RIFLE classification can predict short-term prognosis in critically ill cirrhotic patients
10
Intensive Care Med (2007) 33:1921–1930 DOI 10.1007/s00134-007-0760-6 ORIGINAL Chang-Chyi Jenq Ming-Hung Tsai Ya-Chung Tian Chan-Yu Lin Chun Yang Nai-Jen Liu Jau-Min Lien Yung-Chang Chen Ji-Tseng Fang Pan-Chi Chen Chih-Wei Yang RIFLE classification can predict short-term prognosis in critically ill cirrhotic patients Received: 22 January 2007 Accepted: 4 June 2007 Published online: 30 June 2007 © Springer-Verlag 2007 C.-C. Jenq · M.-H. Tsai · Y.-C. Tian · C.-Y. Lin· Y.-C. Chen (✉) · J.-T. Fang · C.-W. Yang Chang Gung University College of Medicine, Department of Nephrology, Chang Gung Memorial Hospital, 199 Tung Hwa North Road, 105 Taipei, Taiwan e-mail: [email protected] Tel.: 886-3-3281200 ext 8181 Fax: 886-3-3282173 C. Yang · N.-J. Liu · J.-M. Lien · P.-C. Chen Chang Gung University College of Medicine, Division of Gastroenterology, Chang Gung Memorial Hospital, Taipei, Taiwan Abstract Objective: End-stage liver disease is frequently complicated by renal function disturbances. Cirrhotic patients with renal failure admitted to intensive care units (ICUs) have high mortality rates. This study analyzed the outcomes of critically ill cirrhotic patients and identified the association between prognosis and RIFLE (risk of renal failure, injury to kidney, failure of kidney function, loss of kidney function, and end-stage renal failure) classification, in comparison with other five scor- ing systems. Design: Prospective, clinical study. Setting: Ten-bed spe- cialized hepatogastroenterology ICU in a university hospital in Taiwan. Patients and participants: One hun- dred and thirty-four cirrhotic patients consecutively admitted to ICU during a 1.5-year period. Interventions: Thirty-two demographic, clinical and laboratory variables were analyzed as predictors of survival. Measurements and main results: Overall hospital mortality was 65.7%. There was a progressive and significant increase (χ 2 for trend: p < 0.001) in mortal- ity based on RIFLE classification severity. Multiple logistic regres- sion analysis indicated that RIFLE classification and Sequential Organ Failure Assessment (SOFA) score on the first day of ICU admission were independent risk factors for hospital mortality. By using the areas under the receiver operating characteristic curve (AUROC), the RIFLE category and SOFA both indicated a good discriminative power (AUROC 0.837 ± 0.036 and 0.917 ± 0.025; p < 0.001). Cumulative survival rates at 6-month follow-up differed signif- icantly ( p < 0.05) for non-ARF vs. RIFLE-R, RIFLE-I, and RIFLE-F. Conclusion: Both SOFA and RIFLE category showed high discriminative power in predicting hospital mortal- ity in critically ill patients with cir- rhosis. The RIFLE classification is a simple and easily applied evalu- ative tool with good prognostic abilities. Keywords Acute renal failure · ICU · APACHE · SOFA · MELD Introduction A feature of liver cirrhosis is the existence of disturbances in systemic circulation characterized by marked arterial vasodilation that occurs principally in the splanchnic circulation and generates a reduction in total peripheral vascular resistance and arterial pressure and a secondary increase in cardiac output. These abnormalities are central to the development of several major complications of cir- rhosis, such as hepatorenal syndrome, ascites, spontaneous bacterial peritonitis, dilutional hyponatremia, and hep- atopulmonary syndrome. Renal failure is the most clinical relevant of these conditions as its appearance generally indicates very poor prognosis [1–9]. Elevated serum creatinine (SCr) levels of > 1.3 or 1.5 mg/dl have been identified as a predictor of poor
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of RIFLE classification can predict short-term prognosis in critically ill cirrhotic patients

Intensive Care Med (2007) 33:1921–1930DOI 10.1007/s00134-007-0760-6 O R I G I N A L
Chang-Chyi JenqMing-Hung TsaiYa-Chung TianChan-Yu LinChun YangNai-Jen LiuJau-Min LienYung-Chang ChenJi-Tseng FangPan-Chi ChenChih-Wei Yang
RIFLE classification can predict short-termprognosis in critically ill cirrhotic patients
Received: 22 January 2007Accepted: 4 June 2007Published online: 30 June 2007© Springer-Verlag 2007
C.-C. Jenq · M.-H. Tsai · Y.-C. Tian ·C.-Y. Lin · Y.-C. Chen (�) · J.-T. Fang ·C.-W. YangChang Gung University College ofMedicine, Department of Nephrology,Chang Gung Memorial Hospital,199 Tung Hwa North Road, 105 Taipei,Taiwane-mail: [email protected].: 886-3-3281200 ext 8181Fax: 886-3-3282173
C. Yang · N.-J. Liu · J.-M. Lien · P.-C. ChenChang Gung University College ofMedicine, Division of Gastroenterology,Chang Gung Memorial Hospital,Taipei, Taiwan
Abstract Objective: End-stage liverdisease is frequently complicated byrenal function disturbances. Cirrhoticpatients with renal failure admittedto intensive care units (ICUs) havehigh mortality rates. This studyanalyzed the outcomes of criticallyill cirrhotic patients and identifiedthe association between prognosisand RIFLE (risk of renal failure,injury to kidney, failure of kidneyfunction, loss of kidney function, andend-stage renal failure) classification,in comparison with other five scor-ing systems. Design: Prospective,clinical study. Setting: Ten-bed spe-cialized hepatogastroenterology ICUin a university hospital in Taiwan.Patients and participants: One hun-dred and thirty-four cirrhotic patientsconsecutively admitted to ICU duringa 1.5-year period. Interventions:Thirty-two demographic, clinical andlaboratory variables were analyzed aspredictors of survival. Measurementsand main results: Overall hospitalmortality was 65.7%. There wasa progressive and significant increase(χ2 for trend: p < 0.001) in mortal-
ity based on RIFLE classificationseverity. Multiple logistic regres-sion analysis indicated that RIFLEclassification and Sequential OrganFailure Assessment (SOFA) score onthe first day of ICU admission wereindependent risk factors for hospitalmortality. By using the areas underthe receiver operating characteristiccurve (AUROC), the RIFLE categoryand SOFA both indicated a gooddiscriminative power (AUROC0.837 ± 0.036 and 0.917 ± 0.025;p < 0.001). Cumulative survival ratesat 6-month follow-up differed signif-icantly (p < 0.05) for non-ARF vs.RIFLE-R, RIFLE-I, and RIFLE-F.Conclusion: Both SOFA and RIFLEcategory showed high discriminativepower in predicting hospital mortal-ity in critically ill patients with cir-rhosis. The RIFLE classification isa simple and easily applied evalu-ative tool with good prognosticabilities.
