
Heterotopic and orthotopic autologous chondrocyte implantation using a minipig chondral defect model
Upload
independentCategory
view
0download
0
HEPATOCELLULAR CARCINOMA IN AN ORTHOTOPIC MOUSEMODEL METASTASIZES INTRAHEPATICALLY IN CIRRHOTICBUT NOT IN NORMAL LIVERShigeki KURIYAMA *, Masaharu YAMAZAKI , Akira MITORO, Tatsuhiro TSUJIMOTO, Masaji KIKUKAWA , Hirohisa TSUJINOUE,Toshiya NAKATANI , Yasunori TOYOKAWA, Hitoshi YOSHIJI and Hiroshi FUKUI
Third Department of Internal Medicine, Nara Medical University, Nara, Japan
Prognosis of hepatocellular carcinoma (HCC) still remainspoor mainly because of intrahepatic metastasis. In the majority ofcases, HCC is found in conjunction with liver cirrhosis. It is,therefore, of great importance to investigate the invasive andmetastatic behavior of HCC in cirrhotic liver. To examine this, aliver cirrhosis model was produced by injecting thioacetamide i.p.into mice. Murine HCC cells were labeled with the fluorescentcarbocyanine dye, DiI, and implanted directly under the capsuleof cirrhotic and normal livers of syngeneic mice. DiI-labeled HCCcells in the liver were observed under fluorescent and confocalmicroscopy. Histological analysis of cirrhotic and normal liversrevealed that implanted HCC cells migrated to and invaded theadjacent periportal regions, but not the adjacent centrolobularareas. This characteristic behavior of HCC was more evident incirrhotic liver than in normal liver. Furthermore, intrahepaticmetastasis to unimplanted hepatic lobes was observed in cir-rhotic liver as early as 7 days after implantation, while it was notdetected in normal liver even 4 weeks later. Thus, an orthotopicanimal model for HCC with cirrhosis described here may besuitable for investigating the invasive and metastatic behavior ofHCC. Importantly, labeling tumor cells with a fluorescent dyebefore orthotopic implantation may be a convenient and usefulmethod to investigate the invasive and metastatic behavior ofvarious types of cancer. Int. J. Cancer 80:471–476, 1999.r 1999 Wiley-Liss, Inc.
Although primary cancers of the liver include multiple histologicsub-types, hepatocellular carcinoma (HCC) accounts for more than 90%of primary hepatic malignancies. The incidence of HCC is quite variableworldwide, related to variable distribution of predisposing factors. Inlow-incidence areas, such as the United States and Western Europe,HCC has an incidence of 3 to 7 cases per 100,000 population. HCC ismuch more frequently seen in areas of sub-SaharanAfrica and SoutheastAsia, where the reported incidence approaches 150 cases per 100,000(Simonettiet al., 1991). In Japan, approximately 85% of malignantneoplasms in the liver are assumed to be hepatocellular carcinoma. Thedeath rate from HCC has gradually increased both for males and forfemales during the past 3 decades. HCC is responsible for approxi-mately 27,000 fatalities a year, and represents the third and fourth mostfrequent causes of malignant-neoplasm-related deaths in males andfemales, respectively (Hatori, 1994).
Any patient with chronic liver disease is at increased risk for thedevelopment of HCC. Predisposing factors for HCC include cirrhosis,chronic hepatitis and various carcinogens, and a minority of HCCs arethought to arisede novoin non-cirrhotic livers. In the majority of cases(70–90%), HCC is found in conjunction with liver cirrhosis. HCC isknown to have a poor prognosis because of the high frequency ofmultiple hepatic tumors, although patients rarely have distant metastasesat the time of surgery.Although some cases of HCC have a multicentricorigin, multiple lesions in HCC have been attributed mainly to intrahe-patic metastases (Okuda and Nakashima, 1981). Intrahepatic metastaseswere found in approximately 30% of cases of surgically resected smallHCC with a diameter of,3 cm and in almost 80% of HCC autopsycases (Yukiet al.,1990). Early and liver-specific recurrences have alsobeen seen frequently in cases of HCC treated by liver transplantation(McPeakeet al.,1993). These findings indicate that the liver is the maintarget organ of HCC metastasis.
