
Radial approach for percutaneous coronary interventions on chronic total occlusions: technical...
11
Interventional Rounds Radial Approach for Percutaneous Coronary Interventions on Chronic Total Occlusions: Technical Issues and Data Review Francesco Burzotta, 1 * MD, PHD, Maria De Vita, 2 MD, PHD, Thierry Lefevre, 3 MD, Antonella Tommasino, 1 MD, Yves Louvard, 3 MD, and Carlo Trani, 1 MD Objective: To overview the scientific data and the technical details regarding percutane- ous coronary interventions (PCI) on chronic total occlusions (CTO) by radial approach. Background: Trans-femoral approach is commonly regarded as the standard for PCI on CTO. Methods: A systematic search in Medline and in the main international websites was realized. Key data were extracted and analyzed using standard meta-analytic techniques. Bench test assessment of compatibility between different combinations of interventional devices (required for CTO recanalization techniques) and the following guiding catheters was performed: 5 Fr, Sheathless 6.5 Fr, 6 Fr, Sheathless 7.5 Fr and 8 Fr. Results: No prospective randomized study was found, whereas 13 observational studies on 3,501 CTOs treated by radial approach were identified. Overall, the crossover to femoral access rate ranged between 0 and 5.8%. Access site complications were noted in <1% of cases and in-hospital major adverse events were reported in 0–3.8% of patients. PCI success was significantly influenced by the learning curve: In the five stud- ies comparing the success rates between a first and a later period of practice, a signifi- cant improvement was observed (OR, 95% CI: 0.30, 0.39–0.51; P < 0.001). The technical details relevant to approach a CTO by transradial access are discussed, and the original results of bench tests provide details regarding the compatibility of various CTO recana- lization techniques with specific guiding catheter sizes. Conclusions: The transradial access represents a promising alternative to trans-femoral access to treat patients undergoing CTO PCI in high-volume transradial centres. The presented data may be useful to plan transradial PCI attempts on CTO lesions. V C 2013 Wiley Periodicals, Inc. Key words: transradial approach; chronic total occlusion; percutaneous coronary inter- vention; vascular complications INTRODUCTION Chronic total occlusion (CTO) percutaneous coro- nary intervention (PCI) represents an evolving field of interventional cardiology [1–8]. According to the standard practice of the majority of CTO-dedicated centres and operators, PCI on CTO are attempted using large guiding catheters and trans-femoral approach (TFA). Yet, transradial approach (TRA) is a valuable 1 Institute of Cardiology, , Catholic University of Sacred Heart, Rome, Italy 2 Interventional Cardiology, Morgagni-Pierantoni Hospital, Forl ı, Italy 3 Interventional Cardiology, Istitut Cardiovasculaire Paris Sud, Massy, France Conflict of interest: Nothing to report. *Correspondence to: Francesco Burzotta, MD, PhD; Institute of Car- diology, Catholic University of Sacred Heart, L.go Gemelli 1, 00168 Rome, Italy. E-mail: [email protected] Revised 23 June 2013; Revision accepted 27 June 2013 DOI: 10.1002/ccd.25118 Published online 5 July 2013 in Wiley Online Library (wileyonlinelibrary.com). V C 2013 Wiley Periodicals, Inc. Catheterization and Cardiovascular Interventions 83:47–57 (2014)
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Radial approach for percutaneous coronary interventions on chronic total occlusions: technical...

Interventional Rounds
Radial Approach for Percutaneous CoronaryInterventions on Chronic Total Occlusions:
Technical Issues and Data Review
Francesco Burzotta,1* MD, PHD, Maria De Vita,2 MD, PHD, Thierry Lefevre,3 MD,Antonella Tommasino,1 MD, Yves Louvard,3 MD, and Carlo Trani,1 MD
Objective: To overview the scientific data and the technical details regarding percutane-ous coronary interventions (PCI) on chronic total occlusions (CTO) by radial approach.Background: Trans-femoral approach is commonly regarded as the standard for PCI onCTO. Methods: A systematic search in Medline and in the main international websiteswas realized. Key data were extracted and analyzed using standard meta-analytictechniques. Bench test assessment of compatibility between different combinations ofinterventional devices (required for CTO recanalization techniques) and the followingguiding catheters was performed: 5 Fr, Sheathless 6.5 Fr, 6 Fr, Sheathless 7.5 Fr and 8Fr. Results: No prospective randomized study was found, whereas 13 observationalstudies on 3,501 CTOs treated by radial approach were identified. Overall, the crossoverto femoral access rate ranged between 0 and 5.8%. Access site complications werenoted in <1% of cases and in-hospital major adverse events were reported in 0–3.8% ofpatients. PCI success was significantly influenced by the learning curve: In the five stud-ies comparing the success rates between a first and a later period of practice, a signifi-cant improvement was observed (OR, 95% CI: 0.30, 0.39–0.51; P < 0.001). The technicaldetails relevant to approach a CTO by transradial access are discussed, and the originalresults of bench tests provide details regarding the compatibility of various CTO recana-lization techniques with specific guiding catheter sizes. Conclusions: The transradialaccess represents a promising alternative to trans-femoral access to treat patientsundergoing CTO PCI in high-volume transradial centres. The presented data may beuseful to plan transradial PCI attempts on CTO lesions. VC 2013 Wiley Periodicals, Inc.
Key words: transradial approach; chronic total occlusion; percutaneous coronary inter-vention; vascular complications
INTRODUCTION
Chronic total occlusion (CTO) percutaneous coro-nary intervention (PCI) represents an evolving field ofinterventional cardiology [1–8]. According to the
standard practice of the majority of CTO-dedicated
centres and operators, PCI on CTO are attempted using
large guiding catheters and trans-femoral approach
(TFA). Yet, transradial approach (TRA) is a valuable
1Institute of Cardiology, , Catholic University of Sacred Heart,Rome, Italy2Interventional Cardiology, Morgagni-Pierantoni Hospital, Forl�ı,Italy3Interventional Cardiology, Istitut Cardiovasculaire Paris Sud,Massy, France
Conflict of interest: Nothing to report.
