Ranibizumab for Macular Edema Due to Retinal Vein Occlusions: Implication of VEGF as a Critical...
9
Ranibizumab for Macular Edema Due to Retinal Vein Occlusions: Implication of VEGF as a Critical Stimulator Peter A Campochiaro 1 , Gulnar Hafiz 1 , Syed Mahmood Shah 1 , Quan Dong Nguyen 1 , Howard Ying 1 , Diana V Do 1 , Edward Quinlan 1 , Ingrid Zimmer-Galler 1 , Julia A Haller 1 , Sharon D Solomon 1 , Jennifer U Sung 1 , Yasmin Hadi 1 , Kashif A Janjua 1 , Nida Jawed 1 , David F Choy 2 and Joseph R Arron 2 1 Department of Ophthalmology, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA; 2 Immunology, Tissue Growth, and Repair Diagnostics and Biomarkers Genentech, Inc., South San Francisco, California, USA Macular edema is a major cause of vision loss in patients with central retinal vein occlusion (CRVO) or branch reti- nal vein occlusion (BRVO). It is not clear how much of the edema is due to hydrodynamic changes from the obstruction and how much is due to chemical media- tors. Patients with macular edema due to CRVO (n = 20) or BRVO (n = 20) were randomized to receive three monthly injections of 0.3 or 0.5 mg of ranibizumab. At the primary endpoint, month 3, the median improve- ment in letters read at 4 m was 17 in the 0.3-mg group and 14 in the 0.5-mg group for CRVO, and 10 and 18, respectively for the BRVO group. Optical coherence tomography (OCT) showed that compared to injections of 0.3 mg, injections of 0.5 mg of ranibizumab tended to cause more rapid reductions of central retinal thickening that lasted longer between injections, but in 3 months, excess central retinal thickening which is a quantita- tive assessment of the macular edema, was reduced by ~90% in all four treatment groups. There was no correla- tion between the amount of improvement and duration of disease or patient age at baseline, but there was some correlation between the aqueous vascular endothelial growth factor (VEGF) level at baseline and amount of improvement. These data indicate that excess produc- tion of VEGF in the retinas of patients with CRVO or BRVO is a major contributor to macular edema and sug- gest that additional studies investigating the efficacy of intraocular injections of ranibizumab are needed. Received 28 September 2007; accepted 7 January 2008; published online 5 February 2008. doi:10.1038/mt.2008.10 INTRODUCTION e pathogenesis of central retinal vein occlusions (CRVOs) is poorly understood. In the early stages, there are scattered hemorr- hages throughout the entire retina, cotton wool patches, a sign of retinal ischemia, and massive edema of the retina. Fluorescein angiography oſten shows delayed filling of retinal veins suggesting reduced blood flow, staining of the walls of retinal veins, and leakage of dye into the retina. It has been concluded that this picture most likely occurs from thrombosis within the central retinal vein caus- ing partial obstruction of blood flow from the eye, increased intra- luminal pressure in the retinal veins, and increased transudation of blood and plasma into the retina. Histopathology has confirmed the presence of a thrombus in the central retinal vein in several cases. 1 e marked increase in interstitial fluid and protein increases interstitial pressure and is likely to be an impediment to capillary perfusion resulting in ischemia. e subacute stage varies among patients depending primarily upon the amount of retinal ischemia, and patients are classified as ischemic or nonischemic, although it is not an all or none dichotomy. In some patients ischemia increases over time and they are viewed as undergoing a transition from nonis- chemic to ischemic. Severe retinal ischemia can be complicated by retinal neovascularization, iris neovascularization, neovascular glau- coma, and a very poor visual outcome. us the amount of retinal ischemia is one of the major determinants of outcome. ose patients classified as nonischemic still have retinal isch- emia, as demonstrated by cotton wool patches and areas of capil- lary nonperfusion seen in fluorescein angiograms. ese patients oſten enter a chronic stage in which they have severe macular edema that may last for many months and oſten years. Eventually the edema may resolve, presumably because there is resolution of the venous obstruction due to recanalization and/or formation of collateral vessels, but generally the visual outcome is poor due to damage to macular photoreceptors from the chronic edema, poor perfusion of perifoveal capillaries, or both. 2 Hypertension is a major risk factor for branch retinal vein occlusions (BRVOs). 3 Chronic hypertension leads to thickening of the walls of retinal arterioles and since retinal arterioles and veins share a common adventitia at crossings, this may cause constriction of retinal veins that can lead to occlusions. 4,5 e complications of BRVOs are similar to those for CRVOs but more limited in scope, because only part of the retina is drained by the involved branch vein. ere is increased luminal pressure distal to the obstruction resulting in increased transudation of blood and plasma, increased interstitial fluid pressure, and reduced Correspondence: Peter A. Campochiaro, Maumenee 719, The Wilmer Eye Institute, The Johns Hopkins University School of Medicine, 600 North Wolfe Street, Baltimore, Maryland 21287-9277, USA. E-mail: [email protected] © The American Society of Gene Therapy original article Molecular Therapy vol. 16 no. 4, 791–799 april 2008 791
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Ranibizumab for Macular Edema Due to Retinal Vein Occlusions: Implication of VEGF as a Critical...

