
Antisecretory effects of three omeprazole regimens for maintenance treatment in duodenal ulcer
10
Digestive Diseases and Sciences, I/ol. 39, No. 7 (July 1994), pp. 1473-1482 Antisecretory Effects of Three Omeprazole Regimens for Maintenance Treatment in Duodenal Ulcer VINCENZO SAVARINO, MD, GIUSEPPE SANDRO MELA, MD, PATRIZIA ZENTILIN, MD, PATRIZIA CUTELA, MD, MARIA RAFFAELLA MELE, MD, DANIELE PERILLI, MD, AMBROGIO VASSALLO, MD, ADRIANA ZAMBOTTI, MD, CARLO MANSI, MD, and GUIDO CELLE, MD This study was carried out to assess the antisecretory effects and their possible changes over time of three different dose regimens of omeprazole that could be proposed for maintenance treatment in duodenal ulcer. Forty-five patients with endoscopically proven duodenal ulcer were studied by means of 24-hr gastric pH-metry both in basal conditions and on the fifth day of acute treatment with omeprazole 20 mg in the morning. Ulcers healed after four weeks (in three cases after eight weeks) and afterwards, 15 patients were randomized to receive orally at 0800 hr in single-blind fashion omeprazole 10 mg daily (group A), 15 to receive omeprazole 40 mg on Saturday and Sunday followed by a five-day period without medication (group B), and 15 to receive omeprazole 20 mg every other day (group C) for up to three months. On the 20th and 80th days of these maintenance treatments 24-hr gastric pH-metry was repeated to assess the antisecretory effectiveness of each regimen over a two-month period. In patients of group B these tests began at 1700 hr on Friday, the last of five days off treatment, and in those of group C at 1700 hr of the day off medication. All three dose regimens of omeprazole were able to raise pH values significantly (P < 0.01-0.001) compared to basal levels. Omeprazole 20 mg every other day was more effective (P < 0.01) than omeprazole 40 mg weekend, but did not differ significantly from omeprazole 10 mg daily. The durations of acid inhibition (pH > 3.0 units/24 hr) were 12.44, 10.00, and 17.38 hr with groups A, B, and C, respectively. There was no significant difference between the pH profiles of the 20th and 80th days with every dose regimen. It is concluded that all three dose regimens of omeprazole are effective in reducing gastric acidity and their pharmacodynamic action does not change with time. Therefore they are suitable to be assessed in large clinical trials aimed at verifying the prevention of duodenal ulcer recurrence for longer periods. KEY WORDS: duodenal ulcer; maintenance therapy; omeprazole; pH monitoring. Duodenal ulcer is a chronic disease characterized by high tendency to heal and to recur. H2-receptor Manuscript received November 11, 1992; revised manuscript received June 29, 1993; accepted August 13, 1993. From the Dipartimento di Medicina Interna, Cattedra di Gas- troenterologia, and Clinica Medica R, Universith Degli Studi di Genova, Italy. Address for reprint requests: Prof. Vincenzo Savarino, DIMI, Cattedra di Gastroenterologia, Universitg di Genova, Viale Benedetto XV, n 6, 6132 Genova, Italy. antagonists, administered at half the dose com- monly used for acute ulcer healing, have been rec- ommended as maintenance treatment in the attempt to keep the ulcer healed (1). They have been shown to reduce the one-year relapse rate from 75-80% obtained with placebo to 25-30% (2), thus diminish- ing absenteeism from work and improving the qual- ity of life for ulcer sufferers (3). Omeprazole, the first substituted benzimidazole inhibitor of H+,K +- Digestive Diseases and Sciences, VoL 39, No. 7 (July 1994) 0163-2116/94/0700-1473$07.00/0 © 1994 Plenum Publishing Corporation 1473
Transcript of Antisecretory effects of three omeprazole regimens for maintenance treatment in duodenal ulcer
Digestive Diseases and Sciences, I/ol. 39, No. 7 (July 1994), pp. 1473-1482
Antisecretory Effects of Three Omeprazole Regimens for Maintenance Treatment in
Duodenal Ulcer VINCENZO SAVARINO, MD, GIUSEPPE SANDRO MELA, MD, PATRIZIA ZENTILIN, MD,
PATRIZIA CUTELA, MD, MARIA RAFFAELLA MELE, MD, DANIELE PERILLI, MD, AMBROGIO VASSALLO, MD, ADRIANA ZAMBOTTI, MD, CARLO MANSI, MD,
and GUIDO CELLE, MD
This study was carried out to assess the antisecretory effects and their possible changes over time of three different dose regimens of omeprazole that could be proposed for maintenance treatment in duodenal ulcer. Forty-five patients with endoscopically proven duodenal ulcer were studied by means of 24-hr gastric pH-metry both in basal conditions and on the fifth day of acute treatment with omeprazole 20 mg in the morning. Ulcers healed after four weeks (in three cases after eight weeks) and afterwards, 15 patients were randomized to receive orally at 0800 hr in single-blind fashion omeprazole 10 mg daily (group A), 15 to receive omeprazole 40 mg on Saturday and Sunday followed by a five-day period without medication (group B), and 15 to receive omeprazole 20 mg every other day (group C) for up to three months. On the 20th and 80th days of these maintenance treatments 24-hr gastric pH-metry was repeated to assess the antisecretory effectiveness of each regimen over a two-month period. In patients of group B these tests began at 1700 hr on Friday, the last of five days off treatment, and in those of group C at 1700 hr of the day off medication. All three dose regimens of omeprazole were able to raise pH values significantly (P < 0.01-0.001) compared to basal levels. Omeprazole 20 mg every other day was more effective (P < 0.01) than omeprazole 40 mg weekend, but did not differ significantly from omeprazole 10 mg daily. The durations of acid inhibition (pH > 3.0 units/24 hr) were 12.44, 10.00, and 17.38 hr with groups A, B, and C, respectively. There was no significant difference between the pH profiles of the 20th and 80th days with every dose regimen. It is concluded that all three dose regimens of omeprazole are effective in reducing gastric acidity and their pharmacodynamic action does not change with time. Therefore they are suitable to be assessed in large clinical trials aimed at verifying the prevention of duodenal ulcer recurrence for longer periods.
KEY WORDS: duodenal ulcer; maintenance therapy; omeprazole; pH monitoring.
Duodenal ulcer is a chronic disease characterized by high tendency to heal and to recur. H2-receptor
Manuscript received November 11, 1992; revised manuscript received June 29, 1993; accepted August 13, 1993.
From the Dipartimento di Medicina Interna, Cattedra di Gas- troenterologia, and Clinica Medica R, Universith Degli Studi di Genova, Italy.