Keywords Acute renal failure ·ICU · APACHE · SOFA · MELD
Introduction
A feature of liver cirrhosis is the existence of disturbancesin systemic circulation characterized by marked arterialvasodilation that occurs principally in the splanchniccirculation and generates a reduction in total peripheralvascular resistance and arterial pressure and a secondaryincrease in cardiac output. These abnormalities are central
to the development of several major complications of cir-rhosis, such as hepatorenal syndrome, ascites, spontaneousbacterial peritonitis, dilutional hyponatremia, and hep-atopulmonary syndrome. Renal failure is the most clinicalrelevant of these conditions as its appearance generallyindicates very poor prognosis [1–9].
Elevated serum creatinine (SCr) levels of > 1.3 or1.5 mg/dl have been identified as a predictor of poor

1922
prognosis in patients with advanced liver cirrhosis [10,11]. Serum creatinine level is a poor marker because it isaffected not only by urinary clearance of creatinine, butalso by the rate of production and volume of distribution.Furthermore, SCr concentration does not correctly reflectglomerular filtration rate (GFR) in the non-steady-statecondition of patients with acute renal failure (ARF).To date, no consensus exists regarding the definitionof ARF in critically ill patients. Consequently, morethan 35 different definitions have been proposed in theliterature [12]. The wide-ranging definitions for ARFcause clinical confusion and make comparative studiesdifficult [13–16]. The common used scoring systems forpredicting the outcome in critically ill cirrhotic patients,such as Child–Pugh score [17], Sequential Organ FailureAssessment (SOFA) [18], Model for End-stage Liver Dis-ease (MELD) [19], and Acute Physiology, Age, ChronicHealth Evaluation II (APACHE II) [20], either omit theevaluation or evaluate renal function only according to theSCr.
The RIFLE (risk of renal failure, injury to the kidney,failure of kidney function, loss of kidney function, andend-stage renal failure) classification was first proposed bythe Acute Dialysis Quality Initiative (ADQI) group at thesecond ADQI conference in Vicenza, Italy, in May 2002,in an attempt to standardize the study of ARF [21]. TheRIFLE criteria classify ARF into three groups (risk, in-jury, and failure) according to changes in SCr and urineoutput (UO). To date, the RIFLE classification has beenapplied in critical ill patients receiving renal replacementtherapy, cardiac surgery patients, heterogeneous patientsfrom intensive care units (ICUs), heterogeneous popula-tion of hospitalized patients, and unique populations suchas patients requiring extracorporeal membrane oxygena-tion for post-cardiotomy cardiogenic shock [22, 23].
Renal failure is common in critically ill patientswith cirrhosis, and its occurrence is associated withan extremely high mortality rate. The objective of thisprospective study was to identify the association betweenhospital mortality/short-term prognosis and RIFLE criteriain this homogeneous critically ill cirrhotic patient group.Other scoring systems, including the Child–Pugh score,SOFA, MELD, and APACHE II and APACHE III [24]were also applied for comparison with the RIFLEclassification.
Methods
Patient information and data collection
The local ethics committee approved the study protocol.Formal consent was obtained from the next of kin. Thisinvestigation was performed in a 10-bed specializedhepatogastroenterology ICU at a 2000-bed universityhospital in Taiwan, between January 2005 and June 2006.
In total, 134 consecutive patients with hepatic cirrhosisrequiring intensive monitoring and/or treatment that couldnot be provided outside the ICU were enrolled. Exclusioncriteria were as follows: pediatric patients (aged ≤ 18years); uremic patients undergoing renal replacementtherapy; duration of hospital stay < 24 h; patients who hadundergone liver transplantation. Readmitted patients werealso excluded from this study.
Prospectively collected data were as follows: demo-graphics; reason for ICU admission; acute diagnosis;illness severity; RIFLE classification, SOFA, MELD, andAPACHE II & APACHE III scores on the first day ofICU admission; duration of hospitalization; and, outcome.The primary study outcome was hospital mortality rate.Follow-up at 6 months after hospital discharge wasperformed via a telephone interview. When necessary,the registry office provided information regarding patientsurvival or date of death.
Definitions
Diagnosis of cirrhosis was based on liver histology (25patients) or on a combination of physical signs andbiochemical and ultrasonographic findings (109 patients).Respiratory failure is defined as respiratory rate ≤ 5/minor ≥ 50/min and/or mechanical ventilation for ≥ 3 daysand/or fraction of inspired oxygen (FiO2) > 0.4 and/orpositive end-expiratory pressure > 5 cmH2O [25–27].