Although it has been suggested, from clinical observation, thatintrahepatic metastasis may be generated by cell implantation viathe portal venous system (Nakashima, 1976), the mechanism and
pathogenesis of the high frequency of intrahepatic metastasis andportal invasion in HCC are not well understood. To investigate themechanism of intrahepatic invasion of HCC, we employed afluorescent-dye-labeling technique. We have shown that whenmurine HCC cells labeled with the fluorescent carbocyanine dye,1,18-dioctadecyl-3,3,38,38-tetramethylindocarbocyanine (DiI), wereimplanted into the liver of syngeneic mice, HCC cells preferen-tially migrated to and invaded the adjacent periportal regions,known as Rappaport’s Zone 1, but not the adjacent centrolobularareas, Zone 3 (Kuriyamaet al., 1998). DiI enters hydrophobiccompartments and is stable, non-metabolized and non-diffusible,not only in vitro but alsoin vivo (Ledleyet al.,1992). This methodenables us to distinguish a single HCC cell in the liver, conse-quently it is possible to trace the early invasive and metastaticfootprints of HCC in the liver.
In the present study, to investigate the invasive and metastaticbehavior of HCC in cirrhotic liver, we implanted DiI-labeled murineHCC cells under the capsule of the left-lateral hepatic lobe of cirrhoticmice produced by i.p. administration of thioacetamide (TAA). Weinvestigated whether HCC preferentially invades adjacent Zone 1 butnot adjacent Zone 3 in cirrhotic liver; also, we examined whether HCCmetastasizes to unimplanted hepatic lobes in cirrhotic liver.
MATERIAL AND METHODS
Cell culture
The murine HCC cell line BNL1ME A.7R.1, which was originallyestablished from a BALB/c mouse, was purchased from the ATCC(Rockville, MD). Cells were cultured in RPMI-1640 medium supple-mentedwith10%(vol/vol) heat-inactivatedFCS,0.3mg/mlL-glutamine,100 units/ml ampicillin and 100 µg/ml streptomycin at 37°C in ahumidified atmosphere containing 5% CO2 in air.
Labeling of cellsDiI was purchased from Molecular Probes (Eugene, OR) and
prepared as a 2.0 mg/ml solution in 99.5% ethanol. The DiIsolution was then passed through a 0.22-µm-pore filter (Millipore,Bedford, MA), and routinely sonicated prior to application to cells.Optimal conditions for labeling murine HCC cells and hepatocyteshave been described (Kuriyamaet al.,1998). Briefly, cells culturedat 37°C were trypsinized and suspended in culture medium withoutserum at a concentration of 53 106 cells/ml, and stained byincubating with 20 µg/ml DiI for 60 min at 37°C with gentleagitation at 10-min intervals. After staining, the cells were washed3 times by centrifugation to remove the dye not incorporated in thecells and re-suspended in the culture medium or in PBS. Cellviability was assessed by Trypan-blue exclusion.
Grant sponsor: Japanese Ministry of Education, Science, Sports andCulture; Grant numbers: B-07457141 and B-10470140.
*Correspondence to: Third Department of Internal Medicine, NaraMedical University, 840 Shijo-cho, Kashihara, Nara 634-8522, Japan. Fax:(81) 744-24-7122.
Received 25 June 1998; Revised 14 August 1998
Int. J. Cancer:80,471–476 (1999)
r 1999 Wiley-Liss, Inc.
Publication of the International Union Against CancerPublication de l’Union Internationale Contre le Cancer

Production of a murine liver-cirrhosis modelFemale BALB/c mice 8 weeks old were purchased from Japan
SLC (Hamamatsu, Japan). They were kept at a constant roomtemperature of 246 2°C under a 12-hr light/dark cycle. Cirrhosiswas induced in mice by i.p. injections of various doses of TAA(0.2–0.6 mg/g body weight) suspended in PBS twice weekly for 24weeks, beginning at 10 weeks of age. Control mice received i.p.injections of the same volume of PBS at the same time points.Animal experiments were performed with approved protocols andin accordance with recommendations for the proper care and use oflaboratory animals.
Histological analysisA stock of 100% Avertin was prepared by mixing 10 g of
tribromoethyl alcohol with 10 ml of tertiary amyl alcohol, and wasdiluted to 2.5% in isotonic saline. To isolate livers, mice wereanesthetized by i.p. administration of 2.5% Avertin (0.012 ml/gbody weight) and the abdomen was opened. The liver was thenperfused with PBS to clear it of blood and fixed in 10%neutral-buffered formalin. After fixation, tissues were embedded inparaffin for hematoxylin-eosin staining and azan staining.
