Training in Percutaneous Nephrolithotomy—A Critical Review
10
Review – Endo-urology Training in Percutaneous Nephrolithotomy—A Critical Review Jean J.M.C.H. de la Rosette a, *, Maria P. Laguna a , Jens J. Rassweiler b , Pierre Conort c a Department of Urology, AMC University Hospital, Amsterdam, The Netherlands b SLK Klinikun, Heilbronn, Germany c Hopital La Pitie – Salpetriere, Paris, France 1. Introduction In an active urologic department, 30% of the surgical working load is known to be related to treatment of renal and ureteral stones [1(R)]. Percutaneous nephrolithotomy (PCNL) has a well-defined role in the treatment of renal stones, specifically for large stones [1,2 (2/B)]. Worldwide, PCNL represents 5% of european urology 54 (2008) 994–1003 available at www.sciencedirect.com journal homepage: www.europeanurology.com Article info Article history: Accepted March 18, 2008 Published online ahead of print on March 28, 2008 Keywords: Percutaneous surgery Training Urinary stones Abstract Aim: To study factors influencing training and maintaining skills in performing percutaneous nephrolithotomy (PCNL). Methods: We matched key words, throughout Medline, MeSH, and Cochrane databases including: renal stone, percutaneous, nephrostomy, endourology, educational, training, learning curve, expertise, skill, resi- dency, practice, survey, simulator, and robotics. For this topic we defined,if possible, levels of evidence based on International Consultation on Urolo- gical Diseases (ICUD) and World Health Organization recommendations. Results: Obtaining renal access is one of the most important factors in training for PCNL. A resident has to perform about 24 PCNL procedures to obtain a good proficiency during the residence period. Competence at performing PCNL is reached after 60 cases and excellence is obtained at >100 cases. Stone centers providing all the endoscopic treatment options seem to provide the best conditions to ensure a sufficient volume of patients recruited. Virtual reality simulators may have a potential in training for PCNL. To maintain one’s expertise, participation in continu- ing educational programs is recommended. Conclusion: PCNL is currently the most complicated stone surgery tech- nique to teach. The steep learning curve is mainly related to obtaining renal access. The traditional method of acquiring surgical skills is by apprenticeship in the absence of validated virtual simulators. Given the complexity of the treatment of renal stones, one may consider a cen- tralized renal stone treatment in dedicated stone centers. # 2008 European Association of Urology. Published by Elsevier B.V. All rights reserved. * Corresponding author. Department of Urology G4-105, AMC University Hospital, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands. E-mail address: [email protected] (J.J.M.C.H. de la Rosette). 0302-2838/$ – see back matter # 2008 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2008.03.052
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Training in Percutaneous Nephrolithotomy—A Critical Review
Review – Endo-urology
Training in Percutaneous Nephrolithotomy—A Critical Review
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 9 4 – 1 0 0 3
avai lable at www.sc iencedi rect .com
journal homepage: www.europeanurology.com
,
.
Jean J.M.C.H. de la Rosette a,*, Maria P. Laguna a, Jens J. Rassweiler b, Pierre Conort c
aDepartment of Urology, AMC University Hospital, Amsterdam, The Netherlandsb SLK Klinikun, Heilbronn, GermanycHopital La Pitie – Salpetriere, Paris, France
Article info
Article history:Accepted March 18, 2008Published online ahead ofprint on March 28, 2008
Keywords:Percutaneous surgeryTrainingUrinary stones
Abstract
Aim: To study factors influencing training and maintaining skills inperforming percutaneous nephrolithotomy (PCNL).Methods: We matched key words, throughout Medline, MeSH, andCochrane databases including: renal stone, percutaneous, nephrostomyendourology, educational, training, learning curve, expertise, skill, resi-dency,practice,survey,simulator,androbotics.Forthistopicwedefined,ifpossible, levels of evidence based on International Consultation on Urolo-gical Diseases (ICUD) and World Health Organization recommendationsResults: Obtaining renal access is one of the most important factors intraining for PCNL. A resident has to perform about 24 PCNL procedures toobtain a good proficiency during the residence period. Competence atperforming PCNL is reached after 60 cases and excellence is obtained at>100 cases. Stone centers providing all the endoscopic treatment optionsseem to provide the best conditions to ensure a sufficient volume ofpatients recruited. Virtual reality simulators may have a potential intraining for PCNL. To maintain one’s expertise, participation in continu-ing educational programs is recommended.Conclusion: PCNL is currently the most complicated stone surgery tech-nique to teach. The steep learning curve is mainly related to obtainingrenal access. The traditional method of acquiring surgical skills is byapprenticeship in the absence of validated virtual simulators. Given the
e treatment of renal stones, one may consider a cen-
complexity of th tralized renal stone treatment in dedicated stone centers.# 2008 European Association of Urology. Published by Elsevier B.V. All rights reserved.* Corresponding author. Department of Urology G4-105, AMC University Hospital,Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands.E-mail address: [email protected] (J.J.M.C.H. de la Rosette).
1. Introduction
In an active urologic department, 30% of the surgicalworking load is known to be related to treatment of
0302-2838/$ – see back matter # 2008 European Association of Urology. Publis
renal and ureteral stones [1(R)]. Percutaneousnephrolithotomy (PCNL) has a well-defined role inthe treatment of renal stones, specifically for largestones [1,2 (2/B)]. Worldwide, PCNL represents 5% of
hed by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2008.03.052

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 9 4 – 1 0 0 3 995
renal stone surgery [1 (R)]. The last European surveyshowed that a significant number of urologistsperform PCNL, but geographical variations areimportant and the number of mean proceduresfor year is low [3 (3a/B)]. With >25 yr of worldwidepractice, PCNL remains a milestone technique witha very low major complication rate and a very highsuccess rate. All these data induce the motivation tolearn this procedure.
