Systemic Treatment for Metastatic Biliary Tract Cancer - MDPI

jnci.oxfordjournals.org JNCI | Articles 21
DOI: 10.1093/jnci/djq456 © The Author 2010. Published by Oxford University Press. All rights reserved.Advance Access publication on December 1, 2010 For Permissions, please e-mail: [email protected].
Colorectal carcinoma is one of the most common cancers in Western countries (1,2), and a considerable proportion of colo-rectal cancer patients die as a result of the metastatic spread of their disease. The availability of three active cytotoxic agents (fluoropy-rimidines, irinotecan, and oxaliplatin), two classes of biological agents (monoclonal antibodies that block vascular endothelial growth factor and epidermal growth factor receptor), and the ex-panded indications for surgical resection of metastases have consid-erably improved the prognosis of patients with metastatic colorectal cancer (3,4). Nevertheless, the long-term outcomes of these patients are still unsatisfactory given their median survival of just more than 20 months and a 5-year survival of less than 10% (5).
Chemotherapy remains the primary therapeutic option for patients with metastatic colorectal cancer, and the development of more efficacious chemotherapy regimens is of crucial interest. An
additional critical and unresolved issue is the optimal duration of chemotherapy. Indeed, in the large majority of clinical trials, treat-ment was continued until progression of disease, whereas in clin-ical practice, treatment is often discontinued after a definite period of time (6,7). Although several randomized trials (8–10) have dem-onstrated that intermittent treatment did not result in worse out-comes compared with continuous treatment until progression of disease, the two optimized leucovorin–fluorouracil–oxaliplatin (OPTIMOX) trials (11,12) that evaluated oxaliplatin discontinua-tion and reintroduction in a stop-and-go strategy have suggested that a complete chemotherapy-free interval after 3 months of in-duction chemotherapy may be detrimental compared with contin-uous maintenance therapy.
In this context, we studied a 6-month induction treatment by using a three-drug regimen comprising 5-fluorouracil (by
ARTICLE
Randomized Trial of Two Induction Chemotherapy Regimens in Metastatic Colorectal Cancer: An Updated AnalysisGianluca Masi, Enrico Vasile, Fotios Loupakis, Samanta Cupini, Lorenzo Fornaro, Giacomo Baldi, Lisa Salvatore, Chiara Cremolini, Irene Stasi, Isa Brunetti, Maria Agnese Fabbri, Martina Puglisi, Patrizia Trenta, Cristina Granetto, Silvana Chiara, Luisa Fioretto, Giacomo Allegrini, Lucio Crinò, Michele Andreuccetti, Alfredo Falcone
Manuscript received February 8, 2010; revised September 22, 2010; accepted October 18, 2010.
Correspondence to: Alfredo Falcone, MD, U.O. Oncologia Medica 2 Universitaria – Polo Oncologico, Azienda Ospedaliero-Universitaria Pisana, Via Roma, 67 - 56126 Pisa, Italy (e-mail: [email protected]).
Background In a randomized trial with a median follow-up of 18.4 months, 6 months of induction chemotherapy with a three-drug regimen comprising 5-fluorouracil (by continuous infusion)–leucovorin, irinotecan, and oxaliplatin (FOLFOXIRI) demonstrated statistically significant improvements in response rate, radical surgical resection of metastases, progression-free survival, and overall survival compared with 6 months of induction chemotherapy with fluorouracil–leucovorin and irinotecan (FOLFIRI).
Methods From November 14, 2001, to April 22, 2005, we enrolled 244 patients with metastatic colorectal cancer. To eval-uate if the superiority of FOLFOXIRI is maintained in the long term, we updated the overall and progression-free survival data to include events that occurred up to February 12, 2009, with a median follow-up of 60.6 months. We performed a subgroup and a risk-stratified analysis to examine whether outcomes differed in specific patient subgroups, and we analyzed the results of treatment after progression. Survival curves were estimated by the Kaplan–Meier method. Multivariable Cox regression models were fit to estimate hazard ratios (HRs) and 95% confidence intervals (CIs). All statistical tests were two-sided.
Results FOLFOXIRI demonstrated statistically significant improvements in median progression-free survival (9.8 vs 6.8 months, HR for progression = 0.59, 95% CI = 0.45 to 0.76, P < .001) and median overall survival (23.4 vs 16.7 months, HR for death = 0.74, 95% CI = 0.56 to 0.96, P = .026) with a 5-year survival rate of 15% (95% CI = 9% to 23%) vs 8% (95% CI = 4% to 14%). The improvements in progression-free survival and, to a lesser extent, in overall survival were evident even when the analysis excluded patients who received radical resection of metas-tases. With regard to the risk-stratified analysis, FOLFOXIRI results in longer progression-free survival and over-all survival than FOLFIRI in all risk subgroups.
Conclusions Six months of induction chemotherapy with FOLFOXIRI is associated with a clinically significant improvement in the long-term outcome compared with FOLFIRI with an absolute benefit in survival at 5 years of 7%.
