
Radiation Therapy in the Management of Early Stage Breast ...
83
Radiation Therapy Radiation Therapy in the Management of in the Management of Early Stage Breast Cancer Early Stage Breast Cancer Jennifer L. Peterson, M.D. Jennifer L. Peterson, M.D. Department of Radiation Oncology Department of Radiation Oncology Mayo Clinic, Jacksonville Mayo Clinic, Jacksonville
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Radiation Therapy in the Management of Early Stage Breast ...
Radiation TherapyRadiation Therapyin the Management ofin the Management of
Early Stage Breast CancerEarly Stage Breast Cancer
Jennifer L. Peterson, M.D.Jennifer L. Peterson, M.D.Department of Radiation OncologyDepartment of Radiation OncologyMayo Clinic, JacksonvilleMayo Clinic, Jacksonville
No commercial interestNo commercial interestor off label usageor off label usage
to discloseto disclose
ObjectivesObjectives
�� To discuss surgical options for early stageTo discuss surgical options for early stagebreast cancerbreast cancer
�� To understand the role of radiation in theTo understand the role of radiation in thetreatment of early stage breast cancertreatment of early stage breast cancer
�� To demonstrate theTo demonstrate the technical aspects oftechnical aspects ofradiotherapy planningradiotherapy planning
�� To review the rationale and patient selectionTo review the rationale and patient selectionfor partial breast radiotherapyfor partial breast radiotherapy

Early Stage Breast CancerEarly Stage Breast Cancer
�� Early StageEarly Stage–– Stage I or IIStage I or II–– Tumors < 5 cm in sizeTumors < 5 cm in size–– Negative or 1Negative or 1--3 positive lymph nodes3 positive lymph nodes
�� At diagnosisAt diagnosis–– 94% of women have tumors < 5cm94% of women have tumors < 5cm–– 64% of women are node negative64% of women are node negative
Early Stage Breast CancerEarly Stage Breast Cancer
�� Two major treatment optionsTwo major treatment options–– MastectomyMastectomy–– Breast conserving therapyBreast conserving therapy
�� MarginMargin--negative lumpectomynegative lumpectomy�� Adjuvant radiation therapyAdjuvant radiation therapy
�� Adjuvant therapyAdjuvant therapy–– Dependent on pathologic variablesDependent on pathologic variables
�� ChemotherapyChemotherapy�� Hormonal therapyHormonal therapy

What are the surgicalWhat are the surgicaloptions for early stageoptions for early stage
breast cancer?breast cancer?

MastectomyMastectomy
�� Total or simple mastectomyTotal or simple mastectomy–– Removal of all breast tissueRemoval of all breast tissue
�� Modified radical mastectomyModified radical mastectomy–– Removal of breast tissue and axillary level I/IIRemoval of breast tissue and axillary level I/II
lymph nodeslymph nodes�� Skin sparing mastectomySkin sparing mastectomy
–– Total or modified radical mastectomy withTotal or modified radical mastectomy withpreservation of the native skin through apreservation of the native skin through acircumareolar incisioncircumareolar incision
–– Performed in conjunction with immediatePerformed in conjunction with immediatereconstructionreconstruction

MastectomyMastectomy
�� Nipple sparingNipple sparingmastectomymastectomy–– Total or modified radicalTotal or modified radical
mastectomy withmastectomy withpreservation of thepreservation of thenipplenipple--areolar complexareolar complex
–– Performed inPerformed inconjunction withconjunction withimmediateimmediatereconstructionreconstruction
–– Controversial, notControversial, notstandard of carestandard of care
Courtesy of S. McLaughlin, Mayo Clinic

Nipple SparingNipple SparingMastectomyMastectomy�� Nonrandomized comparisonNonrandomized comparison�� Follow up 4.9 yearsFollow up 4.9 years�� All tumors > 2cm from nippleAll tumors > 2cm from nipple--areolarareolar
complexcomplex
Gerber, et al. Ann Surg, 2003
3 (5%)3 (5%)6161NSMNSM
3 (6%)3 (6%)5151SSMSSM
11 (8%)11 (8%)134134MRMMRM
Local recurrenceLocal recurrenceNo. of patientsNo. of patientsType of mastectomyType of mastectomy
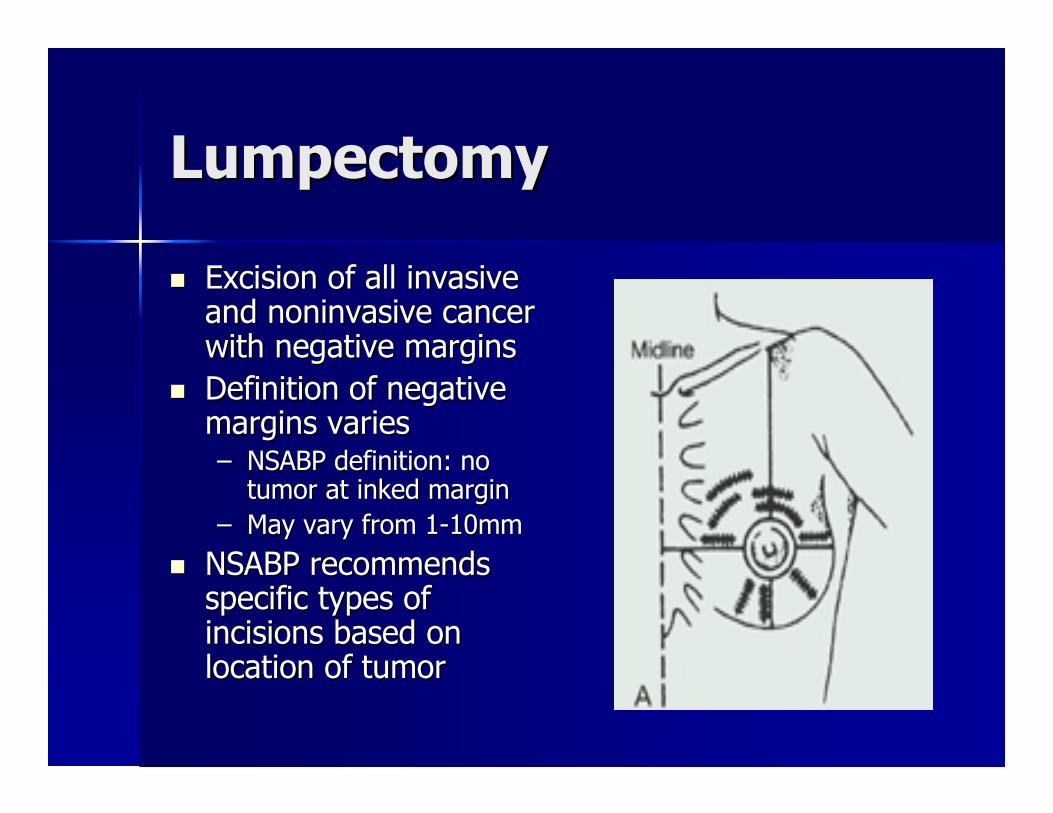
LumpectomyLumpectomy
�� Excision of all invasiveExcision of all invasiveand noninvasive cancerand noninvasive cancerwith negative marginswith negative margins
�� Definition of negativeDefinition of negativemargins variesmargins varies–– NSABP definition: noNSABP definition: no
tumor at inked margintumor at inked margin–– May vary from 1May vary from 1--10mm10mm
�� NSABP recommendsNSABP recommendsspecific types ofspecific types ofincisions based onincisions based onlocation of tumorlocation of tumor
Indications forIndications forReRe--excisionexcision�� Initial surgical procedure was less than aInitial surgical procedure was less than a
complete lumpectomycomplete lumpectomy�� Residual calcifications on postResidual calcifications on post--excisionexcision
mammogrammammogram–– 6060--85% chance of detecting residual disease on85% chance of detecting residual disease on
rere--excisionexcision–– Increased risk of local recurrence w/o removal ofIncreased risk of local recurrence w/o removal of
residual calcificationsresidual calcifications–– Lally, et al. Cancer 2005Lally, et al. Cancer 2005
�� 9% vs. 19% local recurrence rate9% vs. 19% local recurrence rate
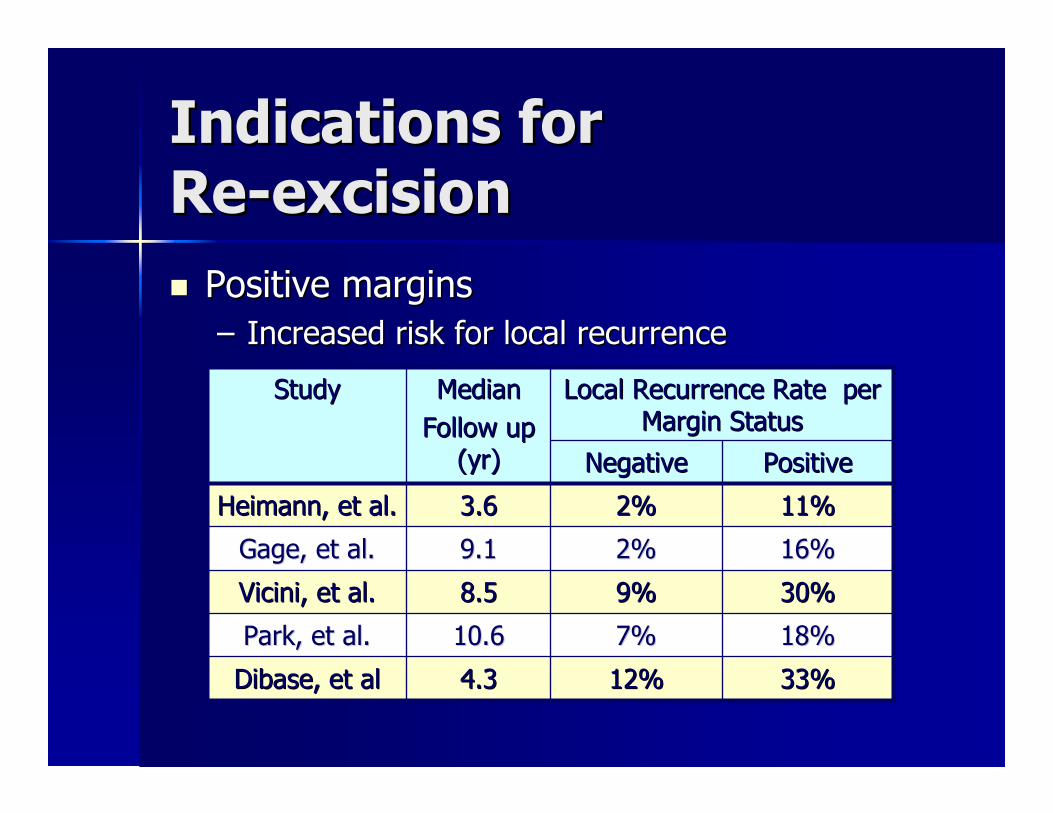
Indications forIndications forReRe--excisionexcision�� Positive marginsPositive margins
–– Increased risk for local recurrenceIncreased risk for local recurrence
33%33%12%12%4.34.3DibaseDibase, et al, et al
18%18%7%7%10.610.6Park, et al.Park, et al.
30%30%9%9%8.58.5Vicini, et al.Vicini, et al.
16%16%2%2%9.19.1Gage, et al.Gage, et al.
11%11%2%2%3.63.6Heimann, et al.Heimann, et al.
PositivePositiveNegativeNegative
Local Recurrence Rate perLocal Recurrence Rate perMargin StatusMargin Status
MedianMedianFollow upFollow up
(yr)(yr)
StudyStudy

Surgical Management ofSurgical Management ofLymph NodesLymph Nodes�� Surgical evaluation is a important component ofSurgical evaluation is a important component of
pathological stagingpathological staging–– 30% of clinically node negative pts. have + nodes30% of clinically node negative pts. have + nodes
pathologicallypathologically�� Historically, axillary dissection was part of standardHistorically, axillary dissection was part of standard
surgerysurgery�� Currently, sentinel lymph node biopsy eliminatesCurrently, sentinel lymph node biopsy eliminates
need for axillary dissection in biopsy negativeneed for axillary dissection in biopsy negativepatientspatients
�� In patients with positive sentinel lymph nodeIn patients with positive sentinel lymph nodebiopsy, completion axillary dissection isbiopsy, completion axillary dissection isrecommendedrecommended–– Defines prognosisDefines prognosis–– Decreases risk of axillary recurrenceDecreases risk of axillary recurrence