Transplantation of cells into the liverNormal and cirrhotic mice were anesthetized by i.p. administra-
tion of 2.5% Avertin (0.012 ml/g body weight) for laparotomy, and4 3 105 DiI-labeled cells suspended in 10 µl of PBS wereimplanted directly under the capsule of the left-lateral hepatic lobeunder direct visualization, by means of a 10-µl Hamilton syringewith a 26-gauge needle over a period of 2 to 3 min.
Analysis of fluorescent-dye-labeled HCC cells in the liverSix mice were killed as a group of experiments and systemically
perfused from the portal vein with 4% paraformaldehyde and 0.5%glutaraldehyde in PBS. From our preliminary experimental results,this fixative was shown not to affect the fluorescent intensity ofDiI-stained cells. After post-fixation with the same fixative for 30min, the liver was sliced into 25-µm-thick sections with a micro-slicer (DTK-3000; DOSAKA EM, Kyoto, Japan). Liver slices wereobserved by an inverted fluorescent microscope with a rhodaminefilter (IMT2-RFC; Olympus, Tokyo, Japan), also by an InSIGHTp-lus-IQ laser-scanning confocal microscope (Meridian, Okemos,MI) including an argon-ion laser (488 nm).
Quantitation of fluorescent intensity in the liverLiver slices prepared as above were estimated for the fluorescent
intensity by the confocal microscope. Each group consisted of 6mice. At least 20 different areas within 1 mm from the margin of theimplantation site of DiI-stained HCC cells were randomly selected
from Zone 1 and from Zone 3 of each animal. The fluorescentintensity of each area was quantitated by the confocal microscope.
StatisticsResults are expressed as means6 SD. Data were analyzed for
statistical significance by Student’st-test. p values of,0.05 wereconsidered to indicate statistically significant differences between groups.
RESULTS
Survival rate of mice treated with i.p. injection of TAA
Of 3 groups of 10 mice each that received i.p. injections of TAA atdoses of 0.2, 0.4 and 0.6 mg/g body weight, 2, 5 and 7 respectively diedwithin 3 days after the first TAA administration. However, a significantnumber of animals did not die thereafter, and survival rates after a10-week treatment with TAA twice weekly at doses of 0.2, 0.4 and 0.6mg/g body weight were 70%, 30% and 20% respectively. Consequently,a TAA dose of 0.2 mg/g body weight twice weekly was selected andused for subsequent experiments (Fig. 1).
TAA-induced liver cirrhosis in miceI.p. administration of TAA to mice is known to cause liver
cirrhosis, characterized by hepatocellular necrosis, increased con-
FIGURE 1 – Survival rate of mice injected i.p. with TAA. Micereceived i.p. injections of TAA at doses of 0.2 (bold line, n5 10), 0.4(thin line, n5 10) or 0.6 (dotted line, n5 10) mg/g body weight twiceweekly for 10 weeks.
FIGURE 2 – Histological analysis of the liver of TAA-treated mice.Mice were given i.p. injections of TAA at a dose of 0.2 mg/g bodyweight twice weekly. After 10 and 20 weeks, animals were killed andtheir livers were removed for histological analysis. Representativepictures of azan staining for liver sections of animals treated with TAAfor 10 weeks(a) and 20 weeks(b) are shown. Scale bars: 300 µm.
472 KURIYAMA ET AL.
nective tissue and formation of regenerative nodules. Histologicalanalysis by hematoxylin-eosin staining of the livers of mice treatedwith i.p. administration of TAA for 10 weeks revealed that thenormally radial liver-cell alignment disappeared and that most ofthe hepatocytes represented the hyperplastic type with nuclearenlargement (data not shown). Azan staining of the liver demon-
strated that the fibrotic septa were thin and predominantly restrictedto Zone 1 (Fig. 2a). Azan staining of sections from the liver after20-week TAA administration revealed that cirrhosis was mani-fested by increase and thickening of the fibrotic septa, traversingthe lobular parenchyma by porto-venous or porto-portal bridging,thus promoting the formation of pseudolobuli (Fig. 2b).
