Editorial - Peshawar Medical College
98
Ophthalmology Update Vol. 10. No. 3, July-September 2012 209 Diabetic Retinopathy – Update Editorial T he number of diabetics worldwide is likely to grow to 429 million by 2030, owing to the rising frequency of obesity, increasing life span, and improved methods of detection of the disease. The increase in Diabetes Mellitus (DM) denotes an urgency to prevent retinopathy which requires both a better under-standing of the mechanism and improved means of detecting retinopathy. The treatment relies almost exclusively on managing the deranged metabolism in DM until the severity of vascular lesions, which warrants laser treatment. Intensive metabolic control remains a highly effective means of controlling retinopathy and other diabetes-related complications. Recent research has identified the central role of vascular endothelial growth factor (VEGF) in the vascular lesions and the use of new agents that block VEGF action. Despite advances in diabetes care, complications persist for various reasons. Proliferative DR and other complications develop even after 30 years in up to 20% of persons with diabetes who have been treated with intensive metabolic control. The fact that treatment of vascular complications in the retina preserves vision in diabetics, highlights the interconnectedness of the neural retina with the retinal vasculature and the functional neurovascular unit which is considered to be the basis of molecular interaction of neural, glial and vascular cells in the retina. Past and Present: The features of DR as detected by ophthalmoscopy, were described in the 19th century. They begin with micro-aneurysms and progress into exudative changes (leakage of lipoproteins-hard exudates) and blood (blot hemorrhages) that lead to macular edema. The clinical features of DR are ischemic changes (infarcts of the nerve-fiber layer- cotton-wool spots), collateralization (intra-retinal microvascular abnormalities), dilatation of venules (venous beading), and proliferative changes (abnormal vessels on the optic disc and retina, proliferation of fibroblasts, and vitreous hemorrhage). Persons with mild to moderate non-proliferative retinopathy have impaired contrast sensitivity and visual fields that cause difficulty with driving, reading and other activities of daily life. Visual acuity declines when the macula is affected by edema, ischemia, epiretinal membranes and retinal detachment. Fifty years ago PDR was treated by means of pituitary ablation resulting in complications related to hypopituitarism including death, prompted the development of pan-retinal photocoagulation which showed the dramatic effects and significantly reduced the severe visual loss. The incidence and the risk of progression of diabetic retinopathy have both declined over the past 30 years from 90% to 50%. The population- based Wisconsin Epidemiologic Study showed that from 1980 to 2007, the estimated incidence of proliferative diabetic retinopathy (PDR) has decreased by 77% and vision impairment decreased by 57% with type 1 diabetes and much lower risk of PDR, macular edema, and visual impairment. These improvements have resulted from the introduction of new devices for self-monitoring of blood-glucose levels, administration of insulin, new medications, surgical interventions (including vitrectomy), an increased awareness for intensive control of glycemia and blood pressure with implementation of educational and screening programs; yet the benefits of intensive control are negated by a 33% increase in the frequency of hypoglycemia and a 100% increase in the prevalence of obesity. The percentage of persons with type 2 diabetes who meet the target levels for glycated hemoglobin, blood pressure, or serum total cholesterol have increased by 30 to 50% from 2000 to 2006, but it remains uncertain whether the lifestyle changes and
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Editorial - Peshawar Medical College

Ophthalmology Update Vol. 10. No. 3, July-September 2012 209
Diabetic Retinopathy – Update
Editorial
The number of diabetics worldwide is likely togrow to 429 million by 2030, owing to the risingfrequency of obesity, increasing life span, and
improved methods of detection of the disease. Theincrease in Diabetes Mellitus (DM) denotes an urgencyto prevent retinopathy which requires both a betterunder-standing of the mechanism and improvedmeans of detecting retinopathy. The treatment reliesalmost exclusively on managing the derangedmetabolism in DM until the severity of vascular lesions,which warrants laser treatment. Intensive metaboliccontrol remains a highly effective means of controllingretinopathy and other diabetes-related complications.Recent research has identified the central role ofvascular endothelial growth factor (VEGF) in thevascular lesions and the use of new agents that blockVEGF action. Despite advances in diabetes care,complications persist for various reasons. ProliferativeDR and other complications develop even after 30 yearsin up to 20% of persons with diabetes who have beentreated with intensive metabolic control.
The fact that treatment of vascular complicationsin the retina preserves vision in diabetics, highlightsthe interconnectedness of the neural retina with theretinal vasculature and the functional neurovascularunit which is considered to be the basis of molecularinteraction of neural, glial and vascular cells in theretina.Past and Present:
The features of DR as detected byophthalmoscopy, were described in the 19th century.They begin with micro-aneurysms and progress intoexudative changes (leakage of lipoproteins-hardexudates) and blood (blot hemorrhages) that lead tomacular edema. The clinical features of DR areischemic changes (infarcts of the nerve-fiber layer-cotton-wool spots), collateralization (intra-retinalmicrovascular abnormalities), dilatation of venules
(venous beading), and proliferative changes (abnormalvessels on the optic disc and retina, proliferation offibroblasts, and vitreous hemorrhage). Persons withmild to moderate non-proliferative retinopathy haveimpaired contrast sensitivity and visual fields that causedifficulty with driving, reading and other activities ofdaily life. Visual acuity declines when the macula isaffected by edema, ischemia, epiretinal membranes andretinal detachment.
Fifty years ago PDR was treated by means ofpituitary ablation resulting in complications related tohypopituitarism including death, prompted thedevelopment of pan-retinal photocoagulation whichshowed the dramatic effects and significantly reducedthe severe visual loss. The incidence and the risk ofprogression of diabetic retinopathy have both declinedover the past 30 years from 90% to 50%. The population-based Wisconsin Epidemiologic Study showed thatfrom 1980 to 2007, the estimated incidence ofproliferative diabetic retinopathy (PDR) has decreasedby 77% and vision impairment decreased by 57% withtype 1 diabetes and much lower risk of PDR, macularedema, and visual impairment.
These improvements have resulted from theintroduction of new devices for self-monitoring ofblood-glucose levels, administration of insulin, newmedications, surgical interventions (includingvitrectomy), an increased awareness for intensivecontrol of glycemia and blood pressure withimplementation of educational and screeningprograms; yet the benefits of intensive control arenegated by a 33% increase in the frequency ofhypoglycemia and a 100% increase in the prevalenceof obesity. The percentage of persons with type 2diabetes who meet the target levels for glycatedhemoglobin, blood pressure, or serum total cholesterolhave increased by 30 to 50% from 2000 to 2006, but itremains uncertain whether the lifestyle changes and
210 Ophthalmology Update Vol. 10. No. 3, July-September 2012
Editorial
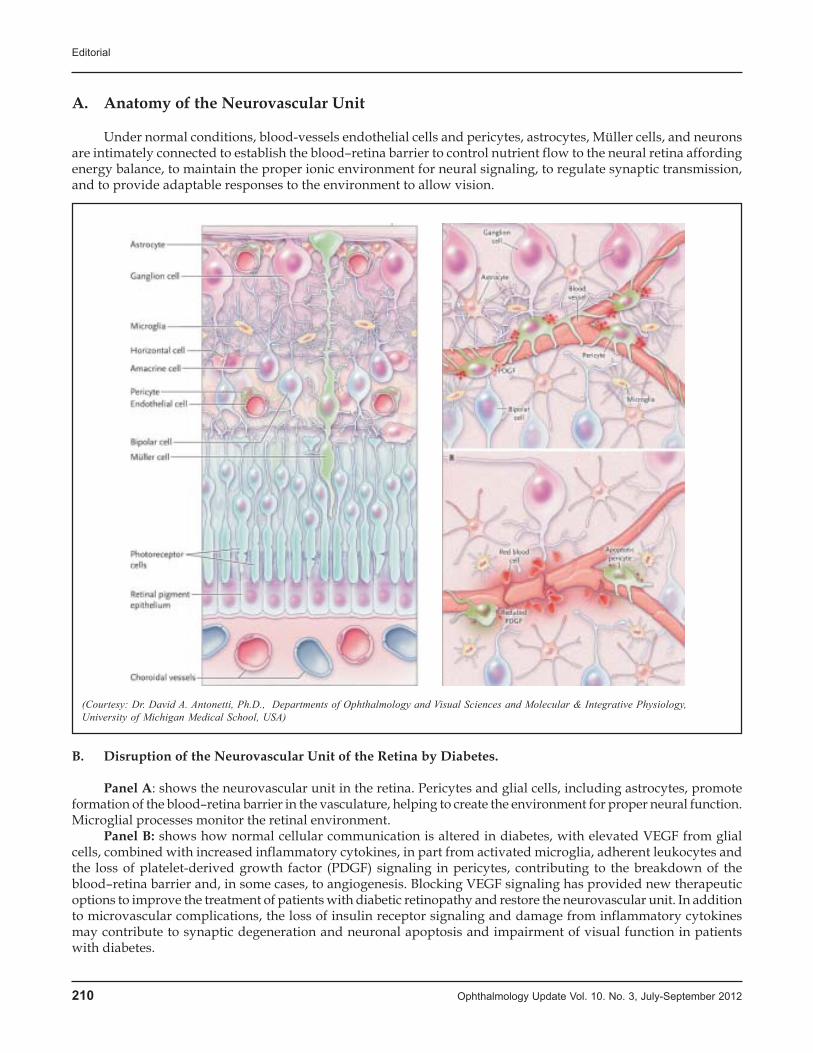
A. Anatomy of the Neurovascular Unit
Under normal conditions, blood-vessels endothelial cells and pericytes, astrocytes, Müller cells, and neuronsare intimately connected to establish the blood–retina barrier to control nutrient flow to the neural retina affordingenergy balance, to maintain the proper ionic environment for neural signaling, to regulate synaptic transmission,and to provide adaptable responses to the environment to allow vision.
B. Disruption of the Neurovascular Unit of the Retina by Diabetes.
Panel A: shows the neurovascular unit in the retina. Pericytes and glial cells, including astrocytes, promoteformation of the blood–retina barrier in the vasculature, helping to create the environment for proper neural function.Microglial processes monitor the retinal environment.
Panel B: shows how normal cellular communication is altered in diabetes, with elevated VEGF from glialcells, combined with increased inflammatory cytokines, in part from activated microglia, adherent leukocytes andthe loss of platelet-derived growth factor (PDGF) signaling in pericytes, contributing to the breakdown of theblood–retina barrier and, in some cases, to angiogenesis. Blocking VEGF signaling has provided new therapeuticoptions to improve the treatment of patients with diabetic retinopathy and restore the neurovascular unit. In additionto microvascular complications, the loss of insulin receptor signaling and damage from inflammatory cytokinesmay contribute to synaptic degeneration and neuronal apoptosis and impairment of visual function in patientswith diabetes.
(Courtesy: Dr. David A. Antonetti, Ph.D., Departments of Ophthalmology and Visual Sciences and Molecular & Integrative Physiology,University of Michigan Medical School, USA)

Ophthalmology Update Vol. 10. No. 3, July-September 2012 211
urbanization in developing countries will result inuncontrolled glycemia, blood pressure, and lipid levels.
Major Pharmacologic studies have revealed thatthe metabolic control, the renin–angiotensin system,peroxisome proliferator activated receptor á (PPAR-á),and VEGF contribute to human pathophysiology.Notably, renin–angiotensin system inhibitors reducethe incidence and risk of progression of DR in personswith type-1 diabetes and is now a standard therapy.The PPAR-á agonist fenofibrate, reduces the risk ofprogression by 40% among patients with non-proliferative retinopathy.However, the mechanism ofaction underlying this preventive effect of fenofibrateis related to its lipid-lowering action remains unclear.
Use of the VEGF-neutralizing antibodiesbevacizumab and ranibizumab improves visual acuityin 25 to 30% of patients. These improvements aresignificantly better than the results of laser treatmentalone. Sustained intravitreal delivery ofglucocorticoidssuch as fluocinolone yields a similar improvement witha 60% increase in the risk of glaucoma and a 33%increase in cataract. The same implant technologydelivering a lower dose of fluocinolone did not increasethe risk of cataract or glaucoma, it certainly reducesretinal inflammation and may restore the integrity ofthe blood–retina barrier. These initial treatments for DRreflect the gains in our understanding of how diabetesimpairs vision and set the stage for further advances.The Neurovascular Unit:
New insights into retinal physiology suggest thatthe retinal dysfunction associated with diabetes maybe viewed as a change in the retinal neurovascular unit,refers to the physical and biochemical relationshipamong neurons, glia and specialized vasculature andthe close interdependency of these tissues in the centralnervous system.The glial-cell, pericyte, and neuralinteractions promote formation of the blood–brain andblood–retina barriers, which control the flux of fluidsand bloodborne metabolites into the neuralparenchyma. Neurodegenerative conditions such asAlzheimer’s and Parkinson’s disease alter theneurovascular unit, with changes in neural function,neurotransmitter metabolism and loss of the blood–brain barrier. If the neurovascular unit is similarlyinvolved in diabetes, then new therapeutic approachesaddressing both vascular dysfunction and neuraldegeneration may be required.
The fact that treatment of vascular complicationspreserving visual acuity, highlights the intercon-nectedness of the neural retina with the retinalvasculature - the functional neurovascular unit whichis considered to be the basis of molecular interactionof neural, glial and vascular cells in the retina.
Improved outcomes of treatment for cancer have
resulted from advances in clinical trial end points thatreflect the pathophysiology of the disease, such asmolecular biomarkers of tumor activity and positron-emission–tomographic scanning. Likewise, new endpoints reflecting the pathophysiological features ofdiabetic retinopathy are needed for sensitive,quantitative, and predictive assessment of the severityof retinopathy. Vascular lesions change slowly, andphotographic staging alone cannot facilitate short-term(<1 year) proof-of-concept trials to evaluatepathophysiological mechanisms and therapies.
Standard measures are now being supplementedwith sensitive indexes of retinal function and structureto determine the nature of early retinopathy.Flavoprotein spectrophotometry reveals defects inmitochondrial metabolism. Reduced electroretino-graphic responses suggest reduced cellular signaltransmission, predict subsequent microvascular lesionsand responses to improved metabolic control. Subtledefects in visual function are detected by contrastsensitivity and visual-field defects.Optical coherencetomography (OCT) detects thinning of the neuronal andsynaptic layers of mild retinopathy. In fact, the retinalarchitecture confers unique characteristics to theneurovascular unit. The inner retina has capillary bedsin the ganglion-cell and inner nuclear layers. Theneurovascular unit includes astrocytes and Müllercells,amacrine and ganglion neurons which reside inclose proximity to microvascular segments that deliveroxygen and nutrientsSummary:
Molecular causes of diabetic retinopathy revealschanges affecting all cells within the retina, includingthose in the microvasculature, glia, neurons, andmicroglia. These changes in the retina, which can beviewed as a disruption of the neurovascular unit,contribute to the pathophysiology of diabeticretinopathy. Intraocular administration of VEGFinhibitors and glucocorticoids has launched an era ofbiologically based pharmacologic treatment thatcomplements surgical approaches for advanced stagesof retinopathy. Further advances require anunderstanding of how the metabolic changes indiabetes disrupt the neurovascular unit, as well asfocused efforts to develop clinical-trial end points andbiomarkers. The expected increase in diabeticretinopathy due to the increasing incidence of type 2diabetes requires the elimination of socioeconomicbarriers so that research advances can be translated intoeffective and accessible care for all persons withdiabetes.Continued epidemiologic surveillance isneeded to determine trends, properly allocateresources, and develop cost-effective preventiveinterventions.
Editorial

212 Ophthalmology Update Vol. 10. No. 3, July-September 2012
Editorial
REFERENCES1. Photocoagulation treatment of proliferative diabetic
retinopathy: the second report of Diabetic Retinopathy Studyfindings. Ophthalmology 1978;85:82-105
2. Photocoagulation for diabetic macular edema: EarlyTreatment Diabetic Retinopathy Study report number 1. ArchOphthalmol 1985;103:1796-1806
3. Hovind P, Tarnow L, Rossing K, et al. Decreasing incidenceof severe diabetic microangiopathy in type 1 diabetes.Diabetes Care 2003;26:1258-1264
4. Nordwall M, Bojestig M, Arnqvist HJ, Ludvigsson J.Declining incidence of severe retinopathy and persistingdecrease of nephropathy in an unselected population of Type1 diabetes — the Linkoping Diabetes Complications Study.Diabetologia 2004;47:1266-1272
5. Kempen JH, O’Colmain BJ, Leske MC, et al. The prevalenceof diabetic retinopathy among adults in the United States.Arch Ophthalmol 2004;122:552-563
6. Sloan FA, Belsky D, Ruiz D Jr, Lee P. Changes in incidenceof diabetes mellitus-related eye disease among US elderlypersons, 1994-2005. Arch Ophthalmol 2008;126:1548-1553
7. Klein R, Klein BE. Are individuals with diabetes seeingbetter? A long-term epidemiological perspective. Diabetes
2010;59:1853-18608. UK Prospective Diabetes Study (UKPDS) Group. Intensive
blood-glucose control with sulphonylureas or insulincompared with conventional treatment and risk ofcomplications in patients with type 2 diabetes (UKPDS 33).Lancet 1998;352:837-853[Erratum, Lancet 1999;354:602.]
9. Mauer M, Zinman B, Gardiner R, et al. Renal and retinaleffects of enalapril and losartan in type 1 diabetes. N Engl JMed 2009;361:40-51
10. Mann DM, Woodward M, Ye F, Krousel-Wood M, MuntnerP. Trends in medication use among US adults with diabetesmellitus: glycemic control at the expense of controllingcardiovascular risk factors. Arch Intern Med 2009;169:1718-1720
Prof. M. Yasin Khan DurraniMBBS., DO., MD., FRCOphth(Lond)Editor in Chief267-A, St: 53, F-10/4, Islamabad, Pakistan.E.Mail>[email protected]: 0092 333 5158885

Ophthalmology Update Vol. 10. No. 3, July-September 2012 213
–––––––––––––––––––––––––––––––––––––––––––––––––––––*This study was carried out at the Department of Ophthalmology,Services Institute of Medical Sciences & Services Hospital, Lahore.–––––––––––––––––––––––––––––––––––––––––––––––––––––1Registrar in Eye Unit I, Services Institute of Medical Sciences /Services Hospital, Lahore, 2Assistant Professor, 3Senior Registrar,4Medical Officer, 5Head of Ophthalmology–––––––––––––––––––––––––––––––––––––––––––––––––––––Address for correspondence: Dr. Amber Zahid, FCPS., C-44/A OldOfficers Colony, Zarar Shaheed Road, Lahore Cantt. Tel: 0321-4089696 E.Mail>[email protected], Registrar in Eye UnitI, Services Institute of Medical Sciences / Services Hospital, Lahore.–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: March’ 2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
INTRODUCTIONPhacoemulsification with foldable intraocular lens
is the standard and popular surgical procedure ofcataract extraction over the past two decades.1 The aimof modern cataract surgery is rapid visual rehabilitationand the best uncorrected visual acuity both for distanceand near.2 Currently available monofocal intraocularlens focus at one fixed distance either far or near.Therefore no matter what’s the age of patient is, hisnear visual acuity is significantly impaired after surgicalintervention despite good recovery of distance visualacuity due to loss of accommodation.3 Even with bestsurgical results patient requires spectacle correction fornear vision postoperatively.
To overcome this problem different types ofintraocular lenses have been evolved. One of them ismulti-focal intraocular lens that provide refractivecorrection for both distance and near simultaneously.4
The original concept of multi-focal IOL was based onthe principle that pupil tends to constrict for near taskso central portion of lens was designed for near andouter portion for distance.5 The disadvantage was thatin bright light when pupil constricts the distancecorrection was not available. Now current designs solvethis problem by having central and outer zones fordistance correction and intermediate zones for nearcorrection.
Array is the first multi-focal intraocular lensapproved by Federal drug administration for use aftercataract extraction It uses five refractive concentriczones on its anterior surface to provide distance,intermediate and near vision. The rationale of this studywas that mostly mono-focal intraocular lenses areimplanted in patients after cataract surgery but postoperatively patients require spectacle correction fornear vision. This study was designed in our set up toevaluate array multfocal lens in terms of improvementof vision both for distance and near with reducedspectacle dependence.MATERIAL AND METHODS
This interventional, quasi experimental study wasconducted at department of Ophthalmology, ServicesInstitute Of Medical Sciences & Services Hospital,Lahore form 21-01-2009 to 21-04-2010.Thirty eyes of 26patients were recruited from outpatient department bynon-probability purposive sampling who were advisedphaco-emulsification with foldable intraocular lensabove the age of 20 years. Patients were excluded from
Visual Outcome for Distance & Nearwithout Glasses after Phacoemulsification
with Array Multifocal Intraocular Lens*
Amber Zahid FCPS1, Intzar Hussain FCPS, FRCS2, SaqibSiddiq FCPS3
Khalid Jamal MBBS4, Prof M Tayyib FRCS, FRCOphth5
ABSTRACT:Purpose of Study: To assess the visual outcome for distance and near without glasses after phacoemulsification withimplantation of Array multifocal Intraocular lens implantation.Patients and Methods:This quasi experimental study was carried out at department of ophthalmology, Services Instituteof Medical Sciences & Services Hospital Lahore from 21st January 2009 to 21st April 2010.Thirty eyes of twenty sixpatients were operated for cataract by phacoemulsification with Array multifocal IOL.Results: Age of patients ranged from 22-80 years with mean of 58.1 ± 14.8 years. Preoperative best corrected distancevisual acuity ranged from 6/9 to counting fingers. Postoperatively 100% patients achieved uncorrected distance visualacuity from 6/6-6/12 and 100% achieved uncorrected near visual acuity from N6-N10. Spectacle independence wasencountered in 40% eyes. 60% eyes had uncorrected near vision range from N8-N10. Most of patients were satisfiedwith their vision post operatively however 32% reported different visual aberrations at night.Conclusion: Array multifocal intraocular lens improves functional vision both for distance and nearKey Words: Phacoemulsification, multifocal intraocular lens, cataract surgery.
Original Article
Dr. Amber

214 Ophthalmology Update Vol. 10. No. 3, July-September 2012
the study having any co-existing ocular disease,traumatic cataract or who had any complication duringsurgical procedure. Professional night drivers,obsessive or highly critical patients, professionals withhigh visual demands and patients expected highresidual postoperative astigmatism were also excluded.Demographic profile for various patients including age,gender and address were noted.
A detailed history was taken from the patients.Detailed ocular examination was performed includingmeasurement of visual acuity by Snellen chart with orwithout glasses, slit lamp for detailed anterior segmentexamination, IOP measurement and dilated fundusexamination. Maximum pupillary dilatation was alsodetermined. The type and density of lens opacities werenoted.
A written consent was taken. Standardpreoperative biometric measurement was taken usingautomated keratometry and A scan. The IOL power wascalculated with SRK/T formula. Phaco-emulsificationwith Array multifocal intraocular lens implant wasdone by one surgeon so as to maintain uniformity andcontrol the confounding variables. The procedure wascarried out under local anaesthesia. Patients wereadvised to use combination of dexamethasone andTobramycine topically in tapering dose postoperatively.
Postoperative follow up was done on 1st
postoperative day, 1st postoperative week,1st and 3rd
postoperative month.At each visit, distance vision using Snellen chart
and near vision using near vision chart was measured.Slit lamp examination was also performed for anteriorsegment on each visit.Data was analysed with the helpof computer software program, Statistical Package forSocial Sciences (SPSS) Version 10.0.RESULTS
There were twenty six patients of whom thirtyeyes underwent phaco-emulsification, Four patientshad bilateral Array multifocal IOL implants while intwenty two patients only one eye was operated. Theage of patients ranged from 22-80 years with mean of58.1±14.8 years (Table-1). Sixteen were male (61.53%)and ten were female (38.46%) as shown in graph 1.Nosurgical complication such as posterior capsularrupture, suprachoroidal haemorrhage andendophthalmitis was reported among the patients.
Preoperative best corrected distance vision rangewas from6/9 to counting finger whereas near visionranged from N8 to worse than N36. The best correcteddistance visual acuity that could be achieved was 6/6and near visual acuity was N6 at three months. Postoperative unaided distance visual acuity at 1st week was6/18 in two eyes (6.66%), 6/12 in four eyes(13.33%), 6/9 in eight eyes(26.66%) and 6/6 in sixteen eyes.(53.33%)
At first and third month postoperative follow upunaided distance vision improved to 6/12 in five eyes(16.66%), 6/9 in seven eyes (23.33%) and 6/6 in eighteeneyes (60%). Final visual acuity that was at 3 monthspost operatively is shown in graph 2. This showseighteen eyes (60%) had 6/6 unaided distance vision.The remaining twelve eyes (40%) also improved to 6/6with glasses. Eighteen out of thirty eyes (60%) haduncorrected near vision range from N8-N10. Theyimproved to N6 with correction. Twelve eyes (40%)were N6 without correction (graph 3). Five patientsreported glare at night (16%), three patients reportedhalos around light (10%) and two patients reportedstreaks of lights (6%). These visual symptoms weremore troublesome at night (graph 4). Total spectacleindependence was achieved in twelve eyes (40%). Thefrequency of spectacle wear post operatively wasmeasured at 3 levels. Spectacle dependence wasencountered in 7 eyes (23.33%) for near most of the time.In 11 eyes (36.66%) of 11 patients spectacles wererequired sometimes for near (Table 2).DISCUSSION
The goal of modern cataract surgery is rapidvisual rehabilitation without complication and low orno postoperative refractive error.Conventional mono-focal IOL offer excellent distance visual rehabilitation,however most patients require reading glasses for neartask. The restoration of near vision in pseudophakicpatients without spectacles is the most challenging taskof modern cataract surgery.
Multi-focal IOLs overcome this problem using theprinciple of simultaneous vision1. Clinically multi-focalIOL have been reported to provide patients withfunctional near and distance vision with acceptablesatisfaction2
A study by Weghaupt et al3 has showed that
Table 1. Distribution of patients according to the age
Age Group Number Percent
<40 Years 2 7.7
41 – 55 Years 10 38.4
56 – 70 Years 8 30.8
> 70 Years 6 23.1
Total 26 100.0
Table 2. Spectacle dependence (Eyes)
Distance Near
Sometimes 0 11
Most of the time 0 7
All the time 0 0
Visual Outcome for Distance & Near without Glasses after Phacoemulsification with Array Multifocal Intraocular Lens

Ophthalmology Update Vol. 10. No. 3, July-September 2012 215
results for distance and near visual acuity are verysatisfactory with a diffractive multi-focal IOL, whereasfor intermediate distance visual acuity may be limitedto activities that do not require optimal vision.In ourstudy Array SA 40N refractive multi-focal IOL wereimplanted in thirty eyes. The results are comparable toresults reported in literature in terms of efficacy andsafety at three months after surgery. Our study showedtotal spectacle independence in about 40% of patients.
Evidence reported by Shoji et al4 showed thatimplantation of Array IOL in the dominant eye couldhave a better visual outcome as compared to non-dominant eye. In our study we couldn’t draw thisconclusion, because the numbers of eyes dealt withwere small and dominance of eyes with unilateralimplantation couldn’t be ascertained.
Good performance on static reading chart cannotsimulate the real performance of an IOL. Patientsimplanted with Array SA 40 multi-focal IOL havereported that they can read fine print in magazines andcan perform various tasks with out glasses5.Our studydemonstrated that almost all our patients could performdaily living tasks without glasses after Arrayimplantation, but for fine work like reading, sewingetc, patients require near glasses most of the time.Although our patients achieved satisfactory level ofunaided distance and near vision, frequent complaintwas about experiencing mild halos around light,slightgeneral blur and overall reduction in clarity.Sen HN etal in 2004 also reported in their study about increasedperception of halos and lower contrast sensitivity bysubjects with Array multi-focal intraocular lensimplants6.However they found that slightly lowercontrast sensitivity and increased perception of halosappeared to be an acceptable compromise to enhancednear and distance vision in subjects with multifocal lensimplant7.
For the implantation of multi-focal lens besidesgood surgical strategy, patients education andcounselling is very important8. In our study it isobserved that younger patients adapted to this newvisual environment more readily as compared to olderpatients. Finally patients need to have reasonableexpectation. The multi-focal IOL implantation reducedthe dependency on spectacles, but not completelyeliminating them9. CillinoS et al10 reported in theircomparative study about spectacle independence. Itwas 20% in monofocal IOL group, 53.3% in refractivemultifocal IOL group and 87.5% in diffractivemultifocal IOL group. They found that in comparisonto monofocal IOL, multifocal IOL provide greater depthof focus and higher patient satisfaction.Steinart et al15
reported that a significantly higher proportion ofbilateral multi-focal (81%) could function comfortably
Graph 1 – Gender distribution
Graph 2 – Post operative uncorrected distant vision at 3 months
Graph 4 – Postoperative visual phenomena
Graph 3 – Post operative uncorrected near vision at 3 months
Visual Outcome for Distance & Near without Glasses after Phacoemulsification with Array Multifocal Intraocular Lens

216 Ophthalmology Update Vol. 10. No. 3, July-September 2012
without glasses at near compared with mono-focalsubjects. However we found in our study that unilateralmulti-focal implant also function as comfortable as thebilateral multi-focal implant.
In our study Array multifocal IOL which is arefractive IOL yields total spectacle independence inabout 40%. It improves the quality of life in active andmotivated patients who wish to reduce theirdependence on glasses. With on-going innovations inIOL technology patients will benefit from better qualityof vision and enjoy less dependence on spectacles.CONCLUSION
Array multifocal intraocular lens improvesfunctional vision both for distance and near aftercataract surgery.REFERENCES1. Dada VK ,Sindu N .Management of cataract- A revolutionary
change that occurred during last two decades. J Indian MedAssoc 1999;97(8):313-7
2. HussainM,DuraniJ,Nisar A. Phacoemulsification-A reviewof 210 cases .Pak J Ophthalmol 1996;12:38-9
3. Langenbucher A, Huber S, Nguyen NW, Seitz B, Gusek-Schneider GC, Kuchle M. Measurement of accommodationafter implantation of an accommodating posterior chamberintraocular lens. J Cataract Refract Surg 2003; 29: 677-85.
4. Fernandez AP, Jaramillo J, Celis V, Vargas J, Distacio M,Galindez A, et al. Refractive outcomes after bilateralmultifocal intraocular lens implantation. J Cataract RefractSurg 2004; 30: 685-8.
5. Artigas JM, Menezo JL, PerisC,Felipe A, Diaz-Llopis M.Image quality with multifocal intraocular lenses and theeffect of pupil size : Comparison of refractive and hybridrefractive –diffractive designs. J Cataract Refract Surg2007;33(7):2111-7
6. Leyland M Zinicola E. Multifocal versus monofocalintraocular lenses in cataract surgery- a systematic review.Ophthalmology 2003;110:1789-98
7. Javitt JC, Wang F, TrentacostDJ.RoweM,Tarantino NOutcomes of cataract extraction with multifocal intraocularlens implantation:functional status and quality of life.Ophthalmology 1997;104:589-99
8. Weghaupt H ,Pieh S, Skorpik C. Comparison of pseudoaccommodation and visual quality between a diffractive andrefractive multi-focal intraocular lens. J Cataract Refract Surg1998;24:663-5
9. Shoji N, Shimizu K. Binocular function of the patient withrefractive multi-focal intraocular lens. J cataract Refract Surg2002; 28:1012-22
10. Cillion S, Casuccio A, Di Pace F,Morreale R, Pillitteri F,Cillino G, Lodato G.One year outcomes with new generationmultifocal intraocular lenses. Ophthalmology 2008; 115(9):1508-16
11. Sen HN, Sarikkola AU, Uusitalo RJ, Laatikainen L. Qualityof Vision after AMO Array Multi-focal intraocular lensimplantation. J Cataract Refract Surg. 2004;30(12):2483-93.
12. PiehS,LacknerB,HanselmayerG.Halo size under distance andnear conditions in refractive multifocal lenses.Br JOphthalmol 2001;85:816-21
13. avitt HJ, Brauweiler HP, Jacobi KW, Klemen U, Kohnen S,Quentin CD,TepingC,PhamT,KnorzMC,Poetzsch D. Cataractextraction with multifocal intraocular lens implantation.Clinical, functional and quality of life outcomes.Multi-centerclinical trial in Germany and Austria. J Cataract Refract Surg2000; 26:1356-1366.
14. Bellucci R. Multi-focal intraocular lenses. Curr OpinOphthalmol 2005; 16:33-37
15. Steinert RF, Aker BL,Trentacost DJ, Smith PJ,Tarantino N.Aprospective comparative study of AMO Array zonalprogressive multifocal silicon intraocular lens and amonofocal intraocular lens. Ophthalmology 1999; 106: 1243-55
Visual Outcome for Distance & Near without Glasses after Phacoemulsification with Array Multifocal Intraocular Lens

Ophthalmology Update Vol. 10. No. 3, July-September 2012 217
–––––––––––––––––––––––––––––––––––––––––––––––––––––1Assistant Professor Ophthalmology, 2ENT Surgeon–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Dr. Hashim Imran, Assistant ProfessorOphthalmology, Sargodha Medical College, University of SargodhaE.Mail>[email protected] House:4, Buglaow:10, CivilLines, Sargodha. 0321 6032085–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: March”2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
INTRODUCTIONNasolacrimal duct obstruction can occur
anywhere in the lacrimal drainage system. It mostcommonly occurs at the distal end of the nasolacrimalduct at the membrane of Hasner (ie, the unopened valveof Hasner). Patients with Nasolacrimal duct obstructionpresent with a history of chronic or intermittent tearing,debris on the eyelashes (mattering), and occasionallyredness of the conjunctiva.. On physical examination,there may be an increase in the size of the tear meniscus.Palpation of the lacrimal sac may cause reflux of tearsand/or mucoid discharge onto the eye through thepuncta. If tearing is intermittent, and none of the abovesigns are present at the time of examination, the dyedisappearance test can be performed to help confirmthe diagnosis1.
A dacryocystocele (also known as dacryocele,amniotocele, or nasolacrimal duct cyst) is producedwhen both the proximal and distal portions of thenasolacrimal system are obstructed. The proximal
obstruction typically occurs in the common canaliculusor at the valve of Rosenmuller . The proximalobstruction is a one-way valve that permits tears toenter, but not to reflux out of the canaliculi of thelacrimal drainage system. Dacryocystoceles usually arenoted at or shortly after birth. A bluish swelling of theskin overlying the lacrimal sac and superiordisplacement of the medial canthal tendon occurs. Thediagnosis can be confirmed by CT, though the diagnosisis usually obvious clinically and further work-upunnecessary. Acute dacryocystitis, indicated byerythema and tenderness of the dacryocystocele,swelling and fever , or altered behavior. Acutedacryocystitis is a medical emergency in a newborninfant, and it must be treated promptly to prevent thedevelopment of secondary preseptal or orbital cellulitis,sepsis, meningitis, or brain abscess2. Distension of themucosal lining of the nasolacrimal duct through theentrapment of tears. The swelling may distend intothe nose, forming a mucocele, which can lead to nasalobstruction and respiratory distress in infants who areobligate nose breathers 3,4.
Decompression of a dacryocystocele usually canbe achieved with digital massage or probing of thelacrimal canaliculus and duct. Untreated, infectionoften ensues. The Nasolacrimal duct obstructioncomponent is treated as it is in older children. Inaddition, intranasal mucoceles, if present, must bedrained to relieve nasal obstruction. Drainage of
Analysis and Efficacy of Dacryocystorhinostomyperformed with Nasal Endoscope & its Advantage
over External Dacryocystorhinostomy
Hashim Imran1, Rizwan Ullah Chattha2, Sarfraz Latif3, Naveed Aslam4
ABSTRACT :Objectives : To analyze the results of Dacryocystorhinostomy performed with nasal endoscope by performing the followup for one year and detecting its advantages over the conventional methods.Study design: Hospital based prospective interventional study .Place and duration of study: This study was conducted at Eye & ENT departments of Sargodha Medical CollegeSargodha and Sheikh Zayed Hospital, Lahore between January 2008 to July 2011Method: The study group comprised of 30 patients who were referred by Ophthalmologist. 28 of them were females, ageranging from 12 to 60 years. These Patients were not ready to give consent for external scar. Their presentation was withcomplaints of epiphora, sac swelling and pain around medial canthus. These patients underwent endoscopicDacryocystorhinostomy and tried to preserve the mucosal flap.Results: These 30 patients remained in one year follow up and success rate was seen about 76%Conclusion : Endoscopic Dacryocystorhinostomy is good choice to avoid external facial scars in females. Other nasalpathologies are addressed simultaneously.The procedure is safe and having less complications. It is highly indicated inyoung femalesKey words: Nasal endoscope, dacryocystitis, epiphora, dacyocystorhinostomy, Nasolacrimal duct.
Original Article
Dr. HashimImran

218 Ophthalmology Update Vol. 10. No. 3, July-September 2012
intranasal mucoceles is typically performed in theoperating room under general anesthesia, with the aidof a nasal endoscope 5,6
Adeo Toti was the first surgeon who describedthe external Dacryocystorhinostomy in 1904. Theoriginal intranasal approach was described byCaldwellin 19837. Endoscopic dacryocystorhinostomywas first performed by Rice in 1988. Since thisdescription, a number of modifications8 using LASERhave also been described as a useful tool in endoscopicDacryocystorhinostomy. In external Dacryocysto-rhinostomy surgeon is unaware of the size of middleturbinate, infected ethmoid sinuses, deflected nasalseptum9.In endoscopic Dacryocystorhinostomy we cansave the external skin incision and medial canthalanatomy10. This procedure is gaining popularity dueto availability of endoscopes having different angles.By routine use of nasal endoscopes ENT surgeon arewell familiar with the anatomy of lateral wall of Nose.MATERIAL AND METHODS:
30 patients were presented to Ophthalmologist forcomplaint of epiphora8 and/ or medial canthal swelling,28 of them were females. All patients underwentdetailed nasal examination with rigid nasal endoscopein OPD. Patients with deflected nasal septum, nasaladhesions and inflamed Ager Nasi cells were includedin study. The cases with pre-saccal blockage wereexcluded.
All patients were operated under G/A at DHQTeaching Hospital Sargodha and at Shaikh ZayedHospital, Lahore. 30 minutes before the surgerybilateral nasal packing was performed which wasimpregnated with 4% xylocaine and 1:10000 adrenaline.After G/A induction, detailed examination of the nosewas performed with 0 and then 30 degree nasalendoscopes. Lateral wall of nose on diseased sideinjected with 2% xylocaine with adrenaline in 1:200,000.Aim is to perform hydrostatic dissection and localvasoconstriction.
With the help of sickle knife, incision is givenstarting from anterior to axilla of middle turbinate indownward direction in the form of curve. With Frèreselevator, mucosal flap elevated. Karrison bone punchis made to push on bone and let it enter in to thin boneoverlying the sac area. Pieces of bone are removed bitby bit. The job of bone removal is performed frominferior to superior direction. While reaching at axillaof middle turbinate , there is hard bone of frontalprocess of maxilla, sometimes it is very difficult toremove with punch, chisel and hammer can be usedfor removal of hard piece of bone. Electric drill isanother good option.After removal of bone, irrigationand suction is performed inside the nasal cavity andmedial wall of sac is tried to visualized. Sac is confirmed
by putting pressure on medial canthus and sacmovements are observed. With sickle knife verticalincision is given lumen of sac visualized. Blunt probeis inserted inside the lumen and adhesions cleared ifany. With the help of Blaksleys forceps , wall of sacand mucosal flap trimmed. Now the surgeon performswater irrigation in to canaliculated and free flow ofwater is seen inside the nasal cavity.
Clinical features of NLD obstruction may includechronic or intermittent tearing, debris on the eyelashes,increased tear meniscus, reflux of tears and mucoiddischarge through the puncta with palpation of thelacrimal sac, and redness of the conjunctiva. Clinicalfeatures of dacryocystoceles include a bluish swellingof the skin overlying the lacrimal sac and superiordisplacement of the medial canthal tendon. Acutedacryocystitis, manifest by erythema, swelling, warmth,and/or tenderness of the lacrimal sac, which can bemanaged in consultation with an ophthalmologist.RESULTS
30 cases were collected and underwentendoscopic dacryocystorhinostomy, all of them hadfree flow of saline through newly built window. Thiswas considered as successful criteria. Patient kept infollow up for one year and observed for epiphora andsac swelling. 8 patients had recurrence of symptoms in6 months follow up. Endoscopic examination revealedeither they were having adhesions or granulationsinside the stoma. Out of these 8 patients 3 patients gottheir symptoms relieved by removal of adhesions orgranulations under L/A.
Complaints No of cases ResultsEpiphora 21 19Acute infection 5 4Sac abscess 4 2Success rate is 76%
DISCUSSIONThe lacrimal drainage system begins by forming
at approximately 6 weeks of gestational age as adepression, teemed the lacrimal groove. A solid cordof ectoderm is eventually buried as the mesodermdevelops and extends from the eyelid to Nose.Canalization of the cord begins at approximately 3.5months of gestational age and is usually completed ator near the time of birth, with the lower level of thesystem being last to open. Anomalies may occur anywhere in the course of system 11.
Atresia of the nasolacrimal duct or dacryostenosisis the most common cause of epiphora in paediatricpopulation. It is thought to result from failure of the
Analysis and Efficacy of Dacryocystorhinostomy performed with Nasal Endoscope & its Advantage over External Dacryocystorhinostomy

Ophthalmology Update Vol. 10. No. 3, July-September 2012 219
canalization of the column of epithelial cells that formthe nasolacrimal duct. The most common site ofobstruction is at the mucosal entrance in to the noseunder the inferior turbinate.12 Probing of thenasolacrimal duct is the standard therapeutic procedurein the management of nasolacrimal duct obstruction,if it fails then further can be proceeded to invasiveprocedures12.In eye clinics epiphora is a commoncomplaint. Most of the Ophthalmologist refer such casesto ENT colleagues for nasal examination. Some13
Ophthalmologist try to perform syringing and passageof saline on irrigation is shared with ENT consultant.Inpresent study, we collected 30 patients and all of themwere females, ranging from 12 to 60 years.
The success rate of 76% depends upon providinga wide intranasal stoma with removal of adequate bonearound the stomal area. The complications13 likesecondary canalicular stenosis, sump syndrome, distalstenosis and adhesions between septum and lateral wallwere not seen.Endoscopic dacryocystorhinostomyavoids external incision hence save the facial skin fromscar. It preserves the pumping action of orbicularis oculimuscle. In our study we also found that 20% of patientsneeded concomitant nasal procedures. Although ifthere are reports of successful DCR with poweredinstruments and laser but in our study we performedall cases with conventional instruments without usinglaser14.CONCLUSION:
Endoscopic Dacryocystorhinostomy is goodchoice to avoid external facial scars in females. Othernasal pathologies are addressed simultaneously.Although it is having failure in reasonable percentagebut with the help of powered instruments and LASERwe can improve it further.REFERENCES1. Paysse EA, Coats DK, Bernstein JM, et al. Management and
complications of congenital dacryocele with concurrentintranasal mucocele. J AAPOS 2000; 4:46.
2. Paysse EA, Coats DK, Bernstein JM, et al. Management andcomplications of congenital dacryocele with concurrentintranasal mucocele. J AAPOS 2000; 4:46.
3. Edmond JC, Keech RV. Congenital nasolacrimal sacmucocele associated with respiratory distress. JPediatrOphthalmol Strabismus 1991; 28:287.
4. Duval M, Alsabah BH, Carpineta L, Daniel SJ. Respiratorydistress secondary to bilateral nasolacrimal ductmucocelesin a newborn. Otolaryngol Head Neck Surg 2007; 137:353.
5. Yee SW, Seibert RW, Bower CM, Glasier CM. Congenitalnasolacrimal duct mucocele: a cause of respiratory distress.Int J PediatrOtorhinolaryngol 1994; 29:151.
6. Leonard DS, O’Keefe M, Rowley H, Hughes JP. Neonatalrespiratory distress secondary to bilateralintranasaldacryocystocoeles. Int J PediatrOtorhinolaryngol2008; 72:1873
7. Caldwell GW (1893) Two new operations for obstruction ofthe nasal duct. N Y Med J 57:581-582
8. Massaro BM, Gonnesing RS, Harris GJ (1990) Endonasal laserdacryocystorhinostomy. A new approach to nasolacrimalduct obstruction. Arch Opthalmol 108(8):1172-76
9. Hartikainen J, Antila J, Varpula M (1998): prospectiverandomized comparison of endonasal endoscopicdacryocystorhinostomy and external dacryocystor-hinostomy . Laryngoscope 108 : 1861-1866
10. Kupper DS, Dermarco RC, Resende R, Anselmo-lima WT,Valera FC Morib I (2005) Endoscopic nasaldacryo-cystorhinostomy :results and advantages over externalapproach. Rev Bras otorhinolaryngol.Ophthalmology111:837-845
11. Jackson TL. Moorfields Manual of Ophthalmology , Mosby(2008);55-69
12. kerstein RC. Congenital nasolacrimal abnormalities In:Principles and practice of Opthalmic Plastic andReconstructive surgery. W B Saunders Company ;1996.Vol 2,p 731- 747
13. Fayet B, Racy E, Assouline M (2004) Complications ofstandard endonasal dacrycystorhinostomy withunciformectomy. Ophthalmology 111:837-845
14. Kirukov AL, Davydov DV, Kravchenko AV, (2005) domestic1.44 mcmNdYag laser in combined treatment ofdacryocystitiscomplicated by abscess formation.VestenOtorhinolaryngol (6):14-17
Analysis and Efficacy of Dacryocystorhinostomy performed with Nasal Endoscope & its Advantage over External Dacryocystorhinostomy

220 Ophthalmology Update Vol. 10. No. 3, July-September 2012
–––––––––––––––––––––––––––––––––––––––––––––––––––––*Professor of Ophthalmology–––––––––––––––––––––––––––––––––––––––––––––––––––––Corresponding address: 7Ap, 1Entr, 26 Sayat-Nova Avenue,Yerevan, 0001, Republic of ArmeniaE-mail: [email protected] Tel: (37410) 523 468–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: March”2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
INTRODUCTION:Retinal vein occlusion (RVO) is the most common
visually disabling disease affecting the retina afterdiabetic retinopathy.1 Although it is more common inthe middle-aged and elderly population, no age groupis immune to it 2.
In spite of the fact that the clinical entity of RVOhas been known since 1878 3, its management stillremains highly controversial. The pathogenesis of RVOis multifactorial with both local factors and systemicdiseases being etiologically important. Many case-control studies have examined the clinical features andrisk factors in this disorder 4,,9. Known risk factors forRVO include systemic vascular disease, hypertension,diabetes mellitus, hyperlipidemia and glaucoma.Hypercoagulable states are associated with RVO. Theseinclude primary hypercoagulable states with a defectin the physiological anticoagulant mechanism andsecondary hypercoagulable states, which areconditions, associated with an increased risk ofthrombosis. There are still gaps in understanding theaetiology and pathogenesis of circulatory disorders ofthe central retinal vein and its branches.
Although various new therapeutic approacheshave been developed in the past few years, existing
therapy forms are subject to controversy and availabledata to same extent inconsistent. Over the years, manytreatments have been advocated enthusiastically andsuccess has been claimed. Except for a few prospectivestudies, all the reports are based on retrospectivecollection of information or on limited personalexperience. Most of the reported studies have a varietyof limitations, which make it hard to evaluate theclaimed benefits.
Macular edema is the main reason for decreasedvisual acuity in RVO. Macular edema is a common sight–threatening response of the retina. It involves thebreakdown of the inner blood-retinal barrier andconsists of an abnormal vascular permeability resultingin fluid accumulation and macular thickening,detectable by optical coherence tomography (OCT).
The objective of this review is to evaluate newmedical and surgical treatment modalities aimed atreducing macular edema due to central retinal veinocclusion (CRVO) and branch retinal vein occlusion(BRVO), and to discuss controversies and futuretreatment options. The main treatments can be dividedinto three categories: medical, surgical and laser.MATERIAL & METHODSMEDICAL TREATMENTi) Intravitreal Drug Administration:
Recently the vitreous cavity has increasingly beenused as a reservoir of drugs for the direct treatment ofmacular edema through intravitreal injection route.ii) Intravitreal tissue plasminogen activator:
In a retrospective review of 17 eyes with BRVOMurakami et al.10 treated subjects with the fibrinolyticagent intravitreal tissue plasminogen activator (tPA)
Treatment of Macular Edema inRetinal Vein Occlusion :How Forward we are?
Prof. Marianne L. Shahsuvaryan*Yerevan State Medical University ,Yerevan, Armenia
ABSTRACT: Retinal Vein Occlusion (RVO) is the most common visually disabling disease affecting the retina afterdiabetic retinopathy. Although the disease entity has long been known, its management is still controversial. Macularedema is the main reason for decreased visual acuity in RVO. Recently the vitreous cavity has increasingly been used asa reservoir of drugs for the direct treatment of macular edema through intravitreal injection route. The most widelyinjected drugs so far has been triamcinolone acetonide and bevacizumab. The objective of this review is to evaluate newmedical and surgical treatment modalities aimed at reducing macular edema due to central retinal vein occlusion (CRVO)and branch retinal vein occlusion (BRVO), including intraocular injections of steroids and anti-vascular endothelial growthfactor agents, vitrectomy, sheathotomy, and to discuss controversies and future treatment options.Keywords: retina, central retinal vein, branch retinal vein, occlusion, secondary macular edema, surgical treatment,medical treatment, intravitreal injections.
Original Article
Prof. Marianne

Ophthalmology Update Vol. 10. No. 3, July-September 2012 221
and claimed that visual acuity (VA) significantlyimproved and foveal thickness significantly decreased.They concluded that intravitreal tPA injection may bean effective treatment for resolving macular edema andimproving the VA in BRVO. This report is based onretrospective collection of information and on limitedpersonal experience.iii) Intravitreal Corticosteroidsa) Triamcinolone Acetonide
The SCORE ( Standard care vs. Corticosteroid forretinal vein occlusion) study, sponsored by the NationalEye Institute (NEI) consists of 2 multi-centerrandomized, controlled clinical trials comparing thesafety and efficacy of standard care with IVTA in eithera 1 or 4 mg dose for vision loss associated with macularedema secondary to CRVO or BRVO11,12. In the CRVOtrial, standard care therapy is observation. Retreatmentsare considered for persistent or new macular edema at4-month intervals.
The SCORE-CRVO study61 showed that bothtriamcinolone groups were superior to observation withrespect to VA. The visual benefit of IVTA wasdemonstrated as early as 4 months and continued to 24months; although there was less power at this point,the benefit appears to persist. However, in all 3 groups(1mg IVTA, 4mg IVTA or observation, there was areduction of central retinal thickness from baseline to24 months. Therefore, the visual benefit of IVTA maybe due not only to macular edema decrease, but also toother effects, such as anti-inflammatory orneuroprotective effects. The study report 5 alsoevidenced the superior safety profile of the 1-mg dosecompared with the 4 mg dose, particularly with respectto glaucoma and cataract, rendering in the preferreddose in CRVO11.
In SCORE-BRVO12 IVTA injections was not foundto be associated with improved VA outcomes comparedwith grid photocoagulation, being the standard care.The rates of adverse events were highest in the 4mgtriamcinolone group. The rates of adverse events inthe 1 mg TA group were similar, with respect to surgicalintervention for cataract and glaucoma, to the lasergroup, but laser treatment excluded any possibility ofinjection related adverse events. The SCORE StudyInvestigative Group concluded that grid photo-coagulation should remain the benchmark againstwhich other treatments are compared in clinical trialsfor eyes with vision loss associated with macular edemasecondary to BRVO.b) DexamethasoneThe Ozurdex ( Allergan Inc., Irvine, CA, USA)dexamethasone drug delivery system (DDS) wasrecently developed and approved by the FDA as abiodegradable intravitreal implant to provide sustained
delivery of 0.7 mg dexamethasone for the treatment ofmacular edema associated with RVO13,14.
Haller et al.13 concluded that for patients who haverelatively short duration of macular edema, Ozurdexshould be considered a viable treatment option.Increases in IOP were generally transient and similarfollowing each treatment. Cataract adverse eventsoccurred in 26% of patients treated with two injectionsand in 5% of patients who received no treatment overthe 12-month study.c) Posterior Sub-tenon injection of triamcinolone
acetonideSome authors15,16 have recently advocated the
posterior sub-Tenon (PST) injection of 40 mg TA undertopic anesthesia, based on claims that IOP elevationmay be less common after PST injection than afterintravitreal injection, however Iwao et al.66 have foundthat PST TA injection is associated with high rates ofsteroid-induced IOP elevation in eyes with previouslynormal IOP.
Lin et al.15, in a prospective study of 18 eyes withCRVO treated by three biweekly PST TA injections,claimed that this treatment is effective in reversingcystoid macular edema (CME) and improving VA inrecent onset CRVO in the first 9 months beforelongstanding macular edema results in irreversiblephotoreceptor damage. No cataract progression or othercomplications were observed. They stated that patientswith non-ischaemic CRVO may respond morefavorably than patients with ischaemic CRVO andfurther study with longer follow-up period is necessary.
Recently Mizumo et al.17 in the experimental studyhave found that the periocular injection of TAeffectively decreased retinal thickness and inhibitedleukocyte-endothelium interactions in the retina afterischemia. Down regulation of adhesion molecules ofretinal vascular endothelium induced by TA may playa role in the course.iv) Anti-VEGF therapyApplication of vascular endothelial growth factor(VEGF) inhibitors represents a treatment option formacular edema secondary to RVO that targets thedisease at the causal molecular level.
Over the past years, ophthalmologists haveattempted to treat RVO-associated edema triggered byhypoxia-induced expression of VEGF with ranibizumab(Lucentis®), bevacizumab (Avastin®), and pegaptanibsodium (Macugen®).a) Ranibizumab has received FDA approval for thetreatment of macular edema due to both CRVO andBRVO, and it is the only available FDA-approvedtherapy. With ranibizumab, Pieramici et al.18 designeda study following the scheme of the PIER Study, i.e.the first 3 injections monthly and then after 6 and 9
Macular Edema Treatment in Retinal Vein Occlusion : How Forward we are?