J Natl Cancer Inst 2011;103:21–30
by guest on February 19, 2011jnci.oxfordjournals.org
Dow
nloaded from

22 Articles | JNCI Vol. 103, Issue 1 | January 5, 2011
continuous infusion)–leucovorin, irinotecan, and oxaliplatin (ie, FOLFOXIRI) (13,14) in an attempt to expose all patients with metastatic colorectal cancer to the three active cytotoxic agents with the goals of improving tumor response rates, increasing the rate of radical surgery of metastases, and improving survival. There are data from patients with metastatic colorectal cancer that sup-port an association between tumor response to chemotherapy and efficacy (15,16). In addition, a direct correlation was demonstrated between the activity of chemotherapy (in terms of response rate) and the rate of radical resection of metastases among patients with unresectable metastatic disease at presentation (17) (and this strategy of chemotherapy followed by radical surgical resection of metastases led to better long-term survival). Moreover, the “expo-sure” of patients with advanced colorectal cancer to all three active cytotoxic agents is associated with survival (18). As previously reported (19), on behalf of the Gruppo Oncologico Nord Ovest (GONO), we conducted a randomized trial comparing FOLFOXIRI with fluorouracil (by infusion)–leucovorin and irinotecan (FOLFIRI) as a first-line treatment in patients with metastatic co-lorectal cancer. On the basis of the current knowledge and standard clinical practice at the time the study was designed, we scheduled a
maximum of 6 months of induction chemotherapy (20). The trial demonstrated an increased activity and efficacy of the three-drug regimen. After a median follow-up of 18.4 months (19), the con-firmed response rate was statistically significantly higher in the FOLFOXIRI arm than in the FOLFIRI arm (60% vs 34%, P < .001), as was the rate of secondary radical surgical resection of metastases among all patients (15% vs 6%, P = .03) and among patients with liver metastases only (36% vs 12%, P = .017). Median progression-free survival was longer in the FOLFOXIRI arm than in the FOLFIRI arm (9.8 vs 6.9 months; hazard ratio [HR] of disease progression = 0.63, 95% confidence interval [CI] = 0.47 to 0.81, P = .006), as was median overall survival (22.6 vs 16.7 months; HR of death = 0.70, 95% CI = 0.50 to 0.97, P = .03). Compared with FOLFIRI, FOLFOXIRI was associated with a modest increase in the incidence of grade 2 or 3 peripheral neurotoxicity (0% vs 19%, P = .001) and of grade 3 or 4 neutropenia (28% vs 50%, P = .001), but the incidence of febrile neutropenia (3% vs 5%) and of grade 3 or 4 diarrhea (12% vs 20%) were not statistically significantly different, and there were no treatment-related deaths.
Here we report the final analysis of this trial, after a median follow-up of 5 years, to evaluate whether the superiority of FOLFOXIRI was maintained in the long term. We also performed subgroup and risk-stratified analyses, with risk defined according to the Kohne prognostic model (21), to explore whether any clin-ical factor predicts differential likelihood of benefit from the treat-ment. Finally, we analyzed the outcomes of patients who received treatment after disease progression to examine whether they were negatively affected by FOLFOXIRI.
Patients and MethodsStudy OverviewFrom November 14, 2001 to April 22, 2005, we enrolled a total of 244 patients from 15 Italian centers (Figure 1). The main inclusion criteria were as follows: adenocarcinoma of the colon or rectum; unresectable metastatic disease; no previous palliative chemotherapy for metastatic disease; age 18–75 years; an Eastern Cooperative Oncology Group (ECOG) performance status (22) of 2 or lower for patients aged 70 years or younger or an ECOG performance status of 0 for patients aged 71–75 years; measurable disease according to World Health Organization criteria (23); and adequate bone marrow, liver, cardiac, and renal functions defined as white blood cell count greater than 3500/mm3, neutrophil count greater than 1500/mm3, platelet count greater than 100 000/mm3, serum creati-nine level less than 1.2 mg/dL, serum bilirubin level less than 1.5 mg/dL, and serum aspartate aminotransferase, alanine amino-transferase, and alkaline phosphatase levels less than 2.5 times nor-mal values (<5 times normal values if liver metastases were present). The protocol was approved by the ethics committee of all partici-pating institutions. All patients were informed of the investigational nature of the study and provided written informed consent before registration. Eligible patients were assigned to a treatment arm with the use of a dynamic randomization algorithm that was designed to achieve overall balance between the arms. Randomization was cen-tralized. Patients were stratified according to study center, ECOG performance status (0 vs 1 or 2), and history of adjuvant therapy (yes vs no), and then were randomly assigned to receive irinotecan at 180
CONTEXT AND CAVEATS
Prior knowledgeIn a randomized trial with a median follow-up of 18.4 months, patients with metastatic colorectal cancer who underwent 6 months of induction chemotherapy with 5-fluorouracil (by contin-uous infusion)–leucovorin, irinotecan, and oxaliplatin (FOLFOXIRI) had statistically significant improvements in response rate, rate of radical surgical resection of metastases, progression-free survival, and overall survival compared with those who underwent 6 months of induction chemotherapy with fluorouracil–leucovorin and irinotecan (FOLFIRI).
Study designAn updated analysis of overall and progression-free survival data, with a median follow-up of 60.6 months, to evaluate if the superi-ority of FOLFOXIRI is maintained in the long term.
ContributionSix months of induction chemotherapy with FOLFOXIRI is associ-ated with a clinically significant improvement in the long-term outcome compared with FOLFIRI with an absolute benefit in sur-vival at 5 years of 7%. The improvements in progression-free sur-vival and overall survival were evident even when the analysis excluded patients who received radical resection of metastases.
ImplicationsFOLFOXIRI is a therapeutic option that should be considered in rou-tine practice as a conversion therapy for fit patients with potentially resectable metastatic colorectal cancer or as a palliative therapy for patients with diffuse aggressive or symptomatic disease.
LimitationsThe sample size of the trial was small and the statistical power was low. The results may not produce a change in the current standard of care because the trial was conducted before monoclonal anti-bodies were included in the standard of care.
