

The Benefit of Pacemaker Therapy in Patients with ... - CiteSeerX
25
DOI: 10.1161/CIRCEP.113.001103 1 The Benefit of Pacemaker Therapy in Patients with Presumed Neurally- Mediated Syncope and Documented Asystole is Greater when Tilt Test is Negative. An Analysis from the Third International Study on Syncope of Uncertain Etiology (ISSUE-3) Running title: Brignole et al.; Pacemaker efficacy and tilt test responses Michele Brignole, MD 1 ; Paolo Donateo, MD 1 ; Marco Tomaino, MD 2 ; Riccardo Massa, MD 3 ; Matteo Iori, MD 4 ; Xulio Beiras, MD 5 ; Angel Moya, MD 6 ; Teresa Kus, MD, PhD 7 ; Jean Claude Deharo, MD 8 ; Silvia Giuli, MSc 9 ; Alessandra Gentili, MSc 9 ; Richard Sutton, DSc 10 on behalf of the International Study on Syncope of Uncertain Etiology 3 (ISSUE-3) Investigators Department of Cardiology, 1 Ospedali del Tigullio, Lavagna; 2 Ospedale di Bolzano, Bolzano; 3 Ospedale SS. Antonio e Biagio e Cesare Arrigo, Alessandria; 4 Arcispedale S. Maria Nuova, Reggio Emilia, Italy; 5 Hospital Xeral de Vigo, Vigo; 6 Hospital Universitario Vall d’Hebron, Barcelona, Spain; 7 Hopital du Sacre-Coeur de Montreal, Montreal; Canada; 8 Hopital La Timone Adultes , Marseille, France; 9 EMEA Regional Clinical Center, Medtronic Clinical Research Institute, Italy; 10 St.Mary’s Hospital, Imperial College Healthcare NHS Trust, London, United Kingdom Investigators in the ISSUE-3 study are listed in the Data Supplement. Correspondence: Michele Brignole, MD Arrhythmologic Centre, Department of Cardiology Ospedali del Tigullio 16033 Lavagna Italy Tel: +39 0185 329569 Fax: +39 0185 306506 E-mail: [email protected] Journal Subject Codes: [33] Other diagnostic testing, [106] Electrophysiology, [120] Pacemaker, [5] Arrhythmias, clinical electrophysiology, drugs Su Su Su Sutt tt tt tton on on on , , , , DS DS DS DSc c c c 10 10 o o o on n n n be be be beh h h h SUE- E- 3) 3) 3) I Inv nves esti ti ti t ga ga ga to to to tors rs m n R I o 7 t e I Mary’s Hospital, Imperial College Healthcare NHS Trust, London, United Kingdom me me me ment of Card d dio io iolo ogy y y y, 1 1 1 1 Os Os Os Ospe pe p pe dali l l li de e el Tig gul llio, L Lav v v va ag a na na na n ; ; ; 2 2 2 2 Os Os Ospeda d d l le d d d di i i B B Bol l l za za zano o o , Bo Bo Bo Bolz lz lz lzan S S S SS. S. S. Antonio e B Biag g gio o e Ce Ce Cesare Arr r rri igo, , A A Aless ssandr dr dr dria ia ia ia ; 4 Ar rci ci cisped da ale S S. S Mar ar ria a i N Nu uov va va, , R Ital al ly; y; y; y; 5 Ho Ho Ho Hosp sp sp spit it it tal al al a X X X Xer er er eral al al l d d de Vi Vi Vi Vigo go go go, Vi Vigo go go go; ; ; 6 6 6 Ho Ho Ho Hosp sp sp s it it ital al al a U U U Uni ni ni n ve ve ve vers rs rs r it it it tar ar ar rio io io o V V Val al al all d’ d’ d’He He He Hebr br br b on on on o , Ba Ba Ba Barc rc rc r el el el e o Hop p p it it it tal du Sa S S cre e e -C -C -Coeur d d d de e e Montreal, Mo Mo Mo ont nt nt n re re re r al; Ca Ca Cana nada; 8 Ho Ho Ho H pi tal La La La La Tim im im i one Adult e, Fra ra ra r nc nc nce e e ; 9 9 9 9 EM EM EMEA EA EA EA R R Reg eg egio io iona na nal l l l C Cl C in n n nic ic ical al al C C C Ce en e te te te t r, r, r, M M M Med ed ed dtr tr tr t on on on o ic ic ic C C C Cli li li lini ni nica ca cal l l Re Re Re Rese se sear ar ar arch ch ch I I I Ins ns nsti ti titu tu tu ut t t te, I M M Mar ar ary’ y y s s s Ho Ho Hosp sp spit ital al, Im Im Impe pe peri rial al C C Col olle lege ge ge H H Hea ea ealt lthc hcar ar are e e NH NH NHS S S Tr Tr Trus us ust t t, L L Lon on ondo don n n, U U Uni nite te ted d Ki King ng ngdo dom m m Inve e est st st stig ig ig igat at at a or or or ors s s s in in in in t t t the he he he I I I ISS S S SUE UE UE UE -3 3 3 3 s s s stu tu tu tudy dy dy dy a a a are re re re l l lis is is iste e e ed d d d in in in n t t t the he he he D D D Dat at at ata a a Su Su Su Supp pp pp ple le le leme me me ment nt nt nt. by guest on May 8, 2016 http://circep.ahajournals.org/ Downloaded from by guest on May 8, 2016 http://circep.ahajournals.org/ Downloaded from by guest on May 8, 2016 http://circep.ahajournals.org/ Downloaded from by guest on May 8, 2016 http://circep.ahajournals.org/ Downloaded from by guest on May 8, 2016 http://circep.ahajournals.org/ Downloaded from by guest on May 8, 2016 http://circep.ahajournals.org/ Downloaded from by guest on May 8, 2016 http://circep.ahajournals.org/ Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of The Benefit of Pacemaker Therapy in Patients with ... - CiteSeerX
DOI: 10.1161/CIRCEP.113.001103
1
The Benefit of Pacemaker Therapy in Patients with Presumed Neurally-Mediated Syncope and Documented Asystole is Greater when Tilt Test is Negative. An Analysis from the Third International Study on Syncope of
Uncertain Etiology (ISSUE-3)
Running title: Brignole et al.; Pacemaker efficacy and tilt test responses
Michele Brignole, MD1; Paolo Donateo, MD1; Marco Tomaino, MD2; Riccardo Massa, MD3;
Matteo Iori, MD4; Xulio Beiras, MD5; Angel Moya, MD6; Teresa Kus, MD, PhD7; Jean Claude
Deharo, MD8; Silvia Giuli, MSc9; Alessandra Gentili, MSc9; Richard Sutton, DSc10 on behalf of
the International Study on Syncope of Uncertain Etiology 3 (ISSUE-3) Investigators
Department of Cardiology, 1Ospedali del Tigullio, Lavagna; 2Ospedale di Bolzano, Bolzano;3Ospedale SS. Antonio e Biagio e Cesare Arrigo, Alessandria; 4Arcispedale S. Maria Nuova, Reggio
Emilia, Italy; 5Hospital Xeral de Vigo, Vigo; 6Hospital Universitario Vall d’Hebron, Barcelona, Spain; 7Hopital du Sacre-Coeur de Montreal, Montreal; Canada; 8Hopital La Timone Adultes ,
Marseille, France; 9EMEA Regional Clinical Center, Medtronic Clinical Research Institute, Italy;10St.Mary’s Hospital, Imperial College Healthcare NHS Trust, London, United Kingdom
Investigators in the ISSUE-3 study are listed in the Data Supplement.
Correspondence:
Michele Brignole, MD
Arrhythmologic Centre, Department of Cardiology
Ospedali del Tigullio
16033 Lavagna
Italy
Tel: +39 0185 329569
Fax: +39 0185 306506
E-mail: [email protected]
Journal Subject Codes: [33] Other diagnostic testing, [106] Electrophysiology, [120] Pacemaker, [5] Arrhythmias, clinical electrophysiology, drugs
SuSuSuSuttttttttonononon,,,, DSDSDSDScccc1010 oooonnn n bebebebehhhh
SUE-E-3)3)3) IInvnvesestititit gagagag totototorsrs
m nR
I o7 te IMary’s Hospital, Imperial College Healthcare NHS Trust, London, United Kingdom
mememement of Cardddioioioloogyyyy, 1111OsOsOsOspepeppedddalillli deeel Tiggulllio, LLavvvvaaga nananan ;;; 2222OsOsOspedadd lle ddddi i i BBBolllzazazanooo, BoBoBoBolzlzlzlzanSSSSS.S.S. Antonio e BBiagggioo e CeCeCesare Arrrrriigo,, AAAlessssandrdrdrdriaiaiaia; 4ArArrcicicispeddaale SS.S Mararriaai NNuuovvava,, RItalally;y;y;y; 5HoHoHoHospspspspititittalalala XXXXererereralalall ddde ViViViVigogogogo, ViViVigogogogo; ; ; 666HoHoHoHospspsps itititalalala UUUUnininin veveveversrsrsr ititittarararrioioioo VVValalalall d’d’d’HeHeHeHebrbrbrb ononono , ,, BaBaBaBarcrcrcr elelele oHopppititittal du SaSS creee-C-C-Coeur dddde ee Montreal,,, MoMoMoontntntn rererer al; CaCaCananada; 8HoHoHoH pipp tal LaLaLaLa Timimimi one Adult
e, Frararar ncncnceee; 9999EMEMEMEAEAEAEA RRRegegegioioionananallll CClC innnnicicicalalal CCCCeene tetetet r,r,r, MMMMedededdtrtrtrt ononono icicic CCCClilililinininicacacal l l ReReReReseseseararararchchch IIIInsnsnstitititututuutttte, IMMMararary’yy sss HoHoHospspspititalal, ImImImpepeperirialal CCColollelegegege HHHeaeaealtlthchcararareee NHNHNHSSS TrTrTrusususttt, LLLononondodonnn, UUUninitetetedd KiKingngngdodommm
Inveeeststststigigigigatatata ororororssss inininin tttthehehehe IIIISSSSSUEUEUEUE-3333 sssstutututudydydydy aaaarererere lllisisisisteeeeddd d inininn tttthehehehe DDDDatatatata aa SuSuSuSuppppppplelelelemememementntntnt.
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCEP.113.001103
2
Abstract:
Background - In the Third International Study on Syncope of Uncertain Etiology (ISSUE-3)
cardiac pacing was effective in reducing recurrence of syncope in patients with presumed
neurally-mediated syncope (NMS) and documented asystole but syncope still recurred in 25% of
them at 2 years. We have investigated the role of tilt testing (TT) in predicting recurrences.
