Rate Modulation by Arm Movements of the Respiratory Dependent Rate Responsive Pacemaker
10
Rate Modulation by Arm Movements of the Respiratory Dependent Rate Responsive Pacemaker CHU-PAK LAU, DON RITCHE,* GHAZWAN S. BUTROUS, DAVID E. WARD, and A. JOHN CAMM From the Department of Cardiological Sciences, St. George's Hospital Medical School, Blackshaw Road, London SW17 ORE, United Kingdom LAU, C-P, ET AL.: Rate modulation by arm movements of the respriratory-dependent rate responsive pacemaker. The rate response to arm movements o/(he respiratory dependent rate responsive pacemaker {RDP3, Biotec) was assessed in four patients implanted with this pacemaker. The pacemaker was impJanted in the left prepectoraJ region and the auxiliary impedance measuring electrode positioned subcutaneousiy over the right second intercostal space with its tip lateral to the mid-ciavicular line. The lower rate of the pacemaker was programmed to 75 bpm. While holding the breath, swinging arm movements (30 times) resulted in rate acceleration. The peak rate was /aster when the arm on the side of the auxiliary electrode was swung (mean ± SEM, 117 ±8 compared to 130 ±5 bpm, P < 0.5). The mean rate response of the subjects to brie/treadmill exercise (Bruce stage 1) performed with both hands holding the support rails, swinging the right arm only, swinging left arm only and swinging both arms were 108, 140, 135 and 128 bpm respec- tively. Impedance measurement confirmed the significant influence of arm movements on thoracic "im- pedance" changes, which was mainly caused by electrode motion artifacts affecting the two electrode measuring system. This effect was dependent on the relative positions of the impedance measuring elec- trodes (i.e., between the pacemaker casing the auxiliary lead). Subsequently the auxiliary lead of the respiratory pacemaker (MB-1, and Biorate) was implanted in the lower part of the chest on the right sternal edge in another patient. Rate acceleration was only observed when the arm on the side of the pacemaker was swung. As arm movements often accompany physical activities, pacing rate can be affected and should be considered when programming this pacemaker. (PACE, Vol. 11, June 1988] rate responsive pacemaker, respiratory sensing, thoracic impedance Introduction Rossi et al.^ have shown that the change in respiratory rate during exercise is significantly related to the change in heart rate. Futhermore it has also been suggested that this relation is valid in patients with lung diseases,^ The sensing of re- spiratory changes during exercise has been uti- lized in the construction of rate responsive pace- makers.^'^ "Principal Physics Technician, Department of Medical Phys- ics, St. George's Hospital Address for reprints: Chu-pak Lau. MB. Department of Car- diological Sciences. St. George's Hospital Medical School, Blackshaw Road, London SW17 ORE. United Kingdom. Received July 13. 1987; accepted August 25, 1987, The respiratory dependent rate responsive pacemaker (RDP3, MB-1, Biorate, Biotec, Interna- tional, Bologna, Italy) measures respiratory rate by means of an auxiliary lead implanted subcuta- neousiy across the chest. Thoracic impedance is measured by a bipolar electrode configuration, using the pacemaker casing as the active elec- trode and the auxiliary lead as the passive elec- trode.^ Respiratory movement above a program- mable level is detected and the sensed respiratory rate is converted into a pacing rate by a program- mable slope of rate response. The MB-1 is similar to the RDP3 but offers more basic pacemaker pro- grammable features and some telemetry func- tions. Satisfactory rate responses have been claimed, although most of the studies used leg exercises as a means of 744 June 1988 PACE, Vol, 11
Transcript of Rate Modulation by Arm Movements of the Respiratory Dependent Rate Responsive Pacemaker

Rate Modulation by Arm Movementsof the Respiratory Dependent RateResponsive Pacemaker