222 Ophthalmology Update Vol. 10. No. 3, July-September 2012
months, if needed (persistent macular edema). Theyfound that ranibizumab is generally well tolerated andmay improve BCVA and decrease central retinalthickness in OCT. But the efficacy was lost after theloading phase, so an interval of 3 months betweeninjections may be too long. In addition, Spaide et al.19
and Rouvas et al.20 demonstrated in two prospectivestudies that the patients with RVO have animprovement in VA, but with a mean of 7.4–8.5injections in 1 year of follow-up.
Nowadays two phase III multicenter, prospectiveclinical trials are under way, assessing the safety,tolerability and efficacy of intravitreal ranibizumabinjections in the treatment of macular edema secondaryto BRVO and CRVO 71. They are called BRAVO (studyof the efficacy and safety of ranibizumab injectioncompared with sham in patients with macular edemadue to BRVO) and CRUISE (study of the efficacy andsafety of ranibizumab injection compared with shamin patients with macular edema due to CRVO). Duringthe first 6 months, the patients monthly received either0.3 or 0.5 mg of ranibizumab or sham injection. Duringthe second 6 month period, the patients were evaluatedmonthly and treated on an as-needed basis; meanwhile,patients in the sham group received 0.5 mgranibizumab. In addition, in the BRAVO study, rescuelaser therapy was performed if criteria were met. Forthe first 6 months, results are available. Regardingefficacy, at the primary endpoint (mean change frombaseline BCVA at month 6), there is a rapid andsustained improvement in BCVA in patients withmacular edema due to BRVO or CRVO. They show astatistically significant number of patients who gained>15 letters from baseline at month 6, in the study groupcompared to the control group, as well as a change frombaseline central foveal thickness over time to month 6.In the BRVO group, more patients in the sham groupreceived rescue grid laser, compared with the 0.3 or0.5 mg ranibizumab groups. Besides, intravitrealranibizumab seems to have a safety profile consistentwith previous phase III trials, and low rates of ocularand non-ocular safety events22,23,24. Moreover, these twotrials demonstrate that the duration of the disease doesnot matter for taking the decision of treating. Treatedpatients did always better than sham-treated patients.Therefore, treatment for RVO can also be delayed by 3months25,26. The latest results from open-label extensiontrial of the 12-month ranibizumab assessing long-termsafety and efficacy in BRAVO and CRUISE trials26
evidenced that in patients who completed month 12,the mean number of injections (excluding month 12injection) in the sham/0.5-, 0.3/0.5-, and 0.5-mg groupswas 2.0, 2.4, and 2.1 (branch RVO) and 2.9, 3.8, and 3.5(central RVO), respectively. The incidence of study eye
ocular serious adverse events and systemic adverseevents potentially related to systemic vascularendothelial growth factor inhibition across treatmentarms was 2% to 9% and 1% to 6%, respectively. Themean change from baseline BCVA letter score at month12 in branch RVO patients was 0.9 (sham/0.5 mg), 2.3(0.3/0.5 mg), and 0.7 (0.5 mg), respectively. The meanchange from baseline BCVA at month 12 in central RVOpatients was 4.2 (sham/0.5 mg), 5.2 (0.3/0.5 mg), and4.1 (0.5 mg), respectively. The authors concluded thatno new safety events were identified with long-termuse of ranibizumab; rates of systemic adverse eventspotentially related to treatment were consistent withprior ranibizumab trials. Reduced follow up and fewerranibizumab injections in the second year of treatmentwere associated with a decline in vision in central RVOpatients, but vision in branch RVO patients remainedstable. Results suggest that during the second year ofranibizumab treatment of RVO patients, follow up andinjections should be individualized and, on average,central RVO patients may require more frequent follow-up than every 3 months.b) Bevacizuma(Avastin®), Bevacizumab is arecombinant humanized monoclonal antibody directedagainst VEGF. There have been several studies withbevacizumab and RVO, retrospective or prospective,all showing improvements in VA and optical coherencetomography (OCT) outcomes, but also short-termefficacy and high recurrence rate. The dosage variesbetween 1 and 2.5 mg, there are no different outcomes27-
86. The Pan-American Collaborative Retina Study groupconcluded that intravitreal injections of bevacizumabat doses up to 2.5 mg were more effective in improvingVA and reducing macular edema at 6 months(compared to 1.25 mg), but the study had no controlgroup [82]. By contrast, no statistically significantdifferences were found between the doses, when thegroup presented the results at 24 months37. In addition,Ach et al.38 found that CRVO patients who benefit fromtherapy were significantly younger and had lowercentral retinal thickness at baseline, while BRVOpatients showed no predictive factors for effectivenessof bevacizumab therapy.
Recently, Ghayoor et al.39 evaluated the effect ofAvastin (mean 2.8 claimed that significantimprovement in best corrected VA was observed at 6th
week of follow-up. At 6th month more than 60% showedimprovement in best corrected visual acuity, similarly70% patients had complete resolution of macularedema. The authors concluded that anti-VEGF therapyshould be further evaluated in large, prospective,controlled clinical studies.
Epstein et al40 conducted the latest prospectivedouble-masked clinical trial of 60 patients with macular
Macular Edema Treatment in Retinal Vein Occlusion : How Forward we are?

Ophthalmology Update Vol. 10. No. 3, July-September 2012 223
edema secondary to CRVO randomized 1:1 to receiveintraocular injections of bevacizumab or sham injectionevery 6 weeks for 6 months. Results evidenced that thetreatment improve VA and reduce macular edemasignificantly compared with sham.c) Pegaptanib Sodium (Macugen®).
The pegaptanib sodium is a selective anti-VEGFand it is still not well studied in RVO. Bennet41
performed a pilot study where Macugen treatmentachieved a decrease in macular thickness and animprovement in VA and retinal perfusion. But thisstudy had enrolled only 7 patients with 6 months offollow-up and it had no control group. On the otherhand, Wroblewski et al.42 conducted a study wheresubjects with BRVO were randomized 3:1 to intravitrealinjections of pegaptanib 0.3 or 1 mg at baseline and atweeks 6 and 12 with subsequent injections at 6-weekintervals at the discretion of the investigator until week48. He also found improvements in VA and macularthickness in this study with a 54 week follow-up.Therefore, the authors consider that intravitrealpegaptanib offers a promising alternative for macularedema secondary to BRVO.d) VEGF Trap
The VEGF trap is another novel anti-VEGF agent.It is essentially a small fully human, soluble VEGFreceptor that acts as a decoy receptor binding freeVEGF.93 The VEGF trap eye is currently underevaluation in two phase III studies on CRVO (GALILEOand COPERNICUS Studies) with 6-monthly injectionsof drug or sham-controlled injections. The latest six-months results of the phase III from COPERNICUSStudy multicenter, randomized, prospective, controlledtrial44 assessing the efficacy and safety of intravitrealtrap-eye in one hundred eighty-nine eyes with macularedema secondary to central retinal vein occlusion(CRVO) randomized 3:2 to receive VEGF trap-eye 2 mgor sham injection monthly for 6 months evidenced thatat week 24, 56.1% of VEGF trap-eye treated eyes gained15 letters or more from baseline versus 12.3% of sham-treated eyes (P<0.001). The VEGF Trap-Eye treated eyesgained a mean of 17.3 letters versus sham-treated eyes,which lost 4.0 letters (P<0.001). Central retinal thicknessdecreased by 457.2 mm in eyes treated with VEGF Trap-Eye versus 144.8 mm in sham-treated eyes (P<0.001),and progression to any neovascularization occurred in0 and 5 (6.8%) of eyes treated with VEGF Trap-Eye andsham-treated eyes, respectively (P= 0.006). Conjunctivalhemorrhage, reduced visual acuity, and eye pain werethe most common adverse events .Serious ocular werereported by 3.5% of VEGF trap-eye patients and 13.5%of sham patients. Incidences of nonocular seriousadverse events generally were well balanced betweenboth groups.
The authors concluded that at 24 weeks, monthlyintravitreal injection of VEGF Trap-Eye 2 mg in eyeswith macular edema resulting from CRVO improvedvisual acuity and central retinal thickness, eliminatedprogression resulting from neovascularization, and wasassociated with a low rate of ocular adverse eventsrelated to treatment.
The general consensus is that the intravitrealinjections turned out to be promising in recent clinicaltrials and appear to be an additional therapeuticoption45-54. But there are limits in efficacy, need formultiple injections, rebound effect of macular edemaand non-responders. There are still many unclearpoints, such as: the correct time to start injections andthe specific moment to finish them, the number ofinjections, the long-term efficacy and safety, ocular andsystemic side effects.
The International Intravitreal Bevacizumab SafetySurvey gathered adverse events from doctors aroundthe world via the internet and showed all ocular andsystemic side effects to be under 0.21%55 includingcorneal abrasion, lens injury, endophthalmitis, retinaldetachment, uveitis, cataract progression, acute visionloss, central retinal artery occlusion, sub-retinalhaemorrhage, retinal pigment epithelium tears, bloodpressure elevation, transient ischaemic attack,cerebrovascular accident and death.
The latest study56 revealed that endophthalmitisfollowing intravitreal injection is associated with anincreased incidence of Streptococcus spp. infection,earlier presentation and poorer visual outcomes whencompared with endophthalmitis following cataractsurgery. While used intravitreally, the systemicabsorption is minimal, however, a trend has beenobserved towards a higher risk of stroke among patientswith a history of heart disease42. In conclusion, patientsshould discuss the potential risks and benefits ofintravitreal pharmacotherapy with their physiciansbefore receiving treatment.SURGICAL TREATMENTi) Radial optic neurotomy (RON)
Radial optic neurotomy, a new surgical techniquehas been recently proposed for treatingCRVO 57,65 andhemicentral RVO66,68. It is hypothesized that CRVOconstitutes a neurovascular compartment syndrome atthe site of the lamina cribrosa, which can be alleviatedby performing a radial incision at the nasal part of theoptic nerve head, relaxing the cribriform plate and theadjacent sclera.
Recently, Opremcak et al.57,60 claimed that surgicaldecompression of the vein in CRVO by making a radialcut from the vitreous side in the optic nerve headextending all the way down to the lamina cribrosa,adjacent sclera and cutting the arterial circle of Zinn
Macular Edema Treatment in Retinal Vein Occlusion : How Forward we are?

224 Ophthalmology Update Vol. 10. No. 3, July-September 2012
and Haller by a procedure they called “radial opticneurotomy” (RON) is a technically feasible and safeprocedure that was associated with anatomicalresolution of CRVO in 95% patients and improvedvisual function in 71%. Some authors also haveadvocated RON for CRVO58,59,61-63, 66,67 and hemicentralRVO65, however Horio and Horiguchi59 in a study of 7patients with CRVO underwent RON have found thatVA was better than the preoperative VA by two or morelines in three out of seven eyes, and was worse in twoeyes, macular edema was improved, but stated that theycannot exclude the possibility that the changesrepresent the natural course of this disease.
Garcia Arumi et al. comparing of outcome afterRON in younger vs older patients concluded thatfunctional results were better in younger patientsalthough functional improvement remained limited inthose with low baseline VA. Recently, Rizvi et al.67
presented an intervention case series of 11 patients withCRVO treated by RON. The authors concluded that arandomized study with a larger number of patients isnecessary to establish the factors important fordeveloping collateral circulation that allows for blooddrainage beyond the occluded vessel.
Hayreh have studied the anatomy and bloodsupply of the optic nerve head and its ischaemicdisorders in detail69 and have found that the claim madeby some authors that RON is a safe procedure is totallyunwarranted, for the following reasons: 1) RON is goingto cut the arterial circle of Zinn and Haller, which isone of the sources of blood supply to optic nerve head.Therefore, this procedure is bound to cut off bloodsupply to the optic nerve head, resulting in acuteischemia of the optic nerve head and visual loss. 2) RONis also going to cut a large number of nerve fibers inthe optic nerve head, and that is found to produce visualloss and visual field defects. 3) There is a risk of cuttingor damaging the central retinal artery and/or centralretinal vein during RON because the two structures liein close apposition in the optic nerve head. Thus,Hayreh concluded that RON cannot be considered asafe procedure by any standard.
Visual field defects were associated withRON61,65,68, Hasselbach et al.61 found various defects in86.8 % of all cases. Takaya et al.71 presented a case ofarterial bleeding from the incision site during RON inpatient with CRVO and following haemorrhagic retinaldetachment and vitreous haemorrhage.
To avoid complications following a deeperincision in RON Wrede et al.64 have found that thedevelopment of a knife with a fixed penetration depthwould be helpful. Voger et al.72 examinedhistopathologic findings in a human eye after RON forischaemic CRVO and enucleated due to neovascular
glaucoma and concluded that they do not provideevidence for the postulated mechanism of action and itappears prudent to further evaluate this techniquebefore its general implementation in the managementof CRVO. In conclusion, there is not much scientificallyvalid evidence of the beneficial effects of this procedure.ii) Vitrectomy
Hvarfner and Larsson73 evaluated the effect ofvitrectomy in eyes with non-ischaemic macular edemasecondary to hemi and CRVO and concluded that ithas the potential to reduce macular edema and improveVA in the early postoperative phase but does not seemto improve the long term outcome of the disease.Furukawa et al.74 have found that vitrectomy with thecreation of a posterior vitreous detachment also appearsto be a possibly effective treatment in some eyes withCME associated with non-ischaemic CRVO.
Some authors have advocated vitrectomy withinternal limited membrane (ILM) peeling for macularedema secondary for RVO75-77, claiming rapidlyreduction of macular edema with improvement in VA.
Recently, Mandelcorn et al.76 claimed enthusi-astically that in CRVO and BRVO cases maculardecompression by ILM peeling may reduce macularedema and haemorrhage and improve visual acuity byrelieving elevated intra-retinal tissue pressure andfacilitating egress of blood and extracellular fluid outof inner retinal layers into the vitrectomized vitreouscavity.
In conclusion, further randomized and controlledstudies are needed to confirm these results and tocompare them to the natural course of the disease.iii) Arteriovenous adventitial sheathotomy
Most branch retinal vein occlusions occur at anarteriovenous crossing site78. It has been proposed thatconditions such as hypertension or arteriosclerosis maycompress the lumen of the venule, which may in turnlead to occlusion, and that relieving the compressionby surgical sheathotomy may improve the outcome ofBRVO. The principle steps of this procedure are a parsplana vitrectomy, following which the overlying arteryis separated from the vein by creating an incision inthe adventitial sheath adjacent to the arterio-venouscrossing and then separating the adhesions.
Although the study by Mason et al.79 reported abeneficial effect on VA in those patients undergoingsurgery compared with those receiving laser or notreatment, the study was not randomized and waspartly retrospective, introducing sources of potentialbias. Feltgen et al.80 in the prospective study of 35patients with BRVO have evaluated effect of arterio-venous dissection on VA and concluded that visualimprovement was found irrespective of the successfuldissection of vessels. The cataract formation rate and
Macular Edema Treatment in Retinal Vein Occlusion : How Forward we are?

Ophthalmology Update Vol. 10. No. 3, July-September 2012 225
additional surgery was a shortcoming of this procedure.Rodanant and Thoongsuwan81 and Wrigstad andAlgvere82 in a case reports have found that sheathotomymay improve vision and decrease macular edema inselected cases of BRVO. In conclusion, there is currentlyno evidence from randomized clinical trials supportingthe routine use of adventitial sheathotomy to improveVA in eyes with BRVO.COMBINATION THERAPYi) RON and intraocular TASome authors83,84 have advocated RON withsimultaneous, adjunctive intraocular TA for CRVO.Opremcak et al.84 claimed enthusiastically that clinicalimprovement was noted in 93% of patients followingRON and intraocular TA, which paralleled outcomesfollowing RON alone, but combined procedure wasassociated with a higher incidence of elevated IOP andendophthalmitis.ii) Vitrectomy and intraocular TA
Vitrectomy and intraocular TA were also used inmacular edema secondary to RVO75,84-86. Nkeme et al.,in a study of 4 patients with nonischaemic RVO andTsujikawa et al.86 in a study of 17 patients with BRVOhave found that an intraoperative injection of TA incombination with pars plana vitrectomy has thepotential to facilitate the absorption of macular edema.Simultaneous peeling of ILM was done by someauthors75, 74.
Yamashita et al.87 also have evaluated long-termIOP response after this combined procedure and statedthat a dose-dependent IOP elevation was observed,starting from early postoperative days and returningto normal values after several months.iii) Vitrectomy and sheathotomy
Mason et al.79 compared vitrectomy combinedwith adventitial sheathotomy with a concurrent controlgroup in which patients with BRVO were treated withlaser or no treatment. The surgical group also had astatistically significant increase in VA when comparedwith control patients, with an average increase of 4.55lines compared with 1.55 lines in the control group.Sohn and Song88, in a study of 22 patients with BRVOand recurrent macular edema, found visualimprovement in 10 eyes (45%) and decrease of foveathickness and concluded that vitrectomy withsheathotomy can be one treatment option for thesepatients. Kumagai et al.89 comparing the long-termeffect of vitrectomy with or without sheathotomy formacular edema secondary for BRVO, have found thatadditional arteriovenous sheathotomy did not lead toa distinct functional benefit, but early surgicalintervention may result in better visual outcomes.iv) Vitrectomy and endovascular lysis
Feltgen et al.90, in a prospective study of 13
patients with ischaemic CRVO performed endovascularlysis by injecting a fibrinolytic agent directly into acannulated retinal vein after vitrectomy and have foundthat CRVO patients did not profit from this procedureand the number of postoperative complications isunacceptably high.
In conclusion, in spite of various claims made invarious studies about the beneficial effect of surgery inmacular edema secondary to RVO, there is littlescientifically valid evidence of its effectiveness, sinceto date no randomized controlled trials on surgicalprocedures have been conducted and any evidencesupporting these procedures has been based on clinicalcase series.v) Laser Treatment
The Central Vein Occlusion Study91, a largeprospective randomized clinical trial, did not showstatistically significant VA benefit from grid laserphotocoagulation for macular edema. Two randomizedclinical trials investigated the efficacy of grid macularlaser treatment for macular edema secondary toBRVO72,73. The Branch Vein Occlusion Study (BVOS)Group have found that patients treated with grid lasergained an average of 1.33 lines at the third year studyvisit from baseline compared with 0.23 lines in thecontrol group. The grid laser group had statisticallysignificant improvements in VA with 65 % treatedversus 37 % controls gaining 2 or more lines of visionover consecutive visits. Battaglia Parodi et al. in otherrandomized clinical study assessing the effect of gridmacular laser photocoagulation on macular edema inBRVO have found that improvement in VA was relatedto natural history rather than laser photocoagulationin patients with very early (less than 15 days) onset ofBRVO.
In conclusion, grid laser photocoagulation is notrecommended for macular edema secondary to CRVOand is recommended as an effective treatment to reducemacular edema and to improve VA in BRVO withmacular edema after 3 months of onset, allowing forany spontaneous resolution, reduction in haemorrhage,and VA of 20/40 or less.CONCLUSION:
In conclusion, studies evaluating interventions formacular edema secondary to RVO have lackedsufficient sample size and power, are not controlled orlack an adequate control using placebo or best practiceintervention, combine one interventional therapy withanother, did not have insufficient follow-up times forlong-term assessment of outcomes, or a combinationthereof. Therefore, definitive conclusions cannot bereached. In spite of enthusiastic claims of success forvarious therapies, the reality is that the currentlyavailable treatments are associated with visual
Macular Edema Treatment in Retinal Vein Occlusion : How Forward we are?

226 Ophthalmology Update Vol. 10. No. 3, July-September 2012
improvement in only a subset of patients and theapproach to treatment of macular edema secondary toRVO is not evidence-based yet. The benefits and risksof therapy should be weighted in all treatmentdecisions. There is a need for large well-designedprospective randomized controlled trials with a long-term follow-up of new drugs taken in a non-invasiveway.REFERENCE:1. Shahid H, Hossain P, Amoaku WM. The management of
retinal vein occlusion: is interventional ophthalmology theway forward? Br J Ophthalmol 2006; 90(5): 627-39.
2. Hayreh SS, Zimmerman MB, Podhajsky P. Incidence ofvarious types of retinal vein occlusion and their recurrenceand demographic characteristics. Am J Ophthalmol 1994; 117:429-41.
3. Michel J. Ueber die anatomischen Ursachen vonVeraenderungen des Augenhintergrundes bei einigenAllgemeinerkrankungen. Dtsch Arch Klin Med 1878; 22: 339-45.
4. Sperduto RD, Hiller R, Chew E et al.Risk factors forhemiretinal vein occlusion: comparison with risk factors forcentral and branch retinal vein occlusion: the eye diseasecase-control study. Ophthalmology 1998;105(5):765-71
5. Koizumi H, Ferrara DC, Bruè C, Spaide RF. Central retinalvein occlusion case-control study. Am J Ophthalmol2007;144(6):858-863
6. The Eye Disease Case-Control Study Group. Risk factors forcentral retinal vein occlusion. Arch Ophthalmol 1996; 114:545-54.
7. Lang GE, Spraul CW. Risk factors for retinal vein occlusivediseases. Klin Monatsbl Augenheilkd 1997; 211: 217-26.
8. Shahsuvaryan ML, Melkonyan AK. Central retinal veinocclusion risk profile: a case-control study. Eur J Ophthalmol2003; 13: 445-52.
9. Arakawa S, Yasuda M, Nagata M, et al. Nine-year incidenceand risk factors for retinal vein occlusion in a generalJapanese population: the Hisayama Study. InvestOphthalmol Vis Sci; 2011;52(8):5905-9.
10. Murakami T, Takagi H, Kita M et al. Intravitreal tissueplasminogen activator to treat macular edema associatedwith branch retinal vein occlusion. Am J Ophthalmol 2006;142(2): 318-20.
11. The SCORE Study Research Group: A randomized trialcomparing the efficacy and safety of intravitrealtriamcinolone with observation to treat vision loss associatedwith macular edema secondary to central retinal veinocclusion (SCORE) study report 5. Arch Ophthalmol2009;127:1101–1114.
12. The SCORE Study Research Group: A randomized trialcomparing the efficacy and safety of intravitrealtriamcinolone with standard care to treat vision lossassociated with macular edema secondary to branch retinalvein occlusion: the standard care vs corticosteroid for retinalvein occlusion (SCORE) study report 6. Arch Ophthalmol2009;127:1115–1128.
13. Haller JA, Bandello F, Belfort R. et al. OZURDEX GENEVAS tudy Group: Randomized, sham-controlled trial ofdexamethasone intravitreal implant in patients with macularedema due to retinal vein occlusion. Ophthalmology 2010;117:1134-46.
14. London NJ, Chiang A, Haller JA.The dexamethasone drugdelivery system: indications and evidence. Adv Ther.2011;28(5):351-66.
15. Lin JM, Chiu YT, Hung PT, Tsai YY. Early treatment of severe
cystoid macular edema in central retinal vein occlusion withposterior sub-tenon triamcinolone acetonide. Retina 2007;27(2): 180-9.
16. Iwao K, Inatani M, Kawaji T, Koga T, Mawatari Y, TaniharaH. Frequency and risk factors for intraocular pressureelevation after posterior sub-Tenon capsule triamcinoloneacetonide injection. J Glaucoma 2007; 16(2): 251-6.
17. Mizuno S, Nishiwaki A, Morita H, Mivake T, Ogura Y. Effectsof periocular administration of triamcinolone acetonide onleukocyte-endothelium interactions in the ischaemic retina.Invest Ophthalmol Vis Sci 2007; 48(6): 2831-6.
18. Pieramici DJ, Rabena M, Castellarin AA, Nasir M, See R,Norton T, Sanchez A, Risard S, Avery RL: Ranibizumab forthe treatment of macular edema associated with perfusedcentral retinal vein occlusion. Ophthalmology 2008;115:e47–e54.
19. Spaide RF, Chang LK, Klancnik JM, Yannuzzi LA, SorensonJ, Slakter JS, Freund KB, Klein R: Prospective study ofranibizumab as a treatment of decreased visual acuitysecondary to central retinal vein occlusion. Am J Ophthalmol2009;147:298–306.
20. Rouvas A, Petrou P, Vergados I, Pechtasides D, Liarakos V,Mitsopoulou M, Ladas I: Intravitreal ranibizumab (Lucentis)for treatment of central retinal vein occlusion: a prospectivestudy. Graefes Arch Clin Exp Ophthalmol 2009;247:1609–1616.
21. Pieramici DJ: Intravitreal ranibizumab for treatment ofmacular edema secondary to retinal vein occlusion. RetinaToday 2009;4:44–46.
22. Campochiaro PA, Heier JS, Feiner L, Gray S, Saroj N, RundleAC, Murahashi WY, Rubio RG, BRAVO Investigators:Ranibizumab for macular edema following branch retinalvein occlusion six-month primary end point results of a phaseIII study. Ophthalmology 2010;117:1102–1112.
23. Brown DM, Campochiaro PA, Singh RP, Li Z, Saroj N, RundleAC, Rubio RG, Murahashi WY, CRUISE Investigators:Ranibizumab for macular edema following central retinalvein occlusion six-month primary end point results of a phaseIII study. Ophthalmology 2010;117:1124–1133.
24. Garnock-Jones KP Ranibizumab: in macular oedemafollowing retinal vein occlusion. Drugs. 2011 ;5;71(4):455-63.
25. Brown DM: Clinical implications of the BRAVO and CRUISEtrials. Retina Today 2010;5:38–40.
26. Heier JS, Campochiaro PA, Yau L, Li Z, Saroj N, Rubio RG,Lai P. Ranibizumab for Macular Edema Due to Retinal VeinOcclusions Long-term Follow-up in the HORIZON Trial.Ophthalmology 2012;11 (2):145-57.
27. Iturralde D, Spaide RF, Meyerle CB, Klancnik JM, YannuzziLA, Fisher YL, Sorenson J, Slakter JS, Freund KB, Cooney M,Fine HF: Intravitreal bevacizumab (Avastin) treatment ofmacular edema in central retinal vein occlusion. A short-termstudy. Retina 2006;26:279–284.
28. Costa RA, Jorge R, Calucci D, Melo LA Jr, Cardillo JA, ScottIU: Intravitreal bevacizumab (Avastin) for central and retinalvein occlusions. IBeVo study. Retina 2007;27:141–149.
29. Fish GE: Intravitreous bevacizumab in the treatment ofmacular edema from branch retinal vein occlusion andhemisphere retinal vein occlusion (an AOS thesis). Trans AmOphthalmol Soc 2008;106:276–300.
30. Rabena MD, Pieramici DJ, Castellarin AA, Nasir MA, AveryRL: Intravitreal bevacizumab (Avastin) in the treatment ofmacular edema secondary to branch retinal vein occlusion.Retina 2007;27:419–425.
31. Badalá F: The treatment of branch retinal vein occlusion withbevacizumab. Curr Opin Ophthalmol 2008;19:234–238.
32. Wu L, Arevalo JF, Roca JA, Maia M, Berrocal MH, RodriguezFJ, Evans T, Costa RA, Cardillo J: Comparison of two doses
Macular Edema Treatment in Retinal Vein Occlusion : How Forward we are?
Ophthalmology Update Vol. 10. No. 3, July-September 2012 227
of intravitreal bevacizumab (Avastin) for treatment ofmacular edema secondary to branch retinal vein occlusion:results from the Pan-American Collaborative Retina Study(PACORES) Group at 6 months of follow-up. Retina2008;28:212–219.
33. Chung EJ, Hong YT, Lee SC, Kwon OW, Koh HJ: Prognosticfactors for visual outcome after intravitreal bevacizumab formacular edema due to branch retinal vein occlusion. GraefesArch Clin Exp Ophthalmol 2008;246:1241–1247.
34. Ahmadi AA, Chou JY, Banashkevich A, Ma PE, MaberleyDA: The effects of intravitreals bevacizumab on patients withmacular edema secondary to branch retinal vein occlusion.Can J Ophthalmol 2009;44:154–159.
35. Prager F, Michels S, Kriechbaum K, Georgopoulos M, FunkM, Geitzenauer W, Polak K, Schmidt-Erfurth U: Intravitrealbevacizumab (Avastin) for macular oedema secondary toretinal vein occlusion: 12-month results of a prospectiveclinical trial. Br J Ophthalmol 2009;93:452–456.
36. Kondo M, Kondo N, Ito Y, Achi S, Kikuchi M, Yasuma TR,Ota I, Miyake K, Terasaki H: Intravitreal injection ofbevacizumab for macular edema secondary to branch retinalvein occlusion. Results after 12 months and multipleregression analysis. Retina 2000;29:1242–1248.
37. Wu L, Arevalo JF, Berrocal MH, Maia M, Roca JA, Morales-Cantón V, Alezzandrini AA, Díaz-Llopis MJ: Comparisonof two doses of intravitreal bevacizumab as primarytreatment of macular edema secondary to branch retinal veinocclusions: results from the Pan-American CollaborativeRetina Study (PACORES) Group at 24 months. Retina2009;29:1396–1403.
38. Ach T, Hoeh AE, Schaal KB, Scheuerle AF, Dithmar S:Predictive factors for changes in macular edema inintravitreal bevacizumab therapy of retinal vein occlusion.Graefes Arch Clin Exp Ophthalmol 2010;248:155–159.
39. Ghayoor I, Bokhari SA, Kamil Z, Shakir M, Zafar S, KhanMA. To assess the effect of intravitreal Bevacizumab(Avastin) in the treatment of macular edema secondary toretinal vein occlusion. Ophthalmology Update 2012;10(1):7-13.
40. Epstein DL, Algvere PV, von Wendt G, Seregard S, KvantaA. Bevacizumab for Macular Edema in Central Retinal VeinOcclusion: A Prospective, Randomized, Double-MaskedClinical Study. Ophthalmology (Mar 2012)
41. Bennet MD: Pegaptanib for the treatment of ischemicretinopathy in patients with diabetes and retinal vascularocclusive disorders. Retina Today 2009;4:63–66.
42. Wroblewski JJ, Wells JA 3rd, Gonzales CR: Pegaptanibsodium for macular edema secondary to branch retinal veinocclusion. Am J Ophthalmol 2010;149:147–154.
43. Pieramici DJ, Rabena MD: Anti-VEGF therapy: comparisonof current and future agents. Eye 2008;22;1330–1336
44. Boyer D, Heier J, Brown DM, Clark WL, Vitti R, Berliner AJ,Groetzbach G, Zeitz O, Sandbrink R, Zhu X, Beckmann K,Haller JA. Vascular Endothelial Growth Factor Trap-Eye forMacular Edema Secondary to Central Retinal Vein Occlusion:Six-Month Results of the Phase 3 COPERNICUS Study.Ophthalmology 2012; Mar 20.
45. Braithwaite T, Nanji AA, Greenberg PB. Cochrane DatabaseSyst Rev. Anti-vascular endothelial growth factor for macularedema secondary to central retinal vein occlusion.2010;(10):CD007325
46. Jonas J, Paques M, Mones J, Glacet-Bernard A. Retinal veinocclusions. Dev Ophthalmol 2010;47:111-35.
47. Rehak M, Wiedemann P. Retinal vein thrombosis:pathogenesis and management. J Thromb Haemost. 2010;8(9):1886-94.
48. Scott IU. Macular edema associated with retinal vein
occlusion. Retina today 2010; 4:54-5.49. Ehlers JP, Fekrat S. Retinal vein occlusion: beyond the acute
event. Surv Ophthalmol. 2011;56(4):281-99.50. Laouri M, Chen E, Looman M, Gallagher M. The burden of
disease of retinal vein occlusion: review of the literature. Eye(Lond). 2011;25(8):981-8.
51. London NJ, Brown G. Update and review of central retinalvein occlusion. Curr Opin Ophthalmol. 2011;22(3):159-65.
52. Wells JA. The Paradigm Shifts in the Management of RetinalVein Occlusion. Retinal physician, November 2011
53. Lattanzio R, Torres Gimeno A, Battaglia Parodi M, BandelloF. Retinal vein occlusion: current treatment.Ophthalmologica. 2011;225(3):135-43.
54. Hahn P, Fekrat S. Best practices for treatment of retinal veinocclusion.Curr Opin Ophthalmol 2012 Mar 23.
55. Lynch SS, Cheng CM. Bevacizumab for neovascular oculardiseases. Ann Pharmacother 2007; 41(4): 614-25.
56. Simunovic MP, Rush RB, Hunyor AP, Chang AA.Endophthalmitis following intravitreal injection versusendophthalmitis following cataract surgery: clinical features,causative organisms and post-treatment outcomes. Br JOphthalmol published 24 March 2012, 10.1136/bjophthalmol-2011-301439
57. Opremcak EM, Bruce RA, Lomeo MD, Ridenour CD, LetsonAD, Rehmar AJ. Radial optic neurotomy for central retinalvein occlusion: A retrospective pilot study of 11 consecutivecases. Retina 2001; 21: 408-15.
58. Kolar P, Vlkova E, Vyslouzilova D. Radial neurotomy of theoptic nerve in central retinal vein occlusion (case reports).Cesk Slov Oftalmol 2005; 61(5): 321-9.
59. Horio N, Horiguchi M. Retinal blood flow and macularedema after radial optic neurotomy for central retinal veinocclusion. Am J Ophthalmol 2006; 141(1): 31-34.
60. Opremcak EM, Rehmar AJ, Reidenour CD, Kurz DE. Radialoptic neurotomy for central retinal vein occlusion: 117consecutive cases. Retina 2006; 26(3): 297-305.
61. Hasselbach HC, Ruefer F, Feltgen N. et al. Treatment ofcentral retinal vein occlusion by radial optic neurotomy in107 cases. Graefes Arch Clin Exp Ophthalmol 2007; Epubahead of print.
62. Garcia-Arumi J, Boixadera A, Martinez-Castillo V, MontolioM, Verdugo A, Corcostegui B. Radial optic neurotomy incentral retinal vein occlusion: comparison of outcome inyounger vs older patients. Am J Ophthalmol 2007; 143(1):134-140. Epub 2006 Oct 9.
63. Binder S, Aggermann T, Brunner S. Long-term effects ofradial optic neurotomy for central retinal vein occlusionconsecutive interventional case series. Graefes Arch Clin ExpOphthalmol 2007; Epub ahead of print.
64. Wrede J, Varadi G, Volcker HE, Dithmar S. Radial opticneurotomy for central retinal vein occlusion – how deepshould it be? Ophthalmologe 2006; 103(4): 321-4.
65. Barak A, Kesler A, Gold D, Loewenstein A. Visual fielddefects after radial optic neurotomy for central retinal veinocclusion. Retina 2006; 26(5): 549-54.
66. Garcia-Arumi J, Boixadera A, Martinez-Castillo V, Blasco H,Lavaque A, Corcostegui B. Radial optic neurotomy formanagement of hemicentral retinal vein occlusion. ArchOphthalmol 2006; 124(5): 690-5.
67. Rizvi F, Kamil Z, Bokhari SA, Zafar S, Shakir M. Radial OpticNeurotomy (RON) in cases of central retinal vein occlusion.Ophthalmology Update 2012; 10(1):14-17.
68. Sakaguchi H, Ohji M, Kamei M. et al. Radial optic neurotomyfor the management of hemicentral retinal vein occlusion:long-term follow-up study. Retina 2006; 26(5): 555-61.
69. Hayreh SS. The blood supply of the optic nerve head andthe evaluation of it – myth and reality. Prog Retin Eye Res
Macular Edema Treatment in Retinal Vein Occlusion : How Forward we are?
228 Ophthalmology Update Vol. 10. No. 3, July-September 2012
2001; 20: 563-93.70. Hayreh SS. Central retinal vein occlusion. Ophthalmol Clin
North Am 1998; 11:559-90.71. Takaya K, Suzuki Y, Nakazawa M. Massive haemorrhagic
retinal detachment during radial optic neurotomy. GraefesArch Clin Exp Ophthalmol 2006; 244(2): 265-7. Epub @005Jul 23.
72. Vogel A, Holz FG, Loeffler KU. Histopathologic findingsafter radial optic neurotomy in central retinal vein occlusion.Am J Ophthalmol 2006; 141(1): 203-5.
73. Hvarfner C, Larsson J. Vitrectomy for non-ischaemic macularoedema in retinal vein occlusion. Acta Ophthalmol Scand2006; 84(6): 812-4.
74. Furukawa M, Kumagai K, Ogino N, Uemura N, Larson E.Long-term visual outcomes of vitrectomy for cystoid macularedema due to nonischaemic central retinal vein occlusion.Eur J Ophthalmol 2006; 16(6): 841-6.
75. Nkeme J, Glaccet-Bernard A, Gnikpingo K. et al. Surgicaltreatment of persistent macular edema in retinal veinocclusion. J Fr Ophtalmol 2006; 29(7): 808-14.
76. Mandelcorn MS, Mandelcorn E, Guan K, Adatia FA. Surgicalmacular decompression for macular edema in retinal veinocclusion, Can J Ophthalmol 2007; 42(1): 116-22.
77. Liang XL, Chen HY, Huang YS. et al. Pars plana vitrectomyand internal limiting membrane peeling for macular oedemasecondary to retinal vein occlusion: a pilot study. Ann AcadMed Singapore 2007; 36(4): 293-7.
78. Weinberg D, Dodwell DG, Fern SA. Anatomy of arterio-venous crossings in branch retinal vein occlusion. Am JOphthalmol 1990; 109: 298-302.
79. Mason J III, Feist R, White M Jr. et al. Sheathotomy todecompress branch retinal vein occlusion. A matched controlstudy. Ophthalmology 2004; 111: 540-5.
80. Feltgen N, Herrmann J, Agostini H, Sammain A, Hansen LL.Arterio-venous dissection after isovolaemic haemodilutionin branch retinal vein occlusion: a non-randomizedprospective study. Graefes Arch Clin Exp Ophthalmol 2006;244(7): 829-35.
81. Rodanant N, Thoongsuwan S. Sheathotomy withoutseparation of venule overlying arteriole at occlusion site inuncommon branch retinal vein occlusion. J Med Assoc Thai2005; 88 Suppl 9: S143-50.
82. Wrigstad A, Algvere P. Arteriovenous adventitialsheathotomy for branch retinal vein occlusion: report of a
Macular Edema Treatment in Retinal Vein Occlusion : How Forward we are?
case with long-term follow-up. Acta Ophthalmol Scand 2006;84(5): 699-702.
83. Furino C, Ferrari TM, Boscia F. et al. Combined radial opticneurotomy, internal limiting membrane peeling, andintravitreal triamcinolone acetonide for central retinal veinocclusion. Ophthalmic Surg Lasers Imaging 2005; 36(5): 422-5.
84. Opremcak EM, Rehmar AJ, Ridenour CD, Kurz DE,Borkowski LM. Radial optic neurotomy with adjunctiveintraocular triamcinolone for central retinal vein occlusion:63 consecutive cases. Retina 2006; 26(3): 306-13.
85. Shah GK, Rosenblatt BJ, Blinder KJ, Grand MG, Smith M.Triamcinolone-assisted internal limiting membrane peeling.Retina 2005; 25(8): 972-5.
86. Tsujikawa A, Fujihara M, Iwawaki T, Yamamoto K, KurimotoY. Triamcinolone acetonide with vitrectomy for treatmentof macular edema associated with branch retinal veinocclusion. Retina 2005; 25(7): 861-7.
87. Yamashita T, Uemura A, Kita H, Sakamoto T. Intraocularpressure after intravitreal injection of triamcinoloneacetonide following virtectomy for macular edema. JGlaucoma 2007; 16(2): 220-4.
88. Sohn JH, Song SJ. Arteriovenous sheathotomy for persistentmacular edema in branch retinal vein occlusion. Korean JOphthalmol 2006; 20(4): 210-4.
89. Kumagai K, Furukawa M, Ogino N, Uemura A, Larson E.Long-term outcomes of vitrectomy with or withoutarteriovenous sheathotomy in branch retinal vein occlusion.Retina 2007; 27(1): 49-54.
90. Feltgen N, Junker B,Agostini H, Hansen LL. Retinalendovascular lysis in ischaemic central retinal vein occlusion:one-year results of a pilot study. Ophthalmology 2007; 114(4):716-23.
91. Central Retinal Vein Occlusion Study Group: Evaluation ofgrid pattern photocoagulation for macular edema in centralvein occlusion. The Central Retinal Vein Occlusion StudyGroup M report. Ophthalmology 1995; 102: 1425-33.
92. Branch Vein Occlusion Study Group. Argon laserphotocoagulation for macular edema in branch retinal veinocclusion. Am J Ophthalmol 1984; 98: 271-82.
93. Battaglia Parodi M, Saviano S, Bergamini L, Ravalico G. Gridlaser treatment of macular edema in macular branch retinalvein occlusion. Doc Ophthalmol 1999; 97: 427-31.

Ophthalmology Update Vol. 10. No. 3, July-September 2012 229
–––––––––––––––––––––––––––––––––––––––––––––––––––––*The study was carried out at the Department of Ophthalmology,Baqai Medical University Karachi–––––––––––––––––––––––––––––––––––––––––––––––––––––1. Professor of Ophthalmology2.3Registrars–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Prof. Dr. Syed AmjadRizvi Department ofOphthalmology, Baqai Medical University, superhighway, Karachi.Cell: 0313-2321942. Fax 021-363118109.E. Mail: [email protected]: A-11, Block - 9 Federal B Area, Karachi.,–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: March”2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
INTRODUCTIONGlaucoma is characterized by progressive
ganglion cell death, which clinically manifests as typicalvisual field (VF), optic nerve head (ONH) and retinalnerve fibre layer (RNFL) damage. As yet, the diagnosisand / or progression of glaucoma are established byanalyzing these manifestations. As the visual fielddefects may appear later then the damage in the ONHand NFL damage,1 the focus is currently on scrutinizingthe later two structures for the management ofglaucoma. As a result, sophisticated devices have beendeveloped to study these structures.2 However, thesetechnologies are expensive and most eye departments,especially those in the developing countries, cannotafford to use them for documenting all the glaucomacases. Simpler methods like determining the cup to discratio are too crude to be useful.3A need therefore exists
for a method to document the ONH changes whichshould be accurate, but simple and cost effective.
Spaeth and colleagues proposed an ONH gradingsystem, the Disc Damage Likelihood Scale (DDLS),4
which takes into account the size of the optic disc andthe narrowest neuro-retinal rim (NRR), therebyproviding, not only a standardized and accuratemethod of ONH documentation, but also someinformation regarding the likelihood of glaucomatousdamage. The system’s diagnostic power,5,6,7,8
reproducibility9 and ability to detect glaucomaprogression,10 have been validated over time.A studywas done to determine how the disc damage likelihoodscale correlates with the visual field damage, regardlessof the actual aetiology of the optic disc damage.MATERIALS AND METHODS
In this observational case series, all the patientsattending the Baqai University Hospital and itsaffiliated centres between August 2010 to February2011, whose automated VF analysis results, and stereo-photographs of the ONH (SPs) were available, wereincluded in the study. The patients with unreliable VFresults ((>20% fixation errors, >33% false-positives, and>33% false-negatives), and / or poor quality SPs, wereexcluded. As the correlation of the DDLS grade andvisual field defects was to be studied without otherinfluences, the individual eyes were used forcomputation of statistical correlation rather than the
Correlation of Visual Field Damage &the Disc Damage likelihood Scale*
Prof. Syed Amjad Rizvi FCPS1, Uroob Mirza Barlas MBBS2
Lal Mohammad Khan MBBS3
ABSTRACTTitle: Correlation of visual field damage and disc damage likelihood scale.Purpose:To determine how the disc damage likelihood scale ((DDLS) correlates with the visual field (VFs) damage,regardless of the actual aetiology of the optic disc damage. Study design:Retrospective, observational case series.Subjects and Methods:After approval from the competent authorities, the records of the patients attending the outpatientclinics of the Eye Department of the Baqai University Hospital and its associated eye centres (between between August2010 to February 2011), whose reliable VF test results and stereo-photographs (SPs) of the optic discs were available,were searched and the severity of the defects in the VFs as represented by the mean deviation (MD), was correlated withthe grade of DDLS, as determined from the SPs. The data was analysed using Pearson product-moment correlationcoefficient, and the significance determined by 2-tailed t test, using the SPSS software.Results:Altogether 42 eyes of 21 patients (15 males and 6 females) were included in the study. The means (MD + / - SD)of 42 eyes for the DDLS grades and VF MD was, 5.6 +/- 2.2 (range from 1 to 9), and -6.5 DB +/- 4.7 (range 1 to 18)respectively. There was a strong positive correlation between the grades of the DDLS and amount of visual field damage(r = 0.85) which was highly significant (p <0.01). Two discs which were definitely non-glaucomatous were also graded asdamaged in the DDLS.Conclusion:DDLS is significantly correlated to the visual field defects in a positive, linear manner. However, otherevidence of glaucoma must be sought for before establishing the diagnosis.Key words: Glaucoma, Optic Disc, visual filed defects, Diagnosis
Original Article
Prof.Rizvi

230 Ophthalmology Update Vol. 10. No. 3, July-September 2012
patients. No attempt was made to classify the eyes asglaucomatous or non glaucomatous. (This is the topicof another ongoing study yet to be published).However, for the purpose of listing the frequencydistribution, the diagnosis, age and sex were noted. Allother variables were disregarded.
The procedure for determination of DDLS hasbeen described previously.8 Briefly, the process includesdetermination of the ONH size using a slit lamp beamand a high plus lens e.g. 60 D, 78 D, or 90 D, andmultiplying it with the multiplication factor (MF) of thelens used (e.g. the MF of Volk 90 D lens is 1.3), whilethe degree and extent of narrowest part of the NRR isestimated clinically, using the same equipment or adirect ophthalmoscope. The ratio between thenarrowest part of the rim and the disc diameter in thatmeridian is then determined. If the NRR is absent atsome place, its extent is determined in clock hours. Thedisc is then graded into 1 to 10, according to the rim /disc ratio or the extent of the absent NRR. For the discssmaller (<1.5 mm) or larger (>2.0 mm) then the average,the grade is increased or decreased by one respectively.The details of the grading system are given in table 1.
In this study the size of the disc was determinedusing a slit lamp with a Volk 90 D lens. However,instead of clinical estimation, SPs of the ONHs wereused to determine the rim / disc ratio in order tomaintain reproducibility, as has been done previously.9
Sequential digital SPs were obtained using Canon 60Sfundus camera (Canon Inc., Tokyo, Japan), fitted withan Olympus E330 Digital SLR (Olympus Corp., Tokyo.Japan) camera body. The SPs were viewed using an on-screen stereo-viewer, and measurements done bymeans of a ruler.Visual fields testing was done using
Table 1
The disc damage likelihood scale8, narrowest width of rim (rim/disc ratio)
New DDLS For small disc For average size disc For large disc
Stage <1.50 mm 1.50–2.00 mm > 2.00 mm
1 0.5 or more 0.4 or more 0.3 or more
2 0.4 to 0.49 0.3 to 0.39 0.2 to 0.29
3 0.3 to 0.39 0.2 to 0.29 0.1 to 0.19
4 0.2 to 0.29 0.1 to 0.19 less than 0.1
5 0.1 to 0.19 less than 0.1 0 for less than 45°
6 less than 0.1 0 for less than 45° 0 for 46° to 90°
7 0 for less than 45° 0 for 46° to 90° 0 for 91° to 180°
8 0 for 46° to 90° 0 for 91° to 180° 0 for 181° to 270°
9 0 for 91° to 180° 0 for 181° to 270° 0 for more than270°
10 0 for more than 180° 0 for more than 270°
Humphrey (Carl Zeiss Meditec, Dublin, CA) 30-2 fullthreshold program, within a month of obtaining the SPs.Mean deviation (MD) was taken as the amount of fielddamage and used for statistical analysis.
The statistics software SPSS (IBM,) was used todetermine the correlation between the DDLS grades andamount of VF damage by Pearson product-momentcorrelation coefficient, as this is known to be a linearcorrelation without outliers. Correlation was to besignificant at the 0.01 level (2-tailedRESULTS
Altogether 42 eyes of 21 patients (15 males and6 females) were included in the study.
The means (MD + / - SD) of 42 eyes for the DDLSgrades and VF MD was, 5.6 +/- 2.2 (range from 1 to 9),and -6.5 DB +/- 4.7 (range 1 to 18) respectively.
There was a strong positive correlation betweenthe grades of the DDLS and amount of visual fielddamage (r = 0.85) which was highly significant (<0.01)
An incidental finding was that two of the discs,which were definitely not glaucomatous, were gradedas substantially damaged according to the DDLS. Onewas a case of tilted discs with minor VF defects (Figure1), and the other was a myopic disc with negligible VFdamage (Figure 2). Previous SPs of both the cases wereavailable for three and four years respectively, and hadshown no change.DISCUSSION
This study is in agreement with the earlier studiesin demonstrating the strong correlation between theDDLS and the VF defects. This fact could be useful forthe screening of glaucoma, which is not satisfactoryeven in advanced countries.11Clinical disc examinationof the optic disc is a convenient, cost effective, and
Correlation of Visual Field Damage & the Disc Damage likelihood Scale

Ophthalmology Update Vol. 10. No. 3, July-September 2012 231
potentially accurate method of glaucoma detection.However it can be quite inaccurate if only the cup todisc ratio is considered. Standardizing DDLS as auniform protocol for disc examination may enable eventhe junior ophthalmologists to detect glaucoma in earlystages.
This study is different from the previous studieson this topic in that the DDLS was correlated with theVF defects, irrespective of the VF defects beingglaucomatous or not. This was useful in determining ifthe DDLS can give false positive results; a fact whichcan help in determining it’s role as a screening tool infuture studies. Indeed, in this study, two cases whichwere definitely not glaucoma were classified asdamaged, demonstrating the relatively low specificityof the DDLS. This observation stresses the necessity tothoroughly evaluate the patient, considering all aspects,before making a diagnosis of glaucoma. The DDLS may
be more helpful as a screening tool rather than adiagnostic utility; the DDLS based abnormal casesdetected by non-ophthalmologists or non-glaucomaspecialists can be referred to a glaucoma specialist forfurther scrutiny.
One weakness of the study was the relativelysmall number of subjects. This is because of the factthat the availability of reliable visual fields test resultswas much less than the unreliable results and manyeyes had to be excluded from the study. This is acommon observation in our Country, especially amongthe less educated patients who generally visit thecharity or public sector eye departments.
Another shortcoming of the study was that MDwas used as a measure of visual field loss instead ofmore elaborate calculations. This was done to avoidcomplex computations, and due to the fact that theoverall damage of VF, rather than localized VF defects,was to be correlated to the DDLS. MD has been usedfor this purpose in many good studies.9, 12
There were more males in the study then thefemales. Although not statistically analyzed, this wassimply due to the fact that reliable results were availablemore for males then the females, and does not in anyway reflect the prevalence of glaucomatous damageamong the sexes.CONCLUSION:
DDLS is significantly correlated to the visual fielddefects in a positive, linear manner. However, otherevidence of glaucoma must be sought for beforeestablishing the diagnosisREFERENCES1) D Kamal, AViswanathan, D Garway-Heath, R Hitchings, D
Poinoosawmy, and C Bunce. Detection of optic disc changewith the Heidelberg retina tomograph before confirmedvisual field change in ocular hypertensives converting toearly glaucoma. Br J Ophthalmol. 1999;83(3):290–294.
2) Mansouri K, Leite MT, Medeiros FA, Leung CK, WeinrebRN. Assessment of rates of structural change in glaucomausing imaging technologies. Eye 2011;25(3):269-77
3) Wolfs RC, Ramrattan RS, Hofman A, de Jong PT. Cup-to-disc ratio: ophthalmoscopy versus automated measurementin a general population: the Rotterdam study.Ophthalmology. 1999;106(8):1597-601.
4) Bayer A, Harasymowycz P, Henderer JD, et al. Validity of anew disk grading scale for estimating glaucomatous damage:correlation with visual field damage. Am J Ophthalmol2002;133:758–763.
5) Abdul Majid AS, Kwag JH, Jung SH, Yim HB, Kim YD, KangKD. Correlation between disc damage likelihood scale andoptical coherence tomography in the diagnosis of glaucoma.Ophthalmologica. 2010;224(5):274-82.
6) Hornova J, Kuntz Navarro JB, Prasad A, Freitas DG, NunesCM. Correlation of Disc Damage Likelihood Scale, visualfield, and Heidelberg Retina Tomograph II in patients withglaucoma. Eur J Ophthalmol. 2008;18(5):739-47.
7) Danesh-Meyer HV, Gaskin BJ, Jayusundera T, Donaldson M,Gamble GD. Comparison of disc damage likelihood scale,cup to disc ratio, and Heidelberg retina tomograph in the
Correlation of Visual Field Damage & the Disc Damage likelihood Scale
Fig. 2. Stereograph of the myopic disc.
Fig. 1. Stereograph of the tilted disc.
232 Ophthalmology Update Vol. 10. No. 3, July-September 2012
diagnosis of glaucoma. Br J Ophthalmol. 2006;90(4):437-41.8) Henderer JD. Disc damage likelihood scale. Br J Ophthalmol.
2006;90(4):395-6.9) Spaeth GL, Henderer J, Liu C, Kesen M, Altangerel U, Bayer
A, Katz LJ, Myers J, Rhee D, Steinmann W. The disc damagelikelihood scale: reproducibility of a new method ofestimating the amount of optic nerve damage caused byglaucoma. Trans Am Ophthalmol Soc. 2002;100:181-5.
10) Henderer J, Wang Y, Bayer A, Altangerel U, Schwartz L,Schmidt C. Evaluating a new disc staging scale for
glaucomatous damage: the ability to detect change over time.Eur J Ophthalmol. 2009;19(3):404-10
11) Taylor H. Glaucoma screening in the real world.Ophthalmology. 2011;118(5):1008.
12) Yokoyama Y, Aizawa N, Chiba N, et al. Significantcorrelations between optic nerve head microcirculation andvisual field defects and nerve fiber layer loss in glaucomapatients with myopic glaucomatous disk. ClinOphthalmol.2011;5:1721-7
Correlation of Visual Field Damage & the Disc Damage likelihood Scale

