Single port laparoscopic access surgery
10
Single port laparoscopic access surgery Manoel Galvao Neto, MD, a Almino Ramos, MD, a Josemberg Campos, PhD b a Gastro Obeso Center, Sao Paulo, Brazil. b Federal University of Pernambuco, Recife, Brazil. Since the introduction of Natural Orifice Translumenal Surgery (NOTES), experimental and human series of new access way to abdominal cavity are being described. Some are the resurrection of mini-site and some are single access umbilical laparoscopy. NOTES still on experimental field in most of its applications, but transumbilical single access seems to be better accepted for immediate clinical use. Nomenclature of this approach varies in many ways as: Natural Orifice Transumbilical Surgery (NOTUS), Single-Port Access (SPA) and Laparoendoscopic Single-site Surgery (LESS). Those are the most popular names. From the initial umbilical single access procedures it was a natural evolution the development of single trocars that could accommodate all instruments in a single incision, the Single Port Access Surgery. This article will present and discuss the differences of the technique when compared with laparoscopy, the different models of single trocar devices and the literature available on this matter. Authors experience with single incision, multiple trocars and single trocar procedures comes from 21 consecutive single incision, multiple trocars cholecystectomies and 25 single trocar cholecystectomies from 2008 to 2009 (retrospective analysis). Single incision group had 16 female patients within 22 to 58y (M 42 y), single port group had 19 female patients within 26 to 60 y (M 44 y). Operative time was 32 to 100 min (M 59 min) and 32 to 205 min (M 85.2 min) respectively. Intra-op complication happened as 1 cystic artery bleeding on single access group. Post-op complication appears as 2 seromas on single port group. No conversion or mortality was registered. Single port access devices and procedures represents a promising opportunity at its beginning of clinical experience. Proper training should be offered and more comparative data is requested. © 2009 Elsevier Inc. All rights reserved. KEYWORDS: Laparoendoscopic Single-site Surgery (LESS); Single-Port Access (SPA); Natural Orifice Transumbilical Surgery (NOTUS); Natural Orifice Translumenal Surgery (NOTES); Laparoscopy; Laparoscopic cholecystectomy The introduction of natural orifice translumenal endo- scopic surgery (NOTES) by Kalloo 1 has stimulated in- terest in a less invasive new approach to laparoscopic surgery. Single-port access umbilical laparoscopic sur- gery has advantages of a more cosmetic and less invasive approach than standard laparoscopy. As NOTES is still experimental, single-port transumbilical access may be more acceptable for immediate clinical use. Unlike NOTES, single-port surgery provides a better comfort zone for most surgeons because the instruments and techniques are similar to standard laparoscopic surgery. Not withstanding the claim that the umbilicus is a form of a natural orifice, it is a location where multiple instru- ments can be placed through an incision without a visible scar because it is already a “scar.” It is logical that the experience of open surgical, single- incision umbilical procedures, such as cholecystectomy, nephrectomy, and appendectomy, will support the develop- ment of laparoscopic trocars that could accommodate mul- tiple instruments in a single incision. The nomenclature for this approach has been quite variable and includes natural orifice transumbilical surgery (NOTUS), single-port access (SPA), one-port umbilical surgery (OPUS), transumbili- cal endoscopic surgery (TUES), single-site laparoscopy (SSL), single-incision laparoscopic surgery (SILS), sin- gle-instrument port laparoscopic surgery (SIMPL), and laparoendoscopic single-site (LESS) surgery. In this ar- ticle, the differences in techniques and devices as com- pared with laparoscopy will be reviewed. The authors report no direct financial interests that might pose a conflict of interest with the submitted manuscript. Address reprint requests to Manoel Galvao Neto, MD, Gastro Obeso Center, Rua Barata Ribeiro 237, São Paulo - SP, 01308000, Brazil. E-mail: [email protected] Techniques in GASTROINTESTINAL ENDOSCOPY www.techgiendoscopy.com Techniques in Gastrointestinal Endoscopy (2009) 11, 84-93 1096-2883/09/$-see front matter © 2009 Elsevier Inc. All rights reserved. doi:10.1016/j.tgie.2009.06.007
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Single port laparoscopic access surgery

Single port laparoscopic access surgeryManoel Galvao Neto, MD,a Almino Ramos, MD,a Josemberg Campos, PhDb
aGastro Obeso Center, Sao Paulo, Brazil.bFederal University of Pernambuco, Recife, Brazil.
Since the introduction of Natural Orifice Translumenal Surgery (NOTES), experimental and humanseries of new access way to abdominal cavity are being described. Some are the !resurrection! ofmini-site and some are single access umbilical laparoscopy. NOTES still on experimental field in mostof its applications, but transumbilical single access seems to be better accepted for immediate clinicaluse. Nomenclature of this approach varies in many ways as: Natural Orifice Transumbilical Surgery(NOTUS), Single-Port Access (SPA) and Laparoendoscopic Single-site Surgery (LESS). Those are themost popular names. From the initial umbilical single access procedures it was a natural evolution thedevelopment of single trocars that could accommodate all instruments in a single incision, the Single PortAccess Surgery. This article will present and discuss the differences of the technique when compared withlaparoscopy, the different models of single trocar devices and the literature available on this matter. Authorsexperience with single incision, multiple trocars and single trocar procedures comes from 21 consecutivesingle incision, multiple trocars cholecystectomies and 25 single trocar cholecystectomies from 2008 to 2009(retrospective analysis). Single incision group had 16 female patients within 22 to 58y (M " 42 y), singleport group had 19 female patients within 26 to 60 y (M " 44 y). Operative time was 32 to 100 min (M "59 min) and 32 to 205 min (M " 85.2 min) respectively. Intra-op complication happened as 1 cystic arterybleeding on single access group. Post-op complication appears as 2 seromas on single port group. Noconversion or mortality was registered. Single port access devices and procedures represents a promisingopportunity at its beginning of clinical experience. Proper training should be offered and more comparativedata is requested.© 2009 Elsevier Inc. All rights reserved.