CHU-PAK LAU, DON RITCHE,* GHAZWAN S. BUTROUS,DAVID E. WARD, and A. JOHN CAMM
From the Department of Cardiological Sciences, St. George's Hospital Medical School,Blackshaw Road, London SW17 ORE, United Kingdom
LAU, C-P, ET AL.: Rate modulation by arm movements of the respriratory-dependent rate responsivepacemaker. The rate response to arm movements o/(he respiratory dependent rate responsive pacemaker{RDP3, Biotec) was assessed in four patients implanted with this pacemaker. The pacemaker was impJantedin the left prepectoraJ region and the auxiliary impedance measuring electrode positioned subcutaneousiyover the right second intercostal space with its tip lateral to the mid-ciavicular line. The lower rate of thepacemaker was programmed to 75 bpm. While holding the breath, swinging arm movements (30 times)resulted in rate acceleration. The peak rate was /aster when the arm on the side of the auxiliary electrodewas swung (mean ± SEM, 117 ±8 compared to 130 ±5 bpm, P < 0.5). The mean rate response of the subjectsto brie/treadmill exercise (Bruce stage 1) performed with both hands holding the support rails, swinging theright arm only, swinging left arm only and swinging both arms were 108, 140, 135 and 128 bpm respec-tively. Impedance measurement confirmed the significant influence of arm movements on thoracic "im-pedance" changes, which was mainly caused by electrode motion artifacts affecting the two electrodemeasuring system. This effect was dependent on the relative positions of the impedance measuring elec-trodes (i.e., between the pacemaker casing the auxiliary lead). Subsequently the auxiliary lead of therespiratory pacemaker (MB-1, and Biorate) was implanted in the lower part of the chest on the right sternaledge in another patient. Rate acceleration was only observed when the arm on the side of the pacemakerwas swung. As arm movements often accompany physical activities, pacing rate can be affected andshould be considered when programming this pacemaker. (PACE, Vol. 11, June 1988]
rate responsive pacemaker, respiratory sensing, thoracic impedance
Introduction
Rossi et al.̂ have shown that the change inrespiratory rate during exercise is significantlyrelated to the change in heart rate. Futhermore ithas also been suggested that this relation is validin patients with lung diseases,^ The sensing of re-spiratory changes during exercise has been uti-lized in the construction of rate responsive pace-makers.^'^
"Principal Physics Technician, Department of Medical Phys-ics, St. George's Hospital
Address for reprints: Chu-pak Lau. MB. Department of Car-diological Sciences. St. George's Hospital Medical School,Blackshaw Road, London SW17 ORE. United Kingdom.
Received July 13. 1987; accepted August 25, 1987,
The respiratory dependent rate responsivepacemaker (RDP3, MB-1, Biorate, Biotec, Interna-tional, Bologna, Italy) measures respiratory rateby means of an auxiliary lead implanted subcuta-neousiy across the chest. Thoracic impedance ismeasured by a bipolar electrode configuration,using the pacemaker casing as the active elec-trode and the auxiliary lead as the passive elec-trode.^ Respiratory movement above a program-mable level is detected and the sensed respiratoryrate is converted into a pacing rate by a program-mable slope of rate response. The MB-1 is similarto the RDP3 but offers more basic pacemaker pro-grammable features and some telemetry func-tions. Satisfactory rate responses have beenclaimed, although most of the studies used legexercises as a means of
744 June 1988 PACE, Vol, 11
RESPIRATORY-DEPENDENT RATE RESPONSIVE PACEMAKER
In a preliminary report, Webb et al,^ baveshown tbat rate acceleration of patients with thispacemaker can be caused by arm movements.However, it is not clear wbether tbis effect wasmediated by respiratory cbanges during arm ex-ercise. We bave investigated this phenomenon infive patients with this pacemaker and thoracicimpedance cbanges were also measured in a nor-mal subject during arm movements.