However, there is a known steep learning curve forPCNL and urologists remain reluctant to perform thiskind of surgery [4–6 (3a/B)]. Although the major andmost difficult step of PCNL seems to be the ability toobtain an appropriate access to the renal cavities,which reduces the risk of vascular injury and leads toa better stone-free rate [8 (3a/B)], other outcomes asstone-free rate and the need for ancillary proceduresmay also be used to categorize the performance.Therefore, the most important issue concerningPCNL represents its learning curve [9 (3b/C)].
There are very few data on the teaching of renalpercutaneous access and PCNL. In addition to theapprenticeship, inanimate simulators, virtual real-ity (VR) simulators, and robotics provide newperspectives in the 21st century.
In this paper we aim to provide insight into thefactors influencing the training in percutaneousstone surgery and to include a proposal for aminimum training curriculum on PCNL. In addition,we want to provide specific recommendations fortraining and the number of PCNL procedures (peryear) required to maintain a surgical proficiency.
2. Methods
A critical non-structured review of the literature regarding the
training for PCNL was conducted. We matched key words,
throughout Medline, MeSH, and Cochrane databases: renal or
urinary stone, percutaneous, nephrostomy, endourology,
educational, training, learning curve, expertise, skill, resi-
dency, practice, survey, simulator, and robotics. For this topic
Table 1 – Key issues, level of evidence, and recommendations ain percutaneous renal stone surgery
Key issues Evidence
Creation of renal access Few urologists perform access themselve
Trend to become increasingly involved
Definition of learning curve No clear definition of which outcomes
should be used as surrogate markers
Quality of training Performing PCNL during residency increa
the chances to perform routine PCNL aft
Training models Scarcity of animal and inanimate models
VR may help in training
PCNL = percutaneous nephrolithotomy; VR = virtual reality.
we have defined, when possible, levels and grades of evidence
based on 2001 recommendations of the Oxford Center for
evidence-based medicine (http://minerva.minervation.com/
cebm/docs/level.html).
3. Results
The following key factors related to training of PCNLwere found: learning renal access, the definition oflearning curve, quality of training, and differentforms of training (Table 1). Levels of evidence arestated in the corresponding sections for each one ofthe key factors.
3.1. Who creates the renal access?
A recent report confirmed that up to 69.6% of theurologists perform percutaneous procedures with amean of 16.8 PCNLs per month. However, PCNL forstone management is mainly performed in EasternEuropean countries and in non-European countries[3 (3a/B)] gaining a proper percutaneous renal accessis an integral step in percutaneous renal drainageand percutaneous nephrolithotomy [10 (R)]. Obtain-ing renal access in the operating room remains achallenging task for many urologists. Inaccurateplacement of the needle can cause injuries inthe kidney and adjacent organs, thus compromisingthe planned percutaneous procedure, as well as theclinical outcome of the patient [7 (3a/C),8 (3a/B)].
A recent American survey revealed that only 11%of urologists performing PCNL routinely obtainedpercutaneous access by themselves [8 (3a/B)].Reasons for this trend may include the lack oftraining, a personal comfort level and other param-eters as may the availability of better equipment inthe radiology suite or the costs related to the extratime to obtain access [11 (3b/C)]. Nevertheless, thedevelopment of techniques to establish a safe andreliable percutaneous access has provided signifi-cant progress in percutaneous intrarenal procedures
s cornerstones for training and maintaining surgical skills
Recommendation
s Include radiologic access to renal cavities in the
current residency programs
Definition of outcomes to be used as end points
of the training
ses
er training
Defining a minimum training curriculum and
fellowships in endourology in reference stone centers
Development and validation of simulation models

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 9 4 – 1 0 0 3996
[9 (3b/C)]. Urologists are increasingly obtainingaccess themselves because this eliminates relianceon a second ‘‘surgeon’’ and increases flexibility withrespect to procedure timing and the location of theaccess tract [10 (R)]. Moreover, different techniquesincluding the use of a flexible ureterorenoscopeand the supine position for access may furtherfacilitate renal access and familiarity with newtechnologies [12 (R)]. In addition one can gain moreexperience in percutaneous renal access by includ-ing other percutaneous manipulations, such asinsertion of percutaneous nephrostomy, antegradeendopyelotomy, and procedures for antegrade ure-teric stenting in the training program.
3.2. Definition of learning curve
The surgical learning curve remains primarily atheoretical concept; actual curves based on surgicaloutcome data, mostly in the field of radicalprostatectomy, are rarely presented for other tech-niques [13(R)]. The PCNL procedure has a steeplearning curve leading to a higher complication ratein the beginning of the experience [14 (3/C)].
The first aim is to determine surrogate markers toevaluate the surgical expertise and the number ofprocedures needed to gain surgical competence inthe PCNL procedures. In urology, studies definingthe learning curve are mostly focused on cancersurgery and specifically on laparoscopic procedures.There are very few publications on this topic.