KEYWORDS:LaparoendoscopicSingle-site Surgery (LESS);Single-Port Access (SPA);Natural OrificeTransumbilical Surgery(NOTUS);Natural OrificeTranslumenal Surgery(NOTES);Laparoscopy;Laparoscopiccholecystectomy
The introduction of natural orifice translumenal endo-scopic surgery (NOTES) by Kalloo1 has stimulated in-terest in a less invasive new approach to laparoscopicsurgery. Single-port access umbilical laparoscopic sur-gery has advantages of a more cosmetic and less invasiveapproach than standard laparoscopy. As NOTES is stillexperimental, single-port transumbilical access may bemore acceptable for immediate clinical use. UnlikeNOTES, single-port surgery provides a better comfortzone for most surgeons because the instruments andtechniques are similar to standard laparoscopic surgery.
Not withstanding the claim that the umbilicus is a form ofa natural orifice, it is a location where multiple instru-ments can be placed through an incision without a visiblescar because it is already a “scar.”
It is logical that the experience of open surgical, single-incision umbilical procedures, such as cholecystectomy,nephrectomy, and appendectomy, will support the develop-ment of laparoscopic trocars that could accommodate mul-tiple instruments in a single incision. The nomenclature forthis approach has been quite variable and includes naturalorifice transumbilical surgery (NOTUS), single-port access(SPA), one-port umbilical surgery (OPUS), transumbili-cal endoscopic surgery (TUES), single-site laparoscopy(SSL), single-incision laparoscopic surgery (SILS), sin-gle-instrument port laparoscopic surgery (SIMPL), andlaparoendoscopic single-site (LESS) surgery. In this ar-ticle, the differences in techniques and devices as com-pared with laparoscopy will be reviewed.
The authors report no direct financial interests that might pose a conflictof interest with the submitted manuscript.
Address reprint requests to Manoel Galvao Neto, MD, Gastro ObesoCenter, Rua Barata Ribeiro 237, São Paulo - SP, 01308000, Brazil. E-mail:[email protected]
Techniques inGASTROINTESTINAL
ENDOSCOPY
www.techgiendoscopy.com
Techniques in Gastrointestinal Endoscopy (2009) 11, 84-93
1096-2883/09/$-see front matter © 2009 Elsevier Inc. All rights reserved.doi:10.1016/j.tgie.2009.06.007
Single-port laparoscopyversus standard laparoscopy
Laparoscopic surgical techniques are based primarily ontraction and counter traction forces that allow triangulationof forces from two different points. Inserting the laparo-scopic instruments from a single-site port prevents triangu-lation when using standard laparoscopic instruments whileproviding an in-line instrument deployment and visualiza-tion of the operating field (Fig. 1). Once not desirable for agood visualization of laparoscopic procedures, in-line viewis gaining acceptance among surgeons as they become moreproficient with advanced endoscopy and NOTES proce-
dures where using flexible endoscopy where in-line view isthe rule.
Triangulation from a single port can be achieved witharticulated or steerable instruments (Fig. 2), like the ones fromCambridge Endo (Framingham, MA), the RealHand line fromNovare Surgical Systems (Cupertino, CA), the Roticulatorfrom Covidien (Norwalk, CT), and the SITRACC system fromEDLO (Porto Alegre, RS, Brazil). One way to improve visu-alization is by using articulated optics like the Endoeye (Olym-pus America, Center Valley, PA) or flexible endoscopes.
With single-port laparoscopy, the surgeon must dealwith the “sword fight” of instruments located on theexterior of the abdomen that compete for the relatively
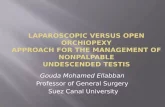
Figure 1 In-line disposition on instruments at a single port also competing for the same space. (Color version of figure isavailable online at www.techgiendoscopy.com.)
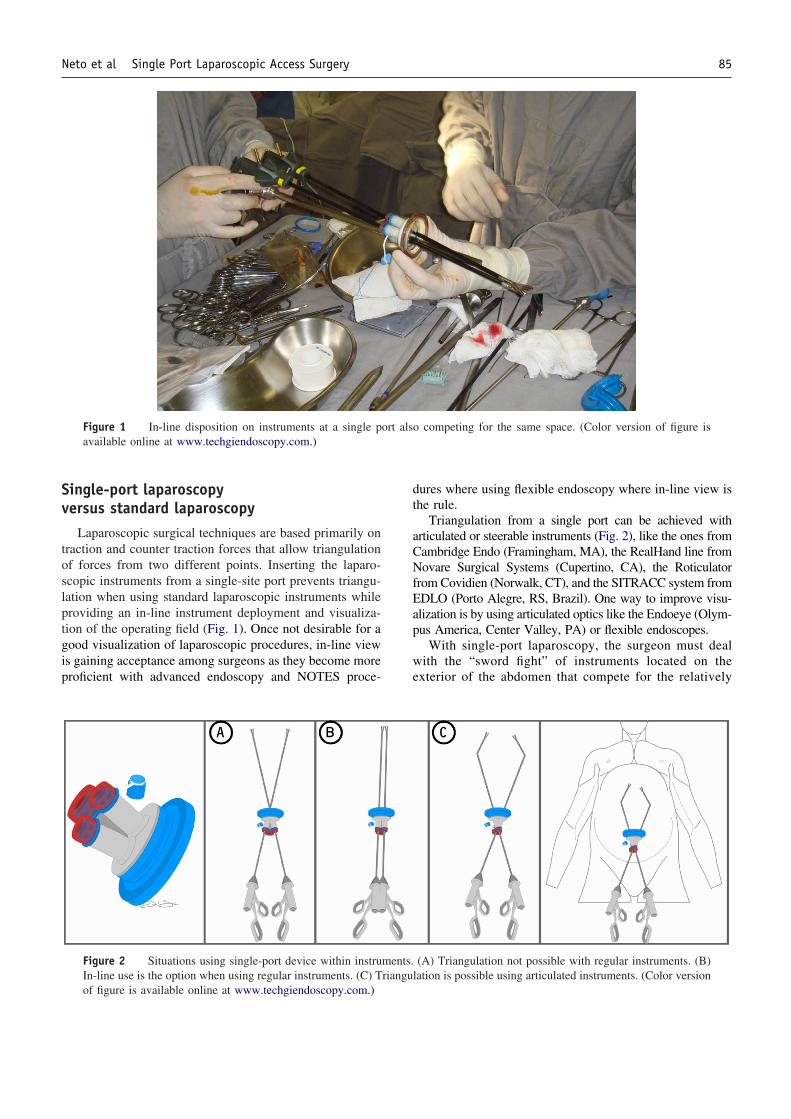
Figure 2 Situations using single-port device within instruments. (A) Triangulation not possible with regular instruments. (B)In-line use is the option when using regular instruments. (C) Triangulation is possible using articulated instruments. (Color versionof figure is available online at www.techgiendoscopy.com.)
