
Prolonged discordant xenograft survival and delayed xenograft rejection in a pig-to-baboon...
8
PROLONGED DISCORDANT XENOGRAFT SURVIVAL AND DELAYED XENOGRAFT REJECTION IN A PIG-TO-BABOON ORTHOTOPIC CARDIAC XENOGRAFT MODEL He Xu, MD a Steven R. Gundry, MD a Wayne W. Hancock, MD b Goro Matsumiya, MD a Craig W. Zuppan, MD c Toro Morimoto, MD a James Slater, MD d Leonard L. Bailey, MD a Objective: Our objectives were to study delayed xenograft rejection and the effectiveness of pretransplantation total lymphoid irradiation combined with immunosuppression on rejection in a pig-to-baboon cardiac xenograft model. Methods: Baboons were treated with pretransplantation total lym- phoid irradiation, cyclosporine A (INN: ciclosporin), and methotrexate. Orthotopic pig-to-baboon cardiac transplantations were performed after depletion of circulating xenoreactive natural antibody by pretransplanta- tion donor organ hemoperfusion. Tissue samples were collected for immu- nologic and immunopathologic evaluation. Results: Pig cardiac xenografts survived more than 18 and 19 days without evidence of hyperacute rejection. Immunologic analysis of serum samples demonstrated that circulating xenoreactive natural antibody levels did not return to pretrans- plantation levels. The production of xenoreactive natural antibodies from the recipient’s splenocytes was inhibited completely. Histologic examina- tion of xenografts showed the feature of acute vascular rejection. Immuno- histochemical studies demonstrated infiltration of cardiac xenografts by large numbers of macrophages, small numbers of natural killer cells, and a few T cells. The infiltrating macrophages also showed expression of interleukin-1 and tumor necrosis factor. Diffuse deposition of immunoglob- ulin G, C1Q, C3, and fibrin on xenograft vasculature was observed. Interleukin-2 expression was not found in rejected cardiac xenografts. Xenograft endothelial cells also showed evidence of activation (expression of cytokines interleukin-1 and tumor necrosis factor). Conclusions: This study demonstrates prolonged discordant cardiac xenograft survival and delayed xenograft rejection in a pig-to-baboon model. The delayed xeno- graft rejection is mediated by both humoral and cellular mechanisms. Pretransplantation total lymphoid irradiation combined with cyclosporine A and methotrexate can inhibit xenoreactive natural antibody production but not elicited antipig antibody production and the xenoreactivity of macrophages. (J Thorac Cardiovasc Surg 1998;115:1342-9) C linical cardiac allotransplantation has been lim- ited by a critical shortage of donor organs. 1 Cross-species transplantation has been proposed as an alternative to allograft transplantation. Unlike concordant xenografts (transplantation between closely related species), discordant xenografts (transplantation between widely disparate species) are usually hyperacutely rejected; the pathogenesis of hyperacute rejection is believed to be mediated by the binding of circulating xenoreactive natural anti- bodies to xenograft endothelium and activation of the classical complement pathway resulting in endo- thelial cell injury. 2 To prevent hyperacute rejection, early investiga- tions have focused on xenoreactive natural anti- From the Cardiac Transplantation Research Laboratory, Divi- sion of Cardiothoracic Surgery, Department of Surgery, a the Department of Pathology, c and the Department of Radiation Medicine, d Loma Linda University Medical Center, Loma Linda, Calif., and the Sandoz Center for Immunobiology, New England Deaconess Hospital, Harvard Medical School, Boston, Mass. b Presented in part at the Fourth International Congress for Xenotransplantation, Sept. 7-11, 1997, Nantes, France. Received for publication Dec. 5, 1997; accepted for publication Jan. 15, 1998. Address for reprints: Steven R. Gundry, MD, Department of Surgery, Loma Linda University Medical Center, 11234 Anderson St., Loma Linda, CA 92354. Copyright © 1998 by Mosby, Inc. 0022-5223/98 $5.00 1 0 12/1/88941 1342
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Prolonged discordant xenograft survival and delayed xenograft rejection in a pig-to-baboon...