The RIFLE classification system comprises individualcriteria for SCr levels and UO. A patient can fulfillRIFLE criteria via changes in SCr concentrations orchanges to UO, or both [21]. The criteria resulting inworst possible classification were employed. Patients wereclassified into three severity categories (risk, injury, andfailure) and two clinical outcome categories (loss andend-stage renal disease). Notably, the F component ofRIFLE is present even if the increase in SCr is < 3-foldwhen the subsequent SCr is > 4.0 mg/dl (350 µmol/l)in the setting of an acute increase of at least 0.5 mg/dl(44 µmol/l). Baseline SCr was the first value measuredduring hospitalization. The MDRD formula was appliedto estimate baseline SCr concentrations in 15 patients whowere admitted directly to the ICU and whose previousSCr levels were thus unknown [21]. Patients were groupedaccording to the risk, injury and failure categories ofthe RIFLE classification. No patient met the criteriafor loss or end-stage renal disease. A simple model formortality—non-ARF (0 points), RIFLE-R (1 point),RIFLE-I (2 points), and RIFLE-F (3 points) for day 1 ofICU admission—was developed (Table 1) [22].
Severity of liver disease on ICU admission was gradedusing the Child–Pugh system. Illness severity also wasassessed using the SOFA, MELD, APACHE II, andAPACHE III scoring systems. These systems have beenvalidated to predict the outcomes of critically ill patients

1923
Table 1 RIFLE classification for acute renal failure
GFR criteria Urine output Score Beta Standard Odds ratio pcriteria used coefficient error (95% CI)
Non-ARF GFR decrease ≤ 25% UO ≥ 0.5 ml/kg/h 0 0 – 1 (reference) –Risk Increase SCr × 1.5 or UO < 0.5 ml/kg/h 1 1.539 0.614 4.659 0.012
GFR decrease > 25% × 6 h (1.397–15.534)Injury Increase SCr × 2 or UO < 0.5 ml/kg/h 2 1.667 0.877 5.294 0.050
GFR decrease > 50% × 12 h (1.0–30.111)Failure Increase SCr × 3 or UO < 0.3 ml/kg/h 3 3.659 0.662 38.824 < 0.001
GFR decrease > 75% × 24 h (10.609–142.072)or SCr > 4 mg/dl or anuria × 12 h
Loss Complete loss – – – – –of kidney function> 4 weeks
ESRD End-stage renal – – – – –disease (> 3 months)
Constant – –0.750 0.294 – 0.011
GFR, glomerular filtration rate; CI, confidence intervals; ARF, acute renal failure; UO, urine output; SCr, serum creatinine
with cirrhosis [19, 26, 28, 29]. The worst physiologicaland biochemical values during the first day of ICUadmission were recorded.
Statistical analysis
Continuous variables were summarized using means andstandard error. The primary analysis compared hospitalsurvivors with nonsurvivors. All variables were testedfor normal distribution using the Kolmogorov–Smirnovtest. Student’s t-test was employed to compare the meansof continuous variables and normally distributed data;otherwise, the Mann–Whitney U-test was employed.Categorical data were tested using the chi-square test.The analysis of variance (ANOVA) test with Tukey testpost-hoc for numerical values and the chi-square test fortrends were utilized to assess categorical data associatedwith RIFLE classifications. Finally, risk factors wereassessed with univariate analysis, and variables that werestatistically significant ( p < 0.05) in the univariate anal-ysis were included in multivariate analysis by applyinga multiple logistic regression based on forward eliminationof data.
In this study, two methods were adopted to test calibra-tion (i. e., the degree of correspondence between predictedand observed mortality over the entire range of risks).First, calibration was graphically displayed by plottingobserved and predicted mortality for all patients across allrisk ranges. Second, goodness-of-fit testing was applied todetermine calibration using the Hosmer–Lemeshow test.
Discrimination (i. e., the model’s ability to differenti-ate between patients who died and those who survived)was examined using the area under a receiver operatingcharacteristic curve (AUROC). To compare the areas under
the two resulting AUROC curves we used a nonparamet-ric approach [30]. AUROC analysis was also performedto calculate the cut-off values, sensitivity, specificity, over-all correctness, and positive and negative predictive values.Finally, cut-off points were calculated by obtaining the bestYouden index (sensitivity + specificity – 1) [31].
Cumulative survival curves as a function of time wereproduced utilizing the Kaplan–Meier approach and com-pared with the log rank test. All statistical tests were two-tailed; a value of p < 0.05 was considered statistically sig-nificant. Data were analyzed using SPSS 12.0 for Windows95 (SPSS, Chicago, IL, USA).
Results
Subject characteristics
Between January 2005 and June 2006, 134 cirrhotic pa-tients at the specialized hepatogastroenterology ICU wereenrolled. Their median age was 55 years; 100 patientswere male (74.6%) and 34 were female (25.4%). Theoverall in-hospital mortality rate for the entire group was65.7% (88/134). Table 2 presents patient demographicdata and clinical characteristics of survivors and non-survivors. Table 3 lists the cause of cirrhosis and reasonsfor ICU admission. Liver disease was largely attributed tohepatitis B viral infection; the most frequent reason forICU admission was upper gastrointestinal bleeding.