Ranibizumab for Macular Edema Due to Retinal Vein Occlusions: Implication of VEGF as a Critical StimulatorPeter A Campochiaro1, Gulnar Hafiz1, Syed Mahmood Shah1, Quan Dong Nguyen1, Howard Ying1, Diana V Do1, Edward Quinlan1, Ingrid Zimmer-Galler1, Julia A Haller1, Sharon D Solomon1, Jennifer U Sung1, Yasmin Hadi1, Kashif A Janjua1, Nida Jawed1, David F Choy2 and Joseph R Arron2
1Department of Ophthalmology, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA; 2Immunology, Tissue Growth, and Repair Diagnostics and Biomarkers Genentech, Inc., South San Francisco, California, USA
Macular edema is a major cause of vision loss in patients with central retinal vein occlusion (CRVO) or branch reti-nal vein occlusion (BRVO). It is not clear how much of the edema is due to hydrodynamic changes from the obstruction and how much is due to chemical media-tors. Patients with macular edema due to CRVO (n = 20) or BRVO (n = 20) were randomized to receive three monthly injections of 0.3 or 0.5 mg of ranibizumab. At the primary endpoint, month 3, the median improve-ment in letters read at 4 m was 17 in the 0.3-mg group and 14 in the 0.5-mg group for CRVO, and 10 and 18, respectively for the BRVO group. Optical coherence tomography (OCT) showed that compared to injections of 0.3 mg, injections of 0.5 mg of ranibizumab tended to cause more rapid reductions of central retinal thickening that lasted longer between injections, but in 3 months, excess central retinal thickening which is a quantita-tive assessment of the macular edema, was reduced by ~90% in all four treatment groups. There was no correla-tion between the amount of improvement and duration of disease or patient age at baseline, but there was some correlation between the aqueous vascular endothelial growth factor (VEGF) level at baseline and amount of improvement. These data indicate that excess produc-tion of VEGF in the retinas of patients with CRVO or BRVO is a major contributor to macular edema and sug-gest that additional studies investigating the efficacy of intraocular injections of ranibizumab are needed.
Received 28 September 2007; accepted 7 January 2008; published online 5 February 2008. doi:10.1038/mt.2008.10
IntroductIonThe pathogenesis of central retinal vein occlusions (CRVOs) is poorly understood. In the early stages, there are scattered hemorrhages throughout the entire retina, cotton wool patches, a sign of retinal ischemia, and massive edema of the retina. Fluorescein angiography often shows delayed filling of retinal veins suggesting
reduced blood flow, staining of the walls of retinal veins, and leakage of dye into the retina. It has been concluded that this picture most likely occurs from thrombosis within the central retinal vein causing partial obstruction of blood flow from the eye, increased intraluminal pressure in the retinal veins, and increased transudation of blood and plasma into the retina. Histopathology has confirmed the presence of a thrombus in the central retinal vein in several cases.1 The marked increase in interstitial fluid and protein increases interstitial pressure and is likely to be an impediment to capillary perfusion resulting in ischemia. The subacute stage varies among patients depending primarily upon the amount of retinal ischemia, and patients are classified as ischemic or nonischemic, although it is not an all or none dichotomy. In some patients ischemia increases over time and they are viewed as undergoing a transition from nonischemic to ischemic. Severe retinal ischemia can be complicated by retinal neovascularization, iris neovascularization, neovascular glaucoma, and a very poor visual outcome. Thus the amount of retinal ischemia is one of the major determinants of outcome.
Those patients classified as nonischemic still have retinal ischemia, as demonstrated by cotton wool patches and areas of capillary nonperfusion seen in fluorescein angiograms. These patients often enter a chronic stage in which they have severe macular edema that may last for many months and often years. Eventually the edema may resolve, presumably because there is resolution of the venous obstruction due to recanalization and/or formation of collateral vessels, but generally the visual outcome is poor due to damage to macular photoreceptors from the chronic edema, poor perfusion of perifoveal capillaries, or both.2
Hypertension is a major risk factor for branch retinal vein occlusions (BRVOs).3 Chronic hypertension leads to thickening of the walls of retinal arterioles and since retinal arterioles and veins share a common adventitia at crossings, this may cause constriction of retinal veins that can lead to occlusions.4,5 The complications of BRVOs are similar to those for CRVOs but more limited in scope, because only part of the retina is drained by the involved branch vein. There is increased luminal pressure distal to the obstruction resulting in increased transudation of blood and plasma, increased interstitial fluid pressure, and reduced
Correspondence: Peter A. Campochiaro, Maumenee 719, The Wilmer Eye Institute, The Johns Hopkins University School of Medicine, 600 North Wolfe Street, Baltimore, Maryland 21287-9277, USA. E-mail: [email protected]
© The American Society of Gene Therapy original article
Molecular Therapy vol. 16 no. 4, 791–799 april 2008 791

792 www.moleculartherapy.org vol. 16 no. 4 april 2008
© The American Society of Gene TherapyRanibizumab for Macular Edema in Vein Occlusions
capillary perfusion causing ischemia. Since the area of ischemic retina tends to be much less than that in patients with CRVO, iris neovascularization and neovascular glaucoma are rare, but retinal neovascularization adjacent to the ischemic retina can occur and can cause vitreous hemorrhages necessitating scatter photocoagulation to the ischemic retina. The most common cause of reduced vision is macular edema, but nonperfusion of perifoveal capillaries can also be another contributing factor. Grid laser photocoagulation to the poorly perfused retina adjacent to the fovea can help to resolve macular edema and improve vision.6
Thus, in both CRVO and BRVO, retinal ischemia occurs and serves as an exacerbating factor. The ischemic retina releases vascular endothelial growth factor (VEGF) which underlies neovascular complications, but also causes excessive vascular permeability.7,8 Hence, the release of VEGF is likely to contribute to macular edema. In this study, we investigated the potential contribution of VEGF to macular edema in patients with CRVO and BRVO by testing the effects of intraocular injections of ranibizumab (Lucentis; Genentech, South San Francisco, CA), an Fab fragment that binds and neutralizes all isoforms of VEGFA.9
resultsBaseline characteristics of study patientsThe baseline characteristics of patients are shown in Table 1. For CRVO patients, the 0.5mg group was somewhat older than the 0.3mg group and had a longer duration of disease.
