
Tecnologia e processo produttivo: i rifiuti e gli scarti di cava
Upload
mumbaiunivercityCategory
view
3download
0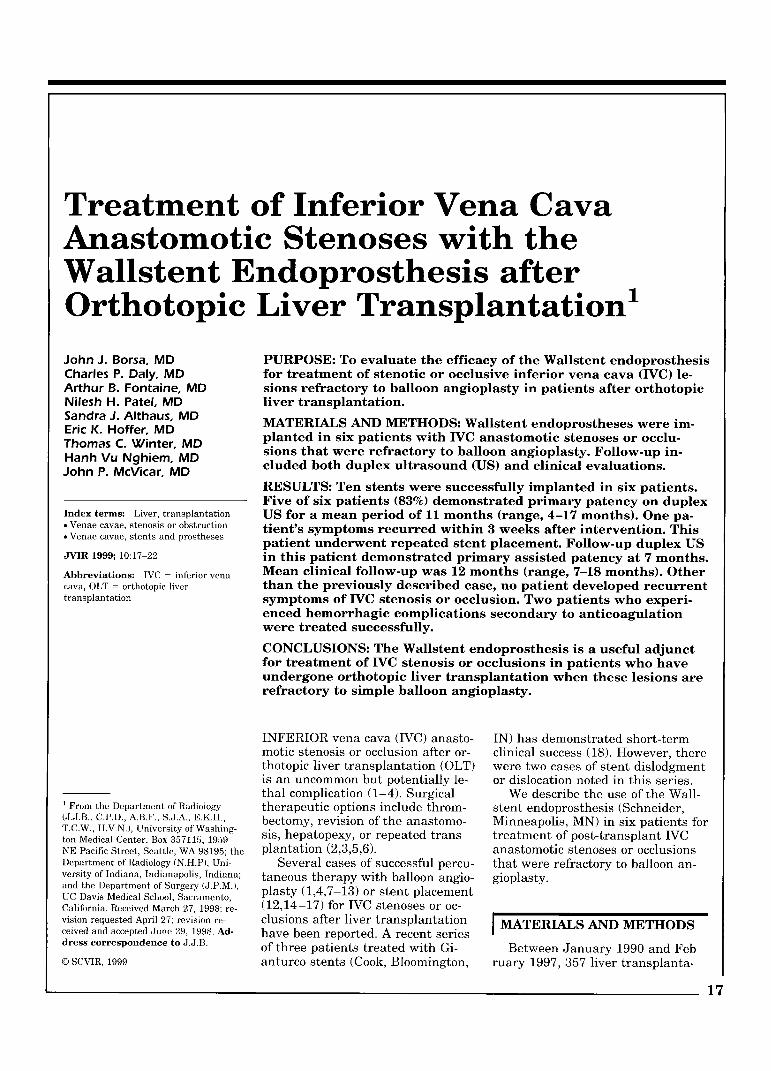
Treatment of Inferior Vena Cava Anastornotic Stenoses with the Wallstent Endoprosthesis after Orthotopic Liver ~rans~lantation' John J. Borsa, MD PURPOSE: To evaluate the efficacy of the Wallstent endoprosthesis Charles P. Daly, MD for treatment of stenotic or occlusive inferior vena cava (IVC) le- Arthur B. Fontaine, MD sions refractory to balloon angioplasty in patients after orthotopic Nilesh H. Patel, MD liver transplantation. Sandra J. Althaus, MD Eric K. Hoffer, MD MATERIALS AND METHODS: Wallstent endoprostheses were im-
Thomas C. Winter, MD planted in six patients with IVC anastomotic stenoses or occlu-
Hanh Vu Nghiem, MD sions that were refractory to balloon angioplasty. Follow-up in-
John P. McVicar, MD cluded both duplex ultrasound (US) and clinical evaluations.
RESULTS: Ten stents were successfully implanted in six patients. Five of six patients (83%) demonstrated primary patency on duplex
Index terms: Liver, transplantation US for a mean period of 11 months (range, 4-17 months). One pa- * Venae cavae, stenosis Or obstruction tient's symptoms recurred within 3 weeks after intervention. This . Venae cavae, stents and prostheses
patient underwent repeated stent placement. Follow-up duplex US JVIR 1999; 10:17-22 in this patient demonstrated primary assisted patency at 7 months. Abbreviations: IVC = inferior vena Mean clinical follow-up was 12 months (range, 7-18 months). Other cava, OLT = orthotopic liver than the previously described case, no patient developed recurrent transplantation symptoms of IVC stenosis or occlusion. Two patients who experi-
enced hemorrhagic complications secondary to anticoagulation were treated successfully.