Ophthalmology Update Vol. 10. No. 3, July-September 2012 233
–––––––––––––––––––––––––––––––––––––––––––––––––––––*Department of Ophthalmology, Hospital Sant Joan. UniversityRovira & Virgili, Institut de Investigació Sanitaria Pere Virgili (IISPV),Reus (Spain).–––––––––––––––––––––––––––––––––––––––––––––––––––––1Director, 2Chief of the Clinic,3Fellow of Department ofOphthalmology, 4Professor of Department of Basic Sciences,Instituto de Salud Carlos III (ISCIII), Spain 5Fellow of Departmentof Ophthalmology, 6Resident of Department of Ophthalmology,–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Prof. Pedro Romero-Aroca, Department ofOphthalmology, Hospital Sant Joan. University Rovira & Virgili,Institut de Investigació Sanitaria Pere Virgili (IISPV), Reus (Spain).–––––––––––––––––––––––––––––––––––––––––––––––––––––Acknowledgment: The management of Opthalmology Updatethanks Prof. Pedro for permitting to take the excerpts from hisoriginal article.–––––––––––––––––––––––––––––––––––––––––––––––––––––
INTRODUCTIONEndophthalmitis remains a serious complication
after cataract surgery, although prophylactic measuresintroduced in recent years have reduced the numberof patients with this complication.
Currently there are two streams of opiniontowards endophthalmitis prophylaxis, the use of fourth-generation quinolones (gatifloxacin and moxifloxacin)topically,1–4 or the introduction of intracameralcephalosporins, the latter being cefuroxime (a secondgeneration cephalosporin), which is the most widelyused and accepted.5–10 However, our study group,11 aswell as Garat et al,2,13 prefers the use of cefazolin (a firstgeneration cephalosporin). Having previously studiedthe bacteria that cause endophthalmitis in ourenvironment most frequently, we prefer cefazolinbecause of its higher frequency of gram-positive
bacteria in our medium, and because it best coversinfections by such bacteria. Furthermore, cefazolinshows no corneal toxicity at doses of 1 mg or 2 mg; itstoxicity was established when doses of 5 mg or morewere injected. We consider the risk of an infectioncaused by a cefazolin-resistant bacterium low, basedon the bacteria cultured since 1994 and theirantibiogram. We consider there not to be any risk ofcoverage of gram-negative bacteria by cefazolin, andits incidence in endophthalmitis was low in our HealthCare District.
Our two groups are included in the BarcelonaEndophthalmitis Group (GEB), formed by 38 public andprivate Hospitals in Catalonia (Spain), who have beenstudying the epidemiological factors of postoperativeendophtalmitis and assessing the prophylaxis andtreatment of endophtalmitis in our country since 2000.
This study will present the results obtained afterseven years of using intracameral cefazolin aftercataract surgery at doses of 1 mg in 0.1 ml.MATERIAL & METHODS
Since 1996, there has been an ongoing registrationof all postoperative endophthalmitis patients atHospital St Joan (Table 1). All cases of postoperativeendophthalmitis were studied in the epidemiologicalunit of the hospital in order to determine their origin.
A prospective observational study. Thepopulation comprised all patients submitted to un-combined cataract surgery in the period from January1996 to December 2009. All cases of postoperativeendophthalmitis were related. Only patients withphacoemulsification were included in the study in order
Results at Seven Years after the Use ofIntracamerul Cefazolin as an
Endophthalmitis Prophylaxis in Cataract Surgery*
Prof. Pedro Romero-Aroca1 Isabel Méndez-Marin2Merce Salvat-Serra3
Prof. Juan Fernández-Ballart4Matias Almena-Garcia5 Javier Reyes-Torres6
ABSTRACTBackground To evaluate results after seven years using prophylactic intracameral cefazolin for the prevention ofendophthalmitis in cataract surgery.Methods A prospective, observational study of all patients submitted to cataract surgery over the period January 1996 toDecember 2009. All cases of postoperative endophthalmitis over that period were reviewed. The patients were classifiedin two groups: Group 1 (11,696 patients) operated on between January 1996 and December 2002, Group 2 (13,305patients) between January 2003 and December 2009 (in whom a 1 mg/0.1 bolus of intracameral cefazolin was instilled).Results During the study period, 76 cases of endophthalmitis were observed in Group 1, and seven in Group 2. The rateof postoperative endophthalmitis reduced from 0.63% to 0.05% with a cefazolin injection. The relative risk (RR) forendophthalmitis in Group 1 against group 2 was 11.45 [95% CI 5.72–22.84, p < 0.001].Conclusions An intracameral bolus injection of cefazolin (1 mg in 0.1 ml solution) at the conclusion of the cataractsurgery significantly reduced the rate of postoperative endophthalmitis.
Original Article
Prof.Pedro
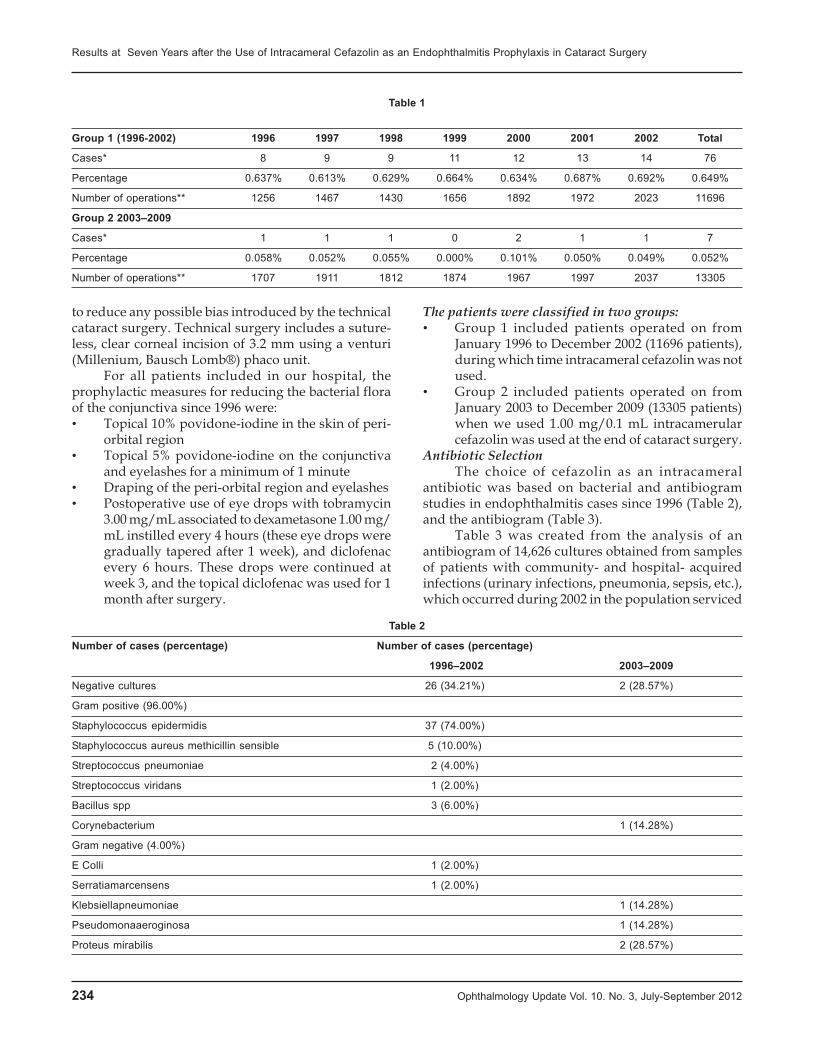
234 Ophthalmology Update Vol. 10. No. 3, July-September 2012
to reduce any possible bias introduced by the technicalcataract surgery. Technical surgery includes a suture-less, clear corneal incision of 3.2 mm using a venturi(Millenium, Bausch Lomb®) phaco unit.
For all patients included in our hospital, theprophylactic measures for reducing the bacterial floraof the conjunctiva since 1996 were:• Topical 10% povidone-iodine in the skin of peri-
orbital region• Topical 5% povidone-iodine on the conjunctiva
and eyelashes for a minimum of 1 minute• Draping of the peri-orbital region and eyelashes• Postoperative use of eye drops with tobramycin
3.00 mg/mL associated to dexametasone 1.00 mg/mL instilled every 4 hours (these eye drops weregradually tapered after 1 week), and diclofenacevery 6 hours. These drops were continued atweek 3, and the topical diclofenac was used for 1month after surgery.
The patients were classified in two groups:• Group 1 included patients operated on from
January 1996 to December 2002 (11696 patients),during which time intracameral cefazolin was notused.
• Group 2 included patients operated on fromJanuary 2003 to December 2009 (13305 patients)when we used 1.00 mg/0.1 mL intracamerularcefazolin was used at the end of cataract surgery.
Antibiotic SelectionThe choice of cefazolin as an intracameral
antibiotic was based on bacterial and antibiogramstudies in endophthalmitis cases since 1996 (Table 2),and the antibiogram (Table 3).
Table 3 was created from the analysis of anantibiogram of 14,626 cultures obtained from samplesof patients with community- and hospital- acquiredinfections (urinary infections, pneumonia, sepsis, etc.),which occurred during 2002 in the population serviced
Table 1
Group 1 (1996-2002) 1996 1997 1998 1999 2000 2001 2002 Total
Cases* 8 9 9 11 12 13 14 76
Percentage 0.637% 0.613% 0.629% 0.664% 0.634% 0.687% 0.692% 0.649%
Number of operations** 1256 1467 1430 1656 1892 1972 2023 11696
Group 2 2003–2009
Cases* 1 1 1 0 2 1 1 7
Percentage 0.058% 0.052% 0.055% 0.000% 0.101% 0.050% 0.049% 0.052%
Number of operations** 1707 1911 1812 1874 1967 1997 2037 13305
Table 2
Number of cases (percentage) Number of cases (percentage)
1996–2002 2003–2009
Negative cultures 26 (34.21%) 2 (28.57%)
Gram positive (96.00%)
Staphylococcus epidermidis 37 (74.00%)
Staphylococcus aureus methicillin sensible 5 (10.00%)
Streptococcus pneumoniae 2 (4.00%)
Streptococcus viridans 1 (2.00%)
Bacillus spp 3 (6.00%)
Corynebacterium 1 (14.28%)
Gram negative (4.00%)
E Colli 1 (2.00%)
Serratiamarcensens 1 (2.00%)
Klebsiellapneumoniae 1 (14.28%)
Pseudomonaaeroginosa 1 (14.28%)
Proteus mirabilis 2 (28.57%)
Results at Seven Years after the Use of Intracameral Cefazolin as an Endophthalmitis Prophylaxis in Cataract Surgery
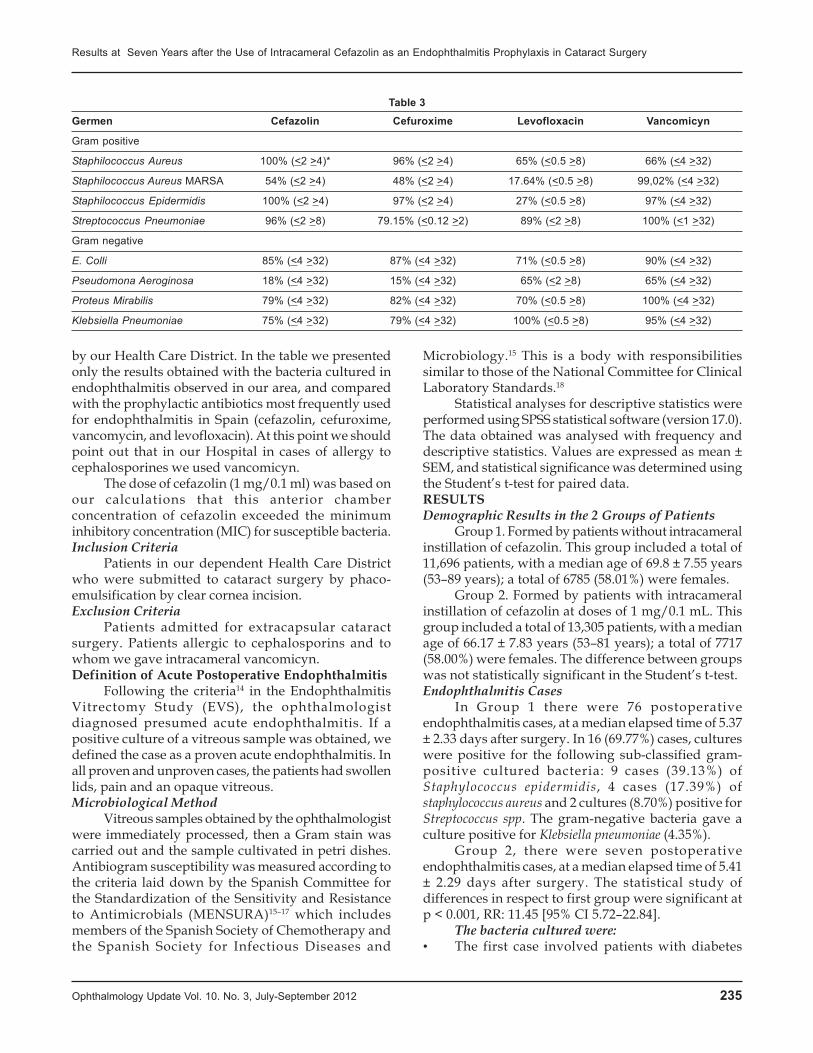
Ophthalmology Update Vol. 10. No. 3, July-September 2012 235
by our Health Care District. In the table we presentedonly the results obtained with the bacteria cultured inendophthalmitis observed in our area, and comparedwith the prophylactic antibiotics most frequently usedfor endophthalmitis in Spain (cefazolin, cefuroxime,vancomycin, and levofloxacin). At this point we shouldpoint out that in our Hospital in cases of allergy tocephalosporines we used vancomicyn.
The dose of cefazolin (1 mg/0.1 ml) was based onour calculations that this anterior chamberconcentration of cefazolin exceeded the minimuminhibitory concentration (MIC) for susceptible bacteria.Inclusion Criteria
Patients in our dependent Health Care Districtwho were submitted to cataract surgery by phaco-emulsification by clear cornea incision.Exclusion Criteria
Patients admitted for extracapsular cataractsurgery. Patients allergic to cephalosporins and towhom we gave intracameral vancomicyn.Definition of Acute Postoperative Endophthalmitis
Following the criteria14 in the EndophthalmitisVitrectomy Study (EVS), the ophthalmologistdiagnosed presumed acute endophthalmitis. If apositive culture of a vitreous sample was obtained, wedefined the case as a proven acute endophthalmitis. Inall proven and unproven cases, the patients had swollenlids, pain and an opaque vitreous.Microbiological Method
Vitreous samples obtained by the ophthalmologistwere immediately processed, then a Gram stain wascarried out and the sample cultivated in petri dishes.Antibiogram susceptibility was measured according tothe criteria laid down by the Spanish Committee forthe Standardization of the Sensitivity and Resistanceto Antimicrobials (MENSURA)15–17 which includesmembers of the Spanish Society of Chemotherapy andthe Spanish Society for Infectious Diseases and
Microbiology.15 This is a body with responsibilitiessimilar to those of the National Committee for ClinicalLaboratory Standards.18
Statistical analyses for descriptive statistics wereperformed using SPSS statistical software (version 17.0).The data obtained was analysed with frequency anddescriptive statistics. Values are expressed as mean ±SEM, and statistical significance was determined usingthe Student’s t-test for paired data.RESULTSDemographic Results in the 2 Groups of Patients
Group 1. Formed by patients without intracameralinstillation of cefazolin. This group included a total of11,696 patients, with a median age of 69.8 ± 7.55 years(53–89 years); a total of 6785 (58.01%) were females.
Group 2. Formed by patients with intracameralinstillation of cefazolin at doses of 1 mg/0.1 mL. Thisgroup included a total of 13,305 patients, with a medianage of 66.17 ± 7.83 years (53–81 years); a total of 7717(58.00%) were females. The difference between groupswas not statistically significant in the Student’s t-test.Endophthalmitis Cases
In Group 1 there were 76 postoperativeendophthalmitis cases, at a median elapsed time of 5.37± 2.33 days after surgery. In 16 (69.77%) cases, cultureswere positive for the following sub-classified gram-positive cultured bacteria: 9 cases (39.13%) ofStaphylococcus epidermidis, 4 cases (17.39%) ofstaphylococcus aureus and 2 cultures (8.70%) positive forStreptococcus spp. The gram-negative bacteria gave aculture positive for Klebsiella pneumoniae (4.35%).
Group 2, there were seven postoperativeendophthalmitis cases, at a median elapsed time of 5.41± 2.29 days after surgery. The statistical study ofdifferences in respect to first group were significant atp < 0.001, RR: 11.45 [95% CI 5.72–22.84].
The bacteria cultured were:• The first case involved patients with diabetes
Table 3
Germen Cefazolin Cefuroxime Levofloxacin Vancomicyn
Gram positive
Staphilococcus Aureus 100% (<2 >4)* 96% (<2 >4) 65% (<0.5 >8) 66% (<4 >32)
Staphilococcus Aureus MARSA 54% (<2 >4) 48% (<2 >4) 17.64% (<0.5 >8) 99,02% (<4 >32)
Staphilococcus Epidermidis 100% (<2 >4) 97% (<2 >4) 27% (<0.5 >8) 97% (<4 >32)
Streptococcus Pneumoniae 96% (<2 >8) 79.15% (<0.12 >2) 89% (<2 >8) 100% (<1 >32)
Gram negative
E. Colli 85% (<4 >32) 87% (<4 >32) 71% (<0.5 >8) 90% (<4 >32)
Pseudomona Aeroginosa 18% (<4 >32) 15% (<4 >32) 65% (<2 >8) 65% (<4 >32)
Proteus Mirabilis 79% (<4 >32) 82% (<4 >32) 70% (<0.5 >8) 100% (<4 >32)
Klebsiella Pneumoniae 75% (<4 >32) 79% (<4 >32) 100% (<0.5 >8) 95% (<4 >32)
Results at Seven Years after the Use of Intracameral Cefazolin as an Endophthalmitis Prophylaxis in Cataract Surgery
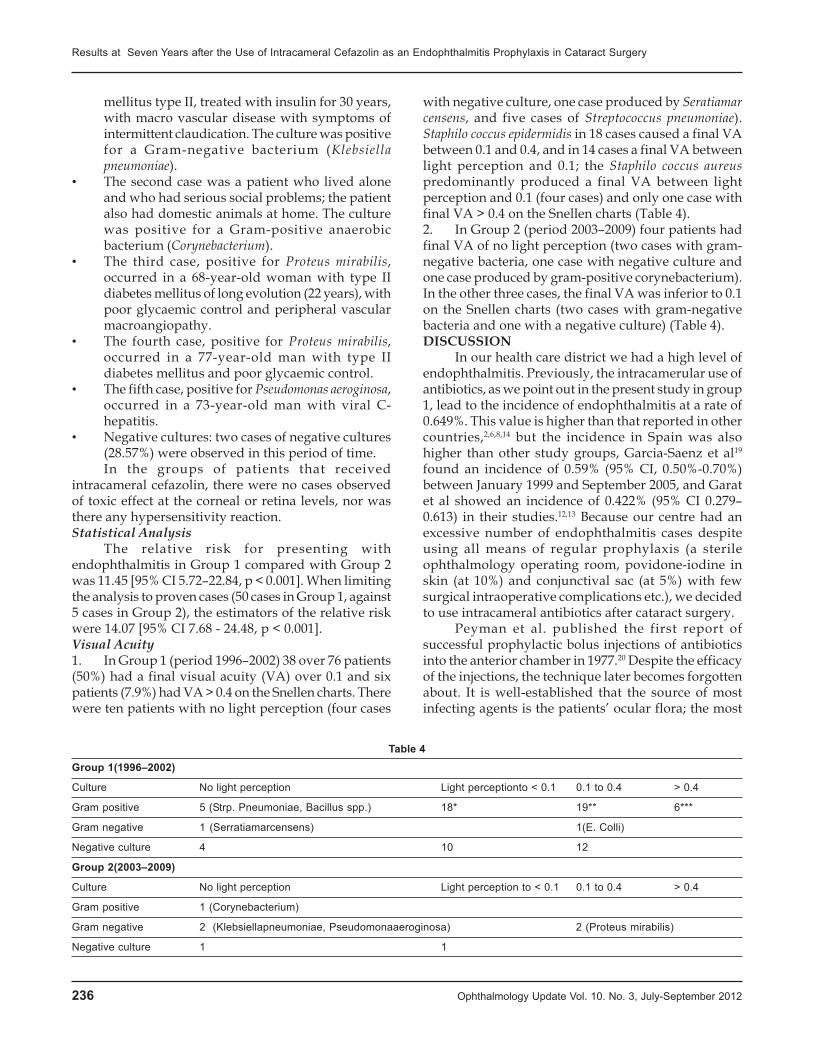
236 Ophthalmology Update Vol. 10. No. 3, July-September 2012
mellitus type II, treated with insulin for 30 years,with macro vascular disease with symptoms ofintermittent claudication. The culture was positivefor a Gram-negative bacterium (Klebsiellapneumoniae).
• The second case was a patient who lived aloneand who had serious social problems; the patientalso had domestic animals at home. The culturewas positive for a Gram-positive anaerobicbacterium (Corynebacterium).
• The third case, positive for Proteus mirabilis,occurred in a 68-year-old woman with type IIdiabetes mellitus of long evolution (22 years), withpoor glycaemic control and peripheral vascularmacroangiopathy.
• The fourth case, positive for Proteus mirabilis,occurred in a 77-year-old man with type IIdiabetes mellitus and poor glycaemic control.
• The fifth case, positive for Pseudomonas aeroginosa,occurred in a 73-year-old man with viral C-hepatitis.
• Negative cultures: two cases of negative cultures(28.57%) were observed in this period of time.In the groups of patients that received
intracameral cefazolin, there were no cases observedof toxic effect at the corneal or retina levels, nor wasthere any hypersensitivity reaction.Statistical Analysis
The relative risk for presenting withendophthalmitis in Group 1 compared with Group 2was 11.45 [95% CI 5.72–22.84, p < 0.001]. When limitingthe analysis to proven cases (50 cases in Group 1, against5 cases in Group 2), the estimators of the relative riskwere 14.07 [95% CI 7.68 - 24.48, p < 0.001].Visual Acuity1. In Group 1 (period 1996–2002) 38 over 76 patients(50%) had a final visual acuity (VA) over 0.1 and sixpatients (7.9%) had VA > 0.4 on the Snellen charts. Therewere ten patients with no light perception (four cases
with negative culture, one case produced by Seratiamarcensens, and five cases of Streptococcus pneumoniae).Staphilo coccus epidermidis in 18 cases caused a final VAbetween 0.1 and 0.4, and in 14 cases a final VA betweenlight perception and 0.1; the Staphilo coccus aureuspredominantly produced a final VA between lightperception and 0.1 (four cases) and only one case withfinal VA > 0.4 on the Snellen charts (Table 4).2. In Group 2 (period 2003–2009) four patients hadfinal VA of no light perception (two cases with gram-negative bacteria, one case with negative culture andone case produced by gram-positive corynebacterium).In the other three cases, the final VA was inferior to 0.1on the Snellen charts (two cases with gram-negativebacteria and one with a negative culture) (Table 4).DISCUSSION
In our health care district we had a high level ofendophthalmitis. Previously, the intracamerular use ofantibiotics, as we point out in the present study in group1, lead to the incidence of endophthalmitis at a rate of0.649%. This value is higher than that reported in othercountries,2,6,8,14 but the incidence in Spain was alsohigher than other study groups, Garcia-Saenz et al19
found an incidence of 0.59% (95% CI, 0.50%-0.70%)between January 1999 and September 2005, and Garatet al showed an incidence of 0.422% (95% CI 0.279–0.613) in their studies.12,13 Because our centre had anexcessive number of endophthalmitis cases despiteusing all means of regular prophylaxis (a sterileophthalmology operating room, povidone-iodine inskin (at 10%) and conjunctival sac (at 5%) with fewsurgical intraoperative complications etc.), we decidedto use intracameral antibiotics after cataract surgery.
Peyman et al. published the first report ofsuccessful prophylactic bolus injections of antibioticsinto the anterior chamber in 1977.20 Despite the efficacyof the injections, the technique later becomes forgottenabout. It is well-established that the source of mostinfecting agents is the patients’ ocular flora; the most
Table 4
Group 1(1996–2002)
Culture No light perception Light perceptionto < 0.1 0.1 to 0.4 > 0.4
Gram positive 5 (Strp. Pneumoniae, Bacillus spp.) 18* 19** 6***
Gram negative 1 (Serratiamarcensens) 1(E. Colli)
Negative culture 4 10 12
Group 2(2003–2009)
Culture No light perception Light perception to < 0.1 0.1 to 0.4 > 0.4
Gram positive 1 (Corynebacterium)
Gram negative 2 (Klebsiellapneumoniae, Pseudomonaaeroginosa) 2 (Proteus mirabilis)
Negative culture 1 1
Results at Seven Years after the Use of Intracameral Cefazolin as an Endophthalmitis Prophylaxis in Cataract Surgery

Ophthalmology Update Vol. 10. No. 3, July-September 2012 237
frequently reported being bacteria gram-positive,coagulase-negative, or positive staphylococcus.
Swedish physicians have pioneered the use ofintracameral cefuroxime since 2002, with excellentoutcomes in 400,000 surgical interventions. Montan etal. published the efficacy of cefuroxime 1 mgintracameral,5,6 a practice that has lowered the rate ofpostoperative endophthalmitis from 0.26% to 0.06%.The large, prospective, multi-centred study, theEuropean Society of Cataract Refractive Surgeons(ESCRS) confirmed the Swedish experience, findingthat an injection of cefuroxime at the end of the surgeryreduced endophthalmitis rates to just 0.05%.8–10
We chose to use cefazolin, which is recommendedby the Department of Microbiology and the InfectiousDiseases Committee of our Hospital, rather thancefuroxime because it is a first generation cephalosporinand has a wide range of activity against gram-positivebacteria in our Health Care District, rather than asecond-generation cephalosporin, such as cefuroxime.A study in our Health Care District by Vila-Corcoles etal,21 showed an increased resistance of Streptococcuspneumoniae to cefuroxime but not to cefazolin.
It is interesting to observe in Table 3 that cefazolinand cefuroxime present a similar antibiotic resistancepattern, with regard to both gram-positive and gram-negative bacteria. Therefore, we still believe thatcefazolin is a good option as a prophylaxis forendophthalmitis, and its substitution for cefuroxime isnot important for reducing the number of cases ofendophthalmitis. However, by using cefazolin, thereis still a risk of infection by gram-negative bacteria,which is why the majority of proven cases ofendophthalmitis in Group 2 (4/5 cases were gram-negative) were caused by this type of bacteria. This isclearly a limitation in the use of cefazolin as aprophylaxis for endophthalmitis.
The lack of availability of eye-drops of fourthgeneration quinolones in Spain is the most obviousreason for the preference for intracameral antibioticsin the prophylaxis of endophthalmitis. Since June 2010,a moxifloxacin eye-drop has been available in Spain,with more possibilities of prophylaxis.
Results show that final VA was worse in Group 2than in group 1. The explanation for this can be foundin the type of bacteria that cause endophthalmitis. Wefound Corynebacterium, Klebsiella pneumonia,Pseudomonaa eroginosa, and Proteus mirabilis in group 2.All these bacteria were poorly sensitive to cefazolin.Negative culture was observed in a 34.21% of cases ingroup 1 and 28.57% in Group 2, similar to other studies,such as the EndophthalmitisVitrectomy Study (EVS),with values near to 30%.CONCLUSIONS
Intracameral bolus injection of cefazolin incataract surgery demonstrated prophylactic efficacy indiminishing the rate of postoperative endophthalmitisin our hospital, at two doses of 1 mg in 0.1 ml solution.
Furthermore, a close relationship between withthe Department of Microbiology, and the InfectiousDiseases Committee of our Hospital is essential fordeveloping a proper antibiotic prophylaxis.
Further studies are needed with a larger numberof patients in order to fully determine the effectivenessof cefazolin and its non-toxicity at corneal endotheliumlevel.REFERENCES:1. Jensen MK, Fiscella RG, Moshirfar M, Mooney B: Third- and
fourth generation fluoroquinolones: retrospectivecomparison of endophthalmitis after cataract surgeryperformed over 10 years. J Cataract Refract Surg 2008, 34:1460–7.
2. O’Brien TP, Arshinoff SA, Mah FS: Perspectives on antibioticsfor postoperative endophthalmitis prophylaxis: potential roleof moxifloxacin. J Cataract Refract Surg 2007, 33:1790–800.
3. Kowalski RP, Romanowski EG, Mah FS, Yates KA, GordonYJ: Topical 0.5% moxifloxacin prevents endophthalmitis inan intravitreal injection rabbit model. J OculPharmacolTher2008, 24:1–7.
4. Hariprasad SM, Blinder KJ, Shah GK, Apte RS, Rosenblatt B,Holekamp NM, Thomas MA, Mieler WF, Chi J, Prince RA:Penetration pharmacokinetics of topically administered 0.5%moxifloxacin ophthalmic solution in human aqueous andvitreous. Arch Ophthalmol 2005, 123:39–44.
5. Montan PG, Wejde G, Koranyi G, Rylander M: Prophylacticintracameral cefuroxime. Efficacy in preventingendophthalmitis after cataract surgery.J Cataract Refract Surg2002, 28:977–81.
6. Montan P, Lundström M, Stenevi U, Thorburn W:Endophthalmitis following cataract surgery in Sweden:national prospective survey 1999–2001. InActaOphthalmolScand Edited by Wejde G. 2005, 83:7–10.
7. García-Sáenz MC, Arias-Puente A, Rodríguez-Caravaca G,Bañuelos JB: Effectiveness of intracameral cefuroxime inpreventing endophthalmitis after cataract surgery Ten-yearcomparative study. J Cataract Refract Surg 2010, 36:203–7.
8. ESCRS study of prophylaxis of postoperativeendophthalmitis after cataract surgery: Case for a Europeanmulticenter study, Seal DV, Barry P, Gettinby G, Lees F,Peterson M, Revie CW, Wilhelmus KR: ESCRSEndophthalmitis Study Group. J Cataract Refract Surg 2006,32:396–406. Erratum in: J Cataract Refract Surg. 2006,32:709
9. ESCRS study of prophylaxis of postoperativeendophthalmitis after cataract surgery: Preliminary reportof principal results from a European multicenter study, BarryP, Seal DV, Gettinby G, Lees F, Peterson M, Revie CW: ESCRSEndophthalmitis Study Group. J Cataract Refract Surg 2006,32:407–10.
10. ESCRSEndophthalmitis Study Group: Prophylaxis ofpostoperative endophthalmitis following cataract surgery:results of the ESCRS multicenter study and identification ofrisk factors. J Cataract Refract Surg 2007, 33:978–88.
11. Romero P, Méndez I, Salvat M, Fernández J, Almena M:Intracameralcefazolin as prophylaxis againstendophthalmitis in cataract surgery. J Cataract Refract Surg2006, 32:438–41.
12. Garat M, Moser CL, Alonso-Tarrés C, Martín-Baranera M,Alberdi A: Intracameralcefazolin to prevent endophthalmitis
Results at Seven Years after the Use of Intracameral Cefazolin as an Endophthalmitis Prophylaxis in Cataract Surgery
238 Ophthalmology Update Vol. 10. No. 3, July-September 2012
in cataract surgery: 3-year retrospective study. J CataractRefract Surg 2005, 31:2230–4.
13. Garat M, Moser CL, Martín-Baranera M, Alonso-Tarrés C,Alvarez-Rubio L: Prophylactic intracameralcefazolin aftercataract surgery: endophthalmitis risk reduction and safetyresults in a 6-year study. J Cataract Refract Surg 2009, 35:637–42.
14. Endophthalmitisvitrectomy study group: Result of theendophthlmitisvitrectomy study. A randomised trial ofimmediate vitrectomy and of intravenous antibiotics for thetreatment of postoperative bacterial endophthalmitis.ArchOphthlmol 1995, 1:1479–96.
15. Peter Barry, Susanne Gardner, David Seal, George Gettinby,Fiona Lees, Magnus Peterson, Crawford Revie, for the ESCRSEndophthalmitis Study Group: Clinical observationsassociated with proven and unproven cases in the ESCRSstudy of prophylaxis of postoperative endophthalmitis aftercataract surgery. J Cataract Refract Surg 2009, 35:1523–31.
16. Baquero F, Martínez-Beltrán J, Cantón R, Grupo MENSURA:Criterios del grupo MENSURA para la definición de los
Results at Seven Years after the Use of Intracameral Cefazolin as an Endophthalmitis Prophylaxis in Cataract Surgery
puntoscríticos de sensibilidad a los antibióticos. RevEspQuimiot 1997, 10:303–13.
17. Baquero F, Martínez-Beltrán J, Cantón R: y losrestantesmiembros de la Mesa Española de Normalizaciónde la Sensibilidad y Resistencia a los Antimicrobianos(MENSURA). Criterios del grupo MENSURA para ladefinición de los puntoscríticos de sensibilidad a losantibióticos.EnfInfecMicrobiolClin 1998, 16:85–92.
18. National Committee for Clinical Laboratory Standards:Performance Standards for Antimicrobial Disk Susceptibility Tests:Approved Standard. NCCLS document M2-A7.7thedition.Edited by Wayne, PA.National Committee forClinical Laboratory Standards; 2002.
19. García-Sáenz MC, Arias-Puente A, Rodríguez-Caravaca G,Andrés Alba Y, BañuelosBañuelos J: Endophthalmitis aftercataract surgery: epidemiology, clinical features andantibiotic prophylaxis. Arch SocEspOftalmol 2010, 85:263–7.
20. Peyman GA, Sathar ML, May DR: Intra ocular gentamicineas intra operative prophylaxis in South India eye camps. Br JOphthalmol 1977, 61:260–2.

Ophthalmology Update Vol. 10. No. 3, July-September 2012 239
–––––––––––––––––––––––––––––––––––––––––––––––––––––1.Registrar, Ophthalmology, Hayatabad Medical Complex,Peshawar2,3. Postgraduate Trainees, Hayatabad Medical Complex,Peshawar4. Associate Professor Ophthalmology Hayatabad MedicalComplex, Peshawar. 5Assistant Profesor ophthalmology, BannuMedical College, Bannu,6. Head Department of OphthalmologyHayatabad Medical Complex, Peshawar.–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Dr Mushtaq Ahmad House No 31B, street No2, sector N4, Phase 4, Hayatabad, PeshawarE.Mail>[email protected] 03339119605–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: March’2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
Phacoemulsification: Effect of Intraocular IrrigatingSolutions on the Corneal Endothelium
Mushtaq Ahmad FCPS1. Yousaf Jamal Mahsood2. Muhammad Naeem3
Sofia Iqbal MRCOph. FRCS4.Nazullah FCPS5. Prof. Nasir Saeed FCPS6
ABSTRACTObjective: To compare corneal integrity after phacoemulsification with Balanced Salt Solution Plus (BSS Plus) versusLactated Ringer’s (Ringer) solution.Material and Methods: Sixty patients undergoing phacoemulsification were randomised to either BSS Plus (n=30) orRinger (n=30) as the irrigating solution. Patients were examined at baseline and at 15 and 30days postoperatively.Evaluations included specular microscopy to evaluate endothelial cell density (ECD) and endothelial cell size variability(CV).Results: Groups were well balanced regarding baseline ECD and CV (p>0.05). There was no statistically significantdifference between ECD reduction in group BSS Plus 15 ±2.0% and Ringer 11.1±1.9% (p<0.05) at day 30 or on any visit.There was no statistically significant difference between CV increase in group BSS Plus 20.0±3.0% and Ringer 27.2±4.0%(p<0.05) at day 60 or on any visit. Interestingly, there were statistically significant correlations between ECD loss andphacoemulsification time (p<0.0001) and ECD loss and irrigation solution volume (p<0.0001) in the Ringer group, but notin the BSS Plus group.Conclusions: Ringers solution was similar to BSS Plus for corneal preservation in atraumatic cataract surgery. However,our study demonstrates that there is a trend towards lower postoperative endothelial cell density for surgeries with longerphacoemulsification time and higher irrigation volumes if Ringer is used.Keywords: phacoemulsification, corneal integrity, irrigating solutions
Original Article
Dr. Mushtaq
INTRODUCTION:The corneal endothelium consists of a monolayer
of cells on the posterior corneal surface that has limitedregenerating capability after injury. The normalthickness and transparency of the cornea aremaintained by a barrier function and the active fluidpump of corneal endothelial cells.1 The natural loss ofhuman endothelial cells is approximately 0.6% eachyear.2 Intraocular manipulation, such as that duringphacoemulsification cataract surgery, causes fluid andlens fragment turbulence that can lead to endothelialcell damage.3
Solutions initially used for cataract surgery weresalt solution, Ringer’s solution and plasma-lyte 148.Subsequently, in 1960, more physiological solutionswith ionic composition, pH and osmorality similar toaqueous humour were developed and received the
name of balanced salt solution (BSS).4 In 1973, a thirdgeneration of irrigation solution, named BSS Plus, wasdeveloped after studies by Edelhauser and coauthors,5-
7 who verified that the addition of glutathione, glucoseand bicarbonate to the irrigation solution wouldcontribute to endothelial cell function and survival invitro. Further, some in vivo studies using differentirrigating solutions show that postoperative cornealthickness and endothelial cell count do not depend onirrigation volume and time but rather depend on thesolution’s chemical composition.8–11 In fact, studies showthat enriched balanced salt solutions such as BSS Plus(glucose glutathione bicarbonate solution) providecharacteristics similar to those of the aqueous humourto maintain constant intraocular conditions.8,12,13
However, dextrose bicarbonate Lactated Ringer’ssolution for irrigation has been reported to be aseffective as enriched BSS during cataract surgery,14 andsome authors consider operating time and irrigationvolume to be important clinical factors for endothelialcell loss during phacoemulsification cataractsurgery.15,16
Based on the above presented conflictinginformation and the necessity for optimising costs incataract surgery, especially for very poor regions fromdeveloping countries, and considering that LactatedRinger’s is 30 times cheaper than BSS Plus, 17 wedesigned this prospective masked trial to investigate

240 Ophthalmology Update Vol. 10. No. 3, July-September 2012
for differences in preservation of corneal integrity afterphacoemulsification cataract surgery using twointraocular irrigating solutions.MATERIALS AND METHODS
A randomized clinical trial was conducted atOphthalmology Department Hayatabad MedicalComplex, Peshawar from August 2011 to November2011.
Participation in a prospective, double-maskedtrial was offered to all patients with age-related cataractscheduled to undergo phacoemulsification withintraocular lens (IOL) implantation.Exclusion criteria included: (1) types of cataract other than age-related (eg, secondary
or congenital)(2) previous ocular surgery(3) previous corneal disease(4) anterior chamber cells or flare(5) any condition that impeded corneal evaluation by
specular microscopy and pachymetry or follow-up. Allpatients underwent an initial screening visit whichincluded a detailed ophthalmic evaluation with SnellenBCVA measurement, applanation tonometry measuredwith a Goldmann tonometer, biomicroscopy of theanterior segment, dilated biomicroscopic fundusexamination and binocular indirect ophthalmoscopy.Patients who met the eligibility criteria were
informed verbally and in writing of the potential risksand benefits of the use of the two irrigation solutions,and those patients who agreed to participate signed awritten informed consent form. For patients whoaccepted study participation, the screening visit wasused as the baseline examination, which occurred 1–
7days before surgery. If both eyes were eligible for studyparticipation, the eye with worse BCVA was includedin the study.
The corneal endothelium was examined with anon-contact specular microscope (Topcon SP2000P).Three photographs were taken per eye at eachexamination, and the mean of measurements wascalculated. With this semiautomatic method, theoperator hand-digitised the centre of each cell (centremethod). Corneal endothelial morphology wascalculated from a cluster of 55 cells from each photo asdescribed elsewhere18 The following variables weremeasured: (1) central endothelial cell density (ECD)defined as the number of cells per mm2; (2) centralendothelial cell size variability or the coefficient ofvariation (CV).
This variable is defined as SD/ìCS (where SD isthe standard deviation of the cell size, and ìCS is themean cell size) and is expressed as a percentage. Afterbaseline evaluation, patients were randomised ingroups of five. The technician was asked to pick up one
of two identical opaque envelopes, one containing thedesignation for phacoemulsification surgery using BSSPlus irrigation solution (BSS Plus group; BSS Plus,Alcon, Fortworth, Texas) and the other containing thedesignation for phacoemulsification surgery usingLactated Ringer’s solution (Ringer group; RingerLactato, Baxter, São Paulo, Brazil).
The next five included patients wereautomatically assigned to the treatment group specifiedin the second envelope. The time of ultrasound use andits potency (kept at 60% for all cases), volume ofirrigation solution used and operating time were notedfor each surgery procedure, as well as intraoperativecomplications such as Descemet detachment, iristrauma and posterior capsule rupture. All surgerieswere performed by the same physician (DRL) understerile conditions. The physician was not masked andknew the type of irrigation solution that was being usedfor each patient. Postoperatively, 0.3% ciprofloxacinthree times per day and prednisolone acetate 1% fourtimes per day were used for 4weeks. Patients werescheduled for follow-up examinations at postoperativedays 1,15 (±1) and 30 (±2).
At these visits, patients underwent completeophthalmic examination using the same procedures asat baseline. All baseline and postoperative evaluationswere performed by a masked ophthalmologist (MSAL)who was not aware of the irrigation solution usedduring surgery. Comparisons between groups atbaseline (ie, patient age, surgery duration, etc) wereperformed with non-paired t tests. Cataract nucleusscores were compared with a contingency analysisfollowed by a Pearson ÷2 test. For data retrieved atpostoperative days 1, 15 and 30 intra-individualdifferences from baseline were calculated, and astatistically significant effect was defined as a differencefor zero for intra-individual mean differences. Statisticalanalyses have been performed using JMP 7.0.2 (SASInstitute 2007; SAS Institute, Cary, North Carolina)software.
Considering the mean and SD (16% and 4%respectively) for the intra-individual difference inendothelial cell density found in a previous study, 19
we could estimate that, with a sample of 50 patientsper group, the minimal detectable difference would be2.4% (power=80%), which isRESULTS
Ten patients (five from the BSS Plus group andfive from the Ringer group) were excluded because theyhad two consecutive missed visits. There were nosignificant differences between groups with respect topatient’s age, gender, baseline visual acuity, intraocularpressure, cataract grading, time for ultrasound use andvolume of irrigation solution employed (table 1).
Phacoemulsification: Effect of Intraocular Irrigating Solutions on the Corneal Endothelium
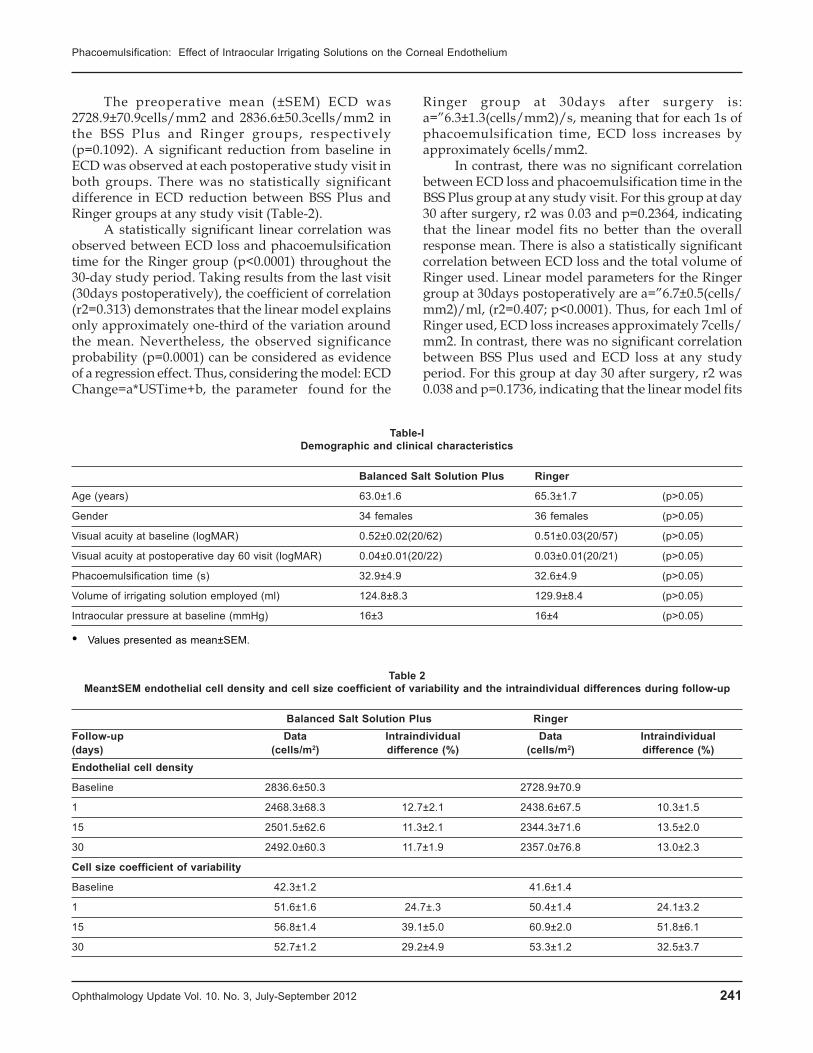
Ophthalmology Update Vol. 10. No. 3, July-September 2012 241
Table 2Mean±SEM endothelial cell density and cell size coefficient of variability and the intraindividual differences during follow-up
Balanced Salt Solution Plus RingerFollow-up Data Intraindividual Data Intraindividual(days) (cells/m2) difference (%) (cells/m2) difference (%)Endothelial cell density
Baseline 2836.6±50.3 2728.9±70.9
1 2468.3±68.3 12.7±2.1 2438.6±67.5 10.3±1.5
15 2501.5±62.6 11.3±2.1 2344.3±71.6 13.5±2.0
30 2492.0±60.3 11.7±1.9 2357.0±76.8 13.0±2.3
Cell size coefficient of variability
Baseline 42.3±1.2 41.6±1.4
1 51.6±1.6 24.7±.3 50.4±1.4 24.1±3.2
15 56.8±1.4 39.1±5.0 60.9±2.0 51.8±6.1
30 52.7±1.2 29.2±4.9 53.3±1.2 32.5±3.7
The preoperative mean (±SEM) ECD was2728.9±70.9cells/mm2 and 2836.6±50.3cells/mm2 inthe BSS Plus and Ringer groups, respectively(p=0.1092). A significant reduction from baseline inECD was observed at each postoperative study visit inboth groups. There was no statistically significantdifference in ECD reduction between BSS Plus andRinger groups at any study visit (Table-2).
A statistically significant linear correlation wasobserved between ECD loss and phacoemulsificationtime for the Ringer group (p<0.0001) throughout the30-day study period. Taking results from the last visit(30days postoperatively), the coefficient of correlation(r2=0.313) demonstrates that the linear model explainsonly approximately one-third of the variation aroundthe mean. Nevertheless, the observed significanceprobability (p=0.0001) can be considered as evidenceof a regression effect. Thus, considering the model: ECDChange=a*USTime+b, the parameter found for the
Table-IDemographic and clinical characteristics
Balanced Salt Solution Plus Ringer
Age (years) 63.0±1.6 65.3±1.7 (p>0.05)
Gender 34 females 36 females (p>0.05)
Visual acuity at baseline (logMAR) 0.52±0.02(20/62) 0.51±0.03(20/57) (p>0.05)
Visual acuity at postoperative day 60 visit (logMAR) 0.04±0.01(20/22) 0.03±0.01(20/21) (p>0.05)
Phacoemulsification time (s) 32.9±4.9 32.6±4.9 (p>0.05)
Volume of irrigating solution employed (ml) 124.8±8.3 129.9±8.4 (p>0.05)
Intraocular pressure at baseline (mmHg) 16±3 16±4 (p>0.05)
• Values presented as mean±SEM.
Ringer group at 30days after surgery is:a=”6.3±1.3(cells/mm2)/s, meaning that for each 1s ofphacoemulsification time, ECD loss increases byapproximately 6cells/mm2.
In contrast, there was no significant correlationbetween ECD loss and phacoemulsification time in theBSS Plus group at any study visit. For this group at day30 after surgery, r2 was 0.03 and p=0.2364, indicatingthat the linear model fits no better than the overallresponse mean. There is also a statistically significantcorrelation between ECD loss and the total volume ofRinger used. Linear model parameters for the Ringergroup at 30days postoperatively are a=”6.7±0.5(cells/mm2)/ml, (r2=0.407; p<0.0001). Thus, for each 1ml ofRinger used, ECD loss increases approximately 7cells/mm2. In contrast, there was no significant correlationbetween BSS Plus used and ECD loss at any studyperiod. For this group at day 30 after surgery, r2 was0.038 and p=0.1736, indicating that the linear model fits
Phacoemulsification: Effect of Intraocular Irrigating Solutions on the Corneal Endothelium

242 Ophthalmology Update Vol. 10. No. 3, July-September 2012
no better than the overall response mean .The preoperative mean CV was 42.3±1.2% and
41.6±1.4% in the BSS Plus and Ringer groups,respectively (p=0.6503). There was a significant increasein CV in both groups at 1, 15 and 30 days after surgery.There was no statistically significant difference in CVbetween the groups at any study visit.There was nostatistically significant correlation between CV changeand phacoemulsification time or total volume ofirrigation volume used in either group. There were nocases of Descemet membrane detachment, iris trauma,posterior capsule rupture or endophthalmitis duringthe study.DISCUSSION
The results of the current study show that BSS Plusis similar to Lactated Ringer’s with respect to the clinicalparameters (ECD and CV) that reflect preservation ofcorneal integrity following phacoemulsification cataractsurgery with posterior chamber IOL implantation. It isimportant to point out that this study includeduncomplicated cases performed by an experiencedsurgeon, who performed all surgeries with less than180s of phacoemulsification time (phacoemulsificationpower at 60%) and with less than 150ml for all surgeries.Kiss et al 20 and Puckett et al 14 reported similarendothelial preservation with the use of BSS Plus orLactated Ringer’s as irrigating solutions for atraumaticcataract surgery by phacoemulsification andextracapsular extraction, respectively. However, theresults of these latter two studies are in contrast to datafrom a study by Joussen et al, 21 who reported thatcorneas irrigated with BSS Plus duringphacoemulsification were less swollen than corneasirrigated with Ringer’s solution on the firstpostoperative day.
Another study, by Vasavada et al, 22 also reportedthe same finding, although in this Indian study,standard BSS was used. On the other hand, thesteepness of the endothelial cell density reduction slopein relation to phacoemulsification time and irrigationvolume used in the Ringer group demonstrates thetrend towards reduced endothelial cell density forsurgeries with longer phacoemulsification time andhigher volumes of irrigation; this is in contrast to theBSS Plus group, for which the endothelial cell densityreduction slope is not so steep, and there is nosignificant correlation with phacoemulsification timeand irrigation volume used. This is consistent with dataobtained in studies from Edelhauser et al,6 7 Matsuda etal 8 and Yagoubi et al, 23 which demonstrated that thecorneal endothelium can be better preserved by usingsolutions with a composition similar to that of aqueoushumour. In fact, BSS Plus and Lactated Ringer’s havecommon aqueous humour constituents: sodium
chloride, potassium chloride, calcium chloride.However, just BSS Plus has magnesium, sodiumphosphate, sodium bicarbonate, dextrose andglutathione, which are also present in aqueous humour.
The rationale for the above-mentionedcomposition differences that theoretically favour BSSPlus would be: magnesium is essential for the Mg-ATPase endothelial pump; the addition of dextrosewould be justified as a natural energy source forendothelial cells24, sodium phosphate and bicarbonateare physiological buffers found in aqueous humour,25,26
and glutathione is a peptide which is important as anantioxidant and as an agent maintaining theintercellular junctions.5,7,8,14,21 In addition, aqueoushumour, BSS Plus and Lactated Ringer’s pH andosmolarity are 7.38/304; 7.40/305 and 6.4/260,respectively.7,14,21,27
Consequently, Lactated Ringer’s solution ishypotonic and slightly acidic when compared with BSSPlus, which seems to be more physiological, since it haspH and osmolarity values closer to aqueous humourvalues. In summary, for uncomplicatedphacoemulsification cataract surgeries, Ringer’ssolution is associated with a corneal endothelial cellreduction similar to BSS Plus, if the surgeon uses limitedphacoemulsification time and irrigation volume. Giventhe 30-fold higher cost of BSS Plus compared withLactated Ringer’s solution, the findings of our studymay have a substantial impact on the cost of providingcataract surgery for atraumatic cases. On the otherhand, for cataract operations that may require a highervolume of irrigation solution or longerphacoemulsification time, such as dislocated lens, densecataracts and inexperienced surgeons cases, BSS Plusmay contribute to lower endothelial cell loss.CONCLUSIONS:
Ringers solution was similar to BSS Plus forcorneal preservation in atraumatic cataract surgery.However, our study demonstrates that there is a trendtowards lower postoperative endothelial cell densityfor surgeries with longer phacoemulsification time andhigher irrigation volumes if Ringer is used.REFERENCES1. Mishima S. Clinical investigations on the corneal
endothelium. Ophthalmology 1982;89:525–30.2. Bourne WM, Nelson LR, Hodge DO. Central corneal
endothelial cell changes over a ten-year period. InvestOphthalmol Vis Sci 1997;38:779–82.
3. Dick HB, Kohnen T, Jacobi FK. Long-term endothelial cellloss following phacoemulsification through a temporal clearcorneal incision. J Cataract Refract Surg 1996;22:63–71.
4. Merrill DL, Fleming TC, Girard LJ. The effects of physiologicbalanced salt solutions and normal saline on intraocular andextraocular tissues. Am J Ophthalmol 1960;49:895.
5. McCarey BE, Edelhauser HF, Van Horn DL. Functional andstructural changes in the corneal endothelium during in vitroperfusion. Invest Ophthalmol 1973;12:410–17.
Phacoemulsification: Effect of Intraocular Irrigating Solutions on the Corneal Endothelium

