Percutaneous and Laparoscopic Cryoablation of Small Renal Masses
7
Percutaneous and Laparoscopic Cryoablation of Small Renal Masses David S. Finley,* Shawn Beck, Geoffrey Box, William Chu, Leslie Deane, Duane J. Vajgrt, Elspeth M. McDougall† and Ralph V. Clayman‡ From the Departments of Urology (DSF, SB, GB, WC, LD, EMM, RVC) and Radiology (DJV), University of California Irvine Medical Center, Orange, California Purpose: We reviewed our 4-year experience with percutaneous cryoablation and laparoscopy for treating small renal masses. Materials and Methods: After institutional review board approval we retrospectively analyzed renal cryoablation proce- dures performed between March 2003 and October 2007. An in-depth analysis was performed concerning demographics, hospital course and short-term outcome with respect to percutaneous vs laparoscopic cryoablation. Results: A total of 37 patients underwent treatment for 43 renal masses. Of the 37 patients 19 underwent laparoscopic cryoablation (24 tumors) and 18 underwent percutaneous cryoablation (19 tumors) using computerized tomography fluoros- copy. For percutaneous cryoablation a saline instillation was used in 58% of cases to move nonrenal vital structures away from the targeted renal mass. There were 5 cases of hemorrhage requiring transfusion, all of which were associated with the use of multiple cryoprobes. The transfusion rate in the percutaneous and laparoscopic cryoablation groups was 11.1% and 27.8%, respectively. Operative time was significantly longer in the laparoscopic cryoablation group compared to the percu- taneous cryoablation group at 147 (range 89 to 209) vs 250.2 (range 151 to 360) minutes, respectively. The overall complication rate (including transfusion) was lower in the percutaneous cryoablation group compared to the laparoscopic cryoablation group (4 of 18 [22.2%] vs 8 of 20 [40%], respectively). Hospital stay was significantly shorter in the percutaneous vs laparoscopic cryoablation group at 1.3 vs 3.1 days, p 0.0001, respectively. Narcotic use in the percutaneous cryoablation group was more than half that used by the laparoscopic cryoablation group (5.1 vs 17.8 mg, p 0.03, respectively). Among patients with biopsy proven renal cell carcinoma during a median followup of 11.4 and 13.4 months in the percutaneous and laparoscopic cryoablation groups, cancer specific survival was 100% and 100%, respectively, and the treatment failure rate was 5.3% and 4.2%, respectively. Conclusions: Percutaneous cryoablation is an efficient, minimally morbid method for the treatment of small renal masses and it appears to be superior to the laparoscopic approach. Short-term followup has shown no difference in tumor recurrence or need for re-treatment. Of note, hemorrhage was solely associated with the use of multiple probes. Key Words: cryosurgery; carcinoma, renal cell; kidney; laparoscopy; administration, cutaneous I n 2007 it was estimated that 51,000 renal masses would be detected in the United States. 1 Advances in renal imaging and needle ablation have allowed minimally invasive techniques to become an option for the treatment of small renal masses. Since 2003 we have treated select renal lesions with a laparoscopic or more recently a percutaneous approach. We present our experience with both modalities. METHODS After institutional review board approval we performed a retrospective chart review of 37 consecutive cases of renal cryoablation (19 laparoscopic for 24 tumors and 18 percuta- neous for 19 tumors) performed at the University of Califor- nia Irvine Medical Center from March 2003 to October 2007. Clinical, pathological and radiological data were entered into a database and reviewed. Complications were classified according to the Clavien system. 2 Probe Planning For select cases a computer assisted 3-dimensional model (ADAC 3D Pinnacle-3®) for probe planning was generated from the preoperative CT to predict the optimal number of probes necessary to treat a given mass. Isotherms We used an argon based cryoablation system (CryoCare™). Five different probes were used measuring 1.7, 2.4, 3.8, 5.0 and 8.0 mm. The 5 and 8 mm probes were used early in our experience and were abandoned when smaller probes be- came available. The reported 20C isotherm (iceball) di- mensions of the 1.7, 2.4 and 3.8 mm probes are 2.1 4.2, 2.4 4.4 and 3.3 4.9 cm, respectively. At 40C the isotherms measure 1.4 3.5, 1.6 3.6 and 2.4 4.4 cm, respectively. Submitted for publication December 11, 2007. Study received institutional review board approval. * Correspondence: Department of Urology, University of Califor- nia Irvine Medical Center, 101 The City Dr., Building 55, Room 304, Orange, California 92868 (telephone: 562-897-2221; FAX: 714-456- 5062; e-mail: fi[email protected]). † Financial interest and/or other relationship with Endocare, METI Inc., Astellas, Storz Endoscopy, Simbionix, Intuitive Surgical and Ethicon Endo-Surgery. ‡ Financial interest and/or other relationship with Applied Urol- ogy, Cook Urological, EndoCare, Greenwald Inc., Microvasive, Or- thopedic Systems Inc., Astellas, Boston Scientific and Karl Storz Endoscopy. 0022-5347/08/1802-0492/0 Vol. 180, 492-498, August 2008 THE JOURNAL OF UROLOGY ® Printed in U.S.A. Copyright © 2008 by AMERICAN UROLOGICAL ASSOCIATION DOI:10.1016/j.juro.2008.04.019 492
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Percutaneous and Laparoscopic Cryoablation of Small Renal Masses

Percutaneous and Laparoscopic Cryoablation of Small Renal MassesDavid S. Finley,* Shawn Beck, Geoffrey Box, William Chu, Leslie Deane, Duane J. Vajgrt,Elspeth M. McDougall† and Ralph V. Clayman‡From the Departments of Urology (DSF, SB, GB, WC, LD, EMM, RVC) and Radiology (DJV), University of California Irvine MedicalCenter, Orange, California
Purpose: We reviewed our 4-year experience with percutaneous cryoablation and laparoscopy for treating small renal masses.Materials and Methods: After institutional review board approval we retrospectively analyzed renal cryoablation proce-dures performed between March 2003 and October 2007. An in-depth analysis was performed concerning demographics,hospital course and short-term outcome with respect to percutaneous vs laparoscopic cryoablation.Results: A total of 37 patients underwent treatment for 43 renal masses. Of the 37 patients 19 underwent laparoscopiccryoablation (24 tumors) and 18 underwent percutaneous cryoablation (19 tumors) using computerized tomography fluoros-copy. For percutaneous cryoablation a saline instillation was used in 58% of cases to move nonrenal vital structures awayfrom the targeted renal mass. There were 5 cases of hemorrhage requiring transfusion, all of which were associated with theuse of multiple cryoprobes. The transfusion rate in the percutaneous and laparoscopic cryoablation groups was 11.1% and27.8%, respectively. Operative time was significantly longer in the laparoscopic cryoablation group compared to the percu-taneous cryoablation group at 147 (range 89 to 209) vs 250.2 (range 151 to 360) minutes, respectively. The overallcomplication rate (including transfusion) was lower in the percutaneous cryoablation group compared to the laparoscopiccryoablation group (4 of 18 [22.2%] vs 8 of 20 [40%], respectively). Hospital stay was significantly shorter in the percutaneousvs laparoscopic cryoablation group at 1.3 vs 3.1 days, p �0.0001, respectively. Narcotic use in the percutaneous cryoablationgroup was more than half that used by the laparoscopic cryoablation group (5.1 vs 17.8 mg, p � 0.03, respectively). Amongpatients with biopsy proven renal cell carcinoma during a median followup of 11.4 and 13.4 months in the percutaneous andlaparoscopic cryoablation groups, cancer specific survival was 100% and 100%, respectively, and the treatment failure ratewas 5.3% and 4.2%, respectively.Conclusions: Percutaneous cryoablation is an efficient, minimally morbid method for the treatment of small renal massesand it appears to be superior to the laparoscopic approach. Short-term followup has shown no difference in tumor recurrenceor need for re-treatment. Of note, hemorrhage was solely associated with the use of multiple probes.