PROLONGED DISCORDANT XENOGRAFT SURVIVAL AND DELAYED XENOGRAFT REJECTION INA PIG-TO-BABOON ORTHOTOPIC CARDIAC XENOGRAFT MODEL
He Xu, MDa
Steven R. Gundry, MDa
Wayne W. Hancock, MDb
Goro Matsumiya, MDa
Craig W. Zuppan, MDc
Toro Morimoto, MDa
James Slater, MDd
Leonard L. Bailey, MDa
Objective: Our objectives were to study delayed xenograft rejection and theeffectiveness of pretransplantation total lymphoid irradiation combinedwith immunosuppression on rejection in a pig-to-baboon cardiac xenograftmodel. Methods: Baboons were treated with pretransplantation total lym-phoid irradiation, cyclosporine A (INN: ciclosporin), and methotrexate.Orthotopic pig-to-baboon cardiac transplantations were performed afterdepletion of circulating xenoreactive natural antibody by pretransplanta-tion donor organ hemoperfusion. Tissue samples were collected for immu-nologic and immunopathologic evaluation. Results: Pig cardiac xenograftssurvived more than 18 and 19 days without evidence of hyperacuterejection. Immunologic analysis of serum samples demonstrated thatcirculating xenoreactive natural antibody levels did not return to pretrans-plantation levels. The production of xenoreactive natural antibodies fromthe recipient’s splenocytes was inhibited completely. Histologic examina-tion of xenografts showed the feature of acute vascular rejection. Immuno-histochemical studies demonstrated infiltration of cardiac xenografts bylarge numbers of macrophages, small numbers of natural killer cells, anda few T cells. The infiltrating macrophages also showed expression ofinterleukin-1 and tumor necrosis factor. Diffuse deposition of immunoglob-ulin G, C1Q, C3, and fibrin on xenograft vasculature was observed.Interleukin-2 expression was not found in rejected cardiac xenografts.Xenograft endothelial cells also showed evidence of activation (expressionof cytokines interleukin-1 and tumor necrosis factor). Conclusions: Thisstudy demonstrates prolonged discordant cardiac xenograft survival anddelayed xenograft rejection in a pig-to-baboon model. The delayed xeno-graft rejection is mediated by both humoral and cellular mechanisms.Pretransplantation total lymphoid irradiation combined with cyclosporineA and methotrexate can inhibit xenoreactive natural antibody productionbut not elicited antipig antibody production and the xenoreactivity ofmacrophages. (J Thorac Cardiovasc Surg 1998;115:1342-9)
Clinical cardiac allotransplantation has been lim-ited by a critical shortage of donor organs.1
Cross-species transplantation has been proposed asan alternative to allograft transplantation. Unlikeconcordant xenografts (transplantation betweenclosely related species), discordant xenografts(transplantation between widely disparate species)are usually hyperacutely rejected; the pathogenesisof hyperacute rejection is believed to be mediated bythe binding of circulating xenoreactive natural anti-bodies to xenograft endothelium and activation ofthe classical complement pathway resulting in endo-thelial cell injury.2
To prevent hyperacute rejection, early investiga-tions have focused on xenoreactive natural anti-
From the Cardiac Transplantation Research Laboratory, Divi-sion of Cardiothoracic Surgery, Department of Surgery,a theDepartment of Pathology,c and the Department of RadiationMedicine,d Loma Linda University Medical Center, LomaLinda, Calif., and the Sandoz Center for Immunobiology,New England Deaconess Hospital, Harvard Medical School,Boston, Mass.b
Presented in part at the Fourth International Congress forXenotransplantation, Sept. 7-11, 1997, Nantes, France.
Received for publication Dec. 5, 1997; accepted for publicationJan. 15, 1998.
Address for reprints: Steven R. Gundry, MD, Department ofSurgery, Loma Linda University Medical Center, 11234Anderson St., Loma Linda, CA 92354.
Copyright © 1998 by Mosby, Inc.0022-5223/98 $5.00 1 0 12/1/88941
1 3 4 2

bodies and complement depletion using plasma ex-change,3 donor organ hemoperfusion,4 and inhibitionof complement.5 Despite these measures, only limitedxenograft survival has been achieved. Although hyper-acute rejection of discordant xenografts has beenovercome, the late phase of xenograft rejection,termed delayed xenograft rejection, has become themajor barrier to the long-term xenograft survival.6
Cooper and associates4 have demonstrated severeacute cellular rejection in one heterotopically trans-planted heart xenograft that survived more than 5days.4 Blakeley, Hancock, and their associates6 haveextensively evaluated the pathogenesis of delayedxenograft rejection in a guinea pig–to–rat cardiacxenograft model; and endothelial cell activation andmacrophages appear important in the delayed xeno-graft rejection. In addition, Millan and coworkers7
have recently demonstrated evidence of porcine endo-thelial cell activation in response to human macro-phages/monocytes in an in vitro study.
In a pig-to-baboon cardiac xenotransplant model,we8 have shown prolonged xenograft survival anddelayed xenograft rejection. Immunologic analysisof blood samples also demonstrated increased levelsof xenoreactive natural antibodies after transplanta-tion, suggesting that these antibodies play an impor-tant role in delayed xenograft rejection. In thecurrent study, we extended our investigation toexamine the effectiveness of pretransplantation totallymphoid irradiation (TLI) combined with immuno-suppression in inhibiting delayed xenograft rejectionin a pig-to-baboon model of orthotopic cardiacxenotransplantation. We have also attempted to
characterize the delayed xenograft rejection in theorthotopic cardiac xenograft model using immuno-histochemical staining.