Ophthalmology Update Vol. 10. No. 3, July-September 2012 243
6. Edelhauser HF, Gonnering R, Van Horn DL. Intraocularirrigating solutions—a comparative study of BSS Plus andLactated Ringer’s solution. Arch Ophthalmol 1978;96:516–20.
7. Edelhauser HF, Van Horn DL, Hyndiuk RA. Intraocularirrigating solutions. Their effect on the corneal endothelium.Arch Ophthalmol 1975;93:648–57.
8. Matsuda M, Kinoshita S, Ohashi Y. Comparison of the effectsof intraocular irrigating solutions on the corneal endotheliumin intraocular lens implantation. Br J Ophthalmol1991;75:476–9.
9. Araie M, Shirasawa E, Hikita M. Effect of oxidizedglutathione on the barrier function of the cornealendothelium. Invest Ophthalmol Vis Sci 1988;29:1884–7.
10. Whikehart DR, Edelhauser HF. Glutathione in rabbit cornealendothelia: the effects of selected perfusion fluids. InvestOphthalmol Vis Sci 1978;17:455–64.
11. Matsuda M, Tano Y, Edelhauser HF. Comparison ofintraocular irrigating solutions used for pars planavitrectomy and prevention of endothelial cell loss. Jpn JOphthalmol 1984;28:230–8.
12. Glasser DB, Matsuda M, Ellis JG. Effects of intraocularirrigating solutions on the corneal endothelium after in vivoanterior chamber irrigation. Am J Ophthalmol 1985;99:321–8.
13. Araie M. Barrier function of corneal endothelium and theintraocular irrigating solutions. Arch Ophthalmol1986;104:435–8.
14. Puckett TR, Peele KA, Howard RS. Intraocular irrigatingsolutions—a randomized clinical trial of balanced saltsolution plus and dextrose bicarbonate lactated ringer’ssolution. Ophthalmology 1995;102:291–6.
15. O’Grady GE, Alfonso E, Lee W. Comparison of low andhigh volume irrigation-aspiration systems for extracapsularcataract surgery. Am J Ophthalmol 1986;102:91–4.
16. Sugar J, Mitchelson J, Kraff M. The effect ofphacoemulsification on corneal endothelial cell density. Arch
Ophthalmol 1978;96:446–8.17. Brasindice pharmaceutical guide. 2009. http://
www.brasindice.com.br. Year 45.18. Behndig A, Karlsson K, Brannstrom T. Corneal endothelial
integrity in mice lacking extracellular superoxide dismutase.Invest Ophthalmol Vis Sci 2001;42:2784–8.
19. Ventura ACS, Walti R, Bohnke M . Corneal thickness andendothelial density before and after cataract surgery. Br JOphthalmol 2001;85:18–20.
20. Kiss B, Findl O, Menapace R. Corneal endothelial cellprotection with a dispersive viscoelastic material and airrigating solution during phacoemulsification. Low-costversus expensive combination. J Cataract Refract Surg2003;29:733–40.
21. Joussen AM, Barth U, Çubuk H. Effect of irrigating solutionand irrigation temperature on the cornea and pupil duringphacoemulsification. J Cataract Refract Surg 2000;26:392–7.
22. Vasavada V, Dixit NV, Raj SM. Comparison between Ringer’slactate and balanced salt solution on postoperative outcomesafter phacoemulsification: a randomized clinical trial. IndianJ Ophthalmol 2009;57:191–5.
23. Yagoubi MI, Armitage WJ, Diamond J. Effects of irrigationsolutions on corneal endothelial function. Br J Ophthalmol1994;78:302–6.
24. Edelhauser HF. The resiliency of the corneal endothelium torefractive and intraocular surgery. Cornea 2000;19:263–73.
25. McCarey BE, Polack FM, Marshall W. Thephacoemulsification procedure. I. The effect of intraocularirrigating solutions on the corneal endothelium. InvestOphthalmol 1976;15:449–57
26. McEnerney JK, Peyman GA. Simplification of glutathione-bicarbonate–Ringer solution: its effect on corneal thickness.Invest Ophthalmol Vis Sci 1977;16:657–60.
27. Nuyts RMMA, Edelhauser HF, Holley GP . Intraocularirrigating solutions: a comparison of Hartmann’s lactatedRinger’s solution, BSS and BSS Plus. Graefe’s Arch Clin ExpOphthalmol 1995;233:655–61.
Phacoemulsification: Effect of Intraocular Irrigating Solutions on the Corneal Endothelium
244 Ophthalmology Update Vol. 10. No. 3, July-September 2012
–––––––––––––––––––––––––––––––––––––––––––––––––––––1.Post graduate Trainee.2. Registrar. 3.Associate Professor4,5.Assistant Prof. 6. Head Department of Ophthalmology–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Dr Muhammad Naeem House No 31B, streetNo 2, Sector N4, Phase 4, Hayatabad, PeshawarE.Mail>[email protected] Cell: 03339114435–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: February’2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
INTRODUCTION:Several worldwide studies suggest that the
prevalence of blindness is approximately 11%.1 Reviewof these studies shows that cataract is the main causeof blindness, as some studies have reported about 79%of bilateral blindness is due to cataract.2 The WorldHealth Organization (WHO) estimates that 161 millionpeople worldwide have visual impairment, including37 million blind and 124 million with visualimpairment. Cataract is the leading cause of worldwideblindness. Globally, it accounts for almost 16 millioncases of blindness and 50 million cases of low vision.3
In South Asian countries like India and Nepal around70% of cases of blindness are due to cataract.
In Pakistan, 66% of the blindness is due tocataract.4 An estimated 2.5 million people are blind dueto cataract in one eye and 1.5 million in both eyes.5 Thetreatment for cataract is surgical removal, usuallyfollowed by replacement of the cataractous lens with
an intraocular lens (IOL) implant. There are severaltechniques for cataract extraction.6 Out of these,phacoemulsification is now the gold standard. Ascompared to conventional extracapsular cataractextraction (ECCE), phacoemulsification offers theadvantages of faster, more predictable wound healing,reduced discomfort to patients, fewer woundcomplications and less chances of post-operativeastigmatism.
These advantages are mainly due to the smallerincision (usually 3.5 mm or less) that is used inphacoemulsification. The sutureless clear cornealincision was first described 1992 and is currently thepreferred incision for phacoemulsification cataractsurgery. The wound generally does not require anyhydrations as it is watertight. Sutureless surgery hasgenerally been shown to be associated with lessastigmatism compared with conventional ECCE.
Larger incisions made to insert non foldable lOLsare likely to require at least one stitch. In addition, somesurgeons simply prefer the wound hydrations, even ifthe incision is already watertight. Wound instability isassociated with wound leak, endopthalmitis, and otherfeared complications of cataract surgery.7 We report thefindings of a study which compared the rates ofsignificant post operative wound leak and anteriorchamber (AC) reaction in patients undergoing
Wound Leakage and Anterior Chamber Reaction afterPhacoemulsification with & without Ports Hydration
Muhammad Naeem1, Mushtaq Ahmad FCPS2, Sofia Iqbal MRCOph.,FRCS3
Sana Ullah Jan FCPS4, Mohammad Naeem Khan5, Prof. Nasir SaeedFCPS6
Ophthalmology Department Hayatabad Medical Complex, Peshawar
ABSTRACTPurpose: To compare the rates of significant post operative wound leak and anterior chamber (AC) reaction in patientsundergoing phacoemulsification cataract surgery with and without hydrations of corneal incisions.Material and Methods: All eyes scheduled to have phacoemulsification surgery by two surgeons were selected. The firstgroup of eyes underwent phacoemulsification surgery with 3.25 mm superior and two side ports at right angle to the mainclear corneal incision. The incisions were hydrated with 27 gage cannula. The second group of eyes underwent anidentical surgery, but the incisions were not hydrated at the end of surgery. Patients were followed up at 24 hours, and 1week and evaluated by slit lamp for wound leak (using Seidel’s Test), AC cells and flare.Results: Twenty four eyes underwent surgery with ports hydrations and 25 eyes underwent no ports hydrations at theend of surgery. The mean age of patients in groups I and II were 61.2 years and 63.3 years, respectively. Followingsurgery, none of the patients in two groups showed wound leak at 1 day and 1 week. At the first post-op day, only 14.6%of eyes in group 1 showed AC reaction, compared to 32.0 % in group II (p = 0.04). At one week postop,16.7% and 20.0%of eyes in Groups I and II showed AC reaction, respectively. However, the difference was not statistically significant (p =0.67).Conclusions: The incidence of postoperative wound leakage and anterior chamber reaction in patients undergoingphacoemulsification cataract surgery with and without corneal incisions hydrations are not different. Thus ports hydrationsat the end of surgery offers no added advantages.Keywords: Phacoemulsification, cataract, Anterior chamber reactions, Wound leakage
Original Article
Dr. Naeem

Ophthalmology Update Vol. 10. No. 3, July-September 2012 245
phacoemulsification cataract surgery with and withoutports hydrations at the end of surgery.MATERIALS AND METHODS
All eyes that were scheduled to havephacoemulsification surgery at OphthalmologyDepartment Hayatabad Medical Complex (HMC),Peshawar from December 2010 to December 2011 wereincluded in the study. Eyes with very dark browncataracts were excluded because of a likelihood ofconverting to ECCE or prolonged phacoemulsificationtime.
Eyes with phacoemulsification time greater than1.5 minutes were also excluded. Post-operatively, eyeswith corneal edema were excluded as this interferedwith the evaluation of anterior chamber reaction. Thefirst group of eyes underwent uncomplicatedphacoemulsification surgery with 3.25 mm superior andtwo side ports at right angle to the main clear cornealincision.and. The incisions were hydrated using a 27gage cannula.
The second group of eyes underwent an identicalsurgery, but the incisions were not hydrated. Patientswere followed up at 24 hours, and 1 week and evaluatedby slit lamp for the presence of wound leak (usingSeidel’s test), and AC cells and flare.
A Seidel’s test includes application of a fluoresceinstrip with local anesthetic into the conjunctival sac andthen examination of the wound using a cobalt blue filter.If fluid appears to flow from the wound, there’s a leak.Anterior chamber (AC) reaction was assessed using slitlamp to determine the number of cells and the amountof flare in the anterior chamber. AC reaction was calledsignificant if the number of cells in one field, with anyamount of flare, were > 10. Surgeons who operated,assessed the patients postoperatively and recorded thefindings. The data were entered and analyzed usingSPSS software (version 11.5; SPPS Inc., Chicago, USA).Means (± SD) were calculated for continuous variablesand frequencies and proportions for categoricalvariables. Chi-square test was used to compare the ratesof wound leak and AC reaction in the two groups.RESULTS
Twenty four eyes of 21 patients, 14 men and sevenwomen, underwent surgery with ports hydrations and25 eyes of 22 patients, 13 men and 10 women,underwent no ports hydrations after surgery. The meanages of patients in groups 1 and II were 61.2 years and63.3 years, respectively. Following surgery, none of thepatients in two groups showed wound leak at 24 hoursand the first week. In addition, at 24 hours only 14.6%of eyes in group 1 showed AC reaction, compared to32.0 % in group II (p = 0.04). At one week post-op, 16.7%and 20.0% of eyes in Groups I and II showed ACreaction, respectively. However, the difference was not
statistically significant (p = 0.67).DISCUSSION
To the best of our knowledge, this is the first studyin Pakistan to compare the rates of postoperativewound leak and anterior chamber reaction in patientsundergoing phacoemulsification cataract surgery withand without ports hydrations after surgery. We foundthat that there were no statistically significantdifferences in the rates of postoperative wound leakand anterior chamber reaction in the two groups at 24hours and one week. Logically wound hydration sealthe eye and reduce the chances of wound leak and mostof the surgeons prefer to hydrate the incision afterphacoemulsification for their own satisfaction althoughour study showed no added advantage of this practice.Comparison with other studies
An extensive review of national and internationalliterature revealed there were no studies that directlycompared the rates of postoperative wound leak andanterior chamber reaction in the two groups we studied.However, there were several studies that comparedpostoperative astigmatism between sutured andunsutured phaco surgery. We plan to address these inour future studies.Our study had the following limitations:
First, the sample size was small, especially for theassessment of wound leak which is a relatively rareoutcome. Second, participants were not assigned to thetwo interventions randomly. Randomization eliminatesselection biases.
We conclude that the rates of postoperativewound leak and anterior chamber reaction inphacoemulsification are not different in both groups.Thus ports hydrations at the end of surgery offers noadded advantages.REFERENCE1. Sapkota YD, Pokharel GP, Nirmalan PK, et al. Prevalence of
blindness and cataract surgery in Gandaki Zone, Nepal. Br JOphthalmol 2006;90(4):411-6.
2. Chandrashekhar TS, Bhat HV, Pai RP, Nair SK. Prevalenceof blindness and its causes among those aged 50 years andabove in rural Karnataka, South India. Trop Doct2007;37(1):18-21.
3. Resnikoff S, Pascolini D, Etya’ale D, et al. Global data onvisual impairment in the year 2002. Bull World Health Organ2004; 82: 844-51.
4. Memon MS: Prevalence and causes of blindness in Pakistan.J Pak Med Assoc 1992; 42: 196-8.
5. Ahmad K, Khan MD, Qureshi MB, et al. Prevalence andcauses of blindness and low vision in a rural setting inPakistan. Ophthalmic Epidemiol. 2005; 12: 19-23.
6. Snellingen T, Evans JR, Ravilla T, et al. Surgical interventionsfor age-related cataract. Cochrane Database Syst Rev 2002:CD001323.
7. Buratto L, Werner L, Zanini M, et al. Phacoemulsification:Principles and Techniques, Slack Incorporated, Thorafore NJ,USA; 2003.
Wound Leakage and Anterior Chamber Reaction after Phacoemulsification with & without Ports Hydration

246 Ophthalmology Update Vol. 10. No. 3, July-September 2012
–––––––––––––––––––––––––––––––––––––––––––––––––––––1.Registrar Ophthalmology Department, Hayatabad MedicalComplex, Peshawar. 2.Assistant Professor Ophthalmology BannuMedical College, Bannu3. Medical Officer, Hayatabad MedicalComplex, Peshawar 4.Associate Professor OphthalmologyDepartment, Hayatabad Medical Complex, Peshawar–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Dr Mushtaq Ahmad House no 31B, street no 2,sector N4, Phase 4, Hayatabad, PeshawarE.mail >[email protected] Cell: 03339119605–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: Jan’2012 Accepted: May’ 2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
Phacoemulsification Vs Small IncisionCataract Surgery (SICS)
Mushtaq Ahmed FCPS1, Sanallah Khan FCPS2, Muhammad Naeem3
Sofia Iqbal MRCOphth, FRCS4
ABSTRACTObjectives: To compare the safety and efficacy of phacoemulsification versus small incision cataract surgery (SICS) inmature cataract.Material and methods: A prospective randomized controlled trial was carried out involving 79 and 71 patients withmature senile cataract selected for phacoemulsification and SICS respectively. All patients underwent slit lamp examination.Phaco-suitable mature senile cataracts were included for this study. Study variables included surgeon’s time, intraoperative/postoperative complications, postoperative uncorrected visual acuity and surgery-induced astigmatism on the firstpostoperative day. Mean values with standard deviations were calculated. P value of less than 0.05 was consideredsignificant.Results: There was no difference between the groups in terms of gender, age and pre-operative visual acuity (p = 0.09).In phacoemulsification group (n=79) more than three quarters and in SICS group (n=71) more than two thirds of thepatients had good visual outcome (6/6-6/18) on first postoperative day p=0.065). Poor outcome (<6/60) was recorded in1% (phacoemulsification group) and 3% (small incision cataract surgery group). Mean visual acuity was 0.53 ± 0.27 inphacoemulsification group and 0.47 ± 0.24 in SICS group. Mean surgery time was significantly shorter in SICS group(p=0.003). Data were computed and analyzed using the SPSS software program vs 10. The p value of < 0.05 wasconsidered significant.Conclusion: Performing SICS is significantly cheaper, faster and is a suitable alternative option for the treatment ofimmature senile cataracts. Although the complication rate is high in group B but there is no significant difference in visualoutcome on the first postoperative day between Phaco and SICS techniques.Keywords: phacoemulsification, small incision cataract surgery (SICS)
Original Article
Dr. Mushtaq
INTRODUCTIONSeveral worldwide studies suggest that the
prevalence of blindness is approximately 11%1 incataract surgery. Review of these studies shows thatcataract is the main cause of blindness, as some studieshave reported about 79% of bilateral blindness is dueto cataract.2 Insufficient financial resources,inaccessibility and lack of awareness about existing eyecare facilities are some of the barriers underprivilegedpeople face in utilizing available eye care services inpoor countries.3 Phacoemulsification is the preferredtechnique for cataract surgery in developed countries,but large-scale implementation in developing countriesmay prove to be a challenge.4 An alternative surgicaltechnique, manual sutureless small incision cataractsurgery, has been increasing in popularity, as the
technique has been shown to yield similar surgicaloutcomes as phacoemulsification.5 Several comparablestudies have shown similar visual outcome of the twosurgical techniques (Ruit et al 2007; Schwab, 2007;Gogate et al 2007; Spencer, 2006) but none of thoseprevious studies had compared the surgical procedureson phaco mature cataracts.6,7,8,9
This prospective randomized controlled trial wasdone to compare the efficacy of these two methods ofcataract extraction on phaco mature cataract indeveloping countries.MATERIALS AND METHODS
A randomized clinical trial was conducted atOphthalmology Department Hayatabad MedicalComplex, Peshawar from August 2011 to November2011. All patients underwent slit lamp examination.Phaco-suitable mature senile cataracts were includedfor this study. Mature cataract was defined as total lensopacity. All other types of cataracts were excluded fromthis study. An informed consent was obtained from allthe patients before including them in the study. Ethicalclearance was obtained from the Institutional ResearchCommittee. The patients with mature senile cataractwere divided into two groups before receivingretrobulbar anaesthesia. Randomization was done withthe help of random number tables. All patients wereoperated by a single surgeon well experienced in

Ophthalmology Update Vol. 10. No. 3, July-September 2012 247
performing cataract surgery with both techniques formore than ten years.
All cases were operated and examined in thepostoperative period by a single surgeon. A manual(Topcon) keratometer was used for the purpose ofkeratometry and a A-Scan ultrasound (Sonomed) forthe purpose of axial length measurement. The powerof the intra-ocular lens was calculated with the modifiedSRK II formula. After pupil dilatation with tropicamideand phenylephrine eye drops, a retrobulbar injectionwas given in sitting position and the patient requestedto press the eye ball with the palm of the hand over apiece of a cotton gauge to soften the eyeball.Preoperative povidone-iodine 5 % solution was usedfor disinfection of the periocular skin area. All thesurgeries were done via the superior approach. Threeincisions made in phaco patients (3.2mm superior andtwo side ports). A phacoemulsification machine(Universal-II) with tubings, hand pieces and Phaco tips,irrigation and aspiration cannulas was used forperforming phacoemulsification surgery in this study.The Acrylic hydrophilic foldable lens with a 6 mm opticwas implanted in the bag.
The SICS was performed using the tunnel incision2mm from the limbus and 7 mm enlarged. In all SICScases, a large capsulorrhexis was made before nucleusdelivery to ensure the placement of the intraocular lensin the bag. The rigid poly- methylmethacrylateintraocular lens with a 6 mm optic was implanted inthe bag. The surgical time was measured from thepreparation of the sclera-corneal incision to the
application of the eye pad.Study variables included surgeon’s time,
intraoperative/ postoperative complications,postoperative uncorrected visual acuity and surgery-induced astigmatism on the first postoperative day.Postoperative uncorrected visual acuity was taken witha Snellen chart at a 6 meter distance and was convertedinto decimals.RESULTS
Total of 150 patients included in the study, 79 wereoperated with the phacoemulsification technique(Group A) and 71 were operated with the SICStechnique (Group B).
Baseline characteristics were similar in bothgroups as shown in table 1.
Mean intraocular lens power was similar in bothgroups, phaco group: 22.2 ± 1.8 D and SICS group: 22.02± 1.31 D. In group A, one patient had zonular dialysisduring hydro-dissection procedure. In group B, twopatients had posterior capsule rupture (PCR) withvitreous loss. One patient underwent anteriorvitrectomy and PCIOL was placed in the ciliary sulcus.The other patient, who had a nucleus drop, was referredto the Retina Unit of our hospital. Dropped nucleus wasremoved and PCIOL was implanted in ciliary sulcusby the vitreo-retina surgeon.
Mean time spent by the surgeon per surgery was11 minutes in group A and 8 minute 18 seconds in groupB. In group A, 56.2 % patients and in group B 19.9 %had surgery time of more than 9 minutes (p value <0.003).
Table 1 Baseline characteristics
Variables Phacoemulsification SICS P value
(Group A) n=79 (group B) n=71
Age (Mean± SD) 58.7±12.5 yr 58.3±11.3yr
Male 56.2 % 50.2 % 0.0968
Female 43.8% 49.8% 0.0987
VA (HM orworse) 6.7 % 11.9 % 0.2336
Mean VA (remaining patients) 0.11±0.05 0.076±0.11
Table 2 Intra-operative findings
Parameters Phaco surgery (Group A) SICS (Group B)
Mean IOL power 22.2 ± 1.8 D 22.02 ± 1.31 D
Intra-operative complications Zonular dialysis during PCR + vitreous loss: 1
hydrodissection: 1 PCR + Nucleus drop: 1
Mean surgerytime > 9 min 56.2% 19.9% p value <0.003
Phacoemulsification Vs Small Incision Cataract Surgery (SICS)

248 Ophthalmology Update Vol. 10. No. 3, July-September 2012
Postoperatively, uncorrected visual acuity wasmeasured on the first postoperative day immediatelyafter removal of the eye pad. In group A, 90% morethan two third and in group B 75% nearly two thirds ofpatients had good visual outcome (6/6-6/18).
Mean visual acuity was 0.53 ± 0.27 D in group Aand 0.47 ± 0.24 in group B. Poor outcome (unaidedvisual acuity <6/60) was noticed in 1% patients fromgroup A and in 3% patients from group B.
Postoperatively, four patients had corneal edemain group A and three patients in group B. one patienthad increased anterior chamber reactions due topostoperative uveitis and eight patients had hyphemain group B (Table 4). All patients with corneal edemaresponded to treatment with antibiotic and steroid(Tobramycine and Dexamethasone) containing eyedrops and all the patients with hyphema hadspontaneous resolution with in a two days. Cornealastigmatism are more in group B as compared to groupA. All the patients were discharged on the third postoperative day.DISCUSSION
In this randomized clinical trial only maturecataracts were included, so the outcomes cannot begeneralized for all types of cataract. Operated patientswere advised to apply antibiotic and steroid containing(Tobramycine and Dexamethasone) eye drops regularlyon a tapering regime for six weeks. It is a commontendency that though we advise our patients to reviewafter six weeks. All surgeries were performed by asingle surgeon (SKS), who is experienced in both thetechniques. After the phacoemulsification procedure a
6 mm optic hydrophilic foldable lens was implanted inthe bag and after the fish hook SICS surgery a 6 mmoptic PMMA lens was implanted in the bag. Usually inSICS, the internal opening of the sclero-corneal woundis larger than the outer opening. On the first post-operative day, more than three quarters of all thepatients in group A and more than two thirds of thepatients in group B had a good visual outcome.
Mean visual outcome and mean inducedkeratometric astigmatism were comparable in bothgroups on the first post operative day. A frown shapedtemporal incision of SICS with phaco resulted in almostsimilar visual outcome with equal amount ofpostoperative astigmatism.
Mean surgery time was 10 minutes in group Aand 8 minutes and 18 seconds in group B. Mean surgerytime of more than 9 minutes was observed in 85% ofpatients in group A and 11 % of patients in group B (Pvalue <0.003). Shorter in toto nucleus extraction timecompared to phacoemulsification of nucleus, fasterepinucleus removal and faster cortex aspiration bysimcoe cannula compared to irrigation and aspirationcannula resulted in faster surgery by the SICS method.Complications like hyphema and against the ruleastigmatism are more frequently observed in group B.Though the cost difference between the phaco and SICSwith rigid lens is very low (Gogate et al, 2007) in highvolume set up, consumable cost of phaco surgery witha rigid PMMA lens is higher due to increased use ofviscoelastics and irrigating solution. A hospital basedstudy done by Hennig et al (2007) in similar setting atSagarmatha Choudhary Eye Hospital, Nepal showed
Table 3 Visual outcome on the first postoperative day
Parameters Phacoemulsification SICS P value
(Group A)n=79 (Group B)n=71
Good (6/6-6/18) 90.7% 75% 0.0655
Borderline (6/24-6/60) 26% 22%
Poor (<6/60) 1% 3%
Mean visual outcome 0.53 ± 0.27 0.47 ± 0.24
Table 4 Postoperative findings on the first post-operative day
Parameters Group A SICSGroup B
Postoperativecomplications Corneal edema 4 3
AC reaction 0 1
Hyphema 0 8
Mean induced Kastigmatism ( diopter) 0.12 (SD 0.82) 0.81(SD 0.84)
Phacoemulsification Vs Small Incision Cataract Surgery (SICS)

Ophthalmology Update Vol. 10. No. 3, July-September 2012 249
a consumable cost difference of USD 0.50 between SICSand phaco with rigid lens. The fixed cost associated withthe establishment of a phaco set-up is much highercompared to SICS. The cost of the phaco machine usedin this study was Euro 20,000. The depreciation of thephaco machine and the running cost associated withthe consumables and tips make phaco surgeryexpensive as compared to SICS.
Phacoemulsification has a long learning curve,requires expensive equipments, has a high consumablecost and needs expensive foldable lenses to maximizethe benefit associated with the small incision (Thomas,2009). Despite these facts, there is a growing demandfor phaco surgery in the developing world and manypatients are willing to pay more for it (Thomas et al,2008). To meet the demand and to make it affordableto the people of all socioeconomic levels,phacoemulsification is being performed withimplantation of foldable and rigid IOLs as well in thedeveloping countries.
In the high volume set-up of the BEH where asingle surgeon operates on two tables, six surgical setsof instruments, hand pieces, phaco tips, sleeves andirrigation-aspiration cannulas are required to performphacoemulsification faster. The cost associated withphaco hand pieces, phaco tips, sleeves, irrigation andaspiration cannulas are high and increase the fixed costand consumable cost associated with phaco-emulsification. Reusable tubings, cassettes, phaco tipsand hand pieces can help to lower the cost ofphacoemulsification surgery. There are certainguidelines given by the company about the maximumnumber of autoclaving cycles for the tubings, tips andhand pieces. Often these accessories are autoclaved andreused many more times than recommended (Thomas,2008). Only in a very few ophthalmic theatres indeveloping countries do they change phaco handpieces, phaco tips, sleeves and tubings for each surgery(Thomas, 2009). Various practices like changing onlythe tips and sleeves between surgery and dipping phacotips and cannulas in antiseptic solution after eachsurgery are common practices in developing countriesto cut down the cost. But none of the above-mentionedprocedures meet the recommended sterilization
standards and therefore, should be avoided (Thomas,2009). Easily available, inexpensive surgicalinstruments allow surgeons to follow standardrecommended procedures of sterilization for SICSwhereas the same is not true for phacoemulsification.Although there is hyphema and against the ruleastigmatism in significant number of patients in groupB but this study clearly shows that there is no additionalvisual and surgical benefit on the first postoperativeday with phaco technique with foldable IOLs ascompared to SICS with rigid IOLs.CONCLUSION
Performing SICS is significantly cheaper, fasterand is a suitable alternative option for the treatment ofimmature senile cataracts. Although the complicationrate is high in group B but there is no significantdifference in visual outcome on the first postoperativeday between phaco and SICS techniques.REFRENCES:1. Sapkota YD, Pokharel GP, Nirmalan PK, et al. Prevalence of
blindness and cataract surgery in Gandaki Zone, Nepal. Br JOphthalmol 2006;90(4):411-6.
2. Chandrashekhar TS, Bhat HV, Pai RP, Nair SK. Prevalenceof blindness and its causes among those aged 50 years andabove in rural Karnataka, South India. Trop Doct2007;37(1):18-21.
3. De Lima D M, Ventura L O, Brandt C T. Barriers in the accessto senile cataract treatment at Altino Ventura Foundation.Arq Bras Oftalmol 2005; 68:357-62.
4. Tabin G, Chen M, Espandar L. Cataract surgery for thedeveloping world. Curr Opin Ophthalmol 2008;19(1):55-9.
5. Hennig A, Kumar J, Yorston D, Foster A. Sutureless cataractsurgery with nucleus extraction: outcome of a prospectivestudy in Nepal. Br J Ophthalmol 2003; 87:266-70.
6. Ruit S, Tabin G, Chang D, Bajracharya L, Kline D C,RichheimerW, Shrestha M, PaudyalG. A prospectiverandomized clinical trial of phacoemulsification vs manualsutureless smallincision extracapsular cataract surgery inNepal. AmJ Ophthalmol 2007; 143:32-38.
7. Schwab L. A prospective randomized clinical trial ofphacoemulsification vs manual sutureless small-incisionextracapsular surgery in Nepal. Am J Ophthalmol 2007;143:1069.
8. Gogate P, Deshpande M, Nirmalan P K. Why dophacoemulsification? Manual small-incision cataract surgeryis almost as effective, but less expensive. Ophthalmology2007; 114:965-8.
9. Spencer M. Phaco vs. small-incision. Ophthalmology 2006;113:353.
Phacoemulsification Vs Small Incision Cataract Surgery (SICS)

250 Ophthalmology Update Vol. 10. No. 3, July-September 2012
–––––––––––––––––––––––––––––––––––––––––––––––––––––1,3.Post graduate TraineeOphthalmology. 2Registrar, Ophthalmology4Post graduate Trainee, Radiology. 5Assistant Prof. Ophthalmology–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Dr Muhammad Naeem, House No 31B, StreetNo 2, Sector N4, Phase 4, Hayatabad, Peshawar E.Mail>[email protected] Cell: 03339114435–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: February’2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
Comparision Between Topical Anesthesia alonevs Topical with Intracameral Anesthesia
in Phacoemulsification
Muhammad Naeem1, Mushtaq Ahmad FCPS2, Yousaf Jamal Mehsood3
Hina Mehwish Khan4, Mohammad Naeem Khan FCPS5
Ophthalmology Department, Hayatabad Medical Complex, Peshawar
ABSTRACTPurpose: To compare and determine patients and surgeon’s comfort and satisfaction in Phacoemulsification undertopical anesthesia with proparacain hydrochloride 0.5% versus topical with intracameral xylocaine 2% (preservativefree).Material and Methods: The study was conducted in the department of Ophthalmology Hayat abad MedicalComplex,Peshawar from May 2010 to June 2011. 96 patients of cataract divided into two groups, A and B each containing48 patients were included in this study. Phacoemulsification was performed on group A under topical anesthesia withproparacaine hydrochloride 0.5% and on group B under topical anesthesia along with intracameral xylocaine1% . All thepatients in both groups were operated by the same surgeon. The surgeon and patients satisfaction score was entered ina standardized performa.Results: 43 patients (89.58%) in group A, felt no pain while 5 patients(10.41%) felt pain up to the extent that 0.5 cc of 2% lignocaine was needed to inject in the anterior chamber and then the procedure of phacoemulsification was completedcomfortably and pain free in one patient (2.08%) in group A, the nucleus dropped into the vitreous and was referred tovitroretinal surgeon for further management. The mean phaco time was 2.2 minutes while mean operation time was 22minutes. In group B, the patients were operated after infiltration of 0.5 cc 2 % lignocaine injection in the anterior chamber.All patients operated under topical with intracameral were pain free and remained comfortable during surgery except intwo cases in group A,who felt pain during implanting folding lens. The mean phaco time was 2.1 minutes and meanoperation time was 22.0 minutes. The extension of CCC was seen in 5 patients(10.41% ) in group A and 2 patients(4.16%)in group B .The posterior capsule rent was seen in 2 patients (4.16%) in A group and in 2 patients(4.16% ) in group B.Conclusion: The intracameral injection of 2% lignocaine into the anterior chamber is superior to topical anesthesiaalone with proparacaine hydrochloride during phacoemulsification in ensuring patient’s and surgeon’s comfort. None ofthe patients in any group showed the complications as sometimes seen in periocular or retrobulbar anesthesia.
Original Article
INTRODUCTIONCataract blindness has been recognized for many
centuries with potential surgical intervention varyingfrom couching, extra capsular by needle pricking firstECCE, than intra capsular cataract extraction, with theintroduction of cryo-extraction, this became mostpopular method. These obtained limited success dueto the complications like vitreous prolapse, retinaldetachment, macular edema, aphakic glaucoma1.
Early surgeons, performing couching had no ideaof pushing something behind the pupil was the humanlens. In 16th century Atoine Jan and Michel Pierreidentified from autopsy specimen that the cataract was
truly the crystalline lens itself2.
The written proof of couching came from Susrutaan Indian surgeon3.Daviel performed extracapsularextraction from inferior limbus in sitting position4.Pierre Francos shifted incision to the upper limbuswhile sitting on head side of patient. Thepharmacological mydriasis and planned iridectomywas introduced by Carl Himly5.
The next breakthrough came in intracapsularsurgery with the development of chemical zonulysisusing an enzyme ?-chymotrysin6. Aphakic correctionwith contact lens started from 1940. Harold Ridlelyimplanted first synthetic lens on November 29, 19497.First feeling of intact supports for IOL was urged byCornelius Binkhorst. Kelman introduced hisphacoemulsifier in 1967 but many intracapsularsurgeons were not convinced8. After that RobertSinskey and John Sheets were more popular in smallincision ultrasonic surgery9. Howard Gimbelintroduced capsulorhexis first time10. Small incisionclosing sutures were introduced by John Shepherd and
Dr. Naeem

Ophthalmology Update Vol. 10. No. 3, July-September 2012 251
later by Howard Fine11.
Kelman performed phacoemulsification intoanterior chamber and D. Calvard, Kratz.,T performedphacoemulsification into the papillary plane12.Endocapsular phacoemulsification was introduced byShephard13. Several studies have demonstrated thattopical anesthesia provides satisfactory analgesia,comparable with regional blocks (retrobulbar,peribulbar and sub-tenon, anesthesia)14. This studywas conducted to assess and compare the advantagesof topical with intracameral anesthesia over topicalanesthesia alone in phacoemulsification surgery.MATERIALS AND METHODS
The ninety six patients having cataract weredivided into two groups A and B each having 48patients. The age of patients ranged between 50 to 70years. Both male and female patients with anterior,posterior, nuclear, cortical or grade 1 to 3 cataract wereincluded in the study.
Following patients were excluded from the study;• Having history of trauma and ocular surgery• Having corneal opacity• Un-cooperative patients• Claustrophobic patients
Pre-operative ocular and systemic assessmentsalong with routine investigations were carried out. Allthe surgeries were done by the same doctor. Thepreoperative medicines included,1 tab. diamox, 1 tab.Neo-k,1 tab. valium 5 mg, 1 tab. levoflaxacine and thesewere given an hour before starting surgery to eachpatient. Every patient’s pupil was dilated with eyedrops of Alcaine, Mydracyl and Isonephrine, half anhour before start of surgery. A written informed consentwas obtained from each patient on the day of surgery.The out come measures and criteria consisted of;1. Patient satisfaction;
a. Very happyb. Happyc. Angry
2. Ease of surgerya. Phaco timeb. Operative timec. Conversion to ECCE
3. Complicationsa. Extension of CCCb. Posterior capsule rentc. Vitreous loss and nucleus dropThe group A patients were operated under topical
anesthesia (proparacaine hydrochloride 0.5%, Alcaine)instilled 6 times with interval of 5 minutes between eachdrop, after dilating the pupil before start of surgery.Patients were instructed to keep their eyes closed after
instilling drops. The patients were instructed to liesupine on operating table with opened eyes while atthe same time keeping their eyes stable. At operatingtable no topical, intracameral or subconjunctivalanesthesia was given. One limbal 3.2 mm phaco portand two side ports about 0.8 mm were fashioned. TheCCC was done with cystitome after filling anteriorchamber with methyl cellulose. Hydro dissection andhydro delineation were done properly and then phacostarted with observation of good phaco techniques andtips. Total phaco and surgery completion time,complications if any and satisfaction score was notedand recorded in the performa.
The patients in group B were prepared in the samemanner as above except in addition a 0.5 cc 2%lignocaine was injected intracameraly. No other typeof analgesia was given. Then phaco time, total operationtime, complications and satisfaction points wererecorded in the performa.RESULTS
There were 48 patients in group A. The age of thepatients was between 50 to 70 years (detail is shown inthe table). Out of 48 in group A only 5 patients (10.41%)felt pain so severe that they required injection of 0.5 ccof 2 % lignocaine intracameraly and then the procedurewas carried out. The extension of ccc was seen in 5patients (10.41%) out of total 48 patients while posteriorcapsule rent was seen in 2 patients (4.16%) thiscomplication was managed with anterior vitrectomyand implantation of 6.5 mm IOL in the sulcus andincision was closed with 3 interrupted 10/0 sutures. Inone patient nucleus dropped in the vitreous and wasreferred to vitreoretinal surgeon for furthermanagement. The average phaco time was 2.2 minuteswhile total operative time was 22 minutes. In group Bthere were 48 patients and all of them were given 0.5 ccinjection of lignocaine intracameraly. None of thepatients felt remarkable pain. The extension of ccc wasseen in 2 cases (4.16%) while posterior capsule rent wasseen in 2 patients (4.16%) that was managed withvitrectomy and 6.5 mm IOL in the sulcus and the closureof incision was done with 3 interrupted 10.0 stitches.No nucleus was dropped in the vitreous. The averagephaco time 2 minutes and total operative time was 22minutes.
Age and Sex determination
Group Age range Age n (%) Sex n (%)
Group A 50-60 23 (47.91) 35 (72.91)
61-70 25 (52.08) 13 (27.08)
Group B 50-60 22 (45.83) 28 ((58.33)
61-70 26 (54.16) 20 (41.66)
Comparision Between Topical Anesthesia alone vs Topical with Intracameral Anesthesi in Phacoemulsification
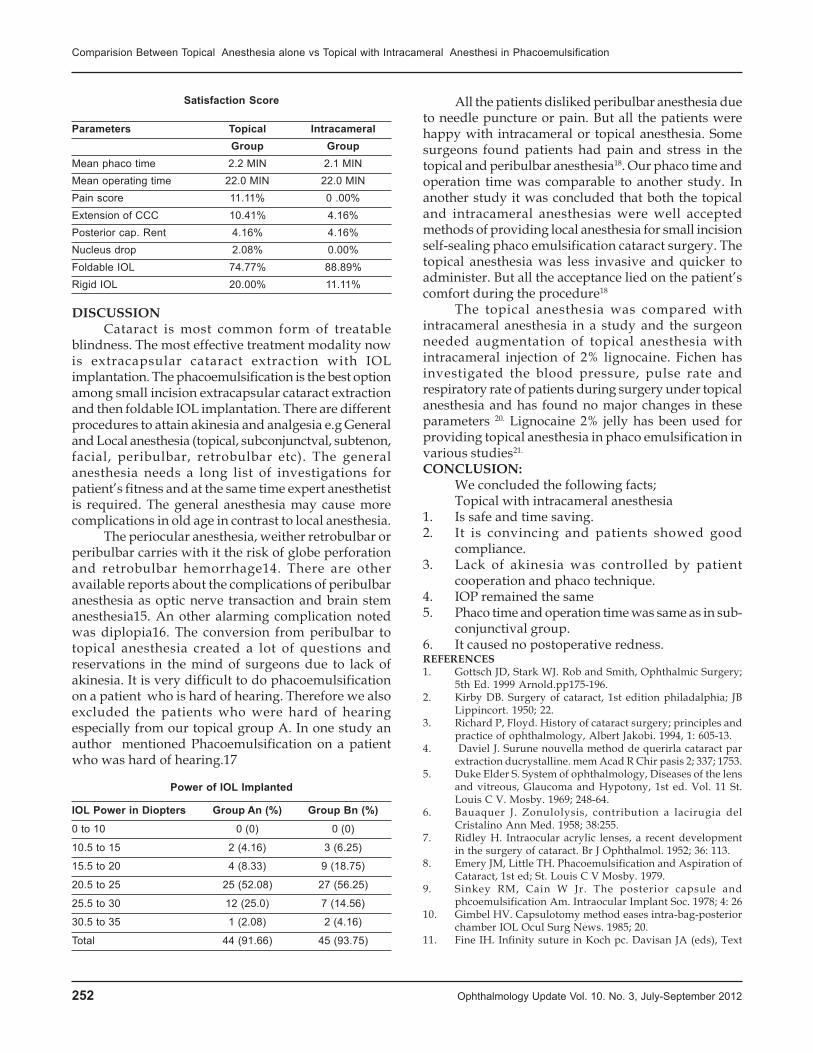
252 Ophthalmology Update Vol. 10. No. 3, July-September 2012
Satisfaction Score
Parameters Topical IntracameralGroup Group
Mean phaco time 2.2 MIN 2.1 MINMean operating time 22.0 MIN 22.0 MINPain score 11.11% 0 .00%Extension of CCC 10.41% 4.16%Posterior cap. Rent 4.16% 4.16%Nucleus drop 2.08% 0.00%Foldable IOL 74.77% 88.89%Rigid IOL 20.00% 11.11%
DISCUSSIONCataract is most common form of treatable
blindness. The most effective treatment modality nowis extracapsular cataract extraction with IOLimplantation. The phacoemulsification is the best optionamong small incision extracapsular cataract extractionand then foldable IOL implantation. There are differentprocedures to attain akinesia and analgesia e.g Generaland Local anesthesia (topical, subconjunctval, subtenon,facial, peribulbar, retrobulbar etc). The generalanesthesia needs a long list of investigations forpatient’s fitness and at the same time expert anesthetistis required. The general anesthesia may cause morecomplications in old age in contrast to local anesthesia.
The periocular anesthesia, weither retrobulbar orperibulbar carries with it the risk of globe perforationand retrobulbar hemorrhage14. There are otheravailable reports about the complications of peribulbaranesthesia as optic nerve transaction and brain stemanesthesia15. An other alarming complication notedwas diplopia16. The conversion from peribulbar totopical anesthesia created a lot of questions andreservations in the mind of surgeons due to lack ofakinesia. It is very difficult to do phacoemulsificationon a patient who is hard of hearing. Therefore we alsoexcluded the patients who were hard of hearingespecially from our topical group A. In one study anauthor mentioned Phacoemulsification on a patientwho was hard of hearing.17
Power of IOL Implanted
IOL Power in Diopters Group An (%) Group Bn (%)
0 to 10 0 (0) 0 (0)
10.5 to 15 2 (4.16) 3 (6.25)
15.5 to 20 4 (8.33) 9 (18.75)
20.5 to 25 25 (52.08) 27 (56.25)
25.5 to 30 12 (25.0) 7 (14.56)
30.5 to 35 1 (2.08) 2 (4.16)
Total 44 (91.66) 45 (93.75)
All the patients disliked peribulbar anesthesia dueto needle puncture or pain. But all the patients werehappy with intracameral or topical anesthesia. Somesurgeons found patients had pain and stress in thetopical and peribulbar anesthesia18. Our phaco time andoperation time was comparable to another study. Inanother study it was concluded that both the topicaland intracameral anesthesias were well acceptedmethods of providing local anesthesia for small incisionself-sealing phaco emulsification cataract surgery. Thetopical anesthesia was less invasive and quicker toadminister. But all the acceptance lied on the patient’scomfort during the procedure18
The topical anesthesia was compared withintracameral anesthesia in a study and the surgeonneeded augmentation of topical anesthesia withintracameral injection of 2% lignocaine. Fichen hasinvestigated the blood pressure, pulse rate andrespiratory rate of patients during surgery under topicalanesthesia and has found no major changes in theseparameters 20. Lignocaine 2% jelly has been used forproviding topical anesthesia in phaco emulsification invarious studies21.
CONCLUSION:We concluded the following facts;Topical with intracameral anesthesia
1. Is safe and time saving.2. It is convincing and patients showed good
compliance.3. Lack of akinesia was controlled by patient
cooperation and phaco technique.4. IOP remained the same5. Phaco time and operation time was same as in sub-
conjunctival group.6. It caused no postoperative redness.REFERENCES1. Gottsch JD, Stark WJ. Rob and Smith, Ophthalmic Surgery;
5th Ed. 1999 Arnold.pp175-196.2. Kirby DB. Surgery of cataract, 1st edition philadalphia; JB
Lippincort. 1950; 22.3. Richard P, Floyd. History of cataract surgery; principles and
practice of ophthalmology, Albert Jakobi. 1994, 1: 605-13.4. Daviel J. Surune nouvella method de querirla cataract par
extraction ducrystalline. mem Acad R Chir pasis 2; 337; 1753.5. Duke Elder S. System of ophthalmology, Diseases of the lens
and vitreous, Glaucoma and Hypotony, 1st ed. Vol. 11 St.Louis C V. Mosby. 1969; 248-64.
6. Bauaquer J. Zonulolysis, contribution a lacirugia delCristalino Ann Med. 1958; 38:255.
7. Ridley H. Intraocular acrylic lenses, a recent developmentin the surgery of cataract. Br J Ophthalmol. 1952; 36: 113.
8. Emery JM, Little TH. Phacoemulsification and Aspiration ofCataract, 1st ed; St. Louis C V Mosby. 1979.
9. Sinkey RM, Cain W Jr. The posterior capsule andphcoemulsification Am. Intraocular Implant Soc. 1978; 4: 26
10. Gimbel HV. Capsulotomy method eases intra-bag-posteriorchamber IOL Ocul Surg News. 1985; 20.
11. Fine IH. Infinity suture in Koch pc. Davisan JA (eds), Text
Comparision Between Topical Anesthesia alone vs Topical with Intracameral Anesthesi in Phacoemulsification
Ophthalmology Update Vol. 10. No. 3, July-September 2012 253
book of advanced phacoemulsification techniques 1st ed.Tholofare N J Slack. 1991; 383.
12. Calvard Dm, Kratz RP. Endothelial cell loss followingphacoemulsification in the papillary plane. J Am Intraocularimplant Soc T. 1981; 334.
13. Shephard J. In Situ fracture phacoemulsification method,phaco, PI. 1989.
14. Haider SA, Khaqan HA. Topical versus periocular anesthesiafor cataract surgery what is best? Pak J Ophthalmol. 2005,21: 1- 5.
15. Hay A, Flynn HW, Hoffmann JI, et al. Needle perforation ofthe globe during retrobulbar and peribubar injection,Ophthalmology. 1991; 98: 1017-24.
16. Gomez –Arnou JI, Yan gucla J, Gozalez A, et al. Anesthesiarelated diplopia after cataract surgery. Br J Anesthesia. 2003;90: 189-93.
17. 18-19-Nielsen PJ. A Prospective evaluation of anxiety andpain with topical analgesia or retrobulbar anesthesia for smallincision cataract surgery. Eur J Implant Refract Surgery. 1995;7: 6-10.
18. H B Chitlenden, WR, Meacock J AA. Govan topical anesthesiawith oxybuprocain versus sub-tenon,s infiltration 2%lignocaine for small incision cataract surgery. Br JOphthalmol. 1997; 81: 288-90.
19. Manners TD, Burton RL. Randomised Trial of topical versussubtenant’s local anesthesia for small incision cataractsurgery, Eye. 1996; 367-70.
20. Fichman RA. Use of topical anesthesia alone in cataractsurgery. J Cataract Refract Surg. 1996; 22: 612-4.
21. Barequet IS, Soriano FS, Green WRO, et al. Provision ofanesthesia with single application of lidocaine 2% gell. JCataract Refract Surg.1999; 25: 828-31
Comparision Between Topical Anesthesia alone vs Topical with Intracameral Anesthesi in Phacoemulsification

254 Ophthalmology Update Vol. 10. No. 3, July-September 2012
–––––––––––––––––––––––––––––––––––––––––––––––––––––1,3. postgraduate trainee, Eye Department , Hayatabad MedicalComplex, Peshawar2. RegistrarEye Department , HayatabadMedical Complex, Peshawar–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence:Dr. Yousaf Jamal Mahsood,H: No: 289, StreetNo: 7,Sector: H-1, Phase 2,Hayatabad, Peshawar.E-mail: [email protected] Ph: No: 0092-91-5810370Res) 03339102980 (Cell)–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: Jan’2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
Effect of Ophthalmic Visco-elastic Deviceon Corneal Endothelial Cell Count
after Phacoemulsification
Yousaf Jamal Mahsood1, Mushtaq Ahmad FCPS2, Muhammad Naeem3
ABSTRACTObjective: To compare the effect of cohesive and dispersive ophthalmic viscoelastic devices (OVDs) on cornealendothelium cell count after in-the-bag phacoemulsification with implantation of a foldable posterior chamber intraocularlens (IOL).Materials and Methods:This study was conducted at department of ophthalmology, Hayatabad Medical Complex,Peshawar from 1st May 2010 to 31st April 2011. It was a prospective single-masked randomized study and included 50eyes of 50 cataract patients. Two groups were compared each consisting of 25 patients, with dispersive sodium hyaluronate(dispersive-NaHa) used in one group while cohesive sodium hyaluronate (cohesive-NaHa) in other group. The cornealresponse to surgery was evaluated by measuring the endothelial cell loss. Data were recorded preoperatively and 2months postoperatively.Results:Preoperatively, no significant difference was observed in cell count between the groups. Postoperatively, boththe groups had a significant decrease in cell count, but the decrease was significantly less in the dispersive-NaHa group(6.97%) than cohesive-NaHa group (18.46%).Conclusions: Choosing a dispersive OVD during the phaco procedure may allow better protection of the endothelialcells while suppressing the formation of free radicals. This may be the reason for the superior protective effect on thecorneal endothelial cells of dispersive-NaHa compared with cohesive-NaHa.Keywords: Ophthalmic viscoelastic devices, phacoemulsification, corneal endothelial cell.
Original Article
INTRODUCTION:The development of new surgical phaco-
emulsification techniques aims at restoring visual acuity(VA) with a faster return to normal social life and work.Advancements in the technique and instrumentationlike small-incision phaco procedures have minimizedpostoperative astigmatism and have reduced theincidence of postoperative endophthalmitis. However,corneal edema can lead to compromised VA in thesepatients because of a decrease in endothelial pumpfunction. Different factors have been reported to causeendothelial cell damage during phacoemulsificationlike: phacoemulsification technique,1 hardness of thenucleus,2 incision size and design,3 amount of totalultrasonic energy,4 the composition of the irrigationfluids,5 and formation of free radicals.6 To decreasepostoperative corneal endothelial cell loss, differentOVDs have been tried to facilitate surgical maneuvers,
maintain space during surgery, and protect theendothelial cells. Researchers have provided enoughevidence of endothelial cell protection duringphacoemulsification in humans.7The endothelial cellpump is primarily responsible for clear cornea.8 Thecritical endothelial cell density is estimated to be 600–800 cells/mm2. If the number of cells decrease belowthis level, corneal edema appears.
Adult human corneal endothelium behaves as anon-replicative tissue and throughout life there is anatural decrease in endothelial cell density, from 4000cells/mm2 in childhood to 2500 cells/mm2 in peopleaged 80 years and over.9 Increased age and oculartraumas such as cataract surgery cause the endothelialcell area to become less uniform.9 The cornealendothelium acts as a barrier between the anteriorchamber and the corneal stroma. If this barrier functionis damaged during cataract surgery, swelling of thecornea will occur. An increase in central cornealthickness in the first postoperative week, measured bypachymetry, may be a useful clinical predictor of long-term endothelial cell loss,10although the correlationbetween corneal thickness and endothelial cell count isnot quite clear.11
The aim of our study was to evaluate the efficacyof dispersive-NaHa and cohesive-NaHa in protectingthe corneal endothelium during in-the-bagphacoemulsification with implantation of a foldable
Dr Yousaf