*Correspondence to: Francesco Burzotta, MD, PhD; Institute of Car-
diology, Catholic University of Sacred Heart, L.go Gemelli 1,
00168 Rome, Italy. E-mail: [email protected]
Revised 23 June 2013; Revision accepted 27 June 2013
DOI: 10.1002/ccd.25118
Published online 5 July 2013 in Wiley Online Library
(wileyonlinelibrary.com).
VC 2013 Wiley Periodicals, Inc.
Catheterization and Cardiovascular Interventions 83:47–57 (2014)
alternative to TFA, which has been shown to reducevascular complications [9,10] and possibly be associ-ated to a better clinical outcome [11–13]. For such rea-sons, radial access is going to widespread not only inroutine coronary procedures, but also, thank to recenttechnological advances, in fields like complex PCIsand peripheral interventions [14–18]. As a conse-quence, radial approach may nowadays be successfullyused for the most complex CTO PCI like retrograde re-canalization of left main [19].
In the current study, we aimed at providing a com-prehensive overview of the scientific data and the tech-nical details that may be relevant for interventionalistsapproaching CTO by TRA. Moreover, because theissue of technique compatibility with different guidingcatheters may be pivotal, original bench tests were per-formed and reported.
SCIENTIFIC DATA ON THE FEASIBILITY ANDSAFETY OF TRA FOR CTO PCI
Study Search Strategy, Data Extraction, andStatistical Analysis
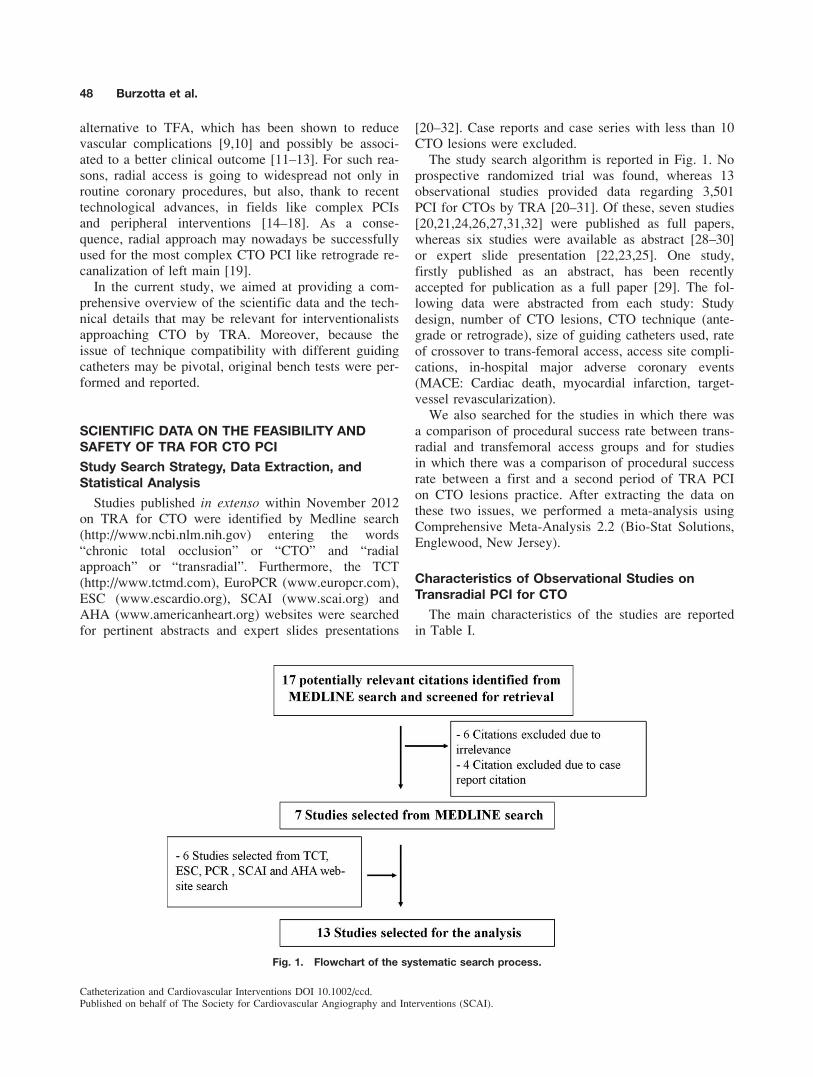
Studies published in extenso within November 2012on TRA for CTO were identified by Medline search(http://www.ncbi.nlm.nih.gov) entering the words“chronic total occlusion” or “CTO” and “radialapproach” or “transradial”. Furthermore, the TCT(http://www.tctmd.com), EuroPCR (www.europcr.com),ESC (www.escardio.org), SCAI (www.scai.org) andAHA (www.americanheart.org) websites were searchedfor pertinent abstracts and expert slides presentations
[20–32]. Case reports and case series with less than 10CTO lesions were excluded.
The study search algorithm is reported in Fig. 1. Noprospective randomized trial was found, whereas 13observational studies provided data regarding 3,501PCI for CTOs by TRA [20–31]. Of these, seven studies[20,21,24,26,27,31,32] were published as full papers,whereas six studies were available as abstract [28–30]or expert slide presentation [22,23,25]. One study,firstly published as an abstract, has been recentlyaccepted for publication as a full paper [29]. The fol-lowing data were abstracted from each study: Studydesign, number of CTO lesions, CTO technique (ante-grade or retrograde), size of guiding catheters used, rateof crossover to trans-femoral access, access site compli-cations, in-hospital major adverse coronary events(MACE: Cardiac death, myocardial infarction, target-vessel revascularization).
We also searched for the studies in which there wasa comparison of procedural success rate between trans-radial and transfemoral access groups and for studiesin which there was a comparison of procedural successrate between a first and a second period of TRA PCIon CTO lesions practice. After extracting the data onthese two issues, we performed a meta-analysis usingComprehensive Meta-Analysis 2.2 (Bio-Stat Solutions,Englewood, New Jersey).
Characteristics of Observational Studies onTransradial PCI for CTO
The main characteristics of the studies are reportedin Table I.
Fig. 1. Flowchart of the systematic search process.
48 Burzotta et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

TA
BL
EI.
