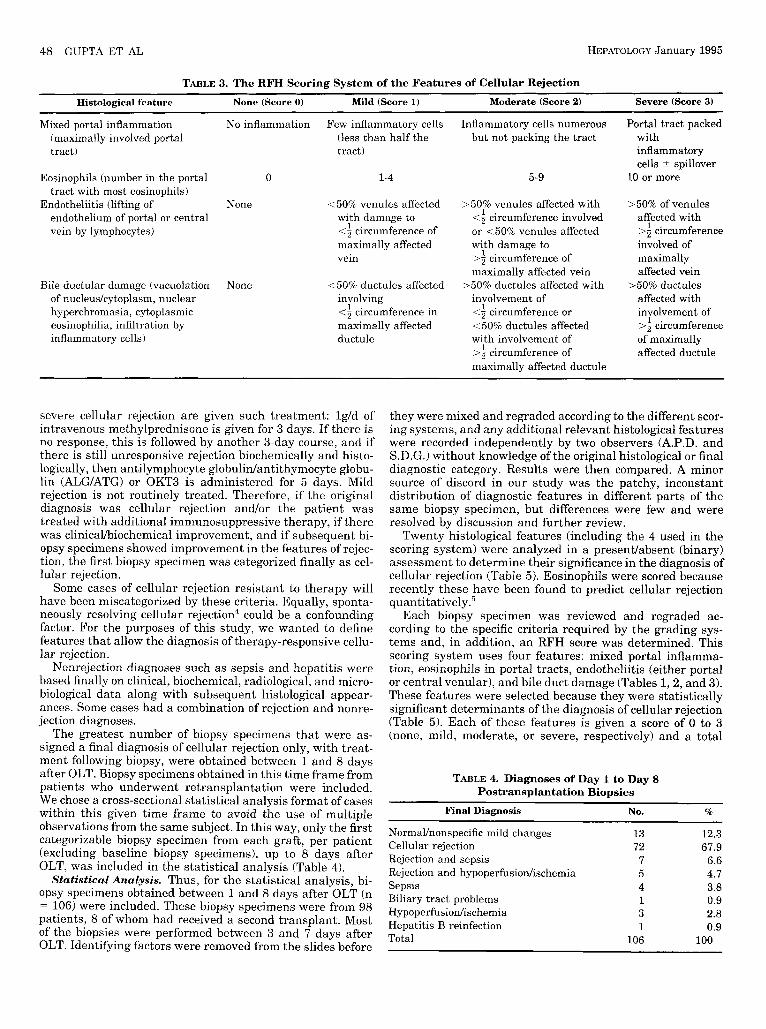
TABLE 3. The RFH Scoring System of the Features of Cellular Rejection Histological feature None (Score 0 ) Mild (Score 1) Moderate (Score 2) Severe (Score 3)
Mixed portal inflammation (maximally involved portal tract)
Eosinophils (number in the portal tract with most eosinophils)
Endotheliitis (lifting of endothelium of portal or central vein by lymphocytes)
Bile ductular damage (vacuolation of nucleus/cytoplasm, nuclear hyperchromasia, cytoplasmic eosinophilia, infiltration by inflammatory cells)
No inflammation Few inflammatory cells (less than half the tract)
0 1-4
None <50% venules affected with damage to <a circumference of maximally affected vein
None 150%; ductules affected involving <f circumference in maximally affected ductule
Inflammatory cells numerous but not packing the tract
5-9
>50% venules affected with <f circumference involved or <50% venules affected with damage to >f circumference of maximally affected vein
>50% ductules affected with involvement of <f circumference or 1 5 0 % ductules affected with involvement of >f circumference of maximally affected ductule
Portal tract packed with inflammatory cells 2 spillover
10 or more
>50% of venules affected with >f circumference involved of maximally affected vein
>50% ductules affected with involvement of >f circumference of maximally affected ductule
severe cellular rejection are given such treatment: lg/d of intravenous methylprednisone is given for 3 days. If there is no response, this is followed by another 3-day course, and if there is still unresponsive rejection biochemically and histo- logically, then antilymphocyte globulidantithymocyte globu- lin (ALG/ATG) or OKT3 is administered for 5 days. Mild rejection is not routinely treated. Therefore, if the original diagnosis was cellular rejection and/or the patient was treated with additional immunosuppressive therapy, if there was clinicaUbiochemica1 improvement, and if subsequent bi- opsy specimens showed improvement in the features of rejec- tion, the first biopsy specimen was categorized finally as cel- lular rejection.
Some cases of cellular rejection resistant to therapy will have been miscategorized by these criteria. Equally, sponta- neously resolving cellular rejection4 could be a confounding factor. For the purposes of this study, we wanted to define features that allow the diagnosis of therapy-responsive cellu- lar rejection.
Nonrejection diagnoses such as sepsis and hepatitis were based finally on clinical, biochemical, radiological, and micro- biological data along with subsequent histological appear- ances. Some cases had a combination of rejection and nonre- jection diagnoses.
The greatest number of biopsy specimens that were as- signed a final diagnosis of cellular rejection only, with treat- ment following biopsy, were obtained between 1 and 8 days after OLT. Biopsy specimens obtained in this time frame from patients who underwent retransplantation were included. We chose a cross-sectional statistical analysis format of cases within this given time frame to avoid the use of multiple observations from the same subject. In this way, only the first categorizable biopsy specimen from each graft, per patient (excluding baseline biopsy specimens), up to 8 days after OLT, was included in the statistical analysis (Table 4).
Statistical Analysis. Thus, for the statistical analysis, bi- opsy specimens obtained between 1 and 8 days after OLT (n
106) were included. These biopsy specimens were from 98 patients, 8 of whom had received a second transplant. Most of the biopsies were performed between 3 and 7 days after OLT. Identifying factors were removed from the slides before
they were mixed and regraded according to the different scor- ing systems, and any additional relevant histological features were recorded independently by two observers (A.P.D. and S.D.G.) without knowledge of the original histological or final diagnostic category. Results were then compared. A minor source of discord in our study was the patchy, inconstant distribution of diagnostic features in different parts of the same biopsy specimen, but differences were few and were resolved by discussion and further review.