To define the learning curve for PCNL there aresome potential surrogate markers (or outcomes).Although the most relevant clinical end points forPCNL are the stone clearance and the complicationrate, they may not be the best tools for assessing thelearning curve in the PCNL procedure [9 (3b/C)]. Allenet al used operation and fluoroscopic screening timesand also radiation dose. With these markers thelearning curve of a single surgeon suggests thatcompetence at performing PCNL is reached after 60cases and excellence is obtained after 115 [15 (3b/C)].Taniverdi et al have studied the learning curve of onesurgeon prospectively, using many parameters,including stone-free rate and complication rate.The two markers showing improvement were theoperation time and the fluoroscopic screening times.No further decrease in the operation time wasobserved after case number 60. A drop in the meanfluoroscopy screening time was observedfrom a peakof 17.5 � 3.2 min in the first 15 cases to 8.9 � 4.3 minfor cases 46 through 60. This decline continued incases 61–104 but was not significant. These authorssuggested that competence in PCNL is obtained after60 cases [9 (3b/C)].
However, the number of PCNL cases required togain surgical proficiency in the treatment of renalstone disease is uncertain [9 (3b/C)]. A survey in theUnited States showed that residents are comfortablewith percutaneous access after an average of21.2 � 4.5 access procedures [11 (3b/C)]. Conversely,urologists who were comfortable performing percu-taneous access after residency had performedsignificantly more percutaneous access proceduresduring their residency than those who wereuncomfortable (24.4 � 5.6 and 10.6 � 3.1 procedures,respectively; p = 0.046) [11 (3b/C)]. Therefore, theauthors suggested that performing �24 percuta-neous access procedures during residency mightincrease resident proficiency immediately afterresidency.
3.3. Quality of training
Another objective is to determine if the practiceafter residency is related to the training. Bird et alreported an interesting survey of 1102 urologistsregarding the treatment of large renal stones. Fromthe 564 responders, 73% of the urologists werecomfortable performing PCNL procedures and thosetrained to perform PCNL during residency weremore often comfortable with this procedure thanthose who did not receive training in PCNL duringresidency [16 (3b/C)].
The current method of acquiring surgical skills inPCNL is by traditional apprenticeship and involvesan extensive period of training with patients. Thelearning process of surgical skills begins with thetheoretical approach written in books and journals.The next step is mentored practice on patients untilthe moment that the trainee is considered matureenough to perform the surgical procedure alone.Nevertheless, an enormous gap exists between whatcan be read in books or taught by experts and thereality encountered when operating on patients.Since the introduction of audiovisual technology,after theoretical learning the apprentice has theopportunity to watch recorded real proceduresbefore switching to real practice.
3.4. Training models
Surprisingly few models have been developed totrain urologists in percutaneous renal access [10 (R)].Animal models allow surgical training in an envi-ronment more akin to reality. The porcine modelhas been used but training on animals is difficult toorganize and not close enough to human reality; inaddition, the cost is high. Surgical simulation isincreasingly being considered for training and
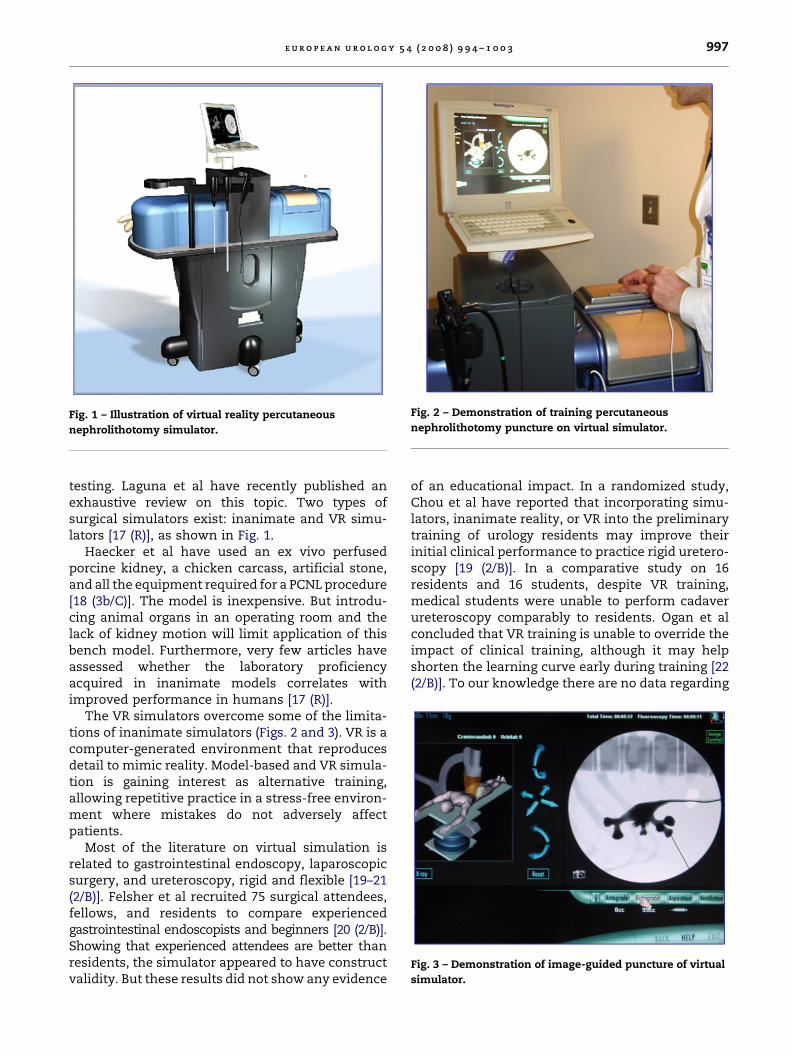
Fig. 1 – Illustration of virtual reality percutaneous
nephrolithotomy simulator.