Ma
inF
ea
ture
so
fS
tud
ies
on
Tra
nsra
dia
lP
CI
inC
TO
Le
sio
ns
Auth
or
Stu
dy
des
ign
Full
pap
erC
TO
lesi
on
num
ber
GC�
6F
r
Ret
rogra
de
tech
niq
ue
Double
Rad
ial
Appro
ach
Cro
ssover
toF
emora
l
Pro
cedure
succ
ess
“Rel
evan
t”
acce
sssi
te
com
pli
cati
ons
In-H
MA
CE
Sai
toet
al.
(20)
Sin
gle
centr
e,
retr
osp
ecti
ve
regis
try
Yes
181
72%
a0%
NA
NA
78%
NA
0%
a
Kim
etal
.(2
1)
Sin
gle
centr
e,
retr
osp
ecti
ve
regis
try
Yes
87
81%
0%
NA
5.7
%66%
None
1.1
%
Wu
etal
.(2
2)
Sin
gle
centr
e,
retr
osp
ecti
ve
regis
try
Ora
lP
rese
nta
tion
TC
T2008
909
NA
0%
NA
NA
77%
NA
NA
Ques
ada
etal
.(2
3)
Sin
gle
centr
e,
retr
osp
ecti
ve
regis
try
Ora
lP
rese
nta
tion
TC
T2008
129
85%
NA
2.3
%2.3
%79%
NA
NA
Rat
hore
etal
.(2
4)
Sin
gle
centr
e,
retr
osp
ecti
ve
regis
try
Yes
318
“Mai
nly
”0%
NA
3.3
%82%
Noneb
3.8
%
Kat
suki
(25)
Sin
gle
centr
e,
retr
osp
ecti
ve
regis
try
Ora
lP
rese
nta
tion
TC
T2009
165
98%
NA
NA
NA
76%
NA
NA
Yan
get
al.
(26)
Sin
gle
centr
e,
retr
osp
ecti
ve
regis
try
Yes
400
91%
0%
NA
NA
69%
NA
3%
Liu
etal
.(2
7)
Sin
gle
centr
e,
retr
osp
ecti
ve
regis
try
Yes
120
78%
5.8
%N
A0%
80%
None
0.8
%
Fer
rante
etal
.(2
8)
Sin
gle
centr
e,
retr
osp
ecti
ve
regis
try
Ora
lP
rese
nta
tion
TC
T2012
848
99%
6.5
%N
AN
A73%
NA
NA
Burz
ott
aet
al.
(29)
Sin
gle
centr
e,
retr
osp
ecti
ve
regis
try
Ora
lP
rese
nta
tion
PC
R2012,
Full
pap
er
inpre
ss
167
95%
3%
31%
1.2
%74
0.8
%0%
Asg
edom
etal
.(3
0)
Sin
gle
centr
e,
retr
osp
ecti
ve
regis
try
Ora
lP
rese
nta
tion
TC
T2012
93
NA
Mai
nly
ante
gra
de
NA
NA
84%
None
NA
Wu
etal
.(3
1)
Sin
gle
centr
e,
retr
osp
ecti
ve
regis
try
Yes
85
91%
(ante
gra
de)
20%
(ret
rogra
de)
100%
100%
Bi-
fore
arm
appro
ach.
(Ante
gra
de:
radia
l95%
uln
ar/b
rach
ial
5%
;R
etro
gra
de:
radia
l89%
uln
ar/b
rach
ial
11%
)
NA
87%
Nonec
3.6
%
Rin
fret
etal
.(3
2)
Sin
gle
oper
ator,
retr
osp
ecti
ve
regis
try
Yes
42
71%
(ante
gra
de)
91%
(ret
rogra
de)
100%
88%
NA
88%
None
2%
aD
ata
from
the
phas
e2
of
the
study
(CT
OP
CI
per
form
edbet
wee
nJa
nuar
yan
dA
ugust
2001)
and
from
all
the
study
popula
tion
(80
pat
ients
;69%
TR
A).
b3.5
%R
ate
of
smal
l(<
2cm
)hem
atom
are
port
ed;
no
larg
ehem
atom
asor
oth
eren
try
site
com
pli
cati
ons
wer
eobse
rved
.c3.5
%R
ate
of
fore
arm
ecch
ym
osi
s.
NA
,not
avai
lable
.
Transradial Approach for CTO 49
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

Of note, all studies [20–32] were single centre [20–32] and were conducted by operators reporting to havea specific experience in TRA PCI. The majority ofthe studies adopted mainly the antegrade technique(Table I), whereas two registries [31,32] reportedrespectively a single centre and a single operator expe-rience with retrograde bi-radial technique (Table I).
An important issue reflecting the feasibility of TRAfor CTO lesions is represented by the specific criteriaadopted to select patients in which TRA procedures isattempted. Of note, five studies [21–23,27,29] for a totalof 550 CTO lesions were retrospective registries report-ing the data on CTO lesions treated by radial accesswithout mentioning the rate of CTO lesions treatedusing the femoral (or others) route in the same period.Three studies only [21,29,32] reported the criteria usedto exclude patients from TRA and these were: NegativeAllen’s (and or Barbeau) test for both wrists and chronicrenal failure requiring dialysis. Eight studies [22,24–26,28,30–32] reported the rate of femoral access [22,24–26,28,30,32] or brachial access [31] use during the studyperiod and this ranged between 4.5 and 42%. The rea-sons for exclusion from radial artery access reported infour (out of such eight) studies were: Discretion of theindividual operator [24,26], radial artery too small for a6-Fr introducer, negative Allen’s test, absent or weak ra-dial pulse, haemodialysis [20,31]. Interestingly, threestudies [20,29,30] reported a selective choice of radialartery access in the first period of the study and a rou-tine radial artery access use in a second study period.These data suggest that (sometimes unclear) patients’selections were performed in the available studies onTRA CTO PCI and that with increased experience therelevance of patient’s selection may be reduced.
Another important issue reflecting the feasibility ofTRA CTO PCI is represented by the need of crossoverto another access after having attempted firstly the ra-dial artery approach. The crossover to TFA rate hasbeen reported in six studies [20,22,23,27,29] andresulted to be highly variable ranging between 0 and5.8% (Table I). According to the results reported in thetwo articles providing details regarding this issue[20,24], crossovers were mainly due to anatomical var-iants of radial and subclavian arteries affecting the ra-dial artery cannulation, the coronary ostia engagementand the guiding catheters support.
