Editorial Board - Infection & Chemotherapy
66
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Editorial Board - Infection & Chemotherapy
Editorial Board
Editor-in-Chief
Dong-Gun Lee
The Catholic University of Korea, Korea
Associate Editors
Byung Chul Chun
Korea University, Korea
Dae Sun Jo
Chonbuk National University, Korea
Baek-Nam Kim
Inje University, Korea
Heejung Kim
Yonsei University, Korea
Sun Hee Lee
Pusan National University, Korea Kyoung Un Park
Seoul National University, Korea
Wan Beom Park
Seoul Natoinal University, Korea
Eui-Cheol Shin
KAIST, Korea
Editorial Board
Yagob Al-Mazrou Saudi Health Council, Saudi Arabia
Lucille Blumberg National Institute for Communicable Diseases, South Africa
Yi Ann Louis Chai National University Health System, Singapore
Mee Soo Chang Seoul National University, Korea Remi Charrel Aix-Marseille University, France
Yee-Chun Chen National Taiwan University, Taiwan
Hee Jin Cheong Korea University, Korea
Hee Jung Choi Ehwa Womans University, Korea
Min-Ho Choi Seoul National University, Korea
Sang-Ho Choi University of Ulsan, Korea
Young Hwa Choi Ajou University, Korea
Doo Ryeon Chung Sungkyunkwan University, Korea
Benjamin Cowie WHO Collaborating Centre for Viral Hepatitis, Australia
Byung Wook Eun Eulji University, Korea
Nohynek Hanna National Institute for Health and Welfare, Finland
Sue Huang Institute of Environmental Science and Research, New Zealand Eung-Soo Hwang Seoul National University, Korea
Youngmee Jee Korea Center for Disease Control and Prevention, Korea
Joseph F John, Jr Medical University of South Carolina, USA
Bum-Joon Kim Seoul National University, Korea
Hong Bin Kim Seoul National University, Korea
Nam Joong Kim Seoul National University, Korea Ichiro Kurane National Institute of Infectious Diseases, Japan
Hyuck Lee Dong-A Medical Center, Korea
Sang-Oh Lee University of Ulsan, Korea
Anna Lena Lopez University of the Philippines, Philippines
Moon H. Nahm University of Alabama at Birmingham, USA
John M Nicholls Hong Kong University, China
Hyunjoo Pai Hanyang University, Korea
Kyong Ran Peck Sungkyunkwan University, Korea
Raymund R. Razonable Mayo Clinic, USA
Jeong Hwan Shin Inje University, Korea
Adebayo Shittu Obafemi Awolowo University, Nigeria
Robert Leo Skov Statens Serum Institut, Denmark
Joon Young Song Korea University, Korea
Young Goo Song Yonsei University, Korea
Vincent H. Tam University of Houston, USA
Tomohiko Takasaki Kanagawa Prefectural Institute of Public Health, Japan
Visanu Thamlikitkul Mahidol University, Thailand
Thomas J. Walsh Weill Cornell Medicine of Cornell University, USA
Eun Jeong Won Chonnam National University, Korea
Statistics Editor Jun-Pyo Myong The Catholic University of Korea, Korea
Manuscript Editor Ji Hee Lee [email protected]

The Korean Society for AIDS
2020 대한에이즈학회 학술대회
Vol. 52 • Sup3 • November 2020
Aims and Scope
Infection & Chemotherapy (Infect Chemother) is an international, peer-reviewed, and open-access journal in English, which pub-
lishes the current research on issues posed by infectious diseases worldwide. This journal, which is published quarterly (on the last
day of March, June, September, and December) in both print and online (https://icjournal.org) versions, is the only official pub-
lication of the Korean Society of Infectious Diseases, Korean Society for Antimicrobial Therapy, and the Korean Society for AIDS.
It publishes review articles, original articles, brief communications, correspondences, case reports, editorials, and special articles
covering an extensive range of clinical descriptions on infectious diseases, public health issues, microbiology including emerging
resistance, parasitology and immunity to microbes, current and novel treatments, and the promotion of optimal practices or guide-
lines for diagnoses and treatments. As the world continues to shrink as a result of globalization, it is necessary that appropriate
communication is maintained among countries for timely sharing of information on infectious diseases. This is an important topic
because such diseases tend to have unique biologic features according to the regions in which they develop, and these diseases can
easily become niduses that may spread globally at any time. Based on these factors, the aim of this publication is to facilitate com-
munication among societies and countries, enabling the worldwide sharing of information on infectious diseases. The scope of this
journal is to link basic and clinical research in the field of infectious diseases, in reference to relevant evidence. The journal con-
tinuously attempts to publish current global and regional topics concerning infectious diseases and their diagnoses and manage-
ments to create awareness of related issues and link various developing and developed countries.
• Manuscripts of articles for publication should be submitted online through the Infection & Chemotherapy e-submission system
at http://www.editorialmanager.com/ic
• Open Access, everyone everywhere can read your research without cost.
• Full text PDF files are available at https://www.icjournal.org
• Infection & Chemotherapy is indexed/tracked/covered by Emerging Sources Citation Index (ESCI), PubMed, PubMed Central,
SCOPUS, CrossRef and DOI, DOAJ, EMBASE, CAS, Google Scholar, CABI, KoreaMed, Synapse, KoMCI.
• It has been published since 1969.
Editor in Chief Dong-Gun Lee
Editorial Office#806, Seocho Town Trapalace, 23 Seocho-daero 74-gil, Seocho-gu, Seoul 06621, Korea Tel. +82-2-532-6003 / Fax. +82-2-535-2494 / E-mail. [email protected] / Web. https://icjournal.org
Printed by CAPSTONE Co.
21, Baekbeom-ro 31-gil, Mapo-gu, Seoul, KoreaTel: +82-2-6010-8500, Fax: +82-50-4187-5550, E-mail: [email protected]
This journal was supported by the Korean Federation of Science and Technology Societies Grant funded by the Korean Government
(Ministry of Education).
© Infection & Chemotherapy◯CC It is identical to the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0).
◯CC This paper meets the requirements of KS X ISO 9706, ISO 9706-1994 & ANSI/NISO Z.39.48-1992 (Permanence of Paper)
E-poster session분야 발표번호 제목 발표자 Page
Basic and translational research
P-01Comparison of T cell subsets between virally-suppressed HIV-infected
patients receiving antiretroviral therapy and normal control김윤정 / 253
Basic and translational research
P-02
Potassium acetate alleviates HIV-1 Tat-induced pro-inflammatory
chemokines expression by suppressing the HDAC6-ROS-MAPK-NF-kB
axis in astrocytes
윤기수 / 254
Basic and translational research
P-03Improvement of latent HIV-1 infection model by blocking pyroptosis-
mediated cell death김동은 / 255
Basic and translational research
P-04
Construction and examination of a new type of Brec1
Recombinase derivatives for the Elimination of HIV Proviral DNA
from the Host Genome
배준현 / 256
Basic and translational research
P-05The novel biological function of FBXW4 in Human
Immunodeficiency Virus Type-1 (HIV-1) replication유경리 / 257
Basic and translational research
P-06Aristolactam derivatives against Human Immunodeficiency
virsus-1 with inhibition of Tat-mediated viral transcription신영현 / 258
Basic and translational research
P-07Enhanced Anti-viral effect of SCOTIN derivatives on Human
Immunodeficiency Virus-1(HIV-1) production김가나 / 259
Basic and translational research
P-08Ack1, a novel Nef binding partner, play a key role in CD4
down-regulation by HIV-1 infection김정아 / 260
Basic and translational research
P-09Discovery of Effective HIV-1 Transcription Inhibitory Antiviral
Peptides김해인 / 261
Basic and translational research
P-10
Sequence length of HIV-1 subtype B increases over time: a
longitudinal analysis of a Korean hemophiliac cohort over 30
years
조영걸 / 262
Clinical research P-11Age at which subclinical atherosclerosis occurs in people living
with HIV in Korea박성희 / 263
Clinical research P-12
Evaluation of lipid profile in HIV patients on dolutegravir,
abacavir, lamivudine, and elvitegravir, cobicistat, emtricitabine,
tenofovir alafenamide - a single center clinical experience
배상운 / 264
Clinical research P-13Rate of and risk factors for loss to follow up in HIV-infected
patients in South Korea: Korean HIV/AIDS cohort study성 혜 / 265
Clinical research P-14
Integrase strand transfer inhibitor treatment does not increase
the incidence of immune reconstitution inflammatory
syndrome in HIV-infected Koreans
김 진 / 276
Clinical research P-15Lenacapavir Resistance Analysis in a Phase 1b Clinical Proof-Of-
Concept Study이정아 / 277

The Korean Society for AIDS
2020 대한에이즈학회 학술대회
분야 발표번호 제목 발표자 Page
Clinical research P-16 코로나19가 감염인 상담에 미치는 영향 : case study 서아영 / 278
Clinical research P-17
Starting or switching to bictegravir/emtricitabine/tenofovir alafenamide
(B/F/TAF) in clinical practice: pooled 12-month (12M) results from
the global BICSTaR study
이정아 / 280
Clinical research P-18
Durable Efficacy of Dolutegravir (DTG) Plus Lamivudine (3TC)
in Antiretroviral Treatment-Naïve Adults With HIV-1 Infection
–3-Year Results From the GEMINI Studies
권성신 / 281
Clinical research P-19Safety and Efficacy of Cabotegravir + Rilpivirine Long-Acting
With and Without Oral Lead-In: FLAIR Week 124 Results권성신 / 283
Clinical research P-20 HIV 감염자에서 발생한 항문암 4례와 인간유두종바이러스와의 관련성 백예지 / 286
Clinical research P-21
Pooled Analysis of 4 International Trials of Bictegravir/Emtricitabine/
Tenofovir Alafenamide (B/F/TAF) in Adults Aged ≥ 65 or Older
Demonstrating Safety and Efficacy: Week 48 Results
이정아 / 289
Clinical research P-22
Switching to DTG/3TC Fixed-Dose Combination (FDC) Is Non-Inferior
to Continuing a TAF-Based Regimen (TBR) in Maintaining Virologic
Suppression Through 96 Weeks (TANGO Study)
권성신 / 290
Epidemiology and social research
P-23
Assessment of disease burden and immunization rates for
vaccine- preventable diseases in people living with HIV: The
Korea HIV/AIDS Cohort study
성 혜 / 292
Epidemiology and social research
P-24의료기관감염인상담사업 지표로 본 감염인 건강관리 현황 : 2015년~2019
년 시계열 분석최재필 / 301
Epidemiology and social research
P-25 남성 동성애자 대상 성 건강 결정 영향요인 양혜진 / 303
Epidemiology and social research
P-26
Stuck in Neutral: Identifying opportunities to make progress in
addressing HIV-related stigma and other emotional and
psychosocial unmet needs among people living with HIV in
South Korea
권성신 / 304

E-poster session
2020The Korean Society for AIDS
대한에이즈학회 학술대회

E-poster session
2020 대한에이즈학회 학술대회 253
P-01 Basic and translational research
Comparison of T cell subsets between virally-suppressed
HIV-infected patients receiving antiretroviral therapy and
normal control
Youn Jeong Kim , Si-Hyun Kim , Yeon Jeong Jeong , Yoon Hee Jun , Sang Il Kim , Yang Ree Kim
Division of Infectious disease, Department of Internal Medicine, The Catholic University of Korea, College of Medicine, Seoul, Korea
Introduction: With the introduction of antiretroviral therapy (ART), the majority of HIV-infected
individuals fully suppress viral load and display a progressive increase in CD4 counts resulting in
improvement in their health. However HIV infection results in changes T cell phenotype and function
which may persist even during effective ART. The aim of this study was to determine profiles of T cells
in virally suppressive HIV-infected patients after ART.
Methods: We included HIV-infected subjects receiving ART with VL<40 copies/mL for at least one year,
and compared with healthy control. Selected panels of immunological markers of T were evaluated by
flow cytometry.
Results: Nineteen HIV-infected patients and twenty-five healthy controls were included. The mean age
was 44.8±14.6 years among the HIV-infected and 61.3±5.2 years old among the control (p=0.0001).
HIV-infected subjects had a mean duration of viral suppression of 2759.8±2139.7 days prior to
enrollment). The mean CD4+ count at the time of enrollment was 639.1±153.7 cells/mm3
The proportion of CD4+ CD161+ T cells (8.5±5.5 vs. 4.9±3.6, p=0.01) CD57+CD28- (0.6±0.6 vs.
0.3±0.3, p=0.04) were higher in HIV-infected group. The proportion of CD4+ CD45RA+CCR7+
(49.4±16.6 vs. 28.9±15.7, p=0.001) were higher and the proportion of CD4+ CD45RA-CCR7-
(10.2±5.6 vs. 23.1±10.3, p=0.0001) and CD45RA+CCR7- (1.8±1.4 vs. 6.9±8.0, p=0.005) were lower
in HIV-infected group.
The proportion of CD8+ CD45RA+CCR7- (29.9 ±13.5 vs. 17.9±16.0, p=0.01) were higher in
HIV-infected group.
In the analysis of subgroups over 50 years of age, the proportion of CD4+ CD28- expressing CD57+
(p=0.01) and CD8+ CD28- expressing CD57+ (p=0.009) was higher in HIV-infected group. And the
proportion of CD4+CD45RA-CCR7- was significantly lower in HIV-infected group (p=0.001).
Conclusion: Our results showed that dysfunctional phenotype including late-differentiated peripheral
blood CD4+ and CD8+ T cell may take place despite of successful ART.
Keywords: HIV, T cell, phenotype, ART
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
254 2020 대한에이즈학회 학술대회
P-02 Basic and translational research
Potassium acetate alleviates HIV-1 Tat-induced
pro-inflammatory chemokines expression by suppressing
the HDAC6-ROS-MAPK-NF-kB axis in astrocytes
Donggyu Kim, Hyundong Jo, Gi Soo Youn, Soo Young Choi, Jinseu Park
Department of Biomedical Science and Research Institute for Bioscience & Biotechnology, Hallym University, Chunchon 200-702, Republic of Korea
Background: HIV-1 trans-activator of transcription (Tat) activates NADPH oxidase resulting in the
generation of reactive oxygen species (ROS), leading to extensive neuroinflammation in the central
nervous system and progress to AIDS-related encephalitis or dementia. Astrocytes, the major glial cells
in the central nervous system, contribute to immune regulation by expressing chemokines, cytokines,
and adhesion molecules. This report explored potassium acetate (PA) regulatory activity on HIV-1
Tat-mediated chemokine production and its mode of action in astrocytes.
Methods: These experiments used human astrocyte cell line CRT-MG cells. HIV-1 Tat purification
followed the Glutathione S-transferase fusion protein purification method, and the GST-Tat fusion
protein was digested with thrombin to get the Tat protein. Potassium acetate was pre-treated before
HIV-1 Tat treated 1 hour.
Results: Potassium acetate significantly suppressed HIV-1 Tat-mediated production of
pro-inflammatory chemokines, such as CCL2, CXCL8, and CXCL10. Potassium acetate inhibited the
expression of HDAC6, which is an important regulator in HIV-1 Tat-mediated chemokine production.
Potassium acetate diminished HIV-1 Tat-mediated reactive oxygen species (ROS) generation and
NADPH oxidase activation. Furthermore, inhibited HIV-1 Tat-mediated signaling cascades, including the
HDAC6-ROS-MAPK-NF-kB axis.
Conclusion: Overall, these results showed that Potassium acetate regulates HIV-1 Tat-induced
pro-inflammatory mediator expression via blockage of the HDAC6-ROS-MAPK-NF-kB axis in
astrocytes. Therefore, suggest that potassium acetate is a therapeutic compound candidate against
AIDS-related encephalitis or dementia.
Keywords: HIV-1 Tat, chemokines, inflammation, HDAC6, NADPH oxidase
E-poster session
2020 대한에이즈학회 학술대회 255
P-03 Basic and translational research
Improvement of latent HIV-1 infection model by blocking
pyroptosis-mediated cell death
Dong-eun Kim, Cheol-Hee Yoon, Young Hyun Shin, Byeong-Sun Choi
Division of Chronic Viral Disease Research, Center for Emerging Virus Research, National Institute of Infectious Disease, Chungbuk, Korea
Background: The highly active antiretroviral therapy (HAART) efficiently controls HIV infection and
prevents the AIDS progression, but this treatment cannot completely eliminate HIV reservoir. Several
studies developed the ex vivo models for HIV-1 latency to determine the specific characteristics of the
reservoirs. However, these models using non-replicative viruses could not represent the latent in vivo
infection. Here, we improved a primary latent HIV-1 infection model using replication-competent virus
by inhibiting pyroptosis.
Methods: Naive CD4 T cells were isolated from the PBMCs and the cells were then activated and
polarized to TCM for 7 days. After differentiation, cells were infected with replication-competent HIVNL4-3
(MOI 1). For 2 days, the infected cells were treated with inhibitors of caspase-1, capase-3 and viral
infection. At day 4, 6 and 8 post-infection, the cell viability was analyzed. At day 6 post-infection, cells
were reactivated and assessed p24 level to determine the population of latently infected cells.
Results: In an assay for cell viability, It was observed that the cell viability were markedly increased
about two fold in the cells treated with caspase-1 inhibitor compared to vehicle. At same time, latently
HIV-1 infected cells were countered using anti-p24 antibody conjugated with FITC after T cell
activation. The population of p24 positive cells was increased about two-fold in cells treated with
caspase-1 inhibitor compared to vehicle-treated cells. The enhanced p24+ cell number might be caused
by enhanced cell viability. In a LDH release assay for detecting pyroptosis, the amount of LDH released
from HIV-1 infected were definitely reduced about 40% in the cells treated with caspase-1 inhibitor.
Conclusion: Taken together, we improved the latent HIV-1 infection model using replication-competent
virus which may be helpful to define characteristics of latent HIV-1 infection.
This work was supported by Grant No. 2019-NI-067-01 from the KNIH
Keywords: HIV-1, latency model, pyrotosis, caspase-1

The Korean Society for AIDS
2020 대한에이즈학회 학술대회
256 2020 대한에이즈학회 학술대회
P-04 Basic and translational research
Construction and examination of a new type of Brec1
Recombinase derivatives for the Elimination of HIV Proviral
DNA from the Host Genome
Jun-Hyun Bae, Ji-Chang You
National Research Laboratory for Molecular Virology, Department of Pathology, School of Medicine, The Catholic University of Korea, Seoul.
Background: Even though combinatorial antiretroviral therapies (cART), which are used to treat HIV-1
infection, can effectively suppress and relieve symptoms of AIDS, but it does not completely eliminate
HIV-1 infection. In order to effectively cure HIV-1 infection, it is needed that the integrated proviral
DNA must be removed from the virus-infected host genome.
Methods: Toward the goal, We set to develop a therapeutic protein drug using Broad-range
recombinase 1 (Brec1) and a novel advanced cell-penetrating peptide (ACP). The Brec1 has previously
been known to efficiently and safely remove integrated provirus from HIV-1 infected cells. However, it
in its current form is difficult to being used as for a protein drug as it cannot get into cells by itself. To
overcome this problem, we fused the Brec1 with ACP, which can be easily internalized into cells and
might capable of targeting integrated proviral DNA in HIV-1 infected cells.
Results: We observed that the overexpression of ACP-Brec1 lead to the excision of co-transfected
proviral DNA in HIV-integrated cell lines. Virus production was also found to be significantly reduced by
HIV-1 p24 ELISA and western blot assay.
Conclusion: This novel approach using a combination of Brec1 and ACP might have a great potential to
develop a novel fundamentally curative HIV-1 therapy.
Keywords: HIV-1, Provirus

E-poster session
2020 대한에이즈학회 학술대회 257
P-05 Basic and translational research
The novel biological function of FBXW4 in Human
Immunodeficiency Virus Type-1 (HIV-1) replication
Kyung-Lee Yu, Ji Chang You
National Research Laboratory for Molecular Virology, Department of Pathology, College of Medicine, The Catholic University of Korea, Seoul, Korea 137-701
Background: The HIV-1 nucleocapsid (NC) is an essential viral protein containing two highly conserved
retroviral-type zinc finger (ZF) motifs, which functions in multiple stages of the HIV-1 life cycle. We
have screened several host cell factors interacting with NC protein through in vitro pull-down assay and
yeast two-hybrid assay. Among them, F-box/WD repeat domain-containing protein 4 (FBXW4) was
identified.
FBXW4 is a component of SCF (SKp1, Cullin, F-box protein)-type ubiquitin ligase, which mediates
ubiquitination of proteins targeted for degradation by the proteasome. So far, no target protein has been
identified for FBXW4, and little research has been done on the molecular or biochemical function of
FBXW4.
To identify the biological function of interaction between NC and FBXW4, we confirmed the effects of
FBXW4 on HIV-1 replication.
Methods and Materials: To overexpression of FBXW4, HA tagging FBXW4 plasmid were constructed. In
293T cells, we confirmed the effect either FBXW4 overexpression or knock-down in virus replication by
measuring the HIV-1 production by p24 ELISA assay and confirmed the Gag protein expression level by
western blot. In HeLa cells, we confirmed the subcellular localization of FBXW4 under conditions of
HIV-1 expression and absence.
Results: Both overexpression and knock-down of FBXW4 reduce the virus replication. In HIV-1
expression cells, co-localization between the Gag and FBXW4 at cell plasma membrane.
Conclusions: Our data show that HIV-1 requires the FBXW4 to replication properly, but if FBXW4
becomes overloaded, it causes suppression. We are working on a study to determine the exact
mechanism of FBXW4 role in HIV-1 replication.
Keywords: HIV-1, Nucleocapsid, FBXW4,

The Korean Society for AIDS
2020 대한에이즈학회 학술대회
258 2020 대한에이즈학회 학술대회
P-06 Basic and translational research
Aristolactam derivatives against Human Immunodeficiency
virsus-1 with inhibition of Tat-mediated viral transcription
YoungHyun Shin1, Hong Gi Kim2, Chul Min Park2, Dong-Eun Kim1, Jeong-Ah Kim1, Byeong-Sun Choi1, Cheol-Hee Yoon1
1Division of Chronic Viral Disease Research, Center for New Infectious Diseases Research, National Institute of Infectious Diseases, Korea National Institute of Health, Chungbuk, Republic of Korea2Center for Convergent Research of Emerging Virus Infection, Korea Research Institute of Chemical Technology, Daejeon, 34114, Republic of Korea
Background: Despite the success of antiretroviral therapy (ART), an effort to develop new class of
anti-HIV-1 agent have been ongoing with emergence of the drug resistances. Dibenso/indole-based
aristolactams are compounds isolated from various plants species which have multiple clinically relevant
effects including anti-inflammatory, antiplatelet and anti-mycobacterial effects, but it has not been
elucidated in anti-HIV-1 effect.
Methods: In this study, aristolactam derivative bearing dibenzo[cd,f]indol-4(5H)-one showed a potent
anti-HIV-1 effect for the first time. Subsequently, the structure–activity relationship (SAR) study using
nine synthetic derivatives of aristolactam revealed that residue substitutions had different effects on
HIV-1 infection and cell viability.
Results: Among the compounds tested, the 1,2,8,9-tetramethoxy-5-(2-(piperidinyl)ethyl)-dibenzo[cd,
f]indol-4(5H)-one (ID 183341) exhibited the most potent activity by inhibiting HIV-1 infection with a
half-maximal inhibitory concentration (IC50) of 1.03 μM and CC50 of 16.91 μM (Selective index 16.45).
Their inhibitory effect on HIV-1 infection linked to inhibition of viral life cycle in the T cell lines and
PBMCs. In a sequential study for defining the mode of action, the aristolactam derivatives did not affect
the revers-transcription and integration required in HIV-1 infection, while they inhibited viral
transcription with closely similar to pattern shown in their inhibition of HIV-1 infection without
nonspecific transcriptional inhibition.
Conclusion: Taken together, these findings suggested that several aristolactam derivatives impaired
HIV-1 infection by inhibiting the activity of Tat-mediated viral transcription and these derivatives may
be considerable candidates for the development of antiretroviral agents.
This research was supported by intramural fund (Grant No. 2019-NI-066-01) from the Korea National
Institute of Health.
Keywords: Aristolactam, HIV-1 Tat, HIV-1 Transcriptional inhibitors, Anti-HIV-1 effects
E-poster session
2020 대한에이즈학회 학술대회 259
P-07 Basic and translational research
Enhanced Anti-viral effect of SCOTIN derivatives on
Human Immunodeficiency Virus-1(HIV-1) production.
Ga-Na Kim, Kyung-Lee Yu, Ji-Chang You
National Research Laboratory for Molecular Virology, Department of Pathology, School of Medicine, The Catholic University of Korea, Seoul.
Background: The cell penetration peptide (CPP) composed of typically 5-30 amino acids can be used to
improve the probability of molecular transfer, including drugs. Also, it provides the potential to increase
the therapeutic effect of the disease. Lately, Unpublished Advanced Cell Penetration-Peptide (ACP) is
studying in our laboratory has established a novel CPP, named ACP, which shows a better delivery
activity than well-known CPP such as Tat of HIV-1. In addition, we have also demonstrated that
SHISA5 gene has an anti-virus effect against HIV-1. Here, we have examined whether anti-viral
activity of SCOTIN against HIV-1 production could be enhanced and delivered by fusing the ACP.
Method: We have made expression vectors of SCOTIN and ACP fusion SCOTIN. The protein expression
level of each vector was verified by western blot assay and Fluorescence. Next, they were
co-transfected with NL4-3_GFP DNA to 293T cells, and viral production level was measured by
Western blot assay and enzyme-linked immunosorbent assay. Viral infectivity was also determined by
GFP signal. The same volume of virus-containing each culture supernatant was used to infect MT4
cells.
Results: The protein expression level of ACP-SCOTIN and SCOTIN-ACP was compared with SCOTIN.
We observed the separation of ACP and SCOTIN by a signal sequence of SCOTIN in the expression of
ACP-SCOTIN. Overexpression of each recombinant significantly reduced the p24 level than SCOTIN
alone. Also, we confirmed that the level of GFP was further reduced in the ACP fusion SCOTIN
expression. As a result, our study showed that ACP fusion form of SCOTIN inhibited and reduced
infectivity of progeny virus and production of HIV-1 quite efficiently.
Conclusion: Taken together, these results suggested that ACP could enhance the effect of anti-HIV-1
by SCOTIN. Thus, this approach might be a useful approach for the development of a new anti-HIV-1
drug molecule.
Keywords: AIDS, HIV-1, CPP, ACP, SCOTIN
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
260 2020 대한에이즈학회 학술대회
P-08 Basic and translational research
Ack1, a novel Nef binding partner, play a key role in CD4
down-regulation by HIV-1 infection
Jeong-Ah kim, YoungHyun Shin, Dong-Eun Kim, Eun-ji Kim, Cheol-Hee Yoon
Division of Chronic Viral Disease Research, Center for New Infectious Diseases Research, National Institute of Infectious Diseases, Korea National Institute of Health, Korea Disease Control and Prevention Agency, Chungbuk, Korea
Background: Nef is a key factor inducing HIV-1 virulence, which is commonly defective in HIV-1s
isolated from long term non-progressors. Numerous studies determined the virulence mechanism
underlying the molecular biology of Nef including CD4 and MHC-I/II down-regulation and increased
viral infectivity, but the detailed mechanism of Nef-induced virulence is not understood fully. Here, we
report that Ack1 is a novel Nef-interacting partner that plays a crucial role in CD4 down-regulation
during viral infection
Methods: To identify Nef binding partners, we performed yeast two hybrid method and confirmed their
interaction in 293T cells by co-immunoprecipitation (Co-IP). In order to identify the Nef binding domain
on ACK1, we constructed deleted forms of Ack1 and determined the binding domain by co-IP.
Additionally, to test whether Ack1 is a necessary factor for Nef-induced down-regulation of surface
immune molecule, shRNA knock-down of ACK1 was conducted in Tzm-bl cells expressing CD4,
CXCR4 and CCR5.
Results: We discovered 60 kinds of Nef-binding host proteins using yeast two-hybrid screening
method. Among these, TNK2, also called ACK1 (Activated Cdc42-associated kinase). In the Nef
expressing cells, the level of Ack1 mRNA was not changed, whereas the protein level was significantly
reduced. In a mapping assay, Nef specifically binds to the SH3 domain of Ack1. To determine whether
the interaction of ACK1-Nef influence on down-regulation of surface immune molecules, shRNA
knock-down of ACK1 was conducted in TZM-bl cells. The ACK1 knock-down significantly
down-regulated the expression of CD4 as well as co-receptors, similarly to shown in HIV-1 infected
cells.
Conclusion: Taken together, Nef facilitates the degradation of ACK1 protein by direct Nef-ACK1
interaction, which may trigger down-regulation of immune molecules including CD4, CCR5 and CXCR4
on the host cell surface linked to HIV-1-induced virulence.
This work was supported by Grant No. 2019-NI-066-01 from the KNIH
Keywords: Nef, ACK1, HIV-1 virulence, CD4 down-regulation