Address for reprint requests: Prof. Vincenzo Savarino, DIMI, Cattedra di Gastroenterologia, Universitg di Genova, Viale Benedetto XV, n 6, 6132 Genova, Italy.
antagonists, administered at half the dose com- monly used for acute ulcer healing, have been rec- ommended as maintenance treatment in the attempt to keep the ulcer healed (1). They have been shown to reduce the one-year relapse rate from 75-80% obtained with placebo to 25-30% (2), thus diminish- ing absenteeism from work and improving the qual- ity of life for ulcer sufferers (3). Omeprazole, the first substituted benzimidazole inhibitor of H+,K +-
Digestive Diseases and Sciences, VoL 39, No. 7 (July 1994) 0163-2116/94/0700-1473$07.00/0 © 1994 Plenum Publishing Corporation
1473
SAVARINO ET AL
ATPase in the parietal cell to be used clinically, produces a more profound and prolonged inhibition of gastric acidity than HE-receptor antagonists (4), and this sustained ant isecretory effect promotes faster duodenal ulcer healing (5). This potent drug has been poorly assessed in the long-term treatment of duodenal ulcer, and large trials comparing ome- prazole and HE-receptor antagonists in the preven- tion of ulcer relapse are lacking. This scarce expe- rience is mainly due to the worldwide reluctance to treat chronically ulcer patients with a drug poten- tially associated with the development of important undesirable side effects (mainly gastric carcinoid tumors) because of its marked acid inhibition (6, 7). However , the increasing number of clinical reports that exclude relevant and persistent changes in the amount or distribution of argyrophilic cells in the gastric oxynt ic mucosa of patients t reated with omeprazole for many consecut ive months and even years (8-11), seems to encourage studies on main- tenance treatment of duodenal ulcer with this com- pound. In this connect ion, omeprazole is also fa- vored by the fact that its action is irreversible until new enzyme is synthesized, and therefore acid in- hibitioh takes several days to pass off (12, 13). The ability of omeprazole to accumulate in the parietal cell and the car ryover effect on subsequent days of dosing make possible the use of intermittent instead of eve ryday administration of the drug, and this might contribute to obviating the potential risk of undesirable side effects.
This s tudy was undertaken to assess the an- t isecretory action of three different dose regimens of omeprazole that could be suitable for mainte- nance treatment in duodenal ulcer and to ver i fy whether their effectiveness in controlling acid se- cretion changes over a two-month period of dosage.
MATERIALS AND METHODS
Patients. Forty-five consecutive patients (31 males and 14 females) with endoscopically proven duodenal ulcer were recruited for this study. At the time of inclusion, physical examination and laboratory baseline tests were normal. None had undergone previous ulcer surgery or had significant gastrointestinal bleeding, requiring a trans- fusion within the seven days preceding the trial. Patients who had been treated with antacids, HE-receptor antago- nists, omeprazole, or other antiulcer drugs were entered in the study providing that such therapies were with- drawn at least two weeks before the endoscopic diagnosis of ulcer. Other exclusion criteria were the following: history of Zollinger-Ellison syndrome, severe symptom- atic reflux esophagitis, inflammatory bowel disease,
chronic systemic medical disorders, regular intake of antidepressants, phenothiazines, corticosteroids, nonste- roidal antiinflammatory drugs, salicylates, any condition associated with poor patient compliance, pregnant or lactating women, and pyloric stenosis. Informed consent was obtained from each patient and the study was ap- proved by the local ethics committee.
Study Design. If all entry criteria were satisfied, each patient underwent continuous 24-hr intragastric pH mon- itoring in basal conditions within three days of ulcer detection. Thereafter a course of omeprazole 20 mg, given orally at 0800 hr immediately before breakfast in single-blind fashion (patient), was begun in all cases. As this drug takes from three to five days to reach a steady state (14), a second pH-metry was performed on the fifth day of treatment in order to assess the individual re- sponse to the full omeprazole dosage. Then, therapy was continued until the 28th day, when endoscopy was re- peated to check for ulcer healing. In three patients duo- denal ulcer did not heal at this time and a supplementary course of four weeks of omeprazole 20 mg was necessary to obtain complete repair of the lesion.
Once ulcer healing was confirmed, patients were ran- domized using a computer-generated list to receive main- tenance treatment with three different dose regimens of omeprazole: group A, omeprazole 10 mg/day given orally at 0800 hr before breakfast; group B, omeprazole 40 mg taken for two consecutive mornings at 0800 hr before breakfast on Saturday and Sunday (weekend) followed by a five-day period without medication; and group C, ome- prazole 20 mg administered at 0800 hr before breakfast every other day.
Medication was given single-blind (patient) as enteric- coated granules in hard gelatin capsules containing either 10 rag, 20 mg, or 40 mg of the active drug or placebo. Capsules were delivered in weekly blister packs, which were arranged in order to allow patients of groups B and C to take placebo capsules from Monday to Friday and every other day, respectively. Each patient was supplied every time with four weekly blister packs until three months of treatment were completed. Returned study capsules were counted at the end of each month and patients later found to have taken less than three quarters of the active capsules per study period were regarded as noncompliant with the study protocol.
To allow patients to reach steady-state conditions, par- ticularly with the weekend regimen, the assessment of acid suppression achieved with each dosage schedule of omeprazole was carried out at the third week of mainte- nance treatment. In patients treated with omeprazole 40 mg weekend, pH monitoring started at 1700 hr on Friday, that is, on the fifth day after the last Sunday dose of the drug, and stopped at 1700 hr on Saturday, the first day of dosing during the weekend. So it was possible to record gastric acidity changes on the final phase of the five-day period without medication and on the initial part of the two-day period of treatment. In patients treated with omeprazole 20 mg every other day, intragastric pH-metry started at 1700 hr on the day off treatment and lasted for 24 hr until 1700 hr of the day on treatment. In this way, the evening and nocturnal pH fluctuations of the day
1474 Digestive Diseases and Sciences, VoL 39, No. 7 (July 1994)
OMEPRAZOLE REGIMENS TO PREVENT ULCER RELAPSE
without medication and the daytime pH changes of the day with medication were monitored.
At the end of an additional two-month period of main- tenance treatment (80th day), intragastric pH-metry was repeated in order to evaluate whether the action of ome- prazole changes with time. Within 7 - 3 days of this fourth pH-metry, another upper endoscopy was per- formed in order to check for the existence of ulcer re- lapse. Each patient was also assessed clinically on the basis of diary cards that were supplied at the beginning of the period of maintenance treatment.
pH Monitoring. The technique for measuring 24-hr gas- tric acidity has been validated by this group (15, 16) prior to being routinely employed. In brief, intragastric pH was monitored with a combined glass electrode (Ingold 440 M4, Urdorf, Switzerland) connected to a portable appa- ratus (Proxima light 2, Synectics Medical, Stockholm, Sweden). A sampling rate of 6 sec was selected. At the beginning of each test, the pH electrode was accurately calibrated at 37°C using buffer solutions of pH 1.0 and pH 7.0 (Merck, Darmstadt, Germany). Each electrode was periodically controlled with appropriate in vitro stability tests over 24 hr (17), and faulty electrodes were dis- carded. Each electrode was replaced with a new one after every 20 examinations. Only drifts less than -+0.3 pH units were tolerated. Four examinations were repeated because of technical failure. After calibration, the elec- trode was passed through an anesthetized nostril and positioned about 10 cm below the cardia under rapid fluoroscopic control. The distance from tip to nostrils was recorded and kept constant for all study days in each duodenal ulcer patient, pH measurements started at 1700 hr and lasted for 24 hr until 1700 hr on the following day. Each patient was given three daily meals, which were standardized for timing (dinner at 1800 hr, breakfast at 0800 hr and lunch at noon) and composition (18). Extra food was not allowed. During the tests patients were fully ambulatory. Smoker patients were asked to record the timing and number of cigarettes consumed during the first examination and to repeat them during the following three tests.