CONCLUSIONS: The Wallstent endoprosthesis is a useful adjunct for treatment of IVC stenosis or occlusions in patients who have undergone orthotopic liver transplantation when these lesions are refractory to simple balloon angioplasty.
INFERIOR vena cava (IVC) anasto- IN) has demonstrated short-term motic stenosis or occlusion after or- clinical success (18). However, there thotopic liver transplantation (OLT) were two cases of stent dislodgment is an uncommon but potentially le- or dislocation noted in this series. thal complication (1-4). Surgical We describe the use of the Wall-
' From the Department of Radiology therapeutic options include throm- stent endoprosthesis (Schneider, (J.J.B., C.P.D., A.B.F., S.J.A., E.K.H., T.C.W., H.V.N.), University of Washing-
bectomy, revision of the anastomo- Minneapolis, MN) in six patients for ton Medical Center, Box 357115, 1959 sis, hepatopexy, or repeated trans- treatment of post-transplant IVC NE Pacific Street, Seattle, WA 98195; the plantation (2,3,5,6). anastornotic stenoses or O C C ~ U S ~ O ~ S Department of Radiology (N.H.P), Uni- Several cases of successful percu- that were refractory to balloon an- versity of Indiana, Indianapolis, Indiana; taneous therapy with balloon angio- gioplasty. and the Department of Surgery (J.P.M.), UC Davis Medical School, Sacramento, plasty (1,4,7-13) or stent placement California. Received March 27, 1998; re- (12,14-17) for IVC stenoses or oc- vision requested April 27; revision re- clusions after liver transplantation MATERIALS AND METHODS ceived and accepted June 29, 1998. Ad- have been reported. A recent series dress correspondence to J.J.B. of three patients treated with Gi- Between January 1990 and Feb- o SCVIR, 1999 anturco stents (Cook, Bloomington, ruary 1997, 357 liver transplanta-
17
18 Treatment of Inferior Vena Cava Anastomotic Stenoses
January 1999 JVIR
tions were performed a t our institu- tion. Nine of these patients (2.5%) were referred to us for evaluation and treatment of IVC anastomotic stenosis or occlusion. Of these nine patients, two underwent successful angioplasty of their stenoses, while a third underwent unsuccessful an- gioplasty followed by Gianturco stent placement. Unfortunately, stent migration in this patient re- quired surgical retrieval followed by operative revision of the suprahe- patic anastomotic stenosis.
Six patients had stenoses or oc- clusions refractory to balloon angio- plasty that were subsequently treated with placement of the Wall- stent endoprosthesis (three men and three women; age range, 27-68 years [mean, 48 years]).
Three of the patients were re- ferred early (within 12 days of transplantation). They all had their IVC stenosis created intraopera- tively and experienced intraopera- tive and postoperative hemody- namic instability secondary to inad- equate blood return to the heart. All three patients also demon- strated deteriorating hepatic and renal function postoperatively. These three patients required pres- sor support until their IVC lesions were treated.
Three patients were referred later. Two patients were referred approximately 1 month after liver transplantation with ascites, lower extremity edema, and renal insuffi- ciency. The final patient was re- ferred 6 months after transplanta- tion while hospitalized for abdomi- nal pain and diarrhea. Duplex sonography a t this time demon- strated poor flow within his intra- hepatic IVC; this was also evident on computed tomography (CT) of the abdomen (Figs 1-4).