E-poster session
2020 대한에이즈학회 학술대회 261
P-09 Basic and translational research
Discovery of Effective HIV-1 Transcription Inhibitory
Antiviral Peptides
Hae-In Kim, Ji-Chang You
National Research Laboratory for Molecular Virology, Department of Pathology, School of Medicine, The Catholic University of Korea, Seoul.
Background: P-TEFb is comprised of CycT1 and CDK9, and it is required for transcription elongation for
both HIV and host gene expression. The 7SK snRNP complex not only plays an essential role in the
regulation of transcription by RNA Pol II but also regulates P-TEFb activity. One of the 7SK snRNP
components, HEXIM1, binds to P-TEFb and inhibits the cyclin-dependent kinase activity of P-TEFb by
concealing the substrate-binding site of CDK9. Viral trans-activator Tat can hijack P-TEFb from 7SK
snRNP and convey it to TAR, which induces enhanced gene expression from the HIV promoter by
engaging RNA Pol II. Recently, it has been shown that the chimeric protein HEXIM1-Tat (HT) impedes
viral transcription, by contending with Tat for TAR binding. We conducted the present research to
develop antiviral agents that could more effectively inhibit virus transcription.
Methods: We fused HT with Advanced cell-penetrating protein (ACP), a novel peptide identified and
developed in our laboratory. NL43-eGFP co-transfected with ACP-HT, HT-ACP, or HT into 293T cells.
The resulting cell lysates were used for Western blot and the supernatants were also collected for
ELISA and for infection of MT4 cells. The LTR assay was performed in the T-REx 293 cell to examine
the inhibition of viral transcription.
Results: Stable expression of ACP-HT or HT-ACP inhibited viral protein expression more effectively
than HT itself. ACP-HT and HT-ACP depleted the p24 level of the supernatant up to 95.7% and 81.3%,
while HT reduced only up to 52.2 %. Also, the expression of ACP-HT or HT-ACP induces a decrease in
virus-infected cells and LTR activity. The results suggested that ACP-HT or HT-ACP could inhibit virus
production and restrain the infectivity of the progeny virus.
Conclusion: We found the potential for the new fusion proteins to outperform the antiviral effects of HT.
These novel chimeric proteins inhibit HIV-1 replication efficiently and denote new candidates for novel
anti-HIV-1 therapy.
Keywords: HIV-1 transcription, antiviral drug, HEXIM1, Tat

The Korean Society for AIDS
2020 대한에이즈학회 학술대회
262 2020 대한에이즈학회 학술대회
P-10 Basic and translational research
Sequence length of HIV-1 subtype B increases over time:
a longitudinal analysis of a Korean hemophiliac cohort over
30 years
Young-Keol Cho, Jung-Eun Kim
Departments of Microbiology, University of Ulsan College of Medicine, Seoul, Korea.
Objective: The aim of this study was to investigate whether sequence length of HIV-1 increases over
time.
Design: A longitudinal analysis of near full-length HIV-1 sequences (FLs) in an outbreak of HIV-1
infection among Korean hemophiliacs and local controls previously identified as infected with Korean
subclade B (KSB).
Methods: Genes amplified by overlapping RT-PCR or nested PCR were subjected to direct sequencing.
One hundred twenty-five FLs were sequentially determined over 30 years in 62 KSB-infected patients.
Sequence length over time was compared with HIV Sequence Database at Los Alamos National
Laboratory.
Results: Phylogenetic analysis indicated that within KSB, two FLs from plasma donors O and P
comprised two clusters together with eight hemophiliacs and twelve hemophiliacs, respectively
(bootstrap values, all 100%). Signature pattern analysis for the KSB of HIV-1 revealed signature
nucleotide residues 1.05% (91 residues), compared with local controls. In addition, in-depth FLs
sequence analysis over 30 years in KSB indicates that the sequence length of HIV-1 significantly
increases over time before combined antiretroviral therapy (cART) and do not increase on cART.
Furthermore, the increase in sequence length over time occurred in subtypes B and C, but, suprisinlgy,
it did not occur in about 4-fold rapidly progressing subtype D. Consequently, sequence length of
subtype D was significantly shorter than all subtypes we analyzed.
Conclusion: Phylogenetic and signature pattern analysis revealed the epidemiological linkage between
plasma donors and hemophiliacs. Sequence length of HIV-1 subtypes B and C increases over time
before cART.
Keywords: full-length HIV-1, Korean subclade B; subtypes B, C and D; sequence length; hemophiliacs
E-poster session
2020 대한에이즈학회 학술대회 263
P-11 Clinical research
Age at which subclinical atherosclerosis occurs in people
living with HIV in Korea
Sunghee Park1, Eunyoung Lee2, Se Yoon Park3, Eunjung Lee3 , Tae Hyong Kim3
1Division of Infectious Diseases, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea; 2Division of Infectious Diseases, Seoul National University Boramae Medical Center, Seoul, Republic of Korea; 3Division of Infectious Diseases, Soonchunhyang University College of Medicine, Seoul, Republic of Korea
Background and Objectives: People living with human immunodeficiency virus (PLHIV) are known to
have an increased risk of atherosclerosis and cardiovascular disease (CVD). Carotid intima-media
thickness (IMT) is often measured as a surrogate marker for cardiovascular risk, but such data on Asian
PLHIV is limited. In this study, we aimed to identify the risk factors of increased carotid IMT in PLHIV
living in South Korea.
Methods: A total of 225 PLHIV who underwent carotid IMT in a teaching hospital in Seoul, Republic of
Korea between January 2017 and January 2020 were analyzed. The participants were then divided into
the subclinical atherosclerosis group and the control group. Data on clinical characteristics, underlying
diseases, laboratory findings, and antiretroviral therapy regimens, along with carotid IMT measurements
were compared between the two groups.
Results: Among the study population, 123 (54.7%) had subclinical atherosclerosis. The subclinical
atherosclerosis group was older than the control group (46 vs. 35.1 years, p<.001), had more
hypertension (33.3% vs. 19.6%, p=0.021), dyslipidemia (56.9% vs. 16.7%, p<.001), and CVD history
(6.5% vs. 0%, p=0.009). The cut-off level of age to predict subclinical atherosclerosis was 39.5 (area
under the curve 0.79, p<0.001). Subclinical atherosclerosis group also had longer HIV infection duration
(85.4 vs. 67.2 months, p=0.006) albeit it was not associated significantly after adjust other variables.
Conclusions: Conventional risk factors including age, hypertension, dyslipidemia were associated with
subclinical atherosclerosis in PLHIV. Particularly, age 39.5 was a cut-off level.
Keywords: HIV, atherosclerosis , carotid intima-media thickness, risk factors, Republic of Korea