Data Processing and Statistics. Raw pH measurements were off-loaded into a MS-DOS personal computer and then transferred to a HP 332 calculator for further elabo- ration only when all recordings were complete. Working files of 1440 data points/24 hr were created by averaging the values of every 10 consecutive pH readings (1 min), because this data compression has been shown to be optimal to describe changes in gastric acidity over the circadian cycle in any clinical condition (19). Measure- ments obtained in basal conditions and after each treat- ment were plotted as 24-hr mean pH profiles and the means (_+ SD) of pH values (20) were calculated during the 24-hr time interval (1700-1659 hr). The mean times (in minutes) spent above 3.0 pH units during the same time interval were also calculated, as this threshold has been thought to be an additional, helpful index of acid suppres- sion in pharmacological studies on gastric antisecretory drugs (21). Only in patients of group B, the above calcu- lations were carried out for an additional time segment (1700-0759 hr) in order to assess whether there is residual pharmacological effect at the end of the treatment-free
TABLE 1. DEMOGRAPHIC CHARACTERISTICS OF PATIENTS
Group A Group B Group C
Age (mean - sn) 48.5 -+ 15.3 50.2 - 12.2 48.3 _+ 11.8 Sex (M/F) 10:5 10:5 11:4 Smokers 9 8 10 Alcohol consumers 10 12 10 Coffee users 9 10 12 Ulcer size (cm) 12.6 -+ 4.2 12.2 _+ 2.6 12.8 -+ 2.7
(mean _+ sn) Previous 2 0 1
complications Length of history 7.1 - 8.5 8.7 -+ 7.9 9.3 - 8.8
(yr) (mean --- SD)
period by comparing pH values measured on the fifth day without medication with those of the corresponding pe- riod of the basal curve.
Data were compared by means of analysis of variance, and P values were corrected for multiple testing, where appropriate. Significance was assessed at the 5% level. Furthermore, the density distributions of pH values dur- ing the circadian cycle (1700-1659 hr) were calculated with 0.1 pH incremental steps for all measurements. Demographic data pertaining to the three groups of duo- denal ulcer patients on maintenance treatment were com- pared by means of Student's t test and chi-square test. The power of the study was calculated taking as the primary objective the difference in mean pH values be- tween basal and maintenance treatment tracings. This difference should be of at least +-1.0 pH unit to have clinical relevance. On the basis of preliminary data, 15 patients per treatment arm would be needed to give a test power (1 - 13) of 0.9 to detect a true difference of 1.2 pH units with a common SD of -+ 1.0 pH unit, with a two- tailed ct probability level of 0.05. All programs were written by G.S.M.
RESULTS
The three groups of duodenal ulcer patients did not differ significantly as regards any of the demo- graphic variables displayed in Table 1. No relevant adverse events were reported during and at the end of the study. The only complaints, which, however, did not lead to stopping maintenance treatment, were itching in one patient receiving omeprazole 10 mg daily and diarrhea in one patient receiving ome- prazole 40 mg two days a week.
Four patients were lost to follow-up for various reasons: two patients, receiving 10 mg daily and 40 mg weekend of omeprazole, were noncompliant regarding the s tudy medication; one patient treated with omeprazole 10 mg daily was withdrawn be- cause of the appearance of severe symptoms, and one patient given omeprazole 20 mg every other day refused to undergo gastric pH-metry while on main, tenance treatment.
Digestive Diseases and Sciences, Vol. 39, No. 7 (July 1994) 1475
SAVARINO ET AL
IoH
O m e p r a z o l e 10
Basal
PH I OME 18 mg on 21tth day (long-term) 7 r
5
4
3
2
1
13 21 23 I 3 5 ? 9 11 13 IS
rng e v e r y day OME 20 m9 on 5th day (acute)
OME Ig mg on BOth day {long-term)
19 21 23 I 3 5 7 9 11 13 15 h
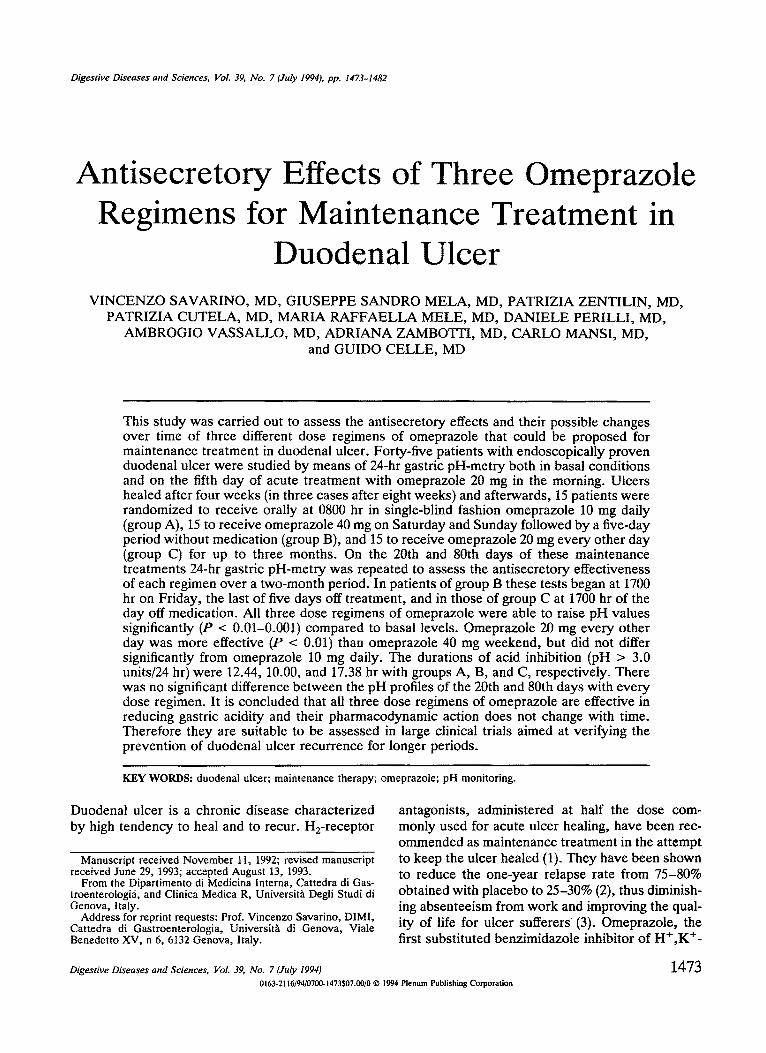
Fig 1. The 24-hr mean pH profiles of the four scheduled experimental times in duodenal ulcer patients on maintenance treatment with omeprazole 10 mg daily.
The 24-hr mean pH profiles of the four scheduled experimental times in the three treatment groups are reported in Figures 1-3. In each group, the acidity patterns obtained in basal conditions are characterized by prolonged periods of low pH val- ues with small pH increases after meals, while those pertaining to the antisecretory effects of omepra- zole 20 mg on the fifth day of acute treatment show a profound and long-lasting acid inhibition.