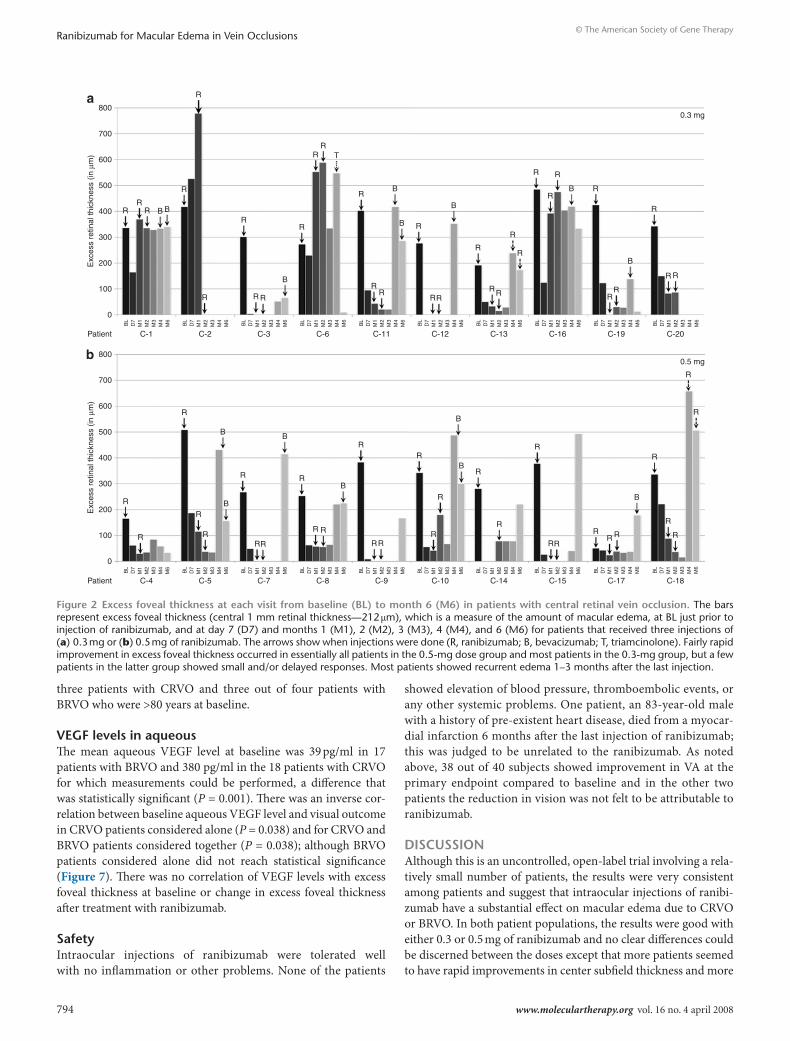
effect of ranibizumab on central retinal (foveal) thickeningFigure 1 shows optical coherence tomography (OCT) scans at all time points up to the primary endpoint for five randomly selected patients with CRVO randomized to each dose. Although the response varied somewhat among patients in each group, most patients showed substantial reduction in central retinal thickness over time. Within 7 days of the first injection, 8 out of 10 patients in the 0.3mg group and 9 out of 10 in the 0.5mg group had a substantial improvement in edema as assessed by OCT (Figure 2a and b). Four patients in the 0.3mg group showed a worsening of the thickening between the time points of 1 week and 1 month but improved after the next two injections, while the other six showed persistent improvement 1 month after the first injection that improved further with subsequent injections (Figure 2a). All the patients in the 0.5mg dose group showed the latter pattern of response (Figure 2b). Figure 3 shows the OCT scans of the five randomly selected patients with BRVO randomized to each group. They tended to show rapid and sustained responses after the first injection of 0.3 or 0.5 mg of ranibizumab with further improvement after subsequent injections. Measurements of central retinal thickening confirmed that this was the case for most patients, but two in the 0.3mg group and one in the 0.5mg group showed slight worsening between the time points of 1 week and 1 month (Figure 4).
In patients with CRVO, the median excess foveal thickness was 340 µm at baseline in the 0.3mg group and 7 days after the first injection it improved to 124 µm, thus eliminating 64% of the edema (Figure 5a). In the 0.5mg group, the median excess foveal thickness improved from 309 µm at baseline to 53 µm 1 week after
the first injection, thus eliminating 83% of the edema (Figure 5b). At the primary endpoint of 3 months, excess foveal thickness was reduced to 25 µm (eliminating 93% of the edema) in the 0.3mg group, and 35 µm (eliminating 89% of the edema), in the 0.5mg group. Thus, in patients with CRVO, edema was reduced to a greater extent and the reduction was more sustained after a single injection of 0.5 mg of ranibizumab compared to 0.3 mg, but after three injections of either dose, most of the edema, i.e., ~90%, had been eliminated.
In patients with macular edema due to BRVO, the median excess foveal thickness was 270 µm at baseline in the 0.3mg group and 7 days after the first injection it improved to 48 µm, thus eliminating 82% of the edema (Figure 5c). In the 0.5mg group, the median excess foveal thickness was 294 µm at baseline and 7 days after the first injection it improved to 51 µm, eliminating 83% of the edema (Figure 5d). At the primary endpoint, excess foveal thickness was essentially eliminated in each group.
The last injection was at the time point of month 2; by month 4 in some patients and month 6 in most patients there was recurrent edema in patients with CRVO and worsening of the edema
table 1 Baseline characteristics
crVo BrVo
0.3 mg 0.5 mg 0.3 mg 0.5 mg
Age (years)
Mean ± SD 63 ± 17 68 ± 13 69 ± 13 65 ± 10
Median 69 70 68 65
Range 34–83 48–83 43–84 50–82
Duration of disease (months)
Mean ± SD 9 ± 7 16 ± 17 5 ± 3 3 ± 2
Median 7.4 13 5 3
Range 1–26 0.5–53 0.4–9 0.8–6
Systemic disease
Diabetes 3 3 3 3
Hypertension 5 6 9 8
Hyperlipidema 4 7 7 3
Elevated homocysteine 1 3 3 6
Ocular disease
Glaucoma 1 3 0 1
Other 2 5 5 3
Prior treatment
Bevacizumab 0 0 1 2
Steroids 1 2 2 2
Laser 1 3 4 3
Visual acuity (ETDRS letters read at 4 m)
Mean ± SD 16 ± 13 23 ± 15 26 ± 12 20 ± 14
Median 18 26 29 23
Excess foveal thickness (in μm)
Mean ± SD 346 ± 88 297 ± 126 252 ± 104 288 ± 101
Median 340 309 270 294
Abbreviations: BRVO, branch retinal vein occlusion; CRVO, central retinal vein occlusion; ETDRS, Early Treatment Diabetic Retinopathy Study.