85Neto et al Single Port Laparoscopic Access Surgery
tight space of the single port (Figs. 1 and 2). Ideally theinstruments should have different lengths, the handlesmust have a more opened angle than the regular 90°, therigid angled optic should be longer with the light sourcein-line, and also the camera couple must have its cablein-line and the coupler on a low profile. To divide vessels,regular 5-mm clip appliers—Harmonic Scalpel (EthiconEndo-Surgery, Cincinnati, OH), LigaSure vessel sealing
system (Covidien), and SonoSurg (Olympus America)—arethe ones that are mainly used but are not articulated.
Suturing is especially challenging with single-port lapa-roscopy. Instruments like the Endostitch from Covidientogether with knot pushers and endoloops are useful. Sta-plers have the challenge of having a relatively larger diam-eter that can compromise vision. Therefore, when an oversuture is necessary along the staple line, it will be difficult
0306090
120150180210
PT 1 PT 3 PT5 PT7 PT9PT1
1PT1
3PT1
5PT1
7PT1
9PT2
1
SINGLE ACCESSMULTIPLE TROCARS
SITRACC
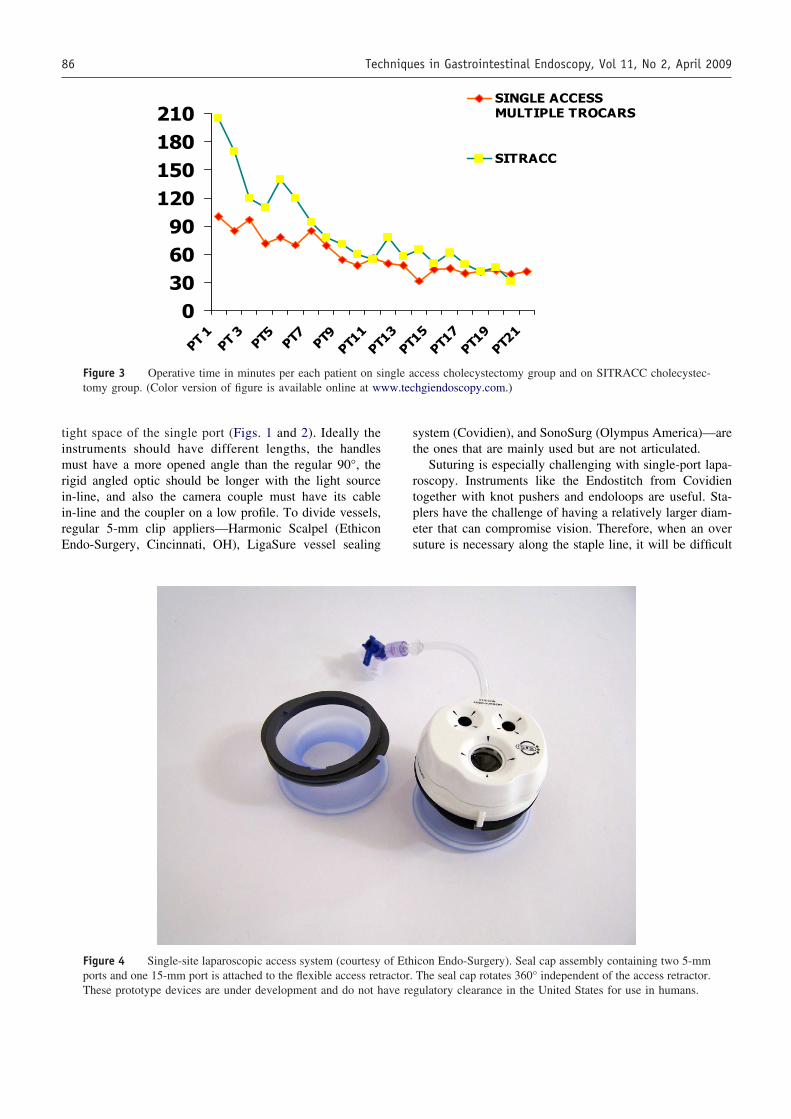
Figure 3 Operative time in minutes per each patient on single access cholecystectomy group and on SITRACC cholecystec-tomy group. (Color version of figure is available online at www.techgiendoscopy.com.)