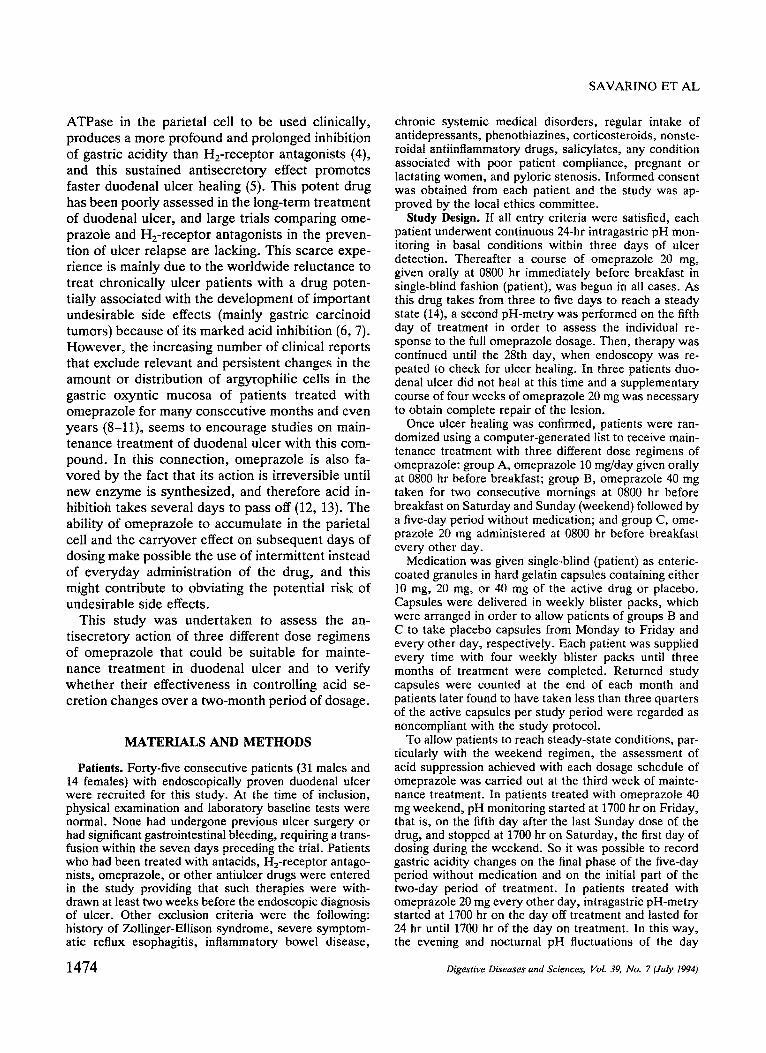
On the 20th day of maintenance treatment, the mean pH profile of omeprazole 10 mg daily (lower left corner of Figure 1) is mainly represented by low pH values from about 2200 to 0300 hr and a marked increase in pH levels during the second half of the night and in postprandial periods. In patients re- ceiving omeprazole 40 mg weekend (lower left cor- ner of Figure 2), there are low pH values during the evening and the first half of the night, while the
RH
il
Omeprazole 4 0 mg Basal
OlIE 41] mg on 21]th day (long-term)
w e e k - e n d ONE 2B mg on 5th day (acute)
OME 4fl mg on BBth day (long-term)
I s 21 2 3 z 3 S 7 9 l z 13 z s h 13 2 z 2 3 I 3 5 7 3 11 13 Is h
Fig 2. The 24-hr mean pH profiles of the four scheduled experimental times in duodenal ulcer patients on maintenance treatment with omeprazole 40 mg weekend.
1476 Digestive Diseases and Sciences, VoL 39, No. 7 (July 1994)
OMEPRAZOLE REGIMENS TO PREVENT ULCER RELAPSE
O m e p r a z o l e 20 mg ,,e,,very other d a y 014E 2g mg on 5th day (acute)
~ * 1 . ¢ . 1 . 1 . 1 . 1 . J . I . t . I ~ I ~ 1 . I . 1 . 1 . 1 . I . I , I , I . I ,
PH t 0ME ?8 mg on ?Bth d~y (long-term)
s
s
1 p ~ = I . I . I . 1 .1 .1 . t . t . 11 l l l = } . t . t . l . l . l . I . I . 18 8 S 12
OE 28 mg on I]l]th day (long-term)
IB B S 1;~
Fig 3. The 24-hr mean pH profiles of the four scheduled experimental times in duodenal ulcer patients on maintenance treatment with omeprazole 20 mg every other day.
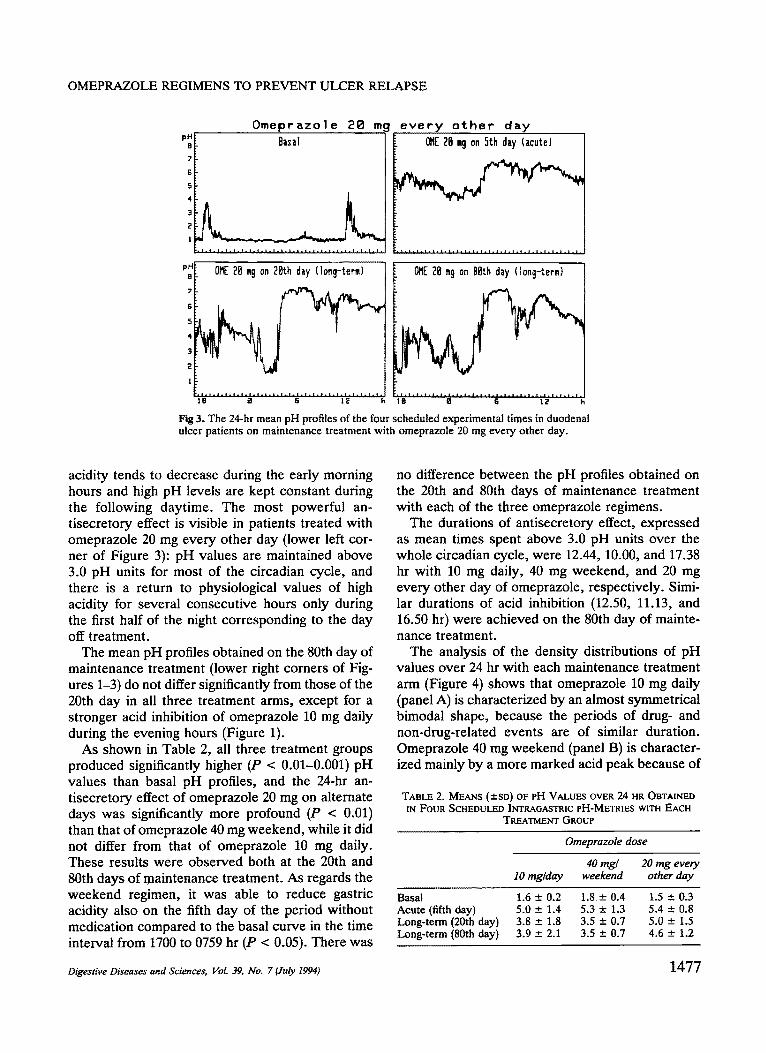
acidity tends to decrease during the early morning hours and high pH levels are kept constant during the following daytime. The most powerful an- tisecretory effect is visible in patients treated with omeprazole 20 mg every other day (lower left cor- ner of Figure 3): pH values are maintained above 3.0 pH units for most of the circadian cycle, and there is a return to physiological values of high acidity for several consecutive hours only during the first half of the night corresponding to the day off treatment.