Sentinel Lymph NodeSentinel Lymph NodeBiopsyBiopsy�� TechnetiumTechnetium--99 sulfur99 sulfur
colloid and/or blue dyecolloid and/or blue dyeinjected into breastinjected into breastskin or tissueskin or tissuesurrounding tumorsurrounding tumor
�� Intraoperative cytologyIntraoperative cytologyto determine statusto determine status
�� NSABP B32NSABP B32–– SLNB alone vs.SLNB alone vs.
SLNB/ALNDSLNB/ALND–– 10% false negative rate10% false negative rate–– 97% accuracy97% accuracy
Krag, et al. Lancet Oncol 2007
Lumpectomy orLumpectomy orMastectomy?Mastectomy?
How do you determine theHow do you determine thebest approach?best approach?
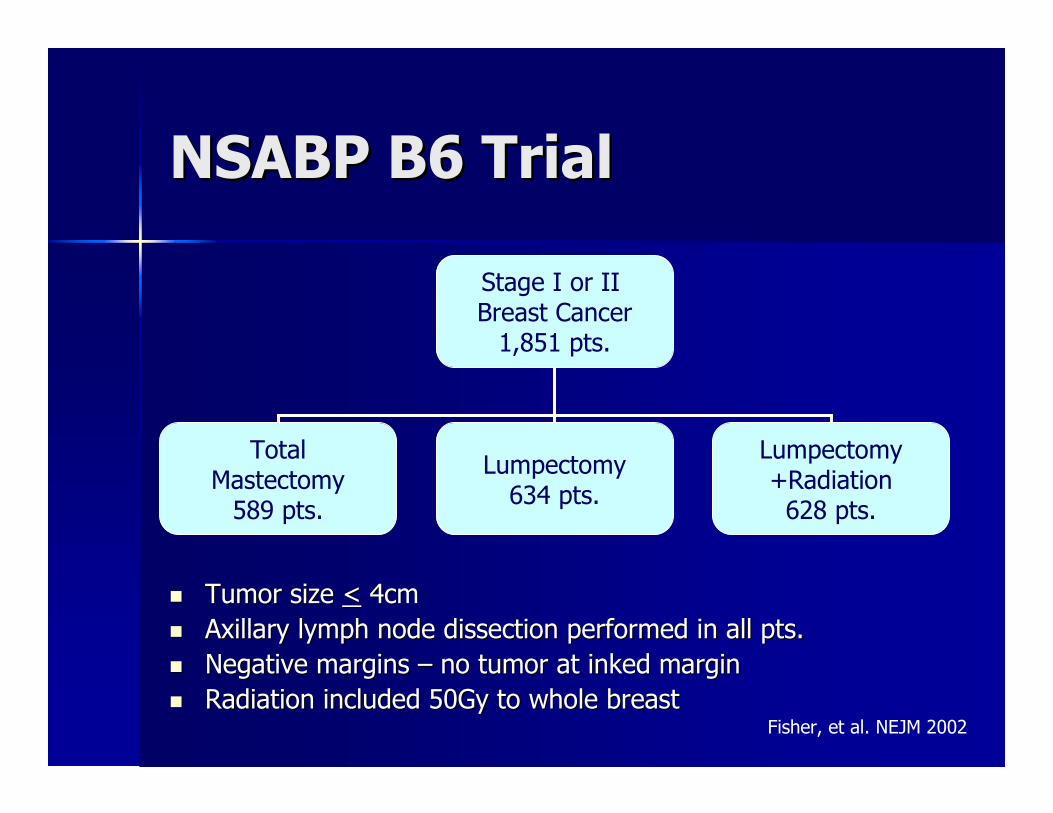
NSABP B6 TrialNSABP B6 Trial
Stage I or IIBreast Cancer
1,851 pts.
TotalMastectomy
589 pts.
Lumpectomy634 pts.
Lumpectomy+Radiation
628 pts.
�� Tumor sizeTumor size << 4cm4cm�� Axillary lymph node dissection performed in all pts.Axillary lymph node dissection performed in all pts.�� Negative marginsNegative margins –– no tumor at inked marginno tumor at inked margin�� Radiation included 50Gy to whole breastRadiation included 50Gy to whole breast
Fisher, et al. NEJM 2002
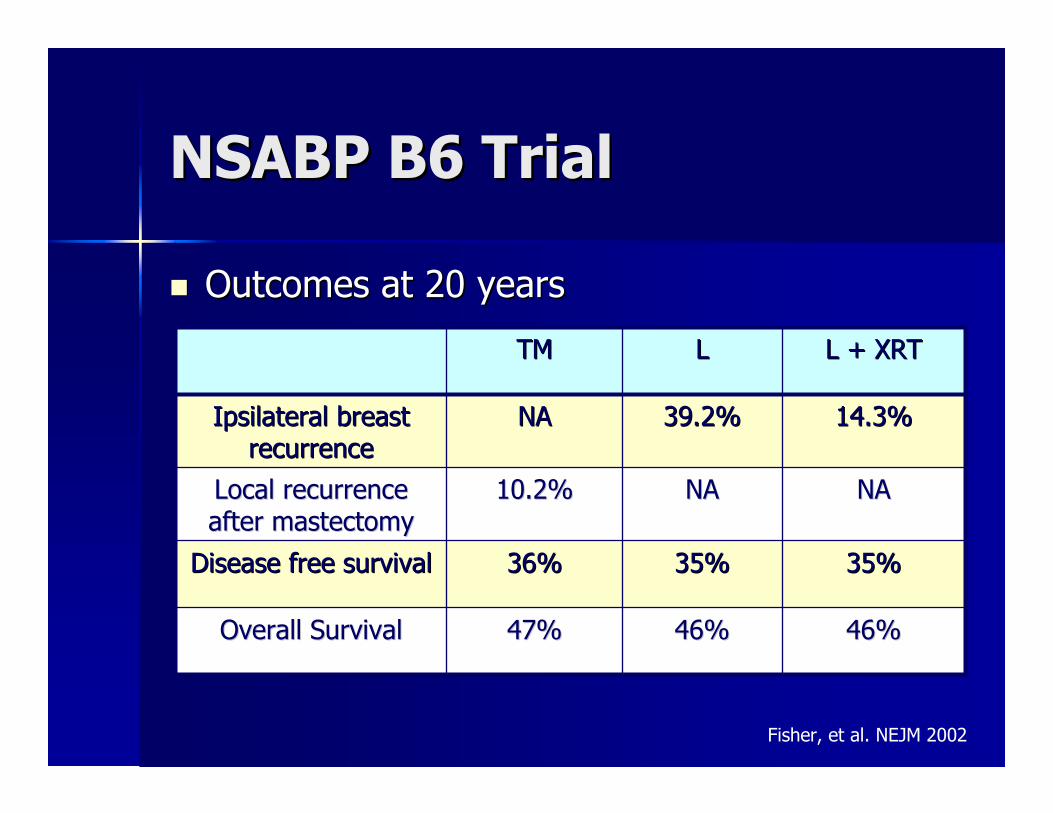
NSABP B6 TrialNSABP B6 Trial
�� Outcomes at 20 yearsOutcomes at 20 years
46%46%46%46%47%47%Overall SurvivalOverall Survival
35%35%35%35%36%36%Disease free survivalDisease free survival
NANANANA10.2%10.2%Local recurrenceLocal recurrenceafter mastectomyafter mastectomy
14.3%14.3%39.2%39.2%NANAIpsilateral breastIpsilateral breastrecurrencerecurrence
L + XRTL + XRTLLTMTM
Fisher, et al. NEJM 2002
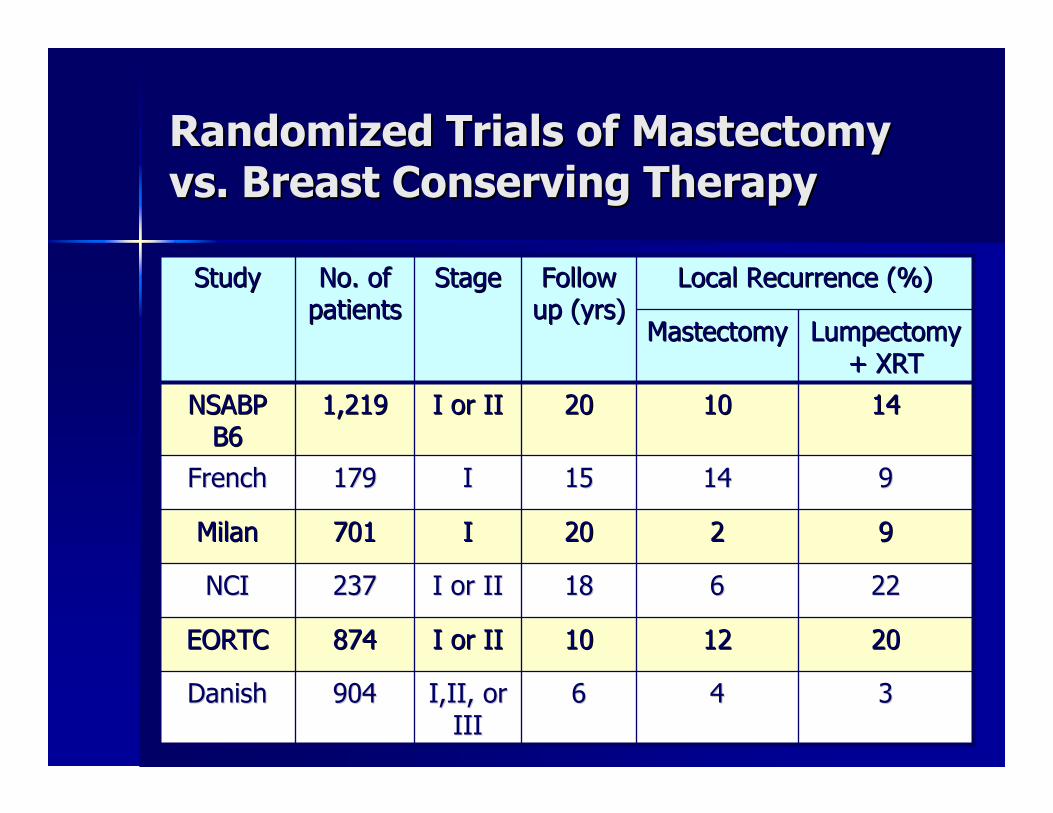
Randomized Trials of MastectomyRandomized Trials of Mastectomyvs. Breast Conserving Therapyvs. Breast Conserving Therapy
334466I,II, orI,II, orIIIIII
904904DanishDanish
202012121010I or III or II874874EORTCEORTC
2222661818I or III or II237237NCINCI
99222020II701701MilanMilan
9914141515II179179FrenchFrench
141410102020I or III or II1,2191,219NSABPNSABPB6B6
LumpectomyLumpectomy+ XRT+ XRT
MastectomyMastectomy
Local Recurrence (%)Local Recurrence (%)FollowFollowup (yrs)up (yrs)
StageStageNo. ofNo. ofpatientspatients
StudyStudy
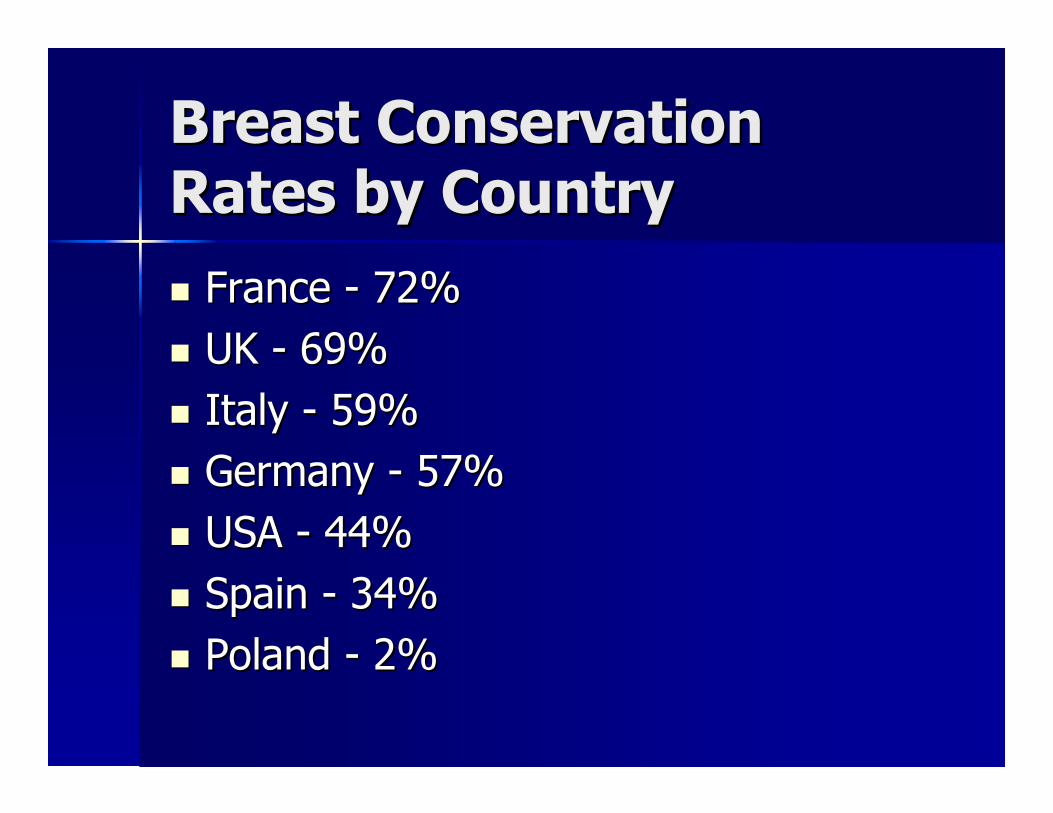
Breast ConservationBreast ConservationRates by CountryRates by Country�� FranceFrance -- 72%72%�� UKUK -- 69%69%�� ItalyItaly -- 59%59%�� GermanyGermany -- 57%57%�� USAUSA -- 44%44%�� SpainSpain -- 34%34%�� PolandPoland -- 2%2%
Cosmetic OutcomeCosmetic Outcome
Courtesy of L. Vallow, Mayo Clinic
Cosmetic OutcomeCosmetic Outcome
Courtesy of L. Vallow, Mayo Clinic
Barriers to BreastBarriers to BreastConservationConservation�� Stage at diagnosisStage at diagnosis�� Lack of screeningLack of screening�� Physician and patient attitudesPhysician and patient attitudes�� Access to radiotherapyAccess to radiotherapy
Indications forIndications forMastectomyMastectomy�� Multicentric diseaseMulticentric disease�� Anticipated poor cosmetic outcome withAnticipated poor cosmetic outcome with
lumpectomylumpectomy�� Persistent positive marginsPersistent positive margins�� Diffuse microcalcificationsDiffuse microcalcifications�� Contraindications to radiation therapyContraindications to radiation therapy
–– PregnancyPregnancy–– Collagen vascular diseaseCollagen vascular disease–– Prior radiation therapyPrior radiation therapy