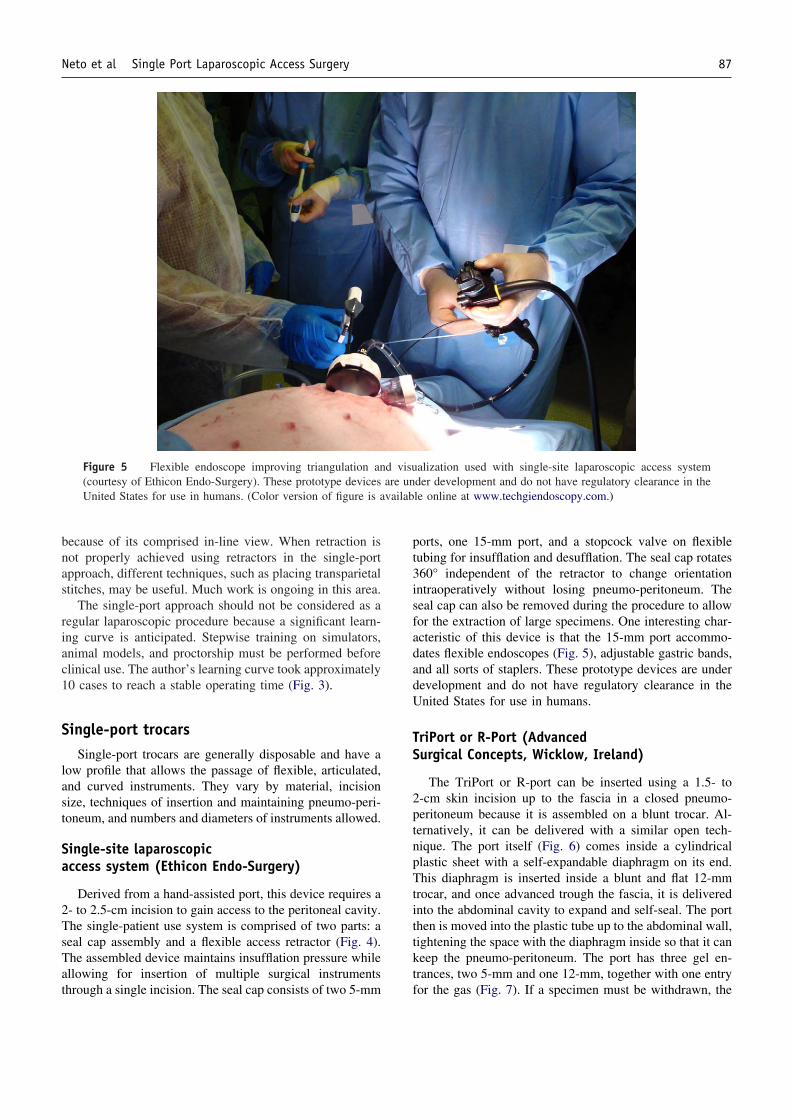
Figure 4 Single-site laparoscopic access system (courtesy of Ethicon Endo-Surgery). Seal cap assembly containing two 5-mmports and one 15-mm port is attached to the flexible access retractor. The seal cap rotates 360° independent of the access retractor.These prototype devices are under development and do not have regulatory clearance in the United States for use in humans.
86 Techniques in Gastrointestinal Endoscopy, Vol 11, No 2, April 2009
because of its comprised in-line view. When retraction isnot properly achieved using retractors in the single-portapproach, different techniques, such as placing transparietalstitches, may be useful. Much work is ongoing in this area.
The single-port approach should not be considered as aregular laparoscopic procedure because a significant learn-ing curve is anticipated. Stepwise training on simulators,animal models, and proctorship must be performed beforeclinical use. The author’s learning curve took approximately10 cases to reach a stable operating time (Fig. 3).
Single-port trocarsSingle-port trocars are generally disposable and have a
low profile that allows the passage of flexible, articulated,and curved instruments. They vary by material, incisionsize, techniques of insertion and maintaining pneumo-peri-toneum, and numbers and diameters of instruments allowed.
Single-site laparoscopicaccess system (Ethicon Endo-Surgery)
Derived from a hand-assisted port, this device requires a2- to 2.5-cm incision to gain access to the peritoneal cavity.The single-patient use system is comprised of two parts: aseal cap assembly and a flexible access retractor (Fig. 4).The assembled device maintains insufflation pressure whileallowing for insertion of multiple surgical instrumentsthrough a single incision. The seal cap consists of two 5-mm
ports, one 15-mm port, and a stopcock valve on flexibletubing for insufflation and desufflation. The seal cap rotates360° independent of the retractor to change orientationintraoperatively without losing pneumo-peritoneum. Theseal cap can also be removed during the procedure to allowfor the extraction of large specimens. One interesting char-acteristic of this device is that the 15-mm port accommo-dates flexible endoscopes (Fig. 5), adjustable gastric bands,and all sorts of staplers. These prototype devices are underdevelopment and do not have regulatory clearance in theUnited States for use in humans.
TriPort or R-Port (AdvancedSurgical Concepts, Wicklow, Ireland)
The TriPort or R-port can be inserted using a 1.5- to2-cm skin incision up to the fascia in a closed pneumo-peritoneum because it is assembled on a blunt trocar. Al-ternatively, it can be delivered with a similar open tech-nique. The port itself (Fig. 6) comes inside a cylindricalplastic sheet with a self-expandable diaphragm on its end.This diaphragm is inserted inside a blunt and flat 12-mmtrocar, and once advanced trough the fascia, it is deliveredinto the abdominal cavity to expand and self-seal. The portthen is moved into the plastic tube up to the abdominal wall,tightening the space with the diaphragm inside so that it cankeep the pneumo-peritoneum. The port has three gel en-trances, two 5-mm and one 12-mm, together with one entryfor the gas (Fig. 7). If a specimen must be withdrawn, the
Figure 5 Flexible endoscope improving triangulation and visualization used with single-site laparoscopic access system(courtesy of Ethicon Endo-Surgery). These prototype devices are under development and do not have regulatory clearance in theUnited States for use in humans. (Color version of figure is available online at www.techgiendoscopy.com.)