Key Words: cryosurgery; carcinoma, renal cell; kidney; laparoscopy; administration, cutaneous
In 2007 it was estimated that 51,000 renal masses wouldbe detected in the United States.1 Advances in renalimaging and needle ablation have allowed minimally
invasive techniques to become an option for the treatment ofsmall renal masses. Since 2003 we have treated select renallesions with a laparoscopic or more recently a percutaneousapproach. We present our experience with both modalities.
METHODS
After institutional review board approval we performed aretrospective chart review of 37 consecutive cases of renal
Submitted for publication December 11, 2007.Study received institutional review board approval.* Correspondence: Department of Urology, University of Califor-
nia Irvine Medical Center, 101 The City Dr., Building 55, Room 304,Orange, California 92868 (telephone: 562-897-2221; FAX: 714-456-5062; e-mail: [email protected]).
† Financial interest and/or other relationship with Endocare,METI Inc., Astellas, Storz Endoscopy, Simbionix, Intuitive Surgicaland Ethicon Endo-Surgery.
‡ Financial interest and/or other relationship with Applied Urol-ogy, Cook Urological, EndoCare, Greenwald Inc., Microvasive, Or-
thopedic Systems Inc., Astellas, Boston Scientific and Karl StorzEndoscopy.0022-5347/08/1802-0492/0THE JOURNAL OF UROLOGY®
Copyright © 2008 by AMERICAN UROLOGICAL ASSOCIATION
492
cryoablation (19 laparoscopic for 24 tumors and 18 percuta-neous for 19 tumors) performed at the University of Califor-nia Irvine Medical Center from March 2003 to October 2007.Clinical, pathological and radiological data were enteredinto a database and reviewed. Complications were classifiedaccording to the Clavien system.2
Probe PlanningFor select cases a computer assisted 3-dimensional model(ADAC 3D Pinnacle-3®) for probe planning was generatedfrom the preoperative CT to predict the optimal number ofprobes necessary to treat a given mass.
IsothermsWe used an argon based cryoablation system (CryoCare™).Five different probes were used measuring 1.7, 2.4, 3.8, 5.0and 8.0 mm. The 5 and 8 mm probes were used early in ourexperience and were abandoned when smaller probes be-came available. The reported �20C isotherm (iceball) di-mensions of the 1.7, 2.4 and 3.8 mm probes are 2.1 � 4.2, 2.4� 4.4 and 3.3 � 4.9 cm, respectively. At �40C the isotherms
measure 1.4 � 3.5, 1.6 � 3.6 and 2.4 � 4.4 cm, respectively.Vol. 180, 492-498, August 2008Printed in U.S.A.
DOI:10.1016/j.juro.2008.04.019

PERCUTANEOUS AND LAPAROSCOPIC CRYOABLATION OF SMALL RENAL MASSES 493
Anesthesia ManeuversRespiration was held during needle and probe insertion tominimize renal movement. In cases where the lesion wasnear the inferior recess of the ipsilateral pleural space, se-lective intubation of the contralateral lung was used to min-imize inflation of the ipsilateral lung. For this type of ven-tilation the patient was placed in the ipsilateral decubitusposition.
Laparoscopic ApproachFor anterior and anteromedial lesions transperitoneal ac-cess was established. The patient is placed in the lateraldecubitus position and a Veress needle insufflation wasachieved via a 12 mm incision just off the iliac crest. A 12mm port was placed superior to the umbilicus just off thepararectus line. Another 12 mm port was placed subcostal inthe midclavicular line. A third port, 5 mm, was placed sub-costal in the anterior axillary line.
For posterior and posterolateral lesions not amenable topercutaneous treatment due to the presence of adjacentorgans a retroperitoneoscopic approach was used. A 1 inchincision was made below the tip of the 12th rib and thelumbodorsal fascia was incised. A finger was placed retro-peritoneally to palpate the psoas muscle and confirm properlocation. A balloon dilator was inflated twice to expand theretroperitoneum cephalad and caudal. A 12 mm port wasplaced in the posterior axillary line. Another 12 mm portwas placed in Petit’s triangle and a 5 mm port subcostal inthe anterior axillary line. A blunt port was placed in theinitial incision and the balloon was inflated.