The Korean Society for AIDS
2020 대한에이즈학회 학술대회
264 2020 대한에이즈학회 학술대회
P-12 Clinical research
Evaluation of lipid profile in HIV patients on dolutegravir,
abacavir, lamivudine, and elvitegravir, emtricitabine,
tenofovir alafenamide - A single center clinical experience
Sang Woon Bae, Youn Jeong Kim, Sang Il Kim, Yoon Hee Jun
Division of Infectious Diseases, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea
Background: As an era that HIV infection treated with excellent anti-retroviral therapy (ART) such as
dolutegravir and elvitegravir is a long term maintained disease, HIV specialists have to care for people
living with HIV; who would have healthier and longer elderly life, being concerned about their
dyslipidemia, overweight, and cardio- and cerebrovascular diseases.
Method: A total of 299 patient medical records were reviewed. All of them are on single-pill ART,
including dolutegravir, abacavir, lamivudine (DTG/ABC/3TC), or elvitegravir, emtricitabine, tenofovir
alafenamide (EVG/ FTC/TAF). We used the Cox proportional hazards model to determine associations
between ART treatment regimen and lipid profile changes. Increased total cholesterol (TC) was defined
when the difference of TC levels on baseline and event dates equals to or greater than 20 mg/dl.
Increased low-density lipoprotein cholesterol (LDL) was defined likewise. We defined body-weight gain
as a five percentile gain between the baseline and event dates.
Results: DTG/ABC/3TC group (n=136) and EVG/FTC/TAF (n=123) group did not differ in terms of age
(p=0.26), CD4 T cell count (p=0.26), eGFR (p=0.19), baseline LDL (p=0.81), triglyceride (p=0.25), and
HDL (p=0.12). Treatment duration was significantly longer in DTG/ABC/3TC group compared with
EVG/FTC/TAF group (median 428.5 vs. 321, p=7.182E-08).
In the Cox regression analyses, increased LDL levels were associated with EVG/FTC/TAF (HR=3.17)
and less than 200 mg/dl of baseline TC level (HR=4.35). Also, increased TC was associated with
EVG/FTC/TAF (HR=3.26), less than 200 mg/dl of baseline TC level (HR=3.16), and well-controlled viral
copy (HR=0.47).
Conclusion: EVG/FTC/TAF has increased LDL and total cholesterol levels compared to DTG/ABC/3TC.
Baseline cholesterol is also an essential factor in lipid profile change during ART, while body weight
showed no significance in this study.
Keywords: HIV Integrase Inhibitors, Dyslipidemias, HIV
E-poster session
2020 대한에이즈학회 학술대회 265
P-13 Clinical research
Rate of and risk factors for loss to follow up in
HIV-infected patients in South Korea: The Korea HIV/AIDS
Cohort study
Hye Seong1,2,4, Yunsu Choi3, Min Jeong Kim4, Joon Young Song5, Shin-Woo Kim6, Sang Il Kim7, Mee-Kyung Kee8, Bo Youl
Choi3, Jun-Yong Choi1,2
1Department of Internal Medicine; 2AIDS Research Institute, Yonsei University College of Medicine, Seoul; 3Department of Preventive Medicine, Hanyang University College of Medicine; 4Institute for Health and Society, Hanyang University, Seoul, Korea; 5Department of Internal Medicine, Korea University College of Medicine, Seoul; 6Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu; 7Department of Internal Medicine, Catholic University College of Medicine, Seoul; 8Division of Viral Disease Research, Korea Centers for Disease Control and Prevention, Cheongju, Korea
Background/Aims: Owing to antiretroviral therapy (ART), the acquired immune deficiency syndrome
(AIDS)-related mortality has significantly decreased. Retaining care is an essential step for HIV care
cascade. This study investigated the incidence of and risk factors for loss to follow-up (LTFU) in Korean
people living with HIV (PLWH).
Methods: Data from the Korea HIV/AIDS cohort study (including prospective interval cohort and
retrospective clinical cohort) were analyzed. LTFU was defined as not visiting clinic more than 1 year.
Risk factors for LTFU were identified using Cox regression hazard model.
Results: The study enrolled 3,172 adult HIV patients (median age, 36 years; male 92.97%). The median
CD4 T cell count at enrollment was 234 cells/mm3 (interquartile range [IQR], 85- 373) and median viral
load at enrollment was 56,100 copies/mL (IQR, 15,000-203,992). The total follow-up duration was
16,487 person-years, and the overall incidence rate of LTFU was 85/1000 person-years.
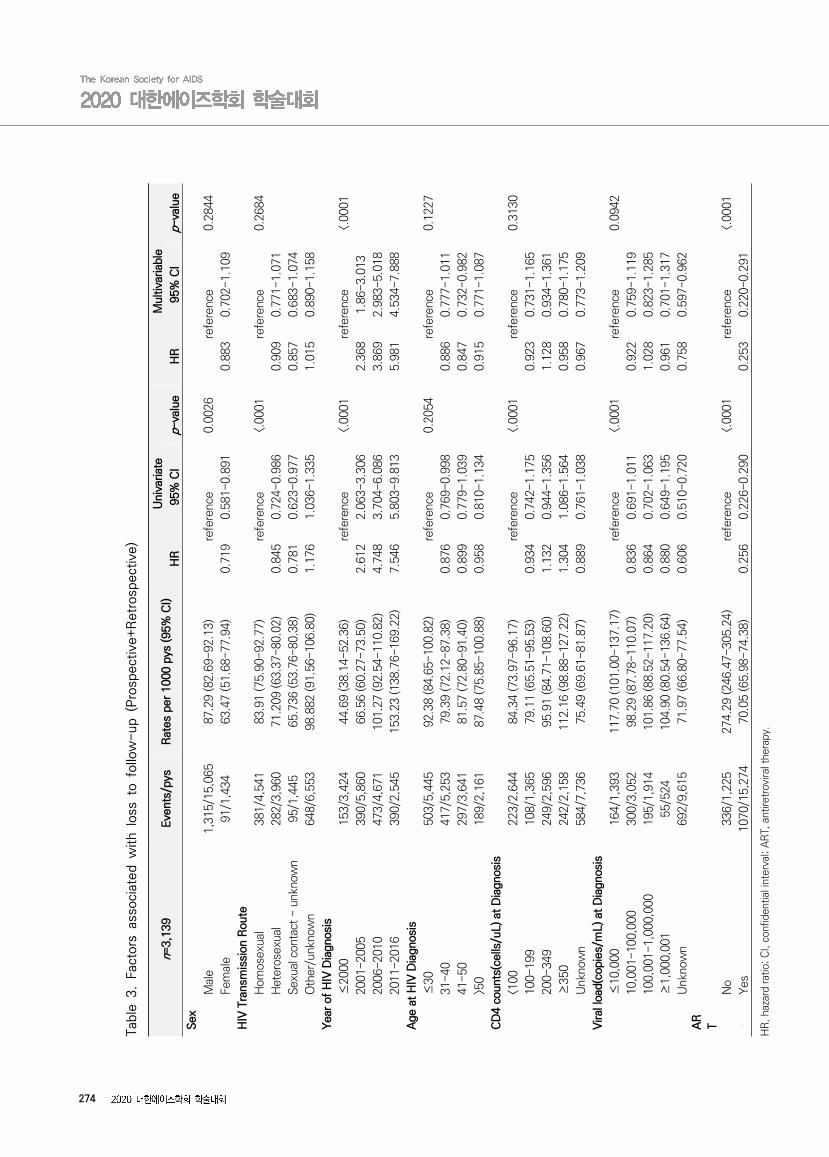
In the multivariable Cox regression model, subjects on ART were less likely to have LTFU than subjects not
on ART (hazard ratio [HR]= 0.253, 95% confidence interval [CI]: 0.220-0.291, p<0.0001). Among PLWH on
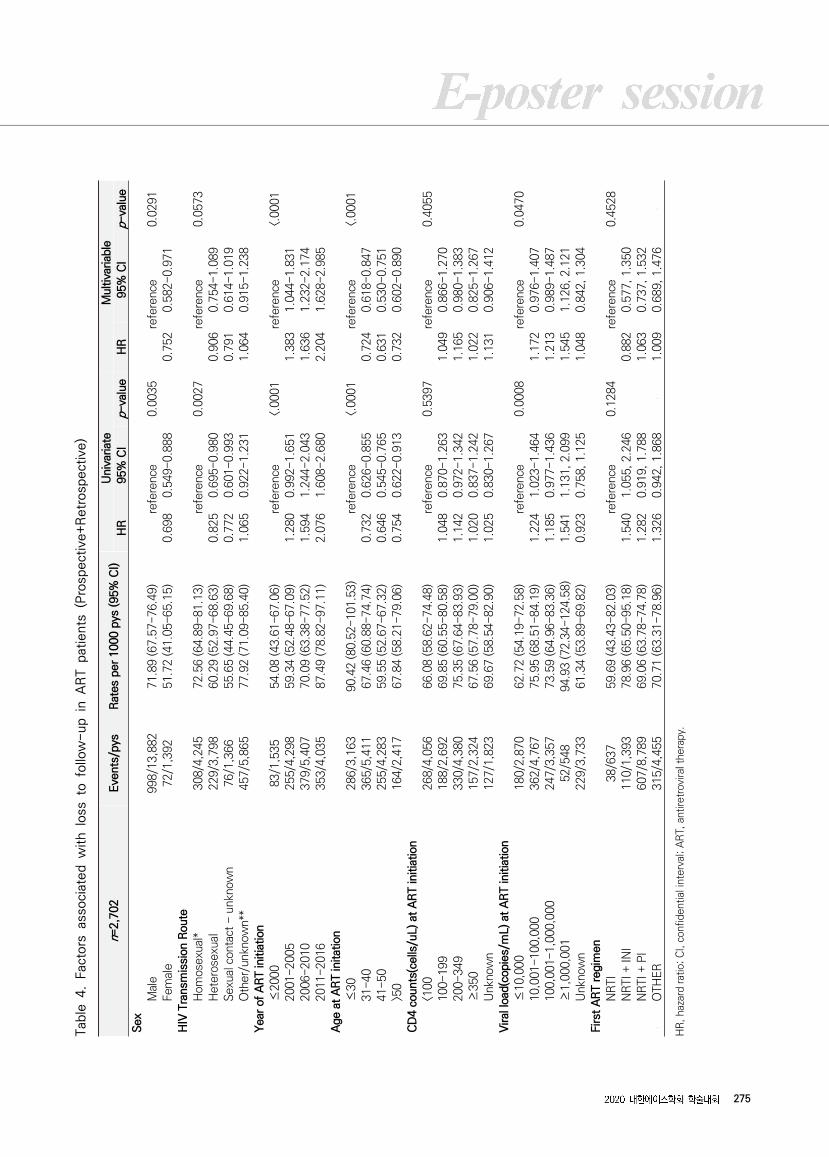
ART, female sex (HR = 0.752, 95 % CI: 0.582-0.971, p=0.0291) and older age (>50: HR = 0.732, 95% CI:
0.602-0.890; 41-50: HR = 0.634, 95% CI:0.530-0.750; 31-40: HR = 0.724, 95% CI: 0.618-0.847; ≤30:
reference, p<0.0001) were associated with lower rate of LTFU. A recent viral load ≥1,000,001 (HR = 1.545,
95 % CI: 1.126-2.121, ≤10,000: reference) was associated with higher rate of LTFU.
Conclusion: Young and male PLWH may have higher rate of LTFU, and increased rate of LTFU may
induce virologic failure.
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
266 2020 대한에이즈학회 학술대회
Keywords: antiretroviral therapy, human immunodeficiency virus, loss to follow up, Korea HIV/AIDS
cohort, risk factor
267
Exc
lude
d (N
=23
7)
Hop
e to
withd
raw
a(n=
94)
rans
ferr
ed t
o an
othe
r cl
inic
(n=
69)
Em
igra
tion
(n=
3)H
ospi
tal
withd
raw
al (
n=70
) et
c (n
=1)
Pat
ient
s w
ho h
ave
basi
c in
form
atio
nN
=3,
729
Exc
lude
d (N
=379)
Mis
sing
of
the
birt
h da
te (
n=4)
Mis
sing
of
the
firs
t H
IV d
iagn
osis
dat
e (n
=130
) M
issi
ng o
f H
IV
tran
smis
sion
ro
ute
(n=123
) M
issi
ng
of
the
AR
T
initia
tion
dat
e (n
=110)
Mis
sing
of
the
firs
t vi
sit
date
(n=
8)M
issi
ng o
f th
e la
st v
isit d
ate
(n=1)
Age
und
er
18 (
n=3)
Tota
l (P
rosp
ective
+R
etr
ospe
ctiv
e, ~
2016
)N
=4,
108
(100
.00%
)
Exc
ulde
d (N
=32
0)D
eath
(n=
225)
who
vis
ited
onl
y on
e tim
e d
urin
g f/
u pe
riod
(n=
95)
In C
are
N=1,
766
(55.
67%
)Lo
ss t
o fo
llow
-up
N=1,
407(
44.3
3%
)
Stu
dy P
opul
atio
nN
=3,
172(
77.2
2%)
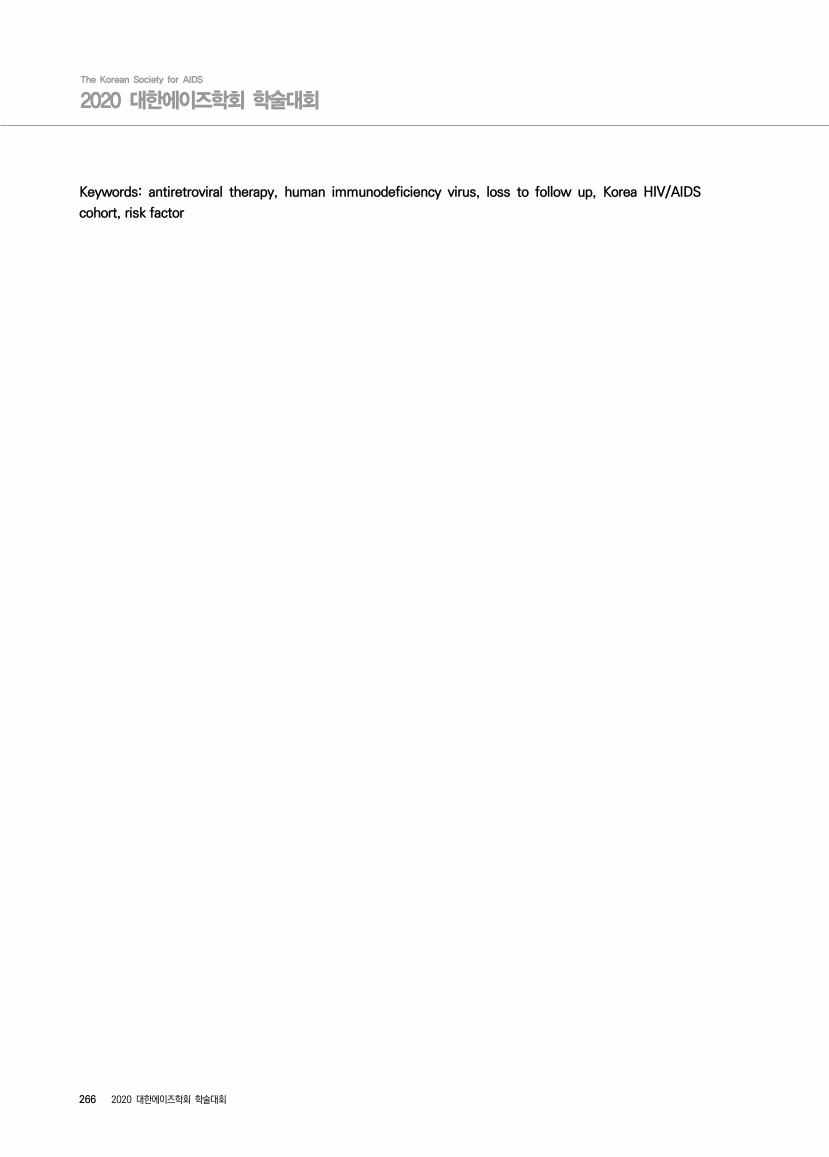
Fig
ure
1.
A F
low
char
t desc
ribin
g t
he p
atie
nts
enro
lled i
nto
Kore
an H
IV/A
IDS
cohort
, 1987-2016.
268
(a)
(b)
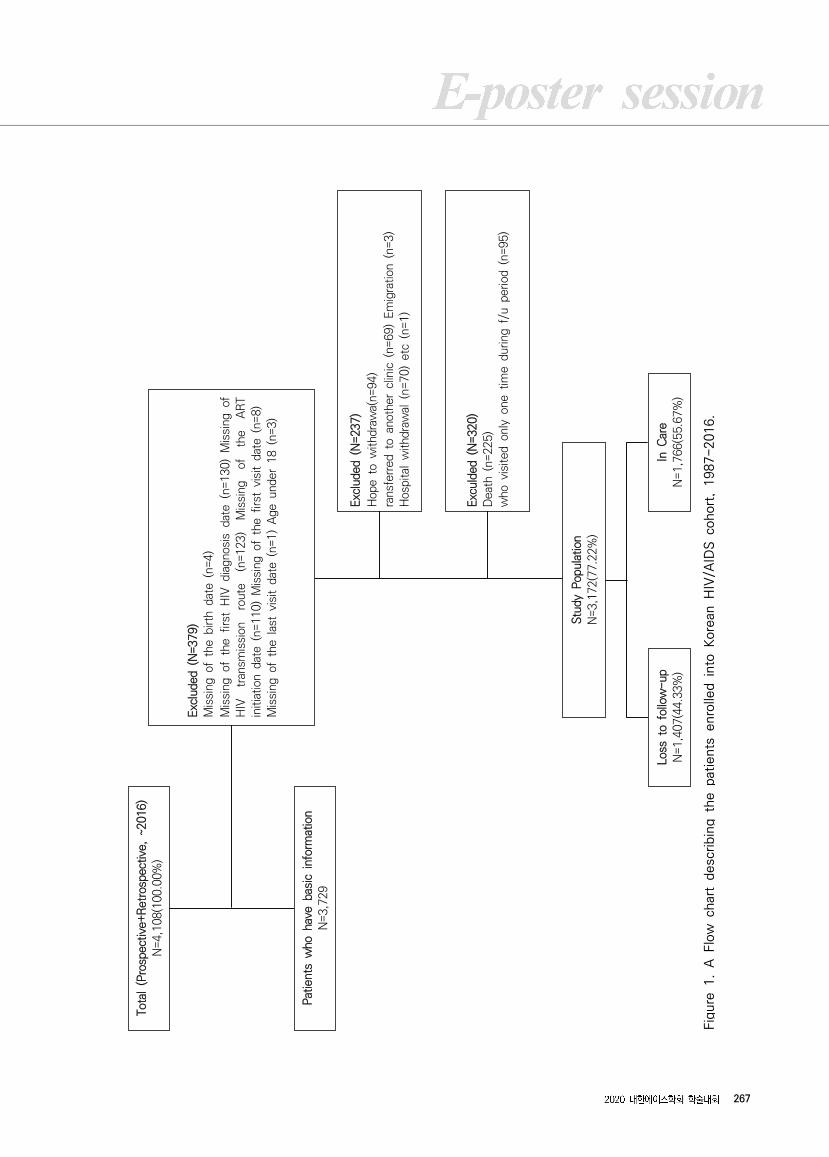
Fig
ure
2.
Num
ber
of
loss
to f
ollo
w-up (
LTFU
) pat
ients
and L
TFU
inci
dence
rat
es.
(a)
LTFU
inci
dence
rat
es
by
follo
w-up d
ura
tion;
(b)
LTFU
inci
dence
rat
es
by
loss
to f
ollo
w- u
p y
ear
.
(a)
(b)
Fig
ure
3.
Kap
lan-M
eie
r cu
rves
for
loss
to f
ollo
w-up (
LTFU
) st
ratified b
y risk
fac
tors
. (a
) LTFU
rat
es
by
HIV
dia
gnosi
s ye
ar;
(b)
LTFU
rate
s by
antire
trovi
ral
thera
py.
269
(a)
(b)
(a)
(b)
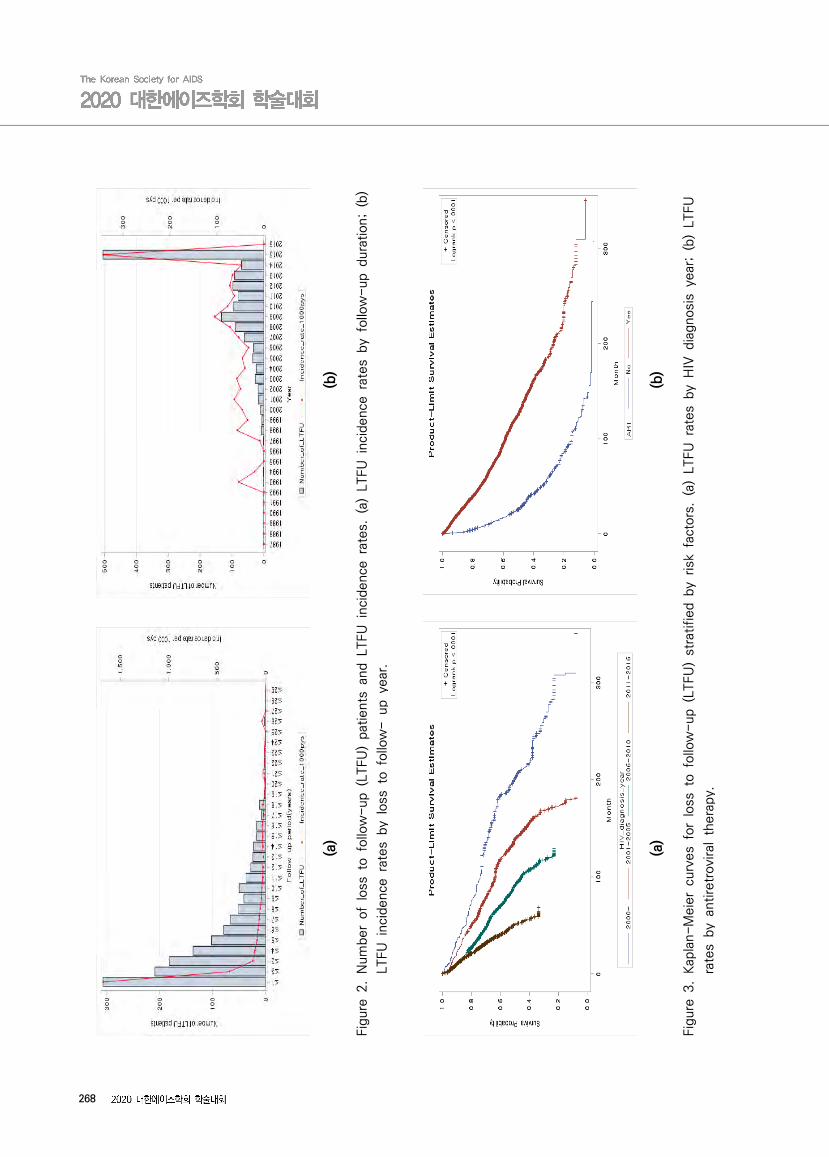
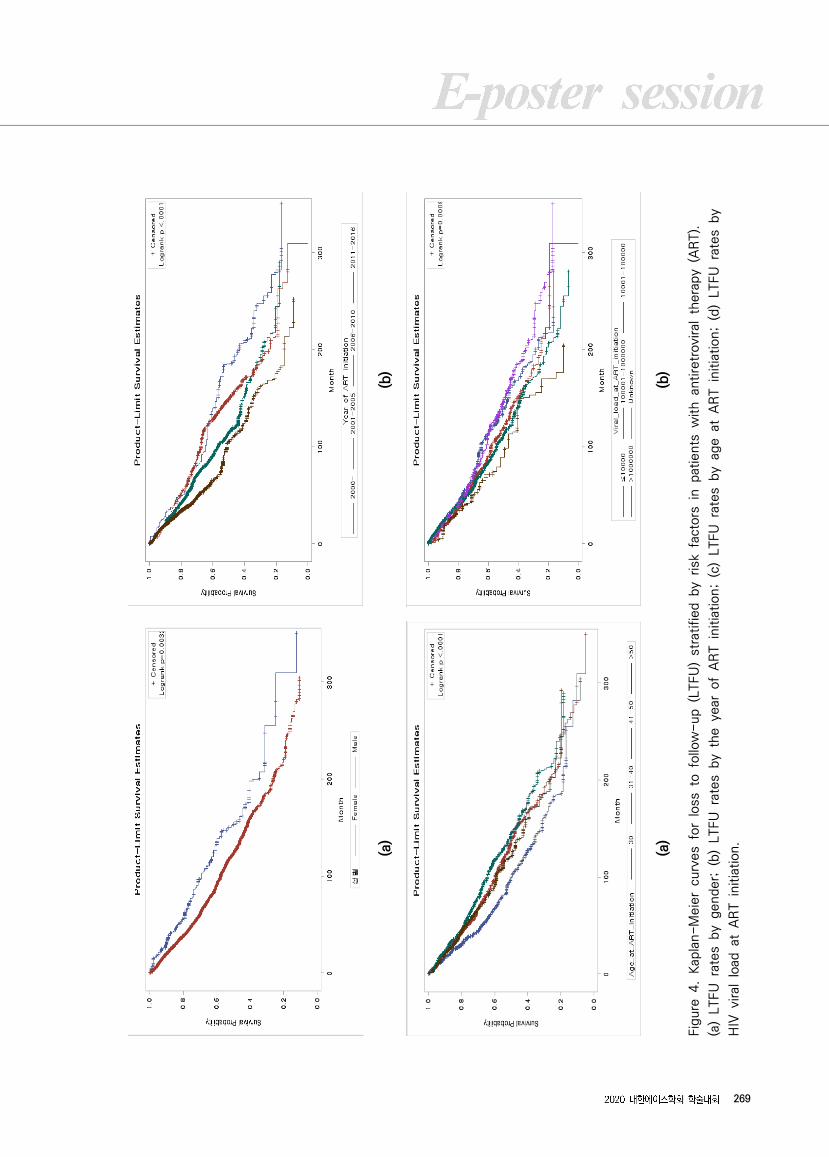
Fig
ure
4.
Kap
lan-M
eie
r cu
rves
for
loss
to f
ollo
w-up (
LTFU
) st
ratified b
y risk
fac
tors
in p
atie
nts
with a
ntire
trovi
ral
thera
py
(AR
T).
(a)
LTFU
rat
es
by
gender;
(b)
LTFU
rat
es
by
the y
ear
of
AR
T i
nitia
tion;
(c)
LTFU
rat
es
by
age a
t A
RT i
nitia
tion;
(d)
LTFU
rat
es
by
HIV
viral
load
at
AR
T i
nitia
tion.
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
270 2020 대한에이즈학회 학술대회
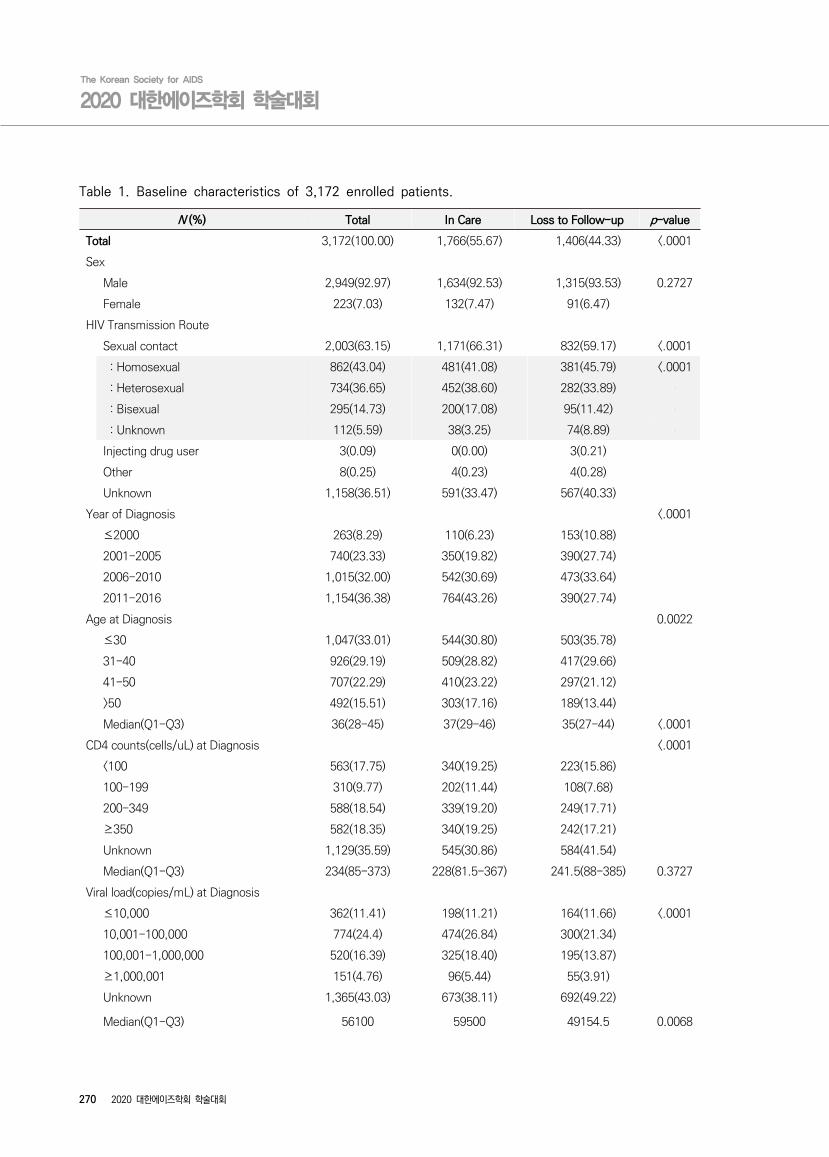
N (%) Total In Care Loss to Follow-up p-value
Total 3,172(100.00) 1,766(55.67) 1,406(44.33) <.0001
Sex
Male 2,949(92.97) 1,634(92.53) 1,315(93.53) 0.2727
Female 223(7.03) 132(7.47) 91(6.47)
HIV Transmission Route
Sexual contact 2,003(63.15) 1,171(66.31) 832(59.17) <.0001
: Homosexual 862(43.04) 481(41.08) 381(45.79) <.0001
: Heterosexual 734(36.65) 452(38.60) 282(33.89)
: Bisexual 295(14.73) 200(17.08) 95(11.42)
: Unknown 112(5.59) 38(3.25) 74(8.89)
Injecting drug user 3(0.09) 0(0.00) 3(0.21)
Other 8(0.25) 4(0.23) 4(0.28)
Unknown 1,158(36.51) 591(33.47) 567(40.33)
Year of Diagnosis <.0001
≤2000 263(8.29) 110(6.23) 153(10.88)
2001-2005 740(23.33) 350(19.82) 390(27.74)
2006-2010 1,015(32.00) 542(30.69) 473(33.64)
2011-2016 1,154(36.38) 764(43.26) 390(27.74)
Age at Diagnosis 0.0022
≤30 1,047(33.01) 544(30.80) 503(35.78)
31-40 926(29.19) 509(28.82) 417(29.66)
41-50 707(22.29) 410(23.22) 297(21.12)
>50 492(15.51) 303(17.16) 189(13.44)
Median(Q1-Q3) 36(28-45) 37(29-46) 35(27-44) <.0001
CD4 counts(cells/uL) at Diagnosis <.0001
<100 563(17.75) 340(19.25) 223(15.86)
100-199 310(9.77) 202(11.44) 108(7.68)
200-349 588(18.54) 339(19.20) 249(17.71)
≥350 582(18.35) 340(19.25) 242(17.21)
Unknown 1,129(35.59) 545(30.86) 584(41.54)
Median(Q1-Q3) 234(85-373) 228(81.5-367) 241.5(88-385) 0.3727
Viral load(copies/mL) at Diagnosis
≤10,000 362(11.41) 198(11.21) 164(11.66) <.0001
10,001-100,000 774(24.4) 474(26.84) 300(21.34)
100,001-1,000,000 520(16.39) 325(18.40) 195(13.87)
≥1,000,001 151(4.76) 96(5.44) 55(3.91)
Unknown 1,365(43.03) 673(38.11) 692(49.22)
Median(Q1-Q3) 56100 59500 49154.5 0.0068
Table 1. Baseline characteristics of 3,172 enrolled patients.
E-poster session
2020 대한에이즈학회 학술대회 271
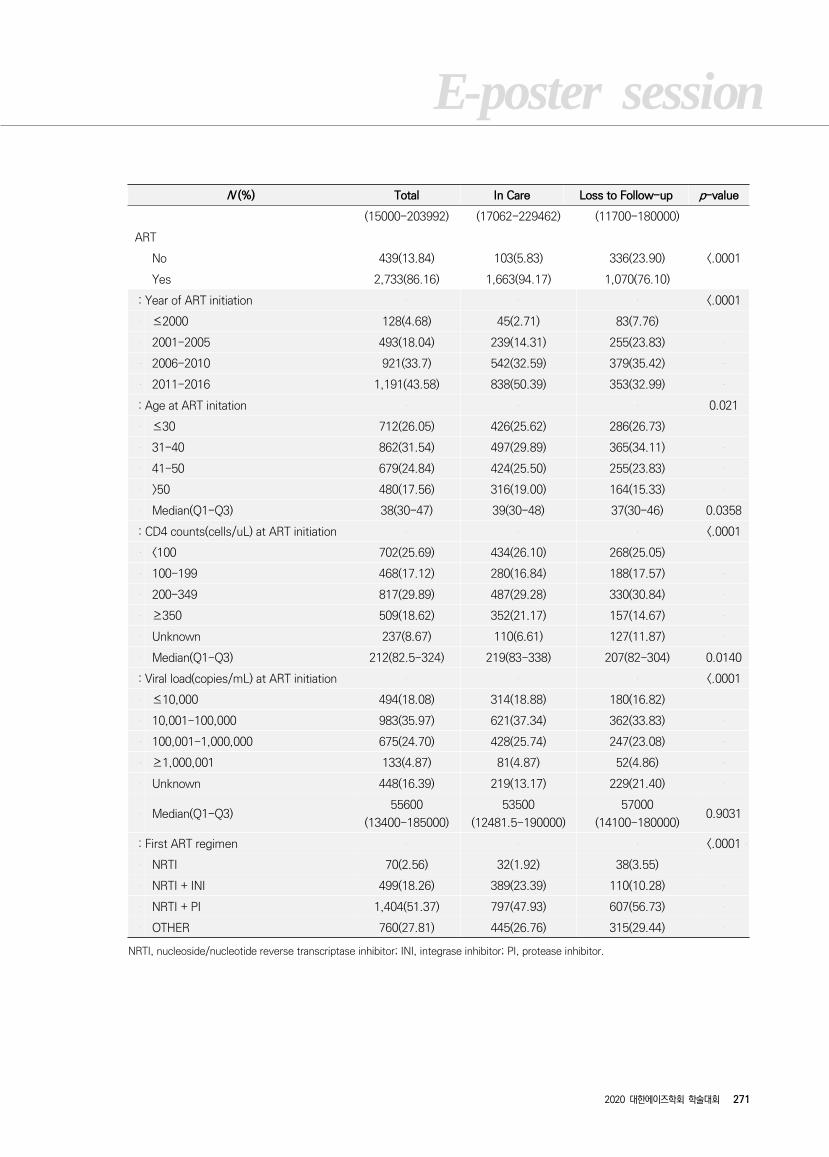
N (%) Total In Care Loss to Follow-up p-value
(15000-203992) (17062-229462) (11700-180000)
ART
No 439(13.84) 103(5.83) 336(23.90) <.0001
Yes 2,733(86.16) 1,663(94.17) 1,070(76.10)
: Year of ART initiation <.0001
≤2000 128(4.68) 45(2.71) 83(7.76)
2001-2005 493(18.04) 239(14.31) 255(23.83)
2006-2010 921(33.7) 542(32.59) 379(35.42)
2011-2016 1,191(43.58) 838(50.39) 353(32.99)
: Age at ART initation 0.021
≤30 712(26.05) 426(25.62) 286(26.73)
31-40 862(31.54) 497(29.89) 365(34.11)
41-50 679(24.84) 424(25.50) 255(23.83)
>50 480(17.56) 316(19.00) 164(15.33)
Median(Q1-Q3) 38(30-47) 39(30-48) 37(30-46) 0.0358
: CD4 counts(cells/uL) at ART initiation <.0001
<100 702(25.69) 434(26.10) 268(25.05)
100-199 468(17.12) 280(16.84) 188(17.57)
200-349 817(29.89) 487(29.28) 330(30.84)
≥350 509(18.62) 352(21.17) 157(14.67)
Unknown 237(8.67) 110(6.61) 127(11.87)
Median(Q1-Q3) 212(82.5-324) 219(83-338) 207(82-304) 0.0140
: Viral load(copies/mL) at ART initiation <.0001
≤10,000 494(18.08) 314(18.88) 180(16.82)
10,001-100,000 983(35.97) 621(37.34) 362(33.83)
100,001-1,000,000 675(24.70) 428(25.74) 247(23.08)
≥1,000,001 133(4.87) 81(4.87) 52(4.86)
Unknown 448(16.39) 219(13.17) 229(21.40)
Median(Q1-Q3)55600
(13400-185000)
53500
(12481.5-190000)
57000
(14100-180000)0.9031
: First ART regimen <.0001
NRTI 70(2.56) 32(1.92) 38(3.55)
NRTI + INI 499(18.26) 389(23.39) 110(10.28)
NRTI + PI 1,404(51.37) 797(47.93) 607(56.73)
OTHER 760(27.81) 445(26.76) 315(29.44)
NRTI, nucleoside/nucleotide reverse transcriptase inhibitor; INI, integrase inhibitor; PI, protease inhibitor.
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
272 2020 대한에이즈학회 학술대회
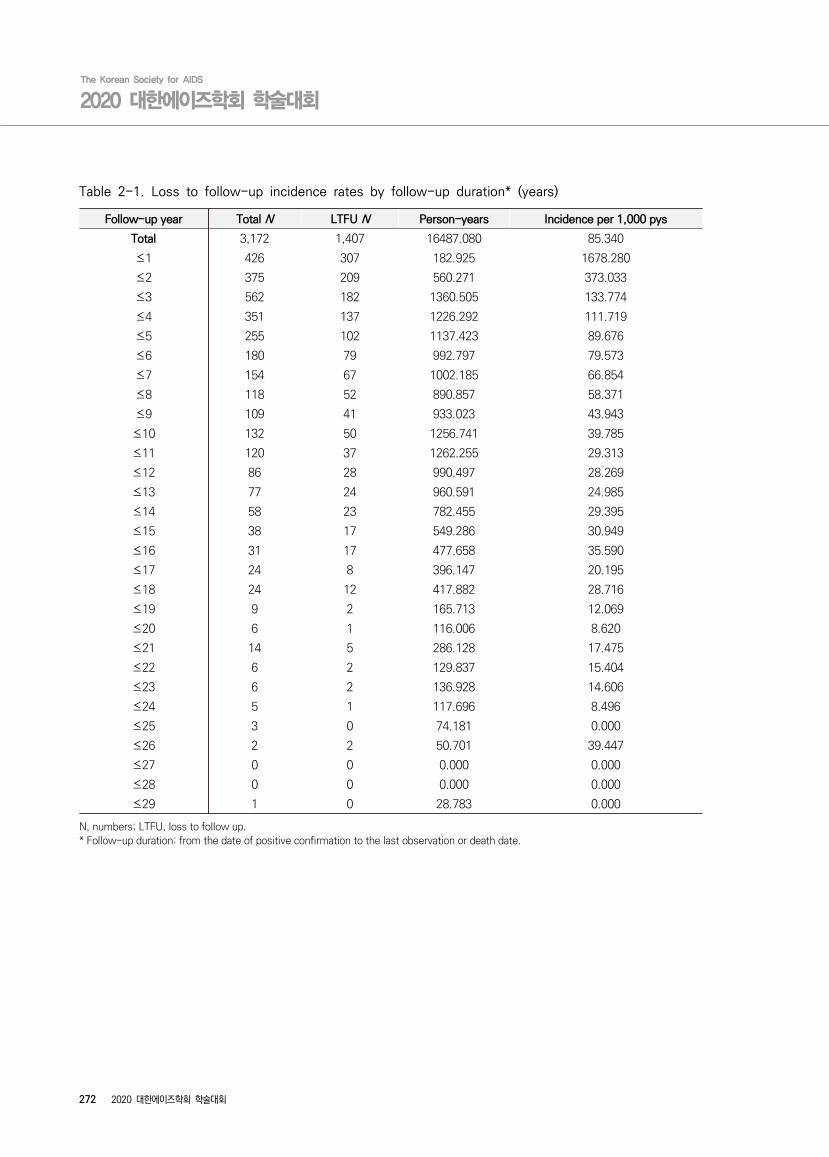
Follow-up year Total N LTFU N Person-years Incidence per 1,000 pys
Total 3,172 1,407 16487.080 85.340
≤1 426 307 182.925 1678.280
≤2 375 209 560.271 373.033
≤3 562 182 1360.505 133.774
≤4 351 137 1226.292 111.719
≤5 255 102 1137.423 89.676
≤6 180 79 992.797 79.573
≤7 154 67 1002.185 66.854
≤8 118 52 890.857 58.371
≤9 109 41 933.023 43.943
≤10 132 50 1256.741 39.785
≤11 120 37 1262.255 29.313
≤12 86 28 990.497 28.269
≤13 77 24 960.591 24.985
≤14 58 23 782.455 29.395
≤15 38 17 549.286 30.949
≤16 31 17 477.658 35.590
≤17 24 8 396.147 20.195
≤18 24 12 417.882 28.716
≤19 9 2 165.713 12.069
≤20 6 1 116.006 8.620
≤21 14 5 286.128 17.475
≤22 6 2 129.837 15.404
≤23 6 2 136.928 14.606
≤24 5 1 117.696 8.496
≤25 3 0 74.181 0.000
≤26 2 2 50.701 39.447
≤27 0 0 0.000 0.000
≤28 0 0 0.000 0.000
≤29 1 0 28.783 0.000
N, numbers; LTFU, loss to follow up.* Follow-up duration: from the date of positive confirmation to the last observation or death date.
Table 2-1. Loss to follow-up incidence rates by follow-up duration* (years)
E-poster session
2020 대한에이즈학회 학술대회 273
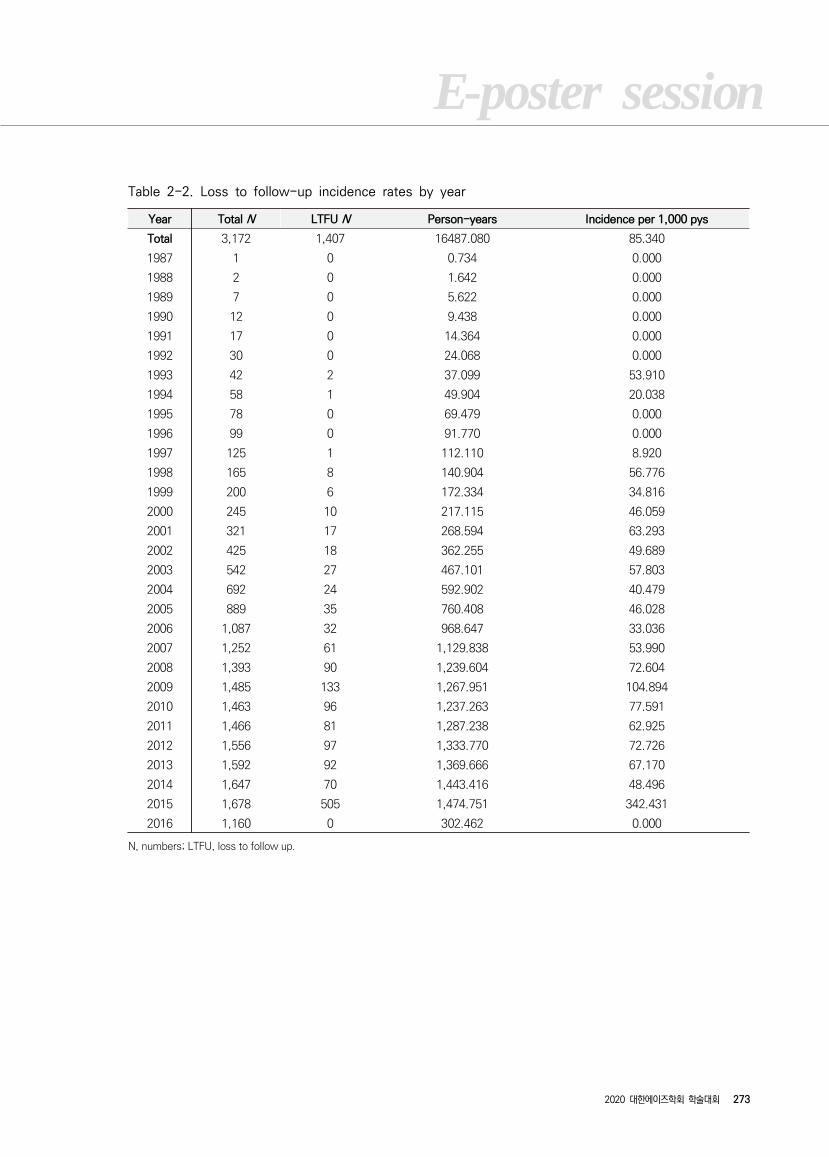
Year Total N LTFU N Person-years Incidence per 1,000 pys
Total 3,172 1,407 16487.080 85.340
1987 1 0 0.734 0.000
1988 2 0 1.642 0.000
1989 7 0 5.622 0.000
1990 12 0 9.438 0.000
1991 17 0 14.364 0.000
1992 30 0 24.068 0.000
1993 42 2 37.099 53.910
1994 58 1 49.904 20.038
1995 78 0 69.479 0.000
1996 99 0 91.770 0.000
1997 125 1 112.110 8.920
1998 165 8 140.904 56.776
1999 200 6 172.334 34.816
2000 245 10 217.115 46.059
2001 321 17 268.594 63.293
2002 425 18 362.255 49.689
2003 542 27 467.101 57.803
2004 692 24 592.902 40.479
2005 889 35 760.408 46.028
2006 1,087 32 968.647 33.036
2007 1,252 61 1,129.838 53.990
2008 1,393 90 1,239.604 72.604
2009 1,485 133 1,267.951 104.894
2010 1,463 96 1,237.263 77.591
2011 1,466 81 1,287.238 62.925
2012 1,556 97 1,333.770 72.726
2013 1,592 92 1,369.666 67.170
2014 1,647 70 1,443.416 48.496
2015 1,678 505 1,474.751 342.431
2016 1,160 0 302.462 0.000
N, numbers; LTFU, loss to follow up.
Table 2-2. Loss to follow-up incidence rates by year
274
n=3,
139
Eve
nts/
pys
Rat
es p
er
1000
pys
(95
% C
I) U
niva
riat
e
M
ultiv
aria
ble
HR
95%
CI
p-va
lue
HR
95%
CI
p-va
lue
Sex
Mal
e1,3
15/
15,0
65
87.
29 (82.
69-92.
13)
refe
renc
e0.
0026
refe
renc
e0.
284
4
Fem
ale
91/
1,43
463.
47 (51.
68-77.
94)
0.7
19
0.5
81-
0.89
10.8
83
0.7
02-1.1
09
HIV
Tra
nsm
issi
on R
oute
Hom
osex
ual
381/
4,5
4183.
91 (75.
90-92.
77)
refe
renc
e<.
000
1re
fere
nce
0.268
4
Het
eros
exua
l28
2/3,9
6071
.209
(63.
37-
80.0
2)0.8
45
0.7
24-
0.98
60.9
09
0.7
71-1.0
71
Sex
ual c
onta
ct -
unk
now
n95/
1,44
565
.736
(53.
76-
80.3
8)0.7
81
0.6
23-
0.97
70.8
57
0.6
83-1.0
74
Oth
er/u
nknow
n64
8/6,5
5398.8
82 (91.
56-106.
80)
1.1
76
1.0
36-
1.33
51.0
15
0.8
90-1.1
58
Yea
r of
HIV
Dia
gnos
is
≤2000
153/
3,4
2444.
69 (38.
14-52.
36)
refe
renc
e<.
000
1
refe
renc
e<.
0001
2001-
2005
390/
5,8
6066.
56 (60.
27-73.
50)
2.6
12
2.0
63-
3.30
62.3
68
1.8
6-3.0
13
2006-
2010
473/
4,6
71101.
27 (92.
54-110.
82)
4.7
48
3.7
04-
6.08
63.8
69
2.9
83-5.0
18
2011-
2016
390/
2,5
45153
.23 (13
8.76-
169.
22)
7.5
46
5.8
03-
9.81
35.9
81
4.5
34-7.8
88
Age
at
HIV
Dia
gnos
is
≤30
503/
5,4
4592
.38 (84
.65-
100
.82)
refe
renc
e0.
2054
refe
renc
e0.
122
7
31-40
417/
5,2
5379.
39 (72.
12-87.
38)
0.8
76
0.7
69-
0.99
80.8
86
0.7
77-1.0
11
41-50
297/
3,6
4181.
57 (72.
80-91.
40)
0.8
99
0.7
79-
1.03
90.8
47
0.7
32-0.9
82
>50
189/
2,1
6187
.48 (75
.85-
100
.88)
0.9
58
0.8
10-
1.13
40.9
15
0.7
71-1.0
87
CD
4 co
unts
(cel
ls/u
L) a
t D
iagn
osis
<100
223/
2,6
4484.
34 (73.
97-96.
17)
refe
renc
e<.
000
1re
fere
nce
0.313
0
100-
199
108/
1,3
6579.
11 (65.
51-95.
53)
0.9
34
0.7
42-
1.17
50.9
23
0.7
31-1.1
65
200-
349
249/
2,5
9695
.91 (84
.71-
108
.60)
1.1
32
0.9
44-
1.35
61.1
28
0.9
34-1.3
61
≥350
242/
2,1
58112.
16 (98.
88-127.
22)
1.3
04
1.0
86-
1.56
40.9
58
0.7
80-1.1
75
Unk
now
n58
4/7,7
3675.
49 (69.
61-81.
87)
0.8
89
0.7
61-
1.03
80.9
67
0.7
73-1.2
09
Viral
load
(cop
ies/
mL)
at
Dia
gnos
is
≤10,
000
164/
1,3
93117
.70 (10
1.00-
137.
17)
refe
renc
e<.
000
1re
fere
nce
0.094
2
10,0
01-
100,
000
300/
3,0
5298
.29 (87
.78-
110
.07)
0.8
36
0.6
91-
1.01
10.9
22
0.7
59-1.1
19
100,
001
-1,0
00,
000
195/
1,9
14101.
86 (88.
52-117.
20)
0.8
64
0.7
02-
1.06
31.0
28
0.8
23-1.2
85
≥1,0
00,
001
55/
524
104.
90 (80.
54-136.
64)
0.8
80
0.6
49-
1.19
50.9
61
0.7
01-1.3
17
Unk
now
n69
2/9,6
1571.
97 (66.
80-77.
54)
0.6
06
0.5
10-
0.72
00.7
58
0.5
97-0.9
62
AR
TN
o33
6/1,2
25274
.29 (24
6.47-
305.
24)
refe
renc
e<.
000
1re
fere
nce
<.0001
Yes
107
0/15,
274
70.
05 (65.
98-74.
38)
0.2
56
0.2
26-
0.29
0
0.2
53
0.2
20-0.2
91
HR
, ha
zard
rat
io; C
I, c
onfide
ntia
l int
erva
l; A
RT,
ant
iret
rovi
ral t
hera
py.
Tab
le 3
. Fac
tors
ass
oci
ated w
ith l
oss
to f
ollo
w-up (
Pro
spect
ive+
Retr
osp
ect
ive)
275
n=2,7
02
Eve
nts/
pys
Rat
es p
er
1000
pys
(95
% C
I) U
niva
riat
e
M
ultiva
riab
le
HR
95%
CI
p-va
lue
HR
95%
CI
p-va
lue
Sex
Mal
e998
/13,8
8271.
89 (67.
57-76.
49)
refe
renc
e0.
0035
refe
renc
e0.
029
1
Fem
ale
72/1
,392
51.
72 (41.
05-65.
15)
0.6
98
0.549
-0.8
88
0.75
2
0.5
82-
0.97
1H
IV T
rans
mis
sion
Rou
teH
omos
exua
l*308/
4,24
572.
56 (64.
89-81.
13)
refe
renc
e0.
0027
refe
renc
e0.
057
3
Het
eros
exua
l229/
3,79
860.
29 (52.
97-68.
63)
0.8
25
0.695
-0.9
80
0.90
6
0.7
54-
1.08
9Sex
ual c
onta
ct -
unk
now
n76
/1,3
66
55.
65 (44.
45-69.
68)
0.7
72
0.601
-0.9
93
0.79
1
0.6
14-
1.01
9O
ther
/unk
now
n**
457/
5,86
577.
92 (71.
09-85.
40)
1.0
65
0.922
-1.2
31
1.06
4
0.9
15-
1.23
8Y
ear
of A
RT
initia
tion
≤200
083
/1,5
35
54.
08 (43.
61-67.
06)
refe
renc
e<.
000
1re
fere
nce
<.0001
2001
-2005
255/
4,29
859.
34 (52.
48-67.
09)
1.2
80
0.992
-1.6
51
1.38
3
1.0
44-
1.83
12006
-2010
379/
5,40
770.
09 (63.
38-77.
52)
1.5
94
1.244
-2.0
43
1.63
6
1.2
32-
2.17
42011
-2016
353/
4,03
587.
49 (78.
82-97.
11)
2.0
76
1.608
-2.6
80
2.20
4
1.6
28-
2.98
5A
ge a
t A
RT
initat
ion
≤30
286/
3,16
390
.42 (80
.52-
101
.53)
refe
renc
e<.
000
1re
fere
nce
<.0001
31-
40
365/
5,41
167.
46 (60.
88-74.
74)
0.7
32
0.626
-0.8
55
0.72
4
0.6
18-
0.84
741-
50
255/
4,28
359.
55 (52.
67-67.
32)
0.6
46
0.545
-0.7
65
0.63
1
0.5
30-
0.75
1>5
0164/
2,41
767.
84 (58.
21-79.
06)
0.7
54
0.622
-0.9
13
0.73
2
0.6
02-
0.89
0C
D4
coun
ts(c
ells
/uL)
at
AR
T in
itia
tion
<100
268/
4,05
666.
08 (58.
62-74.
48)
refe
renc
e0.
5397
refe
renc
e0.
405
5
100-
199
188/
2,69
269.
85 (60.
55-80.
58)
1.0
48
0.870
-1.2
63
1.04
9
0.8
66-
1.27
0200-
349
330/
4,38
075.
35 (67.
64-83.
93)
1.1
42
0.972
-1.3
42
1.16
5
0.9
80-
1.38
3≥
350
157/
2,32
467.
56 (57.
78-79.
00)
1.0
20
0.837
-1.2
42
1.02
2
0.8
25-
1.26
7U
nkno
wn
127/
1,82
369.
67 (58.
54-82.
90)
1.0
25
0.830
-1.2
67
1.13
1
0.9
06-
1.41
2V
iral
load
(cop
ies/
mL)
at
AR
T in
itia
tion
≤10,
000
180/
2,87
062.
72 (54.
19-72.
58)
refe
renc
e0.
0008
refe
renc
e0.
047
0
10,0
01-100,
000
362/
4,76
775.
95 (68.
51-84.
19)
1.2
24
1.023
-1.4
64
1.17
2
0.9
76-
1.40
7100,
001-
1,0
00,0
00
247/
3,35
773.
59 (64.
96-83.
36)
1.1
85
0.977
-1.4
36
1.21
3
0.9
89-
1.48
7≥
1,0
00,0
01
52/5
48
94.9
3 (72
.34-
124
.58)
1.5
41
1.1
31,
2.0
991.
545
1.12
6, 2
.121
Unk
now
n229/
3,73
361.
34 (53.
89-69.
82)
0.9
23
0.7
58,
1.1
251.
048
0.84
2, 1
.304
Firs
t A
RT
regi
men
NR
TI38
/637
59.
69 (43.
43-82.
03)
refe
renc
e0.
1284
refe
renc
e0.
452
8
NR
TI +
IN
I110/
1,39
378.
96 (65.
50-95.
18)
1.5
40
1.0
55,
2.2
460.
882
0.57
7, 1
.350
NR
TI +
PI
607/
8,78
969.
06 (63.
78-74.
78)
1.2
82
0.9
19,
1.7
881.
063
0.73
7, 1
.532
O
THER
315/
4,45
570.
71 (63.
31-78.
96)
1.3
26
0.9
42,
1.8
68
1.00
9
0.68
9, 1
.476
HR
, ha
zard
rat
io; C
I, c
onfide
ntia
l int
erva
l; A
RT,
ant
iret
rovi
ral t
hera
py.
Tab
le 4
. Fac
tors
ass
oci
ated w
ith l
oss
to f
ollo
w-up i
n A
RT p
atie
nts
(P
rosp
ect
ive+
Retr
osp
ect
ive)