From the Editors
by guest on February 19, 2011jnci.oxfordjournals.org
Dow
nloaded from

jnci.oxfordjournals.org JNCI | Articles 23
mg/m2 in 250 mL normal saline given over 1 hour on day 1, leu-covorin at 100 mg/m2 in 250 mL 5% dextrose given over 2 hours, followed immediately by 5-fluorouracil at 400 mg/m2 (bolus) and 5-fluorouracil at 600 mg/m2 by 22-hour infusion on days 1 and 2 (FOLFIRI) (24) or irinotecan at 165 mg/m2 in 250 mL normal saline over 1 hour on day 1, followed immediately by oxaliplatin at 85 mg/m2 in 250 mL 5% dextrose and leucovorin at 200 mg/m2 in 250 mL 5% dextrose infused concomitantly over 2 hours via a Y-connector on day 1, followed immediately by 5-fluorouracil at 3200 mg/m2 infused continuously over 48 hours starting on day 1 (FOLFOXIRI). Treatment was administered biweekly for a maximum of 12 cycles (fewer cycles were administered in cases where there was evidence
of disease progression, unacceptable toxicity, or withdrawal of con-sent). This trial is registered at ClinicalTrials.gov (ClinicalTrials.gov identifier: NCT01219920).
Study MeasuresThe primary study endpoint was the response rate, which was exter-nally reviewed. Secondary endpoints were progression-free survival, overall survival, radical surgical resection of metastases after chemo-therapy, safety, and quality of life. Responses and progressions were evaluated according to World Health Organization criteria (23). In particular, to evaluate responses and progressions, a computed tomography scan was required at baseline (within 4 weeks before
Excluded n = 39
- Did not meet inclusion criteria n=35- Refused to participate n=4
Analyzed n = 122
Excluded from analysis n = 0
Allocated to FOLFIRI n=122
Received allocated intervention n = 122Allocation
Analysis
Follow-Up
Enrollment
Patients randomlyassigned n = 244
FOLFIRI
Allocated to FOLFOXIRI n=122
Received allocated intervention n = 122
FOLFOXIRI
Analyzed n = 122
Excluded from analysis n = 0
Lost to follow-up n = 3
Study site could not locate patient
Discontinued intervention n = 58
Adverse event n = 4Toxicity n = 5Consent withdrawn n = 8Progressive disease n = 41
Lost to follow-up n = 5
Study site could not locate patient
Discontinued intervention n = 45
Adverse event n = 6Toxicity n = 11Consent withdrawn n = 12Progressive disease n = 16
Assessed foreligibility n = 283
Figure 1. Consort flowchart. FOLFOXIRI = oxaliplatin, irinotecan, fluorouracil, and leucovorin; FOLFIRI = irinotecan, fluorouracil, and leucovorin; FOLFOX = oxaliplatin, fluorouracil, and leucovorin.
by guest on February 19, 2011jnci.oxfordjournals.org
Dow
nloaded from

24 Articles | JNCI Vol. 103, Issue 1 | January 5, 2011
Table 1. Characteristics of patients*
Characteristic FOLFIRI FOLFOXIRI
No. of patients (%) 122 (100) 122 (100)Median age, y (range) 64 (21–75) 62 (27–75)Sex, No. (%) Male 69 (57) 75 (61) Female 53 (43) 47 (39)ECOG performance status, No. (%) 0 74 (61) 74 (61) 1 41 (34) 45 (37) 2 7 (6) 3 (2)Primary tumor, No. (%) Colon 95 (78) 81 (66) Rectum 27 (22) 41 (34)Previous adjuvant chemotherapy, No. (%) Yes 29 (24) 29 (24) No 93 (76) 93 (76)Time from diagnosis to randomization, No. (%) <3 mo 79 (65) 79 (65) 3 mo 43 (35) 43 (35)No. of metastatic sites, No. (%) 1 67 (55) 65 (53) >1 55 (45) 57 (47)Liver only metastases, No. (%) Yes 42 (34) 39 (32) No 80 (66) 83 (68)Liver involvement, No. (%) No 28 (23) 31 (25) <25% 40 (33) 43 (35) >25% 54 (44) 48 (40)Serum alkaline phosphatase, No. (%) <300 U/L 69 (57) 86 (71) 300 U/L 53 (43) 36 (29)Serum lactate dehydrogenase, No. (%) <UNL 81 (66) 86 (71) UNL 41 (34) 36 (29)Serum carcinoembryonic antigen, No. (%) <100 ng/mL 81 (66) 85 (70) 100 ng/mL 41 (34) 37 (30)
* FOLFIRI = fluorouracil, leucovorin, and irinotecan; FOLFOXIRI = fluorouracil, leucovorin, oxaliplatin, and irinotecan; ECOG = Eastern Cooperative Oncology Group; ULN = upper limit of normal.
randomization) and every 8 weeks during treatment and after treat-ment completion throughout follow-up. Adverse events were evalu-ated according to National Cancer Institute’s Common Toxicity Criteria (version 2.0) (25). The progression-free interval was mea-sured from the date of random assignment to the documentation of disease progression or death from any cause, whichever occurred first, with censoring of patients at the date at which they were last known to be free of progression. Overall survival time was measured from the date of random assignment to the date of death from any cause, with censoring of patients at the last date they were known to be alive.
Statistical AnalysisOverall survival and progression-free survival were updated to include events that occurred up to February 12, 2009. Survival curves were estimated by the Kaplan–Meier method and compared by using the log-rank test. Cox proportional hazards modeling was used to calcu-late hazard ratios (HRsand 95% confidence intervals (CIs). The pro-portional hazard assumption was verified using the method proposed by Schoenfeld (26). The assumption of proportional hazards was ap-propriate because cumulative hazard plots estimated for FOLFIRI and FOLFOXIRI showed a parallel trend. For the risk-stratified analysis, we compared overall survival and progression-free survival between the treatment arms for each risk group. All analyses were done on the intention-to-treat population, which was defined as all randomly assigned subjects. Assuming an !-error of 0.05, the trial had a power of 0.80 to demonstrate an improvement of 20% in response rate and a prolongation in progression-free survival of 3 months. A multivariable logistic regression model was used to identify predic-tive factors for objective response and for radical surgical resection. A factor was considered potentially associated with the outcome of interest if its univariate P value was less than or equal to .05; such factors were retained in the multivariable models. The statistical analysis was performed using SPSS statistical software (version 16.0 for Windows; SPSS, Chicago, IL). All statistical tests were two-sided.