Twenty histological features (including the 4 used in the scoring system) were analyzed in a presenvabsent (binary) assessment to determine their significance in the diagnosis of cellular rejection (Table 5 ) . Eosinophils were scored because recently these have been found to predict cellular rejection quantitatively.5
Each biopsy specimen was reviewed and regraded ac- cording to the specific criteria required by the grading sys- tems and, in addition, an RFH score was determined. This scoring system uses four features: mixed portal inflamma- tion, eosinophils in portal tracts, endotheliitis (either portal or central venular), and bile duct damage (Tables 1 , 2 , and 3). These features were selected because they were statistically significant determinants of the diagnosis of cellular rejection (Table 5 ) . Each of these features is given a score of 0 to 3 (none, mild, moderate, or severe, respectively) and a total
TABLE 4. Diagnoses of Day 1 to Day 8 Postransplantation Biopsies
Final Diagnosis No. %
Normalhonspecific mild changes 13 12.3 Cellular rejection 72 67.9 Rejection and sepsis 7 6.6
Sepsis 4 3.8
Hypoperfusiodischemia 3 2.8
Rejection and hypoperfusiodischemia 5 4.7
Biliary tract problems 1 0.9
Hepatitis B reinfection 1 0.9 Total 106 100
GUPTA ET AL 49 HEPATOLOGY Vol. 21, NO. 1, 1995
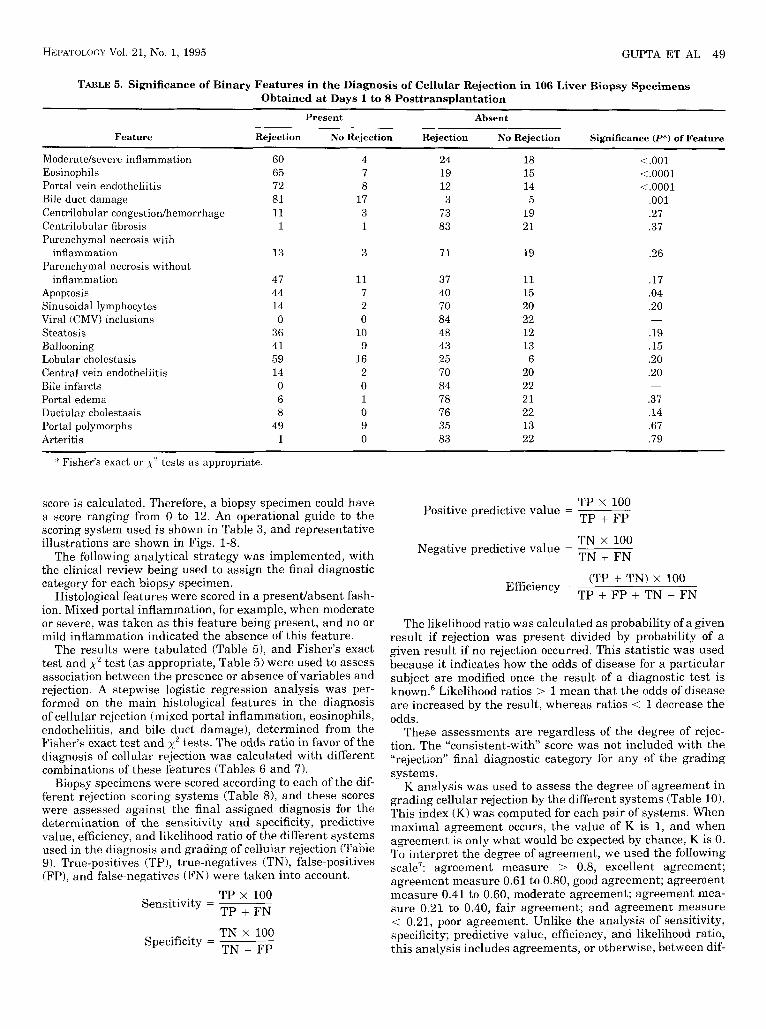
TABLE 5. Significance of Binary Features in the Diagnosis of Cellular Rejection in 106 Liver Biopsy Specimens Obtained at Days 1 to 8 Posttransplantation
Present Absent
Feature Rejection No Rejection Rejection No Rejection Significance (P*) of Feature
Moderatekevere inflammation 60 4 24 18 <.001 Eosinophils 65 7 19 15 <.0001 Portal vein endotheliitis 72 8 12 14 <.0001 Bile duct damage 81 17 3 5 ,001 Centrilobular congestionhemorrhage 11 3 73 19 .27 Centrilobular fibrosis 1 1 83 21 .37 Parenchymal necrosis with
inflammation 13 3 71 19 .26 Parenchymal necrosis without
inflammation 47 11 37 11 .17 Apoptosis 44 7 40 15 .04 Sinusoidal lymphocytes 14 2 70 20 .20 Viral ICMV) inclusions 0 0 84 22 -
Steatosis 36 10 48 12 .19 Ballooning 41 9 43 13 .15 Lobular cholestasis 59 16 25 6 .20 Central vein endotheliitis 14 2 70 20 .20 Bile infarcts 0 0 84 22 Portal edema 6 1 78 21 .37 Ductular cholestasis 8 0 76 22 .14 Portal polymorphs 49 9 35 13 .67 Arteritis 1 0 83 22 .79
-
:I Fisher’s exact or ,y2 tests as appropriate.
score is calculated. Therefore, a biopsy specimen could have a score ranging from 0 to 12. An operational guide to the scoring system used is shown in Table 3, and representative illustrations are shown in Figs. 1-8.
The following analytical strategy was implemented, with the clinical review being used to assign the final diagnostic category for each biopsy specimen.
Histological features were scored in a presentlabsent fash- ion. Mixed portal inflammation, for example, when moderate or severe, was taken as this feature being present, and no or mild inflammation indicated the absence of this feature.