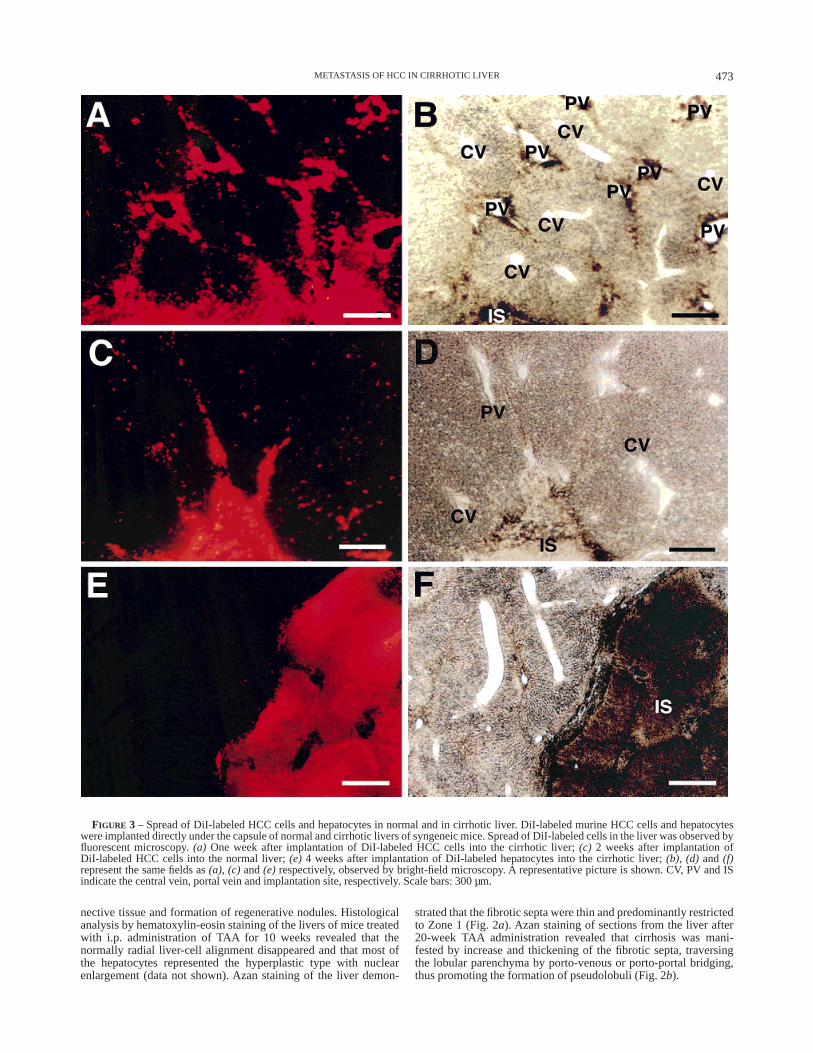
FIGURE 3 – Spread of DiI-labeled HCC cells and hepatocytes in normal and in cirrhotic liver. DiI-labeled murine HCC cells and hepatocyteswere implanted directly under the capsule of normal and cirrhotic livers of syngeneic mice. Spread of DiI-labeled cells in the liver was observed byfluorescent microscopy.(a) One week after implantation of DiI-labeled HCC cells into the cirrhotic liver;(c) 2 weeks after implantation ofDiI-labeled HCC cells into the normal liver;(e) 4 weeks after implantation of DiI-labeled hepatocytes into the cirrhotic liver;(b), (d) and (f)represent the same fields as(a), (c) and(e) respectively, observed by bright-field microscopy. A representative picture is shown. CV, PV and ISindicate the central vein, portal vein and implantation site, respectively. Scale bars: 300 µm.
473METASTASIS OF HCC IN CIRRHOTIC LIVER

Analysis of invasive behavior of HCC in normaland in cirrhotic liver
DiI-labeled murine HCC cells were implanted under the capsuleof normal and cirrhotic liver of syngeneic mice, and liver sliceswere prepared as described above. Invasive behavior of HCC cellsin the liver was observed under fluorescent microscopy. As shownin Figure 3a,b, 1 week after the implantation of DiI-labeled HCCcells into cirrhotic liver an irregularly shaped HCC tumor withintensive fluorescence was observed at the implantation site.Marked migration of HCC cells from the implantation site to Zone1, but not to Zone 3, was apparent. Conversely, when DiI-labeledHCC cells were implanted into normal liver in the same way, atumor mass with less irregularity and much less migration from theimplantation site to adjacent Zone 1 was observed even 2 weeksafter the implantation (Fig. 3c,d). Migration of HCC cells toadjacent Zone 3 was much less apparent then that to Zone 1, incirrhotic and in normal liver. In both cases, protruding spread ofDiI-labeled HCC cells from the implantation site was not observed4 hr after implantation (data not shown). When hepatocytesisolated from syngeneic mice were labeled with DiI and implantedinto the liver in the same way as HCC cells, DiI-labeled hepato-cytes did not show migration either to adjacent Zone 3 or toadjacent Zone 1 in normal liver (data not shown). Furthermore,DiI-labeled hepatocytes did not migrate in cirrhotic liver 1 weekafter implantation (data not shown) and as much as 4 weeks afterimplantation (Fig. 3e,f ).