After the kidney was mobilized Gerota’s fascia was in-cised and circumferentially released from the surface of thekidney to completely expose the tumor. The perinephric fatwas sent for pathological analysis. Probe insertion was thenperformed. A coaxial system was developed to protect thetract from seeding/freezing and to facilitate the delivery ofadjunctive hemostatic agents. A stab incision was made witha scalpel through which, depending on the size of the cryo-probe, an 8/10Fr coaxial ureteral dilator kit (Cook Urologi-cal, Spencer, Indiana) or 12/14Fr Flexor® access sheath wasplaced under direct vision in near contact with the lesion.After multiple central and peripheral biopsies were obtainedwith a Temno Evolution™ 18 gauge coaxial biopsy system,the cryoprobe(s) were placed to the appropriate depth andfreezing was initiated. Intraoperative ultrasound was usedto guide probe placement just beyond the far border of thelesion and to monitor the advancing iceball. For single probeapplications the probe was inserted in center of the lesion.Multiprobe configurations usually consisted of a centrallyplaced probe along the Z-axis of the tumor, and other probesplaced perpendicular or tangential to this depending on thesize and shape of the lesion. An Endoholder (Codman Inc.,Raynham, Massachusetts) or CIVCO retractor (CIVCO Inc.,Sarasota, Florida) was used to stabilize the cryoprobes. Af-ter a double freeze-thaw cycle the iceball was melted byapplying irrigant until no ice was visible. The cryosite wasobserved under a 5 mm Hg pneumoperitoneum for a mini-mum of 10 minutes. Bleeding was often delayed after cryoa-blation and, thus, the period of observation had to be suffi-ciently lengthy to assess for this potential event. If bleedingwas noted then argon beam coagulation and placement of
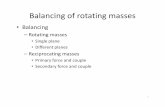
hemostatic agents Floseal™ or Surgicel™ ensued.Percutaneous ApproachPosterior lesions with a clear treatment window were se-lected for percutaneous treatment. Percutaneous procedureswere completed by an interventional radiologist (DV) and aurologist (RVC, EM). After induction of general anesthesiathe patient was placed prone or in the lateral decubitusposition on the CT scanner. Tumor localization was done byserial transaxial images using noncontrast 10 mm slicethickness. In select cases perinephric saline was infused tophysically separate the kidney from the adjacent chest wall,spleen, colon or spine. In these cases a 5Fr 10 cm Yuehcentesis needle was advanced under CT fluoroscopic guid-ance incrementally into the perinephric space (fig. 1). Oncethe needle position was confirmed up to 400 ml sterile salinewere interposed between the kidney and adjacent structures(fig. 2). Repeat imaging was then obtained using 5 mm slicethickness to allow proper positioning and percutaneous ac-cess to the mass. To enhance the definition of the mass 75 ccnonionic contrast were given intravenously before repeatearly and late phase 5 mm imaging. With the lesion ade-quately identified an appropriate skin entry site was deter-mined.
Following routine skin preparation, sterile draping andinfusion of a local anesthetic, an 18 gauge needle was ad-vanced percutaneously during a breath hold under CT fluo-roscopic guidance to the center of the mass. The needleposition was confirmed with subsequent transaxial imagesbefore then inserting the stiff end of an Amplatz SuperStiff™ Guidewire to the surface of the lesion. The needle wasremoved. A measurement was determined for the distancefrom the skin surface to the surface of the lesion (d1) (fig. 3).Following this a stab incision was made with a scalpelthrough which, depending on the size of the cryoprobe, an8/10Fr (for use with 1.7 and 2.4 mm cryoprobes) coaxialureteral dilator kit (Cook Urological) or 12/14Fr (for usewith 3.8 mm cryoprobes) Flexor access sheath was placed inclose proximity to the lesion. The sheath position was con-firmed with transaxial images before performing a core bi-opsy. The biopsy was obtained using the Temno 18 gaugecoaxial biopsy system. Three or 4 core samples were ob-
FIG. 1. Positioning of Yueh centesis needle for saline floating ofbowel away from kidney. Note some air has been introduced
through needle which now surrounds shaft of needle (arrow). Lesionis outlined.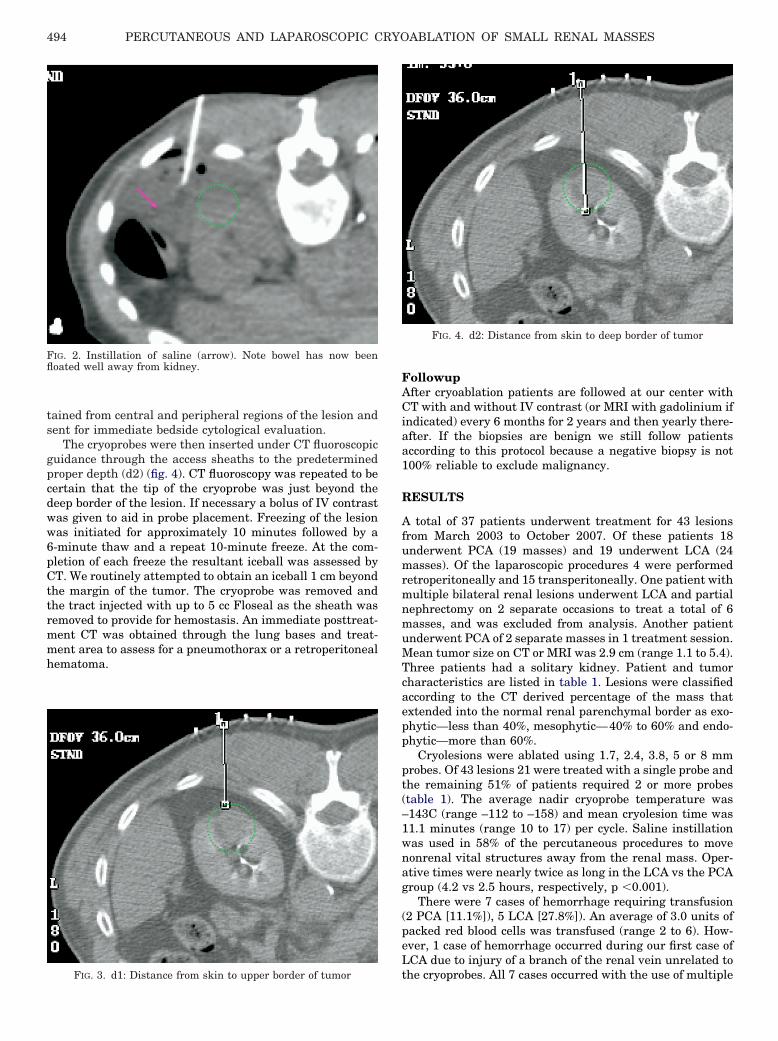
PERCUTANEOUS AND LAPAROSCOPIC CRYOABLATION OF SMALL RENAL MASSES494
tained from central and peripheral regions of the lesion andsent for immediate bedside cytological evaluation.