87Neto et al Single Port Laparoscopic Access Surgery
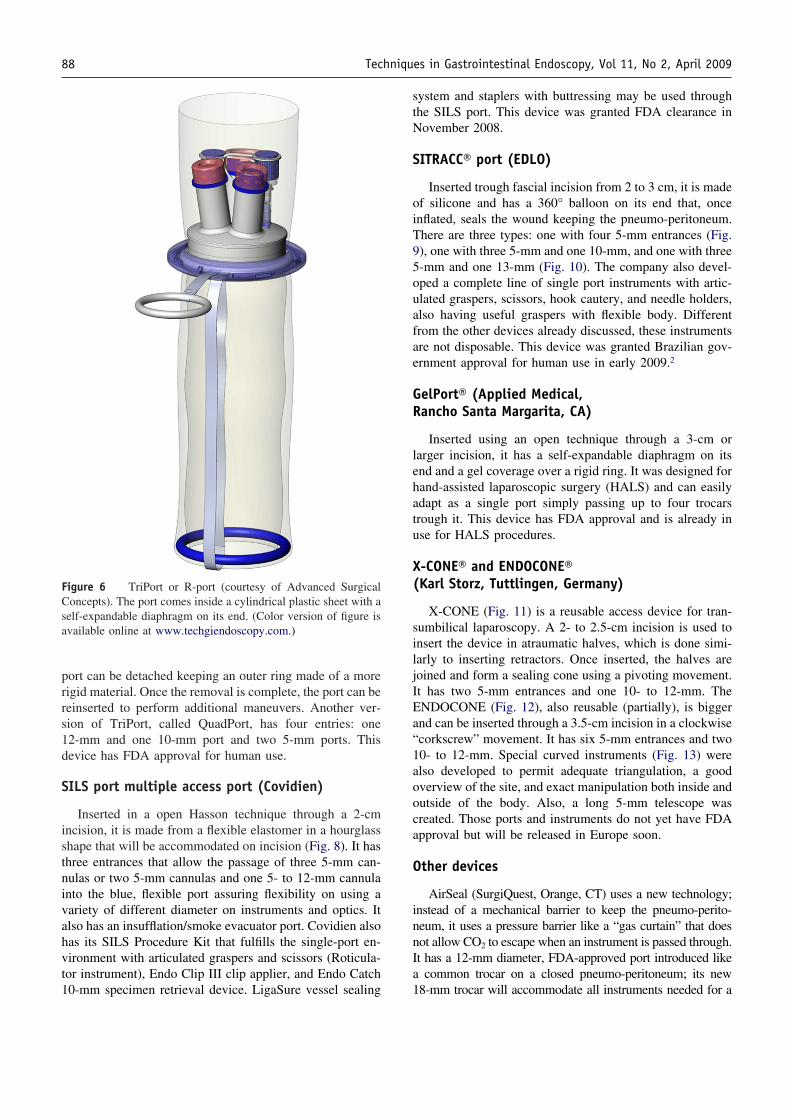
port can be detached keeping an outer ring made of a morerigid material. Once the removal is complete, the port can bereinserted to perform additional maneuvers. Another ver-sion of TriPort, called QuadPort, has four entries: one12-mm and one 10-mm port and two 5-mm ports. Thisdevice has FDA approval for human use.
SILS port multiple access port (Covidien)
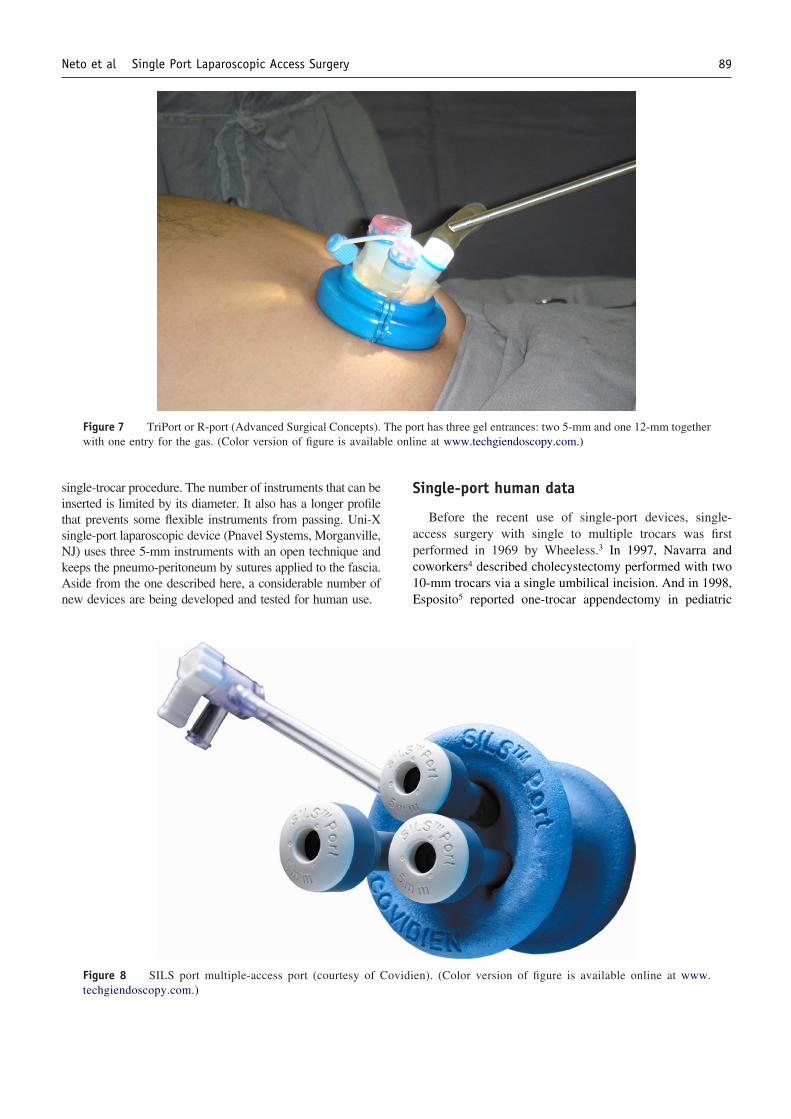
Inserted in a open Hasson technique through a 2-cmincision, it is made from a flexible elastomer in a hourglassshape that will be accommodated on incision (Fig. 8). It hasthree entrances that allow the passage of three 5-mm can-nulas or two 5-mm cannulas and one 5- to 12-mm cannulainto the blue, flexible port assuring flexibility on using avariety of different diameter on instruments and optics. Italso has an insufflation/smoke evacuator port. Covidien alsohas its SILS Procedure Kit that fulfills the single-port en-vironment with articulated graspers and scissors (Roticula-tor instrument), Endo Clip III clip applier, and Endo Catch10-mm specimen retrieval device. LigaSure vessel sealing
system and staplers with buttressing may be used throughthe SILS port. This device was granted FDA clearance inNovember 2008.