Is adjuvant radiationIs adjuvant radiationalways indicated afteralways indicated after
lumpectomy?lumpectomy?
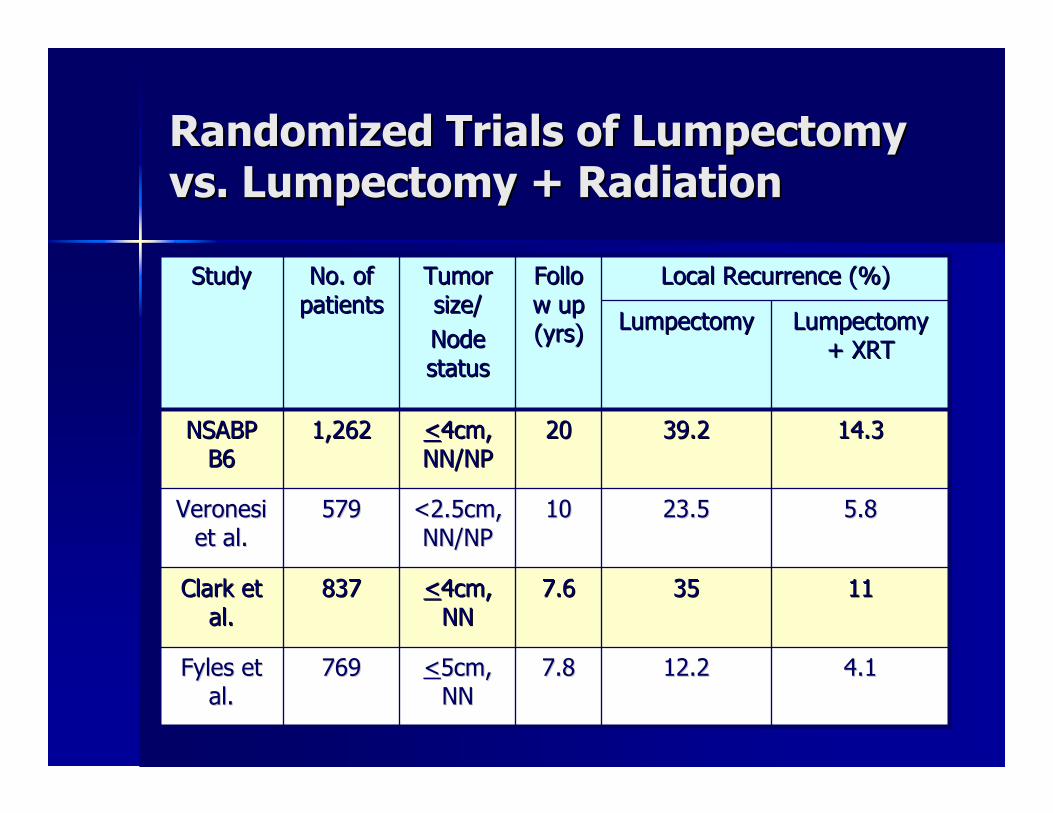
Randomized Trials of LumpectomyRandomized Trials of Lumpectomyvs. Lumpectomy + Radiationvs. Lumpectomy + Radiation
4.14.112.212.27.87.8<<5cm,5cm,NNNN
769769FylesFyles etetal.al.
111135357.67.6<<4cm,4cm,NNNN
837837Clark etClark etal.al.
5.85.823.523.51010<2.5cm,<2.5cm,NN/NPNN/NP
579579VeronesiVeronesiet al.et al.
14.314.339.239.22020<<4cm,4cm,NN/NPNN/NP
1,2621,262NSABPNSABPB6B6
LumpectomyLumpectomy+ XRT+ XRT
LumpectomyLumpectomy
Local Recurrence (%)Local Recurrence (%)FolloFollow upw up(yrs)(yrs)
TumorTumorsize/size/NodeNodestatusstatus
No. ofNo. ofpatientspatients
StudyStudy
Early Breast Cancer TrialistsEarly Breast Cancer TrialistsCollaborative GroupCollaborative Group
�� MetaMeta--analysis of trials comparinganalysis of trials comparingradiation vs. no radiation after BCSradiation vs. no radiation after BCS–– 7,300 patients7,300 patients–– 5 year risk of local recurrence5 year risk of local recurrence
�� 7% with XRT vs. 26% w/o XRT7% with XRT vs. 26% w/o XRT�� 19% absolute reduction19% absolute reduction
–– 5.4% absolute reduction in breast cancer5.4% absolute reduction in breast cancermortalitymortality
Clark et al., Lancet 2005
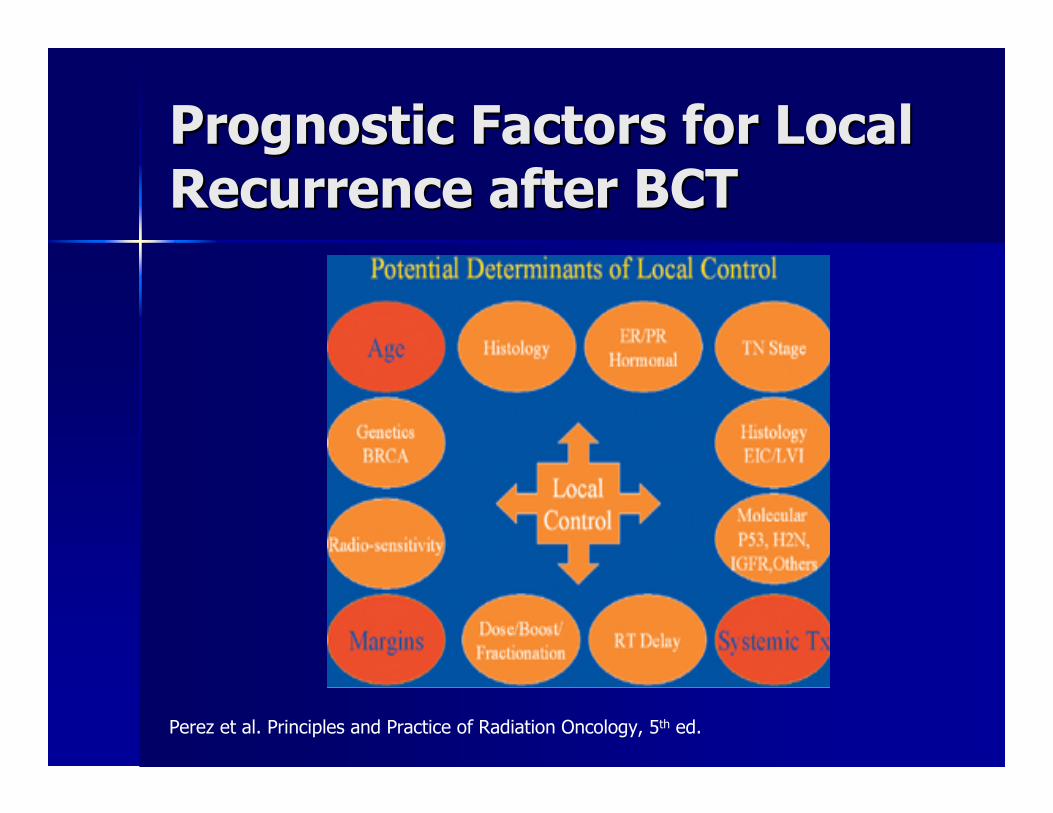
Prognostic Factors for LocalPrognostic Factors for LocalRecurrence after BCTRecurrence after BCT
Perez et al. Principles and Practice of Radiation Oncology, 5th ed.
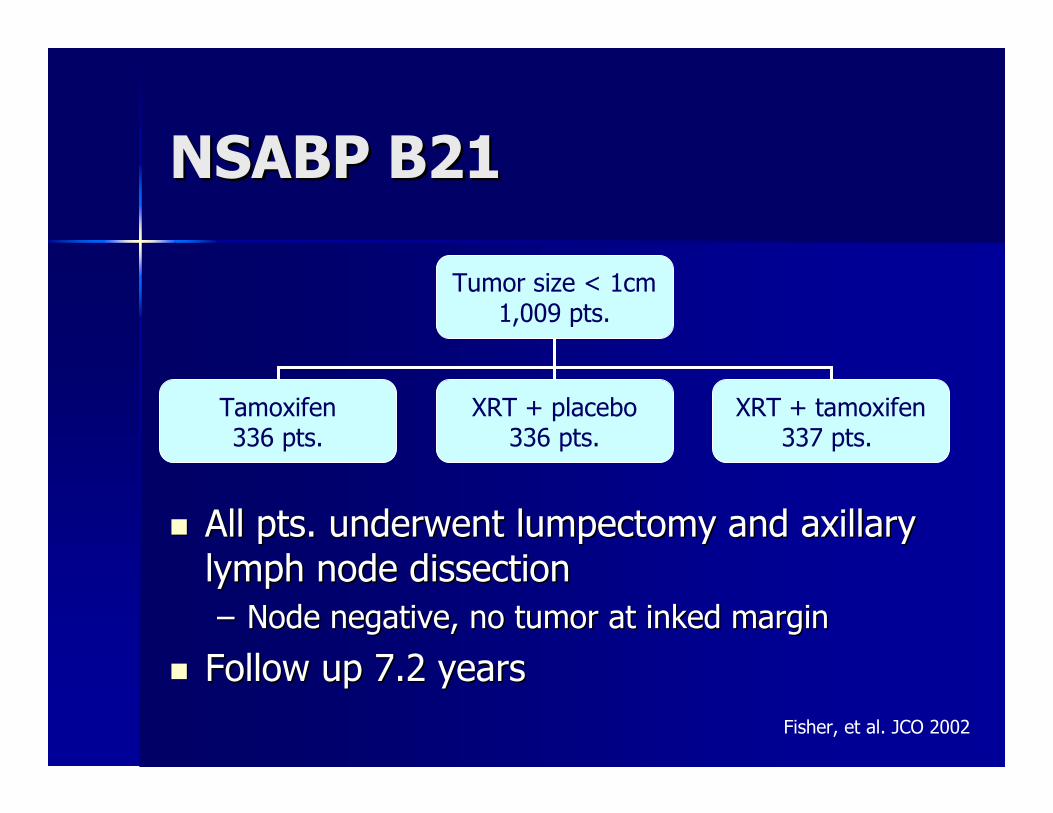
NSABP B21NSABP B21
�� All pts. underwent lumpectomy and axillaryAll pts. underwent lumpectomy and axillarylymph node dissectionlymph node dissection–– Node negative, no tumor at inked marginNode negative, no tumor at inked margin
�� Follow up 7.2 yearsFollow up 7.2 years
Tumor size < 1cm1,009 pts.
Tamoxifen336 pts.
XRT + placebo336 pts.
XRT + tamoxifen337 pts.
Fisher, et al. JCO 2002
NSABP B21NSABP B21
�� Incidence of local relapse at 8 yearsIncidence of local relapse at 8 years–– Tamoxifen group: 16.5%Tamoxifen group: 16.5%–– XRT group: 9.3%XRT group: 9.3%–– XRT + tamoxifen group: 2.8%XRT + tamoxifen group: 2.8%
�� Overall survivalOverall survival–– 93% both arms93% both arms
Fisher, et al. JCO 2002

CALGB TrialCALGB Trial
�� Follow up 8.2 yearsFollow up 8.2 years�� Local recurrenceLocal recurrence
–– 1.3% with XRT1.3% with XRT–– 7.2% w/o XRT7.2% w/o XRT
�� No difference inNo difference inmastectomy rate,mastectomy rate,distant metastases,distant metastases,breast cancer specificbreast cancer specificsurvival, or overallsurvival, or overallsurvivalsurvival
> 70 yrs old< 2cm, node
negative,ER +/?
636 pts.
Lumpectomy+ tamoxifen
319 pts.
Lumpectomy+ tamoxifen
+ XRT317 pts.
Hughes, et al NEJM 2004, updated
Are there indications forAre there indications forradiation after mastectomyradiation after mastectomy
for early stage breastfor early stage breastcancer?cancer?

Radiation AfterRadiation AfterMastectomyMastectomy�� Retrospective review from BritishRetrospective review from British
ColumbiaColumbia�� Reviewed 1,505 pts.Reviewed 1,505 pts.
–– T1T1--2N0 tumors2N0 tumors–– Mastectomy with clear margins, no XRTMastectomy with clear margins, no XRT
�� Median follow up 7 yearsMedian follow up 7 years�� Performed a recursive partitioningPerformed a recursive partitioning
analysis to predict who may benefitanalysis to predict who may benefitfrom XRTfrom XRT
Truong et al., IJROBP 2005

What are the currentWhat are the currenttechniques fortechniques for
whole breast irradiation?whole breast irradiation?
Treatment PositionTreatment Position
�� SupineSupine–– Arms abducted 90Arms abducted 90ºº or greateror greater–– Immobilization devicesImmobilization devices
�� Alpha cradles, breast boards, plastic moldsAlpha cradles, breast boards, plastic molds
�� ProneProne–– Improve dosimetry in large, pendulous breastsImprove dosimetry in large, pendulous breasts–– Reduction of lung volume in fieldReduction of lung volume in field–– Reduction of scatter to opposite breastReduction of scatter to opposite breast
�� Lateral decubitusLateral decubitus–– Improve dosimetry in large, pendulous breastsImprove dosimetry in large, pendulous breasts
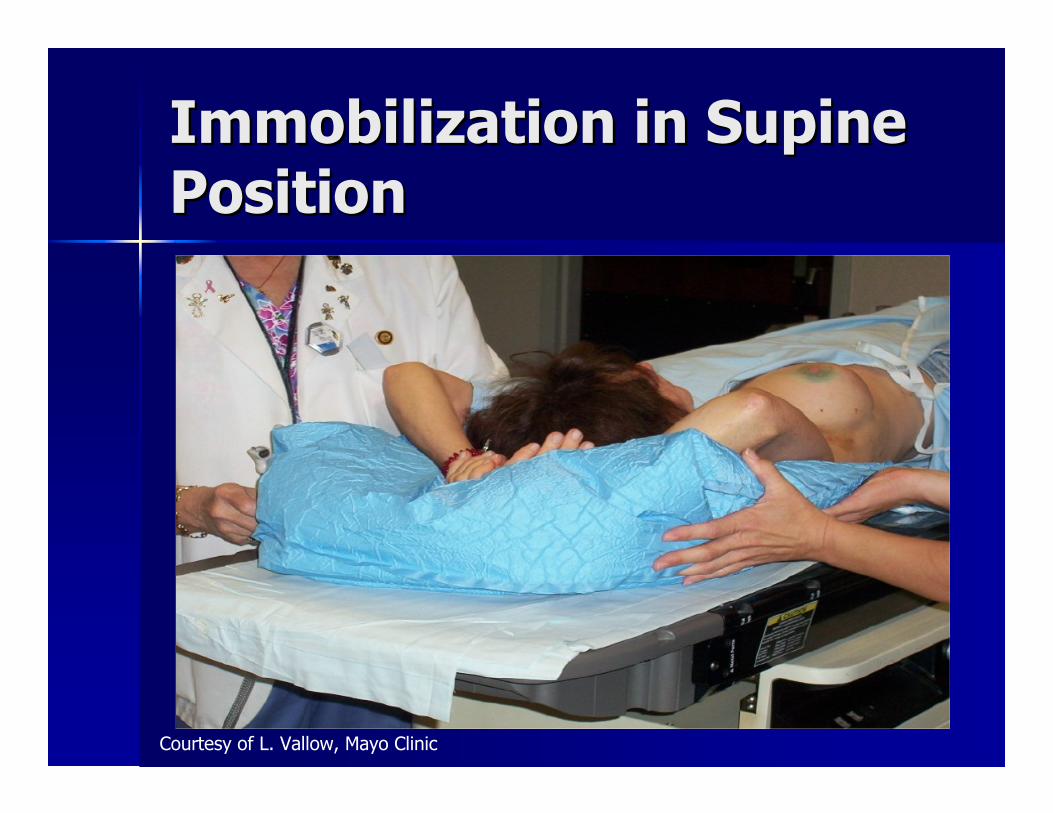
Immobilization in SupineImmobilization in SupinePositionPosition
Courtesy of L. Vallow, Mayo Clinic

Immobilization in SupineImmobilization in SupinePositionPosition
Perez et al. Principles and Practice of Radiation Oncology, 5th ed.
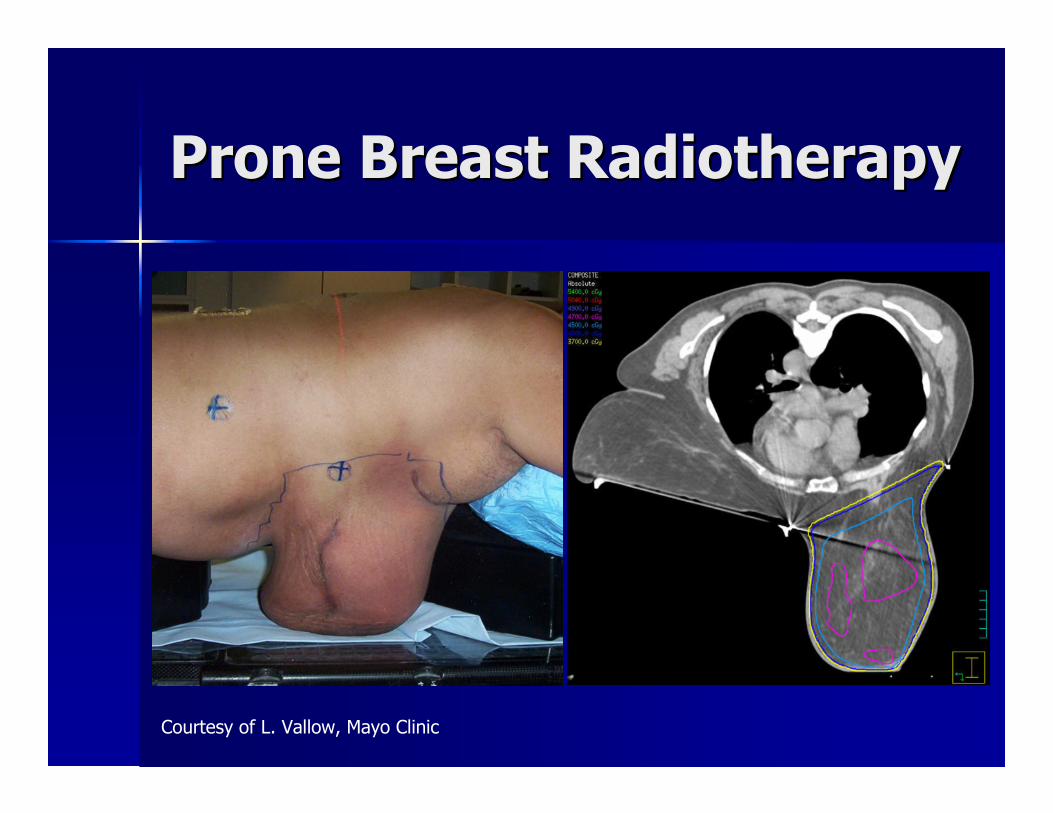
Prone Breast RadiotherapyProne Breast Radiotherapy
Courtesy of L. Vallow, Mayo Clinic
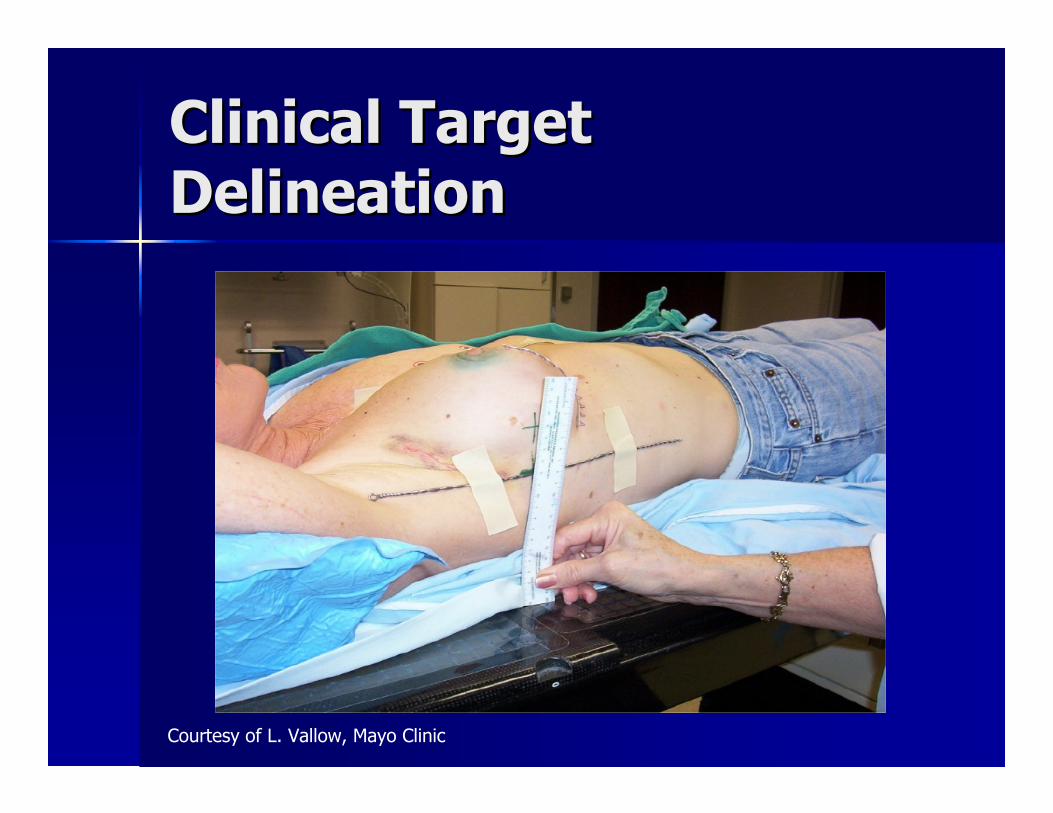
Clinical TargetClinical TargetDelineationDelineation�� Radiopaque wires placed at time ofRadiopaque wires placed at time of
simulation to clinically outline breastsimulation to clinically outline breasttissuetissue–– Superior border: head of the clavicleSuperior border: head of the clavicle–– Medial border: MidlineMedial border: Midline–– Lateral border: 1Lateral border: 1--2cm beyond palpable2cm beyond palpable
breast tissue or posterior to midbreast tissue or posterior to mid--axillaryaxillarylineline
–– Inferior border: 1Inferior border: 1--2cm below2cm belowinframammary foldinframammary fold