Materials and methods
Animals. Three juvenile baboons, 1 to 2 years of ageand weighing 2.5 to 3.5 kg, were used as recipients.Newborn piglets, weighing 3 to 4 kg, were used as heartdonors. Three pigs, weighing 10 kg, were used as organhemoperfusion donors (lung donors). All animals weremaintained with humane care in compliance with the“Guide for the Care and Use of Laboratory Animals”prepared by the Institute of Laboratory Animal Resourcesand published by the National Institutes of Health (NIHPublication No. 86-23, revised 1985).
Immunosuppression. Recipients were treated with 80cGy from a 60 Co source twice a week for 5 weeks (total800 cGy) in the Department of Radiation Medicine, LomaLinda University Medical Center. One recipient receivedan additional 400 cGy (100 cGy for 4 consecutive days) of
Fig. 1. Change of xenoreactive natural antibody levels inrecipients before and after donor organ hemoperfusion.
Fig. 2. Change of xenoreactive natural antibody levels inrecipients before and after orthotopic pig cardiac xeno-transplantation.
The Journal of Thoracic andCardiovascular SurgeryVolume 115, Number 6
Xu et al. 1 3 4 3
splenic irradiation after completion of TLI. Pretransplan-tation immunosuppression consisted of intravenous meth-otrexate twice a week (2 mg/kg) for 4 weeks and intra-muscular cyclosporine A (INN: ciclosporin), 15 mg/kg perday for 1 week. All recipients received perioperativeantithymocyte globulin at 15 mg/kg per day from day 3 to4 and methylprednisolone intravenously (125 mg/day) for3 days after orthotopic cardiac transplantation. Posttrans-plantation immunosuppression was maintained with intra-venous methotrexate, 2 mg/kg twice a week, and cyclo-sporine A, 15 mg/kg per day intramuscularly. Recipientswere treated with additional intravenous methylpred-nisolone (125 mg/day) when rejection occurred.
Depletion of xenoreactive natural antibodies and ortho-topic cardiac transplantation. Both heart and lung do-nors were sedated with ketamine hydrochloride (10 mg/kg), and sedation was maintained with inhalationalhalothane (0.5% to 3%) and oxygen after endotrachealintubation. Donors were monitored by electrocardiogra-
phy. Donor hearts were exposed through a median ster-notomy and preserved with cold cardioplegic solution(Roe’s solution, 50 ml/kg), and donor lungs were pre-served with 500 ml cold Collins solution containing 500 mgaprostadil (prostaglandin E1). Both the heart and lungswere stored in cold saline solution until donor organhemoperfusion and cardiac transplantation.
Anesthesia in the recipients was induced and main-tained with inhalational fluroxane (1% to 3%) and oxy-gen. The recipients’ hearts were exposed through a me-dian sternotomy and removed after cardiopulmonarybypass had been established. Donor lungs were placed inthe cardiopulmonary bypass line and the pulmonary arterywas perfused for 60 minutes with the recipients’ blood toremove xenoreactive natural antibodies before transplan-tation. Blood egressing from the pulmonary veins of thelungs was returned to the bypass circuit. Blood sampleswere collected before and after donor organ hemoperfu-sion for analysis of xenoreactive natural antibodies. Pig-to-baboon orthotopic cardiac transplantation was per-formed according to techniques previously described.9
Packed baboon red blood cells were added to the cardio-pulmonary bypass circuit before rewarming.
Posttransplantation monitoring. Pig cardiac xenograftswere monitored daily by two-dimensional echocardiogra-phy. Blood samples were collected for analysis of xenore-active natural antibodies. At the time of cessation ofxenografts, myocardial tissue was collected for histologicand immunohistochemical analysis. Recipients’ spleenswere also harvested so that the production of xenoreactiveantibodies could be studied.