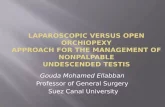
The cryoprobes were then inserted under CT fluoroscopicguidance through the access sheaths to the predeterminedproper depth (d2) (fig. 4). CT fluoroscopy was repeated to becertain that the tip of the cryoprobe was just beyond thedeep border of the lesion. If necessary a bolus of IV contrastwas given to aid in probe placement. Freezing of the lesionwas initiated for approximately 10 minutes followed by a6-minute thaw and a repeat 10-minute freeze. At the com-pletion of each freeze the resultant iceball was assessed byCT. We routinely attempted to obtain an iceball 1 cm beyondthe margin of the tumor. The cryoprobe was removed andthe tract injected with up to 5 cc Floseal as the sheath wasremoved to provide for hemostasis. An immediate posttreat-ment CT was obtained through the lung bases and treat-ment area to assess for a pneumothorax or a retroperitonealhematoma.
FIG. 2. Instillation of saline (arrow). Note bowel has now beenfloated well away from kidney.
FIG. 3. d1: Distance from skin to upper border of tumor
FollowupAfter cryoablation patients are followed at our center withCT with and without IV contrast (or MRI with gadolinium ifindicated) every 6 months for 2 years and then yearly there-after. If the biopsies are benign we still follow patientsaccording to this protocol because a negative biopsy is not100% reliable to exclude malignancy.
RESULTS
A total of 37 patients underwent treatment for 43 lesionsfrom March 2003 to October 2007. Of these patients 18underwent PCA (19 masses) and 19 underwent LCA (24masses). Of the laparoscopic procedures 4 were performedretroperitoneally and 15 transperitoneally. One patient withmultiple bilateral renal lesions underwent LCA and partialnephrectomy on 2 separate occasions to treat a total of 6masses, and was excluded from analysis. Another patientunderwent PCA of 2 separate masses in 1 treatment session.Mean tumor size on CT or MRI was 2.9 cm (range 1.1 to 5.4).Three patients had a solitary kidney. Patient and tumorcharacteristics are listed in table 1. Lesions were classifiedaccording to the CT derived percentage of the mass thatextended into the normal renal parenchymal border as exo-phytic—less than 40%, mesophytic—40% to 60% and endo-phytic—more than 60%.
Cryolesions were ablated using 1.7, 2.4, 3.8, 5 or 8 mmprobes. Of 43 lesions 21 were treated with a single probe andthe remaining 51% of patients required 2 or more probes(table 1). The average nadir cryoprobe temperature was–143C (range –112 to –158) and mean cryolesion time was11.1 minutes (range 10 to 17) per cycle. Saline instillationwas used in 58% of the percutaneous procedures to movenonrenal vital structures away from the renal mass. Oper-ative times were nearly twice as long in the LCA vs the PCAgroup (4.2 vs 2.5 hours, respectively, p �0.001).
There were 7 cases of hemorrhage requiring transfusion(2 PCA [11.1%]), 5 LCA [27.8%]). An average of 3.0 units ofpacked red blood cells was transfused (range 2 to 6). How-ever, 1 case of hemorrhage occurred during our first case ofLCA due to injury of a branch of the renal vein unrelated to
FIG. 4. d2: Distance from skin to deep border of tumor
the cryoprobes. All 7 cases occurred with the use of multiple
PERCUTANEOUS AND LAPAROSCOPIC CRYOABLATION OF SMALL RENAL MASSES 495
probes (average 3.6, range 2 to 7, table 2). Excluding thepreviously mentioned case with the use of multiple probes inthe LCA and PCA groups the bleeding rates were 33.3% (4 of12) and 22.2% (2 of 9), respectively. For the PCA groupmedian tumor size associated with bleeding was signifi-cantly larger than in those that did not bleed (4.2 [range 3.6to 4.7] vs 2.6 cm [range 2.4 to 3.3], respectively, p � 0.005).Among LCA cases median tumor size associated with hem-orrhage was not significantly different (3.2 [range 2.7 to 3.4]vs 3.4 cm [range 1.2 to 5.4], respectively, p � 0.70). The mostcommonly used probe size in cases of hemorrhage was 2.4mm. With the use of a single probe the bleeding rate forlaparoscopic and percutaneous procedures was 0% (0 of 12)and 0% (0 of 10 cases), respectively.
There were no conversions to open surgery, acute or de-layed embolization for renal bleeding and no deaths. Therewas no significant difference between the mean preoperative(1.2, 1.2 mg/dl), postoperative day 1 (1.2, 1.5 mg/dl) or lastfollowup (1.2, 1.4 mg/dl) serum creatinine for the PCA or theLCA group (p � 0.93, p � 0.29, p � 0.43). The Charlsonindex scores of patients in the PCA and LCA groups weresimilar (5.2 vs 5.5). The average Charlson index score ofpatients who experienced complications in each group was 9and 6.3. Overall there were 8 grade 2 complications (6 bloodtransfusions, 1 DVT [PCA], 1 internal jugular vein thrombus[LCA]), 1 grade 3b small bowel injury (LCA) and 1 grade IVcomplication (loss of kidney [PCA]) based on the Clavienclassification system (table 1).2