Ophthalmology Update Vol. 10. No. 3, July-September 2012 255
acrylic lens. Cohesive-NaHa was used as the referencegold standard.MATERIALS AND METHODS:
We designed a clinical prospective, randomizedstudy including 50 eyes of 50 consecutive patientsscheduled to undergo cataract surgery at departmentof ophthalmology, Hayatabad Medical Complex,Peshawar from 1st May 2010 31st April 2011. The studyprotocol was approved by the local ethical committee.All patients gave full informed consent. The 50 patientswere randomly assigned into two groups based on theOVDs used: dispersive-NaHa or cohesive-NaHa. Thetwo viscoelastics differ from each other in molecularweight, concentration, viscosity, pseudoplasticity,cohesiveness and coatability. The rheological andclinical features of the two OVDs are presented in Table1.
Exclusion criteria were corneal dystrophies,traumatic or old infected corneal scars or previousintraocular surgery, history of intraocularinflammation, diabetes, preoperative pupil dilatation< 5 mm, age less than 45 years, preoperative endothelialcell count <2000 cells/mm2 and surgical complicationsthat may lead to excessive compromise of cornealendothelium. Preoperatively, all patients’ best correctedvisual acuity (BCVA) and intraocular pressure (IOP)were measured followed by detailed slit lampexamination and dilated fundus examination. Theendothelial cell parameters including cell density wasrecorded using a non-contact specular microscope.Specular microscopy was repeated 2 monthspostoperatively.
All the surgeries were carried out by one surgeonfollowing a standardized procedure: sterile drapingwith Povidine-iodine (PVD-iodine) 5%; peribulbaranesthesia; a 3.2-mm, self-sealing, superior, clearcorneal incision; followed by one of the two OVDs;capsulorhexis with rhexis forceps; phaco stop and chopremoval of the nucleus; cortical clean-up; implantationof a foldable acrylic lens using an injector system, andaspiration of the OVD. At the end of the operation all
patients received a subconjunctival injection of 1ccdexamethasone followed by steroid-antibioticcombination ointment in conjunctival sac. No sutureswere applied.
The surgeon used same phaco machine, phacomachine parameters and standard phaco tips in allcases. The patients were dismissed from ourdepartment on 1st postoperative day. Postoperatively,steroid-antibiotic combination eye drops were used 4times a day. The two observer who performed the pre-and postoperative measurements was unaware awareof the OVD used.Statistical analysis:
Statistical analysis was carried out by using SPSSsoftware version 17. Tests for difference between thegroups in demographic and clinical characteristics werecarried out using chi-square tests for categoricalvariables and one-way analysis of variance (anova)tables for continuous variables. If differences wereobserved using anova, least significant difference testswere performed between all pairs of groups. Snellen’sVA was converted to logMAR for statistical purposes.A p-value of less than 0.05 was considered significant.For the power calculation a clinical important changein cell count was defined as a loss of one standarddeviation (300 cells/mm2).RESULTS:
Fifty patients were enrolled but three patientscouldn’t come for follow-up due to personal reasons.The remainder 47 patients (23 patients in dispersive-NaHa and 24 patients in cohesive-NaHa groups) camefor last follow-up. Baseline preoperative data is givenin Table 2. There were no statistically significantdifferences between the two groups regarding their age,gender, visual acuity or IOP (Table 2). No significantdifference was observed preoperatively between twogroups (Table 3).
Postoperatively, both groups had a significantdecrease in endothelial cells (Table 3). The meanendothelial cell loss was 190 cells/mm2 (7.39%) in the
Table 1Characteristics of the two viscoelastics
Classification Dispersive CohesiveIngredient Na-hyaluronate Na-hyaluronateConcentration mg/ml 3% 1%Molecular weight (Dalton) 600 000 4 000 000Viscosity (V0) 40 000 400 000Viscosity (V1000) 310 110Pseudoplasticity (V0/V1000) 129.0 3636.3Cohesiveness Moderate HighCoatability High Low
Table 2Preoperative findings
Dispersive- Cohesive- p-valueNaHa NaHa
No. of patients 23 24Age, years (SD) 66.2 (6.3) 65.4 (7.1) 0.92†Gender, male/female 15/8 15/9 0.94*Visual acuity,logMAR (SD) 0.30 (0.19) 0.32 (0.18) 0.83†Intraocular pressure,mmHg (SD) 15.0 (2.7) 15.2 (2.4) 0.65†
*Chi-square test; † anova test
Effect of Ophthalmic Visco-elastic Device on Corneal Endothelial Cell Count after Phacoemulsification

256 Ophthalmology Update Vol. 10. No. 3, July-September 2012
dispersive-NaHa group, and 530 cells/mm2 (19.6%) inthe cohesive-NaHa group. The dispersive-NaHa grouphad a significantly lower rate of cell loss than the othergroup (anova, p = 0.04). There was an equal increase inVA. Postoperative IOP did not differ significantly frompreoperative IOP within any of the groups or betweenthe two groups.DISCUSSION:
In our study, we investigated the effect ofphacoemulsification on the corneal endothelium withimplantation of a posterior foldable acrylic lens usingtwo different OVDs. Preoperatively, demographic aswell as endothelial cell parameters were similar in thetwo groups, indicating that no sampling bias waspresent. Loss of endothelial cells is compensated bycellular enlargement, cell gliding, rearrangement andcell coalescence.9 Postoperatively, both groups had asignificant decrease in cell density, but the cell loss wassignificantly lower in the dispersive-NaHa group thanin the other group. Several factors may explain thisobservation.
Ophthalmic viscoelastic devices (OVDs) havebeen shown to decrease endothelial cell damage duringphacoemulsification by facilitating the surgicalmaneuvers, maintaining space and protecting theendothelial cells during surgery. The visco-elastics varyin their properties (Table 1). However, in clinical life itis more convenient to divide OVDs into two maingroups of cohesive and dispersive OVDs according totheir behavior during surgery.12 A cohesive hyaluronateOVD with high molecular weight contains longpolysaccharide chains with glycosides connections,which gives it higher viscosity, pseudoplasticity andcohesiveness. Cohesive OVDs are good at maintainingspace and stabilizing tissue during surgery.
They are easy to inject and easy to remove fromthe anterior chamber.13 However, the vulnerable aspectof these OVDs concerns their tendency to escape fromthe anterior chamber as a solid mass duringphacoemulsification, leaving the endothelial cells
without sufficient protection.11 Dispersive hyaluronatesand methylcellulose OVDs such as have lowermolecular weight and shorter, weaker chains whichgive them less viscosity, pseudoplasticity andcohesiveness. Dispersive OVDs do not maintain spaceas well as the cohesive agents. However, they are lessentangled, so they do not leave the anterior chamberduring surgery as easily as cohesive OVDs, whichmeans dispersive OVDs are better able to coat andprotect the corneal endothelium.11,13 This ability isconvenient during surgery, but it is more difficult toremove dispersive OVDs from the anterior chamber atthe end of the operation. The complete removal of theseOVDs may prolong aspiration/irrigation time and beresponsible for increased endothelial cell loss.7This hasbeen demonstrated in another study using the Miyakevideo technique.14 Less cell loss was observed withdispersive-NaHa. This may be explained by the abilityof dispersive-NaHa to reduce formation of free radicals.Phacoemulsification produces free hydroxyl radicalsand reports suggest that these are destructive to cornealendothelial cells.15 The amount of free radicals isproportional to phaco time.15 Hyaluronate OVDs havebeen shown to suppress the formation of free radicalsand exert anti-inflammatory properties.16 It has beendemonstrated that dispersive hyaluronate OVDssuppress free radicals better than cohesive hyaluronateOVDs.17 Others have shown that cohesive hyaluronateOVDs suppress the formation of free radicalssignificantly more than methylcellulose.18
RESULTSSimilar to ours have been published for the
dispersive which reported that there was significantlybetter endothelial protection was observed usingdispersive OVD as compared to a cohesive OVD.11 Anew group of OVDs, the viscoadaptives, behavedifferently from both the cohesive and the dispersiveOVDs because they are able to change from beinghighly viscous cohesive to fracturable pseudo-dispersive according to the flow rate.19 It has beensuggested that these new viscoadaptives may offerbetter protection of endothelial cells because they arewell retained during lower flow rates, and are easilyevacuated under higher flow at the conclusion of theoperation.20 Viscoadaptives OVDs have been comparedwith the dispersive OVDs and seem to offer comparableprotection to endothelial cells.21
In summary, a dispersive-NaHa OVD which iswell retained in the anterior chamber during thephacoemulsification procedure, and thus offersmechanical protection to endothelial cells whilesuppressing the formation of free radicals. Theseabilities may explain the better protection provided bydispersive-NaHa compared to cohesive-NaHa. Our
Table 3Preoperativeand postoperativeendothelial cell count by group
Dispersive- Cohesive- p-valueNaHa NaHa
PreoperativeCells/mm2 (SD) 2570 (290) 2698 (376) 0.30*PostoperativeCells/mm2 (SD) 2380 (410) 2168 (589) 0.35*Mean cell loss
Cells/mm2 (%) 190 (7.39) 530 (19.6) 0.04*
*anova and leastg significant difference as post hoc test.
Effect of Ophthalmic Visco-elastic Device on Corneal Endothelial Cell Count after Phacoemulsification
Ophthalmology Update Vol. 10. No. 3, July-September 2012 257
results encourage further investigations of theprotective characteristics of dispersive-NaHa andsimilar dispersive, low molecular, hyaluronate OVDs.REFERENCES1. Pirazzoli G, D’Eliseo D, Ziosi M , Acciarri R. Effects of
phacoemulsification time on the corneal endothelium usingphacofracture and phaco chop techniques. J Cataract RefractSurg . 1996;22:967–9.
2. Hayashi K, Hayashi H, Nakao F, Hayashi F. Risk factors forcorneal endothelial injury during phacoemulsification. JCataract Refract Surg. 1996;22:1079–84.
3. Dick HB, Kohnen T, Jacobi FK, Jacobi KW. Longtermendothelial cell loss following phacoemulsification througha temporal clear corneal incision. J Cataract Refract Surg.1996;22:63–71.
4. Hayashi K, Nakao F, Hayashi F. Corneal endothelial cell lossafter phacoemulsification using nuclear cracking procedures.J Cataract Refract Surg. 1994;20:44–7.
5. Joussen AM, Barth U, Cubuk H, Koch HR. Effect of irrigatingsolution and irrigation temperature on the cornea and pupilduring phacoemulsification. J Cataract Refract Surg.2000;26:392–7.
6. Cameron MD, Poyer JF, Aust SD. Identification of freeradicals produced during phacoemulsification. J CataractRefract Surg. 2001;27:463–70.
7. Holzer MP, Tetz MR, Auffarth GU, Welt R, Volcker HE. Effectof Healon5 and four other viscoelastic substances onintraocular pressure and endothelium after cataract surgery.J Cataract Refract Surg. 2001;27:213–8.
8. Shaw EL, Rao GN, Arthur EJ, Aquavella JV. The functionalreserve of corneal endothelium. Ophthalmology.1978;85:640–9.
9. Yee RW, Matsuda M, Schultz RO, Edelhauser HF. Changesin the normal corneal endothelial cellular pattern as afunction of age. Curr Eye Res. 1985;4:671–8.
10. Beneyto P, Gutierrez R, Perez TM. Comparative study ofthree methods of evaluation of the corneal endothelium inpseudophakic patients: fluorophotometry, specularmicroscopy and pachymetry. Graefes Arch
ClinExpOphthalmol. 1996;234:623–7.11. Koch DD, Liu JF, Glasser DB, Merin LM, Haft E. A
comparison of corneal endothelial changes after use ofHealon or Viscoat during phacoemulsification. Am JOphthalmol. 1993;115:188–201.
12. Liesegang TJ. Viscoelastic substances in ophthalmology.SurvOphthalmol. 1990;34:268–93.
13. McDermott ML, Hazlett LD, Barrett RP, Lambert RJ.Viscoelastic adherence to corneal endothelium followingphacoemulsification. J Cataract Refract Surg. 1998;24:678–83.
14. Assia EI, Apple DJ, Lim ES, Morgan RC, Tsai JC. Removal ofviscoelastic materials after experimental cataract surgery invitro. J Cataract Refract Surg. 1992;18:3–6.
15. Holst A, Rolfsen W, Svensson B, Ollinger K, Lundgren B.Formation of free radicals during phacoemulsification. CurrEye Res. 1993;12:359–65.
16. Camillieri G, Nastasi A, Gulino P, Bucolo C, Drago F. Effectsof hyaluronan on free-radical formation, cornealendothelium damage and inflammation parameters afterphacoemulsification in rabbits. J OculPharmacolTher.2004;20:151–7.
17. Takahashi H, Sakamoto A, Takahashi R, Ohmura T,Shimmura S, Ohara K. Free radicals in phacoemulsificationand aspiration procedures. Arch Ophthalmol. 2002;120:1348–52.
18. Augustin AJ, Dick HB. Oxidative tissue damage afterphacoemulsification: influence of ophthalmic viscosurgicaldevices. J Cataract Refract Surg. 2004;30:424–7.
19. Arshinoff SA, Jafari M. New classification of ophthalmicviscosurgical devices. J Cataract Refract Surg. 2005;31: 2167–71.
20. Arshinoff SA, Wong E. Understanding, retaining andremoving dispersive and pseudodispersive ophthalmicviscosurgical devices. J Cataract Refract Surg. 2003;29:2318–23.
21. Vajpayee RB, Verma K, Sinha R. Comparative evaluation ofefficacy and safety of ophthalmic viscosurgical devices inphacoemulsification. BMC Ophthalmol. 2005;5:17–22.
Effect of Ophthalmic Visco-elastic Device on Corneal Endothelial Cell Count after Phacoemulsification

258 Ophthalmology Update Vol. 10. No. 3, July-September 2012
–––––––––––––––––––––––––––––––––––––––––––––––––––––1.Postgraduate Trainees Radiology Deptt., Hayatabad MedicalComplex, Peshawar, 2Registrar, Ophthalmology Hayatabad MedicalComplex, Peshawar, 3Postgraduate Trainee Ophthalmology,4Associate Professor Ophthalmology, Hayatabad Medical Complex,Peshawar. 5Assistant Profesor Ophthalmology, Bannu MedicalCollege, Bannu,6Head Department of OphthalmologyHayatabadMedical Complex, Peshawar.–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Dr. Hina Mehwish Khan, House no 31B, streetno 2, sector N4, Phase 4, Hayatabad,PeshawarE.Mail>[email protected]–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: March’2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
Role of CT Scan in Diagnosis of Orbital Masses
Hina Mehwish Khan1, Mushtaq Ahmad2, Muhammad Naeem3, Sofia Iqbal4Radiology Department, Hayatabad Medical Complex, Peshawar.
ABSTRACTObjectives: To analyze the diagnostic role of CT scan in evaluation of orbital massesMaterial and Methods:26 patients presenting with proptosis were evaluated by CT scan. Role of CT was evaluated indefining the cause of exophthalmos and the nature and extent of the lesions causing exophthalmos.Results: .The most common lesion causing exophthalmos were tumours (46%) and infections (28%) followed byinflammation (18%), trauma (6%) and vascular (2%). CT scan findings in relation with the age of the patient, theclinical picture and laboratory investigations were able to give a correct diagnosis in 82% patients.Conclusion: CT scan can be considered as a cost effective, non invasive, reliable diagnostic tool for evaluation ofexophthalmos.Keywords: CT scan, exophthalmos
Original Article
INTRODUCTIONThe term exophthalmos has been derived from
Greek, literally meaning with prominent eyes. It refersto the protrusion of one or both eyes. It is often usedinterchangeably with the term proptosis although somereserve the term exophthalmos for endocrine-relatedprotruding eyeball and proptosis for other causes.1
Exophthalmos is a clinical sign of orbital disease andmay be accompanied by other signs. The orbital diseasemay be isolated (e.g. orbital varices) or may be amanifestation of a more proximal problem (e.g. carotid-cavernous fistula) or systemic disease (e.g. Graves’disease).2 The evaluation of proptosis include a detailedclinical history, ocular examination, laboratoryinvestigations and imaging studies .As far as theradiological investigations are concerned, findings onplain radiographs and ultrasonography are notpathognomonic of most of the orbital disease processthough some help can be obtained in characterizationof lesion in certain cases. Advent of MRIand CT hasrevolutionized the diagnostic imaging of orbit anditscontents. MRI with its superb soft tissue contrastandmultiplanar ability provides excellent rendering of
orbital anatomy but is limited by lack of wideravailability and high cost. On the other hand easyavailability and operability, good maintenance andspeed makes CT scan an affordable diagnostic tool inorbital diseases under existing circumstances andpresent set up.MATERIAL AND METHODS
26 patients of various age groups and both sexeswith unilateral or bilateral exophthalmos were thesubjects for the study. Before commencing for CTexamination, all the preceding history, clinical,laboratory data were recorded. A CT scanner(SIEMENS SOMATOM AR.T) was used for the study.The technique was to obtain a lateral scannogram withthe patient supine and contiguous axial sections withslice thickness of 3 mm and interslice gap of 3 mm wereobtained. Coronal 3-5 mm sections were obtained asand when required with the patient in prone position.The scans were obtained both prior to and afteradministration of non ionic intravenous contrast. Allpatients with globe protrusion >21mm anterior to theinterzygomatic line on axial scans at the level of lenswere evaluated .CT findings were correlated with finaldiagnosis based on clinical, laboratory findings,operative findings , histopathological study or responseto treatment.RESULTS
The patients included were from 2 to 80 yrs. ofage. The majority of patients (22%) were between 31-40 yrs. of age. man/woman ratio was 1.08: 1. The mostcommon lesion causing exophthalmos weretumoursand infections. Various lesions causing exophthalmosare grouped in the table.Tumours
Lymphomas were the most common orbital
Dr Hina
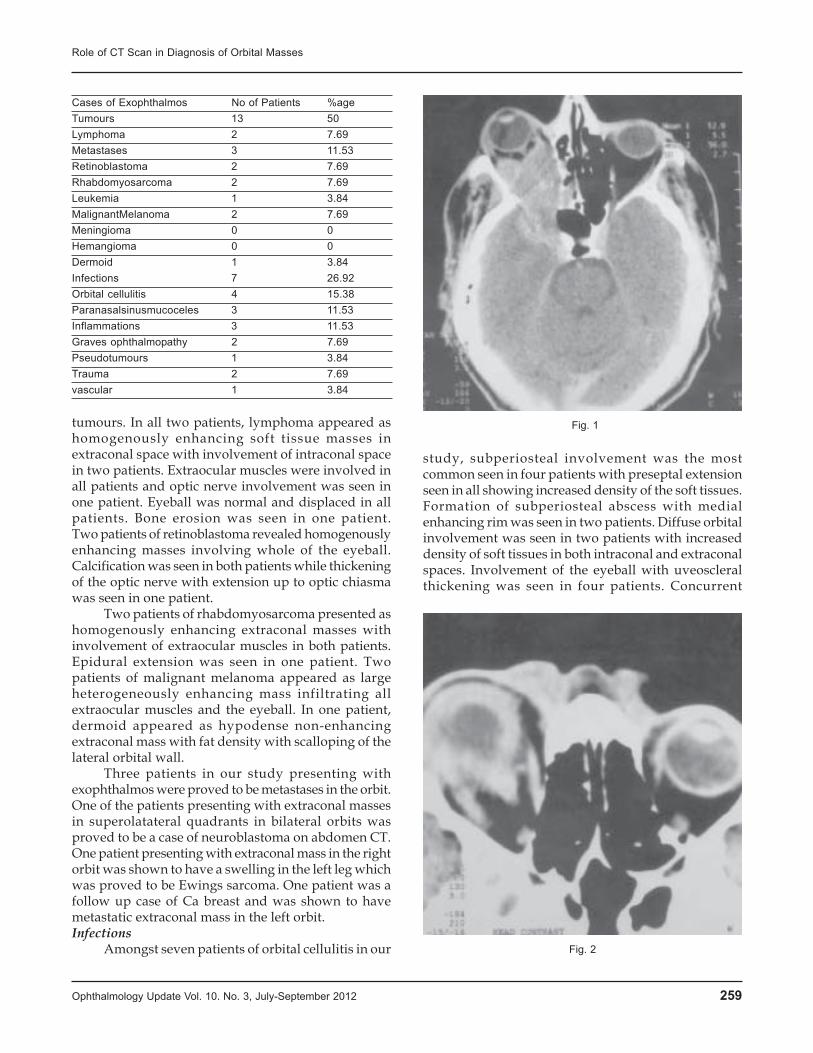
Ophthalmology Update Vol. 10. No. 3, July-September 2012 259
tumours. In all two patients, lymphoma appeared ashomogenously enhancing soft tissue masses inextraconal space with involvement of intraconal spacein two patients. Extraocular muscles were involved inall patients and optic nerve involvement was seen inone patient. Eyeball was normal and displaced in allpatients. Bone erosion was seen in one patient.Two patients of retinoblastoma revealed homogenouslyenhancing masses involving whole of the eyeball.Calcification was seen in both patients while thickeningof the optic nerve with extension up to optic chiasmawas seen in one patient.
Two patients of rhabdomyosarcoma presented ashomogenously enhancing extraconal masses withinvolvement of extraocular muscles in both patients.Epidural extension was seen in one patient. Twopatients of malignant melanoma appeared as largeheterogeneously enhancing mass infiltrating allextraocular muscles and the eyeball. In one patient,dermoid appeared as hypodense non-enhancingextraconal mass with fat density with scalloping of thelateral orbital wall.
Three patients in our study presenting withexophthalmos were proved to be metastases in the orbit.One of the patients presenting with extraconal massesin superolatateral quadrants in bilateral orbits wasproved to be a case of neuroblastoma on abdomen CT.One patient presenting with extraconal mass in the rightorbit was shown to have a swelling in the left leg whichwas proved to be Ewings sarcoma. One patient was afollow up case of Ca breast and was shown to havemetastatic extraconal mass in the left orbit.Infections
Amongst seven patients of orbital cellulitis in our
study, subperiosteal involvement was the mostcommon seen in four patients with preseptal extensionseen in all showing increased density of the soft tissues.Formation of subperiosteal abscess with medialenhancing rim was seen in two patients. Diffuse orbitalinvolvement was seen in two patients with increaseddensity of soft tissues in both intraconal and extraconalspaces. Involvement of the eyeball with uveoscleralthickening was seen in four patients. Concurrent
Cases of Exophthalmos No of Patients %ageTumours 13 50Lymphoma 2 7.69Metastases 3 11.53Retinoblastoma 2 7.69Rhabdomyosarcoma 2 7.69Leukemia 1 3.84MalignantMelanoma 2 7.69Meningioma 0 0Hemangioma 0 0Dermoid 1 3.84Infections 7 26.92Orbital cellulitis 4 15.38Paranasalsinusmucoceles 3 11.53Inflammations 3 11.53Graves ophthalmopathy 2 7.69Pseudotumours 1 3.84Trauma 2 7.69vascular 1 3.84
Role of CT Scan in Diagnosis of Orbital Masses
Fig. 1
Fig. 2

260 Ophthalmology Update Vol. 10. No. 3, July-September 2012
ethmoid sinusitis was seen in seven patients andmaxillary sinusitis in one patient. One patient presentedwith soft tissue density in peripheral orbital space withmass in the nasal cavity and ethmoid sinuses witherosion of the medial orbital wall which was proved tobe mucormycosison histopathology.
Amongst three patients of mucoceles of paranasalsinuses invading the orbit, involvement of frontal sinuswas most common followed by front oethmoidinvolvement. All patients had a non enhancingextraconal cystic mass in superomedial quadrant of theorbit with evidence of expansion of the bone in all anderosion of bone in two patients. Optic nervecompression was seen in one patient.Inflammation
Amongst three patients of Grave’s disease,bilateral involvement was seen in two patients andunilateral involvement in one. Extraocular muscleenlargement was seen in all patients with multiplemuscle involvement being more common than singlemuscle involvement. Inferior rectus muscle was mostcommonly enlarged followed by medial rectus andsuperior rectus. In inflammatory pseudotumor of theorbit, unilateral involvement was seen. Muscleenlargement was diffuse involving the tendinousinsertions. Soft tissue infiltration of orbital fat was alsoseen. Optic nerve was infiltrated. Eyeball was involvedin a patient showing uveoscleral thickening withenhancement.Trauma
Two patients of orbital trauma had intraorbitalhaemorrhage (retrobulbar and preseptal). Fracture ofthe bony orbit was seen in both of the patients withevidence of haemorrhage in paranasal sinuses. Therewas extradural haematoma in temporal lobe in onepatient.Vascular
In our study there was one patient of carotidcavernous fistula presenting as pulsatile exophthalmos
after trauma. CT findings included proptosis,asymmetry and distension of affected cavernous sinusand congestion and asymmetrical dilatation of superiorophthalmic vein.DISCUSSION
The most common lesion causing proptosis in ourstudy were tumours (46%).Our findings correlated wellwith the findings of Masud MZ et al (2006) 3whodescribed neoplasms (33%) as the most common causesof proptosis in their study. Lymphomas were the mostcommon orbital tumours in our study. Margo CE et al(1998) 4 reported orbital lymphoma to be the mostcommon malignant orbital tumours. The most commonparaorbital tumor invading the orbit in our study wasmaxillary carcinoma similar to that described byJohnson LN et al (1984).5 Out of 23 patients of tumoursCT diagnosis correlated with the histopathologicaldiagnosis in 18 patients (78.26%). In a study by Usha etal (2005) there was 56.6% correlation between the CTdiagnosis and histopathological diagnosis in case ofneoplasms (Conference proceedings: All Indianophthalmological society: 2005).
Infectious pathology accounted for 28% patientsof exophthalmos in our study while in study by MasudMZ et al (2006)3 infections accounted for 20% patientsof exophthalmos. CT provided an accurate diagnosisin 88.8% patients of orbital cellulitis in our study. ClaryRA et al (1992) 6analysed the accuracy of CT in orbitalcellulitis in children and showed correlation betweenradiological and operative findings in 84.21% cases.
Graves disease accounted for 10% patients ofexophthalmos in our study compared to the study byM K Narula et al (1994) 7 where Graves diseaseaccounted for 6% patients of exophthalmos. Inferiorrectus muscle was most commonly enlarged followedby medial rectus and superior rectus similar to the studyby Murakami Y et al (2001).8 Correct diagnosis ofGraves disease was made in 4 out of 5 (80%) patientson CT in the present study. In a study by Ozgen A et al(1999) 9 diagnosis of Graves ophthalmopathy was madein 69 of 87 (79%) patients using CT.
Pseudotumor accounted for 8% patients ofexophthalmos in our study compared to the study byM K Narula et al (1994) 7where pseudotumor accountedfor 11% patients of exophthalmos.Correct diagnosis ofpseudotumour was made in 50% patients in our studyin view of the non specific radiological findings asstated by Alfred L Weber et al (1999).10
Trauma was the cause in 6% patients of proptosisin the present study. Our results are similar to the studydone by Masud MZ et al (2006) 3 where trauma was thecause of exophthalmos in 5% patients. In our studyvascular lesions were the least common accounting for2% patients of while in a study by Masud MZ et al (2006)
Role of CT Scan in Diagnosis of Orbital Masses
Fig. 3

Ophthalmology Update Vol. 10. No. 3, July-September 2012 261
3 7 % cases of proptosis were caused by vascular lesions.In the present study overall CT diagnosis was
found to be correct in 41 patients (82%). Our results aresimilar to the study of Zahir Shah Mahsud et al (2004).11
In their study the diagnostic accuracy of CT scan inevaluation of proptosis was 80%. CT scan is highlyuseful in describing the precise location and extent ofthe lesion and is fairly accurate in lesioncharacterization. In view of non specific findings incases of orbital tumours and pseudotumours, anevaluation of clinical and laboratory data is essentialto arrive at a precise diagnosis.CONCLUSION
CT is useful to characterize: the precise locationof the lesion - the intraconal space (including muscles& Optic nerve), the extraconal space (associated or notto an extra orbital lesion), or the eyeball; the features ofthe lesion (density, calcification, enhancement.). Thesefindings are helpful to generate a differential diagnosis.CT is also useful to demonstrate the precise extensionof the orbital lesion, the involvement of adjacentparanasal sinuses and nasal cavity, the evidence of boneerosion and intracranial extension which helps in pre-treatment evaluation andpost treatment follow up. To
conclude CT scan can be considered as a cost effective,non-invasive, reliable diagnostic tool for evaluationoforbital masses.REFRENCES1. Mercandetti M; Exophthalmos, eMedicine, Feb 20102. Kanski J. Clinical Ophthalmology, A Systematic Approach,
5th Ed, 2003, Butterworth Heinemann.3. Masud MZ, Babar TF, Iqbal A et al, Proptosis- etiology and
demographic patterns. J. Coll. Physicians Surg. Pak. 2006;16(1): 38-41
4. Margo CE, Mulla ZD, Malignant tumors of the orbit.Ophthalmology 1998; 105: 185
5. Johnson LN, Krohel GB, Yeon EB, Parnes SM, Sinus tumorsinvading the orbit. Ophthalmology 1984; 91(3): 209-17.
6. Clary RA, Cunningham MJ, Eavey RD, Orbital complicationsof acute sinusitis- Comparison of CT scan & surgical findings.Ann. Otol. Rhinol. Laryngol. 1992; 101 (7): 598-600
7. Narula M. K. et al, Ultrasound evaluation of proptosis. IJRI1994; 4: 203-206
8. Murakami Y, KanamotoT, Tuboi T et al, Evaluation ofextraocular muscle enlargement in dysthyroidophthalmopathy. Jpn J Ophthal. 2001; 45(6): 622-7
9. Ozgen A, Alp MN, Ariyurek M, Tutuncu NB, CanI, GunalpI, Quantitative CT of orbit in Graves disease. Br. J.Radiol.1999; 72 (860): 757-6
10. Alfred L. Weber, Laura Vitale Romo,Nelson R. Sabates,Pseudotumor of the orbit RCNA Jan 1999; 37:1: 151-166
11. Zahir Shah Mahsud, SurayaBano, Diagnostic role of CT scanin proptosis in pediatric age group. JPMI 2004; 18: 3: 439-446
Role of CT Scan in Diagnosis of Orbital Masses

262 Ophthalmology Update Vol. 10. No. 3, July-September 2012
–––––––––––––––––––––––––––––––––––––––––––––––––––––1.Medical Officer,Ophthalmology Department, District Head QuarterHospital, Swabi.(KPK) 2Senior Registrar, Khyber Institute ofOphthalmic Medical Sciences, Hayatabad Medical Complex,Peshawar.–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence :Dr. Omer Khan Orakzai, House No; 279, Street10, Sector E-2, Phase- 1, Hayatabad, Peshawar. Cell: 0333- 911-6370. E.Mail>dcasif@ yahoo.Com.–––––––––––––––––––––––––––––––––––––––––––––––––––––Received; Jan’2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
INTRODUCTION:Epiphora and acute or chronic dacryosystitis are
the most common symptoms of acquired nasolacrimalduct obstruction.Epiphora due to nasolacrimal ductobstruction is a common ophthalmological problem andaccounts for approximately 3% of all ophthalmologicclinic visits1. Acquired nasolacrimal duct obstructionis a common disorder that occurs more frequently infemales than in males 2.In Pakistan the disease morecommonly occurs in adult females. DCR allowsfistulization of lacrimal sac into nasal cavity,bypassingthe blocked nasolacrimal duct.Previous studies show
the success rate for this procedure is about 90%4.Toti(1904,Italy) first described the technique of externalDCR5. Dupy-Dutemps and Baerrget (1921, France)described the modern external flap DCR technique6.Over the years the external dacryocystorhinostomy(Ext-DCR) has underwent many modifications for abetter surgical outcome without altering its basicconcept.
The two most frequent causes of DCR failure areobstruction of common canaliculus and fibrous closureof the osteotomy site 7. Most Ophthalmic surgeons nowthink that the success rate of Ext-DCR may be increasedby intraoperative use of anti-proliferative agents toinhibit the fibrous tissue growth and scarring over theanastomosed flaps and osteotomy site 9.
Mitomytcin-C(MMC) is useful in DCR because itreduces the scarring process and prevents the occlusionof osteotomy site due to fibrosis .Intraoperative MMChas been used by Liao in 2000, You in 2001, Roozitalabin 2004 and Akhund in 2005 and reported the successrate of 97.5%, 100%, 90.5% and 99% respectively10.MMC is isolated from Streptomyces caespitosus, is an
External Dacryocystorhinostomy with & withoutIntraoperative Mitomycin-C Application in Adults
Asif Iqbal1, Omer Khan2
ABSTRACTObjective:To compare the results of external dacryocystorhinostomy with and without intraoperative mitomycin-Capplication in adults.Material and Methods:This was hospital based prospective randomized controlled study. 60 consecutive eyes of thepatients above 20 years of age, diagnosed with uncomplicated nasolacrimal duct obstruction or chronic dacryocystitis(CDC).The patients were randomly divided by simple random technique into two equal groups;a conventionaldacryocystorhinostomy (DCR) group and an external dacryocystorhinostomy with mitomycin-C (DCR with MMC) group,in which mitomycin- C(MMC) was used during surgery. The surgical procedures in both groups were exactly the same,except that in DCR with MMC group, a piece of neurosurgical cottonoid soaked with 0.2 mg/ml MMC was applied to theosteotomy site for 10 minutes. The patients were followed for 6 months. The results of surgeries were evaluated byasking patients about conditions of tearing improvement, irrigation and height of tear meniscus.Results: 60 eyes were included in this study.10 patients (16.7%) were male and 50 patients (83.3%) were female. In56.7% right side was involved and in 43.3% left side was involved. In DCR with MMC group,26 cases(86.7%) showedcomplete improvement, 3 cases(10%) showed partial improvement while 1 case(3.3%) showed no improvement ofsymptoms. In conventional group, 23 cases(76.7%)showed complete improvement, 1 case(3.3%) partial improvementand 6 cases(20%) showed no improvement. The difference between two groups was significant. The tear meniscus inDCR with MMC group was normal in 28 cases(93.3%), moderate in 1 case(3.3%) and high in 1 case(3.3%).In conventionalgroup, tear meniscus was normal in 24 cases(80%),moderate in 2cases(6.7%)and high in 4 cases(13.3%). The differencebetween two groups was statistically significant. Irrigation(syringing test),in DCR with MMC group showed patent pathwayin 29 cases(96.7%) and pathway obstruction in 1 case(3.3%).In conventional group, irrigation showed patent pathway in24 cases(80%) and pathway obstruction in 6 cases(20%). The difference between two groups was statisticallysignificant.Complications like nasal bleeding was observed on 1stpost operative day in 2 cases in DCR with MMC group,while one case in same group showed delayed wound healing at 10thpost operative day.Conclusion: Intraoperative MMC is effective in increasing the success rate and a safe adjunct to achieve good results ofExt-DCR surgery.Key words :External dacryocystorhinostomy(Ext-DCR), Mitomycin-C(MMC), Nasolacrimal duct obstruction,Chronicdacryocystitis(CDC)
Original Article
Dr. Asif

Ophthalmology Update Vol. 10. No. 3, July-September 2012 263
antineoplastic antibiotic that acts by the inhibition ofDNA synthesis, RNA and cellular proteins. It decreasescollagen synthesis in fibroblasts by inhibiting thesynthesis of RNA dependent DNA, thus inhibitingfibrous tissue growth and scarring11.MMC has widelybeen used in pterygium excision and trabeculectomywith favorable results12.The objective of the study wasto evaluate the success rate of intraoperativemitomycin-C in external DCR.MATERIAL AND METHOD:
This was a prospective randomized control studywhich was undertaken at Ophthalmology DepartmentDistrict Head Quarter Hospital,Swabi (KPK) fromFebruary 2010 to September 2011.There were sixtyconsecutive patients from 20- 60 years of age withchronic dacryocystitis with or without lacrimal sacfistula, primary acquired nasolacrimal duct obstructionand mucocele of lacrimal sac were included. Youngpatients(<20 years), patients with canalicularobstruction(common or individual),previously failedDCR and patients with associated nasal pathology wereexcluded from the study.
Patients fulfilling the criteria were included in thestudy.An informed consent was taken from all patientsincluded in study.Patients were then randomly dividedinto two groups. A specific proforma was designed withdetailed record of all the parameters of the diseaseincluding detailed history, complete clinicalexamination(ocular,nasal, systemic), laboratory andradiological investigations. Nasal examination wasdone in ENT department of DHQ Swabi.
Surgery was performed by single surgeon andunder local anaesthesia. All patients underwentstandard Ext-DCR. Technique for the two procedureswas essentially the same, except that a neurosurgicalcottonoid soaked in 0.2mg/ ml was placed at osteotomysite for 10 minutes in Ext-DCR with MMC group.Incision site was infiltrated with 2% xylocainwithadrenaline 1:100,000 injections. Nasal packing was donewith gauze soaked in xylocain 4% and adrenaline(1:1000). A vertically straight bone deep incision wasgiven about 8 mm medial to the medial canthus. Bonewas exposed by blunt dissection of the orbicularismuscle,medial palpebral ligament and periosteumwasdivided and sac exposed.Osteotomy was made usingbone nibbler.Lacrimal sac was exposed and an anteriorand posterior lacrimal sac flaps were made. Posteriorflap was excised but the anterior flap was secured bypassing two stitches either with 4/0 catgut or 6/0 vicryl.H-shaped nasal mucosal flaps were made. Anteriornasal flap was sutured to the anterior flap of the lacrimalsac.A piece of neurosurgical cottonoid soaked with0.2mg/mIMitomycin-C was placed under theanastomosed anterior flaps and osteotomy site with the
long thread passing out through the nostril. The anteriornasal and lacrimal sac flaps were sutured with 3-4interrupted 6/0 vicryl sutures. After 10 minutes at theconclusion of surgery, the cotton swab was removedtransnasally by pulling out the long thread from thenostril. The orbicularis oculi and the skin were closedin separate layers. Wound was then closed in layers.Antibiotic ointment was then applied over the woundas well as to external ocular surface and firm pressurepad applied to the eye for 24 hours.
Most of the patients were discharged on the firstpostoperative day. Two patients had significantpostoperative bleeding, were managed promptly anddischarged after 48 hours. After discharge each patientwas reviewed on the 10th postoperative day, at 3months and finally at 6 months following the surgery.Skin stitches were removed on tenth postoperative day.At each visit patients were evaluated for relief ofsymptoms and any complications they might haddeveloped. The outcome of surgery was measuredaccording to the symptomatic relief, regurgitation test,irrigation in selected cases,height of tear meniscus. Theheight of tear meniscus was measured with fluoresceinstain under cobalt blue light at slit lamp for each patientand graded it as normal tear meniscus (<0.1 mm),moderate tear meniscus (0.1-0.2mm) and high tearmeniscus (>0.2mm).Record of each visit was made tothe data collection proforma.RESULTS:
There were 60 patients included in this study;30in DCR with MMC group and 30 in conventional group.Age range was from 20- 60 years. There was nosignificant difference in age between the twogroups(p>0.1).10 patients were male(16.7%)and 50patients were female(83.3%).The male to female ratiowas 1:5.In 34 cases(56.7%)right side was involvedandin 26 cases(43.3%)left side was involved. All cases weredone under local anaesthesia.Most common presentingcomplaint was watering in 49 cases(81.7%),followed byrecurrent infection in 7 cases(11.7%) and swelling alongmedial canthus in 4 cases(6.7%).The patients werefollowed for six months. In DCR with MMC group, 26cases(86.7%) showed complete improvement, 3cases(10%) showed partial improvement while 1case(3.3%) showed no improvement of symptoms. Inconventional group, 23 cases(76.7%)showed completeimprovement, 1 case(3.3%) partial improvement and 6cases(20%) showed no improvement in symptoms aftersix months.
As far as objective symptoms were concerned, thetear meniscus in DCR withMMC group was normal in28 cases(93.3%), moderate in 1 case(3.3%) and high in1 case(3.3%).In conventional group, tear meniscus wasnormal in 24 cases(80%), moderate in 2 cases(6.7%) and
External Dacryocystorhinostomy with & without Intraoperative Mitomycin-C Application in Adults

264 Ophthalmology Update Vol. 10. No. 3, July-September 2012
high in 4 cases(13.3%) after 6 months follow up, thedifference between two groups is statisticallysignificant.
Irrigation (syringing test), in DCR with MMCgroup showed patent pathway in 29 cases (96.7%) andpathway obstruction in 1 case(3.3%), whereas inconventional group, irrigation showed patent pathwayin 24 cases(80%) while pathway obstruction in 6cases(20%).
During the follow up period, complications likenasal bleeding was observed on 1st post-operative dayin 2 cases in DCR with MMC group, while one case insame group showed delayed wound healing at 10th
post-operative day. The delayed wound healing wasdue to accidental contact of MMC soaked sponge toedges of skin wound. In all patients the wound healedcompletely leaving a barely visible scar at 3 monthsfollow up.The final success rate in DCR with MMCgroup was 96.7% compared to 80% in conventionalgroup. There was significant difference in success oftwo groups. P value was 0.045(p<0.05).DISCUSSION:
External DCR is a highly successful procedure inmanaging epiphora due to nasolacrimal ductobstruction.The reported success rate varies between85% to 99%. Traditional DCR has its own limitationswith reported failure rates of 0 to 18%. To overcomethis, different modifications have occurred in thistechnique from time to time13.Failure is generallydefined as persistent tearing with the inability to irrigatethe lacrimal drainage system. McPherson and Egelstonnoted dense scar tissue obstructing the osteotomy site14.Pico found occluding membrane obstructing the newdrainage channels. On histopathology, the granulationtissue formed the occluding membrane 15. Granulationtissue obstructing the distal part of common canaliculusand osteotomy scarring was also reported by Allen andBerliner 7.
The above literature review shows that fibroustissue growth, scarring and granulation tissueformation during the healing process results in thestenosis or complete obstruction of osteotomy site,leading to surgical failure. This implies that the successrate can be increased dy reducing fibrous proliferation
at the osteotomy site of anastomosed flaps.Mitomycin-C(MMC) is an antineoplastic
antibiotic, isolated from Streptomyces caespitosus;itinhibits the synthesis of DNA, cellular RNA andproteins in rapidly growing cells. It has the ability tosuppress the vascular growth and fibrosissignificantly,hence can reduce possibility of stenosis ofnewly created osteotomy in DCR.
To suppress the fibrous proliferation, MMC0.2mg/ ml was used in this study at the osteotomy siteand anastomosed flaps. Theoretically, this modificationshould reduce fibrous tissue growth and scarring at theosteotomy site as well as around the opening ofcommon canaliculus. Ugurbas et al concluded thatMMC application can result in a decrease in densityand cellularity of mucosa and enhance the success ofDCR surgery 16.Similarly Yeatts and Neves alsorecommended that adjunctive use of MMC mayincrease the success rate of repeat DCR17. In our study,0.2mg/ ml MMC was applied to osteotomy site for 10minutes. The drug was applied without intubation withthe success rate of 96.7%.
In this study, nasolacrimal duct obstruction wasmost commonly noted in middle age females, morecomparable with the studies of Lee-wing, Ashenhurst18
Figure 1. Gender distribution
Table- 1: Age distribution
Age in years DCR with MMC Conventionaln = 30 n = 30
20- 30 10 1031- 40 10 1041- 50 5 551- 60 5 5
Table- 2: Symptomatic improvement after 6 months
Symptoms DCR with MMC Conventional groupn = 30 n = 30
Improved completely 26 (86.7%) 23(76.7%)Partial improvement 3(10%) 1(3.3%)No improvement 1(3.3%) 6(20%)
Table-3 :Height of tear meniscus
Tear Meniscus DCR with MMC Convential Groupn = 30 n = 30
Normal 28(93.3%) 24(80%)Moderate 1(3.3%) 2(6.7%)High 1(3.3%) 4(13.3%)
Table- 4: Syringing after 6 months
Irrigation DCR with MMC Conventional Groupn = 30 n = 30
Pathway patent 29(96.7%) 24(80%)Pathway obstruction 1(3.3%) 6(20%)
External Dacryocystorhinostomy with & without Intraoperative Mitomycin-C Application in Adults
Ophthalmology Update Vol. 10. No. 3, July-September 2012 265
and Baiget al19. The nasolacrimal duct and lacrimal fossaforms greater angle on the right side than on left side 20
.In our study 34 cases(56.7%) had unilateralinvolvement of right side. Most common presentingcomplaint was epiphora in 49 cases(81.7%). Thiscompares well with Baber et al21.
In this study,epiphora completely improved in 26cases(86.7%), partial improvement in 3 cases(10%)while no improvement in 1 case(3.3%)in DCR withMMC group. In conventional group, 23 cases(76.7%)showed complete improvement, 1 case (3.3%)partial improvement and 6 cases(20%) showed noimprovement in epiphora. There was a significantdifference between the two groups according tosymptoms reported by patients.
The height of the tear meniscus was also measuredand compared between two groups.In DCR withMMCgroup height of the tear meniscus was normal in 28cases(93.3%), moderate in 1 case(3.3%) and high in 1case(3.3%).In conventional group, tear meniscus wasnormal in 24 cases(80%),moderate in 2cases(6.7%)andhigh in 4 cases(13.3%) after 6 months follow up. Thedifference between two groups is statisticallysignificant.
Patency of lacrimal drainage system showed thatin DCR with MMC group 29 cases (96.7%)had patentpathway in and 1 case (3.3%) had pathway obstruction.In conventional group, irrigation showed patentpathway in 24 cases(80%) and pathway obstruction in6 cases (20%). The patency rate of lacrimal drainagesystem was 96.7% in DCR with MMC groupcomparedto 80% in conventional group. The differencebetween the success rate of two procedures wasstatistically significant.
In this study, no significant complication wasnoted due to MMC. Two cases showed nasal bleedingin early post-operative period in DCR with MMCgroup. While one case showed delayed wound healingat the 10th post-operative day. Kao et al pointed outvarious possible complications due to intraoperativeuse of MMC22. You et al23 and Yeattset al17 reported nocomplications due to MMC application in Ext-DCR.CONCLUSION :
Dacryocystitis and nasolacrimal duct obstructionis primarily a disease of middle age females. Right sideis more commonly involved. Intraoperative MMC inExt-DCR is safe and effective adjunct that helps toachieve good results of DCR surgery.This modificationsignificantly improves the success rate over traditionalDCR.it is cheap and less time consuming procedurehaving minimal complications.REFRENCES:1. Traquair H. Chronic dacryocystitis: its causation and
treatment. Arch Ophthalmol 1941; 26: 165–80.
2. Shigeta K, Takegoshi H, Kikuchi S. Sex and age differencesin the bony nasolacrimal canal. Arch Ophthalmol 2007; 125: 1677–81.
3. Dareshani S, Niazi JH, Saeed M, Memon MS, Mahmood T.Dacryocystorhinostomy, Importance of anastomosis betweenanterior and posterior flaps. Pak J Ophthalmol1996; 12:129-31.
4. Tarbet KJ, Custer PL. External dacryocystorhinostomy:surgical success, patient satisfaction and economic cost.Ophthalmology 1995;102:1065–70.
5. Toti A. Nuovometodo conservative di cura radicalledellesupporazioni chronicle del saccolacrimale. Clin ModFirenze 1904;10:385–9.
6. Dupuy-Dutemps L, Boureguet J. Procedeplastique dedacryocystorhinostomy et sesresultants.AnnOculJ. 1921;158:241–61.
7. Allen K, Berlin AJ. Dacrocystorhinostomy failure associationwith nasolacrimal silicone intubation OphthalSurg 1989; 20:486-9.
8. Mc Lachlan DL, Shannon GM, Flanagan JC. Results ofDacrocystorhinostomy: analysis of thereoperations.OphthalSurg 1980; 11: 427-30.
9. Liao SL, Kao SCS, Tesng JHS, et al. Results ofintraoperativeMitomycin C application indacryocystorhinostomy. Br J Ophthalmol 2000; 84:903-4.
10. Rahman A, Channa S, Niazi JH, MemonMS.Dacryocystorhinostomy without intubation withintraoperative mitomycin-C. JCPSP 2006; 16(7): 476- 78.
11. Abraham LM, Selva D, Casson R, Leibovitch I. Mytomycin:clinical application in ophthalmic practice. Drugs 2006; 66:321-40.
12. Dar AJ, Chaudhary NH, Masud H, Khan MW. Role ofMitomycin-C in prevention ofpterygium recurrence. Pak JOphthalmoI2001; 7:814.
13. Deka A, Saikia SP, Bhuyan SK. Combined posterior flap andanterior suspended flap dacryocystorhinostomy: Amodification of external dacryocystorhinostomy. Oman JOphthalmol. 2010; 3(1): 18- 20.
14. McPherson SD, Egelston D. Dacryocystorhinostomy: areview of 106 patients. Am J Ophthalmol1959 ;47 : 328- 31.
15. Pico GA. Modified techniques of externaldacryocystorhinostomy. Am J Ophthalmol 1971; 72: 679-90.
16. Ugurbas SH, Zileliogo G, Sargon MF, et al. Histopathologiceffects of Mitomycin C on endoscopictransnasaldacryocystorhmostomy.OphthalmicSurg Lasers1997; 28:300-4.
17. Yeatts RP, Neves RB. Use of Mitomycin-C in repeatdacryocystorhinostomy. Ophthalmic Plast Recons Surg 1999;15:19- 22.
18. Lee-Wing MW, Ashenhurst ME. Clinicopathologic analysisof 166 patients with primary acquired nasolacrimal ductobstruction. Ophthalmology 2001;108:2038-40.
19. Baig MSA, Shaikh ZA, Aziz M. Externaldacryocystorhinostomy with silicone tube intubation. Pak JOphthalmol 2000;16:90-3.
20. Bartley GB. Acquired lacrimal drainage obstruction: anetiologic classification system, case reports and review of theliterature. Ophthalmic Plast Recons Surg 1992; 8: 237- 42.
21. Baber TF, Masud MZ, Saeed N, Khan MD. An analysis ofpatients with chronic dacryocystitis. Pak J Ophthalmol 2003;19: 77- 83.
22. Kao SCS, Liao SL, Tseng JHS, et al. Dacryocystorhinostomywith intraoperative Mitomycin-c. Ophthalmology 1997; 104:86-91.
23. You YA, Fang CT. IntrnoperativeMitomycin C indaCtyocystorhinostomy. Ophthalmic Plast Recons Surg 2001;17:115-9.
External Dacryocystorhinostomy with & without Intraoperative Mitomycin-C Application in Adults
266 Ophthalmology Update Vol. 10. No. 3, July-September 2012
–––––––––––––––––––––––––––––––––––––––––––––––––––––1.Registrar, 2Senior Registrar, 3Medical Officer–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence : Dr. Nuzhat Rahil, Registrar, Eye Unit, LRHPeshawar . Cell no: 0321 9036959E.Mail:>[email protected]–––––––––––––––––––––––––––––––––––––––––––––––––––––Received; March’2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
INTRODUCTIONEvisceration is a standard surgical treatment
modality for many end-stage eye diseases. Indicationsfor evisceration vary with changing trends in diseasemanagement. Von Graefe first advocated the use ofevisceration in the presence of severe endophthalmitisas a means of preventing intracranial spread ofinfection1,2. Over the years, indications for eviscerationhave expanded to include both infectious andnoninfectious intraocular inflammation resulting intotal loss of vision with no potential for any usefulvision, end-stage glaucoma, and post traumatic severeocular injuries. With the advent of modern technologyand rapid access to modern eye care in the developedcountries, many eyes with endophthalmitis, glaucoma,and severe ocular trauma are being saved without theneed for evisceration or enucleation. However, indeveloping countries, because of the delay in access tomodern health care and appropriate diagnostic andtherapeutic intervention, many eyes lose visualpotential. Eventually, many of these patients presentwith end-stage diseases; therefore, evisceration or
enucleation may be the only available option. Thepurpose of this study was to determine the underlyingocular conditions leading to evisceration in a majortertiary eye care center in Khyber Pukhtoonkhawa andto correlate it clinically.MATERIAL AND METHODS
Clinical records of all the patients who underwentevisceration from April 2010 till April 2011 at LadyReading Hospital, PGMI, Peshawar, a tertiary centerfor referral of the patients were retrospectivelyreviewed. Information regarding patient history,duration of disease, diagnosis , investigation, any priortreatment were evaluated. Additional information forprevious trauma, the objects causing trauma, earliertreatment, length of time before seeking medical help,history of any prior surgery, the place of surgery andany complication during surgery and presence ofsystemic disease was obtained. For the purpose of datacollection, indications were assigned on the basis of themost recent clinical diagnosis. Results of diagnosticinvestigation, such as ultrasonography (U/S) orcomputed tomography (CT), anterior chamber tap andvitreous tap or biopsy were collected where available.Indications for evisceration for each operated eye wereobtained. The predisposing causes for the finaldiagnosis were categorized as panophthalmitis,severely traumatized eye, cosmetically disfigured eyeswith corneal perforation, postsurgical, and others. Allpatients were further categorized by age and divided
Evisceration: Frequency, Indications andClinical Correlation in a Tertiary Care Hospital
Nuzhat Rahil1, Rahil Aumir Malik2, Shams Ul Haq3
Lady Reading Hospital, Peshawar (KPK)
ABSTRACTPurpose: To analyze the frequency, clinical indications and clinical correlation for evisceration in patients at a tertiarycare centre in KPK.Materials and Methods: It was a retrospective hospital-based case series study of all the patients who underwentevisceration at Lady Reading Hospital, PGMI Peshawar from April 2010 till April 2011.The parameters evaluated were theage and sex distribution, The clinical features and the indications for evisceration, the etiological factors responsible forevisceration were determined on the basis of history, clinical examination and investigations as determined from previousrecords. An attempt was made to classify eyes to the original underlying disorder that led to the need for evisceration. Results: Total number of eyes which were eviscerated was 49 in one year. Males outnumbered females in a ratio of1.9:1 (32 males and 17 females) .The most common age group affected was between 51 to 60 years and the second onewas above 60 years. Panophthalmitis was the major clinical indication in 24 patients and in these patients , post cataractendophthalmitis was responsible for 18 cases. Old neglected perforated corneal opacities, keratitis and descematoceleswere the indication of evisceration in 14 cases. Post trauma evisceration was carried out in 11 patients. Clinicopathologicalcorrelation was 100% in cases with definite clinical diagnosis of post operative and post traumatic endophthalmitis.Conclusion: Panophthalmitis, old neglected corneal opacities and severe ocular injuries were the major indications ofevisceration in our tertiary care hospital.
Original Article
Dr. Nuzhat