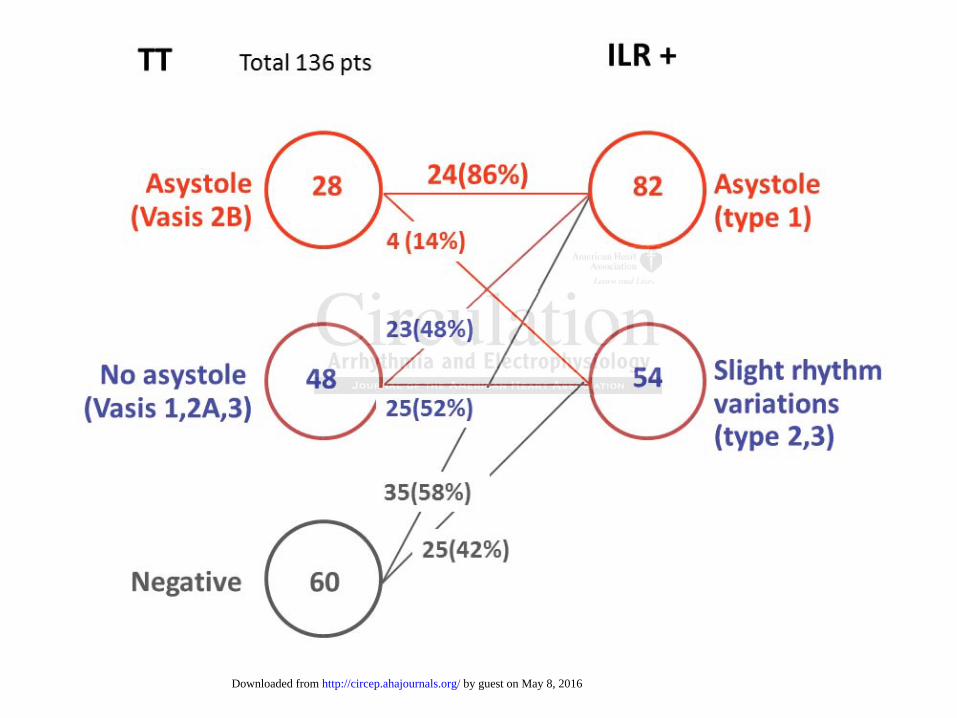
Methods and Results - In 136 patients enrolled in the ISSUE-3, TT was positive in 76 and
negative in 60. An asystolic response predicted a similar asystolic form during implantable loop
recorder monitoring, with a positive predictive value of 86%. The corresponding values were
48% in patients with non-asystolic TT and 58% in patients with negative TT (p=0.001 vs
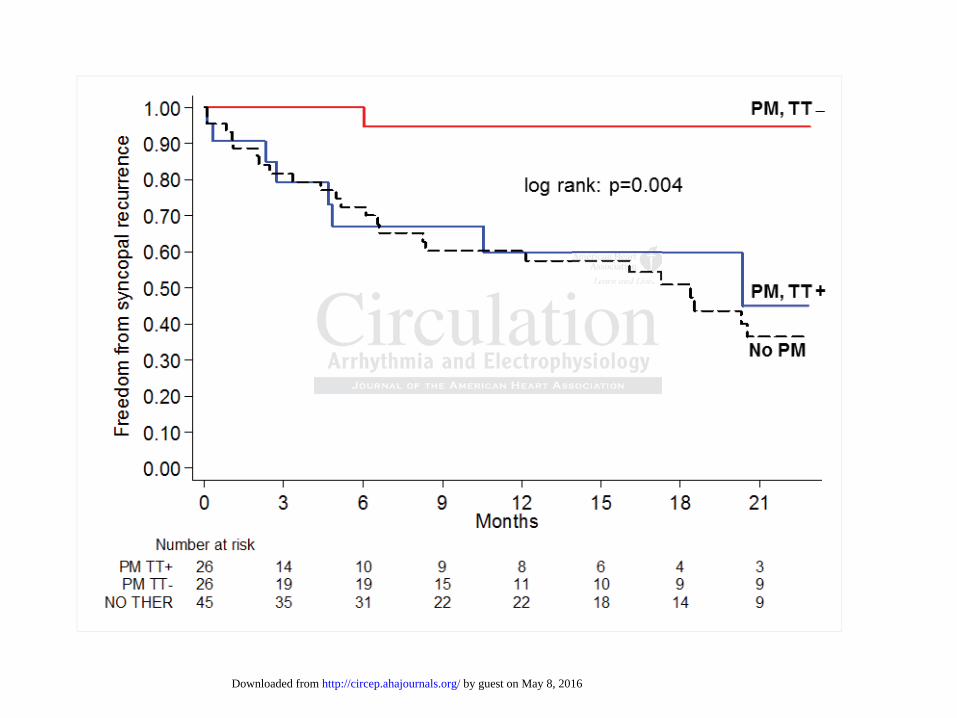
asystolic TT). Fifty-two patients (26 TT+ and 26 TT–) with asystolic NMS received a
pacemaker. Syncope recurred in 8 TT+ and in 1 TT – patients. At 21 months, the estimated
product-limit syncope recurrence rates were 55% and 5%, respectively (p=0.004). The TT+
recurrence rate was similar to that seen in 45 untreated patients (control group), which was 64%
(p=0.75). The recurrence rate was similar between 14 patients with asystolic and 12 with non-
asystolic responses during tilt testing (p=0.53).
Conclusions - Cardiac pacing was very effective in NMS patients with documented asystolic
episodes in whom TT was negative; conversely, there was insufficient evidence of efficacy from
this dataset in patients with a positive TT even when spontaneous asystole was documented.
Present observations are unexpected and need to be confirmed by other studies
Clinical Trial Registration - clinicaltrials.gov; Identifier: NCT01463358.
Key words: arrhythmia, syncope, reflexes, cardiovascular, nervous system, autonomic, pacemaker, implantable loop recorder, tilt table test
NMNMNMNMS S S S rerererececececeivivivivedededed aaa
montnttthshshh , ththththee esestitimamamamatttete
mit syncope recurrence rates were 55% and 5%, respectively (p=0.004). The TT+
rate was similar to that seen in 45 untreated patients (control group), which was
The recurrence rate was similar between 14 patients with asystolic and 12 with no
e
n l
n y
mit syysyncncncopopope e e reecucuccurrence rates were 55% annnd dd 5%, respectivelyyyly (p=0.004). The TT+
rrrratatatateeee was siiiimimimim lalalaar tooto ttthahahaat ttt seseeenenenen iin n 454545 uuuntntntrerr attedd pppatattatieieieientnnn s (c(c(c(cononontrtrtrolololo groooupupupup),),), wwwhihiihichchch wwwwas
Thhhhe recurrencee rrateee wwas sisisis milar bebbetweeeeen 1414 patatatieieieientnn ss wwwittth asysystooliici annndn 122 witthth no
esponnnnsessesss dddud riiiing ttttilillilttt tttesting ggg (p(p(p=0.5553)3)3)3).
ns --- CaCaCaC rdrdrdiaiaiacc c papapaacicicicingngngn wwwasasas vvvereerery efefefe fefefectctctivivivive inininin NNNMSMSMSMS ppppatatata ieieientntntn ss wiwiwiththth ddddococoocumumummenenentetetetedd d d asasasyyyystol
n whom TTTTTTT wawawawassss nenenenegagagagatiiiiveveveve; cococonvnvnvnvererere seseseselylyyly, , , ththththerererere e e e wawawawas ss inininnsususuufffffficcicicieieieientntntnt eeeevivivividedededencncnce e e e ofofofof efficacy
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCEP.113.001103
3
The randomized, double-blind, Third International Study on Syncope of Uncertain Etiology
(ISSUE-3) showed that dual-chamber permanent pacing was effective in reducing the recurrence
neurally-mediated syncope (NMS)
documented by implantable loop recorder (ILR) 1. Nevertheless, patients who had received
pacing therapy had an estimated syncopal recurrence rate of 25% at 2 years. Previous
randomized controlled trials 2,3,4,5,6 enrolled patients with a positive (TT). In ISSUE-3 only about
a half the patients had a positive test. Owing to its sequential design, the study lacked the power
to make any subgroup analysis. The aim of this study was to investigate the role of TT response
in predicting syncopal recurrence in the whole ISSUE-3 population
Methods
Patient selection
The multicenter, prospective ISSUE-3 study included patients s old who
syncopal episodes with a clinically assessed neurally-mediated mechanism (presumed) in the
previous 2 years. NMS was defined as reflex syncope, with the exception of carotid sinus
syndrome, with a sufficiently severe clinical presentation to warrant specific treatment. These
individuals received an ILR and were followed up. In accordance with the guidelines of the
European Society of Cardiology 7, NMS was diagnosed when the clinical history was consistent
with NMS and competing diagnoses had been excluded. Detailed inclusion criteria and study
protocol has been previously published 1,8.
TT was recommended, but its result was not taken into account in the subsequent
management. The Italian protocol 9 was recommended, which consists of 60°-70º passive tilting
for 20 minutes or until syncope occurs. If the passive tilt phase did not induce syncope, 0.4 mg
te the role of TT rrrresesesespp
l
pisodes ith a clinicall assessed ne rall mediated mechanism (pres med) in th
lectioioioonnn
enter, prpp ospepp ctctctctive ISISISSUSUSUEEE-3333 studydydy iiincludeddd dd d papp tiiients ssss lold dd whhho
ipi dde iithth lili ini llll ded llll didi tat ded hha ini (( ded)) iin tthh
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCEP.113.001103
4
sublingual nitroglycerine spray was administered to the patient while the table was maintained in
the same position; the test was continued for 15 minutes after pharmacological challenge. TT
was considered positive if syncope occurred in presence of hypotension with or without
bradycardia; positive responses were classified according to the New VASIS classification 10 as
an asystolic or VASIS 2B form ( ) or mixed or vasodepressor forms
(all the other forms without asystole). TT was considered negative if syncope did not occur.
Study protocol
After ILR implantation, all patients were followed up quarterly until the first documented
syncopal recurrence, occurrence of a diagnostic arrhythmic event or the end of the study. Events
were classified according to the ISSUE classification 11 as: type 1 (asystole >3 s), type 2
(bradycardia), type 3 (slight or no rhythm variations) and type 4 (tachycardia).
For the purpose of this study, the selected group consisted of those patients who had
performed a TT and had a diagnosis established by means of ILR documentation. Those with
asystolic episodes received a DDD pacemaker which was programmed in rate drop response
pacing mode (lower rate of 40/min, drop size of 20 beats with a drop rate of 50/min within a
detection window of 1 minute) and were followed up quarterly for 24 months or up to the first
episode of recurrence of syncope. The control group consisted of those patients who, despite an
established diagnosis, did not receive active treatment; there were 31 asystolic NMS patient (29
of whom assigned to inactive pacemaker arm of the randomized trial) and 14 not asystolic NMS.
The protocol was approved by a research ethics board at each center and each patient
provided signed informed consent.