Biopsy results were nondiagnostic in 8 of 43 lesions
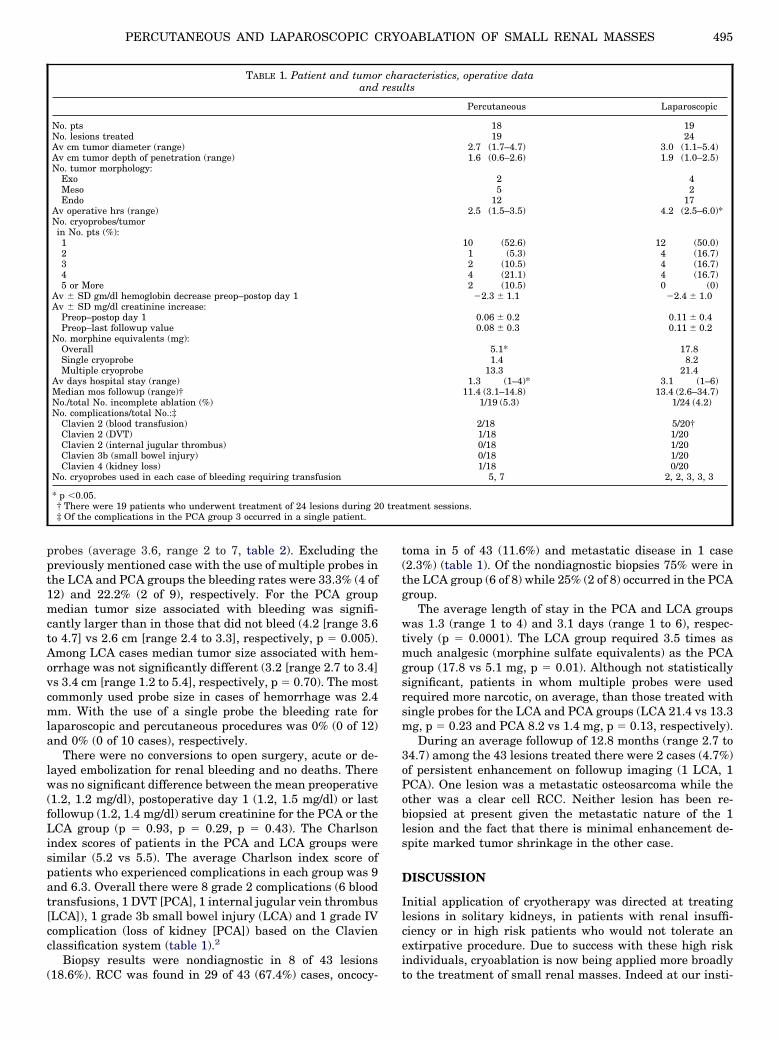
TABLE 1. Patient and tumorand
No. ptsNo. lesions treatedAv cm tumor diameter (range)Av cm tumor depth of penetration (range)No. tumor morphology:
ExoMesoEndo
Av operative hrs (range)No. cryoprobes/tumorin No. pts (%):12345 or More
Av � SD gm/dl hemoglobin decrease preop–postop day 1Av � SD mg/dl creatinine increase:
Preop–postop day 1Preop–last followup value
No. morphine equivalents (mg):OverallSingle cryoprobeMultiple cryoprobe
Av days hospital stay (range)Median mos followup (range)†No./total No. incomplete ablation (%)No. complications/total No.:‡
Clavien 2 (blood transfusion)Clavien 2 (DVT)Clavien 2 (internal jugular thrombus)Clavien 3b (small bowel injury)Clavien 4 (kidney loss)
No. cryoprobes used in each case of bleeding requiring transfusion
* p �0.05.† There were 19 patients who underwent treatment of 24 lesions during 2‡ Of the complications in the PCA group 3 occurred in a single patient.
(18.6%). RCC was found in 29 of 43 (67.4%) cases, oncocy-
toma in 5 of 43 (11.6%) and metastatic disease in 1 case(2.3%) (table 1). Of the nondiagnostic biopsies 75% were inthe LCA group (6 of 8) while 25% (2 of 8) occurred in the PCAgroup.
The average length of stay in the PCA and LCA groupswas 1.3 (range 1 to 4) and 3.1 days (range 1 to 6), respec-tively (p � 0.0001). The LCA group required 3.5 times asmuch analgesic (morphine sulfate equivalents) as the PCAgroup (17.8 vs 5.1 mg, p � 0.01). Although not statisticallysignificant, patients in whom multiple probes were usedrequired more narcotic, on average, than those treated withsingle probes for the LCA and PCA groups (LCA 21.4 vs 13.3mg, p � 0.23 and PCA 8.2 vs 1.4 mg, p � 0.13, respectively).
During an average followup of 12.8 months (range 2.7 to34.7) among the 43 lesions treated there were 2 cases (4.7%)of persistent enhancement on followup imaging (1 LCA, 1PCA). One lesion was a metastatic osteosarcoma while theother was a clear cell RCC. Neither lesion has been re-biopsied at present given the metastatic nature of the 1lesion and the fact that there is minimal enhancement de-spite marked tumor shrinkage in the other case.
DISCUSSION
Initial application of cryotherapy was directed at treatinglesions in solitary kidneys, in patients with renal insuffi-ciency or in high risk patients who would not tolerate anextirpative procedure. Due to success with these high riskindividuals, cryoablation is now being applied more broadly
racteristics, operative datalts
Percutaneous Laparoscopic
18 1919 24
2.7 (1.7–4.7) 3.0 (1.1–5.4)1.6 (0.6–2.6) 1.9 (1.0–2.5)
2 45 2
12 172.5 (1.5–3.5) 4.2 (2.5–6.0)*
10 (52.6) 12 (50.0)1 (5.3) 4 (16.7)2 (10.5) 4 (16.7)4 (21.1) 4 (16.7)2 (10.5) 0 (0)
�2.3 � 1.1 �2.4 � 1.0
0.06 � 0.2 0.11 � 0.40.08 � 0.3 0.11 � 0.2
5.1* 17.81.4 8.2
13.3 21.41.3 (1–4)* 3.1 (1–6)
11.4 (3.1–14.8) 13.4 (2.6–34.7)1/19 (5.3) 1/24 (4.2)
2/18 5/20†1/18 1/200/18 1/200/18 1/201/18 0/20
5, 7 2, 2, 3, 3, 3
tment sessions.
charesu
0 trea
to the treatment of small renal masses. Indeed at our insti-
PERCUTANEOUS AND LAPAROSCOPIC CRYOABLATION OF SMALL RENAL MASSES496
tution it is now the most commonly performed procedure forall patients presenting with a small renal mass regardless ofcircumstances.
Our technique for PCA has evolved in the last 2 years. Inthis regard we have developed a novel modified Seldingertechnique for PCA and LCA.3 We use a protective cryoprobesheath through which we can obtain multiple biopsies,thereby in theory minimizing the chance of tumor seeding.In addition, using the cryoprobe in this manner precludesany untoward freezing of surrounding normal tissues of theback (eg nerve, skin or muscle injury).4 In point of fact, thetemperature of the tissue abutting the sheath is only 5Caccording to studies done in our laboratory vs minus 15Cwhen a sheath is not used. Finally, after freezing is completethe sheath serves as a conduit for the injection of hemostaticFloseal into the cryotract. This method of Floseal deliverywas adapted from tubeless percutaneous nephrostolitho-tomy where its effectiveness has been demonstrated.5 An-other technique described by others which we have usedextensively is the instillation of a saline barrier (floating)around the target to move surrounding structures such asthe bowel or spleen away from the renal mass.6 In our seriessaline floating was used in 58% of percutaneous cases. Therewere no instances of injury to nearby visceral structuresduring percutaneous cryoablation.