Preparation of splenocytes. Baboon spleens were col-lected in cold (4° C) RPMI-1640 medium (Gibco Labora-tories, Grand Island, N.Y.). The spleens were minced, anda fine sterile steel mesh filter was used to remove theconnective tissue capsule. The cells were washed threetimes with cold Hanks medium (Gibco) and then resus-
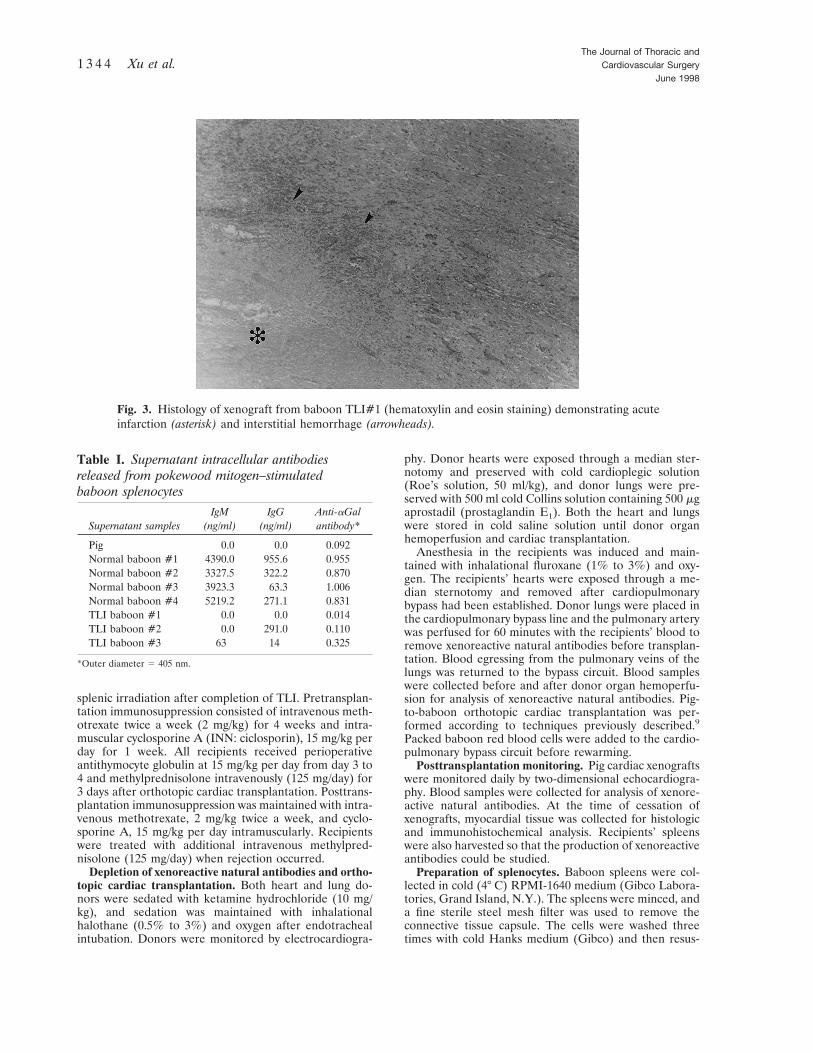
Fig. 3. Histology of xenograft from baboon TLI#1 (hematoxylin and eosin staining) demonstrating acuteinfarction (asterisk) and interstitial hemorrhage (arrowheads).
Table I. Supernatant intracellular antibodiesreleased from pokewood mitogen–stimulatedbaboon splenocytes
Supernatant samplesIgM
(ng/ml)IgG
(ng/ml)Anti-aGalantibody*
Pig 0.0 0.0 0.092Normal baboon #1 4390.0 955.6 0.955Normal baboon #2 3327.5 322.2 0.870Normal baboon #3 3923.3 63.3 1.006Normal baboon #4 5219.2 271.1 0.831TLI baboon #1 0.0 0.0 0.014TLI baboon #2 0.0 291.0 0.110TLI baboon #3 63 14 0.325
*Outer diameter 5 405 nm.
The Journal of Thoracic andCardiovascular Surgery
June 19981 3 4 4 Xu et al.

pended in 0.83% buffered hypotonic TRIS-ammoniumchloride at 4° C to lyse red blood cells. The splenocyteswere rewashed three times with RPMI-1640 medium andtheir viability was examined by trypan blue exclusion to90%.
Pokeweed mitogen stimulation of splenocytes. Cryo-preserved splenocytes were thawed and washed twice inRPMI-1640 medium. The cells were then resuspended incomplete media (RPMI-1640, 20% fetal bovine serum,glutamate 2 mmol/L, 200 IU penicillin/100 mg streptomy-cin, pyruvate 1 mmol/L, ITS (insulin, transferrin, andsodium selenite), and 50 mg b-mercaptoethanol) andadjusted to a concentration of 2 3 106 cells per milliliter.The cells were than placed in an incubator with humidi-fied 5% carbon dioxide at 37° C and rested overnight. Thecells were harvested and resuspended at 2 3 106 cells permilliliter in complete media containing pokeweed mitogen500 mg/ml (Sigma, St Louis, Mo.) and then incubated for7 days. At the end of incubation, cells were harvested,centrifuged, and the supernatant was collected. Aliquotswere frozen and stored at –70° C.