In all patients, the presence of IVC stenosis or occlusion was con- firmed by means of venography as follows: a 5-F pigtail catheter was introduced into the lower IVC from the femoral approach with use of the Seldinger technique. Single plane, digital subtraction images were obtained after injection of Op- tiray 320 (Mallinckrodt, St. Louis, MO) a t a rate of 15-20 ml/sec for a
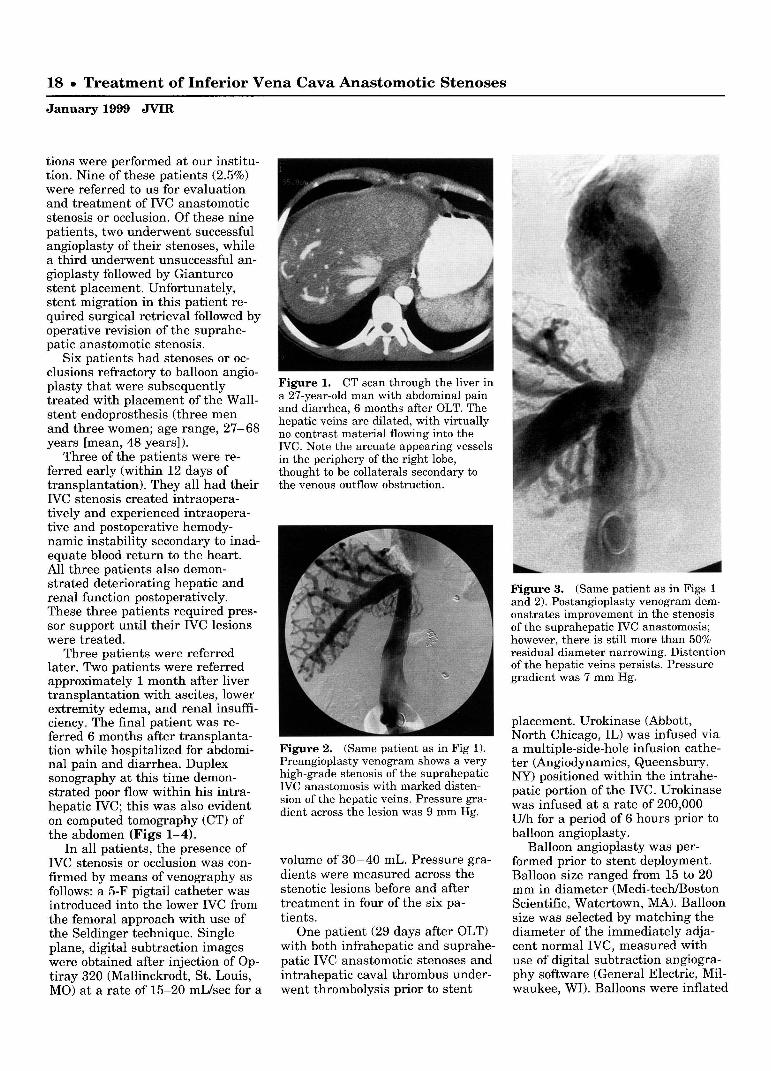
Figure 1. CT scan through the liver in a 27-year-old man with abdominal pain and diarrhea, 6 months after OLT. The hepatic veins are dilated, with virtually no contrast material flowing into the IVC. Note the arcuate appearing vessels in the periphery of the right lobe, thought to be collaterals secondary to the venous outflow obstruction.
Figure 2. (Same patient as in Fig 1). Preangioplasty venogram shows a very high-grade stenosis of the suprahepatic IVC anastomosis with marked disten- sion of the hepatic veins. Pressure gra- dient across the lesion was 9 mm Hg.
volume of 30-40 mL. Pressure gra- dients were measured across the stenotic lesions before and after treatment in four of the six pa- tients.
One patient (29 days after OLT) with both infrahepatic and suprahe- patic IVC anastomotic stenoses and intrahepatic caval thrombus under- went thrombolysis prior to stent
Figure 3. (Same patient as in Figs 1 and 2). Postangioplasty venogram dem- onstrates improvement in the stenosis of the suprahepatic IVC anastomosis; however, there is still more than 50% residual diameter narrowing. Distention of the hepatic veins persists. Pressure gradient was 7 mm Hg.
placement. Urokinase (Abbott, North Chicago, IL) was infused via a multiple-side-hole infusion cathe- ter (Angiodynamics, Queensbury, NY) positioned within the intrahe- patic portion of the IVC. Urokinase was infused a t a rate of 200,000 U/h for a period of 6 hours prior to balloon angioplasty.
Balloon angioplasty was per- formed prior to stent deployment. Balloon size ranged from 15 to 20 mm in diameter (Medi-techBoston Scientific, Watertown, MA). Balloon size was selected by matching the diameter of the immediately adja- cent normal IVC, measured with use of digital subtraction angiogra- phy software (General Electric, Mil- waukee, WI). Balloons were inflated

Borsa et a1 19
Volume 10 Number 1
Figure 4. (Same patient as in Figs 1-3). Venogram after stent placement demonstrates wide patency of the supra- hepatic IVC anastomosis with brisk for- ward flow into the right atrium. There is still some filling of the hepatic veins. Pressure gradient was 2 mm Hg.
to 3-4 atm and left inflated for 15-30 seconds. Inadequate response to balloon dilation was defined as persistent caval narrowing (>50% luminal diameter) with poor for- ward flow into the right atrium. Wallstents were then immediately placed.