Fig. 2 – Demonstration of training percutaneous
nephrolithotomy puncture on virtual simulator.
Fig. 3 – Demonstration of image-guided puncture of virtual
simulator.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 9 4 – 1 0 0 3 997
testing. Laguna et al have recently published anexhaustive review on this topic. Two types ofsurgical simulators exist: inanimate and VR simu-lators [17 (R)], as shown in Fig. 1.
Haecker et al have used an ex vivo perfusedporcine kidney, a chicken carcass, artificial stone,and all the equipment required for a PCNL procedure[18 (3b/C)]. The model is inexpensive. But introdu-cing animal organs in an operating room and thelack of kidney motion will limit application of thisbench model. Furthermore, very few articles haveassessed whether the laboratory proficiencyacquired in inanimate models correlates withimproved performance in humans [17 (R)].
The VR simulators overcome some of the limita-tions of inanimate simulators (Figs. 2 and 3). VR is acomputer-generated environment that reproducesdetail to mimic reality. Model-based and VR simula-tion is gaining interest as alternative training,allowing repetitive practice in a stress-free environ-ment where mistakes do not adversely affectpatients.
Most of the literature on virtual simulation isrelated to gastrointestinal endoscopy, laparoscopicsurgery, and ureteroscopy, rigid and flexible [19–21(2/B)]. Felsher et al recruited 75 surgical attendees,fellows, and residents to compare experiencedgastrointestinal endoscopists and beginners [20 (2/B)].Showing that experienced attendees are better thanresidents, the simulator appeared to have constructvalidity. But these results did not show any evidence
of an educational impact. In a randomized study,Chou et al have reported that incorporating simu-lators, inanimate reality, or VR into the preliminarytraining of urology residents may improve theirinitial clinical performance to practice rigid uretero-scopy [19 (2/B)]. In a comparative study on 16residents and 16 students, despite VR training,medical students were unable to perform cadaverureteroscopy comparably to residents. Ogan et alconcluded that VR training is unable to override theimpact of clinical training, although it may helpshorten the learning curve early during training [22(2/B)]. To our knowledge there are no data regarding

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 9 4 – 1 0 0 3998
the evaluation of VR simulators for PCNL as has beendone for ureteroscopy [23 (2/B)]. A VR simulator,which may aid in training for PCNL procedures, iscurrently being developed [11 (3b/C)].
4. Discussion
4.1. The safest access technique
The renal cavities have a huge variability in theirthree-dimensional (3D) presentation. Despite thefact that main calices are more or less in the samearea in the orthotopic kidney, two identical caliceal3D positions are not likely to be found. Thus, it is noteasy to standardize a precise and reliable techniquewithout the help of an expert to adapt the procedureto the patient’s anatomy.
Percutaneous access to the kidney requires a trueexpert system, using or not additional tools such as acomputer. Currently, the routine 3D computedtomography, performed before most of PCNL proce-dures, provides excellent representations of thisanatomy and allows a preplanning step [24 (3b/C)].However, the 3D rendering shape of the cavities isobtained by the maximum intensity projection,which does not show the relationship between thecalices and the different organs, such as colon inparticular, and the kidney motion. Limitation withrobot-assisted percutaneous renal access (PAKY) isrelated to the mobile kidney within the retroperito-neum during respiratory variation and to the varioustissue interfaces that the needle must traverse beforereaching the collecting system [7 (3a/C)].
Table 2 – Proposal for the minimal requirements for a curricu
Competence
Medical expertise Theoretical and practical kn
Technical expertise Access and lithotripsy perfo
strict supervision
Complete or part of proced
Judgment/clinical decision-making Correct anamnesis with spe
Correct assessment of risk
Communication To be able to communicate
as well as alternatives, poss
Collaboration To be able to contact the di
diathesis as well those who
Management and leadership Coordination of the procedu
appropriate time frame
Health advocacy To be able to counsel patien
Scholar and teacher Participate in continuing m
and implement new techni
Professionalism To be able to apply the ethi
the patient to a more quali
limitations
PCNL = percutaneous nephrolithotomy.
Additional real-time control, such as ultrasound,should be the safest technique in an expert system[25,26 (3b/C)]. Montanari et al reported a 98% successrate in their experience of 330 percutaneous renalaccess procedures under ultrasound fluoroscopicguidance [25 (3b/C)]. The urologist has to be theexpert, feeling the different interfaces from the skinto the cavities and the resistance during the motionof the nephroscope and tools.
4.2. The optimal training
Today, urologists still must learn how to performsafely and effectively the percutaneous access bythemselves [11 (3b/C)]. Training in the more tech-nically challenging aspects of endoscopic lithotripsymust be encouraged. VR simulators may have a realfuture in this field. Simulation must provide tactilefeedback to recreate an optimal surgical environ-ment. Despite current limitations, it is likely that inthe near future improvements in computers willprovide the right tactile information [17 (R)]. Meas-urement tools of force and visual dexterity will beincorporated into the simulators allowing for anobjective assessment of the trainee’s skills [17 (R)].Furthermore, real instruments can be incorporatedinto the endoscopic (hybrid) simulation making iteasier to generate a realistic sensation of pressureand force [17 (R)].