Quantitative analysis of intrahepatic invasion of HCC in normaland in cirrhotic liver
DiI-labeled HCC cells were implanted directly into normal andcirrhotic livers of syngeneic mice as described above. Each groupconsisted of 6 animals. One and 2 weeks after the implantation,animals were killed and their livers were sliced into 25-µm-thicksections. At least 20 different areas within 1 mm from the margin ofthe implantation site of DiI-stained HCC cells were randomlyselected from Zone 1 and from Zone 3 of each mouse. Quantitationof DiI-labeled HCC cells in Zone 1 and Zone 3 was estimated bymeasuring the fluorescent intensity of each area under confocalmicroscopy. As shown in Figure 4, the fluorescent intensity of Zone1 adjacent to the implantation site was much higher than that ofZone 3 adjacent to the implantation site 1 and 2 weeks after theimplantation of HCC cells, not only in cirrhotic liver but also innormal liver, indicating that HCC preferentially migrates to andinvades the adjacent portal vein. Furthermore, the fluorescentintensity of Zone 1 was higher in cirrhotic liver than in normalliver, while that of Zone 3 was lower in cirrhotic liver than innormal liver, indicating that HCC preferentially migrates to andinvades the adjacent portal vein in cirrhotic liver rather than innormal liver.
Analysis of intrahepatic metastasis of HCC in normaland in cirrhotic liver
DiI-labeled murine HCC cells were implanted under the capsuleof the left-lateral hepatic lobe of normal and cirrhotic mice, andliver slices were prepared as described above. Metastasis of HCCcells to the right-median hepatic lobe was examined by fluorescentmicroscope. There were no detectable DiI-labeled HCC cells in thenormal liver 4 weeks after implantation (data not shown). Con-versely, clusters of DiI-labeled HCC cells were observed in Zone 1but not in Zone 3 of cirrhotic liver even 1 week after implantation(Fig. 5a,b).
Quantitative analysis of intrahepatic metastasis of HCC in normaland in cirrhotic liver
One and 2 weeks after implantation of DiI-labeled HCC cellsunder the capsule of the left-lateral hepatic lobe, animals werekilled and the right-median hepatic lobe was sliced into 25-µm-thick sections. Each group consisted of 6 animals. At least 20different areas were randomly selected from Zone 1 and from Zone3 of each mouse. Quantitation of DiI-labeled HCC cells in Zone 1
and Zone 3 was estimated from the fluorescent intensity of eacharea as measured by confocal microscopy. As shown in Figure 6,the fluorescent intensity of Zone 1 of cirrhotic liver was exclusivelyhigher 1 and 2 weeks after implantation. The fluorescent intensityof Zone 3 of cirrhotic liver as well as that of Zones 1 and 3 ofnormal liver was not significantly different from that of thebackground.
DISCUSSION
Invasion and metastasis are the major obstacles to successfulcancer treatment. Relevant animal models for human cancer are ofgreat help, not only to investigate invasive and metastatic mecha-nisms of a cancer but also to evaluate the usefulness of newtherapies for human cancer. Ectopic sub-cutaneous-tumor modelshave frequently been utilized, since they are easily produced by s.c.implanting established human cell lines derived from various typesof cancer or human tumors obtained directly from surgery intonude mice. S.c. tumor models are, however, definitely differentfrom clinical manifestations. Furthermore, human tumors growns.c. in nude mice rarely metastasize, although they closely resemblethe original tumors morphologically, biologically and biochemi-cally. It has been shown that implantation of human tumor cellsorthotopically into the corresponding organ of nude mice results inmuch higher metastatic rates (Manzottiet al., 1993). Orthotopicanimal models are, therefore, much more suitable for investigatingthe invasive and metastatic behavior of various types of cancer. Sunet al. (1996) have shown that orthotopic implantation of histologi-cally intact human HCC specimens into nude mice resulted in localgrowth, regional invasion and spontaneous intrahepatic metastasis.However, since it appears difficult to distinguish a small number ofhuman HCC cells in mouse liver, they did not demonstrate howearly intrahepatic invasion and metastasis of HCC occurs. Lindsayet al. (1997) have shown morphological evidence of intravasculartumor growth after tumor invasion and spread through the intrahe-patic portal venous system, using a monkey HCC model withoutcirrhosis induced by a chemical carcinogen. We have shown thatHCC cells preferentially migrated to and invaded Zone 1 but notZone 3 of normal liver, when murine HCC cells labeled with DiIwere implanted orthotopically into syngeneic mice (Kuriyamaet
FIGURE 4 – Quantitative analysis of DiI-labeled HCC cells in theliver. DiI-labeled HCC cells were implanted under the capsule ofnormal and of cirrhotic liver. One and 2 weeks after implantation,animals were killed and their livers were sliced into 25-µm-thicksections. At least 20 different areas within 1 mm from the margin of theimplantation site of DiI-stained HCC cells were randomly selectedfrom Zone 1 and from Zone 3 of each mouse. Each group consisted of 6animals. Quantitation of DiI-labeled HCC cells in Zones 1 and 3 wasestimated by measuring the fluorescent intensity of each area byconfocal microscopy. The open bars and diagonally striped barsrepresent the results of cirrhotic and normal mice, respectively. Valuesare means6 SD of 6 animals. The asterisk indicates values signifi-cantly different among groups, as indicated by Student’st-test.