Wallstent endoprostheses were deployed across the lesions and then dilated with an appropriately sized balloon catheter to achieve their nominal diameter. Wallstent sizes were selected by matching the diameter of t h e immediately adja- cent normal IVC. (In one case, 14-mm Wallstents were overdilated to 20 mm because larger Wallstents were not available at that time). Final stent position was confirmed with venography.
After stent placement, five pa- tients were anticoagulated with heparin sodium (Elkins-Sinn, Cherry Hill, NJ), consisting of an initial bolus of 80 U k g intrave- nously followed by a continuous in- fusion of 10-15 U/kg/h intrave- nously titrated to maintain the par- tial thromboplastin time between 2 and 2.5 times the control. Two of these five patients developed hem- orrhagic complications, and antico- agulation was stopped immediately. The other three patients received
warfarin for 3 months. One patient (our most recent) was not anticoag- ulated at all. All patients were pre- treated with aspirin and main- tained on one adult aspirin per day thereafter.
Follow-up included physical ex- amination to rule out development of lower extremity edema or ascites. In addition, ultrasonographic (US) interrogation of the stents for possi- ble focal increased velocity was done. The hepatic veins were also evaluated for patency and direction of flow.
I RESULTS Initial venograms demonstrated
two patients with suprahepatic IVC anastomotic occlusions, two patients with suprahepatic IVC anastomotic stenosis, and two patients with both suprahepatic and infrahepatic IVC anastomotic stenoses, one of which had some intrahepatic caval throm- bus present. The mean pressure gradient across the IVC lesions ob- tained prior to balloon angioplasty was 11 mm Hg, with a range of 8-14 mm Hg.
Results of urokinase infusion in the one patient (29 days after OLT) with intrahepatic caval thrombus demonstrated little change in ap- pearance after 6 hours of urokinase delivery (200,000 Uk), indicating that the thrombus was predomi- nantly chronic in nature.
Balloon angioplasty was unsuc- cessful in all six patients. While complete expansion of the balloon was easily achieved in all cases, elastic recoil was evident on postan- gioplasty venograms, demonstrated by persistent caval narrowing (>50% luminal diameter) and poor forward flow into the right atrium. The mean pressure gradient ob- tained after angioplasty was 10 mm Hg, with a range of 7-12 mm Hg.
Nine stents were initially placed in the six patients. The two patients with both infrahepatic and suprahe- patic IVC stenoses required two stents each, one at each anastomo- sis (20 mm x 40 mm, 22 mm x 45 mm; and 16 mm X 60 mm, 16 mm x 60 mm). Another patient,
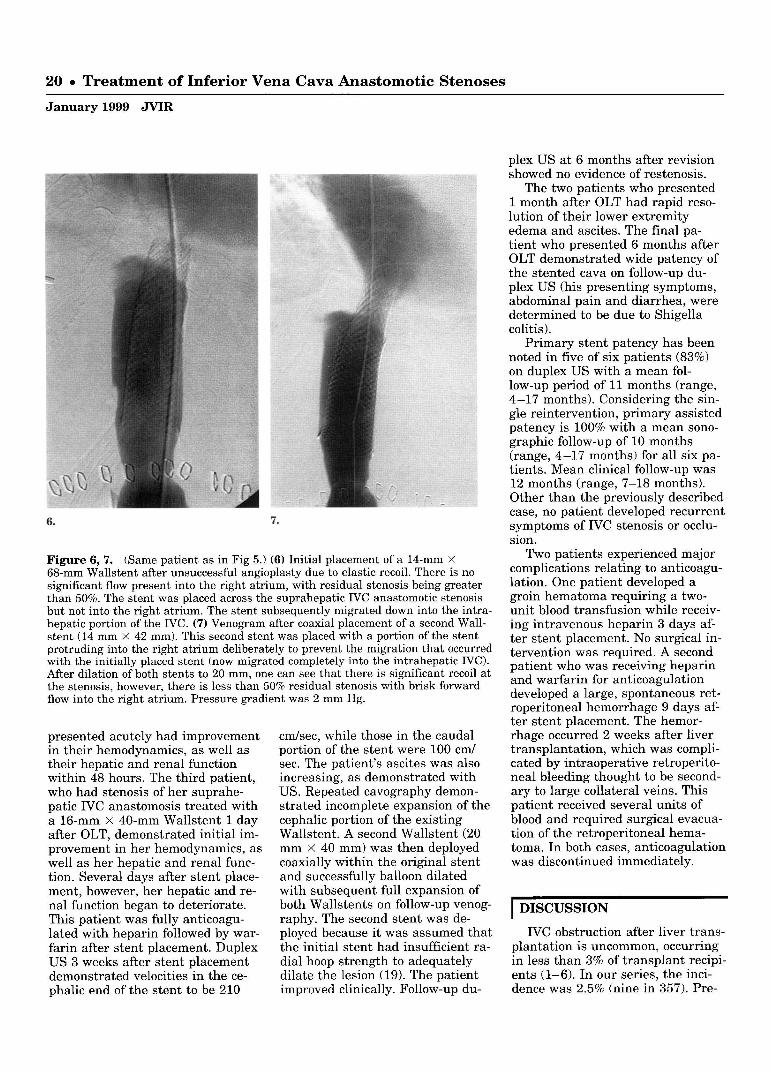
Figure 5. A 68-year-old man 12 days after OLT with hypotension and de- creasing renal and hepatic function. In- ferior vena cavogram demonstrates oc- clusion a t the suprahepatic anastomosis with retrograde filling of the hepatic veins. Pressure gradient across the le- sion was 13 mm Hg.