The mean pH profiles obtained on the 80th day of maintenance treatment (lower right corners of Fig- ures 1-3) do not differ significantly from those of the 20th day in all three treatment arms, except for a stronger acid inhibition of omeprazole 10 mg daily during the evening hours (Figure 1).
As shown in Table 2, all three treatment groups produced significantly higher (P < 0.01-0.001) pH values than basal pH profiles, and the 24-hr an- tisecretory effect of omeprazole 20 mg on alternate days was significantly more profound (P < 0.01) than that of omeprazole 40 mg weekend, while it did not differ from that of omeprazole 10 mg daily. These results were observed both at the 20th and 80th days of maintenance treatment. As regards the weekend regimen, it was able to reduce gastric acidity also on the fifth day of the period without medication compared to the basal curve in the time interval from 1700 to 0759 hr (P < 0.05). There was
no difference between the pH profiles obtained on the 20th and 80th days of maintenance treatment with each of the three omeprazole regimens.
The durations of antisecretory effect, expressed as mean times spent above 3.0 pH units over the whole circadian cycle, were 12.44, 10.00, and 17.38 hr with 10 mg daily, 40 mg weekend, and 20 mg every other day of omeprazole, respectively. Simi- lar durations of acid inhibition (12.50, 11.13, and 16.50 hr) were achieved on the 80th day of mainte- nance treatment.
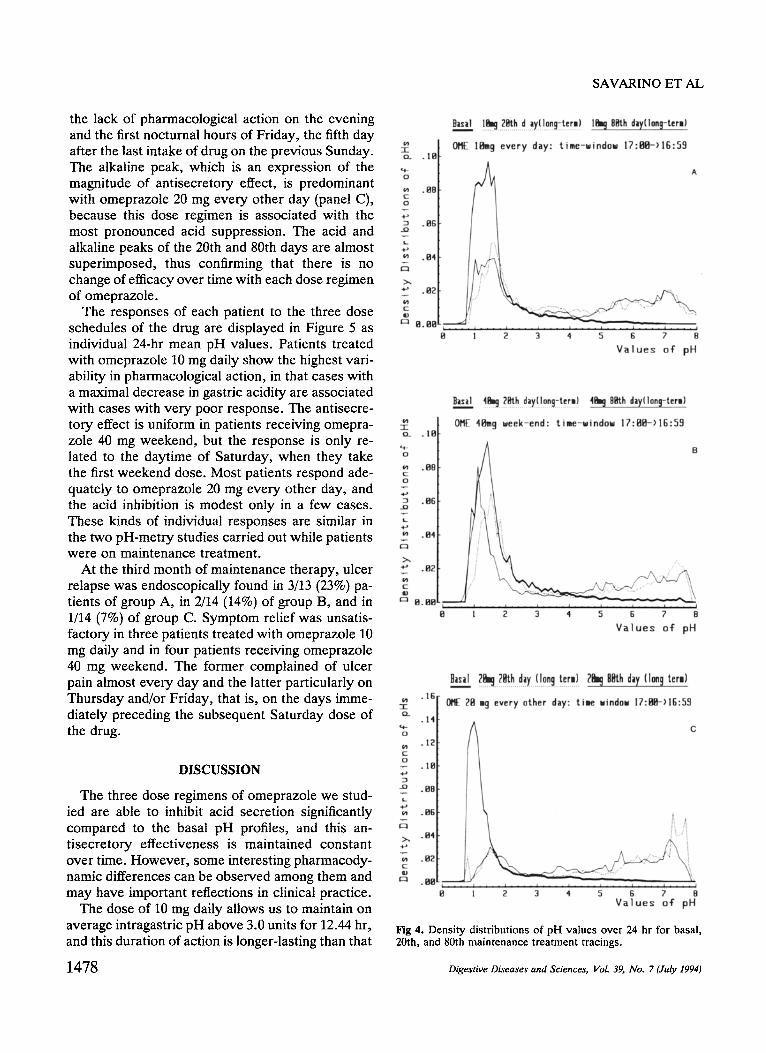
The analysis of the density distributions of pH values over 24 hr with each maintenance treatment arm (Figure 4) shows that omeprazole 10 mg daily (panel A) is characterized by an almost symmetrical bimodal shape, because the periods of drug- and non-drug-related events are of similar duration. Omeprazole 40 mg weekend (panel B) is character- ized mainly by a more marked acid peak because of
TABLE 2. MEANS (±SD) OF PH VALUES OVER 24 HR OBTAINED IN FOUR SCHEDULED INTRAGASTRIC PH-METRIES WITH EACH
TREATMENT GROUP
Omeprazole dose
40 mg/ 20 mg every 10 rag~day weekend other day
Basal 1.6 ± 0.2 1.8 --- 0.4 1.5 ± 0.3 Acute (fifth day) 5.0 ± 1.4 5.3 ± 1.3 5.4 ± 0.8 Long-term (20th day) 3.8 ± 1.8 3.5 ± 0.7 5.0 ± 1.5 Long-term (80th day) 3.9 ± 2.1 3.5 ± 0.7 4.6 ± 1.2
Digestive Diseases and Sciences, Vol. 39, No. 7 (July 1994) 1477
SAVARINO ET AL
the lack of pharmacological action on the evening and the first nocturnal hours of Friday, the fifth day after the last intake of drug on the previous Sunday. The alkaline peak, which is an expression of the magnitude of antisecretory effect, is predominant with omeprazole 20 mg every other day (panel C), because this dose regimen is associated with the most pronounced acid suppression. The acid and alkaline peaks of the 20th and 80th days are almost superimposed, thus confirming that there is no change of efficacy over time with each dose regimen of omeprazole.
