Posterior Lumbar Vein Off the Retrohepatic Inferior Vena Cava: A Novel Anatomical Variant With...
6
Posterior Lumbar Vein Off the Retrohepatic Inferior Vena Cava: A Novel Anatomical Variant With Surgical Implications Ammara Abbasi, Timothy V. Johnson, Renee Kleris, Kai Ying, Michael Y. Bonner, Shishir K. Maithel, David A. Kooby, Fray F. Marshall and Viraj A. Master From the Departments of Urology (AA, TVJ, RK, KY, MYB, FFM, VAM) and Surgery (SKM, DAK) and Winship Cancer Institute (SKM, VAM), Emory University, Atlanta, Georgia Abbreviation and Acronym IVC inferior vena cava Submitted for publication March 23, 2011. Purpose: Resection of tumors involving the inferior vena cava requires vascular control of posteriorly draining lumbar veins to ensure a bloodless field. Surgical texts and atlases assert that lumbar veins do not insert into the inferior vena cava superior to the renal hilum. However, at our institution we have encoun- tered patients undergoing inferior vena cava tumor thrombectomy who have a posterior lumbar vein cephalad to the renal veins. Since this represents an unrecognized source of hemorrhage, we investigated the frequency of a superior lumbar vein in cadaveric dissection. Materials and Methods: Retroperitoneal cadaveric dissection of the inferior vena cava was done to assess the frequency of a lumbar vein draining into the inferior vena cava cephalad to the renal veins. Results: Of the 49 cadaveric dissections performed 19 (38.8%) showed a single posterior lumbar vein between the diaphragm and the renal hilum. Of these 19 cadavers 15 (78.9%) were male. This vein was located an average SD of 7.4 0.6 cm cephalad to the right renal vein and it was 3.7 1.6 cm in diameter. In all cadavers this vein inserted within 30 degrees to the left or right of the posterior (also termed dorsal) aspect of the inferior vena cava. Conclusions: The identification of a lumbar vein between the renal hilum and the diaphragm represents an important anatomical variant that occurs in a significant percent of individuals. Surgeons will benefit from the knowledge of this variant of inferior vena cava vasculature and should anticipate the presence of this vein to prevent unnecessary morbidity and mortality secondary to unex- pected hemorrhage, particularly in male patients. Key Words: kidney; cava, inferior vena; blood supply; lumbosacral region; dissection TUMORS arising from the IVC are rare. 1 However, cancer, such as renal cell, adrenocortical and hepatocellu- lar carcinoma, can also have exten- sion of tumor thrombus into the IVC and rarely into the right atrium. 1–3 Complete vascular control of the IVC is needed to achieve a bloodless field so that tumor excision occurs under direct visualization in a safe, expedi- ent manner. 3–5 This necessitates proxi- mal and distal occlusion of the IVC with Rummel tourniquets or vascular clamps. All feeding tributary vessels to the IVC within the operative field must also be controlled. More extensive tu- mor spread cephalad may require the exclusion of hepatic venous drainage via direct control or suprahepatic IVC occlusion combined with a Pringle- type maneuver. 6,7 Incomplete vascu- 296 www.jurology.com 0022-5347/12/1871-0296/0 Vol. 187, 296-301, January 2012 THE JOURNAL OF UROLOGY ® Printed in U.S.A. © 2012 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH,INC. DOI:10.1016/j.juro.2011.09.009
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Posterior Lumbar Vein Off the Retrohepatic Inferior Vena Cava: A Novel Anatomical Variant With...

Posterior Lumbar Vein Off the Retrohepatic Inferior Vena Cava:A Novel Anatomical Variant With Surgical Implications
Ammara Abbasi, Timothy V. Johnson, Renee Kleris, Kai Ying, Michael Y. Bonner,Shishir K. Maithel, David A. Kooby, Fray F. Marshall and Viraj A. MasterFrom the Departments of Urology (AA, TVJ, RK, KY, MYB, FFM, VAM) and Surgery (SKM, DAK) and Winship Cancer Institute (SKM, VAM),Emory University, Atlanta, Georgia
Abbreviation
and Acronym
IVC � inferior vena cava
Submitted for publication March 23, 2011.