Patient and Methods
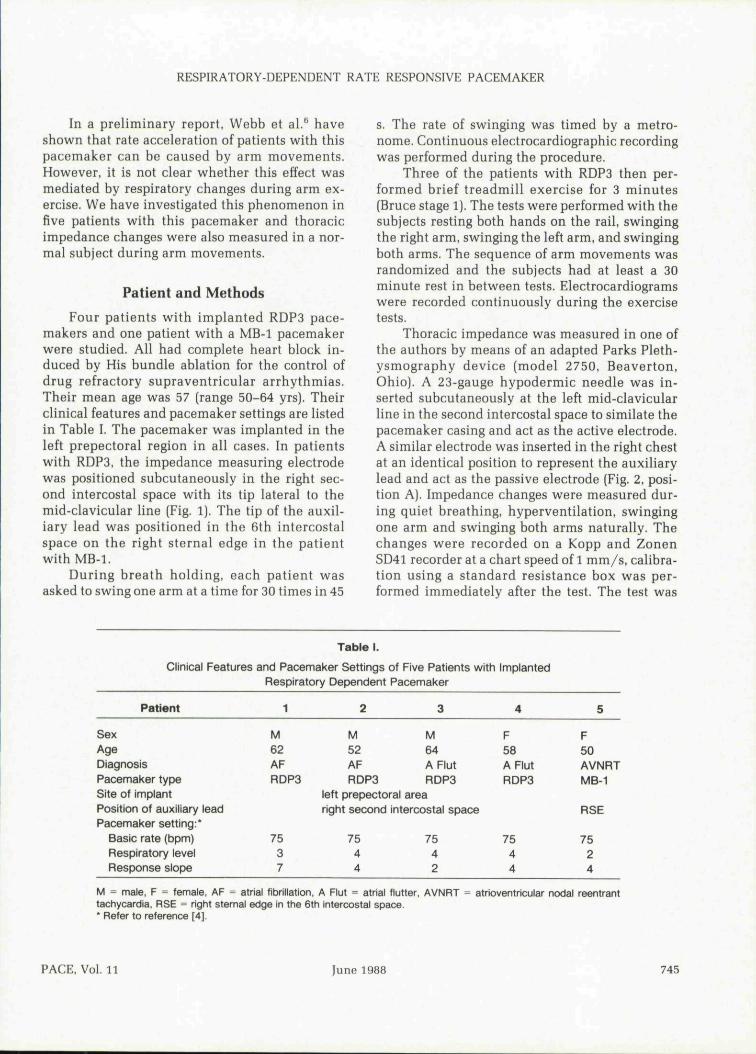
Four patients witb implanted RDP3 pace-makers and one patient witb a MB-1 pacemakerwere studied. All had complete heart block in-duced by His bundle ablation for the control ofdrug refractory supraventricular arrhytbmias.Tbeir mean age was 57 (range 50-64 yrs). Theirclinical features and pacemaker settings are listedin Table I. Tbe pacemaker was implanted in tbeleft prepectoral region in all cases. In patientswith RDP3, the impedance measuring electrodewas positioned subcutaneously in tbe right sec-ond intercostal space with its tip lateral to tbemid-clavicular line (Fig, 1). Tbe tip of tbe auxil-iary lead was positioned in the 6tb intercostalspace on tbe right sternal edge in tbe patientwith MB-1.
During breath holding, eacb patient wasasked to swing one arm at a time for 30 times in 45
s. Tbe rate of swinging was timed by a metro-nome. Continuous electrocardiograpbic recordingwas performed during the procedure.
Tbree of the patients witb RDP3 tben per-formed brief treadmill exercise for 3 minutes(Bruce stage 1). Tbe tests were performed witb tbesubjects resting both hands on the rail, swingingthe rigbt arm, swinging the left arm, and swingingbotb arms. Tbe sequence of arm movements wasrandomized and tbe subjects had at least a 30minute rest in between tests. Electrocardiogramswere recorded continuously during tbe exercisetests.