Risk factors for hospital mortality
Univariate analysis identified 17 of the 32 variables asprognostically valuable (Table 4). Multivariate analysis

1924
Table 2 Patient demographic data and clinical characteristics
All patients Survivors Non-survivors p-value(n = 134) (n = 46) (n = 88)
Age (years) 56 ± 1 55 ± 2 57 ± 1 NS (0.505)Gender (M/F) 100/34 38/8 62/26 NS (0.125)Body weight on ICU admission (kg) 64 ± 1 62 ± 2 65 ± 2 NS (0.399)Length of ICU stay (days) 6.9 ± 0.7 5.4 ± 0.7 7.7 ± 0.9 NS (0.104)Length of hospital stay (days) 18.5 ± 1.2 21.7 ± 2.1 16.8 ± 1.4 0.048DM (yes/no) 34/100 10/36 24/64 NS (0.485)Ascites, ICU first day (yes/no) 67/67 21/25 46/42 NS (0.467)SBP, ICU first day (yes/no) 27/107 7/39 20/68 NS (0.303)Hepatic encephalopathy, ICU first day (yes/no) 79/55 22/24 57/31 NS (0.058)EV bleeding, ICU first day (yes/no) 60/74 28/18 32/56 0.007Peptic ulcer bleeding, ICU first day (yes/no) 46/88 12/34 34/54 NS (0.146)Previous hepatoma (yes/no) 42/92 11/35 31/57 NS (0.180)Bilirubin, ICU first day (mg/dl) 11.6 ± 1.0 5.7 ± 1.1 14.7 ± 1.4 < 0.001Albumin, ICU first day (g/l) 2.4 ± 0.0 2.5 ± 0.1 2.4 ± 0.1 NS (0.313)PT prolongation, ICU first day (s) 14 ± 2 6 ± 1 18 ± 3 < 0.001AST, ICU first day (units/l) 475 ± 115 160 ± 38 622 ± 166 0.008ALT, ICU first day (units/l) 216 ± 48 72 ± 22 291 ± 72 0.004Platelets, ICU first day (×109/l) 98 ± 6 98 ± 9 98 ± 9 NS (0.983)Leukocytes, ICU first day (×109/l) 12.9 ± 0.7 11.5 ± 1.1 13.6 ± 0.8 NS (0.131)Hemoglobin, ICU first day (g/dl) 9.0 ± 0.2 9.2 ± 0.2 9.0 ± 0.3 NS (0.491)Serum creatinine on admission (mg/dl) 2.2 ± 0.2 1.7 ± 0.2 2.5 ± 0.2 0.030Serum creatinine, ICU first day (mg/dl) 3.0 ± 0.2 1.6 ± 0.2 3.8 ± 0.2 < 0.001Daily urine output, ICU first day (ml/day) 868 ± 67 1281 ± 104 662 ± 76 < 0.001RIFLE classification, ICU first day 1.5 ± 0.1 0.4 ± 0.1 2.1 ± 0.1 < 0.001MAP on ICU admission (mmHg) 74 ± 2 85 ± 2 69 ± 2 < 0.001Respiratory failure, ICU first day (yes/no) 55/79 10/36 45/43 0.001Child–Pugh category (A/B/C; n) 5/25/104 3/16/27 2/9/77 0.001Child–Pugh score, ICU first day (mean ± SE) 11.5 ± 0.2 10.5 ± 0.4 12.1 ± 0.2 < 0.001MELD score, ICU first day (mean ± SE) 28.4 ± 1.2 18.2 ± 1.3 34.5 ± 1.2 < 0.001APACHE II, ICU first day (mean ± SE) 24.2 ± 0.8 17.8 ± 1.0 27.6 ± 0.9 < 0.001APACHE III, ICU first day (mean ± SE) 102.0 ± 3.4 67.6 ± 4.3 120.1 ± 3.3 < 0.001SOFA, ICU first day (mean ± SE) 10.9 ± 0.4 6.9 ± 0.4 12.9 ± 0.4 < 0.001
NS, not significant; ICU, intensive care unit; DM, diabetes mellitus; SBP, spontaneous bacterial peritonitis; EV, esophageal varices; PT, pro-thrombin time; AST, aspartate aminotransferase; ALT, alanine aminotransferase; MAP, mean arterial pressure; SE, standard error; MELD,model for end-stage liver disease; APACHE, Acute Physiology and Chronic Health Evaluation; SOFA, sequential organ failure assessment
Table 3 Causes of cirrhosis and reasons for ICU admission
All patients Hospital survivors Hospital non- pn (%) n (%) survivors n (%)
Cause of cirrhosisAlcoholic 26 (19) 14 (30) 12 (14) 0.023Hepatitis B 55 (41) 9 (20) 46 (52) < 0.001Hepatitis C 23 (17) 8 (17) 15 (17) NS (1.000)Alcoholic + Hepatitis B 16 (12) 6 (13) 10 (11) NS (0.784)Alcoholic + Hepatitis C 1 (1) 1 (2) 0 (0) NS (0.343)Hepatitis B + Hepatitis C 4 (3) 3 (7) 1 (1) NS (0.117)Hepatitis B + Hepatitis D 1 (1) 1 (2) 0 (0) NS (0.343)Alcoholic + Hepatitis B + Hepatitis C 1 (1) 1 (2) 0 (0) NS (0.343)Other causes a 7 (5) 3 (7) 4 (5) NS (0.691)
Primary ICU admissionSevere UGI bleeding 47 (35) 25 (54) 22 (25) 0.001Severe sepsis 33 (25) 4 (9) 29 (33) 0.002Hepatic encephalopathy 24 (18) 12 (26) 12 (14) NS (0.074)Respiratory failure 13 (10) 3 (7) 10 (11) NS (0.369)Acute renal failure require renal replacement 11 (8) 2 (4) 9 (10) NS (0.239)Hepatoma rapture 6 (4) 0 (0) 6 (7) NS (0.074)
NS, not significant; ICU, intensive care unit; UGI, upper gastrointestinal; a Primary biliary cirrhosis, autoimmune hepatitis

1925
Table 4 Prognostically significant variables
Parameter Beta coefficient Standard error Odds ratio (95% CI) p
Univariate logistic regressionSerum creatinine on admission (mg/dl) 0.369 0.170 1.447 (1.036–2.021) 0.030Serum creatinine, ICU first day (mg/dl) 0.953 0.197 2.594 (1.762–3.818) < 0.001Daily urine output, ICU first day (ml/day) –0.001 0.000 0.999 (0.998–0.999) < 0.001RIFLE classification, ICU first day 1.183 0.206 3.264 (2.181–4.886) < 0.001EV bleeding, ICU first day –1.001 0.375 0.367 (0.176–0.766) 0.008Bilirubin, ICU first day (mg/dl) 0.100 0.027 1.105 (1.048–1.166) < 0.001PT prolongation, ICU first day (second) 0.116 0.036 1.004 (1.000–1.008) 0.001AST, ICU first day (units/l) 0.001 0.001 1.001 (1.000–1.003) 0.043ALT, ICU first day (units/l) 0.004 0.002 1.105 (1.048–1.166) 0.035MAP on ICU admission (mmHg) –0.061 0.014 0.941 (0.916–0.967) 0.002Respiratory failure, ICU first day 1.326 0.416 3.767 (1.666–8.518) 0.001Child–Pugh category 1.222 0.376 3.393 (1.625–7.086) 0.001Child–Pugh score 0.354 0.092 1.424 (1.190–1.704) < 0.001MELD score, ICU first day 0.168 0.030 1.183 (1.115–1.255) < 0.001APACHE II, ICU first day 0.174 0.034 1.190 (1.114–1.272) < 0.001APACHE III, ICU first day 0.059 0.010 1.061 (1.040–1.083) < 0.001SOFA, ICU first day 0.771 0.145 2.161 (1.626–2.872) < 0.001