SITRACC® port (EDLO)
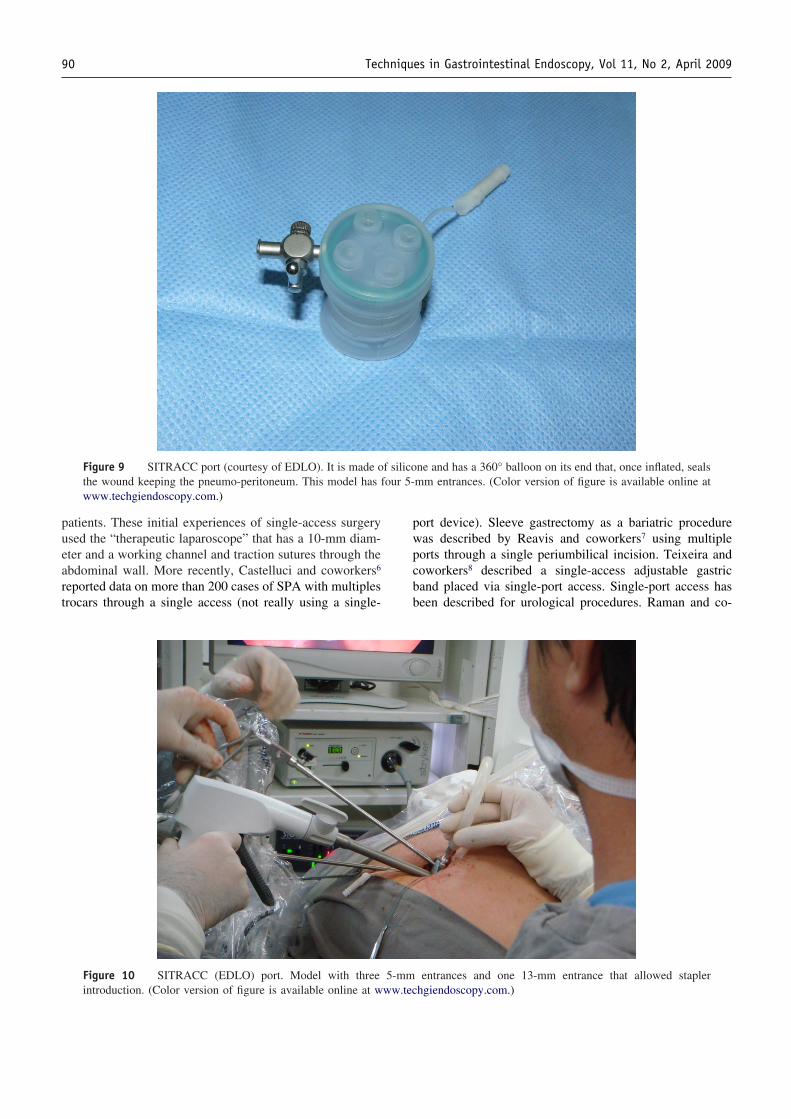
Inserted trough fascial incision from 2 to 3 cm, it is madeof silicone and has a 360° balloon on its end that, onceinflated, seals the wound keeping the pneumo-peritoneum.There are three types: one with four 5-mm entrances (Fig.9), one with three 5-mm and one 10-mm, and one with three5-mm and one 13-mm (Fig. 10). The company also devel-oped a complete line of single port instruments with artic-ulated graspers, scissors, hook cautery, and needle holders,also having useful graspers with flexible body. Differentfrom the other devices already discussed, these instrumentsare not disposable. This device was granted Brazilian gov-ernment approval for human use in early 2009.2
GelPort® (Applied Medical,Rancho Santa Margarita, CA)
Inserted using an open technique through a 3-cm orlarger incision, it has a self-expandable diaphragm on itsend and a gel coverage over a rigid ring. It was designed forhand-assisted laparoscopic surgery (HALS) and can easilyadapt as a single port simply passing up to four trocarstrough it. This device has FDA approval and is already inuse for HALS procedures.
X-CONE® and ENDOCONE®(Karl Storz, Tuttlingen, Germany)
X-CONE (Fig. 11) is a reusable access device for tran-sumbilical laparoscopy. A 2- to 2.5-cm incision is used toinsert the device in atraumatic halves, which is done simi-larly to inserting retractors. Once inserted, the halves arejoined and form a sealing cone using a pivoting movement.It has two 5-mm entrances and one 10- to 12-mm. TheENDOCONE (Fig. 12), also reusable (partially), is biggerand can be inserted through a 3.5-cm incision in a clockwise“corkscrew” movement. It has six 5-mm entrances and two10- to 12-mm. Special curved instruments (Fig. 13) werealso developed to permit adequate triangulation, a goodoverview of the site, and exact manipulation both inside andoutside of the body. Also, a long 5-mm telescope wascreated. Those ports and instruments do not yet have FDAapproval but will be released in Europe soon.
Other devices
AirSeal (SurgiQuest, Orange, CT) uses a new technology;instead of a mechanical barrier to keep the pneumo-perito-neum, it uses a pressure barrier like a “gas curtain” that doesnot allow CO2 to escape when an instrument is passed through.It has a 12-mm diameter, FDA-approved port introduced likea common trocar on a closed pneumo-peritoneum; its new18-mm trocar will accommodate all instruments needed for a
Figure 6 TriPort or R-port (courtesy of Advanced SurgicalConcepts). The port comes inside a cylindrical plastic sheet with aself-expandable diaphragm on its end. (Color version of figure isavailable online at www.techgiendoscopy.com.)
88 Techniques in Gastrointestinal Endoscopy, Vol 11, No 2, April 2009
single-trocar procedure. The number of instruments that can beinserted is limited by its diameter. It also has a longer profilethat prevents some flexible instruments from passing. Uni-Xsingle-port laparoscopic device (Pnavel Systems, Morganville,NJ) uses three 5-mm instruments with an open technique andkeeps the pneumo-peritoneum by sutures applied to the fascia.Aside from the one described here, a considerable number ofnew devices are being developed and tested for human use.
Single-port human data
Before the recent use of single-port devices, single-access surgery with single to multiple trocars was firstperformed in 1969 by Wheeless.3 In 1997, Navarra andcoworkers4 described cholecystectomy performed with two10-mm trocars via a single umbilical incision. And in 1998,Esposito5 reported one-trocar appendectomy in pediatric
Figure 7 TriPort or R-port (Advanced Surgical Concepts). The port has three gel entrances: two 5-mm and one 12-mm togetherwith one entry for the gas. (Color version of figure is available online at www.techgiendoscopy.com.)