Clinical TargetClinical TargetDelineationDelineation
Courtesy of L. Vallow, Mayo Clinic
Clinical TargetClinical TargetDelineationDelineation
Courtesy of L. Vallow, Mayo Clinic
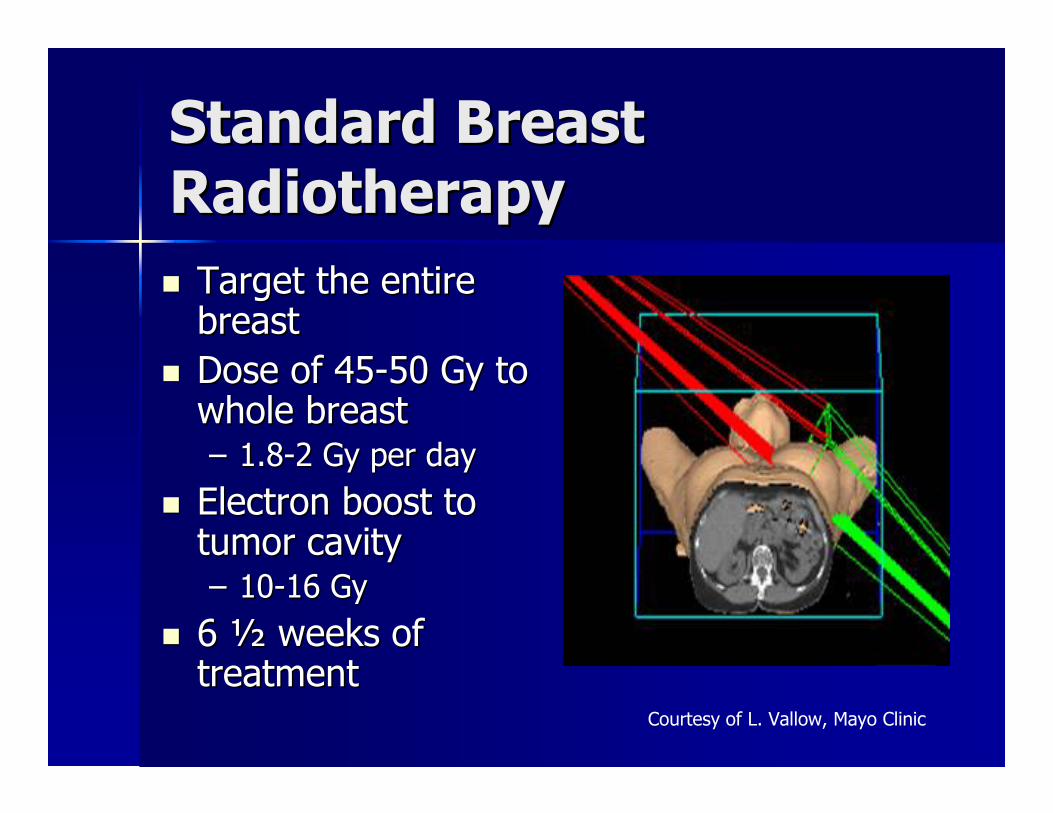
Standard BreastStandard BreastRadiotherapyRadiotherapy�� Target the entireTarget the entire
breastbreast�� Dose of 45Dose of 45--50 Gy to50 Gy to
whole breastwhole breast–– 1.81.8--2 Gy per day2 Gy per day
�� Electron boost toElectron boost totumor cavitytumor cavity–– 1010--16 Gy16 Gy
�� 66 ½½ weeks ofweeks oftreatmenttreatment
Courtesy of L. Vallow, Mayo Clinic
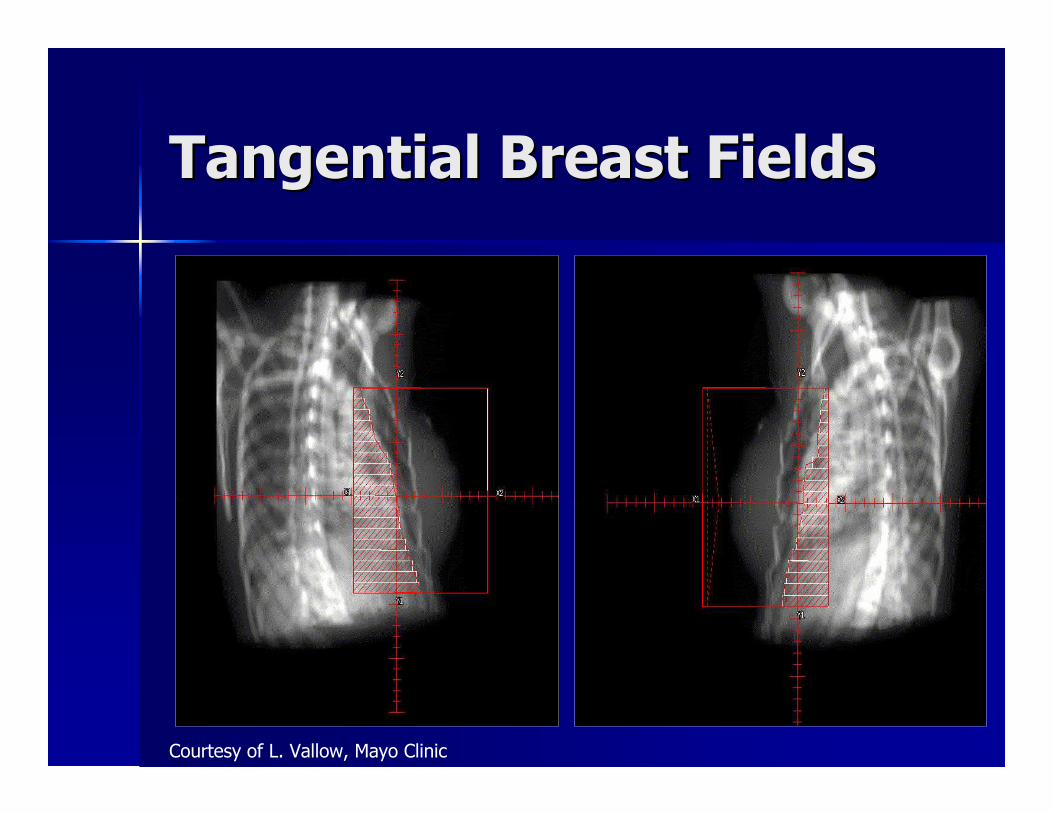
Tangential Breast FieldsTangential Breast Fields
Courtesy of L. Vallow, Mayo Clinic
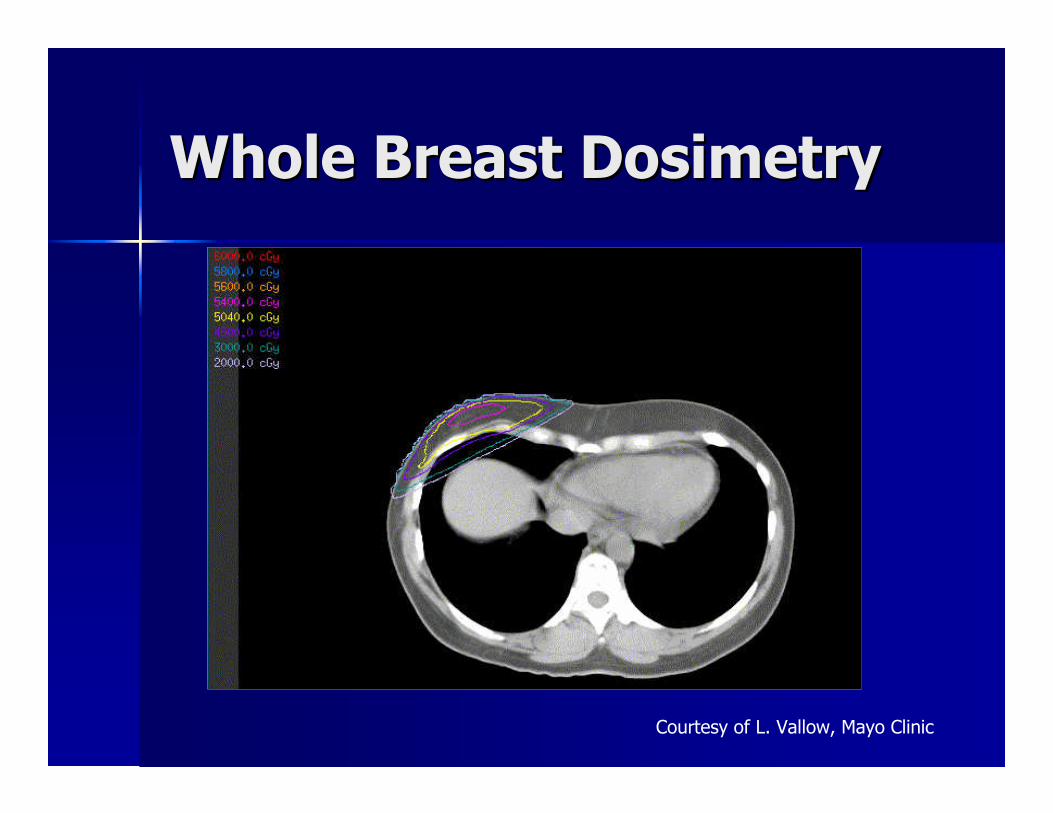
Whole Breast DosimetryWhole Breast Dosimetry
Courtesy of L. Vallow, Mayo Clinic
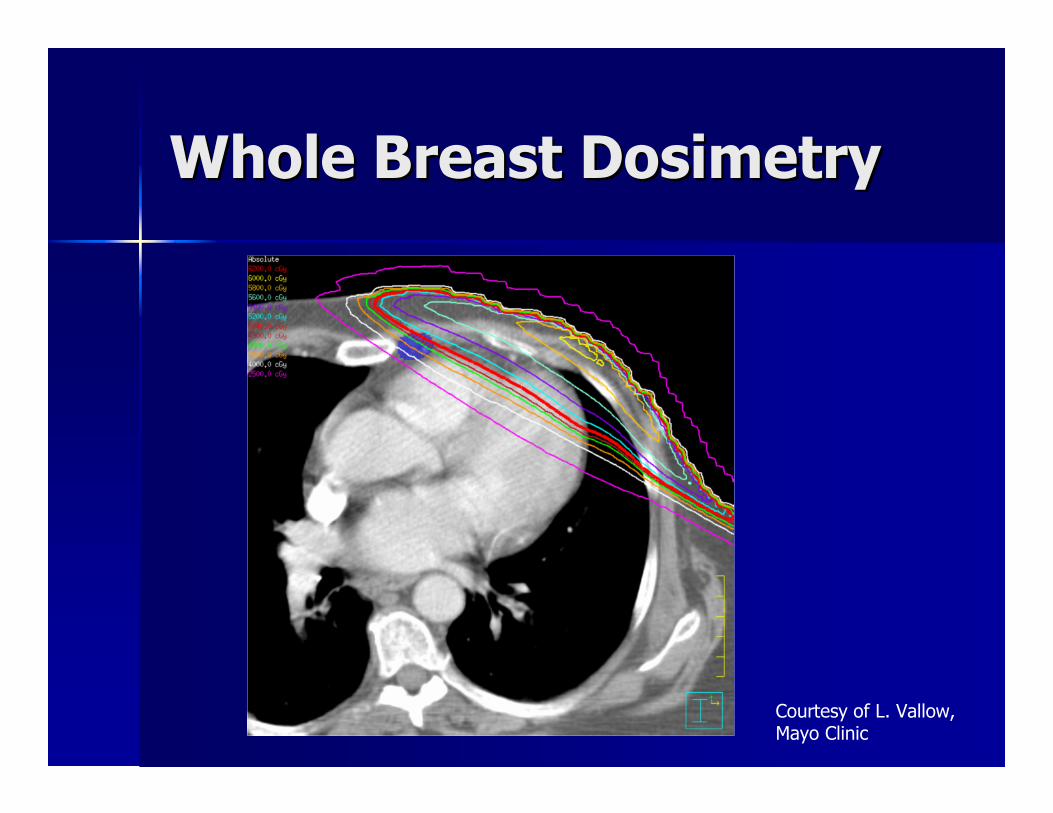
Courtesy of L. Vallow,Mayo Clinic
Whole Breast DosimetryWhole Breast Dosimetry