Procedural Efficacy and Clinical Results ofTransradial PCI for CTO
The clinical efficacy of vascular access selection inCTO PCI procedures may be evaluated by means ofprocedural success rates, by the rate of vascular com-plications and by the postprocedural MACE.
Of note, the definition of procedural success was notavailable in some studies [20,22,23,25,27,28,30,32] anddiffered significantly across studies providing it.Indeed, procedural success was defined as either:
1. PCI completion by TRA with a residual stenosis<30% and no major cardiovascular complications [21];
2. Final TIMI flow 3 and no major cardiovascularcomplications [26];
3. Residual stenosis< 20% and final TIMI flow 3[29];
4. Residual stenosis< 30% and final TIMI flow 3 [31];5. Successful lesion crossing with wire and balloon
with a residual stenosis <70% [24].
Besides such heterogeneity in its definition, thereported TRA CTO procedural success rate was highlyvariable among the studies in which mainly an ante-grade approach is used, ranging between 65% [22] and84% [30] (Table I). Such variability seems to be simi-lar to that encountered across studies on TFA CTOPCI [5,8,33–36] and is probably related to differentdefinitions of procedural success, different complexityof attempted lesions and different study periods.
Two studies provided statistical analysis on the pre-dictors of TRA PCI failure [20,21]. In such studies,nontapered stump, longer and older lesions [20,21]were associated to the inability to cross the occlusionwith a guidewire or a balloon [20,21], thus suggestingthat the procedural complexity markers are not differ-ent compared to TFA-CTO studies [5,8,33–37].
Five studies [20–22,29,32] provided data regardingthe comparison of success rates between a first and alater period of the study. As shown in Fig. 2, the suc-cess rate significantly improved in all the studies sothat an overall increased success has been observedwith increased experience (overall OR,95% CI:0.30,0.39–0.51; P< 0.001).
Finally, the overall clinical safety of TRA CTO PCIseems to be supported by the rarity of vascular compli-cations as well as by the overall clinical outcomereported in the available studies. Indeed, as shown inTable I, access-site complications were rarely reported(being constantly below 1% rate), whereas the rates ofin-hospital MACE ranged between 0 and 3.8% (TableI). Such results seems in line with the in-hospitalMACE observed in the major studies on CTO PCI per-formed by TFA [5,8,33–36].
Results of Observational Studies ComparingTransradial and Trans-Femoral PCI for CTO
Five studies reported a direct comparison betweenTRA and TFA for PCI on CTO [20,24,26,28,30]. As
50 Burzotta et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

shown in Fig. 3, the results obtained by TRA comparedfavourably with that obtained by TFA (OR: 0.82; 95%CI: 0.68–0.99: P¼ 0.046). Such finding may be relatedwith a selection of patients with lower complexity forTRA PCI. This hypothesis is supported by the study byFerrante et al. [28] who reported a significantly lowerprevalence of difficult CTO lesions in the TRA groupas compared to the TFA group (39.4 vs. 48.4%;P¼ 0.001).
Regarding resource consumption, the contrast vol-ume [24,30], the procedure time [24] and the radiation
dose [30] were all found to be similar in TRAand TFA groups in the (few) studies reporting theseparameters.
The rate of entry site complications, reported byRathore et al. [24], was significantly higher in TFAgroup as compared to TRA group (3.5% TRA groupversus 11.3% TFA group; P< 0.001). Similar findingswere reported by Asgedom et al. [30].
Finally, in two studies who provided such data[24,30], early MACE resulted to be similar betweenTRA group and TFA group. However, it should
Fig. 2. Forrest plot of odds ratio (ORs) of procedural success of PCI in CTO lesions bytransradial in the comparison between first and second period of time. Statistical analysisperformed using Comprehensive Meta-Analysis 2.2 (Bio-Stat Solutions, Englewood, New Jer-sey).
Fig. 3. Forrest plot of odds ratio (ORs) of procedural success of PCI in CTO lesions in thecomparison between radial and femoral approach. Statistical analysis performed using Com-prehensive Meta-Analysis 2.2 (Bio-Stat Solutions, Englewood, New Jersey).
Transradial Approach for CTO 51
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

emphasized that such studies were clearly underpoweredto compare clinical outcomes.
TECHNICAL ISSUES OF TRA FOR CTO PCI
The radial approach is associated with some specifictechnical characteristics which may render the PCI pro-cedure quite different from that performed by the fem-oral approach.
Guiding Catheter Size
First of all, although large sized guiding catheters(GC) may safely be inserted in the radial arteries ofselected patients [38,39], only 5 and 6 Fr GC may rou-tinely be used in transradial PCI. As summarized inTable I, radial operators often select 6 Fr GC for CTOPCI to avoid excessive injury to the small sized radialartery. This attitude differs from that of many femoraloperators who like to have a large GC size (7 and 8Fr) allowing for free CTO technique selection in thecourse of CTO PCI procedure. Indeed, various techni-ques requiring the manipulation of various combina-tions of devices have been developed to improve thesuccess of CTO interventions [1–3]. Thus, in the set-ting of CTO interventions operators adopting the TRAshould focus their attention on materials’ compatibilitymuch more compared with those using systematicallylarge GC by TFA. This issue is complicated by the factthat same materials (for example same size balloons) ofdifferent manufactures may have different width thusinfluencing their possibility to be inserted in GC togetherwith other devices. As a consequence, the knowledge ofthe combination of materials that can fit into each GCtype may come from the direct or indirect experienceonly. Recently, the border between larger (7 and 8 Fr)and smaller (5 and 6 Fr) GC has been challenged by anew family of GC not requiring the insertion of asheath, commonly called “Sheathless” GC (first avail-able type: Eucath, Asahi, Japan). Again, no exhaustiveinformation regarding the compatibility of different de-vice combinations with the Sheathless GC is available.