The Korean Society for AIDS
2020 대한에이즈학회 학술대회
276 2020 대한에이즈학회 학술대회
P-14 Clinical research
Incidence and Risk factor of Human Immunodeficiency
Virus-Associated Immune Reconstitution Inflammatory
Syndrome in South Korea; for Integrase strand transfer
Inhibitors versus other antiretrovirals
Jin Kim1, Hyun-Ju Nam1, Yu-Jin Jung3, Hye-Jung Lee3, Sook-In Jung1, Yeon-Sook Kim2, Hyun-Ha Chang3, Shin-Woo Kim3,
Kyung-Hwa Park1
1Department of Infectious Diseases, Chonnam National University Hospital, Gwangju, Republic of Korea, 2Department of Internal Medicine, Chungnam National Hospital, Deajeon, Republic of Korea, 3Department of Internal Medicine, Kyungpook National Hospital, Daegu, Republic of Korea
Background: Immune reconstitution inflammatory syndrome (IRIS) is a major concern when starting
antiretroviral therapy (ART) in patients with advanced HIV infection. We determined the incidence and
risk factors of IRIS in HIV-infected Koreans initiating ART, and whether integrase strand transfer
inhibitor (INSTI) increases the risk of IRIS.
Methods: This retrospective analysis included adults living with HIV, seen at four university-affiliated
hospitals in South Korea, who were naïve to ART and had a CD4+ T-cell count < 200 cells/mm3 between
January 2004 and May 2019. IRIS was determined through a medical record review within 6 months of
ART initiation.
Results: The study included 501 patients; 192 were assigned to the INSTI group, who started ART after
INSTI as the initial treatment. There were opportunistic infections (OI) in 253 (50.5%) cases before ART
initiation. The three most common OIs were Pneumocystis jirovecii pneumonia (PCP), candidiasis, and
tuberculosis (TB). We identified 47 cases of IRIS; TB-IRIS was the most type. The incidence of IRIS
within 6 months of ART initiation was 9.4%, and the incidence of IRIS was the same between the
non-INSTI and INSTI groups. The risk factors for IRIS were pre-ART CD4+ T-cell count (< 30 cells/mm3),
higher pre-ART viral load (≥ 75,000 copies/mL), and TB-OI.
Conclusions: The incidence of IRIS was 9.4% in Korean HIV patients. The INSTI regimen was not related
to IRIS occurrence.
Keywords: Human immunodeficiency virus, immune reconstitution inflammatory syndrome, integrase
strand transfer inhibitor, antiretroviral therapy, tuberculosis
E-poster session
2020 대한에이즈학회 학술대회 277
P-15 Clinical research
Lenacapavir Resistance Analysis in a Phase 1b Clinical
Proof-Of-Concept Study
Nicolas Margot , Jeong-a Lee , Renee Ram , PC Parvangada , Ross Martin , Rob Hyland , Martin Rhee , Christian Callebaut
Gilead Sciences, Inc., Foster City, California, USA
Background: Lenacapavir (LEN, GS-6207) is a first-in-class subcutaneous (SC) long acting inhibitor of
HIV-1 capsid function, which can be administered every 6 months. In vitro resistance selections with
LEN have identified 7 mutations in HIV-1 capsid protein (CA) associated with reduced susceptibility to
LEN. We conducted a phase 1b proof-of-concept study in which people living with HIV (PLWH)
received a single SC injection of LEN 20, 50, 150, 450, or 750 mg. LEN demonstrated potent antiviral
activity with up to 2.3 log10 decline in HIV-1 RNA after 9 days of monotherapy.
Methods: Study 4072 is a double-blind, placebo-controlled, dose-ranging, randomized (3:1; n=8/group)
study in PLWH who were capsid inhibitor-naive. Resistance analyses were performed for all
participants prior to study entry and at the end of monotherapy using genotypic and phenotypic Gag-Pro
assays (Monogram Biosciences) and next-generation sequencing (NGS; Seq-IT). Samples were
evaluated for the emergence of CA mutations and/or change in phenotypic susceptibility to LEN.
Results: Thirty-nine PLWH enrolled in the study, 29 receiving LEN and 10 receiving placebo. All PLWH
responded to LEN with no rebound. In the pre-treatment analysis, none had HIV-1 harboring resistance
mutations to LEN, with all having wild-type (WT) phenotypic susceptibility to LEN. Post-monotherapy
analyses revealed the emergence of CA mutation Q67H at Day 10 in 2 participants. One participant (20
mg group) had a Q67Q/H mixture detected both by population and NGS analysis, and another
participant (50 mg group) had a Q67H mutation, detected only by the NGS analysis. No other
substitutions were observed in the CA protein.
Conclusions: Overall, emergence of resistance to LEN was rare and only occurred well below exposures
expected to be achieved in Ph2/3 studies, with the emergence of a single mutation Q67H. These
results support further evaluation of LEN as a long-acting antiretroviral agent in PLWH.
Keywords: HIV, long-acting ART
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
278 2020 대한에이즈학회 학술대회
P-16 Clinical research
코로나19 지역사회 발생이 감염인 상담에 미치는 영향
서아영, 이정휘, 이수연, 최재필, 오동현, 안미영
서울특별시 서울의료원 감염내과
배경: 코로나-19 는 2019 년 12 월 중국 우한에서 처음 발생한 이후 중국 전역과 전 세계로 확산된, 새로운 유형의 코로
나바이러스(SARS-CoV-2)에 의한 호흡기 감염질환이다. 이에 정기적으로 의료기관을 방문해야 하는 감염인들의 의료
기관 방문이 어렵고, 기존 진행되던 상담사업의 내담자의 수와 상담 횟수를 감소시켜 감염인의 건강 관리지표가 악화될
가능성이 높다.
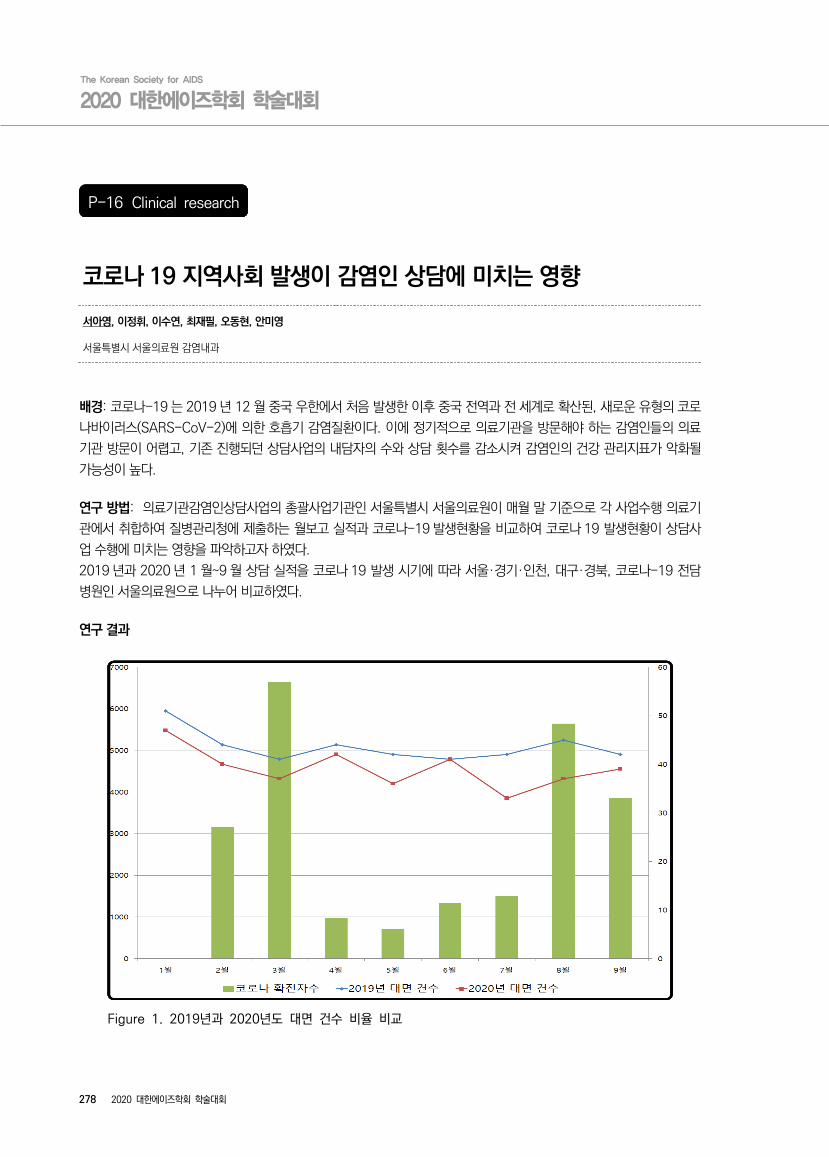
연구 방법: 의료기관감염인상담사업의 총괄사업기관인 서울특별시 서울의료원이 매월 말 기준으로 각 사업수행 의료기
관에서 취합하여 질병관리청에 제출하는 월보고 실적과 코로나-19 발생현황을 비교하여 코로나 19 발생현황이 상담사
업 수행에 미치는 영향을 파악하고자 하였다.
2019 년과 2020 년 1 월~9 월 상담 실적을 코로나 19 발생 시기에 따라 서울·경기·인천, 대구·경북, 코로나-19 전담
병원인 서울의료원으로 나누어 비교하였다.
연구 결과
Figure 1. 2019년과 2020년도 대면 건수 비율 비교
E-poster session
2020 대한에이즈학회 학술대회 279
- 서울·경기·인천 지역의 경우 5 월 (이태원 클럽 사례), 8 월 (사랑제일교회 및 광화문 집회사례)에는 서울·경기·인천
지역에 위치한 의료기관의 대면상담 건수가 1 월 기준 11.9%, 20.9%로 낮아 졌다.
- 대구·경북 지역에 위치한 의료기관의 경우 1 월 기준 3 월(신천지 대구 교회 사례) 대면 상담건수가 89 건(64.3%)으
로 감소, 전화ㆍ온라인 상담은 270 건(58%)으로 증가하였다.
- 코로나 전담병원인 서울의료원의 경우 1 월 기준 5 월(이태원 클럽 사례), 8 월(사랑제일교회 및 광화문 집회사례)에는
대면 건수가 40 건(58.4%), 34 건(64.6%)으로 감소하였다.
- 의료기관감염인상담사업 40copies/ml 기준 바이러스 억제비율은 2019 년 최종보고서 93.8% 과 2020 년 중간보
고서 93.2%로 차이가 없었다.
- 2019 년도와 2020 년도의 총 상담건수의 소계 차이는 크게 없지만 상담의 형태가 바뀐 것을 알 수 있다. 2019 년은
대면상담의 건수가 높은 반면 2020 년은 코로나-19 의 영향으로 2019 년 대비 대면보다는 전화, 온라인상담의 건수
가 높다.
결론: 코로나-19 로 인해 상담유형이 대면이 줄고 비대면 방법(전화, 온라인)이 증가하여 상담건수는 유지되었다. 감염
인들의 의료기관 방문이 어려워졌음에도 불구하고 다양한 상당방법의 관리로 바이러스억제비율 또한 유지할 수 있었던
것으로 판단된다. 지속되는 코로나-19 상황에서 HIV/AIDS 감염인의 병원이용, 효과적인 상담 방법에 대한 다양한 연
구가 필요하다.