Purpose: Resection of tumors involving the inferior vena cava requires vascularcontrol of posteriorly draining lumbar veins to ensure a bloodless field. Surgicaltexts and atlases assert that lumbar veins do not insert into the inferior venacava superior to the renal hilum. However, at our institution we have encoun-tered patients undergoing inferior vena cava tumor thrombectomy who have aposterior lumbar vein cephalad to the renal veins. Since this represents anunrecognized source of hemorrhage, we investigated the frequency of a superiorlumbar vein in cadaveric dissection.Materials and Methods: Retroperitoneal cadaveric dissection of the inferior venacava was done to assess the frequency of a lumbar vein draining into the inferiorvena cava cephalad to the renal veins.Results: Of the 49 cadaveric dissections performed 19 (38.8%) showed a singleposterior lumbar vein between the diaphragm and the renal hilum. Of these 19cadavers 15 (78.9%) were male. This vein was located an average � SD of 7.4 �0.6 cm cephalad to the right renal vein and it was 3.7 � 1.6 cm in diameter. In allcadavers this vein inserted within 30 degrees to the left or right of the posterior(also termed dorsal) aspect of the inferior vena cava.Conclusions: The identification of a lumbar vein between the renal hilum andthe diaphragm represents an important anatomical variant that occurs in asignificant percent of individuals. Surgeons will benefit from the knowledge ofthis variant of inferior vena cava vasculature and should anticipate the presenceof this vein to prevent unnecessary morbidity and mortality secondary to unex-pected hemorrhage, particularly in male patients.
Key Words: kidney; cava, inferior vena; blood supply;
lumbosacral region; dissection296 www.jurology.com
TUMORS arising from the IVC arerare.1 However, cancer, such as renalcell, adrenocortical and hepatocellu-lar carcinoma, can also have exten-sion of tumor thrombus into the IVCand rarely into the right atrium.1–3
Complete vascular control of the IVCis needed to achieve a bloodless fieldso that tumor excision occurs underdirect visualization in a safe, expedi-
ent manner.3–5 This necessitates proxi-0022-5347/12/1871-0296/0THE JOURNAL OF UROLOGY®
© 2012 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RES
mal and distal occlusion of the IVCwith Rummel tourniquets or vascularclamps.
All feeding tributary vessels to theIVC within the operative field mustalso be controlled. More extensive tu-mor spread cephalad may require theexclusion of hepatic venous drainagevia direct control or suprahepatic IVCocclusion combined with a Pringle-
type maneuver.6,7 Incomplete vascu-Vol. 187, 296-301, January 2012Printed in U.S.A.
EARCH, INC. DOI:10.1016/j.juro.2011.09.009

POSTERIOR LUMBAR VEIN OFF RETROHEPATIC INFERIOR VENA CAVA AND SURGICAL IMPLICATIONS 297
lar control may lead to substantial hemorrhage,which can limit visibility, compromise complete tu-mor excision and most importantly increase the riskto the patient with a threat of exsanguination.