TABLE 2. Cryoablation probe and tumor characteristics
LesionSize (cm) Site Morphology
Incursion(cm)
CryoprobeSize (mm)
No.Probes
BleedUnits
Percutaneous:1.5 pLMP Meso 0.8 2.4 1 —1.7 pLMP Endo 1.2 2.4 1 —1.9 pLUP Endo 1.7 3.8 1 —2.2 aRUP Endo 1.7 2.4 1 —2.3 pLMP Exo 0.6 3.8 1 —2.4 pRLP Endo 2.3 1.7 1 —2.4 pRMP Meso 1.0 2.4 5 �32.4 pLUP Meso 1.2 1.7 4 —2.4 pLMP Exo 0.9 3.8 1 —2.4 pLLP Endo 2.4 2.0 2 —2.6 pLUP Endo 1.9 2.4 4 —2.6 pLMP Endo 2.3 2.4 3 —2.7 pLMP Meso 1.1 3.8 1 —3.1 pLLP Endo 1.4 3.8 1 —3.1 pRMP Endo 2.0 2.4 3 —3.3 pLUP Endo 2.6 2.4 4 —3.6 pLLP Endo 2.0 2.4 7 �64.0 pLMP Endo 1.7 3.8 1 —4.7 pLUP Meso 2.4 3.8 3 —
2.4 1Laparoscopic:
1.2 aLLP Endo 1.0 1.7 2 —1.5 aRLP Endo 1.2 1.7 1 —1.6 aRLP Endo 1.6 3.8 1 —1.6 pRUP Endo 1.0 5.0 1 —1.7 aLLP Endo 1.6 5.0 1 —2.0 lRMP Endo 2.0 3.8 1 —2.6 pRMP Endo 2.5 3.8 1 —2.7 pRUP Endo 1.8 2.4 2 �22.9 aRUP Endo 2.0 3.8 2 �4*3.2 pLUP Exo 1.2 2.4 3 �23.3 hRMP Endo 2.1 3.8 1 —3.4 aRLP Endo 2.2 2.4 3 �23.5 lRUP Endo 2.4 2.4 3 �23.8 hLUP Exo 1.0 3.8 4 —
2.4 13.9 aRMP Meso 2.0 8.0 1 —4.4 aLUP Meso 2.0 3.8 1 —
2.4 34.7 aLMP Endo 2.5 1.7 4 —5.4 lRMP Exo 1.7 2.4 4 —
* Bleeding due to avulsion of branch of renal vein, not from cryoprobe.
For larger or nonspherical tumors we generated a 3-di-mensional treatment plan using the ADAC 3D Pinnacle-3Treatment Planner. This software, traditionally used forradiation therapy treatment planning, reconstructs datagathered from CT into 3-dimensional images allowing formore accurate determination of the shape of the lesion.Optimal cryoprobe placement is then determined accordingto the established elliptical isotherm of each probe to ensurea minimum margin of 5 mm beyond the edge of the lesion at�20C. Multiprobe configurations result in fusion of the ice-balls into a conglomerate which produces larger zones ofablation according to studies in a porcine model.7
Unlike with partial nephrectomy there are no surgicalmargins indicating complete extirpation for pathologicalanalysis after cryoablation. The surgeon’s only margin is theextent of the �20C area beyond the perimeter of the mass.As such, meticulous followup of these patients is essential.Our series only had a average followup of 10 months. How-ever, intermediate term oncological outcome data are nowemerging for cryoablation therapy with excellent results.8 Ina recent review that only included studies with 3 to 5-yearfollowup the cancer specific survival ranged from 97% to100% with cryoablation.9 The overall survival rate was 82%to 90.2%. Local recurrence rates ranged from 1.4% to 12.5%.We successfully ablated 41 of 43 lesions (95.3%). Persistentenhancement was found in 2 of 43 (4.7%) lesions on followup.One of these failures was a metastatic osteosarcoma and thesecond failure exhibited a 7 mm central focus of enhance-ment which was thought to represent a pseudoaneurysm orpossibly residual disease. Regarding the latter case followupscans are pending with a plan to re-biopsy and re-treat if theenhancement appears more prominent or if there is growthof the lesion.
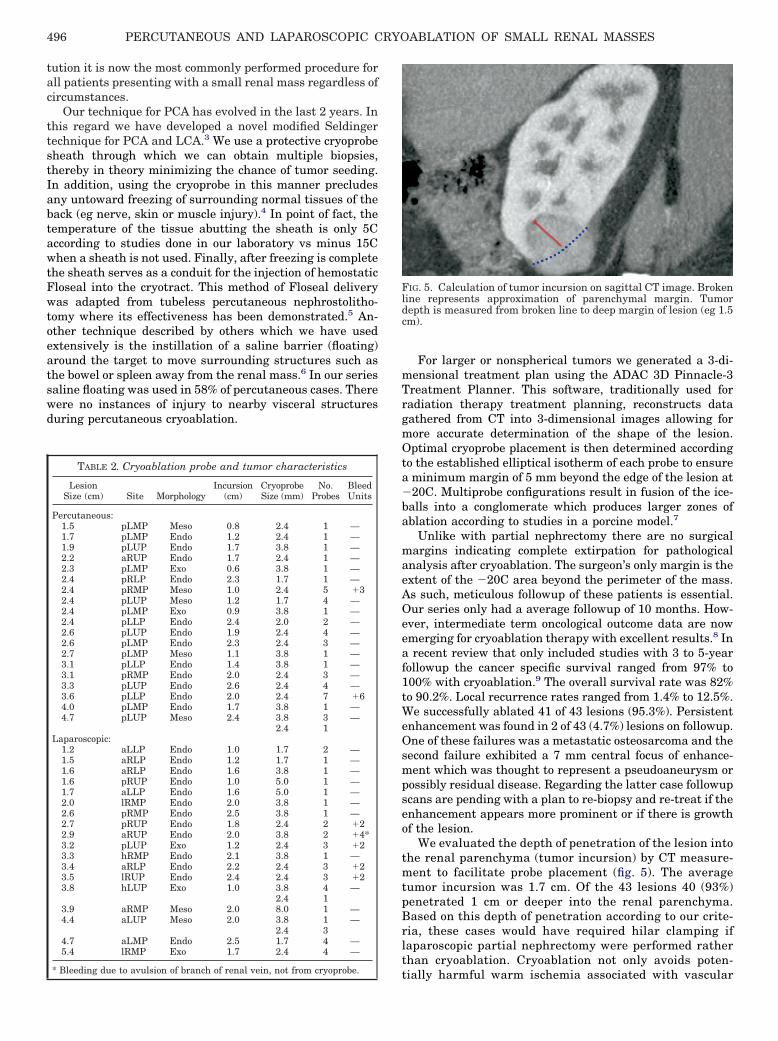
We evaluated the depth of penetration of the lesion intothe renal parenchyma (tumor incursion) by CT measure-ment to facilitate probe placement (fig. 5). The averagetumor incursion was 1.7 cm. Of the 43 lesions 40 (93%)penetrated 1 cm or deeper into the renal parenchyma.Based on this depth of penetration according to our crite-ria, these cases would have required hilar clamping iflaparoscopic partial nephrectomy were performed ratherthan cryoablation. Cryoablation not only avoids poten-
FIG. 5. Calculation of tumor incursion on sagittal CT image. Brokenline represents approximation of parenchymal margin. Tumordepth is measured from broken line to deep margin of lesion (eg 1.5cm).