The Korean Society for AIDS
2020 대한에이즈학회 학술대회
280 2020 대한에이즈학회 학술대회
P-17 Clinical research
Starting or switching to bictegravir/emtricitabine/tenofovir
alafenamide (B/F/TAF) in clinical practice: Pooled
12-month (12M) results from the global BICSTaR study
Christoph Spinner1, Jeong-a Lee12, Albrecht Stoehr2, Alex Wong3, Joss de Wet4, Jérémy Zeggagh5, Laurent Hocqueloux6, Berend van Welzen7, Marion Heinzkill8, Sabrinel Sahali9, Almudena Torres Cornejo10, Heribert Ramroth11, Richard Haubrich12,
David Thorpe11, Connie Kim13
1Technical University of Munich, School of Medicine, University Hospital Rechts der Isar, Munich, Germany; 2IFI Studien und Projekte GmbH, Hamburg, Germany; 3Department of Medicine, University of Saskatchewan, Regina, Canada; 4Spectrum Health, Vancouver, Canada; 5Service des Maladies Infectieuses, Hôpital Saint Louis, APHP, Paris, France; 6Service des Maladies Infectieuses et Tropicales, CHR d'Orléans, Orléans, France; 7University Medical Centre, Utrecht, Netherlands; 8Gilead Sciences GmbH, Munich, Germany; 9Gilead Sciences, Boulogne-Billancourt, France; 10Gilead Sciences, Amsterdam, Netherlands; 11Gilead Sciences Ltd, London, UK; 12Gilead Sciences USA, Foster City, USA; 13Gilead Sciences Canada Inc, Ontario, Canada, 12Gilead Korea, Seoul, Korea
Background: The ongoing observational BICSTaR study aims to demonstrate effectiveness, safety and tolerability of B/F/TAF in routine clinical practice in at least 1400 antiretroviral treatment (ART)?na?ve (TN) and ART?experienced (TE) people living with HIV (PLHIV).
Materials and Methods: This 12M analysis of PLHIV receiving B/F/TAF in Europe and Canada assessed HIV?1 RNA (missing data=excluded analysis), drug?related (DR) adverse events (AEs), persistence and weight/body-mass index (BMI) change.
Results: At the time of data cut-off (Mar 2020), 513 participants (n=84 TN/n=429 TE) completed a 12M visit. Prevalence of comorbidities at baseline was 76%; the most common were neuropsychiatric (28%), hyperlipidemia (18%) and hypertension (18%). 71%/18%/13% of TE participants switched from INSTI/NNRTI/PI-based regimens, respectively (26% TDF); 8% had a history of prior virologic failure. Baseline primary resistance prevalence by historical genotype was 9% (n=43/513)At M12, 100% of TN (n=74/74) and 96% (n=357/373) TE participants had viral load (VL) <50 copies/ml. Comparable and high effectiveness was observed in both male and female participants, including older individuals (Table). No major resistance substitutions to the components of B/F/TAF emerged.DRAEs occurred in 14% (n=12/84) of TN and 15% (n=64/429) of TE participants, with the most common being gastrointestinal (5%) and neuropsychiatric (4%); discontinuations due to DRAE were low (TN 3.6% and 7.2% TE). Serious DRAEs were rare (0.4%; all in TE participants [n=2 depression]).At 12M, median (Q1, Q3) weight change was +2.5 kg (0.5, 6.3) for TN (n=48) and +0.9 kg (?1.0, 3.0) for TE (n=269). Weight increase >10% was observed in 19% (n=9/48) and 5% (n=15/269) of TN and TE participants, respectively.
Conclusions: The use of B/F/TAF in this real-world clinical cohort was associated with a high level of effectiveness and safety through 12M, inclusive of male, female and older PLHIV.
Keywords: B/F/TAF, real world evidence
E-poster session
2020 대한에이즈학회 학술대회 281
P-18 Clinical research
Durable Efficacy of Dolutegravir (DTG) Plus Lamivudine
(3TC) in Antiretroviral Treatment-Naïve Adults With HIV-1 Infection -3-Year Results From the GEMINI Studies
P Cahn1, J Sierra Madero2, J Arribas3, A Antinori4, R Ortiz5, A Clarke6, C-C Hung7, J Rockstroh8, P-M Girard9, J Sievers10, C
Man11, R Urbaityte12, M Underwood11, K Pappa11, B Wynne11, M Gartland11, M Aboud10, J van Wyk10, K Smith11, S Kwon13
1Fundación Huésped, Buenos Aires, Argentina; 2Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico; 3Hospital La Paz, Madrid, Spain; 4Istituto Nazionale per le Malattie Infettive Lazzaro Spallanzani, Rome, Italy; 5Bliss Healthcare Services, Orlando, FL, USA; 6Royal Sussex County Hospital and Brighton & Sussex Medical School, Brighton, UK; 7National Taiwan University Hospital, Taipei, Taiwan; 8Rheinische Friedrich-Wilhelms Universität, Bonn, Germany; 9Hôpital Saint Antoine, Paris, France; 10ViiV Healthcare, Brentford, UK; 11ViiV Healthcare, Research Triangle Park, NC, USA; 12GlaxoSmithKline, Stockley Park, UK; 13GlaxoSmithKline, Seoul, South Korea
Background: Two-drug regimens (2DR) have the potential to reduce cumulative drug exposure during
life-long antiretroviral therapy in HIV-1 infected patients. In GEMINI-1 and GEMINI-2 (ClinicalTrials.gov:
NCT02831673/NCT02831764), the efficacy of the 2DR of DTG+3TC was non-inferior to DTG+
tenofovir/emtricitabine (TDF/FTC) at weeks 48 and 96 in treatment-naïve adults.
Method: GEMINI-1&2 are identical double-blind, multicentre Phase III studies. Participants with HIV-1
RNA ≤500,000c/mL at screening were randomised 1:1 (stratified by plasma HIV-1 RNA and CD4+ cell
count) to once-daily treatment with DTG+3TC or DTG+TDF/FTC. The primary endpoint was the
proportion of participants with plasma HIV-1 RNA < 50c/mL at week 48 (Snapshot algorithm). We
present efficacy and safety data from prespecified 144-week secondary analyses. Estimates and
confidence intervals were based on a stratified analysis using Cochran-Mantel-Haenszel weights.
Results: 714 and 719 adults were randomised and treated in GEMINI-1&2, respectively. At baseline,
20% had HIV-1 RNA >100,000c/mL, 8% had CD4+ <200cells/mm3. At week 144, DTG+3TC was
non-inferior to DTG+TDF/FTC in both GEMINI-1&2 and in the pooled analysis (using a 10%
non-inferiority margin) [Table]. Response rates in participants with baseline HIV-1 RNA >100,000c/mL
were high and similar between arms. Consistent with week 48 and 96 outcomes, response remained
lower in DTG+3TC participants with CD4+ <200cells/mm3. Across both studies, 12 participants on
DTG+3TC (1 since week 96) and 9 on DTG+TDF/FTC (2 since week 96) met protocol-defined confirmed
virologic withdrawal (CVW) criteria through week 144; none had treatment-emergent integrase strand
transfer inhibitor or NRTI resistance mutations. One non-CVW DTG+3TC participant with reported
non-adherence developed M184V (week 132; HIV-1 RNA 61,927c/mL) and added R263R/K at week
144 (135c/mL), conferring a 1.8-fold change in DTG susceptibility. Overall rates of AEs were similar,

The Korean Society for AIDS
2020 대한에이즈학회 학술대회
282 2020 대한에이즈학회 학술대회
with low rates of withdrawals due to AEs in both arms. DTG+3TC had a significantly lower rate of
drug-related AEs than DTG+TDF/FTC (20% vs 27%; relative risk ratio,0.76;95%CI:0.63-0.92).
Post-baseline changes in markers of bone and renal function favoured DTG+3TC through week 144.
Conclusion: DTG+3TC remains non-inferior to DTG+TDF/FTC in treatment-naïve adults at week 144.
Both regimens were well tolerated. The results demonstrate durable efficacy and potency of DTG+3TC,
further supporting it as a first-line option for HIV treatment.
Keywords: HIV Dolutegravir
GEMINI-1 GEMINI-2 Pooled
Snapshot responders DTG+3TC 281/356 (79%) 303/360 (84%) 584/716 (82%)
DTG+TDF/FTC 296/358 (83%) 303/359 (84%) 599/717 (84%)
Adjusted Difference (95% CI) -3.6 (-9.4, 2.1) 0.0 (-5.3, 5.3) -1.8 (-5.8, 2.1)
[Proportion of participants with plasma HIV-1 RNA <50 c/mL at week 144: Snapshot analysis – ITT-E population]
Data from this abstract were previously presented in full at HIV Drug Therapy Glasgow 2020; October
5-8, 2020; Virtual.
E-poster session
2020 대한에이즈학회 학술대회 283
P-19 Clinical research
Safety and Efficacy of Cabotegravir + Rilpivirine
Long-Acting With and Without Oral Lead-In: FLAIR Week
124 Results
Ronald D’Amico1, Chloe Orkin2, Enrique Bernal Morell3, Darrell H.S. Tan4, Harold Katner5, Yashna Singh6, Hans-Jürgen Stellbrink7, Elena Belonosova8, Rebecca DeMoor9, Sandy Griffith1, Shanker Thiagarajah9, Rodica Van Solingen-Ristea10, Herta
Crauwels10, Susan L. Ford11, Parul Patel1, Amy Cutrell1, Kimberly Y. Smith1, Kati Vandermeulen10, David A. Margolis1, Marty St.
Clair1, William R. Spreen1, Sungshin Kwon12
1ViiV Healthcare, Research Triangle Park, NC, USA; 2Queen Mary University, London, UK; 3Hospital General Universitario Reina Sofía, Murcia, Spain; 4Division of Infectious Diseases, St. Michael's Hospital, Toronto, Canada; 5Mercer University Medical School, Macon, GA, USA; 6Desmond Tutu HIV Foundation, Cape Town, South Africa; 7ICH Study Center, Hamburg, Germany; 8Orel Regional Center for AIDS, Orel, Russia; 9GlaxoSmithKline, London, UK; 10Janssen Research and Development, Beerse, Belgium; 11GlaxoSmithKline, NC, USA; 12GlaxoSmithKline, Seoul, Korea
Background: FLAIR (NCT02938520), a phase III, randomized, open-label study, established
noninferiority of switching virologically suppressed participants (pts) from daily oral DTG/ABC/3TC
(CAR) to monthly CAB+RPV LA following CAB+RPV oral lead-in (OLI) over 2 y. We report results from
the Extension Phase on efficacy, safety, and tolerability of switching CAR arm pts to LA therapy ± OLI.
Method: ART-naive pts achieving virologic suppression (HIV-1 RNA <50c/mL) with CAR during the
20-wk Induction Phase were randomized (1:1) to continue CAR or switch to LA (n=283 each). Pts
randomized to LA therapy received an OLI of CAB+RPV once daily for ≥4 wk before receiving monthly
injectable CAB+RPV LA. At W100, CAR pts could switch to LA therapy (Extension Switch population),
either directly (Direct to Inject [DTI] arm) or with a 4-wk OLI (OLI arm), or withdraw. Endpoints
assessed at W124 for Extension Switch population included plasma HIV-1 RNA ≥50c/mL and
<50c/mL, CVF (2 consecutive HIV-1 RNA ≥200c/mL), safety, and tolerability.
Results: In total, 111 and 121 CAR arm pts transitioned to CAB+RPV LA, entering the DTI or OLI arms,
respectively. At W124, 1 pt (<1%) in each arm had HIV-1 RNA ≥50c/mL (Table; Figure). Further, 99%
and 93% of pts in the DTI and OLI arms maintained virologic suppression (HIV-1 RNA <50c/mL),
respectively. 1 pt in the DTI arm developed CVF at W112. AEs leading to withdrawal were infrequent.
There was 1 grade 4 drug-related AE in the DTI arm (mixed cellularity Hodgkin lymphoma). The number
of pts experiencing serious AEs was comparable between arms. Overall, CAB+RPV LA was well
tolerated; injection-site reactions were the most common AE, with most classified as mild/moderate in
severity.
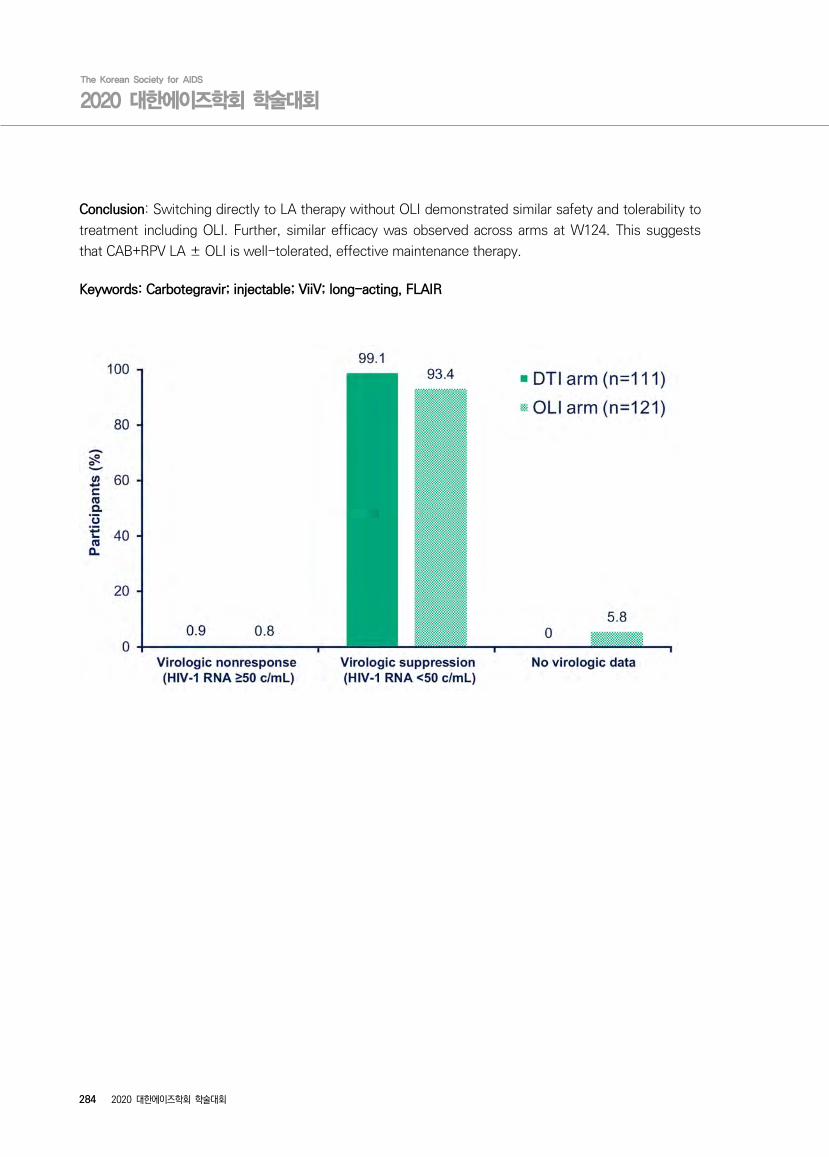
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
284 2020 대한에이즈학회 학술대회
Conclusion: Switching directly to LA therapy without OLI demonstrated similar safety and tolerability to
treatment including OLI. Further, similar efficacy was observed across arms at W124. This suggests
that CAB+RPV LA ± OLI is well-tolerated, effective maintenance therapy.
Keywords: Carbotegravir; injectable; ViiV; long-acting, FLAIR
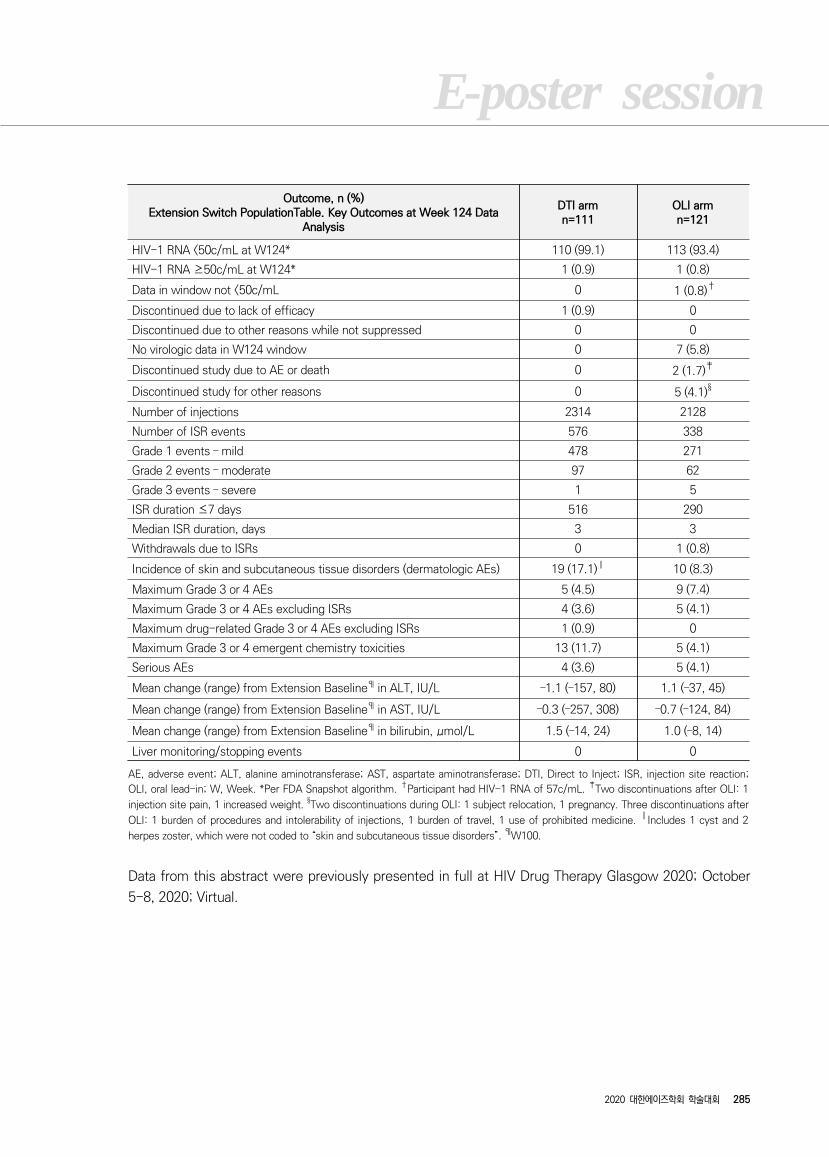
E-poster session
2020 대한에이즈학회 학술대회 285
Outcome, n (%)Extension Switch PopulationTable. Key Outcomes at Week 124 Data
Analysis
DTI armn=111
OLI armn=121
HIV-1 RNA <50c/mL at W124* 110 (99.1) 113 (93.4)
HIV-1 RNA ≥50c/mL at W124* 1 (0.9) 1 (0.8)
Data in window not <50c/mL 0 1 (0.8)†
Discontinued due to lack of efficacy 1 (0.9) 0
Discontinued due to other reasons while not suppressed 0 0
No virologic data in W124 window 0 7 (5.8)
Discontinued study due to AE or death 0 2 (1.7)‡
Discontinued study for other reasons 0 5 (4.1)§
Number of injections 2314 2128
Number of ISR events 576 338
Grade 1 events – mild 478 271
Grade 2 events – moderate 97 62
Grade 3 events – severe 1 5
ISR duration ≤7 days 516 290
Median ISR duration, days 3 3
Withdrawals due to ISRs 0 1 (0.8)
Incidence of skin and subcutaneous tissue disorders (dermatologic AEs) 19 (17.1)║ 10 (8.3)
Maximum Grade 3 or 4 AEs 5 (4.5) 9 (7.4)
Maximum Grade 3 or 4 AEs excluding ISRs 4 (3.6) 5 (4.1)
Maximum drug-related Grade 3 or 4 AEs excluding ISRs 1 (0.9) 0
Maximum Grade 3 or 4 emergent chemistry toxicities 13 (11.7) 5 (4.1)
Serious AEs 4 (3.6) 5 (4.1)
Mean change (range) from Extension Baseline¶ in ALT, IU/L –1.1 (–157, 80) 1.1 (–37, 45)
Mean change (range) from Extension Baseline¶ in AST, IU/L –0.3 (–257, 308) –0.7 (–124, 84)
Mean change (range) from Extension Baseline¶ in bilirubin, μmol/L 1.5 (–14, 24) 1.0 (–8, 14)
Liver monitoring/stopping events 0 0
AE, adverse event; ALT, alanine aminotransferase; AST, aspartate aminotransferase; DTI, Direct to Inject; ISR, injection site reaction;
OLI, oral lead-in; W, Week. *Per FDA Snapshot algorithm. †Participant had HIV-1 RNA of 57c/mL. ‡Two discontinuations after OLI: 1
injection site pain, 1 increased weight. §Two discontinuations during OLI: 1 subject relocation, 1 pregnancy. Three discontinuations after
OLI: 1 burden of procedures and intolerability of injections, 1 burden of travel, 1 use of prohibited medicine. ║Includes 1 cyst and 2
herpes zoster, which were not coded to “skin and subcutaneous tissue disorders”. ¶W100.
Data from this abstract were previously presented in full at HIV Drug Therapy Glasgow 2020; October
5-8, 2020; Virtual.

The Korean Society for AIDS
2020 대한에이즈학회 학술대회
286 2020 대한에이즈학회 학술대회
P-20 Clinical research
HIV 감염자에서 발생한 인간유두종바이러스 관련 항문암 4 례
백예지1, 조윤숙 1, 현종훈 1, 김무현 1, 손유진 1, 김정호 1, 안진영 1, 정수진 1, 염준섭 1, 김현기 2, 최준용 1
1 연세대학교 의과대학 내과학 교실, 2 연세대학교 의과대학 병리학 교실
배경: 인간면역결핍바이러스(HIV) 감염 환자들은 항문암의 발생이 일반 인구보다 15~60 배 높은 것으로 알려져 있다.
일반적으로 항문암의 84%는 인간유두종바이러스(HPV)의 아형 중 고위험군에 의한 것으로, 변형대의 점막 이형성세포
를 유발하여 암으로 진행하는 것으로 알려져 있다. 본 연구에서는 HIV 로 항레트로바이러스 치료 중 항문암을 진단받은
4 명의 환자를 기술하고 HPV 와의 관련성을 확인해보고자 하였다.
증례: 증례 1. 34 세부터 HIV 치료하였고, 과거에 치루절제술 하였던 분이다. 50 세에 항문의 불편감으로 내원하여 첨부
콘딜로마 확인되었는데 고등급상피내병변으로 항문연 절제술 시행하였다. 5 년 후 치루 확인 위하여 시행한 대장내시경
에서 첨부콘딜로마 보였고, 편평상피세포암 진단되어 절제술 후 현재 항암방사선치료 예정이다.
증례 2. 28 세에 HIV 진단되어 33 세에 설사와 가스차는 증상으로 시행한 대장 내시경에서 첨부콘딜로마 확인되었다.
항문연 절제술 후 조직검사 상 고등급상피내병변으로 항문상피내종양에 합당하였으며, p16 양성이었다. 이후 첨부콘딜
로마 확인되었으나 저절로 관해되었고 추적 관찰 중에 있다.
증례 3. 43 세부터 HIV 치료 중 51 세에 항문의 미만성대 B 세포림프종 진단되어 항암치료 받고 추적관찰 중이던 분이
다. 5 년 후 항문 통증 및 혈변으로 내시경 시행하여 항문의 편평상피세포의 고분화이형성 및 침범 소견으로 항암방사선
치료를 시작하였으나, 이후 만져지는 종괴에서 편평상피세포암 진단되어 2013 년 수술 후 항암방사선 치료하였다. 현재
는 편도의 편평상피세포암으로 항암방사선 치료 후 추적관찰 중이다.
증례 4. 29 세에 HIV 진단 후 55 세에 점점 커지는 항문연의 종괴로 조직검사 시행하여 편평상피세포암을 확인, 항문암
3 기로 진단되어 술전 항암방사선치료 후 진행 소견으로 수술을 시행하고 보조항암화학요법 및 방사선 치료를 시행하였
고 현재는 호스피스 치료 중에 있다.
결과: 4 증례 모두 항레트로바이러스 치료 중 증상이 있어 대장 내시경을 시행하여 항문암 혹은 항문상피내종양이 확인
된 공통점이 있으나, 증례 1, 2 에서만 p16 IHC 양성, 고위험군 HPV 와 관련이 있는 것으로 나타났다. 증례 3, 4 에서
는 저위험군 HPV 이 발견되었으나 p16 IHC 는 음성이었다.
결론: 항문암은 느리게 진행하는 암이지만 증상 발생 후 진단하면 진행성으로 예후가 불량할 수 있으므로, 고위험군인
HIV 환자들에게서 항문 내시경, 항문 부위 세포진 및 HPV DNA 검사 등의 조기 검사 및 정기적 추적관찰이 중요할 것으
로 생각되며 이에 대한 추가 연구가 필요할 것이다. 또한, 많은 종류의 HPV 의 감염을 예방할 수 있는 HPV 예방접종을
실시하는 것이 도움이 될 것이다.