The results were tabulated (Table 51, and Fisher’s exact test and ,y2 test (as appropriate, Table 5 ) were used to assess association between the presence or absence of variables and rejection. A stepwise logistic regression analysis was per- formed on the main histological features in the diagnosis of cellular rejection (mixed portal inflammation, eosinophils, endotheliitis, and bile duct damage), determined from the Fisher’s exact test and x2 tests. The odds ratio in favor of the diagnosis of cellular rejection was calculated with different combinations of these features (Tables 6 and 7).
Biopsy specimens were scored according to each of the dif- ferent rejection scoring systems (Table 8) , and these scores were assessed against the final assigned diagnosis for the determination of the sensitivity and specificity, predictive value, efficiency, and likelihood ratio of the different systems used in the diagnosis and grading of cellular rejection (Table 9). True-positives (TP), true-negatives (TN), false-positives (FP), and false-negatives (FN) were taken into account.
TP x 100 TP + FN
Sensitivity =
TN x 100 TN + FP
Specificity =
TP x 100 TP + FP
Positive predictive value =
TN x 100 TN + FN
Negative predictive value =
(TP + TN) x 100 TP + FP + TN + FN
Efficiency =
The likelihood ratio was calculated as probability of a given result if rejection was present divided by probability of a given result if no rejection occurred. This statistic was used because it indicates how the odds of disease for a particular subject are modified once the result of a diagnostic test is known.6 Likelihood ratios > 1 mean that the odds of disease are increased by the result, whereas ratios < 1 decrease the odds.
These assessments are regardless of the degree of rejec- tion. The “consistent-with score was not included with the “rejection” final diagnostic category for any of the grading systems.
K analysis was used to assess the degree of agreement in grading cellular rejection by the different systems (Table 10). This index (K) was computed for each pair of systems. When maximal agreement occurs, the value of K is 1, and when agreement is only what would be expected by chance, K is 0. To interpret the degree of agreement, we used the following scale7: agreement measure > 0.8, excellent agreement; agreement measure 0.61 to 0.80, good agreement; agreement measure 0.41 to 0.60, moderate agreement; agreement mea- sure 0.21 to 0.40, fair agreement; and agreement measure < 0.21, poor agreement. Unlike the analysis of sensitivity, specificity; predictive value, efficiency, and likelihood ratio, this analysis includes agreements, or otherwise, between dif-

50 GUPTAETAL HEPATOLOGY January 1995
vein endotheliitis, and there was no instance of central vein endotheliitis without portal vein endotheliitis.
The stepwise logistic regression analysis performed on the above four features showed that bile duct dam- age did not make a significant independent contribu- tion (P = .27) to the diagnosis of cellular rejection, but the other three features did.
Tables 6 and 7 show how the number of features present contributes to the diagnosis of rejection. When portal inflammation, endotheliitis, and eosinophils are used, likelihood ratios were 0.11 for none of the fea- tures present, 0.52 for one feature, and 3.61 €or two or three features. When bile duct damage is added, the likelihood ratios were 0 for no features, 0.2 for one feature, 0.52 for two features, and 3.61 for three or four features. Thus, bile duct damage adds little to the identification of cellular rejection in this analysis, but
FIG. 1. A biopsy specimen obtained 3 days after OLT. There is little inflammation, and very few lymphocytes can be observed in the biliary epithelium of the duct in the middle of the figure. The portal vein endothelium is normal. No eosinophils were identified. This appearance corresponds to RFH score 2, Snover grade 0, and Demetris grade 1 (consistent with rejection). (Hematoxylin-eosin; magnification X140.)
ferent degrees (grades) of histological rejection, not taking into consideration the final assigned diagnostic category.
RESULTS As shown in Table 4, during the period ranging from
1 to 8 days after OLT, of 106 biopsy specimens, cellular rejection was finally diagnosed in 84 cases (79.2%), of which 72 cases (67.9%) had cellular rejection only and 12 cases (11.3%) had cellular rejection associated with sepsis or hypoperfusiodischemic episodes.
Examination of the 20 binary features to determine
showed that four features are Observed signifi- cantly more often in rejection than in nOnreJeCtiOn cases. These four features (Table 5) were portal vein endotheliitis ( p < .0001), portal tract eosinophils ( p < 'oool), moderate-to-severe mixed portal inflammation ( p < .001), and bile duct damage ( p = .ool). Central vein endotheliitis was observed less often than portal
their importance in rejec- FIG, 2, A protocol liver biopsy specimen obtained 3 days after OLT. There is moderate bile duct damage, mild inflammation, includ- ing four eosinophils (not appreciable a t this magnification and in monochrome), and approximately half of the circumference of the portal vein shows endotheliitis. This produces an RFH score of 5 and corresponds to Snover grade 1 and Demetris grade 2. Thus, all of the scoring systems indicate mild cellular rejection, but they arrive a t this conclusion having used different specific grading criteria. (He- matoxylin-eosin; magnification x 140.)