Multivariate logistic regressionRIFLE classification, ICU first day 0.758 0.277 2.134 (1.239–3.676) 0.006SOFA, ICU first day 0.671 0.185 1.957 (1.362–2.812) < 0.001Constant –6.781 1.823 0.001 < 0.001
CI, confidence intervals; ICU, intensive care; EV, esophageal varices; PT, prothrombin time; AST, aspartate aminotransferase; ALT, alanineaminotransferase; MAP, mean arterial pressure; MELD, model for end-stage liver disease; APACHE, Acute Physiology and Chronic HealthEvaluation; SOFA, sequential organ failure assessment
identified the following variables as of independentprognostic significance: RIFLE classification andSOFA score (Table 4). Regression coefficients ofthese variables were utilized to calculate a logit ofdeath for each patient as follows: Logarithm of oddsof death = –6.781 + 0.758 × RIFLE classification (non-ARF = 0, RIFLE-R = 1, RIFLE-I = 2, RIFLE-F = 3) +0.671 × SOFA score.
Hospital mortality and severity of illness scoring systems
The data needed to calculate RIFLE classification on day 1of ICU admission were available for all 134 patients. Hos-pital mortality was 32.1% (17/53) for non-ARF patients,68.8% (11/16) for RIFLE-R (risk), 71.4% (5/7) for RIFLE-I (injury), and 94.8% (55/58) for RIFLE-F (failure) (χ2
for trend: p < 0.001). A progressive and significant ele-vation in mortality was correlated with increasing RIFLEclassification severity among all patients. Odds ratios forRIFLE criteria were 4.659 ( p = 0.012) for RIFLE-R vs.non-ARF, 5.294 ( p = 0.05) for RIFLE-I vs. non-ARF, and38.824 ( p < 0.001) for RIFLE-F vs. non-ARF (Table 1).
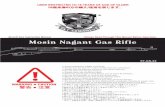
Figure 1 illustrates the calibration curve for RIFLEclassification. This curve revealed that, generally, theproportion of patients who died increased with in-creasing risk of hospital mortality predicted utilizingthe two prognostic approaches. Calibration for RIFLEclassification [Hosmer–Lemeshow chi-square = 1.196,
2 degrees of freedom (df), p = 0.550] and the RIFLEclassification calibration curve were close to the line ofperfect predictive ability. Goodness-of-fit, as measured bythe Hosmer–Lemeshow chi-square statistic of predictedmortality risk, the predictive accuracy of the RIFLEclassification, Child–Pugh score, MELD, APACHE II,APACHE III, and SOFA scores are listed in Table 5.Table 5 also gives the discrimination for the RIFLEclassification, Child–Pugh score, MELD, APACHE II,
Fig. 1 Calibration curves for RIFLE classifications. The diagonalline is the line of ideal prediction (predicted mortality = observedmortality) for RIFLE classification

1926
Table 5 Calibration and discrimination for the scoring methods in predicting hospital mortality
Calibration DiscriminationGoodness of fit (χ2) df p AUROC ± SE 95% CI p
RIFLE classification 1.196 2 0.550 0.837 ± 0.036 0.766–0.908 < 0.001Child–Pugh score 8.260 6 0.220 0.699 ± 0.051 0.599–0.798 < 0.001MELD score 12.153 8 0.145 0.878 ± 0.031* 0.816–0.939 < 0.001APACHE II 10.977 8 0.203 0.810 ± 0.038 0.734–0.885 < 0.001APACHE III 5.780 8 0.672 0.885 ± 0.030* 0.827–0.944 < 0.001SOFA 8.481 8 0.388 0.917 ± 0.025* 0.868–0.966 < 0.001
df, degrees of freedom; AUROC, areas under the receiver operating characteristic curve; SE, standard error; CI, confidence intervals; MELD,model for end-stage liver disease; APACHE, Acute Physiology and Chronic Health Evaluation; SOFA, sequential organ failure assessment* p < 0.05 vs. Child–Pugh score
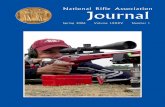
Fig. 2 a Acute Physiology, Age,Chronic Health Evaluation II(APACHE II); b APACHE III;c Model for end-stage liverdisease (MELD); d Sequentialorgan failure assessment (SOFA)scores according to RIFLEclassification on ICU day 1(* p < 0.05 vs. non-ARF;ˆp < 0.05vs. RIFLE-R; ! p < 0.05 vs.RIFLE-I)
Table 6 Subsequent hospital mortality predicted on the first day of ICU admission
Predictive Cut-off Youden Sensitivity Specificity Overall PPV NPVfactors point index (%) (%) correctness (%) (%) (%)
RIFLE category Non-ARF a 0.59 81 78 80 79 80Child–Pugh score 12 a 0.39 72 67 70 69 71MELD score 19 a 0.62 97 64 81 73 96APACHE II 21 a 0.46 81 65 73 70 77APACHE III 87 a 0.63 89 74 82 77 87SOFA 8 a 0.69 95 74 85 79 94
PPV, positive predictive value; NPV, negative predictive value; ARF, acute renal failure; MELD, model for end-stage liver disease; APACHE,Acute Physiology and Chronic Health Evaluation; SOFA, sequential organ failure assessment; a Value giving the best Youden index
APACHE III, and SOFA scores. Computation for theAUROC verified the significantly better discriminatory
power ( p < 0.05) of the MELD, APACHE III, and SOFAscores compared with Child–Pugh score.