287
case
C
urre
nt
age(
yr)
Sex
MSM
Com
orbi
dity
Dat
e of
di
agno
sis
Firs
t sy
mpt
omA
nal
carc
inom
a gra
dep1
6H
PV
Gen
otyp
eC
D4
coun
t (/
uL)
on d
iagn
osis
Op.
CC
RTx
155
MY
Syp
hilis
,
Ana
l fis
tula
2015
.06.2
6A
nal d
isco
mfo
rtH
SIL
+35
810
YN
2020
.07.2
8A
nal f
istu
laSqC
C, M
D+
35,6
194
6Y
Y
235
MY
Urt
icar
ia2018
.02.2
6D
iarr
hea,
blo
atin
gH
SIL
+6,1
1,1
8,40
,43,6
660
5Y
N
364
MY
DLB
CL,
orop
hary
nx
SqC
C
2012
.01.3
0H
emat
oche
zia,
Ana
l pai
nSqC
C, W
D-
632
5Y
Y
457
MY
HTN
, Syp
hilis
2018
.02.0
8M
ass
SqC
C, W
D-
11&
5458
4Y
Y
Abb
revi
atio
n: M
SM
, M
ale-
to-m
ale
sex;
Op.
, op
erat
ion;
CC
RT,
con
curr
ent
chem
orad
ioth
erap
y; M
, m
ale;
DLB
CL,
diffu
se lar
ge B
cel
l ly
mph
oma;
HSIL
, hi
gh g
rade
squ
amou
s in
trae
pith
elia
l le
sion
; SqC
C, sq
uam
ous
cell
carc
inom
a; M
D, m
oder
ate
diff
eren
tiat
ed; W
D, w
ell d
iffe
rent
iate
d;
*bol
d nu
mbe
rs r
epre
sent
hig
h-risk
typ
es o
f H
PV
Tab
le 1
. C
har
acte
rist
ics
of
HIV
pat
ients
who w
ere
dia
gnose
d w
ith a
nal
car
cinom
a
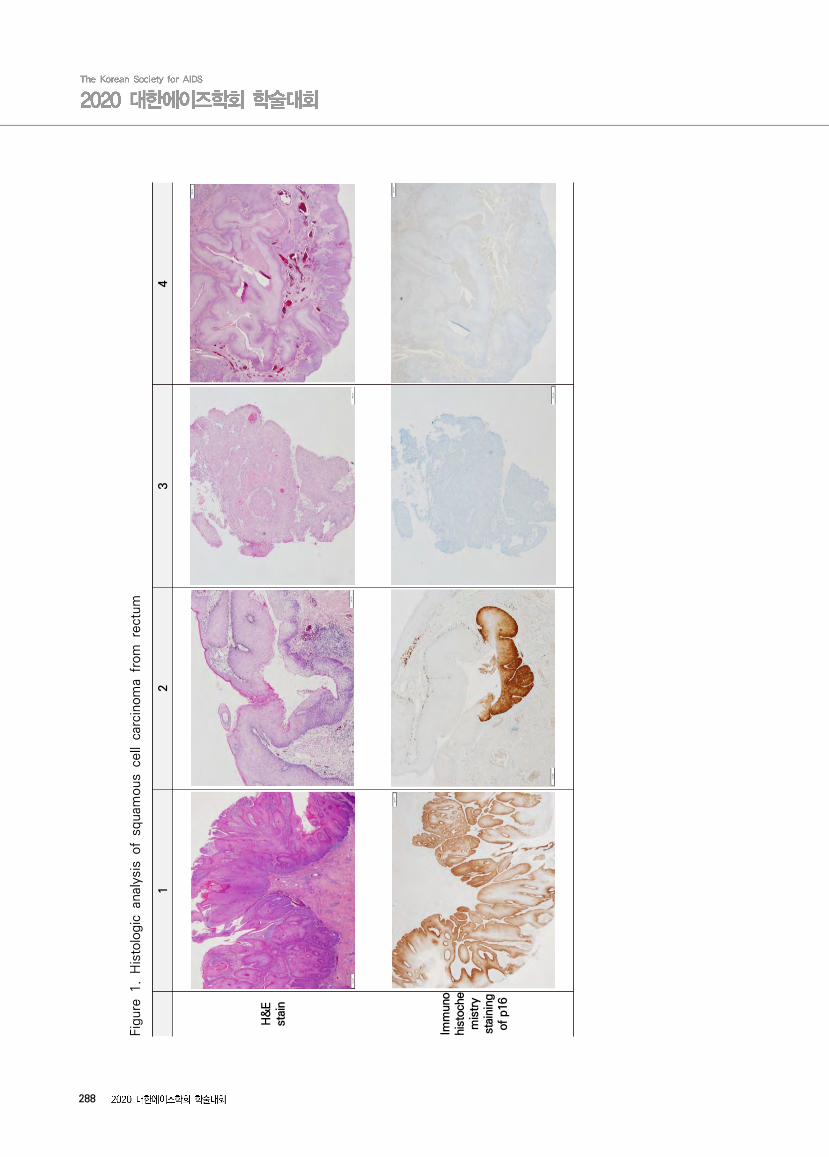
288
12
34
H&
E
stai
n
Imm
uno
hist
oche
mis
try
stai
ning
of
p16
Fig
ure
1.
His
tolo
gic
anal
ysis
of
squam
ous
cell
carc
inom
a fr
om
rect
um
E-poster session
2020 대한에이즈학회 학술대회 289
P-21 Clinical research
Pooled Analysis of 4 International Trials of Bictegravir/
Emtricitabine/Tenofovir Alafenamide (B/F/TAF) in Adults
Aged ≥ 65 or Older Demonstrating Safety and Efficacy:
Week 48 Results
Ramgopal M1, Jeong-a Lee2, Maggiolo F3, Ward D4, Lebouche B5, Rizzardini G6, Molina JM7, Brinson C8, Wang H9, Gallant J9,
Collins S9, McNicholl I9, Martin H9
1Midway Research, Fort Pierce, FL, USA; 2Gilead Korea, Seoul, Korea; 3Division of Infectious Diseases, ASST Papa Giovanni XXIII, Bergamo, Italy; 4Dupont Circle Physicians Group, Washington, DC, USA; 5Research Institute, McGill University Health Centre, Montreal, Canada; 6Division of Infectious Diseases, Luigi Sacco Hospital, ASST Fatebenefratelli Sacco, Milan, Italy; 7Department of Infectious Diseases, Saint Louis Hospital, University Paris Diderot, France; 8Central Texas Clinical Research, Austin, TX, USA; 9Gilead Sciences, Inc., Foster City, CA, USA
Objectives: As life expectancy for people with HIV increases, optimizing antiretroviral therapy to fit the needs of older adults, including those with comorbidities and multiple medications, is paramount. B/F/TAF is a small single-tablet regimen with few drug-drug interactions, a high barrier to resistance and may provide a beneficial option for older patients.
Methods: In this pooled analysis of 4 international trials (Studies 1844, 1878, 4030 and 4449) of virologically suppressed (HIV-1 RNA<50 copies/mL), treatment-experienced adults, we evaluated the efficacy and safety of switching to B/F/TAF for participants ≥65 years. Primary endpoint was HIV-1 RNA<50 copies/mL at Week 48 as defined by the Food and Drug Administration Snapshot algorithm.
Results: 140 participants were age ≥65 years at study enrollment. Median age (Q1, Q3) was 68 years (66, 72), 14% were female, and 88% were White. Medical history at baseline was significant for diabetes 22%, hypertension 55%, cardiovascular disease 24% and dyslipidemia 59%. At W48, the proportion with HIV RNA<50 copies/mL was 92% (129/140). No participant had virologic failure. Most common adverse events (AEs) were nasopharyngitis and arthralgia (7% each). Eleven participants (8%) had a study drug related AE, all were either Grade 1 or Grade 2. There were no Grade 3-4 study drug-related AEs. Four participants had AEs that led to premature study drug discontinuation. Median changes from baseline in fasting lipids were: total fasting cholesterol (-7mg/dL), LDL (-2mg/dL), HDL (0mg/dL), triglycerides (-15mg/dL) and total cholesterol:HDL (-0.1). Median weight change was 1.0 kg (IQR -0.9, 3.0).
Conclusion: Switching to B/F/TAF in older adults was well tolerated and safe while maintaining high rates of virologic suppression through 48 weeks. These data support the use of B/F/TAF for treatment of adults ≥65 years who could benefit from a small tablet with few drug-drug interactions and an established safety profile.
Keywords: B/F/TAF elderly patients
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
290 2020 대한에이즈학회 학술대회
P-22 Clinical research
Switching to DTG/3TC Fixed-Dose Combination (FDC) Is
Non-Inferior to Continuing a TAF-Based Regimen (TBR) in
Maintaining Virologic Suppression Through 96 Weeks
(TANGO Study)
J van Wyk1, F Ajana2, F Bisshop3, S De Wit4, O Osiyemi5, J Portilla6, J-P Routy7, C Wyen8, M Ait-Khaled1, M-C Nascimento1,
KA Pappa9, R Wang9, J Wright10, B Wynne9, M Aboud1, KY Smith9, S Kwon11
1ViiV Healthcare, Brentford, UK; 2Centre Hospitalier de Tourcoing, Tourcoing, France; 3Holdsworth House Medical Brisbane, Queensland, Australia; 4CHU St-Pierre, Brussels, Belgium; 5Triple O Research Institute PA, West Palm Beach, FL, USA; 6Hospital General Universitario de Alicante, Alicante Spain; 7McGill University Health Center, Montreal, QC, Canada; 8Praxis am Ebertplatz, Cologne, Germany; 9ViiV Healthcare, Research Triangle Park, NC, USA; 10GlaxoSmithKline, Stockley Park, UK; 11GlaxoSmithKline, Seoul, South Korea
Background: DTG/3TC 2-drug regimen (2DR) was non-inferior to a TAF-based 3/4DR through the
Week 48 primary endpoint in TANGO. Here we present Week 96 secondary endpoint analyses.
Methods: TANGO, a randomized, open-label, non-inferiority phase III study evaluates the efficacy and
safety of switching to once-daily DTG/3TC in HIV-1–infected, virologically suppressed (>6 months, no
prior virologic failure, no major NRTI or INSTI resistance) adults vs remaining on a TBR, over 148 weeks.
Participants were randomized 1:1, stratified by baseline third agent class: PI, NNRTI, INSTI. Week 96
analysis assessed non-inferiority with a 4% non-inferiority margin for Snapshot virologic failure (VF) and
8% for virologic success (VS; FDA Snapshot algorithm, intention-to-treat–exposed [ITT-E] population).
Results: 741 randomized/exposed participants (DTG/3TC: 369; TBR: 372). For Snapshot VF, switching
to DTG/3TC was non-inferior to continuing TBR at Week 96 in the ITT-E analysis: 0.3% vs 1.1%;
adjusted difference: −0.8% (95% CI: −2.0%, 0.4%) and superior to TBR in the per-protocol analysis:
0% vs 1.1%; adjusted difference: −1.1% (95% CI: −2.3, −0.0); P=0.044 (two-sided). Snapshot VS
was high in both arms and demonstrated non-inferiority (Table 1). Forty-four participants (5.9%) had
missing data in the Week 96 window due to COVID-19 impact. Zero participants on DTG/3TC and 3
(<1%) on TBR met protocol-defined VF with no resistance observed at failure. Overall adverse event
rates were similar between arms, with more drug-related AEs in the DTG/3TC arm (Table 1). TC,
LDL-cholesterol, and triglycerides improved significantly with DTG/3TC while HDL-cholesterol changes
significantly favored TBR, with no difference in TC/HDL-C ratio between arms. Decreases in GFR by
cystatin C were observed with a significantly lower decrease in the DTG/3TC arm; proximal tubular
function marker changes were small and similar across arms.
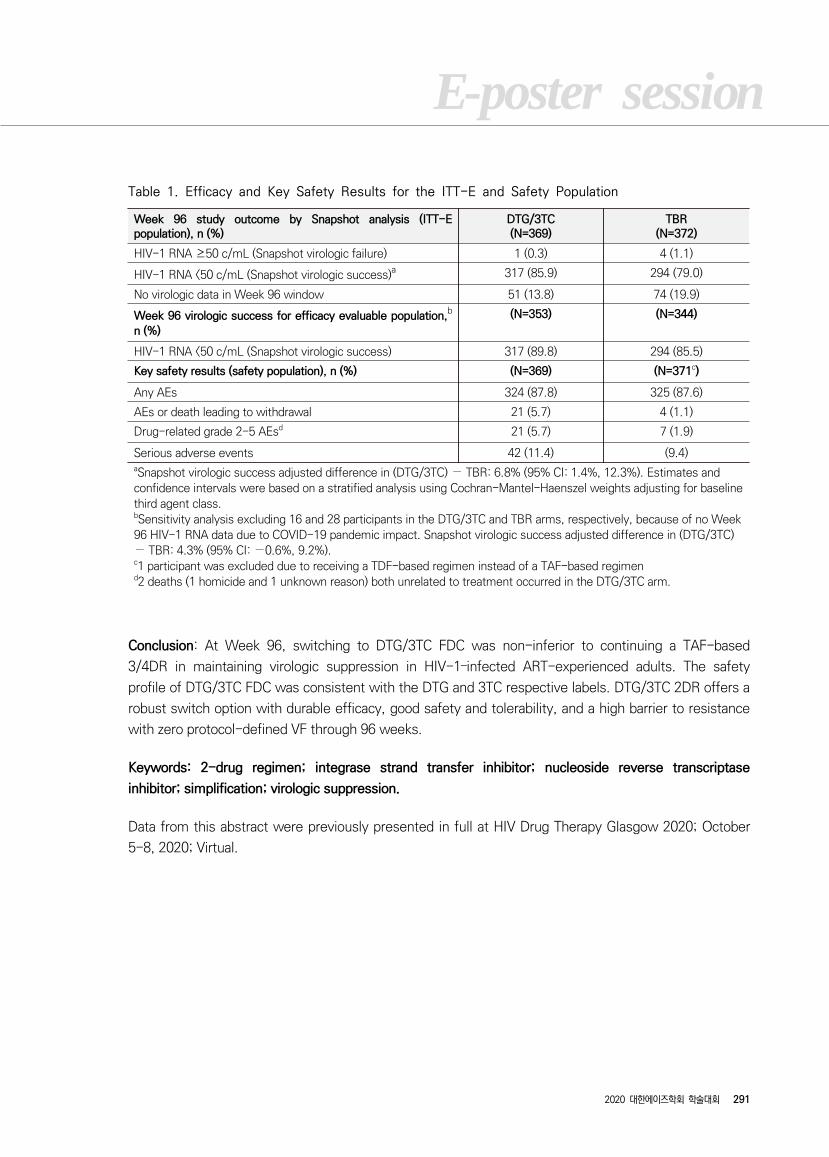
E-poster session
2020 대한에이즈학회 학술대회 291
Week 96 study outcome by Snapshot analysis (ITT-E population), n (%)
DTG/3TC(N=369)
TBR(N=372)
HIV-1 RNA ≥50 c/mL (Snapshot virologic failure) 1 (0.3) 4 (1.1)
HIV-1 RNA <50 c/mL (Snapshot virologic success)a 317 (85.9) 294 (79.0)
No virologic data in Week 96 window 51 (13.8) 74 (19.9)
Week 96 virologic success for efficacy evaluable population,b n (%)
(N=353) (N=344)
HIV-1 RNA <50 c/mL (Snapshot virologic success) 317 (89.8) 294 (85.5)
Key safety results (safety population), n (%) (N=369) (N=371c)
Any AEs 324 (87.8) 325 (87.6)
AEs or death leading to withdrawal 21 (5.7) 4 (1.1)
Drug-related grade 2-5 AEsd 21 (5.7) 7 (1.9)
Serious adverse events 42 (11.4) (9.4)aSnapshot virologic success adjusted difference in (DTG/3TC) − TBR: 6.8% (95% CI: 1.4%, 12.3%). Estimates and confidence intervals were based on a stratified analysis using Cochran-Mantel-Haenszel weights adjusting for baseline third agent class.bSensitivity analysis excluding 16 and 28 participants in the DTG/3TC and TBR arms, respectively, because of no Week 96 HIV-1 RNA data due to COVID-19 pandemic impact. Snapshot virologic success adjusted difference in (DTG/3TC) − TBR: 4.3% (95% CI: −0.6%, 9.2%).c1 participant was excluded due to receiving a TDF-based regimen instead of a TAF-based regimend2 deaths (1 homicide and 1 unknown reason) both unrelated to treatment occurred in the DTG/3TC arm.
Table 1. Efficacy and Key Safety Results for the ITT-E and Safety Population
Conclusion: At Week 96, switching to DTG/3TC FDC was non-inferior to continuing a TAF-based
3/4DR in maintaining virologic suppression in HIV-1–infected ART-experienced adults. The safety
profile of DTG/3TC FDC was consistent with the DTG and 3TC respective labels. DTG/3TC 2DR offers a
robust switch option with durable efficacy, good safety and tolerability, and a high barrier to resistance
with zero protocol-defined VF through 96 weeks.
Keywords: 2-drug regimen; integrase strand transfer inhibitor; nucleoside reverse transcriptase
inhibitor; simplification; virologic suppression.
Data from this abstract were previously presented in full at HIV Drug Therapy Glasgow 2020; October
5-8, 2020; Virtual.
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
292 2020 대한에이즈학회 학술대회
P-23 Epidemiology and social research
Assessment of disease burden and immunization rates for
vaccine-preventable diseases in people living with HIV:
The Korea HIV/AIDS Cohort study
Hye Seong1, Yunsu Choi2, Kyounghwan Ahn3, Jun-Yong Choi4,5, Shin-Woo Kim6, Sang Il Kim7, Mee-Kyung Kee8, Bo Youl Choi2,
Hak Jun Hyun1, Jin Gu Yoon1, Ji Yun Noh1,9, Hee Jin Cheong1,9, Woo Joo Kim1,9, Joon Young Song1,9
1Department of Internal Medicine, Korea University College of Medicine, Seoul; 2Department of Preventive Medicine, Hanyang University College of Medicine; 3Institute for Health and Society, Hanyang University, Seoul, Korea; 4Department of Internal Medicine, Yonsei University College of Medicine, Seoul; 5AIDS Research Institute, Yonsei University College of Medicine, Seoul; 6Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu; 7Department of Internal Medicine, Catholic University College of Medicine, Seoul; 8Division of Viral Disease Research, Korea Centers for Disease Control and Prevention, Cheongju, Korea; 9Asian Pacific Influenza Institute (APII), Seoul, Republic of Korea
Backgrounds: Prophylactic immunization is important for HIV-infected patients, but there is insufficient
data on the disease burden of vaccine-preventable diseases (VPD), vaccination rates or influencing
factors to be vaccinated.
Methods: The incidence and prevalence of VPDs were estimated in HIV-infected patients using the
Korea HIV/AIDS cohort database between 2006 and 2017. In addition, we evaluated the vaccination
rates and analyzed influencing factors to get vaccinated in HIV-infected patients through multilevel
analysis for the clinico-epidemiological factors, immune status, psychological status, etc. A
questionnaire survey was also conducted for experts whether they recommended vaccination to
HIV-infected patients or not.
Results: The incidence rates of HBV, herpes zoster, anogenital wart were 1.74, 7.38, and 10.85 per
1000 person-year, respectively. The prevalence of HBV and anogenital wart at enrollment was 4.8%
and 8.6%, respectively, which increased to 5.3% and 12.0% cumulatively by 2017. HBV (21.7% in 2008,
56.3% in 2013, and 75.4% in 2017) and pneumococcal (3.0% in 2015, 7.6% in 2016, and 9.6% in 2017)
vaccination rates increased by year, while annual influenza vaccination rates were similar by season
(33.9 - 34.4%).
In the multi-level analysis, influencing factors for pneumococcal and HBV vaccination were HIV viral
load and CD4 T-cell count, respectively. Influenza vaccination was related to male sex and the number
of antiretroviral therapy (ART) line, but not significantly associated with CD4 T-cell count or HIV viral
load. In questionnaire survey, most experts recommended HBV (92.9%), HAV (95.7%), pneumococcal
(81.4% for PCV13 and 75.4% for PPSV23) and influenza (100%) vaccination routinely, but they did not
for HPV (12.9%) and zoster (27.1%) vaccination.