In subgroup analyses, we assessed associations between the fol-lowing baseline (ie, at randomization) clinical factors for patients treated on each study arm and overall survival, progression-free survival, response rate, and the rate of radical surgical resection of metastases after chemotherapy: treatment (FOLFOXIRI vs FOLFIRI), sex, age (< 65 or 65 years), ECOG performance status (0 or 1–2), site of primary tumor (colon or rectum), number of met-astatic sites (1 or 2), location of metastatic sites (liver only or other sites), liver involvement (<25% or 25%), time from first diagnosis to first metastasis (0–3, 3–12, or >12 months), previous adjuvant therapy (yes or no), baseline serum lactate dehydrogenase level (nor-mal or upper limit of normal [laboratory-specific]), baseline serum carcinoembryonic antigen level (<100 or 100 ng/mL), baseline white blood cell count (<10 000 or 10 000 per mm3), baseline hemoglobin level (<10 or 10 g/dL), and baseline serum alkaline phosphatase level (<300 or 300 U/L). Categories and cut points were chosen according to their prognostic value in metastatic colo-rectal cancer based on other randomized trials in this setting (27).
In the risk-stratified analysis, patients were assigned to three risk groups as defined by Kohne et al. (21) according to the following baseline variables: white blood cell count, number of metastatic sites, serum alkaline phosphatase level, and ECOG performance status. The low-risk group included patients with an ECOG perfor-
mance status of 0 or 1 and one site of metastatic disease. The intermediate-risk group included patients with an ECOG perfor-mance status of 0 or 1, more than one site of metastatic disease, and a serum alkaline phosphatase level less than 300 U/L and patients with an ECOG performance status greater than 1, a white blood cell count less than 10 000/mm3, and one site of metastatic disease. The high-risk group included patients with an ECOG performance status of 0 or 1, more than one site of metastatic disease, and a serum alkaline phosphatase level equal to or greater than 300 U/L; patients with an ECOG performance status greater than 1 and a white blood cell count greater than 10,000/mm3; and patients with an ECOG performance status greater than 1, a white blood cell count less than 10,000/mm3, and more than one site of metastatic disease.
by guest on February 19, 2011jnci.oxfordjournals.org
Dow
nloaded from

jnci.oxfordjournals.org JNCI | Articles 25
ResultsThe 244 enrolled patients were randomly assigned to FOLFIRI (n = 122) or FOLFOXIRI (n = 122). The characteristics of the patients at baseline were well balanced between the treatment arms (Table 1).
Progression-Free Survival and Overall SurvivalAfter a median follow-up of 60.6 months, 115 patients in the FOLFOXIRI arm and 121 patients in the FOLFIRI arm experi-enced disease progression. The median progression-free interval was statistically significantly longer for FOLFOXIRI than for FOLFIRI (9.8 months vs 6.8 months; HR for progression = 0.59, 95% CI = 0.45 to 0.76, P < .001) (Figure 2). The corresponding 5-year progression-free survival rates were 5% (95% CI = 1% to 8%) for FOLFOXIRI and 1% (95% CI = 0% to 3%) for FOLFIRI. In addition, the median progression-free interval remained longer for FOLFOXIRI compared with FOLFIRI when we excluded patients who had undergone radical surgery on metastases from the analysis (9.5 months vs 6.6 months; HR of progression = 0.59, 95% CI = 0.44 to 0.76, P < .001).
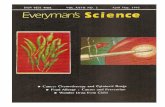
There were 104 deaths in the FOLFOXIRI arm and 112 deaths in the FOLFIRI arm. The median overall survival was statistically significantly longer for FOLFOXIRI compared with FOLFIRI (23.4 months vs 16.7 months; HR for death = 0.74, 95% CI = 0.56 to 0.96, P = .026) (Figure 3). The 5-year survival rates were 15% (95% CI = 9% to 23%) for FOLFOXIRI and 8% (95% CI = 4% to 14%) for FOLFIRI. When we excluded patients who had undergone radical surgery on metastases from the analysis, the survival benefit of FOLFOXIRI was maintained but was no longer
statistically significant (median overall survival, FOLFOXIRI vs FOLFIRI: 20.2 months vs 15.9 months; HR for death = 0.80 95% CI = 0.61 to 1.05; P = .12) (Figure 4).
Prognostic Factors, Subgroup Analysis, and Risk-Stratified AnalysisThe analysis of the treatment effect in the 15 aforementioned subgroups of patients demonstrated that treatment with FOLFOXIRI is associated with improvements in both progression-free survival and overall survival in all subgroups (data not shown).
The Cox multivariable analysis demonstrated that independent prognostic factors for reduction of the risk of progression were treatment with FOLFOXIRI (HR = 0.63, 95% CI = 0.48 to 0.82, P < .001), male sex (HR = 0.75, 95% CI = 0.57 to 0.98, P = .03), serum carcinoembryonic antigen level less than 100 ng/mL (HR = 0.66, 95% CI = 0.48 to 0.92, P = .01), and white blood cell count less than 10 000/mm3 (HR = 0.72, 95% CI = 0.52 to 0.99, P = .05). Independent prognostic factors for reduction of the risk of death were baseline hemoglobin level greater than or equal to 10 g/dL (HR = 0.59, 95% CI = 0.40 to 0.87, P = .008) and baseline serum alkaline phosphatase level less than 300 U/L (HR = 0.57, 95% CI = 0.41 to 0.78, P = .001).