Statistical Analysis
Continuous data are shown as averages±SDs or medians (25th–75th percentile), as appropriate,
he first documenteteeed d d d
he endnddd ooffff ththththee tststtududddy.y.yy EE
i 11
i
d
i
pisodes recei ed a DDD pacemaker hich as programmed in rate drop respons
ifieeeddd acacaca cocooordrdrdding gg g tot the ISSUE classificatioooon nn 11 as: type 1 (asysysysy tole >3 s), type 2
iaaaa),,, type 3 (sliighht oroor no rhrhrhhythmhmhmh vvvaariattiooonss) andddd ttttypypypypee 4 (tttachyhyccardrdrdr ia).
the ppppurururpppopose offf ththththisiii sttut dyy, thhththe selelelelectctctctededded ggroupup cccononononsisisiststststedddd oooof fff thththose papapapatitititients whohhh hhhhadddd
a TTTTTTT a ddnd hhhadadad aaaa ddddiaii gngg osisii estabbbblilili hshhedddd by yy means fofff IIILRLRLRR ddddocumumummentatiitiion. ThThThThosososose wi
iis dod ii ded DDDDDD kak hihi hch dd iin tat ddr
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCEP.113.001103
5
while absolute and relative frequencies were used to describe categorical data. The Shapiro-Wilk
test was performed to check the skewness of distributions. Continuous variables were compared
by unpaired Student’s t test or e non-parametric Mann-Whitney test, depending on data
distribution. Fisher’s exact test was used to compare proportions. Differences with a p value
<0.05 were indicated. The time to the first recurrence of syncope was analyzed by means of
Kaplan – Meier survival curves, which were compared by using the log-rank test. Analyses were
carried out by means of SAS 9.3.
Results
Study participants were enrolled from July 2006 to November 2010 and follow-up was
concluded in November 2012. During the observation period, 162 of 504 patients had a
presumed diagnosis of NMS documented by ILR, which showed an ECG pattern consistent with
a reflex mechanism (i.e., types 1, 2 and 3 of the ISSUE classification 11). In another 25 patients,
the ILR documented an event that was inconsistent with the diagnosis of NMS (e.g., persistent
AV block, brady-tachy syndrome, atrial or ventricular tachyarrhythmias); these patients were
therefore excluded from the analysis.
Among the 162 patients with presumed NMS, TT was positive in 76 (during the passive
phase in 22 and during drug challenge in 54) and negative in 60 (not performed in 26). Their
clinical characteristics are listed in Table 1. Patients with positive and negative TT had very
similar characteristics; apart from TT response, the two groups were indistinguishable. An
asystolic response (type 2B of the VASIS classification) predicted a similar asystolic form
during ILR monitoring (type 1 of the ISSUE classification), with a positive predictive value of
86% (95% CI: 70%-95%) (Figure 1). The corresponding values were 48% in patients with non-
i
d
e i
c mented an e ent that as inconsistent ith the diagnosis of NMS (e g persist
icipppanananantssts wwwwereere enenenenrolled from July 2006 too NoNNovember 201110 anananand dd follow-up was
innnn NNNoN vember 2001222. Durrrininining ththththe oboobservrvvatioonn peeeriririodododd, 1666222 of 50404 pppatientntntn ss s hahad a a r
diagnnnnosoosisissis of NMNMNMNMS SSS dddocumeeeenttntnted bbby yyy ILLILILRRRR, whhhiiici hhhh sssshohohohowewww d ddd ananana ECECECECGGGG paaaattttttteeere n consisii ttten
echa iniism (((i.ii e., ytytypepp s 11,1 222 a dndd 3333 of ff thhthhe ISSSSSUSUSUEE EE llclas iisiffif catitiiion 111111).).).) IIInI ano hththherrrr 2222555 papap ti
tnt ded tnt thth tat iin iistte tnt itithh thth didi isi fof NNMSMS (( iistt
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.113.001103
6
asystolic TT (p=0.001 vs asystolic TT) and 58% in patients with negative TT (p=0.001 vs
asystolic TT).
Fifty-two patients (26 TT+ and 26 TT –) with asystole documented by ILR received a
pacemaker (Figure 2). Apart from TT response, the two groups had similar clinical
characteristics (Table 2). Syncope recurred in 8 (31%) TT+ and in 1 (4%) TT– patients: it
occurred in standing or sitting positions in all and was preceded by a prodrome in 8. At
multivariable analysis, TT+ and total number of events were the only independent predictor of
syncope recurrence (see supplementary web file table W1). At the 21st month, the estimated
product-limit syncope recurrence rates were 55% (95%CI 29-85) and 5% (95%CI 1-32),
respectively (p=0.004). The recurrence rate in TT+ patients was similar to that seen in 45
untreated controls (table 2 and supplementary web figure W1), which was 64% (95%CI 48-80),
p=0.75. The 14 TT+ patients with an asystolic Vasis 2B response had a recurrence rate of 35%
(95%CI 13-75) at 12 months and of 57% (95%CI 24-93) at 21 months; these rates were similar
to those observed in 12 non-asystolic TT+ patients, p=0.53. There was a trend toward a longer
median time to first syncope recurrence in the 4 asystolic TT+ patients who suffered syncopal
recurrence than in the 4 non-asystolic TT+ patients who suffered syncopal recurrence: 8 (4-15)
and 2 (0-4) months, p=0.1 (Figure 3). Finally, 10 patients who had not performed TT had
asystole documented by ILR and received a pacemaker: 1 had syncopal recurrence (estimated
product-limit syncope recurrence rate at 21 months of 14% [95%CI 2-67]).
Discussion
The study was able to provide some insight into pacing failure observed in a quarter of patients
in the double-blind, randomized, ISSUE-3 trial. Indeed, we found that the benefit of pacemaker
t month, the estimmatatatatede
5% (9(9(9(95%5%5%5%CICICICI 1111-3-3332)2)2)2),,
y
c
h 3
m
bser ed in 12 non as stolic TT+ patients p 0 53 There as a trend to ard a lon
y (((p=p=p=p=0.00 00000004)4)4)4 . ThThThThe recurrence rate in TT+++ papap tients was simi illllararara to that seen in 45
coooonttttrols (table 2 annnd supppplppp emmeentaarry wweeeb ffigigureee WWW1W )), wwwhhhichh wwasasas 664%%%% (((95959 %%CIII 4448
he 1444 TTTTT+T+T+T+ ppattttieii tttnts iiiwithtt an nnn aasasystolililiiccc VaVaVaV siiis 2B2B2B2B rrresesesespopopoponnse ee hahahahad dd a recuuuurrrrrrrreence r tttate fffof 3
-75)5)5)5 at 1222 monononnthhhhs and dd foff 55557%7%7%% (9(9(95%5%5%%CCIC 2222444-9993)3)3)3 at 2121212 monoono thhhs;;; ththththese rates wewewewerereree sim
bb ded ii 1212 tst loliic TTT+T+ tatiie tnt 00 5533 ThTh tt dnd tt dd llo
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCEP.113.001103
7
therapy in patients with presumed NMS and documented asystole was not substantial in those
with a positive TT. Syncope recurrence was independent from the type of response during TT.
Although an asystolic response during TT predicted spontaneous asystole, we were unable to
show a benefit greater than in patients with non-asystolic responses. Therefore, we speculate
that pacing failure was due to hypotensive syncope (either vasodepressor NMS or orthostatic
hypotension), which is disclosed by TT susceptibility and which cannot be prevented by cardiac
pacing. It is commonly accepted that hypotension plays a major role in all forms of TT-induced
NMS and that it precedes (and perhaps triggers) bradycardia and syncope in the vast majority of
patients even in those with cardioinhibitory syncope according to the modified VASIS
classification 12, 13.
TT+ and TT– patients had similar clinical characteristics, similar outcomes and similar
ECG patterns when an episode was documented by ILR (Table 1). These findings had already
emerged from the ISSUE 1 and ISSUE 2 studies 14,15 and other studies in the literature 16,17,18,19.
Even though the two groups were indistinguishable in terms of clinical characteristics, the
different effect of pacing prompts us to infer that the underlying mechanism of syncope is
different, i.e. that a vasodepressive mechanism is dominant in TT+ patients while a
cardioinhibitory mechanism is dominant in TT– patients. Thus, the utility of TT shifts from that
of a tool for clinical diagnosis to a tool for pathophysiological classification, with obvious
therapeutic implications. Before the ISSUE-3 trial, cardiac pacing for NMS had only been
evaluated in randomized trials which enrolled patients with TT+ 2,3,4,5,6, TT being considered the
standard means of diagnosing NMS; no indication for pacing in TT– NMS patients existed.
ISSUE-2 enrolled both TT+ and TT- patients but the outcome was not considered separately 15.
ISSUE-3 included both TT+ and TT– patients, and clinical history and initial evaluation were
oppe in the vast maaaajojojojorir
modiiiififififieddded VVVVASASASASIISISI
o 12 13
+ m
r a
r ,
gh the t o gro ps ere indisting ishable in terms of clinical characteristics the
on 12212, 131313.
++++ annndn TT– pattieentsss hhhad sisisiimilalalal r cccliiniccalll chharractctctererrrisisisstiics, sssimiilaar ouooutcommmmeees anand siim
rns whwhwhw ennenen an epiiisodddde was ddddocococumenenennteteteted dd bbybyb IIILRLRLRLR ((((TaTaTaT blblblblee 1)1)1)1 . ThThThT ese finininndidididingngs hahhh dddd alllrea
rom thehh ISSSSSSUEUEUEE 1111 anddd IIISSSSSSUEUEUEU 222 studididiies 1444 1,11555 a ddnd othhthher stuuuudididid ess iiiin hththe lililliteratuuuurererere 11161 ,17,
hh thth tt ii dndiistiti ii hsh bablle iin tt ff lcliiniic lal hha tct iistiti thth
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCEP.113.001103
8
regarded as the standard for diagnosis. By showing that TT– NMS patients are those who
benefit most from cardiac pacing, the present study inverts previous knowledge on indications
for pacing.
In this subanalysis of ISSUE-3 study, pacemaker therapy in TT+ patients showed no
benefit, despite the documentation of a long asystole at the time of a spontaneous event; the
syncopal recurrence rate was also similar to the 37% and 57% rates observed at 1 and 2 years in
the pacemaker-off arm of ISSUE-3. This result was largely unexpected as previous five major
multicenter, randomized, controlled trials 2,3,4,5,6 performed on TT+ showed some efficacy of
pacing even in the absence of documentation of spontaneous asystole. When pooled together, the
five trials evaluated 318 patients; syncope recurred in 21% of the paced patients and in 44% of
unpaced patients (P <0.001). A meta-analysis suggested a non-significant 17% reduction in
syncope in the double-blind studies and a 84% reduction in the studies in which the control
group did not receive a pacemaker 20. Our study group was small and the confidence interval of
the probability of recurrence of syncope at 21st month ranged from 29% to 85%. We cannot
therefore exclude a type II error; some benefit of pacing may still be possible, especially in
patients with an asystolic TT+ response. What we have observed here in NMS patients is similar
to what was observed in patients paced for carotid sinus syndrome. In Gaggioli et al’s study 21
patients with carotid sinus syndrome and TT+ had a 2.7-fold increased risk of syncopal
recurrence compared with carotid sinus syndrome and TT- : at a mean follow-up of 33 months,
syncope recurred in 21% of 70 patients versus 9% of 99 patients (p=0.02); positive TT was the
only independent predictor of syncopal recurrence. Solari et al, 22, in 141 patients affected by
carotid sinus syndrome, found a mixed or vasodepressor response to TT was the only
independent predictor of syncopal recurrence (HR=1.8; p=0.01). In conclusion, in the light of the
owed some efficaacycycycy o
Whehenn popoololll dededd ttttogogoggetetetethhhh
e %
a n
the double-blind studies and a 84% reduction in the studies in which the control
n v
ilit of rec rrence of s ncope at 21st month ranged from 29% to 85% We canno
evalalaluauauauatetedddd 333118 ppppata ients; syncope recurred ddd ininii 21% of the pacececeeddd patients and in 44%ddd
atttit eenene ts (P( <0.0001). AAA meeettta-ananalyyysiis suuggggeestted dd aa nononononn-siiigggnifiicaantttt 1171 % reeeduucctiooon inP
the ddddouououblblblb e-blblblb iiind ddd ttst ddudies anananandddd a 848444%%%% rerredddu ttctiiioi n inininin tttthehehehe stututuudididiies iiiin whwhwhwhicicicichhhh thhhhe co ttntrol
not receiivi e a papapaacemakkker 202020. OOuO r studdddy yy grgg ouppp was smalllll aaana d dd thththhe co fnfffidididi enceeee iiiintntntnterv
ililitit fof fof tt 2121stst thth dd ffr 229%9% tt 8585%% WW o
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.113.001103
9
present study and of the above literature, it is clear that cardiac pacing is very effective when TT
is negative while syncope can frequently recur when TT is positive.