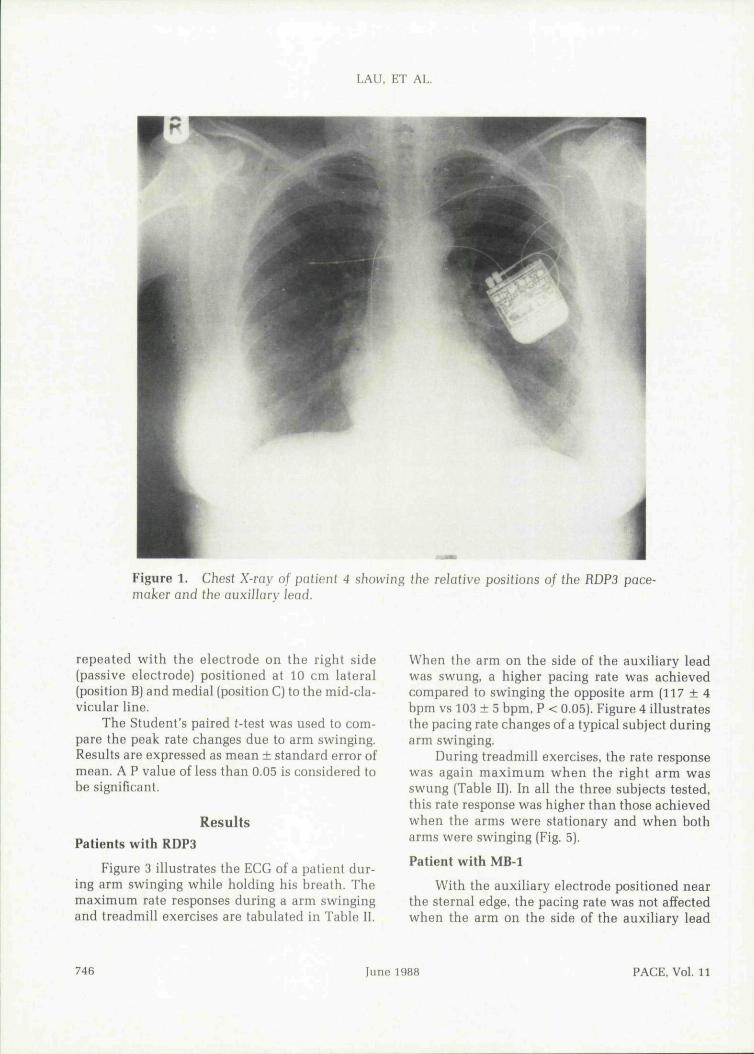
Thoracic impedance was measured in one ofthe authors by means of an adapted Parks Pletb-ysmograpby device [model 2750, Beaverton,Ohio), A 23-gauge hypodermic needle was in-serted subcutaneously at tbe left mid-clavicularline in tbe second intercostal space to similate tbepacemaker casing and act as tbe active electrode.A similar electrode was inserted in the right cbestat an identical position to represent the auxiliarylead and act as the passive electrode (Fig. 2, posi-tion A). Impedance cbanges were measured dur-ing quiet breathing, byperventilation, swingingone arm and swinging botb arms naturally. Thechanges were recorded on a Kopp and ZonenSD41 recorder at a chart speed of 1 mm/s, calibra-tion using a standard resistance box was per-formed immediately after the test. Tbe test was
Table I.
Clinical Features and Pacemaker Settings of Five Patients with ImplantedRespiratory Dependent Pacemaker
Patient
SexAgeDiagnosisPacemaker typeSite of implantPosition of auxiliary leadPacemaker setting:*
Basic rate (bpm)Respiratory levelResponse slope
1
M62AFRDP3
7537
2
M52AFRDP3
left prepectoral
3
M64AFlutRDP3
arearight second intercostal space
7544
7542
4
F58AFlutRDP3
7544
5
F50AVNRTMB-1
RSE
7524
M = male, F = female, AF = atrial fibrillation, A Flut = atrial flutter, AVNRT = atrioventricular nodal reentranttachycardia. RSE = right sternal edge in the 6th intercostal space.' Refer to reference [4],
PACE, Vol. 11 June 1988 745
LAU, ET AL,
Figure 1. ChesI X-ray 0/ pnfjenf 4 showing (he relative positions 0/ the RDP3 pace-maker and the auxiliary lead.
repeated with the electrode on the right side(passive electrode) positioned at 10 cm lateral(position B) and medial (position C) to the mid-cla-vicular line.
The Student's paired t-test was used to com-pare the peak rate changes due to arm swinging.Results are expressed as mean ± standard error ofmean. A P value of less than 0.05 is considered tobe significant.
ResultsPatients with RDP3
Figure 3 illustrates the ECG of a patient dur-ing arm swinging while holding his breath. Themaximum rate responses during a arm swingingand treadmill exercises are tabulated in Table II.