HEPATOLOGY VoI. 21, No. 1, 1995 GUF’TAETAL 51
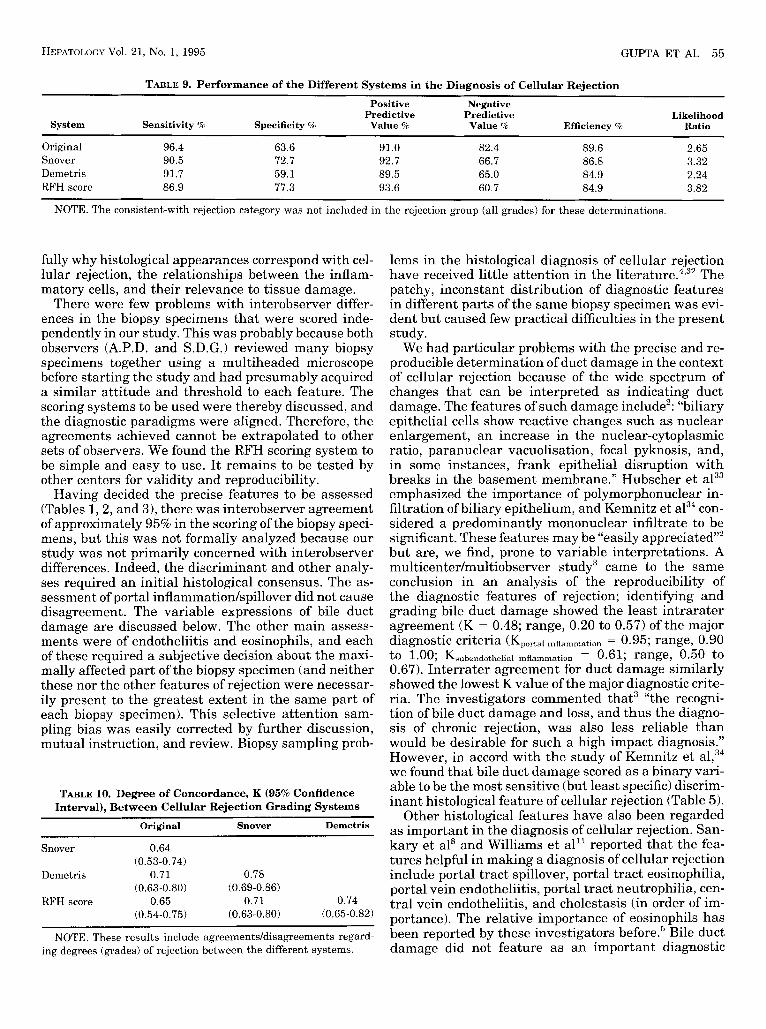
RFH scores were more efficient (3.32 and 3.82, respec- tively) in diagnosing rejection than were the other two scores (original, 2.65; and Demetris, 2.24).
K analysis showed good agreement between the dif- ferent grading systems (Table 10).
DISCUSSION In this work we have applied discriminant analysis
to define four histological features in liver biopsy speci- mens (mixed portal inflammation, endotheliitis, eosino- phils, and bile duct damage), which are informative regarding cellular rejection. These features were used to formulate a rejection scoring system that appeared to compare favorably with existing rejection grading systems when K analysis of the degree of agreement between these schemes was performed. As far as we are aware, this is a novel study strategy in these respects. Reassuringly, the individual informative histological elements that comprise our scoring system have all
FIG. 3. Protocol liver biopsy specimen obtained 3 days after OLT. The portal tract in the center field is moderately inflamed, whereas the nearby portal tract at the upper right of the figure shows little inflammation. The more inflamed portal tract contains three eosino- phils, the bile duct shows mild intraepithelial inflammation, and there is moderate endotheliitis. Not all of these features can be fully appreciated at this magnification. The total RFH score is 6 (mild rejection), corresponding to Snover grade 1 and Demetris grade 2 (mild rejection), when the same biopsy specimen was scored for the separate criteria required by these two classifications. (Hematoxylin- eosin; magnification X 140.)
its absence, along with the absence of the three other features, increases the evidence against cellular rejec- tion.
The results of the overall grading of the 106 liver biopsy specimens obtained from 1 to 8 days after trans- plantation are given in Table 8. The sensitivity, speci- ficity, predictive values, efficiency, and likelihood ratios of the different grading systems are enumerated in Ta- ble 9. Each of the grading schemes had a high sensitiv- ity (87% to 96%) in diagnosing cellular rejection. How- ever, the specificity varied from 59% to 77%. The specificity of the original, routine diagnosis (63.6%) was similar to that of the Demetris system (59.1%), and the Snover (72.7%) and RFH scoring (77.3%) systems had similar specificities for diagnosing cellular rejection. The derived likelihood ratios showed the Snover and
FIG. 4. A biopsy specimen obtained 5 days after OLT. There is packing of the portal tract by inflammatory cells, with little spillover into the parenchyma. There are six eosinophils and moderate endo- theliitis with moderate bile duct damage overall. The total RFH score is 9, amounting to moderate rejection. This biopsy specimen was scored separately as Snover grade 2 (moderate rejection) and De- metris grade 2 (mild rejection). (Hematoxylin-eosin; magnification X 140.)

52 GUPTA ET AL HEPATOLOGY January 1995
treatment, including immunosuppression in patients with presumptive cellular rejection.
Fortunately, the majority of episodes of cellular rejec- tion are responsive to immunosuppression.2 L ~ d w i g , ~ referring to the response of rejection-related inflam- mation, endotheliitis, and duct damage to immunosup- pressive therapy, states that “improvement or disap- pearance of these ‘acute lesions’ can be considered the most reliable confirmation of the diagnosis.” Neverthe- less, our study is still limited by the lack of a diagnostic option more reliable than, and independent of, histopa- thology. Our work in more precise terms is of statisti- cally significant histological features of immunosup- pression-responsive cellular rejection from 1 to 8 days after OLT only. Until we have the ability to diagnose cellular rejection with certainty and without recourse to histology, these limitations will be difficult to over- come.
FIG. 5. A liver biopsy specimen obtained 6 days after OLT. The portal tract in the upper field is packed with inflammatory cells, and it contains four eosinophils. There is severe endotheliitis (see Fig. 6) and moderate duct damage overall. Therefore, the RFH score is 9 (moderate cellular rejection). There is also endotheliitis of the central venule (lower part of the field) and focal parenchymal necrosis (mid- dle field). (Hematoxylin-eosin; magnification x 140.)
been previously recognized as important components of cellular rejection.1,2,5 In a single previous study using stepwise logistic regression analysis, portal tract spill- over, eosinophilia, portal vein endotheliitis, neutro- philia, central vein endotheliitis, and cholestasis were identified as significant histological variables affecting the diagnosis of rejection.8
The main aim of our study was to identify those histo- logical features that contribute significantly to a diag- nosis of cellular rejection. Because we wanted to use a statistical approach, certain constraints were neces- sary. Our discriminant analysis only applies to the time frame selected (1 to 8 days after OLT) and to those of our relatively “uncomplicated biopsy specimens that could be categorized clinically with confidence (be- cause, obviously, we were unable to use the features in the biopsy specimens under study for the diagnostic assignment). Part of this assessment is response to
FIG. 6. The same biopsy specimen as in Fig. 5. This central vein shows endotheliitis of most of its circumference. There is hemorrhage into the surrounding acinar zone 3 (many of the small dark cells in this field are red blood cells) with liver cell loss and ballooning of the surviving adjacent liver cells. In combination with the features shown in Fig. 5 this biopsy specimen, therefore, shows rejection grade 3 according to the Snover grading system and Demetris grade 4 (severe rejection). (Hematoxylin-eosin; magnification x 140.)