Limitations
As discussed above, the study group was small with a large confidence interval of the probability
of recurrence of syncope. Some benefit of pacing may still be possible in patients with positive
TT response. For example, we observed a 4-fold longer median time to syncope recurrence (8
versus 2 months) in asystolic than in non-asystolic TT+ patients on pacemaker treatment. The
same finding was observed in the SYNPACE trial 6, in which the time to the first syncope
recurrence was longer on pacemaker therapy than on placebo in patients who had shown an
asystolic (ventricular pause of 13±8 s) response during tilt table testing: 97 versus 11 days,
p=0.06. We did not evaluate the effect of cardiac pacing in asystolic TT+ patients who did not
achieve the end-point of an ILR event documentation; theoretically, these patients could have a
better outcome with a pacemaker.
It is not completely clear that all of patients had NMS. It is important to acknowledge that
the ISSUE-3 population is by no means the typical NMS type of patients. Many ISSUE-3
patients were old and had atypical presentation with no or subtle prodrome and lack of
recognizable triggers. NMS could not be confirmed by TT which was negative in half patients. It
is possible that these patients simply had an intermittent form of extreme bradycardia (i.e.,
asystole) different from NMS. A great overlap between extrinsic sinus node dysfunction and
dysautonomic conditions exists 23,24. Idiopathic paroxysmal AV block has been recently
described as a different cause of unexplained syncope in patients without structural heart disease
25.
Compared with TT-, TT+ patients treated with a pacemaker had a longer history of more
to the first syny coopepepepe
nts whwhhhoo hhhahaddd d shshhhowown n nn aaan
v
e did not evaluate the effect of cardiac pacing in asystolic TT+ patients who did
e a
o
s not completel clear that all of patients had NMS It is important to ackno ledg
vennnntrtrtrtricicici ulululu ararara ppauuuussess of 13±8 s) response durururininini g tilt table tesee tingngngng: 97 versus 11 days,
eeee dddiiidi not evaluuaate thththe effffefefefect oofff f cccarrdiaacc pacicing iiin n n n aaasa yysttotolic TTTT++ ppap tiennnntststs wwhho dddiiid
e endddd p-p-poioiioint of fff an IIILRLRLRLR eventntntn ddddocummmmenenentattatatitiiion; ththhtheoeoeoeoreeetiititicallllllyyy, ttthehh se patataatieieieients coullld ddd hhhha
ome witii h hh a papapacccec makkek r.
tt llettell lle tthhatt lalll fof tatiie tnt hhadd NMNMSS ItIt ii iim trt tt tto kck ll ded
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.113.001103
10
syncopal episodes during life (but not in the last 2 years) and fewer were males. Albeit marginal,
these differences, could indicate a different susceptibility to NMS and partly influence pacing
results.
Finally, this study suggests a strategy of pacing indication largely based on the result of
TT despite TT being regarded as having questionable diagnostic accuracy and reproducibility
17,19.
For all the above reasons, the findings of the present study cannot be taken as conclusive;
the largely unexpected prompt future studies which may show similar results to ours.
Conclusions
In the present study, cardiac pacing was very effective in NMS patients with documented
asystolic episodes in whom TT was negative; conversely, there was insufficient evidence of
efficacy from this dataset in patients with a positive TT even when spontaneous asystole was
documented. Present observations are unexpected and need to be confirmed by other studies
Conflict of Interest Disclosures: M. Brignole reports receiving modest consultancy fees from
Medtronic and being a direct shareholder of F2 solutions; R. Sutton is a consultant to Medtronic,
receiving modest fees, and is a paid lecturer for St Jude Medical; A. Moya reports receiving
modest consultancy fees from Medtronic; Dr Deharo reports receiving limited consultant fees
from Medtronic; Beiras reports receiving limited consultant fees from Medtronic and St Jude
Medical; S. Giuli and A. Gentili are employees of Medtronic; the other authors have no financial
disclosures.
References:
1. Brignole M, Menozzi C, Moya A, Andresen D, Blanc JJ, Krahn AD, Wieling W, Beiras X, Deharo JC, Russo V, Tomaino M, Sutton R. Pacemaker therapy in patients with neurally
results to ours.
n
e
p o
o
ed Present obser ations are ne pected and need to be confirmed b other st die
ns
entntntnt study, carddiaac pappacingngngg wass veeeryy efffeeectiivee innnn NNNMSMMM pppaaatienntss wwwiw ttht doocoo umumu eenteeeddd
pisodododdesees iiiinn whhhhom TTTTTTT was nenenenegativeeee;;;; cooonverselyy, thththt ererereree wawawaas inii sufficieieieiennnnt eviiidddence o
om hthhiiis dddatasetetett iin papp iitients with hhh a popp isiitive TTTT TTT even whehheh nnn n sppponononntaneous asysysysystototot lelll w
ded PPr tt bob tatiio ttedd dd ded tt bbe fifi ded bb tothhe tst ddiie
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.113.001103
11
mediated syncope and documented asystole: Third International Study on Syncope of Uncertain Etiology (ISSUE-3): a randomized trial. Circulation. 2012;125:2566-2571.
2. Sutton R, Brignole M, Menozzi C, Raviele A, Alboni P, Giani P, Moya. Dual-chamber pacing in the treatment of neurally mediated tilt-positive cardioinhibitory syncope : pacemaker versus no therapy: a multicenter randomized study. Circulation. 2000;102:294-299.
3. Connolly SJ, Sheldon R, Roberts RS, Gent M. Vasovagal pacemaker study investigators. The North American vasovagal pacemaker study (VPS): a randomized trial of permanent cardiac pacing for the prevention of vasovagal syncope. J Am Coll Cardiol. 1999;33:16–20.
4. Ammirati F Colvicchi F, Santini M. Permanent cardiac pacing versus medical treatment for the prevention of recurrent vasovagal syncope: a multicenter, randomized, controlled trial. Circulation. 2001;104:52-57.
5. Connolly SJ, Sheldon R, Thorpe KE, Roberts RS, Ellenbogen KA, Wilkoff BL, MorilloC, Gent M. Pacemaker therapy for prevention of syncope in patients with recurrent severe vasovagal syncope: Second Vasovagal Pacemaker Study (VPS II). JAMA. 2003;289:2224-2229.
6. Raviele A, Giada F, Menozzi C, Speca G, Orazi S, Gasparini G, Sutton R, Brignole M. The vasovagal syncope and pacing trial (Synpace). A randomized placebo-controlled study of permanent pacing for treatment of recurrent vasovagal syncope. Eur Heart J. 2004:25:1741–1748.
7. Brignole M, Alboni P, Benditt D, Bergfeldt L, Blanc JJ, Thomsen PE, Gert van Dijk J, Fitzpatrick A, Hohnloser S, Janousek J, Kapoor W, Kenny RA, Kulakowski P, Masotti G, Moya A, Raviele A, Sutton R, Theodorakis G, Ungar A, Wieling W, Priori SG, Garcia MA, Budaj A, Cowie M, Deckers J, Burgos EF, Lekakis J, Lindhal B, Mazzotta G, Morais J, Oto A, Smiseth O, Menozzi C, Ector H, Vardas P. Guidelines on management (diagnosis and treatment) of syncope – Update 2004. Europace. 2004;6,467-537.
8. The Steering Committee of the ISSUE 3 Study. International study on syncope of uncertain aetiology 3(ISSUE 3): pacemaker therapy for patients with asystolic neurally-mediated syncope: rationale and study design. Europace. 2007;9:25–30.
9. Bartoletti A, Alboni P, Ammirati F, Brignole M, Del Rosso A, Foglia Manzillo G, Menozzi C, Raviele A, Sutton R. The Italian protocol: a simplified head-up tilt testing potentiated with oral nitroglycerin to assess patients with unexplained syncope. Europace. 2000;2:339–342.
10. Brignole M, Menozzi C, Del Rosso A, Costa S, Gaggioli G, Bottoni N, Bartoli P, Sutton R. New classification of haemodynamics of vasovagal syncope: beyond the VASIS classification. Analysis of the pre-syncopal phase of the tilt test without and with nitroglycerin challenge. Europace. 2000;2:66-76.
WWWWililililkokokokoffffffff BBBBL,L,L,L, MMMMooororilililillolloloCCCCh recururrerentnttt sseveverere eMA 2020202003030303;2;2;2;289898989:2:22222222222444 2
A, Giada F, Menozzi C, Speca G, Orazi S, Gasparini G, Sutton R, Brignole M. Ts
1
eA, Hohnloser S, Janousek J, Kapoor W, Kenny RA, Kulakowski P, Masotti G, MA S tton R Theodorakis G Ungar A Wieling W Priori SG Garcia MA B da
AAAA, GGiGG ada F,FFF MMMeneee ozozozzizizi CCCC, SpSpSppececece a G,G,G, OOOrararaziz SS, Gaaaspsppspararararini i ii G,G,G,G SSSutututttott n R,R,R,R BBBBrirr gngngnolololo ee e M.MMM Tsyyyynnncn ope and ppacinng trialalal (Synpn aaacee). A AA randndommmizizizedededed plaaaccceboo-cconnntrtrolleeeed dd sttuddy ofofof papapacicicing forrr tttreattmeeennt of f f reeecurrrrrrrenennt vasososovagagal sysyssynnncopopopo e. EEEur HeHearrrrt J.JJJ 20000000 4:225:11177741
e M,M AAAlblblbonii i PPP, BBBBendididitt DDD, BBBeB rgggfffeldldldt LLL,L BBBBlllanc JJ,JJ TTTThohh mssen PPPE,EEE GGGGert t van DiDiDiDijkjkjkjk J, A, Hohnlnlnlosososo ererere SSSS,,,, JaJaJaJanonononoususususekeekek JJJJ,,, , KaKaKaKapopopopoorororr WWWW,,, KeKeKeKennnnny y y y RARARARA,,, KuuKuKulalalaakokokokowswswswskikikiki PPPP, ,, MaMaMaMasotti G, MAA SS tttt RR ThTh ddo kiki GG UU AA WiWi leliin WW PP iri ii SGSG GGa iia MMAA BB dda
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.113.001103
12
11. Brignole M, Moya A, Menozzi C, Garcia-Civera R, Sutton R. Proposed electrocardiographic classification of spontaneous syncope documented by an implantable loop recorder. Europace.2005;7:14-18
12. Schroeder C, Jens Tank J, Heusser K, Diedrich A, Luft F, Jordan J. Physiological phenomenology of neurally-mediated syncope with management implications PLoS One.2011;6:e26489
13. Verheyden B, Liu J, van Dijk N, Westerhof BE, Reybrouck T, Aubert AE, Wieling W. Steep fall in cardiac output is main determinant of hypotension during drug-free and nitroglycerine-induced orthostatic vasovagal syncope. Heart Rhythm. 2008;5:1695–1701.