Molecular Therapy vol. 16 no. 4 april 2008 793
© The American Society of Gene TherapyRanibizumab for Macular Edema in Vein Occlusions
tended to occur sooner after the last injection in the 0.3mg group compared to the 0.5mg group. In the 0.3mg/CRVO group, seven, and then five patients were given another treatment (usually an offlabel injection of bevacizumab) at the time points of months 4 and 6, respectively. In the 0.5mg/CRVO group, three, and then six patients received additional injections at the time points of months 4 and 6, respectively. In patients with BRVO, recurrent edema was somewhat less frequent than in patients with CRVO, but still occurred in several patients. In the 0.3mg/BRVO group, one, and then two patients received additional injections at the time points of months 4 and 6, respectively, and in the 0.5mg/BRVO group, four patients, and then one, received additional injections at time points of months 4 and 6, respectively.
effect of ranibizumab on visual acuityIn the CRVO group at the primary endpoint, the change from baseline (in the median number of letters read on an Early Treatment Diabetic Retinopathy Study chart) at 4 m was 17 and 14 in patients treated with 0.3 or 0.5 mg of ranibizumab, respectively (Figure 5a and b). All the patients in the 0.3mg group and eight patients in the 0.5mg group showed improvement in vision at the primary endpoint compared to baseline. One of the patients showed a reduction of 16 letters at the endpoint of 3 months, that was back to baseline at 4 months. The other patient showed a reduction of 11 letters at the endpoint of 3 months that was judged to be due to progression of edema despite administration of ranibizumab; there was no evidence of ischemia or any other problem that could be attributed to the drug. The percentage of patients with
clinically significant visual improvement defined as an improvement of ≥15 letters was 70% in the 0.3mg group and 40% in the 0.5mg group.
At the primary endpoint in patients with macular edema due to BRVO, the median change in visual acuity (VA) from baseline was 10 letters in the 0.3mg group, and 18 in the 0.5mg dose group (Figure 5c and d). One patient in the 0.5mg dose group showed a reduction in VA of three letters at the primary endpoint, but all other patients showed improved vision. The percentage of patients with clinically significant visual improvement defined as an improvement of ≥15 letters was 40% in the 0.3mg group and 70% in the 0.5mg group.
effect of duration of disease and patient’s age on visual outcomeFigure 6 shows scatter plots of change from baseline in VA versus the patient’s age or duration of disease for patients with CRVO or BRVO treated with ranibizumab. There was no correlation between the amount of improvement in VA and duration of edema. There were four patients who had edema from CRVO for >2 years prior to starting injections of ranibizumab and three of them improved in VA by >15 letters. Three patients had edema from BRVO for >2 years at baseline and they showed improvements of 41, 21, and 14 letters in 3 months. Therefore, chronic edema from a vein occlusion does not preclude visual improvement as a result of intraocular injections of ranibizumab. There was no correlation between the patient’s age and visual improvement; improvement in VA of >15 letters occurred in two out of
a C-1 C-3 C-6 C-16 C-19
C-5
BL
D7
M1
M2
M3
BL
D7
M1
M2
M3
C-8 C-10 C-15 C-17b
Figure 1 cross sections through the fovea obtained by optical coherence tomography in patients with central retinal vein occlusion. The hori-zontal cross sections at baseline (BL), day 7 (D7), month 1 (M1), month 2 (M2), and month 3 (M3, primary endpoint) are shown for five randomly selected patients of the 10 patients treated with (a) 0.3 mg or (b) 0.5 mg of ranibizumab.
794 www.moleculartherapy.org vol. 16 no. 4 april 2008
© The American Society of Gene TherapyRanibizumab for Macular Edema in Vein Occlusions
three patients with CRVO and three out of four patients with BRVO who were >80 years at baseline.
VeGF levels in aqueousThe mean aqueous VEGF level at baseline was 39 pg/ml in 17 patients with BRVO and 380 pg/ml in the 18 patients with CRVO for which measurements could be performed, a difference that was statistically significant (P = 0.001). There was an inverse correlation between baseline aqueous VEGF level and visual outcome in CRVO patients considered alone (P = 0.038) and for CRVO and BRVO patients considered together (P = 0.038); although BRVO patients considered alone did not reach statistical significance (Figure 7). There was no correlation of VEGF levels with excess foveal thickness at baseline or change in excess foveal thickness after treatment with ranibizumab.
safetyIntraocular injections of ranibizumab were tolerated well with no inflammation or other problems. None of the patients
showed elevation of blood pressure, thromboembolic events, or any other systemic problems. One patient, an 83yearold male with a history of preexistent heart disease, died from a myocardial infarction 6 months after the last injection of ranibizumab; this was judged to be unrelated to the ranibizumab. As noted above, 38 out of 40 subjects showed improvement in VA at the primary endpoint compared to baseline and in the other two patients the reduction in vision was not felt to be attributable to ranibizumab.
dIscussIonAlthough this is an uncontrolled, openlabel trial involving a relatively small number of patients, the results were very consistent among patients and suggest that intraocular injections of ranibizumab have a substantial effect on macular edema due to CRVO or BRVO. In both patient populations, the results were good with either 0.3 or 0.5 mg of ranibizumab and no clear differences could be discerned between the doses except that more patients seemed to have rapid improvements in center subfield thickness and more
0
Patient
BL
D7
M1
M2
C-1 C-2 C-3 C-6 C-11 C-12 C-13 C-16 C-19 C-20
0.3 mg
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
100
200
300
400 R
R
R
R
R
R
B
R
B B
R
R R
B
RR
R
B
BR
R
R
RR
RR R
B
R
R
R
R
R
RRRRR
RR B B
R
R
R
R
R R
B
R
RR
T
R
RR
B
B R
B
R
RR
R
R
R
R
R
B R
RR
B
R
R R
RR
500
600
Exc
ess
retin
al th
ickn
ess
(in µ
m)
700
800a
0
Patient
BL
D7
M1
M2
C-4 C-5 C-7 C-8 C-9 C-10 C-14 C-15 C-17 C-18
0.5 mg
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
100
200
300
400
500
600
Exc
ess
retin
al th
ickn
ess
(in µ
m)
700
800b
Figure 2 excess foveal thickness at each visit from baseline (Bl) to month 6 (M6) in patients with central retinal vein occlusion. The bars represent excess foveal thickness (central 1 mm retinal thickness—212 µm), which is a measure of the amount of macular edema, at BL just prior to injection of ranibizumab, and at day 7 (D7) and months 1 (M1), 2 (M2), 3 (M3), 4 (M4), and 6 (M6) for patients that received three injections of (a) 0.3 mg or (b) 0.5 mg of ranibizumab. The arrows show when injections were done (R, ranibizumab; B, bevacizumab; T, triamcinolone). Fairly rapid improvement in excess foveal thickness occurred in essentially all patients in the 0.5-mg dose group and most patients in the 0.3-mg group, but a few patients in the latter group showed small and/or delayed responses. Most patients showed recurrent edema 1–3 months after the last injection.