E-poster session
2020 대한에이즈학회 학술대회 293
Conclusion: CD4 T-cell count, HIV viral load, and the number of ART line were influencing factors to get
vaccination. There was a discordance between clinical practice and experts' opinions.
Keywords: HIV, disease burden, vaccination, risk factor, Korean HIV/AIDS cohort study
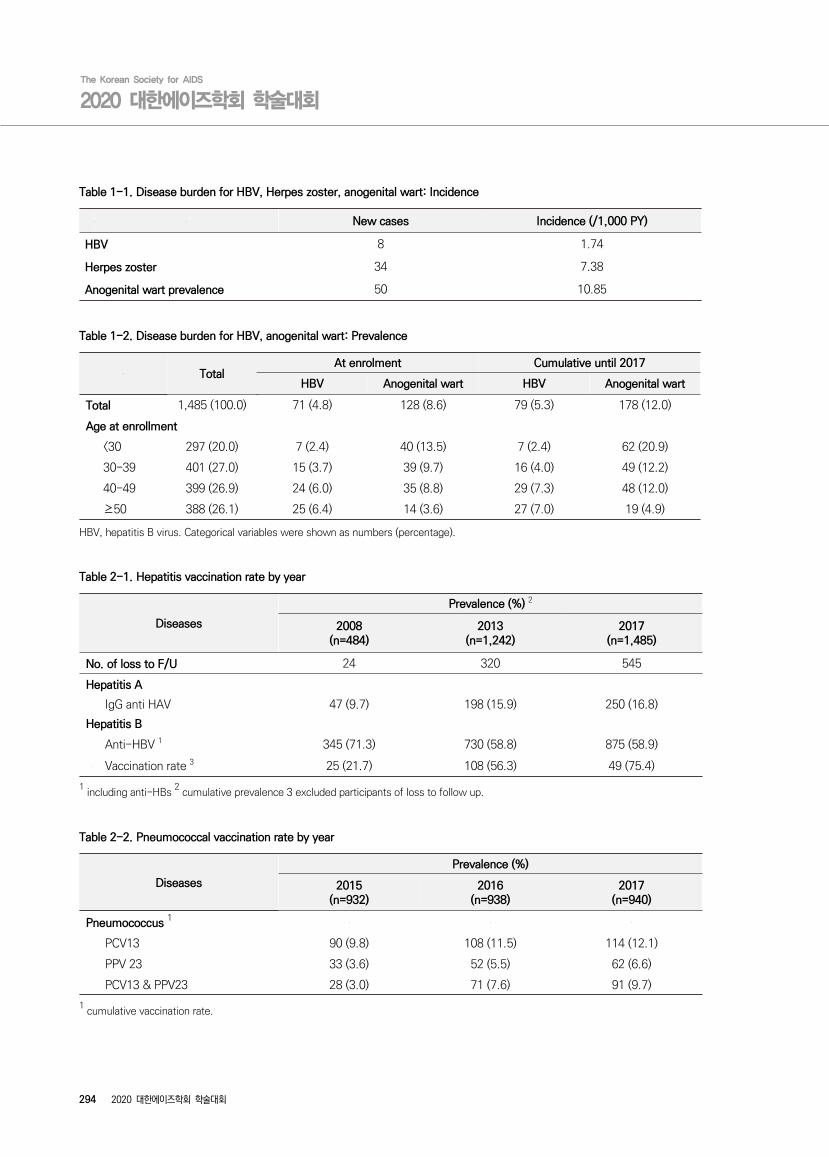
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
294 2020 대한에이즈학회 학술대회
New cases Incidence (/1,000 PY)
HBV 8 1.74
Herpes zoster 34 7.38
Anogenital wart prevalence 50 10.85
Table 1-1. Disease burden for HBV, Herpes zoster, anogenital wart: Incidence
TotalAt enrolment Cumulative until 2017
HBV Anogenital wart HBV Anogenital wart
Total 1,485 (100.0) 71 (4.8) 128 (8.6) 79 (5.3) 178 (12.0)
Age at enrollment
<30 297 (20.0) 7 (2.4) 40 (13.5) 7 (2.4) 62 (20.9)
30-39 401 (27.0) 15 (3.7) 39 (9.7) 16 (4.0) 49 (12.2)
40-49 399 (26.9) 24 (6.0) 35 (8.8) 29 (7.3) 48 (12.0)
≥50 388 (26.1) 25 (6.4) 14 (3.6) 27 (7.0) 19 (4.9)
HBV, hepatitis B virus. Categorical variables were shown as numbers (percentage).
Table 1-2. Disease burden for HBV, anogenital wart: Prevalence
Diseases
Prevalence (%) 2
2008(n=484)
2013(n=1,242)
2017(n=1,485)
No. of loss to F/U 24 320 545
Hepatitis A
IgG anti HAV 47 (9.7) 198 (15.9) 250 (16.8)
Hepatitis B
Anti-HBV 1 345 (71.3) 730 (58.8) 875 (58.9)
Vaccination rate 3 25 (21.7) 108 (56.3) 49 (75.4)
1 including anti-HBs
2 cumulative prevalence 3 excluded participants of loss to follow up.
Table 2-1. Hepatitis vaccination rate by year
Diseases
Prevalence (%)
2015(n=932)
2016(n=938)
2017(n=940)
Pneumococcus 1
PCV13 90 (9.8) 108 (11.5) 114 (12.1)
PPV 23 33 (3.6) 52 (5.5) 62 (6.6)
PCV13 & PPV23 28 (3.0) 71 (7.6) 91 (9.7)
1 cumulative vaccination rate.
Table 2-2. Pneumococcal vaccination rate by year
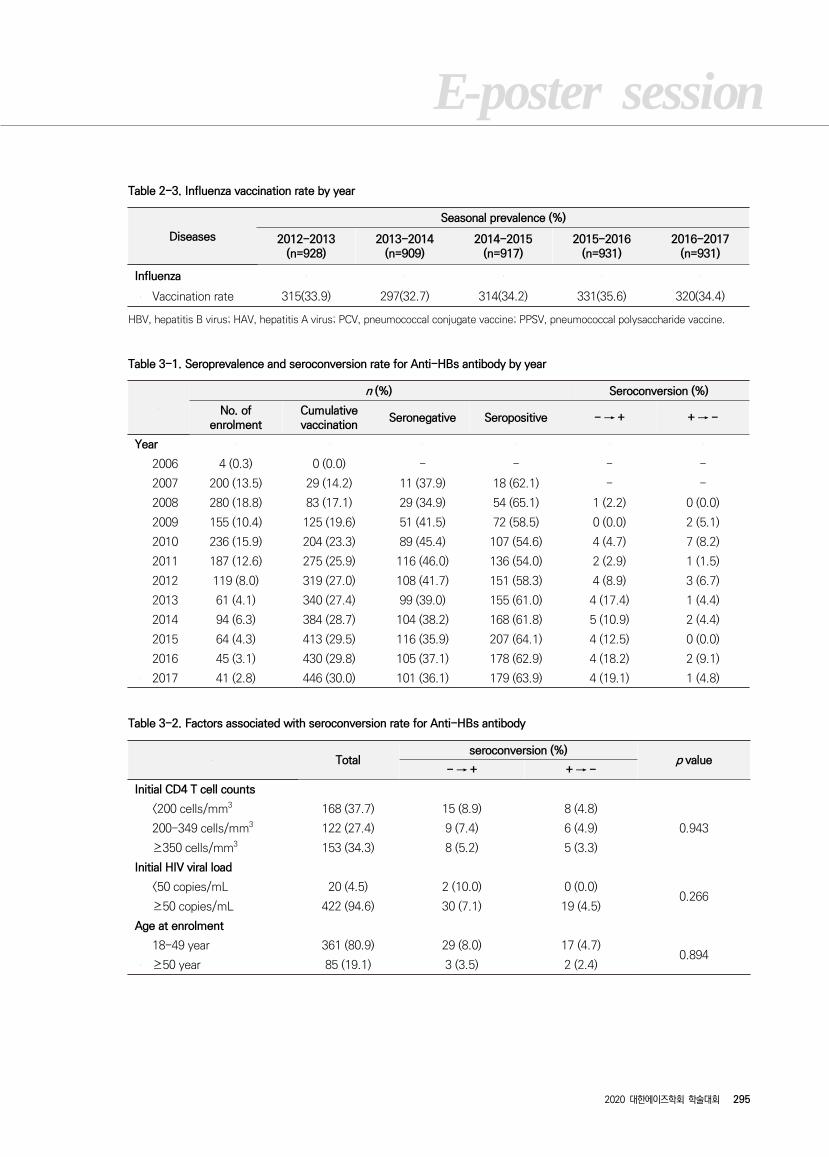
E-poster session
2020 대한에이즈학회 학술대회 295
Diseases
Seasonal prevalence (%)
2012-2013(n=928)
2013-2014(n=909)
2014-2015(n=917)
2015-2016(n=931)
2016-2017(n=931)
Influenza
Vaccination rate 315(33.9) 297(32.7) 314(34.2) 331(35.6) 320(34.4)
HBV, hepatitis B virus; HAV, hepatitis A virus; PCV, pneumococcal conjugate vaccine; PPSV, pneumococcal polysaccharide vaccine.
Table 2-3. Influenza vaccination rate by year
n (%) Seroconversion (%)
No. of enrolment
Cumulative vaccination
Seronegative Seropositive - → + + → -
Year
2006 4 (0.3) 0 (0.0) - - - -
2007 200 (13.5) 29 (14.2) 11 (37.9) 18 (62.1) - -
2008 280 (18.8) 83 (17.1) 29 (34.9) 54 (65.1) 1 (2.2) 0 (0.0)
2009 155 (10.4) 125 (19.6) 51 (41.5) 72 (58.5) 0 (0.0) 2 (5.1)
2010 236 (15.9) 204 (23.3) 89 (45.4) 107 (54.6) 4 (4.7) 7 (8.2)
2011 187 (12.6) 275 (25.9) 116 (46.0) 136 (54.0) 2 (2.9) 1 (1.5)
2012 119 (8.0) 319 (27.0) 108 (41.7) 151 (58.3) 4 (8.9) 3 (6.7)
2013 61 (4.1) 340 (27.4) 99 (39.0) 155 (61.0) 4 (17.4) 1 (4.4)
2014 94 (6.3) 384 (28.7) 104 (38.2) 168 (61.8) 5 (10.9) 2 (4.4)
2015 64 (4.3) 413 (29.5) 116 (35.9) 207 (64.1) 4 (12.5) 0 (0.0)
2016 45 (3.1) 430 (29.8) 105 (37.1) 178 (62.9) 4 (18.2) 2 (9.1)
2017 41 (2.8) 446 (30.0) 101 (36.1) 179 (63.9) 4 (19.1) 1 (4.8)
Table 3-1. Seroprevalence and seroconversion rate for Anti-HBs antibody by year
Totalseroconversion (%)
p value- → + + → -
Initial CD4 T cell counts
<200 cells/mm3 168 (37.7) 15 (8.9) 8 (4.8)
0.943200-349 cells/mm3 122 (27.4) 9 (7.4) 6 (4.9)
≥350 cells/mm3 153 (34.3) 8 (5.2) 5 (3.3)
Initial HIV viral load
<50 copies/mL 20 (4.5) 2 (10.0) 0 (0.0)0.266
≥50 copies/mL 422 (94.6) 30 (7.1) 19 (4.5)
Age at enrolment
18-49 year 361 (80.9) 29 (8.0) 17 (4.7)0.894
≥50 year 85 (19.1) 3 (3.5) 2 (2.4)
Table 3-2. Factors associated with seroconversion rate for Anti-HBs antibody
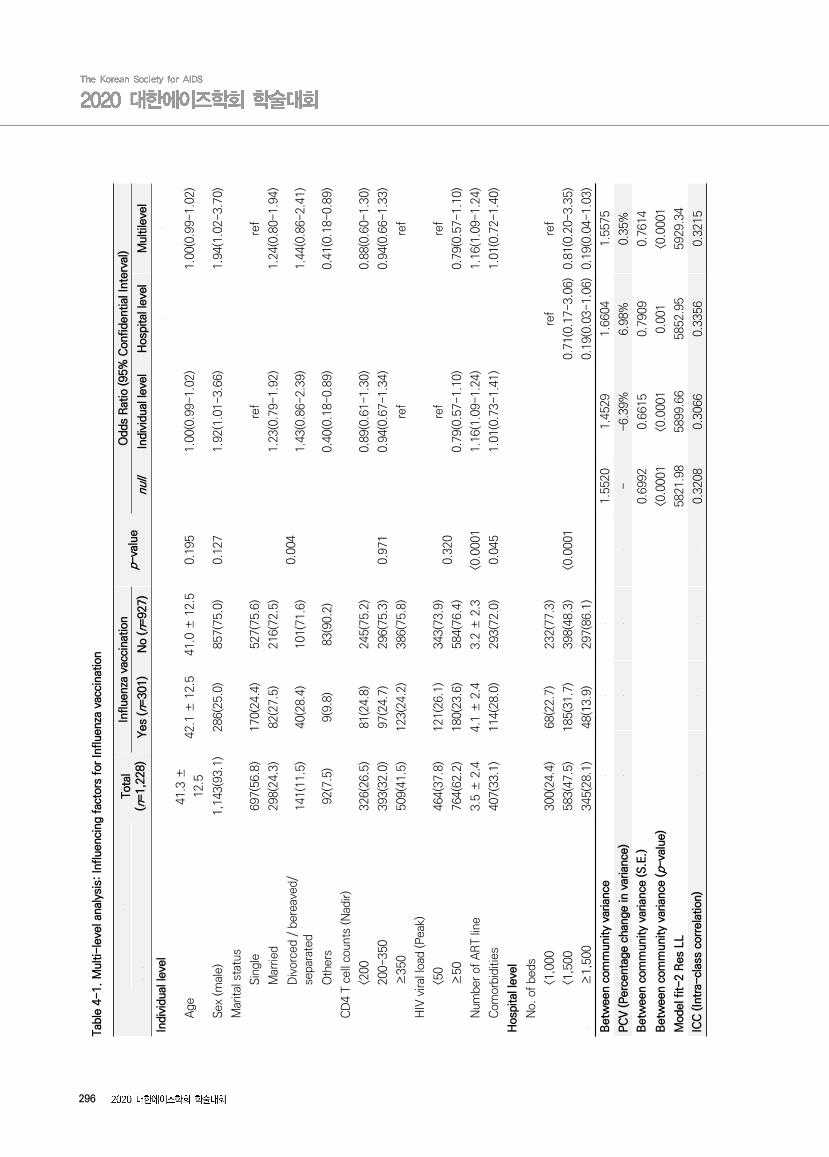
296
To
tal
(n=1,2
28)
Influe
nza
vacc
inat
ion
p-va
lue
Odd
s R
atio
(95%
Con
fide
ntia
l Int
erva
l)
Yes
(n=
301)
No
(n=927)
null
Indi
vidu
al le
vel
Hos
pita
l lev
elM
ultile
vel
Indi
vidu
al le
vel
Age
41.
3 ±
12.
542.1
± 1
2.5
41.
0 ±
12.5
0.1
951.
00(0
.99-
1.02
)1.
00(
0.9
9-1.
02)
Sex
(m
ale)
1,143
(93.
1)286(
25.0
)857
(75.
0)0.1
271.
92(1
.01-
3.66
)1.
94(
1.0
2-3.
70)
Mar
ital
sta
tus
Sin
gle
697
(56.
8)170(
24.4
)527
(75.
6)
0.0
04
ref
ref
Mar
ried
298
(24.
3)82
(27.
5)216
(72.
5)1.
23(0
.79-
1.92
)1.
24(
0.8
0-1.
94)
Div
orce
d /
bere
aved
/ se
para
ted
141
(11.
5)40
(28.
4)101
(71.
6)1.
43(0
.86-
2.39
)1.
44(
0.8
6-2.
41)
Oth
ers
92(7
.5)
9(9
.8)
83(
90.2
)0.
40(0
.18-
0.89
)0.
41(
0.1
8-0.
89)
CD
4 T
cell
coun
ts (N
adir)
<200
326
(26.
5)81
(24.
8)245
(75.
2)
0.9
71
0.89
(0.6
1-1.
30)
0.88(
0.6
0-1.
30)
200-
350
393
(32.
0)97
(24.
7)296
(75.
3)0.
94(0
.67-
1.34
)0.
94(
0.6
6-1.
33)
≥350
509
(41.
5)123(
24.2
)386
(75.
8)re
fre
f
HIV
viral
load
(Pea
k)
<50
464
(37.
8)121(
26.1
)343
(73.
9)0.3
20re
fre
f
≥50
764
(62.
2)180(
23.6
)584
(76.
4)0.
79(0
.57-
1.10
)0.
79(
0.5
7-1.
10)
Num
ber
of A
RT
line
3.5
± 2
.44.1
± 2
.43.
2 ±
2.3
<0.0
001
1.16
(1.0
9-1.
24)
1.16(
1.0
9-1.
24)
Com
orbi
dities
407
(33.
1)114(
28.0
)293
(72.
0)0.0
451.
01(0
.73-
1.41
)1.
01(
0.7
2-1.
40)
Hos
pita
l lev
el
No.
of
beds
<1,0
00
300
(24.
4)68
(22.
7)232
(77.
3)
<0.0
001
ref
ref
<1,5
00
583
(47.
5)185(
31.7
)398
(48.
3)0.7
1(0.
17-3.0
6)0.
81(
0.2
0-3.
35)
≥1,5
00
345
(28.
1)48
(13.
9)297
(86.
1)0.1
9(0.
03-1.0
6)0.
19(
0.0
4-1.
03)
Bet
wee
n co
mm
unity
varian
ce
1.
552
01.4
529
1.6
604
1.55
75
PC
V (Perc
enta
ge c
hang
e in
var
ianc
e)
-
-6.
39%
6.9
8%0.
35%
Bet
wee
n co
mm
unity
varian
ce (S.E
.)0.
699
20.6
615
0.7
909
0.76
14
Bet
wee
n co
mm
unity
varian
ce (p-
valu
e)<0
.0001
<0.0
001
0.0
01
<0.0
001
Mod
el f
it-2 R
es L
L58
21.
98589
9.6
658
52.
955929
.34
ICC
(In
tra-
clas
s co
rrel
atio
n)
0.
320
80.3
066
0.3
356
0.32
15
Tabl
e 4-
1. M
ulti-le
vel a
naly
sis:
Inf
luen
cing
fac
tors
for
Influe
nza
vacc
inat
ion

297
Tota
l(n
=1,1
58)
Pne
umoc
occa
l vac
cina
tion
p-va
lue
Odd
s R
atio
(95%
Con
fide
ntia
l Int
erva
l)
Y
es (n=
248
)N
o (n
=910
)nu
llIn
divi
dual
leve
lH
ospi
tal l
evel
Mul
tile
vel
Indi
vidu
al le
vel
Age
41.
3 ±
12.5
41.9
± 1
1.5
41.1
± 1
2.7
0.3
501.0
1(0.
99-1.0
3)1.
01(0
.99-
1.03
)
Sex
(m
ale)
1,076
(92.
9)22
9(21
.3)
847(
78.7
)0.6
880.6
3(0.
33-1.2
2)0.
63(0
.33-
1.22
)
Mar
ital s
tatu
s
Sin
gle
658
(56.
8)14
9(22
.6)
509(
77.4
)
0.0
08
ref
ref
Mar
ried
283
(24.
5)65(
23.0
)21
8(77
.0)
0.7
7(0.
46-1.2
8)0.
77(0
.47-
1.29
)
Div
orce
d /
bere
aved
/ se
para
ted
130
(11.
2)28(
21.5
)10
2(78
.5)
0.7
2(0.
39-1.3
4)0.
72(0
.39-
1.35
)
Oth
ers
87(7
.5)
6(6.9
)81(
93.
1)0.3
4(0.
13-0.9
0)0.
34(0
.13-
0.89
)
CD
4 T
cell
coun
ts (N
adir)
<200
316
(27.
3)64(
20.2
)25
2(79
.8)
0.0
14
0.9
2(0.
60-1.4
2)0.
92(0
.59-
1.42
)
200
-350
375
(32.
4)65(
17.3
)31
0(82
.7)
0.7
0(0.
46-1.0
6)0.
70(0
.46-
1.06
)
≥35
0467
(40.
3)11
9(25
.5)
348(
74.5
)re
fre
f
HIV
vira
l loa
d (P
eak)
<50
430
(37.
1)12
0(27
.9)
310(
72.1
)<0
.0001
ref
ref
≥50
728
(62.
9)12
8(17
.6)
600(
82.4
)0.6
3(0.
43-0.9
2)0.
63(0
.43-
0.92
)
Hos
pita
l lev
el
No.
of
beds
<1,0
00290
(25.
0)43(
14.8
)24
7(85
.2)
<0.0
001
ref
ref
<1,5
00551
(47.
6)15
8(28
.7)
393(
71.3
)1.4
4(0.3
1-6.6
1)1.
59(0
.36-
7.05
)
≥1,
500
317
(27.
4)47(
14.8
)27
0(85
.2)
0.5
8(0.0
9-3.5
9)0.
55(0
.09-
3.47
)
Bet
wee
n co
mm
unity
varian
ce
1.6
222
1.558
61.
7377
1.6
386
PC
V (Per
cent
age
chan
ge in
var
ianc
e)
-
-4%
7%
1%
Bet
wee
n co
mm
unity
varian
ce (S.E
.)0.7
044
0.681
00.
7913
0.7
561
Bet
wee
n co
mm
unity
varian
ce (p-
valu
e)<0
.000
10.0
05
<0.0
001
0.01
0
Mod
el f
it-2 R
es L
L579
2.84
5888.
745806
.79
590
2.22
ICC
(In
tra-
clas
s co
rrel
atio
n)
0.3
305
0.321
70.
3459
0.3
327
Tabl
e 4-
2. M
ulti-le
vel a
naly
sis:
Inf
luen
cing
fac
tors
for
Pne
umoc
occa
l vac
cina
tion

298
Tota
l(n
=962)
Hep
atitis
B v
acci
nation
p-va
lue
Odd
s R
atio
(95
% C
onfide
ntia
l Int
erva
l)
Y
es (n=
405)
No
(n=55
7)nu
llIn
divi
dual
leve
lH
ospi
tal l
evel
Mul
tile
vel
Indi
vidu
al le
vel
Age
41.
1 ±
12.
239.1
± 1
1.7
42.
6 ±
12.4
<0.0
001
0.98(
0.9
7-1.
00)
0.9
8(0.
97-1.0
0)
Sex
(m
ale)
895(
93.
0)381(
42.6
)514
(57.
4)0.2
81
0.92(
0.5
1-1.
65)
0.9
2(0.
51-1.6
5)
Mar
ital
sta
tus
Sin
gle
559(
58.
1)269(
48.1
)290
(51.
9)
<0.0
001
ref
ref
Mar
ried
242(
25.
2)82
(33.
9)160
(66.
1)0.
78(
0.5
1-1.
20)
0.7
8(0.
51-1.2
0)
Div
orce
d /
bere
aved
/ se
para
ted
112(
11.
6)41
(36.
6)71(
63.4
)0.
81(
0.4
8-1.
36)
0.8
1(0.
48-1.3
5)
Oth
ers
49(
5.1
)13
(26.
5)36(
74.5
)0.
79(
0.3
8-1.
65)
0.8
0(0.
38-1.6
8)
CD
4 T
cell
coun
ts (N
adir)
<200
256(
26.
6)105(
41.0
)151
(59.
0)
<0.0
001
0.88(
0.6
1-1.
27)
0.8
8(0.
61-1.2
7)
200
-350
301(
31.
3)100(
33.2
)201
(66.
8)0.
54(
0.3
9-0.
77)
0.5
4(0.
39-0.7
6)
≥35
0405(
42.
1)200(
49.4
)205
(50.
6)re
fre
f
HIV
vira
l loa
d (P
eak)
<50
370(
38.
5)171(
46.2
)199
(53.
8)0.0
41
ref
ref
≥50
592(
61.
5)234(
39.5
)358
(60.
5)0.
87(
0.6
4-1.
20)
0.8
8(0.
64-1.2
0)
Num
ber
of A
RT
line
3.4 ±
2.2
3.1
± 2
.23.
5 ±
2.2
0.0
05
0.96(
0.9
0-1.
02)
0.9
6(0.
90-1.0
2)
Hos
pita
l lev
el
No.
of
beds
<1,0
00244(
25.
3)92
(37.
7)152
(62.
3)
0.1
69
ref
ref
<1,5
00448(
46.
6)189(
42.2
)259
(57.
8)0.
59(0
.16-
2.16
)0.5
2(0.
14-1.9
6)
≥1,
500
270(
28.
1)124(
45.9
)146
(54.
1)1.
25(0
.28-
5.52
)1.2
5(0.
27-5.6
8)
Bet
wee
n co
mm
unity
varian
ce
1.1
519
1.21
86
1.3
412
1.390
6
PC
V (Perc
enta
ge c
hang
e in
var
ianc
e)
-
6%16%
21%
Bet
wee
n co
mm
unity
varian
ce (S.E
.)0.5
270
0.56
28
0.6
274
0.653
6
Bet
wee
n co
mm
unity
varian
ce (p-
valu
e)0.4
12
0.014
0.81
70.0
16
Mod
el f
it-2 R
es L
L41
99.
274278
.83
420
7.2
642
88.
04IC
C (In
tra-
clas
s co
rrel
atio
n)
0.2
595
0.27
05
0.2
898
0.297
3
Tabl
e 4-
3. M
ulti-le
vel a
naly
sis:
Inf
luen
cing
fac
tors
for
Hep
atitis
B v
acci
nation
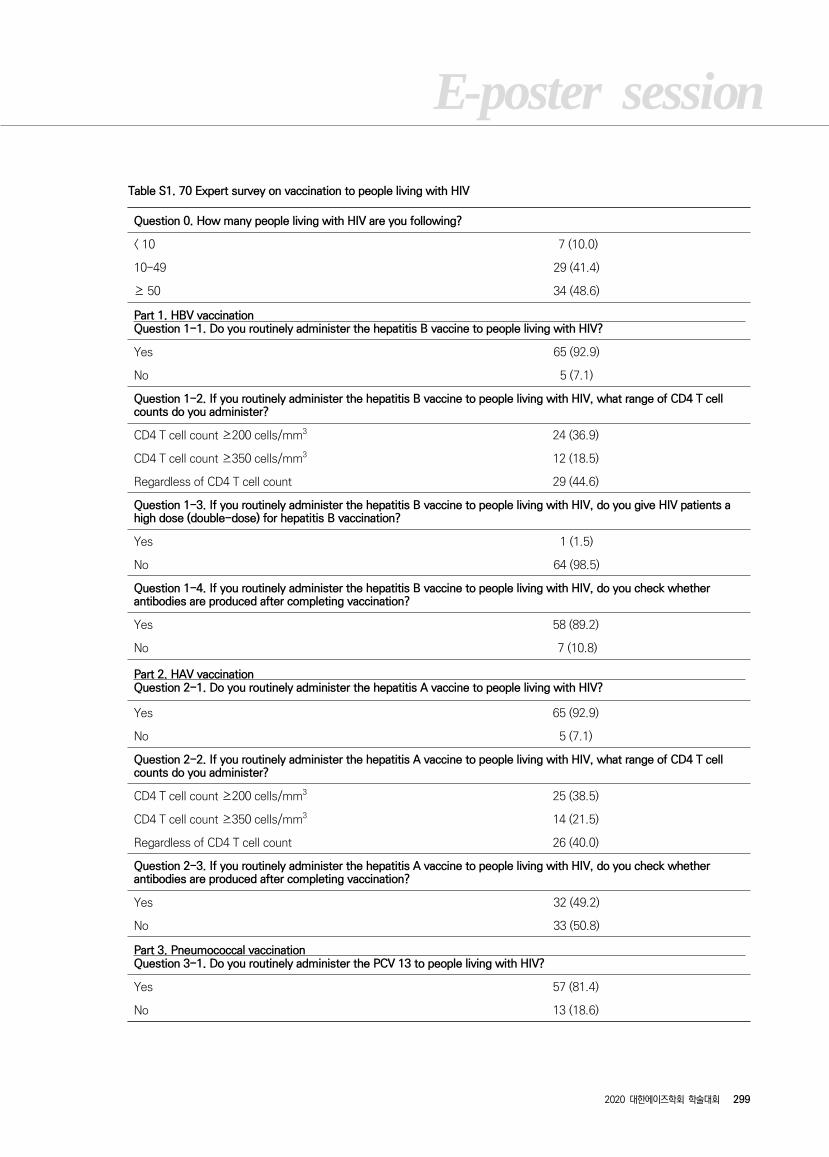
E-poster session
2020 대한에이즈학회 학술대회 299
Question 0. How many people living with HIV are you following?
< 10 7 (10.0)
10-49 29 (41.4)
≥ 50 34 (48.6)
Part 1. HBV vaccinationQuestion 1-1. Do you routinely administer the hepatitis B vaccine to people living with HIV?
Yes 65 (92.9)
No 5 (7.1)
Question 1-2. If you routinely administer the hepatitis B vaccine to people living with HIV, what range of CD4 T cell counts do you administer?
CD4 T cell count ≥200 cells/mm3 24 (36.9)
CD4 T cell count ≥350 cells/mm3 12 (18.5)
Regardless of CD4 T cell count 29 (44.6)
Question 1-3. If you routinely administer the hepatitis B vaccine to people living with HIV, do you give HIV patients a high dose (double-dose) for hepatitis B vaccination?
Yes 1 (1.5)
No 64 (98.5)
Question 1-4. If you routinely administer the hepatitis B vaccine to people living with HIV, do you check whether antibodies are produced after completing vaccination?
Yes 58 (89.2)
No 7 (10.8)
Part 2. HAV vaccinationQuestion 2-1. Do you routinely administer the hepatitis A vaccine to people living with HIV?
Yes 65 (92.9)
No 5 (7.1)
Question 2-2. If you routinely administer the hepatitis A vaccine to people living with HIV, what range of CD4 T cell counts do you administer?
CD4 T cell count ≥200 cells/mm3 25 (38.5)
CD4 T cell count ≥350 cells/mm3 14 (21.5)
Regardless of CD4 T cell count 26 (40.0)
Question 2-3. If you routinely administer the hepatitis A vaccine to people living with HIV, do you check whether antibodies are produced after completing vaccination?
Yes 32 (49.2)
No 33 (50.8)
Part 3. Pneumococcal vaccinationQuestion 3-1. Do you routinely administer the PCV 13 to people living with HIV?
Yes 57 (81.4)
No 13 (18.6)
Table S1. 70 Expert survey on vaccination to people living with HIV
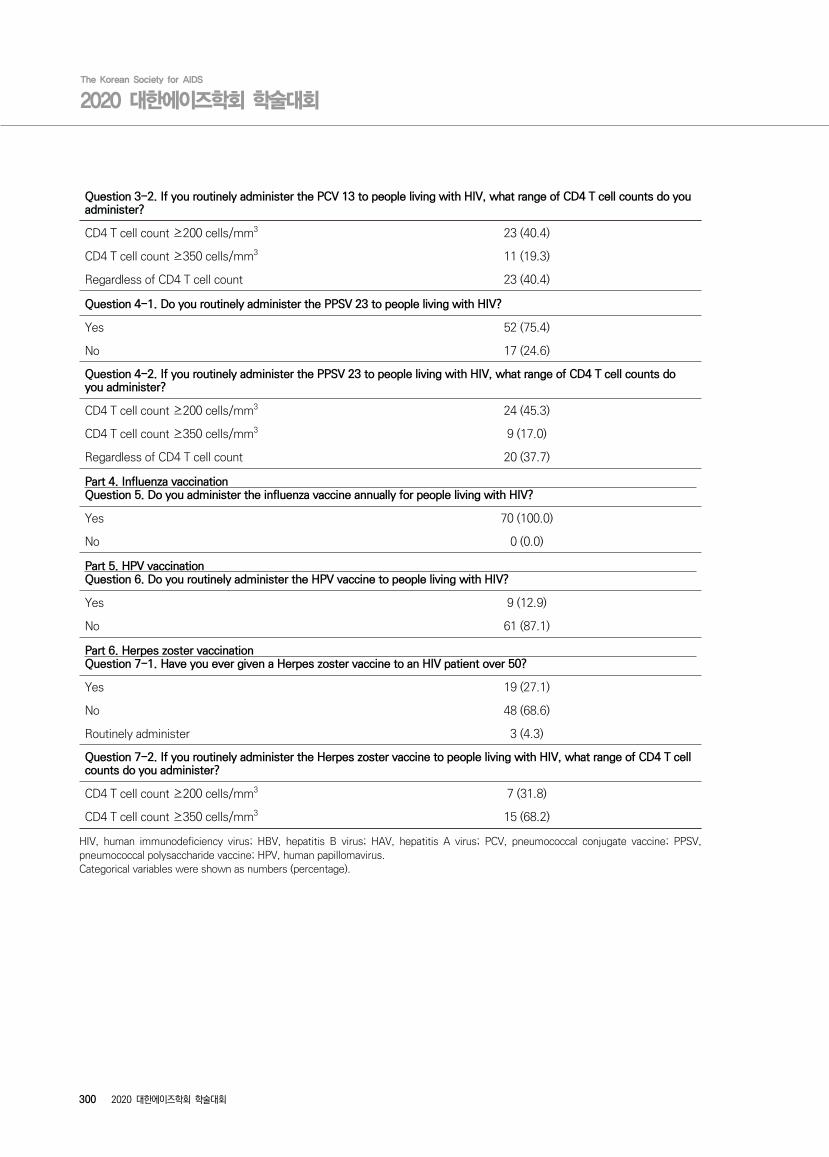
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
300 2020 대한에이즈학회 학술대회
Question 3-2. If you routinely administer the PCV 13 to people living with HIV, what range of CD4 T cell counts do you administer?
CD4 T cell count ≥200 cells/mm3 23 (40.4)
CD4 T cell count ≥350 cells/mm3 11 (19.3)
Regardless of CD4 T cell count 23 (40.4)
Question 4-1. Do you routinely administer the PPSV 23 to people living with HIV?
Yes 52 (75.4)
No 17 (24.6)
Question 4-2. If you routinely administer the PPSV 23 to people living with HIV, what range of CD4 T cell counts do you administer?
CD4 T cell count ≥200 cells/mm3 24 (45.3)
CD4 T cell count ≥350 cells/mm3 9 (17.0)
Regardless of CD4 T cell count 20 (37.7)
Part 4. Influenza vaccinationQuestion 5. Do you administer the influenza vaccine annually for people living with HIV?
Yes 70 (100.0)
No 0 (0.0)
Part 5. HPV vaccinationQuestion 6. Do you routinely administer the HPV vaccine to people living with HIV?
Yes 9 (12.9)
No 61 (87.1)
Part 6. Herpes zoster vaccinationQuestion 7-1. Have you ever given a Herpes zoster vaccine to an HIV patient over 50?
Yes 19 (27.1)
No 48 (68.6)
Routinely administer 3 (4.3)
Question 7-2. If you routinely administer the Herpes zoster vaccine to people living with HIV, what range of CD4 T cell counts do you administer?
CD4 T cell count ≥200 cells/mm3 7 (31.8)
CD4 T cell count ≥350 cells/mm3 15 (68.2)
HIV, human immunodeficiency virus; HBV, hepatitis B virus; HAV, hepatitis A virus; PCV, pneumococcal conjugate vaccine; PPSV, pneumococcal polysaccharide vaccine; HPV, human papillomavirus.Categorical variables were shown as numbers (percentage).

