A Dosimetric Comparison of IORT Techniques in Limited-Stage Breast Cancer
7
342 Strahlenther Onkol 2006 · No. 6 © Urban & Vogel Strahlentherapie und Onkologie Original Article A Dosimetric Comparison of IORT Techniques in Limited-Stage Breast Cancer Olaf Nairz 1 , Heinz Deutschmann 1 , Michael Kopp 1 , Karl Wurstbauer 1 , Gerhard Kametriser 1 , Gerd Fastner 1 , Florian Merz 1 , Roland Reitsamer 2 , Christian Menzel 2 , Felix Sedlmayer 1 Background and Purpose: For intraoperative radiotherapy (IORT) during breast-conserving treatment four different techniques have been addressed: interstitial brachytherapy, an inflatable balloon with a central high-dose-rate source (MammoSite), a min- iature orthovolt system (Intrabeam), and linac-based electron radiotherapy (IOERT). The dosimetric properties of these methods are compared. Material and Methods: Planning target volumes (PTVs) of the same size but of different shapes are assumed, corresponding to the technique’s specific situs. Dose distributions for the PTVs and for surrounding tissues are demonstrated by dose-volume his- tograms and a list of physical parameters. A dose inhomogeneity index (DII) is introduced to describe the deviation of a delivered from the prescribed dose, reaching its minimal value 0 in case of perfect homogeneity. Results: In terms of DII, IOERT reaches the lowest value followed by the MammoSite, the Intrabeam and interstitial implants. The surrounding tissues receive the smallest average dose with IOERT, closely followed by the orthovolt system. Conclusion: When comparing simplified geometric figures, IOERT delivers the most homogeneous dose distributions. However, in clinical reality PTVs often present asymmetric shapes instead of ideal geometries. Due to a strictly centric dose fall-off, any system with a round central applicator will have technical limits. During IOERT margin-directed applicator guidance is possible and in- terstitial brachytherapy allows for polygonal dose shaping. These techniques seem to be superior for asymmetric PTV irradia- tion. Key Words: Breast cancer · Intraoperative radiotherapy · IORT · PTV · Dosimetry Strahlenther Onkol 2006;182:342–8 DOI 10.1007/s00066-006-1580-2 Dosimetrischer Vergleich von IORT-Techniken beim konservativ operierten Mammakarzinom Hintergrund und Ziel: Für die intraoperative Radiotherapie (IORT) des konservativ operierten Mammakarzinoms sind vier Tech- niken in Gebrauch: die interstitielle Brachytherapie, ein aufblasbarer Ballon mit einer zentralen High-Dose-Rate-Quelle (Mammo- Site), ein Miniatur-Orthovoltsystem (Intrabeam) sowie Elektronen am Linac (IOERT). Die dosimetrischen Eigenschaften dieser Methoden werden verglichen. Material und Methodik: Für jede dieser Techniken werden Planungszielvolumina (PTVs) des gleichen Volumens, aber unter- schiedlicher Form angenommen, die dem jeweiligen typischen Situs zum Zeitpunkt der Applikation entsprechen (Abbildung 1, Tabellen 1 und 2). Die Dosisverteilungen (Abbildung 2) inner- und außerhalb der PTVs werden mittels Dosis-Volumen-Histogram- men und einer Reihe von Parametern miteinander verglichen (Abbildung 3, Tabelle 3). Ein Dosisinhomogenitätsindex (DII) wird vorgestellt, der die Abweichung einer verabreichten von einer vorgeschriebenen Dosis beschreibt und im Fall einer perfekten Homogenität den Minimalwert 0 erreicht. Ergebnisse: In Bezug auf den DII erreicht die IOERT den niedrigsten Wert, gefolgt von MammoSite, dem Orthovoltsystem und den interstitiellen Implantaten. Das umgebende Gewebe erhält die geringste mittlere Dosis mittels IOERT, knapp gefolgt vom Intra- beam (Abbildung 3, Tabelle 3). Schlussfolgerung: Die IOERT zeigt die homogenste Dosisverteilung. In der klinischen Realität weisen PTVs aber häufig asymme- trische anstelle idealgeometrischer Formen auf. Durch den strikten zentralen Dosisabfall bestehen bei Systemen mit runden zentralen Applikatoren technische Limitationen. Während einer IOERT ist eine asymmetrische Applikatorführung möglich, die interstitielle Brachytherapie erlaubt eine polygonale Dosisformung, weshalb diese beiden Verfahren zur Erfassung asymmetrischer PTVs überlegen scheinen (Abbildung 4). Schlüsselwörter: Mammakarzinom · Intraoperative Radiotherapie · IORT · PTV · Dosimetrie Received: March 15, 2006; accepted: March 20, 2006 1 Department of Radio-Oncology, Salzburger Landeskliniken and Paracelsus Private Medical University (PMU), Salzburg, Austria, 2 Department of Special Gynecology, Salzburger Landeskliniken and Paracelsus Private Medical University (PMU), Salzburg, Austria.