Ophthalmology Update Vol. 10. No. 3, July-September 2012 267
into seven groups of 10 years each. Mean and standarddeviation was calculated for quantitative variable likeage. Chi square test was applied to find the correlationof diagnoses and indication. P value < 0.05 wasconsidered as significant value.RESULTS
The total admission in one year (April 2010 toApril 2011) in our eye unit was 2446. Out of these 49patients between the age of 0 and 70 years and abovewere operated for evisceration in one year. Thesepatients were included in the study. Male constituted32 (63.5%) and females 17 (34.6%) in number. Out ofthese 49 cases, 6 (12.24%) patients were in the age group0 to 10 years. Age group 11 to 20 years had no patientwhile 4 (8.16%) patients were in age group of 21 to 30years and in the age group 31 to 40 years 3 patients(6.12%) underwent evisceration, 41 to 50 years agegroup included 6 (12.2%) patients. The most commongroup admitted was between 51 to 60 years included19 (38.77%); the other group of 60 years and aboveincluded 11 (22.48%).
Panophthalmitis was the major etiology forevisceration of 24 (48.97%) eyes. Post cataract surgerypanophthalmitis was responsible in 18 eyes to beeviscerated because of trauma included 6 patients ofthe total. Trauma from bomb blast injuries, FAI, stonesand sticks as well as road traffic accidents andpenetrating sharp objects, mostly in young males, wereresponsible for devastating ocular injuries andsubsequently had eviscerations in 11 (22.44%) patients.The number of evisceration done for old cornealopacities with spontaneous perforation were in 10 eyes(20.40%).These opacities were years old and some weresince childhood. The other common indication forevisceration was keratitis. These keratitis led toendophthalmitis and 4(8.16%) had perforated cornealulcer. These perforation led to uveal prolapse and wereunable to be treated conservatively, and as a last resortevisceration was done. The indications for eviscerationis shown in the table.
Table 1
Indication for Evisceration PercentagePost Operative Panophthalmitis 36.73%Post traumatic Panophthalmitis 12.24%Trauma 22.04%Perforated corneal opacities 20.40%Keratitis 8.16%
DISCUSSIONEvisceration although a surgical procedure which
mostly cannot be justified and explained to the patientsand in our opinion the indication for evisceration aremostly unexplainable to the patients .The need of this
study was to find out the commonest indication forevisceration in tertiary set up and why with all theavailable sources we had to opt for this surgery. In ourstudy the number of the male patients were more thanthe female As in other case series, there waspredominance of males undergoing evisceration .2,3,4,5
Predominance of males undergoing enucleation hasalso been reported in previous studies6,7 This may berelated to males being more prone to trauma becauseof their high-risk professions and outdoor activities.
The commonest age group affected was above 50years and the reason was that most of the patient hadpanophthalmitis after age related cataract surgery.Panophthalmits and untreatable endophthalmitisfollowed by unsightly eyes emerged as the majorreasons for patients presenting for evisceration in thepresent study. Blind painful eyes occurred primarilydue to endophthalmitis post operatively and posttrauma, ocular injury, neglected corneal ulcers andopacities. Panophthalmitis was responsible forevisceration in 24 (48.97%) patients in our study. In theliterature, depending on the geographic location,endophthalmitis has been reported to be the cause forevisceration in 23.3%–78.6% of cases 2. Classically, theclearest indication for an evisceration has been in casesof virulent endophthalmitis, to reduce the risk of theinfection spreading via the optic nerve sheath3.
The number of endophthalmitis cases have beenon the decline lately in developing countries. Forexample, a recent study from India reported asignificant decrease in eviscerations due toendophthalmitis from 91.2% during the first 5-yearperiod (1990–1994) to 50% during the second 5-yearperiod (1996–2000)2. The authors’ rationale for thisdecline was improvement in ophthalmic care,introduction of newer antibiotics, availability of bettertrained health care professionals, and better access tohealth care. The data presented in our study has beencollected from a tertiary eye care center where the casesreferred to us were at the end stage of the diseaseprocess. That is why the results of our study regardingpost operative and post trauma do not correlate withthe rest of international studies. The reason is that wereceive cases from all over the province and we mostlyreceive those cases which were operated in lessequipped, and by less trained professionals.
The other bigger issue is trauma, which is muchmore common as compared to other studies and thisinclude trauma due to war on terror as well .Traumafrom bomb blast injuries, FAI, stones and sticks as wellas road traffic accidents and penetrating sharp objects,mostly in young males, was responsible for devastatingocular injuries and subsequent eviscerations in 16(32.65%) patients of cases in our study. This was similar
Evisceration: Frequency, Indications and Clinical Correlation in a Tertiary Care Hospital
268 Ophthalmology Update Vol. 10. No. 3, July-September 2012
to the results previously reported by other observersin India, Ireland, and Sweden.2,4,5 Panophthalmitis wasthe most common indication for evisceration (78.6%)followed by irreparable globe injury (21.3%),by a studydone Dada et al 2. .In a study done by Limbu et al theindications for evisceration included ruptured eyeball, Panophthalmitis and painful blind eyes8 .
In our study 4 (8.40%) of the eyes were evisceratedbecause they had perforating keratitis. In study doneby Constantinou et al corneal ulcers that result in theloss of eye in elderly population are frequentlyassociated with glaucoma and persistent epithelialdefects. The majority of these cases have non-healingmicrobial keratitis caused by Pseudomonas aeruginos9. The indications for evisceration or enucleation wereextensive non-healing microbial keratitis (22/47) andcorneal perforation secondary to microbial keratitis (17/47)9
One of the major indications for evisceration wasold perforated corneal scars and opacities. It is incorrelation with other international studies6,7. 9,10. Mostof these patient had these corneal opacities since agesand a trivial trauma leads for the indication ofevisceration.CONCLUSION & RECOMMENDATIONS.
Panophthalmitis, old neglected corneal opacitiesand severe ocular injury are the major indications ofevisceration in our tertiary care hospital.
Public education, health safety regulations,implementation of safe working and livingenvironments, along with early diagnosis of the eye
diseases and timely intervention by well trained healthcare workers, may prevent loss of vision. It is expectedthat with improvement in eye care, the advent ofmodern surgical techniques, and the use of newerantibiotics, many of these eyes can be saved fromevisceration or enucleation in the future.REFERENCES1. Dortzbach RK, Woog JJ. Choice of procedure: Enucleation,
evisceration, or prosthetic fitting over globes.Ophthalmology1985; 92:1249–1255.
2. Dada T, Ray M, Tandon R, Vajpayee RB. A study of theindications and changing trends of evisceration in northIndia. Clin Exp Ophthalmol. 2002; 30:120–123.
3. Hansen B, Petersen C, Heegaard S, Prause U. Review of 1028bulbar eviscerations and enucleations. ActaOphthalmol.1999;77:331–335.
4. Canavan YM, O’Flaherty MJ, Archer DB, Elword JH. A 10-year survey of the eye injuries in Northern Ireland 1967-1976.Br J Ophthalmol.1980;64:618–625.
5. Monestam E, Bjornstig U. Eye injuries in Northern Sweden.Acta Ophthalmol. 1991;69:1–5.
6. Vemuganti GK, Jalali S, Honavar SG, Shekar GC. Enucleationin a tertiary eye care centre in India: prevalence, currentindications and Clinicopathological correlation. Eye.2001;15:760–765.
7. Singurdsson H, Thorisdottir S, Bjornsoon JK. Enucleation andevisceration in Iceland 1964-1992. Study in a definedpopulation. Acta Ophthalmol. 1998;76:103–107.
8. B Limbu, R Saiju and S Ruit Kathmandu Univ Med J(KUMJ).A retrospective study on the causes for eviscerationat Tilganga Eye Centre.7(26):115-9 (2009).
9. Constantinou M, Jhanji V, William TL and Vajpayee B.Clinical review of corneal ulcers resulting in evisceration andenucleation in elderly population Graefes Arch Clin ExpOphthalmol 247(10):1389-93 (2009)
10. Wagoner MD, al-Rajhi AA. Ophthalmology in the Kingdomof Saudi Arabia. Arch Ophthalmol. 2001;119:1539–1543.
Evisceration: Frequency, Indications and Clinical Correlation in a Tertiary Care Hospital

Ophthalmology Update Vol. 10. No. 3, July-September 2012 269
–––––––––––––––––––––––––––––––––––––––––––––––––––––1.Trainee Medical Officer 2. Asstt. Professor, 3.Senior Registrar4.Registrar,5 Medical Officer–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Dr Zakir Hussain, H.No. 86, St. No. 9, Sector: J-1, Phase II, Hayatabad, Peshawar. Ph: 0092-091-5811020,03339314643 0334 0123070 Email: [email protected]/o Marwat Optico, Ghazni Khel Market, Main Lorry Addah, LakkiMarwat (KPK)–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: March’2012 Accepted May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
Optic Neuritis in Children
Zakir Hussain FCPS1, Dr. Sana ullah Jan FCPS, FRCS 2, Afzal Qader FCPS3
Mohammad Sabir FCPS4. Samina Karim FCPS5
Ophthalmology Deptt., Khyber Institute of Ophthalmic Medical Sciences,Hayatabad Medical Complex, Peshawar.
ABSTRACTObjectives: To study the clinical characteristics of optic neuritis in children.Place and duration of study: The study was carried out at Department of Clinical Ophthalmology, Khyber Institute ofOphthalmic Medical Sciences (KIOMS), Postgraduate Medical Institute (PGMI), Hayatabad Medical Complex (HMC),Peshawar from November 1st, 2007 to March 31st, 2011.Patients and Methods: A retrospective review of the medical charts of 18 patients who were diagnosed with opticneuritis before age 10 was conducted in this study. Data were collected on the demographics, clinical features, use ofintravenous corticosteroids, neuroimaging, and diagnosis of multiple sclerosis.Results: Eighteen patients were identified with optic neuritis, 13 of whom were girls (72.2%) and the remaining 5, boys.Mean age at diagnosis was 7.2 ± 1.5 years (range, 4 to 10 years). Eleven patients were diagnosed with bilateral diseases(61.1%). All patients (100%) exhibited visual acuity worse than 6/60. However, 14 patients (77.7%) recovered to a visualacuity level better than 6/12. Fifteen patients received the corticosteroid treatment. Disc swelling was observed in 75.8%of eyes (25 eyes). The mean follow-up period was 24.9 ± 22.3 months (range, 6 to 69 months). During that time, 3patients developed multiple sclerosis.Conclusions: In children with optic neuritis, it was found that there was a profound decrease in initial visual acuity andrapid recovery of visual acuity. Corticosteroid treatment resulted in a beneficial effect on visual outcomes, but had noeffect on the risk of multiple sclerosis.Key words: Optic neuritis, Multiple sclerosis.
Original Article
INTRODUCTIONOptic neuritis (ON) is an acute inflammatory
condition affecting the optic nerve. The most commoncause of ON is demyelination of the optic nerve (eitheridiopathic or due to multiple sclerosis), although thereare other possible etiologies, including para-infectiousresponses, infections and vasculitides.1 Attack of opticneuritis in childhood are usually bilateral.2 Childhoodoptic neuritis is a rare condition that differs from adult-onset optic neuritis in some clinical aspects. It is widelyaccepted that in children, attacks of optic neuritisusually occur following a febrile illness, tend to affectboth eyes, are frequently associated with swollen discs,improve rapidly, and have a low conversion rate tomultiple sclerosis (MS).3-5 The relationship betweenoptic neuritis and multiple sclerosis (MS) has been well-established, and several articles have noted a lower
incidence of MS in children with optic neuritis. 4,6-12 Sincethere have been no studies of childhood optic neuritiscomparable to the Optic Neuritis Treatment Trial(ONTT), a multi-center, randomized, placebo-controlled trial for adult optic neuritis, the previousresults regarding childhood optic neuritis cannot beviewed as complete or definitive.
In previous studies on childhood optic neuritis,the study populations were heterogeneous in nature,owing to the broad age distributions of the subjectchildren. Some previous reports have suggested thathormonal effects and puberty affected the clinicalmanifestations of the condition . 5,7-13 Working from thisperspective, several authors have focused on pre-pubertal patients, however, the number of studypatients was small . 13,14
In this study, we describe the clinicalcharacteristics of optic neuritis in young children whowere diagnosed before the age of 13.MATERIAL AND METHODS
Our study reviewed patients younger than 13years of age that visited the Eye unit of HayatabadMedical Complex, Peshawar and were diagnosed withoptic neuritis between November 1st, 2007 and March31st, 2011. Optic neuritis was diagnosed on the basis ofthe following clinical symptoms and signs: acute lossof visual acuity or visual field lasting 8 days or less,
Dr. Zakir

270 Ophthalmology Update Vol. 10. No. 3, July-September 2012
relative afferent pupillary defect, and abnormal colorvision. Additionally, bilateral disease was defined as aloss of vision in the other eye occurring within twoweeks after the initial attack. The following data wererecorded: demographics (age at diagnosis, sex), clinicalprofiles (laterality, initial visual acuity, worst visualacuity, final visual acuity, duration between initialsymptom and recovery), ophthalmologic characteristics(disc swelling, results of color vision test and visualfield test), presumed or definite viral infection orvaccination preceding visual loss, findings in brainmagnetic resonance images (MRI), development of MS,and the use of steroid treatment. We considered 6/12as functionally good visual acuity, and the duration ofvisual recovery to 6/12 was checked. We used SPSSver. 17.0 for the analysis, and regarded the result asstatistically significant when the p-value was less than0.05.RESULTS:
We identified 18 patients, 13 of whom were girls(72.2%) and the remaining 5, boys. Mean age atdiagnosis was 7.2 ± 1.5 years (range, 4 to 10 years).Eleven patients were diagnosed with bilateral diseases(61.1%). All patients (100%) exhibited visual acuityworse than 6/60. However, 14 patients (77.7%)recovered to a visual acuity level better than 6/12.. Theduration between the worst visual acuity and 6/12 was2.50 ± 2.90 months (6 days to 8 months). Four patientsshowed no recovery of visual acuity, 3 (16.6%) patientsshowed bilateral disease, and 3 patients did not receivecorticosteroid treatment.
We administered a regimen of 10 to 30 milligramsof methylprednisolone per kilogram per day. Fifteenpatients received this treatment. Based on previousreports of corticosteroid treatment favorable visualoutcomes in childhood optic neuritis, we recommendedthe treatment to every parent. However, 3 patientsrefused the therapy and underwent a follow-up.Compared to the non-treated subjects, patients whoreceived intravenous corticosteroid treatment resultedin better visual outcomes (p = 0.043). Disc swelling wasobserved in 75.8% of eyes (25 eyes). Color vision testswere done on 10 eligible patients. Color vision defectwas present in all the 10 patients. Goldmann perimetrywas done with the same 10 patients. Four of the patientsexperienced central and paracentral scotomas, 4patients had diffuse decreased central sensitivity, 1patient showed a paracentral island, and the otherpatient reported no generalized depression. Six patientsreported suffering from febrile disease before the onsetof acute visual loss, and 2 patients had received thevaccine for measles, mumps, and rubella prior to theattack.
With the exception of 2 patients, all children had
a baseline brain MRI. MRI abnormalities are shown inTable II. Six of the patients showed no abnormalities.Three patients showed optic nerve enhancement and 4patients had high signal lesions in the white matter.On the MRI of the other 3 patients, both high signals inthe optic nerve and white matter lesions in the brainwere observed.
The mean follow-up period was 24.9 ± 22.3months (range, 6 to 69 months). During that time, 3patients developed multiple sclerosis. Two of thepatients were female, and one did not initially receiveintravenous corticosteroid treatment for optic neuritis.
Table IGender distribution
Gender Number of cases (%)
Male 5 (27.77%)
Female 13 (72.23%)
Total 18 (100%)
Table IIMRI abnormalities
(n=16)MRI= Magnetic Resonance Imaging, n= number
MRI Abnormalities Number of cases
No abnormalities 6
Optic nerve enhancement 3
High signal lesion in white matter 4
Optic nerve enhancement + high signa
Lesion in white matter 3
Total 16
DISCUSSION:Attacks of optic neuritis in childhood are usually
bilateral and often associated with a febrile illness.Visual symptoms tend to improve rapidly, especiallywith steroid therapy, and visual acuities are oftennormal within 4-6 weeks of onset.15,16 The frequency ofmultiple sclerosis after optic neuritis in childhoodappears to be low. 2-5According to the ONTT, femalepredominance was observed in adulthood opticneuritis, that is, 77% of the enrolled patients werefemale. 17 With regards to its dominance in childhood,there has been some controversy regarding a femalepredilection for the condition, and the ratio of femalesto males affected was 2:3 to 4. 2,7,8,18 Some authorsreported that no sex preponderance , but the female-to-male ratio increased to 2:1 after puberty.5,7,13 In aprevious study conducted in Thailand, the proportionsof females were 59% and 71% of patients with opticneuritis age under 10 and between 10 and 12,
Optic Neuritis in Children

Ophthalmology Update Vol. 10. No. 3, July-September 2012 271
respectively. 14 However, in our study, a femalepredominance was detected with 72.2% of the patientsbeing female.
Childhood optic neuritis was considered to bebilateral in nature. Contrary to the inclusion criteria ofthe ONTT, which covers only patients with unilateralvisual acuity loss17, some authors have recruitedchildren with bilateral optic neuritis18, while otherauthors did not attempt to exclusively include bilateraldiseases, but exclusively reported cases in which theconditions were bilateral. 12.19There were 11 cases ofbilateral disease among our 18 patients, which wasconsistent with previous articles where bilateral diseasewas reported in the range of 42% to 87%. 3,7,20
Initial profound visual loss occurred morecommonly in children than adults. The authors reportedthat 84% to 100% of childhood patients experiencedvisual acuity of 20 / 200 or worse upon presentation.7,11
According to the ONTT, initial visual acuity was betterthan 20 / 200 in 64.1% of the 454 patients .21 In our study,all patients (100%) exhibited visual acuity worse than6/60. Despite severe visual loss at the initial phase,visual prognosis was good to excellent in the childhoodoptic neuritis patients. Previous articles reported that53% to 92% of patients recovered visual acuity betterthan 20 / 40.3,13,18 The ONTT provided long-term follow-up results of visual prognosis: 72% of the affected eyeshad a visual acuity of 20 / 20 or better, and 66% ofpatients had a visual acuity of 20 / 20 or better in botheyes at 15-years’ follow-up.22 In this study, 14 patients(77.7%) recovered to a visual acuity level better than6/12,while 4 patients exhibited no recovery of theirvisual acuity. The duration between the worst visualacuity and 6/12 was 2.50 ± 2.90 months (6 days to 8months).
This study was not a controlled study, and thenumber of study patients was small. However, we wereable to identify significant beneficial effects ofintravenous corticosteroid therapy on the visualoutcomes. We employed the regimen of 10 to 30milligrams of methylprednisolone per kilogram perday, which was consistent with previous articles thatreported satisfactory visual outcomes withcorticosteroid therapy.3,5 Of course, there have also beenreports showing no correlation between the use ofsteroids and the final visual outcomes, making thedecision of corticosteroid treatment on young childrendifficult and controversial.7,13 However, it is both logicaland ethical to treat optic neuritis patients withcorticosteroids when taking the suspected autoimmunemechanism underlying the pathogenesis of opticneuritis into account . 1
Many reports have focused on the associationbetween optic neuritis and MS. According to the ONTT,
the aggregate cumulative probabilities of developingMS were 30%, 38%, and 50% with 5-year, 10-year, and15-year follow-ups, respectively.23 In a study ofchildhood optic neuritis, Lucchinetti et al.6 estimatedthe risk of MS to be 13%, 19%, 22%, and 26% after 10,20, 30, and 40 years from the onset of optic neuritis. Inanother case series, the risk of developing MS wasestimated to be 8% to 50%.4,7,12 In our study, during themean follow-up period of 24.9 ± 22.3 months (range, 6to 69 months), 3 patients (16.6%) were diagnosed withMS. After the ONTT reports, it became commonlyaccepted that steroid therapy did not alter the visualoutcomes or the risk of MS in adults. In addition, wefind no significance in corticosteroids preventing MS.Only the presence of MRI lesions, the most importantrisk factor in the ONTT, affected the risk of MS. In ourstudy, only patients who showed abnormalities in thebaseline MRI developed MS. This finding wascomparable to the findings of the ONTT, whichreported the risk of MS after 15 years increasing 25% to72% in cases where the baseline MRI showed one ormore lesions 23, and the findings of the study on patientswere younger than 18 years of age.24
This study has the same disadvantage as otherstudies concerning childhood optic neuritis: the studypopulation is too small to fully analyze the prognosisdepending on the treatment and risk factors of multiplesclerosis. The prevalence of optic neuritis in children isknown to be less than in adults, and thus the possibilityof studying large population of patients is consideredfairly low. Nevertheless, we found that steroidtreatment exerted a significant effect on visualoutcomes, and the presence of MRI lesions had astatistically significant effect on the risk of MS. Thisstudy recruited a large number of patients who wereyounger than 10 years when diagnosed with opticneuritis, and thus created a distinction between ourresults and the previous articles. Previous reportsregarding childhood optic neuritis that studied such abroad age group or such a small study populationexhibited insignificant results. In this study, wedemonstrated the clinical characteristics of opticneuritis in young children. In particular, the patientsin this age group tended to be female, have bilateraldisease, and despite initial deep visual loss, recoveredtheir visual acuity within a few months. Corticosteroidtreatment appeared to exert a helpful effect on the visualoutcomes, and in cases involving MRI lesions atbaseline, the risk of developing MS tended to be higher.CONCLUSION:
In children with optic neuritis, it was found thatthere was a profound decrease in initial visual acuityand rapid recovery of visual acuity. Corticosteroidtreatment resulted in a beneficial effect on visual
Optic Neuritis in Children

272 Ophthalmology Update Vol. 10. No. 3, July-September 2012
outcomes, but had no effect on the risk of multiplesclerosis.REFERENCES:1. Walsh FB, Hoyt WF, Miller NR. Walsh and Hoyt’s clinical
neuro-ophthalmology. 4th ed. Vol. 1. Baltimore: Williams &Wilkins; 1982
2. Boomer JA, Siatkowski RM. Optic neuritis in adults andchildren. Semin Ophthalmol 2003;18:174–80.
3. Hwang JM, Lee YJ, Kim MK. Optic neuritis in Asian children.J Pediatr Ophthalmol Strabismus 2002;39:26–32.
4. Riikonen R. The role of infection and vaccination in thegenesis of optic neuritis and multiple sclerosis in children.Acta Neurol Scand 1989;80:425–431.
5. Farris BK, Pickard DJ. Bilateral postinfectious optic neuritisand intravenous steroid therapy in children. Ophthalmology1990;97:339–345
6. Lucchinetti CF, Kiers L, O’Duffy A, et al. Risk factors fordeveloping multiple sclerosis after childhood optic neuritis.Neurology 1997;49:1413–1418
7. Morales DS, Siatkowski RM, Howard CW, Warman R. Opticneuritis in children. J Pediatr Ophthalmol Strabismus2000;37:254–25
8. Hierons R, Lyle TK. Bilateral retrobulbar optic neuritis. Brain1959;82:56–67.
9. Kriss A, Francis DA, Cuendet F, et al. Recovery after opticneuritis in childhood. J Neurol Neurosurg Psychiatry1988;51:1253–1258.
10. Alper G, Wang L. Demyelinating optic neuritis in children. JChild Neurol 2009;24:45–48.
11. Kennedy C, Carroll FD. Optic neuritis in children. ArchOphthalmol 1960;63:747–755.
12. Good WV, Muci-Mendoza R, Berg BO, et al. Optic neuritisin children with poor recovery of vision. Aust N Z JOphthalmol 1992;20:319–323.
13. Brady KM, Brar AS, Lee AG, et al. Optic neuritis in children:clinical features and visual outcome. J AAPOS 1999;3:98–103.
14. Chirapapaisan N, Borchert MS. Pediatric optic neuritis. J MedAssoc Thai 2008;91:323–330.
15. McDonald WI, Compston A, Edan G, et al. Recommendeddiagnostic criteria for multiple sclerosis: guidelines from theInternational Panel on the diagnosis of multiple sclerosis.Ann Neurol 2001;50:121–127.
16. Polman CH, Reingold SC, Edan G, et al. Diagnostic criteriafor multiple sclerosis: 2005 revisions to the “McDonaldCriteria”. Ann Neurol 2005;58:840–846.
17. Beck RW. The optic neuritis treatment trial. Arch Ophthalmol1988;106:1051–1053.
18. Hwang JS, Kim SJ, Yu YS, Chung H. Clinical characteristicsof multiple sclerosis and associated optic neuritis in Koreanchildren. J AAPOS 2007;11:559–563.
19. Nakao Y, Omuto T, Shimomura Y. Optic neuritis in children.Folia Ophthalmol Jpn 1983;34:496–498
20. Wilejto M, Shroff M, Buncic JR, et al. The clinical features,MRI findings, and outcome of optic neuritis in children.Neurology 2006;67:258–262.
21. Beck RW, Cleary PA, Anderson MM Jr, et al. The OpticNeuritis Study Group. A randomized, controlled trial ofcorticosteroids in the treatment of acute optic neuritis. N EnglJ Med 1992;326:581–588.
22. Optic Neuritis Study Group. Visual function 15 years afteroptic neuritis: a final follow-up report from the Optic NeuritisTreatment Trial. Ophthalmology 2008;115:1079–1082.e5.
23. Optic Neuritis Study Group. Multiple sclerosis risk after opticneuritis: final optic neuritis treatment trial follow-up. ArchNeurol 2008;65:727–732.
24. Bonhomme GR, Waldman AT, Balcer LJ, et al. Pediatric opticneuritis: brain MRI abnormalities and risk of multiplesclerosis. Neurology 2009;72:881–885.
Optic Neuritis in Children
Ophthalmology Update Vol. 10. No. 3, July-September 2012 273
––––––––––––––––––––––––––––––––––––––––––––––––––––– (Note: The Article is basically a ‘review article’, but on the requestof Prof. Naimatullah Khan Kundi, Head of Ophthalmology, KhyberTeaching Hospital, Peshawar, it is being published as an ‘OriginalArticle’, as all the 62 patients were operated in his Department,under his supervision as all these patients were closely observed.The management of Ophthalmology Update has the policy ofpromoting the culture of research by encouraging young andbudding ophthalmologists to undertake various topics of their choicewhile maintaining the originality of their work).–––––––––––––––––––––––––––––––––––––––––––––––––––––*Department of Ophthalmology, Khyber Teaching Hospital,Peshawar (KPK) 1.,Senior Registrar2.Associate professor, 3.Registrar,4.Senior registrar RMI, 5. Medical officer–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Dr Zakir Hussain, H.No. 86, St. No. 9, Sector: J-1, Phase II, Hayatabad, Peshawar. Ph: 0092-091-5811020,03339314643 0334 0123070 Email: [email protected]/o Marwat Optico, Ghazni Khel Market, Main Lorry Addah, LakkiMarwat (KPK)–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: March’2012 Accepted May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
Phacoemulsification with Topical Anaesthesia VsPeribulbar Anaesthesia*
Zaman Shah1, Sadia Sethi2, Saber Mohammad3, Mohammad Rafiq Afridi4Shafqatullah Khan Marwat5
Abstract: Objective: To investigate the level of pain perceived by patients undergoing phacoemulsification under topicalanaesthesia, in comparison with peribulbar technique.Material and methods: This study was conduct in the department of ophthalmology Khyber Teaching Hospital Peshawarfrom 1stJune 2011 to 30th December 2011. 62 consecutive patients undergoing phacoemulsification under local anaesthesiawere established. The study was done in two groups, group 1 consist of 31 patients (11 male, 20 female) were operatedon topical anaesthesia. Group 2 consist of 31 patients (15 male, 16 female) underwent phako surgery using peribulbarinjection.Results: The study groups showed the distribution of pain score at the time of induction, per-operative and postoperative.On induction score ranged from 0-3 for group 1 and 0-10 for group 2. Per operative pain score was 0-3 in both groups.Post operative pain ranged from 0-3 for group 1 and 0-5 for group 2.Conclusion: Phacoemulsification with topical anaesthesia is quite successful with minimum or no pain during procedureand this avoid the dreadful complications of peribulbar/ retrobulbar injection.
Original Article
INTRODUCTIONAlthough phacoemulsification with only topical
anaesthesia is possible, the level of any discomfortperceived by the patients is unknown. Topicalanaesthesia eliminates any risk of inadvertent ocularor orbital injury. With the advent of phaco-emulsification, cataract surgery using only topicalanaesthesia has become a reality1. This form ofanaesthesia has several advantages over regionalinfiltrative techniques such as peribulbar, retrobulbarand sub-tennon injection, the foremost of which is theabolition of any risk of inadvertent injury to the globeor orbital contents2.The drops are instilled just a fewminute before surgery and anaesthesia is sufficient to
perform phacoemulsification through a sclera or cornealpockets without a superior rectus sutures, typically witha single dose.
In topical anaesthesia, patients’ education andcooperation is needed because ocular motility andsurgeon’s tension are all there. As iris is one of the mostsensitive structures, inadvertent touching of the iris willresult in to severe pain. Pupil should be widely dilatedbefore proceeding the surgical procedure. In miosedpupil the surgery is not only difficult but frequenttouching of the iris with chopper and grasping of theiris into the phako probe is common. One should notcarry out phako surgery on long standing dilated pupilbecause the pupil may get constrict during theprocedure.MATERIAL AND METHODS
This study was conducted in the department ofOphthalmology Khyber Teaching Hospital Peshawarfrom 1st June 2011 to 30 December 2011. 62 consecutivepatients underwent phacoemulsification under localanaesthesia. Group 1 consist of 31 patients (11 male, 20female) were operated on topical anaesthesia. Group 2consist of 31 patients (15 male, 16 female) underwentphako surgery using peribulbar injection.
In group 1 topical anaesthesia was administeredin the form of proparacaine eye drop instilled to thesuperior conjunctival fornix once the patient waspositioned on the operating table. The patient wasasked to report when the stinging sensation subsided.In group 2 peribulbaran aesthesia consisted ofxylocain2% with adrenaline. This was divided in to twoinjections, half was injected inferior temporally and halfsuperiorly.
Dr ZamanShah
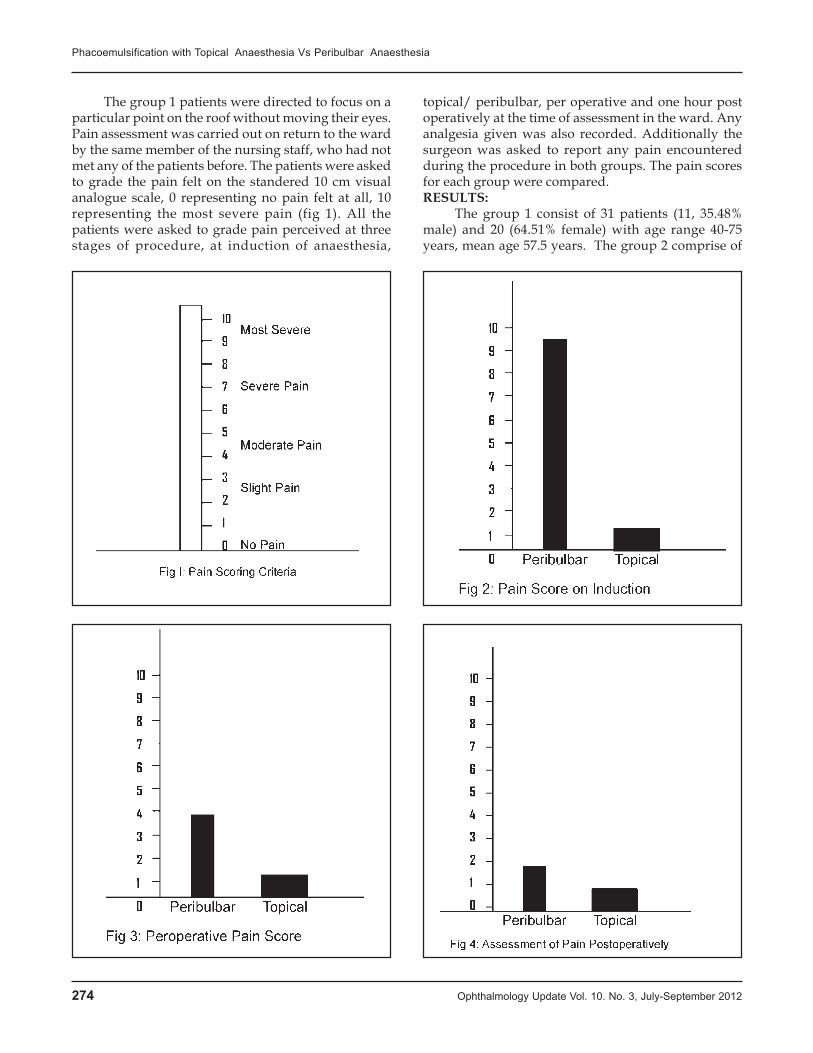
274 Ophthalmology Update Vol. 10. No. 3, July-September 2012
The group 1 patients were directed to focus on aparticular point on the roof without moving their eyes.Pain assessment was carried out on return to the wardby the same member of the nursing staff, who had notmet any of the patients before. The patients were askedto grade the pain felt on the standered 10 cm visualanalogue scale, 0 representing no pain felt at all, 10representing the most severe pain (fig 1). All thepatients were asked to grade pain perceived at threestages of procedure, at induction of anaesthesia,
topical/ peribulbar, per operative and one hour postoperatively at the time of assessment in the ward. Anyanalgesia given was also recorded. Additionally thesurgeon was asked to report any pain encounteredduring the procedure in both groups. The pain scoresfor each group were compared.RESULTS:
The group 1 consist of 31 patients (11, 35.48%male) and 20 (64.51% female) with age range 40-75years, mean age 57.5 years. The group 2 comprise of
Phacoemulsification with Topical Anaesthesia Vs Peribulbar Anaesthesia

Ophthalmology Update Vol. 10. No. 3, July-September 2012 275
31 patients, 15(48.38%) male, 16(51.61%) female, agerange 30-80 years and mean age 55 years.
A fig 2 shows the distribution of pain scores atthe time of induction. Score ranges from 0-3 for group1 and 0-10 for group 2. There was a significant differencebetween the pain perceived with instillation of dropsand that with peribulbar injection.Per operative painscore was shown in fig 3, score ranged from 0-3 in bothgroups and most of the score in each group representingslight pain or less.Fig 4 showed the pain scores postoperatively, score ranged from 0-3 for group 1 and 0-5for group 2. The median scores were 0 for the group 1and 1 for group 2 and most of the scores in each groupagain represented slight pain or less. Only 2 patientsneeded analgesia in group 1 and 05 patients in group 2in the ward.DISCUSSION:
Topical anaesthesia in the form 5% cocaine wasdescribed as pre-eminently useful for cataract extractionby Knapp in 1884(3). He reported that pain was feltonly when iris was grasped to perform an iredectomy.Nucleus extraction is likely to produce pain due tostretching of iris, particularly when dialatation is poor.By fragmenting the nucleus in situ, phacoemulsificationobviates the need to touch the iris during cataractextraction, provided the pupil is well dilated. Duringthe introduction of phako probe at the start of surgerythe patients may feel slight pain due to iris stretchingand deepening of the anterior chamber.
Cataract surgery under topical anaesthesiarequires full co-operation of the patient during theprocedure, to prevent undesirable movement of theglobe and this requires particular effort by the surgeonto win the patient’s confidence.A detail discussion isneeded to explain the procedure to the patient and evenmultiple visits may be arranged to get the patientconfidence. Superior rectus suture may be omitted inmost of the cases which may well contribute to lowerincidence of post operative diplopia and ptosis4. Thepatient needs to be asked to try to keep the eyeparticularly still for a moment to perform capsullorhexisand at the time of intra ocular lens implantation. Theglobe is adequately fixated by phacoemulsificationprobe and chopper during the procedure. The idealanaesthetic technique should produce an adequate levelof analgesia for the proposed surgical procedure, inflictthe minimum pain or toxicity on the patient top workeasily, whilst both the peribulbar and retrobulbartechniques are effective5. There is a small risk of globeperforation (0.006%)6, retrobulbar hemorrhage(0.072%)3
and damage to extra ocular muscles with these. Asubdural injection may also occur with retrobulbarinjection which may result in brain stem anaesthesia ordeath7. Optic atrophy and central retinal vein and artery
occlusion have also been reported8. Most of the risksare eliminated by the use of a subtennon injection asdescribed by Stevens9.
Topical anaesthesia is rapid and straight forwardto perform, it is also likely to be more acceptable topatients and large proportion of whom are afraid ofneedle. There is no risk of damage to the globe or orbitalcontents and therefore topical anaestheisa is stronglyindicated in the presence of large styphylomatous globewith synechiae especially associated with bleedingtendency. The absence of akinesia, whilst increasing thetechnical difficulty for the surgeon, also avoid anytransient post operative diplopia experience by thepatient. Diplopia may still occur if the cataract hasimpaired the patient’s fusion4. The mydriasis andcycloplegia are now limiting factors on immediate postoperative vision. Finally the cost of topical anaestheticagent like proparacaine is less than lignocaine andbupivicain mixture.
A reasonable degree of experience is required toperform phacoemulsification under topical anaesthesia.It will be very difficult to convert it to traditional extracapsular cataract extraction once you get any problemin the procedure. The capsullorhexis has to beperformed reasonably quick to minimize the risk ofunfavorable effect of patient movement, as this is thefirst step for successful phacoemulsification. One mustavoid touching the unanaesthetized iris with anyinstruments so that to minimize the per operativemiosis. In my study all those patients operated ontopical anaesthesia did not require any pad for coveringthe eye and the post-operative medications includingtopical steroid and antibiotic started and these patientshave good visual acuity just post operatively andregarding the pain most of the patients said at the endof procedure that they had enjoyed the surgicalprocedure. To abolish the effect of mydriatics, I usuallyinject intracameral miochol at the end of surgery on allgroup 1 patients so that to have a good vision just postoperatively.CONCLUSION:
The study is concluded with the remarks thatphacoemulsification with topical anaesthesia is quitesuccessful with minimum or no pain during theprocedure and slight pain afterward, which avoids thedreadful complications of peribulbar or retrobulbarinjection. The best line of anaesthesia recommended inthis study for cataract surgery is topical anaesthesia.REFERENCES:1. Grabow HB. Topical anaesthesia for cataract surgery.Eur J
Implant Surg 1993;5:20-4.2. Hamilton RC, Gimbel HV, Javitt JC. The prevention of
complications of regional anaesthesia for Ophthalmology.In Zahl K, KeltzerMA(eds). Ophthalmology clinics of NorthAmerica, vol 3.Regional anaesthesia for intra ocular surgery.
Phacoemulsification with Topical Anaesthesia Vs Peribulbar Anaesthesia

276 Ophthalmology Update Vol. 10. No. 3, July-September 2012
Philadelphia: WB Saunders, 1990:111-25.3. Knapp H. on cocaine and it uses in Ophthalmic Surgery.
Arch Ophthalmol 1884;13:402-48.4. Wylie J, Henderson M, Doyle M, Hickey-Dweyer M.
Persistent binocular diplopia following cataract surgery:etiology and management. Eye 1994;8:543-6.
5. Murdoch IE. Peribulbar versus retrobulbar anaesthesia. Eye1990;4:445-9.
6. Davis DB, Mandel MR. Efficiency and complication rate of
16224 consecutive peribulbar blocks. J Cataract Refract Surg1994;20:327-37.
7. Hamilton RC. Braing stem anaesthesia following retrobulbarblockade. Anaesthesiology 1985;63:688-90.
8. Berry CB, Murphy PM. Regional anaesthesia for cataractsurgery. Br J Hosp Med 1993;49:680-701.
9. Steven JD. A new local anaesthesia technique for cataractextraction by one quadrant subtennon’s infiltration. Br JOphthalmol 1992;76:670-4.
Phacoemulsification with Topical Anaesthesia Vs Peribulbar Anaesthesia

Ophthalmology Update Vol. 10. No. 3, July-September 2012 277
–––––––––––––––––––––––––––––––––––––––––––––––––––––*This study was financed by Fred Hollows Foundation Australia–––––––––––––––––––––––––––––––––––––––––––––––––––––1Optometrist (Orthoptist) 2.Associate Professor3 Senior Registrar4Registrar–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Ayat Shah Optometrist (Orthoptist) Departmentof Ophthalmology Khyber Teaching Hospital, Peshawar Cell No.0321-9030996 E. Mail> gohar said [email protected]–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: March2012 Accepted June:2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
Ratio between Refractive Error & Strabismusamong its different Types in Children
attending Eye DepartmentKhyber Teaching Hospital, Peshawar*
Ayat Shah1, Sadia SethiFCPS2, Zaman ShahFCPS3, Saber MohammadFCPS4
Department of Ophthalmology, Khyber Teaching Hospital, Peshawar
ABSTRACT:Objectives: The objectives of the study were to find out the ratio between refractive error and strabismus and amongdifferent types of refractive errors. in children up to 16 years age.Material and Methods: This study was conducted in the Department of Ophthalmology, Khyber Teaching HospitalPeshawar from 1st Jan 2011 to 31st Dec 2011.All patients of refractive error and strabismus under 16 years visiting OutPatient Department Khyber Teaching Hospital were examined. A total of 1535 patients were included in the study, fulfillingthe inclusion criteria. All the patients were examined according to the protocol.Results: A total of 1535 patients of refractive error and squint below 16 years were examined. Out of these patients 860(56.03%) were of refractive error, 588(38.31%) patients were of squint and 87(5.67%) patients were excluded from study.Among these refractive error 860 patients, 396(46.05%) were astigmatism, 176(20.46%) patients were myopic, 149(17.32%)patients were hypermetropic, 58(6.74%) patients were aphakic, 57(6.63%) patients had nystagmus and 24(2.79%) patientswere anisometropic amblyopic. In squint patients out of 588, 205(34.86%) were Accommodative esotropia, 125(21.26%)patients were of exotropia, 107(18.20%) patients were of infantile esotropia, 73(12.41%) patients were of straibismicamblyopia, 33(5.61%) patients were of pseudo-squint, 23(3.9%) patients were of exophoria, 22(3.74%) patients were ofparalytic squint. Total amblyopic patients were 97(6.32%). Local patients of Peshawar were 1012(65.93%) and non localpatients were 523(34.07%). Out of total patients 59(3.84%) from Khyber Agency, 46(3.0%) patients were from Afghanistan.A total 808(52.64%) patients were male, 727(47.36%) patients were female.Conclusion: The study shows that the ratio of refractive error was greater than strabismus. In refractive error the ratio ofastigmatism was higher than other types of refractive error. Myopia, hypermetropia, aphakia, nystagmus and anisometropiahave descending ratio respectively. In squint the ratio of esotropia were greater than exotropia. Accommodative esotropiahave high ratio in all types of strabismus. Infantile esotropia, exotropia, pseudo squint, exophoria, paralytic squint havedescending ratio respectively. The ratio of local patients was greater than non local.The ratio of male was greater thanfemale.Key Words: Astigmatism, Myopia, Hypermetropia, Esotropia, Exotropia, Exophoria, Amblyopia.
Original Article
INTRODUCTION:Vision 2020 declared by WHO as the “right to
sight” and global initiative to eliminate the five majorocular causes of avoidable blindness by the year 2020known as vision 2020. These are cataract, trachoma,onchocerciasis, vitamin -A deficiency and refractiveerror1. Refractive error in Pakistan is 11.4% accordingto the national survey conducted in 1987-1990 andfound that the refractive error was the largest cause ofavoidable blindness2. Refractive error which account
mostly for low vision and visual handicap was thelargest cause of preventable blindness in Pakistan3.
Strabismus is the misalignment of visual axis ofone or both eyes. Convergent squint is the mostcommon form of strabismus constituting 2 to b of allmisaligned eyes4. Strabismus is a common disorder thataffects 3% to 5% of children5. The overall estimatedprevalence of strabismus in Pakistan is 5.4%6. In Ireland,it was found that esotropia was five times more thanexotropia7. Accommodative esotropia is the mostcommon type of comitant convergent squint about36.5%8.MATERIAL AND METHODS:
This study was conducted in the department ofOphthalmology Khyber Teaching Hospital Peshawarfrom 1st Jan 2011 to 31st Dec 2011.The study includes1535 patients of refractive errors and strabismus under16 years, all the patients were examined in detail. Toestimate the ratio of refractive error and strabismus andratio among its different types under the age of 16 years
Ayat Shah
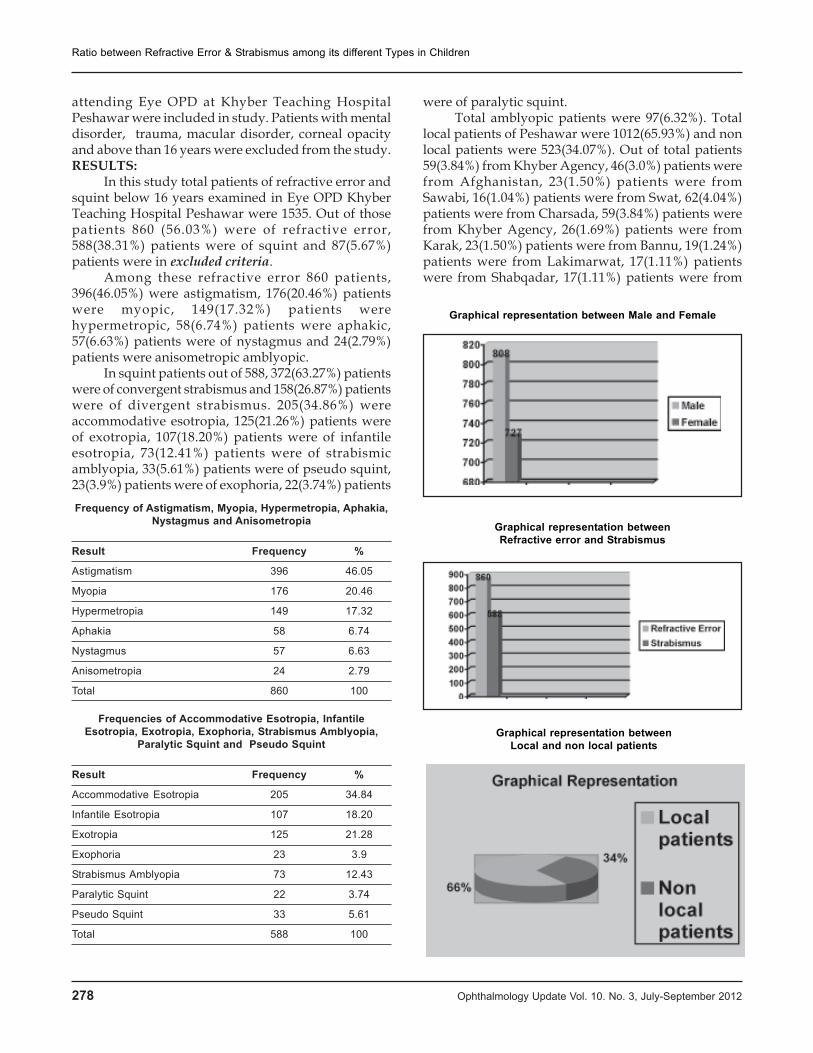
278 Ophthalmology Update Vol. 10. No. 3, July-September 2012
attending Eye OPD at Khyber Teaching HospitalPeshawar were included in study. Patients with mentaldisorder, trauma, macular disorder, corneal opacityand above than 16 years were excluded from the study.RESULTS:
In this study total patients of refractive error andsquint below 16 years examined in Eye OPD KhyberTeaching Hospital Peshawar were 1535. Out of thosepatients 860 (56.03%) were of refractive error,588(38.31%) patients were of squint and 87(5.67%)patients were in excluded criteria.
Among these refractive error 860 patients,396(46.05%) were astigmatism, 176(20.46%) patientswere myopic, 149(17.32%) patients werehypermetropic, 58(6.74%) patients were aphakic,57(6.63%) patients were of nystagmus and 24(2.79%)patients were anisometropic amblyopic.
In squint patients out of 588, 372(63.27%) patientswere of convergent strabismus and 158(26.87%) patientswere of divergent strabismus. 205(34.86%) wereaccommodative esotropia, 125(21.26%) patients wereof exotropia, 107(18.20%) patients were of infantileesotropia, 73(12.41%) patients were of strabismicamblyopia, 33(5.61%) patients were of pseudo squint,23(3.9%) patients were of exophoria, 22(3.74%) patients
Frequency of Astigmatism, Myopia, Hypermetropia, Aphakia,Nystagmus and Anisometropia
Result Frequency %
Astigmatism 396 46.05
Myopia 176 20.46
Hypermetropia 149 17.32
Aphakia 58 6.74
Nystagmus 57 6.63
Anisometropia 24 2.79
Total 860 100
Frequencies of Accommodative Esotropia, InfantileEsotropia, Exotropia, Exophoria, Strabismus Amblyopia,
Paralytic Squint and Pseudo Squint
Result Frequency %
Accommodative Esotropia 205 34.84
Infantile Esotropia 107 18.20
Exotropia 125 21.28
Exophoria 23 3.9
Strabismus Amblyopia 73 12.43
Paralytic Squint 22 3.74
Pseudo Squint 33 5.61
Total 588 100
were of paralytic squint.Total amblyopic patients were 97(6.32%). Total
local patients of Peshawar were 1012(65.93%) and nonlocal patients were 523(34.07%). Out of total patients59(3.84%) from Khyber Agency, 46(3.0%) patients werefrom Afghanistan, 23(1.50%) patients were fromSawabi, 16(1.04%) patients were from Swat, 62(4.04%)patients were from Charsada, 59(3.84%) patients werefrom Khyber Agency, 26(1.69%) patients were fromKarak, 23(1.50%) patients were from Bannu, 19(1.24%)patients were from Lakimarwat, 17(1.11%) patientswere from Shabqadar, 17(1.11%) patients were from
Graphical representation between Male and Female
Graphical representation betweenRefractive error and Strabismus
Graphical representation betweenLocal and non local patients
Ratio between Refractive Error & Strabismus among its different Types in Children