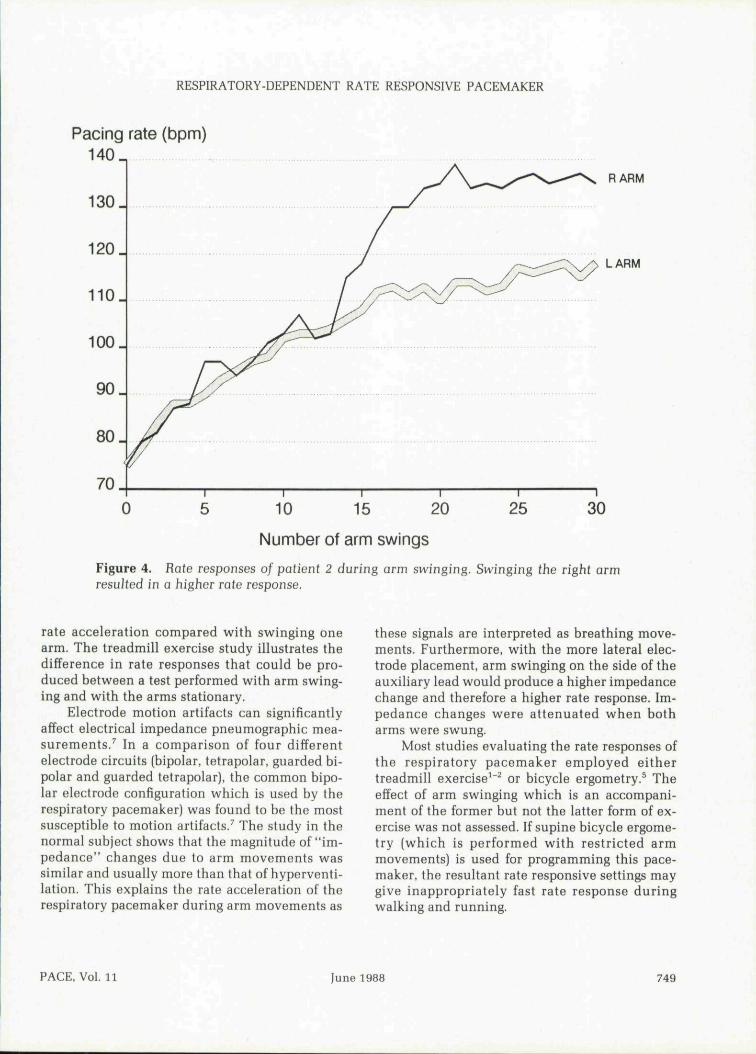
When the arm on the side of the auxiliary leadwas swung, a higher pacing rate was achievedcompared to swinging the opposite arm (117 ± 4bpm vs 103 ± 5 bpm, P < 0.05). Figure 4 illustratesthe pacing rate changes of a typical subject duringarm swinging.
During treadmill exercises, the rate responsewas again maximum when the right arm wasswung (Table II). In all the three subjects tested,this rate response was higher than those achievedwhen the arms were stationary and when botharms were swinging (Fig. 5).
Patient with MB-1
With the auxiliary electrode positioned nearthe sternal edge, the pacing rate was not affectedwhen the arm on the side of the auxiliary lead
746 June 1988 PACE, Vol. 11
RESPIRATORY-DEPENDENT RATE RESPONSIVE PACEMAKER
Figure 2. Electrode position during impedance measurement of the normal subject. Anactive electrode X was inserted at the left second space in the mid-ciavicuJar line tosimiJate the pacemaker, A second electrode (passive) was inserted at the right secondspace in the mid-cJavicuIar line (position A). This electrode was later moved to positionB and position C, respectively 10 cm lateral and medial to position A for repeat pedancerecording.
was swung. Instead swinging the arm on the sideof the pacemaker gave a pacing rate of 135 hpm.
Study on the Normal Subject
The impedance changes recorded in the nor-mal subject are summarized in Figure 6. In posi-tion A (with roughly symmetrical electrode place-ment), arm swinging of either arm introducednearly identical impedance changes. This washigher than the changes during hyperventilationand when both arms were swung. With the pas-sive electrode inserted more laterally (position B),swinging the right arm produced higher imped-ance changes than those achieved when the leftarm or both arms were swung. With a medialelectrode placement (position C). the highest im-
pedance changes were achieved when the leftarm was swung. In all cases, the impedancechanges recorded were similar or more than thechanges induced by hyperventilation.