Supernatant immunoglobulin quantification. Immu-noglobulin levels in cell culture supernatants were deter-mined by an enzyme-linked immunosorbent assay(ELISA). Mouse monoclonal antibodies to either baboonimmunoglobulin M or G (IgM or IgG, PharMingen, SanDiego, Calif.) were adsorbed onto the surface of a micro-titer plate at 4° C overnight. The plates were washed threetimes with triethanolamine-buffered saline solution(TBS), and nonspecific binding sites were blocked withSuperBlock Blocking Buffer in TBS and then air dried.The plates were then washed three times with TBS-Tweenfollowed by the addition of standards and cell culturesupernatants to the appropriate wells. After 2 hours’incubation, the plates were washed three times withTBS-Tween solution and the appropriate secondary anti-bodies were added (alkaline phosphatase–labeled mono-
clonal mouse antihuman IgM, PharMingen, San Diego,Calif., and IgG, Fisher, Pittsburgh, Pa.). The plates wereincubated at room temperature for 2 hours. After a finalwash with TBS-Tween solution, the substrate was added.The absorbance of each well was measured at 405 nmwithin 1 hour.
Measurement of xenoreactive natural antibodies in theserum and supernatant. The supernatant and serum lev-els of xenoreactive natural antibodies were measured byan ELISA using the method described by Kujundzic andassociates.10 Gal antigens-aGal(1-3)bGal(1-4)GlcNac-BSA (V-LABS, Inc., Covington, La.) were adsorbed ontothe surface of a microtiter plate at 4° C for 17 hours. Theplates were washed three times with TBS, and nonspecificbinding sites were blocked with SuperBlock BlockingBuffer in TBS. Immediately before the assay, the plateswere washed three times with TBS-Tween solution. Cellculture supernatants from pokeweed mitogen–stimulatedsplenocytes and serum samples were added to the wellsand incubated for 2 hours at room temperature. Theplates were washed four times with TBS-Tween solutionfollowed by addition of the secondary antibody (alkalinephosphatase–labeled antihuman IgM and IgG, Fisher,Pittsburgh, Pa.). After 2 hours of incubation at roomtemperature, the plates were rewashed four times withTBS-Tween solution. Substrate was added to the wells andafter 1 hour the absorbance of each well was measured at405 nm.
Histology and immunohistology. Biopsy specimens ofthe cardiac xenografts were collected and fixed in 10%neutral-buffered formalin. Standard paraffin sections wereprepared and stained with routine hematoxylin and eosinstain and examined microscopically. Small pieces of car-diac xenografts were snap-frozen in ornithine carbamyl-transferase (OCT) medium and then stored at –70° C untilimmunohistologic analysis. After cryostat sections werefixed with paraformaldehyde-lysineperiodate, tissue sec-
Fig. 4. Photomicrograph of xenograft from baboon TLI#2 demonstrating microvascular thrombosis(some marked with asterisks).
The Journal of Thoracic andCardiovascular SurgeryVolume 115, Number 6
Xu et al. 1 3 4 5

tions were than stained with antibodies to IgM, IgG, C1q,C3, and fibrin to determine humoral rejection; monoclo-nal antibodies to macrophages, T cells, B cells, to identifythe types of infiltrating baboon leukocytes; and an anti-body to the cytokine IL-1 and IL-2, tumor necrosis factor(TNF-a), as previously described.6
Results
Xenograft survival and natural antibody titers.Two recipients (TLI#1 and TLI#2) fully recoveredfrom orthotopic cardiac transplantation withouttechnical failure, and all xenografts functioned wellwithout any evidence of hyperacute rejection. Onerecipient (TLI#3) died 3 hours after transplantationbecause of multiple arrhythmias and hemodynamicinstability but lacked evidence of immediate hyper-acute rejection. Pig cardiac xenograft survival timeswere 18 and 19 days before death.
Serum levels of xenoreactive natural antibodieswere reduced significantly after pretransplantationdonor organ hemoperfusion without returning topretransplantation levels (Fig. 1). Very low levels ofxenoreactive natural antibodies in serum samplesobtained after transplantation were observed; thislow level was maintained until the recipients died(Fig. 2).
Xenoreactive natural antibody production andrelease from baboon splenocytes. Table I summa-rizes production and release of intracellular anti-
bodies from baboon splenocytes. As positive con-trols, normal baboon splenocytes released very highlevels of IgM and IgG antibodies. ELISA demon-strated that these intracellular antibodies directlyrecognized and bound to pig xenoantigens at veryhigh levels. In contrast, the recipients’ splenocytesfailed to produce and release high levels of antibod-ies including xenoreactive natural antibodies. Onlyone recipient showed IgG antibody formation. Thebinding levels of xenoreactive natural antibodies topig xenoantigens remained very low.
Immunopathology of xenografts. At the time ofcessation of cardiac xenografts, gross appearance ofxenografts included swollen, thickened cardiac wallsand hemorrhage. Histologic study revealed evidenceof acute vascular rejection, which included intersti-tial edema and hemorrhage, microvascular throm-bosis, and acute infarction (Figs. 3 and 4).