To try clarify which are the techniques that can beapplied using different GC, we tested in the bench thecompatibility of different CTO techniques (requiringdifferent combinations of devices) with 5, 6, 7, and 8Fr GC and with 6.5 and 7.5 Fr sheathless GC. Theresults of these tests are reported in the Table II. Over-all, it is evident that the selection of 6 Fr GC may pro-foundly limit the freedom to select some CTOtechniques, so that 7 Fr are required when some com-plex, specific techniques are needed. Of note, the feasi-bility of standard large GC use in selected patientsundergoing TRA complex procedures [39] has been
previously reported. Thus, radial approach by itselfcannot be considered an absolute exclusion criteria forthe selection of 7 or 8 Fr GC and individual patientevaluation is needed (a large sheath TRA PCI on CTOis shown in Fig. 4). Moreover, as shown in Table II,the 7.5 Fr Sheathless GC technology seems to poten-tially offer a major advance which may overcomealmost completely the drawback of using a small arteryaccess like the radial. It should be underlined thatsheathless GC are still not available in some countrieslike United States of America and that the use ofsheathless GC requires specific experience because ofthe highly hydrophilic coating which may increasecatheter instability.
A further important issue specifically associated withbi-radial retrograde techniques is represented by theGC length. Indeed, the use of the 150 cm devices (likeCorsair catheter or long-shaft over the wire balloons)for retrograde access may need GC shorter than 100cm, especially when the patient is taller than 175 cm[31,32]. Actually, short 90 cm GC, but not sheathlessGC, are available in different curvature and size[31,32]. An alternative possibility to overcome theproblem of shorter GC need is to cut the standard GCand different effective techniques to cut standard GChave been described [31,32]. Finally, the last possibleoption is to perform an high radial stick (puncture site10 cm proximal to styloid process) for the retrograderadial artery access [31]. Yet, it should be emphasizedthat at that level radial artery travels deep so thathemostasis can be difficult and deserves meticulousattention to minimise the local bleeding risks.
Guiding Catheter Support
Another relevant issue related with the TRA forCTO intervention is represented by the need of GCback up to push wires, microcatheters and balloonsacross the occlusive lesion. The “passive” back up isthe support offered by the GC itself and is increasedwith increasing GC size. Of difference compared tofemoral operators, TRA interventional cardiologists useto gain the maximal “active” backup from the usuallysmaller GC. A series of specific points may optimizethe “active” support. Firstly, when dealing with aCTO, it may be important to achieve a stable coronarycannulation with the guiding catheter. Because of thewide spectrum of anatomical variations encounteredbetween the forearm and the aortic root [40], multiplepoints of contact can affect the guiding catheter torquetransmission from a radial access. Accordingly, thelearning curve of individual radial operators is charac-terized by the development of an appropriate selectionof guiding catheter shape and radial approach side
52 Burzotta et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

(right or left) to achieve the best cannulation in thevarious clinical conditions. Beside these considerations,for CTOs located in the left coronary, the right radialapproach may be considered a valuable option as this“opposite” radial entry site warrants, especially withextra backup GC shapes, a strong support (see Fig. 4for example). Of difference, when dealing with theright coronary artery (RCA) CTOs, the right radialapproach is sometimes suboptimal as Ikary et al.showed increased back up force with left vs right ra-dial approach for RCA cannulation [41]. Thus, whenthe need of high support from the GC is anticipated,we consider the possibility to electively select the“opposite” left radial access for CTO on the RCA(Fig. 5).
It is important to recognize that the “passive back-up” offered by the same GC when inserted by radial orfemoral approach is strongly influenced by the GCshape. For example, when dealing with a RCA CTO,some GC shapes (Judkins) have wider and others have
smaller (Ikary and Amplatz Left) back up force differ-ence comparing their radial or femoral insertion [41].
Another important issue which may potentiallyreduce the drawback of using small sized GC is relatedwith the possibility to perform the “deep intubationtechnique” in the case of CTO with distal location[20,21]. This technique is more easily and efficientlyperformed with GC without complex curves (for exam-ple, Judkins, Hockey stick for the RCA) and is facili-tated by 5 or 6 Fr GC (Fig. 5).
Finally, it should be emphasized that specific devi-ces have been designed to improve the support ofsmall sized GC. Among these, the “five in sixtechnique” (or “mother and child technique”) has beenreported to be effective in the setting of CTO interven-tions [42–44]. This technique is facilitated by the avail-ability of specifically designed 5 Fr GC compatiblewith 6 Fr GC (Heartrail Terumo) or by a novel 6 Fr(and 7 Fr) GC extensor (Guideliner, Vascular solu-tions). Of note, the use of such devices may be
TABLE II. Compatibility of CTO PCI Techniques With Different Guiding Catheters
GUIDING CATHETERS
5 Fr Sheath
þ GC
6 Fr Sheath
þ GC
6.5 Fr
Sheathless
7 Fr Sheath
þ GC
7.5 Fr
Sheathless
8 Fr Sheath
þ GC
Internal diameter (inches) 0.56–0.58 0.70–0.71 0.70 0.78–0.81 0.81 0.88–0.90
External diameter at the arterial access site (mm) 2.30 2.52–2.60 2.16 2.85–3.10 2.49 3.20–3.50
Parallel Wire Technique (Antegrade CTO PCI Technique)
Wire þ 1 microcatheter Yes Yes Yes Yes Yes Yes
2 microcatheters No Yes Yes Yes Yes Yes
1 microcatheter þ 1 OTW balloon No No No Yes Yes Yes
2 OTW balloons No No No No No Yes
Side-Branch Anchoring Balloon and Balloon Trapping (Useful for Both Antegrade and Retrograde CTO PCI Techniques)
1 monorail balloon þ 1 microcatheter No Yesa Yesa Yes Yes Yes
1 monorail balloon þ 1 OTW balloon No Yesb Yesb Yes Yes Yes
CTO PCI: IVUS-Guidance (Useful for Both Antegrade and Retrograde CTO PCI Techniques)
With simultaneous wire inside Yes Yes Yes Yes Yes Yes
With simultaneous microcatheter inside No No No Yes Yes Yes
Adjunctive Devices (Useful for Both Antegrade and Retrograde CTO PCI Techniques)
Rotablator 1.25–1.75 mm burr No Yesc Yes Yes Yes Yes
Rotablator 2.0–2.25 mm burr No No No Yes Yes Yes
Laser 0.9–1.4 mm Yes Yes Yes Yes Yes Yes
Laser 1.7–2.2 mm No No No Yes Yes Yes
Tornus 2.1 F No Yes Yes Yes Yes Yes
Tornus 2.6 F No Yes Yes Yes Yes Yes
Corsair No Yes Yes Yes Yes Yes
CrossBoss Catheter No Yes Yes Yes Yes Yes
Stingray CTO Re-entry device No Yes Yes Yes Yes Yes
Data from bench testing with the following materials:
Guiding Catheters (GC): 5, 6, 7, and 8 Fr Vista Brite Tip (Cordis) and Sherpa NX Active and Launcher (medtronic), Eucath Sheathless 6.5 and 7.5
Fr (Asahi).