-
Upload
ecomedicine -
Category
Documents
-
view
1 -
download
0
Transcript of A Dosimetric Comparison of IORT Techniques in Limited-Stage Breast Cancer

342 Strahlenther Onkol 2006 · No. 6 © Urban & Vogel
Strahlentherapie und Onkologie Original Article
A Dosimetric Comparison of IORT Techniques in Limited-Stage Breast CancerOlaf Nairz1, Heinz Deutschmann1, Michael Kopp1, Karl Wurstbauer1, Gerhard Kametriser1, Gerd Fastner1, Florian Merz1, Roland Reitsamer2, Christian Menzel2, Felix Sedlmayer1
Background and Purpose: For intraoperative radiotherapy (IORT) during breast-conserving treatment four different techniques have been addressed: interstitial brachytherapy, an inflatable balloon with a central high-dose-rate source (MammoSite), a min-iature orthovolt system (Intrabeam), and linac-based electron radiotherapy (IOERT). The dosimetric properties of these methods are compared.Material and Methods: Planning target volumes (PTVs) of the same size but of different shapes are assumed, corresponding to the technique’s specific situs. Dose distributions for the PTVs and for surrounding tissues are demonstrated by dose-volume his-tograms and a list of physical parameters. A dose inhomogeneity index (DII) is introduced to describe the deviation of a delivered from the prescribed dose, reaching its minimal value 0 in case of perfect homogeneity.Results: In terms of DII, IOERT reaches the lowest value followed by the MammoSite, the Intrabeam and interstitial implants. The surrounding tissues receive the smallest average dose with IOERT, closely followed by the orthovolt system.Conclusion: When comparing simplified geometric figures, IOERT delivers the most homogeneous dose distributions. However, in clinical reality PTVs often present asymmetric shapes instead of ideal geometries. Due to a strictly centric dose fall-off, any system with a round central applicator will have technical limits. During IOERT margin-directed applicator guidance is possible and in-terstitial brachytherapy allows for polygonal dose shaping. These techniques seem to be superior for asymmetric PTV irradia-tion.
Key Words: Breast cancer · Intraoperative radiotherapy · IORT · PTV · Dosimetry
Strahlenther Onkol 2006;182:342–8 DOI 10.1007/s00066-006-1580-2
Dosimetrischer Vergleich von IORT-Techniken beim konservativ operierten Mammakarzinom
Hintergrund und Ziel: Für die intraoperative Radiotherapie (IORT) des konservativ operierten Mammakarzinoms sind vier Tech-niken in Gebrauch: die interstitielle Brachytherapie, ein aufblasbarer Ballon mit einer zentralen High-Dose-Rate-Quelle (Mammo-Site), ein Miniatur-Orthovoltsystem (Intrabeam) sowie Elektronen am Linac (IOERT). Die dosimetrischen Eigenschaften dieser Methoden werden verglichen.Material und Methodik: Für jede dieser Techniken werden Planungszielvolumina (PTVs) des gleichen Volumens, aber unter-schiedlicher Form angenommen, die dem jeweiligen typischen Situs zum Zeitpunkt der Applikation entsprechen (Abbildung 1, Tabellen 1 und 2). Die Dosisverteilungen (Abbildung 2) inner- und außerhalb der PTVs werden mittels Dosis-Volumen-Histogram-men und einer Reihe von Parametern miteinander verglichen (Abbildung 3, Tabelle 3). Ein Dosisinhomogenitätsindex (DII) wird vorgestellt, der die Abweichung einer verabreichten von einer vorgeschriebenen Dosis beschreibt und im Fall einer perfekten Homogenität den Minimalwert 0 erreicht.Ergebnisse: In Bezug auf den DII erreicht die IOERT den niedrigsten Wert, gefolgt von MammoSite, dem Orthovoltsystem und den interstitiellen Implantaten. Das umgebende Gewebe erhält die geringste mittlere Dosis mittels IOERT, knapp gefolgt vom Intra-beam (Abbildung 3, Tabelle 3).Schlussfolgerung: Die IOERT zeigt die homogenste Dosisverteilung. In der klinischen Realität weisen PTVs aber häufig asymme-trische anstelle idealgeometrischer Formen auf. Durch den strikten zentralen Dosisabfall bestehen bei Systemen mit runden zentralen Applikatoren technische Limitationen. Während einer IOERT ist eine asymmetrische Applikatorführung möglich, die interstitielle Brachytherapie erlaubt eine polygonale Dosisformung, weshalb diese beiden Verfahren zur Erfassung asymmetrischer PTVs überlegen scheinen (Abbildung 4).