With regard to the risk-stratified analysis based on the Kohne prognostic model (21), in this series, this model discriminated well between the high-risk group and the low- and intermediate-risk group. Indeed, when analyzing the entire study population, regard-less of treatment arm, we observed statistically significant differ-ences in the log-rank P values (P < .001 for both progression-free
Figure 2. Kaplan–Meier analysis of progression-free survival (PFS) for all randomly assigned patients. HR = hazard ratio; CI = confidence interval. The P value (two-sided) was calculated using the log-rank test.
by guest on February 19, 2011jnci.oxfordjournals.org
Dow
nloaded from

26 Articles | JNCI Vol. 103, Issue 1 | January 5, 2011
FOLFIRI FOLFOXIRIEntered 122 122
Died 112 104
Median OS 16.7 mo 23.4 mo
95%CI 13.8 to 19.4 mo 19.8 to 25.6 mo
5-year OS rate 8% 15%
95%CI 4% to 14% 9% to 23%
HR = 0.74 (95% CI = 0.56 to 0.96)
Log-rank P = 0.026
Patients at riskOS rate (95% CI)
FOLFOXIRI 122100%
9980% (72% to 86%)
5948% (39% to 57%)
2924% (17% to 32%)
2221% (13% to 29%)
1015% (9% to 23%)
FOLFIRI 122100%
8267% (58% to 74%)
4334% (26% to 43%)
2620% (14% to 28%)
1614% (8% to 20%)
78% (4% to 14%)
0 12 24 36 48 600
10
20
30
40
50
60
70
80
90
100
Time (months)
Ove
rall
surv
ival
(%)
Figure 3. Kaplan–Meier analysis of overall survival (OS) for all randomly assigned patients. HR = hazard ratio; CI = confidence interval. The P value (two-sided) was calculated using the log-rank test.
survival and overall survival) for comparisons between high-risk and low-risk groups and for comparisons between high-risk and intermediate-risk groups. By contrast, the differences in progression-free survival and overall survival between the low-risk group and the intermediate-risk group were not statistically signif-icant. In the risk-stratified analysis, compared with FOLFIRI, FOLFOXIRI resulted in longer progression-free survival and longer overall survival in all risk subgroups (Table 2).
Treatment After ProgressionA total of 93 patients (76%) in the FOLFIRI arm and 89 patients (73%) in the FOLFOXIRI arm received second-line treatment with chemotherapy after experiencing disease progression (Table 3). The majority (87%) of patients in the FOLFIRI arm who experienced disease progression had second-line treatment with FOLFOX, whereas only 4% received FOLFIRI again as second-line treatment. A total of 18% of patients in the FOLFOXIRI arms who experienced disease progression had second-line treatment again with FOLFOXIRI. For patients in the FOLFIRI arm, the median treatment-free interval was 3.1 months (95% CI = 2.3 to 4.0 months), and second-line treatment resulted in a response rate of 16% (95% CI = 9% to 24%), a median progression-free interval of 4.0 months (95% CI = 3.0 to 4.9 months), and a median overall survival of 9.4 months (95% CI = 6.7 to 12.0 months). For patients in the FOLFOXIRI arm, the median treatment-free interval was 5.0 months (95% CI = 4.1 to 6.2 months), and the response rate to second-line treatment was 17% (95% CI = 9% to 25%), the median
progression-free interval was 5.3 months (95% CI = 4.0 to 6.3 months), and median overall survival was 11.7 months (95% CI = 7.9 to 15.4 months). Patients who received second-line treatment with FOLFOXIRI had a response rate of 27% (95% CI = 6% to 49%), a median progression-free interval of 8.1 months (95% CI = 5.1 to 11.0 months), and median overall survival of 22.4 months (95% CI = 4.2 to 40.6 months) from the start of second-line FOLFOXIRI and 36.6 months (95% CI = 8.7 to 64.4 months) from the start of induction FOLFOXIRI. Notably, only a small propor-tion of patients received cetuximab or bevacizumab after disease progression (1% of patients in the FOLFIRI arm received both monoclonal antibodies, while in the FOLFOXIRI arm 8% of patients received cetuximab and no patient received bevacizumab).
DiscussionThis updated analysis of a randomized trial of first-line treatment for patients with metastatic colorectal cancer showed that 6 months of induction chemotherapy with FOLFOXIRI is associ-ated with a clinically significant improvement in the long-term outcome compared with FOLFIRI, with an absolute benefit in survival at 5 years of 7%. Moreover, improvements in progression-free survival and overall survival were maintained with long-term follow-up.
Current treatment of metastatic colorectal cancer is based on three main therapeutic options: chemotherapy, targeted therapies, and surgical resection of metastases. The aim of treatment may
by guest on February 19, 2011jnci.oxfordjournals.org
Dow
nloaded from

jnci.oxfordjournals.org JNCI | Articles 27
Figure 4. Kaplan–Meier analysis of progression-free survival (PFS) and overall survival (OS) after excluding patients who underwent radical sur-gical resection of metastases. A) PFS. B) OS. HR = hazard ratio; CI = confidence interval. The P value (two-sided) was calculated using the log-rank test.
by guest on February 19, 2011jnci.oxfordjournals.org
Dow
nloaded from

28 Articles | JNCI Vol. 103, Issue 1 | January 5, 2011
Table 3. Second-line treatments*
Second-line treatment
FOLFIRI (N = 122)
FOLFOXIRI (N = 122)
N (%) N (%)
Any 93 (76) 89 (73)FOLFOX 80 (87) 15 (17)FOLFIRI 4 (4) 20 (22)FOLFOXIRI 1 (1) 16 (18)5FU by protracted infusion 3 (3) 11 (12)Mytomicin-C ± 5FU 0 (0) 16 (18)Cetuximab ± chemotherapy 1 (1) 7 (8)Bevacizumab ± chemotherapy 1 (1) 0 (0)Other† 3 (3) 4 (5)
* FOLFOXIRI = oxaliplatin, irinotecan, fluorouracil, and leucovorin; FOLFIRI = irinotecan, fluorouracil, and leucovorin; FOLFOX = oxaliplatin, fluorouracil, and leucovorin; 5FU = fluorouracil.