with suprahepatic IVC occlusion (Fig 5), required placement of a second stent because of migration of the first stent down into the intra- hepatic IVC after deployment (Figs 6, 7). This was our first patient treated; the second Wallstent de- ployed in this patient and all suc- cessive Wallstent deployments across the suprahepatic IVC anasto- mosis were positioned with a signif- icant portion of the stent protruding into the right atrium to prevent such migration. Fourteen-millime- ter-diameter stents (14 mm X 42 mm, 14 mm X 68 mm) were placed in this first patient (IVC measured 20 mm) and overdilated to 20 mm because larger diameter Wallstents were not available a t the time. The remaining three patients each re- quired a single Wallstent initially (16 mm X 40 mm, 16 mm X 40 mm, 16 mm X 60 mm). Venograms obtained after deployment demon- strated wide patency of the stented portions of the IVC and brisk for- ward flow into the right atrium in all patients. The mean pressure gradient obtained after stent de- ployment was 2 mm Hg, with a range of 0-2 mm Hg.
Two of the three patients who
20 . Treatment of Inferior Vena Cava Anastomotic Stenoses
January 1999 JVIR
Figure 6, 7. (Same patient as in Fig 5.) (6) Initial placement of a 14-mm X 68-mm Wallstent after unsuccessful angioplasty due to elastic recoil. There is no significant flow present into the right atrium, with residual stenosis being greater than 50%. The stent was placed across the suprahepatic IVC anastomotic stenosis but not into the right atrium. The stent subsequently migrated down into the intra- hepatic portion of the IVC. (7) Venogram after coaxial placement of a second Wall- stent (14 mm X 42 mm). This second stent was placed with a portion of the stent protruding into the right atrium deliberately to prevent the migration that occurred with the initially placed stent (now migrated completely into the intrahepatic IVC). After dilation of both stents to 20 mm, one can see that there is significant recoil at the stenosis, however, there is less than 50% residual stenosis with brisk forward flow into the right atrium. Pressure gradient was 2 mm Hg.
presented acutely had improvement in their hemodynamics, as well as their hepatic and renal function within 48 hours. The third patient, who had stenosis of her suprahe- patic IVC anastomosis treated with a 16-mm x 40-mm Wallstent 1 day after OLT, demonstrated initial im- provement in her hemodynamics, as well as her hepatic and renal func- tion. Several days after stent place- ment, however, her hepatic and re- nal function began to deteriorate. This patient was fully anticoagu- lated with heparin followed by war- farin after stent placement. Duplex US 3 weeks after stent placement demonstrated velocities in the ce- phalic end of the stent to be 210
cmlsec, while those in the caudal portion of the stent were 100 cml sec. The patient's ascites was also increasing, as demonstrated with US. Repeated cavography demon- strated incomplete expansion of the cephalic portion of the existing Wallstent. A second Wallstent (20 mm x 40 mm) was then deployed coaxially within the original stent and successfully balloon dilated with subsequent full expansion of both Wallstents on follow-up venog- raphy. The second stent was de- ployed because it was assumed that the initial stent had insufficient ra- dial hoop strength to adequately dilate the lesion (19). The patient improved clinically. Follow-up du-
plex US a t 6 months after revision showed no evidence of restenosis.
The two patients who presented 1 month after OLT had rapid reso- lution of their lower extremity edema and ascites. The final pa- tient who presented 6 months after OLT demonstrated wide patency of the stented cava on follow-up du- plex US (his presenting symptoms, abdominal pain and diarrhea, were determined to be due to Shigella colitis).