Ophthalmology Update Vol. 10. No. 3, July-September 2012 279
Nowshehra and a little number from other areas likeWaziristan, Dara, Malakand, Chitral etc. A total808(52.64%) patients were male, 727(47.36%) patientswere female.DISCUSSION:
In our study 860 patients (children) were ofrefractive error (56.03%), 588 patients were havingstrabismus (38.31%) and 87 patients were of othercondition which causes refractive error and squint likeTrauma etc (5.66%). Out of 1535 patients, 808 Patientswere male (52.64%) and 727 patients were female(47.36%).
In refractive error the ratio of Astigmatism wasgreater 396(46.05%) followed by myopia 176(20.46%),hypermetropia 149(17.32%), aphakia 58(6.74%),nystagmus 57(6.63%) and anisometropic amblyopia24(2.79%). In squint patients the ratio ofaccommodative esoptropia was greater 205(34.86%)followed by infantile esotropia 107(18.20%), exotropia125(21.28%), strabismic amblyopia 73(12.43%), pseudosquint 33(5.61%), exophoria 23(3.9%), paralytic squint23(3.74%).
Total amblyopic patients were 97(6.32%).Comitant esotropia was found in 372(63.27%) patientsand comitant exotropia was found in 158(26.87%)patients. Refractive errors are among the leading causesof visual impairment worldwide and are responsiblefor high rates of low vision and blindness in certainareas9.
According to the study done in Khyber TeachingHospital Peshawar the prevalence of astigmatism was46.6%, myopia 28.6%, hypermetropia 25%10. Accordingto another study done among school going children inDezfal, Iran revealed overall rate of myopia in studentsup to 15 years 3.4%, hypermetropia 16.6% andastigmatism 18.7%11.
In our study anisometriopic amblyopia was found2.79% (24.75%) and strabismus amblyopia was found6.32 %( 75.25%). While according the study done inKhyber Teaching Hospital Peshawar anisometropiawas found 21%, combined amblyopia 16%, ammetropicamblyopia 6% and stimulus deprivation amblyopia2%12.
Strabismus is a significant cause of ocularmorbidity leading to amblyopia and psychosocialdistress13. According to our study esotropia was found63.27% and exotropia 26.87% in all types of strabismuswhich has no big different with another study done inHMC Peshawar.
According to the study done in Department of
Ophthalmology Hayatabad Medical ComplexPeshawar, esotropia was found 74.35% and exotropia25.64% in children14. In a population base study WoodRuff on 961 children with amblyopia in UnitedKingdom15, found that 57% of amblyopia was due tostrabismus. While according to our study 75.25%amblyopia was due to strabismus.CONCLUSION:
Our study showed that the ratio of refractive errorwas greater than strabismus in children. Astigmatismwas found the most common type of refractive errorwhich is greater more than twice times of myopia andhypermetropia. Accommodative esotropia wasapproximately twice times of infantile esotropia andexotropia. Esotropia was greater in proportion thanexotropia. The ratio of male patients was greater thanfemale. Local patients were approximately twice timesof non local patients.REFRENCES:1. Christan Garms, the Global Initiative: Launch of vision 2020,
Journal of Community Eyes Health 28, Volume 11, 1998.2. Memon MS, Prevalence in Causes of blindness in Pakistan,
JPMA August 1992.3. Durani J. blindness statistics for Pakistan, Pak j Ophthalmol,
1999; 15:1-2.4. Pai A and Mitchalt P. Prevalence of amblyopia and
strabismus. Volume; 116, Issue 2: American Academy ofOphthalmology 2012: 365-660.
5. Mohney BG. Common forms of childhood esotropia.Ophthalmology 2009; 108; 805.
6. Khan A. child and adult health (Eds) National health surveyof Pakistan, Islamabad: Pakistan Medical Research Council.1996; 19-22.
7. Morgan RE. Pattern of eye diseases in children seen at josuniversity teaching hospital. Bar J Ophthalmology 2007; 91:1337.
8. Greenberg A, Mohney BG, Diehl NN, Burke JP, incidenceand ty0pes of childhood esotropia: a population-based study.Ophthalmology. 2007; 114(1): 1700-174.
9. Dandona R, Dandona L. Refractive error blindness. Bullworld health organization. 2001; 79:237-43.
10. Sethi.S, Sethi MJ, Hussain I; Khan T. Refractive error inchildren Pak Armed forces Med J 2008; 58(4): 424-428.
11. Fotouchi A, Hashami H, Khaibazkhoob M, Mohammad K.The Prevalence of refractive errors among school children inDezful, Iran, Br J Ophthalmol. 2007; 91:287-92.
12. Sethi S, Hussain I, Sethi M J, Kundi NK, Cause of amblyopiain children coming to ophthalmology Out PatientDepartment Khyber Teaching Hospital, Peshawar. JPMA2008; 58:125.
13. Von Noorden GK. Binocular Vision and ocular Motility 6th
ed. St Lauis; Mosby; 2002.14. Ahmed-M, Iqbal-S, Jehangir-N, Nazullah. Amblyopia in
Strabismic children Ophthalmology update Jan-Mar 2012;Vol. 10, 57.
15. Dandona R, Dandona L, Srinivas M, Sahare P, Narsaiah S,Munoz SR, et al. Refractive errors in children in ruralpopulation. Invest Oph Visc Sci 2002; 43: 615-22.
Ratio between Refractive Error & Strabismus among its different Types in Children
280 Ophthalmology Update Vol. 10. No. 3, July-September 2012
–––––––––––––––––––––––––––––––––––––––––––––––––––––1.Assistant Professor Ophthalmology Department Bannu MedicalCollege/KGN Hospital, Bannu, 2.Registrar OphthalmologyDepartment Hayatabad Medical Complex, Peshawar3,4,5 MedicalOfficer Ophthalmology, Khyber Teaching Hospital, Peshawar4.
–––––––––––––––––––––––––––––––––––––––––––––––––––––Address for correspondence: Dr Nazullah FCPS AssistantProfessor Ophthalmology Department,l Bannu Medical College/KGN Hospital, Bannu E.Mail>[email protected] Cell.03339288040–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: May’2012 Accepted: June 2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
INTRODUCTIONTrabeculectomy, since its introduction in 1968, has
become the gold standard surgical procedure forprogressive open angle glaucoma1 .Trabeculectomy isthe most common operative procedure for the treatmentof medically uncontrolled glaucoma2 and is a betteroption than medical treatment in many cases3.Trabeculectomy lowers intraocular pressure by creationof a new channel for aqueous outflow between theanterior chamber and sub-tenon space4. Recentlysurgery for glaucoma is being performed at early stagesof the disease when the vision is still fairly good. Manypatients report subjective changes in vision followingtrabeculectomy.
Two types of astigmatic changes are usually foundfollowing trabeculectomy. Majority of patients showsvertical steepening and ‘with the rule’ astigmatism,while some patients shows vertical flattening and‘against the rule’ astigmatism5. Corneal astigmatismalso occur after trabeculectomy and combinedoperation with various surgical techniques6.The
surgically induced astigmatism is more in the early postoperative period and it decreases with the passage oftime. The astigmatism usually corrects within the initialperiod of three months postoperatively7. Small flaptrabeculectomy produces smaller changes in cornealcurvature that resolve sooner than previous reports oflarger flap technique8. Various explanations have beengiven regarding the effect of trabeculectomy on cornealcurvatures.
1. The more posterior placement of the incision intrabeculectomy may also explain the observed behavioras the size and location of the incision have a profoundimpact on the postoperative visual results9.
2. Another explanation is that in trabeculectomy,when a piece of tissue is removed from under the scleralflap and the flap then sutured back, the flapapproximates corneal edge of the trabeculectomyopening to the scleral edge and also allows theunsupported corneal edge of the opening to sinkslightly. Both of these mechanisms would have theeffect of shortening the vertical corneal radius ofcurvature. A few months onwards the tension in thesclera sutures may start to weaken and allow the freecorneal edge of the sclerostomy opening to resume itspreoperative position10.
3. The cause of induced astigmatism may berelated to the use of cautery during surgery, producinga contraction of the sclera in the meridian of surgeryand leading to the ‘with the rule’ astigmatism.11Whenthe surgery is augmented with topical application ofanti-metabolite which have antifibroblastic activity,this will have less astigmatism as noted by Honj YJ12
Keratometeric changes after Primary Trabeculectomy
Nazullah FCPS1. Mushtaq Ahmad FCPS2. Javed Rasul FCPS3. Abdul Baseer4.
Sabir Mohammad5.
ABSTRACTPurpose: The main objective of this study was to evaluate the effects of trabeculectomy on corneal astigmatism.Material and methods: The study was conducted in the Department of Ophthalmology, Khyber Teaching Hospital PeshawarPakistan. The duration was one year starting from August 2009 to September 2010. It was a prospective, comparativestudy. The patients admitted for primary trabeculectomy to the eye department was included in this study. Special proformawas made for information of the patients. The pre and post-operative assessment of the patient regarding the type ofGlaucoma, intra ocular pressure, and manual keratometry readings were recorded. The surgery was performed with localanesthesia. Informed consent was taken from each patient included in this study. The patients were followed up for twoweeks postoperatively.Results Total 33 eyes of the 23 patients with trabeculectomy were studied. 10 patients were having bilateral surgery. Outof these, 52% were male and 48 % were female patients. Two types of astigmatic changes were found followingtrabeculectomy. Seventy two percent of cases showed vertical steepening (with the rule astigmatism) while 28 % showedvertical flattening (against the rule astigmatism). The results are assessed on SPSS version 10.Conclusion The impact of the procedure on the visual prognosis of the glaucoma patient must therefore be carefullyevaluated and should be explained to the patient beforehand.
Original Article
Dr. Nazullah

Ophthalmology Update Vol. 10. No. 3, July-September 2012 281
and Zarnowski T13.MATERIAL AND METHODS
The study was conducted in the Department ofOphthalmology, Khyber Teaching Hospital Peshawar,Pakistan. It was spanned over one year durationstarting from August 2009 to September 2010. It was aprospective and comparative study. The patientsadmitted for primary trabeculectomy to the eyedepartment was included in this study. The pre andpost-operative assessment of the patient regarding thetype of Glaucoma, intra ocular pressure, and manualkeratometry readings were recorded. Shin Nipponmanual Keratometer was used.
The surgery was performed with local anesthesia.In all the patients a limbal based conjunctival flap wasraised and reflected forward. A square partial-thicknessscleral flap (approximately 4 x4 mm) was dissectedtowards the limbus, and a wedge of trabecular tissue(1x2 mm ) was excised from beneath this. A peripheraliridectomy was performed, and the scleral flap wassecured back with two 10/0 nylon sutures at thecorners. The conjunctiva was also closed withinterrupted 10/0 suture. All post operative keratometryreadings were compared with that of the pre-operativereadings. Special proforma was made for informationof the patients. Informed consent was taken from eachpatient included in this study.
The inclusion criteria were; 1. Adult patient’s age 17 years and above. 2. All patients with diagnosis of primary
open angle glaucoma, uncontrolled with maximalmedical therapy and needing filtration surgery.
The exclusion criteria were: 1. Congenital /juvenile glaucoma. 2. Previous intraocular surgeries. 3. Significant corneal opacification. 4. All types of lens induced and neovascular
glaucoma. 5. Patients who were not willing to give
consent of being included into this study. 6. Patients with no follow up.The patients were followed 15days after the
operation so that the operative inflammation is reduced.RESULTS
Total 33 eyes of the 23 patients withtrabeculectomy were studied. 52% patients were maleand 48% were female. Ten patients were havingbilateral operations, the rest were having surgery onone eye only. Patient’s demography given in Table I.Out of these 33 cases 24 (73%) eyes were having verticalsteepening with the rule astigmatism and the 9 (27%)were having vertical flattening against the ruleastigmatism. In the early post operative days thedifference was more between the preoperative and
postoperative keratometeries and the average verticalsteepening was 2.25D and flattening was 2.50D.Results are assessed on Statistical Package for SocialStudies (SPSS) version 10. P-value in group 1 (verticalsteepening) is 0.000 which is highly significant as it isless than 0.05 and in group II P value is 0.02 which isalso significant. Details are given in Table II and III
Table IDemographic data of patients with trabeculectomy
No of patients %age
Mean age (years (SD) 52 + 017 yrsMale 12 52.0%
Female 11 48.0%
Unilateral 13 56.5%
Bilateral 10 43.5%
Table IIKeratometry changes in Steepening group
Stage Diopters Mean ± S.D P – Value
Pre-operative 43.52
Post-operative 45.772.25 0.00
Table IIIKeratometry changes in Flattening group
Stage Diopters Mean ± S.D P – Value
Pre-operative 44.45
Post-operative 41.95 2.50 0.020
DISCUSSIONIn our study total 33 cases were included. 72%
eyes were having vertical steepening i.e. with the ruleastigmatism and the 28% were having vertical flatteningi.e. against the rule astigmatism. Our observationsclosely correlate with the Hugkulstone9 who in 1991found similar changes in the vertical corneal radius ofcurvature following trabeculectomy in 10 patients.
Rosen11 also found that five of eight (62.5%) eyesdeveloped 1.50 to 2.50 diopters of steepening in the 90-degree meridian following trabeculectomy. A studydone by Cunliffe IA10 also discovered that the changein vertical corneal curvature after trabeculectomy isconsistent with the with-the-rule change in cornealastigmatism. Claridge14 in 1995 suggested that thereappear to be two broad patterns of topographicvariation following trabeculectomy, the most commonbeing a postoperative steepening of the cornealcurvature though a smaller number of patientsdeveloped a superior corneal flattening .
Liu15 found that trabeculectomy may cause certain
Keratometeric changes after Primary Trabeculectomy
282 Ophthalmology Update Vol. 10. No. 3, July-September 2012
with-the-rule corneal astigmatism which in most of thecases may decrease as time passes by. Dietze7 concludedthat by 12 weeks after trabeculectomy, visual acuityreturned to preoperative levels in all patients and thecorneal topographic changes returned to within 1diopter of preoperative values in 12 of 13 (92%) patients.In 2005 S K Law6 observed that there is with the rulecorneal astigmatism, after trabeculectomy Ourobservations are also supported by another studyrecently conducted by Mehmooda Ashai5 in 2007 inSrinagar India. They have observed 87% with the ruleastigmatism and 13% against the rule.CONCLUSION
Surgically induced astigmatism is becoming animportant issue because it delays visual rehabilitationand exerts a negative effect on the final visual outcome.Hence the effect of the procedure should be explainedto the patient before the operation.REFRENCES:1. Cairns JE. Trabeculectomy: preliminary report of a method.
Am J Ophthalmol 1968; 66:673–9.2. B. O. Adegbehingbe and T. Majemgbasan. A review of
trabeculectomies at a Nigerian Teaching Hospital . Ghanamedical journal 2007;41(4): 176-80.
3. Anand A,Negi S, Khokhar S. Role of early trabeculectomyin primary open angle in developing world,Eye.2007;21(1):40-5.
4. Hanan F, Shah M A, Javaid M, Mohammad S. Effectivenessof trabe in primary open angle glaucoma. JPMI 2007; 21(03):209-211.
5. S K Law, A M Mansury, D Vasudev and J Caprioli. Effects ofcombined cataract surgery and trabeculectomy withmitomycin C on ocular dimensions. Br J phthalmol 2005; 89;1021-1025.
6. Dietze PJ, Oram O, Kohnen T, Feldam RM ,Koch DD , GrossRL. Visual function following trabeculectomy: effect oncorneal topography and contrast sensitivity. J Glaucoma1997;6:99–103.
7. Vernon SA, Zambarakji HJ, Potgieter F, Evans J, Chell PB.Topographic and keratometric astigmatism upto 1 yearfollowing small flap trabeculectomy (microtrabeculectomy).Br J Ophthalmol 1999; 83(7): 779-82.
8. Charles E Hugkulstone. Changes in keratometry followingtrabeculectomy BritishJournal of Ophthalmology,1991,75,217-218
9. Cunliffe IA , Dapling RB , West J , Longstaff S . A prospectivestudy examining the changes in factors that affect visualacuity following trabeculectomy . Eye 1992 ; 6(Pt 6) : 618-22.
10. Rosen WJ , Mannis MJ , Brandt JD. The effect oftrabeculectomy on corneal topography. Ophthalmic Surg1992 ; 23 (6) : 395-8.
11. Honj YJ , Choe CM , Lee YG , Chung HS, Kim HK. The effectof mitomycin –C on postoperative corneal astigmatism intrabeculectomy and a triple procedure. Ophthalmic SurgLasers. 1998; 29(6): 484-9.
12. Zarnowski T, Haszcz D, Rakowska E, Zagórski Z.Cornealastigmatism after trabeculectomy. (Article in Polish) KlinOczna. 1997; 99(5):313-5 (PubMed Online)
13. Claridge KG, Galbraith JK, Karmel V, Bates AK. The effectof trabeculectomy on refraction, keratometry and cornealtopography. Eye 1995;9:292–8.
14. Liu H, Peng D, Chen J. Corneal astigmatism followingtrabeculectomy . Zhonghua Yan Ke Za Zhi. 1996; 32(5): 355-8.
Keratometeric changes after Primary Trabeculectomy

Ophthalmology Update Vol. 10. No. 3, July-September 2012 283
–––––––––––––––––––––––––––––––––––––––––––––––––––––1.Registrar2.Senior Registrar 3.Medical Officer–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence, Dr Afzal Qadir, Registrar OphthalmologyDepartment ,Hayatabad Medical Complex PeshawarEmail >[email protected] Cell No. 0321-9128247Fax. 091-9217189, House no 40, Street 2, N/4, Phase 4, Hayatabad,Peshawar–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: March ’2012 Accepted: June’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
To determine the Diagnostic use of B-Scan in thedetection of Vitreoretinal Pathologies
in patients with poor Posterior Segment View
Afzal Qadir FCPS1, Umer Khan FCPS2, Zakir Hussain FCPS3
Department of Ophthalmology, Hayatabad Medical Complex, Peshawar (KPK)
ABSTRACTObjectives: To determine the diagnostic use of B-Scan in the detection of vitreoretinal pathologies in patients with poorposterior segment view.Material and Methods: The study was conducted in the Department of ophthalmology Hayatabad Medical ComplexPeshawar from September 2011 to February 2012. In this study evaluation of over a period of six months, 240 eyes of240 patients with vitreous opacities and poor retinal visualization were investigated with B-Scan ultrasound. Patientswere selected from the retina clinic of the Department of Ophthalmology. The B-Scan machine used was US Scan- 3300Results: Total 240 scans performed, RR/D 117 eyes, TR/D 8, 91 had vitreous hemorrhage, 22 had endophthalmitis,IOFB in 21 eyes, intraocular tumor in 8 eyes, PVD in 5 eyes, Asteroid hylosis in 5 eyes. Dropped nucleus in 1 eye.Dropped IOL in 1 patient, and choroidal detachment 2 eyes. Seven patients had traumatic scleral perforation. Six Patientswere diagnosed as cases of PHPV.Conclusion:B-scan ultrasound is a very useful diagnostic tool in detection and evaluation of vitreo-retinal pathologies inpatients with opacities in the vitreous cavity.Key words: B Scan, Vitreoretinal pathologies.
Original Article
Dr. Afzal Qadir
INTRODUCTIONUltrasound is an acoustic wave that consists of
an oscillation of particles within a medium. Ultrasoundwas first used in ophthalmology in 1956 by Americanophthalmologists Mundt and Hughes.1 They used A-scan mode to evaluate an intraocular tumor. B-scan wasintroduced in ophthalmic practice by Baum andGreenwood in 1958.2 Both A-scan and B-scan techniquesare important for the diagnosis of intraocular diseases.B (Brightness) mode is useful for a better demonstrationof the shape and topographic relationship of lesions inthe posterior segment.3 B-scan provides cross sectionaldisplay of diseased tissues and is valuable in detectingunsuspected posterior segment diseases.4 Thefrequency used in the diagnostic ophthalmic ultrasoundfor posterior segment is 8-10 MHz. Over the last 30 yearsultrasonography has greatly advanced and this hasenabled us to study posterior segment of the eye in thepresence of opaque media.4 The purpose of this studyis to evaluate the nature of intraocular pathologies
detected by ultrasound examination in patients withvitreous opacity.MATERIAL AND METHODS
Over a period of six months (September 2011 toFebruary 2012), 240 eyes of 240 patients were selectedfrom the retina clinic of the Department ofOphthalmology at the Hayatabad Medical ComplexPeshawar. There was poor visualization of fundus usingslit lamp and indirect ophthalmoscope in all the patientsdue to vitreous opacities. B-scan ultrasound wasadvised for the evaluation of vitreous opacities and todetect any underlying posterior segment pathology.Patients were explained about the procedure. Topicalanaesthetic eye drop was used to achieve ocular surfaceanesthesia. The B-Scan machine used was US Scan- 3300(NIDEK). Hydroxypropyl methyl cellulose was usedas the coupling material. Patient was kept in supine orseated in comfortable position and the patient was soadjusted that the examiner could see the eye underevaluation and the monitor at the same time. Basicscreening was performed initially at high gain (i.e. 80dB) setting followed by examination under lowersensitivity. Kinetic echography was done by keepingthe probe still and asking the patient to move the eyesin different gazes to determine the after movements ofmembranous structures. Any solid lesion detected wasevaluated topographically. Quantitative echographywas performed to determine the internal reflectivity ofa solid lesion. The clinical and ultrasound findings wererecorded in proforma.
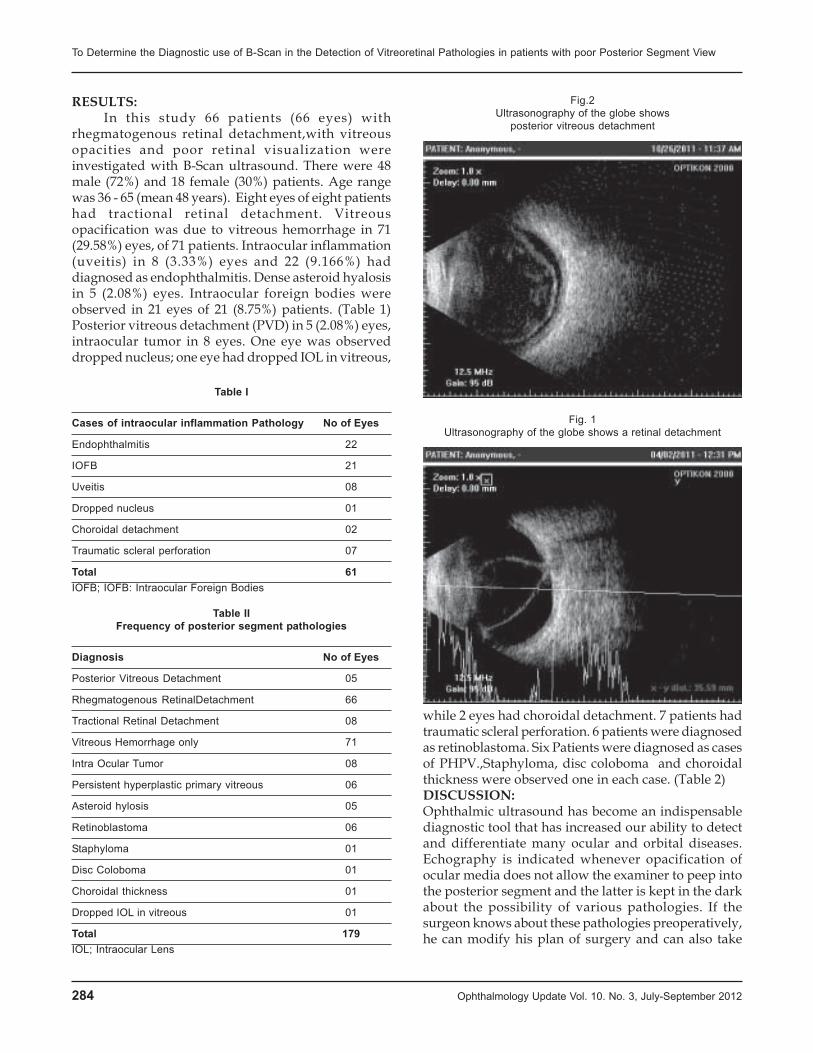
284 Ophthalmology Update Vol. 10. No. 3, July-September 2012
RESULTS:In this study 66 patients (66 eyes) with
rhegmatogenous retinal detachment,with vitreousopacities and poor retinal visualization wereinvestigated with B-Scan ultrasound. There were 48male (72%) and 18 female (30%) patients. Age rangewas 36 - 65 (mean 48 years). Eight eyes of eight patientshad tractional retinal detachment. Vitreousopacification was due to vitreous hemorrhage in 71(29.58%) eyes, of 71 patients. Intraocular inflammation(uveitis) in 8 (3.33%) eyes and 22 (9.166%) haddiagnosed as endophthalmitis. Dense asteroid hyalosisin 5 (2.08%) eyes. Intraocular foreign bodies wereobserved in 21 eyes of 21 (8.75%) patients. (Table 1)Posterior vitreous detachment (PVD) in 5 (2.08%) eyes,intraocular tumor in 8 eyes. One eye was observeddropped nucleus; one eye had dropped IOL in vitreous,
while 2 eyes had choroidal detachment. 7 patients hadtraumatic scleral perforation. 6 patients were diagnosedas retinoblastoma. Six Patients were diagnosed as casesof PHPV.,Staphyloma, disc coloboma and choroidalthickness were observed one in each case. (Table 2)DISCUSSION:Ophthalmic ultrasound has become an indispensablediagnostic tool that has increased our ability to detectand differentiate many ocular and orbital diseases.Echography is indicated whenever opacification ofocular media does not allow the examiner to peep intothe posterior segment and the latter is kept in the darkabout the possibility of various pathologies. If thesurgeon knows about these pathologies preoperatively,he can modify his plan of surgery and can also take
Fig.2Ultrasonography of the globe shows
posterior vitreous detachment
Fig. 1Ultrasonography of the globe shows a retinal detachment
Table I
Cases of intraocular inflammation Pathology No of Eyes
Endophthalmitis 22
IOFB 21
Uveitis 08
Dropped nucleus 01
Choroidal detachment 02
Traumatic scleral perforation 07
Total 61IOFB; IOFB: Intraocular Foreign Bodies
Table IIFrequency of posterior segment pathologies
Diagnosis No of Eyes
Posterior Vitreous Detachment 05
Rhegmatogenous RetinalDetachment 66
Tractional Retinal Detachment 08
Vitreous Hemorrhage only 71
Intra Ocular Tumor 08
Persistent hyperplastic primary vitreous 06
Asteroid hylosis 05
Retinoblastoma 06
Staphyloma 01
Disc Coloboma 01
Choroidal thickness 01
Dropped IOL in vitreous 01
Total 179IOL; Intraocular Lens
To Determine the Diagnostic use of B-Scan in the Detection of Vitreoretinal Pathologies in patients with poor Posterior Segment View

Ophthalmology Update Vol. 10. No. 3, July-September 2012 285
measures to combat various predictable complications.7
In this study, 240 eyes of 240 patients with vitreousopacities were examined. In all the cases, vitreousopacities were dense enough to preclude adequateassessment of retina and any underlying pathology.
Vitreous opacification was because of vitreoushemorrhage in 91 eyes, intraocular inflammation in 8eyes and asteroid hyalosis in five eyes. 22 eyes werediagnosed as endophthalmitis in which 14 were postoperative endohthalmitis and eight were post traumaticendophthalmitis. The distinction between the opacitieswas clinical as well as echographic. Fresh vitreoushemorrhage appears as dots and short lines on B-scan.The more dense the hemorrhage, the more opacities areseen on B-scan. Organized blood produces largermembranous surfaces on B scan. Inflammatory cells invitreous give similar echogenic appearance as freshvitreous hemorrhage; however, certain feature on B-scan can help differentiate posterior vitreousdetachment (PVD) is more extensive in vitreoushemorrhage; inflammatory cells are evenly distributedwhile vitreous hemorrhage settles inferiorly due togravity.6
In asteroid hyalosis, calcium soaps produce brightechos on B-scan with clear vitreous gel located betweenasteroid opacities and retina.6 Out of 91 eyes withvitreous hemorrhage, 4 eyes showed associatedposterior segment pathologies rhegmatogenous RD wasdetected. It produces a bright continuous foldedmembrane that inserts into optic disc and/or oraserrata.8 In contrast PVD produces a smooth membranethat shows low reflectivity as compared to RD. Andnine eyes had IOFB with vitreous hemorrhage. Kinetic
echography is helpful in differentiating these 2conditions; in PVD there is very fluid undulating aftermovement on Bscan, whereas RD exhibits a moretethered and restricted after movement. However thereare situations in which the acoustic behavior of PVD issimilar to RRD and the distinction may be quitechallenging. Peripheral retinal tear was detected withB-scan in 2 eyes; this appears on B-scan as a retinal flap;with a PVD or vitreous strand attached to it. Eight eyeswith tractional RD and vitreous hemorrhage wereexamined. The causes of TRD in our patients wereadvanced diabetic eye disease in 4 eyes, penetratingocular trauma in 3 eyes andin 1 eye due toinflammatory processes. Both tent like and table topconfigurations were observed on B-scan. Whereas tentlike TRD is produced by a point like adherence, thetable top detachment is the result of a broadervitreoretinal adherence. A thorough echographicexamination is very helpful before vitrectomy in eyeswith TRD; it demonstrates the safest region to breakthe posterior hyaloid, allows the surgeon to anticipateareas of vitreoretinal traction and provide reasonableassessment of expected visual prognosis.9
In our study, 23 patients had penetrating oculartrauma with vitreous hemorrhage and 16 retainedintraocular foreign body. Standardized echography isinvaluable in precise localization of IOFB and todetermine the extent of intraocular damage, even whena foreign body (FB) has been previously localized withCT scan. Typical metallic FB produces a very brightsignal on B-scan that persists at low sensitivity; alsothere is marked shadowing of ocular and orbitalstructures just posterior to it.10 One patient had severeblunt trauma and presented with hemorrhagicchemosis and dense vitreous hemorrhage. B-scanshowed RD and features suggestive of posterior scleralrupture i.e. irregular scleral contour and low reflectivityin the area of rupture along with vitreous incarcerationand episcleral hemorrhage.6 Eight patients withintraocular tumor were scanned; the features wereconsistent with choroidal melanoma in 1 patient i.e.mushroom shape growth showing acoustic hollowness,choroidal excavation and orbital shadowing.11Sixpatients had retinoblastoma, and one patient wasreferred for fine needle biopsy and for metastaticworkup. Endophthalmitis was diagnosed in 22patients; 14 of these were postoperative eyes, 8 hadtraumatic endophthalmitis, with corneal ulcer/abscessin anterior chamber full of hypopion.
Ultrasound is useful to determine the severity andextent of inflammation in clinically suspected cases ofendophthalmitis. When the presence of infection isquestionable from clinical appearance, B-scan may helpto differentiate whether the vitreous opacities are
Fig. 3Ultrasonography of the globe shows IOFB
with vitreous hemorrhage
To Determine the Diagnostic use of B-Scan in the Detection of Vitreoretinal Pathologies in patients with poor Posterior Segment View

286 Ophthalmology Update Vol. 10. No. 3, July-September 2012
secondary to inflammation or to vitreous hemorrhage,as already discussed16 One postoperative patientshowed vitreous opacities and membranes along witha dropped nucleus that appeared as an oval sphericalmass adhered to the retina or floating in the vitreouscavity. Two postoperative patient with history ofchoroidal detachment during surgery, large domeshaped membranes, extending from the periphery tothe posterior pole along with echogenic shadows offresh and clotted blood in the supra-choroidal space.Echography is useful in following the course ofhemorrhagic choroidal detachment and in determiningthe appropriate time for drainage.6
CONCLUSION:B-scan ultrasound is very important for
demonstrating the nature and extent of abnormalitiesin eyes with vitreous opacification.13It is also useful formonitoring progression of retinal diseases. In eyes withvitreous haze that are being considered for vitrectomy,ultrasonic evaluation helps to diagnose the underlyingpathology, to determine the timing of surgery, inoptimal placement of vitrectomy instruments and topredict the visual outcome.REFERENCES:1. Mundt GH, Hughes WF. Ultrasonics in ocular diagnosis.Am
J Ophthalmol.1956; 41: 488-98.
2. Baum G, Greenwood I. the application of ultrasonic locatingtechnique to ophthalmology. Arch Ophthalmol.1958; 60: 263-79.
3. Till P, Osoining KC. Ten year study on clinical echographyin intraocular disease. BiblOphthalmol. 1975; 83: 49-62.
4. Hodes BL. Eye disorders: Using ultrasound in ophthalmicdiagnosis. Post grad Med. 1976; 59: 197-203.
5. Zafar D, Sajad AM, Qadeer A. role of B- Scan ultrasonographyfor posterior segmet lesions. JLUMHS.2008; 07: 7-12.
6. Freeman HM. Diagnostic ophthalmic ultrasound. In: RyanSJ, editor. Retina. vol. 3, 3rd ed. St: Louis: Mosby, 1989: 280-306.
7. Imtiaz SA, Rehman HU. Role of B-Scan in PreoperativeDetection of Posterior Segment Pathologies in CataractPatients. Pak J Ophthalmol. 1997; 13: 108-12.
8. Kerman BM, Coleman DJ: B- Scan ultrasonography of retinaldetachments. Ann Ophthalmol. 1978; 10: 903-11.
9. Bigar F, Bosshard C, Kolti R. combined A- and B- scanechography: preoperative evaluation of vitrectomy patients.Mod ProblOphthalmol.1977; 18: 2-11.
10. Awaschalom L, Meyers SM: Ultrasonography of vitrealforeign bodies in eyes obtained at autopsy. ArchOphthalmol.1982; 100: 979-80.
11. Ossoining KC. Standardized echography: basic principles,clinical applications and results. IntOphthalmolClin. 1979;19: 127-210.
12. Valencia M, Green RL, Lopez PF. Echographic findings inhemorrhagic disciform lesions. Ophthalmology.1994; 101:1379-83.
13. McLeod D, Restori M. Ultrasonic examination in severediabetic eye disease. Br J Ophthalmol.1979; 63: 533-8.
To Determine the Diagnostic use of B-Scan in the Detection of Vitreoretinal Pathologies in patients with poor Posterior Segment View

Ophthalmology Update Vol. 10. No. 3, July-September 2012 287
–––––––––––––––––––––––––––––––––––––––––––––––––––––1.Assistant Professor, Bannu Medical College / Khalifa Gul NawazHospital, Bannu2. Registrar Eye A Ward,Department ofOphthalmology Khyber Teaching Hospital, Peshawar3. AssistantProfessor Bannu Medical College / Khalifa Gul Nawaz Hospital,Bannu4. Assistant Professor Kohat Medical College.5. Registrar6
Asssistant Prof. Patholog, Bannu Medical College, KGN Hospital–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Dr. Sanaullah, FCPS, MPH Assistant ProfessorBannu Medical College / Khalifa Gul Nawaz Hospital, BannuMob.no.0333-9107871, A-one Optico Skakeel Plaza in front ofIslamia College Naimat Mahal PeshawarEmail: [email protected]–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: March’2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
INTRODUCTIONViral hepatitis also called infectious hepatitis–an
inflammation of the liver caused by virus and is a majorhealth problem affecting approximately two billionpeople worldwide. The hepatitis B virus (HBV) hasinfected more than 2 billions people and 350 millionpeople are carrier of the virus. Approximately onemillion people die from hepatitis B, makes it one of thecause of morbidity and mortality1. Hepatitis C virus(HCV) infection is increasing even more rapidly andhas occurred in endemic situation in most part of theworld, with a prevalence of about 3% world wide.2
Hepatitis C virus infection progresses slowly and carrieshigh risk of chronic liver disease (70-80%) and later livermalignancy.3 The prevalence of hepatitis B and C is alsoincreasing in our country.4 Surgeons and paramedicalstaff have a high occupational risk of acquiring HBSand HCV from infected patients.5 Due to this
occupational risk of disease, we want to carried out andevaluate the presence of HBC and HCV infection inpatients underwent cataract surgeries in differentoperation theatre in Bannu district.MATERIALS AND METHODS:
The observational study was carried out at districtBannu from March 2011 to March 2012. During thisperiod 500 patients undergoing eye surgery wereevaluated for hepatitis B and C antibody. After takinghistory, examination and investigations patients werescreened for HBS and HCV with chromatography (kit)method. The details were recorded on proforma anddata was compiled and analyzed for age and sex meanvalues. Special emphases were put on age, sex, andoccupation. All patients of either sex who were operatedas elective cases were included in the study.RESULTS:
In this study, 500 patients who underwent eyesurgery at district Bannu were screened for HBS andHCV. There were 234 (46.8%) male and 266 (53.2%)female patients shown in Fig: 1. Mean age of thepatients were 60 years. The range of age was 40 to 80years shown in (Table 1). Total 20 patients were foundpositive for HBS and HCV. Amongst them 12 werepositive for hepatitis B (2.4%) and 8 for hepatitis C(1.6%) shown in Fig 2. Hepatitis B was found in 07(1.4%) male and 05 (1.0%) female patients. Hepatitis Cwas predominant in females 6 (1.2%) while it was foundin 2 (0.4%) male patients. Both hepatitis B and C werefound in 20 (4%) patients. Amongst them 9 (45%) weremale and 11 (55%) were females shown in Fig: 3.
Frequency of Hepatitis B & C in patientsUndergoing Ocular Surgeries in Bannu District (KPK)
Sanaullah FCPS, MPH1. Saber Mohammad, FCPS2 Nazullah Khan, FCPS3
Awalia Jan FCPS4. Waseem ullah Memon, MCPS, MPH5, Mir Attaullah DCP6
ABSTRACTObjectives: To know the frequency of Hepatitis B and C viral infection in the patients undergoing different ocular surgeriesin district Bannu.MATERIAL & METHODSStudy design: It was a retrospective study.SETTING:Duration of study: It was one year study conducted from March 2011 to March 2012.Sample size: Sample size was 500 patients.Results: Five hundred patients were operated for different ocular surgeries at district Bannu. Mean age of the patientswas 60 years. 234 (46.8%) were male and 266 (53.2%) were female. Out of them 7 (1.4%) were male and 5 (1.0%) werefemale positive for HBS antibodies, while HCV antibodies were found in 2 (0.4%) male patients and 6 (1.2%) femalepatients.Conclusion:The prevalence rate of Hepatitis B and C antibody in district Bannu is alarming sign not only for the generalpopulation but also for the general health care personals. Steps needs to be taken to stop this preventable diseases.
Original Article
Dr. Sanaullah
288 Ophthalmology Update Vol. 10. No. 3, July-September 2012
Figure 2
Figure 3
DISCUSSION:The incident of hepatitis B and C has achieved
endemic situation in many countries of the world,especially in underdeveloped countries. Pakistan is ofno exception, as the disease has been recorded to analarming level in most parts of the countries especiallyrural areas, as can be seen from table 1 and 2. In Pakistana large proportion of the population is already infectedwith hepatitis B and C with the prevalence of 10% forhepatitis B and 4-7% for hepatitis C. In certain partsespecially in the rural areas the percentage of infectedindividuals is significantly higher than the abovequoted figures 6,7. The transmission of virus is throughthe blood and secretions. Most common source ofspread of these infections is through the use ofunsterilized syringes or instrument especially dentalinstruments or unchecked blood transfusion. Otherfactors involved in the spread of infections are personswho have their arm-pits or face shaved by street barberor those involved in sexual abuse8,9,10.
In this study 2.4% patients had hepatitis B and1.6% patients had hepatitis C. According to Cloud Hayand his colleagues11 the prevalence of hepatitis C was11.26% which is higher than our study. Ali and hisassociates reported 5.1% patients suffering fromhepatitis C in their study at Gadap area. The carrierstate of HBS Ag is around 10% in different segments ofPakistani people7 which is higher than our study. Studydone by Shiekh and his colleagues13 carrier state of HBSAg was found to be 2.8%.Wies and his co-workers14
reported 35% cases of HCV and 4% cases of HBV intheir study of patients operated at John Hopkins. Ourstudy showed that the prevalence of hepatitis is quitelow as compared to other studies carried out abroad.CONCLUSION:
With such a rate of HBV and HCV as reported inour study suggests screening of all the patients whoare selected for surgery. At the same time the print andelectronic media is required to aware the public aboutthe methods of the spread of the disease to preventfurther transmission. It is the prime duty of doctors andparamedical staff to counsel the patients and use ethicalpractice.REFERENCES:1. Kane M. Global programme for control of hepatitis B
infection, vaccine. 1995;47-9.2. Dubios F, Desenclos JC, Merriote N. Gondean A, and the
cooaboration study group. Hepatitus C in a Frenchpopulation-based surgery, 1994. Sero prevalence surgery ofviremia, genotype distribution and prognostic risk factors.Hepatol. 1997;25;1940-6.
3. Supras VE, Hadjipashali E, Hatzakis A. Prevalence of riskfctors and evaluation of a screening strategy for hepatitis Band C viral infections in healthy company employees. Eurol Epidemiol. 2001;17:721.
4. Khohkar N, Gill ML, Malik GL. General seroprevance of
Figure 1
Frequency of Hepatitis B & C in patients Undergoing Ocular Surgeries in Bannu District (KPK)
Table 1: Age Group
No. of Patients 500
Age Group 40 – 80 years
Mean age 60 years
Ophthalmology Update Vol. 10. No. 3, July-September 2012 289
hepatitis B and C infections in the populations and sergeonsPak, 2004; 14:534.
5. Bell DM. Occupational risk of HBV,HCV and HIV infectionsin health care workers. An overview. J med. 1997; 102:9-15.
6. Malik IA, Kaleem SA, Tarique WUZ. Hepatitus C infectionin prospective, where do we stand? J college of Physiciansand Surgeons Pakistan. 1999; 9:234-7.
7. Yousaf A, Mohammad A, Ishaque M, et al. Can we efford tooperate on a patients without HBS ag screening? J college ofPhysician and surgeons Pak. 1996; 9:98-100.
8. Luby S. The relationship between therapeutic injections &high prevalence of hepatitis C infection in Hafizabad,Pakistan. Epidemiol infection.1997; 119:349-56.
9. Khuwaja Ak, Qureshi R, Fatimi Z. Knowledge and attitudeabout hepatitis B & C among patients attending family
medicine clinics in Karachi. Eastern Mediterranean HealthJ.2002;8:1-6.
10. Thornburn D, Roy K, Camerson SO. Risk of hepatitis C virustransmission from patients to surgeons. Gut 2003;52:1333-8.
11. Chaudhary IA, Khan SA, Samiullah. Should we do thehepatitis B and C screening on each patient before surgery.Pak J Med Sci.2005; 21:278-80.
12. Ali SA, Sheikh FA, Ahmed K. Prevalence of hepatitis B andC virus in surgical patients. Pak J surgery. 2007;23:109-12.
13. Shaikh MH, Shams K. Prevalence of HBV in health carepersonnel and methods of control. J College of Physician andSurgeons Pak.1995;5:19-21.
14. Makary ESW, Weis MA. Prevalence of blood borne pathogensin an urban university based general surgical practice. AnnSurg.2005;24:803-9.
Frequency of Hepatitis B & C in patients Undergoing Ocular Surgeries in Bannu District (KPK)

290 Ophthalmology Update Vol. 10. No. 3, July-September 2012
–––––––––––––––––––––––––––––––––––––––––––––––––––––1.Registrar2.Senior Registrar 3.Medical Officer–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence, Dr AfzalQadir, Registrar OphthalmologyDepartment ,Hayatabad Medical Complex PeshawarEmail >[email protected] Cell No. 0321-9128247Fax. 091-9217189,House no 40, Street 2, N/4, Phase 4, Hayatabad, Peshawar–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: Dec’2012 Accepted: March’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
Frequency of Raised Intraocular Pressureafter ND: YAG Laser Capsulotomy
Afzal Qadir FCPS1, Umer Khan FCPS2, ZakirHussain FCPS3
Department of Ophthalmology, Hayatabad Medical Complex, Peshawar (KPK)
ABSTRACTObjective : To measure the rise of intraocular pressure immediate after Nd: YAG laser in posterior capsulotomy inpsuedophakic patients.Study design: prospective studyMaterial and method: A total number of 100 patients referred to the laser room of department of ophthalmology, LadyReading Hospital, Peshawar fulfilling the inclusion and exclusion criteria were included in this study. With Nd: YAG laserabout 4mm hole was created in the posterior capsule. Intraocular pressure was measured before and after laser withnon-contact air puff tonometer.Results: Out of 100 patients 69 (69%) were male and 31 (31%) were females. Their mean age was (52 years) rangingfrom 5 years to 70 years. Sixty three patients had normal or low intraocular pressure, 24% patients had rise of 2 – 3 mmHg in intraocular pressure. While 13 patients had a significantly raised intraocular pressure of more than 5 mm Hg onehour after YAG laser capsulotomy. The rise in intraocular pressure was noticed in patients after Nd: YAG laser capsulotomy.Conclusion: IOP rise was noticed, immediately after Nd: YAG laser capsulotomy. Hence it is advisable to start pressurelowering drugs before capsulotomy.
Original Article
Dr. Afzal Qadir
INTRODUCTIONPosterior capsule opacification is the commonest
complication of cataract surgery with an incidence ofbetween 10% to 50% by two years postoperatively. Itcauses reduction in visual acuity and contrastsensitivity by obstructing the view or by scattering thelight that is perceived by the patient as glare.2Interesthas been shown to prevent this visually disablingcomplication by introducing intraocular lenses ofdifferent material and different design or surgicalprocedure. Daniel Aron Rosa first described theprocedure of Nd: YAG laser capsulatomy.3Nd: YAGlaser is a photodisruptive laser, producing extremeamount of heat of about 10,000 Celsius along with anacoustic shock wave at the site being focused on.3 Itdisrupts the tissue and the property is used inophthalmology to perform YAG laser capsulatomyperipheral iridotomy in glaucoma and to cut vitreousbands.4
Standard treatment for posterior capsuleopacification consist of opening the posterior capsuleusing a Neodymium Yatrium-Aluminium-Garnet laser
(Nd:YAG laser).5Nd: YAG laser is widely available forposterior capsulotomy, and although complicationssuch as transient rise in intraocular pressure, uveitis,retinal detachment, and cystoid macular oedema,intraocular lens damage and IOL subluxation has beenreported.6-8The purpose of this study was to record anyrise of intraocular pressure immediate after YAG lasercapsulotomy.MATERIAL AND METHODS
This prospective study was conducted indepartment of ophthalmology PGMI, Leady ReadingHospital Peshawar, Khyber institute of OphthalmicMedical Sciences from January 2011 to June 2011 onehundred pseudophakic patients with posteriorcapsularopacification referred from consultant OPD forNd: YAG laser capsulotomy were included in thisstudy. Patients having other ocular diseases likeglaucoma, inflammatory diseases, and who hadundergone pars planavitrectomy were excluded fromthis study.Before capsulotomy all patient had athorough ophthalmic examination including bestcorrected visual acuity, slit lamp examination,gonioscopy, and intraocular pressure with non-contactair puff tonometer, the pupil was dilated with 1%tropicamide eye drops. A minimum energy of 3.4mj/shot was used to create a 3 – 4 mm hole in the posteriorcapsule.
The intraocular pressure was measured 1 hourafter laser. A rise in intraocular pressure of more than5mm Hg post laser capsulotomy was recorded asashaving raised intraocular pressure.

Ophthalmology Update Vol. 10. No. 3, July-September 2012 291
RESULTOut of 100 patients 69 (69%) were male and 31
(31%) were females. Their mean age was (52 years)ranging from 5 years to 70 years. Sixty three patientshave normal or low intraocular pressure, 24% patientshad rise of 2 – 3 mm Hg in intraocular pressure. While13 patients had a significantly raised intraocularpressure of more than 5 mm Hg one hour after YAGlaser capsulatomy.DISCUSSION
Cataract is the most common cause of blindnessworldwide, posterior capsularopacification (PCO) orsecondary cataract is an extremely common cause aswell.9opacification of the posterior capsule is thecommon time related complication of extra-capsularcataract extraction more frequently in children andyounger adults.10 In Pakistan it is possible for about 36%of patients.11 Posterior capsularopacification has notonly medical but social and economic implication overthe life of the patients’ family and society as a whole.12
The incidence of posterior capsularopacification (PCO)has been reported different in different studies. AppleDJ has noted the incidence of PCO up to 50% by thetwo years postoperatively.13 While other authors havereported the incidence of PCO up to 43% in five yearsduration after extra-capsular extraction, due to suchhigh incidence of PCO after cataract surgery differentmodalities and techniques have been developed andadopted to alter the incidence of the disease(sequaely).14
Capsular opacification started from continued
viability of lens epithelial cells remaining after removalof the nucleus and cortex.15With the recognition of therole of lens epithelial cells in PCO, a wide verity oftechnique have also been directed to remove residualcell during surgery. The fact that none of thesetechniques has been utilized as a routine surgicalprocedure reflect the difficulty in totally removing alllens epithelial cells. As a result of clinical failure of bothlens epithelial cells removal and pharmacologicalintervention to reduce PCO. Emphasis has been shiftedtowards IOL, its material and design, as a practicalsolution. Recent work worldwide strongly suggests thatlens implant design rather than lens material maybethe more important factor in the prevention of PCO. Arecent systematic study review based onCochranemethodology including 26 randomized controlled trialswith a follow up of at least 12 months showed that thePCO score was significantly lower with sharp-edgedIOL but did not different with 1 piece open lope IOLs.16
Neodymium YAG laser has become popular non-invasive technique of creating posterior capsulotomyin both psuedophakic and aphakic eyes with posteriorcapsularopacification. Nowadays PCO is treated withNd: YAGlaser which is safe and effective as out-patientdepartment procedure. Although Nd: YAG lasercapsulotomy is a widespread and popular approachfor the treatment of posterior capsule opacification ,some complication have been reported such as increaseintraocular pressure (IOP), hyphaema, cystoid macularedema, retinal detachment, endophthalmitis, anteriorvitreous opacification, posterior sub-laxation of IOL,IOL pitting. A transient rise in IOP after Nd; YAG lasercapsulotomy has been well documented.18
Although this IOP elevation, whichcharacteristically reaches a peak within the first threepostoperative hours, usually resolves without squally,it may lead to visual field loss and or loss of centralvision particularly in the eyes with pre-existingglaucomatous damage. In our study of 100 patients weincluded the rise in intraocular pressure one hour afterNd: YAG laser capsulotomy in eyes free from otherpathologies. Among them 69% were male and 31%female while similar study by Rafiq et al 80% of thepatient were male and 20% patient were female.19 WhileIOP is higher 13% in my study as compare to Richter etal.18
CONCLUSION:IOP rise was noticed, immediately after Nd:
YAG laser capsulotomy. Hence it is advisable to startpressure lowering drugs before capsulotomy.REFERENCES1) Hollick EJ, Spalton DS, Uresll PG, Pande MV. Lens epithelial
cell regression on the posterior capsule with differentintraocular lens materials. Br J ophthalmol (1998;82;1182-88).
2) Tan CH, Spalton DJ, Arden GB. Comparison of methods to
Table
IOP Number of Patient Percentage
Normal or low IOP 63 63%
Slightly rise IOP 24 24%
Significantly rise IOP 13 13%
Total 100 100%IOP: Intraocular Pressure
Gender Distributiuon
Frequency of Raised Intraocular Pressure after ND: YAG Laser Capsulotomy
292 Ophthalmology Update Vol. 10. No. 3, July-September 2012
assess visual impairment from glare and light scattering withposterior capsule opacification. J Cataract and refract surg.1998, 24: 1626-31.
3) Aron-Rosa D, Cohan HC and Arora JJ. The French use of apulsed PICO neodymium YAG laser in endo ocular surgery.In Wayne Marched; Adranees in ophthalmic laser therapy;Bermingham Alabama Aeseulapiuus publishing. 1998, P 11-7.
4) Majeed A, Bangash T, Muzzafar W, Durani O. Macularhaemorrhage : An unusual complication of Nd; YAG lasercapsulatomy. Pak J ophthalmol 1998; 14 (3) 118.
5) Aslam TM, Denlin H, Denlin B, use of ND; YAG lasercapsulatoy :survOPhthalmol 2003; 48; 594 – 612.
6) Winslomrl, Taylor BC, Retinal complications following YAGlaser capsulatomy ophthalmology 1985; 92: 785.
7) Holmeger RR, Marefat B. Intraocular pressure changes afterNeodymium: YAG laser capsulatomy. J cataract Refract surg1997; 23: 115 – 21.
8) Hu CY, Woung LC, Wang MC. Change in the area of laserposterior capsulatony. J cataract Refract sury 2001; 27: 537 –42.
9) Panday SK, Apple DJ, Wernevl, Maloof AJ, Milverton EJ.Posterior capsule opacification clinical studies and factorsfor prevention. Highlights of ophthalmology 2004; 32 (4) :14 – 20.
10) Evie JC, Harding pal, Hodge DO. Effect of intraocular lensdesign on neodymium m: YAG laser capsulatomy rate. Jcataract Refract surg 1998; 24 : 1239 – 42.
11) Dineen B, Bourne RR, Jado on Z, Shah SP, Khan MA, ForterA, Gilbert CE, Khan MD; Pakistan nation eye survey group.
Causes of blindness and visual impairment in Pakistan. ThePakistan national blindness and visual impairment survey.Br J ophthalmol 2007 Aug; 91 (8): 1005 – 1 pub jan 17.
12) Shaikh A, shaikh B, AJR, shaikh AZ. Prevelance of differentNd:YAG laser induced complication in the patient withsignificant posterior capsule opicification and theircorrelation with final duration after standard cataractsurgery. Int.Med. Med Scivol 12(1) Pd-012-017, January 2010.
13) Apple DJ,SolomonKD,Tetz MR. posterior capsuleopicificationsurvophthalmol 1992, 37:73-116.
14) Sundelin K, Sjostand J. posterior capsule opacification 5 yearafter extra capsular cataract extraction. J cataract Refract surg1999; 25:246-50.
15) M.MuhammadR.Kashif AH Anwar. Posterior capsuleopicification after PMMA and Hydrophobic Acrylic Intraocular Lens implication. Pak J Ophthalmol 2009, vol:25 No.4.
16) Buehl W, Findlo. Effect of Intraocular lens design on posteriorcapsule opacification . J cataract refract surg 2008;34: 1976-85.
17) Baratz KH, cook BE, Hodge DO. Probability of Nd-YAG lasercapsulotomy after cataract surgery in Olmted countMinnesota. Am J Ophthalmol 2001; 31:161-66.
18) Richter CU, Arzeno G, Pappal HR, Steinert RF, Publiafito C,Epstein D, Intraocular pressure elevation following Nd-YAGlaser posterior capsulotomy . Ophthalmology 1985; 92:636-40.
19) Rafiq M, Shah Z, Sethi S, Kundi N. Nd:YAG laser posteriorcapsulotomy& its complication. Ophthalmology updateVo:9; No:1 March 2011; 18-20.
Frequency of Raised Intraocular Pressure after ND: YAG Laser Capsulotomy