Molecular Therapy vol. 16 no. 4 april 2008 795
© The American Society of Gene TherapyRanibizumab for Macular Edema in Vein Occlusions
had improvements that lasted for a month after the initial injection in the 0.5mg groups compared to the 0.3mg groups. However, at the 3month primary endpoint, 1 month after the third injection, ~90% of excess foveal thickness was eliminated in both patient populations with either dose. In addition, improvements from baseline in VA were large in both dose groups for patients with macular edema due to CRVO or BRVO. These results are very encouraging and strongly support the performance of larger, more definitive studies.
The Central Retinal Vein Occlusion Study was a large multicenter trial that investigated the effect of grid laser photocoagulation in patients with macular edema due to CRVO.10 Although 69% of patients in the treated group compared to 0% in the untreated group showed reduction of fluorescein leakage in the macula at the end of 1 year, there was no difference in the final VA (20/200 in treated patients versus 20/160 in untreated patients). It has been felt that a possible explanation is that chronic edema due to CRVO leads to permanent visual loss. Our data demonstrate that visual improvement is possible in some patients who have had edema for >1 year and in some cases several years. In fact, there was no inverse correlation between duration of edema at baseline and improvement in VA after three injections of ranibizumab, suggesting that patients with chronic edema should not be excluded from treatment based solely upon the duration of edema. Our data suggest that chronicity of edema and the relatively slow resolution of edema after grid laser therapy are not likely to explain the poor visual results after grid laser therapy. Our data also suggest that elderly patients with macular edema due to CRVO or BRVO should not be excluded from treatment with intraocular
ranibizumab, because the patient’s age being advanced at baseline did not negatively impact the outcome.
No drugrelated adverse effects such as elevation of blood pressure, thromboembolic events, or any other systemic problems were observed. This provides some preliminary data, suggesting that intraocular injections of ranibizumab are welltolerated in patients with retinal vein occlusions just as they are in patients with neovascular agerelated macular degeneration.11,12
Measurement of VEGF levels in aqueous demonstrated a higher mean level in patients with CRVO compared to patients with BRVO. In patients with CRVO there was an inverse correlation with VEGF level at baseline and the visual outcome. Further work is needed to determine the predictive value of baseline aqueous levels of VEGF and to determine the range of VEGF levels that occur in other disease processes such as neovascular agerelated macular degeneration and diabetic macular edema.
In addition to grid laser therapy, several treatments have been tried in patients with macular edema due to CRVO including the use of anticoagulants, fibrinolytics, steroids, acetozolamide, isovolemic hemodilution, surgically induced retinochoroidal anastamoses or laserinduced retinochoroidal anastamoses, and radial optic neurotomy. A recent metaanalysis of all published randomized clinical trials concluded that there is no convincing evidence that any of these treatments provide benefit.13 In contrast, grid laser therapy provides modest benefit in patients with macular edema due to BRVO;6 after 3 years, patients treated with grid laser photocoagulation improved by 1.33 lines from baseline compared to an improvement of 0.23 lines in the control group. There are several case series suggesting possible benefit
a B-6 B-7 B-8 B-14 B-17
B-2
BL
D7
M1
M2
M3
BL
D7
M1
M2
M3
B-5 B-9 B-10 B-13b
Figure 3 cross sections through the fovea obtained by optical coherence tomography in patients with branch retinal vein occlusion. The hori-zontal cross sections at baseline (BL), day 7 (D7), month 1 (M1), month 2 (M2), and month 3 (M3, primary endpoint) are shown for five randomly selected patients of the ten patients treated with (a) 0.3 mg or (b) 0.5 mg of ranibizumab.

796 www.moleculartherapy.org vol. 16 no. 4 april 2008
© The American Society of Gene TherapyRanibizumab for Macular Edema in Vein Occlusions
from intraocular steroids and the ongoing Standard Care vs. Corticosteroid for Retinal Vein Occlusion Study should determine if there truly is benefit. There are also case series suggesting possible benefit from intraocular injections of bevacizumab.14–18 When examined together, these reports and our study suggest that VEGF plays an important role in the development of macular edema in retinal vein occlusions. Hemodynamic changes from the vascular occlusion lead to reduced retinal perfusion and ischemia causing increased production of VEGF. The increased production of VEGF is the major cause of macular edema, because blockade of the VEGF results in substantial improvement in the edema.
The results of our study are very encouraging because of the magnitude and consistency of response among patients and the rarity of spontaneous improvements in patients with macular edema due to CRVO;10 however, they are not definitive because of the relatively small number of patients studied, the lack of a control group, and the short followup. A major unanswered question is the duration of treatment that will be needed. Three injections was not sufficient in achieving longterm benefit in most of our patients and it is important to determine if and when injections
can be terminated without recurrent edema. The CRUISE and BRAVO phase III trials investigating the effect of ranibizumab in patients with macular edema due to CRVO or BRVO are underway and should provide a definitive answer as to the usefulness of intraocular ranibizumab in these conditions.