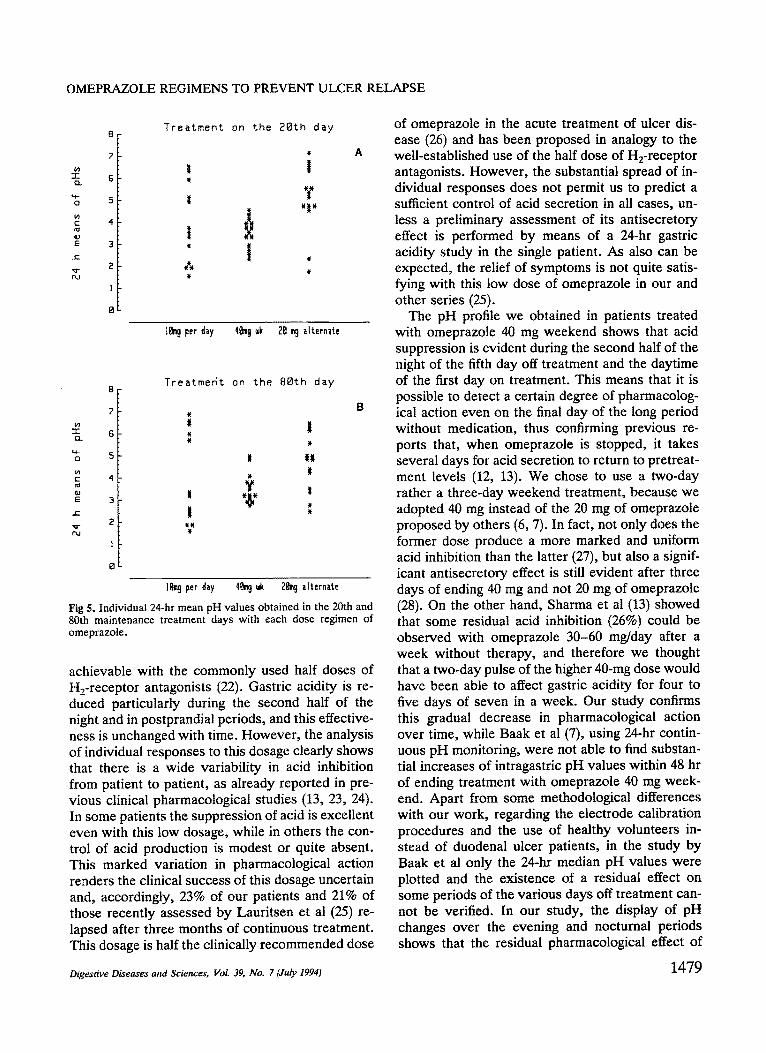
The responses of each patient to the three dose schedules of the drug are displayed in Figure 5 as individual 24-hr mean pH values. Patients treated with omeprazole 10 mg daily show the highest vari- ability in pharmacological action, in that cases with a maximal decrease in gastric acidity are associated with cases with very poor response. The antisecre- tory effect is uniform in patients receiving omepra- zole 40 mg weekend, but the response is only re- lated to the daytime of Saturday, when they take the first weekend dose. Most patients respond ade- quately to omeprazole 20 mg every other day, and the acid inhibition is modest only in a few cases. These kinds of individual responses are similar in the two pH-metry studies carried out while patients were on maintenance treatment.
At the third month of maintenance therapy, ulcer relapse was endoscopically found in 3/13 (23%) pa- tients of group A, in 2/14 (14%) of group B, and in 1/14 (7%) of group C. Symptom relief was unsatis- factory in three patients treated with omeprazole 10 mg daily and in four patients receiving omeprazole 40 mg weekend. The former complained of ulcer pain almost every day and the latter particularly on Thursday and/or Friday, that is, on the days imme- diately preceding the subsequent Saturday dose of the drug.
DISCUSSION
The three dose regimens of omeprazole we stud- ied are able to inhibit acid secretion significantly compared to the basal pH profiles, and this an- tisecretory effectiveness is maintained constant over time. However, some interesting pharmacody- namic differences can be observed among them and may have important reflections in clinical practice.
The dose of 10 mg daily allows us to maintain on average intragastric pH above 3.0 units for 12.44 hr, and this duration of action is longer-lasting than that
1478
~_ . le
.88 o
.84
Bmsil .!.bj. 2~.h.~d..ay.!!.0ng-tcrm) Ibj 8~h day(1on~-ter,)
OF/ IBmg every day: t i ~e -u indau 17:g2-) lK:59
A
g I ~ 3 4 5 6 7 8
V a l u e s of" pH
01~ 41~ 9 meek-end: t i = e - u i n d 0 u 17:Bfl-) lG:59 o_ . IB
B
.fib o
L
.B4
~>" .112
t-~ 8.BB I I
fl :~ 3 4 5 fi 7 8
V a l u e s oT pH
.16
~L .14
o .IE
_o .BB
>~ oH4
. a~
u
n,,,__= nnth (vm t,,,)
0RE Z8 =9 every other day: t i e uindou 17:flS-)lG:59
C
, i
1 2 3 4 5 6 7 8 V a l u e s o f pH
Fig 4. Density distributions of pH values over 24 hr for basal, 20th, and 80th maintenance treatment tracings.
Digestive Diseases and Sciences, VoL 39, No. 7 (July 1994)
OMEPRAZOLE REGIMENS TO PREVENT ULCER RELAPSE
7-
(n
Q,I E
T~
8
7
15
5
4
3
2
I
O
Trea tment on the 2Bth day
, A
t
¢, w
IBm 9 per day 4~ 9 wk 2B m@ alternate
sis c~
E d~
T rea tme6t on the BOth day
#
t ~w w
#
÷
I
## #
# w
16rob per day 4~m9 ~k 2~@ alternate
Fig 5. Individual 24-hr mean pH values obtained in the 20th and 80th maintenance treatment days with each dose regimen of omeprazole.
achievable with the commonly used half doses of H2-receptor antagonists (22). Gastric acidity is re- duced particularly during the second half of the night and in postprandial periods, and this effective- ness is unchanged with time. However, the analysis of individual responses to this dosage clearly shows that there is a wide variability in acid inhibition from patient to patient, as already reported in pre- vious clinical pharmacological studies (13, 23, 24). In some patients the suppression of acid is excellent even with this low dosage, while in others the con- trol of acid production is modest or quite absent. This marked variation in pharmacological action renders the clinical success of this dosage uncertain and, accordingly, 23% of our patients and 21% of those recently assessed by Lauritsen et al (25) re- lapsed after three months of continuous treatment. This dosage is half the clinically recommended dose
of omeprazole in the acute treatment of ulcer dis- ease (26) and has been proposed in analogy to the well-established use of the half dose of H2-receptor antagonists. However, the substantial spread of in- dividual responses does not permit us to predict a sufficient control of acid secretion in all cases, un- less a preliminary assessment of its ant#secretory effect is performed by means of a 24-hr gastric acidity study in the single patient. As also can be expected, the relief of symptoms is not quite satis- fying with this low dose of omeprazole in our and other series (25).
The pH profile we obtained in patients treated with omeprazole 40 mg weekend shows that acid suppression is evident during the second half of the night of the fifth day off treatment and the daytime of the first day on treatment. This means that it is possible to detect a certain degree of pharmacolog- ical action even on the final day of the long period without medication, thus confirming previous re- ports that, when omeprazole is stopped, it takes several days for acid secretion to return to pretreat- ment levels (12, 13). We chose to use a two-day rather a three-day weekend treatment, because we adopted 40 mg instead of the 20 mg of omeprazole proposed by others (6, 7). In fact, not only does the former dose produce a more marked and uniform acid inhibition than the latter (27), but also a signif- icant ant#secretory effect is still evident after three days of ending 40 mg and not 20 mg of omeprazole (28). On the other hand, Sharma et al (13) showed that some residual acid inhibition (26%) could be observed with omeprazole 30-60 mg/day after a week without therapy, and therefore we thought that a two-day pulse of the higher 40-mg dose would have been able to affect gastric acidity for four to five days of seven in a week. Our study confirms this gradual decrease in pharmacological action over time, while Baak et al (7), using 24-hr contin- uous pH monitoring, were not able to find substan- tial increases of intragastric pH values within 48 hr of ending treatment with omeprazole 40 mg week- end. Apart from some methodological differences with our work, regarding the electrode calibration procedures and the use of healthy volunteers in- stead of duodenal ulcer patients, in the study by Baak et al only the 24-hr median pH values were plotted and the existence of a residual effect on some periods of the various days off treatment can- not be verified. In our study, the display of pH changes over the evening and nocturnal periods shows that the residual pharmacological effect of
Digestive Diseases and Sciences, Vol. 39, No. 7 (July 1994) 1479

omeprazole 40 mg weekend is strictly confined to the early morning hours, and this time interval cor- responds to that during which Sharma et al (13) also found a reduction in gastric acidity one week after the cessation of omeprazole therapy. The replica- tion of this finding in the pH profile we achieved on the 80th day of treatment is further confirmation of the reliability of our data.