Figure 8 SILS port multiple-access port (courtesy of Covidien). (Color version of figure is available online at www.techgiendoscopy.com.)
89Neto et al Single Port Laparoscopic Access Surgery
patients. These initial experiences of single-access surgeryused the “therapeutic laparoscope” that has a 10-mm diam-eter and a working channel and traction sutures through theabdominal wall. More recently, Castelluci and coworkers6
reported data on more than 200 cases of SPA with multiplestrocars through a single access (not really using a single-
port device). Sleeve gastrectomy as a bariatric procedurewas described by Reavis and coworkers7 using multipleports through a single periumbilical incision. Teixeira andcoworkers8 described a single-access adjustable gastricband placed via single-port access. Single-port access hasbeen described for urological procedures. Raman and co-
Figure 10 SITRACC (EDLO) port. Model with three 5-mm entrances and one 13-mm entrance that allowed staplerintroduction. (Color version of figure is available online at www.techgiendoscopy.com.)
Figure 9 SITRACC port (courtesy of EDLO). It is made of silicone and has a 360° balloon on its end that, once inflated, sealsthe wound keeping the pneumo-peritoneum. This model has four 5-mm entrances. (Color version of figure is available online atwww.techgiendoscopy.com.)
90 Techniques in Gastrointestinal Endoscopy, Vol 11, No 2, April 2009
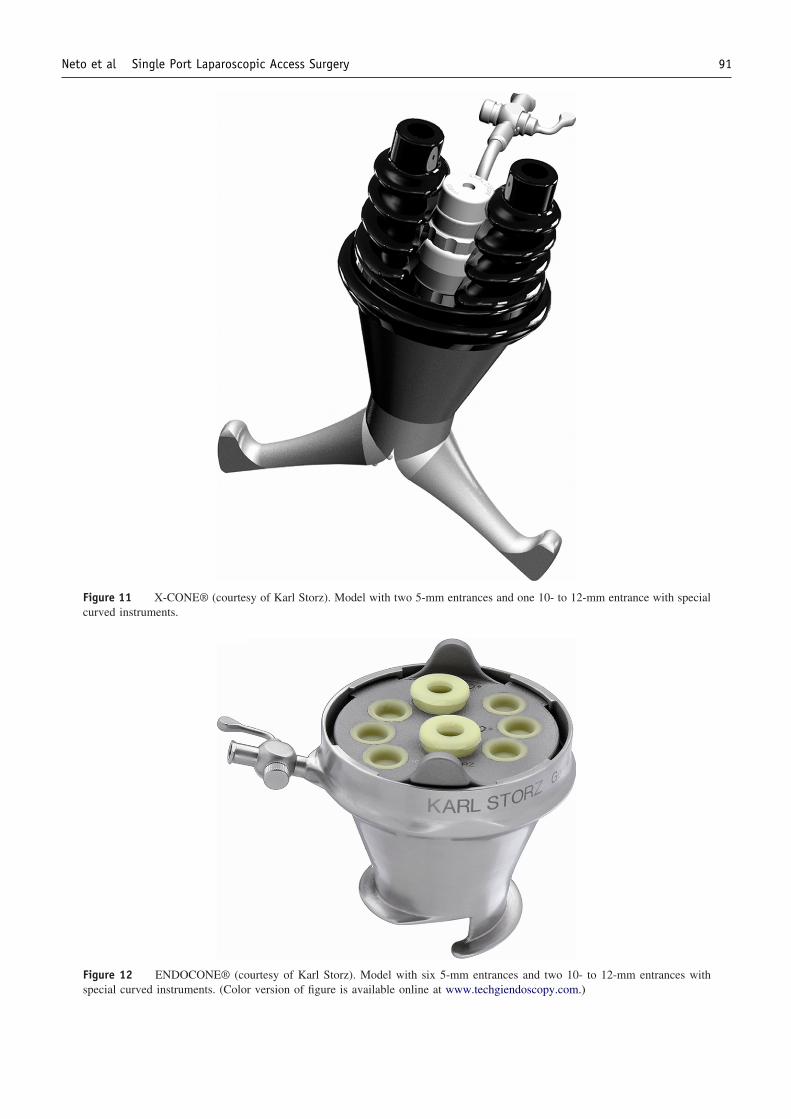
Figure 11 X-CONE® (courtesy of Karl Storz). Model with two 5-mm entrances and one 10- to 12-mm entrance with specialcurved instruments.
Figure 12 ENDOCONE® (courtesy of Karl Storz). Model with six 5-mm entrances and two 10- to 12-mm entrances withspecial curved instruments. (Color version of figure is available online at www.techgiendoscopy.com.)
91Neto et al Single Port Laparoscopic Access Surgery

workers9 described the first comparative study of laparo-scopic versus single-access nephrectomy, showing that sin-gle-access surgery had significantly less blood loss (withoutchanges in clinical outcomes).
Single-port access surgery, like single-access surgery, isrelatively new and there is a lack comparative studies withconventional laparoscopy. Kagaya and coworkers10 in 2001described a series of cholecystectomies performed using asingle-port device with two entrances. Using the TriPort orR-port (Advanced Surgical Concepts), there are reports ofprocedures like cholecystectomy,11,12 and nephrectomy.13
With the GelPort (Applied Medical), a series of cholecys-tectomy, hemicolectomy, adjustable gastric banding, sleevegastrectomy, and esophagectomy was presented.14 Usingthe Uni-X single-port laparoscopic device (Pnavel Sys-tems), urological procedures like radical prostatectomy15
and nephrectomy16 have been described. The AirSeal(SurgiQuest) device was used for cholecystectomy.17 TheSILS Port (Covidien) recently got FDA clearance, and theresults of first trials and procedures are pending.