MaterIals and MethodsThe protocol for this study was designed to test the effect of two doses of ranibizumab, 0.3 and 0.5 mg, in patients with macular edema due to CRVO or BRVO and was approved by the Federal Drug Administration under a physicianinitiated investigational new drug application and by the Institutional Review Board of the Johns Hopkins Medical Institutions. This study was conducted in compliance with the Declaration of Helsinki, US Code 21 of Federal Regulations, and the Harmonized Tripartite Guidelines for Good Clinical Practice (1996). Twenty patients with CRVO and 20 patients with BRVO were randomized 1:1 to receive three monthly intraocular injections of 0.3 or 0.5 mg of ranibizumab, with both patients and investigators masked with respect to treatment group. The primary endpoint was 3 months after the first injection and 1 month after the third injection. The primary outcome measure was the percentage of patients who achieved an improvement in VA from baseline for ≥15 letters read on an Early Treatment Diabetic Retinopathy Study VA chart at 4 m. Secondary outcome
0
Patient
BL
D7
M1
M2
B-3 B-6 B-7 B-8 B-11 B-14 B-15 B-17 B-19 B-20
0.3 mg
0.5 mg
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
100
200
300
400
500
600
Exc
ess
retin
al th
ickn
ess
(in µ
m)
700
800a
0
Patient
BL
D7
M1
M2
B-1 B-2 B-4 B-5 B-9 B-10 B-12 B-13 B-16 B-18
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
BL
D7
M1
M2
M3
M4
M6
100
200
300
400
500
600
Exc
ess
retin
al th
ickn
ess
(in µ
m)
700
800b
R
R
R
R
R
R
R
R
R R
R
RR B
R
RR
R
R R
R
RR
R
RR
R
RR
RR
B B
R
RR
R
RR
R
R R
R
RR
R
RR
R
RR
R
RR
RR
R
R
R R
R
R R
L
B
BB
B
B
Figure 4 excess foveal thickness at each visit from baseline (Bl) to month 6 (M6) in patients with branch retinal vein occlusion. The bars represent excess foveal thickness (central 1 mm retinal thickness—212 µm), which is a measure of the amount of macular edema, at BL just prior to injection of ranibizumab, and at day 7 (D7) and months 1 (M1), 2 (M2), 3 (M3), 4 (M4), and 6 (M6) for patients who received three injections of (a) 0.3 mg or (b) 0.5 mg of ranibizumab. The arrows show when injections of ranibizumab were done. The response was uniformly good in all patients of both groups. Several patients in each group showed recurrent edema 1–3 months after the last injection.

Molecular Therapy vol. 16 no. 4 april 2008 797
© The American Society of Gene TherapyRanibizumab for Macular Edema in Vein Occlusions
measures were mean and median change in VA at several time points after study entry and change in excess foveal thickness measured by OCT.19,20
Inclusion and exclusion criteria. Patients >18 years with VA between 20/30 and 20/400 from macular edema due to CRVO or BRVO were eligible if foveal thickness (central subfield) was >250 µm and none of the following exclusion criteria were present: (i) VA <20/400 in the fellow eye, (ii) a sign of possible permanent vision loss in the study eye such as atrophy or prominent pigmentary change in the macula, (iii) laser photocoagulation or intraocular surgery within the previous 3 months, (iv) intraocular injection of a VEGF antagonist within the previous 3 months, (v) intraocular steroids within the previous 4 months, or (vi) vitreomacular traction or an epiretinal membrane.
Study protocol. Consenting patients were screened for the study by taking down their medical history, conducting a physical examination, measuring bestcorrected VA by an experienced examiner using the Early Treatment Diabetic Retinopathy Study protocol,21 conducting a complete eye examination, an OCT, doing a fluorescein angiogram, and laboratory tests on blood and urine. Patients who entered the study underwent an anterior chamber tap and were randomized to receive an intraocular injection of 0.3 or 0.5 mg of ranibizumab. Patients returned 1 week later for a repeat examination and OCT. Intraocular injections of ranibizumab were given at time points of 1 and 2 months, and the primary endpoint was at 3 months. Safety evaluations, measurement of bestcorrected VA,
eye examinations, and OCTs were done at all study visits, and fluorescein angiograms were done at baseline and 3 months.
Administration of study drug. Povidone iodine was used to clean the lids and a lid speculum was inserted. Topical anesthesia was applied and the conjunctiva was irrigated with 5% povidone iodine. A 30gauge needle was inserted through the pars plana and 0.05 ml of ranibizumab was injected into the vitreous cavity. Funduscopic examination was done to confirm retinal perfusion.
OCTs. OCT scans were performed by an experienced investigator with a StratusOCT3 (Carl Zeiss Meditec, Dublin, CA) using the fast macular scan protocol. This protocol consists of six line scans that are 6.0mm long centered on fixation and spaced 30° apart around the circumference of a circle. Each line consists of 128 Ascan measurements. With each Ascan, the OCT software measures the distance between the inner surface of the retina and the anterior border of retinal pigmented epitheliumchoriocapillaris complex based on changes in reflectivity. In some cases the retinal pigmented epithelium/choriocapillaris layer is obscured due to excessive edema and StratusOCT software misinterprets the outer boundary of the retina. We used the RetinaTomographer (version 1.1; RIRRC, Baltimore, MD) to correct the outer boundary of the retina for cases in which StratusOCT software identified it erroneously.