However, despite the fact that numerous deviceshave evolved as educational tools in a variety offields, and especially in endourology, whether thesetools can be used for validation of physicians’ skillshas yet to be determined.
lum of percutaneous nephrolithotomy
Level to be reached
owledge of the technique and its indications
rmance in simple/medium complicated cases under
ure may be done under supervision depending on trainee skills
cial emphasis on the previous stone history and operations
and benefits of the different lithiasis interventions and of PCNL
with the patient and relatives the nature of the procedure
ible complications, and consequences
fferent specialists involved in the management of the stone
can be potentially involved in the procedure
re resulting in an effective, safe, and efficient treatment in the
ts and take adequate preventive measures
edical education and be able to identify ways to update knowledge
cal skills
cal principles that drive the patient–doctor relationship and to refer
fied colleague when indicated. To recognize their own professional

Fig. 4 – Master class in percutaneous nephrolithotomy
showing a live demonstrating of an expert with
endourology fellow.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 9 4 – 1 0 0 3 999
Urologists have to embrace the new trainingtechnologies and remain active participants intheir applications to the care of the urologic patient[7 (3a/C)]. There is a strong need for a definedcurriculum for PCNL training. However, while someof the basic competences such as knowledge andcommunication should be completely fulfilled at theend of the residency, the level of surgical skills andperformance is going to be guided by the case load ofthe training center, the trainee’s individual skills,and preferences. The minimum level of expertisewill be defined by the different national urologicorganizations. Neither literature nor a comprehen-sive current curriculum defines the level of skills tobe reached at the end of the training [27]. Table 2presents an example of a proposal including theminimal requirements for a training curriculum forPCNL.
Once trained, it is important to maintain a highlevel of PCNL performance in one’s daily practice.The maintenance of sufficient skills in percutaneousaccess may require continuing education to reg-ularly refresh the urologist’s technique after resi-dency [11 (3b/C)]. Emphasis should be placed onproviding and attending continuing educationopportunities to maintain competency in thisimportant technique. Although urologists trainedin percutaneous access were significantly morelikely to perform percutaneous surgical proceduresthan those not trained in percutaneous access (88%and 38%, respectively, p = 0.04) [11 (3b/C)], only 27%of the urologists trained in percutaneous accesscontinued to perform percutaneous renal accesscompared to 11% of those untrained ( p = 0.33) [11(3b/C)].
The survey conducted by Lee et al has shown thaturologists trained in access perform a mean of 14 � 4percutaneous renal procedures annually whilethose untrained perform 3.3 � 1.7 procedures( p = 0.02) [11 (3b/C)]. These results are similar tothose of the European survey published by Michelet al, showing a mean of 16 PCNLs performed peryear after the training phase [4 (3a/B)]. Conse-quently, it is suggested that a minimum of 14–16PCNL procedures per year could be required tomaintain a urologist’s competence. There is arelationship between training in percutaneousaccess and a significant increase in the numberand complexity of PCNLs being performed by theurologist [11 (3b/C)]. Beside the traditional stagesand theoretical courses, master class workshops inPCNL are a powerful tool of continuing medicaleducation. These master classes offer trainingopportunities to residents and junior urologists andinclude intense real-life hands-on training and
blackboard teaching by experts in the field of renalstone management in a short period of time (Fig. 4).
To define minimum requirements for training inPCNL and minimal requirements to maintain certi-fication, however, is a major challenge as is thedefinition of the learning curve in PCNL. Currently,no validated surrogate markers define the learningcurve, and consequently data on continuing educa-tion markers cannot be extrapolated. The meannumber of procedures performed after the trainingrepresents only a bare figure and does not provideany information on complexity of the procedure orquality of the performance [4 (3a/B)–11(3b/C)].
In surgery both the traditional apprenticeshipsand the modern curriculums firmly support thatcases of increased complexity should be the secondline of the training. Those cases are usuallyperformed by and with experts in academic dedi-cated urologic centers. It is also expected that in thenear future simulators and robots may simulatepathology of increased difficulty and become usefuland important tools in training and in postgraduatecontinuing education [17 (R)]. It remains unan-swered in what extension will simulation substitutethe conventional training in the operating theaterand if it will ultimately result in greater efficiencyand lower morbidity.
4.3. From training to continuing education: the
contribution of stone centers
Training in the more technically challenging aspectsof endoscopic lithotripsy must be encouraged. Thenumber of simple PCNL procedures has a tendencyto decrease in the era of flexible ureteroscopy andrepresents about 5–10% of all the treatments forurinary stones. PCNL is mostly performed for large

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 9 4 – 1 0 0 31000
or complex stones in the departments of urologywhere it has to be taught. Regardless of thepercutaneous access and related complexity of thestone, PCNL has become more difficult to learn. Aresident should perform around 24 PCNL proceduresto obtain good proficiency during the residencyperiod. Considering the increasing number of com-plex cases to be performed by the seniors, anacademic Department of Urology, with only onenew resident per year, should recruit approximately500 cases of renal stone cases per year to ensure atraining program. Such an enormous caseload canbe reached only by a very few centers worldwide,which will limit to the minimum the number ofresidents trained.
Because data show that performance is directlyrelated to the volume of activity of each surgeon peryear, post-residency dedicated fellowships in stonecenters providing all the endoscopic treatmentoptions would provide the best conditions to ensureboth a sufficient volume of patients recruited andproper training of a selected, but sufficient number,to cover the incidence of PCNL and number oftrainees.