HEPATOLOGY Vol. 21, No. 1, 1995 GUPTA ET AL 53
FIG. 7. Liver biopsy specimen obtained 5 days after OLT. The portal area is expanded with a marked inflammatory infiltrate with spillover into the adjacent parenchyma. There are 15 eosinophils in this portal tract, marked ductulitis, and moderate endotheliitis overall. The degree of endotheliitis of the portal vein is difficult to assess with this degree of inflammation, and in this situation assess- ment of endotheliitis is better made by examination of central ve- nules. The total RFH score in this biopsy specimen is 11, the Snover grade is 3, and the Demetris grade is 4 (severe rejection). (Hematoxy- lin-eosin; magnification X 140.)
In this study an inherent bias in favor of the original diagnosis could have been a problem, because this was instrumental in deciding the therapy. This potential bias was not substantiated, however; as shown in Table 9, the original, routine diagnosis had the second small- est (albeit acceptable) likelihood ratio. Therefore, we are confident that the criteria used for making the final diagnosis of immunosuppression-responsive cellular rejection in this study were independent of the biopsy specimens under study and reasonably free of bias.
Acute cellular rejection is common early after OLT. It is estimated that 70% of patients experience at least one episode of acute cellular rejection, and this occurs in 50% to 90% of hepatic allograft^.*,^^-'^ Cellular rejec- tion is recognized by a combination of clinical, biochem- ical, and histopathological finding^.',^,'^ Histological evaluation seems to be the best means at present of
FIG. 8. With lesser degrees of portal tract inflammation as ob- served here, inflammation of bile ducts (center field) and portal vein endotheliitis (upper field) are easier to appreciate. (Hematoxylin- eosin; magnification ~ 3 5 0 . )
identifying cellular rejection in the liver a l l ~ g r a f t . ~ , ~ ~ , ' ~ The histopathological appearance that indicates cellu- lar rejection consists of a mixed inflammatory cell in- filtrate, inflammatory damage of bile ducts, and endo- theliitis.'
Lymphocytic infiltration and endothelial damage were recognized as characteristic histological features
TABLE 6. Diagnosis of Rejection According to the Presence of ModeratdSevere Portal Inflammation,
Endotheliitis, and Eosinophils
No. of Histological
Features No Rejection Likelihood Present Rejection Present Total Ratio
0 12 5 17 0.11 1 5 10 15 0.52
2 3 4 1 20 49 Ei 13.61
Total 22 84 106

54 GUPTA ET AL HEPATOLOGY January 1995
TABLE 7. Diagnosis of Rejection According to the Presence of ModerateBevere Portal Inflammation, Endotheliitis,
Eosinophils, and Bile Duct Damage
No. of Histological
Features No Rejection Likelihood Present Reiection Present Total Ratio
0 4 0 4 0 1 9 7 16 0.2 2 4 8 12 0.52 3 1 21 4 4 48
22
Total 22 84 106 52 13.61
in early studies of cellular reje~tion.’~,’~ Porter” also pointed out that tissue damage caused by graft isch- emia consequent on immunologic vascular compromise was probably important in the pathogenesis of the re- jection process. Eggink et al” and Williams et al” em- phasized the importance of portal inflammation and its severity, and Fennell,” Portmann et a1,2‘ and Vierling and Fenne1lz3 documented the relevance of bile duct damage.
Currently established systems of rejection grading depend primarily on the histological diagnostic triad of mixed portal inflammation, “endothelialitis,” and bile duct damage,’ but include other features currently re- garded as components of chronic rejection and is- chemia: arteritis, paucity of ducts, and loss of zone 3 hepatocytes.’,’ The dilemma of whether to include the latter or not has been expressed as “If the severity of rejection is based solely on the degree of inflammation, the pathologist fails to take into account architectural damage that may arise as a consequence of rejection- related ischemia,”2 on the one hand, and “apparent his- tological markers of acute ischemic damage. . . . may be nonspecific or even unrelated to rejection,”‘ on the other.
The immune reaction responsible for cellular rejec- tion is principally cell mediated, and the target tissues are mainly interlobular bile ducts and vascular endo- thelium.” Early acute cellular rejection is probably ma- jor histocompatibility complex (MHC) class I-depen- dent, whereas later episodes as well as chronic rejection are mediated by a class I1 MHC mechanism.13 Patterns of MHC expression are variable, and these correlations are not a b ~ o l u t e . ~ ~ ~ ~ Approximately equal
numbers of CD4+ and CD8+ T lymphocytes are pres- ent in portal tracts in acute reje~tion.’~ Parenchymal CD8+ T cells increase in chronic rejection, and lympho- cytes infiltrating biliary epithelium are mainly of the CD8+ phen~type.’~ Portal lymphocytic infiltrates rich in CD4+ T cells have been found to be indicative of steroid-responsive cellular rejection. In one study this infiltrate preceded and predicted histological and bio- chemical features of rejection by 12 days.25
The mixed inflammatory infiltrate indicating cellular rejection consists of lymphoblasts, lymphocytes, neu- trophils, and eosinophils. Although the latter have al- ways been noted,’ the question of their significance has not been addressed until recently. Formerly, a predom- inance of eosinophils was thought to indicate an ad- verse drug reaction, even within the setting of allograft rejection.“ More recently, morphometric quantification of portal tract eosinophilia has been found to be pre- dictive of acute rejection with a high sensitivity (80%) and specificity Furthermore, tissue eosino- philia persists when therapy for rejection is unsuccess- ful, and it decreases with successful Eosin- ophils have been implicated in tissue damage,30 possibly via the production of eosinophil cationic pro- teins. A recent study showed the expression of the che- motactic cytokine regulation activation, normal T cells, expressed and secreted (RANTES) by mononuclear cells and renal tubular epithelium in cell-mediated re- nal transplant reje~tion.~’ This cytokine is specifically chemotactic for T cells, monocytes, and eosinophils. This sort of mechanism could explain the concurrence of the eosinophilic and lymphoid infiltrate observed in previous studies of liver transplant rejection, as well as in our own.