The center point thickness, also known as the foveolar thickness, is a mean value generated by the StratusOCT software from the six central
350E
xces
s re
tinal
thic
knes
s (in
µm
)25
D7 M1 M2 M3 M4 M6Baseline
20
15
10
5
0
300
250
200 3 Lines
CRVO: 0.3 mg
2 Lines150
100
50
0
340
0
10
FTH
0=212 µm
∆ VA
N
7 7 15 17 13 11
810 9101010
124 64 26 334 12025
a
25
D7 M1 M2 M3 M4 M6Baseline0=212 µm
20
15
10
5
0
350
2 Lines
3 Lines
300
250
200
150
100
50
0
Exc
ess
retin
al th
ickn
ess
(in µ
m)
1010101010
0 6.5
269.5
N
∆ VA
FTH 47.5
10 14 9.5
0 42 56
157.5
0.530.5
10 9
BRVO: 0.3 mgc
25350
300
250
200
150
100
50
D7 M1 M2 M3 M4 M60
Baseline
20
15
10
5
0
Cha
nge
from
bas
elin
e in
Va
309
0 4 8 11 14
10
4
10
3
1010101010
53 28 38 35 69 223
3 Lines
CRVO: 0.5 mg
2 Lines
FTH
0=212 µm
∆ VA
N
b
25350
300
250
200
150
100
50
D7
0
294
M1 M2 M3 M4 M6Baseline
20
15
10
5
0
3 Lines
2 Lines
0
Cha
nge
from
bas
elin
e in
Va
0=212 µm
N
∆ VA
FTH
10 10 10 10 10
1517.518.514.57.5
50.5 19 18 12.5 103.5 79.5
10 10
14.5
BRVO: 0.5 mgd
Figure 5 Median excess foveal thickness and median change from baseline in visual acuity (Va) for patients in each of the four treatment groups. The bars show the median excess foveal thickness at baseline, day 7 (D7), and months 1 (M1), 2 (M2), 3 (M3), 4 (M4), and 6 (M6) for patients with central retinal vein occlusion (CRVO) who received three injections of (a) 0.3 or (b) 0.5 mg of ranibizumab or patients with branch retinal vein occlusion (BRVO) who received (c) 0.3 or (d) 0.5 mg of ranibizumab. The scale, in microns, for excess foveal thickness is shown along the left side of each graph. The median number of letters for VA that has improved from baseline is shown by the points connected by lines and the scale is located along the right side of each graph. The arrows show when injections of ranibizumab were done. Substantial improvements in edema and VA occurred in each group. After injections were stopped, recurrent edema was more substantial in the CRVO patients, particularly those treated with 0.3 mg of ranibizumab. FTH, foveal thickness.

798 www.moleculartherapy.org vol. 16 no. 4 april 2008
© The American Society of Gene TherapyRanibizumab for Macular Edema in Vein Occlusions
Ascan thickness values of each of the radial lines comprising the fast macular thickness map. We did not use this value generated from only six data points for our primary measure of central retinal thickness, but instead used the foveal or central 1mm thickness, which is an average interpolated value based on central 21 scans of each of the six lines passing through the patient’s fixation (126 data points). Macular volume throughout the entire 6mm zone was calculated using extrapolated values between the line scans. Excess foveal thickness was calculated by subtracting the measured foveal thickness value from the normal mean value of 212 µm calculated from measurements on a large population of subjects.22
Measurement of VEGF in aqueous samples. A 30gauge needle was inserted into the anterior chamber and 0.1 ml of aqueous was removed just prior to each injection of ranibizumab and 1 hour after each injection. This report focuses on the level of VEGF in the aqueous at baseline prior to the first injection of ranibizumab. It was measured by a highly sensitive sandwich enzymelinked immunosorbent assay designed to detect all isoforms of VEGFA.23 Briefly, we used two monoclonal mouse capture antibodies and a biotinylated detection antibody against human VEGFA. Aqueous humor samples were diluted tenfold in enzymelinked immunosorbent assay diluent for accurate quantification. VEGF levels were measured by fluorometry for the detection of βgalactosidase conversion of 4methyllumbelliferylβdgalactopyranoside. A fourparameter cure fit program was used to generate a standard curve from which sample and control concentrations were interpolated.
Statistical analysis. Statistical analyses were performed using statistical package for the social sciences (SPSS, Chicago, IL). The likelihood that the change
25
20
15
10
30 40 50
Cha
nge
in V
A b
etw
een
base
line
and
mon
th 3
Cha
nge
in V
A b
etw
een
base
line
and
mon
th 3
60 70 80 90
30 40 50 60 70 80 90
CRVO
BRVO
CRVO
y = 0.066x + 8.088R2 = 0.016
y = 0.171x + 6.073R2 = 0.052
BRVO
y = 0.333x + 15.86R2 = 0.004
y = −0.225x + 15.01R2 = 0.093
5
0
–5
–10
–15
–20
25
20
15
10
0 10 20 30 40 50 60
5
0
–5
–10
–15
–20
45
40
35
30
25
20
15
10
5
00 1 2 3 4 5 6 7 8 9 10
–5
–10
45
40
35
30
25
20
15
10
5
0
–5
–10Age (in years) Duration of disease (in months)
a
c
b
d
Figure 6 Impact of patient age and duration of disease on visual outcome. (a) Visual outcome (expressed as change in visual acuity between baseline and month 3 in number of letters read at 4 m by standardized protocol) was plotted versus patient age for central retinal vein occlusion (CRVO) patients. (b) Visual outcome (expressed as change in visual acuity between baseline and month 3 in number of letters read at 4 m by standardized protocol) was plotted versus duration of disease for CRVO. (c) Visual outcome (expressed as change in visual acuity between baseline and month 3 in number of letters read at 4 m by standardized protocol) was plotted versus patient age for branch retinal vein occlusion (BRVO) patients. (d) Visual outcome (expressed as change in visual acuity between baseline and month 3 in number of letters read at 4 m by standardized protocol) was plotted versus duration of disease for BRVO patients. There was no inverse correlation for either indicating that neither age nor duration of disease had a negative impact on visual outcome.
100
10
11 10
Baseline aqueous humor VEGF (pg/ml)
Cha
nge
in V
A b
etw
een
base
line
and
mon
th 3
100 1,000
CRVO BRVO
10,000
Spearmans rank correlationRVO P = 0.0378CRVO P = 0.0381BRVO P = 0.2779
Figure 7 negative correlation between baseline aqueous vascular endothelial growth factor (VeGF) levels and change in visual acuity (Va) between baseline and month 3. The aqueous humor levels of VEGF at baseline are plotted against the change in VA between baseline and month 3 for all patients for whom measurements could be made [n = 18 for central retinal vein occlusion (CRVO); n = 17 for branch retinal vein occlusion (BRVO)]. Two CRVO patients and one BRVO patient experi-enced a net loss of VA at 3 months and were included in the analysis, but are not depicted in the graph, as negative values cannot be plotted on a logarithmic scale. Spearman rank order correlation analysis was conducted and a significant correlation was observed for CRVO alone (P = 0.038) and for CRVO and BRVO considered together (P = 0.038); although BRVO alone did not reach statistical significance (P = 0.278). CRVO patients are depicted as closed squares, BRVO patients are depicted as open squares.