474 KURIYAMA ET AL.

al., 1998). However, it should be noticed that HCC is found inconjunction with liver cirrhosis in the majority of cases, and theunderlying liver cirrhosis is a major obstacle for achievingsuccessful treatment for HCC. Therefore, a strict animal model forhuman HCC must have HCC in the cirrhotic liver. In the presentstudy, we produced cirrhotic mice by i.p. administration of TAAand orthotopically implanted HCC cells into cirrhotic mice.
We have demonstrated here that HCC preferentially migrates toand invades the adjacent portal vein but not the adjacent centralvein in cirrhotic liver as well as in normal liver. Dissemination ofthe fluorescent marker substance is considered to involve somemigration of macrophages that phagocytized necrotic tumor cellslabeled with DiI. Moreover, it is not completely impossible thatlymphatic drainage of the lipophilic dye from the sub-capsularimplantation site could contribute to dissemination of the markersubstance. Therefore, as a control experiment, we implantedDiI-labeled hepatocytes sub-capsularly into the liver as DiI-labeledHCC cells, and demonstrated that there was no migration ofDiI-labeled hepatocytes from the implantation site. These resultsindicate that dissemination of the fluorescent substance is substan-
tially mediated by the invasive and metastatic behavior of HCCcells.
The stream in the liver pours to the central vein from the portalspace. Hepatocytes nascent at the portal space were shown togradually stream toward the central vein where they were probablyeliminated by apoptosis (Zajiceket al., 1985). The migration ofHCC cells is, however, shown to be against the stream in the liver.HCC cells are shown to migrate to Rappaport’s Zone 1 of the liverand to invade the portal vein. This characteristic behavior of HCC,more apparent in cirrhotic than in normal liver, may be considered amain cause of intrahepatic metastasis of HCC. It has been shown inclinical observations that HCC has a propensity for vascularinvasion: portal-vein-tumor thrombosis occurs in 44% of cases andinferior vena cava and hepatic vein invasion occurs much lesscommonly with the incidence being 4% and 5.9% respectively(Mathieu et al., 1988; Freenyet al., 1992). The results demon-strated here may support the clinical consensus that intrahepaticmetastasis of HCC occurs by way of the portal vein.
Intrahepatic metastasis of HCC has already been shown to occurvia the portal vein by implanting HCC cells into the spleen(Nakashima, 1976) or into the portal venous system (Osadaet al.,1996). These approaches, however, result in scattering HCC cellsin the peripheral portal vein, so that it appears pointless to provethat intrahepatic metastasis of HCC occurs by invading the portalvenous system. We therefore implanted DiI-labeled HCC cellssuspended in a small inoculum volume directly under the capsuleof cirrhotic liver, and trace the invasive and metastatic footprints ofHCC cells. Although the present study demonstrated that HCCmore preferentially migrates to Zone 1 of the liver and invades theportal vein in cirrhotic liver rather than in normal liver, themechanism of this characteristic invasive pattern of HCC remainsunknown. A plausible explanation is that this phenomenon occursdue to structural differences in the liver. The normally radialliver-cell alignment is destroyed and fibrotic septa transversing thelobular parenchyma are present in the cirrhosis. These structuralchanges may provide more space for HCC cells to invade.