Schlüsselwörter: Mammakarzinom · Intraoperative Radiotherapie · IORT · PTV · Dosimetrie
Received: March 15, 2006; accepted: March 20, 2006
1 Department of Radio-Oncology, Salzburger Landeskliniken and Paracelsus Private Medical University (PMU), Salzburg, Austria,2 Department of Special Gynecology, Salzburger Landeskliniken and Paracelsus Private Medical University (PMU), Salzburg, Austria.

Nairz O, et al. IORT Techniques for Breast Cancer
343Strahlenther Onkol 2006 · No. 6 © Urban & Vogel
IntroductionIntraoperative radiotherapy (IORT) to the tumor bed during breast-conserving surgery has become a booming field of in-terest for partial-breast irradiation, either as anticipated boost or as sole treatment in limited-stage breast cancer [24, 25]. The aim of breast IORT is an utmost precise dose delivery to the area at highest risk for contamination with subclinical tumor cells [1, 6, 7, 12, 27, 31]. This has given rise to the development of different technical approaches, with the term “IORT” used for the following techniques: perioperative multicatheter brachytherapy, endocavitary brachytherapy, an orthovolt sys-tem, and intraoperative radiotherapy with electrons on linear accelerators (IOERT).
Perioperative multicatheter brachytherapy corresponds to classic interstitial brachytherapy by flexible needles, applied during open sight of the excision hole [14, 19–21, 28, 33]. Endo-cavitary IORT, the so-called MammoSite, is performed by an inflatable balloon which is placed into the lumpectomy cavity and filled with sterile saline to a size that fills the cavity com-pletely, typically 4 cm in diameter. A high-dose-rate source is guided into the balloon’s center with the dose normally pre-scribed 1 cm from the surface of the balloon [5, 9, 13]. For both brachytherapy techniques only the applicators’ positionings are true intraoperative maneuvers, with the irradiation being performed postoperatively, thus allowing for fractionated treatments.
In contrast to these brachytherapy techniques, IOERT and orthovolt treatments are IORTs sensu stricto. The orthovolt sys-tem (Intrabeam) consists of a miniature electron-driven low-en-ergy X-ray source, emitting an isotropic X-ray spectrum. For breast irradiations spheric applicators, chosen according to the excision cavity’s size, are put at the top of the source, resulting in a similar configuration as for the MammoSite system: a point source at the center within a spheric applicator [15, 29, 30].
Finally, IOERT is possible with various electron energies, with the walls of the excision hole temporarily approximated by central sutures to bring the target volume into reach for the electron beam, which is applied by round tubes of different diameters [2, 4, 8, 16, 18, 19, 22, 26, 32].
The aim of our study was to investigate the dose distribu-tions of these four techniques for identical clinical precondi-tions and the analysis of their dosimetric properties. One pa-rameter quantifying the homogeneity of the dose distribution with a simple and intuitive interpretation will be defined and discussed.
Material and MethodsPlanning Target Volume (PTV) and Surrounding Tissue Shapes
The PTV size was generally assumed with roughly 80 ml, which is in accordance with frequently reported treatment volumes [10]. For all IORT techniques typical PTV shapes were created which correspond to their specific surgical situs at the time of the IORT maneuver (Figure 1).
In case of the MammoSite and the Intrabeam system, the PTV is treated by a round central applicator and therefore supposed to be a shell around its surface. For both techniques we assumed an applicator’s diameter of 4 cm and a shell thick-ness of 1 cm. In case of perioperative brachytherapy three dif-ferent shapes were allowed to study the possible influence of central seromas of various sizes: the first assumption was a spherical shell of 1 cm thickness with a 4-cm seroma, resulting in the identical PTV shape as for the MammoSite and the In-trabeam. Furthermore, we calculated for two oblate spher-oids, one without and one with an elliptical seroma inside. By contrast, IOERT will have to encompass PTV shapes which have rather the shape of half prolate spheroids according to the surgical preparation technique.
Table 1 gives a summary of the shapes and dimensions of the target volumes for the different IORT techniques. For do-simetric comparisons not only PTVs but also the surrounding tissues were considered. They were assumed to have a volume of roughly 400 ml for all cases. Their shapes and dimensions are summarized in Table 2.
Dose Calculation The dose distribution for interstitial brachytherapy and the MammoSite system was calculated by assuming 192Ir point sources and the dose to be applied to water. In this approxima-tion the dose at a distance r from the source is given by
D(r)g(r)
r2∝ (equation 1)with g(r) the water perturbation correction, which was ap-proximated by a fourth-order polynomial [17].
PTV
Applicator/ seroma
ST
a b
c d
PTVSeroma
ST
PTVST
PTVST
Figures 1a to 1d. Idealized shapes for the target volumes and surround-ing tissues for the different techniques of intraoperative irradiation. Dimensions given in Tables 1 and 2. a) MammoSite, Intrabeam and brachytherapy five-layer; b) brachytherapy three-layer; c) brachyther-apy two-layer; d) IOERT.