1927
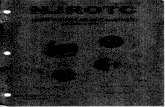
Fig. 3 Cumulative survival rate for 134 critically ill cirrhotic patients based on their a RIFLE classification and b SOFA score on day 1 ofICU admission
Figure 2a–d show APACHE II, III, MELD, and SOFAscores according to RIFLE classification on ICU day 1.RIFLE classification severity among our patients is corre-lated to those scores.
Indices for predicting short-term prognosis
To assess the predictive values of selected cut-off pointsfor predicting hospital mortality, the sensitivity, specificity,overall correctness of prediction, and positive and nega-tive predictive values were determined. Table 6 lists thesedata calculated using the cut-off point providing the bestYouden index. The SOFA score had the best Youden in-dex and highest overall correctness of prediction. Cumula-tive survival rates differed significantly ( p < 0.05) for non-ARF vs. RIFLE-R, RIFLE-I, and RIFLE-F (Fig. 3a). Fig-ure 3b shows the cumulative rates of survival for the studygroup dichotomized by SOFA score ≤ 8/SOFA score ≥ 9( p < 0.001).
Discussion
The overall mortality rate in this investigation was 65.7%,and is in agreement with previous reports indicating thatcirrhotic patients admitted to an ICU have a very poorprognosis [22, 23, 25, 26, 33, 38]. This investigationidentified that RIFLE classification and SOFA score on the
first day of ICU admission were prognostically significantvariables for critically ill cirrhotic patients (Table 4).Analytical results suggest that for critically ill cirrhoticpatients, variables estimating the advanced liver diseasessuperimposed on one episode of bleeding or infection withmultiple organs failure and/or changes in GFR and UOcriteria are extremely useful prognostically—better thanthe Child–Pugh and APACHE II scores, SCr on admissionor ICU day 1, and UO on ICU day 1.
Several recent studies have verified the importanceof renal failure when assessing the prognosis of cirrhoticpatients [34, 35]. A state of intense renal vasoconstric-tion develops, leading to renal failure in the absenceof any organic renal disease [36]. ARF in critically illpatients is frequently related to progressive multipleorgan failure and sepsis [37, 38]. Past ARF criteria wereused an absolute cut-off value for SCr and/or oliguriato define ARF. However, as some patients with chronicrenal dysfunction received diuretics, or had systemichemodynamic changes, such criteria must have severalstepwise cut-off values for SCr and UO to accompany itsincrement. As demonstrated in our previous study [34],86.6% of critically ill cirrhotic patients with renal failuredied during hospitalization. Renal failure was defined asa SCr level > 1.5 mg/dl (132.6 µmol/l) or a 50% increasein SCr after correcting for prerenal causes and mechanicalobstructions, or an acute need for renal replacementtherapy [34, 35]. A cut-off value of 1.5 mg/dl for SCrwas applied as previous investigations have demonstrated

1928
that patients with cirrhosis and SCr levels > 1.5 mg/dlhave markedly decreased GFR [39], and this also is thecut-off level utilized to define hepatorenal syndrome [40].This work determined that the RIFLE classification is anindependent predictor of hospital mortality rather thanSCr on admission or on ICU day 1, and UO on ICU day 1.The RIFLE criteria include various levels of ARF severity(risk, injury, and failure). This study found that for ICUcirrhotic patients, these categorical groups had significantodds ratios for hospital mortality with a stepwise increase(risk 4.659; injury 5.294; failure 38.824) (Table 1). In ourpatients, renal dysfunction was related to APACHE II,APACHE III, MELD, and SOFA scores and may havecontributed to mortality (Fig. 2). The RIFLE classifica-tion’s failure to measure the extrarenal parameters mayaccount for its inferiority to the MELD, APACHE III, andSOFA scores in discriminative capability (Table 5). TheRIFLE criteria provide diagnostic definitions for the stageat which kidney injury can be prevented (risk stratum),when the kidney has been damaged (injury), and whenrenal failure occurs (failure) [41]. The RIFLE criteria havealso been tested in clinical practice and seem to be at leastcoherent with regard to outcome of patients with acutekidney injury [22, 23, 42–45].
In a previous report, the discriminatory power of theSOFA for predicting short-term mortality in criticallyill patients with cirrhosis was superior to that of theAPACHE II and Child–Pugh systems [28]. In critically illcirrhotic patients, calculation of the area under the ROCcurve in this study also confirmed the superiority of SOFAto APACHE II and Child–Pugh score. The SOFA classi-fication ignores diagnosis, age and co-morbid conditions.The SOFA score probably reflects the unique characteris-tics of the present patient group, whose prognosis couldbe predicted without considering age and diagnosis. Theinfluence of age on outcome has been demonstrated todecrease with increasing disease severity [25, 26, 29].
This could, at least partially, explain why age did notsubstantially influence the probability of mortality in thiswork.
Despite the encouraging results, this study has severallimitations. First, this study was conducted at just oneinstitution; consequently, the results may not be directlyextrapolated to other patient populations. Second, thepatient population contained high proportions of hep-atitis B patients (57.5%; Table 3) and hepatoma patients(31.3%; Table 2), and may present as a special subgroupin the cirrhotic patients. Third, the predictive accuracy oflogistic regression models has its own limitations. Fourth,sequential measurement of these scoring systems (forexample, daily, weekly) may reflect the dynamic aspectsof clinical diseases, thus providing superior informationon mortality risk. Finally, the prognostic instruments weretested on patients already admitted to ICUs, rather thanapplied as a preadmission screening tool; this may haveskewed the measured results.