tially harmful warm ischemia associated with vascular

PERCUTANEOUS AND LAPAROSCOPIC CRYOABLATION OF SMALL RENAL MASSES 497
clamping but also appears to be associated with a loweroverall complication rate compared to laparoscopic partialnephrectomy. Indeed Desai et al found laparoscopic par-tial nephrectomy resulted in twice the blood loss (211 vs101 ml) and a 5-fold higher incidence of overall (intraop-erative, postoperative, late) complications (32% vs 6.7%)compared with cryoablation.10 Hruby et al showed a sim-ilar trend in complication rates when comparing laparo-scopic partial nephrectomy and laparoscopic cryoablationfor hilar tumors.11 The higher complication rate associ-ated with laparoscopic partial nephrectomy is probablydue to the increased technical difficulty of the procedure. In1 study operative times for the laparoscopic partial nephrec-tomy group were nearly 40% longer than the LCA times, andthe laparoscopic partial nephrectomy group also resulted in13 conversions to open vs no conversions in the cryoablationgroup.12
Overall complication rates from cryoablation are rela-tively low. In our series there were no deaths. Serious com-plications in the LCA group (ie Clavien 3 or 4) occurred inonly 2 patients (4.7%). If LCA is more sanguine than lapa-roscopic partial nephrectomy, PCA is far more favorablethan the laparoscopic approach. PCA was associated with astatistically significant decrease in operative time, hospitalstay, analgesic use and a trend toward fewer complicationswith an equivalent outcome. Limited bleeding is one of themost frequently recognized complications of cryoablation.Post-cryoablation transfusion rates for percutaneous proce-dures are reported in 0.9% to 8.3% of patients.9 LCA appearsto have a slightly lower rate of transfusion.10,12 Our overalltransfusion rate was 17.1%.
Of note, we found bleeding occurred in our series onlywhen multiple probes were used. Similarly the 2 cases ofhemorrhage in the series by Atwell et al of PCA occurredwith the use of 6 and 7 cryoprobes to treat 6.7 and 7.2 cmtumors.13 In our PCA group bleeding tended to occur notonly with multiple probes but also with larger tumors.However, the treatment of larger tumors invariably alsorequires the use of additional cryoprobes, so it is difficultto tell whether it is the size of the lesion alone or theinteraction between 2 or more growing iceballs that leadsto the bleeding. We favor the latter hypothesis because inour laparoscopic cohort bleeding was seen secondary torenal fracture after thawing. We believe that a synergisticiceball formed from a multiprobe configuration may resultin renal parenchymal fracture secondary to stress due toplate tectonic type motion during thawing (fig. 6). Inter-estingly in the LCA group we found no correlation be-tween hemorrhage and tumor size, further supporting thehypothesis that the problem occurs due to the growth orthawing of multiple iceballs rather than the size of thetumor itself. Among our laparoscopic cases none requiredreoperation for bleeding or angiographic embolization.Likewise among the patients with retroperitoneal bleed-ing after a percutaneous procedure this was always self-limited, requiring no intervention other than transfusion.Transfusions were in many cases dictated by surgeonpreference based on a combination of hematocrit trendsand patient comorbidities and not due to hemodynamicinstability. The average postoperative decrease in hemo-globin was comparable for the percutaneous and laparo-
scopic routes (2.6 and 2.4 gm/dl, respectively). Althoughwe hypothesized that the application of Floseal could beuseful as adjunctive hemostatics, our bleeding rate was nodifferent than that in other series in which a hemostaticagent was not used after cryoablation.
In addition to hemorrhage we experienced 1 complica-tion (Clavien 3b) of a small bowel perforation from atrocar requiring small bowel resection. This injury oc-curred in a patient with extensive intraperitoneal adhe-sions after radiation. The second major complication (Cla-vien 4) occurred in a high risk patient who presented witha postoperative DVT and re-bled due to anticoagulationmismanagement and a supratherapeutic internationalnormalized ratio. Our overall complication rate was 11.1%in the PCA group and 38.9% in the LCA group. However,8 of the 10 complications were minor Clavien 2 complica-tions.
To date we have not observed many of the more seriouscomplications described in the literature. Specifically wehave not seen freeze injury to the collecting system withsubsequent urinary extravasation as reported after cryo-ablation by others.8,14 Also, cryoinduced colorenal fistulaand splenic hematoma have been reported.15,16 To mini-mize this risk in select cases we instilled several hundredml saline into the pararenal space to float the bowel orspleen out of the ablation zone, and to create a salinebuffer between the renal mass and the surrounding struc-tures.6
PCA has become the treatment of choice for renalmasses less than 3 cm at our institution. Posterior, lateraland selected anterior lesions are all considered viablecandidates for this approach with or without saline infu-sion. While we have shied away from treating hilar le-sions, the experience of Hruby et al in this regard hasbeen favorable, albeit all done with a laparoscopic ap-proach.11 Lastly, we consider anterior lesions of the rightkidney in the vicinity of the duodenum off-limits for PCAbecause it is our impression that unlike the colon or otherorgans, the duodenum may not be as easily displaced from
FIG. 6. Following laparoscopic treatment of renal mass with 3, 2.4mm probes, thawing of iceball revealed large stellate crack in pa-renchyma remote to insertion site of any of probes. All 3 probes wereactivated simultaneously during procedure.
the kidney.