DiscussionThis study demonstrates that rate responses
of the respiratory dependent pacemaker can beprofoundly affected by arm movements. Therewas a laterality of the effect of arm movementson the rate responses. With the electrode place-ment in patients with RDP3, a higher rate re-sponse was produced when the arm on the sameside as the auxiliary lead was swung. The con-verse occurred in the patient with MB-1 wherethe auxiliary lead was positioned in the right
PACE, Vol. n June 1988 747

75 bpm 1 1 5 b p m
- • [
• ! • • • i 1 '
..iXa..X.I._.Jj-I..._.a!' • 11 "̂ r T"!
RDPiEP
Figure 3. ECG recording of patient 2 during left arm swinging while holding his breath.The electrode corresponding to V2 and V3 were placed respectively on Ihe right fflA) andleft (LA) arm. Swinging arm movements (numbered] were recorded hy the /luctuafion inthe baseline of the LA recording.
sternal edge. Webb et al.^ have reported rate ac-celeration durng arm swinging, which was morewhen the arm on the side of the pacemaker was
swung. However, the placement of the auxiliaryleads in their patients were not specified. Wehave shown that swinging both arms reduced the
Table II.
Maximum Rate Responses (bpm) of Patients with RDP3 to Arm Swinging and Treadmill Exercises.Patient 1 Did Not Perform Treadmill Exercise as he was Suffering from an Infection of the
Pacemaker Pocket at the Time of the Study. The Pacemaker was Subsequently Removed
Patient
Arm swinging while holding their breaths:Right armLeft arm
Treadmill exercises:1. Both hands on rails2. Swing right arm3. Swinging left arm4. Swinging both arms
1
11098
————
2
139115
104140134118
3
115103
104140132130
4
10297
117140140135
Mean
117103
108140135128
748 June 1988 PACE, Vol. 11
RESPIRATORY-DEPENDENT RATE RESPONSIVE PACEMAKER
Pacing rate (bpm)140^
130 _
120.
100 _
90 _
80 _
70
RARM
LARM
0 10 15 20
Number of arm swings
25 30
Figure 4. Rate responses of patient 2 during arm swinging. Swinging the right armresulted in a higher rafe response.
rate acceleration compared with swinging onearm. The treadmill exercise study illustrates thedifference in rate responses that could be pro-duced between a test performed with arm swing-ing and with the arms stationary.
Electrode motion artifacts can significantlyaffect electrical impedance pneumographic mea-surements,^ In a comparison of four differentelectrode circuits (bipolar, tetrapolar, guarded bi-polar and guarded tetrapolar), the common bipo-lar electrode configuration which is used by therespiratory pacemaker) was found to be the mostsusceptible to motion artifacts.^ The study in thenormal subject shows that the magnitude of "im-pedance" changes due to arm movements wassimilar and usually more than that of hyperventi-lation. This explains the rate acceleration of therespiratory pacemaker during arm movements as
these signals are interpreted as breathing move-ments. Furthermore, with the more lateral elec-trode placement, arm swinging on the side of theauxiliary lead would produce a higher impedancechange and therefore a higher rate response. Im-pedance changes were attenuated when botharms were swung.
Most studies evaluating the rate responses ofthe respiratory pacemaker employed eithertreadmill exercise^^^ or bicycle ergometry.^ Theeffect of arm swinging which is an accompani-ment of the former but not the latter form of ex-ercise was not assessed. If supine bicycle ergome-try (which is performed with restricted armmovements) is used for programming this pace-maker, the resultant rate responsive settings maygive inappropriately fast rate response duringwalking and running.
PACE, Vol. 11 June 1988 749

LAU. ET AL.
Pacing rate (bpm)
140 ,
130.
120.
110.
100.
90_
80 _
70
Swinging RA
Swinging LA
ing both
Arms on railing
0.0 0.5 2.5 3.01.0 1.5 2.0Time on treadmill (mins)
Figure 5. Mean rate responses of 3 patients with RDP3 during treadmill exercises. Thehighest rate response was achieved when the right arm was swung, followed by the leftarm, the swinging of both arms and with the hands resting on the support rails. RA= right arm, LA = left arm.