14. Moya A, Brignole M, Menozzi C, Menozzi C, Garcia-Civera R, Wieling W,Andresen D, Benditt DG, Garcia-Sacrista´n JF, Beiras X, Grovale N, Vardas P. Mechanism of syncope in patients with isolated syncope and in patients with tilt-positive syncope. Circulation.2001;104:1261–1267.
15. Brignole M, Sutton R, Menozzi C, Garcia-Civera R, Moya A, Wieling W, Andresen D, Benditt DG, Vardas P. Early application of an Implantable Loop Recorder allows a mechanism-based effective therapy in patients with recurrent suspected neurally-mediated syncope. Eur Heart J. 2006;27:1085–1092.
16. Grimm W, Degenhardt M, Hoffman J, Menz V, Wirths A, Maisch B. Syncope recurrence can better be predicted by history than by head-up tilt testing in untreated patients with suspected neurally mediated syncope. Eur Heart J. 1997;18:1465–1469.
17. Sheldon R, Rose S, Koshman ML. Comparison of patients with syncope of unknown cause having negative or positive tilt-table tests. Am J Cardiol. 1997;80:581–585.
18. Sheldon R, Rose S, Connolly S, Ritchie D, Koshman ML, Frenneaux M. Diagnostic criteria for vasovagal syncope based on a quantitative history. Eur Heart J. 2006;27:344–350.
19. Sheldon R. Tilt table testing and implantable loop recorders for syncope. Cardiol Clin. 2013;31:67–74.
20. Sud S, Massel D, Klein GJ, Gula L, Yee R, Krahn A. The expectation effect and cardiac pacing for refractory vasovagal syncope. Am J Med. 2007;120:54-62.
21. Gaggioli G, Brignole M, Menozzi C, Devoto G, Oddone D, Gianfranchi L, Gostoli E, Lolli G. Positive response to head-up tilt testing predicts syncopal recurrence in carotid sinus syndrome patients with permanent pacemakers. Am J Cardiol. 1995;76:720–722.
22. Solari D, Maggi R, Oddone D, Solano A, Croci F, Donateo P, Brignole M. Clinical context and outcome of carotid sinus syndrome diagnosed by means of the “method of symptoms”. Europace. 2013: Sep 20. [Epub ahead of print]
e. Circulation.
eling WWWW AAAAndndndndrerereresesesesennnn DDDG, Vardas P. Early application of an Implantable Loop Recorder allows a mechanc0
m W, Degenhardt M, Hoffman J, Menz V, Wirths A, Maisch B. Syncope recurrenr ee
n R Rose S Koshman ML Comparison of patients ith s ncope of nkno n ca
G, VaVaVaVardrdrdrdasasss PPP. EaEaEaarlrr y application of an Implplplplanana table Loop RRRecororororder allows a mechanctttiviviviveeee therappppy y y ininnin patatatieieientntntts sss wiwiiwithththh rrecececuruu reeentntnt sussppectttedededed nnnneueurrrralllllll yyy-m-mm-medee iaateteteted d d d sysysyyncncncopopopopeee. EuEE006060606;27:1085–110092.
m W, DDDDegggegenhardddttt M,M,M HHHHoffmfmfmfmaanan J, MeMeMeMenznznz VVVV, WiWiWiW rtttthshshshs AAAA, MaMaMaMaisisisi chhh BBBB. SySySyyncncncncoppe recurrenredicccctetetet d d d d bybybyb hhhhisisisi tototot ryryryy ttthahahahan nnn bybybyby hhheaaaaddd---upupupup tttiilt teteteesttinininng g g g inininin uuuntntntntrererereatatata ededed ppppatatatatieieieientntnts ss s wiwiwithththth ssssusususpepepep cteediatedd d syyyncopopoppe. EuEE r HHHeart J. 111999999777;1118:1114646465–555 14141446969696 .
RR RR SS KK hhm MMLL CC iri fof tatiie tnt iithth ff kkn
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.113.001103
13
23. Brignole M, Menozzi C, Gianfranchi L, Oddone D, Lolli G, Bertulla A. Neurally mediated syncope detected by carotid sinus massage and head-up tilt test. Am J Cardiol. 1991;68:1032-1036.
24. Alboni P, Menozzi C, Brignole M, Paparella N, Lolli G, Oddone D, Dinelli M. An abnormal neural reflex plays a role in causing syncope in sinus bradycardia. J Am Coll Cardiol.1993;22:1130-1134.
25. Brignole M, Deharo JC, De Roy L, Menozzi C, Blommaert D, Dabiri L, Ruf J, Guieu R. Syncope due to idiopathic paroxysmal atrioventricular block: long-term follow-up of a distinct form of atrioventricular block. J Am Coll Cardiol. 2011;58:167–173.
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCEP.113.001103
14
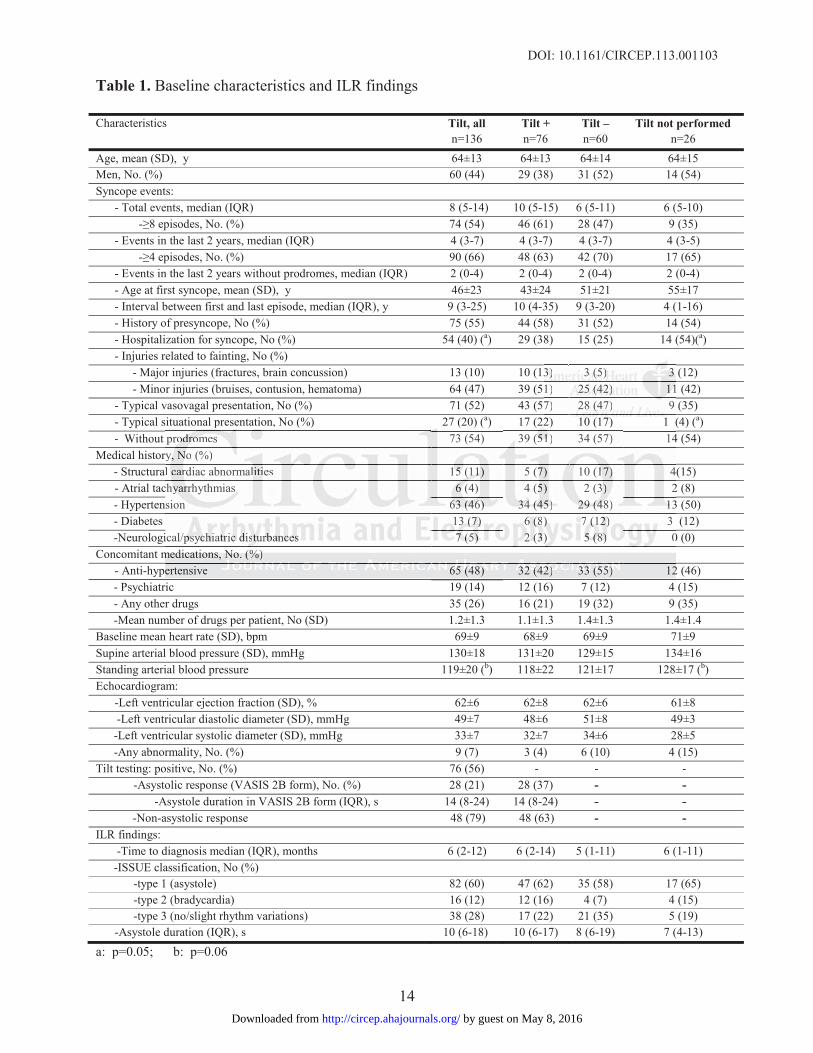
Table 1. Baseline characteristics and ILR findings
Characteristics Tilt, alln=136
Tilt +n=76
Tilt –n=60
Tilt not performedn=26
Age, mean (SD), y 64±13 64±13 64±14 64±15Men, No. (%) 60 (44) 29 (38) 31 (52) 14 (54)Syncope events:
- Total events, median (IQR) 8 (5-14) 10 (5-15) 6 (5-11) 6 (5-10) - No. (%) 74 (54) 46 (61) 28 (47) 9 (35)- Events in the last 2 years, median (IQR) 4 (3-7) 4 (3-7) 4 (3-7) 4 (3-5) - No. (%) 90 (66) 48 (63) 42 (70) 17 (65)- Events in the last 2 years without prodromes, median (IQR) 2 (0-4) 2 (0-4) 2 (0-4) 2 (0-4)- Age at first syncope, mean (SD), y 46±23 43±24 51±21 55±17- Interval between first and last episode, median (IQR), y 9 (3-25) 10 (4-35) 9 (3-20) 4 (1-16)- History of presyncope, No (%) 75 (55) 44 (58) 31 (52) 14 (54)- Hospitalization for syncope, No (%) 54 (40) (a) 29 (38) 15 (25) 14 (54)(a)- Injuries related to fainting, No (%)
- Major injuries (fractures, brain concussion) 13 (10) 10 (13) 3 (5) 3 (12)- Minor injuries (bruises, contusion, hematoma) 64 (47) 39 (51) 25 (42) 11 (42)
- Typical vasovagal presentation, No (%) 71 (52) 43 (57) 28 (47) 9 (35)- Typical situational presentation, No (%) 27 (20) (a) 17 (22) 10 (17) 1 (4) (a)- Without prodromes 73 (54) 39 (51) 34 (57) 14 (54)
Medical history, No (%)- Structural cardiac abnormalities 15 (11) 5 (7) 10 (17) 4(15)- Atrial tachyarrhythmias 6 (4) 4 (5) 2 (3) 2 (8)- Hypertension 63 (46) 34 (45) 29 (48) 13 (50)- Diabetes 13 (7) 6 (8) 7 (12) 3 (12)-Neurological/psychiatric disturbances 7 (5) 2 (3) 5 (8) 0 (0)
Concomitant medications, No. (%)- Anti-hypertensive 65 (48) 32 (42) 33 (55) 12 (46)- Psychiatric 19 (14) 12 (16) 7 (12) 4 (15)- Any other drugs 35 (26) 16 (21) 19 (32) 9 (35)-Mean number of drugs per patient, No (SD) 1.2±1.3 1.1±1.3 1.4±1.3 1.4±1.4
Baseline mean heart rate (SD), bpm 69±9 68±9 69±9 71±9Supine arterial blood pressure (SD), mmHg 130±18 131±20 129±15 134±16Standing arterial blood pressure 119±20 (b) 118±22 121±17 128±17 (b)Echocardiogram:
-Left ventricular ejection fraction (SD), % 62±6 62±8 62±6 61±8-Left ventricular diastolic diameter (SD), mmHg 49±7 48±6 51±8 49±3
-Left ventricular systolic diameter (SD), mmHg 33±7 32±7 34±6 28±5-Any abnormality, No. (%) 9 (7) 3 (4) 6 (10) 4 (15)