In conclusion, this investigation demonstrated that theprognosis for cirrhotic patients admitted to ICU is poor.This study also elucidated the predictors of RIFLE classi-fication and SOFA score that are independently associatedwith hospital mortality. We found that RIFLE criteriaclassified 60.4% of ICU cirrhotic patients as having somedegree of ARF. Analytical data also showed the gooddiscriminative power of RIFLE categories in predictinghospital mortality of critically ill patients with cirrhosis.Considering the economy and ease of implementation,we suggest that RIFLE classification can increase theaccuracy of short-term prognosis in this homogeneoussubset of patients.
Acknowledgements. This work was supported by the Chang GungMedical Research Fund CMRPG-32064, Chang Gung MemorialHospital, Linkou, Taiwan, and in part by the National ScienceCouncil of Taiwan (NSC 94–2314-B-182A-129).
References
1. Schrier RW, Arroyo V, Bernardi M,Epstein M, Henriksen JH, Rodés J(1988) Peripheral arterial vasodilationhypothesis: a proposal for the initiationof sodium and water retention incirrhosis. Hepatology 8:1151–1157
2. Gines P, Cardenas A, Arroyo V, Rodes J(2004) Management of cirrhosis andascites. N Engl J Med 350:1646–1654
3. Iwakiri Y, Groszmann RJ (2006) Thehyperdynamic circulation of chronicliver diseases: from the patient to themolecule. Hepatology 43:S121–S131
4. Martin PY, Ginès P, Schrier RW(1998) Nitric oxide as a mediatorof hemodynamic abnormalities andsodium and water retention in cirrhosis.N Engl J Med 339:533–541
5. Xu L, Carter EP, Ohara M, Martin PY,Rogachev B, Morris K, Cadnapa-phornchai M, Knotek M, Schrier RW(2000) Neuronal nitric oxide syn-thase and systemic vasodilation inrats with cirrhosis. Am J PhysiolRenal Physiol 279:F1110–F1115
6. Chen YC, Gines P, Yang J, Summer SN,Falk S, Russell NS, Schrier RW (2004)Increased vascular heme oxygenase-1expression contributes to arterial va-sodilation in experimental cirrhosis inrats. Hepatology 39:1075–1087
7. Andrews P, Azoulay E, Antonelli M,Brochard L, Brun-Buisson C, Dobb G,Fagon JY, Gerlach H, Groeneveld J,Mancebo J, Metnitz P, Nava S, Pugin J,Pinsky M, Radermacher P, Richard C,Tasker R, Vallet B (2005) Year inreview in intensive care medicine, 2004.I. Respiratory failure, infection, andsepsis. Intensive Care Med 31:28–40

1929
8. Andrews P, Azoulay E, Antonelli M,Brochard L, Brun-Buisson C, Dobb G,Fagon JY, Gerlach H, Groeneveld J,Mancebo J, Metnitz P, Nava S, Pugin J,Pinsky M, Radermacher P, Richard C,Tasker R, Vallet B (2005) Year in reviewin intensive care medicine, 2004. III.Outcome, ICU organisation, scoring,quality of life, ethics, psychologicalproblems and communication in theICU, immunity and hemodynamicsduring sepsis, pediatric and neonatalcritical care, experimental studies.Intensive Care Med 31:356–372
9. Andrews P, Azoulay E, Antonelli M,Brochard L, Brun-Buisson C,Backer DD, Dobb G, Fagon JY,Gerlach H, Groeneveld J, Mancebo J,Metnitz P, Nava S, Pugin J, Pinsky M,Radermacher P, Richard C, Tasker R(2006) Year in review in intensive caremedicine. 2005. I. Acute respiratoryfailure and acute lung injury, ventila-tion, hemodynamics, education, renalfailure. Intensive Care Med 32:207–216
10. Shellman RG, Fulkerson WJ, De-Long E, Piantadosi CA (1998)Prognosis of patients with cirrho-sis and chronic liver disease admittedto the medical intensive care unit.Crit Care Med 16:671–678
11. Chen YC, Tsai MH, Hsu CW, Ho YP,Lien JM, Chang MY, Fang JT,Huang CC, Chen PC (2003) Role ofserum creatinine and prognostic scoringsystems in assessing hospital mortal-ity in critically ill cirrhotic patientswith upper gastrointestinal bleeding.J Nephrol 16:558–565
12. Kellum JA, Levin N, Bouman C,Lameire N (2002) Develop-ing a consensus classificationsystem for acute renal failure.Curr Opin Crit Care 8:509–514
13. Mehta RL, Chertow GM (2003)Acute renal failure definitions andclassification: time for change?J Am Soc Nephrol 14:2178–2187
14. Schrier RW, Wang W, Poole B,Mitra A (2004) Acute renalfailure: definitions, diagnosis,pathogenesis, and therapy.J Clin Invest 114:5–14
15. Lameire N, Van Biesen W, Van-holder R (2005) Acute renal failure.Lancet 365:417–430
16. Bellomo R (2006) The epidemiology ofacute renal failure: 1975 versus 2005.Curr Opin Crit Care 12:557–560
17. Pugh RN, Murray-Lyon IM, Daw-son JL, Pietroni MC, Williams R(1973) Transection of the esopha-gus for bleeding esophageal varices.Br J Surg 60:646–649
18. Vincent JL, Moreno R, Takala J,Willatts S, De Mendonca A, Bruining H(1996) The SOFA (Sepsis-relatedOrgan Failure Assessment) score todescribe organ dysfunction/failure. Onbehalf of the Working Group on Sepsis-Related Problems of the EuropeanSociety of Intensive Care Medicine.Intensive Care Med 22:707–710
19. Kamath PS, Wiesner RH, Malinchoc M,Kremers W, Therneau TM, Kosberg CL,D’Amico G, Dickson ER, Kim WR(2001) A model to predict survival inpatients with end-stage liver disease.Hepatology 33:464–470