Operations on the IVC typically necessitate con-trol of the lumbar veins. Surgical and anatomicaltexts describe lumbar veins as paired vessels thattravel anterior to the spinous process and drain thevertebrae and muscles of the back.8–10 Lumbarveins drain posterior into the IVC and connect theazygous and hemiazygous system to the IVC.10–12
Typically there are 4 or 5 paired lumbar veins andtheir termination can vary, especially for the firstand second lumbar veins.11 The first 2 lumbar veinscan be connected to the IVC, to the ascending lum-bar vein, to lumbar azygous veins or to eachother.11,13 Usually the first lumbar vein does notdrain into the IVC directly but rather angles down-ward to feed into the second lumbar vein. The thirdand fourth lumbar veins are much more predictableand typically drain into the IVC as paired struc-tures.11,13 The fifth lumbar vein commonly ends inthe iliolumbar vein.8,13 Sources assert that theselumbar veins exist only below the renal hilum andthere are no posteriorly located tributaries fromthe insertion of the renal veins to the hepaticveins.8,11,14
METHODS
This study obtained exemption from review by the EmoryUniversity institutional review board. Cadaveric dissec-tions were done at Emory University, Mercer UniversitySchool of Medicine, Medical College of Georgia, the Geor-gia State Physician Assistant Anatomy Department andMorehouse School of Medicine. Cadavers without an in-tact inferior vena cava from the renal hilum to the hepaticconfluence due to prior dissection were excluded fromstudy. Cause of death was not an exclusion criterion.
Anatomical Dissection
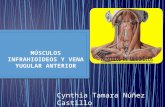
Dissection of the IVC from the renal hilum to the hepaticvein confluence was done in systematic fashion. The venacava was opened anterior with a longitudinal venotomyfrom below the renal veins extending cephalad to thehepatic vein confluence. The ostia for the renal and theright adrenal veins were identified and marked. The pos-terior IVC was carefully inspected for an ostium or anopening. When an ostium was detected, it was bluntlyprobed to confirm that there was an obvious vascularchannel (figs. 1 and 2). When a posterior ostium wasidentified, the IVC was completely dissected off the ante-rior spinous ligament and crus of the diaphragm to clearlyidentify the tributary vein into the posterior vena cava.Photographs were taken of the dissections except at 1institution, which did not allow photography of cadaveric
specimens.MeasurementsIf an ostium was present, its diameter, radial site anddistance from the right renal vein ostium were recorded.Radial site positions were numbered in clockwise fashionwith the 12 o’clock position at the midline anterior IVCand the 6 o’clock position at the midline posterior IVC. Theexact radial position of the lumbar vein was not recordedin 3 of the initial cadavers in which it was identified.Instead it was only noted that it was located posterior. Thegender of each cadaveric specimen was also recorded. Themean � SD was used as a descriptive measure to definevariation among cases.
RESULTS
A total of 49 cadavers with an intact IVC wereexamined, of which 29 (59%) were male. Of the ca-davers 19 (38.8%) showed a variant unpaired lum-bar vein that drained posterior into the IVC ceph-alad to the renal hilum. Of the 19 cadavers with theanomaly 15 (78.9%) were male. The variant lumbarvein was identified in 20% of females and 52% ofmales. Mean diameter of the variant vein ostiumwas 3.7 � 1.6 mm (maximum 7). Mean distance ofthe variant lumbar vein from the right renal veinwas 7.4 � 0.6 cm. The mean radial site of the variantlumbar vein was between the 6 and 7 o’clock posi-tions.
DISCUSSION
General surgery, surgical oncology, liver transplan-tation and urology texts describe lumbar veins as
Figure 1
dorsal tributaries from the lumbar muscles and skin

igure 2
POSTERIOR LUMBAR VEIN OFF RETROHEPATIC INFERIOR VENA CAVA AND SURGICAL IMPLICATIONS298
that join with the azygous and hemiazygous sys-tems.10,15–18 However, the texts make no mention ofvenous anomalies that drain into the posterior IVCsuperior to the renal vein ostia. In our practice wehave occasionally observed substantial bleeding af-ter opening the suprarenal IVC despite having prox-imal and distal control of the IVC, suggesting suchan anomalous draining posterior lumbar vein. Sincethis can have a profound impact on the operation, weperformed this cadaveric study to assess the fre-quency of this anomaly.