Abbildungen 1a bis 1d. Idealisierte Geometrien für die Planungsziel-volumina und das umgebende Gewebe für die verschiedenen intra-operativen Bestrahlungstechniken. Abmessungen s. Tabellen 1 und 2. a) MammoSite, Intrabeam und fünflagiges Brachyimplantat; b) drei-lagiges Brachyimplantat; c) zweilagiges Brachyimplantat; d) IOERT.
Nairz O, et al. IORT Techniques for Breast Cancer
344 Strahlenther Onkol 2006 · No. 6 © Urban & Vogel
For interstitial brachytherapy, we designed five-, three- and two-layer implants with 14, 9 and 13 needles, respectively, in order to achieve best coverage of the three target volumes. The needles were arranged to form equilateral triangles with a side length of 1.5 cm. The step size of the source inside the ap-plicators was assumed to be 2.5 mm. All source positions were equally weighted and only positions inside the borders of the PTV were loaded. In order to exclude infinite contributions to the dose matrix, the radius of the needles and thus the mini-mum distance between source and tissue was assumed to be 1 mm. In that way we avoided unphysical dose peaks and the quotation of the maximum dose value for interstitial brachy-therapy becomes more meaningful.
The dose distribution matrix of the MammoSite system resulted from a single point source at the center of the balloon. The balloon was assumed to be filled with water yielding a homogeneous transition to the surrounding tissues. The maxi-mum dose is applied to the tissue at the applicator’s surface.
For the orthovolt system a dose fall-off obeying a 1/r3-law was reported in the literature [3] – with r the distance from the target at the tip of the drift tube – but for the case that no appli-cator is used. An applicator modifies the dose distribution and a correction term of the general form exp(a + b · r 0.5 + c · r –1.5) has to be multiplied to the 1/r3-term, the parameters a, b and c depending on the applicator’s diameter [11]. Since, to our
knowledge, no data exist in the literature for the case of a 4-cm applicator, we derived these parameters from the data re-ported for a 3.5-cm applicator [29], assuming that these pa-rameters will be the same for a 4-cm applicator. Investigations by Herskind et al. [11] suggest that no significant quantitative error may be introduced by this procedure. The correction to the 1/r3-fall-off was lower than 10% for both the PTV and the surrounding tissue.
For IOERT the dose distribution matrix was derived from an actually measured dose applied to water by a linear accelera-tor (Elekta SL 18). For our study situation we assumed that the surgeon prepared the tissue to be irradiated in a shape of half of a prolate spheroid with a diameter of 6 cm and a depth of 4.2 cm. The best coverage for that situation was achieved by taking a tube of 7 cm in diameter and 25 cm in length, which corresponds to a focus-surface distance of 118 cm, and the tissue irradiated by energies of 12 and 15 MeV weighted in a relation of 1 : 2.2.
Dose Comparison The dose matrices of all these six situations were multiplied with a factor so that the points of the minimum dose inside the target volumes got the value of 90. This value is interpreted as the per-centage of the reference dose and fixed as the minimum dose re-quired. So the comparison of dose distributions of different tech-niques regardless of absolute dose deliveries becomes possible.
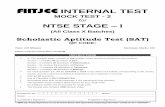
Table 1. Dimensions of the planning target volumes (PTV) for the IORT techniques. IOERT: intraoperative electron radiotherapy; NA: not applicable.
Tabelle 1. Abmessungen der Zielvolumina (PTV) für die verschiedenen intraoperativen Bestrahlungstechniken. IOERT: intraoperative Radiothera-pie mit Elektronen; NA: nicht anwendbar.
IORT technique PTV shape PTV inner dimensions (cm) PTV outer dimensions (cm) PTV volume (ml) Semimajor axis Semiminor axis Semimajor axis Semiminor axis
MammoSite Spherical shell 2 2 3 3 79.6Intrabeam Spherical shell 2 2 3 3 79.6Brachy five-layer Spherical shell 2 2 3 3 79.6Brachy three-layer Oblate spheroid shell 1.5 1.0 3.2 2.1 80.7Brachy two-layer Oblate spheroid NA NA 4.0 1.2 80.4IOERT Half prolate spheroid NA NA 4.2 3.0 79.2
Table 2. Dimensions of the surrounding tissues (ST) for the different techniques (rounded to one digit). IOERT: intraoperative electron radio-therapy.
Tabelle 2. Abmessungen des umgebenden Gewebes (ST) für die verschiedenen Bestrahlungstechniken (auf eine Kommastelle gerundet). IOERT: intraoperative Radiotherapie mit Elektronen.