Alternative FractionationAlternative Fractionation
�� Pathological node negativePathological node negative�� Negative margin, no tumor at inked marginNegative margin, no tumor at inked margin�� TumorTumor << 5cm5cm�� No boost in either armNo boost in either arm�� Maximum width of breast tissueMaximum width of breast tissue << 25cm25cm
1234 womenS/p lumpectomy
XRT50 Gy in 25 fx.
XRT42.5 Gy in 16 fx.
Whelan, et al. J Natl Cancer Inst 2002
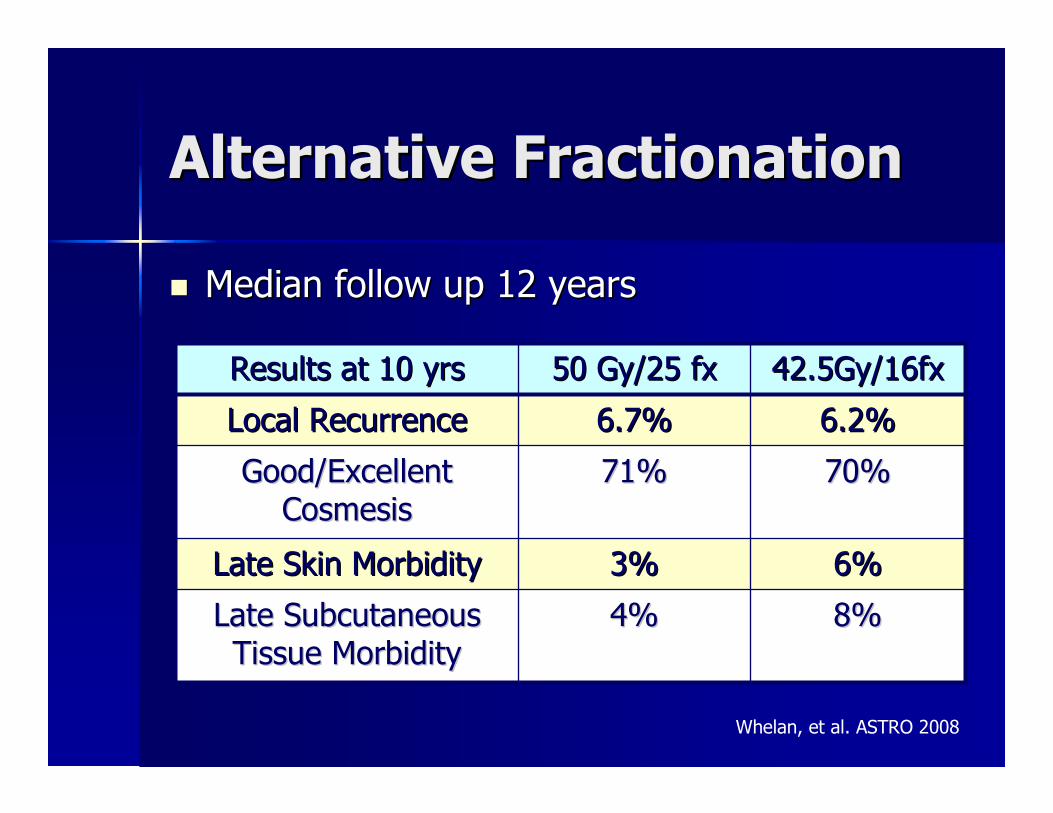
Alternative FractionationAlternative Fractionation
�� Median follow up 12 yearsMedian follow up 12 years
Whelan, et al. ASTRO 2008
8%8%4%4%Late SubcutaneousLate SubcutaneousTissue MorbidityTissue Morbidity
6%6%3%3%Late Skin MorbidityLate Skin Morbidity
70%70%71%71%Good/ExcellentGood/ExcellentCosmesisCosmesis
6.2%6.2%6.7%6.7%Local RecurrenceLocal Recurrence
42.5Gy/16fx42.5Gy/16fx50 Gy/25 fx50 Gy/25 fxResults at 10 yrsResults at 10 yrs

Boost to Tumor CavityBoost to Tumor Cavity
�� Lyons TrialLyons Trial–– Randomized 1,024 patients to boost ofRandomized 1,024 patients to boost of
10Gy to tumor bed vs. no boost after 50Gy10Gy to tumor bed vs. no boost after 50Gyto whole breastto whole breast
–– Included invasive T1Included invasive T1--2, N02, N0--1 tumors1 tumors–– << 3cm, negative margins3cm, negative margins–– Median follow up 3.3 yearsMedian follow up 3.3 years–– Local recurrence at 5 years 3.6% vs. 4.5%Local recurrence at 5 years 3.6% vs. 4.5%
in favor of boostin favor of boost–– Disease free survival at 5 years 82% vs.Disease free survival at 5 years 82% vs.
86% in favor of boost86% in favor of boost
Romestaing, et al. JCO 1997
Boost to Tumor CavityBoost to Tumor Cavity
�� EORTC 22881EORTC 22881–– Randomized 5,318 patients to boostRandomized 5,318 patients to boost
of 16Gy to tumor bed vs. no boostof 16Gy to tumor bed vs. no boostafter 50Gy to whole breastafter 50Gy to whole breast
–– Included invasive T1Included invasive T1--2, N02, N0--1 tumors1 tumors–– Negative marginsNegative margins–– Median follow up 10.8 yearsMedian follow up 10.8 years–– Local recurrence at 10 years 10.2%Local recurrence at 10 years 10.2%
vs. 6.2% in favor of boostvs. 6.2% in favor of boostBartelink, et al. JCO 2007
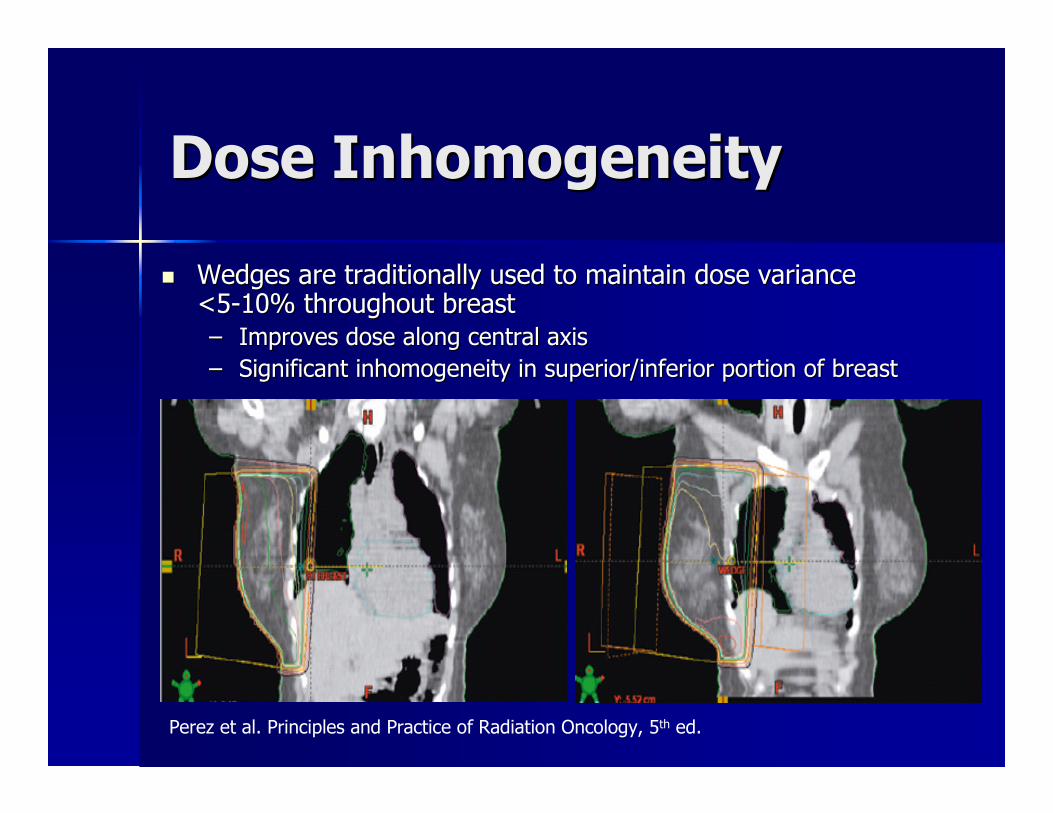
Dose InhomogeneityDose Inhomogeneity
�� Wedges are traditionally used to maintain dose varianceWedges are traditionally used to maintain dose variance<5<5--10% throughout breast10% throughout breast–– Improves dose along central axisImproves dose along central axis–– Significant inhomogeneity in superior/inferior portion of breastSignificant inhomogeneity in superior/inferior portion of breast
Perez et al. Principles and Practice of Radiation Oncology, 5th ed.

IMRT for BreastIMRT for BreastRadiotherapyRadiotherapy�� Optimize dose homogeneityOptimize dose homogeneity�� Avoid unnecessary normal tissueAvoid unnecessary normal tissue
radiationradiation�� Improve target volume coverageImprove target volume coverage
IMRT for BreastIMRT for BreastRadiotherapyRadiotherapy
Courtesy of L. Vallow,Mayo Clinic
IMRT for BreastIMRT for BreastRadiotherapyRadiotherapy�� Review of 281 women with Stage 0Review of 281 women with Stage 0--IIII
breast cancer treated with BCTbreast cancer treated with BCT�� Static, multileaf collimator IMRTStatic, multileaf collimator IMRT
techniquetechnique–– Median planning time: 40Median planning time: 40--45 minutes45 minutes–– Median # of sMLC segments: 6Median # of sMLC segments: 6–– Median treatment time: <10minMedian treatment time: <10min–– Median % of treatment with open field:Median % of treatment with open field:
83%83%Vicini, et al. IJROBP, 2002Vicini, et al. IJROBP, 2002

IMRT for BreastIMRT for BreastRadiotherapyRadiotherapy�� OutcomesOutcomes
–– Median volume of breast receiving % ofMedian volume of breast receiving % ofprescribed doseprescribed dose�� 105% prescribed dose: 11%105% prescribed dose: 11%�� 110% prescribed dose : 0%110% prescribed dose : 0%�� 115% prescribed dose : 0%115% prescribed dose : 0%
–– 1% grade 3 toxicity1% grade 3 toxicity–– 99% good or excellent cosmesis99% good or excellent cosmesis
Vicini, et al. IJROBP, 2002Vicini, et al. IJROBP, 2002
IMRT for BreastIMRT for BreastRadiotherapyRadiotherapy
�� All patients received lumpectomy followed by 50GyAll patients received lumpectomy followed by 50Gyin 25fxin 25fx–– Stratified use of boost and breast sizeStratified use of boost and breast size
�� Significant reduction in VSignificant reduction in V105105, V, V107107, V, V110110, V, V115115
�� Decrease in moist desquamation, 31% vs. 48%Decrease in moist desquamation, 31% vs. 48%
Pignol, et al. JCO 2008
331 pts.Early stage breast cancer
Breast IMRT Standard XRT withwedge compensation
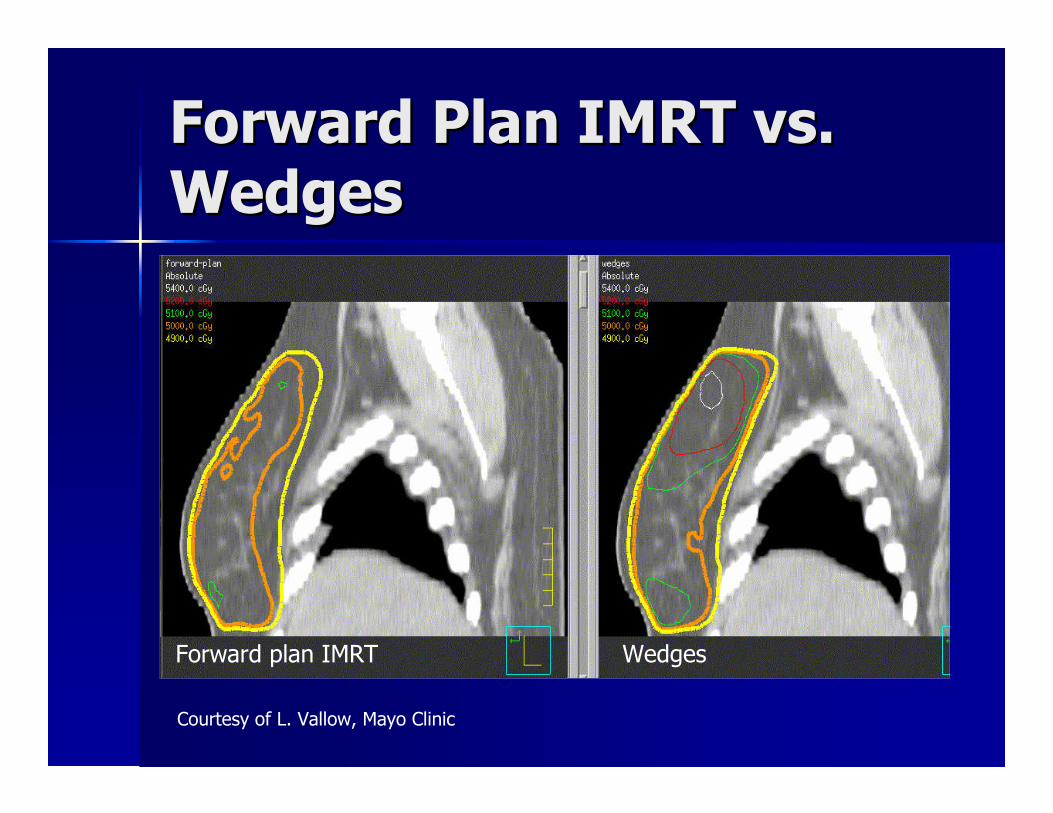
Forward Plan IMRT vs.Forward Plan IMRT vs.WedgesWedges
Forward plan IMRT Wedges
Courtesy of L. Vallow, Mayo Clinic
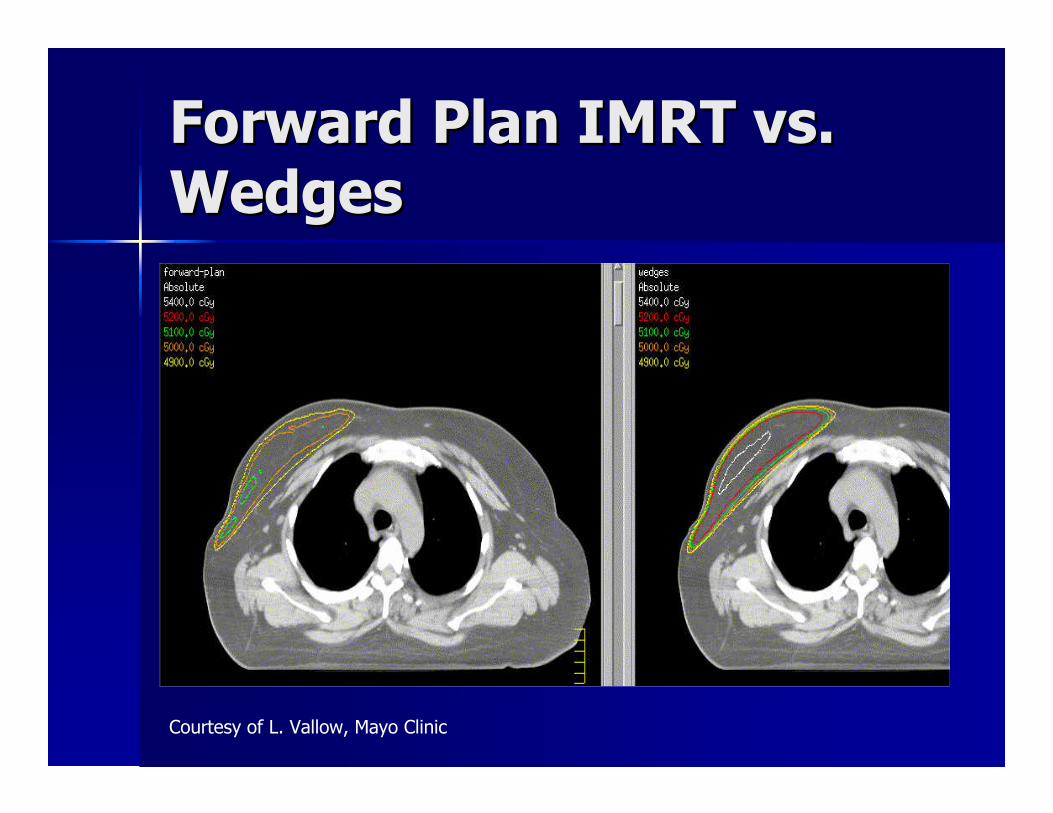
Forward Plan IMRT vs.Forward Plan IMRT vs.WedgesWedges
Courtesy of L. Vallow, Mayo Clinic
What is the rationale forWhat is the rationale forpartial breastpartial breastirradiation?irradiation?