Immunohistochemical staining of rejected xeno-grafts demonstrated deposition of baboon IgM, IgG,C1q, C3, and fibrin on the surface of xenograftendothelial cells, suggesting humoral rejection (Fig.5). The infiltrate of cardiac xenografts consisted oflarge numbers of macrophages and smaller numbersof natural killer (NK) cells (10% to 20%). Very fewT cells were seen in xenografts (Fig. 6). The infil-trating macrophages showed expression of IL-1band TNF-a, and the expression of IL- 1b and TNF-a
Fig. 5. Immunopathologic studies of rejected pig hearts from baboons showed diffuse endothelialmembrane staining for IgG (left, arrows) and complement C3 (right, arrows).
The Journal of Thoracic andCardiovascular Surgery
June 19981 3 4 6 Xu et al.
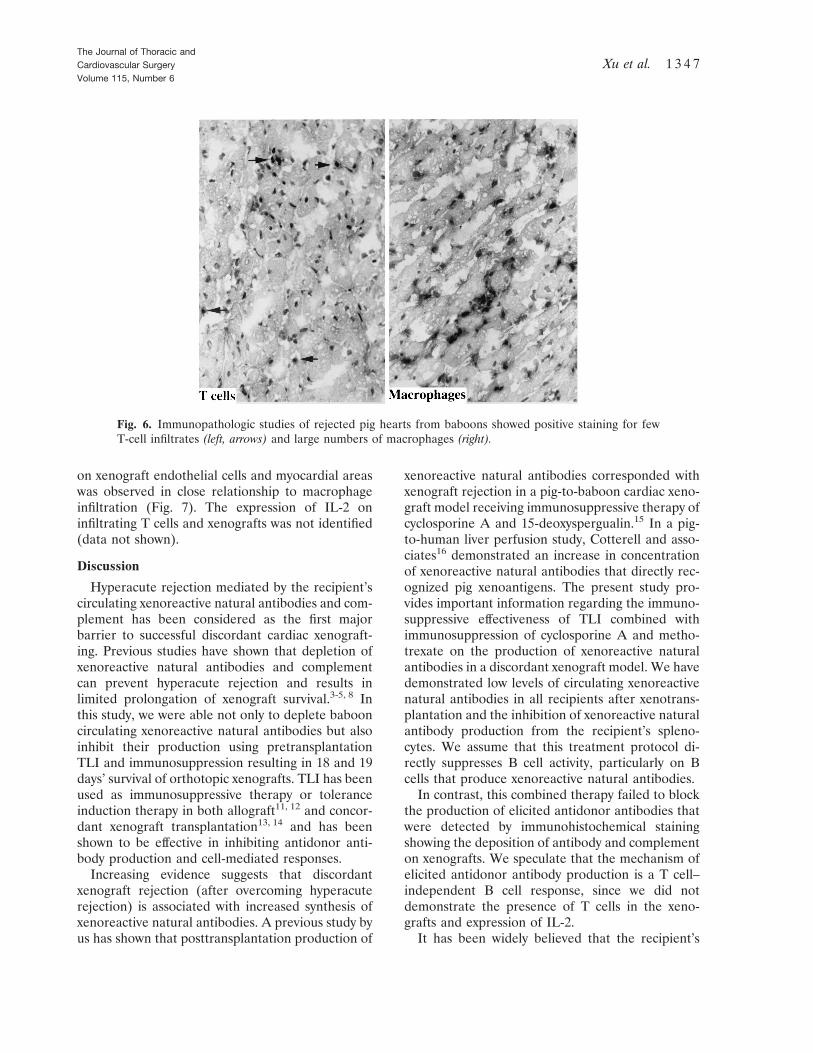
on xenograft endothelial cells and myocardial areaswas observed in close relationship to macrophageinfiltration (Fig. 7). The expression of IL-2 oninfiltrating T cells and xenografts was not identified(data not shown).
Discussion
Hyperacute rejection mediated by the recipient’scirculating xenoreactive natural antibodies and com-plement has been considered as the first majorbarrier to successful discordant cardiac xenograft-ing. Previous studies have shown that depletion ofxenoreactive natural antibodies and complementcan prevent hyperacute rejection and results inlimited prolongation of xenograft survival.3-5, 8 Inthis study, we were able not only to deplete babooncirculating xenoreactive natural antibodies but alsoinhibit their production using pretransplantationTLI and immunosuppression resulting in 18 and 19days’ survival of orthotopic xenografts. TLI has beenused as immunosuppressive therapy or toleranceinduction therapy in both allograft11, 12 and concor-dant xenograft transplantation13, 14 and has beenshown to be effective in inhibiting antidonor anti-body production and cell-mediated responses.