Currently, definitive data are lacking on howmany procedures need to be performed to gain andmaintain surgical competence in PCNL procedures.Besides gaining access one of the biggest challengesis to obtain a stone-free status in one single PCNLsession. In addition to this stone-free status, thenumber of second-look PCNL sessions, auxiliaryprocedures, and complication rates are crucialparameters in performing PCNL with excellence.Continuing education in percutaneous access maybenefit from the incorporation of teleproctoring,teleconferencing, or VR simulation [10,28 (2/C)]. Toguarantee the role of the urologist as major player inthe complete armamentarium of renal stone treat-ment, we recommend a critical appraisal of the keyissues identified and summarized in Table 1. Therecommendations provided by the authors reflectthe lacks identified in the present review andprovide an option to guarantee complete masteringof the procedure
5. Conclusions
Training in PCNL has a steep learning curve that ismainly related to obtaining renal access. The qualityof training during residency is likely related to therecruitment of patients in the training center and theavailability of complete up-to-date equipment.Learning curves published for PCNL reach a plateauafter 40–60 procedures performed solo. It seems quite
clear that new forms of training must be incorporatedinto learning the surgical skills. In addition, partici-pation in continuing education programs is recom-mended to maintain one’s proficiency.
Author contributions: Jean J.M.C.H. de la Rosette had full access
to all the data in the study and takes responsibility for the
integrity of the data and the accuracy of the data analysis.
Study concept and design: de la Rosette, Laguna, Rassweiler,
Concort.
Acquisition of data: de la Rosette, Laguna, Rassweiler, Concort.
Analysis and interpretation of data: de la Rosette, Laguna,
Rassweiler, Concort.
Drafting of the manuscript: de la Rosette, Concort.
Critical revision of the manuscript for important intellectual content:
de la Rosette, Laguna, Rassweiler, Concort.
Statistical analysis: Not applicable.
Obtaining funding: Not applicable.
Administrative, technical, or material support: Not applicable.
Supervision: Not applicable.
Other (specify): None.
Financial disclosures: I certify that all conflicts of interest,
including specific financial interests and relationships and
affiliations relevant to the subject matter or materials
discussed in the manuscript (eg, employment/affiliation,
grants or funding, consultancies, honoraria, stock ownership
or options, expert testimony, royalties, or patents filed,
received, or pending), are the following: None.
Funding/Support and role of the sponsor: None.
References
[1] Alken P, Bellman G, Flam T, et al. Treatment of renal
stones. In: Segura J, Conort P, Khoury S, PAK C, Preminger
GM, Tolley D, eds. International Consultation on Stone
Disease, Paris 2001, July 4–5. Proc Ed 2003;21:173–210 (R).
[2] Skolarikos A, Alivizatos G, de la Rosette JJMCH. Percuta-
neous nephrolithotomy and its legacy. Eur Urol 2005;47:
22–8 (2/B).
[3] Kauer PC, Laguna MP, Alivizatos G, et al., on behalf of the
members of ESUT. Present practice and treatment stra-
tegies in endourological stone management: results of a
survey of the European Society of Uro-technology (ESUT).
Eur Urol 2005;48:182–8 (3a/B).
[4] Michel MS, Trojan L, Rassweiler JJ. Complications in per-
cutaneous nephrolithotomy. Eur Urol 2007;51:899–906
(3a/B).
[5] Kukreja R, Desai M, Patel S, Bapat S, Desai M. Factors
affecting blood loss during percutaneous nephrolitho-
tomy: a prospective study. J Endourol 2004;18:715–22 (3a/B).
[6] Sreenevasan G. Urinary stones in Malaysia—its incidence
and management. Med J Malaysia 1990;45:92–112 (3a/B).
[7] Su LM, Stoianovici D, Jarrett TW, et al. Robotic percuta-
neous access to the kidney: comparison with standard
manual access. J Endourol 2002;16:471–5 (3a/C).

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 9 4 – 1 0 0 3 1001
[8] Watterson JD, Soon S, Jana K. Access related complica-
tions during percutaneous nephrolithotomy: urology ver-
sus radiology at a single academic institution. J Urol
2006;176:142–5 (3a/B).
[9] Tanriverdi O, Boylu U, Kendirci M, Kadihasanoglu M,
Horasanli K, Miroglu C. The learning curve in the training
of percutaneous nephrolithotomy. Eur Urol 2007;52:206–
12 (3b/C).
[10] Stern J, Zeltser IS, Pearle MS. Percutaneous renal access
simulators. J Endourol 2007;21:270–3 (R).
[11] Lee CL, Anderson JK, Monga M. Residency training in
percutaneous renal access: does it affect urological prac-
tice? J Urol 2004;171:592–5 (3b/C).
[12] Deane LA, Clayman RV. Advances in percutaneous
nephrolithotomy. Urol Clin North Am 2007;34:383–95 (R).
[13] Vickers AJ, Bianco FJ, Serio AM, et al. The surgical learning
curve for prostate cancer control after radical prostatec-
tomy. J Natl Cancer Inst 2007;99:1171–7 (R).
[14] Jemni M, Bacha K, Ben Hassine L, Karray MS, Ayed M. Le
resultat du traitement de la lithiase renale par nephro-
lithotomie percutanee: a propos de 115 cas. Prog Urol
1999;9:52–60 (3/C).
[15] Allen D, O’Brien T, Tiptaft R, Glass J. Defining the learning
curve for percutaneous nephrolithotomy. J Endourol
2005;19:279–82 (3b/C).
[16] Bird VG, Fallon B, Winfield HN. Practice patterns in the
treatment of large renal stones. J Endourol 2003;17:355–63
(3b/C).
[17] Laguna MP, Hatzinger M, Rassweiler J. Simulators and
endourological training. Curr Opin Urol 2002;12:209–15 (R).