Molecular Therapy vol. 16 no. 4 april 2008 799
© The American Society of Gene TherapyRanibizumab for Macular Edema in Vein Occlusions
in foveal thickness or VA from baseline to month 3 was due to ranibizumab rather than chance was determined by the Wilcoxon signedrank test. To assess the relationship between baseline aqueous VEGF level and visual outcome, Spearman’s rank order correlation coefficient was calculated.
acknowledGMentsSupported by an Investigator Initiated Study grant from Genentech, J.A.H. is the Katharine Graham Professor of Ophthalmology. P.A.C. is the George S. and Dolores Doré Eccles Professor of Ophthalmology and Neuroscience and recipient of a Senior Scientist Award from Research to Prevent Blindness, New York, NY.
reFerences1. Green, WR, Chan, CC, Hutchins, GM and Terry, JM (1981). Central retinal vein
occlusion: a prospective histopathologic study of 29 eyes in 28 cases. Trans Am Ophthalmol Soc 79: 371–422.
2. The Central Vein Occlusion Study Group (1997). Natural history and clinical management of central retinal vein occlusion. Arch Ophthalmol 115: 486–491.
3. The Eye Disease Case-control Study Group (1993). Risk factors for branch retinal vein occlusion. Am J Ophthalmol 116: 286–296.
4. Weinberg, D, Dodwell, DG and Fern, SA (1990). Anatomy of arteriovenous crossings in branch retinal vein occlusion. Am J Ophthalmol 109: 298–302.
5. Zhao, J, Sastry, SM Sperduto, RD, Chew, EY and Remaley, NA (1993). Arteriovenous crossing patterns in branch retinal vein occlusion. The Eye Disease Case-control Study Group. Ophthalmology 100: 423–428.
6. The Branch Vein Occlusion Study Group (1984). Argon laser photocoagulation for macular edema in branch vein occlusion. Am J Ophthalmol 98: 271–282.
7. Ozaki, H, Hayashi, H, Vinores, SA, Moromizato, Y, Campochiaro, PA and Oshima, K (1997). Intravitreal sustained release of VEGF causes retinal neovascularization in rabbits and breakdown of the blood-retinal barrier in rabbits and primates. Exp Eye Res 64: 505–517.
8. Derevjanik, NL, Vinores, SA, Xiao, WH, Mori, K, Turon, T, Hudish, T et al. (2002). Quantitative assessment of the integrity of the blood-retinal barrier in mice. Invest Ophthalmol Vis Sci 43: 2462–2467.
9. Ferrara, N, Damico, L, Shams, N, Lowman, H and Kim, R (2006). Development of ranibizumab, an anti-vascular endothelial growth factor antigen binding fragment, as therapy for neovascular age-related macular degeneration. Retina 26: 859–870.
10. The Central Vein Occlusion Study Group (1995). Evaluation of grid pattern photocoagulation for macular edema in central vein occlusion. The Central Vein Occlusion Study Group M report. Ophthalmology 102: 1425–1433.
11. Rosenfeld, PJ, Brown, DM, Heier, JS, Boyer, DS, Kaiser, PK, Chung, CY et al. (2006). Ranibizumab for neovascular age-related macular degeneration. N Engl J Med 355: 1419–1431.
12. Brown, DM, Kaiser, PK, Michels, M, Soubrane, G, Heier, JS, Kim, RY et al. (2006). Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med 355: 1432–1444.
13. Mohamed, Q, McIntosh, RL, Saw, SM and Wong, TY (2007). Interventions for central retinal vein occlusion: an evidence-based systematic review. Ophthalmology 114: 507–519, 524.
14. Iturralde, D, Spaide, RF, Meyerle, CB, Klancnik, JM, Yannuzzi, LA, Fisher, YL et al. (2006). Intravitreal bevacizumab (Avastin) treatment of macular edema in central retinal vein occlusion: a short-term study. Retina 26: 279–284.
15. Costa, RA, Jorge, R, Calucci, D, Melo, LA Jr, Cardillo, JA and Scott, IU (2007). Intravitreal bevacizumab (Avastin) for central and hemicentral retinal vein occlusions: the IBeVO study. Retina 27: 141–149.
16. Rabena, MD, Pieramici, DJ, Castellarin, AA, Nasir, MA and Avery, RL (2007). Intravitreal bevacizumab (Avastin) in the treatment of macular edema secondary to branch retinal vein occlusion. Retina 27: 419–425.
17. Pai, SA, Shetty, R, Vijayan, PB, Venkatasubramaniam, G, Yadav, NK, Shetty, BK et al. (2007). Clinical, anatomic, and electrophysiologic evaluation following intravitreal bevacizumab for macular edema in retinal vein occlusion. Am J Ophthalmol 143: 601–606.
18. Stahl, A, Agostini, H, Hansen, LL and Feltgen, N (2007). Bevacizumab in retinal vein occlusion-results of a prospective case series. Graefes Arch Clin Exp Ophthalmol 245: 1429–1436.
19. Huang, D, Swanson, EA, Lin, CP, Schuman, JS, Stinson, WG, Chang, W et al. (1991). Optical coherence tomography. Science 254: 1178–1181.
20. Hee, MR, Izatt, JA, Swanson, EA, Huang, D, Schuman, JS, Lin, CP et al. (1995). Optical coherence tomography of the human retina. Arch Ophthalmol 113: 325–332.
21. The Diabetic Retinopathy Study Research Group (1985). Early vitrectomy for severe vitreous hemorrhage in diabetic retinopathy. Two-year results of a randomized trial. Diabetic Retinopathy Vitrectomy Study report 2. Arch Ophthalmol 103: 1644–1652.
22. Chan, A, Duker, JS, Ko, TH, Fujimoto, JG and Schuman, JS (2006). Normal macular thickness measurements in healthy eyes using Stratus optical coherence tomography. Arch Ophthalmol 124: 193–198.
23. Rodriguez, CR, Fei, DT, Keyt, B and Baly, DL (1998). A sensitive fluorometric enzyme-linked immunosorbent assay that measures vascular endothelial growth facto165 in human plasma. J Immunol Methods 219: 45–55.