† Intravenous raltitrexed, oral uracil and tegafur, floxuridine through hepatic arterial infusion.
Table 2. Risk-stratified analysis*
Treatment arm by risk group
Progression-free survival Overall survival
No. of patients Median, mo HR (95% CI) Median, mo HR (95% CI)
Low risk FOLFOXIRI 63 9.8 0.68 (0.47 to 0.96) 24.3 0.90 (0.62 to 1.32) FOLFIRI 64 6.9 1.00 (Referent) 19.9 1.00 (Referent)Intermediate risk FOLFOXIRI 41 11.1 0.56 (0.34 to 0.92) 24.8 0.58 (0.35 to 0.96) FOLFIRI 28 9.2 1.00 (Referent) 17.6 1.00 (Referent)High risk FOLFOXIRI 18 8.3 0.44 (0.24 to 0.82) 14.1 0.78 (0.43 to 1.41) FOLFIRI 30 4.4 1.00 (Referent) 11.7 1.00 (Referent)
* HR = hazard ratio; CI = confidence interval; FOLFOXIRI = oxaliplatin, irinotecan, fluorouracil, and leucovorin; FOLFIRI = irinotecan, fluorouracil, and leucovorin.
range from cure (by achieving a definitive disease eradication), to maximal disease control (by improving progression-free and over-all survival), to palliation (by improving quality of life). The major challenge today is how best to integrate these treatment options to give patients the opportunity to receive and benefit from all avail-able effective therapies. Considering that surgery alone is an op-tion only for a minority of patients and that inhibitors of vascular endothelial growth factor and epidermal growth factor receptor have limited activity in monotherapy, chemotherapy remains the primary therapeutic strategy for the majority of patients.
Our results demonstrate that compared with 6 months of induction treatment with the doublet FOLFIRI, 6 months of in-duction treatment with the three-drug combination FOLFOXIRI provides a clinically relevant improvement in 5-year survival (15% vs 8%). In our opinion, these data provide useful information about a treatment option (FOLFOXIRI) that should be considered in routine clinical practice. As we previously reported (19), the three-drug regimen that we developed and used in this trial is not only more efficacious than FOLFIRI but is also feasible and has manageable toxic effects (with acceptable levels of neutropenia and peripheral neurotoxicity). In addition, it is important to note that this analysis demonstrates that FOLFOXIRI was not only associ-ated with a higher rate of patients who received radical resection
of metastases but also with better outcomes in patients with meta-static disease who did not undergo radical resection. Moreover, the improvements in progression-free survival, and, to a lesser extent, in overall survival were evident even when we excluded patients who received radical resection of metastases from the analysis. However, the greater proportion of patients in the FOLFOXIRI arm who received radical resection probably explains the better 5-year survival in this arm. In addition, FOLFOXIRI was associ-ated with improvements in both progression-free survival and overall survival in all subgroups as well as in all Kohne risk cate-gories we tested. To our knowledge, a confirmed response rate of 60%, a median progression-free interval of 9.8 months, a median overall survival of 23.4 months, and a 5-year survival of 15%, as reported here for the FOLFOXIRI arm, are among the highest rates reported in a randomized trial of chemotherapy in metastatic colorectal cancer (28,29), whereas the results obtained for the FOLFIRI arm are in line with those reported in several other con-temporary randomized studies with 5-fluorouracil–based doublets (30). It is important to note that in this study, only a small propor-tion of patients received cetuximab after disease progression and only one patient was treated with bevacizumab. Therefore, these results were obtained in a “biologic-free” population, and thus they could be viewed as a benchmark to assess the efficacy of che-motherapy alone in metastatic colorectal cancer.
Several concerns have been raised (31) about the use of a triple cytotoxic combination as first-line treatment for metastatic colo-rectal cancer. The first concern is the risk of excessive toxicity. Our results are reassuring: In a fit population (defined according to the inclusion criteria used in this study), the FOLFOXIRI regimen was feasible and had a manageable safety profile. Moreover, an analysis of hepatic toxicity in patients who underwent surgery on metastases revealed no relevant liver damage (32). The second concern is the possibility that first-line treatment with a triple cytotoxic combination could reduce the efficacy of second-line treatments. Our results show that induction chemotherapy with FOLFOXIRI did not have a negative impact on the outcomes of patients who received treatment after disease progression, and, moreover, the data in terms of disease control compare well with the results usually achieved with second-line treatments. Previous studies showed that the most important variable associated with a failure to receive and benefit from second-line therapy is the lack of response to frontline therapy (33), thus supporting the concept
by guest on February 19, 2011jnci.oxfordjournals.org
Dow
nloaded from

jnci.oxfordjournals.org JNCI | Articles 29
that a more active first-line chemotherapy is not detrimental to the results of second-line therapies.
This trial was not designed to address the issue of the optimal duration of treatment. The results we reported with FOLFOXIRI suggest that 6 months of induction chemotherapy is appropriate for most patients and that the increased activity of the induction treatment also produces improvements in long-term survival. Furthermore, our data underline the importance of rechallenging patients who responded to first-line treatment with the same agents used in first-line, as has been suggested previously (8,34,35).
Is the combination of the three cytotoxic agents better or worse than two cytotoxic agents plus one biological agent? So far, to our knowledge, no study has addressed this question. However, we do not believe that this is a relevant comparison because the triplet should not be viewed as an alternative to biological agents but rather as an agent that should be studied in combination with bio-logical agents . Results of recent randomized trials of chemotherapy doublets in association with inhibitors of vascular endothelial growth factor (36–38) or epidermal growth factor receptor (39) show that the median survival of patients is still approximately 20 months, which suggests that further improvements are still needed. Results of a phase II trial evaluating the combination of FOLFOXIRI and bevacizumab were promising with a response rate of 77%, a disease control rate of 100%, a median progression-free interval of 13.1 months, and a median survival of 30.9 months (40).