In the present study, four histological features were found to be significantly discriminating in diagnosing cellular rejection histologically. Consistent with previ- ous observations, these features were mixed portal in- flammation, eosinophils, endotheliitis, and bile duct damage. The first two features could be considered the histological reflections of the immunologic cellular in- filtrate, causing cellular rejection according to the pathophysiological observations described above, and the second two features could well represent the major damage caused. Our present understanding of the pathophysiology of cellular rejection is incomplete. His- tological analysis alone is bound to be immunologically limited, and further work is necessary to appreciate
TABLE 8. Overall Diagnosis of Cellular Rejection in 106 Post-OLT (Days 1 to 8) Biopsy Specimens Using Different Grading Systems*
Grade of Rejection No Rejection Consistent With Rejection Mild Rejection Moderate Rejection Severe Rejection
31 51 7 Original 17 - Snover 10 14 35 36 11 D e m e t r i s 12 8 43 37 6 RFH score 5 23 42 23 13
* These are purely histological assignments (Tables 1,2 , and 3) and do not necessarily correspond to the final clinical diagnostic categories (Table 41, having been scored “blind” according to morphological features alone.
HEPATOLOGY Vol. 21, No. 1, 1995 GUPTA ET AL 55
TABLE 9. Performance of the Different Systems in the Diagnosis of Cellular Rejection
Positive Negative Predictive Predictive Likelihood
System Sensitivity % Specificity 9% Value % Value % Efficiency % Ratio ~~
0 r i gi n a 1 96.4 63.6 91.0 82.4 89.6 2.65 Snover 90.5 72.7 92.7 66.7 86.8 3.32 Demetris 91.7 59.1 89.5 65.0 84.9 2.24 RFH score 86.9 77.3 93.6 60.7 84.9 3.82
NOTE. The consistent-with rejection category was not included in the rejection group (all grades) for these determinations.
fully why histological appearances correspond with cel- lular rejection, the relationships between the inflam- matory cells, and their relevance to tissue damage.
There were few problems with interobserver differ- ences in the biopsy specimens that were scored inde- pendently in our study. This was probably because both observers (A.P.D. and S.D.G.) reviewed many biopsy specimens together using a multiheaded microscope before starting the study and had presumably acquired a similar attitude and threshold to each feature. The scoring systems to be used were thereby discussed, and the diagnostic paradigms were aligned. Therefore, the agreements achieved cannot be extrapolated to other sets of observers. We found the RFH scoring system to be simple and easy to use. It remains to be tested by other centers for validity and reproducibility.
Having decided the precise features to be assessed (Tables 1,2, and 3), there was interobserver agreement of approximately 95% in the scoring of the biopsy speci- mens, but this was not formally analyzed because our study was not primarily concerned with interobserver differences. Indeed, the discriminant and other analy- ses required an initial histological consensus. The as- sessment of portal inflammatiodspillover did not cause disagreement. The variable expressions of bile duct damage are discussed below. The other main assess- ments were of endotheliitis and eosinophils, and each of these required a subjective decision about the maxi- mally affected part of the biopsy specimen (and neither these nor the other features of rejection were necessar- ily present to the greatest extent in the same part of each biopsy specimen). This selective attention sam- pling bias was easily corrected by further discussion, mutual instruction, and review. Biopsy sampling prob-
TABLE 10. Degree of Concordance, K (95% Confidence Interval), Between Cellular Rejection Grading Systems
~~ ~
Original Snover Demetris
Snover 0.64
Demetris 0.71 0.78
RFH score 0.65 0.71 0.74
(0.53-0.74)
(0.63-0.80) (0.69-0.86)
(0.54-0.75) (0.63-0.80) (0.65-0.82)
NOTE. These results include agreementddisagreements regard- ing degrees (grades) of rejection between the different systems.
lems in the histological diagnosis of cellular rejection have received little attention in the l i t e r a t~ re .~ .~ ’ The patchy, inconstant distribution of diagnostic features in different parts of the same biopsy specimen was evi- dent but caused few practical difficulties in the present study.
We had particular problems with the precise and re- producible determination of duct damage in the context of cellular rejection because of the wide spectrum of changes that can be interpreted as indicating duct damage. The features of such damage include’: “biliary epithelial cells show reactive changes such as nuclear enlargement, an increase in the nuclear-cytoplasmic ratio, paranuclear vacuolisation, focal pyknosis, and, in some instances, frank epithelial disruption with breaks in the basement membrane.” Hubscher et a133 emphasized the importance of polymorphonuclear in- filtration of biliary epithelium, and Kemnitz et a134 con- sidered a predominantly mononuclear infiltrate to be significant. These features may be “easily appreciated”’ but are, we find, prone to variable interpretations. A multicenter/multiobserver study3 came to the same conclusion in an analysis of the reproducibility of the diagnostic features of rejection; identifying and grading bile duct damage showed the least intrarater agreement ( K = 0.48; range, 0.20 to 0.57) of the major diagnostic criteria (Kporta, = 0.95; range, 0.90 to 1.00; Ksubendothelial inflammation = 0.61; range, 0.50 to 0.67). Interrater agreement for duct damage similarly showed the lowest K value of the major diagnostic crite- ria. The investigators commented that3 “the recogni- tion of bile duct damage and loss, and thus the diagno- sis of chronic rejection, was also less reliable than would be desirable for such a high impact diagnosis.” However, in accord with the study of Kemnitz et we found that bile duct damage scored as a binary vari- able to be the most sensitive (but least specific) discrim- inant histological feature of cellular rejection (Table 5 ) .