Increasing evidence suggests that discordantxenograft rejection (after overcoming hyperacuterejection) is associated with increased synthesis ofxenoreactive natural antibodies. A previous study byus has shown that posttransplantation production of
xenoreactive natural antibodies corresponded withxenograft rejection in a pig-to-baboon cardiac xeno-graft model receiving immunosuppressive therapy ofcyclosporine A and 15-deoxyspergualin.15 In a pig-to-human liver perfusion study, Cotterell and asso-ciates16 demonstrated an increase in concentrationof xenoreactive natural antibodies that directly rec-ognized pig xenoantigens. The present study pro-vides important information regarding the immuno-suppressive effectiveness of TLI combined withimmunosuppression of cyclosporine A and metho-trexate on the production of xenoreactive naturalantibodies in a discordant xenograft model. We havedemonstrated low levels of circulating xenoreactivenatural antibodies in all recipients after xenotrans-plantation and the inhibition of xenoreactive naturalantibody production from the recipient’s spleno-cytes. We assume that this treatment protocol di-rectly suppresses B cell activity, particularly on Bcells that produce xenoreactive natural antibodies.
In contrast, this combined therapy failed to blockthe production of elicited antidonor antibodies thatwere detected by immunohistochemical stainingshowing the deposition of antibody and complementon xenografts. We speculate that the mechanism ofelicited antidonor antibody production is a T cell–independent B cell response, since we did notdemonstrate the presence of T cells in the xeno-grafts and expression of IL-2.
It has been widely believed that the recipient’s
Fig. 6. Immunopathologic studies of rejected pig hearts from baboons showed positive staining for fewT-cell infiltrates (left, arrows) and large numbers of macrophages (right).
The Journal of Thoracic andCardiovascular SurgeryVolume 115, Number 6
Xu et al. 1 3 4 7

immune system will recognize and respond to xeno-grafts once hyperacute rejection is overcome, result-ing in so-called delayed xenograft rejection. Thepresent study demonstrates the pathogenic mecha-nisms of delayed xenograft rejection in an ortho-topic pig-to-baboon cardiac xenograft model. Thisstudy has found evidence of both humoral andcellular rejection mechanisms in xenografts under-going delayed xenograft rejection, including deposi-tion of antibody and complement and cellular infil-tration. Unlike allografts or concordant xenografts,the majority of infiltrating lymphoid cells were mac-rophages, 10% to 20% NK cells, but very smallnumbers of T cells, suggesting that macrophages/NKcells play an important role in delayed xenograftrejection. Blakeley, Hancock, and their associates6
showed progressive infiltration of macrophages in aguinea pig–to–rat cardiac xenograft model that wastreated with cobra venom factor. However, thisguinea pig–to–rat model did not demonstrate hu-moral rejection resulting from the complement de-pletion by cobra venom factor.6 Candinas and co-workers17 demonstrated that macrophages/NK cell–mediated delayed xenograft rejection is not alteredby the presence or absence of T cells. In an in vitrostudy, Vallee and colleagues18 have shown de-creased lymphocyte proliferation in response to pigendothelial cells after depletion of macrophaged
monocytes. In our study, although a small number ofT cells were present in xenografts, there was a lackof IL-2 expression on xenografts. This evidencesuggests that T cells do not play an important role inthe early phase of delayed xenograft rejection indiscordant xenografts.
In this study, pig xenografts undergoing delayedrejection demonstrated evidence of xenograft vascu-lar endothelial activation and activated macro-phages/NK cells. The expression of IL-1, TNF-a,and E-selectin was observed and could be associatedwith macrophage xenoreactivity. A previous studyshowed type II endothelial cell activation in delayedxenograft rejection, including expression of P-selec-tin, E-selectin, and von Willebrand factor. Theexpression of selectin is associated with productionof interferon, TNF-a, IL-1, and other cytokines.6
Furthermore, in a recent in vitro study, Millan andcoworkers7 demonstrated that direct contact ofmonocytes/macrophages and porcine endothelialcells can induce E-selectin expression on porcineendothelial cells, and human IL-1 a induces expres-sion of E-selectin on endothelial cells. These find-ings suggest that activation of macrophages/NK cellsand xenograft vascular endothelial cells play animportant role in delayed xenograft rejection ofdiscordant xenotransplantation.
As an alternative to clinical allotransplantation,
Fig. 7. Immunopathologic studies of rejected pig hearts from baboons showed expression of TNF-a (left)and IL-1b (right) by infiltrating macrophages. TNF-a staining includes the area surrounding macrophages,as well as adjacent endothelial cells and focal myocardial areas. IL-1b was observed in close relationshipto macrophages, plus locally on the surfaces of endothelial cells (arrows).
The Journal of Thoracic andCardiovascular Surgery
June 19981 3 4 8 Xu et al.