We show here that the early occurrence of intrahepatic metasta-sis of HCC to other hepatic lobes was observed in cirrhotic liver butnot in normal liver. Mitsunobuet al.(1996), who directly injected aradiopaque material into surgically resected HCC tumors, sug-gested that tumor spread in HCC progresses from capsular invasion
FIGURE 5 – Analysis of intrahepatic metastasis of HCC in cirrhoticliver. DiI-labeled murine HCC cells were implanted under the capsuleof the left-lateral hepatic lobe of cirrhotic mice. Metastasis of HCCcells to the right-median hepatic lobe was examined by fluorescentmicroscopy.(a) Clusters of DiI-labeled HCC cells were observed inZone 1 but not in Zone 3 of cirrhotic liver even 1 week afterimplantation. (b) The same fields as(a), observed by bright-fieldmicroscopy. The figure shows a representative picture. CV and PVindicate the central and portal veins, respectively. Scale bars: 100 µm.
FIGURE 6 – Quantitative analysis of intrahepatic metastasis of HCCin normal and in cirrhotic liver. DiI-labeled HCC cells were implantedunder the capsule of the left-lateral hepatic lobe of normal and cirrhoticmice. One and 2 weeks after implantation, animals were killed andtheir right-median hepatic lobes were sliced into 25-µm-thick sections.At least 20 different areas were randomly selected from Zone 1 andfrom Zone 3 of each mouse. Each group consisted of 6 animals.Quantitation of DiI-labeled HCC cells in Zone 1 or Zone 3 wasestimated by measuring the fluorescent intensity of each area byconfocal microscopy. Open bars and diagonally striped bars representthe results of cirrhotic and of normal mice, respectively. Values aremeans6 SD of 6 animals.
475METASTASIS OF HCC IN CIRRHOTIC LIVER

to intrahepatic invasion and that the portal vein may act as anefferent tumor vessel. They also demonstrated that the use of theportal vein as an efferent vessel was more marked when HCC wassuperimposed on cirrhosis. This communication with the portalcirculation in HCC could be responsible for the early occurrence ofintrahepatic metastasis in cirrhotics. It has been shown that portalflow velocity and the portal blood flow are significantly decreasedin patients with liver cirrhosis (Chawlaet al., 1998), also thatforward/backward or even continuous backward flow of the portalblood was observed in cirrhotic patients with tumor thrombus orblood-clot thrombus of the portal vein (Furuseet al.,1992). Thesefindings taken together suggest, as a mechanism of intrahepaticmetastasis of HCC in cirrhotic liver, that HCC preferentiallyinvades the portal vein, forms the tumor thrombus in the portalvein, and that HCC cells in the portal vein are then transported to
the peripheral portal vein in the same or other hepatic lobes by theforward/backward flow of the portal blood.
Despite the development of novel treatment modalities for HCC,the prognosis of HCC remains relatively poor. The feasibility ofgene therapy for HCC has therefore been investigated using animalmodels (Kuriyamaet al.,1995, 1997; Caoet al.,1997), since theseare important for evaluating new treatment modalities for HCC.Orthotopic animal models for HCC are likewise useful for analyz-ing the invasive and metastatic mechanisms of HCC. An animalmodel for HCC described here may be suitable for these purposes,while orthotopic implantation of DiI-labeled tumor cells into thecorresponding organs is a convenient and practical method ofinvestigating the invasive and metastatic behavior of various typesof cancer.
REFERENCES