Primary stent patency has been noted in five of six patients (83%) on duplex US with a mean fol- low-up period of 11 months (range, 4-17 months). Considering the sin- gle reintervention, primary assisted patency is 100% with a mean sono- graphic follow-up of 10 months (range, 4-17 months) for all six pa- tients. Mean clinical follow-up was 12 months (range, 7-18 months). Other than the previously described case, no patient developed recurrent symptoms of IVC stenosis or occlu- sion.
Two patients experienced major complications relating to anticoagu- lation. One patient developed a groin hematoma requiring a two- unit blood transfusion while receiv- ing intravenous heparin 3 days af- ter stent placement. No surgical in- tervention was required. A second patient who was receiving heparin and warfarin for anticoagulation developed a large, spontaneous ret- roperitoneal hemorrhage 9 days af- ter stent placement. The hemor- rhage occurred 2 weeks after liver transplantation, which was compli- cated by intraoperative retroperito- neal bleeding thought to be second- ary to large collateral veins. This patient received several units of blood and required surgical evacua- tion of the retroperitoneal hema- toma. In both cases, anticoagulation was discontinued immediately.
1 DISCUSSION
IVC obstruction after liver trans- plantation is uncommon, occurring in less than 3% of transplant recipi- ents (1-6). In our series, the inci- dence was 2.5% (nine in 357). Pre-

Borsa et a1 21
Volume 10 Number 1
senting signs and symptoms of post- operative caval compromise include deteriorating hepatic and renal function, hypotension, decreasing cardiac output, lower extremity edema, and ascites. Surgical ther- apy has included thrombectomy, anastomotic revision, retransplanta- tion, and hepatopexy (to alleviate torsion or kinking of the caval anas- tomosis) (2,3,5,6). Brouwers et a1 suggested that percutaneous ther- apy has a limited role in these pa- tients because of the risk for ~ulmo- nary emboli from caval thrombus (5). On the other hand. Pfammatter e t a1 has described the' successful outcome of primary stent placement in a patient with a thrombosed IVC 2 days after transplantation (12). Unfortunately, this patient died; at autopsy (7 days after stent place- ment), no evidence of pulmonary embolism was found.
We did have one case of intrahe- patic caval thrombus 29 days after OLT. Thrombolytic therapy was performed prior to angioplasty and stent placement. There was no clini- cal sign of pulmonary embolism. The patient developed a groin he- matoma secondary to anticoagula- tion 3 days after the procedure, which required a two-unit blood transfusion.
When IVC obstruction occurs im- mediately after surgery, it is usu- ally due to a technical problem, such as anastomotic stricture from a tight suture line, donor-recipient size discrepancy, anastomotic tor- sion, anastomotic kinking, or caval compression from a large graft (1,2,4-6). We have observed, along with others, a high degree of elastic recoil of anastomotic stenoses when balloon angioplasty is attempted in the acute post-transplant period (12,14-16,18). This finding is not unexpected, considering the possible mechanisms of obstruction (anasto- motic stricture from a tight suture line, donor-recipient size discrep- ancy, anastomotic torsion, anasto- motic kinking, or caval compression from a large graft). Percutaneous stent placement is an attractive so- lution for these patients because the stent adds permanent support to the lumen of the IVC and coun-
teracts the elastic recoil inherent in the mechanisms of acute anasto- motic stenosis. Primary stent place- ment could, in fact, be considered in these acute postoperative patients, however, we are in agreement with Pfammatter et a1 (20) that initial angioplasty of these lesions defines their distensibility, demonstrated by the amount of expansion achieved with the balloon. With a distensible lesion, immediate failure of angioplasty is most likely second- ary to elastic recoil, and stent place- ment should have a high rate of success. One must be very cautious, however, when performing angio- plasty on these fresh anastomoses because aggressive dilation of an anastomotic stricture secondary to a tight suture line may possibly re- sult in disruption of the anastomo- sis. In such cases, it is important for the interventional radiologist to have good communication with the transplant team; if the surgeon be- lieves that the anastomosis was strictured because of an overly tight suture line, angioplasty should probably not be attempted.
IVC obstruction that presents later (weeks, months) may be caused by fibrosislscarring or inti- ma1 hyperplasia at the anastomotic site (11,13,21,22). Balloon angio- plasty alone has been described as successful in these patients (1,4,7- 13). Maintenance of primary as- sisted patency, however, may neces- sitate multiple angioplasty revisions (1,4,7,9-11,13). We found a high degree of elastic recoil present in such stenoses with a poor response to balloon angioplasty. Stent deploy- ment was necessary to maintain caval patency.