IORT technique ST shape ST inner dimensions (cm) ST outer dimensions (cm) ST volume (ml) Semimajor axis Semiminor axis Semimajor axis Semiminor axis
MammoSite Spherical shell 3 3 5.0 5.0 401Intrabeam Spherical shell 3 3 5.0 5.0 401Brachy five-layer Spherical shell 3 3 5.0 5.0 401Brachy three-layer Oblate spheroid shell 3.2 2.1 5.6 3.7 400Brachy two-layer Oblate spheroid shell 4.0 1.2 7.3 2.2 401IOERT Half prolate spheroid shell 4.2 3.0 7.6 5.5 402

Nairz O, et al. IORT Techniques for Breast Cancer
345Strahlenther Onkol 2006 · No. 6 © Urban & Vogel
For each technique we specified several prominent pa-rameters both for the PTV and the surrounding tissues as the minimum, the maximum, the mean, the median dose, and the volume-related doses D90 and D10. D90 (D10) is obtained when from all dose matrix elements of the considered volume that subset is taken, which represents 90% (10%) of the volume and contains the highest values. From this subset the smallest value is picked.
Furthermore, we tried to summarize the main characte-ristics of the dose distribution in one single parameter, which will be called dose inhomogeneity index (DII). It is defined as the mean deviation of the dose inside the PTV from the prescribed dose
DII =Da,Vx, y, z – Dp,Vx, y, z dVx, y, z
Dp,Vx, y, z
1
VV
(equation 2)
or in its discrete form
DII = =
Da,Vi – Dp,Vin
i=1Σ
n
i=1Σ
·Vi Vi
Vi
Dp,Vi Da,Vi – Dp,Vin
i=1Σ
Dp,Vi
1
n
= const.
(equation 3)
where Da,V and Dp,V are the actual and prescribed dose in the corresponding voxel, respectively, Vi the size of the vox-el, and n the number of voxels of the considered volume.
In the most common case that all voxels have the same size, the absolute values of the deviations per voxel dose are added and divided by the number of voxels. Taking the absolute value guar-antees that no compensation of under-dosage by an overdosage in another re-gion is possible. In the ideal case of a completely homogeneous irradiation, where the whole PTV receives the pre-scribed dose, the DII becomes 0. It be-comes larger with growing dose inhomo-geneity. The DII multiplied with 100 gives the mean absolute deviation from the prescribed dose in the PTV in percent.
Results A visualization of the dose distributions is given in the two-dimensional plots in Figure 2. In Figure 3 the dose-volume histograms (DVHs) of the target vol-umes and the surrounding tissues are shown. It is evident that for IOERT the steepest DVH is achieved, whereas the
dose spread is highest for the two-layer implant. For the sur-rounding tissues the DVHs show that the minimum dose is lowest for IOERT, whereas the high-dose region has the smallest volume using Intrabeam.
A summary of all above-mentioned parameters is given in Table 3. With respect to the PTV, IOERT delivers the most homogeneous dose distribution, being free from any dose peaks which are most pronounced in interstitial brachythera-py and the orthovolt system. In terms of DII, IOERT reaches a value of 0.047, followed with a clear gap by the MammoSite system (0.295), orthovolt treatment (0.505), and the intersti-tial implants (0.648–1.581). Furthermore, IOERT has an aver-age dose inside the target volume closest to the prescribed dose and the smallest maximum dose. The surrounding tissues receive the highest doses with the interstitial implants and, to-gether with the MammoSite system, also the highest minimum dose. The minimum dose is lowest with IOERT and also the average dose is smallest with this technique, closely followed by the Intrabeam system.
Discussion and ConclusionWhen comparing tele- with brachytherapeutic maneuvers for IORT, it is possibly misleading to consider single isolated
200
150
100
50
0
Dose (
% o
f re
fere
nce d
ose)
22
0−2−2
Dose distribution brachytherapy 5-layer
a
0
300
200
100
0
Dose (
% o
f re
fere
nce d
ose)
2
y-axis x-axisy-axis x-axis2
0−2−2
Dose distribution IOERT
b
0
300
200
100
0
Dose (%
of
refe
ren
ce d
ose)
2
y-axis x-axis2
0−2−2
c
0
100
50
0
Dose (%
of
refe
ren
ce d
ose)
2
y-axis x-axis2
0−2−2
d
0
Dose distribution MammoSite Dose distribution orthovolt
Figures 2a to 2d. Dose distribution in the equatorial plane of the MammoSite system (a), the Intrabeam system (b), and interstitial brachytherapy for the case of spheric seroma (c). The graph for IOERT (d) shows the dose distribution in a plane containing the beam central axis. The dose inside the applicator for the Intrabeam system and inside the balloon for the Mam-moSite system was set to 0.