Variant IVC Anatomy
We identified a posteriorly draining lumbar veinabove the renal hilum in 30.9% of cadaveric spec-imens. This unpaired vein was located an averageof 7.4 cm cephalad to the right renal vein betweenthe radial sites at the 6 and 7 o’clock positions. Ithad an average ostial diameter of 3.7 mm. Al-though we have occasionally noted this vein in theoperating room, the prevalence of this suprarenalvein in anatomical dissections was much higherthan anticipated. In fact, it appears that this vari-ant lumbar vein occurs substantially more oftenthan other commonly described anomalies of theIVC, namely 0.69% for a left IVC, 1.03% to 3.0%for a duplicated IVC and 0.8% for azygous vein
F
continuation.19,20 Thus, we believe that this ve-
nous tributary should be considered a variant ofnormal anatomy rather than merely as an occa-sionally encountered anomaly. There also appearsto be a male predominance of this variant veinsince 52% of males but only 20% of females hadthe variant lumbar vein.
Variant Lumbar Vein Distinctive Features
Certain characteristics attest to the unique natureof this variant posterior lumbar vein compared toother lumbar veins. 1) The variant vein that wedescribe is unpaired. Although different configura-tions of infrarenal lumbar veins have been de-scribed, generally most texts describe them as sym-metrical and paired structures.11,12,21 2) Pastcadaveric studies with retroperitoneal dissection re-vealed a predominance of lumbar veins on the leftand right sides of the IVC, although this variantvein generally has a central posterior location.11,13,21
Lumbar Vein Historical Studies
Termination of lumbar veins into the IVC were de-scribed as early as 1543 in the seminal work byVesalius.13 In 1749 Winslow further described vari-ations of lumbar veins22 but they remained unclas-sified until the series by Seib centuries later.13 An-son23 and Davis13 et al performed hundreds of
thorough dissections that focused on the vertebral
POSTERIOR LUMBAR VEIN OFF RETROHEPATIC INFERIOR VENA CAVA AND SURGICAL IMPLICATIONS 299
vasculature and described the contributions of otheranatomists to the understanding of lumbar venousanatomy. Despite this we still lacked an accuratedescription of lumbar vein anatomy.11 More recentlyurologists who performed more than 2,000 retroper-itoneal dissections for testicular carcinoma formallydescribed the distribution and site of lumbar veins,and documented the specific frequency of commonanomalies.24,25
Most studies of the anatomy of the retrohepaticIVC have focused on its anterior aspect, likely sincethis area is most relevant to mobilizing the liverfrom the IVC.11,15,16,26,27 To our knowledge no grouphas carefully examined the posterior aspect of theretrohepatic IVC to specifically describe posteriorlydraining lumbar veins above the renal hilum. Thisvoid may be due to the scarcity of tumors involvingthe vena cava and procedures that necessitate com-plete vascular control of the retrohepatic IVC.1,3,4 Infact, Donohue et al omitted the suprarenal compo-nent from retroperitoneal dissections describing IVCanatomy, likely since that area is not usually in-volved with metastatic disease.24,25,28
The method by which cadaveric dissections aredone may partly have a role in the persistent ambi-guity of posterior IVC anatomy above the renal hi-lum. Posterior longitudinal venotomy is often madewhen investigating the anterior aspect to assess he-patic vein drainage into the IVC.26 Also, instructionduring medical school anatomy courses usually in-volves transection of the IVC just below the edge ofthe liver.29 These maneuvers preclude adequate ex-amination of the posterior aspect of the IVC. In fact,many cadavers that we wished to evaluate for thisstudy were not eligible due to prior transection ofthe vena cava.