the application of discordant cardiac xenografts tohuman beings is still limited by delayed xenograftrejection. However, consistent 21⁄2 weeks’ orthotopicdiscordant cardiac xenograft survival can beachieved using TLI and novel but conventionalimmunosuppression in this pig-to-baboon model.This study demonstrates that induced antipig (rath-er than naturally occurring) antibody productionand macrophages/NK cells are responsible for thedelayed xenograft rejection. This information fur-ther strengthens our hypothesis that pig-to-humanheart xenotransplantation may eventually be feasi-ble when activation of xenograft endothelial cellsand delayed xenograft rejection can be overcome.
R E F E R E N C E S1. McManus RP, O’Hair DP, Beitzinger JM, et al. Patients who
die awaiting heart transplantation. J Heart Lung Transplant1993;12:159-72.
2. Platt JL, Vercellotti GM, Dalmasso AP, Matas AJ, BolmanRM, Najarian JS, et al. Transplantation of discordant xeno-grafts: a review of progress. Immunol Today 1990;11:450-6.
3. Reding R, Davies H, White D, et al. Effect of plasmaexchange on guinea pig–to–rat heart xenografts. TransplantProc 1989;21:534.
4. Cooper DKC, Human PA, Lexer G, et al. Effects ofcyclosporine and antibody adsorption on pig cardiac xeno-graft survival in the baboon. J Heart Transplant 1988;7:238-46.
5. Leventhal JR, Dalmasso AP, Cromwell JW, et al. Prolonga-tion of cardiac xenograft survival by depletion of comple-ment. Transplantation 1993;55:857-66.
6. Blakely ML, Van Der Werf WL, Berndt MC, et al. Activationof intragraft endothelial and mononuclear cells during dis-cordant xenograft rejection. Transplantation 1994;58:1059-66.
7. Millan MT, Geczy C, Stuhlmeier KM, Goodman DJ,Ferran C, Bach FH. Human monocytes activate porcineendothelial cells, resulting in increased E-selectin, inter-leukin-8, monocyte chemotactic protein-1, and plasmino-
gen activator inhibitor-type-1 expression. Transplantation1997;63:421-9.
8. Fukushima N, Gundry SR, Matsumiya G, Bouchart F, Zup-pan C, Bailey LL. Histological findings in heart grafts afterorthotopic pig to baboon cardiac transplantation. TransplantProc 1996;28:788-90.
9. Bailey LL, Jang J, Johnson W, Jolley WB. Orthotopic cardiacxenografting in the newborn goat. J Thorac Cardiovasc Surg1985;89:242-9.
10. Kujundzic M, Koren E, Neethling FA, et al. Variability ofanti-aGal antibodies in human serum and their relation toserum cytotoxicity against pig cells. Xenotransplantation1994;1:58.
11. Gottlieb M, Strober S, Hoppe RT, Grumet FC, Kaplan HS.Engraftment of allogeneic bone marrow without graft-versus-host disease in mongrel dogs using total lymphoid irradiation.Transplantation 1980;29:487-91.
12. Myburgh JA, Smit JA, Hill RR, Browde S. Transplantationtolerance in primates following total lymphoid irradiationand allogeneic bone marrow injection. II. Renal allografts.Transplantation 1980;29:405-8.
13. Roslin MS, Tranbaugh RE, Panza A, et al. One-year monkeyheart xenograft survival in cyclosporine-treated baboons.Transplantation 1992;54:949-55.
14. Myburgh JA, Smit JA, Stark JH. Transplantation tolerancefollowing total lymphoid irradiation in baboon–to–vervetmonkey kidney xenotransplantation. Transplant Proc 1994;26:1081.
15. Fukushima N, Bouchart F, Gundry SR, et al. The role ofanti-pig antibody in pig-to-baboon cardiac xenotransplantrejection. Transplantation 1994;57:923-8.
16. Cotterell AH, Collins BH, Parker W, Harland RC, PlattJL. The humoral immune response in humans followingcross-perfusion of porcine organs. Transplantation 1995;60:861-8.
17. Candinas D, Koyamada N, Miyatake T, et al. T cell-indepen-dence of macrophage and NK cell infiltration, cytokineproduction and endothelial activation during delayed xeno-graft rejection. Transplantation 1996;62:1920-8.
18. Vallee I, Watier H, Thibault G, et al. Evidence of nonin-volvement of swine MHC class II in the in vitro proliferativeresponse of human lymphocytes to porcine endothelial cells.Transplantation 1995;59:897-901.
The Journal of Thoracic andCardiovascular SurgeryVolume 115, Number 6
Xu et al. 1 3 4 9












![Mapping muscarinic receptors in human and baboon brain using [N-11C-methyl]-benztropine](https://static.fdokumen.com/doc/165x107/6344f35df474639c9b049d90/mapping-muscarinic-receptors-in-human-and-baboon-brain-using-n-11c-methyl-benztropine.jpg)