Abbildungen 2a bis 2d. Dosisverteilung in der Äquatorialebene beim MammoSite-System (a), beim Intrabeam-System (b) und bei der fünflagigen interstitiellen Brachytherapie mit kugel-förmigem Serom (c). Der Graph für die IOERT (d) zeigt die Dosisverteilung in einer den Zentral-strahl enthaltenden Ebene. Die Dosis innerhalb des Applikators beim Intrabeam- und Mam-moSite-System wurde auf 0 gesetzt.

Nairz O, et al. IORT Techniques for Breast Cancer
346 Strahlenther Onkol 2006 · No. 6 © Urban & Vogel
numbers. Therefore, we introduced a single parameter, the DII, to characterize the dosimetric dignity of the implant. It is important to note that the DII is not merely a measure of the spread of the values of the dose matrix but is also a measure of the deviation of the dose values from the prescribed dose. This distinguishes the DII from the standard deviation: the standard deviation is a measure of the deviation from the av-erage dose, but the average dose is in general different from the prescribed dose.
With respect to typical and idealized geometric PTV shapes, the physical dose comparison clearly revealed IOERT to be by far best suited of all IORT techniques, both in terms
of dose homogeneity within the PTV and at the same time sparing surround-ing tissues also the best. However, be-fore overemphasizing the role of physi-cal dose homogeneity, the dignity of IORT maneuvers has also to be judged with respect to intraoperative clinical re-ality, which might differ enormously from ideal geometric conditions. A dis-cussion about advantages and pitfalls of IORT techniques has to consider their adaptability to an individual surgical si-tus where asymmetric instead of sym-metric PTVs have to be encompassed. Neither does tumor spread follow strict-ly equidistant concentric growth, nor will the surgeon be able to perform a tu-
mor removal which is perfectly equidistant in all directions in terms of normal-tissue margins (Figure 4). The shape of a re-maining PTV which is assumed to be subclinically contami-nated with tumor cells resembles a “sickle room” rather than a shell, demanding for asymmetric spatial dose delivery. Due to a strictly centric dose fall-off, any system with a round cen-tral applicator will have technical limits which cannot always be compensated by surgical preparation techniques. During IOERT, excentric applicator guidance is possible. However, the histopathologic information about the extent of free mar-gins has to be provided during the operation, emphasizing the role of telepathology in this setting. In situ components will
100
90
80
70
60
50
40
30
20
10
0
100
90
80
70
60
50
40
30
20
10
0
Vo
lum
e (
%)
Vo
lum
e (
%)
0 50 100 150 200 250 300 350 0 10 20 30 40 50 60 70 80 90 100
Dose (%)a b Dose (%)
MammoSiteOrthovoltBrachy 5-layerBrachy 2-layerBrachy 3-layerIOERT
MammoSiteOrthovoltBrachy 5-layerBrachy 2-layerBrachy 3-layerIOERT
Figures 3a and 3b. Dose-volume histograms for the target volume (a) and the surrounding tissue (b).
Abbildungen 3a und 3b. Dosis-Volumen-Histogramme für das Zielvolumen (a) und das umge-bende Gewebe (b).
Table 3. Summary of the most important statistical parameters characterizing the dose distributions inside the target volumes (PTV) and the sur-rounding tissues (ST). Dmin: minimal dose in the considered volume (was set to 90% for all cases); Dmax: maximal dose in the considered volume; D90: minimal dose to 90% of the considered volume which receives the highest doses; D10: minimal dose to 10% of the considered volume which receives the highest doses; Dav: average dose; Dmedian: median dose; DII: dose inhomogeneity index (average absolute value of deviation from pre-scribed dose); IOERT: intraoperative electron radiotherapy.
Tabelle 3. Zusammenfassung der wichtigsten statistischen Parameter, die die Dosisverteilung im Zielvolumen (PTV) und im umgebenden Gewe-be (ST) charakterisieren. Dmin: Minimaldosis im betrachteten Volumen (wurde für alle betrachteten Fälle auf 90% gesetzt); Dmax: Maximaldosis im betrachteten Volumen; D90: Minimaldosis für den Teil des Volumens, der die höchste Dosis erhält und 90% des gesamten Volumens umfasst; D10: Minimaldosis für den Teil des Volumens, der die höchste Dosis erhält und 10% des gesamten Volumens umfasst; Dav: durchschnittliche Dosis; Dmedian: mediane Dosis; DII: Dosisinhomogenitätsindex (durchschnittliche absolute Abweichung von der vorgeschriebenen Dosis); IOERT: intra-operative Radiotherapie mit Elektronen.