Tilt testing: positive, No. (%) 76 (56) - - --Asystolic response (VASIS 2B form), No. (%) 28 (21) 28 (37) - - -Asystole duration in VASIS 2B form (IQR), s 14 (8-24) 14 (8-24) - --Non-asystolic response 48 (79) 48 (63) - -
ILR findings:-Time to diagnosis median (IQR), months 6 (2-12) 6 (2-14) 5 (1-11) 6 (1-11)
-ISSUE classification, No (%)-type 1 (asystole) 82 (60) 47 (62) 35 (58) 17 (65)-type 2 (bradycardia) 16 (12) 12 (16) 4 (7) 4 (15)-type 3 (no/slight rhythm variations) 38 (28) 17 (22) 21 (35) 5 (19)
-Asystole duration (IQR), s 10 (6-18) 10 (6-17) 8 (6-19) 7 (4-13)
a: p=0.05; b: p=0.06
3333)))) 3333 (5(5(5(5))) 33331) 25252525 ((((42424242)))) 111111117) 2828282 ((((47)) 9
0
p , ( ) ( ) ( ) ( ) ( ) (4
rl 4
c 23
ime 2
p , ( ) ( ) ( ) ( ) ( ) (prododododrorororomes 73 (54) 39 (((51515151) 34 (57) 14
ry,y,y, NNNoN (%)l carrrdiac abnormallitiies 1515155 (((111111) 5 (77) 10 (11711 ))) 4
chyyyyarrrrhr ythmiass 6 66 6 (4) 4 (55) 2 (333) 2sion 63636363 ((((4646464 )))) 34343434 (((454545)))) 29292929 ((((4848484 ) 13111
133 ((((7)7)7) 6 6 6 6 (8(8(8))) 7 (1(1(1( 2)2)22 3 ical/ppppsysyychchchiaiaiatrtrtriccc dddisisistututuurbrbrbbananancececesss 7 77 (5(5(5( ))) 22 2 (3(3(3))) 555 (8(8(8( ))) 0mememedidicacacatitionononsss, NoNo. (%(%))ertensive 65555 ((((48484848)))) 3232322 (((42424242)))) 3333333 (((55555555))) 12
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCEP.113.001103
15
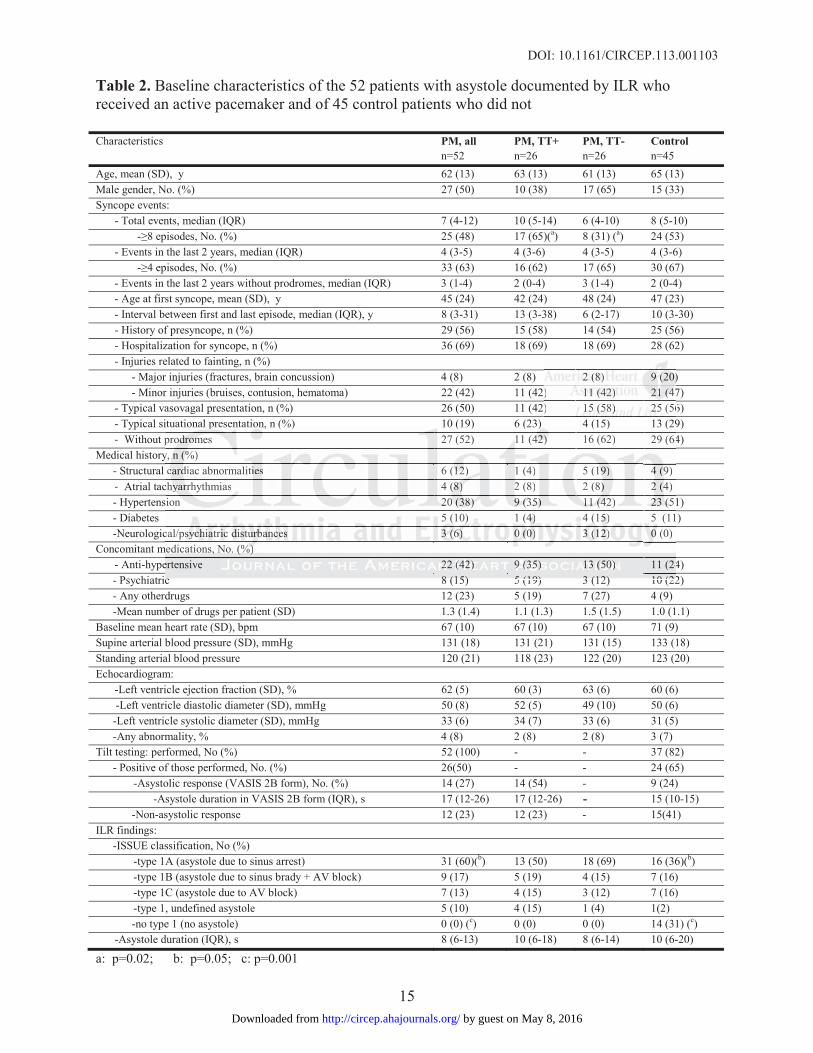
Table 2. Baseline characteristics of the 52 patients with asystole documented by ILR who received an active pacemaker and of 45 control patients who did not
Characteristics PM, all n=52
PM, TT+n=26
PM, TT-n=26
Control n=45
Age, mean (SD), y 62 (13) 63 (13) 61 (13) 65 (13)Male gender, No. (%) 27 (50) 10 (38) 17 (65) 15 (33)Syncope events:
- Total events, median (IQR) 7 (4-12) 10 (5-14) 6 (4-10) 8 (5-10) - No. (%) 25 (48) 17 (65)(a) 8 (31) (a) 24 (53)- Events in the last 2 years, median (IQR) 4 (3-5) 4 (3-6) 4 (3-5) 4 (3-6) - No. (%) 33 (63) 16 (62) 17 (65) 30 (67)- Events in the last 2 years without prodromes, median (IQR) 3 (1-4) 2 (0-4) 3 (1-4) 2 (0-4)- Age at first syncope, mean (SD), y 45 (24) 42 (24) 48 (24) 47 (23)- Interval between first and last episode, median (IQR), y 8 (3-31) 13 (3-38) 6 (2-17) 10 (3-30)- History of presyncope, n (%) 29 (56) 15 (58) 14 (54) 25 (56)- Hospitalization for syncope, n (%) 36 (69) 18 (69) 18 (69) 28 (62)- Injuries related to fainting, n (%) - Major injuries (fractures, brain concussion) 4 (8) 2 (8) 2 (8) 9 (20) - Minor injuries (bruises, contusion, hematoma) 22 (42) 11 (42) 11 (42) 21 (47)- Typical vasovagal presentation, n (%) 26 (50) 11 (42) 15 (58) 25 (56)- Typical situational presentation, n (%) 10 (19) 6 (23) 4 (15) 13 (29)- Without prodromes 27 (52) 11 (42) 16 (62) 29 (64)
Medical history, n (%)- Structural cardiac abnormalities 6 (12) 1 (4) 5 (19) 4 (9)- Atrial tachyarrhythmias 4 (8) 2 (8) 2 (8) 2 (4)- Hypertension 20 (38) 9 (35) 11 (42) 23 (51)- Diabetes 5 (10) 1 (4) 4 (15) 5 (11)-Neurological/psychiatric disturbances 3 (6) 0 (0) 3 (12) 0 (0)
Concomitant medications, No. (%)- Anti-hypertensive 22 (42) 9 (35) 13 (50) 11 (24)- Psychiatric 8 (15) 5 (19) 3 (12) 10 (22)- Any otherdrugs 12 (23) 5 (19) 7 (27) 4 (9)-Mean number of drugs per patient (SD) 1.3 (1.4) 1.1 (1.3) 1.5 (1.5) 1.0 (1.1)
Baseline mean heart rate (SD), bpm 67 (10) 67 (10) 67 (10) 71 (9)Supine arterial blood pressure (SD), mmHg 131 (18) 131 (21) 131 (15) 133 (18)Standing arterial blood pressure 120 (21) 118 (23) 122 (20) 123 (20)Echocardiogram:
-Left ventricle ejection fraction (SD), % 62 (5) 60 (3) 63 (6) 60 (6)-Left ventricle diastolic diameter (SD), mmHg 50 (8) 52 (5) 49 (10) 50 (6)
-Left ventricle systolic diameter (SD), mmHg 33 (6) 34 (7) 33 (6) 31 (5)-Any abnormality, % 4 (8) 2 (8) 2 (8) 3 (7)
Tilt testing: performed, No (%) 52 (100) - - 37 (82)- Positive of those performed, No. (%) 26(50) - - 24 (65)
-Asystolic response (VASIS 2B form), No. (%) 14 (27) 14 (54) - 9 (24) -Asystole duration in VASIS 2B form (IQR), s 17 (12-26) 17 (12-26) - 15 (10-15)
-Non-asystolic response 12 (23) 12 (23) - 15(41)ILR findings:
-ISSUE classification, No (%)-type 1A (asystole due to sinus arrest) 31 (60)(b) 13 (50) 18 (69) 16 (36)(b)-type 1B (asystole due to sinus brady + AV block) 9 (17) 5 (19) 4 (15) 7 (16)-type 1C (asystole due to AV block) 7 (13) 4 (15) 3 (12) 7 (16)-type 1, undefined asystole 5 (10) 4 (15) 1 (4) 1(2)
-no type 1 (no asystole) 0 (0) (c) 0 (0) 0 (0) 14 (31) (c)-Asystole duration (IQR), s 8 (6-13) 10 (6-18) 8 (6-14) 10 (6-20)
a: p=0.02; b: p=0.05; c: p=0.001
2222 (8(8(8(8)))) 9 999 (2(2(2(20)0)0)0)) 11111111 ((((42424242)))) 21212121 ((((444747) 151515 ((((58585858)))) 25252525 ((56
ituational presentation, n (%) 10 (19) 6 (23) 4 (15) 13 (29p 4y
cs
1c
me 4c 8 (15) 5 (19) 3 (12) 10 (22
ituational prpp esentation, n (%) 10 (19) 6 (23)))) 4 (15) 13 (29prododdodroooommmmes 27 (52) 11 (4242422)))) 16 (62) 29 (64y, nn ((((%%%%)cccardddid ac abnormalitiiess 6 (1(11122)2 1 (4) 5 (19)999 444 4 ((99)
chyhyhyhyarrrrhrr ythmias 4 (8(88(8))) 222 (8) 2 (8)))) 222 (444)sion 202020 (((3838388))) 9 9 9 9 (3(3(335)5)) 11111 (((442424 ) 232232 (((55
5 (1( 0))) 1 (44(44))) 4 (1(( 5)5)55 5 (11cal/psysysychchcchiaiaiatrtricicic dddisistututurbrbrbrbananncecees 3 3 3 3 (6(6(6(6))) 0 0 0 (0(0(0)) 3333 (1(1(1( 2)2)2 0 000 (0)
medications,,, No. (%%(%)))ertensive 22222 (((4242422))) 9 9 9 9 (3(3(335)5)5)5) 1311313 (((50505050)))) 11 (24c 88 (1(15)5) 55 (1(19)9) 33 (1(12)2) 1010 ((2222
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCEP.113.001103
16
Figure Legends:
Figure 1. Correlation between tilt test responses and the mechanism of syncope, as documented
by ILR
Figure 2. Kaplan-Meier freedom from syncope recurrence after pacemaker therapy in tilt-
negative asystolic NMS and in tilt-positive asystolic NMS patients. The curve of a control group
of untreated patients is also superimposed
Figure 3. Kaplan-Meier freedom from syncope recurrence after pacemaker therapy in patients
who had had an asystolic response during TT (VASIS 2B) and in those who had not.