This study had several limitations. The sample of randomly assigned patients studied was small and therefore the power of statistical analysis performed was low. In addition, this trial was conducted before the inclusion of monoclonal antibodies to stan-dard of care, and thus the control arm was not optimized to present practice. As a consequence, our results cannot produce a clear change in the current standard of care.
In conclusion, considering the heterogeneity of the clinical course of metastatic colorectal cancer, we think that FOLFOXIRI should represent one of the therapeutic options to be considered in the treatment plan of patients with metastatic colorectal cancer. We believe that this regimen is appropriate as a conversion therapy for fit patients (as defined herein) who have potentially resectable disease or as a palliative therapy for patients with dif-fuse aggressive or symptomatic disease. The combination of FOLFOXIRI with targeted biological agents is of particular in-terest and, on behalf of GONO, we are now conducting a phase III randomized trial comparing 6 months of induction therapy with FOLFOXIRI plus bevacizumab with FOLFIRI plus bevaci-zumab (TRIBE trial).
References
1. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58(2):71–96.
2. Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P. Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol. 2000;18(3):581–592.
3. Loupakis F, Masi G, Vasile E, Falcone A. First-line chemotherapy in metastatic colorectal cancer: new approaches and therapeutic algorithms. Always hit hard first? Curr Opin Oncol. 2008;20(4):459–465.
4. Kopetz S, Chang GJ, Overman MJ, et al. Improved survival in metastatic colorectal cancer is associated with adoption of hepatic resection and improved chemotherapy. J Clin Oncol. 2009;27(22):3677–3683.
5. O’Neil BH, Goldberg RM. Innovations in chemotherapy for metastatic colorectal cancer: an update of recent clinical trials. Oncologist. 2008;13(10):1074–1083.
6. Seymour MT, Stenning SP, Cassidy J. Attitudes and practice in the man-agement of metastatic colorectal cancer in Britain. Clin Oncol (R Coll Radiol). 1997;9(4):248–251.
7. Hochster HS. Stop and go: yes or no? J Clin Oncol. 2009;27(34):5677–5679.
8. Hejna M, Kornek GV, Raderer M, et al. Reinduction therapy with the same cytostatic regimen in patients with advanced colorectal cancer. Br J Cancer. 1998;78(6):760–764.
9. Maughan TS, James RD, Kerr DJ, et al. Comparison of intermittent and continuous palliative chemotherapy for advanced colorectal cancer: a multicentre randomised trial. Lancet. 2003;361(9356):457–464.
10. Labianca R, Floriani I, Cortesi E, et al. Alternating versus continuous “FOLFIRI” in advanced colorectal cancer (ACC): a randomized “GISCAD” trial. J Clin Oncol. 2006;24(18s):147s. (suppl; abstr 3505).
11. Tournigand C, Cervantes A, Figer A, et al. OPTIMOX1: A randomized study of FOLFOX4 or FOLFOX7 with oxaliplatin in a stop-and-go fash-ion in advanced colorectal cancer a GERCOR study. J Clin Oncol. 2006;24(3):394–400.
12. Chibaudel B, Maindrault-Goebel F, Lledo G, et al. Can chemotherapy be discontinued in unresectable metastatic colorectal cancer? The GERCOR OPTIMOX2 study. J Clin Oncol. 2009;27(34):5727–5733.
13. Falcone A, Masi G, Allegrini G, et al. Biweekly chemotherapy with oxali-platin, irinotecan, infusional fluorouracil, and leucovorin: a pilot study in patients with metastatic colorectal cancer. J Clin Oncol. 2002;20(19):4006–4014.
14. Masi G, Allegrini G, Cupini S, et al. First-line treatment of metastatic colorectal cancer with irinotecan, oxaliplatin and 5-fluorouracil/leucovo-rin (FOLFOXIRI): results of phase II study with a simplified biweekly schedule. Ann Oncol. 2004;15(12):1766–1772.
15. Buyse M, Thirion P, Carlson RW, Burzykowski T, Molenberghs G, Piedbois P. Relation between tumor response to first-line chemotherapy and survival in advanced colorectal cancer: a meta-analysis. Lancet. 2000;356(9227):373–378.
16. Johnson RK, Ringland C, Stokes JB, et al. Response rate or time to progres-sion as predictors of survival in trials of metastatic colorectal cancer or non-small-cell lung cancer: a meta-analysis. Lancet Oncol. 2006;7(9):741–746.
17. Folprecht G, Grothey A, Alberts S, Raab HR, Kohne CH. Neoadjuvant treatment of unresectable colorectal liver metastases: correlation between tumour response and resection rates. Ann Oncol. 2005;16(8):1311–1319.
18. Grothey A, Sargent D, Goldberg RM, Schmoll HJ. Survival of patients with advanced colorectal cancer improves with the availability of fluoro-uracil-leucovorin, irinotecan, and oxaliplatin in the course of treatment. J Clin Oncol. 2004;22(7):1209–1214.
19. Falcone A, Ricci S, Brunetti I, et al. Phase III trial of infusional fluoro-uracil, leucovorin, oxaliplatin, and irinotecan (FOLFOXIRI) compared with infusional fluorouracil, leucovorin, and irinotecan (FOLFIRI) as first-line treatment for metastatic colorectal cancer: the Gruppo Oncologico Nord Ovest. J Clin Oncol. 2007;25(13):1670–1676.
20. Cunningham D, Atkin W, Lenz HJ, et al. Colorectal cancer. Lancet. 2010;375(9719):1030–1047.
21. Kohne CH, Cunningham D, Di Costanzo F, et al. Clinical determinants of survival in patients with 5-fluorouracil-based treatment for metastatic colorectal cancer: results of a multivariate analysis of 3825 patients. Ann Oncol. 2002;13(2):308–317.
22. Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649–655.