[18] Hacker A, Wendt-Nordahl G, Honeck P, Michel MS, Alken
P, Knoll T. A biological model to teach percutaneous
nephrolithotomy technique with ultrasound- and fluoro-
scopy-guided access. J Endourol 2007;21:545–50 (3b/C).
[19] Chou DS, Abdelshehid C, Clayman RV, McDougall EM.
Comparison of results of virtual-reality simulator and
Editorial Comment on: Training in PercutaneousNephrolithotomy—A Critical ReviewAlberto BredaDivision of Endourology, Department of Urology,David Geffen School of Medicine at UCLA,United [email protected]
What is the learning curve? The concept of thelearning curve was introduced by the 19th centuryGerman psychologist Heramn Ebbinghaus in hisstudy of the efficiency of memorization. Ebbing-haus tested his long-term memory by attemptingto memorize a series of nonsense syllables.He found that the more he repeated the series,the more syllables he could remember, until finallyhe could recall the whole list. Furthermore, hereported rapid progress in syllable recall during theinitial stages, followed by lessening improvements
training model for basic ureteroscopy training. J Endourol
2006;20:266–71 (2/B).
[20] Felsher JJ, Olesevich M, Farres H, et al. Validation of a
flexible endoscopy simulator. Am J Surg 2005;189:497–500
(2/B).
[21] Watterson JD, Beiko DT, Kuan JK, Denstedt JD. Rando-
mized prospective blinded study validating acquisition
of ureteroscopy skills using computer based virtual
reality endourological simulator. J Urol 2002;168:1928–32
(2/B).
[22] Ogan K, Jacomides L, Shulman MJ, Roehrborn CG,
Cadeddu JA, Pearle MS. Virtual ureteroscopy predicts
ureteroscopic proficiency of medical students on a cada-
ver. J Urol 2004;172:667–71 (2/B).
[23] Knoll T, Trojan L, Haecker A, Alken P, Michel MS. Valida-
tion of computer-based training in ureteroscopy. BJU Int
2003;95:1276–9 (2/B).
[24] Thiruchelvam N, Mostafid H, Ubhayakar G. Planning per-
cutaneous nephrolithotomy using multidetector computer
tomography urography, multiplanar reconstruction and
three-dimensional reformatting. BJU Int 2005;95:1280–4
(3b/C).
[25] Montanari E, Serrago M, Esposito N, et al. Ultrasound-
fluoroscopy guided access to the intrarenal excretory
system. Ann Urol 1999;33:168–81 (3b/C).
[26] Mozer P, Conort P, Leroy A, et al. Aid to percutaneous renal
access by virtual projection of the ultrasound puncture
tract onto fluoroscopic images. J Endourol 2007;21:460–5
(3b/C).
[27] Miller GE. The assessment of clinical skills/competence/
performance. Acad Med 1990;65:563–7.
[28] Challacombe BJ, Patriciu A, Glass J, et al. A randomized
controlled trial of human versus robotic and telerobotic
access to the kidney as the first step in percutaneous
nephrolithotomy. Comput Aided Surg 2005;10:165–71,
(2/C).
with further practice [1]. If we wanted to transferEbbinghaus’ experience to surgery, we would needto draw a slope, and the definition of learning curvewould be the point at which the slope changes. Thequestion is: Is it possible to determine how manyprocedures are required before seeing a change inthe slope? Specifically, is this possible for percu-taneous nephrolithotomy (PCNL)? From the studiespublished in the literature on this topic, one mayconclude that the learning curve for PCNL reachesa plateau after 40 to 60 cases [2,3]. Unfortunately, Ifind it difficult to believe that one specific numberof cases can be extrapolated to a group of surgeons.In general, surgery has a dynamic learning curvewith many variables to consider, including differ-ent skill levels among surgeons that may justifydifferent learning curves [4]. Furthermore, there isa constant evolution in technology, periodicallychanging the way we practice medicine and per-

form surgery [5]. Therefore it will remain challen-ging to objectively define education. Will this ever bepossible? In the United States, the American Collegeof Surgeons (www.facs.org/education) is trying toenhance the care of surgical patients and activelypromote patient safety through standardization ofeducational programs and products for surgeons.In this review, the authors have suggested a modelthat tries to standardize the requirements for atraining curriculum for PCNL [2]. I believe thisrepresents a valid initial model. Hopefully thisreview will generate further investigations.
References
[1] Ebbinghaus H. Memory: A Contribution to Experimental
Psychology. Ruger HA and Bussenius CE, trans. NY:
Columbia University Teacher’s College, 1913.
[2] de la Rosette JJMCH, Laguna MP, Rassweiler JJ, Conort P.
Training in percutaneous nephrolithotomy—a critical
review. Eur Urol 2008;54:994–1003.
[3] Tanriverdi O, Boylu U, Kendirci M, Kadihasanoglu M,
Horasanli K, Miroglu C. The learning curve in the train-
ing of percutaneous nephrolithotomy. Eur Urol 2007;
52:206–12.
[4] Vickers AJ, Bianco FJ, Gonen M, et al. Effects of pathologic
stage on the learning curve for radical prostatectomy:
evidence that recurrence in organ-confined cancer is
largely related to inadequate surgical technique. Eur
Urol 2008;53:960–6.
[5] Frede T, Hammady A, Klein J, et al. The radius surgical
system—a new device for complex minimally invasive
procedures in urology? Eur Urol 2007;51:1015–22, discus-
sion 1022.