Authors’ experience withsingle-port access devices
Our group first performed NOTES in 2006 with a seriesof a hybrid transgastric cholecystectomy, removing the gall-
bladder by the stomach with a flexible endoscope. In 2007,the transvaginal route was used with a double-channel flex-ible endoscope except for a single 3- to 5-mm port on theumbilicus for traction transvaginal trial.18 Although feasibleand safe, it was time-demanding and complex. In 2008, weperformed “video-assisted” NOTES transvaginal cholecys-tectomy with rigid instruments,19 which were also found tobe feasible and safe. On track with pursuing procedures asa bridge to NOTES, we began single-access procedures witha series of 21 consecutive cholecystectomies using 3 trocarsvia a 2-cm incision on umbilicus, 1 central trocar of 10 mm,and the 2 lateral of 5 mm. By the time we had the TriPort(Advanced Surgical Concepts) available, we had performed5 consecutive cases. In 2009, we joined the SITRACC(EDLO) Brazilian multicentric trial and are performing 20consecutive cases in a group comprised of 3 institutions(Gastro Obeso Center, Sao Paulo; San Rafael Hospital,Salvador; Federal University of Pernambuco, Recife).These results (Fig. 3, Table 1) are partial and derived fromthe authors. All procedures were done without extra ports.As intraoperative complication, one cystic artery bleedingoccurred on single-access (multiple trocars) cholecystec-tomy group and was controlled with clips. As postoperativecomplication, one seroma at SITRACC cholecystectomygroup and one on TriPort cholecystectomy group weretreated with fine-needle aspiration. No mortality was regis-
Figure 13 X-CONE® (courtesy of Karl Storz) with special curved instruments that allows triangulation.
92 Techniques in Gastrointestinal Endoscopy, Vol 11, No 2, April 2009

tered. The authors also performed 2 cases of SITRACCSleeve gastrectomy in patients with BMI of 42 and 45 witha 3-mm liver retractor introduced without a trocar (Fig. 14).
ConclusionsSingle-port access devices and procedures are a promis-
ing form of minimally invasive surgery currently in theinitial stages of clinical experience. There is growing ac-ceptance and enthusiasm among surgeons, patients, andindustry. However we should be cautious as suggested bythe editorial of Connor,20 which serves as a reminder of thehigh incidence of biliary tract injury with the introductionof laparoscopic cholecystectomy in the early 1990s. Weshould not allow that history to be repeated. A compellingneed exists for proper training and more controlled trialsbefore widespread use of this technique is advocated.
References1. Kalloo AN, Singh VK, Jagannath SB, et al: Flexible transgastric perito-
neoscopy: A novel approach to diagnostic and therapeutic interventions inthe peritoneal cavity. Gastrointest Endosc 60:114-117, 2004
2. Martins MV, Skinovsky J, Coelho D, et al: SITRACC—Single TrocarAccess: A new device for a new surgical approach. Bras J Video-Sur2:061-063, 2008
3. Wheeless CR: A rapid, inexpensive, and effective method of surgicalsterilization by laparoscopy. J Reprod Med 5:255, 1969
4. Navarra G, Pozza E, Occhionorelli S, et al: One-wound laparoscopiccholecystectomy. Br J Surg 84:695, 1997
5. Esposito C: One-trocar appendectomy in pediatric surgery. Surg En-dosc 12:177-178, 1998
6. Castellucci SA, Curcillo PG, Ginsberg PC, et al: Single-port accessadrenalectomy. J Endourol 22:1573-1576, 2008
7. Reavis KM, Hinojosa MW, Smith BR, et al: Single laparoscopic-incision transabdominal surgery sleeve gastrectomy. Obes Surg 18:1492-1494, 2008
8. Teixeira J, McGill K, Binenbaum S, et al: Laparoscopic single-sitesurgery for placement of an adjustable gastric band: Initial experience.Surg Endosc 23:1409-1414, 2009
9. Raman JD, Cadeddu JA, Rao P, et al: Single-incision laparoscopicsurgery: initial urological experience and comparison with natural-orifice transluminal endoscopic surgery. BJU 101:1493-1496, 2008
10. Kagaya T: Laparoscopic cholecystectomy via two ports, using the“Twin-Port” system. J Hepatobiliary Pancreat Surg 8:76-80, 2001
11. Langwieler TE, Nimmesgern T, Back M: Single-port access in lapa-roscopic cholecystectomy. Surg Endosc 23:1138-1141, 2009
12. Romanelli JR, Mark L, Omotosho PA: Single port laparoscopic cho-lecystectomy with the TriPort system: A case report. Surg Innov15:223-228, 2008
13. Rané A, Rao P, Rao P: Single-port-access nephrectomy and otherlaparoscopic urologic procedures using a novel laparoscopic port (R-port). Urology 72:260-263, discussion 263-264, 2008
14. Merchant AM, Cook MW, White BC, et al: Transumbilical Gelportaccess technique for performing single-incision laparoscopic Surgery(SILS). J Gastrointest Surg 13:159-162, 2009
15. Kaouk JH, Goel RK, Haber GP, et al: Single-port laparoscopic radicalprostatectomy. Urology 72:1190-1193, 2008
16. Kaouk JH, Haber GP, Goel RK, et al: Single-port laparoscopic surgeryin urology: Initial experience. Urology 71:3-6, 2008
17. Earle DB, Jones D, Schwaitzberg S, et al: Air-Seal: A minimallyinvasive access port that enhances patient safety and enables newoperative approaches. SAGES abstract book, Emerging TechnologyForum, 2008 (ET016)
18. Mottin C, Galvao Neto M, Ramos A, et al: Transvaginal cholecystec-tomy: A case report. Rev Bras Videocir 5:139-143, 2007
19. Ramos A, Murakami A, Galvao Neto M, et al: NOTES transvaginalvideo-assisted cholecystectomy: First series. Endoscopy 40:572-575,2008
20. Connor S: Single-port-access cholecystectomy: History should not beallowed to repeat. World J Surg 33:1020-1021, 2009
Figure 14 SITRACC sleeve gastrectomy procedure highlighting the vertical stapling of stomach. (Color version of figure isavailable online at www.techgiendoscopy.com.)
93Neto et al Single Port Laparoscopic Access Surgery