MammoSite Intrabeam Brachy five-layer Brachy three-layer Brachy two-layer IOERT
PTV Dmin 90 90 90 90 90 90 Dmax 200 276 635 709 969 110 D90 94 96 111 122 136 100 D10 174 228 226 262 371 109 Dav 127 149 165 189 258 104 Dmedian 120 135 150 173 243 105 DII 0.295 0.505 0.648 0.893 1.581 0.047ST Dmin 33 22 33 22 25 4 Dmax 90 90 486 852 540 102 D90 35 24 37 28 30 6 D10 74 68 90 142 89 85 Dav 50 40 58 71 55 37 Dmedian 46 35 51 53 47 28

Nairz O, et al. IORT Techniques for Breast Cancer
347Strahlenther Onkol 2006 · No. 6 © Urban & Vogel
not be judgable by frozen sections only, which may lead to discrepancies with the final histological assessments. In our own early series, up to 10% of the patients were referred to reexcisions and/or secondary mastectomies [22, 23, 26]. Peri-operative interstitial brachytherapy has the advantage that definitive histopathologic information might already be avail-able at the beginning of treatment, allowing also for asymmet-ric spatial dose shaping.
References 1. Bartelink H, Horiot JC, Poortmans P, et al. Recurrence rates after treatment
of breast cancer with standard radiotherapy with or without additional ra-diation. N Engl J Med 2001;345:1378–87.
2. Battle JA, DuBois JB, Merrick HW, et al. IORT for breast cancer. In: Gunderson LL, Willett CG, Harrison LB, et al., eds. Current clinical oncology: intraopera-tive irradiation techniques and results. Totowa: Humana Press, 1999:521–6.
3. Beatty J, Biggs PJ, Gall K, et al. A new miniature x-ray device for interstitial radiosurgery: dosimetry. Med Phys 1996;23:53–62.
4. DuBois JB, Hay M, Gely S, et al. IORT in breast carcinoma. Front Radiat Ther Oncol 1997;31:131–7.
5. Edmundson GK, Vicini FA, Chen PY, et al. Dosimetric characterisation of the MammoSite RTS, a new breast brachytherapy applicator. Int J Radiat Oncol Biol Phys 2002;52:1132–9.
6. Faverly DR, Hendriks JH, Holland R. Breast carcinomas of limited extent: frequency, radiologic-pathologic characteristics, and surgical margin re-quirements. Cancer 2001;91:647–59.
7. Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a random-ized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 2002; 347:1233–41.
8. Gatzemeier W, Orecchia R, Gatti G, et al. Intraoperative radiotherapy (IORT) in treatment of breast carcinoma – a new therapeutic alternative within the scope of breast-saving therapy? Current status and future prospects. Report of experiences from the European Institute of Oncology (EIO), Mailand. Strahlenther Onkol 2001;177:330–7.
9. Gittleman M, Vigneri P, Carlson D, et al. Clinical evaluation of the Mam-moSite breast brachytherapy catheter: an analysis of technical reproduc-ibility, acute toxicity, and patient demographics. Int J Radiat Oncol Biol Phys 2003;57:365–6.
Figures 4a to 4d. Typical surgical situs and its influence on IORT ma-neuvers. Green lines: coverage by reference dose. a) Non-equidistant surgical removal of the tumor leaves asymmetric PTV shapes (“sickle rooms”). b) Round central applicators are at risk of leaving tumor cells out of reach. c) With IOERT margin-directed applicator guidance is pos-sible. d) Interstitial brachytherapy allows for polygonal dose shaping.
Abbildungen 4a bis 4d. Typischer chirurgischer Situs und sein Einfluss auf das IORT-Manöver. Grüne Linien: Abdeckung mit Referenzdosis. a) Nicht-äquidistantes chirurgisches Entfernen des Tumors hinterlässt asymmetrische Zielvolumina („Sichelraum“). b) Bei kugelförmigen Applikatoren besteht dabei die Gefahr, dass Tumorzellen nicht erreicht werden. c) Resektionsrand und durch den Applikator festgesetztes Zielvolumen können bei IOERT in Deckung gebracht werden. d) Poly-gonale Dosisformung ist bei interstitieller Brachytherapie möglich.
a b
c d
10. Hammer J, Mazeron JJ, van Limbergen E. Breast boost – why, how, when? Strahlenther Onkol 1999;175:478–83.
11. Herskind C, Steil V, Kraus-Tiefenbacher U, et al. Radiobiological aspects of intraoperative radiotherapy (IORT) with isotropic low-energy X-rays for early-stage breast cancer. Radiat Res 2005;163:208–15.
12. Holland R, Connolly JL, Gelman R, et al. The presence of an extensive intraductal component following a limited excision correlates with prom-inent residual disease in the remainder of the breast. J Clin Oncol 1990; 8:113–8.
13. Keisch M, Vicini F, Kuske RR, et al. Initial clinical experience with the Mam-moSite breast brachytherapy applicator in women with early-stage breast cancer treated with breast-conserving therapy. Int J Radiat Oncol Biol Phys 2003;55:289–93.
14. King TA, Bolton JS, Kuske RR, et al. Long-term results of wide-field brachy-therapy as the sole method of radiation therapy after segmental mastec-tomy for T(is,1,2) breast cancer. Am J Surg 2000;180:299–304.