DOI: 10.1016/j.eururo.2008.03.053
DOI of original article: 10.1016/j.eururo.2008.03.052
Editorial Comment on: Training in PercutaneousNephrolithotomy—A Critical ReviewChristian SeitzDepartment of Urology, General Hospital Bolzano, [email protected]
This is a well-written critical review focusing ontraining in percutaneous nephrolithotomy (PCNL).To date there are very few data on educationalconcepts in the teaching of PCNL in Europe. Theauthors are to be commended for providing insightinto factors influencing training, and including aproposal for a minimum training curriculum togain and to maintain surgical proficiency [1].However, it is a challenge to define minimumrequirements for training in PCNL. Although theauthors stated correctly that obtaining renal accessis a crucial step within the learning curve, andstone clearance combined with complication ratesare most relevant clinical end points, the numberof procedures necessary to achieve surgical com-petence represents a number without informationon the complexity of the procedure performed. Anestimated case load of 60 patients is necessary toachieve competence in PCNL. Those data are basedon two studies, each including one surgeon only[2,3]. But how to define competence? In bothstudies operation time reached a plateau after 60cases and was one criterion to define competence.If the stone-free rates were regarded as end point, itwas achieved at the very initial cases, and thelearning curve was a horizontal line [3]. Hence,
surrogate markers defining the learning curve needto be defined.
At present, due to a limited case load, only someresidents in urology will be able to gain surgicalcompetence for PCNL, especially for complicatedcases with staghorn stones and a complex anat-omy. This raises the controversial question ofwhether PCNL education and treatment for com-plex cases should follow the current trend inmedicine of centralization in dedicated centers,where technical requirements are met and thenumber of necessary cases is achieved to maintainand to teach surgical proficiency.
References
[1] de la Rosette JJMCH, Laguna PM, Rassweiler JJ, Conort P.
Training in percutaneous nephrolithotomy—a critical
review. Eur Urol 2008;54:994–1003.
[2] Allen D, O’Brien T, Tiptaft R, Glass J. Defining the learn-
ing curve for percutaneous nephrolithotomy. J Endourol
2005;19:279–82.
[3] Tanriverdi O, Boylu U, Kendirci M, Kadihasanoglu M,
Horasanli K, Miroglu C. The learning curve in the train-
ing of percutaneous nephrolithotomy. Eur Urol 2007;52:
206–12.
DOI:10.1016/j.eururo.2008.03.054
DOI of original article: 10.1016/j.eururo.2008.03.052
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 9 4 – 1 0 0 31002

Editorial Comment on: Training in PercutaneousNephrolithotomy—A Critical ReviewThomas KnollDepartment of Urology, Mannheim University Hospital,Mannheim, [email protected]
Percutaneous nephrolithotomy (PNL) achievesexcellent stone-free rates (SFR) with acceptablecomplication rates and is therefore still the treat-ment of choice for large renal calculi [1]; however,the reported complications rates in the literaturediffer widely, with transfusion rates up to 20% andincluding even more severe cases. It is generallyagreed that the establishment of a proper accesstract is the crucial step, and it has been demon-strated that both SFR and complication rates aresuperior when renal access is achieved by theurologist [2].
Because PNL is a difficult surgical techniquewith reported learning curves of up to 50 proce-dures, it is clear that standardized, continuoustraining options are necessary to teach youngurologists and to maintain proficiency [3]. Thepaper of de la Rosette and colleagues highlightsthese issues [4]. The traditional way of acquiringsurgical skills through apprenticeship should bedisplaced in the near future by training on modelsor simulators. Today, only animal organ modelsoffer training in the whole procedure; currentvirtual reality (VR) simulators just allow placementof percutaneous nephrostomies and do not provideultrasound guidance (which significantly reducesaccess-related complications) [5]. Furthermore,costs limit the distribution of VR models.
Without any doubt, VR has the potential toovercome the limitations of organ models and will
be the future standard. Until then, each modeloffers individual advantages. Most importantly,training under the supervision of a dedicated,experienced trainer will most effectively reducethe learning curve. Participation in educationalprograms at experienced stone centres offers idealopportunities to achieve competence in PNL. Theobservation of rising PNL frequencies worldwideunderscores the need for such programs to main-tain satisfactory surgical standards.
References
[1] Osman M, Wendt-Nordahl G, Heger K, Michel MS,
Alken P, Knoll T. Percutaneous nephrolithotomy with
ultrasonography-guided renal access: experience from
over 300 cases. BJU Int 2005;96:875–8.
[2] Watterson JD, Soon S, Jana K. Access related complica-
tions during percutaneous nephrolithotomy: urology
versus radiology at a single academic institution. J Urol
2006;176:142–5.
[3] Tanriverdi O, Boylu U, Kendirci M, Kadihasanoglu M,
Horasanli K, Miroglu C. The learning curve in the train-
ing of percutaneous nephrolithotomy. Eur Urol 2007;52:
206–12.
[4] de la Rosette JJMCH, Laguna MP, Rassweiler JJ, Conort P.
Training in percutaneous nephrolithotomy—a critical
review. Eur Urol 2008;54:994–1003.
[5] Mozer P, Conort P, Leroy A,et al. Aid to percutaneous renal
access by virtual projection of the ultrasound puncture
tract onto fluoroscopic images. J Endourol 2007;21:460–5.
DOI:10.1016/j.eururo.2008.03.055
DOI of original article: 10.1016/j.eururo.2008.03.052
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 9 9 4 – 1 0 0 3 1003