Partial Breast IrradiationPartial Breast Irradiation
�� 6565--80% of breast tumor recurrences80% of breast tumor recurrencesrecur around the primary siterecur around the primary site
�� Incidence of elsewhere failures withinIncidence of elsewhere failures withinthe breast are equivalent in womenthe breast are equivalent in womenwith or without XRT after lumpectomywith or without XRT after lumpectomy
�� Adjuvant XRT can be completed withinAdjuvant XRT can be completed within5 days5 days
Partial Breast IrradiationPartial Breast Irradiation
�� MultiMulti--catheter brachytherapycatheter brachytherapy�� MammoSite brachytherapyMammoSite brachytherapy�� 3D3D--Conformal external beam radiationConformal external beam radiation
therapytherapy
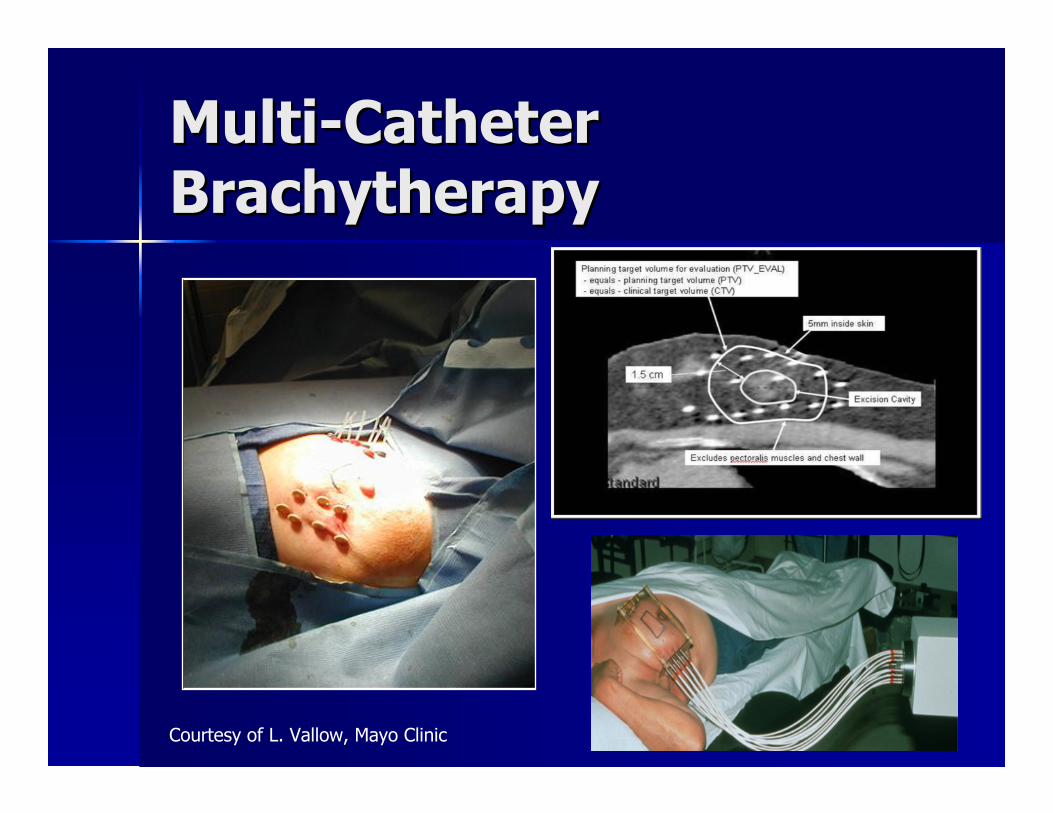
MultiMulti--CatheterCatheterBrachytherapyBrachytherapy
Courtesy of L. Vallow, Mayo Clinic

MultiMulti--CatheterCatheterBrachytherapyBrachytherapy
4.4%4.4%70704545NIO, HungaryNIO, HungaryPhase I/IIPhase I/II
3%3%44449999RTOG 95RTOG 95--1717
2.5%2.5%8484160160Ochsner ClinicOchsner Clinic
1.2%1.2%6565199199WilliamWilliamBeaumontBeaumont
5 yr. Local5 yr. Localrecurrencerecurrence
Follow upFollow up(months)(months)
No. ofNo. ofpatientspatients
StudyStudy
Keisch et al., The Breast Journal 2005
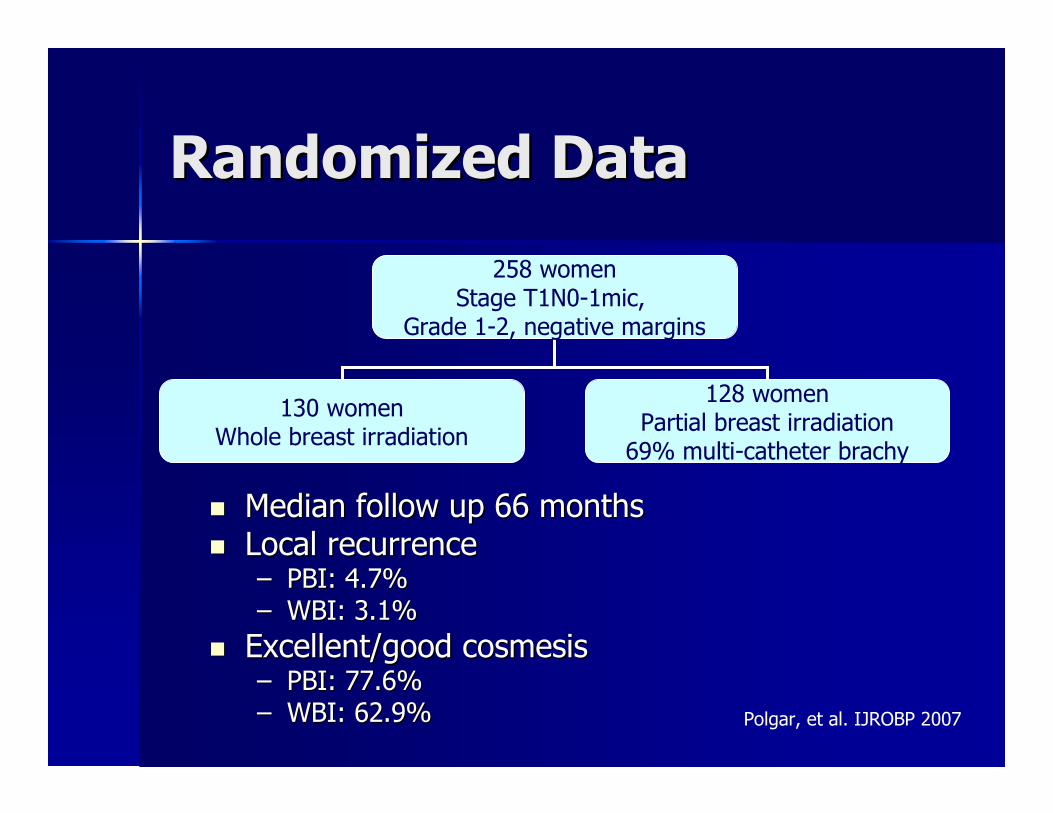
Randomized DataRandomized Data
�� Median follow up 66 monthsMedian follow up 66 months�� Local recurrenceLocal recurrence
–– PBI: 4.7%PBI: 4.7%–– WBI: 3.1%WBI: 3.1%
�� Excellent/good cosmesisExcellent/good cosmesis–– PBI: 77.6%PBI: 77.6%–– WBI: 62.9%WBI: 62.9%
258 womenStage T1N0-1mic,
Grade 1-2, negative margins
130 womenWhole breast irradiation
128 womenPartial breast irradiation
69% multi-catheter brachy
Polgar, et al. IJROBP 2007