K e
a
Kaplplplananana -MeMeMeMeieii r frfrfrf eedom from syncope recccuuru rrence after pappp cemammm ker therapy in patie
addd d aaana asystolicc rrespopponsee e ddudd riiingn TTTTT (VVAAASISIS 2B)B)B)B aaaandnndn innn thossee whwhwhw o haaad ddd nonon t..
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from

Moya, Teresa Kus, Jean Claude Deharo, Silvia Giuli, Alessandra Gentili and Richard SuttonMichele Brignole, Paolo Donateo, Marco Tomaino, Riccardo Massa, Matteo Iori, Xulio Beiras, Angel
International Study on Syncope of Uncertain Etiology (ISSUE-3)Documented Asystole is Greater when Tilt Test is Negative. An Analysis from the Third
The Benefit of Pacemaker Therapy in Patients with Presumed Neurally-Mediated Syncope and
Print ISSN: 1941-3149. Online ISSN: 1941-3084 Copyright © 2013 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Arrhythmia and Electrophysiology
published online December 12, 2013;Circ Arrhythm Electrophysiol.
http://circep.ahajournals.org/content/early/2013/12/12/CIRCEP.113.001103World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circep.ahajournals.org/content/suppl/2013/12/12/CIRCEP.113.001103.DC1.htmlData Supplement (unedited) at:
http://circep.ahajournals.org//subscriptions/
is online at: Circulation: Arrhythmia and Electrophysiology Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answerinformation about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Arrhythmia and Electrophysiology Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 8, 2016http://circep.ahajournals.org/Downloaded from

1
Supplemental material
Appendix Steering committee: Michele Brignole (Chairman), Dietrich Andresen, David Benditt, Jean Jacques Blanc, Roberto Garcia‐Civera, Andrew Krahn, Carlo Menozzi, Angel Moya, Richard Sutton, Panos Vardas, Wouter Wieling. End‐point committee: Michele Brignole, Richard Sutton, Andrea Ungar, Angel Moya. The following centers and investigators participated in this ISSUE‐3 substudy: Italy: Ospedali del Tigullio, Lavagna ‐ P.Donateo and D. Oddone; Ospedale di Bolzano, Bolzano ‐ M. Tomaino, C. Romeo, P. Sgobino and F. Pescoller; Ospedale SS. Antonio e Biagio e Cesare Arrigo, Alessandria – E. Vitale and R. Massa; Arcispedale S.Maria Nuova, Reggio Emilia ‐ C. Menozzi, F. Quartieri, M. Iori and G. Lolli; Ospedale Santa Croce, Moncalieri ‐ F. Rabjoli and C. Cecchinato; Ospedale di Manduria, Taranto ‐ V. Russo, Dr. F. Pierri and M.G. Matino; Ospedale S.Giovanni Battista Le Molinette, Torino ‐ M. Iorfida and P. Golzio; Ospedale S. Pietro Igneo, Fucecchio ‐ A. Del Rosso and V. Guernaccia; Azienda Ospedaliera Villa Scassi, Genova ‐ G. Gaggioli and M. Laffi; AO di Rilievo Nazionale e di Alta Specializzazione Garibaldi, Catania ‐ M. Gulizia and M. Francese; Ospedale di Venere, Bari ‐ M. Palella and C.D'Agostino; Ospedale Santa Croce e Carle, Cuneo ‐ A. Vado and A. Menardi; Ospedale S. Gerardo ‐ Monza, A. Vincenti and S. De Ceglia; Ospedale San Giovanni di Dio, Firenze ‐ A. Bartoletti and Domenico Rossi; Spain: Complejo Hospitalario Universitario de Vigo, Vigo ‐ X. Beiras Torrado and E.G. Campo; Hospital Universitario Vall d’Hebron, Barcelona ‐ Á. Moya, I. Roca, N. Rivas, J. Perez, G. Senador and C. Alonso; Consorcio Hospitalario Provincial de Castellón, Castellón ‐ L. Fácila Rubio, F. Perez Alcalá, V. Montagud Balaguer, A. Peset and T. Mut; Hospital Universitario Puerta de Hierro, Madrid ‐ J.Toquero Ramos, I. F. Lozano and V. Castro; Complejo Hospitalario Universitario de Albacete, Albacete ‐ J.F. García Sacristán, R. Ceres and J. Enero; Hospital General de Granollers, Granollers ‐ E. Chueca and J. Mercader; Hospital Clínico Universitario de Valencia, Valencia ‐ R. Garcia Civera, R. Ruiz Granell and S. Morell Cabedo. Germany: Vivantes Klinikum Am Urban, Berlin ‐ D. Andresen, G. Wedegärtner and I. Atmowihardjo; Kardiologiske Gemeinschaftspraxis, Riesa – H.H. Ebert and G. Stenzel; Vivantes Humboldt, Berlin – U. Bach and J. Ohler; Charité ‐ Campus Benjamin Franklin, Berlin – S. Spencker and A. Schirdewahn; Klinikum der Universität München ‐ Großhadern und Innenstadt, München – S. Kääb and M.F. Sinner; Kreiskrankenhaus Hameln, Hameln‐Pyrmont – H. Topp. United Kingdom: St Mary's Hospital, London ‐ R. Sutton and D. Francis; William Harvey Hospital, Kent ‐ K. Kamalvand and M. Asgari. Canada: Hôpital du Sacré‐Coeur de Montreal , Montreal – T. Kus and M. Strurmer; The Netherland: Academisch Medisch Centrum, Amsterdam ‐ W. Wieling and R.E. Knops; Atrium Medisch Centrum, Heerlen ‐ A.J.J. Aerst; Catharina Ziekenhuis, Eindhoven ‐ L.R.C Dekker and P.H. van der Voort; Medisch Centrum Alkmaar, Alkmaar ‐ J.H. Ruiter and J.J.C.M. Romme. France: Hôpital de la Timone, Marseille ‐ J.C. Deharo and E. Peyrouse; Switzerland: Centre Hôpitalier Universitaire Vaudois – Lausanne – E. Pruvot and D. Graf. Austria: A.ö. Bezirkskrankenhaus Hall, Hall in Tirol – W. Grander and P. Eller.
2
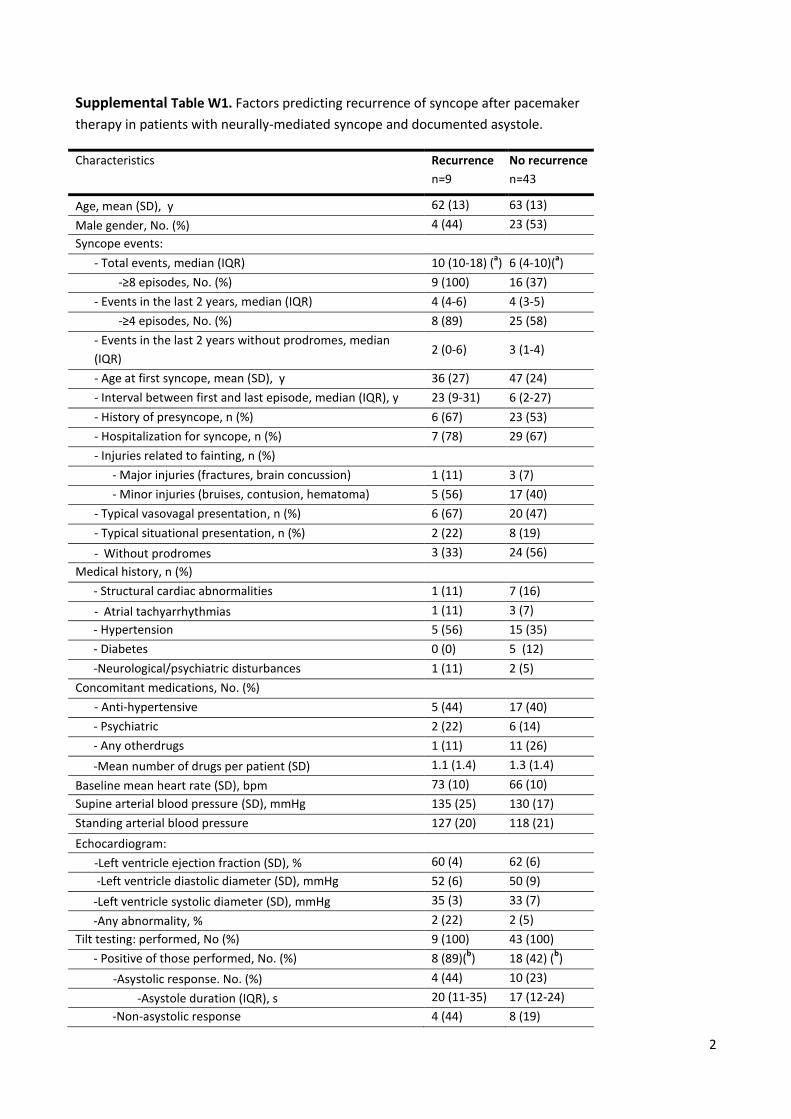
Supplemental Table W1. Factors predicting recurrence of syncope after pacemaker
therapy in patients with neurally-mediated syncope and documented asystole.