15. Kraus-Tiefenbacher U, Steil V, Bauer L, et al. A novel mobile device for in-traoperative radiotherapy (IORT). Onkologie 2003;26:596–8.
16. Merrick HW, Battle JA, Padgett BJ, et al. IORT for early breast cancer: a re-port on long term results. Front Radiat Ther Oncol 1997;31:126–30.
17. Nath R, Anderson LL, Luxton G, et al. Dosimetry of interstitial brachythera-py sources: recommendations of the AAPM Radiation Therapy Committee Task Group No. 43. Med Phys 1995;22:209–34.
18. Orecchia R, Ciocca M, Lazzari R, et al. Intraoperative radiation therapy with electrons (ELIOT) in early-stage breast cancer. Breast 2003;12:483–90.
19. Ott OJ, Potter R, Hammer J, et al. Accelerated partial breast irradiation with iridium-192 multicatheter PDR/HDR brachytherapy. Preliminary re-sults of the German-Austrian Multicenter Trial. Strahlenther Onkol 2004; 180:642–9.
20. Polgar C, Fodor J, Major T, et al. Radiotherapy confined to the tumor bed following breast conserving surgery – current status, controversies, and future projects. Strahlenther Onkol 2002;178:597–606.
21. Polgar C, Major T, Fodor J, et al. High-dose-rate brachytherapy alone versus whole breast radiotherapy with or without tumor bed boost after breast-conserving surgery: seven-year results of a comparative study. Int J Radiat Oncol Biol Phys 2004;60:1173–81.
22. Reitsamer R, Peintinger F, Kopp M, et al. Local recurrence rates in breast cancer patients treated with intraoperative electron-boost radiotherapy versus postoperative external-beam electron-boost irradiation. A sequen-tial intervention study. Strahlenther Onkol 2004;180:38–44.
23. Reitsamer R, Peintinger F, Kopp M, et al. The Salzburg concept of intraop-erative radiotherapy for breast cancer: results and considerations. Int J Cancer 2006;118:2882–7.

Nairz O, et al. IORT Techniques for Breast Cancer
348 Strahlenther Onkol 2006 · No. 6 © Urban & Vogel
24. Sauer G, Strnad V, Kurzeder C, et al. Partial breast irradiation after breast-conserving surgery. Strahlenther Onkol 2005;181:1–8.
25. Sauer R, Wenz F, Strnad V, et al. Teilbrustbestrahlung nach brusterhaltender Operation bei Brustkrebs. Stellungnahme der Deutschen Gesellschaft für Radioonkologie, der Deutschen Gesellschaft für Senologie und der Arbeits-gemeinschaft Gynäkologische Onkologie der Deutschen Krebsgesellschaft. Strahlenther Onkol 2005;181:417–23.
26. Sedlmayer F, Reitsamer R, Menzel C, et al. IORT with electrons in limited-stage breast cancer – a novel boost strategy during breast conserving ther-apy. In: Kogelnik HD, Lukas P, Sedlmayer F, eds. Progress in radio-oncology VII. Bologna: Monduzzi, 2002:323–32.
27. Sinn HP, Anton HW, Magener A, et al. Extensive and predominant in situ component in breast carcinoma: their influence on treatment results after breast-conserving therapy. Eur J Cancer 1998;34:646–53.
28. Strnad V, Ott O, Potter R, et al. Interstitial brachytherapy alone after breast conserving surgery: interim results of a German-Austrian multicenter phase II trial. Brachytherapy 2004;3:115–9.
29. Vaidya JS, Baum M, Tobias JS, et al. Targeted intra-operative radiotherapy (Targit): an innovative method of treatment for early breast cancer. Ann Oncol 2001;12:1075–80.
30. Vaidya JS, Tobias JS, Baum M, et al. Intraoperative radiotherapy for breast cancer. Lancet Oncol 2004;5:165–73.
31. Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a ran-domized study comparing breast-conserving surgery with radical mastec-tomy for early breast cancer. N Engl J Med 2002;347:1227–32.
32. Veronesi U, Orecchia R, Luini A, et al. A preliminary report of intraoperative radiotherapy (IORT) in limited-stage breast cancers that are conservatively treated. Eur J Cancer 2001;37:2178–83.
33. Vicini F, Arthur D, Polgar C, et al. Defining the efficacy of accelerated partial breast irradiation: the importance of proper patient selection, optimal quality assurance, and common sense. Int J Radiat Oncol Biol Phys 2003;57:1210–3.
Address for Correspondence Dr. Olaf Nairz Salzburger Landeskliniken und Paracelsus Medizinische Universität (PMU) Muellner Hauptstraße 48 5020 Salzburg Austria Phone (+43/662) 4482-3949, Fax -3903
e-mail: [email protected]