PERCUTANEOUS AND LAPAROSCOPIC CRYOABLATION OF SMALL RENAL MASSES498
CONCLUSIONS
Renal cryoablation is effectively delivered percutaneouslyor via a laparoscopic approach with acceptable morbidity.However, patient comfort and hospital stay are signifi-cantly better with a percutaneous approach. Posttreat-ment bleeding is an ongoing concern and in this regard wenow routinely use a single larger 3.8 mm probe in ratherthan multiple smaller probes whenever possible. To besure, longer followup for PCA is needed. However, reportsat 5 years are encouraging and appear to equal the lapa-roscopic experience with cryoablation or partial nephrec-tomy. At our institution PCA has become the procedure ofchoice for the majority of posterior, lateral and selectanterior renal masses 3 cm or smaller.
Abbreviations and Acronyms
a � anteriorCT � computerized tomography
DVT � deep vein thrombosisendo � endophytic
exo � exophytich � hilar
IV � intravenousl � lateral
LCA � laparoscopic cryoablationLLP � left lower poleLMP � left mid poleLUP � left upper polemeso � mesophyticMRI � magnetic resonance imaging
p � posteriorPCA � percutaneous cryoablationRCC � renal cell carcinomaRLP � right lower poleRMP � right mid poleRUP � right upper pole
REFERENCES
1. Jemal A, Siegel R, Ward E, Murray T, Xu J and Thun MJ:Cancer statistics, 2007. CA Cancer J Clin 2007; 57: 43.
2. Dindo D, Demartines N and Clavien PA: Classification of sur-gical complications: a new proposal with evaluation in acohort of 6336 patients and results of a survey. Ann Surg2004; 240: 205.
3. Abraham JB, Gamboa AJ, Finley DS, Lee HJ, Santos RJ,Deane LA et al: The Seldinger technique for percutaneousrenal cryoablation: protecting the tract and achieving he-mostasis. Unpublished data.
4. Lokken RP, Gervais DA, Arellano RS, Tuncali K, Morrison PR,Tatli S et al: Inflammatory nodules mimic applicator trackseeding after percutaneous ablation of renal tumors. AJRAm J Roentgenol 2007; 189: 845.
5. Lee DI, Uribe C, Eichel L, Khonsari S, Basillote J, Park HK etal: Sealing percutaneous nephrolithotomy tracts with gela-tin matrix hemostatic sealant: initial clinical use. J Urol2004; 171: 575.
6. Milner J, Borge M, Sharma S, Turk T and Perry K: Percuta-neous CT guided saline mobilization of colon to facilitaterenal cryoablation. J Urol, suppl., 2005; 173: 320, abstract1181.
7. Weld KJ, Hruby G, Humphrey PA, Ames CD and Landman J:
Precise characterization of renal parenchymal response tosingle and multiple cryoablation probes. J Urol 2006; 176:784.
8. Hegarty NJ, Gill IS, Desai MM, Remer EM, O’Malley CM andKaouk JH: Probe-ablative nephron-sparing surgery: cryoa-blation versus radiofrequency ablation. Urology 2006; 68: 7.
9. Hafron J and Kaouk JH: Cryosurgical ablation of renal cellcarcinoma. Cancer Control 2007; 14: 211.
10. Desai MM, Aron M and Gill IS: Laparoscopic partial nephrec-tomy versus laparoscopic cryoablation for the small renaltumor. Urology 2005; 66: 23.
11. Hruby G, Reisiger K, Venkatesh R, Yan Y and Landman J:Comparison of laparoscopic partial nephrectomy and lapa-roscopic cryoablation for renal hilar tumors. Urology 2006;67: 50.
12. O’Malley RL, Berger AD, Kanofsky JA, Phillips CK, StifelmanM and Taneja SS: A matched-cohort comparison of laparo-scopic cryoablation and laparoscopic partial nephrectomyfor treating renal masses. BJU Int 2007; 99: 395.
13. Atwell TD, Farrell MA, Callstrom MR, Charboneau JW, Lei-bovich BC, Patterson DE et al: Percutaneous cryoablationof 40 solid renal tumors with US guidance and CT moni-toring: initial experience. Radiology 2007; 243: 276.
14. Bandi G, Wen C, Hedican S, Moon T, Lee F and Nakada SY:Cryoablation of small renal masses: assessment of the out-come at one institution. BJU Int 2007; 100: 798.
15. Vanderbrink BA, Rastinehad A, Caplin D, Ost MC, Lobko Iand Lee BR: Successful conservative management of colo-renal fistula after percutaneous cryoablation of renal-cellcarcinoma. J Endourol 2007; 21: 726.
16. Gill IS, Remer EM, Hasan WA, Strzempkowski B, SpalivieroM, Steinberg AP et al: Renal cryoablation: outcome at 3years. J Urol 2005; 173: 1903.
EDITORIAL COMMENT
The authors present a strong argument for the use of per-cutaneous cryoablation in the treatment of posterior/lateraland select anterior renal masses 3 cm or smaller. Mosturologists will not be enthralled about the prospect of losingoperative cases to other specialties. However, as surgicalprocedures continue to evolve into more minimally invasiveapproaches it becomes imperative that the urologist con-tinue to evolve as well. Many centers including institutionssuch as Johns Hopkins, Long Island Jewish Medical Centerand the University of California at Irvine have establishedstrong allegiances with their interventional radiology col-leagues. These institutions do these procedures coopera-tively on a procedural or medical level but also with com-bined billing. This allows for a mutually beneficialrelationship without financial compromise and with ulti-mate benefit for the individual patient. At the same time wemust also be wary of giving up too much. Examples includedonor nephrectomies which were historically performed byurologists, and are now shared or solely performed by gen-eral surgeons and transplant surgeons. In addition, brachy-therapy and even prostate biopsies are being performedsolely by radiation oncologists. Even cystoscopy is performedby gynecologists and family practice physicians. With thethreat of a shortage of physicians, particularly urologists, inthe next decade we must continue to strive to stay involvedand remain primary.
Michael A. PaleseDepartment of Urology
The Mount Sinai Medical Center
New York, New York