Other histological features have also been regarded as important in the diagnosis of cellular rejection. San- kary et als and Williams et all’ reported that the fea- tures helpful in making a diagnosis of cellular rejection include portal tract spillover, portal tract eosinophilia, portal vein endotheliitis, portal tract neutrophilia, cen- tral vein endotheliitis, and cholestasis (in order of im- portance). The relative importance of eosinophils has been reported by these investigators b e f ~ r e . ~ Bile duct damage did not feature as an important diagnostic

56 GUPTA ET AL HEPATOLOGY January 1995
variable in their list. Intralobular lymphocytic infiltra- tion4 and small areas of perivenular hepatocyte necro- sis:j5 can also be considered as features of rejection.
The present analysis showed that of the 20 binary histological features studied, 4 (moderatelsevere mixed portal inflammation, eosinophils, portal vein endotheli- itis, and bile duct injury) were present in a significant number of biopsy specimens confirmed as having acute cellular rejection (Table 5 ) . Other features did not have a statistically significant discriminant value. There was no case of central vein endotheliitis without portal vein endotheliitis in our study. Thus, the diagnosis of cellular rejection can be made predominantly on fea- tures identifiable in the portal tract.
The stepwise logistic regression analysis showed that four major binary features, moderatelsevere portal in- flammation, eosinophils, endotheliitis, and duct dam- age, indicate cellular rejection. Therefore, we agree with Sankary et al,8 Williams et al,” and with Foster et al”7.30 that eosinophils are an important histological feature of cellular rejection. The RFH scoring system based on the four major histological discriminant fea- tures was highly sensitive (86.9%) and specific (77.3%). It agreed with Snover’s and Demetris’s systems (Table 10). Superficially, our scoring system could be consid- ered to have similarities with the Knodell et a136 system for scoring the activity of chronic hepatitis. This sort of evaluation was used by Eggink et all9 and Williams et a12” in their assessment of rejection. The features that are assessed in the RFH system and the way in which they were chosen for assessment are different from these previous studies. The application of a num- ber to a subjective assessment of severity is a common method of semiquantification. In our system, we have not attempted to give any particular weight to any of the parameters, and our numerical scales are continu- ous, in contrast with the Knodell et a136 scoring scheme.
The overall score in the RFH system can be broadly subdivided into five grades comparable with the other systems (none, consistent with, mild, moderate, and severe cellular rejection). These divisions led to a pro- portion (21.7%) of biopsy specimens being graded in the consistent-with category. Of the 23 biopsy specimens in this group, 11 biopsy specimens (with follow-up infor- mation) had cellular rejection (1 of which had sepsis in addition), and 12 were nonrejectors. With the method of Snover et al, in the category of consistent-with (grade 0) 6 of 14 patients (including 1 with sepsis) had cases of cellular rejection. By the Demetris method, five of eight patients (including 1 each with additional sepsis and hypoperfusion) were rejectors. Thus, with all three methods, approximately half of the patients in a cate- gory consistent-with includes cases of cellular rejection. This situation was recognized by Kemnitz et a134 as well, who noted that 65% of their consistent-with-rejec- tion category had therapy-requiring rejection. This group of patients requires a more careful scrutiny with clinical and biochemical parameters before deciding whether or not to implement further immunosuppres- sive therapy. At present, at the RFH, patients with
mild cellular rejection histologically are not usually considered to require increased immunosuppression. Therefore, the treatment given to the lesser categories of cellular rejection needs to be reconsidered. In the present study, the consistent-with-rejection category was not included in the rejection group for any of the scoring systems performance determinations (Table 9).
All of the schemes that we studied had similar sensi- tivities, probably because all incorporated major histo- logical discriminant features, portal inflammation, en- dotheliitis, and duct damage, for the diagnosis of cellular rejection. This is also the most likely explana- tion for the good-to-excellent agreement between these systems.
In conclusion, we have confirmed that four histologi- cal features are important discriminants in the diagno- sis of acute cellular rejection-moderatelsevere mixed portal inflammation, endotheliitis, eosinophils in the portal tract, and bile duct damage. Based on the semi- quantitative assessment of these four features, we have formulated a numerical scoring system. This system has a high sensitivity and specificity, and compares favorably with the established grading schemes of Snover et all and Demetris et a1.’ A simple, widely acceptable, reproducible scoring system would permit more reliable follow-up of serial biopsies, allow compar- ison of results between different centers, and perhaps help in the fine tuning of immunosuppressive therapy in the future. Further prospective studies are neces- sary to validate and assess the reproducibility of the RFH scoring system.
Acknowledgment: This study was performed while S.D.G. was a visiting British Council Research Fellow at the RFHSM. We thank Lynette Bannister and Rod Conrad for helping to prepare the manuscript and Francis Moll for photographic help.
1.
2.
3.
4.
5.
6.
7.
8.
9.
REFERENCES Snover DC, Freese DK, Sharp HL, Bloomer JR, Najarian JA, Ascher NL. Liver allograft rejection: an analysis of the use of biopsy in determining outcome of rejection. Am J Surg Pathol
Demetris AJ, Qian S, Sun H, Fung JJ . Liver allograft rejection: an overview of morphological findings. Am J Surg Pathol 1990; 14(suppl 1):49-63. Demetris AJ, Belle SH, Hart J, Lewin K, Ludwig J , Snover DC, Tillery GW, et al. Intraobserver and interobserver variation in the histopathological assessment of liver allograft rejection. HEP-
Hubscher SG. Histological findings in liver allograft rejection- new insights into the pathogenesis of hepatocellular damage in liver allografts. Histopathology 1991; 18:377-383. Foster PF, Sankary H, Williams JW. Study of eosinophilia and hepatic dysfunction as a predictor of rejection in human liver transplantation. Transplant Proc 1988; 20:676-677. Altman DG. Practical statistics for medical research. Ed 1. Lon- don: Chapman & Hall, 1991. Fleiss JL. Statistical methods for rates and proportions. Ed 2. New York: Wiley, 1981. Sankary H, Foster P, Hart M, Ashmann M, Schwartz D, Wil- liams JW. An analysis of the determinants of hepatic allograft rejection using stepwise logistic regression. Transplantation 1989;47:74-77. Ludwig J. Histopathology of the liver following transplantation.
1987; 11:1-10.
ATOLOGY 1991; 14:751-755.