Pressure gradients across caval lesions present an attractive method of determining both the sig- nificance of caval stenosis. as well as measuring their response to an- gioplasty (with the subsequent need for stent placement in angioplasty failures). At present, there is no consensus regarding what degree of IVC pressure gradient is hemody- namically significant in these pa- tients. Rossi et a1 (23) suggest that a gradient is not significant until it reaches the range of 7-10 mm Hg,
while Raby et a1 (9) suggests that a gradient greater than 10 mm Hg is significant in these patients. In our series, the mean preangioplasty pressure gradient obtained was 11 mm Hg, with a range of 8-14 mm Hg. All patients were symptomatic and we, therefore, concur with pre- vious investigators that pressure gradients of 11 mm Hg or greater are hemodynamically significant. In addition, we suggest that a pressure gradient of 8 mm Hg (our lowest gradient) may also be hemodynami- cally significant. In further support of this, all of our patients became asymptomatic after treatment with mean pressure gradients of 2 mm Hg (range, 0-2 mm Hg).
Stent placement in or about the caval anastomosis of a liver trans- plant does raise the concern of cov- ering or compromising hepatic ve- nous drainage. Potential adverse sequela may include thrombosis of the excluded vein(s). There are sev- eral reports in the literature of cov- ering venous origins with IVC stents without evidence of side branch thrombosis in non-OLT pa- tients (24-26). Anecdotally, we fre- quently place Wallstents across the origin of the left (or less frequently, the right) portal vein during tran- sjugular intrahepatic portosystemic shunt procedures with patency of the excluded portal vein demon- strated on follow-up duplex US. Nonetheless, our first five patients were given anticoagulants in an ef- fort to prevent hepatic vein throm- bosis after IVC stent placement. In two of these patients, anticoagula- tion was stopped very early because of bleeding. Patency of their hepatic veins on follow-up duplex US led to our decision to cease administering anticoagulants altogether. There- fore, three of our six patients were not maintained on long-term antico- agulation. All of our patients had 100% hepatic venous patency as de- termined with duplex US, with an average follow-up of 10 months (range, 4-17 months).
Another sequela of covering the hepatic veins with an IVC stent is their exclusion from further inter- vention via the IVC (eg, for subse- quent hepatic vein stenosis, throm-

22 Treatment of Inferior Ve !na Cava Anastomotic Stenoses
January 1999 JVIR
bosis, and so forth). If subsequent intervention in a hepatic vein is re- quired, a percutaneous transhepatic route could be utilized for access.
Another concern with IVC stent placement is that it may potentially increase the technical difficulty of retransplantation, particularly if a portion of a stent placed across a suprahepatic IVC anastomosis is protruding into the right atrium.
In summary, we describe six cases of OLT complicated by IVC stenosis or occlusion that were suc- cessfully treated with use of the Wallstent endoprosthesis in the set- ting of failed balloon angioplasty. Technical success was 100%. Pri- mary assisted patency was loo%, at a mean clinical follow-up of 12 months. There were two hemor- rhagic complications and one case of stent migration with no permanent clinical sequela from either. The Wallstent endoprosthesis is a useful adjunct for the treatment of post- transplantation caval stenoses or occlusions in the setting of failed balloon angioplasty.
References 1. Koneru B, Tzakis AG, Bowman J ,
Cassavilla A, Zajko AB, Starzl TE. Postoperative surgical complica- tions. Gastroenterol Clin North Am 1988; 17:71-91.
2. Lerut J , Gordon RD, Iwatsuki S, Starzl TE. Surgical complications in human orthotopic liver transplan- tation. Acta Chir Belg 1987; 87:193- 204.
3. Lerut J , Tzakis AG, Bron K, e t al. Complications of venous reconstruc- tion in human orthotopic liver transplantation. Ann Surg 1987; 205:404-414.
4. Orons PD, Zajko AB. Angiography and interventional procedures in liver transplantation. Radiol Clin North Am 1995; 33:541-558.
5. Brouwers MA, de Jong KP, Peeters PM, Bijleveld CM, Klompmaker IJ, Slooff MJ. Inferior vena cava ob- struction after orthotopic liver transplantation. Clin Transplant 1994; 8:19-22.
6. Boillot 0 , Sarfati PO, Bringier J, Moncorge CI, Houssin D, Chapuis Y. Orthotopic liver transplantation and pathology of the inferior vena cava. Transplant Proc 1990; 22:1567-1568.
7. Karatzas T, Lykaki-Karatzas E, Webb M, et al. Vascular complica- tions, treatment, and outcome fol- lowing orthotopic liver transplanta- tion. Transplant Proc 1997; 29:2853-2855.