Although the hemodynamic advantages ofrate responsive pacing over constant frequencyventricular pacing is well established,*'^ an idealsensor for physiological demands have not beenestablisbed. The clinically used systems such asthe activity sensing and QT sensing pacemakershave tbeir advantages and limitations.^""'^ Tbelimitations of tbe respiratory pacemakers includethe lack of programmability of tbe RDP3 (whichhas been partially improved in the newer modelMB-1), tbe relatively low correlation between therespiratory and sinus rates, tbe irregularity ofpacing rate wben subjects are exercised above theanaerobic threshold^^ and tbe potential for delete-rious positive feedback in heart rate responseduring tachypnea induced by beart failure. It has
been suggested tbat the response of the respira-tory pacemakers to arm movements may repre-sent a dual sensor system for more physiologicalrate response.^ Although the motion artifact-in-duced impedance changes may improve thespeed of response during exercise like walkingand running, it may lead to inappropriate rateacceleration during arm exercises especially if theexercise involves only one arm. Also it is depen-dent on tbe position of tbe auxiliary lead makingits reliable use difficult.
The use of a larger impedance electrode or atetrapolar recording system may reduce motion-induced artifacts^ but these may make implanta-tion difficult. Recently, intravascular impedancebas been sbown to be a feasible means of measur-
750 June 1988 PACE, Vol. 11

RESPIRATORY-DEPENDENT RATE RESPONSIVE PACEMAKER
Impedance (ohms)2 2 ,
20-
Lateral(B)
Central(A)
Medial(C)
RA LA BA HVFigure 6. Average impedance changes during arm movements at the three electrodepositions. See discussion in text. HA = right arm, LA ^ left arm, BA = swinging botharms, HV ^ hyperventiiation.
ing minute ventilation changes.^ This is expectedto reduce the influence of motion artifacts on tho-racic impedance measurements.
Medical Physics and Clinical Engineering, Royal HallamshireHospital. Sheffield for advice on impedance measurementsand interpretation. The lechnical assistance of Miss S. King-well and Mrs. M. Leigh-Jones of the Technical Unit. St.George's Hospital are gratefully acknowledged.
Acknowiedgments; We wish to express our gratitude toProfessor B.H, Brown and Mr. N.D. Harris of the Department of
References
Rossi P, Plicchi G. Canducci GC, et al. Respiratoryrate as a determinant of optimal pacing rate. InProc Cardiostim. Cardiac Pacing Present and Fu-ture Problems. PACE 1983; 6:502.Rossi P, Plicchi G, Canducci GC, et al. Respirationas a reliable physiological sensor for the control ofcardiac pacing rate. Br Heart I 1985; 51;7.Nappholtz T, Valenta H. Maloney I. et al. Elec-trode configuration for respiratory impedancemeasurement suitable for rate responsive pacing.PACE 1986; 9:960.
4. Biorate RDP3 physician menu. Biotec. 1986.5. Zegelman M, Beyersdorf E, Kreuzer I, et al. Rate
responsive pacemakers: assessment after twoyears. PACE 1986; 9:1005.
6. Webb SC, Lewis LM, Morris-Thurgood fA, et al.Rate responsive pacing: is there already a dualsensor system (abstract). Br Heart I 1987; 57:585.
7. Sahakian AV, Tompkins WI, Webster JG. Elec-trode motion artifacts in electrical impedancepneumography, IEEE Trans Bio-Med Eng 1985;32:448.
PACE, Vol. 11 June 1988 751
LAU. ET AL.
10.
Karloff L Hemodynamic effect of atrial triggeredversus fixed rate pacing at rest and during exer-cise in complete heart block. Acta Med Scand1975; 197:195.Fananapazir E, Maurius R, Bennett DH. Reliabilityof the evoked response in determining the pacedventricular rate and performace of the QT or rateresponsive T(X) pacemaker, PACE 1985; 8:701.Lau CP. Mehta D, Toff W, et al. Limitations of rateresponse of activity sensing rate responsive pacingto different forms of activity, PACE, 1988; 11:141.
11. Mehta D, Lau CP, Davies W, et al. Comparativeevaluation of rate responses between activity andQT sensing rate responsive pacing to different ac-tivities (abstract). PACE 1987; 10:419.
12. Maisch B, Langenfe!d H. Rate adaptive pacing—clinical experience with three different pacingsystems. PACE 1986; 9:997.
13. Rossi P. State of art on rate responsive pacing: aninternational survey. In M Santilli, M Pistolese, AAlliegro (eds): Progress in Clinical Pacing, Rome,1986.
752 June 1988 PACE, Vol. 11