HEPATOLOGY Vol. 21, No. 1, 1995 GUPTA ET AL 57
In: Maddrey WC, ed. Transplantation of the liver. New York: Elsevier, 1988:191-218.
10. Adams DH, Neuberger JM. Patterns of graft rejection following liver transplantation. J Hepatol 1990; 10:113-119.
11. Williams JW, Foster PF, Sankary HN. Role of liver allograft biopsy in patient management. Semin Liver Dis 1992; 1250-72.
12. Vierling JM. Iinmunologic mechanisms of hepatic allograft rejec- tion. Semin Liver Dis 1992; 12: 16-27.
13. Starzl TE, Demetris AJ, Van Thiel D. Liver transplantation: rejection and histocompatibility. N Engl J Med 1989; 321: 1092- 1093.
14. Colina F, Molleja M, Moreno E, Alberti N, Garcia I, Gomez-Sanz R, Castellano G. Effectiveness of histopathological diagnoses in dysfunction of hepatic transplantation-review of 146 histologi- cal studies from 53 transplants. Arch Pathol Lab Med
15. Henley KS, Lucey MR, Appelman HD, Baliga P, Brown KA, Burtch GD, Campbell DA, Jr , et al. Biochemical and histopatho- logical correlation in liver transplant: the first 180 days. HEPA- TOLOGY 1992; 16:688-693.
16. Wight DGD, Portmann B. Pathology of liver transplantation. In: Calne R, ed. Liver transplantation. Ed 2. Philadelphia: Grune & Stratton, 1987:385-435.
17. Porter KA. Pathology of liver transplantation. Transplant Rev
18. Porter KA. Pathology of the orthotopic homograft and hetero- graft. In: Starzl TE, ed. Experience in hepatic transplantation. Philadelphia: Saunders, 1969:422-471.
19. Eggink HF, Hofstee N, Gips CH, Krom RAF, Houthoff HJ. Histo- pathology of serial graft biopsies from liver transplant recipients. Am J Pathol 1984;114:18-31.
20. Williams JW, Peters TG, Vera SR, Britt LG, Van Voorst SJ, Haggitt RC. Biopsy-directed immunosuppression following he- patic transplantation in man. Transplantation 1985; 39:589-596.
21. Fennell RH. Ductular damage in liver transplant rejection. Pa- tho1 Ann 1981; 16:289-294.
22. Portmann B, Neuberger JM, Williams R. Intrahepatic bile duct lesions, In: Calne RV, ed. Liver transplantation. Philadelphia: Grune & Stratton, 1983:279-287.
23. Vierling JM, Fennell RH. Histopathology of early and late hu- man hepatic allograft rejection: evidence of progressive destruc- tion of interlobular bile ducts. HEPATOLOGY 1985; 5 : 1076-1082.
24. McCaughan GW, Stewart Davies J, Waugh JA, Bishop A, Hall BM, Gallagher ND, Thompson JF , et al. A quantitative analysis of T-lymphocyte populations in human liver allografts undergo-
1991; 115x998-1005.
1969; 21129-170.
ing rejection: the use of monoclonal antibodies and double immu- nolabelling. HEPATOLOCY 1990; 12:1305-1313.
25. Perkins JD, Rakela J , Sterioff S, Banks PM, Weisner RH, Krom RAF. Immunohistologic pattern of the portal T-lymphocyte infil- tration in hepatic allograft rejection. Mayo Clin Proc
26. Snover DC, Sibley RK, Freese DK, Sharp HL, Bloomer JR, Na- jarian JS, Ascher NL. Orthotopic liver transplantation: a patho- logical study of 63 serial liver biopsies from 17 patients with special reference to the diagnostic features and natural history of rejection. HEPATOLOGY 1984;4:1212-1222.
27. Foster PF, Sankary HN, Williams JW, Bhattacharyya A, Cole- man J , Ashmann M. Morphometric inflammatory cell analysis of human liver allograft biopsies. Transplantation 1991; 51373- 876.
28. Foster PF, Sankary HN, McChesney L, Williams JW. Morpho- metric analysis of serial liver allograft biopsies predicts ade- quacy of acute rejection treatment [Abstract]. HEPATOLOGY 1991; 14:281A.
29. Foster PF, Sankary HN, Bhattacharyya A, Novich K, Xiao F, Williams JW. Morphometric analysis of liver allograft biopsies following treatment of acute rejection [Abstract]. HEPATOLOGY 1990; 12:1015.
30. Foster PF, Bhattacharyya A, Sankary HN, Coleman J , Ashmann M, Williams JW. Eosinophil cationic protein’s role in human hepatic allograft rejection. HEPATOLOGY 1991; 13:1117-1125.
31. Pattison J, Nelson PJ, Huie P, von Leuttichau I, Farshid G, Sibley RK, Krensky AM. RANTES chemokine expression in cell- mediated transplant rejection of the kidney. Lancet 1994; 343:209-2 11.
32. Thung SN, Gerber MA. Histological features of liver allograft rejection: do you see what I see? HEPATOLOGY 1991; 14:949-951.
33. Hubscher SG, Clements D, Elias E, McMaster P. Biopsy findings in cases of rejection of liver allograft. J Clin Pathol1985;38: 1366- 1373.
34. Kemnitz J , Ringe B, Cohnert TR, Gubernatis G, Choritz H, Geor- gii A. Bile duct injury as part of diagnostic criteria for liver allograft rejection. Hum Pathol 1989;20:132-143.
35. Demetris AJ, Lasky S, Van Thiel DH, Starzl TE, Dekker A. Pathology of hepatic transplantation: a review of 62 adult allo- graft recipients immunosuppressed with a cyclosporine/steroid regimen. Am J Pathol 1985; 118:151-161.
36. Knodell RG, Ishak KG, Black WC, Chen TS, Craig R, Kaplowitz N, Kiernan TW, et al. Formulation and application of a numeri- cal scoring system for assessing histological activity in asymp- tomatic chronic active hepatitis. HEPATOLOGY 1981; 1:431-435.
1989;64:565-569.



