Microcatheters: Finecross (Terumo); Quickcross (Spectranetis); over-the-wire (OTW).
Monorail Balloons: Sprinter Legend 1.25 mm (Medtronic); Mini Trek 1.20 mm (Abbott), Ryujin 1.25 mm (Terumo), Emerge 1.25mm (Boston).
IVUS: Atlantis Pro (Boston Scientific).aFeasible with Finecross, Quick cross, Tornus 2.1 Fr microcatheters but not with Corsair and Bridgepoint device.bFeasible but not advisable (too much friction)cWith 1.75 mm burr feasible but not advisable (too much friction)
GC, guiding catheter.
Transradial Approach for CTO 53
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

facilitated by less complex guiding catheter curves (forexample, JR 4 instead of Amplatz for RCA CTO).
UPCOMING IMPROVEMENTS
The process of angioplasty equipment miniaturiza-tion is actually ongoing and is expected to improvethe feasibility of TRA CTO interventions by increas-ing the number of techniques which can be performedthrough small sheaths. The avenues of research aredouble: To develop smaller GC with sufficient inter-nal lumen and to realize smaller interventional devi-ces (wires, balloons, stents) reducing the GC lumenrequirement.
Among the GC improvements, two novel types havebeen developed and their use reported for CTOs. A 5Fr Sheathless guiding catheter (Virtual 3 Fr, Medikit,Japan) with inner diameter comparable to a standard 5Fr GC and outer diameter comparable to a 3-Fr intro-ducer has been successfully used to treat by radialapproach two patients with CTO [43]. Moreover, anovel GC (Kiwami, Heartrail II, Terumo) compatiblewith a 4-Fr introducer with an inner diameter of 0.05000
has been tested in four CTO (as well as in other lesiontypes) [46].
In the field of coronary interventional devices, a rev-olutionary advancement is potentially constituted by0.01000 guidewires and 0.01000-compatible balloons. Thefirst series of such devices is represented by the“Slender System” (Japan Lifeline) and two studiesreported their use in the setting of CTO [25,47].
STUDY LIMITATIONS
The main limitation of this literature review on TRAin CTO PCI is that all the studies entered the revieware registries because no randomized data are presenton TRA use in CTO lesions PCI. Moreover, all regis-tries are single centre or single operator and are con-ducted by operators with a specific experience in TRAPCI so that the reported results cannot be extended todifferent settings.
Other important limitations are the lack of a consist-ent classification of the type of CTO lesions treated,the different definitions of procedural success and TRAcross-over among the studies, the lack of a systematic
Fig. 4. Example of radial approach for PCI on an left anterior descending CTO with no visi-ble stump. (A and B) Left radial approach is used for right coronary cannulation, whereasright radial approach is used for left coronary cannulation with 8 Fr extra backup 3.5 guidingcatheter. The CTO has no stump and is located immediately after diagonal branch take off.(C) IVUS-guided proximal cap puncture using Miracle 3 guidewire supported by Finecrossmicrocatheter. (D) Final result after stenting.
54 Burzotta et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

comparison between TRA and TFA and the incompletereporting of access-site complications (like radial arteryocclusion).
CONCLUSIONS
The radial access constitutes a valuable alternativeto trans-femoral approach to treat patients undergoingCTO PCI in centres with high volume of transradialprocedures. A specific knowledge in the material com-patibility and techniques to gain support is needed.
REFERENCES
1. Ochiai M, Ashida K, Araki H, Ogata N, Okabayashi H, Obara
C. The latest wire technique for chronic total occlusion. Ital
Heart J 2005;6:489–493.
2. Rathore S, Matsuo H, Terashima M, Kinoshita Y, Kimura M,
Tsuchikane E, Nasu K, Ehara M, Asakura Y, Katoh O, Suzuki
T. Procedural and in-hospital outcomes after percutaneous coro-
nary intervention for chronic total occlusions of coronary
arteries 2002–2008: Impact of novel guidewire techniques.
JACC Cardiovasc Interv 2009;2:489–497.
3. Kimura M, Katoh O, Tsuchikane E, Nasu K, Kinoshita Y,
Ehara M, Terashima M, Matsuo H, Matsubara T, Asakura K,
Asakura Y, Nakamura S, Oida A, Takase S, Reifart N, Di
Mario C, Suzuki T. The efficacy of a bilateral approach for
treating lesions with chronic total occlusions the CART (con-
trolled antegrade and retrograde subintimal tracking) registry.
JACC Cardiovasc Interv 2009;2:1135–1141.
4. Suttorp MJ, Laarman GJ, Rahel BM, Kelder JC, Bosschaert
MA, Kiemeneij F, Ten Berg JM, Bal ET, Rensing BJ, Eefting
FD, Mast EG. Primary stenting of totally occluded native coro-
nary arteries II (PRISON II): A randomized comparison of bare
metal stent implantation with sirolimus-eluting stent implanta-
tion for the treatment of total coronary occlusions. Circulation
2006;114:921–928.
5. Suero JA, Marso SP, Jones PG, Laster SB, Huber KC, Giorgi LV,
Johnson WL, Rutherford BD. Procedural outcomes and long-term
survival among patients undergoing percutaneous coronary inter-
vention of a chronic total occlusion in native coronary arteries: A
20-year experience. J Am Coll Cardiol 2001;38:409–414.