8. Rose BS, Van Aman ME, Simon DC, Sommer BG, Ferguson RM, Henry ML. Transluminal balloon angio- plasty of infrahepatic caval anasto- motic stenosis following liver trans- plantation: case report. Cardiovasc Intervent Radiol 1988; 11:79-81.
9. Raby N, Karani J , Thomas S, O'Grady J , Williams R. Stenoses of vascular anastomoses after hepatic transplantation: treatment with bal- loon angioplasty. AJR 1991; 157: 167-171.
10. Fujimoto M, Moriyasu F, Someda H, e t al. Recovery of graft circulation following percutaneous transluminal angioplasty for stenotic venous com- plications in pediatric liver trans- plantation: assessment with Doppler ultrasound. Transpl Int 1995; 8:119-125.
11. Zajko AB, Sheng R, Bron K, Reyes J , Nour B, Tzakis A. Percutaneous transluminal angioplasty of venous anastomotic stenoses complicating liver transplantation: intermediate- term results. JVIR 1994; 5:121-126.
12. Pfammatter T, Williams DM, Lane KL, Campbell DAJ, Cho KJ. Su- prahepatic caval anastomotic steno- sis complicating orthotopic liver transplantation: treatment with per- cutaneous transluminal angioplasty, Wallstent placement, or both. AJR 1997; 168:477-480.
13. Zajko AB, Claus D, Clapuyt P, et al. Obstruction to hepatic venous drain- age after liver transplantation: treatment with balloon angioplasty. Radiology 1989; 170(3 Pt 1):763- 765.
14. Althaus SJ, Perkins JD, Soltes G, Glickerman D. Use of a Wallstent in successful treatment of IVC ob- struction following liver transplan- tation. Transplantation 1996; 61: 669-672.
15. Berger H, Hilbertz T, Zuhlke K, Forst H, Pratschke E. Balloon di- latation and stent placement of su- prahepatic caval anastomotic steno- sis following liver transplantation. Cardiovasc Intervent Radiol 1993; 16:384-387.
16. Zulke C, Berger H, Anthuber M, Jauch KW. Detection of suprahe-
patic caval stenosis following liver transplantation and treatment via balloon-expandable intravascular stent (letter). Transpl Int 1995; 8:330-332.
17. Orons PD, Hari AK, Zajko AB, Marsh JW. Thrombolysis and en- dovascular stent placement for infe- rior vena caval thrombosis in a liver transplant recipient. Transplanta- tion 1997; 64:1357-1361.
18. Simo G, Echenagusia A, Camunez F, et al. Stenosis of the inferior vena cava after liver transplanta- tion: treatment with Gianturco ex- pandable metallic stents. Cardiovasc Intervent Radiol 1995; 18:212-216.
19. Lossef SV, Lutz RJ, Mundorf J , Barth KH. Comparison of mechan- ical deformation properties of metal- lic stents with use of stress-strain analysis. JVIR 1994; 5:341-349.
20. Pfammatter T, Williams DM, Lane KL, Campbell DAJ, Cho KJ. Su- prahepatic caval anastomotic steno- sis complicating orthotopic liver transplantation: treatment with per- cutaneous transluminal angioplasty, Wallstent placement, or-both. AJR 1997; 168:477-480.
21. Cardella JF , Amplatz K. Postoper- ative angiographic and interven- tional radiologic evaluation of liver recipients. Radiol Clin North Am 1987; 25:309-321.
22. Cardella JF , Castaneda-Zuniga WR, Hunter D, Young A, Amplatz K. Angiographic and interventional ra- diologic considerations in liver transplantation. AJR 1986; 146:143-153.
23. Rossi AR, Pozniak MA, Zarvan NP. Upper inferior vena caval anasto- motic stenosis in liver transplant recipients: Doppler US diagnosis. Radiology 1993; 187:387-389.
24. Entwisle KG, Watkinson AF', Hib- bert J , Adam A. The use of the Wallstent endovascular prosthesis in the treatment of malignant infe- rior vena cava obstruction. Clin Ra- diol 1995; 50:310-313.
25. Charnsangavej C, Carrasco CH, Wallace S, et al. Stenosis of the vena cava: preliminary assessment of treatment with expandable me- tallic stents. Radiology 1986; 161: 295-298.
26. Furui S, Sawada S, Irie T, et al. Hepatic inferior vena cava obstruc- tion: treatment of two types with Gianturco expandable metallic stents (see comments). Radiology 1990; 176:665-670.
Copyright © 2022 FDOKUMEN




