Variant Lumbar Vein
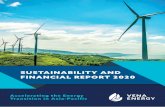
Embryogenesis. A deeper understanding of IVCembryogenesis offers an explanation for a variant
Figure 3
posterior lumber vein. IVC formation is a complexprocess that occurs during the 6th to 8th week ofgestation. It involves a balance of proliferation, for-mation of new venous connections and regressionamong 3 paired embryonic veins, including the pos-terior cardinal, the supracardinal and the subcardi-nal veins.8,13,20,30 The suprarenal IVC, where thevariant vein is located, is divided into 2 distinctembryological structures, that is the pars hepaticaand the pars renalis. The pars hepatica forms themore cephalad IVC and is embryologically derivedfrom a connection between the subcardinal andomphalomesenteric veins.30 The pars renalis, whichis caudal to the pars hepatica, lies just above therenal hilum and is derived from the subcardinalveins.30 Joining the subcardinal veins are supracar-dinal veins that eventually regress to form pairedlumbar veins below the renal hilum, which are dis-tinct from the azygous and hemiazygous venous sys-tems. It is conceivable that the variant vein resultsfrom a persistent suprarenal connection between asupracardinal and a subcardinal vein (fig. 3).
Clinical implications. Hemorrhage from an unrec-ognized lumbar vein can be life threatening.12,21
This situation can be particularly difficult to controlsince attempts to expose and control the bleedingmay exacerbate a tear in the thin walled vein andcause enlargement, avulsion or extension into theIVC.21 Although the advent of improved preopera-tive imaging facilitates the recognition of vascularanomalies before surgery, there are numerous in-stances in which this vein may be underappreciatedor not visualized on cross-sectional imaging. Thus,knowledge of the potential presence of this variantposterior lumbar vein when operating on the su-prarenal IVC will be of tremendous benefit to theoperating surgeon and the patient. Figure 4 showsthe variant posterior lumbar vein in dorsoventraland side views.

igure 4
POSTERIOR LUMBAR VEIN OFF RETROHEPATIC INFERIOR VENA CAVA AND SURGICAL IMPLICATIONS300
We hope that the description of this variant lum-bar vein enables others to successfully avoid majorbleeding by early vascular control of this variantvein with circumferential mobilization of the IVC orwith intraluminal control using a Fogarty ballooncatheter. This anatomical variant should have par-ticular significance for surgeons who perform proce-dures in which the suprarenal IVC must be com-pletely isolated and controlled.
Study Limitations
The formaldehyde preservation routinely used forcadavers can alter the dimensions of vessels andbody tissue. Variant lumbar vein diameter, distancefrom the renal hilum and radial site in a living
F
patient may possibly differ slightly from the mea-
REFERENCES
tumor thrombus in the renal and inferior vena Ann Surg 2006; 244: 80.
surements reported in our study. However, we havefound that the measurements correlate well withour intraoperative findings.
CONCLUSIONS
An unpaired lumbar vein draining into the posteriorsuprarenal IVC appears to be present in approxi-mately 39% of individuals with a predilection inmales. It is prudent for surgeons operating on ornear the suprarenal IVC to be aware of this variantlumbar vein to prevent the morbidity and mortalityof substantial bleeding. Further anatomical, embry-ological and radiological studies should be done tobetter characterize this variant posterior lumbar
vein.1. Aguilar IC, Benavente VA, Pow-Sang MR et al:Leiomyosarcoma of the inferior vena cava; a casereport and review of the literature. Urol Oncol2005; 23: 22.
2. Marshall VF, Middleton RG, Holswade GR et al:Surgery for renal cell carcinoma in the vena cava.J Urol 1970; 103: 414.
3. Ciancio G, Livingstone AS and Soloway M: Sur-gical management of renal cell carcinoma with
cava: the University of Miami experience in usingliver transplantation techniques. Eur Urol 2007;51: 988.
4. Zini L, Haulon S, Decoence C et al: Renal cellcarcinoma associated with tumor thrombus in theinferior vena cava: surgical strategies. Ann VascSurg 2005; 19: 552.
5. Azoulay D, Andeani P, Maggi U et al: Combinedliver resection and reconstruction of the supra-renal vena cava: the Paul Brousse experience.
6. Delis SG, Madariaga J and Ciancio G: Combinesliver and inferior vena cava resection of hepaticmalignancy. J Surg Oncol 2007; 96: 258.