The lack of differences in the pattern of acid inhibition between the two pH profiles obtained while patients were on maintenance therapy with omeprazole 40 mg weekend seems to confirm that this drug keeps unaltered its pharmacological action also with a five-day period free of medication during each week. In other words, the bioavailability of this acid-labile compound does not seem to be re- duced even if only a two-day weekend pulse is used, and this further encourages the use of this dose regimen in the clinical setting. However, in our series, 14% of ulcers relapsed after three months of treatment and symptom relief was not quite satisfactory, because four patients com- plained of mild ulcer pain on Thursday and/or Fri- day, probably as a consequence of the return to high acidity levels during most of the circadian cycle after the first three or four days of the long period without medication.
In patients treated with omeprazole 20 mg on alternate days, the antisecretory effect was remark- able and only slightly inferior to that achievable with the same dose given daily (see Figure 3). In fact, the 24-hr mean pH was 5.0 units on the 20th day of maintenance treatment compared to 5.4 pH units on the fifth day of acute treatment, and the only difference was a more marked and longer- lasting decline in pH values with the former regimen during the late evening and the first half of the night. This reduced effectiveness over several nocturnal hours exaggerates the well-known tendency of ome- prazole 20 mg daily to decrease its antisecretory action during this period of the circadian cycle (29), as result of a poorly understood mechanism. Using this dosage schedule, acid secretion is controlled more than with the other two regimens of omepra- zole we tested, although the difference is significant only with omeprazole 40 mg weekend. Accordingly, the relief of symptoms was good in all patients and the three-month relapse rate was minimal (7%) with this regimen in our study. The individual response was adequate in the majority of patients, both at the 20th and 80th days of maintenance treatment, but a poor acid inhibition can be expected in some cases
SAVARINO ET AL
and this may result in clinical failure to control ulcer relapses.
Finally, it is worth emphasizing that low or inter- mittent doses of omeprazole also have the advan- tage of preventing high levels of gastrinemia (6, 7, 25) and permitting a rapid sterilization of gastric contents (30), by leaving the acid gastric milieu undisturbed during many hours of the circadian cycle. This consideration is reinforced by the grow- ing evidence that hypergastrinemia is of little, if any, clinical significance even during daily omepra- zole treatment (31). Therefore, frequent monitoring of plasma gastrin levels is no more strongly recom- mended in patients treated with short- or long-term omeprazole.
Among the different strategies that are now avail- able for preventing duodenal ulcer recurrences, maintenance treatment with antisecretory drugs has been shown to decrease substantially both the re- lapse rate and the risk of hemorrhage or perforation (32). Although long-term therapy has been pro- posed for all patients with duodenal ulcer by some authors (33), others (34, 35) have highlighted that it should be performed only in carefully selected sub- groups of patients, such as those with history of complications, frequent relapses per year, refrac- tory ulceration, continuation of NSAIDs, and heavy smoking. If this option is chosen in all or some duodenal ulcer patients, the regimens of ome- prazole we tested can be a valid alternative to the traditional He-antagonist treatment. In light of this, omeprazole also has the advantage that its efficacy does not decrease with time, as our study confirms. H2 antagonists, in fact, have been shown to develop tolerance few days after start of treatment (36, 37), even though the good results obtained in long-term management of peptic ulcer (2) seem to greatly diminish the clinical relevance of this phenomenon.
In recent years treatment regimens designed to eradicate Helicobacterpylori have been regarded as the best alternative to prolonged maintenance ther- apy, because they seem to be able to cure duodenal ulcer (38). Although there is no doubt that this germ is an important factor in the development of ulcer recurrence (39), at present its eradication cannot be recommended as standard therapy in all patients with this disease because current treatment is com- plex, patient compliance is poor, resistance to an- tibiotics develops rapidly, and even triple therapy fails in up to 20% of patients (32). We still need rigorous controlled studies aimed at assessing the drug combination capable to eradicate this bacte-
1480 Digestive Diseases and Sciences, VoL 39, No. 7 (July 1994)
OMEPRAZOLE REGIMENS TO PREVENT ULCER RELAPSE
rium with fewer side effects, better compliance, and lower costs. While waiting for the results of these studies, maintenance treatment remains a safe and effective option for managing duodenal ulcer pa- tients, and the omeprazole regimens evaluated in this study can be a valid alternative to those using H 2 blockers. It cannot be excluded that the partic- ular pharmacodynamic properties of omeprazole emerging from our experiments may also lead to a better clinical response than that obtained with H2 antagonists.
In conclusion, the three dose regimens of ome- prazole we assessed in our study seem to be suit- able for maintenance treatment of duodenal ulcer patients, because they produce a substantial de- crease of gastric acidity compared to basal pH pro- files and their antisecretory effect does not tend to change over time. The doses of omeprazole 10 mg daily and omeprazole 40 mg weekend are likely to be beneficial in clinically mild or moderate duodenal ulcer, while the dose of omeprazole 20 mg every other day could be more indicated in the control of the most severe forms of this disease. If future large clinical trials confirm the therapeutic efficacy of these regimens in terms of symptom relief and pre- vention of ulcer relapse and complications, the ad- ministration of low or intermittent dosage schedules of omeprazole can be a valid and safe regimen in the maintenance treatment of duodenal ulcer.