Ophthalmology Update Vol. 10. No. 3, July-September 2012 293
–––––––––––––––––––––––––––––––––––––––––––––––––––––1.Registrar Eye A ward, Department of Ophthalmology KhyberTeaching Hospital, Peshawar 2.Assistant Professor Khalifa GulNawaz Hospital, Bannu. 3.Senior Registrar Eye A ward, KhyberTeaching Hospital, Peshawar 4.Assistant Professor Khyber TeachingHospital, Peshawar. 5.6.Medical Officers, Department ofOphthalmology Hayatabad Medical Complex,Peshawar 7.Professor& Head of department of Ophthalmology, Khyber Teaching Hospital,Peshawar–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Dr. Saber Mohammad Flat No, 13 New. DoctorColony Khyber Teaching Hospital, PeshawarEmail> [email protected] Tel No. 0346-9155303–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: March ’2012 Accepted: June’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
INTRODUCTION:Congenital cataract is the most common cause of
treatable childhood blindness accounting for 5% to 20%of blindness in children worldwide. The prevalence ofblindness from cataract is higher, about 1 to 4 per 10,000children in developing countries.4In the developedworld, most of the causes of bilateral congenital cataractis idiopathic and about one third of cases are hereditary,without any systemic diseases.5, 6 Rare causes ofchildhood cataracts are metabolic disorders such asgalactosemia and hypocalcemia.
Unilateral congenital cataract is generally notassociated with systemic disease and is rarely
inherited.7 Rubella virus infection (TORCHES infection)occurring in pregnant women during the first trimesterof pregnancy may often result in the development ofcongenital rubella syndrome of the new born producingone or more severe congenital defects like congenitalcataract6 and commonly associated with mentalretardation. Pediatric cataract is always a challenge forthe ophthalmologist. It is not only the surgicalmanagement of the cataract but also the post op visualrehabilitation, which is an even bigger challenge. Inrecent years, lot of advances have been made in themanagement of pediatric cataracts in terms of surgicalmethods employed as well as the various means to treataphakia especially with intraocular lenses. In spite ofthis, the long term safety of intraocular lenses especiallyin a child less than one year of age is still uncertain8.However these advancements have made it possible totackle the problem of congenital cataract in a smoothway. In addition to the small size of the child’s eye,decreased scleral rigidity and increased tissue reactivityleading to excessive postoperative inflammation andcapsular opacification make pediatric IOL implantationparticularly challenging.MATERIALS AND METHODS:
65 cases of congenital cataract were included in
Audit of 65 Congenital Cataract Patientspresented to the Department of Ophthalmology
Khyber Teaching Hospital Peshawar
Saber Mohammad FCPS1, Sanaullah Khan, FCPS2 Zaman Shah FCPS,3
Tajamul Khan., FCPS4., Samina Karim FCPS5., Zakir Hussain FCPS6
Prof. Naimat ullah Khan Kundi FCPS,7
ABSTRACTObjectives: To point out age, sex distribution, laterality, surgical management and postoperative visual rehabilitation ofcongenital cataract patients presented to eye A ward Khyber Teaching Hospital Peshawar.MATERIAL & METHODSSetting: This was a retrospective study conducted on 65 patients of congenital cataract presented to the department ofclinical ophthalmology, Eye A ward Khyber Teaching Hospital Peshawar. Both sexes were included between the ages ofone month to 11 years. Pre-operatively, a detailed history including family history, past visual status and trauma weretaken. The workup included thorough systemic and local examination, visual acuity with or without best correction (whenpossible) was recorded. A complete silt lamp examination of the anterior segment was performed where possible. Posteriorsegment was assessed by direct and indirect ophthalmoscopy and ultrasonography. All patients gave informed consent.Surgery was performed under general anesthesia.Duration: Study duration was one-year from 01/06/2010 to 01/06/2011Sample size: Sixty five patients included in our study.Results: The surgical managements of each case were on individual basis and included lens aspiration (56.9%) and lensaspiration with IOL implantation (42.2%) while one patient refused surgery (1.53%). Post op visual rehabilitation wasmainly in the form of spectacles (62%), while intraocular lenses (IOL) were implanted in 38% of patients where appropriate.Conclusion: Congenital cataract is the most treatable cause of childhood blindness. Early detection and surgical treatmentfollowed by visual rehabilitation is very important.
Original Article
Dr.Saber
294 Ophthalmology Update Vol. 10. No. 3, July-September 2012
this retrospective study. Both the sexes were includedbetween the ages of one month to 11 years. Pre-operatively, a detailed history including family history,past visual status and trauma were taken. The workupincluded thorough systemic and local examination,visual acuity with or without best correction (whenpossible) was recorded. A complete slit lampexamination or examination under anesthesia (EUA)of the anterior and posterior segment was performedwhere possible. Posterior segment was assessed bydirect and indirect ophthalmoscopy and ultrasono-graphy. All patients gave informed consent. Surgerywas performed under general anesthesia. Pupils weredilated with 1% cyclopentolate and 2.5% phenylephrineeye drops preoperatively. All the patients undergoinglens aspiration without IOL implantation had aperipheral iridectomy. Vitrectomy was done in the caseswith posterior capsule rupturing and vitreous loss.RESULTS:
65 patients could be identified from the case notes,and the total number of eyes enrolled in this study was119 eyes. The number of patients between the age of 2-11 months were 23 (35.38%), 12 were male and 11 werefemale given in (Figure No, 1) while between 1-11years,total number of patients were 42 (64.61%), 26 were maleand 16 were female. (Figure No, 2). The number ofunilateral case were 11(17.8%) in which 7 were maleand 4 were female and the number of bilateral caseswere 54(83.0%) in which 31 were male and 23 werefemale shown in (Figure No, 3). In the surgicalmanagement, 37 (56.9%) eyes under-went simple lensaspiration with spectacles correction and 27 (42.2%)patients were implanted intraocular lens (IOL) and onepatient refused any surgical intervention shown in(Figure No, 4). Post op visual rehabilitation included37(56.9%) eyes treated with spectacles while 27(42.2%)eyes were treated with intraocular lenses implantation(Figure No, 5).
Figure 1. (No. of patients 23)
Figure 3.
Figure 1. (No. of patients 42)
Figure 4. (No. of patients 65)
DISCUSSION:There are an estimated 200,000 children blind
from cataract worldwide; 20,000 to 40,000 children withcongenital cataracts are born each year. In thedeveloping world there is a need to improve earlydetection and referral services and to establish centerswith expertise in the assessment, surgical treatment,
Audit of 65 Congenital Cataract Patients presented to the Department of Ophthalmology Khyber Teaching Hospital Peshawar

Ophthalmology Update Vol. 10. No. 3, July-September 2012 295
Figure 5.
and long term management of the child with cataract.9Ifwe compare the etiology of cataracts betweenindustrialized and developing countries, there is nodifference of etiology in case of bilateral cataracts.However in case of unilateral cataracts, it is mainlyidiopathic in industrialized countries where as indeveloping countries trauma is the leading cause ofunilateral cataracts. In our study, 23 patients werebetween the age of 2-11months and 42 patients werebetween 1- 11 years of age. In 23 patients of age 2-11months, 12 were male and 11 were female. In 42 patientsof age 1-11 years, 26 were male and 16 were female. Inour study, the number of bilateral and unilateralcataract were 54 (83%) and 11(17.8%) respectively,which is similar to the study conducted by OndracekO and Lokaj M.in 2003 in which 55 were bilateral and53 were unilateral in 108 patients1.
In our study, the maximum number of cases weredevelopmental 37(56.92%) followed congenital28(43.07%) which is similar, studied by Iqbal Z et al inwhich 60.30% were developmental and 13.70% werecongenital in 110 cases of pediatric cataracts.2 A childborn with cataracts has to fight both aphakia as well asamblyopia. Timing is very crucial for the managementof paediatric cataract.
In our study the protocol was to implant IOL atthe age of 2years or above which is different fromstudied by Sidky M.A et al in which they implantedIOL under 2years of age.3 Congenital cataractmanagement depend on the density of lens opacity andmust be removed as early as possible in order todevelop binocular vision.11 It is now about four decadeswhen scheie first introduced the surgical method of lensaspiration.12 It is still performed nowadays, howevernewer surgical techniques are practiced especially toretard the most dreaded post-op complication ofposterior capsule opacification in children. Some ofthese techniques with posterior continued curvilinear
capsulorhexis (PCCC), with or without anteriorvitrectomy.
In our study 37(56.9%) children eyes underwentplain lens aspiration with peripheral iridectomy, 27(42.2%) underwent lens aspiration with IOLimplantation while 01(1.53%) patient refused surgery.For the post-op visual rehabilitation, basically theophthalmologist has to choose between spectacles,contact lenses and IOL’s. Spectacles are usually usedfor bilateral aphakia. In case of IOL, a lot of work isbeing done especially in terms of material, which inturn hinders the process of PCO. IOL implantation inan infant’s eye is further confounded by the rapidgrowth of the eye during the first two years of life.13 Toavoid the complication of induced myopia in childrenwhich might warrant an IOL exchange in adult life, itis better to under correct a child younger than 2yearsby 20% while children between 2 and 8 years of ageshould be under corrected by 10%14. Out of the 65patient’s eyes, 37(56.9%) were treated with spectacles,27(42.2%) had IOL’s implantation while none of themwere given contact lens. Once the ophthalmologist hadtreated the cataract and rehabilitated the child in termsof vision, he still has to overcome the obstacles of post-op complications which range from posterior capsularopacification (PCO)15, papillary membrane13,16,17,aphakicglaucoma,18,19 strabismus,20 uveitis,8 IOLdecentration,21,22 retinal detachment,23and cystoidmacular oedema24.As this was a retrospective study wehad not followed the patients for the complications.CONCLUSION:
Early detection and surgical treatment followedby visual rehabilitation is very important to preventamblyopia. Congenital cataract is the most treatablecause of childhood blindness. The importance of regularfollow-ups must be stressed, with assessment andtreatment of posterior capsule opacification, glaucoma,refractive errors and amblyopia undertaken if goodvisual outcome is to be achieved.9
REFRENCES1. ONDRACEK O, LOKAJ M.Visual out come after congenital
cataract surgery. Long term clinical results.Scripta Medica(BRNO)-76(2):95-102, April 2003.
2. Iqbal Z et al. Management of paediatric cataract at Khyberteaching hospital.JPMI-Vol.17 (1):70-74.
3. Sidky M.A. et al.The outcome of congenital cataract surgeryin Kuwait. Saudi J of Ophthalmology (2011)25,295-299.
4. Foster A, Gilbert C, Rahi J.Epidemiology of cataract inchildhood: a global perspective. J Cataract Refract surg1997;23:601-604.
5. Bardelli AM, Lasorella G, Vanni M.Cngenital anddevelopmental cataracts and multimalformation syndromes.Ophthalmic Paediatr Genet 1989;10:293-298.
6. Merin S, Crawford Js.The etiology of congenital cataracts; asurvey of 386 cases. Can J Ophthalmol 1971;6:178-182.
7. Katow S. Rubella virus genome diagnosis during pregnancyand mechanism of congenital rubella Intervirology 1998;
Audit of 65 Congenital Cataract Patients presented to the Department of Ophthalmology Khyber Teaching Hospital Peshawar

296 Ophthalmology Update Vol. 10. No. 3, July-September 2012
41(4-5):163-9.8. Wilson-Holt N, Hing S, Taylor DS. Bilateral blinding uveitis
in a child after secondary intraocular lens implantation forunilateral congenital cataract. J Paediatr OphthalmolStrabismus 1991; 28:116.
9. Allen Foster. Epidemiology of cataract in childhood; A globeperspective. J Cataract refract Surg 1997; 23:601.
10. Shirable H. Visual functions following unilateral cataractsurgery. Am Orthopt j 1998; 48:97.
11. Tailor D. Amblyopia in bilateral infantile and juvenilecataract. Relationship To timing of treatment. TransOphthalmol Soc UK 1970; 99:170.
12. Sheie HG. Aspiration of congenital or soft cataracts: a newtechnique. Am J Ophthalmol 1960; 50:1048.
13. Sinskey RM, Amin PA, Lingua R. Cataract extraction andintraocular lens implantation in an infant with a monocularcongenital cataract. J cataract Refract Surg 1994; 20:647.
14. Elie Dahan. Choice of lens and diopteric power in paediatricpseudophakia, J cataract Refract Surg 1997; 23:618.
15. Apple DJ. Posterior capsular opacification. Surv Ophthalmol1992; 37:73.
16. Hiles DA. Watson BA. Complications of implant surgery inchildren. Am Intra-Ocular Implant Soc J 1979; 5:24.
17. Brady KM, Atkinson CS, Kilty LA, Hiles DA. Cataractsurgery and intraocular lens implantation in children. Am JOphthalmol 1995; 120:1.
18. Mills MD, Robb Rm. Glaucoma following childhood cataractsurgery. J Paediatr Ophthalmol Strabismus 1994; 31:355.
19. Tomey KF, Traverso CE. The glaucoma’s in aphakia andpseudophakia. Surv Ophthalmol 1991; 36:79.
20. Francois J. Late result of congenital cataract surgery,Ophthalmology 1979; 86:1586.
21. Buckley EG, Klombers LA, Seaber JH et al. Management ofthe posterior capsule during paediatric intraocularimplantation. An J Ophthalmol 1993; 115:722.
22. Vasvada A, Chauhan H. IOL implantation in congenitalcataracts. J Cataract Refract Surg 1994; 20:592.
23. Chrouseos GA, Parks MM, O’ Neill JF. Incidence of chronicglaucoma, retinal detachment and secondary membranesurgery in paediatric Aphakic patients. Ophthalmology 1984;91:1238.
24. Hoyt CS, Nickel B. Aphakic cystoid macular oedema;occurrence in infants and children after transpupillarylensectomy and anterior vitrectomy. Arch Ophthalmol 1982;100:746.
Audit of 65 Congenital Cataract Patients presented to the Department of Ophthalmology Khyber Teaching Hospital Peshawar
Where all of
Ophthalmologygoes to connect the trusted source of
information in visual sciences.Where evidence meets experience,
you will find‘Ophthalmology Update’

Ophthalmology Update Vol. 10. No. 3, July-September 2012 297
–––––––––––––––––––––––––––––––––––––––––––––––––––––*Islamic International Medical College, Pakistan Railways Hospital,Rawalpindi–––––––––––––––––––––––––––––––––––––––––––––––––––––1.2.Senior Registrars–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Dr. Sohail Zia, E-mail: [email protected]: 0321-5288182.–––––––––––––––––––––––––––––––––––––––––––––––––––––Received: Feb’2012 Accepted: May’2012–––––––––––––––––––––––––––––––––––––––––––––––––––––
Postoperative Wound Leakagein Sutured & Sutureless Corneal Incisions
after Phacoemulsification and Rigid IOL Implantation*
Sohail Zia FCPS1, Yasir Iqbal FCPS2
ABSTRACTBackground: Phacoemulsification is the gold standard cataract surgery these days. Foldable IOL is an expensive optionin our settings. Rigid IOL can be implanted after extending the incision. The purpose of this study is to compare the rateof wound leakage in two groups who underwent phacoemulsification with rigid IOL, sutured and unsutured corneal incision.The study would be important in decision making regarding the safety of the two techniques.Material and Methods: It was a non-randomized clinical intervention study conducted from January 2011 to December2011 in REDO Eye Hospital, Rawalpindi.75 patients in group A underwent phacoemulsification with sutured cornealincision and 75 patients in group B underwent phacoemulsification with sutureless corneal incision. Rigid IOL was implantedin all cases. Rate of wound leakage was noted in both groups at 24 hours and one week postoperatively.Results: Only one case in group B showed wound leakage at 24 hours postoperatively. No case of wound leakage wasseen in group A. Difference was statistically insignificant.Conclusion: Both sutured and sutureless corneal incisions after phacoemulsification with rigid IOL implantation are safetechniques regarding wound leakage. Sutureless corneal incision is less time consuming and cost effective. Suturedcorneal incision provides no additional benefit.
Original Article
INTRODUCTIONCataract is the world leading cause of avoidable
blindness affecting about 20 million people worldwide1.In Pakistan 52% of total blindness is due to cataract2.Cataract surgery is the leading ocular surgeryperformed these days3.
Many techniques are employed for cataractsurgery including conventional extracapsular cataractextraction and phacoemulsification4. Phacoemulsi-fication is the gold standard treatment and is almostuniversally used today5. Phacoemulsification providesminimal post operative complications and swift visualrehabilitation6. These advantages are mainly due tosmall incision usually about 3.2 mm.
In developed countries phacoemulsification isfollowed by foldable Intra Ocular Lens (IOL) but indeveloping countries like ours foldable IOL is not acommon practice in public sector due its high cost7.Therefore rigid PMMA IOL is implanted after enlargingthe initial incision to 5.5mm. Wound closure either bysimple hydration of incision or by applying a suturehas been reported in studies8,9. The purpose of applying
suture is to prevent wound leak leakage which can leadto endophthalmitis and other serious complications.8
In this study we report the findings of rate of postoperative wound leaks in patients undergoingphacoemulsification with rigid PMMA IOL with sutureand sutureless wound closure.MATERIAL AND METHODS
This clinical interventional study withconvenience (non-probability) sampling was conductedat Redo Eye Hospital, Rawalpindi from Jan 2011 to Dec2011. The patients were first allotted the hospitalregistration number before proceeding for examination.Complete eye examination was performed includingSnellen’s best corrected visual acuity, intraocularpressure measurement by Goldmann’s applanationtonometry, slit-lamp biomicroscopy , indirectophthalmoscopy and biometry for IOL powercalculation.
The study procedure and its aim were explainedto all the patients before beginning the treatment andthey had to sign an informed written consent form.
75 patients were selected for study in each group.Eyes with senile uncomplicated cataracts were selected.Dark brown cataracts were excluded because of alikelihood of converting to ECCE or prolongedphacoemulsification time. All eyes underwentuncomplicated phacoemulsification surgery with 3.25mm superior corneal incision. After completion ofphacoemulsification, incision was enlarged to 5.5 mmand a 5.5mm rigid PMMA IOL was implanted in thecapsular bag. Wound closure in Group A was done with
Dr. Sohail Zia
298 Ophthalmology Update Vol. 10. No. 3, July-September 2012
a single 10/0 monofilament nylon suture and in GroupB without suture with stromal hydration only.
Patients were followed up at 24 hours and 1 weekpostoperatively. Seidel’s test was performed at slit lampfor the presence of wound leakage. Seidel’s test includesapplication of a sterilized fluorescein strip moistenedwith topical anesthetic into the conjunctival sac and thenexamination of the wound using a cobalt blue filter. Iffluid appears to flow from the wound, that indicateswound leakage.
The data were entered and analyzed using SPSSsoftware version 13. The quantitative variables like age,was also presented as mean and standard deviation.Chi-square test was used to compare the rates of woundleak. A p value of < 0.005 was taken as significant. RESULTS
The study was completed in one year. Total of150 patients, 34 (45%) male and female 41(54%)underwent surgery with sutured corneal incision(group A) and 39(52%) men and 36(48%) femaleunderwent surgery without suture in (group B). Meanages of patients were 61.2 years and 63.3 years in groupsA and B, respectively. Following surgery, none of thepatients in group A showed wound leakage at 24 hoursand 1 week whereas only one case in group B showedleakage at 24 hours which was a sutured on the sameday. Statistical test was applied. However, the
Table-1Gender distribution Group A (N=75)
Male 34 (45%)
Female 41 (54%)
Table-2Gender distribution Group B (N=75)
Male 39 (52%)
Female 36 (48%)
Table-3 Mean Age (years)
Group A 61.2
Group B 63.3
Table-4Cases with wound leak (N=150)
24 hours 1st weekpostoperative postoperative
Group A(N=75) NIL NIL
Group B (N=75) 01(1.3%) NIL
difference was not statistically significant (p = 0.65).DISCUSSION
After thorough literature review we conclude thatthis is the first study in Pakistan to compare the ratesof postoperative wound leakage in patients undergoingphacoemulsification cataract surgery with sutured andsutureless corneal incisions, with rigid PMMA IOL. Wefound that there were no statistically significantdifferences in the rates of postoperative wound leakagein the two groups at 24 hours and one week. A studyhas been conducted by Chaudhary TA8 which comparesthe rate of wound leakage after phacoemulsificationwith foldable IOL. Another study done by Iftikhar S.Kiani SA,10 showed wound leakage in two cases ofphacoemulsification with implantation of rigid 6mmIOL without sutures. Our results are comparable withresults shown in above mentioned studies.
As foldable IOL are expensive option in oursettings, our study may have significant implications.For example, sutureless surgery is less time-consumingand cost effective. Surgically induced astigmatism,which increased with suture9 can be avoided, providingbetter and early uncorrected visual rehabilitation.CONCLUSION
Despite of small sample size and non-randomization we conclude that our results areencouraging for opting sutureless surgery as suturedsurgery gives no additional benefit. Multicenter studieswith larger sample size are recommended.REFERENCES1. Roodhooft J.M. Leading causes of blindness worldwide. Bull
Soc Belge Ophtalmol 2002; 283:19-25.2. Awan ZH, Mahar PS, Memon MS. Blindness and poverty.
Pak J Ophthalmol 2011; 27(3):165-70.3. Qazi ZA. Corneal endothelium tissue that demands respect
[editorial]. Pak J Ophthalmol 2003; 19:1-2.4. Snellingen T, Evans JR, Ravilla T, et al. Surgical interventions
for age-related cataract. Cochrane Database Syst Rev2002:CD001323.
5. Olali CA, Ahmed S, Gupta M. Surgical outcome followingbreach rhexis. Eur J Ophthalmol 2007; 17(4):565-70.
6. Pershing S, Kumar A. Phacoemulsification versusextracapsular cataract extraction? Where do we stand? CurrOpin Ophthalmol 2010; 22: 37-42.
7. Gogate PM, Deshpande M, Wormald RP.Is manual smallincision cataract surgery affordable in the developingcountries? A cost comparison with extracapsular cataractextraction.Br J Ophthalmol 2003; 87:843–6.
8. ChaudhryTA , Shahzad MH, Khan S, Ahmad K.Postoperative wound leak and anterior chamber reaction inpatients undergoing phacoemulsification cataract surgerywith sutured and sutureless corneal incisions.Pak JOphthalmol 2007 ; 23 (3):114-16.
9. Iqbal CJ, Gul R, Arshad MS, Hussain M. Comparative studyof post-operative astigmatism following phacoemulsificationwith sutured versus un-sutured wound. Pak J Med HealthSci 2011; 5(2):243-7.
10. Iftikhar S, Kiani SA. Sutureless Phacoemulsification withimplantation of 6mm PMMA IOLs. Pak J Ophthalmol 2004;20:74-6.
Postoperative Wound Leakage in Sutured & Sutureless Corneal Incisions after Phacoemulsification and Rigid IOL Implantation

Ophthalmology Update Vol. 10. No. 3, July-September 2012 299
–––––––––––––––––––––––––––––––––––––––––––––––––––––Correspondence: Dr.Syed S. Hasnain M.D.General Ophthalmologist560 W. Putnam Ave. Suite #6 Porterville, CA 93257.–––––––––––––––––––––––––––––––––––––––––––––––––––––Email: [email protected], California, USATel: 559.781.7482 Fax: 559.781.8446 Web: www.hasnaineye–––––––––––––––––––––––––––––––––––––––––––––––––––––
Unlikely, it is widely published that glaucomamay be a neurodegenerative disease such asAlzheimer’s, Parkinson’s, and ALS1, 2
. The reason,glaucoma is considered a neurodegenerative diseaseis due to unexplained death of neurons in the lateralgeniculate nucleus (LGN) and of the neurons in thevisual cortex occurring concurrently with the death ofthe retinal ganglion cells (RGCs). Based upon theforthcoming arguments, this article will attempt todemonstrate glaucoma not to be a disease with suchneuro-degenerative pathophysiology.
It is an established fact in glaucoma, that thearcuate and peripheral vision fibers are selectivelydestroyed first, whereas the central vision fibers remainuntil the end-stage of the disease. In other words, theRCGs are being destroyed in a specific sequence andin an orderly fashion in glaucoma.
On the other hand, in neurodegenerative diseaseslike Parkinson’s, Alzheimer’s or ALS, the degenerationof the neurons occurs randomlyand haphazardly— notfollowing any specific sequence as occurring inglaucoma. If glaucoma is a neurodegenerative disease,we face another dilemma: why, in glaucoma, doesneurodegeneration always start precisely first withthose RGCs which serve the peripheral vision and notoccur randomly? The random destruction of theneurons is characteristic of a neurodegenerative disease,as a result the course of such a disease varies in eachindividual. Therefore, this distinction alone should keepglaucoma distanced from the group of neuro-degenerative diseases.
I would like to mention briefly about history ofterm ‘cupping’ of the optic disc which seems to be the
core problem in glaucoma. The term cupping was givenby Heinrich Muller in 1856 and endorsed by themajority of the ophthalmologists of the time. It wasbelieved that the optic disc was being cupped orexcavated by the direct mechanical pressure of highIOP. However, there was one dissenter. In 1864, Dr.Dixon disagreed that cupping was caused by directeffect of raised IOP. He argued that if the mechanicalforce of high IOP was strong enough to cause cuppingof the disc, then the same force should have alsodisplaced the lens and iris forward as well. But hisopinion was turned down by another prominentophthalmologist, Sir William Bowman, and since thenthe term cupping has become synonymous withglaucoma. One hundred years later (1960s), weintroduced the term ‘cup-to-disc ratio’ which gavefurther credence to cupping theory.
I believe the term cupping was mistakenly given150 years ago which has misguided and put us on awrong path. We are deeply indoctrinated with the‘cupping disc’ paradigm and unless we replace it, wemay never discover the true pathogenesis of glaucoma.If cupping is indeed occurring, then I salute those whogave us this term by using their rudimentaryophthalmoscope (without electricity/battery) in theearly stages of ophthalmology.
Returning to the subject of Neuro-degeneration:why are the RGCs and neurons of the LGN beingdestroyed simultaneously in glaucoma? In order toanswer this question, we have to first replace thepresent cupping disc paradigm of glaucoma with a‘sinking disc’ paradigm. The phenomenon of cuppingimplies that the problem starts from the center of theoptic disc and extends peripherally. As we know, thecentral vision fibers originate closer to the disc and liesuperficial (closer to vitreous) and exit from the centralpart of the disc. In contrast, the peripheral vision fibersoriginate from the distant retina or farther from the opticdisc and lie deeper (closer to sclera) and exit closer to
Is Glaucoma a Neurodegenerative Disease?Could it be a mechanical problem and
not a neurodegenerative disease?
Syed S. Hasnain M.D.General Ophthalmologist, California &
Abbas S. HasnainDr Syed S.Hasnain
Abbas S.Hasnain
Current Research

300 Ophthalmology Update Vol. 10. No. 3, July-September 2012
the edge of the scleral opening. If cupping wasoccurring, then the central vision fibers should bedestroyed first, and peripheral vision fibers last, butthe opposite is occurring in glaucoma.
Now the further question arises as to why theperipheral fibers being destroyed first in glaucoma. Toanswer this, I hypothesize that the optic disc may besinking 3, 4, not cupping in glaucoma. Due to sinking ofthe disc, the prelaminar nerve fibers, prior to their entryin the lamina, are being stretched as one end is attachedto the RGC and the other end anchored in the sinkingoptic disc and thus ultimately severed against thescleral edge. Since the peripheral nerve fibers lie deeperand exit closer to the scleral edge, the peripheral fiberswould be the first to be affected and severed whereasthe central fibers later if sinking of the disc is occurring.This is exactly what is revealed by glaucomatous visualfields. Furthermore, severing of the axons would resultin retrograde degeneration of the RGC and Walleriandegeneration of the distal axon leading to the death ofthe neurons of the LGN. Wallerian degeneration mayexplain the death of the neurons in the LGN and alsoin the visual cortex. Sinking of the disc would becomeself-propagated due to progressive severance of 360degrees of nerve fibers which also provide anchorageto the disc as roots do to a tree. The process of sinkingdisc would continue until all the nerve fibers are cutagainst the scleral edge.
Since I have proposed that nerve fibers are beingsevered, not atrophied in glaucoma: Do we have anyevidence for it? Before we discuss this issue I wouldlike to define the atrophy of an organ. Atrophy isdefined as an abnormal decrease in size or mass of adeveloped organ or a tissue due to disease. Atrophicorgans though shrunk in mass are normally visible anddon’t disappear unless the involved tissue is very smalland has atrophied to microscopic level. On the otherhand, severance is simply the cutting of an organ ortissue leading to its immediate total disappearance. Anexample would be whether the leg is atrophied due tostroke or severed (amputated) due to gangrene. It willbe important to keep this distinction in mind for ensuingdiscussion whether the nerve fibers are being atrophiedor severed in glaucoma.
Returning to the evidence for severing of the nervefiber: Although we may never see the actual processof severing of the nerve fibers, we may conclude thisby deductive reasoning of the events taking place inglaucomatous disc. The continuous severing of thenerve fibers is supported by the phenomenon ofprogressive thinning of the RNFL as observed on opticalcoherence tomography (OCT). The end-stage histologyof glaucomatous disc resembles an empty bean-pot. Instudying the histology of the bean-pot; its opening
appears to be that of scleral opening; its dilated belly isformed by dura mater and its base composed of necrotictissue. Interestingly, the bean-pot appears quite hugecompared to the size of original disc. Is this large bean-pot really a deeply cupped disc (lamina)? Is the laminaso distensible that its excavation has assumed the shapeof a large bean-pot? If so, then the lamina should beforming the walls of the bean-pot, if not, then wheredid the lamina and atrophied nerve fibers disappear?Why don’t we see atrophied nerve fibers in bean-potas we see in the histology of optic atrophy such as dueto multiple sclerosis? I believe the bean-pot is not adeeply cupped disc. The empty bean-pot appears to bethe left over area which once housed the disc. Mostlikely, the lamina is lying at the bottom after all thenerve fibers have been cut and disappeared. Thus, theend-stage glaucomatous disc resembling a bean-pot canonly be explained by severance, not due to atrophy ofthe nerve fibers
In studying the optic atrophy caused by multiplesclerosis or other conditions, the atrophic discs in theseconditions are flat (non-excavated). There is neithersloping/kinking of the blood vessels at the disc marginnor excavation of the disc indicating that flat atrophicdiscs are not associated with sinking. Since these discsare not sinking, there is no severing of the nerve fibersand thus no excavation is occurring in these conditions.The histology of the flat disc atrophy reveals shrunkenand collapsed nerve fibers, but no empty bean-pot asin glaucoma. Therefore, histologically, flat disc atrophyand glaucomatous disc are distinctly different. Inconclusion, the nerve fibers are being atrophied in flatdisc atrophy whereas the nerve fibers are severed inglaucomatous disc.
Regarding arcuate field defects: How is it possiblethat raised IOP or neurodegeneration or any otherpathology would cause the degeneration only of thesuperior and inferior arcuate fibers or their RGCs solely,leaving others unscathed in the early stages ofglaucoma? The severing, not atrophy, of the nerve fibersmay explain the sharply defined arcuate field defectsoccurring in the early stages of glaucoma. Due toinherent temporal tilt of the optic disc, the entire groupof temporal fibers (macular, sup., and inf. arcuate) arebeing stretched and severed. However, the superiorand inferior arcuate fibers being fewer in numbercompared to the macular fibers will be depleted earlier,resulting in arcuate fielddefects/ring scotoma. Thewedge shaped defects in retina which sometime we seein glaucoma patients are empty spaces created by theseverance and thus disappearance of the arcuate nervefibers, not due to their atrophy. We do not observesuch empty gaps in flat disc atrophy conditions suchas due to multiple sclerosis and other conditions.
Is Glaucoma a Neurodegenerative Disease? Could it be a mechanical problem and not a neurodegenerative disease?

Ophthalmology Update Vol. 10. No. 3, July-September 2012 301
The vertical enlargement of the physiological cupmay be due to severance and depletion of the sup. andinf. arcuate fibers which occurs in early stages ofglaucoma. The enlarged vertical cup/disc ratio may notbe a risk factor but may be representing cases in whichglaucoma has already been initiated. Otherwise, howdo we explain that vertical, and not the horizontal cup/disc ratio, is a risk factor for glaucoma? Severing of themacular fibers occurring concurrently with the sup.andinf. arcuate fibers from the very early stages ofglaucoma may explain the thinning of the macularganglion cell complex as observed on OCT. There aretwo events which appear to be taking place inglaucoma. First, the sinking of the disc, second, thesevering of the nerve fibers as a result of sinking disc,the severance of the nerve fibers and excavation of thedisc are unique features of glaucoma. In view of theabove rationale, chronic glaucoma may not be an opticdisc neuropathy but an optic disc axotomy.
So, do we have any scientific evidence of theSinking Disc? I believe we do.
First, the photographs of the glaucomatous opticdiscs vividly reveal sloping and kinking of the bloodvessels at the disc margin prior to any change in thecontour of the physiological cup. This suggests that theoptic disc may be sinking, not cupping in glaucoma.The physiological cup may not be truly enlarging, butinstead, disintegrating due to severance of the nervefibers. Second, the new enhanced imaging techniqueof the optic disc (EDI-SD-OCT) has enabled us tovisualize the deeper structures in the scleral canal wellbeyond the entire width of the lamina cribrosa whichwas previously not possible with standard SD-OCT.Therefore, EDI technique has opened a new chapter andprovided us with very valuable information of the
glaucomatous disc. EDI of the glaucomatous optic discin vivo has shown the posterior migration of the laminacribrosa from the very early stages of glaucoma as farback as pia mater or in other words total slidingoutward of the lamina from the scleral opening 5,6,7,8.This is very significant discovery as it suggests thatlamina (optic disc) is detachable from the scleral walland is able to slide posteriorly (sink) in the scleral canal.If the lamina is detachable from the scleral wall, thenhow can a loose and rigid lamina cribrosa also becomecupped at the same time? EDI findings support thephenomenon of sinking, not cupping of the disc. If true,then chronic glaucoma may be a mechanical problem,a herniation of the disc, not a neurodegenerativedisease.REFERENCES: 1. Levin LA, Peeples( February 2006) “History of
neuroprotection and rationale as a therapy for glaucoma”Am J Manag Care 14; S11-4.
2. Osborn NN, et al (August 1999) “Ganglion cell death inglaucoma; what do we reall know” Br JOphthalmol83(8):980-6
3. Hasnain SS. Optic Disc may be Sinking in Chronic glaucoma.Ophthalmology Update. Oct-Dec. 2010; 8 (4); 22-28
4. Hasnain SS. Scleral edge, not optic disc or retina is theprimary site of injury in chronic glaucoma. MedicalHypothesis 2006; 67(6) ;1320-1325
5. Anderson, DR Probing the Floor of the Optic Nerve Head inGlaucoma Ophthalmology 2012;119:1-2
6. Yang H. et al. Posterior(outward) migration of the laminacribrosa and early cupping in monkey experimentalglaucoma. Invest Ophthalmol Vis Sci 2011;52:7109-21
7. Yang H. Optic Nerve Head (ONH) Lamina Cribrosa InsertionMigration andPialization in Early Non-Human PrimateExperimental Glaucoma. Poster Presentation ARVO meetingMay 03, 2010.
8. Park SC et al. In-vivo, 3-dimentional imaging of the laminacribrosa horizontal central ridge in normals and laminacribrosa deformation in glaucoma. Invest.Ophthalmol Vis Sci2011;52:3063
Is Glaucoma a Neurodegenerative Disease? Could it be a mechanical problem and not a neurodegenerative disease?

302 Ophthalmology Update Vol. 10. No. 3, July-September 2012
Current Research
Glaucoma may Involve the entire Visual Pathway,not just the Eye
Elma Chang, MD, & Jeffrey Goldberg, MD, PhD,Bascom Palmer Eye Institute
University of Miami Miller School of Medicine, Florida USA.Prof. Robert Weinreb, MD,
Chairman, Department of OphthalmologyDirector, Shiley Eye Center, University of California, San Diego, USA.
Syed S. Hasnain M.D.General Ophthalmologist ,California, USA
Edited by: Dr. Rashad Qamar Bahawalpur(on line)
Dr. Chang Dr Goldberg
Glaucoma, long held to be a disease primarily ofelevated intraocular pressure, in reality may be adisease primarily of neuro-degeneration. In an articlepublished online February 18 in Ophthalmology, ElmaChang, present a view of glaucoma focused on thedegeneration of retinal ganglion cells (RGCs) and theiraxons in the optic nerve, with an eye toward potentialneuroprotective, neuroregenerative, and neuro-enhancing strategies.
Dr. Elma ChangAll glaucoma treatments to date have been aimed atlowering the risk factor of elevated intraocular pressure,which works well in most patients, especially when thediagnosis is made early in the disease. However, Dr.Goldberg expressed “Fundamentally, the disease isn’tthe pressure. It’s the susceptibility to the pressure, andthat’s what we don’t understand.” For example, onepatient may get into trouble at a given pressure, butanother will not. “With progress in understanding that,we can bring what we’ve learned into new treatmentsthat have nothing to do with the pressure, but havesomething to do with the underlying susceptibility,”Dr. Goldberg predicted.
There are myriad pathophysiologic mechanismsto explore, including glutamate excito-toxicity, reactiveoxygen species, vascular effects and ischemia, defectiveaxonal transport, glial dysfunction, loss of neurotrophicfactors, cell survival, and apoptotic mechanisms.Unraveling these intertwined factors may lead totherapies that provide neuroprotection, neuro-enhancement (improved functioning of neurons), andeven neuroregeneration.Mechanisms of Retinal Ganglion Cells (RGC) Damageand Death:
In addition to the observable structural damageat the optic nerve head, glaucoma leads to changes inthe central visual pathway from the retina to the brain’slateral geniculate nucleus and the visual cortex. Theprimary lesion is found in the axons in the optic nerve.“It may then activate additional degeneration processesin the retina and in the brain, but the progression of thedisease has to be happening in the optic nerve head,”Dr. Goldberg explained. Therefore, the spread of RGCdamage does not propagate in the retina, but occursaccording to the distribution of RGC axons in the opticnerve. Adjacent RGC cell bodies in the retina may thushave different fates.
The authors discussed several mechanisms bywhich RGC cells may die in glaucoma. For example,acute and chronic ischemia from vasospasm, defectivevascular regulation, or microvascular compression atthe lamina cribrosa may limit perfusion of the opticnerve head, resulting in metabolic imbalances andoxidative stress. Treatments including antioxidants andanti-vasospastic drugs such as calcium channel blockershave been studied.
Another possibility is that excite-toxicity fromcompounds such as glutamate released from dying cellsmay activate N-methyl-D-aspartate (NMDA)-sensitiveglutamate channels, causing deleterious rises inintracellular calcium as well as other harmful pathwaysin adjacent neurons or other functionally supportivecells. Wherever the harm occurs, bystander RGCsultimately take the hit.
Finally, increased intraocular pressure that ismechanically deforming the optic nerve head or causingmetabolic disruptions may lead to defective axonaltransport. “Axonal cargoes” normally shuttle up anddown the axon. These include neurotrophic survival

Ophthalmology Update Vol. 10. No. 3, July-September 2012 303
factors and growth signals, such as brain-derivedneurotrophic factor. RGCs may also become lessresponsive to these signals once they are injured, andendoplasmic reticulum stress may occur fromabnormally folded proteins resulting from othermetabolic defects. Whatever the pathophysiologicinsults to the RGCs, their final common pathway isapoptosis: programmed cell death with degradation ofintracellular components and eventual phagocyticclean-up. Better understanding of these processes maytherefore lead to anti-apoptotic therapies “independentof what the initiating factors are,” Dr. Goldbergpredicted.
Pressure to find Treatments not focused on Pressure:
Dr. Jeffrey GoldbergDr. Goldberg said he is focusing on translating
knowledge into new treatment approaches “that don’thave anything to do with pressure but, rather,...withkeeping the cells in the eye and optic nerve functioningat full capacity and giving them a boost and protectingthem from dying.” In this regard, treatments cangenerally be considered neuroprotective, neuro-regenerative, and neuro-enhancing.
During development, the retina and optic nerveare an outgrowth of the brain, so these organs sharemany properties with the rest of the central nervoussystem, such as a lack of a regenerative response undernormal circumstances. “We know fundamentally that[glaucoma is] a neurodegeneration like the rest of theneurodegenerative diseases. It stretches across multipleparts of the brain,” Dr. Goldberg said. Therefore, manyapproaches currently used in other neurodegenerativeconditions may also have potential in glaucoma.
Neuroprotection focuses on preventing the deathof neurons and maintaining their function. Oneexample is the use of memantine, which is approvedfor the treatment of the symptoms of Alzheimer’sdisease. Memantine is an NMDA antagonist and blocksglutamate excitotoxicity, and animal models haveshown that it protects against RGC loss. In a clinicaltrial in glaucoma, however, it failed to meet its primaryefficacy endpoint, the authors note. Other approacheshave targeted alpha-adrenergic receptors, inhibition ofnitric oxide synthesis, immune modulation, and the useof traditional neurotrophic factors. Various methods ofthe inhibition of caspases, enzymes that mediateapoptosis, are in clinical trials.
Another potential therapy, optic nerve axonregeneration, aims at remediating long-standing insultsto the nerve. Glial cells release molecules that stop RGCaxons from growing, and inhibiting these signals is oneapproach to regeneration. Targeted gene therapy,
including modulating transcription factors, is another.Many growth control pathways are potential targetsfor modulation by genetic, immune, small molecule,and electrical means. Small surgical manipulations maystimulate the release of prosurvival and progrowthfactors. Coaxing stem cells to differentiate into RGCsand make proper connections may be a long way off,but in the nearer term, they may hold promise assources of beneficial chemical mediators.
Neuroe nhancement may be a more realistic goalin the short run compared with neuro-regeneration.Neuroenhancement in glaucoma refers to short-termimprovements in RGC function, similar to the effectsof acetyl cholinesterase inhibitors and memantine inAlzheimer’s disease. Somewhere between cell injuryand cell death, there may be opportunity to improvecell function. Electrophysiologic testing has alreadyshown reversible dysfunction after acute lowering ofintraocular pressure in glaucoma, especially early inthe disease.
Beyond pressure-lowering treatments, neuro-trophic factors may improve RGC function. Smallmolecules involved in the production of membranelipids have shown some positive effects. Electricalstimulation may be another way to protect RGCs andenhance their function. The RGCs die if their electricalactivity is blocked with tetrodotoxin, but electricalactivity enhances RGC survival both in vitro and invivo. A contact lens electrode has promoted RGCsurvival after optic nerve injury in an animal model.
The Barrier for TestingA large remaining challenge is how to test new
therapies. At this time, the second endpoints that theUS Food and Drug Administration will accept forglaucoma therapy trials are the lowering of intraocularpressure and visual field testing. “Glaucoma tends tobe a slow neurodegeneration,” Dr. Goldberg noted, andhalf of RGCs may be lost before there are changes invisual field testing, which is a relatively insensitiveendpoint.
Therefore, a major area of research is finding anddefining other biomarkers of disease progression “togive us outcomes that can be measured in a shorterterm, and allow these trials to proceed in a more realisticand affordable fashion,” he said. Some possibilities arephysiologic measures such as pattern electroretino-grams and structural measurement techniques such asretinal stereo photography, confocal scanning lasertomography, scanning laser polarimetry, and opticalcoherence tomography. These modalities are all moreobjective than visual field testing, but even with them,it may take years to confirm the efficacy of candidateneuroprotective drugs.
Glaucoma may Involve the Entire Visual Pathway – Not just Eye

304 Ophthalmology Update Vol. 10. No. 3, July-September 2012
Showing neuroenhancement may be somethingless of a challenge. “If we have a drug that acutelyimproves visual function, which never happens in thenatural course of glaucoma, it might be something thatwe could measure very quickly and easily in patients,which would facilitate bringing treatments to clinicaluse”.
Given the time frame and the barriers to clinicaltesting, the great variety of possible pathophysiologicmechanisms, and the wide array of potential targetsand means of hitting them, Dr. Goldberg says there isstill a message of hope in viewing glaucoma as asusceptibility of RGCs to neurodegeneration. “We’regoing to wait to see when the dust settles which if anyof these new approaches ends up working and reallyhelping patients”. “But we’re starting to realize someof the hope that a better understanding of the diseasecan lead us to new therapies.”
Prof. Robert Weinreb.He extended the discussion beyond RGCs, saying
that the damage seen in glaucoma reaches into thevisual pathways of the brain — a subject that he hasbeen investigating for 15 years. “the axons are dying,then it’s likely that the cells that they connect to mightalso be deprived of electrical and chemical signals andwould not be healthy”. His research in non humanprimates found loss of neurons in the visual pathwayin the brainstem and in the visual cortex.
”This could potentially be a problem withneuroprotection, too”. “It could potentially be anotherbarrier because you might protect the retinal ganglioncells, but if the neurodegenerative process has alreadybeen ongoing, by protecting the ganglion cells or evenregrowing the ganglion cells you might not be affectingthe relay neurons, the neurons that are within thecentral visual pathways.” He cautioned that this lineof reasoning is still speculative, but that it brings up anissue of whether one could restore vision with an eyedrop or an intravitreal injection if there is secondaryneurodegeneration that is already occurring in thevisual pathways. “Is it possible you might need a pillthat influences the neurons in the eye, as well as in theentire visual pathway?” he asked.
Going even further, Dr. Weinreb stated thatglaucoma is not just a disease of the eye but also of thecentral nervous system. With 60 to 80 million patientsworldwide, “you can make the case that it’s probablythe most prevalent neurodegenerative disease of all,”
he said, and although elevated intraocular pressuremay lead to glaucoma, “It’s entirely plausible to methat there’s a subset of glaucomas where the initiationmight be somewhere else in the visual pathway,” whichis a controversial and speculative point, he admitted.
He lauded Dr. Goldberg for talking aboutglaucoma as a collection of conditions, rather than asingle disease or phenotype, “but it appears to be a largegroup of different conditions with a final commonpathway that has a phenotype with characteristicchanges” in the optic nerve and the visual field.
Whereas Dr. Goldberg pinpointed the RGCs as acentral target in glaucoma, Dr. Weinreb saidsurrounding cell types, such as astrocytes and retinalamacrine cells, also probably have a role, “and thereare people who have hypothesized that the primarydamage might be to those cells, and then the retinalganglion cell is a bystander that gets injured in thecourse of the primary cell getting injured.”
Dr. S.S. HasnainResearchers have been speculating about
glaucoma, being a neurodegenerative disease for a longtime and some have even suggested that glaucomastarts in the midbrain. In my humble opinion we havefailed in understanding glaucoma because we aredeeply embedded in wrong paradigm of “cuppingdisc”which was mistakenly given 150 years ago. Theterm “cupping” was given by Heinrich Muller in 1856(Duke-Elder) and since then the term cupping hasbecome synonymous with glaucoma. I believe, unlesswe abandon the ‘cupping disc’ paradigm we may neverdiscover the true pathogenesis of glaucoma. If ‘cupping’is indeed taking place, then I salute those who gave usthe term ‘cupping’ by using their rudimentaryophthalmoscope devoid of electricity in the early stagesof ophthalmology.
Interestingly, even though the researchers aretalking about true pathogenesis of glaucoma being aneurodegenerative disease, they still don’t seem toabandon the terms “cupping” and cup/disc ratio. Inmy response in the article “Is glaucoma aneurodegenerative disease” you may agree with myhypothesis that chronic glaucoma may not be an opticdisc neuropathy but an optic disc axotomy with astrong scientific evidence of sinking disc,thusdiscovering the true pathogenesis and correcttreatment of glaucoma.
Glaucoma may Involve the Entire Visual Pathway – Not just Eye

Ophthalmology Update Vol. 10. No. 3, July-September 2012 305
Ophthalmology Notebook
News, Views, and Events
Letter to the EditorDear Prof. Durrani,
With great interest I have read the latest issue ofOphthalmology Update covering a wide spectrum oftopics, including central serious chorio-retinopathy,clinical usage of Povidone-iodine. I personally use1.25% solution for Bacterial Keratitis. I am veryimpressed by your hard work as an Editor-in-Chief tokeep the high level of publications, and really thecontents of Journal entirely reflects its name. I am veryimpressed by your Editorial on the Over-indulgenceof Computer. You have highlighted extremely updatedtopic. I agree with you entirely.
You have also highlighted the cutting edge ofmodern reality and evidenced the current problem. Onemore time reading your journal confirms my feelingwhen I have acquainted with it that the contents ofjournal entirely reflects the largest scope of problems. Iimagine your hard and fruitful work to keep this highlevel.
Thank you very much for your kind words andpresentation of my work to the readers. Hoping thatmy second paper also meets your requirements.
May I take this opportunity of wishing you all thevery best and prosperity in all spheres of your activityincluding exciting scientific journal under yourEditorship.
I have just finished my second paper and as Ipromised I am sending it to you hoping that it meetsyour requirements, reflecting the cutting edgeachievements in ophthalmology, that is why my newpaper contains the latest findings on the matter.Wising you further fruitful work, prosperity and allthe very best,with warmest regards.
Prof. Marianne ShahsuvrayanMD, Ph.D, D.Sc
Professor of OphthalmologyRepublic of Armenia
–––––––––––––––––––
Dear Prof Durrani
I really appreciate the new crisp Ophthal-mology Update copy, handed over to me by a drugcompany (Jan-March’2012 issue). I had seen previousissues and have always appreciated. I have now, seenthis new type of format of big size for the first time.The articles which I saw are of really good quality. Ipay my heartiest congratulations to you and your teamespecially Dr. Jahanzeb Durrani for this achievement. Ifully understand the amount of hard work it needs tokeep up the standard. Also I must update about myself.As you know CPSP introduced its second fellowshipin Vitreo-retinal surgery and I am the first candidate topass this fellowship in VR in December 2011. It was areally hard task. Allah, The Beneficial helped me topass this. I thank you for sharing the scientific materialwith the Ophthalmic community by publishing thisjournal.
Dr. Kashif Iqbal, FCPS FRCS.(Ed)Fellowship in Vitreoretinal Ophthalmology (CPSP)
Consultant Ophthalmologist LRBT Lahore
Dear Dr. Kahif Iqbal!
Please accept heartiest congratulations on successfullycompleting the Fellowship in Vitreo-retinal surgery. We donot have many V-R surgeons in the country and it is highlycreditable of you to be the one to qualify the examinationwith flying colors. It certainly speaks volumes of yourprofessional dedication. May Allah bless you enough strengthand vigor to continue serving the profession andameliorating the ailing humanity to your best. Amin! Themanagement of Ophthalmology Update especially Dr.Jahanzeb joins me in congratulating you on your creditableachievement……. Chief Editor)
–––––––––––––––––––

306 Ophthalmology Update Vol. 10. No. 3, July-September 2012
To
Prof. Dr. Nadeem Qureshi., FCPSHead of Vitreo-Retinal Unit,Al-Shifa Trust Eye Hospital,RAWALPINDI
CONGRATULATIONS
My Dear Prof. Nadeem,
Please accept heartiest congratulations from themanagement and editorial staff of OphthalmologyUpdate on the award of a highest and prestigiousscientific award of gold medal by the OphthalmologicalSociety of Pakistan, as an outstanding Vitreo-RetinalSurgeon. You have, indeed, a brilliant record ofacademic eminence in the pursuit of knowledge in yourfield which speaks volumes of your dedication anddevotion to achieve professional excellence and aprestigious place in the comity of veneratedacademicians.
May Allah bless you enough strength and vigorto continue serving the profession and ameliorating thesufferings of ailing humanity to your best. Amin! wishesthe happiest moments in future life.
Prof. Dr. M. Yasin Khan DurraniEditor in Chief
–––––––––––––––––––
News, Views, Letters & Events
Carrot – A Sight Booster?Zainab Inam, Nowshera (KPK)
According to popular wisdom Carrot has longbeen used for its efficacy in improving eye sight, butscientifically speaking is it really a sight booster or justa lore?
Carrot is found in Pakistan in fantastic colors of pinkishred, purple and yellowish pink (popularly known as ‘CheeniGajar’ China Carrot) used in popular Chinese dishes andPakistani cuisine- a most delicious biryani. Carrot belongs tothe family of Umbelliferae with coriander, parsley and cuminas its members. The vegetable has long been touted for itsefficacy in improving eye sight, but is it really a sight boosteras popular wisdom asserts and believed by different systemsof practicing medicine. The purported link between carrotand markedly acute vision, is it a matter of scientific wisdomor mere a lore?
Carrot contains 87% of water and it is rich in fiber, whichprotects against the cancer of colon. It has high content ofluxuriously rich beta-carotene, Vitamin-B, calcium, iron andvitamin-C. It is also very effective in the fight againstcardiovascular diseases, cataract and macular degeneration.It promotes skin complexion and maintains its elasticity byelimination pimples. Hippocrates described the use of carrotseeds as an oral contraceptive. Quite interestingly, the anti-laxative property of carrots has also helped Greek soldierssurvived the prolonged hide out inside the Trojan horse. HenryFord convinced that it held the secret of longevity.
Because it contains more sugar than any othervegetable, carrots have been used in sweet cakes ‘thePassion Cake’ popularly known as Gajar ka halwa, whichhas now become a standard dessert in winter so much sopeople in California hold exclusive February Festival and relishby promoting the consumption of carrots. The extract of purplecarrot, popularly known a kalonji is used over this sub-continent as a carminative against digestive ailments.Interestingly, in 2010, a $25 million marketing campaign waslaunched to promote baby-cut carrots as an alternative to junkfoods.
During the worldwar II, soldiers were chanting ‘a carrota day keeps the black out at bay’. Walt Disney in his famousmovie “Dr. Carrot” people were lure into belief that the carrotroots helped British Pilots develop the ‘cat eyes’ required tosee Nazi bombers attacking at night, a bit more vision-relatedcachet. Even more amusingly, carrots can not only be eaten,but also be played. Thanks to Flutenveg, a group of talentedAustralian individuals who make musical instruments out ofcarrots and thus promote health dietary habits. Making carrotsall the more distinct is the latest endeavor of the astronautswho promised to make the ability to grow the vitamin-A richcarrots in space in order to incorporate natural antioxidantsinto their diet to combat the effects of radiation. Moreover,scientists now believe that bio-fuels, harnessed from thecarrots will be able to supplement our energy demands whenthe oil runs out.
(Note: Zainab Inam is a matric student, daughter of a notedophthalmologist Dr. Inamul Haq Khan from Nowshera. Sheis a versatile writer on various subjects. We haverequested her to feature vision-related articles for theinterest of our readers…… Editor)
More on LineRead the latest
research inOphthalmologyat the following
website,www.ophthalmologyupdate.com