7. Ho KJ, Owens CD, Ledbetter SM et al: Renalvenous diversion: an unusual treatment for renalvein thrombosis. J Vasc Surg 2006; 43: 1283.
8. Gray H: Anatomy: Descriptive and Surgical. Lon-don: John W. Parker and Son 1858.
9. Hollinstead W: Anatomy for Surgeons. New York:
Harper and Row 1971.
POSTERIOR LUMBAR VEIN OFF RETROHEPATIC INFERIOR VENA CAVA AND SURGICAL IMPLICATIONS 301
10. Moore K, Dalley A and Agur A: Clinically OrientedAnatomy, 6th ed. Philadelphia: Lippincott Williams &Wilkins 2010.
11. Baniel J, Foster RS and Donohue JP: Surgicalanatomy of the lumbar vessels: implications forretroperitoneal surgery. J Urol 1995; 153: 1422.
12. Wein AJ, Kavoussi LR, Novick AC et al: Camp-bell-Walsh Urology, 9th ed. Philadelphia: Saun-ders Elsevier 2007.
13. Davis RA, Milloy FJ and Anson BJ: Lumbar, renal,and associated parietal and visceral veins basedupon a study of 100 specimens. Surg GynecolObstet 1958; 107: 1.
14. Agur A and Dalley A: Atlas of Anatomy. Balti-more: Lippincott Williams & Wilkins 2005.
15. Duty B and Daneshmand S: Venous resection inurological surgery. J Urol 2008; 180: 2338.
16. Gaujoux S, Douard R, Ettorre GM et al: Liverhanging maneuver: an anatomic and clinical re-view. Ann Surg 2007; 73: 1193.
17. Woodburne R and Burkel W: Essentials of HumanAnatomy. New York: Oxford University Press
1988.18. Stranding S: Gray’s Anatomy: The AnatomicalBasis of Clinical Practice. Edinburgh: ElsevierChurchill Livingstone 2005.
19. Ueda J, Hara K, Kobayashi Y et al: Anomaly ofthe inferior vena cava observed by CT. ComputRadiol 1983; 7: 145.
20. Downey RS, Sicard GA and Anderson CB: Majorretroperitoneal venous anomalies: surgical con-siderations. Surgery 1990; 107: 359.
21. Miles RM, Flowers BF, Parsons HL et al: Somesurgical implications of the anatomy of the cava-iliofemoral system. Ann Surg 1973; 177: 740.
22. Winslow JB: An Anatomical Exposition of theStructure of the Human Body, 3rd ed. London1749.
23. Anson BJ, Cauldwell EW, Pick J et al: The anat-omy of the pararenal system of veins, with com-ments on the renal arteries. J Urol 1948; 60: 714.
24. Donohue JP, Thornhill JA, Foster RS et al: Vas-cular considerations in postchemotherapy retro-peritoneal lymph-node dissection: part II. World
J Urol 1994; 12: 187.25. Donohue JP: Retroperitoneal lymphadenectomy:the anterior approach including bilateral suprare-nal-hilar dissection. Urol Clin North Am 1977; 4:509.
26. Camargo AM, Teixeira GG and Ortale JR: Anat-omy of the ostia venae hepaticae and the retrohepatic segment of the inferior vena cava. J Anat1989; 188: 59.
27. Banner RL and Brasfield RD: Surgical anatomy ofthe hepatic veins. Cancer 1973; 11: 22.
28. Donohue JP: Evolution of retroperitoneal lymph-adenectomy (RPLND) in the management of non-seminomatous testicular cancer (NSGCT). UrolOncol 1995; 21: 129.
29. Clemente C: Clemente’s Anatomy Dissector, 2nded. Philadelphia: Lippincott Williams & Wilkins2007.
30. Mathews R, Smith PA, Fishman EK et al: Anom-alies of the inferior vena cava and renal reins:embryological and surgical consideration. Urology
1999; 53: 873.