CAO, G., KURIYAMA , S., DU, P., SAKAMOTO, T., KONG, X., MASUI, K. and QI,Z., Complete regression of established murine hepatocellular carcinoma byin vivo tumor necrosis factora gene transfer.Gastroenterology,112,501–510 (1997).CHAWLA , Y., SANTA, N., DHIMAN , R.K. and DILAWARI , J.B., Portalhemodynamics by duplex Doppler sonography in different grades ofcirrhosis.Dig. Dis. Sci.,43,354–357 (1998).FREENY, P.C., BARON, R.L. and TEEFEY, S.A., Hepatocellular carcinoma:reduced frequency of typical findings with dynamic contrast-enhanced CTin a non-Asian population.Radiology,182,143–148 (1992).FURUSE, J., MATSUTANI, S., YOSHIKAWA, M., EBARA, M., SAISHO, H.,TSUCHIYA, Y. and OHTO, M., Diagnosis of portal vein tumor thrombus bypulsed Doppler ultrasonography.J. clin. Ultrasound,20,439–446 (1992).HATORI, N., Epidemiology of liver cancer in Japan.J. clin. exp. Med.,171,1097–1104 (1994).KURIYAMA , S., NAKATANI , T., MASUI, K., SAKAMOTO, T., TOMINAGA, K.,YOSHIKAWA, M., FUKUI, H., IKENAKA , K. and TSUJII, T., Bystander effectcaused by suicide gene expression indicates the feasibility of gene therapyfor hepatocellular carcinoma.Hepatology,22,1838–1846 (1995).KURIYAMA , S., SAKAMOTO, T., MASUI, K., NAKATANI , T., TOMINAGA, K.,KIKUKAWA , M., YOSHIKAWA, M., IKENAKA , K., FUKUI, H. and TSUJII, T.,Tissue-specific expression of HSV-tk gene can induce efficient antitumoreffect and protective immunity to wild-type hepatocellular carcinoma.Int.J. Cancer,71,470–475 (1997).KURIYAMA , S., YAMAZAKI , M., MITORO, A., TSUJIMOTO, T., KIKUKAWA , M.,OKUDA, H., TSUJINOUE, H., NAKATANI , T., YOSHIJI, H., TOYOKAWA, Y.,NAGAO, S. and FUKUI, H., Analysis of intrahepatic invasion of hepatocellu-lar carcinoma using fluorescent dye-labeled cells in mice.Anticancer Res.(1998). (In press).LEDLEY, F.D., SORIANO, H.E., O’MALLEY, B.W., JR., LEWIS, D., DARLING-TON, G.J. and FINEGOLD, M., DiI as a marker for cellular transplantation intosolid organs.BioTechniques,13,581–587 (1992).LINDSAY, C.K., SINHA, C.C. and THORGEIRSSON, U.P., Morphological studyof vascular dissemination in a metastatic hepatocellular carcinoma model inthe monkey.Hepatology,26,1209–1215 (1997).
MANZOTTI, C., AUDISIO, R.A. and PRATESI, G., Importance of orthotopicimplantation for human tumours as model system: relevance to metastasisand invasion.Clin. exp. Metastasis,11,5–14 (1993).MATHIEU, D., GUINET, C., BOUKLIA -HASSANE, A. and VASILE, N., Hepaticvein involvement in hepatocellular carcinoma.Gastrointest. Radiol.,13,55–60 (1988).MCPEAKE, J.R., O’GRADY, J.G., ZAMAN , S., PORTMANN, B., WIGHT, D.G.,TAN, K.C., CALNE, R.Y. and WILLIAMS , R., Liver transplantation for primaryhepatocellular carcinoma: tumor size and number determine outcome.J.Hepatol.,18,226–234 (1993).MITSUNOBU, M., TOYOSAKA, A., ORIYAMA , T., OKAMOTO, E. and NAKAO, N.,Intrahepatic metastases in hepatocellular carcinoma: the role of the portalvein as an efferent vessel.Clin. exp. Metastasis,14,520–529 (1996).NAKASHIMA , T., Vascular changes and hemodynamics in hepatocellularcarcinoma.In K. Okuda and R.L. Peter (eds.),Hepatocellular carcinoma,pp. 169–203, Wiley, New York (1976).OKUDA, K. and NAKASHIMA , T., Hepatocellular carcinoma: a review of therecent studies and development.In H. Popper and F. Schaffner (eds.),Progress in liver diseases.Vol. IV, pp. 639–650, Grune and Strantton, NewYork (1981).OSADA, T., SAKAMOTO, M., INO, Y., IWAMATSU, A., MATSUNO, Y., MUTO, T.and HIROHASHI, S., E-cadherin is involved in the intrahepatic metastasis ofhepatocellular carcinoma.Hepatology,24,1460–1467 (1996).SIMONETTI, R.G., CAMMA , C., FIORELLO, F., POLITI, F., D’AMICO, G. andPAGLIARO, L., Hepatocellular carcinoma: a worldwide problem and themajor risk factors.Dig. Dis. Sci.,36,962–972 (1991).SUN, F.X., TANG, Z.Y., LIU, K.D., XUE, Q., GAO, D.M., YU, Y.Q., ZHOU,X.D. and MA, Z.C., Metastatic models of human liver cancer in nude miceorthotopically constructed by using histologically intact patient specimens.J. Cancer Res. clin. Oncol.,122,397–402 (1996).YUKI, K., HIROHASHI, S., SAKAMOTO, M., KANAI , T. and SHIMOSATO, Y.,Growth and spread of hepatocellular carcinoma: a review of 240 consecu-tive autopsy cases.Cancer,66,2174–2179 (1990).ZAJICEK, G., OREN, R. and WEINREB, M., JR., The streaming liver.Liver, 5,293–300 (1985).
476 KURIYAMA ET AL.
Copyright © 2022 FDOKUMEN




