E-poster session
2020 대한에이즈학회 학술대회 301
의료기관감염인상담사업 2015 2016 2017 2018 2019
내원
감염인
전체 내원감염인 5927 6629 7236 8873 9978
성별
N (%)
male490
(92.6)
6143
(93)
6708
(93)
8206
(92.5)
9247
(92.7)
female 437(7.4) 486(7) 528(7) 667(7.5) 723(7.3)
나이
N (%)
0~9 2(0) 0(0) 0(0) 2(0) 2(0)
10~19 48(0.8) 37(0.5) 34(1) 35(0.4) 27(0.3)
20~29996
(16.8)
1231
(18.5)
1356
(19)
1530
(17.4)
1635
(16.4)
30~391448
(24.4)
1605
(24)
1678
(23)
2064
(23.5)
2457
(24.6)
40~491621
(27.3)
1735
(26)
1876
(26)
2160
(24.6)
2409
(24.1)
50~591111
(18.7)
1295
(20)
1419
(20)
1792
(20.4)
2064
(20.7)
60 이상701
(11.8)
724
(11)
649
(9)
1189
(13.6)
1384
(13.9)
P-24 Epidemiology and social research
의료기관감염인상담사업 지표로 본 감염인 건강관리 현황
: 2015 년~2019 년 시계열 분석
최재필1, 이정휘 1, 서아영 1, 의료기관감염인상담사업단 2
1 서울의료원 감염내과, 226 개 의료기관감염인상담사업 사업책임자 및 상담간호사, 코디네이터
배경: 의료기관감염인상담사업은 2006 년부터 본사업을 시작하여 2020 년 14 년차로 26 개의 의료기관에서 수행되고
있다. 의료기관에서 HIV 관련 상담간호사의 전문적인 상담을 통해 감염인의 질병적응과 건강관리를 돕고 심리적 안정을
도모하여 복약 순응도를 높이고 궁극적으로 감염인의 삶의 질 향상과 HIV 전파 예방을 위하여 시행되고 있다. 자료는 1
년 단위로 보고서형태로 작성되고만 있어 본 연구에서는 최근 5 개년도의 보고서 자료를 이용하여 지표변화를 시계열 분
석하고자 한다.
방법: 2015 년~2019 년 상담사업 최종보고 자료와 2020 년 사업중간보고 자료를 이용하여 기본적인 인구학적 지표,
사업지표인 복약순응도, 우울ㆍ불안 중재율, 바이러스 미검출을 비교하였다.
결과: 2015 년 5927 명(전국 생존감염인 대비 56.4%)에서 증가하여 2020 년 9,978 명(72%)의 감염인이 상담사업
의료기관을 방문하고, 그중 89.9%의 감염인이 상담을 이용하고 있다.
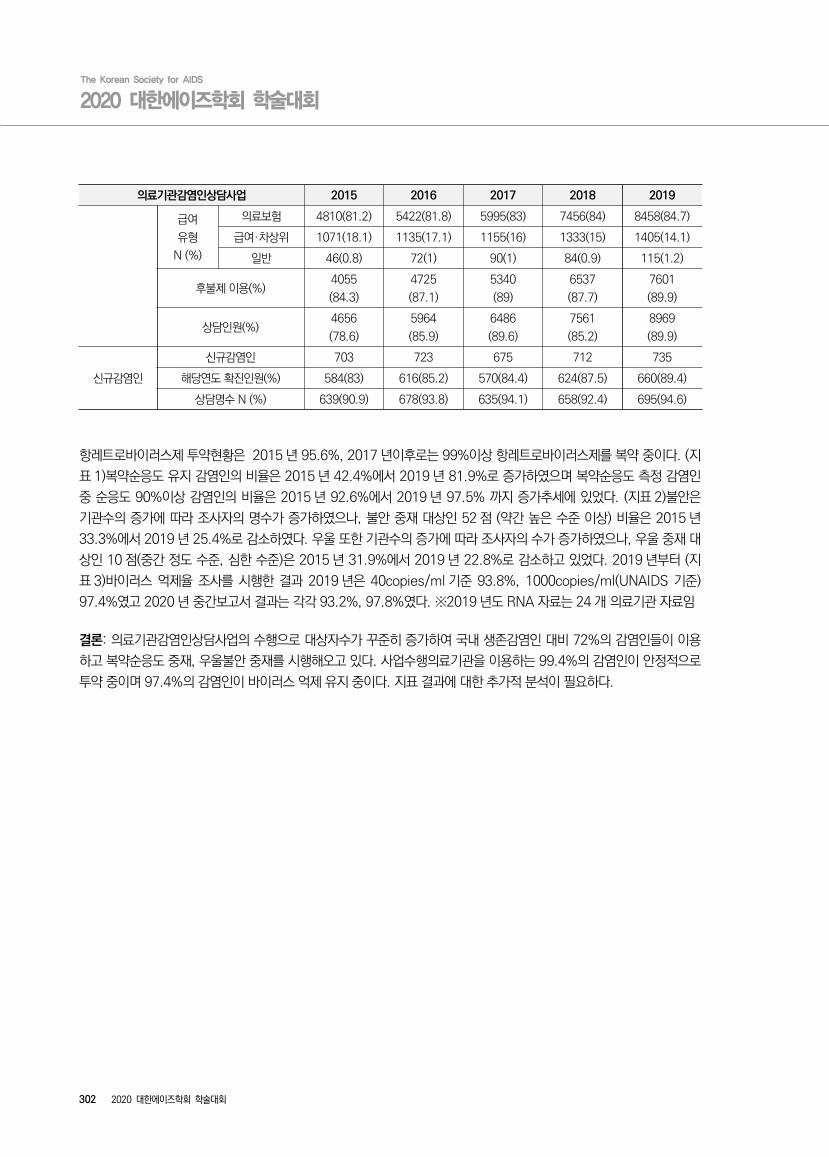
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
302 2020 대한에이즈학회 학술대회
의료기관감염인상담사업 2015 2016 2017 2018 2019
급여
유형
N (%)
의료보험 4810(81.2) 5422(81.8) 5995(83) 7456(84) 8458(84.7)
급여·차상위 1071(18.1) 1135(17.1) 1155(16) 1333(15) 1405(14.1)
일반 46(0.8) 72(1) 90(1) 84(0.9) 115(1.2)
후불제 이용(%)4055
(84.3)
4725
(87.1)
5340
(89)
6537
(87.7)
7601
(89.9)
상담인원(%)4656
(78.6)
5964
(85.9)
6486
(89.6)
7561
(85.2)
8969
(89.9)
신규감염인
신규감염인 703 723 675 712 735
해당연도 확진인원(%) 584(83) 616(85.2) 570(84.4) 624(87.5) 660(89.4)
상담명수 N (%) 639(90.9) 678(93.8) 635(94.1) 658(92.4) 695(94.6)
항레트로바이러스제 투약현황은 2015 년 95.6%, 2017 년이후로는 99%이상 항레트로바이러스제를 복약 중이다. (지
표 1)복약순응도 유지 감염인의 비율은 2015 년 42.4%에서 2019 년 81.9%로 증가하였으며 복약순응도 측정 감염인
중 순응도 90%이상 감염인의 비율은 2015 년 92.6%에서 2019 년 97.5% 까지 증가추세에 있었다. (지표 2)불안은
기관수의 증가에 따라 조사자의 명수가 증가하였으나, 불안 중재 대상인 52 점 (약간 높은 수준 이상) 비율은 2015 년
33.3%에서 2019 년 25.4%로 감소하였다. 우울 또한 기관수의 증가에 따라 조사자의 수가 증가하였으나, 우울 중재 대
상인 10 점(중간 정도 수준, 심한 수준)은 2015 년 31.9%에서 2019 년 22.8%로 감소하고 있었다. 2019 년부터 (지
표 3)바이러스 억제율 조사를 시행한 결과 2019 년은 40copies/ml 기준 93.8%, 1000copies/ml(UNAIDS 기준)
97.4%였고 2020 년 중간보고서 결과는 각각 93.2%, 97.8%였다. ※2019 년도 RNA 자료는 24 개 의료기관 자료임
결론: 의료기관감염인상담사업의 수행으로 대상자수가 꾸준히 증가하여 국내 생존감염인 대비 72%의 감염인들이 이용
하고 복약순응도 중재, 우울불안 중재를 시행해오고 있다. 사업수행의료기관을 이용하는 99.4%의 감염인이 안정적으로
투약 중이며 97.4%의 감염인이 바이러스 억제 유지 중이다. 지표 결과에 대한 추가적 분석이 필요하다.

E-poster session
2020 대한에이즈학회 학술대회 303
P-25 Epidemiology and social research
남성 동성애자 대상 성 건강 결정 영향요인
양혜진
건양대학교 간호대학 간호학과
연구배경: 우리나라는 2004 년 성매매특별법이 시행되고, 과거 유교문화에서 개방적인 성문화로 변모하면서 자유로운
성적 교류가 확산되면서 성 매개 감염병의 발생빈도가 높아지고, 그 중 바이러스성 성 매개 감염병은 지속적으로 증가하
는 추세에 있으며, 매질, 임질과 같은 성 매개 감염병은 HIV 의 전파 및 감염의 위험성을 2-3 배 증가시킨다.
우리나라는 주로 남성 동성애자들 간의 성 접촉을 통해 확산되는 1 단계이며, HIV/AIDS 유병률은 0.1%로, 다른 나라
에 비해서 유병율이 낮은 편이다. 하지만, 국가의 치료비 지원정책에 있어서는 경제적 장벽이 낮음에도 불구하고 남성 동
성애자의 HIV 수검율은 2008 년 22%로낮은 편이다.
이에 HIV 감염 및 성매개감염병 취약군인 남성 동성애자 대상으로 성 건강 자기결정에 영향요인으로 예측되는 주요변수
인 성 건강지식, 성태도, 성정체성, 성적 자율성을 중심으로 이 요인들이 남성 동성애자 대상의 성 건강 자기결정성에 미
치는 영향요인을 파악함으로써 남성 동성애자 대상 상담 및 교육프로그램의 기초자료로 활용하고자 한다.
연구방법:이반시티(IVANCITY) 홈페이지에 접속하는 남성 동성애자 대상으로 성 건강지식, 성 태도, 성 정체성, 성적 자
율성, 성 건강 자기결정의 정도를 알아보고, 그들 간의 관계를 살펴보면서, 성 건강 자기결정서에 영향을 주는 요인을 알
아보기 위한 서술적 단면조사연구이다.
연구결과: 총 217 명에 대해 분석하였으며, 대상자의 212 명(97.7%)가 남성이었으며, 대상자의 연령은 평균 연령은
37.42±9.95 세였다. 이변량 분석에서 성 지식에 영향을 미친 요인으로는 교육수준과 성 정체감에 통계적으로 유의한
차이가 있는 것으로 나타났고, 성 허용성에서는 거주지역, 성 태도에서는 도시지역유무, 성 정체감, 성 자율성과 성 건강
결정성에서 성 정체성에서 통계적으로 유의한 차이가 있는 것으로 나타났다. 남성 동성애자 대상으로 성 건강 결정에 영
향을 미치는 요인을 확인하기 위해 성 정체성과 성 자율성 단계적 다중회귀분석을 실시한 결과, 성적 자율성이 54%의
설명력을 보여주었다.
결론: 남성 동성애자 대상으로 성 건강 결정에 영향을 미치는 요인으로 성적 자율성이 영향을 미치는 것으로 확인되었다.
추후 이들 대상으로 성교육 프로그램 개발 및 운영 시 필요한 교육전략의 기초자료를 마련할 수 있을 것으로 생각된다.
Keywords: 지식, 태도, 자율성, 성 건강 결정, 남성 동성애자
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
304 2020 대한에이즈학회 학술대회
P-26 Epidemiology and social research
Stuck in Neutral: Identifying opportunities to make
progress in addressing HIV-related stigma and other
emotional and psychosocial unmet needs among people
living with HIV in South Korea
Sungshin Kwon1, Benjamin Young2, Ki Hyon Kim3, Piotr Budnik4, Dannae Brown5, Nathalie Dang3, Chinyere Okoli4, Patricia de
los Rios6
1GSK Healthcare, Seoul Korea; 2ViiV Healthcare Research Triangle NC US; 3ViiV Healthcare, Singapore; 4ViiV Healthcare Brentford Middlesex England; 5ViiV Healthcare Abbotsford Australia; 6ViiV Healthcare Quebec Canada
Background: Much progress has been made in HIV prevention and control in South Korea in recent
years. During 2017, there were 1,307 new diagnoses of HIV, down from a peak of 3,496 in the year
2000. Of the estimated 25,557 people living with HIV (PLHIV) in the country in 2017, HIV-specific
mortality rate in that year was less than 1%, attesting to high uptake and utilization of antiretroviral
therapy (ART). Yet, major barriers to HIV care remain, including HIV stigma and homophobia. Delivering
HIV care in a manner that helps PLHIV rise above these challenges is critical to ensuring retention in
care, adherence, and improved quality of life. The World Health Organization’s definition of health as
well as the proposed “fourth 90” target both go beyond merely ensuring “absence of disease or
infirmity”, rather, they focus on promoting health-related quality of life. We investigated the extent of
physical, emotional, and psychosocial challenges of ART among PLHIV in South Korea.
Methods: We analyzed self-reported data for 50 PLHIV aged 18+ years on ART in South Korea who
participated in the 2019 Positive Perspectives study, an international, web-based survey conducted in a
total of 25 countries. Data were collected regarding ART-related experiences and perceptions, including
whether participants had ever disguised/hidden their HIV medication to avoid sharing their HIV status,
perceived comfort with sharing their HIV status, individuals they had shared their HIV status with, as
well as reasons for ever refusing to share. Participants were also asked a series of questions regarding
perceptions towards daily oral intake of ART, number of times they missed ART within the past month,
and reasons for missing. We computed overall prevalence estimates for South Korea to quantify the
diverse treatment challenges. We further examined differences in stigma experiences by sexual
orientation in South Korea and contrasted that with other Asian countries in the Positive Perspectives
study (Japan, n = 75; Taiwan, n = 55; China, n = 50). Prevalence differences in markers of perceived
structural stigma between PLHIV identifying as heterosexual vs as homosexual/other sexual orientation

E-poster session
2020 대한에이즈학회 학술대회 305
were calculated; larger differences were taken as greater stigma among the disadvantaged group.
Prevalence estimates were compared with c2 tests at p<0.05.
Results: Mean age of participants in South Korea was 36.3 (SD=11.2) years; mean HIV duration was 5.2
(SD=5.0) years. Overall, 58%[29/50] identified as men and 68%[34/50] as heterosexual. Of all
participants, 84%[42/50] had ever disguised their HIV medications in the past 6 months, and
62%[31/50] indicated they would be very anxious if someone were to see their HIV medication.
Furthermore, 46%[23/50] experienced side effects from their HIV medicines, 56%[28/50] had difficulty
swallowing pills, and 62%[31/50] admitted that the overall impact of HIV on their life was negative.
Regarding emotional challenges related to daily ART within the overall South Korean sample,
48%[24/50] felt it limited their life, 56%[28/50] were stressed by it, 58%[29/50] said it reminded them
of their HIV, 44%[22/50] associated it with bad memories, 46%[23/50] were worried of forgetting to
take their ART as prescribed, and 56%[28/50] were concerned that taking HIV medicines every day
increased the chances of someone knowing their HIV status. Disparities existed in perceived stigma by
sexual orientation in South Korea; PLHIV identifying as homosexual/other sexual orientation were eight
times more likely than those identifying as heterosexual to report they had ever refused to share their
HIV status because "I was worried about my physical safety/potential violence" (25%[4/16] vs
3%[1/34], p = 0.015). They were also more likely to be concerned (2-3 times higher, all p<0.05) about
being treated differently (94%[15/16] vs 44%[15/34]), of losing their friendships from sharing their
status (88%[14/16] vs 26%[9/34]), of losing their jobs if their HIV status became known (69%[11/16] vs
24%[8/34]), that sharing their HIV status might affect their romantic relationships (50%[8/16] vs
15%[5/34]), and of being excluded from social activities because of their HIV (63%[10/16] vs
29%[10/34]). Interestingly, none of these differences were statistically significant by gender (men vs
women). For each of these markers of perceived structural stigma, the inequality by sexual orientation
was highest in South Korea compared to the other countries in the Asian region. Of all participants in
South Korea, 70%[35/50] were interested in a nondaily ART regimen.
Conclusion: Physical, emotional, and psychosocial challenges are common among PLHIV. Perceived
stigma was prominent along the lines of sexual orientation, but not gender. Participants identifying as
homosexual/other sexual orientation reported disproportionately higher stigma experience compared to
heterosexual, and this gap was wider in South Korea than other Asian countries surveyed. It is
important to recalibrate social norms regarding HIV stigma and homophobia. In addition, treatment
alternatives that make HIV a less conspicuous part of the lives of PLHIV (e.g., nondaily regimens) may
reduce perceived disruption of their lives from HIV or HIV treatment, thereby potentially improving
health-related quality of life as espoused in the “fourth 90” target.
Keywords: Antiretrovirals, Difficulty swallowing, Privacy, Quality of life, Stigma
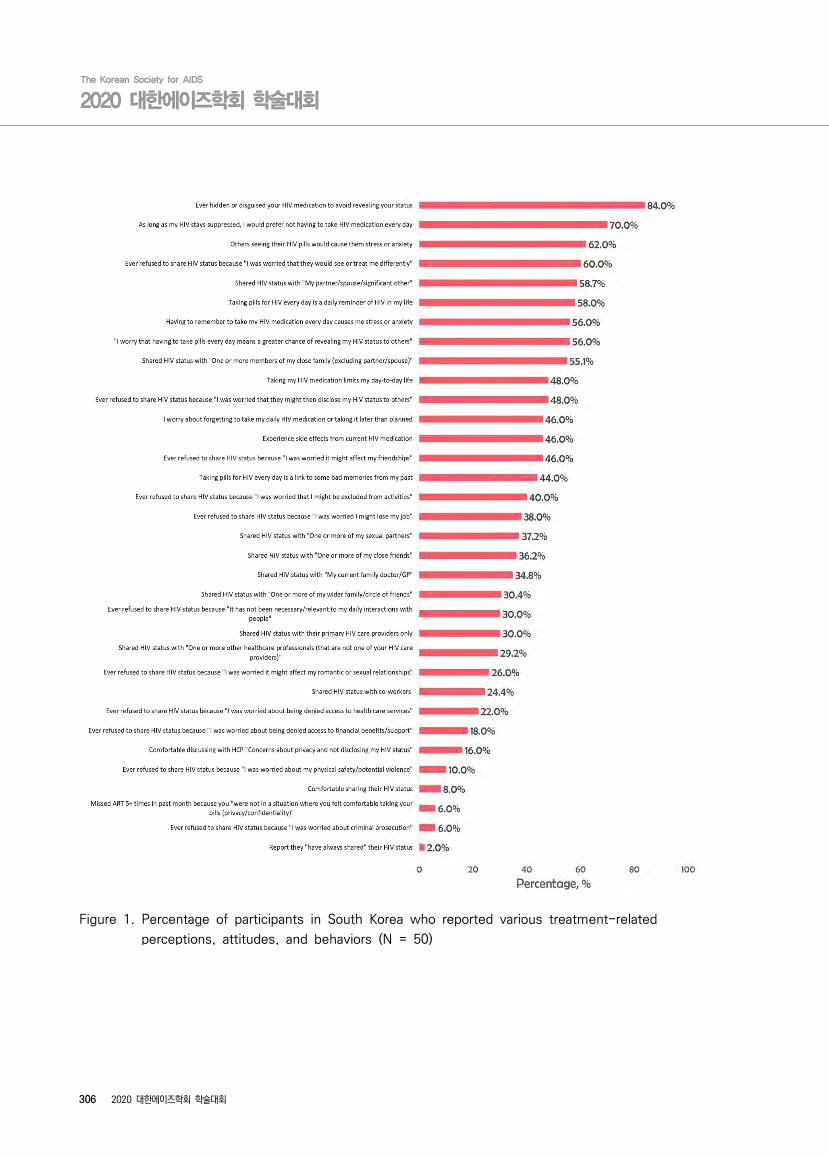
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
306 2020 대한에이즈학회 학술대회
Figure 1. Percentage of participants in South Korea who reported various treatment-related
perceptions, attitudes, and behaviors (N = 50)

E-poster session
2020 대한에이즈학회 학술대회 307
Figure 2. Indicators of perceived stigma, stratified by sexual orientation, among people living with
HIV in South Korea (N = 50)
Note: Asterisks indicate p < 0.05 based on chi-squared tests
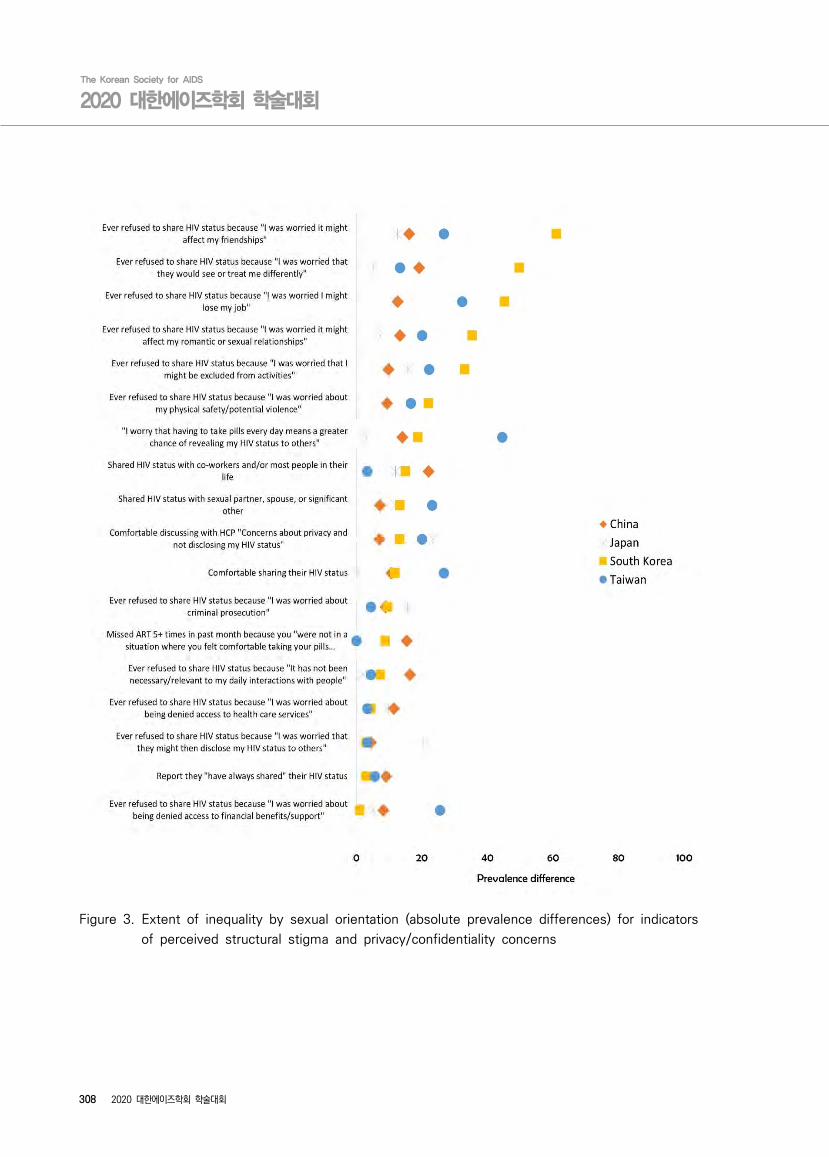
The Korean Society for AIDS
2020 대한에이즈학회 학술대회
308 2020 대한에이즈학회 학술대회
Figure 3. Extent of inequality by sexual orientation (absolute prevalence differences) for indicators
of perceived structural stigma and privacy/confidentiality concerns
2020 대한에이즈학회
학술대회인 쇄
발 행
발 행 처
편 집 제 작
2020년 11월 20일
2020년 11월 20일
대한에이즈학회서울시 서초구 서초대로 74길 23서초타운트라팰리스 806Tel: 02-3487-1755, Fax: 02-6499-1755E-mail: [email protected]: www.kosaids.or.kr
(주) 캡스톤 그룹 (CAPSTONE Group)(04147) 서울특별시 마포구 백범로 31길 21 본관6층Tel : 02-6010-8500E-mail : [email protected]