REFERENCES
1. Sontag SJ: Current status of maintenance therapy in peptic ulcer disease. Am J Gastroenterol 83:607-617, 1988
2. Bianchi Porro G, Parente F: Long term treatment of duode- nal ulcer. A review of management options. Drugs 7:482- 487, 1991
3. Jensen DM: Economic and health aspects of peptic ulcer disease and Hz-receptor antagonists. Am J Med 81(suppl 4B):42-48, 1986
4. Lanzon Miller S, Pounder RE, Hamilton MR, Ball S, Chro- nos NAF, Raymond F, Olausson M, Cederberg C: Twenty- four-hour intragastric acidity and plasma gastrin concentra- tion before and during treatment with either ranitidine and omeprazole. Aliment Pharmacol Ther 1:239-251, 1987
5. Maton PN: Omeprazole. N Engl J Med 324:965-975, 1991 6. Hewson EG, Yeomans ND, Angus PW, Shulkes A, Brook
CW, Sewell RB, Smallwood RA: Effect of "weekend ther- apy" with omeprazole on basal and stimulated acid secretion and fasting plasma gastrin in duodenal ulcer patients. Gut 29:1715-1720, 1988
7. Baak LC, Jansen JBMJ, Biemond I, Lamers CBHW: Week- end treatment with 20 and 40 mg omeprazole: Effect on intragastric pH, fasting and postprandial serum gastrin, and serum pepsinogens. Gut 32:977-982, 1991
8. Lamberts R, Creutzfeldt Stockmann F, Jacubaschke U,
Maas S, Brunner G: Long-term omeprazole treatment in man: Effects on gastric endocrine cell populations. Digestion 38:126-135, 1988
9. Solcia E, Rindi G, Havu N, Elm G: Qualitative studies of gastric endocrine cells in patients treated long-term with omeprazole. Scand J Gastroenterol 24(suppl 166):129-137, 1989
10. Dayal Y, Berlin R, Collen M, Bhatnager R: Does prolonged omeprazole administration affect enterochromaltin-like cell populations in hypersecretors? Gastroenterology 96:Al13, 1989
11. Lundell L, Backman L, Ekstrom P, Enander L-K, Faikner S, Fausa O, Grimelius L, Havu N, Lind T, Lonroth H, Sandmark S, Sandzen B, Unge P, Westin IH: Prevention of relapse of reflux oesophagitis after endoscopic healing: The efficacy and safety of omeprazole compared with ranitidine. Scand J Gastroenterol 26:248-256, 1991
12. Lind T, Cederberg C, Ekenved G, Haglund U, Olbe L: Effect of omeprazole--a gastric proton pump inhibitor---on pentagastrin stimulated acid secretion in man. Gut 24:270- 276, 1983
13. Sharma BK, Walt RP, Pounder RE, Gomes MD, Wood EC, Logan RH: Optimal dose of oral omeprazole for maximal 24 hour decrease of intragastric acidity. Gut 25:957-964, 1984
14. Miiller P, Dammann HG, Seitz H, Simon B: Effect of re- peated, once daily, oral omeprazole on gastric secretion. Lancet 1:66, 1983
15. Savarino V, Mela GS, Scalabrini P, Magnolia MR, Percario G, Di Timoteo E, Celle G: 24 hour comparison between pH values of continuous intraluminal recording and simultane- ous gastric aspiration. Scand J Gastroenterol 22:135-140, 1987
16. Savarino V, Mela GS, Zentilin P, Magnolia MR, Scalabrini P, Valle F, Moretti M, Bonifacino G, Celle G: Gastric aspiration versus antimony and glass pH electrodes. A si- multaneous comparative in vivo study. Scand J Gastroen- terol 24:434-439, 1989
17. Mela GS, Savarino V, Moretti M, Sumberaz A, Bonifacino G, Zentilin P, Caputo E, Villa G, Celle G: Antimony and glass pH electrodes can be used interchangeability in 24- hour studies of gastric acidity. Dig Dis Sci 36:1473-1481, 1990
18. Savarino V, Mela GS, Scalabrini P, Magnolia MR, Di Tim- oteo E, Percario G, Celle G: Continuous intragastric pH monitoring: Focus on its reproducibility in duodenal ulcer patients. A preliminary report. Gastroenterol Clin Biol 10:826-830, 1986
19. Meta GS, Savarino V, Moretti M, Bonifacino G, Sumberaz A, Zentilin P: Clinical relevance of sampling rate in the characterization and analysis of 24-hour gastric acidity. A report on 413 cases. Scand J Gastroenterol 24:683-687, 1989
20. Mela GS, Savarino V, Sumberaz A, Bonifacino G, Zentilin P, Villa G, Caputo E: Continuous acidity monitoring in the study of gastric antisecretory drugs: pH or antilog transfor- mation of pH, mean or median? Am J Gastroenterol 85:1105-1108, 1990
21. Mela GS, Savarino V: Relationship between ulcer healing and acid suppression. Gastroenterology 100:1482-1483, 1991
22. Savarino V, Mela GS, Zentilin P, Bonifacino G, Moretti M, Valle F, Celle G: Low bedtime doses of H2-receptor antag- onists for acute treatment of duodenal ulcer. Dig Dis Sci 34:1043-1046, 1989
Digestive Diseases and Sciences, Vol. 39, No. 7 (July 1994) 1481

SAVARINO ET AL
23. Howden CW, Derodra JK, Burget DW, Hunt RH: Effects of low dose omeprazole on gastric secretion and plasma gastrin in patients with healed duodenal ulcer. Hepato-Gastroen- terol 33:267-270, 1986
24. Hemery P, Galmiche JP, Roze C, Isal J-P, Brutey des Varennes S, Lavignolle A, Le Bodic L: Low dose omepra- zole effects on gastric acid secretion in normal man. Gastro- enterol Clin Biol 11:148-153, 1987
25. Lauritsen K, Andersen BN, Laursen LS, Hansen J, Have- lund T, Eriksen J, Rehfeld JF, Kjaergaard J, Rask-Madsen J: Omeprazole 20 mg three days a week and 10 mg daily in prevention of duodenal ulcer relapse. Double-blind compar- ative trial. Gastroenterology 100:663-669, 1991
26. McTavish D, Buckley MM-T, Heel RC: Omeprazole. An updated review of its pharmacology and therapeutic use in acid-related disorders. Drugs 42:138-170, 1991
27. Savarino V, Mela GS, Zentilin P, Cuteta P, Mele MR, Vigneri S, Celle G: Variability in individual response to various doses of omeprazole: Implications for antiulcer ther- apy. Dig Dis Sci (in press)
28. Lind T, Cederberg C, Forssell H, Olausson M, Olbe L: Relationship between reduction of gastric acid secretion and plasma gastrin concentration during omeprazole treatment. Scand J Gastroenterol 23:1259-1266, 1988
29. Savarino V, Mela GS, Zentilin P, Celle G: Ulcer healing: does omeprazole efficacy depend on daytime or 24-hour acid inhibition? Gastroenterology 99:1858-1860, 1990
30. Hunt RH: The protective role of gastric acid. Scand J Gas- troenterol 23(suppl 146):34-39, 1988
31. Freston JW: Clinical significance of hypergastrinemia: Rel- evance to gastrin monitoring during omeprazole therapy. Digestion 51(suppl 1):102-114, 1992
32. Penston JG, Wormsley KG: Review article: Maintenance treatment with H2-receptor antagonists for peptic ulcer dis- ease. Aliment Pharmacol Ther 6:3-29, 1992
33. Penston JG, Wormsley KG: Nine years of maintenance treatment with ranitidine for patients with duodenal ulcer disease. Aliment Pharmacol Ther 6:629-645, 1992
34. Howden CW: Maintenance treatment with H2 receptor an- tagonists in patients with peptic ulcer disease: Rarely justi- fied in terms of cost or patient benefit. Br Med J 297:1393- 1394, 1988
35. Bardhan KD, Hollander D, Festen HPM, Bianchi Porro G: Changing strategies for peptic ulcer disease. Gastroenterol Int 3:3-21, 1990
36. Smith JTL, Gavey C, Nwokolo CU, Pounder RE: Tolerance during 8 days of high-dose Hz-blockade: Placebo-controlled studies of 24-h acidity and gastrin. Aliment Pharmacol Ther 4S:47-64, 1990
37. Wilder-Smith CH, Ernst T, Gennoni M, Zeyen B, Halter F, Merki HS: Tolerance to oral Hz-receptor antagonists. Dig Dis Sci 35:976-983, 1990
38. Rauws EAJ, Tytgat GNJ: Cure of duodenal ulcer associated with eradication of Helicobacterpylori. Lancet 2:1233-1235, 1990
39. Peterson WL: Helicobacterpylori and peptic ulcer disease. N Engl J Med 324:1043-1048, 1991
1.482 Digestive Diseases and Sciences, Vol. 39, No. 7 (July 1994)




