23. Miller AB, Hoogstraten B, Staquet M, et al. Reporting results of cancer treatment. Cancer. 1981;47(1):207–214.
24. Douillard JY, Cunningham D, Roth AD, et al. Irinotecan combined with fluorouracil compared with fluorouracil alone as first-line treatment for metastatic colorectal cancer: a multicentre randomised trial. Lancet. 2000;355(9209):1041–1047.
25. Cancer Therapy Evaluation Program NCI. Common Terminology Criteria for Adverse Events (CTCAE) v2.0 Online Instructions and
by guest on February 19, 2011jnci.oxfordjournals.org
Dow
nloaded from

30 Articles | JNCI Vol. 103, Issue 1 | January 5, 2011
Guidelines. https://webapps.ctep.nci.nih.gov/webobjs/ctc/webhelp/welcome_ to_ctcae.htm. Accessed February 4, 2010.
26. Schoenfeld DA. Partial residuals for the proportional hazards regression model. Biometrika. 1982;39(2):499–503.
27. Sorbye H, Köhne CH, Sargent DJ, et al. Patient characteristics and strat-ification in medical treatment studies for metastatic colorectal cancer: a proposal for standardization of patient characteristic reporting and strati-fication. Ann Oncol. 2007;18(10):1666–1672.
28. Tournigand C, Andre T, Achille E, et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a ran-domized GERCOR study. J Clin Oncol. 2004;22(2):229–237.
29. Sanoff H, Sargent D, Campbell M, et al. Five-year data and prognostic factor analysis of oxaliplatin and irinotecan combinations for advanced colorectal cancer: N9741. J Clin Oncol. 2008;26(35):5721–5727.
30. Pessino A, Sobrero A. Optimal treatment of metastatic colorectal cancer. Expert Rev Anticancer Ther. 2006;6(5):801–812.
31. Koopman M, Punt CJ. Chemotherapy, which drugs and when. Eur J Cancer. 2009;45(suppl 1):50–56.
32. Masi G, Loupakis F, Pollina L, et al. Long-term outcome of initially unre-sectable metastatic colorectal cancer patients treated with 5-fluorouracil/leucovorin, oxaliplatin, and irinotecan (FOLFOXIRI) followed by radical surgery of metastases. Ann Surg. 2009;249(3):420–425.
33. Gallagher DJ, Kemeny N. Second-line management of metastatic colo-rectal cancer. Clin Colorectal Cancer. 2008;7(1):25–32.
34. Yeoh C, Chau I, Cunningham D, Norman AR, Hill M, Ross PJ. Impact of 5-fluorouracil rechallenge on subsequent response and survival in advanced colorectal cancer: pooled analysis from three consecutive ran-domized controlled trials. Clin Colorectal Cancer. 2003;3(2):102–107.
35. De Gramont A, Buyse M, Abrahantes JC, et al. Reintroduction of oxalipla-tin is associated with improved survival in advanced colorectal cancer. J Clin Oncol. 2007;25(22):3224–3229.
36. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irino-tecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350(23):2335–2342.
37. Saltz LB, Clarke S, Diaz-Rubio E, et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colo-rectal cancer: a randomized phase III study. J Clin Oncol. 2008;26(12):2013–2019.
38. Tol J, Koopman M, Cats A, et al. Chemotherapy, bevacizumab, and cetux-imab in metastatic colorectal cancer. N Engl J Med. 2009;360(6):563–572.
FundingThis work was supported in part by the Fondazione Associazione Ricerca e Cura in Oncologia (A.R.C.O).
39. Van Cutsem E, Köhne CH, Hitre E, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360(14):1408–1417.
40. Masi G, Vasile E, Loupakis F, et al. Bevacizumab (BV) in combination with FOLFOXIRI (irinotecan, oxaliplatin and infusional 5FU/LV) as first-line treatment of metastatic colorectal cancer (mCRC): a phase II trial by the GONO group. Ann Oncol. 2009;20(suppl 7);viii12 (abstract#O-0017).
NotesThe authors had full responsibility for designing and analyzing the study, inter-preting the data, writing the manuscript, and submitting it for publication. The Fondazione Associazione Ricerca e Cura in Oncologia had no role in the design of the study; the collection, analysis, or interpretation of the data; the writing of the manuscript; or the decision to submit the manuscript for publication.
The authors thank Dr Luca Boni for helpful statistical insights and Mrs Simona Giannace and Mrs Etleva Beijta for data management and technical assistance.
Affiliations of authors: U.O. Oncologia Medica 2 Universitaria, Azienda Ospedaliero-Universitaria Pisana, Istituto Toscano Tumori, Pisa, Italy (GM, EV, FL, LF, GB, LS, CC, MA, AF); U.O. Oncologia Medica, Azienda USL 6 di Livorno, Istituto Toscano Tumori, Livorno, Italy (SC, IS); U.O. Oncologia Medica 1, Azienda Ospedaliero-Universitaria Pisana, Istituto Toscano Tumori, Pisa, Italy (IB); U.O. Oncologia B, Dipartimento di Medicina Sperimentale, Università di Roma “Sapienza”, Roma, Italy (MAF, MP, PT); U.O. Oncologia Medica, Ospedale S. Croce e Carle, Cuneo, Italy (CG); U.O. Oncologia Medica, Istituto Nazionale Tumori, Genova, Italy (SC); S.C. Oncologia Medica, Azienda Sanitaria di Firenze, Istituto Toscano Tumori, Firenze, Italy (LF); U.O. Oncologia Medica, Azienda USL-5, Istituto Toscano Tumori, Pisa, Italy (GA); U.O. Oncologia Medica, Ospedale S. Andrea delle Fratte, Perugia, Italy (LC).
by guest on February 19, 2011jnci.oxfordjournals.org
Dow
nloaded from
Copyright © 2022 FDOKUMEN