6. Isobe N, Sugawara M, Taniguchi K, Oshima S, Hoshizaki H,
Toyama T, Adachi H, Naito S. Delayed recovery of left ventric-
ular regional work after coronary angioplasty in patients with
opposite wall old myocardial infarction. Heart Vessels 2003;18:
61–66.
7. Warren RJ, Black AJ, Valentine PA, Manolas EG, Hunt D. Cor-
onary angioplasty for chronic total occlusion reduces the need
for subsequent coronary bypass surgery. Am Heart J 1990;120:
270–274.
8. Ivanhoe RJ, Weintraub WS, Douglas JS Jr, Lembo NJ, Furman
M, Gershony G, Cohen CL, King SB III. Percutaneous translu-
minal coronary angioplasty of chronic total occlusions: Primary
success, restenosis, and long-term clinical follow-up. Circulation
1992;85:106–115.
Fig. 5. Example of radial approach for PCI on a right coronary artery CTO. (A) Right radialapproach is used for left coronary cannulation, whereas left radial approach is used for rightcoronary cannulation with 6 Fr Judkins Right guiding catheter. (B) Fielder XT wire navigatesthe CTO (with support of Finecross microcatheter). (C) After successful wiring, during theadvancement of the small over-the-wire balloon, the guiding catheter is deeply intubated. (D)Final result after stenting.
Transradial Approach for CTO 55
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

9. Agostoni P, Biondi-Zoccai GG, de Benedictis ML, Rigattieri S,
Turri M, Anselmi M, Vassanelli C, Zardini P, Louvard Y,
Hamon M. Radial versus femoral approach for percutaneous
coronary diagnostic and interventional procedures: Systematic
overview and meta-analysis of randomized trials. J Am Coll
Cardiol 2004;44:349–356.
10. Jolly SS, Amlani S, Hamon M, Yusuf S, Mehta SR. Radial ver-
sus femoral access for coronary angiography or intervention and
the impact on major bleeding and ischemic events: A systematic
review and meta-analysis of randomized trials. Am Heart J
2009;157:132–140.
11. Chase AJ, Fretz EB, Warburton WP, Klinke WP, Carere RG, Pi
D, Berry B, Hilton JD. Association of the arterial access site at
angioplasty with transfusion and mortality: The M.O.R.T.A.L
study (Mortality benefit Of Reduced Transfusion after percuta-
neous coronary intervention via the Arm or Leg). Heart 2008;
94:1019–1025.
12. Pristipino C, Trani C, Nazzaro MS, Berni A, Patti G, Patrizi R,
Pironi B, Mazzarotto P, Gioffre G, Biondi-Zoccai GG, Richichi
G; Prospective REgistry of Vascular Access in Interventions in
Lazio Region Study Group. Major improvement of percutaneous
cardiovascular procedure outcomes with radial artery catheter-
isation: Results from the PREVAIL study. Heart 2009;95:476–
482.
13. Sciahbasi A, Pristipino C, Ambrosio G, Sperduti I, Scabbia EV,
Greco C, Ricci R, Ferraiolo G, Di Clemente D, Giombolini C,
Lioy E, Tubaro M. Arterial access-site-related outcomes of
patients undergoing invasive coronary procedures for acute coro-
nary syndromes (from the ComPaRison of Early Invasive and
Conservative Treatment in Patients With Non-ST-ElevatiOn
Acute Coronary Syndromes [PRESTO-ACS] Vascular Sub-
study). Am J Cardiol 2009;103:796–800.
14. Burzotta F, Hamon M, Trani C, Kiemeneij F. Direct coronary
stenting by transradial approach: Rationale and technical issues.
Catheter Cardiovasc Interv 2004;63:215–219.
15. Burzotta F, Trani C, Hamon M, Amoroso G, Kiemeneij F.
Transradial approach for coronary angiography and interventions
in patients with coronary bypass grafts: Tips and tricks. Catheter
Cardiovasc Interv 2008;72:263–272.
16. Trani C, Tommasino A, Burzotta F. Transradial renal stenting:
Why and how. Catheter Cardiovasc Interv 2009;74:951–956.
17. Trani C, Burzotta F, Tommasino A, Giammarinaro M. Transra-
dial approach to treat superficial femoral artery in-stent resteno-
sis. Catheter Cardiovasc Interv 2009;74:494–498.
18. Trani C, Burzotta F, Coroleu SF. Transradial carotid artery
stenting with proximal embolic protection. Catheter Cardiovasc
Interv 2009;74:267–272.
19. Burzotta F, Trani C, Coroleu S. Retrograde recanalization of
left main from saphenous vein graft supported by percutaneous
Impella Recover LP 2.5 assist device. J Invasive Cardiol 2009;
21:E147–E150.
20. Saito S, Tanaka S, Hiroe Y, Miyashita Y, Takahashi S, Satake
S, Tanaka K. Angioplasty for chronic total occlusion by using
tapered-tip guidewires. Catheter Cardiovasc Interv 2003;59:305–
311.
21. Kim JY, Lee SH, Choe HM, Yoo BS, Yoon J, Choe KH. The
feasibility of percutaneous transradial coronary intervention for
chronic total occlusion. Yonsei Med J 2006;31:680–687.
22. Wu CJ. Feasibility of bilateral radial access antegrade and retro-
grade approach for CTO lesions: Single center experience. Perso-
nal communication TCT 2008. Available at: www. tctmd.com.
23. Quesada R. Transradial approach to CTO: Techniques, results
and why. Personal communication TCT 2008. Available at:
www. tctmd.com.
24. Rathore S, Hakeem A, Pauriah M, Roberts E, Beaumont A,
Morris JL. A comparison of the transradial and the trans-
femoral approach in chronic total occlusion percutaneous coro-
nary intervention. Catheter Cardiovasc Interv 2009;73:883–887.
25. Katsuki T. Is the transradial approach a reasonable option for
most CTOs? Personal communication TCT 2009. Available at:
www. tctmd.com.
26. Yang CH, Guo GB, Chen SM, Yip HK, Hsieh K, Fang CY,
Chen CJ, Hang CL, Chen MC, Wu CJ. Feasibility and safety of
a transradial approach in intervention for chronic total occlusion
of coronary arteries: A single-center experience. Chang Gung
Med J 2010;33:639–645.