Characteristics Recurrence
n=9
No recurrence
n=43
Age, mean (SD), y 62 (13) 63 (13)
Male gender, No. (%) 4 (44) 23 (53)
Syncope events:
- Total events, median (IQR) 10 (10-18) (a) 6 (4-10)(
a)
-≥8 episodes, No. (%) 9 (100) 16 (37)
- Events in the last 2 years, median (IQR) 4 (4-6) 4 (3-5)
-≥4 episodes, No. (%) 8 (89) 25 (58)
- Events in the last 2 years without prodromes, median
(IQR) 2 (0-6) 3 (1-4)
- Age at first syncope, mean (SD), y 36 (27) 47 (24)
- Interval between first and last episode, median (IQR), y 23 (9-31) 6 (2-27)
- History of presyncope, n (%) 6 (67) 23 (53)
- Hospitalization for syncope, n (%) 7 (78) 29 (67)
- Injuries related to fainting, n (%)
- Major injuries (fractures, brain concussion) 1 (11) 3 (7)
- Minor injuries (bruises, contusion, hematoma) 5 (56) 17 (40)
- Typical vasovagal presentation, n (%) 6 (67) 20 (47)
- Typical situational presentation, n (%) 2 (22) 8 (19)
- Without prodromes 3 (33) 24 (56)
Medical history, n (%)
- Structural cardiac abnormalities 1 (11) 7 (16)
- Atrial tachyarrhythmias 1 (11) 3 (7)
- Hypertension 5 (56) 15 (35)
- Diabetes 0 (0) 5 (12)
-Neurological/psychiatric disturbances 1 (11) 2 (5)
Concomitant medications, No. (%)
- Anti-hypertensive 5 (44) 17 (40)
- Psychiatric 2 (22) 6 (14)
- Any otherdrugs 1 (11) 11 (26)
-Mean number of drugs per patient (SD) 1.1 (1.4) 1.3 (1.4)
Baseline mean heart rate (SD), bpm 73 (10) 66 (10)
Supine arterial blood pressure (SD), mmHg 135 (25) 130 (17)
Standing arterial blood pressure 127 (20) 118 (21)
Echocardiogram:
-Left ventricle ejection fraction (SD), % 60 (4) 62 (6)
-Left ventricle diastolic diameter (SD), mmHg 52 (6) 50 (9)
-Left ventricle systolic diameter (SD), mmHg 35 (3) 33 (7)
-Any abnormality, % 2 (22) 2 (5)
Tilt testing: performed, No (%) 9 (100) 43 (100)
- Positive of those performed, No. (%) 8 (89)(b) 18 (42) (
b)
-Asystolic response. No. (%) 4 (44) 10 (23)
-Asystole duration (IQR), s 20 (11-35) 17 (12-24)
-Non-asystolic response 4 (44) 8 (19)
3
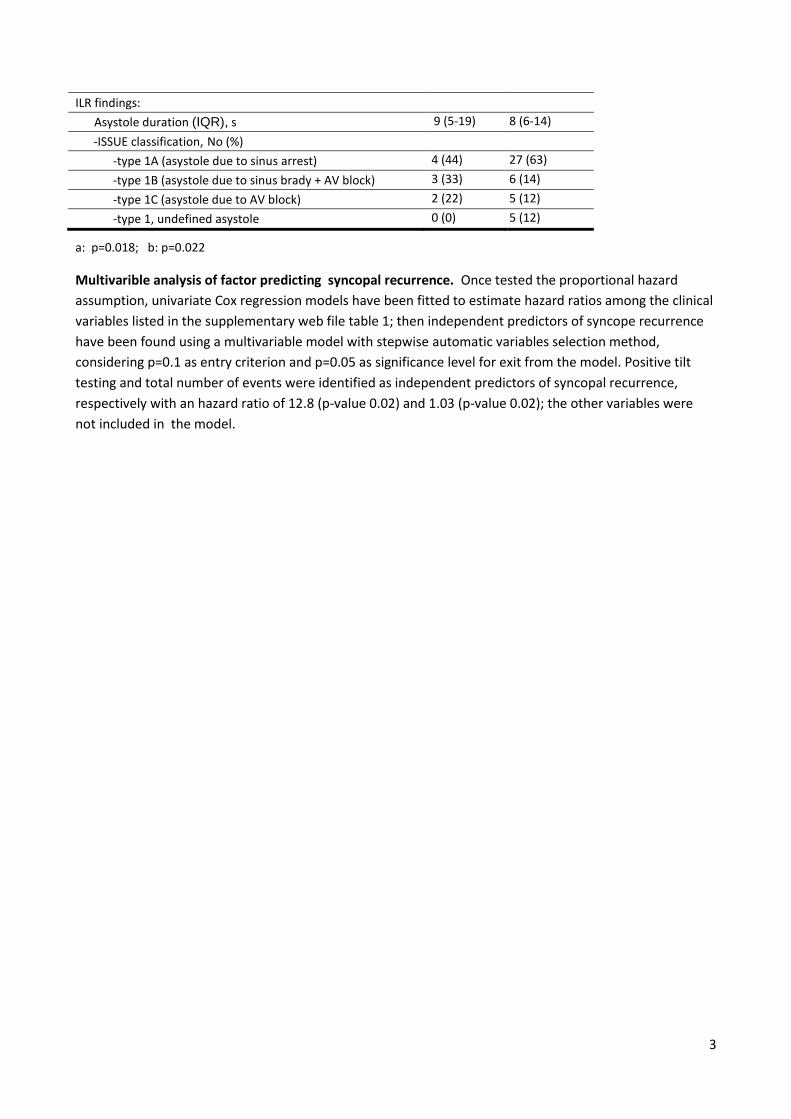
ILR findings:
Asystole duration (IQR), s 9 (5-19) 8 (6-14)
-ISSUE classification, No (%)
-type 1A (asystole due to sinus arrest) 4 (44) 27 (63)
-type 1B (asystole due to sinus brady + AV block) 3 (33) 6 (14)
-type 1C (asystole due to AV block) 2 (22) 5 (12)
-type 1, undefined asystole 0 (0) 5 (12)
a: p=0.018; b: p=0.022
Multivarible analysis of factor predicting syncopal recurrence. Once tested the proportional hazard
assumption, univariate Cox regression models have been fitted to estimate hazard ratios among the clinical
variables listed in the supplementary web file table 1; then independent predictors of syncope recurrence
have been found using a multivariable model with stepwise automatic variables selection method,
considering p=0.1 as entry criterion and p=0.05 as significance level for exit from the model. Positive tilt
testing and total number of events were identified as independent predictors of syncopal recurrence,
respectively with an hazard ratio of 12.8 (p-value 0.02) and 1.03 (p-value 0.02); the other variables were
not included in the model.

4
Supplemental table W2. Kaplan-Meier 3-monthly freedom from syncope recurrence (average and 95%
confidence interval) after pacemaker therapy in tilt-negative asystolic NMS and tilt-positive asystolic NMS
patients and in controls untreated patients.
PM TT+ 3 6 9 12 15 18 21 months
# pts at risk 14 10 9 8 6 4 3
Failure estimate % (95% CI)
21 (8-47) 33 (16-60) 33 (16-60) 40(21-67) 40(21-67) 40(21-67) 55(29-85)
PM TT- 3 6 9 12 15 18 21 months
# pts at risk 19 19 15 11 10 9 9
Failure estimate % (95% CI)
--- --- 5 (1-32) 5 (1-32) 5 (1-32) 5 (1-32) 5 (1-32)
NO THERAPY 3 6 9 12 15 18 21 months
# pts at risk 35 31 22 22 18 14 9
Failure estimate % (95% CI)
18 (10-33) 28 (17-44) 40 (27-56) 40 (27-56) 43 (29-59) 49 (35-66) 64 (47-80)
5
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
Fre
ed
om
fro
m s
yn
cop
al re
curr
ence
31 22 18 16 16 13 10 6Asystole
14 13 13 6 6 5 4 3No Asystole
Number at risk
0 3 6 9 12 15 18 21Months
log rank: p=0.68
No PM, no asystole
No PM, asystole
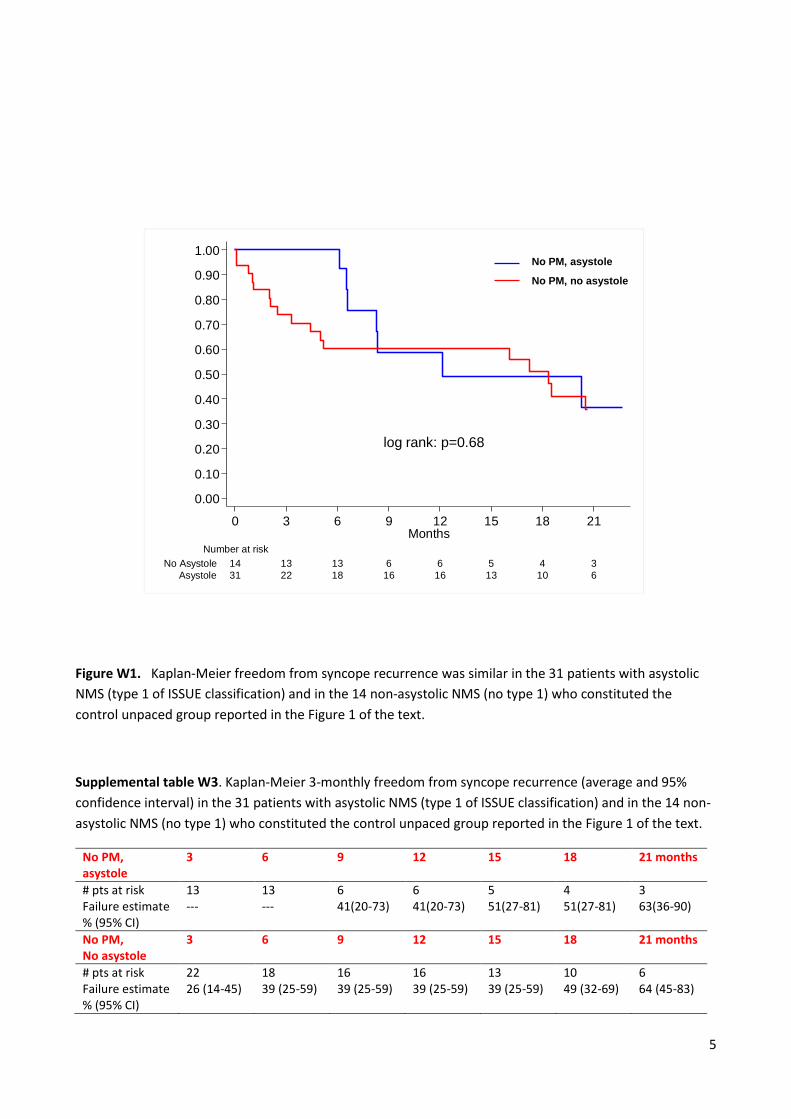
Figure W1. Kaplan-Meier freedom from syncope recurrence was similar in the 31 patients with asystolic
NMS (type 1 of ISSUE classification) and in the 14 non-asystolic NMS (no type 1) who constituted the
control unpaced group reported in the Figure 1 of the text.
Supplemental table W3. Kaplan-Meier 3-monthly freedom from syncope recurrence (average and 95%
confidence interval) in the 31 patients with asystolic NMS (type 1 of ISSUE classification) and in the 14 non-
asystolic NMS (no type 1) who constituted the control unpaced group reported in the Figure 1 of the text.
No PM, asystole
3 6 9 12 15 18 21 months
# pts at risk 13 13 6 6 5 4 3 Failure estimate % (95% CI)
--- --- 41(20-73) 41(20-73) 51(27-81) 51(27-81) 63(36-90)
No PM, No asystole
3 6 9 12 15 18 21 months
# pts at risk 22 18 16 16 13 10 6 Failure estimate % (95% CI)
26 (14-45) 39 (25-59) 39 (25-59) 39 (25-59) 39 (25-59) 49 (32-69) 64 (45-83)




