MammoSiteMammoSiteBrachytherapyBrachytherapy
Courtesy of L. Vallow, Mayo Clinic
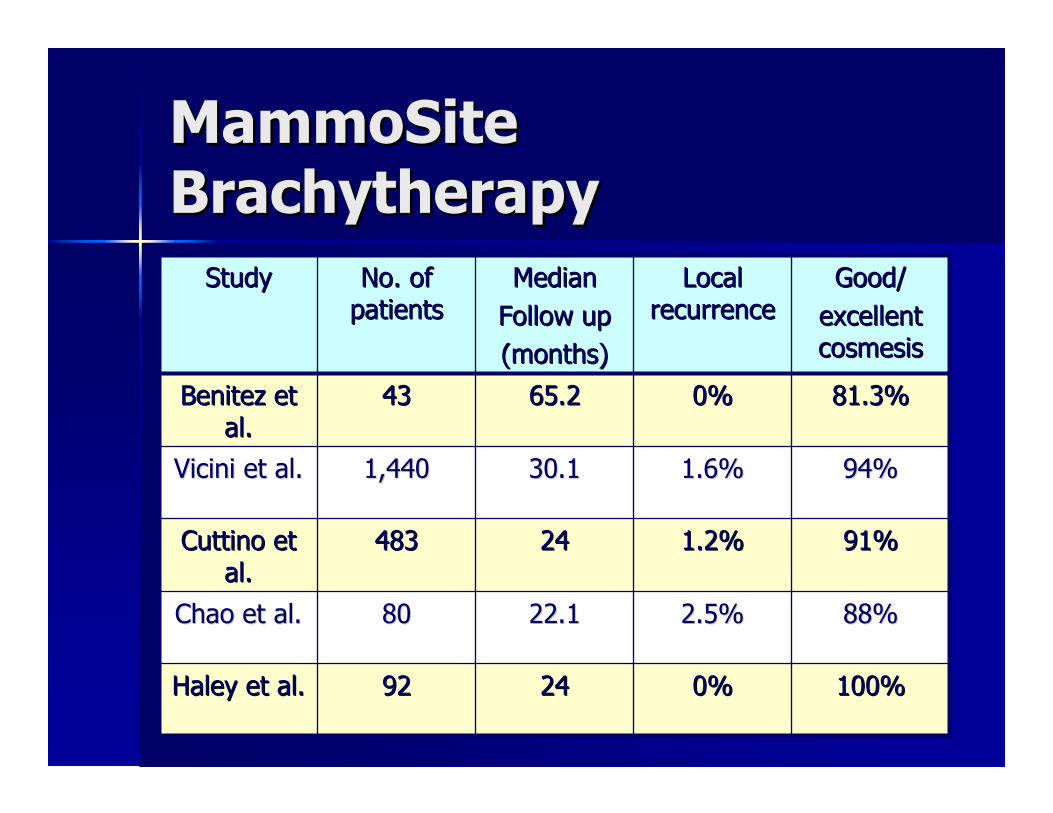
MammoSiteMammoSiteBrachytherapyBrachytherapy
100%100%0%0%24249292Haley et al.Haley et al.
88%88%2.5%2.5%22.122.18080Chao et al.Chao et al.
91%91%1.2%1.2%2424483483Cuttino etCuttino etal.al.
94%94%1.6%1.6%30.130.11,4401,440Vicini et al.Vicini et al.
81.3%81.3%0%0%65.265.24343Benitez etBenitez etal.al.
Good/Good/excellentexcellentcosmesiscosmesis
LocalLocalrecurrencerecurrence
MedianMedianFollow upFollow up(months)(months)
No. ofNo. ofpatientspatients
StudyStudy
Technical AspectsTechnical Aspects
�� Placement of catheterPlacement of catheter–– Open technique: placed at the time of surgeryOpen technique: placed at the time of surgery
�� Increased seroma formationIncreased seroma formation
–– Closed technique: placed postClosed technique: placed post--lumpectomylumpectomy�� Decreased risk of infectionDecreased risk of infection
�� Technical requirements verified by CTTechnical requirements verified by CT–– Skin spacingSkin spacing >> 5mm5mm–– BalloonBalloon--cavity conformance, > 90%cavity conformance, > 90%–– AsymmetryAsymmetry
�� MammoSite explantation rate ~ 10MammoSite explantation rate ~ 10--20%20%
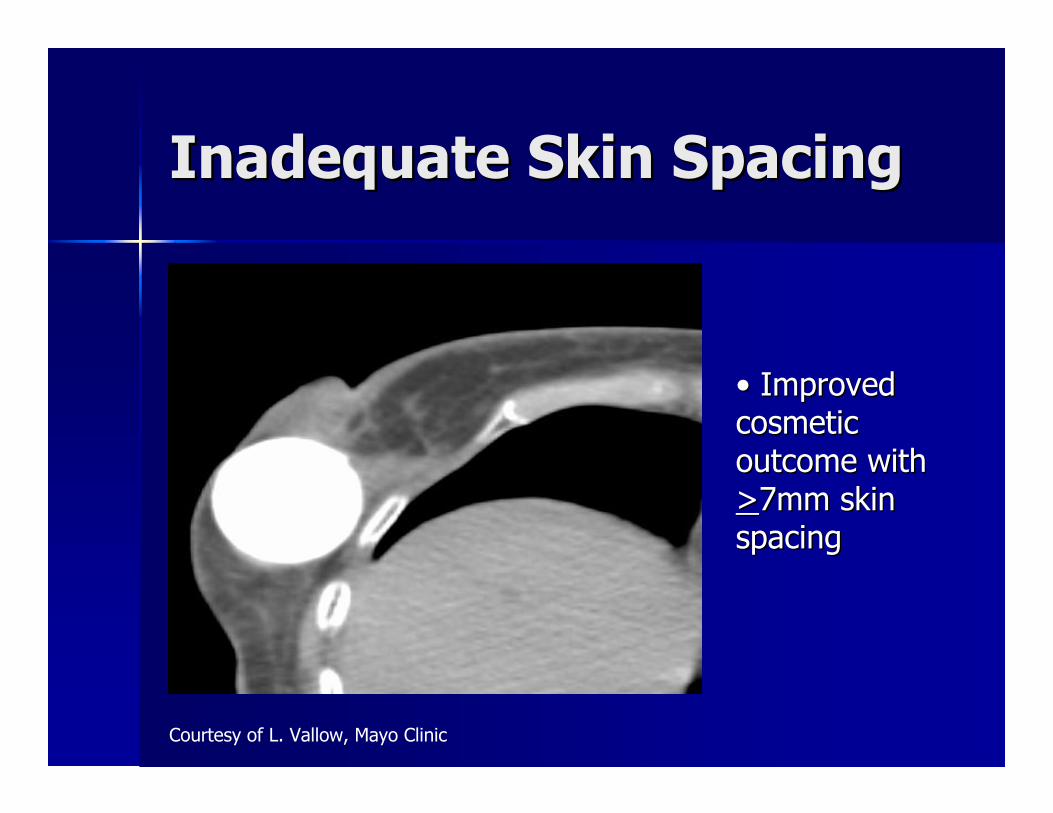
Inadequate Skin SpacingInadequate Skin Spacing
Courtesy of L. Vallow, Mayo Clinic
•• ImprovedImprovedcosmeticcosmeticoutcome withoutcome with>>7mm skin7mm skinspacingspacing
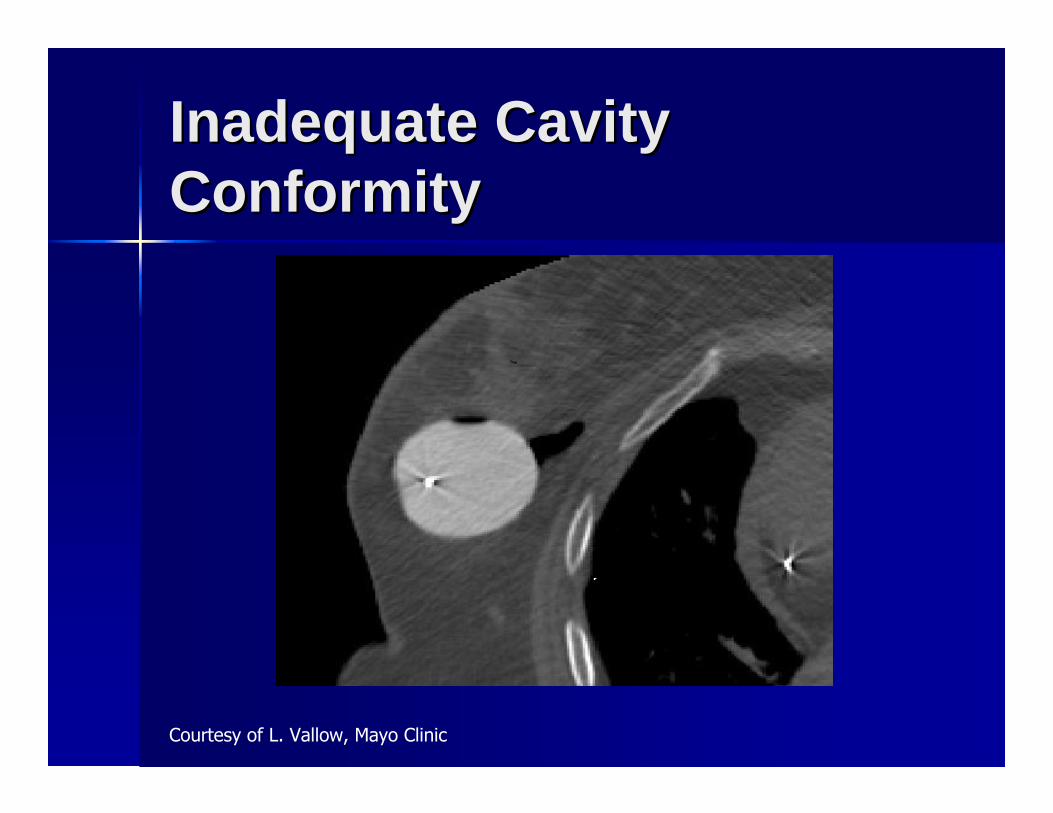
Inadequate CavityInadequate CavityConformityConformity
Courtesy of L. Vallow, Mayo Clinic
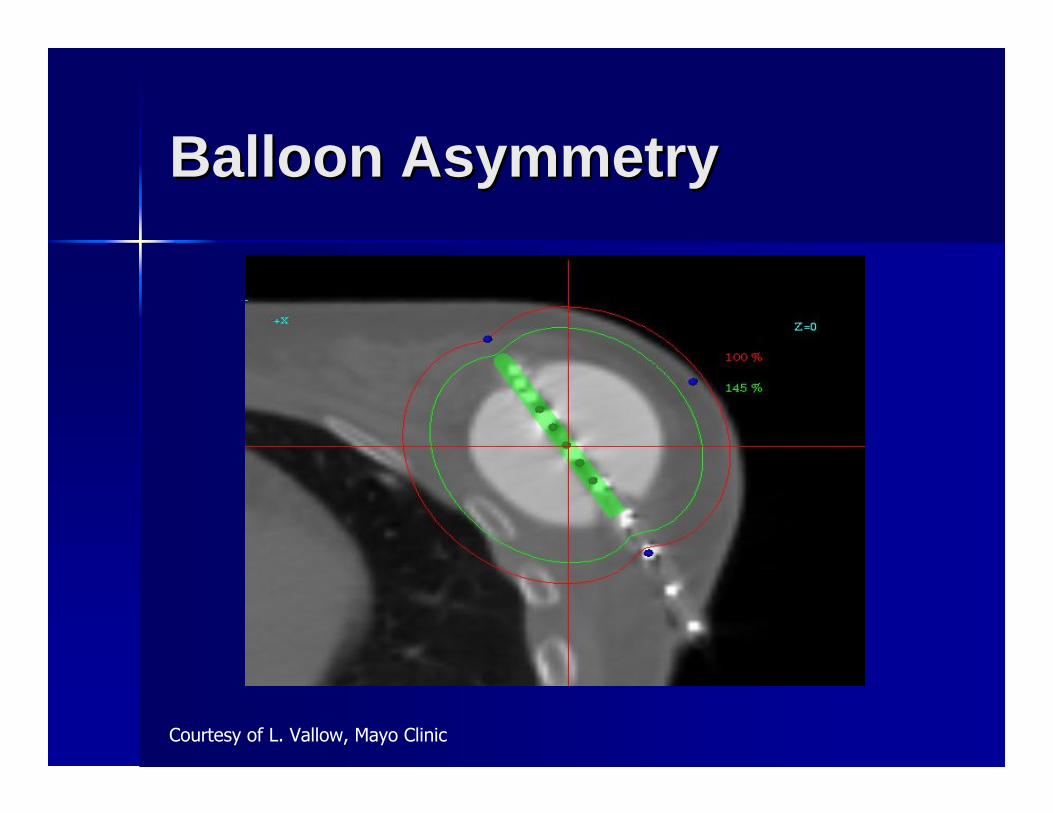
Balloon AsymmetryBalloon Asymmetry
Courtesy of L. Vallow, Mayo Clinic
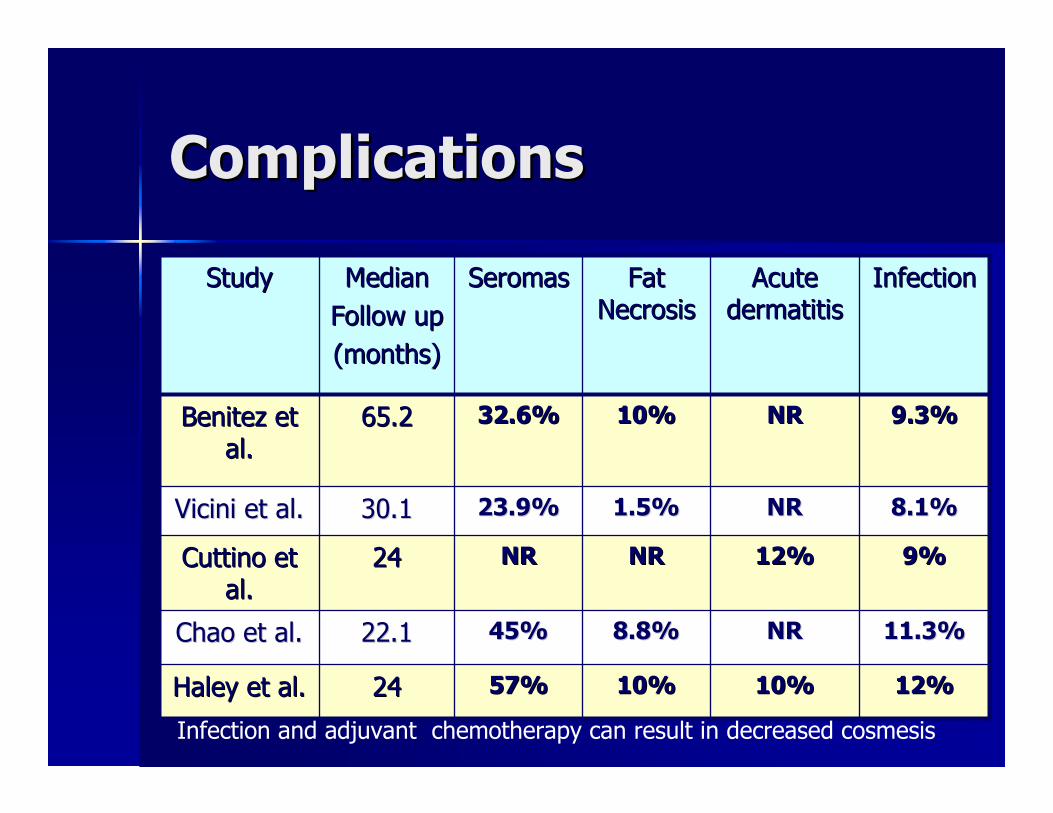
ComplicationsComplications
11.3%11.3%NRNR8.8%8.8%45%45%22.122.1Chao et al.Chao et al.
StudyStudy MedianMedianFollow upFollow up(months)(months)
SeromasSeromas FatFatNecrosisNecrosis
AcuteAcutedermatitisdermatitis
InfectionInfection
Benitez etBenitez etal.al.
65.265.2 32.6%32.6% 10%10% NRNR 9.3%9.3%
Vicini et al.Vicini et al. 30.130.1 23.9%23.9% 1.5%1.5% NRNR 8.1%8.1%
Cuttino etCuttino etal.al.
2424 NRNR NRNR 12%12% 9%9%
Haley et al.Haley et al. 2424 57%57% 10%10% 10%10% 12%12%
Infection and adjuvant chemotherapy can result in decreased cosmesis
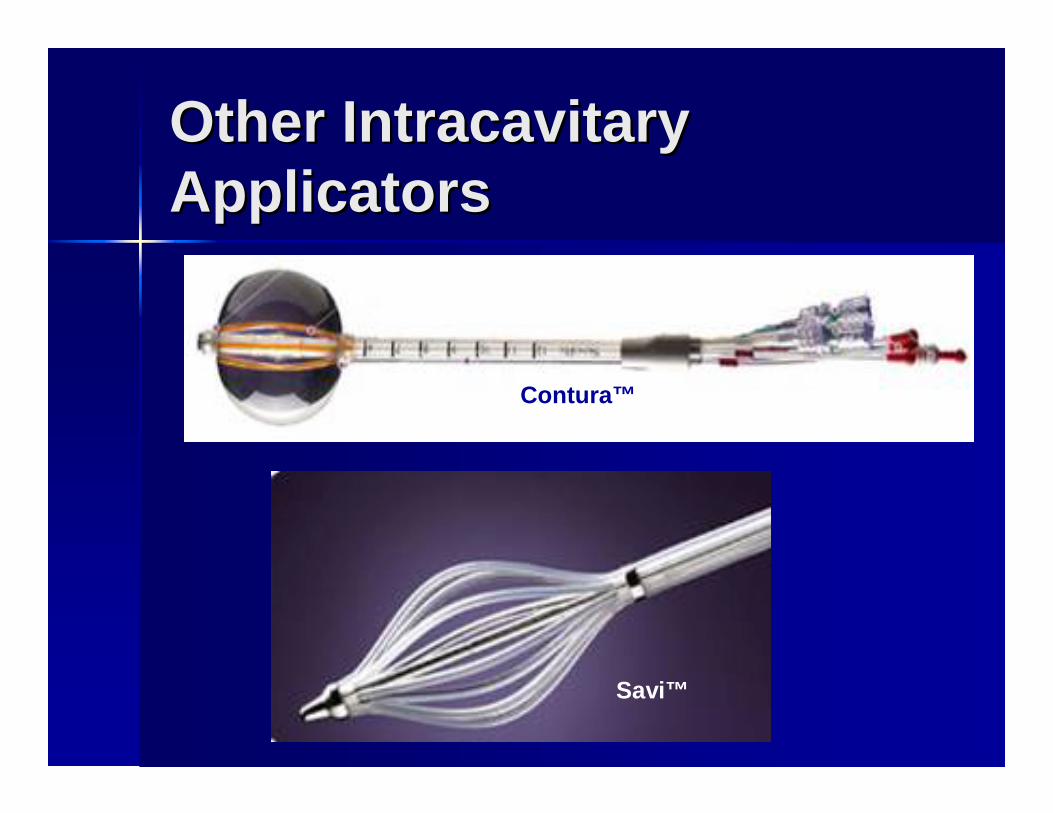
Other IntracavitaryOther IntracavitaryApplicatorsApplicators
Contura™
Savi™
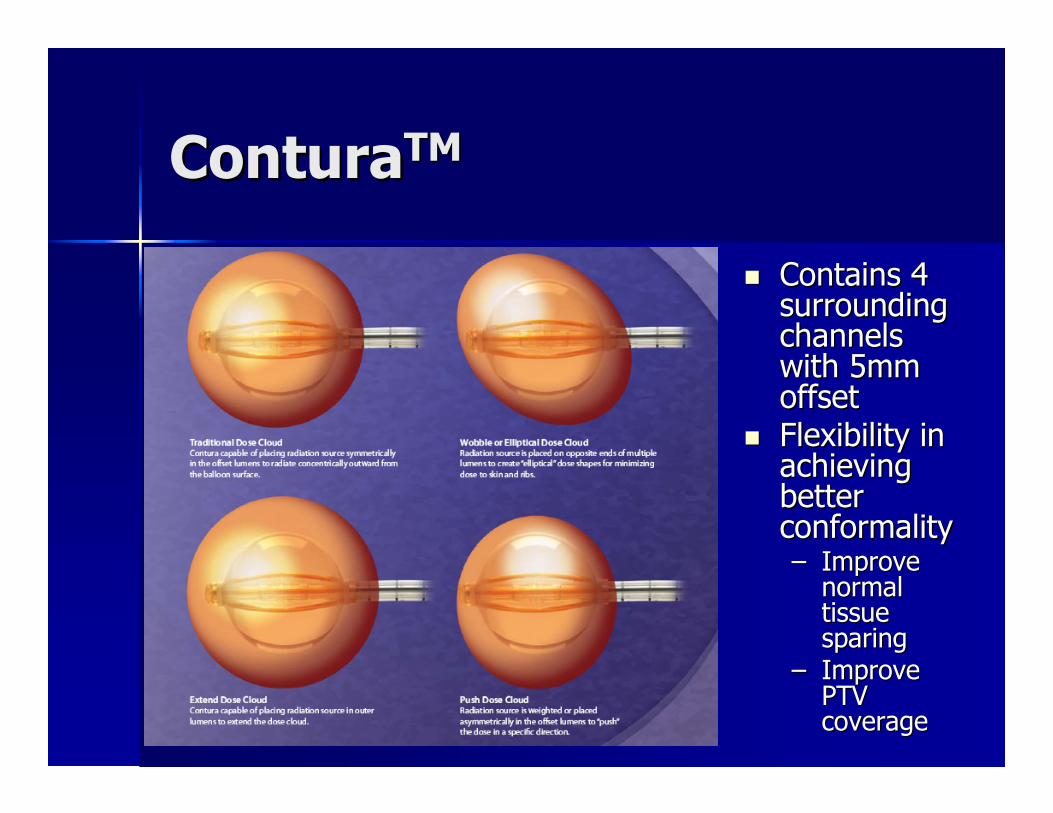
ConturaConturaTMTM
�� Contains 4Contains 4surroundingsurroundingchannelschannelswith 5mmwith 5mmoffsetoffset
�� Flexibility inFlexibility inachievingachievingbetterbetterconformalityconformality–– ImproveImprove
normalnormaltissuetissuesparingsparing
–– ImproveImprovePTVPTVcoveragecoverage