27. Liu W, Wagatsuma K, Toda M, Amano H, Nii H, Utida Y,
Nakanishi R. Short- and long-term follow-up of percutaneous
coronary intervention for chronic total occlusion through trans-
radial approach: Tips for successful procedure from a single-
center experience. J Interv Cardiol 2011;24:137–143.
28. Ferrante G, Louvard Y, Hayashid K, Benamer H, Hovasse T,
Unterseeh T, Garot P, Lefevre T. Radial versus femoral access
for percutaneous coronary interventions in patients with chronic
total occlusions. J Am Coll Cardiol 2012;60(Suppl 7):B128.
29. Burzotta F, Trani C, Tommasino A, Brancati MF, Saffioti S,
Pirozzolo G, Niccoli G, Leone AM, Schiavoni G, Crea F.
Impact of operator experience and wiring technique on proce-
dural efficacy of trans-radial percutaneous chronic total occlu-
sion recanalization performed by dedicated radialists. Cardiol J
2013 [Epub ahead of print]
30. Asgedom S, Bjornstad P, Patten R, McAdam B, Sheahan R,
Foley D. Radial approach to CTO recanalization is as successful
and safer than femoral: Single centre observational study. J Am
Coll Cardiol 2012;60(Suppl 7):B131.
31. Wu CJ, Fang HY, Cheng CI, Hussein H, Abdou SM, Youssef
AA, Bhasin A, Yang CH, Chen CJ, Hsieh YK, Yip HK, Fang
CY. The safety and feasibility of bilateral radial approach in
chronic total occlusion percutaneous coronary intervention. Int
Heart J 2011;52:131–138.
32. Rinfret S, Joyal D, Nguyen CM, Bagur R, Hui W, Leung R,
Larose E, Love MP, Mansour S. Retrograde recanalization of
chronic total occlusions from the transradial approach: Early Ca-
nadian experience. Catheter Cardiovasc Interv 2011;78:366–374.
33. Noguchi T, Miyazaki MD S, Morii I, Daikoku S, Goto Y, NonogiH. Percutaneous transluminal coronary angioplasty of chronic totalocclusions: Determinants of primary success and long-term clinicaloutcome. Catheter Cardiovasc Interv 2000;49:258–264.
34. Hoye A, van Domburg RT, Sonnenschein K, Serruys PW. Per-cutaneous coronary intervention for chronic total occlusions:The Thoraxcenter experience 1992–2002. Eur Heart J 2005;26:2630–2636.
35. Han YL, Wang SL, Jing QM, Li Y, Zhang J, Ma YY, Luan B.Percutaneous coronary intervention for chronic total occlusionin 1263 patients: A single-center report. Chin Med J 2006;119:1165–1170.
36. Kinoshita I, Katoh O, Nariyama J, Otsuji S, Tateyama H,Kobayashi T, Shibata N, Ishihara T, Ohsawa N. Coronary angio-plasty of chronic total occlusions with bridging collateral ves-sels: Immediate and follow-up outcome from a large single-center experience. J Am Coll Cardiol 1995;26:409–415.
37. Tan KH, Sulke N, Taub NA, Watts E, Karani S, Sowton E.
Determinants of success of coronary angioplasty in patients with
a chronic total occlusion: A multiple logistic regression model
to improve selection of patients. Br Heart J 1993;70:126–131.
38. Saito S, Ikei H, Hosokawa G, Tanaka S. Influence of the ratio
between radial artery inner diameter and sheath outer diameter
on radial artery flow after transradial coronary intervention.
Catheter Cardiovasc Interv 1999;46:173–178.
56 Burzotta et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

39. Coroleu SF, Burzotta F, Fern�andez-G�omez C, Tommasino A,
Giammarinaro M, Coluccia V, Di Noi P, Schiavoni G, Trani C.
Feasibility of complex coronary and peripheral interventions by
trans-radial approach using large sheaths. Catheter Cardiovasc
Interv 2012;79:597–600.
40. Burzotta F, Trani C, De Vita M, Crea F. A new operative classi-
fication of both anatomic vascular variants and physiopathologic
conditions affecting transradial cardiovascular procedures. Int J
Cardiol 2010;145:120–122.
41. Ikari Y, Masuda N, Matsukage T, Ogata N, Nakazawa G,
Tanabe T, Morino Y. Backup force of guiding catheters for the
right coronary artery in trans-femoral and transradial interven-
tions. J Invasive Cardiol 2009;21:570–574.
42. Takahashi S, Saito S, Tanaka S, Miyashita Y, Shiono T, Arai F,
Domae H, Satake S, Itoh T. New method to increase a backup
support of a 6 French guiding coronary catheter. Catheter Cardi-
ovasc Interv 2004;63:452–456.
43. Takeshita S, Shishido K, Sugitatsu K, Okamura N, Mizuno S,
Yaginuma K, Suenaga H, Tanaka Y, Matsumi J, Takahashi S, Saito
S. In vitro and human studies of a 4F double-coaxial technique
(“mother-child” configuration) to facilitate stent implantation in re-
sistant coronary vessels. Circ Cardiovasc Interv 2011;4:155–161.
44. Hayashida K, Louvard Y, Lefevre T. Transradial complex coro-
nary interventions using a five-in-six system. Catheter Cardio-
vasc Interv 2011;77:63–68.
45. Takeshita S, Saito S. Transradial coronary intervention using a
novel 5-Fr sheathless guiding catheter. Catheter Cardiovasc
Interv 2009;74:862–865.
46. Takeshita S, Shiono T, Takagi A, Ito T, Saito S. Percutaneous
coronary intervention using a novel 4-French coronary accessor.
Catheter Cardiovasc Interv 2008;72:222–227.
47. Masutani M, Yoshimachi F, Matsukage T, Ikari Y, Saito S. Use
of slender catheters for transradial angiography and interven-
tions. Indian Heart J 2008;60(Suppl 1):A22–A26.
Transradial Approach for CTO 57
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).




