20. Knaus WA, Draper EA, Wagner DP,Zimmerman JE (1985) APACHE II:a severity of disease classificationsystem. Crit Care Med 13:818–824
21. Bellomo R, Ronco C, Kellum JA,Mehta RL, Palevsky P, Acute DialysisQuality Initiative Workgroup (2004)Acute renal failure—definition, out-come measures, animal models, fluidtherapy and information technologyneeds: the Second International Consen-sus Conference of the Acute DialysisQuality Initiative (ADQI) Group.Crit Care 8:R204–R212
22. Lin CY, Chen YC, Tsai FC, Tian YC,Jenq CC, Fang JT, Yang CW (2006)RIFLE classification is predic-tive of short-term prognosis incritically ill patients with acuterenal failure supported by extra-corporeal membrane oxygenation.Nephrol Dial Transplant 21:2867–2873
23. Bellomo R, Kellum JA, Ronco C (2007)Defining and classifying acute renalfailure: from advocacy to consensusand validation of the RIFLE criteria.Intensive Care Med 33:409–413
24. Knaus WA, Wagner DP, Draper EA,Zimmerman JE, Bergner M, Bastos PG(1991) The APACHE III prognosticsystem: risk prediction of hospitalmortality for critically ill hospitalizedadults. Chest 100:1619–1636
25. Tsai MH, Chen YC, Ho YP, Fang JT,Lien JM, Chiu CT, Liu NJ, Chen PC(2003) Organ system failure scoringsystem can predict hospital mortal-ity in critically ill cirrhotic patients.J Clin Gastroenterol 37:251–257
26. Cholongitas E, Senzolo M, Patch D,Shaw S, Hui C, Burroughs AK (2006)Scoring systems for assessing prognosisin critically ill adult cirrhotics. AlimentPharmacol Ther 24:453–464
27. Knaus WA, Draper EA, Wagner DP,Zimmerman JE (1985) Progno-sis in acute organ-system failure.Ann Surg 202:685–693
28. Wehler M, Kokoska J, Reulbach U,Hahn EG, Strauss R (2001) Short-termprognosis in critically ill patients withcirrhosis assessed by prognostic scoringsystems. Hepatology 34:255–261
29. Chen YC, Tian YC, Liu NJ, Ho YP,Yang C, Chu YY, Chen PC, Fang JT,Hsu CW, Yang CW, Tsai MH (2006)Prospective cohort study comparingSOFA and APACHE III scoring sys-tems for hospital mortality predictionin critically ill cirrhotic patients.Int J Clin Pract 60:160–166
30. DeLong E, DeLong D, Clarke-Pearson D (1988) Comparing theareas under two or more correlatedreceiver operating characteristiccurves: a non-parametric approach.Biometrics 44:837–844
31. Youden WJ (1950) Index for ratingdiagnosis tests. Cancer 3:32–35
32. du Cheyron D, Bouchet B, Pari-enti JJ, Ramakers M, Charbonneau P(2005) The attributable mortalityof acute renal failure in criticallyill patients with liver cirrhosis.Intensive Care Med 31:1693–1699
33. Tsai MH, Peng YS, Chen YC, Liu NJ,Ho YP, Fang JT, Lien JM, Yang C,Chen PC, Wu CS (2006) Adrenalinsufficiency in critically ill cirrhoticpatients with severe sepsis and septicshock. Hepatology 43:673–681
34. Chen YC, Tsai MH, Ho YP, Hsu CW,Lin HH, Fang JT, Huang CC, Chen PC(2004) Comparison of the severity ofillness scoring systems for criticallyill cirrhotic patients with renal failure.Clin Nephrol 61:111–118
35. Cardenas A, Gines P, Uriz J, Bessa X,Salmeron JM, Mas A (2001) Renal fail-ure after upper gastrointestinal bleedingin cirrhosis: incidence, clinical course,predictive factors, and short-termprognosis. Hepatology 34:671–676
36. Gines P, Guevara M, Arroyo V,Rodes J (2003) Hepatorenal syndrome.Lancet 362:1819–1827
37. Parker RA, Himmelfarb J, Tolkoff-Rubin N, Chandran P, Wingard RL,Hakim RM (1998) Prognosis of pa-tients with acute renal failure requiringdialysis: results of a multicenter study.Am J Kidney Dis 32:432–442
38. Cosentino F, Chaff C, Piedmonte M(1994) Risk factors influencing survivalin ICU acute renal failure. Nephrol DialTransplant 9(4):179–182
39. Bataller R, Gines P, Guevara M, Ar-royo V (1997) Hepatorenal syndrome.Semin Liver Dis 17:233–247

1930
40. Arroyo V, Gines P, Gerbes AL, Dud-ley FJ, Gentilini P, Laffi G (1996)Definition and diagnostic criteria ofrefractory ascites and hepatorenalsyndrome in cirrhosis. InternationalAscites Club. Hepatology 23:164–176
41. Uchino S, Bellomo R, Goldsmith D,Bates S, Ronco C (2006) An assess-ment of the RIFLE criteria for acuterenal failure in hospitalized patients.Crit Care Med 34:1913–1917
42. Bell M, Liljestam E, Granath F,Fryckstedt J, Ekbom A, Martling CR(2005) Optimal follow-up time aftercontinuous renal replacement therapyin actual renal failure patients stratifiedwith the RIFLE criteria. Nephrol DialTransplant 20:354–360
43. Hoste EA, Clermont G, Kersten A,Venkataraman R, Angus DC, DeBacquer D, Kellum JA (2006) RIFLEcriteria for acute kidney injury areassociated with hospital mortality incritically ill patients: A cohort analysis.Crit Care 10:R73–R83
44. Kuitunen A, Vento A, Suojaranta-Ylinen R, Pettila V (2006) Acuterenal failure after cardiac surgery:Evaluation of the RIFLE classification.Ann Thorac Surg 81:542–546
45. Lerolle N, Guerot E, Faisy C,Bornstain C, Diehl JL, Fagon JY(2006) Renal failure in septicshock: predictive value of Doppler-based renal arterial resistive index.Intensive Care Med 32:1553–1559