ConturaConturaTMTM
�� Vacuum port allows for improved conformityVacuum port allows for improved conformity
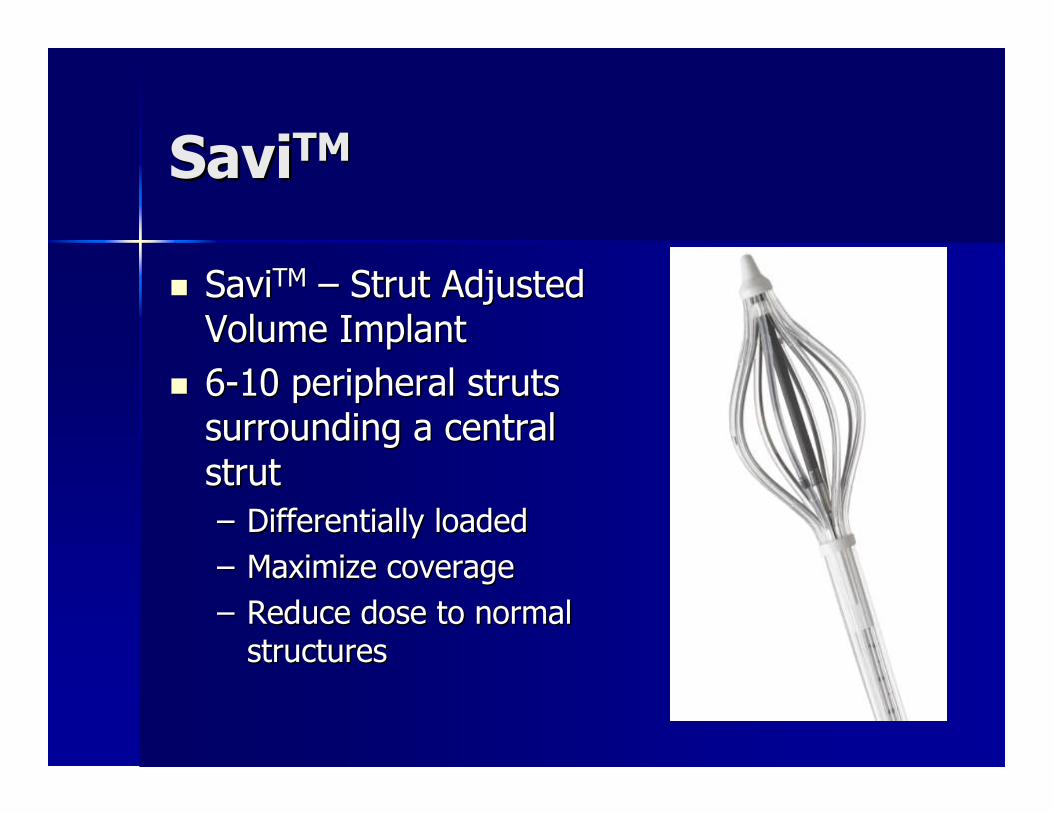
SaviSaviTMTM
�� SaviSaviTMTM –– Strut AdjustedStrut AdjustedVolume ImplantVolume Implant
�� 66--10 peripheral struts10 peripheral strutssurrounding a centralsurrounding a centralstrutstrut–– Differentially loadedDifferentially loaded–– Maximize coverageMaximize coverage–– Reduce dose to normalReduce dose to normal
structuresstructures
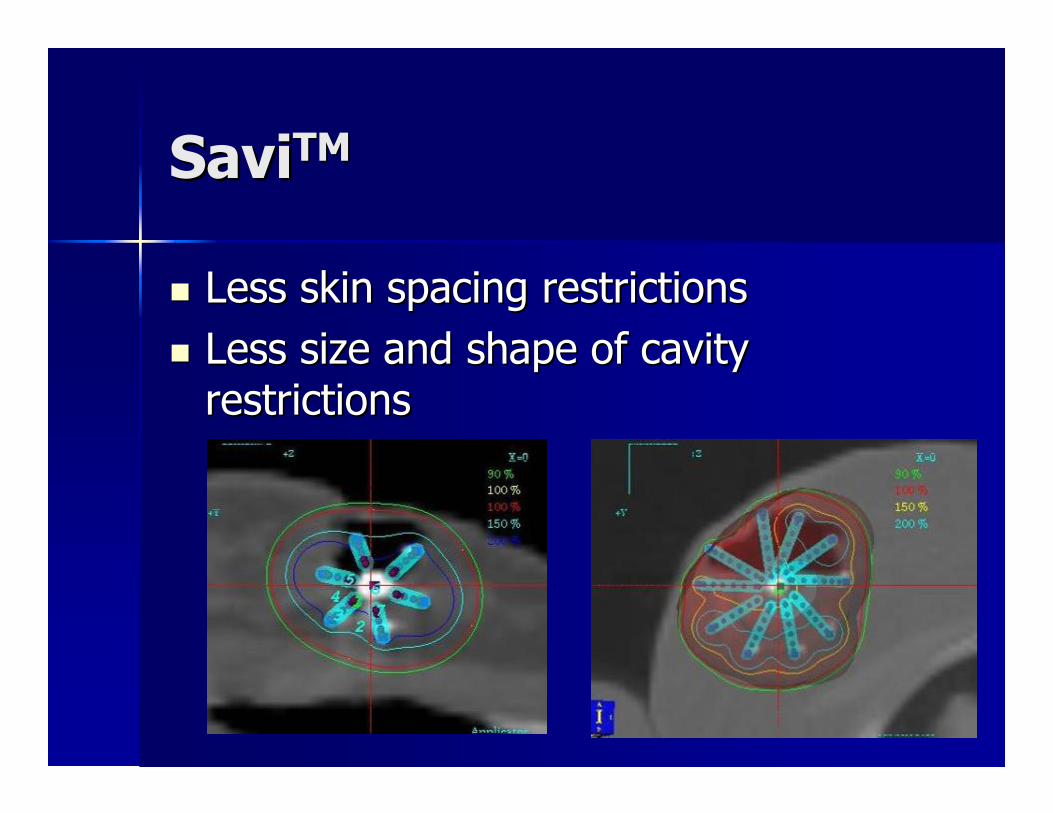
SaviSaviTMTM
�� Less skin spacing restrictionsLess skin spacing restrictions�� Less size and shape of cavityLess size and shape of cavity
restrictionsrestrictions

SaviSaviTMTM
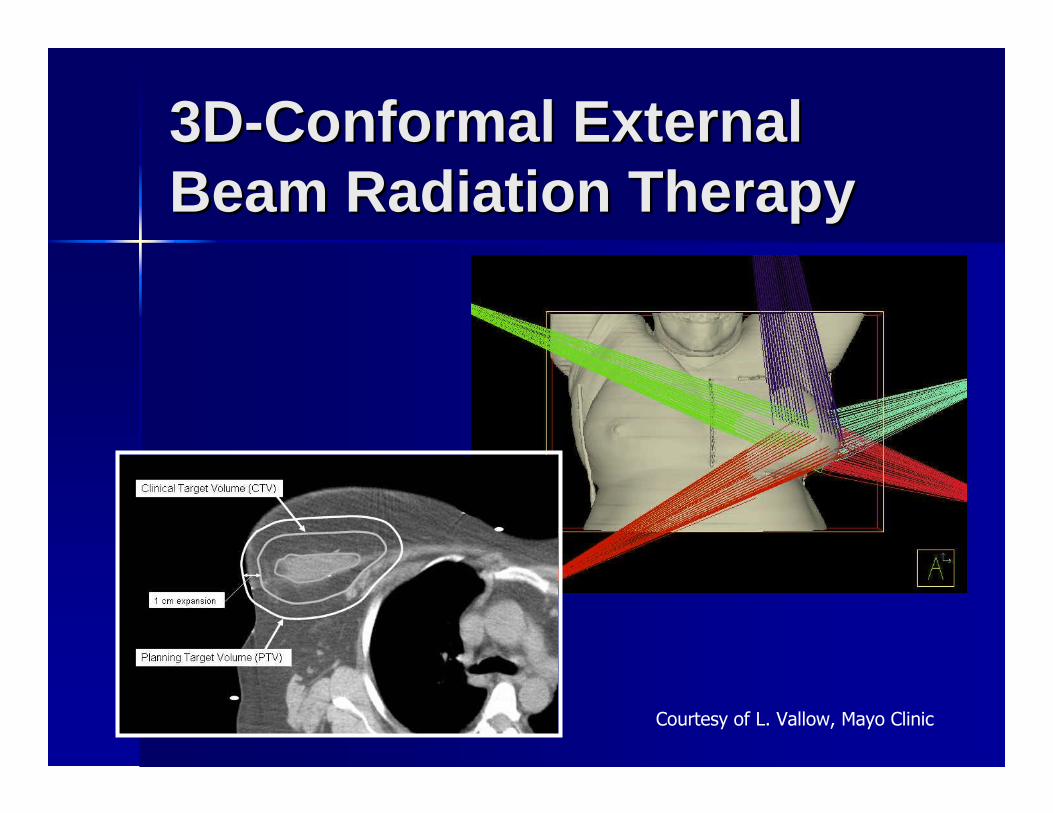
3D3D--Conformal ExternalConformal ExternalBeam Radiation TherapyBeam Radiation Therapy
Courtesy of L. Vallow, Mayo Clinic

Dosimetric ComparisonDosimetric Comparison
Weed, et al. Brachytherapy 2005
5%5%0%0%0%0%Lung VLung V2020
48%48%18%18%26%26%NormalNormalbreast 50%breast 50%
PDPD
100%100%91%91%68%68%PTV VPTV V9090
100%100%76%76%58%58%PTV VPTV V100100
3D3Dconformalconformal
EBRTEBRT
MammoSiteMammoSitebrachytherapybrachytherapy
MultiMulti--cathetercatheterbrachytherapybrachytherapy
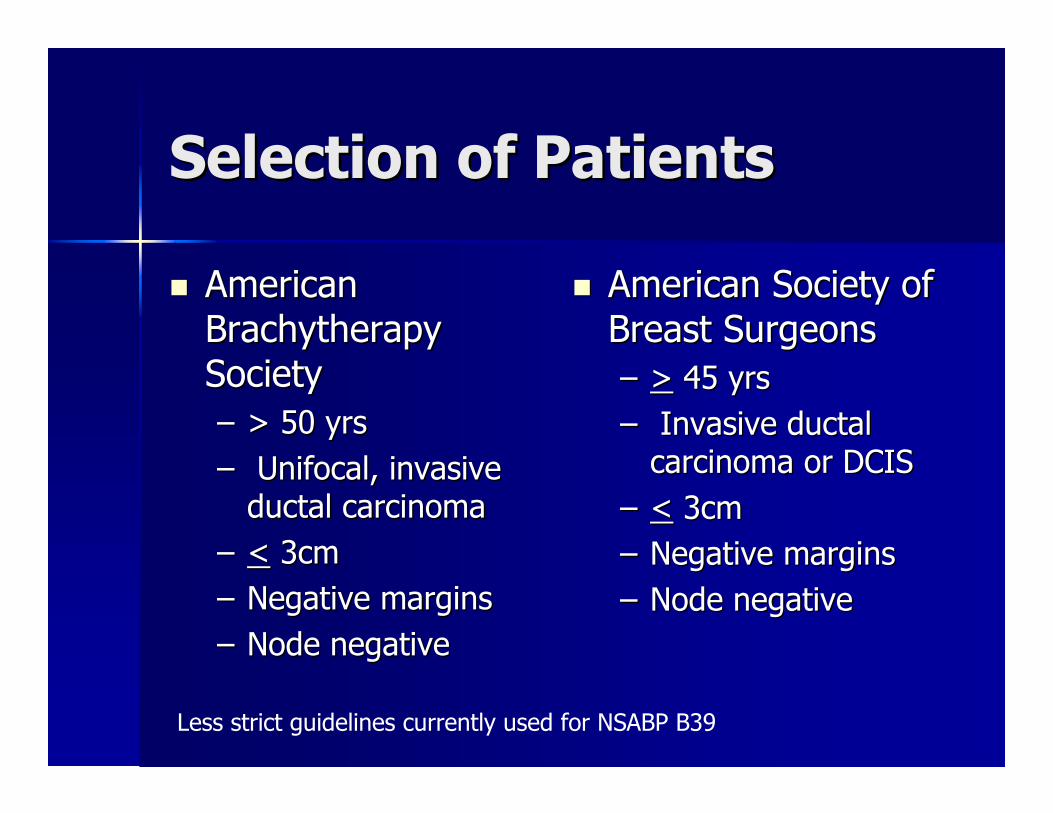
Selection of PatientsSelection of Patients
�� AmericanAmericanBrachytherapyBrachytherapySocietySociety–– > 50 yrs> 50 yrs–– Unifocal, invasiveUnifocal, invasive
ductal carcinomaductal carcinoma–– << 3cm3cm–– Negative marginsNegative margins–– Node negativeNode negative
�� American Society ofAmerican Society ofBreast SurgeonsBreast Surgeons–– >> 45 yrs45 yrs–– Invasive ductalInvasive ductal
carcinoma or DCIScarcinoma or DCIS–– << 3cm3cm–– Negative marginsNegative margins–– Node negativeNode negative
Less strict guidelines currently used for NSABP B39
Selection of PatientsSelection of Patients
�� Breast sizeBreast size
�� Lumpectomy cavity siteLumpectomy cavity site–– Medial,Medial, parasternalparasternal
–– Inframammary foldInframammary fold
–– RetroareolarRetroareolar
�� ImplantsImplants
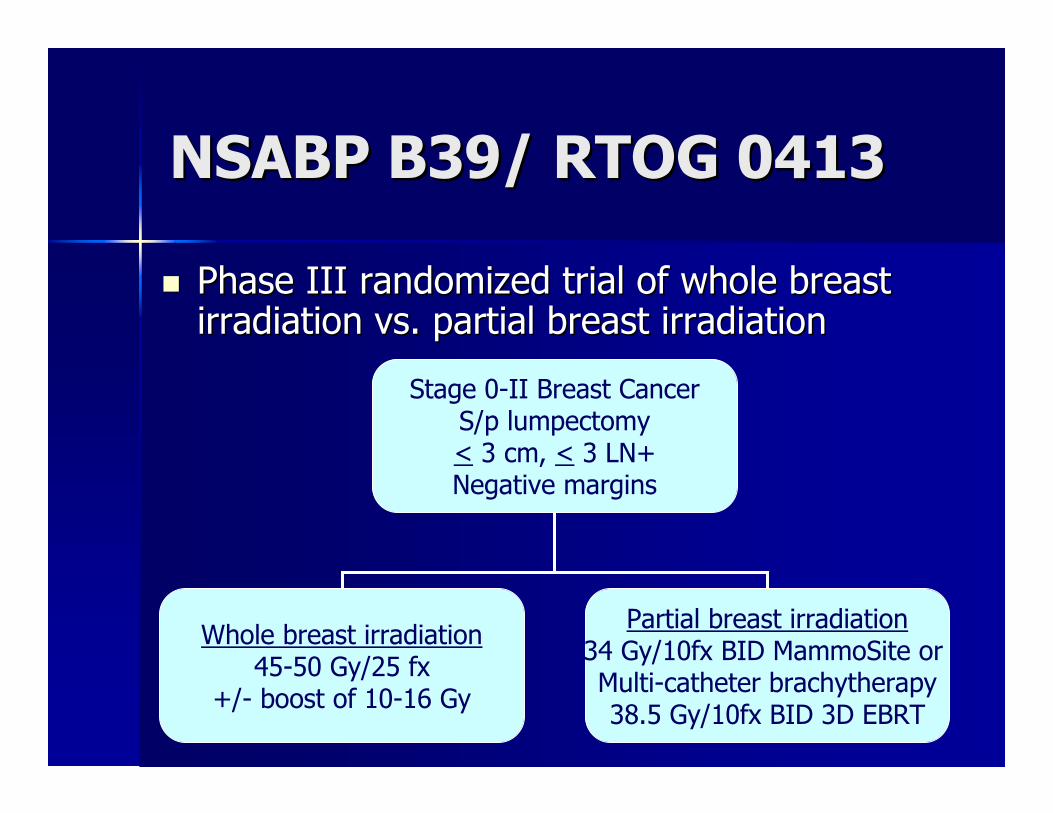
NSABP B39/ RTOG 0413NSABP B39/ RTOG 0413
�� Phase III randomized trial of whole breastPhase III randomized trial of whole breastirradiation vs. partial breast irradiationirradiation vs. partial breast irradiation
Stage 0-II Breast CancerS/p lumpectomy< 3 cm, < 3 LN+Negative margins
Whole breast irradiation45-50 Gy/25 fx
+/- boost of 10-16 Gy
Partial breast irradiation34 Gy/10fx BID MammoSite orMulti-catheter brachytherapy38.5 Gy/10fx BID 3D EBRT

ConclusionsConclusions
�� Early stage breast cancer can be treatedEarly stage breast cancer can be treatedwith lumpectomy and radiation therapy inwith lumpectomy and radiation therapy inthe majority of patients with good outcomesthe majority of patients with good outcomesand cosmesisand cosmesis
�� Technical advances in radiotherapyTechnical advances in radiotherapyplanning may allow the benefit of radiationplanning may allow the benefit of radiationwith less morbiditywith less morbidity
�� Outcomes with long term followOutcomes with long term follow--up fromup fromNSABP B39 will further clarify the role ofNSABP B39 will further clarify the role ofPBIPBI
Questions?Questions?




















